User login
Sunshine Act – a reminder
Last year, when the Physician Payment Sunshine Act became law, I recommended that all physicians involved in any sort of financial relationship with the pharmaceutical industry review the data reported about them prior to public posting of the information. Since that posting is due to occur at the end of this month, a reminder is in order.
Under a new bureaucracy created by the Affordable Care Act – formally called the Open Payments program – all manufacturers of drugs, devices, and medical supplies covered by federal health care programs must report any financial interactions with physicians and teaching hospitals to the Centers for Medicare & Medicaid Services (CMS).
Reportable interactions include consulting; food; ownership or investment interest; direct compensation for speakers at education programs; and research. Compensation for conducting clinical trials must be reported, but will not be posted on the website until the product receives approval from the Food and Drug Administration or until 4 years after the payment, whichever is earlier. Payments for trials involving a new indication for an approved drug will be posted immediately.
There are a number of specific exclusions, such as certified and accredited continuing medical education activities funded by manufacturers, and product samples for patient use. Medical students and residents are excluded entirely.
Under the law, you are allowed to review your data and seek corrections before it is published. Publication is scheduled to occur on Sept. 30, so if you have not yet done this, there is no time to waste. Although you will have an additional 2 years to pursue corrections after the online content goes live, any erroneous information will remain on the site until corrections can be made, so the best time to find and fix errors is now.
If you don’t see drug reps, accept sponsored lunches, or give sponsored talks, don’t assume that you won’t be on the website. Check anyway; you might be indirectly involved in a compensation situation that you were not aware of, or you may have been reported in error.
To review your data, register at the CMS Enterprise Portal, and request access to the Open Payments system.
Once you are satisfied that your interactions have been reported accurately, the question of what effect the law will have on research, continuing education, and private practice remains. The short answer is that no one knows. Much will depend on how the public interprets the data – if they take notice at all.
Sunshine laws have been in effect for several years in six states: California, Colorado, Massachusetts, Minnesota, Vermont, and West Virginia; plus the District of Columbia. (Maine repealed its law in 2011.) Observers disagree on their impact. Studies in Maine and West Virginia showed no significant public reaction or changes in prescribing patterns, according to a 2012 article in Archives of Internal Medicine (Arch. Intern. Med. 2012;172:819-21).
Potential effects on physician-patient interactions are equally unclear. Do patients think less of doctors who accept the occasional industry-sponsored lunch for their employees? Do they think more of doctors who speak at meetings or conduct industry-sponsored clinical research? There are no objective data, as far as I know.
My guess is that attorneys, activists, and the occasional reporter will data-mine the website on a regular basis, and perhaps use their findings as ammunition in any agenda that they might be pushing, but few patients will ever bother to visit. Nevertheless, you should review each year’s reportage to ensure the accuracy of anything posted about you.
The data must be reported to CMS by March 31 each year, so you will need to set aside time each April or May to review it. If you have many or complex industry relationships, you should probably contact each company in January or February and ask to see the data before it is submitted. Then, review it again once CMS gets it, to be sure nothing was changed. A free app is available to help physicians track payments and other reportable industry interactions; search for "Open Payments" at your favorite app store.
Maintaining accurate financial records has always been important, but it will be even more so now, to effectively dispute any inconsistencies. While the extra work may turn out to have been unnecessary, it is still a prudent precaution, given the possible consequences of any increased government or public scrutiny that may (or may not) result.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
Last year, when the Physician Payment Sunshine Act became law, I recommended that all physicians involved in any sort of financial relationship with the pharmaceutical industry review the data reported about them prior to public posting of the information. Since that posting is due to occur at the end of this month, a reminder is in order.
Under a new bureaucracy created by the Affordable Care Act – formally called the Open Payments program – all manufacturers of drugs, devices, and medical supplies covered by federal health care programs must report any financial interactions with physicians and teaching hospitals to the Centers for Medicare & Medicaid Services (CMS).
Reportable interactions include consulting; food; ownership or investment interest; direct compensation for speakers at education programs; and research. Compensation for conducting clinical trials must be reported, but will not be posted on the website until the product receives approval from the Food and Drug Administration or until 4 years after the payment, whichever is earlier. Payments for trials involving a new indication for an approved drug will be posted immediately.
There are a number of specific exclusions, such as certified and accredited continuing medical education activities funded by manufacturers, and product samples for patient use. Medical students and residents are excluded entirely.
Under the law, you are allowed to review your data and seek corrections before it is published. Publication is scheduled to occur on Sept. 30, so if you have not yet done this, there is no time to waste. Although you will have an additional 2 years to pursue corrections after the online content goes live, any erroneous information will remain on the site until corrections can be made, so the best time to find and fix errors is now.
If you don’t see drug reps, accept sponsored lunches, or give sponsored talks, don’t assume that you won’t be on the website. Check anyway; you might be indirectly involved in a compensation situation that you were not aware of, or you may have been reported in error.
To review your data, register at the CMS Enterprise Portal, and request access to the Open Payments system.
Once you are satisfied that your interactions have been reported accurately, the question of what effect the law will have on research, continuing education, and private practice remains. The short answer is that no one knows. Much will depend on how the public interprets the data – if they take notice at all.
Sunshine laws have been in effect for several years in six states: California, Colorado, Massachusetts, Minnesota, Vermont, and West Virginia; plus the District of Columbia. (Maine repealed its law in 2011.) Observers disagree on their impact. Studies in Maine and West Virginia showed no significant public reaction or changes in prescribing patterns, according to a 2012 article in Archives of Internal Medicine (Arch. Intern. Med. 2012;172:819-21).
Potential effects on physician-patient interactions are equally unclear. Do patients think less of doctors who accept the occasional industry-sponsored lunch for their employees? Do they think more of doctors who speak at meetings or conduct industry-sponsored clinical research? There are no objective data, as far as I know.
My guess is that attorneys, activists, and the occasional reporter will data-mine the website on a regular basis, and perhaps use their findings as ammunition in any agenda that they might be pushing, but few patients will ever bother to visit. Nevertheless, you should review each year’s reportage to ensure the accuracy of anything posted about you.
The data must be reported to CMS by March 31 each year, so you will need to set aside time each April or May to review it. If you have many or complex industry relationships, you should probably contact each company in January or February and ask to see the data before it is submitted. Then, review it again once CMS gets it, to be sure nothing was changed. A free app is available to help physicians track payments and other reportable industry interactions; search for "Open Payments" at your favorite app store.
Maintaining accurate financial records has always been important, but it will be even more so now, to effectively dispute any inconsistencies. While the extra work may turn out to have been unnecessary, it is still a prudent precaution, given the possible consequences of any increased government or public scrutiny that may (or may not) result.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
Last year, when the Physician Payment Sunshine Act became law, I recommended that all physicians involved in any sort of financial relationship with the pharmaceutical industry review the data reported about them prior to public posting of the information. Since that posting is due to occur at the end of this month, a reminder is in order.
Under a new bureaucracy created by the Affordable Care Act – formally called the Open Payments program – all manufacturers of drugs, devices, and medical supplies covered by federal health care programs must report any financial interactions with physicians and teaching hospitals to the Centers for Medicare & Medicaid Services (CMS).
Reportable interactions include consulting; food; ownership or investment interest; direct compensation for speakers at education programs; and research. Compensation for conducting clinical trials must be reported, but will not be posted on the website until the product receives approval from the Food and Drug Administration or until 4 years after the payment, whichever is earlier. Payments for trials involving a new indication for an approved drug will be posted immediately.
There are a number of specific exclusions, such as certified and accredited continuing medical education activities funded by manufacturers, and product samples for patient use. Medical students and residents are excluded entirely.
Under the law, you are allowed to review your data and seek corrections before it is published. Publication is scheduled to occur on Sept. 30, so if you have not yet done this, there is no time to waste. Although you will have an additional 2 years to pursue corrections after the online content goes live, any erroneous information will remain on the site until corrections can be made, so the best time to find and fix errors is now.
If you don’t see drug reps, accept sponsored lunches, or give sponsored talks, don’t assume that you won’t be on the website. Check anyway; you might be indirectly involved in a compensation situation that you were not aware of, or you may have been reported in error.
To review your data, register at the CMS Enterprise Portal, and request access to the Open Payments system.
Once you are satisfied that your interactions have been reported accurately, the question of what effect the law will have on research, continuing education, and private practice remains. The short answer is that no one knows. Much will depend on how the public interprets the data – if they take notice at all.
Sunshine laws have been in effect for several years in six states: California, Colorado, Massachusetts, Minnesota, Vermont, and West Virginia; plus the District of Columbia. (Maine repealed its law in 2011.) Observers disagree on their impact. Studies in Maine and West Virginia showed no significant public reaction or changes in prescribing patterns, according to a 2012 article in Archives of Internal Medicine (Arch. Intern. Med. 2012;172:819-21).
Potential effects on physician-patient interactions are equally unclear. Do patients think less of doctors who accept the occasional industry-sponsored lunch for their employees? Do they think more of doctors who speak at meetings or conduct industry-sponsored clinical research? There are no objective data, as far as I know.
My guess is that attorneys, activists, and the occasional reporter will data-mine the website on a regular basis, and perhaps use their findings as ammunition in any agenda that they might be pushing, but few patients will ever bother to visit. Nevertheless, you should review each year’s reportage to ensure the accuracy of anything posted about you.
The data must be reported to CMS by March 31 each year, so you will need to set aside time each April or May to review it. If you have many or complex industry relationships, you should probably contact each company in January or February and ask to see the data before it is submitted. Then, review it again once CMS gets it, to be sure nothing was changed. A free app is available to help physicians track payments and other reportable industry interactions; search for "Open Payments" at your favorite app store.
Maintaining accurate financial records has always been important, but it will be even more so now, to effectively dispute any inconsistencies. While the extra work may turn out to have been unnecessary, it is still a prudent precaution, given the possible consequences of any increased government or public scrutiny that may (or may not) result.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.

Common Coding Mistakes Hospitalists Should Avoid

Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
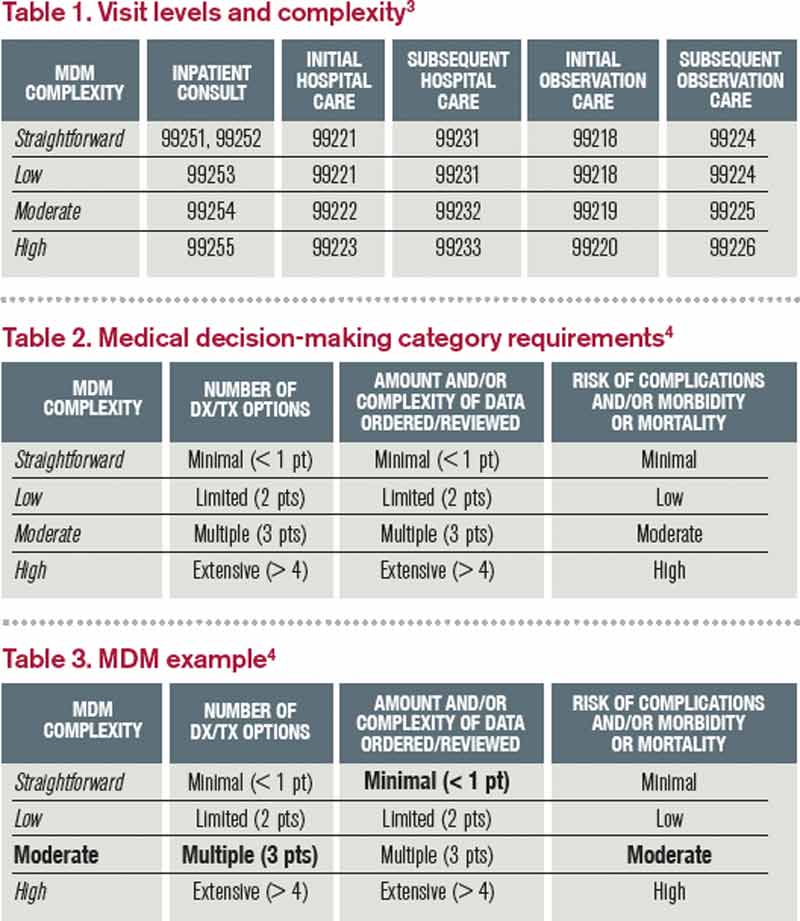
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical Decision-Making: Avoid These Common Coding & Documentation Mistakes
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Medical decision-making (MDM) mistakes are common. Here are the coding and documentation mistakes hospitalists make most often, along with some tips on how to avoid them.
Listing the problem without a plan. Healthcare professionals are able to infer the acuity and severity of a case without superfluous or redundant documentation, but auditors may not have this ability. Adequate documentation for every service date helps to convey patient complexity during a medical record review. Although the problem list may not change dramatically from day to day during a hospitalization, the auditor only reviews the service date in question, not the entire medical record.
Hospitalists should be sure to formulate a complete and accurate description of the patient’s condition with an analogous plan of care for each encounter. Listing problems without a corresponding plan of care does not corroborate physician management of that problem and could cause a downgrade of complexity. Listing problems with a brief, generalized comment (e.g. “DM, CKD, CHF: Continue current treatment plan”) equally diminishes the complexity and effort put forth by the physician.
Clearly document the plan. The care plan represents problems the physician personally manages, along with those that must also be considered when he or she formulates the management options, even if another physician is primarily managing the problem. For example, the hospitalist can monitor the patient’s diabetic management while the nephrologist oversees the chronic kidney disease (CKD). Since the CKD impacts the hospitalist’s diabetic care plan, the hospitalist may also receive credit for any CKD consideration if the documentation supports a hospitalist-related care plan, or comment about CKD that does not overlap or replicate the nephrologist’s plan. In other words, there must be some “value-added” input by the hospitalist.
Credit is given for the quantity of problems addressed as well as the quality. For inpatient care, an established problem is defined as one in which a care plan has been generated by the physician (or same specialty group practice member) during the current hospitalization. Established problems are less complex than new problems, for which a diagnosis, prognosis, or care plan has not been developed. Severity of the problem also influences complexity. A “worsening” problem is considered more complex than an “improving” problem, since the worsening problem likely requires revisions to the current care plan and, thus, more physician effort. Physician documentation should always:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined;
- Indicate the management/treatment option(s) for each problem; and
- Note management options to be continued somewhere in the progress note for that encounter (e.g. medication list) when documentation indicates a continuation of current management options (e.g. “continue meds”).
Considering relevant data. “Data” is organized as pathology/laboratory testing, radiology, and medicine-based diagnostic testing that contributes to diagnosing or managing patient problems. Pertinent orders or results may appear in the medical record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note. To receive credit:
- Specify tests ordered and rationale in the physician’s progress note, or make an entry that refers to another auditor-accessible location for ordered tests and studies; however, this latter option jeopardizes a medical record review due to potential lack of awareness of the need to submit this extraneous information during a payer record request or appeal.
- Document test review by including a brief entry in the progress note (e.g. “elevated glucose levels” or “CXR shows RLL infiltrates”); credit is not given for entries lacking a comment on the findings (e.g. “CXR reviewed”).
- Summarize key points when reviewing old records or obtaining history from someone other than the patient, as necessary; be sure to identify the increased efforts of reviewing the considerable number of old records by stating, “OSH (outside hospital) records reviewed and shows…” or “Records from previous hospitalization(s) reveal….”
- Indicate when images, tracings, or specimens are “personally reviewed,” or the auditor will assume the physician merely reviewed the written report; be sure to include a comment on the findings.
- Summarize any discussions of unexpected or contradictory test results with the physician performing the procedure or diagnostic study.
Data credit may be more substantial during the initial investigative phase of the hospitalization, before diagnoses or treatment options have been confirmed. Routine monitoring of the stabilized patient may not yield as many “points.”
Undervaluing the patient’s complexity. A general lack of understanding of the MDM component of the documentation guidelines often results in physicians undervaluing their services. Some physicians may consider a case “low complexity” simply because of the frequency with which they encounter the case type. The speed with which the care plan is developed should have no bearing on how complex the patient’s condition really is. Hospitalists need to better identify the risk involved for the patient.
Patient risk is categorized as minimal, low, moderate, or high based on pre-assigned items pertaining to the presenting problem, diagnostic procedures ordered, and management options selected. The single highest-rated item detected on the Table of Risk determines the overall patient risk for an encounter.1 Chronic conditions with exacerbations and invasive procedures offer more patient risk than acute, uncomplicated illnesses or noninvasive procedures. Stable or improving problems are considered “less risky” than progressing problems; conditions that pose a threat to life/bodily function outweigh undiagnosed problems where it is difficult to determine the patient’s prognosis; and medication risk varies with the administration (e.g. oral vs. parenteral), type, and potential for adverse effects. Medication risk for a particular drug is invariable whether the dosage is increased, decreased, or continued without change. Physicians should:
- Provide status for all problems in the plan of care and identify them as stable, worsening, or progressing (mild or severe), when applicable; don’t assume that the auditor can infer this from the documentation details.
- Document all diagnostic or therapeutic procedures considered.
- Identify surgical risk factors involving co-morbid conditions that place the patient at greater risk than the average patient, when appropriate.
- Associate the labs ordered to monitor for medication toxicity with the corresponding medication; don’t assume that the auditor knows which labs are used to check for toxicity.
Varying levels of complexity. Remember that decision-making is just one of three components in evaluation and management (E&M) services, along with history and exam. MDM is identical for both the 1995 and 1997 guidelines, rooted in the complexity of the patient’s problem(s) addressed during a given encounter.1,2 Complexity is categorized as straightforward, low, moderate, or high, and directly correlates to the content of physician documentation.
Each visit level represents a particular level of complexity (see Table 1). Auditors only consider the care plan for a given service date when reviewing MDM. More specifically, the auditor reviews three areas of MDM for each encounter (see Table 2), and the physician receives credit for: a) the number of diagnoses and/or treatment options; b) the amount and/or complexity of data ordered/reviewed; c) the risk of complications/morbidity/mortality.
To determine MDM complexity, each MDM category is assigned a point level. Complexity correlates to the second-highest MDM category. For example, if the auditor assigns “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician attains moderate complexity decision-making (see Table 3).
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
References
- Centers for Medicare and Medicaid Services. 1995 Documentation Guidelines for Evaluation and Management Services. Available at: www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/95Docguidelines.pdf. Accessed July 7, 2014.
- Centers for Medicare and Medicaid Services. 1997 Documentation Guidelines for Evaluation and Management Services. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed July 7, 2014.
- American Medical Association. Current Procedural Terminology: 2014 Professional Edition. Chicago: American Medical Association; 2013:14-21.
- Novitas Solutions. Novitas Solutions documentation worksheet. Available at: www.novitas-solutions.com/webcenter/content/conn/UCM_Repository/uuid/dDocName:00004966. Accessed July 7, 2014.
Could thorough documentation have changed the outcome of this trial?
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |


Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
| Joseph S. Sanfilippo, MD, MBA Professor, Department of Obstetrics, Gynecology, and Reproductive Sciences, University of Pittsburgh, and Director, Reproductive Endocrinology & Infertility at Magee-Womens Hospital, Pittsburgh, Pennsylvania. He also serves on the OBG Management Board of Editors. |
| Steven R. Smith, JD |
| Shirley M. Pruitt, BSN, JD |
Disclosures
Dr. Sanfilippo reports being on the advisory board for Bayer Healthcare Pharmaceuticals and Smith and Nephew. Mr. Smith and Ms. Pruitt report no financial relationships relevant to this article.
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.
Case: Did the gynecologist have the right to not remove the ovaries?
A 36-year-old woman (G3 P3003) presented to her gynecologist with dysmenorrhea and abnormal uterine bleeding. She reported a family history of ovarian cancer for two generations. She was evaluated and underwent physical examination and preoperative ultrasound examination of pelvic organs. All findings were unremarkable. The gynecologist prescribed oral contraceptives (OCs). After an initial excellent response, the patient reported a reoccurrence of pelvic pain and abnormal bleeding 6 years later. The gynecologist suggested options including operative hysteroscopy, dilatation and curettage (D&C), endometrial ablation, off-label use of an intrauterine contraceptive system, or hysterectomy performed via a minimally invasive, vaginal, or abdominal approach. The patient opted for hysteroscopy, D&C, and endometrial ablation and operative laparoscopy. The patient received a diagnosis of stage I endometriosis, which was treated with fulguration.
Two years later, she reported menorrhagia and pelvic pain. The gynecologist suggested trying an OC again, and the patient was given a prescription for a low-dose estrogen/desogestrel combination pill. The patient then changed her mind within 72 hours, never took the OC, and contacted her gynecologist to schedule surgery with him. Upon a return visit to the office, the patient and gynecologist decided to proceed with laparoscopic-assisted vaginal hysterectomy (LAVH) with bilateral salpingo-oophorectomy (BSO). The written consent included laparoscopic hysterectomy with removal of ovary or ovaries and bilateral fallopian tubes, with a possibility of abdominal hysterectomy.
The gynecologist met with the patient preoperatively to update the history, which was unchanged from her prior office visit. In the operating room, “time out” occurred and was documented appropriately—concerns were to be provided to the gynecologist; none were noted.
Intraoperatively, the ovaries were normal in appearance and no endometriosis was noted. The gynecologist proceeded with LAVH and, because the ovaries were normal, did not remove them or the fallopian tubes.
The patient sued the gynecologist on the grounds that, because the originally planned BSO was not performed, she was fearful of developing ovarian cancer in the future.
Preoperative documentation was “sketchy”at best and did not reflect the preoperative discussion and options presented to the patient. There was no documentation of anyone accompanying the patient at the preoperative office visit.
The case went to trial.
What’s the verdict?
CASE: Final verdict was for the patient
The jury awarded damages to the patient based on the absence of adequate consent and failure to perform what was preoperatively agreed to in the consent form.
Legal takeaways from this case
This is an unusual case. Absent something else, it is unusual for there to be liability for not doing a procedure, where the procedure seemed medically unnecessary based on observations during surgery and where language of the signed written consent form created ambiguity about the plan for the removal of the ovaries. Here the patient alleged that her consent was not “informed.” Although informed consent claims are fairly common in malpractice litigation, they are generally appended to an underlying count (or counts) of negligent care; it is uncommon for there to be recovery of damages based solely on the absence of informed consent.
A signed consent form may not be sufficient. In general, a patient’s signature on a consent form alone is not sufficient evidence of informed consent. Whether the patient was truly informed will be judged by the circumstances during which the patient’s consent was obtained.
State laws vary on the specifics of informed consent. Many states have specific statutes or regulations dealing with informed consent. The “informed” part of informed consent generally requires that the patient be informed of:
- the nature of the procedure proposed
- the risks and benefits of the procedure
- the alternative forms of treatment
- the consequences of not undertaking the proposed procedure or an alternative.
In this case, the lawsuit alleges damages based on the fear of future ovarian cancer. It is likely that the patient offered credible testimony that she decided to proceed with surgery specifically because of her fear of ovarian cancer. The patient may have offered testimony about her specific request for her ovaries to be removed because of this fear, or she may have offered testimony about her belief or understanding that the ovaries were going to be removed based on her preoperative discussion with the gynecologist.
Related article: Sound strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Written consent must reflect the actual preoperative discussion
The written consent stated: “hysterectomy with removal of ovary or ovaries,” creating some ambiguity regarding whether the gynecologist had latitude in deciding whether or not to remove the ovaries. However, certain “facts” in this case scenario support the claim that the written consent form was meant to have reflected a decision and agreement between the doctor and patient that the ovaries were to be removed, including:
- the patient had a significant family history of ovarian cancer, making the fear of future ovarian cancer reasonable
- the patient opted out of a conservative treatment plan within 3 days and asked instead to schedule major surgery.
The gynecologist may have testified that the preoperative discussion included only the possibility of removing the ovaries, to be determined based upon what was observed in the course of the surgery. However, in the case description, we are told that the “preoperative documentation was ‘sketchy’ at best.” The jury may have concluded that the gynecologist did not know the wishes of the patient in the event that the ovaries appeared normal during the surgery.
We also know that when the patient returned to the gynecologist’s office after requesting surgery, a “discussion occurred to ‘proceed with LAVH with BSO.’” If this precise language was noted in the patient’s chart, the jury may have concluded that the gynecologist ignored the patient’s wishes!
A claim that the patient was adequately informed prior to treatment can be difficult to address if the informed consent process has not been adequately documented. Often in litigation the decisive question is not whether the right thing was done but whether that can be demonstrated. This case emphasizes the need for good documentation reflecting the specific discussions with the patient.
Litigation prevention rule #1: Thorough documentationVital elements to document | |
| Preoperative office-visit records
Written consent form
| Operative report
Postoperative office-visit records
|
*In the event of an adverse outcome, your actions will be judged on whether you were acting reasonably and using your best judgment. Your documentation needs to explain in detail what you did and why you did it that way. If what you did was a “variance,” explain why. | |
Clinical takeaways
The importance of a good rapport with patients as well as clear discussion of clinical findings, test results, and options for treatment remains paramount. This includes documentation of discussions, recording of who is present during the discussion (including witnesses), as well as the patient’s response to various treatment offerings.
The informed consent process from the clinician’s perspective should reflect discussion of risks, benefits, alternatives, sequelae of complications, and an appropriate risk of refusal. It is most important to pay attention to detail, and record that detail which will reflect your effort to be thorough. Make sure that the surgical consent form includes the operating physician’s name, the name(s) of the assisting physician(s), and no blank spaces.
Related article: More strategies to avoid malpractice hazards on labor and delivery. Martin L. Gimovsky, MD, and Alexis C. Gimosky, MD (Professional Liability; January 2011)
Open communication plus complete documentation are key
A well-designed history form—without blanks but with documentation of the physical examination and reflection of the impression and plan—can serve to avert litigation. Ideally, the operative report will reflect not only what was done but also the intraoperative decision-making process on the part of the gynecologist. Documentation of the physician’s thoroughness with intraoperative assessment may well avoid acceptance of a case by a patient’s attorney. Most importantly, transparent postoperative discussions with the patient and family detailing what occurred and the intraoperative decision-making process may convince the patient and family that the clinician has nothing to hide and has the patient’s best interest in mind.
WE WANT TO HEAR FROM YOU! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Please include the city and state in which you practice.

HIPAA: One last deadline looms
Last July, I summarized the significant changes in the Health Insurance Portability and Accountability Act (HIPAA). With the last of the deadlines mandated by those changes fast approaching, and a significant enforcement action levied against a dermatology group in the interim, an update is warranted.
The deadline is Sept. 23; by then, all of your business associate (BA) agreements must be modified to reflect the new privacy rules. A recent enforcement action involved a Massachusetts dermatology group that was hit with a substantial fine for violating one of those rules, sending a clear signal from the Centers for Medicare & Medicaid Services (CMS) and its enforcer, the Office for Civil Rights, that these tighter regulations cannot be taken lightly.
The criteria for identifying BAs remain the same: Nonemployees, performing "functions or activities" on behalf of the "covered entity" (your practice), that involve "creating, receiving, maintaining, or transmitting" personal health information (PHI).
Typical BAs include answering and billing services, independent transcriptionists, hardware and software companies, and any other vendors involved in creating or maintaining your medical records. Practice management consultants, attorneys, companies that store or microfilm medical records, and record-shredding services are BAs if they must have direct access to PHI in order to do their jobs.
Mail carriers, package delivery people, cleaning services, copier repairmen, bank employees, and the like are not considered BAs, even though they might conceivably come in contact with PHI on occasion. You are required to use "reasonable diligence" in limiting the PHI that these folks may encounter, but you do not need to enter into written BA agreements with them.
Independent contractors who work within your practice – aestheticians and physical therapists, for example – are not considered BAs either, and do not need to sign a BA agreement; just train them, as you do your employees. (More on HIPAA and OSHA training soon.)
What is new is the additional onus placed on physicians for confidentiality breaches committed by their BAs. It’s not enough to simply have a BA contract; you are expected to use "reasonable diligence" in monitoring the work of your BAs. BAs and their subcontractors are directly responsible for their own actions, but the primary responsibility is yours. Furthermore, you must now assume the worst-case scenario. Previously, when PHI was compromised, you would only have to notify affected patients (and the government) if there was a "significant risk of financial or reputational harm," but now, any incident involving patient records is assumed to be a breach, and must be reported.
Failure to report could subject your practice, as well as the contractor, to significant fines. That is where the Massachusetts group had trouble: It lost a thumb drive containing unencrypted PHI, and was forced to pay a $150,000 fine early this year as a result. There is no excuse for not encrypting HIPAA-protected information; encryption software is cheap, readily available, and easy to use. Had the drive lost in Massachusetts been encrypted, according to the CMS, the incident would not have been considered a breach, because its contents would not have been viewable by the finder. Stay tuned for a list of popular encryption programs. (As always, I have no financial interest in any company or product that I mention in this column.)
Patients have new rights under the new rules as well; they may now restrict any PHI shared with third-party insurers and health plans, if they pay for the services themselves. They also have the right to request copies of their electronic health records. You can bill the costs of responding to such requests. If you have EHRs, work out a system for doing this, because the response time has been decreased from 90 days to 30 – and is even shorter in some states.
If you haven’t yet revised your Notice of Privacy Practices (NPP) to explain your relationships with BAs, and their status under the new rules, do it now. You need to explain the breach notification process, as well as the new patient rights mentioned above. You must post your revised NPP in your office, and make copies available there; but you need not mail a copy to every patient.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
Last July, I summarized the significant changes in the Health Insurance Portability and Accountability Act (HIPAA). With the last of the deadlines mandated by those changes fast approaching, and a significant enforcement action levied against a dermatology group in the interim, an update is warranted.
The deadline is Sept. 23; by then, all of your business associate (BA) agreements must be modified to reflect the new privacy rules. A recent enforcement action involved a Massachusetts dermatology group that was hit with a substantial fine for violating one of those rules, sending a clear signal from the Centers for Medicare & Medicaid Services (CMS) and its enforcer, the Office for Civil Rights, that these tighter regulations cannot be taken lightly.
The criteria for identifying BAs remain the same: Nonemployees, performing "functions or activities" on behalf of the "covered entity" (your practice), that involve "creating, receiving, maintaining, or transmitting" personal health information (PHI).
Typical BAs include answering and billing services, independent transcriptionists, hardware and software companies, and any other vendors involved in creating or maintaining your medical records. Practice management consultants, attorneys, companies that store or microfilm medical records, and record-shredding services are BAs if they must have direct access to PHI in order to do their jobs.
Mail carriers, package delivery people, cleaning services, copier repairmen, bank employees, and the like are not considered BAs, even though they might conceivably come in contact with PHI on occasion. You are required to use "reasonable diligence" in limiting the PHI that these folks may encounter, but you do not need to enter into written BA agreements with them.
Independent contractors who work within your practice – aestheticians and physical therapists, for example – are not considered BAs either, and do not need to sign a BA agreement; just train them, as you do your employees. (More on HIPAA and OSHA training soon.)
What is new is the additional onus placed on physicians for confidentiality breaches committed by their BAs. It’s not enough to simply have a BA contract; you are expected to use "reasonable diligence" in monitoring the work of your BAs. BAs and their subcontractors are directly responsible for their own actions, but the primary responsibility is yours. Furthermore, you must now assume the worst-case scenario. Previously, when PHI was compromised, you would only have to notify affected patients (and the government) if there was a "significant risk of financial or reputational harm," but now, any incident involving patient records is assumed to be a breach, and must be reported.
Failure to report could subject your practice, as well as the contractor, to significant fines. That is where the Massachusetts group had trouble: It lost a thumb drive containing unencrypted PHI, and was forced to pay a $150,000 fine early this year as a result. There is no excuse for not encrypting HIPAA-protected information; encryption software is cheap, readily available, and easy to use. Had the drive lost in Massachusetts been encrypted, according to the CMS, the incident would not have been considered a breach, because its contents would not have been viewable by the finder. Stay tuned for a list of popular encryption programs. (As always, I have no financial interest in any company or product that I mention in this column.)
Patients have new rights under the new rules as well; they may now restrict any PHI shared with third-party insurers and health plans, if they pay for the services themselves. They also have the right to request copies of their electronic health records. You can bill the costs of responding to such requests. If you have EHRs, work out a system for doing this, because the response time has been decreased from 90 days to 30 – and is even shorter in some states.
If you haven’t yet revised your Notice of Privacy Practices (NPP) to explain your relationships with BAs, and their status under the new rules, do it now. You need to explain the breach notification process, as well as the new patient rights mentioned above. You must post your revised NPP in your office, and make copies available there; but you need not mail a copy to every patient.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
Last July, I summarized the significant changes in the Health Insurance Portability and Accountability Act (HIPAA). With the last of the deadlines mandated by those changes fast approaching, and a significant enforcement action levied against a dermatology group in the interim, an update is warranted.
The deadline is Sept. 23; by then, all of your business associate (BA) agreements must be modified to reflect the new privacy rules. A recent enforcement action involved a Massachusetts dermatology group that was hit with a substantial fine for violating one of those rules, sending a clear signal from the Centers for Medicare & Medicaid Services (CMS) and its enforcer, the Office for Civil Rights, that these tighter regulations cannot be taken lightly.
The criteria for identifying BAs remain the same: Nonemployees, performing "functions or activities" on behalf of the "covered entity" (your practice), that involve "creating, receiving, maintaining, or transmitting" personal health information (PHI).
Typical BAs include answering and billing services, independent transcriptionists, hardware and software companies, and any other vendors involved in creating or maintaining your medical records. Practice management consultants, attorneys, companies that store or microfilm medical records, and record-shredding services are BAs if they must have direct access to PHI in order to do their jobs.
Mail carriers, package delivery people, cleaning services, copier repairmen, bank employees, and the like are not considered BAs, even though they might conceivably come in contact with PHI on occasion. You are required to use "reasonable diligence" in limiting the PHI that these folks may encounter, but you do not need to enter into written BA agreements with them.
Independent contractors who work within your practice – aestheticians and physical therapists, for example – are not considered BAs either, and do not need to sign a BA agreement; just train them, as you do your employees. (More on HIPAA and OSHA training soon.)
What is new is the additional onus placed on physicians for confidentiality breaches committed by their BAs. It’s not enough to simply have a BA contract; you are expected to use "reasonable diligence" in monitoring the work of your BAs. BAs and their subcontractors are directly responsible for their own actions, but the primary responsibility is yours. Furthermore, you must now assume the worst-case scenario. Previously, when PHI was compromised, you would only have to notify affected patients (and the government) if there was a "significant risk of financial or reputational harm," but now, any incident involving patient records is assumed to be a breach, and must be reported.
Failure to report could subject your practice, as well as the contractor, to significant fines. That is where the Massachusetts group had trouble: It lost a thumb drive containing unencrypted PHI, and was forced to pay a $150,000 fine early this year as a result. There is no excuse for not encrypting HIPAA-protected information; encryption software is cheap, readily available, and easy to use. Had the drive lost in Massachusetts been encrypted, according to the CMS, the incident would not have been considered a breach, because its contents would not have been viewable by the finder. Stay tuned for a list of popular encryption programs. (As always, I have no financial interest in any company or product that I mention in this column.)
Patients have new rights under the new rules as well; they may now restrict any PHI shared with third-party insurers and health plans, if they pay for the services themselves. They also have the right to request copies of their electronic health records. You can bill the costs of responding to such requests. If you have EHRs, work out a system for doing this, because the response time has been decreased from 90 days to 30 – and is even shorter in some states.
If you haven’t yet revised your Notice of Privacy Practices (NPP) to explain your relationships with BAs, and their status under the new rules, do it now. You need to explain the breach notification process, as well as the new patient rights mentioned above. You must post your revised NPP in your office, and make copies available there; but you need not mail a copy to every patient.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.

Survey: ObGyns’ salaries rose slightly in 2013
The 2014 Medscape Compensation Report surveyed more than 24,000 physicians in 25 specialties. Five percent of respondents were ObGyns, whose mean income rose slightly to $243,000 in 2013 from $242,000 in 2012, up from $220,000 in 2011.1–3 The highest ObGyn earners lived in the Great Lakes and North Central regions.1
Survey findings
Men make more than women. In 2013, male ObGyns reported earning $256,000; female ObGyns reported $229,000 in mean income. However, women felt more satisfied with their salary (47% of women vs 38% of men). Regardless of gender, ObGyns were slightly less happy with their income than all physicians (50% satisfied).1
Among all female physicians, more were employed than self-employed; the opposite was true for male physicians.4 Half of all graduating physicians are now female, and demographics show that 62% of all female physicians are younger than age 45.1
Practice settings are key to income. Sixty percent of ObGyns indicated they would choose medicine again as a career; 43% would choose their own specialty. However, only 25% of ObGyns would make the same decision about practice setting.1
In 2013, employed and self-employed ObGyns reported nearly the same mean income: $243,000 versus $246,000, respectively. However, when broken down by specific practice setting, the highest earners were ObGyns who worked for health-care organizations, at $273,000. Additional 2013 mean earnings ranked by work setting were1:
- multispecialty office-based group practices, $271,000
- single-specialty office-based group practices, $255,000
- hospitals, $228,000
- solo office-based practices, $212,000
- outpatient clinics, $207,000.
In 2013, 49% of employed physicians worked in hospitals or in groups owned by a hospital, while 21% were employed by private groups. Other employment situations included community health centers, corporate laboratories, correction institutions, military bases, and nursing homes.4
ACO participation grows. In 2013, 37% of ObGyns either participated in an Accountable Care Organization (ACO) or planned on joining an ACO within the next year.1 This was an increase from 25% in 2012.2,3
In the most recent report, 2% chose concierge practices (also known as direct primary care) and 5% opted for cash-only practices.1 In 2012, only 1% of ObGyns opted for concierge practices, and 3% for cash-only practices.2,3
Related article: Is private ObGyn practice on its way out? Lucia DiVenere, MA (October 2011)
Employment over private practice? In 2013, physicians were enticed to seek employment by the financial challenges of private practice (38%); not having to be concerned about administrative issues (29%); and working shorter and more regular hours (19%). Other reported benefits of employment were academic opportunities, better life−work balance, more vacation time, and no loss of income during vacation. More than half (53%) of employed physicians who were previously self-employed felt that patient care was superior now that they were employed, and 37% thought it was about the same.4
Related article: Mean income for ObGyns increased in 2012. Deborah Reale (News for your Practice; August 2013)
Career satisfaction
ObGyns were close to the bottom among all physicians (48%) when it came to overall career satisfaction, tied with nephrologists, surgeons, and pulmonologists. The most satisfied physicians were dermatologists (65%); the least satisfied were plastic surgeons (45%).1
What drives you? In 2013, more ObGyns (41%) than all physicians (33%) reported that the most rewarding part of their job was their relationships with patients. Thirty percent of ObGyns chose being good at their jobs; 8% chose making good money; and 2% found nothing rewarding about the job.1
How much patient time do you spend? The majority (58%) of ObGyns reported spending more than 40 hours per week with patients and 16 minutes or less (66%) per patient.1 In 2012, 60% of ObGyn respondents reported spending 16 minutes or less per patient.2,3
Anticipating the effects of the Affordable Care Act
Under the Affordable Care Act (ACA), an organization’s revenue will still be determined largely by the volume generated by physicians. The percentage of ObGyns who saw 50 to 124 patients per week increased from 57% in 2012 to 69% in 2013 (TABLE).1,2
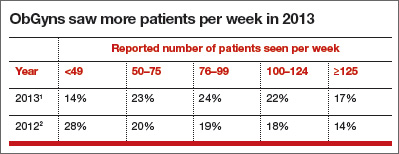
In 2013, 53% of ObGyns still were undecided about health-insurance exchange participation—the same percentage as all survey respondents. Among ObGyns, 30% would participate, and 17% would not participate.1
Related article: As the Affordable Care Act comes of age, a look behind the headlines. Lucia DiVenere, MA (Practice Management; January 2014)
Almost half (49%) of ObGyns expect their income under the ACA to decrease. About 45% of ObGyns did not foresee any change, and 5% believed their incomes would increase (1% didn’t know) under the ACA. ObGyns also anticipated a higher workload, a decline in quality of patient care and access, and reduced ability to make decisions.1
Almost one-third of ObGyns dropped poorly paying insurers. In 2013, 29% of ObGyns said they regularly drop insurers who pay poorly, but 46% said they keep their insurers year after year. In 2012, 26% of ObGyns said they drop insurers who pay the least or create the most trouble; 29% said they keep all insurers.2,3 Private insurance paid for 63% of patient visits to ObGyns in 2013.1
Fewer ObGyns indicated they would see Medicare and Medicaid patients. In 2013, 20% of self-employed and 5% of employed ObGyns said that they plan to stop taking new Medicare or Medicaid patients. More employed (72%) than self-employed (46%) ObGyns reported that they would continue seeing new and current Medicare and Medicaid patients.1
Related article: Medicare and Medicaid are on the brink of insolvency, and you’re not just a bystander. Robert L. Barbieri, MD (Editorial; October 2011)
In 2012, 15% of ObGyn respondents planned to stop taking new Medicare or Medicaid patients, but 53% of ObGyn respondents said they would continue to see current patients and would take on new Medicare or Medicaid patients.2,3
TELL US WHAT YOU THINK! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
- Peckham C. Medscape OB/GYN Compensation Report 2014. Medscape Web site. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 15, 2014. Accessed June 2, 2014.
- Medscape News. Ob/Gyn Compensation Report 2013. Medscape Web site. http://www.medscape.com/features/slideshow/compensation/2013/womenshealth. Accessed June 30, 2013.
- Reale D. Mean income for ObGyns increased in 2012. OBG Manag. 2013;25(8):34–36.
- Kane L. Employed vs self-employed: Who is better off? Medscape Web site. http://www.medscape.com/features/slideshow/public/employed-doctors. Published March 11, 2014. Accessed June 2, 2014.
The 2014 Medscape Compensation Report surveyed more than 24,000 physicians in 25 specialties. Five percent of respondents were ObGyns, whose mean income rose slightly to $243,000 in 2013 from $242,000 in 2012, up from $220,000 in 2011.1–3 The highest ObGyn earners lived in the Great Lakes and North Central regions.1
Survey findings
Men make more than women. In 2013, male ObGyns reported earning $256,000; female ObGyns reported $229,000 in mean income. However, women felt more satisfied with their salary (47% of women vs 38% of men). Regardless of gender, ObGyns were slightly less happy with their income than all physicians (50% satisfied).1
Among all female physicians, more were employed than self-employed; the opposite was true for male physicians.4 Half of all graduating physicians are now female, and demographics show that 62% of all female physicians are younger than age 45.1
Practice settings are key to income. Sixty percent of ObGyns indicated they would choose medicine again as a career; 43% would choose their own specialty. However, only 25% of ObGyns would make the same decision about practice setting.1
In 2013, employed and self-employed ObGyns reported nearly the same mean income: $243,000 versus $246,000, respectively. However, when broken down by specific practice setting, the highest earners were ObGyns who worked for health-care organizations, at $273,000. Additional 2013 mean earnings ranked by work setting were1:
- multispecialty office-based group practices, $271,000
- single-specialty office-based group practices, $255,000
- hospitals, $228,000
- solo office-based practices, $212,000
- outpatient clinics, $207,000.
In 2013, 49% of employed physicians worked in hospitals or in groups owned by a hospital, while 21% were employed by private groups. Other employment situations included community health centers, corporate laboratories, correction institutions, military bases, and nursing homes.4
ACO participation grows. In 2013, 37% of ObGyns either participated in an Accountable Care Organization (ACO) or planned on joining an ACO within the next year.1 This was an increase from 25% in 2012.2,3
In the most recent report, 2% chose concierge practices (also known as direct primary care) and 5% opted for cash-only practices.1 In 2012, only 1% of ObGyns opted for concierge practices, and 3% for cash-only practices.2,3
Related article: Is private ObGyn practice on its way out? Lucia DiVenere, MA (October 2011)
Employment over private practice? In 2013, physicians were enticed to seek employment by the financial challenges of private practice (38%); not having to be concerned about administrative issues (29%); and working shorter and more regular hours (19%). Other reported benefits of employment were academic opportunities, better life−work balance, more vacation time, and no loss of income during vacation. More than half (53%) of employed physicians who were previously self-employed felt that patient care was superior now that they were employed, and 37% thought it was about the same.4
Related article: Mean income for ObGyns increased in 2012. Deborah Reale (News for your Practice; August 2013)
Career satisfaction
ObGyns were close to the bottom among all physicians (48%) when it came to overall career satisfaction, tied with nephrologists, surgeons, and pulmonologists. The most satisfied physicians were dermatologists (65%); the least satisfied were plastic surgeons (45%).1
What drives you? In 2013, more ObGyns (41%) than all physicians (33%) reported that the most rewarding part of their job was their relationships with patients. Thirty percent of ObGyns chose being good at their jobs; 8% chose making good money; and 2% found nothing rewarding about the job.1
How much patient time do you spend? The majority (58%) of ObGyns reported spending more than 40 hours per week with patients and 16 minutes or less (66%) per patient.1 In 2012, 60% of ObGyn respondents reported spending 16 minutes or less per patient.2,3
Anticipating the effects of the Affordable Care Act
Under the Affordable Care Act (ACA), an organization’s revenue will still be determined largely by the volume generated by physicians. The percentage of ObGyns who saw 50 to 124 patients per week increased from 57% in 2012 to 69% in 2013 (TABLE).1,2
In 2013, 53% of ObGyns still were undecided about health-insurance exchange participation—the same percentage as all survey respondents. Among ObGyns, 30% would participate, and 17% would not participate.1
Related article: As the Affordable Care Act comes of age, a look behind the headlines. Lucia DiVenere, MA (Practice Management; January 2014)
Almost half (49%) of ObGyns expect their income under the ACA to decrease. About 45% of ObGyns did not foresee any change, and 5% believed their incomes would increase (1% didn’t know) under the ACA. ObGyns also anticipated a higher workload, a decline in quality of patient care and access, and reduced ability to make decisions.1
Almost one-third of ObGyns dropped poorly paying insurers. In 2013, 29% of ObGyns said they regularly drop insurers who pay poorly, but 46% said they keep their insurers year after year. In 2012, 26% of ObGyns said they drop insurers who pay the least or create the most trouble; 29% said they keep all insurers.2,3 Private insurance paid for 63% of patient visits to ObGyns in 2013.1
Fewer ObGyns indicated they would see Medicare and Medicaid patients. In 2013, 20% of self-employed and 5% of employed ObGyns said that they plan to stop taking new Medicare or Medicaid patients. More employed (72%) than self-employed (46%) ObGyns reported that they would continue seeing new and current Medicare and Medicaid patients.1
Related article: Medicare and Medicaid are on the brink of insolvency, and you’re not just a bystander. Robert L. Barbieri, MD (Editorial; October 2011)
In 2012, 15% of ObGyn respondents planned to stop taking new Medicare or Medicaid patients, but 53% of ObGyn respondents said they would continue to see current patients and would take on new Medicare or Medicaid patients.2,3
TELL US WHAT YOU THINK! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
The 2014 Medscape Compensation Report surveyed more than 24,000 physicians in 25 specialties. Five percent of respondents were ObGyns, whose mean income rose slightly to $243,000 in 2013 from $242,000 in 2012, up from $220,000 in 2011.1–3 The highest ObGyn earners lived in the Great Lakes and North Central regions.1
Survey findings
Men make more than women. In 2013, male ObGyns reported earning $256,000; female ObGyns reported $229,000 in mean income. However, women felt more satisfied with their salary (47% of women vs 38% of men). Regardless of gender, ObGyns were slightly less happy with their income than all physicians (50% satisfied).1
Among all female physicians, more were employed than self-employed; the opposite was true for male physicians.4 Half of all graduating physicians are now female, and demographics show that 62% of all female physicians are younger than age 45.1
Practice settings are key to income. Sixty percent of ObGyns indicated they would choose medicine again as a career; 43% would choose their own specialty. However, only 25% of ObGyns would make the same decision about practice setting.1
In 2013, employed and self-employed ObGyns reported nearly the same mean income: $243,000 versus $246,000, respectively. However, when broken down by specific practice setting, the highest earners were ObGyns who worked for health-care organizations, at $273,000. Additional 2013 mean earnings ranked by work setting were1:
- multispecialty office-based group practices, $271,000
- single-specialty office-based group practices, $255,000
- hospitals, $228,000
- solo office-based practices, $212,000
- outpatient clinics, $207,000.
In 2013, 49% of employed physicians worked in hospitals or in groups owned by a hospital, while 21% were employed by private groups. Other employment situations included community health centers, corporate laboratories, correction institutions, military bases, and nursing homes.4
ACO participation grows. In 2013, 37% of ObGyns either participated in an Accountable Care Organization (ACO) or planned on joining an ACO within the next year.1 This was an increase from 25% in 2012.2,3
In the most recent report, 2% chose concierge practices (also known as direct primary care) and 5% opted for cash-only practices.1 In 2012, only 1% of ObGyns opted for concierge practices, and 3% for cash-only practices.2,3
Related article: Is private ObGyn practice on its way out? Lucia DiVenere, MA (October 2011)
Employment over private practice? In 2013, physicians were enticed to seek employment by the financial challenges of private practice (38%); not having to be concerned about administrative issues (29%); and working shorter and more regular hours (19%). Other reported benefits of employment were academic opportunities, better life−work balance, more vacation time, and no loss of income during vacation. More than half (53%) of employed physicians who were previously self-employed felt that patient care was superior now that they were employed, and 37% thought it was about the same.4
Related article: Mean income for ObGyns increased in 2012. Deborah Reale (News for your Practice; August 2013)
Career satisfaction
ObGyns were close to the bottom among all physicians (48%) when it came to overall career satisfaction, tied with nephrologists, surgeons, and pulmonologists. The most satisfied physicians were dermatologists (65%); the least satisfied were plastic surgeons (45%).1
What drives you? In 2013, more ObGyns (41%) than all physicians (33%) reported that the most rewarding part of their job was their relationships with patients. Thirty percent of ObGyns chose being good at their jobs; 8% chose making good money; and 2% found nothing rewarding about the job.1
How much patient time do you spend? The majority (58%) of ObGyns reported spending more than 40 hours per week with patients and 16 minutes or less (66%) per patient.1 In 2012, 60% of ObGyn respondents reported spending 16 minutes or less per patient.2,3
Anticipating the effects of the Affordable Care Act
Under the Affordable Care Act (ACA), an organization’s revenue will still be determined largely by the volume generated by physicians. The percentage of ObGyns who saw 50 to 124 patients per week increased from 57% in 2012 to 69% in 2013 (TABLE).1,2
In 2013, 53% of ObGyns still were undecided about health-insurance exchange participation—the same percentage as all survey respondents. Among ObGyns, 30% would participate, and 17% would not participate.1
Related article: As the Affordable Care Act comes of age, a look behind the headlines. Lucia DiVenere, MA (Practice Management; January 2014)
Almost half (49%) of ObGyns expect their income under the ACA to decrease. About 45% of ObGyns did not foresee any change, and 5% believed their incomes would increase (1% didn’t know) under the ACA. ObGyns also anticipated a higher workload, a decline in quality of patient care and access, and reduced ability to make decisions.1
Almost one-third of ObGyns dropped poorly paying insurers. In 2013, 29% of ObGyns said they regularly drop insurers who pay poorly, but 46% said they keep their insurers year after year. In 2012, 26% of ObGyns said they drop insurers who pay the least or create the most trouble; 29% said they keep all insurers.2,3 Private insurance paid for 63% of patient visits to ObGyns in 2013.1
Fewer ObGyns indicated they would see Medicare and Medicaid patients. In 2013, 20% of self-employed and 5% of employed ObGyns said that they plan to stop taking new Medicare or Medicaid patients. More employed (72%) than self-employed (46%) ObGyns reported that they would continue seeing new and current Medicare and Medicaid patients.1
Related article: Medicare and Medicaid are on the brink of insolvency, and you’re not just a bystander. Robert L. Barbieri, MD (Editorial; October 2011)
In 2012, 15% of ObGyn respondents planned to stop taking new Medicare or Medicaid patients, but 53% of ObGyn respondents said they would continue to see current patients and would take on new Medicare or Medicaid patients.2,3
TELL US WHAT YOU THINK! Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
- Peckham C. Medscape OB/GYN Compensation Report 2014. Medscape Web site. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 15, 2014. Accessed June 2, 2014.
- Medscape News. Ob/Gyn Compensation Report 2013. Medscape Web site. http://www.medscape.com/features/slideshow/compensation/2013/womenshealth. Accessed June 30, 2013.
- Reale D. Mean income for ObGyns increased in 2012. OBG Manag. 2013;25(8):34–36.
- Kane L. Employed vs self-employed: Who is better off? Medscape Web site. http://www.medscape.com/features/slideshow/public/employed-doctors. Published March 11, 2014. Accessed June 2, 2014.
- Peckham C. Medscape OB/GYN Compensation Report 2014. Medscape Web site. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 15, 2014. Accessed June 2, 2014.
- Medscape News. Ob/Gyn Compensation Report 2013. Medscape Web site. http://www.medscape.com/features/slideshow/compensation/2013/womenshealth. Accessed June 30, 2013.
- Reale D. Mean income for ObGyns increased in 2012. OBG Manag. 2013;25(8):34–36.
- Kane L. Employed vs self-employed: Who is better off? Medscape Web site. http://www.medscape.com/features/slideshow/public/employed-doctors. Published March 11, 2014. Accessed June 2, 2014.

Moving forward with ICD-10: Capitalize on this extra time

Yes, we have been here before. Another day, another delay in implementing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). But, do not expect another postponement. If you are already conducting training sessions to move to the new system come next October, continue to do so. If you have not yet started, now is the time to start. ICD-10-CM is coming to your practice, and it will change everything.
“Why the switch?” you ask?
This change in our diagnostic coding system is required to allow coding for increased specificity in the reporting of diseases and recently recognized conditions as well as to maintain our status with respect to the rest of the world (which has been using ICD-10 for years). It also will be essential to use this coding system with the electronic medical record (EMR), so that meaningful use can be demonstrated more easily. Keep in mind that failure to show meaningful use will lead to penalties in the future. This new system offers improvements over ICD-9-CM in coding primary care encounters, external causes of injury, mental disorders, neoplasms, obstetric complications, and preventive health. It also allows physicians to demonstrate severity of illness in a way that is not possible with ICD-9-CM.
There will be 65,000 more codes than currently exist in ICD-9-CM. No physician will be able to keep all of these code numbers handy, but by making changes to clinician documentation and applying diagnostic coding guidelines correctly within the framework of the new system, the transition will not be onerous. And consider that, while the number of new codes is great, the number of codes used in the typical ObGyn practice will be a fraction of that number.
Related article: As ICD-10 conversion nears, keep these factors in mind to ensure proper reimbursements in 2014. Barbara S. Levy, MD (Audiocast, January 2014)
For ICD-10, documentation is paramount
The most important issue when considering overall coding and practice changes will be recognizing that clinician documentation will be the key to coding the highest level of specificity—and this high level of specificity may be required by most payers when deciding to reimburse for treatments rendered. Complete documentation sets the stage for the severity of illness and should in fact result in fewer denials for medical necessity.
For the new process to work efficiently, however, without a lot of delays due to coders and billers having to get more information from clinician offices before sending out claims, your understanding of and “buy-in” to the more clinically specific documentation will be essential.
To explain, under ICD-9-CM coding, simply documenting amenorrhea was acceptable. But when we switch to ICD-10-CM, documentation will need to specify whether the amenorrhea was primary or secondary. This more specific diagnostic coding will make a difference in the health statistics we collect. These data are used for research and to make decisions about allocation of resources—all essential components to excellent quality patient care.
The codes themselves will look different, which may be why some are resisting the change. Instead of the up to five digits required in ICD-9-CM, ICD-10-CM will require up to seven characters. All of the ICD-10-CM codes begin with a letter, may require a placeholder code of “x” as part of the code number, and the seventh character can be either a number or a letter. For instance, with some ICD-10-CM diagnoses reported by ObGyns, a seventh character might require documentation of the encounter as being initial, subsequent, or a sequel; in other cases, that seventh character will be used to identify which fetus has the problem identified by the diagnostic code.
Related article: The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century. Q&A with Barbara S. Levy, MD (Practice Management; February 2013)
Your understanding, although not a necessity, is best for all involved
In truth, most clinicians are not familiar with code formats and code numbers within our current ICD-9-CM code set. The expectation that you will suddenly become fluent in ICD-10-CM “code speak” is not realistic. But an understanding of the new codes in relation to documentation expectations will go a long way to making this transition as smooth as possible. For instance, when a patient currently presents reporting vaginal pain that is found to be due to erosion of a previously placed mesh, the code 628.31 (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue) is reported. But in ICD-10-CM, the documentation would need to include whether this was an initial encounter and the code would become T83.711A (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue, initial encounter).
Smart search. The good news is that most EMR products will have a “smart search” program available for clinicians to pick the correct code based on the search criteria. The bad news is that you will have to be a bit more exact in the search terms you use to make the process easy. For instance, the patient has pelvic pain but you search only on the term “pain.” That term by itself will result in about 100 codes to select from, and the order of the codes may mean that the correct code for pelvic pain is 25 codes down the list. However, if you instead search on the term “pelvic pain,” the one and only code for this condition will be listed and you can simply select it and move on.
Develop cheat sheets. Health-care professionals who are not using an EMR or some sort of computerized code search program will have a harder time, but the use of multiple paper “cheat sheets” for general gynecology, family planning, surgical cases, urology, infertility, obstetrics, etc., will ease that burden. Practice management staff can develop these forms, built on the codes that are currently being reported by the clinician. Place all of the options to replace the older code on the sheet so the correct selection can be made.
For instance, if the provider previously had reported vaginitis with one code, when we move to ICD-10-CM the code would expand to four code selections based on documentation of acute vaginitis, subacute and chronic vaginitis, acute vulvitis, or subacute and chronic vulvitis. If you only had documented vaginitis in the medical record, this gives you the opportunity to refine the documentation to something more specific that supports selection of the correct code and supports the medical need for management options.
Related article: Dos, don’ts, and dollars: Making the switch to an HER. Neil H. Baum, MD; Paul Kepper, MS. (Practice Management; November 2013)
Take advantage of the extra time
Now that we have a delay in the rollout, take this time to critically examine your documentation styles, and practice selecting ICD-10-CM codes before it counts toward payment or nonpayment of a claim. When the time comes, your practice will be fluent in the new system and there will be no delays in getting claims out the door or payment due to incorrect diagnostic coding. In other words, practice makes perfect.
In fact, some ObGyn practices that were ready for the new system have decided to switch to ICD-10-CM coding as of October 1, 2014. They will code each encounter by reporting both the ICD-9-CM code and the ICD-10-CM code on the revised CMS claim form or electronic billing format that permits dual diagnostic coding. This type of experience will ensure that all physicians and other health-care professionals in the practice have ample opportunity to improve their documentation and make any adjustments before the 2015 deadline.
Related article: The 2014 CPT and Medicare code changes affecting ObGyn practice. Melanie Witt, RN, CPC, COBGC, MA (Reimbursement Adviser; January 2014)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Yes, we have been here before. Another day, another delay in implementing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). But, do not expect another postponement. If you are already conducting training sessions to move to the new system come next October, continue to do so. If you have not yet started, now is the time to start. ICD-10-CM is coming to your practice, and it will change everything.
“Why the switch?” you ask?
This change in our diagnostic coding system is required to allow coding for increased specificity in the reporting of diseases and recently recognized conditions as well as to maintain our status with respect to the rest of the world (which has been using ICD-10 for years). It also will be essential to use this coding system with the electronic medical record (EMR), so that meaningful use can be demonstrated more easily. Keep in mind that failure to show meaningful use will lead to penalties in the future. This new system offers improvements over ICD-9-CM in coding primary care encounters, external causes of injury, mental disorders, neoplasms, obstetric complications, and preventive health. It also allows physicians to demonstrate severity of illness in a way that is not possible with ICD-9-CM.
There will be 65,000 more codes than currently exist in ICD-9-CM. No physician will be able to keep all of these code numbers handy, but by making changes to clinician documentation and applying diagnostic coding guidelines correctly within the framework of the new system, the transition will not be onerous. And consider that, while the number of new codes is great, the number of codes used in the typical ObGyn practice will be a fraction of that number.
Related article: As ICD-10 conversion nears, keep these factors in mind to ensure proper reimbursements in 2014. Barbara S. Levy, MD (Audiocast, January 2014)
For ICD-10, documentation is paramount
The most important issue when considering overall coding and practice changes will be recognizing that clinician documentation will be the key to coding the highest level of specificity—and this high level of specificity may be required by most payers when deciding to reimburse for treatments rendered. Complete documentation sets the stage for the severity of illness and should in fact result in fewer denials for medical necessity.
For the new process to work efficiently, however, without a lot of delays due to coders and billers having to get more information from clinician offices before sending out claims, your understanding of and “buy-in” to the more clinically specific documentation will be essential.
To explain, under ICD-9-CM coding, simply documenting amenorrhea was acceptable. But when we switch to ICD-10-CM, documentation will need to specify whether the amenorrhea was primary or secondary. This more specific diagnostic coding will make a difference in the health statistics we collect. These data are used for research and to make decisions about allocation of resources—all essential components to excellent quality patient care.
The codes themselves will look different, which may be why some are resisting the change. Instead of the up to five digits required in ICD-9-CM, ICD-10-CM will require up to seven characters. All of the ICD-10-CM codes begin with a letter, may require a placeholder code of “x” as part of the code number, and the seventh character can be either a number or a letter. For instance, with some ICD-10-CM diagnoses reported by ObGyns, a seventh character might require documentation of the encounter as being initial, subsequent, or a sequel; in other cases, that seventh character will be used to identify which fetus has the problem identified by the diagnostic code.
Related article: The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century. Q&A with Barbara S. Levy, MD (Practice Management; February 2013)
Your understanding, although not a necessity, is best for all involved
In truth, most clinicians are not familiar with code formats and code numbers within our current ICD-9-CM code set. The expectation that you will suddenly become fluent in ICD-10-CM “code speak” is not realistic. But an understanding of the new codes in relation to documentation expectations will go a long way to making this transition as smooth as possible. For instance, when a patient currently presents reporting vaginal pain that is found to be due to erosion of a previously placed mesh, the code 628.31 (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue) is reported. But in ICD-10-CM, the documentation would need to include whether this was an initial encounter and the code would become T83.711A (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue, initial encounter).
Smart search. The good news is that most EMR products will have a “smart search” program available for clinicians to pick the correct code based on the search criteria. The bad news is that you will have to be a bit more exact in the search terms you use to make the process easy. For instance, the patient has pelvic pain but you search only on the term “pain.” That term by itself will result in about 100 codes to select from, and the order of the codes may mean that the correct code for pelvic pain is 25 codes down the list. However, if you instead search on the term “pelvic pain,” the one and only code for this condition will be listed and you can simply select it and move on.
Develop cheat sheets. Health-care professionals who are not using an EMR or some sort of computerized code search program will have a harder time, but the use of multiple paper “cheat sheets” for general gynecology, family planning, surgical cases, urology, infertility, obstetrics, etc., will ease that burden. Practice management staff can develop these forms, built on the codes that are currently being reported by the clinician. Place all of the options to replace the older code on the sheet so the correct selection can be made.
For instance, if the provider previously had reported vaginitis with one code, when we move to ICD-10-CM the code would expand to four code selections based on documentation of acute vaginitis, subacute and chronic vaginitis, acute vulvitis, or subacute and chronic vulvitis. If you only had documented vaginitis in the medical record, this gives you the opportunity to refine the documentation to something more specific that supports selection of the correct code and supports the medical need for management options.
Related article: Dos, don’ts, and dollars: Making the switch to an HER. Neil H. Baum, MD; Paul Kepper, MS. (Practice Management; November 2013)
Take advantage of the extra time
Now that we have a delay in the rollout, take this time to critically examine your documentation styles, and practice selecting ICD-10-CM codes before it counts toward payment or nonpayment of a claim. When the time comes, your practice will be fluent in the new system and there will be no delays in getting claims out the door or payment due to incorrect diagnostic coding. In other words, practice makes perfect.
In fact, some ObGyn practices that were ready for the new system have decided to switch to ICD-10-CM coding as of October 1, 2014. They will code each encounter by reporting both the ICD-9-CM code and the ICD-10-CM code on the revised CMS claim form or electronic billing format that permits dual diagnostic coding. This type of experience will ensure that all physicians and other health-care professionals in the practice have ample opportunity to improve their documentation and make any adjustments before the 2015 deadline.
Related article: The 2014 CPT and Medicare code changes affecting ObGyn practice. Melanie Witt, RN, CPC, COBGC, MA (Reimbursement Adviser; January 2014)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Yes, we have been here before. Another day, another delay in implementing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). But, do not expect another postponement. If you are already conducting training sessions to move to the new system come next October, continue to do so. If you have not yet started, now is the time to start. ICD-10-CM is coming to your practice, and it will change everything.
“Why the switch?” you ask?
This change in our diagnostic coding system is required to allow coding for increased specificity in the reporting of diseases and recently recognized conditions as well as to maintain our status with respect to the rest of the world (which has been using ICD-10 for years). It also will be essential to use this coding system with the electronic medical record (EMR), so that meaningful use can be demonstrated more easily. Keep in mind that failure to show meaningful use will lead to penalties in the future. This new system offers improvements over ICD-9-CM in coding primary care encounters, external causes of injury, mental disorders, neoplasms, obstetric complications, and preventive health. It also allows physicians to demonstrate severity of illness in a way that is not possible with ICD-9-CM.
There will be 65,000 more codes than currently exist in ICD-9-CM. No physician will be able to keep all of these code numbers handy, but by making changes to clinician documentation and applying diagnostic coding guidelines correctly within the framework of the new system, the transition will not be onerous. And consider that, while the number of new codes is great, the number of codes used in the typical ObGyn practice will be a fraction of that number.
Related article: As ICD-10 conversion nears, keep these factors in mind to ensure proper reimbursements in 2014. Barbara S. Levy, MD (Audiocast, January 2014)
For ICD-10, documentation is paramount
The most important issue when considering overall coding and practice changes will be recognizing that clinician documentation will be the key to coding the highest level of specificity—and this high level of specificity may be required by most payers when deciding to reimburse for treatments rendered. Complete documentation sets the stage for the severity of illness and should in fact result in fewer denials for medical necessity.
For the new process to work efficiently, however, without a lot of delays due to coders and billers having to get more information from clinician offices before sending out claims, your understanding of and “buy-in” to the more clinically specific documentation will be essential.
To explain, under ICD-9-CM coding, simply documenting amenorrhea was acceptable. But when we switch to ICD-10-CM, documentation will need to specify whether the amenorrhea was primary or secondary. This more specific diagnostic coding will make a difference in the health statistics we collect. These data are used for research and to make decisions about allocation of resources—all essential components to excellent quality patient care.
The codes themselves will look different, which may be why some are resisting the change. Instead of the up to five digits required in ICD-9-CM, ICD-10-CM will require up to seven characters. All of the ICD-10-CM codes begin with a letter, may require a placeholder code of “x” as part of the code number, and the seventh character can be either a number or a letter. For instance, with some ICD-10-CM diagnoses reported by ObGyns, a seventh character might require documentation of the encounter as being initial, subsequent, or a sequel; in other cases, that seventh character will be used to identify which fetus has the problem identified by the diagnostic code.
Related article: The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century. Q&A with Barbara S. Levy, MD (Practice Management; February 2013)
Your understanding, although not a necessity, is best for all involved
In truth, most clinicians are not familiar with code formats and code numbers within our current ICD-9-CM code set. The expectation that you will suddenly become fluent in ICD-10-CM “code speak” is not realistic. But an understanding of the new codes in relation to documentation expectations will go a long way to making this transition as smooth as possible. For instance, when a patient currently presents reporting vaginal pain that is found to be due to erosion of a previously placed mesh, the code 628.31 (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue) is reported. But in ICD-10-CM, the documentation would need to include whether this was an initial encounter and the code would become T83.711A (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue, initial encounter).
Smart search. The good news is that most EMR products will have a “smart search” program available for clinicians to pick the correct code based on the search criteria. The bad news is that you will have to be a bit more exact in the search terms you use to make the process easy. For instance, the patient has pelvic pain but you search only on the term “pain.” That term by itself will result in about 100 codes to select from, and the order of the codes may mean that the correct code for pelvic pain is 25 codes down the list. However, if you instead search on the term “pelvic pain,” the one and only code for this condition will be listed and you can simply select it and move on.
Develop cheat sheets. Health-care professionals who are not using an EMR or some sort of computerized code search program will have a harder time, but the use of multiple paper “cheat sheets” for general gynecology, family planning, surgical cases, urology, infertility, obstetrics, etc., will ease that burden. Practice management staff can develop these forms, built on the codes that are currently being reported by the clinician. Place all of the options to replace the older code on the sheet so the correct selection can be made.
For instance, if the provider previously had reported vaginitis with one code, when we move to ICD-10-CM the code would expand to four code selections based on documentation of acute vaginitis, subacute and chronic vaginitis, acute vulvitis, or subacute and chronic vulvitis. If you only had documented vaginitis in the medical record, this gives you the opportunity to refine the documentation to something more specific that supports selection of the correct code and supports the medical need for management options.
Related article: Dos, don’ts, and dollars: Making the switch to an HER. Neil H. Baum, MD; Paul Kepper, MS. (Practice Management; November 2013)
Take advantage of the extra time
Now that we have a delay in the rollout, take this time to critically examine your documentation styles, and practice selecting ICD-10-CM codes before it counts toward payment or nonpayment of a claim. When the time comes, your practice will be fluent in the new system and there will be no delays in getting claims out the door or payment due to incorrect diagnostic coding. In other words, practice makes perfect.
In fact, some ObGyn practices that were ready for the new system have decided to switch to ICD-10-CM coding as of October 1, 2014. They will code each encounter by reporting both the ICD-9-CM code and the ICD-10-CM code on the revised CMS claim form or electronic billing format that permits dual diagnostic coding. This type of experience will ensure that all physicians and other health-care professionals in the practice have ample opportunity to improve their documentation and make any adjustments before the 2015 deadline.
Related article: The 2014 CPT and Medicare code changes affecting ObGyn practice. Melanie Witt, RN, CPC, COBGC, MA (Reimbursement Adviser; January 2014)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]

Pre-Order Your State of Hospital Medicine Report Now
The State of Hospital Medicine Report is the authoritative source for hospitalists to compare and contrast their staffing, productivity, and compensation with other HM groups across the country. SHM publishes the State of Hospital Medicine every two years. SHM is accepting pre-orders now. For more information, visit www.hospitalmedicine.org/sohm.
The State of Hospital Medicine Report is the authoritative source for hospitalists to compare and contrast their staffing, productivity, and compensation with other HM groups across the country. SHM publishes the State of Hospital Medicine every two years. SHM is accepting pre-orders now. For more information, visit www.hospitalmedicine.org/sohm.
The State of Hospital Medicine Report is the authoritative source for hospitalists to compare and contrast their staffing, productivity, and compensation with other HM groups across the country. SHM publishes the State of Hospital Medicine every two years. SHM is accepting pre-orders now. For more information, visit www.hospitalmedicine.org/sohm.
Blue towel left in abdomen: $7.2M verdict

Blue towel left in abdomen: $7.2M verdict
When a 61-year-old woman underwent laparoscopic hysterectomy, her gynecologist, Dr. A, was assisted by another gynecologist (Dr. B), a nurse, and a technician. When Dr. A noted that the uterine artery had been injured, he converted to an open procedure, retracted the bowel, repaired the artery, and completed the operation.
Postdischarge, the patient was febrile and developed abdominal pain and an odorous vaginal discharge. A month later, exploratory surgery revealed a retained blue towel that had been used for bowel retraction. The patient required open healing of the surgical wound and a temporary colostomy. She developed an incisional hernia after colostomy reversal, and hernia repair required resection of a small portion of the bowel.
PATIENT’S CLAIM It was negligent to use a blue towel to retract the bowel. The towel should have been removed from her abdomen before closure.
DEFENDANTS’ DEFENSE The technician claimed that she did not provide the towel, did not see the towel used, and that she was not told that the towel had to be tracked. She noted that its color indicated that it lacked a radiopaque tag, and that hospital policy forbade use of untagged towels in an open wound.
Dr. A claimed that he specifically requested a blue towel because it was absorbent, that the technician provided the towel, and that the towel’s use prevented the patient from bleeding to death.
VERDICT A $7.2 million New York verdict was returned against both gynecologists and the hospital as the technician’s employer.
MISCARRIAGE AFTER D&C
A few days after a woman thought she miscarried, her family practi-tioner (FP) performed a dilation and curettage (D&C).
The patient was at work 12 days later when she expelled a fully formed 14-week fetus into a toilet. She was taken to the emergency department (ED), where the cord was cut. Later that day, she passed placental tissue; a repeat D&C was performed the next day.
PATIENT'S CLAIM The FP did not properly perform the first D&C. Although the pathology report was available to the FP prior to the patient’s postoperative visit, the FP failed to inform the patient that no fetal parts had been extracted.
PHYSICIAN’S DEFENSE Because the FP thought that the fetus had been passed prior to the D&C, she believed the pathology report was appropriate.
The patient had been informed of the possibility of retained products of conception after the D&C. The FP had ordered a blood pregnancy test that would have revealed the presence of retained products of conception, but the patient did not have the test. The patient did not contact the FP to report symptoms that felt like labor pains on the day that she passed the fetus.
VERDICT A bench trial resulted in a $51,000 California verdict.
PREGNANT WOMAN COMPLAINS OF LEG PAIN; DIES OF DVT
A 23-year-old woman went to the ED with pain and swelling in her lower left leg and calf. The symptoms were reported to her ObGyn, who examined and then discharged her within a few hours, with instructions to come for her regularly scheduled prenatal visit.
The patient died 2 weeks later. The cause of death was determined to be a pulmonary embolus from a thrombus of the left popliteal vein.
ESTATE’S CLAIM The ObGyn was negligent in failing to test the patient for thrombosis in her left leg when she was in the ED or several days later at the office, when she continued to report leg pain.
PHYSICIAN’S DEFENSE The patient did not have signs of thrombosis at the ED or at the subsequent office visit. The pathologist reported that the clot that caused the embolus appeared fresh. The ObGyn surmised that it had formed after the patient’s last appointment.
VERDICT A Texas defense verdict was returned.

Mother took topiramate; child born with cleft lip and palate: $3M verdict
When a woman learned she was pregnant in December 2007, she was taking topiramate (Topamax) to treat migraine headaches. She discussed tapering off but not discontinuing topiramate usage with her neurologist. The patient’s ObGyn told her that topiramate was safe to take during pregnancy. The child was born with a cleft lip and palate.
PARENTS’ CLAIM Janssen Pharmaceuticals, manufacturer of Topamax, failed to provide adequate warnings about the potential risks associated with Topamax until labeling was changed in March 2011. Janssen knew of potential birth defects associated with Topamax use during pregnancy more than a decade before the labeling change; Janssen’s associate director of regulatory affairs had testified in an earlier hearing that there was knowledge of related birth defects as early as 1996.
DEFENDANTS’ DEFENSE There is uncertainty as to whether exposure to Topamax during pregnancy causes birth defects. The neurologist had warned the patient of possible risks associated with taking Topamax during pregnancy, but the patient had refused to discontinue the drug.
VERDICT A $3 million Pennsylvania verdict was returned.
Related articles:
• Is it time to rethink the use of oral contraceptives in premenopausal women with migraine? Anne H. Calhoun, MD (Audiocast; October 2013)
• How to choose a contraceptive for a patient who has headaches. Kristina M. Tocce, MD; Stephanie B. Teal, MD, MPH (February 2011)
• The gynecologist’s role in managing menstrual migraine. Anne H. Calhoun, MD (April 2010)
WAS MOTHER’S HISTORY OF INCOMPETENT CERVIX IGNORED?
Early in her second pregnancy, a woman told her ObGyn that she had previously miscarried due to an incompetent cervix.
At 24 weeks’ gestation, the patient was admitted to the hospital with back and pelvic pain and vaginal bleeding. Shortly after admission, the ObGyn performed a vaginal examination and ordered ultrasonography (US), which showed that the fetus was in the transverse position and the membranes were bulging.
The ObGyn performed an emergency cesarean delivery, but the premature infant died within 2 hours.
PARENTS’ CLAIM The ObGyn should have performed a cervical cerclage because of the mother’s history of an incompetent cervix. The mother should have been placed on bed rest and monitored every 2 weeks for cervical dilation.
PHYSICIAN’S DEFENSE The patient underwent regular prenatal evaluations for an incompetent cervix, and the findings were always normal.
VERDICT A Florida defense verdict was returned.
Related article:
A stepwise approach to cervical cerclage. Katrin Karl, MD; Michael Katz, MD (Surgical Technique; June 2012)
ObGyn unresponsive to patient’s postsurgical phone calls
In 2009, a 50-year-old woman reported occasional right lower quadrant pain to her ObGyn. US results were normal. The menopausal patient’s history included three cesarean deliveries, a total abdominal hysterectomy, and a laparoscopic ovarian cystectomy.
When the patient saw her ObGyn in December 2010, she reported intermittent, progressive right lower quadrant pain that radiated down her right leg. She also reported urine loss with coughing or sneezing, and slight pain on intercourse. The ObGyn prescribed oxybutynin chloride (Ditropan) to treat the patient’s incontinence.
Three weeks later, the patient reported bilateral lower quadrant pain to her ObGyn, with minor improvement in incontinence.
The ObGyn performed bilateral salpingo-oophorectomy (BSO) in January 2011. Surgery took 3.5 hours due to extensive adhesiolysis.
After discharge, the patient felt ill and vomited. She attempted to reach the ObGyn by phone several times. That evening, the ObGyn prescribed a suppository to treat nausea and vomiting.
The patient went to the ED later that night and was found to have a perforated colon. Emergency surgery to repair the injury included creation of a colostomy, which was repaired 20 months later.
PATIENT’S CLAIM A proper workup of her symptoms was not performed; BSO was unnecessary. The ObGyn was negligent for failing to respond in a timely manner to her post-discharge phone calls, and did not properly evaluate her postoperative symptoms.
PHYSICIAN’S DEFENSE BSO was warranted. Colon injury is a known complication of the procedure.
VERDICT A $716,976 California verdict was returned, but was reduced to $591,967 under the state cap.

Who delayed delivery? $32.8M verdict for child with CP
An 18-year-old woman at 38 weeks’ gestation went to the hospital in labor. After 3.5 hours, the fetal heart rate dropped to 60 bpm. A nurse repositioned the patient, administered oxygen, and increased intravenous fluids. When the nurse rang the emergency call bell, a second nurse responded. Eighteen minutes after the fetal heart rate first dropped, a nurse rang the call bell again and the on-call ObGyn appeared.
The ObGyn performed a vaginal examination and repositioned the patient. She noted that the fetal heart-rate monitor was not working correctly, and called for an emergency cesarean delivery. The baby was born 42 minutes after the fetal heart rate initially dropped.
The child received a diagnosis of spastic-quadriplegia cerebral palsy (CP). She requires a wheelchair and has severe speech deficits and developmental delays.
PARENT’S CLAIM Cesarean delivery was not performed in a timely manner; the delivery delay was responsible for the injury that caused CP. The ObGyn was negligent in not responding to the initial emergency call. The nurses should have summoned the ObGyn earlier.
DEFENDANTS’ DEFENSE The hospital argued that the nurses followed proper protocol. Furthermore, the hospital noted that the ObGyn did not respond to the first call, and did not request a cesarean delivery for 17 minutes.
The ObGyn claimed that she made the decision to perform cesarean delivery within 5 minutes of her arrival, but it took another 15 minutes to gather the surgical team.
VERDICT A $32,882,860 Pennsylvania verdict was returned against the hospital. The ObGyn was vindicated.
DIFFICULT DELIVERY: ZAVANELLI MANEUVER
At 38 5/7 weeks’ gestation, a woman went to the hospital for induction of labor. Twenty-four hours later, she began to push. After an hour of pushing, the mother was exhausted and had a low-grade fever, and the fetal heart rate was slowing. Her ObGyn, Dr. A, attempted vacuum extraction and performed a midline episiotomy. Shoulder dystocia was encountered and maneuvers were used, but without success. Another ObGyn, Dr. B, arrived to assist and also attempted the maneuvers.
The physicians agreed to try the Zavanelli maneuver, which involves pushing the baby’s head back inside the vagina and performing a cesarean delivery.
The baby was sent to the neonatal intensive care unit, where her breathing quickly normalized without supplemental oxygen. The child has a brachial plexus injury.
PARENTS’ CLAIM Dr. A should have performed an earlier cesarean delivery. Excessive traction was used when shoulder dystocia maneuvers were attempted.
PHYSICIANS’ DEFENSE The ObGyns’ actions saved the baby’s life and prevented serious injury to both mother and baby.
VERDICT An Alabama defense verdict was returned.
Related article:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
PLACENTA PREVIA FOUND EARLY, BUT FETUS DIES
A woman's first pregnancy was complicated by complete placenta previa. A cesarean delivery was scheduled at 36 weeks’ gestation. However, before that date, the mother developed vaginal bleeding and was taken to the ED. The covering ObGyn was notified of the mother’s arrival within 15 minutes, but did not come to the hospital for 2.5 hours. After examining her, the ObGyn ordered US evaluation and transferred the mother to the obstetric floor. Nursing notes indicate that the fetal heart rate was 120 bpm at that time.
There are no notes from the ObGyn between 5:30 am and mid-afternoon. There is no record of the fetal heart rate when the mother was taken for US in the afternoon, which revealed fetal demise and a large extraovular hematoma. A cesarean delivery was performed. It was determined that the fetus died from placental abruption.
PARENTS’ CLAIM The mother was not adequately evaluated and monitored, which led to fetal demise. Delivery could have proceeded while the fetus was still alive.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $495,000 Massachusetts settlement was reached.
Related articles:
• What is the optimal time to deliver a woman who has placenta previa? John T. Repke, MD (Examining the Evidence; April 2011)
• Act fast when confronted by a coagulopathy postpartum. Robert L. Barbieri, MD (Editorial; March 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK! Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state. Stay in touch! Your feedback is important to us!
Blue towel left in abdomen: $7.2M verdict
When a 61-year-old woman underwent laparoscopic hysterectomy, her gynecologist, Dr. A, was assisted by another gynecologist (Dr. B), a nurse, and a technician. When Dr. A noted that the uterine artery had been injured, he converted to an open procedure, retracted the bowel, repaired the artery, and completed the operation.
Postdischarge, the patient was febrile and developed abdominal pain and an odorous vaginal discharge. A month later, exploratory surgery revealed a retained blue towel that had been used for bowel retraction. The patient required open healing of the surgical wound and a temporary colostomy. She developed an incisional hernia after colostomy reversal, and hernia repair required resection of a small portion of the bowel.
PATIENT’S CLAIM It was negligent to use a blue towel to retract the bowel. The towel should have been removed from her abdomen before closure.
DEFENDANTS’ DEFENSE The technician claimed that she did not provide the towel, did not see the towel used, and that she was not told that the towel had to be tracked. She noted that its color indicated that it lacked a radiopaque tag, and that hospital policy forbade use of untagged towels in an open wound.
Dr. A claimed that he specifically requested a blue towel because it was absorbent, that the technician provided the towel, and that the towel’s use prevented the patient from bleeding to death.
VERDICT A $7.2 million New York verdict was returned against both gynecologists and the hospital as the technician’s employer.
MISCARRIAGE AFTER D&C
A few days after a woman thought she miscarried, her family practi-tioner (FP) performed a dilation and curettage (D&C).
The patient was at work 12 days later when she expelled a fully formed 14-week fetus into a toilet. She was taken to the emergency department (ED), where the cord was cut. Later that day, she passed placental tissue; a repeat D&C was performed the next day.
PATIENT'S CLAIM The FP did not properly perform the first D&C. Although the pathology report was available to the FP prior to the patient’s postoperative visit, the FP failed to inform the patient that no fetal parts had been extracted.
PHYSICIAN’S DEFENSE Because the FP thought that the fetus had been passed prior to the D&C, she believed the pathology report was appropriate.
The patient had been informed of the possibility of retained products of conception after the D&C. The FP had ordered a blood pregnancy test that would have revealed the presence of retained products of conception, but the patient did not have the test. The patient did not contact the FP to report symptoms that felt like labor pains on the day that she passed the fetus.
VERDICT A bench trial resulted in a $51,000 California verdict.
PREGNANT WOMAN COMPLAINS OF LEG PAIN; DIES OF DVT
A 23-year-old woman went to the ED with pain and swelling in her lower left leg and calf. The symptoms were reported to her ObGyn, who examined and then discharged her within a few hours, with instructions to come for her regularly scheduled prenatal visit.
The patient died 2 weeks later. The cause of death was determined to be a pulmonary embolus from a thrombus of the left popliteal vein.
ESTATE’S CLAIM The ObGyn was negligent in failing to test the patient for thrombosis in her left leg when she was in the ED or several days later at the office, when she continued to report leg pain.
PHYSICIAN’S DEFENSE The patient did not have signs of thrombosis at the ED or at the subsequent office visit. The pathologist reported that the clot that caused the embolus appeared fresh. The ObGyn surmised that it had formed after the patient’s last appointment.
VERDICT A Texas defense verdict was returned.
Mother took topiramate; child born with cleft lip and palate: $3M verdict
When a woman learned she was pregnant in December 2007, she was taking topiramate (Topamax) to treat migraine headaches. She discussed tapering off but not discontinuing topiramate usage with her neurologist. The patient’s ObGyn told her that topiramate was safe to take during pregnancy. The child was born with a cleft lip and palate.
PARENTS’ CLAIM Janssen Pharmaceuticals, manufacturer of Topamax, failed to provide adequate warnings about the potential risks associated with Topamax until labeling was changed in March 2011. Janssen knew of potential birth defects associated with Topamax use during pregnancy more than a decade before the labeling change; Janssen’s associate director of regulatory affairs had testified in an earlier hearing that there was knowledge of related birth defects as early as 1996.
DEFENDANTS’ DEFENSE There is uncertainty as to whether exposure to Topamax during pregnancy causes birth defects. The neurologist had warned the patient of possible risks associated with taking Topamax during pregnancy, but the patient had refused to discontinue the drug.
VERDICT A $3 million Pennsylvania verdict was returned.
Related articles:
• Is it time to rethink the use of oral contraceptives in premenopausal women with migraine? Anne H. Calhoun, MD (Audiocast; October 2013)
• How to choose a contraceptive for a patient who has headaches. Kristina M. Tocce, MD; Stephanie B. Teal, MD, MPH (February 2011)
• The gynecologist’s role in managing menstrual migraine. Anne H. Calhoun, MD (April 2010)
WAS MOTHER’S HISTORY OF INCOMPETENT CERVIX IGNORED?
Early in her second pregnancy, a woman told her ObGyn that she had previously miscarried due to an incompetent cervix.
At 24 weeks’ gestation, the patient was admitted to the hospital with back and pelvic pain and vaginal bleeding. Shortly after admission, the ObGyn performed a vaginal examination and ordered ultrasonography (US), which showed that the fetus was in the transverse position and the membranes were bulging.
The ObGyn performed an emergency cesarean delivery, but the premature infant died within 2 hours.
PARENTS’ CLAIM The ObGyn should have performed a cervical cerclage because of the mother’s history of an incompetent cervix. The mother should have been placed on bed rest and monitored every 2 weeks for cervical dilation.
PHYSICIAN’S DEFENSE The patient underwent regular prenatal evaluations for an incompetent cervix, and the findings were always normal.
VERDICT A Florida defense verdict was returned.
Related article:
A stepwise approach to cervical cerclage. Katrin Karl, MD; Michael Katz, MD (Surgical Technique; June 2012)
ObGyn unresponsive to patient’s postsurgical phone calls
In 2009, a 50-year-old woman reported occasional right lower quadrant pain to her ObGyn. US results were normal. The menopausal patient’s history included three cesarean deliveries, a total abdominal hysterectomy, and a laparoscopic ovarian cystectomy.
When the patient saw her ObGyn in December 2010, she reported intermittent, progressive right lower quadrant pain that radiated down her right leg. She also reported urine loss with coughing or sneezing, and slight pain on intercourse. The ObGyn prescribed oxybutynin chloride (Ditropan) to treat the patient’s incontinence.
Three weeks later, the patient reported bilateral lower quadrant pain to her ObGyn, with minor improvement in incontinence.
The ObGyn performed bilateral salpingo-oophorectomy (BSO) in January 2011. Surgery took 3.5 hours due to extensive adhesiolysis.
After discharge, the patient felt ill and vomited. She attempted to reach the ObGyn by phone several times. That evening, the ObGyn prescribed a suppository to treat nausea and vomiting.
The patient went to the ED later that night and was found to have a perforated colon. Emergency surgery to repair the injury included creation of a colostomy, which was repaired 20 months later.
PATIENT’S CLAIM A proper workup of her symptoms was not performed; BSO was unnecessary. The ObGyn was negligent for failing to respond in a timely manner to her post-discharge phone calls, and did not properly evaluate her postoperative symptoms.
PHYSICIAN’S DEFENSE BSO was warranted. Colon injury is a known complication of the procedure.
VERDICT A $716,976 California verdict was returned, but was reduced to $591,967 under the state cap.
Who delayed delivery? $32.8M verdict for child with CP
An 18-year-old woman at 38 weeks’ gestation went to the hospital in labor. After 3.5 hours, the fetal heart rate dropped to 60 bpm. A nurse repositioned the patient, administered oxygen, and increased intravenous fluids. When the nurse rang the emergency call bell, a second nurse responded. Eighteen minutes after the fetal heart rate first dropped, a nurse rang the call bell again and the on-call ObGyn appeared.
The ObGyn performed a vaginal examination and repositioned the patient. She noted that the fetal heart-rate monitor was not working correctly, and called for an emergency cesarean delivery. The baby was born 42 minutes after the fetal heart rate initially dropped.
The child received a diagnosis of spastic-quadriplegia cerebral palsy (CP). She requires a wheelchair and has severe speech deficits and developmental delays.
PARENT’S CLAIM Cesarean delivery was not performed in a timely manner; the delivery delay was responsible for the injury that caused CP. The ObGyn was negligent in not responding to the initial emergency call. The nurses should have summoned the ObGyn earlier.
DEFENDANTS’ DEFENSE The hospital argued that the nurses followed proper protocol. Furthermore, the hospital noted that the ObGyn did not respond to the first call, and did not request a cesarean delivery for 17 minutes.
The ObGyn claimed that she made the decision to perform cesarean delivery within 5 minutes of her arrival, but it took another 15 minutes to gather the surgical team.
VERDICT A $32,882,860 Pennsylvania verdict was returned against the hospital. The ObGyn was vindicated.
DIFFICULT DELIVERY: ZAVANELLI MANEUVER
At 38 5/7 weeks’ gestation, a woman went to the hospital for induction of labor. Twenty-four hours later, she began to push. After an hour of pushing, the mother was exhausted and had a low-grade fever, and the fetal heart rate was slowing. Her ObGyn, Dr. A, attempted vacuum extraction and performed a midline episiotomy. Shoulder dystocia was encountered and maneuvers were used, but without success. Another ObGyn, Dr. B, arrived to assist and also attempted the maneuvers.
The physicians agreed to try the Zavanelli maneuver, which involves pushing the baby’s head back inside the vagina and performing a cesarean delivery.
The baby was sent to the neonatal intensive care unit, where her breathing quickly normalized without supplemental oxygen. The child has a brachial plexus injury.
PARENTS’ CLAIM Dr. A should have performed an earlier cesarean delivery. Excessive traction was used when shoulder dystocia maneuvers were attempted.
PHYSICIANS’ DEFENSE The ObGyns’ actions saved the baby’s life and prevented serious injury to both mother and baby.
VERDICT An Alabama defense verdict was returned.
Related article:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
PLACENTA PREVIA FOUND EARLY, BUT FETUS DIES
A woman's first pregnancy was complicated by complete placenta previa. A cesarean delivery was scheduled at 36 weeks’ gestation. However, before that date, the mother developed vaginal bleeding and was taken to the ED. The covering ObGyn was notified of the mother’s arrival within 15 minutes, but did not come to the hospital for 2.5 hours. After examining her, the ObGyn ordered US evaluation and transferred the mother to the obstetric floor. Nursing notes indicate that the fetal heart rate was 120 bpm at that time.
There are no notes from the ObGyn between 5:30 am and mid-afternoon. There is no record of the fetal heart rate when the mother was taken for US in the afternoon, which revealed fetal demise and a large extraovular hematoma. A cesarean delivery was performed. It was determined that the fetus died from placental abruption.
PARENTS’ CLAIM The mother was not adequately evaluated and monitored, which led to fetal demise. Delivery could have proceeded while the fetus was still alive.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $495,000 Massachusetts settlement was reached.
Related articles:
• What is the optimal time to deliver a woman who has placenta previa? John T. Repke, MD (Examining the Evidence; April 2011)
• Act fast when confronted by a coagulopathy postpartum. Robert L. Barbieri, MD (Editorial; March 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK! Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state. Stay in touch! Your feedback is important to us!
Blue towel left in abdomen: $7.2M verdict
When a 61-year-old woman underwent laparoscopic hysterectomy, her gynecologist, Dr. A, was assisted by another gynecologist (Dr. B), a nurse, and a technician. When Dr. A noted that the uterine artery had been injured, he converted to an open procedure, retracted the bowel, repaired the artery, and completed the operation.
Postdischarge, the patient was febrile and developed abdominal pain and an odorous vaginal discharge. A month later, exploratory surgery revealed a retained blue towel that had been used for bowel retraction. The patient required open healing of the surgical wound and a temporary colostomy. She developed an incisional hernia after colostomy reversal, and hernia repair required resection of a small portion of the bowel.
PATIENT’S CLAIM It was negligent to use a blue towel to retract the bowel. The towel should have been removed from her abdomen before closure.
DEFENDANTS’ DEFENSE The technician claimed that she did not provide the towel, did not see the towel used, and that she was not told that the towel had to be tracked. She noted that its color indicated that it lacked a radiopaque tag, and that hospital policy forbade use of untagged towels in an open wound.
Dr. A claimed that he specifically requested a blue towel because it was absorbent, that the technician provided the towel, and that the towel’s use prevented the patient from bleeding to death.
VERDICT A $7.2 million New York verdict was returned against both gynecologists and the hospital as the technician’s employer.
MISCARRIAGE AFTER D&C
A few days after a woman thought she miscarried, her family practi-tioner (FP) performed a dilation and curettage (D&C).
The patient was at work 12 days later when she expelled a fully formed 14-week fetus into a toilet. She was taken to the emergency department (ED), where the cord was cut. Later that day, she passed placental tissue; a repeat D&C was performed the next day.
PATIENT'S CLAIM The FP did not properly perform the first D&C. Although the pathology report was available to the FP prior to the patient’s postoperative visit, the FP failed to inform the patient that no fetal parts had been extracted.
PHYSICIAN’S DEFENSE Because the FP thought that the fetus had been passed prior to the D&C, she believed the pathology report was appropriate.
The patient had been informed of the possibility of retained products of conception after the D&C. The FP had ordered a blood pregnancy test that would have revealed the presence of retained products of conception, but the patient did not have the test. The patient did not contact the FP to report symptoms that felt like labor pains on the day that she passed the fetus.
VERDICT A bench trial resulted in a $51,000 California verdict.
PREGNANT WOMAN COMPLAINS OF LEG PAIN; DIES OF DVT
A 23-year-old woman went to the ED with pain and swelling in her lower left leg and calf. The symptoms were reported to her ObGyn, who examined and then discharged her within a few hours, with instructions to come for her regularly scheduled prenatal visit.
The patient died 2 weeks later. The cause of death was determined to be a pulmonary embolus from a thrombus of the left popliteal vein.
ESTATE’S CLAIM The ObGyn was negligent in failing to test the patient for thrombosis in her left leg when she was in the ED or several days later at the office, when she continued to report leg pain.
PHYSICIAN’S DEFENSE The patient did not have signs of thrombosis at the ED or at the subsequent office visit. The pathologist reported that the clot that caused the embolus appeared fresh. The ObGyn surmised that it had formed after the patient’s last appointment.
VERDICT A Texas defense verdict was returned.
Mother took topiramate; child born with cleft lip and palate: $3M verdict
When a woman learned she was pregnant in December 2007, she was taking topiramate (Topamax) to treat migraine headaches. She discussed tapering off but not discontinuing topiramate usage with her neurologist. The patient’s ObGyn told her that topiramate was safe to take during pregnancy. The child was born with a cleft lip and palate.
PARENTS’ CLAIM Janssen Pharmaceuticals, manufacturer of Topamax, failed to provide adequate warnings about the potential risks associated with Topamax until labeling was changed in March 2011. Janssen knew of potential birth defects associated with Topamax use during pregnancy more than a decade before the labeling change; Janssen’s associate director of regulatory affairs had testified in an earlier hearing that there was knowledge of related birth defects as early as 1996.
DEFENDANTS’ DEFENSE There is uncertainty as to whether exposure to Topamax during pregnancy causes birth defects. The neurologist had warned the patient of possible risks associated with taking Topamax during pregnancy, but the patient had refused to discontinue the drug.
VERDICT A $3 million Pennsylvania verdict was returned.
Related articles:
• Is it time to rethink the use of oral contraceptives in premenopausal women with migraine? Anne H. Calhoun, MD (Audiocast; October 2013)
• How to choose a contraceptive for a patient who has headaches. Kristina M. Tocce, MD; Stephanie B. Teal, MD, MPH (February 2011)
• The gynecologist’s role in managing menstrual migraine. Anne H. Calhoun, MD (April 2010)
WAS MOTHER’S HISTORY OF INCOMPETENT CERVIX IGNORED?
Early in her second pregnancy, a woman told her ObGyn that she had previously miscarried due to an incompetent cervix.
At 24 weeks’ gestation, the patient was admitted to the hospital with back and pelvic pain and vaginal bleeding. Shortly after admission, the ObGyn performed a vaginal examination and ordered ultrasonography (US), which showed that the fetus was in the transverse position and the membranes were bulging.
The ObGyn performed an emergency cesarean delivery, but the premature infant died within 2 hours.
PARENTS’ CLAIM The ObGyn should have performed a cervical cerclage because of the mother’s history of an incompetent cervix. The mother should have been placed on bed rest and monitored every 2 weeks for cervical dilation.
PHYSICIAN’S DEFENSE The patient underwent regular prenatal evaluations for an incompetent cervix, and the findings were always normal.
VERDICT A Florida defense verdict was returned.
Related article:
A stepwise approach to cervical cerclage. Katrin Karl, MD; Michael Katz, MD (Surgical Technique; June 2012)
ObGyn unresponsive to patient’s postsurgical phone calls
In 2009, a 50-year-old woman reported occasional right lower quadrant pain to her ObGyn. US results were normal. The menopausal patient’s history included three cesarean deliveries, a total abdominal hysterectomy, and a laparoscopic ovarian cystectomy.
When the patient saw her ObGyn in December 2010, she reported intermittent, progressive right lower quadrant pain that radiated down her right leg. She also reported urine loss with coughing or sneezing, and slight pain on intercourse. The ObGyn prescribed oxybutynin chloride (Ditropan) to treat the patient’s incontinence.
Three weeks later, the patient reported bilateral lower quadrant pain to her ObGyn, with minor improvement in incontinence.
The ObGyn performed bilateral salpingo-oophorectomy (BSO) in January 2011. Surgery took 3.5 hours due to extensive adhesiolysis.
After discharge, the patient felt ill and vomited. She attempted to reach the ObGyn by phone several times. That evening, the ObGyn prescribed a suppository to treat nausea and vomiting.
The patient went to the ED later that night and was found to have a perforated colon. Emergency surgery to repair the injury included creation of a colostomy, which was repaired 20 months later.
PATIENT’S CLAIM A proper workup of her symptoms was not performed; BSO was unnecessary. The ObGyn was negligent for failing to respond in a timely manner to her post-discharge phone calls, and did not properly evaluate her postoperative symptoms.
PHYSICIAN’S DEFENSE BSO was warranted. Colon injury is a known complication of the procedure.
VERDICT A $716,976 California verdict was returned, but was reduced to $591,967 under the state cap.
Who delayed delivery? $32.8M verdict for child with CP
An 18-year-old woman at 38 weeks’ gestation went to the hospital in labor. After 3.5 hours, the fetal heart rate dropped to 60 bpm. A nurse repositioned the patient, administered oxygen, and increased intravenous fluids. When the nurse rang the emergency call bell, a second nurse responded. Eighteen minutes after the fetal heart rate first dropped, a nurse rang the call bell again and the on-call ObGyn appeared.
The ObGyn performed a vaginal examination and repositioned the patient. She noted that the fetal heart-rate monitor was not working correctly, and called for an emergency cesarean delivery. The baby was born 42 minutes after the fetal heart rate initially dropped.
The child received a diagnosis of spastic-quadriplegia cerebral palsy (CP). She requires a wheelchair and has severe speech deficits and developmental delays.
PARENT’S CLAIM Cesarean delivery was not performed in a timely manner; the delivery delay was responsible for the injury that caused CP. The ObGyn was negligent in not responding to the initial emergency call. The nurses should have summoned the ObGyn earlier.
DEFENDANTS’ DEFENSE The hospital argued that the nurses followed proper protocol. Furthermore, the hospital noted that the ObGyn did not respond to the first call, and did not request a cesarean delivery for 17 minutes.
The ObGyn claimed that she made the decision to perform cesarean delivery within 5 minutes of her arrival, but it took another 15 minutes to gather the surgical team.
VERDICT A $32,882,860 Pennsylvania verdict was returned against the hospital. The ObGyn was vindicated.
DIFFICULT DELIVERY: ZAVANELLI MANEUVER
At 38 5/7 weeks’ gestation, a woman went to the hospital for induction of labor. Twenty-four hours later, she began to push. After an hour of pushing, the mother was exhausted and had a low-grade fever, and the fetal heart rate was slowing. Her ObGyn, Dr. A, attempted vacuum extraction and performed a midline episiotomy. Shoulder dystocia was encountered and maneuvers were used, but without success. Another ObGyn, Dr. B, arrived to assist and also attempted the maneuvers.
The physicians agreed to try the Zavanelli maneuver, which involves pushing the baby’s head back inside the vagina and performing a cesarean delivery.
The baby was sent to the neonatal intensive care unit, where her breathing quickly normalized without supplemental oxygen. The child has a brachial plexus injury.
PARENTS’ CLAIM Dr. A should have performed an earlier cesarean delivery. Excessive traction was used when shoulder dystocia maneuvers were attempted.
PHYSICIANS’ DEFENSE The ObGyns’ actions saved the baby’s life and prevented serious injury to both mother and baby.
VERDICT An Alabama defense verdict was returned.
Related article:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
PLACENTA PREVIA FOUND EARLY, BUT FETUS DIES
A woman's first pregnancy was complicated by complete placenta previa. A cesarean delivery was scheduled at 36 weeks’ gestation. However, before that date, the mother developed vaginal bleeding and was taken to the ED. The covering ObGyn was notified of the mother’s arrival within 15 minutes, but did not come to the hospital for 2.5 hours. After examining her, the ObGyn ordered US evaluation and transferred the mother to the obstetric floor. Nursing notes indicate that the fetal heart rate was 120 bpm at that time.
There are no notes from the ObGyn between 5:30 am and mid-afternoon. There is no record of the fetal heart rate when the mother was taken for US in the afternoon, which revealed fetal demise and a large extraovular hematoma. A cesarean delivery was performed. It was determined that the fetus died from placental abruption.
PARENTS’ CLAIM The mother was not adequately evaluated and monitored, which led to fetal demise. Delivery could have proceeded while the fetus was still alive.
PHYSICIAN’S DEFENSE The case was settled during the trial.
VERDICT A $495,000 Massachusetts settlement was reached.
Related articles:
• What is the optimal time to deliver a woman who has placenta previa? John T. Repke, MD (Examining the Evidence; April 2011)
• Act fast when confronted by a coagulopathy postpartum. Robert L. Barbieri, MD (Editorial; March 2012)
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK! Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state. Stay in touch! Your feedback is important to us!

To MU or not to MU, that is the question
If you are still on the fence on meaningful use – our government’s motivational strategy for popularizing electronic health records – the point of no return is rapidly approaching: If you want to qualify for at least a portion of the incentive money, plus avoid a 1% penalty (eventually rising to 5%) on your Medicare Part B reimbursements, this year is your final opportunity to join the party. And, unfortunately, it is not simply a matter of adopting an electronic record system.
Each year, you must attest to demonstrating "meaningful use" (MU) of that system. To do that, you must continually monitor your progress toward meeting the necessary percentage benchmarks, making course corrections as you go. If the numbers are not there when your practice is ready to attest, it will have all been for naught, and a major waste of time and resources.
That being the case, private practitioners who have not yet taken the plunge – and those who have, but are undecided on progressing to stage 2 – must ask themselves whether the significant temporal and monetary investment is worth the trouble.
Many, apparently, have decided that it is not. While a substantial percentage of eligible practitioners signed up for stage 1, approximately 20% of them stopped participating in 2013. And according to the Centers for Medicare & Medicaid Services’ own data, only 4 hospitals and 50 individual practitioners in the entire country had attested to stage 2 through March of 2014.
The American Medical Association has little faith in the program, at least in its current form. In an open letter to the CMS in May 2014, they predicted significantly higher dropout rates unless major modifications are made. Specifically, they singled out the requirement that providers meet all requirements at each stage. Rather than "all or nothing," they proposed a 75% achievement level to receive incentive payments, and a 50% minimum to avoid financial penalties. The AMA also recommended eliminating all benchmarks beyond physicians’ control, such as the stage 2 goal of 5% patient participation on the practice’s electronic health record (EHR) portal.
Another problem that falls outside the control of physicians is maintenance of EHR software. Nearly one EHR-equipped office in five, according to the CMS, is running software that does not meet stage 2 standards. The unfortunate owners of systems that cannot be upgraded before the stage 2 deadline will – through no fault of their own – be faced with a Morton’s fork of replacing their EHR on short notice or abandoning their quest for stage 2 attestation.
While the CMS has not yet indicated whether it has any inclination to address these issues or ease any of the requirements, one official did announce that the agency will be more flexible with its hardship exemptions on a case-by-case basis. Currently, such exemptions are available to new providers, those recovering from natural disasters, and others, such as pathologists, who do not interact face-to-face with patients.
So the question remains: Is the investment of time and resources needed to capture all of the data necessary for successful MU attestation worth making? Is it justified by the promise of MU incentive dollars and the benefits to your practice and your patients? And what exactly are those purported benefits, anyway?
Proponents maintain that integrated EHR will lead to improved documentation, which in turn should lead to improvements in patient care. Errors would be more easily identified because entries from generalists, specialists, labs, and others would be available to all at any time. All involved providers, theoretically, would be on the same page with every individual patient. The downside, of course, is that the real world seldom reflects the ideal situation envisioned by bureaucrats.
Ultimately, the choice is yours: Each private practitioner must decide whether starting (or continuing) meaningful use is worth the financial and time burden in his or her particular situation. If you are still undecided, time is almost up: You must begin your 90-day stage 1 reporting period in July 2014 in order to attest by the final deadline of October 1. The last calendar quarter to begin stage 2 reporting starts on October 1 as well. Detailed instructions for meeting stage 1 and stage 2 deadlines are available from many sources, including the American Academy of Dermatology website.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
If you are still on the fence on meaningful use – our government’s motivational strategy for popularizing electronic health records – the point of no return is rapidly approaching: If you want to qualify for at least a portion of the incentive money, plus avoid a 1% penalty (eventually rising to 5%) on your Medicare Part B reimbursements, this year is your final opportunity to join the party. And, unfortunately, it is not simply a matter of adopting an electronic record system.
Each year, you must attest to demonstrating "meaningful use" (MU) of that system. To do that, you must continually monitor your progress toward meeting the necessary percentage benchmarks, making course corrections as you go. If the numbers are not there when your practice is ready to attest, it will have all been for naught, and a major waste of time and resources.
That being the case, private practitioners who have not yet taken the plunge – and those who have, but are undecided on progressing to stage 2 – must ask themselves whether the significant temporal and monetary investment is worth the trouble.
Many, apparently, have decided that it is not. While a substantial percentage of eligible practitioners signed up for stage 1, approximately 20% of them stopped participating in 2013. And according to the Centers for Medicare & Medicaid Services’ own data, only 4 hospitals and 50 individual practitioners in the entire country had attested to stage 2 through March of 2014.
The American Medical Association has little faith in the program, at least in its current form. In an open letter to the CMS in May 2014, they predicted significantly higher dropout rates unless major modifications are made. Specifically, they singled out the requirement that providers meet all requirements at each stage. Rather than "all or nothing," they proposed a 75% achievement level to receive incentive payments, and a 50% minimum to avoid financial penalties. The AMA also recommended eliminating all benchmarks beyond physicians’ control, such as the stage 2 goal of 5% patient participation on the practice’s electronic health record (EHR) portal.
Another problem that falls outside the control of physicians is maintenance of EHR software. Nearly one EHR-equipped office in five, according to the CMS, is running software that does not meet stage 2 standards. The unfortunate owners of systems that cannot be upgraded before the stage 2 deadline will – through no fault of their own – be faced with a Morton’s fork of replacing their EHR on short notice or abandoning their quest for stage 2 attestation.
While the CMS has not yet indicated whether it has any inclination to address these issues or ease any of the requirements, one official did announce that the agency will be more flexible with its hardship exemptions on a case-by-case basis. Currently, such exemptions are available to new providers, those recovering from natural disasters, and others, such as pathologists, who do not interact face-to-face with patients.
So the question remains: Is the investment of time and resources needed to capture all of the data necessary for successful MU attestation worth making? Is it justified by the promise of MU incentive dollars and the benefits to your practice and your patients? And what exactly are those purported benefits, anyway?
Proponents maintain that integrated EHR will lead to improved documentation, which in turn should lead to improvements in patient care. Errors would be more easily identified because entries from generalists, specialists, labs, and others would be available to all at any time. All involved providers, theoretically, would be on the same page with every individual patient. The downside, of course, is that the real world seldom reflects the ideal situation envisioned by bureaucrats.
Ultimately, the choice is yours: Each private practitioner must decide whether starting (or continuing) meaningful use is worth the financial and time burden in his or her particular situation. If you are still undecided, time is almost up: You must begin your 90-day stage 1 reporting period in July 2014 in order to attest by the final deadline of October 1. The last calendar quarter to begin stage 2 reporting starts on October 1 as well. Detailed instructions for meeting stage 1 and stage 2 deadlines are available from many sources, including the American Academy of Dermatology website.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
If you are still on the fence on meaningful use – our government’s motivational strategy for popularizing electronic health records – the point of no return is rapidly approaching: If you want to qualify for at least a portion of the incentive money, plus avoid a 1% penalty (eventually rising to 5%) on your Medicare Part B reimbursements, this year is your final opportunity to join the party. And, unfortunately, it is not simply a matter of adopting an electronic record system.
Each year, you must attest to demonstrating "meaningful use" (MU) of that system. To do that, you must continually monitor your progress toward meeting the necessary percentage benchmarks, making course corrections as you go. If the numbers are not there when your practice is ready to attest, it will have all been for naught, and a major waste of time and resources.
That being the case, private practitioners who have not yet taken the plunge – and those who have, but are undecided on progressing to stage 2 – must ask themselves whether the significant temporal and monetary investment is worth the trouble.
Many, apparently, have decided that it is not. While a substantial percentage of eligible practitioners signed up for stage 1, approximately 20% of them stopped participating in 2013. And according to the Centers for Medicare & Medicaid Services’ own data, only 4 hospitals and 50 individual practitioners in the entire country had attested to stage 2 through March of 2014.
The American Medical Association has little faith in the program, at least in its current form. In an open letter to the CMS in May 2014, they predicted significantly higher dropout rates unless major modifications are made. Specifically, they singled out the requirement that providers meet all requirements at each stage. Rather than "all or nothing," they proposed a 75% achievement level to receive incentive payments, and a 50% minimum to avoid financial penalties. The AMA also recommended eliminating all benchmarks beyond physicians’ control, such as the stage 2 goal of 5% patient participation on the practice’s electronic health record (EHR) portal.
Another problem that falls outside the control of physicians is maintenance of EHR software. Nearly one EHR-equipped office in five, according to the CMS, is running software that does not meet stage 2 standards. The unfortunate owners of systems that cannot be upgraded before the stage 2 deadline will – through no fault of their own – be faced with a Morton’s fork of replacing their EHR on short notice or abandoning their quest for stage 2 attestation.
While the CMS has not yet indicated whether it has any inclination to address these issues or ease any of the requirements, one official did announce that the agency will be more flexible with its hardship exemptions on a case-by-case basis. Currently, such exemptions are available to new providers, those recovering from natural disasters, and others, such as pathologists, who do not interact face-to-face with patients.
So the question remains: Is the investment of time and resources needed to capture all of the data necessary for successful MU attestation worth making? Is it justified by the promise of MU incentive dollars and the benefits to your practice and your patients? And what exactly are those purported benefits, anyway?
Proponents maintain that integrated EHR will lead to improved documentation, which in turn should lead to improvements in patient care. Errors would be more easily identified because entries from generalists, specialists, labs, and others would be available to all at any time. All involved providers, theoretically, would be on the same page with every individual patient. The downside, of course, is that the real world seldom reflects the ideal situation envisioned by bureaucrats.
Ultimately, the choice is yours: Each private practitioner must decide whether starting (or continuing) meaningful use is worth the financial and time burden in his or her particular situation. If you are still undecided, time is almost up: You must begin your 90-day stage 1 reporting period in July 2014 in order to attest by the final deadline of October 1. The last calendar quarter to begin stage 2 reporting starts on October 1 as well. Detailed instructions for meeting stage 1 and stage 2 deadlines are available from many sources, including the American Academy of Dermatology website.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
