User login
Administration reports ACA enrollment at over 7 million
Just over 7 million Americans signed up for private health insurance plans through federal and state insurance marketplaces during the Affordable Care Act’s first open enrollment period, according to preliminary figures released by the White House April 1.
The number is a bit of a surprise since only 4.2 million individuals had signed up for health plans as of March 1. A last minute surge helped the administration meet enrollment projections that were made before the technical glitches plagued the start of healthcare.gov in October and November.
Complete enrollment numbers, as well information on how many people have actually paid their premiums, will not be available for a few more weeks, administration officials said.
In the meantime, President Obama pointed to the enrollment number as proof that the health care law is working. And he blasted opponents who have spent the last several months trying to repeal or undermine the law.
"I will always work with anyone who is willing to make this law work even better," President Obama said from the Rose Garden. "But the debate over repealing this law is over. The Affordable Care Act is here to stay."
On Twitter @maryellenny
Just over 7 million Americans signed up for private health insurance plans through federal and state insurance marketplaces during the Affordable Care Act’s first open enrollment period, according to preliminary figures released by the White House April 1.
The number is a bit of a surprise since only 4.2 million individuals had signed up for health plans as of March 1. A last minute surge helped the administration meet enrollment projections that were made before the technical glitches plagued the start of healthcare.gov in October and November.
Complete enrollment numbers, as well information on how many people have actually paid their premiums, will not be available for a few more weeks, administration officials said.
In the meantime, President Obama pointed to the enrollment number as proof that the health care law is working. And he blasted opponents who have spent the last several months trying to repeal or undermine the law.
"I will always work with anyone who is willing to make this law work even better," President Obama said from the Rose Garden. "But the debate over repealing this law is over. The Affordable Care Act is here to stay."
On Twitter @maryellenny
Just over 7 million Americans signed up for private health insurance plans through federal and state insurance marketplaces during the Affordable Care Act’s first open enrollment period, according to preliminary figures released by the White House April 1.
The number is a bit of a surprise since only 4.2 million individuals had signed up for health plans as of March 1. A last minute surge helped the administration meet enrollment projections that were made before the technical glitches plagued the start of healthcare.gov in October and November.
Complete enrollment numbers, as well information on how many people have actually paid their premiums, will not be available for a few more weeks, administration officials said.
In the meantime, President Obama pointed to the enrollment number as proof that the health care law is working. And he blasted opponents who have spent the last several months trying to repeal or undermine the law.
"I will always work with anyone who is willing to make this law work even better," President Obama said from the Rose Garden. "But the debate over repealing this law is over. The Affordable Care Act is here to stay."
On Twitter @maryellenny
Hospital Medicine Group Leaders Need Not Work Clinical Shifts to Achieve Respect
Hospitalist Group Leaders Need Not Work Clinical Shifts to Achieve Respect
The “Survey Insights” article by Dr. Rachel Lovins (“Physician Practice Leaders,” November 2013) makes excellent points about the importance of leadership in hospital medicine groups but perpetuates a fallacy that undercuts the effectiveness of physician leaders. Dr. Lovins states that hospitalist leaders need to work as clinical hospitalists to achieve respect. Consider the example of professional sports, where athletes are highly skilled and earn more than doctors, but the concept of a player/coach has essentially disappeared. The difference is that athletes understand that they are playing on a team that needs a cohesive vision to succeed. They value the insights of a coach who can watch their performance from the sidelines and help them improve, even though that person’s own playing skills may have been undistinguished.
Dr. Lovins states that hospitalist leaders need to experience firsthand the frustrations of hospital practice. Would it not be better to replace anecdotal evidence with systematic communication and analysis of experiences from the entire group? The demand by physicians that their leaders be active clinicians is really a way to ensure that those individuals are unable to secure the time and perspective needed to become effective coaches, and it encroaches upon the autonomy of the individuals.
HM cannot achieve its potential until it develops leaders who can move beyond the level of chief resident and engage meaningfully with the concerns of senior hospital leaders to drive the performance of their teams. Hospitalists must understand that they are part of an organization that will be led by persons with different skill sets than those required to diagnose and treat disease.
—Richard Rohr, MD, SFHM, team leader, United Health Group, Broomall, Pa.
Hospitalist Group Leaders Need Not Work Clinical Shifts to Achieve Respect
The “Survey Insights” article by Dr. Rachel Lovins (“Physician Practice Leaders,” November 2013) makes excellent points about the importance of leadership in hospital medicine groups but perpetuates a fallacy that undercuts the effectiveness of physician leaders. Dr. Lovins states that hospitalist leaders need to work as clinical hospitalists to achieve respect. Consider the example of professional sports, where athletes are highly skilled and earn more than doctors, but the concept of a player/coach has essentially disappeared. The difference is that athletes understand that they are playing on a team that needs a cohesive vision to succeed. They value the insights of a coach who can watch their performance from the sidelines and help them improve, even though that person’s own playing skills may have been undistinguished.
Dr. Lovins states that hospitalist leaders need to experience firsthand the frustrations of hospital practice. Would it not be better to replace anecdotal evidence with systematic communication and analysis of experiences from the entire group? The demand by physicians that their leaders be active clinicians is really a way to ensure that those individuals are unable to secure the time and perspective needed to become effective coaches, and it encroaches upon the autonomy of the individuals.
HM cannot achieve its potential until it develops leaders who can move beyond the level of chief resident and engage meaningfully with the concerns of senior hospital leaders to drive the performance of their teams. Hospitalists must understand that they are part of an organization that will be led by persons with different skill sets than those required to diagnose and treat disease.
—Richard Rohr, MD, SFHM, team leader, United Health Group, Broomall, Pa.
Hospitalist Group Leaders Need Not Work Clinical Shifts to Achieve Respect
The “Survey Insights” article by Dr. Rachel Lovins (“Physician Practice Leaders,” November 2013) makes excellent points about the importance of leadership in hospital medicine groups but perpetuates a fallacy that undercuts the effectiveness of physician leaders. Dr. Lovins states that hospitalist leaders need to work as clinical hospitalists to achieve respect. Consider the example of professional sports, where athletes are highly skilled and earn more than doctors, but the concept of a player/coach has essentially disappeared. The difference is that athletes understand that they are playing on a team that needs a cohesive vision to succeed. They value the insights of a coach who can watch their performance from the sidelines and help them improve, even though that person’s own playing skills may have been undistinguished.
Dr. Lovins states that hospitalist leaders need to experience firsthand the frustrations of hospital practice. Would it not be better to replace anecdotal evidence with systematic communication and analysis of experiences from the entire group? The demand by physicians that their leaders be active clinicians is really a way to ensure that those individuals are unable to secure the time and perspective needed to become effective coaches, and it encroaches upon the autonomy of the individuals.
HM cannot achieve its potential until it develops leaders who can move beyond the level of chief resident and engage meaningfully with the concerns of senior hospital leaders to drive the performance of their teams. Hospitalists must understand that they are part of an organization that will be led by persons with different skill sets than those required to diagnose and treat disease.
—Richard Rohr, MD, SFHM, team leader, United Health Group, Broomall, Pa.
Copper Considered Safe, Effective in Preventing Hospital-Acquired Infections
Concern about Copper’s Effectiveness in Preventing Hospital-Acquired Infections
As public knowledge about the benefits of antimicrobial copper touch surfaces in healthcare facilities continues to grow, questions about this tool naturally arise. Can this copper surface really continuously kill up to 83% of bacteria it comes in contact with? Can it really reduce patient infections by more than half? Can this metal really keep people safer? The answer is “yes,” as has been reported in the Journal of Infection Control, in Hospital Epidemiology, and in the Journal of Clinical Microbiology.
In his “Letter to the Editor (“Concern about Copper’s Effectiveness in Preventing Hospital-Acquired Infections,” November 2013), Dr. Rod Duraski voices cautions about human sensitivity to copper—noting that implanted copper-nickel alloy devices have the potential for severe allergic reactions; however, implanted devices are not part of the EPA-approved products list of antimicrobial copper and, therefore, are not being proposed for use in the fight against hospital infections. Although some patients might experience sensitivity to jewelry, zippers, or buttons, if made from nickel-containing copper alloys, these reactions will be the result of prolonged skin contact, and when removed, the sensitivity will dissipate. The touch-surface components proposed in Karen Appold’s story, “Copper,” (September 2013) come into very brief and intermittent contact with the skin. And, sensitivities are not life-threatening; hospital-acquired infections are.
In fact, three of the four major coin denominations (nickel, dime, quarter) are made from copper-nickel alloys. If these metals are suitable for the everyday exposure we all experience with coinage, they are just as safe when it comes to touch surface components in hospitals. In many instances, the benefits of copper outweigh the relative risk of a rash caused by nickel sensitivity.
Like any surface, copper alloys should be cleaned regularly—especially in hospitals. Copper alloys are compatible with all hospital grade cleaners and disinfectants when the cleaners are used according to manufacturer label instructions. But more importantly, the antimicrobial effect of this metal is not inhibited if the surfaces tarnish. In 2005, a study (www.antimicrobialcopper.com/media/69850/infectious_disease.pdf) found tarnish to be a non-issue when researchers tested the bacterial load on three separate copper alloys, all of which had developed tarnish over time. Additionally, manufacturers are offering components made from tarnish-resistant alloys.
—Harold Michels, PhD, senior vice president of technology and technical services, Copper Development Association, Inc.
Correction: April 4, 2014
A version of this article appeared in print in the April 2014 issue of The Hospitalist. Changes have since been made to the online article per the request of the author.
Concern about Copper’s Effectiveness in Preventing Hospital-Acquired Infections
As public knowledge about the benefits of antimicrobial copper touch surfaces in healthcare facilities continues to grow, questions about this tool naturally arise. Can this copper surface really continuously kill up to 83% of bacteria it comes in contact with? Can it really reduce patient infections by more than half? Can this metal really keep people safer? The answer is “yes,” as has been reported in the Journal of Infection Control, in Hospital Epidemiology, and in the Journal of Clinical Microbiology.
In his “Letter to the Editor (“Concern about Copper’s Effectiveness in Preventing Hospital-Acquired Infections,” November 2013), Dr. Rod Duraski voices cautions about human sensitivity to copper—noting that implanted copper-nickel alloy devices have the potential for severe allergic reactions; however, implanted devices are not part of the EPA-approved products list of antimicrobial copper and, therefore, are not being proposed for use in the fight against hospital infections. Although some patients might experience sensitivity to jewelry, zippers, or buttons, if made from nickel-containing copper alloys, these reactions will be the result of prolonged skin contact, and when removed, the sensitivity will dissipate. The touch-surface components proposed in Karen Appold’s story, “Copper,” (September 2013) come into very brief and intermittent contact with the skin. And, sensitivities are not life-threatening; hospital-acquired infections are.
In fact, three of the four major coin denominations (nickel, dime, quarter) are made from copper-nickel alloys. If these metals are suitable for the everyday exposure we all experience with coinage, they are just as safe when it comes to touch surface components in hospitals. In many instances, the benefits of copper outweigh the relative risk of a rash caused by nickel sensitivity.
Like any surface, copper alloys should be cleaned regularly—especially in hospitals. Copper alloys are compatible with all hospital grade cleaners and disinfectants when the cleaners are used according to manufacturer label instructions. But more importantly, the antimicrobial effect of this metal is not inhibited if the surfaces tarnish. In 2005, a study (www.antimicrobialcopper.com/media/69850/infectious_disease.pdf) found tarnish to be a non-issue when researchers tested the bacterial load on three separate copper alloys, all of which had developed tarnish over time. Additionally, manufacturers are offering components made from tarnish-resistant alloys.
—Harold Michels, PhD, senior vice president of technology and technical services, Copper Development Association, Inc.
Correction: April 4, 2014
A version of this article appeared in print in the April 2014 issue of The Hospitalist. Changes have since been made to the online article per the request of the author.
Concern about Copper’s Effectiveness in Preventing Hospital-Acquired Infections
As public knowledge about the benefits of antimicrobial copper touch surfaces in healthcare facilities continues to grow, questions about this tool naturally arise. Can this copper surface really continuously kill up to 83% of bacteria it comes in contact with? Can it really reduce patient infections by more than half? Can this metal really keep people safer? The answer is “yes,” as has been reported in the Journal of Infection Control, in Hospital Epidemiology, and in the Journal of Clinical Microbiology.
In his “Letter to the Editor (“Concern about Copper’s Effectiveness in Preventing Hospital-Acquired Infections,” November 2013), Dr. Rod Duraski voices cautions about human sensitivity to copper—noting that implanted copper-nickel alloy devices have the potential for severe allergic reactions; however, implanted devices are not part of the EPA-approved products list of antimicrobial copper and, therefore, are not being proposed for use in the fight against hospital infections. Although some patients might experience sensitivity to jewelry, zippers, or buttons, if made from nickel-containing copper alloys, these reactions will be the result of prolonged skin contact, and when removed, the sensitivity will dissipate. The touch-surface components proposed in Karen Appold’s story, “Copper,” (September 2013) come into very brief and intermittent contact with the skin. And, sensitivities are not life-threatening; hospital-acquired infections are.
In fact, three of the four major coin denominations (nickel, dime, quarter) are made from copper-nickel alloys. If these metals are suitable for the everyday exposure we all experience with coinage, they are just as safe when it comes to touch surface components in hospitals. In many instances, the benefits of copper outweigh the relative risk of a rash caused by nickel sensitivity.
Like any surface, copper alloys should be cleaned regularly—especially in hospitals. Copper alloys are compatible with all hospital grade cleaners and disinfectants when the cleaners are used according to manufacturer label instructions. But more importantly, the antimicrobial effect of this metal is not inhibited if the surfaces tarnish. In 2005, a study (www.antimicrobialcopper.com/media/69850/infectious_disease.pdf) found tarnish to be a non-issue when researchers tested the bacterial load on three separate copper alloys, all of which had developed tarnish over time. Additionally, manufacturers are offering components made from tarnish-resistant alloys.
—Harold Michels, PhD, senior vice president of technology and technical services, Copper Development Association, Inc.
Correction: April 4, 2014
A version of this article appeared in print in the April 2014 issue of The Hospitalist. Changes have since been made to the online article per the request of the author.
Delays, Controversy Muddle CMS’ Two-Midnight Rule for Hospital Patient Admissions
A new rule issued by the Centers for Medicare & Medicaid Services (CMS) is at the center of controversy fueled by competing interests and lack of clarity. And, for the fourth time since the two-midnight rule was introduced in the 2014 Hospital Inpatient Prospective Payment System, its implementation has been delayed. Hospitals and providers have until March 31, 2015, before auditors begin scrutinizing patient admission statuses for reimbursement determination.
The rule requires Medicare and Medicaid patients spending fewer than two midnights receiving hospital care to be classified as outpatient or under observation. Patients spending more than two midnights will be considered inpatient. Only physicians can make the determination, and the clock begins ticking the moment care begins.
The rule also cuts hospital inpatient reimbursement by 0.2%, because CMS believes the number of inpatient admissions will increase.

–Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association
The rule pits private Medicare auditors (Medicare Administrative Contractors, MACs, and Recovery Audit Contractors, RACs), who have a financial stake in denying inpatient claims, against hospitals and physicians. It does little to clear confusion for patients when it comes time for them to pay their bills.
Patients generally are unaware whether they’ve been admitted or are under observation. But observation status leaves them on the hook for any skilled nursing care they receive following discharge and for the costs of routine maintenance drugs hospitals give them for chronic conditions.
Beneficiaries also are not eligible for Medicare Part A skilled nursing care coverage if they were an inpatient for fewer than 72 hours, and observation days do not count toward the three-day requirement. The two-midnight rule adds another “layer” to the equation, says Bradley Flansbaum, DO, MPH, FACP, a hospitalist and clinical assistant professor of medicine at NYU School of Medicine in New York City.
At the same time, hospitals now face penalties for patients readmitted within 30 days of discharge for a similar episode of care. Observation status offers a measure of protection in the event patients return.
The number of observation patients increased 69% between 2006 and 2011, according to federal data cited by Kaiser Health News, and the number of observation patients staying more than 48 hours increased from 3% to 8% during this same period.
“The concern is that [the two-midnight rule] sets an arbitrary time threshold that dictates where a patient should be placed,” says Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association. The AHA opposes aspects of the rule and was involved in legislation to delay implementation.
“We feel time should not be the only factor taken into account,” Hiatt Kim adds. “It should be a decision a physician reaches based on a patient’s condition.”
Good Intentions
The rule states that hospital stays fewer than two midnights are generally medically inappropriate for inpatient designation. The services provided are not at issue, but CMS believes those administered during a short stay could be provided on a less expensive outpatient basis.
Dr. Flansbaum, a member of SHM’s Public Policy Committee, says the language of medical necessity that designates status is unclear, though CMS has given physicians the benefit of the doubt.
“We are looking for clear signals from providers for how we determine when someone is appropriately inpatient and when they’re observation,” he explains.
Although medical needs can be quantified, there are often other, nonmedical factors that put patients at risk and influence when and whether a patient is admitted. Physicians routinely weigh these factors on behalf of their patients.
“Risk isn’t necessarily implied by just a dangerous blood value,” Dr. Flansbaum says. “If something is not right in the transition zone or in the community, I think those [factors] need to be taken into account.”
Physicians are being given “a lot of latitude” in CMS’ new rule, he notes.
Clarification
In recent clarification, CMS highlighted exceptions to the rule. If “unforeseen circumstances” shorten the anticipated stay of someone initially deemed inpatient—transfer to another hospital, death, or clinical improvement in fewer than two midnights, for example—CMS can advise auditors to approve the inpatient claim.
Additionally, CMS will maintain a list of services considered “inpatient only,” regardless of stay duration.
But creating a list of every medically necessary service is an “administrative black hole,” says Dr. Flansbaum, though he believes that with enough time and clarity, compliance with the two-midnight rule is possible.
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
A new rule issued by the Centers for Medicare & Medicaid Services (CMS) is at the center of controversy fueled by competing interests and lack of clarity. And, for the fourth time since the two-midnight rule was introduced in the 2014 Hospital Inpatient Prospective Payment System, its implementation has been delayed. Hospitals and providers have until March 31, 2015, before auditors begin scrutinizing patient admission statuses for reimbursement determination.
The rule requires Medicare and Medicaid patients spending fewer than two midnights receiving hospital care to be classified as outpatient or under observation. Patients spending more than two midnights will be considered inpatient. Only physicians can make the determination, and the clock begins ticking the moment care begins.
The rule also cuts hospital inpatient reimbursement by 0.2%, because CMS believes the number of inpatient admissions will increase.
–Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association
The rule pits private Medicare auditors (Medicare Administrative Contractors, MACs, and Recovery Audit Contractors, RACs), who have a financial stake in denying inpatient claims, against hospitals and physicians. It does little to clear confusion for patients when it comes time for them to pay their bills.
Patients generally are unaware whether they’ve been admitted or are under observation. But observation status leaves them on the hook for any skilled nursing care they receive following discharge and for the costs of routine maintenance drugs hospitals give them for chronic conditions.
Beneficiaries also are not eligible for Medicare Part A skilled nursing care coverage if they were an inpatient for fewer than 72 hours, and observation days do not count toward the three-day requirement. The two-midnight rule adds another “layer” to the equation, says Bradley Flansbaum, DO, MPH, FACP, a hospitalist and clinical assistant professor of medicine at NYU School of Medicine in New York City.
At the same time, hospitals now face penalties for patients readmitted within 30 days of discharge for a similar episode of care. Observation status offers a measure of protection in the event patients return.
The number of observation patients increased 69% between 2006 and 2011, according to federal data cited by Kaiser Health News, and the number of observation patients staying more than 48 hours increased from 3% to 8% during this same period.
“The concern is that [the two-midnight rule] sets an arbitrary time threshold that dictates where a patient should be placed,” says Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association. The AHA opposes aspects of the rule and was involved in legislation to delay implementation.
“We feel time should not be the only factor taken into account,” Hiatt Kim adds. “It should be a decision a physician reaches based on a patient’s condition.”
Good Intentions
The rule states that hospital stays fewer than two midnights are generally medically inappropriate for inpatient designation. The services provided are not at issue, but CMS believes those administered during a short stay could be provided on a less expensive outpatient basis.
Dr. Flansbaum, a member of SHM’s Public Policy Committee, says the language of medical necessity that designates status is unclear, though CMS has given physicians the benefit of the doubt.
“We are looking for clear signals from providers for how we determine when someone is appropriately inpatient and when they’re observation,” he explains.
Although medical needs can be quantified, there are often other, nonmedical factors that put patients at risk and influence when and whether a patient is admitted. Physicians routinely weigh these factors on behalf of their patients.
“Risk isn’t necessarily implied by just a dangerous blood value,” Dr. Flansbaum says. “If something is not right in the transition zone or in the community, I think those [factors] need to be taken into account.”
Physicians are being given “a lot of latitude” in CMS’ new rule, he notes.
Clarification
In recent clarification, CMS highlighted exceptions to the rule. If “unforeseen circumstances” shorten the anticipated stay of someone initially deemed inpatient—transfer to another hospital, death, or clinical improvement in fewer than two midnights, for example—CMS can advise auditors to approve the inpatient claim.
Additionally, CMS will maintain a list of services considered “inpatient only,” regardless of stay duration.
But creating a list of every medically necessary service is an “administrative black hole,” says Dr. Flansbaum, though he believes that with enough time and clarity, compliance with the two-midnight rule is possible.
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
A new rule issued by the Centers for Medicare & Medicaid Services (CMS) is at the center of controversy fueled by competing interests and lack of clarity. And, for the fourth time since the two-midnight rule was introduced in the 2014 Hospital Inpatient Prospective Payment System, its implementation has been delayed. Hospitals and providers have until March 31, 2015, before auditors begin scrutinizing patient admission statuses for reimbursement determination.
The rule requires Medicare and Medicaid patients spending fewer than two midnights receiving hospital care to be classified as outpatient or under observation. Patients spending more than two midnights will be considered inpatient. Only physicians can make the determination, and the clock begins ticking the moment care begins.
The rule also cuts hospital inpatient reimbursement by 0.2%, because CMS believes the number of inpatient admissions will increase.
–Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association
The rule pits private Medicare auditors (Medicare Administrative Contractors, MACs, and Recovery Audit Contractors, RACs), who have a financial stake in denying inpatient claims, against hospitals and physicians. It does little to clear confusion for patients when it comes time for them to pay their bills.
Patients generally are unaware whether they’ve been admitted or are under observation. But observation status leaves them on the hook for any skilled nursing care they receive following discharge and for the costs of routine maintenance drugs hospitals give them for chronic conditions.
Beneficiaries also are not eligible for Medicare Part A skilled nursing care coverage if they were an inpatient for fewer than 72 hours, and observation days do not count toward the three-day requirement. The two-midnight rule adds another “layer” to the equation, says Bradley Flansbaum, DO, MPH, FACP, a hospitalist and clinical assistant professor of medicine at NYU School of Medicine in New York City.
At the same time, hospitals now face penalties for patients readmitted within 30 days of discharge for a similar episode of care. Observation status offers a measure of protection in the event patients return.
The number of observation patients increased 69% between 2006 and 2011, according to federal data cited by Kaiser Health News, and the number of observation patients staying more than 48 hours increased from 3% to 8% during this same period.
“The concern is that [the two-midnight rule] sets an arbitrary time threshold that dictates where a patient should be placed,” says Joanna Hiatt Kim, vice president of payment policy for the American Hospital Association. The AHA opposes aspects of the rule and was involved in legislation to delay implementation.
“We feel time should not be the only factor taken into account,” Hiatt Kim adds. “It should be a decision a physician reaches based on a patient’s condition.”
Good Intentions
The rule states that hospital stays fewer than two midnights are generally medically inappropriate for inpatient designation. The services provided are not at issue, but CMS believes those administered during a short stay could be provided on a less expensive outpatient basis.
Dr. Flansbaum, a member of SHM’s Public Policy Committee, says the language of medical necessity that designates status is unclear, though CMS has given physicians the benefit of the doubt.
“We are looking for clear signals from providers for how we determine when someone is appropriately inpatient and when they’re observation,” he explains.
Although medical needs can be quantified, there are often other, nonmedical factors that put patients at risk and influence when and whether a patient is admitted. Physicians routinely weigh these factors on behalf of their patients.
“Risk isn’t necessarily implied by just a dangerous blood value,” Dr. Flansbaum says. “If something is not right in the transition zone or in the community, I think those [factors] need to be taken into account.”
Physicians are being given “a lot of latitude” in CMS’ new rule, he notes.
Clarification
In recent clarification, CMS highlighted exceptions to the rule. If “unforeseen circumstances” shorten the anticipated stay of someone initially deemed inpatient—transfer to another hospital, death, or clinical improvement in fewer than two midnights, for example—CMS can advise auditors to approve the inpatient claim.
Additionally, CMS will maintain a list of services considered “inpatient only,” regardless of stay duration.
But creating a list of every medically necessary service is an “administrative black hole,” says Dr. Flansbaum, though he believes that with enough time and clarity, compliance with the two-midnight rule is possible.
Kelly April Tyrrell is a freelance writer in Wilmington, Del.
Hospitalists’ Skill Sets, Work Experience Perfect for Hospitals' C-Suite Positions
Steve Narang, MD, a pediatrician, hospitalist, and the then-CMO at Banner Health’s Cardon Children’s Medical Center in Phoenix, was attending a leadership summit where all of Banner’s top officials were gathered. It was his third day in his new job.
Banner’s President, Peter Fine, gave a presentation in the future of healthcare and asked for questions. Dr. Narang stepped up to the microphone, asked a question, and made remarks about how the organization needed to ready itself for the changing landscape. Kathy Bollinger, president of the Arizona West Region of Banner, was struck by those remarks. Less than two years later, she made Dr. Narang the CEO at Arizona’s largest teaching hospital, Good Samaritan Medical Center.
His hospitalist background was an important ingredient in the kind of leader Dr. Narang has become, she says.
“The correlation is that hospitalists are leading teams; they are quarterbacking care,” Bollinger adds. “A good hospitalist brings the team together.”
Physicians with a background in hospital medicine are no strangers to C-suite level positions at hospitals. In April, Brian Harte, MD, SFHM, was named president of South Pointe Hospital in Warrenville Heights, Ohio, a center within the Cleveland Clinic system. In January, Patrick Cawley, MD, MBA, MHM, a former SHM president, was named CEO at the Medical University of South Carolina Medical Center in Charleston.
Other recent C-suite arrivals include Nasim Afsar, MD, SFHM, an SHM board member who is associate CMO at UCLA Hospitals in Los Angeles, and Patrick Torcson, MD, MMM, FACP, SFHM, another SHM board member, vice president, and chief integration officer at St. Tammany Parish Hospital in Covington, La.
Although their paths to the C-suite have differed, each agrees that their experience in hospital medicine gave them the knowledge of the system that was required to begin an ascent to the highest levels of leadership. Just as important, or maybe more so, their exposure to the inner workings of a hospital awakened within them a desire to see the system function better. And the necessity of working with all types of healthcare providers within the complicated hospital setting helped them recognize—or at least get others to recognize—their potential for leadership, and helped hone the teamwork skills that are vital in top administrative roles.
They also say that, when they were starting out, they never aspired to high leadership positions. Rather, it was simply following their own interests that ultimately led them there.
By the time Dr. Narang stepped up to the microphone that day in Phoenix, he had more than a dozen years under his belt working as a hospitalist for a children’s hospital and as part of a group that created a pediatric hospitalist company in Louisiana.
And that work helped lay the foundation for him, he says.
“Being a hospitalist was a key strength of my background,” Dr. Narang explains. “Hospitalists are so well-positioned…to get truly at the intersection of operations and find value in a complex puzzle. Hospitalists are able to do that.
“At the end of the day, it’s about leadership. And I learned that from day one as a hospitalist.”
His confidence and sense of the big picture were not lost on Bollinger that day at the leadership summit.
“I thought that took a fair amount of courage,” she says, “on Day 3, to stand up to the mic and have [a] specific conversation with the president of the company. In my mind, he was very enlightened. His comments were very enlightened.”
Firm Foundation
Robert Zipper, MD, MMM, SFHM, chair of SHM’s Leadership Committee, and CMO of Sound Physicians’ West Region, says it’s probably not realistic for a hospitalist to vault up immediately to a chief executive officer position. Pursuing lower-level leadership roles would be a good starting point for hospitalists with C-suite aspirations, he says.
“For those just starting out, I would recommend that they seek out opportunities to lead or be a part of managing change in their hospitals. The right opportunities should feel like a bit of a stretch, but not overwhelming. This might be work in quality, medical staff leadership, etc.,” Dr. Zipper says.
For hospitalists with leadership experience, CMO and vice president of medical affairs have the closest translation, he adds. He also says jobs like chief informatics officer and roles in quality improvement are highly suitable for hospitalists.
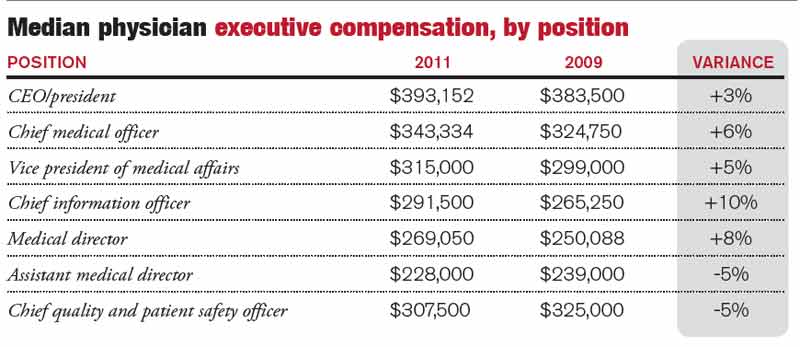
According to the 2011 Cejka Executive Search Physician Executive Compensation Survey, a survey of the American College of Physician Executives’ membership of physicians in management, the median salary of physicians in CEO positions was $393,152. That figure was $343,334 for CMO and $307,500 for chief quality and patient safety officer. The median for all physician executive positions was $305,000. Compensation was typically higher in academic medical centers and lower for hospitals and multi-specialty groups.
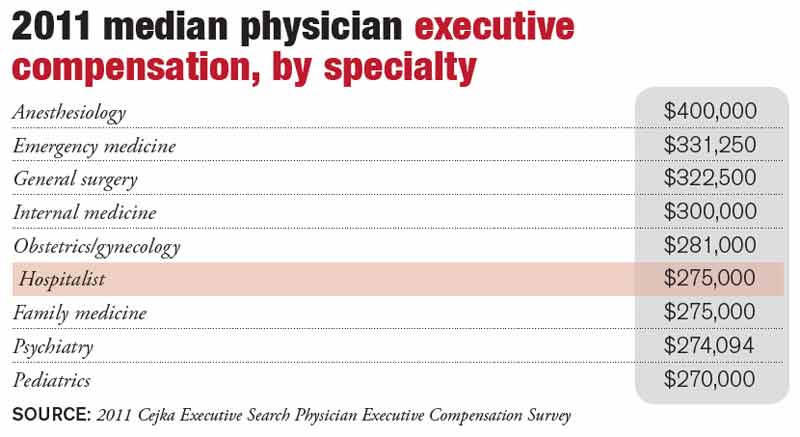
Hospitalists in executive positions had a 2011 median income of $275,000, according to the survey.
The survey also showed a wide range of compensation, typically dependent on the size of the institution. Some hospitalist leaders with more than 75% of their full-time-equivalent hours worked clinically “might actually take a small pay cut to make a move,” Dr. Zipper says.
Natural Progression
The hospitalist executives interviewed, for the most part, were emphatic that C-suite level leadership was not something that they imagined for themselves when they began their medical careers.
“In 2007, I could never imagine doing anything less than 100 percent clinical hospitalist work,” UCLA Hospitals’ Dr. Afsar says. “But once I started working and doing my hospitalist job day in and day out, I realized that there were many aspects of our care where I knew we could do better.”
Dr. Harte, president of South Pointe Hospital in Cleveland, says he never really thought about hospital administration as a career ambition. But, “opportunities presented themselves.”
Dr. Torcson says he was so firmly disinterested in administrative positions that when he was asked to join the Medical Executive Committee at his hospital, his first thought was “no way … I’m a doctor, not an administrator.” But after talking to some senior colleagues about it, they reminded him that he was basically obliged to say “yes.” And it ended up being a crucial component in his ascent through the ranks.
Dr. Narang imagined having a career that impacted value fairly early on, after making observations during his pediatric residency. But even he was surprised when he got the call to be CEO, after less than two years on the job.
Now, in retrospect, they all see their years working as a rank-and-file hospitalist as formative.
As a leader in a hospital, you have to be good at recruiting physicians, retaining them and developing them professionally, Dr. Harte says. That requires having clinical credibility, being a decent mentor, being a good role model, and “wearing your integrity on your sleeve.”
“I think one of the things that makes hospitalists fairly natural fits for the hospital leadership positions is that a hospital is a very complicated environment,” Dr. Harte notes. “You have pockets of enormous expertise that sometimes function like silos.
“Being a hospitalist actually trains you well for those things. By nature of what we do, we tend to be folks who do multi-disciplinary rounds. We can sit around a table or walk rounds with nurses, case managers, physical therapists, respiratory therapists, and the like, and actually develop a plan of care that recognizes the expertise of the other individuals within that group. That is a very good incubator for that kind of thinking.”
Hospital leaders also have to know how everything works together within the hospital.
“Hospital medicine has this overlap with that domain as it is,” Dr. Harte continues. “We work in hospitals. It is not such a stretch then, to think that we could be running a hospital.”
Golden Opportunity
Dr. Torcson says the opportunities to lead in the hospital setting abound. A former internist, he says hospitalists are primed to “improve quality and service at the hospital level because of the system-based approach to hospital care.”
Dealing with incomplete information and uncertainty are important challenges for hospital leaders, something Dr. Afsar says are daily hurdles for hospitalists.
“By nature when you’re a hospitalist, you are a problem solver,” she says. “You don’t shy away from problems that you don’t understand.”
That problem-solver outlook is what prompted Neil Martin, MD, chief of neurosurgery at UCLA, to ask Dr. Afsar to join a quality improvement program within the department—first as a participant and then as its leader.
“She was always one of the most active and vocal and solution-oriented people on the committees that I was participating in,” Dr. Martin says. “She was not the kind of person who would describe all of the problems and leave it at that. But, rather, [she] would help identify problems and then propose solutions and then help follow through to implement solutions.”
Hospitalist C-suiters describe days dominated by meetings with executive teams, staff, and individual physicians or groups. Meetings are a necessity, as executives are tasked with crafting a vision, constantly assessing progress, and refining the approach when necessary.
Continuing at least some clinical work is important, Dr. Harte says. It depends on the organization, but he says he sees benefits that help him in his administrative duties.
“It changes the dynamic of the interaction with some of the naysayers on the medical staff,” he says. “That’s still something that I enjoy doing. I think it’s important for me, it’s important for the credibility of my job, and particularly for the organization that I work at.”
A lot of C-suiters sought out formal training in administrative areas—though not necessarily an MBA—once they realized they had an interest in administration.
Dr. Torcson says getting a master’s in medical management degree was “absolutely invaluable.”
“It was obvious to me that I had some needs to develop some additional competencies and capabilities, a different skill set than I gained in medical school and residency,” he says. “The same skill set that makes one a successful or quality physician isn’t necessarily the same skill set that you need to be an effective manager or administrator.”
Dr. Afsar completed an advanced quality improvement training program at Intermountain Healthcare, and Dr. Narang received a master’s in healthcare management from Harvard.
Dr. Harte, who does not have an advanced management degree, says that at some institutions, such as Cleveland Clinic, you can learn on the job the non-clinical areas needed to be a top leader in a hospital, including finance and strategy.
Dr. Zipper says a related degree can be a big leg up.
“If one is specifically looking to enter the C-suite, an advanced business or management degree will make that barrier a lot lower,” he says. Whether that degree is a master’s in business administration, healthcare administration, medical management, or a similar degree doesn’t seem to matter much, he adds.
When she was looking for a new CEO for Good Samaritan Medical Center, Bollinger says that she preferred to hire a physician. That candidate, she says, had to have certain leadership qualities, including the ability to create a suitable vision, curiosity, an “executive presence,” and a “tolerance of ambiguity.”
As it turns out, the value of having a physician CEO has been “probably three times what I anticipated,” she says.
If you’re a hospitalist and have an interest in rising up the leadership ladder, getting involved and getting exposure to areas of interest is where it begins.
“I would say go for it,” Dr. Afsar says. “Raising your hand and being willing to take on responsibility are kind of the first steps in getting involved. I think it’s just as much making sure that you’re the right fit for that type of work, as it is to excel and do well. Not everyone, I think, will thrive and enjoy this type of work. So I think having the opportunity to get exposed to it and see if it’s something that you enjoy is a critical piece.”
Tom Collins is a freelance writer in Florida.
Steve Narang, MD, a pediatrician, hospitalist, and the then-CMO at Banner Health’s Cardon Children’s Medical Center in Phoenix, was attending a leadership summit where all of Banner’s top officials were gathered. It was his third day in his new job.
Banner’s President, Peter Fine, gave a presentation in the future of healthcare and asked for questions. Dr. Narang stepped up to the microphone, asked a question, and made remarks about how the organization needed to ready itself for the changing landscape. Kathy Bollinger, president of the Arizona West Region of Banner, was struck by those remarks. Less than two years later, she made Dr. Narang the CEO at Arizona’s largest teaching hospital, Good Samaritan Medical Center.
His hospitalist background was an important ingredient in the kind of leader Dr. Narang has become, she says.
“The correlation is that hospitalists are leading teams; they are quarterbacking care,” Bollinger adds. “A good hospitalist brings the team together.”
Physicians with a background in hospital medicine are no strangers to C-suite level positions at hospitals. In April, Brian Harte, MD, SFHM, was named president of South Pointe Hospital in Warrenville Heights, Ohio, a center within the Cleveland Clinic system. In January, Patrick Cawley, MD, MBA, MHM, a former SHM president, was named CEO at the Medical University of South Carolina Medical Center in Charleston.
Other recent C-suite arrivals include Nasim Afsar, MD, SFHM, an SHM board member who is associate CMO at UCLA Hospitals in Los Angeles, and Patrick Torcson, MD, MMM, FACP, SFHM, another SHM board member, vice president, and chief integration officer at St. Tammany Parish Hospital in Covington, La.
Although their paths to the C-suite have differed, each agrees that their experience in hospital medicine gave them the knowledge of the system that was required to begin an ascent to the highest levels of leadership. Just as important, or maybe more so, their exposure to the inner workings of a hospital awakened within them a desire to see the system function better. And the necessity of working with all types of healthcare providers within the complicated hospital setting helped them recognize—or at least get others to recognize—their potential for leadership, and helped hone the teamwork skills that are vital in top administrative roles.
They also say that, when they were starting out, they never aspired to high leadership positions. Rather, it was simply following their own interests that ultimately led them there.
By the time Dr. Narang stepped up to the microphone that day in Phoenix, he had more than a dozen years under his belt working as a hospitalist for a children’s hospital and as part of a group that created a pediatric hospitalist company in Louisiana.
And that work helped lay the foundation for him, he says.
“Being a hospitalist was a key strength of my background,” Dr. Narang explains. “Hospitalists are so well-positioned…to get truly at the intersection of operations and find value in a complex puzzle. Hospitalists are able to do that.
“At the end of the day, it’s about leadership. And I learned that from day one as a hospitalist.”
His confidence and sense of the big picture were not lost on Bollinger that day at the leadership summit.
“I thought that took a fair amount of courage,” she says, “on Day 3, to stand up to the mic and have [a] specific conversation with the president of the company. In my mind, he was very enlightened. His comments were very enlightened.”
Firm Foundation
Robert Zipper, MD, MMM, SFHM, chair of SHM’s Leadership Committee, and CMO of Sound Physicians’ West Region, says it’s probably not realistic for a hospitalist to vault up immediately to a chief executive officer position. Pursuing lower-level leadership roles would be a good starting point for hospitalists with C-suite aspirations, he says.
“For those just starting out, I would recommend that they seek out opportunities to lead or be a part of managing change in their hospitals. The right opportunities should feel like a bit of a stretch, but not overwhelming. This might be work in quality, medical staff leadership, etc.,” Dr. Zipper says.
For hospitalists with leadership experience, CMO and vice president of medical affairs have the closest translation, he adds. He also says jobs like chief informatics officer and roles in quality improvement are highly suitable for hospitalists.
According to the 2011 Cejka Executive Search Physician Executive Compensation Survey, a survey of the American College of Physician Executives’ membership of physicians in management, the median salary of physicians in CEO positions was $393,152. That figure was $343,334 for CMO and $307,500 for chief quality and patient safety officer. The median for all physician executive positions was $305,000. Compensation was typically higher in academic medical centers and lower for hospitals and multi-specialty groups.
Hospitalists in executive positions had a 2011 median income of $275,000, according to the survey.
The survey also showed a wide range of compensation, typically dependent on the size of the institution. Some hospitalist leaders with more than 75% of their full-time-equivalent hours worked clinically “might actually take a small pay cut to make a move,” Dr. Zipper says.
Natural Progression
The hospitalist executives interviewed, for the most part, were emphatic that C-suite level leadership was not something that they imagined for themselves when they began their medical careers.
“In 2007, I could never imagine doing anything less than 100 percent clinical hospitalist work,” UCLA Hospitals’ Dr. Afsar says. “But once I started working and doing my hospitalist job day in and day out, I realized that there were many aspects of our care where I knew we could do better.”
Dr. Harte, president of South Pointe Hospital in Cleveland, says he never really thought about hospital administration as a career ambition. But, “opportunities presented themselves.”
Dr. Torcson says he was so firmly disinterested in administrative positions that when he was asked to join the Medical Executive Committee at his hospital, his first thought was “no way … I’m a doctor, not an administrator.” But after talking to some senior colleagues about it, they reminded him that he was basically obliged to say “yes.” And it ended up being a crucial component in his ascent through the ranks.
Dr. Narang imagined having a career that impacted value fairly early on, after making observations during his pediatric residency. But even he was surprised when he got the call to be CEO, after less than two years on the job.
Now, in retrospect, they all see their years working as a rank-and-file hospitalist as formative.
As a leader in a hospital, you have to be good at recruiting physicians, retaining them and developing them professionally, Dr. Harte says. That requires having clinical credibility, being a decent mentor, being a good role model, and “wearing your integrity on your sleeve.”
“I think one of the things that makes hospitalists fairly natural fits for the hospital leadership positions is that a hospital is a very complicated environment,” Dr. Harte notes. “You have pockets of enormous expertise that sometimes function like silos.
“Being a hospitalist actually trains you well for those things. By nature of what we do, we tend to be folks who do multi-disciplinary rounds. We can sit around a table or walk rounds with nurses, case managers, physical therapists, respiratory therapists, and the like, and actually develop a plan of care that recognizes the expertise of the other individuals within that group. That is a very good incubator for that kind of thinking.”
Hospital leaders also have to know how everything works together within the hospital.
“Hospital medicine has this overlap with that domain as it is,” Dr. Harte continues. “We work in hospitals. It is not such a stretch then, to think that we could be running a hospital.”
Golden Opportunity
Dr. Torcson says the opportunities to lead in the hospital setting abound. A former internist, he says hospitalists are primed to “improve quality and service at the hospital level because of the system-based approach to hospital care.”
Dealing with incomplete information and uncertainty are important challenges for hospital leaders, something Dr. Afsar says are daily hurdles for hospitalists.
“By nature when you’re a hospitalist, you are a problem solver,” she says. “You don’t shy away from problems that you don’t understand.”
That problem-solver outlook is what prompted Neil Martin, MD, chief of neurosurgery at UCLA, to ask Dr. Afsar to join a quality improvement program within the department—first as a participant and then as its leader.
“She was always one of the most active and vocal and solution-oriented people on the committees that I was participating in,” Dr. Martin says. “She was not the kind of person who would describe all of the problems and leave it at that. But, rather, [she] would help identify problems and then propose solutions and then help follow through to implement solutions.”
Hospitalist C-suiters describe days dominated by meetings with executive teams, staff, and individual physicians or groups. Meetings are a necessity, as executives are tasked with crafting a vision, constantly assessing progress, and refining the approach when necessary.
Continuing at least some clinical work is important, Dr. Harte says. It depends on the organization, but he says he sees benefits that help him in his administrative duties.
“It changes the dynamic of the interaction with some of the naysayers on the medical staff,” he says. “That’s still something that I enjoy doing. I think it’s important for me, it’s important for the credibility of my job, and particularly for the organization that I work at.”
A lot of C-suiters sought out formal training in administrative areas—though not necessarily an MBA—once they realized they had an interest in administration.
Dr. Torcson says getting a master’s in medical management degree was “absolutely invaluable.”
“It was obvious to me that I had some needs to develop some additional competencies and capabilities, a different skill set than I gained in medical school and residency,” he says. “The same skill set that makes one a successful or quality physician isn’t necessarily the same skill set that you need to be an effective manager or administrator.”
Dr. Afsar completed an advanced quality improvement training program at Intermountain Healthcare, and Dr. Narang received a master’s in healthcare management from Harvard.
Dr. Harte, who does not have an advanced management degree, says that at some institutions, such as Cleveland Clinic, you can learn on the job the non-clinical areas needed to be a top leader in a hospital, including finance and strategy.
Dr. Zipper says a related degree can be a big leg up.
“If one is specifically looking to enter the C-suite, an advanced business or management degree will make that barrier a lot lower,” he says. Whether that degree is a master’s in business administration, healthcare administration, medical management, or a similar degree doesn’t seem to matter much, he adds.
When she was looking for a new CEO for Good Samaritan Medical Center, Bollinger says that she preferred to hire a physician. That candidate, she says, had to have certain leadership qualities, including the ability to create a suitable vision, curiosity, an “executive presence,” and a “tolerance of ambiguity.”
As it turns out, the value of having a physician CEO has been “probably three times what I anticipated,” she says.
If you’re a hospitalist and have an interest in rising up the leadership ladder, getting involved and getting exposure to areas of interest is where it begins.
“I would say go for it,” Dr. Afsar says. “Raising your hand and being willing to take on responsibility are kind of the first steps in getting involved. I think it’s just as much making sure that you’re the right fit for that type of work, as it is to excel and do well. Not everyone, I think, will thrive and enjoy this type of work. So I think having the opportunity to get exposed to it and see if it’s something that you enjoy is a critical piece.”
Tom Collins is a freelance writer in Florida.
Steve Narang, MD, a pediatrician, hospitalist, and the then-CMO at Banner Health’s Cardon Children’s Medical Center in Phoenix, was attending a leadership summit where all of Banner’s top officials were gathered. It was his third day in his new job.
Banner’s President, Peter Fine, gave a presentation in the future of healthcare and asked for questions. Dr. Narang stepped up to the microphone, asked a question, and made remarks about how the organization needed to ready itself for the changing landscape. Kathy Bollinger, president of the Arizona West Region of Banner, was struck by those remarks. Less than two years later, she made Dr. Narang the CEO at Arizona’s largest teaching hospital, Good Samaritan Medical Center.
His hospitalist background was an important ingredient in the kind of leader Dr. Narang has become, she says.
“The correlation is that hospitalists are leading teams; they are quarterbacking care,” Bollinger adds. “A good hospitalist brings the team together.”
Physicians with a background in hospital medicine are no strangers to C-suite level positions at hospitals. In April, Brian Harte, MD, SFHM, was named president of South Pointe Hospital in Warrenville Heights, Ohio, a center within the Cleveland Clinic system. In January, Patrick Cawley, MD, MBA, MHM, a former SHM president, was named CEO at the Medical University of South Carolina Medical Center in Charleston.
Other recent C-suite arrivals include Nasim Afsar, MD, SFHM, an SHM board member who is associate CMO at UCLA Hospitals in Los Angeles, and Patrick Torcson, MD, MMM, FACP, SFHM, another SHM board member, vice president, and chief integration officer at St. Tammany Parish Hospital in Covington, La.
Although their paths to the C-suite have differed, each agrees that their experience in hospital medicine gave them the knowledge of the system that was required to begin an ascent to the highest levels of leadership. Just as important, or maybe more so, their exposure to the inner workings of a hospital awakened within them a desire to see the system function better. And the necessity of working with all types of healthcare providers within the complicated hospital setting helped them recognize—or at least get others to recognize—their potential for leadership, and helped hone the teamwork skills that are vital in top administrative roles.
They also say that, when they were starting out, they never aspired to high leadership positions. Rather, it was simply following their own interests that ultimately led them there.
By the time Dr. Narang stepped up to the microphone that day in Phoenix, he had more than a dozen years under his belt working as a hospitalist for a children’s hospital and as part of a group that created a pediatric hospitalist company in Louisiana.
And that work helped lay the foundation for him, he says.
“Being a hospitalist was a key strength of my background,” Dr. Narang explains. “Hospitalists are so well-positioned…to get truly at the intersection of operations and find value in a complex puzzle. Hospitalists are able to do that.
“At the end of the day, it’s about leadership. And I learned that from day one as a hospitalist.”
His confidence and sense of the big picture were not lost on Bollinger that day at the leadership summit.
“I thought that took a fair amount of courage,” she says, “on Day 3, to stand up to the mic and have [a] specific conversation with the president of the company. In my mind, he was very enlightened. His comments were very enlightened.”
Firm Foundation
Robert Zipper, MD, MMM, SFHM, chair of SHM’s Leadership Committee, and CMO of Sound Physicians’ West Region, says it’s probably not realistic for a hospitalist to vault up immediately to a chief executive officer position. Pursuing lower-level leadership roles would be a good starting point for hospitalists with C-suite aspirations, he says.
“For those just starting out, I would recommend that they seek out opportunities to lead or be a part of managing change in their hospitals. The right opportunities should feel like a bit of a stretch, but not overwhelming. This might be work in quality, medical staff leadership, etc.,” Dr. Zipper says.
For hospitalists with leadership experience, CMO and vice president of medical affairs have the closest translation, he adds. He also says jobs like chief informatics officer and roles in quality improvement are highly suitable for hospitalists.
According to the 2011 Cejka Executive Search Physician Executive Compensation Survey, a survey of the American College of Physician Executives’ membership of physicians in management, the median salary of physicians in CEO positions was $393,152. That figure was $343,334 for CMO and $307,500 for chief quality and patient safety officer. The median for all physician executive positions was $305,000. Compensation was typically higher in academic medical centers and lower for hospitals and multi-specialty groups.
Hospitalists in executive positions had a 2011 median income of $275,000, according to the survey.
The survey also showed a wide range of compensation, typically dependent on the size of the institution. Some hospitalist leaders with more than 75% of their full-time-equivalent hours worked clinically “might actually take a small pay cut to make a move,” Dr. Zipper says.
Natural Progression
The hospitalist executives interviewed, for the most part, were emphatic that C-suite level leadership was not something that they imagined for themselves when they began their medical careers.
“In 2007, I could never imagine doing anything less than 100 percent clinical hospitalist work,” UCLA Hospitals’ Dr. Afsar says. “But once I started working and doing my hospitalist job day in and day out, I realized that there were many aspects of our care where I knew we could do better.”
Dr. Harte, president of South Pointe Hospital in Cleveland, says he never really thought about hospital administration as a career ambition. But, “opportunities presented themselves.”
Dr. Torcson says he was so firmly disinterested in administrative positions that when he was asked to join the Medical Executive Committee at his hospital, his first thought was “no way … I’m a doctor, not an administrator.” But after talking to some senior colleagues about it, they reminded him that he was basically obliged to say “yes.” And it ended up being a crucial component in his ascent through the ranks.
Dr. Narang imagined having a career that impacted value fairly early on, after making observations during his pediatric residency. But even he was surprised when he got the call to be CEO, after less than two years on the job.
Now, in retrospect, they all see their years working as a rank-and-file hospitalist as formative.
As a leader in a hospital, you have to be good at recruiting physicians, retaining them and developing them professionally, Dr. Harte says. That requires having clinical credibility, being a decent mentor, being a good role model, and “wearing your integrity on your sleeve.”
“I think one of the things that makes hospitalists fairly natural fits for the hospital leadership positions is that a hospital is a very complicated environment,” Dr. Harte notes. “You have pockets of enormous expertise that sometimes function like silos.
“Being a hospitalist actually trains you well for those things. By nature of what we do, we tend to be folks who do multi-disciplinary rounds. We can sit around a table or walk rounds with nurses, case managers, physical therapists, respiratory therapists, and the like, and actually develop a plan of care that recognizes the expertise of the other individuals within that group. That is a very good incubator for that kind of thinking.”
Hospital leaders also have to know how everything works together within the hospital.
“Hospital medicine has this overlap with that domain as it is,” Dr. Harte continues. “We work in hospitals. It is not such a stretch then, to think that we could be running a hospital.”
Golden Opportunity
Dr. Torcson says the opportunities to lead in the hospital setting abound. A former internist, he says hospitalists are primed to “improve quality and service at the hospital level because of the system-based approach to hospital care.”
Dealing with incomplete information and uncertainty are important challenges for hospital leaders, something Dr. Afsar says are daily hurdles for hospitalists.
“By nature when you’re a hospitalist, you are a problem solver,” she says. “You don’t shy away from problems that you don’t understand.”
That problem-solver outlook is what prompted Neil Martin, MD, chief of neurosurgery at UCLA, to ask Dr. Afsar to join a quality improvement program within the department—first as a participant and then as its leader.
“She was always one of the most active and vocal and solution-oriented people on the committees that I was participating in,” Dr. Martin says. “She was not the kind of person who would describe all of the problems and leave it at that. But, rather, [she] would help identify problems and then propose solutions and then help follow through to implement solutions.”
Hospitalist C-suiters describe days dominated by meetings with executive teams, staff, and individual physicians or groups. Meetings are a necessity, as executives are tasked with crafting a vision, constantly assessing progress, and refining the approach when necessary.
Continuing at least some clinical work is important, Dr. Harte says. It depends on the organization, but he says he sees benefits that help him in his administrative duties.
“It changes the dynamic of the interaction with some of the naysayers on the medical staff,” he says. “That’s still something that I enjoy doing. I think it’s important for me, it’s important for the credibility of my job, and particularly for the organization that I work at.”
A lot of C-suiters sought out formal training in administrative areas—though not necessarily an MBA—once they realized they had an interest in administration.
Dr. Torcson says getting a master’s in medical management degree was “absolutely invaluable.”
“It was obvious to me that I had some needs to develop some additional competencies and capabilities, a different skill set than I gained in medical school and residency,” he says. “The same skill set that makes one a successful or quality physician isn’t necessarily the same skill set that you need to be an effective manager or administrator.”
Dr. Afsar completed an advanced quality improvement training program at Intermountain Healthcare, and Dr. Narang received a master’s in healthcare management from Harvard.
Dr. Harte, who does not have an advanced management degree, says that at some institutions, such as Cleveland Clinic, you can learn on the job the non-clinical areas needed to be a top leader in a hospital, including finance and strategy.
Dr. Zipper says a related degree can be a big leg up.
“If one is specifically looking to enter the C-suite, an advanced business or management degree will make that barrier a lot lower,” he says. Whether that degree is a master’s in business administration, healthcare administration, medical management, or a similar degree doesn’t seem to matter much, he adds.
When she was looking for a new CEO for Good Samaritan Medical Center, Bollinger says that she preferred to hire a physician. That candidate, she says, had to have certain leadership qualities, including the ability to create a suitable vision, curiosity, an “executive presence,” and a “tolerance of ambiguity.”
As it turns out, the value of having a physician CEO has been “probably three times what I anticipated,” she says.
If you’re a hospitalist and have an interest in rising up the leadership ladder, getting involved and getting exposure to areas of interest is where it begins.
“I would say go for it,” Dr. Afsar says. “Raising your hand and being willing to take on responsibility are kind of the first steps in getting involved. I think it’s just as much making sure that you’re the right fit for that type of work, as it is to excel and do well. Not everyone, I think, will thrive and enjoy this type of work. So I think having the opportunity to get exposed to it and see if it’s something that you enjoy is a critical piece.”
Tom Collins is a freelance writer in Florida.
Malpractice Counsel
Postpartum Shortness of Breath
A 35-year-old woman presented to the ED after referral by her obstetrician. Six days prior, the patient had given birth to twins without incident. On postpartum hospital day 2, however, she developed mild shortness of breath, and a chest X-ray was ordered. Since there was concern for possible pneumonia, the patient was prescribed oral antibiotics and discharged home on hospital day 4. She continued to complain of shortness of breath following discharge; at that time, the obstetrician referred the patient to the ED for further evaluation.
The patient was evaluated by the EP, who ordered a chest X-ray. He was also concerned that patient had pneumonia and prescribed a different class of antibiotic before discharging the patient home.
One week later, the patient presented back to the same ED with continued shortness of breath. On this visit, she was seen by a physician assistant (PA). Following the history taking and physical examination, a chest X-ray and rapid flu and rapid strep tests were ordered. Both the PA and supervising EP reviewed the chest X-ray and were concerned for pneumonia; however, both the flu and strep tests were negative. A third class of antibiotic was prescribed, and the patient was discharged home.
The chest X-ray on the second ED visit was not interpreted by a radiologist until 3 days later (The patient was seen on a Friday evening and the films were not read until the following Monday morning). The radiologist’s interpretation was “worsening congestive heart failure” (CHF). Two days later (5 days following the second ED visit), the EP was notified of the interpretation discrepancy and made multiple attempts to contact the patient, which included leaving a voice-mail message on her home phone.
The patient returned the call the following day and spoke with one of the ED nurses, who encouraged her to return immediately to the ED. The patient returned to the ED the next day (1 week after her second ED visit) and was admitted to the hospital for CHF secondary to postpartum cardiomyopathy. Unfortunately, she developed an embolus to her kidney, followed by an ischemic cerebrovascular accident, and died 3 weeks after admission.
The patient’s family filed a malpractice lawsuit against the hospital, the EPs, and the PA for negligent delay in making the correct diagnosis, stating that patient’s subsequent stroke and death were a direct result of this delay. Following deliberations, all of the EPs involved in the case were found free of negligence; the PA and the hospital ED, however, were found guilty.
Discussion
Interestingly, the majority of successful malpractice suits against physicians involve cognitive errors and system issues; this case is no exception. Making the correct diagnosis in a patient is a complex process, involving data gathering and synthesis, intuition, clinical experience, and logical thinking. Unfortunately, biases can occur during this process and result in misdiagnosis or delayed diagnosis. These biases include anchoring bias, confirmation bias, premature closure, and diagnosis momentum.1
Anchoring Bias. This occurs when a physician relies too heavily on the first piece of information or one’s initial impression.1 Despite evidence to the contrary, the physician keeps returning to the initial diagnosis (ie, he or she is “anchored” to it).
Confirmation Bias. Related to anchoring bias, in confirmation bias, the physician ignores or discounts evidence that contradicts one’s initial impression and focuses solely on the evidence supporting it.1
Both anchoring bias and confirmation bias appear to have played a role in this case. The differential diagnosis was never broadened beyond pneumonia, despite the fact that one must also consider pulmonary embolism (ie, a hypercoagulable state) and CHF (ie, postpartum cardiomyopathy) in a patient complaining of dyspnea in the postpartum period.
Premature Closure. This occurs when the physician finds a cause that fits the clinical picture and ceases to search for other diagnostic possibilities.1,2
Diagnosis Momentum. A bias that occurs when the diagnosis considered a possibility by one physician becomes a definitive diagnosis as it is passed from one physician to the next; it then becomes accepted without question by physicians down the line.1 This type of bias also seems to have played a role in this case.
There are a few strategies to help prevent or minimize these types of errors. First, as new data are gathered, one should reconsider and reprioritize the differential diagnosis. When certain data points do not fit neatly with an earlier diagnosis, careful attention must be paid to them. This is especially true for the patient receiving appropriate treatment but not showing clinical improvement. While it is usually helpful to know previous working diagnoses, the clinician must try to keep an open mind and consider alternative diagnoses. At the end of the day, the lesson is the need to develop a broad differential diagnosis.2
The system error in this case involves the lack of timely overread of radiology studies. Emergency medicine is a 24-hour, 7-day-a-week specialty; therefore, support services to the ED need to be similarly available. With today’s teleradiology and dedicated night readers, it is difficult to justify not providing such a service. This situation explains, in part, the negligent verdict against the hospital.
Chest Pain in a Man With Type 2 Diabetes
A 54-year-old man presented to the ED with a several-hour history of chest pain and shortness of breath. His medical history was remarkable for type 2 diabetes mellitus. He denied any associated nausea, vomiting, or diaphoresis. He smoked one pack of cigarettes per day and drank alcohol on occasion. The patient further denied having experienced similar symptoms in the past. All vital signs were normal, and he appeared comfortable and in no acute distress. His physical examination was completely unremarkable.
An electrocardiogram (ECG) revealed Q-waves in the anterior leads, but was otherwise nondiagnostic. The results of a portable chest X-ray were interpreted as normal. Cardiac enzyme testing revealed a positive troponin I, but a normal creatine phosphokinase-MB (CPK-MB). The patient’s complete blood count and coagulation studies were normal, and a basic metabolic profile was remarkable only for a blood sugar of 540 mg/dL; his serum bicarbonate value was normal.
The patient was placed on oxygen via nasal cannula, administered an aspirin (325 mg), and given subcutaneous regular insulin for hyperglycemia. The EP contacted a hospitalist to admit the patient. The hospitalist accepted the patient and admitted him to the telemetry floor.
Upon arrival at telemetry, the patient was examined by a nurse who noted rhonchi bilaterally on lung auscultation. Shortly afterward, he became anxious, and the nurse consulted the hospitalist, who ordered administration of lorazepam. Approximately 20 minutes later, the patient went into cardiac arrest and died.
This patient was never examined by the hospitalist prior to coding. An autopsy revealed evidence of severe coronary artery disease, a previous infarction that was at least a few months old with scarring of the left ventricle, and a recent infarction that had begun at least 12 hours prior to death.
The family sued all of the providers involved in the care of the patient. At trial, there was a factual dispute regarding whether the EP informed the hospitalist of the elevated troponin I level. The defendants argued that the patient had sustained irreversible heart damage prior to his arrival at the hospital, and that nothing any of the defendants could have done would have saved his life. The jury deliberated for approximately 2 hours before delivering a verdict in favor of the defense.
Discussion
Clearly, this verdict could have gone the other way. This patient was experiencing a non-ST segment elevation myocardial infarction (MI). The nondiagnostic ECG, coupled with the elevated troponin I, indicated damage of heart muscle from an acute interruption of coronary blood flow.
There are several problems with the management of this case. First, this patient required a cardiology consult for risk stratification. Several scoring systems could have been used to determine whether this patient was a candidate for early (ie, within 4-48 hours) invasive treatments such as percutaneous intervention or a more conservative approach.
Second, having sustained an MI, this patient was at high risk for complications such as ventricular arrhythmias, heart failure, cardiogenic shock, and other serious adverse events. Patients with acute MI should be admitted to the critical care or intensive care unit. In addition to aspirin, this patient should have received nitroglycerin and anticoagulation therapy. Either heparin or a low molecular weight heparin, such as enoxaparin, would have been appropriate if no contraindications existed. Finally, additional therapy including glycoprotein IIB/IIIA inhibitors, clopidogrel, etc, may have been indicated depending upon the timing of percutaneous intervention.1
It appears that both the EP and the hospitalist either failed to appreciate the significance of the elevated troponin I or overlooked it. This patient had normal renal function, so the only explanation—especially in the setting of a middle-aged man complaining of chest pain—was that myocardial damage had occurred.
Alcohol Detoxification in a Young Man
A young man was brought to the ED by a friend. The patient’s sole complaint was the need for help with his alcohol dependency. In addition to alcohol abuse, his medical history was remarkable only for an admission 1 month prior for suicidal ideation. The patient denied suicidal or homicidal ideations on this presentation. The physical examination revealed stable vital signs, but conjunctival injection, slurred speech, and a strong odor of alcohol. A blood alcohol test showed a concentration level of 0.36 g/dL. The patient, however, was alert and able to ambulate without assistance. He was medically cleared by the EP and arrangements were made to admit him to a local detoxification center.
Approximately 4 hours after his arrival, while waiting for transport to the detoxification center, the patient became impatient with the delay, removed his intravenous line, and told the nurse that he was going home via taxi. The nurse encouraged him to call a friend to take him home, to which to the patient agreed. The nurse left the patient to inform the EP of his desire to go home; when she returned, she discovered that the patient had already left the hospital. The physician notified hospital security but not the police. Approximately 2 hours later, the patient was struck by a car and seriously injured.
The patient sued the EP and the hospital for negligence and medical malpractice. The suit alleged that the physician and the hospital should have prevented the patient from leaving the ED. The physician and the hospital requested a dismissal, arguing that the patient did not exhibit any suicidal or homicidal ideation, presented on his own volition, and, though intoxicated, could still make decisions for himself. An appellate court granted the motion, holding that the defendants “lacked authority to confine the plaintiff upon his departure” from the ED.
Discussion
When a patient attempts to leave the ED against medical advice, the treating physician should make an attempt to convince him or her to remain for treatment. Often, something as simple as offering a cup of coffee will change a patient’s mind. In other instances, the use of chemical or physical restraint may be required. The handling of the case ultimately becomes a question of whether the patient was competent to make decisions and whether he presented a danger to himself or others. The extent of intoxication varies by the degree and does not of itself constitute incapability to make decisions. All practicing EPs have cared for patients with blood alcohol levels above the legal limit for driving, but who were functionally sober and able to make decisions. If a patient is competent and does not present a danger to self or others, he or she can decide to leave the ED without further management. However, it is best to release the patient in the company of friends or family, as was urged by the nurse in this case. Obviously, such a patient should not be allowed to drive himself home.
When a patient does leave against medical advice, the physician and nurse should document in the ED record their conversations urging him or her to stay. Alternatively, when a patient is found incompetent of making decisions or is a danger to self or others, he or she must be prevented from leaving the ED. This includes use of the minimal amount of physical or chemical restraint needed to keep the patient from leaving. When there is doubt that the patient is able to make a competent decision, it is better to err on the side of caution and keep him or her in the ED for his own safety and the safety of others.
Postpartum Shortness of Breath
- Penney FT, Datal AK: Understanding diagnostic error. Hospital Medicine Clinics. 2013;2(2):e292-e303.
- Ely JW, Kaldjian LC, D’Alessandro DM. Diagnostic errors in primary care: lessons learned. J Am Board Fam Med. 2012;25(1):87-97.
Chest Pain in a Man With Type 2 Diabetes
- Anantharam V, Lim SH. Treatment of NSTEMI (Non-ST elevation myocardial infarction). Curr Emerg Hosp Med Rep. 2013;1(1):18-28.
Postpartum Shortness of Breath
A 35-year-old woman presented to the ED after referral by her obstetrician. Six days prior, the patient had given birth to twins without incident. On postpartum hospital day 2, however, she developed mild shortness of breath, and a chest X-ray was ordered. Since there was concern for possible pneumonia, the patient was prescribed oral antibiotics and discharged home on hospital day 4. She continued to complain of shortness of breath following discharge; at that time, the obstetrician referred the patient to the ED for further evaluation.
The patient was evaluated by the EP, who ordered a chest X-ray. He was also concerned that patient had pneumonia and prescribed a different class of antibiotic before discharging the patient home.
One week later, the patient presented back to the same ED with continued shortness of breath. On this visit, she was seen by a physician assistant (PA). Following the history taking and physical examination, a chest X-ray and rapid flu and rapid strep tests were ordered. Both the PA and supervising EP reviewed the chest X-ray and were concerned for pneumonia; however, both the flu and strep tests were negative. A third class of antibiotic was prescribed, and the patient was discharged home.
The chest X-ray on the second ED visit was not interpreted by a radiologist until 3 days later (The patient was seen on a Friday evening and the films were not read until the following Monday morning). The radiologist’s interpretation was “worsening congestive heart failure” (CHF). Two days later (5 days following the second ED visit), the EP was notified of the interpretation discrepancy and made multiple attempts to contact the patient, which included leaving a voice-mail message on her home phone.
The patient returned the call the following day and spoke with one of the ED nurses, who encouraged her to return immediately to the ED. The patient returned to the ED the next day (1 week after her second ED visit) and was admitted to the hospital for CHF secondary to postpartum cardiomyopathy. Unfortunately, she developed an embolus to her kidney, followed by an ischemic cerebrovascular accident, and died 3 weeks after admission.
The patient’s family filed a malpractice lawsuit against the hospital, the EPs, and the PA for negligent delay in making the correct diagnosis, stating that patient’s subsequent stroke and death were a direct result of this delay. Following deliberations, all of the EPs involved in the case were found free of negligence; the PA and the hospital ED, however, were found guilty.
Discussion
Interestingly, the majority of successful malpractice suits against physicians involve cognitive errors and system issues; this case is no exception. Making the correct diagnosis in a patient is a complex process, involving data gathering and synthesis, intuition, clinical experience, and logical thinking. Unfortunately, biases can occur during this process and result in misdiagnosis or delayed diagnosis. These biases include anchoring bias, confirmation bias, premature closure, and diagnosis momentum.1
Anchoring Bias. This occurs when a physician relies too heavily on the first piece of information or one’s initial impression.1 Despite evidence to the contrary, the physician keeps returning to the initial diagnosis (ie, he or she is “anchored” to it).
Confirmation Bias. Related to anchoring bias, in confirmation bias, the physician ignores or discounts evidence that contradicts one’s initial impression and focuses solely on the evidence supporting it.1
Both anchoring bias and confirmation bias appear to have played a role in this case. The differential diagnosis was never broadened beyond pneumonia, despite the fact that one must also consider pulmonary embolism (ie, a hypercoagulable state) and CHF (ie, postpartum cardiomyopathy) in a patient complaining of dyspnea in the postpartum period.
Premature Closure. This occurs when the physician finds a cause that fits the clinical picture and ceases to search for other diagnostic possibilities.1,2
Diagnosis Momentum. A bias that occurs when the diagnosis considered a possibility by one physician becomes a definitive diagnosis as it is passed from one physician to the next; it then becomes accepted without question by physicians down the line.1 This type of bias also seems to have played a role in this case.
There are a few strategies to help prevent or minimize these types of errors. First, as new data are gathered, one should reconsider and reprioritize the differential diagnosis. When certain data points do not fit neatly with an earlier diagnosis, careful attention must be paid to them. This is especially true for the patient receiving appropriate treatment but not showing clinical improvement. While it is usually helpful to know previous working diagnoses, the clinician must try to keep an open mind and consider alternative diagnoses. At the end of the day, the lesson is the need to develop a broad differential diagnosis.2
The system error in this case involves the lack of timely overread of radiology studies. Emergency medicine is a 24-hour, 7-day-a-week specialty; therefore, support services to the ED need to be similarly available. With today’s teleradiology and dedicated night readers, it is difficult to justify not providing such a service. This situation explains, in part, the negligent verdict against the hospital.
Chest Pain in a Man With Type 2 Diabetes
A 54-year-old man presented to the ED with a several-hour history of chest pain and shortness of breath. His medical history was remarkable for type 2 diabetes mellitus. He denied any associated nausea, vomiting, or diaphoresis. He smoked one pack of cigarettes per day and drank alcohol on occasion. The patient further denied having experienced similar symptoms in the past. All vital signs were normal, and he appeared comfortable and in no acute distress. His physical examination was completely unremarkable.
An electrocardiogram (ECG) revealed Q-waves in the anterior leads, but was otherwise nondiagnostic. The results of a portable chest X-ray were interpreted as normal. Cardiac enzyme testing revealed a positive troponin I, but a normal creatine phosphokinase-MB (CPK-MB). The patient’s complete blood count and coagulation studies were normal, and a basic metabolic profile was remarkable only for a blood sugar of 540 mg/dL; his serum bicarbonate value was normal.
The patient was placed on oxygen via nasal cannula, administered an aspirin (325 mg), and given subcutaneous regular insulin for hyperglycemia. The EP contacted a hospitalist to admit the patient. The hospitalist accepted the patient and admitted him to the telemetry floor.
Upon arrival at telemetry, the patient was examined by a nurse who noted rhonchi bilaterally on lung auscultation. Shortly afterward, he became anxious, and the nurse consulted the hospitalist, who ordered administration of lorazepam. Approximately 20 minutes later, the patient went into cardiac arrest and died.
This patient was never examined by the hospitalist prior to coding. An autopsy revealed evidence of severe coronary artery disease, a previous infarction that was at least a few months old with scarring of the left ventricle, and a recent infarction that had begun at least 12 hours prior to death.
The family sued all of the providers involved in the care of the patient. At trial, there was a factual dispute regarding whether the EP informed the hospitalist of the elevated troponin I level. The defendants argued that the patient had sustained irreversible heart damage prior to his arrival at the hospital, and that nothing any of the defendants could have done would have saved his life. The jury deliberated for approximately 2 hours before delivering a verdict in favor of the defense.
Discussion
Clearly, this verdict could have gone the other way. This patient was experiencing a non-ST segment elevation myocardial infarction (MI). The nondiagnostic ECG, coupled with the elevated troponin I, indicated damage of heart muscle from an acute interruption of coronary blood flow.
There are several problems with the management of this case. First, this patient required a cardiology consult for risk stratification. Several scoring systems could have been used to determine whether this patient was a candidate for early (ie, within 4-48 hours) invasive treatments such as percutaneous intervention or a more conservative approach.
Second, having sustained an MI, this patient was at high risk for complications such as ventricular arrhythmias, heart failure, cardiogenic shock, and other serious adverse events. Patients with acute MI should be admitted to the critical care or intensive care unit. In addition to aspirin, this patient should have received nitroglycerin and anticoagulation therapy. Either heparin or a low molecular weight heparin, such as enoxaparin, would have been appropriate if no contraindications existed. Finally, additional therapy including glycoprotein IIB/IIIA inhibitors, clopidogrel, etc, may have been indicated depending upon the timing of percutaneous intervention.1
It appears that both the EP and the hospitalist either failed to appreciate the significance of the elevated troponin I or overlooked it. This patient had normal renal function, so the only explanation—especially in the setting of a middle-aged man complaining of chest pain—was that myocardial damage had occurred.
Alcohol Detoxification in a Young Man
A young man was brought to the ED by a friend. The patient’s sole complaint was the need for help with his alcohol dependency. In addition to alcohol abuse, his medical history was remarkable only for an admission 1 month prior for suicidal ideation. The patient denied suicidal or homicidal ideations on this presentation. The physical examination revealed stable vital signs, but conjunctival injection, slurred speech, and a strong odor of alcohol. A blood alcohol test showed a concentration level of 0.36 g/dL. The patient, however, was alert and able to ambulate without assistance. He was medically cleared by the EP and arrangements were made to admit him to a local detoxification center.
Approximately 4 hours after his arrival, while waiting for transport to the detoxification center, the patient became impatient with the delay, removed his intravenous line, and told the nurse that he was going home via taxi. The nurse encouraged him to call a friend to take him home, to which to the patient agreed. The nurse left the patient to inform the EP of his desire to go home; when she returned, she discovered that the patient had already left the hospital. The physician notified hospital security but not the police. Approximately 2 hours later, the patient was struck by a car and seriously injured.
The patient sued the EP and the hospital for negligence and medical malpractice. The suit alleged that the physician and the hospital should have prevented the patient from leaving the ED. The physician and the hospital requested a dismissal, arguing that the patient did not exhibit any suicidal or homicidal ideation, presented on his own volition, and, though intoxicated, could still make decisions for himself. An appellate court granted the motion, holding that the defendants “lacked authority to confine the plaintiff upon his departure” from the ED.
Discussion
When a patient attempts to leave the ED against medical advice, the treating physician should make an attempt to convince him or her to remain for treatment. Often, something as simple as offering a cup of coffee will change a patient’s mind. In other instances, the use of chemical or physical restraint may be required. The handling of the case ultimately becomes a question of whether the patient was competent to make decisions and whether he presented a danger to himself or others. The extent of intoxication varies by the degree and does not of itself constitute incapability to make decisions. All practicing EPs have cared for patients with blood alcohol levels above the legal limit for driving, but who were functionally sober and able to make decisions. If a patient is competent and does not present a danger to self or others, he or she can decide to leave the ED without further management. However, it is best to release the patient in the company of friends or family, as was urged by the nurse in this case. Obviously, such a patient should not be allowed to drive himself home.
When a patient does leave against medical advice, the physician and nurse should document in the ED record their conversations urging him or her to stay. Alternatively, when a patient is found incompetent of making decisions or is a danger to self or others, he or she must be prevented from leaving the ED. This includes use of the minimal amount of physical or chemical restraint needed to keep the patient from leaving. When there is doubt that the patient is able to make a competent decision, it is better to err on the side of caution and keep him or her in the ED for his own safety and the safety of others.
Postpartum Shortness of Breath
A 35-year-old woman presented to the ED after referral by her obstetrician. Six days prior, the patient had given birth to twins without incident. On postpartum hospital day 2, however, she developed mild shortness of breath, and a chest X-ray was ordered. Since there was concern for possible pneumonia, the patient was prescribed oral antibiotics and discharged home on hospital day 4. She continued to complain of shortness of breath following discharge; at that time, the obstetrician referred the patient to the ED for further evaluation.
The patient was evaluated by the EP, who ordered a chest X-ray. He was also concerned that patient had pneumonia and prescribed a different class of antibiotic before discharging the patient home.
One week later, the patient presented back to the same ED with continued shortness of breath. On this visit, she was seen by a physician assistant (PA). Following the history taking and physical examination, a chest X-ray and rapid flu and rapid strep tests were ordered. Both the PA and supervising EP reviewed the chest X-ray and were concerned for pneumonia; however, both the flu and strep tests were negative. A third class of antibiotic was prescribed, and the patient was discharged home.
The chest X-ray on the second ED visit was not interpreted by a radiologist until 3 days later (The patient was seen on a Friday evening and the films were not read until the following Monday morning). The radiologist’s interpretation was “worsening congestive heart failure” (CHF). Two days later (5 days following the second ED visit), the EP was notified of the interpretation discrepancy and made multiple attempts to contact the patient, which included leaving a voice-mail message on her home phone.
The patient returned the call the following day and spoke with one of the ED nurses, who encouraged her to return immediately to the ED. The patient returned to the ED the next day (1 week after her second ED visit) and was admitted to the hospital for CHF secondary to postpartum cardiomyopathy. Unfortunately, she developed an embolus to her kidney, followed by an ischemic cerebrovascular accident, and died 3 weeks after admission.
The patient’s family filed a malpractice lawsuit against the hospital, the EPs, and the PA for negligent delay in making the correct diagnosis, stating that patient’s subsequent stroke and death were a direct result of this delay. Following deliberations, all of the EPs involved in the case were found free of negligence; the PA and the hospital ED, however, were found guilty.
Discussion
Interestingly, the majority of successful malpractice suits against physicians involve cognitive errors and system issues; this case is no exception. Making the correct diagnosis in a patient is a complex process, involving data gathering and synthesis, intuition, clinical experience, and logical thinking. Unfortunately, biases can occur during this process and result in misdiagnosis or delayed diagnosis. These biases include anchoring bias, confirmation bias, premature closure, and diagnosis momentum.1
Anchoring Bias. This occurs when a physician relies too heavily on the first piece of information or one’s initial impression.1 Despite evidence to the contrary, the physician keeps returning to the initial diagnosis (ie, he or she is “anchored” to it).
Confirmation Bias. Related to anchoring bias, in confirmation bias, the physician ignores or discounts evidence that contradicts one’s initial impression and focuses solely on the evidence supporting it.1
Both anchoring bias and confirmation bias appear to have played a role in this case. The differential diagnosis was never broadened beyond pneumonia, despite the fact that one must also consider pulmonary embolism (ie, a hypercoagulable state) and CHF (ie, postpartum cardiomyopathy) in a patient complaining of dyspnea in the postpartum period.
Premature Closure. This occurs when the physician finds a cause that fits the clinical picture and ceases to search for other diagnostic possibilities.1,2
Diagnosis Momentum. A bias that occurs when the diagnosis considered a possibility by one physician becomes a definitive diagnosis as it is passed from one physician to the next; it then becomes accepted without question by physicians down the line.1 This type of bias also seems to have played a role in this case.
There are a few strategies to help prevent or minimize these types of errors. First, as new data are gathered, one should reconsider and reprioritize the differential diagnosis. When certain data points do not fit neatly with an earlier diagnosis, careful attention must be paid to them. This is especially true for the patient receiving appropriate treatment but not showing clinical improvement. While it is usually helpful to know previous working diagnoses, the clinician must try to keep an open mind and consider alternative diagnoses. At the end of the day, the lesson is the need to develop a broad differential diagnosis.2
The system error in this case involves the lack of timely overread of radiology studies. Emergency medicine is a 24-hour, 7-day-a-week specialty; therefore, support services to the ED need to be similarly available. With today’s teleradiology and dedicated night readers, it is difficult to justify not providing such a service. This situation explains, in part, the negligent verdict against the hospital.
Chest Pain in a Man With Type 2 Diabetes
A 54-year-old man presented to the ED with a several-hour history of chest pain and shortness of breath. His medical history was remarkable for type 2 diabetes mellitus. He denied any associated nausea, vomiting, or diaphoresis. He smoked one pack of cigarettes per day and drank alcohol on occasion. The patient further denied having experienced similar symptoms in the past. All vital signs were normal, and he appeared comfortable and in no acute distress. His physical examination was completely unremarkable.
An electrocardiogram (ECG) revealed Q-waves in the anterior leads, but was otherwise nondiagnostic. The results of a portable chest X-ray were interpreted as normal. Cardiac enzyme testing revealed a positive troponin I, but a normal creatine phosphokinase-MB (CPK-MB). The patient’s complete blood count and coagulation studies were normal, and a basic metabolic profile was remarkable only for a blood sugar of 540 mg/dL; his serum bicarbonate value was normal.
The patient was placed on oxygen via nasal cannula, administered an aspirin (325 mg), and given subcutaneous regular insulin for hyperglycemia. The EP contacted a hospitalist to admit the patient. The hospitalist accepted the patient and admitted him to the telemetry floor.
Upon arrival at telemetry, the patient was examined by a nurse who noted rhonchi bilaterally on lung auscultation. Shortly afterward, he became anxious, and the nurse consulted the hospitalist, who ordered administration of lorazepam. Approximately 20 minutes later, the patient went into cardiac arrest and died.
This patient was never examined by the hospitalist prior to coding. An autopsy revealed evidence of severe coronary artery disease, a previous infarction that was at least a few months old with scarring of the left ventricle, and a recent infarction that had begun at least 12 hours prior to death.
The family sued all of the providers involved in the care of the patient. At trial, there was a factual dispute regarding whether the EP informed the hospitalist of the elevated troponin I level. The defendants argued that the patient had sustained irreversible heart damage prior to his arrival at the hospital, and that nothing any of the defendants could have done would have saved his life. The jury deliberated for approximately 2 hours before delivering a verdict in favor of the defense.
Discussion
Clearly, this verdict could have gone the other way. This patient was experiencing a non-ST segment elevation myocardial infarction (MI). The nondiagnostic ECG, coupled with the elevated troponin I, indicated damage of heart muscle from an acute interruption of coronary blood flow.
There are several problems with the management of this case. First, this patient required a cardiology consult for risk stratification. Several scoring systems could have been used to determine whether this patient was a candidate for early (ie, within 4-48 hours) invasive treatments such as percutaneous intervention or a more conservative approach.
Second, having sustained an MI, this patient was at high risk for complications such as ventricular arrhythmias, heart failure, cardiogenic shock, and other serious adverse events. Patients with acute MI should be admitted to the critical care or intensive care unit. In addition to aspirin, this patient should have received nitroglycerin and anticoagulation therapy. Either heparin or a low molecular weight heparin, such as enoxaparin, would have been appropriate if no contraindications existed. Finally, additional therapy including glycoprotein IIB/IIIA inhibitors, clopidogrel, etc, may have been indicated depending upon the timing of percutaneous intervention.1
It appears that both the EP and the hospitalist either failed to appreciate the significance of the elevated troponin I or overlooked it. This patient had normal renal function, so the only explanation—especially in the setting of a middle-aged man complaining of chest pain—was that myocardial damage had occurred.
Alcohol Detoxification in a Young Man
A young man was brought to the ED by a friend. The patient’s sole complaint was the need for help with his alcohol dependency. In addition to alcohol abuse, his medical history was remarkable only for an admission 1 month prior for suicidal ideation. The patient denied suicidal or homicidal ideations on this presentation. The physical examination revealed stable vital signs, but conjunctival injection, slurred speech, and a strong odor of alcohol. A blood alcohol test showed a concentration level of 0.36 g/dL. The patient, however, was alert and able to ambulate without assistance. He was medically cleared by the EP and arrangements were made to admit him to a local detoxification center.
Approximately 4 hours after his arrival, while waiting for transport to the detoxification center, the patient became impatient with the delay, removed his intravenous line, and told the nurse that he was going home via taxi. The nurse encouraged him to call a friend to take him home, to which to the patient agreed. The nurse left the patient to inform the EP of his desire to go home; when she returned, she discovered that the patient had already left the hospital. The physician notified hospital security but not the police. Approximately 2 hours later, the patient was struck by a car and seriously injured.
The patient sued the EP and the hospital for negligence and medical malpractice. The suit alleged that the physician and the hospital should have prevented the patient from leaving the ED. The physician and the hospital requested a dismissal, arguing that the patient did not exhibit any suicidal or homicidal ideation, presented on his own volition, and, though intoxicated, could still make decisions for himself. An appellate court granted the motion, holding that the defendants “lacked authority to confine the plaintiff upon his departure” from the ED.
Discussion
When a patient attempts to leave the ED against medical advice, the treating physician should make an attempt to convince him or her to remain for treatment. Often, something as simple as offering a cup of coffee will change a patient’s mind. In other instances, the use of chemical or physical restraint may be required. The handling of the case ultimately becomes a question of whether the patient was competent to make decisions and whether he presented a danger to himself or others. The extent of intoxication varies by the degree and does not of itself constitute incapability to make decisions. All practicing EPs have cared for patients with blood alcohol levels above the legal limit for driving, but who were functionally sober and able to make decisions. If a patient is competent and does not present a danger to self or others, he or she can decide to leave the ED without further management. However, it is best to release the patient in the company of friends or family, as was urged by the nurse in this case. Obviously, such a patient should not be allowed to drive himself home.
When a patient does leave against medical advice, the physician and nurse should document in the ED record their conversations urging him or her to stay. Alternatively, when a patient is found incompetent of making decisions or is a danger to self or others, he or she must be prevented from leaving the ED. This includes use of the minimal amount of physical or chemical restraint needed to keep the patient from leaving. When there is doubt that the patient is able to make a competent decision, it is better to err on the side of caution and keep him or her in the ED for his own safety and the safety of others.
Postpartum Shortness of Breath
- Penney FT, Datal AK: Understanding diagnostic error. Hospital Medicine Clinics. 2013;2(2):e292-e303.
- Ely JW, Kaldjian LC, D’Alessandro DM. Diagnostic errors in primary care: lessons learned. J Am Board Fam Med. 2012;25(1):87-97.
Chest Pain in a Man With Type 2 Diabetes
- Anantharam V, Lim SH. Treatment of NSTEMI (Non-ST elevation myocardial infarction). Curr Emerg Hosp Med Rep. 2013;1(1):18-28.
Postpartum Shortness of Breath
- Penney FT, Datal AK: Understanding diagnostic error. Hospital Medicine Clinics. 2013;2(2):e292-e303.
- Ely JW, Kaldjian LC, D’Alessandro DM. Diagnostic errors in primary care: lessons learned. J Am Board Fam Med. 2012;25(1):87-97.
Chest Pain in a Man With Type 2 Diabetes
- Anantharam V, Lim SH. Treatment of NSTEMI (Non-ST elevation myocardial infarction). Curr Emerg Hosp Med Rep. 2013;1(1):18-28.
Senate passes 1-year SGR patch; delays ICD-10 until 2015
In a last-minute move, Congress averted a scheduled 24% cut to Medicare physician fees slated to start on April 1, while simultaneously delaying the move to the ICD-10 coding sets.
On March 31, the Senate voted 64 to 35 to approve H.R. 4302, a bill that replaces the scheduled cut called for by the Medicare Sustainable Growth Rate formula with a 0.5% fee increase through the end of 2014 and a pay freeze from Jan. 1, 2015 through March 15, 2015. The bill also bars the Health and Human Services (HHS) department from implementing ICD-10 until Oct. 1, 2015.

The House passed the same legislation on March 27. It now heads to the White House for President Obama’s signature.
At first glance, the bill looks like good news for physicians, who will get relief from both a hefty Medicare fee cut and a costly new regulatory requirement. But many physician organizations, led by the American Medical Association, have campaigned against the temporary patch, saying that it essentially stops the work to permanently repeal the SGR.
"It appears that an unprecedented, bipartisan agreement on Medicare reform is on the verge of being cast aside because elected leaders are unwilling to make tough choices to strengthen programs serving 50 million Americans," the AMA and more than 50 other medical societies wrote to congressional leaders before the House vote.
Several physician groups had endorsed a bipartisan legislative package that would have eliminated the SGR and replaced it with a combination of small fee increases and delivery system reforms. The hurdle to passing the legislation was finding a way to pay for it that would appeal to both Democrats and Republicans.
Recently, the House passed H.R. 4015, which would have funded the permanent SGR repeal package with a 5-year delay of the Affordable Care Act’s individual insurance mandate. But that bill is unlikely to be considered in the Democratic-controlled Senate. And an attempt by Sen. Ron Wyden (D.-Ore.) to move the permanent SGR repeal forward and pay for it using the savings from the end of the wars in Iraq and Afghanistan failed to gain enough votes in the Senate.
Before the March 31 vote, Sen. Wyden chided fellow lawmakers for continuing to pass temporary fixes to the SGR problem rather than replacing it and moving to a payment system that incentivizes quality improvement. "It can’t be ducked much longer," he said.
But Sen. Orrin Hatch (R.-Utah), who worked on the bipartisan bill to replace the SGR, said he objects to the funding mechanism that Sen. Wyden proposed. He said the 12-month SGR patch will give lawmakers more time to agree on how to pay for a permanent fix. "I’m not going to make the perfect the enemy of the good," he said on the Senate floor.
On Twitter @maryellenny
In a last-minute move, Congress averted a scheduled 24% cut to Medicare physician fees slated to start on April 1, while simultaneously delaying the move to the ICD-10 coding sets.
On March 31, the Senate voted 64 to 35 to approve H.R. 4302, a bill that replaces the scheduled cut called for by the Medicare Sustainable Growth Rate formula with a 0.5% fee increase through the end of 2014 and a pay freeze from Jan. 1, 2015 through March 15, 2015. The bill also bars the Health and Human Services (HHS) department from implementing ICD-10 until Oct. 1, 2015.
The House passed the same legislation on March 27. It now heads to the White House for President Obama’s signature.
At first glance, the bill looks like good news for physicians, who will get relief from both a hefty Medicare fee cut and a costly new regulatory requirement. But many physician organizations, led by the American Medical Association, have campaigned against the temporary patch, saying that it essentially stops the work to permanently repeal the SGR.
"It appears that an unprecedented, bipartisan agreement on Medicare reform is on the verge of being cast aside because elected leaders are unwilling to make tough choices to strengthen programs serving 50 million Americans," the AMA and more than 50 other medical societies wrote to congressional leaders before the House vote.
Several physician groups had endorsed a bipartisan legislative package that would have eliminated the SGR and replaced it with a combination of small fee increases and delivery system reforms. The hurdle to passing the legislation was finding a way to pay for it that would appeal to both Democrats and Republicans.
Recently, the House passed H.R. 4015, which would have funded the permanent SGR repeal package with a 5-year delay of the Affordable Care Act’s individual insurance mandate. But that bill is unlikely to be considered in the Democratic-controlled Senate. And an attempt by Sen. Ron Wyden (D.-Ore.) to move the permanent SGR repeal forward and pay for it using the savings from the end of the wars in Iraq and Afghanistan failed to gain enough votes in the Senate.
Before the March 31 vote, Sen. Wyden chided fellow lawmakers for continuing to pass temporary fixes to the SGR problem rather than replacing it and moving to a payment system that incentivizes quality improvement. "It can’t be ducked much longer," he said.
But Sen. Orrin Hatch (R.-Utah), who worked on the bipartisan bill to replace the SGR, said he objects to the funding mechanism that Sen. Wyden proposed. He said the 12-month SGR patch will give lawmakers more time to agree on how to pay for a permanent fix. "I’m not going to make the perfect the enemy of the good," he said on the Senate floor.
On Twitter @maryellenny
In a last-minute move, Congress averted a scheduled 24% cut to Medicare physician fees slated to start on April 1, while simultaneously delaying the move to the ICD-10 coding sets.
On March 31, the Senate voted 64 to 35 to approve H.R. 4302, a bill that replaces the scheduled cut called for by the Medicare Sustainable Growth Rate formula with a 0.5% fee increase through the end of 2014 and a pay freeze from Jan. 1, 2015 through March 15, 2015. The bill also bars the Health and Human Services (HHS) department from implementing ICD-10 until Oct. 1, 2015.
The House passed the same legislation on March 27. It now heads to the White House for President Obama’s signature.
At first glance, the bill looks like good news for physicians, who will get relief from both a hefty Medicare fee cut and a costly new regulatory requirement. But many physician organizations, led by the American Medical Association, have campaigned against the temporary patch, saying that it essentially stops the work to permanently repeal the SGR.
"It appears that an unprecedented, bipartisan agreement on Medicare reform is on the verge of being cast aside because elected leaders are unwilling to make tough choices to strengthen programs serving 50 million Americans," the AMA and more than 50 other medical societies wrote to congressional leaders before the House vote.
Several physician groups had endorsed a bipartisan legislative package that would have eliminated the SGR and replaced it with a combination of small fee increases and delivery system reforms. The hurdle to passing the legislation was finding a way to pay for it that would appeal to both Democrats and Republicans.
Recently, the House passed H.R. 4015, which would have funded the permanent SGR repeal package with a 5-year delay of the Affordable Care Act’s individual insurance mandate. But that bill is unlikely to be considered in the Democratic-controlled Senate. And an attempt by Sen. Ron Wyden (D.-Ore.) to move the permanent SGR repeal forward and pay for it using the savings from the end of the wars in Iraq and Afghanistan failed to gain enough votes in the Senate.
Before the March 31 vote, Sen. Wyden chided fellow lawmakers for continuing to pass temporary fixes to the SGR problem rather than replacing it and moving to a payment system that incentivizes quality improvement. "It can’t be ducked much longer," he said.
But Sen. Orrin Hatch (R.-Utah), who worked on the bipartisan bill to replace the SGR, said he objects to the funding mechanism that Sen. Wyden proposed. He said the 12-month SGR patch will give lawmakers more time to agree on how to pay for a permanent fix. "I’m not going to make the perfect the enemy of the good," he said on the Senate floor.
On Twitter @maryellenny

Initial MARQUIS results offer lessons in med reconciliation
LAS VEGAS – Tired of getting a patient medication list that isn’t reliable? A 3-year study on medication reconciliation could offer a roadmap for improving that list and reducing potentially harmful errors.
Preliminary results from MARQUIS (the Multi-Center Medication Reconciliation Quality Improvement Study) indicate that hospitals are able to reduce unintentional medication discrepancies by implementing a menu of interventions ranging from training providers to take a better medication history to stationing a designated provider in the emergency department to reconcile the patient’s information with pharmacies and primary care offices. But outside forces, such as problems with an electronic health record (EHR) system, can offset those effects.

The 3-year study, which will wrap up in the next few months, is sponsored by the Society of Hospital Medicine, with $1.5 million in funding from the Agency for Healthcare Research and Quality.
In the first phase of the study, researchers identified evidence-based techniques for taking the best possible medication history from hospitalized patients and synthesized them into a toolkit for clinicians. The free toolkit includes how-to videos and pocket cards. The second phase of the study is the mentored implementation of the techniques at five sites: two academic medical centers, two community hospitals, and one Veterans Affairs medical center.
Initial results from two of the five sites show that training on how to take a better medication history and clarity about who should be working on reconciling the medication list can help improve medication discrepancies. But while the interventions are promising, the initial case studies show mixed results.
While one community hospital site was able to lower medication discrepancies significantly, a second community hospital site had a spike in its medication discrepancies as it underwent a problematic implementation of a new EHR system.
Eighteen minutes to win it
At the first site, a Medication Reconciliation Assistant (MRA) program was used to improve the reliability of medication lists. The MRA is stationed in the emergency department and interviews patients about their medications and then verifies that list with the pharmacy, the primary care physician, or the skilled nursing facility. That new medication list is then handed off to the admitting physician. The process usually takes about 18-20 minutes.
They MRA program is staffed by four full-time employees, all pharmacy technicians with experience in retail pharmacies, who work 8-hour shifts throughout the week.
"It doesn’t have to be a pharmacy technician," said Dr. Jason Stein, a MARQUIS coinvestigator and a professor of medicine at Emory University, Atlanta, at the annual meeting of the Society of Hospital Medicine. "But somebody needs to be spending that 18 minutes doing something that roughly looks like this."
At that first site, unintentional medication discrepancies from either history or reconciliation errors dropped from 4.5 per patient at the in the preintervention period to 3.4 per patient. And the total number of potentially harmful discrepancies was reduced from 0.25 to 0.09 per patient.
At the second site, a smaller community hospital, the quality improvement team provided training to front-line providers on medication history taking and counseling at discharge and created a new hospital policy that clarified expectations about who would perform medication reconciliation and when they would do it. And recently, they began stationing a provider in the emergency department 5 days a week to work on medication reconciliation.
But shortly after the second hospital began implementing the MARQUIS interventions, the hospital launched a new EHR system that created problems for medication reconciliation. For instance, with the paper system, the admitting physician was accountable for the initial medication history. But under the electronic system, that accountability was lost. Also, the new EHR was unable to group medications as "continued," "changed," "stopped," or "new," making it difficult to perform discharge medication counseling.
The result was that, after some initial success, unintentional medication discrepancies spiked. In the preintervention period, unintentional medication discrepancies were 2.0 per patient, but they rose to nearly 5 discrepancies per patient after the rollout of the new EHR system. They have since fallen back down to 3.8 per patient. Similarly, the total of potentially harmful discrepancies rose from 0.20 to 1.11 per patient.
The free MARQUIS toolkit is available online.
On Twitter @maryellenny
LAS VEGAS – Tired of getting a patient medication list that isn’t reliable? A 3-year study on medication reconciliation could offer a roadmap for improving that list and reducing potentially harmful errors.
Preliminary results from MARQUIS (the Multi-Center Medication Reconciliation Quality Improvement Study) indicate that hospitals are able to reduce unintentional medication discrepancies by implementing a menu of interventions ranging from training providers to take a better medication history to stationing a designated provider in the emergency department to reconcile the patient’s information with pharmacies and primary care offices. But outside forces, such as problems with an electronic health record (EHR) system, can offset those effects.
The 3-year study, which will wrap up in the next few months, is sponsored by the Society of Hospital Medicine, with $1.5 million in funding from the Agency for Healthcare Research and Quality.
In the first phase of the study, researchers identified evidence-based techniques for taking the best possible medication history from hospitalized patients and synthesized them into a toolkit for clinicians. The free toolkit includes how-to videos and pocket cards. The second phase of the study is the mentored implementation of the techniques at five sites: two academic medical centers, two community hospitals, and one Veterans Affairs medical center.
Initial results from two of the five sites show that training on how to take a better medication history and clarity about who should be working on reconciling the medication list can help improve medication discrepancies. But while the interventions are promising, the initial case studies show mixed results.
While one community hospital site was able to lower medication discrepancies significantly, a second community hospital site had a spike in its medication discrepancies as it underwent a problematic implementation of a new EHR system.
Eighteen minutes to win it
At the first site, a Medication Reconciliation Assistant (MRA) program was used to improve the reliability of medication lists. The MRA is stationed in the emergency department and interviews patients about their medications and then verifies that list with the pharmacy, the primary care physician, or the skilled nursing facility. That new medication list is then handed off to the admitting physician. The process usually takes about 18-20 minutes.
They MRA program is staffed by four full-time employees, all pharmacy technicians with experience in retail pharmacies, who work 8-hour shifts throughout the week.
"It doesn’t have to be a pharmacy technician," said Dr. Jason Stein, a MARQUIS coinvestigator and a professor of medicine at Emory University, Atlanta, at the annual meeting of the Society of Hospital Medicine. "But somebody needs to be spending that 18 minutes doing something that roughly looks like this."
At that first site, unintentional medication discrepancies from either history or reconciliation errors dropped from 4.5 per patient at the in the preintervention period to 3.4 per patient. And the total number of potentially harmful discrepancies was reduced from 0.25 to 0.09 per patient.
At the second site, a smaller community hospital, the quality improvement team provided training to front-line providers on medication history taking and counseling at discharge and created a new hospital policy that clarified expectations about who would perform medication reconciliation and when they would do it. And recently, they began stationing a provider in the emergency department 5 days a week to work on medication reconciliation.
But shortly after the second hospital began implementing the MARQUIS interventions, the hospital launched a new EHR system that created problems for medication reconciliation. For instance, with the paper system, the admitting physician was accountable for the initial medication history. But under the electronic system, that accountability was lost. Also, the new EHR was unable to group medications as "continued," "changed," "stopped," or "new," making it difficult to perform discharge medication counseling.
The result was that, after some initial success, unintentional medication discrepancies spiked. In the preintervention period, unintentional medication discrepancies were 2.0 per patient, but they rose to nearly 5 discrepancies per patient after the rollout of the new EHR system. They have since fallen back down to 3.8 per patient. Similarly, the total of potentially harmful discrepancies rose from 0.20 to 1.11 per patient.
The free MARQUIS toolkit is available online.
On Twitter @maryellenny
LAS VEGAS – Tired of getting a patient medication list that isn’t reliable? A 3-year study on medication reconciliation could offer a roadmap for improving that list and reducing potentially harmful errors.
Preliminary results from MARQUIS (the Multi-Center Medication Reconciliation Quality Improvement Study) indicate that hospitals are able to reduce unintentional medication discrepancies by implementing a menu of interventions ranging from training providers to take a better medication history to stationing a designated provider in the emergency department to reconcile the patient’s information with pharmacies and primary care offices. But outside forces, such as problems with an electronic health record (EHR) system, can offset those effects.
The 3-year study, which will wrap up in the next few months, is sponsored by the Society of Hospital Medicine, with $1.5 million in funding from the Agency for Healthcare Research and Quality.
In the first phase of the study, researchers identified evidence-based techniques for taking the best possible medication history from hospitalized patients and synthesized them into a toolkit for clinicians. The free toolkit includes how-to videos and pocket cards. The second phase of the study is the mentored implementation of the techniques at five sites: two academic medical centers, two community hospitals, and one Veterans Affairs medical center.
Initial results from two of the five sites show that training on how to take a better medication history and clarity about who should be working on reconciling the medication list can help improve medication discrepancies. But while the interventions are promising, the initial case studies show mixed results.
While one community hospital site was able to lower medication discrepancies significantly, a second community hospital site had a spike in its medication discrepancies as it underwent a problematic implementation of a new EHR system.
Eighteen minutes to win it
At the first site, a Medication Reconciliation Assistant (MRA) program was used to improve the reliability of medication lists. The MRA is stationed in the emergency department and interviews patients about their medications and then verifies that list with the pharmacy, the primary care physician, or the skilled nursing facility. That new medication list is then handed off to the admitting physician. The process usually takes about 18-20 minutes.
They MRA program is staffed by four full-time employees, all pharmacy technicians with experience in retail pharmacies, who work 8-hour shifts throughout the week.
"It doesn’t have to be a pharmacy technician," said Dr. Jason Stein, a MARQUIS coinvestigator and a professor of medicine at Emory University, Atlanta, at the annual meeting of the Society of Hospital Medicine. "But somebody needs to be spending that 18 minutes doing something that roughly looks like this."
At that first site, unintentional medication discrepancies from either history or reconciliation errors dropped from 4.5 per patient at the in the preintervention period to 3.4 per patient. And the total number of potentially harmful discrepancies was reduced from 0.25 to 0.09 per patient.
At the second site, a smaller community hospital, the quality improvement team provided training to front-line providers on medication history taking and counseling at discharge and created a new hospital policy that clarified expectations about who would perform medication reconciliation and when they would do it. And recently, they began stationing a provider in the emergency department 5 days a week to work on medication reconciliation.
But shortly after the second hospital began implementing the MARQUIS interventions, the hospital launched a new EHR system that created problems for medication reconciliation. For instance, with the paper system, the admitting physician was accountable for the initial medication history. But under the electronic system, that accountability was lost. Also, the new EHR was unable to group medications as "continued," "changed," "stopped," or "new," making it difficult to perform discharge medication counseling.
The result was that, after some initial success, unintentional medication discrepancies spiked. In the preintervention period, unintentional medication discrepancies were 2.0 per patient, but they rose to nearly 5 discrepancies per patient after the rollout of the new EHR system. They have since fallen back down to 3.8 per patient. Similarly, the total of potentially harmful discrepancies rose from 0.20 to 1.11 per patient.
The free MARQUIS toolkit is available online.
On Twitter @maryellenny
EXPERT ANALYSIS FROM HOSPITAL MEDICINE 14

House passes temporary SGR fix, 1-year ICD-10 delay
Legislation to delay the 24% Medicare pay cut based on the Sustainable Growth Rate formula passed the House by a voice vote March 27, despite the objections of a large coalition of physician organizations.
The Protecting Access to Medicare Act (H.R. 4302) would delay the SGR-mandated cut slated to take effect March 31, replace it with a 0.5% pay increase through the end of 2014, and freeze Medicare pay at that rate for the first quarter of 2015. The bill also would delay implementation of ICD-10 for 1 year.

At press time, it was uncertain if the Senate would take up the bill.
Physicians organizations favor full repeal of the SGR and would like to see it replaced with a payment and delivery system reform policy that passed the House earlier this month as H.R. 4015. Financing for that legislation depended on a 5-year delay on the Affordable Care Act’s individual mandate, something most Democratic lawmakers do not support. H.R. 4015 had not been taken up by the Senate as the March 31 deadline loomed.
Prior to the vote, a coalition of 58 organizations called on the House to vote against the legislation.
"Instead of reforming the Medicare physician payment system, Congress seems intent on imposing yet another round of arbitrary provider payment reductions to maintain a corrosive policy that essentially every member of Congress says should be scrapped," the coalition wrote in a letter to House Speaker John Boehner (R-Ohio) and Minority Leader Nancy Pelosi (D-Calif.). "The endless cycle of short-term remedies that serve to support a failed policy are no longer acceptable."
[email protected]
On Twitter @denisefulton
Legislation to delay the 24% Medicare pay cut based on the Sustainable Growth Rate formula passed the House by a voice vote March 27, despite the objections of a large coalition of physician organizations.
The Protecting Access to Medicare Act (H.R. 4302) would delay the SGR-mandated cut slated to take effect March 31, replace it with a 0.5% pay increase through the end of 2014, and freeze Medicare pay at that rate for the first quarter of 2015. The bill also would delay implementation of ICD-10 for 1 year.
At press time, it was uncertain if the Senate would take up the bill.
Physicians organizations favor full repeal of the SGR and would like to see it replaced with a payment and delivery system reform policy that passed the House earlier this month as H.R. 4015. Financing for that legislation depended on a 5-year delay on the Affordable Care Act’s individual mandate, something most Democratic lawmakers do not support. H.R. 4015 had not been taken up by the Senate as the March 31 deadline loomed.
Prior to the vote, a coalition of 58 organizations called on the House to vote against the legislation.
"Instead of reforming the Medicare physician payment system, Congress seems intent on imposing yet another round of arbitrary provider payment reductions to maintain a corrosive policy that essentially every member of Congress says should be scrapped," the coalition wrote in a letter to House Speaker John Boehner (R-Ohio) and Minority Leader Nancy Pelosi (D-Calif.). "The endless cycle of short-term remedies that serve to support a failed policy are no longer acceptable."
[email protected]
On Twitter @denisefulton
Legislation to delay the 24% Medicare pay cut based on the Sustainable Growth Rate formula passed the House by a voice vote March 27, despite the objections of a large coalition of physician organizations.
The Protecting Access to Medicare Act (H.R. 4302) would delay the SGR-mandated cut slated to take effect March 31, replace it with a 0.5% pay increase through the end of 2014, and freeze Medicare pay at that rate for the first quarter of 2015. The bill also would delay implementation of ICD-10 for 1 year.
At press time, it was uncertain if the Senate would take up the bill.
Physicians organizations favor full repeal of the SGR and would like to see it replaced with a payment and delivery system reform policy that passed the House earlier this month as H.R. 4015. Financing for that legislation depended on a 5-year delay on the Affordable Care Act’s individual mandate, something most Democratic lawmakers do not support. H.R. 4015 had not been taken up by the Senate as the March 31 deadline loomed.
Prior to the vote, a coalition of 58 organizations called on the House to vote against the legislation.
"Instead of reforming the Medicare physician payment system, Congress seems intent on imposing yet another round of arbitrary provider payment reductions to maintain a corrosive policy that essentially every member of Congress says should be scrapped," the coalition wrote in a letter to House Speaker John Boehner (R-Ohio) and Minority Leader Nancy Pelosi (D-Calif.). "The endless cycle of short-term remedies that serve to support a failed policy are no longer acceptable."
[email protected]
On Twitter @denisefulton

Line up credit now for possible ICD-10 cash crunch, experts advise
Cash shortfalls related to the Oct. 1 switchover to ICD-10 "could be potentially devastating for a lot of practices," according to Dr. Barbara McAneny. That’s why she is setting up a $4 million line of credit to pay the bills and protect her practice in case claims are rejected and income is held up.
Health IT expert Stanley Nachimson agreed with her: Now is the time to prepare financially for the coming of ICD-10.
A plan has to be developed well before Oct. 1, said Mr. Nachimson, who has studied the cost of ICD-10 implementation for the American Medical Association.
"You have got to prepare for ICD-10 or you risk significant payment disruptions," he said at the AMA National Advocacy Conference in Washington.
Dr. McAneny, managing partner and chief executive officer of the New Mexico Cancer Center in Albuquerque, said that she’s already started talking to her local banker. She said she has very little faith that the ICD-10 transition will be smooth, given her experience in moving from the Health Insurance Portability and Accountability Act 4010 standard to the 5010 standard in 2011.

"That was a much smaller event," said Dr. McAneny, who is also a member of the AMA Board of Trustees . And, with the change in HIPAA standards, the Centers for Medicare & Medicaid Services allowed for several transitional periods, where the old format continued to be accepted.
Dr. McAneny recalled that in 2011, the test runs were fine, and that both the clearinghouse and payer said that her practice was ready. But when the transition started, "we got denials like mad," she said in an interview. Some payers made no payments for 2-3 months.
This time, a substantial line of credit should be enough to cover 4 months of payroll, she said, adding that she anticipates hiring more coders and paying her billing staff extra to potentially chase denials.
"This transition has the potential to be a major disrupter," Dr. McAneny said.
Robert M. Tennant, senior policy adviser at the Medical Group Management Association (MGMA), said that physicians need to figure out soon how they will cover cash shortfalls, in part, because they may have to jump through a lot of hoops to satisfy a bank’s demands. "The days of supereasy credit are probably gone," he said in an interview.
He suggested arranging a line of credit to cover at least 2 months of operating expenses. A bank’s willingness to extend credit will depend on several variables, including the age of the practice, how long it’s been in its location, whether the practice owns or rents space, and what type of collateral is available to secure the line. In some cases, physicians might need to put up personal collateral.
"The hope, of course, is that you won’t have to tap into that line of credit very much, if at all," he said.
And it’s important to find out sooner rather than later how much credit can be secured. If it’s not enough to cover a few months’ expenses, practices might want to increase their cash reserves, Mr. Tennant said.
It’s important to "clear the decks" of any claims for services prior to Oct. 1, he said. Health plans will likely be overwhelmed by the transition, and that could lead to delays in payment for ICD-9 claims.
Mr. Nachimson said that practices should reach out to their major payers to get as much information as possible on changes in coverage policies and reimbursement for unspecified codes. "What they’re doing has a major impact on you," said Mr Nachimson.
Although many are still hoping for a delay in ICD-10, Mr. Tennant urged physicians to plan for the Oct. 1 implementation, "It’s too big a gamble for the practice to assume the date is going to be moved," he said. "If you bet the house and you lose, you’re going to be in a world of financial hurt."
The MGMA is suggesting that physicians "assume the worst and hope for the best," especially since there’s no real downside to improving documentation of diagnoses and getting staff better training in coding, he said.
On Twitter @aliciaault
Cash shortfalls related to the Oct. 1 switchover to ICD-10 "could be potentially devastating for a lot of practices," according to Dr. Barbara McAneny. That’s why she is setting up a $4 million line of credit to pay the bills and protect her practice in case claims are rejected and income is held up.
Health IT expert Stanley Nachimson agreed with her: Now is the time to prepare financially for the coming of ICD-10.
A plan has to be developed well before Oct. 1, said Mr. Nachimson, who has studied the cost of ICD-10 implementation for the American Medical Association.
"You have got to prepare for ICD-10 or you risk significant payment disruptions," he said at the AMA National Advocacy Conference in Washington.
Dr. McAneny, managing partner and chief executive officer of the New Mexico Cancer Center in Albuquerque, said that she’s already started talking to her local banker. She said she has very little faith that the ICD-10 transition will be smooth, given her experience in moving from the Health Insurance Portability and Accountability Act 4010 standard to the 5010 standard in 2011.
"That was a much smaller event," said Dr. McAneny, who is also a member of the AMA Board of Trustees . And, with the change in HIPAA standards, the Centers for Medicare & Medicaid Services allowed for several transitional periods, where the old format continued to be accepted.
Dr. McAneny recalled that in 2011, the test runs were fine, and that both the clearinghouse and payer said that her practice was ready. But when the transition started, "we got denials like mad," she said in an interview. Some payers made no payments for 2-3 months.
This time, a substantial line of credit should be enough to cover 4 months of payroll, she said, adding that she anticipates hiring more coders and paying her billing staff extra to potentially chase denials.
"This transition has the potential to be a major disrupter," Dr. McAneny said.
Robert M. Tennant, senior policy adviser at the Medical Group Management Association (MGMA), said that physicians need to figure out soon how they will cover cash shortfalls, in part, because they may have to jump through a lot of hoops to satisfy a bank’s demands. "The days of supereasy credit are probably gone," he said in an interview.
He suggested arranging a line of credit to cover at least 2 months of operating expenses. A bank’s willingness to extend credit will depend on several variables, including the age of the practice, how long it’s been in its location, whether the practice owns or rents space, and what type of collateral is available to secure the line. In some cases, physicians might need to put up personal collateral.
"The hope, of course, is that you won’t have to tap into that line of credit very much, if at all," he said.
And it’s important to find out sooner rather than later how much credit can be secured. If it’s not enough to cover a few months’ expenses, practices might want to increase their cash reserves, Mr. Tennant said.
It’s important to "clear the decks" of any claims for services prior to Oct. 1, he said. Health plans will likely be overwhelmed by the transition, and that could lead to delays in payment for ICD-9 claims.
Mr. Nachimson said that practices should reach out to their major payers to get as much information as possible on changes in coverage policies and reimbursement for unspecified codes. "What they’re doing has a major impact on you," said Mr Nachimson.
Although many are still hoping for a delay in ICD-10, Mr. Tennant urged physicians to plan for the Oct. 1 implementation, "It’s too big a gamble for the practice to assume the date is going to be moved," he said. "If you bet the house and you lose, you’re going to be in a world of financial hurt."
The MGMA is suggesting that physicians "assume the worst and hope for the best," especially since there’s no real downside to improving documentation of diagnoses and getting staff better training in coding, he said.
On Twitter @aliciaault
Cash shortfalls related to the Oct. 1 switchover to ICD-10 "could be potentially devastating for a lot of practices," according to Dr. Barbara McAneny. That’s why she is setting up a $4 million line of credit to pay the bills and protect her practice in case claims are rejected and income is held up.
Health IT expert Stanley Nachimson agreed with her: Now is the time to prepare financially for the coming of ICD-10.
A plan has to be developed well before Oct. 1, said Mr. Nachimson, who has studied the cost of ICD-10 implementation for the American Medical Association.
"You have got to prepare for ICD-10 or you risk significant payment disruptions," he said at the AMA National Advocacy Conference in Washington.
Dr. McAneny, managing partner and chief executive officer of the New Mexico Cancer Center in Albuquerque, said that she’s already started talking to her local banker. She said she has very little faith that the ICD-10 transition will be smooth, given her experience in moving from the Health Insurance Portability and Accountability Act 4010 standard to the 5010 standard in 2011.
"That was a much smaller event," said Dr. McAneny, who is also a member of the AMA Board of Trustees . And, with the change in HIPAA standards, the Centers for Medicare & Medicaid Services allowed for several transitional periods, where the old format continued to be accepted.
Dr. McAneny recalled that in 2011, the test runs were fine, and that both the clearinghouse and payer said that her practice was ready. But when the transition started, "we got denials like mad," she said in an interview. Some payers made no payments for 2-3 months.
This time, a substantial line of credit should be enough to cover 4 months of payroll, she said, adding that she anticipates hiring more coders and paying her billing staff extra to potentially chase denials.
"This transition has the potential to be a major disrupter," Dr. McAneny said.
Robert M. Tennant, senior policy adviser at the Medical Group Management Association (MGMA), said that physicians need to figure out soon how they will cover cash shortfalls, in part, because they may have to jump through a lot of hoops to satisfy a bank’s demands. "The days of supereasy credit are probably gone," he said in an interview.
He suggested arranging a line of credit to cover at least 2 months of operating expenses. A bank’s willingness to extend credit will depend on several variables, including the age of the practice, how long it’s been in its location, whether the practice owns or rents space, and what type of collateral is available to secure the line. In some cases, physicians might need to put up personal collateral.
"The hope, of course, is that you won’t have to tap into that line of credit very much, if at all," he said.
And it’s important to find out sooner rather than later how much credit can be secured. If it’s not enough to cover a few months’ expenses, practices might want to increase their cash reserves, Mr. Tennant said.
It’s important to "clear the decks" of any claims for services prior to Oct. 1, he said. Health plans will likely be overwhelmed by the transition, and that could lead to delays in payment for ICD-9 claims.
Mr. Nachimson said that practices should reach out to their major payers to get as much information as possible on changes in coverage policies and reimbursement for unspecified codes. "What they’re doing has a major impact on you," said Mr Nachimson.
Although many are still hoping for a delay in ICD-10, Mr. Tennant urged physicians to plan for the Oct. 1 implementation, "It’s too big a gamble for the practice to assume the date is going to be moved," he said. "If you bet the house and you lose, you’re going to be in a world of financial hurt."
The MGMA is suggesting that physicians "assume the worst and hope for the best," especially since there’s no real downside to improving documentation of diagnoses and getting staff better training in coding, he said.
On Twitter @aliciaault
