User login
Burden of thyroid cancer: Substantial and increasing
in many developed countries, including the Unites States, concluded a new analysis based on 30 years of observational data.
“We report overall increases in the burden of thyroid cancer across the majority of EU15+ countries between 1990 and 2019, evidenced by plateaus in incidence rates and reductions in mortality and DALY [disability-adjusted life-years] rates,” the authors reported.
“However, in a number of countries, including the U.S., there are unfavorable increasing mortality and DALY trends over this time period ... [and] a better understanding of the trends in the disease burden of thyroid cancer may help to inform future health system planning,” they added.
The study was published online March 10, 2022, in JAMA Otolaryngology–Head & Neck Surgery.
Trends in thyroid cancer
For the analysis, James Schuster-Bruce, MBChB, from St. George’s University Hospital NHS Foundation Trust, London, and colleagues compared trends in thyroid cancer across 30 years of follow-up among 15 countries of the (pre-2004) European Union as well as those in the United States, Australia, Canada, and Norway (EU15+).
Data from the Global Burden of Disease study database were used to track these trends. “We extracted age-standardized incidence rates (ASIRs), age-standardized mortality rates (ASMRs), and DALYs for thyroid cancer from EU15+ countries between 1990 and 2019 using the dedicated GBD study results tool,” the investigators explained.
In 2019, ASIRs were highest in Italy at 6.36 per 100,000 population, followed by the United States at a rate of 5.59 per 100,000 population – although incidence rates of thyroid cancer have actually recently decreased in U.S. women, they noted.
“Thirteen of 19 countries showed an average annual percentage increase in ASIR across the study period,” the investigators added. Out of all the EU15+ countries, the average annual percentage change (AAPC) was the highest in Australia at 2.5 per 100,000 population and the United States at 1.2 per 100,000.
On the other hand, a largely plateauing trend in incidence rates across the majority of EU15+ nations has been observed since 1990, as reflected by incidence rates ranging from –0.8 to 0.8 per 100,000 in the most recent period, the researchers added. ASMRs ranged from a 0.40 per 100,000 in Greece to 0.57 per 100,000 in Luxembourg.
In the United States, the ASMR in 2019 was 0.43 per 100,000 population while the ASMR was the lowest in the United Kingdom in the same year at 0.38 per 100,000 population.
Australia, Denmark, and the United States were the only countries showing positive AAPC changes, the team observed. For example, in the most recent period to 2019, Denmark and Australia had reductions in ASMR trends, whereas in the United States, the trend was toward increasing ASMRs
In 2019, the DALYs of the EU15+ nations ranged from 9.63 per 100,000 in the United Kingdom to 14.46 per 100,000 in Luxembourg. In the most recent period, a downward trend in DALYs was observed in Australia and Denmark while it plateaued in the United States.
“Overall, we identified improvements in thyroid cancer mortality and DALYs, but overall increases in thyroid cancer incidence in EU15+ countries over the past 3 decades,” the investigators commented.
It has been widely suggested that improvements in diagnostic techniques have contributed significantly to increasing incidence rates of thyroid cancer, but there is concern about overdiagnosis. Newer diagnostic techniques detect significant numbers of slow-growing, subclinical papillary thyroid cancers that make up at least one quarter of all thyroid cancer subtypes, the authors pointed out.
“It has therefore been suggested that an increase in subclinical disease has inflated the data to look more substantial than the clinical reality,” the authors wrote. However, they insisted that overdiagnosis alone is unlikely to account entirely for increasing incidence trends in the current analysis.
Rather, their concern for countries with high incidence rates of thyroid cancer is the surveillance burden of disease that does not affect mortality. “Close observation of future time trends in thyroid cancer disease burden should be performed in the context of recent changes in international clinical practice guidelines, which have suggested more conservative diagnostic and management strategies,” the authors suggested.
“In the context of the more conservative treatment guidelines and reported increase in true disease, it is important to closely observe mortality and DALYs over the coming years to ensure optimum thyroid cancer management in these nations,” they added.
The study had no specific funding. Dr. Schuster-Bruce disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
in many developed countries, including the Unites States, concluded a new analysis based on 30 years of observational data.
“We report overall increases in the burden of thyroid cancer across the majority of EU15+ countries between 1990 and 2019, evidenced by plateaus in incidence rates and reductions in mortality and DALY [disability-adjusted life-years] rates,” the authors reported.
“However, in a number of countries, including the U.S., there are unfavorable increasing mortality and DALY trends over this time period ... [and] a better understanding of the trends in the disease burden of thyroid cancer may help to inform future health system planning,” they added.
The study was published online March 10, 2022, in JAMA Otolaryngology–Head & Neck Surgery.
Trends in thyroid cancer
For the analysis, James Schuster-Bruce, MBChB, from St. George’s University Hospital NHS Foundation Trust, London, and colleagues compared trends in thyroid cancer across 30 years of follow-up among 15 countries of the (pre-2004) European Union as well as those in the United States, Australia, Canada, and Norway (EU15+).
Data from the Global Burden of Disease study database were used to track these trends. “We extracted age-standardized incidence rates (ASIRs), age-standardized mortality rates (ASMRs), and DALYs for thyroid cancer from EU15+ countries between 1990 and 2019 using the dedicated GBD study results tool,” the investigators explained.
In 2019, ASIRs were highest in Italy at 6.36 per 100,000 population, followed by the United States at a rate of 5.59 per 100,000 population – although incidence rates of thyroid cancer have actually recently decreased in U.S. women, they noted.
“Thirteen of 19 countries showed an average annual percentage increase in ASIR across the study period,” the investigators added. Out of all the EU15+ countries, the average annual percentage change (AAPC) was the highest in Australia at 2.5 per 100,000 population and the United States at 1.2 per 100,000.
On the other hand, a largely plateauing trend in incidence rates across the majority of EU15+ nations has been observed since 1990, as reflected by incidence rates ranging from –0.8 to 0.8 per 100,000 in the most recent period, the researchers added. ASMRs ranged from a 0.40 per 100,000 in Greece to 0.57 per 100,000 in Luxembourg.
In the United States, the ASMR in 2019 was 0.43 per 100,000 population while the ASMR was the lowest in the United Kingdom in the same year at 0.38 per 100,000 population.
Australia, Denmark, and the United States were the only countries showing positive AAPC changes, the team observed. For example, in the most recent period to 2019, Denmark and Australia had reductions in ASMR trends, whereas in the United States, the trend was toward increasing ASMRs
In 2019, the DALYs of the EU15+ nations ranged from 9.63 per 100,000 in the United Kingdom to 14.46 per 100,000 in Luxembourg. In the most recent period, a downward trend in DALYs was observed in Australia and Denmark while it plateaued in the United States.
“Overall, we identified improvements in thyroid cancer mortality and DALYs, but overall increases in thyroid cancer incidence in EU15+ countries over the past 3 decades,” the investigators commented.
It has been widely suggested that improvements in diagnostic techniques have contributed significantly to increasing incidence rates of thyroid cancer, but there is concern about overdiagnosis. Newer diagnostic techniques detect significant numbers of slow-growing, subclinical papillary thyroid cancers that make up at least one quarter of all thyroid cancer subtypes, the authors pointed out.
“It has therefore been suggested that an increase in subclinical disease has inflated the data to look more substantial than the clinical reality,” the authors wrote. However, they insisted that overdiagnosis alone is unlikely to account entirely for increasing incidence trends in the current analysis.
Rather, their concern for countries with high incidence rates of thyroid cancer is the surveillance burden of disease that does not affect mortality. “Close observation of future time trends in thyroid cancer disease burden should be performed in the context of recent changes in international clinical practice guidelines, which have suggested more conservative diagnostic and management strategies,” the authors suggested.
“In the context of the more conservative treatment guidelines and reported increase in true disease, it is important to closely observe mortality and DALYs over the coming years to ensure optimum thyroid cancer management in these nations,” they added.
The study had no specific funding. Dr. Schuster-Bruce disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
in many developed countries, including the Unites States, concluded a new analysis based on 30 years of observational data.
“We report overall increases in the burden of thyroid cancer across the majority of EU15+ countries between 1990 and 2019, evidenced by plateaus in incidence rates and reductions in mortality and DALY [disability-adjusted life-years] rates,” the authors reported.
“However, in a number of countries, including the U.S., there are unfavorable increasing mortality and DALY trends over this time period ... [and] a better understanding of the trends in the disease burden of thyroid cancer may help to inform future health system planning,” they added.
The study was published online March 10, 2022, in JAMA Otolaryngology–Head & Neck Surgery.
Trends in thyroid cancer
For the analysis, James Schuster-Bruce, MBChB, from St. George’s University Hospital NHS Foundation Trust, London, and colleagues compared trends in thyroid cancer across 30 years of follow-up among 15 countries of the (pre-2004) European Union as well as those in the United States, Australia, Canada, and Norway (EU15+).
Data from the Global Burden of Disease study database were used to track these trends. “We extracted age-standardized incidence rates (ASIRs), age-standardized mortality rates (ASMRs), and DALYs for thyroid cancer from EU15+ countries between 1990 and 2019 using the dedicated GBD study results tool,” the investigators explained.
In 2019, ASIRs were highest in Italy at 6.36 per 100,000 population, followed by the United States at a rate of 5.59 per 100,000 population – although incidence rates of thyroid cancer have actually recently decreased in U.S. women, they noted.
“Thirteen of 19 countries showed an average annual percentage increase in ASIR across the study period,” the investigators added. Out of all the EU15+ countries, the average annual percentage change (AAPC) was the highest in Australia at 2.5 per 100,000 population and the United States at 1.2 per 100,000.
On the other hand, a largely plateauing trend in incidence rates across the majority of EU15+ nations has been observed since 1990, as reflected by incidence rates ranging from –0.8 to 0.8 per 100,000 in the most recent period, the researchers added. ASMRs ranged from a 0.40 per 100,000 in Greece to 0.57 per 100,000 in Luxembourg.
In the United States, the ASMR in 2019 was 0.43 per 100,000 population while the ASMR was the lowest in the United Kingdom in the same year at 0.38 per 100,000 population.
Australia, Denmark, and the United States were the only countries showing positive AAPC changes, the team observed. For example, in the most recent period to 2019, Denmark and Australia had reductions in ASMR trends, whereas in the United States, the trend was toward increasing ASMRs
In 2019, the DALYs of the EU15+ nations ranged from 9.63 per 100,000 in the United Kingdom to 14.46 per 100,000 in Luxembourg. In the most recent period, a downward trend in DALYs was observed in Australia and Denmark while it plateaued in the United States.
“Overall, we identified improvements in thyroid cancer mortality and DALYs, but overall increases in thyroid cancer incidence in EU15+ countries over the past 3 decades,” the investigators commented.
It has been widely suggested that improvements in diagnostic techniques have contributed significantly to increasing incidence rates of thyroid cancer, but there is concern about overdiagnosis. Newer diagnostic techniques detect significant numbers of slow-growing, subclinical papillary thyroid cancers that make up at least one quarter of all thyroid cancer subtypes, the authors pointed out.
“It has therefore been suggested that an increase in subclinical disease has inflated the data to look more substantial than the clinical reality,” the authors wrote. However, they insisted that overdiagnosis alone is unlikely to account entirely for increasing incidence trends in the current analysis.
Rather, their concern for countries with high incidence rates of thyroid cancer is the surveillance burden of disease that does not affect mortality. “Close observation of future time trends in thyroid cancer disease burden should be performed in the context of recent changes in international clinical practice guidelines, which have suggested more conservative diagnostic and management strategies,” the authors suggested.
“In the context of the more conservative treatment guidelines and reported increase in true disease, it is important to closely observe mortality and DALYs over the coming years to ensure optimum thyroid cancer management in these nations,” they added.
The study had no specific funding. Dr. Schuster-Bruce disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA OTOLARYNGOLOGY–HEAD & NECK SURGERY.
Radioactive iodine shows no benefit in low-risk thyroid cancer
, suggesting these patients can be spared the previously common treatment.
The study’s take-home message for clinicians should be to “stop systematic radioiodine ablation administration in low-risk thyroid cancer patients,” lead author Sophie Leboulleux, MD, PhD, said in an interview.
The results were first reported at ENDO 2021 and have now been published in the New England Journal of Medicine by Dr. Leboulleux, of the department of nuclear medicine and endocrine oncology, Gustave Roussy Cancer Institute, Villejuif, France, and colleagues.
While American Thyroid Association (ATA) guidelines already indicate that radioiodine ablation is not routinely recommended after thyroidectomy for patients with low-risk thyroid cancer, the guidance is only a “weak recommendation,” supported by “low-quality evidence.”
However, the new findings should give that level of evidence a much-needed boost, said one expert. “I think the main contribution of this paper is to change the evidence level to ‘high quality,’ therefore making the recommendation ‘strong,’ rather than ‘weak,’ ” David S. Cooper, MD, said in an interview.
Dr. Cooper, professor of medicine and radiology at Johns Hopkins University, Baltimore, wrote an editorial that accompanies Dr. Leboulleux’s study.
The ability to safely spare patients the radioiodine ablation step after thyroidectomy has important benefits in terms of cost and convenience, Dr. Cooper stressed.
ESTIMABL2 trial
The new findings are from the prospective, randomized, phase 3 Essai Stimulation Ablation 2 (ESTIMABL2) trial, in which 730 patients at 35 centers in France with low-risk DTC scheduled to undergo thyroidectomy were enrolled between May 2013 and March 2017.
Patients were randomized to receive either postoperative radioiodine ablation (1.1 GBq) after injections of recombinant human thyrotropin (n = 363) or no postoperative radioiodine (n = 367).
Patients were a mean age of 52 years and 83% were women. About 96% had papillary tumors, and pathological tumor node (pTN) stages were mostly pT1b thyroid with a nodal status of N0 or Nx (81.1%). It is these patients in particular in whom retrospective studies of the use of radioiodine ablation have yielded inconsistent results, Dr. Leboulleux and colleagues noted. Hence, their decision to look at this prospectively.
Outcomes were based on the groups’ rates of events, defined as the presence of abnormal foci of radioiodine uptake on whole-body scanning that required treatment (in the radioiodine group only), abnormal findings on neck ultrasonography, or increased levels of thyroglobulin or thyroglobulin antibodies.
After a 3-year follow-up, the rates of having no events in both groups were very high – and nearly identical – at 95.6% among those receiving no radioiodine ablation and 95.9% in the radioiodine group, for a between-group difference of –0.3 percentage points, which met the criteria for noninferiority for the no-radioiodine group.
Likewise, the events that did occur were nearly equally split between the no-radioiodine group (16 events, 4.4%) and the radioiodine group (15 events, 4.1%).
Among patients who had events, subsequent treatments, including surgery, radioiodine administration, or both, were necessary for four patients in the no-radioiodine group and 10 in the radioiodine group, and additional treatments were not necessary for the other patients who experienced events.
There were no differences between those who did and did not experience events in terms of molecular alterations, and 50 of the tumors had BRAF mutations, with no significant differences between groups.
Of the adverse events that occurred in 30 patients, none were determined to be related to treatment, and there were no thyroid-related deaths.
The recurrence rates align with the rates observed overall with low-risk thyroid cancer, the authors noted.
“We observed that less than 5% of the patients in the two groups had events that included abnormal findings on whole-body scanning or neck ultrasonography or elevated levels of thyroglobulin or thyroglobulin antibodies during the first 3 years of follow-up,” they reported.
“This rate is concordant with the definition of low-risk thyroid cancer, and our trial showed that the risk of events was not higher in the absence of postoperative administration of radioiodine.”
Patients spared costs, work losses
Dr. Cooper elaborated on the advantages, for patients, of avoiding radioiodine ablation.
For one thing, the recombinant human TSH that is necessary to prepare for radioiodine therapy is very expensive, ranging from $2,000 to $3,000, with patients often having a copay, he explained.
“Patients usually have to take time off work, which is also an expense to society and to them if they don’t get paid for days that they don’t work,” Dr. Cooper added.
A possible study limitation is the question of whether 3 years is an ample follow-up period to detect events. However, Dr. Cooper said he considers the period to be sufficient.
“As the authors point out, most recurrences of thyroid cancer are detected within the first 3-5 years of initial treatment, so ... the 3-year window is still clinically relevant,” he said.
Regarding the study’s inclusion of centers only in France, Dr. Cooper added, “I do not think that this is a study limitation. There is nothing specific about the French population that would lead me to conclude that the results were not generalizable to all populations with low-risk papillary thyroid cancer.”
Some continue radioiodine use, but lobectomies add to decline
Despite the mounting evidence of the lack of benefit of radioiodine ablation in low-risk patients, some centers, particularly in Europe, continue the practice, which was standard in the treatment of DTC until relatively recently.
“[While] U.S. guidelines changed in 2015 in favor of no radioiodine in low-risk differentiated thyroid cancer patients, this study should help to change European guidelines,” Dr. Leboulleux said. “The results will help to change practice both in the U.S. and in Europe.”
In addition to awareness of guidelines and new evidence, another reason for the decline in radioiodine ablation for low-risk DTC is the increasing use of thyroid lobectomy, which does not involve the use of radioiodine ablation, rather than total thyroidectomy, Dr. Cooper noted.
“The [new] NEJM paper will hopefully decrease the inappropriate use of radioiodine in low-risk patients even further,” he concluded.
The study received support from the French Ministry of Health through a grant from the National Cancer Institute. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, suggesting these patients can be spared the previously common treatment.
The study’s take-home message for clinicians should be to “stop systematic radioiodine ablation administration in low-risk thyroid cancer patients,” lead author Sophie Leboulleux, MD, PhD, said in an interview.
The results were first reported at ENDO 2021 and have now been published in the New England Journal of Medicine by Dr. Leboulleux, of the department of nuclear medicine and endocrine oncology, Gustave Roussy Cancer Institute, Villejuif, France, and colleagues.
While American Thyroid Association (ATA) guidelines already indicate that radioiodine ablation is not routinely recommended after thyroidectomy for patients with low-risk thyroid cancer, the guidance is only a “weak recommendation,” supported by “low-quality evidence.”
However, the new findings should give that level of evidence a much-needed boost, said one expert. “I think the main contribution of this paper is to change the evidence level to ‘high quality,’ therefore making the recommendation ‘strong,’ rather than ‘weak,’ ” David S. Cooper, MD, said in an interview.
Dr. Cooper, professor of medicine and radiology at Johns Hopkins University, Baltimore, wrote an editorial that accompanies Dr. Leboulleux’s study.
The ability to safely spare patients the radioiodine ablation step after thyroidectomy has important benefits in terms of cost and convenience, Dr. Cooper stressed.
ESTIMABL2 trial
The new findings are from the prospective, randomized, phase 3 Essai Stimulation Ablation 2 (ESTIMABL2) trial, in which 730 patients at 35 centers in France with low-risk DTC scheduled to undergo thyroidectomy were enrolled between May 2013 and March 2017.
Patients were randomized to receive either postoperative radioiodine ablation (1.1 GBq) after injections of recombinant human thyrotropin (n = 363) or no postoperative radioiodine (n = 367).
Patients were a mean age of 52 years and 83% were women. About 96% had papillary tumors, and pathological tumor node (pTN) stages were mostly pT1b thyroid with a nodal status of N0 or Nx (81.1%). It is these patients in particular in whom retrospective studies of the use of radioiodine ablation have yielded inconsistent results, Dr. Leboulleux and colleagues noted. Hence, their decision to look at this prospectively.
Outcomes were based on the groups’ rates of events, defined as the presence of abnormal foci of radioiodine uptake on whole-body scanning that required treatment (in the radioiodine group only), abnormal findings on neck ultrasonography, or increased levels of thyroglobulin or thyroglobulin antibodies.
After a 3-year follow-up, the rates of having no events in both groups were very high – and nearly identical – at 95.6% among those receiving no radioiodine ablation and 95.9% in the radioiodine group, for a between-group difference of –0.3 percentage points, which met the criteria for noninferiority for the no-radioiodine group.
Likewise, the events that did occur were nearly equally split between the no-radioiodine group (16 events, 4.4%) and the radioiodine group (15 events, 4.1%).
Among patients who had events, subsequent treatments, including surgery, radioiodine administration, or both, were necessary for four patients in the no-radioiodine group and 10 in the radioiodine group, and additional treatments were not necessary for the other patients who experienced events.
There were no differences between those who did and did not experience events in terms of molecular alterations, and 50 of the tumors had BRAF mutations, with no significant differences between groups.
Of the adverse events that occurred in 30 patients, none were determined to be related to treatment, and there were no thyroid-related deaths.
The recurrence rates align with the rates observed overall with low-risk thyroid cancer, the authors noted.
“We observed that less than 5% of the patients in the two groups had events that included abnormal findings on whole-body scanning or neck ultrasonography or elevated levels of thyroglobulin or thyroglobulin antibodies during the first 3 years of follow-up,” they reported.
“This rate is concordant with the definition of low-risk thyroid cancer, and our trial showed that the risk of events was not higher in the absence of postoperative administration of radioiodine.”
Patients spared costs, work losses
Dr. Cooper elaborated on the advantages, for patients, of avoiding radioiodine ablation.
For one thing, the recombinant human TSH that is necessary to prepare for radioiodine therapy is very expensive, ranging from $2,000 to $3,000, with patients often having a copay, he explained.
“Patients usually have to take time off work, which is also an expense to society and to them if they don’t get paid for days that they don’t work,” Dr. Cooper added.
A possible study limitation is the question of whether 3 years is an ample follow-up period to detect events. However, Dr. Cooper said he considers the period to be sufficient.
“As the authors point out, most recurrences of thyroid cancer are detected within the first 3-5 years of initial treatment, so ... the 3-year window is still clinically relevant,” he said.
Regarding the study’s inclusion of centers only in France, Dr. Cooper added, “I do not think that this is a study limitation. There is nothing specific about the French population that would lead me to conclude that the results were not generalizable to all populations with low-risk papillary thyroid cancer.”
Some continue radioiodine use, but lobectomies add to decline
Despite the mounting evidence of the lack of benefit of radioiodine ablation in low-risk patients, some centers, particularly in Europe, continue the practice, which was standard in the treatment of DTC until relatively recently.
“[While] U.S. guidelines changed in 2015 in favor of no radioiodine in low-risk differentiated thyroid cancer patients, this study should help to change European guidelines,” Dr. Leboulleux said. “The results will help to change practice both in the U.S. and in Europe.”
In addition to awareness of guidelines and new evidence, another reason for the decline in radioiodine ablation for low-risk DTC is the increasing use of thyroid lobectomy, which does not involve the use of radioiodine ablation, rather than total thyroidectomy, Dr. Cooper noted.
“The [new] NEJM paper will hopefully decrease the inappropriate use of radioiodine in low-risk patients even further,” he concluded.
The study received support from the French Ministry of Health through a grant from the National Cancer Institute. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, suggesting these patients can be spared the previously common treatment.
The study’s take-home message for clinicians should be to “stop systematic radioiodine ablation administration in low-risk thyroid cancer patients,” lead author Sophie Leboulleux, MD, PhD, said in an interview.
The results were first reported at ENDO 2021 and have now been published in the New England Journal of Medicine by Dr. Leboulleux, of the department of nuclear medicine and endocrine oncology, Gustave Roussy Cancer Institute, Villejuif, France, and colleagues.
While American Thyroid Association (ATA) guidelines already indicate that radioiodine ablation is not routinely recommended after thyroidectomy for patients with low-risk thyroid cancer, the guidance is only a “weak recommendation,” supported by “low-quality evidence.”
However, the new findings should give that level of evidence a much-needed boost, said one expert. “I think the main contribution of this paper is to change the evidence level to ‘high quality,’ therefore making the recommendation ‘strong,’ rather than ‘weak,’ ” David S. Cooper, MD, said in an interview.
Dr. Cooper, professor of medicine and radiology at Johns Hopkins University, Baltimore, wrote an editorial that accompanies Dr. Leboulleux’s study.
The ability to safely spare patients the radioiodine ablation step after thyroidectomy has important benefits in terms of cost and convenience, Dr. Cooper stressed.
ESTIMABL2 trial
The new findings are from the prospective, randomized, phase 3 Essai Stimulation Ablation 2 (ESTIMABL2) trial, in which 730 patients at 35 centers in France with low-risk DTC scheduled to undergo thyroidectomy were enrolled between May 2013 and March 2017.
Patients were randomized to receive either postoperative radioiodine ablation (1.1 GBq) after injections of recombinant human thyrotropin (n = 363) or no postoperative radioiodine (n = 367).
Patients were a mean age of 52 years and 83% were women. About 96% had papillary tumors, and pathological tumor node (pTN) stages were mostly pT1b thyroid with a nodal status of N0 or Nx (81.1%). It is these patients in particular in whom retrospective studies of the use of radioiodine ablation have yielded inconsistent results, Dr. Leboulleux and colleagues noted. Hence, their decision to look at this prospectively.
Outcomes were based on the groups’ rates of events, defined as the presence of abnormal foci of radioiodine uptake on whole-body scanning that required treatment (in the radioiodine group only), abnormal findings on neck ultrasonography, or increased levels of thyroglobulin or thyroglobulin antibodies.
After a 3-year follow-up, the rates of having no events in both groups were very high – and nearly identical – at 95.6% among those receiving no radioiodine ablation and 95.9% in the radioiodine group, for a between-group difference of –0.3 percentage points, which met the criteria for noninferiority for the no-radioiodine group.
Likewise, the events that did occur were nearly equally split between the no-radioiodine group (16 events, 4.4%) and the radioiodine group (15 events, 4.1%).
Among patients who had events, subsequent treatments, including surgery, radioiodine administration, or both, were necessary for four patients in the no-radioiodine group and 10 in the radioiodine group, and additional treatments were not necessary for the other patients who experienced events.
There were no differences between those who did and did not experience events in terms of molecular alterations, and 50 of the tumors had BRAF mutations, with no significant differences between groups.
Of the adverse events that occurred in 30 patients, none were determined to be related to treatment, and there were no thyroid-related deaths.
The recurrence rates align with the rates observed overall with low-risk thyroid cancer, the authors noted.
“We observed that less than 5% of the patients in the two groups had events that included abnormal findings on whole-body scanning or neck ultrasonography or elevated levels of thyroglobulin or thyroglobulin antibodies during the first 3 years of follow-up,” they reported.
“This rate is concordant with the definition of low-risk thyroid cancer, and our trial showed that the risk of events was not higher in the absence of postoperative administration of radioiodine.”
Patients spared costs, work losses
Dr. Cooper elaborated on the advantages, for patients, of avoiding radioiodine ablation.
For one thing, the recombinant human TSH that is necessary to prepare for radioiodine therapy is very expensive, ranging from $2,000 to $3,000, with patients often having a copay, he explained.
“Patients usually have to take time off work, which is also an expense to society and to them if they don’t get paid for days that they don’t work,” Dr. Cooper added.
A possible study limitation is the question of whether 3 years is an ample follow-up period to detect events. However, Dr. Cooper said he considers the period to be sufficient.
“As the authors point out, most recurrences of thyroid cancer are detected within the first 3-5 years of initial treatment, so ... the 3-year window is still clinically relevant,” he said.
Regarding the study’s inclusion of centers only in France, Dr. Cooper added, “I do not think that this is a study limitation. There is nothing specific about the French population that would lead me to conclude that the results were not generalizable to all populations with low-risk papillary thyroid cancer.”
Some continue radioiodine use, but lobectomies add to decline
Despite the mounting evidence of the lack of benefit of radioiodine ablation in low-risk patients, some centers, particularly in Europe, continue the practice, which was standard in the treatment of DTC until relatively recently.
“[While] U.S. guidelines changed in 2015 in favor of no radioiodine in low-risk differentiated thyroid cancer patients, this study should help to change European guidelines,” Dr. Leboulleux said. “The results will help to change practice both in the U.S. and in Europe.”
In addition to awareness of guidelines and new evidence, another reason for the decline in radioiodine ablation for low-risk DTC is the increasing use of thyroid lobectomy, which does not involve the use of radioiodine ablation, rather than total thyroidectomy, Dr. Cooper noted.
“The [new] NEJM paper will hopefully decrease the inappropriate use of radioiodine in low-risk patients even further,” he concluded.
The study received support from the French Ministry of Health through a grant from the National Cancer Institute. The authors have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Evaluating phantom hCG and low-level hCG elevations in the nonpregnant patient
A human chorionic gonadotropin (hCG) test is commonly ordered by gynecologists prior to surgical procedures, in the workup of bleeding abnormalities, and in the follow-up of ectopic and molar pregnancies, to name a few indications. In doing so, occasionally clinicians will find themselves in the diagnostic dilemma of discovering an inexplicable low-level elevation in hCG, such as in a postmenopausal patient. This clinical picture can be confusing and can be concerning for conditions such as postmolar gestational trophoblastic neoplasia (GTN). However, there can be benign causes of this phenomenon.1 To prevent unnecessary worry, investigation of treatments is important. In fact, misdiagnosis and inappropriate treatment of benign, low-level hCG levels with unnecessary chemotherapy is problematic mismanagement of gestational trophoblastic disease (GTD), and a major cause of litigation.

Human chorionic gonadotropin is a glycoprotein hormone with two subunits (alpha and beta). It can come from multiple sources, including trophoblastic cells, malignant trophoblastic cells, the pituitary gland, and exogenous sources.1 Its alpha-subunit is identical to that of follicle stimulating hormone (FSH), luteinizing hormone (LH), and thyroid-stimulating hormone (TSH). Its beta-subunit is unique, though very similar to that of LH. The free hCG beta subunit can be produced by nontrophoblastic neoplasms. The gene for the beta subunit of hCG is in close proximity to the beta subunit of LH and increases in gonadotropin-releasing hormone (GnRH) in menopause can result in the stimulation of both genes. Understanding the sources of hCG-like glycoproteins and mechanisms for testing is important when considering possible causes for falsely elevated hCG.
Most commercially available serum hCG assays detect normal intact hCG and free beta subunits. They are typically sandwich assays utilizing antibody binding sites in which a solid-phase anti-hCG antibody to a specific hCG target is then mixed with the patient’s serum, trapping or binding the hCG, which is then treated with an indicator antibody. After being washed with the indicator or “capture” antibody, its relative (quantitative) levels can be measured.1
Urine hCG testing (such as urine pregnancy tests) work through capillary action, drawing the patient’s urine across absorbent pads before reaching a pad which contains anti-hCG antibodies (the detection zone) in the test line. These tests are less sensitive than serum tests, but many can detect hCG levels <15-20 mIU/mL.1
When ob.gyns. are asked to consult on or evaluate persistently low-level elevations of hCG in nonpregnant patients they should consider both malignant and nonmalignant etiologies. Malignant causes include GTN or quiescent GTD (e.g., after treatment of a molar pregnancy or GTN), choriocarcinoma (e.g., ovarian germ cell tumors), and nonchoriocarcinoma malignancies (such as cervical, pancreatic, breast, renal). Nonmalignant causes of hCG elevations in nonpregnant patients include pituitary hCG (in postmenopausal patients), exogenous hCG, and phantom hCG.
The first step in diagnostic workup is to perform a urine pregnancy test. Provided that the serum hCG level is > 20 mIU/mL, the urine HCG should be positive unless the cause of elevated levels is “phantom hCG” from heterophilic antibodies. When patients are exposed to animal antigens (such as in vaccines) they can develop antibodies such as human anti-mouse antibody. These antibodies have affinity to the binding antibodies used in many hCG sandwich assays and form a linkage between the solid phase antibody and the detection antibody creating a false-positive result. This false-positive test is only present in serum testing but not urine tests because the patient’s heterophilic antibodies are not excreted by the kidney and thus not available to create a false-positive result. An alternative method to make the diagnosis of phantom hCG is to request that the hCG testing be run at a different lab with a different assay (which may not react with the same affinity to the patient’s anti-animal heterophile antibodies), or to request that the lab perform serial dilutions. If phantom hCG from heterophile antibodies is at play, serial dilutions will result in a nonlinear dilution response.
If the patient’s urine hCG test is positive, then pregnancy should be ruled out with a transvaginal ultrasound. If negative, an ectopic pregnancy should still be considered (unless not medically plausible, such as in postmenopausal women or women who have undergone hysterectomy). In the absence of an intrauterine or ectopic pregnancy, a positive serum and urine pregnancy test could be from exogenous hCG, from malignancy or pituitary hCG. Use of exogenous hCG can be ruled out by taking a thorough history, with particular focus on asking about weight loss medications and muscle building therapies.
If pregnancy and exogenous hCG are ruled out, clinicians should assess for an occult hCG-secreting malignancy. The lab should be asked to measure the proportion of the free beta subunit of hCG, as this is typically what is secreted by malignancies. CT imaging of the chest, abdomen, and pelvis to search for an occult primary tumor should take place. If the patient has been recently treated for molar pregnancy or GTN, and serum hCG levels reside between 100 and 300 mIU/mL, quiescent GTD should be considered the diagnosis. Determination of the proportion of hyperglycosylated hCG to total hCG can help differentiate active choriocarcinoma from quiescent GTD. After restaging imaging has been done to confirm no measurable metastatic foci, observation can follow with monthly hCG measurements. The majority of these cases will eventually resolve without intervention within a year. Quiescent GTD and persistent low-level HCG in the absence of measurable GTN on imaging or symptoms does not require treatment with chemotherapy or hysterectomy, particularly in women who desire future fertility.2
Once occult malignancy has been ruled out, the remaining potential source of hCG is the pituitary gland. As mentioned earlier, hCG shares its morphology with TSH, LH, and FSH. This can result in cross reactivity and false positives. In the menopausal state, GnRH levels increase and thus so do pituitary LH and hCG levels. To confirm that the pituitary is the source of the low-level hCG levels, the provider should prescribe a course of hormonal treatment such as an oral contraceptive pill for a 2- to 3-month period. This should result in suppression of pituitary hCG, and serum hCG levels, as part of a negative feedback loop. Pituitary source of hCG is a benign condition, and, like quiescent GTD, phantom hCG or exogenous hCG does not require intervention.
Getting to the bottom of persistent low-level hCG elevations can be challenging. By following the step-wise algorithm listed here, clinicians can sequentially test for urine hCG, heterophilic antibodies, elevated free beta-subunit, occult malignancy, and pituitary hCG.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest. Email her at [email protected].
References
1. Oyatogun O et al. Ther Adv Reprod Health 2021 Jun 13. doi: 10.1177/2F26334941211016412.
2. Soper JT. Obstet Gynecol. 2021 Feb 1;137(2):355-70.
A human chorionic gonadotropin (hCG) test is commonly ordered by gynecologists prior to surgical procedures, in the workup of bleeding abnormalities, and in the follow-up of ectopic and molar pregnancies, to name a few indications. In doing so, occasionally clinicians will find themselves in the diagnostic dilemma of discovering an inexplicable low-level elevation in hCG, such as in a postmenopausal patient. This clinical picture can be confusing and can be concerning for conditions such as postmolar gestational trophoblastic neoplasia (GTN). However, there can be benign causes of this phenomenon.1 To prevent unnecessary worry, investigation of treatments is important. In fact, misdiagnosis and inappropriate treatment of benign, low-level hCG levels with unnecessary chemotherapy is problematic mismanagement of gestational trophoblastic disease (GTD), and a major cause of litigation.
Human chorionic gonadotropin is a glycoprotein hormone with two subunits (alpha and beta). It can come from multiple sources, including trophoblastic cells, malignant trophoblastic cells, the pituitary gland, and exogenous sources.1 Its alpha-subunit is identical to that of follicle stimulating hormone (FSH), luteinizing hormone (LH), and thyroid-stimulating hormone (TSH). Its beta-subunit is unique, though very similar to that of LH. The free hCG beta subunit can be produced by nontrophoblastic neoplasms. The gene for the beta subunit of hCG is in close proximity to the beta subunit of LH and increases in gonadotropin-releasing hormone (GnRH) in menopause can result in the stimulation of both genes. Understanding the sources of hCG-like glycoproteins and mechanisms for testing is important when considering possible causes for falsely elevated hCG.
Most commercially available serum hCG assays detect normal intact hCG and free beta subunits. They are typically sandwich assays utilizing antibody binding sites in which a solid-phase anti-hCG antibody to a specific hCG target is then mixed with the patient’s serum, trapping or binding the hCG, which is then treated with an indicator antibody. After being washed with the indicator or “capture” antibody, its relative (quantitative) levels can be measured.1
Urine hCG testing (such as urine pregnancy tests) work through capillary action, drawing the patient’s urine across absorbent pads before reaching a pad which contains anti-hCG antibodies (the detection zone) in the test line. These tests are less sensitive than serum tests, but many can detect hCG levels <15-20 mIU/mL.1
When ob.gyns. are asked to consult on or evaluate persistently low-level elevations of hCG in nonpregnant patients they should consider both malignant and nonmalignant etiologies. Malignant causes include GTN or quiescent GTD (e.g., after treatment of a molar pregnancy or GTN), choriocarcinoma (e.g., ovarian germ cell tumors), and nonchoriocarcinoma malignancies (such as cervical, pancreatic, breast, renal). Nonmalignant causes of hCG elevations in nonpregnant patients include pituitary hCG (in postmenopausal patients), exogenous hCG, and phantom hCG.
The first step in diagnostic workup is to perform a urine pregnancy test. Provided that the serum hCG level is > 20 mIU/mL, the urine HCG should be positive unless the cause of elevated levels is “phantom hCG” from heterophilic antibodies. When patients are exposed to animal antigens (such as in vaccines) they can develop antibodies such as human anti-mouse antibody. These antibodies have affinity to the binding antibodies used in many hCG sandwich assays and form a linkage between the solid phase antibody and the detection antibody creating a false-positive result. This false-positive test is only present in serum testing but not urine tests because the patient’s heterophilic antibodies are not excreted by the kidney and thus not available to create a false-positive result. An alternative method to make the diagnosis of phantom hCG is to request that the hCG testing be run at a different lab with a different assay (which may not react with the same affinity to the patient’s anti-animal heterophile antibodies), or to request that the lab perform serial dilutions. If phantom hCG from heterophile antibodies is at play, serial dilutions will result in a nonlinear dilution response.
If the patient’s urine hCG test is positive, then pregnancy should be ruled out with a transvaginal ultrasound. If negative, an ectopic pregnancy should still be considered (unless not medically plausible, such as in postmenopausal women or women who have undergone hysterectomy). In the absence of an intrauterine or ectopic pregnancy, a positive serum and urine pregnancy test could be from exogenous hCG, from malignancy or pituitary hCG. Use of exogenous hCG can be ruled out by taking a thorough history, with particular focus on asking about weight loss medications and muscle building therapies.
If pregnancy and exogenous hCG are ruled out, clinicians should assess for an occult hCG-secreting malignancy. The lab should be asked to measure the proportion of the free beta subunit of hCG, as this is typically what is secreted by malignancies. CT imaging of the chest, abdomen, and pelvis to search for an occult primary tumor should take place. If the patient has been recently treated for molar pregnancy or GTN, and serum hCG levels reside between 100 and 300 mIU/mL, quiescent GTD should be considered the diagnosis. Determination of the proportion of hyperglycosylated hCG to total hCG can help differentiate active choriocarcinoma from quiescent GTD. After restaging imaging has been done to confirm no measurable metastatic foci, observation can follow with monthly hCG measurements. The majority of these cases will eventually resolve without intervention within a year. Quiescent GTD and persistent low-level HCG in the absence of measurable GTN on imaging or symptoms does not require treatment with chemotherapy or hysterectomy, particularly in women who desire future fertility.2
Once occult malignancy has been ruled out, the remaining potential source of hCG is the pituitary gland. As mentioned earlier, hCG shares its morphology with TSH, LH, and FSH. This can result in cross reactivity and false positives. In the menopausal state, GnRH levels increase and thus so do pituitary LH and hCG levels. To confirm that the pituitary is the source of the low-level hCG levels, the provider should prescribe a course of hormonal treatment such as an oral contraceptive pill for a 2- to 3-month period. This should result in suppression of pituitary hCG, and serum hCG levels, as part of a negative feedback loop. Pituitary source of hCG is a benign condition, and, like quiescent GTD, phantom hCG or exogenous hCG does not require intervention.
Getting to the bottom of persistent low-level hCG elevations can be challenging. By following the step-wise algorithm listed here, clinicians can sequentially test for urine hCG, heterophilic antibodies, elevated free beta-subunit, occult malignancy, and pituitary hCG.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest. Email her at [email protected].
References
1. Oyatogun O et al. Ther Adv Reprod Health 2021 Jun 13. doi: 10.1177/2F26334941211016412.
2. Soper JT. Obstet Gynecol. 2021 Feb 1;137(2):355-70.
A human chorionic gonadotropin (hCG) test is commonly ordered by gynecologists prior to surgical procedures, in the workup of bleeding abnormalities, and in the follow-up of ectopic and molar pregnancies, to name a few indications. In doing so, occasionally clinicians will find themselves in the diagnostic dilemma of discovering an inexplicable low-level elevation in hCG, such as in a postmenopausal patient. This clinical picture can be confusing and can be concerning for conditions such as postmolar gestational trophoblastic neoplasia (GTN). However, there can be benign causes of this phenomenon.1 To prevent unnecessary worry, investigation of treatments is important. In fact, misdiagnosis and inappropriate treatment of benign, low-level hCG levels with unnecessary chemotherapy is problematic mismanagement of gestational trophoblastic disease (GTD), and a major cause of litigation.
Human chorionic gonadotropin is a glycoprotein hormone with two subunits (alpha and beta). It can come from multiple sources, including trophoblastic cells, malignant trophoblastic cells, the pituitary gland, and exogenous sources.1 Its alpha-subunit is identical to that of follicle stimulating hormone (FSH), luteinizing hormone (LH), and thyroid-stimulating hormone (TSH). Its beta-subunit is unique, though very similar to that of LH. The free hCG beta subunit can be produced by nontrophoblastic neoplasms. The gene for the beta subunit of hCG is in close proximity to the beta subunit of LH and increases in gonadotropin-releasing hormone (GnRH) in menopause can result in the stimulation of both genes. Understanding the sources of hCG-like glycoproteins and mechanisms for testing is important when considering possible causes for falsely elevated hCG.
Most commercially available serum hCG assays detect normal intact hCG and free beta subunits. They are typically sandwich assays utilizing antibody binding sites in which a solid-phase anti-hCG antibody to a specific hCG target is then mixed with the patient’s serum, trapping or binding the hCG, which is then treated with an indicator antibody. After being washed with the indicator or “capture” antibody, its relative (quantitative) levels can be measured.1
Urine hCG testing (such as urine pregnancy tests) work through capillary action, drawing the patient’s urine across absorbent pads before reaching a pad which contains anti-hCG antibodies (the detection zone) in the test line. These tests are less sensitive than serum tests, but many can detect hCG levels <15-20 mIU/mL.1
When ob.gyns. are asked to consult on or evaluate persistently low-level elevations of hCG in nonpregnant patients they should consider both malignant and nonmalignant etiologies. Malignant causes include GTN or quiescent GTD (e.g., after treatment of a molar pregnancy or GTN), choriocarcinoma (e.g., ovarian germ cell tumors), and nonchoriocarcinoma malignancies (such as cervical, pancreatic, breast, renal). Nonmalignant causes of hCG elevations in nonpregnant patients include pituitary hCG (in postmenopausal patients), exogenous hCG, and phantom hCG.
The first step in diagnostic workup is to perform a urine pregnancy test. Provided that the serum hCG level is > 20 mIU/mL, the urine HCG should be positive unless the cause of elevated levels is “phantom hCG” from heterophilic antibodies. When patients are exposed to animal antigens (such as in vaccines) they can develop antibodies such as human anti-mouse antibody. These antibodies have affinity to the binding antibodies used in many hCG sandwich assays and form a linkage between the solid phase antibody and the detection antibody creating a false-positive result. This false-positive test is only present in serum testing but not urine tests because the patient’s heterophilic antibodies are not excreted by the kidney and thus not available to create a false-positive result. An alternative method to make the diagnosis of phantom hCG is to request that the hCG testing be run at a different lab with a different assay (which may not react with the same affinity to the patient’s anti-animal heterophile antibodies), or to request that the lab perform serial dilutions. If phantom hCG from heterophile antibodies is at play, serial dilutions will result in a nonlinear dilution response.
If the patient’s urine hCG test is positive, then pregnancy should be ruled out with a transvaginal ultrasound. If negative, an ectopic pregnancy should still be considered (unless not medically plausible, such as in postmenopausal women or women who have undergone hysterectomy). In the absence of an intrauterine or ectopic pregnancy, a positive serum and urine pregnancy test could be from exogenous hCG, from malignancy or pituitary hCG. Use of exogenous hCG can be ruled out by taking a thorough history, with particular focus on asking about weight loss medications and muscle building therapies.
If pregnancy and exogenous hCG are ruled out, clinicians should assess for an occult hCG-secreting malignancy. The lab should be asked to measure the proportion of the free beta subunit of hCG, as this is typically what is secreted by malignancies. CT imaging of the chest, abdomen, and pelvis to search for an occult primary tumor should take place. If the patient has been recently treated for molar pregnancy or GTN, and serum hCG levels reside between 100 and 300 mIU/mL, quiescent GTD should be considered the diagnosis. Determination of the proportion of hyperglycosylated hCG to total hCG can help differentiate active choriocarcinoma from quiescent GTD. After restaging imaging has been done to confirm no measurable metastatic foci, observation can follow with monthly hCG measurements. The majority of these cases will eventually resolve without intervention within a year. Quiescent GTD and persistent low-level HCG in the absence of measurable GTN on imaging or symptoms does not require treatment with chemotherapy or hysterectomy, particularly in women who desire future fertility.2
Once occult malignancy has been ruled out, the remaining potential source of hCG is the pituitary gland. As mentioned earlier, hCG shares its morphology with TSH, LH, and FSH. This can result in cross reactivity and false positives. In the menopausal state, GnRH levels increase and thus so do pituitary LH and hCG levels. To confirm that the pituitary is the source of the low-level hCG levels, the provider should prescribe a course of hormonal treatment such as an oral contraceptive pill for a 2- to 3-month period. This should result in suppression of pituitary hCG, and serum hCG levels, as part of a negative feedback loop. Pituitary source of hCG is a benign condition, and, like quiescent GTD, phantom hCG or exogenous hCG does not require intervention.
Getting to the bottom of persistent low-level hCG elevations can be challenging. By following the step-wise algorithm listed here, clinicians can sequentially test for urine hCG, heterophilic antibodies, elevated free beta-subunit, occult malignancy, and pituitary hCG.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest. Email her at [email protected].
References
1. Oyatogun O et al. Ther Adv Reprod Health 2021 Jun 13. doi: 10.1177/2F26334941211016412.
2. Soper JT. Obstet Gynecol. 2021 Feb 1;137(2):355-70.
White House unveils plan to combat endocrine-disrupting PFAS pollution
The federal government is stepping up actions to protect Americans from per- and polyfluoroalkyl substances that continue to threaten health through pollution in the air, water, and foods, according to a statement from the White House on Oct. 18.

The comprehensive plan includes efforts to prevent per- and polyfluoroalkyl substances (PFAS) from being released into the air, drinking and ground water, and the food supply chain, according to the statement. Other efforts will expand cleanup and remediation of the impact of PFAS already present in the environment.
PFAS are a category of endocrine-disrupting chemicals (EDCs) that have been used for decades in a range of consumer products including cookware, stain-resistant clothes, fast food wrappers, treatments for carpets and furniture, and firefighting foams. PFAS can be released into the air, and also into surface water, drinking water, and ground water, because of how they are disposed, according to a 2020 report from the Endocrine Society and the International Pollutants Elimination Network. The report suggested that creation of more plastic products will likely increase exposure to PFAS and other EDCs.
The Environmental Protection Agency will take the lead on the Biden administration’s PFAS reduction efforts. The agency announced a PFAS Roadmap, which outlines actions to control PFAS over the next 3 years. The Roadmap’s goals include keeping PFAS out of the environment, holding polluters accountable for their actions, investing in scientific research to learn more about the impact of PFAS on human health, and prioritizing protection for disadvantaged communities. The EPA described its approach to PFAS as three pronged (Research, Restrict, Remediate). Planned actions noted on the EPA website include publication of a national PFAS testing strategy, establishing an improved review process for new PFAS, reviewing existing PFAS, and enhancing reporting to track sources and quantities of PFAS.
White House statement noted that other agencies committed to controlling PFAS include the Department of Defense, which will conduct cleanups and assessments at DOD and National Guard locations; the Food and Drug Administration, which will to expand its food supply testing to estimate dietary exposure to PFAS; and the Department of Agriculture, which is investigating causes and impacts of PFAS in the food system, and supporting research on environmental contaminants including PFAS.
The Department of Homeland Security has conducted an inventory of PFAS use, notably the use of PFAS in firefighting foams, and established an Emerging Contaminants Working Group to remediate PFAS and other contaminants. In addition, the Department of Health & Human Services monitors the evolving science on human health and PFAS and anticipates a report by the Centers for Disease Control and Prevention on the health effects of PFAS exposure, with data from eight states.
The American Chemistry Council (ACC), a trade association for American chemistry companies, issued a statement in response to the EPA’s PFAS Strategic Roadmap in which they supported the value of science-based regulation, but emphasized that PFAS are distinct from one another, and should not be grouped together for regulation purposes.
“According to EPA, approximately 600 PFAS substances are manufactured or in use today, each with its own unique properties and uses, from cellphones to solar panels, for which alternatives are not always available,” according to the ACC statement. “EPA’s Roadmap reinforces the differences between these chemistries and that they should not all be grouped together.” The newly formed Interagency Policy Committee on PFAS will coordinate PFAS response efforts across agencies and “help develop new policy strategies to support research, remediation, and removal of PFAS in communities across the country,” according to the White House statement.
The federal government is stepping up actions to protect Americans from per- and polyfluoroalkyl substances that continue to threaten health through pollution in the air, water, and foods, according to a statement from the White House on Oct. 18.
The comprehensive plan includes efforts to prevent per- and polyfluoroalkyl substances (PFAS) from being released into the air, drinking and ground water, and the food supply chain, according to the statement. Other efforts will expand cleanup and remediation of the impact of PFAS already present in the environment.
PFAS are a category of endocrine-disrupting chemicals (EDCs) that have been used for decades in a range of consumer products including cookware, stain-resistant clothes, fast food wrappers, treatments for carpets and furniture, and firefighting foams. PFAS can be released into the air, and also into surface water, drinking water, and ground water, because of how they are disposed, according to a 2020 report from the Endocrine Society and the International Pollutants Elimination Network. The report suggested that creation of more plastic products will likely increase exposure to PFAS and other EDCs.
The Environmental Protection Agency will take the lead on the Biden administration’s PFAS reduction efforts. The agency announced a PFAS Roadmap, which outlines actions to control PFAS over the next 3 years. The Roadmap’s goals include keeping PFAS out of the environment, holding polluters accountable for their actions, investing in scientific research to learn more about the impact of PFAS on human health, and prioritizing protection for disadvantaged communities. The EPA described its approach to PFAS as three pronged (Research, Restrict, Remediate). Planned actions noted on the EPA website include publication of a national PFAS testing strategy, establishing an improved review process for new PFAS, reviewing existing PFAS, and enhancing reporting to track sources and quantities of PFAS.
White House statement noted that other agencies committed to controlling PFAS include the Department of Defense, which will conduct cleanups and assessments at DOD and National Guard locations; the Food and Drug Administration, which will to expand its food supply testing to estimate dietary exposure to PFAS; and the Department of Agriculture, which is investigating causes and impacts of PFAS in the food system, and supporting research on environmental contaminants including PFAS.
The Department of Homeland Security has conducted an inventory of PFAS use, notably the use of PFAS in firefighting foams, and established an Emerging Contaminants Working Group to remediate PFAS and other contaminants. In addition, the Department of Health & Human Services monitors the evolving science on human health and PFAS and anticipates a report by the Centers for Disease Control and Prevention on the health effects of PFAS exposure, with data from eight states.
The American Chemistry Council (ACC), a trade association for American chemistry companies, issued a statement in response to the EPA’s PFAS Strategic Roadmap in which they supported the value of science-based regulation, but emphasized that PFAS are distinct from one another, and should not be grouped together for regulation purposes.
“According to EPA, approximately 600 PFAS substances are manufactured or in use today, each with its own unique properties and uses, from cellphones to solar panels, for which alternatives are not always available,” according to the ACC statement. “EPA’s Roadmap reinforces the differences between these chemistries and that they should not all be grouped together.” The newly formed Interagency Policy Committee on PFAS will coordinate PFAS response efforts across agencies and “help develop new policy strategies to support research, remediation, and removal of PFAS in communities across the country,” according to the White House statement.
The federal government is stepping up actions to protect Americans from per- and polyfluoroalkyl substances that continue to threaten health through pollution in the air, water, and foods, according to a statement from the White House on Oct. 18.
The comprehensive plan includes efforts to prevent per- and polyfluoroalkyl substances (PFAS) from being released into the air, drinking and ground water, and the food supply chain, according to the statement. Other efforts will expand cleanup and remediation of the impact of PFAS already present in the environment.
PFAS are a category of endocrine-disrupting chemicals (EDCs) that have been used for decades in a range of consumer products including cookware, stain-resistant clothes, fast food wrappers, treatments for carpets and furniture, and firefighting foams. PFAS can be released into the air, and also into surface water, drinking water, and ground water, because of how they are disposed, according to a 2020 report from the Endocrine Society and the International Pollutants Elimination Network. The report suggested that creation of more plastic products will likely increase exposure to PFAS and other EDCs.
The Environmental Protection Agency will take the lead on the Biden administration’s PFAS reduction efforts. The agency announced a PFAS Roadmap, which outlines actions to control PFAS over the next 3 years. The Roadmap’s goals include keeping PFAS out of the environment, holding polluters accountable for their actions, investing in scientific research to learn more about the impact of PFAS on human health, and prioritizing protection for disadvantaged communities. The EPA described its approach to PFAS as three pronged (Research, Restrict, Remediate). Planned actions noted on the EPA website include publication of a national PFAS testing strategy, establishing an improved review process for new PFAS, reviewing existing PFAS, and enhancing reporting to track sources and quantities of PFAS.
White House statement noted that other agencies committed to controlling PFAS include the Department of Defense, which will conduct cleanups and assessments at DOD and National Guard locations; the Food and Drug Administration, which will to expand its food supply testing to estimate dietary exposure to PFAS; and the Department of Agriculture, which is investigating causes and impacts of PFAS in the food system, and supporting research on environmental contaminants including PFAS.
The Department of Homeland Security has conducted an inventory of PFAS use, notably the use of PFAS in firefighting foams, and established an Emerging Contaminants Working Group to remediate PFAS and other contaminants. In addition, the Department of Health & Human Services monitors the evolving science on human health and PFAS and anticipates a report by the Centers for Disease Control and Prevention on the health effects of PFAS exposure, with data from eight states.
The American Chemistry Council (ACC), a trade association for American chemistry companies, issued a statement in response to the EPA’s PFAS Strategic Roadmap in which they supported the value of science-based regulation, but emphasized that PFAS are distinct from one another, and should not be grouped together for regulation purposes.
“According to EPA, approximately 600 PFAS substances are manufactured or in use today, each with its own unique properties and uses, from cellphones to solar panels, for which alternatives are not always available,” according to the ACC statement. “EPA’s Roadmap reinforces the differences between these chemistries and that they should not all be grouped together.” The newly formed Interagency Policy Committee on PFAS will coordinate PFAS response efforts across agencies and “help develop new policy strategies to support research, remediation, and removal of PFAS in communities across the country,” according to the White House statement.
Although inconclusive, CV safety study of cancer therapy attracts attention
The first global trial to compare the cardiovascular (CV) safety of two therapies for prostate cancer proved inconclusive because of inadequate enrollment and events, but the study is a harbinger of growth in the emerging specialty of cardio-oncology, according to experts.

“Many new cancer agents have extended patient survival, yet some of these agents have significant potential cardiovascular toxicity,” said Renato D. Lopes, MD, in presenting a study at the annual congress of the European Society of Cardiology.
In the context of improving survival in patients with or at risk for both cancer and cardiovascular disease, he suggested that the prostate cancer study he led could be “a model for interdisciplinary collaboration” needed to address the relative and sometimes competing risks of these disease states.
This point was seconded by several pioneers in cardio-oncology who participated in the discussion of the results of the trial, called PRONOUNCE.
“We know many drugs in oncology increase cardiovascular risk, so these are the types of trials we need,” according Thomas M. Suter, MD, who leads the cardio-oncology service at the University Hospital, Berne, Switzerland. He was the ESC-invited discussant for PRONOUNCE.
More than 100 centers in 12 countries involved
In PRONOUNCE, 545 patients with prostate cancer and established atherosclerotic cardiovascular disease were randomized to degarelix, a gonadotropin-releasing hormone antagonist, or leuprolide, a GnRH agonist. The patients were enrolled at 113 participating centers in 12 countries. All of the patients had an indication for an androgen-deprivation therapy (ADT).

In numerous previous studies, “ADT has been associated with higher CV morbidity and mortality, particularly in men with preexisting CV disease,” explained Dr. Lopes, but the relative cardiovascular safety of GnRH agonists relative to GnRH antagonists has been “controversial.”
The PRONOUNCE study was designed to resolve this issue, but the study was terminated early because of slow enrollment (not related to the COVID-19 pandemic). The planned enrollment was 900 patients.
In addition, the rate of major adverse cardiovascular events (MACE), defined as myocardial infarction, stroke, or death, was lower over the course of follow-up than anticipated in the study design.
No significant difference on primary endpoint
At the end of 12 months, MACE occurred in 11 (4.1%) of patients randomized to leuprolide and 15 (5.5%) of those randomized to degarelix. The greater hazard ratio for MACE in the degarelix group did not approach statistical significance (hazard ratio, 1.28; P = .53).
As a result, the question of the relative CV safety of these drugs “remains unresolved,” according to Dr. Lopes, professor of medicine at Duke University Medical Center, Durham, N.C.
This does not diminish the need to answer this question. In the addition to the fact that cancer is a malignancy primarily of advancing age when CV disease is prevalent – the mean age in this study was 73 years and 44% were over age 75 – it is often an indolent disease with long periods of survival, according to Dr. Lopes. About half of prostate cancer patients have concomitant CV disease, and about half will receive ADT at some point in their treatment.
In patients receiving ADT, leuprolide is far more commonly used than GnRH antagonists, which are offered in only about 4% of patients, according to data cited by Dr. Lopes. The underlying hypothesis of this study was that leuprolide is associated with greater CV risk, which might have been relevant to a risk-benefit calculation, if the hypothesis had been confirmed.
Cancer drugs can increase CV risk
Based on experimental data, “there is concern the leuprolide is involved in plaque destabilization,” said Dr. Lopes, but he noted that ADTs in general are associated with adverse metabolic changes, including increases in LDL cholesterol, insulin resistance, and body fat, all of which could be relevant to CV risk.
It is the improving rates of survival for prostate cancer as well for other types of cancer that have increased attention to the potential for cancer drugs to increase CV risk, another major cause of early mortality. For these competing risks, objective data are needed to evaluate a relative risk-to-benefit ratio for treatment choices.
This dilemma led the ESC to recently establish its Council on Cardio-Oncology, and many centers around the world are also creating interdisciplinary groups to guide treatment choices for patients with both diseases.
“You will certainly get a lot of referrals,” said Rudolf de Boer, MD, professor of translational cardiology, University Medical Center, Groningen, Netherlands. Basing his remark on his own experience starting a cardio-oncology clinic at his institution, he called this work challenging and agreed that the need for objective data is urgent.
“We need data to provide common ground on which to judge relative risks,” Dr. de Boer said. He also praised the PRONOUNCE investigators for their efforts even if the data failed to answer the question posed.
The PRONOUNCE results were published online in Circulation at the time of Dr. Lopes’s presentation.
The study received funding from Ferring Pharmaceuticals. Dr. Lopes reports financial relationships with Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi. Dr. Suter reports financial relationships with Boehringer Ingelheim, GlaxoSmithKline, and Roche. Dr. de Boer reports financial relationships with AstraZeneca, Abbott, Bristol-Myers Squibb, Novartis, Novo Nordisk, and Roche.
The first global trial to compare the cardiovascular (CV) safety of two therapies for prostate cancer proved inconclusive because of inadequate enrollment and events, but the study is a harbinger of growth in the emerging specialty of cardio-oncology, according to experts.
“Many new cancer agents have extended patient survival, yet some of these agents have significant potential cardiovascular toxicity,” said Renato D. Lopes, MD, in presenting a study at the annual congress of the European Society of Cardiology.
In the context of improving survival in patients with or at risk for both cancer and cardiovascular disease, he suggested that the prostate cancer study he led could be “a model for interdisciplinary collaboration” needed to address the relative and sometimes competing risks of these disease states.
This point was seconded by several pioneers in cardio-oncology who participated in the discussion of the results of the trial, called PRONOUNCE.
“We know many drugs in oncology increase cardiovascular risk, so these are the types of trials we need,” according Thomas M. Suter, MD, who leads the cardio-oncology service at the University Hospital, Berne, Switzerland. He was the ESC-invited discussant for PRONOUNCE.
More than 100 centers in 12 countries involved
In PRONOUNCE, 545 patients with prostate cancer and established atherosclerotic cardiovascular disease were randomized to degarelix, a gonadotropin-releasing hormone antagonist, or leuprolide, a GnRH agonist. The patients were enrolled at 113 participating centers in 12 countries. All of the patients had an indication for an androgen-deprivation therapy (ADT).
In numerous previous studies, “ADT has been associated with higher CV morbidity and mortality, particularly in men with preexisting CV disease,” explained Dr. Lopes, but the relative cardiovascular safety of GnRH agonists relative to GnRH antagonists has been “controversial.”
The PRONOUNCE study was designed to resolve this issue, but the study was terminated early because of slow enrollment (not related to the COVID-19 pandemic). The planned enrollment was 900 patients.
In addition, the rate of major adverse cardiovascular events (MACE), defined as myocardial infarction, stroke, or death, was lower over the course of follow-up than anticipated in the study design.
No significant difference on primary endpoint
At the end of 12 months, MACE occurred in 11 (4.1%) of patients randomized to leuprolide and 15 (5.5%) of those randomized to degarelix. The greater hazard ratio for MACE in the degarelix group did not approach statistical significance (hazard ratio, 1.28; P = .53).
As a result, the question of the relative CV safety of these drugs “remains unresolved,” according to Dr. Lopes, professor of medicine at Duke University Medical Center, Durham, N.C.
This does not diminish the need to answer this question. In the addition to the fact that cancer is a malignancy primarily of advancing age when CV disease is prevalent – the mean age in this study was 73 years and 44% were over age 75 – it is often an indolent disease with long periods of survival, according to Dr. Lopes. About half of prostate cancer patients have concomitant CV disease, and about half will receive ADT at some point in their treatment.
In patients receiving ADT, leuprolide is far more commonly used than GnRH antagonists, which are offered in only about 4% of patients, according to data cited by Dr. Lopes. The underlying hypothesis of this study was that leuprolide is associated with greater CV risk, which might have been relevant to a risk-benefit calculation, if the hypothesis had been confirmed.
Cancer drugs can increase CV risk
Based on experimental data, “there is concern the leuprolide is involved in plaque destabilization,” said Dr. Lopes, but he noted that ADTs in general are associated with adverse metabolic changes, including increases in LDL cholesterol, insulin resistance, and body fat, all of which could be relevant to CV risk.
It is the improving rates of survival for prostate cancer as well for other types of cancer that have increased attention to the potential for cancer drugs to increase CV risk, another major cause of early mortality. For these competing risks, objective data are needed to evaluate a relative risk-to-benefit ratio for treatment choices.
This dilemma led the ESC to recently establish its Council on Cardio-Oncology, and many centers around the world are also creating interdisciplinary groups to guide treatment choices for patients with both diseases.
“You will certainly get a lot of referrals,” said Rudolf de Boer, MD, professor of translational cardiology, University Medical Center, Groningen, Netherlands. Basing his remark on his own experience starting a cardio-oncology clinic at his institution, he called this work challenging and agreed that the need for objective data is urgent.
“We need data to provide common ground on which to judge relative risks,” Dr. de Boer said. He also praised the PRONOUNCE investigators for their efforts even if the data failed to answer the question posed.
The PRONOUNCE results were published online in Circulation at the time of Dr. Lopes’s presentation.
The study received funding from Ferring Pharmaceuticals. Dr. Lopes reports financial relationships with Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi. Dr. Suter reports financial relationships with Boehringer Ingelheim, GlaxoSmithKline, and Roche. Dr. de Boer reports financial relationships with AstraZeneca, Abbott, Bristol-Myers Squibb, Novartis, Novo Nordisk, and Roche.
The first global trial to compare the cardiovascular (CV) safety of two therapies for prostate cancer proved inconclusive because of inadequate enrollment and events, but the study is a harbinger of growth in the emerging specialty of cardio-oncology, according to experts.
“Many new cancer agents have extended patient survival, yet some of these agents have significant potential cardiovascular toxicity,” said Renato D. Lopes, MD, in presenting a study at the annual congress of the European Society of Cardiology.
In the context of improving survival in patients with or at risk for both cancer and cardiovascular disease, he suggested that the prostate cancer study he led could be “a model for interdisciplinary collaboration” needed to address the relative and sometimes competing risks of these disease states.
This point was seconded by several pioneers in cardio-oncology who participated in the discussion of the results of the trial, called PRONOUNCE.
“We know many drugs in oncology increase cardiovascular risk, so these are the types of trials we need,” according Thomas M. Suter, MD, who leads the cardio-oncology service at the University Hospital, Berne, Switzerland. He was the ESC-invited discussant for PRONOUNCE.
More than 100 centers in 12 countries involved
In PRONOUNCE, 545 patients with prostate cancer and established atherosclerotic cardiovascular disease were randomized to degarelix, a gonadotropin-releasing hormone antagonist, or leuprolide, a GnRH agonist. The patients were enrolled at 113 participating centers in 12 countries. All of the patients had an indication for an androgen-deprivation therapy (ADT).
In numerous previous studies, “ADT has been associated with higher CV morbidity and mortality, particularly in men with preexisting CV disease,” explained Dr. Lopes, but the relative cardiovascular safety of GnRH agonists relative to GnRH antagonists has been “controversial.”
The PRONOUNCE study was designed to resolve this issue, but the study was terminated early because of slow enrollment (not related to the COVID-19 pandemic). The planned enrollment was 900 patients.
In addition, the rate of major adverse cardiovascular events (MACE), defined as myocardial infarction, stroke, or death, was lower over the course of follow-up than anticipated in the study design.
No significant difference on primary endpoint
At the end of 12 months, MACE occurred in 11 (4.1%) of patients randomized to leuprolide and 15 (5.5%) of those randomized to degarelix. The greater hazard ratio for MACE in the degarelix group did not approach statistical significance (hazard ratio, 1.28; P = .53).
As a result, the question of the relative CV safety of these drugs “remains unresolved,” according to Dr. Lopes, professor of medicine at Duke University Medical Center, Durham, N.C.
This does not diminish the need to answer this question. In the addition to the fact that cancer is a malignancy primarily of advancing age when CV disease is prevalent – the mean age in this study was 73 years and 44% were over age 75 – it is often an indolent disease with long periods of survival, according to Dr. Lopes. About half of prostate cancer patients have concomitant CV disease, and about half will receive ADT at some point in their treatment.
In patients receiving ADT, leuprolide is far more commonly used than GnRH antagonists, which are offered in only about 4% of patients, according to data cited by Dr. Lopes. The underlying hypothesis of this study was that leuprolide is associated with greater CV risk, which might have been relevant to a risk-benefit calculation, if the hypothesis had been confirmed.
Cancer drugs can increase CV risk
Based on experimental data, “there is concern the leuprolide is involved in plaque destabilization,” said Dr. Lopes, but he noted that ADTs in general are associated with adverse metabolic changes, including increases in LDL cholesterol, insulin resistance, and body fat, all of which could be relevant to CV risk.
It is the improving rates of survival for prostate cancer as well for other types of cancer that have increased attention to the potential for cancer drugs to increase CV risk, another major cause of early mortality. For these competing risks, objective data are needed to evaluate a relative risk-to-benefit ratio for treatment choices.
This dilemma led the ESC to recently establish its Council on Cardio-Oncology, and many centers around the world are also creating interdisciplinary groups to guide treatment choices for patients with both diseases.
“You will certainly get a lot of referrals,” said Rudolf de Boer, MD, professor of translational cardiology, University Medical Center, Groningen, Netherlands. Basing his remark on his own experience starting a cardio-oncology clinic at his institution, he called this work challenging and agreed that the need for objective data is urgent.
“We need data to provide common ground on which to judge relative risks,” Dr. de Boer said. He also praised the PRONOUNCE investigators for their efforts even if the data failed to answer the question posed.
The PRONOUNCE results were published online in Circulation at the time of Dr. Lopes’s presentation.
The study received funding from Ferring Pharmaceuticals. Dr. Lopes reports financial relationships with Bristol-Myers Squibb, GlaxoSmithKline, Medtronic, Pfizer, and Sanofi. Dr. Suter reports financial relationships with Boehringer Ingelheim, GlaxoSmithKline, and Roche. Dr. de Boer reports financial relationships with AstraZeneca, Abbott, Bristol-Myers Squibb, Novartis, Novo Nordisk, and Roche.
FROM ESC 2021
Possible obesity effect detected in cancer death rates
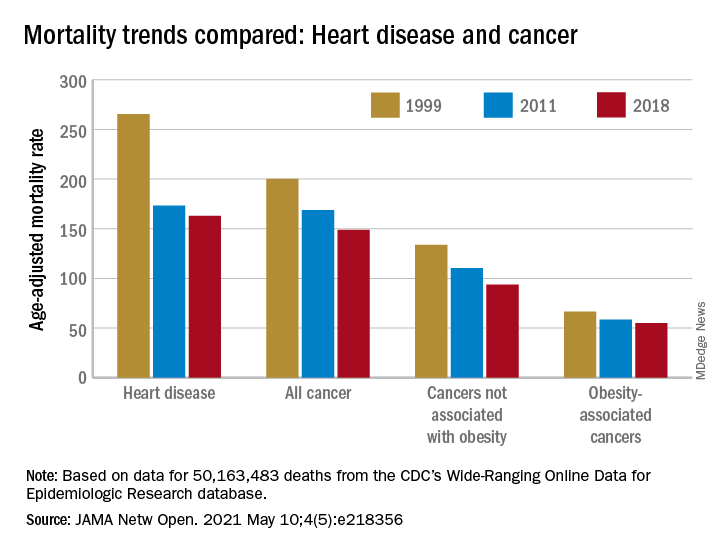
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
“By integrating 20 years of cancer mortality data, we demonstrated that trends in obesity-associated cancer mortality showed signs of recent deceleration, consistent with recent findings for heart disease mortality,” Christy L. Avery, PhD, and associates wrote in JAMA Network Open.
Improvements in mortality related to heart disease slowed after 2011, a phenomenon that has been associated with rising obesity rates. The age-adjusted mortality rate (AAMR) declined at an average of 3.8 deaths per 100,000 persons from 1999 to 2011 but only 0.7 deaths per 100,000 from 2011 to 2018, based on data from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (WONDER).
To understand trends in cancer mortality and their possible connection with obesity, data for 1999-2018 from the WONDER database were divided into obesity-associated and non–obesity-associated categories and compared with heart disease mortality, they explained. The database included more than 50 million deaths that matched inclusion criteria.
The analysis showed there was difference between obesity-associated and non–obesity-associated cancers that was obscured when all cancer deaths were considered together. The average annual change in AAMR for obesity-associated cancers slowed from –1.19 deaths per 100,000 in 1999-2011 to –0.83 in 2011-2018, Dr. Avery and associates reported.
For non–obesity-associated cancers, the annual change in AAMR increased from –1.62 per 100,000 for 1999-2011 to –2.29 for 2011-2018, following the trend for all cancers: –1.48 per 100,000 during 1999-2011 and –1.77 in 2011-2018, they said.
“The largest mortality decreases were observed for melanoma of the skin and lung cancer, two cancers not associated with obesity. For obesity-associated cancers, stable or increasing mortality rates have been observed for liver and pancreatic cancer among both men and women as well as for uterine cancer among women,” the investigators wrote.
Demographically, however, the slowing improvement in mortality for obesity-associated cancers did not follow the trend for heart disease. The deceleration for cancer was more pronounced for women and for non-Hispanic Whites and not seen at all in non-Hispanic Asian/Pacific Islander individuals. “For heart disease, evidence of a deceleration was consistent across sex, race, and ethnicity,” they said.
There are “longstanding disparities in obesity” among various populations in the United States, and the recent trend of obesity occurring earlier in life may be having an effect. “Whether the findings of decelerating mortality rates potentially signal a changing profile of cancer and heart disease mortality as the consequences of the obesity epidemic are realized remains to be seen,” they concluded.
The investigators reported receiving grants from the National Institutes of Health during the conduct of the study, but no other disclosures were reported.
FROM JAMA NETWORK OPEN
AHA statement flags CV risk of hormonal cancer therapies
Hormonal therapies for the treatment of hormone-dependent breast and prostate cancer could raise the risk for myocardial infarction and stroke, and patients need to be closely monitored to allow early detection and treatment of cardiovascular disease (CVD), the American Heart Association says in a new scientific statement.
“The statement provides data on the risks of each type of hormonal therapy so clinicians can use it as a guide to help manage cardiovascular risks during cancer treatment,” Tochi Okwuosa, DO, chair of the writing group, said in a news release.
“A team-based approach to patient care that includes the oncology team, cardiologist, primary care clinician, dietitian, endocrinologist, and other health care professionals as appropriate is needed to work with each patient to manage and reduce the increased risk of heart disease and strokes associated with hormonal therapy in breast and prostate cancer treatment,” said Dr. Okwuosa, director of cardio-oncology services, Rush University Medical Center, Chicago.
The scientific statement was published online April 26 in Circulation: Genomic and Precision Medicine.
Hormone-dependent cancers, such as prostate and breast cancer, are the most common noncutaneous cancers in the United States and around the world. As hormonal therapies have markedly improved survival in these patients, CVD has emerged as a leading cause illness and death.
The increased CVD burden might be explained by the increasing average age of cancer survivors, leading to higher rates of age-related CV risk factors and coronary artery disease.
The writing group reviewed existing evidence from observational studies and randomized controlled trials on the cardiovascular impact of anticancer hormonal therapies.
Among the key findings:
- In patients with breast cancer, has been shown to increase the risk for venous thromboembolic events, but to have somewhat protective to neutral effects on CVD risk burden and CVD events. Conversely, aromatase inhibitors have been shown to increase the risk for CVD risk factors and events, including MI and stroke.
- Androgen-deprivation therapy for prostate cancer appears to increase the risk for CV events, although gonadotrophin-releasing hormone (GnRH) antagonists are associated with a lower risk for CV events than are GnRH agonists. The oral antiandrogens appear to be associated with increased CVD risk as well, particularly when used for complete androgen blockade as combination GnRH/anti-androgen therapy.
- The duration of hormonal therapies has a significant impact on CVD risk; the longer patients receive hormonal therapy, the greater the risk. More research is needed to better define the risks associated with duration of treatment.
- The data are mixed on the impact of preexisting CV risk factors and CVD on CV events associated with hormonal therapy. Although the presence of baseline CV risk factors and CVD can increase CV events associated with aromatase inhibitors, it is not clear that tamoxifen does.
- Studies suggest that patients with prostate cancer and baseline CVD and CV risk factors have increased rates of CV events when treated with androgen-deprivation therapy.
- Although the prolonged use of some hormonal therapies worsens CV risk factors and , the effects of the duration of therapy on CV events are less clear.
The writing group noted that there are no definitive guidelines for the monitoring and management of hormonal therapy-related CVD risks.
The authors encourage clinicians to be alert for worsening CV problems in those with preexisting heart disease or risk factors, and to recognize that even patients without preexisting CV problems are at higher risk because of their exposure to hormonal therapies.
“For patients who have two or more cardiovascular risk factors, it is likely that referral to a cardiologist would be appropriate prior to beginning hormone treatment. For patients already receiving hormonal therapies, a discussion with the oncology team can help to determine if a cardiology referral is recommended,” Dr. Okwuosa said in the news release.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardio-Oncology Subcommittee of the Council on Clinical Cardiology and the Council on Genomic and Precision Medicine; the Council on Arteriosclerosis, Thrombosis, and Vascular Biology; and the Council on Cardiovascular Radiology and Intervention.
The research had no commercial funding. Dr. Okwuosa has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hormonal therapies for the treatment of hormone-dependent breast and prostate cancer could raise the risk for myocardial infarction and stroke, and patients need to be closely monitored to allow early detection and treatment of cardiovascular disease (CVD), the American Heart Association says in a new scientific statement.
“The statement provides data on the risks of each type of hormonal therapy so clinicians can use it as a guide to help manage cardiovascular risks during cancer treatment,” Tochi Okwuosa, DO, chair of the writing group, said in a news release.
“A team-based approach to patient care that includes the oncology team, cardiologist, primary care clinician, dietitian, endocrinologist, and other health care professionals as appropriate is needed to work with each patient to manage and reduce the increased risk of heart disease and strokes associated with hormonal therapy in breast and prostate cancer treatment,” said Dr. Okwuosa, director of cardio-oncology services, Rush University Medical Center, Chicago.
The scientific statement was published online April 26 in Circulation: Genomic and Precision Medicine.
Hormone-dependent cancers, such as prostate and breast cancer, are the most common noncutaneous cancers in the United States and around the world. As hormonal therapies have markedly improved survival in these patients, CVD has emerged as a leading cause illness and death.
The increased CVD burden might be explained by the increasing average age of cancer survivors, leading to higher rates of age-related CV risk factors and coronary artery disease.
The writing group reviewed existing evidence from observational studies and randomized controlled trials on the cardiovascular impact of anticancer hormonal therapies.
Among the key findings:
- In patients with breast cancer, has been shown to increase the risk for venous thromboembolic events, but to have somewhat protective to neutral effects on CVD risk burden and CVD events. Conversely, aromatase inhibitors have been shown to increase the risk for CVD risk factors and events, including MI and stroke.
- Androgen-deprivation therapy for prostate cancer appears to increase the risk for CV events, although gonadotrophin-releasing hormone (GnRH) antagonists are associated with a lower risk for CV events than are GnRH agonists. The oral antiandrogens appear to be associated with increased CVD risk as well, particularly when used for complete androgen blockade as combination GnRH/anti-androgen therapy.
- The duration of hormonal therapies has a significant impact on CVD risk; the longer patients receive hormonal therapy, the greater the risk. More research is needed to better define the risks associated with duration of treatment.
- The data are mixed on the impact of preexisting CV risk factors and CVD on CV events associated with hormonal therapy. Although the presence of baseline CV risk factors and CVD can increase CV events associated with aromatase inhibitors, it is not clear that tamoxifen does.
- Studies suggest that patients with prostate cancer and baseline CVD and CV risk factors have increased rates of CV events when treated with androgen-deprivation therapy.
- Although the prolonged use of some hormonal therapies worsens CV risk factors and , the effects of the duration of therapy on CV events are less clear.
The writing group noted that there are no definitive guidelines for the monitoring and management of hormonal therapy-related CVD risks.
The authors encourage clinicians to be alert for worsening CV problems in those with preexisting heart disease or risk factors, and to recognize that even patients without preexisting CV problems are at higher risk because of their exposure to hormonal therapies.
“For patients who have two or more cardiovascular risk factors, it is likely that referral to a cardiologist would be appropriate prior to beginning hormone treatment. For patients already receiving hormonal therapies, a discussion with the oncology team can help to determine if a cardiology referral is recommended,” Dr. Okwuosa said in the news release.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardio-Oncology Subcommittee of the Council on Clinical Cardiology and the Council on Genomic and Precision Medicine; the Council on Arteriosclerosis, Thrombosis, and Vascular Biology; and the Council on Cardiovascular Radiology and Intervention.
The research had no commercial funding. Dr. Okwuosa has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Hormonal therapies for the treatment of hormone-dependent breast and prostate cancer could raise the risk for myocardial infarction and stroke, and patients need to be closely monitored to allow early detection and treatment of cardiovascular disease (CVD), the American Heart Association says in a new scientific statement.
“The statement provides data on the risks of each type of hormonal therapy so clinicians can use it as a guide to help manage cardiovascular risks during cancer treatment,” Tochi Okwuosa, DO, chair of the writing group, said in a news release.
“A team-based approach to patient care that includes the oncology team, cardiologist, primary care clinician, dietitian, endocrinologist, and other health care professionals as appropriate is needed to work with each patient to manage and reduce the increased risk of heart disease and strokes associated with hormonal therapy in breast and prostate cancer treatment,” said Dr. Okwuosa, director of cardio-oncology services, Rush University Medical Center, Chicago.
The scientific statement was published online April 26 in Circulation: Genomic and Precision Medicine.
Hormone-dependent cancers, such as prostate and breast cancer, are the most common noncutaneous cancers in the United States and around the world. As hormonal therapies have markedly improved survival in these patients, CVD has emerged as a leading cause illness and death.
The increased CVD burden might be explained by the increasing average age of cancer survivors, leading to higher rates of age-related CV risk factors and coronary artery disease.
The writing group reviewed existing evidence from observational studies and randomized controlled trials on the cardiovascular impact of anticancer hormonal therapies.
Among the key findings:
- In patients with breast cancer, has been shown to increase the risk for venous thromboembolic events, but to have somewhat protective to neutral effects on CVD risk burden and CVD events. Conversely, aromatase inhibitors have been shown to increase the risk for CVD risk factors and events, including MI and stroke.
- Androgen-deprivation therapy for prostate cancer appears to increase the risk for CV events, although gonadotrophin-releasing hormone (GnRH) antagonists are associated with a lower risk for CV events than are GnRH agonists. The oral antiandrogens appear to be associated with increased CVD risk as well, particularly when used for complete androgen blockade as combination GnRH/anti-androgen therapy.
- The duration of hormonal therapies has a significant impact on CVD risk; the longer patients receive hormonal therapy, the greater the risk. More research is needed to better define the risks associated with duration of treatment.
- The data are mixed on the impact of preexisting CV risk factors and CVD on CV events associated with hormonal therapy. Although the presence of baseline CV risk factors and CVD can increase CV events associated with aromatase inhibitors, it is not clear that tamoxifen does.
- Studies suggest that patients with prostate cancer and baseline CVD and CV risk factors have increased rates of CV events when treated with androgen-deprivation therapy.
- Although the prolonged use of some hormonal therapies worsens CV risk factors and , the effects of the duration of therapy on CV events are less clear.
The writing group noted that there are no definitive guidelines for the monitoring and management of hormonal therapy-related CVD risks.
The authors encourage clinicians to be alert for worsening CV problems in those with preexisting heart disease or risk factors, and to recognize that even patients without preexisting CV problems are at higher risk because of their exposure to hormonal therapies.
“For patients who have two or more cardiovascular risk factors, it is likely that referral to a cardiologist would be appropriate prior to beginning hormone treatment. For patients already receiving hormonal therapies, a discussion with the oncology team can help to determine if a cardiology referral is recommended,” Dr. Okwuosa said in the news release.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Cardio-Oncology Subcommittee of the Council on Clinical Cardiology and the Council on Genomic and Precision Medicine; the Council on Arteriosclerosis, Thrombosis, and Vascular Biology; and the Council on Cardiovascular Radiology and Intervention.
The research had no commercial funding. Dr. Okwuosa has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
ATA risk stratification for DTC performs well in real-world cohort
NEW ORLEANS – The 2015 American Thyroid Association risk stratification system for patients with differentiated thyroid cancer performed well in a real-world cohort with a high proportion of high-risk patients, according to a study presented at the annual meeting of the Endocrine Society.
“The 2015 ATA Risk Stratification System is an excellent predictor of both persisting disease and survival,” wrote Evert F.S. van Velsen, MD, and his colleagues at Erasmus Medical Center, Rotterdam, the Netherlands, in a poster accompanying the presentation.
Among a group of 236 patients with differentiated thyroid cancer (DTC), Dr. van Velsen and his coauthors looked at how the ATA high-risk criteria influenced patient response to therapy. By the end of the 14-year study period, initial gross extrathyroidal disease extension meant patients were much less likely to have an excellent response (odds ratio, 0.26; P less than .001), and much more likely to have persistent disease (OR, 2.57; P = .001).
Odds of having an excellent response were reduced by having high postoperative thyroglobulin levels (OR, 0.21; P less than .001), and persistent disease was more likely (OR, 2.39; P = .002).
Other high-risk criteria associated with significantly lower odds of excellent response included distant metastases (OR, 0.36), incomplete resection (OR, 0.51), and having follicular thyroid carcinoma (FTC) with extensive vascular invasion (OR, 0.27). All these risk factors also were associated with higher odds of persistent disease.
“Recurrence after no evidence of disease occurred in 14%” of the study population, said Dr. van Velsen and his coauthors, adding, “Clinicians should be aware of the relatively high recurrence risk, even after an excellent response to therapy.”
The study aimed to evaluate the 2015 ATA risk stratification system’s prognostic value in a population that included a relatively large proportion of high-risk DTC patients, to include many FTC patients. This work, they noted, augments previous assessments of the risk stratification system in lower-risk populations.
The authors noted that, in addition to predicting disease recurrence, the risk stratification system also worked as a predictor of disease-specific survival. Patients with structural incomplete response fared the worst, with a survival probability below 0.5 at 200 months on a Kaplan-Meier curve of disease-specific survival. Survival probability remained at 1.0 for patients with excellent response after first therapy and was intermediate for those with indeterminate response and biochemical incomplete response.
Overall mortality was higher in FTC patients. Over the study period, 31 of the 76 FTC patients (41%) died, compared with 39 of the PTC patients (24%; P = .010). In all, 28% of the FTC patients and 18% of the PTC patients died of thyroid cancer, but this difference didn’t reach statistical significance.
The retrospective study included adults with DTC meeting the 2015 ATA high-risk criteria who were diagnosed and/or treated at Erasmus Medical Center over a 13-year span ending in December 2015.
Overall, the investigators found 236 patients meeting inclusion criteria; 160 had papillary thyroid cancer (PTC), and the remaining 76 had FTC. The latter group were significantly older at baseline than PTC patients (64 versus 53 years), and were significantly less likely to undergo neck dissection (22% versus 55%).
In the full cohort, 96 patients (41%) had one high-risk factor, and an additional 74 (31%) had two risk factors. The remaining patients had three or more risk factors.
There was no between-group difference in the likelihood of receiving radioactive iodine treatment, but those with FTC had a lower cumulative radiation dose (195 versus 298 mCi; P less than .001).
More than half of patients (58%) had persistent disease after completing their first therapy. Of these, 51% had structural incomplete response and 7% had biochemical incomplete response. The response was indeterminate for about a quarter of the cohort, and the remaining 17% had an excellent initial response.
By the end of the study period, 55% of patients had persistent disease, and 51% had structural incomplete response (a more likely result for those with FTC than PTC). Just 4% had a biochemical incomplete response, and the response was indeterminate for 16%. Response was judged excellent for 29% of patients.
Dr. van Velsen and his coauthors reported that they had no relevant disclosures.
SOURCE: van Velsen EFS et al. ENDO 2019, Abstract MON-549.
NEW ORLEANS – The 2015 American Thyroid Association risk stratification system for patients with differentiated thyroid cancer performed well in a real-world cohort with a high proportion of high-risk patients, according to a study presented at the annual meeting of the Endocrine Society.
“The 2015 ATA Risk Stratification System is an excellent predictor of both persisting disease and survival,” wrote Evert F.S. van Velsen, MD, and his colleagues at Erasmus Medical Center, Rotterdam, the Netherlands, in a poster accompanying the presentation.
Among a group of 236 patients with differentiated thyroid cancer (DTC), Dr. van Velsen and his coauthors looked at how the ATA high-risk criteria influenced patient response to therapy. By the end of the 14-year study period, initial gross extrathyroidal disease extension meant patients were much less likely to have an excellent response (odds ratio, 0.26; P less than .001), and much more likely to have persistent disease (OR, 2.57; P = .001).
Odds of having an excellent response were reduced by having high postoperative thyroglobulin levels (OR, 0.21; P less than .001), and persistent disease was more likely (OR, 2.39; P = .002).
Other high-risk criteria associated with significantly lower odds of excellent response included distant metastases (OR, 0.36), incomplete resection (OR, 0.51), and having follicular thyroid carcinoma (FTC) with extensive vascular invasion (OR, 0.27). All these risk factors also were associated with higher odds of persistent disease.
“Recurrence after no evidence of disease occurred in 14%” of the study population, said Dr. van Velsen and his coauthors, adding, “Clinicians should be aware of the relatively high recurrence risk, even after an excellent response to therapy.”
The study aimed to evaluate the 2015 ATA risk stratification system’s prognostic value in a population that included a relatively large proportion of high-risk DTC patients, to include many FTC patients. This work, they noted, augments previous assessments of the risk stratification system in lower-risk populations.
The authors noted that, in addition to predicting disease recurrence, the risk stratification system also worked as a predictor of disease-specific survival. Patients with structural incomplete response fared the worst, with a survival probability below 0.5 at 200 months on a Kaplan-Meier curve of disease-specific survival. Survival probability remained at 1.0 for patients with excellent response after first therapy and was intermediate for those with indeterminate response and biochemical incomplete response.
Overall mortality was higher in FTC patients. Over the study period, 31 of the 76 FTC patients (41%) died, compared with 39 of the PTC patients (24%; P = .010). In all, 28% of the FTC patients and 18% of the PTC patients died of thyroid cancer, but this difference didn’t reach statistical significance.
The retrospective study included adults with DTC meeting the 2015 ATA high-risk criteria who were diagnosed and/or treated at Erasmus Medical Center over a 13-year span ending in December 2015.
Overall, the investigators found 236 patients meeting inclusion criteria; 160 had papillary thyroid cancer (PTC), and the remaining 76 had FTC. The latter group were significantly older at baseline than PTC patients (64 versus 53 years), and were significantly less likely to undergo neck dissection (22% versus 55%).
In the full cohort, 96 patients (41%) had one high-risk factor, and an additional 74 (31%) had two risk factors. The remaining patients had three or more risk factors.
There was no between-group difference in the likelihood of receiving radioactive iodine treatment, but those with FTC had a lower cumulative radiation dose (195 versus 298 mCi; P less than .001).
More than half of patients (58%) had persistent disease after completing their first therapy. Of these, 51% had structural incomplete response and 7% had biochemical incomplete response. The response was indeterminate for about a quarter of the cohort, and the remaining 17% had an excellent initial response.
By the end of the study period, 55% of patients had persistent disease, and 51% had structural incomplete response (a more likely result for those with FTC than PTC). Just 4% had a biochemical incomplete response, and the response was indeterminate for 16%. Response was judged excellent for 29% of patients.
Dr. van Velsen and his coauthors reported that they had no relevant disclosures.
SOURCE: van Velsen EFS et al. ENDO 2019, Abstract MON-549.
NEW ORLEANS – The 2015 American Thyroid Association risk stratification system for patients with differentiated thyroid cancer performed well in a real-world cohort with a high proportion of high-risk patients, according to a study presented at the annual meeting of the Endocrine Society.
“The 2015 ATA Risk Stratification System is an excellent predictor of both persisting disease and survival,” wrote Evert F.S. van Velsen, MD, and his colleagues at Erasmus Medical Center, Rotterdam, the Netherlands, in a poster accompanying the presentation.
Among a group of 236 patients with differentiated thyroid cancer (DTC), Dr. van Velsen and his coauthors looked at how the ATA high-risk criteria influenced patient response to therapy. By the end of the 14-year study period, initial gross extrathyroidal disease extension meant patients were much less likely to have an excellent response (odds ratio, 0.26; P less than .001), and much more likely to have persistent disease (OR, 2.57; P = .001).
Odds of having an excellent response were reduced by having high postoperative thyroglobulin levels (OR, 0.21; P less than .001), and persistent disease was more likely (OR, 2.39; P = .002).
Other high-risk criteria associated with significantly lower odds of excellent response included distant metastases (OR, 0.36), incomplete resection (OR, 0.51), and having follicular thyroid carcinoma (FTC) with extensive vascular invasion (OR, 0.27). All these risk factors also were associated with higher odds of persistent disease.
“Recurrence after no evidence of disease occurred in 14%” of the study population, said Dr. van Velsen and his coauthors, adding, “Clinicians should be aware of the relatively high recurrence risk, even after an excellent response to therapy.”
The study aimed to evaluate the 2015 ATA risk stratification system’s prognostic value in a population that included a relatively large proportion of high-risk DTC patients, to include many FTC patients. This work, they noted, augments previous assessments of the risk stratification system in lower-risk populations.
The authors noted that, in addition to predicting disease recurrence, the risk stratification system also worked as a predictor of disease-specific survival. Patients with structural incomplete response fared the worst, with a survival probability below 0.5 at 200 months on a Kaplan-Meier curve of disease-specific survival. Survival probability remained at 1.0 for patients with excellent response after first therapy and was intermediate for those with indeterminate response and biochemical incomplete response.
Overall mortality was higher in FTC patients. Over the study period, 31 of the 76 FTC patients (41%) died, compared with 39 of the PTC patients (24%; P = .010). In all, 28% of the FTC patients and 18% of the PTC patients died of thyroid cancer, but this difference didn’t reach statistical significance.
The retrospective study included adults with DTC meeting the 2015 ATA high-risk criteria who were diagnosed and/or treated at Erasmus Medical Center over a 13-year span ending in December 2015.
Overall, the investigators found 236 patients meeting inclusion criteria; 160 had papillary thyroid cancer (PTC), and the remaining 76 had FTC. The latter group were significantly older at baseline than PTC patients (64 versus 53 years), and were significantly less likely to undergo neck dissection (22% versus 55%).
In the full cohort, 96 patients (41%) had one high-risk factor, and an additional 74 (31%) had two risk factors. The remaining patients had three or more risk factors.
There was no between-group difference in the likelihood of receiving radioactive iodine treatment, but those with FTC had a lower cumulative radiation dose (195 versus 298 mCi; P less than .001).
More than half of patients (58%) had persistent disease after completing their first therapy. Of these, 51% had structural incomplete response and 7% had biochemical incomplete response. The response was indeterminate for about a quarter of the cohort, and the remaining 17% had an excellent initial response.
By the end of the study period, 55% of patients had persistent disease, and 51% had structural incomplete response (a more likely result for those with FTC than PTC). Just 4% had a biochemical incomplete response, and the response was indeterminate for 16%. Response was judged excellent for 29% of patients.
Dr. van Velsen and his coauthors reported that they had no relevant disclosures.
SOURCE: van Velsen EFS et al. ENDO 2019, Abstract MON-549.
REPORTING FROM ENDO 2019
Key clinical point: in a cohort of high-risk patients.
Major finding: Gross extrathyroidal disease extension and high postoperative thyroglobulin levels predicted poor response (OR for excellent response, 0.26 and 0.21, respectively).
Study details: Retrospective single-center study of 236 patients with DTC meeting American Thyroid Association criteria for high risk.
Disclosures: The authors reported no external sources of funding and that they had no conflicts of interest.
Source: van Velsen EFS et al. ENDO 2019, Abstract MON-549.
PCOS linked to increased cancer risk in premenopausal women
based on an analysis of nearly 3.5 million women in a large Swedish database.
Women with PCOS had a sixfold increased risk of endometrial cancer, a tripling of endocrine gland cancers, and more than a doubling in the risk of ovarian and pancreatic cancers. Once women reached menopausal status, however, their cancer risk was comparable to that of women without a history of PCOS.
“Several carcinogenic processes are associated with PCOS, including dyslipidemia, hyperinsulinemia, and chronic inflammation,” wrote Weimin Ye, MD, PhD, of the Karolinska Institutet, Stockholm, and his colleagues. “Our study indicates that cancer may need to be added to the spectrum of long-term health consequences of PCOS and warrants increased surveillance among those patients.”
The research letter was published online in JAMA Oncology.
The team examined the relationship between PCOS and primary cancers in about 3.5 million women over a span of up to 24 years (1985-2009), although the mean follow-up time was not mentioned. To examine the potential impact of menopause, they conducted separate multivariate logistic regression analyses for those younger than 51 years, and those aged 51 years or older. The analyses controlled for use of some medications (metformin, oral contraceptives, and hormone therapy); as well as educational level (a proxy for socioeconomic status); smoking; parity (a proxy for fertility); parental cancers; and diabetes.
Overall, 14,764 women had been diagnosed with PCOS; they were a mean of 28 years at baseline and 182 developed a primary cancer 1 year or more after PCOS diagnosis.
These women had a 15% overall increased risk of cancer, compared with women without PCOS.
The risks for specific cancers also were increased, compared with women without PCOS, including endometrial (hazard ratio, 2.62), ovarian (HR, 2.16), endocrine (HR, 1.92), pancreatic (HR, 3.4), kidney (HR, 3.0), and skeletal and hematopoietic (HR, 1.69) cancers.
The risks were associated with younger age, however. In the group under age 51 years, the overall risk was 22% higher. The increased risk of specific cancers were endometrial (HR, 6.45), ovarian (HR, 2.55), pancreatic (HR, 6.68), kidney (HR, 4.57), and endocrine (not thyroid) gland (HR, 2.9) cancers.
The authors had no relevant financial disclosures.
SOURCE: Yin W et al. JAMA Oncol. 2018 Nov 29. doi:10.1001/jamaoncol.2018.5188.
based on an analysis of nearly 3.5 million women in a large Swedish database.
Women with PCOS had a sixfold increased risk of endometrial cancer, a tripling of endocrine gland cancers, and more than a doubling in the risk of ovarian and pancreatic cancers. Once women reached menopausal status, however, their cancer risk was comparable to that of women without a history of PCOS.
“Several carcinogenic processes are associated with PCOS, including dyslipidemia, hyperinsulinemia, and chronic inflammation,” wrote Weimin Ye, MD, PhD, of the Karolinska Institutet, Stockholm, and his colleagues. “Our study indicates that cancer may need to be added to the spectrum of long-term health consequences of PCOS and warrants increased surveillance among those patients.”
The research letter was published online in JAMA Oncology.
The team examined the relationship between PCOS and primary cancers in about 3.5 million women over a span of up to 24 years (1985-2009), although the mean follow-up time was not mentioned. To examine the potential impact of menopause, they conducted separate multivariate logistic regression analyses for those younger than 51 years, and those aged 51 years or older. The analyses controlled for use of some medications (metformin, oral contraceptives, and hormone therapy); as well as educational level (a proxy for socioeconomic status); smoking; parity (a proxy for fertility); parental cancers; and diabetes.
Overall, 14,764 women had been diagnosed with PCOS; they were a mean of 28 years at baseline and 182 developed a primary cancer 1 year or more after PCOS diagnosis.
These women had a 15% overall increased risk of cancer, compared with women without PCOS.
The risks for specific cancers also were increased, compared with women without PCOS, including endometrial (hazard ratio, 2.62), ovarian (HR, 2.16), endocrine (HR, 1.92), pancreatic (HR, 3.4), kidney (HR, 3.0), and skeletal and hematopoietic (HR, 1.69) cancers.
The risks were associated with younger age, however. In the group under age 51 years, the overall risk was 22% higher. The increased risk of specific cancers were endometrial (HR, 6.45), ovarian (HR, 2.55), pancreatic (HR, 6.68), kidney (HR, 4.57), and endocrine (not thyroid) gland (HR, 2.9) cancers.
The authors had no relevant financial disclosures.
SOURCE: Yin W et al. JAMA Oncol. 2018 Nov 29. doi:10.1001/jamaoncol.2018.5188.
based on an analysis of nearly 3.5 million women in a large Swedish database.
Women with PCOS had a sixfold increased risk of endometrial cancer, a tripling of endocrine gland cancers, and more than a doubling in the risk of ovarian and pancreatic cancers. Once women reached menopausal status, however, their cancer risk was comparable to that of women without a history of PCOS.
“Several carcinogenic processes are associated with PCOS, including dyslipidemia, hyperinsulinemia, and chronic inflammation,” wrote Weimin Ye, MD, PhD, of the Karolinska Institutet, Stockholm, and his colleagues. “Our study indicates that cancer may need to be added to the spectrum of long-term health consequences of PCOS and warrants increased surveillance among those patients.”
The research letter was published online in JAMA Oncology.
The team examined the relationship between PCOS and primary cancers in about 3.5 million women over a span of up to 24 years (1985-2009), although the mean follow-up time was not mentioned. To examine the potential impact of menopause, they conducted separate multivariate logistic regression analyses for those younger than 51 years, and those aged 51 years or older. The analyses controlled for use of some medications (metformin, oral contraceptives, and hormone therapy); as well as educational level (a proxy for socioeconomic status); smoking; parity (a proxy for fertility); parental cancers; and diabetes.
Overall, 14,764 women had been diagnosed with PCOS; they were a mean of 28 years at baseline and 182 developed a primary cancer 1 year or more after PCOS diagnosis.
These women had a 15% overall increased risk of cancer, compared with women without PCOS.
The risks for specific cancers also were increased, compared with women without PCOS, including endometrial (hazard ratio, 2.62), ovarian (HR, 2.16), endocrine (HR, 1.92), pancreatic (HR, 3.4), kidney (HR, 3.0), and skeletal and hematopoietic (HR, 1.69) cancers.
The risks were associated with younger age, however. In the group under age 51 years, the overall risk was 22% higher. The increased risk of specific cancers were endometrial (HR, 6.45), ovarian (HR, 2.55), pancreatic (HR, 6.68), kidney (HR, 4.57), and endocrine (not thyroid) gland (HR, 2.9) cancers.
The authors had no relevant financial disclosures.
SOURCE: Yin W et al. JAMA Oncol. 2018 Nov 29. doi:10.1001/jamaoncol.2018.5188.
FROM JAMA ONCOLOGY
Key clinical point: Polycystic ovarian syndrome may be associated with increased cancer risks among younger women.
Major finding: Among premenopausal women, there was a sixfold increased risk of endometrial cancer, a tripling of endocrine gland cancers, and a more than doubling in the risk of ovarian and pancreatic cancers
Study details: The study examined risks in 3.5 million women with up to 24 years of follow-up.
Disclosures: The study authors had no financial disclosures.
Source: Yin W et al. JAMA Oncol. 2018 Nov 29. doi:10.1001/jamaoncol.2018.5188.
CTCs linked to late recurrence in HER2–, HR+ breast cancer
Circulating tumor cells could be used to stratify patients with hormone receptor (HR)–positive, HER2-negative breast cancer for late recurrence risk, results of a secondary analysis of a randomized clinical trial suggest.
Risk of late clinical recurrence was about 13-fold higher among HR-positive patients with a positive circulating tumor cell (CTC) assay result, according to results of the study, published in JAMA Oncology.
“This prospectively conducted study offers a high level of evidence supporting the association between a positive CTC assay result and risk of clinical recurrence,” said Joseph A. Sparano, MD, of Albert Einstein College of Medicine, New York, and his coauthors.
The present study is the first to show that this CTC assay may play a role in determining late clinical recurrence after local and systemic adjuvant therapy, according to the investigators.
The study is a secondary analysis of E5103, a phase 3 trial of adjuvant doxorubicin and cyclophosphamide followed by paclitaxel with bevacizumab in patients with HER2-negative stage II-III breast cancer. Investigators included a total of 547 patients who had no clinical evidence of recurrence between 4.5 and 7.5 years of registration in that trial.
Positive CTC assay results occurred in 26 of those patients (4.8%), they found.
At a median follow-up of 2.6 years, 24 patients had a clinical recurrence, including 23 HR-positive patients and just 1 HR-negative patient. Accordingly, the investigators focused most of their further analysis on the HR-positive subset.
A total of 7 of 23 patients with HR-positive disease (30.4%) had a positive CTC assay result.
A positive CTC result in HR-positive patients was associated with a 13.1-fold increased risk of recurrence, multivariate analysis showed.
Higher CTC burden appeared to be associated with a numerically higher recurrence risk in HR-positive patients, the investigators found. They saw recurrences in 16 of 335 patients with a CTC count of 0 cells per 7.5 mL blood (4.8%), compared with 2 of 12 patients with 1 cell per 7.5 mL blood (16.7%), and 5 of 6 patients with 2 or more cells per 7.5 mL (83.3%).
Taken together, these results provided proof of concept to support additional investigations of the CTC assay and other blood-based biomarker tests in the setting of late clinical recurrence in HR-positive patients, the researchers said.
They acknowledged several limitations of this study: It was small, it had relatively short follow-up, and it did not evaluate the CTC assay in the context of other assays.
“Notwithstanding proof of concept, further evaluation is required to confirm the clinical validity and determine the clinical utility of performing the CTC assay in this context,” Dr. Sparano and his coauthors wrote.
Late recurrences, or those that occur more than 5 years after diagnosis, account for about half of all recurrences among HR-positive receptive breast cancers, Dr. Sparano and his colleagues said.
The researchers had no conflicts of interest to report. The study was supported by grants from the National Cancer Institute, National Institutes of Health, Breast Cancer Research Foundation, and Susan G. Komen Foundation.
SOURCE: Sparano J et al. JAMA Oncol. 2018 Jul 26. doi: 10.1001/jamaoncol.2018.2574.
Circulating tumor cells could be used to stratify patients with hormone receptor (HR)–positive, HER2-negative breast cancer for late recurrence risk, results of a secondary analysis of a randomized clinical trial suggest.
Risk of late clinical recurrence was about 13-fold higher among HR-positive patients with a positive circulating tumor cell (CTC) assay result, according to results of the study, published in JAMA Oncology.
“This prospectively conducted study offers a high level of evidence supporting the association between a positive CTC assay result and risk of clinical recurrence,” said Joseph A. Sparano, MD, of Albert Einstein College of Medicine, New York, and his coauthors.
The present study is the first to show that this CTC assay may play a role in determining late clinical recurrence after local and systemic adjuvant therapy, according to the investigators.
The study is a secondary analysis of E5103, a phase 3 trial of adjuvant doxorubicin and cyclophosphamide followed by paclitaxel with bevacizumab in patients with HER2-negative stage II-III breast cancer. Investigators included a total of 547 patients who had no clinical evidence of recurrence between 4.5 and 7.5 years of registration in that trial.
Positive CTC assay results occurred in 26 of those patients (4.8%), they found.
At a median follow-up of 2.6 years, 24 patients had a clinical recurrence, including 23 HR-positive patients and just 1 HR-negative patient. Accordingly, the investigators focused most of their further analysis on the HR-positive subset.
A total of 7 of 23 patients with HR-positive disease (30.4%) had a positive CTC assay result.
A positive CTC result in HR-positive patients was associated with a 13.1-fold increased risk of recurrence, multivariate analysis showed.
Higher CTC burden appeared to be associated with a numerically higher recurrence risk in HR-positive patients, the investigators found. They saw recurrences in 16 of 335 patients with a CTC count of 0 cells per 7.5 mL blood (4.8%), compared with 2 of 12 patients with 1 cell per 7.5 mL blood (16.7%), and 5 of 6 patients with 2 or more cells per 7.5 mL (83.3%).
Taken together, these results provided proof of concept to support additional investigations of the CTC assay and other blood-based biomarker tests in the setting of late clinical recurrence in HR-positive patients, the researchers said.
They acknowledged several limitations of this study: It was small, it had relatively short follow-up, and it did not evaluate the CTC assay in the context of other assays.
“Notwithstanding proof of concept, further evaluation is required to confirm the clinical validity and determine the clinical utility of performing the CTC assay in this context,” Dr. Sparano and his coauthors wrote.
Late recurrences, or those that occur more than 5 years after diagnosis, account for about half of all recurrences among HR-positive receptive breast cancers, Dr. Sparano and his colleagues said.
The researchers had no conflicts of interest to report. The study was supported by grants from the National Cancer Institute, National Institutes of Health, Breast Cancer Research Foundation, and Susan G. Komen Foundation.
SOURCE: Sparano J et al. JAMA Oncol. 2018 Jul 26. doi: 10.1001/jamaoncol.2018.2574.
Circulating tumor cells could be used to stratify patients with hormone receptor (HR)–positive, HER2-negative breast cancer for late recurrence risk, results of a secondary analysis of a randomized clinical trial suggest.
Risk of late clinical recurrence was about 13-fold higher among HR-positive patients with a positive circulating tumor cell (CTC) assay result, according to results of the study, published in JAMA Oncology.
“This prospectively conducted study offers a high level of evidence supporting the association between a positive CTC assay result and risk of clinical recurrence,” said Joseph A. Sparano, MD, of Albert Einstein College of Medicine, New York, and his coauthors.
The present study is the first to show that this CTC assay may play a role in determining late clinical recurrence after local and systemic adjuvant therapy, according to the investigators.
The study is a secondary analysis of E5103, a phase 3 trial of adjuvant doxorubicin and cyclophosphamide followed by paclitaxel with bevacizumab in patients with HER2-negative stage II-III breast cancer. Investigators included a total of 547 patients who had no clinical evidence of recurrence between 4.5 and 7.5 years of registration in that trial.
Positive CTC assay results occurred in 26 of those patients (4.8%), they found.
At a median follow-up of 2.6 years, 24 patients had a clinical recurrence, including 23 HR-positive patients and just 1 HR-negative patient. Accordingly, the investigators focused most of their further analysis on the HR-positive subset.
A total of 7 of 23 patients with HR-positive disease (30.4%) had a positive CTC assay result.
A positive CTC result in HR-positive patients was associated with a 13.1-fold increased risk of recurrence, multivariate analysis showed.
Higher CTC burden appeared to be associated with a numerically higher recurrence risk in HR-positive patients, the investigators found. They saw recurrences in 16 of 335 patients with a CTC count of 0 cells per 7.5 mL blood (4.8%), compared with 2 of 12 patients with 1 cell per 7.5 mL blood (16.7%), and 5 of 6 patients with 2 or more cells per 7.5 mL (83.3%).
Taken together, these results provided proof of concept to support additional investigations of the CTC assay and other blood-based biomarker tests in the setting of late clinical recurrence in HR-positive patients, the researchers said.
They acknowledged several limitations of this study: It was small, it had relatively short follow-up, and it did not evaluate the CTC assay in the context of other assays.
“Notwithstanding proof of concept, further evaluation is required to confirm the clinical validity and determine the clinical utility of performing the CTC assay in this context,” Dr. Sparano and his coauthors wrote.
Late recurrences, or those that occur more than 5 years after diagnosis, account for about half of all recurrences among HR-positive receptive breast cancers, Dr. Sparano and his colleagues said.
The researchers had no conflicts of interest to report. The study was supported by grants from the National Cancer Institute, National Institutes of Health, Breast Cancer Research Foundation, and Susan G. Komen Foundation.
SOURCE: Sparano J et al. JAMA Oncol. 2018 Jul 26. doi: 10.1001/jamaoncol.2018.2574.
FROM JAMA ONCOLOGY
Key clinical point: Circulating tumor cells (CTC) may help to evaluate late recurrence risk in patients with HER2-negative breast cancer.
Major finding: A positive CTC result was associated with a 13.1-fold increased risk of recurrence in hormone receptor–positive patients.
Study details: Secondary analysis of a randomized clinical trial including 547 patients with HER2-negative stage II-III breast cancer.
Disclosures: The study was supported by grants from the National Cancer Institute, National Institutes of Health, Breast Cancer Research Foundation, and Susan G. Komen Foundation. The authors reported no conflicts of interest.
Source: Sparano J et al. JAMA Oncol. 2018 Jul 26. doi: 10.1001/jamaoncol.2018.2574.