User login
New approval in early breast cancer: First advance in 20 years
Abemaciclib had already been approved for use in the treatment of HR+, HER2– advanced or metastatic breast cancer.
Now it is also approved for use in HR+, HER2– early breast cancer for patients who have high-risk, node-positive disease and whose tumors have a Ki-67 score of 20% or higher, as determined by a U.S. Food and Drug Administration–approved test.
The FDA also approved the Ki-67 IHC MIB-1 pharmDx (Dako Omnis) assay for use as a companion diagnostic test.
This is the first CDK4/6 inhibitor to be approved for use in this patient population.
Approximately 70% of all breast cancers are of the HR+, HER2– subtype.
The approval is based on some of the results from the monarchE study, which was presented last year at the annual meeting of the European Society of Medical Oncology and was simultaneously published in the Journal of Clinical Oncology.
The results showed that the addition of abemaciclib to endocrine therapy (tamoxifen or aromatase inhibitors) significantly improved invasive disease-free survival (IDFS), which was defined on the basis of the length of time before breast cancer comes back, any new cancer develops, or death.
The 2-year IDFS rates were 92.2% with the combination vs. 88.7% for endocrine therapy alone for the overall patient population.
“This is the first time in more than 20 years that we have seen an advance in the adjuvant treatment of this form of breast cancer,” lead investigator Stephen Johnston, MD, PhD, from the Royal Marsden Hospital NHS Foundation Trust, London, said at the meeting, as reported at the time by this news organization.
Reacting to the findings, Giuseppe Curigliano, MD, PhD, head of the division of early drug development at the European Institute of Oncology, Milan, said, “This is a very important trial and the findings will change practice.”
He predicted that once the drug is approved for use in high-risk HR+, HER2– early breast cancer, “the new standard of care for these patients will be to add 2 years of abemaciclib to endocrine therapy.”
In a press release about the new approval from the manufacturer (Lilly), another investigator on the monarchE study, Sara M. Tolaney, MD, MPH, Harvard Medical School and the Dana-Farber Cancer Institute, Boston, agreed that the results are practice changing. She said that the combination of abemaciclib and endocrine therapy is a potential new standard of care for this patient population. “We are encouraged by the marked reduction in the risk of recurrence even beyond the 2-year treatment period in these patients, and I’m grateful to be able to offer this as a treatment option to my patients,” she said.
On Twitter, she commented that restricting the indication to patients who show Ki67 ≥20% is “interesting,” inasmuch as benefits were seen in patients with both low and high Ki67.
Hal Burstein, MD, from Dana-Farber, also found this detail “interesting, as Ki67 testing remains a very controversial topic and difficult to standardize.”
Replying, Pedro Exman, MD, from the Hospital Alemão Oswaldo Cruz, in São Paulo, said: “Does it make sense to approve only in a subset of patients based in a positive subgroup analysis of a positive ITT study that was not even described in the JCO publication?”
Other experts said they were eagerly awaiting further results, particularly on overall survival, from the monarchE trial. New data are due to be presented on Oct. 14 at an ESMO virtual plenary session.
Commenting late last year about these results, George W. Sledge Jr, MD, professor of medicine at Stanford University Medical Center, Palo Alto, Calif., said that the median follow-up time “is still quite short for a study of ER+ adjuvant therapy, where the majority of recurrences and deaths occur after 5 years in many studies.”
Consequently, “we still have a long way to go to understand the ultimate effects of CDK4/6 inhibition on early-stage ER+ breast cancer, particularly on late recurrences,” he told this news organization at the time.
Agreed, said C. Kent Osborne, MD, codirector of the San Antonio Breast Cancer Symposium and founding director of the Duncan Cancer Center at Baylor College of Medicine, Houston, Tex. The results are “very encouraging, especially in the subgroup of tumors with high proliferation” (identified by the K1-67 score).
However, Dr. Osborne also urged caution in the interpretation of the results, “given the still rather short follow-up, given that that ER+ disease is known for its persistent recurrence rate, even past 10 years.”
He also noted that “this class of inhibitors is likely cytostatic, rather than cytocidal, meaning that it blocks cell proliferation rather than killing the cells.” Questions therefore remain over whether the survival curves for combination therapy will come together with those for endocrine therapy alone once patients stop taking the drug.
Study details
The monarchE trial involved patients with HR+, HER2–, high-risk early breast cancer who had undergone surgery and, as indicated, radiotherapy and/or adjuvant/neoadjuvant chemotherapy. Patients with four or more positive nodes or one to three nodes and either tumors of size ≥5 cm, histologic grade 3, or central Ki-67 ≥20% were eligible; 5,637 patients were randomly assigned in a 1:1 ratio to receive standard-of-care adjuvant endocrine therapy (ET) with or without abemaciclib (150 mg twice daily for 2 years).
A preplanned interim analysis was carried out after 323 IDFS events were observed in the intent-to-treat population. The results, as published last year in the Journal of Clinical Oncology, show that abemaciclib plus ET yielded superior IDFS in comparison with ET alone (P = .01; hazard ratio, 0.75; 95% confidence interval, 0.60-0.93), with 2-year IDFS rates of 92.2% vs. 88.7%.
In the press release announcing the approval of the new indication, the manufacturer notes that the approval was based on the results from a subgroup of 2,003 patients whose tumors had a Ki-67 score of ≥20% and who were also at high risk for recurrence (≥four positive axillary lymph nodes [ALN], or one-three positive ALN with grade 3 disease and/or tumor size ≥5 cm).
There was a statistically significant improvement in IDFS for this prespecified subgroup of patients (HR, 0.643; 95% CI, 0.475-0.872; P = .0042).
With additional follow-up, conducted post hoc, the results showed a 37% decrease in the risk for breast cancer recurrence or death, compared with ET alone (HR, 0.626; 95% CI, 0.49-0.80) and an absolute benefit in IDFS event rate of 7.1% at 3 years. IDFS was 86.1% for abemaciclib plus ET vs. 79.0% for ET alone.
Adverse reactions from monarchE were consistent with the known safety profile for abemaciclib, the company noted. Safety and tolerability were evaluated in 5,591 patients. The most common adverse reactions reported (≥10%) with abemaciclib plus ET vs. ET alone were diarrhea (84% vs. 9%), infections (51% vs. 39%), neutropenia (46% vs. 6%), fatigue (41% vs. 18%), leukopenia (38% vs. 7%), nausea (30% vs. 9%), anemia (24% vs. 4%), headache (20% vs. 15%), vomiting (18% vs. 4.6%), stomatitis (14% vs. 5%), lymphopenia (14% vs. 3%), thrombocytopenia (13% vs. 2%), decreased appetite (12% vs. 2.4%), increased ALT (12% vs. 6%), increased AST (12% vs. 5%), dizziness (11% vs. 7%), rash (11% vs. 4.5%), and alopecia (11% vs. 2.7 %).
A version of this article first appeared on Medscape.com.
Abemaciclib had already been approved for use in the treatment of HR+, HER2– advanced or metastatic breast cancer.
Now it is also approved for use in HR+, HER2– early breast cancer for patients who have high-risk, node-positive disease and whose tumors have a Ki-67 score of 20% or higher, as determined by a U.S. Food and Drug Administration–approved test.
The FDA also approved the Ki-67 IHC MIB-1 pharmDx (Dako Omnis) assay for use as a companion diagnostic test.
This is the first CDK4/6 inhibitor to be approved for use in this patient population.
Approximately 70% of all breast cancers are of the HR+, HER2– subtype.
The approval is based on some of the results from the monarchE study, which was presented last year at the annual meeting of the European Society of Medical Oncology and was simultaneously published in the Journal of Clinical Oncology.
The results showed that the addition of abemaciclib to endocrine therapy (tamoxifen or aromatase inhibitors) significantly improved invasive disease-free survival (IDFS), which was defined on the basis of the length of time before breast cancer comes back, any new cancer develops, or death.
The 2-year IDFS rates were 92.2% with the combination vs. 88.7% for endocrine therapy alone for the overall patient population.
“This is the first time in more than 20 years that we have seen an advance in the adjuvant treatment of this form of breast cancer,” lead investigator Stephen Johnston, MD, PhD, from the Royal Marsden Hospital NHS Foundation Trust, London, said at the meeting, as reported at the time by this news organization.
Reacting to the findings, Giuseppe Curigliano, MD, PhD, head of the division of early drug development at the European Institute of Oncology, Milan, said, “This is a very important trial and the findings will change practice.”
He predicted that once the drug is approved for use in high-risk HR+, HER2– early breast cancer, “the new standard of care for these patients will be to add 2 years of abemaciclib to endocrine therapy.”
In a press release about the new approval from the manufacturer (Lilly), another investigator on the monarchE study, Sara M. Tolaney, MD, MPH, Harvard Medical School and the Dana-Farber Cancer Institute, Boston, agreed that the results are practice changing. She said that the combination of abemaciclib and endocrine therapy is a potential new standard of care for this patient population. “We are encouraged by the marked reduction in the risk of recurrence even beyond the 2-year treatment period in these patients, and I’m grateful to be able to offer this as a treatment option to my patients,” she said.
On Twitter, she commented that restricting the indication to patients who show Ki67 ≥20% is “interesting,” inasmuch as benefits were seen in patients with both low and high Ki67.
Hal Burstein, MD, from Dana-Farber, also found this detail “interesting, as Ki67 testing remains a very controversial topic and difficult to standardize.”
Replying, Pedro Exman, MD, from the Hospital Alemão Oswaldo Cruz, in São Paulo, said: “Does it make sense to approve only in a subset of patients based in a positive subgroup analysis of a positive ITT study that was not even described in the JCO publication?”
Other experts said they were eagerly awaiting further results, particularly on overall survival, from the monarchE trial. New data are due to be presented on Oct. 14 at an ESMO virtual plenary session.
Commenting late last year about these results, George W. Sledge Jr, MD, professor of medicine at Stanford University Medical Center, Palo Alto, Calif., said that the median follow-up time “is still quite short for a study of ER+ adjuvant therapy, where the majority of recurrences and deaths occur after 5 years in many studies.”
Consequently, “we still have a long way to go to understand the ultimate effects of CDK4/6 inhibition on early-stage ER+ breast cancer, particularly on late recurrences,” he told this news organization at the time.
Agreed, said C. Kent Osborne, MD, codirector of the San Antonio Breast Cancer Symposium and founding director of the Duncan Cancer Center at Baylor College of Medicine, Houston, Tex. The results are “very encouraging, especially in the subgroup of tumors with high proliferation” (identified by the K1-67 score).
However, Dr. Osborne also urged caution in the interpretation of the results, “given the still rather short follow-up, given that that ER+ disease is known for its persistent recurrence rate, even past 10 years.”
He also noted that “this class of inhibitors is likely cytostatic, rather than cytocidal, meaning that it blocks cell proliferation rather than killing the cells.” Questions therefore remain over whether the survival curves for combination therapy will come together with those for endocrine therapy alone once patients stop taking the drug.
Study details
The monarchE trial involved patients with HR+, HER2–, high-risk early breast cancer who had undergone surgery and, as indicated, radiotherapy and/or adjuvant/neoadjuvant chemotherapy. Patients with four or more positive nodes or one to three nodes and either tumors of size ≥5 cm, histologic grade 3, or central Ki-67 ≥20% were eligible; 5,637 patients were randomly assigned in a 1:1 ratio to receive standard-of-care adjuvant endocrine therapy (ET) with or without abemaciclib (150 mg twice daily for 2 years).
A preplanned interim analysis was carried out after 323 IDFS events were observed in the intent-to-treat population. The results, as published last year in the Journal of Clinical Oncology, show that abemaciclib plus ET yielded superior IDFS in comparison with ET alone (P = .01; hazard ratio, 0.75; 95% confidence interval, 0.60-0.93), with 2-year IDFS rates of 92.2% vs. 88.7%.
In the press release announcing the approval of the new indication, the manufacturer notes that the approval was based on the results from a subgroup of 2,003 patients whose tumors had a Ki-67 score of ≥20% and who were also at high risk for recurrence (≥four positive axillary lymph nodes [ALN], or one-three positive ALN with grade 3 disease and/or tumor size ≥5 cm).
There was a statistically significant improvement in IDFS for this prespecified subgroup of patients (HR, 0.643; 95% CI, 0.475-0.872; P = .0042).
With additional follow-up, conducted post hoc, the results showed a 37% decrease in the risk for breast cancer recurrence or death, compared with ET alone (HR, 0.626; 95% CI, 0.49-0.80) and an absolute benefit in IDFS event rate of 7.1% at 3 years. IDFS was 86.1% for abemaciclib plus ET vs. 79.0% for ET alone.
Adverse reactions from monarchE were consistent with the known safety profile for abemaciclib, the company noted. Safety and tolerability were evaluated in 5,591 patients. The most common adverse reactions reported (≥10%) with abemaciclib plus ET vs. ET alone were diarrhea (84% vs. 9%), infections (51% vs. 39%), neutropenia (46% vs. 6%), fatigue (41% vs. 18%), leukopenia (38% vs. 7%), nausea (30% vs. 9%), anemia (24% vs. 4%), headache (20% vs. 15%), vomiting (18% vs. 4.6%), stomatitis (14% vs. 5%), lymphopenia (14% vs. 3%), thrombocytopenia (13% vs. 2%), decreased appetite (12% vs. 2.4%), increased ALT (12% vs. 6%), increased AST (12% vs. 5%), dizziness (11% vs. 7%), rash (11% vs. 4.5%), and alopecia (11% vs. 2.7 %).
A version of this article first appeared on Medscape.com.
Abemaciclib had already been approved for use in the treatment of HR+, HER2– advanced or metastatic breast cancer.
Now it is also approved for use in HR+, HER2– early breast cancer for patients who have high-risk, node-positive disease and whose tumors have a Ki-67 score of 20% or higher, as determined by a U.S. Food and Drug Administration–approved test.
The FDA also approved the Ki-67 IHC MIB-1 pharmDx (Dako Omnis) assay for use as a companion diagnostic test.
This is the first CDK4/6 inhibitor to be approved for use in this patient population.
Approximately 70% of all breast cancers are of the HR+, HER2– subtype.
The approval is based on some of the results from the monarchE study, which was presented last year at the annual meeting of the European Society of Medical Oncology and was simultaneously published in the Journal of Clinical Oncology.
The results showed that the addition of abemaciclib to endocrine therapy (tamoxifen or aromatase inhibitors) significantly improved invasive disease-free survival (IDFS), which was defined on the basis of the length of time before breast cancer comes back, any new cancer develops, or death.
The 2-year IDFS rates were 92.2% with the combination vs. 88.7% for endocrine therapy alone for the overall patient population.
“This is the first time in more than 20 years that we have seen an advance in the adjuvant treatment of this form of breast cancer,” lead investigator Stephen Johnston, MD, PhD, from the Royal Marsden Hospital NHS Foundation Trust, London, said at the meeting, as reported at the time by this news organization.
Reacting to the findings, Giuseppe Curigliano, MD, PhD, head of the division of early drug development at the European Institute of Oncology, Milan, said, “This is a very important trial and the findings will change practice.”
He predicted that once the drug is approved for use in high-risk HR+, HER2– early breast cancer, “the new standard of care for these patients will be to add 2 years of abemaciclib to endocrine therapy.”
In a press release about the new approval from the manufacturer (Lilly), another investigator on the monarchE study, Sara M. Tolaney, MD, MPH, Harvard Medical School and the Dana-Farber Cancer Institute, Boston, agreed that the results are practice changing. She said that the combination of abemaciclib and endocrine therapy is a potential new standard of care for this patient population. “We are encouraged by the marked reduction in the risk of recurrence even beyond the 2-year treatment period in these patients, and I’m grateful to be able to offer this as a treatment option to my patients,” she said.
On Twitter, she commented that restricting the indication to patients who show Ki67 ≥20% is “interesting,” inasmuch as benefits were seen in patients with both low and high Ki67.
Hal Burstein, MD, from Dana-Farber, also found this detail “interesting, as Ki67 testing remains a very controversial topic and difficult to standardize.”
Replying, Pedro Exman, MD, from the Hospital Alemão Oswaldo Cruz, in São Paulo, said: “Does it make sense to approve only in a subset of patients based in a positive subgroup analysis of a positive ITT study that was not even described in the JCO publication?”
Other experts said they were eagerly awaiting further results, particularly on overall survival, from the monarchE trial. New data are due to be presented on Oct. 14 at an ESMO virtual plenary session.
Commenting late last year about these results, George W. Sledge Jr, MD, professor of medicine at Stanford University Medical Center, Palo Alto, Calif., said that the median follow-up time “is still quite short for a study of ER+ adjuvant therapy, where the majority of recurrences and deaths occur after 5 years in many studies.”
Consequently, “we still have a long way to go to understand the ultimate effects of CDK4/6 inhibition on early-stage ER+ breast cancer, particularly on late recurrences,” he told this news organization at the time.
Agreed, said C. Kent Osborne, MD, codirector of the San Antonio Breast Cancer Symposium and founding director of the Duncan Cancer Center at Baylor College of Medicine, Houston, Tex. The results are “very encouraging, especially in the subgroup of tumors with high proliferation” (identified by the K1-67 score).
However, Dr. Osborne also urged caution in the interpretation of the results, “given the still rather short follow-up, given that that ER+ disease is known for its persistent recurrence rate, even past 10 years.”
He also noted that “this class of inhibitors is likely cytostatic, rather than cytocidal, meaning that it blocks cell proliferation rather than killing the cells.” Questions therefore remain over whether the survival curves for combination therapy will come together with those for endocrine therapy alone once patients stop taking the drug.
Study details
The monarchE trial involved patients with HR+, HER2–, high-risk early breast cancer who had undergone surgery and, as indicated, radiotherapy and/or adjuvant/neoadjuvant chemotherapy. Patients with four or more positive nodes or one to three nodes and either tumors of size ≥5 cm, histologic grade 3, or central Ki-67 ≥20% were eligible; 5,637 patients were randomly assigned in a 1:1 ratio to receive standard-of-care adjuvant endocrine therapy (ET) with or without abemaciclib (150 mg twice daily for 2 years).
A preplanned interim analysis was carried out after 323 IDFS events were observed in the intent-to-treat population. The results, as published last year in the Journal of Clinical Oncology, show that abemaciclib plus ET yielded superior IDFS in comparison with ET alone (P = .01; hazard ratio, 0.75; 95% confidence interval, 0.60-0.93), with 2-year IDFS rates of 92.2% vs. 88.7%.
In the press release announcing the approval of the new indication, the manufacturer notes that the approval was based on the results from a subgroup of 2,003 patients whose tumors had a Ki-67 score of ≥20% and who were also at high risk for recurrence (≥four positive axillary lymph nodes [ALN], or one-three positive ALN with grade 3 disease and/or tumor size ≥5 cm).
There was a statistically significant improvement in IDFS for this prespecified subgroup of patients (HR, 0.643; 95% CI, 0.475-0.872; P = .0042).
With additional follow-up, conducted post hoc, the results showed a 37% decrease in the risk for breast cancer recurrence or death, compared with ET alone (HR, 0.626; 95% CI, 0.49-0.80) and an absolute benefit in IDFS event rate of 7.1% at 3 years. IDFS was 86.1% for abemaciclib plus ET vs. 79.0% for ET alone.
Adverse reactions from monarchE were consistent with the known safety profile for abemaciclib, the company noted. Safety and tolerability were evaluated in 5,591 patients. The most common adverse reactions reported (≥10%) with abemaciclib plus ET vs. ET alone were diarrhea (84% vs. 9%), infections (51% vs. 39%), neutropenia (46% vs. 6%), fatigue (41% vs. 18%), leukopenia (38% vs. 7%), nausea (30% vs. 9%), anemia (24% vs. 4%), headache (20% vs. 15%), vomiting (18% vs. 4.6%), stomatitis (14% vs. 5%), lymphopenia (14% vs. 3%), thrombocytopenia (13% vs. 2%), decreased appetite (12% vs. 2.4%), increased ALT (12% vs. 6%), increased AST (12% vs. 5%), dizziness (11% vs. 7%), rash (11% vs. 4.5%), and alopecia (11% vs. 2.7 %).
A version of this article first appeared on Medscape.com.
True or false: Breast density increases breast cancer risk
Which of the following statements about breast density is TRUE?
Text copyright DenseBreast-info.org.
Answer
D. The risks associated with dense breast tissue are 2-fold: Dense tissue can mask cancer on a mammogram, and having dense breasts also increases the risk of developing breast cancer. As breast density increases, the sensitivity of mammography decreases, and the risk of developing breast cancer increases.
A woman’s breast density is usually determined by a radiologist’s visual evaluation of the mammogram. Breast density also can be measured quantitatively by computer software or estimated on computed tomography scan or magnetic resonance imaging. Breast density cannot be determined by the way a breast looks or feels.
Breast density and mammographic sensitivity
Cancers can be hidden or “masked” by dense tissue. On a mammogram, cancer is white. Normal dense tissue also appears white. If a cancer develops in an area of normal dense tissue, it can be harder or sometimes impossible to see it on the mammogram, like trying to see a snowman in a blizzard. As breast density increases, the ability to see cancer on mammography decreases (FIGURE 1).
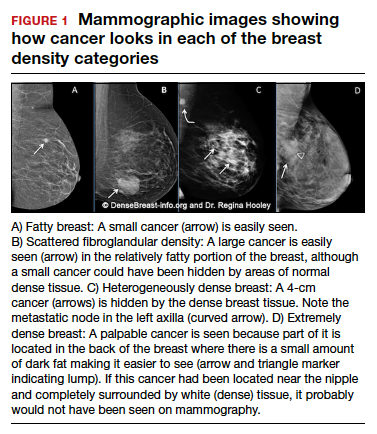
Standard 2D mammography has been shown to miss about 40% of cancers present in women with extremely dense breasts and 25% of cancers present in women with heterogeneously dense breasts.1-6 A cancer still can be masked on tomosynthesis (3D mammography) if it occurs in an area of dense tissue (where breast cancers more commonly occur), and tomosynthesis does not improve cancer detection appreciably in women with extremely dense breasts. To find cancer in a woman with dense breasts, additional screening beyond mammography should be considered.
Breast density and breast cancer risk
Dense breast tissue not only reduces mammography effectiveness, it also is a risk factor for the development of breast cancer: the denser the breast, the higher the risk.7 A meta-analysis across many studies concluded that magnitude of risk increases with each increase in density category, and women with extremely dense breasts (category D) have a 4-fold greater risk of developing breast cancer than do women with fatty breasts (category A), with upper limit of nearly 6-fold greater risk (FIGURE 2).8
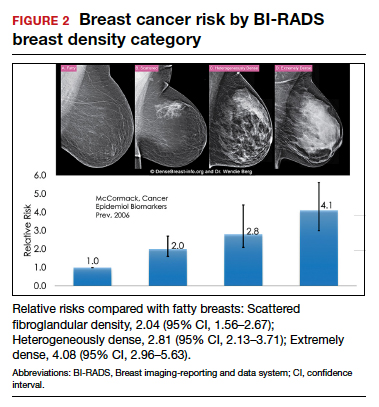
Most women do not have fatty breasts, however. More women have breasts with scattered fibroglandular density.9 Women with heterogeneously dense breasts (category C) have about a 1.5-fold greater risk of developing breast cancer than those with scattered fibroglandular density (category B), while women with extremely dense breasts (category D) have about a 2-fold greater risk.
There are probably several reasons that dense tissue increases breast cancer risk. One is that cancers arise microscopically in the glandular tissue. The more glandular tissue, the more susceptible tissue where cancer can develop. Glandular cells divide with hormonal stimulation throughout a woman’s lifetime, and each time a cell divides, “mistakes” can be made. An accumulation of mistakes can result in cancer. The more glandular the tissue, the greater the breast cancer risk. Women who have had breast reduction experience a reduced risk for breast cancer: thus, even a reduced absolute amount of glandular tissue reduces the risk for breast cancer. The second is that the local environment around the glands may produce certain growth hormones that stimulate cells to divide, and this is observed with fibrous breast tissue more than fatty breast tissue. ●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012;307:1394-1404. doi: 10.1001 /jama.2012.388.
- Destounis S, Johnston L, Highnam R, et al. Using volumetric breast density to quantify the potential masking risk of mammographic density. AJR Am J Roentgenol. 2017;208:222-227. doi: 10.2214/AJR.16.16489.
- Kerlikowske K, Scott CG, Mahmoudzadeh AP, et al. Automated and clinical breast imaging reporting and data system density measures predict risk for screen-detected and interval cancers: a case-control study. Ann Intern Med. 2018;168:757-765. doi: 10.7326/M17-3008.
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225:165-175. doi: 10.1148/radiol.2251011667.
- Mandelson MT, Oestreicher N, Porter PL, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst. 2000;92:1081-1087. doi: 10.1093/jnci/92.13.1081.
- Wanders JOP, Holland K, Karssemeijer N, et al. The effect of volumetric breast density on the risk of screen-detected and interval breast cancers: a cohort study. Breast Cancer Res. 2017;19:67. doi: 10.1186/s13058-017-0859-9.
- Society AC. Breast Cancer Facts & Figures 2019-2020. American Cancer Society, Inc. https://www.cancer.org/content/dam/cancer-org/research/cancer -facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts -and-figures-2019-2020.pdf. Published 2019. Accessed September 23, 2021.
- McCormack VA, dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2006;15:1159-1169. doi: 10.1158/1055-9965.EPI-06-0034.
- Kerlikowske K, Cook AJ, Buist DS, et al. Breast cancer risk by breast density, menopause, and postmenopausal hormone therapy use. J Clin Oncol. 2010;28:3830-3837. doi: 10.1200/JCO.2009.26.4770.
Which of the following statements about breast density is TRUE?
Text copyright DenseBreast-info.org.
Answer
D. The risks associated with dense breast tissue are 2-fold: Dense tissue can mask cancer on a mammogram, and having dense breasts also increases the risk of developing breast cancer. As breast density increases, the sensitivity of mammography decreases, and the risk of developing breast cancer increases.
A woman’s breast density is usually determined by a radiologist’s visual evaluation of the mammogram. Breast density also can be measured quantitatively by computer software or estimated on computed tomography scan or magnetic resonance imaging. Breast density cannot be determined by the way a breast looks or feels.
Breast density and mammographic sensitivity
Cancers can be hidden or “masked” by dense tissue. On a mammogram, cancer is white. Normal dense tissue also appears white. If a cancer develops in an area of normal dense tissue, it can be harder or sometimes impossible to see it on the mammogram, like trying to see a snowman in a blizzard. As breast density increases, the ability to see cancer on mammography decreases (FIGURE 1).
Standard 2D mammography has been shown to miss about 40% of cancers present in women with extremely dense breasts and 25% of cancers present in women with heterogeneously dense breasts.1-6 A cancer still can be masked on tomosynthesis (3D mammography) if it occurs in an area of dense tissue (where breast cancers more commonly occur), and tomosynthesis does not improve cancer detection appreciably in women with extremely dense breasts. To find cancer in a woman with dense breasts, additional screening beyond mammography should be considered.
Breast density and breast cancer risk
Dense breast tissue not only reduces mammography effectiveness, it also is a risk factor for the development of breast cancer: the denser the breast, the higher the risk.7 A meta-analysis across many studies concluded that magnitude of risk increases with each increase in density category, and women with extremely dense breasts (category D) have a 4-fold greater risk of developing breast cancer than do women with fatty breasts (category A), with upper limit of nearly 6-fold greater risk (FIGURE 2).8
Most women do not have fatty breasts, however. More women have breasts with scattered fibroglandular density.9 Women with heterogeneously dense breasts (category C) have about a 1.5-fold greater risk of developing breast cancer than those with scattered fibroglandular density (category B), while women with extremely dense breasts (category D) have about a 2-fold greater risk.
There are probably several reasons that dense tissue increases breast cancer risk. One is that cancers arise microscopically in the glandular tissue. The more glandular tissue, the more susceptible tissue where cancer can develop. Glandular cells divide with hormonal stimulation throughout a woman’s lifetime, and each time a cell divides, “mistakes” can be made. An accumulation of mistakes can result in cancer. The more glandular the tissue, the greater the breast cancer risk. Women who have had breast reduction experience a reduced risk for breast cancer: thus, even a reduced absolute amount of glandular tissue reduces the risk for breast cancer. The second is that the local environment around the glands may produce certain growth hormones that stimulate cells to divide, and this is observed with fibrous breast tissue more than fatty breast tissue. ●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
Which of the following statements about breast density is TRUE?
Text copyright DenseBreast-info.org.
Answer
D. The risks associated with dense breast tissue are 2-fold: Dense tissue can mask cancer on a mammogram, and having dense breasts also increases the risk of developing breast cancer. As breast density increases, the sensitivity of mammography decreases, and the risk of developing breast cancer increases.
A woman’s breast density is usually determined by a radiologist’s visual evaluation of the mammogram. Breast density also can be measured quantitatively by computer software or estimated on computed tomography scan or magnetic resonance imaging. Breast density cannot be determined by the way a breast looks or feels.
Breast density and mammographic sensitivity
Cancers can be hidden or “masked” by dense tissue. On a mammogram, cancer is white. Normal dense tissue also appears white. If a cancer develops in an area of normal dense tissue, it can be harder or sometimes impossible to see it on the mammogram, like trying to see a snowman in a blizzard. As breast density increases, the ability to see cancer on mammography decreases (FIGURE 1).
Standard 2D mammography has been shown to miss about 40% of cancers present in women with extremely dense breasts and 25% of cancers present in women with heterogeneously dense breasts.1-6 A cancer still can be masked on tomosynthesis (3D mammography) if it occurs in an area of dense tissue (where breast cancers more commonly occur), and tomosynthesis does not improve cancer detection appreciably in women with extremely dense breasts. To find cancer in a woman with dense breasts, additional screening beyond mammography should be considered.
Breast density and breast cancer risk
Dense breast tissue not only reduces mammography effectiveness, it also is a risk factor for the development of breast cancer: the denser the breast, the higher the risk.7 A meta-analysis across many studies concluded that magnitude of risk increases with each increase in density category, and women with extremely dense breasts (category D) have a 4-fold greater risk of developing breast cancer than do women with fatty breasts (category A), with upper limit of nearly 6-fold greater risk (FIGURE 2).8
Most women do not have fatty breasts, however. More women have breasts with scattered fibroglandular density.9 Women with heterogeneously dense breasts (category C) have about a 1.5-fold greater risk of developing breast cancer than those with scattered fibroglandular density (category B), while women with extremely dense breasts (category D) have about a 2-fold greater risk.
There are probably several reasons that dense tissue increases breast cancer risk. One is that cancers arise microscopically in the glandular tissue. The more glandular tissue, the more susceptible tissue where cancer can develop. Glandular cells divide with hormonal stimulation throughout a woman’s lifetime, and each time a cell divides, “mistakes” can be made. An accumulation of mistakes can result in cancer. The more glandular the tissue, the greater the breast cancer risk. Women who have had breast reduction experience a reduced risk for breast cancer: thus, even a reduced absolute amount of glandular tissue reduces the risk for breast cancer. The second is that the local environment around the glands may produce certain growth hormones that stimulate cells to divide, and this is observed with fibrous breast tissue more than fatty breast tissue. ●
For more information, visit medically sourced DenseBreast-info.org. Comprehensive resources include a free CME opportunity, Dense Breasts and Supplemental Screening.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012;307:1394-1404. doi: 10.1001 /jama.2012.388.
- Destounis S, Johnston L, Highnam R, et al. Using volumetric breast density to quantify the potential masking risk of mammographic density. AJR Am J Roentgenol. 2017;208:222-227. doi: 10.2214/AJR.16.16489.
- Kerlikowske K, Scott CG, Mahmoudzadeh AP, et al. Automated and clinical breast imaging reporting and data system density measures predict risk for screen-detected and interval cancers: a case-control study. Ann Intern Med. 2018;168:757-765. doi: 10.7326/M17-3008.
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225:165-175. doi: 10.1148/radiol.2251011667.
- Mandelson MT, Oestreicher N, Porter PL, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst. 2000;92:1081-1087. doi: 10.1093/jnci/92.13.1081.
- Wanders JOP, Holland K, Karssemeijer N, et al. The effect of volumetric breast density on the risk of screen-detected and interval breast cancers: a cohort study. Breast Cancer Res. 2017;19:67. doi: 10.1186/s13058-017-0859-9.
- Society AC. Breast Cancer Facts & Figures 2019-2020. American Cancer Society, Inc. https://www.cancer.org/content/dam/cancer-org/research/cancer -facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts -and-figures-2019-2020.pdf. Published 2019. Accessed September 23, 2021.
- McCormack VA, dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2006;15:1159-1169. doi: 10.1158/1055-9965.EPI-06-0034.
- Kerlikowske K, Cook AJ, Buist DS, et al. Breast cancer risk by breast density, menopause, and postmenopausal hormone therapy use. J Clin Oncol. 2010;28:3830-3837. doi: 10.1200/JCO.2009.26.4770.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012;307:1394-1404. doi: 10.1001 /jama.2012.388.
- Destounis S, Johnston L, Highnam R, et al. Using volumetric breast density to quantify the potential masking risk of mammographic density. AJR Am J Roentgenol. 2017;208:222-227. doi: 10.2214/AJR.16.16489.
- Kerlikowske K, Scott CG, Mahmoudzadeh AP, et al. Automated and clinical breast imaging reporting and data system density measures predict risk for screen-detected and interval cancers: a case-control study. Ann Intern Med. 2018;168:757-765. doi: 10.7326/M17-3008.
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225:165-175. doi: 10.1148/radiol.2251011667.
- Mandelson MT, Oestreicher N, Porter PL, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst. 2000;92:1081-1087. doi: 10.1093/jnci/92.13.1081.
- Wanders JOP, Holland K, Karssemeijer N, et al. The effect of volumetric breast density on the risk of screen-detected and interval breast cancers: a cohort study. Breast Cancer Res. 2017;19:67. doi: 10.1186/s13058-017-0859-9.
- Society AC. Breast Cancer Facts & Figures 2019-2020. American Cancer Society, Inc. https://www.cancer.org/content/dam/cancer-org/research/cancer -facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts -and-figures-2019-2020.pdf. Published 2019. Accessed September 23, 2021.
- McCormack VA, dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2006;15:1159-1169. doi: 10.1158/1055-9965.EPI-06-0034.
- Kerlikowske K, Cook AJ, Buist DS, et al. Breast cancer risk by breast density, menopause, and postmenopausal hormone therapy use. J Clin Oncol. 2010;28:3830-3837. doi: 10.1200/JCO.2009.26.4770.
Quiz developed in collaboration with 
Biomarker testing in metastatic breast cancer management: ‘Essential’
Identifying biomarkers in metastatic breast cancer (MBC) has become an integral part of choosing treatments and understanding disease progression. The American Society of Clinical Oncology Clinical Practice Guideline, published in 2015, recommends an initial biopsy to confirm estrogen receptor (ER), progesterone receptor (PR), or human epidermal growth factor receptor 2 (HER2) status as well as repeat biopsies to watch for receptor status changes over time.
“Decisions concerning the initiation of systemic therapy or selection of systemic therapy for metastatic breast cancer should be guided by ER, PR, and HER2 status in conjunction with clinical evaluation, judgment, and the patient’s goals for care,” according to the guideline authors.This news organization reached out to Kelly McCann, MD, PhD, a hematologist and oncologist in the department of medicine at the David Geffen School of Medicine, University of California, Los Angeles, to explore the role biomarker testing plays in managing MBC.
Question: How important is biomarker testing in guiding MBC treatments? Is there a standard or recommended process?
Dr. McCann: Biomarker testing is essential to breast cancer treatment and the development of targeted therapies. Oncologists typically identify a tumor’s canonical biomarkers — ER, PR, and HER2 — using immunohistochemistry or fluorescence in situ hybridization (FISH) testing and then try to match the tumor biology to drugs that target that subtype.

For tumors that lack canonical biomarkers — for example, triple-negative breast cancer (TNBC) — I send the tumor tissue for next-generation sequencing at the time of metastatic diagnosis to identify a wider range of potential targets or oncogenic drivers, such as somatic or germline mutations in homologous recombination repair genes ( BRCA1, BRCA2, and PALB2 ) or mutations in the PI3K/AKT/mTOR pathway.
In our attempts to define tumor biology and design a treatment strategy, two additional issues quickly arise. First, tumors are heterogeneous from the start. Second, tumors evolve.
Let’s start with how we define or subtype a tumor. Would you walk us through this process?
Defining a breast tumor can be tricky because these cancers often don’t fit neatly into predefined categories. Let’s take the estrogen receptor. In clinical trials, we need to define the cutoff for what constitutes ER-positive MBC or TNBC. Some trials define ER-positive as 1% or greater, others define it as 10% or greater.
But is a PR- and HER2-negative tumor with 1% or even 5% ER expression really ER-positive in the biological or prognostic sense? Probably not. A tumor with less than 10% ER expression, for instance, will actually behave like a triple-negative tumor. Instead of choosing a regimen targeting the ER-positive cells, I’ll lean more toward cytotoxic chemotherapy, the standard treatment for TNBC.
Tumors may have multiple drivers as well. What are some aberrations in addition to the main subtypes?
Tumors also often harbor more than one targetable driver. For instance, PIK3CA gene mutations are present in about 40% of hormone receptor–positive, HER2-negative tumors. Activating mutations in ESR1 develop in anywhere from 10% to 50% of MBCs as a resistance mechanism to estrogen deprivation therapy, conferring estrogen independence to the cells. Activating mutations in ERBB2, which essentially turns HER2 into an active receptor, are found in 2%-4% of breast cancers, including ER-positive, HER2-mutant breast cancers, and are enriched in lobular breast cancers, which are typically ER positive, HER2 negative.
What about tumor evolution, given the growing body of evidence that biomarker status in MBC can change over time?
Patients with MBC often have several active areas of cancer, and these areas will evolve differently. During each line of treatment, some metastases will develop resistance and others won’t. For instance, if my patient’s liver metastases start to grow, I will change therapy immediately. If, however, a single bone metastasis begins to grow and the liver metastases have responded well, I might consider local therapy — such as radiation — to target that bone metastasis, though this particular approach hasn’t been formally studied.
Ultimately, we can expect tumors to change over time as they become more biologically aggressive or resistant to current therapy. The most common biomarker change is probably loss of ER or PR expression, but the frequency of ER, PR, or HER2 biomarker changes is still not well understood.
Resistance mutations can also happen. When, for instance, activating mutations in ESR1 occur, the estrogen receptor becomes independent of estrogen and tumors then develop resistance to endocrine therapies. We see a similar problem arise in metastatic prostate cancer. With chronic testosterone deprivation, eventually the androgen receptor evolves to become independent of testosterone in a stage known as castrate-resistant prostate cancer.
Which biomarkers or combinations of biomarkers can be paired with an approved treatment?
We have a range of treatments targeting ER-positive and HER2-positive MBC in particular. For tumors harboring additional targetable mutations, preliminary data suggest that HER2-targeted tyrosine kinase inhibitors (TKIs), such as tucatinib and neratinib, are effective against activating mutations in ERBB2.
The PI3K inhibitor alpelisib in combination with fulvestrant has been approved for patients with ER-positive, HER2-negative MBC and mutations in PIK3CA. The mTOR inhibitor everolimus plus exemestane is an option for patients with ER-positive, HER2-negative. And for those with activating mutations in ESR1, I switch patients to a selective estrogen receptor degrader, such as fulvestrant.
PARP inhibitors, including olaparib or talazoparib, target metastatic HR-positive disease or TNBC with deleterious germline BRCA1 or BRCA2 mutations. Sacituzumab govitecan has been approved for treating metastatic TNBC and targets the cell surface protein TROP2, expressed in almost 90% of TNBC tumors.
What targets, on the other hand, are less informative for treatment choice?
When we order next-generation sequencing, we also will get a list of possible targets for which there are currently no therapeutic options, but there may be in the future. I find this knowledge is helpful. For example, an activating mutation in KRAS tells me that the cancer has a very strong oncogenic driver that I won›t be able to target. I know that activating KRAS mutations in lung cancer and colon cancer portend a poorer prognosis, which helps me to prepare the patient and family.
Atezolizumab in combination with paclitaxel has been FDA-approved for PD-L1 TNBC in the first-line setting, though data show that immune checkpoint inhibitors may be effective even without PD-L1 expression. Although cell surface protein TROP2 has emerged as a target in recent years, its expression is so common in TNBC that confirmatory testing for TROP2 expression is not required to prescribe sacituzumab govitecan.
What factors do you weigh when selecting among the large number of tests available for tumor testing?
We have many biomarker tests available, but the National Comprehensive Cancer Network does not have guidelines for tumor genetics testing in breast cancer. That means insurance does not have to cover the cost, and many companies don’t. Ultimately, though, drug companies and some testing companies have an incentive to cover the cost themselves because a companion diagnostic might be linked to their drug — therascreen PIK3CA RGQ PCR kit for alpelisib, for instance.
I tend not to use a companion diagnostic test because I want more information with a wider panel. The tumor tests I often use are FoundationOne CDx, Caris Molecular Intelligence, and Tempus. I use Tempus because their financial aid is very generous and almost all of my patients qualify to be tested for less than $100. For germline genetic testing, Invitae, Myriad, and Color are also options. Invitae and Color are about $250 out of pocket without insurance. Many academic centers have their own gene panels as well.
How far have we come in identifying biomarkers in MBC?
Targeted treatment for breast cancer has advanced significantly since doing my PhD research in cancer biology about 15 years ago. Of course, targeted therapies for ER-positive and HER2-amplified cancers were available at that point, but many more have been developed. The most significant advance has been the development of efficient and affordable genome sequencing, which has led to these large panels and identification of therapeutic targets. We’ve also expanded our knowledge of genetic predispositions for breast cancer beyond BRCA1 and BRCA2, which not only allows us to preemptively advise patients and their families about cancer risks and recommendations for cancer screening, but also to select a therapy to target a cancer’s DNA repair deficits.
I feel that we are in an exciting discovery phase in oncology. We currently rely on biomarkers to manage MBC and will continue to refine our strategies and develop more effective drug therapies as we identify more oncogenic drivers, tumor-specific proteins, and cancer cell vulnerabilities.
Identifying biomarkers in metastatic breast cancer (MBC) has become an integral part of choosing treatments and understanding disease progression. The American Society of Clinical Oncology Clinical Practice Guideline, published in 2015, recommends an initial biopsy to confirm estrogen receptor (ER), progesterone receptor (PR), or human epidermal growth factor receptor 2 (HER2) status as well as repeat biopsies to watch for receptor status changes over time.
“Decisions concerning the initiation of systemic therapy or selection of systemic therapy for metastatic breast cancer should be guided by ER, PR, and HER2 status in conjunction with clinical evaluation, judgment, and the patient’s goals for care,” according to the guideline authors.This news organization reached out to Kelly McCann, MD, PhD, a hematologist and oncologist in the department of medicine at the David Geffen School of Medicine, University of California, Los Angeles, to explore the role biomarker testing plays in managing MBC.
Question: How important is biomarker testing in guiding MBC treatments? Is there a standard or recommended process?
Dr. McCann: Biomarker testing is essential to breast cancer treatment and the development of targeted therapies. Oncologists typically identify a tumor’s canonical biomarkers — ER, PR, and HER2 — using immunohistochemistry or fluorescence in situ hybridization (FISH) testing and then try to match the tumor biology to drugs that target that subtype.
For tumors that lack canonical biomarkers — for example, triple-negative breast cancer (TNBC) — I send the tumor tissue for next-generation sequencing at the time of metastatic diagnosis to identify a wider range of potential targets or oncogenic drivers, such as somatic or germline mutations in homologous recombination repair genes ( BRCA1, BRCA2, and PALB2 ) or mutations in the PI3K/AKT/mTOR pathway.
In our attempts to define tumor biology and design a treatment strategy, two additional issues quickly arise. First, tumors are heterogeneous from the start. Second, tumors evolve.
Let’s start with how we define or subtype a tumor. Would you walk us through this process?
Defining a breast tumor can be tricky because these cancers often don’t fit neatly into predefined categories. Let’s take the estrogen receptor. In clinical trials, we need to define the cutoff for what constitutes ER-positive MBC or TNBC. Some trials define ER-positive as 1% or greater, others define it as 10% or greater.
But is a PR- and HER2-negative tumor with 1% or even 5% ER expression really ER-positive in the biological or prognostic sense? Probably not. A tumor with less than 10% ER expression, for instance, will actually behave like a triple-negative tumor. Instead of choosing a regimen targeting the ER-positive cells, I’ll lean more toward cytotoxic chemotherapy, the standard treatment for TNBC.
Tumors may have multiple drivers as well. What are some aberrations in addition to the main subtypes?
Tumors also often harbor more than one targetable driver. For instance, PIK3CA gene mutations are present in about 40% of hormone receptor–positive, HER2-negative tumors. Activating mutations in ESR1 develop in anywhere from 10% to 50% of MBCs as a resistance mechanism to estrogen deprivation therapy, conferring estrogen independence to the cells. Activating mutations in ERBB2, which essentially turns HER2 into an active receptor, are found in 2%-4% of breast cancers, including ER-positive, HER2-mutant breast cancers, and are enriched in lobular breast cancers, which are typically ER positive, HER2 negative.
What about tumor evolution, given the growing body of evidence that biomarker status in MBC can change over time?
Patients with MBC often have several active areas of cancer, and these areas will evolve differently. During each line of treatment, some metastases will develop resistance and others won’t. For instance, if my patient’s liver metastases start to grow, I will change therapy immediately. If, however, a single bone metastasis begins to grow and the liver metastases have responded well, I might consider local therapy — such as radiation — to target that bone metastasis, though this particular approach hasn’t been formally studied.
Ultimately, we can expect tumors to change over time as they become more biologically aggressive or resistant to current therapy. The most common biomarker change is probably loss of ER or PR expression, but the frequency of ER, PR, or HER2 biomarker changes is still not well understood.
Resistance mutations can also happen. When, for instance, activating mutations in ESR1 occur, the estrogen receptor becomes independent of estrogen and tumors then develop resistance to endocrine therapies. We see a similar problem arise in metastatic prostate cancer. With chronic testosterone deprivation, eventually the androgen receptor evolves to become independent of testosterone in a stage known as castrate-resistant prostate cancer.
Which biomarkers or combinations of biomarkers can be paired with an approved treatment?
We have a range of treatments targeting ER-positive and HER2-positive MBC in particular. For tumors harboring additional targetable mutations, preliminary data suggest that HER2-targeted tyrosine kinase inhibitors (TKIs), such as tucatinib and neratinib, are effective against activating mutations in ERBB2.
The PI3K inhibitor alpelisib in combination with fulvestrant has been approved for patients with ER-positive, HER2-negative MBC and mutations in PIK3CA. The mTOR inhibitor everolimus plus exemestane is an option for patients with ER-positive, HER2-negative. And for those with activating mutations in ESR1, I switch patients to a selective estrogen receptor degrader, such as fulvestrant.
PARP inhibitors, including olaparib or talazoparib, target metastatic HR-positive disease or TNBC with deleterious germline BRCA1 or BRCA2 mutations. Sacituzumab govitecan has been approved for treating metastatic TNBC and targets the cell surface protein TROP2, expressed in almost 90% of TNBC tumors.
What targets, on the other hand, are less informative for treatment choice?
When we order next-generation sequencing, we also will get a list of possible targets for which there are currently no therapeutic options, but there may be in the future. I find this knowledge is helpful. For example, an activating mutation in KRAS tells me that the cancer has a very strong oncogenic driver that I won›t be able to target. I know that activating KRAS mutations in lung cancer and colon cancer portend a poorer prognosis, which helps me to prepare the patient and family.
Atezolizumab in combination with paclitaxel has been FDA-approved for PD-L1 TNBC in the first-line setting, though data show that immune checkpoint inhibitors may be effective even without PD-L1 expression. Although cell surface protein TROP2 has emerged as a target in recent years, its expression is so common in TNBC that confirmatory testing for TROP2 expression is not required to prescribe sacituzumab govitecan.
What factors do you weigh when selecting among the large number of tests available for tumor testing?
We have many biomarker tests available, but the National Comprehensive Cancer Network does not have guidelines for tumor genetics testing in breast cancer. That means insurance does not have to cover the cost, and many companies don’t. Ultimately, though, drug companies and some testing companies have an incentive to cover the cost themselves because a companion diagnostic might be linked to their drug — therascreen PIK3CA RGQ PCR kit for alpelisib, for instance.
I tend not to use a companion diagnostic test because I want more information with a wider panel. The tumor tests I often use are FoundationOne CDx, Caris Molecular Intelligence, and Tempus. I use Tempus because their financial aid is very generous and almost all of my patients qualify to be tested for less than $100. For germline genetic testing, Invitae, Myriad, and Color are also options. Invitae and Color are about $250 out of pocket without insurance. Many academic centers have their own gene panels as well.
How far have we come in identifying biomarkers in MBC?
Targeted treatment for breast cancer has advanced significantly since doing my PhD research in cancer biology about 15 years ago. Of course, targeted therapies for ER-positive and HER2-amplified cancers were available at that point, but many more have been developed. The most significant advance has been the development of efficient and affordable genome sequencing, which has led to these large panels and identification of therapeutic targets. We’ve also expanded our knowledge of genetic predispositions for breast cancer beyond BRCA1 and BRCA2, which not only allows us to preemptively advise patients and their families about cancer risks and recommendations for cancer screening, but also to select a therapy to target a cancer’s DNA repair deficits.
I feel that we are in an exciting discovery phase in oncology. We currently rely on biomarkers to manage MBC and will continue to refine our strategies and develop more effective drug therapies as we identify more oncogenic drivers, tumor-specific proteins, and cancer cell vulnerabilities.
Identifying biomarkers in metastatic breast cancer (MBC) has become an integral part of choosing treatments and understanding disease progression. The American Society of Clinical Oncology Clinical Practice Guideline, published in 2015, recommends an initial biopsy to confirm estrogen receptor (ER), progesterone receptor (PR), or human epidermal growth factor receptor 2 (HER2) status as well as repeat biopsies to watch for receptor status changes over time.
“Decisions concerning the initiation of systemic therapy or selection of systemic therapy for metastatic breast cancer should be guided by ER, PR, and HER2 status in conjunction with clinical evaluation, judgment, and the patient’s goals for care,” according to the guideline authors.This news organization reached out to Kelly McCann, MD, PhD, a hematologist and oncologist in the department of medicine at the David Geffen School of Medicine, University of California, Los Angeles, to explore the role biomarker testing plays in managing MBC.
Question: How important is biomarker testing in guiding MBC treatments? Is there a standard or recommended process?
Dr. McCann: Biomarker testing is essential to breast cancer treatment and the development of targeted therapies. Oncologists typically identify a tumor’s canonical biomarkers — ER, PR, and HER2 — using immunohistochemistry or fluorescence in situ hybridization (FISH) testing and then try to match the tumor biology to drugs that target that subtype.
For tumors that lack canonical biomarkers — for example, triple-negative breast cancer (TNBC) — I send the tumor tissue for next-generation sequencing at the time of metastatic diagnosis to identify a wider range of potential targets or oncogenic drivers, such as somatic or germline mutations in homologous recombination repair genes ( BRCA1, BRCA2, and PALB2 ) or mutations in the PI3K/AKT/mTOR pathway.
In our attempts to define tumor biology and design a treatment strategy, two additional issues quickly arise. First, tumors are heterogeneous from the start. Second, tumors evolve.
Let’s start with how we define or subtype a tumor. Would you walk us through this process?
Defining a breast tumor can be tricky because these cancers often don’t fit neatly into predefined categories. Let’s take the estrogen receptor. In clinical trials, we need to define the cutoff for what constitutes ER-positive MBC or TNBC. Some trials define ER-positive as 1% or greater, others define it as 10% or greater.
But is a PR- and HER2-negative tumor with 1% or even 5% ER expression really ER-positive in the biological or prognostic sense? Probably not. A tumor with less than 10% ER expression, for instance, will actually behave like a triple-negative tumor. Instead of choosing a regimen targeting the ER-positive cells, I’ll lean more toward cytotoxic chemotherapy, the standard treatment for TNBC.
Tumors may have multiple drivers as well. What are some aberrations in addition to the main subtypes?
Tumors also often harbor more than one targetable driver. For instance, PIK3CA gene mutations are present in about 40% of hormone receptor–positive, HER2-negative tumors. Activating mutations in ESR1 develop in anywhere from 10% to 50% of MBCs as a resistance mechanism to estrogen deprivation therapy, conferring estrogen independence to the cells. Activating mutations in ERBB2, which essentially turns HER2 into an active receptor, are found in 2%-4% of breast cancers, including ER-positive, HER2-mutant breast cancers, and are enriched in lobular breast cancers, which are typically ER positive, HER2 negative.
What about tumor evolution, given the growing body of evidence that biomarker status in MBC can change over time?
Patients with MBC often have several active areas of cancer, and these areas will evolve differently. During each line of treatment, some metastases will develop resistance and others won’t. For instance, if my patient’s liver metastases start to grow, I will change therapy immediately. If, however, a single bone metastasis begins to grow and the liver metastases have responded well, I might consider local therapy — such as radiation — to target that bone metastasis, though this particular approach hasn’t been formally studied.
Ultimately, we can expect tumors to change over time as they become more biologically aggressive or resistant to current therapy. The most common biomarker change is probably loss of ER or PR expression, but the frequency of ER, PR, or HER2 biomarker changes is still not well understood.
Resistance mutations can also happen. When, for instance, activating mutations in ESR1 occur, the estrogen receptor becomes independent of estrogen and tumors then develop resistance to endocrine therapies. We see a similar problem arise in metastatic prostate cancer. With chronic testosterone deprivation, eventually the androgen receptor evolves to become independent of testosterone in a stage known as castrate-resistant prostate cancer.
Which biomarkers or combinations of biomarkers can be paired with an approved treatment?
We have a range of treatments targeting ER-positive and HER2-positive MBC in particular. For tumors harboring additional targetable mutations, preliminary data suggest that HER2-targeted tyrosine kinase inhibitors (TKIs), such as tucatinib and neratinib, are effective against activating mutations in ERBB2.
The PI3K inhibitor alpelisib in combination with fulvestrant has been approved for patients with ER-positive, HER2-negative MBC and mutations in PIK3CA. The mTOR inhibitor everolimus plus exemestane is an option for patients with ER-positive, HER2-negative. And for those with activating mutations in ESR1, I switch patients to a selective estrogen receptor degrader, such as fulvestrant.
PARP inhibitors, including olaparib or talazoparib, target metastatic HR-positive disease or TNBC with deleterious germline BRCA1 or BRCA2 mutations. Sacituzumab govitecan has been approved for treating metastatic TNBC and targets the cell surface protein TROP2, expressed in almost 90% of TNBC tumors.
What targets, on the other hand, are less informative for treatment choice?
When we order next-generation sequencing, we also will get a list of possible targets for which there are currently no therapeutic options, but there may be in the future. I find this knowledge is helpful. For example, an activating mutation in KRAS tells me that the cancer has a very strong oncogenic driver that I won›t be able to target. I know that activating KRAS mutations in lung cancer and colon cancer portend a poorer prognosis, which helps me to prepare the patient and family.
Atezolizumab in combination with paclitaxel has been FDA-approved for PD-L1 TNBC in the first-line setting, though data show that immune checkpoint inhibitors may be effective even without PD-L1 expression. Although cell surface protein TROP2 has emerged as a target in recent years, its expression is so common in TNBC that confirmatory testing for TROP2 expression is not required to prescribe sacituzumab govitecan.
What factors do you weigh when selecting among the large number of tests available for tumor testing?
We have many biomarker tests available, but the National Comprehensive Cancer Network does not have guidelines for tumor genetics testing in breast cancer. That means insurance does not have to cover the cost, and many companies don’t. Ultimately, though, drug companies and some testing companies have an incentive to cover the cost themselves because a companion diagnostic might be linked to their drug — therascreen PIK3CA RGQ PCR kit for alpelisib, for instance.
I tend not to use a companion diagnostic test because I want more information with a wider panel. The tumor tests I often use are FoundationOne CDx, Caris Molecular Intelligence, and Tempus. I use Tempus because their financial aid is very generous and almost all of my patients qualify to be tested for less than $100. For germline genetic testing, Invitae, Myriad, and Color are also options. Invitae and Color are about $250 out of pocket without insurance. Many academic centers have their own gene panels as well.
How far have we come in identifying biomarkers in MBC?
Targeted treatment for breast cancer has advanced significantly since doing my PhD research in cancer biology about 15 years ago. Of course, targeted therapies for ER-positive and HER2-amplified cancers were available at that point, but many more have been developed. The most significant advance has been the development of efficient and affordable genome sequencing, which has led to these large panels and identification of therapeutic targets. We’ve also expanded our knowledge of genetic predispositions for breast cancer beyond BRCA1 and BRCA2, which not only allows us to preemptively advise patients and their families about cancer risks and recommendations for cancer screening, but also to select a therapy to target a cancer’s DNA repair deficits.
I feel that we are in an exciting discovery phase in oncology. We currently rely on biomarkers to manage MBC and will continue to refine our strategies and develop more effective drug therapies as we identify more oncogenic drivers, tumor-specific proteins, and cancer cell vulnerabilities.
MRI screening cost effective for women with dense breasts
Alternatively, if a woman worries that the 4-year screening interval is too long, screening mammography may be offered every 2 years, with MRI screening offered for the second 2-year interval, according to the findings. This strategy would still require the patient to undergo MRI breast cancer screening every 4 years.
“MRI is more effective not only for selected patients. It is actually more effective than mammography for all women,” editorialist Christiane Kuhl, MD, PhD, University of Aachen (Germany), said in an interview.
“But the superior diagnostic accuracy of MRI is more often needed for women who are at higher risk for breast cancer, and therefore the cost-effectiveness is easier to achieve in women who are at higher risk,” she added.
The study was published online Sept. 29 in the Journal of the National Cancer Institute.
DENSE trial
The simulation model used for the study was based on results from the Dense Tissue and Early Breast Neoplasm Screening (DENSE) trial, which showed that additional MRI screening for women with extremely dense breast tissue led to significantly fewer interval cancers in comparison with mammography alone (P < .001). In the DENSE trial, MRI participants underwent mammography plus MRI at 2-year intervals; the control group underwent mammography alone at 2-year intervals.
In the current study, “screening strategies varied in the number of MRIs and mammograms offered to women aged 50-75 years,” explains Amarens Geuzinge, MSc, University Medical Center, Rotterdam, the Netherlands, and colleagues, “and incremental cost-effectiveness ratios (ICERs) were calculated ... with a willingness-to-pay threshold of 22,000 euros (>$25,000 U.S.),” the investigators add.
Analyses indicated that screening every 2 years with mammography alone cost the least of all strategies that were evaluated, but it also resulted in the lowest number of quality-adjusted life years (QALYs) – in other words, it delivered the least amount of benefit for patients, coauthor Eveline Heijnsdijk, PhD, University Medical Center, Rotterdam, the Netherlands, explained to this news organization.
Offering an additional MRI every 2 years resulted in the highest costs but not the highest number of QALYs and was inferior to the other screening strategies analyzed, she added. Alternating mammography with MRI breast cancer screening, each conducted every 2 years, came close to providing the same benefits to patients as the every-4-year MRI screening strategy, Dr. Heijnsdijk noted.
However, when the authors applied the National Institute for Health and Care Excellence (NICE) threshold, MRI screening every 4 years yielded the highest acceptable incremental cost-effectiveness ratio (ICER), at 15,620 euros per QALYs, whereas screening every 3 years with MRI alone yielded an ICER of 37,181 euros per QALY.
If decision-makers are willing to pay more than 22,000 euros per QALY gained, “MRI every 2 or 3 years can also become cost effective,” the authors add.
Asked how acceptable MRI screening might be if performed only once every 4 years, Dr. Heijnsdijk noted that, in another of their studies, most of the women who had undergone MRI screening for breast cancer said that they would do so again. “MRI is not a pleasant test, but mammography is also not a pleasant test,” she said.
“So many women prefer MRI above mammography, especially because the detection rate with MRI is better than mammography,” she noted. Dr. Heijnsdijk also said that the percentage of women with extremely dense breasts who would be candidates for MRI screening is small – no more than 10% of women.
At a unit cost of slightly under 300 euros for MRI screening – compared with about 100 euros for screening mammography in the Netherlands – the cost of offering 10% of women MRI instead of mammography might increase, but any additional screening costs could be offset by reductions in the need to treat late-stage breast cancer more aggressively.
‘Interval’ cancers
Commenting further on the study, Dr. Kuhl pointed out that from 25% to 45% of cancers that occur in women who have undergone screening mammography are diagnosed as “interval” cancers, even among women who participate in the best mammography programs. “For a long time, people argued that these interval cancers developed only after the last respective mammogram, but that’s not true at all, because we know that with MRI screening, we can reduce the interval cancer rate down to zero,” Dr. Kuhl emphasized.
This is partially explained by the fact that mammography is “particularly blind” when it comes to detecting rapidly growing tumors. “The fact is that mammography has a modality-inherent tendency to preferentially detect slow-growing cancers, whereas rapidly growing tumors are indistinguishable from ubiquitous benign changes like cysts. [This] is why women who undergo screening mammography are frequently not diagnosed with the cancers that we really need to find,” she said.
Although there is ample talk about overdiagnosis when it comes to screening mammography, the overwhelmingly important problem is underdiagnosis. Even in exemplary mammography screening programs, at least 20% of tumors that are diagnosed on mammography have already advanced to a stage that is too late, Dr. Kuhl noted.
This means that at least half of women do not benefit from screening mammography nearly to the extent that they – and their health care practitioners – believe they should, she added. Dr. Kuhl underscored that this does not mean that clinicians should abandon screening mammography.
What it does mean is that physicians need to abandon the one-size-fits-all approach to screening mammography and start stratifying women on the basis of their individual risk of developing breast cancer by taking a family or personal history. Most women do undergo screening mammography at least once, Dr. Kuhl pointed out. From that mammogram, physicians can use information on breast density and breast architecture to better determine individual risk.
“We have good ideas about how to achieve risk stratification, but we’re not using them, because as long as mammography is the answer for everybody, there isn’t much motivation to dig deeper into the issue of how to determine risk,” Dr. Kuhl said.
“But we have to ensure the early diagnosis of aggressive cancers, and it’s exactly MRI that can do this, and we should start with women with very dense breasts because they are doubly underserved by mammography,” she said.
The study was supported by the University Medical Center Utrecht, Bayer HealthCare Medical Care, Matakina, and others. Ms. Geuzinge, Dr. Heijnsdijk, and Dr. Kuhl have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Alternatively, if a woman worries that the 4-year screening interval is too long, screening mammography may be offered every 2 years, with MRI screening offered for the second 2-year interval, according to the findings. This strategy would still require the patient to undergo MRI breast cancer screening every 4 years.
“MRI is more effective not only for selected patients. It is actually more effective than mammography for all women,” editorialist Christiane Kuhl, MD, PhD, University of Aachen (Germany), said in an interview.
“But the superior diagnostic accuracy of MRI is more often needed for women who are at higher risk for breast cancer, and therefore the cost-effectiveness is easier to achieve in women who are at higher risk,” she added.
The study was published online Sept. 29 in the Journal of the National Cancer Institute.
DENSE trial
The simulation model used for the study was based on results from the Dense Tissue and Early Breast Neoplasm Screening (DENSE) trial, which showed that additional MRI screening for women with extremely dense breast tissue led to significantly fewer interval cancers in comparison with mammography alone (P < .001). In the DENSE trial, MRI participants underwent mammography plus MRI at 2-year intervals; the control group underwent mammography alone at 2-year intervals.
In the current study, “screening strategies varied in the number of MRIs and mammograms offered to women aged 50-75 years,” explains Amarens Geuzinge, MSc, University Medical Center, Rotterdam, the Netherlands, and colleagues, “and incremental cost-effectiveness ratios (ICERs) were calculated ... with a willingness-to-pay threshold of 22,000 euros (>$25,000 U.S.),” the investigators add.
Analyses indicated that screening every 2 years with mammography alone cost the least of all strategies that were evaluated, but it also resulted in the lowest number of quality-adjusted life years (QALYs) – in other words, it delivered the least amount of benefit for patients, coauthor Eveline Heijnsdijk, PhD, University Medical Center, Rotterdam, the Netherlands, explained to this news organization.
Offering an additional MRI every 2 years resulted in the highest costs but not the highest number of QALYs and was inferior to the other screening strategies analyzed, she added. Alternating mammography with MRI breast cancer screening, each conducted every 2 years, came close to providing the same benefits to patients as the every-4-year MRI screening strategy, Dr. Heijnsdijk noted.
However, when the authors applied the National Institute for Health and Care Excellence (NICE) threshold, MRI screening every 4 years yielded the highest acceptable incremental cost-effectiveness ratio (ICER), at 15,620 euros per QALYs, whereas screening every 3 years with MRI alone yielded an ICER of 37,181 euros per QALY.
If decision-makers are willing to pay more than 22,000 euros per QALY gained, “MRI every 2 or 3 years can also become cost effective,” the authors add.
Asked how acceptable MRI screening might be if performed only once every 4 years, Dr. Heijnsdijk noted that, in another of their studies, most of the women who had undergone MRI screening for breast cancer said that they would do so again. “MRI is not a pleasant test, but mammography is also not a pleasant test,” she said.
“So many women prefer MRI above mammography, especially because the detection rate with MRI is better than mammography,” she noted. Dr. Heijnsdijk also said that the percentage of women with extremely dense breasts who would be candidates for MRI screening is small – no more than 10% of women.
At a unit cost of slightly under 300 euros for MRI screening – compared with about 100 euros for screening mammography in the Netherlands – the cost of offering 10% of women MRI instead of mammography might increase, but any additional screening costs could be offset by reductions in the need to treat late-stage breast cancer more aggressively.
‘Interval’ cancers
Commenting further on the study, Dr. Kuhl pointed out that from 25% to 45% of cancers that occur in women who have undergone screening mammography are diagnosed as “interval” cancers, even among women who participate in the best mammography programs. “For a long time, people argued that these interval cancers developed only after the last respective mammogram, but that’s not true at all, because we know that with MRI screening, we can reduce the interval cancer rate down to zero,” Dr. Kuhl emphasized.
This is partially explained by the fact that mammography is “particularly blind” when it comes to detecting rapidly growing tumors. “The fact is that mammography has a modality-inherent tendency to preferentially detect slow-growing cancers, whereas rapidly growing tumors are indistinguishable from ubiquitous benign changes like cysts. [This] is why women who undergo screening mammography are frequently not diagnosed with the cancers that we really need to find,” she said.
Although there is ample talk about overdiagnosis when it comes to screening mammography, the overwhelmingly important problem is underdiagnosis. Even in exemplary mammography screening programs, at least 20% of tumors that are diagnosed on mammography have already advanced to a stage that is too late, Dr. Kuhl noted.
This means that at least half of women do not benefit from screening mammography nearly to the extent that they – and their health care practitioners – believe they should, she added. Dr. Kuhl underscored that this does not mean that clinicians should abandon screening mammography.
What it does mean is that physicians need to abandon the one-size-fits-all approach to screening mammography and start stratifying women on the basis of their individual risk of developing breast cancer by taking a family or personal history. Most women do undergo screening mammography at least once, Dr. Kuhl pointed out. From that mammogram, physicians can use information on breast density and breast architecture to better determine individual risk.
“We have good ideas about how to achieve risk stratification, but we’re not using them, because as long as mammography is the answer for everybody, there isn’t much motivation to dig deeper into the issue of how to determine risk,” Dr. Kuhl said.
“But we have to ensure the early diagnosis of aggressive cancers, and it’s exactly MRI that can do this, and we should start with women with very dense breasts because they are doubly underserved by mammography,” she said.
The study was supported by the University Medical Center Utrecht, Bayer HealthCare Medical Care, Matakina, and others. Ms. Geuzinge, Dr. Heijnsdijk, and Dr. Kuhl have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Alternatively, if a woman worries that the 4-year screening interval is too long, screening mammography may be offered every 2 years, with MRI screening offered for the second 2-year interval, according to the findings. This strategy would still require the patient to undergo MRI breast cancer screening every 4 years.
“MRI is more effective not only for selected patients. It is actually more effective than mammography for all women,” editorialist Christiane Kuhl, MD, PhD, University of Aachen (Germany), said in an interview.
“But the superior diagnostic accuracy of MRI is more often needed for women who are at higher risk for breast cancer, and therefore the cost-effectiveness is easier to achieve in women who are at higher risk,” she added.
The study was published online Sept. 29 in the Journal of the National Cancer Institute.
DENSE trial
The simulation model used for the study was based on results from the Dense Tissue and Early Breast Neoplasm Screening (DENSE) trial, which showed that additional MRI screening for women with extremely dense breast tissue led to significantly fewer interval cancers in comparison with mammography alone (P < .001). In the DENSE trial, MRI participants underwent mammography plus MRI at 2-year intervals; the control group underwent mammography alone at 2-year intervals.
In the current study, “screening strategies varied in the number of MRIs and mammograms offered to women aged 50-75 years,” explains Amarens Geuzinge, MSc, University Medical Center, Rotterdam, the Netherlands, and colleagues, “and incremental cost-effectiveness ratios (ICERs) were calculated ... with a willingness-to-pay threshold of 22,000 euros (>$25,000 U.S.),” the investigators add.
Analyses indicated that screening every 2 years with mammography alone cost the least of all strategies that were evaluated, but it also resulted in the lowest number of quality-adjusted life years (QALYs) – in other words, it delivered the least amount of benefit for patients, coauthor Eveline Heijnsdijk, PhD, University Medical Center, Rotterdam, the Netherlands, explained to this news organization.
Offering an additional MRI every 2 years resulted in the highest costs but not the highest number of QALYs and was inferior to the other screening strategies analyzed, she added. Alternating mammography with MRI breast cancer screening, each conducted every 2 years, came close to providing the same benefits to patients as the every-4-year MRI screening strategy, Dr. Heijnsdijk noted.
However, when the authors applied the National Institute for Health and Care Excellence (NICE) threshold, MRI screening every 4 years yielded the highest acceptable incremental cost-effectiveness ratio (ICER), at 15,620 euros per QALYs, whereas screening every 3 years with MRI alone yielded an ICER of 37,181 euros per QALY.
If decision-makers are willing to pay more than 22,000 euros per QALY gained, “MRI every 2 or 3 years can also become cost effective,” the authors add.
Asked how acceptable MRI screening might be if performed only once every 4 years, Dr. Heijnsdijk noted that, in another of their studies, most of the women who had undergone MRI screening for breast cancer said that they would do so again. “MRI is not a pleasant test, but mammography is also not a pleasant test,” she said.
“So many women prefer MRI above mammography, especially because the detection rate with MRI is better than mammography,” she noted. Dr. Heijnsdijk also said that the percentage of women with extremely dense breasts who would be candidates for MRI screening is small – no more than 10% of women.
At a unit cost of slightly under 300 euros for MRI screening – compared with about 100 euros for screening mammography in the Netherlands – the cost of offering 10% of women MRI instead of mammography might increase, but any additional screening costs could be offset by reductions in the need to treat late-stage breast cancer more aggressively.
‘Interval’ cancers
Commenting further on the study, Dr. Kuhl pointed out that from 25% to 45% of cancers that occur in women who have undergone screening mammography are diagnosed as “interval” cancers, even among women who participate in the best mammography programs. “For a long time, people argued that these interval cancers developed only after the last respective mammogram, but that’s not true at all, because we know that with MRI screening, we can reduce the interval cancer rate down to zero,” Dr. Kuhl emphasized.
This is partially explained by the fact that mammography is “particularly blind” when it comes to detecting rapidly growing tumors. “The fact is that mammography has a modality-inherent tendency to preferentially detect slow-growing cancers, whereas rapidly growing tumors are indistinguishable from ubiquitous benign changes like cysts. [This] is why women who undergo screening mammography are frequently not diagnosed with the cancers that we really need to find,” she said.
Although there is ample talk about overdiagnosis when it comes to screening mammography, the overwhelmingly important problem is underdiagnosis. Even in exemplary mammography screening programs, at least 20% of tumors that are diagnosed on mammography have already advanced to a stage that is too late, Dr. Kuhl noted.
This means that at least half of women do not benefit from screening mammography nearly to the extent that they – and their health care practitioners – believe they should, she added. Dr. Kuhl underscored that this does not mean that clinicians should abandon screening mammography.
What it does mean is that physicians need to abandon the one-size-fits-all approach to screening mammography and start stratifying women on the basis of their individual risk of developing breast cancer by taking a family or personal history. Most women do undergo screening mammography at least once, Dr. Kuhl pointed out. From that mammogram, physicians can use information on breast density and breast architecture to better determine individual risk.
“We have good ideas about how to achieve risk stratification, but we’re not using them, because as long as mammography is the answer for everybody, there isn’t much motivation to dig deeper into the issue of how to determine risk,” Dr. Kuhl said.
“But we have to ensure the early diagnosis of aggressive cancers, and it’s exactly MRI that can do this, and we should start with women with very dense breasts because they are doubly underserved by mammography,” she said.
The study was supported by the University Medical Center Utrecht, Bayer HealthCare Medical Care, Matakina, and others. Ms. Geuzinge, Dr. Heijnsdijk, and Dr. Kuhl have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Many patients, doctors unaware of advancements in cancer care
This is the main finding from two studies presented at the 2021 European Society for Medical Oncology Congress.
The survey of patients found that most don’t understand how immunotherapy works, and the survey of doctors found that many working outside of the cancer field are using information on survival that is wildly out of date.
When a patient is first told they have cancer, counseling is usually done by a surgeon or general medical doctor and not an oncologist, said Conleth Murphy, MD, of Bon Secours Hospital Cork, Ireland, and coauthor of the second study.
Noncancer doctors often grossly underestimate patients’ chances of survival, Dr. Murphy’s study found. This suggests that doctors who practice outside of cancer care may be working with the same information they learned in medical school, he said.
“These patients must be spared the traumatic effects of being handed a death sentence that no longer reflects the current reality,” Dr. Murphy said.
After receiving a diagnosis of cancer, “patients often immediately have pressing questions about what it means for their future,” he noted. A common question is: “How long do I have left?”
Nononcologists should refrain from answering patients’ questions with numbers, Dr. Murphy said.
Family doctors are likely to be influenced by the experience they have had with specific cancer patients in their practice, said Cyril Bonin, MD, a general practitioner in Usson-du-Poitou, France, who has 900 patients in his practice.
He sees about 10 patients with a new diagnosis of cancer each year. In addition, about 50 of his patients are in active treatment for cancer or have finished treatment and are considered cancer survivors.
“It is not entirely realistic for us to expect practitioners who deal with hundreds of different diseases to keep up with every facet of a rapidly changing oncology landscape,” said Marco Donia, MD, an expert in immunotherapy from the University of Copenhagen.
That landscape has changed dramatically in recent years, particularly since immunotherapy was added to the arsenal. Immunotherapy is a way to fine-tune your immune system to fight cancer.
For example, in the past, patients with metastatic melanoma would have an average survival of about 1 year. But now, some patients who have responded to immunotherapy are still alive 10 years later.
Findings from the patient survey
It is important that patients stay well informed because immunotherapy is a “complex treatment that is too often mistaken for a miracle cure,” said Paris Kosmidis, MD, the co-author of the patient survey.
“The more patients know about it, the better the communication with their medical team and thus the better their outcomes are likely to be,” said Dr. Kosmidis, who is co-founder and chief medical officer of CareAcross, an online service that provides personalized education for cancer patients
The survey was of 5,589 patients with cancer who were recruited from CareAcross clients from the United Kingdom, France, Italy, Spain, and Germany.
The survey asked them about how immunotherapy works, what it costs, and its side effects.
Almost half responded “not sure/do not know,” but about a third correctly answered that immunotherapy “activates the immune system to kill cancer cells.”
Similarly, more than half thought that immunotherapy started working right away, while only 20% correctly answered that it takes several weeks to become effective.
“This is important because patients need to start their therapy with realistic expectations, for example to avoid disappointment when their symptoms take some time to disappear,” Dr. Kosmidis said.
A small group of 24 patients with lung cancer who had been treated with immunotherapy got many correct answers, but they overestimated the intensity of side effects, compared with other therapies.
“Well-informed patients who know what to expect can do 90% of the job of preventing side effects from becoming severe by having them treated early,” said Dr. Donia, of the University of Copenhagen.
Most cancer patients were also unaware of the cost of immunotherapy, which can exceed $100,000 a year, Dr. Kosmidis said.
Results of the doctor survey
The other survey presented at the meeting looked at how much doctors know about survival for 12 of the most common cancers.
Dr. Murphy and colleagues asked 301 noncancer doctors and 46 cancer specialists to estimate the percentage of patients who could be expected to live for 5 years after diagnosis (a measure known as the 5-year survival rate).
Answers from the two groups were compared and graded according to cancer survival statistics from the National Cancer Registry of Ireland.
Both groups of doctors had a hard time estimating the survival of common cancers.
Nononcologists accurately predicted 5-year survival for just two of the cancer types, while the cancer specialists got it right for four cancer types.
However, the noncancer doctors had a more pessimistic outlook on cancer survival generally and severely underestimated the chances of survival in specific cancers, particularly stage IV breast cancer. The survival for this cancer has “evolved considerably over time and now reaches 40% in Ireland,” Dr. Murphy pointed out.
“These results are in line with what we had expected because most physicians’ knowledge of oncology dates back to whatever education they received during their years of training, so their perceptions of cancer prognosis are likely to lag behind the major survival gains achieved in the recent past,” Dr. Murphy said.
A version of this article first appeared on Medscape.com.
This is the main finding from two studies presented at the 2021 European Society for Medical Oncology Congress.
The survey of patients found that most don’t understand how immunotherapy works, and the survey of doctors found that many working outside of the cancer field are using information on survival that is wildly out of date.
When a patient is first told they have cancer, counseling is usually done by a surgeon or general medical doctor and not an oncologist, said Conleth Murphy, MD, of Bon Secours Hospital Cork, Ireland, and coauthor of the second study.
Noncancer doctors often grossly underestimate patients’ chances of survival, Dr. Murphy’s study found. This suggests that doctors who practice outside of cancer care may be working with the same information they learned in medical school, he said.
“These patients must be spared the traumatic effects of being handed a death sentence that no longer reflects the current reality,” Dr. Murphy said.
After receiving a diagnosis of cancer, “patients often immediately have pressing questions about what it means for their future,” he noted. A common question is: “How long do I have left?”
Nononcologists should refrain from answering patients’ questions with numbers, Dr. Murphy said.
Family doctors are likely to be influenced by the experience they have had with specific cancer patients in their practice, said Cyril Bonin, MD, a general practitioner in Usson-du-Poitou, France, who has 900 patients in his practice.
He sees about 10 patients with a new diagnosis of cancer each year. In addition, about 50 of his patients are in active treatment for cancer or have finished treatment and are considered cancer survivors.
“It is not entirely realistic for us to expect practitioners who deal with hundreds of different diseases to keep up with every facet of a rapidly changing oncology landscape,” said Marco Donia, MD, an expert in immunotherapy from the University of Copenhagen.
That landscape has changed dramatically in recent years, particularly since immunotherapy was added to the arsenal. Immunotherapy is a way to fine-tune your immune system to fight cancer.
For example, in the past, patients with metastatic melanoma would have an average survival of about 1 year. But now, some patients who have responded to immunotherapy are still alive 10 years later.
Findings from the patient survey
It is important that patients stay well informed because immunotherapy is a “complex treatment that is too often mistaken for a miracle cure,” said Paris Kosmidis, MD, the co-author of the patient survey.
“The more patients know about it, the better the communication with their medical team and thus the better their outcomes are likely to be,” said Dr. Kosmidis, who is co-founder and chief medical officer of CareAcross, an online service that provides personalized education for cancer patients
The survey was of 5,589 patients with cancer who were recruited from CareAcross clients from the United Kingdom, France, Italy, Spain, and Germany.
The survey asked them about how immunotherapy works, what it costs, and its side effects.
Almost half responded “not sure/do not know,” but about a third correctly answered that immunotherapy “activates the immune system to kill cancer cells.”
Similarly, more than half thought that immunotherapy started working right away, while only 20% correctly answered that it takes several weeks to become effective.
“This is important because patients need to start their therapy with realistic expectations, for example to avoid disappointment when their symptoms take some time to disappear,” Dr. Kosmidis said.
A small group of 24 patients with lung cancer who had been treated with immunotherapy got many correct answers, but they overestimated the intensity of side effects, compared with other therapies.
“Well-informed patients who know what to expect can do 90% of the job of preventing side effects from becoming severe by having them treated early,” said Dr. Donia, of the University of Copenhagen.
Most cancer patients were also unaware of the cost of immunotherapy, which can exceed $100,000 a year, Dr. Kosmidis said.
Results of the doctor survey
The other survey presented at the meeting looked at how much doctors know about survival for 12 of the most common cancers.
Dr. Murphy and colleagues asked 301 noncancer doctors and 46 cancer specialists to estimate the percentage of patients who could be expected to live for 5 years after diagnosis (a measure known as the 5-year survival rate).
Answers from the two groups were compared and graded according to cancer survival statistics from the National Cancer Registry of Ireland.
Both groups of doctors had a hard time estimating the survival of common cancers.
Nononcologists accurately predicted 5-year survival for just two of the cancer types, while the cancer specialists got it right for four cancer types.
However, the noncancer doctors had a more pessimistic outlook on cancer survival generally and severely underestimated the chances of survival in specific cancers, particularly stage IV breast cancer. The survival for this cancer has “evolved considerably over time and now reaches 40% in Ireland,” Dr. Murphy pointed out.
“These results are in line with what we had expected because most physicians’ knowledge of oncology dates back to whatever education they received during their years of training, so their perceptions of cancer prognosis are likely to lag behind the major survival gains achieved in the recent past,” Dr. Murphy said.
A version of this article first appeared on Medscape.com.
This is the main finding from two studies presented at the 2021 European Society for Medical Oncology Congress.
The survey of patients found that most don’t understand how immunotherapy works, and the survey of doctors found that many working outside of the cancer field are using information on survival that is wildly out of date.
When a patient is first told they have cancer, counseling is usually done by a surgeon or general medical doctor and not an oncologist, said Conleth Murphy, MD, of Bon Secours Hospital Cork, Ireland, and coauthor of the second study.
Noncancer doctors often grossly underestimate patients’ chances of survival, Dr. Murphy’s study found. This suggests that doctors who practice outside of cancer care may be working with the same information they learned in medical school, he said.
“These patients must be spared the traumatic effects of being handed a death sentence that no longer reflects the current reality,” Dr. Murphy said.
After receiving a diagnosis of cancer, “patients often immediately have pressing questions about what it means for their future,” he noted. A common question is: “How long do I have left?”
Nononcologists should refrain from answering patients’ questions with numbers, Dr. Murphy said.
Family doctors are likely to be influenced by the experience they have had with specific cancer patients in their practice, said Cyril Bonin, MD, a general practitioner in Usson-du-Poitou, France, who has 900 patients in his practice.
He sees about 10 patients with a new diagnosis of cancer each year. In addition, about 50 of his patients are in active treatment for cancer or have finished treatment and are considered cancer survivors.
“It is not entirely realistic for us to expect practitioners who deal with hundreds of different diseases to keep up with every facet of a rapidly changing oncology landscape,” said Marco Donia, MD, an expert in immunotherapy from the University of Copenhagen.
That landscape has changed dramatically in recent years, particularly since immunotherapy was added to the arsenal. Immunotherapy is a way to fine-tune your immune system to fight cancer.
For example, in the past, patients with metastatic melanoma would have an average survival of about 1 year. But now, some patients who have responded to immunotherapy are still alive 10 years later.
Findings from the patient survey
It is important that patients stay well informed because immunotherapy is a “complex treatment that is too often mistaken for a miracle cure,” said Paris Kosmidis, MD, the co-author of the patient survey.
“The more patients know about it, the better the communication with their medical team and thus the better their outcomes are likely to be,” said Dr. Kosmidis, who is co-founder and chief medical officer of CareAcross, an online service that provides personalized education for cancer patients
The survey was of 5,589 patients with cancer who were recruited from CareAcross clients from the United Kingdom, France, Italy, Spain, and Germany.
The survey asked them about how immunotherapy works, what it costs, and its side effects.
Almost half responded “not sure/do not know,” but about a third correctly answered that immunotherapy “activates the immune system to kill cancer cells.”
Similarly, more than half thought that immunotherapy started working right away, while only 20% correctly answered that it takes several weeks to become effective.
“This is important because patients need to start their therapy with realistic expectations, for example to avoid disappointment when their symptoms take some time to disappear,” Dr. Kosmidis said.
A small group of 24 patients with lung cancer who had been treated with immunotherapy got many correct answers, but they overestimated the intensity of side effects, compared with other therapies.
“Well-informed patients who know what to expect can do 90% of the job of preventing side effects from becoming severe by having them treated early,” said Dr. Donia, of the University of Copenhagen.
Most cancer patients were also unaware of the cost of immunotherapy, which can exceed $100,000 a year, Dr. Kosmidis said.
Results of the doctor survey
The other survey presented at the meeting looked at how much doctors know about survival for 12 of the most common cancers.
Dr. Murphy and colleagues asked 301 noncancer doctors and 46 cancer specialists to estimate the percentage of patients who could be expected to live for 5 years after diagnosis (a measure known as the 5-year survival rate).
Answers from the two groups were compared and graded according to cancer survival statistics from the National Cancer Registry of Ireland.
Both groups of doctors had a hard time estimating the survival of common cancers.
Nononcologists accurately predicted 5-year survival for just two of the cancer types, while the cancer specialists got it right for four cancer types.
However, the noncancer doctors had a more pessimistic outlook on cancer survival generally and severely underestimated the chances of survival in specific cancers, particularly stage IV breast cancer. The survival for this cancer has “evolved considerably over time and now reaches 40% in Ireland,” Dr. Murphy pointed out.
“These results are in line with what we had expected because most physicians’ knowledge of oncology dates back to whatever education they received during their years of training, so their perceptions of cancer prognosis are likely to lag behind the major survival gains achieved in the recent past,” Dr. Murphy said.
A version of this article first appeared on Medscape.com.
Novel trastuzumab duocarmazine significantly improved survival in advanced HER2-positive breast cancer
Based on significant progression-free survival (PFS) benefits shown in the phase 3 TULIP trial, trastuzumab duocarmazine (SYD985) may provide a new treatment option among HER2-positive metastatic breast cancer patients, according to Cristina Saura, MD, head of the breast cancer program at Vall d’Hebron University Hospital, Barcelona. Dr. Saura presented the results of the TULIP trial (abstract LBA15) on Sept. 19 at the 2021 European Society for Medical Oncology Congress.
Trastuzumab duocarmazine is a novel HER2-targeting antibody-drug conjugate that consists of trastuzumab and a drug containing duocarmycin. Its three-way mechanism of action includes uptake of the antibody-drug conjugate by internalization and intracellular release of duocarmycin with two bystander effects: proteolytic cleavage and subsequent release of payload in the tumor microenvironment and diffusion of active payload to neighboring tumor cells.
While one physician described the results as encouraging, another said the treatment is not nearly ready for primetime.
“It is encouraging to observe clinically meaningful and potentially practice changing progression-free survival improvements in patients receiving treatment in the third line and beyond,” said Aditya Bardia, MD, Massachusetts General Hospital, Boston. “Several agents have been approved as treatments for HER2-positive metastatic breast cancer in recent years including T-DXd, neratinib, tucatinib, and margetuximab. Trastuzumab duocarmazine could eventually be another option.”
Fatima Cardoso, MD, director of the breast cancer unit at the Breast Cancer Research Foundation, New York, said: “At this time there is only a minor 2-month difference in progression-free survival and a nonsignificant overall difference. With the high incidence of ocular toxicity and four toxic deaths, we cannot recommend this drug for clinical practice, in my opinion.”
Two or more prior therapies for metastatic breast cancer
TULIP investigators enrolled 437 patients from 83 sites in 11 countries with HER2-positive locally advanced or metastatic breast cancer who had received two or more therapies for metastatic disease (treatment for brain metastases allowed). They were randomized 2:1 to trastuzumab duocarmazine (1.2 mg/kg every 21 days, 291 patients) or physician’s choice (146 patients) of one of three trastuzumab-containing combinations or lapatinib plus capecitabine. Treatment was continued until progression or unacceptable toxicity. The primary endpoint was centrally assessed PFS.
Longer PFS with trastuzumab duocarmazine
Median age was 57 years, and the median number of prior metastatic breast cancer regimens was 4.7. Centrally reviewed PFS was significantly longer in the trastuzumab duocarmazine group at 7.0 months versus 4.9 months for physicians choice treatment (hazard ratio, 0.64; 95% confidence interval, 0.49-0.84; P = .002). Subgroup analysis, also centrally reviewed, revealed numerical advantage for trastuzumab duocarmazine over physician’s choice across all categories (except for Eastern Cooperative Oncology Group status 2). Analysis of PFS by investigators showed a similar benefit for trastuzumab duocarmazine (6.9 months vs. 4.6 months; HR, 0.60; P < .001).
A first look at median overall survival showed a nonsignificant advantage for trastuzumab duocarmazine (20.4 months vs. 16.3 months (HR, 0.83; 95% CI, 0.62-1.09, P = .153). The overall response rate (partial or complete response) was similar between groups at 27.8% for trastuzumab duocarmazine and 29.5% for physician’s choice with reductions in target lesion measurement at 70.2% and 32.2% for trastuzumab duocarmazine and physician’s choice, respectively. The clinical benefit rates were 38.5% for trastuzumab duocarmazine and 32.2% for physician’s choice.
Ocular toxicity
Most patients had at least one treatment-related adverse event (96.5% SD985, 96.4% PC), and grade 3 or higher event rates were similar between groups (52.8% SYD985, 48.2% PC). The most frequently reported adverse events for trastuzumab duocarmazine were ocular toxicity, with conjunctivitis reported in 38.2%, and keratitis in 38.2%, with fatigue at 33.3%; for physician’s choice these were diarrhea (35.8%), nausea (31.4%) and fatigue (29.9%). Interstitial lung disease pneumonitis was reported for 7.6% (5.2% grade 1-2) of patients treated with trastuzumab duocarmazine, including two grade 5 events.
Eye toxicity led to discontinuations in 20.8% of trastuzumab duocarmazine patients, dose modifications in 22.9%, with dose modifications for interstitial lung disease/pneumonitis in 5.2% of trastuzumab duocarmazine patients. Six fatalities (2.1%) were reported in the trastuzumab duocarmazine group, with four attributed to treatment. Assessment of health-related quality of life showed no significant difference between groups.
Dr. Manich outlined risk mitigation strategies. Patients with prior keratitis were excluded and patients were given prophylactic lubricating eye drops and regular eye exams by ophthalmologists. Treatment was discontinued if grade 3 or higher keratitis developed, and was delayed if grade 3 conjunctivitis developed until it reduced to grade 2. Also, patients with prior pneumonitis were excluded and CT lung scans were evaluated for lung changes. New or worsening respiratory symptoms triggered a full diagnostic workup. Treatment was discontinued for grade 2 or higher pneumonitis and delayed until resolution for grade 1 pneumonitis.
TULIP was funded by Byondis. Dr. Saura disclosed numerous financial interests including support from AstraZeneca and Daiichi Sankyo.
Based on significant progression-free survival (PFS) benefits shown in the phase 3 TULIP trial, trastuzumab duocarmazine (SYD985) may provide a new treatment option among HER2-positive metastatic breast cancer patients, according to Cristina Saura, MD, head of the breast cancer program at Vall d’Hebron University Hospital, Barcelona. Dr. Saura presented the results of the TULIP trial (abstract LBA15) on Sept. 19 at the 2021 European Society for Medical Oncology Congress.
Trastuzumab duocarmazine is a novel HER2-targeting antibody-drug conjugate that consists of trastuzumab and a drug containing duocarmycin. Its three-way mechanism of action includes uptake of the antibody-drug conjugate by internalization and intracellular release of duocarmycin with two bystander effects: proteolytic cleavage and subsequent release of payload in the tumor microenvironment and diffusion of active payload to neighboring tumor cells.
While one physician described the results as encouraging, another said the treatment is not nearly ready for primetime.
“It is encouraging to observe clinically meaningful and potentially practice changing progression-free survival improvements in patients receiving treatment in the third line and beyond,” said Aditya Bardia, MD, Massachusetts General Hospital, Boston. “Several agents have been approved as treatments for HER2-positive metastatic breast cancer in recent years including T-DXd, neratinib, tucatinib, and margetuximab. Trastuzumab duocarmazine could eventually be another option.”
Fatima Cardoso, MD, director of the breast cancer unit at the Breast Cancer Research Foundation, New York, said: “At this time there is only a minor 2-month difference in progression-free survival and a nonsignificant overall difference. With the high incidence of ocular toxicity and four toxic deaths, we cannot recommend this drug for clinical practice, in my opinion.”
Two or more prior therapies for metastatic breast cancer
TULIP investigators enrolled 437 patients from 83 sites in 11 countries with HER2-positive locally advanced or metastatic breast cancer who had received two or more therapies for metastatic disease (treatment for brain metastases allowed). They were randomized 2:1 to trastuzumab duocarmazine (1.2 mg/kg every 21 days, 291 patients) or physician’s choice (146 patients) of one of three trastuzumab-containing combinations or lapatinib plus capecitabine. Treatment was continued until progression or unacceptable toxicity. The primary endpoint was centrally assessed PFS.
Longer PFS with trastuzumab duocarmazine
Median age was 57 years, and the median number of prior metastatic breast cancer regimens was 4.7. Centrally reviewed PFS was significantly longer in the trastuzumab duocarmazine group at 7.0 months versus 4.9 months for physicians choice treatment (hazard ratio, 0.64; 95% confidence interval, 0.49-0.84; P = .002). Subgroup analysis, also centrally reviewed, revealed numerical advantage for trastuzumab duocarmazine over physician’s choice across all categories (except for Eastern Cooperative Oncology Group status 2). Analysis of PFS by investigators showed a similar benefit for trastuzumab duocarmazine (6.9 months vs. 4.6 months; HR, 0.60; P < .001).
A first look at median overall survival showed a nonsignificant advantage for trastuzumab duocarmazine (20.4 months vs. 16.3 months (HR, 0.83; 95% CI, 0.62-1.09, P = .153). The overall response rate (partial or complete response) was similar between groups at 27.8% for trastuzumab duocarmazine and 29.5% for physician’s choice with reductions in target lesion measurement at 70.2% and 32.2% for trastuzumab duocarmazine and physician’s choice, respectively. The clinical benefit rates were 38.5% for trastuzumab duocarmazine and 32.2% for physician’s choice.
Ocular toxicity
Most patients had at least one treatment-related adverse event (96.5% SD985, 96.4% PC), and grade 3 or higher event rates were similar between groups (52.8% SYD985, 48.2% PC). The most frequently reported adverse events for trastuzumab duocarmazine were ocular toxicity, with conjunctivitis reported in 38.2%, and keratitis in 38.2%, with fatigue at 33.3%; for physician’s choice these were diarrhea (35.8%), nausea (31.4%) and fatigue (29.9%). Interstitial lung disease pneumonitis was reported for 7.6% (5.2% grade 1-2) of patients treated with trastuzumab duocarmazine, including two grade 5 events.
Eye toxicity led to discontinuations in 20.8% of trastuzumab duocarmazine patients, dose modifications in 22.9%, with dose modifications for interstitial lung disease/pneumonitis in 5.2% of trastuzumab duocarmazine patients. Six fatalities (2.1%) were reported in the trastuzumab duocarmazine group, with four attributed to treatment. Assessment of health-related quality of life showed no significant difference between groups.
Dr. Manich outlined risk mitigation strategies. Patients with prior keratitis were excluded and patients were given prophylactic lubricating eye drops and regular eye exams by ophthalmologists. Treatment was discontinued if grade 3 or higher keratitis developed, and was delayed if grade 3 conjunctivitis developed until it reduced to grade 2. Also, patients with prior pneumonitis were excluded and CT lung scans were evaluated for lung changes. New or worsening respiratory symptoms triggered a full diagnostic workup. Treatment was discontinued for grade 2 or higher pneumonitis and delayed until resolution for grade 1 pneumonitis.
TULIP was funded by Byondis. Dr. Saura disclosed numerous financial interests including support from AstraZeneca and Daiichi Sankyo.
Based on significant progression-free survival (PFS) benefits shown in the phase 3 TULIP trial, trastuzumab duocarmazine (SYD985) may provide a new treatment option among HER2-positive metastatic breast cancer patients, according to Cristina Saura, MD, head of the breast cancer program at Vall d’Hebron University Hospital, Barcelona. Dr. Saura presented the results of the TULIP trial (abstract LBA15) on Sept. 19 at the 2021 European Society for Medical Oncology Congress.
Trastuzumab duocarmazine is a novel HER2-targeting antibody-drug conjugate that consists of trastuzumab and a drug containing duocarmycin. Its three-way mechanism of action includes uptake of the antibody-drug conjugate by internalization and intracellular release of duocarmycin with two bystander effects: proteolytic cleavage and subsequent release of payload in the tumor microenvironment and diffusion of active payload to neighboring tumor cells.
While one physician described the results as encouraging, another said the treatment is not nearly ready for primetime.
“It is encouraging to observe clinically meaningful and potentially practice changing progression-free survival improvements in patients receiving treatment in the third line and beyond,” said Aditya Bardia, MD, Massachusetts General Hospital, Boston. “Several agents have been approved as treatments for HER2-positive metastatic breast cancer in recent years including T-DXd, neratinib, tucatinib, and margetuximab. Trastuzumab duocarmazine could eventually be another option.”
Fatima Cardoso, MD, director of the breast cancer unit at the Breast Cancer Research Foundation, New York, said: “At this time there is only a minor 2-month difference in progression-free survival and a nonsignificant overall difference. With the high incidence of ocular toxicity and four toxic deaths, we cannot recommend this drug for clinical practice, in my opinion.”
Two or more prior therapies for metastatic breast cancer
TULIP investigators enrolled 437 patients from 83 sites in 11 countries with HER2-positive locally advanced or metastatic breast cancer who had received two or more therapies for metastatic disease (treatment for brain metastases allowed). They were randomized 2:1 to trastuzumab duocarmazine (1.2 mg/kg every 21 days, 291 patients) or physician’s choice (146 patients) of one of three trastuzumab-containing combinations or lapatinib plus capecitabine. Treatment was continued until progression or unacceptable toxicity. The primary endpoint was centrally assessed PFS.
Longer PFS with trastuzumab duocarmazine
Median age was 57 years, and the median number of prior metastatic breast cancer regimens was 4.7. Centrally reviewed PFS was significantly longer in the trastuzumab duocarmazine group at 7.0 months versus 4.9 months for physicians choice treatment (hazard ratio, 0.64; 95% confidence interval, 0.49-0.84; P = .002). Subgroup analysis, also centrally reviewed, revealed numerical advantage for trastuzumab duocarmazine over physician’s choice across all categories (except for Eastern Cooperative Oncology Group status 2). Analysis of PFS by investigators showed a similar benefit for trastuzumab duocarmazine (6.9 months vs. 4.6 months; HR, 0.60; P < .001).
A first look at median overall survival showed a nonsignificant advantage for trastuzumab duocarmazine (20.4 months vs. 16.3 months (HR, 0.83; 95% CI, 0.62-1.09, P = .153). The overall response rate (partial or complete response) was similar between groups at 27.8% for trastuzumab duocarmazine and 29.5% for physician’s choice with reductions in target lesion measurement at 70.2% and 32.2% for trastuzumab duocarmazine and physician’s choice, respectively. The clinical benefit rates were 38.5% for trastuzumab duocarmazine and 32.2% for physician’s choice.
Ocular toxicity
Most patients had at least one treatment-related adverse event (96.5% SD985, 96.4% PC), and grade 3 or higher event rates were similar between groups (52.8% SYD985, 48.2% PC). The most frequently reported adverse events for trastuzumab duocarmazine were ocular toxicity, with conjunctivitis reported in 38.2%, and keratitis in 38.2%, with fatigue at 33.3%; for physician’s choice these were diarrhea (35.8%), nausea (31.4%) and fatigue (29.9%). Interstitial lung disease pneumonitis was reported for 7.6% (5.2% grade 1-2) of patients treated with trastuzumab duocarmazine, including two grade 5 events.
Eye toxicity led to discontinuations in 20.8% of trastuzumab duocarmazine patients, dose modifications in 22.9%, with dose modifications for interstitial lung disease/pneumonitis in 5.2% of trastuzumab duocarmazine patients. Six fatalities (2.1%) were reported in the trastuzumab duocarmazine group, with four attributed to treatment. Assessment of health-related quality of life showed no significant difference between groups.
Dr. Manich outlined risk mitigation strategies. Patients with prior keratitis were excluded and patients were given prophylactic lubricating eye drops and regular eye exams by ophthalmologists. Treatment was discontinued if grade 3 or higher keratitis developed, and was delayed if grade 3 conjunctivitis developed until it reduced to grade 2. Also, patients with prior pneumonitis were excluded and CT lung scans were evaluated for lung changes. New or worsening respiratory symptoms triggered a full diagnostic workup. Treatment was discontinued for grade 2 or higher pneumonitis and delayed until resolution for grade 1 pneumonitis.
TULIP was funded by Byondis. Dr. Saura disclosed numerous financial interests including support from AstraZeneca and Daiichi Sankyo.
FROM ESMO 2021
Treatment shows 'important improvements' in triple-negative breast cancer
But as a subanalysis of data from the randomized, phase 3 study showed, sacituzumab govitecan was associated with significantly better progression-free survival (PFS) and overall survival among patients without an initial TNBC diagnosis, with efficacy similar to that seen in the overall study population and in patients without known brain metastases, reported Joyce O’Shaughnessy, MD, at the 2021 European Society for Medical Oncology Congress. In her presentation (abstract 258P), Dr. O’Shaughnessy, who is an oncologist with the Texas Oncology–Baylor Charles A. Sammons Cancer Center in Dallas, said that it’s not uncommon to see acquired triple-negative breast cancer in patients who have hormone receptor–positive disease initially and then later on, develop triple-negative breast cancer.
“That is why at the time of metastatic diagnosis we always say that patients should have repeat receptor [testing], because it’s been well described that a subset of hormone receptor–positive breast can become triple negative under pressure from endocrine therapy,” said ASCENT coinvestigator Aditya Bardia, MD, MPH, Massachusetts General Hospital, Boston, in an interview
Coinvestigator Kevine Punie, MD, from University Hospitals Leuven (Belgium), said that “triple-negative breast cancer is a diagnosis of exclusion. This is a heterogenous disease where several biological subsets are merged.”
“It was important to perform this subgroup analysis to reassure us that the treatment effect we see from [sacituzumab govitecan] in the overall population is also observed in this specific subgroup of patients where biologically we’re treating a different disease,” he said in an interview.
Antibody-drug conjugate
Sacituzumab govitecan consists of an antibody targeted to the trophoblast antigen 2 cell surface receptor found on most breast cancer cells, plus the topoisomerase-1 inhibitor SN-38 as its toxic payload.
In the primary intent-to-treat (ITT) analysis of ASCENT, sacituzumab significantly prolonged PFS with a median of 4.8 versus 1.7 months for patients treated with the physician’s choice of either capecitabine, eribulin, vinorelbine, or gemcitabine. The difference translated into an HR for progression with the antibody-drug conjugate of 0.41 (P < .00001).
The subgroup analysis looked at outcomes for 70 patients randomized to sacituzumab govitecan and 78 randomized to single-agent chemotherapy who did not have an initial diagnosis of TNBC.
In all, 27% of patients in this subgroup in the sacituzumab arm and 29% in the chemotherapy arm had received a prior line of treatment with a CDK4/6 inhibitor.
At the time of data cutoff in March 2020, four patients (6%) in the sacituzumab arm remained on treatment versus no patient in the chemotherapy arm. The most common reason for treatment discontinuation was disease progression, which occurred in 84% and 72% of patients, respectively.
The median treatment duration was 5.1 months in the sacituzumab and 1.2 months in the chemotherapy arm. The median duration of follow-up was 10.6 and 6.1 months, respectively.
Progression-free survival, overall survival results
For all patients without an initial TNBC diagnosis, the median PFS was 4.6 months with sacituzumab versus 2.3 months with chemotherapy, which translated into a hazard ratio for progression of 0.48 (95% confidence interval, 0.32-0.72). The progression-free benefit with the antibody-drug conjugate was similar to that seen in the intent-to-treat population, as noted before, and among the overall population of patients in the study with no known brain metastases (HR, 5.6 vs. 1.7, respectively; P < .001).
The objective response rates were 21% in the sacituzumab and 5% in the chemotherapy arm. Objective responses were not affected by the prior use of CDK 4/6 inhibitors.
Median overall survival in this subgroup was 12.4 months with the antibody-drug conjugate versus 6.7 months with chemotherapy (95% CI, 0.30-0.64).
The investigators reported that the safety profile was manageable in this subgroup of patients, with a low rate of treatment discontinuations because of adverse events (5%) and no treatment-related deaths with sacituzumab govitecan.
Health-related quality of life
In a separate poster (abstract 257P) presented at the meeting, the ASCENT investigators reported health-related quality of life results in the overall population.
The mean European Organization for the Research and Treatment of Cancer quality of life questionnaire subscale scores at baseline were similar between treatment arms.
For the major domains of global health status, physical and emotional functioning as well as lower symptomatic impact of fatigue, pain, dyspnea, and insomnia, sacituzumab govitecan showed “significantly and meaningfully greater improvement” than the physician’s choice of chemotherapy, the investigators found.
Of individual symptoms, only diarrhea was worse with the antibody-drug conjugate.
“These were important improvements,” Dr. Punie said, “because we saw improvements in the primary health-related quality of life domains such as global health status. We also saw that the time to clinically meaningful deterioration of quality of life domains were significantly longer for patients treated with [sacituzumab govitecan].”
“Patients who received sacituzumab govitecan had better health-related quality of life as compared to the control arm, and that’s a very important result, because in the metastatic setting our goal is twofold: We want to prolong survival, and we want patients to have improved quality of life,” Dr. Bardia said.
The Ascent trial is sponsored by Gilead Sciences. Dr. Punie disclosed relationships with multiple companies/organizations, not including Gilead. Dr. Bardia disclosed contracted research for Gilead and others, as well as other relationships.
But as a subanalysis of data from the randomized, phase 3 study showed, sacituzumab govitecan was associated with significantly better progression-free survival (PFS) and overall survival among patients without an initial TNBC diagnosis, with efficacy similar to that seen in the overall study population and in patients without known brain metastases, reported Joyce O’Shaughnessy, MD, at the 2021 European Society for Medical Oncology Congress. In her presentation (abstract 258P), Dr. O’Shaughnessy, who is an oncologist with the Texas Oncology–Baylor Charles A. Sammons Cancer Center in Dallas, said that it’s not uncommon to see acquired triple-negative breast cancer in patients who have hormone receptor–positive disease initially and then later on, develop triple-negative breast cancer.
“That is why at the time of metastatic diagnosis we always say that patients should have repeat receptor [testing], because it’s been well described that a subset of hormone receptor–positive breast can become triple negative under pressure from endocrine therapy,” said ASCENT coinvestigator Aditya Bardia, MD, MPH, Massachusetts General Hospital, Boston, in an interview
Coinvestigator Kevine Punie, MD, from University Hospitals Leuven (Belgium), said that “triple-negative breast cancer is a diagnosis of exclusion. This is a heterogenous disease where several biological subsets are merged.”
“It was important to perform this subgroup analysis to reassure us that the treatment effect we see from [sacituzumab govitecan] in the overall population is also observed in this specific subgroup of patients where biologically we’re treating a different disease,” he said in an interview.
Antibody-drug conjugate
Sacituzumab govitecan consists of an antibody targeted to the trophoblast antigen 2 cell surface receptor found on most breast cancer cells, plus the topoisomerase-1 inhibitor SN-38 as its toxic payload.
In the primary intent-to-treat (ITT) analysis of ASCENT, sacituzumab significantly prolonged PFS with a median of 4.8 versus 1.7 months for patients treated with the physician’s choice of either capecitabine, eribulin, vinorelbine, or gemcitabine. The difference translated into an HR for progression with the antibody-drug conjugate of 0.41 (P < .00001).
The subgroup analysis looked at outcomes for 70 patients randomized to sacituzumab govitecan and 78 randomized to single-agent chemotherapy who did not have an initial diagnosis of TNBC.
In all, 27% of patients in this subgroup in the sacituzumab arm and 29% in the chemotherapy arm had received a prior line of treatment with a CDK4/6 inhibitor.
At the time of data cutoff in March 2020, four patients (6%) in the sacituzumab arm remained on treatment versus no patient in the chemotherapy arm. The most common reason for treatment discontinuation was disease progression, which occurred in 84% and 72% of patients, respectively.
The median treatment duration was 5.1 months in the sacituzumab and 1.2 months in the chemotherapy arm. The median duration of follow-up was 10.6 and 6.1 months, respectively.
Progression-free survival, overall survival results
For all patients without an initial TNBC diagnosis, the median PFS was 4.6 months with sacituzumab versus 2.3 months with chemotherapy, which translated into a hazard ratio for progression of 0.48 (95% confidence interval, 0.32-0.72). The progression-free benefit with the antibody-drug conjugate was similar to that seen in the intent-to-treat population, as noted before, and among the overall population of patients in the study with no known brain metastases (HR, 5.6 vs. 1.7, respectively; P < .001).
The objective response rates were 21% in the sacituzumab and 5% in the chemotherapy arm. Objective responses were not affected by the prior use of CDK 4/6 inhibitors.
Median overall survival in this subgroup was 12.4 months with the antibody-drug conjugate versus 6.7 months with chemotherapy (95% CI, 0.30-0.64).
The investigators reported that the safety profile was manageable in this subgroup of patients, with a low rate of treatment discontinuations because of adverse events (5%) and no treatment-related deaths with sacituzumab govitecan.
Health-related quality of life
In a separate poster (abstract 257P) presented at the meeting, the ASCENT investigators reported health-related quality of life results in the overall population.
The mean European Organization for the Research and Treatment of Cancer quality of life questionnaire subscale scores at baseline were similar between treatment arms.
For the major domains of global health status, physical and emotional functioning as well as lower symptomatic impact of fatigue, pain, dyspnea, and insomnia, sacituzumab govitecan showed “significantly and meaningfully greater improvement” than the physician’s choice of chemotherapy, the investigators found.
Of individual symptoms, only diarrhea was worse with the antibody-drug conjugate.
“These were important improvements,” Dr. Punie said, “because we saw improvements in the primary health-related quality of life domains such as global health status. We also saw that the time to clinically meaningful deterioration of quality of life domains were significantly longer for patients treated with [sacituzumab govitecan].”
“Patients who received sacituzumab govitecan had better health-related quality of life as compared to the control arm, and that’s a very important result, because in the metastatic setting our goal is twofold: We want to prolong survival, and we want patients to have improved quality of life,” Dr. Bardia said.
The Ascent trial is sponsored by Gilead Sciences. Dr. Punie disclosed relationships with multiple companies/organizations, not including Gilead. Dr. Bardia disclosed contracted research for Gilead and others, as well as other relationships.
But as a subanalysis of data from the randomized, phase 3 study showed, sacituzumab govitecan was associated with significantly better progression-free survival (PFS) and overall survival among patients without an initial TNBC diagnosis, with efficacy similar to that seen in the overall study population and in patients without known brain metastases, reported Joyce O’Shaughnessy, MD, at the 2021 European Society for Medical Oncology Congress. In her presentation (abstract 258P), Dr. O’Shaughnessy, who is an oncologist with the Texas Oncology–Baylor Charles A. Sammons Cancer Center in Dallas, said that it’s not uncommon to see acquired triple-negative breast cancer in patients who have hormone receptor–positive disease initially and then later on, develop triple-negative breast cancer.
“That is why at the time of metastatic diagnosis we always say that patients should have repeat receptor [testing], because it’s been well described that a subset of hormone receptor–positive breast can become triple negative under pressure from endocrine therapy,” said ASCENT coinvestigator Aditya Bardia, MD, MPH, Massachusetts General Hospital, Boston, in an interview
Coinvestigator Kevine Punie, MD, from University Hospitals Leuven (Belgium), said that “triple-negative breast cancer is a diagnosis of exclusion. This is a heterogenous disease where several biological subsets are merged.”
“It was important to perform this subgroup analysis to reassure us that the treatment effect we see from [sacituzumab govitecan] in the overall population is also observed in this specific subgroup of patients where biologically we’re treating a different disease,” he said in an interview.
Antibody-drug conjugate
Sacituzumab govitecan consists of an antibody targeted to the trophoblast antigen 2 cell surface receptor found on most breast cancer cells, plus the topoisomerase-1 inhibitor SN-38 as its toxic payload.
In the primary intent-to-treat (ITT) analysis of ASCENT, sacituzumab significantly prolonged PFS with a median of 4.8 versus 1.7 months for patients treated with the physician’s choice of either capecitabine, eribulin, vinorelbine, or gemcitabine. The difference translated into an HR for progression with the antibody-drug conjugate of 0.41 (P < .00001).
The subgroup analysis looked at outcomes for 70 patients randomized to sacituzumab govitecan and 78 randomized to single-agent chemotherapy who did not have an initial diagnosis of TNBC.
In all, 27% of patients in this subgroup in the sacituzumab arm and 29% in the chemotherapy arm had received a prior line of treatment with a CDK4/6 inhibitor.
At the time of data cutoff in March 2020, four patients (6%) in the sacituzumab arm remained on treatment versus no patient in the chemotherapy arm. The most common reason for treatment discontinuation was disease progression, which occurred in 84% and 72% of patients, respectively.
The median treatment duration was 5.1 months in the sacituzumab and 1.2 months in the chemotherapy arm. The median duration of follow-up was 10.6 and 6.1 months, respectively.
Progression-free survival, overall survival results
For all patients without an initial TNBC diagnosis, the median PFS was 4.6 months with sacituzumab versus 2.3 months with chemotherapy, which translated into a hazard ratio for progression of 0.48 (95% confidence interval, 0.32-0.72). The progression-free benefit with the antibody-drug conjugate was similar to that seen in the intent-to-treat population, as noted before, and among the overall population of patients in the study with no known brain metastases (HR, 5.6 vs. 1.7, respectively; P < .001).
The objective response rates were 21% in the sacituzumab and 5% in the chemotherapy arm. Objective responses were not affected by the prior use of CDK 4/6 inhibitors.
Median overall survival in this subgroup was 12.4 months with the antibody-drug conjugate versus 6.7 months with chemotherapy (95% CI, 0.30-0.64).
The investigators reported that the safety profile was manageable in this subgroup of patients, with a low rate of treatment discontinuations because of adverse events (5%) and no treatment-related deaths with sacituzumab govitecan.
Health-related quality of life
In a separate poster (abstract 257P) presented at the meeting, the ASCENT investigators reported health-related quality of life results in the overall population.
The mean European Organization for the Research and Treatment of Cancer quality of life questionnaire subscale scores at baseline were similar between treatment arms.
For the major domains of global health status, physical and emotional functioning as well as lower symptomatic impact of fatigue, pain, dyspnea, and insomnia, sacituzumab govitecan showed “significantly and meaningfully greater improvement” than the physician’s choice of chemotherapy, the investigators found.
Of individual symptoms, only diarrhea was worse with the antibody-drug conjugate.
“These were important improvements,” Dr. Punie said, “because we saw improvements in the primary health-related quality of life domains such as global health status. We also saw that the time to clinically meaningful deterioration of quality of life domains were significantly longer for patients treated with [sacituzumab govitecan].”
“Patients who received sacituzumab govitecan had better health-related quality of life as compared to the control arm, and that’s a very important result, because in the metastatic setting our goal is twofold: We want to prolong survival, and we want patients to have improved quality of life,” Dr. Bardia said.
The Ascent trial is sponsored by Gilead Sciences. Dr. Punie disclosed relationships with multiple companies/organizations, not including Gilead. Dr. Bardia disclosed contracted research for Gilead and others, as well as other relationships.
FROM ESMO 2021
Better survival with extended letrozole in early-stage breast cancer
The approach “should be considered among the optimal standard endocrine treatments for postmenopausal patients with hormone receptor–positive breast cancer, regardless of the nodal status at diagnosis,” concluded investigators led by Lucia Del Mastro, MD, a medical oncologist at the University of Genoa, Italy.
Clinical practice guidelines recommend an individualized approach to decide the duration of treatment based on relapse risk and tolerability because no study until now has shown an overall survival benefit with extended aromatase inhibitor therapy. Based on “our results ... this statement is no longer supported by the evidence and should be updated,” they wrote.
The optimal duration or type of endocrine therapy has been uncertain; the team sought to bring more clarity to the issue.
Following 2-3 years of adjuvant tamoxifen, they randomized evenly 2,056 women at 69 hospitals in Italy to either 2-3 years or letrozole 2.5 mg once daily – the usual care control group – or 5 years. Women in the trial, dubbed GIM4, had stage I-III histologically proven and operable invasive cancer, with no signs of disease recurrence.
Twelve-year overall survival was 88% with extended letrozole, but 84% in the control arm (HR 0.77, 95% confidence interval, 0.60-0.98; P = 0.036).
Twelve-year disease-free survival was 67% in the extended group versus 62% in the control arm (HR 0.78, 95% CI, 0.65-0.93; P = 0.0064).
At a median follow-up of 11.7 years, disease-free survival (DFS) events occurred in 25.4% of control patients, but only 20.7% with extended aromatase inhibitor treatment.
It took 9.5 years for the survival curves to separate, suggesting “that the effect of letrozole takes several years to be seen,” the investigators said.
With the disease-free survival benefits shown in earlier trials and now better overall survival as well, it’s looking like “7-8 years of adjuvant therapy, including at least 5 years with an aromatase inhibitor, could be the optimal duration of adjuvant endocrine therapy in postmenopausal patients with breast cancer.” It probably represents “the best compromise between efficacy and side-effects,” they said.
Breast cancer oncologists Rachel L. Yung, MD, and Nancy E. Davidson, MD, both of the Fred Hutchinson Cancer Research Center, Seattle, agreed in an editorial.
For now, “the currently available data seem to recommend 5 years of aromatase inhibitor for postmenopausal women who have already completed 2-3 years of tamoxifen,” they said.
However, with 19.5% of control patients and 37.1% in the extended stopping treatment early, “GIM4 highlights that early therapy discontinuation remains a crucial issue ... better ways to promote adherence are sorely needed. Another area of focus is the identification of biomarkers that could [better] inform the optimal duration of therapy,” they said.
Longer duration of letrozole was associated with an increased incidence of arthralgia, myalgia, hypertension, and osteoporosis; however, there was no difference in the incidence of bone fractures.
There was also a slightly higher number of cardiovascular events (1% in the extended group, but fewer in the control arm) which is a known issue with aromatase inhibitors. There were three serious treatment-related adverse events in the control arm and eight in the extended group, but no deaths. The Italian investigators noted that because they enrolled only patients free of recurrence after 2-3 years of tamoxifen, the population with early relapse who were likely to be node-positive, was excluded, leaving only patients with a better prognosis. “On the other hand, patients with node-negative disease relapse later and are therefore captured by this trial with a long follow-up.”
The work was funded by Novartis and the Italian Ministry of Health. The investigators had numerous industry ties, including Dr. Del Mastro, who reported honoraria and nonfinancial support from Novartis, Roche, Pfizer, and others. The editorialists didn’t have any competing interests.
The approach “should be considered among the optimal standard endocrine treatments for postmenopausal patients with hormone receptor–positive breast cancer, regardless of the nodal status at diagnosis,” concluded investigators led by Lucia Del Mastro, MD, a medical oncologist at the University of Genoa, Italy.
Clinical practice guidelines recommend an individualized approach to decide the duration of treatment based on relapse risk and tolerability because no study until now has shown an overall survival benefit with extended aromatase inhibitor therapy. Based on “our results ... this statement is no longer supported by the evidence and should be updated,” they wrote.
The optimal duration or type of endocrine therapy has been uncertain; the team sought to bring more clarity to the issue.
Following 2-3 years of adjuvant tamoxifen, they randomized evenly 2,056 women at 69 hospitals in Italy to either 2-3 years or letrozole 2.5 mg once daily – the usual care control group – or 5 years. Women in the trial, dubbed GIM4, had stage I-III histologically proven and operable invasive cancer, with no signs of disease recurrence.
Twelve-year overall survival was 88% with extended letrozole, but 84% in the control arm (HR 0.77, 95% confidence interval, 0.60-0.98; P = 0.036).
Twelve-year disease-free survival was 67% in the extended group versus 62% in the control arm (HR 0.78, 95% CI, 0.65-0.93; P = 0.0064).
At a median follow-up of 11.7 years, disease-free survival (DFS) events occurred in 25.4% of control patients, but only 20.7% with extended aromatase inhibitor treatment.
It took 9.5 years for the survival curves to separate, suggesting “that the effect of letrozole takes several years to be seen,” the investigators said.
With the disease-free survival benefits shown in earlier trials and now better overall survival as well, it’s looking like “7-8 years of adjuvant therapy, including at least 5 years with an aromatase inhibitor, could be the optimal duration of adjuvant endocrine therapy in postmenopausal patients with breast cancer.” It probably represents “the best compromise between efficacy and side-effects,” they said.
Breast cancer oncologists Rachel L. Yung, MD, and Nancy E. Davidson, MD, both of the Fred Hutchinson Cancer Research Center, Seattle, agreed in an editorial.
For now, “the currently available data seem to recommend 5 years of aromatase inhibitor for postmenopausal women who have already completed 2-3 years of tamoxifen,” they said.
However, with 19.5% of control patients and 37.1% in the extended stopping treatment early, “GIM4 highlights that early therapy discontinuation remains a crucial issue ... better ways to promote adherence are sorely needed. Another area of focus is the identification of biomarkers that could [better] inform the optimal duration of therapy,” they said.
Longer duration of letrozole was associated with an increased incidence of arthralgia, myalgia, hypertension, and osteoporosis; however, there was no difference in the incidence of bone fractures.
There was also a slightly higher number of cardiovascular events (1% in the extended group, but fewer in the control arm) which is a known issue with aromatase inhibitors. There were three serious treatment-related adverse events in the control arm and eight in the extended group, but no deaths. The Italian investigators noted that because they enrolled only patients free of recurrence after 2-3 years of tamoxifen, the population with early relapse who were likely to be node-positive, was excluded, leaving only patients with a better prognosis. “On the other hand, patients with node-negative disease relapse later and are therefore captured by this trial with a long follow-up.”
The work was funded by Novartis and the Italian Ministry of Health. The investigators had numerous industry ties, including Dr. Del Mastro, who reported honoraria and nonfinancial support from Novartis, Roche, Pfizer, and others. The editorialists didn’t have any competing interests.
The approach “should be considered among the optimal standard endocrine treatments for postmenopausal patients with hormone receptor–positive breast cancer, regardless of the nodal status at diagnosis,” concluded investigators led by Lucia Del Mastro, MD, a medical oncologist at the University of Genoa, Italy.
Clinical practice guidelines recommend an individualized approach to decide the duration of treatment based on relapse risk and tolerability because no study until now has shown an overall survival benefit with extended aromatase inhibitor therapy. Based on “our results ... this statement is no longer supported by the evidence and should be updated,” they wrote.
The optimal duration or type of endocrine therapy has been uncertain; the team sought to bring more clarity to the issue.
Following 2-3 years of adjuvant tamoxifen, they randomized evenly 2,056 women at 69 hospitals in Italy to either 2-3 years or letrozole 2.5 mg once daily – the usual care control group – or 5 years. Women in the trial, dubbed GIM4, had stage I-III histologically proven and operable invasive cancer, with no signs of disease recurrence.
Twelve-year overall survival was 88% with extended letrozole, but 84% in the control arm (HR 0.77, 95% confidence interval, 0.60-0.98; P = 0.036).
Twelve-year disease-free survival was 67% in the extended group versus 62% in the control arm (HR 0.78, 95% CI, 0.65-0.93; P = 0.0064).
At a median follow-up of 11.7 years, disease-free survival (DFS) events occurred in 25.4% of control patients, but only 20.7% with extended aromatase inhibitor treatment.
It took 9.5 years for the survival curves to separate, suggesting “that the effect of letrozole takes several years to be seen,” the investigators said.
With the disease-free survival benefits shown in earlier trials and now better overall survival as well, it’s looking like “7-8 years of adjuvant therapy, including at least 5 years with an aromatase inhibitor, could be the optimal duration of adjuvant endocrine therapy in postmenopausal patients with breast cancer.” It probably represents “the best compromise between efficacy and side-effects,” they said.
Breast cancer oncologists Rachel L. Yung, MD, and Nancy E. Davidson, MD, both of the Fred Hutchinson Cancer Research Center, Seattle, agreed in an editorial.
For now, “the currently available data seem to recommend 5 years of aromatase inhibitor for postmenopausal women who have already completed 2-3 years of tamoxifen,” they said.
However, with 19.5% of control patients and 37.1% in the extended stopping treatment early, “GIM4 highlights that early therapy discontinuation remains a crucial issue ... better ways to promote adherence are sorely needed. Another area of focus is the identification of biomarkers that could [better] inform the optimal duration of therapy,” they said.
Longer duration of letrozole was associated with an increased incidence of arthralgia, myalgia, hypertension, and osteoporosis; however, there was no difference in the incidence of bone fractures.
There was also a slightly higher number of cardiovascular events (1% in the extended group, but fewer in the control arm) which is a known issue with aromatase inhibitors. There were three serious treatment-related adverse events in the control arm and eight in the extended group, but no deaths. The Italian investigators noted that because they enrolled only patients free of recurrence after 2-3 years of tamoxifen, the population with early relapse who were likely to be node-positive, was excluded, leaving only patients with a better prognosis. “On the other hand, patients with node-negative disease relapse later and are therefore captured by this trial with a long follow-up.”
The work was funded by Novartis and the Italian Ministry of Health. The investigators had numerous industry ties, including Dr. Del Mastro, who reported honoraria and nonfinancial support from Novartis, Roche, Pfizer, and others. The editorialists didn’t have any competing interests.
FROM THE LANCET ONCOLOGY
TULIP trial shows extended survival in HER2+ metastatic breast cancer
, according to Cristina Saura Manich, MD, Hospital Universitario Valle de Hebrón, Barcelona. In TULIP, trastuzumab duocarmazine (SYD985, Byondis B.V., NL) was compared with physician’s choice of chemotherapy, Dr. Saura said at the virtual European Society for Medical Oncology Congress 2021 on Sept. 18 (abstract LBA15).
Trastuzumab duocarmazine, Dr. Manich noted, is a novel HER2-targeting antibody–drug conjugate based on trastuzumab and a cleavable linker-duocarmycin (vc-seco-DUBA) payload. Its three-way mechanism of action includes uptake of the antibody–drug conjugate by internalization and intracellular release of the payload, and two bystander effects: proteolytic cleavage and subsequent release of payload in the tumor microenvironment and diffusion of active payload to neighboring tumor cells.
Two or more prior therapies for metastatic breast cancer
TULIP investigators enrolled 437 patients from 83 sites in 11 countries with HER2-positive locally advanced or metastatic breast cancer who had received two or more therapies for metastatic disease (treatment for brain metastases allowed). They were randomized 2:1 to SYD985 (1.2 mg/kg IV every 21 days [n = 291]) or physician’s choice (PC) [n = 146] of one of three trastuzumab-containing combinations or lapatinib plus capecitabine. Treatment was continued until progression or unacceptable toxicity. The primary endpoint was centrally assessed PFS.
Longer progression-free survival with SYD985
Median age was 57 years, and the median number of prior metastatic breast cancer regimens was 4.7. Centrally reviewed progression-free survival was significantly longer in the SYD985 group at 7.0 months (5.4-7.2) versus 4.9 months (4.0-5.5) for PC (hazard ratio [HR], 0.64, 95% confidence interval [CI], 0.49-0.84, P = .002). Subgroup analysis, also centrally reviewed, revealed numerical advantage for SYD985 over physician choice across all categories (except for ECOG status 2). Analysis of progression-free survival by investigators showed a similar benefit for SYD985 (6.9 months versus 4.6 months, HR, 0.60, P < .001).
A first look at median overall survival showed a nonsignificant advantage for SYD985 (20.4 months versus 16.3 months (HR, 0.83, 95% CI, 0.62-1.09, P = .153). The overall response rate (partial or complete response) was similar between groups at 27.8% for SYD985 and 29.5% for PC, with reductions in target lesion measurement at 70.2% and 32.2% for SYD985 and physician choice, respectively. The clinical benefit rates were 38.5% for SYD985 and 32.2% for physician choice.
Ocular toxicity
Most patients had at least one treatment-related adverse event (96.5% SD985, 96.4% PC), and grade 3 or higher event rates were similar between groups (52.8% SYD985, 48.2% PC). The most frequently reported adverse events for SYD985 were ocular toxicity, with conjunctivitis reported in 38.2%, and keratitis in 38.2%, with fatigue at 33.3%; for physician’s choice these were diarrhea (35.8%), nausea (31.4%), and fatigue (29.9%). Interstitial lung disease pneumonitis was reported for 7.6% (5.2% grade 1-2) of patients treated with SYD985, including two grade 5 events. Eye toxicity led to discontinuations in 20.8% of SYD985 patients, dose modifications in 22.9%, with dose modifications for interstitial lung disease/pneumonitis in 5.2% of SYD985 patients. Six fatalities (2.1%) were reported in the SYD985 group, with four attributed to treatment. Assessment of health-related quality of life showed no significant difference between groups.
Dr. Manich outlined risk mitigation strategies. Patients with prior keratitis were excluded and patients were given prophylactic lubricating eye drops and regular eye exams by ophthalmologists. Treatment was discontinued if grade 3 or higher keratitis developed, and was delayed if grade 3 conjunctivitis developed until it reduced to grade 2. Also, patients with prior pneumonitis were excluded and CT lung scans were evaluated for lung changes. New or worsening respiratory symptoms triggered a full diagnostic workup. Treatment was discontinued for grade 2 or higher pneumonitis and delayed until resolution for grade 1 pneumonitis.
Another option
“It is encouraging to observe clinically meaningful and potentially practice changing PFS improvements in patients receiving treatment in the third line and beyond,” said Aditya Bardia, MD, of Massachusetts General Hospital and Harvard Medical School, Boston. “Several agents have been approved as treatments for HER2-positive metastatic breast cancer in recent years – including T-DXd, neratinib, tucatinib, and margetuximab – and [vic-]trastuzumab duocarmazine could eventually be another option.”
“At this time, there is only a minor 2-month difference in progression-free survival and a nonsignificant overall survival difference,” said Fatima Cardoso, MD, of Champalimaud Cancer Center, Lisbon, Portugal. “With the high incidence of ocular toxicity and four toxic deaths, we cannot recommend this drug for clinical practice, in my opinion.”
Dr. Manich concluded, “SYD985 can provide a new treatment option for patients with pretreated locally advanced or metastatic HER2-positive metastatic breast cancer.”
The study was funded by Byondis B.V. The authors disclosed numerous pharmaceutical-related financial interests.
This article was updated Sept. 24, 2021.
, according to Cristina Saura Manich, MD, Hospital Universitario Valle de Hebrón, Barcelona. In TULIP, trastuzumab duocarmazine (SYD985, Byondis B.V., NL) was compared with physician’s choice of chemotherapy, Dr. Saura said at the virtual European Society for Medical Oncology Congress 2021 on Sept. 18 (abstract LBA15).
Trastuzumab duocarmazine, Dr. Manich noted, is a novel HER2-targeting antibody–drug conjugate based on trastuzumab and a cleavable linker-duocarmycin (vc-seco-DUBA) payload. Its three-way mechanism of action includes uptake of the antibody–drug conjugate by internalization and intracellular release of the payload, and two bystander effects: proteolytic cleavage and subsequent release of payload in the tumor microenvironment and diffusion of active payload to neighboring tumor cells.
Two or more prior therapies for metastatic breast cancer
TULIP investigators enrolled 437 patients from 83 sites in 11 countries with HER2-positive locally advanced or metastatic breast cancer who had received two or more therapies for metastatic disease (treatment for brain metastases allowed). They were randomized 2:1 to SYD985 (1.2 mg/kg IV every 21 days [n = 291]) or physician’s choice (PC) [n = 146] of one of three trastuzumab-containing combinations or lapatinib plus capecitabine. Treatment was continued until progression or unacceptable toxicity. The primary endpoint was centrally assessed PFS.
Longer progression-free survival with SYD985
Median age was 57 years, and the median number of prior metastatic breast cancer regimens was 4.7. Centrally reviewed progression-free survival was significantly longer in the SYD985 group at 7.0 months (5.4-7.2) versus 4.9 months (4.0-5.5) for PC (hazard ratio [HR], 0.64, 95% confidence interval [CI], 0.49-0.84, P = .002). Subgroup analysis, also centrally reviewed, revealed numerical advantage for SYD985 over physician choice across all categories (except for ECOG status 2). Analysis of progression-free survival by investigators showed a similar benefit for SYD985 (6.9 months versus 4.6 months, HR, 0.60, P < .001).
A first look at median overall survival showed a nonsignificant advantage for SYD985 (20.4 months versus 16.3 months (HR, 0.83, 95% CI, 0.62-1.09, P = .153). The overall response rate (partial or complete response) was similar between groups at 27.8% for SYD985 and 29.5% for PC, with reductions in target lesion measurement at 70.2% and 32.2% for SYD985 and physician choice, respectively. The clinical benefit rates were 38.5% for SYD985 and 32.2% for physician choice.
Ocular toxicity
Most patients had at least one treatment-related adverse event (96.5% SD985, 96.4% PC), and grade 3 or higher event rates were similar between groups (52.8% SYD985, 48.2% PC). The most frequently reported adverse events for SYD985 were ocular toxicity, with conjunctivitis reported in 38.2%, and keratitis in 38.2%, with fatigue at 33.3%; for physician’s choice these were diarrhea (35.8%), nausea (31.4%), and fatigue (29.9%). Interstitial lung disease pneumonitis was reported for 7.6% (5.2% grade 1-2) of patients treated with SYD985, including two grade 5 events. Eye toxicity led to discontinuations in 20.8% of SYD985 patients, dose modifications in 22.9%, with dose modifications for interstitial lung disease/pneumonitis in 5.2% of SYD985 patients. Six fatalities (2.1%) were reported in the SYD985 group, with four attributed to treatment. Assessment of health-related quality of life showed no significant difference between groups.
Dr. Manich outlined risk mitigation strategies. Patients with prior keratitis were excluded and patients were given prophylactic lubricating eye drops and regular eye exams by ophthalmologists. Treatment was discontinued if grade 3 or higher keratitis developed, and was delayed if grade 3 conjunctivitis developed until it reduced to grade 2. Also, patients with prior pneumonitis were excluded and CT lung scans were evaluated for lung changes. New or worsening respiratory symptoms triggered a full diagnostic workup. Treatment was discontinued for grade 2 or higher pneumonitis and delayed until resolution for grade 1 pneumonitis.
Another option
“It is encouraging to observe clinically meaningful and potentially practice changing PFS improvements in patients receiving treatment in the third line and beyond,” said Aditya Bardia, MD, of Massachusetts General Hospital and Harvard Medical School, Boston. “Several agents have been approved as treatments for HER2-positive metastatic breast cancer in recent years – including T-DXd, neratinib, tucatinib, and margetuximab – and [vic-]trastuzumab duocarmazine could eventually be another option.”
“At this time, there is only a minor 2-month difference in progression-free survival and a nonsignificant overall survival difference,” said Fatima Cardoso, MD, of Champalimaud Cancer Center, Lisbon, Portugal. “With the high incidence of ocular toxicity and four toxic deaths, we cannot recommend this drug for clinical practice, in my opinion.”
Dr. Manich concluded, “SYD985 can provide a new treatment option for patients with pretreated locally advanced or metastatic HER2-positive metastatic breast cancer.”
The study was funded by Byondis B.V. The authors disclosed numerous pharmaceutical-related financial interests.
This article was updated Sept. 24, 2021.
, according to Cristina Saura Manich, MD, Hospital Universitario Valle de Hebrón, Barcelona. In TULIP, trastuzumab duocarmazine (SYD985, Byondis B.V., NL) was compared with physician’s choice of chemotherapy, Dr. Saura said at the virtual European Society for Medical Oncology Congress 2021 on Sept. 18 (abstract LBA15).
Trastuzumab duocarmazine, Dr. Manich noted, is a novel HER2-targeting antibody–drug conjugate based on trastuzumab and a cleavable linker-duocarmycin (vc-seco-DUBA) payload. Its three-way mechanism of action includes uptake of the antibody–drug conjugate by internalization and intracellular release of the payload, and two bystander effects: proteolytic cleavage and subsequent release of payload in the tumor microenvironment and diffusion of active payload to neighboring tumor cells.
Two or more prior therapies for metastatic breast cancer
TULIP investigators enrolled 437 patients from 83 sites in 11 countries with HER2-positive locally advanced or metastatic breast cancer who had received two or more therapies for metastatic disease (treatment for brain metastases allowed). They were randomized 2:1 to SYD985 (1.2 mg/kg IV every 21 days [n = 291]) or physician’s choice (PC) [n = 146] of one of three trastuzumab-containing combinations or lapatinib plus capecitabine. Treatment was continued until progression or unacceptable toxicity. The primary endpoint was centrally assessed PFS.
Longer progression-free survival with SYD985
Median age was 57 years, and the median number of prior metastatic breast cancer regimens was 4.7. Centrally reviewed progression-free survival was significantly longer in the SYD985 group at 7.0 months (5.4-7.2) versus 4.9 months (4.0-5.5) for PC (hazard ratio [HR], 0.64, 95% confidence interval [CI], 0.49-0.84, P = .002). Subgroup analysis, also centrally reviewed, revealed numerical advantage for SYD985 over physician choice across all categories (except for ECOG status 2). Analysis of progression-free survival by investigators showed a similar benefit for SYD985 (6.9 months versus 4.6 months, HR, 0.60, P < .001).
A first look at median overall survival showed a nonsignificant advantage for SYD985 (20.4 months versus 16.3 months (HR, 0.83, 95% CI, 0.62-1.09, P = .153). The overall response rate (partial or complete response) was similar between groups at 27.8% for SYD985 and 29.5% for PC, with reductions in target lesion measurement at 70.2% and 32.2% for SYD985 and physician choice, respectively. The clinical benefit rates were 38.5% for SYD985 and 32.2% for physician choice.
Ocular toxicity
Most patients had at least one treatment-related adverse event (96.5% SD985, 96.4% PC), and grade 3 or higher event rates were similar between groups (52.8% SYD985, 48.2% PC). The most frequently reported adverse events for SYD985 were ocular toxicity, with conjunctivitis reported in 38.2%, and keratitis in 38.2%, with fatigue at 33.3%; for physician’s choice these were diarrhea (35.8%), nausea (31.4%), and fatigue (29.9%). Interstitial lung disease pneumonitis was reported for 7.6% (5.2% grade 1-2) of patients treated with SYD985, including two grade 5 events. Eye toxicity led to discontinuations in 20.8% of SYD985 patients, dose modifications in 22.9%, with dose modifications for interstitial lung disease/pneumonitis in 5.2% of SYD985 patients. Six fatalities (2.1%) were reported in the SYD985 group, with four attributed to treatment. Assessment of health-related quality of life showed no significant difference between groups.
Dr. Manich outlined risk mitigation strategies. Patients with prior keratitis were excluded and patients were given prophylactic lubricating eye drops and regular eye exams by ophthalmologists. Treatment was discontinued if grade 3 or higher keratitis developed, and was delayed if grade 3 conjunctivitis developed until it reduced to grade 2. Also, patients with prior pneumonitis were excluded and CT lung scans were evaluated for lung changes. New or worsening respiratory symptoms triggered a full diagnostic workup. Treatment was discontinued for grade 2 or higher pneumonitis and delayed until resolution for grade 1 pneumonitis.
Another option
“It is encouraging to observe clinically meaningful and potentially practice changing PFS improvements in patients receiving treatment in the third line and beyond,” said Aditya Bardia, MD, of Massachusetts General Hospital and Harvard Medical School, Boston. “Several agents have been approved as treatments for HER2-positive metastatic breast cancer in recent years – including T-DXd, neratinib, tucatinib, and margetuximab – and [vic-]trastuzumab duocarmazine could eventually be another option.”
“At this time, there is only a minor 2-month difference in progression-free survival and a nonsignificant overall survival difference,” said Fatima Cardoso, MD, of Champalimaud Cancer Center, Lisbon, Portugal. “With the high incidence of ocular toxicity and four toxic deaths, we cannot recommend this drug for clinical practice, in my opinion.”
Dr. Manich concluded, “SYD985 can provide a new treatment option for patients with pretreated locally advanced or metastatic HER2-positive metastatic breast cancer.”
The study was funded by Byondis B.V. The authors disclosed numerous pharmaceutical-related financial interests.
This article was updated Sept. 24, 2021.
FROM ESMO 2021
Study supports add-on therapy for germline and wildtype BRCA mutations
The initial improvement that was seen in pathologic complete response (pCR) rates with the addition of carboplatin to paclitaxel and standard neoadjuvant chemotherapy translated into improved event-free survival (EFS) rates in patients with resectable TNBC more than 4 years after surgery.
The benefits of adding carboplatin to paclitaxel, followed by four cycles of AC (doxorubicin and cyclophosphamide) chemotherapy, were seen both in patients with germline BRCA mutations and those with wildtype BRCA.
The trial results also demonstrated, however, that there were no short- or long-term benefits to adding veliparib (ABT-888), a poly (ADP-ribose) polymerase (PARP) inhibitor, to the mix.
Although pCR and EFS rates were significantly improved with the combination of paclitaxel and carboplatin compared with paclitaxel alone, there were no significant differences when veliparib was added in either pCR, EFS, or overall survival (OS).
“These findings overall support the inclusion of carboplatin into neoadjuvant chemotherapy for stage 2 and 3 triple-negative breast cancer patients, regardless of germline BRCA status,” concluded lead author Sibylle Loibl, MD, PhD, chief executive officer and chair of the German Breast Group.
She presented the new data during an oral session at the virtual European Society for Medical Oncology (ESMO) Congress 2021.
The BrighTNess results show that “neoadjuvant carboplatin plus paclitaxel is superior to paclitaxel alone, with high pCR rates and benefit of event-free survival rates with manageable toxicity and no safety signals,” commented invited discussant Monica Arnedos, MD, PhD, head of the breast cancer research program at the Institut Bergonié in Bordeaux, France.
The findings also put to rest the notion that patients with germline BRCA mutations would not benefit from carboplatin treatment because of extreme sensitivity to standard neoadjuvant chemotherapy.
“The BrighTNess study says otherwise,” Dr. Arnedos said. “Today we’ve seen that the pCR improved event-free survival regardless of the germline BRCA mutated status, so BRCA-mutated germline patients require neoadjuvant carboplatin.”
The new data may lead to changes in breast cancer guidelines, she suggested.
Prior to these results, the evidence was that “platinum salts as neoadjuvant chemotherapy increased pCR rates in triple-negative breast cancer patients, but this was associated with more toxicity, and with higher rates of treatment discontinuation and dose reduction, without strong evidence of long-term benefit. This led to a lack of consensus to recommend platinum salts in this setting between the different breast cancer guidelines.”
The new BrighTNess data showed that the improved pCR rates translated into an EFS benefit in both platinum-containing groups of the trial, a finding that is consistent with the KEYNOTE-522 trial, which showed that adding pembrolizumab (Keytruda) to chemotherapy improved pCR in patients with early TNBC.
The BrighTNess results suggest that patients with high- or moderate-risk TNBC could be treated in the neoadjuvant setting with paclitaxel and carboplatin followed by standard chemotherapy concurrently with pembrolizumab, followed by surgery, and adjuvant therapy with pembrolizumab plus olaparib (Lynparza) for patients with germline BRCA mutations, or capecitabine for patients without mutations, Dr. Arnedos proposed.
BrighTNess study details
The BrighTNess trial involved 634 patients with previously untreated histologically or cytologically confirmed stage 2-3 TNBC who were candidates for potentially curative surgery and had a good performance status. They were randomly assigned to receive either paclitaxel plus carboplatin and veliparib, paclitaxel plus carboplatin only, or paclitaxel alone prior to four cycles of chemotherapy with doxorubicin and cyclophosphamide (AC).
Initial results, published in 2018 in The Lancet Oncology, showed that the addition of veliparib to carboplatin and paclitaxel improved pCR rates compared with paclitaxel alone but not paclitaxel plus carboplatin. The trial data supported the addition of carboplatin to standard neoadjuvant chemotherapy but not veliparib, the investigators stated at the time.
Now at the ESMO meeting, Dr. Loibl presented longer follow-up results.
After a median follow-up of 4.5 years, the hazard ratio (HR) for event-free survival with the paclitaxel/carboplatin/veliparib combination compared with paclitaxel alone was 0.63 (P = .016). In a post-hoc analysis, the adjusted HR was 0.57 (P = .018).
In a subgroup of 309 patients who had initial pCRs, the HR for EFS compared with patients without a pCR was 0.26 (P < .0001). Among patients with germline BRCA mutation, the HR for EFS for those who had a pCR was 0.14 (P = .0004), and among those with germline wildtype BRCA and a pCR the HR was 0.29 (P < .0001).
However, there were no significant differences in OS a median of 4.5 years after surgery.
An analysis of the frequency of myelodysplastic syndrome, acute myeloid leukemia, or other second primary malignancies also showed no significant differences between the groups, Dr. Loibl noted.
Although there were higher rates of hematologic malignancies with the addition of carboplatin, with or without veliparib, these adverse events did not compromise either treatment delivery of the benefits of carboplatin on the primary pCR endpoint, she added.
The BrighTNess trial was supported by AbbVie. Dr. Loibl has reported receiving grants and honoraria from AbbVie and others, including Medscape. Dr. Arnedos has reported receiving honoraria, travel grants, and/or research grants from AstraZeneca, Novartis, Pfizer, and Roche.
A version of this article first appeared on Medscape.com.
The initial improvement that was seen in pathologic complete response (pCR) rates with the addition of carboplatin to paclitaxel and standard neoadjuvant chemotherapy translated into improved event-free survival (EFS) rates in patients with resectable TNBC more than 4 years after surgery.
The benefits of adding carboplatin to paclitaxel, followed by four cycles of AC (doxorubicin and cyclophosphamide) chemotherapy, were seen both in patients with germline BRCA mutations and those with wildtype BRCA.
The trial results also demonstrated, however, that there were no short- or long-term benefits to adding veliparib (ABT-888), a poly (ADP-ribose) polymerase (PARP) inhibitor, to the mix.
Although pCR and EFS rates were significantly improved with the combination of paclitaxel and carboplatin compared with paclitaxel alone, there were no significant differences when veliparib was added in either pCR, EFS, or overall survival (OS).
“These findings overall support the inclusion of carboplatin into neoadjuvant chemotherapy for stage 2 and 3 triple-negative breast cancer patients, regardless of germline BRCA status,” concluded lead author Sibylle Loibl, MD, PhD, chief executive officer and chair of the German Breast Group.
She presented the new data during an oral session at the virtual European Society for Medical Oncology (ESMO) Congress 2021.
The BrighTNess results show that “neoadjuvant carboplatin plus paclitaxel is superior to paclitaxel alone, with high pCR rates and benefit of event-free survival rates with manageable toxicity and no safety signals,” commented invited discussant Monica Arnedos, MD, PhD, head of the breast cancer research program at the Institut Bergonié in Bordeaux, France.
The findings also put to rest the notion that patients with germline BRCA mutations would not benefit from carboplatin treatment because of extreme sensitivity to standard neoadjuvant chemotherapy.
“The BrighTNess study says otherwise,” Dr. Arnedos said. “Today we’ve seen that the pCR improved event-free survival regardless of the germline BRCA mutated status, so BRCA-mutated germline patients require neoadjuvant carboplatin.”
The new data may lead to changes in breast cancer guidelines, she suggested.
Prior to these results, the evidence was that “platinum salts as neoadjuvant chemotherapy increased pCR rates in triple-negative breast cancer patients, but this was associated with more toxicity, and with higher rates of treatment discontinuation and dose reduction, without strong evidence of long-term benefit. This led to a lack of consensus to recommend platinum salts in this setting between the different breast cancer guidelines.”
The new BrighTNess data showed that the improved pCR rates translated into an EFS benefit in both platinum-containing groups of the trial, a finding that is consistent with the KEYNOTE-522 trial, which showed that adding pembrolizumab (Keytruda) to chemotherapy improved pCR in patients with early TNBC.
The BrighTNess results suggest that patients with high- or moderate-risk TNBC could be treated in the neoadjuvant setting with paclitaxel and carboplatin followed by standard chemotherapy concurrently with pembrolizumab, followed by surgery, and adjuvant therapy with pembrolizumab plus olaparib (Lynparza) for patients with germline BRCA mutations, or capecitabine for patients without mutations, Dr. Arnedos proposed.
BrighTNess study details
The BrighTNess trial involved 634 patients with previously untreated histologically or cytologically confirmed stage 2-3 TNBC who were candidates for potentially curative surgery and had a good performance status. They were randomly assigned to receive either paclitaxel plus carboplatin and veliparib, paclitaxel plus carboplatin only, or paclitaxel alone prior to four cycles of chemotherapy with doxorubicin and cyclophosphamide (AC).
Initial results, published in 2018 in The Lancet Oncology, showed that the addition of veliparib to carboplatin and paclitaxel improved pCR rates compared with paclitaxel alone but not paclitaxel plus carboplatin. The trial data supported the addition of carboplatin to standard neoadjuvant chemotherapy but not veliparib, the investigators stated at the time.
Now at the ESMO meeting, Dr. Loibl presented longer follow-up results.
After a median follow-up of 4.5 years, the hazard ratio (HR) for event-free survival with the paclitaxel/carboplatin/veliparib combination compared with paclitaxel alone was 0.63 (P = .016). In a post-hoc analysis, the adjusted HR was 0.57 (P = .018).
In a subgroup of 309 patients who had initial pCRs, the HR for EFS compared with patients without a pCR was 0.26 (P < .0001). Among patients with germline BRCA mutation, the HR for EFS for those who had a pCR was 0.14 (P = .0004), and among those with germline wildtype BRCA and a pCR the HR was 0.29 (P < .0001).
However, there were no significant differences in OS a median of 4.5 years after surgery.
An analysis of the frequency of myelodysplastic syndrome, acute myeloid leukemia, or other second primary malignancies also showed no significant differences between the groups, Dr. Loibl noted.
Although there were higher rates of hematologic malignancies with the addition of carboplatin, with or without veliparib, these adverse events did not compromise either treatment delivery of the benefits of carboplatin on the primary pCR endpoint, she added.
The BrighTNess trial was supported by AbbVie. Dr. Loibl has reported receiving grants and honoraria from AbbVie and others, including Medscape. Dr. Arnedos has reported receiving honoraria, travel grants, and/or research grants from AstraZeneca, Novartis, Pfizer, and Roche.
A version of this article first appeared on Medscape.com.
The initial improvement that was seen in pathologic complete response (pCR) rates with the addition of carboplatin to paclitaxel and standard neoadjuvant chemotherapy translated into improved event-free survival (EFS) rates in patients with resectable TNBC more than 4 years after surgery.
The benefits of adding carboplatin to paclitaxel, followed by four cycles of AC (doxorubicin and cyclophosphamide) chemotherapy, were seen both in patients with germline BRCA mutations and those with wildtype BRCA.
The trial results also demonstrated, however, that there were no short- or long-term benefits to adding veliparib (ABT-888), a poly (ADP-ribose) polymerase (PARP) inhibitor, to the mix.
Although pCR and EFS rates were significantly improved with the combination of paclitaxel and carboplatin compared with paclitaxel alone, there were no significant differences when veliparib was added in either pCR, EFS, or overall survival (OS).
“These findings overall support the inclusion of carboplatin into neoadjuvant chemotherapy for stage 2 and 3 triple-negative breast cancer patients, regardless of germline BRCA status,” concluded lead author Sibylle Loibl, MD, PhD, chief executive officer and chair of the German Breast Group.
She presented the new data during an oral session at the virtual European Society for Medical Oncology (ESMO) Congress 2021.
The BrighTNess results show that “neoadjuvant carboplatin plus paclitaxel is superior to paclitaxel alone, with high pCR rates and benefit of event-free survival rates with manageable toxicity and no safety signals,” commented invited discussant Monica Arnedos, MD, PhD, head of the breast cancer research program at the Institut Bergonié in Bordeaux, France.
The findings also put to rest the notion that patients with germline BRCA mutations would not benefit from carboplatin treatment because of extreme sensitivity to standard neoadjuvant chemotherapy.
“The BrighTNess study says otherwise,” Dr. Arnedos said. “Today we’ve seen that the pCR improved event-free survival regardless of the germline BRCA mutated status, so BRCA-mutated germline patients require neoadjuvant carboplatin.”
The new data may lead to changes in breast cancer guidelines, she suggested.
Prior to these results, the evidence was that “platinum salts as neoadjuvant chemotherapy increased pCR rates in triple-negative breast cancer patients, but this was associated with more toxicity, and with higher rates of treatment discontinuation and dose reduction, without strong evidence of long-term benefit. This led to a lack of consensus to recommend platinum salts in this setting between the different breast cancer guidelines.”
The new BrighTNess data showed that the improved pCR rates translated into an EFS benefit in both platinum-containing groups of the trial, a finding that is consistent with the KEYNOTE-522 trial, which showed that adding pembrolizumab (Keytruda) to chemotherapy improved pCR in patients with early TNBC.
The BrighTNess results suggest that patients with high- or moderate-risk TNBC could be treated in the neoadjuvant setting with paclitaxel and carboplatin followed by standard chemotherapy concurrently with pembrolizumab, followed by surgery, and adjuvant therapy with pembrolizumab plus olaparib (Lynparza) for patients with germline BRCA mutations, or capecitabine for patients without mutations, Dr. Arnedos proposed.
BrighTNess study details
The BrighTNess trial involved 634 patients with previously untreated histologically or cytologically confirmed stage 2-3 TNBC who were candidates for potentially curative surgery and had a good performance status. They were randomly assigned to receive either paclitaxel plus carboplatin and veliparib, paclitaxel plus carboplatin only, or paclitaxel alone prior to four cycles of chemotherapy with doxorubicin and cyclophosphamide (AC).
Initial results, published in 2018 in The Lancet Oncology, showed that the addition of veliparib to carboplatin and paclitaxel improved pCR rates compared with paclitaxel alone but not paclitaxel plus carboplatin. The trial data supported the addition of carboplatin to standard neoadjuvant chemotherapy but not veliparib, the investigators stated at the time.
Now at the ESMO meeting, Dr. Loibl presented longer follow-up results.
After a median follow-up of 4.5 years, the hazard ratio (HR) for event-free survival with the paclitaxel/carboplatin/veliparib combination compared with paclitaxel alone was 0.63 (P = .016). In a post-hoc analysis, the adjusted HR was 0.57 (P = .018).
In a subgroup of 309 patients who had initial pCRs, the HR for EFS compared with patients without a pCR was 0.26 (P < .0001). Among patients with germline BRCA mutation, the HR for EFS for those who had a pCR was 0.14 (P = .0004), and among those with germline wildtype BRCA and a pCR the HR was 0.29 (P < .0001).
However, there were no significant differences in OS a median of 4.5 years after surgery.
An analysis of the frequency of myelodysplastic syndrome, acute myeloid leukemia, or other second primary malignancies also showed no significant differences between the groups, Dr. Loibl noted.
Although there were higher rates of hematologic malignancies with the addition of carboplatin, with or without veliparib, these adverse events did not compromise either treatment delivery of the benefits of carboplatin on the primary pCR endpoint, she added.
The BrighTNess trial was supported by AbbVie. Dr. Loibl has reported receiving grants and honoraria from AbbVie and others, including Medscape. Dr. Arnedos has reported receiving honoraria, travel grants, and/or research grants from AstraZeneca, Novartis, Pfizer, and Roche.
A version of this article first appeared on Medscape.com.