User login
Traditional Hand Hygiene Audits Can Lead to Inaccurate Conclusions about Physician Performance
Clinical Question: Does direct observation underestimate physician compliance with hand hygiene (HH) compared to other professional groups due to the Hawthorne effect?

Background: Although it is well-known that HH is imperative to infection control, physician compliance remains suboptimal and is often reported to be below that of nurses. The Hawthorne effect may be contributing to this perceived difference because nurses, who work on the same unit consistently, may more readily recognize hospital auditors.
Study Design: Observational.
Setting: 800-bed acute-care academic hospital in Canada.
Synopsis: Two students were trained to covertly observe physician and nursing HH compliance on inpatient units. For two months, students rotated units every week to minimize risk of discovery. Their findings were compared with data gathered by hospital auditors over the same time period.
Covertly observed HH compliance was 50% (799/1,597 opportunities) compared with 83.7% (2,769/3,309) reported by hospital auditors (P<0.0002). The difference in physician compliance was 19% (73.2% compliance with overt observation versus 54.2% with covert observation). The difference was much higher for nurses at 40.7% (85.8% compliance with overt observation versus 45.1% with covert observation). Attending physician behaviors heavily influenced team behaviors—79.5% of trainees were compliant if their attending was compliant compared with 18.9% if attending was not (P<0.0002).
Bottom Line: Traditional HH audit findings that physicians are less compliant than nurses may be at least partially due to the Hawthorne effect. Nonetheless, all healthcare providers have substantial room for improvement, and attending physicians are powerful role models to effect this change.
Citation: Kovacs-Litman A, Wong K, Shojania KJ, Callery S, Vearncombe M, Leis J. Do physicians clean their hands? Insights from a covert observational study [published online ahead of print July 5, 2016]. J Hosp Med.
Clinical Question: Does direct observation underestimate physician compliance with hand hygiene (HH) compared to other professional groups due to the Hawthorne effect?
Background: Although it is well-known that HH is imperative to infection control, physician compliance remains suboptimal and is often reported to be below that of nurses. The Hawthorne effect may be contributing to this perceived difference because nurses, who work on the same unit consistently, may more readily recognize hospital auditors.
Study Design: Observational.
Setting: 800-bed acute-care academic hospital in Canada.
Synopsis: Two students were trained to covertly observe physician and nursing HH compliance on inpatient units. For two months, students rotated units every week to minimize risk of discovery. Their findings were compared with data gathered by hospital auditors over the same time period.
Covertly observed HH compliance was 50% (799/1,597 opportunities) compared with 83.7% (2,769/3,309) reported by hospital auditors (P<0.0002). The difference in physician compliance was 19% (73.2% compliance with overt observation versus 54.2% with covert observation). The difference was much higher for nurses at 40.7% (85.8% compliance with overt observation versus 45.1% with covert observation). Attending physician behaviors heavily influenced team behaviors—79.5% of trainees were compliant if their attending was compliant compared with 18.9% if attending was not (P<0.0002).
Bottom Line: Traditional HH audit findings that physicians are less compliant than nurses may be at least partially due to the Hawthorne effect. Nonetheless, all healthcare providers have substantial room for improvement, and attending physicians are powerful role models to effect this change.
Citation: Kovacs-Litman A, Wong K, Shojania KJ, Callery S, Vearncombe M, Leis J. Do physicians clean their hands? Insights from a covert observational study [published online ahead of print July 5, 2016]. J Hosp Med.
Clinical Question: Does direct observation underestimate physician compliance with hand hygiene (HH) compared to other professional groups due to the Hawthorne effect?
Background: Although it is well-known that HH is imperative to infection control, physician compliance remains suboptimal and is often reported to be below that of nurses. The Hawthorne effect may be contributing to this perceived difference because nurses, who work on the same unit consistently, may more readily recognize hospital auditors.
Study Design: Observational.
Setting: 800-bed acute-care academic hospital in Canada.
Synopsis: Two students were trained to covertly observe physician and nursing HH compliance on inpatient units. For two months, students rotated units every week to minimize risk of discovery. Their findings were compared with data gathered by hospital auditors over the same time period.
Covertly observed HH compliance was 50% (799/1,597 opportunities) compared with 83.7% (2,769/3,309) reported by hospital auditors (P<0.0002). The difference in physician compliance was 19% (73.2% compliance with overt observation versus 54.2% with covert observation). The difference was much higher for nurses at 40.7% (85.8% compliance with overt observation versus 45.1% with covert observation). Attending physician behaviors heavily influenced team behaviors—79.5% of trainees were compliant if their attending was compliant compared with 18.9% if attending was not (P<0.0002).
Bottom Line: Traditional HH audit findings that physicians are less compliant than nurses may be at least partially due to the Hawthorne effect. Nonetheless, all healthcare providers have substantial room for improvement, and attending physicians are powerful role models to effect this change.
Citation: Kovacs-Litman A, Wong K, Shojania KJ, Callery S, Vearncombe M, Leis J. Do physicians clean their hands? Insights from a covert observational study [published online ahead of print July 5, 2016]. J Hosp Med.

Long-Term Mortality in Nondiabetic Patients Favors Coronary Artery Bypass Over Intervention with Drug-Eluting Stents
Clinical Question: Is there a mortality difference in nondiabetic patients with multivessel coronary artery disease (CAD) treated with coronary artery bypass graft (CABG) versus percutaneous coronary intervention (PCI)?
Background: Randomized clinical trials have shown a mortality benefit of CABG over PCI with drug-eluting stents (DES) for diabetic patients. The best strategy for nondiabetics, however, has not been well established.
Study Design: Pooled individual patient data from two large randomized clinical trials.
Setting: Multicenter, multinational (Europe, United States, Asia).
Synopsis: Excluding patients with left main disease, a total of 1,275 nondiabetic patients with two- or three-vessel CAD were analyzed. After median follow-up of 61 months, the CABG group had significantly fewer deaths from any cause (hazard ratio [HR], 0.65; 95% CI, 0.43–0.98; P=0.039) as well as fewer deaths from cardiac causes (HR, 0.41; 95% CI, 0.25–0.78; P=0.005) when compared to PCI with DES. The benefit was primarily seen at five-year follow-up in patients with intermediate to severe disease, with a nonsignificant difference detected in patients with less severe disease.
Despite the increasing popularity of DES, this study suggests that for nondiabetic patients with CAD, there is a mortality benefit at five years favoring CABG over PCI with DES. However, in this study stents used for PCI included both older and newer generation DES; a study using only newer DES may reduce the differences in outcomes between the groups.
Bottom Line: Five-year mortality is lower in nondiabetic patients with multivessel CAD treated with CABG compared with PCI with DES.
Citation: Chang M, Ahn JM, Lee CW, et al. Long-term mortality after coronary revascularization in nondiabetic patients with multivessel disease. J Am Coll Cardiol. 2016;68(1):29-36.
Clinical Question: Is there a mortality difference in nondiabetic patients with multivessel coronary artery disease (CAD) treated with coronary artery bypass graft (CABG) versus percutaneous coronary intervention (PCI)?
Background: Randomized clinical trials have shown a mortality benefit of CABG over PCI with drug-eluting stents (DES) for diabetic patients. The best strategy for nondiabetics, however, has not been well established.
Study Design: Pooled individual patient data from two large randomized clinical trials.
Setting: Multicenter, multinational (Europe, United States, Asia).
Synopsis: Excluding patients with left main disease, a total of 1,275 nondiabetic patients with two- or three-vessel CAD were analyzed. After median follow-up of 61 months, the CABG group had significantly fewer deaths from any cause (hazard ratio [HR], 0.65; 95% CI, 0.43–0.98; P=0.039) as well as fewer deaths from cardiac causes (HR, 0.41; 95% CI, 0.25–0.78; P=0.005) when compared to PCI with DES. The benefit was primarily seen at five-year follow-up in patients with intermediate to severe disease, with a nonsignificant difference detected in patients with less severe disease.
Despite the increasing popularity of DES, this study suggests that for nondiabetic patients with CAD, there is a mortality benefit at five years favoring CABG over PCI with DES. However, in this study stents used for PCI included both older and newer generation DES; a study using only newer DES may reduce the differences in outcomes between the groups.
Bottom Line: Five-year mortality is lower in nondiabetic patients with multivessel CAD treated with CABG compared with PCI with DES.
Citation: Chang M, Ahn JM, Lee CW, et al. Long-term mortality after coronary revascularization in nondiabetic patients with multivessel disease. J Am Coll Cardiol. 2016;68(1):29-36.
Clinical Question: Is there a mortality difference in nondiabetic patients with multivessel coronary artery disease (CAD) treated with coronary artery bypass graft (CABG) versus percutaneous coronary intervention (PCI)?
Background: Randomized clinical trials have shown a mortality benefit of CABG over PCI with drug-eluting stents (DES) for diabetic patients. The best strategy for nondiabetics, however, has not been well established.
Study Design: Pooled individual patient data from two large randomized clinical trials.
Setting: Multicenter, multinational (Europe, United States, Asia).
Synopsis: Excluding patients with left main disease, a total of 1,275 nondiabetic patients with two- or three-vessel CAD were analyzed. After median follow-up of 61 months, the CABG group had significantly fewer deaths from any cause (hazard ratio [HR], 0.65; 95% CI, 0.43–0.98; P=0.039) as well as fewer deaths from cardiac causes (HR, 0.41; 95% CI, 0.25–0.78; P=0.005) when compared to PCI with DES. The benefit was primarily seen at five-year follow-up in patients with intermediate to severe disease, with a nonsignificant difference detected in patients with less severe disease.
Despite the increasing popularity of DES, this study suggests that for nondiabetic patients with CAD, there is a mortality benefit at five years favoring CABG over PCI with DES. However, in this study stents used for PCI included both older and newer generation DES; a study using only newer DES may reduce the differences in outcomes between the groups.
Bottom Line: Five-year mortality is lower in nondiabetic patients with multivessel CAD treated with CABG compared with PCI with DES.
Citation: Chang M, Ahn JM, Lee CW, et al. Long-term mortality after coronary revascularization in nondiabetic patients with multivessel disease. J Am Coll Cardiol. 2016;68(1):29-36.
Prolonged Ceftaroline Exposure Associated with High Incidence of Neutropenia
Clinical Question: What is the incidence of neutropenia in patients treated with prolonged courses of ceftaroline?
Background: Ceftaroline, a new broad-spectrum cephalosporin antibiotic, is FDA approved for the treatment of skin and soft-tissue infections and community-acquired pneumonia (CAP). Other than a few case reports, previous studies have not assessed the incidence of neutropenia in patients receiving ceftaroline for off-label indications or for prolonged courses.
Study Design: Retrospective chart review.
Setting: Brigham and Women’s Hospital and Massachusetts General Hospital in Boston.
Synopsis: The authors identified 67 patients who received ceftaroline for seven or more consecutive days. Overall, ceftaroline exposure for two or more weeks was associated with a 10%–14% incidence of neutropenia (absolute neutrophil count less than 1,800 cells/mm3), and ceftaroline exposure for three or more weeks was associated with a 21% incidence of neutropenia. Both the mean duration of ceftaroline exposure and the total number of ceftaroline doses were associated with incident neutropenia.
This is the first study to systematically assess the incidence of ceftaroline-associated neutropenia. The data support a correlation between cumulative ceftaroline exposure and neutropenia. Hospitalists managing patients with prolonged courses of ceftaroline should carefully monitor hematologic studies during treatment.
Bottom Line: The overall rate of neutropenia in patients receiving prolonged courses of ceftaroline is significant, and it is associated with duration of ceftaroline exposure and total number of doses received.
Citation: Furtek KJ, Kubiak DW, Barra M, Varughese C, Ashbaugh CD, Koo S. High incidence of neutropenia in patients with prolonged ceftaroline exposure. J Antimicrob Chemother. 2016;71(7):2010-2013.
Short Take
New Guidelines from IDSA/ATS for Patients with Community-Acquired Pneumonia Can Safely Be Implemented for Hospitalized Patients
A multicenter, non-inferiority randomized clinical trial of 312 patients with community-acquired pneumonia (CAP) found that stopping antibiotics after five days was not associated with worse outcomes and may reduce readmissions.
Citation: Uranga A, España PP, Bilbao A, et al. Duration of antibiotic treatment in community-acquired pneumonia: a multicenter randomized clinical trial. JAMA Intern Med. 2016;176(9):1257-1265.
Clinical Question: What is the incidence of neutropenia in patients treated with prolonged courses of ceftaroline?
Background: Ceftaroline, a new broad-spectrum cephalosporin antibiotic, is FDA approved for the treatment of skin and soft-tissue infections and community-acquired pneumonia (CAP). Other than a few case reports, previous studies have not assessed the incidence of neutropenia in patients receiving ceftaroline for off-label indications or for prolonged courses.
Study Design: Retrospective chart review.
Setting: Brigham and Women’s Hospital and Massachusetts General Hospital in Boston.
Synopsis: The authors identified 67 patients who received ceftaroline for seven or more consecutive days. Overall, ceftaroline exposure for two or more weeks was associated with a 10%–14% incidence of neutropenia (absolute neutrophil count less than 1,800 cells/mm3), and ceftaroline exposure for three or more weeks was associated with a 21% incidence of neutropenia. Both the mean duration of ceftaroline exposure and the total number of ceftaroline doses were associated with incident neutropenia.
This is the first study to systematically assess the incidence of ceftaroline-associated neutropenia. The data support a correlation between cumulative ceftaroline exposure and neutropenia. Hospitalists managing patients with prolonged courses of ceftaroline should carefully monitor hematologic studies during treatment.
Bottom Line: The overall rate of neutropenia in patients receiving prolonged courses of ceftaroline is significant, and it is associated with duration of ceftaroline exposure and total number of doses received.
Citation: Furtek KJ, Kubiak DW, Barra M, Varughese C, Ashbaugh CD, Koo S. High incidence of neutropenia in patients with prolonged ceftaroline exposure. J Antimicrob Chemother. 2016;71(7):2010-2013.
Short Take
New Guidelines from IDSA/ATS for Patients with Community-Acquired Pneumonia Can Safely Be Implemented for Hospitalized Patients
A multicenter, non-inferiority randomized clinical trial of 312 patients with community-acquired pneumonia (CAP) found that stopping antibiotics after five days was not associated with worse outcomes and may reduce readmissions.
Citation: Uranga A, España PP, Bilbao A, et al. Duration of antibiotic treatment in community-acquired pneumonia: a multicenter randomized clinical trial. JAMA Intern Med. 2016;176(9):1257-1265.
Clinical Question: What is the incidence of neutropenia in patients treated with prolonged courses of ceftaroline?
Background: Ceftaroline, a new broad-spectrum cephalosporin antibiotic, is FDA approved for the treatment of skin and soft-tissue infections and community-acquired pneumonia (CAP). Other than a few case reports, previous studies have not assessed the incidence of neutropenia in patients receiving ceftaroline for off-label indications or for prolonged courses.
Study Design: Retrospective chart review.
Setting: Brigham and Women’s Hospital and Massachusetts General Hospital in Boston.
Synopsis: The authors identified 67 patients who received ceftaroline for seven or more consecutive days. Overall, ceftaroline exposure for two or more weeks was associated with a 10%–14% incidence of neutropenia (absolute neutrophil count less than 1,800 cells/mm3), and ceftaroline exposure for three or more weeks was associated with a 21% incidence of neutropenia. Both the mean duration of ceftaroline exposure and the total number of ceftaroline doses were associated with incident neutropenia.
This is the first study to systematically assess the incidence of ceftaroline-associated neutropenia. The data support a correlation between cumulative ceftaroline exposure and neutropenia. Hospitalists managing patients with prolonged courses of ceftaroline should carefully monitor hematologic studies during treatment.
Bottom Line: The overall rate of neutropenia in patients receiving prolonged courses of ceftaroline is significant, and it is associated with duration of ceftaroline exposure and total number of doses received.
Citation: Furtek KJ, Kubiak DW, Barra M, Varughese C, Ashbaugh CD, Koo S. High incidence of neutropenia in patients with prolonged ceftaroline exposure. J Antimicrob Chemother. 2016;71(7):2010-2013.
Short Take
New Guidelines from IDSA/ATS for Patients with Community-Acquired Pneumonia Can Safely Be Implemented for Hospitalized Patients
A multicenter, non-inferiority randomized clinical trial of 312 patients with community-acquired pneumonia (CAP) found that stopping antibiotics after five days was not associated with worse outcomes and may reduce readmissions.
Citation: Uranga A, España PP, Bilbao A, et al. Duration of antibiotic treatment in community-acquired pneumonia: a multicenter randomized clinical trial. JAMA Intern Med. 2016;176(9):1257-1265.
Making Fall Prevention “Routine”
Every second of every day in the U.S. an older adult falls, according to CDC data. Falls are the number one cause of injuries and deaths from injury among older Americans. The report cites 29 million falls in 2014 alone.
“Older adult falls are increasing and, sadly, often herald the end of independence,” said CDC Director Tom Frieden, MD, MPH. But he adds: “Health care providers can make fall prevention a routine part of care in their practice, and older adults can take steps to protect themselves.”
Related: Preventing Falls and Saving Costs
The CDC created Stopping Elderly Accidents, Deaths, and Injuries (STEADI), an initiative to make fall prevention routine in health care. The program provides information on how to screen for falls, online training for providers, videos on conducting functional assessments, and brochures for health care providers (HCPs), patients, and caregivers.
Among the suggestions for HCPs:
- Ask patients whether they have fallen in the past year, feel unsteady, or worry about falling
- Review medications and stop, switch, or reduce medicines that could increase the risk of falls
- Recommend vitamin D supplements
For older adults, the CDC recommends:
- Talk to a HCP about falls and fall prevention
- Tell a HCP if you have fallen—fewer than half of Americans who fall tell their doctor
- Have your eyes checked, and update eye prescriptions
- Participate in evidence-based programs like tai chi to improve balance and strengthen legs
- Get rid of fall hazards in your home
Every second of every day in the U.S. an older adult falls, according to CDC data. Falls are the number one cause of injuries and deaths from injury among older Americans. The report cites 29 million falls in 2014 alone.
“Older adult falls are increasing and, sadly, often herald the end of independence,” said CDC Director Tom Frieden, MD, MPH. But he adds: “Health care providers can make fall prevention a routine part of care in their practice, and older adults can take steps to protect themselves.”
Related: Preventing Falls and Saving Costs
The CDC created Stopping Elderly Accidents, Deaths, and Injuries (STEADI), an initiative to make fall prevention routine in health care. The program provides information on how to screen for falls, online training for providers, videos on conducting functional assessments, and brochures for health care providers (HCPs), patients, and caregivers.
Among the suggestions for HCPs:
- Ask patients whether they have fallen in the past year, feel unsteady, or worry about falling
- Review medications and stop, switch, or reduce medicines that could increase the risk of falls
- Recommend vitamin D supplements
For older adults, the CDC recommends:
- Talk to a HCP about falls and fall prevention
- Tell a HCP if you have fallen—fewer than half of Americans who fall tell their doctor
- Have your eyes checked, and update eye prescriptions
- Participate in evidence-based programs like tai chi to improve balance and strengthen legs
- Get rid of fall hazards in your home
Every second of every day in the U.S. an older adult falls, according to CDC data. Falls are the number one cause of injuries and deaths from injury among older Americans. The report cites 29 million falls in 2014 alone.
“Older adult falls are increasing and, sadly, often herald the end of independence,” said CDC Director Tom Frieden, MD, MPH. But he adds: “Health care providers can make fall prevention a routine part of care in their practice, and older adults can take steps to protect themselves.”
Related: Preventing Falls and Saving Costs
The CDC created Stopping Elderly Accidents, Deaths, and Injuries (STEADI), an initiative to make fall prevention routine in health care. The program provides information on how to screen for falls, online training for providers, videos on conducting functional assessments, and brochures for health care providers (HCPs), patients, and caregivers.
Among the suggestions for HCPs:
- Ask patients whether they have fallen in the past year, feel unsteady, or worry about falling
- Review medications and stop, switch, or reduce medicines that could increase the risk of falls
- Recommend vitamin D supplements
For older adults, the CDC recommends:
- Talk to a HCP about falls and fall prevention
- Tell a HCP if you have fallen—fewer than half of Americans who fall tell their doctor
- Have your eyes checked, and update eye prescriptions
- Participate in evidence-based programs like tai chi to improve balance and strengthen legs
- Get rid of fall hazards in your home
Some Patients With Diabetes Aren’t Getting Needed Weight Advice
About two-thirds of overweight and obese patients are not getting the advice they need from their health care providers (HCPs) about weight management, according to a study by Arizona State researchers, reported in the CDC’s Preventing Chronic Disease.
The researchers conducted a phone survey of 1,109 overweight or obese adults, asking whether a HCP had in the previous 12 months given them advice about their weight. A “concerning” finding, the researchers say: Only 35% of the respondents reported getting advice.
Related: Confronting the Diabetes Epidemic
As body mass index (BMI) increased, so did the likelihood of receiving weight-loss advice: 22% of those with a BMI of 25.0 to 29.9 received advice vs 63% of those with a BMI of 40.0 or higher. Hispanics were the most likely of the 3 racial/ethnic groups to report receiving advice from a HCP. The researchers say other studies have suggested that a higher prevalence of weight problems among African Americans and Hispanics draws more attention from HCPs for counseling.
High-risk patients, such as the extremely obese or those with comorbidities, are most likely to receive weight-loss advice, the researchers say. But demographic factors also come into play: People with high levels of education are more likely than those with low levels to receive advice, and middle-aged people are more likely to get advice than are younger or older patients.
Related: Diabetes Report: The News Isn’t Good
Patients in the lowest-income groups had significantly lower odds of receiving weight-loss advice compared with those in higher income groups. Adjusting for health insurance did not change the results. That finding is “problematic,” the researchers say, because people with the lowest incomes tend to have poorer health outcomes than that of those with higher incomes.
About two-thirds of overweight and obese patients are not getting the advice they need from their health care providers (HCPs) about weight management, according to a study by Arizona State researchers, reported in the CDC’s Preventing Chronic Disease.
The researchers conducted a phone survey of 1,109 overweight or obese adults, asking whether a HCP had in the previous 12 months given them advice about their weight. A “concerning” finding, the researchers say: Only 35% of the respondents reported getting advice.
Related: Confronting the Diabetes Epidemic
As body mass index (BMI) increased, so did the likelihood of receiving weight-loss advice: 22% of those with a BMI of 25.0 to 29.9 received advice vs 63% of those with a BMI of 40.0 or higher. Hispanics were the most likely of the 3 racial/ethnic groups to report receiving advice from a HCP. The researchers say other studies have suggested that a higher prevalence of weight problems among African Americans and Hispanics draws more attention from HCPs for counseling.
High-risk patients, such as the extremely obese or those with comorbidities, are most likely to receive weight-loss advice, the researchers say. But demographic factors also come into play: People with high levels of education are more likely than those with low levels to receive advice, and middle-aged people are more likely to get advice than are younger or older patients.
Related: Diabetes Report: The News Isn’t Good
Patients in the lowest-income groups had significantly lower odds of receiving weight-loss advice compared with those in higher income groups. Adjusting for health insurance did not change the results. That finding is “problematic,” the researchers say, because people with the lowest incomes tend to have poorer health outcomes than that of those with higher incomes.
About two-thirds of overweight and obese patients are not getting the advice they need from their health care providers (HCPs) about weight management, according to a study by Arizona State researchers, reported in the CDC’s Preventing Chronic Disease.
The researchers conducted a phone survey of 1,109 overweight or obese adults, asking whether a HCP had in the previous 12 months given them advice about their weight. A “concerning” finding, the researchers say: Only 35% of the respondents reported getting advice.
Related: Confronting the Diabetes Epidemic
As body mass index (BMI) increased, so did the likelihood of receiving weight-loss advice: 22% of those with a BMI of 25.0 to 29.9 received advice vs 63% of those with a BMI of 40.0 or higher. Hispanics were the most likely of the 3 racial/ethnic groups to report receiving advice from a HCP. The researchers say other studies have suggested that a higher prevalence of weight problems among African Americans and Hispanics draws more attention from HCPs for counseling.
High-risk patients, such as the extremely obese or those with comorbidities, are most likely to receive weight-loss advice, the researchers say. But demographic factors also come into play: People with high levels of education are more likely than those with low levels to receive advice, and middle-aged people are more likely to get advice than are younger or older patients.
Related: Diabetes Report: The News Isn’t Good
Patients in the lowest-income groups had significantly lower odds of receiving weight-loss advice compared with those in higher income groups. Adjusting for health insurance did not change the results. That finding is “problematic,” the researchers say, because people with the lowest incomes tend to have poorer health outcomes than that of those with higher incomes.
Why Aren’t Doctors Following Guidelines?

One recent paper in Clinical Pediatrics, for example, chronicled low adherence to the 2011 National Heart, Lung, and Blood Institute lipid screening guidelines in primary-care settings.1 Another cautioned providers to “mind the (implementation) gap” in venous thromboembolism prevention guidelines for medical inpatients.2 A third found that lower adherence to guidelines issued by the American College of Cardiology/American Heart Association for acute coronary syndrome patients was significantly associated with higher bleeding and mortality rates.3
Both clinical trials and real-world studies have demonstrated that when guidelines are applied, patients do better, says William Lewis, MD, professor of medicine at Case Western Reserve University and director of the Heart & Vascular Center at MetroHealth in Cleveland. So why aren’t they followed more consistently?
Experts in both HM and other disciplines cite multiple obstacles. Lack of evidence, conflicting evidence, or lack of awareness about evidence can all conspire against the main goal of helping providers deliver consistent high-value care, says Christopher Moriates, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California, San Francisco.

“In our day-to-day lives as hospitalists, for the vast majority probably of what we do there’s no clear guideline or there’s a guideline that doesn’t necessarily apply to the patient standing in front of me,” he says.
Even when a guideline is clear and relevant, other doctors say inadequate dissemination and implementation can still derail quality improvement efforts.
“A lot of what we do as physicians is what we learned in residency, and to incorporate the new data is difficult,” says Leonard Feldman, MD, SFHM, a hospitalist and associate professor of internal medicine and pediatrics at Johns Hopkins School of Medicine in Baltimore.

Dr. Feldman believes many doctors have yet to integrate recently revised hypertension and cholesterol guidelines into their practice, for example. Some guidelines have proven more complex or controversial, limiting their adoption.
“I know I struggle to keep up with all of the guidelines, and I’m in a big academic center where people are talking about them all the time, and I’m working with residents who are talking about them all the time,” Dr. Feldman says.
Despite the remaining gaps, however, many researchers agree that momentum has built steadily over the past two decades toward a more systematic approach to creating solid evidence-based guidelines and integrating them into real-world decision making.
Emphasis on Evidence and Transparency

The term “evidence-based medicine” was coined in 1990 by Gordon Guyatt, MD, MSc, FRCPC, distinguished professor of medicine and clinical epidemiology at McMaster University in Hamilton, Ontario. It’s played an active role in formulating guidelines for multiple organizations. The guideline-writing process, Dr. Guyatt says, once consisted of little more than self-selected clinicians sitting around a table.
“It used to be that a bunch of experts got together and decided and made the recommendations with very little in the way of a systematic process and certainly not evidence based,” he says.
Cincinnati Children’s Hospital Medical Center was among the pioneers pushing for a more systematic approach; the hospital began working on its own guidelines in 1995 and published the first of many the following year.

“We started evidence-based guidelines when the docs were still saying, ‘This is cookbook medicine. I don’t know if I want to do this or not,’” says Wendy Gerhardt, MSN, director of evidence-based decision making in the James M. Anderson Center for Health Systems Excellence at Cincinnati Children’s.
Some doctors also argued that clinical guidelines would stifle innovation, cramp their individual style, or intrude on their relationships with patients. Despite some lingering misgivings among clinicians, however, the process has gained considerable support. In 2000, an organization called the GRADE Working Group (Grading of Recommendations, Assessment, Development and Evaluation) began developing a new approach to raise the quality of evidence and strength of recommendations.
The group’s work led to a 2004 article in BMJ, and the journal subsequently published a six-part series about GRADE for clinicians.4 More recently, the Journal of Clinical Epidemiology also delved into the issue with a 15-part series detailing the GRADE methodology.5 Together, Dr. Guyatt says, the articles have become a go-to guide for guidelines and have helped solidify the focus on evidence.
Cincinnati Children’s and other institutions also have developed tools, and the Institute of Medicine has published guideline-writing standards.
“So it’s easier than it’s ever been to know whether or not you have a decent guideline in your hand,” Gerhardt says.
Likewise, medical organizations are more clearly explaining how they came up with different kinds of guidelines. Evidence-based and consensus guidelines aren’t necessarily mutually exclusive, though consensus building is often used in the absence of high-quality evidence. Some organizations have limited the pool of evidence for guidelines to randomized controlled trial data.
“Unfortunately, for us in the real world, we actually have to make decisions even when there’s not enough data,” Dr. Feldman says.
Sometimes, the best available evidence may be observational studies, and some committees still try to reach a consensus based on that evidence and on the panelists’ professional opinions.
Dr. Guyatt agrees that it’s “absolutely not” true that evidence-based guidelines require randomized controlled trials. “What you need for any recommendation is a thorough review and summary of the best available evidence,” he says.
As part of each final document, Cincinnati Children’s details how it created the guideline, when the literature searches occurred, how the committee reached a consensus, and which panelists participated in the deliberations. The information, Gerhardt says, allows anyone else to “make some sensible decisions about whether or not it’s a guideline you want to use.”
Guideline-crafting institutions are also focusing more on the proper makeup of their panels. In general, Dr. Guyatt says, a panel with more than 10 people can be unwieldy. Guidelines that include many specific recommendations, however, may require multiple subsections, each with its own committee.
Dr. Guyatt is careful to note that, like many other experts, he has multiple potential conflicts of interest, such as working on the anti-thrombotic guidelines issued by the American College of Chest Physicians. Committees, he says, have become increasingly aware of how properly handling conflicts (financial or otherwise) can be critical in building and maintaining trust among clinicians and patients. One technique is to ensure that a diversity of opinions is reflected among a committee whose experts have various conflicts. If one expert’s company makes drug A, for example, then the committee also includes experts involved with drugs B or C. As an alternative, some committees have explicitly barred anyone with a conflict of interest from participating at all.
But experts often provide crucial input, Dr. Guyatt says, and several committees have adopted variations of a middle-ground approach. In an approach that he favors, all guideline-formulating panelists are conflict-free but begin their work by meeting with a separate group of experts who may have some conflicts but can help point out the main issues. The panelists then deliberate and write a draft of the recommendations, after which they meet again with the experts to receive feedback before finalizing the draft.
In a related approach, experts sit on the panel and discuss the evidence, but those with conflicts recuse themselves before the group votes on any recommendations. Delineating between discussions of the evidence and discussions of recommendations can be tricky, though, increasing the risk that a conflict of interest may influence the outcome. Even so, Dr. Guyatt says the model is still preferable to other alternatives.
Getting the Word Out
Once guidelines have been crafted and vetted, how can hospitalists get up to speed on them? Dr. Feldman’s favorite go-to source is Guideline.gov, a national guideline clearinghouse that he calls one of the best compendiums of available information. Especially helpful, he adds, are details such as how the guidelines were created.
To help maximize his time, he also uses tools like NEJM Journal Watch, which sends daily emails on noteworthy articles and weekend roundups of the most important studies.
“It is a way of at least trying to keep up with what’s going on,” he says. Similarly, he adds, ACP Journal Club provides summaries of important new articles, The Hospitalist can help highlight important guidelines that affect HM, and CME meetings or online modules like SHMconsults.com can help doctors keep pace.
For the past decade, Dr. Guyatt has worked with another popular tool, a guideline-disseminating service called UpToDate. Many alternatives exist, such as DynaMed Plus.
“I think you just need to pick away,” Dr. Feldman says. “You need to decide that as a physician, as a lifelong learner, that you are going to do something that is going to keep you up-to-date. There are many ways of doing it. You just have to decide what you’re going to do and commit to it.”
Researchers are helping out by studying how to present new guidelines in ways that engage doctors and improve patient outcomes. Another trend is to make guidelines routinely accessible not only in electronic medical records but also on tablets and smartphones. Lisa Shieh, MD, PhD, FHM, a hospitalist and clinical professor of medicine at Stanford University Medical Center, has studied how best-practice alerts, or BPAs, impact adherence to guidelines covering the appropriate use of blood products. Dr. Shieh, who splits her time between quality improvement and hospital medicine, says getting new information and guidelines into clinicians’ hands can be a logistical challenge.
“At Stanford, we had a huge official campaign around the guidelines, and that did make some impact, but it wasn’t huge in improving appropriate blood use,” she says. When the medial center set up a BPA through the electronic medical record system, however, both overall and inappropriate blood use declined significantly. In fact, the percentage of providers ordering blood products for patients with a hemoglobin count above 8 g/dL dropped from 60% to 25%.6
One difference maker, Dr. Shieh says, was providing education at the moment a doctor actually ordered blood. To avoid alert fatigue, the “smart BPA” fires only if a doctor tries to order blood and the patient’s hemoglobin is greater than 7 or 8 g/dL, depending on the diagnosis. If the doctor still wants to transfuse, the system requests a clinical indication for the exception.
Despite the clear improvement in appropriate use, the team wanted to understand why 25% of providers were still ordering blood products for patients with a hemoglobin count greater than 8 despite the triggered BPA and whether additional interventions could yield further improvements. Through their study, the researchers documented several reasons for the continued ordering. In some cases, the system failed to properly document actual or potential bleeding as an indicator. In other cases, the ordering reflected a lack of consensus on the guidelines in fields like hematology and oncology.
One of the most intriguing reasons, though, was that residents often did the ordering at the behest of an attending who might have never seen the BPA.
“It’s not actually reaching the audience making the decision; it might be reaching the audience that’s just carrying out the order,” Dr. Shieh says.
The insight, she says, may provide an opportunity to talk with attending physicians who may not have completely bought into the guidelines and to involve the entire team in the decision-making process.
Hospitalists, she says, can play a vital role in guideline development and implementation, especially for strategies that include BPAs.
“I think they’re the perfect group to help use this technology wisely because they are at the front lines taking care of patients so they’ll know the best workflow of when these alerts fire and maybe which ones happen the most often,” Dr. Shieh says. “I think this is a fantastic opportunity to get more hospitalists involved in designing these alerts and collaborating with the IT folks.”
Even with widespread buy-in from providers, guidelines may not reach their full potential without a careful consideration of patients’ values and concerns. Experts say joint deliberations and discussions are especially important for guidelines that are complicated, controversial, or carrying potential risks that must be weighed against the benefits.
Some of the conversations are easy, with well-defined risks and benefits and clear patient preferences, but others must traverse vast tracts of gray area. Fortunately, Dr. Feldman says, more tools also are becoming available for this kind of shared decision making. Some use pictorial representations to help patients understand the potential outcomes of alternative courses of action or inaction.
“Sometimes, that pictorial representation is worth the 1,000 words that we wouldn’t be able to adequately describe otherwise,” he says.
Similarly, Cincinnati Children’s has developed tools to help to ease the shared decision-making process.
“We look where there’s equivocal evidence or no evidence and have developed tools that help the clinician have that conversation with the family and then have them informed enough that they can actually weigh in on what they want,” Gerhardt says. One end product is a card or trifold pamphlet that might help parents understand the benefits and side effects of alternate strategies.
“Typically, in medicine, we’re used to telling people what needs to be done,” she says. “So shared decision making is kind of a different thing for clinicians to engage in.” TH
Bryn Nelson, PhD, is a freelance writer in Seattle.
References
- Valle CW, Binns HJ, Quadri-Sheriff M, Benuck I, Patel A. Physicians’ lack of adherence to National Heart, Lung, and Blood Institute guidelines for pediatric lipid screening. Clin Pediatr. 2015;54(12):1200-1205.
- Maynard G, Jenkins IH, Merli GJ. Venous thromboembolism prevention guidelines for medical inpatients: mind the (implementation) gap. J Hosp Med. 2013;8(10):582-588.
- Mehta RH, Chen AY, Alexander KP, Ohman EM, Roe MT, Peterson ED. Doing the right things and doing them the right way: association between hospital guideline adherence, dosing safety, and outcomes among patients with acute coronary syndrome. Circulation. 2015;131(11):980-987.
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ. 2004;328:1490
- Andrews JC, Schünemann HJ, Oxman AD, et al. GRADE guidelines: 15. Going from evidence to recommendation—determinants of a recommendation’s direction and strength. J Clin Epidemiol. 2013;66(7):726-735.
- 6. Chen JH, Fang DZ, Tim Goodnough L, Evans KH, Lee Porter M, Shieh L. Why providers transfuse blood products outside recommended guidelines in spite of integrated electronic best practice alerts. J Hosp Med. 2015;10(1):1-7.
One recent paper in Clinical Pediatrics, for example, chronicled low adherence to the 2011 National Heart, Lung, and Blood Institute lipid screening guidelines in primary-care settings.1 Another cautioned providers to “mind the (implementation) gap” in venous thromboembolism prevention guidelines for medical inpatients.2 A third found that lower adherence to guidelines issued by the American College of Cardiology/American Heart Association for acute coronary syndrome patients was significantly associated with higher bleeding and mortality rates.3
Both clinical trials and real-world studies have demonstrated that when guidelines are applied, patients do better, says William Lewis, MD, professor of medicine at Case Western Reserve University and director of the Heart & Vascular Center at MetroHealth in Cleveland. So why aren’t they followed more consistently?
Experts in both HM and other disciplines cite multiple obstacles. Lack of evidence, conflicting evidence, or lack of awareness about evidence can all conspire against the main goal of helping providers deliver consistent high-value care, says Christopher Moriates, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California, San Francisco.
“In our day-to-day lives as hospitalists, for the vast majority probably of what we do there’s no clear guideline or there’s a guideline that doesn’t necessarily apply to the patient standing in front of me,” he says.
Even when a guideline is clear and relevant, other doctors say inadequate dissemination and implementation can still derail quality improvement efforts.
“A lot of what we do as physicians is what we learned in residency, and to incorporate the new data is difficult,” says Leonard Feldman, MD, SFHM, a hospitalist and associate professor of internal medicine and pediatrics at Johns Hopkins School of Medicine in Baltimore.
Dr. Feldman believes many doctors have yet to integrate recently revised hypertension and cholesterol guidelines into their practice, for example. Some guidelines have proven more complex or controversial, limiting their adoption.
“I know I struggle to keep up with all of the guidelines, and I’m in a big academic center where people are talking about them all the time, and I’m working with residents who are talking about them all the time,” Dr. Feldman says.
Despite the remaining gaps, however, many researchers agree that momentum has built steadily over the past two decades toward a more systematic approach to creating solid evidence-based guidelines and integrating them into real-world decision making.
Emphasis on Evidence and Transparency
The term “evidence-based medicine” was coined in 1990 by Gordon Guyatt, MD, MSc, FRCPC, distinguished professor of medicine and clinical epidemiology at McMaster University in Hamilton, Ontario. It’s played an active role in formulating guidelines for multiple organizations. The guideline-writing process, Dr. Guyatt says, once consisted of little more than self-selected clinicians sitting around a table.
“It used to be that a bunch of experts got together and decided and made the recommendations with very little in the way of a systematic process and certainly not evidence based,” he says.
Cincinnati Children’s Hospital Medical Center was among the pioneers pushing for a more systematic approach; the hospital began working on its own guidelines in 1995 and published the first of many the following year.
“We started evidence-based guidelines when the docs were still saying, ‘This is cookbook medicine. I don’t know if I want to do this or not,’” says Wendy Gerhardt, MSN, director of evidence-based decision making in the James M. Anderson Center for Health Systems Excellence at Cincinnati Children’s.
Some doctors also argued that clinical guidelines would stifle innovation, cramp their individual style, or intrude on their relationships with patients. Despite some lingering misgivings among clinicians, however, the process has gained considerable support. In 2000, an organization called the GRADE Working Group (Grading of Recommendations, Assessment, Development and Evaluation) began developing a new approach to raise the quality of evidence and strength of recommendations.
The group’s work led to a 2004 article in BMJ, and the journal subsequently published a six-part series about GRADE for clinicians.4 More recently, the Journal of Clinical Epidemiology also delved into the issue with a 15-part series detailing the GRADE methodology.5 Together, Dr. Guyatt says, the articles have become a go-to guide for guidelines and have helped solidify the focus on evidence.
Cincinnati Children’s and other institutions also have developed tools, and the Institute of Medicine has published guideline-writing standards.
“So it’s easier than it’s ever been to know whether or not you have a decent guideline in your hand,” Gerhardt says.
Likewise, medical organizations are more clearly explaining how they came up with different kinds of guidelines. Evidence-based and consensus guidelines aren’t necessarily mutually exclusive, though consensus building is often used in the absence of high-quality evidence. Some organizations have limited the pool of evidence for guidelines to randomized controlled trial data.
“Unfortunately, for us in the real world, we actually have to make decisions even when there’s not enough data,” Dr. Feldman says.
Sometimes, the best available evidence may be observational studies, and some committees still try to reach a consensus based on that evidence and on the panelists’ professional opinions.
Dr. Guyatt agrees that it’s “absolutely not” true that evidence-based guidelines require randomized controlled trials. “What you need for any recommendation is a thorough review and summary of the best available evidence,” he says.
As part of each final document, Cincinnati Children’s details how it created the guideline, when the literature searches occurred, how the committee reached a consensus, and which panelists participated in the deliberations. The information, Gerhardt says, allows anyone else to “make some sensible decisions about whether or not it’s a guideline you want to use.”
Guideline-crafting institutions are also focusing more on the proper makeup of their panels. In general, Dr. Guyatt says, a panel with more than 10 people can be unwieldy. Guidelines that include many specific recommendations, however, may require multiple subsections, each with its own committee.
Dr. Guyatt is careful to note that, like many other experts, he has multiple potential conflicts of interest, such as working on the anti-thrombotic guidelines issued by the American College of Chest Physicians. Committees, he says, have become increasingly aware of how properly handling conflicts (financial or otherwise) can be critical in building and maintaining trust among clinicians and patients. One technique is to ensure that a diversity of opinions is reflected among a committee whose experts have various conflicts. If one expert’s company makes drug A, for example, then the committee also includes experts involved with drugs B or C. As an alternative, some committees have explicitly barred anyone with a conflict of interest from participating at all.
But experts often provide crucial input, Dr. Guyatt says, and several committees have adopted variations of a middle-ground approach. In an approach that he favors, all guideline-formulating panelists are conflict-free but begin their work by meeting with a separate group of experts who may have some conflicts but can help point out the main issues. The panelists then deliberate and write a draft of the recommendations, after which they meet again with the experts to receive feedback before finalizing the draft.
In a related approach, experts sit on the panel and discuss the evidence, but those with conflicts recuse themselves before the group votes on any recommendations. Delineating between discussions of the evidence and discussions of recommendations can be tricky, though, increasing the risk that a conflict of interest may influence the outcome. Even so, Dr. Guyatt says the model is still preferable to other alternatives.
Getting the Word Out
Once guidelines have been crafted and vetted, how can hospitalists get up to speed on them? Dr. Feldman’s favorite go-to source is Guideline.gov, a national guideline clearinghouse that he calls one of the best compendiums of available information. Especially helpful, he adds, are details such as how the guidelines were created.
To help maximize his time, he also uses tools like NEJM Journal Watch, which sends daily emails on noteworthy articles and weekend roundups of the most important studies.
“It is a way of at least trying to keep up with what’s going on,” he says. Similarly, he adds, ACP Journal Club provides summaries of important new articles, The Hospitalist can help highlight important guidelines that affect HM, and CME meetings or online modules like SHMconsults.com can help doctors keep pace.
For the past decade, Dr. Guyatt has worked with another popular tool, a guideline-disseminating service called UpToDate. Many alternatives exist, such as DynaMed Plus.
“I think you just need to pick away,” Dr. Feldman says. “You need to decide that as a physician, as a lifelong learner, that you are going to do something that is going to keep you up-to-date. There are many ways of doing it. You just have to decide what you’re going to do and commit to it.”
Researchers are helping out by studying how to present new guidelines in ways that engage doctors and improve patient outcomes. Another trend is to make guidelines routinely accessible not only in electronic medical records but also on tablets and smartphones. Lisa Shieh, MD, PhD, FHM, a hospitalist and clinical professor of medicine at Stanford University Medical Center, has studied how best-practice alerts, or BPAs, impact adherence to guidelines covering the appropriate use of blood products. Dr. Shieh, who splits her time between quality improvement and hospital medicine, says getting new information and guidelines into clinicians’ hands can be a logistical challenge.
“At Stanford, we had a huge official campaign around the guidelines, and that did make some impact, but it wasn’t huge in improving appropriate blood use,” she says. When the medial center set up a BPA through the electronic medical record system, however, both overall and inappropriate blood use declined significantly. In fact, the percentage of providers ordering blood products for patients with a hemoglobin count above 8 g/dL dropped from 60% to 25%.6
One difference maker, Dr. Shieh says, was providing education at the moment a doctor actually ordered blood. To avoid alert fatigue, the “smart BPA” fires only if a doctor tries to order blood and the patient’s hemoglobin is greater than 7 or 8 g/dL, depending on the diagnosis. If the doctor still wants to transfuse, the system requests a clinical indication for the exception.
Despite the clear improvement in appropriate use, the team wanted to understand why 25% of providers were still ordering blood products for patients with a hemoglobin count greater than 8 despite the triggered BPA and whether additional interventions could yield further improvements. Through their study, the researchers documented several reasons for the continued ordering. In some cases, the system failed to properly document actual or potential bleeding as an indicator. In other cases, the ordering reflected a lack of consensus on the guidelines in fields like hematology and oncology.
One of the most intriguing reasons, though, was that residents often did the ordering at the behest of an attending who might have never seen the BPA.
“It’s not actually reaching the audience making the decision; it might be reaching the audience that’s just carrying out the order,” Dr. Shieh says.
The insight, she says, may provide an opportunity to talk with attending physicians who may not have completely bought into the guidelines and to involve the entire team in the decision-making process.
Hospitalists, she says, can play a vital role in guideline development and implementation, especially for strategies that include BPAs.
“I think they’re the perfect group to help use this technology wisely because they are at the front lines taking care of patients so they’ll know the best workflow of when these alerts fire and maybe which ones happen the most often,” Dr. Shieh says. “I think this is a fantastic opportunity to get more hospitalists involved in designing these alerts and collaborating with the IT folks.”
Even with widespread buy-in from providers, guidelines may not reach their full potential without a careful consideration of patients’ values and concerns. Experts say joint deliberations and discussions are especially important for guidelines that are complicated, controversial, or carrying potential risks that must be weighed against the benefits.
Some of the conversations are easy, with well-defined risks and benefits and clear patient preferences, but others must traverse vast tracts of gray area. Fortunately, Dr. Feldman says, more tools also are becoming available for this kind of shared decision making. Some use pictorial representations to help patients understand the potential outcomes of alternative courses of action or inaction.
“Sometimes, that pictorial representation is worth the 1,000 words that we wouldn’t be able to adequately describe otherwise,” he says.
Similarly, Cincinnati Children’s has developed tools to help to ease the shared decision-making process.
“We look where there’s equivocal evidence or no evidence and have developed tools that help the clinician have that conversation with the family and then have them informed enough that they can actually weigh in on what they want,” Gerhardt says. One end product is a card or trifold pamphlet that might help parents understand the benefits and side effects of alternate strategies.
“Typically, in medicine, we’re used to telling people what needs to be done,” she says. “So shared decision making is kind of a different thing for clinicians to engage in.” TH
Bryn Nelson, PhD, is a freelance writer in Seattle.
References
- Valle CW, Binns HJ, Quadri-Sheriff M, Benuck I, Patel A. Physicians’ lack of adherence to National Heart, Lung, and Blood Institute guidelines for pediatric lipid screening. Clin Pediatr. 2015;54(12):1200-1205.
- Maynard G, Jenkins IH, Merli GJ. Venous thromboembolism prevention guidelines for medical inpatients: mind the (implementation) gap. J Hosp Med. 2013;8(10):582-588.
- Mehta RH, Chen AY, Alexander KP, Ohman EM, Roe MT, Peterson ED. Doing the right things and doing them the right way: association between hospital guideline adherence, dosing safety, and outcomes among patients with acute coronary syndrome. Circulation. 2015;131(11):980-987.
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ. 2004;328:1490
- Andrews JC, Schünemann HJ, Oxman AD, et al. GRADE guidelines: 15. Going from evidence to recommendation—determinants of a recommendation’s direction and strength. J Clin Epidemiol. 2013;66(7):726-735.
- 6. Chen JH, Fang DZ, Tim Goodnough L, Evans KH, Lee Porter M, Shieh L. Why providers transfuse blood products outside recommended guidelines in spite of integrated electronic best practice alerts. J Hosp Med. 2015;10(1):1-7.
One recent paper in Clinical Pediatrics, for example, chronicled low adherence to the 2011 National Heart, Lung, and Blood Institute lipid screening guidelines in primary-care settings.1 Another cautioned providers to “mind the (implementation) gap” in venous thromboembolism prevention guidelines for medical inpatients.2 A third found that lower adherence to guidelines issued by the American College of Cardiology/American Heart Association for acute coronary syndrome patients was significantly associated with higher bleeding and mortality rates.3
Both clinical trials and real-world studies have demonstrated that when guidelines are applied, patients do better, says William Lewis, MD, professor of medicine at Case Western Reserve University and director of the Heart & Vascular Center at MetroHealth in Cleveland. So why aren’t they followed more consistently?
Experts in both HM and other disciplines cite multiple obstacles. Lack of evidence, conflicting evidence, or lack of awareness about evidence can all conspire against the main goal of helping providers deliver consistent high-value care, says Christopher Moriates, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California, San Francisco.
“In our day-to-day lives as hospitalists, for the vast majority probably of what we do there’s no clear guideline or there’s a guideline that doesn’t necessarily apply to the patient standing in front of me,” he says.
Even when a guideline is clear and relevant, other doctors say inadequate dissemination and implementation can still derail quality improvement efforts.
“A lot of what we do as physicians is what we learned in residency, and to incorporate the new data is difficult,” says Leonard Feldman, MD, SFHM, a hospitalist and associate professor of internal medicine and pediatrics at Johns Hopkins School of Medicine in Baltimore.
Dr. Feldman believes many doctors have yet to integrate recently revised hypertension and cholesterol guidelines into their practice, for example. Some guidelines have proven more complex or controversial, limiting their adoption.
“I know I struggle to keep up with all of the guidelines, and I’m in a big academic center where people are talking about them all the time, and I’m working with residents who are talking about them all the time,” Dr. Feldman says.
Despite the remaining gaps, however, many researchers agree that momentum has built steadily over the past two decades toward a more systematic approach to creating solid evidence-based guidelines and integrating them into real-world decision making.
Emphasis on Evidence and Transparency
The term “evidence-based medicine” was coined in 1990 by Gordon Guyatt, MD, MSc, FRCPC, distinguished professor of medicine and clinical epidemiology at McMaster University in Hamilton, Ontario. It’s played an active role in formulating guidelines for multiple organizations. The guideline-writing process, Dr. Guyatt says, once consisted of little more than self-selected clinicians sitting around a table.
“It used to be that a bunch of experts got together and decided and made the recommendations with very little in the way of a systematic process and certainly not evidence based,” he says.
Cincinnati Children’s Hospital Medical Center was among the pioneers pushing for a more systematic approach; the hospital began working on its own guidelines in 1995 and published the first of many the following year.
“We started evidence-based guidelines when the docs were still saying, ‘This is cookbook medicine. I don’t know if I want to do this or not,’” says Wendy Gerhardt, MSN, director of evidence-based decision making in the James M. Anderson Center for Health Systems Excellence at Cincinnati Children’s.
Some doctors also argued that clinical guidelines would stifle innovation, cramp their individual style, or intrude on their relationships with patients. Despite some lingering misgivings among clinicians, however, the process has gained considerable support. In 2000, an organization called the GRADE Working Group (Grading of Recommendations, Assessment, Development and Evaluation) began developing a new approach to raise the quality of evidence and strength of recommendations.
The group’s work led to a 2004 article in BMJ, and the journal subsequently published a six-part series about GRADE for clinicians.4 More recently, the Journal of Clinical Epidemiology also delved into the issue with a 15-part series detailing the GRADE methodology.5 Together, Dr. Guyatt says, the articles have become a go-to guide for guidelines and have helped solidify the focus on evidence.
Cincinnati Children’s and other institutions also have developed tools, and the Institute of Medicine has published guideline-writing standards.
“So it’s easier than it’s ever been to know whether or not you have a decent guideline in your hand,” Gerhardt says.
Likewise, medical organizations are more clearly explaining how they came up with different kinds of guidelines. Evidence-based and consensus guidelines aren’t necessarily mutually exclusive, though consensus building is often used in the absence of high-quality evidence. Some organizations have limited the pool of evidence for guidelines to randomized controlled trial data.
“Unfortunately, for us in the real world, we actually have to make decisions even when there’s not enough data,” Dr. Feldman says.
Sometimes, the best available evidence may be observational studies, and some committees still try to reach a consensus based on that evidence and on the panelists’ professional opinions.
Dr. Guyatt agrees that it’s “absolutely not” true that evidence-based guidelines require randomized controlled trials. “What you need for any recommendation is a thorough review and summary of the best available evidence,” he says.
As part of each final document, Cincinnati Children’s details how it created the guideline, when the literature searches occurred, how the committee reached a consensus, and which panelists participated in the deliberations. The information, Gerhardt says, allows anyone else to “make some sensible decisions about whether or not it’s a guideline you want to use.”
Guideline-crafting institutions are also focusing more on the proper makeup of their panels. In general, Dr. Guyatt says, a panel with more than 10 people can be unwieldy. Guidelines that include many specific recommendations, however, may require multiple subsections, each with its own committee.
Dr. Guyatt is careful to note that, like many other experts, he has multiple potential conflicts of interest, such as working on the anti-thrombotic guidelines issued by the American College of Chest Physicians. Committees, he says, have become increasingly aware of how properly handling conflicts (financial or otherwise) can be critical in building and maintaining trust among clinicians and patients. One technique is to ensure that a diversity of opinions is reflected among a committee whose experts have various conflicts. If one expert’s company makes drug A, for example, then the committee also includes experts involved with drugs B or C. As an alternative, some committees have explicitly barred anyone with a conflict of interest from participating at all.
But experts often provide crucial input, Dr. Guyatt says, and several committees have adopted variations of a middle-ground approach. In an approach that he favors, all guideline-formulating panelists are conflict-free but begin their work by meeting with a separate group of experts who may have some conflicts but can help point out the main issues. The panelists then deliberate and write a draft of the recommendations, after which they meet again with the experts to receive feedback before finalizing the draft.
In a related approach, experts sit on the panel and discuss the evidence, but those with conflicts recuse themselves before the group votes on any recommendations. Delineating between discussions of the evidence and discussions of recommendations can be tricky, though, increasing the risk that a conflict of interest may influence the outcome. Even so, Dr. Guyatt says the model is still preferable to other alternatives.
Getting the Word Out
Once guidelines have been crafted and vetted, how can hospitalists get up to speed on them? Dr. Feldman’s favorite go-to source is Guideline.gov, a national guideline clearinghouse that he calls one of the best compendiums of available information. Especially helpful, he adds, are details such as how the guidelines were created.
To help maximize his time, he also uses tools like NEJM Journal Watch, which sends daily emails on noteworthy articles and weekend roundups of the most important studies.
“It is a way of at least trying to keep up with what’s going on,” he says. Similarly, he adds, ACP Journal Club provides summaries of important new articles, The Hospitalist can help highlight important guidelines that affect HM, and CME meetings or online modules like SHMconsults.com can help doctors keep pace.
For the past decade, Dr. Guyatt has worked with another popular tool, a guideline-disseminating service called UpToDate. Many alternatives exist, such as DynaMed Plus.
“I think you just need to pick away,” Dr. Feldman says. “You need to decide that as a physician, as a lifelong learner, that you are going to do something that is going to keep you up-to-date. There are many ways of doing it. You just have to decide what you’re going to do and commit to it.”
Researchers are helping out by studying how to present new guidelines in ways that engage doctors and improve patient outcomes. Another trend is to make guidelines routinely accessible not only in electronic medical records but also on tablets and smartphones. Lisa Shieh, MD, PhD, FHM, a hospitalist and clinical professor of medicine at Stanford University Medical Center, has studied how best-practice alerts, or BPAs, impact adherence to guidelines covering the appropriate use of blood products. Dr. Shieh, who splits her time between quality improvement and hospital medicine, says getting new information and guidelines into clinicians’ hands can be a logistical challenge.
“At Stanford, we had a huge official campaign around the guidelines, and that did make some impact, but it wasn’t huge in improving appropriate blood use,” she says. When the medial center set up a BPA through the electronic medical record system, however, both overall and inappropriate blood use declined significantly. In fact, the percentage of providers ordering blood products for patients with a hemoglobin count above 8 g/dL dropped from 60% to 25%.6
One difference maker, Dr. Shieh says, was providing education at the moment a doctor actually ordered blood. To avoid alert fatigue, the “smart BPA” fires only if a doctor tries to order blood and the patient’s hemoglobin is greater than 7 or 8 g/dL, depending on the diagnosis. If the doctor still wants to transfuse, the system requests a clinical indication for the exception.
Despite the clear improvement in appropriate use, the team wanted to understand why 25% of providers were still ordering blood products for patients with a hemoglobin count greater than 8 despite the triggered BPA and whether additional interventions could yield further improvements. Through their study, the researchers documented several reasons for the continued ordering. In some cases, the system failed to properly document actual or potential bleeding as an indicator. In other cases, the ordering reflected a lack of consensus on the guidelines in fields like hematology and oncology.
One of the most intriguing reasons, though, was that residents often did the ordering at the behest of an attending who might have never seen the BPA.
“It’s not actually reaching the audience making the decision; it might be reaching the audience that’s just carrying out the order,” Dr. Shieh says.
The insight, she says, may provide an opportunity to talk with attending physicians who may not have completely bought into the guidelines and to involve the entire team in the decision-making process.
Hospitalists, she says, can play a vital role in guideline development and implementation, especially for strategies that include BPAs.
“I think they’re the perfect group to help use this technology wisely because they are at the front lines taking care of patients so they’ll know the best workflow of when these alerts fire and maybe which ones happen the most often,” Dr. Shieh says. “I think this is a fantastic opportunity to get more hospitalists involved in designing these alerts and collaborating with the IT folks.”
Even with widespread buy-in from providers, guidelines may not reach their full potential without a careful consideration of patients’ values and concerns. Experts say joint deliberations and discussions are especially important for guidelines that are complicated, controversial, or carrying potential risks that must be weighed against the benefits.
Some of the conversations are easy, with well-defined risks and benefits and clear patient preferences, but others must traverse vast tracts of gray area. Fortunately, Dr. Feldman says, more tools also are becoming available for this kind of shared decision making. Some use pictorial representations to help patients understand the potential outcomes of alternative courses of action or inaction.
“Sometimes, that pictorial representation is worth the 1,000 words that we wouldn’t be able to adequately describe otherwise,” he says.
Similarly, Cincinnati Children’s has developed tools to help to ease the shared decision-making process.
“We look where there’s equivocal evidence or no evidence and have developed tools that help the clinician have that conversation with the family and then have them informed enough that they can actually weigh in on what they want,” Gerhardt says. One end product is a card or trifold pamphlet that might help parents understand the benefits and side effects of alternate strategies.
“Typically, in medicine, we’re used to telling people what needs to be done,” she says. “So shared decision making is kind of a different thing for clinicians to engage in.” TH
Bryn Nelson, PhD, is a freelance writer in Seattle.
References
- Valle CW, Binns HJ, Quadri-Sheriff M, Benuck I, Patel A. Physicians’ lack of adherence to National Heart, Lung, and Blood Institute guidelines for pediatric lipid screening. Clin Pediatr. 2015;54(12):1200-1205.
- Maynard G, Jenkins IH, Merli GJ. Venous thromboembolism prevention guidelines for medical inpatients: mind the (implementation) gap. J Hosp Med. 2013;8(10):582-588.
- Mehta RH, Chen AY, Alexander KP, Ohman EM, Roe MT, Peterson ED. Doing the right things and doing them the right way: association between hospital guideline adherence, dosing safety, and outcomes among patients with acute coronary syndrome. Circulation. 2015;131(11):980-987.
- GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ. 2004;328:1490
- Andrews JC, Schünemann HJ, Oxman AD, et al. GRADE guidelines: 15. Going from evidence to recommendation—determinants of a recommendation’s direction and strength. J Clin Epidemiol. 2013;66(7):726-735.
- 6. Chen JH, Fang DZ, Tim Goodnough L, Evans KH, Lee Porter M, Shieh L. Why providers transfuse blood products outside recommended guidelines in spite of integrated electronic best practice alerts. J Hosp Med. 2015;10(1):1-7.
Evaluation of a Dementia Resource Fair for Veterans, Caregivers, and Staff
Due to the increasing number of older adults, the annual number of new cases of Alzheimer disease and other types of dementia is projected to double by 2050.1 The cost of caring for persons with dementia is rising as well. In 2015, the expected health care cost for persons with dementia in the U.S. is estimated to be $226 billion.1 There is a growing awareness of the needs of persons with dementia and of the importance of providing caregivers with support and education that enables them to keep their loved ones at home as long as possible. Additionally, caregiver stress adversely affects health and increases mortality risk.2-4 Efficacious interventions that teach caregivers to cope with challenging behaviors and functional decline are also available.5,6 Yet many caregivers encounter barriers that prevent access to these interventions. Some may not be able to access interventions due to lack of insurance plan coverage; others may not have the time to participate in these programs.7,8
The VA has requested that its VISNs and VAMCs develop dementia committees so that VA employees can establish goals focused on improving dementia care. The VA Palo Alto Health Care System (VAPAHCS) Dementia Committee determined that veterans, caregivers, and staff needed simple, clear information about dementia, based on consensus opinion. In 2013, one of the committee co-chairs, a clinical nurse specialist in the Geriatric Research Education and Clinical Center (GRECC), introduced the concept of a dementia resource fair. There is evidence supporting the use of interdisciplinary health fairs to educate allied health trainees (eg, nursing students and social workers) through service learning.9 But to the authors’ knowledge, the use of such a fair to provide dementia information has not been evaluated.
The fair drew from the evidence base for formal psychoeducational interventions for caregiversand for those with dementia or cognitive impairment.10,11 The goal of the fair was to provide information about resources for and management of dementia to veterans, families, staff, caregivers, and the community, using printed material and consultation with knowledgeable staff. The GRECC staff also initiated a systematic evaluation of this new initiative and collaborated with the Stanford/VA Alzheimer’s Research Center staff on the evaluation process.
Initial Plan
A subcommittee, composed of interdisciplinary professionals who work with veterans diagnosed with dementia, planned the initial dementia resource fair. The subcommittee representatives included geriatric medicine, nursing, occupational therapy, pharmacy, psychology, recreational therapy, and social work. Subcommittee members were charged with developing VA-branded handouts as educational tools to address key issues related to dementia, such as advance directive planning, behavioral management, home safety, and medication management. The subcommittee met monthly for 6 months and focused on logistics, identification of resource tables, creation of educational materials, advertising, and development of an evaluation. Table 1 provides an overview of the planning time line for the 2013 fair held in San Jose. Findings from a systematic evaluation of the 2013 fair were used to improve the 2015 fair held in Menlo Park. A discussion about the evaluation method and results follows.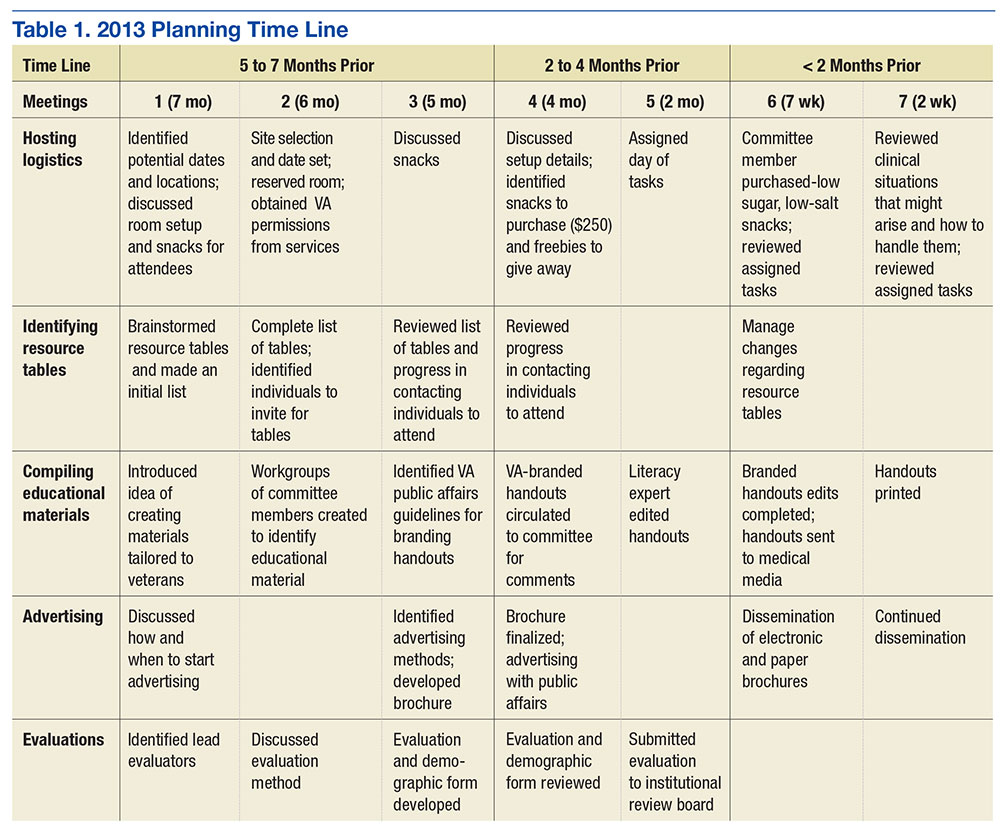
Methods
The first fair was held at a VA community-based outpatient clinic in a small conference room with 13 resource tables. Feedback from attendees in 2013 included suggestions for having more tables, larger event space, more publicity, and alternate locations for the fair. In response to the feedback, the 2015 fair was held at a division of the main VAMC in a large conference room and hosted 20 tables arranged in a horseshoe shape. The second fair included an activity table staffed by a psychology fellow and recreation therapist who provided respite to caregivers if their loved one with dementia accompanied them to the event. Both the 2013 and 2015 fairs were 4 hours long.
A 1-page, anonymous survey was developed to assess attendees’ opinions about the fair. The survey included information about whether attendees were caregivers, veterans, or VA staff but did not ask other demographic questions to preserve anonymity. In 2013, the survey asked attendees to choose the category that best described them, but in 2015, the survey asked attendees to indicate the number of individuals from each category in their party. The 2015 survey assessed 2 additional categories (family member, other) and added a question about the number of people in each party to better estimate attendance. Both surveys also asked attendees to check which resource tables they visited.
The following assessment questions were consistent across both fairs to allow for comparisons. The authors assessed attitudes and learning as a result of the fair, using 2 statements that were rated with a 5-point Likert scale. The authors asked 3 open-ended questions to ascertain the helpful aspects of the fair, unmet needs, and suggestions for improvement. The Stanford University Institutional Review Board (IRB) reviewed this program evaluation plan and determined that the program evaluation project did not require IRB approval.
When attendees arrived at the fair, they received a folder containing branded handouts, a reusable bag, and a survey. Committee members asked that 1 person per party complete the survey at the end of the visit. Attendees visited tables, obtained written materials, and spoke with subcommittee members who staffed the tables. Snacks and light refreshments were provided. The reusable bag was provided by the VAMC Suicide Prevention Program to increase awareness of the VAPAHCS Suicide Prevention Program. As attendees were leaving, they were reminded to complete the survey. Attendees deposited completed surveys in a box to ensure anonymity.
Results
Thirty-six individuals attended the 2013 fair, and 138 individuals attended the 2015 fair. Thirty-one surveys were completed in 2013, yielding an 86% response rate. One hundred six surveys were returned and represented responses for 129 individuals in 2015, yielding a 94% response rate in 2015. Most of the 2013 attendees were caregivers, followed by veterans, VA staff, and outside staff (Table 2). In contrast, most of the 2015 attendees were VA staff, followed by veterans, caregivers/family members, outside staff, and others. Distributions of attendees differed significantly across the fairs: χ2(4) = 12.66; P = .01.
The surveys assessed which tables attendees visited and their perceptions of the fair. The most frequently visited resource table for both 2013 and 2015 fairs was the Alzheimer’s Association table. Other popular resource tables were VA Benefits and VA Caregiver Support in 2013 and Home Safety and End of Life Care in 2015. Ninety-six percent of 2013 attendees and 100% of 2015 attendees strongly agreed or agreed that “attending the dementia fair was worth my time and effort.” Eighty-three percent of 2013 attendees and 100% of 2015 attendees felt that they had learned something useful at the fair. The proportion of individuals reporting that they had learned something useful significantly increased from 2013 to 2015: χ2(2) = 18.07; P = .0001.
To summarize the open-ended responses to the question “What was most helpful about the fair?” the authors constructed a word cloud that displays the 75 most frequently used words in attendees’ descriptions of the 2015 fair (Figure). Attendees provided suggestions about additional information and resources they desired, which included VA benefits enrollment, books and movies about dementia (eg, Still Alice), speech and swallowing disorders representatives, varied types of advance directives, class discussion, question-and-answer time with speakers, and resources for nonveteran older adults. General suggestions for future fairs included hosting the fair at the main division of the VA health care system, having more room between tables, inviting more vendors, using more visual posters at the tables, and additional advertising for VA services.
Discussion
Dementia is a costly disease with detrimental health and well-being effects on caregivers. The dementia resource fairs aimed to connect caregivers with resources for veterans with dementia in the VA and in the community. Given that nearly half the 2015 fair attendees were VA staff, there is an apparent need for increasing dementia education and access to care resource for this VAMC’s workforce. The high proportion of staff attendees at the 2015 fair may be attributed to the 2 VA community living centers at the VAMC site where the fair was held. This unexpected finding points to the importance of informal and interactive education opportunities for staff, particularly those working with veterans with dementia. The fair served an important role for VA staff seeking information on dementia for professional and personal reasons. This systematic evaluation of the fair demonstrated a need for improving access to information about dementia.
The idea of hosting a dementia resource fair was met with enthusiasm from attendees and subcommittee members in 2013. Feedback helped refine the second fair. The increase in self-reported learning from 2013 to 2015 suggests improvements may have been made between the first and second fair; however, this must be interpreted in light of the different compositions of the attendees at each fair and the absence of a control group. Attendees desired even more information about dementia at the second fair, as evidenced by suggestions to have presentations, speakers, and class discussions. These responses suggest that other sites may wish to consider holding similar events. Next steps include researching the effectiveness of low-cost, pragmatic educational initiatives for caregivers. In fact, randomized, controlled trials of dementia caregiver education and skill-building interventions are underway at VAPAHCS.
Conclusion
The primary lesson learned from the most recent fair was that marketing is the key to success. The authors created an efficient hospital publicity plan in 2015 that included (1) flyers posted throughout 2 main medical center campuses; (2) announcements on closed-circuit VA waiting room televisions; (3) e-mail announcements sent to staff; and (4) VA social media announcements. Flyers also were mailed to known caregivers, and announcements of the event were provided to local community agencies. This focus on publicity likely contributed to the substantial increase in participation from the 2013 to 2015 fair.
Future fairs may be improved by providing more detailed information about dementia through formal presentations. The authors aim to increase the number of family caregivers in attendance possibly through coordinating the fair to coincide with primary care clinic hours, advertising the availability of brief respite at the fair, and conducting additional outreach to veterans.
This systematic evaluation of the dementia resource fair confirmed that providing resources in a drop-in setting resulted in self-reported learning about resources available for veterans with dementia. VA dementia care providers are encouraged to use the authors’ time line and lessons learned to develop dementia resource fairs for their sites.
Acknowledgments
The authors wish to acknowledge the members of the 2013 and 2015 Dementia Resource Fair Committees, chaired by Betty Wexler and Kathleen McConnell, respectively. Dr. Gould is supported by the U.S. Department of Veterans Affairs (IK2 RX001478) and by Ellen Schapiro & Gerald Axelbaum through a 2014 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. Dr. Scanlon is supported by the U.S. Department of Veterans Affairs (IK2 RX001240; I21 RX001710), U.S. Department of Defense (W81XWH-15-1-0246), Sierra-Pacific Mental Illness Research Education and Clinical Center, and Stanford/VA Alzheimer’s Research Center. Drs. Gould and Scanlon also receive support from Palo Alto Veterans Institute for Research.
1. Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3)332-384.
2. Schulz R, Beach SR, Cook TB, Martire LM, Tomlinson JM, Monin JK. Predictors and consequences of perceived lack of choice in becoming an informal caregiver. Aging Ment Health. 2012;16(6):712-721.
3. Cooper C, Mukadam N, Katona C, et al; World Federation of Biological Psychiatry – Old Age Taskforce. Systematic review of the effectiveness of non-pharmacological interventions to improve quality of life of people with dementia. Int Psychogeriatr. 2012;24(6):856-870.
4. Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA. 1991;282(23):2215-2219.
5. Brodaty H, Arasaratnam C. Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia. Am J Psychiatry. 2012;169(9):946-953.
6. Gitlin LN. Good news for dementia care: caregiver interventions reduce behavioral symptoms in people with dementia and family distress. Am J Psychiatry. 2012;169(9):894-897.
7. Ho A, Collins SR, Davis K, Doty MM. A look at working-age caregivers roles, health concerns, and need for support. Issue Brief (Commonw Fund). 2005;(854):1-12.
8. Joling KJ, van Marwijk HWJ, Smit F, et al. Does a family meetings intervention prevent depression and anxiety in family caregivers of dementia patients? A randomized trial. PLoS One. 2012;7(1):e30936.
9. Kolomer S, Quinn ME, Steele K. Interdisciplinary health fairs for older adults and the value of interprofessional service learning. J Community Pract. 2010;18(2-3):267-279.
10. Jensen M, Agbata IN, Canavan M, McCarthy G. Effectiveness of educational interventions for informal caregivers of individuals with dementia residing in the community: systematic review and meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry. 2015;30(2):130-143.
11. Quinn C, Toms G, Anderson D, Clare L. A review of self-management interventions for people with dementia and mild cognitive impairment. J Appl Gerontol. 2015;pii:0733464814566852.
Due to the increasing number of older adults, the annual number of new cases of Alzheimer disease and other types of dementia is projected to double by 2050.1 The cost of caring for persons with dementia is rising as well. In 2015, the expected health care cost for persons with dementia in the U.S. is estimated to be $226 billion.1 There is a growing awareness of the needs of persons with dementia and of the importance of providing caregivers with support and education that enables them to keep their loved ones at home as long as possible. Additionally, caregiver stress adversely affects health and increases mortality risk.2-4 Efficacious interventions that teach caregivers to cope with challenging behaviors and functional decline are also available.5,6 Yet many caregivers encounter barriers that prevent access to these interventions. Some may not be able to access interventions due to lack of insurance plan coverage; others may not have the time to participate in these programs.7,8
The VA has requested that its VISNs and VAMCs develop dementia committees so that VA employees can establish goals focused on improving dementia care. The VA Palo Alto Health Care System (VAPAHCS) Dementia Committee determined that veterans, caregivers, and staff needed simple, clear information about dementia, based on consensus opinion. In 2013, one of the committee co-chairs, a clinical nurse specialist in the Geriatric Research Education and Clinical Center (GRECC), introduced the concept of a dementia resource fair. There is evidence supporting the use of interdisciplinary health fairs to educate allied health trainees (eg, nursing students and social workers) through service learning.9 But to the authors’ knowledge, the use of such a fair to provide dementia information has not been evaluated.
The fair drew from the evidence base for formal psychoeducational interventions for caregiversand for those with dementia or cognitive impairment.10,11 The goal of the fair was to provide information about resources for and management of dementia to veterans, families, staff, caregivers, and the community, using printed material and consultation with knowledgeable staff. The GRECC staff also initiated a systematic evaluation of this new initiative and collaborated with the Stanford/VA Alzheimer’s Research Center staff on the evaluation process.
Initial Plan
A subcommittee, composed of interdisciplinary professionals who work with veterans diagnosed with dementia, planned the initial dementia resource fair. The subcommittee representatives included geriatric medicine, nursing, occupational therapy, pharmacy, psychology, recreational therapy, and social work. Subcommittee members were charged with developing VA-branded handouts as educational tools to address key issues related to dementia, such as advance directive planning, behavioral management, home safety, and medication management. The subcommittee met monthly for 6 months and focused on logistics, identification of resource tables, creation of educational materials, advertising, and development of an evaluation. Table 1 provides an overview of the planning time line for the 2013 fair held in San Jose. Findings from a systematic evaluation of the 2013 fair were used to improve the 2015 fair held in Menlo Park. A discussion about the evaluation method and results follows.
Methods
The first fair was held at a VA community-based outpatient clinic in a small conference room with 13 resource tables. Feedback from attendees in 2013 included suggestions for having more tables, larger event space, more publicity, and alternate locations for the fair. In response to the feedback, the 2015 fair was held at a division of the main VAMC in a large conference room and hosted 20 tables arranged in a horseshoe shape. The second fair included an activity table staffed by a psychology fellow and recreation therapist who provided respite to caregivers if their loved one with dementia accompanied them to the event. Both the 2013 and 2015 fairs were 4 hours long.
A 1-page, anonymous survey was developed to assess attendees’ opinions about the fair. The survey included information about whether attendees were caregivers, veterans, or VA staff but did not ask other demographic questions to preserve anonymity. In 2013, the survey asked attendees to choose the category that best described them, but in 2015, the survey asked attendees to indicate the number of individuals from each category in their party. The 2015 survey assessed 2 additional categories (family member, other) and added a question about the number of people in each party to better estimate attendance. Both surveys also asked attendees to check which resource tables they visited.
The following assessment questions were consistent across both fairs to allow for comparisons. The authors assessed attitudes and learning as a result of the fair, using 2 statements that were rated with a 5-point Likert scale. The authors asked 3 open-ended questions to ascertain the helpful aspects of the fair, unmet needs, and suggestions for improvement. The Stanford University Institutional Review Board (IRB) reviewed this program evaluation plan and determined that the program evaluation project did not require IRB approval.
When attendees arrived at the fair, they received a folder containing branded handouts, a reusable bag, and a survey. Committee members asked that 1 person per party complete the survey at the end of the visit. Attendees visited tables, obtained written materials, and spoke with subcommittee members who staffed the tables. Snacks and light refreshments were provided. The reusable bag was provided by the VAMC Suicide Prevention Program to increase awareness of the VAPAHCS Suicide Prevention Program. As attendees were leaving, they were reminded to complete the survey. Attendees deposited completed surveys in a box to ensure anonymity.
Results
Thirty-six individuals attended the 2013 fair, and 138 individuals attended the 2015 fair. Thirty-one surveys were completed in 2013, yielding an 86% response rate. One hundred six surveys were returned and represented responses for 129 individuals in 2015, yielding a 94% response rate in 2015. Most of the 2013 attendees were caregivers, followed by veterans, VA staff, and outside staff (Table 2). In contrast, most of the 2015 attendees were VA staff, followed by veterans, caregivers/family members, outside staff, and others. Distributions of attendees differed significantly across the fairs: χ2(4) = 12.66; P = .01.
The surveys assessed which tables attendees visited and their perceptions of the fair. The most frequently visited resource table for both 2013 and 2015 fairs was the Alzheimer’s Association table. Other popular resource tables were VA Benefits and VA Caregiver Support in 2013 and Home Safety and End of Life Care in 2015. Ninety-six percent of 2013 attendees and 100% of 2015 attendees strongly agreed or agreed that “attending the dementia fair was worth my time and effort.” Eighty-three percent of 2013 attendees and 100% of 2015 attendees felt that they had learned something useful at the fair. The proportion of individuals reporting that they had learned something useful significantly increased from 2013 to 2015: χ2(2) = 18.07; P = .0001.
To summarize the open-ended responses to the question “What was most helpful about the fair?” the authors constructed a word cloud that displays the 75 most frequently used words in attendees’ descriptions of the 2015 fair (Figure). Attendees provided suggestions about additional information and resources they desired, which included VA benefits enrollment, books and movies about dementia (eg, Still Alice), speech and swallowing disorders representatives, varied types of advance directives, class discussion, question-and-answer time with speakers, and resources for nonveteran older adults. General suggestions for future fairs included hosting the fair at the main division of the VA health care system, having more room between tables, inviting more vendors, using more visual posters at the tables, and additional advertising for VA services.
Discussion
Dementia is a costly disease with detrimental health and well-being effects on caregivers. The dementia resource fairs aimed to connect caregivers with resources for veterans with dementia in the VA and in the community. Given that nearly half the 2015 fair attendees were VA staff, there is an apparent need for increasing dementia education and access to care resource for this VAMC’s workforce. The high proportion of staff attendees at the 2015 fair may be attributed to the 2 VA community living centers at the VAMC site where the fair was held. This unexpected finding points to the importance of informal and interactive education opportunities for staff, particularly those working with veterans with dementia. The fair served an important role for VA staff seeking information on dementia for professional and personal reasons. This systematic evaluation of the fair demonstrated a need for improving access to information about dementia.
The idea of hosting a dementia resource fair was met with enthusiasm from attendees and subcommittee members in 2013. Feedback helped refine the second fair. The increase in self-reported learning from 2013 to 2015 suggests improvements may have been made between the first and second fair; however, this must be interpreted in light of the different compositions of the attendees at each fair and the absence of a control group. Attendees desired even more information about dementia at the second fair, as evidenced by suggestions to have presentations, speakers, and class discussions. These responses suggest that other sites may wish to consider holding similar events. Next steps include researching the effectiveness of low-cost, pragmatic educational initiatives for caregivers. In fact, randomized, controlled trials of dementia caregiver education and skill-building interventions are underway at VAPAHCS.
Conclusion
The primary lesson learned from the most recent fair was that marketing is the key to success. The authors created an efficient hospital publicity plan in 2015 that included (1) flyers posted throughout 2 main medical center campuses; (2) announcements on closed-circuit VA waiting room televisions; (3) e-mail announcements sent to staff; and (4) VA social media announcements. Flyers also were mailed to known caregivers, and announcements of the event were provided to local community agencies. This focus on publicity likely contributed to the substantial increase in participation from the 2013 to 2015 fair.
Future fairs may be improved by providing more detailed information about dementia through formal presentations. The authors aim to increase the number of family caregivers in attendance possibly through coordinating the fair to coincide with primary care clinic hours, advertising the availability of brief respite at the fair, and conducting additional outreach to veterans.
This systematic evaluation of the dementia resource fair confirmed that providing resources in a drop-in setting resulted in self-reported learning about resources available for veterans with dementia. VA dementia care providers are encouraged to use the authors’ time line and lessons learned to develop dementia resource fairs for their sites.
Acknowledgments
The authors wish to acknowledge the members of the 2013 and 2015 Dementia Resource Fair Committees, chaired by Betty Wexler and Kathleen McConnell, respectively. Dr. Gould is supported by the U.S. Department of Veterans Affairs (IK2 RX001478) and by Ellen Schapiro & Gerald Axelbaum through a 2014 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. Dr. Scanlon is supported by the U.S. Department of Veterans Affairs (IK2 RX001240; I21 RX001710), U.S. Department of Defense (W81XWH-15-1-0246), Sierra-Pacific Mental Illness Research Education and Clinical Center, and Stanford/VA Alzheimer’s Research Center. Drs. Gould and Scanlon also receive support from Palo Alto Veterans Institute for Research.
Due to the increasing number of older adults, the annual number of new cases of Alzheimer disease and other types of dementia is projected to double by 2050.1 The cost of caring for persons with dementia is rising as well. In 2015, the expected health care cost for persons with dementia in the U.S. is estimated to be $226 billion.1 There is a growing awareness of the needs of persons with dementia and of the importance of providing caregivers with support and education that enables them to keep their loved ones at home as long as possible. Additionally, caregiver stress adversely affects health and increases mortality risk.2-4 Efficacious interventions that teach caregivers to cope with challenging behaviors and functional decline are also available.5,6 Yet many caregivers encounter barriers that prevent access to these interventions. Some may not be able to access interventions due to lack of insurance plan coverage; others may not have the time to participate in these programs.7,8
The VA has requested that its VISNs and VAMCs develop dementia committees so that VA employees can establish goals focused on improving dementia care. The VA Palo Alto Health Care System (VAPAHCS) Dementia Committee determined that veterans, caregivers, and staff needed simple, clear information about dementia, based on consensus opinion. In 2013, one of the committee co-chairs, a clinical nurse specialist in the Geriatric Research Education and Clinical Center (GRECC), introduced the concept of a dementia resource fair. There is evidence supporting the use of interdisciplinary health fairs to educate allied health trainees (eg, nursing students and social workers) through service learning.9 But to the authors’ knowledge, the use of such a fair to provide dementia information has not been evaluated.
The fair drew from the evidence base for formal psychoeducational interventions for caregiversand for those with dementia or cognitive impairment.10,11 The goal of the fair was to provide information about resources for and management of dementia to veterans, families, staff, caregivers, and the community, using printed material and consultation with knowledgeable staff. The GRECC staff also initiated a systematic evaluation of this new initiative and collaborated with the Stanford/VA Alzheimer’s Research Center staff on the evaluation process.
Initial Plan
A subcommittee, composed of interdisciplinary professionals who work with veterans diagnosed with dementia, planned the initial dementia resource fair. The subcommittee representatives included geriatric medicine, nursing, occupational therapy, pharmacy, psychology, recreational therapy, and social work. Subcommittee members were charged with developing VA-branded handouts as educational tools to address key issues related to dementia, such as advance directive planning, behavioral management, home safety, and medication management. The subcommittee met monthly for 6 months and focused on logistics, identification of resource tables, creation of educational materials, advertising, and development of an evaluation. Table 1 provides an overview of the planning time line for the 2013 fair held in San Jose. Findings from a systematic evaluation of the 2013 fair were used to improve the 2015 fair held in Menlo Park. A discussion about the evaluation method and results follows.
Methods
The first fair was held at a VA community-based outpatient clinic in a small conference room with 13 resource tables. Feedback from attendees in 2013 included suggestions for having more tables, larger event space, more publicity, and alternate locations for the fair. In response to the feedback, the 2015 fair was held at a division of the main VAMC in a large conference room and hosted 20 tables arranged in a horseshoe shape. The second fair included an activity table staffed by a psychology fellow and recreation therapist who provided respite to caregivers if their loved one with dementia accompanied them to the event. Both the 2013 and 2015 fairs were 4 hours long.
A 1-page, anonymous survey was developed to assess attendees’ opinions about the fair. The survey included information about whether attendees were caregivers, veterans, or VA staff but did not ask other demographic questions to preserve anonymity. In 2013, the survey asked attendees to choose the category that best described them, but in 2015, the survey asked attendees to indicate the number of individuals from each category in their party. The 2015 survey assessed 2 additional categories (family member, other) and added a question about the number of people in each party to better estimate attendance. Both surveys also asked attendees to check which resource tables they visited.
The following assessment questions were consistent across both fairs to allow for comparisons. The authors assessed attitudes and learning as a result of the fair, using 2 statements that were rated with a 5-point Likert scale. The authors asked 3 open-ended questions to ascertain the helpful aspects of the fair, unmet needs, and suggestions for improvement. The Stanford University Institutional Review Board (IRB) reviewed this program evaluation plan and determined that the program evaluation project did not require IRB approval.
When attendees arrived at the fair, they received a folder containing branded handouts, a reusable bag, and a survey. Committee members asked that 1 person per party complete the survey at the end of the visit. Attendees visited tables, obtained written materials, and spoke with subcommittee members who staffed the tables. Snacks and light refreshments were provided. The reusable bag was provided by the VAMC Suicide Prevention Program to increase awareness of the VAPAHCS Suicide Prevention Program. As attendees were leaving, they were reminded to complete the survey. Attendees deposited completed surveys in a box to ensure anonymity.
Results
Thirty-six individuals attended the 2013 fair, and 138 individuals attended the 2015 fair. Thirty-one surveys were completed in 2013, yielding an 86% response rate. One hundred six surveys were returned and represented responses for 129 individuals in 2015, yielding a 94% response rate in 2015. Most of the 2013 attendees were caregivers, followed by veterans, VA staff, and outside staff (Table 2). In contrast, most of the 2015 attendees were VA staff, followed by veterans, caregivers/family members, outside staff, and others. Distributions of attendees differed significantly across the fairs: χ2(4) = 12.66; P = .01.
The surveys assessed which tables attendees visited and their perceptions of the fair. The most frequently visited resource table for both 2013 and 2015 fairs was the Alzheimer’s Association table. Other popular resource tables were VA Benefits and VA Caregiver Support in 2013 and Home Safety and End of Life Care in 2015. Ninety-six percent of 2013 attendees and 100% of 2015 attendees strongly agreed or agreed that “attending the dementia fair was worth my time and effort.” Eighty-three percent of 2013 attendees and 100% of 2015 attendees felt that they had learned something useful at the fair. The proportion of individuals reporting that they had learned something useful significantly increased from 2013 to 2015: χ2(2) = 18.07; P = .0001.
To summarize the open-ended responses to the question “What was most helpful about the fair?” the authors constructed a word cloud that displays the 75 most frequently used words in attendees’ descriptions of the 2015 fair (Figure). Attendees provided suggestions about additional information and resources they desired, which included VA benefits enrollment, books and movies about dementia (eg, Still Alice), speech and swallowing disorders representatives, varied types of advance directives, class discussion, question-and-answer time with speakers, and resources for nonveteran older adults. General suggestions for future fairs included hosting the fair at the main division of the VA health care system, having more room between tables, inviting more vendors, using more visual posters at the tables, and additional advertising for VA services.
Discussion
Dementia is a costly disease with detrimental health and well-being effects on caregivers. The dementia resource fairs aimed to connect caregivers with resources for veterans with dementia in the VA and in the community. Given that nearly half the 2015 fair attendees were VA staff, there is an apparent need for increasing dementia education and access to care resource for this VAMC’s workforce. The high proportion of staff attendees at the 2015 fair may be attributed to the 2 VA community living centers at the VAMC site where the fair was held. This unexpected finding points to the importance of informal and interactive education opportunities for staff, particularly those working with veterans with dementia. The fair served an important role for VA staff seeking information on dementia for professional and personal reasons. This systematic evaluation of the fair demonstrated a need for improving access to information about dementia.
The idea of hosting a dementia resource fair was met with enthusiasm from attendees and subcommittee members in 2013. Feedback helped refine the second fair. The increase in self-reported learning from 2013 to 2015 suggests improvements may have been made between the first and second fair; however, this must be interpreted in light of the different compositions of the attendees at each fair and the absence of a control group. Attendees desired even more information about dementia at the second fair, as evidenced by suggestions to have presentations, speakers, and class discussions. These responses suggest that other sites may wish to consider holding similar events. Next steps include researching the effectiveness of low-cost, pragmatic educational initiatives for caregivers. In fact, randomized, controlled trials of dementia caregiver education and skill-building interventions are underway at VAPAHCS.
Conclusion
The primary lesson learned from the most recent fair was that marketing is the key to success. The authors created an efficient hospital publicity plan in 2015 that included (1) flyers posted throughout 2 main medical center campuses; (2) announcements on closed-circuit VA waiting room televisions; (3) e-mail announcements sent to staff; and (4) VA social media announcements. Flyers also were mailed to known caregivers, and announcements of the event were provided to local community agencies. This focus on publicity likely contributed to the substantial increase in participation from the 2013 to 2015 fair.
Future fairs may be improved by providing more detailed information about dementia through formal presentations. The authors aim to increase the number of family caregivers in attendance possibly through coordinating the fair to coincide with primary care clinic hours, advertising the availability of brief respite at the fair, and conducting additional outreach to veterans.
This systematic evaluation of the dementia resource fair confirmed that providing resources in a drop-in setting resulted in self-reported learning about resources available for veterans with dementia. VA dementia care providers are encouraged to use the authors’ time line and lessons learned to develop dementia resource fairs for their sites.
Acknowledgments
The authors wish to acknowledge the members of the 2013 and 2015 Dementia Resource Fair Committees, chaired by Betty Wexler and Kathleen McConnell, respectively. Dr. Gould is supported by the U.S. Department of Veterans Affairs (IK2 RX001478) and by Ellen Schapiro & Gerald Axelbaum through a 2014 NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. Dr. Scanlon is supported by the U.S. Department of Veterans Affairs (IK2 RX001240; I21 RX001710), U.S. Department of Defense (W81XWH-15-1-0246), Sierra-Pacific Mental Illness Research Education and Clinical Center, and Stanford/VA Alzheimer’s Research Center. Drs. Gould and Scanlon also receive support from Palo Alto Veterans Institute for Research.
1. Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3)332-384.
2. Schulz R, Beach SR, Cook TB, Martire LM, Tomlinson JM, Monin JK. Predictors and consequences of perceived lack of choice in becoming an informal caregiver. Aging Ment Health. 2012;16(6):712-721.
3. Cooper C, Mukadam N, Katona C, et al; World Federation of Biological Psychiatry – Old Age Taskforce. Systematic review of the effectiveness of non-pharmacological interventions to improve quality of life of people with dementia. Int Psychogeriatr. 2012;24(6):856-870.
4. Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA. 1991;282(23):2215-2219.
5. Brodaty H, Arasaratnam C. Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia. Am J Psychiatry. 2012;169(9):946-953.
6. Gitlin LN. Good news for dementia care: caregiver interventions reduce behavioral symptoms in people with dementia and family distress. Am J Psychiatry. 2012;169(9):894-897.
7. Ho A, Collins SR, Davis K, Doty MM. A look at working-age caregivers roles, health concerns, and need for support. Issue Brief (Commonw Fund). 2005;(854):1-12.
8. Joling KJ, van Marwijk HWJ, Smit F, et al. Does a family meetings intervention prevent depression and anxiety in family caregivers of dementia patients? A randomized trial. PLoS One. 2012;7(1):e30936.
9. Kolomer S, Quinn ME, Steele K. Interdisciplinary health fairs for older adults and the value of interprofessional service learning. J Community Pract. 2010;18(2-3):267-279.
10. Jensen M, Agbata IN, Canavan M, McCarthy G. Effectiveness of educational interventions for informal caregivers of individuals with dementia residing in the community: systematic review and meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry. 2015;30(2):130-143.
11. Quinn C, Toms G, Anderson D, Clare L. A review of self-management interventions for people with dementia and mild cognitive impairment. J Appl Gerontol. 2015;pii:0733464814566852.
1. Alzheimer’s Association. 2015 Alzheimer’s disease facts and figures. Alzheimers Dement. 2015;11(3)332-384.
2. Schulz R, Beach SR, Cook TB, Martire LM, Tomlinson JM, Monin JK. Predictors and consequences of perceived lack of choice in becoming an informal caregiver. Aging Ment Health. 2012;16(6):712-721.
3. Cooper C, Mukadam N, Katona C, et al; World Federation of Biological Psychiatry – Old Age Taskforce. Systematic review of the effectiveness of non-pharmacological interventions to improve quality of life of people with dementia. Int Psychogeriatr. 2012;24(6):856-870.
4. Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA. 1991;282(23):2215-2219.
5. Brodaty H, Arasaratnam C. Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia. Am J Psychiatry. 2012;169(9):946-953.
6. Gitlin LN. Good news for dementia care: caregiver interventions reduce behavioral symptoms in people with dementia and family distress. Am J Psychiatry. 2012;169(9):894-897.
7. Ho A, Collins SR, Davis K, Doty MM. A look at working-age caregivers roles, health concerns, and need for support. Issue Brief (Commonw Fund). 2005;(854):1-12.
8. Joling KJ, van Marwijk HWJ, Smit F, et al. Does a family meetings intervention prevent depression and anxiety in family caregivers of dementia patients? A randomized trial. PLoS One. 2012;7(1):e30936.
9. Kolomer S, Quinn ME, Steele K. Interdisciplinary health fairs for older adults and the value of interprofessional service learning. J Community Pract. 2010;18(2-3):267-279.
10. Jensen M, Agbata IN, Canavan M, McCarthy G. Effectiveness of educational interventions for informal caregivers of individuals with dementia residing in the community: systematic review and meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry. 2015;30(2):130-143.
11. Quinn C, Toms G, Anderson D, Clare L. A review of self-management interventions for people with dementia and mild cognitive impairment. J Appl Gerontol. 2015;pii:0733464814566852.
VA Treats Patients’ Impatience With Clinical Pharmacists
MADISON, WIS.— Something astonishing has happened in the past year to outpatient treatment at the Veterans Affairs hospital here.
Vets regularly get next-day and even same-day appointments for primary care now, no longer waiting a month or more to see a doctor as many once did.
The reason is they don’t all see doctors. Clinical pharmacists — whose special training permits them to prescribe drugs, order lab tests, make referrals to specialists and do physical examinations — are handling more patients’ chronic care needs. That frees physicians to concentrate on new patients and others with complex needs.
A quarter of primary care appointments at the Madison hospital are now handled by clinical pharmacists since they were integrated in patient care teams in 2015. Several VA hospitals — in El Paso, Texas, and Kansas City, Mo., among them — have followed Madison’s approach and more than 36 others are considering it, according to hospital officials.
“It’s made a tremendous positive impact in improving access,” said Dr. Jean Montgomery, chief of primary care services at the Madison hospital.
That’s critical for the VA, the focus of a national scandal in 2014 after news reports revealed the Phoenix VA hospital had booked primary care appointments months in advance, schedulers falsified wait times to make them look shorter and dozens had died awaiting care. Further investigations uncovered similar problems at other VA facilities. More than two years later, tens of thousands of vets are still waiting a month or two for an appointment, according to the latest data from the VA.
The Obama administration has allowed some veterans to seek care in the private sector if they choose, but VA wait times remain long and more action is needed, theGeneral Accountability Office reported in April.
Expanding clinical pharmacists’ role is a solution.
They receive two more years of education than regular pharmacists and they can handle many primary care needs for patients, particularly after physicians have diagnosed their conditions.
The VA has had them for more than 20 years, but their growing involvement in patient care is more recent. This year it employs 3,185 clinical pharmacists with authority to prescribe medications, order lab tests and perform physical assessments — nearly a 50 percent increase since 2011.
“It’s having a significant impact on reducing wait times and our office is trying to expand more of them nationally to increase access,” said Heather Ourth, national clinical program manager for VA Pharmacy Benefits Management Services.
In 2015, VA clinical pharmacists wrote 1.9 million prescriptions for chronic diseases, according to a report co-authored by Ourth and published in September in the American Journal of Health-System Pharmacy.
A goal is to increase the use of clinical pharmacists to help patients with mental health needs and pain management.
“This helps open up appointment slots for physicians to meet patients with acute care needs,” Ourth said.
Clinical pharmacists’ authority is determined at each VA hospital based on their training and knowledge.
The Madison VA allowed clinical pharmacists to take over management of patients with chronic diseases such as diabetes and high blood pressure, participate in weekly meetings with doctors and other members of patients’ care teams and handle patients’ calls about medications.
They typically see five patients in their office each day, usually for 30 minutes each, and they talk to another 10 by telephone, said Ellina Seckel, the clinical pharmacist who led the changes at the hospital.
Many issues involve adjusting medication dosages such as insulin, which do not require a face-to-face visit. When Seckel sees patients, she often helps them lower the number of drugs they take because they may cause unnecessary complications.
Expanding clinical pharmacists’ role in primary care has cut readmission rates and helped more patients keep their diabetes under control, Seckel said.
VA hospital officials in both Madison and El Paso said they faced challenges initially in persuading doctors to delegate some duties to qualified pharmacists.
“Some physicians feel like it’s a turf war and don’t want to refer their patients because they feel the clinical pharmacist is trying to practice medicine,” said Lanre’ Obisesan, a clinical pharmacist and assistant chief of pharmacy at the El Paso VA.
Even so, the El Paso VA’s average wait time fell from two months to two weeks, he said, after it added several clinical pharmacists and gave them independence to help patients. About 30 percent of the VA patients in El Paso have used clinical pharmacists, Obisesan said.
That share will rise. The hospital now has one clinical pharmacist for every six physicians, but it aims to add more pharmacists to reduce the ratio to 1 to 3.
The Madison VA is close to that ratio now after adding four clinical pharmacist positions in the past year.
Patients there can choose whether to see a doctor or a pharmacist. With approval from primary care physicians, pharmacists took over 27 percent of the follow-up appointments for patients with chronic illnesses, Seckel said.
That shift yields benefits for both doctors and patients, said Montgomery, the head of primary care services at the Madison VA.
Many VA doctors only have time to deal with patients’ acute care issues, such as knee or back pain, with little time to focus on a patient’s multiple chronic illnesses and often a dozen or more medications they may be taking for them.
“The more we can have members of the team to do routine things that do not require a physician’s time the better the quality of the visit and the better patient outcomes,” he said.
Patients seem to like what the hospital is doing.
Stephen Howard Foster saw a clinical pharmacist recently who told him he could stop taking one heartburn medication and switched him to another medicine to reduce side effects. He said he was comfortable with the pharmacist advising him without first consulting his physician and he saved time.
“This is a good idea rather than put up with normal delays,” said Foster, 51.
Another Madison VA patient, Mike Fonger, 71, saw clinical pharmacist Anita Kashyap recently to get a blood pressure check, lab test results, a review of his medications and to change an ointment he was taking for back and shoulder pain. Kashyap also helped him ease the side effects from the cholesterol-lowering drug he takes by cutting his dosage in half.
“I like the extra attention I get here,” Fonger said.
This story was produced by Kaiser Health News, which publishes California Healthline, a service of the California Health Care Foundation.
MADISON, WIS.— Something astonishing has happened in the past year to outpatient treatment at the Veterans Affairs hospital here.
Vets regularly get next-day and even same-day appointments for primary care now, no longer waiting a month or more to see a doctor as many once did.
The reason is they don’t all see doctors. Clinical pharmacists — whose special training permits them to prescribe drugs, order lab tests, make referrals to specialists and do physical examinations — are handling more patients’ chronic care needs. That frees physicians to concentrate on new patients and others with complex needs.
A quarter of primary care appointments at the Madison hospital are now handled by clinical pharmacists since they were integrated in patient care teams in 2015. Several VA hospitals — in El Paso, Texas, and Kansas City, Mo., among them — have followed Madison’s approach and more than 36 others are considering it, according to hospital officials.
“It’s made a tremendous positive impact in improving access,” said Dr. Jean Montgomery, chief of primary care services at the Madison hospital.
That’s critical for the VA, the focus of a national scandal in 2014 after news reports revealed the Phoenix VA hospital had booked primary care appointments months in advance, schedulers falsified wait times to make them look shorter and dozens had died awaiting care. Further investigations uncovered similar problems at other VA facilities. More than two years later, tens of thousands of vets are still waiting a month or two for an appointment, according to the latest data from the VA.
The Obama administration has allowed some veterans to seek care in the private sector if they choose, but VA wait times remain long and more action is needed, theGeneral Accountability Office reported in April.
Expanding clinical pharmacists’ role is a solution.
They receive two more years of education than regular pharmacists and they can handle many primary care needs for patients, particularly after physicians have diagnosed their conditions.
The VA has had them for more than 20 years, but their growing involvement in patient care is more recent. This year it employs 3,185 clinical pharmacists with authority to prescribe medications, order lab tests and perform physical assessments — nearly a 50 percent increase since 2011.
“It’s having a significant impact on reducing wait times and our office is trying to expand more of them nationally to increase access,” said Heather Ourth, national clinical program manager for VA Pharmacy Benefits Management Services.
In 2015, VA clinical pharmacists wrote 1.9 million prescriptions for chronic diseases, according to a report co-authored by Ourth and published in September in the American Journal of Health-System Pharmacy.
A goal is to increase the use of clinical pharmacists to help patients with mental health needs and pain management.
“This helps open up appointment slots for physicians to meet patients with acute care needs,” Ourth said.
Clinical pharmacists’ authority is determined at each VA hospital based on their training and knowledge.
The Madison VA allowed clinical pharmacists to take over management of patients with chronic diseases such as diabetes and high blood pressure, participate in weekly meetings with doctors and other members of patients’ care teams and handle patients’ calls about medications.
They typically see five patients in their office each day, usually for 30 minutes each, and they talk to another 10 by telephone, said Ellina Seckel, the clinical pharmacist who led the changes at the hospital.
Many issues involve adjusting medication dosages such as insulin, which do not require a face-to-face visit. When Seckel sees patients, she often helps them lower the number of drugs they take because they may cause unnecessary complications.
Expanding clinical pharmacists’ role in primary care has cut readmission rates and helped more patients keep their diabetes under control, Seckel said.
VA hospital officials in both Madison and El Paso said they faced challenges initially in persuading doctors to delegate some duties to qualified pharmacists.
“Some physicians feel like it’s a turf war and don’t want to refer their patients because they feel the clinical pharmacist is trying to practice medicine,” said Lanre’ Obisesan, a clinical pharmacist and assistant chief of pharmacy at the El Paso VA.
Even so, the El Paso VA’s average wait time fell from two months to two weeks, he said, after it added several clinical pharmacists and gave them independence to help patients. About 30 percent of the VA patients in El Paso have used clinical pharmacists, Obisesan said.
That share will rise. The hospital now has one clinical pharmacist for every six physicians, but it aims to add more pharmacists to reduce the ratio to 1 to 3.
The Madison VA is close to that ratio now after adding four clinical pharmacist positions in the past year.
Patients there can choose whether to see a doctor or a pharmacist. With approval from primary care physicians, pharmacists took over 27 percent of the follow-up appointments for patients with chronic illnesses, Seckel said.
That shift yields benefits for both doctors and patients, said Montgomery, the head of primary care services at the Madison VA.
Many VA doctors only have time to deal with patients’ acute care issues, such as knee or back pain, with little time to focus on a patient’s multiple chronic illnesses and often a dozen or more medications they may be taking for them.
“The more we can have members of the team to do routine things that do not require a physician’s time the better the quality of the visit and the better patient outcomes,” he said.
Patients seem to like what the hospital is doing.
Stephen Howard Foster saw a clinical pharmacist recently who told him he could stop taking one heartburn medication and switched him to another medicine to reduce side effects. He said he was comfortable with the pharmacist advising him without first consulting his physician and he saved time.
“This is a good idea rather than put up with normal delays,” said Foster, 51.
Another Madison VA patient, Mike Fonger, 71, saw clinical pharmacist Anita Kashyap recently to get a blood pressure check, lab test results, a review of his medications and to change an ointment he was taking for back and shoulder pain. Kashyap also helped him ease the side effects from the cholesterol-lowering drug he takes by cutting his dosage in half.
“I like the extra attention I get here,” Fonger said.
This story was produced by Kaiser Health News, which publishes California Healthline, a service of the California Health Care Foundation.
MADISON, WIS.— Something astonishing has happened in the past year to outpatient treatment at the Veterans Affairs hospital here.
Vets regularly get next-day and even same-day appointments for primary care now, no longer waiting a month or more to see a doctor as many once did.
The reason is they don’t all see doctors. Clinical pharmacists — whose special training permits them to prescribe drugs, order lab tests, make referrals to specialists and do physical examinations — are handling more patients’ chronic care needs. That frees physicians to concentrate on new patients and others with complex needs.
A quarter of primary care appointments at the Madison hospital are now handled by clinical pharmacists since they were integrated in patient care teams in 2015. Several VA hospitals — in El Paso, Texas, and Kansas City, Mo., among them — have followed Madison’s approach and more than 36 others are considering it, according to hospital officials.
“It’s made a tremendous positive impact in improving access,” said Dr. Jean Montgomery, chief of primary care services at the Madison hospital.
That’s critical for the VA, the focus of a national scandal in 2014 after news reports revealed the Phoenix VA hospital had booked primary care appointments months in advance, schedulers falsified wait times to make them look shorter and dozens had died awaiting care. Further investigations uncovered similar problems at other VA facilities. More than two years later, tens of thousands of vets are still waiting a month or two for an appointment, according to the latest data from the VA.
The Obama administration has allowed some veterans to seek care in the private sector if they choose, but VA wait times remain long and more action is needed, theGeneral Accountability Office reported in April.
Expanding clinical pharmacists’ role is a solution.
They receive two more years of education than regular pharmacists and they can handle many primary care needs for patients, particularly after physicians have diagnosed their conditions.
The VA has had them for more than 20 years, but their growing involvement in patient care is more recent. This year it employs 3,185 clinical pharmacists with authority to prescribe medications, order lab tests and perform physical assessments — nearly a 50 percent increase since 2011.
“It’s having a significant impact on reducing wait times and our office is trying to expand more of them nationally to increase access,” said Heather Ourth, national clinical program manager for VA Pharmacy Benefits Management Services.
In 2015, VA clinical pharmacists wrote 1.9 million prescriptions for chronic diseases, according to a report co-authored by Ourth and published in September in the American Journal of Health-System Pharmacy.
A goal is to increase the use of clinical pharmacists to help patients with mental health needs and pain management.
“This helps open up appointment slots for physicians to meet patients with acute care needs,” Ourth said.
Clinical pharmacists’ authority is determined at each VA hospital based on their training and knowledge.
The Madison VA allowed clinical pharmacists to take over management of patients with chronic diseases such as diabetes and high blood pressure, participate in weekly meetings with doctors and other members of patients’ care teams and handle patients’ calls about medications.
They typically see five patients in their office each day, usually for 30 minutes each, and they talk to another 10 by telephone, said Ellina Seckel, the clinical pharmacist who led the changes at the hospital.
Many issues involve adjusting medication dosages such as insulin, which do not require a face-to-face visit. When Seckel sees patients, she often helps them lower the number of drugs they take because they may cause unnecessary complications.
Expanding clinical pharmacists’ role in primary care has cut readmission rates and helped more patients keep their diabetes under control, Seckel said.
VA hospital officials in both Madison and El Paso said they faced challenges initially in persuading doctors to delegate some duties to qualified pharmacists.
“Some physicians feel like it’s a turf war and don’t want to refer their patients because they feel the clinical pharmacist is trying to practice medicine,” said Lanre’ Obisesan, a clinical pharmacist and assistant chief of pharmacy at the El Paso VA.
Even so, the El Paso VA’s average wait time fell from two months to two weeks, he said, after it added several clinical pharmacists and gave them independence to help patients. About 30 percent of the VA patients in El Paso have used clinical pharmacists, Obisesan said.
That share will rise. The hospital now has one clinical pharmacist for every six physicians, but it aims to add more pharmacists to reduce the ratio to 1 to 3.
The Madison VA is close to that ratio now after adding four clinical pharmacist positions in the past year.
Patients there can choose whether to see a doctor or a pharmacist. With approval from primary care physicians, pharmacists took over 27 percent of the follow-up appointments for patients with chronic illnesses, Seckel said.
That shift yields benefits for both doctors and patients, said Montgomery, the head of primary care services at the Madison VA.
Many VA doctors only have time to deal with patients’ acute care issues, such as knee or back pain, with little time to focus on a patient’s multiple chronic illnesses and often a dozen or more medications they may be taking for them.
“The more we can have members of the team to do routine things that do not require a physician’s time the better the quality of the visit and the better patient outcomes,” he said.
Patients seem to like what the hospital is doing.
Stephen Howard Foster saw a clinical pharmacist recently who told him he could stop taking one heartburn medication and switched him to another medicine to reduce side effects. He said he was comfortable with the pharmacist advising him without first consulting his physician and he saved time.
“This is a good idea rather than put up with normal delays,” said Foster, 51.
Another Madison VA patient, Mike Fonger, 71, saw clinical pharmacist Anita Kashyap recently to get a blood pressure check, lab test results, a review of his medications and to change an ointment he was taking for back and shoulder pain. Kashyap also helped him ease the side effects from the cholesterol-lowering drug he takes by cutting his dosage in half.
“I like the extra attention I get here,” Fonger said.
This story was produced by Kaiser Health News, which publishes California Healthline, a service of the California Health Care Foundation.
What to Know about CMS’s New Emergency Preparedness Requirements
Are you ready?
The Centers for Medicare & Medicaid Services (CMS) recently released new emergency preparedness requirements to ensure that providers and suppliers are duly prepared to adequately serve their community during disasters or emergencies. These requirements were stimulated by unexpected and catastrophic events, such as the September 11 terrorist attacks, the 2009 H1N1 pandemic, and innumerable natural disasters (tornados, floods, and hurricanes, to name a few). The CMS final rule issued “requirements that establish a comprehensive, consistent, flexible, and dynamic regulatory approach to emergency preparedness and response that incorporates the lessons learned from the past, combined with the proven best practices of the present.” In the rule, CMS outlines three essential guiding principles that any healthcare facility or supplier would need to preserve in the event of a disaster:
- Safeguard human resources.
- Maintain business continuity.
- Protect physical resources.
4 Ways to Be Prepared
What does having a comprehensive disaster preparedness program mean for hospitalists, regardless of site of practice? CMS recommends having four key elements for an adequate program:
1. Perform a risk assessment that focuses on the capacities and capabilities that are critical for a full spectrum of types of emergencies or disasters. This risk assessment should take into consideration the type and location of the facility as well as the disasters that are most likely to occur in its area. It should include at a minimum “care-related emergencies; equipment and power failures; interruptions in communications, including cyber attacks; loss of a portion or all of a facility; and interruptions in the normal supply of essentials, such as water and food.”
2. Develop and implement policies and procedures that support the emergency plan. Hospitalists should know about organizational policies and procedures that support the implementation of the emergency plan and how their team is factored into that plan.
3. Develop and maintain a communication plan that also complies with state and federal law. All the preparations in the world can be crippled without a robust and clear communication plan. The facility must have primary and backup mechanisms to contact providers, staff, and personnel in a timely fashion; this should include mechanisms to repeatedly update providers as the event evolves so that everyone knows what they are supposed to be doing and when.
4. Develop and maintain a training and testing program for all personnel. This includes onboarding and annual refreshers, including drills and exercises that test the plan and identify any gaps in performance. Hospitalists will undoubtedly be key members in developing, implementing, and receiving such critical training.
Expectations
There isn’t a single U.S. healthcare facility or provider that will not be affected by these provisions. An estimated 72,000 healthcare providers and suppliers (from nursing homes to dialysis facilities to home health agencies) will be expected to comply with these requirements within about a year.
In addition to hospitals, CMS also extended the requirements to many types of facilities and suppliers so that such providers can more likely stay open and provide care during disasters and emergencies, or at least can resume operations as soon as possible, to provide the very best ongoing care to the affected community. In most of these scenarios, the need for complex and varied care goes up, not down, further exacerbating gaps in basic care if ambulatory facilities and home care providers are unavailable.
CMS does acknowledge that these requirements will be more difficult to execute in facilities that previously did not have requirements or in smaller facilities with more limited resources. It also acknowledges that the cost of implementation could reach up to $279 million, which some argue is actually an underestimation. Despite these challenges, it is hard to argue against basic disaster preparedness for any healthcare facility or provider as a standard and positive business practice. While most acute-care hospitals have long had disaster preparedness plans and programs, gaps in these programs have become readily apparent during natural disasters such as Hurricane Katrina and Superstorm Sandy. CMS also stresses the need for a community approach to planning and implementation and that there is no reason during planning, or during an actual event, that facilities should operate in isolation but rather train and respond together as a community.
As hospitalists, regardless of site of practice, we should all be involved in at least understanding, if not developing and implementing, these basic requirements in our facilities. It is without a doubt that hospitalists will be a core group of physicians who will be called upon to serve within or outside healthcare facilities in the event of a disaster or emergency. In fact, in most recent disasters, we already have. It is better, of course, to be prepared and ready to serve than unprepared and regretful.
Reference
- The Centers for Medicare and Medicaid Services. Medicare and Medicaid Programs; Emergency Preparedness Requirements for Medicare and Medicaid Participating Providers and Suppliers. Federal Register website. Accessed October 6, 2016.

Are you ready?
The Centers for Medicare & Medicaid Services (CMS) recently released new emergency preparedness requirements to ensure that providers and suppliers are duly prepared to adequately serve their community during disasters or emergencies. These requirements were stimulated by unexpected and catastrophic events, such as the September 11 terrorist attacks, the 2009 H1N1 pandemic, and innumerable natural disasters (tornados, floods, and hurricanes, to name a few). The CMS final rule issued “requirements that establish a comprehensive, consistent, flexible, and dynamic regulatory approach to emergency preparedness and response that incorporates the lessons learned from the past, combined with the proven best practices of the present.” In the rule, CMS outlines three essential guiding principles that any healthcare facility or supplier would need to preserve in the event of a disaster:
- Safeguard human resources.
- Maintain business continuity.
- Protect physical resources.
4 Ways to Be Prepared
What does having a comprehensive disaster preparedness program mean for hospitalists, regardless of site of practice? CMS recommends having four key elements for an adequate program:
1. Perform a risk assessment that focuses on the capacities and capabilities that are critical for a full spectrum of types of emergencies or disasters. This risk assessment should take into consideration the type and location of the facility as well as the disasters that are most likely to occur in its area. It should include at a minimum “care-related emergencies; equipment and power failures; interruptions in communications, including cyber attacks; loss of a portion or all of a facility; and interruptions in the normal supply of essentials, such as water and food.”
2. Develop and implement policies and procedures that support the emergency plan. Hospitalists should know about organizational policies and procedures that support the implementation of the emergency plan and how their team is factored into that plan.
3. Develop and maintain a communication plan that also complies with state and federal law. All the preparations in the world can be crippled without a robust and clear communication plan. The facility must have primary and backup mechanisms to contact providers, staff, and personnel in a timely fashion; this should include mechanisms to repeatedly update providers as the event evolves so that everyone knows what they are supposed to be doing and when.
4. Develop and maintain a training and testing program for all personnel. This includes onboarding and annual refreshers, including drills and exercises that test the plan and identify any gaps in performance. Hospitalists will undoubtedly be key members in developing, implementing, and receiving such critical training.
Expectations
There isn’t a single U.S. healthcare facility or provider that will not be affected by these provisions. An estimated 72,000 healthcare providers and suppliers (from nursing homes to dialysis facilities to home health agencies) will be expected to comply with these requirements within about a year.
In addition to hospitals, CMS also extended the requirements to many types of facilities and suppliers so that such providers can more likely stay open and provide care during disasters and emergencies, or at least can resume operations as soon as possible, to provide the very best ongoing care to the affected community. In most of these scenarios, the need for complex and varied care goes up, not down, further exacerbating gaps in basic care if ambulatory facilities and home care providers are unavailable.
CMS does acknowledge that these requirements will be more difficult to execute in facilities that previously did not have requirements or in smaller facilities with more limited resources. It also acknowledges that the cost of implementation could reach up to $279 million, which some argue is actually an underestimation. Despite these challenges, it is hard to argue against basic disaster preparedness for any healthcare facility or provider as a standard and positive business practice. While most acute-care hospitals have long had disaster preparedness plans and programs, gaps in these programs have become readily apparent during natural disasters such as Hurricane Katrina and Superstorm Sandy. CMS also stresses the need for a community approach to planning and implementation and that there is no reason during planning, or during an actual event, that facilities should operate in isolation but rather train and respond together as a community.
As hospitalists, regardless of site of practice, we should all be involved in at least understanding, if not developing and implementing, these basic requirements in our facilities. It is without a doubt that hospitalists will be a core group of physicians who will be called upon to serve within or outside healthcare facilities in the event of a disaster or emergency. In fact, in most recent disasters, we already have. It is better, of course, to be prepared and ready to serve than unprepared and regretful.
Reference
- The Centers for Medicare and Medicaid Services. Medicare and Medicaid Programs; Emergency Preparedness Requirements for Medicare and Medicaid Participating Providers and Suppliers. Federal Register website. Accessed October 6, 2016.
Are you ready?
The Centers for Medicare & Medicaid Services (CMS) recently released new emergency preparedness requirements to ensure that providers and suppliers are duly prepared to adequately serve their community during disasters or emergencies. These requirements were stimulated by unexpected and catastrophic events, such as the September 11 terrorist attacks, the 2009 H1N1 pandemic, and innumerable natural disasters (tornados, floods, and hurricanes, to name a few). The CMS final rule issued “requirements that establish a comprehensive, consistent, flexible, and dynamic regulatory approach to emergency preparedness and response that incorporates the lessons learned from the past, combined with the proven best practices of the present.” In the rule, CMS outlines three essential guiding principles that any healthcare facility or supplier would need to preserve in the event of a disaster:
- Safeguard human resources.
- Maintain business continuity.
- Protect physical resources.
4 Ways to Be Prepared
What does having a comprehensive disaster preparedness program mean for hospitalists, regardless of site of practice? CMS recommends having four key elements for an adequate program:
1. Perform a risk assessment that focuses on the capacities and capabilities that are critical for a full spectrum of types of emergencies or disasters. This risk assessment should take into consideration the type and location of the facility as well as the disasters that are most likely to occur in its area. It should include at a minimum “care-related emergencies; equipment and power failures; interruptions in communications, including cyber attacks; loss of a portion or all of a facility; and interruptions in the normal supply of essentials, such as water and food.”
2. Develop and implement policies and procedures that support the emergency plan. Hospitalists should know about organizational policies and procedures that support the implementation of the emergency plan and how their team is factored into that plan.
3. Develop and maintain a communication plan that also complies with state and federal law. All the preparations in the world can be crippled without a robust and clear communication plan. The facility must have primary and backup mechanisms to contact providers, staff, and personnel in a timely fashion; this should include mechanisms to repeatedly update providers as the event evolves so that everyone knows what they are supposed to be doing and when.
4. Develop and maintain a training and testing program for all personnel. This includes onboarding and annual refreshers, including drills and exercises that test the plan and identify any gaps in performance. Hospitalists will undoubtedly be key members in developing, implementing, and receiving such critical training.
Expectations
There isn’t a single U.S. healthcare facility or provider that will not be affected by these provisions. An estimated 72,000 healthcare providers and suppliers (from nursing homes to dialysis facilities to home health agencies) will be expected to comply with these requirements within about a year.
In addition to hospitals, CMS also extended the requirements to many types of facilities and suppliers so that such providers can more likely stay open and provide care during disasters and emergencies, or at least can resume operations as soon as possible, to provide the very best ongoing care to the affected community. In most of these scenarios, the need for complex and varied care goes up, not down, further exacerbating gaps in basic care if ambulatory facilities and home care providers are unavailable.
CMS does acknowledge that these requirements will be more difficult to execute in facilities that previously did not have requirements or in smaller facilities with more limited resources. It also acknowledges that the cost of implementation could reach up to $279 million, which some argue is actually an underestimation. Despite these challenges, it is hard to argue against basic disaster preparedness for any healthcare facility or provider as a standard and positive business practice. While most acute-care hospitals have long had disaster preparedness plans and programs, gaps in these programs have become readily apparent during natural disasters such as Hurricane Katrina and Superstorm Sandy. CMS also stresses the need for a community approach to planning and implementation and that there is no reason during planning, or during an actual event, that facilities should operate in isolation but rather train and respond together as a community.
As hospitalists, regardless of site of practice, we should all be involved in at least understanding, if not developing and implementing, these basic requirements in our facilities. It is without a doubt that hospitalists will be a core group of physicians who will be called upon to serve within or outside healthcare facilities in the event of a disaster or emergency. In fact, in most recent disasters, we already have. It is better, of course, to be prepared and ready to serve than unprepared and regretful.
Reference
- The Centers for Medicare and Medicaid Services. Medicare and Medicaid Programs; Emergency Preparedness Requirements for Medicare and Medicaid Participating Providers and Suppliers. Federal Register website. Accessed October 6, 2016.
Tooth Decay Is the Most Prevalent Disease
There are 2 leading types of dental diseases: tooth decay (dental caries or cavities) and gum disease (periodontal disease). Tooth decay is by far the more prevalent of the 2, causing a greater, needless loss in the quality of life.
Prevalence of Tooth Decay
Dental caries is a major public health problem. Even though in the past 50 years there has been a significant decline in dental caries, it is the most common ailment in the U.S., and large segments of the population experience various barriers to care. Among children and adolescents, dental caries is 4 to 5 times more common than asthma.1,2 Data from the National Health and Nutrition Examination Survey, 2011-2012, show that among children aged 2 to 8 years, 37% had dental caries in their primary teeth. Among adolescents aged 12 to 19 years, the prevalence of dental caries in the permanent teeth was 58%. About 90% of adults aged ≥ 20 years had dental caries.3,4
Unmet Dental Needs
The real disease burden of dental caries is the amount of unmet needs or untreated decay. In recent years, there has been a shift in the peak prevalence of untreated tooth decay from children to adults, possibly attributable to socioecologic factors.3,5 The prevalence of untreated decay in children and adolescents was about 15%. However, the prevalence of untreated decay among adults aged 20 to 64 years was higher: 27% of the adults had decayed teeth that were left untreated.3,4
The rates of untreated decay among these adults were higher among Hispanics (36%) and non-Hispanic blacks (42%) than among non-Hispanic whites (22%) and non-Hispanic Asians (17%).3,4 Despite the decline in dental caries, disparities persist among different racial, ethnic, educational, and income groups; it remains a modern curse for large segments of the population.
Basics of Tooth Decay
Tooth decay is caused by Streptococcus mutans (S mutans) bacterial infection. The cariogenic bacteria are transmissible from mother or caregiver to children.6 After tooth eruption, the mouth is quickly colonized by S mutans. Even though the bacteria are ubiquitous, the disease burden is more concentrated in some populations.
What makes some people more susceptible to tooth decay? Contrary to popular belief, it is not caused by childbirth or low dietary intake of calcium.7,8 Tooth decay typically starts on the chewing surfaces or proximal contacts of teeth.
S mutans is introduced into the mouth principally from another person. The bacteria colonize the mouth and with the formation of plaques, adhere to the teeth. Plaque is the soft, sticky film formed on teeth from food degradation. The biofilm is conducive to bacterial proliferation and teeming with bacteria.
The S mutans bacteria break down sugars and produce lactic acids, which cause tooth decay—a process of demineralization, or loss of calcium phosphate, from the tooth structure.2,9 As a result, the tooth “softens” and eventually collapses on itself, forming a cavity. Tooth decay most commonly occurs at the occlusal (chewing) surfaces and the proximal contacts of teeth. The occlusal aspects of teeth have a natural pit-and-fissure morphology that facilitates bacterial adherence and colonization. The proximal contacts of teeth also facilitate adherence of plaque and bacteria.
A tooth is made up of 3 layers. The outermost layer of the tooth crown is the enamel, which is the hardest or most mineralized part of the tooth—it is harder than bone. The next layer is the dentin, which has a higher percentage of organic material (collagen) and water than the enamel has and is softer. In the center of the tooth is the pulp (consisting of nerves and blood vessels), which keeps the tooth alive and provides sensation to the tooth. The outermost layer of the tooth root is cementum (instead of enamel), followed by dentin, which encases the pulp tissues contained within the root canals (Figure). 
Process of Tooth Loss
At the early stage of tooth decay, when the decay is confined to the enamel, the tooth is asymptomatic, and the damage is reversible. When the decay extends into the dentin, restorations are a consideration. The further the decay extends toward the pulp, the greater the risk of tooth sensitivity and pain. Decay naturally progresses faster in the (less mineralized) dentin than when the decay is still confined to the enamel. If left unchecked, the decay may progress, and the bacteria eventually invade the pulp. At that point, there is risk of not only pain, but also swelling and tooth loss.
At the earlier stage of decay, a tooth may be treated with restorations, which are typically made of dental amalgam, resin (composite), glass ionomer, porcelain, or gold. When the bacteria have invaded the pulp, a dental restoration will not treat the pain and infection. Root canal therapy is needed to remove the infected tissues in the pulp chamber and root canals. Further, if the tooth is too compromised with extensive destruction from the decay or if there are financial or other barriers to root canal therapy, extraction is likely the only option.
Key to Oral Health
Personal daily oral hygiene (brushing and flossing) helps remove plaque from accumulating on tooth surfaces—especially the occlusal surfaces and proximal contacts, which are most prone to decay. Brushing teeth is of limited benefit without the use of fluoride toothpaste.8 The most important time for brushing is before bedtime, because less salivation occurs during sleep. Saliva helps clear fermented bacterial products, buffers the drop in pH, prevents demineralization, and enhances remineralizaton.10
Fluoride benefits children and adults of all ages, and comes in the form of fluoridated tap water, toothpaste, mouth rinse, and professionally applied gel and varnish. Fluoride occurs naturally in the environment, too. Its effect is mainly topical—fluoride gets incorporated into the tooth as fluorapatite, replacing the hydroxyapatite. Fluorapatite is harder than the hydroxyapatite; hence, the tooth is better able to resist demineralization by bacterial acid attacks.11 Professionally applied fluoride is generally recommended for high-risk patients, typically patients with high caries burden, ie, many decayed teeth. The best predictor of future caries is the past caries experience.
Sealants are thin, plastic coatings that are painted on to tooth occlusal surfaces, obliterating the pits and fissures normally found on posterior teeth. The smooth sealants effectively inhibit the colonization of S mutans on the occlusal aspects of teeth.12 Sealants are applied in dental offices (by the dentists or dental hygienists) or in school-based programs.
1. U.S. Department of Health and Human Services. Oral health in America: a report of the Surgeon General. http://www.nidcr.nih.gov/DataStatistics/SurgeonGeneral/Report/ExecutiveSummary.htm. Updated March 7, 2014. Accessed August 22, 2016.
2. Centers for Disease Control and Prevention. Hygiene-related diseases. http://www.cdc.gov/healthywater/hygiene/disease/dental_caries.html. Updated December 16, 2014. Accessed August 22, 2016.
3. Dye BA, Thornton-Evan G, Xianfen L, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011-2012. http://www.cdc.gov/nchs/data/databriefs/db191.pdf. Published March 2015. NCHS Data Brief. Accessed August 22, 2016.
4. Dye BA, Thornton-Evan G, Xianfen L, Iafolla TJ. Dental caries and tooth loss in adults in the United States, 2011-2012. http://www.cdc.gov/nchs/data/databriefs/db197.pdf. NCHS Data Brief. Published May 2015. Accessed August 22, 2016.
5. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. 2015;94(5):650-658.
6. Smith RE, Badner VM, Morse DE, Freeman K. Maternal risk indicators for childhood caries in an inner city population. Community Dent Oral Epidemiol. 2002;30(3):176-181.
7. Boggess KA, Urlaub DM, Moos MK, Polinkovsky M, El-Khorazaty J, Lorenz C. Knowledge and beliefs regarding oral health among pregnant women. J Am Dent Assoc. 2011;142(11):1275-1282.
8. Roberts-Thomson KF, Spencer AJ. Public knowledge of the prevention of dental decay and gum diseases. Aust Dent J. 1999;44(4):253-258.
9. Cochrane NJ, Cai F, Hug NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010;89(11):1187-1197.
10. Prabhakar AR, Dodawad R, Os R. Evaluation of flow Rate, pH, buffering capacity, calcium, total protein and total antioxidant levels of saliva in caries free and caries active children—an in vivo study. Int J Clin Pediatr Dent. 2009;2(1):9-12.
11. Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of remineralization and fluoride in the dynamic process of demineralization and remuneration (part 3). J Clin Pediatr Dent. 2004;28(3):203-214.
12. Azarpazhooh A, Main PA. Pit and fissure sealants in the prevention of dental caries in children and adolescents: a systematic review. J Can Dent Assoc. 2008;74(2):171-177.
There are 2 leading types of dental diseases: tooth decay (dental caries or cavities) and gum disease (periodontal disease). Tooth decay is by far the more prevalent of the 2, causing a greater, needless loss in the quality of life.
Prevalence of Tooth Decay
Dental caries is a major public health problem. Even though in the past 50 years there has been a significant decline in dental caries, it is the most common ailment in the U.S., and large segments of the population experience various barriers to care. Among children and adolescents, dental caries is 4 to 5 times more common than asthma.1,2 Data from the National Health and Nutrition Examination Survey, 2011-2012, show that among children aged 2 to 8 years, 37% had dental caries in their primary teeth. Among adolescents aged 12 to 19 years, the prevalence of dental caries in the permanent teeth was 58%. About 90% of adults aged ≥ 20 years had dental caries.3,4
Unmet Dental Needs
The real disease burden of dental caries is the amount of unmet needs or untreated decay. In recent years, there has been a shift in the peak prevalence of untreated tooth decay from children to adults, possibly attributable to socioecologic factors.3,5 The prevalence of untreated decay in children and adolescents was about 15%. However, the prevalence of untreated decay among adults aged 20 to 64 years was higher: 27% of the adults had decayed teeth that were left untreated.3,4
The rates of untreated decay among these adults were higher among Hispanics (36%) and non-Hispanic blacks (42%) than among non-Hispanic whites (22%) and non-Hispanic Asians (17%).3,4 Despite the decline in dental caries, disparities persist among different racial, ethnic, educational, and income groups; it remains a modern curse for large segments of the population.
Basics of Tooth Decay
Tooth decay is caused by Streptococcus mutans (S mutans) bacterial infection. The cariogenic bacteria are transmissible from mother or caregiver to children.6 After tooth eruption, the mouth is quickly colonized by S mutans. Even though the bacteria are ubiquitous, the disease burden is more concentrated in some populations.
What makes some people more susceptible to tooth decay? Contrary to popular belief, it is not caused by childbirth or low dietary intake of calcium.7,8 Tooth decay typically starts on the chewing surfaces or proximal contacts of teeth.
S mutans is introduced into the mouth principally from another person. The bacteria colonize the mouth and with the formation of plaques, adhere to the teeth. Plaque is the soft, sticky film formed on teeth from food degradation. The biofilm is conducive to bacterial proliferation and teeming with bacteria.
The S mutans bacteria break down sugars and produce lactic acids, which cause tooth decay—a process of demineralization, or loss of calcium phosphate, from the tooth structure.2,9 As a result, the tooth “softens” and eventually collapses on itself, forming a cavity. Tooth decay most commonly occurs at the occlusal (chewing) surfaces and the proximal contacts of teeth. The occlusal aspects of teeth have a natural pit-and-fissure morphology that facilitates bacterial adherence and colonization. The proximal contacts of teeth also facilitate adherence of plaque and bacteria.
A tooth is made up of 3 layers. The outermost layer of the tooth crown is the enamel, which is the hardest or most mineralized part of the tooth—it is harder than bone. The next layer is the dentin, which has a higher percentage of organic material (collagen) and water than the enamel has and is softer. In the center of the tooth is the pulp (consisting of nerves and blood vessels), which keeps the tooth alive and provides sensation to the tooth. The outermost layer of the tooth root is cementum (instead of enamel), followed by dentin, which encases the pulp tissues contained within the root canals (Figure).
Process of Tooth Loss
At the early stage of tooth decay, when the decay is confined to the enamel, the tooth is asymptomatic, and the damage is reversible. When the decay extends into the dentin, restorations are a consideration. The further the decay extends toward the pulp, the greater the risk of tooth sensitivity and pain. Decay naturally progresses faster in the (less mineralized) dentin than when the decay is still confined to the enamel. If left unchecked, the decay may progress, and the bacteria eventually invade the pulp. At that point, there is risk of not only pain, but also swelling and tooth loss.
At the earlier stage of decay, a tooth may be treated with restorations, which are typically made of dental amalgam, resin (composite), glass ionomer, porcelain, or gold. When the bacteria have invaded the pulp, a dental restoration will not treat the pain and infection. Root canal therapy is needed to remove the infected tissues in the pulp chamber and root canals. Further, if the tooth is too compromised with extensive destruction from the decay or if there are financial or other barriers to root canal therapy, extraction is likely the only option.
Key to Oral Health
Personal daily oral hygiene (brushing and flossing) helps remove plaque from accumulating on tooth surfaces—especially the occlusal surfaces and proximal contacts, which are most prone to decay. Brushing teeth is of limited benefit without the use of fluoride toothpaste.8 The most important time for brushing is before bedtime, because less salivation occurs during sleep. Saliva helps clear fermented bacterial products, buffers the drop in pH, prevents demineralization, and enhances remineralizaton.10
Fluoride benefits children and adults of all ages, and comes in the form of fluoridated tap water, toothpaste, mouth rinse, and professionally applied gel and varnish. Fluoride occurs naturally in the environment, too. Its effect is mainly topical—fluoride gets incorporated into the tooth as fluorapatite, replacing the hydroxyapatite. Fluorapatite is harder than the hydroxyapatite; hence, the tooth is better able to resist demineralization by bacterial acid attacks.11 Professionally applied fluoride is generally recommended for high-risk patients, typically patients with high caries burden, ie, many decayed teeth. The best predictor of future caries is the past caries experience.
Sealants are thin, plastic coatings that are painted on to tooth occlusal surfaces, obliterating the pits and fissures normally found on posterior teeth. The smooth sealants effectively inhibit the colonization of S mutans on the occlusal aspects of teeth.12 Sealants are applied in dental offices (by the dentists or dental hygienists) or in school-based programs.
There are 2 leading types of dental diseases: tooth decay (dental caries or cavities) and gum disease (periodontal disease). Tooth decay is by far the more prevalent of the 2, causing a greater, needless loss in the quality of life.
Prevalence of Tooth Decay
Dental caries is a major public health problem. Even though in the past 50 years there has been a significant decline in dental caries, it is the most common ailment in the U.S., and large segments of the population experience various barriers to care. Among children and adolescents, dental caries is 4 to 5 times more common than asthma.1,2 Data from the National Health and Nutrition Examination Survey, 2011-2012, show that among children aged 2 to 8 years, 37% had dental caries in their primary teeth. Among adolescents aged 12 to 19 years, the prevalence of dental caries in the permanent teeth was 58%. About 90% of adults aged ≥ 20 years had dental caries.3,4
Unmet Dental Needs
The real disease burden of dental caries is the amount of unmet needs or untreated decay. In recent years, there has been a shift in the peak prevalence of untreated tooth decay from children to adults, possibly attributable to socioecologic factors.3,5 The prevalence of untreated decay in children and adolescents was about 15%. However, the prevalence of untreated decay among adults aged 20 to 64 years was higher: 27% of the adults had decayed teeth that were left untreated.3,4
The rates of untreated decay among these adults were higher among Hispanics (36%) and non-Hispanic blacks (42%) than among non-Hispanic whites (22%) and non-Hispanic Asians (17%).3,4 Despite the decline in dental caries, disparities persist among different racial, ethnic, educational, and income groups; it remains a modern curse for large segments of the population.
Basics of Tooth Decay
Tooth decay is caused by Streptococcus mutans (S mutans) bacterial infection. The cariogenic bacteria are transmissible from mother or caregiver to children.6 After tooth eruption, the mouth is quickly colonized by S mutans. Even though the bacteria are ubiquitous, the disease burden is more concentrated in some populations.
What makes some people more susceptible to tooth decay? Contrary to popular belief, it is not caused by childbirth or low dietary intake of calcium.7,8 Tooth decay typically starts on the chewing surfaces or proximal contacts of teeth.
S mutans is introduced into the mouth principally from another person. The bacteria colonize the mouth and with the formation of plaques, adhere to the teeth. Plaque is the soft, sticky film formed on teeth from food degradation. The biofilm is conducive to bacterial proliferation and teeming with bacteria.
The S mutans bacteria break down sugars and produce lactic acids, which cause tooth decay—a process of demineralization, or loss of calcium phosphate, from the tooth structure.2,9 As a result, the tooth “softens” and eventually collapses on itself, forming a cavity. Tooth decay most commonly occurs at the occlusal (chewing) surfaces and the proximal contacts of teeth. The occlusal aspects of teeth have a natural pit-and-fissure morphology that facilitates bacterial adherence and colonization. The proximal contacts of teeth also facilitate adherence of plaque and bacteria.
A tooth is made up of 3 layers. The outermost layer of the tooth crown is the enamel, which is the hardest or most mineralized part of the tooth—it is harder than bone. The next layer is the dentin, which has a higher percentage of organic material (collagen) and water than the enamel has and is softer. In the center of the tooth is the pulp (consisting of nerves and blood vessels), which keeps the tooth alive and provides sensation to the tooth. The outermost layer of the tooth root is cementum (instead of enamel), followed by dentin, which encases the pulp tissues contained within the root canals (Figure).
Process of Tooth Loss
At the early stage of tooth decay, when the decay is confined to the enamel, the tooth is asymptomatic, and the damage is reversible. When the decay extends into the dentin, restorations are a consideration. The further the decay extends toward the pulp, the greater the risk of tooth sensitivity and pain. Decay naturally progresses faster in the (less mineralized) dentin than when the decay is still confined to the enamel. If left unchecked, the decay may progress, and the bacteria eventually invade the pulp. At that point, there is risk of not only pain, but also swelling and tooth loss.
At the earlier stage of decay, a tooth may be treated with restorations, which are typically made of dental amalgam, resin (composite), glass ionomer, porcelain, or gold. When the bacteria have invaded the pulp, a dental restoration will not treat the pain and infection. Root canal therapy is needed to remove the infected tissues in the pulp chamber and root canals. Further, if the tooth is too compromised with extensive destruction from the decay or if there are financial or other barriers to root canal therapy, extraction is likely the only option.
Key to Oral Health
Personal daily oral hygiene (brushing and flossing) helps remove plaque from accumulating on tooth surfaces—especially the occlusal surfaces and proximal contacts, which are most prone to decay. Brushing teeth is of limited benefit without the use of fluoride toothpaste.8 The most important time for brushing is before bedtime, because less salivation occurs during sleep. Saliva helps clear fermented bacterial products, buffers the drop in pH, prevents demineralization, and enhances remineralizaton.10
Fluoride benefits children and adults of all ages, and comes in the form of fluoridated tap water, toothpaste, mouth rinse, and professionally applied gel and varnish. Fluoride occurs naturally in the environment, too. Its effect is mainly topical—fluoride gets incorporated into the tooth as fluorapatite, replacing the hydroxyapatite. Fluorapatite is harder than the hydroxyapatite; hence, the tooth is better able to resist demineralization by bacterial acid attacks.11 Professionally applied fluoride is generally recommended for high-risk patients, typically patients with high caries burden, ie, many decayed teeth. The best predictor of future caries is the past caries experience.
Sealants are thin, plastic coatings that are painted on to tooth occlusal surfaces, obliterating the pits and fissures normally found on posterior teeth. The smooth sealants effectively inhibit the colonization of S mutans on the occlusal aspects of teeth.12 Sealants are applied in dental offices (by the dentists or dental hygienists) or in school-based programs.
1. U.S. Department of Health and Human Services. Oral health in America: a report of the Surgeon General. http://www.nidcr.nih.gov/DataStatistics/SurgeonGeneral/Report/ExecutiveSummary.htm. Updated March 7, 2014. Accessed August 22, 2016.
2. Centers for Disease Control and Prevention. Hygiene-related diseases. http://www.cdc.gov/healthywater/hygiene/disease/dental_caries.html. Updated December 16, 2014. Accessed August 22, 2016.
3. Dye BA, Thornton-Evan G, Xianfen L, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011-2012. http://www.cdc.gov/nchs/data/databriefs/db191.pdf. Published March 2015. NCHS Data Brief. Accessed August 22, 2016.
4. Dye BA, Thornton-Evan G, Xianfen L, Iafolla TJ. Dental caries and tooth loss in adults in the United States, 2011-2012. http://www.cdc.gov/nchs/data/databriefs/db197.pdf. NCHS Data Brief. Published May 2015. Accessed August 22, 2016.
5. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. 2015;94(5):650-658.
6. Smith RE, Badner VM, Morse DE, Freeman K. Maternal risk indicators for childhood caries in an inner city population. Community Dent Oral Epidemiol. 2002;30(3):176-181.
7. Boggess KA, Urlaub DM, Moos MK, Polinkovsky M, El-Khorazaty J, Lorenz C. Knowledge and beliefs regarding oral health among pregnant women. J Am Dent Assoc. 2011;142(11):1275-1282.
8. Roberts-Thomson KF, Spencer AJ. Public knowledge of the prevention of dental decay and gum diseases. Aust Dent J. 1999;44(4):253-258.
9. Cochrane NJ, Cai F, Hug NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010;89(11):1187-1197.
10. Prabhakar AR, Dodawad R, Os R. Evaluation of flow Rate, pH, buffering capacity, calcium, total protein and total antioxidant levels of saliva in caries free and caries active children—an in vivo study. Int J Clin Pediatr Dent. 2009;2(1):9-12.
11. Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of remineralization and fluoride in the dynamic process of demineralization and remuneration (part 3). J Clin Pediatr Dent. 2004;28(3):203-214.
12. Azarpazhooh A, Main PA. Pit and fissure sealants in the prevention of dental caries in children and adolescents: a systematic review. J Can Dent Assoc. 2008;74(2):171-177.
1. U.S. Department of Health and Human Services. Oral health in America: a report of the Surgeon General. http://www.nidcr.nih.gov/DataStatistics/SurgeonGeneral/Report/ExecutiveSummary.htm. Updated March 7, 2014. Accessed August 22, 2016.
2. Centers for Disease Control and Prevention. Hygiene-related diseases. http://www.cdc.gov/healthywater/hygiene/disease/dental_caries.html. Updated December 16, 2014. Accessed August 22, 2016.
3. Dye BA, Thornton-Evan G, Xianfen L, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011-2012. http://www.cdc.gov/nchs/data/databriefs/db191.pdf. Published March 2015. NCHS Data Brief. Accessed August 22, 2016.
4. Dye BA, Thornton-Evan G, Xianfen L, Iafolla TJ. Dental caries and tooth loss in adults in the United States, 2011-2012. http://www.cdc.gov/nchs/data/databriefs/db197.pdf. NCHS Data Brief. Published May 2015. Accessed August 22, 2016.
5. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. 2015;94(5):650-658.
6. Smith RE, Badner VM, Morse DE, Freeman K. Maternal risk indicators for childhood caries in an inner city population. Community Dent Oral Epidemiol. 2002;30(3):176-181.
7. Boggess KA, Urlaub DM, Moos MK, Polinkovsky M, El-Khorazaty J, Lorenz C. Knowledge and beliefs regarding oral health among pregnant women. J Am Dent Assoc. 2011;142(11):1275-1282.
8. Roberts-Thomson KF, Spencer AJ. Public knowledge of the prevention of dental decay and gum diseases. Aust Dent J. 1999;44(4):253-258.
9. Cochrane NJ, Cai F, Hug NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010;89(11):1187-1197.
10. Prabhakar AR, Dodawad R, Os R. Evaluation of flow Rate, pH, buffering capacity, calcium, total protein and total antioxidant levels of saliva in caries free and caries active children—an in vivo study. Int J Clin Pediatr Dent. 2009;2(1):9-12.
11. Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries: role of remineralization and fluoride in the dynamic process of demineralization and remuneration (part 3). J Clin Pediatr Dent. 2004;28(3):203-214.
12. Azarpazhooh A, Main PA. Pit and fissure sealants in the prevention of dental caries in children and adolescents: a systematic review. J Can Dent Assoc. 2008;74(2):171-177.