User login
Career Choices: Forensic psychiatry
Editor’s note: Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Saeed Ahmed, MD, Addiction Psychiatry Fellow at Boston University Medical Center/Boston University School of Medicine, talked with Paul S. Appelbaum, MD, Elizabeth K. Dollard Professor of Psychiatry, Medicine, and Law, and Director, Center for Law, Ethics, and Psychiatry, Department of Psychiatry, Columbia University Vagelos College of Physicians and Surgeons. Dr. Appelbaum is currently Chair of the DSM Steering Committee for the American Psychiatric Association, and Co-chair of the Standing Committee on Ethics of the World Psychiatric Association. He performs forensic evaluations in civil and criminal cases, and treats patients with a broad variety of illnesses, including depression, anxiety, and adjustment problems.
Dr. Ahmed: What made you pick the forensic psychiatry track, and how did your training lead you towards this path?
Dr. Appelbaum: I was a debater in high school and college, and a fair number of our topics dealt with legal issues, which I’d always found intriguing. However, on entering medical school, I had assumed that I would need to leave those interests behind me. During the first week of medical school, though, we were all asked to select a behavioral science elective for the semester, and on the list was “Law and Psychiatry.” I didn’t know what it involved, but it sounded interesting, so I signed up. The class was taught by Dr. Alan Stone, a professor at Harvard Law School and the most important figure in the academic study of legal issues in psychiatry. By the end of the first class—on the Friday afternoon of my first week in medical school—I was so excited by the things we were discussing that I pretty much decided this was what I wanted to focus on in my career.
Later in medical school, I joined a research project looking at violence on the inpatient psychiatric units, as a way of broadening my knowledge of the field. During residency—we’re talking about the late 1970s, which was a time of great legal ferment about regulation of psychiatric practice—I persuaded my attending psychiatrist to join me in studying patients who were exercising their newly granted right to refuse treatment. That’s how Dr. Tom Gutheil and I started working together, a collaboration that continues today, with the publication of the 5th edition of our text, Clinical Handbook of Psychiatry and Law. I was also able to get foundation funding to do a study of patients’ decision-making capacities, a topic that has remained a focus of my research to the present day. During my final year of residency, I was able to create a chief residency in legal psychiatry, which allowed me to take law school courses, pursue my research, and supervise the more junior residents in their forensic evaluations.
Today, most people headed toward careers in forensic psychiatry take a fellowship after residency, but [such fellowships] were few and far between in 1980. So I went to Alan Stone for advice, and he said, “Go work with Loren Roth in Pittsburgh for 5 years, and you’ll be able to do anything you want after that.” I tracked down Loren Roth, then the leading empirical researcher on issues related to law and psychiatry, explained that Alan Stone had said I should go work with him, and somehow it all worked out. My first faculty job was with his Law and Psychiatry Program at the University of Pittsburgh.
Dr. Ahmed: What are some of the pros and cons of working in forensic psychiatry?
Continue to: Dr. Appelbaum...
Dr. Appelbaum: It may sound at first as though forensic psychiatry is a narrow subspecialty of psychiatry. But the field is actually immense, and the diversity of experiences that it provides is one of the big pros of a career in forensic psychiatry. On the academic side of the field, topics of research interest include prediction and management of violence, involuntary commitment and treatment, informed consent and decisional capacity, privacy and confidentiality of psychiatric treatment, criminal responsibility, and correctional treatment. Clinically, forensic psychiatrists perform a variety of evaluations, ranging from competence to consent to treatment, testamentary capacity, emotional harms in tort cases, psychiatric malpractice, sexual harassment and work-related disability, to competence to stand trial, voluntariness of confessions, insanity defense, and pre-sentencing assessments. Indeed, after nearly 40 years in the field, I still occasionally get asked to do evaluations of a type that I’ve never done before. Increasingly, forensic psychiatrists are involved in treating offenders, both in correctional facilities and in outpatient settings. Most people trained in forensic psychiatry mix their forensic work with general clinical work, whether inpatient or outpatient. So the flexibility that the field offers to craft a career is one of its great advantages.
On the cons side, a career in forensic psychiatry can mean a life of what Alan Stone called “moral peril.” By that he meant that forensic psychiatrists face constant ethical challenges as they perform evaluations and provide testimony. One challenge is to stay grounded in the evidence base of psychiatry and resist the temptation to draw conclusions that may seem “right” but that go beyond what psychiatric knowledge can actually support. Making that challenge even more difficult in private forensic practice is knowing that the party for whom one is working has specific interests that they are hoping you will support, and very definite ideas about what they want your conclusions to be. It may be in your financial interest to accommodate them, but in the long run, your reputation is your most valuable asset. Staying honest both to one’s beliefs and to the broader evidence base in psychiatry is an ongoing challenge, but a critical necessity.
Dr. Ahmed: Based on your personal experience, what should one consider when choosing a forensic psychiatry program?
Dr. Appelbaum: Having supervised forensic psychiatry fellowships for roughly 30 years, I think one of the most important aspects of a training program is its breadth. Given the diversity of the field, a program with a limited number of training sites that focuses on a restricted set of evaluations (usually related to criminal law) will not offer a fellow an optimal training experience. Diverse placements with a variety of evaluations to be performed under the supervision of experienced forensic psychiatrists, and without excessive service demands, are key aspects of a top-notch program. In addition, not everything can be learned hands-on; didactic training is indispensable. Fellows should be offered sufficient background on legal issues and the research base in forensic psychiatry to ground their subsequent work. Finally, for many fellows their time in fellowship is the last opportunity they may have to engage in research or other scholarly projects under supervision, another valuable component of a training program. A good question to ask of any program: What are your former fellows doing now? If the answers don’t reflect the career path you hope to pursue, that’s not the program for you.
Dr. Ahmed: What are some of the career options and work settings for forensic psychiatrists?
Continue to: Dr. Appelbaum...
Dr. Appelbaum: One of the advantages of forensic psychiatry is the plethora of work settings available. People headed to private practice can often combine clinical practice with forensic work, a necessity when starting one’s career and waiting to establish steady referral pipelines. Psychiatrists with forensic training are in demand in correctional facilities (which often pay higher salaries than comparable jobs in psychiatric facilities), forensic hospitals, and court clinics. Opportunities for academic involvement include directing fellowship programs, teaching residents, and conducting research. With regard to research, although funding is harder to come by than, for example, for studies of the biology of major psychiatric syndromes, determined psychiatrists can often find ways of framing questions related to forensic issues so that they appeal to funders’ priorities. As one gains experience, opportunities for consultation for law enforcement agencies, intelligence agencies, and federal and state mental health agencies may be available. It is rare for a forensic psychiatrist to do just one of these things; most forensic psychiatrists engage in a mix of types of work, including general clinical work. The possibilities are manifold.
Dr. Ahmed: What are some of the challenges in working in this field?
Dr. Appelbaum: I talked already about some of the ethical challenges in forensic psychiatry. In addition, as a subspecialty that applies psychiatric knowledge to legal questions, forensic psychiatry requires its practitioners to stay up-to-date with both advances in psychiatry and changes in the law, not to mention variations across jurisdictions. This is not an area of specialization in which one can pay attention during fellowship and then coast through a career. In my view, it’s also critical for a good forensic psychiatrist to be an excellent clinician; forensic cases frequently offer diagnostic challenges that require the highest level of clinical skills to address. Finally, for people early in their careers, it can take a few years before they are well-enough known to get a steady flow of private forensic cases. So having a plan B during that career phase will be essential.
Dr. Ahmed: Where do you see forensic psychiatry going?
Dr. Appelbaum: Forensic evaluations will need to incorporate new assessment techniques and new knowledge—although not before they have been demonstrated to be valid and reliable. I can foresee increased use of specialized neuroimaging assessments, genomic and other “omic” testing, and measurement of other neurophysiologic parameters. As we know more about the etiology of psychiatric disorders, that will impact everything from evaluations of causation in emotional harms cases to conclusions about which divorcing parent may be better able to handle primary custody of a child. I think there will be exciting opportunities in the coming decades to integrate growing scientific knowledge about psychiatric illnesses into forensic psychiatry.
Continue to: Dr. Ahmed...
Dr. Ahmed: What advice do you have for those contemplating a career in forensic psychiatry?
Dr. Appelbaum: Residents thinking about undertaking training in forensic psychiatry should come to one of the annual meetings of the American Academy of Psychiatry and the Law, the major professional organization of forensic psychiatrists, which takes place every October
Editor’s note: Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Saeed Ahmed, MD, Addiction Psychiatry Fellow at Boston University Medical Center/Boston University School of Medicine, talked with Paul S. Appelbaum, MD, Elizabeth K. Dollard Professor of Psychiatry, Medicine, and Law, and Director, Center for Law, Ethics, and Psychiatry, Department of Psychiatry, Columbia University Vagelos College of Physicians and Surgeons. Dr. Appelbaum is currently Chair of the DSM Steering Committee for the American Psychiatric Association, and Co-chair of the Standing Committee on Ethics of the World Psychiatric Association. He performs forensic evaluations in civil and criminal cases, and treats patients with a broad variety of illnesses, including depression, anxiety, and adjustment problems.
Dr. Ahmed: What made you pick the forensic psychiatry track, and how did your training lead you towards this path?
Dr. Appelbaum: I was a debater in high school and college, and a fair number of our topics dealt with legal issues, which I’d always found intriguing. However, on entering medical school, I had assumed that I would need to leave those interests behind me. During the first week of medical school, though, we were all asked to select a behavioral science elective for the semester, and on the list was “Law and Psychiatry.” I didn’t know what it involved, but it sounded interesting, so I signed up. The class was taught by Dr. Alan Stone, a professor at Harvard Law School and the most important figure in the academic study of legal issues in psychiatry. By the end of the first class—on the Friday afternoon of my first week in medical school—I was so excited by the things we were discussing that I pretty much decided this was what I wanted to focus on in my career.
Later in medical school, I joined a research project looking at violence on the inpatient psychiatric units, as a way of broadening my knowledge of the field. During residency—we’re talking about the late 1970s, which was a time of great legal ferment about regulation of psychiatric practice—I persuaded my attending psychiatrist to join me in studying patients who were exercising their newly granted right to refuse treatment. That’s how Dr. Tom Gutheil and I started working together, a collaboration that continues today, with the publication of the 5th edition of our text, Clinical Handbook of Psychiatry and Law. I was also able to get foundation funding to do a study of patients’ decision-making capacities, a topic that has remained a focus of my research to the present day. During my final year of residency, I was able to create a chief residency in legal psychiatry, which allowed me to take law school courses, pursue my research, and supervise the more junior residents in their forensic evaluations.
Today, most people headed toward careers in forensic psychiatry take a fellowship after residency, but [such fellowships] were few and far between in 1980. So I went to Alan Stone for advice, and he said, “Go work with Loren Roth in Pittsburgh for 5 years, and you’ll be able to do anything you want after that.” I tracked down Loren Roth, then the leading empirical researcher on issues related to law and psychiatry, explained that Alan Stone had said I should go work with him, and somehow it all worked out. My first faculty job was with his Law and Psychiatry Program at the University of Pittsburgh.
Dr. Ahmed: What are some of the pros and cons of working in forensic psychiatry?
Continue to: Dr. Appelbaum...
Dr. Appelbaum: It may sound at first as though forensic psychiatry is a narrow subspecialty of psychiatry. But the field is actually immense, and the diversity of experiences that it provides is one of the big pros of a career in forensic psychiatry. On the academic side of the field, topics of research interest include prediction and management of violence, involuntary commitment and treatment, informed consent and decisional capacity, privacy and confidentiality of psychiatric treatment, criminal responsibility, and correctional treatment. Clinically, forensic psychiatrists perform a variety of evaluations, ranging from competence to consent to treatment, testamentary capacity, emotional harms in tort cases, psychiatric malpractice, sexual harassment and work-related disability, to competence to stand trial, voluntariness of confessions, insanity defense, and pre-sentencing assessments. Indeed, after nearly 40 years in the field, I still occasionally get asked to do evaluations of a type that I’ve never done before. Increasingly, forensic psychiatrists are involved in treating offenders, both in correctional facilities and in outpatient settings. Most people trained in forensic psychiatry mix their forensic work with general clinical work, whether inpatient or outpatient. So the flexibility that the field offers to craft a career is one of its great advantages.
On the cons side, a career in forensic psychiatry can mean a life of what Alan Stone called “moral peril.” By that he meant that forensic psychiatrists face constant ethical challenges as they perform evaluations and provide testimony. One challenge is to stay grounded in the evidence base of psychiatry and resist the temptation to draw conclusions that may seem “right” but that go beyond what psychiatric knowledge can actually support. Making that challenge even more difficult in private forensic practice is knowing that the party for whom one is working has specific interests that they are hoping you will support, and very definite ideas about what they want your conclusions to be. It may be in your financial interest to accommodate them, but in the long run, your reputation is your most valuable asset. Staying honest both to one’s beliefs and to the broader evidence base in psychiatry is an ongoing challenge, but a critical necessity.
Dr. Ahmed: Based on your personal experience, what should one consider when choosing a forensic psychiatry program?
Dr. Appelbaum: Having supervised forensic psychiatry fellowships for roughly 30 years, I think one of the most important aspects of a training program is its breadth. Given the diversity of the field, a program with a limited number of training sites that focuses on a restricted set of evaluations (usually related to criminal law) will not offer a fellow an optimal training experience. Diverse placements with a variety of evaluations to be performed under the supervision of experienced forensic psychiatrists, and without excessive service demands, are key aspects of a top-notch program. In addition, not everything can be learned hands-on; didactic training is indispensable. Fellows should be offered sufficient background on legal issues and the research base in forensic psychiatry to ground their subsequent work. Finally, for many fellows their time in fellowship is the last opportunity they may have to engage in research or other scholarly projects under supervision, another valuable component of a training program. A good question to ask of any program: What are your former fellows doing now? If the answers don’t reflect the career path you hope to pursue, that’s not the program for you.
Dr. Ahmed: What are some of the career options and work settings for forensic psychiatrists?
Continue to: Dr. Appelbaum...
Dr. Appelbaum: One of the advantages of forensic psychiatry is the plethora of work settings available. People headed to private practice can often combine clinical practice with forensic work, a necessity when starting one’s career and waiting to establish steady referral pipelines. Psychiatrists with forensic training are in demand in correctional facilities (which often pay higher salaries than comparable jobs in psychiatric facilities), forensic hospitals, and court clinics. Opportunities for academic involvement include directing fellowship programs, teaching residents, and conducting research. With regard to research, although funding is harder to come by than, for example, for studies of the biology of major psychiatric syndromes, determined psychiatrists can often find ways of framing questions related to forensic issues so that they appeal to funders’ priorities. As one gains experience, opportunities for consultation for law enforcement agencies, intelligence agencies, and federal and state mental health agencies may be available. It is rare for a forensic psychiatrist to do just one of these things; most forensic psychiatrists engage in a mix of types of work, including general clinical work. The possibilities are manifold.
Dr. Ahmed: What are some of the challenges in working in this field?
Dr. Appelbaum: I talked already about some of the ethical challenges in forensic psychiatry. In addition, as a subspecialty that applies psychiatric knowledge to legal questions, forensic psychiatry requires its practitioners to stay up-to-date with both advances in psychiatry and changes in the law, not to mention variations across jurisdictions. This is not an area of specialization in which one can pay attention during fellowship and then coast through a career. In my view, it’s also critical for a good forensic psychiatrist to be an excellent clinician; forensic cases frequently offer diagnostic challenges that require the highest level of clinical skills to address. Finally, for people early in their careers, it can take a few years before they are well-enough known to get a steady flow of private forensic cases. So having a plan B during that career phase will be essential.
Dr. Ahmed: Where do you see forensic psychiatry going?
Dr. Appelbaum: Forensic evaluations will need to incorporate new assessment techniques and new knowledge—although not before they have been demonstrated to be valid and reliable. I can foresee increased use of specialized neuroimaging assessments, genomic and other “omic” testing, and measurement of other neurophysiologic parameters. As we know more about the etiology of psychiatric disorders, that will impact everything from evaluations of causation in emotional harms cases to conclusions about which divorcing parent may be better able to handle primary custody of a child. I think there will be exciting opportunities in the coming decades to integrate growing scientific knowledge about psychiatric illnesses into forensic psychiatry.
Continue to: Dr. Ahmed...
Dr. Ahmed: What advice do you have for those contemplating a career in forensic psychiatry?
Dr. Appelbaum: Residents thinking about undertaking training in forensic psychiatry should come to one of the annual meetings of the American Academy of Psychiatry and the Law, the major professional organization of forensic psychiatrists, which takes place every October
Editor’s note: Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Saeed Ahmed, MD, Addiction Psychiatry Fellow at Boston University Medical Center/Boston University School of Medicine, talked with Paul S. Appelbaum, MD, Elizabeth K. Dollard Professor of Psychiatry, Medicine, and Law, and Director, Center for Law, Ethics, and Psychiatry, Department of Psychiatry, Columbia University Vagelos College of Physicians and Surgeons. Dr. Appelbaum is currently Chair of the DSM Steering Committee for the American Psychiatric Association, and Co-chair of the Standing Committee on Ethics of the World Psychiatric Association. He performs forensic evaluations in civil and criminal cases, and treats patients with a broad variety of illnesses, including depression, anxiety, and adjustment problems.
Dr. Ahmed: What made you pick the forensic psychiatry track, and how did your training lead you towards this path?
Dr. Appelbaum: I was a debater in high school and college, and a fair number of our topics dealt with legal issues, which I’d always found intriguing. However, on entering medical school, I had assumed that I would need to leave those interests behind me. During the first week of medical school, though, we were all asked to select a behavioral science elective for the semester, and on the list was “Law and Psychiatry.” I didn’t know what it involved, but it sounded interesting, so I signed up. The class was taught by Dr. Alan Stone, a professor at Harvard Law School and the most important figure in the academic study of legal issues in psychiatry. By the end of the first class—on the Friday afternoon of my first week in medical school—I was so excited by the things we were discussing that I pretty much decided this was what I wanted to focus on in my career.
Later in medical school, I joined a research project looking at violence on the inpatient psychiatric units, as a way of broadening my knowledge of the field. During residency—we’re talking about the late 1970s, which was a time of great legal ferment about regulation of psychiatric practice—I persuaded my attending psychiatrist to join me in studying patients who were exercising their newly granted right to refuse treatment. That’s how Dr. Tom Gutheil and I started working together, a collaboration that continues today, with the publication of the 5th edition of our text, Clinical Handbook of Psychiatry and Law. I was also able to get foundation funding to do a study of patients’ decision-making capacities, a topic that has remained a focus of my research to the present day. During my final year of residency, I was able to create a chief residency in legal psychiatry, which allowed me to take law school courses, pursue my research, and supervise the more junior residents in their forensic evaluations.
Today, most people headed toward careers in forensic psychiatry take a fellowship after residency, but [such fellowships] were few and far between in 1980. So I went to Alan Stone for advice, and he said, “Go work with Loren Roth in Pittsburgh for 5 years, and you’ll be able to do anything you want after that.” I tracked down Loren Roth, then the leading empirical researcher on issues related to law and psychiatry, explained that Alan Stone had said I should go work with him, and somehow it all worked out. My first faculty job was with his Law and Psychiatry Program at the University of Pittsburgh.
Dr. Ahmed: What are some of the pros and cons of working in forensic psychiatry?
Continue to: Dr. Appelbaum...
Dr. Appelbaum: It may sound at first as though forensic psychiatry is a narrow subspecialty of psychiatry. But the field is actually immense, and the diversity of experiences that it provides is one of the big pros of a career in forensic psychiatry. On the academic side of the field, topics of research interest include prediction and management of violence, involuntary commitment and treatment, informed consent and decisional capacity, privacy and confidentiality of psychiatric treatment, criminal responsibility, and correctional treatment. Clinically, forensic psychiatrists perform a variety of evaluations, ranging from competence to consent to treatment, testamentary capacity, emotional harms in tort cases, psychiatric malpractice, sexual harassment and work-related disability, to competence to stand trial, voluntariness of confessions, insanity defense, and pre-sentencing assessments. Indeed, after nearly 40 years in the field, I still occasionally get asked to do evaluations of a type that I’ve never done before. Increasingly, forensic psychiatrists are involved in treating offenders, both in correctional facilities and in outpatient settings. Most people trained in forensic psychiatry mix their forensic work with general clinical work, whether inpatient or outpatient. So the flexibility that the field offers to craft a career is one of its great advantages.
On the cons side, a career in forensic psychiatry can mean a life of what Alan Stone called “moral peril.” By that he meant that forensic psychiatrists face constant ethical challenges as they perform evaluations and provide testimony. One challenge is to stay grounded in the evidence base of psychiatry and resist the temptation to draw conclusions that may seem “right” but that go beyond what psychiatric knowledge can actually support. Making that challenge even more difficult in private forensic practice is knowing that the party for whom one is working has specific interests that they are hoping you will support, and very definite ideas about what they want your conclusions to be. It may be in your financial interest to accommodate them, but in the long run, your reputation is your most valuable asset. Staying honest both to one’s beliefs and to the broader evidence base in psychiatry is an ongoing challenge, but a critical necessity.
Dr. Ahmed: Based on your personal experience, what should one consider when choosing a forensic psychiatry program?
Dr. Appelbaum: Having supervised forensic psychiatry fellowships for roughly 30 years, I think one of the most important aspects of a training program is its breadth. Given the diversity of the field, a program with a limited number of training sites that focuses on a restricted set of evaluations (usually related to criminal law) will not offer a fellow an optimal training experience. Diverse placements with a variety of evaluations to be performed under the supervision of experienced forensic psychiatrists, and without excessive service demands, are key aspects of a top-notch program. In addition, not everything can be learned hands-on; didactic training is indispensable. Fellows should be offered sufficient background on legal issues and the research base in forensic psychiatry to ground their subsequent work. Finally, for many fellows their time in fellowship is the last opportunity they may have to engage in research or other scholarly projects under supervision, another valuable component of a training program. A good question to ask of any program: What are your former fellows doing now? If the answers don’t reflect the career path you hope to pursue, that’s not the program for you.
Dr. Ahmed: What are some of the career options and work settings for forensic psychiatrists?
Continue to: Dr. Appelbaum...
Dr. Appelbaum: One of the advantages of forensic psychiatry is the plethora of work settings available. People headed to private practice can often combine clinical practice with forensic work, a necessity when starting one’s career and waiting to establish steady referral pipelines. Psychiatrists with forensic training are in demand in correctional facilities (which often pay higher salaries than comparable jobs in psychiatric facilities), forensic hospitals, and court clinics. Opportunities for academic involvement include directing fellowship programs, teaching residents, and conducting research. With regard to research, although funding is harder to come by than, for example, for studies of the biology of major psychiatric syndromes, determined psychiatrists can often find ways of framing questions related to forensic issues so that they appeal to funders’ priorities. As one gains experience, opportunities for consultation for law enforcement agencies, intelligence agencies, and federal and state mental health agencies may be available. It is rare for a forensic psychiatrist to do just one of these things; most forensic psychiatrists engage in a mix of types of work, including general clinical work. The possibilities are manifold.
Dr. Ahmed: What are some of the challenges in working in this field?
Dr. Appelbaum: I talked already about some of the ethical challenges in forensic psychiatry. In addition, as a subspecialty that applies psychiatric knowledge to legal questions, forensic psychiatry requires its practitioners to stay up-to-date with both advances in psychiatry and changes in the law, not to mention variations across jurisdictions. This is not an area of specialization in which one can pay attention during fellowship and then coast through a career. In my view, it’s also critical for a good forensic psychiatrist to be an excellent clinician; forensic cases frequently offer diagnostic challenges that require the highest level of clinical skills to address. Finally, for people early in their careers, it can take a few years before they are well-enough known to get a steady flow of private forensic cases. So having a plan B during that career phase will be essential.
Dr. Ahmed: Where do you see forensic psychiatry going?
Dr. Appelbaum: Forensic evaluations will need to incorporate new assessment techniques and new knowledge—although not before they have been demonstrated to be valid and reliable. I can foresee increased use of specialized neuroimaging assessments, genomic and other “omic” testing, and measurement of other neurophysiologic parameters. As we know more about the etiology of psychiatric disorders, that will impact everything from evaluations of causation in emotional harms cases to conclusions about which divorcing parent may be better able to handle primary custody of a child. I think there will be exciting opportunities in the coming decades to integrate growing scientific knowledge about psychiatric illnesses into forensic psychiatry.
Continue to: Dr. Ahmed...
Dr. Ahmed: What advice do you have for those contemplating a career in forensic psychiatry?
Dr. Appelbaum: Residents thinking about undertaking training in forensic psychiatry should come to one of the annual meetings of the American Academy of Psychiatry and the Law, the major professional organization of forensic psychiatrists, which takes place every October

Prenatal exposure to illegal substances: Exploring alternatives to fetal assault bills
Near completion of my rounds at a residential substance abuse treatment center, my last patient was a 32-year-old mother. She reported she was there because her newborn had tested positive for cocaine. She stated, “I want to do better. I thought this pregnancy would change things, but it was so hard to stop.” Her admission made me reflect on a proposed bill in my state of Tennessee called the Fetal Assault Bill, which if put into law would affect women such as my patient and her newborn child.
The Tennessee Fetal Assault Bill was originally enacted in 2014, expired in 2016, and failed to pass in 2017. The bill was reintroduced for consideration in February 2019. If enacted, it would subject a woman to prosecution if her illegal use of a substance while pregnant causes her child to be born addicted to or harmed by that drug. However, the mother is protected from prosecution if she “enrolled in an addiction recovery program before the child is born, remained in the program after delivery, and successfully completed the program, regardless of whether the child was born addicted to or harmed by the narcotic drug.”1 This bill is based on the premise that the unborn fetus has the same rights as a born child, and that the threat of incarceration will deter pregnant women from using illegal substances while pregnant.
Pregnant women may enroll in a drug treatment program prior to delivery to avoid prosecution; however, there is a paucity of addiction treatment centers available to pregnant women. Moreover, there is limited access in areas where babies are more likely to be born affected by the use of illegal substances. Few provisions have been made to address the additional barriers to treatment these women face, such as a lack of insurance or underinsurance for rehabilitation treatment, lack of transportation, and limited finances. Additional barriers include limited social supports, the need for childcare arrangements for existing children, and social stigma.
A 2017 report by Amnesty International regarding the original enactment of the Tennessee Fetal Assault Bill in 2014 noted some mothers who used illegal substances were afraid of prosecution.2 This fear caused some to delay prenatal care or evade social services in order to prevent being reported. According to Amnesty International, laws such as the one proposed in Tennessee often show disparities in how they are implemented. Research shows that women of lower socioeconomic status and minorities tend to receive more frequent drug testing and harsher punishments.3
There are benefits to dedicating more resources to addiction treatment and other social services for pregnant women who use illegal substances. Reports show that mothers are motivated to stay abstinent in treatment centers where they are housed with their children. This model of treatment is more cost-effective than incarceration, which includes legal costs, prison costs, and foster care bills. Moreover, a possible felony charge may hinder a woman’s job opportunities and further compound her problems and those of her infant.
In the light of these benefits, instead of re-enacting the 2014 law, which did not yield any conclusive benefits for newborns or mothers who used illegal substances, alternatives should be attempted. Early identification of and interventions for women who are at risk for substance use while pregnant should be implemented. Practical, accessible support services will encourage sobriety, prevent fetal exposure to illegal substances, and improve child health outcomes. Research shows that substance abuse treatment during pregnancy reduces the risk of harm before birth and improves the quality of parental care after birth.4 Legislators and clinicians should emphasize improving access to treatment, expanding integrative addiction treatment centers, and encouraging self-reporting early in pregnancy. This goal cannot be achieved with an emphasis on incarcerating mothers.
1. House Bill 1168. 111th Tennessee General Assembly (Tenn 2019). http://www.capitol.tn.gov/Bills/111/Bill/HB1168.pdf. Accessed August 8, 2019.
2. Amnesty International. Criminalizing pregnancy: policing pregnant women who use drugs in the USA. https://www.amnesty.org/download/Documents/AMR5162032017ENGLISH.pdf. Published May 23, 2017. Accessed August 8, 2019.
3. Paltrow LM, Flavin J. Arrests of and forced interventions on pregnant women in the United States, 1973-2005: implications for women’s legal status and public health. J Health Polit Policy Law. 2013;38(2):299-343.
4. Ashley OS, Marsden ME, Brady TM. Effectiveness of substance abuse treatment programming for women: a review. Am J Drug Alcohol Abuse. 2003;29(1):19-53.
Near completion of my rounds at a residential substance abuse treatment center, my last patient was a 32-year-old mother. She reported she was there because her newborn had tested positive for cocaine. She stated, “I want to do better. I thought this pregnancy would change things, but it was so hard to stop.” Her admission made me reflect on a proposed bill in my state of Tennessee called the Fetal Assault Bill, which if put into law would affect women such as my patient and her newborn child.
The Tennessee Fetal Assault Bill was originally enacted in 2014, expired in 2016, and failed to pass in 2017. The bill was reintroduced for consideration in February 2019. If enacted, it would subject a woman to prosecution if her illegal use of a substance while pregnant causes her child to be born addicted to or harmed by that drug. However, the mother is protected from prosecution if she “enrolled in an addiction recovery program before the child is born, remained in the program after delivery, and successfully completed the program, regardless of whether the child was born addicted to or harmed by the narcotic drug.”1 This bill is based on the premise that the unborn fetus has the same rights as a born child, and that the threat of incarceration will deter pregnant women from using illegal substances while pregnant.
Pregnant women may enroll in a drug treatment program prior to delivery to avoid prosecution; however, there is a paucity of addiction treatment centers available to pregnant women. Moreover, there is limited access in areas where babies are more likely to be born affected by the use of illegal substances. Few provisions have been made to address the additional barriers to treatment these women face, such as a lack of insurance or underinsurance for rehabilitation treatment, lack of transportation, and limited finances. Additional barriers include limited social supports, the need for childcare arrangements for existing children, and social stigma.
A 2017 report by Amnesty International regarding the original enactment of the Tennessee Fetal Assault Bill in 2014 noted some mothers who used illegal substances were afraid of prosecution.2 This fear caused some to delay prenatal care or evade social services in order to prevent being reported. According to Amnesty International, laws such as the one proposed in Tennessee often show disparities in how they are implemented. Research shows that women of lower socioeconomic status and minorities tend to receive more frequent drug testing and harsher punishments.3
There are benefits to dedicating more resources to addiction treatment and other social services for pregnant women who use illegal substances. Reports show that mothers are motivated to stay abstinent in treatment centers where they are housed with their children. This model of treatment is more cost-effective than incarceration, which includes legal costs, prison costs, and foster care bills. Moreover, a possible felony charge may hinder a woman’s job opportunities and further compound her problems and those of her infant.
In the light of these benefits, instead of re-enacting the 2014 law, which did not yield any conclusive benefits for newborns or mothers who used illegal substances, alternatives should be attempted. Early identification of and interventions for women who are at risk for substance use while pregnant should be implemented. Practical, accessible support services will encourage sobriety, prevent fetal exposure to illegal substances, and improve child health outcomes. Research shows that substance abuse treatment during pregnancy reduces the risk of harm before birth and improves the quality of parental care after birth.4 Legislators and clinicians should emphasize improving access to treatment, expanding integrative addiction treatment centers, and encouraging self-reporting early in pregnancy. This goal cannot be achieved with an emphasis on incarcerating mothers.
Near completion of my rounds at a residential substance abuse treatment center, my last patient was a 32-year-old mother. She reported she was there because her newborn had tested positive for cocaine. She stated, “I want to do better. I thought this pregnancy would change things, but it was so hard to stop.” Her admission made me reflect on a proposed bill in my state of Tennessee called the Fetal Assault Bill, which if put into law would affect women such as my patient and her newborn child.
The Tennessee Fetal Assault Bill was originally enacted in 2014, expired in 2016, and failed to pass in 2017. The bill was reintroduced for consideration in February 2019. If enacted, it would subject a woman to prosecution if her illegal use of a substance while pregnant causes her child to be born addicted to or harmed by that drug. However, the mother is protected from prosecution if she “enrolled in an addiction recovery program before the child is born, remained in the program after delivery, and successfully completed the program, regardless of whether the child was born addicted to or harmed by the narcotic drug.”1 This bill is based on the premise that the unborn fetus has the same rights as a born child, and that the threat of incarceration will deter pregnant women from using illegal substances while pregnant.
Pregnant women may enroll in a drug treatment program prior to delivery to avoid prosecution; however, there is a paucity of addiction treatment centers available to pregnant women. Moreover, there is limited access in areas where babies are more likely to be born affected by the use of illegal substances. Few provisions have been made to address the additional barriers to treatment these women face, such as a lack of insurance or underinsurance for rehabilitation treatment, lack of transportation, and limited finances. Additional barriers include limited social supports, the need for childcare arrangements for existing children, and social stigma.
A 2017 report by Amnesty International regarding the original enactment of the Tennessee Fetal Assault Bill in 2014 noted some mothers who used illegal substances were afraid of prosecution.2 This fear caused some to delay prenatal care or evade social services in order to prevent being reported. According to Amnesty International, laws such as the one proposed in Tennessee often show disparities in how they are implemented. Research shows that women of lower socioeconomic status and minorities tend to receive more frequent drug testing and harsher punishments.3
There are benefits to dedicating more resources to addiction treatment and other social services for pregnant women who use illegal substances. Reports show that mothers are motivated to stay abstinent in treatment centers where they are housed with their children. This model of treatment is more cost-effective than incarceration, which includes legal costs, prison costs, and foster care bills. Moreover, a possible felony charge may hinder a woman’s job opportunities and further compound her problems and those of her infant.
In the light of these benefits, instead of re-enacting the 2014 law, which did not yield any conclusive benefits for newborns or mothers who used illegal substances, alternatives should be attempted. Early identification of and interventions for women who are at risk for substance use while pregnant should be implemented. Practical, accessible support services will encourage sobriety, prevent fetal exposure to illegal substances, and improve child health outcomes. Research shows that substance abuse treatment during pregnancy reduces the risk of harm before birth and improves the quality of parental care after birth.4 Legislators and clinicians should emphasize improving access to treatment, expanding integrative addiction treatment centers, and encouraging self-reporting early in pregnancy. This goal cannot be achieved with an emphasis on incarcerating mothers.
1. House Bill 1168. 111th Tennessee General Assembly (Tenn 2019). http://www.capitol.tn.gov/Bills/111/Bill/HB1168.pdf. Accessed August 8, 2019.
2. Amnesty International. Criminalizing pregnancy: policing pregnant women who use drugs in the USA. https://www.amnesty.org/download/Documents/AMR5162032017ENGLISH.pdf. Published May 23, 2017. Accessed August 8, 2019.
3. Paltrow LM, Flavin J. Arrests of and forced interventions on pregnant women in the United States, 1973-2005: implications for women’s legal status and public health. J Health Polit Policy Law. 2013;38(2):299-343.
4. Ashley OS, Marsden ME, Brady TM. Effectiveness of substance abuse treatment programming for women: a review. Am J Drug Alcohol Abuse. 2003;29(1):19-53.
1. House Bill 1168. 111th Tennessee General Assembly (Tenn 2019). http://www.capitol.tn.gov/Bills/111/Bill/HB1168.pdf. Accessed August 8, 2019.
2. Amnesty International. Criminalizing pregnancy: policing pregnant women who use drugs in the USA. https://www.amnesty.org/download/Documents/AMR5162032017ENGLISH.pdf. Published May 23, 2017. Accessed August 8, 2019.
3. Paltrow LM, Flavin J. Arrests of and forced interventions on pregnant women in the United States, 1973-2005: implications for women’s legal status and public health. J Health Polit Policy Law. 2013;38(2):299-343.
4. Ashley OS, Marsden ME, Brady TM. Effectiveness of substance abuse treatment programming for women: a review. Am J Drug Alcohol Abuse. 2003;29(1):19-53.

Challenges of Treating Primary Psychiatric Disease in Dermatology
Dermatology patients experience a high burden of mental health disturbance. Psychiatric disease is seen in an estimated 30% to 60% of our patients.1 It can be secondary to or comorbid with dermatologic disorders, or it can be the primary condition that is driving cutaneous disease. Patients with secondary or comorbid psychiatric disorders often are amenable to referral to a mental health provider or are already participating in some form of mental health treatment; however, patients with primary psychiatric disease who present to dermatology generally do not accept these referrals.2 Therefore, if these patients are to receive care anywhere in the health care system, it often must be in the department of dermatology.
What primary psychiatric conditions do we see in dermatology?
Common primary psychiatric conditions seen in dermatology include delusional infestation, obsessive-compulsive disorder and related disorders, and dermatitis artefacta.
Delusional Infestation
Also known as delusions of parasitosis or delusional parasitosis, delusional infestation presents as a fixed false belief that there is an organism or other foreign entity that is present in the skin and is the cause of cutaneous disruption. It often is an isolated delusion but can have a notable psychosocial impact. The term delusional infestation is sometimes preferred, as it is inclusive of delusions focused on any type of organism, not just parasites. It also encompasses delusions of infestation with nonliving matter such as fibers, also known as Morgellons disease.3
Obsessive-Compulsive Disorder and Related Disorders
This broad category includes several conditions encountered in dermatology. Body dysmorphic disorder (BDD), olfactory reference syndrome (ORS), excoriation disorder, and trichotillomania are some of the most common variants. In patients with BDD, skin and hair are the 2 most common preoccupations. It has been estimated that 12% of dermatology patients experience BDD. Unsurprisingly, it is more common in patients presenting to cosmetic dermatology, but general dermatology patients also are affected at a rate of 7%.2 Patients with ORS falsely believe they have body odor and/or halitosis. Excoriation disorder manifests as repetitive skin picking, either of normal skin or of lesions such as pimples and scabs. Trichotillomania presents as repeated hair pulling, and trichophagia (eating the pulled hair) also may be present.
Dermatitis Artefacta
Almost 1 in 4 patients who seek dermatologic evaluation for primarily psychiatric disorders have dermatitis artefacta, the presence of deliberately self-inflicted skin lesions.2 Patients with dermatitis artefacta have unconscious motives for their behavior and should be distinguished from malingering patients who have a conscious goal of secondary gain.
What treatments are available?
Antidepressants
Selective serotonin reuptake inhibitors are one of the first-line treatments for BDD and may be useful in ORS. In excoriation disorder and trichotillomania, selective serotonin reuptake inhibitors are the most commonly prescribed pharmacotherapy, but they have limited efficacy.2
Antipsychotics
The recommended treatment of delusional infestation is antipsychotic pharmacotherapy. Treatment with risperidone and olanzapine has been reported to achieve full or partial remission in more than two-thirds of cases.4 Aripiprazole, a newer antipsychotic, has fewer side effects and has been successful in several case reports.5-7
Cognitive Behavioral Therapy
Psychotherapy, most often in the form of cognitive behavioral therapy, has been reported as effective treatment of several psychocutaneous diseases. Cognitive behavioral therapy is considered first-line treatment of body-focused repetitive behavior disorders such as excoriation disorder and trichotillomania.2 It addresses maladaptive thought patterns to modify behavior.
Who treats patients with neurodermatoses?
If a patient presents to dermatology with a rash found to be related to an underlying thyroid disorder, the treatment plan likely would include referral to an endocrinologist. Similarly, patients with primary psychiatric conditions presenting to dermatology should ideally be referred to psychiatrists or psychotherapists, the providers most thoroughly trained and best equipped to treat them. The challenge in psychodermatology is that patients often are resistant to the assessment that the primary pathology is psychiatric. Patients may deny that they are “crazy” and see numerous providers in search of a dermatologist who “believes” them.8
Referral to mental health professionals almost always is refused by patients with primarily psychiatric neurodermatoses, which presents dermatologists with a dilemma. As the authors of the “Psychotropic Agents” chapter of Comprehensive Dermatologic Drug Therapy put it: “A dermatologist has two choices. The first is to try to ‘look the other way’ and pacify the patient by providing relatively benign, but minimally effective treatments. The other option is to try to directly address the psychological/psychiatric problems.” The chapter then provides a thorough guide for the use of psychotropic medications in the dermatology population, advocating for option 2: treatment by dermatologists.9
Should a dermatologist prescribe psychotropic drugs?
In Dermatology, the principle reference textbook in many dermatology training programs, it is stated that “[a]lthough less comprehensive than treatment delivered in collaboration with a psychiatrist, in the authors’ opinion, management of these issues by a dermatologist is better than no treatment at all.”10 Recent reviews in the dermatologic literature of psychiatric diseases and drugs in dermatology agree that dermatologists should feel comfortable with prescribing pharmacologic treatment.2,8,11 Performance of psychotherapy by dermatologists, on the other hand, is not recommended based on time constraints and lack of training.
Despite the apparent agreement in the texts and literature that pharmacotherapy of psychiatric neurodermatoses is within our scope of practice in dermatology, most dermatologists do not prescribe psychotropic agents. Dermatology residencies generally do not provide thorough training in psychopharmacotherapy.9 Unsurprisingly, a survey of 40 dermatologists at one academic institution found that only 11% felt comfortable prescribing an antidepressant and a mere 3% were comfortable prescribing an antipsychotic.12
Final Thoughts
The challenges involved in managing patients with primary psychiatric disease in dermatology are great and many patients are undertreated despite the availability of effective, evidence-based treatment options. We need to continue to work toward providing better access to these treatments in a way that maximizes the chance that our patients will accept our care.
- Korabel H, Dudek D, Jaworek A, et al. Psychodermatology: psychological and psychiatrical aspects of dermatology [in Polish]. Przegl Lek. 2008;65:244-248.
- Krooks JA, Weatherall AG, Holland PJ. Review of epidemiology, clinical presentation, diagnosis, and treatment of common primary psychiatric causes of cutaneous disease. J Dermatolog Treat. 2018;29:418-427.
- Bewley AP, Lepping P, Freundenmann RW, et al. Delusional parasitosis: time to call it delusional infestation. Br J Dermatol. 2018;163:1-2.
- Freudenmann RW, Lepping P. Second-generation antipsychotics in primary and secondary delusional parasitosis: outcome and efficacy. J Clin Psychopharmacol. 2008;28:500-508.
- Miyamoto S, Miyake N, Ogino S, et al. Successful treatment of delusional disorder with low-dose aripiprazole. Psychiatry Clin Neurosci. 2008;62:369.
- Ladizinski B, Busse KL, Bhutani T, et al. Aripiprazole as a viable alternative for treating delusions of parasitosis. J Drugs Dermatol. 2010;9:1531-1532.
- Huang WL, Chang LR. Aripiprazole in the treatment of delusional parasitosis with ocular and dermatologic presentations. J Clin Psychopharmacol. 2013;33:272-273.
- Campbell EH, Elston DM, Hawthorne JD, et al. Diagnosis and management of delusional parasitosis. J Am Acad Dermatol. 2019;80:1428-1434.
- Bhutani T, Lee CS, Koo JYM. Psychotropic agents. In: Wolverton SE, ed. Comprehensive Dermatologic Drug Therapy. 3rd ed. China: Elsevier Saunders; 2013:375-388.
- Duncan KO, Koo JYM. Psychocutaneous diseases. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018:128-137.
- Shah B, Levenson JL. Use of psychotropic drugs in the dermatology patient: when to start and stop? Clin Dermatol. 2018;36:748-755.
- Gee SN, Zakhary L, Keuthen N, et al. A survey assessment of the recognition and treatment of psychocutaneous disorders in the outpatient dermatology setting: how prepared are we? J Am Acad Dermatol. 2013;68:47-52.
Dermatology patients experience a high burden of mental health disturbance. Psychiatric disease is seen in an estimated 30% to 60% of our patients.1 It can be secondary to or comorbid with dermatologic disorders, or it can be the primary condition that is driving cutaneous disease. Patients with secondary or comorbid psychiatric disorders often are amenable to referral to a mental health provider or are already participating in some form of mental health treatment; however, patients with primary psychiatric disease who present to dermatology generally do not accept these referrals.2 Therefore, if these patients are to receive care anywhere in the health care system, it often must be in the department of dermatology.
What primary psychiatric conditions do we see in dermatology?
Common primary psychiatric conditions seen in dermatology include delusional infestation, obsessive-compulsive disorder and related disorders, and dermatitis artefacta.
Delusional Infestation
Also known as delusions of parasitosis or delusional parasitosis, delusional infestation presents as a fixed false belief that there is an organism or other foreign entity that is present in the skin and is the cause of cutaneous disruption. It often is an isolated delusion but can have a notable psychosocial impact. The term delusional infestation is sometimes preferred, as it is inclusive of delusions focused on any type of organism, not just parasites. It also encompasses delusions of infestation with nonliving matter such as fibers, also known as Morgellons disease.3
Obsessive-Compulsive Disorder and Related Disorders
This broad category includes several conditions encountered in dermatology. Body dysmorphic disorder (BDD), olfactory reference syndrome (ORS), excoriation disorder, and trichotillomania are some of the most common variants. In patients with BDD, skin and hair are the 2 most common preoccupations. It has been estimated that 12% of dermatology patients experience BDD. Unsurprisingly, it is more common in patients presenting to cosmetic dermatology, but general dermatology patients also are affected at a rate of 7%.2 Patients with ORS falsely believe they have body odor and/or halitosis. Excoriation disorder manifests as repetitive skin picking, either of normal skin or of lesions such as pimples and scabs. Trichotillomania presents as repeated hair pulling, and trichophagia (eating the pulled hair) also may be present.
Dermatitis Artefacta
Almost 1 in 4 patients who seek dermatologic evaluation for primarily psychiatric disorders have dermatitis artefacta, the presence of deliberately self-inflicted skin lesions.2 Patients with dermatitis artefacta have unconscious motives for their behavior and should be distinguished from malingering patients who have a conscious goal of secondary gain.
What treatments are available?
Antidepressants
Selective serotonin reuptake inhibitors are one of the first-line treatments for BDD and may be useful in ORS. In excoriation disorder and trichotillomania, selective serotonin reuptake inhibitors are the most commonly prescribed pharmacotherapy, but they have limited efficacy.2
Antipsychotics
The recommended treatment of delusional infestation is antipsychotic pharmacotherapy. Treatment with risperidone and olanzapine has been reported to achieve full or partial remission in more than two-thirds of cases.4 Aripiprazole, a newer antipsychotic, has fewer side effects and has been successful in several case reports.5-7
Cognitive Behavioral Therapy
Psychotherapy, most often in the form of cognitive behavioral therapy, has been reported as effective treatment of several psychocutaneous diseases. Cognitive behavioral therapy is considered first-line treatment of body-focused repetitive behavior disorders such as excoriation disorder and trichotillomania.2 It addresses maladaptive thought patterns to modify behavior.
Who treats patients with neurodermatoses?
If a patient presents to dermatology with a rash found to be related to an underlying thyroid disorder, the treatment plan likely would include referral to an endocrinologist. Similarly, patients with primary psychiatric conditions presenting to dermatology should ideally be referred to psychiatrists or psychotherapists, the providers most thoroughly trained and best equipped to treat them. The challenge in psychodermatology is that patients often are resistant to the assessment that the primary pathology is psychiatric. Patients may deny that they are “crazy” and see numerous providers in search of a dermatologist who “believes” them.8
Referral to mental health professionals almost always is refused by patients with primarily psychiatric neurodermatoses, which presents dermatologists with a dilemma. As the authors of the “Psychotropic Agents” chapter of Comprehensive Dermatologic Drug Therapy put it: “A dermatologist has two choices. The first is to try to ‘look the other way’ and pacify the patient by providing relatively benign, but minimally effective treatments. The other option is to try to directly address the psychological/psychiatric problems.” The chapter then provides a thorough guide for the use of psychotropic medications in the dermatology population, advocating for option 2: treatment by dermatologists.9
Should a dermatologist prescribe psychotropic drugs?
In Dermatology, the principle reference textbook in many dermatology training programs, it is stated that “[a]lthough less comprehensive than treatment delivered in collaboration with a psychiatrist, in the authors’ opinion, management of these issues by a dermatologist is better than no treatment at all.”10 Recent reviews in the dermatologic literature of psychiatric diseases and drugs in dermatology agree that dermatologists should feel comfortable with prescribing pharmacologic treatment.2,8,11 Performance of psychotherapy by dermatologists, on the other hand, is not recommended based on time constraints and lack of training.
Despite the apparent agreement in the texts and literature that pharmacotherapy of psychiatric neurodermatoses is within our scope of practice in dermatology, most dermatologists do not prescribe psychotropic agents. Dermatology residencies generally do not provide thorough training in psychopharmacotherapy.9 Unsurprisingly, a survey of 40 dermatologists at one academic institution found that only 11% felt comfortable prescribing an antidepressant and a mere 3% were comfortable prescribing an antipsychotic.12
Final Thoughts
The challenges involved in managing patients with primary psychiatric disease in dermatology are great and many patients are undertreated despite the availability of effective, evidence-based treatment options. We need to continue to work toward providing better access to these treatments in a way that maximizes the chance that our patients will accept our care.
Dermatology patients experience a high burden of mental health disturbance. Psychiatric disease is seen in an estimated 30% to 60% of our patients.1 It can be secondary to or comorbid with dermatologic disorders, or it can be the primary condition that is driving cutaneous disease. Patients with secondary or comorbid psychiatric disorders often are amenable to referral to a mental health provider or are already participating in some form of mental health treatment; however, patients with primary psychiatric disease who present to dermatology generally do not accept these referrals.2 Therefore, if these patients are to receive care anywhere in the health care system, it often must be in the department of dermatology.
What primary psychiatric conditions do we see in dermatology?
Common primary psychiatric conditions seen in dermatology include delusional infestation, obsessive-compulsive disorder and related disorders, and dermatitis artefacta.
Delusional Infestation
Also known as delusions of parasitosis or delusional parasitosis, delusional infestation presents as a fixed false belief that there is an organism or other foreign entity that is present in the skin and is the cause of cutaneous disruption. It often is an isolated delusion but can have a notable psychosocial impact. The term delusional infestation is sometimes preferred, as it is inclusive of delusions focused on any type of organism, not just parasites. It also encompasses delusions of infestation with nonliving matter such as fibers, also known as Morgellons disease.3
Obsessive-Compulsive Disorder and Related Disorders
This broad category includes several conditions encountered in dermatology. Body dysmorphic disorder (BDD), olfactory reference syndrome (ORS), excoriation disorder, and trichotillomania are some of the most common variants. In patients with BDD, skin and hair are the 2 most common preoccupations. It has been estimated that 12% of dermatology patients experience BDD. Unsurprisingly, it is more common in patients presenting to cosmetic dermatology, but general dermatology patients also are affected at a rate of 7%.2 Patients with ORS falsely believe they have body odor and/or halitosis. Excoriation disorder manifests as repetitive skin picking, either of normal skin or of lesions such as pimples and scabs. Trichotillomania presents as repeated hair pulling, and trichophagia (eating the pulled hair) also may be present.
Dermatitis Artefacta
Almost 1 in 4 patients who seek dermatologic evaluation for primarily psychiatric disorders have dermatitis artefacta, the presence of deliberately self-inflicted skin lesions.2 Patients with dermatitis artefacta have unconscious motives for their behavior and should be distinguished from malingering patients who have a conscious goal of secondary gain.
What treatments are available?
Antidepressants
Selective serotonin reuptake inhibitors are one of the first-line treatments for BDD and may be useful in ORS. In excoriation disorder and trichotillomania, selective serotonin reuptake inhibitors are the most commonly prescribed pharmacotherapy, but they have limited efficacy.2
Antipsychotics
The recommended treatment of delusional infestation is antipsychotic pharmacotherapy. Treatment with risperidone and olanzapine has been reported to achieve full or partial remission in more than two-thirds of cases.4 Aripiprazole, a newer antipsychotic, has fewer side effects and has been successful in several case reports.5-7
Cognitive Behavioral Therapy
Psychotherapy, most often in the form of cognitive behavioral therapy, has been reported as effective treatment of several psychocutaneous diseases. Cognitive behavioral therapy is considered first-line treatment of body-focused repetitive behavior disorders such as excoriation disorder and trichotillomania.2 It addresses maladaptive thought patterns to modify behavior.
Who treats patients with neurodermatoses?
If a patient presents to dermatology with a rash found to be related to an underlying thyroid disorder, the treatment plan likely would include referral to an endocrinologist. Similarly, patients with primary psychiatric conditions presenting to dermatology should ideally be referred to psychiatrists or psychotherapists, the providers most thoroughly trained and best equipped to treat them. The challenge in psychodermatology is that patients often are resistant to the assessment that the primary pathology is psychiatric. Patients may deny that they are “crazy” and see numerous providers in search of a dermatologist who “believes” them.8
Referral to mental health professionals almost always is refused by patients with primarily psychiatric neurodermatoses, which presents dermatologists with a dilemma. As the authors of the “Psychotropic Agents” chapter of Comprehensive Dermatologic Drug Therapy put it: “A dermatologist has two choices. The first is to try to ‘look the other way’ and pacify the patient by providing relatively benign, but minimally effective treatments. The other option is to try to directly address the psychological/psychiatric problems.” The chapter then provides a thorough guide for the use of psychotropic medications in the dermatology population, advocating for option 2: treatment by dermatologists.9
Should a dermatologist prescribe psychotropic drugs?
In Dermatology, the principle reference textbook in many dermatology training programs, it is stated that “[a]lthough less comprehensive than treatment delivered in collaboration with a psychiatrist, in the authors’ opinion, management of these issues by a dermatologist is better than no treatment at all.”10 Recent reviews in the dermatologic literature of psychiatric diseases and drugs in dermatology agree that dermatologists should feel comfortable with prescribing pharmacologic treatment.2,8,11 Performance of psychotherapy by dermatologists, on the other hand, is not recommended based on time constraints and lack of training.
Despite the apparent agreement in the texts and literature that pharmacotherapy of psychiatric neurodermatoses is within our scope of practice in dermatology, most dermatologists do not prescribe psychotropic agents. Dermatology residencies generally do not provide thorough training in psychopharmacotherapy.9 Unsurprisingly, a survey of 40 dermatologists at one academic institution found that only 11% felt comfortable prescribing an antidepressant and a mere 3% were comfortable prescribing an antipsychotic.12
Final Thoughts
The challenges involved in managing patients with primary psychiatric disease in dermatology are great and many patients are undertreated despite the availability of effective, evidence-based treatment options. We need to continue to work toward providing better access to these treatments in a way that maximizes the chance that our patients will accept our care.
- Korabel H, Dudek D, Jaworek A, et al. Psychodermatology: psychological and psychiatrical aspects of dermatology [in Polish]. Przegl Lek. 2008;65:244-248.
- Krooks JA, Weatherall AG, Holland PJ. Review of epidemiology, clinical presentation, diagnosis, and treatment of common primary psychiatric causes of cutaneous disease. J Dermatolog Treat. 2018;29:418-427.
- Bewley AP, Lepping P, Freundenmann RW, et al. Delusional parasitosis: time to call it delusional infestation. Br J Dermatol. 2018;163:1-2.
- Freudenmann RW, Lepping P. Second-generation antipsychotics in primary and secondary delusional parasitosis: outcome and efficacy. J Clin Psychopharmacol. 2008;28:500-508.
- Miyamoto S, Miyake N, Ogino S, et al. Successful treatment of delusional disorder with low-dose aripiprazole. Psychiatry Clin Neurosci. 2008;62:369.
- Ladizinski B, Busse KL, Bhutani T, et al. Aripiprazole as a viable alternative for treating delusions of parasitosis. J Drugs Dermatol. 2010;9:1531-1532.
- Huang WL, Chang LR. Aripiprazole in the treatment of delusional parasitosis with ocular and dermatologic presentations. J Clin Psychopharmacol. 2013;33:272-273.
- Campbell EH, Elston DM, Hawthorne JD, et al. Diagnosis and management of delusional parasitosis. J Am Acad Dermatol. 2019;80:1428-1434.
- Bhutani T, Lee CS, Koo JYM. Psychotropic agents. In: Wolverton SE, ed. Comprehensive Dermatologic Drug Therapy. 3rd ed. China: Elsevier Saunders; 2013:375-388.
- Duncan KO, Koo JYM. Psychocutaneous diseases. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018:128-137.
- Shah B, Levenson JL. Use of psychotropic drugs in the dermatology patient: when to start and stop? Clin Dermatol. 2018;36:748-755.
- Gee SN, Zakhary L, Keuthen N, et al. A survey assessment of the recognition and treatment of psychocutaneous disorders in the outpatient dermatology setting: how prepared are we? J Am Acad Dermatol. 2013;68:47-52.
- Korabel H, Dudek D, Jaworek A, et al. Psychodermatology: psychological and psychiatrical aspects of dermatology [in Polish]. Przegl Lek. 2008;65:244-248.
- Krooks JA, Weatherall AG, Holland PJ. Review of epidemiology, clinical presentation, diagnosis, and treatment of common primary psychiatric causes of cutaneous disease. J Dermatolog Treat. 2018;29:418-427.
- Bewley AP, Lepping P, Freundenmann RW, et al. Delusional parasitosis: time to call it delusional infestation. Br J Dermatol. 2018;163:1-2.
- Freudenmann RW, Lepping P. Second-generation antipsychotics in primary and secondary delusional parasitosis: outcome and efficacy. J Clin Psychopharmacol. 2008;28:500-508.
- Miyamoto S, Miyake N, Ogino S, et al. Successful treatment of delusional disorder with low-dose aripiprazole. Psychiatry Clin Neurosci. 2008;62:369.
- Ladizinski B, Busse KL, Bhutani T, et al. Aripiprazole as a viable alternative for treating delusions of parasitosis. J Drugs Dermatol. 2010;9:1531-1532.
- Huang WL, Chang LR. Aripiprazole in the treatment of delusional parasitosis with ocular and dermatologic presentations. J Clin Psychopharmacol. 2013;33:272-273.
- Campbell EH, Elston DM, Hawthorne JD, et al. Diagnosis and management of delusional parasitosis. J Am Acad Dermatol. 2019;80:1428-1434.
- Bhutani T, Lee CS, Koo JYM. Psychotropic agents. In: Wolverton SE, ed. Comprehensive Dermatologic Drug Therapy. 3rd ed. China: Elsevier Saunders; 2013:375-388.
- Duncan KO, Koo JYM. Psychocutaneous diseases. In: Bolognia JL, Schaffer JV, Cerroni L, eds. Dermatology. 4th ed. China: Elsevier; 2018:128-137.
- Shah B, Levenson JL. Use of psychotropic drugs in the dermatology patient: when to start and stop? Clin Dermatol. 2018;36:748-755.
- Gee SN, Zakhary L, Keuthen N, et al. A survey assessment of the recognition and treatment of psychocutaneous disorders in the outpatient dermatology setting: how prepared are we? J Am Acad Dermatol. 2013;68:47-52.
Resident Pearl
- Patients often present to dermatology with primary psychologic disorders such as delusional infestation or trichotillomania. Treatment of such conditions with antidepressants and antipsychotics can be highly effective and is within our scope of practice. Increased emphasis on psychopharmacotherapy in dermatology training would increase access to appropriate care for this patient population.

A kick to kick off residency
“A leader is someone who helps improve the lives of other people or improve the system they live under.”
— Sam Houston
If my motivation to become a doctor was ever the supposed glamour and prestige conferred once “MD” is added to your name, that delusion was quickly wiped away on my first day of residency; not at work, but on my way there.
I live in New York City—a city that relies on buses and subways, where the wealthy and elite go to work using the same modes of transportation as everyone else. Unfortunately, because the shelter system in New York isn’t nearly large enough to accommodate the vast homeless population, many homeless people sleep in the subway at night. It’s not uncommon to see a still-sleeping homeless person on the subway in the early hours of the morning, and I encountered one on my first official day of work as a doctor.
There I was, dressed for the occasion in a new,
Within seconds of sitting down, the man extended one of his legs and kicked me in the chest while still asleep. Not hard enough to cause pain or injury, but enough to leave a dirty boot print on my shirt. I had to wear that shirt for the rest of the day, and so I spent my first day of residency explaining to hospital staff and patients alike how I was branded by a drunk homeless man on the subway as he slept.
As time wore on in my first year of residency, I learned that encounters with individuals like these were not rare. The majority of the patients I see are people like that man on the subway. “I sleep on the subway” is often the answer when I ask a patient about their living conditions. “I’m on public assistance” is what I hear when questioning what a patient does for money. “I don’t have money to take the bus” is a typical explanation for why they missed their doctor’s appointments and ran out of medicine. And, sadly, “Because I’m lonely” is the main excuse for why patients engage in self-defeating habits such as drug and alcohol abuse.
I didn’t anticipate this part of psychiatry when I applied for residency in this specialty. My notion of this profession was far more romanticized. I was enthralled with the science of neurotransmitters, the parameters of DSM criteria, the interpersonal skills required to elicit information from a patient during an interview, the deliberation in arriving at a diagnosis, and the ever-changing nature of psychopharmacology. That’s the psychiatry I expected to learn when I got on the subway for my first day of residency. It wasn’t until later that I truly considered the human toll that psychiatric illness takes on the individual who suffers from it. To that person, the science behind their illness and the suffering they endure isn’t romantic at all; it’s a burden to be lifted.
Continue to: We use the term...
We use the term “underserved” to identify challenging patient populations, but there are categories of patients that fall below the threshold of merely underserved. I am mortified to know that one-third of homeless people in the United States have a serious and untreated mental illness. Individuals discharged from psychiatric hospitals are 3 times more likely to obtain food from garbage. They are also far more likely to be the victim of a crime than perpetrators of it. As I’ve discovered since starting residency, if a patient doesn’t have a place to live, food to eat, and some semblance of a support system, then it’s often meaningless for them to take pills, regardless of how those pills work in theory.
No definition of sound mental health is complete unless it gives deference to those who lack basic human needs. This is a realization that was literally kicked into me, and one I hope will guide me in the years ahead.
“A leader is someone who helps improve the lives of other people or improve the system they live under.”
— Sam Houston
If my motivation to become a doctor was ever the supposed glamour and prestige conferred once “MD” is added to your name, that delusion was quickly wiped away on my first day of residency; not at work, but on my way there.
I live in New York City—a city that relies on buses and subways, where the wealthy and elite go to work using the same modes of transportation as everyone else. Unfortunately, because the shelter system in New York isn’t nearly large enough to accommodate the vast homeless population, many homeless people sleep in the subway at night. It’s not uncommon to see a still-sleeping homeless person on the subway in the early hours of the morning, and I encountered one on my first official day of work as a doctor.
There I was, dressed for the occasion in a new,
Within seconds of sitting down, the man extended one of his legs and kicked me in the chest while still asleep. Not hard enough to cause pain or injury, but enough to leave a dirty boot print on my shirt. I had to wear that shirt for the rest of the day, and so I spent my first day of residency explaining to hospital staff and patients alike how I was branded by a drunk homeless man on the subway as he slept.
As time wore on in my first year of residency, I learned that encounters with individuals like these were not rare. The majority of the patients I see are people like that man on the subway. “I sleep on the subway” is often the answer when I ask a patient about their living conditions. “I’m on public assistance” is what I hear when questioning what a patient does for money. “I don’t have money to take the bus” is a typical explanation for why they missed their doctor’s appointments and ran out of medicine. And, sadly, “Because I’m lonely” is the main excuse for why patients engage in self-defeating habits such as drug and alcohol abuse.
I didn’t anticipate this part of psychiatry when I applied for residency in this specialty. My notion of this profession was far more romanticized. I was enthralled with the science of neurotransmitters, the parameters of DSM criteria, the interpersonal skills required to elicit information from a patient during an interview, the deliberation in arriving at a diagnosis, and the ever-changing nature of psychopharmacology. That’s the psychiatry I expected to learn when I got on the subway for my first day of residency. It wasn’t until later that I truly considered the human toll that psychiatric illness takes on the individual who suffers from it. To that person, the science behind their illness and the suffering they endure isn’t romantic at all; it’s a burden to be lifted.
Continue to: We use the term...
We use the term “underserved” to identify challenging patient populations, but there are categories of patients that fall below the threshold of merely underserved. I am mortified to know that one-third of homeless people in the United States have a serious and untreated mental illness. Individuals discharged from psychiatric hospitals are 3 times more likely to obtain food from garbage. They are also far more likely to be the victim of a crime than perpetrators of it. As I’ve discovered since starting residency, if a patient doesn’t have a place to live, food to eat, and some semblance of a support system, then it’s often meaningless for them to take pills, regardless of how those pills work in theory.
No definition of sound mental health is complete unless it gives deference to those who lack basic human needs. This is a realization that was literally kicked into me, and one I hope will guide me in the years ahead.
“A leader is someone who helps improve the lives of other people or improve the system they live under.”
— Sam Houston
If my motivation to become a doctor was ever the supposed glamour and prestige conferred once “MD” is added to your name, that delusion was quickly wiped away on my first day of residency; not at work, but on my way there.
I live in New York City—a city that relies on buses and subways, where the wealthy and elite go to work using the same modes of transportation as everyone else. Unfortunately, because the shelter system in New York isn’t nearly large enough to accommodate the vast homeless population, many homeless people sleep in the subway at night. It’s not uncommon to see a still-sleeping homeless person on the subway in the early hours of the morning, and I encountered one on my first official day of work as a doctor.
There I was, dressed for the occasion in a new,
Within seconds of sitting down, the man extended one of his legs and kicked me in the chest while still asleep. Not hard enough to cause pain or injury, but enough to leave a dirty boot print on my shirt. I had to wear that shirt for the rest of the day, and so I spent my first day of residency explaining to hospital staff and patients alike how I was branded by a drunk homeless man on the subway as he slept.
As time wore on in my first year of residency, I learned that encounters with individuals like these were not rare. The majority of the patients I see are people like that man on the subway. “I sleep on the subway” is often the answer when I ask a patient about their living conditions. “I’m on public assistance” is what I hear when questioning what a patient does for money. “I don’t have money to take the bus” is a typical explanation for why they missed their doctor’s appointments and ran out of medicine. And, sadly, “Because I’m lonely” is the main excuse for why patients engage in self-defeating habits such as drug and alcohol abuse.
I didn’t anticipate this part of psychiatry when I applied for residency in this specialty. My notion of this profession was far more romanticized. I was enthralled with the science of neurotransmitters, the parameters of DSM criteria, the interpersonal skills required to elicit information from a patient during an interview, the deliberation in arriving at a diagnosis, and the ever-changing nature of psychopharmacology. That’s the psychiatry I expected to learn when I got on the subway for my first day of residency. It wasn’t until later that I truly considered the human toll that psychiatric illness takes on the individual who suffers from it. To that person, the science behind their illness and the suffering they endure isn’t romantic at all; it’s a burden to be lifted.
Continue to: We use the term...
We use the term “underserved” to identify challenging patient populations, but there are categories of patients that fall below the threshold of merely underserved. I am mortified to know that one-third of homeless people in the United States have a serious and untreated mental illness. Individuals discharged from psychiatric hospitals are 3 times more likely to obtain food from garbage. They are also far more likely to be the victim of a crime than perpetrators of it. As I’ve discovered since starting residency, if a patient doesn’t have a place to live, food to eat, and some semblance of a support system, then it’s often meaningless for them to take pills, regardless of how those pills work in theory.
No definition of sound mental health is complete unless it gives deference to those who lack basic human needs. This is a realization that was literally kicked into me, and one I hope will guide me in the years ahead.

The ABCs of COCs: A Guide for Dermatology Residents on Combined Oral Contraceptives
The American Academy of Dermatology confers combined oral contraceptives (COCs) a strength A recommendation for the treatment of acne based on level I evidence, and 4 COCs are approved for the treatment of acne by the US Food and Drug Administration (FDA).1 Furthermore, when dermatologists prescribe isotretinoin and thalidomide to women of reproductive potential, the iPLEDGE and THALOMID Risk Evaluation and Mitigation Strategy (REMS) programs require 2 concurrent methods of contraception, one of which may be a COC. In addition, COCs have several potential off-label indications in dermatology including idiopathic hirsutism, female pattern hair loss, hidradenitis suppurativa, and autoimmune progesterone dermatitis.
Despite this evidence and opportunity, research suggests that dermatologists underprescribe COCs. The National Ambulatory Medical Care Survey found that between 1993 and 2008, dermatologists in the United States prescribed COCs to only 2.03% of women presenting for acne treatment, which was less often than obstetricians/gynecologists (36.03%) and internists (10.76%).2 More recently, in a survey of 130 US dermatologists conducted from 2014 to 2015, only 55.4% reported prescribing COCs. This survey also found that only 45.8% of dermatologists who prescribed COCs felt very comfortable counseling on how to begin taking them, only 48.6% felt very comfortable counseling patients on side effects, and only 22.2% felt very comfortable managing side effects.3
In light of these data, this article reviews the basics of COCs for dermatology residents, from assessing patient eligibility and selecting a COC to counseling on use and managing risks and side effects. Because there are different approaches to prescribing COCs, readers are encouraged to integrate the information in this article with what they have learned from other sources.
Assess Patient Eligibility
In general, patients should be at least 14 years of age and have waited 2 years after menarche to start COCs. They can be taken until menopause.1,4 Contraindications can be screened for by taking a medical history and measuring a baseline blood pressure (Tables 1 and 2).5 In addition, pregnancy should be excluded with a urine or serum pregnancy test or criteria provided in Box 2 of the 2016 US Selected Practice Recommendations for Contraceptive Use from the Centers for Disease Control and Prevention (CDC).4 Although important for women’s overall health, a pelvic examination is not required to start COCs according to the CDC and the American Academy of Dermatology.1,4
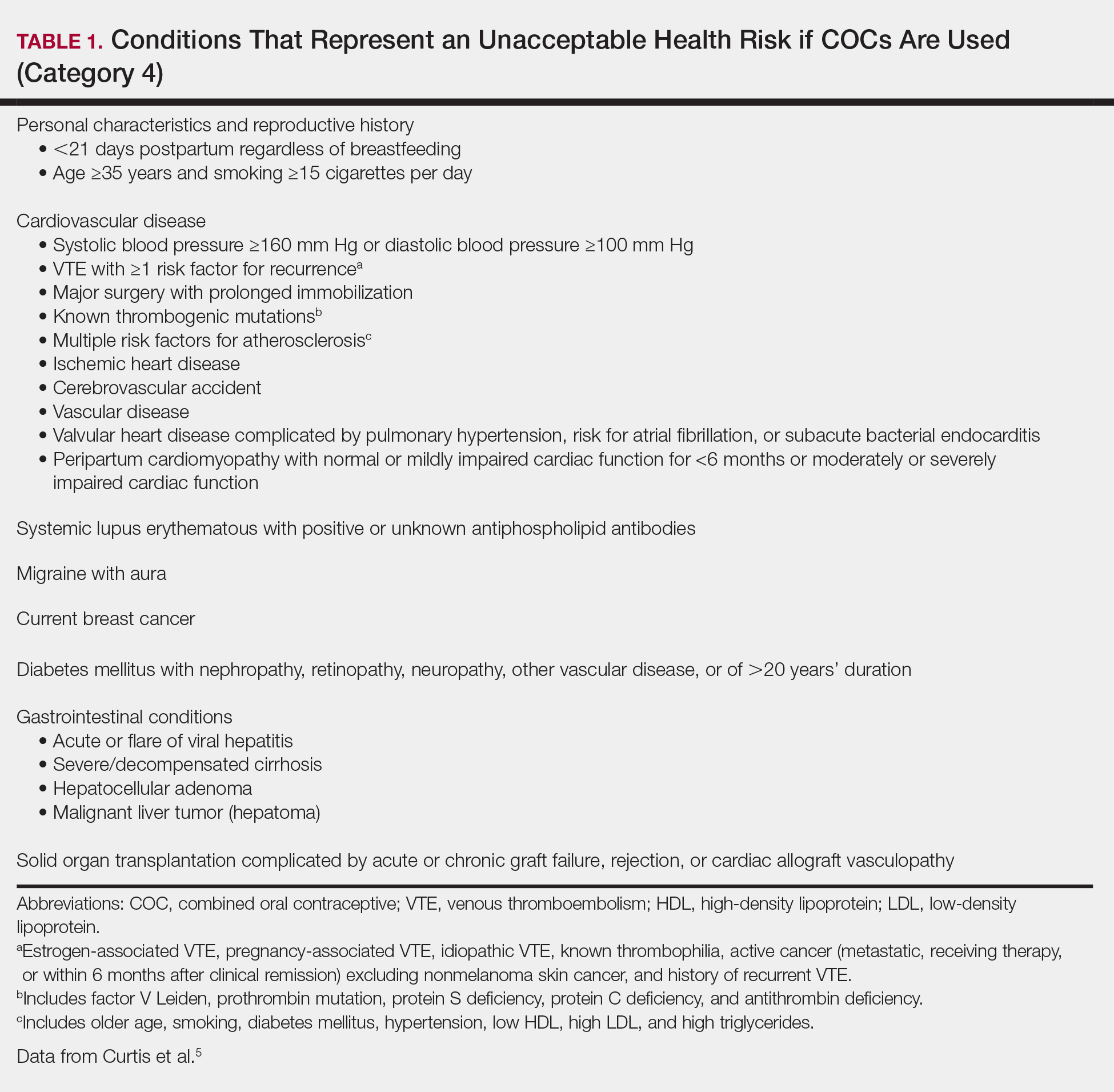
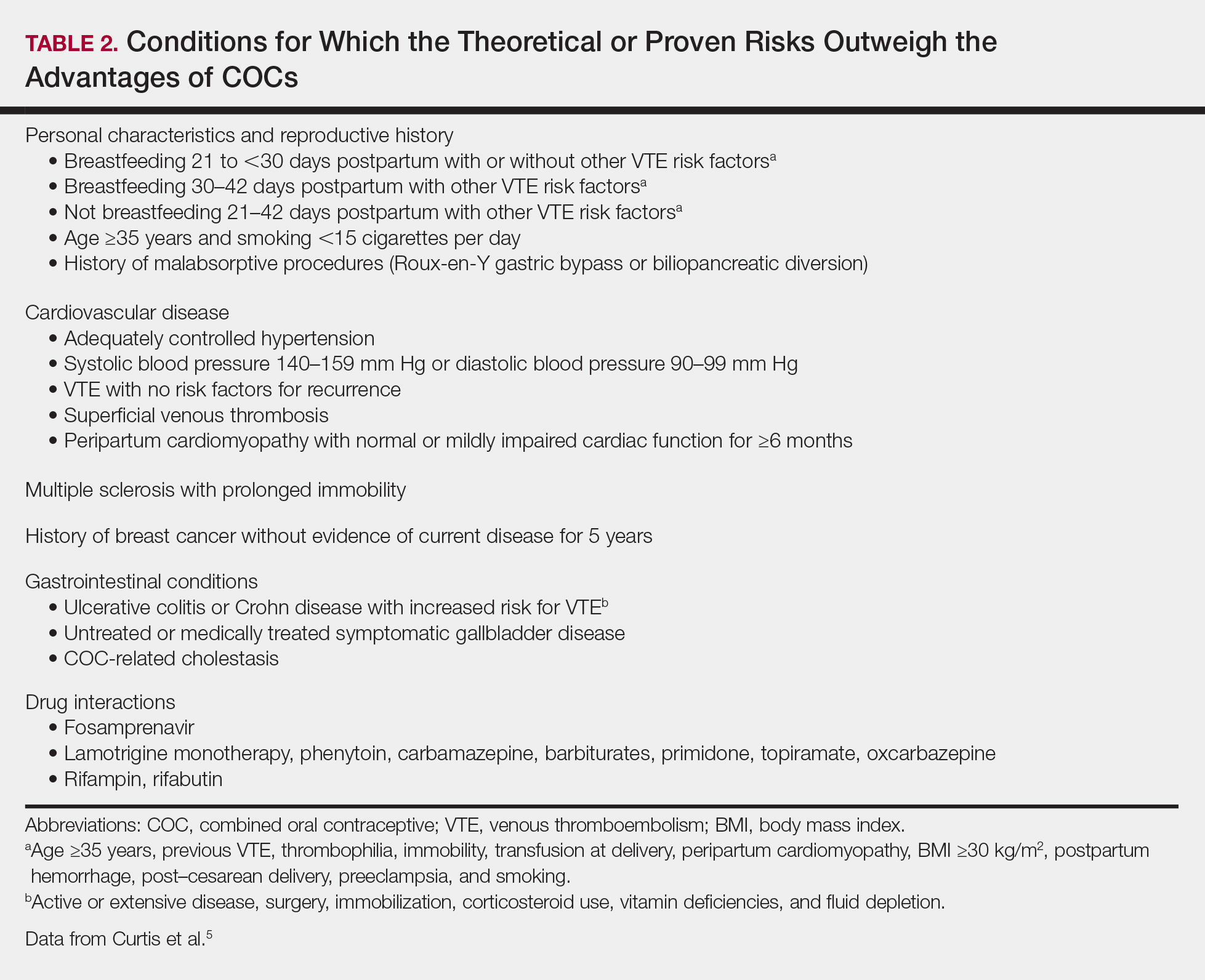
Select the COC
Combined oral contraceptives combine estrogen, usually in the form of ethinyl estradiol, with a progestin. Data suggest that all COCs effectively treat acne, but 4 are specifically FDA approved for acne: ethinyl estradiol–norethindrone acetate–ferrous fumarate, ethinyl estradiol–norgestimate, ethinyl estradiol–drospirenone, and ethinyl estradiol–drospirenone–levomefolate.1 Ethinyl estradiol–desogestrel and ethinyl estradiol–drospirenone are 2 go-to COCs for some of the attending physicians at my residency program. All COCs are FDA approved for contraception. When selecting a COC, one approach is to start with the patient’s drug formulary, then consider the following characteristics.
Monophasic vs Multiphasic
All the hormonally active pills in a monophasic formulation contain the same dose of estrogen and progestin; however, these doses change per pill in a multiphasic formulation, which requires that patients take the pills in a specific order. Given this greater complexity and the fact that multiphasic formulations often are more expensive and lack evidence of superiority, a 2011 Cochrane review recommended monophasic formulations as first line.6 In addition, monophasic formulations are preferred for autoimmune progesterone dermatitis because of the stable progestin dose.
Hormone-Free Interval
Some COCs include placebo pills during which hormone withdrawal symptoms such as bleeding, pelvic pain, mood changes, and headache may occur. If a patient is concerned about these symptoms, choose a COC with no or fewer placebo pills, or have the patient skip the hormone-free interval altogether and start the next pack early7; in this case, the prescription should be written with instructions to allow the patient to get earlier refills from the pharmacy.
Estrogen Dose
To minimize estrogen-related side effects, the lowest possible dose of ethinyl estradiol that is effective and tolerable should be prescribed7,8; 20 μg of ethinyl estradiol generally is the lowest dose available, but it may be associated with more frequent breakthrough bleeding.9 The International Planned Parenthood Federation recommends starting with COCs that contain 30 to 35 μg of estrogen.10 Synthesizing this information, one option is to start with 20 μg of ethinyl estradiol and increase the dose if breakthrough bleeding persists after 3 cycles.
Progestin Type
First-generation progestins (eg, norethindrone), second-generation progestins (eg, norgestrel, levonorgestrel), and third-generation progestins (eg, norgestimate, desogestrel) are derived from testosterone and therefore are variably androgenic; second-generation progestins are the most androgenic, and third-generation progestins are the least. On the other hand, drospirenone, the fourth-generation progestin available in the United States, is derived from 17α-spironolactone and thus is mildly antiandrogenic (3 mg of drospirenone is considered equivalent to 25 mg of spironolactone).
Although COCs with less androgenic progestins should theoretically treat acne better, a 2012 Cochrane review of COCs and acne concluded that “differences in the comparative effectiveness of COCs containing varying progestin types and dosages were less clear, and data were limited for any particular comparison.”11 As a result, regardless of the progestin, all COCs are believed to have a net antiandrogenic effect due to their estrogen component.1
Counsel on Use
Combined oral contraceptives can be started on any day of the menstrual cycle, including the day the prescription is given. If a patient begins a COC within 5 days of the first day of her most recent period, backup contraception is not needed.4 If she begins the COC more than 5 days after the first day of her most recent period, she needs to use backup contraception or abstain from sexual intercourse for the next 7 days.4 In general, at least 3 months of therapy are required to evaluate the effectiveness of COCs for acne.1
Manage Risks and Side Effects
Breakthrough Bleeding
The most common side effect of breakthrough bleeding can be minimized by taking COCs at approximately the same time every day and avoiding missed pills. If breakthrough bleeding does not stop after 3 cycles, consider increasing the estrogen dose to 30 to 35 μg and/or referring to an obstetrician/gynecologist to rule out other etiologies of bleeding.7,8
Nausea, Headache, Bloating, and Breast Tenderness
These symptoms typically resolve after the first 3 months. To minimize nausea, patients should take COCs in the early evening and eat breakfast the next morning.7,8 For headaches that occur during the hormone-free interval, consider skipping the placebo pills and starting the next pack early. Switching the progestin to drospirenone, which has a mild diuretic effect, can help with bloating as well as breast tenderness.7 For persistent symptoms, consider a lower estrogen dose.7,8
Changes in Libido
In a systemic review including 8422 COC users, 64% reported no change in libido, 22% reported an increase, and 15% reported a decrease.12
Weight Gain
Although patients may be concerned that COCs cause weight gain, a 2014 Cochrane review concluded that “available evidence is insufficient to determine the effect of combination contraceptives on weight, but no large effect is evident.”13 If weight gain does occur, anecdotal evidence suggests it tends to be not more than 5 pounds. If weight gain is an issue, consider a less androgenic progestin.8
Venous Thromboembolism
Use the 3-6-9-12 model to contextualize venous thromboembolism (VTE) risk: a woman’s annual VTE risk is 3 per 10,000 women at baseline, 6 per 10,000 women with nondrospirenone COCs, 9 per 10,000 women with drospirenone-containing COCs, and 12 per 10,000 women when pregnant.14 Patients should be counseled on the signs and symptoms of VTE such as unilateral or bilateral leg or arm swelling, pain, warmth, redness, and/or shortness of breath. The British Society for Haematology recommends maintaining mobility as a reasonable precaution when traveling for more than 3 hours.15
Cardiovascular Disease
A 2015 Cochrane review found that the risk for myocardial infarction or ischemic stroke is increased 1.6‐fold in COC users.16 Despite this increased relative risk, the increased absolute annual risk of myocardial infarction in nonsmoking women remains low: increased from 0.83 to 3.53 per 10,000,000 women younger than 35 years and from 9.45 to 40.4 per 10,000,000 women 35 years and older.17
Breast Cancer and Cervical Cancer
Data are mixed on the effect of COCs on the risk for breast cancer and cervical cancer.1 According to the CDC, COC use for 5 or more years might increase the risk of cervical carcinoma in situ and invasive cervical carcinoma in women with persistent human papillomavirus infection.5 Regardless of COC use, women should undergo age-appropriate screening for breast cancer and cervical cancer.
Melasma
Melasma is an estrogen-mediated side effect of COCs.8 A study from 1967 found that 29% of COC users (N=212) developed melasma; however, they were taking COCs with much higher ethinyl estradiol doses (50–100 μg) than typically used today.18 Nevertheless, as part of an overall skin care regimen, photoprotection should be encouraged with a broad-spectrum, water-resistant sunscreen that has a sun protection factor of at least 30. In addition, sunscreens with iron oxides have been shown to better prevent melasma relapse by protecting against the shorter wavelengths of visible light.19
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74:945-973.e933.
- Landis ET, Levender MM, Davis SA, et al. Isotretinoin and oral contraceptive use in female acne patients varies by physician specialty: analysis of data from the National Ambulatory Medical Care Survey. J Dermatolog Treat. 2012;23:272-277.
- Fitzpatrick L, Mauer E, Chen CL. Oral contraceptives for acne treatment: US dermatologists’ knowledge, comfort, and prescribing practices. Cutis. 2017;99:195-201.
- Curtis KM, Jatlaoui TC, Tepper NK, et al. U.S. Selected Practice Recommendations for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65:1-66.
- Curtis KM, Tepper NK, Jatlaoui TC, et al. U.S. Medical Eligibility Criteria for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65:1-103.
- Van Vliet HA, Grimes DA, Lopez LM, et al. Triphasic versus monophasic oral contraceptives for contraception. Cochrane Database Syst Rev. 2011:CD003553.
- Stewart M, Black K. Choosing a combined oral contraceptive pill. Aust Prescr. 2015;38:6-11.
- McKinney K. Understanding the options: a guide to oral contraceptives. https://www.cecentral.com/assets/2097/022%20Oral%20Contraceptives%2010-26-09.pdf. Published November 5, 2009. Accessed June 20, 2019.
- Gallo MF, Nanda K, Grimes DA, et al. 20 microg versus >20 microg estrogen combined oral contraceptives for contraception. Cochrane Database Syst Rev. 2013:CD003989.
- Terki F, Malhotra U. Medical and Service Delivery Guidelines for Sexual and Reproductive Health Services. London, United Kingdom: International Planned Parenthood Federation; 2004.
- Arowojolu AO, Gallo MF, Lopez LM, et al. Combined oral contraceptive pills for treatment of acne. Cochrane Database Syst Rev. 2012:CD004425.
- Pastor Z, Holla K, Chmel R. The influence of combined oral contraceptives on female sexual desire: a systematic review. Eur J Contracept Reprod Health Care. 2013;18:27-43.
- Gallo MF, Lopez LM, Grimes DA, et al. Combination contraceptives: effects on weight. Cochrane Database Syst Rev. 2014:CD003987.
- Birth control pills for acne: tips from Julie Harper at the Summer AAD. Cutis. https://www.mdedge.com/dermatology/article/144550/acne/birth-control-pills-acne-tips-julie-harper-summer-aad. Published August 14, 2017. Accessed June 24, 2019.
- Watson HG, Baglin TP. Guidelines on travel-related venous thrombosis. Br J Haematol. 2011;152:31-34.
- Roach RE, Helmerhorst FM, Lijfering WM, et al. Combined oral contraceptives: the risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev. 2015:CD011054.
- Acute myocardial infarction and combined oral contraceptives: results of an international multicentre case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1997;349:1202-1209.
- Resnik S. Melasma induced by oral contraceptive drugs. JAMA. 1967;199:601-605.
- Boukari F, Jourdan E, Fontas E, et al. Prevention of melasma relapses with sunscreen combining protection against UV and short wavelengths of visible light: a prospective randomized comparative trial. J Am Acad Dermatol. 2015;72:189-190.e181.
The American Academy of Dermatology confers combined oral contraceptives (COCs) a strength A recommendation for the treatment of acne based on level I evidence, and 4 COCs are approved for the treatment of acne by the US Food and Drug Administration (FDA).1 Furthermore, when dermatologists prescribe isotretinoin and thalidomide to women of reproductive potential, the iPLEDGE and THALOMID Risk Evaluation and Mitigation Strategy (REMS) programs require 2 concurrent methods of contraception, one of which may be a COC. In addition, COCs have several potential off-label indications in dermatology including idiopathic hirsutism, female pattern hair loss, hidradenitis suppurativa, and autoimmune progesterone dermatitis.
Despite this evidence and opportunity, research suggests that dermatologists underprescribe COCs. The National Ambulatory Medical Care Survey found that between 1993 and 2008, dermatologists in the United States prescribed COCs to only 2.03% of women presenting for acne treatment, which was less often than obstetricians/gynecologists (36.03%) and internists (10.76%).2 More recently, in a survey of 130 US dermatologists conducted from 2014 to 2015, only 55.4% reported prescribing COCs. This survey also found that only 45.8% of dermatologists who prescribed COCs felt very comfortable counseling on how to begin taking them, only 48.6% felt very comfortable counseling patients on side effects, and only 22.2% felt very comfortable managing side effects.3
In light of these data, this article reviews the basics of COCs for dermatology residents, from assessing patient eligibility and selecting a COC to counseling on use and managing risks and side effects. Because there are different approaches to prescribing COCs, readers are encouraged to integrate the information in this article with what they have learned from other sources.
Assess Patient Eligibility
In general, patients should be at least 14 years of age and have waited 2 years after menarche to start COCs. They can be taken until menopause.1,4 Contraindications can be screened for by taking a medical history and measuring a baseline blood pressure (Tables 1 and 2).5 In addition, pregnancy should be excluded with a urine or serum pregnancy test or criteria provided in Box 2 of the 2016 US Selected Practice Recommendations for Contraceptive Use from the Centers for Disease Control and Prevention (CDC).4 Although important for women’s overall health, a pelvic examination is not required to start COCs according to the CDC and the American Academy of Dermatology.1,4
Select the COC
Combined oral contraceptives combine estrogen, usually in the form of ethinyl estradiol, with a progestin. Data suggest that all COCs effectively treat acne, but 4 are specifically FDA approved for acne: ethinyl estradiol–norethindrone acetate–ferrous fumarate, ethinyl estradiol–norgestimate, ethinyl estradiol–drospirenone, and ethinyl estradiol–drospirenone–levomefolate.1 Ethinyl estradiol–desogestrel and ethinyl estradiol–drospirenone are 2 go-to COCs for some of the attending physicians at my residency program. All COCs are FDA approved for contraception. When selecting a COC, one approach is to start with the patient’s drug formulary, then consider the following characteristics.
Monophasic vs Multiphasic
All the hormonally active pills in a monophasic formulation contain the same dose of estrogen and progestin; however, these doses change per pill in a multiphasic formulation, which requires that patients take the pills in a specific order. Given this greater complexity and the fact that multiphasic formulations often are more expensive and lack evidence of superiority, a 2011 Cochrane review recommended monophasic formulations as first line.6 In addition, monophasic formulations are preferred for autoimmune progesterone dermatitis because of the stable progestin dose.
Hormone-Free Interval
Some COCs include placebo pills during which hormone withdrawal symptoms such as bleeding, pelvic pain, mood changes, and headache may occur. If a patient is concerned about these symptoms, choose a COC with no or fewer placebo pills, or have the patient skip the hormone-free interval altogether and start the next pack early7; in this case, the prescription should be written with instructions to allow the patient to get earlier refills from the pharmacy.
Estrogen Dose
To minimize estrogen-related side effects, the lowest possible dose of ethinyl estradiol that is effective and tolerable should be prescribed7,8; 20 μg of ethinyl estradiol generally is the lowest dose available, but it may be associated with more frequent breakthrough bleeding.9 The International Planned Parenthood Federation recommends starting with COCs that contain 30 to 35 μg of estrogen.10 Synthesizing this information, one option is to start with 20 μg of ethinyl estradiol and increase the dose if breakthrough bleeding persists after 3 cycles.
Progestin Type
First-generation progestins (eg, norethindrone), second-generation progestins (eg, norgestrel, levonorgestrel), and third-generation progestins (eg, norgestimate, desogestrel) are derived from testosterone and therefore are variably androgenic; second-generation progestins are the most androgenic, and third-generation progestins are the least. On the other hand, drospirenone, the fourth-generation progestin available in the United States, is derived from 17α-spironolactone and thus is mildly antiandrogenic (3 mg of drospirenone is considered equivalent to 25 mg of spironolactone).
Although COCs with less androgenic progestins should theoretically treat acne better, a 2012 Cochrane review of COCs and acne concluded that “differences in the comparative effectiveness of COCs containing varying progestin types and dosages were less clear, and data were limited for any particular comparison.”11 As a result, regardless of the progestin, all COCs are believed to have a net antiandrogenic effect due to their estrogen component.1
Counsel on Use
Combined oral contraceptives can be started on any day of the menstrual cycle, including the day the prescription is given. If a patient begins a COC within 5 days of the first day of her most recent period, backup contraception is not needed.4 If she begins the COC more than 5 days after the first day of her most recent period, she needs to use backup contraception or abstain from sexual intercourse for the next 7 days.4 In general, at least 3 months of therapy are required to evaluate the effectiveness of COCs for acne.1
Manage Risks and Side Effects
Breakthrough Bleeding
The most common side effect of breakthrough bleeding can be minimized by taking COCs at approximately the same time every day and avoiding missed pills. If breakthrough bleeding does not stop after 3 cycles, consider increasing the estrogen dose to 30 to 35 μg and/or referring to an obstetrician/gynecologist to rule out other etiologies of bleeding.7,8
Nausea, Headache, Bloating, and Breast Tenderness
These symptoms typically resolve after the first 3 months. To minimize nausea, patients should take COCs in the early evening and eat breakfast the next morning.7,8 For headaches that occur during the hormone-free interval, consider skipping the placebo pills and starting the next pack early. Switching the progestin to drospirenone, which has a mild diuretic effect, can help with bloating as well as breast tenderness.7 For persistent symptoms, consider a lower estrogen dose.7,8
Changes in Libido
In a systemic review including 8422 COC users, 64% reported no change in libido, 22% reported an increase, and 15% reported a decrease.12
Weight Gain
Although patients may be concerned that COCs cause weight gain, a 2014 Cochrane review concluded that “available evidence is insufficient to determine the effect of combination contraceptives on weight, but no large effect is evident.”13 If weight gain does occur, anecdotal evidence suggests it tends to be not more than 5 pounds. If weight gain is an issue, consider a less androgenic progestin.8
Venous Thromboembolism
Use the 3-6-9-12 model to contextualize venous thromboembolism (VTE) risk: a woman’s annual VTE risk is 3 per 10,000 women at baseline, 6 per 10,000 women with nondrospirenone COCs, 9 per 10,000 women with drospirenone-containing COCs, and 12 per 10,000 women when pregnant.14 Patients should be counseled on the signs and symptoms of VTE such as unilateral or bilateral leg or arm swelling, pain, warmth, redness, and/or shortness of breath. The British Society for Haematology recommends maintaining mobility as a reasonable precaution when traveling for more than 3 hours.15
Cardiovascular Disease
A 2015 Cochrane review found that the risk for myocardial infarction or ischemic stroke is increased 1.6‐fold in COC users.16 Despite this increased relative risk, the increased absolute annual risk of myocardial infarction in nonsmoking women remains low: increased from 0.83 to 3.53 per 10,000,000 women younger than 35 years and from 9.45 to 40.4 per 10,000,000 women 35 years and older.17
Breast Cancer and Cervical Cancer
Data are mixed on the effect of COCs on the risk for breast cancer and cervical cancer.1 According to the CDC, COC use for 5 or more years might increase the risk of cervical carcinoma in situ and invasive cervical carcinoma in women with persistent human papillomavirus infection.5 Regardless of COC use, women should undergo age-appropriate screening for breast cancer and cervical cancer.
Melasma
Melasma is an estrogen-mediated side effect of COCs.8 A study from 1967 found that 29% of COC users (N=212) developed melasma; however, they were taking COCs with much higher ethinyl estradiol doses (50–100 μg) than typically used today.18 Nevertheless, as part of an overall skin care regimen, photoprotection should be encouraged with a broad-spectrum, water-resistant sunscreen that has a sun protection factor of at least 30. In addition, sunscreens with iron oxides have been shown to better prevent melasma relapse by protecting against the shorter wavelengths of visible light.19
The American Academy of Dermatology confers combined oral contraceptives (COCs) a strength A recommendation for the treatment of acne based on level I evidence, and 4 COCs are approved for the treatment of acne by the US Food and Drug Administration (FDA).1 Furthermore, when dermatologists prescribe isotretinoin and thalidomide to women of reproductive potential, the iPLEDGE and THALOMID Risk Evaluation and Mitigation Strategy (REMS) programs require 2 concurrent methods of contraception, one of which may be a COC. In addition, COCs have several potential off-label indications in dermatology including idiopathic hirsutism, female pattern hair loss, hidradenitis suppurativa, and autoimmune progesterone dermatitis.
Despite this evidence and opportunity, research suggests that dermatologists underprescribe COCs. The National Ambulatory Medical Care Survey found that between 1993 and 2008, dermatologists in the United States prescribed COCs to only 2.03% of women presenting for acne treatment, which was less often than obstetricians/gynecologists (36.03%) and internists (10.76%).2 More recently, in a survey of 130 US dermatologists conducted from 2014 to 2015, only 55.4% reported prescribing COCs. This survey also found that only 45.8% of dermatologists who prescribed COCs felt very comfortable counseling on how to begin taking them, only 48.6% felt very comfortable counseling patients on side effects, and only 22.2% felt very comfortable managing side effects.3
In light of these data, this article reviews the basics of COCs for dermatology residents, from assessing patient eligibility and selecting a COC to counseling on use and managing risks and side effects. Because there are different approaches to prescribing COCs, readers are encouraged to integrate the information in this article with what they have learned from other sources.
Assess Patient Eligibility
In general, patients should be at least 14 years of age and have waited 2 years after menarche to start COCs. They can be taken until menopause.1,4 Contraindications can be screened for by taking a medical history and measuring a baseline blood pressure (Tables 1 and 2).5 In addition, pregnancy should be excluded with a urine or serum pregnancy test or criteria provided in Box 2 of the 2016 US Selected Practice Recommendations for Contraceptive Use from the Centers for Disease Control and Prevention (CDC).4 Although important for women’s overall health, a pelvic examination is not required to start COCs according to the CDC and the American Academy of Dermatology.1,4
Select the COC
Combined oral contraceptives combine estrogen, usually in the form of ethinyl estradiol, with a progestin. Data suggest that all COCs effectively treat acne, but 4 are specifically FDA approved for acne: ethinyl estradiol–norethindrone acetate–ferrous fumarate, ethinyl estradiol–norgestimate, ethinyl estradiol–drospirenone, and ethinyl estradiol–drospirenone–levomefolate.1 Ethinyl estradiol–desogestrel and ethinyl estradiol–drospirenone are 2 go-to COCs for some of the attending physicians at my residency program. All COCs are FDA approved for contraception. When selecting a COC, one approach is to start with the patient’s drug formulary, then consider the following characteristics.
Monophasic vs Multiphasic
All the hormonally active pills in a monophasic formulation contain the same dose of estrogen and progestin; however, these doses change per pill in a multiphasic formulation, which requires that patients take the pills in a specific order. Given this greater complexity and the fact that multiphasic formulations often are more expensive and lack evidence of superiority, a 2011 Cochrane review recommended monophasic formulations as first line.6 In addition, monophasic formulations are preferred for autoimmune progesterone dermatitis because of the stable progestin dose.
Hormone-Free Interval
Some COCs include placebo pills during which hormone withdrawal symptoms such as bleeding, pelvic pain, mood changes, and headache may occur. If a patient is concerned about these symptoms, choose a COC with no or fewer placebo pills, or have the patient skip the hormone-free interval altogether and start the next pack early7; in this case, the prescription should be written with instructions to allow the patient to get earlier refills from the pharmacy.
Estrogen Dose
To minimize estrogen-related side effects, the lowest possible dose of ethinyl estradiol that is effective and tolerable should be prescribed7,8; 20 μg of ethinyl estradiol generally is the lowest dose available, but it may be associated with more frequent breakthrough bleeding.9 The International Planned Parenthood Federation recommends starting with COCs that contain 30 to 35 μg of estrogen.10 Synthesizing this information, one option is to start with 20 μg of ethinyl estradiol and increase the dose if breakthrough bleeding persists after 3 cycles.
Progestin Type
First-generation progestins (eg, norethindrone), second-generation progestins (eg, norgestrel, levonorgestrel), and third-generation progestins (eg, norgestimate, desogestrel) are derived from testosterone and therefore are variably androgenic; second-generation progestins are the most androgenic, and third-generation progestins are the least. On the other hand, drospirenone, the fourth-generation progestin available in the United States, is derived from 17α-spironolactone and thus is mildly antiandrogenic (3 mg of drospirenone is considered equivalent to 25 mg of spironolactone).
Although COCs with less androgenic progestins should theoretically treat acne better, a 2012 Cochrane review of COCs and acne concluded that “differences in the comparative effectiveness of COCs containing varying progestin types and dosages were less clear, and data were limited for any particular comparison.”11 As a result, regardless of the progestin, all COCs are believed to have a net antiandrogenic effect due to their estrogen component.1
Counsel on Use
Combined oral contraceptives can be started on any day of the menstrual cycle, including the day the prescription is given. If a patient begins a COC within 5 days of the first day of her most recent period, backup contraception is not needed.4 If she begins the COC more than 5 days after the first day of her most recent period, she needs to use backup contraception or abstain from sexual intercourse for the next 7 days.4 In general, at least 3 months of therapy are required to evaluate the effectiveness of COCs for acne.1
Manage Risks and Side Effects
Breakthrough Bleeding
The most common side effect of breakthrough bleeding can be minimized by taking COCs at approximately the same time every day and avoiding missed pills. If breakthrough bleeding does not stop after 3 cycles, consider increasing the estrogen dose to 30 to 35 μg and/or referring to an obstetrician/gynecologist to rule out other etiologies of bleeding.7,8
Nausea, Headache, Bloating, and Breast Tenderness
These symptoms typically resolve after the first 3 months. To minimize nausea, patients should take COCs in the early evening and eat breakfast the next morning.7,8 For headaches that occur during the hormone-free interval, consider skipping the placebo pills and starting the next pack early. Switching the progestin to drospirenone, which has a mild diuretic effect, can help with bloating as well as breast tenderness.7 For persistent symptoms, consider a lower estrogen dose.7,8
Changes in Libido
In a systemic review including 8422 COC users, 64% reported no change in libido, 22% reported an increase, and 15% reported a decrease.12
Weight Gain
Although patients may be concerned that COCs cause weight gain, a 2014 Cochrane review concluded that “available evidence is insufficient to determine the effect of combination contraceptives on weight, but no large effect is evident.”13 If weight gain does occur, anecdotal evidence suggests it tends to be not more than 5 pounds. If weight gain is an issue, consider a less androgenic progestin.8
Venous Thromboembolism
Use the 3-6-9-12 model to contextualize venous thromboembolism (VTE) risk: a woman’s annual VTE risk is 3 per 10,000 women at baseline, 6 per 10,000 women with nondrospirenone COCs, 9 per 10,000 women with drospirenone-containing COCs, and 12 per 10,000 women when pregnant.14 Patients should be counseled on the signs and symptoms of VTE such as unilateral or bilateral leg or arm swelling, pain, warmth, redness, and/or shortness of breath. The British Society for Haematology recommends maintaining mobility as a reasonable precaution when traveling for more than 3 hours.15
Cardiovascular Disease
A 2015 Cochrane review found that the risk for myocardial infarction or ischemic stroke is increased 1.6‐fold in COC users.16 Despite this increased relative risk, the increased absolute annual risk of myocardial infarction in nonsmoking women remains low: increased from 0.83 to 3.53 per 10,000,000 women younger than 35 years and from 9.45 to 40.4 per 10,000,000 women 35 years and older.17
Breast Cancer and Cervical Cancer
Data are mixed on the effect of COCs on the risk for breast cancer and cervical cancer.1 According to the CDC, COC use for 5 or more years might increase the risk of cervical carcinoma in situ and invasive cervical carcinoma in women with persistent human papillomavirus infection.5 Regardless of COC use, women should undergo age-appropriate screening for breast cancer and cervical cancer.
Melasma
Melasma is an estrogen-mediated side effect of COCs.8 A study from 1967 found that 29% of COC users (N=212) developed melasma; however, they were taking COCs with much higher ethinyl estradiol doses (50–100 μg) than typically used today.18 Nevertheless, as part of an overall skin care regimen, photoprotection should be encouraged with a broad-spectrum, water-resistant sunscreen that has a sun protection factor of at least 30. In addition, sunscreens with iron oxides have been shown to better prevent melasma relapse by protecting against the shorter wavelengths of visible light.19
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74:945-973.e933.
- Landis ET, Levender MM, Davis SA, et al. Isotretinoin and oral contraceptive use in female acne patients varies by physician specialty: analysis of data from the National Ambulatory Medical Care Survey. J Dermatolog Treat. 2012;23:272-277.
- Fitzpatrick L, Mauer E, Chen CL. Oral contraceptives for acne treatment: US dermatologists’ knowledge, comfort, and prescribing practices. Cutis. 2017;99:195-201.
- Curtis KM, Jatlaoui TC, Tepper NK, et al. U.S. Selected Practice Recommendations for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65:1-66.
- Curtis KM, Tepper NK, Jatlaoui TC, et al. U.S. Medical Eligibility Criteria for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65:1-103.
- Van Vliet HA, Grimes DA, Lopez LM, et al. Triphasic versus monophasic oral contraceptives for contraception. Cochrane Database Syst Rev. 2011:CD003553.
- Stewart M, Black K. Choosing a combined oral contraceptive pill. Aust Prescr. 2015;38:6-11.
- McKinney K. Understanding the options: a guide to oral contraceptives. https://www.cecentral.com/assets/2097/022%20Oral%20Contraceptives%2010-26-09.pdf. Published November 5, 2009. Accessed June 20, 2019.
- Gallo MF, Nanda K, Grimes DA, et al. 20 microg versus >20 microg estrogen combined oral contraceptives for contraception. Cochrane Database Syst Rev. 2013:CD003989.
- Terki F, Malhotra U. Medical and Service Delivery Guidelines for Sexual and Reproductive Health Services. London, United Kingdom: International Planned Parenthood Federation; 2004.
- Arowojolu AO, Gallo MF, Lopez LM, et al. Combined oral contraceptive pills for treatment of acne. Cochrane Database Syst Rev. 2012:CD004425.
- Pastor Z, Holla K, Chmel R. The influence of combined oral contraceptives on female sexual desire: a systematic review. Eur J Contracept Reprod Health Care. 2013;18:27-43.
- Gallo MF, Lopez LM, Grimes DA, et al. Combination contraceptives: effects on weight. Cochrane Database Syst Rev. 2014:CD003987.
- Birth control pills for acne: tips from Julie Harper at the Summer AAD. Cutis. https://www.mdedge.com/dermatology/article/144550/acne/birth-control-pills-acne-tips-julie-harper-summer-aad. Published August 14, 2017. Accessed June 24, 2019.
- Watson HG, Baglin TP. Guidelines on travel-related venous thrombosis. Br J Haematol. 2011;152:31-34.
- Roach RE, Helmerhorst FM, Lijfering WM, et al. Combined oral contraceptives: the risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev. 2015:CD011054.
- Acute myocardial infarction and combined oral contraceptives: results of an international multicentre case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1997;349:1202-1209.
- Resnik S. Melasma induced by oral contraceptive drugs. JAMA. 1967;199:601-605.
- Boukari F, Jourdan E, Fontas E, et al. Prevention of melasma relapses with sunscreen combining protection against UV and short wavelengths of visible light: a prospective randomized comparative trial. J Am Acad Dermatol. 2015;72:189-190.e181.
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74:945-973.e933.
- Landis ET, Levender MM, Davis SA, et al. Isotretinoin and oral contraceptive use in female acne patients varies by physician specialty: analysis of data from the National Ambulatory Medical Care Survey. J Dermatolog Treat. 2012;23:272-277.
- Fitzpatrick L, Mauer E, Chen CL. Oral contraceptives for acne treatment: US dermatologists’ knowledge, comfort, and prescribing practices. Cutis. 2017;99:195-201.
- Curtis KM, Jatlaoui TC, Tepper NK, et al. U.S. Selected Practice Recommendations for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65:1-66.
- Curtis KM, Tepper NK, Jatlaoui TC, et al. U.S. Medical Eligibility Criteria for Contraceptive Use, 2016. MMWR Recomm Rep. 2016;65:1-103.
- Van Vliet HA, Grimes DA, Lopez LM, et al. Triphasic versus monophasic oral contraceptives for contraception. Cochrane Database Syst Rev. 2011:CD003553.
- Stewart M, Black K. Choosing a combined oral contraceptive pill. Aust Prescr. 2015;38:6-11.
- McKinney K. Understanding the options: a guide to oral contraceptives. https://www.cecentral.com/assets/2097/022%20Oral%20Contraceptives%2010-26-09.pdf. Published November 5, 2009. Accessed June 20, 2019.
- Gallo MF, Nanda K, Grimes DA, et al. 20 microg versus >20 microg estrogen combined oral contraceptives for contraception. Cochrane Database Syst Rev. 2013:CD003989.
- Terki F, Malhotra U. Medical and Service Delivery Guidelines for Sexual and Reproductive Health Services. London, United Kingdom: International Planned Parenthood Federation; 2004.
- Arowojolu AO, Gallo MF, Lopez LM, et al. Combined oral contraceptive pills for treatment of acne. Cochrane Database Syst Rev. 2012:CD004425.
- Pastor Z, Holla K, Chmel R. The influence of combined oral contraceptives on female sexual desire: a systematic review. Eur J Contracept Reprod Health Care. 2013;18:27-43.
- Gallo MF, Lopez LM, Grimes DA, et al. Combination contraceptives: effects on weight. Cochrane Database Syst Rev. 2014:CD003987.
- Birth control pills for acne: tips from Julie Harper at the Summer AAD. Cutis. https://www.mdedge.com/dermatology/article/144550/acne/birth-control-pills-acne-tips-julie-harper-summer-aad. Published August 14, 2017. Accessed June 24, 2019.
- Watson HG, Baglin TP. Guidelines on travel-related venous thrombosis. Br J Haematol. 2011;152:31-34.
- Roach RE, Helmerhorst FM, Lijfering WM, et al. Combined oral contraceptives: the risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev. 2015:CD011054.
- Acute myocardial infarction and combined oral contraceptives: results of an international multicentre case-control study. WHO Collaborative Study of Cardiovascular Disease and Steroid Hormone Contraception. Lancet. 1997;349:1202-1209.
- Resnik S. Melasma induced by oral contraceptive drugs. JAMA. 1967;199:601-605.
- Boukari F, Jourdan E, Fontas E, et al. Prevention of melasma relapses with sunscreen combining protection against UV and short wavelengths of visible light: a prospective randomized comparative trial. J Am Acad Dermatol. 2015;72:189-190.e181.
Resident Pearls
- Screen for contraindications to combined oral contraceptives (COCs) by taking a medical history, measuring a baseline blood pressure, and excluding pregnancy. A baseline pelvic examination is unnecessary.
- Characteristics to consider when selecting a COC include the formulation, hormone-free interval, estrogen dose, and progestin type.
- Combined oral contraceptives can be initiated on any day of the menstrual cycle, with the need for backup contraception based on the number of days since the first day of the patient’s most recent period.
- Management of risks and side effects includes simple lifestyle changes, skipping the hormone-free interval, switching the COC, and referring to an obstetrician/gynecologist.

Career Choices: Academic psychiatry
Editor’s note: Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Saeed Ahmed, MD, Chief Resident at Nassau University Medical Center, East Meadow, New York, talked with Donald W. Black, MD, Professor of Psychiatry, Department of Psychiatry, University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, Iowa. Dr. Black is also Editor-in-Chief of
Dr. Ahmed: What made you choose the academic track, and how did your training lead you towards this path?
Dr. Black: I had always been interested in the idea of working at a medical school, and enjoyed writing and speaking. I was exposed to clinical research as a resident, and that confirmed my interest in academia, because I could envision combining all my interests, along with patient care. I always thought that patients were a major source of ideas for research and writing.
Dr. Ahmed: What are some of the pros and cons of working in academia?
Dr. Black: The pros include being able to influence future physicians through my teaching and writing; being able to pursue important research; and not being isolated from peers. Other advantages are being largely protected from utilization review; having more free time than peers in the private sector, who have difficulty finding coverage; and having defined benefits and a steady salary. I also share call with many peers.
When it comes to the cons, salaries are lower than in the private sector. The cons also include not being my own boss, and sometimes having to bend to the whims of an institution or supervisor.
Continue to: Dr. Ahmed...
Dr. Ahmed: Are you required to conduct research?
Dr. Black: Yes. This is one of the best aspects of my job: being able to make clinical discoveries that I can disseminate through writing and speaking. Over time, this has become increasingly challenging due to the difficulty of obtaining research funding from foundations or the federal government. This has become highly problematic, particularly for clinical researchers, because the National Institutes of Health has clearly been favoring neuroscience.
Dr. Ahmed: What is your typical day like?
Dr. Black: Because of the many hats I wear (or have worn), each day is different from the other. I combine patient care with research, writing, speaking, teaching, and administration. As a tenure-track faculty member, I am expected to write grants, conduct research, and publish. My clinical-track peers primarily provide patient care and teach students and residents.
Dr. Ahmed: What is unique about working in a training institute vs private practice?
Continue to: Dr. Black...
Dr. Black: As an academic psychiatrist, I feel I have the best of both worlds: patient care combined with opportunities my private practice colleagues do not have. Because I have published widely, and have developed a reputation, I am frequently invited to speak at meetings throughout the United States, and sometimes internationally. Travel is a perk of academia, and as someone who loves travel, that is important.
Dr. Ahmed: Where do you see psychiatry going?
Dr. Black: Psychiatry will always be an important specialty because no one else truly cares about patients with psychiatric illnesses. Mental illness will not go away, and society needs highly trained individuals to provide care. There are many “me too” clinicians who now share in caring for patients with psychiatric illnesses, but psychiatrists will always have the most training, and are in a position to provide supervision to others and to direct mental health care teams.
Dr. Ahmed: What advice do you have for residents contemplating a career in academic psychiatry?
Dr. Black: Because most medical schools now have both tenure and clinical tracks, no one needs to feel left out. Those who are interested in scholarly activities will gravitate to the tenure tract, and all that requires in terms of grants and papers, while those who are primarily interested in patient care and teaching will choose the clinical track.
Editor’s note: Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Saeed Ahmed, MD, Chief Resident at Nassau University Medical Center, East Meadow, New York, talked with Donald W. Black, MD, Professor of Psychiatry, Department of Psychiatry, University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, Iowa. Dr. Black is also Editor-in-Chief of
Dr. Ahmed: What made you choose the academic track, and how did your training lead you towards this path?
Dr. Black: I had always been interested in the idea of working at a medical school, and enjoyed writing and speaking. I was exposed to clinical research as a resident, and that confirmed my interest in academia, because I could envision combining all my interests, along with patient care. I always thought that patients were a major source of ideas for research and writing.
Dr. Ahmed: What are some of the pros and cons of working in academia?
Dr. Black: The pros include being able to influence future physicians through my teaching and writing; being able to pursue important research; and not being isolated from peers. Other advantages are being largely protected from utilization review; having more free time than peers in the private sector, who have difficulty finding coverage; and having defined benefits and a steady salary. I also share call with many peers.
When it comes to the cons, salaries are lower than in the private sector. The cons also include not being my own boss, and sometimes having to bend to the whims of an institution or supervisor.
Continue to: Dr. Ahmed...
Dr. Ahmed: Are you required to conduct research?
Dr. Black: Yes. This is one of the best aspects of my job: being able to make clinical discoveries that I can disseminate through writing and speaking. Over time, this has become increasingly challenging due to the difficulty of obtaining research funding from foundations or the federal government. This has become highly problematic, particularly for clinical researchers, because the National Institutes of Health has clearly been favoring neuroscience.
Dr. Ahmed: What is your typical day like?
Dr. Black: Because of the many hats I wear (or have worn), each day is different from the other. I combine patient care with research, writing, speaking, teaching, and administration. As a tenure-track faculty member, I am expected to write grants, conduct research, and publish. My clinical-track peers primarily provide patient care and teach students and residents.
Dr. Ahmed: What is unique about working in a training institute vs private practice?
Continue to: Dr. Black...
Dr. Black: As an academic psychiatrist, I feel I have the best of both worlds: patient care combined with opportunities my private practice colleagues do not have. Because I have published widely, and have developed a reputation, I am frequently invited to speak at meetings throughout the United States, and sometimes internationally. Travel is a perk of academia, and as someone who loves travel, that is important.
Dr. Ahmed: Where do you see psychiatry going?
Dr. Black: Psychiatry will always be an important specialty because no one else truly cares about patients with psychiatric illnesses. Mental illness will not go away, and society needs highly trained individuals to provide care. There are many “me too” clinicians who now share in caring for patients with psychiatric illnesses, but psychiatrists will always have the most training, and are in a position to provide supervision to others and to direct mental health care teams.
Dr. Ahmed: What advice do you have for residents contemplating a career in academic psychiatry?
Dr. Black: Because most medical schools now have both tenure and clinical tracks, no one needs to feel left out. Those who are interested in scholarly activities will gravitate to the tenure tract, and all that requires in terms of grants and papers, while those who are primarily interested in patient care and teaching will choose the clinical track.
Editor’s note: Career Choices features a psychiatry resident/fellow interviewing a psychiatrist about why he or she has chosen a specific career path. The goal is to inform trainees about the various psychiatric career options, and to give them a feel for the pros and cons of the various paths.
In this Career Choices, Saeed Ahmed, MD, Chief Resident at Nassau University Medical Center, East Meadow, New York, talked with Donald W. Black, MD, Professor of Psychiatry, Department of Psychiatry, University of Iowa Roy J. and Lucille A. Carver College of Medicine, Iowa City, Iowa. Dr. Black is also Editor-in-Chief of
Dr. Ahmed: What made you choose the academic track, and how did your training lead you towards this path?
Dr. Black: I had always been interested in the idea of working at a medical school, and enjoyed writing and speaking. I was exposed to clinical research as a resident, and that confirmed my interest in academia, because I could envision combining all my interests, along with patient care. I always thought that patients were a major source of ideas for research and writing.
Dr. Ahmed: What are some of the pros and cons of working in academia?
Dr. Black: The pros include being able to influence future physicians through my teaching and writing; being able to pursue important research; and not being isolated from peers. Other advantages are being largely protected from utilization review; having more free time than peers in the private sector, who have difficulty finding coverage; and having defined benefits and a steady salary. I also share call with many peers.
When it comes to the cons, salaries are lower than in the private sector. The cons also include not being my own boss, and sometimes having to bend to the whims of an institution or supervisor.
Continue to: Dr. Ahmed...
Dr. Ahmed: Are you required to conduct research?
Dr. Black: Yes. This is one of the best aspects of my job: being able to make clinical discoveries that I can disseminate through writing and speaking. Over time, this has become increasingly challenging due to the difficulty of obtaining research funding from foundations or the federal government. This has become highly problematic, particularly for clinical researchers, because the National Institutes of Health has clearly been favoring neuroscience.
Dr. Ahmed: What is your typical day like?
Dr. Black: Because of the many hats I wear (or have worn), each day is different from the other. I combine patient care with research, writing, speaking, teaching, and administration. As a tenure-track faculty member, I am expected to write grants, conduct research, and publish. My clinical-track peers primarily provide patient care and teach students and residents.
Dr. Ahmed: What is unique about working in a training institute vs private practice?
Continue to: Dr. Black...
Dr. Black: As an academic psychiatrist, I feel I have the best of both worlds: patient care combined with opportunities my private practice colleagues do not have. Because I have published widely, and have developed a reputation, I am frequently invited to speak at meetings throughout the United States, and sometimes internationally. Travel is a perk of academia, and as someone who loves travel, that is important.
Dr. Ahmed: Where do you see psychiatry going?
Dr. Black: Psychiatry will always be an important specialty because no one else truly cares about patients with psychiatric illnesses. Mental illness will not go away, and society needs highly trained individuals to provide care. There are many “me too” clinicians who now share in caring for patients with psychiatric illnesses, but psychiatrists will always have the most training, and are in a position to provide supervision to others and to direct mental health care teams.
Dr. Ahmed: What advice do you have for residents contemplating a career in academic psychiatry?
Dr. Black: Because most medical schools now have both tenure and clinical tracks, no one needs to feel left out. Those who are interested in scholarly activities will gravitate to the tenure tract, and all that requires in terms of grants and papers, while those who are primarily interested in patient care and teaching will choose the clinical track.

Residents are drowning in job offers – and debt
Physician search firm Merritt Hawkins did – actually, they heard from 391 residents – and 64% said that they had been contacted too many times by recruiters.
“Physicians coming out of training are being recruited like blue-chip athletes,” Travis Singleton, executive vice president of Merritt Hawkins, said in a statement. “There are simply not enough new doctors to go around.”
Merritt Hawkins asked physicians in their final year of residency about career choices, practice plans, and finances. Most said that they would prefer to be employed by a hospital or group practice, and a majority want to practice in a community with a population of 250,000 or more. More than half of the residents owed over $150,000 in student loans, but there were considerable debt differences between U.S. and international medical graduates.
The specialty distribution of respondents was 50% primary care, 30% internal medicine subspecialty/other, 15% surgical, and 5% diagnostic. About three-quarters were U.S. graduates and one-quarter of the residents were international medical graduates in this latest survey in a series that has been conducted periodically since 1991.
The survey was conducted in April 2018.
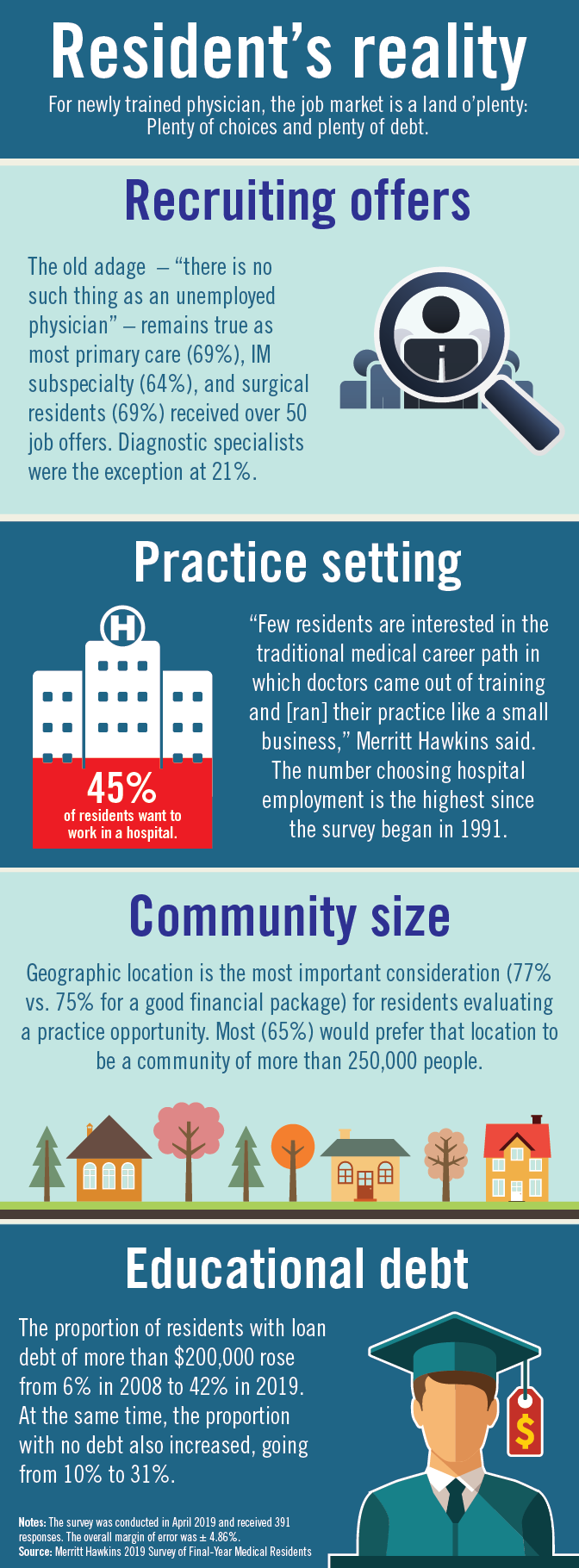
Physician search firm Merritt Hawkins did – actually, they heard from 391 residents – and 64% said that they had been contacted too many times by recruiters.
“Physicians coming out of training are being recruited like blue-chip athletes,” Travis Singleton, executive vice president of Merritt Hawkins, said in a statement. “There are simply not enough new doctors to go around.”
Merritt Hawkins asked physicians in their final year of residency about career choices, practice plans, and finances. Most said that they would prefer to be employed by a hospital or group practice, and a majority want to practice in a community with a population of 250,000 or more. More than half of the residents owed over $150,000 in student loans, but there were considerable debt differences between U.S. and international medical graduates.
The specialty distribution of respondents was 50% primary care, 30% internal medicine subspecialty/other, 15% surgical, and 5% diagnostic. About three-quarters were U.S. graduates and one-quarter of the residents were international medical graduates in this latest survey in a series that has been conducted periodically since 1991.
The survey was conducted in April 2018.
Physician search firm Merritt Hawkins did – actually, they heard from 391 residents – and 64% said that they had been contacted too many times by recruiters.
“Physicians coming out of training are being recruited like blue-chip athletes,” Travis Singleton, executive vice president of Merritt Hawkins, said in a statement. “There are simply not enough new doctors to go around.”
Merritt Hawkins asked physicians in their final year of residency about career choices, practice plans, and finances. Most said that they would prefer to be employed by a hospital or group practice, and a majority want to practice in a community with a population of 250,000 or more. More than half of the residents owed over $150,000 in student loans, but there were considerable debt differences between U.S. and international medical graduates.
The specialty distribution of respondents was 50% primary care, 30% internal medicine subspecialty/other, 15% surgical, and 5% diagnostic. About three-quarters were U.S. graduates and one-quarter of the residents were international medical graduates in this latest survey in a series that has been conducted periodically since 1991.
The survey was conducted in April 2018.
Surgical Dermatoethics for the Trainee
It is an uncomfortable and unavoidable reality as physicians that for every procedure we learn, there must be a first time we perform it. As with any type of skill, it takes practice to become proficient. The unique challenge in medicine is that the practice involves performing procedures on real patients. We cannot avoid the hands-on nature of the training process; we can, however, approach its ethical challenges mindfully. Herein, I will discuss some of the ethical considerations in providing care as a trainee and identify potential barriers to best practices, particularly as they relate to procedural dermatology.
Tell Patients You Are in Training
In every patient encounter, we must introduce ourselves as a trainee. The principle of right to the truth dictates that we are transparent about our level of training and do not misrepresent ourselves to our patients. A statement released by the American Medical Association (AMA) Council on Ethical and Judicial Affairs asserts that “[p]atients should be informed of the identity and training status of individuals involved in their care.”1
Although straightforward in theory, this mandate is not always simple in practice. With patients unfamiliar with the health care system, it could be more onerous to clearly communicate training status than simply introducing oneself as a resident. A study conducted in the emergency department at Vanderbilt University Hospital (Nashville, Tennessee) found that many patients and their family members (N=430) did not understand the various roles and responsibilities of physicians in the teaching hospital setting. For example, 30% believed an attending physician requires supervision by a resident, and an additional 17% of those surveyed were not sure.2 The AMA requests we “refrain from using terms that may be confusing when describing the training status of the students,”1 which evidently is audience specific. Thus, as with any type of patient education, a thorough introduction may require assessment of understanding.
Disclosure of Experience Level With a Particular Procedure
There is a clear professional expectation that we disclose to patients that we are in training; however, a universal standard does not exist for disclosure of our exact level of experience in a particular procedure. Do we need to tell patients if it is our first time performing a given procedure? What if it is our tenth? Multiple studies have found that patients want specifics. In one study of bariatric surgery patients (N=108), 93% felt that they should always be informed if it was the first time a trainee was performing a particular procedure.3 A study conducted in the emergency department setting (N=202) also found that the majority of patients thought they should be informed if a resident was performing a procedure for the first time, but the distribution differed by procedure (66% for suturing vs 82% for lumbar puncture).4
Despite these findings, this degree of specificity is not always discussed with patients and perhaps does not need to be. LaRosa and Grant-Kels5 analyzed a hypothetical scenario in which a dermatology resident is to perform his first excision under attending supervision and concluded that broad disclosure of training status would suffice in the given scenario, as it would not be necessary to state that it was his first time performing an excision. It is unclear if the same conclusion could be drawn for all procedures and levels of experience. Outcome data would help inform the analysis, but the available data are from other specialties including general surgery, gynecology, and urology. Some studies demonstrate an increased risk of adverse outcomes with trainee involvement in procedures such as bariatric surgery and emergency general surgery, but the data are mixed and may not be generalizable to dermatologic procedures.6-8
The appropriate level of detail to disclose regarding a physician’s experience may need to be assessed on a case-by-case basis, and the principles of informed consent can help. Informed consent requires understanding of the diagnosis, the treatment options including nonintervention, and the risks and benefits of each alternative. In obtaining informed consent, we must disclose “any facts which are necessary to form the basis of an intelligent consent by the patient to the proposed treatment.”9 Providers must determine what aspects of a trainee’s experience level are relevant to the risk-benefit analysis in a given set of circumstances. Surely, there is a large degree of subjectivity in this determination as data are limited, but information deemed relevant must be shared. Information that is inconsequential, on the other hand, may be omitted. It could even be argued that more detailed information, especially if it may cause anxiety, would be detrimental to share. For example, we would not list the chemical name of every preservative in every vaccine we recommend for children if there is no evidence of inflicting harm. If the information has not been shown to have clinical impact or affect safety concerns, the anxiety may be undue.
Withholding Information Can Violate Ethical Principles
We must be careful not to withhold details of our experience level with a particular procedure for the wrong reasons. It would be wrong, for example, to withhold information simply to avoid causing anxiety, which could be seen as an invocation of therapeutic privilege, a controversial practice of withholding important information that poses a psychological threat to the patient. A classic example is the physician who defers disclosure of a terminal diagnosis to preserve hope. Although therapeutic privilege theoretically promotes the principle of beneficence, it violates the principles of autonomy and right to truth and therefore generally is regarded as unethically paternalistic in modern medical ethics.9
Patients Can Refuse Trainee Participation
It also is unethical to withhold information to obtain consent and avoid refusal of our care. Refusal of trainee participation is not uncommon. In the aforementioned study of bariatric surgery patients, 92.4% supported their procedure being performed at a teaching hospital, but only 56% would consent to a resident assisting staff during the procedure. A mere 33% of those patients would consent to a resident primarily performing with staff assisting.3 Although the proportion of patients who refuse certainly depends on the type of procedure among other factors, it is a reality in any teaching environment. The training paradigm in medicine depends on being able to practice procedures with supervision before we are independent providers. If patients refuse our care, our training suffers. However, the AMA maintains that “[p]atients are free to choose from whom they receive treatment,”1 and we must respect this aspect of patient autonomy.
Final Thoughts
When it comes to the performance of procedures, there are a few basic principles to keep in mind to provide ethical care to our patients while we are in training. Although we must accept that a crucial part of learning dermatologic procedures is hands on with real patients, we also need to come prepared having learned what we can through reading and practice with cadavers or skin substitutes. Procedures we execute as residents should be performed with adequate supervision, and as we progress through residency, we should be given increased autonomy and graded responsibility to prepare us for independent practice at graduation. Although it is the responsibility of the attending physician to provide appropriate oversight for the resident’s level of training, we should feel empowered to ask for help and have the humility to know when we need it.
- Medical student involvement in patient care: report of the council on ethical and judicial affairs. Virtual Mentor. 2001;3. doi:10.1001/virtualmentor.2001.3.3.code1-0103.
- Santen S, Hemphill RR, Prough E, et al. Do patients understand their physician’s level of training? a survey of emergency department patients. Acad Med. 2004;79:139-143.
- McClellan JM, Nelson D, Porta CR, et al. Bariatric surgery patient perceptions and willingness to consent to resident participation. Surg Obes Relat Dis. 2016;12:1065-1071.
- Santen SA, Hemphill RR, McDonald MF, et al. Patients’ willingness to allow residents to learn to practice medical procedures. Acad Med. 2004;79:144-147.
- LaRosa C, Grant-Kels JM. See one, do one, teach one: the ethical dilemma of residents performing their first procedure on patients. J Am Acad Dermatol. 2016;75:845-848.
- Can MF. The trainee effect on early postoperative surgical outcomes: reflects the effect of resident involvement or hospital capacity to overcome complications? J Invest Surg. 2017;31:67-68.
- Goldberg I, Yang J, Park J, et al. Surgical trainee impact on bariatric surgery safety [published online November 13, 2018]. Surg Endosc. doi:10.1007/s00464-018-6587-0.
- Kasotakis G, Lakha A, Sarkar B, et al. Trainee participation is associated with adverse outcomes in emergency general surgery: an analysis of the National Surgical Quality Improvement Program database. Ann Surg. 2014;3:483-490.
- Richard C, Lajeunesse Y, Lussier MT. Therapeutic privilege: between the ethics of lying and the practice of truth. J Med Ethics. 2010;36:353-357.
It is an uncomfortable and unavoidable reality as physicians that for every procedure we learn, there must be a first time we perform it. As with any type of skill, it takes practice to become proficient. The unique challenge in medicine is that the practice involves performing procedures on real patients. We cannot avoid the hands-on nature of the training process; we can, however, approach its ethical challenges mindfully. Herein, I will discuss some of the ethical considerations in providing care as a trainee and identify potential barriers to best practices, particularly as they relate to procedural dermatology.
Tell Patients You Are in Training
In every patient encounter, we must introduce ourselves as a trainee. The principle of right to the truth dictates that we are transparent about our level of training and do not misrepresent ourselves to our patients. A statement released by the American Medical Association (AMA) Council on Ethical and Judicial Affairs asserts that “[p]atients should be informed of the identity and training status of individuals involved in their care.”1
Although straightforward in theory, this mandate is not always simple in practice. With patients unfamiliar with the health care system, it could be more onerous to clearly communicate training status than simply introducing oneself as a resident. A study conducted in the emergency department at Vanderbilt University Hospital (Nashville, Tennessee) found that many patients and their family members (N=430) did not understand the various roles and responsibilities of physicians in the teaching hospital setting. For example, 30% believed an attending physician requires supervision by a resident, and an additional 17% of those surveyed were not sure.2 The AMA requests we “refrain from using terms that may be confusing when describing the training status of the students,”1 which evidently is audience specific. Thus, as with any type of patient education, a thorough introduction may require assessment of understanding.
Disclosure of Experience Level With a Particular Procedure
There is a clear professional expectation that we disclose to patients that we are in training; however, a universal standard does not exist for disclosure of our exact level of experience in a particular procedure. Do we need to tell patients if it is our first time performing a given procedure? What if it is our tenth? Multiple studies have found that patients want specifics. In one study of bariatric surgery patients (N=108), 93% felt that they should always be informed if it was the first time a trainee was performing a particular procedure.3 A study conducted in the emergency department setting (N=202) also found that the majority of patients thought they should be informed if a resident was performing a procedure for the first time, but the distribution differed by procedure (66% for suturing vs 82% for lumbar puncture).4
Despite these findings, this degree of specificity is not always discussed with patients and perhaps does not need to be. LaRosa and Grant-Kels5 analyzed a hypothetical scenario in which a dermatology resident is to perform his first excision under attending supervision and concluded that broad disclosure of training status would suffice in the given scenario, as it would not be necessary to state that it was his first time performing an excision. It is unclear if the same conclusion could be drawn for all procedures and levels of experience. Outcome data would help inform the analysis, but the available data are from other specialties including general surgery, gynecology, and urology. Some studies demonstrate an increased risk of adverse outcomes with trainee involvement in procedures such as bariatric surgery and emergency general surgery, but the data are mixed and may not be generalizable to dermatologic procedures.6-8
The appropriate level of detail to disclose regarding a physician’s experience may need to be assessed on a case-by-case basis, and the principles of informed consent can help. Informed consent requires understanding of the diagnosis, the treatment options including nonintervention, and the risks and benefits of each alternative. In obtaining informed consent, we must disclose “any facts which are necessary to form the basis of an intelligent consent by the patient to the proposed treatment.”9 Providers must determine what aspects of a trainee’s experience level are relevant to the risk-benefit analysis in a given set of circumstances. Surely, there is a large degree of subjectivity in this determination as data are limited, but information deemed relevant must be shared. Information that is inconsequential, on the other hand, may be omitted. It could even be argued that more detailed information, especially if it may cause anxiety, would be detrimental to share. For example, we would not list the chemical name of every preservative in every vaccine we recommend for children if there is no evidence of inflicting harm. If the information has not been shown to have clinical impact or affect safety concerns, the anxiety may be undue.
Withholding Information Can Violate Ethical Principles
We must be careful not to withhold details of our experience level with a particular procedure for the wrong reasons. It would be wrong, for example, to withhold information simply to avoid causing anxiety, which could be seen as an invocation of therapeutic privilege, a controversial practice of withholding important information that poses a psychological threat to the patient. A classic example is the physician who defers disclosure of a terminal diagnosis to preserve hope. Although therapeutic privilege theoretically promotes the principle of beneficence, it violates the principles of autonomy and right to truth and therefore generally is regarded as unethically paternalistic in modern medical ethics.9
Patients Can Refuse Trainee Participation
It also is unethical to withhold information to obtain consent and avoid refusal of our care. Refusal of trainee participation is not uncommon. In the aforementioned study of bariatric surgery patients, 92.4% supported their procedure being performed at a teaching hospital, but only 56% would consent to a resident assisting staff during the procedure. A mere 33% of those patients would consent to a resident primarily performing with staff assisting.3 Although the proportion of patients who refuse certainly depends on the type of procedure among other factors, it is a reality in any teaching environment. The training paradigm in medicine depends on being able to practice procedures with supervision before we are independent providers. If patients refuse our care, our training suffers. However, the AMA maintains that “[p]atients are free to choose from whom they receive treatment,”1 and we must respect this aspect of patient autonomy.
Final Thoughts
When it comes to the performance of procedures, there are a few basic principles to keep in mind to provide ethical care to our patients while we are in training. Although we must accept that a crucial part of learning dermatologic procedures is hands on with real patients, we also need to come prepared having learned what we can through reading and practice with cadavers or skin substitutes. Procedures we execute as residents should be performed with adequate supervision, and as we progress through residency, we should be given increased autonomy and graded responsibility to prepare us for independent practice at graduation. Although it is the responsibility of the attending physician to provide appropriate oversight for the resident’s level of training, we should feel empowered to ask for help and have the humility to know when we need it.
It is an uncomfortable and unavoidable reality as physicians that for every procedure we learn, there must be a first time we perform it. As with any type of skill, it takes practice to become proficient. The unique challenge in medicine is that the practice involves performing procedures on real patients. We cannot avoid the hands-on nature of the training process; we can, however, approach its ethical challenges mindfully. Herein, I will discuss some of the ethical considerations in providing care as a trainee and identify potential barriers to best practices, particularly as they relate to procedural dermatology.
Tell Patients You Are in Training
In every patient encounter, we must introduce ourselves as a trainee. The principle of right to the truth dictates that we are transparent about our level of training and do not misrepresent ourselves to our patients. A statement released by the American Medical Association (AMA) Council on Ethical and Judicial Affairs asserts that “[p]atients should be informed of the identity and training status of individuals involved in their care.”1
Although straightforward in theory, this mandate is not always simple in practice. With patients unfamiliar with the health care system, it could be more onerous to clearly communicate training status than simply introducing oneself as a resident. A study conducted in the emergency department at Vanderbilt University Hospital (Nashville, Tennessee) found that many patients and their family members (N=430) did not understand the various roles and responsibilities of physicians in the teaching hospital setting. For example, 30% believed an attending physician requires supervision by a resident, and an additional 17% of those surveyed were not sure.2 The AMA requests we “refrain from using terms that may be confusing when describing the training status of the students,”1 which evidently is audience specific. Thus, as with any type of patient education, a thorough introduction may require assessment of understanding.
Disclosure of Experience Level With a Particular Procedure
There is a clear professional expectation that we disclose to patients that we are in training; however, a universal standard does not exist for disclosure of our exact level of experience in a particular procedure. Do we need to tell patients if it is our first time performing a given procedure? What if it is our tenth? Multiple studies have found that patients want specifics. In one study of bariatric surgery patients (N=108), 93% felt that they should always be informed if it was the first time a trainee was performing a particular procedure.3 A study conducted in the emergency department setting (N=202) also found that the majority of patients thought they should be informed if a resident was performing a procedure for the first time, but the distribution differed by procedure (66% for suturing vs 82% for lumbar puncture).4
Despite these findings, this degree of specificity is not always discussed with patients and perhaps does not need to be. LaRosa and Grant-Kels5 analyzed a hypothetical scenario in which a dermatology resident is to perform his first excision under attending supervision and concluded that broad disclosure of training status would suffice in the given scenario, as it would not be necessary to state that it was his first time performing an excision. It is unclear if the same conclusion could be drawn for all procedures and levels of experience. Outcome data would help inform the analysis, but the available data are from other specialties including general surgery, gynecology, and urology. Some studies demonstrate an increased risk of adverse outcomes with trainee involvement in procedures such as bariatric surgery and emergency general surgery, but the data are mixed and may not be generalizable to dermatologic procedures.6-8
The appropriate level of detail to disclose regarding a physician’s experience may need to be assessed on a case-by-case basis, and the principles of informed consent can help. Informed consent requires understanding of the diagnosis, the treatment options including nonintervention, and the risks and benefits of each alternative. In obtaining informed consent, we must disclose “any facts which are necessary to form the basis of an intelligent consent by the patient to the proposed treatment.”9 Providers must determine what aspects of a trainee’s experience level are relevant to the risk-benefit analysis in a given set of circumstances. Surely, there is a large degree of subjectivity in this determination as data are limited, but information deemed relevant must be shared. Information that is inconsequential, on the other hand, may be omitted. It could even be argued that more detailed information, especially if it may cause anxiety, would be detrimental to share. For example, we would not list the chemical name of every preservative in every vaccine we recommend for children if there is no evidence of inflicting harm. If the information has not been shown to have clinical impact or affect safety concerns, the anxiety may be undue.
Withholding Information Can Violate Ethical Principles
We must be careful not to withhold details of our experience level with a particular procedure for the wrong reasons. It would be wrong, for example, to withhold information simply to avoid causing anxiety, which could be seen as an invocation of therapeutic privilege, a controversial practice of withholding important information that poses a psychological threat to the patient. A classic example is the physician who defers disclosure of a terminal diagnosis to preserve hope. Although therapeutic privilege theoretically promotes the principle of beneficence, it violates the principles of autonomy and right to truth and therefore generally is regarded as unethically paternalistic in modern medical ethics.9
Patients Can Refuse Trainee Participation
It also is unethical to withhold information to obtain consent and avoid refusal of our care. Refusal of trainee participation is not uncommon. In the aforementioned study of bariatric surgery patients, 92.4% supported their procedure being performed at a teaching hospital, but only 56% would consent to a resident assisting staff during the procedure. A mere 33% of those patients would consent to a resident primarily performing with staff assisting.3 Although the proportion of patients who refuse certainly depends on the type of procedure among other factors, it is a reality in any teaching environment. The training paradigm in medicine depends on being able to practice procedures with supervision before we are independent providers. If patients refuse our care, our training suffers. However, the AMA maintains that “[p]atients are free to choose from whom they receive treatment,”1 and we must respect this aspect of patient autonomy.
Final Thoughts
When it comes to the performance of procedures, there are a few basic principles to keep in mind to provide ethical care to our patients while we are in training. Although we must accept that a crucial part of learning dermatologic procedures is hands on with real patients, we also need to come prepared having learned what we can through reading and practice with cadavers or skin substitutes. Procedures we execute as residents should be performed with adequate supervision, and as we progress through residency, we should be given increased autonomy and graded responsibility to prepare us for independent practice at graduation. Although it is the responsibility of the attending physician to provide appropriate oversight for the resident’s level of training, we should feel empowered to ask for help and have the humility to know when we need it.
- Medical student involvement in patient care: report of the council on ethical and judicial affairs. Virtual Mentor. 2001;3. doi:10.1001/virtualmentor.2001.3.3.code1-0103.
- Santen S, Hemphill RR, Prough E, et al. Do patients understand their physician’s level of training? a survey of emergency department patients. Acad Med. 2004;79:139-143.
- McClellan JM, Nelson D, Porta CR, et al. Bariatric surgery patient perceptions and willingness to consent to resident participation. Surg Obes Relat Dis. 2016;12:1065-1071.
- Santen SA, Hemphill RR, McDonald MF, et al. Patients’ willingness to allow residents to learn to practice medical procedures. Acad Med. 2004;79:144-147.
- LaRosa C, Grant-Kels JM. See one, do one, teach one: the ethical dilemma of residents performing their first procedure on patients. J Am Acad Dermatol. 2016;75:845-848.
- Can MF. The trainee effect on early postoperative surgical outcomes: reflects the effect of resident involvement or hospital capacity to overcome complications? J Invest Surg. 2017;31:67-68.
- Goldberg I, Yang J, Park J, et al. Surgical trainee impact on bariatric surgery safety [published online November 13, 2018]. Surg Endosc. doi:10.1007/s00464-018-6587-0.
- Kasotakis G, Lakha A, Sarkar B, et al. Trainee participation is associated with adverse outcomes in emergency general surgery: an analysis of the National Surgical Quality Improvement Program database. Ann Surg. 2014;3:483-490.
- Richard C, Lajeunesse Y, Lussier MT. Therapeutic privilege: between the ethics of lying and the practice of truth. J Med Ethics. 2010;36:353-357.
- Medical student involvement in patient care: report of the council on ethical and judicial affairs. Virtual Mentor. 2001;3. doi:10.1001/virtualmentor.2001.3.3.code1-0103.
- Santen S, Hemphill RR, Prough E, et al. Do patients understand their physician’s level of training? a survey of emergency department patients. Acad Med. 2004;79:139-143.
- McClellan JM, Nelson D, Porta CR, et al. Bariatric surgery patient perceptions and willingness to consent to resident participation. Surg Obes Relat Dis. 2016;12:1065-1071.
- Santen SA, Hemphill RR, McDonald MF, et al. Patients’ willingness to allow residents to learn to practice medical procedures. Acad Med. 2004;79:144-147.
- LaRosa C, Grant-Kels JM. See one, do one, teach one: the ethical dilemma of residents performing their first procedure on patients. J Am Acad Dermatol. 2016;75:845-848.
- Can MF. The trainee effect on early postoperative surgical outcomes: reflects the effect of resident involvement or hospital capacity to overcome complications? J Invest Surg. 2017;31:67-68.
- Goldberg I, Yang J, Park J, et al. Surgical trainee impact on bariatric surgery safety [published online November 13, 2018]. Surg Endosc. doi:10.1007/s00464-018-6587-0.
- Kasotakis G, Lakha A, Sarkar B, et al. Trainee participation is associated with adverse outcomes in emergency general surgery: an analysis of the National Surgical Quality Improvement Program database. Ann Surg. 2014;3:483-490.
- Richard C, Lajeunesse Y, Lussier MT. Therapeutic privilege: between the ethics of lying and the practice of truth. J Med Ethics. 2010;36:353-357.
Resident Pearl
- As residents, we must gain experience performing procedures on real patients to enter independent practice as proficient dermatologists. It is important to be mindful of the ethical challenges inherent to the hands-on training process and to understand the ethical principles that guide best practices.
AMA announces final eight recipients of Reimagining Residency initiative
led by medical schools, residency programs, and health systems.
“After establishing a framework for creating the medical schools of the future, the AMA is now supporting innovation projects that will better align residency training with the evolving needs of patients and communities, as well as the workforce needs of the current and future health care system,” AMA CEO and Executive Vice President James L. Madara, MD, stated in a press release.
The projects include curricular innovations to address workforce shortages and address social determinants of health. Other projects will be developed within the framework of innovations and concepts developed and implemented in medical schools over the past 6 years by the AMA’s consortium. These projects include implementing competency-based programs and incorporating Health Systems Science into residency training.
The projects were chosen through a competitive grant process by an advisory panel made up of leading experts in medical education, and selection was based on how well each program met the goals of the initiative: improving the transition from medical school to residency, ensuring readiness for practice through modifications of residency curricula, and optimizing the learning environment to support well-being.
Each of the following projects will receive $1.8 million over 5 years:
- California Oregon Medical Partnership to Address Disparities in Rural Education and Health – Oregon Health & Science University, Portland, and the University of California, Davis
- Fully Integrated Readiness for Service Training: Enhancing the Continuum from Medical School to Residency to Practice – University of North Carolina at Chapel Hill
- NYU Transition to Residency Advantage – New York University
- Promotion in Place: Enhancing Trainee Well-Being and Patient Care Through Time-Variable Graduate Medical Education – Partners HealthCare System, Massachusetts General Hospital, and Brigham and Women’s Hospital, Boston
- Reimagining Residency: Ensuring Readiness for Practice Through Growing Interprofessional Partnerships to Advance Care and Education – Maine Medical Center, Portland
- Residency Training to Effectively Address Social Determinants of Health: Applying a Curricular Framework Across Four Primary Care Specialties – Montefiore Health System, New York
- The Graduate Medical Training “Laboratory”: An Innovative Program to Generate, Implement, and Evaluate Interventions to Improve Resident Burnout and Clinical Skill – Johns Hopkins University, Baltimore; Stanford (Calif.) University; and the University of Alabama at Birmingham
- The GOL2D Project (Goals of Life and Learning Delineated): Collaboration Across Academic Health Systems to Better Align GME with Learner, Patient, and Societal Needs – Vanderbilt University, Nashville, Tenn., and the University of Mississippi, Jackson
An additional three programs will receive a smaller $50,000 planning grant to expedite further exploration and development.
“As the health care landscape and technology rapidly evolve, the AMA will continue working with its community of innovation to drive the future of medicine by supporting significant redesign in physician training. Our goal is to ensure physicians are prepared to adapt, grow, and thrive at every stage of their training and career. Better prepared physicians will deliver more effective and equitable health care,” said Dr. Madara.
led by medical schools, residency programs, and health systems.
“After establishing a framework for creating the medical schools of the future, the AMA is now supporting innovation projects that will better align residency training with the evolving needs of patients and communities, as well as the workforce needs of the current and future health care system,” AMA CEO and Executive Vice President James L. Madara, MD, stated in a press release.
The projects include curricular innovations to address workforce shortages and address social determinants of health. Other projects will be developed within the framework of innovations and concepts developed and implemented in medical schools over the past 6 years by the AMA’s consortium. These projects include implementing competency-based programs and incorporating Health Systems Science into residency training.
The projects were chosen through a competitive grant process by an advisory panel made up of leading experts in medical education, and selection was based on how well each program met the goals of the initiative: improving the transition from medical school to residency, ensuring readiness for practice through modifications of residency curricula, and optimizing the learning environment to support well-being.
Each of the following projects will receive $1.8 million over 5 years:
- California Oregon Medical Partnership to Address Disparities in Rural Education and Health – Oregon Health & Science University, Portland, and the University of California, Davis
- Fully Integrated Readiness for Service Training: Enhancing the Continuum from Medical School to Residency to Practice – University of North Carolina at Chapel Hill
- NYU Transition to Residency Advantage – New York University
- Promotion in Place: Enhancing Trainee Well-Being and Patient Care Through Time-Variable Graduate Medical Education – Partners HealthCare System, Massachusetts General Hospital, and Brigham and Women’s Hospital, Boston
- Reimagining Residency: Ensuring Readiness for Practice Through Growing Interprofessional Partnerships to Advance Care and Education – Maine Medical Center, Portland
- Residency Training to Effectively Address Social Determinants of Health: Applying a Curricular Framework Across Four Primary Care Specialties – Montefiore Health System, New York
- The Graduate Medical Training “Laboratory”: An Innovative Program to Generate, Implement, and Evaluate Interventions to Improve Resident Burnout and Clinical Skill – Johns Hopkins University, Baltimore; Stanford (Calif.) University; and the University of Alabama at Birmingham
- The GOL2D Project (Goals of Life and Learning Delineated): Collaboration Across Academic Health Systems to Better Align GME with Learner, Patient, and Societal Needs – Vanderbilt University, Nashville, Tenn., and the University of Mississippi, Jackson
An additional three programs will receive a smaller $50,000 planning grant to expedite further exploration and development.
“As the health care landscape and technology rapidly evolve, the AMA will continue working with its community of innovation to drive the future of medicine by supporting significant redesign in physician training. Our goal is to ensure physicians are prepared to adapt, grow, and thrive at every stage of their training and career. Better prepared physicians will deliver more effective and equitable health care,” said Dr. Madara.
led by medical schools, residency programs, and health systems.
“After establishing a framework for creating the medical schools of the future, the AMA is now supporting innovation projects that will better align residency training with the evolving needs of patients and communities, as well as the workforce needs of the current and future health care system,” AMA CEO and Executive Vice President James L. Madara, MD, stated in a press release.
The projects include curricular innovations to address workforce shortages and address social determinants of health. Other projects will be developed within the framework of innovations and concepts developed and implemented in medical schools over the past 6 years by the AMA’s consortium. These projects include implementing competency-based programs and incorporating Health Systems Science into residency training.
The projects were chosen through a competitive grant process by an advisory panel made up of leading experts in medical education, and selection was based on how well each program met the goals of the initiative: improving the transition from medical school to residency, ensuring readiness for practice through modifications of residency curricula, and optimizing the learning environment to support well-being.
Each of the following projects will receive $1.8 million over 5 years:
- California Oregon Medical Partnership to Address Disparities in Rural Education and Health – Oregon Health & Science University, Portland, and the University of California, Davis
- Fully Integrated Readiness for Service Training: Enhancing the Continuum from Medical School to Residency to Practice – University of North Carolina at Chapel Hill
- NYU Transition to Residency Advantage – New York University
- Promotion in Place: Enhancing Trainee Well-Being and Patient Care Through Time-Variable Graduate Medical Education – Partners HealthCare System, Massachusetts General Hospital, and Brigham and Women’s Hospital, Boston
- Reimagining Residency: Ensuring Readiness for Practice Through Growing Interprofessional Partnerships to Advance Care and Education – Maine Medical Center, Portland
- Residency Training to Effectively Address Social Determinants of Health: Applying a Curricular Framework Across Four Primary Care Specialties – Montefiore Health System, New York
- The Graduate Medical Training “Laboratory”: An Innovative Program to Generate, Implement, and Evaluate Interventions to Improve Resident Burnout and Clinical Skill – Johns Hopkins University, Baltimore; Stanford (Calif.) University; and the University of Alabama at Birmingham
- The GOL2D Project (Goals of Life and Learning Delineated): Collaboration Across Academic Health Systems to Better Align GME with Learner, Patient, and Societal Needs – Vanderbilt University, Nashville, Tenn., and the University of Mississippi, Jackson
An additional three programs will receive a smaller $50,000 planning grant to expedite further exploration and development.
“As the health care landscape and technology rapidly evolve, the AMA will continue working with its community of innovation to drive the future of medicine by supporting significant redesign in physician training. Our goal is to ensure physicians are prepared to adapt, grow, and thrive at every stage of their training and career. Better prepared physicians will deliver more effective and equitable health care,” said Dr. Madara.
Maternal mortality: Critical next steps in addressing the crisis
As the rest of the industrialized world has seen a decline in maternal mortality, the United States has seen a substantial rise over the last 30 years (FIGURE).1 It is estimated that more than 60% of these pregnancy-related deaths are preventable. Additionally, substantial disparities exist, with African-American women 3 to 4 times more likely to die of pregnancy-related complications than white women.1
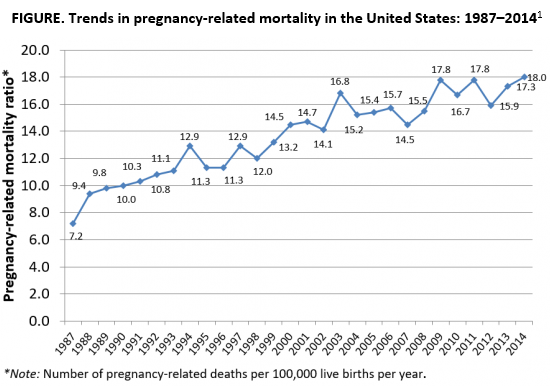
A good first step
The Preventing Maternal Deaths Act was passed by the 115th Congress and signed into law December 2018 in an effort to support and expand maternal mortality review committees (MMRCs) on a state level while allowing the Centers for Disease Control and Prevention (CDC) to further study disparities within maternal mortality. Although these efforts are a good first step to help reduce maternal mortality, more needs to be done to quell this growing epidemic.
We must now improve care access
One strategy to aid in decreasing maternal morbidity and mortality is to improve affordable access to medical care. Medicaid is the largest single payer of maternity care in the United States, covering 42.6% of births. Currently, in many states, Medicaid coverage only lasts until a woman is 60 days postpartum.2 Although 31 states, including the District of Columbia, have adopted Medicaid expansion programs to allow women to extend coverage beyond those 60 days, offering these programs is not a federal law. In the 19 remaining states with no extension options, the vast majority of women will lose their Medicaid coverage just after they are 2 months postpartum and will have no alternative health insurance coverage.2
Why does this coverage cutoff matter? Pregnancy-related deaths are defined as up to 12 months postpartum. A report reviewing 9 MMRCs found that 38% of pregnancy-related deaths occurred while a woman was pregnant, 45% of deaths occurred within 42 days of delivery, and 18% from 43 days to 1 year after delivery.3 Additionally, nearly half of women with Medicaid do not come to their 6-week postpartum visit (for a variety of reasons), missing a critical opportunity to address health concerns.2 Of the deaths that occurred in this later postpartum period, leading causes were cardiomyopathy (32%), mental health conditions (16%), and embolism (11%).3 Prevention and management of these conditions require regular follow-up with an ObGyn, as well as potentially from subspecialists in cardiology, psychiatry, hematology, and other subspecialties. Women not having access to affordable health care during the critical postpartum period greatly increases their risk of death or severe morbidity.
An important next step beyond the Preventing Maternal Deaths Act is to extend Medicaid coverage to 12 months postpartum for all women everywhere. MMRCs have concluded that extending coverage would ensure that “medical and behavioral health conditions [could be] managed and treated before becoming progressively severe.”3 This would presumably help decrease the risk of pregnancy-related death and address worsening morbidity. Additionally, the postpartum period is a well-established time of increased stress and can be an overwhelming and emotional time for many new mothers, especially for those with limited resources for childcare, transportation, stable housing, etc.6 Providing and ensuring ongoing medical care would substantially improve the lives and health of women and the health of their families.
We, as a country, need to make changes
Every step of the way, a woman faces challenges to safely and affordably access health care. Providing access to insurance coverage for 12 months postpartum can help to decrease our country’s rising maternal mortality and morbidity rates.
Take action
Congresswoman Robin Kelly (D-IL) and Senator Dick Durbin (D-IL) have introduced the MOMMA Act (H.R. 1897/S. 916) to help address the rising maternal mortality rate.
This Act would:
- Expand Medicaid coverage to 1 year postpartum.
- Work with the CDC to uniformly collect data to accurately assess maternal mortality and morbidity.
- Ensure the sharing of best practices of care across hospital systems.
- Focus on culturally-competent care to address implicit bias among health care workers.
- Support and expand the Alliance for Innovation on Maternal Health (AIM)—a data-driven initiative to implement safety protocols in hospitals across the country.
To call or contact your representative to co-sponsor this bill, click here. To review if your Congressperson is a co-sponsor, click here. To review if your Senator is a co-sponsor, click here.
- The Centers for Disease Control and Prevention. Pregnancy Mortality Surveillance System, Trends in Pregnancy-Related Deaths. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-mortality-surveillance-system.htm. Accessed May 29, 2019.
- Stuebe A, Moore JE, Mittal P, et al. Extending medicaid coverage for postpartum moms. May 6, 2019. https://www.healthaffairs.org/do/10.1377/hblog20190501.254675/full/. Accessed May 29, 2019.
- Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. 2018. Color/Word_R17_G85_B204http://reviewtoaction.org/Report_from_Nine_MMRCs. Accessed May 29, 2019.
- MacDorman MF, Declercq E, Cabral H, et al. Recent increases in the U.S. maternal mortality rate: disentangling trends from measurement issues. Obstet Gynecol. 2016;128:447-455.
- Martin JA, Hamilton BE, Osterman MJ, et al. Births: final data for 2016. Natl Vital Stat Rep. 2018;67:1-55.
- Vestal C. For addicted women, the year after childbirth is the deadliest. August 14, 2018. https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2018/08/14/for-addicted-women-the-year-after-childbirth-is-the-deadliest. Accessed May 29, 2019.
As the rest of the industrialized world has seen a decline in maternal mortality, the United States has seen a substantial rise over the last 30 years (FIGURE).1 It is estimated that more than 60% of these pregnancy-related deaths are preventable. Additionally, substantial disparities exist, with African-American women 3 to 4 times more likely to die of pregnancy-related complications than white women.1
A good first step
The Preventing Maternal Deaths Act was passed by the 115th Congress and signed into law December 2018 in an effort to support and expand maternal mortality review committees (MMRCs) on a state level while allowing the Centers for Disease Control and Prevention (CDC) to further study disparities within maternal mortality. Although these efforts are a good first step to help reduce maternal mortality, more needs to be done to quell this growing epidemic.
We must now improve care access
One strategy to aid in decreasing maternal morbidity and mortality is to improve affordable access to medical care. Medicaid is the largest single payer of maternity care in the United States, covering 42.6% of births. Currently, in many states, Medicaid coverage only lasts until a woman is 60 days postpartum.2 Although 31 states, including the District of Columbia, have adopted Medicaid expansion programs to allow women to extend coverage beyond those 60 days, offering these programs is not a federal law. In the 19 remaining states with no extension options, the vast majority of women will lose their Medicaid coverage just after they are 2 months postpartum and will have no alternative health insurance coverage.2
Why does this coverage cutoff matter? Pregnancy-related deaths are defined as up to 12 months postpartum. A report reviewing 9 MMRCs found that 38% of pregnancy-related deaths occurred while a woman was pregnant, 45% of deaths occurred within 42 days of delivery, and 18% from 43 days to 1 year after delivery.3 Additionally, nearly half of women with Medicaid do not come to their 6-week postpartum visit (for a variety of reasons), missing a critical opportunity to address health concerns.2 Of the deaths that occurred in this later postpartum period, leading causes were cardiomyopathy (32%), mental health conditions (16%), and embolism (11%).3 Prevention and management of these conditions require regular follow-up with an ObGyn, as well as potentially from subspecialists in cardiology, psychiatry, hematology, and other subspecialties. Women not having access to affordable health care during the critical postpartum period greatly increases their risk of death or severe morbidity.
An important next step beyond the Preventing Maternal Deaths Act is to extend Medicaid coverage to 12 months postpartum for all women everywhere. MMRCs have concluded that extending coverage would ensure that “medical and behavioral health conditions [could be] managed and treated before becoming progressively severe.”3 This would presumably help decrease the risk of pregnancy-related death and address worsening morbidity. Additionally, the postpartum period is a well-established time of increased stress and can be an overwhelming and emotional time for many new mothers, especially for those with limited resources for childcare, transportation, stable housing, etc.6 Providing and ensuring ongoing medical care would substantially improve the lives and health of women and the health of their families.
We, as a country, need to make changes
Every step of the way, a woman faces challenges to safely and affordably access health care. Providing access to insurance coverage for 12 months postpartum can help to decrease our country’s rising maternal mortality and morbidity rates.
Take action
Congresswoman Robin Kelly (D-IL) and Senator Dick Durbin (D-IL) have introduced the MOMMA Act (H.R. 1897/S. 916) to help address the rising maternal mortality rate.
This Act would:
- Expand Medicaid coverage to 1 year postpartum.
- Work with the CDC to uniformly collect data to accurately assess maternal mortality and morbidity.
- Ensure the sharing of best practices of care across hospital systems.
- Focus on culturally-competent care to address implicit bias among health care workers.
- Support and expand the Alliance for Innovation on Maternal Health (AIM)—a data-driven initiative to implement safety protocols in hospitals across the country.
To call or contact your representative to co-sponsor this bill, click here. To review if your Congressperson is a co-sponsor, click here. To review if your Senator is a co-sponsor, click here.
As the rest of the industrialized world has seen a decline in maternal mortality, the United States has seen a substantial rise over the last 30 years (FIGURE).1 It is estimated that more than 60% of these pregnancy-related deaths are preventable. Additionally, substantial disparities exist, with African-American women 3 to 4 times more likely to die of pregnancy-related complications than white women.1
A good first step
The Preventing Maternal Deaths Act was passed by the 115th Congress and signed into law December 2018 in an effort to support and expand maternal mortality review committees (MMRCs) on a state level while allowing the Centers for Disease Control and Prevention (CDC) to further study disparities within maternal mortality. Although these efforts are a good first step to help reduce maternal mortality, more needs to be done to quell this growing epidemic.
We must now improve care access
One strategy to aid in decreasing maternal morbidity and mortality is to improve affordable access to medical care. Medicaid is the largest single payer of maternity care in the United States, covering 42.6% of births. Currently, in many states, Medicaid coverage only lasts until a woman is 60 days postpartum.2 Although 31 states, including the District of Columbia, have adopted Medicaid expansion programs to allow women to extend coverage beyond those 60 days, offering these programs is not a federal law. In the 19 remaining states with no extension options, the vast majority of women will lose their Medicaid coverage just after they are 2 months postpartum and will have no alternative health insurance coverage.2
Why does this coverage cutoff matter? Pregnancy-related deaths are defined as up to 12 months postpartum. A report reviewing 9 MMRCs found that 38% of pregnancy-related deaths occurred while a woman was pregnant, 45% of deaths occurred within 42 days of delivery, and 18% from 43 days to 1 year after delivery.3 Additionally, nearly half of women with Medicaid do not come to their 6-week postpartum visit (for a variety of reasons), missing a critical opportunity to address health concerns.2 Of the deaths that occurred in this later postpartum period, leading causes were cardiomyopathy (32%), mental health conditions (16%), and embolism (11%).3 Prevention and management of these conditions require regular follow-up with an ObGyn, as well as potentially from subspecialists in cardiology, psychiatry, hematology, and other subspecialties. Women not having access to affordable health care during the critical postpartum period greatly increases their risk of death or severe morbidity.
An important next step beyond the Preventing Maternal Deaths Act is to extend Medicaid coverage to 12 months postpartum for all women everywhere. MMRCs have concluded that extending coverage would ensure that “medical and behavioral health conditions [could be] managed and treated before becoming progressively severe.”3 This would presumably help decrease the risk of pregnancy-related death and address worsening morbidity. Additionally, the postpartum period is a well-established time of increased stress and can be an overwhelming and emotional time for many new mothers, especially for those with limited resources for childcare, transportation, stable housing, etc.6 Providing and ensuring ongoing medical care would substantially improve the lives and health of women and the health of their families.
We, as a country, need to make changes
Every step of the way, a woman faces challenges to safely and affordably access health care. Providing access to insurance coverage for 12 months postpartum can help to decrease our country’s rising maternal mortality and morbidity rates.
Take action
Congresswoman Robin Kelly (D-IL) and Senator Dick Durbin (D-IL) have introduced the MOMMA Act (H.R. 1897/S. 916) to help address the rising maternal mortality rate.
This Act would:
- Expand Medicaid coverage to 1 year postpartum.
- Work with the CDC to uniformly collect data to accurately assess maternal mortality and morbidity.
- Ensure the sharing of best practices of care across hospital systems.
- Focus on culturally-competent care to address implicit bias among health care workers.
- Support and expand the Alliance for Innovation on Maternal Health (AIM)—a data-driven initiative to implement safety protocols in hospitals across the country.
To call or contact your representative to co-sponsor this bill, click here. To review if your Congressperson is a co-sponsor, click here. To review if your Senator is a co-sponsor, click here.
- The Centers for Disease Control and Prevention. Pregnancy Mortality Surveillance System, Trends in Pregnancy-Related Deaths. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-mortality-surveillance-system.htm. Accessed May 29, 2019.
- Stuebe A, Moore JE, Mittal P, et al. Extending medicaid coverage for postpartum moms. May 6, 2019. https://www.healthaffairs.org/do/10.1377/hblog20190501.254675/full/. Accessed May 29, 2019.
- Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. 2018. Color/Word_R17_G85_B204http://reviewtoaction.org/Report_from_Nine_MMRCs. Accessed May 29, 2019.
- MacDorman MF, Declercq E, Cabral H, et al. Recent increases in the U.S. maternal mortality rate: disentangling trends from measurement issues. Obstet Gynecol. 2016;128:447-455.
- Martin JA, Hamilton BE, Osterman MJ, et al. Births: final data for 2016. Natl Vital Stat Rep. 2018;67:1-55.
- Vestal C. For addicted women, the year after childbirth is the deadliest. August 14, 2018. https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2018/08/14/for-addicted-women-the-year-after-childbirth-is-the-deadliest. Accessed May 29, 2019.
- The Centers for Disease Control and Prevention. Pregnancy Mortality Surveillance System, Trends in Pregnancy-Related Deaths. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-mortality-surveillance-system.htm. Accessed May 29, 2019.
- Stuebe A, Moore JE, Mittal P, et al. Extending medicaid coverage for postpartum moms. May 6, 2019. https://www.healthaffairs.org/do/10.1377/hblog20190501.254675/full/. Accessed May 29, 2019.
- Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. 2018. Color/Word_R17_G85_B204http://reviewtoaction.org/Report_from_Nine_MMRCs. Accessed May 29, 2019.
- MacDorman MF, Declercq E, Cabral H, et al. Recent increases in the U.S. maternal mortality rate: disentangling trends from measurement issues. Obstet Gynecol. 2016;128:447-455.
- Martin JA, Hamilton BE, Osterman MJ, et al. Births: final data for 2016. Natl Vital Stat Rep. 2018;67:1-55.
- Vestal C. For addicted women, the year after childbirth is the deadliest. August 14, 2018. https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2018/08/14/for-addicted-women-the-year-after-childbirth-is-the-deadliest. Accessed May 29, 2019.
