User login
Proposals Pave the Way for New Drugs
To promote achievable solutions in the ongoing debate on drug financing, Anthem, Inc. and Eli Lilly and Company are offering two policy proposals, which are detailed in “Discovering New Medicines and New Ways to Pay for Them,” published on the Health Affairs blog.
The first proposal calls for clarifying federal regulation to reduce perceived barriers impeding conversations between health benefit companies and biopharmaceutical companies about drugs prior to the drugs being approved for sale.
The second proposal calls for changes to federal laws and regulations to mitigate the barriers that make it difficult to move toward value-based contracting.
“A change in policies could open the door to new opportunities for hospitalists and their employers to create more high-value care,” says Sam Nussbaum, MD, Anthem clinical advisor. “Today, hospitals are paid for seeing patients. What if hospitals participated in a value-based arrangement with manufacturers and insurers that included treating patients with a specific condition with a new therapy proven to be more effective in producing better health outcomes, including keeping patients out of the hospital?”
Reference
- Nussbaum S, Ricks D. Discovering new medicines and new ways to pay for them. Health Policy Lab. Available at: http://healthaffairs.org/blog/2016/01/29/discovering-new-medicines-and-new-ways-to-pay-for-them/. Accessed February 15, 2016.
To promote achievable solutions in the ongoing debate on drug financing, Anthem, Inc. and Eli Lilly and Company are offering two policy proposals, which are detailed in “Discovering New Medicines and New Ways to Pay for Them,” published on the Health Affairs blog.
The first proposal calls for clarifying federal regulation to reduce perceived barriers impeding conversations between health benefit companies and biopharmaceutical companies about drugs prior to the drugs being approved for sale.
The second proposal calls for changes to federal laws and regulations to mitigate the barriers that make it difficult to move toward value-based contracting.
“A change in policies could open the door to new opportunities for hospitalists and their employers to create more high-value care,” says Sam Nussbaum, MD, Anthem clinical advisor. “Today, hospitals are paid for seeing patients. What if hospitals participated in a value-based arrangement with manufacturers and insurers that included treating patients with a specific condition with a new therapy proven to be more effective in producing better health outcomes, including keeping patients out of the hospital?”
Reference
- Nussbaum S, Ricks D. Discovering new medicines and new ways to pay for them. Health Policy Lab. Available at: http://healthaffairs.org/blog/2016/01/29/discovering-new-medicines-and-new-ways-to-pay-for-them/. Accessed February 15, 2016.
To promote achievable solutions in the ongoing debate on drug financing, Anthem, Inc. and Eli Lilly and Company are offering two policy proposals, which are detailed in “Discovering New Medicines and New Ways to Pay for Them,” published on the Health Affairs blog.
The first proposal calls for clarifying federal regulation to reduce perceived barriers impeding conversations between health benefit companies and biopharmaceutical companies about drugs prior to the drugs being approved for sale.
The second proposal calls for changes to federal laws and regulations to mitigate the barriers that make it difficult to move toward value-based contracting.
“A change in policies could open the door to new opportunities for hospitalists and their employers to create more high-value care,” says Sam Nussbaum, MD, Anthem clinical advisor. “Today, hospitals are paid for seeing patients. What if hospitals participated in a value-based arrangement with manufacturers and insurers that included treating patients with a specific condition with a new therapy proven to be more effective in producing better health outcomes, including keeping patients out of the hospital?”
Reference
- Nussbaum S, Ricks D. Discovering new medicines and new ways to pay for them. Health Policy Lab. Available at: http://healthaffairs.org/blog/2016/01/29/discovering-new-medicines-and-new-ways-to-pay-for-them/. Accessed February 15, 2016.
Supreme Court case could expand false claims liability
A case before the U.S. Supreme Court could expand physicians’ liability under the False Claims Act (FCA).
The case of Escobar v. Universal Health Services centers on the theory of implied certification and how that legal test should be used to determine whether a claim for payment is fraudulent.

The case “is an opportunity for the Supreme Court to figure out how far the False Claims Act is going to stretch,” said Lawrence M. Kraus, a Boston health law attorney who attended the April 19 oral arguments. “On the practical level, it may have an impact as to whether [such] cases get dismissed at an early stage or whether they go into the discovery phase, which can be quite long, unpleasant, and expensive.”
The Escobar case arises from the death of a patient who was treated at a Lawrence, Mass., mental health clinic operated by Universal Health Services. The patient died from an alleged adverse reaction to medication prescribed for her by clinic staff, according to allegations by her family. The patient’s father, Julio Escobar, later learned counselors and psychologists involved in his daughter’s treatment were not licensed, were not properly supervised by a physician, and had lied about their medical credentials, according to court documents.
The Massachusetts Department of Public Health found the clinic had violated 14 distinct regulations, including those relating to staff licensure and supervision. As a result of the investigation, the clinic entered into a correction plan with the agency and paid a civil fine.
Mr. Escobar and his wife then filed suit under the FCA and the Massachusetts False Claims Act, claiming that Universal had presented false claims to Medicaid by seeking payments for services provided by unlicensed, unsupervised health care providers. Although the reimbursement claims submitted to the government accurately described the services provided and cited the correct charges, the plaintiffs alleged that because the clinic’s operations violated state requirements to participate in Medicaid, Universal had also violated the FCA. The federal government intervened in the case on behalf of the Escobars.
Universal countered that the FCA suit was invalid because a reimbursement claim cannot be false unless its details are untrue or inaccurate.
The plaintiffs, however, contend that a claim does not have to include explicit false statements to be fraudulent. Rather, their complaint relies on “implied certification,” a theory holding that any submission for government payment includes an implicit certification that the health provider has complied with all applicable contract requirements, laws, and regulations that could be a condition of payment. Universal falsely claimed entitlement when it submitted reimbursement requests that did not conform to applicable laws, the plaintiffs argued.
The 1st U.S. Circuit Court of Appeals ruled in favor of Escobar, and Universal appealed to the Supreme Court.
Circuit courts across the country have split on the issue, Mr. Kraus noted.
“There have been a number of different approaches from appeals courts in the country,” he said. “This is not a new issue, but one that the Supreme Court found important enough to decide.”
Why should doctors care about this case?
A ruling for the plaintiff could increase the chances that physicians are accused of an FCA violation after submitting a claim for payment, said William W. Horton, a Birmingham, Ala., health law attorney and chair of the American Bar Association Health Law Section.

“The problem that this raises for health care providers is: There is an enormous web of laws and regulations out there, many of which don’t have anything to do with whether a particular service was rendered or not,” Mr. Horton said in an interview “If you adopt the implied certification theory and take a broad view, than you significantly enhance the scope of claims that could be pursued under the False Claims Act.”
Mr. Horton provides this example: Take a physician group that has an in-office lab, and assume that for some technical reason, the group doesn’t satisfy the Stark Law exception for in-office ancillary services. If a physician in the group refers a Medicare patient to the lab and the group bills Medicare, that’s a Stark Law violation because the group didn’t meet the Stark exception, even if there’s no dispute over whether the patient needed the test or whether the test was done correctly, or whether the Medicare claim accurately reflected the charges, he said. By broadly applying the implied certification theory to this scenario, a case could be made that the practice violated the FCA in submitting the claim because the group was implicitly certifying that the claim did not result from a referral that violated the Stark Law.
“The group could be found liable for the enormous penalties available under the False Claims Act even though the services rendered were medically necessary and appropriate, and even though the group did not expressly certify, in so many words, that the claim did not result from a referral that violated the Stark Law,” Mr. Horton said.
Medical associations, including the American Medical Association and American Hospital Association have weighed in on the case in favor of Universal Health Services. In its brief, the AMA said there is a “sharp distinction” between statutory, regulatory, or contractual violations and false or fraudulent claims.
“Implied certification claims find no support in the statute and do not resemble claims Congress had in mind when enacting or amending the FCA,” according to the brief. “They deprive contractors of their constitutional rights to have notice that they are engaging in conduct subject to heightened sanctions.”
How might the Supreme Court rule?
During oral arguments on April 19, some justices appeared to indicate which way they are leaning, Mr. Kraus said.
Chief Justice John Roberts seemed concerned about the reach of the FCA under the implied certification theory. He raised questions about how people conducting business with the government would know about each and every regulation that could apply as a condition of payment.
Associate Justice Sonia Sotomayer and Associate Justice Elena Kagan appeared in favor of implied certification, while Associate Justice Samuel Alito Jr., Associate Justice Clarence Thomas, and Associate Justice Ruth Bader-Ginsberg did not display a strong opinion either way, Mr. Kraus said. Associate Justice Stephen Breyer appeared to be conflicted, asking for guidance from Roy T. Englert, an attorney for Universal Health Services.
“I’m asking for advice from you, from your point of view,” Justice Breyer said to Mr. Englert. “What the sentence in the opinion should say that describes the circumstances under which the person who submits a form saying, ‘I want a thousand dollars. I just supplied the guns or the medical care.’ ... When has that person committed fraud? – Or that’s what I want. What is the sentence you want me to write?”
Justices could rule a number of ways. They could uphold the appeals court decision, which would affirm a broad interpretation of implied certification theory. They could rule that the implied certification theory is valid, but it cannot be stretched as far as the appeals court expanded it. Justices could choose to reject the implied certification theory altogether and decide that the government must expressly identify every condition of payment in which a health provider is certifying compliance when they submit a claim, either on the claim form or by regulation. The high court could also split on the issue four to four, leaving intact the range of circuit court interpretations on implied certification across the country.
“There’s a very real question as to whether they’re going to be able to get a majority on any of those decisions because this is not an easy question,” Mr. Horton said. “The court has a pretty wide range of potential rulings available to it, but I don’t know what they’re going to be able to majority around, if they’re going to be able get a majority around any result at all.”
A decision in the case is expected by June.
On Twitter @legal_med
A case before the U.S. Supreme Court could expand physicians’ liability under the False Claims Act (FCA).
The case of Escobar v. Universal Health Services centers on the theory of implied certification and how that legal test should be used to determine whether a claim for payment is fraudulent.
The case “is an opportunity for the Supreme Court to figure out how far the False Claims Act is going to stretch,” said Lawrence M. Kraus, a Boston health law attorney who attended the April 19 oral arguments. “On the practical level, it may have an impact as to whether [such] cases get dismissed at an early stage or whether they go into the discovery phase, which can be quite long, unpleasant, and expensive.”
The Escobar case arises from the death of a patient who was treated at a Lawrence, Mass., mental health clinic operated by Universal Health Services. The patient died from an alleged adverse reaction to medication prescribed for her by clinic staff, according to allegations by her family. The patient’s father, Julio Escobar, later learned counselors and psychologists involved in his daughter’s treatment were not licensed, were not properly supervised by a physician, and had lied about their medical credentials, according to court documents.
The Massachusetts Department of Public Health found the clinic had violated 14 distinct regulations, including those relating to staff licensure and supervision. As a result of the investigation, the clinic entered into a correction plan with the agency and paid a civil fine.
Mr. Escobar and his wife then filed suit under the FCA and the Massachusetts False Claims Act, claiming that Universal had presented false claims to Medicaid by seeking payments for services provided by unlicensed, unsupervised health care providers. Although the reimbursement claims submitted to the government accurately described the services provided and cited the correct charges, the plaintiffs alleged that because the clinic’s operations violated state requirements to participate in Medicaid, Universal had also violated the FCA. The federal government intervened in the case on behalf of the Escobars.
Universal countered that the FCA suit was invalid because a reimbursement claim cannot be false unless its details are untrue or inaccurate.
The plaintiffs, however, contend that a claim does not have to include explicit false statements to be fraudulent. Rather, their complaint relies on “implied certification,” a theory holding that any submission for government payment includes an implicit certification that the health provider has complied with all applicable contract requirements, laws, and regulations that could be a condition of payment. Universal falsely claimed entitlement when it submitted reimbursement requests that did not conform to applicable laws, the plaintiffs argued.
The 1st U.S. Circuit Court of Appeals ruled in favor of Escobar, and Universal appealed to the Supreme Court.
Circuit courts across the country have split on the issue, Mr. Kraus noted.
“There have been a number of different approaches from appeals courts in the country,” he said. “This is not a new issue, but one that the Supreme Court found important enough to decide.”
Why should doctors care about this case?
A ruling for the plaintiff could increase the chances that physicians are accused of an FCA violation after submitting a claim for payment, said William W. Horton, a Birmingham, Ala., health law attorney and chair of the American Bar Association Health Law Section.
“The problem that this raises for health care providers is: There is an enormous web of laws and regulations out there, many of which don’t have anything to do with whether a particular service was rendered or not,” Mr. Horton said in an interview “If you adopt the implied certification theory and take a broad view, than you significantly enhance the scope of claims that could be pursued under the False Claims Act.”
Mr. Horton provides this example: Take a physician group that has an in-office lab, and assume that for some technical reason, the group doesn’t satisfy the Stark Law exception for in-office ancillary services. If a physician in the group refers a Medicare patient to the lab and the group bills Medicare, that’s a Stark Law violation because the group didn’t meet the Stark exception, even if there’s no dispute over whether the patient needed the test or whether the test was done correctly, or whether the Medicare claim accurately reflected the charges, he said. By broadly applying the implied certification theory to this scenario, a case could be made that the practice violated the FCA in submitting the claim because the group was implicitly certifying that the claim did not result from a referral that violated the Stark Law.
“The group could be found liable for the enormous penalties available under the False Claims Act even though the services rendered were medically necessary and appropriate, and even though the group did not expressly certify, in so many words, that the claim did not result from a referral that violated the Stark Law,” Mr. Horton said.
Medical associations, including the American Medical Association and American Hospital Association have weighed in on the case in favor of Universal Health Services. In its brief, the AMA said there is a “sharp distinction” between statutory, regulatory, or contractual violations and false or fraudulent claims.
“Implied certification claims find no support in the statute and do not resemble claims Congress had in mind when enacting or amending the FCA,” according to the brief. “They deprive contractors of their constitutional rights to have notice that they are engaging in conduct subject to heightened sanctions.”
How might the Supreme Court rule?
During oral arguments on April 19, some justices appeared to indicate which way they are leaning, Mr. Kraus said.
Chief Justice John Roberts seemed concerned about the reach of the FCA under the implied certification theory. He raised questions about how people conducting business with the government would know about each and every regulation that could apply as a condition of payment.
Associate Justice Sonia Sotomayer and Associate Justice Elena Kagan appeared in favor of implied certification, while Associate Justice Samuel Alito Jr., Associate Justice Clarence Thomas, and Associate Justice Ruth Bader-Ginsberg did not display a strong opinion either way, Mr. Kraus said. Associate Justice Stephen Breyer appeared to be conflicted, asking for guidance from Roy T. Englert, an attorney for Universal Health Services.
“I’m asking for advice from you, from your point of view,” Justice Breyer said to Mr. Englert. “What the sentence in the opinion should say that describes the circumstances under which the person who submits a form saying, ‘I want a thousand dollars. I just supplied the guns or the medical care.’ ... When has that person committed fraud? – Or that’s what I want. What is the sentence you want me to write?”
Justices could rule a number of ways. They could uphold the appeals court decision, which would affirm a broad interpretation of implied certification theory. They could rule that the implied certification theory is valid, but it cannot be stretched as far as the appeals court expanded it. Justices could choose to reject the implied certification theory altogether and decide that the government must expressly identify every condition of payment in which a health provider is certifying compliance when they submit a claim, either on the claim form or by regulation. The high court could also split on the issue four to four, leaving intact the range of circuit court interpretations on implied certification across the country.
“There’s a very real question as to whether they’re going to be able to get a majority on any of those decisions because this is not an easy question,” Mr. Horton said. “The court has a pretty wide range of potential rulings available to it, but I don’t know what they’re going to be able to majority around, if they’re going to be able get a majority around any result at all.”
A decision in the case is expected by June.
On Twitter @legal_med
A case before the U.S. Supreme Court could expand physicians’ liability under the False Claims Act (FCA).
The case of Escobar v. Universal Health Services centers on the theory of implied certification and how that legal test should be used to determine whether a claim for payment is fraudulent.
The case “is an opportunity for the Supreme Court to figure out how far the False Claims Act is going to stretch,” said Lawrence M. Kraus, a Boston health law attorney who attended the April 19 oral arguments. “On the practical level, it may have an impact as to whether [such] cases get dismissed at an early stage or whether they go into the discovery phase, which can be quite long, unpleasant, and expensive.”
The Escobar case arises from the death of a patient who was treated at a Lawrence, Mass., mental health clinic operated by Universal Health Services. The patient died from an alleged adverse reaction to medication prescribed for her by clinic staff, according to allegations by her family. The patient’s father, Julio Escobar, later learned counselors and psychologists involved in his daughter’s treatment were not licensed, were not properly supervised by a physician, and had lied about their medical credentials, according to court documents.
The Massachusetts Department of Public Health found the clinic had violated 14 distinct regulations, including those relating to staff licensure and supervision. As a result of the investigation, the clinic entered into a correction plan with the agency and paid a civil fine.
Mr. Escobar and his wife then filed suit under the FCA and the Massachusetts False Claims Act, claiming that Universal had presented false claims to Medicaid by seeking payments for services provided by unlicensed, unsupervised health care providers. Although the reimbursement claims submitted to the government accurately described the services provided and cited the correct charges, the plaintiffs alleged that because the clinic’s operations violated state requirements to participate in Medicaid, Universal had also violated the FCA. The federal government intervened in the case on behalf of the Escobars.
Universal countered that the FCA suit was invalid because a reimbursement claim cannot be false unless its details are untrue or inaccurate.
The plaintiffs, however, contend that a claim does not have to include explicit false statements to be fraudulent. Rather, their complaint relies on “implied certification,” a theory holding that any submission for government payment includes an implicit certification that the health provider has complied with all applicable contract requirements, laws, and regulations that could be a condition of payment. Universal falsely claimed entitlement when it submitted reimbursement requests that did not conform to applicable laws, the plaintiffs argued.
The 1st U.S. Circuit Court of Appeals ruled in favor of Escobar, and Universal appealed to the Supreme Court.
Circuit courts across the country have split on the issue, Mr. Kraus noted.
“There have been a number of different approaches from appeals courts in the country,” he said. “This is not a new issue, but one that the Supreme Court found important enough to decide.”
Why should doctors care about this case?
A ruling for the plaintiff could increase the chances that physicians are accused of an FCA violation after submitting a claim for payment, said William W. Horton, a Birmingham, Ala., health law attorney and chair of the American Bar Association Health Law Section.
“The problem that this raises for health care providers is: There is an enormous web of laws and regulations out there, many of which don’t have anything to do with whether a particular service was rendered or not,” Mr. Horton said in an interview “If you adopt the implied certification theory and take a broad view, than you significantly enhance the scope of claims that could be pursued under the False Claims Act.”
Mr. Horton provides this example: Take a physician group that has an in-office lab, and assume that for some technical reason, the group doesn’t satisfy the Stark Law exception for in-office ancillary services. If a physician in the group refers a Medicare patient to the lab and the group bills Medicare, that’s a Stark Law violation because the group didn’t meet the Stark exception, even if there’s no dispute over whether the patient needed the test or whether the test was done correctly, or whether the Medicare claim accurately reflected the charges, he said. By broadly applying the implied certification theory to this scenario, a case could be made that the practice violated the FCA in submitting the claim because the group was implicitly certifying that the claim did not result from a referral that violated the Stark Law.
“The group could be found liable for the enormous penalties available under the False Claims Act even though the services rendered were medically necessary and appropriate, and even though the group did not expressly certify, in so many words, that the claim did not result from a referral that violated the Stark Law,” Mr. Horton said.
Medical associations, including the American Medical Association and American Hospital Association have weighed in on the case in favor of Universal Health Services. In its brief, the AMA said there is a “sharp distinction” between statutory, regulatory, or contractual violations and false or fraudulent claims.
“Implied certification claims find no support in the statute and do not resemble claims Congress had in mind when enacting or amending the FCA,” according to the brief. “They deprive contractors of their constitutional rights to have notice that they are engaging in conduct subject to heightened sanctions.”
How might the Supreme Court rule?
During oral arguments on April 19, some justices appeared to indicate which way they are leaning, Mr. Kraus said.
Chief Justice John Roberts seemed concerned about the reach of the FCA under the implied certification theory. He raised questions about how people conducting business with the government would know about each and every regulation that could apply as a condition of payment.
Associate Justice Sonia Sotomayer and Associate Justice Elena Kagan appeared in favor of implied certification, while Associate Justice Samuel Alito Jr., Associate Justice Clarence Thomas, and Associate Justice Ruth Bader-Ginsberg did not display a strong opinion either way, Mr. Kraus said. Associate Justice Stephen Breyer appeared to be conflicted, asking for guidance from Roy T. Englert, an attorney for Universal Health Services.
“I’m asking for advice from you, from your point of view,” Justice Breyer said to Mr. Englert. “What the sentence in the opinion should say that describes the circumstances under which the person who submits a form saying, ‘I want a thousand dollars. I just supplied the guns or the medical care.’ ... When has that person committed fraud? – Or that’s what I want. What is the sentence you want me to write?”
Justices could rule a number of ways. They could uphold the appeals court decision, which would affirm a broad interpretation of implied certification theory. They could rule that the implied certification theory is valid, but it cannot be stretched as far as the appeals court expanded it. Justices could choose to reject the implied certification theory altogether and decide that the government must expressly identify every condition of payment in which a health provider is certifying compliance when they submit a claim, either on the claim form or by regulation. The high court could also split on the issue four to four, leaving intact the range of circuit court interpretations on implied certification across the country.
“There’s a very real question as to whether they’re going to be able to get a majority on any of those decisions because this is not an easy question,” Mr. Horton said. “The court has a pretty wide range of potential rulings available to it, but I don’t know what they’re going to be able to majority around, if they’re going to be able get a majority around any result at all.”
A decision in the case is expected by June.
On Twitter @legal_med

Opioid reform legislation passes House committee
The House Energy & Commerce Committee has passed a comprehensive package of bills designed to curb the nation’s opioid epidemic.
Eleven opioid-related bills passed the full committee by voice vote on April 27 and April 28. Key provisions of the legislation would:

• Create an interagency task force to review best practices for pain management and prescribing.
• Require annual updates of federal opioid-prescribing guidelines.
• Authorize grants to test coprescribing opioids with buprenorphine or naloxone.
• Limit the number of pills prescribed.
• Increase the number of patients that a qualified addiction treatment specialist could see annually.
• Require an FDA advisory committee to review any new opioid proposed without abuse-deterrent properties.
• Require a detailed assessment of currently available inpatient and outpatient treatment beds.
• Prohibit the sale dextromethorphan-containing products to minors.
The full Senate also has a package of opioid-related bills to consider. On March 17, the Senate Committee on Health, Education, Labor and Pensions moved similar legislation to the Senate floor, including bills that would increase addiction patient panels, require coprescribing, and mandate insurance coverage of addiction treatment as required by current mental health parity laws.
Earlier this year, in a near unanimous vote, the Senate passed the Comprehensive Addiction and Recovery Act, which calls for the creation of a federal pain management best practices interagency task force. No funding was attached to the legislation, however, and companion legislation remains in committee in the House.
Although the opioid bills had bipartisan support in the Energy & Commerce Committee, rancor may yet surface. During mark-up, three amendments were defeated mostly along party lines. The amendments would have increased the number of patients each qualified provider can treat with buprenorphine to a variety of levels – one amendment called for a maximum of 250 patients while others called for as many as 300 or 500. Supporters of the amendments said higher numbers would ensure treatment for many more patients while opponents expressed concern about sacrificing quality of care for quantity.
Another defeated amendment called for a $1 billion appropriation for increased opioid treatment, echoing President Obama’s call earlier this year. Opponents painted the proposal as “fiscally irresponsible.”
At press time, the House had not scheduled consideration on the opioid bills.
On Twitter @whitneymcknight
The House Energy & Commerce Committee has passed a comprehensive package of bills designed to curb the nation’s opioid epidemic.
Eleven opioid-related bills passed the full committee by voice vote on April 27 and April 28. Key provisions of the legislation would:
• Create an interagency task force to review best practices for pain management and prescribing.
• Require annual updates of federal opioid-prescribing guidelines.
• Authorize grants to test coprescribing opioids with buprenorphine or naloxone.
• Limit the number of pills prescribed.
• Increase the number of patients that a qualified addiction treatment specialist could see annually.
• Require an FDA advisory committee to review any new opioid proposed without abuse-deterrent properties.
• Require a detailed assessment of currently available inpatient and outpatient treatment beds.
• Prohibit the sale dextromethorphan-containing products to minors.
The full Senate also has a package of opioid-related bills to consider. On March 17, the Senate Committee on Health, Education, Labor and Pensions moved similar legislation to the Senate floor, including bills that would increase addiction patient panels, require coprescribing, and mandate insurance coverage of addiction treatment as required by current mental health parity laws.
Earlier this year, in a near unanimous vote, the Senate passed the Comprehensive Addiction and Recovery Act, which calls for the creation of a federal pain management best practices interagency task force. No funding was attached to the legislation, however, and companion legislation remains in committee in the House.
Although the opioid bills had bipartisan support in the Energy & Commerce Committee, rancor may yet surface. During mark-up, three amendments were defeated mostly along party lines. The amendments would have increased the number of patients each qualified provider can treat with buprenorphine to a variety of levels – one amendment called for a maximum of 250 patients while others called for as many as 300 or 500. Supporters of the amendments said higher numbers would ensure treatment for many more patients while opponents expressed concern about sacrificing quality of care for quantity.
Another defeated amendment called for a $1 billion appropriation for increased opioid treatment, echoing President Obama’s call earlier this year. Opponents painted the proposal as “fiscally irresponsible.”
At press time, the House had not scheduled consideration on the opioid bills.
On Twitter @whitneymcknight
The House Energy & Commerce Committee has passed a comprehensive package of bills designed to curb the nation’s opioid epidemic.
Eleven opioid-related bills passed the full committee by voice vote on April 27 and April 28. Key provisions of the legislation would:
• Create an interagency task force to review best practices for pain management and prescribing.
• Require annual updates of federal opioid-prescribing guidelines.
• Authorize grants to test coprescribing opioids with buprenorphine or naloxone.
• Limit the number of pills prescribed.
• Increase the number of patients that a qualified addiction treatment specialist could see annually.
• Require an FDA advisory committee to review any new opioid proposed without abuse-deterrent properties.
• Require a detailed assessment of currently available inpatient and outpatient treatment beds.
• Prohibit the sale dextromethorphan-containing products to minors.
The full Senate also has a package of opioid-related bills to consider. On March 17, the Senate Committee on Health, Education, Labor and Pensions moved similar legislation to the Senate floor, including bills that would increase addiction patient panels, require coprescribing, and mandate insurance coverage of addiction treatment as required by current mental health parity laws.
Earlier this year, in a near unanimous vote, the Senate passed the Comprehensive Addiction and Recovery Act, which calls for the creation of a federal pain management best practices interagency task force. No funding was attached to the legislation, however, and companion legislation remains in committee in the House.
Although the opioid bills had bipartisan support in the Energy & Commerce Committee, rancor may yet surface. During mark-up, three amendments were defeated mostly along party lines. The amendments would have increased the number of patients each qualified provider can treat with buprenorphine to a variety of levels – one amendment called for a maximum of 250 patients while others called for as many as 300 or 500. Supporters of the amendments said higher numbers would ensure treatment for many more patients while opponents expressed concern about sacrificing quality of care for quantity.
Another defeated amendment called for a $1 billion appropriation for increased opioid treatment, echoing President Obama’s call earlier this year. Opponents painted the proposal as “fiscally irresponsible.”
At press time, the House had not scheduled consideration on the opioid bills.
On Twitter @whitneymcknight
FROM A HOUSE ENERGY & COMMERCE COMMITTEE HEARING

CMS promises streamlined, flexible program to replace meaningful use
Meaningful use would get a new name and an emphasis on flexibility under a proposal from the Centers for Medicare & Medicaid Services.
“We’re proposing today to replace meaningful use in the physician office with a new effort that moves the emphasis away from the use of information technology to one that supports patient care, supported by better and more connected technology,” CMS Acting Administrator Andy Slavitt said during an April 27 press teleconference to introduce the changes.

“The program, Advancing Care Information, is designed to be far simpler, less burdensome, and more flexible,” Mr. Slavitt said. “If this proposal is finalized, it will replace the current meaningful use program for physician offices and will be effective January 1, 2017, along with the other components of the MACRA implementations.”
Mr. Slavitt and Dr. Karen DeSalvo, National Coordinator for Health Information Technology, noted in a blog postthat the improvements “should increase providers’ ability to use technology in ways that are more relevant to their needs and the needs of their patients.”
The changes come as part of a larger proposed regulation to implement the Medicare Access and CHIP Reauthorization Act, released online April 27 and scheduled for publication in the Federal Register on May 9.
MACRA will create two systems under which doctors will be paid for the quality of care they provide. The changes to the meaningful use program will affect physicians who choose to participate in the Merit-based Incentive Payment System (MIPS). Under the proposed rule, efforts under the new Advancing Care Information program would account for 25% of the score used to determine pay for office-based physicians under Medicare.
The key difference between the proposed program and meaningful use is that physicians will no longer be faced with an all-or-nothing requirement for meeting criteria to qualify for extra payments under the MIPS program.
Advancing Care Information has been divided into two parts. The first is reporting measures and has been streamlined to 11 measures, down from 18. Reporting on computerized physician order entry and clinical decision support measures have been eliminated.
The second part is based on performance measures, with multiple pathways to achieve those targets, which allow physicians to select the measures that best align with their needs.
There also is an opportunity to earn an extra point if a physician is reporting to more than one public health registry.
“We’ve also taken this opportunity to really focus more on aligning quality, on seeing that we are streamlining workflow and creating opportunities for electronic health record and health IT developers to create products that really meet the needs and expectations of clinicians and providers on the front lines,” Dr. DeSalvo said during the April 27 call.
The proposal also emphasizes interoperability, information exchange, and security measures and requires that patients be able to access their health care information easily through the use of apps and other consumer-friendly technology, according to the blog post.
The proposed rule also emphasizes open data sharing and interoperability, something that has been a continual drag on the current meaningful use program.
Comments on the proposed rule can be made at www.regulations.gov and are due June 26.
Meaningful use would get a new name and an emphasis on flexibility under a proposal from the Centers for Medicare & Medicaid Services.
“We’re proposing today to replace meaningful use in the physician office with a new effort that moves the emphasis away from the use of information technology to one that supports patient care, supported by better and more connected technology,” CMS Acting Administrator Andy Slavitt said during an April 27 press teleconference to introduce the changes.
“The program, Advancing Care Information, is designed to be far simpler, less burdensome, and more flexible,” Mr. Slavitt said. “If this proposal is finalized, it will replace the current meaningful use program for physician offices and will be effective January 1, 2017, along with the other components of the MACRA implementations.”
Mr. Slavitt and Dr. Karen DeSalvo, National Coordinator for Health Information Technology, noted in a blog postthat the improvements “should increase providers’ ability to use technology in ways that are more relevant to their needs and the needs of their patients.”
The changes come as part of a larger proposed regulation to implement the Medicare Access and CHIP Reauthorization Act, released online April 27 and scheduled for publication in the Federal Register on May 9.
MACRA will create two systems under which doctors will be paid for the quality of care they provide. The changes to the meaningful use program will affect physicians who choose to participate in the Merit-based Incentive Payment System (MIPS). Under the proposed rule, efforts under the new Advancing Care Information program would account for 25% of the score used to determine pay for office-based physicians under Medicare.
The key difference between the proposed program and meaningful use is that physicians will no longer be faced with an all-or-nothing requirement for meeting criteria to qualify for extra payments under the MIPS program.
Advancing Care Information has been divided into two parts. The first is reporting measures and has been streamlined to 11 measures, down from 18. Reporting on computerized physician order entry and clinical decision support measures have been eliminated.
The second part is based on performance measures, with multiple pathways to achieve those targets, which allow physicians to select the measures that best align with their needs.
There also is an opportunity to earn an extra point if a physician is reporting to more than one public health registry.
“We’ve also taken this opportunity to really focus more on aligning quality, on seeing that we are streamlining workflow and creating opportunities for electronic health record and health IT developers to create products that really meet the needs and expectations of clinicians and providers on the front lines,” Dr. DeSalvo said during the April 27 call.
The proposal also emphasizes interoperability, information exchange, and security measures and requires that patients be able to access their health care information easily through the use of apps and other consumer-friendly technology, according to the blog post.
The proposed rule also emphasizes open data sharing and interoperability, something that has been a continual drag on the current meaningful use program.
Comments on the proposed rule can be made at www.regulations.gov and are due June 26.
Meaningful use would get a new name and an emphasis on flexibility under a proposal from the Centers for Medicare & Medicaid Services.
“We’re proposing today to replace meaningful use in the physician office with a new effort that moves the emphasis away from the use of information technology to one that supports patient care, supported by better and more connected technology,” CMS Acting Administrator Andy Slavitt said during an April 27 press teleconference to introduce the changes.
“The program, Advancing Care Information, is designed to be far simpler, less burdensome, and more flexible,” Mr. Slavitt said. “If this proposal is finalized, it will replace the current meaningful use program for physician offices and will be effective January 1, 2017, along with the other components of the MACRA implementations.”
Mr. Slavitt and Dr. Karen DeSalvo, National Coordinator for Health Information Technology, noted in a blog postthat the improvements “should increase providers’ ability to use technology in ways that are more relevant to their needs and the needs of their patients.”
The changes come as part of a larger proposed regulation to implement the Medicare Access and CHIP Reauthorization Act, released online April 27 and scheduled for publication in the Federal Register on May 9.
MACRA will create two systems under which doctors will be paid for the quality of care they provide. The changes to the meaningful use program will affect physicians who choose to participate in the Merit-based Incentive Payment System (MIPS). Under the proposed rule, efforts under the new Advancing Care Information program would account for 25% of the score used to determine pay for office-based physicians under Medicare.
The key difference between the proposed program and meaningful use is that physicians will no longer be faced with an all-or-nothing requirement for meeting criteria to qualify for extra payments under the MIPS program.
Advancing Care Information has been divided into two parts. The first is reporting measures and has been streamlined to 11 measures, down from 18. Reporting on computerized physician order entry and clinical decision support measures have been eliminated.
The second part is based on performance measures, with multiple pathways to achieve those targets, which allow physicians to select the measures that best align with their needs.
There also is an opportunity to earn an extra point if a physician is reporting to more than one public health registry.
“We’ve also taken this opportunity to really focus more on aligning quality, on seeing that we are streamlining workflow and creating opportunities for electronic health record and health IT developers to create products that really meet the needs and expectations of clinicians and providers on the front lines,” Dr. DeSalvo said during the April 27 call.
The proposal also emphasizes interoperability, information exchange, and security measures and requires that patients be able to access their health care information easily through the use of apps and other consumer-friendly technology, according to the blog post.
The proposed rule also emphasizes open data sharing and interoperability, something that has been a continual drag on the current meaningful use program.
Comments on the proposed rule can be made at www.regulations.gov and are due June 26.

Seven procedures account for most emergency general surgery costs and deaths
A very low number of emergency general surgery procedures account for the majority of all admissions, deaths, complications, and inpatient costs attributable to emergency general surgery procedures nationwide, according to a study published in JAMA Surgery.
“More than half a million patients undergo urgent or emergent general surgery operations annually in the United States, which accounts for more than $6 billion in annual costs. Only seven representative procedures account for approximately 80% of all admissions, deaths, complications, and inpatient costs attributable to operative emergency general surgery nationwide,” said Dr. John W. Scott from the Center for Surgery and Public Health, department of surgery at the Brigham & Women’s Hospital in Boston, and his associates.

The investigators sought to expand the current diagnosis-based definition of emergency general surgery in order to define a standardized, representative set of procedures that comprise the majority of the national clinical burden of emergency general surgery. To accomplish this goal, Dr. Scott and his colleagues examined data from the 2008 to 2011 Healthcare Cost and Utilization Project’s National Inpatient Sample, the largest publicly available all-payers claims database in the United States, from Nov. 15, 2015, to Feb. 16, 2016 (JAMA Surg. 2016 Apr 27. doi: 10.1001/jamasurg.2016.0480).
The results from this nationally representative observational study represented more than 2 million patient encounters, with a final analytic sample that included 137 unique four-digit ICD-9-CM procedure codes that mapped into 35 distinct three-digit procedure group codes. When ordered by burden rank, the cumulative attributable burden for total procedure count, total deaths, total complications, and total costs increased sharply through procedures ranked one to seven (partial colectomy, small-bowel resection, cholecystectomy, operative management of peptic ulcer disease, lysis of peritoneal adhesions, appendectomy, and laparotomy).
In addition, the procedure volumes were found to be highest for cholecystectomy and appendectomy, although the mortality and complication rates for these procedures were comparatively lower than for the other five identified procedures. For example, the frequency of procedures varied from 682,043 primary appendectomies to 9,418 primary laparotomies, but the mortality rate ranged from 0.08% for appendectomy to 23.76% for laparotomy. Similarly, the complication rate ranged from 7.27% for appendectomy to 46.94% for small-bowel resection. Study results also showed that mean inpatient costs ranged from $9,664.30 for appendectomy to $28,450.72 for small-bowel resection.
Based on their study data, Dr. Scott and his associates recommended national quality benchmarks and cost reduction efforts focused on the seven identified common, complicated, and costly emergency general surgery procedures.
No external funding source was disclosed. Coauthor Dr. Adil H. Haider disclosed ties to industry sources. None of the other coauthors reported any conflicts of interest.
A very low number of emergency general surgery procedures account for the majority of all admissions, deaths, complications, and inpatient costs attributable to emergency general surgery procedures nationwide, according to a study published in JAMA Surgery.
“More than half a million patients undergo urgent or emergent general surgery operations annually in the United States, which accounts for more than $6 billion in annual costs. Only seven representative procedures account for approximately 80% of all admissions, deaths, complications, and inpatient costs attributable to operative emergency general surgery nationwide,” said Dr. John W. Scott from the Center for Surgery and Public Health, department of surgery at the Brigham & Women’s Hospital in Boston, and his associates.
The investigators sought to expand the current diagnosis-based definition of emergency general surgery in order to define a standardized, representative set of procedures that comprise the majority of the national clinical burden of emergency general surgery. To accomplish this goal, Dr. Scott and his colleagues examined data from the 2008 to 2011 Healthcare Cost and Utilization Project’s National Inpatient Sample, the largest publicly available all-payers claims database in the United States, from Nov. 15, 2015, to Feb. 16, 2016 (JAMA Surg. 2016 Apr 27. doi: 10.1001/jamasurg.2016.0480).
The results from this nationally representative observational study represented more than 2 million patient encounters, with a final analytic sample that included 137 unique four-digit ICD-9-CM procedure codes that mapped into 35 distinct three-digit procedure group codes. When ordered by burden rank, the cumulative attributable burden for total procedure count, total deaths, total complications, and total costs increased sharply through procedures ranked one to seven (partial colectomy, small-bowel resection, cholecystectomy, operative management of peptic ulcer disease, lysis of peritoneal adhesions, appendectomy, and laparotomy).
In addition, the procedure volumes were found to be highest for cholecystectomy and appendectomy, although the mortality and complication rates for these procedures were comparatively lower than for the other five identified procedures. For example, the frequency of procedures varied from 682,043 primary appendectomies to 9,418 primary laparotomies, but the mortality rate ranged from 0.08% for appendectomy to 23.76% for laparotomy. Similarly, the complication rate ranged from 7.27% for appendectomy to 46.94% for small-bowel resection. Study results also showed that mean inpatient costs ranged from $9,664.30 for appendectomy to $28,450.72 for small-bowel resection.
Based on their study data, Dr. Scott and his associates recommended national quality benchmarks and cost reduction efforts focused on the seven identified common, complicated, and costly emergency general surgery procedures.
No external funding source was disclosed. Coauthor Dr. Adil H. Haider disclosed ties to industry sources. None of the other coauthors reported any conflicts of interest.
A very low number of emergency general surgery procedures account for the majority of all admissions, deaths, complications, and inpatient costs attributable to emergency general surgery procedures nationwide, according to a study published in JAMA Surgery.
“More than half a million patients undergo urgent or emergent general surgery operations annually in the United States, which accounts for more than $6 billion in annual costs. Only seven representative procedures account for approximately 80% of all admissions, deaths, complications, and inpatient costs attributable to operative emergency general surgery nationwide,” said Dr. John W. Scott from the Center for Surgery and Public Health, department of surgery at the Brigham & Women’s Hospital in Boston, and his associates.
The investigators sought to expand the current diagnosis-based definition of emergency general surgery in order to define a standardized, representative set of procedures that comprise the majority of the national clinical burden of emergency general surgery. To accomplish this goal, Dr. Scott and his colleagues examined data from the 2008 to 2011 Healthcare Cost and Utilization Project’s National Inpatient Sample, the largest publicly available all-payers claims database in the United States, from Nov. 15, 2015, to Feb. 16, 2016 (JAMA Surg. 2016 Apr 27. doi: 10.1001/jamasurg.2016.0480).
The results from this nationally representative observational study represented more than 2 million patient encounters, with a final analytic sample that included 137 unique four-digit ICD-9-CM procedure codes that mapped into 35 distinct three-digit procedure group codes. When ordered by burden rank, the cumulative attributable burden for total procedure count, total deaths, total complications, and total costs increased sharply through procedures ranked one to seven (partial colectomy, small-bowel resection, cholecystectomy, operative management of peptic ulcer disease, lysis of peritoneal adhesions, appendectomy, and laparotomy).
In addition, the procedure volumes were found to be highest for cholecystectomy and appendectomy, although the mortality and complication rates for these procedures were comparatively lower than for the other five identified procedures. For example, the frequency of procedures varied from 682,043 primary appendectomies to 9,418 primary laparotomies, but the mortality rate ranged from 0.08% for appendectomy to 23.76% for laparotomy. Similarly, the complication rate ranged from 7.27% for appendectomy to 46.94% for small-bowel resection. Study results also showed that mean inpatient costs ranged from $9,664.30 for appendectomy to $28,450.72 for small-bowel resection.
Based on their study data, Dr. Scott and his associates recommended national quality benchmarks and cost reduction efforts focused on the seven identified common, complicated, and costly emergency general surgery procedures.
No external funding source was disclosed. Coauthor Dr. Adil H. Haider disclosed ties to industry sources. None of the other coauthors reported any conflicts of interest.
FROM JAMA SURGERY
Key clinical point: National quality benchmarks and cost reduction efforts should focus on the seven most common, complicated, and costly emergency general surgery procedures.
Major finding: The majority (80%) of all admissions, deaths, complications, and inpatient costs attributable to emergency general surgery procedures nationwide can be accounted for by seven representative procedures.
Data sources: The 2008-2011 Healthcare Cost and Utilization Project’s National Inpatient Sample claims database.
Disclosures: No external funding source was disclosed. Coauthor Dr. Adil H. Haider disclosed ties to industry sources. None of the other coauthors reported any conflicts of interest.

Attributes of Successful Hospitalist Groups
In the first two installments of my own list of attributes that are important underpinnings of successful hospitalist groups, I covered group culture and decision making, recruiting, the importance of a written policy and procedure manual and performance dashboard, and roles for advanced practice clinicians. I’ll continue numbering from last month and complete the list in this column.
7. Clear Reporting Relationships
Most hospitalists are employed by one entity, usually a hospital subcorporation or staffing company, yet in many respects they report to someone else, such as a hospital CMO. For many, this can feel like serving two masters.
As an example, a hospitalist is employed by St. Excellence Medical Group (SEMG), a subsidiary of St. Excellence Hospital. Yet the hospital CMO is the key person establishing hospitalist performance targets, mediating disagreements between hospitalists and cardiologists, etc. So the hospitalists and CMO might jointly make plans for changes in the hospitalist practice that have staffing or budgetary implications only to find that the SEMG president resists spending more on the hospitalist program. For some hospitalist groups, this problem of being stuck between two masters can be a real barrier to getting things done.
Because the employed physician group nearly always directs most of its attention to outpatient care, the hospitalists are sometimes an afterthought, sort of a like a neglected stepchild. And worse, I’ve worked with more than one organization in which the CMO and physician president of the employed physician group are engaged in a power struggle, with the hospitalist group (and other physician specialties) caught in the middle and suffering as a result.
I think the best way out of this dilemma is for the employed physician group to function as a management services organization, providing human resources (payroll, etc.) and revenue cycle functions to the hospitalist groups. But for nearly all other issues, such as policies and procedures, staffing, strategic planning, hiring and firing, etc., the lead hospitalist should report to the CMO.
8. Well-Organized Group Meetings
My experience is that nearly every hospitalist group has periodic meetings to discuss and make decisions on operational and clinical issues. But the effectiveness of the meetings varies a lot. In some cases, they’re little more than disorganized gripe sessions.
I think most groups should have monthly meetings scheduled for about an hour or a little longer. Attendance at most meetings should be the expectation; that means even those not working clinically that day should be expected to attend unless away on vacation or some other meaningful conflict. Simply not being on clinical service that day should not be a reason to miss the meeting. Attendance by phone periodically is usually fine, especially for those who would otherwise have a long drive to attend in person or have child care duties, etc.
An agenda should be circulated in advance of the meeting; minutes, afterward. The best minutes highlight any “to-do” items, including person responsible and target completion date. Tasks occurring over longer than a month should be tracked in the minutes of every meeting until resolved. All past meeting minutes should be readily accessible via a network computer drive for review by any member of the group at any time.
Although some of every meeting will typically need to be devoted to one-way communication from the group leader or others, ideally in every meeting meaningful time should be devoted to joint problem-solving by all in attendance to ensure all are engaged in the meetings and find them useful. Some one-way communication (e.g., regular reports of performance data) typically can be distributed via email and other means rather than devoting meeting time to review it.
9. Effective Compensation
The amount of compensation should be competitive with your market, but because compensation is typically seen as an entitlement, unusually high compensation amounts usually have little impact on performance. But the method of compensation can matter, that is, the portion of total dollars that are fixed, tied to production, or tied to performance.
I think it’s best if the compensation method is generally similar to the way Medicare and other payors reimburse physician services. As payors tie increasing portions of compensation to performance and bundled payments, it makes sense for these changes to be mirrored in hospitalist compensation formulas to the extent that is practical. As I’ve written in February 2014 and many other times, I think there will always be a role for a portion of compensation tied to individual productivity.
According to SHM’s 2014 State of Hospital Medicine report, 64% of hospitalist groups have some component of compensation tied to citizenship activities such as committee participation, grand rounds presentations, community talks, publications, etc. I described a citizenship bonus program in detail in my November 2011 column. And while I was once an advocate of it, I’m now ambivalent. My anecdotal experience with the group I’m part of and many others I’ve worked with makes me suspect that a bonus for good citizenship might just squash intrinsic motivation as described in Daniel Pink’s book Drive.
If you do tie some portion of compensation to citizenship, I strongly encourage not connecting it to basic expectations like meeting attendance or turning in billing data on time. These are standard parts of the job, and citizenship pay should be reserved for going beyond the basics.
10. Good Social Connections
The way things look to me, doctors across all specialties have historically enjoyed robust and rewarding social connections with one another. But with each passing year, the nature of the work, financial pressures, and even clinical vocabulary become more and more different; that is, our Venn diagrams overlap less and less.
I think doctors in different specialties are becoming less connected, and disagreements or new stresses can more easily divide us.
Although all hospitals and medical groups are working hard to implement operational and technical adjustments to keep up with changing clinical practice and reimbursement models, I see very few deliberately focused on maintaining or strengthening the social connections and feeling of occupational solidarity and shared mission across doctors and other providers (see my June 2010 column). Those that do so—to my way of thinking—will be uniquely positioned to weather the storm of rapid change much more effectively. TH

In the first two installments of my own list of attributes that are important underpinnings of successful hospitalist groups, I covered group culture and decision making, recruiting, the importance of a written policy and procedure manual and performance dashboard, and roles for advanced practice clinicians. I’ll continue numbering from last month and complete the list in this column.
7. Clear Reporting Relationships
Most hospitalists are employed by one entity, usually a hospital subcorporation or staffing company, yet in many respects they report to someone else, such as a hospital CMO. For many, this can feel like serving two masters.
As an example, a hospitalist is employed by St. Excellence Medical Group (SEMG), a subsidiary of St. Excellence Hospital. Yet the hospital CMO is the key person establishing hospitalist performance targets, mediating disagreements between hospitalists and cardiologists, etc. So the hospitalists and CMO might jointly make plans for changes in the hospitalist practice that have staffing or budgetary implications only to find that the SEMG president resists spending more on the hospitalist program. For some hospitalist groups, this problem of being stuck between two masters can be a real barrier to getting things done.
Because the employed physician group nearly always directs most of its attention to outpatient care, the hospitalists are sometimes an afterthought, sort of a like a neglected stepchild. And worse, I’ve worked with more than one organization in which the CMO and physician president of the employed physician group are engaged in a power struggle, with the hospitalist group (and other physician specialties) caught in the middle and suffering as a result.
I think the best way out of this dilemma is for the employed physician group to function as a management services organization, providing human resources (payroll, etc.) and revenue cycle functions to the hospitalist groups. But for nearly all other issues, such as policies and procedures, staffing, strategic planning, hiring and firing, etc., the lead hospitalist should report to the CMO.
8. Well-Organized Group Meetings
My experience is that nearly every hospitalist group has periodic meetings to discuss and make decisions on operational and clinical issues. But the effectiveness of the meetings varies a lot. In some cases, they’re little more than disorganized gripe sessions.
I think most groups should have monthly meetings scheduled for about an hour or a little longer. Attendance at most meetings should be the expectation; that means even those not working clinically that day should be expected to attend unless away on vacation or some other meaningful conflict. Simply not being on clinical service that day should not be a reason to miss the meeting. Attendance by phone periodically is usually fine, especially for those who would otherwise have a long drive to attend in person or have child care duties, etc.
An agenda should be circulated in advance of the meeting; minutes, afterward. The best minutes highlight any “to-do” items, including person responsible and target completion date. Tasks occurring over longer than a month should be tracked in the minutes of every meeting until resolved. All past meeting minutes should be readily accessible via a network computer drive for review by any member of the group at any time.
Although some of every meeting will typically need to be devoted to one-way communication from the group leader or others, ideally in every meeting meaningful time should be devoted to joint problem-solving by all in attendance to ensure all are engaged in the meetings and find them useful. Some one-way communication (e.g., regular reports of performance data) typically can be distributed via email and other means rather than devoting meeting time to review it.
9. Effective Compensation
The amount of compensation should be competitive with your market, but because compensation is typically seen as an entitlement, unusually high compensation amounts usually have little impact on performance. But the method of compensation can matter, that is, the portion of total dollars that are fixed, tied to production, or tied to performance.
I think it’s best if the compensation method is generally similar to the way Medicare and other payors reimburse physician services. As payors tie increasing portions of compensation to performance and bundled payments, it makes sense for these changes to be mirrored in hospitalist compensation formulas to the extent that is practical. As I’ve written in February 2014 and many other times, I think there will always be a role for a portion of compensation tied to individual productivity.
According to SHM’s 2014 State of Hospital Medicine report, 64% of hospitalist groups have some component of compensation tied to citizenship activities such as committee participation, grand rounds presentations, community talks, publications, etc. I described a citizenship bonus program in detail in my November 2011 column. And while I was once an advocate of it, I’m now ambivalent. My anecdotal experience with the group I’m part of and many others I’ve worked with makes me suspect that a bonus for good citizenship might just squash intrinsic motivation as described in Daniel Pink’s book Drive.
If you do tie some portion of compensation to citizenship, I strongly encourage not connecting it to basic expectations like meeting attendance or turning in billing data on time. These are standard parts of the job, and citizenship pay should be reserved for going beyond the basics.
10. Good Social Connections
The way things look to me, doctors across all specialties have historically enjoyed robust and rewarding social connections with one another. But with each passing year, the nature of the work, financial pressures, and even clinical vocabulary become more and more different; that is, our Venn diagrams overlap less and less.
I think doctors in different specialties are becoming less connected, and disagreements or new stresses can more easily divide us.
Although all hospitals and medical groups are working hard to implement operational and technical adjustments to keep up with changing clinical practice and reimbursement models, I see very few deliberately focused on maintaining or strengthening the social connections and feeling of occupational solidarity and shared mission across doctors and other providers (see my June 2010 column). Those that do so—to my way of thinking—will be uniquely positioned to weather the storm of rapid change much more effectively. TH
In the first two installments of my own list of attributes that are important underpinnings of successful hospitalist groups, I covered group culture and decision making, recruiting, the importance of a written policy and procedure manual and performance dashboard, and roles for advanced practice clinicians. I’ll continue numbering from last month and complete the list in this column.
7. Clear Reporting Relationships
Most hospitalists are employed by one entity, usually a hospital subcorporation or staffing company, yet in many respects they report to someone else, such as a hospital CMO. For many, this can feel like serving two masters.
As an example, a hospitalist is employed by St. Excellence Medical Group (SEMG), a subsidiary of St. Excellence Hospital. Yet the hospital CMO is the key person establishing hospitalist performance targets, mediating disagreements between hospitalists and cardiologists, etc. So the hospitalists and CMO might jointly make plans for changes in the hospitalist practice that have staffing or budgetary implications only to find that the SEMG president resists spending more on the hospitalist program. For some hospitalist groups, this problem of being stuck between two masters can be a real barrier to getting things done.
Because the employed physician group nearly always directs most of its attention to outpatient care, the hospitalists are sometimes an afterthought, sort of a like a neglected stepchild. And worse, I’ve worked with more than one organization in which the CMO and physician president of the employed physician group are engaged in a power struggle, with the hospitalist group (and other physician specialties) caught in the middle and suffering as a result.
I think the best way out of this dilemma is for the employed physician group to function as a management services organization, providing human resources (payroll, etc.) and revenue cycle functions to the hospitalist groups. But for nearly all other issues, such as policies and procedures, staffing, strategic planning, hiring and firing, etc., the lead hospitalist should report to the CMO.
8. Well-Organized Group Meetings
My experience is that nearly every hospitalist group has periodic meetings to discuss and make decisions on operational and clinical issues. But the effectiveness of the meetings varies a lot. In some cases, they’re little more than disorganized gripe sessions.
I think most groups should have monthly meetings scheduled for about an hour or a little longer. Attendance at most meetings should be the expectation; that means even those not working clinically that day should be expected to attend unless away on vacation or some other meaningful conflict. Simply not being on clinical service that day should not be a reason to miss the meeting. Attendance by phone periodically is usually fine, especially for those who would otherwise have a long drive to attend in person or have child care duties, etc.
An agenda should be circulated in advance of the meeting; minutes, afterward. The best minutes highlight any “to-do” items, including person responsible and target completion date. Tasks occurring over longer than a month should be tracked in the minutes of every meeting until resolved. All past meeting minutes should be readily accessible via a network computer drive for review by any member of the group at any time.
Although some of every meeting will typically need to be devoted to one-way communication from the group leader or others, ideally in every meeting meaningful time should be devoted to joint problem-solving by all in attendance to ensure all are engaged in the meetings and find them useful. Some one-way communication (e.g., regular reports of performance data) typically can be distributed via email and other means rather than devoting meeting time to review it.
9. Effective Compensation
The amount of compensation should be competitive with your market, but because compensation is typically seen as an entitlement, unusually high compensation amounts usually have little impact on performance. But the method of compensation can matter, that is, the portion of total dollars that are fixed, tied to production, or tied to performance.
I think it’s best if the compensation method is generally similar to the way Medicare and other payors reimburse physician services. As payors tie increasing portions of compensation to performance and bundled payments, it makes sense for these changes to be mirrored in hospitalist compensation formulas to the extent that is practical. As I’ve written in February 2014 and many other times, I think there will always be a role for a portion of compensation tied to individual productivity.
According to SHM’s 2014 State of Hospital Medicine report, 64% of hospitalist groups have some component of compensation tied to citizenship activities such as committee participation, grand rounds presentations, community talks, publications, etc. I described a citizenship bonus program in detail in my November 2011 column. And while I was once an advocate of it, I’m now ambivalent. My anecdotal experience with the group I’m part of and many others I’ve worked with makes me suspect that a bonus for good citizenship might just squash intrinsic motivation as described in Daniel Pink’s book Drive.
If you do tie some portion of compensation to citizenship, I strongly encourage not connecting it to basic expectations like meeting attendance or turning in billing data on time. These are standard parts of the job, and citizenship pay should be reserved for going beyond the basics.
10. Good Social Connections
The way things look to me, doctors across all specialties have historically enjoyed robust and rewarding social connections with one another. But with each passing year, the nature of the work, financial pressures, and even clinical vocabulary become more and more different; that is, our Venn diagrams overlap less and less.
I think doctors in different specialties are becoming less connected, and disagreements or new stresses can more easily divide us.
Although all hospitals and medical groups are working hard to implement operational and technical adjustments to keep up with changing clinical practice and reimbursement models, I see very few deliberately focused on maintaining or strengthening the social connections and feeling of occupational solidarity and shared mission across doctors and other providers (see my June 2010 column). Those that do so—to my way of thinking—will be uniquely positioned to weather the storm of rapid change much more effectively. TH
Reframing the problem seen as way to ease inpatient bed shortage
If an individual with schizophrenia presents to the emergency department, there’s about a 1 in 2 chance that person will wind up in an inpatient psychiatric bed, or transferred to a residential psychiatric facility. As reimbursement to hospitals for psychiatric beds decreases, there’s decreasing incentive for hospitals to maintain inpatient psychiatry services.
Decreasing numbers of hospital beds means strategic thinking about outpatient services is more important than ever, to help avert the crises that bring patients to EDs and to run-ins with the justice system. In some parts of the country, though, the downstream effects of cutbacks and increased demand are overwhelming the system.
For Dr. Carl C. Bell, the combination of shrinking resources and growing need feels like a prescription for disaster in Chicago. Dr. Bell, a psychiatrist who has spent decades providing community mental health services there, saw a relatively robust mental health infrastructure crumble when municipal belt tightening resulted in the consolidation of 13 mental health centers down to just 6.
As individuals with serious mental illness lost access to such outpatient resources as therapy, medication management, supported housing, and employment assistance, jail populations swelled. The Cook County jail became known as “the largest mental health center in the state of Illinois,” said Dr. Bell. He’s not sure he sees a good solution for the near term, but he holds out hope that innovative solutions are on the horizon.
Telepsychiatry offers an eminently workable solution to scarcity and geographic separation in some areas. Dr. David Baldes, a psychiatrist at St. Luke’s Health Care System in Duluth, Minn., “sees” patients via his computer several hours a week. He’s able to care for the sickest of the patients with mental illness served by primary care clinics along the Iron Range in northern Minnesota, helping keep this population out of the emergency department and fending off brushes with the law that are all too common among those with serious mental illnesses such as schizophrenia and severe bipolar disorder.

“The people I see tend to be really sick,” said Dr. Baldes, “and the number of psychiatrists per capita is basically zero” on the Iron Range. Although the area is served by a federally funded community mental health center, it’s extremely difficult to attract and retain psychiatrists to the remote area.
His ability to provide care for patients with serious mental illness helps their primary care providers “not feel so much like they’re on an island,” he said. He enjoys the collaboration and support he’s able to provide for the primary physicians as well.
Getting things started wasn’t hard: “The technology was actually quite simple to set up,” he said, noting that psychiatry is an ideal discipline for virtual care. “We don’t touch the patient. Our exam is our conversation with the patient,” he said.
Another advantage of telepsychiatry, Dr. Baldes said, is that there’s no stigma associated with visiting one’s primary care provider. “My patients go to their regular doctor’s office, they check in with the receptionist, and nobody really knows why they are there.” This can be a particular advantage in some of the more conservative rural communities served by the St. Luke’s program.
This mode of care soon feels completely natural for physician and patient, he said. “Especially for our generation; we’re very comfortable with FaceTime, with Skype, and generally with communicating electronically,” Dr. Baldes said.
“What patients really want is to be able to do these visits from their home,” he said. Because of privacy and security concerns, patients still go to the primary care office to have their virtual visits with Dr. Baldes.
Telepsychiatry’s promise is not limited to rural areas. “Any time people are resource limited, transportation is always an issue,” Dr. Baldes said. The suburbs and exurbs of many American cities are increasingly populated by low-income individuals forced out of gentrifying city centers into areas with fewer mental health resources and fewer transportation options. Telepsychiatry could be useful in many settings, he said.
A more fully integrated suite of services, the Collaborative Care Model (CCM), has been piloted in five locations nationwide and was the subject of an April 14, 2016, congressional briefing. This care model goes beyond co-location and collaboration to encompass a specific set of team members providing specific services, with ongoing tracking of validated outcome measures.
Dr. Erik Vanderlip, professor of psychiatry and medical informatics at the University of Oklahoma, Tulsa, coauthored a recent report sharing evidence of the successful implementation of collaborative care. He said the CCM really represents a shift in thinking. “The lack of psychiatric beds isn’t the problem. The problem is the lack of affordable, accessible, high-quality mental health services,” and collaborative care seeks to meet that need.
Dr. Vanderlip is a double-boarded psychiatrist and family medicine physician; he said that during training, “I discovered quickly that we have to redesign the way we deliver health care services to meet the needs of the most vulnerable.” He began working with Dr. Wayne Katon, now deceased, who pioneered the collaborative care model in Washington state.
In practice, this means that a psychiatrist works with a primary care provider and other team members to provide intensive care and monitoring. Clinical trials have shown impressive results in the treatment of depression, with response rates approaching 70%, Dr. Vanderlip said. “This stuff is the solution,” he said.
“So you have these little ‘teamlets’ of the psychiatrist, the primary care provider, the care manager, and the nurse working together to take care of a cohort of patients,” Dr. Vanderlip said. Typically, a care manager will have from 40 to as many as 100 patients under his or her care.
Key to measuring the success of the care model is an objective, validated measure that changes in relation to improvement or worsening of the target chronic condition. For example, in depression, that measure is the Patient Health Questionnaire (PHQ-9).
In the CCM, a psychiatrist will log in to the secure patient management system and pull up the entire registry of the care manager’s patients. One by one, patients are briefly reviewed, and the care plan and medications are adjusted as needed. The psychiatrist completes a brief note for each patient during the session; notes have a disclaimer that makes clear that the physician did not have a face-to-face encounter with the patient.
The psychiatrists also are available for “curbside” consults to the primary care provider, so they may collaborate on patients’ care plans. For one care manager’s panel of 40-100 patients, a psychiatrist will typically devote about a half day per week of consultative time.
Dr. Vanderlip has found that for some psychiatrists, the new role of “care quarterback” can be a tough sell. “Providers have a hard time comprehending that they are not going to see people directly.” Most psychiatrists involved in collaborative care also see patients in the traditional model as well, he said.
A critical piece of the puzzle for the success of integrated care is reimbursement – and the CCM now has its own CPT code. “There’s reimbursement for the psychiatrist’s time, for the care manager’s time, and for the primary care provider’s time,” Dr. Vanderlip said. The American Psychiatric Association is in discussion with the Centers for Medicare & Medicaid Services and the American Medical Association to fine-tune valuation.
“This is a great candidate for value-based reimbursement,” Dr. Vanderlip said. Depression scores can be tracked over time; successful care teams could be rewarded – and less successful ones docked – depending on patient outcome measures.
As reimbursers seek to find more ways to recognize the burden that chronic care places on the health care system, collaborative care should find more takers. “Collaborative care is chronic care incarnate,” Dr. Vanderlip said. He said he thinks it’s the solution for the care crunch in America. “This is not a bed shortage problem,” he reiterated.
Availability of inpatient services wide ranging
The number of psychiatric hospital beds per capita varies widely by state, as does the availability of psychiatrists and outpatient mental health facilities. In 2011, the American Hospital Association reported that psychiatric bed allocations ranged from a low of about 5 beds per 100,000 persons in Colorado to a high of more than 50 beds per 100,000 persons in both Missouri and Mississippi.
Reported rates of hospital admission among adults with a diagnosis of any mental illness also varies, from 1.1% in Louisiana, to 4.9% in New York (2010-2011 Substance Abuse and Mental Health Services Administration report).
State-by-state estimates of the prevalence of serious mental illness in adults ranges from just under 3% to about 7% (2012 revised SAMHSA report).
On Twitter @karioakes
If an individual with schizophrenia presents to the emergency department, there’s about a 1 in 2 chance that person will wind up in an inpatient psychiatric bed, or transferred to a residential psychiatric facility. As reimbursement to hospitals for psychiatric beds decreases, there’s decreasing incentive for hospitals to maintain inpatient psychiatry services.
Decreasing numbers of hospital beds means strategic thinking about outpatient services is more important than ever, to help avert the crises that bring patients to EDs and to run-ins with the justice system. In some parts of the country, though, the downstream effects of cutbacks and increased demand are overwhelming the system.
For Dr. Carl C. Bell, the combination of shrinking resources and growing need feels like a prescription for disaster in Chicago. Dr. Bell, a psychiatrist who has spent decades providing community mental health services there, saw a relatively robust mental health infrastructure crumble when municipal belt tightening resulted in the consolidation of 13 mental health centers down to just 6.
As individuals with serious mental illness lost access to such outpatient resources as therapy, medication management, supported housing, and employment assistance, jail populations swelled. The Cook County jail became known as “the largest mental health center in the state of Illinois,” said Dr. Bell. He’s not sure he sees a good solution for the near term, but he holds out hope that innovative solutions are on the horizon.
Telepsychiatry offers an eminently workable solution to scarcity and geographic separation in some areas. Dr. David Baldes, a psychiatrist at St. Luke’s Health Care System in Duluth, Minn., “sees” patients via his computer several hours a week. He’s able to care for the sickest of the patients with mental illness served by primary care clinics along the Iron Range in northern Minnesota, helping keep this population out of the emergency department and fending off brushes with the law that are all too common among those with serious mental illnesses such as schizophrenia and severe bipolar disorder.
“The people I see tend to be really sick,” said Dr. Baldes, “and the number of psychiatrists per capita is basically zero” on the Iron Range. Although the area is served by a federally funded community mental health center, it’s extremely difficult to attract and retain psychiatrists to the remote area.
His ability to provide care for patients with serious mental illness helps their primary care providers “not feel so much like they’re on an island,” he said. He enjoys the collaboration and support he’s able to provide for the primary physicians as well.
Getting things started wasn’t hard: “The technology was actually quite simple to set up,” he said, noting that psychiatry is an ideal discipline for virtual care. “We don’t touch the patient. Our exam is our conversation with the patient,” he said.
Another advantage of telepsychiatry, Dr. Baldes said, is that there’s no stigma associated with visiting one’s primary care provider. “My patients go to their regular doctor’s office, they check in with the receptionist, and nobody really knows why they are there.” This can be a particular advantage in some of the more conservative rural communities served by the St. Luke’s program.
This mode of care soon feels completely natural for physician and patient, he said. “Especially for our generation; we’re very comfortable with FaceTime, with Skype, and generally with communicating electronically,” Dr. Baldes said.
“What patients really want is to be able to do these visits from their home,” he said. Because of privacy and security concerns, patients still go to the primary care office to have their virtual visits with Dr. Baldes.
Telepsychiatry’s promise is not limited to rural areas. “Any time people are resource limited, transportation is always an issue,” Dr. Baldes said. The suburbs and exurbs of many American cities are increasingly populated by low-income individuals forced out of gentrifying city centers into areas with fewer mental health resources and fewer transportation options. Telepsychiatry could be useful in many settings, he said.
A more fully integrated suite of services, the Collaborative Care Model (CCM), has been piloted in five locations nationwide and was the subject of an April 14, 2016, congressional briefing. This care model goes beyond co-location and collaboration to encompass a specific set of team members providing specific services, with ongoing tracking of validated outcome measures.
Dr. Erik Vanderlip, professor of psychiatry and medical informatics at the University of Oklahoma, Tulsa, coauthored a recent report sharing evidence of the successful implementation of collaborative care. He said the CCM really represents a shift in thinking. “The lack of psychiatric beds isn’t the problem. The problem is the lack of affordable, accessible, high-quality mental health services,” and collaborative care seeks to meet that need.
Dr. Vanderlip is a double-boarded psychiatrist and family medicine physician; he said that during training, “I discovered quickly that we have to redesign the way we deliver health care services to meet the needs of the most vulnerable.” He began working with Dr. Wayne Katon, now deceased, who pioneered the collaborative care model in Washington state.
In practice, this means that a psychiatrist works with a primary care provider and other team members to provide intensive care and monitoring. Clinical trials have shown impressive results in the treatment of depression, with response rates approaching 70%, Dr. Vanderlip said. “This stuff is the solution,” he said.
“So you have these little ‘teamlets’ of the psychiatrist, the primary care provider, the care manager, and the nurse working together to take care of a cohort of patients,” Dr. Vanderlip said. Typically, a care manager will have from 40 to as many as 100 patients under his or her care.
Key to measuring the success of the care model is an objective, validated measure that changes in relation to improvement or worsening of the target chronic condition. For example, in depression, that measure is the Patient Health Questionnaire (PHQ-9).
In the CCM, a psychiatrist will log in to the secure patient management system and pull up the entire registry of the care manager’s patients. One by one, patients are briefly reviewed, and the care plan and medications are adjusted as needed. The psychiatrist completes a brief note for each patient during the session; notes have a disclaimer that makes clear that the physician did not have a face-to-face encounter with the patient.
The psychiatrists also are available for “curbside” consults to the primary care provider, so they may collaborate on patients’ care plans. For one care manager’s panel of 40-100 patients, a psychiatrist will typically devote about a half day per week of consultative time.
Dr. Vanderlip has found that for some psychiatrists, the new role of “care quarterback” can be a tough sell. “Providers have a hard time comprehending that they are not going to see people directly.” Most psychiatrists involved in collaborative care also see patients in the traditional model as well, he said.
A critical piece of the puzzle for the success of integrated care is reimbursement – and the CCM now has its own CPT code. “There’s reimbursement for the psychiatrist’s time, for the care manager’s time, and for the primary care provider’s time,” Dr. Vanderlip said. The American Psychiatric Association is in discussion with the Centers for Medicare & Medicaid Services and the American Medical Association to fine-tune valuation.
“This is a great candidate for value-based reimbursement,” Dr. Vanderlip said. Depression scores can be tracked over time; successful care teams could be rewarded – and less successful ones docked – depending on patient outcome measures.
As reimbursers seek to find more ways to recognize the burden that chronic care places on the health care system, collaborative care should find more takers. “Collaborative care is chronic care incarnate,” Dr. Vanderlip said. He said he thinks it’s the solution for the care crunch in America. “This is not a bed shortage problem,” he reiterated.
Availability of inpatient services wide ranging
The number of psychiatric hospital beds per capita varies widely by state, as does the availability of psychiatrists and outpatient mental health facilities. In 2011, the American Hospital Association reported that psychiatric bed allocations ranged from a low of about 5 beds per 100,000 persons in Colorado to a high of more than 50 beds per 100,000 persons in both Missouri and Mississippi.
Reported rates of hospital admission among adults with a diagnosis of any mental illness also varies, from 1.1% in Louisiana, to 4.9% in New York (2010-2011 Substance Abuse and Mental Health Services Administration report).
State-by-state estimates of the prevalence of serious mental illness in adults ranges from just under 3% to about 7% (2012 revised SAMHSA report).
On Twitter @karioakes
If an individual with schizophrenia presents to the emergency department, there’s about a 1 in 2 chance that person will wind up in an inpatient psychiatric bed, or transferred to a residential psychiatric facility. As reimbursement to hospitals for psychiatric beds decreases, there’s decreasing incentive for hospitals to maintain inpatient psychiatry services.
Decreasing numbers of hospital beds means strategic thinking about outpatient services is more important than ever, to help avert the crises that bring patients to EDs and to run-ins with the justice system. In some parts of the country, though, the downstream effects of cutbacks and increased demand are overwhelming the system.
For Dr. Carl C. Bell, the combination of shrinking resources and growing need feels like a prescription for disaster in Chicago. Dr. Bell, a psychiatrist who has spent decades providing community mental health services there, saw a relatively robust mental health infrastructure crumble when municipal belt tightening resulted in the consolidation of 13 mental health centers down to just 6.
As individuals with serious mental illness lost access to such outpatient resources as therapy, medication management, supported housing, and employment assistance, jail populations swelled. The Cook County jail became known as “the largest mental health center in the state of Illinois,” said Dr. Bell. He’s not sure he sees a good solution for the near term, but he holds out hope that innovative solutions are on the horizon.
Telepsychiatry offers an eminently workable solution to scarcity and geographic separation in some areas. Dr. David Baldes, a psychiatrist at St. Luke’s Health Care System in Duluth, Minn., “sees” patients via his computer several hours a week. He’s able to care for the sickest of the patients with mental illness served by primary care clinics along the Iron Range in northern Minnesota, helping keep this population out of the emergency department and fending off brushes with the law that are all too common among those with serious mental illnesses such as schizophrenia and severe bipolar disorder.
“The people I see tend to be really sick,” said Dr. Baldes, “and the number of psychiatrists per capita is basically zero” on the Iron Range. Although the area is served by a federally funded community mental health center, it’s extremely difficult to attract and retain psychiatrists to the remote area.
His ability to provide care for patients with serious mental illness helps their primary care providers “not feel so much like they’re on an island,” he said. He enjoys the collaboration and support he’s able to provide for the primary physicians as well.
Getting things started wasn’t hard: “The technology was actually quite simple to set up,” he said, noting that psychiatry is an ideal discipline for virtual care. “We don’t touch the patient. Our exam is our conversation with the patient,” he said.
Another advantage of telepsychiatry, Dr. Baldes said, is that there’s no stigma associated with visiting one’s primary care provider. “My patients go to their regular doctor’s office, they check in with the receptionist, and nobody really knows why they are there.” This can be a particular advantage in some of the more conservative rural communities served by the St. Luke’s program.
This mode of care soon feels completely natural for physician and patient, he said. “Especially for our generation; we’re very comfortable with FaceTime, with Skype, and generally with communicating electronically,” Dr. Baldes said.
“What patients really want is to be able to do these visits from their home,” he said. Because of privacy and security concerns, patients still go to the primary care office to have their virtual visits with Dr. Baldes.
Telepsychiatry’s promise is not limited to rural areas. “Any time people are resource limited, transportation is always an issue,” Dr. Baldes said. The suburbs and exurbs of many American cities are increasingly populated by low-income individuals forced out of gentrifying city centers into areas with fewer mental health resources and fewer transportation options. Telepsychiatry could be useful in many settings, he said.
A more fully integrated suite of services, the Collaborative Care Model (CCM), has been piloted in five locations nationwide and was the subject of an April 14, 2016, congressional briefing. This care model goes beyond co-location and collaboration to encompass a specific set of team members providing specific services, with ongoing tracking of validated outcome measures.
Dr. Erik Vanderlip, professor of psychiatry and medical informatics at the University of Oklahoma, Tulsa, coauthored a recent report sharing evidence of the successful implementation of collaborative care. He said the CCM really represents a shift in thinking. “The lack of psychiatric beds isn’t the problem. The problem is the lack of affordable, accessible, high-quality mental health services,” and collaborative care seeks to meet that need.
Dr. Vanderlip is a double-boarded psychiatrist and family medicine physician; he said that during training, “I discovered quickly that we have to redesign the way we deliver health care services to meet the needs of the most vulnerable.” He began working with Dr. Wayne Katon, now deceased, who pioneered the collaborative care model in Washington state.
In practice, this means that a psychiatrist works with a primary care provider and other team members to provide intensive care and monitoring. Clinical trials have shown impressive results in the treatment of depression, with response rates approaching 70%, Dr. Vanderlip said. “This stuff is the solution,” he said.
“So you have these little ‘teamlets’ of the psychiatrist, the primary care provider, the care manager, and the nurse working together to take care of a cohort of patients,” Dr. Vanderlip said. Typically, a care manager will have from 40 to as many as 100 patients under his or her care.
Key to measuring the success of the care model is an objective, validated measure that changes in relation to improvement or worsening of the target chronic condition. For example, in depression, that measure is the Patient Health Questionnaire (PHQ-9).
In the CCM, a psychiatrist will log in to the secure patient management system and pull up the entire registry of the care manager’s patients. One by one, patients are briefly reviewed, and the care plan and medications are adjusted as needed. The psychiatrist completes a brief note for each patient during the session; notes have a disclaimer that makes clear that the physician did not have a face-to-face encounter with the patient.
The psychiatrists also are available for “curbside” consults to the primary care provider, so they may collaborate on patients’ care plans. For one care manager’s panel of 40-100 patients, a psychiatrist will typically devote about a half day per week of consultative time.
Dr. Vanderlip has found that for some psychiatrists, the new role of “care quarterback” can be a tough sell. “Providers have a hard time comprehending that they are not going to see people directly.” Most psychiatrists involved in collaborative care also see patients in the traditional model as well, he said.
A critical piece of the puzzle for the success of integrated care is reimbursement – and the CCM now has its own CPT code. “There’s reimbursement for the psychiatrist’s time, for the care manager’s time, and for the primary care provider’s time,” Dr. Vanderlip said. The American Psychiatric Association is in discussion with the Centers for Medicare & Medicaid Services and the American Medical Association to fine-tune valuation.
“This is a great candidate for value-based reimbursement,” Dr. Vanderlip said. Depression scores can be tracked over time; successful care teams could be rewarded – and less successful ones docked – depending on patient outcome measures.
As reimbursers seek to find more ways to recognize the burden that chronic care places on the health care system, collaborative care should find more takers. “Collaborative care is chronic care incarnate,” Dr. Vanderlip said. He said he thinks it’s the solution for the care crunch in America. “This is not a bed shortage problem,” he reiterated.
Availability of inpatient services wide ranging
The number of psychiatric hospital beds per capita varies widely by state, as does the availability of psychiatrists and outpatient mental health facilities. In 2011, the American Hospital Association reported that psychiatric bed allocations ranged from a low of about 5 beds per 100,000 persons in Colorado to a high of more than 50 beds per 100,000 persons in both Missouri and Mississippi.
Reported rates of hospital admission among adults with a diagnosis of any mental illness also varies, from 1.1% in Louisiana, to 4.9% in New York (2010-2011 Substance Abuse and Mental Health Services Administration report).
State-by-state estimates of the prevalence of serious mental illness in adults ranges from just under 3% to about 7% (2012 revised SAMHSA report).
On Twitter @karioakes

Medicare delays plans for new star ratings on hospitals
Bowing to pressure from the hospital industry and Congress, the Obama administration on April 20 delayed releasing its new hospital quality rating measure just a day before its planned launch.
The new “overall hospital quality” star rating aimed to combine the government’s disparate efforts to measure hospital care into one easy-to-grasp metric. The Centers for Medicare & Medicaid Services now publishes more than 100 measures of aspects of hospital care, but many of these measures are technical and confusing since hospitals often do well on some and poorly on others. The new star rating boils 62 of the measures down into a unified rating of one to five stars, with five being the best.

But this month, 60 senators and 225 members of the House of Representatives signed letters urging the CMS to delay releasing the star ratings. “We have heard from hospitals in our districts that they do not have the necessary data to replicate or evaluate the CMS’s work to ensure that the methodology is accurate or fair,” the letter from the House members said.
In a notice sent April 20, the CMS told Congress it would delay release of the star ratings on its Hospital Compare website until July 2016. The “CMS is committed to working with hospitals and associations to provide further guidance about star ratings,” the notice said. “After the star ratings go live in their first iteration, we will refine and improve the site as we work together and gain experience.”
But in a conference call with hospital representatives, the CMS officials said they might delay release of the ratings past July if they are still analyzing or revising the methodology, according to people who participated in the call.
Mortality, readmissions, patient experience, and safety of care metrics each accounted for 22% of the star rating, while measures of effectiveness of care, timeliness of care, and efficient use of medical imaging made up 12% in total.

The hospital industry for months has been urging this delay, arguing that many of the measures will not be relevant to patients seeking a specific service. For instance, a hospital’s death rate for Medicare patients might be irrelevant for a woman trying to decide where to give birth.
The industry’s major trade groups said in a letter to the CMS that some hospitals perform poorly because their patients tend to be lower income and don’t have the support at home. Many of the nation’s most prestigious hospitals have been bracing for middling or poor ratings.
Rick Pollack, president of the American Hospital Association, said in a statement that “the delay is a necessary step as hospitals and health systems work with CMS to improve the ratings for patients, and the AHA commends CMS for their decision.”
Last year, the CMS created a star rating to represent the views of patients in surveys. Two sets of researchers recently determined that hospitals with more stars in patient experience tended to have lower death and readmission rates.
Hospital Compare received 3.7 million unique page views last year, according to an April 2016 paper published in the journal Health Affairs. The author, analyst Steven D. Findlay, called the traffic “not at a level commensurate with [the] stature and potential” of the federal government’s health care facility comparison sites.
Dr. Ashish Jha, a Harvard School of Public Health researcher, said consumers will be more likely to use the unified star ratings, but this specific mix of measures raises concerns. “The idea that dying and being readmitted to the hospital are equally important to patients seems funny to me,” he said.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Bowing to pressure from the hospital industry and Congress, the Obama administration on April 20 delayed releasing its new hospital quality rating measure just a day before its planned launch.
The new “overall hospital quality” star rating aimed to combine the government’s disparate efforts to measure hospital care into one easy-to-grasp metric. The Centers for Medicare & Medicaid Services now publishes more than 100 measures of aspects of hospital care, but many of these measures are technical and confusing since hospitals often do well on some and poorly on others. The new star rating boils 62 of the measures down into a unified rating of one to five stars, with five being the best.
But this month, 60 senators and 225 members of the House of Representatives signed letters urging the CMS to delay releasing the star ratings. “We have heard from hospitals in our districts that they do not have the necessary data to replicate or evaluate the CMS’s work to ensure that the methodology is accurate or fair,” the letter from the House members said.
In a notice sent April 20, the CMS told Congress it would delay release of the star ratings on its Hospital Compare website until July 2016. The “CMS is committed to working with hospitals and associations to provide further guidance about star ratings,” the notice said. “After the star ratings go live in their first iteration, we will refine and improve the site as we work together and gain experience.”
But in a conference call with hospital representatives, the CMS officials said they might delay release of the ratings past July if they are still analyzing or revising the methodology, according to people who participated in the call.
Mortality, readmissions, patient experience, and safety of care metrics each accounted for 22% of the star rating, while measures of effectiveness of care, timeliness of care, and efficient use of medical imaging made up 12% in total.
The hospital industry for months has been urging this delay, arguing that many of the measures will not be relevant to patients seeking a specific service. For instance, a hospital’s death rate for Medicare patients might be irrelevant for a woman trying to decide where to give birth.
The industry’s major trade groups said in a letter to the CMS that some hospitals perform poorly because their patients tend to be lower income and don’t have the support at home. Many of the nation’s most prestigious hospitals have been bracing for middling or poor ratings.
Rick Pollack, president of the American Hospital Association, said in a statement that “the delay is a necessary step as hospitals and health systems work with CMS to improve the ratings for patients, and the AHA commends CMS for their decision.”
Last year, the CMS created a star rating to represent the views of patients in surveys. Two sets of researchers recently determined that hospitals with more stars in patient experience tended to have lower death and readmission rates.
Hospital Compare received 3.7 million unique page views last year, according to an April 2016 paper published in the journal Health Affairs. The author, analyst Steven D. Findlay, called the traffic “not at a level commensurate with [the] stature and potential” of the federal government’s health care facility comparison sites.
Dr. Ashish Jha, a Harvard School of Public Health researcher, said consumers will be more likely to use the unified star ratings, but this specific mix of measures raises concerns. “The idea that dying and being readmitted to the hospital are equally important to patients seems funny to me,” he said.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Bowing to pressure from the hospital industry and Congress, the Obama administration on April 20 delayed releasing its new hospital quality rating measure just a day before its planned launch.
The new “overall hospital quality” star rating aimed to combine the government’s disparate efforts to measure hospital care into one easy-to-grasp metric. The Centers for Medicare & Medicaid Services now publishes more than 100 measures of aspects of hospital care, but many of these measures are technical and confusing since hospitals often do well on some and poorly on others. The new star rating boils 62 of the measures down into a unified rating of one to five stars, with five being the best.
But this month, 60 senators and 225 members of the House of Representatives signed letters urging the CMS to delay releasing the star ratings. “We have heard from hospitals in our districts that they do not have the necessary data to replicate or evaluate the CMS’s work to ensure that the methodology is accurate or fair,” the letter from the House members said.
In a notice sent April 20, the CMS told Congress it would delay release of the star ratings on its Hospital Compare website until July 2016. The “CMS is committed to working with hospitals and associations to provide further guidance about star ratings,” the notice said. “After the star ratings go live in their first iteration, we will refine and improve the site as we work together and gain experience.”
But in a conference call with hospital representatives, the CMS officials said they might delay release of the ratings past July if they are still analyzing or revising the methodology, according to people who participated in the call.
Mortality, readmissions, patient experience, and safety of care metrics each accounted for 22% of the star rating, while measures of effectiveness of care, timeliness of care, and efficient use of medical imaging made up 12% in total.
The hospital industry for months has been urging this delay, arguing that many of the measures will not be relevant to patients seeking a specific service. For instance, a hospital’s death rate for Medicare patients might be irrelevant for a woman trying to decide where to give birth.
The industry’s major trade groups said in a letter to the CMS that some hospitals perform poorly because their patients tend to be lower income and don’t have the support at home. Many of the nation’s most prestigious hospitals have been bracing for middling or poor ratings.
Rick Pollack, president of the American Hospital Association, said in a statement that “the delay is a necessary step as hospitals and health systems work with CMS to improve the ratings for patients, and the AHA commends CMS for their decision.”
Last year, the CMS created a star rating to represent the views of patients in surveys. Two sets of researchers recently determined that hospitals with more stars in patient experience tended to have lower death and readmission rates.
Hospital Compare received 3.7 million unique page views last year, according to an April 2016 paper published in the journal Health Affairs. The author, analyst Steven D. Findlay, called the traffic “not at a level commensurate with [the] stature and potential” of the federal government’s health care facility comparison sites.
Dr. Ashish Jha, a Harvard School of Public Health researcher, said consumers will be more likely to use the unified star ratings, but this specific mix of measures raises concerns. “The idea that dying and being readmitted to the hospital are equally important to patients seems funny to me,” he said.
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
FROM KAISER HEALTH NEWS

UnitedHealth Group leaving most ACA marketplaces
UnitedHealth Group will not sell policies next year in most of the health insurance marketplaces created by the Affordable Care Act, CEO Stephen Helmsley announced during an April 19 earnings call.
“Next year, we will remain in only a handful of states, and we will not carry financial exposure from exchanges into 2017,” Mr. Helmsley said, citing the company’s inability to offset the “shorter-term, higher-risk” population covered by the ACA exchange plans with large enough risk pools.

Mr. Helmsley did not say in which state marketplaces UnitedHealth Group (UHG) will continue to offer coverage.
Areas that could be hardest hit by the UHG withdrawal include Alabama, Arizona, Arkansas, Nebraska, North Carolina, and Tennessee, according to an analysis from the Kaiser Family Foundation.
For now, the decision by UHG is not likely to impact the average benchmark premium by more than a 1% increase, according to the analysis. That’s because the insurer was less likely than its competitors to offer lower-cost silver plans; when silver plans were offered, they were offered at or very near to the competitors’ prices. However, in states where the withdrawal of UHG means that two or fewer insurers are participating in the marketplace, benchmark premiums could rise substantially, according to the study.
The long-term effect of the UHG exit from most marketplaces is not clear, according to Kaiser’s analysts. “In areas with limited insurer participation, the remaining plans after a United exit may have more market power relative to providers, but in the absence of insurer competition, those savings may not be passed along to consumers,” they wrote.
ACA measures such as rate reviews and medical loss ratio provisions could mitigate adverse effects on consumers in these markets, giving regulators the power to force insurers to issue rebates if premiums outstrip the cost of care.
The insurer’s decision is simply evidence that typical market forces are in play, according to Jonathan Gold, a spokesperson for the Centers for Medicare & Medicaid Services.
“As with any new market, we expect changes and adjustments in the early years with issuers both entering and exiting states,” Mr. Gold said in an interview. The UHG decision was not unexpected, as company officials said they were contemplating the move last November.
“We have full confidence, based on data, that the marketplaces will continue to thrive for years ahead,” he said, noting that in 2016, 39 insurers exited the marketplace, while 40 entered.
On Twitter @whitneymcknight
UnitedHealth Group will not sell policies next year in most of the health insurance marketplaces created by the Affordable Care Act, CEO Stephen Helmsley announced during an April 19 earnings call.
“Next year, we will remain in only a handful of states, and we will not carry financial exposure from exchanges into 2017,” Mr. Helmsley said, citing the company’s inability to offset the “shorter-term, higher-risk” population covered by the ACA exchange plans with large enough risk pools.
Mr. Helmsley did not say in which state marketplaces UnitedHealth Group (UHG) will continue to offer coverage.
Areas that could be hardest hit by the UHG withdrawal include Alabama, Arizona, Arkansas, Nebraska, North Carolina, and Tennessee, according to an analysis from the Kaiser Family Foundation.
For now, the decision by UHG is not likely to impact the average benchmark premium by more than a 1% increase, according to the analysis. That’s because the insurer was less likely than its competitors to offer lower-cost silver plans; when silver plans were offered, they were offered at or very near to the competitors’ prices. However, in states where the withdrawal of UHG means that two or fewer insurers are participating in the marketplace, benchmark premiums could rise substantially, according to the study.
The long-term effect of the UHG exit from most marketplaces is not clear, according to Kaiser’s analysts. “In areas with limited insurer participation, the remaining plans after a United exit may have more market power relative to providers, but in the absence of insurer competition, those savings may not be passed along to consumers,” they wrote.
ACA measures such as rate reviews and medical loss ratio provisions could mitigate adverse effects on consumers in these markets, giving regulators the power to force insurers to issue rebates if premiums outstrip the cost of care.
The insurer’s decision is simply evidence that typical market forces are in play, according to Jonathan Gold, a spokesperson for the Centers for Medicare & Medicaid Services.
“As with any new market, we expect changes and adjustments in the early years with issuers both entering and exiting states,” Mr. Gold said in an interview. The UHG decision was not unexpected, as company officials said they were contemplating the move last November.
“We have full confidence, based on data, that the marketplaces will continue to thrive for years ahead,” he said, noting that in 2016, 39 insurers exited the marketplace, while 40 entered.
On Twitter @whitneymcknight
UnitedHealth Group will not sell policies next year in most of the health insurance marketplaces created by the Affordable Care Act, CEO Stephen Helmsley announced during an April 19 earnings call.
“Next year, we will remain in only a handful of states, and we will not carry financial exposure from exchanges into 2017,” Mr. Helmsley said, citing the company’s inability to offset the “shorter-term, higher-risk” population covered by the ACA exchange plans with large enough risk pools.
Mr. Helmsley did not say in which state marketplaces UnitedHealth Group (UHG) will continue to offer coverage.
Areas that could be hardest hit by the UHG withdrawal include Alabama, Arizona, Arkansas, Nebraska, North Carolina, and Tennessee, according to an analysis from the Kaiser Family Foundation.
For now, the decision by UHG is not likely to impact the average benchmark premium by more than a 1% increase, according to the analysis. That’s because the insurer was less likely than its competitors to offer lower-cost silver plans; when silver plans were offered, they were offered at or very near to the competitors’ prices. However, in states where the withdrawal of UHG means that two or fewer insurers are participating in the marketplace, benchmark premiums could rise substantially, according to the study.
The long-term effect of the UHG exit from most marketplaces is not clear, according to Kaiser’s analysts. “In areas with limited insurer participation, the remaining plans after a United exit may have more market power relative to providers, but in the absence of insurer competition, those savings may not be passed along to consumers,” they wrote.
ACA measures such as rate reviews and medical loss ratio provisions could mitigate adverse effects on consumers in these markets, giving regulators the power to force insurers to issue rebates if premiums outstrip the cost of care.
The insurer’s decision is simply evidence that typical market forces are in play, according to Jonathan Gold, a spokesperson for the Centers for Medicare & Medicaid Services.
“As with any new market, we expect changes and adjustments in the early years with issuers both entering and exiting states,” Mr. Gold said in an interview. The UHG decision was not unexpected, as company officials said they were contemplating the move last November.
“We have full confidence, based on data, that the marketplaces will continue to thrive for years ahead,” he said, noting that in 2016, 39 insurers exited the marketplace, while 40 entered.
On Twitter @whitneymcknight

Number of malpractice payments down 28% since 2004
The annual number of medical malpractice payment reports fell 28% from 2004 to 2014, according to the Agency for Healthcare Research and Quality.
The total number of medical malpractice payment reports (MMPRs) for 2014 was 12,699, a decrease of 28% since 2004, when there were 17,641. The total had gone down every year until a slight increase in 2013, but the number held steady in 2014, the AHRQ reported in the Chartbook on Patient Safety.
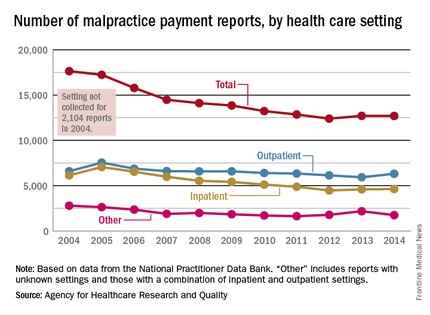
Since 2004, MMPRs related to inpatient settings have been dropping slightly faster than outpatient-related MMPRs, with the exception, again, of 2013, when the number of inpatient MMPRs went up while the outpatient total dropped. Both types went up in 2014, but the category of “other” – reports related to unknown settings and those from a combination of the two – dropped in 2014 to keep the overall number from going up again, data from the National Practitioner Data Bank show.
Looking at the types of allegation leading to MMPRs, treatment was highest, accounting for 27.4% of the total from 2004 to 2014, with diagnosis right behind at 27.1%, followed by surgery at 23.5% and obstetrics at 6.7%. Medication-related cases represented 5.3% of all MMPRs over that period, the AHRQ noted.
The annual number of medical malpractice payment reports fell 28% from 2004 to 2014, according to the Agency for Healthcare Research and Quality.
The total number of medical malpractice payment reports (MMPRs) for 2014 was 12,699, a decrease of 28% since 2004, when there were 17,641. The total had gone down every year until a slight increase in 2013, but the number held steady in 2014, the AHRQ reported in the Chartbook on Patient Safety.
Since 2004, MMPRs related to inpatient settings have been dropping slightly faster than outpatient-related MMPRs, with the exception, again, of 2013, when the number of inpatient MMPRs went up while the outpatient total dropped. Both types went up in 2014, but the category of “other” – reports related to unknown settings and those from a combination of the two – dropped in 2014 to keep the overall number from going up again, data from the National Practitioner Data Bank show.
Looking at the types of allegation leading to MMPRs, treatment was highest, accounting for 27.4% of the total from 2004 to 2014, with diagnosis right behind at 27.1%, followed by surgery at 23.5% and obstetrics at 6.7%. Medication-related cases represented 5.3% of all MMPRs over that period, the AHRQ noted.
The annual number of medical malpractice payment reports fell 28% from 2004 to 2014, according to the Agency for Healthcare Research and Quality.
The total number of medical malpractice payment reports (MMPRs) for 2014 was 12,699, a decrease of 28% since 2004, when there were 17,641. The total had gone down every year until a slight increase in 2013, but the number held steady in 2014, the AHRQ reported in the Chartbook on Patient Safety.
Since 2004, MMPRs related to inpatient settings have been dropping slightly faster than outpatient-related MMPRs, with the exception, again, of 2013, when the number of inpatient MMPRs went up while the outpatient total dropped. Both types went up in 2014, but the category of “other” – reports related to unknown settings and those from a combination of the two – dropped in 2014 to keep the overall number from going up again, data from the National Practitioner Data Bank show.
Looking at the types of allegation leading to MMPRs, treatment was highest, accounting for 27.4% of the total from 2004 to 2014, with diagnosis right behind at 27.1%, followed by surgery at 23.5% and obstetrics at 6.7%. Medication-related cases represented 5.3% of all MMPRs over that period, the AHRQ noted.