User login
Smoking, inactivity most powerful post-MI lifestyle risk factors
PARIS – All lifestyle-related cardiovascular risk factors aren’t equal in power when it comes to secondary prevention after a first acute MI, according to a massive Swedish registry study.

Insufficient physical activity and current smoking were consistently the strongest risk factors for all-cause mortality, major adverse cardiovascular events, and other key adverse outcomes in an analysis from the SWEDEHEART registry. The study included 65,002 patients discharged after a first MI and 325,010 age- and sex-matched controls with no prior MI followed for a median of 5.5 years and maximum of 12, Emil Hagstrom, MD, PhD, reported at the annual congress of the European Society of Cardiology.
Strongest lifestyle risk factors
The study examined the long-term relative importance of control of six major lifestyle risk factors for secondary cardiovascular prevention: current smoking, insufficient physical activity, blood pressure of 140/90 mm Hg or more, obesity, a fasting blood glucose of at least 126 mg/dL, and an LDL cholesterol of 70 mg/dL or more. Notably, two risk factors that physicians often emphasize in working with their patients with known coronary heart disease – an elevated LDL cholesterol and obesity – barely moved the needle. Out of the six risk factors scrutinized, those two consistently showed the weakest association with long-term risk of adverse outcomes. Occupying the middle ground in terms of predictive strength were hypertension and elevated blood glucose, according to Dr. Hagstrom, a cardiologist at Uppsala (Sweden) University.
Risk factor status was assessed 6-10 weeks post MI. Insufficient physical activity was defined as not engaging in at least 30 minutes of moderate-intensity exercise on at least 5 days per week. And when Dr. Hagstrom recalculated the risk of adverse outcomes using an LDL cholesterol threshold of 55 mg/dL rather than using 70 mg/dL, as recommended in new ESC secondary prevention guidelines released during the congress, the study results remained unchanged.
Cumulative effects
A key SWEDEHEART finding underscoring the importance of lifestyle in secondary prevention was that a linear stepwise relationship existed between the number of risk factors at target levels and the risk of all of the various adverse outcomes assessed, including stroke and heart failure hospitalization as well as all-cause mortality, cardiovascular mortality, and major bleeding.
Moreover, patients with none of the six risk factors outside of target when assessed after their MI had the same risks of all-cause mortality, cardiovascular mortality, and stroke as the matched controls.
For example, in an analysis adjusted for comorbid cancer, chronic obstructive pulmonary disease, and dementia, post-MI patients with zero risk factors had the same long-term risk of cardiovascular mortality as controls without a history of MI at baseline. With one risk factor not at target, a patient had a 41% increased risk compared with controls, a statistically significant difference. With two out-of-whack risk factors, the risk climbed to 102%. With three, 185%. With four risk factors not at target, the all-cause mortality risk jumped to 291%. And patients with more than four of the six risk factors not at target had a 409% greater risk of all-cause mortality than controls who had never had a heart attack.
When Dr. Hagstrom stratified subjects by age at baseline – up to 55, 56-64, 65-70, and 70-75 years – he discovered that, regardless of age, patients with zero risk factors had the same risk of all-cause mortality and other adverse outcomes as controls. However, when risk factors were present, younger patients consistently had a higher risk of all adverse outcomes than older patients with the same number of risk factors. When asked for an explanation of this phenomenon, Dr. Hagstrom noted that younger patients with multiple risk factors have a longer time to be exposed to and accumulate risk.
Follow-up of the study cohort will continue for years to come, the cardiologist promised.
At an ESC congress highlights session that closed out the meeting, Eva Prescott, MD, put the SWEDEHEART study at the top of her list of important developments in preventive cardiology arising from the congress.
“This is an excellent national registry I think we’re all envious of,” commented Dr. Prescott, a cardiologist at Copenhagen University. “The conclusion of this registry-based data, I think, is that lifestyle really remains at the core of prevention of cardiovascular events still today.”
The SWEDEHEART study analysis was funded free of commercial support. Dr. Hagstrom reported serving as a consultant to or receiving speakers’ fees from Amgen, AstraZeneca, Bayer, Novo Nordisk, and Sanofi.
PARIS – All lifestyle-related cardiovascular risk factors aren’t equal in power when it comes to secondary prevention after a first acute MI, according to a massive Swedish registry study.
Insufficient physical activity and current smoking were consistently the strongest risk factors for all-cause mortality, major adverse cardiovascular events, and other key adverse outcomes in an analysis from the SWEDEHEART registry. The study included 65,002 patients discharged after a first MI and 325,010 age- and sex-matched controls with no prior MI followed for a median of 5.5 years and maximum of 12, Emil Hagstrom, MD, PhD, reported at the annual congress of the European Society of Cardiology.
Strongest lifestyle risk factors
The study examined the long-term relative importance of control of six major lifestyle risk factors for secondary cardiovascular prevention: current smoking, insufficient physical activity, blood pressure of 140/90 mm Hg or more, obesity, a fasting blood glucose of at least 126 mg/dL, and an LDL cholesterol of 70 mg/dL or more. Notably, two risk factors that physicians often emphasize in working with their patients with known coronary heart disease – an elevated LDL cholesterol and obesity – barely moved the needle. Out of the six risk factors scrutinized, those two consistently showed the weakest association with long-term risk of adverse outcomes. Occupying the middle ground in terms of predictive strength were hypertension and elevated blood glucose, according to Dr. Hagstrom, a cardiologist at Uppsala (Sweden) University.
Risk factor status was assessed 6-10 weeks post MI. Insufficient physical activity was defined as not engaging in at least 30 minutes of moderate-intensity exercise on at least 5 days per week. And when Dr. Hagstrom recalculated the risk of adverse outcomes using an LDL cholesterol threshold of 55 mg/dL rather than using 70 mg/dL, as recommended in new ESC secondary prevention guidelines released during the congress, the study results remained unchanged.
Cumulative effects
A key SWEDEHEART finding underscoring the importance of lifestyle in secondary prevention was that a linear stepwise relationship existed between the number of risk factors at target levels and the risk of all of the various adverse outcomes assessed, including stroke and heart failure hospitalization as well as all-cause mortality, cardiovascular mortality, and major bleeding.
Moreover, patients with none of the six risk factors outside of target when assessed after their MI had the same risks of all-cause mortality, cardiovascular mortality, and stroke as the matched controls.
For example, in an analysis adjusted for comorbid cancer, chronic obstructive pulmonary disease, and dementia, post-MI patients with zero risk factors had the same long-term risk of cardiovascular mortality as controls without a history of MI at baseline. With one risk factor not at target, a patient had a 41% increased risk compared with controls, a statistically significant difference. With two out-of-whack risk factors, the risk climbed to 102%. With three, 185%. With four risk factors not at target, the all-cause mortality risk jumped to 291%. And patients with more than four of the six risk factors not at target had a 409% greater risk of all-cause mortality than controls who had never had a heart attack.
When Dr. Hagstrom stratified subjects by age at baseline – up to 55, 56-64, 65-70, and 70-75 years – he discovered that, regardless of age, patients with zero risk factors had the same risk of all-cause mortality and other adverse outcomes as controls. However, when risk factors were present, younger patients consistently had a higher risk of all adverse outcomes than older patients with the same number of risk factors. When asked for an explanation of this phenomenon, Dr. Hagstrom noted that younger patients with multiple risk factors have a longer time to be exposed to and accumulate risk.
Follow-up of the study cohort will continue for years to come, the cardiologist promised.
At an ESC congress highlights session that closed out the meeting, Eva Prescott, MD, put the SWEDEHEART study at the top of her list of important developments in preventive cardiology arising from the congress.
“This is an excellent national registry I think we’re all envious of,” commented Dr. Prescott, a cardiologist at Copenhagen University. “The conclusion of this registry-based data, I think, is that lifestyle really remains at the core of prevention of cardiovascular events still today.”
The SWEDEHEART study analysis was funded free of commercial support. Dr. Hagstrom reported serving as a consultant to or receiving speakers’ fees from Amgen, AstraZeneca, Bayer, Novo Nordisk, and Sanofi.
PARIS – All lifestyle-related cardiovascular risk factors aren’t equal in power when it comes to secondary prevention after a first acute MI, according to a massive Swedish registry study.
Insufficient physical activity and current smoking were consistently the strongest risk factors for all-cause mortality, major adverse cardiovascular events, and other key adverse outcomes in an analysis from the SWEDEHEART registry. The study included 65,002 patients discharged after a first MI and 325,010 age- and sex-matched controls with no prior MI followed for a median of 5.5 years and maximum of 12, Emil Hagstrom, MD, PhD, reported at the annual congress of the European Society of Cardiology.
Strongest lifestyle risk factors
The study examined the long-term relative importance of control of six major lifestyle risk factors for secondary cardiovascular prevention: current smoking, insufficient physical activity, blood pressure of 140/90 mm Hg or more, obesity, a fasting blood glucose of at least 126 mg/dL, and an LDL cholesterol of 70 mg/dL or more. Notably, two risk factors that physicians often emphasize in working with their patients with known coronary heart disease – an elevated LDL cholesterol and obesity – barely moved the needle. Out of the six risk factors scrutinized, those two consistently showed the weakest association with long-term risk of adverse outcomes. Occupying the middle ground in terms of predictive strength were hypertension and elevated blood glucose, according to Dr. Hagstrom, a cardiologist at Uppsala (Sweden) University.
Risk factor status was assessed 6-10 weeks post MI. Insufficient physical activity was defined as not engaging in at least 30 minutes of moderate-intensity exercise on at least 5 days per week. And when Dr. Hagstrom recalculated the risk of adverse outcomes using an LDL cholesterol threshold of 55 mg/dL rather than using 70 mg/dL, as recommended in new ESC secondary prevention guidelines released during the congress, the study results remained unchanged.
Cumulative effects
A key SWEDEHEART finding underscoring the importance of lifestyle in secondary prevention was that a linear stepwise relationship existed between the number of risk factors at target levels and the risk of all of the various adverse outcomes assessed, including stroke and heart failure hospitalization as well as all-cause mortality, cardiovascular mortality, and major bleeding.
Moreover, patients with none of the six risk factors outside of target when assessed after their MI had the same risks of all-cause mortality, cardiovascular mortality, and stroke as the matched controls.
For example, in an analysis adjusted for comorbid cancer, chronic obstructive pulmonary disease, and dementia, post-MI patients with zero risk factors had the same long-term risk of cardiovascular mortality as controls without a history of MI at baseline. With one risk factor not at target, a patient had a 41% increased risk compared with controls, a statistically significant difference. With two out-of-whack risk factors, the risk climbed to 102%. With three, 185%. With four risk factors not at target, the all-cause mortality risk jumped to 291%. And patients with more than four of the six risk factors not at target had a 409% greater risk of all-cause mortality than controls who had never had a heart attack.
When Dr. Hagstrom stratified subjects by age at baseline – up to 55, 56-64, 65-70, and 70-75 years – he discovered that, regardless of age, patients with zero risk factors had the same risk of all-cause mortality and other adverse outcomes as controls. However, when risk factors were present, younger patients consistently had a higher risk of all adverse outcomes than older patients with the same number of risk factors. When asked for an explanation of this phenomenon, Dr. Hagstrom noted that younger patients with multiple risk factors have a longer time to be exposed to and accumulate risk.
Follow-up of the study cohort will continue for years to come, the cardiologist promised.
At an ESC congress highlights session that closed out the meeting, Eva Prescott, MD, put the SWEDEHEART study at the top of her list of important developments in preventive cardiology arising from the congress.
“This is an excellent national registry I think we’re all envious of,” commented Dr. Prescott, a cardiologist at Copenhagen University. “The conclusion of this registry-based data, I think, is that lifestyle really remains at the core of prevention of cardiovascular events still today.”
The SWEDEHEART study analysis was funded free of commercial support. Dr. Hagstrom reported serving as a consultant to or receiving speakers’ fees from Amgen, AstraZeneca, Bayer, Novo Nordisk, and Sanofi.
REPORTING FROM THE ESC CONGRESS 2019
Daily polypill lowers BP, cholesterol in underserved population
A daily polypill regimen improved cardiovascular risk factors in a socioeconomically vulnerable minority population, in a randomized controlled trial.

Patients at a federally qualified community health center in Alabama who received treatment with a combination pill for 1 year had greater reductions in systolic blood pressure and LDL cholesterol than did patients who received usual care, according to results published online on Sept. 19 in the New England Journal of Medicine.
“The simplicity and low cost of the polypill regimen make this approach attractive” when barriers such as lack of income, underinsurance, and difficulty attending clinic visits are common, said first author Daniel Muñoz, MD, of Vanderbilt University in Nashville, and coinvestigators. The investigators obtained the pills at a cost of $26 per month per participant.
People with low socioeconomic status and those who are nonwhite have high cardiovascular mortality, and the southeastern United States and rural areas have disproportionately high levels of cardiovascular disease burden, according to the investigators. The rates at which people with low socioeconomic status receive treatment for hypertension and hypercholesterolemia – leading cardiovascular disease risk factors – “are strikingly low,” Dr. Muñoz and colleagues said.
To assess the effectiveness of a polypill-based strategy in an underserved population with low socioeconomic status, the researchers conducted the randomized trial.
They enrolled 303 adults without cardiovascular disease, and 148 of the patients were randomized to receive the polypill, which contained generic versions of atorvastatin (10 mg), amlodipine (2.5 mg), losartan (25 mg), and hydrochlorothiazide (12.5 mg). The remaining 155 patients received usual care. All participants scheduled 2-month and 12-month follow-up visits.
The participants had an average age of 56 years, 60% were women, and more than 95% were black. More than 70% had an annual household income of less than $15,000. Baseline characteristics of the treatment groups did not significantly differ.
At baseline, the average BP was 140/83 mm Hg, and the average LDL cholesterol level was 113 mg/dL.
In all, 91% of the participants completed the 12-month trial visit. Average systolic BP decreased by 9 mm Hg in the group that received the polypill, compared with 2 mm Hg in the group that received usual care. Average LDL cholesterol level decreased by 15 mg/dL in the polypill group, versus 4 mg/dL in the usual-care group.
Changes in other medications
Clinicians discontinued or reduced doses of other antihypertensive or lipid-lowering medications in 44% of the patients in the polypill group and none in the usual-care group. Clinicians escalated therapy in 2% of the participants in the polypill group and in 10% of the usual-care group.
Side effects in participants who received the polypill included a 1% incidence of myalgias and a 1% incidence of hypotension or light-headedness. Liver function test results were normal.
Five serious adverse events that occurred during the trial – two in the polypill group and three in the usual-care group – were judged to be unrelated to the trial by a data and safety monitoring board.
The authors noted that limitations of the trial include its open-label design and that it was conducted at a single center.
“It is important to emphasize that use of the polypill does not preclude individualized, add-on therapies for residual elevations in blood-pressure or cholesterol levels, as judged by a patient’s physician,” said Dr. Muñoz and colleagues. “We recognize that a ‘one size fits all’ approach to cardiovascular disease prevention runs counter to current trends in precision medicine, in which clinical, genomic, and lifestyle factors are used for the development of individualized treatment strategies. Although the precision approach has clear virtues, a broader approach may benefit patients who face barriers to accessing the full advantages of precision medicine.”
The study was supported by grants from the American Heart Association Strategically Focused Prevention Research Network and the National Institutes of Health. One author disclosed personal fees from Novartis outside the study.
SOURCE: Muñoz D et al. N Engl J Med. 2019 Sep 18;381(12):1114-23. doi: 10.1056/NEJMoa1815359.
A daily polypill regimen improved cardiovascular risk factors in a socioeconomically vulnerable minority population, in a randomized controlled trial.
Patients at a federally qualified community health center in Alabama who received treatment with a combination pill for 1 year had greater reductions in systolic blood pressure and LDL cholesterol than did patients who received usual care, according to results published online on Sept. 19 in the New England Journal of Medicine.
“The simplicity and low cost of the polypill regimen make this approach attractive” when barriers such as lack of income, underinsurance, and difficulty attending clinic visits are common, said first author Daniel Muñoz, MD, of Vanderbilt University in Nashville, and coinvestigators. The investigators obtained the pills at a cost of $26 per month per participant.
People with low socioeconomic status and those who are nonwhite have high cardiovascular mortality, and the southeastern United States and rural areas have disproportionately high levels of cardiovascular disease burden, according to the investigators. The rates at which people with low socioeconomic status receive treatment for hypertension and hypercholesterolemia – leading cardiovascular disease risk factors – “are strikingly low,” Dr. Muñoz and colleagues said.
To assess the effectiveness of a polypill-based strategy in an underserved population with low socioeconomic status, the researchers conducted the randomized trial.
They enrolled 303 adults without cardiovascular disease, and 148 of the patients were randomized to receive the polypill, which contained generic versions of atorvastatin (10 mg), amlodipine (2.5 mg), losartan (25 mg), and hydrochlorothiazide (12.5 mg). The remaining 155 patients received usual care. All participants scheduled 2-month and 12-month follow-up visits.
The participants had an average age of 56 years, 60% were women, and more than 95% were black. More than 70% had an annual household income of less than $15,000. Baseline characteristics of the treatment groups did not significantly differ.
At baseline, the average BP was 140/83 mm Hg, and the average LDL cholesterol level was 113 mg/dL.
In all, 91% of the participants completed the 12-month trial visit. Average systolic BP decreased by 9 mm Hg in the group that received the polypill, compared with 2 mm Hg in the group that received usual care. Average LDL cholesterol level decreased by 15 mg/dL in the polypill group, versus 4 mg/dL in the usual-care group.
Changes in other medications
Clinicians discontinued or reduced doses of other antihypertensive or lipid-lowering medications in 44% of the patients in the polypill group and none in the usual-care group. Clinicians escalated therapy in 2% of the participants in the polypill group and in 10% of the usual-care group.
Side effects in participants who received the polypill included a 1% incidence of myalgias and a 1% incidence of hypotension or light-headedness. Liver function test results were normal.
Five serious adverse events that occurred during the trial – two in the polypill group and three in the usual-care group – were judged to be unrelated to the trial by a data and safety monitoring board.
The authors noted that limitations of the trial include its open-label design and that it was conducted at a single center.
“It is important to emphasize that use of the polypill does not preclude individualized, add-on therapies for residual elevations in blood-pressure or cholesterol levels, as judged by a patient’s physician,” said Dr. Muñoz and colleagues. “We recognize that a ‘one size fits all’ approach to cardiovascular disease prevention runs counter to current trends in precision medicine, in which clinical, genomic, and lifestyle factors are used for the development of individualized treatment strategies. Although the precision approach has clear virtues, a broader approach may benefit patients who face barriers to accessing the full advantages of precision medicine.”
The study was supported by grants from the American Heart Association Strategically Focused Prevention Research Network and the National Institutes of Health. One author disclosed personal fees from Novartis outside the study.
SOURCE: Muñoz D et al. N Engl J Med. 2019 Sep 18;381(12):1114-23. doi: 10.1056/NEJMoa1815359.
A daily polypill regimen improved cardiovascular risk factors in a socioeconomically vulnerable minority population, in a randomized controlled trial.
Patients at a federally qualified community health center in Alabama who received treatment with a combination pill for 1 year had greater reductions in systolic blood pressure and LDL cholesterol than did patients who received usual care, according to results published online on Sept. 19 in the New England Journal of Medicine.
“The simplicity and low cost of the polypill regimen make this approach attractive” when barriers such as lack of income, underinsurance, and difficulty attending clinic visits are common, said first author Daniel Muñoz, MD, of Vanderbilt University in Nashville, and coinvestigators. The investigators obtained the pills at a cost of $26 per month per participant.
People with low socioeconomic status and those who are nonwhite have high cardiovascular mortality, and the southeastern United States and rural areas have disproportionately high levels of cardiovascular disease burden, according to the investigators. The rates at which people with low socioeconomic status receive treatment for hypertension and hypercholesterolemia – leading cardiovascular disease risk factors – “are strikingly low,” Dr. Muñoz and colleagues said.
To assess the effectiveness of a polypill-based strategy in an underserved population with low socioeconomic status, the researchers conducted the randomized trial.
They enrolled 303 adults without cardiovascular disease, and 148 of the patients were randomized to receive the polypill, which contained generic versions of atorvastatin (10 mg), amlodipine (2.5 mg), losartan (25 mg), and hydrochlorothiazide (12.5 mg). The remaining 155 patients received usual care. All participants scheduled 2-month and 12-month follow-up visits.
The participants had an average age of 56 years, 60% were women, and more than 95% were black. More than 70% had an annual household income of less than $15,000. Baseline characteristics of the treatment groups did not significantly differ.
At baseline, the average BP was 140/83 mm Hg, and the average LDL cholesterol level was 113 mg/dL.
In all, 91% of the participants completed the 12-month trial visit. Average systolic BP decreased by 9 mm Hg in the group that received the polypill, compared with 2 mm Hg in the group that received usual care. Average LDL cholesterol level decreased by 15 mg/dL in the polypill group, versus 4 mg/dL in the usual-care group.
Changes in other medications
Clinicians discontinued or reduced doses of other antihypertensive or lipid-lowering medications in 44% of the patients in the polypill group and none in the usual-care group. Clinicians escalated therapy in 2% of the participants in the polypill group and in 10% of the usual-care group.
Side effects in participants who received the polypill included a 1% incidence of myalgias and a 1% incidence of hypotension or light-headedness. Liver function test results were normal.
Five serious adverse events that occurred during the trial – two in the polypill group and three in the usual-care group – were judged to be unrelated to the trial by a data and safety monitoring board.
The authors noted that limitations of the trial include its open-label design and that it was conducted at a single center.
“It is important to emphasize that use of the polypill does not preclude individualized, add-on therapies for residual elevations in blood-pressure or cholesterol levels, as judged by a patient’s physician,” said Dr. Muñoz and colleagues. “We recognize that a ‘one size fits all’ approach to cardiovascular disease prevention runs counter to current trends in precision medicine, in which clinical, genomic, and lifestyle factors are used for the development of individualized treatment strategies. Although the precision approach has clear virtues, a broader approach may benefit patients who face barriers to accessing the full advantages of precision medicine.”
The study was supported by grants from the American Heart Association Strategically Focused Prevention Research Network and the National Institutes of Health. One author disclosed personal fees from Novartis outside the study.
SOURCE: Muñoz D et al. N Engl J Med. 2019 Sep 18;381(12):1114-23. doi: 10.1056/NEJMoa1815359.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: A daily polypill regimen may improve cardiovascular disease prevention in underserved populations.
Major finding: Mean LDL cholesterol levels decreased by 15 mg/dL in the polypill group, vs. 4 mg/dL in the usual-care group.
Study details: An open-label, randomized trial that enrolled 303 adults without cardiovascular disease at a federally qualified community health center in Alabama.
Disclosures: The study was supported by grants from the American Heart Association Strategically Focused Prevention Research Network and the National Institutes of Health. One author disclosed personal fees from Novartis outside the study.
Source: Muñoz D et al. N Engl J Med. 2019;381(12):1114-23. doi: 10.1056/NEJMoa1815359.
European cholesterol guidelines push LDL targets below 55 mg/dL
PARIS – The 2019 dyslipidemia management guidelines from the European Society of Cardiology set an LDL cholesterol target for very-high-risk people of less than 55 mg/dL (as well as at least a 50% cut from baseline), a class I recommendation. This marks the first time a cardiology society has either recommended a target goal for this measure below 70 mg/dL or endorsed treating patients to still-lower cholesterol once their level was already under 70 mg/dL.*
The guidelines went further by suggesting consideration of an even lower treatment target for LDL-cholesterol in very-high-risk, secondary prevention patients who have already had at least two atherosclerotic cardiovascular disease events during the past 2 years, a setting that could justify an LDL-cholesterol goal of less than 40 mg/dL (along with a cut from baseline of at least 50%), a class IIb recommendation that denotes a “may be considered,” endorsement.
“In all the trials, lower was better. There was no lower level of LDL cholesterol that’s been studied that was not better” for patient outcomes, Colin Baigent, BMBCH, said while presenting the new guideline at the annual congress of the European Society of Cardiology (ESC). “It’s very clear” that the full treatment benefit from lowering LDL-cholesterol extends to getting very-high risk patients below these levels, said Dr. Baigent, professor of cardiology at Oxford (England) University and one of three chairs of the ESC’s dyslipidemia guideline-writing panel.
While this change was seen as a notably aggressive goal and too fixed on a specific number by at least one author of the 2018 American Heart Association/American College of Cardiology cholesterol management guideline (J Am Coll Cardiol. 2019 Jun;73[24]:e285-e350), it was embraced by another U.S. expert not involved in writing the most recent U.S. recommendations.

“A goal for LDL-cholesterol of less than 55 mg/dL is reasonable; it’s well documented” by trial evidence “and I support it,” said Robert H. Eckel, MD, an endocrinologist and professor of medicine at the University of Colorado in Aurora. Dr. Eckel added that he “also supports” an LDL-cholesterol of less than 40 mg/dL in very-high-risk patients with a history of multiple events or with multiple residual risk factors, and he said he has applied this lower LDL-cholesterol goal in his practice for selected patients. But Dr. Eckel acknowledged in an interview that the evidence for it was less clear-cut than was the evidence behind a goal of less than 55 mg/dL. He also supported the concept of including a treatment goal in U.S. lipid recommendations, which in recent versions has been missing. “I fall back on a cholesterol goal for practical purposes” of making the success of cholesterol-lowering treatment easier to track.
The new ESC goal was characterized as “arbitrary” by Neil J. Stone, MD, vice-chair of the panel that wrote the 2018 AHA/ACC guideline, which relied on treating secondary-prevention patients at high risk to an LDL-cholesterol at least 50% less than before treatment, and recommended continued intensification for patients whose LDL-cholesterol level remained at or above 70 mg/dL.

“If the patient is at 58 mg/dL I’m not sure anyone can tell me what the difference is,” compared with reaching less than 55 mg/dL, Dr. Stone said in an interview. “I worry about focusing on a number and not on the concept that people at the very highest risk deserve the most intensive treatment; the Europeans agree, but they have a different way of looking at it. Despite this difference in approach, the new ESC guidelines and the 2018 U.S. guideline “are more similar than different,” stressed Dr. Stone, professor of medicine and preventive medicine at Northwestern University, Chicago.
However, other experts see an important difference in the risk faced by patients who reach the ESC’s recommended treatment goals and those who fall just short.
“It’s hard to lower an LDL-cholesterol that is already relatively low. People who are close to their cholesterol target need the most intensified treatment” to reach their goal, said Rory Collins, F.Med.Sci., professor of epidemiology at Oxford University. He was not on the ESC guidelines panel.

“It’s a mind shift that clinicians need to be most aggressive in treating patients with the highest risk” even when their LDL-cholesterol is low but not yet at the target level, Dr. Collins said during a discussion session at the congress.
The new ESC guidelines is about “both getting the LDL-cholesterol down to a certain level and also about achieving a big [at least 50%] change” from baseline. “I think the ESC guidelines make that crystal clear,” said Marc S. Sabatine, MD, professor of medicine at Harvard Medical School, Boston, and the sole American to participate in the ESC guidelines-writing panel.

The ESC also broke new ground by advocating an aggressive path toward achieving these LDL-cholesterol goals by elevating the newest and most potent class of approved LDL-cholesterol-lowering drugs, the PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors, to a top-tier, class I recommendation (“is recommended”) for secondary prevention in very-high-risk patients not reaching their goal LDL-cholesterol level on a maximally tolerated statin plus ezetimibe. This recommendation to unequivocally add a PCSK9 inhibitor for this patient population contrasts with the 2018 AHA/ACC guideline that deemed adding a PCSK9 inhibitor a IIa recommendation (“is reasonable”).
A similar uptick in treatment aggressiveness appeared in the ESC’s recommendations for managing very-high-risk patients in a primary prevention setting, including those without familial hypercholesterolemia. For these people, the ESC panel, which worked in concert with the European Atherosclerosis Society, pegged adding a PCSK9 inhibitor as a IIb (“may be considered”) recommendation when these very-high-risk people fail to reach their LDL-cholesterol target on a maximally tolerated statin and ezetimibe. Once again, this opening to use a PCSK9 inhibitor contrasted with the 2018 U.S. guideline, which never mentioned an option of adding a PCSK9 inhibitor for primary prevention except when someone also has familial hypercholesterolemia and starts treatment with an LDL level of at least 190 mg/dL (a IIb recommendation). The new European guidelines proposed using a PCSK9 inhibitor as a second-line option to consider when needed for people whose very high risk derives primarily from older age and other factors such as smoking or hypertension that give them at least a 10% 10-year risk for cardiovascular death as estimated with the European-oriented SCORE risk calculator tables.
Updated SCORE risk designations appear in the new ESC dyslipidemia guidelines, and they show, for example, that in lower-risk European countries (mostly Western European nations) virtually all men who are at least 70 years old would fall into the very-high-risk category that makes them potential candidates for treatment with a PCSK9 inhibitor regardless of any other risk they may or may not have. In higher-risk (mostly Eastern European) countries this designation kicks in for most men once they reach the age of 65.
Several Congress attendees who came to a discussion session on the guidelines voiced concerns that the new revision will lead to substantially increased use of the these drugs and hence will significantly boost medical costs, because these drugs today are priced at about $6,000 annually to treat one patient. In response, members of the guideline-writing panel defended their decision as unavoidable given what’s been reported on the clinical impact of PCSK9 inhibitors when lowering LDL cholesterol and cutting atherosclerotic cardiovascular disease events.
“I commend the [ESC] guideline for focusing on the science and on what is best for patients. The U.S. guidelines conflated the science and the cost, and the recommendations got watered down by cost considerations,” said Dr. Sabatine, who has led several studies of PCSK9 inhibitors.
Dr. Baigent added that the panel “deliberated long and hard on cost, but we felt that we had to focus on the evidence. The cost will shift” in the future, he predicted.
Other U.S. physicians highlighted the need to take drug cost into account when writing public health policy documents such as lipid-management guidelines and questioned whether this more liberal use of PCSK9 inhibitors was justified.
“I think that in the absence of familial hypercholesterolemia you need to waffle around the edges to justify a PCSK9 inhibitor,” said Dr. Eckel. “The cost of PCSK9 inhibitors has come down, but at $6,000 per year you can’t ignore their cost.”
“In the U.S. we need to be mindful of the cost of treatment,” said Dr. Stone. “The ESC guidelines are probably more aggressive” than the 2018 U.S. guideline. “They use PCSK9 inhibitors perhaps more than we do; we [in the United States] prefer generic ezetimibe. A lot has to do with the definitions of risk. The European guidelines have a lot of risk definitions that differ” from the U.S. guideline, he said.
Members of the ESC guidelines panel acknowledged that the SCORE risk-assessment charts could overestimate risk in older people who need primary prevention treatment, as well as underestimate the risk in younger adults.
This inherent age bias in the SCORE risk tables make it “extremely important to contextualize” a person’s risk “by considering other risk factors,” advised Brian A. Ference, MD, an interventional cardiologist and professor at Cambridge (England) University who was a member of the ESC guidelines writing group.
The new ESC guidelines say that risk categorization “must be interpreted in light of the clinician’s knowledge and experience, and of the patient’s pretest likelihood” of cardiovascular disease.”
Dr. Baigent has received research funding from Boehringer Ingelheim, Novartis, and Pfizer. Dr. Eckel has been an expert witness on behalf of Sanofi/Regeneron. Dr. Sabatine and Dr. Ference have received honoraria and research funding from several companies including those that market lipid-lowering drugs. Dr. Stone and Dr. Collins had no disclosures.
*Correction, 9/20/19: A previous version of this article incorrectly stated that the ESC guidelines were the first by a medical society to recommend the lower cholesterol goals. The American Association of Clinical Endocrinologists included targets below 55 mg/dL in their 2017 dyslipidemia management guidelines.
SOURCE: Mach F et al. Eur Heart J. 2019 Aug 31. doi: 10.1093/eurheartj/ehz455.
The new ESC dyslipidemia guidelines recently presented at the society’s annual congress are a welcome addition to the lipid disorder treatment guidelines available to clinicians. These guidelines follow the groundbreaking recommendation in 2017 by AACE in their updated guidelines that introduced an LDL goal of <55 mg/dL in “extreme risk” patients. The ESC guidelines now also recommend an LDL goal of <55 mg/dL in “very-high-risk” patients but go further by also requiring a 50% reduction in LDL. Furthermore, they have established an LDL goal of <40 mg/dL in patients who experienced a second vascular event in the past 2 years while on maximally tolerated statin dose.
The ESC very-high-risk category shares many features with AACE’s extreme-risk category but is broader in that it includes patients without a clinical event who display unequivocal evidence of arteriosclerotic cardiovascular disease (ASCVD) on imaging and patients with severe chronic kidney disease (GFR <30 mL/min ) without known ASCVD. There are substantial differences between the ESC and AHA-ACC 2018 guidelines in the very-high-risk category. The AHA very-high-risk is directed toward secondary prevention only and requires two major ASCVD events or one major and at least two high-risk conditions. Moreover, elements of both major ASCVD events and high-risk conditions as well as the very-high-risk eligibility requirements could mean that some patients, who would clearly be classified by both ESC and AACE as candidates for an LDL goal of <55, may not qualify for threshold consideration for maximal LDL lowering below 70 mg/dL including the use of PCSK9 inhibitors. Relative to this point, the AHA-ACC guidelines do not classify past CABG or PCI as a major ASCVD event, nor is a TIA considered a major event or a high-risk condition.
For LDL, “lower is better” is supported by years of statin clinical trial evidence, along with the robust findings in the 2010 Cholesterol Trialists Collaboration. The goal of <55 mg/dL is supported by the IMPROVE-IT, FOURIER, and ODYSSEY trials. The ESC guidelines appropriately take this body of evidence and applies it to an aggressive treatment platform that, like AACE, sets clinically useful LDL goals for clinicians and patients. It takes early, aggressive LDL-lowering treatment to stay ahead of atherosclerotic plaque development in patients who are at very high or extreme risk. Following AACE’s lead, the ESC guidelines are the newest tool available to clinicians addressing this issue with the promise of further decreasing CVD events and extending lives.
Dr. Jellinger is a member of the editorial advisory board for Clinical Endocrinology News. He is professor of clinical medicine on the voluntary faculty at the University of Miami Miller School of Medicine and a practicing endocrinologist at The Center for Diabetes & Endocrine Care in Hollywood, Fla. He is past president of the American Association of Clinical Endocrinologists and the American College of Endocrinology and was chair of the writing committee for the 2017 AACE-ACE lipid guidelines.
The new ESC dyslipidemia guidelines recently presented at the society’s annual congress are a welcome addition to the lipid disorder treatment guidelines available to clinicians. These guidelines follow the groundbreaking recommendation in 2017 by AACE in their updated guidelines that introduced an LDL goal of <55 mg/dL in “extreme risk” patients. The ESC guidelines now also recommend an LDL goal of <55 mg/dL in “very-high-risk” patients but go further by also requiring a 50% reduction in LDL. Furthermore, they have established an LDL goal of <40 mg/dL in patients who experienced a second vascular event in the past 2 years while on maximally tolerated statin dose.
The ESC very-high-risk category shares many features with AACE’s extreme-risk category but is broader in that it includes patients without a clinical event who display unequivocal evidence of arteriosclerotic cardiovascular disease (ASCVD) on imaging and patients with severe chronic kidney disease (GFR <30 mL/min ) without known ASCVD. There are substantial differences between the ESC and AHA-ACC 2018 guidelines in the very-high-risk category. The AHA very-high-risk is directed toward secondary prevention only and requires two major ASCVD events or one major and at least two high-risk conditions. Moreover, elements of both major ASCVD events and high-risk conditions as well as the very-high-risk eligibility requirements could mean that some patients, who would clearly be classified by both ESC and AACE as candidates for an LDL goal of <55, may not qualify for threshold consideration for maximal LDL lowering below 70 mg/dL including the use of PCSK9 inhibitors. Relative to this point, the AHA-ACC guidelines do not classify past CABG or PCI as a major ASCVD event, nor is a TIA considered a major event or a high-risk condition.
For LDL, “lower is better” is supported by years of statin clinical trial evidence, along with the robust findings in the 2010 Cholesterol Trialists Collaboration. The goal of <55 mg/dL is supported by the IMPROVE-IT, FOURIER, and ODYSSEY trials. The ESC guidelines appropriately take this body of evidence and applies it to an aggressive treatment platform that, like AACE, sets clinically useful LDL goals for clinicians and patients. It takes early, aggressive LDL-lowering treatment to stay ahead of atherosclerotic plaque development in patients who are at very high or extreme risk. Following AACE’s lead, the ESC guidelines are the newest tool available to clinicians addressing this issue with the promise of further decreasing CVD events and extending lives.
Dr. Jellinger is a member of the editorial advisory board for Clinical Endocrinology News. He is professor of clinical medicine on the voluntary faculty at the University of Miami Miller School of Medicine and a practicing endocrinologist at The Center for Diabetes & Endocrine Care in Hollywood, Fla. He is past president of the American Association of Clinical Endocrinologists and the American College of Endocrinology and was chair of the writing committee for the 2017 AACE-ACE lipid guidelines.
The new ESC dyslipidemia guidelines recently presented at the society’s annual congress are a welcome addition to the lipid disorder treatment guidelines available to clinicians. These guidelines follow the groundbreaking recommendation in 2017 by AACE in their updated guidelines that introduced an LDL goal of <55 mg/dL in “extreme risk” patients. The ESC guidelines now also recommend an LDL goal of <55 mg/dL in “very-high-risk” patients but go further by also requiring a 50% reduction in LDL. Furthermore, they have established an LDL goal of <40 mg/dL in patients who experienced a second vascular event in the past 2 years while on maximally tolerated statin dose.
The ESC very-high-risk category shares many features with AACE’s extreme-risk category but is broader in that it includes patients without a clinical event who display unequivocal evidence of arteriosclerotic cardiovascular disease (ASCVD) on imaging and patients with severe chronic kidney disease (GFR <30 mL/min ) without known ASCVD. There are substantial differences between the ESC and AHA-ACC 2018 guidelines in the very-high-risk category. The AHA very-high-risk is directed toward secondary prevention only and requires two major ASCVD events or one major and at least two high-risk conditions. Moreover, elements of both major ASCVD events and high-risk conditions as well as the very-high-risk eligibility requirements could mean that some patients, who would clearly be classified by both ESC and AACE as candidates for an LDL goal of <55, may not qualify for threshold consideration for maximal LDL lowering below 70 mg/dL including the use of PCSK9 inhibitors. Relative to this point, the AHA-ACC guidelines do not classify past CABG or PCI as a major ASCVD event, nor is a TIA considered a major event or a high-risk condition.
For LDL, “lower is better” is supported by years of statin clinical trial evidence, along with the robust findings in the 2010 Cholesterol Trialists Collaboration. The goal of <55 mg/dL is supported by the IMPROVE-IT, FOURIER, and ODYSSEY trials. The ESC guidelines appropriately take this body of evidence and applies it to an aggressive treatment platform that, like AACE, sets clinically useful LDL goals for clinicians and patients. It takes early, aggressive LDL-lowering treatment to stay ahead of atherosclerotic plaque development in patients who are at very high or extreme risk. Following AACE’s lead, the ESC guidelines are the newest tool available to clinicians addressing this issue with the promise of further decreasing CVD events and extending lives.
Dr. Jellinger is a member of the editorial advisory board for Clinical Endocrinology News. He is professor of clinical medicine on the voluntary faculty at the University of Miami Miller School of Medicine and a practicing endocrinologist at The Center for Diabetes & Endocrine Care in Hollywood, Fla. He is past president of the American Association of Clinical Endocrinologists and the American College of Endocrinology and was chair of the writing committee for the 2017 AACE-ACE lipid guidelines.
PARIS – The 2019 dyslipidemia management guidelines from the European Society of Cardiology set an LDL cholesterol target for very-high-risk people of less than 55 mg/dL (as well as at least a 50% cut from baseline), a class I recommendation. This marks the first time a cardiology society has either recommended a target goal for this measure below 70 mg/dL or endorsed treating patients to still-lower cholesterol once their level was already under 70 mg/dL.*
The guidelines went further by suggesting consideration of an even lower treatment target for LDL-cholesterol in very-high-risk, secondary prevention patients who have already had at least two atherosclerotic cardiovascular disease events during the past 2 years, a setting that could justify an LDL-cholesterol goal of less than 40 mg/dL (along with a cut from baseline of at least 50%), a class IIb recommendation that denotes a “may be considered,” endorsement.
“In all the trials, lower was better. There was no lower level of LDL cholesterol that’s been studied that was not better” for patient outcomes, Colin Baigent, BMBCH, said while presenting the new guideline at the annual congress of the European Society of Cardiology (ESC). “It’s very clear” that the full treatment benefit from lowering LDL-cholesterol extends to getting very-high risk patients below these levels, said Dr. Baigent, professor of cardiology at Oxford (England) University and one of three chairs of the ESC’s dyslipidemia guideline-writing panel.
While this change was seen as a notably aggressive goal and too fixed on a specific number by at least one author of the 2018 American Heart Association/American College of Cardiology cholesterol management guideline (J Am Coll Cardiol. 2019 Jun;73[24]:e285-e350), it was embraced by another U.S. expert not involved in writing the most recent U.S. recommendations.
“A goal for LDL-cholesterol of less than 55 mg/dL is reasonable; it’s well documented” by trial evidence “and I support it,” said Robert H. Eckel, MD, an endocrinologist and professor of medicine at the University of Colorado in Aurora. Dr. Eckel added that he “also supports” an LDL-cholesterol of less than 40 mg/dL in very-high-risk patients with a history of multiple events or with multiple residual risk factors, and he said he has applied this lower LDL-cholesterol goal in his practice for selected patients. But Dr. Eckel acknowledged in an interview that the evidence for it was less clear-cut than was the evidence behind a goal of less than 55 mg/dL. He also supported the concept of including a treatment goal in U.S. lipid recommendations, which in recent versions has been missing. “I fall back on a cholesterol goal for practical purposes” of making the success of cholesterol-lowering treatment easier to track.
The new ESC goal was characterized as “arbitrary” by Neil J. Stone, MD, vice-chair of the panel that wrote the 2018 AHA/ACC guideline, which relied on treating secondary-prevention patients at high risk to an LDL-cholesterol at least 50% less than before treatment, and recommended continued intensification for patients whose LDL-cholesterol level remained at or above 70 mg/dL.
“If the patient is at 58 mg/dL I’m not sure anyone can tell me what the difference is,” compared with reaching less than 55 mg/dL, Dr. Stone said in an interview. “I worry about focusing on a number and not on the concept that people at the very highest risk deserve the most intensive treatment; the Europeans agree, but they have a different way of looking at it. Despite this difference in approach, the new ESC guidelines and the 2018 U.S. guideline “are more similar than different,” stressed Dr. Stone, professor of medicine and preventive medicine at Northwestern University, Chicago.
However, other experts see an important difference in the risk faced by patients who reach the ESC’s recommended treatment goals and those who fall just short.
“It’s hard to lower an LDL-cholesterol that is already relatively low. People who are close to their cholesterol target need the most intensified treatment” to reach their goal, said Rory Collins, F.Med.Sci., professor of epidemiology at Oxford University. He was not on the ESC guidelines panel.
“It’s a mind shift that clinicians need to be most aggressive in treating patients with the highest risk” even when their LDL-cholesterol is low but not yet at the target level, Dr. Collins said during a discussion session at the congress.
The new ESC guidelines is about “both getting the LDL-cholesterol down to a certain level and also about achieving a big [at least 50%] change” from baseline. “I think the ESC guidelines make that crystal clear,” said Marc S. Sabatine, MD, professor of medicine at Harvard Medical School, Boston, and the sole American to participate in the ESC guidelines-writing panel.
The ESC also broke new ground by advocating an aggressive path toward achieving these LDL-cholesterol goals by elevating the newest and most potent class of approved LDL-cholesterol-lowering drugs, the PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors, to a top-tier, class I recommendation (“is recommended”) for secondary prevention in very-high-risk patients not reaching their goal LDL-cholesterol level on a maximally tolerated statin plus ezetimibe. This recommendation to unequivocally add a PCSK9 inhibitor for this patient population contrasts with the 2018 AHA/ACC guideline that deemed adding a PCSK9 inhibitor a IIa recommendation (“is reasonable”).
A similar uptick in treatment aggressiveness appeared in the ESC’s recommendations for managing very-high-risk patients in a primary prevention setting, including those without familial hypercholesterolemia. For these people, the ESC panel, which worked in concert with the European Atherosclerosis Society, pegged adding a PCSK9 inhibitor as a IIb (“may be considered”) recommendation when these very-high-risk people fail to reach their LDL-cholesterol target on a maximally tolerated statin and ezetimibe. Once again, this opening to use a PCSK9 inhibitor contrasted with the 2018 U.S. guideline, which never mentioned an option of adding a PCSK9 inhibitor for primary prevention except when someone also has familial hypercholesterolemia and starts treatment with an LDL level of at least 190 mg/dL (a IIb recommendation). The new European guidelines proposed using a PCSK9 inhibitor as a second-line option to consider when needed for people whose very high risk derives primarily from older age and other factors such as smoking or hypertension that give them at least a 10% 10-year risk for cardiovascular death as estimated with the European-oriented SCORE risk calculator tables.
Updated SCORE risk designations appear in the new ESC dyslipidemia guidelines, and they show, for example, that in lower-risk European countries (mostly Western European nations) virtually all men who are at least 70 years old would fall into the very-high-risk category that makes them potential candidates for treatment with a PCSK9 inhibitor regardless of any other risk they may or may not have. In higher-risk (mostly Eastern European) countries this designation kicks in for most men once they reach the age of 65.
Several Congress attendees who came to a discussion session on the guidelines voiced concerns that the new revision will lead to substantially increased use of the these drugs and hence will significantly boost medical costs, because these drugs today are priced at about $6,000 annually to treat one patient. In response, members of the guideline-writing panel defended their decision as unavoidable given what’s been reported on the clinical impact of PCSK9 inhibitors when lowering LDL cholesterol and cutting atherosclerotic cardiovascular disease events.
“I commend the [ESC] guideline for focusing on the science and on what is best for patients. The U.S. guidelines conflated the science and the cost, and the recommendations got watered down by cost considerations,” said Dr. Sabatine, who has led several studies of PCSK9 inhibitors.
Dr. Baigent added that the panel “deliberated long and hard on cost, but we felt that we had to focus on the evidence. The cost will shift” in the future, he predicted.
Other U.S. physicians highlighted the need to take drug cost into account when writing public health policy documents such as lipid-management guidelines and questioned whether this more liberal use of PCSK9 inhibitors was justified.
“I think that in the absence of familial hypercholesterolemia you need to waffle around the edges to justify a PCSK9 inhibitor,” said Dr. Eckel. “The cost of PCSK9 inhibitors has come down, but at $6,000 per year you can’t ignore their cost.”
“In the U.S. we need to be mindful of the cost of treatment,” said Dr. Stone. “The ESC guidelines are probably more aggressive” than the 2018 U.S. guideline. “They use PCSK9 inhibitors perhaps more than we do; we [in the United States] prefer generic ezetimibe. A lot has to do with the definitions of risk. The European guidelines have a lot of risk definitions that differ” from the U.S. guideline, he said.
Members of the ESC guidelines panel acknowledged that the SCORE risk-assessment charts could overestimate risk in older people who need primary prevention treatment, as well as underestimate the risk in younger adults.
This inherent age bias in the SCORE risk tables make it “extremely important to contextualize” a person’s risk “by considering other risk factors,” advised Brian A. Ference, MD, an interventional cardiologist and professor at Cambridge (England) University who was a member of the ESC guidelines writing group.
The new ESC guidelines say that risk categorization “must be interpreted in light of the clinician’s knowledge and experience, and of the patient’s pretest likelihood” of cardiovascular disease.”
Dr. Baigent has received research funding from Boehringer Ingelheim, Novartis, and Pfizer. Dr. Eckel has been an expert witness on behalf of Sanofi/Regeneron. Dr. Sabatine and Dr. Ference have received honoraria and research funding from several companies including those that market lipid-lowering drugs. Dr. Stone and Dr. Collins had no disclosures.
*Correction, 9/20/19: A previous version of this article incorrectly stated that the ESC guidelines were the first by a medical society to recommend the lower cholesterol goals. The American Association of Clinical Endocrinologists included targets below 55 mg/dL in their 2017 dyslipidemia management guidelines.
SOURCE: Mach F et al. Eur Heart J. 2019 Aug 31. doi: 10.1093/eurheartj/ehz455.
PARIS – The 2019 dyslipidemia management guidelines from the European Society of Cardiology set an LDL cholesterol target for very-high-risk people of less than 55 mg/dL (as well as at least a 50% cut from baseline), a class I recommendation. This marks the first time a cardiology society has either recommended a target goal for this measure below 70 mg/dL or endorsed treating patients to still-lower cholesterol once their level was already under 70 mg/dL.*
The guidelines went further by suggesting consideration of an even lower treatment target for LDL-cholesterol in very-high-risk, secondary prevention patients who have already had at least two atherosclerotic cardiovascular disease events during the past 2 years, a setting that could justify an LDL-cholesterol goal of less than 40 mg/dL (along with a cut from baseline of at least 50%), a class IIb recommendation that denotes a “may be considered,” endorsement.
“In all the trials, lower was better. There was no lower level of LDL cholesterol that’s been studied that was not better” for patient outcomes, Colin Baigent, BMBCH, said while presenting the new guideline at the annual congress of the European Society of Cardiology (ESC). “It’s very clear” that the full treatment benefit from lowering LDL-cholesterol extends to getting very-high risk patients below these levels, said Dr. Baigent, professor of cardiology at Oxford (England) University and one of three chairs of the ESC’s dyslipidemia guideline-writing panel.
While this change was seen as a notably aggressive goal and too fixed on a specific number by at least one author of the 2018 American Heart Association/American College of Cardiology cholesterol management guideline (J Am Coll Cardiol. 2019 Jun;73[24]:e285-e350), it was embraced by another U.S. expert not involved in writing the most recent U.S. recommendations.
“A goal for LDL-cholesterol of less than 55 mg/dL is reasonable; it’s well documented” by trial evidence “and I support it,” said Robert H. Eckel, MD, an endocrinologist and professor of medicine at the University of Colorado in Aurora. Dr. Eckel added that he “also supports” an LDL-cholesterol of less than 40 mg/dL in very-high-risk patients with a history of multiple events or with multiple residual risk factors, and he said he has applied this lower LDL-cholesterol goal in his practice for selected patients. But Dr. Eckel acknowledged in an interview that the evidence for it was less clear-cut than was the evidence behind a goal of less than 55 mg/dL. He also supported the concept of including a treatment goal in U.S. lipid recommendations, which in recent versions has been missing. “I fall back on a cholesterol goal for practical purposes” of making the success of cholesterol-lowering treatment easier to track.
The new ESC goal was characterized as “arbitrary” by Neil J. Stone, MD, vice-chair of the panel that wrote the 2018 AHA/ACC guideline, which relied on treating secondary-prevention patients at high risk to an LDL-cholesterol at least 50% less than before treatment, and recommended continued intensification for patients whose LDL-cholesterol level remained at or above 70 mg/dL.
“If the patient is at 58 mg/dL I’m not sure anyone can tell me what the difference is,” compared with reaching less than 55 mg/dL, Dr. Stone said in an interview. “I worry about focusing on a number and not on the concept that people at the very highest risk deserve the most intensive treatment; the Europeans agree, but they have a different way of looking at it. Despite this difference in approach, the new ESC guidelines and the 2018 U.S. guideline “are more similar than different,” stressed Dr. Stone, professor of medicine and preventive medicine at Northwestern University, Chicago.
However, other experts see an important difference in the risk faced by patients who reach the ESC’s recommended treatment goals and those who fall just short.
“It’s hard to lower an LDL-cholesterol that is already relatively low. People who are close to their cholesterol target need the most intensified treatment” to reach their goal, said Rory Collins, F.Med.Sci., professor of epidemiology at Oxford University. He was not on the ESC guidelines panel.
“It’s a mind shift that clinicians need to be most aggressive in treating patients with the highest risk” even when their LDL-cholesterol is low but not yet at the target level, Dr. Collins said during a discussion session at the congress.
The new ESC guidelines is about “both getting the LDL-cholesterol down to a certain level and also about achieving a big [at least 50%] change” from baseline. “I think the ESC guidelines make that crystal clear,” said Marc S. Sabatine, MD, professor of medicine at Harvard Medical School, Boston, and the sole American to participate in the ESC guidelines-writing panel.
The ESC also broke new ground by advocating an aggressive path toward achieving these LDL-cholesterol goals by elevating the newest and most potent class of approved LDL-cholesterol-lowering drugs, the PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors, to a top-tier, class I recommendation (“is recommended”) for secondary prevention in very-high-risk patients not reaching their goal LDL-cholesterol level on a maximally tolerated statin plus ezetimibe. This recommendation to unequivocally add a PCSK9 inhibitor for this patient population contrasts with the 2018 AHA/ACC guideline that deemed adding a PCSK9 inhibitor a IIa recommendation (“is reasonable”).
A similar uptick in treatment aggressiveness appeared in the ESC’s recommendations for managing very-high-risk patients in a primary prevention setting, including those without familial hypercholesterolemia. For these people, the ESC panel, which worked in concert with the European Atherosclerosis Society, pegged adding a PCSK9 inhibitor as a IIb (“may be considered”) recommendation when these very-high-risk people fail to reach their LDL-cholesterol target on a maximally tolerated statin and ezetimibe. Once again, this opening to use a PCSK9 inhibitor contrasted with the 2018 U.S. guideline, which never mentioned an option of adding a PCSK9 inhibitor for primary prevention except when someone also has familial hypercholesterolemia and starts treatment with an LDL level of at least 190 mg/dL (a IIb recommendation). The new European guidelines proposed using a PCSK9 inhibitor as a second-line option to consider when needed for people whose very high risk derives primarily from older age and other factors such as smoking or hypertension that give them at least a 10% 10-year risk for cardiovascular death as estimated with the European-oriented SCORE risk calculator tables.
Updated SCORE risk designations appear in the new ESC dyslipidemia guidelines, and they show, for example, that in lower-risk European countries (mostly Western European nations) virtually all men who are at least 70 years old would fall into the very-high-risk category that makes them potential candidates for treatment with a PCSK9 inhibitor regardless of any other risk they may or may not have. In higher-risk (mostly Eastern European) countries this designation kicks in for most men once they reach the age of 65.
Several Congress attendees who came to a discussion session on the guidelines voiced concerns that the new revision will lead to substantially increased use of the these drugs and hence will significantly boost medical costs, because these drugs today are priced at about $6,000 annually to treat one patient. In response, members of the guideline-writing panel defended their decision as unavoidable given what’s been reported on the clinical impact of PCSK9 inhibitors when lowering LDL cholesterol and cutting atherosclerotic cardiovascular disease events.
“I commend the [ESC] guideline for focusing on the science and on what is best for patients. The U.S. guidelines conflated the science and the cost, and the recommendations got watered down by cost considerations,” said Dr. Sabatine, who has led several studies of PCSK9 inhibitors.
Dr. Baigent added that the panel “deliberated long and hard on cost, but we felt that we had to focus on the evidence. The cost will shift” in the future, he predicted.
Other U.S. physicians highlighted the need to take drug cost into account when writing public health policy documents such as lipid-management guidelines and questioned whether this more liberal use of PCSK9 inhibitors was justified.
“I think that in the absence of familial hypercholesterolemia you need to waffle around the edges to justify a PCSK9 inhibitor,” said Dr. Eckel. “The cost of PCSK9 inhibitors has come down, but at $6,000 per year you can’t ignore their cost.”
“In the U.S. we need to be mindful of the cost of treatment,” said Dr. Stone. “The ESC guidelines are probably more aggressive” than the 2018 U.S. guideline. “They use PCSK9 inhibitors perhaps more than we do; we [in the United States] prefer generic ezetimibe. A lot has to do with the definitions of risk. The European guidelines have a lot of risk definitions that differ” from the U.S. guideline, he said.
Members of the ESC guidelines panel acknowledged that the SCORE risk-assessment charts could overestimate risk in older people who need primary prevention treatment, as well as underestimate the risk in younger adults.
This inherent age bias in the SCORE risk tables make it “extremely important to contextualize” a person’s risk “by considering other risk factors,” advised Brian A. Ference, MD, an interventional cardiologist and professor at Cambridge (England) University who was a member of the ESC guidelines writing group.
The new ESC guidelines say that risk categorization “must be interpreted in light of the clinician’s knowledge and experience, and of the patient’s pretest likelihood” of cardiovascular disease.”
Dr. Baigent has received research funding from Boehringer Ingelheim, Novartis, and Pfizer. Dr. Eckel has been an expert witness on behalf of Sanofi/Regeneron. Dr. Sabatine and Dr. Ference have received honoraria and research funding from several companies including those that market lipid-lowering drugs. Dr. Stone and Dr. Collins had no disclosures.
*Correction, 9/20/19: A previous version of this article incorrectly stated that the ESC guidelines were the first by a medical society to recommend the lower cholesterol goals. The American Association of Clinical Endocrinologists included targets below 55 mg/dL in their 2017 dyslipidemia management guidelines.
SOURCE: Mach F et al. Eur Heart J. 2019 Aug 31. doi: 10.1093/eurheartj/ehz455.
REPORTING FROM THE ESC CONGRESS 2019
Statins may do double duty as antidepressants
COPENHAGEN – The tantalizing prospect that statins could be repurposed as adjunctive antidepressant drugs in a defined subgroup of patients with major depression is finally about to undergo rigorous testing.

Several lines of preliminary evidence, including large observational cohort studies as well as three small, short-duration randomized trials, suggest that this might indeed be the case. It’s an extremely attractive possibility, since patients and physicians wish that antidepressant therapy were more effective, statins are among the most widely prescribed drugs worldwide, and their safety profile is thoroughly established. The expectation is that a definitive answer as to whether repurposing of statins as antidepressants is worthwhile will be provided by the SIMCODE trial, recently approved for funding by the German Federal Ministry of Education and Research, Christian Otte, MD, announced at the annual congress of the European College of Neuropsychopharmacology.
SIMCODE is a multicenter, double-blind, placebo-controlled randomized trial to be conducted at eight German academic medical centers. Participants, all of whom must have major depressive disorder and comorbid obesity, will be randomized to simvastatin or placebo on top of standard antidepressant therapy with escitalopram, an SSRI which, like simvastatin, is available as a relatively inexpensive generic, explained Dr. Otte, professor and vice director of the department of psychiatry and psychotherapy at Charite University in Berlin.
For Dr. Otte, SIMCODE will close a circle he helped open with his 2012 report from the Heart and Soul Study, a prospective longitudinal study of nearly 1,000 San Francisco Bay Area patients with coronary heart disease who were assessed annually for depressive symptoms for 6 years. The 65% of patients who were on statin therapy, albeit in nonrandomized fashion, had an adjusted 38% lower risk of developing depression (J Clin Psychiatry. 2012 May;73[5]:610-5).
His was one of seven observational studies involving more than 9,000 patients included in a subsequent meta-analysis showing that statin users were 37% less likely to develop depression than were nonusers (J Affect Disord. 2014 May;160:62-7).
All agreed that the verdict isn’t in yet as to statins’ effectiveness as adjunctive antidepressants, and that the subgroup of patients with major depression who are most likely to gain added antidepressive effect from a statin are those with what the speakers variously described as comorbid cardiometabolic disease, immunometabolic disease, or simply, as in SIMCODE, obesity. These are patients with a high degree of systemic inflammation, which often makes their depression less responsive to standard antidepressant therapies. The working hypothesis is that the pleiotropic anti-inflammatory effects of statins will result in a greater response to conventional antidepressants.
Animal studies point to multiple potential mechanisms by which statins might have antidepressant efficacy in clinical practice, according to Dr. Otte. Beyond their anti-inflammatory effects, these include the drugs’ documented effects on glutamatergic N-methyl-D-aspartate (NMDA) receptors, dopamine receptors, brain-derived neurotrophic factor, glucocorticoid receptors, and hippocampal serotonin 2A receptors.
Ole Kohler, MD, a psychiatrist at Aarhus (Denmark) University, presented highlights of his eye-popping population-based study of more than 872,000 Danes on an SSRI in 1997-2012, more than 113,000 of whom were on a concomitant statin. The key finding: During roughly 3 years of follow-up, the risk of contact with a psychiatric hospital for depression was 36% lower in the group on concomitant SSRI/statin therapy than in those not on a statin (Am J Psychiatry. 2016 Aug 1;173[8]:807-15).

He was quick to observe that a study such as this is vulnerable to various forms of confounding. This risk can be mitigated to a considerable extent by careful propensity score matching. Of note, however, none of the three studies that have been conducted with propensity score matching, including his own recent study of nearly 194,000 statin users and an equal number of matched nonusers, showed a difference in risk of depression between statin users and nonusers. All three studies were performed in general populations without known depression, leading Dr. Kohler to conclude that it’s unlikely that statins have a role in preventing depression in nondepressed individuals.
The focus should instead be on the possible role of statins in reducing the risk of depression in patients with cardiometabolic disease – that is, heart disease, metabolic syndrome, or type 2 diabetes – where more than a half-dozen cohort studies, including the Heart and Soul Study, have found that statins have a favorable impact, he added.
Estela Salagre, MD, a psychiatrist at the University of Barcelona, has carried out a meta-analysis of the three randomized, double-blind, placebo-controlled trials of add-on statin therapy in patients on standard therapies for moderate to severe depression published to date. She found that statin therapy was associated with a 27% greater reduction in scores on the Hamilton Depression Rating Scale, compared with placebo (J Affect Disord. 2016 Aug;200:235-42). Those findings recently were confirmed in a separate meta-analysis by other investigators using different methodologies (J Affect Disord. 2019 Oct 1;257:55-63).

Femke Lamers, PhD, presented evidence based on the nearly 3,000-subject longitudinal Netherlands Study of Depression and Anxiety that roughly one-quarter of individuals with major depressive disorder have a distinct subtype of nonmelancholic depression characterized by a clustering of obesity, inflammation, increased appetite, fatigue, hypersomnia, and increased levels of insulin and leptin. She calls it immunometabolic depression. She and her coinvestigators in the international Psychiatric Genomics Consortium have demonstrated that this phenotypic clustering is associated with a shared genetic vulnerability between major depression and obesity (JAMA Psychiatry. 2017 Dec 1;74[12]:1214-25).

“Major depressive disorder is not a one-size-fits-all disorder. There is an immunometabolic form of depression,” declared Dr. Lamers, an epidemiologist at the University of Amsterdam.
All speakers reported having no financial conflicts of interest.
COPENHAGEN – The tantalizing prospect that statins could be repurposed as adjunctive antidepressant drugs in a defined subgroup of patients with major depression is finally about to undergo rigorous testing.
Several lines of preliminary evidence, including large observational cohort studies as well as three small, short-duration randomized trials, suggest that this might indeed be the case. It’s an extremely attractive possibility, since patients and physicians wish that antidepressant therapy were more effective, statins are among the most widely prescribed drugs worldwide, and their safety profile is thoroughly established. The expectation is that a definitive answer as to whether repurposing of statins as antidepressants is worthwhile will be provided by the SIMCODE trial, recently approved for funding by the German Federal Ministry of Education and Research, Christian Otte, MD, announced at the annual congress of the European College of Neuropsychopharmacology.
SIMCODE is a multicenter, double-blind, placebo-controlled randomized trial to be conducted at eight German academic medical centers. Participants, all of whom must have major depressive disorder and comorbid obesity, will be randomized to simvastatin or placebo on top of standard antidepressant therapy with escitalopram, an SSRI which, like simvastatin, is available as a relatively inexpensive generic, explained Dr. Otte, professor and vice director of the department of psychiatry and psychotherapy at Charite University in Berlin.
For Dr. Otte, SIMCODE will close a circle he helped open with his 2012 report from the Heart and Soul Study, a prospective longitudinal study of nearly 1,000 San Francisco Bay Area patients with coronary heart disease who were assessed annually for depressive symptoms for 6 years. The 65% of patients who were on statin therapy, albeit in nonrandomized fashion, had an adjusted 38% lower risk of developing depression (J Clin Psychiatry. 2012 May;73[5]:610-5).
His was one of seven observational studies involving more than 9,000 patients included in a subsequent meta-analysis showing that statin users were 37% less likely to develop depression than were nonusers (J Affect Disord. 2014 May;160:62-7).
All agreed that the verdict isn’t in yet as to statins’ effectiveness as adjunctive antidepressants, and that the subgroup of patients with major depression who are most likely to gain added antidepressive effect from a statin are those with what the speakers variously described as comorbid cardiometabolic disease, immunometabolic disease, or simply, as in SIMCODE, obesity. These are patients with a high degree of systemic inflammation, which often makes their depression less responsive to standard antidepressant therapies. The working hypothesis is that the pleiotropic anti-inflammatory effects of statins will result in a greater response to conventional antidepressants.
Animal studies point to multiple potential mechanisms by which statins might have antidepressant efficacy in clinical practice, according to Dr. Otte. Beyond their anti-inflammatory effects, these include the drugs’ documented effects on glutamatergic N-methyl-D-aspartate (NMDA) receptors, dopamine receptors, brain-derived neurotrophic factor, glucocorticoid receptors, and hippocampal serotonin 2A receptors.
Ole Kohler, MD, a psychiatrist at Aarhus (Denmark) University, presented highlights of his eye-popping population-based study of more than 872,000 Danes on an SSRI in 1997-2012, more than 113,000 of whom were on a concomitant statin. The key finding: During roughly 3 years of follow-up, the risk of contact with a psychiatric hospital for depression was 36% lower in the group on concomitant SSRI/statin therapy than in those not on a statin (Am J Psychiatry. 2016 Aug 1;173[8]:807-15).
He was quick to observe that a study such as this is vulnerable to various forms of confounding. This risk can be mitigated to a considerable extent by careful propensity score matching. Of note, however, none of the three studies that have been conducted with propensity score matching, including his own recent study of nearly 194,000 statin users and an equal number of matched nonusers, showed a difference in risk of depression between statin users and nonusers. All three studies were performed in general populations without known depression, leading Dr. Kohler to conclude that it’s unlikely that statins have a role in preventing depression in nondepressed individuals.
The focus should instead be on the possible role of statins in reducing the risk of depression in patients with cardiometabolic disease – that is, heart disease, metabolic syndrome, or type 2 diabetes – where more than a half-dozen cohort studies, including the Heart and Soul Study, have found that statins have a favorable impact, he added.
Estela Salagre, MD, a psychiatrist at the University of Barcelona, has carried out a meta-analysis of the three randomized, double-blind, placebo-controlled trials of add-on statin therapy in patients on standard therapies for moderate to severe depression published to date. She found that statin therapy was associated with a 27% greater reduction in scores on the Hamilton Depression Rating Scale, compared with placebo (J Affect Disord. 2016 Aug;200:235-42). Those findings recently were confirmed in a separate meta-analysis by other investigators using different methodologies (J Affect Disord. 2019 Oct 1;257:55-63).
Femke Lamers, PhD, presented evidence based on the nearly 3,000-subject longitudinal Netherlands Study of Depression and Anxiety that roughly one-quarter of individuals with major depressive disorder have a distinct subtype of nonmelancholic depression characterized by a clustering of obesity, inflammation, increased appetite, fatigue, hypersomnia, and increased levels of insulin and leptin. She calls it immunometabolic depression. She and her coinvestigators in the international Psychiatric Genomics Consortium have demonstrated that this phenotypic clustering is associated with a shared genetic vulnerability between major depression and obesity (JAMA Psychiatry. 2017 Dec 1;74[12]:1214-25).
“Major depressive disorder is not a one-size-fits-all disorder. There is an immunometabolic form of depression,” declared Dr. Lamers, an epidemiologist at the University of Amsterdam.
All speakers reported having no financial conflicts of interest.
COPENHAGEN – The tantalizing prospect that statins could be repurposed as adjunctive antidepressant drugs in a defined subgroup of patients with major depression is finally about to undergo rigorous testing.
Several lines of preliminary evidence, including large observational cohort studies as well as three small, short-duration randomized trials, suggest that this might indeed be the case. It’s an extremely attractive possibility, since patients and physicians wish that antidepressant therapy were more effective, statins are among the most widely prescribed drugs worldwide, and their safety profile is thoroughly established. The expectation is that a definitive answer as to whether repurposing of statins as antidepressants is worthwhile will be provided by the SIMCODE trial, recently approved for funding by the German Federal Ministry of Education and Research, Christian Otte, MD, announced at the annual congress of the European College of Neuropsychopharmacology.
SIMCODE is a multicenter, double-blind, placebo-controlled randomized trial to be conducted at eight German academic medical centers. Participants, all of whom must have major depressive disorder and comorbid obesity, will be randomized to simvastatin or placebo on top of standard antidepressant therapy with escitalopram, an SSRI which, like simvastatin, is available as a relatively inexpensive generic, explained Dr. Otte, professor and vice director of the department of psychiatry and psychotherapy at Charite University in Berlin.
For Dr. Otte, SIMCODE will close a circle he helped open with his 2012 report from the Heart and Soul Study, a prospective longitudinal study of nearly 1,000 San Francisco Bay Area patients with coronary heart disease who were assessed annually for depressive symptoms for 6 years. The 65% of patients who were on statin therapy, albeit in nonrandomized fashion, had an adjusted 38% lower risk of developing depression (J Clin Psychiatry. 2012 May;73[5]:610-5).
His was one of seven observational studies involving more than 9,000 patients included in a subsequent meta-analysis showing that statin users were 37% less likely to develop depression than were nonusers (J Affect Disord. 2014 May;160:62-7).
All agreed that the verdict isn’t in yet as to statins’ effectiveness as adjunctive antidepressants, and that the subgroup of patients with major depression who are most likely to gain added antidepressive effect from a statin are those with what the speakers variously described as comorbid cardiometabolic disease, immunometabolic disease, or simply, as in SIMCODE, obesity. These are patients with a high degree of systemic inflammation, which often makes their depression less responsive to standard antidepressant therapies. The working hypothesis is that the pleiotropic anti-inflammatory effects of statins will result in a greater response to conventional antidepressants.
Animal studies point to multiple potential mechanisms by which statins might have antidepressant efficacy in clinical practice, according to Dr. Otte. Beyond their anti-inflammatory effects, these include the drugs’ documented effects on glutamatergic N-methyl-D-aspartate (NMDA) receptors, dopamine receptors, brain-derived neurotrophic factor, glucocorticoid receptors, and hippocampal serotonin 2A receptors.
Ole Kohler, MD, a psychiatrist at Aarhus (Denmark) University, presented highlights of his eye-popping population-based study of more than 872,000 Danes on an SSRI in 1997-2012, more than 113,000 of whom were on a concomitant statin. The key finding: During roughly 3 years of follow-up, the risk of contact with a psychiatric hospital for depression was 36% lower in the group on concomitant SSRI/statin therapy than in those not on a statin (Am J Psychiatry. 2016 Aug 1;173[8]:807-15).
He was quick to observe that a study such as this is vulnerable to various forms of confounding. This risk can be mitigated to a considerable extent by careful propensity score matching. Of note, however, none of the three studies that have been conducted with propensity score matching, including his own recent study of nearly 194,000 statin users and an equal number of matched nonusers, showed a difference in risk of depression between statin users and nonusers. All three studies were performed in general populations without known depression, leading Dr. Kohler to conclude that it’s unlikely that statins have a role in preventing depression in nondepressed individuals.
The focus should instead be on the possible role of statins in reducing the risk of depression in patients with cardiometabolic disease – that is, heart disease, metabolic syndrome, or type 2 diabetes – where more than a half-dozen cohort studies, including the Heart and Soul Study, have found that statins have a favorable impact, he added.
Estela Salagre, MD, a psychiatrist at the University of Barcelona, has carried out a meta-analysis of the three randomized, double-blind, placebo-controlled trials of add-on statin therapy in patients on standard therapies for moderate to severe depression published to date. She found that statin therapy was associated with a 27% greater reduction in scores on the Hamilton Depression Rating Scale, compared with placebo (J Affect Disord. 2016 Aug;200:235-42). Those findings recently were confirmed in a separate meta-analysis by other investigators using different methodologies (J Affect Disord. 2019 Oct 1;257:55-63).
Femke Lamers, PhD, presented evidence based on the nearly 3,000-subject longitudinal Netherlands Study of Depression and Anxiety that roughly one-quarter of individuals with major depressive disorder have a distinct subtype of nonmelancholic depression characterized by a clustering of obesity, inflammation, increased appetite, fatigue, hypersomnia, and increased levels of insulin and leptin. She calls it immunometabolic depression. She and her coinvestigators in the international Psychiatric Genomics Consortium have demonstrated that this phenotypic clustering is associated with a shared genetic vulnerability between major depression and obesity (JAMA Psychiatry. 2017 Dec 1;74[12]:1214-25).
“Major depressive disorder is not a one-size-fits-all disorder. There is an immunometabolic form of depression,” declared Dr. Lamers, an epidemiologist at the University of Amsterdam.
All speakers reported having no financial conflicts of interest.
REPORTING FROM ECNP 2019
Survival at ‘overweight’ BMI surpasses ‘normal’
PARIS – Middle-aged adults with a body mass index of 25-29 kg/m2 had a significantly better adjusted survival during a median follow-up of nearly 10 years than did people with a “normal” body mass index of 20-24 kg/m2 in a worldwide study of more than 140,000. This finding suggests the current, widely accepted definition of normal body mass index is wrong.*
The new findings suggest that the current definition of a “healthy” body mass index (BMI) “should be re-evaluated,” Darryl P. Leong, MBBS, said at the annual Congress of the European Society of Cardiology. The analysis also identified a BMI specifically of 27 kg/m2 as associated with optimal survival among both women and men, “clearly outside the range of 20 to less than 25 kg/m2 that is considered normal,” said Dr. Leong, a cardiologist at McMaster University and the Population Health Research Institute, both in Hamilton, Ont.
Dr. Leong cited three potential explanations for why the new study identified optimal survival with a BMI of 25 to less than 30 kg/m2 among people who were 35-70 years old when they entered the study and were followed for a median of 9.5 years: The current study collected data and adjusted the results using a wider range of potential confounders than in prior studies, the data reflect the impact of contemporary interventions to reduce cardiovascular disease illness and death while past studies relied on data from earlier times when less cardiovascular disease protection occurred, and the current study included people from lower-income countries, although the finding is just as applicable to people who live in high-income countries, who were also included in the study population, noted Salim Yusuf, MBBS, principal investigator for the study.
A BMI of 20-24 kg/m2 “is actually low and harmful,” noted Dr. Yusuf in an interview. Despite recent data consistently showing better survival among people with a BMI of 25-29 kg/m2, panels that have recently written weight guidelines are “ossified” and “refuse to accept” the implications of these findings, said Dr. Yusuf, professor of medicine at McMaster and executive director of the Population Health Research Institute.
The results of the analyses that Dr. Leong reported also showed that BMI paled as a prognosticator for survival when compared with two other assessments of weight: waist/hip ratio, and even more powerful prognostically, a novel measure developed for this analysis that calculates the ratio of hand-grip strength/body weight. Waist/hip ratio adds the dimension of the location of body fat rather than just the amount, and the ratio of grip strength/body weight assesses the contribution of muscle mass to overall weight, noted Dr. Leong. He reported an optimal waist/hip ratio for survival of 0.83 in women and 0.93 in men, and an optimal strength/weight ratio of 0.42 in women and 0.50 in men. This means that a man whose hand-grip strength (measured in kg) is half of the person’s body weight has the best prospect for survival.
The study used data collected in PURE (Prospective Urban Rural Epidemiology Study) on 142,410 people aged 35-70 years from any one of four high-income countries, 12 middle-income countries, and five low-income countries. The study excluded people who had at baseline known coronary artery disease, stroke, heart failure, or cancer, and the adjusted analysis controlled for age, sex, region, education, activity, alcohol and tobacco use, and the baseline prevalence of hypertension and diabetes. During follow-up, 9,712 of these people died.
The researchers saw a nadir for mortality among people with a BMI of 25-29 kg/m2 for both cardiovascular and noncardiovascular deaths. In addition, the link between total mortality and BMI was strongest in the subgroup of people on one or more treatments aimed at preventing cardiovascular disease, while it essentially disappeared among people not receiving any cardiovascular disease preventive measures, highlighting that the relationship now identified depends on a context of overall cardiovascular disease risk reduction, Dr. Leong said. The results also showed a very clear, direct, linear relationship between higher BMI and both the incidence of diabetes and cardiovascular disease, as well as increased all-cause and noncardiovascular mortality among people with a BMI of less than 20 kg/m2.
Dr. Yusuf discussed the results of the analysis in a video interview.
The PURE study has received partial funding from unrestricted grants from several drug companies. Dr. Leong has been an advisor to Ferring Pharmaceuticals and has been a speaker on behalf of Janssen. Dr. Yusuf had no disclosures.
This story was updated 9/19/2019.
PARIS – Middle-aged adults with a body mass index of 25-29 kg/m2 had a significantly better adjusted survival during a median follow-up of nearly 10 years than did people with a “normal” body mass index of 20-24 kg/m2 in a worldwide study of more than 140,000. This finding suggests the current, widely accepted definition of normal body mass index is wrong.*
The new findings suggest that the current definition of a “healthy” body mass index (BMI) “should be re-evaluated,” Darryl P. Leong, MBBS, said at the annual Congress of the European Society of Cardiology. The analysis also identified a BMI specifically of 27 kg/m2 as associated with optimal survival among both women and men, “clearly outside the range of 20 to less than 25 kg/m2 that is considered normal,” said Dr. Leong, a cardiologist at McMaster University and the Population Health Research Institute, both in Hamilton, Ont.
Dr. Leong cited three potential explanations for why the new study identified optimal survival with a BMI of 25 to less than 30 kg/m2 among people who were 35-70 years old when they entered the study and were followed for a median of 9.5 years: The current study collected data and adjusted the results using a wider range of potential confounders than in prior studies, the data reflect the impact of contemporary interventions to reduce cardiovascular disease illness and death while past studies relied on data from earlier times when less cardiovascular disease protection occurred, and the current study included people from lower-income countries, although the finding is just as applicable to people who live in high-income countries, who were also included in the study population, noted Salim Yusuf, MBBS, principal investigator for the study.
A BMI of 20-24 kg/m2 “is actually low and harmful,” noted Dr. Yusuf in an interview. Despite recent data consistently showing better survival among people with a BMI of 25-29 kg/m2, panels that have recently written weight guidelines are “ossified” and “refuse to accept” the implications of these findings, said Dr. Yusuf, professor of medicine at McMaster and executive director of the Population Health Research Institute.
The results of the analyses that Dr. Leong reported also showed that BMI paled as a prognosticator for survival when compared with two other assessments of weight: waist/hip ratio, and even more powerful prognostically, a novel measure developed for this analysis that calculates the ratio of hand-grip strength/body weight. Waist/hip ratio adds the dimension of the location of body fat rather than just the amount, and the ratio of grip strength/body weight assesses the contribution of muscle mass to overall weight, noted Dr. Leong. He reported an optimal waist/hip ratio for survival of 0.83 in women and 0.93 in men, and an optimal strength/weight ratio of 0.42 in women and 0.50 in men. This means that a man whose hand-grip strength (measured in kg) is half of the person’s body weight has the best prospect for survival.
The study used data collected in PURE (Prospective Urban Rural Epidemiology Study) on 142,410 people aged 35-70 years from any one of four high-income countries, 12 middle-income countries, and five low-income countries. The study excluded people who had at baseline known coronary artery disease, stroke, heart failure, or cancer, and the adjusted analysis controlled for age, sex, region, education, activity, alcohol and tobacco use, and the baseline prevalence of hypertension and diabetes. During follow-up, 9,712 of these people died.
The researchers saw a nadir for mortality among people with a BMI of 25-29 kg/m2 for both cardiovascular and noncardiovascular deaths. In addition, the link between total mortality and BMI was strongest in the subgroup of people on one or more treatments aimed at preventing cardiovascular disease, while it essentially disappeared among people not receiving any cardiovascular disease preventive measures, highlighting that the relationship now identified depends on a context of overall cardiovascular disease risk reduction, Dr. Leong said. The results also showed a very clear, direct, linear relationship between higher BMI and both the incidence of diabetes and cardiovascular disease, as well as increased all-cause and noncardiovascular mortality among people with a BMI of less than 20 kg/m2.
Dr. Yusuf discussed the results of the analysis in a video interview.
The PURE study has received partial funding from unrestricted grants from several drug companies. Dr. Leong has been an advisor to Ferring Pharmaceuticals and has been a speaker on behalf of Janssen. Dr. Yusuf had no disclosures.
This story was updated 9/19/2019.
PARIS – Middle-aged adults with a body mass index of 25-29 kg/m2 had a significantly better adjusted survival during a median follow-up of nearly 10 years than did people with a “normal” body mass index of 20-24 kg/m2 in a worldwide study of more than 140,000. This finding suggests the current, widely accepted definition of normal body mass index is wrong.*
The new findings suggest that the current definition of a “healthy” body mass index (BMI) “should be re-evaluated,” Darryl P. Leong, MBBS, said at the annual Congress of the European Society of Cardiology. The analysis also identified a BMI specifically of 27 kg/m2 as associated with optimal survival among both women and men, “clearly outside the range of 20 to less than 25 kg/m2 that is considered normal,” said Dr. Leong, a cardiologist at McMaster University and the Population Health Research Institute, both in Hamilton, Ont.
Dr. Leong cited three potential explanations for why the new study identified optimal survival with a BMI of 25 to less than 30 kg/m2 among people who were 35-70 years old when they entered the study and were followed for a median of 9.5 years: The current study collected data and adjusted the results using a wider range of potential confounders than in prior studies, the data reflect the impact of contemporary interventions to reduce cardiovascular disease illness and death while past studies relied on data from earlier times when less cardiovascular disease protection occurred, and the current study included people from lower-income countries, although the finding is just as applicable to people who live in high-income countries, who were also included in the study population, noted Salim Yusuf, MBBS, principal investigator for the study.
A BMI of 20-24 kg/m2 “is actually low and harmful,” noted Dr. Yusuf in an interview. Despite recent data consistently showing better survival among people with a BMI of 25-29 kg/m2, panels that have recently written weight guidelines are “ossified” and “refuse to accept” the implications of these findings, said Dr. Yusuf, professor of medicine at McMaster and executive director of the Population Health Research Institute.
The results of the analyses that Dr. Leong reported also showed that BMI paled as a prognosticator for survival when compared with two other assessments of weight: waist/hip ratio, and even more powerful prognostically, a novel measure developed for this analysis that calculates the ratio of hand-grip strength/body weight. Waist/hip ratio adds the dimension of the location of body fat rather than just the amount, and the ratio of grip strength/body weight assesses the contribution of muscle mass to overall weight, noted Dr. Leong. He reported an optimal waist/hip ratio for survival of 0.83 in women and 0.93 in men, and an optimal strength/weight ratio of 0.42 in women and 0.50 in men. This means that a man whose hand-grip strength (measured in kg) is half of the person’s body weight has the best prospect for survival.
The study used data collected in PURE (Prospective Urban Rural Epidemiology Study) on 142,410 people aged 35-70 years from any one of four high-income countries, 12 middle-income countries, and five low-income countries. The study excluded people who had at baseline known coronary artery disease, stroke, heart failure, or cancer, and the adjusted analysis controlled for age, sex, region, education, activity, alcohol and tobacco use, and the baseline prevalence of hypertension and diabetes. During follow-up, 9,712 of these people died.
The researchers saw a nadir for mortality among people with a BMI of 25-29 kg/m2 for both cardiovascular and noncardiovascular deaths. In addition, the link between total mortality and BMI was strongest in the subgroup of people on one or more treatments aimed at preventing cardiovascular disease, while it essentially disappeared among people not receiving any cardiovascular disease preventive measures, highlighting that the relationship now identified depends on a context of overall cardiovascular disease risk reduction, Dr. Leong said. The results also showed a very clear, direct, linear relationship between higher BMI and both the incidence of diabetes and cardiovascular disease, as well as increased all-cause and noncardiovascular mortality among people with a BMI of less than 20 kg/m2.
Dr. Yusuf discussed the results of the analysis in a video interview.
The PURE study has received partial funding from unrestricted grants from several drug companies. Dr. Leong has been an advisor to Ferring Pharmaceuticals and has been a speaker on behalf of Janssen. Dr. Yusuf had no disclosures.
This story was updated 9/19/2019.
REPORTING FROM THE ESC CONGRESS 2019
siRNA drug safely halved LDL cholesterol in phase 3 ORION-11
PARIS – A small interfering RNA drug, inclisiran, safely halved LDL cholesterol levels in more than 800 patients in a phase 3, multicenter study, in a big step toward this drug coming onto the market and offering an alternative way to harness the potent cholesterol-lowering power of PCSK9 inhibition.

In the reported study – which enrolled patients with established cardiovascular disease, familial hypercholesterolemia, type 2 diabetes, or a high Framingham Risk Score – participants received inclisiran as a semiannual subcutaneous injection. The safe efficacy this produced showed the viability of a new way to deliver lipid-lowering therapy that guarantees compliance and is convenient for patients.
The prospect of lowering cholesterol with about the same potency as the monoclonal antibodies that block PCSK9 (proprotein convertase subtilisin/kexin type 9) activity but administered as a biannual injection “enables provider control over medication adherence, and may offer patients a meaningful new choice that is safe and convenient and has assured results,” Kausik K. Ray, MD, said at the annual congress of the European Society of Cardiology. The durable effect of the small interfering RNA (siRNA) agent “offers a huge advantage,” and “opens the field,” said Dr. Ray, a cardiologist and professor of public health at Imperial College, London.
He also highlighted the “excellent” safety profile seen in the 811 patients treated with inclisiran, compared with 804 patients in the study who received placebo. After four total injections of inclisiran spaced out over 450 days (about 15 months), the rate of treatment-emergent adverse events and serious events was virtually the same in the two treatment arms, and with no signal of inclisiran causing liver effects, renal or muscle injury, damage to blood components, or malignancy. The serial treatment with inclisiran that patients received – at baseline, 90, 270, and 450 days – produced no severe injection-site reactions, and transient mild or moderate injection-site reactions in just under 5% of patients.

Safety issues, such as more-severe injection-site reactions, thrombocytopenia, hepatotoxicity, and flu-like symptoms, plagued siRNA drugs during their earlier days of development, but more recently next-generation siRNA drugs with modified structures have produced much better safety performance, noted Richard C. Becker, MD, professor of medicine and director of the Heart, Lung, & Vascular Institute at the University of Cincinnati. The new-generation siRNAs such as inclisiran are “very well tolerated,” he said in an interview.
The Food and Drug Administration approved the first siRNA drug in August 2018, and in the year since then a few others have also come onto the U.S. market, Dr. Becker said.
Like other siRNA drugs, the activity of inclisiran comes from a short RNA segment that is antisense to a particular messenger RNA (mRNA) target. In the case of inclisiran, the target is the mRNA for the PCSK9 enzyme produced in hepatocytes, and that decreases the number of LDL cholesterol receptors on the cell’s surface. When the antisense RNA molecule encounters a PCSK9 mRNA, the two bind and the mRNA is then degraded by a normal cell process. This cuts the cell’s production of the PCSK9 protein, resulting in more LDL cholesterol receptors on the cell’s surface that pull more LDL cholesterol from the blood. The blocking of PCSK9 activity by inclisiran is roughly equivalent to the action of the PCSK9 monoclonal antibodies that have now been on the U.S. market for a few years. Also like other siRNA drugs, the RNA of inclisiran is packaged so that, once injected into a patient, the RNA molecules travel to the liver and enter hepatocytes, where they exert their activity.

“No one has concerns about inclisiran being able to lower LDL [cholesterol], and there have been no safety signals. The data we have seen so far look very reassuring, and in particular has been very safe for the liver,” commented Marc S. Sabatine, MD, professor of medicine at Harvard Medical School, Boston, who has led several studies involving PCSK9-targeted drugs and is helping to run ORION-4, a 15,000-patient study of inclisiran designed to assess the drug’s effect on clinical events. Results from ORION-4 are not expected until about 2024.
“The PCSK9 inhibitors in general have been a huge advance for patients, and the more kinds of drugs we have to target PCSK9, the better,” he said in an interview.
The study reported by Dr. Ray, ORION-11, enrolled 1,617 patients with high atherosclerotic disease risk at 70 sites in six European countries and South Africa. The study’s primary efficacy endpoint was reduction from baseline in LDL cholesterol both at 510 days (about 17 months) after the first dose and also throughout the 15-month period that started 3 months after the first dose. The average reduction seen after 510 days was 54%, compared with baseline, and the time-averaged reduction during the 15-month window examined was 50%, Dr. Ray said. The results also showed a consistent reduction in LDL cholesterol in virtually every patient treated with inclisiran.
Two other phase 3 studies of inclisiran with similar design have been completed, and the results will come out before the end of 2019, according to a statement from the Medicines Company, which is developing the drug. The statement also said that the company plans to file their data with the FDA for marketing approval for inclisiran before the end of 2019. In the recent past, the FDA has approved drugs for the indication of lowering LDL cholesterol before evidence is available to prove that the agent has benefits for reducing clinical events.
Future studies of inclisiran will explore the efficacy of a single annual injection of the drug as an approach to primary prevention of cardiovascular disease, Dr. Ray said.
ORION-11 was sponsored by the Medicines Company. Dr. Ray is a consultant to it and to several other companies. Dr. Becker had no relevant disclosures. Dr. Sabatine has received research support from the Medicines Company and several other companies, and has received personal fees from Anthos Therapeutics, Bristol-Myers Squibb, CVS Caremark, Daiichi Sankyo, DalCor Pharmaceuticals, Dyrnamix, and Ionis.
PARIS – A small interfering RNA drug, inclisiran, safely halved LDL cholesterol levels in more than 800 patients in a phase 3, multicenter study, in a big step toward this drug coming onto the market and offering an alternative way to harness the potent cholesterol-lowering power of PCSK9 inhibition.
In the reported study – which enrolled patients with established cardiovascular disease, familial hypercholesterolemia, type 2 diabetes, or a high Framingham Risk Score – participants received inclisiran as a semiannual subcutaneous injection. The safe efficacy this produced showed the viability of a new way to deliver lipid-lowering therapy that guarantees compliance and is convenient for patients.
The prospect of lowering cholesterol with about the same potency as the monoclonal antibodies that block PCSK9 (proprotein convertase subtilisin/kexin type 9) activity but administered as a biannual injection “enables provider control over medication adherence, and may offer patients a meaningful new choice that is safe and convenient and has assured results,” Kausik K. Ray, MD, said at the annual congress of the European Society of Cardiology. The durable effect of the small interfering RNA (siRNA) agent “offers a huge advantage,” and “opens the field,” said Dr. Ray, a cardiologist and professor of public health at Imperial College, London.
He also highlighted the “excellent” safety profile seen in the 811 patients treated with inclisiran, compared with 804 patients in the study who received placebo. After four total injections of inclisiran spaced out over 450 days (about 15 months), the rate of treatment-emergent adverse events and serious events was virtually the same in the two treatment arms, and with no signal of inclisiran causing liver effects, renal or muscle injury, damage to blood components, or malignancy. The serial treatment with inclisiran that patients received – at baseline, 90, 270, and 450 days – produced no severe injection-site reactions, and transient mild or moderate injection-site reactions in just under 5% of patients.
Safety issues, such as more-severe injection-site reactions, thrombocytopenia, hepatotoxicity, and flu-like symptoms, plagued siRNA drugs during their earlier days of development, but more recently next-generation siRNA drugs with modified structures have produced much better safety performance, noted Richard C. Becker, MD, professor of medicine and director of the Heart, Lung, & Vascular Institute at the University of Cincinnati. The new-generation siRNAs such as inclisiran are “very well tolerated,” he said in an interview.
The Food and Drug Administration approved the first siRNA drug in August 2018, and in the year since then a few others have also come onto the U.S. market, Dr. Becker said.
Like other siRNA drugs, the activity of inclisiran comes from a short RNA segment that is antisense to a particular messenger RNA (mRNA) target. In the case of inclisiran, the target is the mRNA for the PCSK9 enzyme produced in hepatocytes, and that decreases the number of LDL cholesterol receptors on the cell’s surface. When the antisense RNA molecule encounters a PCSK9 mRNA, the two bind and the mRNA is then degraded by a normal cell process. This cuts the cell’s production of the PCSK9 protein, resulting in more LDL cholesterol receptors on the cell’s surface that pull more LDL cholesterol from the blood. The blocking of PCSK9 activity by inclisiran is roughly equivalent to the action of the PCSK9 monoclonal antibodies that have now been on the U.S. market for a few years. Also like other siRNA drugs, the RNA of inclisiran is packaged so that, once injected into a patient, the RNA molecules travel to the liver and enter hepatocytes, where they exert their activity.
“No one has concerns about inclisiran being able to lower LDL [cholesterol], and there have been no safety signals. The data we have seen so far look very reassuring, and in particular has been very safe for the liver,” commented Marc S. Sabatine, MD, professor of medicine at Harvard Medical School, Boston, who has led several studies involving PCSK9-targeted drugs and is helping to run ORION-4, a 15,000-patient study of inclisiran designed to assess the drug’s effect on clinical events. Results from ORION-4 are not expected until about 2024.
“The PCSK9 inhibitors in general have been a huge advance for patients, and the more kinds of drugs we have to target PCSK9, the better,” he said in an interview.
The study reported by Dr. Ray, ORION-11, enrolled 1,617 patients with high atherosclerotic disease risk at 70 sites in six European countries and South Africa. The study’s primary efficacy endpoint was reduction from baseline in LDL cholesterol both at 510 days (about 17 months) after the first dose and also throughout the 15-month period that started 3 months after the first dose. The average reduction seen after 510 days was 54%, compared with baseline, and the time-averaged reduction during the 15-month window examined was 50%, Dr. Ray said. The results also showed a consistent reduction in LDL cholesterol in virtually every patient treated with inclisiran.
Two other phase 3 studies of inclisiran with similar design have been completed, and the results will come out before the end of 2019, according to a statement from the Medicines Company, which is developing the drug. The statement also said that the company plans to file their data with the FDA for marketing approval for inclisiran before the end of 2019. In the recent past, the FDA has approved drugs for the indication of lowering LDL cholesterol before evidence is available to prove that the agent has benefits for reducing clinical events.
Future studies of inclisiran will explore the efficacy of a single annual injection of the drug as an approach to primary prevention of cardiovascular disease, Dr. Ray said.
ORION-11 was sponsored by the Medicines Company. Dr. Ray is a consultant to it and to several other companies. Dr. Becker had no relevant disclosures. Dr. Sabatine has received research support from the Medicines Company and several other companies, and has received personal fees from Anthos Therapeutics, Bristol-Myers Squibb, CVS Caremark, Daiichi Sankyo, DalCor Pharmaceuticals, Dyrnamix, and Ionis.
PARIS – A small interfering RNA drug, inclisiran, safely halved LDL cholesterol levels in more than 800 patients in a phase 3, multicenter study, in a big step toward this drug coming onto the market and offering an alternative way to harness the potent cholesterol-lowering power of PCSK9 inhibition.
In the reported study – which enrolled patients with established cardiovascular disease, familial hypercholesterolemia, type 2 diabetes, or a high Framingham Risk Score – participants received inclisiran as a semiannual subcutaneous injection. The safe efficacy this produced showed the viability of a new way to deliver lipid-lowering therapy that guarantees compliance and is convenient for patients.
The prospect of lowering cholesterol with about the same potency as the monoclonal antibodies that block PCSK9 (proprotein convertase subtilisin/kexin type 9) activity but administered as a biannual injection “enables provider control over medication adherence, and may offer patients a meaningful new choice that is safe and convenient and has assured results,” Kausik K. Ray, MD, said at the annual congress of the European Society of Cardiology. The durable effect of the small interfering RNA (siRNA) agent “offers a huge advantage,” and “opens the field,” said Dr. Ray, a cardiologist and professor of public health at Imperial College, London.
He also highlighted the “excellent” safety profile seen in the 811 patients treated with inclisiran, compared with 804 patients in the study who received placebo. After four total injections of inclisiran spaced out over 450 days (about 15 months), the rate of treatment-emergent adverse events and serious events was virtually the same in the two treatment arms, and with no signal of inclisiran causing liver effects, renal or muscle injury, damage to blood components, or malignancy. The serial treatment with inclisiran that patients received – at baseline, 90, 270, and 450 days – produced no severe injection-site reactions, and transient mild or moderate injection-site reactions in just under 5% of patients.
Safety issues, such as more-severe injection-site reactions, thrombocytopenia, hepatotoxicity, and flu-like symptoms, plagued siRNA drugs during their earlier days of development, but more recently next-generation siRNA drugs with modified structures have produced much better safety performance, noted Richard C. Becker, MD, professor of medicine and director of the Heart, Lung, & Vascular Institute at the University of Cincinnati. The new-generation siRNAs such as inclisiran are “very well tolerated,” he said in an interview.
The Food and Drug Administration approved the first siRNA drug in August 2018, and in the year since then a few others have also come onto the U.S. market, Dr. Becker said.
Like other siRNA drugs, the activity of inclisiran comes from a short RNA segment that is antisense to a particular messenger RNA (mRNA) target. In the case of inclisiran, the target is the mRNA for the PCSK9 enzyme produced in hepatocytes, and that decreases the number of LDL cholesterol receptors on the cell’s surface. When the antisense RNA molecule encounters a PCSK9 mRNA, the two bind and the mRNA is then degraded by a normal cell process. This cuts the cell’s production of the PCSK9 protein, resulting in more LDL cholesterol receptors on the cell’s surface that pull more LDL cholesterol from the blood. The blocking of PCSK9 activity by inclisiran is roughly equivalent to the action of the PCSK9 monoclonal antibodies that have now been on the U.S. market for a few years. Also like other siRNA drugs, the RNA of inclisiran is packaged so that, once injected into a patient, the RNA molecules travel to the liver and enter hepatocytes, where they exert their activity.
“No one has concerns about inclisiran being able to lower LDL [cholesterol], and there have been no safety signals. The data we have seen so far look very reassuring, and in particular has been very safe for the liver,” commented Marc S. Sabatine, MD, professor of medicine at Harvard Medical School, Boston, who has led several studies involving PCSK9-targeted drugs and is helping to run ORION-4, a 15,000-patient study of inclisiran designed to assess the drug’s effect on clinical events. Results from ORION-4 are not expected until about 2024.
“The PCSK9 inhibitors in general have been a huge advance for patients, and the more kinds of drugs we have to target PCSK9, the better,” he said in an interview.
The study reported by Dr. Ray, ORION-11, enrolled 1,617 patients with high atherosclerotic disease risk at 70 sites in six European countries and South Africa. The study’s primary efficacy endpoint was reduction from baseline in LDL cholesterol both at 510 days (about 17 months) after the first dose and also throughout the 15-month period that started 3 months after the first dose. The average reduction seen after 510 days was 54%, compared with baseline, and the time-averaged reduction during the 15-month window examined was 50%, Dr. Ray said. The results also showed a consistent reduction in LDL cholesterol in virtually every patient treated with inclisiran.
Two other phase 3 studies of inclisiran with similar design have been completed, and the results will come out before the end of 2019, according to a statement from the Medicines Company, which is developing the drug. The statement also said that the company plans to file their data with the FDA for marketing approval for inclisiran before the end of 2019. In the recent past, the FDA has approved drugs for the indication of lowering LDL cholesterol before evidence is available to prove that the agent has benefits for reducing clinical events.
Future studies of inclisiran will explore the efficacy of a single annual injection of the drug as an approach to primary prevention of cardiovascular disease, Dr. Ray said.
ORION-11 was sponsored by the Medicines Company. Dr. Ray is a consultant to it and to several other companies. Dr. Becker had no relevant disclosures. Dr. Sabatine has received research support from the Medicines Company and several other companies, and has received personal fees from Anthos Therapeutics, Bristol-Myers Squibb, CVS Caremark, Daiichi Sankyo, DalCor Pharmaceuticals, Dyrnamix, and Ionis.
REPORTING FROM THE ESC CONGRESS 2019
In PAD, dropping statins ups death risk 43%
PARIS – , according to new research presented at the annual congress of the European Society of Cardiology.
Patients with peripheral manifestations of cardiovascular disease “are a population with an extremely high risk to suffer a heart attack or a stroke,” said Joern Dopheide, MD, during a press conference at the meeting. Despite the known benefits of statins, including the reduction of all-cause and cardiovascular death and the reduction of morbidity, adherence to guideline-directed statin therapy is far from optimal, said Dr. Dopheide of Bern (Switzerland) University Hospital.
Patients with peripheral artery disease (PAD) not taking statins had a mortality rate of 34%, more than three times that of patients adherent to an intensified statin regimen. More surprisingly, patients who had been on a statin and then stopped the medication also had a mortality rate of 33%, indistinguishable from those who had never been treated with a statin.
Although statin adherence is low in general, it’s especially low in patients with PAD, said Dr. Dopheide. Still, he said, “few systematic data exist on the prognostic value of statin adherence and the correlation between adherence and cardiovascular outcome in PAD patients.”
Accordingly, Dr. Dopheide and his coinvestigators sought to determine the association between statin adherence and survival in PAD patients. The researchers obtained baseline and follow-up data for a cohort of 691 symptomatic PAD patients seen at a single site, looking at statin dosage, LDL cholesterol levels, and survival.
The patients were followed for a period of 50 months. Dr. Dopheide said that “Over the time course, we were able to increase the statin adherence from about 73% to about 81%, and parallel to that, we were able to reduce the LDL cholesterol levels from about 97 to 83 mg/dL, and we were able to increase the intensity of patients on statin therapy.”
Dr. Dopheide said that he and his colleagues saw a dose-response effect, so that the biggest drop in cholesterol was seen in patients on high statin doses, on more potent statins, or both.
Intensity was increased in some cases by upping statin dose – the mean statin dose climbed from 50 to 58 mg daily during the study period. An alternative strategy was to switch to a more potent statin such as atorvastatin or rosuvastatin; sometimes both intensity and dose were boosted.
“We were able to see that patients who were always on their statin therapy had a pretty low mortality rate of about 20%,” a figure that was halved for patients on more intensive statin therapy, who had a mortality rate of 10% across the study period, said Dr. Dopheide. “Patients in whom we started a statin therapy still profited from it, and had only a 15% mortality,” he added.
Some of the most surprising – and disturbing – study findings involved those who reduced their statin dose: “When patients discontinued their usual dose and decreased it, they suffered an even higher mortality rate, of nearly 43%. So that was kind of surprising and shocking to us.”
Identifying these high-risk patients and keeping them adherent is a substantial clinical challenge, but an important goal, said Dr. Dopheide. “We know that patients with peripheral arterial disease are a little more underrepresented in daily practice; it’s hard to identify them, especially when they are asymptomatic,” he acknowledged. However, once a PAD patient is identified, “One should at least keep the patient on the statin dosage they have,” or initiate statins if needed.
Further, warned Dr. Dopheide, “One should never discontinue statin or decrease the dosage,” adding that PAD patients should be informed that they are at “very high risk for myocardial infarction or stroke.” These patients “should regard their statin therapy as one of the most important and life-saving medications they can take,” he said.
Dr. Dopheide reported no outside sources of funding and no conflicts of interest.
SOURCE: Dopheide, J., et al. ESC Congress 2019, Abstract P5363.
PARIS – , according to new research presented at the annual congress of the European Society of Cardiology.
Patients with peripheral manifestations of cardiovascular disease “are a population with an extremely high risk to suffer a heart attack or a stroke,” said Joern Dopheide, MD, during a press conference at the meeting. Despite the known benefits of statins, including the reduction of all-cause and cardiovascular death and the reduction of morbidity, adherence to guideline-directed statin therapy is far from optimal, said Dr. Dopheide of Bern (Switzerland) University Hospital.
Patients with peripheral artery disease (PAD) not taking statins had a mortality rate of 34%, more than three times that of patients adherent to an intensified statin regimen. More surprisingly, patients who had been on a statin and then stopped the medication also had a mortality rate of 33%, indistinguishable from those who had never been treated with a statin.
Although statin adherence is low in general, it’s especially low in patients with PAD, said Dr. Dopheide. Still, he said, “few systematic data exist on the prognostic value of statin adherence and the correlation between adherence and cardiovascular outcome in PAD patients.”
Accordingly, Dr. Dopheide and his coinvestigators sought to determine the association between statin adherence and survival in PAD patients. The researchers obtained baseline and follow-up data for a cohort of 691 symptomatic PAD patients seen at a single site, looking at statin dosage, LDL cholesterol levels, and survival.
The patients were followed for a period of 50 months. Dr. Dopheide said that “Over the time course, we were able to increase the statin adherence from about 73% to about 81%, and parallel to that, we were able to reduce the LDL cholesterol levels from about 97 to 83 mg/dL, and we were able to increase the intensity of patients on statin therapy.”
Dr. Dopheide said that he and his colleagues saw a dose-response effect, so that the biggest drop in cholesterol was seen in patients on high statin doses, on more potent statins, or both.
Intensity was increased in some cases by upping statin dose – the mean statin dose climbed from 50 to 58 mg daily during the study period. An alternative strategy was to switch to a more potent statin such as atorvastatin or rosuvastatin; sometimes both intensity and dose were boosted.
“We were able to see that patients who were always on their statin therapy had a pretty low mortality rate of about 20%,” a figure that was halved for patients on more intensive statin therapy, who had a mortality rate of 10% across the study period, said Dr. Dopheide. “Patients in whom we started a statin therapy still profited from it, and had only a 15% mortality,” he added.
Some of the most surprising – and disturbing – study findings involved those who reduced their statin dose: “When patients discontinued their usual dose and decreased it, they suffered an even higher mortality rate, of nearly 43%. So that was kind of surprising and shocking to us.”
Identifying these high-risk patients and keeping them adherent is a substantial clinical challenge, but an important goal, said Dr. Dopheide. “We know that patients with peripheral arterial disease are a little more underrepresented in daily practice; it’s hard to identify them, especially when they are asymptomatic,” he acknowledged. However, once a PAD patient is identified, “One should at least keep the patient on the statin dosage they have,” or initiate statins if needed.
Further, warned Dr. Dopheide, “One should never discontinue statin or decrease the dosage,” adding that PAD patients should be informed that they are at “very high risk for myocardial infarction or stroke.” These patients “should regard their statin therapy as one of the most important and life-saving medications they can take,” he said.
Dr. Dopheide reported no outside sources of funding and no conflicts of interest.
SOURCE: Dopheide, J., et al. ESC Congress 2019, Abstract P5363.
PARIS – , according to new research presented at the annual congress of the European Society of Cardiology.
Patients with peripheral manifestations of cardiovascular disease “are a population with an extremely high risk to suffer a heart attack or a stroke,” said Joern Dopheide, MD, during a press conference at the meeting. Despite the known benefits of statins, including the reduction of all-cause and cardiovascular death and the reduction of morbidity, adherence to guideline-directed statin therapy is far from optimal, said Dr. Dopheide of Bern (Switzerland) University Hospital.
Patients with peripheral artery disease (PAD) not taking statins had a mortality rate of 34%, more than three times that of patients adherent to an intensified statin regimen. More surprisingly, patients who had been on a statin and then stopped the medication also had a mortality rate of 33%, indistinguishable from those who had never been treated with a statin.
Although statin adherence is low in general, it’s especially low in patients with PAD, said Dr. Dopheide. Still, he said, “few systematic data exist on the prognostic value of statin adherence and the correlation between adherence and cardiovascular outcome in PAD patients.”
Accordingly, Dr. Dopheide and his coinvestigators sought to determine the association between statin adherence and survival in PAD patients. The researchers obtained baseline and follow-up data for a cohort of 691 symptomatic PAD patients seen at a single site, looking at statin dosage, LDL cholesterol levels, and survival.
The patients were followed for a period of 50 months. Dr. Dopheide said that “Over the time course, we were able to increase the statin adherence from about 73% to about 81%, and parallel to that, we were able to reduce the LDL cholesterol levels from about 97 to 83 mg/dL, and we were able to increase the intensity of patients on statin therapy.”
Dr. Dopheide said that he and his colleagues saw a dose-response effect, so that the biggest drop in cholesterol was seen in patients on high statin doses, on more potent statins, or both.
Intensity was increased in some cases by upping statin dose – the mean statin dose climbed from 50 to 58 mg daily during the study period. An alternative strategy was to switch to a more potent statin such as atorvastatin or rosuvastatin; sometimes both intensity and dose were boosted.
“We were able to see that patients who were always on their statin therapy had a pretty low mortality rate of about 20%,” a figure that was halved for patients on more intensive statin therapy, who had a mortality rate of 10% across the study period, said Dr. Dopheide. “Patients in whom we started a statin therapy still profited from it, and had only a 15% mortality,” he added.
Some of the most surprising – and disturbing – study findings involved those who reduced their statin dose: “When patients discontinued their usual dose and decreased it, they suffered an even higher mortality rate, of nearly 43%. So that was kind of surprising and shocking to us.”
Identifying these high-risk patients and keeping them adherent is a substantial clinical challenge, but an important goal, said Dr. Dopheide. “We know that patients with peripheral arterial disease are a little more underrepresented in daily practice; it’s hard to identify them, especially when they are asymptomatic,” he acknowledged. However, once a PAD patient is identified, “One should at least keep the patient on the statin dosage they have,” or initiate statins if needed.
Further, warned Dr. Dopheide, “One should never discontinue statin or decrease the dosage,” adding that PAD patients should be informed that they are at “very high risk for myocardial infarction or stroke.” These patients “should regard their statin therapy as one of the most important and life-saving medications they can take,” he said.
Dr. Dopheide reported no outside sources of funding and no conflicts of interest.
SOURCE: Dopheide, J., et al. ESC Congress 2019, Abstract P5363.
AT ESC CONGRESS 2019
PCSK9 inhibition cuts events in very-high-risk groups
Patients at very high risk of adverse cardiovascular outcomes derive substantial benefit from proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition, according to results of two analyses from the ODYSSEY OUTCOMES trial.
In one prespecified analysis, the PCSK9 inhibitor alirocumab was linked to improved cardiovascular outcomes in patients with prior coronary artery bypass grafting (CABG), while in the other, researchers wrote that alirocumab showed a “large absolute benefit” in patients with polyvascular disease, which they defined as the presence of concomitant peripheral artery disease, cerebrovascular disease, or both.
These reports on alirocumab outcomes in patients with prior CABG and polyvascular disease appear in the Journal of the American College of Cardiology.
Prior CABG and polyvascular disease were both associated with markedly elevated risks of major adverse coronary events (MACE) and death, investigators wrote in the reports.
The ODYSSEY OUTCOMES trial included 18,924 patients with recent acute coronary syndrome (ACS) and high atherogenic lipoproteins despite intensive statin treatment. The primary outcome was MACE, comprising a composite of coronary heart disease death, nonfatal MI, ischemic stroke, or unstable angina requiring hospitalization. During a median 2.8 years of follow-up, this outcome occurred in 9.5% of the overall population randomized to alirocumab and 11.1% of those on placebo, for a statistically significant and clinically meaningful 15% relative risk reduction.
Polyvascular disease
In the trial population, 1,405 patients had polyvascular disease in at least two beds, including a coronary artery, plus either peripheral artery or cerebrovascular, while 149 had polyvascular disease in all three beds. The remainder, including 17,370 patients, were classified as having monovascular disease.
The incidences of MACE for placebo-treated patients with monovascular disease, two-bed polyvascular disease, and three-bed polyvascular disease were 10.0%, 22.2%, and 39.7%, respectively. Alirocumab treatment resulted in an absolute risk reduction for MACE of 1.4%, 1.9%, and 13.0%, for those respective groups (P = .0006).
Similarly, the incidence of the secondary endpoint of death for placebo-treated patients was 3.5%, 10.0%, and 21.8%, and the ARR with alirocumab was 0.4%, 1.3%, and 16.2% (P = .002), according to their reported data.
These results suggest that patients with polyvascular disease are an “easily identifiable subgroup” of ACS patients with a high absolute risk of MACE and death, according to the investigators, led by J. Wouter Jukema, MD, PhD, of Leiden (the Netherlands) University Medical Center.
“The large absolute benefit of PCSK9 inhibition with alirocumab, when added to high-intensity statin therapy, is a potential benefit for this group of patients,” Dr. Jukema and coauthors wrote.
Prior CABG
Of the ODYSSEY OUTCOMES patients, 1,025 had an index CABG after ACS, 1,003 had CABG before ACS, and the remaining 16,896 had no such procedure.
Hazard ratios for both MACE and death in all CABG categories were consistent with the overall results of ODYSSEY OUTCOMES, the investigators wrote. Specifically, alirocumab reduced MACE and death in the overall study, with HRs of 0.85 for both endpoints.
The ARRs in MACE with alirocumab were 1.3% for no CABG, 0.9% for index CABG, and 6.4% for prior CABG (P = .0007), while ARRs in death with the treatment were 0.4%, 0.5%, and 3.6% (P = .03) for those categories, respectively. In this analysis, the investigators calculated the number needed to treat to prevent one primary or secondary endpoint over the median 2.8 years of follow-up. The numbers needed to treat were 16 for prior CABG, 111 for index, and 77 for no prior CABG.
“Although the relative benefit of alirocumab versus placebo is consistent regardless of prior CABG status, those with prior CABG achieve substantially greater absolute risk reduction and consequently lower number needed to treat,” wrote the authors of the analysis, led by Shaun G. Goodman, MD, MSc, of St. Michael’s Hospital, Toronto.
Funding for the ODYSSEY OUTCOMES trial and its subanalyses was provided by Sanofi and Regeneron. Authors of the analyses reported disclosures related to Sanofi, Regeneron, Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and others.
SOURCES: Goodman SG et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.015; Jukema JW et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.03.013.
These two secondary analyses of the ODYSSEY OUTCOMES trial are very important studies that reinforce the usefulness of PCSK9 inhibition in extremely high risk populations.
Although each study has limitations as acknowledged, it provides further evidence that should lead us to strongly consider the use of PCSK9 inhibitors in patients with a previous coronary artery bypass grafting (CABG) or a history of polyvascular disease.
The studies confirm that aggressive lipid-lowering therapy will benefit patients in those high-risk subsets. The significant reductions in mortality associated with lowering LDL cholesterol using alirocumab can no longer be ignored.
Economic analyses would be interesting, as the substantial reductions in major adverse cardiovascular events and all-cause deaths attributed to alirocumab would likely impact health care costs and society at large.
However, it is concerning that patients with prior CABG and those with a high atherosclerosis burden in multiple arterial territories were seemingly less well treated than acute coronary syndrome patients.
An LDL cholesterol level of at least 100 mg/dL was seen in upward of 40% of the high-risk participants at randomization, while 87% had high BP, 40% had diabetes, and 16% were current smokers.
A reasonable first step in the approach to patient care is for physicians to be less complacent and apply, with enthusiasm, secondary prevention guidelines in post-CABG and polyvascular disease patients to strive to eliminate smoking and to enforce lifestyle modifications with known benefits in atherosclerotic cardiovascular disease.
Jacques Genest, MD, and Alexandre M. Bélanger, MD, of McGill University, Montreal, and Mandeep S. Sidhu, MD, of Albany (N.Y.) Medical College made these comments in an accompanying editorial ( J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.016 ). The authors reported disclosures related to Sanofi, Amgen, Pfizer, Aegerion Pharmaceuticals, Valeant Pharmaceuticals, and others.
These two secondary analyses of the ODYSSEY OUTCOMES trial are very important studies that reinforce the usefulness of PCSK9 inhibition in extremely high risk populations.
Although each study has limitations as acknowledged, it provides further evidence that should lead us to strongly consider the use of PCSK9 inhibitors in patients with a previous coronary artery bypass grafting (CABG) or a history of polyvascular disease.
The studies confirm that aggressive lipid-lowering therapy will benefit patients in those high-risk subsets. The significant reductions in mortality associated with lowering LDL cholesterol using alirocumab can no longer be ignored.
Economic analyses would be interesting, as the substantial reductions in major adverse cardiovascular events and all-cause deaths attributed to alirocumab would likely impact health care costs and society at large.
However, it is concerning that patients with prior CABG and those with a high atherosclerosis burden in multiple arterial territories were seemingly less well treated than acute coronary syndrome patients.
An LDL cholesterol level of at least 100 mg/dL was seen in upward of 40% of the high-risk participants at randomization, while 87% had high BP, 40% had diabetes, and 16% were current smokers.
A reasonable first step in the approach to patient care is for physicians to be less complacent and apply, with enthusiasm, secondary prevention guidelines in post-CABG and polyvascular disease patients to strive to eliminate smoking and to enforce lifestyle modifications with known benefits in atherosclerotic cardiovascular disease.
Jacques Genest, MD, and Alexandre M. Bélanger, MD, of McGill University, Montreal, and Mandeep S. Sidhu, MD, of Albany (N.Y.) Medical College made these comments in an accompanying editorial ( J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.016 ). The authors reported disclosures related to Sanofi, Amgen, Pfizer, Aegerion Pharmaceuticals, Valeant Pharmaceuticals, and others.
These two secondary analyses of the ODYSSEY OUTCOMES trial are very important studies that reinforce the usefulness of PCSK9 inhibition in extremely high risk populations.
Although each study has limitations as acknowledged, it provides further evidence that should lead us to strongly consider the use of PCSK9 inhibitors in patients with a previous coronary artery bypass grafting (CABG) or a history of polyvascular disease.
The studies confirm that aggressive lipid-lowering therapy will benefit patients in those high-risk subsets. The significant reductions in mortality associated with lowering LDL cholesterol using alirocumab can no longer be ignored.
Economic analyses would be interesting, as the substantial reductions in major adverse cardiovascular events and all-cause deaths attributed to alirocumab would likely impact health care costs and society at large.
However, it is concerning that patients with prior CABG and those with a high atherosclerosis burden in multiple arterial territories were seemingly less well treated than acute coronary syndrome patients.
An LDL cholesterol level of at least 100 mg/dL was seen in upward of 40% of the high-risk participants at randomization, while 87% had high BP, 40% had diabetes, and 16% were current smokers.
A reasonable first step in the approach to patient care is for physicians to be less complacent and apply, with enthusiasm, secondary prevention guidelines in post-CABG and polyvascular disease patients to strive to eliminate smoking and to enforce lifestyle modifications with known benefits in atherosclerotic cardiovascular disease.
Jacques Genest, MD, and Alexandre M. Bélanger, MD, of McGill University, Montreal, and Mandeep S. Sidhu, MD, of Albany (N.Y.) Medical College made these comments in an accompanying editorial ( J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.016 ). The authors reported disclosures related to Sanofi, Amgen, Pfizer, Aegerion Pharmaceuticals, Valeant Pharmaceuticals, and others.
Patients at very high risk of adverse cardiovascular outcomes derive substantial benefit from proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition, according to results of two analyses from the ODYSSEY OUTCOMES trial.
In one prespecified analysis, the PCSK9 inhibitor alirocumab was linked to improved cardiovascular outcomes in patients with prior coronary artery bypass grafting (CABG), while in the other, researchers wrote that alirocumab showed a “large absolute benefit” in patients with polyvascular disease, which they defined as the presence of concomitant peripheral artery disease, cerebrovascular disease, or both.
These reports on alirocumab outcomes in patients with prior CABG and polyvascular disease appear in the Journal of the American College of Cardiology.
Prior CABG and polyvascular disease were both associated with markedly elevated risks of major adverse coronary events (MACE) and death, investigators wrote in the reports.
The ODYSSEY OUTCOMES trial included 18,924 patients with recent acute coronary syndrome (ACS) and high atherogenic lipoproteins despite intensive statin treatment. The primary outcome was MACE, comprising a composite of coronary heart disease death, nonfatal MI, ischemic stroke, or unstable angina requiring hospitalization. During a median 2.8 years of follow-up, this outcome occurred in 9.5% of the overall population randomized to alirocumab and 11.1% of those on placebo, for a statistically significant and clinically meaningful 15% relative risk reduction.
Polyvascular disease
In the trial population, 1,405 patients had polyvascular disease in at least two beds, including a coronary artery, plus either peripheral artery or cerebrovascular, while 149 had polyvascular disease in all three beds. The remainder, including 17,370 patients, were classified as having monovascular disease.
The incidences of MACE for placebo-treated patients with monovascular disease, two-bed polyvascular disease, and three-bed polyvascular disease were 10.0%, 22.2%, and 39.7%, respectively. Alirocumab treatment resulted in an absolute risk reduction for MACE of 1.4%, 1.9%, and 13.0%, for those respective groups (P = .0006).
Similarly, the incidence of the secondary endpoint of death for placebo-treated patients was 3.5%, 10.0%, and 21.8%, and the ARR with alirocumab was 0.4%, 1.3%, and 16.2% (P = .002), according to their reported data.
These results suggest that patients with polyvascular disease are an “easily identifiable subgroup” of ACS patients with a high absolute risk of MACE and death, according to the investigators, led by J. Wouter Jukema, MD, PhD, of Leiden (the Netherlands) University Medical Center.
“The large absolute benefit of PCSK9 inhibition with alirocumab, when added to high-intensity statin therapy, is a potential benefit for this group of patients,” Dr. Jukema and coauthors wrote.
Prior CABG
Of the ODYSSEY OUTCOMES patients, 1,025 had an index CABG after ACS, 1,003 had CABG before ACS, and the remaining 16,896 had no such procedure.
Hazard ratios for both MACE and death in all CABG categories were consistent with the overall results of ODYSSEY OUTCOMES, the investigators wrote. Specifically, alirocumab reduced MACE and death in the overall study, with HRs of 0.85 for both endpoints.
The ARRs in MACE with alirocumab were 1.3% for no CABG, 0.9% for index CABG, and 6.4% for prior CABG (P = .0007), while ARRs in death with the treatment were 0.4%, 0.5%, and 3.6% (P = .03) for those categories, respectively. In this analysis, the investigators calculated the number needed to treat to prevent one primary or secondary endpoint over the median 2.8 years of follow-up. The numbers needed to treat were 16 for prior CABG, 111 for index, and 77 for no prior CABG.
“Although the relative benefit of alirocumab versus placebo is consistent regardless of prior CABG status, those with prior CABG achieve substantially greater absolute risk reduction and consequently lower number needed to treat,” wrote the authors of the analysis, led by Shaun G. Goodman, MD, MSc, of St. Michael’s Hospital, Toronto.
Funding for the ODYSSEY OUTCOMES trial and its subanalyses was provided by Sanofi and Regeneron. Authors of the analyses reported disclosures related to Sanofi, Regeneron, Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and others.
SOURCES: Goodman SG et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.015; Jukema JW et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.03.013.
Patients at very high risk of adverse cardiovascular outcomes derive substantial benefit from proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition, according to results of two analyses from the ODYSSEY OUTCOMES trial.
In one prespecified analysis, the PCSK9 inhibitor alirocumab was linked to improved cardiovascular outcomes in patients with prior coronary artery bypass grafting (CABG), while in the other, researchers wrote that alirocumab showed a “large absolute benefit” in patients with polyvascular disease, which they defined as the presence of concomitant peripheral artery disease, cerebrovascular disease, or both.
These reports on alirocumab outcomes in patients with prior CABG and polyvascular disease appear in the Journal of the American College of Cardiology.
Prior CABG and polyvascular disease were both associated with markedly elevated risks of major adverse coronary events (MACE) and death, investigators wrote in the reports.
The ODYSSEY OUTCOMES trial included 18,924 patients with recent acute coronary syndrome (ACS) and high atherogenic lipoproteins despite intensive statin treatment. The primary outcome was MACE, comprising a composite of coronary heart disease death, nonfatal MI, ischemic stroke, or unstable angina requiring hospitalization. During a median 2.8 years of follow-up, this outcome occurred in 9.5% of the overall population randomized to alirocumab and 11.1% of those on placebo, for a statistically significant and clinically meaningful 15% relative risk reduction.
Polyvascular disease
In the trial population, 1,405 patients had polyvascular disease in at least two beds, including a coronary artery, plus either peripheral artery or cerebrovascular, while 149 had polyvascular disease in all three beds. The remainder, including 17,370 patients, were classified as having monovascular disease.
The incidences of MACE for placebo-treated patients with monovascular disease, two-bed polyvascular disease, and three-bed polyvascular disease were 10.0%, 22.2%, and 39.7%, respectively. Alirocumab treatment resulted in an absolute risk reduction for MACE of 1.4%, 1.9%, and 13.0%, for those respective groups (P = .0006).
Similarly, the incidence of the secondary endpoint of death for placebo-treated patients was 3.5%, 10.0%, and 21.8%, and the ARR with alirocumab was 0.4%, 1.3%, and 16.2% (P = .002), according to their reported data.
These results suggest that patients with polyvascular disease are an “easily identifiable subgroup” of ACS patients with a high absolute risk of MACE and death, according to the investigators, led by J. Wouter Jukema, MD, PhD, of Leiden (the Netherlands) University Medical Center.
“The large absolute benefit of PCSK9 inhibition with alirocumab, when added to high-intensity statin therapy, is a potential benefit for this group of patients,” Dr. Jukema and coauthors wrote.
Prior CABG
Of the ODYSSEY OUTCOMES patients, 1,025 had an index CABG after ACS, 1,003 had CABG before ACS, and the remaining 16,896 had no such procedure.
Hazard ratios for both MACE and death in all CABG categories were consistent with the overall results of ODYSSEY OUTCOMES, the investigators wrote. Specifically, alirocumab reduced MACE and death in the overall study, with HRs of 0.85 for both endpoints.
The ARRs in MACE with alirocumab were 1.3% for no CABG, 0.9% for index CABG, and 6.4% for prior CABG (P = .0007), while ARRs in death with the treatment were 0.4%, 0.5%, and 3.6% (P = .03) for those categories, respectively. In this analysis, the investigators calculated the number needed to treat to prevent one primary or secondary endpoint over the median 2.8 years of follow-up. The numbers needed to treat were 16 for prior CABG, 111 for index, and 77 for no prior CABG.
“Although the relative benefit of alirocumab versus placebo is consistent regardless of prior CABG status, those with prior CABG achieve substantially greater absolute risk reduction and consequently lower number needed to treat,” wrote the authors of the analysis, led by Shaun G. Goodman, MD, MSc, of St. Michael’s Hospital, Toronto.
Funding for the ODYSSEY OUTCOMES trial and its subanalyses was provided by Sanofi and Regeneron. Authors of the analyses reported disclosures related to Sanofi, Regeneron, Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and others.
SOURCES: Goodman SG et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.015; Jukema JW et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.03.013.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Key clinical point: The PCSK9 inhibitor alirocumab improved cardiovascular outcomes in very-high-risk populations, including patients with previous coronary artery bypass grafting and those with polyvascular disease.
Major findings: In one analysis, the absolute risk reductions in major adverse coronary events with alirocumab were 1.3% for no coronary artery bypass grafting, 0.9% for index CABG, and 6.4% for prior CABG. In another analysis, alirocumab treatment resulted in an ARR for major adverse coronary events of 1.4%, 1.9%, and 13.0% for patients with monovascular disease, two-bed polyvascular disease, and three-bed polyvascular disease, respectively.
Study details: Prespecified analyses of patients with recent acute coronary syndrome and high atherogenic lipoproteins despite intensive statin treatment in the ODYSSEY OUTCOMES trial, which included 18,924 total participants.
Disclosures: Funding for the ODYSSEY OUTCOMES trial and its subanalyses was provided by Sanofi and Regeneron. Authors of the analyses reported disclosures related to Sanofi, Regeneron, Amgen, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, and others.
Sources: Goodman SG et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.07.015; Jukema JW et al. J Am Coll Cardiol. 2019 Aug 26. doi: 10.1016/j.jacc.2019.03.013.
Evinacumab shows promise for HoFH in top line results
(HoFH), according to a release from the company developing the drug.
LDL cholesterol levels were 255 mg/dL on average for patients at the outset of the trial despite treatment with other lipid-lowering therapies; however, combining this drug with lipid-lowering therapies including maximally-tolerated statins, PCSK9 inhibitors, and LDL apheresis, reduced LDL cholesterol by an average of 49% by week 24 relative to treatment with lipid-lowering therapies alone (P less than .0001). Furthermore, 47% of patients taking evinacumab achieved LDL cholesterol levels under 100 mg/dL by that time point versus 23% of those taking lipid-lowering therapies only.
Treatment with evinacumab showed lowering effects as early as the first assessment at 2 weeks, and these effects were maintained.
HoFH is an inherited, rare, but serious condition estimated to affect 1,300 people in the United States; it can lead to early atherosclerotic disease, and even teenagers with this genetic disorder can suffer cardiac events. Further details and data from the trial, called ELIPSE HoFH, will be reported at a future medical meeting, and will be submitted to the Food and Drug Administration for consideration.
Evinacumab is an investigational, fully-human, monoclonal antibody that specifically binds to angiopoietin-like protein 3 (ANGPTL3), which acts as an inhibitor of lipoprotein lipase and endothelial lipase, and appears to play a central role in lipoprotein metabolism.
Evinacumab was granted breakthrough therapy designation for treatment of HoFH by the FDA in 2017, which entails an expedited review and development process for this drug because preliminary results have suggested it could have a substantial effect on a life-threatening or serious condition.
The company’s full release can be read on its website.
(HoFH), according to a release from the company developing the drug.
LDL cholesterol levels were 255 mg/dL on average for patients at the outset of the trial despite treatment with other lipid-lowering therapies; however, combining this drug with lipid-lowering therapies including maximally-tolerated statins, PCSK9 inhibitors, and LDL apheresis, reduced LDL cholesterol by an average of 49% by week 24 relative to treatment with lipid-lowering therapies alone (P less than .0001). Furthermore, 47% of patients taking evinacumab achieved LDL cholesterol levels under 100 mg/dL by that time point versus 23% of those taking lipid-lowering therapies only.
Treatment with evinacumab showed lowering effects as early as the first assessment at 2 weeks, and these effects were maintained.
HoFH is an inherited, rare, but serious condition estimated to affect 1,300 people in the United States; it can lead to early atherosclerotic disease, and even teenagers with this genetic disorder can suffer cardiac events. Further details and data from the trial, called ELIPSE HoFH, will be reported at a future medical meeting, and will be submitted to the Food and Drug Administration for consideration.
Evinacumab is an investigational, fully-human, monoclonal antibody that specifically binds to angiopoietin-like protein 3 (ANGPTL3), which acts as an inhibitor of lipoprotein lipase and endothelial lipase, and appears to play a central role in lipoprotein metabolism.
Evinacumab was granted breakthrough therapy designation for treatment of HoFH by the FDA in 2017, which entails an expedited review and development process for this drug because preliminary results have suggested it could have a substantial effect on a life-threatening or serious condition.
The company’s full release can be read on its website.
(HoFH), according to a release from the company developing the drug.
LDL cholesterol levels were 255 mg/dL on average for patients at the outset of the trial despite treatment with other lipid-lowering therapies; however, combining this drug with lipid-lowering therapies including maximally-tolerated statins, PCSK9 inhibitors, and LDL apheresis, reduced LDL cholesterol by an average of 49% by week 24 relative to treatment with lipid-lowering therapies alone (P less than .0001). Furthermore, 47% of patients taking evinacumab achieved LDL cholesterol levels under 100 mg/dL by that time point versus 23% of those taking lipid-lowering therapies only.
Treatment with evinacumab showed lowering effects as early as the first assessment at 2 weeks, and these effects were maintained.
HoFH is an inherited, rare, but serious condition estimated to affect 1,300 people in the United States; it can lead to early atherosclerotic disease, and even teenagers with this genetic disorder can suffer cardiac events. Further details and data from the trial, called ELIPSE HoFH, will be reported at a future medical meeting, and will be submitted to the Food and Drug Administration for consideration.
Evinacumab is an investigational, fully-human, monoclonal antibody that specifically binds to angiopoietin-like protein 3 (ANGPTL3), which acts as an inhibitor of lipoprotein lipase and endothelial lipase, and appears to play a central role in lipoprotein metabolism.
Evinacumab was granted breakthrough therapy designation for treatment of HoFH by the FDA in 2017, which entails an expedited review and development process for this drug because preliminary results have suggested it could have a substantial effect on a life-threatening or serious condition.
The company’s full release can be read on its website.
Psoriasis patients on biologics show improved heart health
Biologics improved coronary inflammation as well as psoriasis symptoms, according to data from the perivascular fat attenuation index in 134 adults identified using coronary CT angiography.
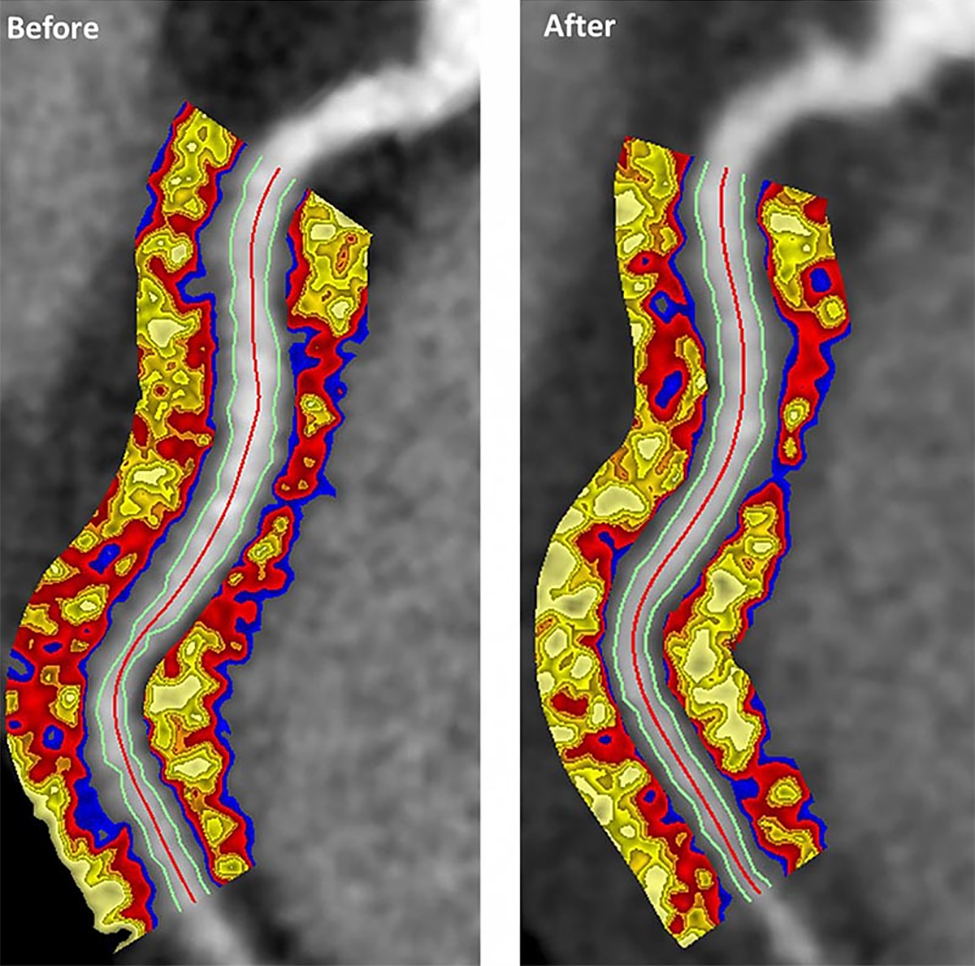
“The perivascular fat attenuation index [FAI] is a [CT]-based, novel, noninvasive imaging technique that allows for direct visualization and quantification of coronary inflammation using differential mapping of attenuation gradients in pericoronary fat,” wrote Youssef A. Elnabawi, MD, of the National Heart, Lung, and Blood Institute and colleagues. Biologics have been associated with reduced noncalcified coronary plaques in psoriasis patients, which suggests possible reduction in coronary inflammation as well.
In a study published in JAMA Cardiology, the researchers analyzed data from 134 adults with moderate to severe psoriasis who received no biologic therapy for at least 3 months before starting the study. Of these, 52 chose not to receive biologics, and served as controls while being treated with topical or light therapies. The participants are part of the Psoriasis Atherosclerosis Cardiometabolic Initiative, an ongoing, prospective cohort study. The average age of the patients was 51 years, and 63% were male.
The 82 patients given biologics received anti–tumor necrosis factor–alpha, anti–interleukin-12/23, or anti-IL-17 for 1 year. Overall, patients on biologics showed a significant decrease in FAI from a median of –71.22 Hounsfield units (HU) at baseline to a median of –76.06 at 1 year. These patients also showed significant improvement in Psoriasis Area and Severity Index scores, from a median of 7.7 at baseline to a median of 3.2 at 1 year. The control patients not on biologics showed no significant changes in FAI, with a median of –71.98 HU at baseline and –72.66 HU at 1 year.
The changes were consistent among the various biologics used, and The median FAI for patients on anti–tumor necrosis factor–alpha changed from –71.25 at baseline to –75.49 at 1 year; median FAI for both IL-12/23 and anti-IL-17 treatment groups changed from –71.18 HU at baseline to –76.92 at 1 year.
In addition, only patients treated with biologics showed a significant reduction in median C-reactive protein levels from baseline (2.2 mg/L vs. 1.3 mg/L). The changes in FAI were not associated with the presence of coronary plaques, the researchers noted.
The study findings were limited by several factors, including the observational design, small size, and lack of data on cardiovascular endpoints. “Future studies will be needed to explore whether the residual CV risk detected by perivascular FAI can be attenuated using targeted anti-inflammatory interventions,” they wrote.
However, the results suggest that biologics impact coronary vasculature at the microenvironmental level, and that FAI can be a noninvasive, cost-effective way to stratify patients at increased risk for cardiovascular disease, the researchers noted.
“We believe that the strength of perivascular FAI in risk stratifying patients with increased coronary inflammation will allow for better identification of patients at increased risk of future myocardial events that are not captured by traditional CV risk factors,” they wrote.
The study was funded by the National Institutes of Health, several research foundations, Elsevier, Colgate-Palmolive, and Genentech. Dr. Elnabawi had no financial conflicts to disclose; several coauthors reported relationships with multiple companies. One coauthor disclosed a pending and licensed patent to a novel tool for cardiovascular risk stratification based on the CT attenuation of perivascular tissue (OxScore) and a pending and licensed patent to perivascular texture index.
SOURCE: Elnabawi YA et al. JAMA Cardiol. 2019 Jul 31. doi: 10.1001/jamacardio.2019.2589.
Biologics improved coronary inflammation as well as psoriasis symptoms, according to data from the perivascular fat attenuation index in 134 adults identified using coronary CT angiography.
“The perivascular fat attenuation index [FAI] is a [CT]-based, novel, noninvasive imaging technique that allows for direct visualization and quantification of coronary inflammation using differential mapping of attenuation gradients in pericoronary fat,” wrote Youssef A. Elnabawi, MD, of the National Heart, Lung, and Blood Institute and colleagues. Biologics have been associated with reduced noncalcified coronary plaques in psoriasis patients, which suggests possible reduction in coronary inflammation as well.
In a study published in JAMA Cardiology, the researchers analyzed data from 134 adults with moderate to severe psoriasis who received no biologic therapy for at least 3 months before starting the study. Of these, 52 chose not to receive biologics, and served as controls while being treated with topical or light therapies. The participants are part of the Psoriasis Atherosclerosis Cardiometabolic Initiative, an ongoing, prospective cohort study. The average age of the patients was 51 years, and 63% were male.
The 82 patients given biologics received anti–tumor necrosis factor–alpha, anti–interleukin-12/23, or anti-IL-17 for 1 year. Overall, patients on biologics showed a significant decrease in FAI from a median of –71.22 Hounsfield units (HU) at baseline to a median of –76.06 at 1 year. These patients also showed significant improvement in Psoriasis Area and Severity Index scores, from a median of 7.7 at baseline to a median of 3.2 at 1 year. The control patients not on biologics showed no significant changes in FAI, with a median of –71.98 HU at baseline and –72.66 HU at 1 year.
The changes were consistent among the various biologics used, and The median FAI for patients on anti–tumor necrosis factor–alpha changed from –71.25 at baseline to –75.49 at 1 year; median FAI for both IL-12/23 and anti-IL-17 treatment groups changed from –71.18 HU at baseline to –76.92 at 1 year.
In addition, only patients treated with biologics showed a significant reduction in median C-reactive protein levels from baseline (2.2 mg/L vs. 1.3 mg/L). The changes in FAI were not associated with the presence of coronary plaques, the researchers noted.
The study findings were limited by several factors, including the observational design, small size, and lack of data on cardiovascular endpoints. “Future studies will be needed to explore whether the residual CV risk detected by perivascular FAI can be attenuated using targeted anti-inflammatory interventions,” they wrote.
However, the results suggest that biologics impact coronary vasculature at the microenvironmental level, and that FAI can be a noninvasive, cost-effective way to stratify patients at increased risk for cardiovascular disease, the researchers noted.
“We believe that the strength of perivascular FAI in risk stratifying patients with increased coronary inflammation will allow for better identification of patients at increased risk of future myocardial events that are not captured by traditional CV risk factors,” they wrote.
The study was funded by the National Institutes of Health, several research foundations, Elsevier, Colgate-Palmolive, and Genentech. Dr. Elnabawi had no financial conflicts to disclose; several coauthors reported relationships with multiple companies. One coauthor disclosed a pending and licensed patent to a novel tool for cardiovascular risk stratification based on the CT attenuation of perivascular tissue (OxScore) and a pending and licensed patent to perivascular texture index.
SOURCE: Elnabawi YA et al. JAMA Cardiol. 2019 Jul 31. doi: 10.1001/jamacardio.2019.2589.
Biologics improved coronary inflammation as well as psoriasis symptoms, according to data from the perivascular fat attenuation index in 134 adults identified using coronary CT angiography.
“The perivascular fat attenuation index [FAI] is a [CT]-based, novel, noninvasive imaging technique that allows for direct visualization and quantification of coronary inflammation using differential mapping of attenuation gradients in pericoronary fat,” wrote Youssef A. Elnabawi, MD, of the National Heart, Lung, and Blood Institute and colleagues. Biologics have been associated with reduced noncalcified coronary plaques in psoriasis patients, which suggests possible reduction in coronary inflammation as well.
In a study published in JAMA Cardiology, the researchers analyzed data from 134 adults with moderate to severe psoriasis who received no biologic therapy for at least 3 months before starting the study. Of these, 52 chose not to receive biologics, and served as controls while being treated with topical or light therapies. The participants are part of the Psoriasis Atherosclerosis Cardiometabolic Initiative, an ongoing, prospective cohort study. The average age of the patients was 51 years, and 63% were male.
The 82 patients given biologics received anti–tumor necrosis factor–alpha, anti–interleukin-12/23, or anti-IL-17 for 1 year. Overall, patients on biologics showed a significant decrease in FAI from a median of –71.22 Hounsfield units (HU) at baseline to a median of –76.06 at 1 year. These patients also showed significant improvement in Psoriasis Area and Severity Index scores, from a median of 7.7 at baseline to a median of 3.2 at 1 year. The control patients not on biologics showed no significant changes in FAI, with a median of –71.98 HU at baseline and –72.66 HU at 1 year.
The changes were consistent among the various biologics used, and The median FAI for patients on anti–tumor necrosis factor–alpha changed from –71.25 at baseline to –75.49 at 1 year; median FAI for both IL-12/23 and anti-IL-17 treatment groups changed from –71.18 HU at baseline to –76.92 at 1 year.
In addition, only patients treated with biologics showed a significant reduction in median C-reactive protein levels from baseline (2.2 mg/L vs. 1.3 mg/L). The changes in FAI were not associated with the presence of coronary plaques, the researchers noted.
The study findings were limited by several factors, including the observational design, small size, and lack of data on cardiovascular endpoints. “Future studies will be needed to explore whether the residual CV risk detected by perivascular FAI can be attenuated using targeted anti-inflammatory interventions,” they wrote.
However, the results suggest that biologics impact coronary vasculature at the microenvironmental level, and that FAI can be a noninvasive, cost-effective way to stratify patients at increased risk for cardiovascular disease, the researchers noted.
“We believe that the strength of perivascular FAI in risk stratifying patients with increased coronary inflammation will allow for better identification of patients at increased risk of future myocardial events that are not captured by traditional CV risk factors,” they wrote.
The study was funded by the National Institutes of Health, several research foundations, Elsevier, Colgate-Palmolive, and Genentech. Dr. Elnabawi had no financial conflicts to disclose; several coauthors reported relationships with multiple companies. One coauthor disclosed a pending and licensed patent to a novel tool for cardiovascular risk stratification based on the CT attenuation of perivascular tissue (OxScore) and a pending and licensed patent to perivascular texture index.
SOURCE: Elnabawi YA et al. JAMA Cardiol. 2019 Jul 31. doi: 10.1001/jamacardio.2019.2589.
FROM JAMA CARDIOLOGY