User login
Permanent SGR fix faces funding hurdle
WASHINGTON – With bipartisan agreement to repeal and replace the Medicare Sustainable Growth Rate formula already on the table, the next battle facing passage of the legislation will be how to pay for it.
Republican leadership of the House Energy and Commerce Health Subcommittee made it clear at a Jan. 21 hearing that a permanent SGR fix would not move forward without offsets to cover the estimated $140 billion price tag for the current agreement.

Finding the offsets “will not be easy, but it is a task we must embrace,” Subcommittee Chairman Joseph Pitts, (R-Pa.), said in opening the first of two days of hearings on SGR repeal. “Some argue that SGR reform does not need to be paid for. I respectfully disagree.”
Rep. Pitts noted that 98% of enacted SGR patches, spanning 120 of the 123 months worth of so-called “doc-fix” legislation, have been paid for with offsets.
Democrats on the subcommittee were critical of that hard line, noting that the House recently passed a bill to change definition of full-time employment in the Affordable Care Act to 40 hours a week, a bill estimated to cost more than $50 billion, without any cost offsets. They also suggested to look elsewhere in government to find the offsets.
“But a fix to the SGR that harms Medicare beneficiaries because of the insistence of offsets that reduce benefits and limit access is not an acceptable tradeoff,” said the subcommittee’s ranking member, Rep. Gene Green, (D-Tex.).
Witnesses who testified on Jan. 21 agreed that it should not be passed without offsets, though the common message was not to put the burden on beneficiaries through higher premiums or reduction of services.
Alice Rivlin, Ph.D., director of the Engelberg Center for Health Care Reform at the Brookings Institution and cochair of the delivery system reform initiative at the Bipartisan Policy Center, offered a number of potential cost-saving reforms, including income-adjusting premiums, accelerating of payment reform, rewarding seniors for choosing generic drugs, more competitive bidding, and accelerating the time frame for higher payments to providers participating in alternative payment mechanisms highlighted in the legislation to 2018 and offering those incentives to all Medicare providers.
“They would move to make Medicare a more efficient program,” Dr. Rivlin, founding director of the Congressional Budget Office, said.
Dr. Rivlin also suggested that strengthening accountable care organizations (ACOs) would help with finding savings offsets, including setting longer-term savings goals rather than resetting baselines every year or eliminating historical or “after-the-fact” attribution of beneficiaries to ACOs.
“The long-term promise of these models won’t be realized if unrealistic short-term pressures for savings make it unlikely that many providers can succeed,” she said. “These are all fixable problems that can be addressed as part of SGR reform.”
Better care coordination also could save Medicare money and contribute to SGR reform funding, according to Marilyn Moon, Ph.D., a fellow at the American Institutes for Research.
Dr. Moon said that there should be incentives that emphasize performing the right care at the right place and at the right time. To that end, she said the notion of bundled payments needs to be carefully examined because of the influence the entity in charge of payments might have.
For example, if a hospital is the lead organization in charge of distributing bundled payments in a coordinated care system, it might be inclined to keep patients in house rather than send them to a more appropriate setting.
There are “a lot of things that need to be worked out,” she said, adding that the SGR legislation could be a good vehicle for it.
On Jan. 22, the Health Subcommittee will hear testimony on SGR reform from a panel of representatives of physician organizations.
WASHINGTON – With bipartisan agreement to repeal and replace the Medicare Sustainable Growth Rate formula already on the table, the next battle facing passage of the legislation will be how to pay for it.
Republican leadership of the House Energy and Commerce Health Subcommittee made it clear at a Jan. 21 hearing that a permanent SGR fix would not move forward without offsets to cover the estimated $140 billion price tag for the current agreement.
Finding the offsets “will not be easy, but it is a task we must embrace,” Subcommittee Chairman Joseph Pitts, (R-Pa.), said in opening the first of two days of hearings on SGR repeal. “Some argue that SGR reform does not need to be paid for. I respectfully disagree.”
Rep. Pitts noted that 98% of enacted SGR patches, spanning 120 of the 123 months worth of so-called “doc-fix” legislation, have been paid for with offsets.
Democrats on the subcommittee were critical of that hard line, noting that the House recently passed a bill to change definition of full-time employment in the Affordable Care Act to 40 hours a week, a bill estimated to cost more than $50 billion, without any cost offsets. They also suggested to look elsewhere in government to find the offsets.
“But a fix to the SGR that harms Medicare beneficiaries because of the insistence of offsets that reduce benefits and limit access is not an acceptable tradeoff,” said the subcommittee’s ranking member, Rep. Gene Green, (D-Tex.).
Witnesses who testified on Jan. 21 agreed that it should not be passed without offsets, though the common message was not to put the burden on beneficiaries through higher premiums or reduction of services.
Alice Rivlin, Ph.D., director of the Engelberg Center for Health Care Reform at the Brookings Institution and cochair of the delivery system reform initiative at the Bipartisan Policy Center, offered a number of potential cost-saving reforms, including income-adjusting premiums, accelerating of payment reform, rewarding seniors for choosing generic drugs, more competitive bidding, and accelerating the time frame for higher payments to providers participating in alternative payment mechanisms highlighted in the legislation to 2018 and offering those incentives to all Medicare providers.
“They would move to make Medicare a more efficient program,” Dr. Rivlin, founding director of the Congressional Budget Office, said.
Dr. Rivlin also suggested that strengthening accountable care organizations (ACOs) would help with finding savings offsets, including setting longer-term savings goals rather than resetting baselines every year or eliminating historical or “after-the-fact” attribution of beneficiaries to ACOs.
“The long-term promise of these models won’t be realized if unrealistic short-term pressures for savings make it unlikely that many providers can succeed,” she said. “These are all fixable problems that can be addressed as part of SGR reform.”
Better care coordination also could save Medicare money and contribute to SGR reform funding, according to Marilyn Moon, Ph.D., a fellow at the American Institutes for Research.
Dr. Moon said that there should be incentives that emphasize performing the right care at the right place and at the right time. To that end, she said the notion of bundled payments needs to be carefully examined because of the influence the entity in charge of payments might have.
For example, if a hospital is the lead organization in charge of distributing bundled payments in a coordinated care system, it might be inclined to keep patients in house rather than send them to a more appropriate setting.
There are “a lot of things that need to be worked out,” she said, adding that the SGR legislation could be a good vehicle for it.
On Jan. 22, the Health Subcommittee will hear testimony on SGR reform from a panel of representatives of physician organizations.
WASHINGTON – With bipartisan agreement to repeal and replace the Medicare Sustainable Growth Rate formula already on the table, the next battle facing passage of the legislation will be how to pay for it.
Republican leadership of the House Energy and Commerce Health Subcommittee made it clear at a Jan. 21 hearing that a permanent SGR fix would not move forward without offsets to cover the estimated $140 billion price tag for the current agreement.
Finding the offsets “will not be easy, but it is a task we must embrace,” Subcommittee Chairman Joseph Pitts, (R-Pa.), said in opening the first of two days of hearings on SGR repeal. “Some argue that SGR reform does not need to be paid for. I respectfully disagree.”
Rep. Pitts noted that 98% of enacted SGR patches, spanning 120 of the 123 months worth of so-called “doc-fix” legislation, have been paid for with offsets.
Democrats on the subcommittee were critical of that hard line, noting that the House recently passed a bill to change definition of full-time employment in the Affordable Care Act to 40 hours a week, a bill estimated to cost more than $50 billion, without any cost offsets. They also suggested to look elsewhere in government to find the offsets.
“But a fix to the SGR that harms Medicare beneficiaries because of the insistence of offsets that reduce benefits and limit access is not an acceptable tradeoff,” said the subcommittee’s ranking member, Rep. Gene Green, (D-Tex.).
Witnesses who testified on Jan. 21 agreed that it should not be passed without offsets, though the common message was not to put the burden on beneficiaries through higher premiums or reduction of services.
Alice Rivlin, Ph.D., director of the Engelberg Center for Health Care Reform at the Brookings Institution and cochair of the delivery system reform initiative at the Bipartisan Policy Center, offered a number of potential cost-saving reforms, including income-adjusting premiums, accelerating of payment reform, rewarding seniors for choosing generic drugs, more competitive bidding, and accelerating the time frame for higher payments to providers participating in alternative payment mechanisms highlighted in the legislation to 2018 and offering those incentives to all Medicare providers.
“They would move to make Medicare a more efficient program,” Dr. Rivlin, founding director of the Congressional Budget Office, said.
Dr. Rivlin also suggested that strengthening accountable care organizations (ACOs) would help with finding savings offsets, including setting longer-term savings goals rather than resetting baselines every year or eliminating historical or “after-the-fact” attribution of beneficiaries to ACOs.
“The long-term promise of these models won’t be realized if unrealistic short-term pressures for savings make it unlikely that many providers can succeed,” she said. “These are all fixable problems that can be addressed as part of SGR reform.”
Better care coordination also could save Medicare money and contribute to SGR reform funding, according to Marilyn Moon, Ph.D., a fellow at the American Institutes for Research.
Dr. Moon said that there should be incentives that emphasize performing the right care at the right place and at the right time. To that end, she said the notion of bundled payments needs to be carefully examined because of the influence the entity in charge of payments might have.
For example, if a hospital is the lead organization in charge of distributing bundled payments in a coordinated care system, it might be inclined to keep patients in house rather than send them to a more appropriate setting.
There are “a lot of things that need to be worked out,” she said, adding that the SGR legislation could be a good vehicle for it.
On Jan. 22, the Health Subcommittee will hear testimony on SGR reform from a panel of representatives of physician organizations.
AT A HOUSE ENERGY AND COMMERCE HEALTH SUBCOMMITTEE HEARING

Justices grill attorneys on right to sue states over Medicaid payments
Some Supreme Court justices appear skeptical about whether physicians and other health providers have the right to sue states over low Medicaid reimbursement.
During oral arguments Jan. 20 in Armstrong v. Exceptional Child Center Inc., Chief Justice John G. Roberts Jr. questioned whether letting providers challenge state-set payment rates would lead to a wave of litigation and force federal judges to make state budgetary decisions.
“There are dozens of different types of providers under the [Social Security] Act,” Justice Roberts said during oral arguments. “Now, what do you do if each of those providers bring a lawsuit similar to yours? The effect, it seems to me, will be putting the setting of budget priorities in the hands of dozens of different federal judges, and I just don’t know what the practical significance of that’s going to be.”

In Armstrong v. Exceptional Child Center Inc., the high court justices are weighing whether the U.S. Constitution’s Supremacy Clause – which establishes the Constitution and federal law as the law of the land – gives health care providers under Medicaid a private “right of action” to enforce Medicaid funding conditions against states. The case originates from a 2009 lawsuit by Exceptional Child Center Inc., of Twin Falls, Idaho, and four other residential habilitation centers against Richard Armstrong, director of the Idaho Department of Health and Welfare.
The centers claimed the state was violating Medicaid’s equal access provision by refusing to raise its payment rates. Under the equal access provision, states that accept federal Medicaid funding are required to set reimbursement rates at levels sufficient to retain enough providers and make sure patients have proper access to care. The Idaho Department of Health and Welfare and its Medicaid division conducted yearly cost studies between 2006 and 2009, developed a new rate-setting methodology, and recommended substantial increases in reimbursement rates for supported living services, according to court documents. However, the new methodology and rate increases were not enacted for budgetary reasons.
A district court ruled in favor of the centers, and the 9th U.S. Circuit Court of Appeals affirmed the ruling. The state petitioned the Supreme Court to resolve the issue.

During arguments, Idaho deputy attorney general Carl J. Withroe argued the courtroom is an incorrect avenue for Medicaid providers to dispute pay rates. If displeased, physicians and other health providers should issue an administrative challenge to the Centers for Medicare & Medicaid Services over its approval of the state’s Medicaid plan. He noted that such state plans – known as waivers – must be approved by the CMS every 5 years.
But Justice Sonia Sotomayor called this pathway an ineffective remedy.
“Let’s assume inflation is going up constantly. What happens 2 years into the plan when providers can’t work for what the state is giving or the state is imposing a tremendous hardship on them, which is happening to a lot of providers who are being underpaid. Where do they go? ... What do they do?”
Other panelists, such as Justice Ruth Bader Ginsberg, expressed doubt that the centers’ case against the state has merit, namely that Idaho is violating Medicaid’s equal access provision.
“According to the district court, all eligible recipients received the services that they needed,” Justice Ginsberg said. “So again, there was no waiting list; nobody’s being kept waiting. These providers, while they say they’re not getting enough, are still providing the service. So where is the [equal access] violation?”
Attorney James M. Piotrowski, who represented the centers, countered that the equal access provision imposes both procedural and substantive requirements. The substantive requirement mandates there must be enough providers to allow access and generate quality care, Mr. Piotrowski said. The procedural requirement entails that the rates be set based upon factors that Congress considers important.
“The violation of [the equal access provision] here was that the state gave no consideration whatsoever to the federal factors,” he said. “They relied only on their own factors.”
The Armstrong case is being closely watched by states, physicians, and patient advocates alike. Twenty-seven states have reached out to the high court in support of Idaho. The states saidthey have been subject to numerous, unwarranted lawsuits because of misguided interpretations of the Supremacy Clause. A number of physician and patient advocacy associations joined a friend-of-the-court brief in support of the centers, including the American Academy of Family Physicians and the American Medical Association. The AMA and other organizations said ongoing violations of Medicaid’s equal access provision by states continue to drive doctors from the program and harm access to care.
A decision by the high court is expected by June.
On Twitter @legal_med
Some Supreme Court justices appear skeptical about whether physicians and other health providers have the right to sue states over low Medicaid reimbursement.
During oral arguments Jan. 20 in Armstrong v. Exceptional Child Center Inc., Chief Justice John G. Roberts Jr. questioned whether letting providers challenge state-set payment rates would lead to a wave of litigation and force federal judges to make state budgetary decisions.
“There are dozens of different types of providers under the [Social Security] Act,” Justice Roberts said during oral arguments. “Now, what do you do if each of those providers bring a lawsuit similar to yours? The effect, it seems to me, will be putting the setting of budget priorities in the hands of dozens of different federal judges, and I just don’t know what the practical significance of that’s going to be.”
In Armstrong v. Exceptional Child Center Inc., the high court justices are weighing whether the U.S. Constitution’s Supremacy Clause – which establishes the Constitution and federal law as the law of the land – gives health care providers under Medicaid a private “right of action” to enforce Medicaid funding conditions against states. The case originates from a 2009 lawsuit by Exceptional Child Center Inc., of Twin Falls, Idaho, and four other residential habilitation centers against Richard Armstrong, director of the Idaho Department of Health and Welfare.
The centers claimed the state was violating Medicaid’s equal access provision by refusing to raise its payment rates. Under the equal access provision, states that accept federal Medicaid funding are required to set reimbursement rates at levels sufficient to retain enough providers and make sure patients have proper access to care. The Idaho Department of Health and Welfare and its Medicaid division conducted yearly cost studies between 2006 and 2009, developed a new rate-setting methodology, and recommended substantial increases in reimbursement rates for supported living services, according to court documents. However, the new methodology and rate increases were not enacted for budgetary reasons.
A district court ruled in favor of the centers, and the 9th U.S. Circuit Court of Appeals affirmed the ruling. The state petitioned the Supreme Court to resolve the issue.
During arguments, Idaho deputy attorney general Carl J. Withroe argued the courtroom is an incorrect avenue for Medicaid providers to dispute pay rates. If displeased, physicians and other health providers should issue an administrative challenge to the Centers for Medicare & Medicaid Services over its approval of the state’s Medicaid plan. He noted that such state plans – known as waivers – must be approved by the CMS every 5 years.
But Justice Sonia Sotomayor called this pathway an ineffective remedy.
“Let’s assume inflation is going up constantly. What happens 2 years into the plan when providers can’t work for what the state is giving or the state is imposing a tremendous hardship on them, which is happening to a lot of providers who are being underpaid. Where do they go? ... What do they do?”
Other panelists, such as Justice Ruth Bader Ginsberg, expressed doubt that the centers’ case against the state has merit, namely that Idaho is violating Medicaid’s equal access provision.
“According to the district court, all eligible recipients received the services that they needed,” Justice Ginsberg said. “So again, there was no waiting list; nobody’s being kept waiting. These providers, while they say they’re not getting enough, are still providing the service. So where is the [equal access] violation?”
Attorney James M. Piotrowski, who represented the centers, countered that the equal access provision imposes both procedural and substantive requirements. The substantive requirement mandates there must be enough providers to allow access and generate quality care, Mr. Piotrowski said. The procedural requirement entails that the rates be set based upon factors that Congress considers important.
“The violation of [the equal access provision] here was that the state gave no consideration whatsoever to the federal factors,” he said. “They relied only on their own factors.”
The Armstrong case is being closely watched by states, physicians, and patient advocates alike. Twenty-seven states have reached out to the high court in support of Idaho. The states saidthey have been subject to numerous, unwarranted lawsuits because of misguided interpretations of the Supremacy Clause. A number of physician and patient advocacy associations joined a friend-of-the-court brief in support of the centers, including the American Academy of Family Physicians and the American Medical Association. The AMA and other organizations said ongoing violations of Medicaid’s equal access provision by states continue to drive doctors from the program and harm access to care.
A decision by the high court is expected by June.
On Twitter @legal_med
Some Supreme Court justices appear skeptical about whether physicians and other health providers have the right to sue states over low Medicaid reimbursement.
During oral arguments Jan. 20 in Armstrong v. Exceptional Child Center Inc., Chief Justice John G. Roberts Jr. questioned whether letting providers challenge state-set payment rates would lead to a wave of litigation and force federal judges to make state budgetary decisions.
“There are dozens of different types of providers under the [Social Security] Act,” Justice Roberts said during oral arguments. “Now, what do you do if each of those providers bring a lawsuit similar to yours? The effect, it seems to me, will be putting the setting of budget priorities in the hands of dozens of different federal judges, and I just don’t know what the practical significance of that’s going to be.”
In Armstrong v. Exceptional Child Center Inc., the high court justices are weighing whether the U.S. Constitution’s Supremacy Clause – which establishes the Constitution and federal law as the law of the land – gives health care providers under Medicaid a private “right of action” to enforce Medicaid funding conditions against states. The case originates from a 2009 lawsuit by Exceptional Child Center Inc., of Twin Falls, Idaho, and four other residential habilitation centers against Richard Armstrong, director of the Idaho Department of Health and Welfare.
The centers claimed the state was violating Medicaid’s equal access provision by refusing to raise its payment rates. Under the equal access provision, states that accept federal Medicaid funding are required to set reimbursement rates at levels sufficient to retain enough providers and make sure patients have proper access to care. The Idaho Department of Health and Welfare and its Medicaid division conducted yearly cost studies between 2006 and 2009, developed a new rate-setting methodology, and recommended substantial increases in reimbursement rates for supported living services, according to court documents. However, the new methodology and rate increases were not enacted for budgetary reasons.
A district court ruled in favor of the centers, and the 9th U.S. Circuit Court of Appeals affirmed the ruling. The state petitioned the Supreme Court to resolve the issue.
During arguments, Idaho deputy attorney general Carl J. Withroe argued the courtroom is an incorrect avenue for Medicaid providers to dispute pay rates. If displeased, physicians and other health providers should issue an administrative challenge to the Centers for Medicare & Medicaid Services over its approval of the state’s Medicaid plan. He noted that such state plans – known as waivers – must be approved by the CMS every 5 years.
But Justice Sonia Sotomayor called this pathway an ineffective remedy.
“Let’s assume inflation is going up constantly. What happens 2 years into the plan when providers can’t work for what the state is giving or the state is imposing a tremendous hardship on them, which is happening to a lot of providers who are being underpaid. Where do they go? ... What do they do?”
Other panelists, such as Justice Ruth Bader Ginsberg, expressed doubt that the centers’ case against the state has merit, namely that Idaho is violating Medicaid’s equal access provision.
“According to the district court, all eligible recipients received the services that they needed,” Justice Ginsberg said. “So again, there was no waiting list; nobody’s being kept waiting. These providers, while they say they’re not getting enough, are still providing the service. So where is the [equal access] violation?”
Attorney James M. Piotrowski, who represented the centers, countered that the equal access provision imposes both procedural and substantive requirements. The substantive requirement mandates there must be enough providers to allow access and generate quality care, Mr. Piotrowski said. The procedural requirement entails that the rates be set based upon factors that Congress considers important.
“The violation of [the equal access provision] here was that the state gave no consideration whatsoever to the federal factors,” he said. “They relied only on their own factors.”
The Armstrong case is being closely watched by states, physicians, and patient advocates alike. Twenty-seven states have reached out to the high court in support of Idaho. The states saidthey have been subject to numerous, unwarranted lawsuits because of misguided interpretations of the Supremacy Clause. A number of physician and patient advocacy associations joined a friend-of-the-court brief in support of the centers, including the American Academy of Family Physicians and the American Medical Association. The AMA and other organizations said ongoing violations of Medicaid’s equal access provision by states continue to drive doctors from the program and harm access to care.
A decision by the high court is expected by June.
On Twitter @legal_med

Supreme Court to decide whether doctors can sue over low Medicaid payments
Physicians are closely watching a U.S. Supreme Court case that could affect their ability to fight low Medicaid payments.
On Jan. 20, the justices will hear arguments in Armstrong v. Exceptional Child Center Inc., a legal dispute that centers on whether physicians and other health care providers have the right to sue states to compel them to raise Medicaid payment rates.
Allowing providers to seek legal action over low Medicaid payments helps to ensure that payment is adequate and that states are held accountable, according to Dr. Reid B. Blackwelder, board chair of the American Academy of Family Physicians. Under the equal access provision of the Medicaid Act, states that accept federal Medicaid funding are required to set reimbursement rates at levels sufficient to retain enough providers and make sure patients have proper access to care.

“States really have the freedom and the will to make [payment] decisions based on their budgets,” Dr. Blackwelder said in an interview. “We feel the only way to create a remedy to the state’s noncompliance [to the equal access provision] is the individual’s right to sue.”
The case stems from a 2009 lawsuit by Exceptional Child Center Inc. of Twin Falls, Idaho, and four other residential habilitation centers against Richard Armstrong, director for the Idaho Department of Health and Welfare. The centers claimed the state should have raised its Medicaid payment rates after studies determined rate increases were necessary. The Idaho Department of Health and Welfare and its Medicaid division had conducted yearly cost studies between 2006 and 2009, developed a new rate-setting methodology, and recommended substantial increases in reimbursement rates for supported living services, according to court documents. However, the new methodology and rate increases were not enacted for budgetary reasons.
A district court ruled in favor of the centers, and the 9th U.S. Circuit Court of Appeals affirmed the ruling. The state petitioned the Supreme Court to resolve the issue. Idaho noted a split among the lower courts as to whether the Constitution’s Supremacy Clause – which establishes the Constitution and federal law as the law of the land – supplies a private right of action to enforce Medicaid funding conditions against states. In a court brief, Idaho Attorney General Lawrence G. Wasden said the Supremacy Clause does not do so and that only Congress has the authority to enforce federal statutes.
Mr. Wasden added that the Centers for Medicare & Medicaid Services had not found issue with Idaho’s payment rates nor had initiated any disciplinary actions against the state.
“If CMS believes a state has failed to correct a deficiency, CMS may initiate a process to withhold federal funds, either entirely or limited to the fund associated with the noncompliant service,” Mr. Wasden said in court documents. “At no time relevant to this case has CMS ever initiated any compliance action or otherwise complained about the state’s rates.”
Twenty-seven states reached out to the high court in support of Idaho. The states said they have been subject to numerous, unwarranted lawsuits because of misguided interpretations of the Supremacy Clause.
A number of physician and patient advocacy associations joined a friend-of-the-court brief in support of the centers, including the AAFP and the American Medical Association. The physicians’ court brief noted that 32 states reduced and/or froze Medicaid rates in 2012, and 23 did the same in 2013. As a result, Medicaid payment rates have often fallen below the average cost to deliver care and make it untenable for physicians to take on Medicaid patients.
“Noncompliance with Medicaid’s equal-access mandate will continue unless private enforcement is allowed to challenge states that adopt Medicaid payment rates based on arbitrary or politically expedient budgetary decisions,” AMA President Dr. Robert M. Wah said in a statement.

The Supreme Court’s decision will have a significant impact on whether physicians and other providers continue to participate in Medicaid and whether patients can find necessary care, added Jane Perkins, legal director of the National Health Law Program, a nonprofit that advocates the rights of low-income patients. The National Health Law Program issued its own friend-of-the-court brief in support of the centers.
“There are a tremendous number of potential ‘bigger picture’ impacts” to the court’s decision, Ms. Perkins said in an interview. “Researchers have found time and again that while many things go into a provider’s decision whether or not to participate in Medicaid, one of the main things is the payment rate. If [Idaho wins], I really fear the already problematic state of provider participation in many places is only going to get worse."
OnTwitter @legal_med
Physicians are closely watching a U.S. Supreme Court case that could affect their ability to fight low Medicaid payments.
On Jan. 20, the justices will hear arguments in Armstrong v. Exceptional Child Center Inc., a legal dispute that centers on whether physicians and other health care providers have the right to sue states to compel them to raise Medicaid payment rates.
Allowing providers to seek legal action over low Medicaid payments helps to ensure that payment is adequate and that states are held accountable, according to Dr. Reid B. Blackwelder, board chair of the American Academy of Family Physicians. Under the equal access provision of the Medicaid Act, states that accept federal Medicaid funding are required to set reimbursement rates at levels sufficient to retain enough providers and make sure patients have proper access to care.
“States really have the freedom and the will to make [payment] decisions based on their budgets,” Dr. Blackwelder said in an interview. “We feel the only way to create a remedy to the state’s noncompliance [to the equal access provision] is the individual’s right to sue.”
The case stems from a 2009 lawsuit by Exceptional Child Center Inc. of Twin Falls, Idaho, and four other residential habilitation centers against Richard Armstrong, director for the Idaho Department of Health and Welfare. The centers claimed the state should have raised its Medicaid payment rates after studies determined rate increases were necessary. The Idaho Department of Health and Welfare and its Medicaid division had conducted yearly cost studies between 2006 and 2009, developed a new rate-setting methodology, and recommended substantial increases in reimbursement rates for supported living services, according to court documents. However, the new methodology and rate increases were not enacted for budgetary reasons.
A district court ruled in favor of the centers, and the 9th U.S. Circuit Court of Appeals affirmed the ruling. The state petitioned the Supreme Court to resolve the issue. Idaho noted a split among the lower courts as to whether the Constitution’s Supremacy Clause – which establishes the Constitution and federal law as the law of the land – supplies a private right of action to enforce Medicaid funding conditions against states. In a court brief, Idaho Attorney General Lawrence G. Wasden said the Supremacy Clause does not do so and that only Congress has the authority to enforce federal statutes.
Mr. Wasden added that the Centers for Medicare & Medicaid Services had not found issue with Idaho’s payment rates nor had initiated any disciplinary actions against the state.
“If CMS believes a state has failed to correct a deficiency, CMS may initiate a process to withhold federal funds, either entirely or limited to the fund associated with the noncompliant service,” Mr. Wasden said in court documents. “At no time relevant to this case has CMS ever initiated any compliance action or otherwise complained about the state’s rates.”
Twenty-seven states reached out to the high court in support of Idaho. The states said they have been subject to numerous, unwarranted lawsuits because of misguided interpretations of the Supremacy Clause.
A number of physician and patient advocacy associations joined a friend-of-the-court brief in support of the centers, including the AAFP and the American Medical Association. The physicians’ court brief noted that 32 states reduced and/or froze Medicaid rates in 2012, and 23 did the same in 2013. As a result, Medicaid payment rates have often fallen below the average cost to deliver care and make it untenable for physicians to take on Medicaid patients.
“Noncompliance with Medicaid’s equal-access mandate will continue unless private enforcement is allowed to challenge states that adopt Medicaid payment rates based on arbitrary or politically expedient budgetary decisions,” AMA President Dr. Robert M. Wah said in a statement.
The Supreme Court’s decision will have a significant impact on whether physicians and other providers continue to participate in Medicaid and whether patients can find necessary care, added Jane Perkins, legal director of the National Health Law Program, a nonprofit that advocates the rights of low-income patients. The National Health Law Program issued its own friend-of-the-court brief in support of the centers.
“There are a tremendous number of potential ‘bigger picture’ impacts” to the court’s decision, Ms. Perkins said in an interview. “Researchers have found time and again that while many things go into a provider’s decision whether or not to participate in Medicaid, one of the main things is the payment rate. If [Idaho wins], I really fear the already problematic state of provider participation in many places is only going to get worse."
OnTwitter @legal_med
Physicians are closely watching a U.S. Supreme Court case that could affect their ability to fight low Medicaid payments.
On Jan. 20, the justices will hear arguments in Armstrong v. Exceptional Child Center Inc., a legal dispute that centers on whether physicians and other health care providers have the right to sue states to compel them to raise Medicaid payment rates.
Allowing providers to seek legal action over low Medicaid payments helps to ensure that payment is adequate and that states are held accountable, according to Dr. Reid B. Blackwelder, board chair of the American Academy of Family Physicians. Under the equal access provision of the Medicaid Act, states that accept federal Medicaid funding are required to set reimbursement rates at levels sufficient to retain enough providers and make sure patients have proper access to care.
“States really have the freedom and the will to make [payment] decisions based on their budgets,” Dr. Blackwelder said in an interview. “We feel the only way to create a remedy to the state’s noncompliance [to the equal access provision] is the individual’s right to sue.”
The case stems from a 2009 lawsuit by Exceptional Child Center Inc. of Twin Falls, Idaho, and four other residential habilitation centers against Richard Armstrong, director for the Idaho Department of Health and Welfare. The centers claimed the state should have raised its Medicaid payment rates after studies determined rate increases were necessary. The Idaho Department of Health and Welfare and its Medicaid division had conducted yearly cost studies between 2006 and 2009, developed a new rate-setting methodology, and recommended substantial increases in reimbursement rates for supported living services, according to court documents. However, the new methodology and rate increases were not enacted for budgetary reasons.
A district court ruled in favor of the centers, and the 9th U.S. Circuit Court of Appeals affirmed the ruling. The state petitioned the Supreme Court to resolve the issue. Idaho noted a split among the lower courts as to whether the Constitution’s Supremacy Clause – which establishes the Constitution and federal law as the law of the land – supplies a private right of action to enforce Medicaid funding conditions against states. In a court brief, Idaho Attorney General Lawrence G. Wasden said the Supremacy Clause does not do so and that only Congress has the authority to enforce federal statutes.
Mr. Wasden added that the Centers for Medicare & Medicaid Services had not found issue with Idaho’s payment rates nor had initiated any disciplinary actions against the state.
“If CMS believes a state has failed to correct a deficiency, CMS may initiate a process to withhold federal funds, either entirely or limited to the fund associated with the noncompliant service,” Mr. Wasden said in court documents. “At no time relevant to this case has CMS ever initiated any compliance action or otherwise complained about the state’s rates.”
Twenty-seven states reached out to the high court in support of Idaho. The states said they have been subject to numerous, unwarranted lawsuits because of misguided interpretations of the Supremacy Clause.
A number of physician and patient advocacy associations joined a friend-of-the-court brief in support of the centers, including the AAFP and the American Medical Association. The physicians’ court brief noted that 32 states reduced and/or froze Medicaid rates in 2012, and 23 did the same in 2013. As a result, Medicaid payment rates have often fallen below the average cost to deliver care and make it untenable for physicians to take on Medicaid patients.
“Noncompliance with Medicaid’s equal-access mandate will continue unless private enforcement is allowed to challenge states that adopt Medicaid payment rates based on arbitrary or politically expedient budgetary decisions,” AMA President Dr. Robert M. Wah said in a statement.
The Supreme Court’s decision will have a significant impact on whether physicians and other providers continue to participate in Medicaid and whether patients can find necessary care, added Jane Perkins, legal director of the National Health Law Program, a nonprofit that advocates the rights of low-income patients. The National Health Law Program issued its own friend-of-the-court brief in support of the centers.
“There are a tremendous number of potential ‘bigger picture’ impacts” to the court’s decision, Ms. Perkins said in an interview. “Researchers have found time and again that while many things go into a provider’s decision whether or not to participate in Medicaid, one of the main things is the payment rate. If [Idaho wins], I really fear the already problematic state of provider participation in many places is only going to get worse."
OnTwitter @legal_med

CMS Administrator Tavenner to step down in February
Centers for Medicare & Medicaid Services Administrator Marilyn Tavenner announced Jan. 16 that she will resign her post at the end of February.
Ms. Tavenner joined CMS in February 2010 and oversaw the implementation of the Affordable Care Act, passed a month into her leadership tenure. She was the first administrator to be confirmed by the U.S. Senate in more than 6 years.

In a Jan. 16 e-mail to CMS staff, Ms. Tavenner highlighted a number of agency achievements during her time as administrator, commending staff’s “hard work, dedication, commitment, and resolve” that are “truly transforming health care in this country.”
Among the achievements she highlighted were improvements in quality of health care delivered, historically overall low growth in health care spending, increased fraud detection, greater transparency, publication of health care data and indicators, and improved access to health care.
“Marilyn led the effort to accelerate the development and expansion of innovative new health care payment and delivery models,” HHS Secretary Sylvia Burwell said Jan. 16 in an e-mail to all CMS staff.
A low point of Tavenner’s tenure was the troubled launch of HealthCare.gov; however, Ms. Burwell commended her for her work to “help right the ship, bringing aboard a systems integrator and overseeing an overhaul of the website.”
Principal Deputy Administrator Andy Slavitt will take over as acting administrator in March, Ms. Burwell said.
Centers for Medicare & Medicaid Services Administrator Marilyn Tavenner announced Jan. 16 that she will resign her post at the end of February.
Ms. Tavenner joined CMS in February 2010 and oversaw the implementation of the Affordable Care Act, passed a month into her leadership tenure. She was the first administrator to be confirmed by the U.S. Senate in more than 6 years.
In a Jan. 16 e-mail to CMS staff, Ms. Tavenner highlighted a number of agency achievements during her time as administrator, commending staff’s “hard work, dedication, commitment, and resolve” that are “truly transforming health care in this country.”
Among the achievements she highlighted were improvements in quality of health care delivered, historically overall low growth in health care spending, increased fraud detection, greater transparency, publication of health care data and indicators, and improved access to health care.
“Marilyn led the effort to accelerate the development and expansion of innovative new health care payment and delivery models,” HHS Secretary Sylvia Burwell said Jan. 16 in an e-mail to all CMS staff.
A low point of Tavenner’s tenure was the troubled launch of HealthCare.gov; however, Ms. Burwell commended her for her work to “help right the ship, bringing aboard a systems integrator and overseeing an overhaul of the website.”
Principal Deputy Administrator Andy Slavitt will take over as acting administrator in March, Ms. Burwell said.
Centers for Medicare & Medicaid Services Administrator Marilyn Tavenner announced Jan. 16 that she will resign her post at the end of February.
Ms. Tavenner joined CMS in February 2010 and oversaw the implementation of the Affordable Care Act, passed a month into her leadership tenure. She was the first administrator to be confirmed by the U.S. Senate in more than 6 years.
In a Jan. 16 e-mail to CMS staff, Ms. Tavenner highlighted a number of agency achievements during her time as administrator, commending staff’s “hard work, dedication, commitment, and resolve” that are “truly transforming health care in this country.”
Among the achievements she highlighted were improvements in quality of health care delivered, historically overall low growth in health care spending, increased fraud detection, greater transparency, publication of health care data and indicators, and improved access to health care.
“Marilyn led the effort to accelerate the development and expansion of innovative new health care payment and delivery models,” HHS Secretary Sylvia Burwell said Jan. 16 in an e-mail to all CMS staff.
A low point of Tavenner’s tenure was the troubled launch of HealthCare.gov; however, Ms. Burwell commended her for her work to “help right the ship, bringing aboard a systems integrator and overseeing an overhaul of the website.”
Principal Deputy Administrator Andy Slavitt will take over as acting administrator in March, Ms. Burwell said.

Fit Direct Observation of Medical Trainees Into Your Day

All of us who work with housestaff understand that a crucial component of teaching clinical medicine is to take the time to both supervise resident work and deliver constructive feedback on its quality. In the assessment of competence, trainees have “direct supervision” when an attending, senior resident, or other individual is physically present and guiding the care in real time or “indirect supervision” when work is being checked after the care has been administered.
Regardless of the level of supervision, checking in with direct observations (watching trainees do the actual work in real time) provides invaluable information for both patient care and resident assessment. Given that assessment and supervision are key components of the Accreditation Council for Graduate Medical Education’s (ACGME) Next Accreditation System, many programs are now placing particular emphasis on the time we spend observing our trainees.
How can faculty fit direct observation into an already busy day? Here are some ideas for how to adapt and leverage your workflow to create new opportunities for resident skills assessment.
Micro-Observations Matter
Gone are the days of sitting in a patient room for an hour observing a long history and physical performed by the resident or student that you are supervising. In spite of time constraints, you should aim to be at the bedside at the same time as the trainee as much as possible. Once there, take note of all that you see. For example, we often observe residents and students during bedside rounds or critical family discussions. Here are additional opportunities for trainee observation that might fit into your workflow:
- First thing in the morning, when the team is pre-rounding (this is perfect for when you are worried about a patient or are scheduled for a busy afternoon). Do NOT interrupt the resident workflow. Instruct them at the beginning of the rotation that you plan to observe unannounced. If they see you, they should continue with their normal activities. Pop in and out to catch key points, and gather the information necessary to guide patient care. Don’t take over to do teaching or feedback; that will come later in the day.
- During a procedure performed by a supervising resident who already has demonstrated technical competence. Bring a computer on wheels into the patient’s room, sit down, and catch up on charting while listening to and observing the explanations, teaching, and interaction between the patient and the resident. You can still intervene if necessary, but take appropriate steps to allow resident autonomy and the observation of high-level communication skills.
- At the bedside of a clinically unstable patient. If you are together with the team when a nurse calls with a concern, you can instruct the resident to go ahead and intervene with close follow-up in a few minutes. This allows residents to get a head start, gather information, and establish themselves as the decision-makers, while still providing an opportunity for close observation by the faculty.
- Finalizing a discharge first thing in the morning. With most hospitals focusing on discharge timeliness, faculty often discuss patients scheduled for discharge prior to or outside of formal rounds. Get to the patient! Observe the resident interacting with the patient and multidisciplinary team, confirming medication reconciliation, finalizing the discharge diagnosis and instructions, and inquiring further about barriers to adherence with the discharge regimen.
Vary Your Approach
Use a variety of formats to tell your learners what was observed. Specific, quick comments made in real time can be encouraging, and brief suggestions are usually welcome in the context of a particular patient. Other observations and feedback that need to be more sensitive or require more time are perfect to wrap up at the end of the day. Finally, the message function in the electronic medical record is another great and timely format for providing feedback on observations related to clinical documentation, differential diagnosis, and management plan.
Real-Time Recordkeeping
Record your observations as you go. Even though you are providing formative feedback throughout the month, you likely also will be expected to translate those observations into a summative end-of-rotation assessment. Whether it is on a notecard with the name of each trainee being supervised or on a printed blank copy of the end of the month assessment or other program-specific assessments, jotting down specific observations will help you recall key information.
When feedback is provided, note the date in order to guide your summative feedback discussion and the final assessment.
Keep in mind that program assessment tools often serve to remind faculty of specific behaviors that have not historically been evaluated. For example, faculty might be in the habit of providing feedback on communication skills after a family meeting but may not specifically listen for trainees to use “teach-back” concepts when explaining the plan for discharge or noting whether they actively seek input from the multidisciplinary team. A tool that lists “teach-back” or “seeks out interprofessional collaboration” as line items on the form can help to remind you of the qualities you are being asked to assess.
Although direct observation is essential in providing useful assessments during the course of supervision of trainees, there are additional ways that faculty can “see” how a trainee is doing. For example, faculty or supervising residents can “observe” an intern’s completed discharge summary in real time for important and key components. Checking this work enables you to provide an assessment of additional skills (i.e., medication reconciliation, medical knowledge, management of clinical conditions, and appropriate handoff to future care providers). As trainees progressively demonstrate competence, the degree of supervision evolves to the point of a quick verification rather than the initial detailed review.
In summary, supervising trainees well means both thinking critically about their care of patients and providing feedback. As much as we have adapted our clinical workflow to meet increasing regulatory, quality, or patient throughput requirements, we must also change our educational workflow to meet the needs of our learners.
This adaptation should not be onerous. A few simple adjustments, as outlined above, can lead to higher-quality assessments and increased satisfaction in your role as teacher. So, get back out on the wards and observe!
Dr. O’Malley is the internal medicine residency program director at Banner Good Samaritan in Phoenix, Ariz., and an assistant professor of medicine at the University of Arizona College of Medicine. She currently serves as SHM’s representative on the Alliance for Academic Internal Medicine’s Internal Medicine Education Redesign Advisory Board, along with Dr. Caverzagie, who is associate dean for educational strategy at the University of Nebraska College of Medicine in Omaha and vice president for education, clinical enterprise of the Nebraska Medical Center. Dr. Caverzagie also was a member of the ABIM and ACGME milestone writing groups.
All of us who work with housestaff understand that a crucial component of teaching clinical medicine is to take the time to both supervise resident work and deliver constructive feedback on its quality. In the assessment of competence, trainees have “direct supervision” when an attending, senior resident, or other individual is physically present and guiding the care in real time or “indirect supervision” when work is being checked after the care has been administered.
Regardless of the level of supervision, checking in with direct observations (watching trainees do the actual work in real time) provides invaluable information for both patient care and resident assessment. Given that assessment and supervision are key components of the Accreditation Council for Graduate Medical Education’s (ACGME) Next Accreditation System, many programs are now placing particular emphasis on the time we spend observing our trainees.
How can faculty fit direct observation into an already busy day? Here are some ideas for how to adapt and leverage your workflow to create new opportunities for resident skills assessment.
Micro-Observations Matter
Gone are the days of sitting in a patient room for an hour observing a long history and physical performed by the resident or student that you are supervising. In spite of time constraints, you should aim to be at the bedside at the same time as the trainee as much as possible. Once there, take note of all that you see. For example, we often observe residents and students during bedside rounds or critical family discussions. Here are additional opportunities for trainee observation that might fit into your workflow:
- First thing in the morning, when the team is pre-rounding (this is perfect for when you are worried about a patient or are scheduled for a busy afternoon). Do NOT interrupt the resident workflow. Instruct them at the beginning of the rotation that you plan to observe unannounced. If they see you, they should continue with their normal activities. Pop in and out to catch key points, and gather the information necessary to guide patient care. Don’t take over to do teaching or feedback; that will come later in the day.
- During a procedure performed by a supervising resident who already has demonstrated technical competence. Bring a computer on wheels into the patient’s room, sit down, and catch up on charting while listening to and observing the explanations, teaching, and interaction between the patient and the resident. You can still intervene if necessary, but take appropriate steps to allow resident autonomy and the observation of high-level communication skills.
- At the bedside of a clinically unstable patient. If you are together with the team when a nurse calls with a concern, you can instruct the resident to go ahead and intervene with close follow-up in a few minutes. This allows residents to get a head start, gather information, and establish themselves as the decision-makers, while still providing an opportunity for close observation by the faculty.
- Finalizing a discharge first thing in the morning. With most hospitals focusing on discharge timeliness, faculty often discuss patients scheduled for discharge prior to or outside of formal rounds. Get to the patient! Observe the resident interacting with the patient and multidisciplinary team, confirming medication reconciliation, finalizing the discharge diagnosis and instructions, and inquiring further about barriers to adherence with the discharge regimen.
Vary Your Approach
Use a variety of formats to tell your learners what was observed. Specific, quick comments made in real time can be encouraging, and brief suggestions are usually welcome in the context of a particular patient. Other observations and feedback that need to be more sensitive or require more time are perfect to wrap up at the end of the day. Finally, the message function in the electronic medical record is another great and timely format for providing feedback on observations related to clinical documentation, differential diagnosis, and management plan.
Real-Time Recordkeeping
Record your observations as you go. Even though you are providing formative feedback throughout the month, you likely also will be expected to translate those observations into a summative end-of-rotation assessment. Whether it is on a notecard with the name of each trainee being supervised or on a printed blank copy of the end of the month assessment or other program-specific assessments, jotting down specific observations will help you recall key information.
When feedback is provided, note the date in order to guide your summative feedback discussion and the final assessment.
Keep in mind that program assessment tools often serve to remind faculty of specific behaviors that have not historically been evaluated. For example, faculty might be in the habit of providing feedback on communication skills after a family meeting but may not specifically listen for trainees to use “teach-back” concepts when explaining the plan for discharge or noting whether they actively seek input from the multidisciplinary team. A tool that lists “teach-back” or “seeks out interprofessional collaboration” as line items on the form can help to remind you of the qualities you are being asked to assess.
Although direct observation is essential in providing useful assessments during the course of supervision of trainees, there are additional ways that faculty can “see” how a trainee is doing. For example, faculty or supervising residents can “observe” an intern’s completed discharge summary in real time for important and key components. Checking this work enables you to provide an assessment of additional skills (i.e., medication reconciliation, medical knowledge, management of clinical conditions, and appropriate handoff to future care providers). As trainees progressively demonstrate competence, the degree of supervision evolves to the point of a quick verification rather than the initial detailed review.
In summary, supervising trainees well means both thinking critically about their care of patients and providing feedback. As much as we have adapted our clinical workflow to meet increasing regulatory, quality, or patient throughput requirements, we must also change our educational workflow to meet the needs of our learners.
This adaptation should not be onerous. A few simple adjustments, as outlined above, can lead to higher-quality assessments and increased satisfaction in your role as teacher. So, get back out on the wards and observe!
Dr. O’Malley is the internal medicine residency program director at Banner Good Samaritan in Phoenix, Ariz., and an assistant professor of medicine at the University of Arizona College of Medicine. She currently serves as SHM’s representative on the Alliance for Academic Internal Medicine’s Internal Medicine Education Redesign Advisory Board, along with Dr. Caverzagie, who is associate dean for educational strategy at the University of Nebraska College of Medicine in Omaha and vice president for education, clinical enterprise of the Nebraska Medical Center. Dr. Caverzagie also was a member of the ABIM and ACGME milestone writing groups.
All of us who work with housestaff understand that a crucial component of teaching clinical medicine is to take the time to both supervise resident work and deliver constructive feedback on its quality. In the assessment of competence, trainees have “direct supervision” when an attending, senior resident, or other individual is physically present and guiding the care in real time or “indirect supervision” when work is being checked after the care has been administered.
Regardless of the level of supervision, checking in with direct observations (watching trainees do the actual work in real time) provides invaluable information for both patient care and resident assessment. Given that assessment and supervision are key components of the Accreditation Council for Graduate Medical Education’s (ACGME) Next Accreditation System, many programs are now placing particular emphasis on the time we spend observing our trainees.
How can faculty fit direct observation into an already busy day? Here are some ideas for how to adapt and leverage your workflow to create new opportunities for resident skills assessment.
Micro-Observations Matter
Gone are the days of sitting in a patient room for an hour observing a long history and physical performed by the resident or student that you are supervising. In spite of time constraints, you should aim to be at the bedside at the same time as the trainee as much as possible. Once there, take note of all that you see. For example, we often observe residents and students during bedside rounds or critical family discussions. Here are additional opportunities for trainee observation that might fit into your workflow:
- First thing in the morning, when the team is pre-rounding (this is perfect for when you are worried about a patient or are scheduled for a busy afternoon). Do NOT interrupt the resident workflow. Instruct them at the beginning of the rotation that you plan to observe unannounced. If they see you, they should continue with their normal activities. Pop in and out to catch key points, and gather the information necessary to guide patient care. Don’t take over to do teaching or feedback; that will come later in the day.
- During a procedure performed by a supervising resident who already has demonstrated technical competence. Bring a computer on wheels into the patient’s room, sit down, and catch up on charting while listening to and observing the explanations, teaching, and interaction between the patient and the resident. You can still intervene if necessary, but take appropriate steps to allow resident autonomy and the observation of high-level communication skills.
- At the bedside of a clinically unstable patient. If you are together with the team when a nurse calls with a concern, you can instruct the resident to go ahead and intervene with close follow-up in a few minutes. This allows residents to get a head start, gather information, and establish themselves as the decision-makers, while still providing an opportunity for close observation by the faculty.
- Finalizing a discharge first thing in the morning. With most hospitals focusing on discharge timeliness, faculty often discuss patients scheduled for discharge prior to or outside of formal rounds. Get to the patient! Observe the resident interacting with the patient and multidisciplinary team, confirming medication reconciliation, finalizing the discharge diagnosis and instructions, and inquiring further about barriers to adherence with the discharge regimen.
Vary Your Approach
Use a variety of formats to tell your learners what was observed. Specific, quick comments made in real time can be encouraging, and brief suggestions are usually welcome in the context of a particular patient. Other observations and feedback that need to be more sensitive or require more time are perfect to wrap up at the end of the day. Finally, the message function in the electronic medical record is another great and timely format for providing feedback on observations related to clinical documentation, differential diagnosis, and management plan.
Real-Time Recordkeeping
Record your observations as you go. Even though you are providing formative feedback throughout the month, you likely also will be expected to translate those observations into a summative end-of-rotation assessment. Whether it is on a notecard with the name of each trainee being supervised or on a printed blank copy of the end of the month assessment or other program-specific assessments, jotting down specific observations will help you recall key information.
When feedback is provided, note the date in order to guide your summative feedback discussion and the final assessment.
Keep in mind that program assessment tools often serve to remind faculty of specific behaviors that have not historically been evaluated. For example, faculty might be in the habit of providing feedback on communication skills after a family meeting but may not specifically listen for trainees to use “teach-back” concepts when explaining the plan for discharge or noting whether they actively seek input from the multidisciplinary team. A tool that lists “teach-back” or “seeks out interprofessional collaboration” as line items on the form can help to remind you of the qualities you are being asked to assess.
Although direct observation is essential in providing useful assessments during the course of supervision of trainees, there are additional ways that faculty can “see” how a trainee is doing. For example, faculty or supervising residents can “observe” an intern’s completed discharge summary in real time for important and key components. Checking this work enables you to provide an assessment of additional skills (i.e., medication reconciliation, medical knowledge, management of clinical conditions, and appropriate handoff to future care providers). As trainees progressively demonstrate competence, the degree of supervision evolves to the point of a quick verification rather than the initial detailed review.
In summary, supervising trainees well means both thinking critically about their care of patients and providing feedback. As much as we have adapted our clinical workflow to meet increasing regulatory, quality, or patient throughput requirements, we must also change our educational workflow to meet the needs of our learners.
This adaptation should not be onerous. A few simple adjustments, as outlined above, can lead to higher-quality assessments and increased satisfaction in your role as teacher. So, get back out on the wards and observe!
Dr. O’Malley is the internal medicine residency program director at Banner Good Samaritan in Phoenix, Ariz., and an assistant professor of medicine at the University of Arizona College of Medicine. She currently serves as SHM’s representative on the Alliance for Academic Internal Medicine’s Internal Medicine Education Redesign Advisory Board, along with Dr. Caverzagie, who is associate dean for educational strategy at the University of Nebraska College of Medicine in Omaha and vice president for education, clinical enterprise of the Nebraska Medical Center. Dr. Caverzagie also was a member of the ABIM and ACGME milestone writing groups.
How to Use Hospitalist Productivity, Compensation Survey Data
The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.

The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.
The 2014 State of Hospital Medicine report (SOHM), published by SHM in the fall of even years, is unquestionably the most robust and informative data available to understand the hospitalist workforce marketplace. And if you are the person who returned a completed survey for your practice, you get a free copy of the report mailed to you.
Keep in mind that the Medical Group Management Association (MGMA) surveys and reports data on hospitalist productivity and compensation every year. And the data acquired by MGMA in even years is simply folded into the SOHM, along with a ton of additional information added by a separate SHM survey, including things like the amount of financial support provided to hospitalist groups by hospitals (now up to a median of $156, 063 per full-time equivalent, or FTE).
I’ve written previously about some of the ways that the data reported in both of these surveys can be tricky to interpret (September 2013 and October 2013), and in this column I’ll go a little deeper into how to use the data reported on number of shifts worked and productivity.
A Common Question
Assume that, to address a staffing shortage or simply as a way to boost their income, some of the doctors in your group are willing to work more shifts than required for full-time status. And, in your group, some portion of a doctor’s compensation is a function of their individual work relevant value unit (wRVU) productivity—for example, a bonus for wRVUs above a certain threshold. You want to know whether the wRVU productivity generated by a doctor on their extra shifts should factor into compensation the same way it does for “regular” shifts.
You might turn to the MGMA and SOHM surveys to see how other groups handle this issue. But here is where it gets tricky.
First, you need to realize that the MGMA surveys, and similar ones from the American Medical Group Association and others, report wRVUs and compensation per physician, not per FTE. So wRVUs generated by these doctors on extra shifts are included, and you can’t tell from the aggregate data what portion of wRVUs came from regular shifts and what portion came from extra shifts.
And it is critical to keep in mind that any doctor who works at least 0.8 FTE as defined by that particular practice is reported as full time. Those working 79% or less of full time are counted by MGMA as part time.
To summarize: The MGMA and similar surveys don’t provide data on wRVU productivity per FTE, even though in most cases that is how everyone describes the data. Instead, the surveys provide data per individual doctor, many of whom work more or less than 1.0 FTE. So, despite the fact that most people, including me, tend to quote data from the surveys as though it is per FTE, as in “The 2014 MGMA data shows median hospitalist compensation is $253,977 per FTE,” we should say “per doctor” instead.
Theoretically, doctors working slightly less than 1.0 FTE should offset the doctors working slightly more than 1.0 FTE. But, while I think that’s a reasonable assumption for most specialties, such a significant portion of hospitalist groups have had chronic staffing shortages that a lot of hospitalists across the country are working extra shifts, probably more than are working between 0.8 and 1.0 FTE. So the hospitalist survey wRVU data is probably at least a little higher than it would be if it were reported per FTE.
Unfortunately, there is no way to confirm my suspicion, because MGMA doesn’t allow any individual doctor to be reported as more than 1.0 FTE, even if he works far more shifts than the number that defines full time for that practice. In other words, extra shifts just aren’t accounted for in the MGMA survey.
Implications of Individual vs. FTE
For most purposes, it probably doesn’t make any difference if you are erroneously thinking about the compensation and productivity survey numbers on a per FTE basis. But, for some purposes, and for those who work significantly more shifts than most hospitalists, it can start to matter.
Now back to the original question. You’re thinking about whether wRVUs generated by the doctors in your group on extra shifts should count toward the wRVU bonus just like those generated on regular shifts. You’d like to handle this the same way as other groups, but, unfortunately, survey data just isn’t helpful here. You’ll have to decide this for yourself.
I think some, but probably not all, extra shift productivity should count toward your wRVU bonus. You might, for example, say that productivity for somewhere between three or five extra shifts per quarter—that’s totally arbitrary, and of course this would be a negotiation between you and hospital leadership—should count toward the productivity target, and the rest wouldn’t, or that those extra shifts above an agreed-upon number would result in an increase in the wRVU target. The biggest problem with this is that it would be a nightmare to administer—essentially impossible for many practices. But you could accomplish the same thing by including the first few shifts per quarter in the “base” FTE calculation and then, after that, adjusting each person’s FTE value up as they work more shifts.
One more thing about productivity targets…
It’s also important to remember that productivity targets make the most sense at the group—not the individual—level. The MGMA data includes hospitalists who work night shifts (including nocturnists) and doctors who work low-production shifts (i.e., pager or ED triage shifts), as well as daytime rounding doctors. So, if you have a doctor who only works days, you would expect him to generate wRVUs in excess of the global target of wRVUs per FTE to make up for the low-productivity shifts that other doctors have to work.
For example, your practice might decide the group as a whole is expected to generate the MGMA yearly median 4,298 wRVUs per doctor, multiplied by the number of FTEs in the group. But the nocturnists would be expected to generate fewer, while those who work most or all of their shifts in a daytime rounder would be expected to generate more. So the threshold to begin paying the wRVU bonus for daytime rounding doctors might be adjusted up to something like 4,500 wRVUs.
The above example is just as an illustration, of course, and there are all kinds of reasons it might be more appropriate to choose different thresholds for your practice. But it’s a good place to start the thinking.
Giving patients ownership of data key to solving health IT woes
Mandating that patients “own” their health care data could open the road to true interoperability of electronic health records and might even help solve other tough health IT problems.
“As a consumer, if I pay for my health care, I go see a provider, and I [should] get my data, whatever it is – doctor’s note, lab test, CT or an MRI, Dr. Samson Jesudass, senior vice president and clinical leader at Ascension Health, said at a panel discussion at the Washington, D.C.,–based Bipartisan Policy Center. “That provider should be able to give that to me at the end of that visit, or whenever at whatever time, in a format that I can probably take and put it anywhere else into any other system.”

Making data portable and, more importantly, giving ownership of it to patients, “might be able to solve the issues” that are affecting the health IT environment, he said. “At the end of the day, if a patient is able to take his or her own data and be able to use it in whatever form or fashion, you actually democratize the whole process of information.”
During the discussion, ownership of data was often cited as a barrier to advancing health IT, particularly with physicians protecting their own data in an effort to protect their practices. But participants noted that language included in the year-end federal continuing resolution and budget bill provides a good opportunity to discuss some of these issues, specifically wording that urges the Office of the National Coordinator for Health Information Technology to exercise its authority to decertify EHR systems from the meaningful use program that block the transfer of data.
“This is a prime opportunity to get the physician’s, health care provider’s, [and] health care facility’s input on what’s going to make this an easier change,” especially for those that have invested in systems that are no longer certified to allow for meaningful use incentive payments, Dr. Rhonda Medows, chief medical officer at Optum, the research arm of UnitedHealth.
Vendors should “listen and serve” more, according to Jon Zimmerman, vice president and general manager of clinical business solutions at GE Healthcare. “We have to engage the clinicians and the business people in the health care delivery systems differently. We have to ask them, not tell them. We have to observe them. We have to assist them. And we really have to dig a little deeper to understand what it is they need to do.”
Mandating that patients “own” their health care data could open the road to true interoperability of electronic health records and might even help solve other tough health IT problems.
“As a consumer, if I pay for my health care, I go see a provider, and I [should] get my data, whatever it is – doctor’s note, lab test, CT or an MRI, Dr. Samson Jesudass, senior vice president and clinical leader at Ascension Health, said at a panel discussion at the Washington, D.C.,–based Bipartisan Policy Center. “That provider should be able to give that to me at the end of that visit, or whenever at whatever time, in a format that I can probably take and put it anywhere else into any other system.”
Making data portable and, more importantly, giving ownership of it to patients, “might be able to solve the issues” that are affecting the health IT environment, he said. “At the end of the day, if a patient is able to take his or her own data and be able to use it in whatever form or fashion, you actually democratize the whole process of information.”
During the discussion, ownership of data was often cited as a barrier to advancing health IT, particularly with physicians protecting their own data in an effort to protect their practices. But participants noted that language included in the year-end federal continuing resolution and budget bill provides a good opportunity to discuss some of these issues, specifically wording that urges the Office of the National Coordinator for Health Information Technology to exercise its authority to decertify EHR systems from the meaningful use program that block the transfer of data.
“This is a prime opportunity to get the physician’s, health care provider’s, [and] health care facility’s input on what’s going to make this an easier change,” especially for those that have invested in systems that are no longer certified to allow for meaningful use incentive payments, Dr. Rhonda Medows, chief medical officer at Optum, the research arm of UnitedHealth.
Vendors should “listen and serve” more, according to Jon Zimmerman, vice president and general manager of clinical business solutions at GE Healthcare. “We have to engage the clinicians and the business people in the health care delivery systems differently. We have to ask them, not tell them. We have to observe them. We have to assist them. And we really have to dig a little deeper to understand what it is they need to do.”
Mandating that patients “own” their health care data could open the road to true interoperability of electronic health records and might even help solve other tough health IT problems.
“As a consumer, if I pay for my health care, I go see a provider, and I [should] get my data, whatever it is – doctor’s note, lab test, CT or an MRI, Dr. Samson Jesudass, senior vice president and clinical leader at Ascension Health, said at a panel discussion at the Washington, D.C.,–based Bipartisan Policy Center. “That provider should be able to give that to me at the end of that visit, or whenever at whatever time, in a format that I can probably take and put it anywhere else into any other system.”
Making data portable and, more importantly, giving ownership of it to patients, “might be able to solve the issues” that are affecting the health IT environment, he said. “At the end of the day, if a patient is able to take his or her own data and be able to use it in whatever form or fashion, you actually democratize the whole process of information.”
During the discussion, ownership of data was often cited as a barrier to advancing health IT, particularly with physicians protecting their own data in an effort to protect their practices. But participants noted that language included in the year-end federal continuing resolution and budget bill provides a good opportunity to discuss some of these issues, specifically wording that urges the Office of the National Coordinator for Health Information Technology to exercise its authority to decertify EHR systems from the meaningful use program that block the transfer of data.
“This is a prime opportunity to get the physician’s, health care provider’s, [and] health care facility’s input on what’s going to make this an easier change,” especially for those that have invested in systems that are no longer certified to allow for meaningful use incentive payments, Dr. Rhonda Medows, chief medical officer at Optum, the research arm of UnitedHealth.
Vendors should “listen and serve” more, according to Jon Zimmerman, vice president and general manager of clinical business solutions at GE Healthcare. “We have to engage the clinicians and the business people in the health care delivery systems differently. We have to ask them, not tell them. We have to observe them. We have to assist them. And we really have to dig a little deeper to understand what it is they need to do.”

Malpractice Counsel
Stroke in a Young Man
A 26-year-old man presented to the ED with the chief complaint of mild right-sided weakness, paresthesias, and slurred speech. He stated the onset was sudden—approximately 30 minutes prior to arrival to the ED. The patient denied any previous similar symptoms and was otherwise in good health; he denied taking any medications. He drank alcohol socially, but denied smoking or illicit drug use.
On physical examination, his vital signs and oxygen saturation were normal. Pulmonary, cardiovascular, and abdominal examinations were also normal. The patient thought his speech was somewhat slurred, but the triage nurse and treating emergency physician (EP) had difficulty detecting any altered speech. He was noted to have mild (4+/5) right upper and lower extremity weakness; no facial droop was detected. The patient did have a mild pronator drift of the right upper extremity. Gait testing revealed a mild limp of the right lower extremity.
The EP consulted the hospitalist, and the patient was admitted to a monitored bed. The following morning, a brain magnetic resonance image revealed an ischemic stroke in the distribution of the left middle cerebral artery. The patient’s hospital course was uncomplicated, but at the time of discharge, he continued to have mild right-sided weakness and required the use of a cane.
The patient sued the hospital and the EP for negligence in failing to treat his condition in a timely manner and for not consulting a neurologist. The plaintiff’s attorneys argued the patient should have been given tissue plasminogen activator (tPA), which would have avoided the residual right-sided weakness. The defense denied negligence and argued the patient’s symptoms could have been due to several things for which tPA would have been an inappropriate treatment. A defense verdict was returned.
Discussion
Stroke in young patients is relatively rare. With “young” defined as aged 18 to 45 years, this population accounts for approximately 2% to 12% of cerebral infarcts.1 In one nationwide US study of stroke in young adults, Ellis2 found that 4.9% of individuals experiencing a stroke in 2007 were between ages 18 and 44 years. Among this group, 78% experienced an ischemic stroke; 11.2% experienced a subarachnoid hemorrhage (SAH); and 10.8% had an intracerebral hemorrhage.2
While the clinical presentation of stroke in young adults is similar to that of older patients, the etiologies and risk factors are very different. In older patients, atherosclerosis is the major cause of ischemic stroke. In studies of young adults with ischemic stroke, cardioembolism was found to be the leading cause. Under this category, a patent foramen ovale (PFO) was considered a common cause, followed by atrial fibrillation, bacterial endocarditis, rheumatic heart disease, and atrial myxoma. There is, however, increasing controversy over the role of PFO as an etiology of stroke. Many investigators think its role has been overstated and is probably more of an incidental finding than a causal relationship.3 Patients with a suspected cardioembolic etiology will usually require an echocardiogram (with saline contrast or a “bubble study” for suspected PFO), cardiac monitoring, and a possible Holter monitor at the time of discharge (to detect paroxysmal arrhythmias).
Following cardioembolic etiologies, arterial dissection is the next most common category.4 In one study of patients aged 31 to 45 years old, arterial dissection was the most common cause of ischemic stroke.4 Clinical features suggesting dissection include a history of head or neck trauma (even minor trauma), headache or neck pain, and local neurological findings (eg, cranial nerve palsy or Horner syndrome).3 Unfortunately, only about 25% of patients volunteer a history of recent neck trauma. If a cervical or vertebral artery dissection is suspected, contrast enhanced magnetic resonance angiography (MRA) is the most sensitive and specific test, followed by carotid ultrasound and CT angiography.3
Traditional risk factors for stroke include hypertension and diabetes mellitus (DM). This is not true for younger adults that experience an ischemic stroke. Cigarette smoking is a very important risk factor for cerebrovascular accident in young adults; in addition, the more one smokes, the greater the risk. Other risk factors in young adults include history of migraine headaches (especially migraine with aura), pregnancy and the postpartum period, and illicit drug use.3
The defense’s argument that there are many causes of stroke in young adults that would be inappropriate for treatment with tPA, such as a PFO, carotid dissection or bacterial endocarditis, is absolutely true. Young patients need to be aggressively worked up for the etiology of their stroke, and may require additional testing, such as an MRA, echocardiogram, or Holter monitoring to determine the underlying cause of their stroke.
Obstruction Following Gastric Bypass Surgery
A 47-year-old woman presented to the ED complaining of severe back and abdominal pain. Onset had been gradual and began approximately 4 hours prior to arrival. She described the pain as crampy and constant. The patient had vomited twice; she denied diarrhea and had a normal bowel movement the previous day. She denied any vaginal or urinary complaints. Her past medical history was significant for hypertension and status post gastric bypass surgery 6 months prior. She had lost 42 pounds to date. She denied smoking or alcohol use.
The patient’s vital signs on physical examination were: blood pressure, 154/92 mm Hg; pulse, 106 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 99˚F. Oxygen saturation was 96% on room air. The patient’s lungs were clear to auscultation bilaterally. The heart was mildly tachycardic, with a regular rhythm and without murmurs, rubs, or gallops. The abdominal examination revealed diffuse tenderness and involuntary guarding. There was no distention or rebound. Bowel sounds were present but hypoactive. Examination of the back revealed bilateral paraspinal muscle tenderness without costovertebral angle tenderness.
The EP ordered a CBC, BMP, serum lipase, and a urinalysis. The patient was given an intravenous (IV) bolus of 250 cc normal saline in addition to IV morphine 4 mg and IV ondansetron 4 mg. Her white blood cell (WBC) count was slightly elevated at 12.2 g/dL, with a normal differential. The remainder of the laboratory studies were normal, except for a serum bicarbonate of 22 mmol/L.
The patient stated she felt somewhat improved, but continued to have abdominal and back pain. The EP admitted her to the hospital for observation and pain control. She died the following day from a bowel obstruction. The family sued the EP for negligence in failing to order appropriate testing and for not consulting with specialists to diagnose the bowel obstruction, which is a known complication of gastric bypass surgery. The jury returned a verdict of $2.4 million against the EP.
Discussion
The frequency of bariatric surgery in the United States continues to increase, primarily due to its success with regard to weight loss, but also because of its demonstrated improvement in hypertension, obstructive sleep apnea, hyperlipidemia, and type 2 DM.1
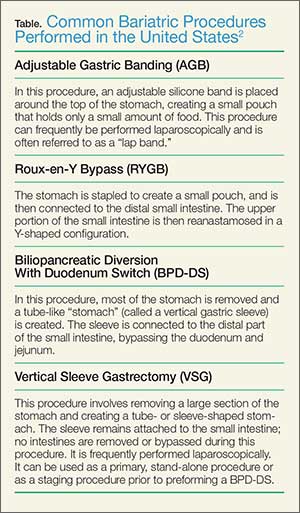
Frequently, the term “gastric bypass surgery” is used interchangeably with bariatric surgery. However, the EP must realize these terms encompass multiple different operations. The four most common types of bariatric surgery in the United Stated are (1) adjustable gastric banding (AGB); (2) the Roux-en-Y gastric bypass (RYGB); (3) biliopancreatic diversion with duodenal switch (BPD-DS); and (4) vertical sleeve gastrectomy (VSG).2 (See the Table for a brief explanation of each type of procedure.)
Since each procedure has its own respective associated complications, it is important for the EP to know which the type of gastric bypass surgery the patient had. For example, leakage is much more frequent following RYGB than in gastric banding, while slippage and obstruction are the most common complications of gastric banding.3,4 It is also very helpful to know the specific type of procedure when discussing the case with the surgical consultant.
Based on a recent review of over 800,000 bariatric surgery patients, seven serious common complications following the surgery were identified.3 These included bleeding, leakage, obstruction, stomal ulceration, pulmonary embolism and respiratory complications, blood sugar disturbances (usually hypoglycemia and/or metabolic acidosis), and nutritional disturbances. While not all-inclusive, this list represents the most common serious complications of gastric bypass surgery.
The complaint of abdominal pain in a patient that has undergone bariatric surgery should be taken very seriously. In addition to determining the specific procedure performed and date, the patient should be questioned about vomiting, bowel movements, and the presence of blood in stool or vomit. Depending upon the degree of pain present, the patient may need to be given IV opioid analgesia to facilitate a thorough abdominal examination. A rectal examination should be performed to identify occult gastrointestinal bleeding.
These patients require laboratory testing, including CBC, BMP, and other laboratory evaluation as indicated by the history and physical examination. Early consultation with the bariatric surgeon is recommended. Many, if not most, patients with abdominal pain and vomiting will require imaging, usually a CT scan with contrast of the abdomen and pelvis. Because of the difficulty in interpreting the CT scan results in these patients, the bariatric surgeon will often want to personally review the films rather than rely solely on the interpretation by radiology services.
Unfortunately, the EP in this case did not appreciate the seriousness of the situation. The presence of severe abdominal pain, tenderness, guarding, mild tachycardia with leukocytosis, and metabolic acidosis all pointed to a more serious etiology than muscle spasm. This patient required IV fluids, analgesia, and imaging, as well as consultation with the bariatric surgeon.
- Chatzikonstantinou A, Wolf ME, Hennerici MG. Ischemic stroke in young adults: classification and risk factors. J Neurol. 2012;259(4):653-659.
- Ellis C. Stroke in young adults. Disabil Health J. 2010;3(3):222-224.
- Ferro JM, Massaro AR, Mas JL. Aetiological diagnosis of ischemic stroke in young adults. Lancet Neurol. 2010;9(11):1085-1096.
- Chan MT, Nadareishvili ZG, Norris JW; Canadian Stroke Consortium. Diagnostic strategies in young patients with ischemic stroke in Canada. Can J Neurol Sci. 2000;27(2):120-124.
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724-1737.
- Livingston EH. Patient guide: Endocrine and nutritional management after bariatric surgery: A patient’s guide. Hormone Health Network Web site. http://www.hormone.org/~/media/Hormone/Files/Patient%20Guides/Mens%20Health/PGBariatricSurgery_2014.pdf. Accessed December 17, 2014.
- Hussain A, El-Hasani S. Bariatric emergencies: current evidence and strategies of management. World J Emerg Surg. 2013;8(1):58.
- Campanille FC, Boru C, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg. 2013;398(5):669-686
Stroke in a Young Man
A 26-year-old man presented to the ED with the chief complaint of mild right-sided weakness, paresthesias, and slurred speech. He stated the onset was sudden—approximately 30 minutes prior to arrival to the ED. The patient denied any previous similar symptoms and was otherwise in good health; he denied taking any medications. He drank alcohol socially, but denied smoking or illicit drug use.
On physical examination, his vital signs and oxygen saturation were normal. Pulmonary, cardiovascular, and abdominal examinations were also normal. The patient thought his speech was somewhat slurred, but the triage nurse and treating emergency physician (EP) had difficulty detecting any altered speech. He was noted to have mild (4+/5) right upper and lower extremity weakness; no facial droop was detected. The patient did have a mild pronator drift of the right upper extremity. Gait testing revealed a mild limp of the right lower extremity.
The EP consulted the hospitalist, and the patient was admitted to a monitored bed. The following morning, a brain magnetic resonance image revealed an ischemic stroke in the distribution of the left middle cerebral artery. The patient’s hospital course was uncomplicated, but at the time of discharge, he continued to have mild right-sided weakness and required the use of a cane.
The patient sued the hospital and the EP for negligence in failing to treat his condition in a timely manner and for not consulting a neurologist. The plaintiff’s attorneys argued the patient should have been given tissue plasminogen activator (tPA), which would have avoided the residual right-sided weakness. The defense denied negligence and argued the patient’s symptoms could have been due to several things for which tPA would have been an inappropriate treatment. A defense verdict was returned.
Discussion
Stroke in young patients is relatively rare. With “young” defined as aged 18 to 45 years, this population accounts for approximately 2% to 12% of cerebral infarcts.1 In one nationwide US study of stroke in young adults, Ellis2 found that 4.9% of individuals experiencing a stroke in 2007 were between ages 18 and 44 years. Among this group, 78% experienced an ischemic stroke; 11.2% experienced a subarachnoid hemorrhage (SAH); and 10.8% had an intracerebral hemorrhage.2
While the clinical presentation of stroke in young adults is similar to that of older patients, the etiologies and risk factors are very different. In older patients, atherosclerosis is the major cause of ischemic stroke. In studies of young adults with ischemic stroke, cardioembolism was found to be the leading cause. Under this category, a patent foramen ovale (PFO) was considered a common cause, followed by atrial fibrillation, bacterial endocarditis, rheumatic heart disease, and atrial myxoma. There is, however, increasing controversy over the role of PFO as an etiology of stroke. Many investigators think its role has been overstated and is probably more of an incidental finding than a causal relationship.3 Patients with a suspected cardioembolic etiology will usually require an echocardiogram (with saline contrast or a “bubble study” for suspected PFO), cardiac monitoring, and a possible Holter monitor at the time of discharge (to detect paroxysmal arrhythmias).
Following cardioembolic etiologies, arterial dissection is the next most common category.4 In one study of patients aged 31 to 45 years old, arterial dissection was the most common cause of ischemic stroke.4 Clinical features suggesting dissection include a history of head or neck trauma (even minor trauma), headache or neck pain, and local neurological findings (eg, cranial nerve palsy or Horner syndrome).3 Unfortunately, only about 25% of patients volunteer a history of recent neck trauma. If a cervical or vertebral artery dissection is suspected, contrast enhanced magnetic resonance angiography (MRA) is the most sensitive and specific test, followed by carotid ultrasound and CT angiography.3
Traditional risk factors for stroke include hypertension and diabetes mellitus (DM). This is not true for younger adults that experience an ischemic stroke. Cigarette smoking is a very important risk factor for cerebrovascular accident in young adults; in addition, the more one smokes, the greater the risk. Other risk factors in young adults include history of migraine headaches (especially migraine with aura), pregnancy and the postpartum period, and illicit drug use.3
The defense’s argument that there are many causes of stroke in young adults that would be inappropriate for treatment with tPA, such as a PFO, carotid dissection or bacterial endocarditis, is absolutely true. Young patients need to be aggressively worked up for the etiology of their stroke, and may require additional testing, such as an MRA, echocardiogram, or Holter monitoring to determine the underlying cause of their stroke.
Obstruction Following Gastric Bypass Surgery
A 47-year-old woman presented to the ED complaining of severe back and abdominal pain. Onset had been gradual and began approximately 4 hours prior to arrival. She described the pain as crampy and constant. The patient had vomited twice; she denied diarrhea and had a normal bowel movement the previous day. She denied any vaginal or urinary complaints. Her past medical history was significant for hypertension and status post gastric bypass surgery 6 months prior. She had lost 42 pounds to date. She denied smoking or alcohol use.
The patient’s vital signs on physical examination were: blood pressure, 154/92 mm Hg; pulse, 106 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 99˚F. Oxygen saturation was 96% on room air. The patient’s lungs were clear to auscultation bilaterally. The heart was mildly tachycardic, with a regular rhythm and without murmurs, rubs, or gallops. The abdominal examination revealed diffuse tenderness and involuntary guarding. There was no distention or rebound. Bowel sounds were present but hypoactive. Examination of the back revealed bilateral paraspinal muscle tenderness without costovertebral angle tenderness.
The EP ordered a CBC, BMP, serum lipase, and a urinalysis. The patient was given an intravenous (IV) bolus of 250 cc normal saline in addition to IV morphine 4 mg and IV ondansetron 4 mg. Her white blood cell (WBC) count was slightly elevated at 12.2 g/dL, with a normal differential. The remainder of the laboratory studies were normal, except for a serum bicarbonate of 22 mmol/L.
The patient stated she felt somewhat improved, but continued to have abdominal and back pain. The EP admitted her to the hospital for observation and pain control. She died the following day from a bowel obstruction. The family sued the EP for negligence in failing to order appropriate testing and for not consulting with specialists to diagnose the bowel obstruction, which is a known complication of gastric bypass surgery. The jury returned a verdict of $2.4 million against the EP.
Discussion
The frequency of bariatric surgery in the United States continues to increase, primarily due to its success with regard to weight loss, but also because of its demonstrated improvement in hypertension, obstructive sleep apnea, hyperlipidemia, and type 2 DM.1
Frequently, the term “gastric bypass surgery” is used interchangeably with bariatric surgery. However, the EP must realize these terms encompass multiple different operations. The four most common types of bariatric surgery in the United Stated are (1) adjustable gastric banding (AGB); (2) the Roux-en-Y gastric bypass (RYGB); (3) biliopancreatic diversion with duodenal switch (BPD-DS); and (4) vertical sleeve gastrectomy (VSG).2 (See the Table for a brief explanation of each type of procedure.)
Since each procedure has its own respective associated complications, it is important for the EP to know which the type of gastric bypass surgery the patient had. For example, leakage is much more frequent following RYGB than in gastric banding, while slippage and obstruction are the most common complications of gastric banding.3,4 It is also very helpful to know the specific type of procedure when discussing the case with the surgical consultant.
Based on a recent review of over 800,000 bariatric surgery patients, seven serious common complications following the surgery were identified.3 These included bleeding, leakage, obstruction, stomal ulceration, pulmonary embolism and respiratory complications, blood sugar disturbances (usually hypoglycemia and/or metabolic acidosis), and nutritional disturbances. While not all-inclusive, this list represents the most common serious complications of gastric bypass surgery.
The complaint of abdominal pain in a patient that has undergone bariatric surgery should be taken very seriously. In addition to determining the specific procedure performed and date, the patient should be questioned about vomiting, bowel movements, and the presence of blood in stool or vomit. Depending upon the degree of pain present, the patient may need to be given IV opioid analgesia to facilitate a thorough abdominal examination. A rectal examination should be performed to identify occult gastrointestinal bleeding.
These patients require laboratory testing, including CBC, BMP, and other laboratory evaluation as indicated by the history and physical examination. Early consultation with the bariatric surgeon is recommended. Many, if not most, patients with abdominal pain and vomiting will require imaging, usually a CT scan with contrast of the abdomen and pelvis. Because of the difficulty in interpreting the CT scan results in these patients, the bariatric surgeon will often want to personally review the films rather than rely solely on the interpretation by radiology services.
Unfortunately, the EP in this case did not appreciate the seriousness of the situation. The presence of severe abdominal pain, tenderness, guarding, mild tachycardia with leukocytosis, and metabolic acidosis all pointed to a more serious etiology than muscle spasm. This patient required IV fluids, analgesia, and imaging, as well as consultation with the bariatric surgeon.
Stroke in a Young Man
A 26-year-old man presented to the ED with the chief complaint of mild right-sided weakness, paresthesias, and slurred speech. He stated the onset was sudden—approximately 30 minutes prior to arrival to the ED. The patient denied any previous similar symptoms and was otherwise in good health; he denied taking any medications. He drank alcohol socially, but denied smoking or illicit drug use.
On physical examination, his vital signs and oxygen saturation were normal. Pulmonary, cardiovascular, and abdominal examinations were also normal. The patient thought his speech was somewhat slurred, but the triage nurse and treating emergency physician (EP) had difficulty detecting any altered speech. He was noted to have mild (4+/5) right upper and lower extremity weakness; no facial droop was detected. The patient did have a mild pronator drift of the right upper extremity. Gait testing revealed a mild limp of the right lower extremity.
The EP consulted the hospitalist, and the patient was admitted to a monitored bed. The following morning, a brain magnetic resonance image revealed an ischemic stroke in the distribution of the left middle cerebral artery. The patient’s hospital course was uncomplicated, but at the time of discharge, he continued to have mild right-sided weakness and required the use of a cane.
The patient sued the hospital and the EP for negligence in failing to treat his condition in a timely manner and for not consulting a neurologist. The plaintiff’s attorneys argued the patient should have been given tissue plasminogen activator (tPA), which would have avoided the residual right-sided weakness. The defense denied negligence and argued the patient’s symptoms could have been due to several things for which tPA would have been an inappropriate treatment. A defense verdict was returned.
Discussion
Stroke in young patients is relatively rare. With “young” defined as aged 18 to 45 years, this population accounts for approximately 2% to 12% of cerebral infarcts.1 In one nationwide US study of stroke in young adults, Ellis2 found that 4.9% of individuals experiencing a stroke in 2007 were between ages 18 and 44 years. Among this group, 78% experienced an ischemic stroke; 11.2% experienced a subarachnoid hemorrhage (SAH); and 10.8% had an intracerebral hemorrhage.2
While the clinical presentation of stroke in young adults is similar to that of older patients, the etiologies and risk factors are very different. In older patients, atherosclerosis is the major cause of ischemic stroke. In studies of young adults with ischemic stroke, cardioembolism was found to be the leading cause. Under this category, a patent foramen ovale (PFO) was considered a common cause, followed by atrial fibrillation, bacterial endocarditis, rheumatic heart disease, and atrial myxoma. There is, however, increasing controversy over the role of PFO as an etiology of stroke. Many investigators think its role has been overstated and is probably more of an incidental finding than a causal relationship.3 Patients with a suspected cardioembolic etiology will usually require an echocardiogram (with saline contrast or a “bubble study” for suspected PFO), cardiac monitoring, and a possible Holter monitor at the time of discharge (to detect paroxysmal arrhythmias).
Following cardioembolic etiologies, arterial dissection is the next most common category.4 In one study of patients aged 31 to 45 years old, arterial dissection was the most common cause of ischemic stroke.4 Clinical features suggesting dissection include a history of head or neck trauma (even minor trauma), headache or neck pain, and local neurological findings (eg, cranial nerve palsy or Horner syndrome).3 Unfortunately, only about 25% of patients volunteer a history of recent neck trauma. If a cervical or vertebral artery dissection is suspected, contrast enhanced magnetic resonance angiography (MRA) is the most sensitive and specific test, followed by carotid ultrasound and CT angiography.3
Traditional risk factors for stroke include hypertension and diabetes mellitus (DM). This is not true for younger adults that experience an ischemic stroke. Cigarette smoking is a very important risk factor for cerebrovascular accident in young adults; in addition, the more one smokes, the greater the risk. Other risk factors in young adults include history of migraine headaches (especially migraine with aura), pregnancy and the postpartum period, and illicit drug use.3
The defense’s argument that there are many causes of stroke in young adults that would be inappropriate for treatment with tPA, such as a PFO, carotid dissection or bacterial endocarditis, is absolutely true. Young patients need to be aggressively worked up for the etiology of their stroke, and may require additional testing, such as an MRA, echocardiogram, or Holter monitoring to determine the underlying cause of their stroke.
Obstruction Following Gastric Bypass Surgery
A 47-year-old woman presented to the ED complaining of severe back and abdominal pain. Onset had been gradual and began approximately 4 hours prior to arrival. She described the pain as crampy and constant. The patient had vomited twice; she denied diarrhea and had a normal bowel movement the previous day. She denied any vaginal or urinary complaints. Her past medical history was significant for hypertension and status post gastric bypass surgery 6 months prior. She had lost 42 pounds to date. She denied smoking or alcohol use.
The patient’s vital signs on physical examination were: blood pressure, 154/92 mm Hg; pulse, 106 beats/minute; respiratory rate, 18 breaths/minute; and temperature, 99˚F. Oxygen saturation was 96% on room air. The patient’s lungs were clear to auscultation bilaterally. The heart was mildly tachycardic, with a regular rhythm and without murmurs, rubs, or gallops. The abdominal examination revealed diffuse tenderness and involuntary guarding. There was no distention or rebound. Bowel sounds were present but hypoactive. Examination of the back revealed bilateral paraspinal muscle tenderness without costovertebral angle tenderness.
The EP ordered a CBC, BMP, serum lipase, and a urinalysis. The patient was given an intravenous (IV) bolus of 250 cc normal saline in addition to IV morphine 4 mg and IV ondansetron 4 mg. Her white blood cell (WBC) count was slightly elevated at 12.2 g/dL, with a normal differential. The remainder of the laboratory studies were normal, except for a serum bicarbonate of 22 mmol/L.
The patient stated she felt somewhat improved, but continued to have abdominal and back pain. The EP admitted her to the hospital for observation and pain control. She died the following day from a bowel obstruction. The family sued the EP for negligence in failing to order appropriate testing and for not consulting with specialists to diagnose the bowel obstruction, which is a known complication of gastric bypass surgery. The jury returned a verdict of $2.4 million against the EP.
Discussion
The frequency of bariatric surgery in the United States continues to increase, primarily due to its success with regard to weight loss, but also because of its demonstrated improvement in hypertension, obstructive sleep apnea, hyperlipidemia, and type 2 DM.1
Frequently, the term “gastric bypass surgery” is used interchangeably with bariatric surgery. However, the EP must realize these terms encompass multiple different operations. The four most common types of bariatric surgery in the United Stated are (1) adjustable gastric banding (AGB); (2) the Roux-en-Y gastric bypass (RYGB); (3) biliopancreatic diversion with duodenal switch (BPD-DS); and (4) vertical sleeve gastrectomy (VSG).2 (See the Table for a brief explanation of each type of procedure.)
Since each procedure has its own respective associated complications, it is important for the EP to know which the type of gastric bypass surgery the patient had. For example, leakage is much more frequent following RYGB than in gastric banding, while slippage and obstruction are the most common complications of gastric banding.3,4 It is also very helpful to know the specific type of procedure when discussing the case with the surgical consultant.
Based on a recent review of over 800,000 bariatric surgery patients, seven serious common complications following the surgery were identified.3 These included bleeding, leakage, obstruction, stomal ulceration, pulmonary embolism and respiratory complications, blood sugar disturbances (usually hypoglycemia and/or metabolic acidosis), and nutritional disturbances. While not all-inclusive, this list represents the most common serious complications of gastric bypass surgery.
The complaint of abdominal pain in a patient that has undergone bariatric surgery should be taken very seriously. In addition to determining the specific procedure performed and date, the patient should be questioned about vomiting, bowel movements, and the presence of blood in stool or vomit. Depending upon the degree of pain present, the patient may need to be given IV opioid analgesia to facilitate a thorough abdominal examination. A rectal examination should be performed to identify occult gastrointestinal bleeding.
These patients require laboratory testing, including CBC, BMP, and other laboratory evaluation as indicated by the history and physical examination. Early consultation with the bariatric surgeon is recommended. Many, if not most, patients with abdominal pain and vomiting will require imaging, usually a CT scan with contrast of the abdomen and pelvis. Because of the difficulty in interpreting the CT scan results in these patients, the bariatric surgeon will often want to personally review the films rather than rely solely on the interpretation by radiology services.
Unfortunately, the EP in this case did not appreciate the seriousness of the situation. The presence of severe abdominal pain, tenderness, guarding, mild tachycardia with leukocytosis, and metabolic acidosis all pointed to a more serious etiology than muscle spasm. This patient required IV fluids, analgesia, and imaging, as well as consultation with the bariatric surgeon.
- Chatzikonstantinou A, Wolf ME, Hennerici MG. Ischemic stroke in young adults: classification and risk factors. J Neurol. 2012;259(4):653-659.
- Ellis C. Stroke in young adults. Disabil Health J. 2010;3(3):222-224.
- Ferro JM, Massaro AR, Mas JL. Aetiological diagnosis of ischemic stroke in young adults. Lancet Neurol. 2010;9(11):1085-1096.
- Chan MT, Nadareishvili ZG, Norris JW; Canadian Stroke Consortium. Diagnostic strategies in young patients with ischemic stroke in Canada. Can J Neurol Sci. 2000;27(2):120-124.
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724-1737.
- Livingston EH. Patient guide: Endocrine and nutritional management after bariatric surgery: A patient’s guide. Hormone Health Network Web site. http://www.hormone.org/~/media/Hormone/Files/Patient%20Guides/Mens%20Health/PGBariatricSurgery_2014.pdf. Accessed December 17, 2014.
- Hussain A, El-Hasani S. Bariatric emergencies: current evidence and strategies of management. World J Emerg Surg. 2013;8(1):58.
- Campanille FC, Boru C, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg. 2013;398(5):669-686
- Chatzikonstantinou A, Wolf ME, Hennerici MG. Ischemic stroke in young adults: classification and risk factors. J Neurol. 2012;259(4):653-659.
- Ellis C. Stroke in young adults. Disabil Health J. 2010;3(3):222-224.
- Ferro JM, Massaro AR, Mas JL. Aetiological diagnosis of ischemic stroke in young adults. Lancet Neurol. 2010;9(11):1085-1096.
- Chan MT, Nadareishvili ZG, Norris JW; Canadian Stroke Consortium. Diagnostic strategies in young patients with ischemic stroke in Canada. Can J Neurol Sci. 2000;27(2):120-124.
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724-1737.
- Livingston EH. Patient guide: Endocrine and nutritional management after bariatric surgery: A patient’s guide. Hormone Health Network Web site. http://www.hormone.org/~/media/Hormone/Files/Patient%20Guides/Mens%20Health/PGBariatricSurgery_2014.pdf. Accessed December 17, 2014.
- Hussain A, El-Hasani S. Bariatric emergencies: current evidence and strategies of management. World J Emerg Surg. 2013;8(1):58.
- Campanille FC, Boru C, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg. 2013;398(5):669-686
Feds release quality data on diabetes, heart disease, infections
Medicare officials have released a slew of new data demonstrating physicians’ and hospitals’ performance on quality measures related to diabetes, cardiovascular care, and hospital-acquired infections and injuries.
The quality data were posted on Medicare’s Physician Compare and Hospital Compare websites, which aim to provide consumers with the information they need to help them select physicians and other health care providers. The information is also available on data.medicare.gov.
“The Compare sites empower consumers with information to help with health care decisions, encourage providers to strive for higher levels of quality, drive overall health system improvement,” Dr. Patrick Conway, chief medical officer and deputy administrator for innovation and quality at the Center for Medicare & Medicaid Services, wrote in a blog post.

For physicians, CMS is posting four measures related to diabetes and heart disease: controlling hemoglobin A1c (less than 8%); controlling blood pressure; prescribing aspirin to patients with diabetes and ischemic vascular disease; and prescribing ACE inhibitors or angiotensin receptor blockers for patients with coronary artery disease and diabetes or left ventricular systolic dysfunction.
The data come from 139 physician group practices, 214 shared savings program accountable care organizations, and 23 Pioneer ACOs.
To make the data more user-friendly, CMS uses stars, followed by a percentage score, to show group performance on individual measures. For instance, if a practice scored 80% on a measure, four stars would be shown along with the 80% score.
This is the second time that CMS officials have added quality data to Physician Compare – the first posting was in February 2014. CMS plans to expand the number of quality measures and the number of providers who are listed on the website. By late 2015, CMS plans to post quality data for group practices of all sizes and some data on individual physicians.
For hospitals, CMS posted performance on reducing hospital-acquired conditions, including central line–associated bloodstream infections, catheter-associated urinary tract infections, pressure ulcers, and accidental punctures and lacerations.
The agency also added data from its Hospital Readmissions Reduction Program, including 30-day readmission rates following elective and primary total hip and/or total knee replacement and the 30-day rate of unplanned readmission for chronic obstructive pulmonary disease.
CMS also released data on payment adjustments made as part of the 2015 Hospital Value-Based Purchasing Program, which ties payment to performance on certain quality measures. In fiscal year 2015 – the third year of the program – 1,714 hospitals will see their payments go up as a result of bonus payments from the program, compared with 1,375 that will see their payments decline, according to CMS.
On Twitter @maryellenny
Medicare officials have released a slew of new data demonstrating physicians’ and hospitals’ performance on quality measures related to diabetes, cardiovascular care, and hospital-acquired infections and injuries.
The quality data were posted on Medicare’s Physician Compare and Hospital Compare websites, which aim to provide consumers with the information they need to help them select physicians and other health care providers. The information is also available on data.medicare.gov.
“The Compare sites empower consumers with information to help with health care decisions, encourage providers to strive for higher levels of quality, drive overall health system improvement,” Dr. Patrick Conway, chief medical officer and deputy administrator for innovation and quality at the Center for Medicare & Medicaid Services, wrote in a blog post.
For physicians, CMS is posting four measures related to diabetes and heart disease: controlling hemoglobin A1c (less than 8%); controlling blood pressure; prescribing aspirin to patients with diabetes and ischemic vascular disease; and prescribing ACE inhibitors or angiotensin receptor blockers for patients with coronary artery disease and diabetes or left ventricular systolic dysfunction.
The data come from 139 physician group practices, 214 shared savings program accountable care organizations, and 23 Pioneer ACOs.
To make the data more user-friendly, CMS uses stars, followed by a percentage score, to show group performance on individual measures. For instance, if a practice scored 80% on a measure, four stars would be shown along with the 80% score.
This is the second time that CMS officials have added quality data to Physician Compare – the first posting was in February 2014. CMS plans to expand the number of quality measures and the number of providers who are listed on the website. By late 2015, CMS plans to post quality data for group practices of all sizes and some data on individual physicians.
For hospitals, CMS posted performance on reducing hospital-acquired conditions, including central line–associated bloodstream infections, catheter-associated urinary tract infections, pressure ulcers, and accidental punctures and lacerations.
The agency also added data from its Hospital Readmissions Reduction Program, including 30-day readmission rates following elective and primary total hip and/or total knee replacement and the 30-day rate of unplanned readmission for chronic obstructive pulmonary disease.
CMS also released data on payment adjustments made as part of the 2015 Hospital Value-Based Purchasing Program, which ties payment to performance on certain quality measures. In fiscal year 2015 – the third year of the program – 1,714 hospitals will see their payments go up as a result of bonus payments from the program, compared with 1,375 that will see their payments decline, according to CMS.
On Twitter @maryellenny
Medicare officials have released a slew of new data demonstrating physicians’ and hospitals’ performance on quality measures related to diabetes, cardiovascular care, and hospital-acquired infections and injuries.
The quality data were posted on Medicare’s Physician Compare and Hospital Compare websites, which aim to provide consumers with the information they need to help them select physicians and other health care providers. The information is also available on data.medicare.gov.
“The Compare sites empower consumers with information to help with health care decisions, encourage providers to strive for higher levels of quality, drive overall health system improvement,” Dr. Patrick Conway, chief medical officer and deputy administrator for innovation and quality at the Center for Medicare & Medicaid Services, wrote in a blog post.
For physicians, CMS is posting four measures related to diabetes and heart disease: controlling hemoglobin A1c (less than 8%); controlling blood pressure; prescribing aspirin to patients with diabetes and ischemic vascular disease; and prescribing ACE inhibitors or angiotensin receptor blockers for patients with coronary artery disease and diabetes or left ventricular systolic dysfunction.
The data come from 139 physician group practices, 214 shared savings program accountable care organizations, and 23 Pioneer ACOs.
To make the data more user-friendly, CMS uses stars, followed by a percentage score, to show group performance on individual measures. For instance, if a practice scored 80% on a measure, four stars would be shown along with the 80% score.
This is the second time that CMS officials have added quality data to Physician Compare – the first posting was in February 2014. CMS plans to expand the number of quality measures and the number of providers who are listed on the website. By late 2015, CMS plans to post quality data for group practices of all sizes and some data on individual physicians.
For hospitals, CMS posted performance on reducing hospital-acquired conditions, including central line–associated bloodstream infections, catheter-associated urinary tract infections, pressure ulcers, and accidental punctures and lacerations.
The agency also added data from its Hospital Readmissions Reduction Program, including 30-day readmission rates following elective and primary total hip and/or total knee replacement and the 30-day rate of unplanned readmission for chronic obstructive pulmonary disease.
CMS also released data on payment adjustments made as part of the 2015 Hospital Value-Based Purchasing Program, which ties payment to performance on certain quality measures. In fiscal year 2015 – the third year of the program – 1,714 hospitals will see their payments go up as a result of bonus payments from the program, compared with 1,375 that will see their payments decline, according to CMS.
On Twitter @maryellenny

Survey: Med students disdain private practice
Almost three-quarters of medical students are aiming for future employment in a large health system or hospital, while just 10% want to work in a solo or partnership practice, according to a survey from Epocrates.
Last year, the numbers were 70% and 17%, respectively.
One cause: Students are not being trained in the business of medicine, said Dr. Anne Meneghetti, executive director of medical information at Epocrates.

“More than half of them are dissatisfied with the training they received in med school on practice management and ownership,” Dr. Meneghetti said in an interview. “The majority feel unprepared to do the billing and coding and other administrative practice functions in this highly regulated environment.”
That finding also plays into another concern future physicians have – work-life balance. A total of 60% of the survey respondents cited that as top concern, moving ahead of being a good physician, which was identified by 50%. In 2013, being a good physician was identified at the top concern by 55% of those surveyed, with work-life balance coming in at 51%.
“Given the choice between a reasonable lifestyle in a large organization versus the hassles of business ownership in this highly regulated field, the choice is really easy for most of them,” Dr. Meneghetti said. “There’s a lot more security and predictability in these larger enterprise settings.”
Nearly all students surveyed “feel it is important to work with extended care teams (which can include registered nurses, physician assistants, specialists, and medical staff)” in order to deliver high quality care and ensure financial success as a physician, according to the report. Two-thirds (66%) said they “feel they are being prepared to tackle the task of care coordination, while 20% feel their training is merely adequate.”
“Younger physicians seem to instinctively know what the entire medical community is realizing – that medicine is a team experience,” Dr. Meneghetti said.
Despite that, the survey found that 65% of medical students feel they don’t know enough about accountable care organizations, down from 72% in the previous year, with 39% unsure about the purpose or structure of ACOs.
The Ninth Future Physicians of America survey report represents the responses of 1,462 medical students surveyed between late August and early September.
Almost three-quarters of medical students are aiming for future employment in a large health system or hospital, while just 10% want to work in a solo or partnership practice, according to a survey from Epocrates.
Last year, the numbers were 70% and 17%, respectively.
One cause: Students are not being trained in the business of medicine, said Dr. Anne Meneghetti, executive director of medical information at Epocrates.
“More than half of them are dissatisfied with the training they received in med school on practice management and ownership,” Dr. Meneghetti said in an interview. “The majority feel unprepared to do the billing and coding and other administrative practice functions in this highly regulated environment.”
That finding also plays into another concern future physicians have – work-life balance. A total of 60% of the survey respondents cited that as top concern, moving ahead of being a good physician, which was identified by 50%. In 2013, being a good physician was identified at the top concern by 55% of those surveyed, with work-life balance coming in at 51%.
“Given the choice between a reasonable lifestyle in a large organization versus the hassles of business ownership in this highly regulated field, the choice is really easy for most of them,” Dr. Meneghetti said. “There’s a lot more security and predictability in these larger enterprise settings.”
Nearly all students surveyed “feel it is important to work with extended care teams (which can include registered nurses, physician assistants, specialists, and medical staff)” in order to deliver high quality care and ensure financial success as a physician, according to the report. Two-thirds (66%) said they “feel they are being prepared to tackle the task of care coordination, while 20% feel their training is merely adequate.”
“Younger physicians seem to instinctively know what the entire medical community is realizing – that medicine is a team experience,” Dr. Meneghetti said.
Despite that, the survey found that 65% of medical students feel they don’t know enough about accountable care organizations, down from 72% in the previous year, with 39% unsure about the purpose or structure of ACOs.
The Ninth Future Physicians of America survey report represents the responses of 1,462 medical students surveyed between late August and early September.
Almost three-quarters of medical students are aiming for future employment in a large health system or hospital, while just 10% want to work in a solo or partnership practice, according to a survey from Epocrates.
Last year, the numbers were 70% and 17%, respectively.
One cause: Students are not being trained in the business of medicine, said Dr. Anne Meneghetti, executive director of medical information at Epocrates.
“More than half of them are dissatisfied with the training they received in med school on practice management and ownership,” Dr. Meneghetti said in an interview. “The majority feel unprepared to do the billing and coding and other administrative practice functions in this highly regulated environment.”
That finding also plays into another concern future physicians have – work-life balance. A total of 60% of the survey respondents cited that as top concern, moving ahead of being a good physician, which was identified by 50%. In 2013, being a good physician was identified at the top concern by 55% of those surveyed, with work-life balance coming in at 51%.
“Given the choice between a reasonable lifestyle in a large organization versus the hassles of business ownership in this highly regulated field, the choice is really easy for most of them,” Dr. Meneghetti said. “There’s a lot more security and predictability in these larger enterprise settings.”
Nearly all students surveyed “feel it is important to work with extended care teams (which can include registered nurses, physician assistants, specialists, and medical staff)” in order to deliver high quality care and ensure financial success as a physician, according to the report. Two-thirds (66%) said they “feel they are being prepared to tackle the task of care coordination, while 20% feel their training is merely adequate.”
“Younger physicians seem to instinctively know what the entire medical community is realizing – that medicine is a team experience,” Dr. Meneghetti said.
Despite that, the survey found that 65% of medical students feel they don’t know enough about accountable care organizations, down from 72% in the previous year, with 39% unsure about the purpose or structure of ACOs.
The Ninth Future Physicians of America survey report represents the responses of 1,462 medical students surveyed between late August and early September.
