User login
MDedge latest news is breaking news from medical conferences, journals, guidelines, the FDA and CDC.
Posttraumatic Stress Disorder May Increase Morbidity Risk in Veterans With HIV
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Posttraumatic stress disorder (PTSD) among veterans living with HIV significantly increased the risk for AIDS and multiple comorbidities, particularly arthritis, cardiovascular disease (CVD), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), and multimorbidity — with the greatest impact seen in the first decade after diagnosis.
METHODOLOGY:
- Researchers conducted a prospective cohort study to assess whether PTSD is associated with increased risk for adverse clinical outcomes in veterans with HIV who received care at the Department of Veterans Affairs.
- They included 3206 veterans (97.4% men; median age at HIV diagnosis, 31.7 years; 42.1% with PTSD) who were deployed in Iraq and Afghanistan while serving in the military and initiated antiretroviral therapy before December 31, 2020.
- Participants were followed-up until December 2022, with censoring at death, the last health care visit, or study termination. The association between PTSD with morbidity and mortality, considering the number of deployments and levels of combat exposure were determined.
TAKEAWAY:
- PTSD significantly increased the overall risks for AIDS by 11% (adjusted hazard ratio [aHR], 1.11), CKD by 21% (aHR, 1.21), COPD by 46% (aHR, 1.46), multimorbidity by 49% (aHR, 1.49), CVD by 57% (aHR, 1.57), and arthritis by two folds (aHR, 1.95; P <.05 for all).
- Among veterans with a single deployment, those with PTSD had 92%, 87%, 80%, 53%, 44%, 32%, and 27% higher risks for asthma, CVD, arthritis, multimorbidity, COPD, liver disease, and AIDS, respectively, than those without PTSD.
- Veterans with PTSD and combat exposure had a lower risk for AIDS but higher risks for multimorbidity, asthma, CVD, and arthritis than those never diagnosed with PTSD and unexposed to combat.
- The associations of PTSD with mortality and morbidity appeared most pronounced in the first decade post-diagnosis, followed by a gradual decline in association strength; however, risks remained elevated.
IN PRACTICE:
“It is recommended that providers who work with VWH [veterans with HIV] consider adopting a trauma-informed model of HIV care and that providers screen veterans for PTSD, so that their unique trauma history can help guide medical decisions and treatment,” the authors wrote.
SOURCE:
This study was led by Kartavya J. Vyas, PhD, Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta. It was published online in AIDS .
LIMITATIONS:
The data could not capture each individual’s true index trauma or the severity of their PTSD. Additionally, the study was limited by considerable loss to follow-up, potential uncontrolled confounding related to homelessness, and a lack of generalizability to veterans with HIV who were not receiving antiretroviral therapy.
DISCLOSURES:
The study did not receive any specific funding. Two authors reported receiving federal research support — one from the Emory Center for AIDS Research and the National Institute of Allergy and Infectious Diseases, and the other from the National Institutes of Health and the CDC — in addition to investigator-initiated grants and consulting fees from various pharmaceutical companies.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Can Patients Really Say No to Life-Saving Cancer Care?
Mrs G.O. is an 80-year-old retired teacher who was widowed a decade ago. With no close relatives, she lives alone, accompanied by only two cats and a dog that she has rescued. “I am alone,” she told Gustavo Kusminsky, MD, consultant in Hematology and Hematopoietic Transplant Service at Austral University Hospital and lecturer in medicine at the Hospital Universitario Austral, Buenos Aires, Argentina. She said this calmly while refusing treatment for life-threatening multiple myeloma. “Doctor, I would rather not,” she added — her words lingering in the quiet consulting room. That moment is now the focus of a recent article in the journal Medicina.
In the article, Kusminsky described how he made an effort to clarify to the patient that she needed cancer treatment. He explained that the treatment was mostly oral, required no initial hospitalization, and that consultations could be spaced out. However, Mrs G.O. maintained her position.
“The patient had no signs of depression, and her argument was logical. Mrs G.O. was already receiving several medications for high blood pressure, was on anticoagulation therapy for atrial fibrillation, and managed dyslipidemia with fenofibrate. But she preferred not to receive treatment for her multiple myeloma.” Kusminsky noted.
“Doctor, I have lived my life. I am old. I am already taking too many medications. I do not have a family, and it would be very difficult to deal with the side effects and be dependent on the hospital. As long as I can take care of myself, I do not want any more treatment, at least not for now. We will talk in a few months if I am still here,” she told him before leaving.
The article mentioned that responses such as Mrs G.O. spark perplexity in modern medicine to the extent that clinicians initiate protocols to rule out depression or other psychological factors when a patient rejects treatments that could prolong their life. On the contrary, no such checks are made when patients agree to treatment, because acceptance is deemed “normal.”
Because of collective assumptions and the war metaphors often used in oncology, Mrs G.O. risked being labeled a “deserter from the battalion” of patients with cancer.
In truth, her decision invites reflection on the doctor-patient relationship, respect for autonomy, and the benefits of modern cancer care offered today, Kusminsky said.
This provides an opportunity to consider the patient’s perspective rather than a purely medical perspective.
Jennifer Hincapié Sánchez, PhD, professor in the Faculty of Medicine at the National Autonomous University of Mexico (UNAM). She is the director of the UNAM University Bioethics Program and coordinates its Institutional Ethics and Bioethics Program for the Faculty of Medicine in Mexico. Although not involved in the article, she regards it as vital. “It’s crucial to remind medical staff that their role is to promote patients’ well-being and that this is related to the life plan that patients have set for themselves, even though this vision is sometimes not aligned with biomedical progress,” she said.
Patient Autonomy
Science-guided medicine aims to prolong life, improve quality, and relieve suffering. However, acceptance or refusal of treatment remains a personal choice for anyone with cancer.
Some evidence showed that patients who decline treatment do not always experience rapid decline. Many can live acceptable, even fulfilling, lives on their own for varying periods, even though they know that there is a possibility of shorter survival. Valuing fewer side effects and better quality of life. This suggested that quality of life is subjective and cannot be measured solely by biomedical standards but also by the meaning each person finds in their existence, even in the face of serious illness.
“There is a myth that quality of life is only valid when defined by objective success. Our task is to explain that it is subjective, and life can be meaningful despite limitations.” Kusminsky said.
Mrs G.O. knew her prognosis and treatment options but chose not to pursue treatment, which, while medically advisable, did not align with her values or vision of life.
Hincapié Sánchez stated that the priority is always to honor the patient’s choice. Clinicians must ensure that the patient has all necessary information that is always appropriate to their sociocultural context before making the decision.
“If the decision persists despite being informed and aware of the effects of the patient’s choice, all we can do is provide support, manage the pain, and seek the patient’s comfort,” she emphasized.
Medical Omnipotence
Physicians should not view the refusal of treatment as an abandonment of the fundamental principles of the profession. Rather, it means respecting patient priorities and recognizing medicine as a dialogue between science and humanity, not as an exercise of control.
However, many clinicians struggle with such decisions because they conflict with their impulse to act and a sense of medical omnipotence. Hincapié Sánchez attributed these difficulties to medical training.
“We are taught to preserve life at all costs. If treatment even slightly prolongs life, many doctors continue to recommend it. The question becomes: Is it valid to extend life when its quality is in doubt?” she asked.
“Medicine is more than a science; it is an art. It is the most human in the sciences and the most scientific in the humanities. Let us not lose sight of the human element that allows us to see the patient as a person, not just a disease to be treated,” Hincapié Sánchez urges.
Kusminsky describes a common therapeutic obstinacy — doctors’ reluctance to stop “doing something,” to avoid “throwing in the towel,” or to uphold “hope is the last thing to be lost.”
“But physicians are growing more aware of these situations, and change is slowly coming,” he said. However, he added: “Of course, there is the issue of the perceived omnipotence of doctors — their words descending with authority to ‘prescribe’ treatment, issue ‘medical orders,’ or dictate ‘pharmacological’ therapy.
For the specialist, such terminology reflects a view of the doctor-patient relationship not as a mutual, two-way exchange, but as a vertical, paternalistic dynamic.
He suggested looking at ancient Greece for perspective. “Hippocrates, or rather the Hippocratic school, taught that the doctor-patient encounter is inherently one of compassion. We must approach this in that way. Reflecting on that bond, improving communication, humanizing relationships, and, above all, being available to listen are key,” Kusminsky said.
Another intersection that has long fascinated Kusminsky is between literature and medicine. This interest led him to explore the field of narrative medicine, serve on the board of directors of the Argentine Society of Narrative Medicine (SAMEN), and join the roster of speakers at the upcoming second SAMEN Conference in Buenos Aires on July 10 and 11, 2025.
“Narrative medicine uses storytelling tools to absorb, process, acknowledge, and empathize with patients’ illness narratives, aiming to restore humanism to practice,” he explained.
According to Kusminsky, the circumstances under which Mrs G.O. expressed her wish not to begin treatment immediately reminded him of a text by Melville’s famous “I would prefer not to” from Bartleby, the Scrivener.
This reflection inspired him to publish an article cited at its beginning. At the same time, it reinforced his belief that what patients say can itself be a form of narrative that extends beyond the confines of clinical history.
Mrs G.O. chose not to pursue treatment for multiple myeloma. However, she returned to Kusminsky’s office approximately 2 months ago. She felt well, and her disease slowly progressed; however, she still had no clinical signs or symptoms.
Kusminsky and Hincapié Sánchez have declared no relevant financial conflicts of interest.
This story was translated from Medscape’s Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Mrs G.O. is an 80-year-old retired teacher who was widowed a decade ago. With no close relatives, she lives alone, accompanied by only two cats and a dog that she has rescued. “I am alone,” she told Gustavo Kusminsky, MD, consultant in Hematology and Hematopoietic Transplant Service at Austral University Hospital and lecturer in medicine at the Hospital Universitario Austral, Buenos Aires, Argentina. She said this calmly while refusing treatment for life-threatening multiple myeloma. “Doctor, I would rather not,” she added — her words lingering in the quiet consulting room. That moment is now the focus of a recent article in the journal Medicina.
In the article, Kusminsky described how he made an effort to clarify to the patient that she needed cancer treatment. He explained that the treatment was mostly oral, required no initial hospitalization, and that consultations could be spaced out. However, Mrs G.O. maintained her position.
“The patient had no signs of depression, and her argument was logical. Mrs G.O. was already receiving several medications for high blood pressure, was on anticoagulation therapy for atrial fibrillation, and managed dyslipidemia with fenofibrate. But she preferred not to receive treatment for her multiple myeloma.” Kusminsky noted.
“Doctor, I have lived my life. I am old. I am already taking too many medications. I do not have a family, and it would be very difficult to deal with the side effects and be dependent on the hospital. As long as I can take care of myself, I do not want any more treatment, at least not for now. We will talk in a few months if I am still here,” she told him before leaving.
The article mentioned that responses such as Mrs G.O. spark perplexity in modern medicine to the extent that clinicians initiate protocols to rule out depression or other psychological factors when a patient rejects treatments that could prolong their life. On the contrary, no such checks are made when patients agree to treatment, because acceptance is deemed “normal.”
Because of collective assumptions and the war metaphors often used in oncology, Mrs G.O. risked being labeled a “deserter from the battalion” of patients with cancer.
In truth, her decision invites reflection on the doctor-patient relationship, respect for autonomy, and the benefits of modern cancer care offered today, Kusminsky said.
This provides an opportunity to consider the patient’s perspective rather than a purely medical perspective.
Jennifer Hincapié Sánchez, PhD, professor in the Faculty of Medicine at the National Autonomous University of Mexico (UNAM). She is the director of the UNAM University Bioethics Program and coordinates its Institutional Ethics and Bioethics Program for the Faculty of Medicine in Mexico. Although not involved in the article, she regards it as vital. “It’s crucial to remind medical staff that their role is to promote patients’ well-being and that this is related to the life plan that patients have set for themselves, even though this vision is sometimes not aligned with biomedical progress,” she said.
Patient Autonomy
Science-guided medicine aims to prolong life, improve quality, and relieve suffering. However, acceptance or refusal of treatment remains a personal choice for anyone with cancer.
Some evidence showed that patients who decline treatment do not always experience rapid decline. Many can live acceptable, even fulfilling, lives on their own for varying periods, even though they know that there is a possibility of shorter survival. Valuing fewer side effects and better quality of life. This suggested that quality of life is subjective and cannot be measured solely by biomedical standards but also by the meaning each person finds in their existence, even in the face of serious illness.
“There is a myth that quality of life is only valid when defined by objective success. Our task is to explain that it is subjective, and life can be meaningful despite limitations.” Kusminsky said.
Mrs G.O. knew her prognosis and treatment options but chose not to pursue treatment, which, while medically advisable, did not align with her values or vision of life.
Hincapié Sánchez stated that the priority is always to honor the patient’s choice. Clinicians must ensure that the patient has all necessary information that is always appropriate to their sociocultural context before making the decision.
“If the decision persists despite being informed and aware of the effects of the patient’s choice, all we can do is provide support, manage the pain, and seek the patient’s comfort,” she emphasized.
Medical Omnipotence
Physicians should not view the refusal of treatment as an abandonment of the fundamental principles of the profession. Rather, it means respecting patient priorities and recognizing medicine as a dialogue between science and humanity, not as an exercise of control.
However, many clinicians struggle with such decisions because they conflict with their impulse to act and a sense of medical omnipotence. Hincapié Sánchez attributed these difficulties to medical training.
“We are taught to preserve life at all costs. If treatment even slightly prolongs life, many doctors continue to recommend it. The question becomes: Is it valid to extend life when its quality is in doubt?” she asked.
“Medicine is more than a science; it is an art. It is the most human in the sciences and the most scientific in the humanities. Let us not lose sight of the human element that allows us to see the patient as a person, not just a disease to be treated,” Hincapié Sánchez urges.
Kusminsky describes a common therapeutic obstinacy — doctors’ reluctance to stop “doing something,” to avoid “throwing in the towel,” or to uphold “hope is the last thing to be lost.”
“But physicians are growing more aware of these situations, and change is slowly coming,” he said. However, he added: “Of course, there is the issue of the perceived omnipotence of doctors — their words descending with authority to ‘prescribe’ treatment, issue ‘medical orders,’ or dictate ‘pharmacological’ therapy.
For the specialist, such terminology reflects a view of the doctor-patient relationship not as a mutual, two-way exchange, but as a vertical, paternalistic dynamic.
He suggested looking at ancient Greece for perspective. “Hippocrates, or rather the Hippocratic school, taught that the doctor-patient encounter is inherently one of compassion. We must approach this in that way. Reflecting on that bond, improving communication, humanizing relationships, and, above all, being available to listen are key,” Kusminsky said.
Another intersection that has long fascinated Kusminsky is between literature and medicine. This interest led him to explore the field of narrative medicine, serve on the board of directors of the Argentine Society of Narrative Medicine (SAMEN), and join the roster of speakers at the upcoming second SAMEN Conference in Buenos Aires on July 10 and 11, 2025.
“Narrative medicine uses storytelling tools to absorb, process, acknowledge, and empathize with patients’ illness narratives, aiming to restore humanism to practice,” he explained.
According to Kusminsky, the circumstances under which Mrs G.O. expressed her wish not to begin treatment immediately reminded him of a text by Melville’s famous “I would prefer not to” from Bartleby, the Scrivener.
This reflection inspired him to publish an article cited at its beginning. At the same time, it reinforced his belief that what patients say can itself be a form of narrative that extends beyond the confines of clinical history.
Mrs G.O. chose not to pursue treatment for multiple myeloma. However, she returned to Kusminsky’s office approximately 2 months ago. She felt well, and her disease slowly progressed; however, she still had no clinical signs or symptoms.
Kusminsky and Hincapié Sánchez have declared no relevant financial conflicts of interest.
This story was translated from Medscape’s Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Mrs G.O. is an 80-year-old retired teacher who was widowed a decade ago. With no close relatives, she lives alone, accompanied by only two cats and a dog that she has rescued. “I am alone,” she told Gustavo Kusminsky, MD, consultant in Hematology and Hematopoietic Transplant Service at Austral University Hospital and lecturer in medicine at the Hospital Universitario Austral, Buenos Aires, Argentina. She said this calmly while refusing treatment for life-threatening multiple myeloma. “Doctor, I would rather not,” she added — her words lingering in the quiet consulting room. That moment is now the focus of a recent article in the journal Medicina.
In the article, Kusminsky described how he made an effort to clarify to the patient that she needed cancer treatment. He explained that the treatment was mostly oral, required no initial hospitalization, and that consultations could be spaced out. However, Mrs G.O. maintained her position.
“The patient had no signs of depression, and her argument was logical. Mrs G.O. was already receiving several medications for high blood pressure, was on anticoagulation therapy for atrial fibrillation, and managed dyslipidemia with fenofibrate. But she preferred not to receive treatment for her multiple myeloma.” Kusminsky noted.
“Doctor, I have lived my life. I am old. I am already taking too many medications. I do not have a family, and it would be very difficult to deal with the side effects and be dependent on the hospital. As long as I can take care of myself, I do not want any more treatment, at least not for now. We will talk in a few months if I am still here,” she told him before leaving.
The article mentioned that responses such as Mrs G.O. spark perplexity in modern medicine to the extent that clinicians initiate protocols to rule out depression or other psychological factors when a patient rejects treatments that could prolong their life. On the contrary, no such checks are made when patients agree to treatment, because acceptance is deemed “normal.”
Because of collective assumptions and the war metaphors often used in oncology, Mrs G.O. risked being labeled a “deserter from the battalion” of patients with cancer.
In truth, her decision invites reflection on the doctor-patient relationship, respect for autonomy, and the benefits of modern cancer care offered today, Kusminsky said.
This provides an opportunity to consider the patient’s perspective rather than a purely medical perspective.
Jennifer Hincapié Sánchez, PhD, professor in the Faculty of Medicine at the National Autonomous University of Mexico (UNAM). She is the director of the UNAM University Bioethics Program and coordinates its Institutional Ethics and Bioethics Program for the Faculty of Medicine in Mexico. Although not involved in the article, she regards it as vital. “It’s crucial to remind medical staff that their role is to promote patients’ well-being and that this is related to the life plan that patients have set for themselves, even though this vision is sometimes not aligned with biomedical progress,” she said.
Patient Autonomy
Science-guided medicine aims to prolong life, improve quality, and relieve suffering. However, acceptance or refusal of treatment remains a personal choice for anyone with cancer.
Some evidence showed that patients who decline treatment do not always experience rapid decline. Many can live acceptable, even fulfilling, lives on their own for varying periods, even though they know that there is a possibility of shorter survival. Valuing fewer side effects and better quality of life. This suggested that quality of life is subjective and cannot be measured solely by biomedical standards but also by the meaning each person finds in their existence, even in the face of serious illness.
“There is a myth that quality of life is only valid when defined by objective success. Our task is to explain that it is subjective, and life can be meaningful despite limitations.” Kusminsky said.
Mrs G.O. knew her prognosis and treatment options but chose not to pursue treatment, which, while medically advisable, did not align with her values or vision of life.
Hincapié Sánchez stated that the priority is always to honor the patient’s choice. Clinicians must ensure that the patient has all necessary information that is always appropriate to their sociocultural context before making the decision.
“If the decision persists despite being informed and aware of the effects of the patient’s choice, all we can do is provide support, manage the pain, and seek the patient’s comfort,” she emphasized.
Medical Omnipotence
Physicians should not view the refusal of treatment as an abandonment of the fundamental principles of the profession. Rather, it means respecting patient priorities and recognizing medicine as a dialogue between science and humanity, not as an exercise of control.
However, many clinicians struggle with such decisions because they conflict with their impulse to act and a sense of medical omnipotence. Hincapié Sánchez attributed these difficulties to medical training.
“We are taught to preserve life at all costs. If treatment even slightly prolongs life, many doctors continue to recommend it. The question becomes: Is it valid to extend life when its quality is in doubt?” she asked.
“Medicine is more than a science; it is an art. It is the most human in the sciences and the most scientific in the humanities. Let us not lose sight of the human element that allows us to see the patient as a person, not just a disease to be treated,” Hincapié Sánchez urges.
Kusminsky describes a common therapeutic obstinacy — doctors’ reluctance to stop “doing something,” to avoid “throwing in the towel,” or to uphold “hope is the last thing to be lost.”
“But physicians are growing more aware of these situations, and change is slowly coming,” he said. However, he added: “Of course, there is the issue of the perceived omnipotence of doctors — their words descending with authority to ‘prescribe’ treatment, issue ‘medical orders,’ or dictate ‘pharmacological’ therapy.
For the specialist, such terminology reflects a view of the doctor-patient relationship not as a mutual, two-way exchange, but as a vertical, paternalistic dynamic.
He suggested looking at ancient Greece for perspective. “Hippocrates, or rather the Hippocratic school, taught that the doctor-patient encounter is inherently one of compassion. We must approach this in that way. Reflecting on that bond, improving communication, humanizing relationships, and, above all, being available to listen are key,” Kusminsky said.
Another intersection that has long fascinated Kusminsky is between literature and medicine. This interest led him to explore the field of narrative medicine, serve on the board of directors of the Argentine Society of Narrative Medicine (SAMEN), and join the roster of speakers at the upcoming second SAMEN Conference in Buenos Aires on July 10 and 11, 2025.
“Narrative medicine uses storytelling tools to absorb, process, acknowledge, and empathize with patients’ illness narratives, aiming to restore humanism to practice,” he explained.
According to Kusminsky, the circumstances under which Mrs G.O. expressed her wish not to begin treatment immediately reminded him of a text by Melville’s famous “I would prefer not to” from Bartleby, the Scrivener.
This reflection inspired him to publish an article cited at its beginning. At the same time, it reinforced his belief that what patients say can itself be a form of narrative that extends beyond the confines of clinical history.
Mrs G.O. chose not to pursue treatment for multiple myeloma. However, she returned to Kusminsky’s office approximately 2 months ago. She felt well, and her disease slowly progressed; however, she still had no clinical signs or symptoms.
Kusminsky and Hincapié Sánchez have declared no relevant financial conflicts of interest.
This story was translated from Medscape’s Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.

2026 VA Budget Bill Narrowly Passed by House Appropriations Committee
2026 VA Budget Bill Narrowly Passed by House Appropriations Committee
The US House Appropriations Committee approved a $453 billion budget to fund the US Department of Veterans (VA), military construction, and other programs in 2026 by a 36-27 vote. The bill includes $34 billion proposed for community care programs, an increase of > 50% from 2025 community care funding levels.
The discretionary funding would also send $2.5 billion to the VA electronic health records modernization program. Mandatory spending includes $53 billion for the Toxic Exposures Fund, which supports benefits and health care costs associated with the PACT Act.
Although VA budget bills are typically bipartisan in nature, this bill passed by a much narrower margin than is typical. Rep. Debbie Wasserman Schultz (D-FL), ranking member of the Military Construction, Veterans Affairs and Related Agencies Appropriations Subcommittee, said the bill “diverts far too many resources away from the vital, VA-based care that veterans consistently tell us they want, and it pushes them into pricier, subpar corporate hospitals.”
Committee Democrats offered dozens of amendments. All amendments were rejected except for a modification that would block staff reductions at the Veterans Crisis Line and other VA suicide prevention programs.
The bill now moves to the full House of Representatives for consideration. House leaders have not yet announced when that vote will take place; the House is in recess the week of June 16, 2025.
The committee also released the Fiscal Year 2026 Military Construction, Veterans Affairs, and Related Agencies Bill, which would spend > $83 million, a 22% increase over the 2025.
The US House Appropriations Committee approved a $453 billion budget to fund the US Department of Veterans (VA), military construction, and other programs in 2026 by a 36-27 vote. The bill includes $34 billion proposed for community care programs, an increase of > 50% from 2025 community care funding levels.
The discretionary funding would also send $2.5 billion to the VA electronic health records modernization program. Mandatory spending includes $53 billion for the Toxic Exposures Fund, which supports benefits and health care costs associated with the PACT Act.
Although VA budget bills are typically bipartisan in nature, this bill passed by a much narrower margin than is typical. Rep. Debbie Wasserman Schultz (D-FL), ranking member of the Military Construction, Veterans Affairs and Related Agencies Appropriations Subcommittee, said the bill “diverts far too many resources away from the vital, VA-based care that veterans consistently tell us they want, and it pushes them into pricier, subpar corporate hospitals.”
Committee Democrats offered dozens of amendments. All amendments were rejected except for a modification that would block staff reductions at the Veterans Crisis Line and other VA suicide prevention programs.
The bill now moves to the full House of Representatives for consideration. House leaders have not yet announced when that vote will take place; the House is in recess the week of June 16, 2025.
The committee also released the Fiscal Year 2026 Military Construction, Veterans Affairs, and Related Agencies Bill, which would spend > $83 million, a 22% increase over the 2025.
The US House Appropriations Committee approved a $453 billion budget to fund the US Department of Veterans (VA), military construction, and other programs in 2026 by a 36-27 vote. The bill includes $34 billion proposed for community care programs, an increase of > 50% from 2025 community care funding levels.
The discretionary funding would also send $2.5 billion to the VA electronic health records modernization program. Mandatory spending includes $53 billion for the Toxic Exposures Fund, which supports benefits and health care costs associated with the PACT Act.
Although VA budget bills are typically bipartisan in nature, this bill passed by a much narrower margin than is typical. Rep. Debbie Wasserman Schultz (D-FL), ranking member of the Military Construction, Veterans Affairs and Related Agencies Appropriations Subcommittee, said the bill “diverts far too many resources away from the vital, VA-based care that veterans consistently tell us they want, and it pushes them into pricier, subpar corporate hospitals.”
Committee Democrats offered dozens of amendments. All amendments were rejected except for a modification that would block staff reductions at the Veterans Crisis Line and other VA suicide prevention programs.
The bill now moves to the full House of Representatives for consideration. House leaders have not yet announced when that vote will take place; the House is in recess the week of June 16, 2025.
The committee also released the Fiscal Year 2026 Military Construction, Veterans Affairs, and Related Agencies Bill, which would spend > $83 million, a 22% increase over the 2025.
2026 VA Budget Bill Narrowly Passed by House Appropriations Committee
2026 VA Budget Bill Narrowly Passed by House Appropriations Committee
Video Capsule Endoscopy Aids Targeted Treatment in Quiescent Crohn’s
A treat-to target (T2T) strategy based on video capsule endoscopy (VCE) identified Crohn’s disease (CD) patients in clinical remission but with small bowel inflammation, resulting in fewer clinical flares versus a treat-by-symptoms standard approach.
“A VCE-guided treat-to-target strategy for patients with CD in remission confers superior clinical outcomes compared with continued standard care,” investigators led by Shomron Ben-Horin, MD, director of gastroenterology at Sheba Medical Center in Ramat-Gan, Israel.
Published in Gastroenterology, the CURE-CD (Comprehensive Individualized Proactive Therapy of Crohn’s Disease), a prospective, temporally blinded, randomized controled trial, looked at 60 adult patients with quiescent CD involving the small bowel (either L1 or L3 iof the terminal ileum and upper colon).
The researchers defined quiescent disease as corticosteroid-free clinical remission with a Crohn’s Disease Activity Index (CDAI) of <50 for the past 3 months on a stable regimen.
Patients ingested a VCE at baseline and those with a Lewis inflammatory score (LS) of ≥350 were designated high risk (n = 40) and randomized to either T2T optimization (n = 20) or continuing standard care (n = 20).
T2T was optimized with repeat VCE results every 6 months. Patients with LS <350 (“low risk”) continued standard care. The primary outcome was the rate of disease exacerbation, demonstrated by a CDAI increase of >70 points and a score >150, or hospitalization/surgery, in high-risk standard care vs T2T groups at 24 months.

Treatment intensification in the high-risk group allocated to a proactive strategy comprised biologic dose escalation (n = 11 of 20), starting a biologic (n = 8 of 20), or swapping biologics (n = 1 of 20).
The primary outcome, clinical flare by 24 months, occurred in 5 of 20 (25%) of high-risk treat-to-target patients vs 14 of 20 (70%) of the high-risk standard-care group (odds ratio [OR], .14; 95% confidence interval [CI], .04–.57, P = .006).
Mucosal healing was significantly more common in the T2T group when determined by a cutoff LS < 350 (OR, 4.5, 95% CI, 1.7–17.4, nominal P value = .03), but not by the combined scores of total LS < 450 and highest-segment LS < 350.
Among all patients continuing standard care (n = 40), baseline LS was numerically higher among relapsers vs nonrelapsers (450, 225–900 vs 225, 135–600, respectively, P = .07).
As to safety, of 221 VCEs ingested, there was a single (.4%) temporary retention, which spontaneously resolved.
“VCE monitoring of CD was approved into government reimbursement in Israel last year, and I know several European countries are also considering the inclusion of this new indication for VCE in their payer reimbursement,” Ben-Horin told GI & Hepatology News. “Uptake in Israel is still baby-stepping. In our center it’s much more common to monitor T2T for small bowel patients, but this approach is still not widely applied.”
The authors cautioned that since the focus was the small bowel, the findings are not necessarily generalizable to patients with Crohn’s colitis.
The study was supported by the Leona M. & Harry B. Helmsley Charitable Trust, Medtronic (USA), AbbVie (Israel), and Takeda. The funders did not intervene in the design or interpretation of the study.
Ben-Horin reported advisory, consulting fees, research support, and/or stocks/options from several pharmaceutical firms. Several coauthors disclosed similar relations with private-sector companies.

As treat-to-target (T2T) strategies continue to redefine inflammatory bowel disease (IBD) care, this randomized controlled trial by Ben-Horin et al. highlights the value of proactive video capsule endoscopy (VCE) monitoring in patients with quiescent small bowel Crohn’s disease (CD).
The study demonstrated that scheduled VCE every six months, used to guide treatment adjustments, significantly reduced clinical flares over 24 months compared to symptom-based standard care. While differences in mucosal healing between groups were less pronounced, the results underscore that monitoring objective inflammation, even in asymptomatic patients, can improve clinical outcomes.
In clinical practice, symptom-driven management remains common, often due to limited access to endoscopy or patient hesitancy toward invasive procedures. VCE offers a non-invasive, well-tolerated alternative that may improve patient adherence to disease monitoring, particularly in small bowel CD. This approach addresses a significant gap in care, as nearly half of IBD patients do not undergo objective disease assessment within a year of starting biologics.

Clinicians should consider integrating VCE into individualized T2T strategies, especially in settings where endoscopic access is constrained. Furthermore, adjunctive non-invasive tools such as intestinal ultrasound (IUS) with biomarkers could further support a non-invasive, patient-centered monitoring approach. As the definition of remission evolves toward more ambitious targets like transmural healing, the integration of cross-sectional imaging modalities such as IUS into routine monitoring protocols may become essential. Aligning monitoring techniques with evolving therapeutic targets and patient preferences will be key to optimizing long-term disease control in CD.
Mariangela Allocca, MD, PhD, is head of the IBD Center at IRCCS Hospital San Raffaele, and professor of gastroenterology at Vita-Salute San Raffaele University, both in Milan, Italy. Silvio Danese, MD, PhD, is professor of gastroenterology at Vita-Salute San Raffaele University and IRCCS San Raffaele Hospital, Milan. Both authors report consulting and/or speaking fees from multiple drug and device companies.
As treat-to-target (T2T) strategies continue to redefine inflammatory bowel disease (IBD) care, this randomized controlled trial by Ben-Horin et al. highlights the value of proactive video capsule endoscopy (VCE) monitoring in patients with quiescent small bowel Crohn’s disease (CD).
The study demonstrated that scheduled VCE every six months, used to guide treatment adjustments, significantly reduced clinical flares over 24 months compared to symptom-based standard care. While differences in mucosal healing between groups were less pronounced, the results underscore that monitoring objective inflammation, even in asymptomatic patients, can improve clinical outcomes.
In clinical practice, symptom-driven management remains common, often due to limited access to endoscopy or patient hesitancy toward invasive procedures. VCE offers a non-invasive, well-tolerated alternative that may improve patient adherence to disease monitoring, particularly in small bowel CD. This approach addresses a significant gap in care, as nearly half of IBD patients do not undergo objective disease assessment within a year of starting biologics.
Clinicians should consider integrating VCE into individualized T2T strategies, especially in settings where endoscopic access is constrained. Furthermore, adjunctive non-invasive tools such as intestinal ultrasound (IUS) with biomarkers could further support a non-invasive, patient-centered monitoring approach. As the definition of remission evolves toward more ambitious targets like transmural healing, the integration of cross-sectional imaging modalities such as IUS into routine monitoring protocols may become essential. Aligning monitoring techniques with evolving therapeutic targets and patient preferences will be key to optimizing long-term disease control in CD.
Mariangela Allocca, MD, PhD, is head of the IBD Center at IRCCS Hospital San Raffaele, and professor of gastroenterology at Vita-Salute San Raffaele University, both in Milan, Italy. Silvio Danese, MD, PhD, is professor of gastroenterology at Vita-Salute San Raffaele University and IRCCS San Raffaele Hospital, Milan. Both authors report consulting and/or speaking fees from multiple drug and device companies.
As treat-to-target (T2T) strategies continue to redefine inflammatory bowel disease (IBD) care, this randomized controlled trial by Ben-Horin et al. highlights the value of proactive video capsule endoscopy (VCE) monitoring in patients with quiescent small bowel Crohn’s disease (CD).
The study demonstrated that scheduled VCE every six months, used to guide treatment adjustments, significantly reduced clinical flares over 24 months compared to symptom-based standard care. While differences in mucosal healing between groups were less pronounced, the results underscore that monitoring objective inflammation, even in asymptomatic patients, can improve clinical outcomes.
In clinical practice, symptom-driven management remains common, often due to limited access to endoscopy or patient hesitancy toward invasive procedures. VCE offers a non-invasive, well-tolerated alternative that may improve patient adherence to disease monitoring, particularly in small bowel CD. This approach addresses a significant gap in care, as nearly half of IBD patients do not undergo objective disease assessment within a year of starting biologics.
Clinicians should consider integrating VCE into individualized T2T strategies, especially in settings where endoscopic access is constrained. Furthermore, adjunctive non-invasive tools such as intestinal ultrasound (IUS) with biomarkers could further support a non-invasive, patient-centered monitoring approach. As the definition of remission evolves toward more ambitious targets like transmural healing, the integration of cross-sectional imaging modalities such as IUS into routine monitoring protocols may become essential. Aligning monitoring techniques with evolving therapeutic targets and patient preferences will be key to optimizing long-term disease control in CD.
Mariangela Allocca, MD, PhD, is head of the IBD Center at IRCCS Hospital San Raffaele, and professor of gastroenterology at Vita-Salute San Raffaele University, both in Milan, Italy. Silvio Danese, MD, PhD, is professor of gastroenterology at Vita-Salute San Raffaele University and IRCCS San Raffaele Hospital, Milan. Both authors report consulting and/or speaking fees from multiple drug and device companies.
A treat-to target (T2T) strategy based on video capsule endoscopy (VCE) identified Crohn’s disease (CD) patients in clinical remission but with small bowel inflammation, resulting in fewer clinical flares versus a treat-by-symptoms standard approach.
“A VCE-guided treat-to-target strategy for patients with CD in remission confers superior clinical outcomes compared with continued standard care,” investigators led by Shomron Ben-Horin, MD, director of gastroenterology at Sheba Medical Center in Ramat-Gan, Israel.
Published in Gastroenterology, the CURE-CD (Comprehensive Individualized Proactive Therapy of Crohn’s Disease), a prospective, temporally blinded, randomized controled trial, looked at 60 adult patients with quiescent CD involving the small bowel (either L1 or L3 iof the terminal ileum and upper colon).
The researchers defined quiescent disease as corticosteroid-free clinical remission with a Crohn’s Disease Activity Index (CDAI) of <50 for the past 3 months on a stable regimen.
Patients ingested a VCE at baseline and those with a Lewis inflammatory score (LS) of ≥350 were designated high risk (n = 40) and randomized to either T2T optimization (n = 20) or continuing standard care (n = 20).
T2T was optimized with repeat VCE results every 6 months. Patients with LS <350 (“low risk”) continued standard care. The primary outcome was the rate of disease exacerbation, demonstrated by a CDAI increase of >70 points and a score >150, or hospitalization/surgery, in high-risk standard care vs T2T groups at 24 months.
Treatment intensification in the high-risk group allocated to a proactive strategy comprised biologic dose escalation (n = 11 of 20), starting a biologic (n = 8 of 20), or swapping biologics (n = 1 of 20).
The primary outcome, clinical flare by 24 months, occurred in 5 of 20 (25%) of high-risk treat-to-target patients vs 14 of 20 (70%) of the high-risk standard-care group (odds ratio [OR], .14; 95% confidence interval [CI], .04–.57, P = .006).
Mucosal healing was significantly more common in the T2T group when determined by a cutoff LS < 350 (OR, 4.5, 95% CI, 1.7–17.4, nominal P value = .03), but not by the combined scores of total LS < 450 and highest-segment LS < 350.
Among all patients continuing standard care (n = 40), baseline LS was numerically higher among relapsers vs nonrelapsers (450, 225–900 vs 225, 135–600, respectively, P = .07).
As to safety, of 221 VCEs ingested, there was a single (.4%) temporary retention, which spontaneously resolved.
“VCE monitoring of CD was approved into government reimbursement in Israel last year, and I know several European countries are also considering the inclusion of this new indication for VCE in their payer reimbursement,” Ben-Horin told GI & Hepatology News. “Uptake in Israel is still baby-stepping. In our center it’s much more common to monitor T2T for small bowel patients, but this approach is still not widely applied.”
The authors cautioned that since the focus was the small bowel, the findings are not necessarily generalizable to patients with Crohn’s colitis.
The study was supported by the Leona M. & Harry B. Helmsley Charitable Trust, Medtronic (USA), AbbVie (Israel), and Takeda. The funders did not intervene in the design or interpretation of the study.
Ben-Horin reported advisory, consulting fees, research support, and/or stocks/options from several pharmaceutical firms. Several coauthors disclosed similar relations with private-sector companies.
A treat-to target (T2T) strategy based on video capsule endoscopy (VCE) identified Crohn’s disease (CD) patients in clinical remission but with small bowel inflammation, resulting in fewer clinical flares versus a treat-by-symptoms standard approach.
“A VCE-guided treat-to-target strategy for patients with CD in remission confers superior clinical outcomes compared with continued standard care,” investigators led by Shomron Ben-Horin, MD, director of gastroenterology at Sheba Medical Center in Ramat-Gan, Israel.
Published in Gastroenterology, the CURE-CD (Comprehensive Individualized Proactive Therapy of Crohn’s Disease), a prospective, temporally blinded, randomized controled trial, looked at 60 adult patients with quiescent CD involving the small bowel (either L1 or L3 iof the terminal ileum and upper colon).
The researchers defined quiescent disease as corticosteroid-free clinical remission with a Crohn’s Disease Activity Index (CDAI) of <50 for the past 3 months on a stable regimen.
Patients ingested a VCE at baseline and those with a Lewis inflammatory score (LS) of ≥350 were designated high risk (n = 40) and randomized to either T2T optimization (n = 20) or continuing standard care (n = 20).
T2T was optimized with repeat VCE results every 6 months. Patients with LS <350 (“low risk”) continued standard care. The primary outcome was the rate of disease exacerbation, demonstrated by a CDAI increase of >70 points and a score >150, or hospitalization/surgery, in high-risk standard care vs T2T groups at 24 months.
Treatment intensification in the high-risk group allocated to a proactive strategy comprised biologic dose escalation (n = 11 of 20), starting a biologic (n = 8 of 20), or swapping biologics (n = 1 of 20).
The primary outcome, clinical flare by 24 months, occurred in 5 of 20 (25%) of high-risk treat-to-target patients vs 14 of 20 (70%) of the high-risk standard-care group (odds ratio [OR], .14; 95% confidence interval [CI], .04–.57, P = .006).
Mucosal healing was significantly more common in the T2T group when determined by a cutoff LS < 350 (OR, 4.5, 95% CI, 1.7–17.4, nominal P value = .03), but not by the combined scores of total LS < 450 and highest-segment LS < 350.
Among all patients continuing standard care (n = 40), baseline LS was numerically higher among relapsers vs nonrelapsers (450, 225–900 vs 225, 135–600, respectively, P = .07).
As to safety, of 221 VCEs ingested, there was a single (.4%) temporary retention, which spontaneously resolved.
“VCE monitoring of CD was approved into government reimbursement in Israel last year, and I know several European countries are also considering the inclusion of this new indication for VCE in their payer reimbursement,” Ben-Horin told GI & Hepatology News. “Uptake in Israel is still baby-stepping. In our center it’s much more common to monitor T2T for small bowel patients, but this approach is still not widely applied.”
The authors cautioned that since the focus was the small bowel, the findings are not necessarily generalizable to patients with Crohn’s colitis.
The study was supported by the Leona M. & Harry B. Helmsley Charitable Trust, Medtronic (USA), AbbVie (Israel), and Takeda. The funders did not intervene in the design or interpretation of the study.
Ben-Horin reported advisory, consulting fees, research support, and/or stocks/options from several pharmaceutical firms. Several coauthors disclosed similar relations with private-sector companies.
FROM GASTROENTEROLOGY
The Essential Guide to Estate Planning for Physicians: Securing Your Legacy and Protecting Your Wealth
As a physician, you’ve spent years building a career that not only provides financial security for your family but also allows you to make a meaningful impact in your community. However, without a comprehensive estate plan in place, much of what you’ve worked so hard to build may not be preserved according to your wishes.

Many physicians delay estate planning, assuming it’s something to consider later in life. However, the most successful estate plans are those that are established early and evolve over time. Proper planning ensures that your assets are protected, your loved ones are provided for, and your legacy is preserved in the most tax-efficient and legally-sound manner possible.1
This article explores why estate planning is particularly crucial for physicians, the key elements of a strong estate plan, and how beginning early can create long-term financial advantages.
Why Estate Planning Matters for Physicians
Physicians are in a unique financial position compared to many other professionals. With high earning potential, specialized assets, and significant liability exposure, their estate planning needs differ from those of the average individual. A well-structured estate plan not only facilitates the smooth transfer of wealth but also protects assets from excessive taxation, legal complications, and potential risks such as malpractice claims.
1. High Net-Worth Considerations
Physicians often accumulate substantial wealth over time. Without a clear estate plan, your estate could face excessive taxation, with a large portion of your assets potentially going to the government rather than your heirs. Estate taxes, probate costs, and legal fees can significantly erode your legacy if not properly planned for.
2. Asset Protection from Liability Risks
Unlike most professionals, physicians are at a higher risk of litigation. A comprehensive estate plan can incorporate asset protection strategies, such as irrevocable trusts, family limited partnerships, or liability insurance, to shield your wealth from lawsuits or creditor claims.
3. Family and Generational Wealth Planning
Many physicians prioritize ensuring their family’s financial stability. Whether you want to provide for your spouse, children, or even charitable causes, estate planning allows you to dictate how your wealth is distributed. Establishing trusts for your children or grandchildren can help manage how and when they receive their inheritance, preventing mismanagement and ensuring financial responsibility.
4. Business and Practice Continuity
If you own a medical practice, succession planning should be part of your estate plan. Without clear directives, the future of your practice may be uncertain in the event of your passing or incapacitation. A well-drafted estate plan provides a roadmap for ownership transition, ensuring continuity for patients, employees, and business partners.
Key Elements of an Effective Estate Plan
Every estate plan should be customized based on your financial situation, goals, and family dynamics. However, certain fundamental components apply to nearly all high-net-worth individuals, including physicians.
1. Revocable Living Trusts
A revocable living trust allows you to manage your assets during your lifetime while providing a clear path for distribution after your passing. Unlike a will, a trust helps your estate avoid probate, ensuring a smoother and more private transition of wealth. You maintain control over your assets while also establishing clear rules for distribution, particularly useful if you have minor children or complex family structures.2
2. Irrevocable Trusts for Asset Protection
For physicians concerned about lawsuits or estate tax exposure, irrevocable trusts can offer robust asset protection. Since assets placed in these trusts are no longer legally owned by you, they are shielded from creditors and legal claims while also reducing your taxable estate.2
3. Powers of Attorney and Healthcare Directives
Estate planning isn’t just about what happens after your passing—it’s also about protecting you and your family if you become incapacitated. A durable power of attorney allows a trusted individual to manage your financial affairs, while a healthcare directive ensures your medical decisions align with your wishes.3
4. Life Insurance Planning
Life insurance is an essential estate planning tool for physicians, providing liquidity to cover estate taxes, debts, or income replacement for your family. A properly structured life insurance trust can help ensure that policy proceeds remain outside of your taxable estate while being efficiently distributed according to your wishes.4
5. Business Succession Planning
If you own a medical practice, a well-designed succession plan can ensure that your business continues to operate smoothly in your absence. This may involve buy-sell agreements, key-person insurance, or identifying a successor to take over your role.5
The Long-Term Benefits of Early Estate Planning
Estate planning is not a one-time event—it’s a process that should evolve with your career, financial growth, and family dynamics. The earlier you begin, the more control you have over your financial future. Here’s why starting early is a strategic advantage:
1. Maximizing Tax Efficiency
Many estate planning strategies, such as gifting assets or establishing irrevocable trusts, are most effective when implemented over time. By spreading out wealth transfers and taking advantage of annual gift exclusions, you can significantly reduce estate tax liability while maintaining financial security.
2. Adjusting for Life Changes
Your financial situation and family needs will change over the years. Marriages, births, career advancements, and new investments all impact your estate planning needs. By starting early, you can make gradual adjustments rather than facing an overwhelming restructuring later in life.1
3. Ensuring Asset Protection Strategies Are in Place
Many asset protection strategies require time to be effective. For instance, certain types of trusts must be in place for a number of years before they fully shield assets from legal claims. Delaying planning could leave your wealth unnecessarily exposed.
4. Creating a Legacy Beyond Wealth
Estate planning is not just about finances—it’s about legacy. Whether you want to support a charitable cause, endow a scholarship, or establish a foundation, early planning gives you the ability to shape your long-term impact.
5. Adapt to Ever Changing Legislation
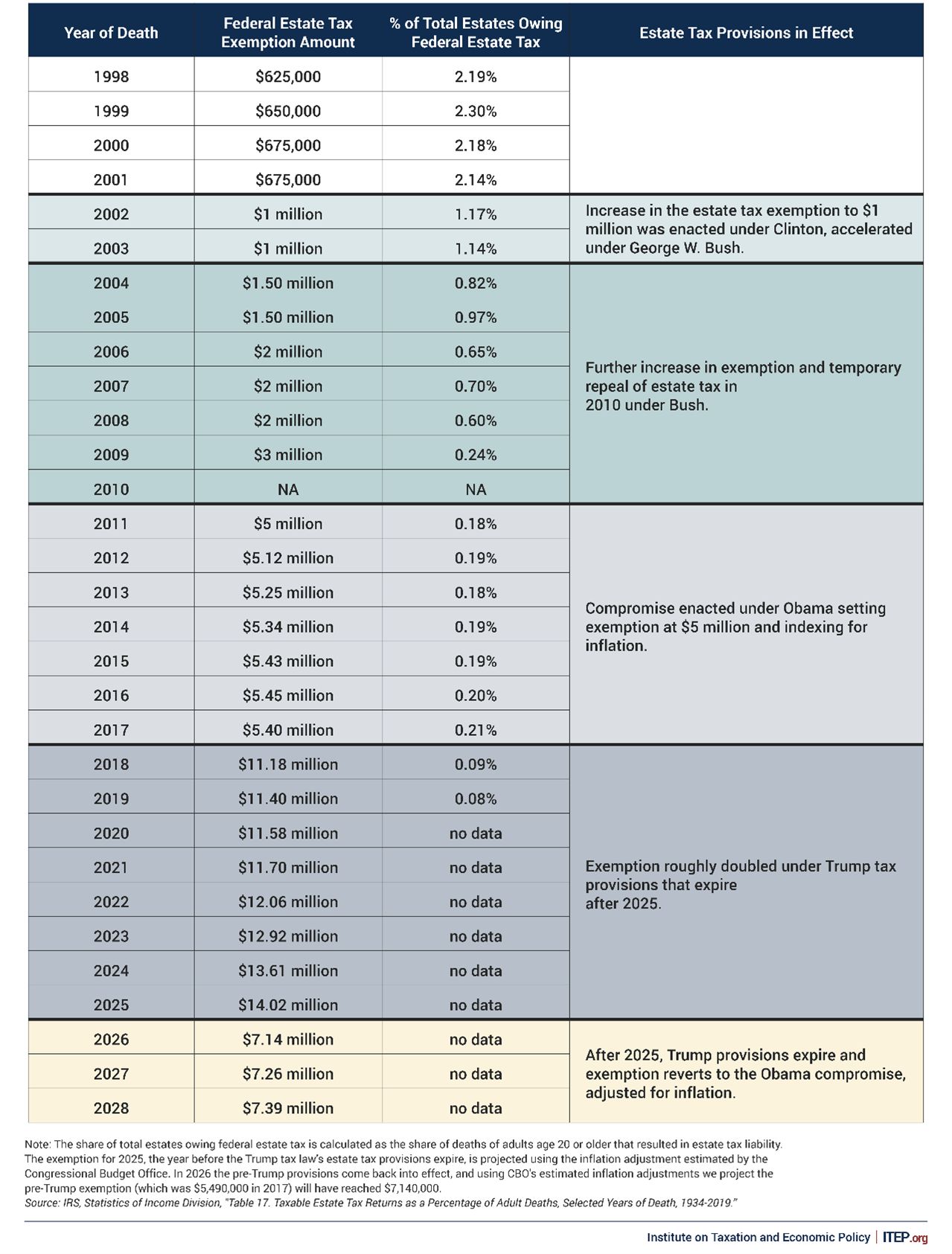
Estate planning needs to be adaptable. The federal government can change the estate tax exemption at any time; this was even a topic of the last election cycle. Early planning allows you to implement necessary changes throughout your life to minimize estate taxes. At present, unless new policy is enacted, the exemption per individual will reduce by half in 2026 (see Figure 1).
Final Thoughts: Taking Action Today
The complexity of physician finances—ranging from high income and significant assets to legal risks—makes individualized estate planning an absolute necessity.
By taking proactive steps today, you can maximize tax efficiency, safeguard your assets, and ensure your wishes are carried out without unnecessary delays or legal battles. Working with a financial advisor and estate planning attorney who understands the unique needs of physicians can help you craft a plan that aligns with your goals and evolves as your career progresses.
Mr. Gardner is a financial advisor at Lifetime Financial Growth, LLC, in Columbus, Ohio, one of the largest privately held wealth management firms in the country. John has had a passion for finance since his early years in college when his tennis coach introduced him. He also has a passion for helping physicians, as his wife is a gastroenterologist at Ohio State University. He reports no relevant disclosures relevant to this article. If you have additional questions, please contact John at 740-403-4891 or [email protected].
References
1. The Law Offices of Diron Rutty, LLC. https://www.dironruttyllc.com/reasons-to-start-estate-planning-early/.
2. Physician Side Gigs. https://www.physiciansidegigs.com/estateplanning.
3. Afshar, A & MacBeth, S. https://www.schwabe.com/publication/estate-planning-for-physicians-why-its-important-and-how-to-get-started/. December 2024.
4. Skeeles, JC. https://ohioline.osu.edu/factsheet/ep-1. July 2012.
5. Rosenfeld, J. Physician estate planning guide. Medical Economics. 2022 Nov. https://www.medicaleconomics.com/view/physician-estate-planning-guide.
As a physician, you’ve spent years building a career that not only provides financial security for your family but also allows you to make a meaningful impact in your community. However, without a comprehensive estate plan in place, much of what you’ve worked so hard to build may not be preserved according to your wishes.
Many physicians delay estate planning, assuming it’s something to consider later in life. However, the most successful estate plans are those that are established early and evolve over time. Proper planning ensures that your assets are protected, your loved ones are provided for, and your legacy is preserved in the most tax-efficient and legally-sound manner possible.1
This article explores why estate planning is particularly crucial for physicians, the key elements of a strong estate plan, and how beginning early can create long-term financial advantages.
Why Estate Planning Matters for Physicians
Physicians are in a unique financial position compared to many other professionals. With high earning potential, specialized assets, and significant liability exposure, their estate planning needs differ from those of the average individual. A well-structured estate plan not only facilitates the smooth transfer of wealth but also protects assets from excessive taxation, legal complications, and potential risks such as malpractice claims.
1. High Net-Worth Considerations
Physicians often accumulate substantial wealth over time. Without a clear estate plan, your estate could face excessive taxation, with a large portion of your assets potentially going to the government rather than your heirs. Estate taxes, probate costs, and legal fees can significantly erode your legacy if not properly planned for.
2. Asset Protection from Liability Risks
Unlike most professionals, physicians are at a higher risk of litigation. A comprehensive estate plan can incorporate asset protection strategies, such as irrevocable trusts, family limited partnerships, or liability insurance, to shield your wealth from lawsuits or creditor claims.
3. Family and Generational Wealth Planning
Many physicians prioritize ensuring their family’s financial stability. Whether you want to provide for your spouse, children, or even charitable causes, estate planning allows you to dictate how your wealth is distributed. Establishing trusts for your children or grandchildren can help manage how and when they receive their inheritance, preventing mismanagement and ensuring financial responsibility.
4. Business and Practice Continuity
If you own a medical practice, succession planning should be part of your estate plan. Without clear directives, the future of your practice may be uncertain in the event of your passing or incapacitation. A well-drafted estate plan provides a roadmap for ownership transition, ensuring continuity for patients, employees, and business partners.
Key Elements of an Effective Estate Plan
Every estate plan should be customized based on your financial situation, goals, and family dynamics. However, certain fundamental components apply to nearly all high-net-worth individuals, including physicians.
1. Revocable Living Trusts
A revocable living trust allows you to manage your assets during your lifetime while providing a clear path for distribution after your passing. Unlike a will, a trust helps your estate avoid probate, ensuring a smoother and more private transition of wealth. You maintain control over your assets while also establishing clear rules for distribution, particularly useful if you have minor children or complex family structures.2
2. Irrevocable Trusts for Asset Protection
For physicians concerned about lawsuits or estate tax exposure, irrevocable trusts can offer robust asset protection. Since assets placed in these trusts are no longer legally owned by you, they are shielded from creditors and legal claims while also reducing your taxable estate.2
3. Powers of Attorney and Healthcare Directives
Estate planning isn’t just about what happens after your passing—it’s also about protecting you and your family if you become incapacitated. A durable power of attorney allows a trusted individual to manage your financial affairs, while a healthcare directive ensures your medical decisions align with your wishes.3
4. Life Insurance Planning
Life insurance is an essential estate planning tool for physicians, providing liquidity to cover estate taxes, debts, or income replacement for your family. A properly structured life insurance trust can help ensure that policy proceeds remain outside of your taxable estate while being efficiently distributed according to your wishes.4
5. Business Succession Planning
If you own a medical practice, a well-designed succession plan can ensure that your business continues to operate smoothly in your absence. This may involve buy-sell agreements, key-person insurance, or identifying a successor to take over your role.5
The Long-Term Benefits of Early Estate Planning
Estate planning is not a one-time event—it’s a process that should evolve with your career, financial growth, and family dynamics. The earlier you begin, the more control you have over your financial future. Here’s why starting early is a strategic advantage:
1. Maximizing Tax Efficiency
Many estate planning strategies, such as gifting assets or establishing irrevocable trusts, are most effective when implemented over time. By spreading out wealth transfers and taking advantage of annual gift exclusions, you can significantly reduce estate tax liability while maintaining financial security.
2. Adjusting for Life Changes
Your financial situation and family needs will change over the years. Marriages, births, career advancements, and new investments all impact your estate planning needs. By starting early, you can make gradual adjustments rather than facing an overwhelming restructuring later in life.1
3. Ensuring Asset Protection Strategies Are in Place
Many asset protection strategies require time to be effective. For instance, certain types of trusts must be in place for a number of years before they fully shield assets from legal claims. Delaying planning could leave your wealth unnecessarily exposed.
4. Creating a Legacy Beyond Wealth
Estate planning is not just about finances—it’s about legacy. Whether you want to support a charitable cause, endow a scholarship, or establish a foundation, early planning gives you the ability to shape your long-term impact.
5. Adapt to Ever Changing Legislation
Estate planning needs to be adaptable. The federal government can change the estate tax exemption at any time; this was even a topic of the last election cycle. Early planning allows you to implement necessary changes throughout your life to minimize estate taxes. At present, unless new policy is enacted, the exemption per individual will reduce by half in 2026 (see Figure 1).
Final Thoughts: Taking Action Today
The complexity of physician finances—ranging from high income and significant assets to legal risks—makes individualized estate planning an absolute necessity.
By taking proactive steps today, you can maximize tax efficiency, safeguard your assets, and ensure your wishes are carried out without unnecessary delays or legal battles. Working with a financial advisor and estate planning attorney who understands the unique needs of physicians can help you craft a plan that aligns with your goals and evolves as your career progresses.
Mr. Gardner is a financial advisor at Lifetime Financial Growth, LLC, in Columbus, Ohio, one of the largest privately held wealth management firms in the country. John has had a passion for finance since his early years in college when his tennis coach introduced him. He also has a passion for helping physicians, as his wife is a gastroenterologist at Ohio State University. He reports no relevant disclosures relevant to this article. If you have additional questions, please contact John at 740-403-4891 or [email protected].
References
1. The Law Offices of Diron Rutty, LLC. https://www.dironruttyllc.com/reasons-to-start-estate-planning-early/.
2. Physician Side Gigs. https://www.physiciansidegigs.com/estateplanning.
3. Afshar, A & MacBeth, S. https://www.schwabe.com/publication/estate-planning-for-physicians-why-its-important-and-how-to-get-started/. December 2024.
4. Skeeles, JC. https://ohioline.osu.edu/factsheet/ep-1. July 2012.
5. Rosenfeld, J. Physician estate planning guide. Medical Economics. 2022 Nov. https://www.medicaleconomics.com/view/physician-estate-planning-guide.
As a physician, you’ve spent years building a career that not only provides financial security for your family but also allows you to make a meaningful impact in your community. However, without a comprehensive estate plan in place, much of what you’ve worked so hard to build may not be preserved according to your wishes.
Many physicians delay estate planning, assuming it’s something to consider later in life. However, the most successful estate plans are those that are established early and evolve over time. Proper planning ensures that your assets are protected, your loved ones are provided for, and your legacy is preserved in the most tax-efficient and legally-sound manner possible.1
This article explores why estate planning is particularly crucial for physicians, the key elements of a strong estate plan, and how beginning early can create long-term financial advantages.
Why Estate Planning Matters for Physicians
Physicians are in a unique financial position compared to many other professionals. With high earning potential, specialized assets, and significant liability exposure, their estate planning needs differ from those of the average individual. A well-structured estate plan not only facilitates the smooth transfer of wealth but also protects assets from excessive taxation, legal complications, and potential risks such as malpractice claims.
1. High Net-Worth Considerations
Physicians often accumulate substantial wealth over time. Without a clear estate plan, your estate could face excessive taxation, with a large portion of your assets potentially going to the government rather than your heirs. Estate taxes, probate costs, and legal fees can significantly erode your legacy if not properly planned for.
2. Asset Protection from Liability Risks
Unlike most professionals, physicians are at a higher risk of litigation. A comprehensive estate plan can incorporate asset protection strategies, such as irrevocable trusts, family limited partnerships, or liability insurance, to shield your wealth from lawsuits or creditor claims.
3. Family and Generational Wealth Planning
Many physicians prioritize ensuring their family’s financial stability. Whether you want to provide for your spouse, children, or even charitable causes, estate planning allows you to dictate how your wealth is distributed. Establishing trusts for your children or grandchildren can help manage how and when they receive their inheritance, preventing mismanagement and ensuring financial responsibility.
4. Business and Practice Continuity
If you own a medical practice, succession planning should be part of your estate plan. Without clear directives, the future of your practice may be uncertain in the event of your passing or incapacitation. A well-drafted estate plan provides a roadmap for ownership transition, ensuring continuity for patients, employees, and business partners.
Key Elements of an Effective Estate Plan
Every estate plan should be customized based on your financial situation, goals, and family dynamics. However, certain fundamental components apply to nearly all high-net-worth individuals, including physicians.
1. Revocable Living Trusts
A revocable living trust allows you to manage your assets during your lifetime while providing a clear path for distribution after your passing. Unlike a will, a trust helps your estate avoid probate, ensuring a smoother and more private transition of wealth. You maintain control over your assets while also establishing clear rules for distribution, particularly useful if you have minor children or complex family structures.2
2. Irrevocable Trusts for Asset Protection
For physicians concerned about lawsuits or estate tax exposure, irrevocable trusts can offer robust asset protection. Since assets placed in these trusts are no longer legally owned by you, they are shielded from creditors and legal claims while also reducing your taxable estate.2
3. Powers of Attorney and Healthcare Directives
Estate planning isn’t just about what happens after your passing—it’s also about protecting you and your family if you become incapacitated. A durable power of attorney allows a trusted individual to manage your financial affairs, while a healthcare directive ensures your medical decisions align with your wishes.3
4. Life Insurance Planning
Life insurance is an essential estate planning tool for physicians, providing liquidity to cover estate taxes, debts, or income replacement for your family. A properly structured life insurance trust can help ensure that policy proceeds remain outside of your taxable estate while being efficiently distributed according to your wishes.4
5. Business Succession Planning
If you own a medical practice, a well-designed succession plan can ensure that your business continues to operate smoothly in your absence. This may involve buy-sell agreements, key-person insurance, or identifying a successor to take over your role.5
The Long-Term Benefits of Early Estate Planning
Estate planning is not a one-time event—it’s a process that should evolve with your career, financial growth, and family dynamics. The earlier you begin, the more control you have over your financial future. Here’s why starting early is a strategic advantage:
1. Maximizing Tax Efficiency
Many estate planning strategies, such as gifting assets or establishing irrevocable trusts, are most effective when implemented over time. By spreading out wealth transfers and taking advantage of annual gift exclusions, you can significantly reduce estate tax liability while maintaining financial security.
2. Adjusting for Life Changes
Your financial situation and family needs will change over the years. Marriages, births, career advancements, and new investments all impact your estate planning needs. By starting early, you can make gradual adjustments rather than facing an overwhelming restructuring later in life.1
3. Ensuring Asset Protection Strategies Are in Place
Many asset protection strategies require time to be effective. For instance, certain types of trusts must be in place for a number of years before they fully shield assets from legal claims. Delaying planning could leave your wealth unnecessarily exposed.
4. Creating a Legacy Beyond Wealth
Estate planning is not just about finances—it’s about legacy. Whether you want to support a charitable cause, endow a scholarship, or establish a foundation, early planning gives you the ability to shape your long-term impact.
5. Adapt to Ever Changing Legislation
Estate planning needs to be adaptable. The federal government can change the estate tax exemption at any time; this was even a topic of the last election cycle. Early planning allows you to implement necessary changes throughout your life to minimize estate taxes. At present, unless new policy is enacted, the exemption per individual will reduce by half in 2026 (see Figure 1).
Final Thoughts: Taking Action Today
The complexity of physician finances—ranging from high income and significant assets to legal risks—makes individualized estate planning an absolute necessity.
By taking proactive steps today, you can maximize tax efficiency, safeguard your assets, and ensure your wishes are carried out without unnecessary delays or legal battles. Working with a financial advisor and estate planning attorney who understands the unique needs of physicians can help you craft a plan that aligns with your goals and evolves as your career progresses.
Mr. Gardner is a financial advisor at Lifetime Financial Growth, LLC, in Columbus, Ohio, one of the largest privately held wealth management firms in the country. John has had a passion for finance since his early years in college when his tennis coach introduced him. He also has a passion for helping physicians, as his wife is a gastroenterologist at Ohio State University. He reports no relevant disclosures relevant to this article. If you have additional questions, please contact John at 740-403-4891 or [email protected].
References
1. The Law Offices of Diron Rutty, LLC. https://www.dironruttyllc.com/reasons-to-start-estate-planning-early/.
2. Physician Side Gigs. https://www.physiciansidegigs.com/estateplanning.
3. Afshar, A & MacBeth, S. https://www.schwabe.com/publication/estate-planning-for-physicians-why-its-important-and-how-to-get-started/. December 2024.
4. Skeeles, JC. https://ohioline.osu.edu/factsheet/ep-1. July 2012.
5. Rosenfeld, J. Physician estate planning guide. Medical Economics. 2022 Nov. https://www.medicaleconomics.com/view/physician-estate-planning-guide.
Lower Gastrointestinal Bleeding: Two Perspectives
Dear colleagues,
: What is the role and optimal timing of colonoscopy? How can we best utilize radiologic studies like CTA or tagged RBC scans? How should we manage patients with recurrent or intermittent bleeding that defies localization?

In this issue of Perspectives, Dr. David Wan, Dr. Fredella Lee, and Dr. Zeyad Metwalli offer their expert insights on these difficult questions. Dr. Wan, drawing on over 15 years of experience as a GI hospitalist, shares – along with his coauthor Dr. Lee – a pragmatic approach to LGIB based on clinical patterns, evolving data, and multidisciplinary collaboration. Dr. Metwalli provides the interventional radiologist’s perspective, highlighting how angiographic techniques can complement GI management and introducing novel IR strategies for patients with recurrent or elusive bleeding.
We hope their perspectives will offer valuable guidance for your practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Management of Lower Gastrointestinal Bleeds: GI Perspective
BY FREDELLA LEE, MD; DAVID WAN, MD

Acute lower gastrointestinal bleeding (LGIB) presents unique challenges. Much of this stems from the natural history of diverticular bleeding, the most common etiology of LGIB.
First, while bleeding can be severe, most will spontaneously stop. Second, despite our best efforts with imaging or colonoscopy, finding an intervenable lesion is rare. Third, LGIB has significant rates of rebleeding that are unpredictable.
While serving as a GI hospitalist for 15 years and after managing over 300 cases of LGIB, I often find myself frustrated and colonoscopy feels futile. So how can we rationally approach these patients? We will focus on three clinical questions to develop a framework for LGIB management.
- What is the role and timing for a colonoscopy?
- How do we best utilize radiologic tests?
- How can we prevent recurrent LGIB?
The Role of Colonoscopy
Traditionally, colonoscopy within 24 hours of presentation was recommended. This was based on retrospective cohort data showing higher endoscopic intervention rates and better clinical outcomes. However, this protocol requires patients to drink a significant volume of bowel preparation over a few hours (often requiring an NGT) to achieve clear rectal effluent. Moreover, one needs to mobilize a team (i.e., nurse, technician, anesthesiologist, and gastroenterologist), and find an appropriate location to scope (i.e., ED, ICU, or OR), Understandably, this is challenging, especially overnight. When the therapeutic yield is relatively low, this approach quickly loses enthusiasm.
Importantly, meta-analyses of the randomized controlled trials, have shown that urgent colonoscopies (<24 hours upon presentation), compared to elective colonoscopies (>24 hours upon presentation), do not improve clinical outcomes such as re-bleeding rates, transfusion requirements, mortality, or length of stay. In these studies, the endoscopic intervention rates were 17-34%, however, observational data shows rates of only 8%. In our practice, we will use a clear cap attachment device and water jet irrigation to increase the odds of detecting an active source of bleeding. Colonoscopy has a diagnostic yield of 95% – despite its low therapeutic yield; and while diverticular bleeds constitute up to 64% of cases, one does not want to miss colorectal cancer or other diagnoses. Regardless, there is generally no urgency to perform a colonoscopy. To quote a colleague, Dr. Elizabeth Ross, “there is no such thing as door-to-butt time.”

The Role of Radiology
Given the limits of colonoscopy, can radiographic tests such as computed tomography angiography (CTA) or tagged red blood cell (RBC) scan be helpful? Multiple studies have suggested using CTA as the initial diagnostic test. The advantages of CTAs are:
- Fast, readily available, and does not require a bowel preparation
- If negative, CTAs portend a good prognosis and make it highly unlikely to detect active extravasation on visceral angiography
- If positive, can localize the source of bleed and increase the success of intervention
Whether a positive CTA should be followed with a colonoscopy or visceral angiography remains unclear. Studies show that positive CTAs increase the detection rate of stigmata of recent hemorrhage on colonoscopy. Positive CTAs can also identify a target for embolization by interventional radiology (IR). Though an important caveat is that the success rate of embolization is highest when performed within 90 minutes of a positive CTA. This highlights that if you have IR availability, it is critical to have clear communication, a well-defined protocol, and collaboration among disciplines (i.e., ED, medical team, GI, and IR).
At our institution, we have implemented a CTA-guided protocol for severe LGIB. Those with positive CTAs are referred immediately to IR for embolization. If the embolization is unsuccessful or CTA is negative, the patient will be planned for a non-urgent inpatient colonoscopy. However, our unpublished data and other studies have shown that the overall CTA positivity rates are only between 16-22%. Moreover, one randomized controlled trial comparing CTA versus colonoscopy as an initial test did not show any meaningful difference in clinical outcomes. Thus, the benefit of CTA and the best approach to positive CTAs remains in question.
Lastly, people often ask about the utility of RBC nuclear scans. While they can detect bleeds at a slower rate (as low as 0.1 mL/min) compared to CTA (at least 0.4 mL/min), there are many limitations. RBC scans take time, are not available 24-7, and cannot precisely localize the site of bleeding. Therefore, we rarely recommend them for LGIB.
Approach to Recurrent Diverticular Bleeding
Unfortunately, diverticular bleeding recurs in the hospital 14% of the time and up to 25% at 5 years. When this occurs, is it worthwhile to repeat another colonoscopy or CTA?
Given the lack of clear data, we have adopted a shared decision-making framework with patients. Oftentimes, these patients are older and have significant co-morbidities, and undergoing bowel preparation, anesthesia, and colonoscopy is not trivial. If the patient is stable and prior work-up has excluded pertinent alternative diagnoses other than diverticular bleeding, then we tell patients the chance of finding an intervenable lesion is low and opt for conservative management. Meanwhile, if the patient has persistent, hemodynamically significant bleeding, we recommend a CTA based on the rationale discussed previously.
The most important clinical decision may not be about scoping or obtaining a CTA – it is medication management. If they are taking NSAIDs, they should be discontinued. If antiplatelet or anticoagulation agents were held, they should be restarted promptly in individuals with significant thrombotic risk given studies showing that while rebleeding rates may increase, overall mortality decreases.
In summary, managing LGIB and altering its natural history with either endoscopic or radiographic means is challenging. More studies are needed to guide the optimal approach. Reassuringly, most bleeding self-resolves and patients have good clinical outcomes.
Dr. Lee is a resident physician at New York Presbyterian Weill Cornell Medical Center, New York, NY. Dr. Wan is associate professor of clinical medicine at Weill Cornell Medicine, New York, N.Y. They declare no conflicts of interest.
Lower Gastrointestinal Bleeding: An Interventional Radiologist’s Perspective
BY ZEYAD METWALLI, MD, FSIR

When colonoscopy fails to localize and/or stop lower gastrointestinal bleeding (LGIB), catheter angiography has been commonly employed as a tool for both diagnosis and treatment of bleeding with embolization. Nuclear medicine or CT imaging studies can serve as useful adjuncts for confirming active bleeding and localizing the site of bleeding prior to angiography, particularly if this information is not provided by colonoscopy. Provocative mesenteric angiography has also become increasingly popular as a troubleshooting technique in patients with initially negative angiography.
Localization of Lower Gastrointestinal Bleeding
Radionuclide technetium-99m-lableled red blood cell scintigraphy (RBCS), also known as tagged RBC scintigraphy, has been in use since the early 1980s for investigation of acute gastrointestinal bleeding. RBCS has a high sensitivity for detection of active bleeding with a theoretical ability to detect bleeding at rates as low as 0.04-0.2 mL/minute.
Imaging protocols vary but should include dynamic images, which may aid in localization of bleeding. The relatively long half-life of the tracer used for imaging allows for delayed imaging 12 to 24 hours after injection. This can be useful to confirm active bleeding, particularly when bleeding is intermittent and is not visible on initial images.
With the advent of computed tomography angiography (CTA), which continues to increase in speed, imaging quality and availability, the use of RBCS for evaluation of LGIB has declined. CTA is quicker to perform than RBCS and allows for detection of bleeding as well as accurate anatomic localization, which can guide interventions.
CTA provides a more comprehensive anatomic evaluation, which can aid in the diagnosis of a wide variety of intra-abdominal issues. Conversely, CTA may be less sensitive than RBCS for detection of slower acute bleeding, detecting bleeding at rates of 0.1-1 mL/min. In addition, intermittent bleeding which has temporarily stopped at the time of CTA may evade detection.
Lastly, CTA may not be appropriate in patients with impaired renal function due to risk of contrast-induced nephropathy, particularly in patients with acute kidney injury, which commonly afflicts hospitalized patients with LGIB. Prophylaxis with normal saline hydration should be employed aggressively in patients with impaired renal function, particularly when eGFR is less than 30 mL/minute. Iodinated contrast should be used judiciously in these patients.
In clinical practice, CTA and RBCS have a similar ability to confirm the presence or absence of clinically significant active gastrointestinal bleeding. Given the greater ability to rapidly localize the bleeding site with CTA, this is generally preferred over RBCS unless there is a contraindication to performing CTA, such as severe contrast allergy or high risk for development of contrast-induced nephropathy.
Role of Catheter Angiography and Embolization
Mesenteric angiography is a well-established technique for both detection and treatment of LGIB. Hemodynamic instability and need for packed RBC transfusion increases the likelihood of positive angiography. Limitations include reduced sensitivity for detection of bleeding slower than 0.5-1 mL/minute as well as the intermittent nature of LGIB, which will often resolve spontaneously. Angiography is variably successful in the literature with a diagnostic yield between 40-80%, which encompasses the rate of success in my own practice.
Once bleeding is identified, microcatheter placement within the feeding vessel as close as possible to the site of bleeding is important to ensure treatment efficacy and to limit risk of complications such as non-target embolization and bowel ischemia. Once the feeding vessel is selected with a microcatheter, embolization can be accomplished with a wide variety of tools including metallic coils, liquid embolic agents, and particles. In the treatment of LGIB, liquid embolic agents (e.g., n-butyl cyanoacrylate or NBCA, ethylene vinyl alcohol copolymer, etc.) and particles should be used judiciously as distal penetration increases the risk of bowel ischemia and procedure-related morbidity. For this reason, metallic coils are often preferred in the treatment of LGIB.
Although the source of bleeding is variable and may include diverticulosis, recent polypectomy, ulcer, tumor or angiodysplasia, the techniques employed are similar. Accurate and distal microcatheter selection is a key driver for successful embolization and minimizing the risk of bowel ischemia. Small intestinal bleeds can be challenging to treat due to the redundant supply of the arterial arcades supplying small bowel and may require occlusion of several branches to achieve hemostasis. This approach must be balanced with the risk of developing ischemia after embolization. Angiodysplasia, a less frequently encountered culprit of LGIB, may also be managed with selective embolization with many reports of successful treatment with liquid embolic agents such as NBCA mixed with ethiodized oil.
Provocative Mesenteric Angiography for Occult Bleeding
When initial angiography in a patient with suspected active LGIB is negative, provocative angiography can be considered to uncover an intermittent bleed. This may be particularly helpful in a patient where active bleeding is confirmed on a prior diagnostic test.
The approach to provocative mesenteric angiography varies by center, and a variety of agents have been used to provoke bleeding including heparin, vasodilators (i.e., nitroglycerin, verapamil, etc.) and thrombolytics (i.e., tPA), often in combination. Thrombolytics can be administered directly into the territory of interest (i.e., superior mesenteric or inferior mesenteric artery) while heparin may be administered systemically or directly into the catheterized artery. Reported success rates for provoking angiographically visible bleeding vary, but most larger series report a 40-50% success rate. The newly detected bleeding can then be treated with either embolization or surgery. A surgeon should be involved and available when provocative angiography is planned should bleeding fail to be controlled by embolization.
In summary, when colonoscopy fails to identify or control lower gastrointestinal bleeding (LGIB), imaging techniques such as RBCS and CTA play a crucial role in localizing active bleeding. While RBCS is highly sensitive, especially for intermittent or slow bleeding, CTA offers faster, more detailed anatomical information and is typically preferred unless contraindicated by renal issues or contrast allergies. Catheter-based mesenteric angiography is a well-established method for both diagnosing and treating LGIB, often using metallic coils to minimize complications like bowel ischemia. In cases where initial angiography is negative, provocative angiography – using agents like heparin or thrombolytics – may help unmask intermittent bleeding, allowing for targeted embolization or surgical intervention.
Dr. Metwalli is associate professor in the Department of Interventional Radiology, Division of Diagnostic Imaging, at The University of Texas MD Anderson Cancer Center, Houston, Texas. He declares no conflicts of interest.
Dear colleagues,
: What is the role and optimal timing of colonoscopy? How can we best utilize radiologic studies like CTA or tagged RBC scans? How should we manage patients with recurrent or intermittent bleeding that defies localization?
In this issue of Perspectives, Dr. David Wan, Dr. Fredella Lee, and Dr. Zeyad Metwalli offer their expert insights on these difficult questions. Dr. Wan, drawing on over 15 years of experience as a GI hospitalist, shares – along with his coauthor Dr. Lee – a pragmatic approach to LGIB based on clinical patterns, evolving data, and multidisciplinary collaboration. Dr. Metwalli provides the interventional radiologist’s perspective, highlighting how angiographic techniques can complement GI management and introducing novel IR strategies for patients with recurrent or elusive bleeding.
We hope their perspectives will offer valuable guidance for your practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Management of Lower Gastrointestinal Bleeds: GI Perspective
BY FREDELLA LEE, MD; DAVID WAN, MD
Acute lower gastrointestinal bleeding (LGIB) presents unique challenges. Much of this stems from the natural history of diverticular bleeding, the most common etiology of LGIB.
First, while bleeding can be severe, most will spontaneously stop. Second, despite our best efforts with imaging or colonoscopy, finding an intervenable lesion is rare. Third, LGIB has significant rates of rebleeding that are unpredictable.
While serving as a GI hospitalist for 15 years and after managing over 300 cases of LGIB, I often find myself frustrated and colonoscopy feels futile. So how can we rationally approach these patients? We will focus on three clinical questions to develop a framework for LGIB management.
- What is the role and timing for a colonoscopy?
- How do we best utilize radiologic tests?
- How can we prevent recurrent LGIB?
The Role of Colonoscopy
Traditionally, colonoscopy within 24 hours of presentation was recommended. This was based on retrospective cohort data showing higher endoscopic intervention rates and better clinical outcomes. However, this protocol requires patients to drink a significant volume of bowel preparation over a few hours (often requiring an NGT) to achieve clear rectal effluent. Moreover, one needs to mobilize a team (i.e., nurse, technician, anesthesiologist, and gastroenterologist), and find an appropriate location to scope (i.e., ED, ICU, or OR), Understandably, this is challenging, especially overnight. When the therapeutic yield is relatively low, this approach quickly loses enthusiasm.
Importantly, meta-analyses of the randomized controlled trials, have shown that urgent colonoscopies (<24 hours upon presentation), compared to elective colonoscopies (>24 hours upon presentation), do not improve clinical outcomes such as re-bleeding rates, transfusion requirements, mortality, or length of stay. In these studies, the endoscopic intervention rates were 17-34%, however, observational data shows rates of only 8%. In our practice, we will use a clear cap attachment device and water jet irrigation to increase the odds of detecting an active source of bleeding. Colonoscopy has a diagnostic yield of 95% – despite its low therapeutic yield; and while diverticular bleeds constitute up to 64% of cases, one does not want to miss colorectal cancer or other diagnoses. Regardless, there is generally no urgency to perform a colonoscopy. To quote a colleague, Dr. Elizabeth Ross, “there is no such thing as door-to-butt time.”
The Role of Radiology
Given the limits of colonoscopy, can radiographic tests such as computed tomography angiography (CTA) or tagged red blood cell (RBC) scan be helpful? Multiple studies have suggested using CTA as the initial diagnostic test. The advantages of CTAs are:
- Fast, readily available, and does not require a bowel preparation
- If negative, CTAs portend a good prognosis and make it highly unlikely to detect active extravasation on visceral angiography
- If positive, can localize the source of bleed and increase the success of intervention
Whether a positive CTA should be followed with a colonoscopy or visceral angiography remains unclear. Studies show that positive CTAs increase the detection rate of stigmata of recent hemorrhage on colonoscopy. Positive CTAs can also identify a target for embolization by interventional radiology (IR). Though an important caveat is that the success rate of embolization is highest when performed within 90 minutes of a positive CTA. This highlights that if you have IR availability, it is critical to have clear communication, a well-defined protocol, and collaboration among disciplines (i.e., ED, medical team, GI, and IR).
At our institution, we have implemented a CTA-guided protocol for severe LGIB. Those with positive CTAs are referred immediately to IR for embolization. If the embolization is unsuccessful or CTA is negative, the patient will be planned for a non-urgent inpatient colonoscopy. However, our unpublished data and other studies have shown that the overall CTA positivity rates are only between 16-22%. Moreover, one randomized controlled trial comparing CTA versus colonoscopy as an initial test did not show any meaningful difference in clinical outcomes. Thus, the benefit of CTA and the best approach to positive CTAs remains in question.
Lastly, people often ask about the utility of RBC nuclear scans. While they can detect bleeds at a slower rate (as low as 0.1 mL/min) compared to CTA (at least 0.4 mL/min), there are many limitations. RBC scans take time, are not available 24-7, and cannot precisely localize the site of bleeding. Therefore, we rarely recommend them for LGIB.
Approach to Recurrent Diverticular Bleeding
Unfortunately, diverticular bleeding recurs in the hospital 14% of the time and up to 25% at 5 years. When this occurs, is it worthwhile to repeat another colonoscopy or CTA?
Given the lack of clear data, we have adopted a shared decision-making framework with patients. Oftentimes, these patients are older and have significant co-morbidities, and undergoing bowel preparation, anesthesia, and colonoscopy is not trivial. If the patient is stable and prior work-up has excluded pertinent alternative diagnoses other than diverticular bleeding, then we tell patients the chance of finding an intervenable lesion is low and opt for conservative management. Meanwhile, if the patient has persistent, hemodynamically significant bleeding, we recommend a CTA based on the rationale discussed previously.
The most important clinical decision may not be about scoping or obtaining a CTA – it is medication management. If they are taking NSAIDs, they should be discontinued. If antiplatelet or anticoagulation agents were held, they should be restarted promptly in individuals with significant thrombotic risk given studies showing that while rebleeding rates may increase, overall mortality decreases.
In summary, managing LGIB and altering its natural history with either endoscopic or radiographic means is challenging. More studies are needed to guide the optimal approach. Reassuringly, most bleeding self-resolves and patients have good clinical outcomes.
Dr. Lee is a resident physician at New York Presbyterian Weill Cornell Medical Center, New York, NY. Dr. Wan is associate professor of clinical medicine at Weill Cornell Medicine, New York, N.Y. They declare no conflicts of interest.
Lower Gastrointestinal Bleeding: An Interventional Radiologist’s Perspective
BY ZEYAD METWALLI, MD, FSIR
When colonoscopy fails to localize and/or stop lower gastrointestinal bleeding (LGIB), catheter angiography has been commonly employed as a tool for both diagnosis and treatment of bleeding with embolization. Nuclear medicine or CT imaging studies can serve as useful adjuncts for confirming active bleeding and localizing the site of bleeding prior to angiography, particularly if this information is not provided by colonoscopy. Provocative mesenteric angiography has also become increasingly popular as a troubleshooting technique in patients with initially negative angiography.
Localization of Lower Gastrointestinal Bleeding
Radionuclide technetium-99m-lableled red blood cell scintigraphy (RBCS), also known as tagged RBC scintigraphy, has been in use since the early 1980s for investigation of acute gastrointestinal bleeding. RBCS has a high sensitivity for detection of active bleeding with a theoretical ability to detect bleeding at rates as low as 0.04-0.2 mL/minute.
Imaging protocols vary but should include dynamic images, which may aid in localization of bleeding. The relatively long half-life of the tracer used for imaging allows for delayed imaging 12 to 24 hours after injection. This can be useful to confirm active bleeding, particularly when bleeding is intermittent and is not visible on initial images.
With the advent of computed tomography angiography (CTA), which continues to increase in speed, imaging quality and availability, the use of RBCS for evaluation of LGIB has declined. CTA is quicker to perform than RBCS and allows for detection of bleeding as well as accurate anatomic localization, which can guide interventions.
CTA provides a more comprehensive anatomic evaluation, which can aid in the diagnosis of a wide variety of intra-abdominal issues. Conversely, CTA may be less sensitive than RBCS for detection of slower acute bleeding, detecting bleeding at rates of 0.1-1 mL/min. In addition, intermittent bleeding which has temporarily stopped at the time of CTA may evade detection.
Lastly, CTA may not be appropriate in patients with impaired renal function due to risk of contrast-induced nephropathy, particularly in patients with acute kidney injury, which commonly afflicts hospitalized patients with LGIB. Prophylaxis with normal saline hydration should be employed aggressively in patients with impaired renal function, particularly when eGFR is less than 30 mL/minute. Iodinated contrast should be used judiciously in these patients.
In clinical practice, CTA and RBCS have a similar ability to confirm the presence or absence of clinically significant active gastrointestinal bleeding. Given the greater ability to rapidly localize the bleeding site with CTA, this is generally preferred over RBCS unless there is a contraindication to performing CTA, such as severe contrast allergy or high risk for development of contrast-induced nephropathy.
Role of Catheter Angiography and Embolization
Mesenteric angiography is a well-established technique for both detection and treatment of LGIB. Hemodynamic instability and need for packed RBC transfusion increases the likelihood of positive angiography. Limitations include reduced sensitivity for detection of bleeding slower than 0.5-1 mL/minute as well as the intermittent nature of LGIB, which will often resolve spontaneously. Angiography is variably successful in the literature with a diagnostic yield between 40-80%, which encompasses the rate of success in my own practice.
Once bleeding is identified, microcatheter placement within the feeding vessel as close as possible to the site of bleeding is important to ensure treatment efficacy and to limit risk of complications such as non-target embolization and bowel ischemia. Once the feeding vessel is selected with a microcatheter, embolization can be accomplished with a wide variety of tools including metallic coils, liquid embolic agents, and particles. In the treatment of LGIB, liquid embolic agents (e.g., n-butyl cyanoacrylate or NBCA, ethylene vinyl alcohol copolymer, etc.) and particles should be used judiciously as distal penetration increases the risk of bowel ischemia and procedure-related morbidity. For this reason, metallic coils are often preferred in the treatment of LGIB.
Although the source of bleeding is variable and may include diverticulosis, recent polypectomy, ulcer, tumor or angiodysplasia, the techniques employed are similar. Accurate and distal microcatheter selection is a key driver for successful embolization and minimizing the risk of bowel ischemia. Small intestinal bleeds can be challenging to treat due to the redundant supply of the arterial arcades supplying small bowel and may require occlusion of several branches to achieve hemostasis. This approach must be balanced with the risk of developing ischemia after embolization. Angiodysplasia, a less frequently encountered culprit of LGIB, may also be managed with selective embolization with many reports of successful treatment with liquid embolic agents such as NBCA mixed with ethiodized oil.
Provocative Mesenteric Angiography for Occult Bleeding
When initial angiography in a patient with suspected active LGIB is negative, provocative angiography can be considered to uncover an intermittent bleed. This may be particularly helpful in a patient where active bleeding is confirmed on a prior diagnostic test.
The approach to provocative mesenteric angiography varies by center, and a variety of agents have been used to provoke bleeding including heparin, vasodilators (i.e., nitroglycerin, verapamil, etc.) and thrombolytics (i.e., tPA), often in combination. Thrombolytics can be administered directly into the territory of interest (i.e., superior mesenteric or inferior mesenteric artery) while heparin may be administered systemically or directly into the catheterized artery. Reported success rates for provoking angiographically visible bleeding vary, but most larger series report a 40-50% success rate. The newly detected bleeding can then be treated with either embolization or surgery. A surgeon should be involved and available when provocative angiography is planned should bleeding fail to be controlled by embolization.
In summary, when colonoscopy fails to identify or control lower gastrointestinal bleeding (LGIB), imaging techniques such as RBCS and CTA play a crucial role in localizing active bleeding. While RBCS is highly sensitive, especially for intermittent or slow bleeding, CTA offers faster, more detailed anatomical information and is typically preferred unless contraindicated by renal issues or contrast allergies. Catheter-based mesenteric angiography is a well-established method for both diagnosing and treating LGIB, often using metallic coils to minimize complications like bowel ischemia. In cases where initial angiography is negative, provocative angiography – using agents like heparin or thrombolytics – may help unmask intermittent bleeding, allowing for targeted embolization or surgical intervention.
Dr. Metwalli is associate professor in the Department of Interventional Radiology, Division of Diagnostic Imaging, at The University of Texas MD Anderson Cancer Center, Houston, Texas. He declares no conflicts of interest.
Dear colleagues,
: What is the role and optimal timing of colonoscopy? How can we best utilize radiologic studies like CTA or tagged RBC scans? How should we manage patients with recurrent or intermittent bleeding that defies localization?
In this issue of Perspectives, Dr. David Wan, Dr. Fredella Lee, and Dr. Zeyad Metwalli offer their expert insights on these difficult questions. Dr. Wan, drawing on over 15 years of experience as a GI hospitalist, shares – along with his coauthor Dr. Lee – a pragmatic approach to LGIB based on clinical patterns, evolving data, and multidisciplinary collaboration. Dr. Metwalli provides the interventional radiologist’s perspective, highlighting how angiographic techniques can complement GI management and introducing novel IR strategies for patients with recurrent or elusive bleeding.
We hope their perspectives will offer valuable guidance for your practice. Join the conversation on X at @AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, and chief of endoscopy at West Haven VA Medical Center, both in Connecticut. He is an associate editor for GI & Hepatology News.
Management of Lower Gastrointestinal Bleeds: GI Perspective
BY FREDELLA LEE, MD; DAVID WAN, MD
Acute lower gastrointestinal bleeding (LGIB) presents unique challenges. Much of this stems from the natural history of diverticular bleeding, the most common etiology of LGIB.
First, while bleeding can be severe, most will spontaneously stop. Second, despite our best efforts with imaging or colonoscopy, finding an intervenable lesion is rare. Third, LGIB has significant rates of rebleeding that are unpredictable.
While serving as a GI hospitalist for 15 years and after managing over 300 cases of LGIB, I often find myself frustrated and colonoscopy feels futile. So how can we rationally approach these patients? We will focus on three clinical questions to develop a framework for LGIB management.
- What is the role and timing for a colonoscopy?
- How do we best utilize radiologic tests?
- How can we prevent recurrent LGIB?
The Role of Colonoscopy
Traditionally, colonoscopy within 24 hours of presentation was recommended. This was based on retrospective cohort data showing higher endoscopic intervention rates and better clinical outcomes. However, this protocol requires patients to drink a significant volume of bowel preparation over a few hours (often requiring an NGT) to achieve clear rectal effluent. Moreover, one needs to mobilize a team (i.e., nurse, technician, anesthesiologist, and gastroenterologist), and find an appropriate location to scope (i.e., ED, ICU, or OR), Understandably, this is challenging, especially overnight. When the therapeutic yield is relatively low, this approach quickly loses enthusiasm.
Importantly, meta-analyses of the randomized controlled trials, have shown that urgent colonoscopies (<24 hours upon presentation), compared to elective colonoscopies (>24 hours upon presentation), do not improve clinical outcomes such as re-bleeding rates, transfusion requirements, mortality, or length of stay. In these studies, the endoscopic intervention rates were 17-34%, however, observational data shows rates of only 8%. In our practice, we will use a clear cap attachment device and water jet irrigation to increase the odds of detecting an active source of bleeding. Colonoscopy has a diagnostic yield of 95% – despite its low therapeutic yield; and while diverticular bleeds constitute up to 64% of cases, one does not want to miss colorectal cancer or other diagnoses. Regardless, there is generally no urgency to perform a colonoscopy. To quote a colleague, Dr. Elizabeth Ross, “there is no such thing as door-to-butt time.”
The Role of Radiology
Given the limits of colonoscopy, can radiographic tests such as computed tomography angiography (CTA) or tagged red blood cell (RBC) scan be helpful? Multiple studies have suggested using CTA as the initial diagnostic test. The advantages of CTAs are:
- Fast, readily available, and does not require a bowel preparation
- If negative, CTAs portend a good prognosis and make it highly unlikely to detect active extravasation on visceral angiography
- If positive, can localize the source of bleed and increase the success of intervention
Whether a positive CTA should be followed with a colonoscopy or visceral angiography remains unclear. Studies show that positive CTAs increase the detection rate of stigmata of recent hemorrhage on colonoscopy. Positive CTAs can also identify a target for embolization by interventional radiology (IR). Though an important caveat is that the success rate of embolization is highest when performed within 90 minutes of a positive CTA. This highlights that if you have IR availability, it is critical to have clear communication, a well-defined protocol, and collaboration among disciplines (i.e., ED, medical team, GI, and IR).
At our institution, we have implemented a CTA-guided protocol for severe LGIB. Those with positive CTAs are referred immediately to IR for embolization. If the embolization is unsuccessful or CTA is negative, the patient will be planned for a non-urgent inpatient colonoscopy. However, our unpublished data and other studies have shown that the overall CTA positivity rates are only between 16-22%. Moreover, one randomized controlled trial comparing CTA versus colonoscopy as an initial test did not show any meaningful difference in clinical outcomes. Thus, the benefit of CTA and the best approach to positive CTAs remains in question.
Lastly, people often ask about the utility of RBC nuclear scans. While they can detect bleeds at a slower rate (as low as 0.1 mL/min) compared to CTA (at least 0.4 mL/min), there are many limitations. RBC scans take time, are not available 24-7, and cannot precisely localize the site of bleeding. Therefore, we rarely recommend them for LGIB.
Approach to Recurrent Diverticular Bleeding
Unfortunately, diverticular bleeding recurs in the hospital 14% of the time and up to 25% at 5 years. When this occurs, is it worthwhile to repeat another colonoscopy or CTA?
Given the lack of clear data, we have adopted a shared decision-making framework with patients. Oftentimes, these patients are older and have significant co-morbidities, and undergoing bowel preparation, anesthesia, and colonoscopy is not trivial. If the patient is stable and prior work-up has excluded pertinent alternative diagnoses other than diverticular bleeding, then we tell patients the chance of finding an intervenable lesion is low and opt for conservative management. Meanwhile, if the patient has persistent, hemodynamically significant bleeding, we recommend a CTA based on the rationale discussed previously.
The most important clinical decision may not be about scoping or obtaining a CTA – it is medication management. If they are taking NSAIDs, they should be discontinued. If antiplatelet or anticoagulation agents were held, they should be restarted promptly in individuals with significant thrombotic risk given studies showing that while rebleeding rates may increase, overall mortality decreases.
In summary, managing LGIB and altering its natural history with either endoscopic or radiographic means is challenging. More studies are needed to guide the optimal approach. Reassuringly, most bleeding self-resolves and patients have good clinical outcomes.
Dr. Lee is a resident physician at New York Presbyterian Weill Cornell Medical Center, New York, NY. Dr. Wan is associate professor of clinical medicine at Weill Cornell Medicine, New York, N.Y. They declare no conflicts of interest.
Lower Gastrointestinal Bleeding: An Interventional Radiologist’s Perspective
BY ZEYAD METWALLI, MD, FSIR
When colonoscopy fails to localize and/or stop lower gastrointestinal bleeding (LGIB), catheter angiography has been commonly employed as a tool for both diagnosis and treatment of bleeding with embolization. Nuclear medicine or CT imaging studies can serve as useful adjuncts for confirming active bleeding and localizing the site of bleeding prior to angiography, particularly if this information is not provided by colonoscopy. Provocative mesenteric angiography has also become increasingly popular as a troubleshooting technique in patients with initially negative angiography.
Localization of Lower Gastrointestinal Bleeding
Radionuclide technetium-99m-lableled red blood cell scintigraphy (RBCS), also known as tagged RBC scintigraphy, has been in use since the early 1980s for investigation of acute gastrointestinal bleeding. RBCS has a high sensitivity for detection of active bleeding with a theoretical ability to detect bleeding at rates as low as 0.04-0.2 mL/minute.
Imaging protocols vary but should include dynamic images, which may aid in localization of bleeding. The relatively long half-life of the tracer used for imaging allows for delayed imaging 12 to 24 hours after injection. This can be useful to confirm active bleeding, particularly when bleeding is intermittent and is not visible on initial images.
With the advent of computed tomography angiography (CTA), which continues to increase in speed, imaging quality and availability, the use of RBCS for evaluation of LGIB has declined. CTA is quicker to perform than RBCS and allows for detection of bleeding as well as accurate anatomic localization, which can guide interventions.
CTA provides a more comprehensive anatomic evaluation, which can aid in the diagnosis of a wide variety of intra-abdominal issues. Conversely, CTA may be less sensitive than RBCS for detection of slower acute bleeding, detecting bleeding at rates of 0.1-1 mL/min. In addition, intermittent bleeding which has temporarily stopped at the time of CTA may evade detection.
Lastly, CTA may not be appropriate in patients with impaired renal function due to risk of contrast-induced nephropathy, particularly in patients with acute kidney injury, which commonly afflicts hospitalized patients with LGIB. Prophylaxis with normal saline hydration should be employed aggressively in patients with impaired renal function, particularly when eGFR is less than 30 mL/minute. Iodinated contrast should be used judiciously in these patients.
In clinical practice, CTA and RBCS have a similar ability to confirm the presence or absence of clinically significant active gastrointestinal bleeding. Given the greater ability to rapidly localize the bleeding site with CTA, this is generally preferred over RBCS unless there is a contraindication to performing CTA, such as severe contrast allergy or high risk for development of contrast-induced nephropathy.
Role of Catheter Angiography and Embolization
Mesenteric angiography is a well-established technique for both detection and treatment of LGIB. Hemodynamic instability and need for packed RBC transfusion increases the likelihood of positive angiography. Limitations include reduced sensitivity for detection of bleeding slower than 0.5-1 mL/minute as well as the intermittent nature of LGIB, which will often resolve spontaneously. Angiography is variably successful in the literature with a diagnostic yield between 40-80%, which encompasses the rate of success in my own practice.
Once bleeding is identified, microcatheter placement within the feeding vessel as close as possible to the site of bleeding is important to ensure treatment efficacy and to limit risk of complications such as non-target embolization and bowel ischemia. Once the feeding vessel is selected with a microcatheter, embolization can be accomplished with a wide variety of tools including metallic coils, liquid embolic agents, and particles. In the treatment of LGIB, liquid embolic agents (e.g., n-butyl cyanoacrylate or NBCA, ethylene vinyl alcohol copolymer, etc.) and particles should be used judiciously as distal penetration increases the risk of bowel ischemia and procedure-related morbidity. For this reason, metallic coils are often preferred in the treatment of LGIB.
Although the source of bleeding is variable and may include diverticulosis, recent polypectomy, ulcer, tumor or angiodysplasia, the techniques employed are similar. Accurate and distal microcatheter selection is a key driver for successful embolization and minimizing the risk of bowel ischemia. Small intestinal bleeds can be challenging to treat due to the redundant supply of the arterial arcades supplying small bowel and may require occlusion of several branches to achieve hemostasis. This approach must be balanced with the risk of developing ischemia after embolization. Angiodysplasia, a less frequently encountered culprit of LGIB, may also be managed with selective embolization with many reports of successful treatment with liquid embolic agents such as NBCA mixed with ethiodized oil.
Provocative Mesenteric Angiography for Occult Bleeding
When initial angiography in a patient with suspected active LGIB is negative, provocative angiography can be considered to uncover an intermittent bleed. This may be particularly helpful in a patient where active bleeding is confirmed on a prior diagnostic test.
The approach to provocative mesenteric angiography varies by center, and a variety of agents have been used to provoke bleeding including heparin, vasodilators (i.e., nitroglycerin, verapamil, etc.) and thrombolytics (i.e., tPA), often in combination. Thrombolytics can be administered directly into the territory of interest (i.e., superior mesenteric or inferior mesenteric artery) while heparin may be administered systemically or directly into the catheterized artery. Reported success rates for provoking angiographically visible bleeding vary, but most larger series report a 40-50% success rate. The newly detected bleeding can then be treated with either embolization or surgery. A surgeon should be involved and available when provocative angiography is planned should bleeding fail to be controlled by embolization.
In summary, when colonoscopy fails to identify or control lower gastrointestinal bleeding (LGIB), imaging techniques such as RBCS and CTA play a crucial role in localizing active bleeding. While RBCS is highly sensitive, especially for intermittent or slow bleeding, CTA offers faster, more detailed anatomical information and is typically preferred unless contraindicated by renal issues or contrast allergies. Catheter-based mesenteric angiography is a well-established method for both diagnosing and treating LGIB, often using metallic coils to minimize complications like bowel ischemia. In cases where initial angiography is negative, provocative angiography – using agents like heparin or thrombolytics – may help unmask intermittent bleeding, allowing for targeted embolization or surgical intervention.
Dr. Metwalli is associate professor in the Department of Interventional Radiology, Division of Diagnostic Imaging, at The University of Texas MD Anderson Cancer Center, Houston, Texas. He declares no conflicts of interest.
Improving Care for Patients from Historically Minoritized and Marginalized Communities with Disorders of Gut-Brain Interaction
Introduction: Cases
Patient 1: A 57-year-old man with post-prandial distress variant functional dyspepsia (FD) was recommended to start nortriptyline. He previously established primary care with a physician he met at a barbershop health fair in Harlem, who referred him for specialty evaluation. Today, he presents for follow-up and reports he did not take this medication because he heard it is an antidepressant. How would you counsel him?
Patient 2: A 61-year-old woman was previously diagnosed with mixed variant irritable bowel syndrome (IBS-M). Her symptoms have not significantly changed. Her prior workup has been reassuring and consistent with IBS-M. Despite this, the patient pushes to repeat a colonoscopy, fearful that something is being missed or that she is not being offered care because of her undocumented status. How do you respond?
Patient 3: A 36-year-old man is followed for the management of generalized anxiety disorder and functional heartburn. He was started on low-dose amitriptyline with some benefit, but follow-up has been sporadic. On further discussion, he reports financial stressors, time barriers, and difficulty scheduling a meeting with his union representative for work accommodations as he lives in a more rural community. How do you reply?
Patient 4: A 74-year-old man with Parkinson’s disease who uses a wheelchair has functional constipation that is well controlled on his current regimen. He has never undergone colon cancer screening. He occasionally notices blood in his stool, so a colonoscopy was recommended to confirm that his hematochezia reflects functional constipation complicated by hemorrhoids. He is concerned about the bowel preparation required for a colonoscopy given his limited mobility, as his insurance does not cover assistance at home. He does not have family members to help him. How can you assist him?
Social determinants of health, health disparities, and DGBIs
Social determinants of health affect all aspects of patient care, with an increasing body of published work looking at potential disparities in organ-based and structural diseases.1,2,3,4 However, little has been done to explore their influence on disorders of gut-brain interaction or DGBIs.

. As DGBIs cannot be diagnosed with a single laboratory or endoscopic test, the patient history is of the utmost importance and physician-patient rapport is paramount in their treatment. Such rapport may be more difficult to establish in patients coming from historically marginalized and minoritized communities who may be distrustful of healthcare as an institution of (discriminatory) power.
Potential DGBI management pitfalls in historically marginalized or minoritized communities
For racial and ethnic minorities in the United States, disparities in healthcare take on many forms. People from racial and ethnic minority communities are less likely to receive a gastroenterology consultation and those with IBS are more likely to undergo procedures as compared to White patients with IBS.6 Implicit bias may lead to fewer specialist referrals, and specialty care may be limited or unavailable in some areas. Patients may prefer seeing providers in their own community, with whom they share racial or ethnic identities, which could lead to fewer referrals to specialists outside of the community.
Historical discrimination contributes to a lack of trust in healthcare professionals, which may lead patients to favor more objective diagnostics such as endoscopy or view being counseled against invasive procedures as having necessary care denied. Due to a broader cultural stigma surrounding mental illness, patients may be more hesitant to utilize neuromodulators, which have historically been used for psychiatric diagnoses, as it may lead them to conflate their GI illness with mental illness.7,8
Since DGBIs cannot be diagnosed with a single test or managed with a single treatment modality, providing excellent care for patients with DGBIs requires clear communication. For patients with limited English proficiency (LEP), access to high-quality language assistance is the foundation of comprehensive care. Interpreter use (or lack thereof) may limit the ability to obtain a complete and accurate clinical history, which can lead to fewer referrals to specialists and increased reliance on endoscopic evaluations that may not be clinically indicated.
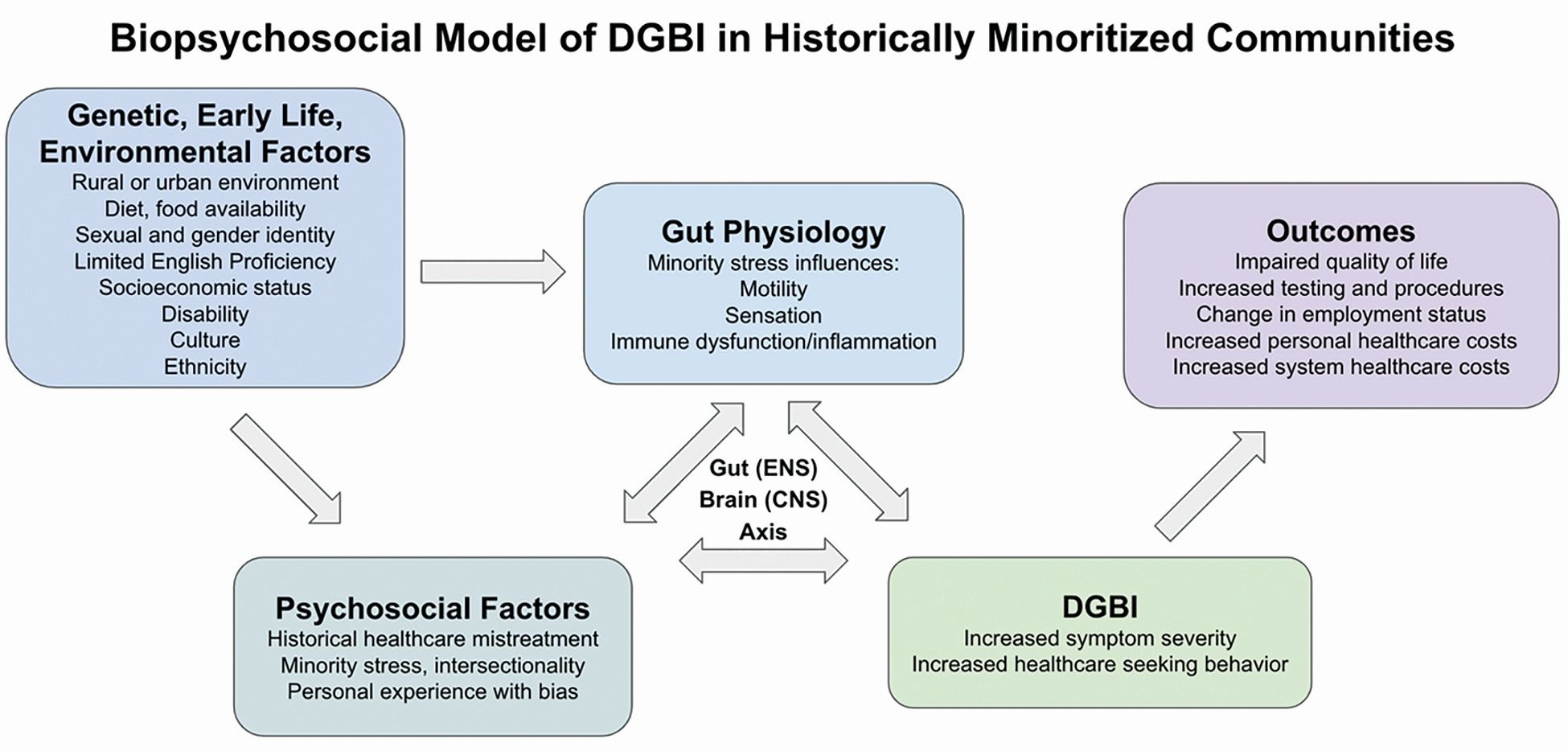
These language barriers affect patients on many levels – in their ability to understand instructions for medication administration, preparation for procedures, and return precautions – which may ultimately lead to poorer responses to therapy or delays in care. LEP alone is broadly associated with fewer referrals for outpatient follow-up, adverse health outcomes and complications, and longer hospital stays.9 These disparities can be mitigated by investing in high-quality interpreter services, providing instructions and forms in multiple languages, and engaging the patient’s family and social supports according to their preferences.
People experiencing poverty (urban and rural) face challenges across multiple domains including access to healthcare, health insurance, stable housing and employment, and more. Many patients seek care at federally qualified health centers, which may face greater difficulties coordinating care with external gastroenterologists.10

Insurance barriers limit access to essential medications, tests, and procedures, and create delays in establishing care with specialists. Significant psychological stress and higher rates of comorbid anxiety and depression contribute to increased IBS severity.11 Financial limitations may limit dietary choices, which can further exacerbate DGBI symptoms. Long work hours with limited flexibility may prohibit them from presenting for regular follow-ups and establishing advanced DGBI care such as with a dietitian or psychologist.
Patients with disabilities face many of the health inequities previously discussed, as well as additional challenges with physical accessibility, transportation, exclusion from education and employment, discrimination, and stigma. Higher prevalence of comorbid mental illness and higher rates of intimate partner violence and interpersonal violence all contribute to DGBI severity and challenges with access to care.12,13 Patients with disabilities may struggle to arrive at appointments, maneuver through the building or exam room, and ultimately follow recommended care plans.
How to approach DGBIs in historically marginalized and minoritized communities
Returning to the patients from the introduction, how would you counsel each of them?
Patient 1: We can discuss with the patient how nortriptyline and other typical antidepressants can and often are used for indications other than depression. These medications modify centrally-mediated pain signaling and many patients with functional dyspepsia experience a significant benefit. It is critical to build on the rapport that was established at the community health outreach event and to explore the patient’s concerns thoroughly.
Patient 2: We would begin by inquiring about her underlying fears associated with her symptoms and seek to understand her goals for repeat intervention. We can review the risks of endoscopy and shift the focus to improving her symptoms. If we can improve her bowel habits or her pain, her desire for further interventions may lessen.
Patient 3: It will be important to work within the realistic time and monetary constraints in this patient’s life. We can validate him and the challenges he is facing, provide positive reinforcement for the progress he has made so far, and avoid disparaging him for the aspects of the treatment plan he has been unable to follow through with. As he reported a benefit from amitriptyline, we can consider increasing his dose as a feasible next step.
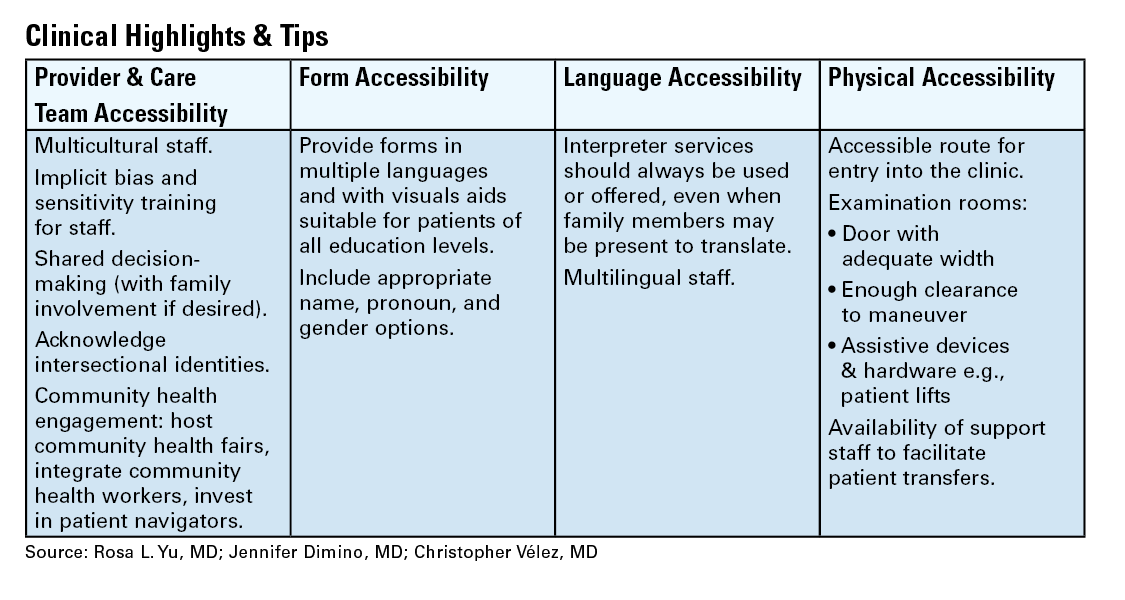
Patient 4: We can encourage the patient to discuss with his primary care physician how they may be able to coordinate an inpatient admission for colonoscopy preparation. Given his co-morbidities, this avenue will provide him dedicated support to help him adequately prep to ensure a higher quality examination and limit the need for repeat procedures.
DGBI care in historically marginalized and minoritized communities: A call to action
Understanding cultural differences and existing disparities in care is essential to improving care for patients from historically minoritized communities with DGBIs. Motivational interviewing and shared decision-making, with acknowledgment of social and cultural differences, allow us to work together with patients and their support systems to set and achieve feasible goals.14

To address known health disparities, offices can take steps to ensure the accessibility of language, forms, physical space, providers, and care teams. Providing culturally sensitive care and lowering barriers to care are the first steps to effecting meaningful change for patients with DGBIs from historically minoritized communities.
Dr. Yu is based at Division of Gastroenterology and Hepatology, Boston Medical Center and Boston University, both in Boston, Massachusetts. Dr. Dimino and Dr. Vélez are based at the Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, both in Boston, Massachusetts. Dr. Yu, Dr. Dimino, and Dr. Vélez do not have any conflicts of interest for this article.
Additional Online Resources
Form Accessibility
- Intake Form Guidance for Providers
- Making Your Clinic Welcoming to LGBTQ Patients
- Transgender data collection in the electronic health record: Current concepts and issues
Language Accessibility
Physical Accessibility
- Access to Medical Care for Individuals with Mobility Disabilities
- Making your medical office accessible
References
1. Zavala VA, et al. Cancer health disparities in racial/ethnic minorities in the United States. Br J Cancer. 2021 Jan. doi: 10.1038/s41416-020-01038-6.
2. Kardashian A, et al. Health disparities in chronic liver disease. Hepatology. 2023 Apr. doi: 10.1002/hep.32743.
3. Nephew LD, Serper M. Racial, Gender, and Socioeconomic Disparities in Liver Transplantation. Liver Transpl. 2021 Jun. doi: 10.1002/lt.25996.
4. Anyane-Yeboa A, et al. The Impact of the Social Determinants of Health on Disparities in Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. 2022 Nov. doi: 10.1016/j.cgh.2022.03.011.
5. Drossman DA. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology. 2016 Feb. doi: 10.1053/j.gastro.2016.02.032.
6. Silvernale C, et al. Racial disparity in healthcare utilization among patients with Irritable Bowel Syndrome: results from a multicenter cohort. Neurogastroenterol Motil. 2021 May. doi: 10.1111/nmo.14039.
7. Hearn M, et al. Stigma and irritable bowel syndrome: a taboo subject? Lancet Gastroenterol Hepatol. 2020 Jun. doi: 10.1016/S2468-1253(19)30348-6.
8. Yan XJ, et al. The impact of stigma on medication adherence in patients with functional dyspepsia. Neurogastroenterol Motil. 2021 Feb. doi: 10.1111/nmo.13956.
9. Twersky SE, et al. The Impact of Limited English Proficiency on Healthcare Access and Outcomes in the U.S.: A Scoping Review. Healthcare (Basel). 2024 Jan. doi: 10.3390/healthcare12030364.
10. Bayly JE, et al. Limited English proficiency and reported receipt of colorectal cancer screening among adults 45-75 in 2019 and 2021. Prev Med Rep. 2024 Feb. doi: 10.1016/j.pmedr.2024.102638.
11. Cheng K, et al. Epidemiology of Irritable Bowel Syndrome in a Large Academic Safety-Net Hospital. J Clin Med. 2024 Feb. doi: 10.3390/jcm13051314.
12. Breiding MJ, Armour BS. The association between disability and intimate partner violence in the United States. Ann Epidemiol. 2015 Jun. doi: 10.1016/j.annepidem.2015.03.017.
13. Mitra M, et al. Prevalence and characteristics of sexual violence against men with disabilities. Am J Prev Med. 2016 Mar. doi: 10.1016/j.amepre.2015.07.030.
14. Bahafzallah L, et al. Motivational Interviewing in Ethnic Populations. J Immigr Minor Health. 2020 Aug. doi: 10.1007/s10903-019-00940-3.
Introduction: Cases
Patient 1: A 57-year-old man with post-prandial distress variant functional dyspepsia (FD) was recommended to start nortriptyline. He previously established primary care with a physician he met at a barbershop health fair in Harlem, who referred him for specialty evaluation. Today, he presents for follow-up and reports he did not take this medication because he heard it is an antidepressant. How would you counsel him?
Patient 2: A 61-year-old woman was previously diagnosed with mixed variant irritable bowel syndrome (IBS-M). Her symptoms have not significantly changed. Her prior workup has been reassuring and consistent with IBS-M. Despite this, the patient pushes to repeat a colonoscopy, fearful that something is being missed or that she is not being offered care because of her undocumented status. How do you respond?
Patient 3: A 36-year-old man is followed for the management of generalized anxiety disorder and functional heartburn. He was started on low-dose amitriptyline with some benefit, but follow-up has been sporadic. On further discussion, he reports financial stressors, time barriers, and difficulty scheduling a meeting with his union representative for work accommodations as he lives in a more rural community. How do you reply?
Patient 4: A 74-year-old man with Parkinson’s disease who uses a wheelchair has functional constipation that is well controlled on his current regimen. He has never undergone colon cancer screening. He occasionally notices blood in his stool, so a colonoscopy was recommended to confirm that his hematochezia reflects functional constipation complicated by hemorrhoids. He is concerned about the bowel preparation required for a colonoscopy given his limited mobility, as his insurance does not cover assistance at home. He does not have family members to help him. How can you assist him?
Social determinants of health, health disparities, and DGBIs
Social determinants of health affect all aspects of patient care, with an increasing body of published work looking at potential disparities in organ-based and structural diseases.1,2,3,4 However, little has been done to explore their influence on disorders of gut-brain interaction or DGBIs.
. As DGBIs cannot be diagnosed with a single laboratory or endoscopic test, the patient history is of the utmost importance and physician-patient rapport is paramount in their treatment. Such rapport may be more difficult to establish in patients coming from historically marginalized and minoritized communities who may be distrustful of healthcare as an institution of (discriminatory) power.
Potential DGBI management pitfalls in historically marginalized or minoritized communities
For racial and ethnic minorities in the United States, disparities in healthcare take on many forms. People from racial and ethnic minority communities are less likely to receive a gastroenterology consultation and those with IBS are more likely to undergo procedures as compared to White patients with IBS.6 Implicit bias may lead to fewer specialist referrals, and specialty care may be limited or unavailable in some areas. Patients may prefer seeing providers in their own community, with whom they share racial or ethnic identities, which could lead to fewer referrals to specialists outside of the community.
Historical discrimination contributes to a lack of trust in healthcare professionals, which may lead patients to favor more objective diagnostics such as endoscopy or view being counseled against invasive procedures as having necessary care denied. Due to a broader cultural stigma surrounding mental illness, patients may be more hesitant to utilize neuromodulators, which have historically been used for psychiatric diagnoses, as it may lead them to conflate their GI illness with mental illness.7,8
Since DGBIs cannot be diagnosed with a single test or managed with a single treatment modality, providing excellent care for patients with DGBIs requires clear communication. For patients with limited English proficiency (LEP), access to high-quality language assistance is the foundation of comprehensive care. Interpreter use (or lack thereof) may limit the ability to obtain a complete and accurate clinical history, which can lead to fewer referrals to specialists and increased reliance on endoscopic evaluations that may not be clinically indicated.
These language barriers affect patients on many levels – in their ability to understand instructions for medication administration, preparation for procedures, and return precautions – which may ultimately lead to poorer responses to therapy or delays in care. LEP alone is broadly associated with fewer referrals for outpatient follow-up, adverse health outcomes and complications, and longer hospital stays.9 These disparities can be mitigated by investing in high-quality interpreter services, providing instructions and forms in multiple languages, and engaging the patient’s family and social supports according to their preferences.
People experiencing poverty (urban and rural) face challenges across multiple domains including access to healthcare, health insurance, stable housing and employment, and more. Many patients seek care at federally qualified health centers, which may face greater difficulties coordinating care with external gastroenterologists.10
Insurance barriers limit access to essential medications, tests, and procedures, and create delays in establishing care with specialists. Significant psychological stress and higher rates of comorbid anxiety and depression contribute to increased IBS severity.11 Financial limitations may limit dietary choices, which can further exacerbate DGBI symptoms. Long work hours with limited flexibility may prohibit them from presenting for regular follow-ups and establishing advanced DGBI care such as with a dietitian or psychologist.
Patients with disabilities face many of the health inequities previously discussed, as well as additional challenges with physical accessibility, transportation, exclusion from education and employment, discrimination, and stigma. Higher prevalence of comorbid mental illness and higher rates of intimate partner violence and interpersonal violence all contribute to DGBI severity and challenges with access to care.12,13 Patients with disabilities may struggle to arrive at appointments, maneuver through the building or exam room, and ultimately follow recommended care plans.
How to approach DGBIs in historically marginalized and minoritized communities
Returning to the patients from the introduction, how would you counsel each of them?
Patient 1: We can discuss with the patient how nortriptyline and other typical antidepressants can and often are used for indications other than depression. These medications modify centrally-mediated pain signaling and many patients with functional dyspepsia experience a significant benefit. It is critical to build on the rapport that was established at the community health outreach event and to explore the patient’s concerns thoroughly.
Patient 2: We would begin by inquiring about her underlying fears associated with her symptoms and seek to understand her goals for repeat intervention. We can review the risks of endoscopy and shift the focus to improving her symptoms. If we can improve her bowel habits or her pain, her desire for further interventions may lessen.
Patient 3: It will be important to work within the realistic time and monetary constraints in this patient’s life. We can validate him and the challenges he is facing, provide positive reinforcement for the progress he has made so far, and avoid disparaging him for the aspects of the treatment plan he has been unable to follow through with. As he reported a benefit from amitriptyline, we can consider increasing his dose as a feasible next step.
Patient 4: We can encourage the patient to discuss with his primary care physician how they may be able to coordinate an inpatient admission for colonoscopy preparation. Given his co-morbidities, this avenue will provide him dedicated support to help him adequately prep to ensure a higher quality examination and limit the need for repeat procedures.
DGBI care in historically marginalized and minoritized communities: A call to action
Understanding cultural differences and existing disparities in care is essential to improving care for patients from historically minoritized communities with DGBIs. Motivational interviewing and shared decision-making, with acknowledgment of social and cultural differences, allow us to work together with patients and their support systems to set and achieve feasible goals.14
To address known health disparities, offices can take steps to ensure the accessibility of language, forms, physical space, providers, and care teams. Providing culturally sensitive care and lowering barriers to care are the first steps to effecting meaningful change for patients with DGBIs from historically minoritized communities.
Dr. Yu is based at Division of Gastroenterology and Hepatology, Boston Medical Center and Boston University, both in Boston, Massachusetts. Dr. Dimino and Dr. Vélez are based at the Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, both in Boston, Massachusetts. Dr. Yu, Dr. Dimino, and Dr. Vélez do not have any conflicts of interest for this article.
Additional Online Resources
Form Accessibility
- Intake Form Guidance for Providers
- Making Your Clinic Welcoming to LGBTQ Patients
- Transgender data collection in the electronic health record: Current concepts and issues
Language Accessibility
Physical Accessibility
- Access to Medical Care for Individuals with Mobility Disabilities
- Making your medical office accessible
References
1. Zavala VA, et al. Cancer health disparities in racial/ethnic minorities in the United States. Br J Cancer. 2021 Jan. doi: 10.1038/s41416-020-01038-6.
2. Kardashian A, et al. Health disparities in chronic liver disease. Hepatology. 2023 Apr. doi: 10.1002/hep.32743.
3. Nephew LD, Serper M. Racial, Gender, and Socioeconomic Disparities in Liver Transplantation. Liver Transpl. 2021 Jun. doi: 10.1002/lt.25996.
4. Anyane-Yeboa A, et al. The Impact of the Social Determinants of Health on Disparities in Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. 2022 Nov. doi: 10.1016/j.cgh.2022.03.011.
5. Drossman DA. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology. 2016 Feb. doi: 10.1053/j.gastro.2016.02.032.
6. Silvernale C, et al. Racial disparity in healthcare utilization among patients with Irritable Bowel Syndrome: results from a multicenter cohort. Neurogastroenterol Motil. 2021 May. doi: 10.1111/nmo.14039.
7. Hearn M, et al. Stigma and irritable bowel syndrome: a taboo subject? Lancet Gastroenterol Hepatol. 2020 Jun. doi: 10.1016/S2468-1253(19)30348-6.
8. Yan XJ, et al. The impact of stigma on medication adherence in patients with functional dyspepsia. Neurogastroenterol Motil. 2021 Feb. doi: 10.1111/nmo.13956.
9. Twersky SE, et al. The Impact of Limited English Proficiency on Healthcare Access and Outcomes in the U.S.: A Scoping Review. Healthcare (Basel). 2024 Jan. doi: 10.3390/healthcare12030364.
10. Bayly JE, et al. Limited English proficiency and reported receipt of colorectal cancer screening among adults 45-75 in 2019 and 2021. Prev Med Rep. 2024 Feb. doi: 10.1016/j.pmedr.2024.102638.
11. Cheng K, et al. Epidemiology of Irritable Bowel Syndrome in a Large Academic Safety-Net Hospital. J Clin Med. 2024 Feb. doi: 10.3390/jcm13051314.
12. Breiding MJ, Armour BS. The association between disability and intimate partner violence in the United States. Ann Epidemiol. 2015 Jun. doi: 10.1016/j.annepidem.2015.03.017.
13. Mitra M, et al. Prevalence and characteristics of sexual violence against men with disabilities. Am J Prev Med. 2016 Mar. doi: 10.1016/j.amepre.2015.07.030.
14. Bahafzallah L, et al. Motivational Interviewing in Ethnic Populations. J Immigr Minor Health. 2020 Aug. doi: 10.1007/s10903-019-00940-3.
Introduction: Cases
Patient 1: A 57-year-old man with post-prandial distress variant functional dyspepsia (FD) was recommended to start nortriptyline. He previously established primary care with a physician he met at a barbershop health fair in Harlem, who referred him for specialty evaluation. Today, he presents for follow-up and reports he did not take this medication because he heard it is an antidepressant. How would you counsel him?
Patient 2: A 61-year-old woman was previously diagnosed with mixed variant irritable bowel syndrome (IBS-M). Her symptoms have not significantly changed. Her prior workup has been reassuring and consistent with IBS-M. Despite this, the patient pushes to repeat a colonoscopy, fearful that something is being missed or that she is not being offered care because of her undocumented status. How do you respond?
Patient 3: A 36-year-old man is followed for the management of generalized anxiety disorder and functional heartburn. He was started on low-dose amitriptyline with some benefit, but follow-up has been sporadic. On further discussion, he reports financial stressors, time barriers, and difficulty scheduling a meeting with his union representative for work accommodations as he lives in a more rural community. How do you reply?
Patient 4: A 74-year-old man with Parkinson’s disease who uses a wheelchair has functional constipation that is well controlled on his current regimen. He has never undergone colon cancer screening. He occasionally notices blood in his stool, so a colonoscopy was recommended to confirm that his hematochezia reflects functional constipation complicated by hemorrhoids. He is concerned about the bowel preparation required for a colonoscopy given his limited mobility, as his insurance does not cover assistance at home. He does not have family members to help him. How can you assist him?
Social determinants of health, health disparities, and DGBIs
Social determinants of health affect all aspects of patient care, with an increasing body of published work looking at potential disparities in organ-based and structural diseases.1,2,3,4 However, little has been done to explore their influence on disorders of gut-brain interaction or DGBIs.
. As DGBIs cannot be diagnosed with a single laboratory or endoscopic test, the patient history is of the utmost importance and physician-patient rapport is paramount in their treatment. Such rapport may be more difficult to establish in patients coming from historically marginalized and minoritized communities who may be distrustful of healthcare as an institution of (discriminatory) power.
Potential DGBI management pitfalls in historically marginalized or minoritized communities
For racial and ethnic minorities in the United States, disparities in healthcare take on many forms. People from racial and ethnic minority communities are less likely to receive a gastroenterology consultation and those with IBS are more likely to undergo procedures as compared to White patients with IBS.6 Implicit bias may lead to fewer specialist referrals, and specialty care may be limited or unavailable in some areas. Patients may prefer seeing providers in their own community, with whom they share racial or ethnic identities, which could lead to fewer referrals to specialists outside of the community.
Historical discrimination contributes to a lack of trust in healthcare professionals, which may lead patients to favor more objective diagnostics such as endoscopy or view being counseled against invasive procedures as having necessary care denied. Due to a broader cultural stigma surrounding mental illness, patients may be more hesitant to utilize neuromodulators, which have historically been used for psychiatric diagnoses, as it may lead them to conflate their GI illness with mental illness.7,8
Since DGBIs cannot be diagnosed with a single test or managed with a single treatment modality, providing excellent care for patients with DGBIs requires clear communication. For patients with limited English proficiency (LEP), access to high-quality language assistance is the foundation of comprehensive care. Interpreter use (or lack thereof) may limit the ability to obtain a complete and accurate clinical history, which can lead to fewer referrals to specialists and increased reliance on endoscopic evaluations that may not be clinically indicated.
These language barriers affect patients on many levels – in their ability to understand instructions for medication administration, preparation for procedures, and return precautions – which may ultimately lead to poorer responses to therapy or delays in care. LEP alone is broadly associated with fewer referrals for outpatient follow-up, adverse health outcomes and complications, and longer hospital stays.9 These disparities can be mitigated by investing in high-quality interpreter services, providing instructions and forms in multiple languages, and engaging the patient’s family and social supports according to their preferences.
People experiencing poverty (urban and rural) face challenges across multiple domains including access to healthcare, health insurance, stable housing and employment, and more. Many patients seek care at federally qualified health centers, which may face greater difficulties coordinating care with external gastroenterologists.10
Insurance barriers limit access to essential medications, tests, and procedures, and create delays in establishing care with specialists. Significant psychological stress and higher rates of comorbid anxiety and depression contribute to increased IBS severity.11 Financial limitations may limit dietary choices, which can further exacerbate DGBI symptoms. Long work hours with limited flexibility may prohibit them from presenting for regular follow-ups and establishing advanced DGBI care such as with a dietitian or psychologist.
Patients with disabilities face many of the health inequities previously discussed, as well as additional challenges with physical accessibility, transportation, exclusion from education and employment, discrimination, and stigma. Higher prevalence of comorbid mental illness and higher rates of intimate partner violence and interpersonal violence all contribute to DGBI severity and challenges with access to care.12,13 Patients with disabilities may struggle to arrive at appointments, maneuver through the building or exam room, and ultimately follow recommended care plans.
How to approach DGBIs in historically marginalized and minoritized communities
Returning to the patients from the introduction, how would you counsel each of them?
Patient 1: We can discuss with the patient how nortriptyline and other typical antidepressants can and often are used for indications other than depression. These medications modify centrally-mediated pain signaling and many patients with functional dyspepsia experience a significant benefit. It is critical to build on the rapport that was established at the community health outreach event and to explore the patient’s concerns thoroughly.
Patient 2: We would begin by inquiring about her underlying fears associated with her symptoms and seek to understand her goals for repeat intervention. We can review the risks of endoscopy and shift the focus to improving her symptoms. If we can improve her bowel habits or her pain, her desire for further interventions may lessen.
Patient 3: It will be important to work within the realistic time and monetary constraints in this patient’s life. We can validate him and the challenges he is facing, provide positive reinforcement for the progress he has made so far, and avoid disparaging him for the aspects of the treatment plan he has been unable to follow through with. As he reported a benefit from amitriptyline, we can consider increasing his dose as a feasible next step.
Patient 4: We can encourage the patient to discuss with his primary care physician how they may be able to coordinate an inpatient admission for colonoscopy preparation. Given his co-morbidities, this avenue will provide him dedicated support to help him adequately prep to ensure a higher quality examination and limit the need for repeat procedures.
DGBI care in historically marginalized and minoritized communities: A call to action
Understanding cultural differences and existing disparities in care is essential to improving care for patients from historically minoritized communities with DGBIs. Motivational interviewing and shared decision-making, with acknowledgment of social and cultural differences, allow us to work together with patients and their support systems to set and achieve feasible goals.14
To address known health disparities, offices can take steps to ensure the accessibility of language, forms, physical space, providers, and care teams. Providing culturally sensitive care and lowering barriers to care are the first steps to effecting meaningful change for patients with DGBIs from historically minoritized communities.
Dr. Yu is based at Division of Gastroenterology and Hepatology, Boston Medical Center and Boston University, both in Boston, Massachusetts. Dr. Dimino and Dr. Vélez are based at the Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, both in Boston, Massachusetts. Dr. Yu, Dr. Dimino, and Dr. Vélez do not have any conflicts of interest for this article.
Additional Online Resources
Form Accessibility
- Intake Form Guidance for Providers
- Making Your Clinic Welcoming to LGBTQ Patients
- Transgender data collection in the electronic health record: Current concepts and issues
Language Accessibility
Physical Accessibility
- Access to Medical Care for Individuals with Mobility Disabilities
- Making your medical office accessible
References
1. Zavala VA, et al. Cancer health disparities in racial/ethnic minorities in the United States. Br J Cancer. 2021 Jan. doi: 10.1038/s41416-020-01038-6.
2. Kardashian A, et al. Health disparities in chronic liver disease. Hepatology. 2023 Apr. doi: 10.1002/hep.32743.
3. Nephew LD, Serper M. Racial, Gender, and Socioeconomic Disparities in Liver Transplantation. Liver Transpl. 2021 Jun. doi: 10.1002/lt.25996.
4. Anyane-Yeboa A, et al. The Impact of the Social Determinants of Health on Disparities in Inflammatory Bowel Disease. Clin Gastroenterol Hepatol. 2022 Nov. doi: 10.1016/j.cgh.2022.03.011.
5. Drossman DA. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology. 2016 Feb. doi: 10.1053/j.gastro.2016.02.032.
6. Silvernale C, et al. Racial disparity in healthcare utilization among patients with Irritable Bowel Syndrome: results from a multicenter cohort. Neurogastroenterol Motil. 2021 May. doi: 10.1111/nmo.14039.
7. Hearn M, et al. Stigma and irritable bowel syndrome: a taboo subject? Lancet Gastroenterol Hepatol. 2020 Jun. doi: 10.1016/S2468-1253(19)30348-6.
8. Yan XJ, et al. The impact of stigma on medication adherence in patients with functional dyspepsia. Neurogastroenterol Motil. 2021 Feb. doi: 10.1111/nmo.13956.
9. Twersky SE, et al. The Impact of Limited English Proficiency on Healthcare Access and Outcomes in the U.S.: A Scoping Review. Healthcare (Basel). 2024 Jan. doi: 10.3390/healthcare12030364.
10. Bayly JE, et al. Limited English proficiency and reported receipt of colorectal cancer screening among adults 45-75 in 2019 and 2021. Prev Med Rep. 2024 Feb. doi: 10.1016/j.pmedr.2024.102638.
11. Cheng K, et al. Epidemiology of Irritable Bowel Syndrome in a Large Academic Safety-Net Hospital. J Clin Med. 2024 Feb. doi: 10.3390/jcm13051314.
12. Breiding MJ, Armour BS. The association between disability and intimate partner violence in the United States. Ann Epidemiol. 2015 Jun. doi: 10.1016/j.annepidem.2015.03.017.
13. Mitra M, et al. Prevalence and characteristics of sexual violence against men with disabilities. Am J Prev Med. 2016 Mar. doi: 10.1016/j.amepre.2015.07.030.
14. Bahafzallah L, et al. Motivational Interviewing in Ethnic Populations. J Immigr Minor Health. 2020 Aug. doi: 10.1007/s10903-019-00940-3.
MASH Driving Global Epidemic of Primary Liver Cancer
Although the incidence of PLC from most etiologies is declining, MASH and alcohol-related liver disease (ALD) are exceptions.
A recent analysis in Clinical Gastroenterology and Hepatology found a near doubling of cases in from 2000 to 2021 in data from the 2024 Global Burden of Disease study.
The analysis assessed age-standardized incidence, mortality, and disability-adjusted life years (DALYs) from MASH-associated PLC, stratified by geographical region, sociodemographic index, age, and sex.
The burden of MASH-associated primary liver cancer (PLC) is rising rapidly while, thanks to effective suppressive treatments, the incidence of PLC from viral hepatitis is declining.
“Given the shifting epidemiology and limited global data, this analysis was timely to provide updated, comprehensive estimates using the GBD 2021 database,” lead authors Ju Dong Yang, MD, MS, and Karn Wijarnpreecha, MD, MPH, told GI & Hepatology News in a joint email. Yang is an associate professor and medical director of the Liver Cancer Program at Cedars-Sinai Medical Center in Los Angeles, and Wijarnpreecha is a transplant hepatologist in the of Division of Gastroenterology at University of Arizona College of Medicine in Phoenix. “Our study helps identify regions, populations, and sex-specific trends that are most affected and informs global policy response.”

Interestingly,the United States ranks among the top three countries worldwide in terms of MASH-associated PLC burden, with nearly 3,400 newly diagnosed cases reported in 2021 alone. The Americas in general experienced the highest percentage increase in age-standardized incidence rate (APC, 2.09%, 95% CI, 2.02–2.16), age-standardized death rate (APC, 1.96%; 95% CI, 1.69–2.23), and age-standardized DALYs (APC, 1.96%; 95% CI, 1.63–2.30) from MASH-associated PLC.
Globally, there were 42,290 incident cases, 40,920 deaths, and 995,470 DALYs from PLC. Global incidence (+98%), death (+93%), and DALYs (+76%) from MASH-associated PLC increased steeply over the study period.
Among different etiologies, the global study found that only MASH-associated PLC had increased mortality rates, for an annual percent change of +0.46 (95% confidence interval [CI], .33%–.59%). Africa and low-sociodemographic index countries exhibited the highest age-standardized incidence, death, and DALYs from MASH-associated PLC.
MASH promotes PLC through chronic liver inflammation, oxidative stress, lipotoxicity, and fibrosis, which together create a procarcinogenic environment even in the absence of cirrhosis. “This distinct pathway makes MASH-associated PLC harder to detect early, especially when cirrhosis is not yet evident,” Yang and Wijarnpreecha said.
By gender, DALYs increased in females (APC, .24%, 95% CI, .06–.42) but remained stable in males. “Males have higher absolute rates of MASH-associated PLC in terms of incidence and DALYs. However, our study found that the rate of increase in MASH-associated PLC-related disability is steeper in females. This suggests a growing burden among women, possibly related to aging, hormonal changes, and cumulative metabolic risk,” the authors said. In terms of age, “while our study did not assess age at onset, separate analyses have shown that both MASH-associated and alcohol-associated liver cancer are rising among younger individuals.”
Yang and Wijarnpreecha emphasized the need for a multi-pronged remedial strategy, including broad public health policies targeting obesity and metabolic syndrome and better risk stratification tools such as no-invasive biomarkers and genetic profiling. They called for investment in liver cancer surveillance, especially in populations at risk, and special attention to sex disparities and health equity across regions.
“We’re entering a new era of liver cancer epidemiology, where MASLD is taking center stage. Clinicians must recognize that MASH can progress to liver cancer even without cirrhosis,” they said. “Early diagnosis and metabolic intervention may be the best tools to curb this trend, and sex-based approaches to risk stratification and treatment may be essential moving forward.”
Yang’s research is supported by the National Institutes of Health. He consults for AstraZeneca, Eisai, Exact Sciences, and FujiFilm Medical Sciences.
Reviewing this study for GI & Hepatology News, but not involved in it, Scott L. Friedman, MD, AGAF, chief emeritus of the Division of Liver Diseases at Mount Sinai Health System in New York City and director of the newly established multidisciplinary Mount Sinai Institute for Liver Research, said the increase in primary liver cancer burden revealed by the research has been recognized for several years, especially among liver specialists, and is worsening, particularly in America.

“This is most evident in the changing composition of liver transplant waiting lists, which include a diminishing number of patients with chronic viral hepatitis, and a growing fraction of patients with steatotic liver disease, either from MASH alone or with concurrent alcohol-associated liver disease,” Friedman said. He noted that apart from the brain, the liver is the body’s least understood organ.
Friedman said that an urgent need exists for increased awareness of and screening for steatotic liver disease in primary care and general medicine practices – especially in patients with type 2 diabetes, about 70% of whom typically have steatosis – as well as those with features of the metabolic syndrome, with obesity, type 2 diabetes, lipid abnormalities and hypertension. “Awareness of metabolic-associated liver disease and MASH among patients and providers is still inadequate,” he said. “However, now that there’s a newly approved drug, Rezdiffra [resmetirom] – and more likely in the coming years – early detection and treatment of MASH will become essential to prevent its progression to cirrhosis and PLC through specific medications.”
Once patients with MASH have more advanced fibrosis, Friedman noted, regular screening for PLC is essential to detect early cancers that are still curable either by liver resection, liver transplant, or direct ablation of small tumors. “Unfortunately, it is not unusual for patients to present with an incurable PLC without realizing they had any underlying liver disease, since MASH is not associated with specific liver symptoms.”
Friedman disclosed no competing interests relevant to his comments.
Reviewing this study for GI & Hepatology News, but not involved in it, Scott L. Friedman, MD, AGAF, chief emeritus of the Division of Liver Diseases at Mount Sinai Health System in New York City and director of the newly established multidisciplinary Mount Sinai Institute for Liver Research, said the increase in primary liver cancer burden revealed by the research has been recognized for several years, especially among liver specialists, and is worsening, particularly in America.
“This is most evident in the changing composition of liver transplant waiting lists, which include a diminishing number of patients with chronic viral hepatitis, and a growing fraction of patients with steatotic liver disease, either from MASH alone or with concurrent alcohol-associated liver disease,” Friedman said. He noted that apart from the brain, the liver is the body’s least understood organ.
Friedman said that an urgent need exists for increased awareness of and screening for steatotic liver disease in primary care and general medicine practices – especially in patients with type 2 diabetes, about 70% of whom typically have steatosis – as well as those with features of the metabolic syndrome, with obesity, type 2 diabetes, lipid abnormalities and hypertension. “Awareness of metabolic-associated liver disease and MASH among patients and providers is still inadequate,” he said. “However, now that there’s a newly approved drug, Rezdiffra [resmetirom] – and more likely in the coming years – early detection and treatment of MASH will become essential to prevent its progression to cirrhosis and PLC through specific medications.”
Once patients with MASH have more advanced fibrosis, Friedman noted, regular screening for PLC is essential to detect early cancers that are still curable either by liver resection, liver transplant, or direct ablation of small tumors. “Unfortunately, it is not unusual for patients to present with an incurable PLC without realizing they had any underlying liver disease, since MASH is not associated with specific liver symptoms.”
Friedman disclosed no competing interests relevant to his comments.
Reviewing this study for GI & Hepatology News, but not involved in it, Scott L. Friedman, MD, AGAF, chief emeritus of the Division of Liver Diseases at Mount Sinai Health System in New York City and director of the newly established multidisciplinary Mount Sinai Institute for Liver Research, said the increase in primary liver cancer burden revealed by the research has been recognized for several years, especially among liver specialists, and is worsening, particularly in America.
“This is most evident in the changing composition of liver transplant waiting lists, which include a diminishing number of patients with chronic viral hepatitis, and a growing fraction of patients with steatotic liver disease, either from MASH alone or with concurrent alcohol-associated liver disease,” Friedman said. He noted that apart from the brain, the liver is the body’s least understood organ.
Friedman said that an urgent need exists for increased awareness of and screening for steatotic liver disease in primary care and general medicine practices – especially in patients with type 2 diabetes, about 70% of whom typically have steatosis – as well as those with features of the metabolic syndrome, with obesity, type 2 diabetes, lipid abnormalities and hypertension. “Awareness of metabolic-associated liver disease and MASH among patients and providers is still inadequate,” he said. “However, now that there’s a newly approved drug, Rezdiffra [resmetirom] – and more likely in the coming years – early detection and treatment of MASH will become essential to prevent its progression to cirrhosis and PLC through specific medications.”
Once patients with MASH have more advanced fibrosis, Friedman noted, regular screening for PLC is essential to detect early cancers that are still curable either by liver resection, liver transplant, or direct ablation of small tumors. “Unfortunately, it is not unusual for patients to present with an incurable PLC without realizing they had any underlying liver disease, since MASH is not associated with specific liver symptoms.”
Friedman disclosed no competing interests relevant to his comments.
Although the incidence of PLC from most etiologies is declining, MASH and alcohol-related liver disease (ALD) are exceptions.
A recent analysis in Clinical Gastroenterology and Hepatology found a near doubling of cases in from 2000 to 2021 in data from the 2024 Global Burden of Disease study.
The analysis assessed age-standardized incidence, mortality, and disability-adjusted life years (DALYs) from MASH-associated PLC, stratified by geographical region, sociodemographic index, age, and sex.
The burden of MASH-associated primary liver cancer (PLC) is rising rapidly while, thanks to effective suppressive treatments, the incidence of PLC from viral hepatitis is declining.
“Given the shifting epidemiology and limited global data, this analysis was timely to provide updated, comprehensive estimates using the GBD 2021 database,” lead authors Ju Dong Yang, MD, MS, and Karn Wijarnpreecha, MD, MPH, told GI & Hepatology News in a joint email. Yang is an associate professor and medical director of the Liver Cancer Program at Cedars-Sinai Medical Center in Los Angeles, and Wijarnpreecha is a transplant hepatologist in the of Division of Gastroenterology at University of Arizona College of Medicine in Phoenix. “Our study helps identify regions, populations, and sex-specific trends that are most affected and informs global policy response.”
Interestingly,the United States ranks among the top three countries worldwide in terms of MASH-associated PLC burden, with nearly 3,400 newly diagnosed cases reported in 2021 alone. The Americas in general experienced the highest percentage increase in age-standardized incidence rate (APC, 2.09%, 95% CI, 2.02–2.16), age-standardized death rate (APC, 1.96%; 95% CI, 1.69–2.23), and age-standardized DALYs (APC, 1.96%; 95% CI, 1.63–2.30) from MASH-associated PLC.
Globally, there were 42,290 incident cases, 40,920 deaths, and 995,470 DALYs from PLC. Global incidence (+98%), death (+93%), and DALYs (+76%) from MASH-associated PLC increased steeply over the study period.
Among different etiologies, the global study found that only MASH-associated PLC had increased mortality rates, for an annual percent change of +0.46 (95% confidence interval [CI], .33%–.59%). Africa and low-sociodemographic index countries exhibited the highest age-standardized incidence, death, and DALYs from MASH-associated PLC.
MASH promotes PLC through chronic liver inflammation, oxidative stress, lipotoxicity, and fibrosis, which together create a procarcinogenic environment even in the absence of cirrhosis. “This distinct pathway makes MASH-associated PLC harder to detect early, especially when cirrhosis is not yet evident,” Yang and Wijarnpreecha said.
By gender, DALYs increased in females (APC, .24%, 95% CI, .06–.42) but remained stable in males. “Males have higher absolute rates of MASH-associated PLC in terms of incidence and DALYs. However, our study found that the rate of increase in MASH-associated PLC-related disability is steeper in females. This suggests a growing burden among women, possibly related to aging, hormonal changes, and cumulative metabolic risk,” the authors said. In terms of age, “while our study did not assess age at onset, separate analyses have shown that both MASH-associated and alcohol-associated liver cancer are rising among younger individuals.”
Yang and Wijarnpreecha emphasized the need for a multi-pronged remedial strategy, including broad public health policies targeting obesity and metabolic syndrome and better risk stratification tools such as no-invasive biomarkers and genetic profiling. They called for investment in liver cancer surveillance, especially in populations at risk, and special attention to sex disparities and health equity across regions.
“We’re entering a new era of liver cancer epidemiology, where MASLD is taking center stage. Clinicians must recognize that MASH can progress to liver cancer even without cirrhosis,” they said. “Early diagnosis and metabolic intervention may be the best tools to curb this trend, and sex-based approaches to risk stratification and treatment may be essential moving forward.”
Yang’s research is supported by the National Institutes of Health. He consults for AstraZeneca, Eisai, Exact Sciences, and FujiFilm Medical Sciences.
Although the incidence of PLC from most etiologies is declining, MASH and alcohol-related liver disease (ALD) are exceptions.
A recent analysis in Clinical Gastroenterology and Hepatology found a near doubling of cases in from 2000 to 2021 in data from the 2024 Global Burden of Disease study.
The analysis assessed age-standardized incidence, mortality, and disability-adjusted life years (DALYs) from MASH-associated PLC, stratified by geographical region, sociodemographic index, age, and sex.
The burden of MASH-associated primary liver cancer (PLC) is rising rapidly while, thanks to effective suppressive treatments, the incidence of PLC from viral hepatitis is declining.
“Given the shifting epidemiology and limited global data, this analysis was timely to provide updated, comprehensive estimates using the GBD 2021 database,” lead authors Ju Dong Yang, MD, MS, and Karn Wijarnpreecha, MD, MPH, told GI & Hepatology News in a joint email. Yang is an associate professor and medical director of the Liver Cancer Program at Cedars-Sinai Medical Center in Los Angeles, and Wijarnpreecha is a transplant hepatologist in the of Division of Gastroenterology at University of Arizona College of Medicine in Phoenix. “Our study helps identify regions, populations, and sex-specific trends that are most affected and informs global policy response.”
Interestingly,the United States ranks among the top three countries worldwide in terms of MASH-associated PLC burden, with nearly 3,400 newly diagnosed cases reported in 2021 alone. The Americas in general experienced the highest percentage increase in age-standardized incidence rate (APC, 2.09%, 95% CI, 2.02–2.16), age-standardized death rate (APC, 1.96%; 95% CI, 1.69–2.23), and age-standardized DALYs (APC, 1.96%; 95% CI, 1.63–2.30) from MASH-associated PLC.
Globally, there were 42,290 incident cases, 40,920 deaths, and 995,470 DALYs from PLC. Global incidence (+98%), death (+93%), and DALYs (+76%) from MASH-associated PLC increased steeply over the study period.
Among different etiologies, the global study found that only MASH-associated PLC had increased mortality rates, for an annual percent change of +0.46 (95% confidence interval [CI], .33%–.59%). Africa and low-sociodemographic index countries exhibited the highest age-standardized incidence, death, and DALYs from MASH-associated PLC.
MASH promotes PLC through chronic liver inflammation, oxidative stress, lipotoxicity, and fibrosis, which together create a procarcinogenic environment even in the absence of cirrhosis. “This distinct pathway makes MASH-associated PLC harder to detect early, especially when cirrhosis is not yet evident,” Yang and Wijarnpreecha said.
By gender, DALYs increased in females (APC, .24%, 95% CI, .06–.42) but remained stable in males. “Males have higher absolute rates of MASH-associated PLC in terms of incidence and DALYs. However, our study found that the rate of increase in MASH-associated PLC-related disability is steeper in females. This suggests a growing burden among women, possibly related to aging, hormonal changes, and cumulative metabolic risk,” the authors said. In terms of age, “while our study did not assess age at onset, separate analyses have shown that both MASH-associated and alcohol-associated liver cancer are rising among younger individuals.”
Yang and Wijarnpreecha emphasized the need for a multi-pronged remedial strategy, including broad public health policies targeting obesity and metabolic syndrome and better risk stratification tools such as no-invasive biomarkers and genetic profiling. They called for investment in liver cancer surveillance, especially in populations at risk, and special attention to sex disparities and health equity across regions.
“We’re entering a new era of liver cancer epidemiology, where MASLD is taking center stage. Clinicians must recognize that MASH can progress to liver cancer even without cirrhosis,” they said. “Early diagnosis and metabolic intervention may be the best tools to curb this trend, and sex-based approaches to risk stratification and treatment may be essential moving forward.”
Yang’s research is supported by the National Institutes of Health. He consults for AstraZeneca, Eisai, Exact Sciences, and FujiFilm Medical Sciences.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Colonoscopy Screening Effective in 45- to 49-Year-Olds
Researchers at Kaiser Permanente Northern California sought to compare yields between the two age groups to assess how a change in guidance in 2021 urging screening in the younger cohort was borne out in a real-world setting.
The researchers published their findings in JAMA, concluding that the results supported screening colonoscopy in 45- to 49-year-olds.
The study compared 4380 individuals aged 45-49 years, with 7651 who were aged 50-54. All of them underwent their first colonoscopy during 2021 to 2024. Thirty-five percent of the younger group and 40% of the older group had any adenoma.
About 4% of each group had an advanced adenoma, 10% had any sessile serrated lesion, a little under 2% had an advanced serrated lesion, and 0.1% in each group had colorectal cancer.
There were no significant differences in neoplasia prevalence between the groups by sex. The authors did note that the study group included more Asian individuals (30%) than in the general population.
Swati G. Patel, MD, MS, director of the Gastrointestinal Hereditary Cancer Program at the University of Colorado Anschutz Medical Center, Denver, said the Kaiser study is important because its data was aggregated after the US Preventive Services Task Force lowered the screening age in 2021.

The Kaiser research “validates the initial studies” done to support that recommendation and the 2022 consensus statement by the US Multi-Society Task Force on Colorectal Cancer, which also advocated screening in 45- to 49-year-olds.
Even though the new JAMA study found a similar rate of cancers and precursor lesions as in previous trials, it provides “reinforcement of the rationale for decreasing the screening age,” Patel, the lead author on the consensus statement, told GI & Hepatology News.
The Kaiser research is “really powerful information,” she said.
“It certainly validates our current guidance to start screening for colorectal cancer at age 45,” said Audrey Calderwood, MD, director of the GI Cancer Risk and Prevention Clinic at the Geisel School of Medicine, Dartmouth, New Hampshire.
The Kaiser data provides granular information to share with younger patients who might think that they don’t need screening because they are healthy and don’t have symptoms, said Calderwood, also director of the Comprehensive Gastroenterology Center at Dartmouth Hitchcock Medical Center.
Colon cancer rates for Americans under age 50 have been steadily rising for the past decade, hitting about 10 cases per 100,000 in 2022, according to the National Cancer Institute (NCI). In 2023, about 73% of eligible 50- to 75-year-olds received colorectal cancer screening based on the most recent guidelines, according to the NCI.
But screening rates in the under-50 age group are much lower. Researchers estimated in a study that only about 34.5% of those aged 45-49 received colorectal cancer screening, which included colonoscopy, stool-based tests, and CT colonography.
Patel said that estimate is “spot on” in terms of other estimates.
“I think there’s a perception that it’s a cancer of older adults and that young healthy people don’t need to worry about it,” she said, adding that getting the word out to younger Americans is a “PR challenge,” in part because of squeamishness about discussing anything to do with stool and changes in how they access information.

Calderwood agreed. Younger people “aren’t chatting to their friends about” colon cancer screening the way they might about mammography, said Calderwood.
Both she and Patel noted that educating the public was an ongoing project, but that a physician’s recommendation was key.
Patel said she hoped that data provided in the Kaiser study might help “dismantle the systemic skepticism around decreasing the age recommendation” for screening.
Calderwood and Patel reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Researchers at Kaiser Permanente Northern California sought to compare yields between the two age groups to assess how a change in guidance in 2021 urging screening in the younger cohort was borne out in a real-world setting.
The researchers published their findings in JAMA, concluding that the results supported screening colonoscopy in 45- to 49-year-olds.
The study compared 4380 individuals aged 45-49 years, with 7651 who were aged 50-54. All of them underwent their first colonoscopy during 2021 to 2024. Thirty-five percent of the younger group and 40% of the older group had any adenoma.
About 4% of each group had an advanced adenoma, 10% had any sessile serrated lesion, a little under 2% had an advanced serrated lesion, and 0.1% in each group had colorectal cancer.
There were no significant differences in neoplasia prevalence between the groups by sex. The authors did note that the study group included more Asian individuals (30%) than in the general population.
Swati G. Patel, MD, MS, director of the Gastrointestinal Hereditary Cancer Program at the University of Colorado Anschutz Medical Center, Denver, said the Kaiser study is important because its data was aggregated after the US Preventive Services Task Force lowered the screening age in 2021.
The Kaiser research “validates the initial studies” done to support that recommendation and the 2022 consensus statement by the US Multi-Society Task Force on Colorectal Cancer, which also advocated screening in 45- to 49-year-olds.
Even though the new JAMA study found a similar rate of cancers and precursor lesions as in previous trials, it provides “reinforcement of the rationale for decreasing the screening age,” Patel, the lead author on the consensus statement, told GI & Hepatology News.
The Kaiser research is “really powerful information,” she said.
“It certainly validates our current guidance to start screening for colorectal cancer at age 45,” said Audrey Calderwood, MD, director of the GI Cancer Risk and Prevention Clinic at the Geisel School of Medicine, Dartmouth, New Hampshire.
The Kaiser data provides granular information to share with younger patients who might think that they don’t need screening because they are healthy and don’t have symptoms, said Calderwood, also director of the Comprehensive Gastroenterology Center at Dartmouth Hitchcock Medical Center.
Colon cancer rates for Americans under age 50 have been steadily rising for the past decade, hitting about 10 cases per 100,000 in 2022, according to the National Cancer Institute (NCI). In 2023, about 73% of eligible 50- to 75-year-olds received colorectal cancer screening based on the most recent guidelines, according to the NCI.
But screening rates in the under-50 age group are much lower. Researchers estimated in a study that only about 34.5% of those aged 45-49 received colorectal cancer screening, which included colonoscopy, stool-based tests, and CT colonography.
Patel said that estimate is “spot on” in terms of other estimates.
“I think there’s a perception that it’s a cancer of older adults and that young healthy people don’t need to worry about it,” she said, adding that getting the word out to younger Americans is a “PR challenge,” in part because of squeamishness about discussing anything to do with stool and changes in how they access information.
Calderwood agreed. Younger people “aren’t chatting to their friends about” colon cancer screening the way they might about mammography, said Calderwood.
Both she and Patel noted that educating the public was an ongoing project, but that a physician’s recommendation was key.
Patel said she hoped that data provided in the Kaiser study might help “dismantle the systemic skepticism around decreasing the age recommendation” for screening.
Calderwood and Patel reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Researchers at Kaiser Permanente Northern California sought to compare yields between the two age groups to assess how a change in guidance in 2021 urging screening in the younger cohort was borne out in a real-world setting.
The researchers published their findings in JAMA, concluding that the results supported screening colonoscopy in 45- to 49-year-olds.
The study compared 4380 individuals aged 45-49 years, with 7651 who were aged 50-54. All of them underwent their first colonoscopy during 2021 to 2024. Thirty-five percent of the younger group and 40% of the older group had any adenoma.
About 4% of each group had an advanced adenoma, 10% had any sessile serrated lesion, a little under 2% had an advanced serrated lesion, and 0.1% in each group had colorectal cancer.
There were no significant differences in neoplasia prevalence between the groups by sex. The authors did note that the study group included more Asian individuals (30%) than in the general population.
Swati G. Patel, MD, MS, director of the Gastrointestinal Hereditary Cancer Program at the University of Colorado Anschutz Medical Center, Denver, said the Kaiser study is important because its data was aggregated after the US Preventive Services Task Force lowered the screening age in 2021.
The Kaiser research “validates the initial studies” done to support that recommendation and the 2022 consensus statement by the US Multi-Society Task Force on Colorectal Cancer, which also advocated screening in 45- to 49-year-olds.
Even though the new JAMA study found a similar rate of cancers and precursor lesions as in previous trials, it provides “reinforcement of the rationale for decreasing the screening age,” Patel, the lead author on the consensus statement, told GI & Hepatology News.
The Kaiser research is “really powerful information,” she said.
“It certainly validates our current guidance to start screening for colorectal cancer at age 45,” said Audrey Calderwood, MD, director of the GI Cancer Risk and Prevention Clinic at the Geisel School of Medicine, Dartmouth, New Hampshire.
The Kaiser data provides granular information to share with younger patients who might think that they don’t need screening because they are healthy and don’t have symptoms, said Calderwood, also director of the Comprehensive Gastroenterology Center at Dartmouth Hitchcock Medical Center.
Colon cancer rates for Americans under age 50 have been steadily rising for the past decade, hitting about 10 cases per 100,000 in 2022, according to the National Cancer Institute (NCI). In 2023, about 73% of eligible 50- to 75-year-olds received colorectal cancer screening based on the most recent guidelines, according to the NCI.
But screening rates in the under-50 age group are much lower. Researchers estimated in a study that only about 34.5% of those aged 45-49 received colorectal cancer screening, which included colonoscopy, stool-based tests, and CT colonography.
Patel said that estimate is “spot on” in terms of other estimates.
“I think there’s a perception that it’s a cancer of older adults and that young healthy people don’t need to worry about it,” she said, adding that getting the word out to younger Americans is a “PR challenge,” in part because of squeamishness about discussing anything to do with stool and changes in how they access information.
Calderwood agreed. Younger people “aren’t chatting to their friends about” colon cancer screening the way they might about mammography, said Calderwood.
Both she and Patel noted that educating the public was an ongoing project, but that a physician’s recommendation was key.
Patel said she hoped that data provided in the Kaiser study might help “dismantle the systemic skepticism around decreasing the age recommendation” for screening.
Calderwood and Patel reported having no relevant financial relationships.
A version of this article appeared on Medscape.com.
Novel Gene Risk Score Predicts Outcomes After RYGB Surgery
SAN DIEGO –
The findings suggested that the MyPhenome test (Phenomix Sciences) can help clinicians identify the patients most likely to benefit from bariatric procedures and at a greater risk for long-term weight regain after surgery.
“Patients with both a high genetic risk score and rare mutations in the leptin-melanocortin pathway (LMP) had significantly worse outcomes, maintaining only 4.9% total body weight loss [TBWL] over 15 years compared to up to 24.8% in other genetic groups,” Phenomix Sciences Co-founder Andres Acosta, MD, PhD, told GI & Hepatology News.

The study included details on the score’s development and predictive capability. It was presented at Digestive Disease Week® (DDW) 2025
‘More Precise Bariatric Care’
The researchers recently developed a machine learning-assisted gene risk score for calories to satiation (CTSGRS), which mainly involves genes in the LMP. To assess the role of the score with or without LMP gene variants on weight loss and weight recurrence after RYGB, they identified 707 patients with a history of bariatric procedures from the Mayo Clinic Biobank. Patients with duodenal switch, revisional procedures, or who used antiobesity medications or became pregnant during follow-up were excluded.
To make predictions for 442 of the patients, the team first collected anthropometric data up to 15 years after RYGB. Then they used a two-step approach: Assessing for monogenic variants in the LMP and defining participants as carriers (LMP+) or noncarriers (LMP-). Then they defined the gene risk score (CTSGRS+ or CTSGRS-).
The result was four groups: LMP+/CTSGRS+, LMP+/CTSGRS-, LMP-/CTSGRS+, and LMP-/CTSGRS-. Multiple regression analysis was used to analyze TBWL percentage (TBWL%) between the groups at different timepoints, adjusting for baseline weight, age, and gender.
At the 10-year follow-up, the LMP+/CTSGRS+ group demonstrated a significantly higher weight recurrence (regain) of TBW% compared to the other groups.
At 15 years post-RYGB, the mean TBWL% for LMP+/CTSGRS+ was -4.9 vs -20.3 for LMP+/CTSGRS-, -18.0 for LMP-/CTSGRS+, and -24.8 for LMP-/CTSGRS-.
Further analyses showed that the LMP+/CTSGRS+ group had significantly less weight loss than LMP+/CTSGRS- and LMP-/CTSGRS- groups.
Based on the findings, the authors wrote, “Genotyping patients could improve the implementation of individualized weight-loss interventions, enhance weight-loss outcomes, and/or may explain one of the etiological factors associated with weight recurrence after RYGB.”
Acosta noted, “We’re actively expanding our research to include more diverse populations by age, sex, and race. This includes ongoing analysis to understand whether certain demographic or physiological characteristics affect how the test performs, particularly in the context of bariatric surgery.”
The team also is investigating the benefits of phenotyping for obesity comorbidities such as heart disease and diabetes, he said, and exploring whether early interventions in high-risk patients can prevent long-term weight regain and improve outcomes.
In addition, Acosta said, the team recently launched “the first prospective, placebo-controlled clinical trial using the MyPhenome test to predict response to semaglutide.” That study is based on earlier findings showing that patients identified with a Hungry Gut phenotype lost nearly twice as much weight on semaglutide compared with those who tested negative.
Overall, he concluded, “These findings open the door to more precise bariatric care. When we understand a patient’s biological drivers of obesity, we can make better decisions about the right procedure, follow-up, and long-term support. This moves us away from a one-size-fits-all model to care rooted in each patient’s unique biology.”
Potentially Paradigm-Shifting
Onur Kutlu, MD, associate professor of surgery and director of the Metabolic Surgery and Metabolic Health Program at the Miller School of Medicine, University of Miami, in Miami, Florida, commented on the study for GI & Hepatology News. “By integrating polygenic risk scores into predictive models, the authors offer an innovative method for identifying patients at elevated risk for weight regain following RYGB.”
“Their findings support the hypothesis that genetic predisposition — particularly involving energy homeostasis pathways — may underlie differential postoperative trajectories,” he said. “This approach has the potential to shift the paradigm from reactive to proactive management of weight recurrence.”
Because current options for treat weight regain are “suboptimal,” he said, “prevention becomes paramount. Preoperative identification of high-risk individuals could inform surgical decision-making, enable earlier interventions, and facilitate personalized postoperative monitoring and support.”
“If validated in larger, prospective cohorts, genetic risk stratification could enhance the precision of bariatric care and improve long-term outcomes,” he added. “Future studies should aim to validate these genetic models across diverse populations and explore how integration of behavioral, psychological, and genetic data may further refine patient selection and care pathways.”
The study was funded by Mayo Clinic and Phenomix Sciences. Gila Therapeutics and Phenomix Sciences licensed Acosta’s research technologies from the University of Florida and Mayo Clinic. Acosta declared receiving consultant fees in the past 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, BI, Currax, Nestle, Phenomix Sciences, Bausch Health, and RareDiseases, as well as funding support from the National Institutes of Health, Vivus Pharmaceuticals, Novo Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, and Rhythm Pharmaceuticals. Kutlu declared having no conflicts of interest.
A version of this article appeared on Medscape.com.
SAN DIEGO –
The findings suggested that the MyPhenome test (Phenomix Sciences) can help clinicians identify the patients most likely to benefit from bariatric procedures and at a greater risk for long-term weight regain after surgery.
“Patients with both a high genetic risk score and rare mutations in the leptin-melanocortin pathway (LMP) had significantly worse outcomes, maintaining only 4.9% total body weight loss [TBWL] over 15 years compared to up to 24.8% in other genetic groups,” Phenomix Sciences Co-founder Andres Acosta, MD, PhD, told GI & Hepatology News.
The study included details on the score’s development and predictive capability. It was presented at Digestive Disease Week® (DDW) 2025
‘More Precise Bariatric Care’
The researchers recently developed a machine learning-assisted gene risk score for calories to satiation (CTSGRS), which mainly involves genes in the LMP. To assess the role of the score with or without LMP gene variants on weight loss and weight recurrence after RYGB, they identified 707 patients with a history of bariatric procedures from the Mayo Clinic Biobank. Patients with duodenal switch, revisional procedures, or who used antiobesity medications or became pregnant during follow-up were excluded.
To make predictions for 442 of the patients, the team first collected anthropometric data up to 15 years after RYGB. Then they used a two-step approach: Assessing for monogenic variants in the LMP and defining participants as carriers (LMP+) or noncarriers (LMP-). Then they defined the gene risk score (CTSGRS+ or CTSGRS-).
The result was four groups: LMP+/CTSGRS+, LMP+/CTSGRS-, LMP-/CTSGRS+, and LMP-/CTSGRS-. Multiple regression analysis was used to analyze TBWL percentage (TBWL%) between the groups at different timepoints, adjusting for baseline weight, age, and gender.
At the 10-year follow-up, the LMP+/CTSGRS+ group demonstrated a significantly higher weight recurrence (regain) of TBW% compared to the other groups.
At 15 years post-RYGB, the mean TBWL% for LMP+/CTSGRS+ was -4.9 vs -20.3 for LMP+/CTSGRS-, -18.0 for LMP-/CTSGRS+, and -24.8 for LMP-/CTSGRS-.
Further analyses showed that the LMP+/CTSGRS+ group had significantly less weight loss than LMP+/CTSGRS- and LMP-/CTSGRS- groups.
Based on the findings, the authors wrote, “Genotyping patients could improve the implementation of individualized weight-loss interventions, enhance weight-loss outcomes, and/or may explain one of the etiological factors associated with weight recurrence after RYGB.”
Acosta noted, “We’re actively expanding our research to include more diverse populations by age, sex, and race. This includes ongoing analysis to understand whether certain demographic or physiological characteristics affect how the test performs, particularly in the context of bariatric surgery.”
The team also is investigating the benefits of phenotyping for obesity comorbidities such as heart disease and diabetes, he said, and exploring whether early interventions in high-risk patients can prevent long-term weight regain and improve outcomes.
In addition, Acosta said, the team recently launched “the first prospective, placebo-controlled clinical trial using the MyPhenome test to predict response to semaglutide.” That study is based on earlier findings showing that patients identified with a Hungry Gut phenotype lost nearly twice as much weight on semaglutide compared with those who tested negative.
Overall, he concluded, “These findings open the door to more precise bariatric care. When we understand a patient’s biological drivers of obesity, we can make better decisions about the right procedure, follow-up, and long-term support. This moves us away from a one-size-fits-all model to care rooted in each patient’s unique biology.”
Potentially Paradigm-Shifting
Onur Kutlu, MD, associate professor of surgery and director of the Metabolic Surgery and Metabolic Health Program at the Miller School of Medicine, University of Miami, in Miami, Florida, commented on the study for GI & Hepatology News. “By integrating polygenic risk scores into predictive models, the authors offer an innovative method for identifying patients at elevated risk for weight regain following RYGB.”
“Their findings support the hypothesis that genetic predisposition — particularly involving energy homeostasis pathways — may underlie differential postoperative trajectories,” he said. “This approach has the potential to shift the paradigm from reactive to proactive management of weight recurrence.”
Because current options for treat weight regain are “suboptimal,” he said, “prevention becomes paramount. Preoperative identification of high-risk individuals could inform surgical decision-making, enable earlier interventions, and facilitate personalized postoperative monitoring and support.”
“If validated in larger, prospective cohorts, genetic risk stratification could enhance the precision of bariatric care and improve long-term outcomes,” he added. “Future studies should aim to validate these genetic models across diverse populations and explore how integration of behavioral, psychological, and genetic data may further refine patient selection and care pathways.”
The study was funded by Mayo Clinic and Phenomix Sciences. Gila Therapeutics and Phenomix Sciences licensed Acosta’s research technologies from the University of Florida and Mayo Clinic. Acosta declared receiving consultant fees in the past 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, BI, Currax, Nestle, Phenomix Sciences, Bausch Health, and RareDiseases, as well as funding support from the National Institutes of Health, Vivus Pharmaceuticals, Novo Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, and Rhythm Pharmaceuticals. Kutlu declared having no conflicts of interest.
A version of this article appeared on Medscape.com.
SAN DIEGO –
The findings suggested that the MyPhenome test (Phenomix Sciences) can help clinicians identify the patients most likely to benefit from bariatric procedures and at a greater risk for long-term weight regain after surgery.
“Patients with both a high genetic risk score and rare mutations in the leptin-melanocortin pathway (LMP) had significantly worse outcomes, maintaining only 4.9% total body weight loss [TBWL] over 15 years compared to up to 24.8% in other genetic groups,” Phenomix Sciences Co-founder Andres Acosta, MD, PhD, told GI & Hepatology News.
The study included details on the score’s development and predictive capability. It was presented at Digestive Disease Week® (DDW) 2025
‘More Precise Bariatric Care’
The researchers recently developed a machine learning-assisted gene risk score for calories to satiation (CTSGRS), which mainly involves genes in the LMP. To assess the role of the score with or without LMP gene variants on weight loss and weight recurrence after RYGB, they identified 707 patients with a history of bariatric procedures from the Mayo Clinic Biobank. Patients with duodenal switch, revisional procedures, or who used antiobesity medications or became pregnant during follow-up were excluded.
To make predictions for 442 of the patients, the team first collected anthropometric data up to 15 years after RYGB. Then they used a two-step approach: Assessing for monogenic variants in the LMP and defining participants as carriers (LMP+) or noncarriers (LMP-). Then they defined the gene risk score (CTSGRS+ or CTSGRS-).
The result was four groups: LMP+/CTSGRS+, LMP+/CTSGRS-, LMP-/CTSGRS+, and LMP-/CTSGRS-. Multiple regression analysis was used to analyze TBWL percentage (TBWL%) between the groups at different timepoints, adjusting for baseline weight, age, and gender.
At the 10-year follow-up, the LMP+/CTSGRS+ group demonstrated a significantly higher weight recurrence (regain) of TBW% compared to the other groups.
At 15 years post-RYGB, the mean TBWL% for LMP+/CTSGRS+ was -4.9 vs -20.3 for LMP+/CTSGRS-, -18.0 for LMP-/CTSGRS+, and -24.8 for LMP-/CTSGRS-.
Further analyses showed that the LMP+/CTSGRS+ group had significantly less weight loss than LMP+/CTSGRS- and LMP-/CTSGRS- groups.
Based on the findings, the authors wrote, “Genotyping patients could improve the implementation of individualized weight-loss interventions, enhance weight-loss outcomes, and/or may explain one of the etiological factors associated with weight recurrence after RYGB.”
Acosta noted, “We’re actively expanding our research to include more diverse populations by age, sex, and race. This includes ongoing analysis to understand whether certain demographic or physiological characteristics affect how the test performs, particularly in the context of bariatric surgery.”
The team also is investigating the benefits of phenotyping for obesity comorbidities such as heart disease and diabetes, he said, and exploring whether early interventions in high-risk patients can prevent long-term weight regain and improve outcomes.
In addition, Acosta said, the team recently launched “the first prospective, placebo-controlled clinical trial using the MyPhenome test to predict response to semaglutide.” That study is based on earlier findings showing that patients identified with a Hungry Gut phenotype lost nearly twice as much weight on semaglutide compared with those who tested negative.
Overall, he concluded, “These findings open the door to more precise bariatric care. When we understand a patient’s biological drivers of obesity, we can make better decisions about the right procedure, follow-up, and long-term support. This moves us away from a one-size-fits-all model to care rooted in each patient’s unique biology.”
Potentially Paradigm-Shifting
Onur Kutlu, MD, associate professor of surgery and director of the Metabolic Surgery and Metabolic Health Program at the Miller School of Medicine, University of Miami, in Miami, Florida, commented on the study for GI & Hepatology News. “By integrating polygenic risk scores into predictive models, the authors offer an innovative method for identifying patients at elevated risk for weight regain following RYGB.”
“Their findings support the hypothesis that genetic predisposition — particularly involving energy homeostasis pathways — may underlie differential postoperative trajectories,” he said. “This approach has the potential to shift the paradigm from reactive to proactive management of weight recurrence.”
Because current options for treat weight regain are “suboptimal,” he said, “prevention becomes paramount. Preoperative identification of high-risk individuals could inform surgical decision-making, enable earlier interventions, and facilitate personalized postoperative monitoring and support.”
“If validated in larger, prospective cohorts, genetic risk stratification could enhance the precision of bariatric care and improve long-term outcomes,” he added. “Future studies should aim to validate these genetic models across diverse populations and explore how integration of behavioral, psychological, and genetic data may further refine patient selection and care pathways.”
The study was funded by Mayo Clinic and Phenomix Sciences. Gila Therapeutics and Phenomix Sciences licensed Acosta’s research technologies from the University of Florida and Mayo Clinic. Acosta declared receiving consultant fees in the past 5 years from Rhythm Pharmaceuticals, Gila Therapeutics, Amgen, General Mills, BI, Currax, Nestle, Phenomix Sciences, Bausch Health, and RareDiseases, as well as funding support from the National Institutes of Health, Vivus Pharmaceuticals, Novo Nordisk, Apollo Endosurgery, Satiogen Pharmaceuticals, Spatz Medical, and Rhythm Pharmaceuticals. Kutlu declared having no conflicts of interest.
A version of this article appeared on Medscape.com.
FROM DDW 2025