User login
The Development of a Comprehensive Wound Care Fellowship Curriculum
The Development of a Comprehensive Wound Care Fellowship Curriculum
Often disguised as comorbid conditions, nonhealing and chronic wounds have emerged as a silent epidemic that affects about 6.5 million Americans.1-3 In 2023, estimated US wound care costs were $126.86 billion.4 About 1% to 2% of individuals worldwide will experience a chronic wound in their lifetime. The Veterans Health Administration reported 277,000 inpatient and outpatient encounters for ulcers in 2011, including chronic ulcers of the lower extremity due to diabetes, venous disease, or arterial disease.5 Associated costs of chronic wounds are expected to increase as the populations of developed countries age.6 Effective treatment of chronic wounds requires a nuanced understanding of complex wound pathophysiology, best practices in interdisciplinary and multidisciplinary wound care, and advanced wound care technologies.7,8
The typical 4-year medical school curriculum, followed by residency, offers little in the way of formal didactic training in wound care.9,10 Without specialized and advanced fellowship training dedicated to wound care, health care will lack specialists prepared to manage complex wounds. As a result, wound care-related difficulties may be exacerbated by prolonged recovery time, increased costs, productivity loss, and increased mortality risk.8 Wound care is a growing field of study and practice, and there is a critical need for rigorous training, research, and quality improvement efforts to enhance outcomes for patients with nonhealing wounds.5
One of the most direct ways to address the need for more physicians with specialty training in wound medicine is to implement a comprehensive training curriculum for advanced wound care practice. Although specialized advanced wound care fellowships are available, the curricula primarily detail rotation names and areas for practice without accompanying competencies, milestones, or entrustable professional activities.11 Furthermore, wound care is not recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME).
This article synthesized the literature and integrated innovative, evidence-based practices into a curriculum for a formal advanced fellowship training program. To our knowledge, no comprehensive wound care curriculum is publicly available that includes rotations, competencies, milestones, entrustable professional activities, and 360-degree evaluation forms.
Program Development
The advanced wound care fellowship program started in January 2014 at the Michael E. DeBakey Veterans Affairs Medical Center in affiliation with the Baylor College of Medicine. The fellowship program was originally designed for geriatrics fellows to extend the 1-year fellowship for an additional year to learn wound care. It has been adjusted to address formal program goals and objectives, competencies, milestones, entrustable professional activities, and evaluations, with the goal of developing an example curriculum for wound care fellowships across specialties. Although the ACGME does not recognize a wound care subspecialty, this curriculum complies with the ACGME 1-year fellowship common program requirements.12,13
Scoping Review
A scoping literature review of Google Scholar and PubMed was performed using the medical subject heading terms “wound care + curriculum” and “wound + care + curriculum” to find advanced wound care medical training, fellowship programs, boards, and related ACGME-accredited specialty curricula. The local wound care fellowship program was initially implemented based on an informal literature review by faculty and their respective contributions to curriculum (ie, process establishing wound care-specific competency domains in accordance with ACGME accreditation competency requirements of 1-year fellowships). 12,13 Standing program practice-based competencies and activities were examined and determined to align with best practices. This scoping review considered additional competencies, competency domains, and entrustable professional activities of reputable wound care fellowship training programs (eg, University of Chicago at Illinois and Wake Forest School of Medicine),8,11,14 a specialty wound care board (American Board of Wound Medicine and Surgery),15 an international wound specialist professional society (European Union of Medical Specialists), 16 and recommended curriculum guidelines for wound care residency programs.17 ACGME-accredited specialty and subspecialty milestones professional activities were examined, including vascular surgery,18 plastic surgery,19 dermatology, 20 foot and ankle,21 orthopedic surgery,22 spinal cord injury,23 and geriatric medicine.24
The competencies, milestones, and entrustable professional activities were compiled and redundancies were eliminated. Wound care specialists from geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy examined the findings and suggested eliminating redundancies, irrelevant content, and content that fell below the minimal expected level of competence for an advanced medical specialist in wound care. An expert consensus meeting further refined items presented to the panel before unanimous consensus resulted in the final set of curriculum competencies, milestones, and entrustable professional activities.
Training Program Feedback
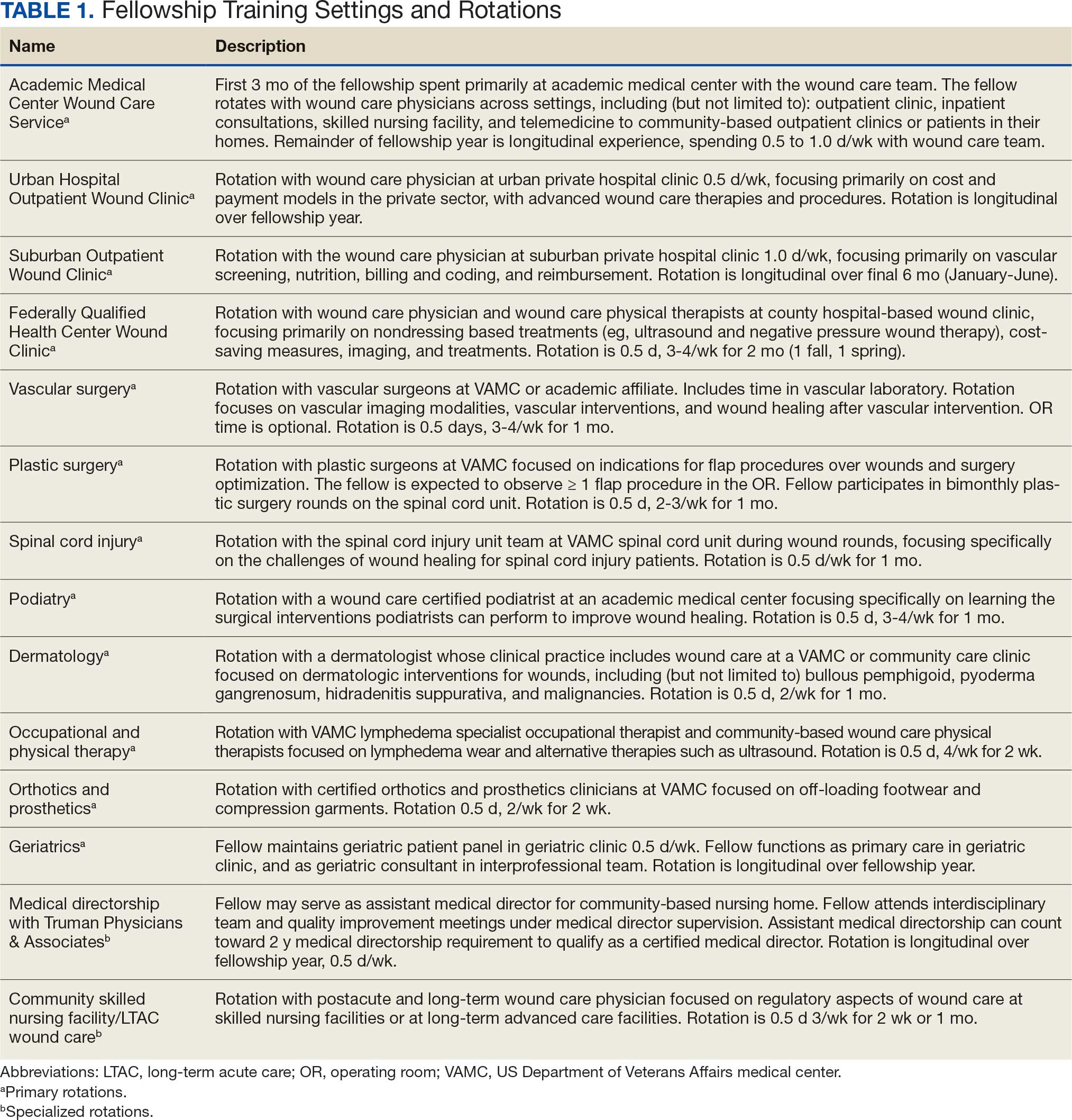
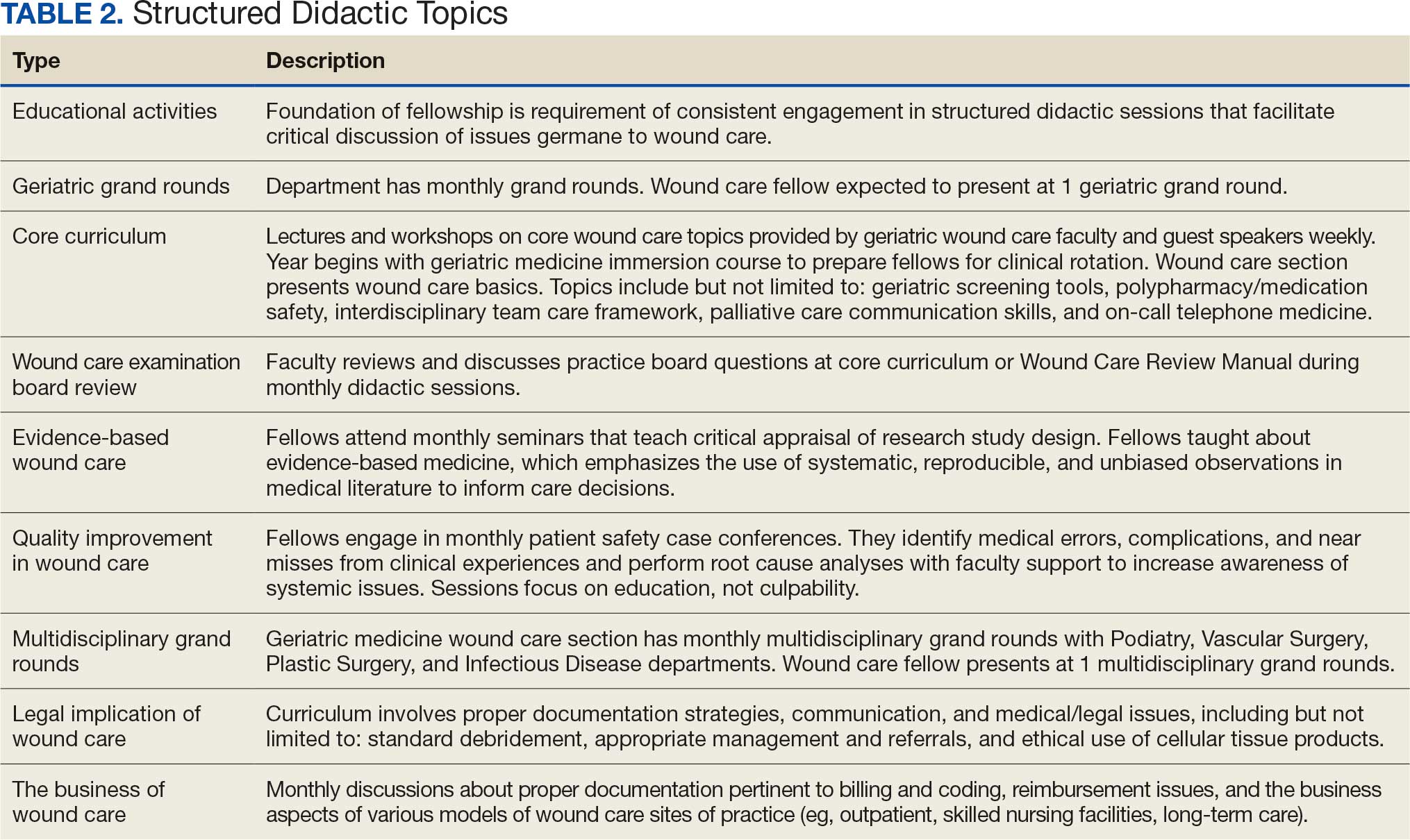
We developed a comprehensive wound care curriculum for an advanced physician fellowship training program based on the streamlined competencies, milestones, and entrustable professional activities (Appendix). Multiple wound care experts from various interdisciplinary backgrounds reached consensus to establish this fellowship curriculum as adaptable for use across training settings. The training program is 12 core rotations and 2 elective rotations (Table 1). Additionally, we developed wound care evaluation forms for faculty-, peer-, and self-assessment of trainees which were adapted from an evidence-based 360-degree evaluation template.25 Suggestions for structured, advanced didactics are in Table 2.
Seventeen fellows have successfully matriculated through the wound care training program. Although wound care certification is not required to work as a wound care specialist, after completion of this fellowship, graduates are able to sit for a wound care certification examination. The American Board of Wound Medicine and Surgery (ABWMS) and the American Board of Wound Management (ABWM) allow physicians to take a certification examination after 1 year of a dedicated wound fellowship program, instead of the typical wound care practice experience ≥ 3 years.
The Clinical Wound Care Fellowship Program collected data for program improvement, and 15 alumni responded (response rate, 88%) to a survey using a 5-point Likert scale. Respondents indicated high mean scores for overall satisfaction (4.7), instructional methods (4.7), program enjoyment (4.7), teaching materials (4.6), and relevance (4.6). All respondents indicated that the fellowship prepared them for a career in wound care as well as their current employment, and 13 of 15 (87%) reported they obtained immediate relevant postfellowship wound care positions and stated that the fellowship prepared them for their current roles. Nine respondents (69%) reported that they were engaged in wound care ≥ 26% of work time. Six respondents (46%) worked in private practice, 3 (23%) at academic medical centers, and 2 (15%) at government- funded hospitals. Four respondents indicated they were board certified in wound care. Program alumni are currently involved in scholarly activities, including 8 in quality improvement and 3 in research.
Discussion
An easily accessible, comprehensive wound care fellowship curriculum has not been previously developed or published. This limited the sources that informed this curriculum. However, the developmental process for this curriculum was robust, as the authors reviewed previously published materials related to wound care, including: 1) descriptive overviews of wound care fellowships; 2) details of month-long rotations for medical students and residents; and 3) practices of the specific environment in which this curriculum was created. Confidence in the practical nature of the curriculum can be assumed, as the experts involved in the development process represented diverse physician specializations, including geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy.
Most wound care clinicians have not completed a formal comprehensive fellowship program. Instead, due to the lack of a comprehensive training curriculum, clinicians have had to use various continuing medical education programs and practice in a wound care setting for ≥ 3 years to be eligible for certification in the specialty. This curriculum will help academic medical centers develop their own fellowship programs, enabling new wound care clinicians to attain certifications more efficiently. As more fellowship programs develop, the goal would be to obtain recognition as an ACGME specialty and standardize the training and competencies for graduates of wound care fellowships.
Conclusions
As new wound care fellowships develop, wound care may become formally acknowledged as its own specialty within medicine and surgery. This will provide wound care with a voice at the national level, particularly in an era of value-based care. Wound care clinicians will be able to advocate for specialty-specific quality metrics and avoid potential penalization for not meeting quality metrics that are irrelevant to wound care.
- Fife CE, Eckert KA, Carter MJ. Publicly Reported wound healing rates: the fantasy and the reality. Adv Wound Care (New Rochelle). 2018;7:77-94. doi:10.1089/wound.2017.0743
- Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care?. Wound Repair Regen. 2010;18:154-158. doi:10.1111/j.1524-475X.2010.00571.x
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771. doi:10.1111/j.1524-475X.2009.00543.x
- Queen D, Harding K. What’s the true costs of wounds faced by different healthcare systems around the world?. Int Wound J. 2023;20:3935-3938. doi:10.1111/iwj.14491
- Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. US Dept of Veterans Affairs; November 2012. https://www.ncbi.nlm.nih.gov/books/NBK132238/
- Simman R, McNevin AJ. Pursuing the path to specialized wound care: the ABWMS perspective. Todays Wound Clin. 2017;8:10,12.
- Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalence in intensive care patients: a cross-sectional study. J Eval Clin Pract. 2008;14:563-568. doi:10.1111/j.1365-2753.2007.00918.x
- Ennis WJ, Valdes W, Meneses P. Wound care specialization: a proposal for a comprehensive fellowship program. Wound Repair Regen. 2004;12:120-128. doi:10.1111/j.1067-1927.2004.012203.x
- Patel NP, Granick MS. Wound education: American medical students are inadequately trained in wound care. Ann Plast Surg. 2007;59:53-55. doi:10.1097/SAP.0b013e31802dd43b
- Patel NP, Granick MS, Kanakaris NK, et al. Comparison of wound education in medical schools in the United States, United Kingdom, and Germany. Eplasty. 2008;8:e8.
- Ennis WJ. Wound care specialization: the current status and future plans to move wound care into the medical community. Adv Wound Care (New Rochelle). 2012;1:184- 188. doi:10.1089/wound.2011.0346
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (fellowship). Updated September 3, 2025. Accessed January 15, 2026. https://www.acgme.org/globalassets/pfassets /programrequirements/2025-reformatted-requirements/cprfellowship_2025_reformatted.pdf
- Accreditation Council for Graduate Medical Education. Program directors’ guide to the common program requirements (fellowship). Updated December 2025. Accessed May 27, 2026. https://www .acgme.org/globalassets/pdfs/guide-to-the-common -program-requirements-fellowship.pdf
- Curriculum overview - wound care and hyperbaric medicine fellowship. Wake Forest University School of Medicine. 2026. Accessed January 5, 2026. https://school .wakehealth.edu/Education-and-Training/Residencies -and-Fellowships/Wound-Care-and-Hyperbaric-Medicine -Fellowship/Curriculum-Overview
- Curriculum overview - American Board of Wound Medicine and Surgery. Core Curriculum for Fellowships in Wound Care. American Board of Wound Medicine and Surgery. 2022. Accessed January 5, 2026. https://abwms.org /curriculum-overview/
- European Wound Management Association. EWMA Wound healing curriculum for physicians. February 13, 2017. Accessed January 15, 2026. https://ewma.org /wp-content/uploads/2024/02/ETR-TF-Wound-Healing -UEMS-approved.pdf
- Accreditation Council for Graduate Medical Education. Recommended Curriculum Guidelines for Family Medicine Residents. Accessed January 5, 2026. https://www.aafp .org/dam/AAFP/documents/medical_education_residency /program_directors/Wound_Care.pdf
- Accreditation Council for Graduate Medical Education. Vascular Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /VascularSurgeryMilestones2.0.pdf
- Accreditation Council for Graduate Medical Education. Plastic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/PlasticSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Dermatology Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /DermatologyMilestones.pdf
- Accreditation Council for Graduate Medical Education. The Foot and Ankle Milestone Project a joint initiative of the Accreditation Council for Graduate Medical Education and the American Board of Orthopaedic Surgery. July 2015. Accessed January 5, 2026. https://www.acgme.org /Portals/0/PDFs/Milestones/FootandAnkleMilestones.pdf
- Accreditation Council for Graduate Medical Education. Orthopaedic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /OrthopaedicSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Spinal Cord Injury Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/SpinalCordInjuryMedicineMilestones.pdf
- Accreditation Council for Graduate Medical Education. Geriatric Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /GeriatricMedicineMilestones.pdf
- Goldhamer ME, Baker K, Anne Rigg DW, et al. Development and implementation of multi-source assessment tools for ACGME residents and fellows. MedEDPORTAL. 2014. Accessed May 14, 2026. doi:10.15766/mep_2374-8265.9839
Often disguised as comorbid conditions, nonhealing and chronic wounds have emerged as a silent epidemic that affects about 6.5 million Americans.1-3 In 2023, estimated US wound care costs were $126.86 billion.4 About 1% to 2% of individuals worldwide will experience a chronic wound in their lifetime. The Veterans Health Administration reported 277,000 inpatient and outpatient encounters for ulcers in 2011, including chronic ulcers of the lower extremity due to diabetes, venous disease, or arterial disease.5 Associated costs of chronic wounds are expected to increase as the populations of developed countries age.6 Effective treatment of chronic wounds requires a nuanced understanding of complex wound pathophysiology, best practices in interdisciplinary and multidisciplinary wound care, and advanced wound care technologies.7,8
The typical 4-year medical school curriculum, followed by residency, offers little in the way of formal didactic training in wound care.9,10 Without specialized and advanced fellowship training dedicated to wound care, health care will lack specialists prepared to manage complex wounds. As a result, wound care-related difficulties may be exacerbated by prolonged recovery time, increased costs, productivity loss, and increased mortality risk.8 Wound care is a growing field of study and practice, and there is a critical need for rigorous training, research, and quality improvement efforts to enhance outcomes for patients with nonhealing wounds.5
One of the most direct ways to address the need for more physicians with specialty training in wound medicine is to implement a comprehensive training curriculum for advanced wound care practice. Although specialized advanced wound care fellowships are available, the curricula primarily detail rotation names and areas for practice without accompanying competencies, milestones, or entrustable professional activities.11 Furthermore, wound care is not recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME).
This article synthesized the literature and integrated innovative, evidence-based practices into a curriculum for a formal advanced fellowship training program. To our knowledge, no comprehensive wound care curriculum is publicly available that includes rotations, competencies, milestones, entrustable professional activities, and 360-degree evaluation forms.
Program Development
The advanced wound care fellowship program started in January 2014 at the Michael E. DeBakey Veterans Affairs Medical Center in affiliation with the Baylor College of Medicine. The fellowship program was originally designed for geriatrics fellows to extend the 1-year fellowship for an additional year to learn wound care. It has been adjusted to address formal program goals and objectives, competencies, milestones, entrustable professional activities, and evaluations, with the goal of developing an example curriculum for wound care fellowships across specialties. Although the ACGME does not recognize a wound care subspecialty, this curriculum complies with the ACGME 1-year fellowship common program requirements.12,13
Scoping Review
A scoping literature review of Google Scholar and PubMed was performed using the medical subject heading terms “wound care + curriculum” and “wound + care + curriculum” to find advanced wound care medical training, fellowship programs, boards, and related ACGME-accredited specialty curricula. The local wound care fellowship program was initially implemented based on an informal literature review by faculty and their respective contributions to curriculum (ie, process establishing wound care-specific competency domains in accordance with ACGME accreditation competency requirements of 1-year fellowships). 12,13 Standing program practice-based competencies and activities were examined and determined to align with best practices. This scoping review considered additional competencies, competency domains, and entrustable professional activities of reputable wound care fellowship training programs (eg, University of Chicago at Illinois and Wake Forest School of Medicine),8,11,14 a specialty wound care board (American Board of Wound Medicine and Surgery),15 an international wound specialist professional society (European Union of Medical Specialists), 16 and recommended curriculum guidelines for wound care residency programs.17 ACGME-accredited specialty and subspecialty milestones professional activities were examined, including vascular surgery,18 plastic surgery,19 dermatology, 20 foot and ankle,21 orthopedic surgery,22 spinal cord injury,23 and geriatric medicine.24
The competencies, milestones, and entrustable professional activities were compiled and redundancies were eliminated. Wound care specialists from geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy examined the findings and suggested eliminating redundancies, irrelevant content, and content that fell below the minimal expected level of competence for an advanced medical specialist in wound care. An expert consensus meeting further refined items presented to the panel before unanimous consensus resulted in the final set of curriculum competencies, milestones, and entrustable professional activities.
Training Program Feedback
We developed a comprehensive wound care curriculum for an advanced physician fellowship training program based on the streamlined competencies, milestones, and entrustable professional activities (Appendix). Multiple wound care experts from various interdisciplinary backgrounds reached consensus to establish this fellowship curriculum as adaptable for use across training settings. The training program is 12 core rotations and 2 elective rotations (Table 1). Additionally, we developed wound care evaluation forms for faculty-, peer-, and self-assessment of trainees which were adapted from an evidence-based 360-degree evaluation template.25 Suggestions for structured, advanced didactics are in Table 2.
Seventeen fellows have successfully matriculated through the wound care training program. Although wound care certification is not required to work as a wound care specialist, after completion of this fellowship, graduates are able to sit for a wound care certification examination. The American Board of Wound Medicine and Surgery (ABWMS) and the American Board of Wound Management (ABWM) allow physicians to take a certification examination after 1 year of a dedicated wound fellowship program, instead of the typical wound care practice experience ≥ 3 years.
The Clinical Wound Care Fellowship Program collected data for program improvement, and 15 alumni responded (response rate, 88%) to a survey using a 5-point Likert scale. Respondents indicated high mean scores for overall satisfaction (4.7), instructional methods (4.7), program enjoyment (4.7), teaching materials (4.6), and relevance (4.6). All respondents indicated that the fellowship prepared them for a career in wound care as well as their current employment, and 13 of 15 (87%) reported they obtained immediate relevant postfellowship wound care positions and stated that the fellowship prepared them for their current roles. Nine respondents (69%) reported that they were engaged in wound care ≥ 26% of work time. Six respondents (46%) worked in private practice, 3 (23%) at academic medical centers, and 2 (15%) at government- funded hospitals. Four respondents indicated they were board certified in wound care. Program alumni are currently involved in scholarly activities, including 8 in quality improvement and 3 in research.
Discussion
An easily accessible, comprehensive wound care fellowship curriculum has not been previously developed or published. This limited the sources that informed this curriculum. However, the developmental process for this curriculum was robust, as the authors reviewed previously published materials related to wound care, including: 1) descriptive overviews of wound care fellowships; 2) details of month-long rotations for medical students and residents; and 3) practices of the specific environment in which this curriculum was created. Confidence in the practical nature of the curriculum can be assumed, as the experts involved in the development process represented diverse physician specializations, including geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy.
Most wound care clinicians have not completed a formal comprehensive fellowship program. Instead, due to the lack of a comprehensive training curriculum, clinicians have had to use various continuing medical education programs and practice in a wound care setting for ≥ 3 years to be eligible for certification in the specialty. This curriculum will help academic medical centers develop their own fellowship programs, enabling new wound care clinicians to attain certifications more efficiently. As more fellowship programs develop, the goal would be to obtain recognition as an ACGME specialty and standardize the training and competencies for graduates of wound care fellowships.
Conclusions
As new wound care fellowships develop, wound care may become formally acknowledged as its own specialty within medicine and surgery. This will provide wound care with a voice at the national level, particularly in an era of value-based care. Wound care clinicians will be able to advocate for specialty-specific quality metrics and avoid potential penalization for not meeting quality metrics that are irrelevant to wound care.
Often disguised as comorbid conditions, nonhealing and chronic wounds have emerged as a silent epidemic that affects about 6.5 million Americans.1-3 In 2023, estimated US wound care costs were $126.86 billion.4 About 1% to 2% of individuals worldwide will experience a chronic wound in their lifetime. The Veterans Health Administration reported 277,000 inpatient and outpatient encounters for ulcers in 2011, including chronic ulcers of the lower extremity due to diabetes, venous disease, or arterial disease.5 Associated costs of chronic wounds are expected to increase as the populations of developed countries age.6 Effective treatment of chronic wounds requires a nuanced understanding of complex wound pathophysiology, best practices in interdisciplinary and multidisciplinary wound care, and advanced wound care technologies.7,8
The typical 4-year medical school curriculum, followed by residency, offers little in the way of formal didactic training in wound care.9,10 Without specialized and advanced fellowship training dedicated to wound care, health care will lack specialists prepared to manage complex wounds. As a result, wound care-related difficulties may be exacerbated by prolonged recovery time, increased costs, productivity loss, and increased mortality risk.8 Wound care is a growing field of study and practice, and there is a critical need for rigorous training, research, and quality improvement efforts to enhance outcomes for patients with nonhealing wounds.5
One of the most direct ways to address the need for more physicians with specialty training in wound medicine is to implement a comprehensive training curriculum for advanced wound care practice. Although specialized advanced wound care fellowships are available, the curricula primarily detail rotation names and areas for practice without accompanying competencies, milestones, or entrustable professional activities.11 Furthermore, wound care is not recognized as a subspecialty by the Accreditation Council for Graduate Medical Education (ACGME).
This article synthesized the literature and integrated innovative, evidence-based practices into a curriculum for a formal advanced fellowship training program. To our knowledge, no comprehensive wound care curriculum is publicly available that includes rotations, competencies, milestones, entrustable professional activities, and 360-degree evaluation forms.
Program Development
The advanced wound care fellowship program started in January 2014 at the Michael E. DeBakey Veterans Affairs Medical Center in affiliation with the Baylor College of Medicine. The fellowship program was originally designed for geriatrics fellows to extend the 1-year fellowship for an additional year to learn wound care. It has been adjusted to address formal program goals and objectives, competencies, milestones, entrustable professional activities, and evaluations, with the goal of developing an example curriculum for wound care fellowships across specialties. Although the ACGME does not recognize a wound care subspecialty, this curriculum complies with the ACGME 1-year fellowship common program requirements.12,13
Scoping Review
A scoping literature review of Google Scholar and PubMed was performed using the medical subject heading terms “wound care + curriculum” and “wound + care + curriculum” to find advanced wound care medical training, fellowship programs, boards, and related ACGME-accredited specialty curricula. The local wound care fellowship program was initially implemented based on an informal literature review by faculty and their respective contributions to curriculum (ie, process establishing wound care-specific competency domains in accordance with ACGME accreditation competency requirements of 1-year fellowships). 12,13 Standing program practice-based competencies and activities were examined and determined to align with best practices. This scoping review considered additional competencies, competency domains, and entrustable professional activities of reputable wound care fellowship training programs (eg, University of Chicago at Illinois and Wake Forest School of Medicine),8,11,14 a specialty wound care board (American Board of Wound Medicine and Surgery),15 an international wound specialist professional society (European Union of Medical Specialists), 16 and recommended curriculum guidelines for wound care residency programs.17 ACGME-accredited specialty and subspecialty milestones professional activities were examined, including vascular surgery,18 plastic surgery,19 dermatology, 20 foot and ankle,21 orthopedic surgery,22 spinal cord injury,23 and geriatric medicine.24
The competencies, milestones, and entrustable professional activities were compiled and redundancies were eliminated. Wound care specialists from geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy examined the findings and suggested eliminating redundancies, irrelevant content, and content that fell below the minimal expected level of competence for an advanced medical specialist in wound care. An expert consensus meeting further refined items presented to the panel before unanimous consensus resulted in the final set of curriculum competencies, milestones, and entrustable professional activities.
Training Program Feedback
We developed a comprehensive wound care curriculum for an advanced physician fellowship training program based on the streamlined competencies, milestones, and entrustable professional activities (Appendix). Multiple wound care experts from various interdisciplinary backgrounds reached consensus to establish this fellowship curriculum as adaptable for use across training settings. The training program is 12 core rotations and 2 elective rotations (Table 1). Additionally, we developed wound care evaluation forms for faculty-, peer-, and self-assessment of trainees which were adapted from an evidence-based 360-degree evaluation template.25 Suggestions for structured, advanced didactics are in Table 2.
Seventeen fellows have successfully matriculated through the wound care training program. Although wound care certification is not required to work as a wound care specialist, after completion of this fellowship, graduates are able to sit for a wound care certification examination. The American Board of Wound Medicine and Surgery (ABWMS) and the American Board of Wound Management (ABWM) allow physicians to take a certification examination after 1 year of a dedicated wound fellowship program, instead of the typical wound care practice experience ≥ 3 years.
The Clinical Wound Care Fellowship Program collected data for program improvement, and 15 alumni responded (response rate, 88%) to a survey using a 5-point Likert scale. Respondents indicated high mean scores for overall satisfaction (4.7), instructional methods (4.7), program enjoyment (4.7), teaching materials (4.6), and relevance (4.6). All respondents indicated that the fellowship prepared them for a career in wound care as well as their current employment, and 13 of 15 (87%) reported they obtained immediate relevant postfellowship wound care positions and stated that the fellowship prepared them for their current roles. Nine respondents (69%) reported that they were engaged in wound care ≥ 26% of work time. Six respondents (46%) worked in private practice, 3 (23%) at academic medical centers, and 2 (15%) at government- funded hospitals. Four respondents indicated they were board certified in wound care. Program alumni are currently involved in scholarly activities, including 8 in quality improvement and 3 in research.
Discussion
An easily accessible, comprehensive wound care fellowship curriculum has not been previously developed or published. This limited the sources that informed this curriculum. However, the developmental process for this curriculum was robust, as the authors reviewed previously published materials related to wound care, including: 1) descriptive overviews of wound care fellowships; 2) details of month-long rotations for medical students and residents; and 3) practices of the specific environment in which this curriculum was created. Confidence in the practical nature of the curriculum can be assumed, as the experts involved in the development process represented diverse physician specializations, including geriatrics, family medicine, internal medicine, undersea and hyperbaric medicine, general surgery, podiatry, and physical therapy.
Most wound care clinicians have not completed a formal comprehensive fellowship program. Instead, due to the lack of a comprehensive training curriculum, clinicians have had to use various continuing medical education programs and practice in a wound care setting for ≥ 3 years to be eligible for certification in the specialty. This curriculum will help academic medical centers develop their own fellowship programs, enabling new wound care clinicians to attain certifications more efficiently. As more fellowship programs develop, the goal would be to obtain recognition as an ACGME specialty and standardize the training and competencies for graduates of wound care fellowships.
Conclusions
As new wound care fellowships develop, wound care may become formally acknowledged as its own specialty within medicine and surgery. This will provide wound care with a voice at the national level, particularly in an era of value-based care. Wound care clinicians will be able to advocate for specialty-specific quality metrics and avoid potential penalization for not meeting quality metrics that are irrelevant to wound care.
- Fife CE, Eckert KA, Carter MJ. Publicly Reported wound healing rates: the fantasy and the reality. Adv Wound Care (New Rochelle). 2018;7:77-94. doi:10.1089/wound.2017.0743
- Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care?. Wound Repair Regen. 2010;18:154-158. doi:10.1111/j.1524-475X.2010.00571.x
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771. doi:10.1111/j.1524-475X.2009.00543.x
- Queen D, Harding K. What’s the true costs of wounds faced by different healthcare systems around the world?. Int Wound J. 2023;20:3935-3938. doi:10.1111/iwj.14491
- Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. US Dept of Veterans Affairs; November 2012. https://www.ncbi.nlm.nih.gov/books/NBK132238/
- Simman R, McNevin AJ. Pursuing the path to specialized wound care: the ABWMS perspective. Todays Wound Clin. 2017;8:10,12.
- Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalence in intensive care patients: a cross-sectional study. J Eval Clin Pract. 2008;14:563-568. doi:10.1111/j.1365-2753.2007.00918.x
- Ennis WJ, Valdes W, Meneses P. Wound care specialization: a proposal for a comprehensive fellowship program. Wound Repair Regen. 2004;12:120-128. doi:10.1111/j.1067-1927.2004.012203.x
- Patel NP, Granick MS. Wound education: American medical students are inadequately trained in wound care. Ann Plast Surg. 2007;59:53-55. doi:10.1097/SAP.0b013e31802dd43b
- Patel NP, Granick MS, Kanakaris NK, et al. Comparison of wound education in medical schools in the United States, United Kingdom, and Germany. Eplasty. 2008;8:e8.
- Ennis WJ. Wound care specialization: the current status and future plans to move wound care into the medical community. Adv Wound Care (New Rochelle). 2012;1:184- 188. doi:10.1089/wound.2011.0346
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (fellowship). Updated September 3, 2025. Accessed January 15, 2026. https://www.acgme.org/globalassets/pfassets /programrequirements/2025-reformatted-requirements/cprfellowship_2025_reformatted.pdf
- Accreditation Council for Graduate Medical Education. Program directors’ guide to the common program requirements (fellowship). Updated December 2025. Accessed May 27, 2026. https://www .acgme.org/globalassets/pdfs/guide-to-the-common -program-requirements-fellowship.pdf
- Curriculum overview - wound care and hyperbaric medicine fellowship. Wake Forest University School of Medicine. 2026. Accessed January 5, 2026. https://school .wakehealth.edu/Education-and-Training/Residencies -and-Fellowships/Wound-Care-and-Hyperbaric-Medicine -Fellowship/Curriculum-Overview
- Curriculum overview - American Board of Wound Medicine and Surgery. Core Curriculum for Fellowships in Wound Care. American Board of Wound Medicine and Surgery. 2022. Accessed January 5, 2026. https://abwms.org /curriculum-overview/
- European Wound Management Association. EWMA Wound healing curriculum for physicians. February 13, 2017. Accessed January 15, 2026. https://ewma.org /wp-content/uploads/2024/02/ETR-TF-Wound-Healing -UEMS-approved.pdf
- Accreditation Council for Graduate Medical Education. Recommended Curriculum Guidelines for Family Medicine Residents. Accessed January 5, 2026. https://www.aafp .org/dam/AAFP/documents/medical_education_residency /program_directors/Wound_Care.pdf
- Accreditation Council for Graduate Medical Education. Vascular Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /VascularSurgeryMilestones2.0.pdf
- Accreditation Council for Graduate Medical Education. Plastic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/PlasticSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Dermatology Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /DermatologyMilestones.pdf
- Accreditation Council for Graduate Medical Education. The Foot and Ankle Milestone Project a joint initiative of the Accreditation Council for Graduate Medical Education and the American Board of Orthopaedic Surgery. July 2015. Accessed January 5, 2026. https://www.acgme.org /Portals/0/PDFs/Milestones/FootandAnkleMilestones.pdf
- Accreditation Council for Graduate Medical Education. Orthopaedic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /OrthopaedicSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Spinal Cord Injury Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/SpinalCordInjuryMedicineMilestones.pdf
- Accreditation Council for Graduate Medical Education. Geriatric Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /GeriatricMedicineMilestones.pdf
- Goldhamer ME, Baker K, Anne Rigg DW, et al. Development and implementation of multi-source assessment tools for ACGME residents and fellows. MedEDPORTAL. 2014. Accessed May 14, 2026. doi:10.15766/mep_2374-8265.9839
- Fife CE, Eckert KA, Carter MJ. Publicly Reported wound healing rates: the fantasy and the reality. Adv Wound Care (New Rochelle). 2018;7:77-94. doi:10.1089/wound.2017.0743
- Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care?. Wound Repair Regen. 2010;18:154-158. doi:10.1111/j.1524-475X.2010.00571.x
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771. doi:10.1111/j.1524-475X.2009.00543.x
- Queen D, Harding K. What’s the true costs of wounds faced by different healthcare systems around the world?. Int Wound J. 2023;20:3935-3938. doi:10.1111/iwj.14491
- Greer N, Foman N, Dorrian J, et al. Advanced Wound Care Therapies for Non-Healing Diabetic, Venous, and Arterial Ulcers: A Systematic Review [Internet]. US Dept of Veterans Affairs; November 2012. https://www.ncbi.nlm.nih.gov/books/NBK132238/
- Simman R, McNevin AJ. Pursuing the path to specialized wound care: the ABWMS perspective. Todays Wound Clin. 2017;8:10,12.
- Shahin ES, Dassen T, Halfens RJ. Pressure ulcer prevalence in intensive care patients: a cross-sectional study. J Eval Clin Pract. 2008;14:563-568. doi:10.1111/j.1365-2753.2007.00918.x
- Ennis WJ, Valdes W, Meneses P. Wound care specialization: a proposal for a comprehensive fellowship program. Wound Repair Regen. 2004;12:120-128. doi:10.1111/j.1067-1927.2004.012203.x
- Patel NP, Granick MS. Wound education: American medical students are inadequately trained in wound care. Ann Plast Surg. 2007;59:53-55. doi:10.1097/SAP.0b013e31802dd43b
- Patel NP, Granick MS, Kanakaris NK, et al. Comparison of wound education in medical schools in the United States, United Kingdom, and Germany. Eplasty. 2008;8:e8.
- Ennis WJ. Wound care specialization: the current status and future plans to move wound care into the medical community. Adv Wound Care (New Rochelle). 2012;1:184- 188. doi:10.1089/wound.2011.0346
- Accreditation Council for Graduate Medical Education. ACGME common program requirements (fellowship). Updated September 3, 2025. Accessed January 15, 2026. https://www.acgme.org/globalassets/pfassets /programrequirements/2025-reformatted-requirements/cprfellowship_2025_reformatted.pdf
- Accreditation Council for Graduate Medical Education. Program directors’ guide to the common program requirements (fellowship). Updated December 2025. Accessed May 27, 2026. https://www .acgme.org/globalassets/pdfs/guide-to-the-common -program-requirements-fellowship.pdf
- Curriculum overview - wound care and hyperbaric medicine fellowship. Wake Forest University School of Medicine. 2026. Accessed January 5, 2026. https://school .wakehealth.edu/Education-and-Training/Residencies -and-Fellowships/Wound-Care-and-Hyperbaric-Medicine -Fellowship/Curriculum-Overview
- Curriculum overview - American Board of Wound Medicine and Surgery. Core Curriculum for Fellowships in Wound Care. American Board of Wound Medicine and Surgery. 2022. Accessed January 5, 2026. https://abwms.org /curriculum-overview/
- European Wound Management Association. EWMA Wound healing curriculum for physicians. February 13, 2017. Accessed January 15, 2026. https://ewma.org /wp-content/uploads/2024/02/ETR-TF-Wound-Healing -UEMS-approved.pdf
- Accreditation Council for Graduate Medical Education. Recommended Curriculum Guidelines for Family Medicine Residents. Accessed January 5, 2026. https://www.aafp .org/dam/AAFP/documents/medical_education_residency /program_directors/Wound_Care.pdf
- Accreditation Council for Graduate Medical Education. Vascular Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /VascularSurgeryMilestones2.0.pdf
- Accreditation Council for Graduate Medical Education. Plastic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/PlasticSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Dermatology Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /DermatologyMilestones.pdf
- Accreditation Council for Graduate Medical Education. The Foot and Ankle Milestone Project a joint initiative of the Accreditation Council for Graduate Medical Education and the American Board of Orthopaedic Surgery. July 2015. Accessed January 5, 2026. https://www.acgme.org /Portals/0/PDFs/Milestones/FootandAnkleMilestones.pdf
- Accreditation Council for Graduate Medical Education. Orthopaedic Surgery Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /OrthopaedicSurgeryMilestones.pdf
- Accreditation Council for Graduate Medical Education. Spinal Cord Injury Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs /Milestones/SpinalCordInjuryMedicineMilestones.pdf
- Accreditation Council for Graduate Medical Education. Geriatric Medicine Milestones the Accreditation Council for Graduate Medical Education. Accessed January 5, 2026. https://www.acgme.org/Portals/0/PDFs/Milestones /GeriatricMedicineMilestones.pdf
- Goldhamer ME, Baker K, Anne Rigg DW, et al. Development and implementation of multi-source assessment tools for ACGME residents and fellows. MedEDPORTAL. 2014. Accessed May 14, 2026. doi:10.15766/mep_2374-8265.9839
The Development of a Comprehensive Wound Care Fellowship Curriculum
The Development of a Comprehensive Wound Care Fellowship Curriculum


Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
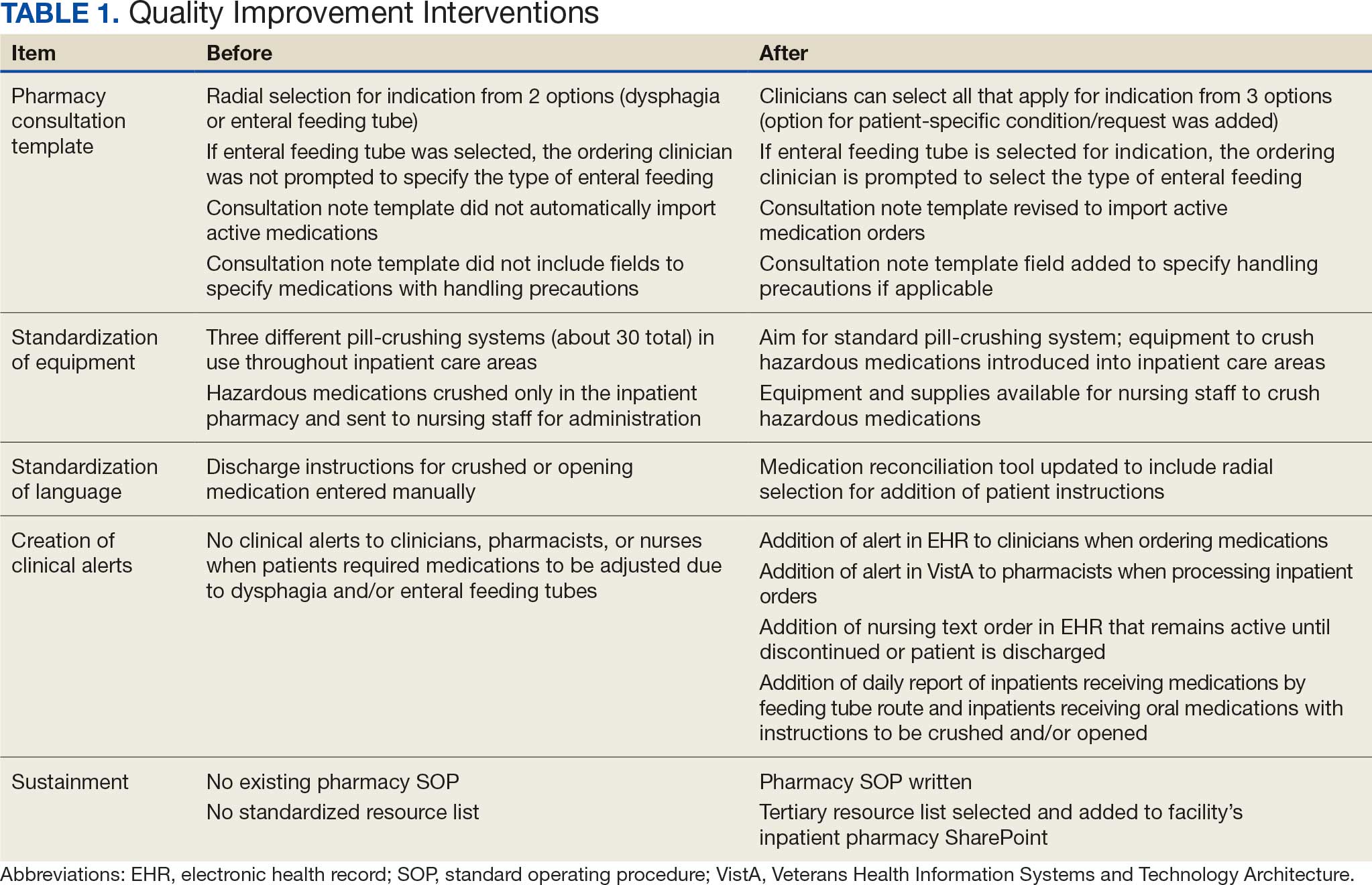
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
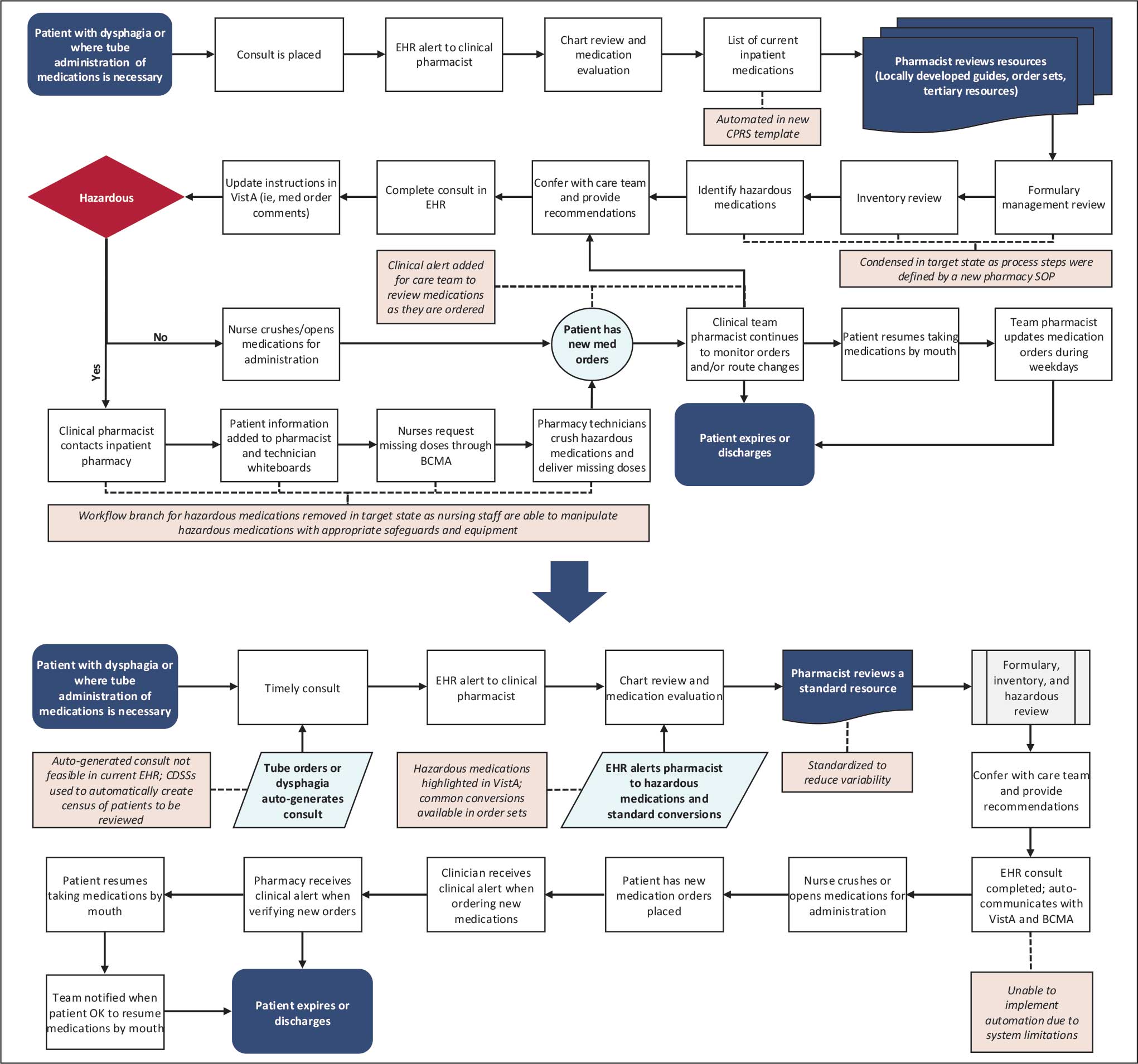
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).

Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
Medication regimens may require adjustment in acute care settings due to dysphagia and/or enteral feeding tubes. When a patient has dysphagia and/or a feeding tube, the health care team must review the pharmacotherapy regimen to assess the appropriateness of medication formulations. Patient anatomy, the type of feeding tube in place, pharmacokinetic and pharmacodynamic properties of medications, risk of feeding tube obstruction, and potential for interactions between enteral nutrition and medications should be considered when clinicians administer medications through feeding tubes. The risk of feeding tube obstruction and clogging rises with increasing tube length and decreasing tube lumen. Incidence of obstructed percutaneous endoscopic gastrotomy tubes is reported to be 23% to 35%.1
A coordinated effort by all members of the health care team is essential to provide safe and effective care to patients with dysphagia and/or enteral feeding tubes. To decrease the risk of feeding tube obstruction, medications should be dissolved in water or administered in liquid form, saline fluids should be avoided, and the tube should be flushed with water before and after administering medications.
The pharmacokinetics of medications can be altered when tablets are crushed or capsules are opened. The bioavailability of dabigatran, for example, increases by 75% when the capsules are opened and pellets are taken orally.2 Medications may become intolerable after manipulation due to taste.3 Others may also increase the risk of feeding tube obstruction, such as omeprazole granules that increase the risk of small-bore feeding tube obstruction.4
Prior assessments of drug administration for patients with dysphagia and/or enteral feeding tubes has shown medication errors are prevalent.5-7 The Institute for Safe Medication Practices (ISMP) issued a Medication Safety Alert that provides a framework for preventing medication errors when preparing and administering medications via enteral feeding tubes.8 Other resources, such as monographs, are also available to guide pharmacotherapy decisions when oral medications require manipulation for administration to patients with dysphagia and/or enteral feeding tubes.9-11
In 2021, the Kansas City Veterans Affairs Medical Center (KCVAMC) was recognized as a Veterans Health Administration (VHA) Shark Tank finalist for improving the safety of medication administration for patients with enteral feeding tubes.12 This involved the addition of a Computerized Patient Record System (CPRS), clinical reminder order check (CROC), and a comprehensive medication review by a pharmacist. After implementing the CROC alert and pharmacy e-consultation workflow, the KCVAMC team reported that the number of inappropriate medications (ie, drugs on the ISMP do not crush list) was reduced from 41 to 6 in 1 year, resulting in an 85.4% reduction in potential medication errors.13
In 2014, the Richard L. Roudebush VAMC (RLRVAMC) created a pharmacy consultation process for patients with dysphagia and/or enteral feeding tubes. Any clinician could place a pharmacy consultation in CPRS. A pharmacist then reviewed patient charts, medication information resources, the VA formulary, and RLRVAMC pharmacy inventory. The pharmacist conferred with the patient’s care team to adjust pharmacotherapy, completed a consultation note, and updated medication order comments in Veterans Health Information Systems and Technology Architecture (VistA). These comments interfaced with the barcode medication administration software for the health care professional administering medications.
Despite the 2014 quality improvement (QI) process, medication errors involving the inappropriate ordering, preparation, and administration of medications for patients with dysphagia and/or enteral feeding tubes continued to be reported. Additionally, anonymous feedback revealed that only 3 of 10 responding pharmacists were satisfied with the existing medication use process for patients with dysphagia and/or enteral feeding tubes. Pharmacists expressed concerns that (1) clinicians were inappropriately crushing and/or manipulating new medications that were ordered after pharmacy consultations; (2) there was a lack of comprehensive documentation in CPRS; and (3) there were too many manual steps in the process. In response, RLRVAMC initiated a new QI initiative to improve the medication use process for patients with dysphagia and/or enteral feeding tubes in the acute care setting.
Quality Improvement Project
This multidisciplinary RLRVAMC QI project began November 2024 to improve pharmacotherapy care for patients with dysphagia and/or enteral feeding tubes in acute care. It was approved by the RLRVAMC Pharmacy Service. This intervention addressed the pharmacy consultation template, standardization of equipment, standardization of language, creation of clinical alerts, and sustainment (Table 1).
RLRVAMC has about 8600 annual inpatient admissions and 159 acute care beds.14 The project charter was drafted, and local stakeholders were identified including pharmacy technicians, pharmacists, nurses, speech language pathologists, and acute care clinicians. Pharmacy consultation workload was retrospectively reviewed to describe the scope of the existing state.
A workshop with 12 QI project stakeholders in December 2024 used A3 methodology to define the current process and the target state, barriers and solutions, prioritize interventions on an impact-effort matrix, perform a gap analysis, identify rapid plan-do-study-act (PDSA) experiments, and develop a completion plan (Figure). Five postworkshop PDSA experiments engaged additional stakeholders, clinical application coordinators, and medical supply representatives to ascertain the feasibility of the tools implemented.
Abbreviations: BCMA, barcode medication administration; CDSS, clinical decision support system; CPRS, Computerized Patient Record System;
EHR, electronic health record; SOP, standard operating procedure; VistA, Veterans Health Information Systems and Technology Architecture.
About 3% of RLRVAMC admissions involve a pharmacy consultation to review medications for dysphagia and/or enteral feeding tubes. Clinicians reviewed 30 preimplementation inpatient pharmacy consultations involving 200 oral medications. Pharmacists were more frequently consulted for inpatients with dysphagia (19 [63%]) than for patients with enteral feeding tubes (11 [37%]) (Table 2).
Pharmacy Consultation Template
The pharmacy consultation was updated in CPRS. Prior to this QI project, the ordering clinician was prompted to select 1 option for the indication: dysphagia or enteral feeding tube. The type of enteral feeding tube was not prompted by the consultation text nor required to be specified in the consultation. The ordering clinician could provide free-text comments. Of 11 preimplementation consultations, the type of enteral feeding tube was specified in 5 (45%). The consultation template entry was updated to include an option to check a box for the consultation indication from 3 options: dysphagia, enteral feeding, or other patient- specific condition/request. If enteral feeding tube is selected, then the clinician is prompted to select the type of enteral feeding tube. Since the completion of the project, there have been no patient safety reports concerning an erroneous or incomplete consultation entry (Supplemental Material).
The note template was updated to import the list of active inpatient medications and provide sections for the adjudicating pharmacist to document which medications can be crushed (or opened), which require adjustment, and which are hazardous and require special handling. Additionally, the revised template added a statement clarifying that the documented recommendations apply only to the medication regimen at the time of the consultation (Supplemental Material).
Standardizations
There are multiple pill-crushing devices used at RLRVAMC that vary in crushing mechanism, corresponding medication pouches, and degree of protection when manipulating hazardous medications. Prior to this QI project, RLRVAMC used 3 pill-crushing devices (about 30 total devices in inpatient care areas). Only 1 device with corresponding closed pouches for preparation of hazardous medications was available, which was stored in the RLRVAMC inpatient pharmacy. This workflow resulted in waste and posed potential risks for delays in care. This project incorporated a standard pill-crushing system with the corresponding medication pouches in all inpatient care areas, which provided safeguards for clinicians to prepare and administer hazardous medications (Supplemental Material).
Patients requiring medications to be crushed or opened on discharge should receive education, written instruction, and have care plans documented in CPRS. RLRVAMC patients receive education and a printed medication list. Prior to this QI project, the instructions for crushing or opening medications could only be entered by free text in the electronic medication reconciliation tool, allowing for the potential for inconsistent language or omissions.
This QI project included an update to the electronic medication reconciliation tool. An optional checkbox selection was added for patients requiring medications to be manipulated. When checked, a radial selection for individual medications is displayed, prompting the clinician and pharmacist to indicate either do not crush tablet or OK to crush tablet. These selections appear in clinical care notes and on the printed medication list provided to the patient (Supplemental Material).
Clinical Alerts
As part of the RLRVAMC QI initiative, a CROC alert was implemented, based on the KCVAMC intervention for patients with enteral feeding tubes.13 The RLRVAMC CROC alert also included patients with dysphagia. A nursing text order was made available in CPRS for patients requiring medications and remains active throughout the duration of the patient’s admission or until discontinued. It generates CROC alerts in CPRS and VistA when new medication orders are entered and reviewed by pharmacists.
Clinicians used clinical decision support systems to create daily lists of patients receiving medications by feeding tube and patients receiving crushed/opened medications due to dysphagia. This allows pharmacists to perform a census review of all inpatients to confirm appropriateness of medication orders. Clinical alerts for patients with enteral feeding tubes are advised by the ISMP and have data demonstrating a reduction in medication errors (Supplemental Material).14,15
Sustainment
During the sustainment phase, process owners were identified and a Pharmacy Service standard operating procedure (SOP) was written. The development of an institutional do not crush medication list was discussed; however, it was determined to be difficult to develop and maintain. An institutional tertiary resource list was selected in favor of a locally developed resource. These resources include the Handbook of Drug Administration via Enteral Feeding Tubes, Third Edition, the Pharmacist’s Letter list, “Meds that Should Not be Crushed,” and the Up- ToDate Lexidrug list, “Oral Medications That Should Not Be Crushed or Altered.”9-11 Links to the resources were added to the RLRVAMC pharmacy service SharePoint. In addition to defining the preferred tertiary resources, the SOP defined the process for reviewing inventory and the process for reviewing medication orders for hazard risk.
Discussion
Continued patient safety reports and low satisfaction rates among pharmacists prompted this QI project to improve safety for patients with dysphagia and/or enteral feeding tubes at RLRVAMC. The project engaged stakeholders and also identified and addressed gaps with potential for patient harm.
The tools implemented by this initiative drew from previous work by the KCVAMC and from framework provided by the ISMP.8,13 We expanded the QI intervention to include acute care patients with dysphagia.
RLRVAMC did not take steps to track the impact of the interventions on medication errors. However, no patient safety reports concerning an erroneous or incomplete pharmacy consultation entry have been reported. We also think that it is reasonable to assume that the adoption of the safety tools described here will have a positive impact on patient safety. RLRVAMC pharmacists have noted an increased appreciation for medication safety when processing medication orders for patients with dysphagia and/or enteral feeding tubes. While the workflow took time to adopt and integrate, clinical pharmacists perceived it as an improvement in patient safety. Our future focus is aimed at translating the process improvement into the Oracle/Cerner electronic health record, which is scheduled to be deployed at the RLRVAMC in August 2026.
Limitations
This QI project did not aim to quantify or compare medication errors before and after the intervention. An accurate number of unreported errors in the medication use process for patients with dysphagia and/or enteral feeding tubes would be challenging to quantify without direct observation. Multiple clinicians are engaged in the medication use process and individual steps may not be documented at all, or documented properly. In addition, medication errors are often underreported and may not reflect the total number of errors and/or potential for errors. That said, reported medication errors in the medication use process for patients with dysphagia and/or enteral feeding tubes are reviewed on a monthly basis by the RLRVAMC Multidisciplinary Medication Safety committee to continuously improve patient safety.
Another potential limitation is the extent to which the project can be adapted at other VHA sites. For example, RLRVAMC uses CPRS; the framework and tools to improve medication safety may not translate to sites using the Oracle/Cerner electronic health record. Furthermore, this QI project included a pharmacy consultation workflow that relied on pharmacists who are available at any hour. Other facilities may not have continuous consultation coverage to review medications for patients with dysphagia and/or enteral feeding tubes.
Conclusions
This QI project drew from ISMP recommendations, previous work within the VHA, local practice, and insight from multiple disciplines on the health care team to revise and create tools to improve medication safety for patients with dysphagia and/or enteral feeding tubes in the acute care setting. These tools included a revised pharmacy consultation workflow with improvements to the pharmacy consultation template, standardization of the pill-crushing devices and language used for patient medication lists, implementation of CROC alerts within the EHR, and development of an SOP.
The RLRVAMC Pharmacy Service intends to continue reviewing patient safety reports, assessing staff perspectives, and refining (and potentially adding) tools for medication safety. Future QI initiatives may focus on improving medication safety for outpatients with dysphagia and/or enteral feeding tubes. We also hope that these tools can be adapted at other VAMCs to promote medication safety for patients with dysphagia and/or enteral feeding tubes.
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
- Blumenstein I, Shastri YM, Stein J. Gastroenteric tube feeding: techniques, problems and solutions. World J Gastroenterol. 2014;20:8505-8524. doi:10.3748/wjg.v20.i26.8505
- Pradaxa (dabigatran etexilate). Prescribing information. Boehringer Ingelheim Pharmaceuticals, Inc; 2025. https:// pro.boehringer-ingelheim.com/us/products/pradaxa/bipdf /pradaxa-capsules-us-pi
- Lovell AG, Protus BM, Dickman JR, et al. Palatability of crushed over-the-counter medications. J Pain Symptom Manage. 2021;61:755-762. doi:10.1016/j.jpainsymman.2020.09.020
- Messaouik D, Sautou-Miranda V, Bagel-Boithias S, et al. Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube. Int J Pharm. 2005;299:65-72. doi:10.1016/j.ijpharm.2005.04.034
- Demirkan K, Bayraktar-Ekincioglu A, Gulhan-Halil M, et al. Assessment of drug administration via feeding tube and the knowledge of health-care professionals in a university hospital. Eur J Clin Nutr. 2017;71:164-168. doi:10.1038/ejcn.2016.147
- Fodil M, Nghiem D, Colas M, et al. Assessment of clinical practices for crushing medication in geriatric units. J Nutr Health Aging. 2017;21:904-908. doi:10.1007/s12603-017-0886-3
- Zhu LL, Xu LC, Wang HQ, et al. Appropriateness of administration of nasogastric medication and preliminary intervention. Ther Clin Risk Manag. 2012;8:393-401. doi:10.2147/TCRM.S37785
- Institute for Safe Medication Practices (ISMP). Preventing errors when preparing and administering medications via enteral feeding tubes. Acute Care ISMP Medication Safety Alert. November 17, 2022. Accessed March 17, 2026. https://nutritioncare.org/wp-content/uploads/2025/02 /ISMP-Safety-Alert_Medications-and-Enteral-Feeding -Tubes.pdf
- White R, Bradnam V. Handbook of Drug Administration via Enteral Feeding Tubes. 3rd ed. Pharmaceutical Press; 2015.
- Clinical resource, meds that should not be crushed. Pharmacist’s Letter/Pharmacy Technician’s Letter/Prescriber Insights. Updated April 2025. Accessed March 17, 2026. https://pharmacist.therapeuticresearch.com/en/Content /Segments/PRL/2014/Aug/Meds-That-Should-Not-Be -Crushed-7309
- Oral medications that should not be crushed or altered. In: Lexidrug. UpToDate, Inc. https://online.lexi.com/lco /action/doc/retrieve/docid/patch_f/4227
- Uttaro E, Zhao F, Schweighardt A. Filling the gaps on the Institute for Safe Medication Practices (ISMP) do not crush list for immediate-release products. Int J Pharm Compd. 2021;25:364-371.
- US Dept of Veterans Affairs. VA Diffusion Marketplace. Improved safety of enteral tube medication administration. Updated 2024. Accessed March 17, 2026. https:// marketplace.va.gov/innovations/improved-safety-of -enteral-tube-medication-administration
- US Dept of Veterans Affairs. About us. VA Indiana Healthcare System. Updated October 17, 2024. Accessed March 2, 2026. https://www.va.gov/indiana-health-care/about-us/
- Wasylewicz ATM, van Grinsven RJB, Bikker JMW, et al. Clinical decision support system-assisted pharmacy intervention reduces feeding tube-related medication errors in hospitalized patients: a focus on medication suitable for feeding-tube administration. JPEN J Parenter Enteral Nutr. 2021;45:625-632. doi:10.1002/jpen.1869
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes
Streamlining the Acute Care Pharmacy Consultation Process for Patients With Dysphagia or Enteral Feeding Tubes

Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
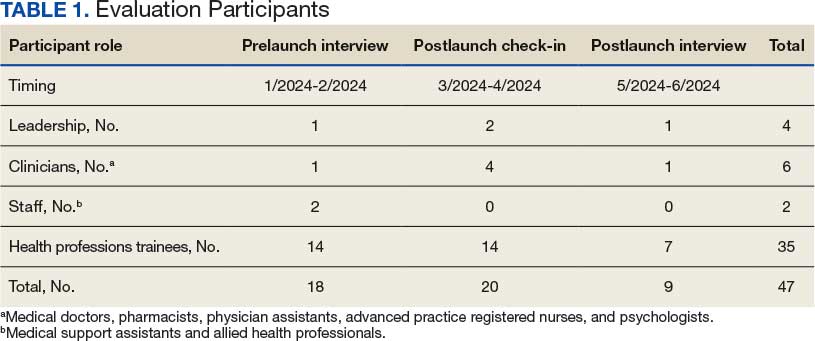
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
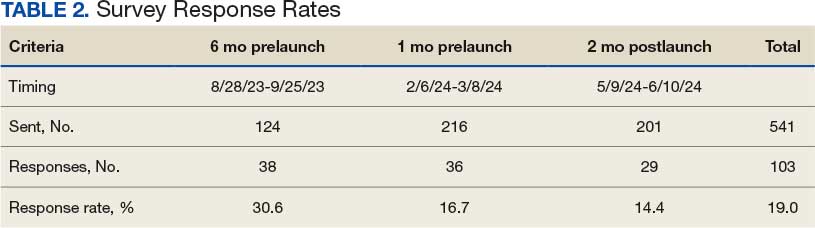
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
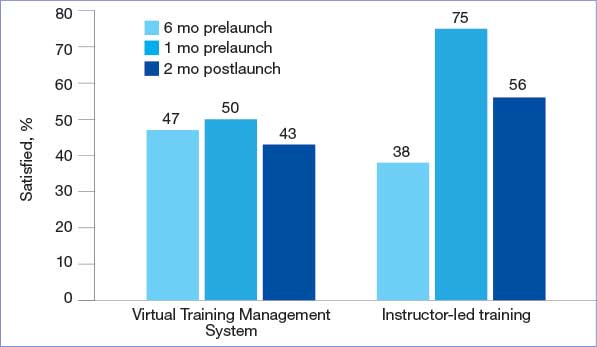
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
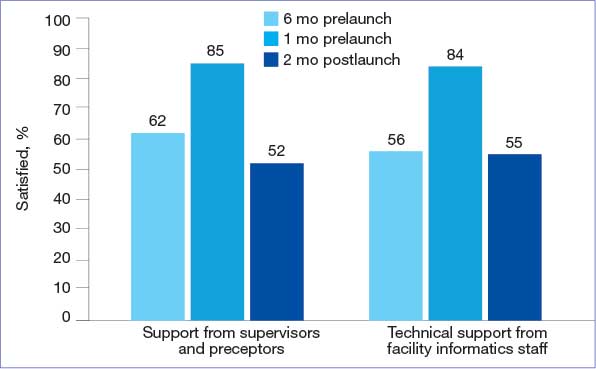
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
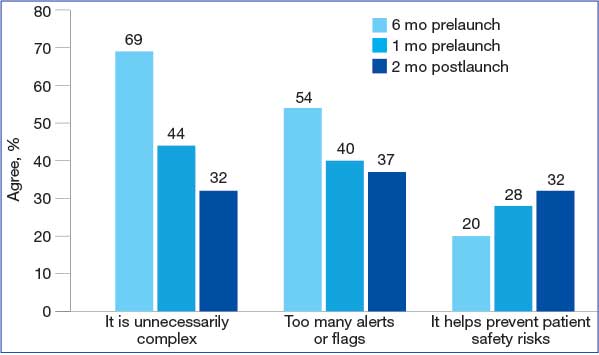
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
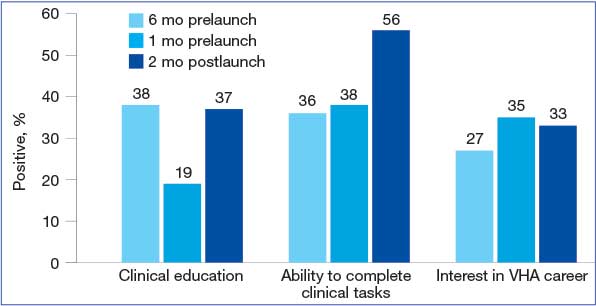
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
The Veterans Health Administration (VHA) is transitioning from its native electronic health record (EHR) Vista/Computerized Patient Record System to the commercial Cerner/Oracle Health EHR. Though this process was temporarily discontinued in April 2023 due to patient safety, usability, and reliability concerns, it resumed in April 2026. It was originally projected to cost $50 billion to implement. 1-3 As of March 9, 2024, 6 sites had transitioned to the new EHR.2 The transition is the largest of its kind in the US, offering an unparalleled opportunity to examine the effects of EHR transitions on an often overlooked part of the workforce: health professions trainees (HPTs).
HPTs serve a central role in VHA. About one-third of patients receive care directly from HPTs who make up about one-third of the VHA workforce. VHA trains > 60 clinical disciplines, comprising > 122,000 trainees annually.4,5 A paucity of literature exists exploring the experiences of HPTs during EHR transitions, and many studies are often limited to single-site or small populations. HPTs face distinct challenges and needs during EHR transitions and are particularly vulnerable to their negative impacts on retention, clinical training, and efficiency and confidence in EHR use.6-10 HPTs at VHA sites that have already transitioned to the Cerner/Oracle Health EHR identified many challenges, including significant delays in gaining EHR access, pervasive perceptions of poor training, concerns that EHR functionality issues limited patient care, and decreased ability to track clinical skill acquisition.6 These challenges may impact some HPTs more than others (eg, students on short rotations are affected more acutely by delayed EHR access and usage).
This quality improvement project evaluated HPT EHR transition experiences at the Captain James A. Lovell Federal Health Care Center (FHCC). This article contributes to the limited literature on HPT transition experiences, identifies opportunities to support HPTs, and informs broader efforts in teaching HPTs new technologies.
Methods
FHCC is jointly operated by the US Department of Defense and US Department of Veterans Affairs (VA). It treats 80,000 inpatient and outpatients annually. FHCC was the sixth VA facility to transition to the new EHR, which went live on March 9, 2024.2,11 About 700 HPTs rotate through FHCC annually. HPTs were eligible for inclusion if they were present during the March 9 transition according to a VA Office of Academic Affiliations database. A total of 216 HPTs were identified for inclusion.
Preparations for the transition included scaling down operations (ie, blocking clinician schedules, not scheduling future appointments that may conflict with the transition, making decisions on new facility- and service-line workflows, required EHR training, and speaking with support staff, including VHA National EHR Modernization Supplemental Staffing Unit [NESSU]). This evaluation was designated nonresearch/quality improvement by the VA Bedford Healthcare System Institutional Review Board.
Surveys
Forty-seven interviews were conducted with HPTs, site leaders, and supervisors from January 2024 to June 2024 (Table 1). Participants were identified by service leads and recruited via email; snowball sampling identified additional participants.
The evaluation team developed semistructured interview guides using grounded probes based on a pilot evaluation and existing research on EHR transitions.12 Questions focused on participant experiences preparing for the EHR transition, learning and using the site’s EHR, and the impact the transition had on clinical training experiences. Interviews were conducted at different times to capture the range of user experiences: 1 month prelaunch, 2 to 6 weeks postlaunch, and 2 months postlaunch. Interviewees were informed of participant rights and provided verbal consent.
HPTs present at FHCC at each survey’s release were emailed invitations and 2 reminders. The anonymous surveys took about 10 minutes to complete. Survey items queried HPTs about their experiences preparing to use the new EHR, perceptions of the current EHR (adapted from the System Usability Scale), satisfaction with VHA training, impact on clinical training, ability to work with preceptors and patients, and experiences with the VHA clinical learning environment (adapted from the VHA Learners Preceptor Survey).13-15 Survey questions used a 5-point Likert response scale.
Analysis
Interviewers completed postinterview summaries for team debriefing and consensus building. Interviews were coded using a priori (from piloting evaluations and relevant literature) and emergent (refined and developed from data) codes. Deductive and inductive content analyses were conducted. 16 Deductive analysis used a priori categories (eg, care coordination, EHR training). Inductive content analysis consisted of open and unstructured coding, capturing data outside a priori categories. Emergent codes captured unidentified categories. Qualitative researchers met weekly to discuss data and reach consensus on interpretation.
Descriptive analysis was conducted using top-2 box scoring (proportion responding within the 2 most favorable responses [agree/ strongly agree]). Survey data were analyzed in SAS.17 The analysis used a merging approach on simultaneously collected qualitative and quantitative data to reach findings consensus.18
Researcher and research team decisions may shape the data collected due to prior assumptions and experience.19 This analysis attempted to integrate reflexivity practices to enhance awareness of the researchers’ assumptions and positionality, including by integrating intent collaborative conversing and memorandum writing into the processes.20,21
Results
This analysis created a survey and fielded responses from HPTs present at FHCC across 3 time points (6 months prelaunch, 1 month prelaunch, and 2 months postlaunch), resulting in a total of 103 responses and an average response rate of 19.0% (Table 2). Six key findings were identified in analysis of responses: (1) critiques of transition management; (2) concerns with training; (3) hope about the EHR; (4) at-the-elbow support was essential; (5) HPTs adjusted to, and later preferred, the new EHR; and (6) transition impacted clinical training, but not overall career plans for HPTs. Findings are presented in this section, with illustrative quantitative data and qualitative data quotes available in the eAppendix.
Critiques of the Transition’s Management
While participants were aware of the transition to the new EHR, most felt they did not have enough information or time to prepare for it, indicating it was “too little, too late.” HPTs felt necessary workflow processes for Cerner/Oracle Health were not determined with enough time to learn them prior to transition. Supervisors shared that important workflow and onboarding decisions remained undecided mere weeks before the transition. Some service lines did not decrease patient loads until right before the transition, making it difficult to manage their schedules and resulting in insufficient time to learn the new EHR.
EHR Training Concerns
Overall, HPTs expressed low satisfaction with computer-based Training Management System (TMS) EHR training, believing it did not prepare them for the new EHR. The percentage of HPTs satisfied or very satisfied with the quality of TMS training was lower than that of instructor-based training pre- and posttransition, with 50% of 36 prelaunch respondents, and 43% of 29 postlaunch respondents expressing satisfaction with computer-based trainings (Figure 1). HPTs were dissatisfied with the training content. They felt it was too general and failed to teach basic tasks in the workflow for their service areas and roles, such as writing a note or order. Furthermore, poor content was exacerbated by poor and unengaging instruction, and HPTs were dissatisfied with the practice EHR used in training, which glitched frequently.
quality of electronic health record training.
EHR Transition Optimism
Even though the transition was stressful, most HPTs hoped it would be a temporary disruption and that they would quickly adjust to the new EHR. Many participants expected that once they switched to the new EHR, they would pick it up quickly. In addition, many anticipated Cerner/Oracle Health would be better and easier to use in the long run.
At-The-Elbow Support Essential
VHA peer support with NESSU was highly valued among HPTs. NESSU staff were highly knowledgeable and could provide both broad and service-line-specific support. NESSU provided prompt answers to EHR questions. This was particularly critical as other forms of in-person support were often inaccessible or absent during the transition.
HPTs found facility support helpful: 85% of 36 respondents reported being satisfied/ very satisfied with support from supervisors and preceptors, and 84% of 36 respondents were satisfied/very satisfied with technical support from facility informatics staff pretransition (n = 36) (Figure 2). NESSU and supervisor support with daily workflows were particularly helpful, as pretransition training only provided a general introduction to the EHR.
health record training.
HPTs Adjusted to and Later Preferred the New EHR
The EHR learning experience was intense but short, with many HPTs feeling able to use it only 2 to 4 weeks posttransition. Confidence grew as HPTs came to view Cerner/Oracle Health as a more integrated and intuitive system than the previous EHR. Most participants preferred the new EHR, even if they criticized some features (eg, no group documentation capabilities). Survey participants frequently rated Cerner/Oracle Health usability higher than the original. A total of 32% of 29 posttransition respondents agreed or strongly agreed that Cerner/Oracle Health helps prevent situations that can lead to patient safety risks—higher than pretransition rates. Additionally, fewer respondents found the new EHR unnecessarily complex or thought it contained too many alerts and flags compared to the original EHR (Figure 3).
health record usability.
Impact on Clinical Training, Not Career Plans
The extensive time and energy the transition demanded of HPTs caused stress and affected their clinical training. Many believed they would have learned more if their training had happened outside the transition.
Concerns that the transition affected learning were most acutely felt pretransition. HPTs reporting that EHR implementation positively affected their clinical education fell from 38% of 36 respondents 6 months pretransition to 19% of 29 respondents 1 month pretransition, but returned to 37% posttransition (Figure 4). However, some HPTs believed there was a silver lining: it provided a learning experience they otherwise would not have had.
new Veterans Health Administration (VHA) electronic health record.
HPTs who believed the transition positively impacted their likelihood of pursuing future career opportunities within the VHA rose to 33% of 29 respondents posttransition. Overall, Cerner/Oracle Health was characterized as a tool: something used in training, but not something that precluded wanting VHA careers or having meaningful experiences, such as caring for patients.
Discussion
This evaluation addressed an underexplored aspect of EHR transitions: their impact on HPTs. It identified HPT challenges, including dissatisfaction with poor transition preparation and EHR training experiences. Promising findings include positive experiences with transition support, EHR uptake, and overall positive educational experiences despite the transition’s disruption.
When EHR users, including HPTs, are dissatisfied with transition preparations, consequent stress can lead to undesired effects, including increased burnout, inappropriate EHR use, and low work satisfaction.22-24 Negative EHR transition experiences shape HPTs’ subsequent EHR adoption, user satisfaction, as well as confidence and career intent.3,25,26 Health systems have strong incentives to implement effective transition change management.
HPTs at previous VHA EHR transition sites reported significantly more disruption to their clinical training compared with HPTs at FHCC. Academic programs were shut down at the first transition site, and HPTs expressed decreased interest in VHA careers at another, even a year posttransition.6,27 These findings are consistent with the limited literature on the adverse impacts that EHR transitions have on HPTs.7,28
HPT retention is critical. VA is mandated to prepare the next generation of HPTs for its needs, and those of the nation. The VA relies heavily on HPT retention to recruit clinicians: > 65% of VHA physicians nationwide participated in VHA training programs prior to recruitment into staff positions.5,29
VHA should invest in transition change management with demonstrated, positive impacts on HPTs, such as in-house support from clinicians. Previous research found that lack of support was a major source of stress and negative outcomes.6,27 Consequently, supporting HPTs through EHR transitions directly contributes to the VHA’s ability to attract high-quality staff from its HPTs. The challenges and promising practices described in this analysis underscore the necessity of understanding how all EHR users are affected by transitions. What happens to them has direct implications for the VA mission to provide safe, efficient care, and its mandate to provide quality clinical training to HPTs.
These findings hold hopeful implications for supporting HPT EHR use, both during and outside EHR transitions. HPTs expressing that an EHR is only 1 part of their clinical training experience suggests that change management can improve EHR transitions. HPT learning can enhance known factors that are important for HPTs in clinical training, including the health care organization’s mission, caring for patients, and personal development.
Further investigations may engage HPTs at future VHA sites making the transition to the new EHR. One focus would involve applying a learning health systems framework to examine the nature of change management efforts—and their effects on HPT transition experiences—iteratively across transition sites to evaluate the effect of the efforts. Another focus may be longitudinal engagement with HPTs at health care systems and sites transitioning to new EHRs. Research has found that disruptions to EHR usability, satisfaction, and care provision can persist for 2 years and beyond following an EHR transition.30 Evaluating the long-term effects of transitions on HPTs is of interest, given their distinct characteristics and differences from employees.
Limitations
Study data came from voluntary participants at 1 highly engaged site, raising the possibility of self-selection bias. HPT experiences at other VA and non-VA sites may differ. Employees and HPTs were engaged during a high-stress event; snowballing recruitment reach was limited by high workloads and limited time for engagement. Statistical data were descriptive and should not be interpreted as causal. Results may reflect, in part, temporal effects, and respondents include HPTs at different stages of training and with different levels of VA experience. Survey sample sizes may limit generalizability; however, merging data streams strengthened the reliability of findings.
Conclusions
The results of this analysis of FHCC HPTs were notably more positive than those of HPTs at previous VHA EHR transition sites. VHA is one of many health care systems that provide clinical training for HPTs and relies on this population to provide patient care. By highlighting challenges and positive experiences of HPTs during an EHR transition, this evaluation produces actionable insights that can inform the actions of health care systems seeking to support HPTs during disruptive EHR transitions.
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
- US Department of Veterans Affairs Office of the Inspector General. VA needs to strengthen controls to address electronic health record system major performance incidents. September 23, 2024. Accessed February 3, 2026. https://www.vaoig.gov/sites/default/files /reports/2024-09/vaoig-22-03591-231.pdf
- EHR deployment schedule. VA EHR Modernization. Updated February 2, 2026. Accessed February 3, 2026. https://digital.va.gov/ehr-modernization/ehr-deployment -schedule/
- Heckman J. VA in 2026 looks to get EHR rollout back on track, embark on health care reorganization. Federal News Network. December 24, 2025. Accessed February 3, 2026. https://federalnewsnetwork.com/veterans-affairs/2025/12 /va-in-2026-looks-to-get-ehr-rollout-back-on-track -embark-on-health-care-reorganization/
- US Department of Veterans Affairs Office of Academic Affiliations. Medical and dental education. Updated September 12, 2025. Accessed February 3, 2026. https://department.va.gov/academic-affiliations /medical-and-dental/
- Functions of Veterans Health Administration: health-care personnel education and training programs. 38 U.S.C. § 7302 (2026). Accessed February 3, 2026. https://uscode.house.gov/view.xhtml ?req=(title:38%20section:7302%20edition:prelim)
- Ahlness EA, Molloy-Paolillo BK, Brunner J, et al. Impacts of an electronic health record transition on Veterans Health Administration health professions trainee experience. J Gen Intern Med. 2023;38:1031-1039. doi:10.1007/s11606-023-08283-4
- Roberts DL, Mishark KJ, Alessandro STD, et al. Impact of electronic medical record transitions on the educational experiences of medical students. J Health Care Finance. 2014;41:1-5.
- Varpio L, Day K, Elliot‐Miller P, et al. The impact of adopting EHRs: how losing connectivity affects clinical reasoning. Med Educ. 2015;49:476-486. doi:10.1111/medu.12665
- Gali HE, Baxter SL, Lander L, et al. Impact of electronic health record implementation on ophthalmology trainee time expenditures. J Acad Ophthalmol (2017). 2019;11:e65-e72. doi:10.1055/s-0039-3401986
- Humphrey‐Murto S, Makus D, Moore S, et al. Training physicians and residents for the use of electronic health records— a comparative case study between two hospitals. Med Educ. 2023;57:337-348. doi:10.1111/medu.14944
- US Department of Defense. Captain James A. Lovell Federal Health Care Center: readying warriors & caring for heroes. Presentation August 10, 2022.
- Sayre G, Young J. Beyond openended questions: purposeful interview guide development to elicit rich, trustworthy data. Patient Aligned Care Teams (PACT) Demonstration Labs cyber seminar. March 21, 2018. Accessed February 3, 2026. https://www.hsrd.research.va.gov/for _researchers/cyber_seminars/catalog/transcripts/2439.doc
- Jordan PW, Thomas B, McClelland IL, Weerdmeester B, eds. Usability Evaluation In Industry. CRC Press; 1996.
- Keitz SA, Holland GJ, Melander EH, et al. The Veterans Affairs Learners’ Perceptions Survey: the foundation for educational quality improvement. Acad Med. 2003;78:910- 917. doi:10.1097/00001888-200309000-00016
- Byrne JM, Chang BK, Gilman SC, et al. The learners’ perceptions survey—primary care: assessing resident perceptions of internal medicine continuity clinics and patient- centered care. J Grad Med Educ. 2013;5:587-593. doi:10.4300/JGME-D-12-00233.1
- Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62:107-115. doi:10.1111/j.1365-2648.2007.04569.x
- Siller AB, Tompkins L. The big four: analyzing complex sample survey data using SAS, SPSS, STATA, and SUDAAN. Poster presented at: 31st Annual SAS Users Group International Conference; March 27, 2006; San Francisco, CA. Accessed February 3, 2026. https://support.sas.com /resources/papers/proceedings/proceedings/sugi31/172 -31.pdf
- Tashakkori A, Johnson RB, Teddlie C. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative Approaches in the Social and Behavioral Sciences. 2nd ed. SAGE Publications, Inc.; 2020.
- Olmos-Vega FM, Stalmeijer RE, Varpio L, et al. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45:241-251. doi:10.1080/0142159X.2022.2057287
- Mezirow J. Fostering Critical Reflection in Adulthood: A Guide to Transformative and Emancipatory Learning. JosseyBass; 1991.
- Probst B, Berenson L. The double arrow: how qualitative social work researchers use reflexivity. Qual Soc Work. 2014;13:813-827. doi:10.1177/1473325013506248
- Huang C, Koppel R, McGreevey JD 3rd, et al. Transitions from one electronic health record to another: challenges, pitfalls, and recommendations. Appl Clin Infor. 2020;11:742-754. doi:10.1055/s-0040-1718535
- Zheng K, Abraham J, Novak LL, et al. A survey of the literature on unintended consequences associated with health information technology: 2014–2015. Yearb Med Inform. 2016;25:13-29. doi:10.15265/IY-2016-036
- Campbell EM, Sittig DF, Ash JS, et al. Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2006;13:547-556. doi:10.1197/jamia.M2042
- Sittig DF, Lakhani P, Singh H. Applying requisite imagination to safeguard electronic health record transitions. JAMA. 2022;29:1014-1018. doi:10.1093/jamia/ocab291
- Ko HH, Lee TK, Leung Y, et al. Factors influencing career choices made by medical students, residents, and practising physicians. B C Med J. 2007;49:482-489.
- Brunner J, Ahlness EA, Anderson E, et al. VA’s EHR transition and health professions trainee programs: findings and impacts of a multistakeholder learning community. Learn Health Sys. 2024;9:e10460. doi:10.1002/lrh2.10460
- Rosdahl JA, Rudd M, Benjamin R, et al. Effect of the adoption of a comprehensive electronic health record on graduate medical education: perceptions of faculty and trainees. South Med J. 2018;111:476-483. doi:10.14423/SMJ.0000000000000847
- Hill C. U.S. Medical education at VA: it’s all about the veterans. VA News. August 18, 2021. Accessed February 3, 2026. https://news.va.gov/93370/medical-education-at-va -its-all-about-the-veterans
- Hanauer DA, Branford GL, Greenberg G, et al. Twoyear longitudinal assessment of physicians’ perceptions after replacement of a longstanding homegrown electronic health record: does a J-curve of satisfaction really exist? J Am Med Inform Assoc. 2017;24:e157-e165. doi:10.1093/jamia/ocw077
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record
Evaluation of Health Professions Trainee Experiences Transitioning to New VHA Electronic Health Record

Median Income and Clinical Outcomes of Hospitalized Persons With COVID-19 at an Urban Veterans Affairs Medical Center
Median Income and Clinical Outcomes of Hospitalized Persons With COVID-19 at an Urban Veterans Affairs Medical Center
Large epidemiologic studies have shown disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status (SES). Racial and ethnic minorities and individuals of lower SES have experienced disproportionately higher rates of intensive care unit (ICU) admission and death. In Washington, DC, Black individuals (47% of the population) accounted for 51% of COVID-19 cases and 75% of deaths. In comparison, White individuals (41% of the population) accounted for 21% of cases and 11% of deaths.1 Place of residence, such as living in socially vulnerable communities, has also been shown to be associated with higher rates of COVID-19 mortality and lower vaccination rates.2-4 Social and structural inequities, such as limited access to health care services and mistrust of the health care system, may explain some of the observed disparities.5 However, data are limited regarding COVID-19 outcomes for individuals with equal access to care.
The Veterans Health Administration (VHA) is the largest integrated US health care system and operates 123 acute care hospitals. Previous research has demonstrated that disparities in outcomes for other diseases are attenuated or erased among veterans receiving VHA care.6,7 Based on literature from the pandemic, markers of health care inequity relating to SES (eg, place of residence, median income) are expected to impact the outcomes of patients acutely hospitalized with COVID-19.4 We hypothesized that the impact on clinical outcomes of infection would be mitigated for veterans receiving VHA care.
This retrospective cohort study included veterans who presented to Washington Veterans Affairs Medical Center (WVAMC) with the goal of determining whether place of residence as a marker of SES, health care access, and median income were predictive of COVID-19 disease severity.
Methods
The WVAMC serves about 125,000 veterans across the metropolitan area, including parts of Maryland and Virginia. It is a high-complexity hospital with 164 acute care beds, 30 psychosocial residential rehabilitation beds, and an adjacent 120-bed community living center providing long-term, hospice, and palliative care.8
The WVAMC developed a dashboard that tracked patients with COVID-19 through on-site testing by admission date, ward, and other key demographics (PowerBi, Corporate Data Warehouse). All patients admitted to WVAMC with a diagnosis of COVID-19 between March 1, 2020, and June 30, 2021, were included in this retrospective review. Using the Computerized Patient Record System (CPRS) and the dashboard, we collected demographic information, baseline clinical diagnoses, laboratory results, and clinical interventions for all patients with documented COVID-19 infection as established by laboratory testing methods available at the time of diagnosis. Veterans treated exclusively outside the WVAMC were excluded. Hospitalization was defined as any acute inpatient admission or transfer recorded within 5 days before and 30 days after the laboratory collection of a positive COVID-19 test. Home testing kits were not widely available during the study period. An ICU stay was defined as any inpatient admission or transfer recorded within 5 days before or 30 days after the laboratory collection of a positive COVID-19 test for which the ward location had the specialty of medical or surgical ICU. Death due to COVID-19 was defined as occurring within 42 days (6 weeks) of a positive COVID-19 test.9 This definition assumed that during the peak of the pandemic, COVID-19 was the attributable cause of death, despite the possible contribution of underlying health conditions.
Patients’ admission periods were based on US Centers for Disease Control and Prevention (CDC) national data and classified as early 2020 (January 2020–April 2020), mid-2020 (May 2020–August 2020), late 2020 (September 2020–December 2020), and early 2021 (January 2021–April 2021).10 We chose to use these time periods as surrogates for the frequent changes in circulating COVID-19 variants, surges in case numbers, therapies and interventions available during the pandemic. The dominant COVID-19 variant during the study period was Alpha (B.1.17). Beta (B.1.351) variants were circulating infrequently, and Delta and Omicron appeared after the study period.11 Treatment strategies evolved rapidly with emerging evidence, including the use of dexamethasone, beginning in June 2020.12 WVAMC followed the Advisory Committee on Immunization Practices guidance on vaccination rollout beginning in December 2020.13
Patients' income was estimated by the median household income of the zip code residence based on US Census Bureau 2021 estimates and was assessed as both a continuous and categorical variable.14 The Charlson Comorbidity Index (CCI) was included in models as a continuous variable.15 Variables contributing to the CCI include myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, hemiplegia or paraplegia, ulcer disease, hepatic disease, diabetes (with or without end-organ damage), chronic obstructive pulmonary disease (COPD), connective tissue disease, leukemia, lymphoma, moderate or severe renal disease, solid tumor (with or without metastases), and HIV/AIDS. The WVAMC Institutional Review Board approved this study (IRB #1573071).
Variables
This study assessed 3 primary outcomes as indicators of disease severity during hospitalization: need for high-flow oxygen (HFO), intubation, and presumed mortality at any time during hospitalization. The following variables were collected as potential social determinants or clinical risk-adjustment predictors of disease severity outcomes: age; sex; race and ethnicity; median income for patient’s zip code residence, state, and county; wards within Washington, DC; comorbidities, CCI; tobacco use; and body mass index.15 Although medications at baseline, treatments during hospitalization for COVID-19, and laboratory parameters during hospitalization are shown in eAppendices 1 and 2, they are beyond the scope of this analysis.
Statistical Analysis
Three types of logistic regression models were calculated for predicting the disease severity outcomes: (1) simple unadjusted models; (2) models predicting from single variables plus age (age-adjusted); and (3) multivariable models using all nonredundant potential predictors with adequate sample sizes (multivariable). Variables were considered to have inadequate sample sizes if there was nontrivial missing data or small numbers within categories, (eg, AIDS, connective tissue disease). Potential predictors for the multivariable model included age, sex, race, median income by zip code residence, CCI, CDC admission period, obesity, hypertension, chronic kidney disease, obstructive sleep apnea (OSA), diabetes, COPD or asthma, liver disease, antibiotics, and acute kidney injury.
For the multivariable models, the following modifications were made to avoid unreliable parameter estimation and computation problems (quasi-separation): age and CCI were included as continuous rather than categorical variables. Race was recoded as a 2-category variable (Black vs other [White, Hispanic, American Indian, Alaska Native, Asian, Native Hawaiian, and Pacific Islander]), and ethnicity was excluded because of the small number of patients in this group (n = 16). Admission period was included. Predicted probability plots were generated for each outcome with continuous independent predictors (income and CCI), both unadjusted and adjusted for age as a continuous covariate. All analyses were performed using SAS version 9.4.
Heat Maps
Heat maps were generated to visualize the geospatial distribution of COVID-19 cases and median incomes across zip codes in the greater Washington, DC area. Patient case data and median income, aggregated by zip code, were imported using ArcGIS Online. A zip code boundary layer from Esri (United States Zip Code Boundaries) was used to spatially align the case data. Data were joined by matching zip codes or median incomes in the patient dataset to those in the boundary layer. The resulting polygon layer was styled using the Counts and Amounts (Color) symbology in ArcGIS Online, with case counts or median income determining the intensity of the color gradient.
Results
Between March 1, 2020, and June 30, 2021, 348 patients were hospitalized with COVID-19 (Table 1). The mean (SD) age was 68.4 (13.9) years, 313 patients (90.2%) were male, 281 patients (83.4%) were Black, 47 patients (13.6%) were White, and 16 patients (4.8%) were Hispanic. One hundred forty patients (40.2%) resided in Washington, DC, 151 (43.4%) in Maryland, and 19 (5.5%) in Virginia. HFO was received by 86 patients (24.7%), 33 (9.5%) required intubation and mechanical ventilation, and 57 (16.4%) died. All intubations and deaths occurred among patients aged > 50 years, with death occurring in 17.8% of patients aged > 50 years.
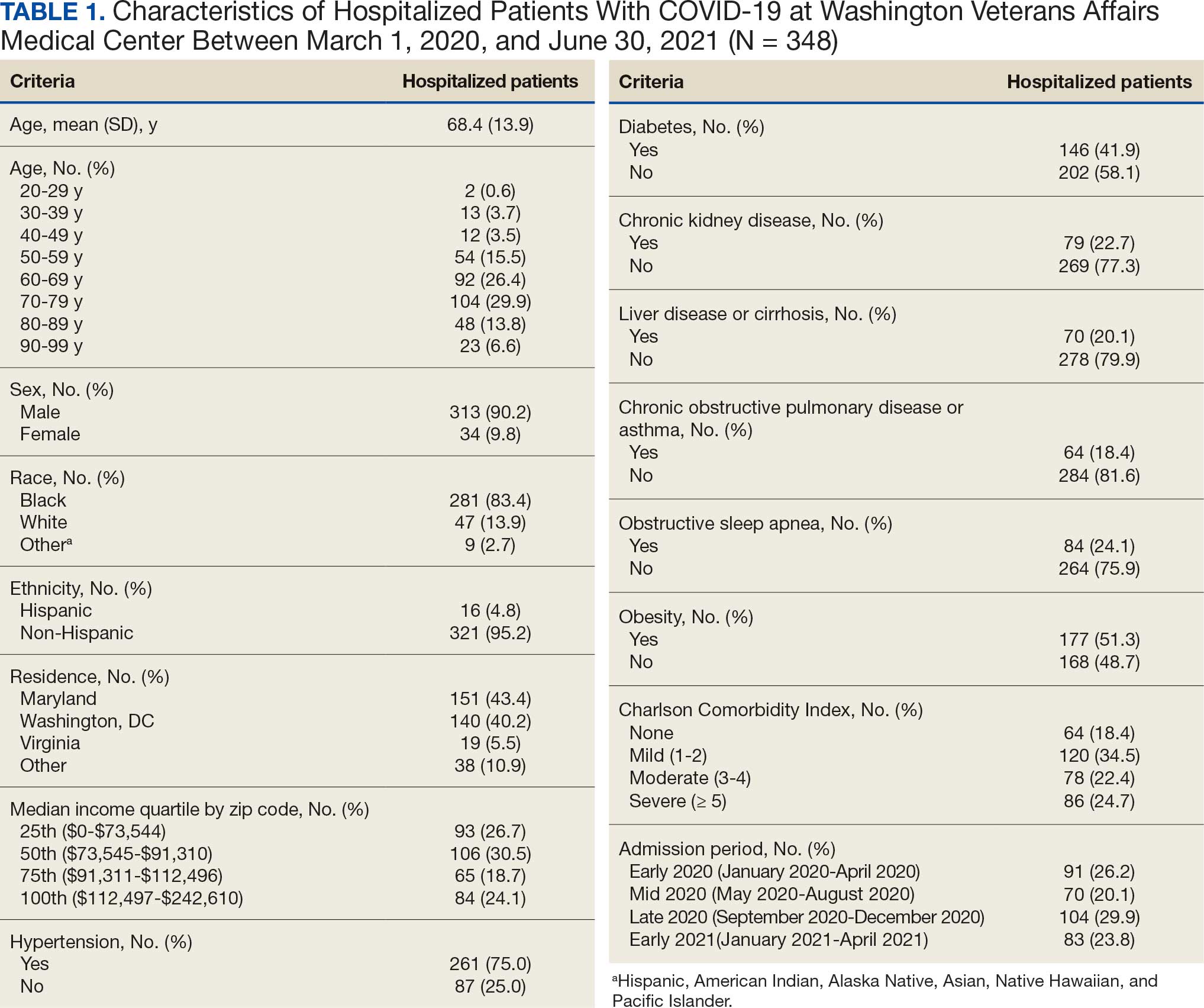
Demographic characteristics and baseline comorbidities associated with COVID-19 disease severity can be found in eAppendix 2. In unadjusted analyses, age was significantly associated with the risk of HFO, with a mean (SD) age of 72.5 (11.7) years among those requiring HFO and 67.1 (14.4) years among patients without HFO (odds ratio [OR], 1.03; 95% CI, 1.01-1.05; P = .002). Although age was not associated with the risk of intubation, it was significantly associated with mortality. Patients who died had a mean (SD) age of 76.8 (11.8) years compared with 66.8 (13.7) years among survivors (OR, 1.06; 95% CI, 1.04-1.09; P < .001).
Compared with patients with no comorbidities, CCI categories of mild, moderate, and severe were associated with increased risk of requiring HFO (eAppendix 3). The adjusted OR (aOR) was highest among patients with severe CCI (aOR, 7.00; 95% CI, 2.42-20.32; P = .0007). In age-adjusted analyses, CCI was not associated with intubation or mortality.
Geospatial Analyses
State of residence, county of residence, and geographic area (including Washington, DC wards, and geographic divisions within counties of residence in Maryland and Virginia) were not associated with the clinical outcomes studied (eAppendix 4). However, zip code-based median income, analyzed as a continuous variable, was associated with a reduced likelihood of receiving HFO (aOR, 0.91; 95% CI, 0.84-0.99; P = .03). Income was not significantly associated with intubation or mortality.
The majority of patients hospitalized for COVID-19 at WVAMC resided in zip codes in eastern Washington, DC, inclusive of wards 7 and 8, and Prince George’s County, Maryland (Figure 1). These areas also corresponded to the lowest median household income by zip code (Figure 2).
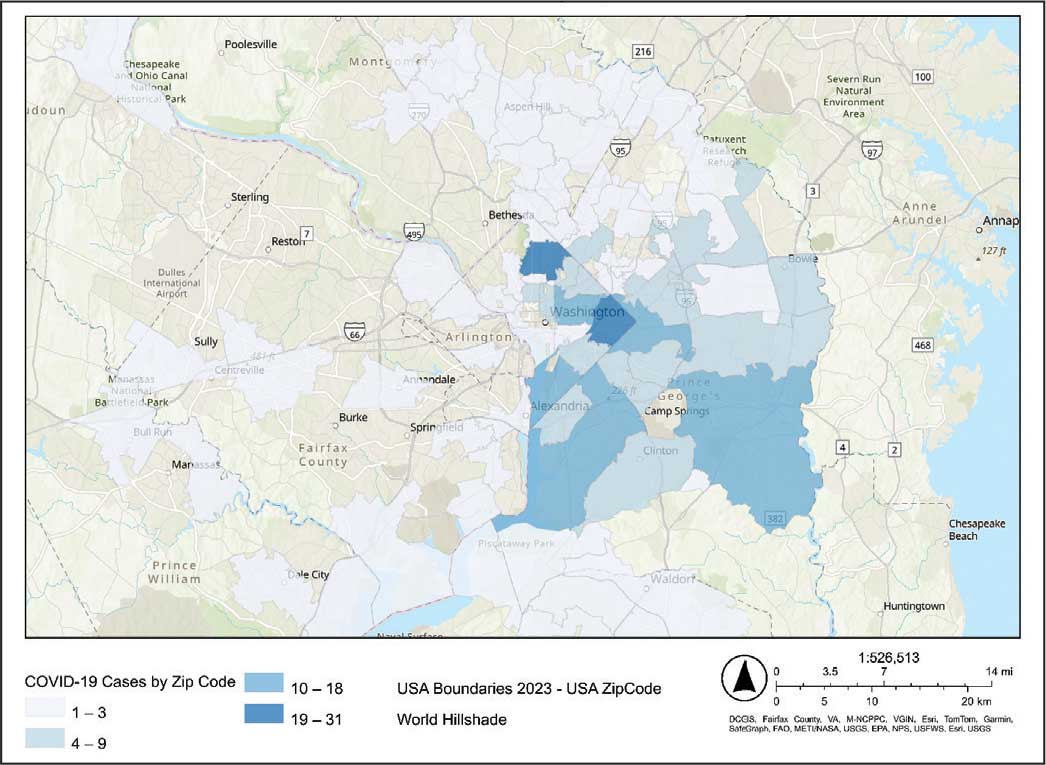
Code
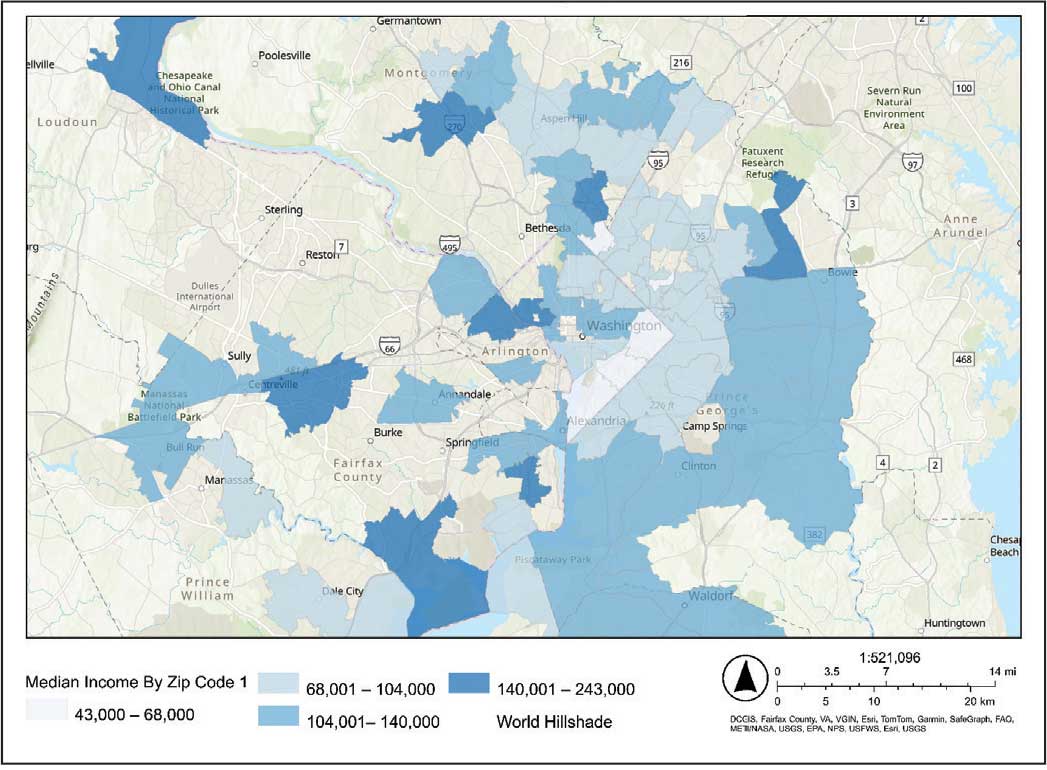
Code
Multivariable Analysis
Significant predictors of HFO requirement included comorbid diabetes (OR, 2.42; 95% CI, 1.27-4.61; P = .006) and liver disease or cirrhosis (OR, 2.19; 95% CI, 1.09-4.39; P = .02) (Table 2). CDC admission period was also associated with HFO need. Patients admitted after early 2020 had lower odds of receiving HFO. Race and median income based on zip code residence were not associated with HFO requirement.
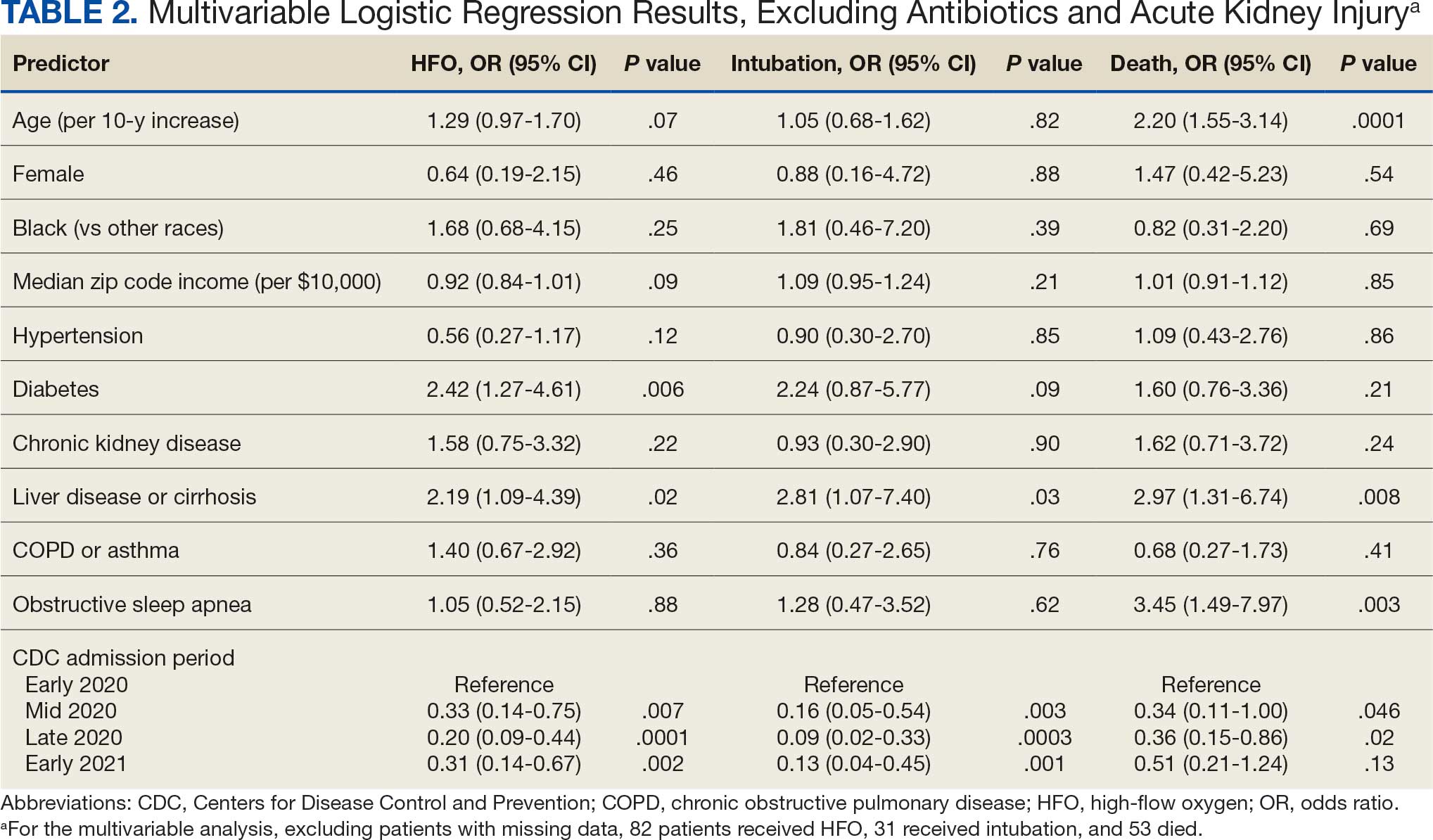
Comorbid liver disease or cirrhosis was a significant predictor of intubation (OR, 2.81; 95% CI, 1.07-7.40; P = .03). CDC admission period was associated with intubation with lower odds of intubation for patients admitted after early 2020. Race and median income by zip code were not associated with intubation.
Significant predictors of mortality included age (OR, 2.20; 95% CI, 1.55-3.14; P = .0001), comorbid liver disease or cirrhosis (OR, 2.97; 95% CI, 1.31-6.74; P = .008), and OSA (OR, 3.45; 95% CI, 1.49-7.97; P = .003). CDC admission period was associated with mortality, with lower odds of intubation for patients admitted in mid- and late 2020. Race and median income by zip code residence were not associated with intubation.
Discussion
In this study of COVID-19 disease severity at a large integrated health care system that provides equal access to care, race, ethnicity, and geographic location were not associated with the need for HFO, intubation, or presumed mortality. Median income by zip code residence was associated with reduced HFO use in univariable analyses but not in multivariable models.
These findings support existing literature suggesting that race and ethnicity alone do not explain disparities in COVID-19 outcomes. Multiple studies have demonstrated that disparities in health outcomes have been reduced for patients receiving VHA care.6,16-19 However, even within a health care system with assumed equal access, the finding of an association between income and need for HFO in the univariable analysis may reflect a greater likelihood of delays in care due to structural barriers. Multiple studies suggest low SES may be an independent risk factor for severe COVID-19 disease. Individuals with low SES have higher rates of chronic diseases of obesity, diabetes, heart disease, and lung disease; thus, they are also at greater risk of serious illness with COVID-19.20-24 Socioeconomic disadvantage may also have limited individuals’ ability to engage in protective behaviors to reduce COVID-19 infection risk, including food stockpiling, social distancing, avoidance of public transportation, and refraining from working in “essential jobs.”21
Beyond SES, place of residence also influences health outcomes. Prior literature supports using zip codes to assess area-based SES status and monitor health disparities.25 The Social Vulnerability Index incorporates SES factors for communities and measures social determinates of health at a zip code level exclusive of race and ethnicity.26 Socially vulnerable communities are known to have higher rates of chronic diseases, COVID-19 mortality, and lower vaccination rates.3 Within a defined geographic area, an individual’s outcome for COVID-19 can be influenced by individual resources such as access to care and median income. Disposable income may mitigate COVID-19 risk by facilitating timely care, reducing occupational exposure, improving housing stability, and supporting health-promoting behaviors.21
Limitations
Due to the evolving nature of the COVID-19 pandemic, variants, treatments, and interventions varied throughout the study period and are not included in this analysis. In late December 2020, COVID-19 vaccination was approved with a tiered allocation for at-risk patients and direct health care professionals. Three of the 4 study periods analyzed in this study were prior to vaccine rollout and therefore vaccination history was not assessed. However, we tried to capture the evolving changes in COVID-19 variants, treatments and interventions, and skill in treating the disease through use of CDC-defined time frames. Another limitation is that some studies have shown that use of median income by zip code residence can underestimate mortality.27 Also, shared resources and access to other sources of disposable income can impact the immediate attainment of social needs. For example, during the COVID-19 pandemic, health care systems in Washington, DC assisted vulnerable individuals by providing food, housing, and other resources.28,29 Finally, the modest sample size limits generalizability and power to detect differences for certain variables, including Hispanic ethnicity.
Conclusions
There have been widely described disparities in disease severity and death during the COVID-19 pandemic. In this urban veteran cohort of hospitalized patients, there was no difference in the need for intubation or mortality associated with race. The findings suggest that a lower median income by zip code residence may be associated with greater disease severity at presentation, but do not predict severe outcomes and mortality overall. VHA care, which provides equal access to care, may mitigate the disparities seen in the private sector.
- District of Columbia: All Race & Ethnicity Data. The COVID Tracking Project. Accessed December 10, 2025. https://covidtracking.com/data/state/district-of-columbia/race-ethnicity
- Freese KE, Vega A, Lawrence JJ, et al. Social vulnerability is associated with risk of COVID-19 related mortality in U.S. counties with confirmed cases. J Health Care Poor Underserved. 2021;32:245-257. doi:10.1353/hpu.2021.0022
- Saulsberry L, Bhargava A, Zeng S, et al. The social vulnerability metric (SVM) as a new tool for public health. Health Serv Res. 2023;58:873-881. doi:10.1111/1475-6773.14102
- Romano SD, Blackstock AJ, Taylor EV, et al. Trends in racial and ethnic disparities in COVID-19 hospitalizations, by region - United States, March-December 2020. MMWR Morb Mortal Wkly Rep. 2021;70:560-565. doi:10.15585/mmwr.mm7015e2
- Kullar R, Marcelin JR, Swartz TH, et al. Racial disparity of coronavirus disease 2019 in African American communities. J Infect Dis. 2020;222:890-893. doi:10.1093/infdis/jiaa372
- Riviere P, Luterstein E, Kumar A, et al. Survival of African American and non-Hispanic White men with prostate cancer in an equal-access health care system. Cancer. 2020;126:1683-1690. doi:10.1002/cncr.32666
- Ohl ME, Richardson Miell K, Beck BF, et al. Mortality among US veterans admitted to community vs Veterans Health Administration hospitals for COVID-19. JAMA Netw Open. 2023;6:e2315902. doi:10.1001/jamanetworkopen.2023.15902
- US Department of Veterans Affairs. VA Washington DC Health Care. Accessed January 16, 2026. https://www.va.gov/washington-dc-health-care/about-us/
- Trottier C, La J, Li LL, et al. Maintaining the utility of coronavirus disease 2019 pandemic severity surveillance: evaluation of trends in attributable deaths and development and validation of a measurement tool. Clin Infect Dis. 2023;77:1247-1256. doi:10.1093/cid/ciad381
- Centers for Disease Control and Prevention. CDC Museum COVID-19 Timeline. Updated July 8, 2024. Accessed January 16, 2026. https://www.cdc.gov/museum/timeline/covid19.html#Early-2020
- Centers for Disease Control and Prevention. Covid-surveillance and data analytics. September 5, 2025. Accessed January 16, 2026. cdc.gov/covid/php/surveillance/index.html12.
- RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704. doi:10.1056/NEJMoa2021436
- Dooling K, Marin M, Wallace M, et al. The Advisory Committee on Immunization Practices’ updated interim recommendation for allocation of COVID-19 Vaccine - United States, December 2020. MMWR Morb Mortal Wkly Rep. 2021;69:1657-1660. doi:10.15585/mmwr.mm695152e2
- US Census Bureau. Explore census data. Accessed December 10, 2025. https://data.census.gov/profile?q=Income%20by%20Zip%20code%20tabulation%20area
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-383. doi:10.1016/0021-9681(87)90171-8
- Zullig LL, Carpenter WR, Provenzale D, Weinberger M, Reeve BB, Jackson GL. Examining potential colorectal cancer care disparities in the Veterans Affairs health care system. J Clin Oncol. 2013;31:3579-3584. doi:10.1200/JCO.2013.50.4753
- Grubaugh AL, Slagle DM, Long M, Frueh BC, Magruder KM. Racial disparities in trauma exposure, psychiatric symptoms, and service use among female patients in Veterans Affairs primary care clinics. Womens Health Issues. 2008;18:433-441. doi:10.1016/j.whi.2008.08.001
- Bosworth HB, Parsey KS, Butterfield MI, et al. Racial variation in wanting and obtaining mental health services among women veterans in a primary care clinic. J Natl Med Assoc. 2000;92:231-236.
- Luo J, Rosales M, Wei G, et al. Hospitalization, mechanical ventilation, and case-fatality outcomes in US veterans with COVID-19 disease between years 2020-2021. Ann Epidemiol. 2022;70:37-44. doi:10.1016/j.annepidem.2022.04.003
- Kondo K, Low A, Everson T, et al. Health disparities in veterans: a map of the evidence. Med Care. 2017;55 Suppl 9 Suppl 2:S9-S15. doi:10.1097/MLR.0000000000000756
- Grosicki GJ, Bunsawat K, Jeong S, Robinson AT. Racial and ethnic disparities in cardiometabolic disease and COVID-19 outcomes in White, Black/African American, and Latinx populations: Social determinants of health. Prog Cardiovasc Dis. 2022;71:4-10. doi:10.1016/j.pcad.2022.04.004
- National Center for Immunization and Respiratory Diseases (U.S.). Division of Viral Diseases. Coronavirus Disease 2019 (COVID-19): COVID-19 in Racial and Ethnic Minority Groups: June 4, 2020. CDC Stacks. June 4, 2020. Accessed January 14, 2026. https://stacks.cdc.gov/view/cdc/88770
- Yancy CW. COVID-19 and African Americans. JAMA. 2020;323:1891-1892. doi:10.1001/jama.2020.6548
- Magesh S, John D, Li WT, et al. Disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status: a systematic-review and meta-analysis. JAMA Netw Open. 2021;4:e2134147. doi:10.1001/jamanetworkopen.2021.34147
- Berkowitz SA, Traore CY, Singer DE, Atlas SJ. Evaluating area-based socioeconomic status indicators for monitoring disparities within health care systems: results from a primary care network. Health Serv Res. 2015;50:398-417. doi:10.1111/1475-6773.12229
- Social Vulnerability Index. Agency for Toxicity and Disease Registry. July 22, 2024. Accessed January 14, 2026. https://www.atsdr.cdc.gov/placeandhealth/svi/index.html
- Moss JL, Johnson NJ, Yu M, Altekruse SF, Cronin KA. Comparisons of individual- and area-level socioeconomic status as proxies for individual-level measures: evidence from the Mortality Disparities in American Communities study. Popul Health Metr. 2021;19:1. doi:10.1186/s12963-020-00244-x
- DC Department of Human Services. Response to COVID-19. Accessed January 14, 2026. https://dhs.dc.gov/page/responsetocovid19
- Wang PG, Brisbon NM, Hubbell H, et al. Is the Gap Closing? Comparison of sociodemographic cisparities in COVID-19 hospitalizations and outcomes between two temporal waves of admissions. J Racial Ethn Health Disparities. 2023;10:593-602. doi:10.1007/s40615-022-01249-y
Large epidemiologic studies have shown disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status (SES). Racial and ethnic minorities and individuals of lower SES have experienced disproportionately higher rates of intensive care unit (ICU) admission and death. In Washington, DC, Black individuals (47% of the population) accounted for 51% of COVID-19 cases and 75% of deaths. In comparison, White individuals (41% of the population) accounted for 21% of cases and 11% of deaths.1 Place of residence, such as living in socially vulnerable communities, has also been shown to be associated with higher rates of COVID-19 mortality and lower vaccination rates.2-4 Social and structural inequities, such as limited access to health care services and mistrust of the health care system, may explain some of the observed disparities.5 However, data are limited regarding COVID-19 outcomes for individuals with equal access to care.
The Veterans Health Administration (VHA) is the largest integrated US health care system and operates 123 acute care hospitals. Previous research has demonstrated that disparities in outcomes for other diseases are attenuated or erased among veterans receiving VHA care.6,7 Based on literature from the pandemic, markers of health care inequity relating to SES (eg, place of residence, median income) are expected to impact the outcomes of patients acutely hospitalized with COVID-19.4 We hypothesized that the impact on clinical outcomes of infection would be mitigated for veterans receiving VHA care.
This retrospective cohort study included veterans who presented to Washington Veterans Affairs Medical Center (WVAMC) with the goal of determining whether place of residence as a marker of SES, health care access, and median income were predictive of COVID-19 disease severity.
Methods
The WVAMC serves about 125,000 veterans across the metropolitan area, including parts of Maryland and Virginia. It is a high-complexity hospital with 164 acute care beds, 30 psychosocial residential rehabilitation beds, and an adjacent 120-bed community living center providing long-term, hospice, and palliative care.8
The WVAMC developed a dashboard that tracked patients with COVID-19 through on-site testing by admission date, ward, and other key demographics (PowerBi, Corporate Data Warehouse). All patients admitted to WVAMC with a diagnosis of COVID-19 between March 1, 2020, and June 30, 2021, were included in this retrospective review. Using the Computerized Patient Record System (CPRS) and the dashboard, we collected demographic information, baseline clinical diagnoses, laboratory results, and clinical interventions for all patients with documented COVID-19 infection as established by laboratory testing methods available at the time of diagnosis. Veterans treated exclusively outside the WVAMC were excluded. Hospitalization was defined as any acute inpatient admission or transfer recorded within 5 days before and 30 days after the laboratory collection of a positive COVID-19 test. Home testing kits were not widely available during the study period. An ICU stay was defined as any inpatient admission or transfer recorded within 5 days before or 30 days after the laboratory collection of a positive COVID-19 test for which the ward location had the specialty of medical or surgical ICU. Death due to COVID-19 was defined as occurring within 42 days (6 weeks) of a positive COVID-19 test.9 This definition assumed that during the peak of the pandemic, COVID-19 was the attributable cause of death, despite the possible contribution of underlying health conditions.
Patients’ admission periods were based on US Centers for Disease Control and Prevention (CDC) national data and classified as early 2020 (January 2020–April 2020), mid-2020 (May 2020–August 2020), late 2020 (September 2020–December 2020), and early 2021 (January 2021–April 2021).10 We chose to use these time periods as surrogates for the frequent changes in circulating COVID-19 variants, surges in case numbers, therapies and interventions available during the pandemic. The dominant COVID-19 variant during the study period was Alpha (B.1.17). Beta (B.1.351) variants were circulating infrequently, and Delta and Omicron appeared after the study period.11 Treatment strategies evolved rapidly with emerging evidence, including the use of dexamethasone, beginning in June 2020.12 WVAMC followed the Advisory Committee on Immunization Practices guidance on vaccination rollout beginning in December 2020.13
Patients' income was estimated by the median household income of the zip code residence based on US Census Bureau 2021 estimates and was assessed as both a continuous and categorical variable.14 The Charlson Comorbidity Index (CCI) was included in models as a continuous variable.15 Variables contributing to the CCI include myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, hemiplegia or paraplegia, ulcer disease, hepatic disease, diabetes (with or without end-organ damage), chronic obstructive pulmonary disease (COPD), connective tissue disease, leukemia, lymphoma, moderate or severe renal disease, solid tumor (with or without metastases), and HIV/AIDS. The WVAMC Institutional Review Board approved this study (IRB #1573071).
Variables
This study assessed 3 primary outcomes as indicators of disease severity during hospitalization: need for high-flow oxygen (HFO), intubation, and presumed mortality at any time during hospitalization. The following variables were collected as potential social determinants or clinical risk-adjustment predictors of disease severity outcomes: age; sex; race and ethnicity; median income for patient’s zip code residence, state, and county; wards within Washington, DC; comorbidities, CCI; tobacco use; and body mass index.15 Although medications at baseline, treatments during hospitalization for COVID-19, and laboratory parameters during hospitalization are shown in eAppendices 1 and 2, they are beyond the scope of this analysis.
Statistical Analysis
Three types of logistic regression models were calculated for predicting the disease severity outcomes: (1) simple unadjusted models; (2) models predicting from single variables plus age (age-adjusted); and (3) multivariable models using all nonredundant potential predictors with adequate sample sizes (multivariable). Variables were considered to have inadequate sample sizes if there was nontrivial missing data or small numbers within categories, (eg, AIDS, connective tissue disease). Potential predictors for the multivariable model included age, sex, race, median income by zip code residence, CCI, CDC admission period, obesity, hypertension, chronic kidney disease, obstructive sleep apnea (OSA), diabetes, COPD or asthma, liver disease, antibiotics, and acute kidney injury.
For the multivariable models, the following modifications were made to avoid unreliable parameter estimation and computation problems (quasi-separation): age and CCI were included as continuous rather than categorical variables. Race was recoded as a 2-category variable (Black vs other [White, Hispanic, American Indian, Alaska Native, Asian, Native Hawaiian, and Pacific Islander]), and ethnicity was excluded because of the small number of patients in this group (n = 16). Admission period was included. Predicted probability plots were generated for each outcome with continuous independent predictors (income and CCI), both unadjusted and adjusted for age as a continuous covariate. All analyses were performed using SAS version 9.4.
Heat Maps
Heat maps were generated to visualize the geospatial distribution of COVID-19 cases and median incomes across zip codes in the greater Washington, DC area. Patient case data and median income, aggregated by zip code, were imported using ArcGIS Online. A zip code boundary layer from Esri (United States Zip Code Boundaries) was used to spatially align the case data. Data were joined by matching zip codes or median incomes in the patient dataset to those in the boundary layer. The resulting polygon layer was styled using the Counts and Amounts (Color) symbology in ArcGIS Online, with case counts or median income determining the intensity of the color gradient.
Results
Between March 1, 2020, and June 30, 2021, 348 patients were hospitalized with COVID-19 (Table 1). The mean (SD) age was 68.4 (13.9) years, 313 patients (90.2%) were male, 281 patients (83.4%) were Black, 47 patients (13.6%) were White, and 16 patients (4.8%) were Hispanic. One hundred forty patients (40.2%) resided in Washington, DC, 151 (43.4%) in Maryland, and 19 (5.5%) in Virginia. HFO was received by 86 patients (24.7%), 33 (9.5%) required intubation and mechanical ventilation, and 57 (16.4%) died. All intubations and deaths occurred among patients aged > 50 years, with death occurring in 17.8% of patients aged > 50 years.
Demographic characteristics and baseline comorbidities associated with COVID-19 disease severity can be found in eAppendix 2. In unadjusted analyses, age was significantly associated with the risk of HFO, with a mean (SD) age of 72.5 (11.7) years among those requiring HFO and 67.1 (14.4) years among patients without HFO (odds ratio [OR], 1.03; 95% CI, 1.01-1.05; P = .002). Although age was not associated with the risk of intubation, it was significantly associated with mortality. Patients who died had a mean (SD) age of 76.8 (11.8) years compared with 66.8 (13.7) years among survivors (OR, 1.06; 95% CI, 1.04-1.09; P < .001).
Compared with patients with no comorbidities, CCI categories of mild, moderate, and severe were associated with increased risk of requiring HFO (eAppendix 3). The adjusted OR (aOR) was highest among patients with severe CCI (aOR, 7.00; 95% CI, 2.42-20.32; P = .0007). In age-adjusted analyses, CCI was not associated with intubation or mortality.
Geospatial Analyses
State of residence, county of residence, and geographic area (including Washington, DC wards, and geographic divisions within counties of residence in Maryland and Virginia) were not associated with the clinical outcomes studied (eAppendix 4). However, zip code-based median income, analyzed as a continuous variable, was associated with a reduced likelihood of receiving HFO (aOR, 0.91; 95% CI, 0.84-0.99; P = .03). Income was not significantly associated with intubation or mortality.
The majority of patients hospitalized for COVID-19 at WVAMC resided in zip codes in eastern Washington, DC, inclusive of wards 7 and 8, and Prince George’s County, Maryland (Figure 1). These areas also corresponded to the lowest median household income by zip code (Figure 2).
Code
Code
Multivariable Analysis
Significant predictors of HFO requirement included comorbid diabetes (OR, 2.42; 95% CI, 1.27-4.61; P = .006) and liver disease or cirrhosis (OR, 2.19; 95% CI, 1.09-4.39; P = .02) (Table 2). CDC admission period was also associated with HFO need. Patients admitted after early 2020 had lower odds of receiving HFO. Race and median income based on zip code residence were not associated with HFO requirement.
Comorbid liver disease or cirrhosis was a significant predictor of intubation (OR, 2.81; 95% CI, 1.07-7.40; P = .03). CDC admission period was associated with intubation with lower odds of intubation for patients admitted after early 2020. Race and median income by zip code were not associated with intubation.
Significant predictors of mortality included age (OR, 2.20; 95% CI, 1.55-3.14; P = .0001), comorbid liver disease or cirrhosis (OR, 2.97; 95% CI, 1.31-6.74; P = .008), and OSA (OR, 3.45; 95% CI, 1.49-7.97; P = .003). CDC admission period was associated with mortality, with lower odds of intubation for patients admitted in mid- and late 2020. Race and median income by zip code residence were not associated with intubation.
Discussion
In this study of COVID-19 disease severity at a large integrated health care system that provides equal access to care, race, ethnicity, and geographic location were not associated with the need for HFO, intubation, or presumed mortality. Median income by zip code residence was associated with reduced HFO use in univariable analyses but not in multivariable models.
These findings support existing literature suggesting that race and ethnicity alone do not explain disparities in COVID-19 outcomes. Multiple studies have demonstrated that disparities in health outcomes have been reduced for patients receiving VHA care.6,16-19 However, even within a health care system with assumed equal access, the finding of an association between income and need for HFO in the univariable analysis may reflect a greater likelihood of delays in care due to structural barriers. Multiple studies suggest low SES may be an independent risk factor for severe COVID-19 disease. Individuals with low SES have higher rates of chronic diseases of obesity, diabetes, heart disease, and lung disease; thus, they are also at greater risk of serious illness with COVID-19.20-24 Socioeconomic disadvantage may also have limited individuals’ ability to engage in protective behaviors to reduce COVID-19 infection risk, including food stockpiling, social distancing, avoidance of public transportation, and refraining from working in “essential jobs.”21
Beyond SES, place of residence also influences health outcomes. Prior literature supports using zip codes to assess area-based SES status and monitor health disparities.25 The Social Vulnerability Index incorporates SES factors for communities and measures social determinates of health at a zip code level exclusive of race and ethnicity.26 Socially vulnerable communities are known to have higher rates of chronic diseases, COVID-19 mortality, and lower vaccination rates.3 Within a defined geographic area, an individual’s outcome for COVID-19 can be influenced by individual resources such as access to care and median income. Disposable income may mitigate COVID-19 risk by facilitating timely care, reducing occupational exposure, improving housing stability, and supporting health-promoting behaviors.21
Limitations
Due to the evolving nature of the COVID-19 pandemic, variants, treatments, and interventions varied throughout the study period and are not included in this analysis. In late December 2020, COVID-19 vaccination was approved with a tiered allocation for at-risk patients and direct health care professionals. Three of the 4 study periods analyzed in this study were prior to vaccine rollout and therefore vaccination history was not assessed. However, we tried to capture the evolving changes in COVID-19 variants, treatments and interventions, and skill in treating the disease through use of CDC-defined time frames. Another limitation is that some studies have shown that use of median income by zip code residence can underestimate mortality.27 Also, shared resources and access to other sources of disposable income can impact the immediate attainment of social needs. For example, during the COVID-19 pandemic, health care systems in Washington, DC assisted vulnerable individuals by providing food, housing, and other resources.28,29 Finally, the modest sample size limits generalizability and power to detect differences for certain variables, including Hispanic ethnicity.
Conclusions
There have been widely described disparities in disease severity and death during the COVID-19 pandemic. In this urban veteran cohort of hospitalized patients, there was no difference in the need for intubation or mortality associated with race. The findings suggest that a lower median income by zip code residence may be associated with greater disease severity at presentation, but do not predict severe outcomes and mortality overall. VHA care, which provides equal access to care, may mitigate the disparities seen in the private sector.
Large epidemiologic studies have shown disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status (SES). Racial and ethnic minorities and individuals of lower SES have experienced disproportionately higher rates of intensive care unit (ICU) admission and death. In Washington, DC, Black individuals (47% of the population) accounted for 51% of COVID-19 cases and 75% of deaths. In comparison, White individuals (41% of the population) accounted for 21% of cases and 11% of deaths.1 Place of residence, such as living in socially vulnerable communities, has also been shown to be associated with higher rates of COVID-19 mortality and lower vaccination rates.2-4 Social and structural inequities, such as limited access to health care services and mistrust of the health care system, may explain some of the observed disparities.5 However, data are limited regarding COVID-19 outcomes for individuals with equal access to care.
The Veterans Health Administration (VHA) is the largest integrated US health care system and operates 123 acute care hospitals. Previous research has demonstrated that disparities in outcomes for other diseases are attenuated or erased among veterans receiving VHA care.6,7 Based on literature from the pandemic, markers of health care inequity relating to SES (eg, place of residence, median income) are expected to impact the outcomes of patients acutely hospitalized with COVID-19.4 We hypothesized that the impact on clinical outcomes of infection would be mitigated for veterans receiving VHA care.
This retrospective cohort study included veterans who presented to Washington Veterans Affairs Medical Center (WVAMC) with the goal of determining whether place of residence as a marker of SES, health care access, and median income were predictive of COVID-19 disease severity.
Methods
The WVAMC serves about 125,000 veterans across the metropolitan area, including parts of Maryland and Virginia. It is a high-complexity hospital with 164 acute care beds, 30 psychosocial residential rehabilitation beds, and an adjacent 120-bed community living center providing long-term, hospice, and palliative care.8
The WVAMC developed a dashboard that tracked patients with COVID-19 through on-site testing by admission date, ward, and other key demographics (PowerBi, Corporate Data Warehouse). All patients admitted to WVAMC with a diagnosis of COVID-19 between March 1, 2020, and June 30, 2021, were included in this retrospective review. Using the Computerized Patient Record System (CPRS) and the dashboard, we collected demographic information, baseline clinical diagnoses, laboratory results, and clinical interventions for all patients with documented COVID-19 infection as established by laboratory testing methods available at the time of diagnosis. Veterans treated exclusively outside the WVAMC were excluded. Hospitalization was defined as any acute inpatient admission or transfer recorded within 5 days before and 30 days after the laboratory collection of a positive COVID-19 test. Home testing kits were not widely available during the study period. An ICU stay was defined as any inpatient admission or transfer recorded within 5 days before or 30 days after the laboratory collection of a positive COVID-19 test for which the ward location had the specialty of medical or surgical ICU. Death due to COVID-19 was defined as occurring within 42 days (6 weeks) of a positive COVID-19 test.9 This definition assumed that during the peak of the pandemic, COVID-19 was the attributable cause of death, despite the possible contribution of underlying health conditions.
Patients’ admission periods were based on US Centers for Disease Control and Prevention (CDC) national data and classified as early 2020 (January 2020–April 2020), mid-2020 (May 2020–August 2020), late 2020 (September 2020–December 2020), and early 2021 (January 2021–April 2021).10 We chose to use these time periods as surrogates for the frequent changes in circulating COVID-19 variants, surges in case numbers, therapies and interventions available during the pandemic. The dominant COVID-19 variant during the study period was Alpha (B.1.17). Beta (B.1.351) variants were circulating infrequently, and Delta and Omicron appeared after the study period.11 Treatment strategies evolved rapidly with emerging evidence, including the use of dexamethasone, beginning in June 2020.12 WVAMC followed the Advisory Committee on Immunization Practices guidance on vaccination rollout beginning in December 2020.13
Patients' income was estimated by the median household income of the zip code residence based on US Census Bureau 2021 estimates and was assessed as both a continuous and categorical variable.14 The Charlson Comorbidity Index (CCI) was included in models as a continuous variable.15 Variables contributing to the CCI include myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, hemiplegia or paraplegia, ulcer disease, hepatic disease, diabetes (with or without end-organ damage), chronic obstructive pulmonary disease (COPD), connective tissue disease, leukemia, lymphoma, moderate or severe renal disease, solid tumor (with or without metastases), and HIV/AIDS. The WVAMC Institutional Review Board approved this study (IRB #1573071).
Variables
This study assessed 3 primary outcomes as indicators of disease severity during hospitalization: need for high-flow oxygen (HFO), intubation, and presumed mortality at any time during hospitalization. The following variables were collected as potential social determinants or clinical risk-adjustment predictors of disease severity outcomes: age; sex; race and ethnicity; median income for patient’s zip code residence, state, and county; wards within Washington, DC; comorbidities, CCI; tobacco use; and body mass index.15 Although medications at baseline, treatments during hospitalization for COVID-19, and laboratory parameters during hospitalization are shown in eAppendices 1 and 2, they are beyond the scope of this analysis.
Statistical Analysis
Three types of logistic regression models were calculated for predicting the disease severity outcomes: (1) simple unadjusted models; (2) models predicting from single variables plus age (age-adjusted); and (3) multivariable models using all nonredundant potential predictors with adequate sample sizes (multivariable). Variables were considered to have inadequate sample sizes if there was nontrivial missing data or small numbers within categories, (eg, AIDS, connective tissue disease). Potential predictors for the multivariable model included age, sex, race, median income by zip code residence, CCI, CDC admission period, obesity, hypertension, chronic kidney disease, obstructive sleep apnea (OSA), diabetes, COPD or asthma, liver disease, antibiotics, and acute kidney injury.
For the multivariable models, the following modifications were made to avoid unreliable parameter estimation and computation problems (quasi-separation): age and CCI were included as continuous rather than categorical variables. Race was recoded as a 2-category variable (Black vs other [White, Hispanic, American Indian, Alaska Native, Asian, Native Hawaiian, and Pacific Islander]), and ethnicity was excluded because of the small number of patients in this group (n = 16). Admission period was included. Predicted probability plots were generated for each outcome with continuous independent predictors (income and CCI), both unadjusted and adjusted for age as a continuous covariate. All analyses were performed using SAS version 9.4.
Heat Maps
Heat maps were generated to visualize the geospatial distribution of COVID-19 cases and median incomes across zip codes in the greater Washington, DC area. Patient case data and median income, aggregated by zip code, were imported using ArcGIS Online. A zip code boundary layer from Esri (United States Zip Code Boundaries) was used to spatially align the case data. Data were joined by matching zip codes or median incomes in the patient dataset to those in the boundary layer. The resulting polygon layer was styled using the Counts and Amounts (Color) symbology in ArcGIS Online, with case counts or median income determining the intensity of the color gradient.
Results
Between March 1, 2020, and June 30, 2021, 348 patients were hospitalized with COVID-19 (Table 1). The mean (SD) age was 68.4 (13.9) years, 313 patients (90.2%) were male, 281 patients (83.4%) were Black, 47 patients (13.6%) were White, and 16 patients (4.8%) were Hispanic. One hundred forty patients (40.2%) resided in Washington, DC, 151 (43.4%) in Maryland, and 19 (5.5%) in Virginia. HFO was received by 86 patients (24.7%), 33 (9.5%) required intubation and mechanical ventilation, and 57 (16.4%) died. All intubations and deaths occurred among patients aged > 50 years, with death occurring in 17.8% of patients aged > 50 years.
Demographic characteristics and baseline comorbidities associated with COVID-19 disease severity can be found in eAppendix 2. In unadjusted analyses, age was significantly associated with the risk of HFO, with a mean (SD) age of 72.5 (11.7) years among those requiring HFO and 67.1 (14.4) years among patients without HFO (odds ratio [OR], 1.03; 95% CI, 1.01-1.05; P = .002). Although age was not associated with the risk of intubation, it was significantly associated with mortality. Patients who died had a mean (SD) age of 76.8 (11.8) years compared with 66.8 (13.7) years among survivors (OR, 1.06; 95% CI, 1.04-1.09; P < .001).
Compared with patients with no comorbidities, CCI categories of mild, moderate, and severe were associated with increased risk of requiring HFO (eAppendix 3). The adjusted OR (aOR) was highest among patients with severe CCI (aOR, 7.00; 95% CI, 2.42-20.32; P = .0007). In age-adjusted analyses, CCI was not associated with intubation or mortality.
Geospatial Analyses
State of residence, county of residence, and geographic area (including Washington, DC wards, and geographic divisions within counties of residence in Maryland and Virginia) were not associated with the clinical outcomes studied (eAppendix 4). However, zip code-based median income, analyzed as a continuous variable, was associated with a reduced likelihood of receiving HFO (aOR, 0.91; 95% CI, 0.84-0.99; P = .03). Income was not significantly associated with intubation or mortality.
The majority of patients hospitalized for COVID-19 at WVAMC resided in zip codes in eastern Washington, DC, inclusive of wards 7 and 8, and Prince George’s County, Maryland (Figure 1). These areas also corresponded to the lowest median household income by zip code (Figure 2).
Code
Code
Multivariable Analysis
Significant predictors of HFO requirement included comorbid diabetes (OR, 2.42; 95% CI, 1.27-4.61; P = .006) and liver disease or cirrhosis (OR, 2.19; 95% CI, 1.09-4.39; P = .02) (Table 2). CDC admission period was also associated with HFO need. Patients admitted after early 2020 had lower odds of receiving HFO. Race and median income based on zip code residence were not associated with HFO requirement.
Comorbid liver disease or cirrhosis was a significant predictor of intubation (OR, 2.81; 95% CI, 1.07-7.40; P = .03). CDC admission period was associated with intubation with lower odds of intubation for patients admitted after early 2020. Race and median income by zip code were not associated with intubation.
Significant predictors of mortality included age (OR, 2.20; 95% CI, 1.55-3.14; P = .0001), comorbid liver disease or cirrhosis (OR, 2.97; 95% CI, 1.31-6.74; P = .008), and OSA (OR, 3.45; 95% CI, 1.49-7.97; P = .003). CDC admission period was associated with mortality, with lower odds of intubation for patients admitted in mid- and late 2020. Race and median income by zip code residence were not associated with intubation.
Discussion
In this study of COVID-19 disease severity at a large integrated health care system that provides equal access to care, race, ethnicity, and geographic location were not associated with the need for HFO, intubation, or presumed mortality. Median income by zip code residence was associated with reduced HFO use in univariable analyses but not in multivariable models.
These findings support existing literature suggesting that race and ethnicity alone do not explain disparities in COVID-19 outcomes. Multiple studies have demonstrated that disparities in health outcomes have been reduced for patients receiving VHA care.6,16-19 However, even within a health care system with assumed equal access, the finding of an association between income and need for HFO in the univariable analysis may reflect a greater likelihood of delays in care due to structural barriers. Multiple studies suggest low SES may be an independent risk factor for severe COVID-19 disease. Individuals with low SES have higher rates of chronic diseases of obesity, diabetes, heart disease, and lung disease; thus, they are also at greater risk of serious illness with COVID-19.20-24 Socioeconomic disadvantage may also have limited individuals’ ability to engage in protective behaviors to reduce COVID-19 infection risk, including food stockpiling, social distancing, avoidance of public transportation, and refraining from working in “essential jobs.”21
Beyond SES, place of residence also influences health outcomes. Prior literature supports using zip codes to assess area-based SES status and monitor health disparities.25 The Social Vulnerability Index incorporates SES factors for communities and measures social determinates of health at a zip code level exclusive of race and ethnicity.26 Socially vulnerable communities are known to have higher rates of chronic diseases, COVID-19 mortality, and lower vaccination rates.3 Within a defined geographic area, an individual’s outcome for COVID-19 can be influenced by individual resources such as access to care and median income. Disposable income may mitigate COVID-19 risk by facilitating timely care, reducing occupational exposure, improving housing stability, and supporting health-promoting behaviors.21
Limitations
Due to the evolving nature of the COVID-19 pandemic, variants, treatments, and interventions varied throughout the study period and are not included in this analysis. In late December 2020, COVID-19 vaccination was approved with a tiered allocation for at-risk patients and direct health care professionals. Three of the 4 study periods analyzed in this study were prior to vaccine rollout and therefore vaccination history was not assessed. However, we tried to capture the evolving changes in COVID-19 variants, treatments and interventions, and skill in treating the disease through use of CDC-defined time frames. Another limitation is that some studies have shown that use of median income by zip code residence can underestimate mortality.27 Also, shared resources and access to other sources of disposable income can impact the immediate attainment of social needs. For example, during the COVID-19 pandemic, health care systems in Washington, DC assisted vulnerable individuals by providing food, housing, and other resources.28,29 Finally, the modest sample size limits generalizability and power to detect differences for certain variables, including Hispanic ethnicity.
Conclusions
There have been widely described disparities in disease severity and death during the COVID-19 pandemic. In this urban veteran cohort of hospitalized patients, there was no difference in the need for intubation or mortality associated with race. The findings suggest that a lower median income by zip code residence may be associated with greater disease severity at presentation, but do not predict severe outcomes and mortality overall. VHA care, which provides equal access to care, may mitigate the disparities seen in the private sector.
- District of Columbia: All Race & Ethnicity Data. The COVID Tracking Project. Accessed December 10, 2025. https://covidtracking.com/data/state/district-of-columbia/race-ethnicity
- Freese KE, Vega A, Lawrence JJ, et al. Social vulnerability is associated with risk of COVID-19 related mortality in U.S. counties with confirmed cases. J Health Care Poor Underserved. 2021;32:245-257. doi:10.1353/hpu.2021.0022
- Saulsberry L, Bhargava A, Zeng S, et al. The social vulnerability metric (SVM) as a new tool for public health. Health Serv Res. 2023;58:873-881. doi:10.1111/1475-6773.14102
- Romano SD, Blackstock AJ, Taylor EV, et al. Trends in racial and ethnic disparities in COVID-19 hospitalizations, by region - United States, March-December 2020. MMWR Morb Mortal Wkly Rep. 2021;70:560-565. doi:10.15585/mmwr.mm7015e2
- Kullar R, Marcelin JR, Swartz TH, et al. Racial disparity of coronavirus disease 2019 in African American communities. J Infect Dis. 2020;222:890-893. doi:10.1093/infdis/jiaa372
- Riviere P, Luterstein E, Kumar A, et al. Survival of African American and non-Hispanic White men with prostate cancer in an equal-access health care system. Cancer. 2020;126:1683-1690. doi:10.1002/cncr.32666
- Ohl ME, Richardson Miell K, Beck BF, et al. Mortality among US veterans admitted to community vs Veterans Health Administration hospitals for COVID-19. JAMA Netw Open. 2023;6:e2315902. doi:10.1001/jamanetworkopen.2023.15902
- US Department of Veterans Affairs. VA Washington DC Health Care. Accessed January 16, 2026. https://www.va.gov/washington-dc-health-care/about-us/
- Trottier C, La J, Li LL, et al. Maintaining the utility of coronavirus disease 2019 pandemic severity surveillance: evaluation of trends in attributable deaths and development and validation of a measurement tool. Clin Infect Dis. 2023;77:1247-1256. doi:10.1093/cid/ciad381
- Centers for Disease Control and Prevention. CDC Museum COVID-19 Timeline. Updated July 8, 2024. Accessed January 16, 2026. https://www.cdc.gov/museum/timeline/covid19.html#Early-2020
- Centers for Disease Control and Prevention. Covid-surveillance and data analytics. September 5, 2025. Accessed January 16, 2026. cdc.gov/covid/php/surveillance/index.html12.
- RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704. doi:10.1056/NEJMoa2021436
- Dooling K, Marin M, Wallace M, et al. The Advisory Committee on Immunization Practices’ updated interim recommendation for allocation of COVID-19 Vaccine - United States, December 2020. MMWR Morb Mortal Wkly Rep. 2021;69:1657-1660. doi:10.15585/mmwr.mm695152e2
- US Census Bureau. Explore census data. Accessed December 10, 2025. https://data.census.gov/profile?q=Income%20by%20Zip%20code%20tabulation%20area
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-383. doi:10.1016/0021-9681(87)90171-8
- Zullig LL, Carpenter WR, Provenzale D, Weinberger M, Reeve BB, Jackson GL. Examining potential colorectal cancer care disparities in the Veterans Affairs health care system. J Clin Oncol. 2013;31:3579-3584. doi:10.1200/JCO.2013.50.4753
- Grubaugh AL, Slagle DM, Long M, Frueh BC, Magruder KM. Racial disparities in trauma exposure, psychiatric symptoms, and service use among female patients in Veterans Affairs primary care clinics. Womens Health Issues. 2008;18:433-441. doi:10.1016/j.whi.2008.08.001
- Bosworth HB, Parsey KS, Butterfield MI, et al. Racial variation in wanting and obtaining mental health services among women veterans in a primary care clinic. J Natl Med Assoc. 2000;92:231-236.
- Luo J, Rosales M, Wei G, et al. Hospitalization, mechanical ventilation, and case-fatality outcomes in US veterans with COVID-19 disease between years 2020-2021. Ann Epidemiol. 2022;70:37-44. doi:10.1016/j.annepidem.2022.04.003
- Kondo K, Low A, Everson T, et al. Health disparities in veterans: a map of the evidence. Med Care. 2017;55 Suppl 9 Suppl 2:S9-S15. doi:10.1097/MLR.0000000000000756
- Grosicki GJ, Bunsawat K, Jeong S, Robinson AT. Racial and ethnic disparities in cardiometabolic disease and COVID-19 outcomes in White, Black/African American, and Latinx populations: Social determinants of health. Prog Cardiovasc Dis. 2022;71:4-10. doi:10.1016/j.pcad.2022.04.004
- National Center for Immunization and Respiratory Diseases (U.S.). Division of Viral Diseases. Coronavirus Disease 2019 (COVID-19): COVID-19 in Racial and Ethnic Minority Groups: June 4, 2020. CDC Stacks. June 4, 2020. Accessed January 14, 2026. https://stacks.cdc.gov/view/cdc/88770
- Yancy CW. COVID-19 and African Americans. JAMA. 2020;323:1891-1892. doi:10.1001/jama.2020.6548
- Magesh S, John D, Li WT, et al. Disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status: a systematic-review and meta-analysis. JAMA Netw Open. 2021;4:e2134147. doi:10.1001/jamanetworkopen.2021.34147
- Berkowitz SA, Traore CY, Singer DE, Atlas SJ. Evaluating area-based socioeconomic status indicators for monitoring disparities within health care systems: results from a primary care network. Health Serv Res. 2015;50:398-417. doi:10.1111/1475-6773.12229
- Social Vulnerability Index. Agency for Toxicity and Disease Registry. July 22, 2024. Accessed January 14, 2026. https://www.atsdr.cdc.gov/placeandhealth/svi/index.html
- Moss JL, Johnson NJ, Yu M, Altekruse SF, Cronin KA. Comparisons of individual- and area-level socioeconomic status as proxies for individual-level measures: evidence from the Mortality Disparities in American Communities study. Popul Health Metr. 2021;19:1. doi:10.1186/s12963-020-00244-x
- DC Department of Human Services. Response to COVID-19. Accessed January 14, 2026. https://dhs.dc.gov/page/responsetocovid19
- Wang PG, Brisbon NM, Hubbell H, et al. Is the Gap Closing? Comparison of sociodemographic cisparities in COVID-19 hospitalizations and outcomes between two temporal waves of admissions. J Racial Ethn Health Disparities. 2023;10:593-602. doi:10.1007/s40615-022-01249-y
- District of Columbia: All Race & Ethnicity Data. The COVID Tracking Project. Accessed December 10, 2025. https://covidtracking.com/data/state/district-of-columbia/race-ethnicity
- Freese KE, Vega A, Lawrence JJ, et al. Social vulnerability is associated with risk of COVID-19 related mortality in U.S. counties with confirmed cases. J Health Care Poor Underserved. 2021;32:245-257. doi:10.1353/hpu.2021.0022
- Saulsberry L, Bhargava A, Zeng S, et al. The social vulnerability metric (SVM) as a new tool for public health. Health Serv Res. 2023;58:873-881. doi:10.1111/1475-6773.14102
- Romano SD, Blackstock AJ, Taylor EV, et al. Trends in racial and ethnic disparities in COVID-19 hospitalizations, by region - United States, March-December 2020. MMWR Morb Mortal Wkly Rep. 2021;70:560-565. doi:10.15585/mmwr.mm7015e2
- Kullar R, Marcelin JR, Swartz TH, et al. Racial disparity of coronavirus disease 2019 in African American communities. J Infect Dis. 2020;222:890-893. doi:10.1093/infdis/jiaa372
- Riviere P, Luterstein E, Kumar A, et al. Survival of African American and non-Hispanic White men with prostate cancer in an equal-access health care system. Cancer. 2020;126:1683-1690. doi:10.1002/cncr.32666
- Ohl ME, Richardson Miell K, Beck BF, et al. Mortality among US veterans admitted to community vs Veterans Health Administration hospitals for COVID-19. JAMA Netw Open. 2023;6:e2315902. doi:10.1001/jamanetworkopen.2023.15902
- US Department of Veterans Affairs. VA Washington DC Health Care. Accessed January 16, 2026. https://www.va.gov/washington-dc-health-care/about-us/
- Trottier C, La J, Li LL, et al. Maintaining the utility of coronavirus disease 2019 pandemic severity surveillance: evaluation of trends in attributable deaths and development and validation of a measurement tool. Clin Infect Dis. 2023;77:1247-1256. doi:10.1093/cid/ciad381
- Centers for Disease Control and Prevention. CDC Museum COVID-19 Timeline. Updated July 8, 2024. Accessed January 16, 2026. https://www.cdc.gov/museum/timeline/covid19.html#Early-2020
- Centers for Disease Control and Prevention. Covid-surveillance and data analytics. September 5, 2025. Accessed January 16, 2026. cdc.gov/covid/php/surveillance/index.html12.
- RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384:693-704. doi:10.1056/NEJMoa2021436
- Dooling K, Marin M, Wallace M, et al. The Advisory Committee on Immunization Practices’ updated interim recommendation for allocation of COVID-19 Vaccine - United States, December 2020. MMWR Morb Mortal Wkly Rep. 2021;69:1657-1660. doi:10.15585/mmwr.mm695152e2
- US Census Bureau. Explore census data. Accessed December 10, 2025. https://data.census.gov/profile?q=Income%20by%20Zip%20code%20tabulation%20area
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-383. doi:10.1016/0021-9681(87)90171-8
- Zullig LL, Carpenter WR, Provenzale D, Weinberger M, Reeve BB, Jackson GL. Examining potential colorectal cancer care disparities in the Veterans Affairs health care system. J Clin Oncol. 2013;31:3579-3584. doi:10.1200/JCO.2013.50.4753
- Grubaugh AL, Slagle DM, Long M, Frueh BC, Magruder KM. Racial disparities in trauma exposure, psychiatric symptoms, and service use among female patients in Veterans Affairs primary care clinics. Womens Health Issues. 2008;18:433-441. doi:10.1016/j.whi.2008.08.001
- Bosworth HB, Parsey KS, Butterfield MI, et al. Racial variation in wanting and obtaining mental health services among women veterans in a primary care clinic. J Natl Med Assoc. 2000;92:231-236.
- Luo J, Rosales M, Wei G, et al. Hospitalization, mechanical ventilation, and case-fatality outcomes in US veterans with COVID-19 disease between years 2020-2021. Ann Epidemiol. 2022;70:37-44. doi:10.1016/j.annepidem.2022.04.003
- Kondo K, Low A, Everson T, et al. Health disparities in veterans: a map of the evidence. Med Care. 2017;55 Suppl 9 Suppl 2:S9-S15. doi:10.1097/MLR.0000000000000756
- Grosicki GJ, Bunsawat K, Jeong S, Robinson AT. Racial and ethnic disparities in cardiometabolic disease and COVID-19 outcomes in White, Black/African American, and Latinx populations: Social determinants of health. Prog Cardiovasc Dis. 2022;71:4-10. doi:10.1016/j.pcad.2022.04.004
- National Center for Immunization and Respiratory Diseases (U.S.). Division of Viral Diseases. Coronavirus Disease 2019 (COVID-19): COVID-19 in Racial and Ethnic Minority Groups: June 4, 2020. CDC Stacks. June 4, 2020. Accessed January 14, 2026. https://stacks.cdc.gov/view/cdc/88770
- Yancy CW. COVID-19 and African Americans. JAMA. 2020;323:1891-1892. doi:10.1001/jama.2020.6548
- Magesh S, John D, Li WT, et al. Disparities in COVID-19 outcomes by race, ethnicity, and socioeconomic status: a systematic-review and meta-analysis. JAMA Netw Open. 2021;4:e2134147. doi:10.1001/jamanetworkopen.2021.34147
- Berkowitz SA, Traore CY, Singer DE, Atlas SJ. Evaluating area-based socioeconomic status indicators for monitoring disparities within health care systems: results from a primary care network. Health Serv Res. 2015;50:398-417. doi:10.1111/1475-6773.12229
- Social Vulnerability Index. Agency for Toxicity and Disease Registry. July 22, 2024. Accessed January 14, 2026. https://www.atsdr.cdc.gov/placeandhealth/svi/index.html
- Moss JL, Johnson NJ, Yu M, Altekruse SF, Cronin KA. Comparisons of individual- and area-level socioeconomic status as proxies for individual-level measures: evidence from the Mortality Disparities in American Communities study. Popul Health Metr. 2021;19:1. doi:10.1186/s12963-020-00244-x
- DC Department of Human Services. Response to COVID-19. Accessed January 14, 2026. https://dhs.dc.gov/page/responsetocovid19
- Wang PG, Brisbon NM, Hubbell H, et al. Is the Gap Closing? Comparison of sociodemographic cisparities in COVID-19 hospitalizations and outcomes between two temporal waves of admissions. J Racial Ethn Health Disparities. 2023;10:593-602. doi:10.1007/s40615-022-01249-y
Median Income and Clinical Outcomes of Hospitalized Persons With COVID-19 at an Urban Veterans Affairs Medical Center
Median Income and Clinical Outcomes of Hospitalized Persons With COVID-19 at an Urban Veterans Affairs Medical Center

Weekends Off on Clinical Rotations? Examining Clinical Opportunity Trends on Weekdays vs Weekends During Internal Medicine Clerkship Rotations in Veterans Health Administration Inpatient Wards
Background
The Accreditation Council for Graduate Medical Education (ACGME) mandates an 80-hour weekly work limit for residents.1 In contrast, decisions regarding undergraduate medical education (UME) are strongly influenced locally, with individual institutions setting academic policy for students. These differences in oversight reflect fundamental differences in residents’ and students’ roles in patient care, power, and responsibility. Considering rotation schedules, internal medicine (IM) clerkship directors have discussed the relative value of weekend vs weekday duty during inpatient rotations, a scheduling topic of interest to students as well, though these conversations are limited by a lack of knowledge regarding admission patterns. Addressing this information gap would inform policy decisions.
The Veterans Health Administration (VHA) is uniquely positioned to address questions about UME clinical experiences nationwide: annually, over 118,000 students representing 97% of US medical schools train at VHA facilities.2,3 We aim to compare the number and variety of patient encounter opportunities presenting during inpatient VHA IM rotations on weekdays versus weekends to inform policy decisions for UME rotation schedules.
Innovation
The VHA Corporate Data Warehouse will be queried for all admissions, diagnoses, and length of stay on inpatient IM services at the 420 VHA hospitals affiliated with US medical schools from 2016-2026. We will aggregate case data for day of week, floor, hospital, and Veteran Integrated Service Network (VISN), and determine number of admissions by weekday (Monday-Friday) and weekend (Saturday-Sunday). Weekday vs. weekend admission data will be compared using generalized mixed effects models for clustered longitudinal data. Heterogeneity across hospitals and VISNs will be explored to examine unique regional trends.
Results
We have drafted strategies to query and curate relevant datasets, developed a preliminary analysis plan, and await data deployment from VHA data stewards.
Conclusions
We believe this will be the first VHA-wide evaluation of patient encounter trends on IM services to examine potential training experiences for medical students. This will increase understanding of the critical role VHA has in developing the nations’ healthcare workforce, and how patterns of opportunities for clinical education may be distributed over time, informing decisions about rotation schedules to maximize students’ abilities to interact with, learn from, and serve our nation’s veterans
- Dimitris KD, Taylor BC, Fankhauser RA. Resident work-week regulations: historical review and modern perspectives. J Surg Educ. 2008;65(4):290-296. doi:10.1016/j.jsurg.2008.05.011
- Health professions education statistics. Veterans Health Administration. Accessed March 19, 2025. https://www.va.gov/oaa/docs/OAACurrentStats.pdf
- Medical education at VA: It’s all about the Veterans. VA News. Updated August 16, 2021. Accessed March 19, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
Background
The Accreditation Council for Graduate Medical Education (ACGME) mandates an 80-hour weekly work limit for residents.1 In contrast, decisions regarding undergraduate medical education (UME) are strongly influenced locally, with individual institutions setting academic policy for students. These differences in oversight reflect fundamental differences in residents’ and students’ roles in patient care, power, and responsibility. Considering rotation schedules, internal medicine (IM) clerkship directors have discussed the relative value of weekend vs weekday duty during inpatient rotations, a scheduling topic of interest to students as well, though these conversations are limited by a lack of knowledge regarding admission patterns. Addressing this information gap would inform policy decisions.
The Veterans Health Administration (VHA) is uniquely positioned to address questions about UME clinical experiences nationwide: annually, over 118,000 students representing 97% of US medical schools train at VHA facilities.2,3 We aim to compare the number and variety of patient encounter opportunities presenting during inpatient VHA IM rotations on weekdays versus weekends to inform policy decisions for UME rotation schedules.
Innovation
The VHA Corporate Data Warehouse will be queried for all admissions, diagnoses, and length of stay on inpatient IM services at the 420 VHA hospitals affiliated with US medical schools from 2016-2026. We will aggregate case data for day of week, floor, hospital, and Veteran Integrated Service Network (VISN), and determine number of admissions by weekday (Monday-Friday) and weekend (Saturday-Sunday). Weekday vs. weekend admission data will be compared using generalized mixed effects models for clustered longitudinal data. Heterogeneity across hospitals and VISNs will be explored to examine unique regional trends.
Results
We have drafted strategies to query and curate relevant datasets, developed a preliminary analysis plan, and await data deployment from VHA data stewards.
Conclusions
We believe this will be the first VHA-wide evaluation of patient encounter trends on IM services to examine potential training experiences for medical students. This will increase understanding of the critical role VHA has in developing the nations’ healthcare workforce, and how patterns of opportunities for clinical education may be distributed over time, informing decisions about rotation schedules to maximize students’ abilities to interact with, learn from, and serve our nation’s veterans
Background
The Accreditation Council for Graduate Medical Education (ACGME) mandates an 80-hour weekly work limit for residents.1 In contrast, decisions regarding undergraduate medical education (UME) are strongly influenced locally, with individual institutions setting academic policy for students. These differences in oversight reflect fundamental differences in residents’ and students’ roles in patient care, power, and responsibility. Considering rotation schedules, internal medicine (IM) clerkship directors have discussed the relative value of weekend vs weekday duty during inpatient rotations, a scheduling topic of interest to students as well, though these conversations are limited by a lack of knowledge regarding admission patterns. Addressing this information gap would inform policy decisions.
The Veterans Health Administration (VHA) is uniquely positioned to address questions about UME clinical experiences nationwide: annually, over 118,000 students representing 97% of US medical schools train at VHA facilities.2,3 We aim to compare the number and variety of patient encounter opportunities presenting during inpatient VHA IM rotations on weekdays versus weekends to inform policy decisions for UME rotation schedules.
Innovation
The VHA Corporate Data Warehouse will be queried for all admissions, diagnoses, and length of stay on inpatient IM services at the 420 VHA hospitals affiliated with US medical schools from 2016-2026. We will aggregate case data for day of week, floor, hospital, and Veteran Integrated Service Network (VISN), and determine number of admissions by weekday (Monday-Friday) and weekend (Saturday-Sunday). Weekday vs. weekend admission data will be compared using generalized mixed effects models for clustered longitudinal data. Heterogeneity across hospitals and VISNs will be explored to examine unique regional trends.
Results
We have drafted strategies to query and curate relevant datasets, developed a preliminary analysis plan, and await data deployment from VHA data stewards.
Conclusions
We believe this will be the first VHA-wide evaluation of patient encounter trends on IM services to examine potential training experiences for medical students. This will increase understanding of the critical role VHA has in developing the nations’ healthcare workforce, and how patterns of opportunities for clinical education may be distributed over time, informing decisions about rotation schedules to maximize students’ abilities to interact with, learn from, and serve our nation’s veterans
- Dimitris KD, Taylor BC, Fankhauser RA. Resident work-week regulations: historical review and modern perspectives. J Surg Educ. 2008;65(4):290-296. doi:10.1016/j.jsurg.2008.05.011
- Health professions education statistics. Veterans Health Administration. Accessed March 19, 2025. https://www.va.gov/oaa/docs/OAACurrentStats.pdf
- Medical education at VA: It’s all about the Veterans. VA News. Updated August 16, 2021. Accessed March 19, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
- Dimitris KD, Taylor BC, Fankhauser RA. Resident work-week regulations: historical review and modern perspectives. J Surg Educ. 2008;65(4):290-296. doi:10.1016/j.jsurg.2008.05.011
- Health professions education statistics. Veterans Health Administration. Accessed March 19, 2025. https://www.va.gov/oaa/docs/OAACurrentStats.pdf
- Medical education at VA: It’s all about the Veterans. VA News. Updated August 16, 2021. Accessed March 19, 2025. https://news.va.gov/93370/medical-education-at-va-its-all-about-the-veterans/
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Deconditioning among hospitalized older adults contributes to significant decline in posthospitalization functional ability, physical performance, and physical activity.1-10 Previous hospital-to-home interventions have targeted improving function and physical activity, including recent programs leveraging home telehealth as a feasible and potentially effective mode of delivering in-home exercise and rehabilitation.11-14 However, pilot interventions have shown mixed effectiveness.11,12,14 This study expands on a previously published intervention describing a pilot home telehealth program for veterans posthospital discharge that demonstrated significant 6-month improvement in physical activity as well as trends in physical function improvement, including among those with cognitive impairment.15 Factors that contribute to improved outcomes are the focus of the present study.
Key factors underlying the complexity of hospital-to-home transitions include hospitalization elements (ie, reason for admission and length of stay), associated posthospital syndromes (ie, postdischarge falls, medication changes, cognitive impairment, and pain), and postdischarge health care application (ie, physical therapy and hospital readmission).16-18 These factors may be associated with postdischarge functional ability, physical performance, and physical activity, but their direct influence on intervention outcomes is unclear (Figure 1).5,7,9,16-20 The objective of this study was to examine the influence of hospitalization, posthospital syndrome, and postdischarge health care application factors on outcomes of a US Department of Veterans Affairs (VA) Video Connect (VVC) intervention to enhance function and physical activity in older adults posthospital discharge.
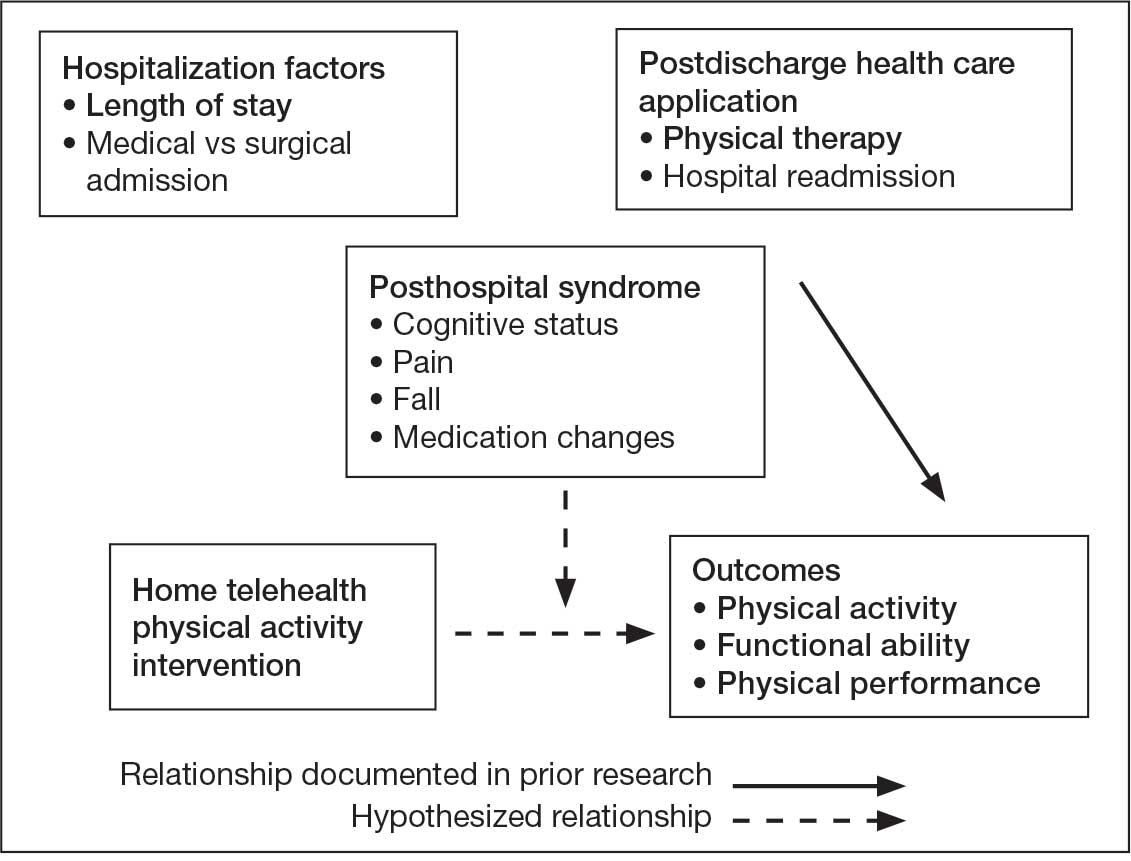
health care application factors on physical activity, functional ability, and
physical performance intervention outcomes.
Methods
The previous analysis reported on patient characteristics, program feasibility, and preliminary outcomes.13,15 The current study reports on relationships between hospitalization, posthospital syndrome, and postdischarge health care application factors and change in key outcomes, namely postdischarge self-reported functional ability, physical performance, and physical activity from baseline to endpoint.
Participants provided written informed consent. The protocol and consent forms were approved by the VA Ann Arbor Healthcare System (VAAAHS) Research and Development Committee, and the project was registered on clinicaltrials.gov (NCT04045054).
Intervention
The pilot program targeted older adults following recent hospital discharge from VAAAHS. Participants were eligible if they were aged ≥ 50 years, had been discharged following an inpatient stay in the past 1 to 2 weeks, evaluated by physical therapy during hospitalization with stated rehabilitation goals on discharge, and followed by a VAAAHS primary care physician. Participants were either recruited during hospital admission or shortly after discharge.13
An experienced physical activity trainer (PAT) supported the progression of participants’ rehabilitation goals via a home exercise program and coached the patient and caregiver to optimize functional ability, physical performance, and physical activity. The PAT was a nonlicensed research assistant with extensive experience in applying standard physical activity enhancement protocols (eg, increased walking) to older adults with comorbidities. Participation in the program lasted about 6 months. Initiation of the PAT program was delayed if the patient was already receiving postdischarge home-based or outpatient physical therapy. The PAT contacted the patient weekly via VVC for the first 6 weeks, then monthly for a total of 6 months. Each contact included information on optimal walking form, injury prevention, program progression, and ways to incorporate sit-to-stand transitions, nonsitting behavior, and walking into daily routines. The initial VVC contact lasted about 60 minutes and subsequent sessions lasted about 30 minutes.13
Demographic characteristics were self-reported by participants and included age, sex, race, years of education, and marital status. Clinical characteristics were obtained from each participant’s electronic health record (EHR), including copay status, index hospitalization length of stay, admission diagnosis, and postsurgery status (postsurgery vs nonpostsurgery). Intervention adherence was tracked as the number of PAT sessions attended.
Posthospital Syndrome Factors
Participant falls (categorized as those who reported a fall vs those who did not) and medication changes (number of changes reported, including new medication, discontinued medication, dose changes, medication changes, or changes in medication schedule) were reported by participants or caregivers during each VVC contact. Participants completed the Montreal Cognitive Assessment (MoCA) at baseline, and were dichotomized into 2 groups: no cognitive impairment (MoCA score ≥ 26) and mild to moderate cognitive impairment (MoCA score 10-25).13,21
Participants rated how much pain interfered with their normal daily activities since the previous VVC session on a 5-point Likert scale (1, not at all; to 5, extremely).22 Similar to prior research, participants were placed into 2 groups based on their mean pain interference score (individuals with scores from 1.0 to 2.0 in 1 group, and individuals with > 2.0 in another).23-25 Participants were separated into a no or mild pain interference group and a moderate to severe pain interference group. Hospital readmissions (VA and non-VA) and postdischarge physical therapy outcomes were obtained from the participant’s EHR, including primary care visits.
Outcomes
Outcomes were collected at baseline (posthospital discharge) and 6 months postenrollment.
Self-Reported Functional Ability. This measure is provided by participants or caregivers and measured by the Katz Index of Independence in Activities of Daily Living (ADL), Lawton and Brody Instrumental ADL Scale (IADL), Nagi Disability Model, and Rosow-Breslau Scale. The Katz ADL assesses the ability to complete 6 self-care activities and awards 1 point for independence and 0 if the individual is dependent (total score range, 0-6).26 The Lawton and Brody IADL measures an individual’s independence in 8 instrumental ADLs; it awards 1 point for independence and 0 if the individual is dependent (total score range, 0-8).27 The Nagi Disability Model evaluates an individual’s difficulty performing 5 tasks (total score range, 0-5) and tallies the number of items with a response other than “no difficulty at all” (higher total score indicates greater difficulty). 28 The Rosow-Breslau Scale is a 3-item measure of mobility disability; individual responses are 0 (no help) and 1 (requires help or unable); higher total score (range, 0-3) indicates greater disability.29
Physical Performance. Measured using the Short Physical Performance Battery (SPPB), which evaluates standing balance, sit to stand, and walking performance. Scores range from 0 to 4 on the balance, gait speed, and chair stand tests, for a total composite score between 0 and 12 (higher score indicates better performance).30
Physical Activity. Measured using actigraphy, namely a physical activity monitor adherent to the thigh (activ-PAL3TM, PAL Technologies Ltd., Glasgow, UK).31 Participants were instructed to wear the activPal for ≥ 1 week. Participants with a minimum of 5 days of wear were included in this analysis.
Data Analyses
Analyses were performed using SPSS software version 29.0.32 Continuous variables were summarized using mean (SD) or median and IQR using the weighted average method; categorical variables were summarized using frequencies and percentages. Baseline scores on outcome variables were compared by categorical hospitalization, posthospital syndrome, and postdischarge health care application factor variables using Mann-Whitney U tests. The differences between outcome variables from baseline to endpoint were then calculated to produce change scores. Relationships between the number of PAT sessions attended and baseline outcomes and outcome change scores were estimated using Spearman correlations. Relationships between categorical factors (hospitalization, posthospital syndrome, and postdischarge health care application) and outcome variable change scores (which were normally distributed) were examined using Mann-Whitney U tests. Relationships with continuous hospitalization (length of stay) and posthospital syndrome factors (medication changes) were estimated using Spearman correlations. Effect sizes (ES) were estimated with Cohen d; small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). Missing data were handled using pairwise deletion.33 Therefore, sample sizes were reported for each analysis. For all statistical tests, P < .05 was considered significant.
Results
Twenty-four individuals completed the pilot intervention.15 Mean (SD) age was 73.6 (8.1) years (range, 64-93 years) and participants were predominantly White males (Table 1). Eight participants had a high school education only and 13 had more than a high school education. Diagnoses at admission included 9 patients with orthopedic/musculoskeletal conditions (6 were for joint replacement), 6 patients with vascular/pulmonary conditions, and 4 with gastrointestinal/renal/urological conditions. Of the 11 postsurgery participants, 7 were orthopedic, 4 were gastrointestinal, and 1 was peripheral vascular.
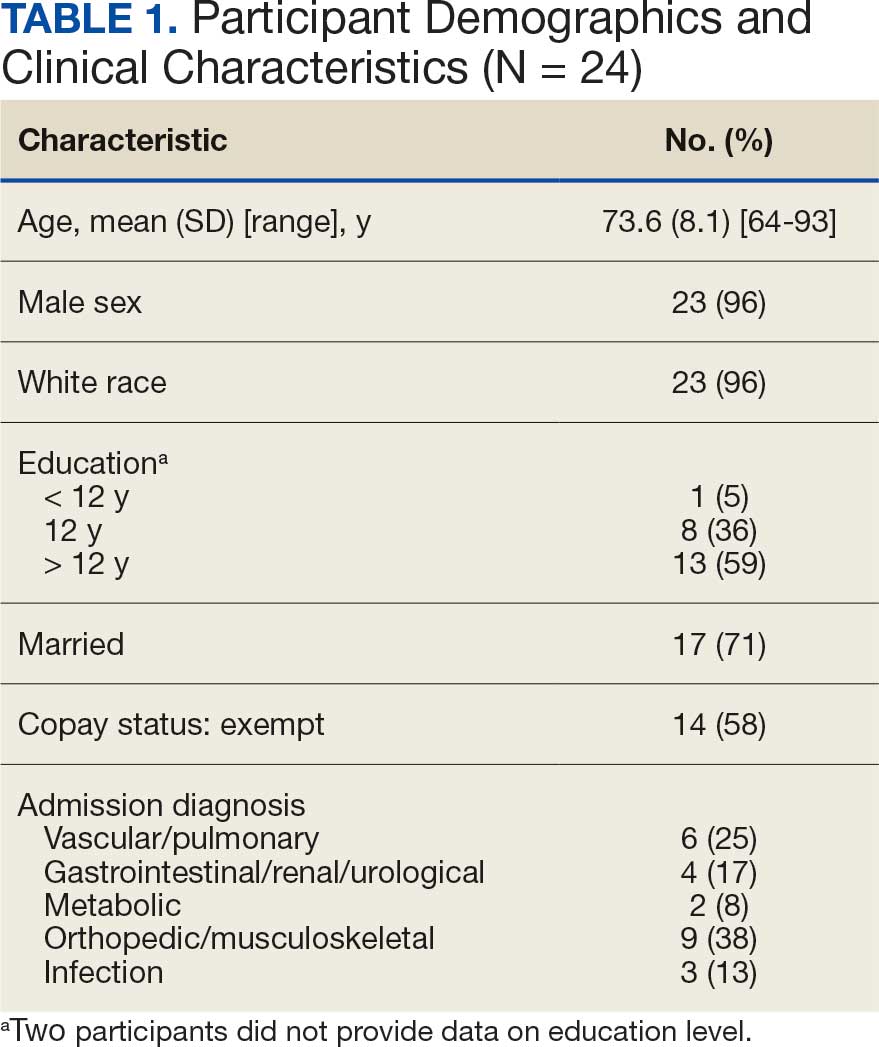
Baseline outcome scores did not differ significantly between groups, except individuals with moderate to severe pain interference reported a significantly lower IADL score (median [IQR] 4 [2-7]) than individuals with mild or moderate pain interference (median [IQR] 8 [7-8]; P = .02) (Table 2). The mean (SD) number of PAT sessions attended was 9.3 (3.7) (range, 3-19). There were no significant relationships between number of sessions attended and any baseline outcome variables or outcome change scores.
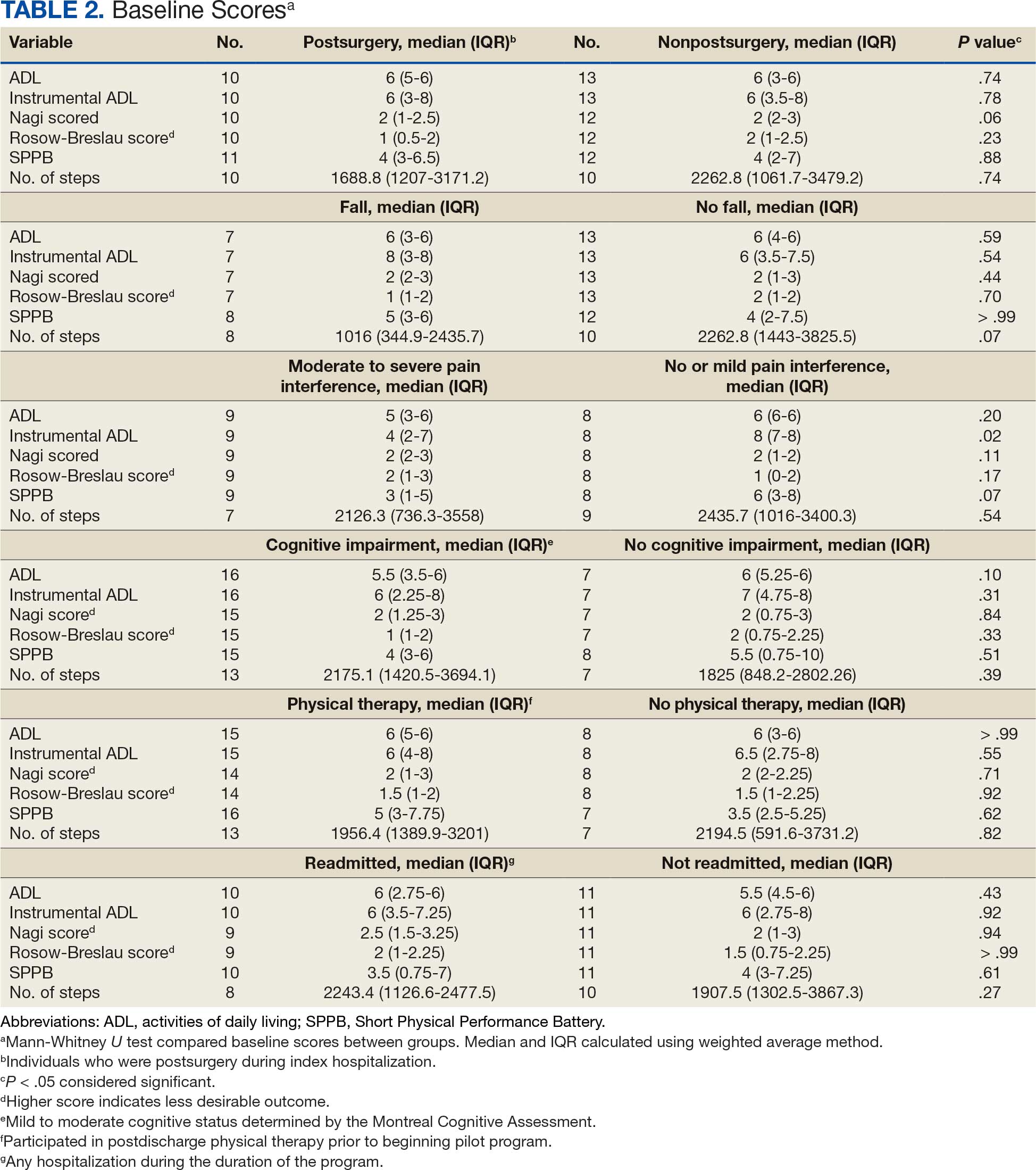
Hospitalization Factors
Participants who were postsurgery tended to have greater improvement than individuals who were nonpostsurgery in ADLs (median [IQR] 0 [0-1.5]; ES, 0.6; P = .10) and SPPB (median [IQR] 2 [1.5-9]; ES, 0.9; P = .07), but the improvements were not statistically significant (Table 3). Mean (SD) length of stay of the index hospitalization was 6.7 (6.1) days. Longer length of stay was significantly correlated with an increase in Nagi score (ρ, 0.45; 95% CI, 0.01-0.75). There were no other significant or trending relationships between length of stay and outcome variables.
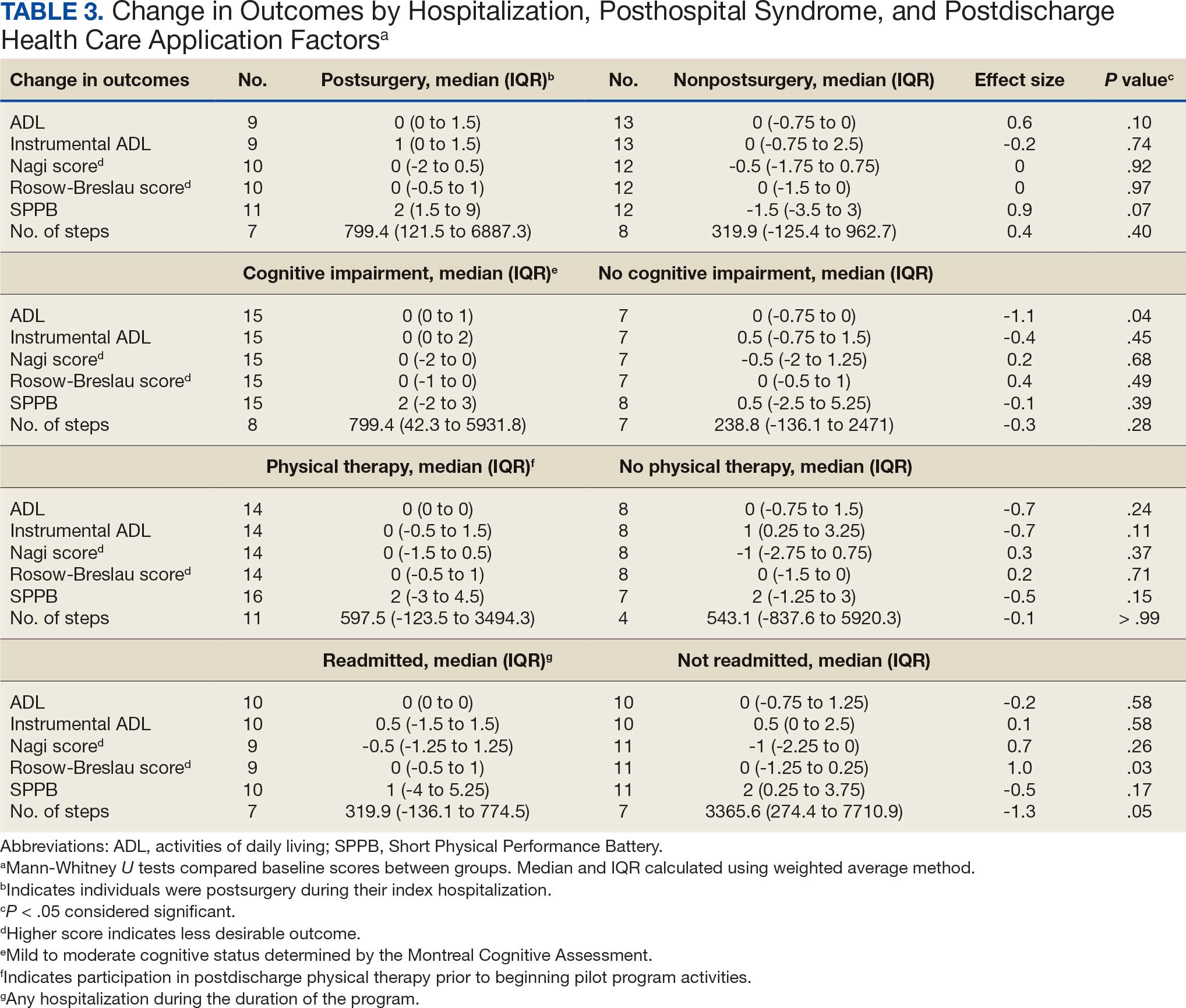
Posthospital Syndrome Factors
The 16 participants with mild to moderate cognitive impairment had less improvement in ADLs (median [IQR] 0 [0-1]) than the 8 participants with no impairment (median [IQR] 0 [-0.75 to 0]; ES, -1.1; P = .04). Change in outcome variables from baseline to endpoint did not significantly differ between the 8 patients who reported a fall compared with the 13 who did not, nor were any trends observed. Change in outcome variables from baseline to endpoint also did not significantly differ between the 8 participants who reported no or mild pain interference compared with the 10 patients with moderate to severe pain interference, nor were any trends observed. Mean (SD) number of medication changes was 2.5 (1.6). Higher number of medication changes was significantly correlated with a decrease in Rosow-Breslau score (ρ, -0.47; 95% CI, -0.76 to -0.02). There were no other significant or trending relationships between number of medication changes and outcome variables.
Postdischarge Health Care Application Factors
The 16 participants who attended posthospital physical therapy trended towards less improvement in IADLs (median [IQR] 0 [-0.5 to 1.5]; ES, -0.7; P = .11) and SPPB (median [IQR] 2 [-3.0 to 4.5]; ES, -0.5; P = .15) than the 8 patients with no postdischarge physical therapy. Eleven participants were readmitted, while 13 had no readmissions in their medical records between baseline and endpoint. Participants with ≥ 1 readmission experienced a greater increase in Rosow-Breslau score (median [IQR] 0 [-0.5 to 1.0]) than those not readmitted (median [IQR] 0 [-1.25 to 0.25]; ES, 1.0; P = .03). Borderline greater improvement in number of steps was found in those not readmitted (median [IQR] 3365.6 [274.4-7710.9]) compared with those readmitted (median [IQR] 319.9 [-136.1 to 774.5]; ES, -1.3; P = .05). Patients who were readmitted also tended to have lower and not statistically significant improvements in SPPB (median [IQR] 1 [-4.0 to 5.3]) compared with those not readmitted (median [IQR] 2 [0.3-3.8]; ES, -0.5; P = .17) (Table 3).
Discussion
This study examined the association between hospitalization, posthospital syndrome, and postdischarge health care use in patients undergoing a VVC-based intervention following hospital discharge. Participants who had no or mild cognitive impairment, no readmissions, higher medication changes, and a shorter hospital length of stay tended to experience lower disability, including in mobility and ADLs. This suggests individuals who are less clinically complex may be more likely to benefit from this type of virtual rehabilitation program. These findings are consistent with clinical experiences; home-based programs to improve physical activity posthospital discharge can be challenging for those who were medically ill (and did not undergo a specific surgical procedure), cognitively impaired, and become acutely ill and trigger hospital readmission. 15 For example, the sample in this study had higher rates of falls, pain, and readmissions compared to previous research.2,3,34-39
The importance of posthospital syndrome in the context of recovery of function and health at home following hospitalization is well documented.16-18 The potential impact of posthospital syndrome on physical activity-focused interventions is less understood. In our analysis, participants with mild or moderate cognitive impairment tended to become more dependent in their ADLs, while those with no cognitive impairment tended to become more independent in their ADLs. This functional decline over time is perhaps expected in persons with cognitive impairment, but the significant difference with a large ES warrants further consideration on how to tailor interventions to better promote functional recovery in these individuals.40,41 While some cognitive decline may not be preventable, this finding supports the need to promote healthy cognitive aging, identify declines in cognition, and work to mitigate additional decline. Programs specifically designed to promote function and physical activity in older adults with cognitive impairment are needed, especially during care transitions.41-43
While participants reported that falls and pain interference did not have a significant impact on change in outcomes between baseline and endpoint, these areas need further investigation. Falls and pain have been associated with function and physical activity in older adults.42-46 Pain is common, yet underappreciated during older adult hospital-to-home transitions.11,12,45,46 There is a need for more comprehensive assessment of pain (including pain intensity) and qualitative research.
Hospitalization and postdischarge health care application factors may have a significant impact on home-telehealth physical activity intervention success. Individuals who were postsurgery tended to have greater improvements in ADLs and physical performance. Most postsurgery participants had joint replacement surgery. Postsurgery status may not be modifiable, but it is important to note expected differences in recovery between medical and surgical admissions and the need to tailor care based on admission diagnosis. Those with a longer length of hospital stay may be considered at higher risk of suboptimal outcomes postdischarge, which indicates an opportunity for targeting resources and support, in addition to efforts of reducing length of stay where possible.47
Readmissions were significantly related to a change in Rosow-Breslau mobility disability score. This may indicate the detrimental impact a readmission can have on increasing mobility and physical activity postdischarge, or the potential of this pilot program to impact readmissions by increasing mobility and physical activity, contrary to prior physical exercise interventions.5,7,9,48 With 5% to 79% of readmissions considered preventable, continued efforts and program dissemination and implementation to address preventable readmissions are warranted.49 Individuals with postdischarge physical therapy (prior to beginning the pilot program) tended to demonstrate less improvement in disability and physical performance. This relationship needs further investigation; the 2 groups did not appear to have significant differences at baseline, albeit with a small sample size. It is possible they experienced initial improvements with postdischarge physical therapy and plateaued or had little further reserve to improve upon entering the VVC program.
Strengths and Limitations
This pilot program provided evaluative data on the use of VVC to enhance function and physical activity in older adults posthospital discharge. It included individual (eg, fall, pain, cognitive impairment) and health service (eg, readmission, physical therapy) level factors as predictors of function and physical activity posthospitalization.5,7,9,15-19
The results of this pilot project stem from a small sample lacking diversity in terms of race, ethnicity, and sex. There was some variation in baseline and endpoints between participants, and when hospitalization, posthospital syndrome, and postdischarge health care application factors were collected. The majority of participants were recruited within a month postdischarge, and the program lasted about 6 months. Data collection was attempted at regular PAT contacts, but there was some variation in when visits occurred based on participant availability and preference. Some participants had missing data, which was handled using pairwise deletion.33 Larger studies are needed to confirm the findings of this study, particularly the trends that did not reach statistical significance. Home health services other than physical therapy (eg, nursing, occupational therapy) were not fully accounted for and should be considered in future research.
Conclusions
In patients undergoing a 6-month pilot VVC-based physical activity intervention posthospital discharge, improvements in mobility and disability were most likely in those who had no cognitive impairment and were not readmitted. Larger sample and qualitative investigations are necessary to optimize outcomes for patients who meet these clinical profiles.
- Liebzeit D, Bratzke L, Boltz M, Purvis S, King B. Getting back to normal: a grounded theory study of function in post-hospitalized older adults. Gerontologist. 2020;60:704-714. doi:10.1093/geront/gnz057
- Ponzetto M, Zanocchi M, Maero B, et al. Post-hospitalization mortality in the elderly. Arch Gerontol Geriatr. 2003;36:83-91. doi:10.1016/s0167-4943(02)00061-4
- Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6:e26951. doi:10.1371/journal.pone.0026951
- Ponzetto M, Maero B, Maina P, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58:1049-1054. doi:10.1093/gerona/58.11.m1049
- Huang HT, Chang CM, Liu LF, Lin HS, Chen CH. Trajectories and predictors of functional decline of hospitalised older patients. J Clin Nurs. 2013;22:1322-1331. doi:10.1111/jocn.12055
- Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171- 2179. doi:10.1111/j.1532-5415.2008.02023.x
- Helvik AS, Selbæk G, Engedal K. Functional decline in older adults one year after hospitalization. Arch Gerontol Geriatr. 2013;57:305-310. doi:10.1016/j.archger.2013.05.008
- Zaslavsky O, Zisberg A, Shadmi E. Impact of functional change before and during hospitalization on functional recovery 1 month following hospitalization. J Gerontol Biol Sci Med Sci. 2015;70:381-386. doi:10.1093/gerona/glu168
- Chen CC, Wang C, Huang GH. Functional trajectory 6 months posthospitalization: a cohort study of older hospitalized patients in Taiwan. Nurs Res. 2008;57:93-100. doi:10.1097/01.NNR.0000313485.18670.e2
- Kleinpell RM, Fletcher K, Jennings BM. Reducing functional decline in hospitalized elderly. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US); 2008. Accessed September 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK2629/
- Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69:2950-2962. doi:10.1111/jgs.17323
- Hladkowicz E, Dumitrascu F, Auais M, et al. Evaluations of postoperative transitions in care for older adults: a scoping review. BMC Geriatr. 2022;22:329. doi:10.1186/s12877-022-02989-6
- Alexander NB, Phillips K, Wagner-Felkey J, et al. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: baseline assessment. BMC Geriatr. 2021;21:502. doi:10.1186/s12877-021-02454-w
- Dawson R, Oliveira JS, Kwok WS, et al. Exercise interventions delivered through telehealth to improve physical functioning for older adults with frailty, cognitive, or mobility disability: a systematic review and meta-analysis. Telemed J E Health. 2024;30:940-950. doi:10.1089/tmj.2023.0177
- Liebzeit D, Phillips KK, Hogikyan RV, Cigolle CT, Alexander NB. A pilot home-telehealth program to enhance functional ability, physical performance, and physical activity in older adult veterans post-hospital discharge. Res Gerontol Nurs. 2024;17:271-279. doi:10.3928/19404921-20241105-01
- Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368:100-102. doi:10.1056/NEJMp1212324
- Caraballo C, Dharmarajan K, Krumholz HM. Post hospital syndrome: is the stress of hospitalization causing harm? Rev Esp Cardiol (Engl Ed). 2019;72:896-898. doi:10.1016/j.rec.2019.04.010
- Rawal S, Kwan JL, Razak F, et al. Association of the trauma of hospitalization with 30-day readmission or emergency department visit. JAMA Intern Med. 2019;179:38- 45. doi:10.1001/jamainternmed.2018.5100
- Dutzi I, Schwenk M, Kirchner M, Jooss E, Bauer JM, Hauer K. Influence of cognitive impairment on rehabilitation received and its mediating effect on functional recovery. J Alzheimers Dis. 2021;84:745-756. doi:10.3233/JAD-210620
- Uriz-Otano F, Uriz-Otano JI, Malafarina V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence ofcognitiveimpairment. JAmMedDirAssoc. 2015;16:215-220. doi:10.1016/j.jamda.2014.09.009
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-699. doi:10.1111/j.1532-5415.2005.53221.x
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- White RS, Jiang J, Hall CB, et al. Higher perceived stress scale scores are associated with higher pain intensity and pain interference levels in older adults. J Am Geriatr Soc. 2014;62:2350-2356. doi:10.1111/jgs.13135
- Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89:127-134. doi:10.1016/s0304-3959(00)00355-9
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain. 2004;110:361-368. doi:10.1016/j.pain.2004.04.017
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919. doi:10.1001/jama.1963.03060120024016
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-186.
- Alexander NB, Guire KE, Thelen DG, et al. Self-reported walking ability predicts functional mobility performance in frail older adults. J Am Geriatr Soc. 2000;48:1408-1413. doi:10.1111/j.1532-5415.2000.tb02630.x
- Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556-559. doi:10.1093/geronj/21.4.556
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85-M94. doi:10.1093/geronj/49.2.m85
- Chan CS, Slaughter SE, Jones CA, Ickert C, Wagg AS. Measuring activity performance of older adults using the activPAL: a rapid review. Healthcare (Basel). 2017;5:94. doi:10.3390/healthcare5040094
- IBM SPSS software. IBM Corp; 2019. Accessed September 3, 2025. https://www.ibm.com/spss
- Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64:402-406. doi:10.4097/kjae.2013.64.5.402
- Epstein AM, Jha AK, Orav EJ. The relationship between hospital admission rates and rehospitalizations. N Engl J Med. 2011;365:2287-2295. doi:10.1056/NEJMsa1101942
- Bogaisky M, Dezieck L. Early hospital readmission of nursing home residents and community-dwelling elderly adults discharged from the geriatrics service of an urban teaching hospital: patterns and risk factors. J Am Geriatr Soc. 2015;63:548-552. doi:10.1111/jgs.13317
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. doi:10.1056/NEJMsa0803563
- Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9:277-282. doi:10.1002/jhm.2152
- Mahoney J, Sager M, Dunham NC, Johnson J. Risk of falls after hospital discharge. J Am Geriatr Soc. 1994;42:269- 274. doi:10.1111/j.1532-5415.1994.tb01750.x
- Hoffman GJ, Liu H, Alexander NB, Tinetti M, Braun TM, Min LC. Posthospital fall injuries and 30-day readmissions in adults 65 years and older. JAMA Netw Open. 2019;2:e194276. doi:10.1001/jamanetworkopen.2019.4276
- Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9:S63-S71. doi:10.1016/j.jalz.2012.10.010
- Auyeung TW, Kwok T, Lee J, Leung PC, Leung J, Woo J. Functional decline in cognitive impairment–the relationship between physical and cognitive function. Neuroepidemiology. 2008;31:167-173. doi:10.1159/000154929
- Patti A, Zangla D, Sahin FN, et al. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine (Baltimore). 2021;100:e25289. doi:10.1097/MD.0000000000025289
- Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017-18). BMC Geriatr. 2022;22:203. doi:10.1186/s12877-022-02879-x
- Ek S, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. 2021;33:2183-2190. doi:10.1007/s40520-020-01747-1
- Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
- Ritchie CS, Patel K, Boscardin J, et al. Impact of persistent pain on function, cognition, and well-being of older adults. J Am Geriatr Soc. 2023;71:26-35. doi:10.1111/jgs.18125
- Han TS, Murray P, Robin J, et al. Evaluation of the association of length of stay in hospital and outcomes. Int J Qual Health Care. 2022;34:mzab160. doi:10.1093/intqhc/ mzab160
- Lærum-Onsager E, Molin M, Olsen CF, et al. Effect of nutritional and physical exercise intervention on hospital readmission for patients aged 65 or older: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act. 2021;18:62. doi:10.1186/s12966-021-01123-w
- Van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183:E391-E402. doi:10.1503/cmaj.101860
Deconditioning among hospitalized older adults contributes to significant decline in posthospitalization functional ability, physical performance, and physical activity.1-10 Previous hospital-to-home interventions have targeted improving function and physical activity, including recent programs leveraging home telehealth as a feasible and potentially effective mode of delivering in-home exercise and rehabilitation.11-14 However, pilot interventions have shown mixed effectiveness.11,12,14 This study expands on a previously published intervention describing a pilot home telehealth program for veterans posthospital discharge that demonstrated significant 6-month improvement in physical activity as well as trends in physical function improvement, including among those with cognitive impairment.15 Factors that contribute to improved outcomes are the focus of the present study.
Key factors underlying the complexity of hospital-to-home transitions include hospitalization elements (ie, reason for admission and length of stay), associated posthospital syndromes (ie, postdischarge falls, medication changes, cognitive impairment, and pain), and postdischarge health care application (ie, physical therapy and hospital readmission).16-18 These factors may be associated with postdischarge functional ability, physical performance, and physical activity, but their direct influence on intervention outcomes is unclear (Figure 1).5,7,9,16-20 The objective of this study was to examine the influence of hospitalization, posthospital syndrome, and postdischarge health care application factors on outcomes of a US Department of Veterans Affairs (VA) Video Connect (VVC) intervention to enhance function and physical activity in older adults posthospital discharge.
health care application factors on physical activity, functional ability, and
physical performance intervention outcomes.
Methods
The previous analysis reported on patient characteristics, program feasibility, and preliminary outcomes.13,15 The current study reports on relationships between hospitalization, posthospital syndrome, and postdischarge health care application factors and change in key outcomes, namely postdischarge self-reported functional ability, physical performance, and physical activity from baseline to endpoint.
Participants provided written informed consent. The protocol and consent forms were approved by the VA Ann Arbor Healthcare System (VAAAHS) Research and Development Committee, and the project was registered on clinicaltrials.gov (NCT04045054).
Intervention
The pilot program targeted older adults following recent hospital discharge from VAAAHS. Participants were eligible if they were aged ≥ 50 years, had been discharged following an inpatient stay in the past 1 to 2 weeks, evaluated by physical therapy during hospitalization with stated rehabilitation goals on discharge, and followed by a VAAAHS primary care physician. Participants were either recruited during hospital admission or shortly after discharge.13
An experienced physical activity trainer (PAT) supported the progression of participants’ rehabilitation goals via a home exercise program and coached the patient and caregiver to optimize functional ability, physical performance, and physical activity. The PAT was a nonlicensed research assistant with extensive experience in applying standard physical activity enhancement protocols (eg, increased walking) to older adults with comorbidities. Participation in the program lasted about 6 months. Initiation of the PAT program was delayed if the patient was already receiving postdischarge home-based or outpatient physical therapy. The PAT contacted the patient weekly via VVC for the first 6 weeks, then monthly for a total of 6 months. Each contact included information on optimal walking form, injury prevention, program progression, and ways to incorporate sit-to-stand transitions, nonsitting behavior, and walking into daily routines. The initial VVC contact lasted about 60 minutes and subsequent sessions lasted about 30 minutes.13
Demographic characteristics were self-reported by participants and included age, sex, race, years of education, and marital status. Clinical characteristics were obtained from each participant’s electronic health record (EHR), including copay status, index hospitalization length of stay, admission diagnosis, and postsurgery status (postsurgery vs nonpostsurgery). Intervention adherence was tracked as the number of PAT sessions attended.
Posthospital Syndrome Factors
Participant falls (categorized as those who reported a fall vs those who did not) and medication changes (number of changes reported, including new medication, discontinued medication, dose changes, medication changes, or changes in medication schedule) were reported by participants or caregivers during each VVC contact. Participants completed the Montreal Cognitive Assessment (MoCA) at baseline, and were dichotomized into 2 groups: no cognitive impairment (MoCA score ≥ 26) and mild to moderate cognitive impairment (MoCA score 10-25).13,21
Participants rated how much pain interfered with their normal daily activities since the previous VVC session on a 5-point Likert scale (1, not at all; to 5, extremely).22 Similar to prior research, participants were placed into 2 groups based on their mean pain interference score (individuals with scores from 1.0 to 2.0 in 1 group, and individuals with > 2.0 in another).23-25 Participants were separated into a no or mild pain interference group and a moderate to severe pain interference group. Hospital readmissions (VA and non-VA) and postdischarge physical therapy outcomes were obtained from the participant’s EHR, including primary care visits.
Outcomes
Outcomes were collected at baseline (posthospital discharge) and 6 months postenrollment.
Self-Reported Functional Ability. This measure is provided by participants or caregivers and measured by the Katz Index of Independence in Activities of Daily Living (ADL), Lawton and Brody Instrumental ADL Scale (IADL), Nagi Disability Model, and Rosow-Breslau Scale. The Katz ADL assesses the ability to complete 6 self-care activities and awards 1 point for independence and 0 if the individual is dependent (total score range, 0-6).26 The Lawton and Brody IADL measures an individual’s independence in 8 instrumental ADLs; it awards 1 point for independence and 0 if the individual is dependent (total score range, 0-8).27 The Nagi Disability Model evaluates an individual’s difficulty performing 5 tasks (total score range, 0-5) and tallies the number of items with a response other than “no difficulty at all” (higher total score indicates greater difficulty). 28 The Rosow-Breslau Scale is a 3-item measure of mobility disability; individual responses are 0 (no help) and 1 (requires help or unable); higher total score (range, 0-3) indicates greater disability.29
Physical Performance. Measured using the Short Physical Performance Battery (SPPB), which evaluates standing balance, sit to stand, and walking performance. Scores range from 0 to 4 on the balance, gait speed, and chair stand tests, for a total composite score between 0 and 12 (higher score indicates better performance).30
Physical Activity. Measured using actigraphy, namely a physical activity monitor adherent to the thigh (activ-PAL3TM, PAL Technologies Ltd., Glasgow, UK).31 Participants were instructed to wear the activPal for ≥ 1 week. Participants with a minimum of 5 days of wear were included in this analysis.
Data Analyses
Analyses were performed using SPSS software version 29.0.32 Continuous variables were summarized using mean (SD) or median and IQR using the weighted average method; categorical variables were summarized using frequencies and percentages. Baseline scores on outcome variables were compared by categorical hospitalization, posthospital syndrome, and postdischarge health care application factor variables using Mann-Whitney U tests. The differences between outcome variables from baseline to endpoint were then calculated to produce change scores. Relationships between the number of PAT sessions attended and baseline outcomes and outcome change scores were estimated using Spearman correlations. Relationships between categorical factors (hospitalization, posthospital syndrome, and postdischarge health care application) and outcome variable change scores (which were normally distributed) were examined using Mann-Whitney U tests. Relationships with continuous hospitalization (length of stay) and posthospital syndrome factors (medication changes) were estimated using Spearman correlations. Effect sizes (ES) were estimated with Cohen d; small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). Missing data were handled using pairwise deletion.33 Therefore, sample sizes were reported for each analysis. For all statistical tests, P < .05 was considered significant.
Results
Twenty-four individuals completed the pilot intervention.15 Mean (SD) age was 73.6 (8.1) years (range, 64-93 years) and participants were predominantly White males (Table 1). Eight participants had a high school education only and 13 had more than a high school education. Diagnoses at admission included 9 patients with orthopedic/musculoskeletal conditions (6 were for joint replacement), 6 patients with vascular/pulmonary conditions, and 4 with gastrointestinal/renal/urological conditions. Of the 11 postsurgery participants, 7 were orthopedic, 4 were gastrointestinal, and 1 was peripheral vascular.
Baseline outcome scores did not differ significantly between groups, except individuals with moderate to severe pain interference reported a significantly lower IADL score (median [IQR] 4 [2-7]) than individuals with mild or moderate pain interference (median [IQR] 8 [7-8]; P = .02) (Table 2). The mean (SD) number of PAT sessions attended was 9.3 (3.7) (range, 3-19). There were no significant relationships between number of sessions attended and any baseline outcome variables or outcome change scores.
Hospitalization Factors
Participants who were postsurgery tended to have greater improvement than individuals who were nonpostsurgery in ADLs (median [IQR] 0 [0-1.5]; ES, 0.6; P = .10) and SPPB (median [IQR] 2 [1.5-9]; ES, 0.9; P = .07), but the improvements were not statistically significant (Table 3). Mean (SD) length of stay of the index hospitalization was 6.7 (6.1) days. Longer length of stay was significantly correlated with an increase in Nagi score (ρ, 0.45; 95% CI, 0.01-0.75). There were no other significant or trending relationships between length of stay and outcome variables.
Posthospital Syndrome Factors
The 16 participants with mild to moderate cognitive impairment had less improvement in ADLs (median [IQR] 0 [0-1]) than the 8 participants with no impairment (median [IQR] 0 [-0.75 to 0]; ES, -1.1; P = .04). Change in outcome variables from baseline to endpoint did not significantly differ between the 8 patients who reported a fall compared with the 13 who did not, nor were any trends observed. Change in outcome variables from baseline to endpoint also did not significantly differ between the 8 participants who reported no or mild pain interference compared with the 10 patients with moderate to severe pain interference, nor were any trends observed. Mean (SD) number of medication changes was 2.5 (1.6). Higher number of medication changes was significantly correlated with a decrease in Rosow-Breslau score (ρ, -0.47; 95% CI, -0.76 to -0.02). There were no other significant or trending relationships between number of medication changes and outcome variables.
Postdischarge Health Care Application Factors
The 16 participants who attended posthospital physical therapy trended towards less improvement in IADLs (median [IQR] 0 [-0.5 to 1.5]; ES, -0.7; P = .11) and SPPB (median [IQR] 2 [-3.0 to 4.5]; ES, -0.5; P = .15) than the 8 patients with no postdischarge physical therapy. Eleven participants were readmitted, while 13 had no readmissions in their medical records between baseline and endpoint. Participants with ≥ 1 readmission experienced a greater increase in Rosow-Breslau score (median [IQR] 0 [-0.5 to 1.0]) than those not readmitted (median [IQR] 0 [-1.25 to 0.25]; ES, 1.0; P = .03). Borderline greater improvement in number of steps was found in those not readmitted (median [IQR] 3365.6 [274.4-7710.9]) compared with those readmitted (median [IQR] 319.9 [-136.1 to 774.5]; ES, -1.3; P = .05). Patients who were readmitted also tended to have lower and not statistically significant improvements in SPPB (median [IQR] 1 [-4.0 to 5.3]) compared with those not readmitted (median [IQR] 2 [0.3-3.8]; ES, -0.5; P = .17) (Table 3).
Discussion
This study examined the association between hospitalization, posthospital syndrome, and postdischarge health care use in patients undergoing a VVC-based intervention following hospital discharge. Participants who had no or mild cognitive impairment, no readmissions, higher medication changes, and a shorter hospital length of stay tended to experience lower disability, including in mobility and ADLs. This suggests individuals who are less clinically complex may be more likely to benefit from this type of virtual rehabilitation program. These findings are consistent with clinical experiences; home-based programs to improve physical activity posthospital discharge can be challenging for those who were medically ill (and did not undergo a specific surgical procedure), cognitively impaired, and become acutely ill and trigger hospital readmission. 15 For example, the sample in this study had higher rates of falls, pain, and readmissions compared to previous research.2,3,34-39
The importance of posthospital syndrome in the context of recovery of function and health at home following hospitalization is well documented.16-18 The potential impact of posthospital syndrome on physical activity-focused interventions is less understood. In our analysis, participants with mild or moderate cognitive impairment tended to become more dependent in their ADLs, while those with no cognitive impairment tended to become more independent in their ADLs. This functional decline over time is perhaps expected in persons with cognitive impairment, but the significant difference with a large ES warrants further consideration on how to tailor interventions to better promote functional recovery in these individuals.40,41 While some cognitive decline may not be preventable, this finding supports the need to promote healthy cognitive aging, identify declines in cognition, and work to mitigate additional decline. Programs specifically designed to promote function and physical activity in older adults with cognitive impairment are needed, especially during care transitions.41-43
While participants reported that falls and pain interference did not have a significant impact on change in outcomes between baseline and endpoint, these areas need further investigation. Falls and pain have been associated with function and physical activity in older adults.42-46 Pain is common, yet underappreciated during older adult hospital-to-home transitions.11,12,45,46 There is a need for more comprehensive assessment of pain (including pain intensity) and qualitative research.
Hospitalization and postdischarge health care application factors may have a significant impact on home-telehealth physical activity intervention success. Individuals who were postsurgery tended to have greater improvements in ADLs and physical performance. Most postsurgery participants had joint replacement surgery. Postsurgery status may not be modifiable, but it is important to note expected differences in recovery between medical and surgical admissions and the need to tailor care based on admission diagnosis. Those with a longer length of hospital stay may be considered at higher risk of suboptimal outcomes postdischarge, which indicates an opportunity for targeting resources and support, in addition to efforts of reducing length of stay where possible.47
Readmissions were significantly related to a change in Rosow-Breslau mobility disability score. This may indicate the detrimental impact a readmission can have on increasing mobility and physical activity postdischarge, or the potential of this pilot program to impact readmissions by increasing mobility and physical activity, contrary to prior physical exercise interventions.5,7,9,48 With 5% to 79% of readmissions considered preventable, continued efforts and program dissemination and implementation to address preventable readmissions are warranted.49 Individuals with postdischarge physical therapy (prior to beginning the pilot program) tended to demonstrate less improvement in disability and physical performance. This relationship needs further investigation; the 2 groups did not appear to have significant differences at baseline, albeit with a small sample size. It is possible they experienced initial improvements with postdischarge physical therapy and plateaued or had little further reserve to improve upon entering the VVC program.
Strengths and Limitations
This pilot program provided evaluative data on the use of VVC to enhance function and physical activity in older adults posthospital discharge. It included individual (eg, fall, pain, cognitive impairment) and health service (eg, readmission, physical therapy) level factors as predictors of function and physical activity posthospitalization.5,7,9,15-19
The results of this pilot project stem from a small sample lacking diversity in terms of race, ethnicity, and sex. There was some variation in baseline and endpoints between participants, and when hospitalization, posthospital syndrome, and postdischarge health care application factors were collected. The majority of participants were recruited within a month postdischarge, and the program lasted about 6 months. Data collection was attempted at regular PAT contacts, but there was some variation in when visits occurred based on participant availability and preference. Some participants had missing data, which was handled using pairwise deletion.33 Larger studies are needed to confirm the findings of this study, particularly the trends that did not reach statistical significance. Home health services other than physical therapy (eg, nursing, occupational therapy) were not fully accounted for and should be considered in future research.
Conclusions
In patients undergoing a 6-month pilot VVC-based physical activity intervention posthospital discharge, improvements in mobility and disability were most likely in those who had no cognitive impairment and were not readmitted. Larger sample and qualitative investigations are necessary to optimize outcomes for patients who meet these clinical profiles.
Deconditioning among hospitalized older adults contributes to significant decline in posthospitalization functional ability, physical performance, and physical activity.1-10 Previous hospital-to-home interventions have targeted improving function and physical activity, including recent programs leveraging home telehealth as a feasible and potentially effective mode of delivering in-home exercise and rehabilitation.11-14 However, pilot interventions have shown mixed effectiveness.11,12,14 This study expands on a previously published intervention describing a pilot home telehealth program for veterans posthospital discharge that demonstrated significant 6-month improvement in physical activity as well as trends in physical function improvement, including among those with cognitive impairment.15 Factors that contribute to improved outcomes are the focus of the present study.
Key factors underlying the complexity of hospital-to-home transitions include hospitalization elements (ie, reason for admission and length of stay), associated posthospital syndromes (ie, postdischarge falls, medication changes, cognitive impairment, and pain), and postdischarge health care application (ie, physical therapy and hospital readmission).16-18 These factors may be associated with postdischarge functional ability, physical performance, and physical activity, but their direct influence on intervention outcomes is unclear (Figure 1).5,7,9,16-20 The objective of this study was to examine the influence of hospitalization, posthospital syndrome, and postdischarge health care application factors on outcomes of a US Department of Veterans Affairs (VA) Video Connect (VVC) intervention to enhance function and physical activity in older adults posthospital discharge.
health care application factors on physical activity, functional ability, and
physical performance intervention outcomes.
Methods
The previous analysis reported on patient characteristics, program feasibility, and preliminary outcomes.13,15 The current study reports on relationships between hospitalization, posthospital syndrome, and postdischarge health care application factors and change in key outcomes, namely postdischarge self-reported functional ability, physical performance, and physical activity from baseline to endpoint.
Participants provided written informed consent. The protocol and consent forms were approved by the VA Ann Arbor Healthcare System (VAAAHS) Research and Development Committee, and the project was registered on clinicaltrials.gov (NCT04045054).
Intervention
The pilot program targeted older adults following recent hospital discharge from VAAAHS. Participants were eligible if they were aged ≥ 50 years, had been discharged following an inpatient stay in the past 1 to 2 weeks, evaluated by physical therapy during hospitalization with stated rehabilitation goals on discharge, and followed by a VAAAHS primary care physician. Participants were either recruited during hospital admission or shortly after discharge.13
An experienced physical activity trainer (PAT) supported the progression of participants’ rehabilitation goals via a home exercise program and coached the patient and caregiver to optimize functional ability, physical performance, and physical activity. The PAT was a nonlicensed research assistant with extensive experience in applying standard physical activity enhancement protocols (eg, increased walking) to older adults with comorbidities. Participation in the program lasted about 6 months. Initiation of the PAT program was delayed if the patient was already receiving postdischarge home-based or outpatient physical therapy. The PAT contacted the patient weekly via VVC for the first 6 weeks, then monthly for a total of 6 months. Each contact included information on optimal walking form, injury prevention, program progression, and ways to incorporate sit-to-stand transitions, nonsitting behavior, and walking into daily routines. The initial VVC contact lasted about 60 minutes and subsequent sessions lasted about 30 minutes.13
Demographic characteristics were self-reported by participants and included age, sex, race, years of education, and marital status. Clinical characteristics were obtained from each participant’s electronic health record (EHR), including copay status, index hospitalization length of stay, admission diagnosis, and postsurgery status (postsurgery vs nonpostsurgery). Intervention adherence was tracked as the number of PAT sessions attended.
Posthospital Syndrome Factors
Participant falls (categorized as those who reported a fall vs those who did not) and medication changes (number of changes reported, including new medication, discontinued medication, dose changes, medication changes, or changes in medication schedule) were reported by participants or caregivers during each VVC contact. Participants completed the Montreal Cognitive Assessment (MoCA) at baseline, and were dichotomized into 2 groups: no cognitive impairment (MoCA score ≥ 26) and mild to moderate cognitive impairment (MoCA score 10-25).13,21
Participants rated how much pain interfered with their normal daily activities since the previous VVC session on a 5-point Likert scale (1, not at all; to 5, extremely).22 Similar to prior research, participants were placed into 2 groups based on their mean pain interference score (individuals with scores from 1.0 to 2.0 in 1 group, and individuals with > 2.0 in another).23-25 Participants were separated into a no or mild pain interference group and a moderate to severe pain interference group. Hospital readmissions (VA and non-VA) and postdischarge physical therapy outcomes were obtained from the participant’s EHR, including primary care visits.
Outcomes
Outcomes were collected at baseline (posthospital discharge) and 6 months postenrollment.
Self-Reported Functional Ability. This measure is provided by participants or caregivers and measured by the Katz Index of Independence in Activities of Daily Living (ADL), Lawton and Brody Instrumental ADL Scale (IADL), Nagi Disability Model, and Rosow-Breslau Scale. The Katz ADL assesses the ability to complete 6 self-care activities and awards 1 point for independence and 0 if the individual is dependent (total score range, 0-6).26 The Lawton and Brody IADL measures an individual’s independence in 8 instrumental ADLs; it awards 1 point for independence and 0 if the individual is dependent (total score range, 0-8).27 The Nagi Disability Model evaluates an individual’s difficulty performing 5 tasks (total score range, 0-5) and tallies the number of items with a response other than “no difficulty at all” (higher total score indicates greater difficulty). 28 The Rosow-Breslau Scale is a 3-item measure of mobility disability; individual responses are 0 (no help) and 1 (requires help or unable); higher total score (range, 0-3) indicates greater disability.29
Physical Performance. Measured using the Short Physical Performance Battery (SPPB), which evaluates standing balance, sit to stand, and walking performance. Scores range from 0 to 4 on the balance, gait speed, and chair stand tests, for a total composite score between 0 and 12 (higher score indicates better performance).30
Physical Activity. Measured using actigraphy, namely a physical activity monitor adherent to the thigh (activ-PAL3TM, PAL Technologies Ltd., Glasgow, UK).31 Participants were instructed to wear the activPal for ≥ 1 week. Participants with a minimum of 5 days of wear were included in this analysis.
Data Analyses
Analyses were performed using SPSS software version 29.0.32 Continuous variables were summarized using mean (SD) or median and IQR using the weighted average method; categorical variables were summarized using frequencies and percentages. Baseline scores on outcome variables were compared by categorical hospitalization, posthospital syndrome, and postdischarge health care application factor variables using Mann-Whitney U tests. The differences between outcome variables from baseline to endpoint were then calculated to produce change scores. Relationships between the number of PAT sessions attended and baseline outcomes and outcome change scores were estimated using Spearman correlations. Relationships between categorical factors (hospitalization, posthospital syndrome, and postdischarge health care application) and outcome variable change scores (which were normally distributed) were examined using Mann-Whitney U tests. Relationships with continuous hospitalization (length of stay) and posthospital syndrome factors (medication changes) were estimated using Spearman correlations. Effect sizes (ES) were estimated with Cohen d; small (d = 0.2), medium (d = 0.5), or large (d ≥ 0.8). Missing data were handled using pairwise deletion.33 Therefore, sample sizes were reported for each analysis. For all statistical tests, P < .05 was considered significant.
Results
Twenty-four individuals completed the pilot intervention.15 Mean (SD) age was 73.6 (8.1) years (range, 64-93 years) and participants were predominantly White males (Table 1). Eight participants had a high school education only and 13 had more than a high school education. Diagnoses at admission included 9 patients with orthopedic/musculoskeletal conditions (6 were for joint replacement), 6 patients with vascular/pulmonary conditions, and 4 with gastrointestinal/renal/urological conditions. Of the 11 postsurgery participants, 7 were orthopedic, 4 were gastrointestinal, and 1 was peripheral vascular.
Baseline outcome scores did not differ significantly between groups, except individuals with moderate to severe pain interference reported a significantly lower IADL score (median [IQR] 4 [2-7]) than individuals with mild or moderate pain interference (median [IQR] 8 [7-8]; P = .02) (Table 2). The mean (SD) number of PAT sessions attended was 9.3 (3.7) (range, 3-19). There were no significant relationships between number of sessions attended and any baseline outcome variables or outcome change scores.
Hospitalization Factors
Participants who were postsurgery tended to have greater improvement than individuals who were nonpostsurgery in ADLs (median [IQR] 0 [0-1.5]; ES, 0.6; P = .10) and SPPB (median [IQR] 2 [1.5-9]; ES, 0.9; P = .07), but the improvements were not statistically significant (Table 3). Mean (SD) length of stay of the index hospitalization was 6.7 (6.1) days. Longer length of stay was significantly correlated with an increase in Nagi score (ρ, 0.45; 95% CI, 0.01-0.75). There were no other significant or trending relationships between length of stay and outcome variables.
Posthospital Syndrome Factors
The 16 participants with mild to moderate cognitive impairment had less improvement in ADLs (median [IQR] 0 [0-1]) than the 8 participants with no impairment (median [IQR] 0 [-0.75 to 0]; ES, -1.1; P = .04). Change in outcome variables from baseline to endpoint did not significantly differ between the 8 patients who reported a fall compared with the 13 who did not, nor were any trends observed. Change in outcome variables from baseline to endpoint also did not significantly differ between the 8 participants who reported no or mild pain interference compared with the 10 patients with moderate to severe pain interference, nor were any trends observed. Mean (SD) number of medication changes was 2.5 (1.6). Higher number of medication changes was significantly correlated with a decrease in Rosow-Breslau score (ρ, -0.47; 95% CI, -0.76 to -0.02). There were no other significant or trending relationships between number of medication changes and outcome variables.
Postdischarge Health Care Application Factors
The 16 participants who attended posthospital physical therapy trended towards less improvement in IADLs (median [IQR] 0 [-0.5 to 1.5]; ES, -0.7; P = .11) and SPPB (median [IQR] 2 [-3.0 to 4.5]; ES, -0.5; P = .15) than the 8 patients with no postdischarge physical therapy. Eleven participants were readmitted, while 13 had no readmissions in their medical records between baseline and endpoint. Participants with ≥ 1 readmission experienced a greater increase in Rosow-Breslau score (median [IQR] 0 [-0.5 to 1.0]) than those not readmitted (median [IQR] 0 [-1.25 to 0.25]; ES, 1.0; P = .03). Borderline greater improvement in number of steps was found in those not readmitted (median [IQR] 3365.6 [274.4-7710.9]) compared with those readmitted (median [IQR] 319.9 [-136.1 to 774.5]; ES, -1.3; P = .05). Patients who were readmitted also tended to have lower and not statistically significant improvements in SPPB (median [IQR] 1 [-4.0 to 5.3]) compared with those not readmitted (median [IQR] 2 [0.3-3.8]; ES, -0.5; P = .17) (Table 3).
Discussion
This study examined the association between hospitalization, posthospital syndrome, and postdischarge health care use in patients undergoing a VVC-based intervention following hospital discharge. Participants who had no or mild cognitive impairment, no readmissions, higher medication changes, and a shorter hospital length of stay tended to experience lower disability, including in mobility and ADLs. This suggests individuals who are less clinically complex may be more likely to benefit from this type of virtual rehabilitation program. These findings are consistent with clinical experiences; home-based programs to improve physical activity posthospital discharge can be challenging for those who were medically ill (and did not undergo a specific surgical procedure), cognitively impaired, and become acutely ill and trigger hospital readmission. 15 For example, the sample in this study had higher rates of falls, pain, and readmissions compared to previous research.2,3,34-39
The importance of posthospital syndrome in the context of recovery of function and health at home following hospitalization is well documented.16-18 The potential impact of posthospital syndrome on physical activity-focused interventions is less understood. In our analysis, participants with mild or moderate cognitive impairment tended to become more dependent in their ADLs, while those with no cognitive impairment tended to become more independent in their ADLs. This functional decline over time is perhaps expected in persons with cognitive impairment, but the significant difference with a large ES warrants further consideration on how to tailor interventions to better promote functional recovery in these individuals.40,41 While some cognitive decline may not be preventable, this finding supports the need to promote healthy cognitive aging, identify declines in cognition, and work to mitigate additional decline. Programs specifically designed to promote function and physical activity in older adults with cognitive impairment are needed, especially during care transitions.41-43
While participants reported that falls and pain interference did not have a significant impact on change in outcomes between baseline and endpoint, these areas need further investigation. Falls and pain have been associated with function and physical activity in older adults.42-46 Pain is common, yet underappreciated during older adult hospital-to-home transitions.11,12,45,46 There is a need for more comprehensive assessment of pain (including pain intensity) and qualitative research.
Hospitalization and postdischarge health care application factors may have a significant impact on home-telehealth physical activity intervention success. Individuals who were postsurgery tended to have greater improvements in ADLs and physical performance. Most postsurgery participants had joint replacement surgery. Postsurgery status may not be modifiable, but it is important to note expected differences in recovery between medical and surgical admissions and the need to tailor care based on admission diagnosis. Those with a longer length of hospital stay may be considered at higher risk of suboptimal outcomes postdischarge, which indicates an opportunity for targeting resources and support, in addition to efforts of reducing length of stay where possible.47
Readmissions were significantly related to a change in Rosow-Breslau mobility disability score. This may indicate the detrimental impact a readmission can have on increasing mobility and physical activity postdischarge, or the potential of this pilot program to impact readmissions by increasing mobility and physical activity, contrary to prior physical exercise interventions.5,7,9,48 With 5% to 79% of readmissions considered preventable, continued efforts and program dissemination and implementation to address preventable readmissions are warranted.49 Individuals with postdischarge physical therapy (prior to beginning the pilot program) tended to demonstrate less improvement in disability and physical performance. This relationship needs further investigation; the 2 groups did not appear to have significant differences at baseline, albeit with a small sample size. It is possible they experienced initial improvements with postdischarge physical therapy and plateaued or had little further reserve to improve upon entering the VVC program.
Strengths and Limitations
This pilot program provided evaluative data on the use of VVC to enhance function and physical activity in older adults posthospital discharge. It included individual (eg, fall, pain, cognitive impairment) and health service (eg, readmission, physical therapy) level factors as predictors of function and physical activity posthospitalization.5,7,9,15-19
The results of this pilot project stem from a small sample lacking diversity in terms of race, ethnicity, and sex. There was some variation in baseline and endpoints between participants, and when hospitalization, posthospital syndrome, and postdischarge health care application factors were collected. The majority of participants were recruited within a month postdischarge, and the program lasted about 6 months. Data collection was attempted at regular PAT contacts, but there was some variation in when visits occurred based on participant availability and preference. Some participants had missing data, which was handled using pairwise deletion.33 Larger studies are needed to confirm the findings of this study, particularly the trends that did not reach statistical significance. Home health services other than physical therapy (eg, nursing, occupational therapy) were not fully accounted for and should be considered in future research.
Conclusions
In patients undergoing a 6-month pilot VVC-based physical activity intervention posthospital discharge, improvements in mobility and disability were most likely in those who had no cognitive impairment and were not readmitted. Larger sample and qualitative investigations are necessary to optimize outcomes for patients who meet these clinical profiles.
- Liebzeit D, Bratzke L, Boltz M, Purvis S, King B. Getting back to normal: a grounded theory study of function in post-hospitalized older adults. Gerontologist. 2020;60:704-714. doi:10.1093/geront/gnz057
- Ponzetto M, Zanocchi M, Maero B, et al. Post-hospitalization mortality in the elderly. Arch Gerontol Geriatr. 2003;36:83-91. doi:10.1016/s0167-4943(02)00061-4
- Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6:e26951. doi:10.1371/journal.pone.0026951
- Ponzetto M, Maero B, Maina P, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58:1049-1054. doi:10.1093/gerona/58.11.m1049
- Huang HT, Chang CM, Liu LF, Lin HS, Chen CH. Trajectories and predictors of functional decline of hospitalised older patients. J Clin Nurs. 2013;22:1322-1331. doi:10.1111/jocn.12055
- Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171- 2179. doi:10.1111/j.1532-5415.2008.02023.x
- Helvik AS, Selbæk G, Engedal K. Functional decline in older adults one year after hospitalization. Arch Gerontol Geriatr. 2013;57:305-310. doi:10.1016/j.archger.2013.05.008
- Zaslavsky O, Zisberg A, Shadmi E. Impact of functional change before and during hospitalization on functional recovery 1 month following hospitalization. J Gerontol Biol Sci Med Sci. 2015;70:381-386. doi:10.1093/gerona/glu168
- Chen CC, Wang C, Huang GH. Functional trajectory 6 months posthospitalization: a cohort study of older hospitalized patients in Taiwan. Nurs Res. 2008;57:93-100. doi:10.1097/01.NNR.0000313485.18670.e2
- Kleinpell RM, Fletcher K, Jennings BM. Reducing functional decline in hospitalized elderly. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US); 2008. Accessed September 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK2629/
- Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69:2950-2962. doi:10.1111/jgs.17323
- Hladkowicz E, Dumitrascu F, Auais M, et al. Evaluations of postoperative transitions in care for older adults: a scoping review. BMC Geriatr. 2022;22:329. doi:10.1186/s12877-022-02989-6
- Alexander NB, Phillips K, Wagner-Felkey J, et al. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: baseline assessment. BMC Geriatr. 2021;21:502. doi:10.1186/s12877-021-02454-w
- Dawson R, Oliveira JS, Kwok WS, et al. Exercise interventions delivered through telehealth to improve physical functioning for older adults with frailty, cognitive, or mobility disability: a systematic review and meta-analysis. Telemed J E Health. 2024;30:940-950. doi:10.1089/tmj.2023.0177
- Liebzeit D, Phillips KK, Hogikyan RV, Cigolle CT, Alexander NB. A pilot home-telehealth program to enhance functional ability, physical performance, and physical activity in older adult veterans post-hospital discharge. Res Gerontol Nurs. 2024;17:271-279. doi:10.3928/19404921-20241105-01
- Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368:100-102. doi:10.1056/NEJMp1212324
- Caraballo C, Dharmarajan K, Krumholz HM. Post hospital syndrome: is the stress of hospitalization causing harm? Rev Esp Cardiol (Engl Ed). 2019;72:896-898. doi:10.1016/j.rec.2019.04.010
- Rawal S, Kwan JL, Razak F, et al. Association of the trauma of hospitalization with 30-day readmission or emergency department visit. JAMA Intern Med. 2019;179:38- 45. doi:10.1001/jamainternmed.2018.5100
- Dutzi I, Schwenk M, Kirchner M, Jooss E, Bauer JM, Hauer K. Influence of cognitive impairment on rehabilitation received and its mediating effect on functional recovery. J Alzheimers Dis. 2021;84:745-756. doi:10.3233/JAD-210620
- Uriz-Otano F, Uriz-Otano JI, Malafarina V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence ofcognitiveimpairment. JAmMedDirAssoc. 2015;16:215-220. doi:10.1016/j.jamda.2014.09.009
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-699. doi:10.1111/j.1532-5415.2005.53221.x
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- White RS, Jiang J, Hall CB, et al. Higher perceived stress scale scores are associated with higher pain intensity and pain interference levels in older adults. J Am Geriatr Soc. 2014;62:2350-2356. doi:10.1111/jgs.13135
- Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89:127-134. doi:10.1016/s0304-3959(00)00355-9
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain. 2004;110:361-368. doi:10.1016/j.pain.2004.04.017
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919. doi:10.1001/jama.1963.03060120024016
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-186.
- Alexander NB, Guire KE, Thelen DG, et al. Self-reported walking ability predicts functional mobility performance in frail older adults. J Am Geriatr Soc. 2000;48:1408-1413. doi:10.1111/j.1532-5415.2000.tb02630.x
- Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556-559. doi:10.1093/geronj/21.4.556
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85-M94. doi:10.1093/geronj/49.2.m85
- Chan CS, Slaughter SE, Jones CA, Ickert C, Wagg AS. Measuring activity performance of older adults using the activPAL: a rapid review. Healthcare (Basel). 2017;5:94. doi:10.3390/healthcare5040094
- IBM SPSS software. IBM Corp; 2019. Accessed September 3, 2025. https://www.ibm.com/spss
- Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64:402-406. doi:10.4097/kjae.2013.64.5.402
- Epstein AM, Jha AK, Orav EJ. The relationship between hospital admission rates and rehospitalizations. N Engl J Med. 2011;365:2287-2295. doi:10.1056/NEJMsa1101942
- Bogaisky M, Dezieck L. Early hospital readmission of nursing home residents and community-dwelling elderly adults discharged from the geriatrics service of an urban teaching hospital: patterns and risk factors. J Am Geriatr Soc. 2015;63:548-552. doi:10.1111/jgs.13317
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. doi:10.1056/NEJMsa0803563
- Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9:277-282. doi:10.1002/jhm.2152
- Mahoney J, Sager M, Dunham NC, Johnson J. Risk of falls after hospital discharge. J Am Geriatr Soc. 1994;42:269- 274. doi:10.1111/j.1532-5415.1994.tb01750.x
- Hoffman GJ, Liu H, Alexander NB, Tinetti M, Braun TM, Min LC. Posthospital fall injuries and 30-day readmissions in adults 65 years and older. JAMA Netw Open. 2019;2:e194276. doi:10.1001/jamanetworkopen.2019.4276
- Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9:S63-S71. doi:10.1016/j.jalz.2012.10.010
- Auyeung TW, Kwok T, Lee J, Leung PC, Leung J, Woo J. Functional decline in cognitive impairment–the relationship between physical and cognitive function. Neuroepidemiology. 2008;31:167-173. doi:10.1159/000154929
- Patti A, Zangla D, Sahin FN, et al. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine (Baltimore). 2021;100:e25289. doi:10.1097/MD.0000000000025289
- Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017-18). BMC Geriatr. 2022;22:203. doi:10.1186/s12877-022-02879-x
- Ek S, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. 2021;33:2183-2190. doi:10.1007/s40520-020-01747-1
- Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
- Ritchie CS, Patel K, Boscardin J, et al. Impact of persistent pain on function, cognition, and well-being of older adults. J Am Geriatr Soc. 2023;71:26-35. doi:10.1111/jgs.18125
- Han TS, Murray P, Robin J, et al. Evaluation of the association of length of stay in hospital and outcomes. Int J Qual Health Care. 2022;34:mzab160. doi:10.1093/intqhc/ mzab160
- Lærum-Onsager E, Molin M, Olsen CF, et al. Effect of nutritional and physical exercise intervention on hospital readmission for patients aged 65 or older: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act. 2021;18:62. doi:10.1186/s12966-021-01123-w
- Van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183:E391-E402. doi:10.1503/cmaj.101860
- Liebzeit D, Bratzke L, Boltz M, Purvis S, King B. Getting back to normal: a grounded theory study of function in post-hospitalized older adults. Gerontologist. 2020;60:704-714. doi:10.1093/geront/gnz057
- Ponzetto M, Zanocchi M, Maero B, et al. Post-hospitalization mortality in the elderly. Arch Gerontol Geriatr. 2003;36:83-91. doi:10.1016/s0167-4943(02)00061-4
- Buurman BM, Hoogerduijn JG, de Haan RJ, et al. Geriatric conditions in acutely hospitalized older patients: prevalence and one-year survival and functional decline. PLoS One. 2011;6:e26951. doi:10.1371/journal.pone.0026951
- Ponzetto M, Maero B, Maina P, et al. Risk factors for early and late mortality in hospitalized older patients: the continuing importance of functional status. J Gerontol A Biol Sci Med Sci. 2003;58:1049-1054. doi:10.1093/gerona/58.11.m1049
- Huang HT, Chang CM, Liu LF, Lin HS, Chen CH. Trajectories and predictors of functional decline of hospitalised older patients. J Clin Nurs. 2013;22:1322-1331. doi:10.1111/jocn.12055
- Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171- 2179. doi:10.1111/j.1532-5415.2008.02023.x
- Helvik AS, Selbæk G, Engedal K. Functional decline in older adults one year after hospitalization. Arch Gerontol Geriatr. 2013;57:305-310. doi:10.1016/j.archger.2013.05.008
- Zaslavsky O, Zisberg A, Shadmi E. Impact of functional change before and during hospitalization on functional recovery 1 month following hospitalization. J Gerontol Biol Sci Med Sci. 2015;70:381-386. doi:10.1093/gerona/glu168
- Chen CC, Wang C, Huang GH. Functional trajectory 6 months posthospitalization: a cohort study of older hospitalized patients in Taiwan. Nurs Res. 2008;57:93-100. doi:10.1097/01.NNR.0000313485.18670.e2
- Kleinpell RM, Fletcher K, Jennings BM. Reducing functional decline in hospitalized elderly. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Agency for Healthcare Research and Quality (US); 2008. Accessed September 3, 2025. http://www.ncbi.nlm.nih.gov/books/NBK2629/
- Liebzeit D, Rutkowski R, Arbaje AI, Fields B, Werner NE. A scoping review of interventions for older adults transitioning from hospital to home. J Am Geriatr Soc. 2021;69:2950-2962. doi:10.1111/jgs.17323
- Hladkowicz E, Dumitrascu F, Auais M, et al. Evaluations of postoperative transitions in care for older adults: a scoping review. BMC Geriatr. 2022;22:329. doi:10.1186/s12877-022-02989-6
- Alexander NB, Phillips K, Wagner-Felkey J, et al. Team VA Video Connect (VVC) to optimize mobility and physical activity in post-hospital discharge older veterans: baseline assessment. BMC Geriatr. 2021;21:502. doi:10.1186/s12877-021-02454-w
- Dawson R, Oliveira JS, Kwok WS, et al. Exercise interventions delivered through telehealth to improve physical functioning for older adults with frailty, cognitive, or mobility disability: a systematic review and meta-analysis. Telemed J E Health. 2024;30:940-950. doi:10.1089/tmj.2023.0177
- Liebzeit D, Phillips KK, Hogikyan RV, Cigolle CT, Alexander NB. A pilot home-telehealth program to enhance functional ability, physical performance, and physical activity in older adult veterans post-hospital discharge. Res Gerontol Nurs. 2024;17:271-279. doi:10.3928/19404921-20241105-01
- Krumholz HM. Post-hospital syndrome—an acquired, transient condition of generalized risk. N Engl J Med. 2013;368:100-102. doi:10.1056/NEJMp1212324
- Caraballo C, Dharmarajan K, Krumholz HM. Post hospital syndrome: is the stress of hospitalization causing harm? Rev Esp Cardiol (Engl Ed). 2019;72:896-898. doi:10.1016/j.rec.2019.04.010
- Rawal S, Kwan JL, Razak F, et al. Association of the trauma of hospitalization with 30-day readmission or emergency department visit. JAMA Intern Med. 2019;179:38- 45. doi:10.1001/jamainternmed.2018.5100
- Dutzi I, Schwenk M, Kirchner M, Jooss E, Bauer JM, Hauer K. Influence of cognitive impairment on rehabilitation received and its mediating effect on functional recovery. J Alzheimers Dis. 2021;84:745-756. doi:10.3233/JAD-210620
- Uriz-Otano F, Uriz-Otano JI, Malafarina V. Factors associated with short-term functional recovery in elderly people with a hip fracture. Influence ofcognitiveimpairment. JAmMedDirAssoc. 2015;16:215-220. doi:10.1016/j.jamda.2014.09.009
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695-699. doi:10.1111/j.1532-5415.2005.53221.x
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
- White RS, Jiang J, Hall CB, et al. Higher perceived stress scale scores are associated with higher pain intensity and pain interference levels in older adults. J Am Geriatr Soc. 2014;62:2350-2356. doi:10.1111/jgs.13135
- Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89:127-134. doi:10.1016/s0304-3959(00)00355-9
- Thomas E, Peat G, Harris L, Wilkie R, Croft PR. The prevalence of pain and pain interference in a general population of older adults: cross-sectional findings from the North Staffordshire Osteoarthritis Project (NorStOP). Pain. 2004;110:361-368. doi:10.1016/j.pain.2004.04.017
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:914-919. doi:10.1001/jama.1963.03060120024016
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-186.
- Alexander NB, Guire KE, Thelen DG, et al. Self-reported walking ability predicts functional mobility performance in frail older adults. J Am Geriatr Soc. 2000;48:1408-1413. doi:10.1111/j.1532-5415.2000.tb02630.x
- Rosow I, Breslau N. A Guttman health scale for the aged. J Gerontol. 1966;21:556-559. doi:10.1093/geronj/21.4.556
- Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49:M85-M94. doi:10.1093/geronj/49.2.m85
- Chan CS, Slaughter SE, Jones CA, Ickert C, Wagg AS. Measuring activity performance of older adults using the activPAL: a rapid review. Healthcare (Basel). 2017;5:94. doi:10.3390/healthcare5040094
- IBM SPSS software. IBM Corp; 2019. Accessed September 3, 2025. https://www.ibm.com/spss
- Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64:402-406. doi:10.4097/kjae.2013.64.5.402
- Epstein AM, Jha AK, Orav EJ. The relationship between hospital admission rates and rehospitalizations. N Engl J Med. 2011;365:2287-2295. doi:10.1056/NEJMsa1101942
- Bogaisky M, Dezieck L. Early hospital readmission of nursing home residents and community-dwelling elderly adults discharged from the geriatrics service of an urban teaching hospital: patterns and risk factors. J Am Geriatr Soc. 2015;63:548-552. doi:10.1111/jgs.13317
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418-1428. doi:10.1056/NEJMsa0803563
- Hoyer EH, Needham DM, Atanelov L, Knox B, Friedman M, Brotman DJ. Association of impaired functional status at hospital discharge and subsequent rehospitalization. J Hosp Med. 2014;9:277-282. doi:10.1002/jhm.2152
- Mahoney J, Sager M, Dunham NC, Johnson J. Risk of falls after hospital discharge. J Am Geriatr Soc. 1994;42:269- 274. doi:10.1111/j.1532-5415.1994.tb01750.x
- Hoffman GJ, Liu H, Alexander NB, Tinetti M, Braun TM, Min LC. Posthospital fall injuries and 30-day readmissions in adults 65 years and older. JAMA Netw Open. 2019;2:e194276. doi:10.1001/jamanetworkopen.2019.4276
- Gill DP, Hubbard RA, Koepsell TD, et al. Differences in rate of functional decline across three dementia types. Alzheimers Dement. 2013;9:S63-S71. doi:10.1016/j.jalz.2012.10.010
- Auyeung TW, Kwok T, Lee J, Leung PC, Leung J, Woo J. Functional decline in cognitive impairment–the relationship between physical and cognitive function. Neuroepidemiology. 2008;31:167-173. doi:10.1159/000154929
- Patti A, Zangla D, Sahin FN, et al. Physical exercise and prevention of falls. Effects of a Pilates training method compared with a general physical activity program. Medicine (Baltimore). 2021;100:e25289. doi:10.1097/MD.0000000000025289
- Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017-18). BMC Geriatr. 2022;22:203. doi:10.1186/s12877-022-02879-x
- Ek S, Rizzuto D, Xu W, Calderón-Larrañaga A, Welmer AK. Predictors for functional decline after an injurious fall: a population-based cohort study. Aging Clin Exp Res. 2021;33:2183-2190. doi:10.1007/s40520-020-01747-1
- Dagnino APA, Campos MM. Chronic pain in the elderly: mechanisms and perspectives. Front Hum Neurosci. 2022;16:736688. doi:10.3389/fnhum.2022.736688
- Ritchie CS, Patel K, Boscardin J, et al. Impact of persistent pain on function, cognition, and well-being of older adults. J Am Geriatr Soc. 2023;71:26-35. doi:10.1111/jgs.18125
- Han TS, Murray P, Robin J, et al. Evaluation of the association of length of stay in hospital and outcomes. Int J Qual Health Care. 2022;34:mzab160. doi:10.1093/intqhc/ mzab160
- Lærum-Onsager E, Molin M, Olsen CF, et al. Effect of nutritional and physical exercise intervention on hospital readmission for patients aged 65 or older: a systematic review and meta-analysis of randomized controlled trials. Int J Behav Nutr Phys Act. 2021;18:62. doi:10.1186/s12966-021-01123-w
- Van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ. 2011;183:E391-E402. doi:10.1503/cmaj.101860
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Factors Influencing Outcomes of a Telehealth-Based Physical Activity Program in Older Veterans Postdischarge
Hospitalists Must Encourage Mental Stimulation for Patients
As a hospitalist, you are in a unique position to notice changes in your hospitalized patients. This frontline perspective can be used to improve inpatient attention and care, and differs from primary care, where a clinician might only see a patient once or twice a year, and subtle, gradual changes may be missed, said George Cao, MD, MBA, a hospitalist at the University of Vermont Medical Center in Burlington and assistant professor at UVM’s Larner College of Medicine.
But in the hospital, Cao said even small shifts — like becoming less active, eating less, or changes in personality — can become much more obvious.
“As hospitalists…we see patients throughout the day, in different situations, and often end up spending more time with them over the course of a week than their primary care provider might in a year,” Cao explained. “This gives us a real advantage in picking up on subtle changes in mental awareness.”
These assessments can also be evaluated with the benefit of daily labs, frequent bedside interactions, and 24–hour observations.
With older adults, Cao said it’s important to go beyond just what’s in the chart.
“I always start by reviewing notes from the primary care provider and previous admissions, but some of the most valuable insights come from talking with family and close friends to get a true sense of the patient’s baseline — how they usually think, move, and interact,” he said.
Why to Watch for Declining Mental Awareness
Declining mental awareness in the inpatient setting is often a sign of an underlying problem — whether that’s a reversible medical condition, unrecognized dementia, or the development of delirium, Cao said.
“On the inpatient side, I pay close attention to more than just memory loss,” he said.
Changes in how patients function day–to–day, shifts in their behavior, or even something as simple as not wanting to get out of bed can be early signs of an aging mind or untreated psychiatric issues, he noted.
“Of course, we always rule out infections and medication side effects, but I also look for other reversible causes like thyroid problems, electrolyte imbalances, low oxygen, pain, urinary retention, constipation, and nutritional deficiencies,” Cao said.
Of note, delirium is the most common cause of sudden mental status changes in the hospital, and “it’s easy to miss if you’re not looking for it.”
He summarized that classic signs are an acute and fluctuating course with changes in alertness, but added there are other red flags too: disorientation, hallucinations, changes in sleep patterns, sporadic unsafe behaviors, mood swings, and changes in activity level, whether that’s agitation or just being unusually quiet.
By combining what he notices bedside and what is learned from the medical record (and from the people who know the patient best), Cao said he’s able to catch these changes early, identify the underlying cause, and work toward the best possible outcome.
“One of the main interventions is providing mental stimulation,” he said.
Why Mental Stimulation Is So Vital
Mental stimulation of the patient is critical to recovery and may prevent prolonged illness, said Meghana R. Medavaram, MD, associate director of consultation liaison and emergency psychiatry at Montefiore Medical Center’s Weiler Hospital in New York City. “Keeping a patient active both physically and mentally can help prevent deconditioning and risks of prolonged immobility,” she said.
It’s important to note that when patients are out of their familiar routines, away from their usual environment and people, and their sleep is fragmented, this can make them even more vulnerable. Keeping patients mentally stimulated during their hospital stay can help maintain their attention, orientation, and a healthy sleep-wake cycle — all things that are easily thrown off in the hospital, Cao said.
“These disruptions hit the pathways that control attention, wakefulness, and the sleep–wake cycle. That’s when you see attention drifting, orientation fading, and circadian rhythms unraveling, especially at night, which is why “sundowning” is so common, Cao said, referring to the syndrome where older adults or people with dementia experience behavioral changes in late afternoon or evening. “Mental stimulation is critical in the hospital because when the brain isn’t active and gets disoriented, it becomes an easy target for delirium.”
He said delirium often develops in older adults when acute stressors like inflammation, low oxygen, metabolic imbalances, or sedating medications disrupt the brain’s arousal systems and networks, especially in older adults.
Therefore, Cao said, encourage your patients to be more engaged during the day through conversation, activities, or regular reorientation. “This supports the brain networks that help prevent inattention and confusion, which are the hallmarks of delirium. Daytime stimulation also helps build up the natural drive for nighttime sleep, so patients are less likely to nap during the day and be awake and disoriented at night.”
To support this, it’s helpful to schedule medications during waking hours instead of around–the–clock dosing that interrupts sleep, and to cluster nighttime care activities to minimize disturbances, Cao explained. Ensuring patients have their glasses, hearing aids, and familiar routines, along with encouraging mobility and hydration, further protects against delirium and supports patients’ cognitive health during hospitalization. “These same principles are just as important in outpatient subacute rehab settings and at home, so it’s essential to take home these strategies after discharge,” he said.
A Family Member or Friend May Help
Hospitalists can suggest straightforward ways to encourage families and friends to keep patients engaged during a hospital stay. Visits and chats can go a long way as conversations are incredibly grounding, Cao said. Other methods could be bringing in favorite foods or snacks, a phone chat or video call, or even showing prerecorded video messages. “These can be effective. Patients respond well to seeing and hearing familiar faces and voices, even if it’s just on a screen,” Cao said.
Beyond that, he said, activities such as watching and discussing the news, reading aloud, using tablets for games, watching movies, doing crossword puzzles, knitting, reminiscing, and playing word games can also be mentally stimulating for patients.
In addition, safe exercises/activities that patients can do in bed — with advice from physical therapy and occupational therapy — are beneficial, Medavaram said. “These often include gentle range–of-motion activities,” she said.
Share Importance of Mental Stimulation With Patients and Caregivers
If a hospitalist wants to motivate patients to keep their minds active, the framing should be simple, positive, and tied directly to their goals of getting better and getting home, said Medavaram. She provided this script suggestion:
“One of the best ways to help your recovery isn’t just taking your medicine, it’s keeping your mind active. When you’re in the hospital, it’s easy to spend the day lying in bed and staring at the TV in your room, but that can make your brain slow down and even cause confusion. Simple things — like reading, talking with visitors, doing puzzles, listening to music you enjoy, or telling a nurse about your favorite memories — can keep your brain sharp. Staying mentally active helps your thinking stay clear and can even help you get home sooner. Think of it like physical therapy for your brain.”
A version of this article first appeared on Medscape.com.
As a hospitalist, you are in a unique position to notice changes in your hospitalized patients. This frontline perspective can be used to improve inpatient attention and care, and differs from primary care, where a clinician might only see a patient once or twice a year, and subtle, gradual changes may be missed, said George Cao, MD, MBA, a hospitalist at the University of Vermont Medical Center in Burlington and assistant professor at UVM’s Larner College of Medicine.
But in the hospital, Cao said even small shifts — like becoming less active, eating less, or changes in personality — can become much more obvious.
“As hospitalists…we see patients throughout the day, in different situations, and often end up spending more time with them over the course of a week than their primary care provider might in a year,” Cao explained. “This gives us a real advantage in picking up on subtle changes in mental awareness.”
These assessments can also be evaluated with the benefit of daily labs, frequent bedside interactions, and 24–hour observations.
With older adults, Cao said it’s important to go beyond just what’s in the chart.
“I always start by reviewing notes from the primary care provider and previous admissions, but some of the most valuable insights come from talking with family and close friends to get a true sense of the patient’s baseline — how they usually think, move, and interact,” he said.
Why to Watch for Declining Mental Awareness
Declining mental awareness in the inpatient setting is often a sign of an underlying problem — whether that’s a reversible medical condition, unrecognized dementia, or the development of delirium, Cao said.
“On the inpatient side, I pay close attention to more than just memory loss,” he said.
Changes in how patients function day–to–day, shifts in their behavior, or even something as simple as not wanting to get out of bed can be early signs of an aging mind or untreated psychiatric issues, he noted.
“Of course, we always rule out infections and medication side effects, but I also look for other reversible causes like thyroid problems, electrolyte imbalances, low oxygen, pain, urinary retention, constipation, and nutritional deficiencies,” Cao said.
Of note, delirium is the most common cause of sudden mental status changes in the hospital, and “it’s easy to miss if you’re not looking for it.”
He summarized that classic signs are an acute and fluctuating course with changes in alertness, but added there are other red flags too: disorientation, hallucinations, changes in sleep patterns, sporadic unsafe behaviors, mood swings, and changes in activity level, whether that’s agitation or just being unusually quiet.
By combining what he notices bedside and what is learned from the medical record (and from the people who know the patient best), Cao said he’s able to catch these changes early, identify the underlying cause, and work toward the best possible outcome.
“One of the main interventions is providing mental stimulation,” he said.
Why Mental Stimulation Is So Vital
Mental stimulation of the patient is critical to recovery and may prevent prolonged illness, said Meghana R. Medavaram, MD, associate director of consultation liaison and emergency psychiatry at Montefiore Medical Center’s Weiler Hospital in New York City. “Keeping a patient active both physically and mentally can help prevent deconditioning and risks of prolonged immobility,” she said.
It’s important to note that when patients are out of their familiar routines, away from their usual environment and people, and their sleep is fragmented, this can make them even more vulnerable. Keeping patients mentally stimulated during their hospital stay can help maintain their attention, orientation, and a healthy sleep-wake cycle — all things that are easily thrown off in the hospital, Cao said.
“These disruptions hit the pathways that control attention, wakefulness, and the sleep–wake cycle. That’s when you see attention drifting, orientation fading, and circadian rhythms unraveling, especially at night, which is why “sundowning” is so common, Cao said, referring to the syndrome where older adults or people with dementia experience behavioral changes in late afternoon or evening. “Mental stimulation is critical in the hospital because when the brain isn’t active and gets disoriented, it becomes an easy target for delirium.”
He said delirium often develops in older adults when acute stressors like inflammation, low oxygen, metabolic imbalances, or sedating medications disrupt the brain’s arousal systems and networks, especially in older adults.
Therefore, Cao said, encourage your patients to be more engaged during the day through conversation, activities, or regular reorientation. “This supports the brain networks that help prevent inattention and confusion, which are the hallmarks of delirium. Daytime stimulation also helps build up the natural drive for nighttime sleep, so patients are less likely to nap during the day and be awake and disoriented at night.”
To support this, it’s helpful to schedule medications during waking hours instead of around–the–clock dosing that interrupts sleep, and to cluster nighttime care activities to minimize disturbances, Cao explained. Ensuring patients have their glasses, hearing aids, and familiar routines, along with encouraging mobility and hydration, further protects against delirium and supports patients’ cognitive health during hospitalization. “These same principles are just as important in outpatient subacute rehab settings and at home, so it’s essential to take home these strategies after discharge,” he said.
A Family Member or Friend May Help
Hospitalists can suggest straightforward ways to encourage families and friends to keep patients engaged during a hospital stay. Visits and chats can go a long way as conversations are incredibly grounding, Cao said. Other methods could be bringing in favorite foods or snacks, a phone chat or video call, or even showing prerecorded video messages. “These can be effective. Patients respond well to seeing and hearing familiar faces and voices, even if it’s just on a screen,” Cao said.
Beyond that, he said, activities such as watching and discussing the news, reading aloud, using tablets for games, watching movies, doing crossword puzzles, knitting, reminiscing, and playing word games can also be mentally stimulating for patients.
In addition, safe exercises/activities that patients can do in bed — with advice from physical therapy and occupational therapy — are beneficial, Medavaram said. “These often include gentle range–of-motion activities,” she said.
Share Importance of Mental Stimulation With Patients and Caregivers
If a hospitalist wants to motivate patients to keep their minds active, the framing should be simple, positive, and tied directly to their goals of getting better and getting home, said Medavaram. She provided this script suggestion:
“One of the best ways to help your recovery isn’t just taking your medicine, it’s keeping your mind active. When you’re in the hospital, it’s easy to spend the day lying in bed and staring at the TV in your room, but that can make your brain slow down and even cause confusion. Simple things — like reading, talking with visitors, doing puzzles, listening to music you enjoy, or telling a nurse about your favorite memories — can keep your brain sharp. Staying mentally active helps your thinking stay clear and can even help you get home sooner. Think of it like physical therapy for your brain.”
A version of this article first appeared on Medscape.com.
As a hospitalist, you are in a unique position to notice changes in your hospitalized patients. This frontline perspective can be used to improve inpatient attention and care, and differs from primary care, where a clinician might only see a patient once or twice a year, and subtle, gradual changes may be missed, said George Cao, MD, MBA, a hospitalist at the University of Vermont Medical Center in Burlington and assistant professor at UVM’s Larner College of Medicine.
But in the hospital, Cao said even small shifts — like becoming less active, eating less, or changes in personality — can become much more obvious.
“As hospitalists…we see patients throughout the day, in different situations, and often end up spending more time with them over the course of a week than their primary care provider might in a year,” Cao explained. “This gives us a real advantage in picking up on subtle changes in mental awareness.”
These assessments can also be evaluated with the benefit of daily labs, frequent bedside interactions, and 24–hour observations.
With older adults, Cao said it’s important to go beyond just what’s in the chart.
“I always start by reviewing notes from the primary care provider and previous admissions, but some of the most valuable insights come from talking with family and close friends to get a true sense of the patient’s baseline — how they usually think, move, and interact,” he said.
Why to Watch for Declining Mental Awareness
Declining mental awareness in the inpatient setting is often a sign of an underlying problem — whether that’s a reversible medical condition, unrecognized dementia, or the development of delirium, Cao said.
“On the inpatient side, I pay close attention to more than just memory loss,” he said.
Changes in how patients function day–to–day, shifts in their behavior, or even something as simple as not wanting to get out of bed can be early signs of an aging mind or untreated psychiatric issues, he noted.
“Of course, we always rule out infections and medication side effects, but I also look for other reversible causes like thyroid problems, electrolyte imbalances, low oxygen, pain, urinary retention, constipation, and nutritional deficiencies,” Cao said.
Of note, delirium is the most common cause of sudden mental status changes in the hospital, and “it’s easy to miss if you’re not looking for it.”
He summarized that classic signs are an acute and fluctuating course with changes in alertness, but added there are other red flags too: disorientation, hallucinations, changes in sleep patterns, sporadic unsafe behaviors, mood swings, and changes in activity level, whether that’s agitation or just being unusually quiet.
By combining what he notices bedside and what is learned from the medical record (and from the people who know the patient best), Cao said he’s able to catch these changes early, identify the underlying cause, and work toward the best possible outcome.
“One of the main interventions is providing mental stimulation,” he said.
Why Mental Stimulation Is So Vital
Mental stimulation of the patient is critical to recovery and may prevent prolonged illness, said Meghana R. Medavaram, MD, associate director of consultation liaison and emergency psychiatry at Montefiore Medical Center’s Weiler Hospital in New York City. “Keeping a patient active both physically and mentally can help prevent deconditioning and risks of prolonged immobility,” she said.
It’s important to note that when patients are out of their familiar routines, away from their usual environment and people, and their sleep is fragmented, this can make them even more vulnerable. Keeping patients mentally stimulated during their hospital stay can help maintain their attention, orientation, and a healthy sleep-wake cycle — all things that are easily thrown off in the hospital, Cao said.
“These disruptions hit the pathways that control attention, wakefulness, and the sleep–wake cycle. That’s when you see attention drifting, orientation fading, and circadian rhythms unraveling, especially at night, which is why “sundowning” is so common, Cao said, referring to the syndrome where older adults or people with dementia experience behavioral changes in late afternoon or evening. “Mental stimulation is critical in the hospital because when the brain isn’t active and gets disoriented, it becomes an easy target for delirium.”
He said delirium often develops in older adults when acute stressors like inflammation, low oxygen, metabolic imbalances, or sedating medications disrupt the brain’s arousal systems and networks, especially in older adults.
Therefore, Cao said, encourage your patients to be more engaged during the day through conversation, activities, or regular reorientation. “This supports the brain networks that help prevent inattention and confusion, which are the hallmarks of delirium. Daytime stimulation also helps build up the natural drive for nighttime sleep, so patients are less likely to nap during the day and be awake and disoriented at night.”
To support this, it’s helpful to schedule medications during waking hours instead of around–the–clock dosing that interrupts sleep, and to cluster nighttime care activities to minimize disturbances, Cao explained. Ensuring patients have their glasses, hearing aids, and familiar routines, along with encouraging mobility and hydration, further protects against delirium and supports patients’ cognitive health during hospitalization. “These same principles are just as important in outpatient subacute rehab settings and at home, so it’s essential to take home these strategies after discharge,” he said.
A Family Member or Friend May Help
Hospitalists can suggest straightforward ways to encourage families and friends to keep patients engaged during a hospital stay. Visits and chats can go a long way as conversations are incredibly grounding, Cao said. Other methods could be bringing in favorite foods or snacks, a phone chat or video call, or even showing prerecorded video messages. “These can be effective. Patients respond well to seeing and hearing familiar faces and voices, even if it’s just on a screen,” Cao said.
Beyond that, he said, activities such as watching and discussing the news, reading aloud, using tablets for games, watching movies, doing crossword puzzles, knitting, reminiscing, and playing word games can also be mentally stimulating for patients.
In addition, safe exercises/activities that patients can do in bed — with advice from physical therapy and occupational therapy — are beneficial, Medavaram said. “These often include gentle range–of-motion activities,” she said.
Share Importance of Mental Stimulation With Patients and Caregivers
If a hospitalist wants to motivate patients to keep their minds active, the framing should be simple, positive, and tied directly to their goals of getting better and getting home, said Medavaram. She provided this script suggestion:
“One of the best ways to help your recovery isn’t just taking your medicine, it’s keeping your mind active. When you’re in the hospital, it’s easy to spend the day lying in bed and staring at the TV in your room, but that can make your brain slow down and even cause confusion. Simple things — like reading, talking with visitors, doing puzzles, listening to music you enjoy, or telling a nurse about your favorite memories — can keep your brain sharp. Staying mentally active helps your thinking stay clear and can even help you get home sooner. Think of it like physical therapy for your brain.”
A version of this article first appeared on Medscape.com.
VA Hospitals Score High in 2025 CMS Quality Survey
The number of US Department of Veterans Affairs (VA) hospitals receiving high scores in the Centers for Medicare & Medicaid Services (CMS) annual survey of quality measures is on the rise.
In 2023, VA hospitals became eligible to receive Overall Hospital Quality Star Ratings from the survey. In 2025, the survey covered 4609 hospitals (VA and non-VA). CMS analyzed 45 hospital quality measures across 5 different groups: mortality, safety of care, readmission, patient experience, and timely and effective care. The better the performance in these areas, the higher the star rating.
In the current ratings, 77% of surveyed VA hospitals earned 4- or 5-star ratings, a double digit increase over the previous 2 years (67% in 2023 and 58% in 2024). No VA hospitals received a 1-star rating, and > 90% of VA hospitals that received ratings maintained or improved on their 2024 mark.
“These ratings highlight the excellent care VA hospitals provide,” VA Secretary Doug Collins said. “Our job is to continue raising the bar for customer service and convenience throughout the department, so VA works better for the Veterans, families, caregivers and survivors we are charged with serving.”
According to a report from the Advisory Board, fewer hospitals are receiving 5-star ratings than ever, possibly due to the COVID-19 pandemic. According to CMS, of all the hospitals that received a rating, 291 earned 5 stars, 90 fewer than in 2024. At the same time, the number of hospitals with 1-star ratings dropped slightly, from 277 in 2024 to 233 in 2025.
The VA publishes its own data on its medical centers. VA Core Hospital Measures have been available from the Joint Commission since 2005. Additional performance measures, including safety, effectiveness, efficiency, timeliness, patient centeredness, and equity, have been published by the VA since 2008. In 2010, the VA began reporting on Hospital Compare, which has information about the quality of care at > 4000 Medicare-certified hospitals, including > 130 VA medical centers and > 50 military hospitals.
The number of US Department of Veterans Affairs (VA) hospitals receiving high scores in the Centers for Medicare & Medicaid Services (CMS) annual survey of quality measures is on the rise.
In 2023, VA hospitals became eligible to receive Overall Hospital Quality Star Ratings from the survey. In 2025, the survey covered 4609 hospitals (VA and non-VA). CMS analyzed 45 hospital quality measures across 5 different groups: mortality, safety of care, readmission, patient experience, and timely and effective care. The better the performance in these areas, the higher the star rating.
In the current ratings, 77% of surveyed VA hospitals earned 4- or 5-star ratings, a double digit increase over the previous 2 years (67% in 2023 and 58% in 2024). No VA hospitals received a 1-star rating, and > 90% of VA hospitals that received ratings maintained or improved on their 2024 mark.
“These ratings highlight the excellent care VA hospitals provide,” VA Secretary Doug Collins said. “Our job is to continue raising the bar for customer service and convenience throughout the department, so VA works better for the Veterans, families, caregivers and survivors we are charged with serving.”
According to a report from the Advisory Board, fewer hospitals are receiving 5-star ratings than ever, possibly due to the COVID-19 pandemic. According to CMS, of all the hospitals that received a rating, 291 earned 5 stars, 90 fewer than in 2024. At the same time, the number of hospitals with 1-star ratings dropped slightly, from 277 in 2024 to 233 in 2025.
The VA publishes its own data on its medical centers. VA Core Hospital Measures have been available from the Joint Commission since 2005. Additional performance measures, including safety, effectiveness, efficiency, timeliness, patient centeredness, and equity, have been published by the VA since 2008. In 2010, the VA began reporting on Hospital Compare, which has information about the quality of care at > 4000 Medicare-certified hospitals, including > 130 VA medical centers and > 50 military hospitals.
The number of US Department of Veterans Affairs (VA) hospitals receiving high scores in the Centers for Medicare & Medicaid Services (CMS) annual survey of quality measures is on the rise.
In 2023, VA hospitals became eligible to receive Overall Hospital Quality Star Ratings from the survey. In 2025, the survey covered 4609 hospitals (VA and non-VA). CMS analyzed 45 hospital quality measures across 5 different groups: mortality, safety of care, readmission, patient experience, and timely and effective care. The better the performance in these areas, the higher the star rating.
In the current ratings, 77% of surveyed VA hospitals earned 4- or 5-star ratings, a double digit increase over the previous 2 years (67% in 2023 and 58% in 2024). No VA hospitals received a 1-star rating, and > 90% of VA hospitals that received ratings maintained or improved on their 2024 mark.
“These ratings highlight the excellent care VA hospitals provide,” VA Secretary Doug Collins said. “Our job is to continue raising the bar for customer service and convenience throughout the department, so VA works better for the Veterans, families, caregivers and survivors we are charged with serving.”
According to a report from the Advisory Board, fewer hospitals are receiving 5-star ratings than ever, possibly due to the COVID-19 pandemic. According to CMS, of all the hospitals that received a rating, 291 earned 5 stars, 90 fewer than in 2024. At the same time, the number of hospitals with 1-star ratings dropped slightly, from 277 in 2024 to 233 in 2025.
The VA publishes its own data on its medical centers. VA Core Hospital Measures have been available from the Joint Commission since 2005. Additional performance measures, including safety, effectiveness, efficiency, timeliness, patient centeredness, and equity, have been published by the VA since 2008. In 2010, the VA began reporting on Hospital Compare, which has information about the quality of care at > 4000 Medicare-certified hospitals, including > 130 VA medical centers and > 50 military hospitals.

Enhancing Workforce Practices to Achieve Commission on Cancer Accreditation
Background
The American College of Surgeons’ Commission on Cancer (CoC) Accreditation requires establishment of a comprehensive cancer program, multi-disciplinary tumor boards, active cancer registry, quality improvement activities and cancer research.
Methods
In 2022, the Tibor Rubin VA Medical Center (TRVAMC) set out to obtain accreditation through enhancing workforce practices. Changes in workforce practices included (1) leadership engagement; (2) acquisition of staff; (3) enhancing staff efficiency and (4) inter-departmental collaboration, leading to CoC accreditation in August 2024. executive leadership team (ELT) buy-in was essential. ELT engagement included communicating the benefits of accreditation, alignment with organizational mission and values, protected time for Cancer Committee members, Chief of Staff presence in Cancer Committee, commitment to recruiting new staff, and membership in the Medical Executive Council to voice cancer program needs. New staff included a cancer program manager, cancer case conference RN care coordinator, certified oncology data specialist and survivorship nurse practitioner. Staff development included structured and focused training. Enhancing staff efficiency included developing standards of work with clear delineation of duties (delegation of specific CoC standards), decentralizing decision making, a shared governance council, and weekly Cancer Program meetings. These changes allowed staff members to be active, autonomous decision-making participants, and increased efficiency. Inter-departmental collaboration involved Hematology/Oncology, Surgery, Radiation Oncology, Pharmacy, Nutrition, Pathology, Palliative Care, Rehabilitation, Chaplaincy and Cancer Research, with key individuals serving as Cancer Committee members. Each department set performance goals and metrics. Each employee’s contribution was rated in annual performance reviews.
Results
TRVAMC thus elevated cancer care delivery standards through structured workforce practices within the framework of CoC standards required for accreditation. Additionally, the accreditation process achieved desirable and measurable outcomes, e.g. 100% growth in oncology dietitian referrals, 75% increase in early palliative care referrals (TRVAMC ranked in the top 5 in the US), and more than 200 patients enrolled in cancer clinical trials (TRVAMC was the highest enrolling VA in the US to NCI trials in 2024).
Conclusions
Our model demonstrates how strategic improvements in healthcare workforce practices at a VA can directly contribute to sustained improvements in quality and delivery of cancer care services.
Background
The American College of Surgeons’ Commission on Cancer (CoC) Accreditation requires establishment of a comprehensive cancer program, multi-disciplinary tumor boards, active cancer registry, quality improvement activities and cancer research.
Methods
In 2022, the Tibor Rubin VA Medical Center (TRVAMC) set out to obtain accreditation through enhancing workforce practices. Changes in workforce practices included (1) leadership engagement; (2) acquisition of staff; (3) enhancing staff efficiency and (4) inter-departmental collaboration, leading to CoC accreditation in August 2024. executive leadership team (ELT) buy-in was essential. ELT engagement included communicating the benefits of accreditation, alignment with organizational mission and values, protected time for Cancer Committee members, Chief of Staff presence in Cancer Committee, commitment to recruiting new staff, and membership in the Medical Executive Council to voice cancer program needs. New staff included a cancer program manager, cancer case conference RN care coordinator, certified oncology data specialist and survivorship nurse practitioner. Staff development included structured and focused training. Enhancing staff efficiency included developing standards of work with clear delineation of duties (delegation of specific CoC standards), decentralizing decision making, a shared governance council, and weekly Cancer Program meetings. These changes allowed staff members to be active, autonomous decision-making participants, and increased efficiency. Inter-departmental collaboration involved Hematology/Oncology, Surgery, Radiation Oncology, Pharmacy, Nutrition, Pathology, Palliative Care, Rehabilitation, Chaplaincy and Cancer Research, with key individuals serving as Cancer Committee members. Each department set performance goals and metrics. Each employee’s contribution was rated in annual performance reviews.
Results
TRVAMC thus elevated cancer care delivery standards through structured workforce practices within the framework of CoC standards required for accreditation. Additionally, the accreditation process achieved desirable and measurable outcomes, e.g. 100% growth in oncology dietitian referrals, 75% increase in early palliative care referrals (TRVAMC ranked in the top 5 in the US), and more than 200 patients enrolled in cancer clinical trials (TRVAMC was the highest enrolling VA in the US to NCI trials in 2024).
Conclusions
Our model demonstrates how strategic improvements in healthcare workforce practices at a VA can directly contribute to sustained improvements in quality and delivery of cancer care services.
Background
The American College of Surgeons’ Commission on Cancer (CoC) Accreditation requires establishment of a comprehensive cancer program, multi-disciplinary tumor boards, active cancer registry, quality improvement activities and cancer research.
Methods
In 2022, the Tibor Rubin VA Medical Center (TRVAMC) set out to obtain accreditation through enhancing workforce practices. Changes in workforce practices included (1) leadership engagement; (2) acquisition of staff; (3) enhancing staff efficiency and (4) inter-departmental collaboration, leading to CoC accreditation in August 2024. executive leadership team (ELT) buy-in was essential. ELT engagement included communicating the benefits of accreditation, alignment with organizational mission and values, protected time for Cancer Committee members, Chief of Staff presence in Cancer Committee, commitment to recruiting new staff, and membership in the Medical Executive Council to voice cancer program needs. New staff included a cancer program manager, cancer case conference RN care coordinator, certified oncology data specialist and survivorship nurse practitioner. Staff development included structured and focused training. Enhancing staff efficiency included developing standards of work with clear delineation of duties (delegation of specific CoC standards), decentralizing decision making, a shared governance council, and weekly Cancer Program meetings. These changes allowed staff members to be active, autonomous decision-making participants, and increased efficiency. Inter-departmental collaboration involved Hematology/Oncology, Surgery, Radiation Oncology, Pharmacy, Nutrition, Pathology, Palliative Care, Rehabilitation, Chaplaincy and Cancer Research, with key individuals serving as Cancer Committee members. Each department set performance goals and metrics. Each employee’s contribution was rated in annual performance reviews.
Results
TRVAMC thus elevated cancer care delivery standards through structured workforce practices within the framework of CoC standards required for accreditation. Additionally, the accreditation process achieved desirable and measurable outcomes, e.g. 100% growth in oncology dietitian referrals, 75% increase in early palliative care referrals (TRVAMC ranked in the top 5 in the US), and more than 200 patients enrolled in cancer clinical trials (TRVAMC was the highest enrolling VA in the US to NCI trials in 2024).
Conclusions
Our model demonstrates how strategic improvements in healthcare workforce practices at a VA can directly contribute to sustained improvements in quality and delivery of cancer care services.
Streamlining Health Care: Inpatient Dashboard as a User-Centric Solution in EHR Enhancement
Streamlining Health Care: Inpatient Dashboard as a User-Centric Solution in EHR Enhancement
Electronic health records (EHRs) are an integral part of modern health care. The 2009, Health Information Technology for Economic and Clinical Health Act established financial incentives for US hospitals to adopt EHRs. In 2009 only 12% of nonfederal acute care hospitals had adopted a certified EHR system, which increased to 96% by 2021.1
EHRs have transformed the way patient data are stored and accessed, streamlining the process of providing quality patient care with improvements in efficiency, effectiveness, patient satisfaction, and safety.2 Despite their widespread adoption and benefits, EHRs have generally been met with mixed physician satisfaction.3 Interactions with EHRs are linked to disproportionate time at the computer and physician burnout.4-6
The US Department of Veterans Affairs (VA) was at the forefront of EHR development, establishing the Veterans Health Information Systems and Technology Architecture (VistA) in the 1970s. The VA released the Computerized Patient Record System (CPRS) in 1997, the first clinical user interface for VistA. In May 2018, the VA signed a $10 billion contract with Cerner (now Oracle Health) to modernize its EHR.7 This was later revised to $16.1 billion, and the Institute for Defense Analyses estimates it will cost $49.8 billion.8 The transition to Oracle Health has been faced with significant challenges, including patient safety risks and workflow inefficiencies, leading to a pause in rollout.9
Due to the known challenges with EHRs and the aging CPRS system (without a scheduled replacement date), innovations that facilitate the synthesis and display of clinical information are needed. To address this gap, the VA Ann Arbor Healthcare System (VAAAHS) developed the Inpatient Dashboard, an online EHR companion tool. The Inpatient Dashboard was designed to draw data from VistA to reduce time spent at the computer by streamlining clinical information presentation, standardizing inpatient notes, improving safety measures, and enhancing overall clinician satisfaction. This study evaluated the adoption and user experience with the Inpatient Dashboard.
INPATIENT DASHBOARD
The Inpatient Dashboard consists of several modules created by a contractor for the VAAAHS that is housed on VA servers with access restricted to individuals with patient health data privileges. As the Inpatient Dashboard draws data from VistA, it can display laboratory information, studies, and notes from all VA sites.
The main dashboard is a snapshot summary of patient information, including patient location, code status, last vital sign readings, vital sign ranges over the previous 24 hours, intake/output, deep vein thrombosis (DVT) prophylaxis, the presence of telemetry orders, or use of Foley or central catheters (Figure). It also includes a customizable to-do list and contact information for the patient’s clinician and nurse. Significant events, such as abnormal vital signs or speciation/sensitivities for blood cultures, are automatically populated on the to-do list. From this main dashboard overview, clinicians can customize which patients are displayed, create and print a rounding list, print a sign-out sheet, or select individual patients to open a progress note module.
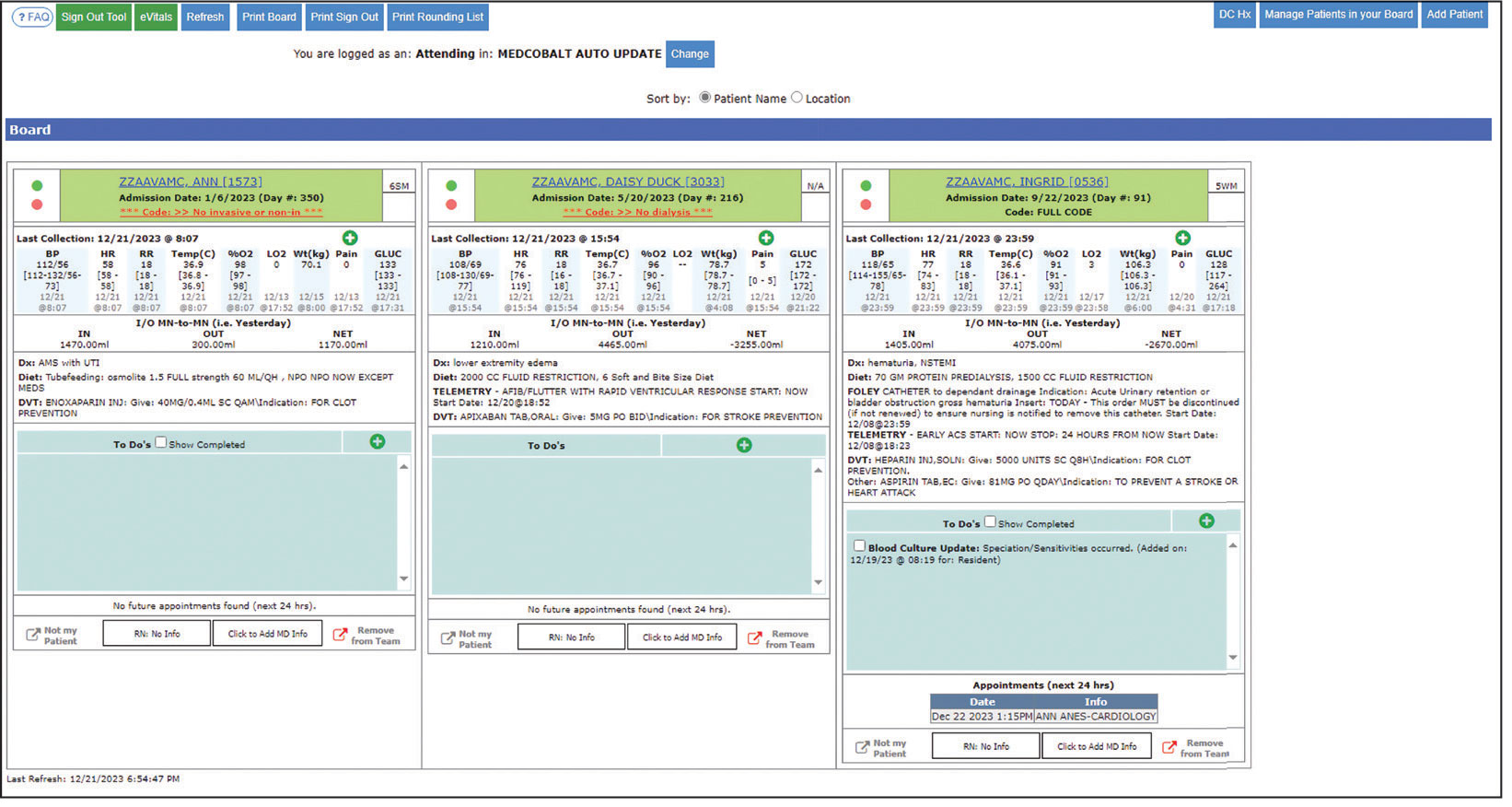
Notes can be written in the patient history and physical module, progress note module, and discharge summary module. The patient history and physical module has text blocks allocated to the traditional components of a history and physical note (ie, chief complaint, history of present illness, review of systems, past medical history, family history, social history, allergies, medications, physical examination, assessment, and plan) (eAppendix 1). Some elements, such as past medical history, family history, and social history are prepopulated if the patient was previously admitted. Vital signs, laboratory results, studies, microbiology/ pathology reports, and other CPRS notes are displayed in this module.
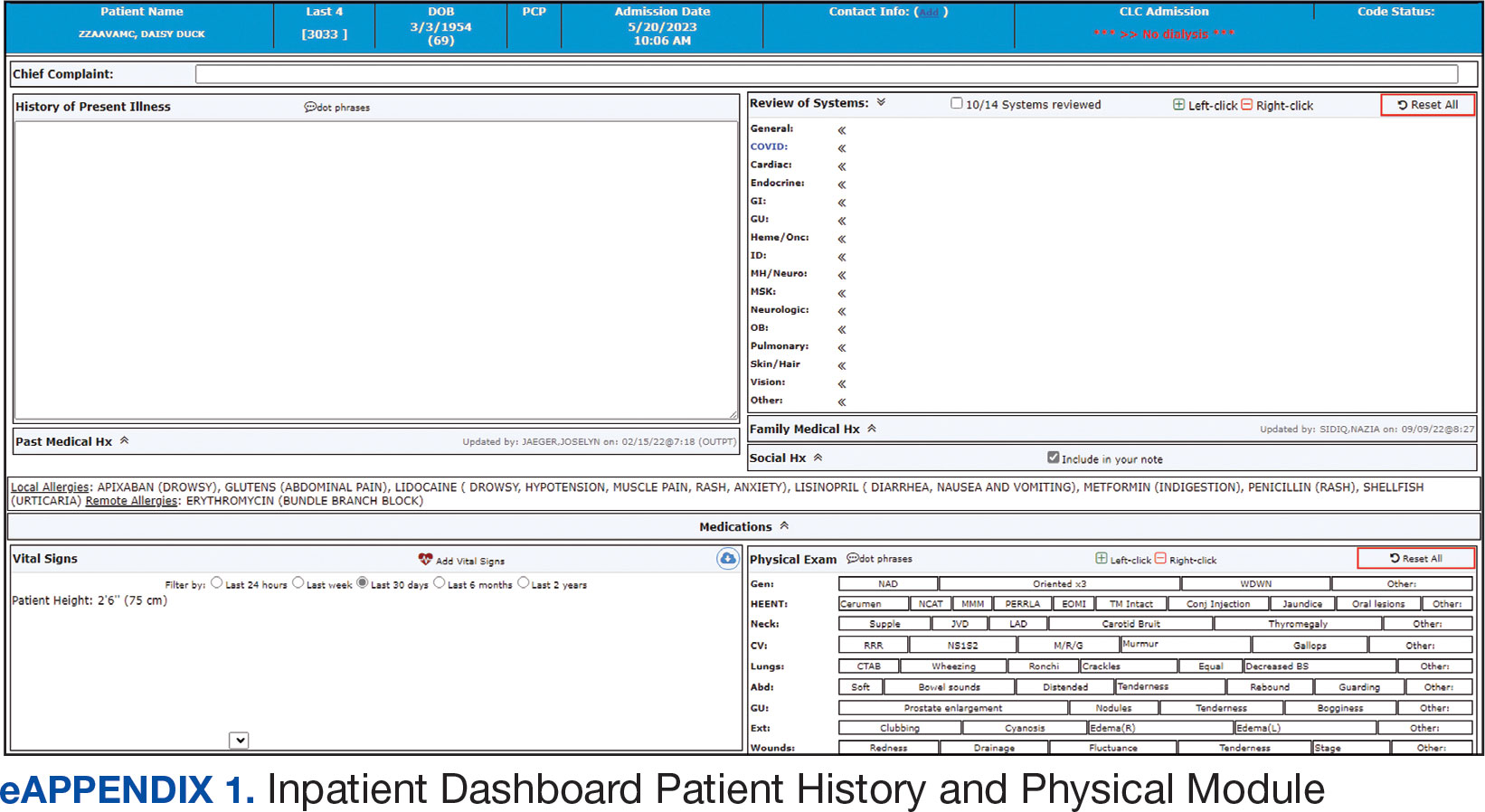
The progress note module contains text blocks allocated to the traditional components of a progress note, such as subjective/interval events, physical examination, assessment, and plan (eAppendix 2). Vital signs, laboratory results, studies, microbiology/ pathology reports, other CPRS notes, and the patient’s medication administration record are also displayed in this module. Lastly, the discharge summary module includes patient follow-up, patient instructions, hospitalization summary, medication reconciliation, laboratory results, and studies/procedures, ensuring a comprehensive discharge summary for patients and clinicians (eAppendix 3).
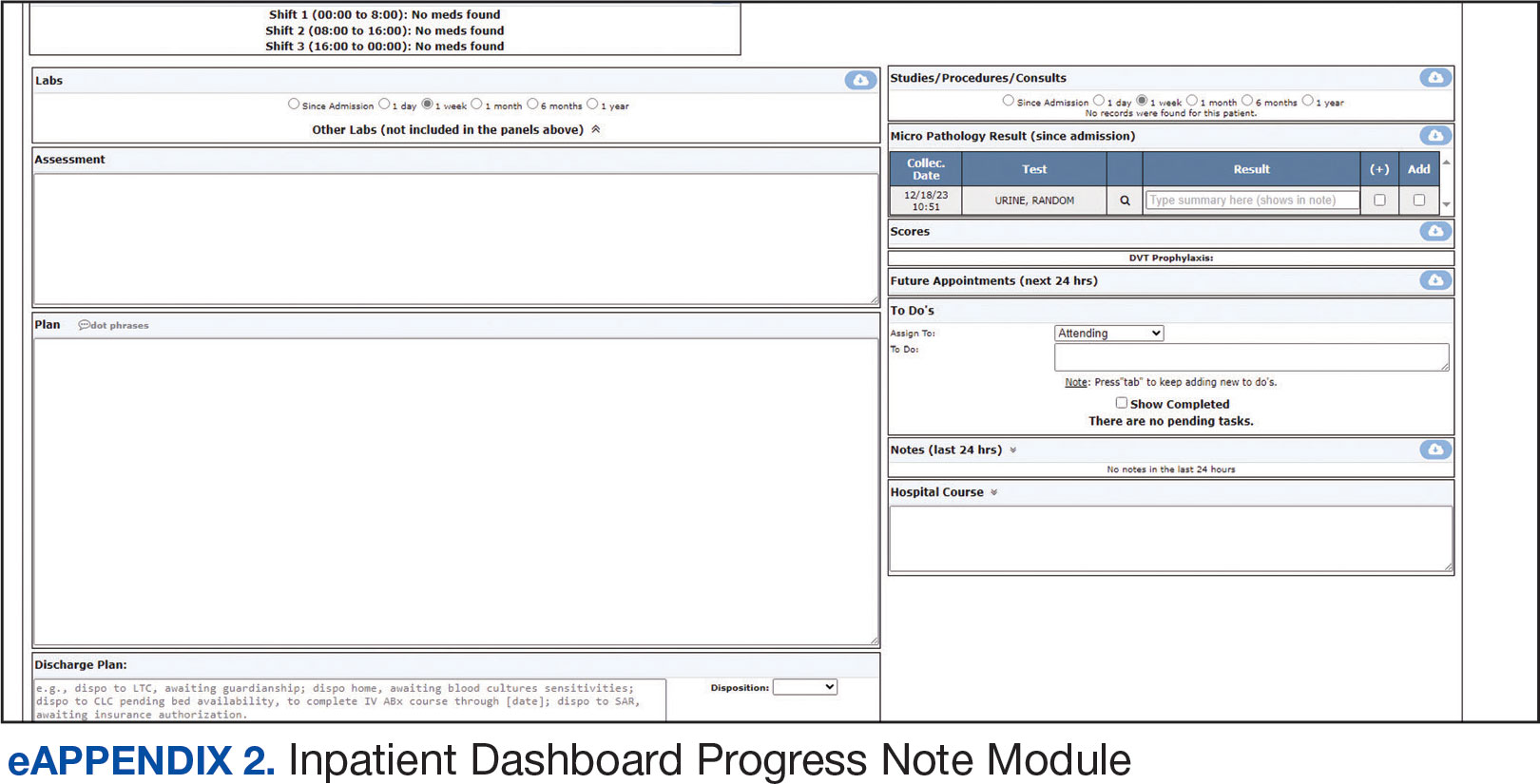
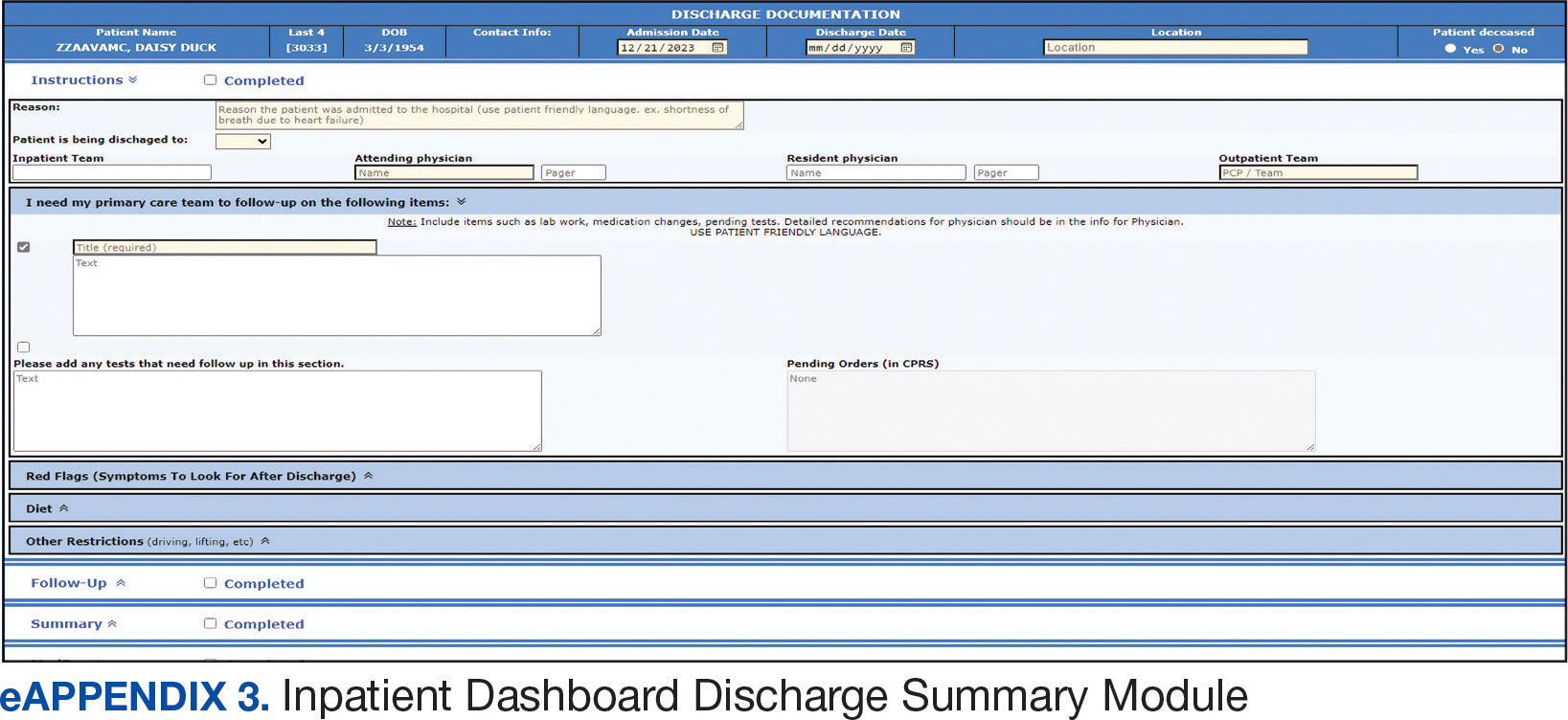
A medication reconciliation tool was embedded within the history and physical and discharge summary modules. This tool has been shown to reduce medication errors in patients admitted from the emergency department to the hospital (eAppendix 4).10 The handoff/sign-out tool (eAppendix 5) accessible through the main dashboard page is modeled on the I-PASS handoff framework.11,12 This includes the patient identifier, interval events, inpatient medications, specific sign-out guidance, sign-out tasks/to-dos, and any other pertinent information.
The Inpatient Dashboard is a team-based construct shared by the attending physicians, residents, and medical students. Each team (eg, general medicine, general surgery) is its own entity; only team members can change the content or add to the documentation. Each facility can have multiple teams caring for the same patient (eg, primary and consulting teams). Additional care members can also be incorporated (eg, pharmacists assist with medication reconciliation for admission and discharge at VAAAHS). The Inpatient Dashboard can export information directly to CPRS for clinicians to review and sign. It can also generate a note that can be pasted into CPRS.
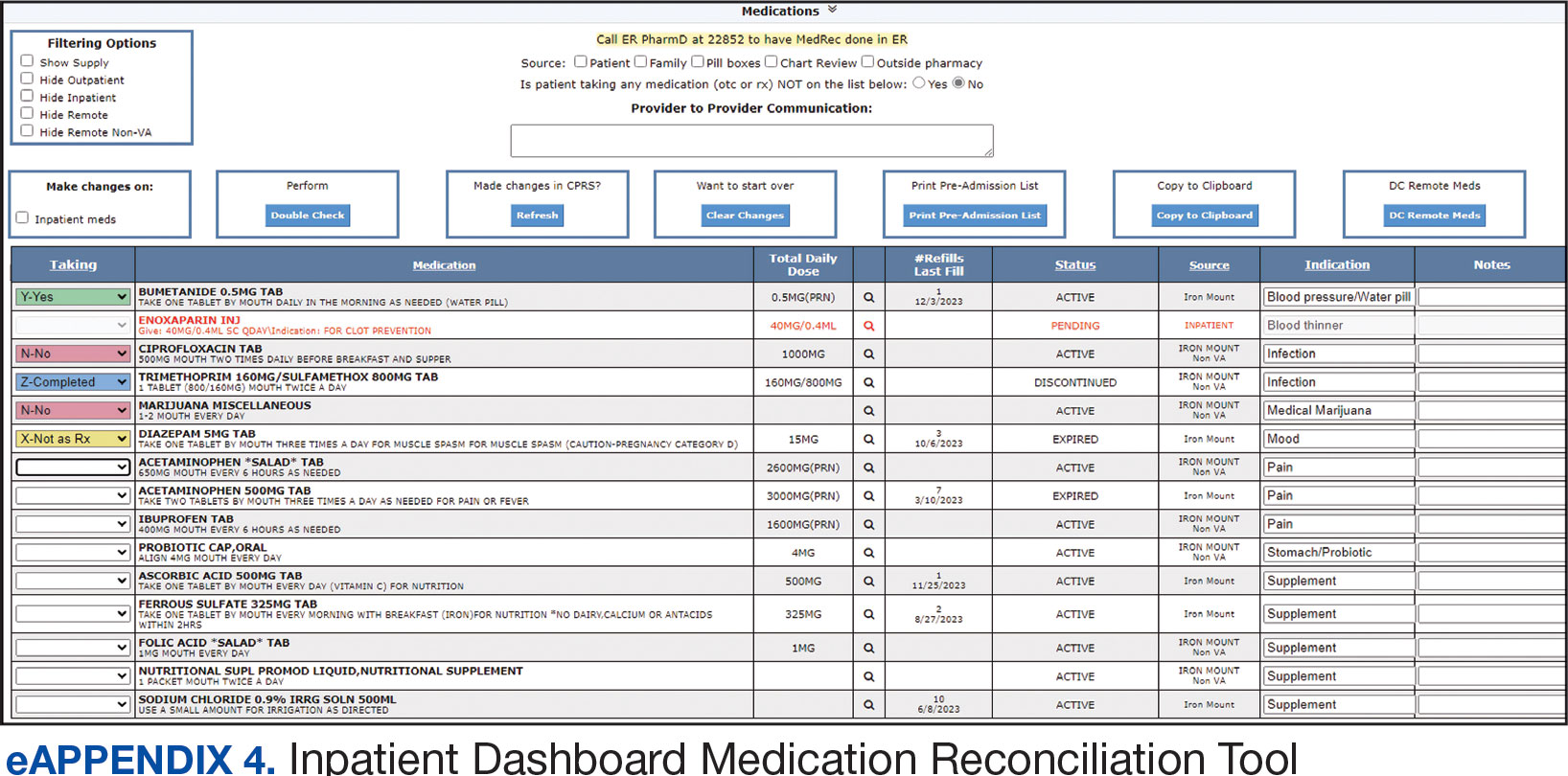
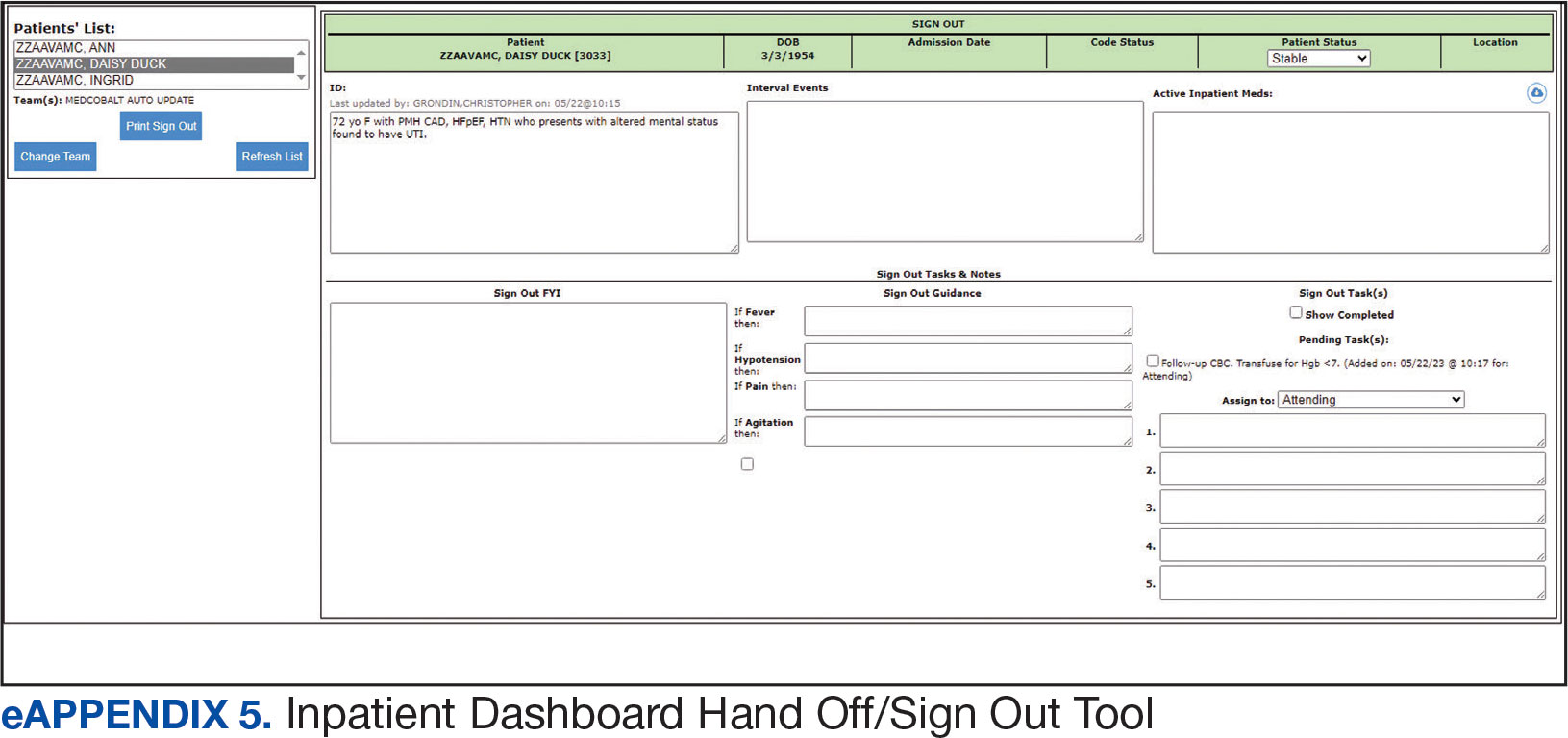
Clinician Feedback and Satisfaction
A survey was developed to evaluate clinician experiences with using the Inpatient Dashboard as an adjunct to the CPRS. The Inpatient Dashboard was made available to general medicine teams in November 2018. The survey was conducted from December 2018 to September 2019. The study was conducted at the VAAAHS and included 4 general medicine teams. Each team included an attending physician, a senior resident, 2 to 3 interns, and 3 to 4 medical students. Eligibility was extended to any team member who used both the CPRS and Inpatient Dashboard. Participation in the survey was voluntary. All respondents were informed of the study’s purpose and encouraged to provide candid feedback to ensure the reliability and validity of the findings.
Data were collected through a semistructured survey administered via the Qualtrics platform. The questionnaire was designed to capture multidimensional insights into clinician experience, with particular focus on satisfaction, efficiency, and perceived safety when using the tool as an adjunct to CPRS compared to using CPRS alone. The questionnaire primarily used a Likert scale for responses. Surveys were emailed at the completion of a team’s 1-month inpatient block. An answer was not required for every question, resulting in slightly different response numbers for some questions.
A question regarding the tool’s impact on workload stress was added halfway through the study period, which resulted in fewer responses. Adoption was assessed by counting the Inpatient Dashboard unique users. Descriptive statistics were used within individual survey responses to report the distribution of responses. Differences in response between levels of training were assessed using a X2 test of independence.
Survey Results
From September 2023 through November 2023, there were 1549 rounding printouts across 144 unique users (5 nurses, 40 medical students, 87 residents, and 12 attending physicians) and 1468 handoff printouts across 148 unique users (5 nurses, 10 medical students, 111 residents, and 22 attending physicians). The clinician survey received 68 responses from users at various levels of medical training: 23 medical students, 31 interns, 12 senior residents, and 2 attending physicians. All 68 participants confirmed they had used the Inpatient Dashboard.
User satisfaction and preference for the Inpatient Dashboard vs CPRS were assessed. Sixty-one respondents (90%) expressed overall satisfaction with the Inpatient Dashboard; 22 (32%) were extremely satisfied, and 39 (57%) were somewhat satisfied (Table 1). Three respondents (4%) were neutral, 2 (3%) were somewhat dissatisfied, and 2 (3%) were extremely dissatisfied with the Inpatient Dashboard. Responses differed by level of training (P = .03), with medical students trending towards higher satisfaction.
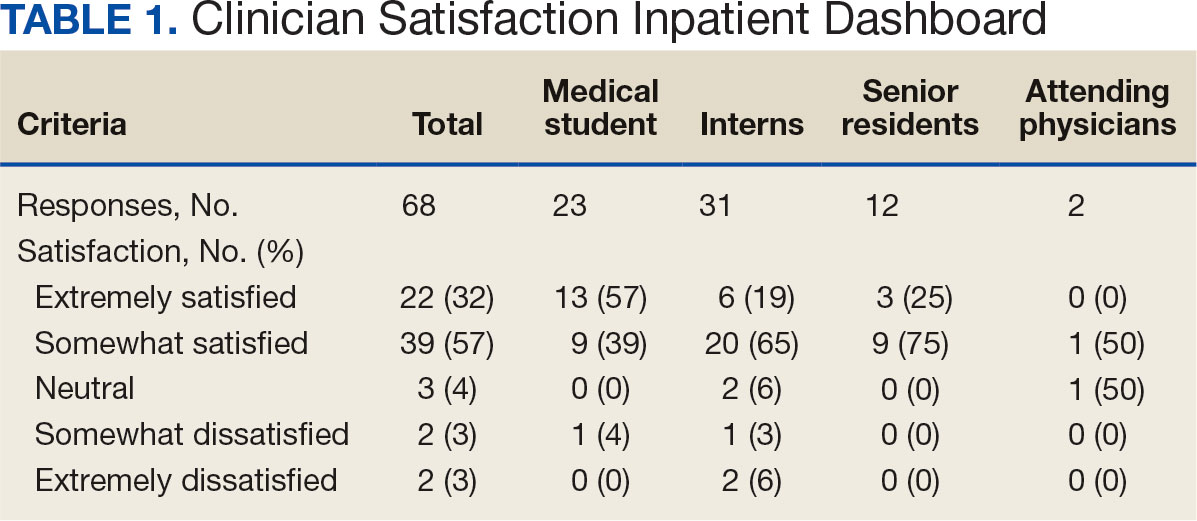
Respondents preferred the Inpatient Dashboard over CPRS for gathering information and writing progress notes; 42 (64%) respondents mostly favored the Inpatient Dashboard, 15 (23%) slightly favored the Inpatient Dashboard over CPRS, and 8 (12%) were neutral. One respondent (2%) slightly favored CPRS to the Inpatient Dashboard (Table 2).
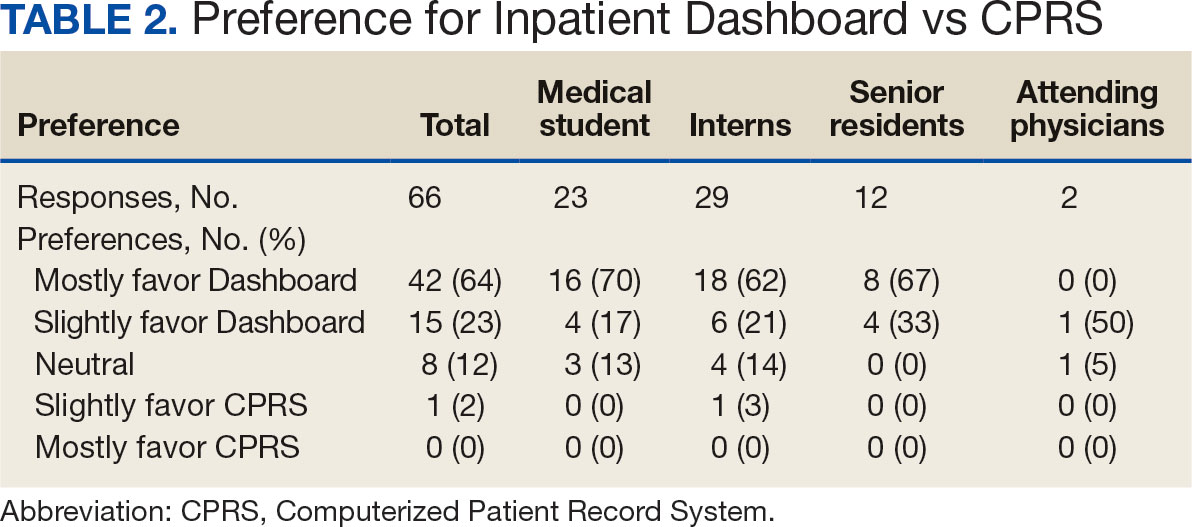
Sixty-five respondents (100%) found the Inpatient Dashboard’s ability to summarize patient information in a central place helpful (Table 3). Among them, 53 (82%) respondents reported it was very or extremely helpful, 10 (15%) respondents reported it was moderately helpful, and 2 (3%) respondents reported it was slightly helpful. This feature positively impacted users’ awareness of patients with DVT prophylaxis or a Foley catheter. Ten (15%) respondents reported being much more aware, and 29 (45%) respondents reporting they were slightly more aware. The remaining 26 (40%) respondents reported no change in awareness.
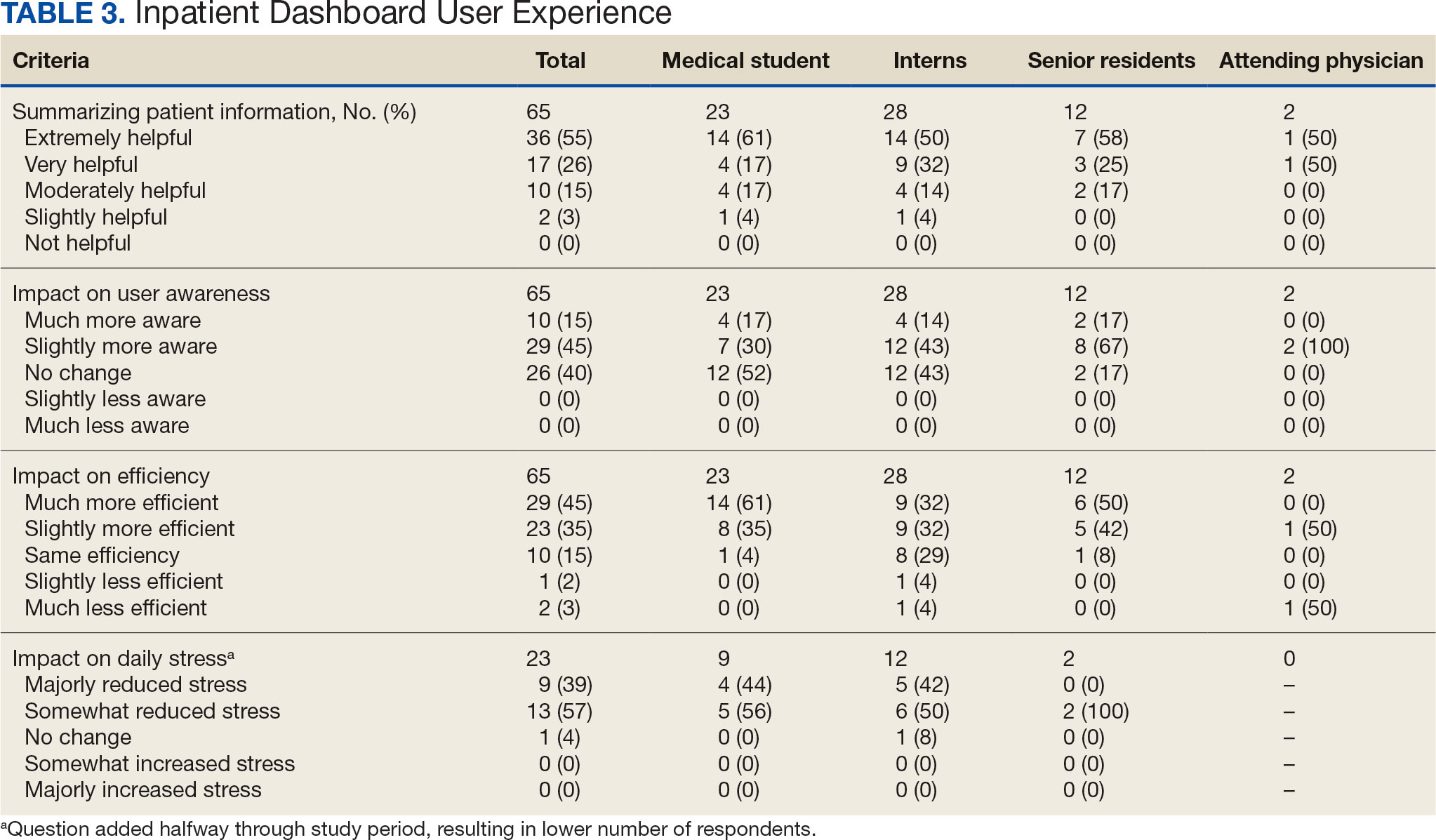
The Inpatient Dashboard was reported to save time preparing for physician rounds by 52 (80%) respondents, contributing to much greater efficiency for 29 (45%) respondents and slightly more efficiency for 23 (35%) respondents. However, 10 (15%) respondents reported no change in efficiency, and 3 (5%) respondents reduced efficiency, with 1 (2%) respondent reporting it slightly less efficient and 2 (3%) respondents reporting it much less efficient. Responses differed by level of training (P = .01), with medical students trending towards higher efficiency. Of the 23 respondents who reported on the Inpatient Dashboard’s impact on daily workload stress level, 22 (96%) indicated the tool had a stress-reducing effect, with 9 (39%) experiencing a major reduction in stress level, and 13 (57%) experiencing somewhat reduced stress level. Only 1 participant (4%) reported no change in stress. No participants reported an increase in stress.
DISCUSSION
The adoption of EHRs has transformed operational modalities in contemporary health care systems, heralding advancements in patient satisfaction, safety, and overall quality and efficiency of care.1,2 However, EHRs still present challenges, predominantly around clinician satisfaction, marked by instances of burnout and increased time spent on computers.2-6 In this context, the Inpatient Dashboard, an online companion to the CPRS, exemplifies how user-centered innovations in EHRs can address and mitigate associated challenges.
The Inpatient Dashboard has been well received with most respondents of the survey conducted in this study indicating they were both satisfied with the instrument and preferring it to CPRS. This high approval aligns with existing literature on the potential advantages of user-centered design in health care technology.13 The tool has gained widespread acceptance at the VAAAHS even in the absence of obligatory usage or institutional incentives. The appeal of the Inpatient Dashboard may stem from its increased efficiency, with most users affirming its timesaving nature. While CPRS can only display local notes, laboratory results, and studies, the Inpatient Dashboard can display data from across all VA sites. The VA Joint Longitudinal Viewer can similarly display data from across all sites, but the display is not streamlined as it is in the Inpatient Dashboard. The Inpatient Dashboard incorporates this clinical information into a single page to facilitate day-to-day workflow and dynamic documentation (ie, reviewing laboratory results, medications, writing notes, and signing out patients). This increased efficiency allows clinicians to counter 2 common barriers to EHR implementation: productivity loss and insufficient time.14
The association between EHRs and improved quality and safety in health care is well-documented.3 The Inpatient Dashboard fortifies this association by enhancing awareness around patient status, evidenced by a majority of respondents, and by integrating a medication reconciliation tool to decrease medication errors on transition from the emergency department to inpatient hospitalization.10
The Inpatient Dashboard’s impact on alleviating daily workload stress is noteworthy, with almost all respondents experiencing reduced stress levels and physician burnout, which has been linked to deteriorating well-being, compromised patient safety, and escalated health care costs.15,16 The heightened susceptibility of physicians to burnout compared to other professionals underscores the imperative for incorporating stress-mitigating interventions in the EHR.17,18
While responses to most questions did not significantly differ by training levels, overall satisfaction with the Inpatient Dashboard and its ability to save time preparing for rounds were rated higher by medical students. This may be attributable to a greater derived benefit from collating and presenting data to learners with less familiarity with the native EHR. It is also notable that the Inpatient Dashboard allows medical students to directly contribute to a patient’s note, which could be another driver in satisfaction. While most interns still felt the Inpatient Dashboard enabled them to save time preparing for rounds, there were a considerable number of ‘no change’ responses, which suggests some interns may not have modified their existing prerounding strategies. These associations are limited by the relatively small number of respondents by learner category, with senior medical residents and attending physicians being underrepresented.
While there are a multitude of dashboards available at the VA, most are made to track certain quality metrics and are used more by administrative and leadership staff. The Inpatient Dashboard was created specifically for frontline clinicians to facilitate their day-to-day workflow and dynamic documentation. This tool can additionally help with quality metrics, though its main purpose was and is to make clinician workflow easier and more efficient.
These results are especially timely because the VA is modernizing its EHR by transitioning to Oracle Health.7 Due to the numerous reports both from veterans and VA clinicians that the Oracle Health EHR is not meeting expectations, deployment at further sites has been halted while improving the experience of the 5 institutions using Oracle Health is prioritized.9 The Inpatient Dashboard, instead of being merely an enhancement to CPRS, could emerge as a potential bridge to Oracle Health if adapted to display data from Oracle Health as it does VistA. This would facilitate a smoother, more integrated transition for those health care institutions employing the Inpatient Dashboard.
Limitations
The reliance on self-reported data inherently carries the risk of bias, and the absence of objective measures, like time-tracking studies, limits the quantifiable assessment of the Inpatient Dashboard efficacy. The single-center nature of the study also may restrict the generalizability of the results.
CONCLUSIONS
Optimal integration of EHRs into health care delivery is critical to high-quality patient care and operational efficiency. The Inpatient Dashboard is an example of an innovative, user-centric solution that integrated and presented clinical information in a way that produced high satisfaction and adoption by users at a VA hospital.
- Office of the National Coordinator for Health Information Technology. National Trends in Hospital and Physician Adoption of Electronic Health Records. HealthIT.gov. Accessed February 5, 2025. https://www.healthit.gov/data/quickstats/national-trends-hospital-and-physician-adoption-electronic-health-records
- Buntin MB, Burke MF, Hoaglin MC, Blumenthal D. The benefits of health information technology: a review of the recent literature shows predominantly positive results. Health Aff (Millwood). 2011;30(3):464-471. doi:10.1377/hlthaff.2011.0178
- Nguyen L, Bellucci E, Nguyen LT. Electronic health records implementation: an evaluation of information system impact and contingency factors. Int J Med Inf. 2014;83(11):779-796. doi:10.1016/j.ijmedinf.2014.06.011
- Alexander AG, Ballou KA. Work-life balance, burnout, and the electronic health record. Am J Med. 2018;131(8):857- 858. doi:10.1016/j.amjmed.2018.02.033
- Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753-760. doi:10.7326/M16-0961
- Chaiyachati KH, Shea JA, Asch DA, et al. Assessment of inpatient time allocation among first-year internal medicine residents using time-motion observations. JAMA Intern Med. 2019;179(6):760-767. doi:10.1001/jamainternmed.2019.0095
- US Department of Veterans Affairs. Statement by Acting Secretary Robert Wilkie - VA signs contract with Cerner for an electronic health record system. New release. May 17, 2018. Accessed February 5, 2025. https://news.va.gov/press-room/statement-by-acting-secretary-robert-wilkie-va-signs-contract-with-cerner-for-an-electronic-health-record-system/
- US Government Publishing Office. VA’s Electronic health record modernization: an update on rollout, cost, and schedule. Subcommittee on Military Construction, Veterans Affairs, and Related Agencies, Committee on Appropriations, United States Senate. 117th Congress, 2nd Session. September 21, 2022. Accessed February 5, 2025. https://www.govinfo.gov/content/pkg/CHRG-117shrg52328/html/CHRG-117shrg52328.htm
- US Department of Veterans Affairs. VA announces reset of electronic health record project. Accessed December 21, 2023. https://news.va.gov/press-room/va-announces-reset-of-electronic-health-record-project/
- Grondin C, Gupta A, Houchens N, et al. Medication reconciliation tool reduces errors in patients admitted from the ED to hospital. Am J Med Qual. 2021;36(2):129. doi:10.1097/01.JMQ.0000741500.33781.eb
- Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803-1812. doi:10.1056/NEJMsa1405556
- Starmer AJ, O’Toole JK, Rosenbluth G, et al. Development, implementation, and dissemination of the I-PASS handoff curriculum: a multisite educational intervention to improve patient handoffs. Acad Med. 2014;89(6):876-884. doi:10.1097/ACM.0000000000000264
- Ratwani RM, Fairbanks RJ, Hettinger AZ, Benda NC. Electronic health record usability: analysis of the user-centered design processes of eleven electronic health record vendors. J Am Med Inform Assoc. 2015;22(6):1179-1182. doi:10.1093/jamia/ocv050
- Kruse CS, Kristof C, Jones B, Mitchell E, Martinez A. Barriers to electronic health record adoption: a systematic literature review. J Med Syst. 2016;40(12):252. doi:10.1007/s10916-016-0628-9
- West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-529. doi:10.1111/joim.12752
- Smeds MR, Janko MR, Allen S, et al. Burnout and its relationship with perceived stress, self-efficacy, depression, social support, and programmatic factors in general surgery residents. Am J Surg. 2020;219(6):907- 912. doi:10.1016/j.amjsurg.2019.07.004
- Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377-1385. doi:10.1001/archinternmed.2012.3199
- Budd J. Burnout related to electronic health record use in primary care. J Prim Care Community Health. 2023;14:21501319231166921. doi:10.1177/21501319231166921
Electronic health records (EHRs) are an integral part of modern health care. The 2009, Health Information Technology for Economic and Clinical Health Act established financial incentives for US hospitals to adopt EHRs. In 2009 only 12% of nonfederal acute care hospitals had adopted a certified EHR system, which increased to 96% by 2021.1
EHRs have transformed the way patient data are stored and accessed, streamlining the process of providing quality patient care with improvements in efficiency, effectiveness, patient satisfaction, and safety.2 Despite their widespread adoption and benefits, EHRs have generally been met with mixed physician satisfaction.3 Interactions with EHRs are linked to disproportionate time at the computer and physician burnout.4-6
The US Department of Veterans Affairs (VA) was at the forefront of EHR development, establishing the Veterans Health Information Systems and Technology Architecture (VistA) in the 1970s. The VA released the Computerized Patient Record System (CPRS) in 1997, the first clinical user interface for VistA. In May 2018, the VA signed a $10 billion contract with Cerner (now Oracle Health) to modernize its EHR.7 This was later revised to $16.1 billion, and the Institute for Defense Analyses estimates it will cost $49.8 billion.8 The transition to Oracle Health has been faced with significant challenges, including patient safety risks and workflow inefficiencies, leading to a pause in rollout.9
Due to the known challenges with EHRs and the aging CPRS system (without a scheduled replacement date), innovations that facilitate the synthesis and display of clinical information are needed. To address this gap, the VA Ann Arbor Healthcare System (VAAAHS) developed the Inpatient Dashboard, an online EHR companion tool. The Inpatient Dashboard was designed to draw data from VistA to reduce time spent at the computer by streamlining clinical information presentation, standardizing inpatient notes, improving safety measures, and enhancing overall clinician satisfaction. This study evaluated the adoption and user experience with the Inpatient Dashboard.
INPATIENT DASHBOARD
The Inpatient Dashboard consists of several modules created by a contractor for the VAAAHS that is housed on VA servers with access restricted to individuals with patient health data privileges. As the Inpatient Dashboard draws data from VistA, it can display laboratory information, studies, and notes from all VA sites.
The main dashboard is a snapshot summary of patient information, including patient location, code status, last vital sign readings, vital sign ranges over the previous 24 hours, intake/output, deep vein thrombosis (DVT) prophylaxis, the presence of telemetry orders, or use of Foley or central catheters (Figure). It also includes a customizable to-do list and contact information for the patient’s clinician and nurse. Significant events, such as abnormal vital signs or speciation/sensitivities for blood cultures, are automatically populated on the to-do list. From this main dashboard overview, clinicians can customize which patients are displayed, create and print a rounding list, print a sign-out sheet, or select individual patients to open a progress note module.
Notes can be written in the patient history and physical module, progress note module, and discharge summary module. The patient history and physical module has text blocks allocated to the traditional components of a history and physical note (ie, chief complaint, history of present illness, review of systems, past medical history, family history, social history, allergies, medications, physical examination, assessment, and plan) (eAppendix 1). Some elements, such as past medical history, family history, and social history are prepopulated if the patient was previously admitted. Vital signs, laboratory results, studies, microbiology/ pathology reports, and other CPRS notes are displayed in this module.
The progress note module contains text blocks allocated to the traditional components of a progress note, such as subjective/interval events, physical examination, assessment, and plan (eAppendix 2). Vital signs, laboratory results, studies, microbiology/ pathology reports, other CPRS notes, and the patient’s medication administration record are also displayed in this module. Lastly, the discharge summary module includes patient follow-up, patient instructions, hospitalization summary, medication reconciliation, laboratory results, and studies/procedures, ensuring a comprehensive discharge summary for patients and clinicians (eAppendix 3).
A medication reconciliation tool was embedded within the history and physical and discharge summary modules. This tool has been shown to reduce medication errors in patients admitted from the emergency department to the hospital (eAppendix 4).10 The handoff/sign-out tool (eAppendix 5) accessible through the main dashboard page is modeled on the I-PASS handoff framework.11,12 This includes the patient identifier, interval events, inpatient medications, specific sign-out guidance, sign-out tasks/to-dos, and any other pertinent information.
The Inpatient Dashboard is a team-based construct shared by the attending physicians, residents, and medical students. Each team (eg, general medicine, general surgery) is its own entity; only team members can change the content or add to the documentation. Each facility can have multiple teams caring for the same patient (eg, primary and consulting teams). Additional care members can also be incorporated (eg, pharmacists assist with medication reconciliation for admission and discharge at VAAAHS). The Inpatient Dashboard can export information directly to CPRS for clinicians to review and sign. It can also generate a note that can be pasted into CPRS.
Clinician Feedback and Satisfaction
A survey was developed to evaluate clinician experiences with using the Inpatient Dashboard as an adjunct to the CPRS. The Inpatient Dashboard was made available to general medicine teams in November 2018. The survey was conducted from December 2018 to September 2019. The study was conducted at the VAAAHS and included 4 general medicine teams. Each team included an attending physician, a senior resident, 2 to 3 interns, and 3 to 4 medical students. Eligibility was extended to any team member who used both the CPRS and Inpatient Dashboard. Participation in the survey was voluntary. All respondents were informed of the study’s purpose and encouraged to provide candid feedback to ensure the reliability and validity of the findings.
Data were collected through a semistructured survey administered via the Qualtrics platform. The questionnaire was designed to capture multidimensional insights into clinician experience, with particular focus on satisfaction, efficiency, and perceived safety when using the tool as an adjunct to CPRS compared to using CPRS alone. The questionnaire primarily used a Likert scale for responses. Surveys were emailed at the completion of a team’s 1-month inpatient block. An answer was not required for every question, resulting in slightly different response numbers for some questions.
A question regarding the tool’s impact on workload stress was added halfway through the study period, which resulted in fewer responses. Adoption was assessed by counting the Inpatient Dashboard unique users. Descriptive statistics were used within individual survey responses to report the distribution of responses. Differences in response between levels of training were assessed using a X2 test of independence.
Survey Results
From September 2023 through November 2023, there were 1549 rounding printouts across 144 unique users (5 nurses, 40 medical students, 87 residents, and 12 attending physicians) and 1468 handoff printouts across 148 unique users (5 nurses, 10 medical students, 111 residents, and 22 attending physicians). The clinician survey received 68 responses from users at various levels of medical training: 23 medical students, 31 interns, 12 senior residents, and 2 attending physicians. All 68 participants confirmed they had used the Inpatient Dashboard.
User satisfaction and preference for the Inpatient Dashboard vs CPRS were assessed. Sixty-one respondents (90%) expressed overall satisfaction with the Inpatient Dashboard; 22 (32%) were extremely satisfied, and 39 (57%) were somewhat satisfied (Table 1). Three respondents (4%) were neutral, 2 (3%) were somewhat dissatisfied, and 2 (3%) were extremely dissatisfied with the Inpatient Dashboard. Responses differed by level of training (P = .03), with medical students trending towards higher satisfaction.
Respondents preferred the Inpatient Dashboard over CPRS for gathering information and writing progress notes; 42 (64%) respondents mostly favored the Inpatient Dashboard, 15 (23%) slightly favored the Inpatient Dashboard over CPRS, and 8 (12%) were neutral. One respondent (2%) slightly favored CPRS to the Inpatient Dashboard (Table 2).
Sixty-five respondents (100%) found the Inpatient Dashboard’s ability to summarize patient information in a central place helpful (Table 3). Among them, 53 (82%) respondents reported it was very or extremely helpful, 10 (15%) respondents reported it was moderately helpful, and 2 (3%) respondents reported it was slightly helpful. This feature positively impacted users’ awareness of patients with DVT prophylaxis or a Foley catheter. Ten (15%) respondents reported being much more aware, and 29 (45%) respondents reporting they were slightly more aware. The remaining 26 (40%) respondents reported no change in awareness.
The Inpatient Dashboard was reported to save time preparing for physician rounds by 52 (80%) respondents, contributing to much greater efficiency for 29 (45%) respondents and slightly more efficiency for 23 (35%) respondents. However, 10 (15%) respondents reported no change in efficiency, and 3 (5%) respondents reduced efficiency, with 1 (2%) respondent reporting it slightly less efficient and 2 (3%) respondents reporting it much less efficient. Responses differed by level of training (P = .01), with medical students trending towards higher efficiency. Of the 23 respondents who reported on the Inpatient Dashboard’s impact on daily workload stress level, 22 (96%) indicated the tool had a stress-reducing effect, with 9 (39%) experiencing a major reduction in stress level, and 13 (57%) experiencing somewhat reduced stress level. Only 1 participant (4%) reported no change in stress. No participants reported an increase in stress.
DISCUSSION
The adoption of EHRs has transformed operational modalities in contemporary health care systems, heralding advancements in patient satisfaction, safety, and overall quality and efficiency of care.1,2 However, EHRs still present challenges, predominantly around clinician satisfaction, marked by instances of burnout and increased time spent on computers.2-6 In this context, the Inpatient Dashboard, an online companion to the CPRS, exemplifies how user-centered innovations in EHRs can address and mitigate associated challenges.
The Inpatient Dashboard has been well received with most respondents of the survey conducted in this study indicating they were both satisfied with the instrument and preferring it to CPRS. This high approval aligns with existing literature on the potential advantages of user-centered design in health care technology.13 The tool has gained widespread acceptance at the VAAAHS even in the absence of obligatory usage or institutional incentives. The appeal of the Inpatient Dashboard may stem from its increased efficiency, with most users affirming its timesaving nature. While CPRS can only display local notes, laboratory results, and studies, the Inpatient Dashboard can display data from across all VA sites. The VA Joint Longitudinal Viewer can similarly display data from across all sites, but the display is not streamlined as it is in the Inpatient Dashboard. The Inpatient Dashboard incorporates this clinical information into a single page to facilitate day-to-day workflow and dynamic documentation (ie, reviewing laboratory results, medications, writing notes, and signing out patients). This increased efficiency allows clinicians to counter 2 common barriers to EHR implementation: productivity loss and insufficient time.14
The association between EHRs and improved quality and safety in health care is well-documented.3 The Inpatient Dashboard fortifies this association by enhancing awareness around patient status, evidenced by a majority of respondents, and by integrating a medication reconciliation tool to decrease medication errors on transition from the emergency department to inpatient hospitalization.10
The Inpatient Dashboard’s impact on alleviating daily workload stress is noteworthy, with almost all respondents experiencing reduced stress levels and physician burnout, which has been linked to deteriorating well-being, compromised patient safety, and escalated health care costs.15,16 The heightened susceptibility of physicians to burnout compared to other professionals underscores the imperative for incorporating stress-mitigating interventions in the EHR.17,18
While responses to most questions did not significantly differ by training levels, overall satisfaction with the Inpatient Dashboard and its ability to save time preparing for rounds were rated higher by medical students. This may be attributable to a greater derived benefit from collating and presenting data to learners with less familiarity with the native EHR. It is also notable that the Inpatient Dashboard allows medical students to directly contribute to a patient’s note, which could be another driver in satisfaction. While most interns still felt the Inpatient Dashboard enabled them to save time preparing for rounds, there were a considerable number of ‘no change’ responses, which suggests some interns may not have modified their existing prerounding strategies. These associations are limited by the relatively small number of respondents by learner category, with senior medical residents and attending physicians being underrepresented.
While there are a multitude of dashboards available at the VA, most are made to track certain quality metrics and are used more by administrative and leadership staff. The Inpatient Dashboard was created specifically for frontline clinicians to facilitate their day-to-day workflow and dynamic documentation. This tool can additionally help with quality metrics, though its main purpose was and is to make clinician workflow easier and more efficient.
These results are especially timely because the VA is modernizing its EHR by transitioning to Oracle Health.7 Due to the numerous reports both from veterans and VA clinicians that the Oracle Health EHR is not meeting expectations, deployment at further sites has been halted while improving the experience of the 5 institutions using Oracle Health is prioritized.9 The Inpatient Dashboard, instead of being merely an enhancement to CPRS, could emerge as a potential bridge to Oracle Health if adapted to display data from Oracle Health as it does VistA. This would facilitate a smoother, more integrated transition for those health care institutions employing the Inpatient Dashboard.
Limitations
The reliance on self-reported data inherently carries the risk of bias, and the absence of objective measures, like time-tracking studies, limits the quantifiable assessment of the Inpatient Dashboard efficacy. The single-center nature of the study also may restrict the generalizability of the results.
CONCLUSIONS
Optimal integration of EHRs into health care delivery is critical to high-quality patient care and operational efficiency. The Inpatient Dashboard is an example of an innovative, user-centric solution that integrated and presented clinical information in a way that produced high satisfaction and adoption by users at a VA hospital.
Electronic health records (EHRs) are an integral part of modern health care. The 2009, Health Information Technology for Economic and Clinical Health Act established financial incentives for US hospitals to adopt EHRs. In 2009 only 12% of nonfederal acute care hospitals had adopted a certified EHR system, which increased to 96% by 2021.1
EHRs have transformed the way patient data are stored and accessed, streamlining the process of providing quality patient care with improvements in efficiency, effectiveness, patient satisfaction, and safety.2 Despite their widespread adoption and benefits, EHRs have generally been met with mixed physician satisfaction.3 Interactions with EHRs are linked to disproportionate time at the computer and physician burnout.4-6
The US Department of Veterans Affairs (VA) was at the forefront of EHR development, establishing the Veterans Health Information Systems and Technology Architecture (VistA) in the 1970s. The VA released the Computerized Patient Record System (CPRS) in 1997, the first clinical user interface for VistA. In May 2018, the VA signed a $10 billion contract with Cerner (now Oracle Health) to modernize its EHR.7 This was later revised to $16.1 billion, and the Institute for Defense Analyses estimates it will cost $49.8 billion.8 The transition to Oracle Health has been faced with significant challenges, including patient safety risks and workflow inefficiencies, leading to a pause in rollout.9
Due to the known challenges with EHRs and the aging CPRS system (without a scheduled replacement date), innovations that facilitate the synthesis and display of clinical information are needed. To address this gap, the VA Ann Arbor Healthcare System (VAAAHS) developed the Inpatient Dashboard, an online EHR companion tool. The Inpatient Dashboard was designed to draw data from VistA to reduce time spent at the computer by streamlining clinical information presentation, standardizing inpatient notes, improving safety measures, and enhancing overall clinician satisfaction. This study evaluated the adoption and user experience with the Inpatient Dashboard.
INPATIENT DASHBOARD
The Inpatient Dashboard consists of several modules created by a contractor for the VAAAHS that is housed on VA servers with access restricted to individuals with patient health data privileges. As the Inpatient Dashboard draws data from VistA, it can display laboratory information, studies, and notes from all VA sites.
The main dashboard is a snapshot summary of patient information, including patient location, code status, last vital sign readings, vital sign ranges over the previous 24 hours, intake/output, deep vein thrombosis (DVT) prophylaxis, the presence of telemetry orders, or use of Foley or central catheters (Figure). It also includes a customizable to-do list and contact information for the patient’s clinician and nurse. Significant events, such as abnormal vital signs or speciation/sensitivities for blood cultures, are automatically populated on the to-do list. From this main dashboard overview, clinicians can customize which patients are displayed, create and print a rounding list, print a sign-out sheet, or select individual patients to open a progress note module.
Notes can be written in the patient history and physical module, progress note module, and discharge summary module. The patient history and physical module has text blocks allocated to the traditional components of a history and physical note (ie, chief complaint, history of present illness, review of systems, past medical history, family history, social history, allergies, medications, physical examination, assessment, and plan) (eAppendix 1). Some elements, such as past medical history, family history, and social history are prepopulated if the patient was previously admitted. Vital signs, laboratory results, studies, microbiology/ pathology reports, and other CPRS notes are displayed in this module.
The progress note module contains text blocks allocated to the traditional components of a progress note, such as subjective/interval events, physical examination, assessment, and plan (eAppendix 2). Vital signs, laboratory results, studies, microbiology/ pathology reports, other CPRS notes, and the patient’s medication administration record are also displayed in this module. Lastly, the discharge summary module includes patient follow-up, patient instructions, hospitalization summary, medication reconciliation, laboratory results, and studies/procedures, ensuring a comprehensive discharge summary for patients and clinicians (eAppendix 3).
A medication reconciliation tool was embedded within the history and physical and discharge summary modules. This tool has been shown to reduce medication errors in patients admitted from the emergency department to the hospital (eAppendix 4).10 The handoff/sign-out tool (eAppendix 5) accessible through the main dashboard page is modeled on the I-PASS handoff framework.11,12 This includes the patient identifier, interval events, inpatient medications, specific sign-out guidance, sign-out tasks/to-dos, and any other pertinent information.
The Inpatient Dashboard is a team-based construct shared by the attending physicians, residents, and medical students. Each team (eg, general medicine, general surgery) is its own entity; only team members can change the content or add to the documentation. Each facility can have multiple teams caring for the same patient (eg, primary and consulting teams). Additional care members can also be incorporated (eg, pharmacists assist with medication reconciliation for admission and discharge at VAAAHS). The Inpatient Dashboard can export information directly to CPRS for clinicians to review and sign. It can also generate a note that can be pasted into CPRS.
Clinician Feedback and Satisfaction
A survey was developed to evaluate clinician experiences with using the Inpatient Dashboard as an adjunct to the CPRS. The Inpatient Dashboard was made available to general medicine teams in November 2018. The survey was conducted from December 2018 to September 2019. The study was conducted at the VAAAHS and included 4 general medicine teams. Each team included an attending physician, a senior resident, 2 to 3 interns, and 3 to 4 medical students. Eligibility was extended to any team member who used both the CPRS and Inpatient Dashboard. Participation in the survey was voluntary. All respondents were informed of the study’s purpose and encouraged to provide candid feedback to ensure the reliability and validity of the findings.
Data were collected through a semistructured survey administered via the Qualtrics platform. The questionnaire was designed to capture multidimensional insights into clinician experience, with particular focus on satisfaction, efficiency, and perceived safety when using the tool as an adjunct to CPRS compared to using CPRS alone. The questionnaire primarily used a Likert scale for responses. Surveys were emailed at the completion of a team’s 1-month inpatient block. An answer was not required for every question, resulting in slightly different response numbers for some questions.
A question regarding the tool’s impact on workload stress was added halfway through the study period, which resulted in fewer responses. Adoption was assessed by counting the Inpatient Dashboard unique users. Descriptive statistics were used within individual survey responses to report the distribution of responses. Differences in response between levels of training were assessed using a X2 test of independence.
Survey Results
From September 2023 through November 2023, there were 1549 rounding printouts across 144 unique users (5 nurses, 40 medical students, 87 residents, and 12 attending physicians) and 1468 handoff printouts across 148 unique users (5 nurses, 10 medical students, 111 residents, and 22 attending physicians). The clinician survey received 68 responses from users at various levels of medical training: 23 medical students, 31 interns, 12 senior residents, and 2 attending physicians. All 68 participants confirmed they had used the Inpatient Dashboard.
User satisfaction and preference for the Inpatient Dashboard vs CPRS were assessed. Sixty-one respondents (90%) expressed overall satisfaction with the Inpatient Dashboard; 22 (32%) were extremely satisfied, and 39 (57%) were somewhat satisfied (Table 1). Three respondents (4%) were neutral, 2 (3%) were somewhat dissatisfied, and 2 (3%) were extremely dissatisfied with the Inpatient Dashboard. Responses differed by level of training (P = .03), with medical students trending towards higher satisfaction.
Respondents preferred the Inpatient Dashboard over CPRS for gathering information and writing progress notes; 42 (64%) respondents mostly favored the Inpatient Dashboard, 15 (23%) slightly favored the Inpatient Dashboard over CPRS, and 8 (12%) were neutral. One respondent (2%) slightly favored CPRS to the Inpatient Dashboard (Table 2).
Sixty-five respondents (100%) found the Inpatient Dashboard’s ability to summarize patient information in a central place helpful (Table 3). Among them, 53 (82%) respondents reported it was very or extremely helpful, 10 (15%) respondents reported it was moderately helpful, and 2 (3%) respondents reported it was slightly helpful. This feature positively impacted users’ awareness of patients with DVT prophylaxis or a Foley catheter. Ten (15%) respondents reported being much more aware, and 29 (45%) respondents reporting they were slightly more aware. The remaining 26 (40%) respondents reported no change in awareness.
The Inpatient Dashboard was reported to save time preparing for physician rounds by 52 (80%) respondents, contributing to much greater efficiency for 29 (45%) respondents and slightly more efficiency for 23 (35%) respondents. However, 10 (15%) respondents reported no change in efficiency, and 3 (5%) respondents reduced efficiency, with 1 (2%) respondent reporting it slightly less efficient and 2 (3%) respondents reporting it much less efficient. Responses differed by level of training (P = .01), with medical students trending towards higher efficiency. Of the 23 respondents who reported on the Inpatient Dashboard’s impact on daily workload stress level, 22 (96%) indicated the tool had a stress-reducing effect, with 9 (39%) experiencing a major reduction in stress level, and 13 (57%) experiencing somewhat reduced stress level. Only 1 participant (4%) reported no change in stress. No participants reported an increase in stress.
DISCUSSION
The adoption of EHRs has transformed operational modalities in contemporary health care systems, heralding advancements in patient satisfaction, safety, and overall quality and efficiency of care.1,2 However, EHRs still present challenges, predominantly around clinician satisfaction, marked by instances of burnout and increased time spent on computers.2-6 In this context, the Inpatient Dashboard, an online companion to the CPRS, exemplifies how user-centered innovations in EHRs can address and mitigate associated challenges.
The Inpatient Dashboard has been well received with most respondents of the survey conducted in this study indicating they were both satisfied with the instrument and preferring it to CPRS. This high approval aligns with existing literature on the potential advantages of user-centered design in health care technology.13 The tool has gained widespread acceptance at the VAAAHS even in the absence of obligatory usage or institutional incentives. The appeal of the Inpatient Dashboard may stem from its increased efficiency, with most users affirming its timesaving nature. While CPRS can only display local notes, laboratory results, and studies, the Inpatient Dashboard can display data from across all VA sites. The VA Joint Longitudinal Viewer can similarly display data from across all sites, but the display is not streamlined as it is in the Inpatient Dashboard. The Inpatient Dashboard incorporates this clinical information into a single page to facilitate day-to-day workflow and dynamic documentation (ie, reviewing laboratory results, medications, writing notes, and signing out patients). This increased efficiency allows clinicians to counter 2 common barriers to EHR implementation: productivity loss and insufficient time.14
The association between EHRs and improved quality and safety in health care is well-documented.3 The Inpatient Dashboard fortifies this association by enhancing awareness around patient status, evidenced by a majority of respondents, and by integrating a medication reconciliation tool to decrease medication errors on transition from the emergency department to inpatient hospitalization.10
The Inpatient Dashboard’s impact on alleviating daily workload stress is noteworthy, with almost all respondents experiencing reduced stress levels and physician burnout, which has been linked to deteriorating well-being, compromised patient safety, and escalated health care costs.15,16 The heightened susceptibility of physicians to burnout compared to other professionals underscores the imperative for incorporating stress-mitigating interventions in the EHR.17,18
While responses to most questions did not significantly differ by training levels, overall satisfaction with the Inpatient Dashboard and its ability to save time preparing for rounds were rated higher by medical students. This may be attributable to a greater derived benefit from collating and presenting data to learners with less familiarity with the native EHR. It is also notable that the Inpatient Dashboard allows medical students to directly contribute to a patient’s note, which could be another driver in satisfaction. While most interns still felt the Inpatient Dashboard enabled them to save time preparing for rounds, there were a considerable number of ‘no change’ responses, which suggests some interns may not have modified their existing prerounding strategies. These associations are limited by the relatively small number of respondents by learner category, with senior medical residents and attending physicians being underrepresented.
While there are a multitude of dashboards available at the VA, most are made to track certain quality metrics and are used more by administrative and leadership staff. The Inpatient Dashboard was created specifically for frontline clinicians to facilitate their day-to-day workflow and dynamic documentation. This tool can additionally help with quality metrics, though its main purpose was and is to make clinician workflow easier and more efficient.
These results are especially timely because the VA is modernizing its EHR by transitioning to Oracle Health.7 Due to the numerous reports both from veterans and VA clinicians that the Oracle Health EHR is not meeting expectations, deployment at further sites has been halted while improving the experience of the 5 institutions using Oracle Health is prioritized.9 The Inpatient Dashboard, instead of being merely an enhancement to CPRS, could emerge as a potential bridge to Oracle Health if adapted to display data from Oracle Health as it does VistA. This would facilitate a smoother, more integrated transition for those health care institutions employing the Inpatient Dashboard.
Limitations
The reliance on self-reported data inherently carries the risk of bias, and the absence of objective measures, like time-tracking studies, limits the quantifiable assessment of the Inpatient Dashboard efficacy. The single-center nature of the study also may restrict the generalizability of the results.
CONCLUSIONS
Optimal integration of EHRs into health care delivery is critical to high-quality patient care and operational efficiency. The Inpatient Dashboard is an example of an innovative, user-centric solution that integrated and presented clinical information in a way that produced high satisfaction and adoption by users at a VA hospital.
- Office of the National Coordinator for Health Information Technology. National Trends in Hospital and Physician Adoption of Electronic Health Records. HealthIT.gov. Accessed February 5, 2025. https://www.healthit.gov/data/quickstats/national-trends-hospital-and-physician-adoption-electronic-health-records
- Buntin MB, Burke MF, Hoaglin MC, Blumenthal D. The benefits of health information technology: a review of the recent literature shows predominantly positive results. Health Aff (Millwood). 2011;30(3):464-471. doi:10.1377/hlthaff.2011.0178
- Nguyen L, Bellucci E, Nguyen LT. Electronic health records implementation: an evaluation of information system impact and contingency factors. Int J Med Inf. 2014;83(11):779-796. doi:10.1016/j.ijmedinf.2014.06.011
- Alexander AG, Ballou KA. Work-life balance, burnout, and the electronic health record. Am J Med. 2018;131(8):857- 858. doi:10.1016/j.amjmed.2018.02.033
- Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753-760. doi:10.7326/M16-0961
- Chaiyachati KH, Shea JA, Asch DA, et al. Assessment of inpatient time allocation among first-year internal medicine residents using time-motion observations. JAMA Intern Med. 2019;179(6):760-767. doi:10.1001/jamainternmed.2019.0095
- US Department of Veterans Affairs. Statement by Acting Secretary Robert Wilkie - VA signs contract with Cerner for an electronic health record system. New release. May 17, 2018. Accessed February 5, 2025. https://news.va.gov/press-room/statement-by-acting-secretary-robert-wilkie-va-signs-contract-with-cerner-for-an-electronic-health-record-system/
- US Government Publishing Office. VA’s Electronic health record modernization: an update on rollout, cost, and schedule. Subcommittee on Military Construction, Veterans Affairs, and Related Agencies, Committee on Appropriations, United States Senate. 117th Congress, 2nd Session. September 21, 2022. Accessed February 5, 2025. https://www.govinfo.gov/content/pkg/CHRG-117shrg52328/html/CHRG-117shrg52328.htm
- US Department of Veterans Affairs. VA announces reset of electronic health record project. Accessed December 21, 2023. https://news.va.gov/press-room/va-announces-reset-of-electronic-health-record-project/
- Grondin C, Gupta A, Houchens N, et al. Medication reconciliation tool reduces errors in patients admitted from the ED to hospital. Am J Med Qual. 2021;36(2):129. doi:10.1097/01.JMQ.0000741500.33781.eb
- Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803-1812. doi:10.1056/NEJMsa1405556
- Starmer AJ, O’Toole JK, Rosenbluth G, et al. Development, implementation, and dissemination of the I-PASS handoff curriculum: a multisite educational intervention to improve patient handoffs. Acad Med. 2014;89(6):876-884. doi:10.1097/ACM.0000000000000264
- Ratwani RM, Fairbanks RJ, Hettinger AZ, Benda NC. Electronic health record usability: analysis of the user-centered design processes of eleven electronic health record vendors. J Am Med Inform Assoc. 2015;22(6):1179-1182. doi:10.1093/jamia/ocv050
- Kruse CS, Kristof C, Jones B, Mitchell E, Martinez A. Barriers to electronic health record adoption: a systematic literature review. J Med Syst. 2016;40(12):252. doi:10.1007/s10916-016-0628-9
- West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-529. doi:10.1111/joim.12752
- Smeds MR, Janko MR, Allen S, et al. Burnout and its relationship with perceived stress, self-efficacy, depression, social support, and programmatic factors in general surgery residents. Am J Surg. 2020;219(6):907- 912. doi:10.1016/j.amjsurg.2019.07.004
- Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377-1385. doi:10.1001/archinternmed.2012.3199
- Budd J. Burnout related to electronic health record use in primary care. J Prim Care Community Health. 2023;14:21501319231166921. doi:10.1177/21501319231166921
- Office of the National Coordinator for Health Information Technology. National Trends in Hospital and Physician Adoption of Electronic Health Records. HealthIT.gov. Accessed February 5, 2025. https://www.healthit.gov/data/quickstats/national-trends-hospital-and-physician-adoption-electronic-health-records
- Buntin MB, Burke MF, Hoaglin MC, Blumenthal D. The benefits of health information technology: a review of the recent literature shows predominantly positive results. Health Aff (Millwood). 2011;30(3):464-471. doi:10.1377/hlthaff.2011.0178
- Nguyen L, Bellucci E, Nguyen LT. Electronic health records implementation: an evaluation of information system impact and contingency factors. Int J Med Inf. 2014;83(11):779-796. doi:10.1016/j.ijmedinf.2014.06.011
- Alexander AG, Ballou KA. Work-life balance, burnout, and the electronic health record. Am J Med. 2018;131(8):857- 858. doi:10.1016/j.amjmed.2018.02.033
- Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016;165(11):753-760. doi:10.7326/M16-0961
- Chaiyachati KH, Shea JA, Asch DA, et al. Assessment of inpatient time allocation among first-year internal medicine residents using time-motion observations. JAMA Intern Med. 2019;179(6):760-767. doi:10.1001/jamainternmed.2019.0095
- US Department of Veterans Affairs. Statement by Acting Secretary Robert Wilkie - VA signs contract with Cerner for an electronic health record system. New release. May 17, 2018. Accessed February 5, 2025. https://news.va.gov/press-room/statement-by-acting-secretary-robert-wilkie-va-signs-contract-with-cerner-for-an-electronic-health-record-system/
- US Government Publishing Office. VA’s Electronic health record modernization: an update on rollout, cost, and schedule. Subcommittee on Military Construction, Veterans Affairs, and Related Agencies, Committee on Appropriations, United States Senate. 117th Congress, 2nd Session. September 21, 2022. Accessed February 5, 2025. https://www.govinfo.gov/content/pkg/CHRG-117shrg52328/html/CHRG-117shrg52328.htm
- US Department of Veterans Affairs. VA announces reset of electronic health record project. Accessed December 21, 2023. https://news.va.gov/press-room/va-announces-reset-of-electronic-health-record-project/
- Grondin C, Gupta A, Houchens N, et al. Medication reconciliation tool reduces errors in patients admitted from the ED to hospital. Am J Med Qual. 2021;36(2):129. doi:10.1097/01.JMQ.0000741500.33781.eb
- Starmer AJ, Spector ND, Srivastava R, et al. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803-1812. doi:10.1056/NEJMsa1405556
- Starmer AJ, O’Toole JK, Rosenbluth G, et al. Development, implementation, and dissemination of the I-PASS handoff curriculum: a multisite educational intervention to improve patient handoffs. Acad Med. 2014;89(6):876-884. doi:10.1097/ACM.0000000000000264
- Ratwani RM, Fairbanks RJ, Hettinger AZ, Benda NC. Electronic health record usability: analysis of the user-centered design processes of eleven electronic health record vendors. J Am Med Inform Assoc. 2015;22(6):1179-1182. doi:10.1093/jamia/ocv050
- Kruse CS, Kristof C, Jones B, Mitchell E, Martinez A. Barriers to electronic health record adoption: a systematic literature review. J Med Syst. 2016;40(12):252. doi:10.1007/s10916-016-0628-9
- West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-529. doi:10.1111/joim.12752
- Smeds MR, Janko MR, Allen S, et al. Burnout and its relationship with perceived stress, self-efficacy, depression, social support, and programmatic factors in general surgery residents. Am J Surg. 2020;219(6):907- 912. doi:10.1016/j.amjsurg.2019.07.004
- Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377-1385. doi:10.1001/archinternmed.2012.3199
- Budd J. Burnout related to electronic health record use in primary care. J Prim Care Community Health. 2023;14:21501319231166921. doi:10.1177/21501319231166921
Streamlining Health Care: Inpatient Dashboard as a User-Centric Solution in EHR Enhancement
Streamlining Health Care: Inpatient Dashboard as a User-Centric Solution in EHR Enhancement