User login
Delayed diagnosis tops breast cancer malpractice claims
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.

“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
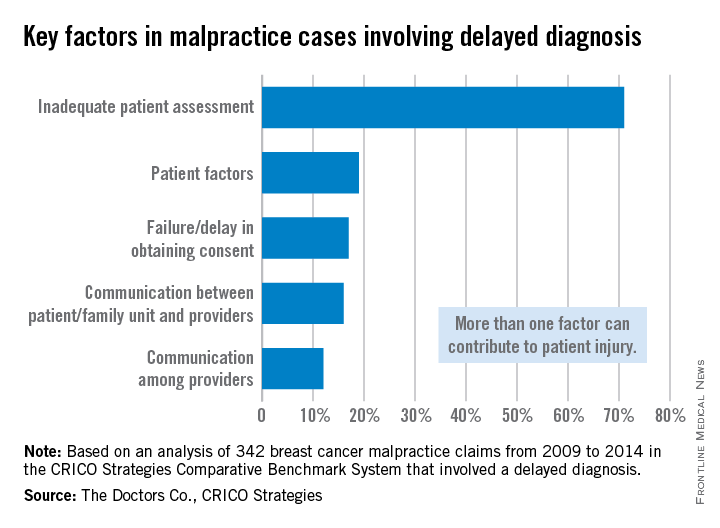
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.
“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med
The majority of medical malpractice lawsuits involving breast cancer result from delayed-diagnosis allegations, but a significant portion also stem from alleged poor management of breast cancer patients, a study showed.
In a review of 562 breast cancer malpractice claims from 2009 to 2014, 61% related to alleged delays in diagnosing breast cancer, and 39% stemmed from purported negligent treatment of patients, according to a joint analysis by medical liability insurers the Doctors Co. and CRICO.
“It was a big surprise to us to see that almost 40% of our cases involved patients who had already been diagnosed and were already receiving treatment,” said study coauthor Darrell Ranum, vice president of patient safety and risk management for the Doctors Co. “Breast cancer has been studied primarily from the angle of the diagnosis issues. We looked at our data, and we discovered there [was] really another very sizable bucket of claims involving breast cancer cases that involved treatment and management of breast cancer.”
The Doctors Co. and CRICO Strategies, a division of CRICO, pooled their databases of claims to conduct the study. Of the 562 breast cancer cases identified, 342 related to alleged delays in diagnosis, and 220 involved the management of breast cancer patients.
Nearly half of the delayed-diagnosis cases involved radiology (48%). But cases involving radiology did not necessarily result from a radiologist’s negligence. In some cases, primary care physicians or other clinicians may have misread or misinterpreted a radiologist’s report, Mr. Ranum said.
Physician offices/clinical care settings accounted for 39% of the delayed-diagnosis cases with family medicine and gynecology being the most common office settings in which cases originated. Common contributing factors to delayed-diagnosis lawsuits were inadequate patient assessment, such as misinterpretation of diagnostic studies. Delay in ordering diagnostic tests or failure to order them also topped contributing factors.
The vast majority of patients who had a delayed diagnosis of breast cancer were seriously harmed, with 70% of cases resulting in very severe outcomes, including 43 patient deaths, according to the report.
Of the 220 breast cancer management claims, 42% were surgery-related allegations. Patients often claimed poor performance of the initial surgery to remove a malignancy, or negligent performance of subsequent surgeries to reconstruct the breast, the study found.
Additional surgical allegations related to patient dissatisfaction with preoperative or postoperative management. The remaining nonsurgical cases related to medication management and minor procedures during the treatment course. The outcome of breast cancer claims involving surgical treatment were primarily of medium severity, with outcomes such as postoperative hematomas, injury to adjacent organs, and postoperative infections.
The analysis highlights opportunities for physicians to improve their care of breast cancer patients, both in the timely diagnosis of the disease and the ongoing management of care, Mr. Ranum said. He stressed that obtaining a timely and accurate diagnosis, including a complete history and interpretation of diagnostic studies, is critical. Equally important is the ongoing management of patients once an accurate diagnosis is made. Physicians should also implement processes, including documentation forms, that support and assist clinicians in providing a comprehensive informed consent process and better alignment of patients’ expectations.
“Systems need to be in place and systems need to be tested to make sure they don’t fail so that the information gets to where it needs to go,” Mr. Ranum said. “Our hope is that physicians will take a look at their own internal processes and track a patient from the time the physician says, ‘We need for you to have a mammogram,’ all the way through every step in that process.”
On Twitter @legal_med

Endocrine therapy in metastatic breast cancer: a closer look at the current clinical practice
How to fix clinical trial accrual
Editor Jame Abraham argues that once there is appropriate clinical trial infrastructure, there is only one person who can increase the clinical trial accrual: the treating oncologist.
Click on the PDF icon at the top of this introduction to read the full article.
Editor Jame Abraham argues that once there is appropriate clinical trial infrastructure, there is only one person who can increase the clinical trial accrual: the treating oncologist.
Click on the PDF icon at the top of this introduction to read the full article.
Editor Jame Abraham argues that once there is appropriate clinical trial infrastructure, there is only one person who can increase the clinical trial accrual: the treating oncologist.
Click on the PDF icon at the top of this introduction to read the full article.
VIDEO: Tomosynthesis soon to be standard of care for breast cancer screening
CHICAGO – The uptake of tomosynthesis has been fairly brisk among the nation’s breast cancer screening centers.
There are good reasons for that. In an interview at the annual clinical congress of the American College of Surgeons, Dr. Sarah Friedewald, division chief of breast and women’s imaging at Northwestern University, Chicago, explained the procedure; its pluses and minuses; and why it’s likely to be the standard of care for breast cancer screening within 5 years.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – The uptake of tomosynthesis has been fairly brisk among the nation’s breast cancer screening centers.
There are good reasons for that. In an interview at the annual clinical congress of the American College of Surgeons, Dr. Sarah Friedewald, division chief of breast and women’s imaging at Northwestern University, Chicago, explained the procedure; its pluses and minuses; and why it’s likely to be the standard of care for breast cancer screening within 5 years.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – The uptake of tomosynthesis has been fairly brisk among the nation’s breast cancer screening centers.
There are good reasons for that. In an interview at the annual clinical congress of the American College of Surgeons, Dr. Sarah Friedewald, division chief of breast and women’s imaging at Northwestern University, Chicago, explained the procedure; its pluses and minuses; and why it’s likely to be the standard of care for breast cancer screening within 5 years.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE ACS CLINICAL CONGRESS

VIDEO: Immediate breast reconstruction results reassuring in select patients
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
CHICAGO – Immediate breast reconstruction did not dramatically increase adverse outcomes in women undergoing mastectomy, a SCOAP database analysis found.
The popularity of immediate breast reconstruction is on the rise. Uptake rates, however, vary considerably across the country, prompting some to question whether concerns about adverse outcomes may be putting some surgeons and patients off the procedure.
Using the Surgical Clinical Outcomes Assessment Program database, researchers examined three key outcomes – 30-day readmissions, surgical complications, and surgical site infections – in 757 women who did or did not undergo breast reconstruction within 30 days of mastectomy for stage 0-3 breast cancer.
The results were reassuring, but should be interpreted within the context that those undergoing immediate reconstruction were a select group of women who were more likely to be nonsmokers and less likely to be obese or to be diagnosed with invasive cancer, observed study author Dr. Meghan Flanagan of the University of Washington in Seattle.
Click here to hear our interview with Dr. Flanagan at the annual clinical congress of the American College of Surgeons, where the data were formally presented.
Dr. Flanagan reported no relevant conflicts of interest.
AT THE ACS ANNUAL CONGRESS

NIH expands cancer research program to include breast density
Officials at the National Institutes of Health are taking a closer look at the role that breast density plays in the development of breast cancer.
As part of the agency’s Breast Cancer and the Environment Research Program (BCERP), grant-funded researchers are being tasked with expanding the study of risk factors that precede breast cancer such as breast density. They will also include more racially and ethnically diverse populations in their studies.
The research will be conducted at six centers: Brigham and Women’s Hospital, Boston; City of Hope/Beckman Research Institute, Duarte, Calif.; Columbia University, New York; Georgetown Lombardi Comprehensive Cancer Center, Washington; Michigan State University, Lansing; University of Massachusetts, Amherst. The research will be coordinated by another center at the University of Wisconsin, Madison.
Breast density is a new area of focus for the NIH. The researchers will consider dense breast tissue as a possible intermediate risk factor for breast cancer with the goal of identifying links between environmental exposures and high breast density, which could provide future prevention strategies.
“These priorities reflect our continued commitment to breast cancer prevention,” Caroline H. Dilworth, Ph.D., BCERP program lead at the National Institute of Environmental Health Sciences, said in a statement. “Our goal is to build on the high-quality science we’ve been funding for more than a decade, while also being responsive to the expert recommendations of the Interagency Breast Cancer and Environmental Research Coordinating Committee] report.”
On Twitter @maryellenny
Officials at the National Institutes of Health are taking a closer look at the role that breast density plays in the development of breast cancer.
As part of the agency’s Breast Cancer and the Environment Research Program (BCERP), grant-funded researchers are being tasked with expanding the study of risk factors that precede breast cancer such as breast density. They will also include more racially and ethnically diverse populations in their studies.
The research will be conducted at six centers: Brigham and Women’s Hospital, Boston; City of Hope/Beckman Research Institute, Duarte, Calif.; Columbia University, New York; Georgetown Lombardi Comprehensive Cancer Center, Washington; Michigan State University, Lansing; University of Massachusetts, Amherst. The research will be coordinated by another center at the University of Wisconsin, Madison.
Breast density is a new area of focus for the NIH. The researchers will consider dense breast tissue as a possible intermediate risk factor for breast cancer with the goal of identifying links between environmental exposures and high breast density, which could provide future prevention strategies.
“These priorities reflect our continued commitment to breast cancer prevention,” Caroline H. Dilworth, Ph.D., BCERP program lead at the National Institute of Environmental Health Sciences, said in a statement. “Our goal is to build on the high-quality science we’ve been funding for more than a decade, while also being responsive to the expert recommendations of the Interagency Breast Cancer and Environmental Research Coordinating Committee] report.”
On Twitter @maryellenny
Officials at the National Institutes of Health are taking a closer look at the role that breast density plays in the development of breast cancer.
As part of the agency’s Breast Cancer and the Environment Research Program (BCERP), grant-funded researchers are being tasked with expanding the study of risk factors that precede breast cancer such as breast density. They will also include more racially and ethnically diverse populations in their studies.
The research will be conducted at six centers: Brigham and Women’s Hospital, Boston; City of Hope/Beckman Research Institute, Duarte, Calif.; Columbia University, New York; Georgetown Lombardi Comprehensive Cancer Center, Washington; Michigan State University, Lansing; University of Massachusetts, Amherst. The research will be coordinated by another center at the University of Wisconsin, Madison.
Breast density is a new area of focus for the NIH. The researchers will consider dense breast tissue as a possible intermediate risk factor for breast cancer with the goal of identifying links between environmental exposures and high breast density, which could provide future prevention strategies.
“These priorities reflect our continued commitment to breast cancer prevention,” Caroline H. Dilworth, Ph.D., BCERP program lead at the National Institute of Environmental Health Sciences, said in a statement. “Our goal is to build on the high-quality science we’ve been funding for more than a decade, while also being responsive to the expert recommendations of the Interagency Breast Cancer and Environmental Research Coordinating Committee] report.”
On Twitter @maryellenny
Race, age, BMI had no impact on pCR rates
SAN FRANCISCO – Age, race, and body mass index (BMI) do not appear to be related to achieving pathologic complete response (pCR) in breast cancer patients, according to data presented at the ASCO Breast Cancer Symposium.
“We did see some suggestions that maybe age and race were associated, but in our modeling, once we accounted for tumor characteristics such as tumor size and lymph node involvement, that association was attenuated to nonsignificance,” said Dr. Erica T. Warner of the Harvard T.H. Chan School of Public Health, Boston.
She noted that some previous research has found a higher pCR among young women and a lower pCR among overweight and obese women.

“Overall we had pretty high pCR rates, much higher than observed in these other studies,” said Dr. Warner. “It is likely due to our definition of pCR, the tumor subtypes that were included in our study, and the studies we included had combination therapy in addition to neoadjuvant therapy.”
Pathologic complete response is an important prognostic indicator and surrogate endpoint, and this is particularly true for patients with hormone receptor–negative breast cancer. Prior research has suggested there may be a differential response to preoperative therapy by age and BMI, although no association has been observed by race.
“Our motivation for this trial was that we know that young age, black race, and obesity are associated with poorer survival, and we wanted to try to better understand the mechanisms behind that,” explained Dr. Warner.
In this study, Dr. Warner and her colleagues conducted an analysis of 1,146 women with breast cancer, who were enrolled in four clinical trials of neoadjuvant chemotherapy (CALGB 40601 and 40603; ACOSOG Z1031 and Z1041). They used logistic regression models to determine the association of race/ethnicity and age at diagnosis with pCR.
Within the cohort, 156 patients (13.6%) were black; 590 tumors (51.5%) were HER2+, 169 (14.7%) were ER+/HER2-, and 387 (33.8%) were triple negative.
In multivariate analyses that controlled for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00), and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR. The researchers found similar associations when they stratified the data by subtype, and found no interaction between age and black race (P = .06), black race and BMI (P = .54), or age and BMI (P = .73).
For the ER+ HER2- subtype, there was a suggestion of an inverse association; per 5-year increase the probability of pCR decreased 17%, but again it was not statistically significant.
There were higher rates of pCR among HER2+ and triple-negative tumors, but there was no difference in pCR according to race (white women, 43.5%; black women, 44.2%; and other/unknown, 46.1%), Dr. Warner pointed out.
There was a lower median age for achieving pCR, as the median age for women who did not achieve pCR was 53, compared with 49 for those who did (P <less than .0001). And for BMI, women who didn’t achieve pCR had an average BMI of 28.6, compared with 28 for those who did (P = .03).
“But there was no association of black race with pCR for any subtype, no association between BMI and pCR for any subtype, and no association for age,” she said.
SAN FRANCISCO – Age, race, and body mass index (BMI) do not appear to be related to achieving pathologic complete response (pCR) in breast cancer patients, according to data presented at the ASCO Breast Cancer Symposium.
“We did see some suggestions that maybe age and race were associated, but in our modeling, once we accounted for tumor characteristics such as tumor size and lymph node involvement, that association was attenuated to nonsignificance,” said Dr. Erica T. Warner of the Harvard T.H. Chan School of Public Health, Boston.
She noted that some previous research has found a higher pCR among young women and a lower pCR among overweight and obese women.
“Overall we had pretty high pCR rates, much higher than observed in these other studies,” said Dr. Warner. “It is likely due to our definition of pCR, the tumor subtypes that were included in our study, and the studies we included had combination therapy in addition to neoadjuvant therapy.”
Pathologic complete response is an important prognostic indicator and surrogate endpoint, and this is particularly true for patients with hormone receptor–negative breast cancer. Prior research has suggested there may be a differential response to preoperative therapy by age and BMI, although no association has been observed by race.
“Our motivation for this trial was that we know that young age, black race, and obesity are associated with poorer survival, and we wanted to try to better understand the mechanisms behind that,” explained Dr. Warner.
In this study, Dr. Warner and her colleagues conducted an analysis of 1,146 women with breast cancer, who were enrolled in four clinical trials of neoadjuvant chemotherapy (CALGB 40601 and 40603; ACOSOG Z1031 and Z1041). They used logistic regression models to determine the association of race/ethnicity and age at diagnosis with pCR.
Within the cohort, 156 patients (13.6%) were black; 590 tumors (51.5%) were HER2+, 169 (14.7%) were ER+/HER2-, and 387 (33.8%) were triple negative.
In multivariate analyses that controlled for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00), and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR. The researchers found similar associations when they stratified the data by subtype, and found no interaction between age and black race (P = .06), black race and BMI (P = .54), or age and BMI (P = .73).
For the ER+ HER2- subtype, there was a suggestion of an inverse association; per 5-year increase the probability of pCR decreased 17%, but again it was not statistically significant.
There were higher rates of pCR among HER2+ and triple-negative tumors, but there was no difference in pCR according to race (white women, 43.5%; black women, 44.2%; and other/unknown, 46.1%), Dr. Warner pointed out.
There was a lower median age for achieving pCR, as the median age for women who did not achieve pCR was 53, compared with 49 for those who did (P <less than .0001). And for BMI, women who didn’t achieve pCR had an average BMI of 28.6, compared with 28 for those who did (P = .03).
“But there was no association of black race with pCR for any subtype, no association between BMI and pCR for any subtype, and no association for age,” she said.
SAN FRANCISCO – Age, race, and body mass index (BMI) do not appear to be related to achieving pathologic complete response (pCR) in breast cancer patients, according to data presented at the ASCO Breast Cancer Symposium.
“We did see some suggestions that maybe age and race were associated, but in our modeling, once we accounted for tumor characteristics such as tumor size and lymph node involvement, that association was attenuated to nonsignificance,” said Dr. Erica T. Warner of the Harvard T.H. Chan School of Public Health, Boston.
She noted that some previous research has found a higher pCR among young women and a lower pCR among overweight and obese women.
“Overall we had pretty high pCR rates, much higher than observed in these other studies,” said Dr. Warner. “It is likely due to our definition of pCR, the tumor subtypes that were included in our study, and the studies we included had combination therapy in addition to neoadjuvant therapy.”
Pathologic complete response is an important prognostic indicator and surrogate endpoint, and this is particularly true for patients with hormone receptor–negative breast cancer. Prior research has suggested there may be a differential response to preoperative therapy by age and BMI, although no association has been observed by race.
“Our motivation for this trial was that we know that young age, black race, and obesity are associated with poorer survival, and we wanted to try to better understand the mechanisms behind that,” explained Dr. Warner.
In this study, Dr. Warner and her colleagues conducted an analysis of 1,146 women with breast cancer, who were enrolled in four clinical trials of neoadjuvant chemotherapy (CALGB 40601 and 40603; ACOSOG Z1031 and Z1041). They used logistic regression models to determine the association of race/ethnicity and age at diagnosis with pCR.
Within the cohort, 156 patients (13.6%) were black; 590 tumors (51.5%) were HER2+, 169 (14.7%) were ER+/HER2-, and 387 (33.8%) were triple negative.
In multivariate analyses that controlled for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00), and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR. The researchers found similar associations when they stratified the data by subtype, and found no interaction between age and black race (P = .06), black race and BMI (P = .54), or age and BMI (P = .73).
For the ER+ HER2- subtype, there was a suggestion of an inverse association; per 5-year increase the probability of pCR decreased 17%, but again it was not statistically significant.
There were higher rates of pCR among HER2+ and triple-negative tumors, but there was no difference in pCR according to race (white women, 43.5%; black women, 44.2%; and other/unknown, 46.1%), Dr. Warner pointed out.
There was a lower median age for achieving pCR, as the median age for women who did not achieve pCR was 53, compared with 49 for those who did (P <less than .0001). And for BMI, women who didn’t achieve pCR had an average BMI of 28.6, compared with 28 for those who did (P = .03).
“But there was no association of black race with pCR for any subtype, no association between BMI and pCR for any subtype, and no association for age,” she said.
FROM THE 2015 ASCO BREAST CANCER SYMPOSIUM
Key clinical point: Race, age, and body mass index do not appear to affect pathologic complete response in breast cancer.
Major finding: In multivariate analyses controlling for tumor characteristics and other factors, black race (OR, 1.07; 95% CI, 0.67-1.70), age (OR, 0.99; 95% CI, 0.97-1.00) and BMI (OR, 0.99; 95% CI, 0.96-1.01) were not significant predictors of pCR.
Data source: An analysis of four clinical trials of neoadjuvant chemotherapy that included 1,146 women with breast cancer.
Disclosures: Dr. Warner had no relevant financial disclosures, and there was no information on outside sponsorship of the study.

Managing menopausal symptoms in women with a BRCA mutation
This audiocast was recorded at the North American Menopause Society Annual Meeting held September 30 to October 3, 2015, in Las Vegas, Nevada
For more on this topic, read Dr. Kaunitz's August 2015 Cases in Menopause article, Is menopausal hormone therapy safe when your patient carries a BRCA mutation?
This audiocast was recorded at the North American Menopause Society Annual Meeting held September 30 to October 3, 2015, in Las Vegas, Nevada
For more on this topic, read Dr. Kaunitz's August 2015 Cases in Menopause article, Is menopausal hormone therapy safe when your patient carries a BRCA mutation?
This audiocast was recorded at the North American Menopause Society Annual Meeting held September 30 to October 3, 2015, in Las Vegas, Nevada
For more on this topic, read Dr. Kaunitz's August 2015 Cases in Menopause article, Is menopausal hormone therapy safe when your patient carries a BRCA mutation?
VIDEO: When to use MRI in breast cancer
CHICAGO – For most women, there’s little role for MRI in screening for and treating breast cancer
However, there are important exceptions. In an interview at the American College of Surgeons Clinical Congress, Dr. Monica Morrow, chief of breast surgery at Memorial Sloan-Kettering Cancer Center in Manhattan, explained what those exceptions are, and how she uses MRI in her practice.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – For most women, there’s little role for MRI in screening for and treating breast cancer
However, there are important exceptions. In an interview at the American College of Surgeons Clinical Congress, Dr. Monica Morrow, chief of breast surgery at Memorial Sloan-Kettering Cancer Center in Manhattan, explained what those exceptions are, and how she uses MRI in her practice.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
CHICAGO – For most women, there’s little role for MRI in screening for and treating breast cancer
However, there are important exceptions. In an interview at the American College of Surgeons Clinical Congress, Dr. Monica Morrow, chief of breast surgery at Memorial Sloan-Kettering Cancer Center in Manhattan, explained what those exceptions are, and how she uses MRI in her practice.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
EXPERT ANALYSIS FROM THE AMERICAN COLLEGE OF SURGEONS CLINICAL CONGRESS

Get smart about dense breasts
It’s a movement that shows no signs of abating. Women in 24 states, encompassing 67% of American women, now receive some level of notification after their mammogram about breast density. Individual patient advocates continue to push for notification, and states are likely to continue to draft bills. On the national level, a federal standard is being pursued through both federal legislation and federal regulation. Clinicians practicing in states with an “inform” law, either already in effect or imminent, will be tasked with engaging in new patient conversations arising from density notification. Are you ready to answer your patients’ questions?
Navigating inconsistent data and expert comments about density and discerning which patients may benefit from additional screening can create challenges in addressing a patient’s questions about the implications of her dense tissue. If you feel less than equipped to address these issues, you are not alone. A recent survey of clinicians, con- ducted after California’s breast density notification law went into effect, showed that only 6% were comfortable answering patients’ questions relating to breast density. Seventy-five percent of respondents indicated they wanted more education on the topic.1
For women having mammography, dense breast tissue is most important because it can mask detection of cancers, and women may want to have additional screening beyond mammography. Women with dense breasts are also at increased risk for developing breast cancer. For clinicians who are on the front lines of care for women undergoing screening, the most important action items are:
- identifying who needs more screening
- weighing the risks and benefits of such additional screening.
To assist you in informing patient discussions, in this article we answer some of the most frequently asked questions of ObGyns.
Which breasts are considered dense?
The American College of Radiology recommends that density be reported in 1 of 4 categories depending on the relative amounts of fat and fibroglandular tissue2:
- almost entirely fatty—on mammography most of the tissue appears dark gray while small amounts of dense (or fibroglandular) tissue display as light gray or white.
- scattered fibroglandular density—scattered areas of dense tissue mixed with fat. Even in breasts with scattered areas of breast tissue, cancers sometimes can be missed when they resemble areas of normal tissue or are within an area of denser tissue.
- heterogeneously dense—there are large portions of the breast where dense tissue could hide masses.
- extremely dense—most of the breast appears to consist of dense tissue, creating a “white out” situation and making it extremely difficult to see through.
Breasts that are either heterogeneously dense or extremely dense are considered “dense.” About 40% of women older than age 40 have dense breasts.3
Case study: Imaging of a cancerous breast mass in a 48-year-old woman with dense breasts
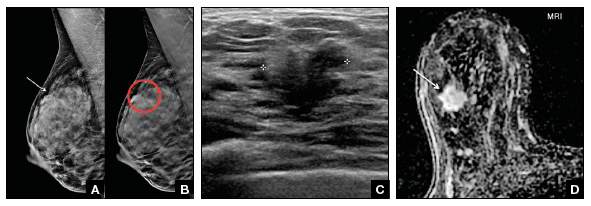
This patient has heterogeneously dense breast tissue. Standard 2D mediolateral oblique (MLO) digital mammogram (A) and MLO tomosynthesis 1-mm slice (B) reveal subtle possible distortion (arrow) in the upper right breast. On tomosynthesis, the distortion is better seen, as is the underlying irregular mass (red circle).
Ultrasound (US) directed to the mass (C) shows an irregular hypoechoic (dark gray) mass (marked by calipers), compatible with cancer. US-guided core needle biopsy revealed grade 2 invasive ductal cancer with associated ductal carcinoma in situ.
Axial magnetic resonance imaging of the right breast obtained after contrast injection, and after computer subtraction of nonenhanced image (D), shows irregular spiculated enhancing (white) mass (arrow) due to the known carcinoma.
Images: Courtesy Wendie Berg, MD, PhD
Who needs more screening?
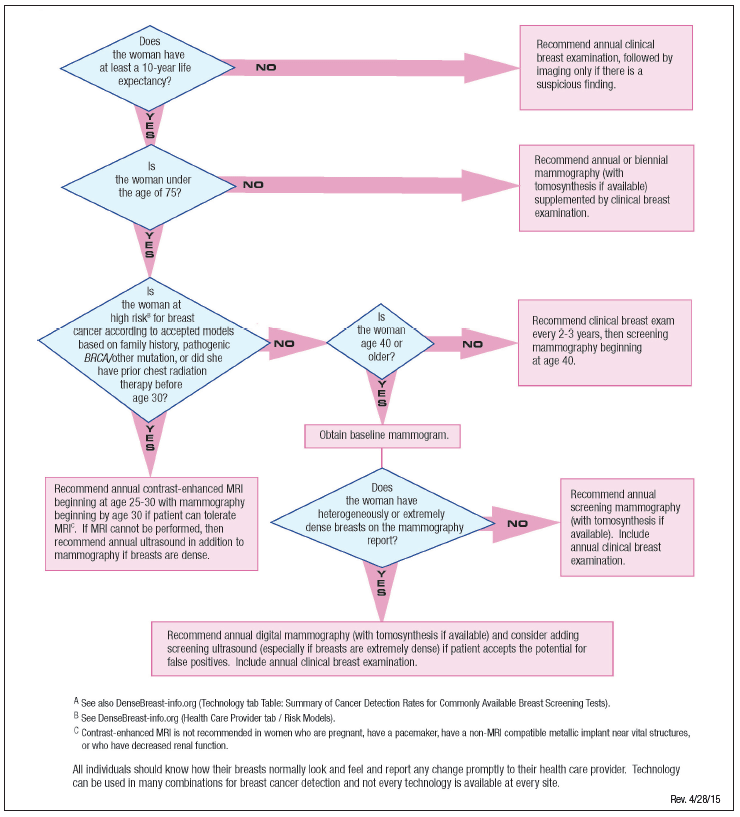
The FIGURE is a screening decision support tool representing the consensus opinion of several medical experts based on the best available scientific evidence to optimize breast cancer detection.
Do dense breasts affect the risk of developing breast cancer?
Yes. Dense breasts are a risk factor for breast cancer. According to the American Cancer Society’s Breast Cancer Facts & Figures 2013−2014, “The risk of breast cancer in-creases with increasing breast density; women with very high breast density have a 4- to 6-fold increased risk of breast cancer compared to women with the least dense breasts.”4,5
There are several reasons that dense tissue increases risk. First, the glands tend to be made up of relatively actively dividing cells that can mutate and become cancerous (the more glandular tissue present, the greater the risk). Second, the local environment around the glands may produce certain growth hormones that stimulate cells to divide, and this seems to occur more in fibrous tissue than in fatty tissue.
Most women have breast density somewhere in the middle range, with their risk for breast cancer falling in between those with extremely dense breasts and those with fatty breasts.6 The risk for developing breast cancer is influenced by a combination of many different factors, including age, family history of cancer (particularly breast or ovarian cancer), and prior atypical breast biopsies. There currently is no reliable way to fully account for the interplay of breast density, family history, prior biopsy results, and other factors in determining overall risk. Importantly, more than half of all women who develop breast cancer have no known risk factors other than being female and aging.
Is your medical support staff “density ready?”
We’re all familiar with the adage that a picture is worth a thousand words. While the medical support personnel in your office are likely quite familiar with imaging reports and the terminology used in describing dense breasts, they may be quite unfamiliar with what a fatty versus dense breast actually looks like on a mammogram, and how cancer may display in each. Illustrated examples, as seen here, are useful for reference.
In the fatty breast (A), a small cancer (arrow) is seen easily. In a breast categorized as scattered fibroglandular density (B), a large cancer is easily seen (arrow) in the relatively fatty portion of the breast, though a small cancer could have been hidden in areas with normal glandular tissue.
In a breast categorized as heterogeneously dense (C), a 4-cm (about 1.5-inch) cancer (arrows) is hidden by the dense breast tissue. This cancer also has spread to a lymph node under the arm (curved arrow).
In an extremely dense breast (D), a cancer is seen because part of it is located in the back of the breast where there is a small amount of dark fat making it easier to see (arrow and triangle marker indicating lump). If this cancer had been located near the nipple and completely surrounded by white (dense) tissue, it probably would not have been seen on mammography.
Image: Courtesy of Dr. Regina Hooley and DenseBreast-info.org
Are screening mammography outcomes different for women with dense versus fatty breasts?
Yes. Cancer is more likely to be clinically detected in the interval between mammography screens (defined as interval cancer) in women with dense breasts. Such interval cancers tend to be more aggressive and have worse outcomes. Compared with those in fatty breasts, cancers found in dense breasts more often7:
- are locally advanced (stage IIb and III)
- are multifocal or multicentric
- require a mastectomy (rather than a lumpectomy).
Does supplemental screening beyond mammography save lives?
Mammography is the only imaging screening modality that has been studied by multiple randomized controlled trials with mortality as an endpoint. Across those trials, mammography has been shown to reduce deaths due to breast cancer. The randomized trials that show a benefit from mammography are those in which mammography increased detection of invasive breast cancers before they spread to lymph nodes.8
No randomized controlled trial has yet been reported on any other imaging screening modality, but it is expected that other screening tests that increase detection of node-negative invasive breast cancers beyond mammography should further reduce breast cancer mortality.
Proving the mortality benefit of any supplemental screening modality would require a very large, very expensive randomized controlled trial with 15 to 20 years of follow-up. Given the speed of technologic developments, any results likely would be obsolete by the trial’s conclusion. What we do know is that women at high risk for breast cancer who undergo annual magnetic resonance imaging (MRI) screening are less likely to have advanced breast cancer than their counterparts who were not screened with MRI.9
We also know that average-risk women who are screened with ultrasonography in addition to mammography are unlikely to have palpable cancer in the interval between screens,10,11 with the rates of such interval cancers similar to women with fatty breasts screened only with mammography. The cancers found only on MRI or ultrasound are mostly small invasive cancers (average size, approximately 1 cm) that are mostly node negative.12,13 MRI also finds some ductal carcinoma in situ (DCIS).
These results suggest that there is a benefit to finding additional cancers with supplemental screening, though it is certainly possible that, as with mammography, some of the cancers found with supplemental screening are slow growing and may never have caused a woman harm even if left untreated.
Dense breasts: Medically sourced resources
Educational Web site
DenseBreast-info.org. This site is a collaborative, multidisciplinary educational resource. It features content for both patients and health care providers with separate data streams for each and includes:
a comprehensive list of FAQs; screening flow charts; a Patient Risk Checklist; an explanation of risks, risk assessment, and links to risk assessment tools; an illustrated round-up of technologies commonly used in screening; and state-by-state legislative analysis of density inform laws across the country.
State-specific Web sites
BreastDensity.info. This site was created by the California Breast Density Information Group (CBDIG), a working group of breast radiologists and breast cancer risk specialists. The content is primarily for health care providers and features screening scenarios as well as FAQs about breast density, breast cancer risk, and the breast density notification law in California.
MIdensebreasts.org. This is a Web-based education resource created for primary care providers by the University of Michigan Health System and the Michigan Department of Health and Human Services. It includes continuing medical education credit.
Medical society materials
American Cancer Society offers Breast Density and Your Mammogram Report for patients: http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-039989.pdf
American College of Obstetricians and Gynecologists’ 2015 Density Policy statement is available online: http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Gynecologic-Practice/Management-of-Women-With-Dense-Breasts-Diagnosed-by-Mammography
American College of Radiology patient brochure details basic information about breast density and can be customized with your center’s information: http://www.acr.org/News-Publications/~/media/180321AF51AF4EA38FEC091461F5B695.pdf
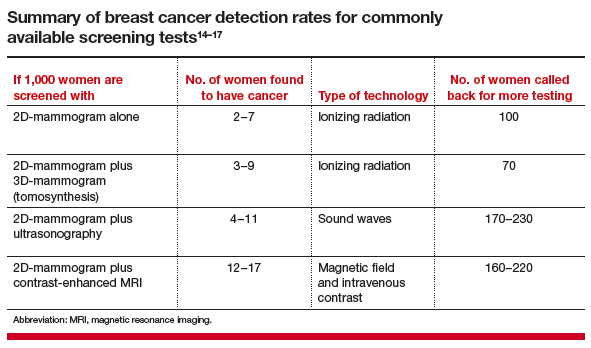
What additional screening tests are available after a 2D mammogram for a woman with dense breasts?
Depending on the patient’s age, risk level, and breast density, additional screening tools—such as tomosynthesis (also known as 3D mammography), ultrasonography, or MRI—may be recommended in addition to mammography. Indeed, in some centers, tomosynthesis is performed alone and the radiologist also reviews computer-generated 2D mammograms.
The addition of another imaging tool after a mammogram will find more cancers than mammography alone (TABLE).14−17 Women at high risk for breast cancer, such as those with pathogenic BRCA mutations, and those who were treated with radiation therapy to their chest (typically for Hodgkin disease) before age 30 and at least 8 years earlier, should be referred for annual MRI in addition to mammography (see Screening Decision Support Tool FIGURE above). If tomosynthesis is performed, the added benefit of ultrasound will be lower; further study on the actual benefit of supplemental ultrasound screening after 3D mammography is needed.
Will insurance cover supplemental screening beyond mammography?
The answer depends on the type of screening, the patient’s insurance and risk factors, the state in which you practice, and whether or not a law is in effect requiring insurance coverage for additional screening. In Illinois, for example, a woman with dense breasts can receive a screening ultrasound without a copay or deductible if it is ordered by a physician. In Connecticut, an ultrasound copay for screening dense breasts cannot exceed $20. Generally, in other states, an ultrasound will be covered if ordered by a physician, but it is subject to the copay and deductible of an individual health plan. In New Jersey, insurance coverage is provided for additional testing if a woman has extremely dense breasts.
Regardless of state, an MRI generally will be covered by insurance (subject to copay and deductible) if the patient meets high-risk criteria. In Michigan, at least one insurance company will cover a screening MRI for normal-risk women with dense breasts at a cost that matches the copay and deductible of a screening mammogram. It is important for patients to check with their insurance carrier prior to having an MRI.
Should women with dense breasts still have mammography screening?
Yes. Mammography is the first step in screening for most women (except for those who are pregnant or breastfeeding, in which case ultrasound can be performed but is usually deferred until several months after the patient is no longer pregnant or breastfeeding). While additional screening may be recommended for women with dense breasts, and for women at high risk for developing breast cancer, there are still some cancers and precancerous changes that will show on a mammogram better than on ultrasound or MRI. Wherever possible, women with dense breasts should have digital mammography rather than film mammography, due to slightly improved cancer detection using digital mammography.18
Does tomosynthesis solve the problem of screening dense breasts?
Tomosynthesis (3D mammography) slightly improves detection of cancers compared with standard digital mammography, but some cancers will remain hidden by overlapping dense tissue. We do not yet know the benefit of annual screening tomosynthesis. Without question, women at high risk for breast cancer still should have MRI if they are able to tolerate it, even if they have had tomosynthesis.
If a patient with dense breasts undergoes screening tomosynthesis, will she also need a screening ultrasound?
Preliminary studies not yet published suggest that, for women with dense breasts, ultrasound does find another 2 to 3 invasive cancers per 1,000 women screened that are not found on tomosynthesis, but further study of this issue is needed.
If recommended for additional screening with ultrasound or MRI, will a patient need that screening every year?
Usually, yes, though age and other medical conditions will change a patient’s personal risk and benefit considerations. Therefore, screening recommendations may change from one year to the next. With technology advancements and evolving guidelines, additional screening recommendations will change in the future.
Prepare yourself and your patients will benefit
The foundation of a successful screening program involves buy-in from both patient and clinician. Patients confused as to what their density notification means may have little understanding as to what next steps should be considered. To allay confusion, your patient will be best served by being provided understandable and actionable information. Advanced preparation for these conversations about the implications of dense tissue will make for more effective patient engagement.
Acknowledgment
Much of the material within this article has been sourced from the educational Web site DenseBreast-info.org. For comprehensive lists of both patient and health care provider frequently asked questions, visit http://www.DenseBreast-info.org.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Khong KA, Hargreaves J, Aminololama-Shakeri S, Lindfors KK. Impact of the California breast density law on primary care physicians. J Am Coll Radiol. 2015;12(3):256–260.
- Sickles EA, D’Orsi CJ, Bassett LW, et al. ACR BI-RADS Mammography. In: ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. Reston, VA: American College of Radiology; 2013.
- Sprague BL, Gangnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 2014;106(10).
- American Cancer Society. Breast Cancer Facts & Figures 2013–2014. http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-042725.pdf. Published 2013. Accessed September 15, 2015.
- Harvey JA, Bovbjerg VE. Quantitative assessment of mammographic breast density: relationship with breast cancer risk. Radiology. 2004;230(1):29–41.
- Kerlikowske K, Cook AJ, Buist DS, et al. Breast cancer risk by breast density, menopause, and postmenopausal hormone therapy use. J Clin Oncol. 2010;28(24):3830–3837.
- Arora N, King TA, Jacks LM, et al. Impact of breast density on the presenting features of malignancy. Ann Surg Oncol. 2010;17(suppl 3):211–218.
- Smith RA, Duffy SW, Gabe R, Tabar L, Yen AM, Chen TH. The randomized trials of breast cancer screening: what have we learned? Radiol Clin North Am. 2004;42(5):793–806, v.
- Warner E, Hill K, Causer P, et al. Prospective study of breast cancer incidence in women with a BRCA1 or BRCA2 mutation under surveillance with and without magnetic resonance imaging. J Clin Oncol. 2011;29(13):1664–1669.
- Corsetti V, Houssami N, Ghirardi M, et al. Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: interval breast cancers at 1 year follow-up. Eur J Cancer. 2011;47(7): 1021–1026.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012;307(13):1394–1404.
- Berg WA. Tailored supplemental screening for breast cancer: what now and what next? AJR Am J Roentgenol. 2009;192(2):390–399.
- Brem RF, Lenihan MJ, Lieberman J, Torrente J. Screening breast ultrasound: past, present, and future. AJR Am J Roentgenol. 2015;204(2):234–240.
- Hooley R. Tomosynthesis. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:2–19.
- Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014;311(24):2499–2507.
- Berg WA. Screening Ultrasound. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:9–43.
- Berg WA. Screening MRI. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:9–49.
- Hooley R. Tomosynthesis. In: Berg WA, Yang WT, eds.Berg WA. Screening Ultrasound. In: Berg WA, Yang WT, eds.Berg WA. Screening MRI. In: Berg WA, Yang WT, eds.Pisano ED, Gatsonis C, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353(17):1773–1783.
Wendie A. Berg, MD, PhD; JoAnn Pushkin; and Cindy Henke-Sarmento

Dr. Berg is Professor of Radiology, University of Pittsburgh School of Medicine, Magee-Womens Hospital of UPMC, Pittsburgh, Pennsylvania, and Chief Scientific Advisor, DenseBreast-info.org.

Ms. Pushkin is Executive Director, DenseBreast-info, Inc.

Ms. Henke-Sarmento is Technology Director, DenseBreast-info, Inc.
Ms. Pushkin and Ms. Henke-Sarmento report that the 501(c)(3) nonprofit, DenseBreast-info, Inc., which supports the Web site DenseBreast-info.org, has received unrestricted educational grants from GE Healthcare and Volpara Solutions Ltd. Dr. Berg reports no financial relationships relevant to this article.
Wendie A. Berg, MD, PhD; JoAnn Pushkin; and Cindy Henke-Sarmento
Dr. Berg is Professor of Radiology, University of Pittsburgh School of Medicine, Magee-Womens Hospital of UPMC, Pittsburgh, Pennsylvania, and Chief Scientific Advisor, DenseBreast-info.org.
Ms. Pushkin is Executive Director, DenseBreast-info, Inc.
Ms. Henke-Sarmento is Technology Director, DenseBreast-info, Inc.
Ms. Pushkin and Ms. Henke-Sarmento report that the 501(c)(3) nonprofit, DenseBreast-info, Inc., which supports the Web site DenseBreast-info.org, has received unrestricted educational grants from GE Healthcare and Volpara Solutions Ltd. Dr. Berg reports no financial relationships relevant to this article.
Wendie A. Berg, MD, PhD; JoAnn Pushkin; and Cindy Henke-Sarmento
Dr. Berg is Professor of Radiology, University of Pittsburgh School of Medicine, Magee-Womens Hospital of UPMC, Pittsburgh, Pennsylvania, and Chief Scientific Advisor, DenseBreast-info.org.
Ms. Pushkin is Executive Director, DenseBreast-info, Inc.
Ms. Henke-Sarmento is Technology Director, DenseBreast-info, Inc.
Ms. Pushkin and Ms. Henke-Sarmento report that the 501(c)(3) nonprofit, DenseBreast-info, Inc., which supports the Web site DenseBreast-info.org, has received unrestricted educational grants from GE Healthcare and Volpara Solutions Ltd. Dr. Berg reports no financial relationships relevant to this article.
It’s a movement that shows no signs of abating. Women in 24 states, encompassing 67% of American women, now receive some level of notification after their mammogram about breast density. Individual patient advocates continue to push for notification, and states are likely to continue to draft bills. On the national level, a federal standard is being pursued through both federal legislation and federal regulation. Clinicians practicing in states with an “inform” law, either already in effect or imminent, will be tasked with engaging in new patient conversations arising from density notification. Are you ready to answer your patients’ questions?
Navigating inconsistent data and expert comments about density and discerning which patients may benefit from additional screening can create challenges in addressing a patient’s questions about the implications of her dense tissue. If you feel less than equipped to address these issues, you are not alone. A recent survey of clinicians, con- ducted after California’s breast density notification law went into effect, showed that only 6% were comfortable answering patients’ questions relating to breast density. Seventy-five percent of respondents indicated they wanted more education on the topic.1
For women having mammography, dense breast tissue is most important because it can mask detection of cancers, and women may want to have additional screening beyond mammography. Women with dense breasts are also at increased risk for developing breast cancer. For clinicians who are on the front lines of care for women undergoing screening, the most important action items are:
- identifying who needs more screening
- weighing the risks and benefits of such additional screening.
To assist you in informing patient discussions, in this article we answer some of the most frequently asked questions of ObGyns.
Which breasts are considered dense?
The American College of Radiology recommends that density be reported in 1 of 4 categories depending on the relative amounts of fat and fibroglandular tissue2:
- almost entirely fatty—on mammography most of the tissue appears dark gray while small amounts of dense (or fibroglandular) tissue display as light gray or white.
- scattered fibroglandular density—scattered areas of dense tissue mixed with fat. Even in breasts with scattered areas of breast tissue, cancers sometimes can be missed when they resemble areas of normal tissue or are within an area of denser tissue.
- heterogeneously dense—there are large portions of the breast where dense tissue could hide masses.
- extremely dense—most of the breast appears to consist of dense tissue, creating a “white out” situation and making it extremely difficult to see through.
Breasts that are either heterogeneously dense or extremely dense are considered “dense.” About 40% of women older than age 40 have dense breasts.3
Case study: Imaging of a cancerous breast mass in a 48-year-old woman with dense breasts
This patient has heterogeneously dense breast tissue. Standard 2D mediolateral oblique (MLO) digital mammogram (A) and MLO tomosynthesis 1-mm slice (B) reveal subtle possible distortion (arrow) in the upper right breast. On tomosynthesis, the distortion is better seen, as is the underlying irregular mass (red circle).
Ultrasound (US) directed to the mass (C) shows an irregular hypoechoic (dark gray) mass (marked by calipers), compatible with cancer. US-guided core needle biopsy revealed grade 2 invasive ductal cancer with associated ductal carcinoma in situ.
Axial magnetic resonance imaging of the right breast obtained after contrast injection, and after computer subtraction of nonenhanced image (D), shows irregular spiculated enhancing (white) mass (arrow) due to the known carcinoma.
Images: Courtesy Wendie Berg, MD, PhD
Who needs more screening?
The FIGURE is a screening decision support tool representing the consensus opinion of several medical experts based on the best available scientific evidence to optimize breast cancer detection.
Do dense breasts affect the risk of developing breast cancer?
Yes. Dense breasts are a risk factor for breast cancer. According to the American Cancer Society’s Breast Cancer Facts & Figures 2013−2014, “The risk of breast cancer in-creases with increasing breast density; women with very high breast density have a 4- to 6-fold increased risk of breast cancer compared to women with the least dense breasts.”4,5
There are several reasons that dense tissue increases risk. First, the glands tend to be made up of relatively actively dividing cells that can mutate and become cancerous (the more glandular tissue present, the greater the risk). Second, the local environment around the glands may produce certain growth hormones that stimulate cells to divide, and this seems to occur more in fibrous tissue than in fatty tissue.
Most women have breast density somewhere in the middle range, with their risk for breast cancer falling in between those with extremely dense breasts and those with fatty breasts.6 The risk for developing breast cancer is influenced by a combination of many different factors, including age, family history of cancer (particularly breast or ovarian cancer), and prior atypical breast biopsies. There currently is no reliable way to fully account for the interplay of breast density, family history, prior biopsy results, and other factors in determining overall risk. Importantly, more than half of all women who develop breast cancer have no known risk factors other than being female and aging.
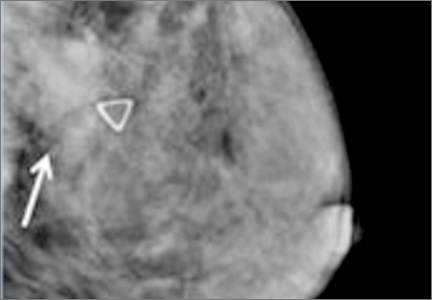
Is your medical support staff “density ready?”
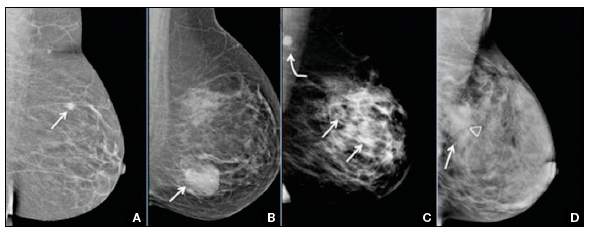
We’re all familiar with the adage that a picture is worth a thousand words. While the medical support personnel in your office are likely quite familiar with imaging reports and the terminology used in describing dense breasts, they may be quite unfamiliar with what a fatty versus dense breast actually looks like on a mammogram, and how cancer may display in each. Illustrated examples, as seen here, are useful for reference.
In the fatty breast (A), a small cancer (arrow) is seen easily. In a breast categorized as scattered fibroglandular density (B), a large cancer is easily seen (arrow) in the relatively fatty portion of the breast, though a small cancer could have been hidden in areas with normal glandular tissue.
In a breast categorized as heterogeneously dense (C), a 4-cm (about 1.5-inch) cancer (arrows) is hidden by the dense breast tissue. This cancer also has spread to a lymph node under the arm (curved arrow).
In an extremely dense breast (D), a cancer is seen because part of it is located in the back of the breast where there is a small amount of dark fat making it easier to see (arrow and triangle marker indicating lump). If this cancer had been located near the nipple and completely surrounded by white (dense) tissue, it probably would not have been seen on mammography.
Image: Courtesy of Dr. Regina Hooley and DenseBreast-info.org
Are screening mammography outcomes different for women with dense versus fatty breasts?
Yes. Cancer is more likely to be clinically detected in the interval between mammography screens (defined as interval cancer) in women with dense breasts. Such interval cancers tend to be more aggressive and have worse outcomes. Compared with those in fatty breasts, cancers found in dense breasts more often7:
- are locally advanced (stage IIb and III)
- are multifocal or multicentric
- require a mastectomy (rather than a lumpectomy).
Does supplemental screening beyond mammography save lives?
Mammography is the only imaging screening modality that has been studied by multiple randomized controlled trials with mortality as an endpoint. Across those trials, mammography has been shown to reduce deaths due to breast cancer. The randomized trials that show a benefit from mammography are those in which mammography increased detection of invasive breast cancers before they spread to lymph nodes.8
No randomized controlled trial has yet been reported on any other imaging screening modality, but it is expected that other screening tests that increase detection of node-negative invasive breast cancers beyond mammography should further reduce breast cancer mortality.
Proving the mortality benefit of any supplemental screening modality would require a very large, very expensive randomized controlled trial with 15 to 20 years of follow-up. Given the speed of technologic developments, any results likely would be obsolete by the trial’s conclusion. What we do know is that women at high risk for breast cancer who undergo annual magnetic resonance imaging (MRI) screening are less likely to have advanced breast cancer than their counterparts who were not screened with MRI.9
We also know that average-risk women who are screened with ultrasonography in addition to mammography are unlikely to have palpable cancer in the interval between screens,10,11 with the rates of such interval cancers similar to women with fatty breasts screened only with mammography. The cancers found only on MRI or ultrasound are mostly small invasive cancers (average size, approximately 1 cm) that are mostly node negative.12,13 MRI also finds some ductal carcinoma in situ (DCIS).
These results suggest that there is a benefit to finding additional cancers with supplemental screening, though it is certainly possible that, as with mammography, some of the cancers found with supplemental screening are slow growing and may never have caused a woman harm even if left untreated.
Dense breasts: Medically sourced resources
Educational Web site
DenseBreast-info.org. This site is a collaborative, multidisciplinary educational resource. It features content for both patients and health care providers with separate data streams for each and includes:
a comprehensive list of FAQs; screening flow charts; a Patient Risk Checklist; an explanation of risks, risk assessment, and links to risk assessment tools; an illustrated round-up of technologies commonly used in screening; and state-by-state legislative analysis of density inform laws across the country.
State-specific Web sites
BreastDensity.info. This site was created by the California Breast Density Information Group (CBDIG), a working group of breast radiologists and breast cancer risk specialists. The content is primarily for health care providers and features screening scenarios as well as FAQs about breast density, breast cancer risk, and the breast density notification law in California.
MIdensebreasts.org. This is a Web-based education resource created for primary care providers by the University of Michigan Health System and the Michigan Department of Health and Human Services. It includes continuing medical education credit.
Medical society materials
American Cancer Society offers Breast Density and Your Mammogram Report for patients: http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-039989.pdf
American College of Obstetricians and Gynecologists’ 2015 Density Policy statement is available online: http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Gynecologic-Practice/Management-of-Women-With-Dense-Breasts-Diagnosed-by-Mammography
American College of Radiology patient brochure details basic information about breast density and can be customized with your center’s information: http://www.acr.org/News-Publications/~/media/180321AF51AF4EA38FEC091461F5B695.pdf
What additional screening tests are available after a 2D mammogram for a woman with dense breasts?
Depending on the patient’s age, risk level, and breast density, additional screening tools—such as tomosynthesis (also known as 3D mammography), ultrasonography, or MRI—may be recommended in addition to mammography. Indeed, in some centers, tomosynthesis is performed alone and the radiologist also reviews computer-generated 2D mammograms.
The addition of another imaging tool after a mammogram will find more cancers than mammography alone (TABLE).14−17 Women at high risk for breast cancer, such as those with pathogenic BRCA mutations, and those who were treated with radiation therapy to their chest (typically for Hodgkin disease) before age 30 and at least 8 years earlier, should be referred for annual MRI in addition to mammography (see Screening Decision Support Tool FIGURE above). If tomosynthesis is performed, the added benefit of ultrasound will be lower; further study on the actual benefit of supplemental ultrasound screening after 3D mammography is needed.
Will insurance cover supplemental screening beyond mammography?
The answer depends on the type of screening, the patient’s insurance and risk factors, the state in which you practice, and whether or not a law is in effect requiring insurance coverage for additional screening. In Illinois, for example, a woman with dense breasts can receive a screening ultrasound without a copay or deductible if it is ordered by a physician. In Connecticut, an ultrasound copay for screening dense breasts cannot exceed $20. Generally, in other states, an ultrasound will be covered if ordered by a physician, but it is subject to the copay and deductible of an individual health plan. In New Jersey, insurance coverage is provided for additional testing if a woman has extremely dense breasts.
Regardless of state, an MRI generally will be covered by insurance (subject to copay and deductible) if the patient meets high-risk criteria. In Michigan, at least one insurance company will cover a screening MRI for normal-risk women with dense breasts at a cost that matches the copay and deductible of a screening mammogram. It is important for patients to check with their insurance carrier prior to having an MRI.
Should women with dense breasts still have mammography screening?
Yes. Mammography is the first step in screening for most women (except for those who are pregnant or breastfeeding, in which case ultrasound can be performed but is usually deferred until several months after the patient is no longer pregnant or breastfeeding). While additional screening may be recommended for women with dense breasts, and for women at high risk for developing breast cancer, there are still some cancers and precancerous changes that will show on a mammogram better than on ultrasound or MRI. Wherever possible, women with dense breasts should have digital mammography rather than film mammography, due to slightly improved cancer detection using digital mammography.18
Does tomosynthesis solve the problem of screening dense breasts?
Tomosynthesis (3D mammography) slightly improves detection of cancers compared with standard digital mammography, but some cancers will remain hidden by overlapping dense tissue. We do not yet know the benefit of annual screening tomosynthesis. Without question, women at high risk for breast cancer still should have MRI if they are able to tolerate it, even if they have had tomosynthesis.
If a patient with dense breasts undergoes screening tomosynthesis, will she also need a screening ultrasound?
Preliminary studies not yet published suggest that, for women with dense breasts, ultrasound does find another 2 to 3 invasive cancers per 1,000 women screened that are not found on tomosynthesis, but further study of this issue is needed.
If recommended for additional screening with ultrasound or MRI, will a patient need that screening every year?
Usually, yes, though age and other medical conditions will change a patient’s personal risk and benefit considerations. Therefore, screening recommendations may change from one year to the next. With technology advancements and evolving guidelines, additional screening recommendations will change in the future.
Prepare yourself and your patients will benefit
The foundation of a successful screening program involves buy-in from both patient and clinician. Patients confused as to what their density notification means may have little understanding as to what next steps should be considered. To allay confusion, your patient will be best served by being provided understandable and actionable information. Advanced preparation for these conversations about the implications of dense tissue will make for more effective patient engagement.
Acknowledgment
Much of the material within this article has been sourced from the educational Web site DenseBreast-info.org. For comprehensive lists of both patient and health care provider frequently asked questions, visit http://www.DenseBreast-info.org.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
It’s a movement that shows no signs of abating. Women in 24 states, encompassing 67% of American women, now receive some level of notification after their mammogram about breast density. Individual patient advocates continue to push for notification, and states are likely to continue to draft bills. On the national level, a federal standard is being pursued through both federal legislation and federal regulation. Clinicians practicing in states with an “inform” law, either already in effect or imminent, will be tasked with engaging in new patient conversations arising from density notification. Are you ready to answer your patients’ questions?
Navigating inconsistent data and expert comments about density and discerning which patients may benefit from additional screening can create challenges in addressing a patient’s questions about the implications of her dense tissue. If you feel less than equipped to address these issues, you are not alone. A recent survey of clinicians, con- ducted after California’s breast density notification law went into effect, showed that only 6% were comfortable answering patients’ questions relating to breast density. Seventy-five percent of respondents indicated they wanted more education on the topic.1
For women having mammography, dense breast tissue is most important because it can mask detection of cancers, and women may want to have additional screening beyond mammography. Women with dense breasts are also at increased risk for developing breast cancer. For clinicians who are on the front lines of care for women undergoing screening, the most important action items are:
- identifying who needs more screening
- weighing the risks and benefits of such additional screening.
To assist you in informing patient discussions, in this article we answer some of the most frequently asked questions of ObGyns.
Which breasts are considered dense?
The American College of Radiology recommends that density be reported in 1 of 4 categories depending on the relative amounts of fat and fibroglandular tissue2:
- almost entirely fatty—on mammography most of the tissue appears dark gray while small amounts of dense (or fibroglandular) tissue display as light gray or white.
- scattered fibroglandular density—scattered areas of dense tissue mixed with fat. Even in breasts with scattered areas of breast tissue, cancers sometimes can be missed when they resemble areas of normal tissue or are within an area of denser tissue.
- heterogeneously dense—there are large portions of the breast where dense tissue could hide masses.
- extremely dense—most of the breast appears to consist of dense tissue, creating a “white out” situation and making it extremely difficult to see through.
Breasts that are either heterogeneously dense or extremely dense are considered “dense.” About 40% of women older than age 40 have dense breasts.3
Case study: Imaging of a cancerous breast mass in a 48-year-old woman with dense breasts
This patient has heterogeneously dense breast tissue. Standard 2D mediolateral oblique (MLO) digital mammogram (A) and MLO tomosynthesis 1-mm slice (B) reveal subtle possible distortion (arrow) in the upper right breast. On tomosynthesis, the distortion is better seen, as is the underlying irregular mass (red circle).
Ultrasound (US) directed to the mass (C) shows an irregular hypoechoic (dark gray) mass (marked by calipers), compatible with cancer. US-guided core needle biopsy revealed grade 2 invasive ductal cancer with associated ductal carcinoma in situ.
Axial magnetic resonance imaging of the right breast obtained after contrast injection, and after computer subtraction of nonenhanced image (D), shows irregular spiculated enhancing (white) mass (arrow) due to the known carcinoma.
Images: Courtesy Wendie Berg, MD, PhD
Who needs more screening?
The FIGURE is a screening decision support tool representing the consensus opinion of several medical experts based on the best available scientific evidence to optimize breast cancer detection.
Do dense breasts affect the risk of developing breast cancer?
Yes. Dense breasts are a risk factor for breast cancer. According to the American Cancer Society’s Breast Cancer Facts & Figures 2013−2014, “The risk of breast cancer in-creases with increasing breast density; women with very high breast density have a 4- to 6-fold increased risk of breast cancer compared to women with the least dense breasts.”4,5
There are several reasons that dense tissue increases risk. First, the glands tend to be made up of relatively actively dividing cells that can mutate and become cancerous (the more glandular tissue present, the greater the risk). Second, the local environment around the glands may produce certain growth hormones that stimulate cells to divide, and this seems to occur more in fibrous tissue than in fatty tissue.
Most women have breast density somewhere in the middle range, with their risk for breast cancer falling in between those with extremely dense breasts and those with fatty breasts.6 The risk for developing breast cancer is influenced by a combination of many different factors, including age, family history of cancer (particularly breast or ovarian cancer), and prior atypical breast biopsies. There currently is no reliable way to fully account for the interplay of breast density, family history, prior biopsy results, and other factors in determining overall risk. Importantly, more than half of all women who develop breast cancer have no known risk factors other than being female and aging.
Is your medical support staff “density ready?”
We’re all familiar with the adage that a picture is worth a thousand words. While the medical support personnel in your office are likely quite familiar with imaging reports and the terminology used in describing dense breasts, they may be quite unfamiliar with what a fatty versus dense breast actually looks like on a mammogram, and how cancer may display in each. Illustrated examples, as seen here, are useful for reference.
In the fatty breast (A), a small cancer (arrow) is seen easily. In a breast categorized as scattered fibroglandular density (B), a large cancer is easily seen (arrow) in the relatively fatty portion of the breast, though a small cancer could have been hidden in areas with normal glandular tissue.
In a breast categorized as heterogeneously dense (C), a 4-cm (about 1.5-inch) cancer (arrows) is hidden by the dense breast tissue. This cancer also has spread to a lymph node under the arm (curved arrow).
In an extremely dense breast (D), a cancer is seen because part of it is located in the back of the breast where there is a small amount of dark fat making it easier to see (arrow and triangle marker indicating lump). If this cancer had been located near the nipple and completely surrounded by white (dense) tissue, it probably would not have been seen on mammography.
Image: Courtesy of Dr. Regina Hooley and DenseBreast-info.org
Are screening mammography outcomes different for women with dense versus fatty breasts?
Yes. Cancer is more likely to be clinically detected in the interval between mammography screens (defined as interval cancer) in women with dense breasts. Such interval cancers tend to be more aggressive and have worse outcomes. Compared with those in fatty breasts, cancers found in dense breasts more often7:
- are locally advanced (stage IIb and III)
- are multifocal or multicentric
- require a mastectomy (rather than a lumpectomy).
Does supplemental screening beyond mammography save lives?
Mammography is the only imaging screening modality that has been studied by multiple randomized controlled trials with mortality as an endpoint. Across those trials, mammography has been shown to reduce deaths due to breast cancer. The randomized trials that show a benefit from mammography are those in which mammography increased detection of invasive breast cancers before they spread to lymph nodes.8
No randomized controlled trial has yet been reported on any other imaging screening modality, but it is expected that other screening tests that increase detection of node-negative invasive breast cancers beyond mammography should further reduce breast cancer mortality.
Proving the mortality benefit of any supplemental screening modality would require a very large, very expensive randomized controlled trial with 15 to 20 years of follow-up. Given the speed of technologic developments, any results likely would be obsolete by the trial’s conclusion. What we do know is that women at high risk for breast cancer who undergo annual magnetic resonance imaging (MRI) screening are less likely to have advanced breast cancer than their counterparts who were not screened with MRI.9
We also know that average-risk women who are screened with ultrasonography in addition to mammography are unlikely to have palpable cancer in the interval between screens,10,11 with the rates of such interval cancers similar to women with fatty breasts screened only with mammography. The cancers found only on MRI or ultrasound are mostly small invasive cancers (average size, approximately 1 cm) that are mostly node negative.12,13 MRI also finds some ductal carcinoma in situ (DCIS).
These results suggest that there is a benefit to finding additional cancers with supplemental screening, though it is certainly possible that, as with mammography, some of the cancers found with supplemental screening are slow growing and may never have caused a woman harm even if left untreated.
Dense breasts: Medically sourced resources
Educational Web site
DenseBreast-info.org. This site is a collaborative, multidisciplinary educational resource. It features content for both patients and health care providers with separate data streams for each and includes:
a comprehensive list of FAQs; screening flow charts; a Patient Risk Checklist; an explanation of risks, risk assessment, and links to risk assessment tools; an illustrated round-up of technologies commonly used in screening; and state-by-state legislative analysis of density inform laws across the country.
State-specific Web sites
BreastDensity.info. This site was created by the California Breast Density Information Group (CBDIG), a working group of breast radiologists and breast cancer risk specialists. The content is primarily for health care providers and features screening scenarios as well as FAQs about breast density, breast cancer risk, and the breast density notification law in California.
MIdensebreasts.org. This is a Web-based education resource created for primary care providers by the University of Michigan Health System and the Michigan Department of Health and Human Services. It includes continuing medical education credit.
Medical society materials
American Cancer Society offers Breast Density and Your Mammogram Report for patients: http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-039989.pdf
American College of Obstetricians and Gynecologists’ 2015 Density Policy statement is available online: http://www.acog.org/Resources-And-Publications/Committee-Opinions/Committee-on-Gynecologic-Practice/Management-of-Women-With-Dense-Breasts-Diagnosed-by-Mammography
American College of Radiology patient brochure details basic information about breast density and can be customized with your center’s information: http://www.acr.org/News-Publications/~/media/180321AF51AF4EA38FEC091461F5B695.pdf
What additional screening tests are available after a 2D mammogram for a woman with dense breasts?
Depending on the patient’s age, risk level, and breast density, additional screening tools—such as tomosynthesis (also known as 3D mammography), ultrasonography, or MRI—may be recommended in addition to mammography. Indeed, in some centers, tomosynthesis is performed alone and the radiologist also reviews computer-generated 2D mammograms.
The addition of another imaging tool after a mammogram will find more cancers than mammography alone (TABLE).14−17 Women at high risk for breast cancer, such as those with pathogenic BRCA mutations, and those who were treated with radiation therapy to their chest (typically for Hodgkin disease) before age 30 and at least 8 years earlier, should be referred for annual MRI in addition to mammography (see Screening Decision Support Tool FIGURE above). If tomosynthesis is performed, the added benefit of ultrasound will be lower; further study on the actual benefit of supplemental ultrasound screening after 3D mammography is needed.
Will insurance cover supplemental screening beyond mammography?
The answer depends on the type of screening, the patient’s insurance and risk factors, the state in which you practice, and whether or not a law is in effect requiring insurance coverage for additional screening. In Illinois, for example, a woman with dense breasts can receive a screening ultrasound without a copay or deductible if it is ordered by a physician. In Connecticut, an ultrasound copay for screening dense breasts cannot exceed $20. Generally, in other states, an ultrasound will be covered if ordered by a physician, but it is subject to the copay and deductible of an individual health plan. In New Jersey, insurance coverage is provided for additional testing if a woman has extremely dense breasts.
Regardless of state, an MRI generally will be covered by insurance (subject to copay and deductible) if the patient meets high-risk criteria. In Michigan, at least one insurance company will cover a screening MRI for normal-risk women with dense breasts at a cost that matches the copay and deductible of a screening mammogram. It is important for patients to check with their insurance carrier prior to having an MRI.
Should women with dense breasts still have mammography screening?
Yes. Mammography is the first step in screening for most women (except for those who are pregnant or breastfeeding, in which case ultrasound can be performed but is usually deferred until several months after the patient is no longer pregnant or breastfeeding). While additional screening may be recommended for women with dense breasts, and for women at high risk for developing breast cancer, there are still some cancers and precancerous changes that will show on a mammogram better than on ultrasound or MRI. Wherever possible, women with dense breasts should have digital mammography rather than film mammography, due to slightly improved cancer detection using digital mammography.18
Does tomosynthesis solve the problem of screening dense breasts?
Tomosynthesis (3D mammography) slightly improves detection of cancers compared with standard digital mammography, but some cancers will remain hidden by overlapping dense tissue. We do not yet know the benefit of annual screening tomosynthesis. Without question, women at high risk for breast cancer still should have MRI if they are able to tolerate it, even if they have had tomosynthesis.
If a patient with dense breasts undergoes screening tomosynthesis, will she also need a screening ultrasound?
Preliminary studies not yet published suggest that, for women with dense breasts, ultrasound does find another 2 to 3 invasive cancers per 1,000 women screened that are not found on tomosynthesis, but further study of this issue is needed.
If recommended for additional screening with ultrasound or MRI, will a patient need that screening every year?
Usually, yes, though age and other medical conditions will change a patient’s personal risk and benefit considerations. Therefore, screening recommendations may change from one year to the next. With technology advancements and evolving guidelines, additional screening recommendations will change in the future.
Prepare yourself and your patients will benefit
The foundation of a successful screening program involves buy-in from both patient and clinician. Patients confused as to what their density notification means may have little understanding as to what next steps should be considered. To allay confusion, your patient will be best served by being provided understandable and actionable information. Advanced preparation for these conversations about the implications of dense tissue will make for more effective patient engagement.
Acknowledgment
Much of the material within this article has been sourced from the educational Web site DenseBreast-info.org. For comprehensive lists of both patient and health care provider frequently asked questions, visit http://www.DenseBreast-info.org.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Khong KA, Hargreaves J, Aminololama-Shakeri S, Lindfors KK. Impact of the California breast density law on primary care physicians. J Am Coll Radiol. 2015;12(3):256–260.
- Sickles EA, D’Orsi CJ, Bassett LW, et al. ACR BI-RADS Mammography. In: ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. Reston, VA: American College of Radiology; 2013.
- Sprague BL, Gangnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 2014;106(10).
- American Cancer Society. Breast Cancer Facts & Figures 2013–2014. http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-042725.pdf. Published 2013. Accessed September 15, 2015.
- Harvey JA, Bovbjerg VE. Quantitative assessment of mammographic breast density: relationship with breast cancer risk. Radiology. 2004;230(1):29–41.
- Kerlikowske K, Cook AJ, Buist DS, et al. Breast cancer risk by breast density, menopause, and postmenopausal hormone therapy use. J Clin Oncol. 2010;28(24):3830–3837.
- Arora N, King TA, Jacks LM, et al. Impact of breast density on the presenting features of malignancy. Ann Surg Oncol. 2010;17(suppl 3):211–218.
- Smith RA, Duffy SW, Gabe R, Tabar L, Yen AM, Chen TH. The randomized trials of breast cancer screening: what have we learned? Radiol Clin North Am. 2004;42(5):793–806, v.
- Warner E, Hill K, Causer P, et al. Prospective study of breast cancer incidence in women with a BRCA1 or BRCA2 mutation under surveillance with and without magnetic resonance imaging. J Clin Oncol. 2011;29(13):1664–1669.
- Corsetti V, Houssami N, Ghirardi M, et al. Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: interval breast cancers at 1 year follow-up. Eur J Cancer. 2011;47(7): 1021–1026.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012;307(13):1394–1404.
- Berg WA. Tailored supplemental screening for breast cancer: what now and what next? AJR Am J Roentgenol. 2009;192(2):390–399.
- Brem RF, Lenihan MJ, Lieberman J, Torrente J. Screening breast ultrasound: past, present, and future. AJR Am J Roentgenol. 2015;204(2):234–240.
- Hooley R. Tomosynthesis. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:2–19.
- Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014;311(24):2499–2507.
- Berg WA. Screening Ultrasound. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:9–43.
- Berg WA. Screening MRI. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:9–49.
- Hooley R. Tomosynthesis. In: Berg WA, Yang WT, eds.Berg WA. Screening Ultrasound. In: Berg WA, Yang WT, eds.Berg WA. Screening MRI. In: Berg WA, Yang WT, eds.Pisano ED, Gatsonis C, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353(17):1773–1783.
- Khong KA, Hargreaves J, Aminololama-Shakeri S, Lindfors KK. Impact of the California breast density law on primary care physicians. J Am Coll Radiol. 2015;12(3):256–260.
- Sickles EA, D’Orsi CJ, Bassett LW, et al. ACR BI-RADS Mammography. In: ACR BI-RADS Atlas, Breast Imaging Reporting and Data System. Reston, VA: American College of Radiology; 2013.
- Sprague BL, Gangnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 2014;106(10).
- American Cancer Society. Breast Cancer Facts & Figures 2013–2014. http://www.cancer.org/acs/groups/content/@research/documents/document/acspc-042725.pdf. Published 2013. Accessed September 15, 2015.
- Harvey JA, Bovbjerg VE. Quantitative assessment of mammographic breast density: relationship with breast cancer risk. Radiology. 2004;230(1):29–41.
- Kerlikowske K, Cook AJ, Buist DS, et al. Breast cancer risk by breast density, menopause, and postmenopausal hormone therapy use. J Clin Oncol. 2010;28(24):3830–3837.
- Arora N, King TA, Jacks LM, et al. Impact of breast density on the presenting features of malignancy. Ann Surg Oncol. 2010;17(suppl 3):211–218.
- Smith RA, Duffy SW, Gabe R, Tabar L, Yen AM, Chen TH. The randomized trials of breast cancer screening: what have we learned? Radiol Clin North Am. 2004;42(5):793–806, v.
- Warner E, Hill K, Causer P, et al. Prospective study of breast cancer incidence in women with a BRCA1 or BRCA2 mutation under surveillance with and without magnetic resonance imaging. J Clin Oncol. 2011;29(13):1664–1669.
- Corsetti V, Houssami N, Ghirardi M, et al. Evidence of the effect of adjunct ultrasound screening in women with mammography-negative dense breasts: interval breast cancers at 1 year follow-up. Eur J Cancer. 2011;47(7): 1021–1026.
- Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA. 2012;307(13):1394–1404.
- Berg WA. Tailored supplemental screening for breast cancer: what now and what next? AJR Am J Roentgenol. 2009;192(2):390–399.
- Brem RF, Lenihan MJ, Lieberman J, Torrente J. Screening breast ultrasound: past, present, and future. AJR Am J Roentgenol. 2015;204(2):234–240.
- Hooley R. Tomosynthesis. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:2–19.
- Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014;311(24):2499–2507.
- Berg WA. Screening Ultrasound. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:9–43.
- Berg WA. Screening MRI. In: Berg WA, Yang WT, eds. Diagnostic Imaging: Breast. 2nd ed. Salt Lake City, UT: Amirsys; 2014:9–49.
- Hooley R. Tomosynthesis. In: Berg WA, Yang WT, eds.Berg WA. Screening Ultrasound. In: Berg WA, Yang WT, eds.Berg WA. Screening MRI. In: Berg WA, Yang WT, eds.Pisano ED, Gatsonis C, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353(17):1773–1783.
In this Article
- Breast mass imaging case study
- Screening decision support tool
- Is your support staff “density” ready?