User login
Rasburicase Use and Glucose-6-Phosphate Dehydrogenase Testing
BACKGROUND/PURPOSE
Tumor lysis syndrome (TLS) occurs when malignant cells rapidly break down. This may lead to hyperuricemia, hyperkalemia, hyperphosphatemia, and/or hypocalcemia. Rasburicase reduces uric acid in cancer patients undergoing anti-cancer therapy. However, caution is required as rasburicase is contraindicated for patients with glucose- 6-phosphate dehydrogenase (G6PD) deficiency due to the increased risk of hemolysis. G6PD deficiency is more prevalent among African Americans (AA), affecting approximately 12% of this population. The FDA recommends testing for G6PD deficiency in higher risk groups before administering rasburicase.
METHODS
A retrospective analysis was conducted at the Louis Stokes Cleveland VAMC from February 1, 2018, to January 31, 2023 addressing appropriate use of rasburicase and incidence of G6PD deficiency and hemolysis. Appropriate use was defined by: TLS (2 or more: uric acid ≥ 8 or 25% increase; K+ ≥ 6.0 or 25% increase; Phos > 4.5mg/dL, or 25% increase; or calcium < 7, or 25% decrease, from baseline) or at high risk for TLS (CLL: venetoclax use w/lymph node > 10cm or WBC > 25k and elevated uric acid; AML: WBC > 100k; ALL: WBC > 100k and LDH 2x ULN; Burkitt lymphoma: LDH 2x ULN).
RESULTS
50 patients were identified who received rasburicase. 21/50 (42%) did not meet criteria for appropriate use. 44/50 (88%) underwent G6PD testing. The average time from G6PD testing order to obtaining the results was 3.4 days; 18/50 patients (36%) had G6PD resulted prior to rasburicase administration, and 26 patients (52%) received rasburicase prior to G6PD results. Overall, 13/50 (26%) were AA. Of the AA pts, 12/13 (92%) were tested for G6PD. Of these 12, 1/12 was found to be G6PD deficient and this patient experienced G6PD deficiency-induced hemolysis after rasburicase. None of the non-AA pts (0/31) tested were found to be G6PD deficient.
IMPLICATIONS
There was a high (42%) level of inappropriate use of rasburicase. G6PD deficiency was uncommon and only found in the AA population. To reduce inappropriate use, rasburicase orders will be restricted to medical oncology. G6PD testing will be limited to AA pts, with pathology to develop a rapid turnaround time for results prior to rasburicase administration to prevent hemolysis.
BACKGROUND/PURPOSE
Tumor lysis syndrome (TLS) occurs when malignant cells rapidly break down. This may lead to hyperuricemia, hyperkalemia, hyperphosphatemia, and/or hypocalcemia. Rasburicase reduces uric acid in cancer patients undergoing anti-cancer therapy. However, caution is required as rasburicase is contraindicated for patients with glucose- 6-phosphate dehydrogenase (G6PD) deficiency due to the increased risk of hemolysis. G6PD deficiency is more prevalent among African Americans (AA), affecting approximately 12% of this population. The FDA recommends testing for G6PD deficiency in higher risk groups before administering rasburicase.
METHODS
A retrospective analysis was conducted at the Louis Stokes Cleveland VAMC from February 1, 2018, to January 31, 2023 addressing appropriate use of rasburicase and incidence of G6PD deficiency and hemolysis. Appropriate use was defined by: TLS (2 or more: uric acid ≥ 8 or 25% increase; K+ ≥ 6.0 or 25% increase; Phos > 4.5mg/dL, or 25% increase; or calcium < 7, or 25% decrease, from baseline) or at high risk for TLS (CLL: venetoclax use w/lymph node > 10cm or WBC > 25k and elevated uric acid; AML: WBC > 100k; ALL: WBC > 100k and LDH 2x ULN; Burkitt lymphoma: LDH 2x ULN).
RESULTS
50 patients were identified who received rasburicase. 21/50 (42%) did not meet criteria for appropriate use. 44/50 (88%) underwent G6PD testing. The average time from G6PD testing order to obtaining the results was 3.4 days; 18/50 patients (36%) had G6PD resulted prior to rasburicase administration, and 26 patients (52%) received rasburicase prior to G6PD results. Overall, 13/50 (26%) were AA. Of the AA pts, 12/13 (92%) were tested for G6PD. Of these 12, 1/12 was found to be G6PD deficient and this patient experienced G6PD deficiency-induced hemolysis after rasburicase. None of the non-AA pts (0/31) tested were found to be G6PD deficient.
IMPLICATIONS
There was a high (42%) level of inappropriate use of rasburicase. G6PD deficiency was uncommon and only found in the AA population. To reduce inappropriate use, rasburicase orders will be restricted to medical oncology. G6PD testing will be limited to AA pts, with pathology to develop a rapid turnaround time for results prior to rasburicase administration to prevent hemolysis.
BACKGROUND/PURPOSE
Tumor lysis syndrome (TLS) occurs when malignant cells rapidly break down. This may lead to hyperuricemia, hyperkalemia, hyperphosphatemia, and/or hypocalcemia. Rasburicase reduces uric acid in cancer patients undergoing anti-cancer therapy. However, caution is required as rasburicase is contraindicated for patients with glucose- 6-phosphate dehydrogenase (G6PD) deficiency due to the increased risk of hemolysis. G6PD deficiency is more prevalent among African Americans (AA), affecting approximately 12% of this population. The FDA recommends testing for G6PD deficiency in higher risk groups before administering rasburicase.
METHODS
A retrospective analysis was conducted at the Louis Stokes Cleveland VAMC from February 1, 2018, to January 31, 2023 addressing appropriate use of rasburicase and incidence of G6PD deficiency and hemolysis. Appropriate use was defined by: TLS (2 or more: uric acid ≥ 8 or 25% increase; K+ ≥ 6.0 or 25% increase; Phos > 4.5mg/dL, or 25% increase; or calcium < 7, or 25% decrease, from baseline) or at high risk for TLS (CLL: venetoclax use w/lymph node > 10cm or WBC > 25k and elevated uric acid; AML: WBC > 100k; ALL: WBC > 100k and LDH 2x ULN; Burkitt lymphoma: LDH 2x ULN).
RESULTS
50 patients were identified who received rasburicase. 21/50 (42%) did not meet criteria for appropriate use. 44/50 (88%) underwent G6PD testing. The average time from G6PD testing order to obtaining the results was 3.4 days; 18/50 patients (36%) had G6PD resulted prior to rasburicase administration, and 26 patients (52%) received rasburicase prior to G6PD results. Overall, 13/50 (26%) were AA. Of the AA pts, 12/13 (92%) were tested for G6PD. Of these 12, 1/12 was found to be G6PD deficient and this patient experienced G6PD deficiency-induced hemolysis after rasburicase. None of the non-AA pts (0/31) tested were found to be G6PD deficient.
IMPLICATIONS
There was a high (42%) level of inappropriate use of rasburicase. G6PD deficiency was uncommon and only found in the AA population. To reduce inappropriate use, rasburicase orders will be restricted to medical oncology. G6PD testing will be limited to AA pts, with pathology to develop a rapid turnaround time for results prior to rasburicase administration to prevent hemolysis.
Implementation of an Interfacility Telehealth Cancer Genetics Clinic
BACKGROUND
Cancer risk assessment and genetic counseling are the processes to identify and counsel people at risk for familial or hereditary cancer syndromes. They serve to inform, educate and empower patients and family members to make informed decisions about testing, cancer screening, and prevention. Additionally, genetic testing can also provide therapeutic options and opportunities for research.
METHODS
Prior to this program initiative, there were no cancer genetics services available at the VA Pittsburgh Medical Center (VAPHS) and 100% of genetics consults were referred to the community. Each year over $100,000 was spent outside of VAPHS on genetic testing and counseling. Community care referral resulted in fragmented care, prolonged wait times of 3 to 5 months, communication issues, and added financial cost to the institution. Corporal Michael J. Crescenz VA Medical Center (CMCVAMC) had previously created a genetics consultation service staffed with an advanced practice nurse that increased access to genetics services and testing rates at the facility-level. VAPHS recently established an interfacility telegenetics clinic with CMCVAMC to provide virtual genetic counseling services to Veterans at VAPHS. Under this program, VAPHS providers place an interfacility consult for Veterans who need cancer genetics services. The consult is received and reviewed by the CMCVAMC team. VAPHS patients are then seen by CMCVAMC providers via VVC or CVT and provide recommendations regarding additional genetic testing and follow-up.
RESULTS
The telegenetics clinic opened in October 2022. The clinic initially focused on patients with metastatic prostate cancer but has since expanded to provide care for all patients for whom genetics testing and/ or counseling is recommended by NCCN guidelines. Since initiation, 29 consults have been placed and 26 have been completed or are in process (89.6%). In the year prior to creation of the clinic, only 31 of 67 (46%) of referred patients completed genetics evaluation.
CONCLUSIONS
Due to the success of the clinic, plans to expand services to the VISN-level and within VAPHS to include high risk breast cancer assessment are underway. Efforts to provide genetic counseling services via virtual care modalities have the potential to increase access to care and to improve outcomes for veterans with cancer.
BACKGROUND
Cancer risk assessment and genetic counseling are the processes to identify and counsel people at risk for familial or hereditary cancer syndromes. They serve to inform, educate and empower patients and family members to make informed decisions about testing, cancer screening, and prevention. Additionally, genetic testing can also provide therapeutic options and opportunities for research.
METHODS
Prior to this program initiative, there were no cancer genetics services available at the VA Pittsburgh Medical Center (VAPHS) and 100% of genetics consults were referred to the community. Each year over $100,000 was spent outside of VAPHS on genetic testing and counseling. Community care referral resulted in fragmented care, prolonged wait times of 3 to 5 months, communication issues, and added financial cost to the institution. Corporal Michael J. Crescenz VA Medical Center (CMCVAMC) had previously created a genetics consultation service staffed with an advanced practice nurse that increased access to genetics services and testing rates at the facility-level. VAPHS recently established an interfacility telegenetics clinic with CMCVAMC to provide virtual genetic counseling services to Veterans at VAPHS. Under this program, VAPHS providers place an interfacility consult for Veterans who need cancer genetics services. The consult is received and reviewed by the CMCVAMC team. VAPHS patients are then seen by CMCVAMC providers via VVC or CVT and provide recommendations regarding additional genetic testing and follow-up.
RESULTS
The telegenetics clinic opened in October 2022. The clinic initially focused on patients with metastatic prostate cancer but has since expanded to provide care for all patients for whom genetics testing and/ or counseling is recommended by NCCN guidelines. Since initiation, 29 consults have been placed and 26 have been completed or are in process (89.6%). In the year prior to creation of the clinic, only 31 of 67 (46%) of referred patients completed genetics evaluation.
CONCLUSIONS
Due to the success of the clinic, plans to expand services to the VISN-level and within VAPHS to include high risk breast cancer assessment are underway. Efforts to provide genetic counseling services via virtual care modalities have the potential to increase access to care and to improve outcomes for veterans with cancer.
BACKGROUND
Cancer risk assessment and genetic counseling are the processes to identify and counsel people at risk for familial or hereditary cancer syndromes. They serve to inform, educate and empower patients and family members to make informed decisions about testing, cancer screening, and prevention. Additionally, genetic testing can also provide therapeutic options and opportunities for research.
METHODS
Prior to this program initiative, there were no cancer genetics services available at the VA Pittsburgh Medical Center (VAPHS) and 100% of genetics consults were referred to the community. Each year over $100,000 was spent outside of VAPHS on genetic testing and counseling. Community care referral resulted in fragmented care, prolonged wait times of 3 to 5 months, communication issues, and added financial cost to the institution. Corporal Michael J. Crescenz VA Medical Center (CMCVAMC) had previously created a genetics consultation service staffed with an advanced practice nurse that increased access to genetics services and testing rates at the facility-level. VAPHS recently established an interfacility telegenetics clinic with CMCVAMC to provide virtual genetic counseling services to Veterans at VAPHS. Under this program, VAPHS providers place an interfacility consult for Veterans who need cancer genetics services. The consult is received and reviewed by the CMCVAMC team. VAPHS patients are then seen by CMCVAMC providers via VVC or CVT and provide recommendations regarding additional genetic testing and follow-up.
RESULTS
The telegenetics clinic opened in October 2022. The clinic initially focused on patients with metastatic prostate cancer but has since expanded to provide care for all patients for whom genetics testing and/ or counseling is recommended by NCCN guidelines. Since initiation, 29 consults have been placed and 26 have been completed or are in process (89.6%). In the year prior to creation of the clinic, only 31 of 67 (46%) of referred patients completed genetics evaluation.
CONCLUSIONS
Due to the success of the clinic, plans to expand services to the VISN-level and within VAPHS to include high risk breast cancer assessment are underway. Efforts to provide genetic counseling services via virtual care modalities have the potential to increase access to care and to improve outcomes for veterans with cancer.
Unlocking the secrets of brown fat
Brown fat, or thermogenic adipose tissue, appears to act as a “nutrient sink,” consuming glucose and lactate, among other metabolites, say U.S. researchers in a mouse study that supports its potential role in tackling obesity and even cancer.
The research, published recently in Nature Metabolism, was led by David A. Guertin, PhD, of the program in molecular medicine, University of Massachusetts, Worcester.
What is adaptive thermogenesis, and why is it important in temperature regulation?
Adaptive thermogenesis is a physiologic process that occurs in a special type of fat cell, called a brown adipocyte, in which intracellular stored lipids and nutrients taken up from the blood are catabolized to generate heat.
The heat generated by these thermogenic adipocytes is critical for warming the blood and maintaining body temperature in cold environments, and is especially critical in human infants and small mammals, which are more sensitive to low temperatures.
The process is stimulated by the sympathetic nervous system, especially in response to feeling cold, but it can be activated by other stresses as well.
While adaptative thermogenesis is also called nonshivering thermogenesis to distinguish it from muscle shivering, both means of generating heat can work together to maintain body temperature.
Why is it considered a potential target for obesity?
Adult humans have brown adipocytes in specific locations in the body called brown adipose tissues (BAT) or, more simply, “brown fat.”
Intriguingly, clinical data show that the more BAT you have, the more likely you are to be protected against cardiometabolic disorders associated with obesity.
Since obesity results from an imbalance between energy intake and energy expenditure, one model proposes that brown adipocytes rebalance this formula by expending the excess energy (calories) as heat rather than storing it.
This has been referred to as the “nutrient sink” model, and the ability to activate this process therapeutically is a very attractive antiobesity strategy.
Why was it important to understand which circulating metabolites BAT uses for thermogenesis?
It is still not clear why brown fat is so beneficial for human health, and thus there is strong rationale for understanding its metabolism and how it cooperates with other tissues in the body.
For example, prior to our work, the field lacked a broad quantitative picture of how much any individual nutrient from the blood was used by brown fat, or which specific nutrients brown fat prefers to use to make heat – such as lipids, glucose, amino acids, etc. Knowing this information helps us identify more precise strategies to activate brown fat.
In addition, circulating metabolites sometimes also have messenger functions, similar to those of hormones, that stimulate physiologic processes such as adaptative thermogenesis. Highly metabolic tissues also put metabolites back into the blood, which can send messages to the brain and other tissues.
We don’t have a lot of information yet on how brown fat might engage in these processes, and so our study also aimed at finding these special metabolite messengers.
You found that glucose and lactate predominate as BAT fuel sources. What does that tell us?
The major fuels used by brown fat have been debated for a long time.
Our study suggests that BAT in mice mainly prefers glucose and lactate, which is generated from glucose. On one hand, this shows us that thermogenic adipocytes may be especially useful in treating hyperglycemia, or even tumors, by reducing the amount of circulating glucose.
It also tells us that we need to focus more on why brown fat needs so much glucose. Other studies suggest that glucose is not just used as a fuel to generate heat but also may have other important functions in keeping brown adipocytes active and healthy.
We need to know that information so that therapeutic strategies targeting brown adipocytes can be optimized to have the best chance of success.
It’s worth noting that we did our study in mice that had free access to food. If the mice were fasting, they would use more lipids from the blood to supplement for the lack of available glucose, but we think that a baseline amount of glucose is still necessary.
What could be the clinical implications of your results if replicated in humans?
They suggest that glucose is an important resource that thermogenic adipocytes cannot do without, and moreover, that glucose is more than just a carbon source.
Resolving those other functions of glucose may provide insight into mechanisms to stimulate these cells or help explain why overweight or obese people who are insulin resistant have less brown fat activity, as insulin stimulates glucose uptake.
Beyond glucose, if any of these other metabolites made or released by brown fat have beneficial messenger functions, there may be ways to pharmacologically mimic them.
How easily do you think your findings could be applied to humans?
On a fundamental level, the basic cellular mechanisms that drive adaptative thermogenesis are likely the same between mice and humans, but the wiring to the sympathetic nervous system is a bit different.
This is why it’s important to look deeply at brown fat metabolism in mouse models to find pathways fundamental to the basic mechanisms of adaptative thermogenesis in both mice and humans, which could reveal unique therapeutic opportunities.
Another big challenge with comparing humans and mice is that humans typically keep their environment warm, so their brown fat is not that active.
In contrast, mice are often raised their entire lives in a facility kept at room temperature, around 22° C (72° F). While comfortable for the humans working with them, it’s cold for a small mouse, and so mice live with constantly active brown fat.
We can change the mouse environment to alter mouse brown fat activity, but that can’t be done with people. This makes comparative studies difficult.
Nevertheless, studies have shown that people who live in cold climates often have more brown fat, and, conversely, mice raised in warmer environments have brown fat that looks a lot more like human brown fat.
What further research do you have planned, or are looking forward to, in this area?
This is the most fun part of what we do, and I’ve been fortunate to have an amazing team passionately working on these questions.
One is to figure out why glucose is so important for these fascinating cells, which will keep us busy for years. We also need to modify the dietary conditions to determine whether the body prioritizes the use of glucose for adaptive thermogenesis even when there isn’t much available.
Another goal is to test whether any of the other metabolites we identified have bioactive functions. We also discovered a unique role for glutamine metabolism in brown fat, through the consumption of amino acids, that we haven’t yet resolved.
Finally, we want to understand how and why brown fat protects other organs from metabolic diseases, and we are just at the tip of the iceberg here.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Alcohol Abuse and Alcoholism; the National Heart, Lung, & Blood Institute; the National Institutes of Health; the AASLD Foundation Pinnacle Research Award in Liver Disease; the Edward Mallinckrodt Jr. Foundation Award; and the Basic Science Research Program of the Ministry of Education (South Korea). No relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
Brown fat, or thermogenic adipose tissue, appears to act as a “nutrient sink,” consuming glucose and lactate, among other metabolites, say U.S. researchers in a mouse study that supports its potential role in tackling obesity and even cancer.
The research, published recently in Nature Metabolism, was led by David A. Guertin, PhD, of the program in molecular medicine, University of Massachusetts, Worcester.
What is adaptive thermogenesis, and why is it important in temperature regulation?
Adaptive thermogenesis is a physiologic process that occurs in a special type of fat cell, called a brown adipocyte, in which intracellular stored lipids and nutrients taken up from the blood are catabolized to generate heat.
The heat generated by these thermogenic adipocytes is critical for warming the blood and maintaining body temperature in cold environments, and is especially critical in human infants and small mammals, which are more sensitive to low temperatures.
The process is stimulated by the sympathetic nervous system, especially in response to feeling cold, but it can be activated by other stresses as well.
While adaptative thermogenesis is also called nonshivering thermogenesis to distinguish it from muscle shivering, both means of generating heat can work together to maintain body temperature.
Why is it considered a potential target for obesity?
Adult humans have brown adipocytes in specific locations in the body called brown adipose tissues (BAT) or, more simply, “brown fat.”
Intriguingly, clinical data show that the more BAT you have, the more likely you are to be protected against cardiometabolic disorders associated with obesity.
Since obesity results from an imbalance between energy intake and energy expenditure, one model proposes that brown adipocytes rebalance this formula by expending the excess energy (calories) as heat rather than storing it.
This has been referred to as the “nutrient sink” model, and the ability to activate this process therapeutically is a very attractive antiobesity strategy.
Why was it important to understand which circulating metabolites BAT uses for thermogenesis?
It is still not clear why brown fat is so beneficial for human health, and thus there is strong rationale for understanding its metabolism and how it cooperates with other tissues in the body.
For example, prior to our work, the field lacked a broad quantitative picture of how much any individual nutrient from the blood was used by brown fat, or which specific nutrients brown fat prefers to use to make heat – such as lipids, glucose, amino acids, etc. Knowing this information helps us identify more precise strategies to activate brown fat.
In addition, circulating metabolites sometimes also have messenger functions, similar to those of hormones, that stimulate physiologic processes such as adaptative thermogenesis. Highly metabolic tissues also put metabolites back into the blood, which can send messages to the brain and other tissues.
We don’t have a lot of information yet on how brown fat might engage in these processes, and so our study also aimed at finding these special metabolite messengers.
You found that glucose and lactate predominate as BAT fuel sources. What does that tell us?
The major fuels used by brown fat have been debated for a long time.
Our study suggests that BAT in mice mainly prefers glucose and lactate, which is generated from glucose. On one hand, this shows us that thermogenic adipocytes may be especially useful in treating hyperglycemia, or even tumors, by reducing the amount of circulating glucose.
It also tells us that we need to focus more on why brown fat needs so much glucose. Other studies suggest that glucose is not just used as a fuel to generate heat but also may have other important functions in keeping brown adipocytes active and healthy.
We need to know that information so that therapeutic strategies targeting brown adipocytes can be optimized to have the best chance of success.
It’s worth noting that we did our study in mice that had free access to food. If the mice were fasting, they would use more lipids from the blood to supplement for the lack of available glucose, but we think that a baseline amount of glucose is still necessary.
What could be the clinical implications of your results if replicated in humans?
They suggest that glucose is an important resource that thermogenic adipocytes cannot do without, and moreover, that glucose is more than just a carbon source.
Resolving those other functions of glucose may provide insight into mechanisms to stimulate these cells or help explain why overweight or obese people who are insulin resistant have less brown fat activity, as insulin stimulates glucose uptake.
Beyond glucose, if any of these other metabolites made or released by brown fat have beneficial messenger functions, there may be ways to pharmacologically mimic them.
How easily do you think your findings could be applied to humans?
On a fundamental level, the basic cellular mechanisms that drive adaptative thermogenesis are likely the same between mice and humans, but the wiring to the sympathetic nervous system is a bit different.
This is why it’s important to look deeply at brown fat metabolism in mouse models to find pathways fundamental to the basic mechanisms of adaptative thermogenesis in both mice and humans, which could reveal unique therapeutic opportunities.
Another big challenge with comparing humans and mice is that humans typically keep their environment warm, so their brown fat is not that active.
In contrast, mice are often raised their entire lives in a facility kept at room temperature, around 22° C (72° F). While comfortable for the humans working with them, it’s cold for a small mouse, and so mice live with constantly active brown fat.
We can change the mouse environment to alter mouse brown fat activity, but that can’t be done with people. This makes comparative studies difficult.
Nevertheless, studies have shown that people who live in cold climates often have more brown fat, and, conversely, mice raised in warmer environments have brown fat that looks a lot more like human brown fat.
What further research do you have planned, or are looking forward to, in this area?
This is the most fun part of what we do, and I’ve been fortunate to have an amazing team passionately working on these questions.
One is to figure out why glucose is so important for these fascinating cells, which will keep us busy for years. We also need to modify the dietary conditions to determine whether the body prioritizes the use of glucose for adaptive thermogenesis even when there isn’t much available.
Another goal is to test whether any of the other metabolites we identified have bioactive functions. We also discovered a unique role for glutamine metabolism in brown fat, through the consumption of amino acids, that we haven’t yet resolved.
Finally, we want to understand how and why brown fat protects other organs from metabolic diseases, and we are just at the tip of the iceberg here.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Alcohol Abuse and Alcoholism; the National Heart, Lung, & Blood Institute; the National Institutes of Health; the AASLD Foundation Pinnacle Research Award in Liver Disease; the Edward Mallinckrodt Jr. Foundation Award; and the Basic Science Research Program of the Ministry of Education (South Korea). No relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
Brown fat, or thermogenic adipose tissue, appears to act as a “nutrient sink,” consuming glucose and lactate, among other metabolites, say U.S. researchers in a mouse study that supports its potential role in tackling obesity and even cancer.
The research, published recently in Nature Metabolism, was led by David A. Guertin, PhD, of the program in molecular medicine, University of Massachusetts, Worcester.
What is adaptive thermogenesis, and why is it important in temperature regulation?
Adaptive thermogenesis is a physiologic process that occurs in a special type of fat cell, called a brown adipocyte, in which intracellular stored lipids and nutrients taken up from the blood are catabolized to generate heat.
The heat generated by these thermogenic adipocytes is critical for warming the blood and maintaining body temperature in cold environments, and is especially critical in human infants and small mammals, which are more sensitive to low temperatures.
The process is stimulated by the sympathetic nervous system, especially in response to feeling cold, but it can be activated by other stresses as well.
While adaptative thermogenesis is also called nonshivering thermogenesis to distinguish it from muscle shivering, both means of generating heat can work together to maintain body temperature.
Why is it considered a potential target for obesity?
Adult humans have brown adipocytes in specific locations in the body called brown adipose tissues (BAT) or, more simply, “brown fat.”
Intriguingly, clinical data show that the more BAT you have, the more likely you are to be protected against cardiometabolic disorders associated with obesity.
Since obesity results from an imbalance between energy intake and energy expenditure, one model proposes that brown adipocytes rebalance this formula by expending the excess energy (calories) as heat rather than storing it.
This has been referred to as the “nutrient sink” model, and the ability to activate this process therapeutically is a very attractive antiobesity strategy.
Why was it important to understand which circulating metabolites BAT uses for thermogenesis?
It is still not clear why brown fat is so beneficial for human health, and thus there is strong rationale for understanding its metabolism and how it cooperates with other tissues in the body.
For example, prior to our work, the field lacked a broad quantitative picture of how much any individual nutrient from the blood was used by brown fat, or which specific nutrients brown fat prefers to use to make heat – such as lipids, glucose, amino acids, etc. Knowing this information helps us identify more precise strategies to activate brown fat.
In addition, circulating metabolites sometimes also have messenger functions, similar to those of hormones, that stimulate physiologic processes such as adaptative thermogenesis. Highly metabolic tissues also put metabolites back into the blood, which can send messages to the brain and other tissues.
We don’t have a lot of information yet on how brown fat might engage in these processes, and so our study also aimed at finding these special metabolite messengers.
You found that glucose and lactate predominate as BAT fuel sources. What does that tell us?
The major fuels used by brown fat have been debated for a long time.
Our study suggests that BAT in mice mainly prefers glucose and lactate, which is generated from glucose. On one hand, this shows us that thermogenic adipocytes may be especially useful in treating hyperglycemia, or even tumors, by reducing the amount of circulating glucose.
It also tells us that we need to focus more on why brown fat needs so much glucose. Other studies suggest that glucose is not just used as a fuel to generate heat but also may have other important functions in keeping brown adipocytes active and healthy.
We need to know that information so that therapeutic strategies targeting brown adipocytes can be optimized to have the best chance of success.
It’s worth noting that we did our study in mice that had free access to food. If the mice were fasting, they would use more lipids from the blood to supplement for the lack of available glucose, but we think that a baseline amount of glucose is still necessary.
What could be the clinical implications of your results if replicated in humans?
They suggest that glucose is an important resource that thermogenic adipocytes cannot do without, and moreover, that glucose is more than just a carbon source.
Resolving those other functions of glucose may provide insight into mechanisms to stimulate these cells or help explain why overweight or obese people who are insulin resistant have less brown fat activity, as insulin stimulates glucose uptake.
Beyond glucose, if any of these other metabolites made or released by brown fat have beneficial messenger functions, there may be ways to pharmacologically mimic them.
How easily do you think your findings could be applied to humans?
On a fundamental level, the basic cellular mechanisms that drive adaptative thermogenesis are likely the same between mice and humans, but the wiring to the sympathetic nervous system is a bit different.
This is why it’s important to look deeply at brown fat metabolism in mouse models to find pathways fundamental to the basic mechanisms of adaptative thermogenesis in both mice and humans, which could reveal unique therapeutic opportunities.
Another big challenge with comparing humans and mice is that humans typically keep their environment warm, so their brown fat is not that active.
In contrast, mice are often raised their entire lives in a facility kept at room temperature, around 22° C (72° F). While comfortable for the humans working with them, it’s cold for a small mouse, and so mice live with constantly active brown fat.
We can change the mouse environment to alter mouse brown fat activity, but that can’t be done with people. This makes comparative studies difficult.
Nevertheless, studies have shown that people who live in cold climates often have more brown fat, and, conversely, mice raised in warmer environments have brown fat that looks a lot more like human brown fat.
What further research do you have planned, or are looking forward to, in this area?
This is the most fun part of what we do, and I’ve been fortunate to have an amazing team passionately working on these questions.
One is to figure out why glucose is so important for these fascinating cells, which will keep us busy for years. We also need to modify the dietary conditions to determine whether the body prioritizes the use of glucose for adaptive thermogenesis even when there isn’t much available.
Another goal is to test whether any of the other metabolites we identified have bioactive functions. We also discovered a unique role for glutamine metabolism in brown fat, through the consumption of amino acids, that we haven’t yet resolved.
Finally, we want to understand how and why brown fat protects other organs from metabolic diseases, and we are just at the tip of the iceberg here.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Alcohol Abuse and Alcoholism; the National Heart, Lung, & Blood Institute; the National Institutes of Health; the AASLD Foundation Pinnacle Research Award in Liver Disease; the Edward Mallinckrodt Jr. Foundation Award; and the Basic Science Research Program of the Ministry of Education (South Korea). No relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
FROM NATURE METABOLISM
Necessary Updates to Skin Cancer Risk Stratification
1. Powers JG, Patel NA, Powers EA, Mayer JE, Stricklin GP, Geller AC. Skin cancer
risk factors and preventative behaviors among United States military veterans deployed to Iraq and Afghanistan. J Invest Dermatol. 2015;135:2871-2873.
2. Balci S, Ayaz L, Gorur A, Yildirim Yaroglu H, Akbayir S, Dogruer Unal N, Bulut B,
Tursen U, Tamer L. microRNA profiling for early detection of nonmelanoma skin cancer. Clin Exp Dermatol. 2016;41(4):346-51. doi:10.1111/ced.12736
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. doi:10.3322/caac.21708
4. Agbai ON, Buster K, Sanchez M, Hernandez C, Kundu RV, Chiu M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-62.
5. Chou SE, Gaysynsky A, Trivedi N, Vanderpool R. Using social media for health: national data from HINTS 2019. Journ of Health Comm. 2019;26(3):184-193. doi:10.1080/10810730.2021.
6. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
7. Dennis LK, et al. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Annals of Epidem. 2008;18(8):614-627. doi:10.1016/j.annepidem.2008.
8. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
9. 2020 Demographics Profile of the military community. US Department of Defense. 2020:iv. Accessed November 15, 2022. 2020 Demographics Profile of the Military Community (militaryonesource.mil)
10. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1-6.
11. Basch CH, Hillyer GC. Skin cancer on Instagram: implications for adolescents and young adults. Int J Adolesc Med Health. 2022;34(3). doi:10.1515/ijamh-2019-0218
1. Powers JG, Patel NA, Powers EA, Mayer JE, Stricklin GP, Geller AC. Skin cancer
risk factors and preventative behaviors among United States military veterans deployed to Iraq and Afghanistan. J Invest Dermatol. 2015;135:2871-2873.
2. Balci S, Ayaz L, Gorur A, Yildirim Yaroglu H, Akbayir S, Dogruer Unal N, Bulut B,
Tursen U, Tamer L. microRNA profiling for early detection of nonmelanoma skin cancer. Clin Exp Dermatol. 2016;41(4):346-51. doi:10.1111/ced.12736
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. doi:10.3322/caac.21708
4. Agbai ON, Buster K, Sanchez M, Hernandez C, Kundu RV, Chiu M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-62.
5. Chou SE, Gaysynsky A, Trivedi N, Vanderpool R. Using social media for health: national data from HINTS 2019. Journ of Health Comm. 2019;26(3):184-193. doi:10.1080/10810730.2021.
6. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
7. Dennis LK, et al. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Annals of Epidem. 2008;18(8):614-627. doi:10.1016/j.annepidem.2008.
8. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
9. 2020 Demographics Profile of the military community. US Department of Defense. 2020:iv. Accessed November 15, 2022. 2020 Demographics Profile of the Military Community (militaryonesource.mil)
10. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1-6.
11. Basch CH, Hillyer GC. Skin cancer on Instagram: implications for adolescents and young adults. Int J Adolesc Med Health. 2022;34(3). doi:10.1515/ijamh-2019-0218
1. Powers JG, Patel NA, Powers EA, Mayer JE, Stricklin GP, Geller AC. Skin cancer
risk factors and preventative behaviors among United States military veterans deployed to Iraq and Afghanistan. J Invest Dermatol. 2015;135:2871-2873.
2. Balci S, Ayaz L, Gorur A, Yildirim Yaroglu H, Akbayir S, Dogruer Unal N, Bulut B,
Tursen U, Tamer L. microRNA profiling for early detection of nonmelanoma skin cancer. Clin Exp Dermatol. 2016;41(4):346-51. doi:10.1111/ced.12736
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7-33. doi:10.3322/caac.21708
4. Agbai ON, Buster K, Sanchez M, Hernandez C, Kundu RV, Chiu M, et al. Skin cancer and photoprotection in people of color: a review and recommendations for physicians and the public. J Am Acad Dermatol. 2014;70(4):748-62.
5. Chou SE, Gaysynsky A, Trivedi N, Vanderpool R. Using social media for health: national data from HINTS 2019. Journ of Health Comm. 2019;26(3):184-193. doi:10.1080/10810730.2021.
6. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-82.
7. Dennis LK, et al. Sunburns and risk of cutaneous melanoma: does age matter? A comprehensive meta-analysis. Annals of Epidem. 2008;18(8):614-627. doi:10.1016/j.annepidem.2008.
8. Wu S, Han J, Laden F, Qureshi AA. Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: a cohort study. Cancer Epidemiol Biomar Prev. 2014;23(6):1080-1089.
9. 2020 Demographics Profile of the military community. US Department of Defense. 2020:iv. Accessed November 15, 2022. 2020 Demographics Profile of the Military Community (militaryonesource.mil)
10. Apalla Z, Lallas A, Sotiriou E, Lazaridou E, Ioannides D. Epidemiological trends in skin cancer. Dermatol Pract Concept. 2017;7:1-6.
11. Basch CH, Hillyer GC. Skin cancer on Instagram: implications for adolescents and young adults. Int J Adolesc Med Health. 2022;34(3). doi:10.1515/ijamh-2019-0218





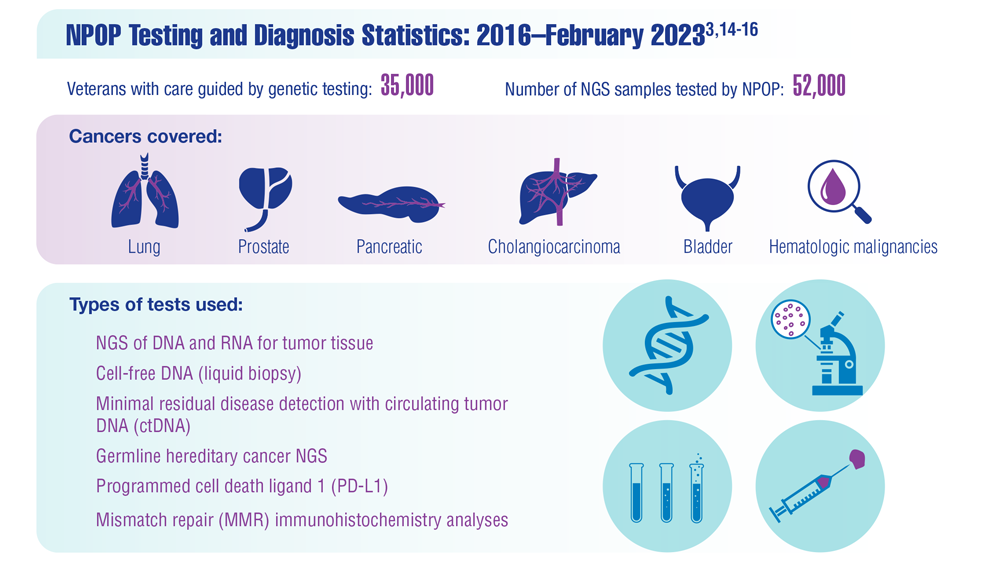
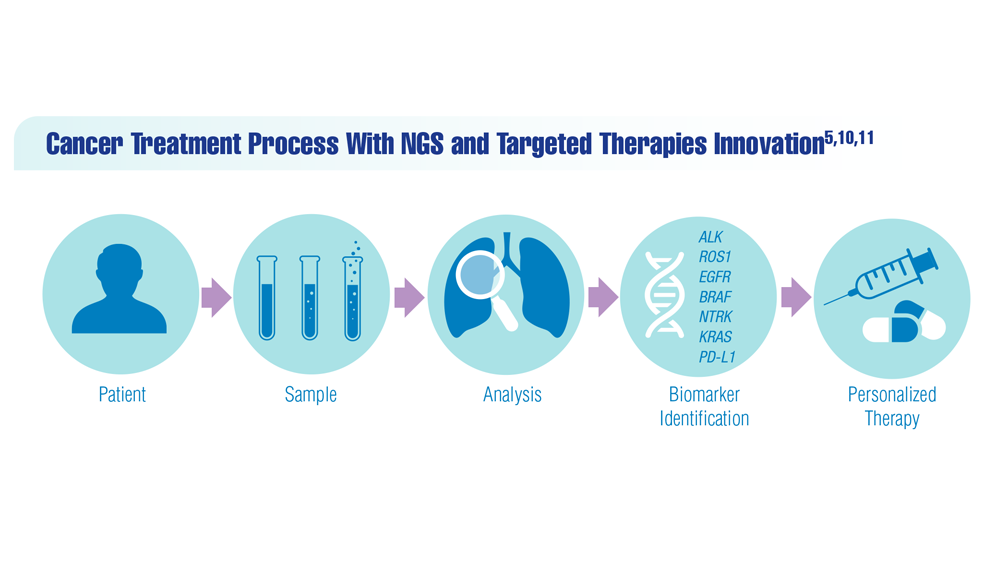
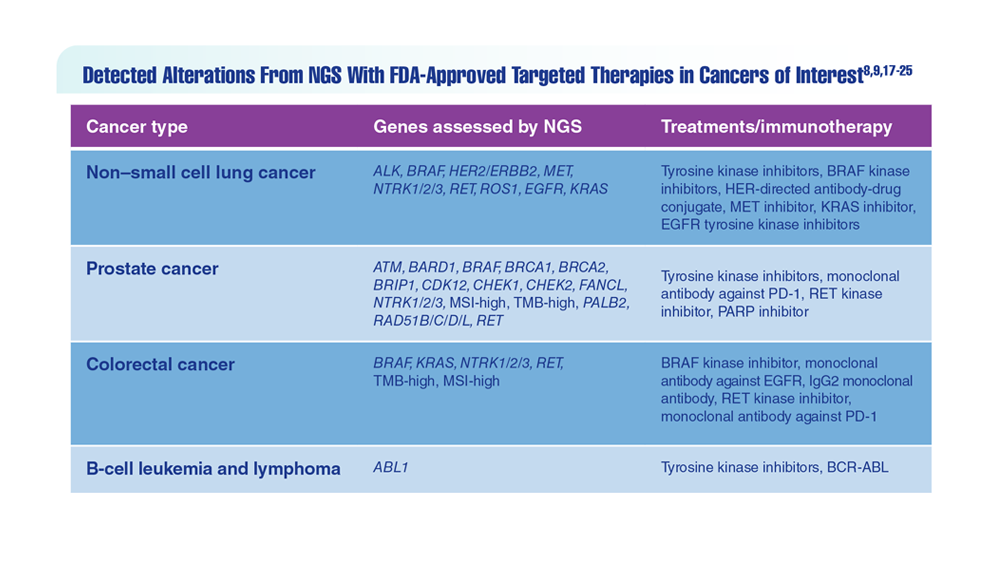
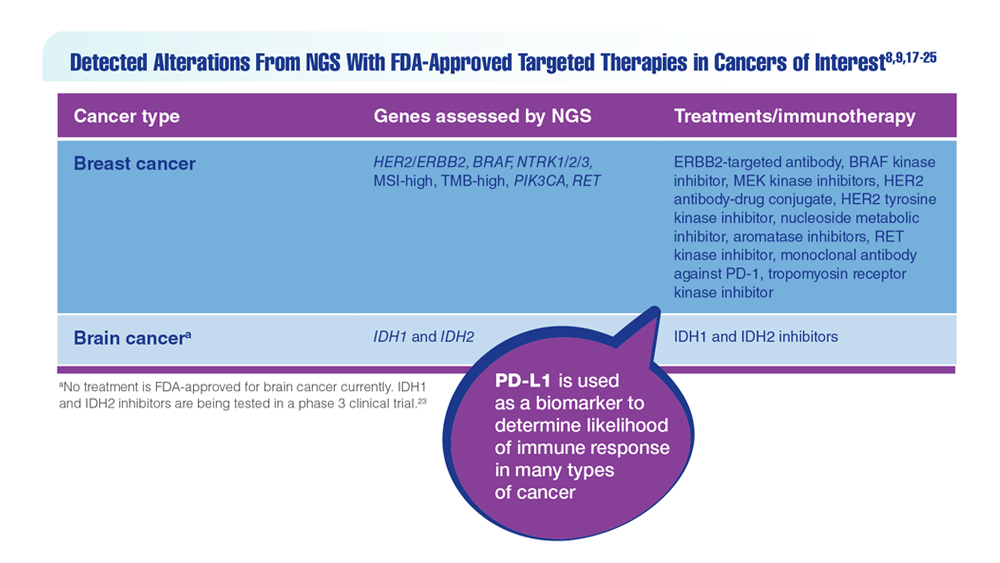
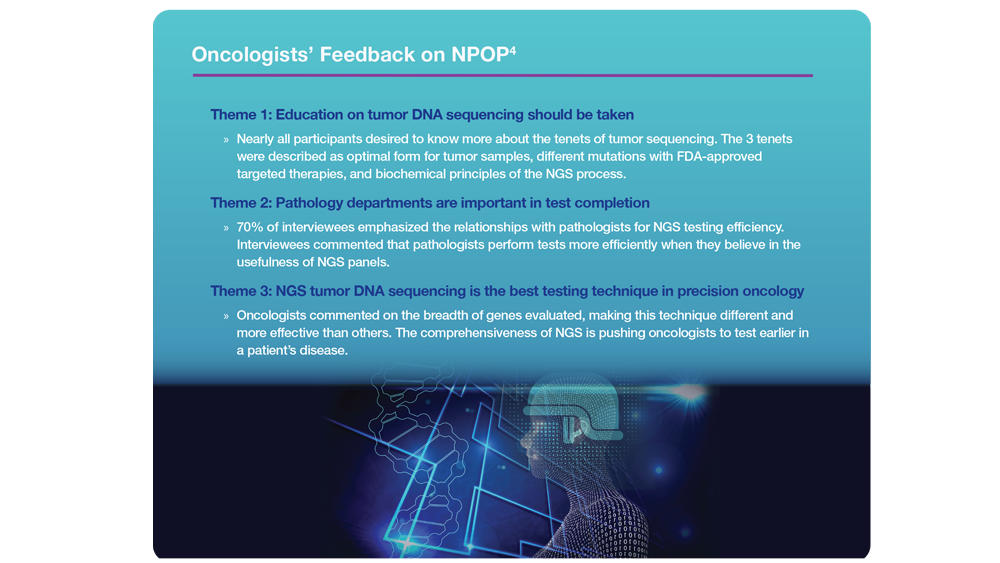
Innovation in Cancer Treatment
- US Department of Veterans Affairs. National Precision Oncology Program (NPOP). June 10, 2019. Accessed December 8, 2022. https://www.cancer.va.gov/CANCER/NPOP.asp
- US Department of Veterans Affairs, Office of Research and Development. VA National Precision Oncology Program brings tailored cancer treatment to veterans. October 3, 2019. Accessed December 8, 2022. https://www.research.va.gov/currents/1019-VA-National-Precision-Oncology-Program-brings-tailored-cancer-treatment-to-Veterans.cfm
- Kelley M, Ahmed S. National Precision Oncology Program (NPOP): right treatment for the right patient at the right time. 2022. Unpublished data.
- Vashistha V et al. PLoS One. 2020;15(7):e0235861. doi:10.1371/journal.pone.0235861
- Dong OM et al. Value Health. 2022;25(4):582-594. doi:10.1016/j.jval.2021.09.017
- Sadik H et al. JCO Precis Oncol. 2022;6:e2200246. doi:10.1200/PO.22.00246
- Petrillo LA et al. J Pain Symptom Manage. 2021;62(3):e65-e74. doi:10.1016/j.jpainsymman.2021.02.010
- Waks AG, Winer EP. JAMA. 2019;321(3):288-300. doi:10.1001/jama.2018.19323
- Mellinghoff IK et al. Clin Cancer Res. 2021;27(16):4491-4499. doi:10.1158/1078-0432.CCR-21-0611
- Debela DT et al. SAGE Open Med. 2021;9:20503121211034366. doi:10.1177/20503121211034366
- Gambardella V et al. Cancers (Basel). 2020;12(4):1009. doi:10.3390/cancers12041009
- US Department of Veterans Affairs, Office of Research and Development. VA Lung Precision Oncology Program (LPOP). Updated January 27, 2022. Accessed January 23, 2023. https://www.research.va.gov/programs/pop/lpop.cfm
- Montgomery B et al. Fed Pract. 2020;37(suppl 4):S48-S53. doi:10.12788/fp.0021
- Kelley MJ. Fed Pract. 2020;37(suppl 4):S22-S27. doi:10.12788/fp.0037
- Poonnen PJ et al. JCO Precis Oncol. 2019;3:PO.19.00075. doi:10.1200/PO.19.00075
- Natera awarded national MRD testing contract by the U.S. Department of Veterans Affairs [press release]. Natera. November 2, 2022. Accessed January 23, 2023. https://www.natera.com/company/news/natera-awarded-national-mrd-testing-contract-by-the-u-s-department-of-veterans-affairs/
- Katsoulakis E et al. JCO Precis Oncol. 2020;4:PO.19.00118. doi:10.1200/PO.19.00118
- Skoulidis F et al. N Engl J Med. 2021;384(25):2371-2381. doi:10.1056/NEJMoa2103695
- To KKW et al. Front Oncol. 2021;11:635007. doi:10.3389/fonc.2021.635007
- Price MJ et al. JCO Precis Oncol. 2022;6(1):e2100461. doi:10.1200/PO.21.00461
- André T et al; KEYNOTE-177 Investigators. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699
- Stivala S, Meyer SC. Cancers (Basel). 2021;13(20):5035. doi:10.3390/cancers13205035
- Konteatis Z et al. ACS Med Chem Lett. 2020;11(2):101-107. doi:10.1021/acsmedchemlett.9b00509
- OncoKB™ - MSK's precision oncology knowledge base. OncoKB. Accessed December 22, 2022. https://www.oncokb.org/actionableGenes
- National Library of Medicine, National Center for Biotechnology Information. PubChem compound database. Accessed December 22, 2022. https://pubchem.ncbi.nlm.nih.gov/
- US Department of Veterans Affairs. National Precision Oncology Program (NPOP). June 10, 2019. Accessed December 8, 2022. https://www.cancer.va.gov/CANCER/NPOP.asp
- US Department of Veterans Affairs, Office of Research and Development. VA National Precision Oncology Program brings tailored cancer treatment to veterans. October 3, 2019. Accessed December 8, 2022. https://www.research.va.gov/currents/1019-VA-National-Precision-Oncology-Program-brings-tailored-cancer-treatment-to-Veterans.cfm
- Kelley M, Ahmed S. National Precision Oncology Program (NPOP): right treatment for the right patient at the right time. 2022. Unpublished data.
- Vashistha V et al. PLoS One. 2020;15(7):e0235861. doi:10.1371/journal.pone.0235861
- Dong OM et al. Value Health. 2022;25(4):582-594. doi:10.1016/j.jval.2021.09.017
- Sadik H et al. JCO Precis Oncol. 2022;6:e2200246. doi:10.1200/PO.22.00246
- Petrillo LA et al. J Pain Symptom Manage. 2021;62(3):e65-e74. doi:10.1016/j.jpainsymman.2021.02.010
- Waks AG, Winer EP. JAMA. 2019;321(3):288-300. doi:10.1001/jama.2018.19323
- Mellinghoff IK et al. Clin Cancer Res. 2021;27(16):4491-4499. doi:10.1158/1078-0432.CCR-21-0611
- Debela DT et al. SAGE Open Med. 2021;9:20503121211034366. doi:10.1177/20503121211034366
- Gambardella V et al. Cancers (Basel). 2020;12(4):1009. doi:10.3390/cancers12041009
- US Department of Veterans Affairs, Office of Research and Development. VA Lung Precision Oncology Program (LPOP). Updated January 27, 2022. Accessed January 23, 2023. https://www.research.va.gov/programs/pop/lpop.cfm
- Montgomery B et al. Fed Pract. 2020;37(suppl 4):S48-S53. doi:10.12788/fp.0021
- Kelley MJ. Fed Pract. 2020;37(suppl 4):S22-S27. doi:10.12788/fp.0037
- Poonnen PJ et al. JCO Precis Oncol. 2019;3:PO.19.00075. doi:10.1200/PO.19.00075
- Natera awarded national MRD testing contract by the U.S. Department of Veterans Affairs [press release]. Natera. November 2, 2022. Accessed January 23, 2023. https://www.natera.com/company/news/natera-awarded-national-mrd-testing-contract-by-the-u-s-department-of-veterans-affairs/
- Katsoulakis E et al. JCO Precis Oncol. 2020;4:PO.19.00118. doi:10.1200/PO.19.00118
- Skoulidis F et al. N Engl J Med. 2021;384(25):2371-2381. doi:10.1056/NEJMoa2103695
- To KKW et al. Front Oncol. 2021;11:635007. doi:10.3389/fonc.2021.635007
- Price MJ et al. JCO Precis Oncol. 2022;6(1):e2100461. doi:10.1200/PO.21.00461
- André T et al; KEYNOTE-177 Investigators. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699
- Stivala S, Meyer SC. Cancers (Basel). 2021;13(20):5035. doi:10.3390/cancers13205035
- Konteatis Z et al. ACS Med Chem Lett. 2020;11(2):101-107. doi:10.1021/acsmedchemlett.9b00509
- OncoKB™ - MSK's precision oncology knowledge base. OncoKB. Accessed December 22, 2022. https://www.oncokb.org/actionableGenes
- National Library of Medicine, National Center for Biotechnology Information. PubChem compound database. Accessed December 22, 2022. https://pubchem.ncbi.nlm.nih.gov/
- US Department of Veterans Affairs. National Precision Oncology Program (NPOP). June 10, 2019. Accessed December 8, 2022. https://www.cancer.va.gov/CANCER/NPOP.asp
- US Department of Veterans Affairs, Office of Research and Development. VA National Precision Oncology Program brings tailored cancer treatment to veterans. October 3, 2019. Accessed December 8, 2022. https://www.research.va.gov/currents/1019-VA-National-Precision-Oncology-Program-brings-tailored-cancer-treatment-to-Veterans.cfm
- Kelley M, Ahmed S. National Precision Oncology Program (NPOP): right treatment for the right patient at the right time. 2022. Unpublished data.
- Vashistha V et al. PLoS One. 2020;15(7):e0235861. doi:10.1371/journal.pone.0235861
- Dong OM et al. Value Health. 2022;25(4):582-594. doi:10.1016/j.jval.2021.09.017
- Sadik H et al. JCO Precis Oncol. 2022;6:e2200246. doi:10.1200/PO.22.00246
- Petrillo LA et al. J Pain Symptom Manage. 2021;62(3):e65-e74. doi:10.1016/j.jpainsymman.2021.02.010
- Waks AG, Winer EP. JAMA. 2019;321(3):288-300. doi:10.1001/jama.2018.19323
- Mellinghoff IK et al. Clin Cancer Res. 2021;27(16):4491-4499. doi:10.1158/1078-0432.CCR-21-0611
- Debela DT et al. SAGE Open Med. 2021;9:20503121211034366. doi:10.1177/20503121211034366
- Gambardella V et al. Cancers (Basel). 2020;12(4):1009. doi:10.3390/cancers12041009
- US Department of Veterans Affairs, Office of Research and Development. VA Lung Precision Oncology Program (LPOP). Updated January 27, 2022. Accessed January 23, 2023. https://www.research.va.gov/programs/pop/lpop.cfm
- Montgomery B et al. Fed Pract. 2020;37(suppl 4):S48-S53. doi:10.12788/fp.0021
- Kelley MJ. Fed Pract. 2020;37(suppl 4):S22-S27. doi:10.12788/fp.0037
- Poonnen PJ et al. JCO Precis Oncol. 2019;3:PO.19.00075. doi:10.1200/PO.19.00075
- Natera awarded national MRD testing contract by the U.S. Department of Veterans Affairs [press release]. Natera. November 2, 2022. Accessed January 23, 2023. https://www.natera.com/company/news/natera-awarded-national-mrd-testing-contract-by-the-u-s-department-of-veterans-affairs/
- Katsoulakis E et al. JCO Precis Oncol. 2020;4:PO.19.00118. doi:10.1200/PO.19.00118
- Skoulidis F et al. N Engl J Med. 2021;384(25):2371-2381. doi:10.1056/NEJMoa2103695
- To KKW et al. Front Oncol. 2021;11:635007. doi:10.3389/fonc.2021.635007
- Price MJ et al. JCO Precis Oncol. 2022;6(1):e2100461. doi:10.1200/PO.21.00461
- André T et al; KEYNOTE-177 Investigators. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699
- Stivala S, Meyer SC. Cancers (Basel). 2021;13(20):5035. doi:10.3390/cancers13205035
- Konteatis Z et al. ACS Med Chem Lett. 2020;11(2):101-107. doi:10.1021/acsmedchemlett.9b00509
- OncoKB™ - MSK's precision oncology knowledge base. OncoKB. Accessed December 22, 2022. https://www.oncokb.org/actionableGenes
- National Library of Medicine, National Center for Biotechnology Information. PubChem compound database. Accessed December 22, 2022. https://pubchem.ncbi.nlm.nih.gov/
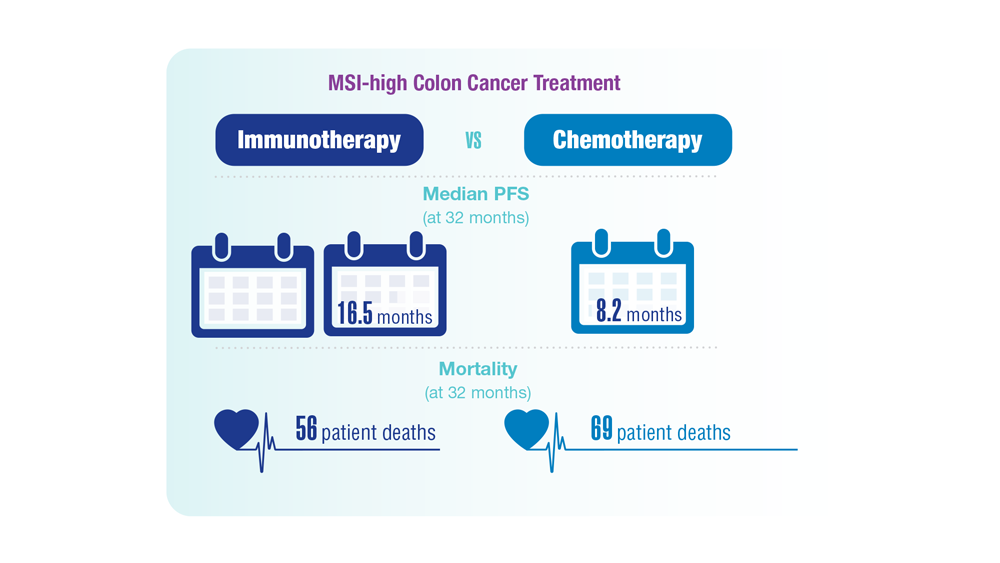
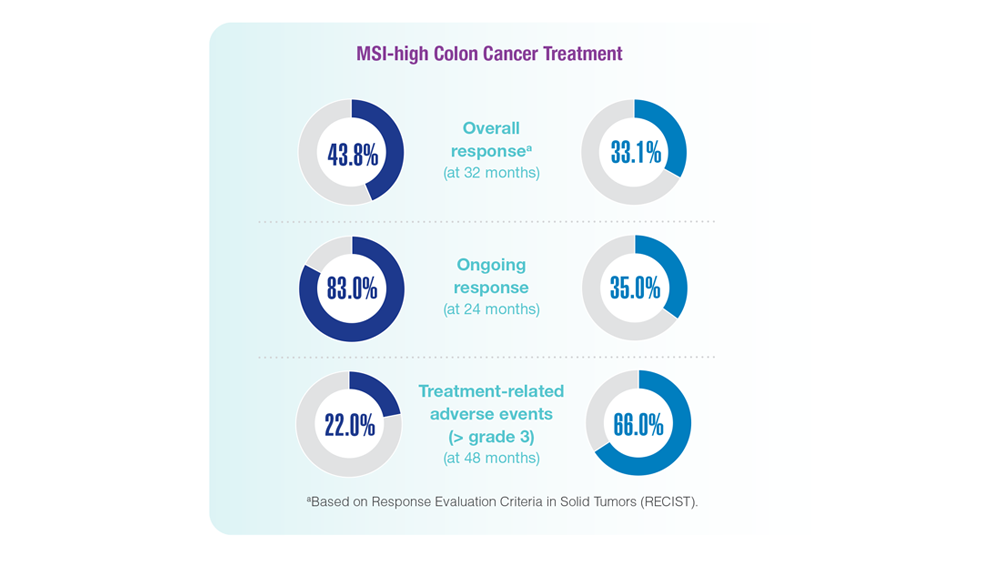
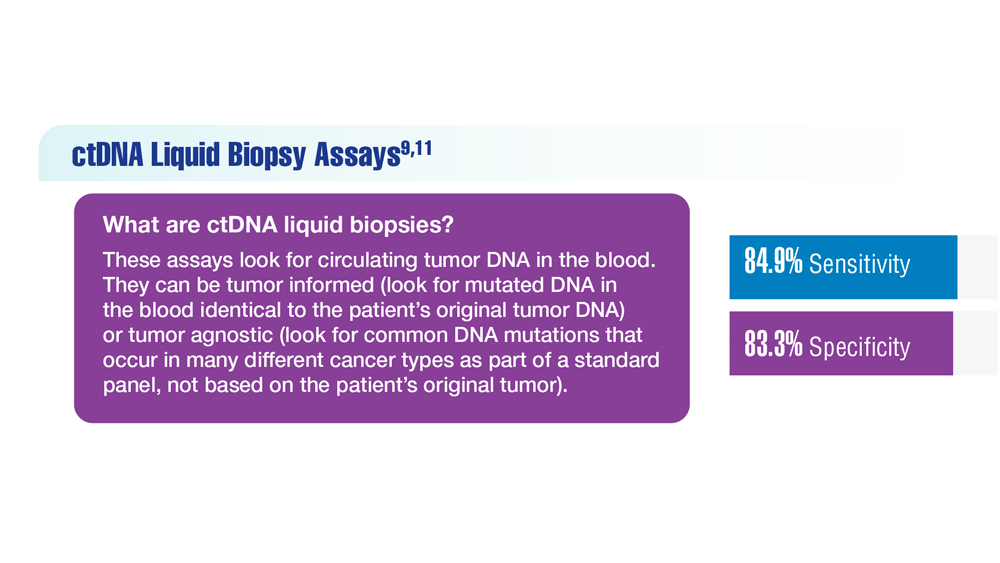
Screening Guideline Updates and New Treatments in Colon Cancer
- Ng K et al. JAMA. 2021;325(19):1943-1945. doi:10.1001/jama.2021.4133
- Xie YH et al. Signal Transduct Target Ther. 2020;5(1):22. doi:10.1038/s41392-020-0116-z
- Muller C et al. Cells. 2021;10(5):1018. doi:10.3390/cells10051018
- Clebak KT et al. Am Fam Physician. 2022;105(2):198-200.
- May FP et al. Dig Dis Sci. 2017;62(8):1923-1932. doi:10.1007/s10620-017-4607-x
- May FP et al. Med Care. 2019;57(10):773-780. doi:10.1097/MLR.0000000000001186
- US Department of Veterans Affairs, National Oncology Program Office. National Precision Oncology Program (NPOP). Updated June 24, 2022. Accessed December 14, 2022. http://www.cancer.va.gov/CANCER/NPOP.asp
- André T et al; KEYNOTE-177 Investigators. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699
- Naidoo M et al. Cancers (Basel). 2021;13(2):346. doi:10.3390/cancers13020346
- Kasi PM et al. BMJ Open. 2021;11(9):e047831. doi:10.1136/bmjopen-2020-047831
- Jin S et al. Proc Natl Acad Sci U S A. 2021;118(5):e2017421118. doi:10.1073/pnas.2017421118
- Ng K et al. JAMA. 2021;325(19):1943-1945. doi:10.1001/jama.2021.4133
- Xie YH et al. Signal Transduct Target Ther. 2020;5(1):22. doi:10.1038/s41392-020-0116-z
- Muller C et al. Cells. 2021;10(5):1018. doi:10.3390/cells10051018
- Clebak KT et al. Am Fam Physician. 2022;105(2):198-200.
- May FP et al. Dig Dis Sci. 2017;62(8):1923-1932. doi:10.1007/s10620-017-4607-x
- May FP et al. Med Care. 2019;57(10):773-780. doi:10.1097/MLR.0000000000001186
- US Department of Veterans Affairs, National Oncology Program Office. National Precision Oncology Program (NPOP). Updated June 24, 2022. Accessed December 14, 2022. http://www.cancer.va.gov/CANCER/NPOP.asp
- André T et al; KEYNOTE-177 Investigators. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699
- Naidoo M et al. Cancers (Basel). 2021;13(2):346. doi:10.3390/cancers13020346
- Kasi PM et al. BMJ Open. 2021;11(9):e047831. doi:10.1136/bmjopen-2020-047831
- Jin S et al. Proc Natl Acad Sci U S A. 2021;118(5):e2017421118. doi:10.1073/pnas.2017421118
- Ng K et al. JAMA. 2021;325(19):1943-1945. doi:10.1001/jama.2021.4133
- Xie YH et al. Signal Transduct Target Ther. 2020;5(1):22. doi:10.1038/s41392-020-0116-z
- Muller C et al. Cells. 2021;10(5):1018. doi:10.3390/cells10051018
- Clebak KT et al. Am Fam Physician. 2022;105(2):198-200.
- May FP et al. Dig Dis Sci. 2017;62(8):1923-1932. doi:10.1007/s10620-017-4607-x
- May FP et al. Med Care. 2019;57(10):773-780. doi:10.1097/MLR.0000000000001186
- US Department of Veterans Affairs, National Oncology Program Office. National Precision Oncology Program (NPOP). Updated June 24, 2022. Accessed December 14, 2022. http://www.cancer.va.gov/CANCER/NPOP.asp
- André T et al; KEYNOTE-177 Investigators. N Engl J Med. 2020;383(23):2207-2218. doi:10.1056/NEJMoa2017699
- Naidoo M et al. Cancers (Basel). 2021;13(2):346. doi:10.3390/cancers13020346
- Kasi PM et al. BMJ Open. 2021;11(9):e047831. doi:10.1136/bmjopen-2020-047831
- Jin S et al. Proc Natl Acad Sci U S A. 2021;118(5):e2017421118. doi:10.1073/pnas.2017421118
Cancer Data Trends 2023
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.

In this issue:
- COVID-19 Outcomes in Veterans With Hematologic Cancers
- Promising New Approaches for Testicular and Prostate Cancer
- Screening Guideline Updates and New Treatments in Colon Cancer
- Exposure-Related Cancers: A Look at the PACT Act
- New Classifications and Emerging Treatments in Brain Cancer
- Gender Disparity in Breast Cancer Among US Veterans
- Lung Cancer Screening in Veterans
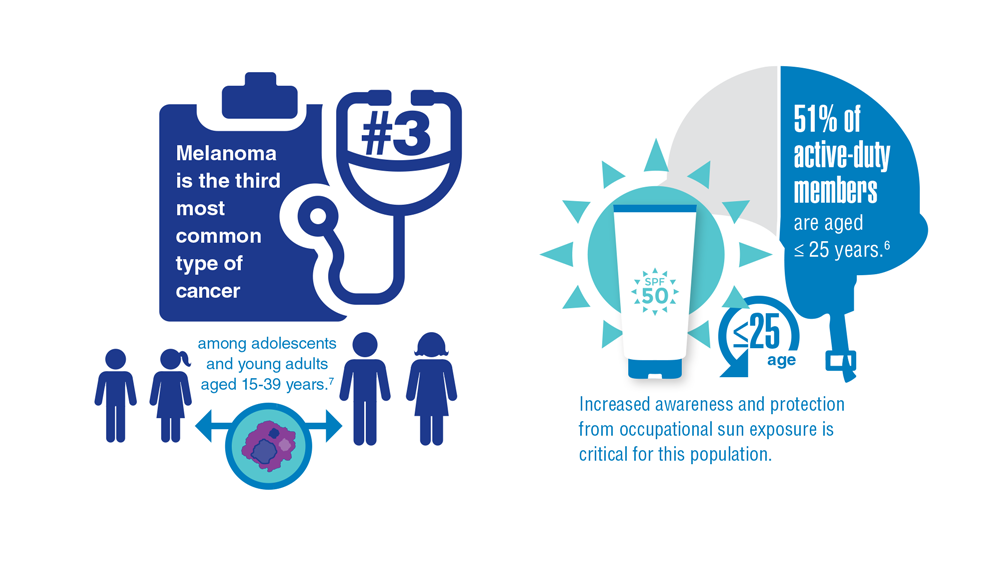
- Necessary Updates to Skin Cancer Risk Stratification
- Innovation in Cancer Treatment
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
In this issue:
- COVID-19 Outcomes in Veterans With Hematologic Cancers
- Promising New Approaches for Testicular and Prostate Cancer
- Screening Guideline Updates and New Treatments in Colon Cancer
- Exposure-Related Cancers: A Look at the PACT Act
- New Classifications and Emerging Treatments in Brain Cancer
- Gender Disparity in Breast Cancer Among US Veterans
- Lung Cancer Screening in Veterans
- Necessary Updates to Skin Cancer Risk Stratification
- Innovation in Cancer Treatment
Federal Practitioner and the Association of VA Hematology/Oncology (AVAHO) present the 2023 edition of Cancer Data Trends (click to view the digital edition). This special issue provides updates on some of the top cancers and related concerns affecting veterans through original infographics and visual storytelling.
In this issue:
- COVID-19 Outcomes in Veterans With Hematologic Cancers
- Promising New Approaches for Testicular and Prostate Cancer
- Screening Guideline Updates and New Treatments in Colon Cancer
- Exposure-Related Cancers: A Look at the PACT Act
- New Classifications and Emerging Treatments in Brain Cancer
- Gender Disparity in Breast Cancer Among US Veterans
- Lung Cancer Screening in Veterans
- Necessary Updates to Skin Cancer Risk Stratification
- Innovation in Cancer Treatment
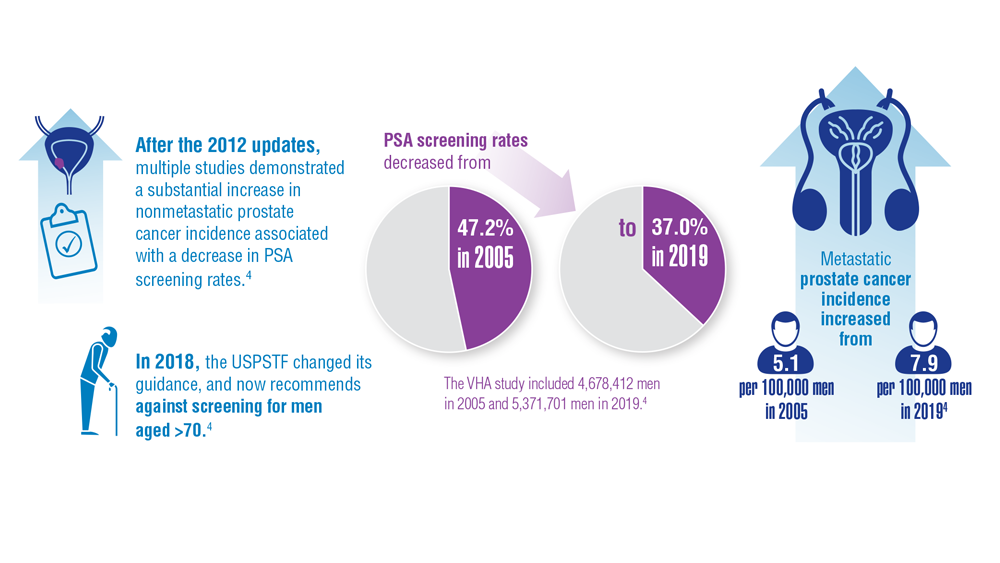
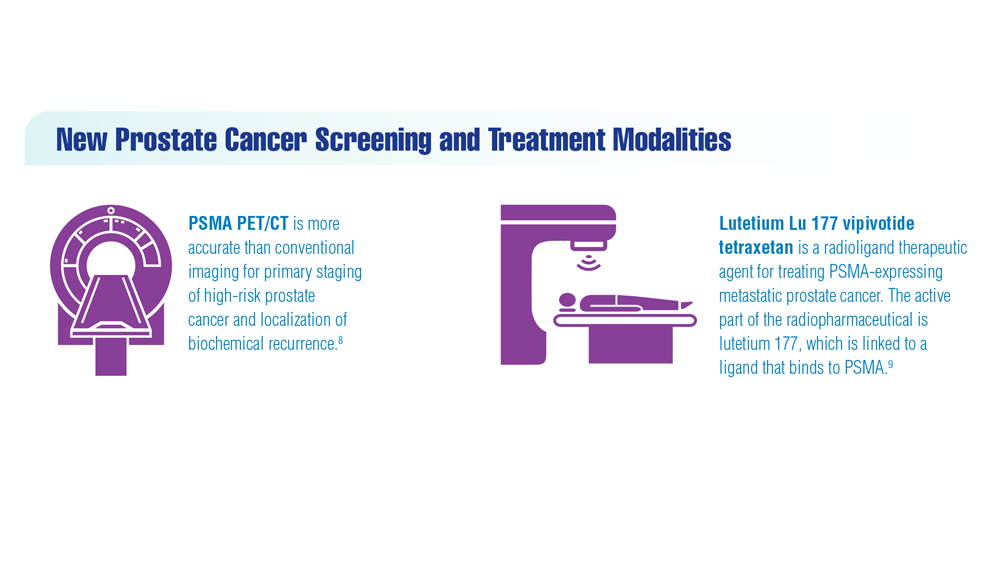
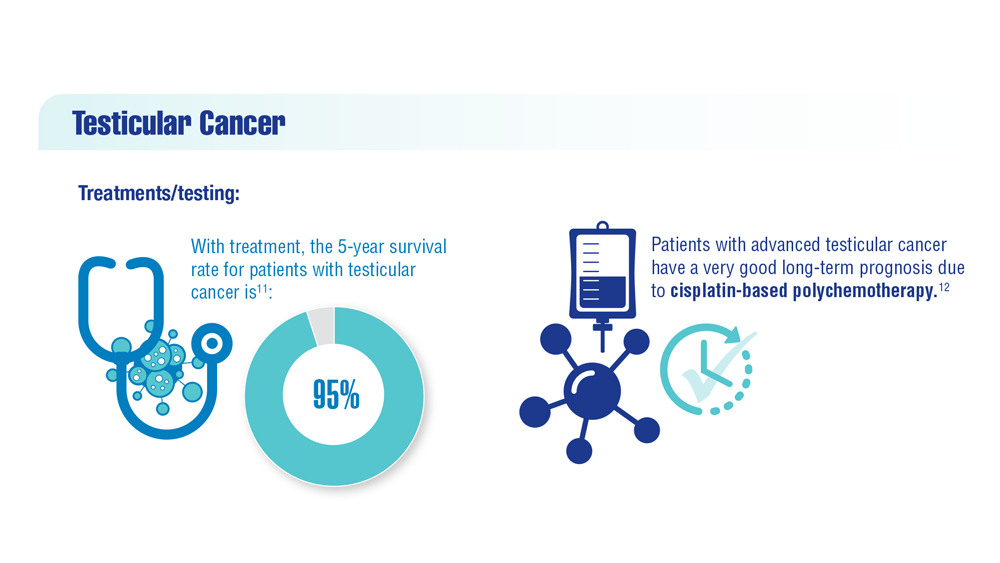
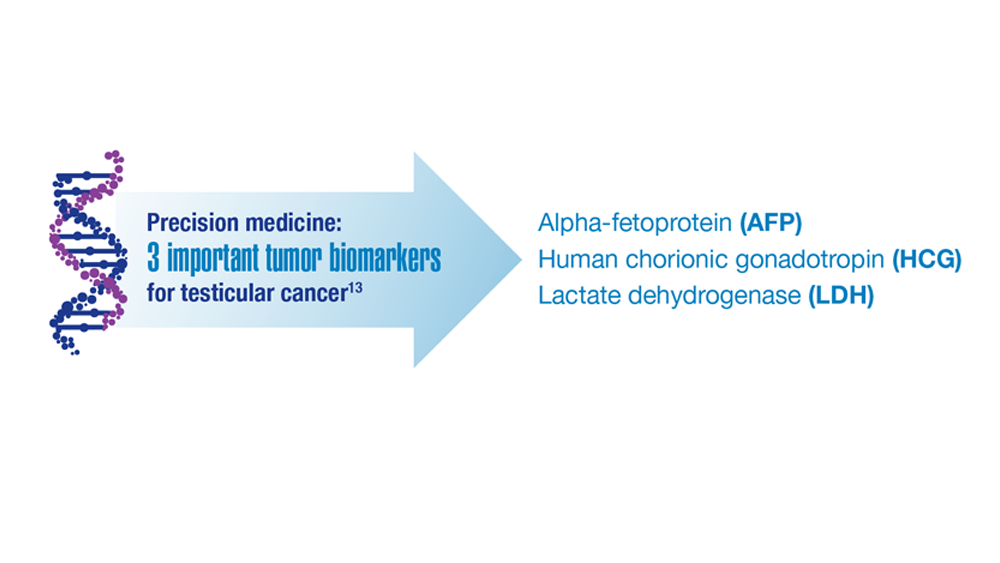
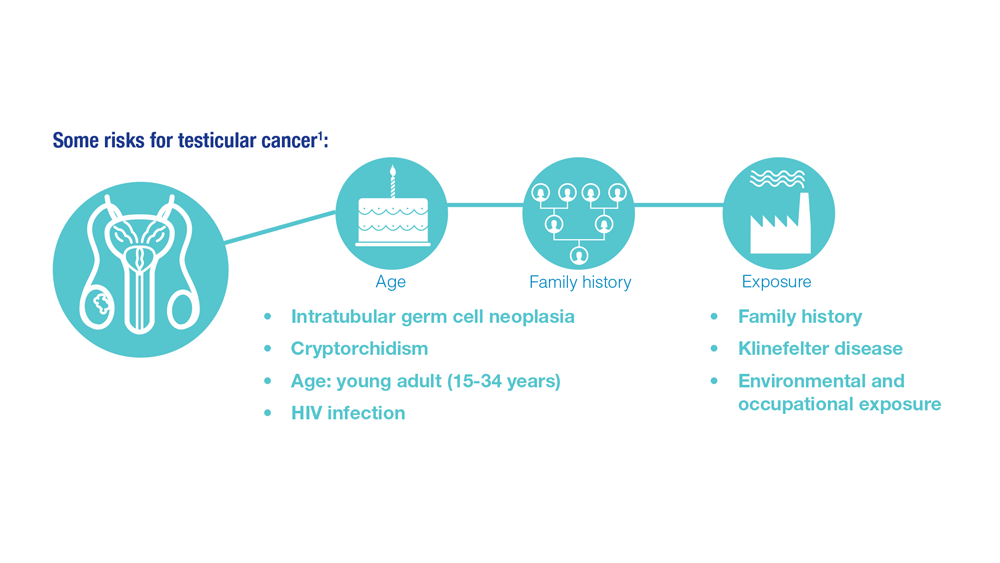
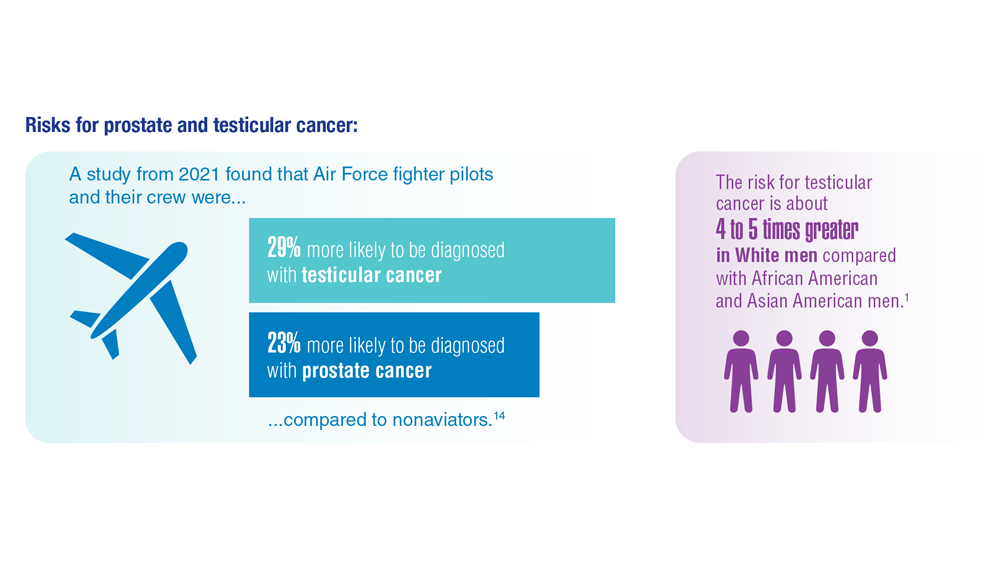
Promising New Approaches for Testicular and Prostate Cancer
- Risk factors for testicular cancer. American Cancer Society. Updated May 17, 2018. Accessed December 15, 2022. https://www.cancer.org/cancer/testicular-cancer/causes-risks-prevention/risk-factors.html
- Chovanec M, Cheng L. BMJ. 2022;379:e070499. doi:10.1136/bmj-2022-070499
- Tavares NT et al. J Pathol. 2022. doi:10.1002/path.6037
- Bryant AK et al. JAMA Oncol. 2022;e224319. doi:10.1001/jamaoncol.2022.4319
- Kabasakal L et al. Nucl Med Commun. 2017;38(2):149-155. doi:10.1097/MNM.0000000000000617
- Sartor O et al; VISION Investigators. N Engl J Med. 2021;385(12):1091-1103. doi:10.1056/NEJMoa2107322
- Rowe SP et al. Annu Rev Med. 2019;70:461-477. doi:10.1146/annurev-med-062117-073027
- Pomykala KL et al. Eur Urol Oncol. 2022;S2588-9311(22)00177-8. doi:10.1016/j.euo.2022.10.007
- Keam SJ. Mol Diagn Ther. 2022;26(4):467-475. doi:10.1007/s40291-022-00594-2
- Lovejoy LA et al. Mil Med. 2022:usac297. doi:10.1093/milmed/usac297
- Smith ZL et al. Med Clin North Am. 2018;102(2):251-264. doi:10.1016/j.mcna.2017.10.003
- Hohnloser JH et al. Eur J Med Res.1996;1(11):509-514.
- Johns Hopkins Medicine website. Testicular Cancer tumor Markers. Accessed December 2022. https://www.hopkinsmedicine.org/health/conditions-and-diseases/testicular-cancer/testicular-cancer-tumor-markers
- Webber BJ et al. J Occup Environ Med. 2022;64(1):71-78. doi:10.1097/JOM.0000000000002353
- Risk factors for testicular cancer. American Cancer Society. Updated May 17, 2018. Accessed December 15, 2022. https://www.cancer.org/cancer/testicular-cancer/causes-risks-prevention/risk-factors.html
- Chovanec M, Cheng L. BMJ. 2022;379:e070499. doi:10.1136/bmj-2022-070499
- Tavares NT et al. J Pathol. 2022. doi:10.1002/path.6037
- Bryant AK et al. JAMA Oncol. 2022;e224319. doi:10.1001/jamaoncol.2022.4319
- Kabasakal L et al. Nucl Med Commun. 2017;38(2):149-155. doi:10.1097/MNM.0000000000000617
- Sartor O et al; VISION Investigators. N Engl J Med. 2021;385(12):1091-1103. doi:10.1056/NEJMoa2107322
- Rowe SP et al. Annu Rev Med. 2019;70:461-477. doi:10.1146/annurev-med-062117-073027
- Pomykala KL et al. Eur Urol Oncol. 2022;S2588-9311(22)00177-8. doi:10.1016/j.euo.2022.10.007
- Keam SJ. Mol Diagn Ther. 2022;26(4):467-475. doi:10.1007/s40291-022-00594-2
- Lovejoy LA et al. Mil Med. 2022:usac297. doi:10.1093/milmed/usac297
- Smith ZL et al. Med Clin North Am. 2018;102(2):251-264. doi:10.1016/j.mcna.2017.10.003
- Hohnloser JH et al. Eur J Med Res.1996;1(11):509-514.
- Johns Hopkins Medicine website. Testicular Cancer tumor Markers. Accessed December 2022. https://www.hopkinsmedicine.org/health/conditions-and-diseases/testicular-cancer/testicular-cancer-tumor-markers
- Webber BJ et al. J Occup Environ Med. 2022;64(1):71-78. doi:10.1097/JOM.0000000000002353
- Risk factors for testicular cancer. American Cancer Society. Updated May 17, 2018. Accessed December 15, 2022. https://www.cancer.org/cancer/testicular-cancer/causes-risks-prevention/risk-factors.html
- Chovanec M, Cheng L. BMJ. 2022;379:e070499. doi:10.1136/bmj-2022-070499
- Tavares NT et al. J Pathol. 2022. doi:10.1002/path.6037
- Bryant AK et al. JAMA Oncol. 2022;e224319. doi:10.1001/jamaoncol.2022.4319
- Kabasakal L et al. Nucl Med Commun. 2017;38(2):149-155. doi:10.1097/MNM.0000000000000617
- Sartor O et al; VISION Investigators. N Engl J Med. 2021;385(12):1091-1103. doi:10.1056/NEJMoa2107322
- Rowe SP et al. Annu Rev Med. 2019;70:461-477. doi:10.1146/annurev-med-062117-073027
- Pomykala KL et al. Eur Urol Oncol. 2022;S2588-9311(22)00177-8. doi:10.1016/j.euo.2022.10.007
- Keam SJ. Mol Diagn Ther. 2022;26(4):467-475. doi:10.1007/s40291-022-00594-2
- Lovejoy LA et al. Mil Med. 2022:usac297. doi:10.1093/milmed/usac297
- Smith ZL et al. Med Clin North Am. 2018;102(2):251-264. doi:10.1016/j.mcna.2017.10.003
- Hohnloser JH et al. Eur J Med Res.1996;1(11):509-514.
- Johns Hopkins Medicine website. Testicular Cancer tumor Markers. Accessed December 2022. https://www.hopkinsmedicine.org/health/conditions-and-diseases/testicular-cancer/testicular-cancer-tumor-markers
- Webber BJ et al. J Occup Environ Med. 2022;64(1):71-78. doi:10.1097/JOM.0000000000002353


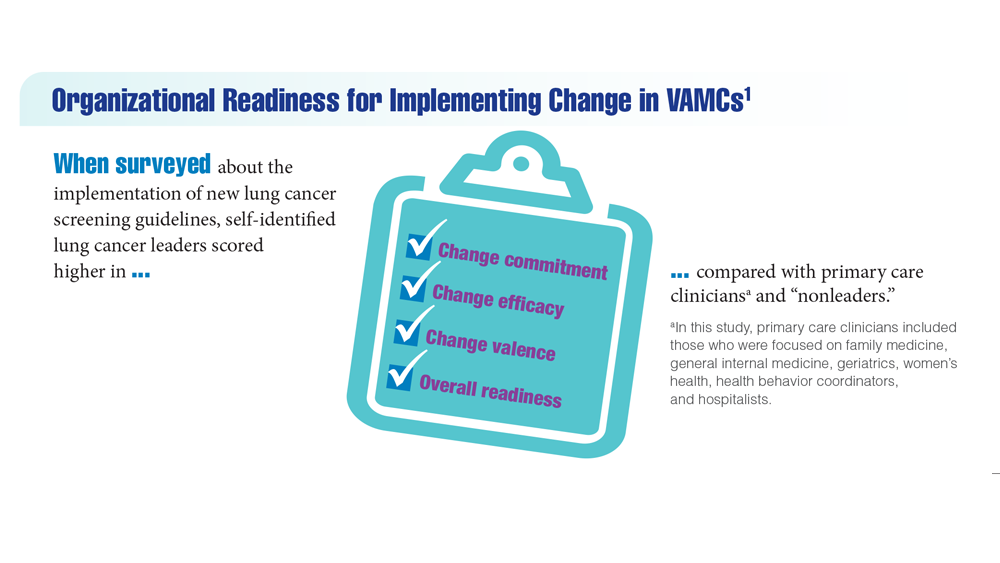
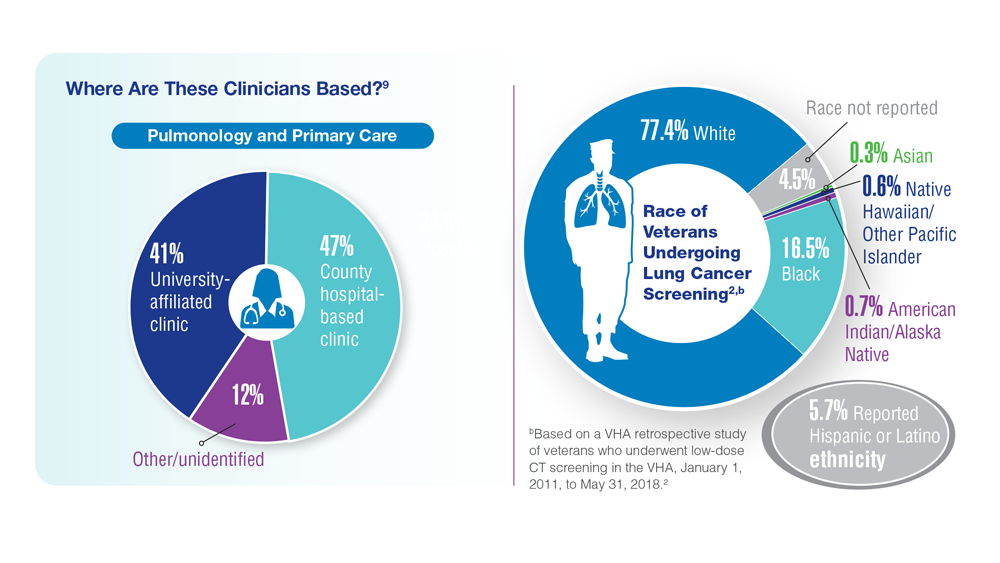
Lung Cancer Screening in Veterans
- Spalluto LB et al. J Am Coll Radiol. 2021;18(6):809-819. doi:10.1016/j.jacr.2020.12.010
- Lewis JA et al. JNCI Cancer Spectr. 2020;4(5):pkaa053. doi:10.1093/jncics/pkaa053
- Wallace C. Largest-ever lung cancer screening study reveals ways to increase screening outreach. Medical University of South Carolina. November 22, 2022. Accessed January 4, 202 https://hollingscancercenter.musc.edu/news/archive/2022/11/22/largest-ever-lung-cancer-screening-study-reveals-ways-to-increase-screening-outreach
- Screening facts & figures. Go2 For Lung Cancer. 2022. Accessed January 4, 2023. https://go2.org/risk-early-detection/screening-facts-figures/
- Dyer O. BMJ. 2021;372:n698. doi:10.1136/bmj.n698
- Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
- Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
- Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
- Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
- Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0
- Spalluto LB et al. J Am Coll Radiol. 2021;18(6):809-819. doi:10.1016/j.jacr.2020.12.010
- Lewis JA et al. JNCI Cancer Spectr. 2020;4(5):pkaa053. doi:10.1093/jncics/pkaa053
- Wallace C. Largest-ever lung cancer screening study reveals ways to increase screening outreach. Medical University of South Carolina. November 22, 2022. Accessed January 4, 202 https://hollingscancercenter.musc.edu/news/archive/2022/11/22/largest-ever-lung-cancer-screening-study-reveals-ways-to-increase-screening-outreach
- Screening facts & figures. Go2 For Lung Cancer. 2022. Accessed January 4, 2023. https://go2.org/risk-early-detection/screening-facts-figures/
- Dyer O. BMJ. 2021;372:n698. doi:10.1136/bmj.n698
- Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
- Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
- Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
- Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
- Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0
- Spalluto LB et al. J Am Coll Radiol. 2021;18(6):809-819. doi:10.1016/j.jacr.2020.12.010
- Lewis JA et al. JNCI Cancer Spectr. 2020;4(5):pkaa053. doi:10.1093/jncics/pkaa053
- Wallace C. Largest-ever lung cancer screening study reveals ways to increase screening outreach. Medical University of South Carolina. November 22, 2022. Accessed January 4, 202 https://hollingscancercenter.musc.edu/news/archive/2022/11/22/largest-ever-lung-cancer-screening-study-reveals-ways-to-increase-screening-outreach
- Screening facts & figures. Go2 For Lung Cancer. 2022. Accessed January 4, 2023. https://go2.org/risk-early-detection/screening-facts-figures/
- Dyer O. BMJ. 2021;372:n698. doi:10.1136/bmj.n698
- Boudreau JH et al. Chest. 2021;160(1):358-367. doi:10.1016/j.chest.2021.02.016
- Maurice NM, Tanner NT. Semin Oncol. 2022;S0093-7754(22)00041-0. doi:10.1053/j.seminoncol.2022.06.001
- Rusher TN et al. Fed Pract. 2022;39(suppl 2):S48-S51. doi:10.12788/fp.0269
- Núñez ER et al. JAMA Netw Open. 2021;4(7):e2116233. doi:10.1001/jamanetworkopen.2021.16233
- Lake M et al. BMC Cancer. 2020;20(1):561. doi:1186/s12885-020-06923-0



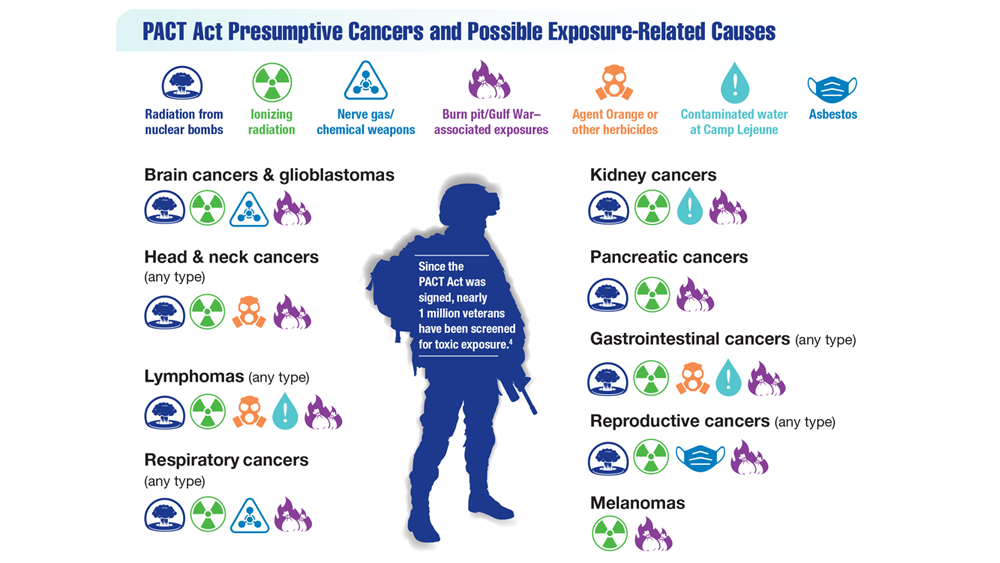
Exposure-Related Cancers: A Look at the PACT Act
- US Department of Veterans Affairs. PACT Act. Updated November 4, 2022. Accessed January 4, 2023. https://www.publichealth.va.gov/exposures/benefits/PACT_Act.asp
- The White House. FACT SHEET: President Biden signs the PACT Act and delivers on his promise to America’s veterans. August 10, 202 Accessed January 10, 2023. https://www.whitehouse.gov/briefing-room/statements-releases/2022/08/10/fact-sheet-president-biden-signs-the-pact-act-and-delivers-on-his-promise-to-americas-veterans/
- US House of Representatives. Honoring our promise to address Comprehensive Toxics Act of 2021. Title I – Expansion of health care eligibility for toxic exposed veterans. House report 117-249. February 22, 2022. Accessed January 19, 202 https://www.govinfo.gov/content/pkg/CRPT-117hrpt249/html/CRPT-117hrpt249-pt1.htm
- VA News. Cancer Moonshot week of action sees VA deploying new clinical pathways. Updated December 7, 2022. Accessed January 19, 2023. https://news.va.gov/111925/cancer-moonshot-clinical-pathways/
- US Department of Veterans Affairs. PACT Act. Updated November 4, 2022. Accessed January 4, 2023. https://www.publichealth.va.gov/exposures/benefits/PACT_Act.asp
- The White House. FACT SHEET: President Biden signs the PACT Act and delivers on his promise to America’s veterans. August 10, 202 Accessed January 10, 2023. https://www.whitehouse.gov/briefing-room/statements-releases/2022/08/10/fact-sheet-president-biden-signs-the-pact-act-and-delivers-on-his-promise-to-americas-veterans/
- US House of Representatives. Honoring our promise to address Comprehensive Toxics Act of 2021. Title I – Expansion of health care eligibility for toxic exposed veterans. House report 117-249. February 22, 2022. Accessed January 19, 202 https://www.govinfo.gov/content/pkg/CRPT-117hrpt249/html/CRPT-117hrpt249-pt1.htm
- VA News. Cancer Moonshot week of action sees VA deploying new clinical pathways. Updated December 7, 2022. Accessed January 19, 2023. https://news.va.gov/111925/cancer-moonshot-clinical-pathways/
- US Department of Veterans Affairs. PACT Act. Updated November 4, 2022. Accessed January 4, 2023. https://www.publichealth.va.gov/exposures/benefits/PACT_Act.asp
- The White House. FACT SHEET: President Biden signs the PACT Act and delivers on his promise to America’s veterans. August 10, 202 Accessed January 10, 2023. https://www.whitehouse.gov/briefing-room/statements-releases/2022/08/10/fact-sheet-president-biden-signs-the-pact-act-and-delivers-on-his-promise-to-americas-veterans/
- US House of Representatives. Honoring our promise to address Comprehensive Toxics Act of 2021. Title I – Expansion of health care eligibility for toxic exposed veterans. House report 117-249. February 22, 2022. Accessed January 19, 202 https://www.govinfo.gov/content/pkg/CRPT-117hrpt249/html/CRPT-117hrpt249-pt1.htm
- VA News. Cancer Moonshot week of action sees VA deploying new clinical pathways. Updated December 7, 2022. Accessed January 19, 2023. https://news.va.gov/111925/cancer-moonshot-clinical-pathways/