User login
FDA sued for access to data on hepatitis C medications
The Global Health Justice Partnership and Treatment Action Group have filed a lawsuit against the Food and Drug Administration for access to data on the hepatitis C drugs sofosbuvir (Sovaldi) and sofosbuvir/ledipasvir (Harvoni), according to a press release from Yale Law School, New Haven, Ct.
Sofosbuvir and sofosbuvir/ledipasvir were given Breakthrough Therapy Designation status by the FDA in December 2013 and October 2014, respectively, and since that time, have been used to treat more than 210,000 people. Both drugs are extremely effective, but their cost is tremendous, with the initial pricing of a 12-week treatment regimen at $84,000 and $94,500, respectively.
The two groups contacted Gilead Sciences for data on both drugs in November 2014, but received no response. In December 2014, GHJP and TAG submitted a Freedom of Information request to the FDA but were informed they would not get a response for 18-24 months and did not guarantee the data would ever be released.
“This lawsuit is about access and answers. The astronomical price of these drugs requires Medicaid programs and other providers to make hard choices about how to allocate their resources. They are making these decisions now. Crucial policy determinations about who has access to treatment are being made on incomplete information,” Karyn Kaplan, TAG’s International Hepatitis/HIV Policy and Advocacy director said in the press release.
Read the full press release on the Yale Law School website.
The Global Health Justice Partnership and Treatment Action Group have filed a lawsuit against the Food and Drug Administration for access to data on the hepatitis C drugs sofosbuvir (Sovaldi) and sofosbuvir/ledipasvir (Harvoni), according to a press release from Yale Law School, New Haven, Ct.
Sofosbuvir and sofosbuvir/ledipasvir were given Breakthrough Therapy Designation status by the FDA in December 2013 and October 2014, respectively, and since that time, have been used to treat more than 210,000 people. Both drugs are extremely effective, but their cost is tremendous, with the initial pricing of a 12-week treatment regimen at $84,000 and $94,500, respectively.
The two groups contacted Gilead Sciences for data on both drugs in November 2014, but received no response. In December 2014, GHJP and TAG submitted a Freedom of Information request to the FDA but were informed they would not get a response for 18-24 months and did not guarantee the data would ever be released.
“This lawsuit is about access and answers. The astronomical price of these drugs requires Medicaid programs and other providers to make hard choices about how to allocate their resources. They are making these decisions now. Crucial policy determinations about who has access to treatment are being made on incomplete information,” Karyn Kaplan, TAG’s International Hepatitis/HIV Policy and Advocacy director said in the press release.
Read the full press release on the Yale Law School website.
The Global Health Justice Partnership and Treatment Action Group have filed a lawsuit against the Food and Drug Administration for access to data on the hepatitis C drugs sofosbuvir (Sovaldi) and sofosbuvir/ledipasvir (Harvoni), according to a press release from Yale Law School, New Haven, Ct.
Sofosbuvir and sofosbuvir/ledipasvir were given Breakthrough Therapy Designation status by the FDA in December 2013 and October 2014, respectively, and since that time, have been used to treat more than 210,000 people. Both drugs are extremely effective, but their cost is tremendous, with the initial pricing of a 12-week treatment regimen at $84,000 and $94,500, respectively.
The two groups contacted Gilead Sciences for data on both drugs in November 2014, but received no response. In December 2014, GHJP and TAG submitted a Freedom of Information request to the FDA but were informed they would not get a response for 18-24 months and did not guarantee the data would ever be released.
“This lawsuit is about access and answers. The astronomical price of these drugs requires Medicaid programs and other providers to make hard choices about how to allocate their resources. They are making these decisions now. Crucial policy determinations about who has access to treatment are being made on incomplete information,” Karyn Kaplan, TAG’s International Hepatitis/HIV Policy and Advocacy director said in the press release.
Read the full press release on the Yale Law School website.
DDW: Single daily pill knocks out HCV in prior nonresponders
WASHINGTON – An investigational once-daily antiviral drug combination produced high rates of sustained viral responses after 12 or 16 weeks of therapy – with or without ribavirin – in patients with chronic hepatitis viral infections for whom prior therapy with peg-interferon and ribavirin had failed, investigators reported.
The rate of sustained viral responses at 12 weeks after the end of treatment (SVR12) was 92% for patients who received the combination of grazoprevir and elbasvir (GZR/EBR, Merck) alone, compared with 94% for patients who received the antivirals plus ribavirin, reported Dr. Paul Kwo of Indiana University Hospital in Indianapolis.

Among patients who received 16 weeks of therapy, the SVR12 rates were 92% without ribavirin, and 97% with ribavirin, Dr. Kwo said at the annual Digestive Disease Week.
“In patients who have failed peg-interferon and ribavirin therapy, 12 weeks of grazoprevir and elbasvir without ribavirin gives outstanding SVR rates in genotype 1b-infected individuals, regardless of treatment response, including those with cirrhosis. If you’re a relapser with genotype 1a or genotype 4 infection, 12 weeks of grazoprevir and elbasvir gives outstanding SVR rates. For genotype 1a, 4 and 6 prior null and partial responders, including those with cirrhosis, 16 weeks of grazoprevir and elbasvir with ribavirin gives outstanding SVR rates with no virologic failures,” he said.
Dr. Kwo presented updated results from the C-EDGE(Study of Efficacy and Safety of Grazoprevir (MK-5172)/Elbasvir (MK-8742) Combination Regimen for Treatment-Naive Participants With Chronic Hepatitis C Virus Genotypes 1, 4, and 6) treatment-experienced trial.
The 12-week C-EDGE results in 316 treatment-naive patients were presented earlier this year in Vienna at the International Liver Congress.
The fixed-dose, once-daily combination is composed of grazoprevir, an inhibitor of the HCV NS3/4a protease, at a dose of 100 mg, and elbasvir, a potent inhibitor of the NS5a protein, at a dose of 50 mg. This combination was shown to have broad activity against most HCV genotypes in vitro, and was efficacious in both treatment-naive and treatment-experienced patients with and without cirrhosis, including those with HIV/HCV coinfections, in the C-WORTHY trial.
The C-EDGE study was a phase III trial of GZR/EBR with or without ribavirin for 12 or 16 weeks for patients for whom prior therapy with peg-interferon and ribavirin had failed because of either null or partial response or viral relapse. The trial included patients with and without cirrhosis, those with HCV genotypes 1, 4, or 6, and those with either HCV mono-infections or HIV coinfections.
A total of 420 patients were enrolled.
As noted before, 97 of 105 patients (92%) on 12 weeks of therapy without ribavirin had an SVR12, although two patients in this group were lost to follow-up or discontinued therapy for reasons other than virologic failure (included as nonresponders). Among patients who received 12 weeks of GZR/EBR plus ribavirin, 98 of 104 (94%) had an SVR12, with no losses to follow-up.
For those patients treated for 16 weeks, 97 of 105 (92%) without ribavirin had an SVR12, compared with 103 of 106 (97%) who received ribavirin in addition to the combination antivirals. In these groups, one and three patients, respectively, were lost to follow-up.
In a subanalysis by HCV genotype or subtype, the combination alone was least effective among patients with genotype 4 treated for 16 weeks, with 3 of 5 patients (60%) having an SVR12, compared with 7 of 9 patients (79%) with genotype 4 treated with no ribavirin for 12 weeks, 14 of 15 (93%) with ribavirin for 12 weeks, and 8 of 8 (100%) treated with ribavirin for 16 weeks. The overall numbers of patients in each subgroup was too small for statistical significance analysis, however.
Among patients with HCV coinfection, the SVR12 rate was 100% in all treatment arms except 16 weeks GZR/EBR without ribavirin (5 of 6; 83%).
A subanalysis by prior response, excluding the 12 total patients who did not complete treatment, showed excellent SVR12 rates in all four treatment arms among patients with a prior relapse, and slightly less robust but still high rates among prior partial or null responders, Dr. Kwo said.
Patients tolerated the regimen well, with the rates of serious adverse events ranging from 2.9% to 3.8%. There were no deaths, and seven discontinuations due to adverse events (one in each in the 12-week arms, and five in the 16-week with ribavirin arm). A total of 31 patients who received ribavirin had hemoglobin reductions below 10 g/dL, and 60 reported fatigue, both common with ribavirin. The majority of adverse events in all arms were fatigue, headache, and nausea.
The combination has received two Breakthrough Therapy designations from the Food and Drug Administration for patients with HCV genotype 4, and for patients with genotype 1 infections who are on hemodialysis for end stage renal disease. The breakthrough designation makes the drug eligible for expedited review.
Dr. Kwo disclosed ties with Merck, which supported the C-EDGE study.
WASHINGTON – An investigational once-daily antiviral drug combination produced high rates of sustained viral responses after 12 or 16 weeks of therapy – with or without ribavirin – in patients with chronic hepatitis viral infections for whom prior therapy with peg-interferon and ribavirin had failed, investigators reported.
The rate of sustained viral responses at 12 weeks after the end of treatment (SVR12) was 92% for patients who received the combination of grazoprevir and elbasvir (GZR/EBR, Merck) alone, compared with 94% for patients who received the antivirals plus ribavirin, reported Dr. Paul Kwo of Indiana University Hospital in Indianapolis.
Among patients who received 16 weeks of therapy, the SVR12 rates were 92% without ribavirin, and 97% with ribavirin, Dr. Kwo said at the annual Digestive Disease Week.
“In patients who have failed peg-interferon and ribavirin therapy, 12 weeks of grazoprevir and elbasvir without ribavirin gives outstanding SVR rates in genotype 1b-infected individuals, regardless of treatment response, including those with cirrhosis. If you’re a relapser with genotype 1a or genotype 4 infection, 12 weeks of grazoprevir and elbasvir gives outstanding SVR rates. For genotype 1a, 4 and 6 prior null and partial responders, including those with cirrhosis, 16 weeks of grazoprevir and elbasvir with ribavirin gives outstanding SVR rates with no virologic failures,” he said.
Dr. Kwo presented updated results from the C-EDGE(Study of Efficacy and Safety of Grazoprevir (MK-5172)/Elbasvir (MK-8742) Combination Regimen for Treatment-Naive Participants With Chronic Hepatitis C Virus Genotypes 1, 4, and 6) treatment-experienced trial.
The 12-week C-EDGE results in 316 treatment-naive patients were presented earlier this year in Vienna at the International Liver Congress.
The fixed-dose, once-daily combination is composed of grazoprevir, an inhibitor of the HCV NS3/4a protease, at a dose of 100 mg, and elbasvir, a potent inhibitor of the NS5a protein, at a dose of 50 mg. This combination was shown to have broad activity against most HCV genotypes in vitro, and was efficacious in both treatment-naive and treatment-experienced patients with and without cirrhosis, including those with HIV/HCV coinfections, in the C-WORTHY trial.
The C-EDGE study was a phase III trial of GZR/EBR with or without ribavirin for 12 or 16 weeks for patients for whom prior therapy with peg-interferon and ribavirin had failed because of either null or partial response or viral relapse. The trial included patients with and without cirrhosis, those with HCV genotypes 1, 4, or 6, and those with either HCV mono-infections or HIV coinfections.
A total of 420 patients were enrolled.
As noted before, 97 of 105 patients (92%) on 12 weeks of therapy without ribavirin had an SVR12, although two patients in this group were lost to follow-up or discontinued therapy for reasons other than virologic failure (included as nonresponders). Among patients who received 12 weeks of GZR/EBR plus ribavirin, 98 of 104 (94%) had an SVR12, with no losses to follow-up.
For those patients treated for 16 weeks, 97 of 105 (92%) without ribavirin had an SVR12, compared with 103 of 106 (97%) who received ribavirin in addition to the combination antivirals. In these groups, one and three patients, respectively, were lost to follow-up.
In a subanalysis by HCV genotype or subtype, the combination alone was least effective among patients with genotype 4 treated for 16 weeks, with 3 of 5 patients (60%) having an SVR12, compared with 7 of 9 patients (79%) with genotype 4 treated with no ribavirin for 12 weeks, 14 of 15 (93%) with ribavirin for 12 weeks, and 8 of 8 (100%) treated with ribavirin for 16 weeks. The overall numbers of patients in each subgroup was too small for statistical significance analysis, however.
Among patients with HCV coinfection, the SVR12 rate was 100% in all treatment arms except 16 weeks GZR/EBR without ribavirin (5 of 6; 83%).
A subanalysis by prior response, excluding the 12 total patients who did not complete treatment, showed excellent SVR12 rates in all four treatment arms among patients with a prior relapse, and slightly less robust but still high rates among prior partial or null responders, Dr. Kwo said.
Patients tolerated the regimen well, with the rates of serious adverse events ranging from 2.9% to 3.8%. There were no deaths, and seven discontinuations due to adverse events (one in each in the 12-week arms, and five in the 16-week with ribavirin arm). A total of 31 patients who received ribavirin had hemoglobin reductions below 10 g/dL, and 60 reported fatigue, both common with ribavirin. The majority of adverse events in all arms were fatigue, headache, and nausea.
The combination has received two Breakthrough Therapy designations from the Food and Drug Administration for patients with HCV genotype 4, and for patients with genotype 1 infections who are on hemodialysis for end stage renal disease. The breakthrough designation makes the drug eligible for expedited review.
Dr. Kwo disclosed ties with Merck, which supported the C-EDGE study.
WASHINGTON – An investigational once-daily antiviral drug combination produced high rates of sustained viral responses after 12 or 16 weeks of therapy – with or without ribavirin – in patients with chronic hepatitis viral infections for whom prior therapy with peg-interferon and ribavirin had failed, investigators reported.
The rate of sustained viral responses at 12 weeks after the end of treatment (SVR12) was 92% for patients who received the combination of grazoprevir and elbasvir (GZR/EBR, Merck) alone, compared with 94% for patients who received the antivirals plus ribavirin, reported Dr. Paul Kwo of Indiana University Hospital in Indianapolis.
Among patients who received 16 weeks of therapy, the SVR12 rates were 92% without ribavirin, and 97% with ribavirin, Dr. Kwo said at the annual Digestive Disease Week.
“In patients who have failed peg-interferon and ribavirin therapy, 12 weeks of grazoprevir and elbasvir without ribavirin gives outstanding SVR rates in genotype 1b-infected individuals, regardless of treatment response, including those with cirrhosis. If you’re a relapser with genotype 1a or genotype 4 infection, 12 weeks of grazoprevir and elbasvir gives outstanding SVR rates. For genotype 1a, 4 and 6 prior null and partial responders, including those with cirrhosis, 16 weeks of grazoprevir and elbasvir with ribavirin gives outstanding SVR rates with no virologic failures,” he said.
Dr. Kwo presented updated results from the C-EDGE(Study of Efficacy and Safety of Grazoprevir (MK-5172)/Elbasvir (MK-8742) Combination Regimen for Treatment-Naive Participants With Chronic Hepatitis C Virus Genotypes 1, 4, and 6) treatment-experienced trial.
The 12-week C-EDGE results in 316 treatment-naive patients were presented earlier this year in Vienna at the International Liver Congress.
The fixed-dose, once-daily combination is composed of grazoprevir, an inhibitor of the HCV NS3/4a protease, at a dose of 100 mg, and elbasvir, a potent inhibitor of the NS5a protein, at a dose of 50 mg. This combination was shown to have broad activity against most HCV genotypes in vitro, and was efficacious in both treatment-naive and treatment-experienced patients with and without cirrhosis, including those with HIV/HCV coinfections, in the C-WORTHY trial.
The C-EDGE study was a phase III trial of GZR/EBR with or without ribavirin for 12 or 16 weeks for patients for whom prior therapy with peg-interferon and ribavirin had failed because of either null or partial response or viral relapse. The trial included patients with and without cirrhosis, those with HCV genotypes 1, 4, or 6, and those with either HCV mono-infections or HIV coinfections.
A total of 420 patients were enrolled.
As noted before, 97 of 105 patients (92%) on 12 weeks of therapy without ribavirin had an SVR12, although two patients in this group were lost to follow-up or discontinued therapy for reasons other than virologic failure (included as nonresponders). Among patients who received 12 weeks of GZR/EBR plus ribavirin, 98 of 104 (94%) had an SVR12, with no losses to follow-up.
For those patients treated for 16 weeks, 97 of 105 (92%) without ribavirin had an SVR12, compared with 103 of 106 (97%) who received ribavirin in addition to the combination antivirals. In these groups, one and three patients, respectively, were lost to follow-up.
In a subanalysis by HCV genotype or subtype, the combination alone was least effective among patients with genotype 4 treated for 16 weeks, with 3 of 5 patients (60%) having an SVR12, compared with 7 of 9 patients (79%) with genotype 4 treated with no ribavirin for 12 weeks, 14 of 15 (93%) with ribavirin for 12 weeks, and 8 of 8 (100%) treated with ribavirin for 16 weeks. The overall numbers of patients in each subgroup was too small for statistical significance analysis, however.
Among patients with HCV coinfection, the SVR12 rate was 100% in all treatment arms except 16 weeks GZR/EBR without ribavirin (5 of 6; 83%).
A subanalysis by prior response, excluding the 12 total patients who did not complete treatment, showed excellent SVR12 rates in all four treatment arms among patients with a prior relapse, and slightly less robust but still high rates among prior partial or null responders, Dr. Kwo said.
Patients tolerated the regimen well, with the rates of serious adverse events ranging from 2.9% to 3.8%. There were no deaths, and seven discontinuations due to adverse events (one in each in the 12-week arms, and five in the 16-week with ribavirin arm). A total of 31 patients who received ribavirin had hemoglobin reductions below 10 g/dL, and 60 reported fatigue, both common with ribavirin. The majority of adverse events in all arms were fatigue, headache, and nausea.
The combination has received two Breakthrough Therapy designations from the Food and Drug Administration for patients with HCV genotype 4, and for patients with genotype 1 infections who are on hemodialysis for end stage renal disease. The breakthrough designation makes the drug eligible for expedited review.
Dr. Kwo disclosed ties with Merck, which supported the C-EDGE study.
AT DDW 2015
Key clinical point: A fixed dose combination of grazoprevir and elbasvir, with or without ribavirin, was effective in patients with previously treated HCV infections.
Major finding: SVR12 was 92% for patients who received the combination of grazoprevir and elbasvir alone, compared with 94% for patients who received the antivirals plus ribavirin for 12 weeks.
Data source: Randomized clinical trial of 420 patients with HCV genotypes 1, 4, and 6 for whom prior therapy with peg-interferon/ribavirin had failed.
Disclosures: Dr. Kwo disclosed ties with Merck, which supported the C-EDGE study.

Significant worker productivity gains with newer hepatitis C drugs
Achieving a cure in hepatitis C infection could result in significant economic gains, with a study estimating that the beneficial effects in terms of improved worker productivity could total around $3.23 billion per year for the United States alone.
Researchers used data on work productivity and activity scores from patients enrolled in clinical trials of the all-oral sofosbuvir and lepidasvir combo to estimate the impact of achieving sustained virologic response at 12 weeks (SVR-12) on workers’ productivity.
They calculated an average work productivity loss of $4,954 for each employed patient with chronic hepatitis C infection per year in the United States and $1,129 per year for the five European Union countries included in the mix.“These new all-oral combinations such as lepidasvir and sofosbuvir have cure rates between 95% and 99% with minimum side effects, [so] treating patients with these combinations results in improved work productivity, improved quality of life, and patient-reported outcomes that can translate into economic benefit,” Dr. Zobair M. Younossi of the Inova Fairfax Medical Campus, Falls Church, Va., said at the annual Digestive Disease Week.
No conflicts of interest were disclosed.
Achieving a cure in hepatitis C infection could result in significant economic gains, with a study estimating that the beneficial effects in terms of improved worker productivity could total around $3.23 billion per year for the United States alone.
Researchers used data on work productivity and activity scores from patients enrolled in clinical trials of the all-oral sofosbuvir and lepidasvir combo to estimate the impact of achieving sustained virologic response at 12 weeks (SVR-12) on workers’ productivity.
They calculated an average work productivity loss of $4,954 for each employed patient with chronic hepatitis C infection per year in the United States and $1,129 per year for the five European Union countries included in the mix.“These new all-oral combinations such as lepidasvir and sofosbuvir have cure rates between 95% and 99% with minimum side effects, [so] treating patients with these combinations results in improved work productivity, improved quality of life, and patient-reported outcomes that can translate into economic benefit,” Dr. Zobair M. Younossi of the Inova Fairfax Medical Campus, Falls Church, Va., said at the annual Digestive Disease Week.
No conflicts of interest were disclosed.
Achieving a cure in hepatitis C infection could result in significant economic gains, with a study estimating that the beneficial effects in terms of improved worker productivity could total around $3.23 billion per year for the United States alone.
Researchers used data on work productivity and activity scores from patients enrolled in clinical trials of the all-oral sofosbuvir and lepidasvir combo to estimate the impact of achieving sustained virologic response at 12 weeks (SVR-12) on workers’ productivity.
They calculated an average work productivity loss of $4,954 for each employed patient with chronic hepatitis C infection per year in the United States and $1,129 per year for the five European Union countries included in the mix.“These new all-oral combinations such as lepidasvir and sofosbuvir have cure rates between 95% and 99% with minimum side effects, [so] treating patients with these combinations results in improved work productivity, improved quality of life, and patient-reported outcomes that can translate into economic benefit,” Dr. Zobair M. Younossi of the Inova Fairfax Medical Campus, Falls Church, Va., said at the annual Digestive Disease Week.
No conflicts of interest were disclosed.
FROM DDW 2015
Key clinical point: Achieving a cure in hepatitis C infection could result in significant economic gains from improved worker productivity.
Major finding: The beneficial effects in terms of improved worker productivity could total around $3.23 billion per year for the United States alone.
Data source: Economic model using data from hepatitis C clinical trials in the United States and Europe.
Disclosures: No conflicts of interest were disclosed.
New drugs saw ‘unprecedented’ spending growth in 2014
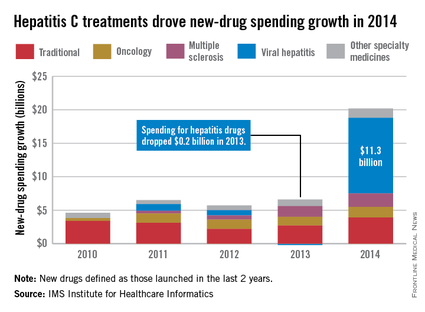
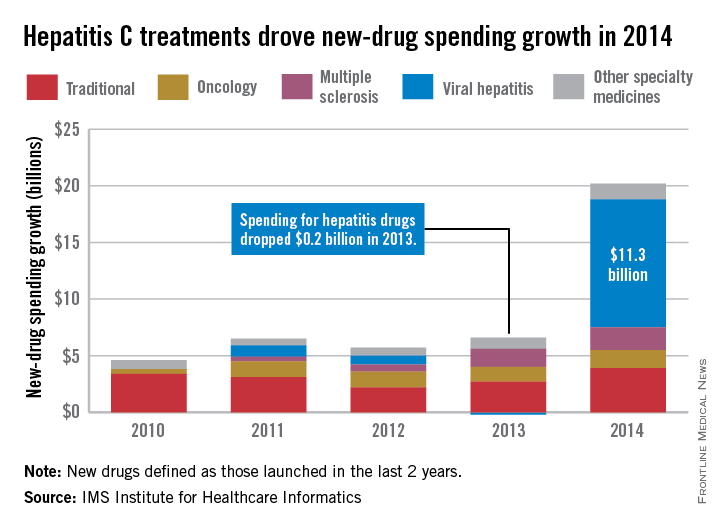
Led by new treatments for hepatitis C, there was an “unprecedented $20.2 billion increase in spending” for new medicines in 2014, which was triple the 2013 level, according to a report from the IMS Institute for Healthcare Informatics.
Compared with 2013, spending for new viral hepatitis drugs was up by $11.3 billion in 2014, accounting for more than half of the total increase. Hepatitis C drugs and other specialty medicines – defined as “products that are often injectable, high-cost, biologic … and include treatment for cancer and other serious chronic conditions” – accounted for 81% of the $20.2 billion, the report noted.
The number of patients who sought treatment for hepatitis C jumped from 17,000 in 2013 to 161,000 in 2014, “owing to new treatments with cure rates over 90% and dramatically fewer side effects,” the IMS Institute said.
Spending on new drugs in the traditional sector, such as those for diabetes, was up by $3.9 billion in 2014. The other leading areas of spending increase in the specialty sector – oncology and multiple sclerosis – were up by $1.6 billion and $2.0 billion, respectively, the report said.
The IMS Institute defines new drugs as those launched in the last 2 years. The report includes data from IMS National Sales Perspectives, which “reports 100% coverage of the retail and nonretail channels for national [non-OTC] pharmaceutical sales at actual transaction prices.”
Led by new treatments for hepatitis C, there was an “unprecedented $20.2 billion increase in spending” for new medicines in 2014, which was triple the 2013 level, according to a report from the IMS Institute for Healthcare Informatics.
Compared with 2013, spending for new viral hepatitis drugs was up by $11.3 billion in 2014, accounting for more than half of the total increase. Hepatitis C drugs and other specialty medicines – defined as “products that are often injectable, high-cost, biologic … and include treatment for cancer and other serious chronic conditions” – accounted for 81% of the $20.2 billion, the report noted.
The number of patients who sought treatment for hepatitis C jumped from 17,000 in 2013 to 161,000 in 2014, “owing to new treatments with cure rates over 90% and dramatically fewer side effects,” the IMS Institute said.
Spending on new drugs in the traditional sector, such as those for diabetes, was up by $3.9 billion in 2014. The other leading areas of spending increase in the specialty sector – oncology and multiple sclerosis – were up by $1.6 billion and $2.0 billion, respectively, the report said.
The IMS Institute defines new drugs as those launched in the last 2 years. The report includes data from IMS National Sales Perspectives, which “reports 100% coverage of the retail and nonretail channels for national [non-OTC] pharmaceutical sales at actual transaction prices.”
Led by new treatments for hepatitis C, there was an “unprecedented $20.2 billion increase in spending” for new medicines in 2014, which was triple the 2013 level, according to a report from the IMS Institute for Healthcare Informatics.
Compared with 2013, spending for new viral hepatitis drugs was up by $11.3 billion in 2014, accounting for more than half of the total increase. Hepatitis C drugs and other specialty medicines – defined as “products that are often injectable, high-cost, biologic … and include treatment for cancer and other serious chronic conditions” – accounted for 81% of the $20.2 billion, the report noted.
The number of patients who sought treatment for hepatitis C jumped from 17,000 in 2013 to 161,000 in 2014, “owing to new treatments with cure rates over 90% and dramatically fewer side effects,” the IMS Institute said.
Spending on new drugs in the traditional sector, such as those for diabetes, was up by $3.9 billion in 2014. The other leading areas of spending increase in the specialty sector – oncology and multiple sclerosis – were up by $1.6 billion and $2.0 billion, respectively, the report said.
The IMS Institute defines new drugs as those launched in the last 2 years. The report includes data from IMS National Sales Perspectives, which “reports 100% coverage of the retail and nonretail channels for national [non-OTC] pharmaceutical sales at actual transaction prices.”
Statins linked to better outcomes in hep C cirrhosis
VIENNA – Patients infected with hepatitis C virus who developed cirrhosis and received statin treatment had significantly lower rates of both death and cirrhosis decompensation, compared with cirrhosis patients who did not receive a statin in a confounder-adjusted analysis of data from more than 2,700 patients in a U.S. Department of Veterans Affairs database.
While this suggestive evidence is not strong enough to warrant routinely prescribing statins to cirrhosis patients, it does highlight the need to prescribe a statin to any cirrhosis patient who qualifies for the drug by standard criteria because of established cardiovascular disease or as part of primary prevention when there is elevated cardiovascular risk, Dr. Arpan Mohanty said at the meeting sponsored by the European Association for the Study of the Liver.

Conventional wisdom has often led to withholding statins from patients with liver disease out of concern for risk of statin-induced hepatotoxicity, said Dr. Mohanty, a gastroenterology researcher at Yale University in New Haven, Conn. But the new findings suggesting such overwhelming benefit from statin treatment in these patients indicates that “statin use should not be avoided” when patients with liver disease would otherwise qualify for statin treatment.
“Statins should be prescribed when required for atherosclerosis,” she said, adding that in New Haven her program has run sessions to educate primary care physicians on this.
The study used data collected during 1996-2009 by the Hepatitis C Virus Clinical Case Registry of the U.S. Department of Veterans Affairs, which includes more than 340,000 veterans, of whom more than 45,000 had been diagnosed with cirrhosis. Further analysis identified 1,323 eligible veterans from this group on statin treatment, and 12,522 not on statin treatment. Propensity score matching narrowed the study group down to 685 hepatitis C virus–infected veterans with cirrhosis who were on statin treatment, and 2,062 closely matched veterans infected with HCV and with cirrhosis but not receiving statin therapy.
The patients averaged 56 years old, 98% were men, and comorbidities were common; a third had a history of coronary artery disease, more than 80% had hypertension, more than half had diabetes, and more than half had alcohol dependency. Among patients with a serum cholesterol level greater than 200 mg/dL, 57% were not on a statin; among those with a serum low-density cholesterol level of about 160 mg/dL, 35% were not receiving a statin. “Statin use is low in patients with cirrhosis, even in those with high cardiovascular risk,” Dr. Mohanty said.
She and her associates tracked the incidence of death for a median of more than 2 years in these patients, and they followed new episodes of cirrhosis decompensation for nearly 2 years.
With adjustment for age, body mass index, serum albumin, and fibrosis-4 and MELD (Model for End-Stage Liver Disease) scores, the rates of both death and cirrhosis decompensation were each a statistically significant 45% lower among the patients on statins, compared with those not on a statin, they reported.
On Twitter @mitchelzoler
VIENNA – Patients infected with hepatitis C virus who developed cirrhosis and received statin treatment had significantly lower rates of both death and cirrhosis decompensation, compared with cirrhosis patients who did not receive a statin in a confounder-adjusted analysis of data from more than 2,700 patients in a U.S. Department of Veterans Affairs database.
While this suggestive evidence is not strong enough to warrant routinely prescribing statins to cirrhosis patients, it does highlight the need to prescribe a statin to any cirrhosis patient who qualifies for the drug by standard criteria because of established cardiovascular disease or as part of primary prevention when there is elevated cardiovascular risk, Dr. Arpan Mohanty said at the meeting sponsored by the European Association for the Study of the Liver.
Conventional wisdom has often led to withholding statins from patients with liver disease out of concern for risk of statin-induced hepatotoxicity, said Dr. Mohanty, a gastroenterology researcher at Yale University in New Haven, Conn. But the new findings suggesting such overwhelming benefit from statin treatment in these patients indicates that “statin use should not be avoided” when patients with liver disease would otherwise qualify for statin treatment.
“Statins should be prescribed when required for atherosclerosis,” she said, adding that in New Haven her program has run sessions to educate primary care physicians on this.
The study used data collected during 1996-2009 by the Hepatitis C Virus Clinical Case Registry of the U.S. Department of Veterans Affairs, which includes more than 340,000 veterans, of whom more than 45,000 had been diagnosed with cirrhosis. Further analysis identified 1,323 eligible veterans from this group on statin treatment, and 12,522 not on statin treatment. Propensity score matching narrowed the study group down to 685 hepatitis C virus–infected veterans with cirrhosis who were on statin treatment, and 2,062 closely matched veterans infected with HCV and with cirrhosis but not receiving statin therapy.
The patients averaged 56 years old, 98% were men, and comorbidities were common; a third had a history of coronary artery disease, more than 80% had hypertension, more than half had diabetes, and more than half had alcohol dependency. Among patients with a serum cholesterol level greater than 200 mg/dL, 57% were not on a statin; among those with a serum low-density cholesterol level of about 160 mg/dL, 35% were not receiving a statin. “Statin use is low in patients with cirrhosis, even in those with high cardiovascular risk,” Dr. Mohanty said.
She and her associates tracked the incidence of death for a median of more than 2 years in these patients, and they followed new episodes of cirrhosis decompensation for nearly 2 years.
With adjustment for age, body mass index, serum albumin, and fibrosis-4 and MELD (Model for End-Stage Liver Disease) scores, the rates of both death and cirrhosis decompensation were each a statistically significant 45% lower among the patients on statins, compared with those not on a statin, they reported.
On Twitter @mitchelzoler
VIENNA – Patients infected with hepatitis C virus who developed cirrhosis and received statin treatment had significantly lower rates of both death and cirrhosis decompensation, compared with cirrhosis patients who did not receive a statin in a confounder-adjusted analysis of data from more than 2,700 patients in a U.S. Department of Veterans Affairs database.
While this suggestive evidence is not strong enough to warrant routinely prescribing statins to cirrhosis patients, it does highlight the need to prescribe a statin to any cirrhosis patient who qualifies for the drug by standard criteria because of established cardiovascular disease or as part of primary prevention when there is elevated cardiovascular risk, Dr. Arpan Mohanty said at the meeting sponsored by the European Association for the Study of the Liver.
Conventional wisdom has often led to withholding statins from patients with liver disease out of concern for risk of statin-induced hepatotoxicity, said Dr. Mohanty, a gastroenterology researcher at Yale University in New Haven, Conn. But the new findings suggesting such overwhelming benefit from statin treatment in these patients indicates that “statin use should not be avoided” when patients with liver disease would otherwise qualify for statin treatment.
“Statins should be prescribed when required for atherosclerosis,” she said, adding that in New Haven her program has run sessions to educate primary care physicians on this.
The study used data collected during 1996-2009 by the Hepatitis C Virus Clinical Case Registry of the U.S. Department of Veterans Affairs, which includes more than 340,000 veterans, of whom more than 45,000 had been diagnosed with cirrhosis. Further analysis identified 1,323 eligible veterans from this group on statin treatment, and 12,522 not on statin treatment. Propensity score matching narrowed the study group down to 685 hepatitis C virus–infected veterans with cirrhosis who were on statin treatment, and 2,062 closely matched veterans infected with HCV and with cirrhosis but not receiving statin therapy.
The patients averaged 56 years old, 98% were men, and comorbidities were common; a third had a history of coronary artery disease, more than 80% had hypertension, more than half had diabetes, and more than half had alcohol dependency. Among patients with a serum cholesterol level greater than 200 mg/dL, 57% were not on a statin; among those with a serum low-density cholesterol level of about 160 mg/dL, 35% were not receiving a statin. “Statin use is low in patients with cirrhosis, even in those with high cardiovascular risk,” Dr. Mohanty said.
She and her associates tracked the incidence of death for a median of more than 2 years in these patients, and they followed new episodes of cirrhosis decompensation for nearly 2 years.
With adjustment for age, body mass index, serum albumin, and fibrosis-4 and MELD (Model for End-Stage Liver Disease) scores, the rates of both death and cirrhosis decompensation were each a statistically significant 45% lower among the patients on statins, compared with those not on a statin, they reported.
On Twitter @mitchelzoler
Unrecognized hepatitis C linked with advanced hepatic fibrosis
VIENNA – Roughly half of American adults with chronic hepatitis C infection are unaware of their infection, and about one-fifth of these people with unsuspected infection likely have advanced liver fibrosis, according to a new analysis of U.S. data.
These findings “strengthen the recommendation for hepatitis C virus (HCV) screening in asymptomatic individuals,” Dr. Prowpanga Udompap said at the meeting sponsored by the European Association for the Study of the Liver.

People infected by HCV with advanced liver fibrosis have top priority for receiving curative drug treatment, according to recommendations by the American Association for the Study of the Liver and the Infectious Diseases Society of America.
People who have HCV-associated liver fibrosis that goes untreated also risk having their infection become more refractory to cure over time, they risk progressive hepatic deterioration that will eventually become symptomatic, and they face increasing risk for developing liver cancer, noted Dr. W. Ray Kim, senior author of the study and professor of medicine and chief of gastroenterology and hepatology at Stanford (Calif.) University.

Dr. Kim said he was surprised that such a large percentage of Americans who have unrecognized HCV infection also probably have substantial hepatic damage. “To me it’s alarming that 20% of people who are not aware of their HCV infection are treatment candidates. These people are out there, but not getting treated,” he said in an interview.
Current U.S. HCV screening recommendations from the Centers for Disease Control and Prevention call for screening all Americans born during 1945-1965, “but there is no incentive to screen” and many U.S. primary care physicians don’t have HCV screening on their radar, he said.
The analysis conducted by Dr. Udompap and Dr. Kim used data collected by the National Health and Nutrition Examination Survey during 2001-2012, when the National Center for Health Statistics administered HCV testing to 45,000 of the 62,000 individuals who participated in the survey then.
Of the 45,000 people tested, 420 (0.9%) screened antibody positive and had infection confirmed by a second, RNA-based test. The HCV-positive patients then received a survey that included a question on whether they were aware of their HCV status before their current test result notification. One hundred sixty-three people (39%) completed and returned the survey: Eighty-three said they had previously been unaware they were HCV positive, and 80 said that they had known about their infection. The 50% rate of awareness of HCV chronic infection is consistent with a previously reported rate (Hepatology 2012;55:1652-61), said Dr. Udompap, a gastroenterology researcher at Stanford.

Individuals who were aware of their infection and those who were not had very similar demographic and clinical parameters. The average age was 53 years, and about two-thirds were men.
Dr. Udompap ran estimates of each respondent’s liver fibrosis and cirrhosis severity using the FIB-4 score and APRI score and data collected during the survey on age, liver enzyme levels, and platelet counts. These calculations showed that 22% of those ignorant of their HCV-positive status had a high probability of having advanced fibrosis, and 11% had a high probability of having cirrhosis, Dr. Udompap reported. These rates tracked close to those of the people who knew about their HCV-positive status, of whom 15% had a high probability of having advanced liver fibrosis and 11% were highly likely to have cirrhosis.
Dr. Udompap reported no financial disclosures. Dr. Kim has been a consultant to several drug companies that market, or are developing, drugs used in HCV.
On Twitter @mitchelzoler
VIENNA – Roughly half of American adults with chronic hepatitis C infection are unaware of their infection, and about one-fifth of these people with unsuspected infection likely have advanced liver fibrosis, according to a new analysis of U.S. data.
These findings “strengthen the recommendation for hepatitis C virus (HCV) screening in asymptomatic individuals,” Dr. Prowpanga Udompap said at the meeting sponsored by the European Association for the Study of the Liver.
People infected by HCV with advanced liver fibrosis have top priority for receiving curative drug treatment, according to recommendations by the American Association for the Study of the Liver and the Infectious Diseases Society of America.
People who have HCV-associated liver fibrosis that goes untreated also risk having their infection become more refractory to cure over time, they risk progressive hepatic deterioration that will eventually become symptomatic, and they face increasing risk for developing liver cancer, noted Dr. W. Ray Kim, senior author of the study and professor of medicine and chief of gastroenterology and hepatology at Stanford (Calif.) University.
Dr. Kim said he was surprised that such a large percentage of Americans who have unrecognized HCV infection also probably have substantial hepatic damage. “To me it’s alarming that 20% of people who are not aware of their HCV infection are treatment candidates. These people are out there, but not getting treated,” he said in an interview.
Current U.S. HCV screening recommendations from the Centers for Disease Control and Prevention call for screening all Americans born during 1945-1965, “but there is no incentive to screen” and many U.S. primary care physicians don’t have HCV screening on their radar, he said.
The analysis conducted by Dr. Udompap and Dr. Kim used data collected by the National Health and Nutrition Examination Survey during 2001-2012, when the National Center for Health Statistics administered HCV testing to 45,000 of the 62,000 individuals who participated in the survey then.
Of the 45,000 people tested, 420 (0.9%) screened antibody positive and had infection confirmed by a second, RNA-based test. The HCV-positive patients then received a survey that included a question on whether they were aware of their HCV status before their current test result notification. One hundred sixty-three people (39%) completed and returned the survey: Eighty-three said they had previously been unaware they were HCV positive, and 80 said that they had known about their infection. The 50% rate of awareness of HCV chronic infection is consistent with a previously reported rate (Hepatology 2012;55:1652-61), said Dr. Udompap, a gastroenterology researcher at Stanford.
Individuals who were aware of their infection and those who were not had very similar demographic and clinical parameters. The average age was 53 years, and about two-thirds were men.
Dr. Udompap ran estimates of each respondent’s liver fibrosis and cirrhosis severity using the FIB-4 score and APRI score and data collected during the survey on age, liver enzyme levels, and platelet counts. These calculations showed that 22% of those ignorant of their HCV-positive status had a high probability of having advanced fibrosis, and 11% had a high probability of having cirrhosis, Dr. Udompap reported. These rates tracked close to those of the people who knew about their HCV-positive status, of whom 15% had a high probability of having advanced liver fibrosis and 11% were highly likely to have cirrhosis.
Dr. Udompap reported no financial disclosures. Dr. Kim has been a consultant to several drug companies that market, or are developing, drugs used in HCV.
On Twitter @mitchelzoler
VIENNA – Roughly half of American adults with chronic hepatitis C infection are unaware of their infection, and about one-fifth of these people with unsuspected infection likely have advanced liver fibrosis, according to a new analysis of U.S. data.
These findings “strengthen the recommendation for hepatitis C virus (HCV) screening in asymptomatic individuals,” Dr. Prowpanga Udompap said at the meeting sponsored by the European Association for the Study of the Liver.
People infected by HCV with advanced liver fibrosis have top priority for receiving curative drug treatment, according to recommendations by the American Association for the Study of the Liver and the Infectious Diseases Society of America.
People who have HCV-associated liver fibrosis that goes untreated also risk having their infection become more refractory to cure over time, they risk progressive hepatic deterioration that will eventually become symptomatic, and they face increasing risk for developing liver cancer, noted Dr. W. Ray Kim, senior author of the study and professor of medicine and chief of gastroenterology and hepatology at Stanford (Calif.) University.
Dr. Kim said he was surprised that such a large percentage of Americans who have unrecognized HCV infection also probably have substantial hepatic damage. “To me it’s alarming that 20% of people who are not aware of their HCV infection are treatment candidates. These people are out there, but not getting treated,” he said in an interview.
Current U.S. HCV screening recommendations from the Centers for Disease Control and Prevention call for screening all Americans born during 1945-1965, “but there is no incentive to screen” and many U.S. primary care physicians don’t have HCV screening on their radar, he said.
The analysis conducted by Dr. Udompap and Dr. Kim used data collected by the National Health and Nutrition Examination Survey during 2001-2012, when the National Center for Health Statistics administered HCV testing to 45,000 of the 62,000 individuals who participated in the survey then.
Of the 45,000 people tested, 420 (0.9%) screened antibody positive and had infection confirmed by a second, RNA-based test. The HCV-positive patients then received a survey that included a question on whether they were aware of their HCV status before their current test result notification. One hundred sixty-three people (39%) completed and returned the survey: Eighty-three said they had previously been unaware they were HCV positive, and 80 said that they had known about their infection. The 50% rate of awareness of HCV chronic infection is consistent with a previously reported rate (Hepatology 2012;55:1652-61), said Dr. Udompap, a gastroenterology researcher at Stanford.
Individuals who were aware of their infection and those who were not had very similar demographic and clinical parameters. The average age was 53 years, and about two-thirds were men.
Dr. Udompap ran estimates of each respondent’s liver fibrosis and cirrhosis severity using the FIB-4 score and APRI score and data collected during the survey on age, liver enzyme levels, and platelet counts. These calculations showed that 22% of those ignorant of their HCV-positive status had a high probability of having advanced fibrosis, and 11% had a high probability of having cirrhosis, Dr. Udompap reported. These rates tracked close to those of the people who knew about their HCV-positive status, of whom 15% had a high probability of having advanced liver fibrosis and 11% were highly likely to have cirrhosis.
Dr. Udompap reported no financial disclosures. Dr. Kim has been a consultant to several drug companies that market, or are developing, drugs used in HCV.
On Twitter @mitchelzoler
Key clinical point: One-fifth of Americans with unrecognized chronic hepatitis C infection likely have advanced hepatic fibrosis.
Major finding: Among U.S. adults with unrecognized chronic hepatitis C infection, 22% had laboratory results indicating a high probability of advanced hepatic fibrosis.
Data source: Data collected from 420 Americans found to have a chronic hepatitis C infection in the National Health and Nutrition Examination Survey during 2001-2012.
Disclosures: Dr. Udompap reported having no financial disclosures. Dr. Kim has been a consultant to several drug companies that market or develop drugs to eradicate hepatitis C infections.
DDW: SVRs slump in real-world use of sofosbuvir drugs
WASHINGTON – Sustained virologic response rates for genotype 1 and 2 patients are lower with sofosbuvir-based hepatitis C virus regimens in routine clinical practice than clinical trials, results from a large observational cohort analysis showed.
Patients with advanced liver disease and those with detectable HCV RNA at 4 weeks were significantly less likely to achieve a sustained virologic response (SVR), study author Dr. Lisa Backus reported at the annual Digestive Disease Week.

SVR rates with sofosbuvir (Sovaldi), which was approved in late 2013 for the treatment of HCV, have been reported in clinical trials generally in the 90%-plus range in genotype 1 (GT1) and 2 (GT2) patients.
“Often, however, it’s apparent that there are differences between the outcomes in clinical trials and routine medical practice,” said Dr. Backus of the VA Palo Alto (Calif.) Health Care System.
As a result, the investigators assessed clinical data from electronic medical records for 4,026 patients with GT1 or GT2 HCV who started sofosbuvir-based therapy for the recommended 12-week duration through the U.S. Department of Veterans Affairs, the largest integrated national provider of HCV care. Roughly a third of the patients were treatment experienced, and their average age was 61 years.
Among 3,203 GT1 patients, 1,302 started sofosbuvir, peginterferon, and ribavirin (SOF+PEG+RBV); 1,559, sofosbuvir plus simeprevir (SOF+SIM; Olysio); and 342, SOF+SIM+RBV. All 823 GT2 patients started SOF+RBV. About 10%-14% of patients did not receive 84 days of drug.
Patients were considered to have no SVR if HCV RNA was detectable on any test after the end of treatment, if they had no test after the end of treatment and HCV RNA was detectable on their last on-treatment test, or if they died before 12 weeks after the end of treatment. In all, 2,417 GT1 patients and 619 GT2 patients had SVR results.
Overall SVR rates were 66.8% with SOF+PEG+RBV, 75.3% with SOF+SIM, and 74.1% with SOF+SIM+RBV in GT1 patients and 79% with SOF+RBV in GT2 patients, Dr. Backus said.
For GT1 patients, SVR rates for treatment-naive vs. treatment-experienced patients were significantly different with SOF+PEG+RBV (73.7% vs. 55.6%; P <.001), but not with SOF+SIM (77.8% vs. 71.2%) or SOF+SIM+RBV (74.7% vs. 73.3%).
SVR rates were also different with SOF+RBV for GT2 treatment-naive vs. treatment-experienced patients (81.6% vs. 70.9%; P <.01), she reported.
Baseline factors associated with significantly lower SVR rates varied in GT1 treatment-naive and treatment-experienced patients by regimen, although an aspartate aminotransferase-to-platelet ratio index (APRI) score >2 was a significant predictor in treatment-naive patients for all three regimens and in treatment-experienced patients on SOF+PEG+RBV or SOF+SIM.
In a multivariate analysis adjusted for age, sex, race, body mass index (BMI), decompensated liver disease, diabetes, treatment experience, APRI score, HCV subtype, and regimen, GT1 patients with a BMI of at least 30 kg/m² had significantly lower odds of achieving a sustained virologic response (odds ratio, 0.64), as did those with decompensated liver disease (OR, 0.51), prior treatment experience (OR, 0.58), or an APRI score >2 (OR, 0.44), or those receiving SOF+PEG+RBV, compared with SOF-SIM (OR, 0.50; P values for all <.001), Dr. Backus said. The odds of achieving a sustained virologic response with SOF+SIM+RBV did not differ from the odds of doing so with SOF+SIM (OR, 1.03; P = .86).
Adding 4-week HCV RNA levels to the model did not change most baseline predictors, but showed that the odds of an SVR were reduced 41% for patients with 4-week HCV RNA <43 IU/mL (OR, 0.59; P <.001) and 58% for those with 4-week HCV RNA ≥43 IU/mL (OR, 0.42; P <.001), compared with patients with undetectable levels.
In GT2 patients, significant baseline predictors of lower SVR rates were an APRI >2 and a fibrosis-4 (FIB-4) index >3.25 in treatment-naive patients and a FIB-4 >3.25 in treatment-experienced patients.Using the first multivariate model, treatment experience (OR, 0.55; P <.01) and an APRI >2 (OR, 0.39; P <.001) predicted markedly lower odds of a sustained virologic response. Both factors remained significant in the second multivariate model, along with 4-week HCV RNA <43 IU/mL (OR, 0.29; P <.001) and ≥43 IU/mL (OR, 0.21; P <.001), Dr. Backus reported.
Study limitations were the lack of treatment randomization, testing and follow-up at the discretion of the provider, the use of surrogate laboratory markers (APRI or FIB-4) since few patients had biopsy or fibroscan results, and the lack of data on Q80K polymorphism status, she said.
Attendees questioned whether compliance could have caused such vastly lower SVR rates than reported in other trial settings. Dr. Backus acknowledged that she and her colleagues did not do chart reviews of actual discontinuation rates, but argued that adherence rates of 70%-80% in regular clinical practice in other fields of medicine, such as infectious diseases, are considered incredibly high.
“I think some of it is people have just gotten really spoiled, and we now think that 95% treatment completion is the real world,” she said. “We just don’t see it. I think one may argue that some of the other supposed real-world trials, the TARGET or TRIO trials, those generally are people getting seen at academic medical centers. … Those kinds of centers, although they’re a version of the real world, it’s not quite the same as my nurse practitioner in some of the VA clinics.”
Dr. Backus had no conflicts of interest.
On Twitter @pwendl
The Department of Veterans Affairs is the largest single provider of hepatitis C care in the United States. Ten percent of veterans born between 1945 and 1965 are infected with hepatitis C and the total number of veterans infected with hepatitis C is more than 200,000. The availability of direct-acting antivirals (DAAs) presented an opportunity to treat more veterans than ever, but also came at great cost to the VA system with most centers focusing the initial use of sofosbuvir-based regimens on those with the most advanced disease. At many centers, the vast majority of treated patients had cirrhosis and many were also treatment experienced. It should therefore come as no surprise that the real-world results of sofosbuvir-based regimens in the veteran population fell short of the results reported in the initial clinical trials.
While it is possible that compliance may have played some role in the lower SVRs reported, the cost of the treatment left most centers selecting patients with demonstrated health care compliance. Additionally, the VA would typically require frequent follow-up visits (as frequent as every 2 weeks at some centers) before dispensing a new round of the costly medications.The new DAA regimens have transcended some of the treatment challenges in the interferon era that are particularly relevant to the veteran population (mental health issues and race). While the real-world results of sofosbuvir-based regimens in veterans may not be ideal, there is still no doubt that DAA regimens represent a major advancement for the health care of veterans.
Dr. Sean Koppe is director of hepatology at the University of Illinois Hospital & Health Sciences System, Chicago. He has no conflicts of interest.
The Department of Veterans Affairs is the largest single provider of hepatitis C care in the United States. Ten percent of veterans born between 1945 and 1965 are infected with hepatitis C and the total number of veterans infected with hepatitis C is more than 200,000. The availability of direct-acting antivirals (DAAs) presented an opportunity to treat more veterans than ever, but also came at great cost to the VA system with most centers focusing the initial use of sofosbuvir-based regimens on those with the most advanced disease. At many centers, the vast majority of treated patients had cirrhosis and many were also treatment experienced. It should therefore come as no surprise that the real-world results of sofosbuvir-based regimens in the veteran population fell short of the results reported in the initial clinical trials.
While it is possible that compliance may have played some role in the lower SVRs reported, the cost of the treatment left most centers selecting patients with demonstrated health care compliance. Additionally, the VA would typically require frequent follow-up visits (as frequent as every 2 weeks at some centers) before dispensing a new round of the costly medications.The new DAA regimens have transcended some of the treatment challenges in the interferon era that are particularly relevant to the veteran population (mental health issues and race). While the real-world results of sofosbuvir-based regimens in veterans may not be ideal, there is still no doubt that DAA regimens represent a major advancement for the health care of veterans.
Dr. Sean Koppe is director of hepatology at the University of Illinois Hospital & Health Sciences System, Chicago. He has no conflicts of interest.
The Department of Veterans Affairs is the largest single provider of hepatitis C care in the United States. Ten percent of veterans born between 1945 and 1965 are infected with hepatitis C and the total number of veterans infected with hepatitis C is more than 200,000. The availability of direct-acting antivirals (DAAs) presented an opportunity to treat more veterans than ever, but also came at great cost to the VA system with most centers focusing the initial use of sofosbuvir-based regimens on those with the most advanced disease. At many centers, the vast majority of treated patients had cirrhosis and many were also treatment experienced. It should therefore come as no surprise that the real-world results of sofosbuvir-based regimens in the veteran population fell short of the results reported in the initial clinical trials.
While it is possible that compliance may have played some role in the lower SVRs reported, the cost of the treatment left most centers selecting patients with demonstrated health care compliance. Additionally, the VA would typically require frequent follow-up visits (as frequent as every 2 weeks at some centers) before dispensing a new round of the costly medications.The new DAA regimens have transcended some of the treatment challenges in the interferon era that are particularly relevant to the veteran population (mental health issues and race). While the real-world results of sofosbuvir-based regimens in veterans may not be ideal, there is still no doubt that DAA regimens represent a major advancement for the health care of veterans.
Dr. Sean Koppe is director of hepatology at the University of Illinois Hospital & Health Sciences System, Chicago. He has no conflicts of interest.
WASHINGTON – Sustained virologic response rates for genotype 1 and 2 patients are lower with sofosbuvir-based hepatitis C virus regimens in routine clinical practice than clinical trials, results from a large observational cohort analysis showed.
Patients with advanced liver disease and those with detectable HCV RNA at 4 weeks were significantly less likely to achieve a sustained virologic response (SVR), study author Dr. Lisa Backus reported at the annual Digestive Disease Week.
SVR rates with sofosbuvir (Sovaldi), which was approved in late 2013 for the treatment of HCV, have been reported in clinical trials generally in the 90%-plus range in genotype 1 (GT1) and 2 (GT2) patients.
“Often, however, it’s apparent that there are differences between the outcomes in clinical trials and routine medical practice,” said Dr. Backus of the VA Palo Alto (Calif.) Health Care System.
As a result, the investigators assessed clinical data from electronic medical records for 4,026 patients with GT1 or GT2 HCV who started sofosbuvir-based therapy for the recommended 12-week duration through the U.S. Department of Veterans Affairs, the largest integrated national provider of HCV care. Roughly a third of the patients were treatment experienced, and their average age was 61 years.
Among 3,203 GT1 patients, 1,302 started sofosbuvir, peginterferon, and ribavirin (SOF+PEG+RBV); 1,559, sofosbuvir plus simeprevir (SOF+SIM; Olysio); and 342, SOF+SIM+RBV. All 823 GT2 patients started SOF+RBV. About 10%-14% of patients did not receive 84 days of drug.
Patients were considered to have no SVR if HCV RNA was detectable on any test after the end of treatment, if they had no test after the end of treatment and HCV RNA was detectable on their last on-treatment test, or if they died before 12 weeks after the end of treatment. In all, 2,417 GT1 patients and 619 GT2 patients had SVR results.
Overall SVR rates were 66.8% with SOF+PEG+RBV, 75.3% with SOF+SIM, and 74.1% with SOF+SIM+RBV in GT1 patients and 79% with SOF+RBV in GT2 patients, Dr. Backus said.
For GT1 patients, SVR rates for treatment-naive vs. treatment-experienced patients were significantly different with SOF+PEG+RBV (73.7% vs. 55.6%; P <.001), but not with SOF+SIM (77.8% vs. 71.2%) or SOF+SIM+RBV (74.7% vs. 73.3%).
SVR rates were also different with SOF+RBV for GT2 treatment-naive vs. treatment-experienced patients (81.6% vs. 70.9%; P <.01), she reported.
Baseline factors associated with significantly lower SVR rates varied in GT1 treatment-naive and treatment-experienced patients by regimen, although an aspartate aminotransferase-to-platelet ratio index (APRI) score >2 was a significant predictor in treatment-naive patients for all three regimens and in treatment-experienced patients on SOF+PEG+RBV or SOF+SIM.
In a multivariate analysis adjusted for age, sex, race, body mass index (BMI), decompensated liver disease, diabetes, treatment experience, APRI score, HCV subtype, and regimen, GT1 patients with a BMI of at least 30 kg/m² had significantly lower odds of achieving a sustained virologic response (odds ratio, 0.64), as did those with decompensated liver disease (OR, 0.51), prior treatment experience (OR, 0.58), or an APRI score >2 (OR, 0.44), or those receiving SOF+PEG+RBV, compared with SOF-SIM (OR, 0.50; P values for all <.001), Dr. Backus said. The odds of achieving a sustained virologic response with SOF+SIM+RBV did not differ from the odds of doing so with SOF+SIM (OR, 1.03; P = .86).
Adding 4-week HCV RNA levels to the model did not change most baseline predictors, but showed that the odds of an SVR were reduced 41% for patients with 4-week HCV RNA <43 IU/mL (OR, 0.59; P <.001) and 58% for those with 4-week HCV RNA ≥43 IU/mL (OR, 0.42; P <.001), compared with patients with undetectable levels.
In GT2 patients, significant baseline predictors of lower SVR rates were an APRI >2 and a fibrosis-4 (FIB-4) index >3.25 in treatment-naive patients and a FIB-4 >3.25 in treatment-experienced patients.Using the first multivariate model, treatment experience (OR, 0.55; P <.01) and an APRI >2 (OR, 0.39; P <.001) predicted markedly lower odds of a sustained virologic response. Both factors remained significant in the second multivariate model, along with 4-week HCV RNA <43 IU/mL (OR, 0.29; P <.001) and ≥43 IU/mL (OR, 0.21; P <.001), Dr. Backus reported.
Study limitations were the lack of treatment randomization, testing and follow-up at the discretion of the provider, the use of surrogate laboratory markers (APRI or FIB-4) since few patients had biopsy or fibroscan results, and the lack of data on Q80K polymorphism status, she said.
Attendees questioned whether compliance could have caused such vastly lower SVR rates than reported in other trial settings. Dr. Backus acknowledged that she and her colleagues did not do chart reviews of actual discontinuation rates, but argued that adherence rates of 70%-80% in regular clinical practice in other fields of medicine, such as infectious diseases, are considered incredibly high.
“I think some of it is people have just gotten really spoiled, and we now think that 95% treatment completion is the real world,” she said. “We just don’t see it. I think one may argue that some of the other supposed real-world trials, the TARGET or TRIO trials, those generally are people getting seen at academic medical centers. … Those kinds of centers, although they’re a version of the real world, it’s not quite the same as my nurse practitioner in some of the VA clinics.”
Dr. Backus had no conflicts of interest.
On Twitter @pwendl
WASHINGTON – Sustained virologic response rates for genotype 1 and 2 patients are lower with sofosbuvir-based hepatitis C virus regimens in routine clinical practice than clinical trials, results from a large observational cohort analysis showed.
Patients with advanced liver disease and those with detectable HCV RNA at 4 weeks were significantly less likely to achieve a sustained virologic response (SVR), study author Dr. Lisa Backus reported at the annual Digestive Disease Week.
SVR rates with sofosbuvir (Sovaldi), which was approved in late 2013 for the treatment of HCV, have been reported in clinical trials generally in the 90%-plus range in genotype 1 (GT1) and 2 (GT2) patients.
“Often, however, it’s apparent that there are differences between the outcomes in clinical trials and routine medical practice,” said Dr. Backus of the VA Palo Alto (Calif.) Health Care System.
As a result, the investigators assessed clinical data from electronic medical records for 4,026 patients with GT1 or GT2 HCV who started sofosbuvir-based therapy for the recommended 12-week duration through the U.S. Department of Veterans Affairs, the largest integrated national provider of HCV care. Roughly a third of the patients were treatment experienced, and their average age was 61 years.
Among 3,203 GT1 patients, 1,302 started sofosbuvir, peginterferon, and ribavirin (SOF+PEG+RBV); 1,559, sofosbuvir plus simeprevir (SOF+SIM; Olysio); and 342, SOF+SIM+RBV. All 823 GT2 patients started SOF+RBV. About 10%-14% of patients did not receive 84 days of drug.
Patients were considered to have no SVR if HCV RNA was detectable on any test after the end of treatment, if they had no test after the end of treatment and HCV RNA was detectable on their last on-treatment test, or if they died before 12 weeks after the end of treatment. In all, 2,417 GT1 patients and 619 GT2 patients had SVR results.
Overall SVR rates were 66.8% with SOF+PEG+RBV, 75.3% with SOF+SIM, and 74.1% with SOF+SIM+RBV in GT1 patients and 79% with SOF+RBV in GT2 patients, Dr. Backus said.
For GT1 patients, SVR rates for treatment-naive vs. treatment-experienced patients were significantly different with SOF+PEG+RBV (73.7% vs. 55.6%; P <.001), but not with SOF+SIM (77.8% vs. 71.2%) or SOF+SIM+RBV (74.7% vs. 73.3%).
SVR rates were also different with SOF+RBV for GT2 treatment-naive vs. treatment-experienced patients (81.6% vs. 70.9%; P <.01), she reported.
Baseline factors associated with significantly lower SVR rates varied in GT1 treatment-naive and treatment-experienced patients by regimen, although an aspartate aminotransferase-to-platelet ratio index (APRI) score >2 was a significant predictor in treatment-naive patients for all three regimens and in treatment-experienced patients on SOF+PEG+RBV or SOF+SIM.
In a multivariate analysis adjusted for age, sex, race, body mass index (BMI), decompensated liver disease, diabetes, treatment experience, APRI score, HCV subtype, and regimen, GT1 patients with a BMI of at least 30 kg/m² had significantly lower odds of achieving a sustained virologic response (odds ratio, 0.64), as did those with decompensated liver disease (OR, 0.51), prior treatment experience (OR, 0.58), or an APRI score >2 (OR, 0.44), or those receiving SOF+PEG+RBV, compared with SOF-SIM (OR, 0.50; P values for all <.001), Dr. Backus said. The odds of achieving a sustained virologic response with SOF+SIM+RBV did not differ from the odds of doing so with SOF+SIM (OR, 1.03; P = .86).
Adding 4-week HCV RNA levels to the model did not change most baseline predictors, but showed that the odds of an SVR were reduced 41% for patients with 4-week HCV RNA <43 IU/mL (OR, 0.59; P <.001) and 58% for those with 4-week HCV RNA ≥43 IU/mL (OR, 0.42; P <.001), compared with patients with undetectable levels.
In GT2 patients, significant baseline predictors of lower SVR rates were an APRI >2 and a fibrosis-4 (FIB-4) index >3.25 in treatment-naive patients and a FIB-4 >3.25 in treatment-experienced patients.Using the first multivariate model, treatment experience (OR, 0.55; P <.01) and an APRI >2 (OR, 0.39; P <.001) predicted markedly lower odds of a sustained virologic response. Both factors remained significant in the second multivariate model, along with 4-week HCV RNA <43 IU/mL (OR, 0.29; P <.001) and ≥43 IU/mL (OR, 0.21; P <.001), Dr. Backus reported.
Study limitations were the lack of treatment randomization, testing and follow-up at the discretion of the provider, the use of surrogate laboratory markers (APRI or FIB-4) since few patients had biopsy or fibroscan results, and the lack of data on Q80K polymorphism status, she said.
Attendees questioned whether compliance could have caused such vastly lower SVR rates than reported in other trial settings. Dr. Backus acknowledged that she and her colleagues did not do chart reviews of actual discontinuation rates, but argued that adherence rates of 70%-80% in regular clinical practice in other fields of medicine, such as infectious diseases, are considered incredibly high.
“I think some of it is people have just gotten really spoiled, and we now think that 95% treatment completion is the real world,” she said. “We just don’t see it. I think one may argue that some of the other supposed real-world trials, the TARGET or TRIO trials, those generally are people getting seen at academic medical centers. … Those kinds of centers, although they’re a version of the real world, it’s not quite the same as my nurse practitioner in some of the VA clinics.”
Dr. Backus had no conflicts of interest.
On Twitter @pwendl
AT DDW® 2015

FDA report provides overview of HCV drug approvals
In a report published in Hepatology, scientists from the FDA’s Division of Antiviral Products in the Center for Drug Evaluation and Research (CDER) have provided a brief overview of the FDA’s scientific approaches and regulatory processes designed to accelerate the approval of drugs to treat hepatitis C virus (HCV).
The decision to publish the paper was made because of concerns regarding the efficacy of new, interferon- and ribavirin-free regimens that have gained traction in the drug marketplace. Publishing the paper should clear up some concerns that the drugs are not being properly evaluated, the authors write.
“This paper intends to provide increased transparency to various stakeholders about FDA’s scientific approaches and regulatory processes that supported drug development and marketing approval of [direct-acting antiviral agents] for the treatment of hepatitis C,” writes lead author Dr. Poonam Mishra, a deputy director in CDER.
Read the full article in Hepatology (doi:10.1002/hep.27880).
In a report published in Hepatology, scientists from the FDA’s Division of Antiviral Products in the Center for Drug Evaluation and Research (CDER) have provided a brief overview of the FDA’s scientific approaches and regulatory processes designed to accelerate the approval of drugs to treat hepatitis C virus (HCV).
The decision to publish the paper was made because of concerns regarding the efficacy of new, interferon- and ribavirin-free regimens that have gained traction in the drug marketplace. Publishing the paper should clear up some concerns that the drugs are not being properly evaluated, the authors write.
“This paper intends to provide increased transparency to various stakeholders about FDA’s scientific approaches and regulatory processes that supported drug development and marketing approval of [direct-acting antiviral agents] for the treatment of hepatitis C,” writes lead author Dr. Poonam Mishra, a deputy director in CDER.
Read the full article in Hepatology (doi:10.1002/hep.27880).
In a report published in Hepatology, scientists from the FDA’s Division of Antiviral Products in the Center for Drug Evaluation and Research (CDER) have provided a brief overview of the FDA’s scientific approaches and regulatory processes designed to accelerate the approval of drugs to treat hepatitis C virus (HCV).
The decision to publish the paper was made because of concerns regarding the efficacy of new, interferon- and ribavirin-free regimens that have gained traction in the drug marketplace. Publishing the paper should clear up some concerns that the drugs are not being properly evaluated, the authors write.
“This paper intends to provide increased transparency to various stakeholders about FDA’s scientific approaches and regulatory processes that supported drug development and marketing approval of [direct-acting antiviral agents] for the treatment of hepatitis C,” writes lead author Dr. Poonam Mishra, a deputy director in CDER.
Read the full article in Hepatology (doi:10.1002/hep.27880).
FROM HEPATOLOGY
VIDEO: Nivolumab puts brakes on advanced liver cancer
CHICAGO – Immune checkpoint inhibition with nivolumab every 2 weeks provides a better response than does standard treatment for advanced liver cancer, phase I/II results suggest.
The overall response rate was 19%, with 8 of the 42 evaluable patients experiencing at least 30% tumor shrinkage.
Moreover, responses to nivolumab (Opdivo) have been durable, with 62% of patients still alive at 12 months, Dr. Anthony El-Khoueiry reported in a press briefing in advance of the formal presentation of the study at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In contrast, just 2% of patients have at least 30% tumor shrinkage with sorafenib (Nexavar) and the average overall survival is about 10-11 months. Sorafenib, a multitargeted tyrosine kinase inhibitor, is currently the only Food and Drug Administration–approved systemic treatment for advanced liver disease, he noted.
Nivolumab, a programmed death-1 (PD-1) inhibitor, is approved for previously treated melanoma and gained a second indication in March for use in previously treated squamous non–small cell lung cancer.
“This is the first study to show antitumor activity of a PD-1 immune checkpoint inhibitor in patients with liver cancer,” said Dr. El-Khoueiry of the University of Southern California Norris Comprehensive Cancer Center, Los Angeles.The durability of those responses was particularly impressive, Dr. Peter Paul Yu, ASCO president, said in an interview.
“This is a small study, but the signal is unusually robust in comparison to what the standard of care would be, which is why this is so promising,” he added.
Press briefing moderator Dr. Lynn Schuchter, chief of hematology-oncology at University of Pennsylvania in Philadelphia, said in a statement, “The fact that this drug might stop advanced liver cancer in its tracks for months, even a year, is great news for patients. To understand the full impact of this approach, however, larger trials are needed.”
Hear more about the promising results from the late-breaking abstract in our interview with Dr. El-Khoueiry.
The study was funded by Bristol-Myers Squibb. Dr. El-Khoueiry reported financial relationships with Bristol-Myers Squibb, GlaxoSmithKline, Genentech/Roche, Amgen, Exelixis, AstraZeneca, and Astex Pharmaceuticals. Several coauthors also had ties to BMS including employment and/or stock ownership. Dr. Schuchter reported institutional research funding from BMS, Genentech, GSK, Merck, and Roche.
On Twitter @pwendl
CHICAGO – Immune checkpoint inhibition with nivolumab every 2 weeks provides a better response than does standard treatment for advanced liver cancer, phase I/II results suggest.
The overall response rate was 19%, with 8 of the 42 evaluable patients experiencing at least 30% tumor shrinkage.
Moreover, responses to nivolumab (Opdivo) have been durable, with 62% of patients still alive at 12 months, Dr. Anthony El-Khoueiry reported in a press briefing in advance of the formal presentation of the study at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In contrast, just 2% of patients have at least 30% tumor shrinkage with sorafenib (Nexavar) and the average overall survival is about 10-11 months. Sorafenib, a multitargeted tyrosine kinase inhibitor, is currently the only Food and Drug Administration–approved systemic treatment for advanced liver disease, he noted.
Nivolumab, a programmed death-1 (PD-1) inhibitor, is approved for previously treated melanoma and gained a second indication in March for use in previously treated squamous non–small cell lung cancer.
“This is the first study to show antitumor activity of a PD-1 immune checkpoint inhibitor in patients with liver cancer,” said Dr. El-Khoueiry of the University of Southern California Norris Comprehensive Cancer Center, Los Angeles.The durability of those responses was particularly impressive, Dr. Peter Paul Yu, ASCO president, said in an interview.
“This is a small study, but the signal is unusually robust in comparison to what the standard of care would be, which is why this is so promising,” he added.
Press briefing moderator Dr. Lynn Schuchter, chief of hematology-oncology at University of Pennsylvania in Philadelphia, said in a statement, “The fact that this drug might stop advanced liver cancer in its tracks for months, even a year, is great news for patients. To understand the full impact of this approach, however, larger trials are needed.”
Hear more about the promising results from the late-breaking abstract in our interview with Dr. El-Khoueiry.
The study was funded by Bristol-Myers Squibb. Dr. El-Khoueiry reported financial relationships with Bristol-Myers Squibb, GlaxoSmithKline, Genentech/Roche, Amgen, Exelixis, AstraZeneca, and Astex Pharmaceuticals. Several coauthors also had ties to BMS including employment and/or stock ownership. Dr. Schuchter reported institutional research funding from BMS, Genentech, GSK, Merck, and Roche.
On Twitter @pwendl
CHICAGO – Immune checkpoint inhibition with nivolumab every 2 weeks provides a better response than does standard treatment for advanced liver cancer, phase I/II results suggest.
The overall response rate was 19%, with 8 of the 42 evaluable patients experiencing at least 30% tumor shrinkage.
Moreover, responses to nivolumab (Opdivo) have been durable, with 62% of patients still alive at 12 months, Dr. Anthony El-Khoueiry reported in a press briefing in advance of the formal presentation of the study at the annual meeting of the American Society of Clinical Oncology.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
In contrast, just 2% of patients have at least 30% tumor shrinkage with sorafenib (Nexavar) and the average overall survival is about 10-11 months. Sorafenib, a multitargeted tyrosine kinase inhibitor, is currently the only Food and Drug Administration–approved systemic treatment for advanced liver disease, he noted.
Nivolumab, a programmed death-1 (PD-1) inhibitor, is approved for previously treated melanoma and gained a second indication in March for use in previously treated squamous non–small cell lung cancer.
“This is the first study to show antitumor activity of a PD-1 immune checkpoint inhibitor in patients with liver cancer,” said Dr. El-Khoueiry of the University of Southern California Norris Comprehensive Cancer Center, Los Angeles.The durability of those responses was particularly impressive, Dr. Peter Paul Yu, ASCO president, said in an interview.
“This is a small study, but the signal is unusually robust in comparison to what the standard of care would be, which is why this is so promising,” he added.
Press briefing moderator Dr. Lynn Schuchter, chief of hematology-oncology at University of Pennsylvania in Philadelphia, said in a statement, “The fact that this drug might stop advanced liver cancer in its tracks for months, even a year, is great news for patients. To understand the full impact of this approach, however, larger trials are needed.”
Hear more about the promising results from the late-breaking abstract in our interview with Dr. El-Khoueiry.
The study was funded by Bristol-Myers Squibb. Dr. El-Khoueiry reported financial relationships with Bristol-Myers Squibb, GlaxoSmithKline, Genentech/Roche, Amgen, Exelixis, AstraZeneca, and Astex Pharmaceuticals. Several coauthors also had ties to BMS including employment and/or stock ownership. Dr. Schuchter reported institutional research funding from BMS, Genentech, GSK, Merck, and Roche.
On Twitter @pwendl
AT THE ASCO ANNUAL MEETING 2015

DDW: Gestational diabetes linked to increased NAFLD risk in middle age
WASHINGTON – Gestational diabetes was identified as a significant, independent risk factor for developing non-alcoholic fatty liver disease later in life, according to a study of more than 1,000 women followed for 25 years.
This study “is the first to show a strong association between gestational diabetes in young adulthood and non-alcoholic fatty liver disease in middle-age,” Dr. Veeral Ajmera of the department of gastroenterology at the University of California, San Francisco, reported at the annual Digestive Disease Week.

The study evaluated 1,115 women from the Coronary Artery Risk Development in Young Adults (CARDIA) study, who had at least one delivery, did not have a diabetes diagnosis before pregnancy, and had a CT evaluation for hepatic steatosis at the 25-year visit, in 2010 and 2011. Women were excluded if they did not have a complete CT scan at that time, they had more than 14 drinks of alcohol per week, used medications associated with steatosis, or had chronic viral hepatitis or HIV infections.
At baseline the median age was 25-26 years, about 55%-56% were black, and the prevalence of hypertension (2%-3%) and dyslipidemia were similar. The CARDIA study enrolled about 5,100 men and women aged 18-30 years at four U.S. medical centers in the mid 1980s. Patients had 7 study visits over a 25-year follow-up period.
Of the 1,115 women evaluated, 124 (11%) went on to develop GDM and 75 (7%) met the CT definition for NAFLD (liver attenuation less than or equal to 40 Hounsfield units on CT scan) by the 25-year follow-up, when they were a median age of 50-51 years.
At 25 years, 14% of those with a history of GDM had NAFLD, compared with 5.8% of those who did not have GDM, for an unadjusted odds ratio of 2.56 (p <0.01), Dr. Ajmera said.
In the statistical analysis, the researchers determined that baseline homeostatic model assessment of insulin resistance (HOMA-IR) and baseline triglycerides were also ”strongly associated” with NAFLD at year 25.
“Importantly,” he noted, the measure of the association between GDM and NAFLD remained statistically significant, after adjusting for these covariates (OR, 2.29). At the start of the study, women who went on to develop GDM had significantly higher body mass index (BMI), HOMA-IR, waist circumference, and triglycerides than those who did not develop GDM, but the magnitude of those differences was small.
Additionally, after adjustment for a diagnosis of diabetes at year 25, the association between a history of GDM and NAFLD was stronger (OR, 1.99) than the association between a diagnosis of diabetes at year 25 and NAFLD (OR, 1.5), he said.
The researchers added BMI to their multivariate analysis to determine whether women with a gestational diabetes history gained more weight, and whether that weight explained the increased prevalence of NAFLD, “and found that the association between gestational diabetes and non-alcoholic fatty liver disease remained,” Dr. Ajmera added.
Evaluations of race, baseline BMI, and baseline HOMA-IR as effect modifiers of the relationship between GDM and NAFLD were not significant.
“Gestational diabetes represents insulin resistance unmasked by the stress of pregnancy, and offers the unique opportunity to identify those at risk of NAFLD at a young age,” Dr. Ajmera concluded.
Limitations of the study included not being able to determine if the women had NAFLD before they were diagnosed with GDM. However, based on the participants’ young age at enrollment, that is unlikely, he said. In addition, the researchers had no information on liver biochemistry tests, which, however, are not sensitive or specific for diagnosing NAFLD. The strengths of the study include the length of follow-up of a large biracial population, with measurement of well-characterized metabolic covariates measured, he added.
Dr. Ajmera reported having no relevant financial disclosures. The CARDIA study is supported by the National Heart, Lung, and Blood Institute, part of the National Institutes of Health.
Nonalcoholic fatty liver disease is the most common and fastest growing liver disease worldwide. Identifying individuals at high risk for NAFLD remains challenging. Dr. Ajmera and his colleagues highlight the association between gestational diabetes mellitus (GDM) and NAFLD. Their work confirms and extends earlier studies that reported increased hepatic fat content and a substantially increased risk for NAFLD, in women with a prior history of GDM. In the present study, a more racially diverse U.S.-based population was followed for a much longer duration than was previous cohorts. After adjusted multivariate analysis, GDM remained a strong, independent predictor of future NAFLD. Indeed, GDM was a a better NAFLD predictor than the diagnosis of diabetes alone was. It is unclear if prepregnancy NAFLD might have affected the risk for GDM, as subjects were not assessed for hepatic steatosis or liver test elevations at baseline. Also, the percentage of 50-year-old women with NAFLD was much lower in this cohort (7%) than in the general U.S. population (at least 25%), perhaps because the study population was enriched with individuals who are typically at low risk for NAFLD (i.e., African Americans, people with low body mass index, and/or low serum triglycerides).
Additional research is needed to clarify these issues and to investigate how maternal GDM affected the health of their children. Intrauterine exposure to metabolic stresses increases the risk for obesity and other metabolic disorders later in life, suggesting that offspring of mothers with GDM may require specialized surveillance or other precautions during childhood. Given that more young women are entering their reproductive years affected by diabetes and obesity, increased attention to these issues will be required to curb the growing public health burden of NAFLD.
Dr. Cynthia A. Moylan, M.H.S., is assistant professor of medicine, Duke University Medical Center and Veterans Affairs Medical Center, Durham, N.C. She is has no relevant financial conflicts of interests.
Nonalcoholic fatty liver disease is the most common and fastest growing liver disease worldwide. Identifying individuals at high risk for NAFLD remains challenging. Dr. Ajmera and his colleagues highlight the association between gestational diabetes mellitus (GDM) and NAFLD. Their work confirms and extends earlier studies that reported increased hepatic fat content and a substantially increased risk for NAFLD, in women with a prior history of GDM. In the present study, a more racially diverse U.S.-based population was followed for a much longer duration than was previous cohorts. After adjusted multivariate analysis, GDM remained a strong, independent predictor of future NAFLD. Indeed, GDM was a a better NAFLD predictor than the diagnosis of diabetes alone was. It is unclear if prepregnancy NAFLD might have affected the risk for GDM, as subjects were not assessed for hepatic steatosis or liver test elevations at baseline. Also, the percentage of 50-year-old women with NAFLD was much lower in this cohort (7%) than in the general U.S. population (at least 25%), perhaps because the study population was enriched with individuals who are typically at low risk for NAFLD (i.e., African Americans, people with low body mass index, and/or low serum triglycerides).
Additional research is needed to clarify these issues and to investigate how maternal GDM affected the health of their children. Intrauterine exposure to metabolic stresses increases the risk for obesity and other metabolic disorders later in life, suggesting that offspring of mothers with GDM may require specialized surveillance or other precautions during childhood. Given that more young women are entering their reproductive years affected by diabetes and obesity, increased attention to these issues will be required to curb the growing public health burden of NAFLD.
Dr. Cynthia A. Moylan, M.H.S., is assistant professor of medicine, Duke University Medical Center and Veterans Affairs Medical Center, Durham, N.C. She is has no relevant financial conflicts of interests.
Nonalcoholic fatty liver disease is the most common and fastest growing liver disease worldwide. Identifying individuals at high risk for NAFLD remains challenging. Dr. Ajmera and his colleagues highlight the association between gestational diabetes mellitus (GDM) and NAFLD. Their work confirms and extends earlier studies that reported increased hepatic fat content and a substantially increased risk for NAFLD, in women with a prior history of GDM. In the present study, a more racially diverse U.S.-based population was followed for a much longer duration than was previous cohorts. After adjusted multivariate analysis, GDM remained a strong, independent predictor of future NAFLD. Indeed, GDM was a a better NAFLD predictor than the diagnosis of diabetes alone was. It is unclear if prepregnancy NAFLD might have affected the risk for GDM, as subjects were not assessed for hepatic steatosis or liver test elevations at baseline. Also, the percentage of 50-year-old women with NAFLD was much lower in this cohort (7%) than in the general U.S. population (at least 25%), perhaps because the study population was enriched with individuals who are typically at low risk for NAFLD (i.e., African Americans, people with low body mass index, and/or low serum triglycerides).
Additional research is needed to clarify these issues and to investigate how maternal GDM affected the health of their children. Intrauterine exposure to metabolic stresses increases the risk for obesity and other metabolic disorders later in life, suggesting that offspring of mothers with GDM may require specialized surveillance or other precautions during childhood. Given that more young women are entering their reproductive years affected by diabetes and obesity, increased attention to these issues will be required to curb the growing public health burden of NAFLD.
Dr. Cynthia A. Moylan, M.H.S., is assistant professor of medicine, Duke University Medical Center and Veterans Affairs Medical Center, Durham, N.C. She is has no relevant financial conflicts of interests.
WASHINGTON – Gestational diabetes was identified as a significant, independent risk factor for developing non-alcoholic fatty liver disease later in life, according to a study of more than 1,000 women followed for 25 years.
This study “is the first to show a strong association between gestational diabetes in young adulthood and non-alcoholic fatty liver disease in middle-age,” Dr. Veeral Ajmera of the department of gastroenterology at the University of California, San Francisco, reported at the annual Digestive Disease Week.
The study evaluated 1,115 women from the Coronary Artery Risk Development in Young Adults (CARDIA) study, who had at least one delivery, did not have a diabetes diagnosis before pregnancy, and had a CT evaluation for hepatic steatosis at the 25-year visit, in 2010 and 2011. Women were excluded if they did not have a complete CT scan at that time, they had more than 14 drinks of alcohol per week, used medications associated with steatosis, or had chronic viral hepatitis or HIV infections.
At baseline the median age was 25-26 years, about 55%-56% were black, and the prevalence of hypertension (2%-3%) and dyslipidemia were similar. The CARDIA study enrolled about 5,100 men and women aged 18-30 years at four U.S. medical centers in the mid 1980s. Patients had 7 study visits over a 25-year follow-up period.
Of the 1,115 women evaluated, 124 (11%) went on to develop GDM and 75 (7%) met the CT definition for NAFLD (liver attenuation less than or equal to 40 Hounsfield units on CT scan) by the 25-year follow-up, when they were a median age of 50-51 years.
At 25 years, 14% of those with a history of GDM had NAFLD, compared with 5.8% of those who did not have GDM, for an unadjusted odds ratio of 2.56 (p <0.01), Dr. Ajmera said.
In the statistical analysis, the researchers determined that baseline homeostatic model assessment of insulin resistance (HOMA-IR) and baseline triglycerides were also ”strongly associated” with NAFLD at year 25.
“Importantly,” he noted, the measure of the association between GDM and NAFLD remained statistically significant, after adjusting for these covariates (OR, 2.29). At the start of the study, women who went on to develop GDM had significantly higher body mass index (BMI), HOMA-IR, waist circumference, and triglycerides than those who did not develop GDM, but the magnitude of those differences was small.
Additionally, after adjustment for a diagnosis of diabetes at year 25, the association between a history of GDM and NAFLD was stronger (OR, 1.99) than the association between a diagnosis of diabetes at year 25 and NAFLD (OR, 1.5), he said.
The researchers added BMI to their multivariate analysis to determine whether women with a gestational diabetes history gained more weight, and whether that weight explained the increased prevalence of NAFLD, “and found that the association between gestational diabetes and non-alcoholic fatty liver disease remained,” Dr. Ajmera added.
Evaluations of race, baseline BMI, and baseline HOMA-IR as effect modifiers of the relationship between GDM and NAFLD were not significant.
“Gestational diabetes represents insulin resistance unmasked by the stress of pregnancy, and offers the unique opportunity to identify those at risk of NAFLD at a young age,” Dr. Ajmera concluded.
Limitations of the study included not being able to determine if the women had NAFLD before they were diagnosed with GDM. However, based on the participants’ young age at enrollment, that is unlikely, he said. In addition, the researchers had no information on liver biochemistry tests, which, however, are not sensitive or specific for diagnosing NAFLD. The strengths of the study include the length of follow-up of a large biracial population, with measurement of well-characterized metabolic covariates measured, he added.
Dr. Ajmera reported having no relevant financial disclosures. The CARDIA study is supported by the National Heart, Lung, and Blood Institute, part of the National Institutes of Health.
WASHINGTON – Gestational diabetes was identified as a significant, independent risk factor for developing non-alcoholic fatty liver disease later in life, according to a study of more than 1,000 women followed for 25 years.
This study “is the first to show a strong association between gestational diabetes in young adulthood and non-alcoholic fatty liver disease in middle-age,” Dr. Veeral Ajmera of the department of gastroenterology at the University of California, San Francisco, reported at the annual Digestive Disease Week.
The study evaluated 1,115 women from the Coronary Artery Risk Development in Young Adults (CARDIA) study, who had at least one delivery, did not have a diabetes diagnosis before pregnancy, and had a CT evaluation for hepatic steatosis at the 25-year visit, in 2010 and 2011. Women were excluded if they did not have a complete CT scan at that time, they had more than 14 drinks of alcohol per week, used medications associated with steatosis, or had chronic viral hepatitis or HIV infections.
At baseline the median age was 25-26 years, about 55%-56% were black, and the prevalence of hypertension (2%-3%) and dyslipidemia were similar. The CARDIA study enrolled about 5,100 men and women aged 18-30 years at four U.S. medical centers in the mid 1980s. Patients had 7 study visits over a 25-year follow-up period.
Of the 1,115 women evaluated, 124 (11%) went on to develop GDM and 75 (7%) met the CT definition for NAFLD (liver attenuation less than or equal to 40 Hounsfield units on CT scan) by the 25-year follow-up, when they were a median age of 50-51 years.
At 25 years, 14% of those with a history of GDM had NAFLD, compared with 5.8% of those who did not have GDM, for an unadjusted odds ratio of 2.56 (p <0.01), Dr. Ajmera said.
In the statistical analysis, the researchers determined that baseline homeostatic model assessment of insulin resistance (HOMA-IR) and baseline triglycerides were also ”strongly associated” with NAFLD at year 25.
“Importantly,” he noted, the measure of the association between GDM and NAFLD remained statistically significant, after adjusting for these covariates (OR, 2.29). At the start of the study, women who went on to develop GDM had significantly higher body mass index (BMI), HOMA-IR, waist circumference, and triglycerides than those who did not develop GDM, but the magnitude of those differences was small.
Additionally, after adjustment for a diagnosis of diabetes at year 25, the association between a history of GDM and NAFLD was stronger (OR, 1.99) than the association between a diagnosis of diabetes at year 25 and NAFLD (OR, 1.5), he said.
The researchers added BMI to their multivariate analysis to determine whether women with a gestational diabetes history gained more weight, and whether that weight explained the increased prevalence of NAFLD, “and found that the association between gestational diabetes and non-alcoholic fatty liver disease remained,” Dr. Ajmera added.
Evaluations of race, baseline BMI, and baseline HOMA-IR as effect modifiers of the relationship between GDM and NAFLD were not significant.
“Gestational diabetes represents insulin resistance unmasked by the stress of pregnancy, and offers the unique opportunity to identify those at risk of NAFLD at a young age,” Dr. Ajmera concluded.
Limitations of the study included not being able to determine if the women had NAFLD before they were diagnosed with GDM. However, based on the participants’ young age at enrollment, that is unlikely, he said. In addition, the researchers had no information on liver biochemistry tests, which, however, are not sensitive or specific for diagnosing NAFLD. The strengths of the study include the length of follow-up of a large biracial population, with measurement of well-characterized metabolic covariates measured, he added.
Dr. Ajmera reported having no relevant financial disclosures. The CARDIA study is supported by the National Heart, Lung, and Blood Institute, part of the National Institutes of Health.
AT DDW® 2015
Key clinical point: Gestational diabetes could be used to identify young women at increased risk of having non-alcoholic fatty liver disease (NAFLD) in middle age.
Major finding: Having been diagnosed with gestational diabetes was associated with about a two-fold increased risk of having NAFLD in middle age.
Data source: The research involved 1,115 women enrolled in the 25-year Coronary Artery Risk Development in Young Adults (CARDIA) study.
Disclosures: Dr. Ajmera reported having no relevant financial disclosures. The CARDIA study is supported by the National Heart, Lung, and Blood Institute.
