User login
Twelve-month overall survival benefit with ribociclib for metastatic breast cancer
“Based on these results, ribociclib and letrozole should be considered the preferred treatment option,” said lead investigator Gabriel N. Hortobagyi, MD, a breast cancer medical oncologist at the University of Texas MD Anderson Cancer Center, Houston.
He presented the definitive overall survival results from MONALESSA-2 which randomized 668 patients equally and in the first line to either ribociclib or placebo on a background of standard dose letrozole.
At a median follow up of 6.6 years, median overall survival with ribociclib was 63.9 months versus 51.4 months in the placebo arm, a 24% reduction in the relative risk of death (P = .004).
It was the first report of a median overall survival (OS) exceeding 5 years in a phase 3 trial for advanced breast cancer. The estimated 6-year OS rate was 44.2% for ribociclib versus 32.0% with placebo.
“These are really impressive results” and support the use of CDK 4/6 inhibitors in the front-line setting,” said study discussant Gonzalo Gomez Abuin, MD, a medical oncologist at Hospital Alemán in Bueno Aires.
Ribociclib and other CDK 4/6 inhibitors have shown consistent progression-free survival benefit for metastatic disease, but ribociclib is the first of the major phase 3 trials with definitive overall survival results. They have “been long awaited,” Dr. Abuin said.
The overall survival benefit in MONALESSA-2 began to emerge at around 20 months and continued to increase over time.
Women had no prior CDK4/6 inhibitor treatment, chemotherapy, or endocrine therapy for metastatic disease. “They represented a pure first-line population,” Dr. Hortobagyi said.
Among other benefits, the time to first chemotherapy was a median of 50.6 months with ribociclib versus 38.9 months with placebo, so patients “had an extra year of delay before chemotherapy was utilized,” he said.
In general, Dr. Abuin said, we “see a consistent benefit with CDK 4/6 inhibitors in metastatic breast cancer across different settings.”
However, “it’s a little intriguing” that in a subgroup analysis of non–de novo disease, the overall survival benefit with ribociclib had a hazard ratio of 0.91, whereas the progression-free survival benefit was robust and statistically significant in an earlier report.
“This has been an important question, but I would caution all of us not to make too much out of the forest plot,” Dr. Hortobagyi said.
“There are a number of hypotheses one could come up with that could explain why the de novo and non–de novo populations faired differently in overall survival as opposed to progression-free survival, but there is also the simple possibility that this is a statistical fluke,” he said.
“We are in the process of analyzing this particular observation. In the meantime, I think we should just take the overall survival results of the entire population as the lead answer, and not follow the subgroup analysis until further information is available,” Dr. Hortobagyi said.
No new ribociclib safety signals were observed in the trial. The most common adverse events were neutropenia and liver function abnormalities, but they were “largely asymptomatic laboratory findings and completely reversible,” he said.
Twice as many patients treated with ribociclib developed prolonged QT intervals, but again, “no clinical consequences of this EKG finding were detected,” Dr. Hortobagyi said.
Less than 1% of patients in the ribociclib arm developed interstitial lung disease. The majority of safety events occurred in the first 12 months of treatment.
The work was funded by Novartis, maker of both ribociclib and letrozole. Dr. Hortobagyi reported receiving an institutional grant from the company and personal fees related to the trial. Other investigators disclosed ties to Novartis. Dr. Abuin reported relationships with many companies, including Novartis.
This article was updated 9/24/21.
“Based on these results, ribociclib and letrozole should be considered the preferred treatment option,” said lead investigator Gabriel N. Hortobagyi, MD, a breast cancer medical oncologist at the University of Texas MD Anderson Cancer Center, Houston.
He presented the definitive overall survival results from MONALESSA-2 which randomized 668 patients equally and in the first line to either ribociclib or placebo on a background of standard dose letrozole.
At a median follow up of 6.6 years, median overall survival with ribociclib was 63.9 months versus 51.4 months in the placebo arm, a 24% reduction in the relative risk of death (P = .004).
It was the first report of a median overall survival (OS) exceeding 5 years in a phase 3 trial for advanced breast cancer. The estimated 6-year OS rate was 44.2% for ribociclib versus 32.0% with placebo.
“These are really impressive results” and support the use of CDK 4/6 inhibitors in the front-line setting,” said study discussant Gonzalo Gomez Abuin, MD, a medical oncologist at Hospital Alemán in Bueno Aires.
Ribociclib and other CDK 4/6 inhibitors have shown consistent progression-free survival benefit for metastatic disease, but ribociclib is the first of the major phase 3 trials with definitive overall survival results. They have “been long awaited,” Dr. Abuin said.
The overall survival benefit in MONALESSA-2 began to emerge at around 20 months and continued to increase over time.
Women had no prior CDK4/6 inhibitor treatment, chemotherapy, or endocrine therapy for metastatic disease. “They represented a pure first-line population,” Dr. Hortobagyi said.
Among other benefits, the time to first chemotherapy was a median of 50.6 months with ribociclib versus 38.9 months with placebo, so patients “had an extra year of delay before chemotherapy was utilized,” he said.
In general, Dr. Abuin said, we “see a consistent benefit with CDK 4/6 inhibitors in metastatic breast cancer across different settings.”
However, “it’s a little intriguing” that in a subgroup analysis of non–de novo disease, the overall survival benefit with ribociclib had a hazard ratio of 0.91, whereas the progression-free survival benefit was robust and statistically significant in an earlier report.
“This has been an important question, but I would caution all of us not to make too much out of the forest plot,” Dr. Hortobagyi said.
“There are a number of hypotheses one could come up with that could explain why the de novo and non–de novo populations faired differently in overall survival as opposed to progression-free survival, but there is also the simple possibility that this is a statistical fluke,” he said.
“We are in the process of analyzing this particular observation. In the meantime, I think we should just take the overall survival results of the entire population as the lead answer, and not follow the subgroup analysis until further information is available,” Dr. Hortobagyi said.
No new ribociclib safety signals were observed in the trial. The most common adverse events were neutropenia and liver function abnormalities, but they were “largely asymptomatic laboratory findings and completely reversible,” he said.
Twice as many patients treated with ribociclib developed prolonged QT intervals, but again, “no clinical consequences of this EKG finding were detected,” Dr. Hortobagyi said.
Less than 1% of patients in the ribociclib arm developed interstitial lung disease. The majority of safety events occurred in the first 12 months of treatment.
The work was funded by Novartis, maker of both ribociclib and letrozole. Dr. Hortobagyi reported receiving an institutional grant from the company and personal fees related to the trial. Other investigators disclosed ties to Novartis. Dr. Abuin reported relationships with many companies, including Novartis.
This article was updated 9/24/21.
“Based on these results, ribociclib and letrozole should be considered the preferred treatment option,” said lead investigator Gabriel N. Hortobagyi, MD, a breast cancer medical oncologist at the University of Texas MD Anderson Cancer Center, Houston.
He presented the definitive overall survival results from MONALESSA-2 which randomized 668 patients equally and in the first line to either ribociclib or placebo on a background of standard dose letrozole.
At a median follow up of 6.6 years, median overall survival with ribociclib was 63.9 months versus 51.4 months in the placebo arm, a 24% reduction in the relative risk of death (P = .004).
It was the first report of a median overall survival (OS) exceeding 5 years in a phase 3 trial for advanced breast cancer. The estimated 6-year OS rate was 44.2% for ribociclib versus 32.0% with placebo.
“These are really impressive results” and support the use of CDK 4/6 inhibitors in the front-line setting,” said study discussant Gonzalo Gomez Abuin, MD, a medical oncologist at Hospital Alemán in Bueno Aires.
Ribociclib and other CDK 4/6 inhibitors have shown consistent progression-free survival benefit for metastatic disease, but ribociclib is the first of the major phase 3 trials with definitive overall survival results. They have “been long awaited,” Dr. Abuin said.
The overall survival benefit in MONALESSA-2 began to emerge at around 20 months and continued to increase over time.
Women had no prior CDK4/6 inhibitor treatment, chemotherapy, or endocrine therapy for metastatic disease. “They represented a pure first-line population,” Dr. Hortobagyi said.
Among other benefits, the time to first chemotherapy was a median of 50.6 months with ribociclib versus 38.9 months with placebo, so patients “had an extra year of delay before chemotherapy was utilized,” he said.
In general, Dr. Abuin said, we “see a consistent benefit with CDK 4/6 inhibitors in metastatic breast cancer across different settings.”
However, “it’s a little intriguing” that in a subgroup analysis of non–de novo disease, the overall survival benefit with ribociclib had a hazard ratio of 0.91, whereas the progression-free survival benefit was robust and statistically significant in an earlier report.
“This has been an important question, but I would caution all of us not to make too much out of the forest plot,” Dr. Hortobagyi said.
“There are a number of hypotheses one could come up with that could explain why the de novo and non–de novo populations faired differently in overall survival as opposed to progression-free survival, but there is also the simple possibility that this is a statistical fluke,” he said.
“We are in the process of analyzing this particular observation. In the meantime, I think we should just take the overall survival results of the entire population as the lead answer, and not follow the subgroup analysis until further information is available,” Dr. Hortobagyi said.
No new ribociclib safety signals were observed in the trial. The most common adverse events were neutropenia and liver function abnormalities, but they were “largely asymptomatic laboratory findings and completely reversible,” he said.
Twice as many patients treated with ribociclib developed prolonged QT intervals, but again, “no clinical consequences of this EKG finding were detected,” Dr. Hortobagyi said.
Less than 1% of patients in the ribociclib arm developed interstitial lung disease. The majority of safety events occurred in the first 12 months of treatment.
The work was funded by Novartis, maker of both ribociclib and letrozole. Dr. Hortobagyi reported receiving an institutional grant from the company and personal fees related to the trial. Other investigators disclosed ties to Novartis. Dr. Abuin reported relationships with many companies, including Novartis.
This article was updated 9/24/21.
FROM ESMO 2021
Call for a move or boycott of big Texas cancer meeting
Docs won’t attend in person
Held annually in December, SABCS is the world’s largest breast cancer meeting and welcomes thousands of attendees every year.
The law banning abortions after 6 weeks, at which time a woman may not even realize that she is pregnant, has been described as the most restrictive in the United States. It also enables private citizens to bring civil lawsuits against people who assist a pregnant person seeking an abortion in violation of the ban.
If the meeting remains in Texas this year, then UCSF’s Laura Esserman, MD, director of the Carol Franc Buck Breast Cancer Center, has said that she and other university faculty and professionals from elsewhere will attend only online — a form of boycotting the in-person event.
Dr. Esserman and UCSF colleague Mary Helen Barcellos-Hoff, PhD, professor of radiation oncology, have emailed conference leaders encouraging them to move the meeting, according to a press statement issued by UCSF.
SABCS organizers told this news organization via email that they “are having serious discussions about this matter” and will update the public via their website and social media channels.
“It’s a terrible law, and it is absolutely not protective of women. I think that if Texas officials understood that when they pass laws inhospitable to women, we will not hold a major conference about women’s health in their state,” said Dr. Esserman.
Dr. Esserman received support for the idea to move the meeting earlier this month from peers on Twitter.
“In light of the Texas law that prohibits abortion past 6 weeks of pregnancy AND promotes vigilantism, directly harming women and their caregivers, the 2021 SABCS breast cancer meeting should be moved out of Texas to a place that supports Women’s rights and public health #sabcs,” tweeted Dr. Esserman on September 5.
The post generated more than 3,300 likes and retweets and 40-plus comments from readers, many of whom were healthcare professionals.
Supporters of the proposed move included Michael Feldman, MD, PhD, pathologist, University of Pennsylvania in Philadelphia; Sarah Sammons, MD, breast medical oncologist, Duke Cancer Center, Durham, N.C.; Anjali Thawani, MD, breast surgeon, Evanston, Ill.; Debora Barton, MD, Carisma Therapeutics, Philadelphia; Jane Hui, MD, surgical oncologist, University of Minnesota, Minneapolis; Erica Leith Mitchell, MD, surgeon, University of Tennessee, Memphis; and Rebecca Shatsky, MD, breast medical oncologist, University of California, San Diego.
Support for boycotting in-person attendance is growing nationally, Dr. Esserman said in the press statement, which also highlighted an “additional concern” about Texas laws prohibiting mandated masking and asking for vaccine status. Conference organizers said local ordinances will be used to require masking.
Notably, a Twitter search using #SABCS21, the meeting’s hashtag, indicates that COVID 19 — and not the restrictive abortion law — is the primary worry of would-be meeting attendees as of the last week or so.
Some said the combination of the two issues was influential in their decision not to attend in person.
Kelly Shanahan, MD, a former ob/gyn living with metastatic breast cancer in South Lake Tahoe, Calif., tweeted: “It’s a hybrid model this year. I was originally going in person but will not now because of their COVID behaviors and now this [the abortion law]. I will tune in virtually but I will not spend the $1500 on the hotel room, the hundreds of $$ on food and drink and Xmas presents. #SayNoToTX #SABCS21.”
Dr. Shanahan also replied to Dr. Esserman’s move-the-meeting-out-of-Texas tweet: “100% agree.”
UCSF’s Dr. Barcellos-Hoff believes moving the meeting would be a high-profile happening. “I think moving a meeting of that size would have an impact, largely because of the visibility of scientists who oppose the law.”
First organized in 1977, SABCS is jointly sponsored by the Cancer Therapy & Research Center at The University of Texas Health Science Center at San Antonio, the American Association for Cancer Research, and Baylor College of Medicine.
A version of this article first appeared on Medscape.com.
Docs won’t attend in person
Docs won’t attend in person
Held annually in December, SABCS is the world’s largest breast cancer meeting and welcomes thousands of attendees every year.
The law banning abortions after 6 weeks, at which time a woman may not even realize that she is pregnant, has been described as the most restrictive in the United States. It also enables private citizens to bring civil lawsuits against people who assist a pregnant person seeking an abortion in violation of the ban.
If the meeting remains in Texas this year, then UCSF’s Laura Esserman, MD, director of the Carol Franc Buck Breast Cancer Center, has said that she and other university faculty and professionals from elsewhere will attend only online — a form of boycotting the in-person event.
Dr. Esserman and UCSF colleague Mary Helen Barcellos-Hoff, PhD, professor of radiation oncology, have emailed conference leaders encouraging them to move the meeting, according to a press statement issued by UCSF.
SABCS organizers told this news organization via email that they “are having serious discussions about this matter” and will update the public via their website and social media channels.
“It’s a terrible law, and it is absolutely not protective of women. I think that if Texas officials understood that when they pass laws inhospitable to women, we will not hold a major conference about women’s health in their state,” said Dr. Esserman.
Dr. Esserman received support for the idea to move the meeting earlier this month from peers on Twitter.
“In light of the Texas law that prohibits abortion past 6 weeks of pregnancy AND promotes vigilantism, directly harming women and their caregivers, the 2021 SABCS breast cancer meeting should be moved out of Texas to a place that supports Women’s rights and public health #sabcs,” tweeted Dr. Esserman on September 5.
The post generated more than 3,300 likes and retweets and 40-plus comments from readers, many of whom were healthcare professionals.
Supporters of the proposed move included Michael Feldman, MD, PhD, pathologist, University of Pennsylvania in Philadelphia; Sarah Sammons, MD, breast medical oncologist, Duke Cancer Center, Durham, N.C.; Anjali Thawani, MD, breast surgeon, Evanston, Ill.; Debora Barton, MD, Carisma Therapeutics, Philadelphia; Jane Hui, MD, surgical oncologist, University of Minnesota, Minneapolis; Erica Leith Mitchell, MD, surgeon, University of Tennessee, Memphis; and Rebecca Shatsky, MD, breast medical oncologist, University of California, San Diego.
Support for boycotting in-person attendance is growing nationally, Dr. Esserman said in the press statement, which also highlighted an “additional concern” about Texas laws prohibiting mandated masking and asking for vaccine status. Conference organizers said local ordinances will be used to require masking.
Notably, a Twitter search using #SABCS21, the meeting’s hashtag, indicates that COVID 19 — and not the restrictive abortion law — is the primary worry of would-be meeting attendees as of the last week or so.
Some said the combination of the two issues was influential in their decision not to attend in person.
Kelly Shanahan, MD, a former ob/gyn living with metastatic breast cancer in South Lake Tahoe, Calif., tweeted: “It’s a hybrid model this year. I was originally going in person but will not now because of their COVID behaviors and now this [the abortion law]. I will tune in virtually but I will not spend the $1500 on the hotel room, the hundreds of $$ on food and drink and Xmas presents. #SayNoToTX #SABCS21.”
Dr. Shanahan also replied to Dr. Esserman’s move-the-meeting-out-of-Texas tweet: “100% agree.”
UCSF’s Dr. Barcellos-Hoff believes moving the meeting would be a high-profile happening. “I think moving a meeting of that size would have an impact, largely because of the visibility of scientists who oppose the law.”
First organized in 1977, SABCS is jointly sponsored by the Cancer Therapy & Research Center at The University of Texas Health Science Center at San Antonio, the American Association for Cancer Research, and Baylor College of Medicine.
A version of this article first appeared on Medscape.com.
Held annually in December, SABCS is the world’s largest breast cancer meeting and welcomes thousands of attendees every year.
The law banning abortions after 6 weeks, at which time a woman may not even realize that she is pregnant, has been described as the most restrictive in the United States. It also enables private citizens to bring civil lawsuits against people who assist a pregnant person seeking an abortion in violation of the ban.
If the meeting remains in Texas this year, then UCSF’s Laura Esserman, MD, director of the Carol Franc Buck Breast Cancer Center, has said that she and other university faculty and professionals from elsewhere will attend only online — a form of boycotting the in-person event.
Dr. Esserman and UCSF colleague Mary Helen Barcellos-Hoff, PhD, professor of radiation oncology, have emailed conference leaders encouraging them to move the meeting, according to a press statement issued by UCSF.
SABCS organizers told this news organization via email that they “are having serious discussions about this matter” and will update the public via their website and social media channels.
“It’s a terrible law, and it is absolutely not protective of women. I think that if Texas officials understood that when they pass laws inhospitable to women, we will not hold a major conference about women’s health in their state,” said Dr. Esserman.
Dr. Esserman received support for the idea to move the meeting earlier this month from peers on Twitter.
“In light of the Texas law that prohibits abortion past 6 weeks of pregnancy AND promotes vigilantism, directly harming women and their caregivers, the 2021 SABCS breast cancer meeting should be moved out of Texas to a place that supports Women’s rights and public health #sabcs,” tweeted Dr. Esserman on September 5.
The post generated more than 3,300 likes and retweets and 40-plus comments from readers, many of whom were healthcare professionals.
Supporters of the proposed move included Michael Feldman, MD, PhD, pathologist, University of Pennsylvania in Philadelphia; Sarah Sammons, MD, breast medical oncologist, Duke Cancer Center, Durham, N.C.; Anjali Thawani, MD, breast surgeon, Evanston, Ill.; Debora Barton, MD, Carisma Therapeutics, Philadelphia; Jane Hui, MD, surgical oncologist, University of Minnesota, Minneapolis; Erica Leith Mitchell, MD, surgeon, University of Tennessee, Memphis; and Rebecca Shatsky, MD, breast medical oncologist, University of California, San Diego.
Support for boycotting in-person attendance is growing nationally, Dr. Esserman said in the press statement, which also highlighted an “additional concern” about Texas laws prohibiting mandated masking and asking for vaccine status. Conference organizers said local ordinances will be used to require masking.
Notably, a Twitter search using #SABCS21, the meeting’s hashtag, indicates that COVID 19 — and not the restrictive abortion law — is the primary worry of would-be meeting attendees as of the last week or so.
Some said the combination of the two issues was influential in their decision not to attend in person.
Kelly Shanahan, MD, a former ob/gyn living with metastatic breast cancer in South Lake Tahoe, Calif., tweeted: “It’s a hybrid model this year. I was originally going in person but will not now because of their COVID behaviors and now this [the abortion law]. I will tune in virtually but I will not spend the $1500 on the hotel room, the hundreds of $$ on food and drink and Xmas presents. #SayNoToTX #SABCS21.”
Dr. Shanahan also replied to Dr. Esserman’s move-the-meeting-out-of-Texas tweet: “100% agree.”
UCSF’s Dr. Barcellos-Hoff believes moving the meeting would be a high-profile happening. “I think moving a meeting of that size would have an impact, largely because of the visibility of scientists who oppose the law.”
First organized in 1977, SABCS is jointly sponsored by the Cancer Therapy & Research Center at The University of Texas Health Science Center at San Antonio, the American Association for Cancer Research, and Baylor College of Medicine.
A version of this article first appeared on Medscape.com.
Patients panic as docs cut off breast cancer drug
The discontinuance appears to be in reaction to an announcement by the manufacturer (Genentech) in late August that it has voluntarily withdrawn its application for accelerated approval of the drug for use in metastatic triple-negative breast cancer (mTNBC).
However, experts stress that discontinuing atezolizumab is not advised if a patient is responding to or is stable on the immune checkpoint inhibitor.
“I think the Genentech announcement has been misinterpreted,” Maryam Lustberg, MD, of Yale Cancer Center, New Haven, Conn., said in an interview. “The consensus opinion from all academic breast oncologists is that people should not be switching off atezolizumab if they are responding. They should not be changing their immunotherapy.”
Dr. Lustberg said the announcement had two major points: “don’t start a new patient on atezolizumab,” and the company is “committed” to supplying the drug to patients whose conditions are stable or responding.
Nevertheless, some patients with mTNBC were recently in a state of escalating emotional upset, said one patient advocate.
“The level of panic among those currently on & responding well to Atezo is growing quickly,” tweeted Janice Cowden on Sept. 5, a former nurse living with mTNBC in Bradenton, Fla.
Ms. Cowden explained that “at least 10-20 patients” were “pulled [off the drug by their oncologists] this past week who have been stable/no evidence of disease/no evidence of disease activity on Tecentriq.”
She estimated that as many as 50 patients in the 2,200-member Triple Negative BC Stage 4 Facebook group who have been responding to the drug were abruptly de-prescribed atezolizumab since the Aug. 27 announcement from Genentech.
Many women learned of the change via patient portals or text messaging, not directly from their physicians, Cowden told Medscape Medical News.
Some of the women had been taking atezolizumab for 2-3 years, including those with no evidence of disease, she said. “Finding out that their oncologist was discontinuing a treatment that was working for them has been driving so much anxiety and stress,” Ms. Cowden emphasized.
Most market withdrawals of drugs are related to safety, but that is not the case with atezolizumab, said Sara Horton, MD, of Howard University, Washington. She was speaking at the recent Facebook webinar on atezolizumab and mTNBC that was sponsored by the TNBC Foundation and the Young Survivors Coalition.
In the case of atezolizumab, it was a question about efficacy that prompted the withdrawal. After the indication was granted an accelerated approval on the basis of response data, a confirmatory trial set out to show clinical benefit. However, the confirmatory phase 3 IMpassion131 trial did not do so: it found that atezolizumab plus paclitaxel did not significantly reduce the risk for cancer progression and death in comparison with paclitaxel plus placebo among patients with TNBC with tumors that were positive for programmed cell death protein–1 (PD-L1), as reported by Medscape Medical News.
These results were discussed by the Food and Drug Administration on the first day of a historic 3-day meeting on accelerated approvals in April 2021. Despite the failure of confirmation of clinical benefit, the advisory panel voted 7-2 in favor of keeping the approval in place for atezolizumab in TNBC. At the same time, it urged Genentech to carry out more studies to show that the drug works in this patient population.
The company apparently decided not to do that and instead voluntarily withdrew the application for the indication some 4 months later.
During the recent TNBC Foundation webinar, Genentech official Lauren Davis said that the company sent letters about this decision to atezolizumab-prescribing physicians and included another letter that was to be shared with patients. Ms. Davis had not responded to this news organization’s request to review the communications at the time this article was published.
At the webinar, Ms. Davis did clarify that current atezolizumab patients (who are responding to the drug), who have commercial insurance, and who benefit from Genentech’s copay program will continue to receive the benefit until June 2022.
In its August announcement, Genentech said it decided to withdraw the atezolizumab approval on the basis of the FDA’s assessment of the “current mTNBC treatment landscape and in accordance with the requirements of the accelerated approval program.”
That landscape presumably includes pembrolizumab (Keytruda), which received a full approval for a TNBC indication similar to that of atezolizumab in July. That full approval was based on findings from the randomized, phase 3 KEYNOTE-522 trial, which showed significantly prolonged event-free survival with the pembrolizumab regimen in comparison with neoadjuvant chemotherapy alone for previously untreated stage II or III TNBC. Details of these clinical data will be presented at the upcoming annual meeting of the European Society of Medical Oncology.
Switching the immunotherapy?
Some U.S. oncologists have been telling patients with mTNBC that the atezolizumab withdrawal is “not an issue” because the new full approval of pembrolizumab in this setting will allow prescriptions to be switched, said patient advocate Ms. Cowden.
However, experts have said that no patient who is responding to or whose condition is stable with atezolizumab should switch immunotherapies. “This is a very aggressive disease,” reminded Dr. Lustberg.
Switching the immunotherapies is complicated by the difference in the respective drugs’ companion biomarker assays used to establish the presence of PD-L1.
Dr. Lustberg explained that patients who are not responding to atezolizumab and who now want to try pembrolizumab will have to be assessed with the CTS assay.
“About 22% of the patients who are positive for the atezolizumab biomarker assay SP-142 are not going to be positive for the CTS,” she said.
In other words, about one in four patients with mTNBC who are taking atezolizumab will not qualify for treatment with pembrolizumab.
Rebecca Shatsky, MD, of the University of California, San Diego, echoed those comments in an email to this news organization – and emphatically discouraged switching off atezolizumab (and going on pembrolizumab) if a patient is having success (i.e., stable disease or positive response).
“The two groups don’t always overlap, so it isn’t an easy switch. That’s why if they are already responding, I would NOT have them stop the drug,” she said.
Not every mTNBC patient receiving – and responding to – atezolizumab has had the unfortunate experience of having their prescription canceled.
Johanna Rauhala, of San Francisco, who is a former middle-school teacher and who writes the blog Pink Stinks, has been taking atezolizumab for 2 years. She has had a partial response and now, after taking the immunotherapy in combination with chemotherapy (gemcitabine and carboplatin), has stable disease. Currently, she is taking single-agent atezolizumab..
Ms. Rauhala has been living with mTNBC for 5 years. She said in an interview that she was “very surprised and concerned” to learn about Genentech’s withdrawal of its accelerated approval. She said that at her next treatment appointment, she was “probably going to ask the oncology nurse first [about the atezolizumab withdrawal] – because they are the front line, and I will then follow-up with my doctor. But I can’t imagine that they will take away something that is working.”
Dr. Shatsky, Dr. Horton, and Dr. Lunsberg report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
The discontinuance appears to be in reaction to an announcement by the manufacturer (Genentech) in late August that it has voluntarily withdrawn its application for accelerated approval of the drug for use in metastatic triple-negative breast cancer (mTNBC).
However, experts stress that discontinuing atezolizumab is not advised if a patient is responding to or is stable on the immune checkpoint inhibitor.
“I think the Genentech announcement has been misinterpreted,” Maryam Lustberg, MD, of Yale Cancer Center, New Haven, Conn., said in an interview. “The consensus opinion from all academic breast oncologists is that people should not be switching off atezolizumab if they are responding. They should not be changing their immunotherapy.”
Dr. Lustberg said the announcement had two major points: “don’t start a new patient on atezolizumab,” and the company is “committed” to supplying the drug to patients whose conditions are stable or responding.
Nevertheless, some patients with mTNBC were recently in a state of escalating emotional upset, said one patient advocate.
“The level of panic among those currently on & responding well to Atezo is growing quickly,” tweeted Janice Cowden on Sept. 5, a former nurse living with mTNBC in Bradenton, Fla.
Ms. Cowden explained that “at least 10-20 patients” were “pulled [off the drug by their oncologists] this past week who have been stable/no evidence of disease/no evidence of disease activity on Tecentriq.”
She estimated that as many as 50 patients in the 2,200-member Triple Negative BC Stage 4 Facebook group who have been responding to the drug were abruptly de-prescribed atezolizumab since the Aug. 27 announcement from Genentech.
Many women learned of the change via patient portals or text messaging, not directly from their physicians, Cowden told Medscape Medical News.
Some of the women had been taking atezolizumab for 2-3 years, including those with no evidence of disease, she said. “Finding out that their oncologist was discontinuing a treatment that was working for them has been driving so much anxiety and stress,” Ms. Cowden emphasized.
Most market withdrawals of drugs are related to safety, but that is not the case with atezolizumab, said Sara Horton, MD, of Howard University, Washington. She was speaking at the recent Facebook webinar on atezolizumab and mTNBC that was sponsored by the TNBC Foundation and the Young Survivors Coalition.
In the case of atezolizumab, it was a question about efficacy that prompted the withdrawal. After the indication was granted an accelerated approval on the basis of response data, a confirmatory trial set out to show clinical benefit. However, the confirmatory phase 3 IMpassion131 trial did not do so: it found that atezolizumab plus paclitaxel did not significantly reduce the risk for cancer progression and death in comparison with paclitaxel plus placebo among patients with TNBC with tumors that were positive for programmed cell death protein–1 (PD-L1), as reported by Medscape Medical News.
These results were discussed by the Food and Drug Administration on the first day of a historic 3-day meeting on accelerated approvals in April 2021. Despite the failure of confirmation of clinical benefit, the advisory panel voted 7-2 in favor of keeping the approval in place for atezolizumab in TNBC. At the same time, it urged Genentech to carry out more studies to show that the drug works in this patient population.
The company apparently decided not to do that and instead voluntarily withdrew the application for the indication some 4 months later.
During the recent TNBC Foundation webinar, Genentech official Lauren Davis said that the company sent letters about this decision to atezolizumab-prescribing physicians and included another letter that was to be shared with patients. Ms. Davis had not responded to this news organization’s request to review the communications at the time this article was published.
At the webinar, Ms. Davis did clarify that current atezolizumab patients (who are responding to the drug), who have commercial insurance, and who benefit from Genentech’s copay program will continue to receive the benefit until June 2022.
In its August announcement, Genentech said it decided to withdraw the atezolizumab approval on the basis of the FDA’s assessment of the “current mTNBC treatment landscape and in accordance with the requirements of the accelerated approval program.”
That landscape presumably includes pembrolizumab (Keytruda), which received a full approval for a TNBC indication similar to that of atezolizumab in July. That full approval was based on findings from the randomized, phase 3 KEYNOTE-522 trial, which showed significantly prolonged event-free survival with the pembrolizumab regimen in comparison with neoadjuvant chemotherapy alone for previously untreated stage II or III TNBC. Details of these clinical data will be presented at the upcoming annual meeting of the European Society of Medical Oncology.
Switching the immunotherapy?
Some U.S. oncologists have been telling patients with mTNBC that the atezolizumab withdrawal is “not an issue” because the new full approval of pembrolizumab in this setting will allow prescriptions to be switched, said patient advocate Ms. Cowden.
However, experts have said that no patient who is responding to or whose condition is stable with atezolizumab should switch immunotherapies. “This is a very aggressive disease,” reminded Dr. Lustberg.
Switching the immunotherapies is complicated by the difference in the respective drugs’ companion biomarker assays used to establish the presence of PD-L1.
Dr. Lustberg explained that patients who are not responding to atezolizumab and who now want to try pembrolizumab will have to be assessed with the CTS assay.
“About 22% of the patients who are positive for the atezolizumab biomarker assay SP-142 are not going to be positive for the CTS,” she said.
In other words, about one in four patients with mTNBC who are taking atezolizumab will not qualify for treatment with pembrolizumab.
Rebecca Shatsky, MD, of the University of California, San Diego, echoed those comments in an email to this news organization – and emphatically discouraged switching off atezolizumab (and going on pembrolizumab) if a patient is having success (i.e., stable disease or positive response).
“The two groups don’t always overlap, so it isn’t an easy switch. That’s why if they are already responding, I would NOT have them stop the drug,” she said.
Not every mTNBC patient receiving – and responding to – atezolizumab has had the unfortunate experience of having their prescription canceled.
Johanna Rauhala, of San Francisco, who is a former middle-school teacher and who writes the blog Pink Stinks, has been taking atezolizumab for 2 years. She has had a partial response and now, after taking the immunotherapy in combination with chemotherapy (gemcitabine and carboplatin), has stable disease. Currently, she is taking single-agent atezolizumab..
Ms. Rauhala has been living with mTNBC for 5 years. She said in an interview that she was “very surprised and concerned” to learn about Genentech’s withdrawal of its accelerated approval. She said that at her next treatment appointment, she was “probably going to ask the oncology nurse first [about the atezolizumab withdrawal] – because they are the front line, and I will then follow-up with my doctor. But I can’t imagine that they will take away something that is working.”
Dr. Shatsky, Dr. Horton, and Dr. Lunsberg report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
The discontinuance appears to be in reaction to an announcement by the manufacturer (Genentech) in late August that it has voluntarily withdrawn its application for accelerated approval of the drug for use in metastatic triple-negative breast cancer (mTNBC).
However, experts stress that discontinuing atezolizumab is not advised if a patient is responding to or is stable on the immune checkpoint inhibitor.
“I think the Genentech announcement has been misinterpreted,” Maryam Lustberg, MD, of Yale Cancer Center, New Haven, Conn., said in an interview. “The consensus opinion from all academic breast oncologists is that people should not be switching off atezolizumab if they are responding. They should not be changing their immunotherapy.”
Dr. Lustberg said the announcement had two major points: “don’t start a new patient on atezolizumab,” and the company is “committed” to supplying the drug to patients whose conditions are stable or responding.
Nevertheless, some patients with mTNBC were recently in a state of escalating emotional upset, said one patient advocate.
“The level of panic among those currently on & responding well to Atezo is growing quickly,” tweeted Janice Cowden on Sept. 5, a former nurse living with mTNBC in Bradenton, Fla.
Ms. Cowden explained that “at least 10-20 patients” were “pulled [off the drug by their oncologists] this past week who have been stable/no evidence of disease/no evidence of disease activity on Tecentriq.”
She estimated that as many as 50 patients in the 2,200-member Triple Negative BC Stage 4 Facebook group who have been responding to the drug were abruptly de-prescribed atezolizumab since the Aug. 27 announcement from Genentech.
Many women learned of the change via patient portals or text messaging, not directly from their physicians, Cowden told Medscape Medical News.
Some of the women had been taking atezolizumab for 2-3 years, including those with no evidence of disease, she said. “Finding out that their oncologist was discontinuing a treatment that was working for them has been driving so much anxiety and stress,” Ms. Cowden emphasized.
Most market withdrawals of drugs are related to safety, but that is not the case with atezolizumab, said Sara Horton, MD, of Howard University, Washington. She was speaking at the recent Facebook webinar on atezolizumab and mTNBC that was sponsored by the TNBC Foundation and the Young Survivors Coalition.
In the case of atezolizumab, it was a question about efficacy that prompted the withdrawal. After the indication was granted an accelerated approval on the basis of response data, a confirmatory trial set out to show clinical benefit. However, the confirmatory phase 3 IMpassion131 trial did not do so: it found that atezolizumab plus paclitaxel did not significantly reduce the risk for cancer progression and death in comparison with paclitaxel plus placebo among patients with TNBC with tumors that were positive for programmed cell death protein–1 (PD-L1), as reported by Medscape Medical News.
These results were discussed by the Food and Drug Administration on the first day of a historic 3-day meeting on accelerated approvals in April 2021. Despite the failure of confirmation of clinical benefit, the advisory panel voted 7-2 in favor of keeping the approval in place for atezolizumab in TNBC. At the same time, it urged Genentech to carry out more studies to show that the drug works in this patient population.
The company apparently decided not to do that and instead voluntarily withdrew the application for the indication some 4 months later.
During the recent TNBC Foundation webinar, Genentech official Lauren Davis said that the company sent letters about this decision to atezolizumab-prescribing physicians and included another letter that was to be shared with patients. Ms. Davis had not responded to this news organization’s request to review the communications at the time this article was published.
At the webinar, Ms. Davis did clarify that current atezolizumab patients (who are responding to the drug), who have commercial insurance, and who benefit from Genentech’s copay program will continue to receive the benefit until June 2022.
In its August announcement, Genentech said it decided to withdraw the atezolizumab approval on the basis of the FDA’s assessment of the “current mTNBC treatment landscape and in accordance with the requirements of the accelerated approval program.”
That landscape presumably includes pembrolizumab (Keytruda), which received a full approval for a TNBC indication similar to that of atezolizumab in July. That full approval was based on findings from the randomized, phase 3 KEYNOTE-522 trial, which showed significantly prolonged event-free survival with the pembrolizumab regimen in comparison with neoadjuvant chemotherapy alone for previously untreated stage II or III TNBC. Details of these clinical data will be presented at the upcoming annual meeting of the European Society of Medical Oncology.
Switching the immunotherapy?
Some U.S. oncologists have been telling patients with mTNBC that the atezolizumab withdrawal is “not an issue” because the new full approval of pembrolizumab in this setting will allow prescriptions to be switched, said patient advocate Ms. Cowden.
However, experts have said that no patient who is responding to or whose condition is stable with atezolizumab should switch immunotherapies. “This is a very aggressive disease,” reminded Dr. Lustberg.
Switching the immunotherapies is complicated by the difference in the respective drugs’ companion biomarker assays used to establish the presence of PD-L1.
Dr. Lustberg explained that patients who are not responding to atezolizumab and who now want to try pembrolizumab will have to be assessed with the CTS assay.
“About 22% of the patients who are positive for the atezolizumab biomarker assay SP-142 are not going to be positive for the CTS,” she said.
In other words, about one in four patients with mTNBC who are taking atezolizumab will not qualify for treatment with pembrolizumab.
Rebecca Shatsky, MD, of the University of California, San Diego, echoed those comments in an email to this news organization – and emphatically discouraged switching off atezolizumab (and going on pembrolizumab) if a patient is having success (i.e., stable disease or positive response).
“The two groups don’t always overlap, so it isn’t an easy switch. That’s why if they are already responding, I would NOT have them stop the drug,” she said.
Not every mTNBC patient receiving – and responding to – atezolizumab has had the unfortunate experience of having their prescription canceled.
Johanna Rauhala, of San Francisco, who is a former middle-school teacher and who writes the blog Pink Stinks, has been taking atezolizumab for 2 years. She has had a partial response and now, after taking the immunotherapy in combination with chemotherapy (gemcitabine and carboplatin), has stable disease. Currently, she is taking single-agent atezolizumab..
Ms. Rauhala has been living with mTNBC for 5 years. She said in an interview that she was “very surprised and concerned” to learn about Genentech’s withdrawal of its accelerated approval. She said that at her next treatment appointment, she was “probably going to ask the oncology nurse first [about the atezolizumab withdrawal] – because they are the front line, and I will then follow-up with my doctor. But I can’t imagine that they will take away something that is working.”
Dr. Shatsky, Dr. Horton, and Dr. Lunsberg report no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Flurry of cancer drug endorsements from EU panel
The CHMP recommended the granting of a conditional marketing authorization for pralsetinib (Gavreto) for the treatment of non–small cell lung cancer (NSCLC).
Specifically, pralsetinib is indicated as monotherapy for the treatment of adult patients with rearranged during transfection (RET) fusion-positive advanced NSCLC not previously treated with a RET inhibitor.
Available as 100 mg capsules, pralsetinib is a RET-receptor tyrosine kinase inhibitor, targeting oncogenic RET fusion proteins (KIF5B-RET and CCDC6-RET).
Pralsetinib’s benefits are its objective response rate and response duration in patients with RET-fusion positive NSCLC, as observed in a pivotal phase 1/2, open-label, multi-cohort, single-arm study.
The most common side effects are anemia, increased aspartate aminotransferase, neutropenia, constipation, musculoskeletal pain, fatigue, leukopenia, increased alanine aminotransferase, and hypertension.
CHMP also recommended ripretinib (Qinlock) for the treatment of adult patients with advanced gastrointestinal stromal tumor (GIST) who have received prior treatment with three or more kinase inhibitors, including imatinib (Gleevec).
Available as 50 mg tablets, ripretinib is a protein kinase inhibitor designed to selectively block the oncogenic KIT and PDGFRA kinases by inhibiting their active conformation.
Ripretinib improved progression-free survival in patients with GIST.
The most common side effects are fatigue, alopecia, nausea, myalgia, constipation, diarrhea, palmar-plantar erythrodysesthesia syndrome, weight loss, and vomiting.
The third drug recommended for approval was zanubrutinib (Brukinsa) for the treatment of adult patients with Waldenström’s macroglobulinemia who have received at least one prior therapy or who are to receive the drug as first-line treatment (and are unsuitable for chemo-immunotherapy).
Available as 80 mg capsules, zanubrutinib is a Bruton’s tyrosine kinase inhibitor that blocks the activity of BTK, inactivating the pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
Zanubrutinib has demonstrated a clinically meaningful rate of very good partial response and/or complete response.
The most common side effects are neutropenia, thrombocytopenia, upper respiratory tract infection, hemorrhage/hematoma, rash, bruising, anemia, musculoskeletal pain, diarrhea, pneumonia, and cough.
Two new indications for already marketed drugs
CHMP also recommended an extension of the indications for two immunotherapies.
Pembrolizumab (Keytruda) will now also have an indication for use in combination with chemotherapy for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumors express PD-L1 with a CPS greater than or equal to 10 and who have not received prior chemotherapy for metastatic disease
Nivolumab (Opdivo) received an extension of indication to include use, in combination with fluoropyrimidine- and platinum-based combination chemotherapy, in the firstline treatment of adult patients with HER2 negative advanced or metastatic gastric, gastroesophageal junction, or esophageal adenocarcinoma whose tumors express PD-L1 with a combined positive score (CPS) greater than or equal to 5.
A version of this article first appeared on Medscape.com.
The CHMP recommended the granting of a conditional marketing authorization for pralsetinib (Gavreto) for the treatment of non–small cell lung cancer (NSCLC).
Specifically, pralsetinib is indicated as monotherapy for the treatment of adult patients with rearranged during transfection (RET) fusion-positive advanced NSCLC not previously treated with a RET inhibitor.
Available as 100 mg capsules, pralsetinib is a RET-receptor tyrosine kinase inhibitor, targeting oncogenic RET fusion proteins (KIF5B-RET and CCDC6-RET).
Pralsetinib’s benefits are its objective response rate and response duration in patients with RET-fusion positive NSCLC, as observed in a pivotal phase 1/2, open-label, multi-cohort, single-arm study.
The most common side effects are anemia, increased aspartate aminotransferase, neutropenia, constipation, musculoskeletal pain, fatigue, leukopenia, increased alanine aminotransferase, and hypertension.
CHMP also recommended ripretinib (Qinlock) for the treatment of adult patients with advanced gastrointestinal stromal tumor (GIST) who have received prior treatment with three or more kinase inhibitors, including imatinib (Gleevec).
Available as 50 mg tablets, ripretinib is a protein kinase inhibitor designed to selectively block the oncogenic KIT and PDGFRA kinases by inhibiting their active conformation.
Ripretinib improved progression-free survival in patients with GIST.
The most common side effects are fatigue, alopecia, nausea, myalgia, constipation, diarrhea, palmar-plantar erythrodysesthesia syndrome, weight loss, and vomiting.
The third drug recommended for approval was zanubrutinib (Brukinsa) for the treatment of adult patients with Waldenström’s macroglobulinemia who have received at least one prior therapy or who are to receive the drug as first-line treatment (and are unsuitable for chemo-immunotherapy).
Available as 80 mg capsules, zanubrutinib is a Bruton’s tyrosine kinase inhibitor that blocks the activity of BTK, inactivating the pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
Zanubrutinib has demonstrated a clinically meaningful rate of very good partial response and/or complete response.
The most common side effects are neutropenia, thrombocytopenia, upper respiratory tract infection, hemorrhage/hematoma, rash, bruising, anemia, musculoskeletal pain, diarrhea, pneumonia, and cough.
Two new indications for already marketed drugs
CHMP also recommended an extension of the indications for two immunotherapies.
Pembrolizumab (Keytruda) will now also have an indication for use in combination with chemotherapy for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumors express PD-L1 with a CPS greater than or equal to 10 and who have not received prior chemotherapy for metastatic disease
Nivolumab (Opdivo) received an extension of indication to include use, in combination with fluoropyrimidine- and platinum-based combination chemotherapy, in the firstline treatment of adult patients with HER2 negative advanced or metastatic gastric, gastroesophageal junction, or esophageal adenocarcinoma whose tumors express PD-L1 with a combined positive score (CPS) greater than or equal to 5.
A version of this article first appeared on Medscape.com.
The CHMP recommended the granting of a conditional marketing authorization for pralsetinib (Gavreto) for the treatment of non–small cell lung cancer (NSCLC).
Specifically, pralsetinib is indicated as monotherapy for the treatment of adult patients with rearranged during transfection (RET) fusion-positive advanced NSCLC not previously treated with a RET inhibitor.
Available as 100 mg capsules, pralsetinib is a RET-receptor tyrosine kinase inhibitor, targeting oncogenic RET fusion proteins (KIF5B-RET and CCDC6-RET).
Pralsetinib’s benefits are its objective response rate and response duration in patients with RET-fusion positive NSCLC, as observed in a pivotal phase 1/2, open-label, multi-cohort, single-arm study.
The most common side effects are anemia, increased aspartate aminotransferase, neutropenia, constipation, musculoskeletal pain, fatigue, leukopenia, increased alanine aminotransferase, and hypertension.
CHMP also recommended ripretinib (Qinlock) for the treatment of adult patients with advanced gastrointestinal stromal tumor (GIST) who have received prior treatment with three or more kinase inhibitors, including imatinib (Gleevec).
Available as 50 mg tablets, ripretinib is a protein kinase inhibitor designed to selectively block the oncogenic KIT and PDGFRA kinases by inhibiting their active conformation.
Ripretinib improved progression-free survival in patients with GIST.
The most common side effects are fatigue, alopecia, nausea, myalgia, constipation, diarrhea, palmar-plantar erythrodysesthesia syndrome, weight loss, and vomiting.
The third drug recommended for approval was zanubrutinib (Brukinsa) for the treatment of adult patients with Waldenström’s macroglobulinemia who have received at least one prior therapy or who are to receive the drug as first-line treatment (and are unsuitable for chemo-immunotherapy).
Available as 80 mg capsules, zanubrutinib is a Bruton’s tyrosine kinase inhibitor that blocks the activity of BTK, inactivating the pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion.
Zanubrutinib has demonstrated a clinically meaningful rate of very good partial response and/or complete response.
The most common side effects are neutropenia, thrombocytopenia, upper respiratory tract infection, hemorrhage/hematoma, rash, bruising, anemia, musculoskeletal pain, diarrhea, pneumonia, and cough.
Two new indications for already marketed drugs
CHMP also recommended an extension of the indications for two immunotherapies.
Pembrolizumab (Keytruda) will now also have an indication for use in combination with chemotherapy for the treatment of locally recurrent unresectable or metastatic triple negative breast cancer in adults whose tumors express PD-L1 with a CPS greater than or equal to 10 and who have not received prior chemotherapy for metastatic disease
Nivolumab (Opdivo) received an extension of indication to include use, in combination with fluoropyrimidine- and platinum-based combination chemotherapy, in the firstline treatment of adult patients with HER2 negative advanced or metastatic gastric, gastroesophageal junction, or esophageal adenocarcinoma whose tumors express PD-L1 with a combined positive score (CPS) greater than or equal to 5.
A version of this article first appeared on Medscape.com.
Immunotherapy for cancer patients with poor PS needs a rethink
The findings have prompted an expert to argue against the use of immunotherapy for such patients, who may have little time left and very little chance of benefiting.
“It is quite clear from clinical practice that most patients with limited PS do very poorly and do not benefit from immune check point inhibitors (ICI),” Jason Luke, MD, UPMC Hillman Cancer Center and the University of Pittsburgh, said in an email.
“So, my strong opinion is that patients should not be getting an immunotherapy just because it might not cause as many side effects as chemotherapy,” he added.
“Instead of giving an immunotherapy with little chance of success, patients and families deserve to have a direct conversation about what realistic expectations [might be] and how we as the oncology community can support them to achieve whatever their personal goals are in the time that they have left,” he emphasized.
Dr. Luke was the lead author of an editorial in which he commented on the study. Both the study and the editorial were published online in JCO Oncology Practice.
Variety of cancers
The study was conducted by Mridula Krishnan, MD, Nebraska Medicine Fred and Pamela Buffett Cancer Center, Omaha, Nebraska, and colleagues.
The team reviewed 257 patients who had been treated with either a programmed cell death protein–1 inhibitor or programmed cell death–ligand-1 inhibitor for a variety of advanced cancers. The drugs included pembrolizumab (Keytruda), nivolumab (Opdivo), atezolizumab (Tecentique), durvalumab (Imfinzi), and avelumab (Bavencio).
Most of the patients (71%) had good PS, with an Eastern Cooperative Oncology Group (ECOG) PS of 0-1 on initiation of immunotherapy; 29% of patients had poor PS, with an ECOG PS of greater than or equal to 2.
“The primary outcome was OS stratified by ECOG PS 0-1 versus ≥2,” note the authors. Across all tumor types, OS was superior for patients in the ECOG 0-1 PS group, the investigators note. The median OS was 12.6 months, compared with only 3.1 months for patients in the ECOG greater than or equal to 2 group (P < .001).
Moreover, overall response rates for patients with a poor PS were low. Only 8%, or 6 of 75 patients with an ECOG PS of greater than or equal to 2, achieved an objective response by RECIST criteria.
This compared to an overall response rate of 23% for patients with an ECOG PS of 0-1, the investigators note (P = .005).
Interestingly, the hospice referral rate for patients with a poor PS (67%) was similar to that of patients with a PS of 1-2 (61.9%), Dr. Krishnan and colleagues observe.
Those with a poor PS were more like to die in-hospital (28.6%) than were patients with a good PS (15.1%; P = .035). The authors point out that it is well known that outcomes with chemotherapy are worse among patients who experience a decline in functional reserve, owing to increased susceptibility to toxicity and complications.
“Regardless of age, patients with ECOG PS >2 usually have poor tolerability to chemotherapy, and this correlates with worse survival outcome,” they emphasize. There is as yet no clear guidance regarding the impact of PS on ICI treatment response, although “there should be,” Dr. Luke believes.
“In a patient with declining performance status, especially ECOG PS 3-4 but potentially 2 as well, there is little likelihood that the functional and immune reserve of the patient will be adequate to mount a robust antitumor response,” he elaborated.
“It’s not impossible, but trying for it should not come at the expense of engaging about end-of-life care and maximizing the palliative opportunities that many only have a short window of time in which to pursue,” he added.
Again, Dr. Luke strongly believes that just giving an ICI without engaging in a frank conversation with the patient and their families – which happens all too often, he feels – is absolutely not the way to go when treating patients with a poor PS and little time left.
“Patients and families might be better served by having a more direct and frank conversation about what the likelihood [is] that ICI therapy will actually do,” Dr. Luke stressed.
In their editorial, Dr. Luke and colleagues write: “Overall, we as an oncology community need to improve our communication with patients regarding goals of care and end-of-life considerations as opposed to reflexive treatment initiation,” he writes.
“Our duty, first and foremost, should focus on the person sitting in front of us – taking a step back may be the best way to move forward with compassionate care,” they add.
The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings have prompted an expert to argue against the use of immunotherapy for such patients, who may have little time left and very little chance of benefiting.
“It is quite clear from clinical practice that most patients with limited PS do very poorly and do not benefit from immune check point inhibitors (ICI),” Jason Luke, MD, UPMC Hillman Cancer Center and the University of Pittsburgh, said in an email.
“So, my strong opinion is that patients should not be getting an immunotherapy just because it might not cause as many side effects as chemotherapy,” he added.
“Instead of giving an immunotherapy with little chance of success, patients and families deserve to have a direct conversation about what realistic expectations [might be] and how we as the oncology community can support them to achieve whatever their personal goals are in the time that they have left,” he emphasized.
Dr. Luke was the lead author of an editorial in which he commented on the study. Both the study and the editorial were published online in JCO Oncology Practice.
Variety of cancers
The study was conducted by Mridula Krishnan, MD, Nebraska Medicine Fred and Pamela Buffett Cancer Center, Omaha, Nebraska, and colleagues.
The team reviewed 257 patients who had been treated with either a programmed cell death protein–1 inhibitor or programmed cell death–ligand-1 inhibitor for a variety of advanced cancers. The drugs included pembrolizumab (Keytruda), nivolumab (Opdivo), atezolizumab (Tecentique), durvalumab (Imfinzi), and avelumab (Bavencio).
Most of the patients (71%) had good PS, with an Eastern Cooperative Oncology Group (ECOG) PS of 0-1 on initiation of immunotherapy; 29% of patients had poor PS, with an ECOG PS of greater than or equal to 2.
“The primary outcome was OS stratified by ECOG PS 0-1 versus ≥2,” note the authors. Across all tumor types, OS was superior for patients in the ECOG 0-1 PS group, the investigators note. The median OS was 12.6 months, compared with only 3.1 months for patients in the ECOG greater than or equal to 2 group (P < .001).
Moreover, overall response rates for patients with a poor PS were low. Only 8%, or 6 of 75 patients with an ECOG PS of greater than or equal to 2, achieved an objective response by RECIST criteria.
This compared to an overall response rate of 23% for patients with an ECOG PS of 0-1, the investigators note (P = .005).
Interestingly, the hospice referral rate for patients with a poor PS (67%) was similar to that of patients with a PS of 1-2 (61.9%), Dr. Krishnan and colleagues observe.
Those with a poor PS were more like to die in-hospital (28.6%) than were patients with a good PS (15.1%; P = .035). The authors point out that it is well known that outcomes with chemotherapy are worse among patients who experience a decline in functional reserve, owing to increased susceptibility to toxicity and complications.
“Regardless of age, patients with ECOG PS >2 usually have poor tolerability to chemotherapy, and this correlates with worse survival outcome,” they emphasize. There is as yet no clear guidance regarding the impact of PS on ICI treatment response, although “there should be,” Dr. Luke believes.
“In a patient with declining performance status, especially ECOG PS 3-4 but potentially 2 as well, there is little likelihood that the functional and immune reserve of the patient will be adequate to mount a robust antitumor response,” he elaborated.
“It’s not impossible, but trying for it should not come at the expense of engaging about end-of-life care and maximizing the palliative opportunities that many only have a short window of time in which to pursue,” he added.
Again, Dr. Luke strongly believes that just giving an ICI without engaging in a frank conversation with the patient and their families – which happens all too often, he feels – is absolutely not the way to go when treating patients with a poor PS and little time left.
“Patients and families might be better served by having a more direct and frank conversation about what the likelihood [is] that ICI therapy will actually do,” Dr. Luke stressed.
In their editorial, Dr. Luke and colleagues write: “Overall, we as an oncology community need to improve our communication with patients regarding goals of care and end-of-life considerations as opposed to reflexive treatment initiation,” he writes.
“Our duty, first and foremost, should focus on the person sitting in front of us – taking a step back may be the best way to move forward with compassionate care,” they add.
The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The findings have prompted an expert to argue against the use of immunotherapy for such patients, who may have little time left and very little chance of benefiting.
“It is quite clear from clinical practice that most patients with limited PS do very poorly and do not benefit from immune check point inhibitors (ICI),” Jason Luke, MD, UPMC Hillman Cancer Center and the University of Pittsburgh, said in an email.
“So, my strong opinion is that patients should not be getting an immunotherapy just because it might not cause as many side effects as chemotherapy,” he added.
“Instead of giving an immunotherapy with little chance of success, patients and families deserve to have a direct conversation about what realistic expectations [might be] and how we as the oncology community can support them to achieve whatever their personal goals are in the time that they have left,” he emphasized.
Dr. Luke was the lead author of an editorial in which he commented on the study. Both the study and the editorial were published online in JCO Oncology Practice.
Variety of cancers
The study was conducted by Mridula Krishnan, MD, Nebraska Medicine Fred and Pamela Buffett Cancer Center, Omaha, Nebraska, and colleagues.
The team reviewed 257 patients who had been treated with either a programmed cell death protein–1 inhibitor or programmed cell death–ligand-1 inhibitor for a variety of advanced cancers. The drugs included pembrolizumab (Keytruda), nivolumab (Opdivo), atezolizumab (Tecentique), durvalumab (Imfinzi), and avelumab (Bavencio).
Most of the patients (71%) had good PS, with an Eastern Cooperative Oncology Group (ECOG) PS of 0-1 on initiation of immunotherapy; 29% of patients had poor PS, with an ECOG PS of greater than or equal to 2.
“The primary outcome was OS stratified by ECOG PS 0-1 versus ≥2,” note the authors. Across all tumor types, OS was superior for patients in the ECOG 0-1 PS group, the investigators note. The median OS was 12.6 months, compared with only 3.1 months for patients in the ECOG greater than or equal to 2 group (P < .001).
Moreover, overall response rates for patients with a poor PS were low. Only 8%, or 6 of 75 patients with an ECOG PS of greater than or equal to 2, achieved an objective response by RECIST criteria.
This compared to an overall response rate of 23% for patients with an ECOG PS of 0-1, the investigators note (P = .005).
Interestingly, the hospice referral rate for patients with a poor PS (67%) was similar to that of patients with a PS of 1-2 (61.9%), Dr. Krishnan and colleagues observe.
Those with a poor PS were more like to die in-hospital (28.6%) than were patients with a good PS (15.1%; P = .035). The authors point out that it is well known that outcomes with chemotherapy are worse among patients who experience a decline in functional reserve, owing to increased susceptibility to toxicity and complications.
“Regardless of age, patients with ECOG PS >2 usually have poor tolerability to chemotherapy, and this correlates with worse survival outcome,” they emphasize. There is as yet no clear guidance regarding the impact of PS on ICI treatment response, although “there should be,” Dr. Luke believes.
“In a patient with declining performance status, especially ECOG PS 3-4 but potentially 2 as well, there is little likelihood that the functional and immune reserve of the patient will be adequate to mount a robust antitumor response,” he elaborated.
“It’s not impossible, but trying for it should not come at the expense of engaging about end-of-life care and maximizing the palliative opportunities that many only have a short window of time in which to pursue,” he added.
Again, Dr. Luke strongly believes that just giving an ICI without engaging in a frank conversation with the patient and their families – which happens all too often, he feels – is absolutely not the way to go when treating patients with a poor PS and little time left.
“Patients and families might be better served by having a more direct and frank conversation about what the likelihood [is] that ICI therapy will actually do,” Dr. Luke stressed.
In their editorial, Dr. Luke and colleagues write: “Overall, we as an oncology community need to improve our communication with patients regarding goals of care and end-of-life considerations as opposed to reflexive treatment initiation,” he writes.
“Our duty, first and foremost, should focus on the person sitting in front of us – taking a step back may be the best way to move forward with compassionate care,” they add.
The authors and editorialists have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
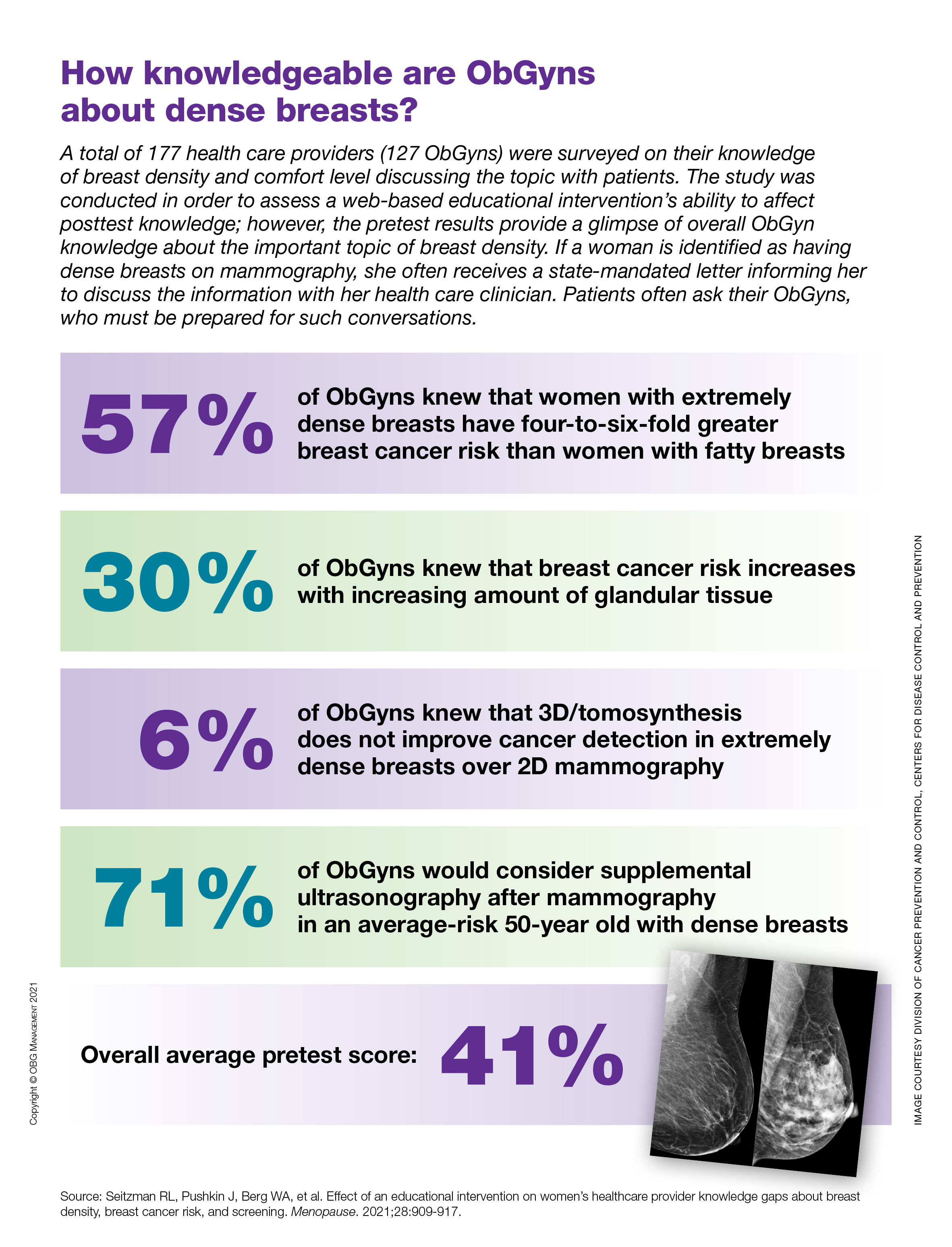
How knowledgeable are ObGyns about dense breasts?
Breast density associated with increased invasive breast cancer risk after age 65
The findings, based on an analysis of Breast Cancer Surveillance Consortium data from Jan. 1, 1996, to Dec. 31, 2012, have potential implications for screening mammography decisions in older women – particularly those aged 75 years and older, for whom screening guidance is limited by a paucity of data, Dejana Braithwaite, PhD, of the University of Florida Health Cancer Center, Gainesville, and colleagues reported in JAMA Network Open.
The investigators analyzed 221,714 screening mammograms from 193,787 women aged 65 and older in the United States. About 65% of the mammograms were from women aged 65-74 years and about 35% were from women aged 75 years and older, who comprised 38% of the study population.
During a mean follow-up of 6.3 years, 5,069 invasive breast cancers were diagnosed, the authors noted.
The 5-year cumulative incidence of invasive breast cancer increased in tandem with increasing breast density among those aged 65-74 years and among those aged 75 and older: The cumulative incidence per 1,000 women aged 65-74 years was 11.3 for those with almost entirely fatty breasts, 17.2 for those with scattered fibroglandular densities, and 23.7 for those with extremely or heterogeneously dense breasts. The cumulative incidence rates for those aged 75 years and older were 13.5, 18.4, and 22.5 per 1,000 women, respectively, they found.
Extreme or heterogeneous breast density was associated with increased risk of breast cancer, compared with scattered fibroglandular breast density, in both age categories (hazard ratios, 1.39 and 1.23 for those aged 65-74 years and 75 years and older, respectively), whereas the risk of invasive breast cancer was about 30% lower among women with almost entirely fatty breasts, compared with women with scattered fibroglandular breast density (HRs, 0.66 and 0.73 for the 65-74 and 75-plus age groups, respectively).
The associations between breast density and breast cancer were statistically significant after adjustment for body mass index (BMI) and other risk factors.
However, no significant differences were seen between breast density and breast cancer risk based on BMI, noted the authors, who investigated this potential association as part of their effort to identify subpopulations of older women who might benefit from screening, “especially because the U.S. Preventive Service Task Force guidelines state that the current evidence is considered insufficient to recommend routine breast cancer screening for women aged 75 years or older,” they wrote.
Further, although breast density is important in risk assessment and could be evaluated in older women, some risk prediction models exclude women aged 75 or older in risk assessments, they noted, adding that this is concerning given “the aging of the population in the U.S. and worldwide.”
“The positive associations found in this study between breast density and breast cancer among women aged 75 years or older suggest that breast density and life expectancy should be considered together when discussing the potential benefits and harms of continued screening mammography in this population,” they concluded.
The new findings supplement those from prior studies and highlight “the intersection of ... two subjects that have garnered considerable lay public, healthy policy, and academic interest” in recent years: screening mammography in older women and the risk of breast cancer caused by breast density in older women, Catherine M. Tuite, MD, of ChristianaCare Helen F. Graham Cancer Center and Research Institute, Newark, Del., wrote in a commentary published with the study.
“Although there is a linear association between age and mammographic density, age is not a perfect surrogate for the latter, and there are meaningful numbers of older women with mammographically dense breast tissue,” she said, noting that a 75-year-old woman in the United States has a life expectancy of 12-14 additional years, and that “continuation of screening mammography in healthy women aged 75 years or older may offer a substantial opportunity to avoid morbidity and mortality from breast cancer in this age group.”
However, overdiagnosis also remains a concern, she said.
“Breast density and age are only a few of the many factors currently under investigation in the drive toward risk-based or personalized breast cancer screening,” she wrote. “We must remain cautious in the application of restrictive screening for women of any age with supposedly lower than average risk ... ultimately, the decision of when to stop screening is personal, and each woman deserves the agency to weigh her own wishes, values, and life experiences with an accurate and unbiased discussion of risks and benefits of screening mammography in making that decision.”
This study was supported by grants from the National Cancer Institute and the Breast Cancer Surveillance Consortium. Cancer and vital status data collection was supported in part by several state public health departments and cancer registries. Dr. Advani and Dr. Tuite each reported having no disclosures.
The findings, based on an analysis of Breast Cancer Surveillance Consortium data from Jan. 1, 1996, to Dec. 31, 2012, have potential implications for screening mammography decisions in older women – particularly those aged 75 years and older, for whom screening guidance is limited by a paucity of data, Dejana Braithwaite, PhD, of the University of Florida Health Cancer Center, Gainesville, and colleagues reported in JAMA Network Open.
The investigators analyzed 221,714 screening mammograms from 193,787 women aged 65 and older in the United States. About 65% of the mammograms were from women aged 65-74 years and about 35% were from women aged 75 years and older, who comprised 38% of the study population.
During a mean follow-up of 6.3 years, 5,069 invasive breast cancers were diagnosed, the authors noted.
The 5-year cumulative incidence of invasive breast cancer increased in tandem with increasing breast density among those aged 65-74 years and among those aged 75 and older: The cumulative incidence per 1,000 women aged 65-74 years was 11.3 for those with almost entirely fatty breasts, 17.2 for those with scattered fibroglandular densities, and 23.7 for those with extremely or heterogeneously dense breasts. The cumulative incidence rates for those aged 75 years and older were 13.5, 18.4, and 22.5 per 1,000 women, respectively, they found.
Extreme or heterogeneous breast density was associated with increased risk of breast cancer, compared with scattered fibroglandular breast density, in both age categories (hazard ratios, 1.39 and 1.23 for those aged 65-74 years and 75 years and older, respectively), whereas the risk of invasive breast cancer was about 30% lower among women with almost entirely fatty breasts, compared with women with scattered fibroglandular breast density (HRs, 0.66 and 0.73 for the 65-74 and 75-plus age groups, respectively).
The associations between breast density and breast cancer were statistically significant after adjustment for body mass index (BMI) and other risk factors.
However, no significant differences were seen between breast density and breast cancer risk based on BMI, noted the authors, who investigated this potential association as part of their effort to identify subpopulations of older women who might benefit from screening, “especially because the U.S. Preventive Service Task Force guidelines state that the current evidence is considered insufficient to recommend routine breast cancer screening for women aged 75 years or older,” they wrote.
Further, although breast density is important in risk assessment and could be evaluated in older women, some risk prediction models exclude women aged 75 or older in risk assessments, they noted, adding that this is concerning given “the aging of the population in the U.S. and worldwide.”
“The positive associations found in this study between breast density and breast cancer among women aged 75 years or older suggest that breast density and life expectancy should be considered together when discussing the potential benefits and harms of continued screening mammography in this population,” they concluded.
The new findings supplement those from prior studies and highlight “the intersection of ... two subjects that have garnered considerable lay public, healthy policy, and academic interest” in recent years: screening mammography in older women and the risk of breast cancer caused by breast density in older women, Catherine M. Tuite, MD, of ChristianaCare Helen F. Graham Cancer Center and Research Institute, Newark, Del., wrote in a commentary published with the study.
“Although there is a linear association between age and mammographic density, age is not a perfect surrogate for the latter, and there are meaningful numbers of older women with mammographically dense breast tissue,” she said, noting that a 75-year-old woman in the United States has a life expectancy of 12-14 additional years, and that “continuation of screening mammography in healthy women aged 75 years or older may offer a substantial opportunity to avoid morbidity and mortality from breast cancer in this age group.”
However, overdiagnosis also remains a concern, she said.
“Breast density and age are only a few of the many factors currently under investigation in the drive toward risk-based or personalized breast cancer screening,” she wrote. “We must remain cautious in the application of restrictive screening for women of any age with supposedly lower than average risk ... ultimately, the decision of when to stop screening is personal, and each woman deserves the agency to weigh her own wishes, values, and life experiences with an accurate and unbiased discussion of risks and benefits of screening mammography in making that decision.”
This study was supported by grants from the National Cancer Institute and the Breast Cancer Surveillance Consortium. Cancer and vital status data collection was supported in part by several state public health departments and cancer registries. Dr. Advani and Dr. Tuite each reported having no disclosures.
The findings, based on an analysis of Breast Cancer Surveillance Consortium data from Jan. 1, 1996, to Dec. 31, 2012, have potential implications for screening mammography decisions in older women – particularly those aged 75 years and older, for whom screening guidance is limited by a paucity of data, Dejana Braithwaite, PhD, of the University of Florida Health Cancer Center, Gainesville, and colleagues reported in JAMA Network Open.
The investigators analyzed 221,714 screening mammograms from 193,787 women aged 65 and older in the United States. About 65% of the mammograms were from women aged 65-74 years and about 35% were from women aged 75 years and older, who comprised 38% of the study population.
During a mean follow-up of 6.3 years, 5,069 invasive breast cancers were diagnosed, the authors noted.
The 5-year cumulative incidence of invasive breast cancer increased in tandem with increasing breast density among those aged 65-74 years and among those aged 75 and older: The cumulative incidence per 1,000 women aged 65-74 years was 11.3 for those with almost entirely fatty breasts, 17.2 for those with scattered fibroglandular densities, and 23.7 for those with extremely or heterogeneously dense breasts. The cumulative incidence rates for those aged 75 years and older were 13.5, 18.4, and 22.5 per 1,000 women, respectively, they found.
Extreme or heterogeneous breast density was associated with increased risk of breast cancer, compared with scattered fibroglandular breast density, in both age categories (hazard ratios, 1.39 and 1.23 for those aged 65-74 years and 75 years and older, respectively), whereas the risk of invasive breast cancer was about 30% lower among women with almost entirely fatty breasts, compared with women with scattered fibroglandular breast density (HRs, 0.66 and 0.73 for the 65-74 and 75-plus age groups, respectively).
The associations between breast density and breast cancer were statistically significant after adjustment for body mass index (BMI) and other risk factors.
However, no significant differences were seen between breast density and breast cancer risk based on BMI, noted the authors, who investigated this potential association as part of their effort to identify subpopulations of older women who might benefit from screening, “especially because the U.S. Preventive Service Task Force guidelines state that the current evidence is considered insufficient to recommend routine breast cancer screening for women aged 75 years or older,” they wrote.
Further, although breast density is important in risk assessment and could be evaluated in older women, some risk prediction models exclude women aged 75 or older in risk assessments, they noted, adding that this is concerning given “the aging of the population in the U.S. and worldwide.”
“The positive associations found in this study between breast density and breast cancer among women aged 75 years or older suggest that breast density and life expectancy should be considered together when discussing the potential benefits and harms of continued screening mammography in this population,” they concluded.
The new findings supplement those from prior studies and highlight “the intersection of ... two subjects that have garnered considerable lay public, healthy policy, and academic interest” in recent years: screening mammography in older women and the risk of breast cancer caused by breast density in older women, Catherine M. Tuite, MD, of ChristianaCare Helen F. Graham Cancer Center and Research Institute, Newark, Del., wrote in a commentary published with the study.
“Although there is a linear association between age and mammographic density, age is not a perfect surrogate for the latter, and there are meaningful numbers of older women with mammographically dense breast tissue,” she said, noting that a 75-year-old woman in the United States has a life expectancy of 12-14 additional years, and that “continuation of screening mammography in healthy women aged 75 years or older may offer a substantial opportunity to avoid morbidity and mortality from breast cancer in this age group.”
However, overdiagnosis also remains a concern, she said.
“Breast density and age are only a few of the many factors currently under investigation in the drive toward risk-based or personalized breast cancer screening,” she wrote. “We must remain cautious in the application of restrictive screening for women of any age with supposedly lower than average risk ... ultimately, the decision of when to stop screening is personal, and each woman deserves the agency to weigh her own wishes, values, and life experiences with an accurate and unbiased discussion of risks and benefits of screening mammography in making that decision.”
This study was supported by grants from the National Cancer Institute and the Breast Cancer Surveillance Consortium. Cancer and vital status data collection was supported in part by several state public health departments and cancer registries. Dr. Advani and Dr. Tuite each reported having no disclosures.
FROM JAMA NETWORK OPEN
Antipsychotics tied to increased breast cancer risk
Use of antipsychotics that increase prolactin levels is significantly associated with an increased risk for breast cancer in women with schizophrenia, new research suggests. However, at least one expert says that, at this point, clinical implications are premature.

Investigators compared data from Finnish nationwide registers on more than 30,000 women diagnosed with schizophrenia. Of those patients, 1,069 were diagnosed with breast cancer. Results showed that long-term exposure to prolactin-increasing antipsychotics was associated with a 56% increased risk of developing breast cancer in comparison with exposure of short duration. No significant association was found with cumulative exposure to prolactin-sparing antipsychotics.
“In case of planning for long-term antipsychotic [therapy], prefer non–prolactin-raising antipsychotics in females and inform patients about a potential risk to allow for informed shared decision-making,” study coauthor Christoph U. Correll, MD, professor of psychiatry and molecular medicine at Hofstra University, Hempstead, N.Y., told this news organization.
“ he said.
The study was published online Aug. 30, 2021, in The Lancet.
A ‘relevant contribution’
Breast cancer is 25% more prevalent among women with schizophrenia than among women in the general population. Antipsychotics have long been suspected as a potential culprit, but research results have been inconsistent, said Dr. Correll.
In addition, high concentrations of prolactin are associated with a higher risk of developing breast cancer, but most previous research did not distinguish between antipsychotics that increased prolactin levels those that did not.
Dr. Correll and colleagues “wanted to add to this literature by utilizing a generalizable nationwide sample with a sufficient large number of patients and sufficiently long follow-up to address the clinically very relevant question whether antipsychotic use could increase the risk of breast cancer.”
They also believed that grouping antipsychotics into prolactin-raising and non–prolactin-raising agents would be “a relevant contribution.”
The researchers drew on data from several large Finnish databases to conduct a nested case-control study of 30,785 women aged at least16 years who were diagnosed with schizophrenia between 1972 and 2014.
Of these patients, 1,069 received an initial diagnosis of invasive breast cancer (after being diagnosed with schizophrenia) between 2000 and 2017. These case patients were compared to 5,339 matched control patients. The mean age of the case patients and the control patients was 62 years. The mean time since initial diagnosis of schizophrenia was 24 years.
Antipsychotic use was divided into three periods: less than 1 year, 1-4 years, and ≥5 years. Antipsychotics were further divided into prolactin-increasing or prolactin-sparing drugs (for example, clozapine, quetiapine, or aripiprazole). Breast cancer was divided into either lobular or ductal adenocarcinoma.
In their statistical analyses, the researchers adjusted for an array of covariates, including previous diagnoses of other medical conditions, drugs that may modify the risk for breast cancer (for example, beta-blockers, calcium channel blockers, spironolactone, loop diuretics, and statins), substance misuse, suicide attempt, parity, and use of hormone replacement therapy (HRT).
‘Clinically meaningful’ risk
Ductal adenocarcinoma was more common than lobular adenocarcinoma (73% vs. 20% among case patients). A higher proportion of case patients used cardiovascular medications and HRT, compared with control patients.
A higher proportion of case patients had used prolactin-increasing antipsychotics for at least 5 years, compared with control patients (71.4% vs. 64.3%; adjusted odds ratio, 1.56; 95% CI, 1.27-1.92; P < .0001) in comparison with minimal exposure (<1 year) to prolactin-increasing antipsychotics.
On the other hand, a similar proportion of case patients and control patients used prolactin-sparing antipsychotics for at least 5 years (8.3 vs. 8.2%; aOR, 1.19; 95% CI, 0.90-1.58); the OR of 1.19 was not deemed significant.
Although exposure of ≥5 years to prolactin-increasing antipsychotics was associated with an increased risk for both types of adenocarcinoma, the risk was higher for lobular than for ductal disease (aOR, 2.36; 95% CI, 1.46-3.82 vs. aOR, 1.42; 95% CI, 1.12-1.80).
“Conservatively, if we subtract the 19% nonsignificantly increased odds with prolactin-sparing antipsychotics from the 56% significantly increased odds with prolactin-increasing antipsychotics, we obtain a 37% relative increase in odds,” the authors noted.
“Using a lifetime incidence of breast cancer in women in the general population of about 12%, with a somewhat higher lifetime incidence in patients with schizophrenia than the general population, this difference between prolactin-increasing versus prolactin-sparing antipsychotics in breast cancer risk upon exposure of 5 or more years would correspond to about a 4% (37% x 12%) increase in absolute breast cancer odds with prolactin-increasing antipsychotic treatment” – a difference the authors call “clinically meaningful.”
Correll noted that although the study was conducted in a Finnish population, the findings are generalizable to other populations.
Clinical implications premature?
Commenting on the study, Anton Pottegård, MScPharm, PhD, DMSc, professor of pharmacoepidemiology, department of public health, University of Southern Denmark, Odense, expressed concern that “this new study is fairly aggressive in its recommendation [that] we need to pay attention to hyperprolactinemia, as this seems to cause breast cancer.”
Dr. Pottegård, who is also the head of research, Hospital Pharmacy Funen, Odense University Hospital, who was not involved with the study, said he does not “think that the full body of the literature supports such a direct conclusion and/or direct inference to clinical practice.”
Although “this is an important study to further this work, I do not think we are at a place (yet) where it should lead to different action from clinicians,” Dr. Pottegård cautioned.
Also commenting on the study, Mary Seeman, MDCM, DSc, professor emeritus of neurosciences and clinical translation, department of psychiatry, University of Toronto, called the question of whether prolactin-increasing antipsychotics increase breast cancer risk “very complicated because the incidence of breast cancer ... is higher in women with schizophrenia than in other women.”
Dr. Seeman, who was not involved with the study, pointed to other reasons for the increased risk, including higher rates of obesity, substance abuse, cigarette smoking, stress, and sedentary behavior, all of which raise prolactin levels. Additionally, “protective factors such as pregnancies and breastfeeding are less frequent in women with schizophrenia than in their peers.” Women with schizophrenia also “tend not to do breast screening, see their doctors less often, follow doctors’ orders less rigorously, and obtain treatment less often.”
The take-home message “is to prescribe prolactin-sparing medication to women if at all possible – but until we know more, that is good advice, although not always possible because the illness for which the antipsychotics are prescribed may not respond to those particular medications,” Dr. Seeman said.
The study was funded by the Finnish Ministry of Social Affairs and Health through the developmental fund for Niuvanniemi Hospital. Funding was also provided to individual researchers by the Academy of Finland, the Finnish Medical Foundation, and the Emil Aaltonen foundation. Dr. Correll has been a consultant or advisor to or has received honoraria from numerous companies. He has provided expert testimony for Janssen and Otsuka; received royalties from UpToDate and is a stock option holder of LB Pharma; served on a data safety monitoring board for Lundbeck, Rovi, Supernus, and Teva; and received grant support from Janssen and Takeda. Dr. Pottegård and Dr. Seeman disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Use of antipsychotics that increase prolactin levels is significantly associated with an increased risk for breast cancer in women with schizophrenia, new research suggests. However, at least one expert says that, at this point, clinical implications are premature.
Investigators compared data from Finnish nationwide registers on more than 30,000 women diagnosed with schizophrenia. Of those patients, 1,069 were diagnosed with breast cancer. Results showed that long-term exposure to prolactin-increasing antipsychotics was associated with a 56% increased risk of developing breast cancer in comparison with exposure of short duration. No significant association was found with cumulative exposure to prolactin-sparing antipsychotics.
“In case of planning for long-term antipsychotic [therapy], prefer non–prolactin-raising antipsychotics in females and inform patients about a potential risk to allow for informed shared decision-making,” study coauthor Christoph U. Correll, MD, professor of psychiatry and molecular medicine at Hofstra University, Hempstead, N.Y., told this news organization.
“ he said.
The study was published online Aug. 30, 2021, in The Lancet.
A ‘relevant contribution’
Breast cancer is 25% more prevalent among women with schizophrenia than among women in the general population. Antipsychotics have long been suspected as a potential culprit, but research results have been inconsistent, said Dr. Correll.
In addition, high concentrations of prolactin are associated with a higher risk of developing breast cancer, but most previous research did not distinguish between antipsychotics that increased prolactin levels those that did not.
Dr. Correll and colleagues “wanted to add to this literature by utilizing a generalizable nationwide sample with a sufficient large number of patients and sufficiently long follow-up to address the clinically very relevant question whether antipsychotic use could increase the risk of breast cancer.”
They also believed that grouping antipsychotics into prolactin-raising and non–prolactin-raising agents would be “a relevant contribution.”
The researchers drew on data from several large Finnish databases to conduct a nested case-control study of 30,785 women aged at least16 years who were diagnosed with schizophrenia between 1972 and 2014.
Of these patients, 1,069 received an initial diagnosis of invasive breast cancer (after being diagnosed with schizophrenia) between 2000 and 2017. These case patients were compared to 5,339 matched control patients. The mean age of the case patients and the control patients was 62 years. The mean time since initial diagnosis of schizophrenia was 24 years.
Antipsychotic use was divided into three periods: less than 1 year, 1-4 years, and ≥5 years. Antipsychotics were further divided into prolactin-increasing or prolactin-sparing drugs (for example, clozapine, quetiapine, or aripiprazole). Breast cancer was divided into either lobular or ductal adenocarcinoma.
In their statistical analyses, the researchers adjusted for an array of covariates, including previous diagnoses of other medical conditions, drugs that may modify the risk for breast cancer (for example, beta-blockers, calcium channel blockers, spironolactone, loop diuretics, and statins), substance misuse, suicide attempt, parity, and use of hormone replacement therapy (HRT).
‘Clinically meaningful’ risk
Ductal adenocarcinoma was more common than lobular adenocarcinoma (73% vs. 20% among case patients). A higher proportion of case patients used cardiovascular medications and HRT, compared with control patients.
A higher proportion of case patients had used prolactin-increasing antipsychotics for at least 5 years, compared with control patients (71.4% vs. 64.3%; adjusted odds ratio, 1.56; 95% CI, 1.27-1.92; P < .0001) in comparison with minimal exposure (<1 year) to prolactin-increasing antipsychotics.
On the other hand, a similar proportion of case patients and control patients used prolactin-sparing antipsychotics for at least 5 years (8.3 vs. 8.2%; aOR, 1.19; 95% CI, 0.90-1.58); the OR of 1.19 was not deemed significant.
Although exposure of ≥5 years to prolactin-increasing antipsychotics was associated with an increased risk for both types of adenocarcinoma, the risk was higher for lobular than for ductal disease (aOR, 2.36; 95% CI, 1.46-3.82 vs. aOR, 1.42; 95% CI, 1.12-1.80).
“Conservatively, if we subtract the 19% nonsignificantly increased odds with prolactin-sparing antipsychotics from the 56% significantly increased odds with prolactin-increasing antipsychotics, we obtain a 37% relative increase in odds,” the authors noted.
“Using a lifetime incidence of breast cancer in women in the general population of about 12%, with a somewhat higher lifetime incidence in patients with schizophrenia than the general population, this difference between prolactin-increasing versus prolactin-sparing antipsychotics in breast cancer risk upon exposure of 5 or more years would correspond to about a 4% (37% x 12%) increase in absolute breast cancer odds with prolactin-increasing antipsychotic treatment” – a difference the authors call “clinically meaningful.”
Correll noted that although the study was conducted in a Finnish population, the findings are generalizable to other populations.
Clinical implications premature?
Commenting on the study, Anton Pottegård, MScPharm, PhD, DMSc, professor of pharmacoepidemiology, department of public health, University of Southern Denmark, Odense, expressed concern that “this new study is fairly aggressive in its recommendation [that] we need to pay attention to hyperprolactinemia, as this seems to cause breast cancer.”
Dr. Pottegård, who is also the head of research, Hospital Pharmacy Funen, Odense University Hospital, who was not involved with the study, said he does not “think that the full body of the literature supports such a direct conclusion and/or direct inference to clinical practice.”
Although “this is an important study to further this work, I do not think we are at a place (yet) where it should lead to different action from clinicians,” Dr. Pottegård cautioned.
Also commenting on the study, Mary Seeman, MDCM, DSc, professor emeritus of neurosciences and clinical translation, department of psychiatry, University of Toronto, called the question of whether prolactin-increasing antipsychotics increase breast cancer risk “very complicated because the incidence of breast cancer ... is higher in women with schizophrenia than in other women.”
Dr. Seeman, who was not involved with the study, pointed to other reasons for the increased risk, including higher rates of obesity, substance abuse, cigarette smoking, stress, and sedentary behavior, all of which raise prolactin levels. Additionally, “protective factors such as pregnancies and breastfeeding are less frequent in women with schizophrenia than in their peers.” Women with schizophrenia also “tend not to do breast screening, see their doctors less often, follow doctors’ orders less rigorously, and obtain treatment less often.”
The take-home message “is to prescribe prolactin-sparing medication to women if at all possible – but until we know more, that is good advice, although not always possible because the illness for which the antipsychotics are prescribed may not respond to those particular medications,” Dr. Seeman said.
The study was funded by the Finnish Ministry of Social Affairs and Health through the developmental fund for Niuvanniemi Hospital. Funding was also provided to individual researchers by the Academy of Finland, the Finnish Medical Foundation, and the Emil Aaltonen foundation. Dr. Correll has been a consultant or advisor to or has received honoraria from numerous companies. He has provided expert testimony for Janssen and Otsuka; received royalties from UpToDate and is a stock option holder of LB Pharma; served on a data safety monitoring board for Lundbeck, Rovi, Supernus, and Teva; and received grant support from Janssen and Takeda. Dr. Pottegård and Dr. Seeman disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Use of antipsychotics that increase prolactin levels is significantly associated with an increased risk for breast cancer in women with schizophrenia, new research suggests. However, at least one expert says that, at this point, clinical implications are premature.
Investigators compared data from Finnish nationwide registers on more than 30,000 women diagnosed with schizophrenia. Of those patients, 1,069 were diagnosed with breast cancer. Results showed that long-term exposure to prolactin-increasing antipsychotics was associated with a 56% increased risk of developing breast cancer in comparison with exposure of short duration. No significant association was found with cumulative exposure to prolactin-sparing antipsychotics.
“In case of planning for long-term antipsychotic [therapy], prefer non–prolactin-raising antipsychotics in females and inform patients about a potential risk to allow for informed shared decision-making,” study coauthor Christoph U. Correll, MD, professor of psychiatry and molecular medicine at Hofstra University, Hempstead, N.Y., told this news organization.
“ he said.
The study was published online Aug. 30, 2021, in The Lancet.
A ‘relevant contribution’
Breast cancer is 25% more prevalent among women with schizophrenia than among women in the general population. Antipsychotics have long been suspected as a potential culprit, but research results have been inconsistent, said Dr. Correll.
In addition, high concentrations of prolactin are associated with a higher risk of developing breast cancer, but most previous research did not distinguish between antipsychotics that increased prolactin levels those that did not.
Dr. Correll and colleagues “wanted to add to this literature by utilizing a generalizable nationwide sample with a sufficient large number of patients and sufficiently long follow-up to address the clinically very relevant question whether antipsychotic use could increase the risk of breast cancer.”
They also believed that grouping antipsychotics into prolactin-raising and non–prolactin-raising agents would be “a relevant contribution.”
The researchers drew on data from several large Finnish databases to conduct a nested case-control study of 30,785 women aged at least16 years who were diagnosed with schizophrenia between 1972 and 2014.
Of these patients, 1,069 received an initial diagnosis of invasive breast cancer (after being diagnosed with schizophrenia) between 2000 and 2017. These case patients were compared to 5,339 matched control patients. The mean age of the case patients and the control patients was 62 years. The mean time since initial diagnosis of schizophrenia was 24 years.
Antipsychotic use was divided into three periods: less than 1 year, 1-4 years, and ≥5 years. Antipsychotics were further divided into prolactin-increasing or prolactin-sparing drugs (for example, clozapine, quetiapine, or aripiprazole). Breast cancer was divided into either lobular or ductal adenocarcinoma.
In their statistical analyses, the researchers adjusted for an array of covariates, including previous diagnoses of other medical conditions, drugs that may modify the risk for breast cancer (for example, beta-blockers, calcium channel blockers, spironolactone, loop diuretics, and statins), substance misuse, suicide attempt, parity, and use of hormone replacement therapy (HRT).
‘Clinically meaningful’ risk
Ductal adenocarcinoma was more common than lobular adenocarcinoma (73% vs. 20% among case patients). A higher proportion of case patients used cardiovascular medications and HRT, compared with control patients.
A higher proportion of case patients had used prolactin-increasing antipsychotics for at least 5 years, compared with control patients (71.4% vs. 64.3%; adjusted odds ratio, 1.56; 95% CI, 1.27-1.92; P < .0001) in comparison with minimal exposure (<1 year) to prolactin-increasing antipsychotics.
On the other hand, a similar proportion of case patients and control patients used prolactin-sparing antipsychotics for at least 5 years (8.3 vs. 8.2%; aOR, 1.19; 95% CI, 0.90-1.58); the OR of 1.19 was not deemed significant.
Although exposure of ≥5 years to prolactin-increasing antipsychotics was associated with an increased risk for both types of adenocarcinoma, the risk was higher for lobular than for ductal disease (aOR, 2.36; 95% CI, 1.46-3.82 vs. aOR, 1.42; 95% CI, 1.12-1.80).
“Conservatively, if we subtract the 19% nonsignificantly increased odds with prolactin-sparing antipsychotics from the 56% significantly increased odds with prolactin-increasing antipsychotics, we obtain a 37% relative increase in odds,” the authors noted.
“Using a lifetime incidence of breast cancer in women in the general population of about 12%, with a somewhat higher lifetime incidence in patients with schizophrenia than the general population, this difference between prolactin-increasing versus prolactin-sparing antipsychotics in breast cancer risk upon exposure of 5 or more years would correspond to about a 4% (37% x 12%) increase in absolute breast cancer odds with prolactin-increasing antipsychotic treatment” – a difference the authors call “clinically meaningful.”
Correll noted that although the study was conducted in a Finnish population, the findings are generalizable to other populations.
Clinical implications premature?
Commenting on the study, Anton Pottegård, MScPharm, PhD, DMSc, professor of pharmacoepidemiology, department of public health, University of Southern Denmark, Odense, expressed concern that “this new study is fairly aggressive in its recommendation [that] we need to pay attention to hyperprolactinemia, as this seems to cause breast cancer.”
Dr. Pottegård, who is also the head of research, Hospital Pharmacy Funen, Odense University Hospital, who was not involved with the study, said he does not “think that the full body of the literature supports such a direct conclusion and/or direct inference to clinical practice.”
Although “this is an important study to further this work, I do not think we are at a place (yet) where it should lead to different action from clinicians,” Dr. Pottegård cautioned.
Also commenting on the study, Mary Seeman, MDCM, DSc, professor emeritus of neurosciences and clinical translation, department of psychiatry, University of Toronto, called the question of whether prolactin-increasing antipsychotics increase breast cancer risk “very complicated because the incidence of breast cancer ... is higher in women with schizophrenia than in other women.”
Dr. Seeman, who was not involved with the study, pointed to other reasons for the increased risk, including higher rates of obesity, substance abuse, cigarette smoking, stress, and sedentary behavior, all of which raise prolactin levels. Additionally, “protective factors such as pregnancies and breastfeeding are less frequent in women with schizophrenia than in their peers.” Women with schizophrenia also “tend not to do breast screening, see their doctors less often, follow doctors’ orders less rigorously, and obtain treatment less often.”
The take-home message “is to prescribe prolactin-sparing medication to women if at all possible – but until we know more, that is good advice, although not always possible because the illness for which the antipsychotics are prescribed may not respond to those particular medications,” Dr. Seeman said.
The study was funded by the Finnish Ministry of Social Affairs and Health through the developmental fund for Niuvanniemi Hospital. Funding was also provided to individual researchers by the Academy of Finland, the Finnish Medical Foundation, and the Emil Aaltonen foundation. Dr. Correll has been a consultant or advisor to or has received honoraria from numerous companies. He has provided expert testimony for Janssen and Otsuka; received royalties from UpToDate and is a stock option holder of LB Pharma; served on a data safety monitoring board for Lundbeck, Rovi, Supernus, and Teva; and received grant support from Janssen and Takeda. Dr. Pottegård and Dr. Seeman disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Data sharing to improve AI used in breast-imaging research
The curated dataset, which consists of 22,032 DBT volumes associated with 5,610 studies from 5,060 patients, was published online in JAMA Network Open. The studies were divided into types: normal studies (91.4%), actionable studies that required additional imaging but no biopsy (5.0%), benign biopsied studies (2.0%), and studies that detected cancer (1.6%).
To develop and evaluate their deep-learning model for the detection of architectural distortions and masses, the researchers used a test set of 460 studies from 418 patients with cancer. Their algorithm reached a breast-based sensitivity of two false positives per DBT volume, or 65%.
“The main focus of this publication is on the dataset, rather than on a specific hypothesis,” said principal researcher Maciej A. Mazurowski, PhD, scientific director of the Duke Center for Artificial Intelligence in Radiology in Durham, N.C.
“We have publicly shared a large dataset of digital breast tomosynthesis images, which are sometimes referred to as 3D mammograms, for more than 5,000 patients. There are two purposes for sharing data like these. One is to improve research and development of machine-learning algorithms. You can train models with these data. The other reason, maybe even more important, is to provide a benchmark to test algorithms,” he said in an interview.
The large-scale sharing of data is a key step toward transparency in science, said Dr. Mazurowski. “It is about making sure results can be easily reproduced and setting benchmarks.”
The dataset includes masses and architectural distortions that were annotated by two experienced radiologists, but does not include annotations for calcifications and/or microcalcifications.
This lack of calcifications is a limitation of the study, said Jean Seely, MD, professor of radiology at the University of Ottawa, who is president of the Canadian Society of Breast Imaging and regional lead for the Ontario Breast Screening Program.
“About 45% of invasive breast cancers are diagnosed based on calcifications,” she explained.
Still, although the sensitivity of the AI algorithm was not high (65%) – the average sensitivity of 2D mammography is 85% – the researchers should be commended for releasing such a large dataset, said Dr. Seely.
“The fact that they have made it publicly available is very, very useful,” she said, adding that the dataset can be leveraged in future breast-imaging research.
Although DBT is much better at identifying breast cancers than mammography, DBT exams take about 30% more time to read.
“There’s a lot of work being done in artificial intelligence in breast imaging to not only improve the workflow for breast radiologists, but also to help with the diagnosis and detection,” she noted. “Anything that helps improve the confidence and the accuracy of the radiologist is really what we’re aiming for right now.”
The size and the content of this dataset will contribute to breast-imaging research, said Jaron Chong, MD, of the department of medical imaging at Western University in London, Ontario, who is chair of the AI Standing Committee at the Canadian Association of Radiologists.
“The contribution could be valuable in the long term because DBT is a rare dataset in comparison to conventional 2D mammography,” said Dr. Chong. “Most existing datasets have focused on two-dimensional imaging. We might see more research papers reference this dataset in the future, iterating and improving upon this article’s algorithm performance.”
Dr. Mazurowski reports serving as an adviser to Gradient Health. Dr. Seely is an unpaid principal investigator for the Ottawa site of the Tomosynthesis Mammographic Imaging Screening Trial (TMIST). Dr. Chong has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The curated dataset, which consists of 22,032 DBT volumes associated with 5,610 studies from 5,060 patients, was published online in JAMA Network Open. The studies were divided into types: normal studies (91.4%), actionable studies that required additional imaging but no biopsy (5.0%), benign biopsied studies (2.0%), and studies that detected cancer (1.6%).
To develop and evaluate their deep-learning model for the detection of architectural distortions and masses, the researchers used a test set of 460 studies from 418 patients with cancer. Their algorithm reached a breast-based sensitivity of two false positives per DBT volume, or 65%.
“The main focus of this publication is on the dataset, rather than on a specific hypothesis,” said principal researcher Maciej A. Mazurowski, PhD, scientific director of the Duke Center for Artificial Intelligence in Radiology in Durham, N.C.
“We have publicly shared a large dataset of digital breast tomosynthesis images, which are sometimes referred to as 3D mammograms, for more than 5,000 patients. There are two purposes for sharing data like these. One is to improve research and development of machine-learning algorithms. You can train models with these data. The other reason, maybe even more important, is to provide a benchmark to test algorithms,” he said in an interview.
The large-scale sharing of data is a key step toward transparency in science, said Dr. Mazurowski. “It is about making sure results can be easily reproduced and setting benchmarks.”
The dataset includes masses and architectural distortions that were annotated by two experienced radiologists, but does not include annotations for calcifications and/or microcalcifications.
This lack of calcifications is a limitation of the study, said Jean Seely, MD, professor of radiology at the University of Ottawa, who is president of the Canadian Society of Breast Imaging and regional lead for the Ontario Breast Screening Program.
“About 45% of invasive breast cancers are diagnosed based on calcifications,” she explained.
Still, although the sensitivity of the AI algorithm was not high (65%) – the average sensitivity of 2D mammography is 85% – the researchers should be commended for releasing such a large dataset, said Dr. Seely.
“The fact that they have made it publicly available is very, very useful,” she said, adding that the dataset can be leveraged in future breast-imaging research.
Although DBT is much better at identifying breast cancers than mammography, DBT exams take about 30% more time to read.
“There’s a lot of work being done in artificial intelligence in breast imaging to not only improve the workflow for breast radiologists, but also to help with the diagnosis and detection,” she noted. “Anything that helps improve the confidence and the accuracy of the radiologist is really what we’re aiming for right now.”
The size and the content of this dataset will contribute to breast-imaging research, said Jaron Chong, MD, of the department of medical imaging at Western University in London, Ontario, who is chair of the AI Standing Committee at the Canadian Association of Radiologists.
“The contribution could be valuable in the long term because DBT is a rare dataset in comparison to conventional 2D mammography,” said Dr. Chong. “Most existing datasets have focused on two-dimensional imaging. We might see more research papers reference this dataset in the future, iterating and improving upon this article’s algorithm performance.”
Dr. Mazurowski reports serving as an adviser to Gradient Health. Dr. Seely is an unpaid principal investigator for the Ottawa site of the Tomosynthesis Mammographic Imaging Screening Trial (TMIST). Dr. Chong has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The curated dataset, which consists of 22,032 DBT volumes associated with 5,610 studies from 5,060 patients, was published online in JAMA Network Open. The studies were divided into types: normal studies (91.4%), actionable studies that required additional imaging but no biopsy (5.0%), benign biopsied studies (2.0%), and studies that detected cancer (1.6%).
To develop and evaluate their deep-learning model for the detection of architectural distortions and masses, the researchers used a test set of 460 studies from 418 patients with cancer. Their algorithm reached a breast-based sensitivity of two false positives per DBT volume, or 65%.
“The main focus of this publication is on the dataset, rather than on a specific hypothesis,” said principal researcher Maciej A. Mazurowski, PhD, scientific director of the Duke Center for Artificial Intelligence in Radiology in Durham, N.C.
“We have publicly shared a large dataset of digital breast tomosynthesis images, which are sometimes referred to as 3D mammograms, for more than 5,000 patients. There are two purposes for sharing data like these. One is to improve research and development of machine-learning algorithms. You can train models with these data. The other reason, maybe even more important, is to provide a benchmark to test algorithms,” he said in an interview.
The large-scale sharing of data is a key step toward transparency in science, said Dr. Mazurowski. “It is about making sure results can be easily reproduced and setting benchmarks.”
The dataset includes masses and architectural distortions that were annotated by two experienced radiologists, but does not include annotations for calcifications and/or microcalcifications.
This lack of calcifications is a limitation of the study, said Jean Seely, MD, professor of radiology at the University of Ottawa, who is president of the Canadian Society of Breast Imaging and regional lead for the Ontario Breast Screening Program.
“About 45% of invasive breast cancers are diagnosed based on calcifications,” she explained.
Still, although the sensitivity of the AI algorithm was not high (65%) – the average sensitivity of 2D mammography is 85% – the researchers should be commended for releasing such a large dataset, said Dr. Seely.
“The fact that they have made it publicly available is very, very useful,” she said, adding that the dataset can be leveraged in future breast-imaging research.
Although DBT is much better at identifying breast cancers than mammography, DBT exams take about 30% more time to read.
“There’s a lot of work being done in artificial intelligence in breast imaging to not only improve the workflow for breast radiologists, but also to help with the diagnosis and detection,” she noted. “Anything that helps improve the confidence and the accuracy of the radiologist is really what we’re aiming for right now.”
The size and the content of this dataset will contribute to breast-imaging research, said Jaron Chong, MD, of the department of medical imaging at Western University in London, Ontario, who is chair of the AI Standing Committee at the Canadian Association of Radiologists.
“The contribution could be valuable in the long term because DBT is a rare dataset in comparison to conventional 2D mammography,” said Dr. Chong. “Most existing datasets have focused on two-dimensional imaging. We might see more research papers reference this dataset in the future, iterating and improving upon this article’s algorithm performance.”
Dr. Mazurowski reports serving as an adviser to Gradient Health. Dr. Seely is an unpaid principal investigator for the Ottawa site of the Tomosynthesis Mammographic Imaging Screening Trial (TMIST). Dr. Chong has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA warns again about robotic mastectomy, breaks new ground
The agency also called out robotically assisted surgical (RAS) device use in the United States that lacks proper federal oversight.
“The FDA is aware of allegations that clinical studies are being conducted” with RAS devices in breast cancer “without the FDA oversight required for such significant risk studies,” the agency said.
The new advisory comes 4 weeks after a Medscape Medical News exclusive story on a set of clinical trials recently underway using RAS devices for nipple-sparing mastectomy, both prophylactically and as a breast cancer treatment.
The report found that investigators are either not collecting cancer outcomes or not doing so as a primary measure – despite a stiff warning in 2019 from the FDA that those outcomes are important.
“Congratulations to the press on doing its job well and informing government. I think this [safety communication] is a direct result of Medscape following up on this issue,” said Hooman Noorchashm, MD, PhD, a patient advocate from Philadelphia. He is a former surgeon and faculty member at the University of Pennsylvania.
In reviewing the FDA’s new warning, Dr. Noorchashm pointed out that the agency also stated unequivocally – after previously hinting – that any study of robotic mastectomy “must include monitoring of long-term clinical outcomes” such as cancer recurrence, disease-free survival, and overall survival.
That’s a change in approach – previously the FDA has typically approved/cleared RAS devices for use in cancer surgery based on 30-day complication rates (compared with standards of care) and had no requirement for cancer-related outcomes data.
“This [new] advisory reiterates the need for a clear focus on primary oncologic outcomes to, at the very least, demonstrate the noninferiority of robotic assisted surgical devices for performing mastectomy procedures,” said Dr. Noorchashm.
In a 2019 warning about robotic mastectomy, the FDA suggested that it would require oncologic measures moving forward, saying that it “anticipates” that any evaluation of new use of robotic devices in women’s cancer “would be supported” by long-term cancer outcomes. But it stopped short of publicly saying so. The new advisory changes that.
Direct comparison with traditional mastectomy needed
There are safety concerns with robotic mastectomy. Experts question whether a surgeon can easily remove a breast tumor in one piece through the small incision (a selling point of the robot). If the tissue cannot be removed in one piece, cancer fragments may be left behind.
As a result, a randomized trial with traditional open mastectomy as a comparator is needed, Dr. Noorchashm stressed. The current batch of clinical trials in the United States are all single-arm studies and as such are “totally inappropriate,” he said.
Julie Margenthaler, MD, a breast surgeon at Washington University in St Louis, also noted the importance of a randomized trial.
“I feel strongly that robotic-assisted mastectomy should only be performed in the setting of a well-designed clinical trial and that oncologic outcomes should be a primary or secondary endpoint analysis as part of that trial,” she said in an email.
Intuitive Surgical, a California-based manufacturer of robotic devices in health care and a pioneer in robot-assisted surgery, is funding one of the current clinical trials of robotic mastectomy in the United States – a single-arm, five-center trial examining use in the prophylactic setting. The two primary outcomes are conversions to open mastectomy (efficacy measure) and the incidence of adverse events during surgery to 42 days after surgery (safety measure).
This news organization previously asked the company, which manufactures the market leader da Vinci robotic surgical equipment, if it planned to conduct a randomized trial.
“Any plans for use of da Vinci Xi surgical system in nipple-sparing mastectomy will be based on these [single-arm] study results as well as other data and evidence,” said a spokesperson, who did not confirm use of a randomized trial.
The new FDA requirement for long-term oncologic outcomes also in part arises from “diminished long-term survival” that was associated with robotic surgery and other minimally invasive surgery for hysterectomy related to cervical cancer.
A version of this article first appeared on Medscape.com.
The agency also called out robotically assisted surgical (RAS) device use in the United States that lacks proper federal oversight.
“The FDA is aware of allegations that clinical studies are being conducted” with RAS devices in breast cancer “without the FDA oversight required for such significant risk studies,” the agency said.
The new advisory comes 4 weeks after a Medscape Medical News exclusive story on a set of clinical trials recently underway using RAS devices for nipple-sparing mastectomy, both prophylactically and as a breast cancer treatment.
The report found that investigators are either not collecting cancer outcomes or not doing so as a primary measure – despite a stiff warning in 2019 from the FDA that those outcomes are important.
“Congratulations to the press on doing its job well and informing government. I think this [safety communication] is a direct result of Medscape following up on this issue,” said Hooman Noorchashm, MD, PhD, a patient advocate from Philadelphia. He is a former surgeon and faculty member at the University of Pennsylvania.
In reviewing the FDA’s new warning, Dr. Noorchashm pointed out that the agency also stated unequivocally – after previously hinting – that any study of robotic mastectomy “must include monitoring of long-term clinical outcomes” such as cancer recurrence, disease-free survival, and overall survival.
That’s a change in approach – previously the FDA has typically approved/cleared RAS devices for use in cancer surgery based on 30-day complication rates (compared with standards of care) and had no requirement for cancer-related outcomes data.
“This [new] advisory reiterates the need for a clear focus on primary oncologic outcomes to, at the very least, demonstrate the noninferiority of robotic assisted surgical devices for performing mastectomy procedures,” said Dr. Noorchashm.
In a 2019 warning about robotic mastectomy, the FDA suggested that it would require oncologic measures moving forward, saying that it “anticipates” that any evaluation of new use of robotic devices in women’s cancer “would be supported” by long-term cancer outcomes. But it stopped short of publicly saying so. The new advisory changes that.
Direct comparison with traditional mastectomy needed
There are safety concerns with robotic mastectomy. Experts question whether a surgeon can easily remove a breast tumor in one piece through the small incision (a selling point of the robot). If the tissue cannot be removed in one piece, cancer fragments may be left behind.
As a result, a randomized trial with traditional open mastectomy as a comparator is needed, Dr. Noorchashm stressed. The current batch of clinical trials in the United States are all single-arm studies and as such are “totally inappropriate,” he said.
Julie Margenthaler, MD, a breast surgeon at Washington University in St Louis, also noted the importance of a randomized trial.
“I feel strongly that robotic-assisted mastectomy should only be performed in the setting of a well-designed clinical trial and that oncologic outcomes should be a primary or secondary endpoint analysis as part of that trial,” she said in an email.
Intuitive Surgical, a California-based manufacturer of robotic devices in health care and a pioneer in robot-assisted surgery, is funding one of the current clinical trials of robotic mastectomy in the United States – a single-arm, five-center trial examining use in the prophylactic setting. The two primary outcomes are conversions to open mastectomy (efficacy measure) and the incidence of adverse events during surgery to 42 days after surgery (safety measure).
This news organization previously asked the company, which manufactures the market leader da Vinci robotic surgical equipment, if it planned to conduct a randomized trial.
“Any plans for use of da Vinci Xi surgical system in nipple-sparing mastectomy will be based on these [single-arm] study results as well as other data and evidence,” said a spokesperson, who did not confirm use of a randomized trial.
The new FDA requirement for long-term oncologic outcomes also in part arises from “diminished long-term survival” that was associated with robotic surgery and other minimally invasive surgery for hysterectomy related to cervical cancer.
A version of this article first appeared on Medscape.com.
The agency also called out robotically assisted surgical (RAS) device use in the United States that lacks proper federal oversight.
“The FDA is aware of allegations that clinical studies are being conducted” with RAS devices in breast cancer “without the FDA oversight required for such significant risk studies,” the agency said.
The new advisory comes 4 weeks after a Medscape Medical News exclusive story on a set of clinical trials recently underway using RAS devices for nipple-sparing mastectomy, both prophylactically and as a breast cancer treatment.
The report found that investigators are either not collecting cancer outcomes or not doing so as a primary measure – despite a stiff warning in 2019 from the FDA that those outcomes are important.
“Congratulations to the press on doing its job well and informing government. I think this [safety communication] is a direct result of Medscape following up on this issue,” said Hooman Noorchashm, MD, PhD, a patient advocate from Philadelphia. He is a former surgeon and faculty member at the University of Pennsylvania.
In reviewing the FDA’s new warning, Dr. Noorchashm pointed out that the agency also stated unequivocally – after previously hinting – that any study of robotic mastectomy “must include monitoring of long-term clinical outcomes” such as cancer recurrence, disease-free survival, and overall survival.
That’s a change in approach – previously the FDA has typically approved/cleared RAS devices for use in cancer surgery based on 30-day complication rates (compared with standards of care) and had no requirement for cancer-related outcomes data.
“This [new] advisory reiterates the need for a clear focus on primary oncologic outcomes to, at the very least, demonstrate the noninferiority of robotic assisted surgical devices for performing mastectomy procedures,” said Dr. Noorchashm.
In a 2019 warning about robotic mastectomy, the FDA suggested that it would require oncologic measures moving forward, saying that it “anticipates” that any evaluation of new use of robotic devices in women’s cancer “would be supported” by long-term cancer outcomes. But it stopped short of publicly saying so. The new advisory changes that.
Direct comparison with traditional mastectomy needed
There are safety concerns with robotic mastectomy. Experts question whether a surgeon can easily remove a breast tumor in one piece through the small incision (a selling point of the robot). If the tissue cannot be removed in one piece, cancer fragments may be left behind.
As a result, a randomized trial with traditional open mastectomy as a comparator is needed, Dr. Noorchashm stressed. The current batch of clinical trials in the United States are all single-arm studies and as such are “totally inappropriate,” he said.
Julie Margenthaler, MD, a breast surgeon at Washington University in St Louis, also noted the importance of a randomized trial.
“I feel strongly that robotic-assisted mastectomy should only be performed in the setting of a well-designed clinical trial and that oncologic outcomes should be a primary or secondary endpoint analysis as part of that trial,” she said in an email.
Intuitive Surgical, a California-based manufacturer of robotic devices in health care and a pioneer in robot-assisted surgery, is funding one of the current clinical trials of robotic mastectomy in the United States – a single-arm, five-center trial examining use in the prophylactic setting. The two primary outcomes are conversions to open mastectomy (efficacy measure) and the incidence of adverse events during surgery to 42 days after surgery (safety measure).
This news organization previously asked the company, which manufactures the market leader da Vinci robotic surgical equipment, if it planned to conduct a randomized trial.
“Any plans for use of da Vinci Xi surgical system in nipple-sparing mastectomy will be based on these [single-arm] study results as well as other data and evidence,” said a spokesperson, who did not confirm use of a randomized trial.
The new FDA requirement for long-term oncologic outcomes also in part arises from “diminished long-term survival” that was associated with robotic surgery and other minimally invasive surgery for hysterectomy related to cervical cancer.
A version of this article first appeared on Medscape.com.