User login
Pyzchiva Receives FDA Approval as Third Ustekinumab Biosimilar
The Food and Drug Administration has approved ustekinumab-ttwe (Pyzchiva) as a biosimilar to ustekinumab (Stelara) for the treatment of multiple inflammatory conditions.
In addition, the agency “provisionally determined” that the medication would be interchangeable with the reference product but that designation would not take hold until the interchangeability exclusivity period for the first approved biosimilar ustekinumab-auub (Wezlana) expires, according to a press release. This designation would, depending on state law, allow a pharmacist to substitute the biosimilar for the reference product without involving the prescribing clinician. It’s unclear when ustekinumab-auub’s interchangeability exclusivity ends.
Ustekinumab-ttwe, a human interleukin (IL)-12 and IL-23 antagonist, is indicated for the treatment of:
- Moderate to severe plaque psoriasis in adults and pediatric patients aged 6 years or older who are candidates for phototherapy or systemic therapy
- Active psoriatic arthritis in adults and pediatric patients aged 6 years or older with moderately to severely active Crohn’s disease or ulcerative colitis
It is administered via subcutaneous injection in 45 mg/0.5 mL and 90 mg/mL prefilled syringes or via intravenous infusion in 130 mg/26 mL (5 mg/mL) single-dose vial.
Developed by Samsung Bioepis, ustekinumab-ttwe will be commercialized by Sandoz in the United States. Besides ustekinumab-auub, the other ustekinumab biosimilar is ustekinumab-aekn (Selarsdi).
Ustekinumab-ttwe is expected to launch in February 2025 “in accordance with the settlement and license agreement with Janssen Biotech,” which manufacturers the reference product, Sandoz said. The other approved ustekinumab biosimilars will launch within a similar time frame.
A version of this article appeared on Medscape.com.
The Food and Drug Administration has approved ustekinumab-ttwe (Pyzchiva) as a biosimilar to ustekinumab (Stelara) for the treatment of multiple inflammatory conditions.
In addition, the agency “provisionally determined” that the medication would be interchangeable with the reference product but that designation would not take hold until the interchangeability exclusivity period for the first approved biosimilar ustekinumab-auub (Wezlana) expires, according to a press release. This designation would, depending on state law, allow a pharmacist to substitute the biosimilar for the reference product without involving the prescribing clinician. It’s unclear when ustekinumab-auub’s interchangeability exclusivity ends.
Ustekinumab-ttwe, a human interleukin (IL)-12 and IL-23 antagonist, is indicated for the treatment of:
- Moderate to severe plaque psoriasis in adults and pediatric patients aged 6 years or older who are candidates for phototherapy or systemic therapy
- Active psoriatic arthritis in adults and pediatric patients aged 6 years or older with moderately to severely active Crohn’s disease or ulcerative colitis
It is administered via subcutaneous injection in 45 mg/0.5 mL and 90 mg/mL prefilled syringes or via intravenous infusion in 130 mg/26 mL (5 mg/mL) single-dose vial.
Developed by Samsung Bioepis, ustekinumab-ttwe will be commercialized by Sandoz in the United States. Besides ustekinumab-auub, the other ustekinumab biosimilar is ustekinumab-aekn (Selarsdi).
Ustekinumab-ttwe is expected to launch in February 2025 “in accordance with the settlement and license agreement with Janssen Biotech,” which manufacturers the reference product, Sandoz said. The other approved ustekinumab biosimilars will launch within a similar time frame.
A version of this article appeared on Medscape.com.
The Food and Drug Administration has approved ustekinumab-ttwe (Pyzchiva) as a biosimilar to ustekinumab (Stelara) for the treatment of multiple inflammatory conditions.
In addition, the agency “provisionally determined” that the medication would be interchangeable with the reference product but that designation would not take hold until the interchangeability exclusivity period for the first approved biosimilar ustekinumab-auub (Wezlana) expires, according to a press release. This designation would, depending on state law, allow a pharmacist to substitute the biosimilar for the reference product without involving the prescribing clinician. It’s unclear when ustekinumab-auub’s interchangeability exclusivity ends.
Ustekinumab-ttwe, a human interleukin (IL)-12 and IL-23 antagonist, is indicated for the treatment of:
- Moderate to severe plaque psoriasis in adults and pediatric patients aged 6 years or older who are candidates for phototherapy or systemic therapy
- Active psoriatic arthritis in adults and pediatric patients aged 6 years or older with moderately to severely active Crohn’s disease or ulcerative colitis
It is administered via subcutaneous injection in 45 mg/0.5 mL and 90 mg/mL prefilled syringes or via intravenous infusion in 130 mg/26 mL (5 mg/mL) single-dose vial.
Developed by Samsung Bioepis, ustekinumab-ttwe will be commercialized by Sandoz in the United States. Besides ustekinumab-auub, the other ustekinumab biosimilar is ustekinumab-aekn (Selarsdi).
Ustekinumab-ttwe is expected to launch in February 2025 “in accordance with the settlement and license agreement with Janssen Biotech,” which manufacturers the reference product, Sandoz said. The other approved ustekinumab biosimilars will launch within a similar time frame.
A version of this article appeared on Medscape.com.
Baricitinib Outperforms TNF Inhibitors in Real-World RA Trial
Baricitinib may be the superior choice to tumor necrosis factor (TNF) inhibitors in patients with rheumatoid arthritis (RA) for whom conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) have failed, according to a new study.
After 12 weeks, patients taking baricitinib achieved a 50% improvement in RA symptoms according to American College of Rheumatology response criteria (ACR50) at twice the rate as in patients assigned to receive TNF inhibitors. In addition, 75% of the baricitinib group achieved a 28-joint Disease Activity Score with C-reactive protein under 2.6, compared with less than half of patients taking TNF inhibitors.
Putting Safety Into the Equation
However, safety concerns also need to be considered when prescribing medication, noted Andrew Wang, MD, PhD, a rheumatologist at Yale School of Medicine in New Haven, Connecticut. He was not involved with the study, called PERFECTRA.
“This category of drugs — JAK-STAT [inhibitors] — are much newer than TNF inhibitors, CTLAs, B-cell depleters, and the other tools we have,” he said, “with relatively less real-world experience and potential downsides in the future.”
Both the ACR and European Alliance of Associations for Rheumatology guidelines recommend that patients who have not achieved target disease activity with csDMARDs can be prescribed either a Janus kinase (JAK) inhibitor or a TNF inhibitor as a treatment option, yet many physicians favor TNF inhibitors because of extensive clinical experience with the drug class and other factors such as biosimilar availability and cost, Celine van de Laar, MSc, of Erasmus University in Rotterdam, the Netherlands, and coauthors explained.
There are also notable safety concerns for using JAK inhibitors: Results from a large postmarketing clinical trial of tofacitinib prompted the US Food and Drug Administration to issue a boxed warning for the medication due to an increased risk for cardiovascular events, cancer, blood clots, and death, in comparison with TNF inhibitors. That warning now includes two other medications in the same drug class: baricitinib and upadacitinib. The European Medicines Agency has also issued guidance to minimize the risk for side effects for these medications.
Some randomized controlled trials have demonstrated that baricitinib “showed significant clinical improvements” in patients with RA, compared with adalimumab and placebo, but these trials do not always reflect treatment in the real world, the study authors wrote. The results were published in RMD Open.
Study Details
In the study, researchers enrolled 199 patients with active RA for which previous use of at least one csDMARD had failed and randomly assigned 97 patients to receive baricitinib and the remainder to receive a TNF inhibitor: 64% started on adalimumab, 33% started on etanercept, and the rest used golimumab or infliximab.
For all patients, the suggested treatment allocation was provided via randomization lists, but physicians and patients ultimately decided treatment via shared decision-making.
Patients were diagnosed less than 5 years ago, had received no previous treatment with biologics or targeted synthetic DMARDs, and had no contraindications for TNF inhibitors or baricitinib. Researchers recruited patients from September 2019 through February 2022 across 15 health centers in the Netherlands and Belgium. The study was funded by Eli Lilly, which manufactures baricitinib, although the study was investigator initiated.
Patients were on average aged 55 years, and about two thirds were women. The average disease duration was 2 years.
At 12 weeks, 42% of the baricitinib group achieved ACR50, compared with 20% of the TNF inhibitor group. All patient-reported outcome measures showed improvement over the study period, favoring baricitinib. More patients receiving baricitinib remained on the medication overall than patients on a TNF inhibitor: At 48 weeks, 70% of patients receiving a TNF inhibitor and 80% of patients receiving baricitinib had continued taking their assigned treatment.
These results are not surprising, Wang noted, as “JAK inhibitors hit many arms of immune signaling, whereas TNF blockers just hit TNF.” However, there is a trade-off between potent, effective drugs and toxicity, he added.
“I would not be as bullish on starting baricitinib in a patient off the bat, in the same way that nobody would want to keep patients on glucocorticoids [any longer than is] minimally necessary.”
While the study was not powered to compare safety between the two drugs, there were no adverse events during the study that had not been previously reported.
“Prescribers have to be aware that cardiovascular and malignant [serious adverse events] are more frequently reported” with JAK inhibitors than with TNF inhibitors, the authors wrote. “Obviously, this has to be considered carefully in risk-benefit discussions with any individual patient.”
Dr. Wang noted that, in general, he and his colleagues would not start with a JAK inhibitor first except for special circumstances: For example, if a patient will not use an injectable medication, or for some reason, it’s impractical for the patient’s lifestyle to use medication that requires constant refrigeration.
“I think the take-home message here is these are, in general, lifelong diseases, and so a rheumatologist and their patients have to develop good relationships to monitor whether or not we’re hitting the sweet spot of keeping disease under control” while also avoiding overmedication and toxicity, he said.
One potential solution, which Dr. Wang has also done in his clinical practice, is to initiate a JAK inhibitor in patients who need it but then switch to a different modality after achieving disease control.
“You can imagine a scenario where you get them to a very low [Disease Activity Score] with baricitinib, for example, and then you switch them to a TNF inhibitor,” he said. “I can imagine that there would be ways that you could get the best of both worlds.”
PERFECTRA was financially supported by an unrestricted grant from Eli Lilly. The authors reported financial relationships with AbbVie, Eli Lilly, Galapagos, and Janssen-Cilag. Dr. Wang serves on NGM Bio’s science advisory board, consults for TCG Labs-Soleil and Seranova Bio, and has received funding from AstraZeneca.
A version of this article first appeared on Medscape.com.
Baricitinib may be the superior choice to tumor necrosis factor (TNF) inhibitors in patients with rheumatoid arthritis (RA) for whom conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) have failed, according to a new study.
After 12 weeks, patients taking baricitinib achieved a 50% improvement in RA symptoms according to American College of Rheumatology response criteria (ACR50) at twice the rate as in patients assigned to receive TNF inhibitors. In addition, 75% of the baricitinib group achieved a 28-joint Disease Activity Score with C-reactive protein under 2.6, compared with less than half of patients taking TNF inhibitors.
Putting Safety Into the Equation
However, safety concerns also need to be considered when prescribing medication, noted Andrew Wang, MD, PhD, a rheumatologist at Yale School of Medicine in New Haven, Connecticut. He was not involved with the study, called PERFECTRA.
“This category of drugs — JAK-STAT [inhibitors] — are much newer than TNF inhibitors, CTLAs, B-cell depleters, and the other tools we have,” he said, “with relatively less real-world experience and potential downsides in the future.”
Both the ACR and European Alliance of Associations for Rheumatology guidelines recommend that patients who have not achieved target disease activity with csDMARDs can be prescribed either a Janus kinase (JAK) inhibitor or a TNF inhibitor as a treatment option, yet many physicians favor TNF inhibitors because of extensive clinical experience with the drug class and other factors such as biosimilar availability and cost, Celine van de Laar, MSc, of Erasmus University in Rotterdam, the Netherlands, and coauthors explained.
There are also notable safety concerns for using JAK inhibitors: Results from a large postmarketing clinical trial of tofacitinib prompted the US Food and Drug Administration to issue a boxed warning for the medication due to an increased risk for cardiovascular events, cancer, blood clots, and death, in comparison with TNF inhibitors. That warning now includes two other medications in the same drug class: baricitinib and upadacitinib. The European Medicines Agency has also issued guidance to minimize the risk for side effects for these medications.
Some randomized controlled trials have demonstrated that baricitinib “showed significant clinical improvements” in patients with RA, compared with adalimumab and placebo, but these trials do not always reflect treatment in the real world, the study authors wrote. The results were published in RMD Open.
Study Details
In the study, researchers enrolled 199 patients with active RA for which previous use of at least one csDMARD had failed and randomly assigned 97 patients to receive baricitinib and the remainder to receive a TNF inhibitor: 64% started on adalimumab, 33% started on etanercept, and the rest used golimumab or infliximab.
For all patients, the suggested treatment allocation was provided via randomization lists, but physicians and patients ultimately decided treatment via shared decision-making.
Patients were diagnosed less than 5 years ago, had received no previous treatment with biologics or targeted synthetic DMARDs, and had no contraindications for TNF inhibitors or baricitinib. Researchers recruited patients from September 2019 through February 2022 across 15 health centers in the Netherlands and Belgium. The study was funded by Eli Lilly, which manufactures baricitinib, although the study was investigator initiated.
Patients were on average aged 55 years, and about two thirds were women. The average disease duration was 2 years.
At 12 weeks, 42% of the baricitinib group achieved ACR50, compared with 20% of the TNF inhibitor group. All patient-reported outcome measures showed improvement over the study period, favoring baricitinib. More patients receiving baricitinib remained on the medication overall than patients on a TNF inhibitor: At 48 weeks, 70% of patients receiving a TNF inhibitor and 80% of patients receiving baricitinib had continued taking their assigned treatment.
These results are not surprising, Wang noted, as “JAK inhibitors hit many arms of immune signaling, whereas TNF blockers just hit TNF.” However, there is a trade-off between potent, effective drugs and toxicity, he added.
“I would not be as bullish on starting baricitinib in a patient off the bat, in the same way that nobody would want to keep patients on glucocorticoids [any longer than is] minimally necessary.”
While the study was not powered to compare safety between the two drugs, there were no adverse events during the study that had not been previously reported.
“Prescribers have to be aware that cardiovascular and malignant [serious adverse events] are more frequently reported” with JAK inhibitors than with TNF inhibitors, the authors wrote. “Obviously, this has to be considered carefully in risk-benefit discussions with any individual patient.”
Dr. Wang noted that, in general, he and his colleagues would not start with a JAK inhibitor first except for special circumstances: For example, if a patient will not use an injectable medication, or for some reason, it’s impractical for the patient’s lifestyle to use medication that requires constant refrigeration.
“I think the take-home message here is these are, in general, lifelong diseases, and so a rheumatologist and their patients have to develop good relationships to monitor whether or not we’re hitting the sweet spot of keeping disease under control” while also avoiding overmedication and toxicity, he said.
One potential solution, which Dr. Wang has also done in his clinical practice, is to initiate a JAK inhibitor in patients who need it but then switch to a different modality after achieving disease control.
“You can imagine a scenario where you get them to a very low [Disease Activity Score] with baricitinib, for example, and then you switch them to a TNF inhibitor,” he said. “I can imagine that there would be ways that you could get the best of both worlds.”
PERFECTRA was financially supported by an unrestricted grant from Eli Lilly. The authors reported financial relationships with AbbVie, Eli Lilly, Galapagos, and Janssen-Cilag. Dr. Wang serves on NGM Bio’s science advisory board, consults for TCG Labs-Soleil and Seranova Bio, and has received funding from AstraZeneca.
A version of this article first appeared on Medscape.com.
Baricitinib may be the superior choice to tumor necrosis factor (TNF) inhibitors in patients with rheumatoid arthritis (RA) for whom conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) have failed, according to a new study.
After 12 weeks, patients taking baricitinib achieved a 50% improvement in RA symptoms according to American College of Rheumatology response criteria (ACR50) at twice the rate as in patients assigned to receive TNF inhibitors. In addition, 75% of the baricitinib group achieved a 28-joint Disease Activity Score with C-reactive protein under 2.6, compared with less than half of patients taking TNF inhibitors.
Putting Safety Into the Equation
However, safety concerns also need to be considered when prescribing medication, noted Andrew Wang, MD, PhD, a rheumatologist at Yale School of Medicine in New Haven, Connecticut. He was not involved with the study, called PERFECTRA.
“This category of drugs — JAK-STAT [inhibitors] — are much newer than TNF inhibitors, CTLAs, B-cell depleters, and the other tools we have,” he said, “with relatively less real-world experience and potential downsides in the future.”
Both the ACR and European Alliance of Associations for Rheumatology guidelines recommend that patients who have not achieved target disease activity with csDMARDs can be prescribed either a Janus kinase (JAK) inhibitor or a TNF inhibitor as a treatment option, yet many physicians favor TNF inhibitors because of extensive clinical experience with the drug class and other factors such as biosimilar availability and cost, Celine van de Laar, MSc, of Erasmus University in Rotterdam, the Netherlands, and coauthors explained.
There are also notable safety concerns for using JAK inhibitors: Results from a large postmarketing clinical trial of tofacitinib prompted the US Food and Drug Administration to issue a boxed warning for the medication due to an increased risk for cardiovascular events, cancer, blood clots, and death, in comparison with TNF inhibitors. That warning now includes two other medications in the same drug class: baricitinib and upadacitinib. The European Medicines Agency has also issued guidance to minimize the risk for side effects for these medications.
Some randomized controlled trials have demonstrated that baricitinib “showed significant clinical improvements” in patients with RA, compared with adalimumab and placebo, but these trials do not always reflect treatment in the real world, the study authors wrote. The results were published in RMD Open.
Study Details
In the study, researchers enrolled 199 patients with active RA for which previous use of at least one csDMARD had failed and randomly assigned 97 patients to receive baricitinib and the remainder to receive a TNF inhibitor: 64% started on adalimumab, 33% started on etanercept, and the rest used golimumab or infliximab.
For all patients, the suggested treatment allocation was provided via randomization lists, but physicians and patients ultimately decided treatment via shared decision-making.
Patients were diagnosed less than 5 years ago, had received no previous treatment with biologics or targeted synthetic DMARDs, and had no contraindications for TNF inhibitors or baricitinib. Researchers recruited patients from September 2019 through February 2022 across 15 health centers in the Netherlands and Belgium. The study was funded by Eli Lilly, which manufactures baricitinib, although the study was investigator initiated.
Patients were on average aged 55 years, and about two thirds were women. The average disease duration was 2 years.
At 12 weeks, 42% of the baricitinib group achieved ACR50, compared with 20% of the TNF inhibitor group. All patient-reported outcome measures showed improvement over the study period, favoring baricitinib. More patients receiving baricitinib remained on the medication overall than patients on a TNF inhibitor: At 48 weeks, 70% of patients receiving a TNF inhibitor and 80% of patients receiving baricitinib had continued taking their assigned treatment.
These results are not surprising, Wang noted, as “JAK inhibitors hit many arms of immune signaling, whereas TNF blockers just hit TNF.” However, there is a trade-off between potent, effective drugs and toxicity, he added.
“I would not be as bullish on starting baricitinib in a patient off the bat, in the same way that nobody would want to keep patients on glucocorticoids [any longer than is] minimally necessary.”
While the study was not powered to compare safety between the two drugs, there were no adverse events during the study that had not been previously reported.
“Prescribers have to be aware that cardiovascular and malignant [serious adverse events] are more frequently reported” with JAK inhibitors than with TNF inhibitors, the authors wrote. “Obviously, this has to be considered carefully in risk-benefit discussions with any individual patient.”
Dr. Wang noted that, in general, he and his colleagues would not start with a JAK inhibitor first except for special circumstances: For example, if a patient will not use an injectable medication, or for some reason, it’s impractical for the patient’s lifestyle to use medication that requires constant refrigeration.
“I think the take-home message here is these are, in general, lifelong diseases, and so a rheumatologist and their patients have to develop good relationships to monitor whether or not we’re hitting the sweet spot of keeping disease under control” while also avoiding overmedication and toxicity, he said.
One potential solution, which Dr. Wang has also done in his clinical practice, is to initiate a JAK inhibitor in patients who need it but then switch to a different modality after achieving disease control.
“You can imagine a scenario where you get them to a very low [Disease Activity Score] with baricitinib, for example, and then you switch them to a TNF inhibitor,” he said. “I can imagine that there would be ways that you could get the best of both worlds.”
PERFECTRA was financially supported by an unrestricted grant from Eli Lilly. The authors reported financial relationships with AbbVie, Eli Lilly, Galapagos, and Janssen-Cilag. Dr. Wang serves on NGM Bio’s science advisory board, consults for TCG Labs-Soleil and Seranova Bio, and has received funding from AstraZeneca.
A version of this article first appeared on Medscape.com.
FROM RMD OPEN
‘Therapeutic Continuums’ Guide Systemic Sclerosis Treatment in Updated EULAR Recommendations
VIENNA – The use of immunosuppressive and antifibrotic drugs to treat skin and lung fibrosis leads updated recommendations from the European Alliance of Associations for Rheumatology (EULAR) for the treatment of systemic sclerosis.
“The most impactful new recommendation relates to the evidence for immunosuppressive agents and antifibrotics for the treatment of skin fibrosis and lung fibrosis,” said Francesco Del Galdo, MD, PhD, professor of experimental medicine, consultant rheumatologist, and scleroderma and connective tissue diseases specialist at Leeds Teaching Hospitals NHS Trust, Leeds, England. Dr. Del Galdo presented the update at the annual European Congress of Rheumatology.
“But there are also new recommendations, including a redefined target population for hematopoietic stem cell transplantation following cyclophosphamide, the upfront combination treatment at the time of diagnosis of pulmonary arterial hypertension [PAH], and a negative recommendation for the use of anticoagulants for pulmonary arterial hypertension,” noted Dr. Del Galdo, highlighting key updates in the 2024 recommendations.
Robert B.M. Landewé, MD, PhD, professor and rheumatologist at Amsterdam University Medical Center, Amsterdam, the Netherlands, and Zuyderland Medical Center, Heerlen, the Netherlands, co-moderated the session on EULAR recommendations. “The management of systemic sclerosis is a field in which a lot is happening,” he said. “The last update goes back to 2017, and in the meantime, many new approaches have seen the light, especially pertaining to skin fibrosis and interstitial lung disease. Six new recommendations have been coined, covering drugs like mycophenolate mofetil, nintedanib, rituximab, and tocilizumab. None of these therapies were present in the 2017 recommendations. It seems the field is now ready to further expand on targeted therapies for the management of musculoskeletal and gastrointestinal manifestations, calcinosis, and the local management of digital ulcers.”
‘Therapeutic Continuums’ Aid Disease Management
Dr. Del Galdo and his colleagues grouped the various interventions across what the recommendations label as evidence-backed “therapeutic continuums.” These span six of the eight different clinical manifestations of systemic sclerosis: Raynaud’s phenomenon, digital ulcers, pulmonary hypertension, musculoskeletal manifestations, skin fibrosis, interstitial lung disease (ILD), and gastrointestinal and renal crisis.
A slide showing the different strengths of evidence for various drugs across the eight manifestations illustrated the principle behind the therapeutic continuums. “These ‘therapeutic continuums’ suggest a common pathogenetic mechanism driving the various manifestations of disease,” said Dr. Del Galdo. For example, he noted, “If rituximab had a positive response in skin and in lung, it suggests that B cells play a role in the clinical manifestations of skin and lung in this disease.”
Dr. Del Galdo highlighted the new immunosuppression continuum and associated treatments for skin and lung fibrosis. “For skin involvement, the task force recommended mycophenolate, methotrexate, and rituximab, with tocilizumab having a lower level of evidence and lower recommendation strength; similarly, in interstitial lung disease, we have rituximab, mycophenolate, cyclophosphamide, and nintedanib, and these all have the highest strength of evidence. Tocilizumab is assigned one strength of evidence below the other drugs.”
He also cited the phosphodiesterase 5 inhibitor (PDE5i) drugs that are used across Raynaud’s phenomenon, digital ulcers, and pulmonary arterial hypertension, which together form a vascular therapeutic continuum.
The complexity of systemic sclerosis and multiple manifestations was a major determinant of the recommendations, Dr. Del Galdo pointed out. “The task force realized that since this is such a complex disease, we cannot recommend one treatment unconditionally. For example, with mycophenolate mofetil, what works for most patients for the skin and lung manifestations might not for someone who experiences severe diarrhea, in which mycophenolate is contraindicated. So, the highest degree of recommendation that the task force felt comfortable with was ‘should be considered.’ ”
Dr. Del Galdo stressed that the complex nature of systemic sclerosis means that “when thinking of treating one manifestation, you also always need to consider all the other clinical manifestations as experienced by the patient, and it is this multifaceted scenario that will ultimately lead to your final choice.”
Turning to new evidence around drug use, Dr. Del Galdo said that rituximab has the highest level of evidence across skin and lung manifestations, nintedanib is new in lung, and tocilizumab is new across both skin and lung.
To treat systemic sclerosis–pulmonary arterial hypertension (SSc-PAH), as long as there are no contraindications, the task force recommends using PDE5i and endothelin receptor antagonists (ERAs) at diagnosis. Data from phase 3 trials show a better outcome when the combination is established early.
The task force suggests avoiding the use of warfarin in PAH. “This is supported by a signal from two trials showing an increase in morbidity and mortality in these patients,” noted Dr. Del Galdo.
He also pointed out that selexipag and riociguat were new and important second-line additions for the treatment of PAH, and — consistent with the ERA approach — the EULAR recommendation supports frequent follow-up to establish a treat-to-target approach to maximizing clinical outcomes in SSc-PAH and SSc-ILD. “Specifically, for the first time, we recommend monitoring the effect of any chosen intervention selected within 3-6 months of starting. The evidence suggests there is a group of patients who respond and some who respond less well and who might benefit from a second-line intervention.”
For example, results of one trial support the approach of adding an antifibrotic agent to reduce progression in people with progressive lung fibrosis. “Similarly, for pulmonary hypertension, we recommend putting patients on dual treatment, and if this fails, place them on selexipag or switch the PDE5i to riociguat,” Dr. Del Galdo said.
Systemic Sclerosis Research Agenda and Recommendations Align
Dr. Del Galdo highlighted the value of therapeutic continuums in advancing disease understanding. “It is starting to teach us what we know and what we don’t and where do we need to build more evidence. Effectively, they determine where the gaps in therapy lie, and this starts to guide the research agenda.
“In fact, what is really interesting about this recommendation update — certainly from the perspective of disease understanding — is that we are starting to have a bird’s-eye view of the clinical manifestations of scleroderma that have so often been dealt with separately. Now we are starting to build a cumulative evidence map of this disease.”
In 2017, the research agenda largely advocated identifying immune-targeting drugs for skin and lung fibrosis, Dr. Del Galdo pointed out. “Now, we’ve done that — we’ve identified appropriate immunosuppressive drugs — and this is testimony to the importance of these recommendations because what prioritized the research agenda 10 years ago ended up informing the clinical trials and made it into the recommendations.”
“We definitely are one step forward compared to this 2017 recommendation and closer to what we would like to do,” he asserted.
Remission Elusive but Getting Closer
In some respects, according to Dr. Del Galdo, research and development is making relatively slow progress, especially compared with other rheumatologic diseases such as rheumatoid arthritis. “We cannot put patients with systemic sclerosis in remission yet. But I think we are one step ahead in that we’ve now established the treat-to-target approach to maximize the efficacy with which we can stall disease progression, but we cannot yet put these patients into remission,” he said. Systemic sclerosis has multiple manifestations, and fibrotic damage cannot be reversed. “Right now, the scar will remain there forever,” he noted.
Until remission is achievable, Dr. Del Galdo advises diagnosing and treating patients earlier to prevent fibrotic manifestations.
Dr. Del Galdo explained the three leading priorities on the systemic sclerosis research agenda. “There are three because it is such a complex disease. The first is considering the patient voice — this is the most important one, and the patients say they want a more holistic approach — so trialing and treating multiple manifestations together.”
Second, Dr. Del Galdo said, he would like to see a patient-reported measure developed that can capture the entire disease.
Third, from a physician’s point of view, Dr. Del Galdo said, “We want to send the patients into remission. We need to continue to further deconvolute the clinical manifestations and find the bottleneck at the beginning of the natural history of disease.
“If we can find a drug that is effective very early on, before the patients start getting the eight different manifestations with different levels of severity, then we will be on the right road, which we hope will end in remission.”
Dr. Del Galdo has served on the speakers bureau for AstraZeneca and Janssen; consulted for AstraZeneca, Boehringer Ingelheim, Capella, Chemomab, Janssen, and Mitsubishi-Tanabe; and received grant or research support from AbbVie, AstraZeneca, Boheringer Ingelheim, Capella, Chemomab, Kymab, Janssen, and Mitsubishi-Tanabe. Dr. Landewé had no relevant disclosures.
A version of this article first appeared on Medscape.com.
VIENNA – The use of immunosuppressive and antifibrotic drugs to treat skin and lung fibrosis leads updated recommendations from the European Alliance of Associations for Rheumatology (EULAR) for the treatment of systemic sclerosis.
“The most impactful new recommendation relates to the evidence for immunosuppressive agents and antifibrotics for the treatment of skin fibrosis and lung fibrosis,” said Francesco Del Galdo, MD, PhD, professor of experimental medicine, consultant rheumatologist, and scleroderma and connective tissue diseases specialist at Leeds Teaching Hospitals NHS Trust, Leeds, England. Dr. Del Galdo presented the update at the annual European Congress of Rheumatology.
“But there are also new recommendations, including a redefined target population for hematopoietic stem cell transplantation following cyclophosphamide, the upfront combination treatment at the time of diagnosis of pulmonary arterial hypertension [PAH], and a negative recommendation for the use of anticoagulants for pulmonary arterial hypertension,” noted Dr. Del Galdo, highlighting key updates in the 2024 recommendations.
Robert B.M. Landewé, MD, PhD, professor and rheumatologist at Amsterdam University Medical Center, Amsterdam, the Netherlands, and Zuyderland Medical Center, Heerlen, the Netherlands, co-moderated the session on EULAR recommendations. “The management of systemic sclerosis is a field in which a lot is happening,” he said. “The last update goes back to 2017, and in the meantime, many new approaches have seen the light, especially pertaining to skin fibrosis and interstitial lung disease. Six new recommendations have been coined, covering drugs like mycophenolate mofetil, nintedanib, rituximab, and tocilizumab. None of these therapies were present in the 2017 recommendations. It seems the field is now ready to further expand on targeted therapies for the management of musculoskeletal and gastrointestinal manifestations, calcinosis, and the local management of digital ulcers.”
‘Therapeutic Continuums’ Aid Disease Management
Dr. Del Galdo and his colleagues grouped the various interventions across what the recommendations label as evidence-backed “therapeutic continuums.” These span six of the eight different clinical manifestations of systemic sclerosis: Raynaud’s phenomenon, digital ulcers, pulmonary hypertension, musculoskeletal manifestations, skin fibrosis, interstitial lung disease (ILD), and gastrointestinal and renal crisis.
A slide showing the different strengths of evidence for various drugs across the eight manifestations illustrated the principle behind the therapeutic continuums. “These ‘therapeutic continuums’ suggest a common pathogenetic mechanism driving the various manifestations of disease,” said Dr. Del Galdo. For example, he noted, “If rituximab had a positive response in skin and in lung, it suggests that B cells play a role in the clinical manifestations of skin and lung in this disease.”
Dr. Del Galdo highlighted the new immunosuppression continuum and associated treatments for skin and lung fibrosis. “For skin involvement, the task force recommended mycophenolate, methotrexate, and rituximab, with tocilizumab having a lower level of evidence and lower recommendation strength; similarly, in interstitial lung disease, we have rituximab, mycophenolate, cyclophosphamide, and nintedanib, and these all have the highest strength of evidence. Tocilizumab is assigned one strength of evidence below the other drugs.”
He also cited the phosphodiesterase 5 inhibitor (PDE5i) drugs that are used across Raynaud’s phenomenon, digital ulcers, and pulmonary arterial hypertension, which together form a vascular therapeutic continuum.
The complexity of systemic sclerosis and multiple manifestations was a major determinant of the recommendations, Dr. Del Galdo pointed out. “The task force realized that since this is such a complex disease, we cannot recommend one treatment unconditionally. For example, with mycophenolate mofetil, what works for most patients for the skin and lung manifestations might not for someone who experiences severe diarrhea, in which mycophenolate is contraindicated. So, the highest degree of recommendation that the task force felt comfortable with was ‘should be considered.’ ”
Dr. Del Galdo stressed that the complex nature of systemic sclerosis means that “when thinking of treating one manifestation, you also always need to consider all the other clinical manifestations as experienced by the patient, and it is this multifaceted scenario that will ultimately lead to your final choice.”
Turning to new evidence around drug use, Dr. Del Galdo said that rituximab has the highest level of evidence across skin and lung manifestations, nintedanib is new in lung, and tocilizumab is new across both skin and lung.
To treat systemic sclerosis–pulmonary arterial hypertension (SSc-PAH), as long as there are no contraindications, the task force recommends using PDE5i and endothelin receptor antagonists (ERAs) at diagnosis. Data from phase 3 trials show a better outcome when the combination is established early.
The task force suggests avoiding the use of warfarin in PAH. “This is supported by a signal from two trials showing an increase in morbidity and mortality in these patients,” noted Dr. Del Galdo.
He also pointed out that selexipag and riociguat were new and important second-line additions for the treatment of PAH, and — consistent with the ERA approach — the EULAR recommendation supports frequent follow-up to establish a treat-to-target approach to maximizing clinical outcomes in SSc-PAH and SSc-ILD. “Specifically, for the first time, we recommend monitoring the effect of any chosen intervention selected within 3-6 months of starting. The evidence suggests there is a group of patients who respond and some who respond less well and who might benefit from a second-line intervention.”
For example, results of one trial support the approach of adding an antifibrotic agent to reduce progression in people with progressive lung fibrosis. “Similarly, for pulmonary hypertension, we recommend putting patients on dual treatment, and if this fails, place them on selexipag or switch the PDE5i to riociguat,” Dr. Del Galdo said.
Systemic Sclerosis Research Agenda and Recommendations Align
Dr. Del Galdo highlighted the value of therapeutic continuums in advancing disease understanding. “It is starting to teach us what we know and what we don’t and where do we need to build more evidence. Effectively, they determine where the gaps in therapy lie, and this starts to guide the research agenda.
“In fact, what is really interesting about this recommendation update — certainly from the perspective of disease understanding — is that we are starting to have a bird’s-eye view of the clinical manifestations of scleroderma that have so often been dealt with separately. Now we are starting to build a cumulative evidence map of this disease.”
In 2017, the research agenda largely advocated identifying immune-targeting drugs for skin and lung fibrosis, Dr. Del Galdo pointed out. “Now, we’ve done that — we’ve identified appropriate immunosuppressive drugs — and this is testimony to the importance of these recommendations because what prioritized the research agenda 10 years ago ended up informing the clinical trials and made it into the recommendations.”
“We definitely are one step forward compared to this 2017 recommendation and closer to what we would like to do,” he asserted.
Remission Elusive but Getting Closer
In some respects, according to Dr. Del Galdo, research and development is making relatively slow progress, especially compared with other rheumatologic diseases such as rheumatoid arthritis. “We cannot put patients with systemic sclerosis in remission yet. But I think we are one step ahead in that we’ve now established the treat-to-target approach to maximize the efficacy with which we can stall disease progression, but we cannot yet put these patients into remission,” he said. Systemic sclerosis has multiple manifestations, and fibrotic damage cannot be reversed. “Right now, the scar will remain there forever,” he noted.
Until remission is achievable, Dr. Del Galdo advises diagnosing and treating patients earlier to prevent fibrotic manifestations.
Dr. Del Galdo explained the three leading priorities on the systemic sclerosis research agenda. “There are three because it is such a complex disease. The first is considering the patient voice — this is the most important one, and the patients say they want a more holistic approach — so trialing and treating multiple manifestations together.”
Second, Dr. Del Galdo said, he would like to see a patient-reported measure developed that can capture the entire disease.
Third, from a physician’s point of view, Dr. Del Galdo said, “We want to send the patients into remission. We need to continue to further deconvolute the clinical manifestations and find the bottleneck at the beginning of the natural history of disease.
“If we can find a drug that is effective very early on, before the patients start getting the eight different manifestations with different levels of severity, then we will be on the right road, which we hope will end in remission.”
Dr. Del Galdo has served on the speakers bureau for AstraZeneca and Janssen; consulted for AstraZeneca, Boehringer Ingelheim, Capella, Chemomab, Janssen, and Mitsubishi-Tanabe; and received grant or research support from AbbVie, AstraZeneca, Boheringer Ingelheim, Capella, Chemomab, Kymab, Janssen, and Mitsubishi-Tanabe. Dr. Landewé had no relevant disclosures.
A version of this article first appeared on Medscape.com.
VIENNA – The use of immunosuppressive and antifibrotic drugs to treat skin and lung fibrosis leads updated recommendations from the European Alliance of Associations for Rheumatology (EULAR) for the treatment of systemic sclerosis.
“The most impactful new recommendation relates to the evidence for immunosuppressive agents and antifibrotics for the treatment of skin fibrosis and lung fibrosis,” said Francesco Del Galdo, MD, PhD, professor of experimental medicine, consultant rheumatologist, and scleroderma and connective tissue diseases specialist at Leeds Teaching Hospitals NHS Trust, Leeds, England. Dr. Del Galdo presented the update at the annual European Congress of Rheumatology.
“But there are also new recommendations, including a redefined target population for hematopoietic stem cell transplantation following cyclophosphamide, the upfront combination treatment at the time of diagnosis of pulmonary arterial hypertension [PAH], and a negative recommendation for the use of anticoagulants for pulmonary arterial hypertension,” noted Dr. Del Galdo, highlighting key updates in the 2024 recommendations.
Robert B.M. Landewé, MD, PhD, professor and rheumatologist at Amsterdam University Medical Center, Amsterdam, the Netherlands, and Zuyderland Medical Center, Heerlen, the Netherlands, co-moderated the session on EULAR recommendations. “The management of systemic sclerosis is a field in which a lot is happening,” he said. “The last update goes back to 2017, and in the meantime, many new approaches have seen the light, especially pertaining to skin fibrosis and interstitial lung disease. Six new recommendations have been coined, covering drugs like mycophenolate mofetil, nintedanib, rituximab, and tocilizumab. None of these therapies were present in the 2017 recommendations. It seems the field is now ready to further expand on targeted therapies for the management of musculoskeletal and gastrointestinal manifestations, calcinosis, and the local management of digital ulcers.”
‘Therapeutic Continuums’ Aid Disease Management
Dr. Del Galdo and his colleagues grouped the various interventions across what the recommendations label as evidence-backed “therapeutic continuums.” These span six of the eight different clinical manifestations of systemic sclerosis: Raynaud’s phenomenon, digital ulcers, pulmonary hypertension, musculoskeletal manifestations, skin fibrosis, interstitial lung disease (ILD), and gastrointestinal and renal crisis.
A slide showing the different strengths of evidence for various drugs across the eight manifestations illustrated the principle behind the therapeutic continuums. “These ‘therapeutic continuums’ suggest a common pathogenetic mechanism driving the various manifestations of disease,” said Dr. Del Galdo. For example, he noted, “If rituximab had a positive response in skin and in lung, it suggests that B cells play a role in the clinical manifestations of skin and lung in this disease.”
Dr. Del Galdo highlighted the new immunosuppression continuum and associated treatments for skin and lung fibrosis. “For skin involvement, the task force recommended mycophenolate, methotrexate, and rituximab, with tocilizumab having a lower level of evidence and lower recommendation strength; similarly, in interstitial lung disease, we have rituximab, mycophenolate, cyclophosphamide, and nintedanib, and these all have the highest strength of evidence. Tocilizumab is assigned one strength of evidence below the other drugs.”
He also cited the phosphodiesterase 5 inhibitor (PDE5i) drugs that are used across Raynaud’s phenomenon, digital ulcers, and pulmonary arterial hypertension, which together form a vascular therapeutic continuum.
The complexity of systemic sclerosis and multiple manifestations was a major determinant of the recommendations, Dr. Del Galdo pointed out. “The task force realized that since this is such a complex disease, we cannot recommend one treatment unconditionally. For example, with mycophenolate mofetil, what works for most patients for the skin and lung manifestations might not for someone who experiences severe diarrhea, in which mycophenolate is contraindicated. So, the highest degree of recommendation that the task force felt comfortable with was ‘should be considered.’ ”
Dr. Del Galdo stressed that the complex nature of systemic sclerosis means that “when thinking of treating one manifestation, you also always need to consider all the other clinical manifestations as experienced by the patient, and it is this multifaceted scenario that will ultimately lead to your final choice.”
Turning to new evidence around drug use, Dr. Del Galdo said that rituximab has the highest level of evidence across skin and lung manifestations, nintedanib is new in lung, and tocilizumab is new across both skin and lung.
To treat systemic sclerosis–pulmonary arterial hypertension (SSc-PAH), as long as there are no contraindications, the task force recommends using PDE5i and endothelin receptor antagonists (ERAs) at diagnosis. Data from phase 3 trials show a better outcome when the combination is established early.
The task force suggests avoiding the use of warfarin in PAH. “This is supported by a signal from two trials showing an increase in morbidity and mortality in these patients,” noted Dr. Del Galdo.
He also pointed out that selexipag and riociguat were new and important second-line additions for the treatment of PAH, and — consistent with the ERA approach — the EULAR recommendation supports frequent follow-up to establish a treat-to-target approach to maximizing clinical outcomes in SSc-PAH and SSc-ILD. “Specifically, for the first time, we recommend monitoring the effect of any chosen intervention selected within 3-6 months of starting. The evidence suggests there is a group of patients who respond and some who respond less well and who might benefit from a second-line intervention.”
For example, results of one trial support the approach of adding an antifibrotic agent to reduce progression in people with progressive lung fibrosis. “Similarly, for pulmonary hypertension, we recommend putting patients on dual treatment, and if this fails, place them on selexipag or switch the PDE5i to riociguat,” Dr. Del Galdo said.
Systemic Sclerosis Research Agenda and Recommendations Align
Dr. Del Galdo highlighted the value of therapeutic continuums in advancing disease understanding. “It is starting to teach us what we know and what we don’t and where do we need to build more evidence. Effectively, they determine where the gaps in therapy lie, and this starts to guide the research agenda.
“In fact, what is really interesting about this recommendation update — certainly from the perspective of disease understanding — is that we are starting to have a bird’s-eye view of the clinical manifestations of scleroderma that have so often been dealt with separately. Now we are starting to build a cumulative evidence map of this disease.”
In 2017, the research agenda largely advocated identifying immune-targeting drugs for skin and lung fibrosis, Dr. Del Galdo pointed out. “Now, we’ve done that — we’ve identified appropriate immunosuppressive drugs — and this is testimony to the importance of these recommendations because what prioritized the research agenda 10 years ago ended up informing the clinical trials and made it into the recommendations.”
“We definitely are one step forward compared to this 2017 recommendation and closer to what we would like to do,” he asserted.
Remission Elusive but Getting Closer
In some respects, according to Dr. Del Galdo, research and development is making relatively slow progress, especially compared with other rheumatologic diseases such as rheumatoid arthritis. “We cannot put patients with systemic sclerosis in remission yet. But I think we are one step ahead in that we’ve now established the treat-to-target approach to maximize the efficacy with which we can stall disease progression, but we cannot yet put these patients into remission,” he said. Systemic sclerosis has multiple manifestations, and fibrotic damage cannot be reversed. “Right now, the scar will remain there forever,” he noted.
Until remission is achievable, Dr. Del Galdo advises diagnosing and treating patients earlier to prevent fibrotic manifestations.
Dr. Del Galdo explained the three leading priorities on the systemic sclerosis research agenda. “There are three because it is such a complex disease. The first is considering the patient voice — this is the most important one, and the patients say they want a more holistic approach — so trialing and treating multiple manifestations together.”
Second, Dr. Del Galdo said, he would like to see a patient-reported measure developed that can capture the entire disease.
Third, from a physician’s point of view, Dr. Del Galdo said, “We want to send the patients into remission. We need to continue to further deconvolute the clinical manifestations and find the bottleneck at the beginning of the natural history of disease.
“If we can find a drug that is effective very early on, before the patients start getting the eight different manifestations with different levels of severity, then we will be on the right road, which we hope will end in remission.”
Dr. Del Galdo has served on the speakers bureau for AstraZeneca and Janssen; consulted for AstraZeneca, Boehringer Ingelheim, Capella, Chemomab, Janssen, and Mitsubishi-Tanabe; and received grant or research support from AbbVie, AstraZeneca, Boheringer Ingelheim, Capella, Chemomab, Kymab, Janssen, and Mitsubishi-Tanabe. Dr. Landewé had no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
Nurse-Led Care for Gout Generates Best Uric Acid Control
VIENNA — To maintain gout in remission, nurses in a rheumatology service do better than doctors in implementing a straightforward treat-to-target (T2T) strategy, according to a randomized study that showed a consistent advantage across subgroups.
“Our study provides evidence that nurse-led therapy for gout leads to better uric acid control, which is an important consideration with the increasing incidence and the increasing costs of managing this condition,” said Jesper W. Larsen, a registered nurse affiliated with the Department of Rheumatology at North Denmark Regional Hospital, Hjørring, Denmark. He presented the study at the annual European Congress of Rheumatology.
The advantage of nurse-led care was seen across every subgroup evaluated. Moreover, more patients in the nurse-led group than in the usual care group remained on urate-lowering therapy at the end of the 2-year study.
The optimal management of gout is based on the treatment goal of lowering serum uric acid (sUA) to below the physiologic level of 0.36 mmol/L (6 mg/dL), a strategy called T2T that is endorsed by both EULAR and the American College of Rheumatology.
“This target can be reached in most patients with commonly used therapies, including allopurinol, which is relatively inexpensive,” Mr. Larsen said. Given that disease control and sustained remission are largely based on this target, he and his colleagues tested the hypothesis that nurses working in a rheumatology service could provide efficient and cost-effective care.
A total of 286 patients with gout defined by microscopy who were treated between 2015 and 2021 were enrolled in the study. Of these, 100 patients who had been enrolled before the introduction of nurse-led care received and were maintained on usual care, which generally included diagnosis by an orthopedist, an emergency room physician, or an internist, with subsequent treatment and follow-up with a general practitioner.
Of 186 patients treated after nurse-led care was implemented, 72 were transitioned to usual care, and the remaining 114 continued receiving nurse-led care over the next 2 years of follow-up. In the nurse-led care arm, nurses who specialized in rheumatology and were trained in gout management monitored a structured T2T strategy. They were available for consultation, provided patient education, and followed laboratory values, including sUA, which they used to adjust treatments.
Except in the case of complications, “there was no more contact with physicians” once care was transferred to the nurse, Mr. Larsen said. Most of the nurse management was based on sUA laboratory values and performed by telephone.
At 2 years, 112 patients in the nurse-led care group were compared with the 144 in the usual care group. Two of the 114 patients who entered the nurse-care cohort and 28 of the 172 in the usual care cohort died before the study ended.
(83% vs 44%). This was also true of patients aged 70 years or older (84% vs 45%), patients with tophi (60% vs 33%), and patients with sUA > 0.5 mmol/L at baseline (84% vs 44%). Nurse-led care also kept a greater proportion of patients at target who entered the study with an estimated glomerular filtration rate < 60 mL/min per 1.73 m2 (84% vs 52%) or were taking diuretics (89% vs 52%). All differences reached statistical significance (P < .05).
The reason for the lower mortality at 2 years in the nurse-led group (4% vs 23%; P < .001) is unclear, according to Mr. Larsen. In addition to considering a selection bias that might have channeled patients with more severe disease to usual care, he and his coinvestigators are also considering whether the lower rates of sUA control in the usual care group might have led to a higher rate of cardiovascular events.
Because of some baseline imbalances, a selection bias cannot be ruled out, but the imbalances did not uniformly favor nurse-led care. For example, the proportion of patients with diabetes (23% vs 13%) or a baseline cancer diagnosis (11% vs 5%) was higher in the nurse-led care group. The proportion of patients with atrial fibrillation (45% vs 35%) or on diuretics (47% vs 33%) at baseline was higher in the usual care group.
The median age of 69 years was the same in the two groups, although the nurse-led group included a higher proportion of men to women (86% vs 76%).
Within a T2T strategy, nurses focused on reaching the target might do a better job than physicians in consistently monitoring and adjusting therapies as needed, but Mr. Larsen also speculated that nurses might offer a more collaborative approach and provide greater support through patient education and regular telephone contact.
Potential Advantages of Nurse-Led Care
Clinicians concerned about nurses missing nuances in disease progression or being slow to recognize complications might be surprised to learn about the advantage of nurse-led care, but Mwidimi Ndosi, PhD, an associate professor in rheumatology nursing at the University of the West of England, Bristol, England, was not.
“There is quite a large literature to show that nursing care is often superior to physician-led patient management in the appropriate circumstances,” Mr. Ndosi said. In this specific instance of gout management, he said that the treatment target is clear, and nurses are often able to devote more time to a specific goal, like T2T, than clinicians balancing more priorities.

“In this trial, the care was administered by nurse specialists who presumably are skilled in this disease and know their limitations if a consultation with a physician is needed,” he said.
Mr. Ndosi, like Mr. Larsen, considers it likely that nurse-led programs for a T2T gout protocol will be implemented elsewhere. Mr. Ndosi pointed out that patients who are concerned about the quality of nurse-led care are generally convinced of its merits over time.
Because of factors such as nurses’ ability to spend more clinical time with patients and greater willingness to engage in resolving obstacles to self-care, compared with physicians, “there are many studies to show that patients are often more satisfied with care provided by nurses,” he said.
Mr. Larsen and Mr. Ndosi reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — To maintain gout in remission, nurses in a rheumatology service do better than doctors in implementing a straightforward treat-to-target (T2T) strategy, according to a randomized study that showed a consistent advantage across subgroups.
“Our study provides evidence that nurse-led therapy for gout leads to better uric acid control, which is an important consideration with the increasing incidence and the increasing costs of managing this condition,” said Jesper W. Larsen, a registered nurse affiliated with the Department of Rheumatology at North Denmark Regional Hospital, Hjørring, Denmark. He presented the study at the annual European Congress of Rheumatology.
The advantage of nurse-led care was seen across every subgroup evaluated. Moreover, more patients in the nurse-led group than in the usual care group remained on urate-lowering therapy at the end of the 2-year study.
The optimal management of gout is based on the treatment goal of lowering serum uric acid (sUA) to below the physiologic level of 0.36 mmol/L (6 mg/dL), a strategy called T2T that is endorsed by both EULAR and the American College of Rheumatology.
“This target can be reached in most patients with commonly used therapies, including allopurinol, which is relatively inexpensive,” Mr. Larsen said. Given that disease control and sustained remission are largely based on this target, he and his colleagues tested the hypothesis that nurses working in a rheumatology service could provide efficient and cost-effective care.
A total of 286 patients with gout defined by microscopy who were treated between 2015 and 2021 were enrolled in the study. Of these, 100 patients who had been enrolled before the introduction of nurse-led care received and were maintained on usual care, which generally included diagnosis by an orthopedist, an emergency room physician, or an internist, with subsequent treatment and follow-up with a general practitioner.
Of 186 patients treated after nurse-led care was implemented, 72 were transitioned to usual care, and the remaining 114 continued receiving nurse-led care over the next 2 years of follow-up. In the nurse-led care arm, nurses who specialized in rheumatology and were trained in gout management monitored a structured T2T strategy. They were available for consultation, provided patient education, and followed laboratory values, including sUA, which they used to adjust treatments.
Except in the case of complications, “there was no more contact with physicians” once care was transferred to the nurse, Mr. Larsen said. Most of the nurse management was based on sUA laboratory values and performed by telephone.
At 2 years, 112 patients in the nurse-led care group were compared with the 144 in the usual care group. Two of the 114 patients who entered the nurse-care cohort and 28 of the 172 in the usual care cohort died before the study ended.
(83% vs 44%). This was also true of patients aged 70 years or older (84% vs 45%), patients with tophi (60% vs 33%), and patients with sUA > 0.5 mmol/L at baseline (84% vs 44%). Nurse-led care also kept a greater proportion of patients at target who entered the study with an estimated glomerular filtration rate < 60 mL/min per 1.73 m2 (84% vs 52%) or were taking diuretics (89% vs 52%). All differences reached statistical significance (P < .05).
The reason for the lower mortality at 2 years in the nurse-led group (4% vs 23%; P < .001) is unclear, according to Mr. Larsen. In addition to considering a selection bias that might have channeled patients with more severe disease to usual care, he and his coinvestigators are also considering whether the lower rates of sUA control in the usual care group might have led to a higher rate of cardiovascular events.
Because of some baseline imbalances, a selection bias cannot be ruled out, but the imbalances did not uniformly favor nurse-led care. For example, the proportion of patients with diabetes (23% vs 13%) or a baseline cancer diagnosis (11% vs 5%) was higher in the nurse-led care group. The proportion of patients with atrial fibrillation (45% vs 35%) or on diuretics (47% vs 33%) at baseline was higher in the usual care group.
The median age of 69 years was the same in the two groups, although the nurse-led group included a higher proportion of men to women (86% vs 76%).
Within a T2T strategy, nurses focused on reaching the target might do a better job than physicians in consistently monitoring and adjusting therapies as needed, but Mr. Larsen also speculated that nurses might offer a more collaborative approach and provide greater support through patient education and regular telephone contact.
Potential Advantages of Nurse-Led Care
Clinicians concerned about nurses missing nuances in disease progression or being slow to recognize complications might be surprised to learn about the advantage of nurse-led care, but Mwidimi Ndosi, PhD, an associate professor in rheumatology nursing at the University of the West of England, Bristol, England, was not.
“There is quite a large literature to show that nursing care is often superior to physician-led patient management in the appropriate circumstances,” Mr. Ndosi said. In this specific instance of gout management, he said that the treatment target is clear, and nurses are often able to devote more time to a specific goal, like T2T, than clinicians balancing more priorities.
“In this trial, the care was administered by nurse specialists who presumably are skilled in this disease and know their limitations if a consultation with a physician is needed,” he said.
Mr. Ndosi, like Mr. Larsen, considers it likely that nurse-led programs for a T2T gout protocol will be implemented elsewhere. Mr. Ndosi pointed out that patients who are concerned about the quality of nurse-led care are generally convinced of its merits over time.
Because of factors such as nurses’ ability to spend more clinical time with patients and greater willingness to engage in resolving obstacles to self-care, compared with physicians, “there are many studies to show that patients are often more satisfied with care provided by nurses,” he said.
Mr. Larsen and Mr. Ndosi reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
VIENNA — To maintain gout in remission, nurses in a rheumatology service do better than doctors in implementing a straightforward treat-to-target (T2T) strategy, according to a randomized study that showed a consistent advantage across subgroups.
“Our study provides evidence that nurse-led therapy for gout leads to better uric acid control, which is an important consideration with the increasing incidence and the increasing costs of managing this condition,” said Jesper W. Larsen, a registered nurse affiliated with the Department of Rheumatology at North Denmark Regional Hospital, Hjørring, Denmark. He presented the study at the annual European Congress of Rheumatology.
The advantage of nurse-led care was seen across every subgroup evaluated. Moreover, more patients in the nurse-led group than in the usual care group remained on urate-lowering therapy at the end of the 2-year study.
The optimal management of gout is based on the treatment goal of lowering serum uric acid (sUA) to below the physiologic level of 0.36 mmol/L (6 mg/dL), a strategy called T2T that is endorsed by both EULAR and the American College of Rheumatology.
“This target can be reached in most patients with commonly used therapies, including allopurinol, which is relatively inexpensive,” Mr. Larsen said. Given that disease control and sustained remission are largely based on this target, he and his colleagues tested the hypothesis that nurses working in a rheumatology service could provide efficient and cost-effective care.
A total of 286 patients with gout defined by microscopy who were treated between 2015 and 2021 were enrolled in the study. Of these, 100 patients who had been enrolled before the introduction of nurse-led care received and were maintained on usual care, which generally included diagnosis by an orthopedist, an emergency room physician, or an internist, with subsequent treatment and follow-up with a general practitioner.
Of 186 patients treated after nurse-led care was implemented, 72 were transitioned to usual care, and the remaining 114 continued receiving nurse-led care over the next 2 years of follow-up. In the nurse-led care arm, nurses who specialized in rheumatology and were trained in gout management monitored a structured T2T strategy. They were available for consultation, provided patient education, and followed laboratory values, including sUA, which they used to adjust treatments.
Except in the case of complications, “there was no more contact with physicians” once care was transferred to the nurse, Mr. Larsen said. Most of the nurse management was based on sUA laboratory values and performed by telephone.
At 2 years, 112 patients in the nurse-led care group were compared with the 144 in the usual care group. Two of the 114 patients who entered the nurse-care cohort and 28 of the 172 in the usual care cohort died before the study ended.
(83% vs 44%). This was also true of patients aged 70 years or older (84% vs 45%), patients with tophi (60% vs 33%), and patients with sUA > 0.5 mmol/L at baseline (84% vs 44%). Nurse-led care also kept a greater proportion of patients at target who entered the study with an estimated glomerular filtration rate < 60 mL/min per 1.73 m2 (84% vs 52%) or were taking diuretics (89% vs 52%). All differences reached statistical significance (P < .05).
The reason for the lower mortality at 2 years in the nurse-led group (4% vs 23%; P < .001) is unclear, according to Mr. Larsen. In addition to considering a selection bias that might have channeled patients with more severe disease to usual care, he and his coinvestigators are also considering whether the lower rates of sUA control in the usual care group might have led to a higher rate of cardiovascular events.
Because of some baseline imbalances, a selection bias cannot be ruled out, but the imbalances did not uniformly favor nurse-led care. For example, the proportion of patients with diabetes (23% vs 13%) or a baseline cancer diagnosis (11% vs 5%) was higher in the nurse-led care group. The proportion of patients with atrial fibrillation (45% vs 35%) or on diuretics (47% vs 33%) at baseline was higher in the usual care group.
The median age of 69 years was the same in the two groups, although the nurse-led group included a higher proportion of men to women (86% vs 76%).
Within a T2T strategy, nurses focused on reaching the target might do a better job than physicians in consistently monitoring and adjusting therapies as needed, but Mr. Larsen also speculated that nurses might offer a more collaborative approach and provide greater support through patient education and regular telephone contact.
Potential Advantages of Nurse-Led Care
Clinicians concerned about nurses missing nuances in disease progression or being slow to recognize complications might be surprised to learn about the advantage of nurse-led care, but Mwidimi Ndosi, PhD, an associate professor in rheumatology nursing at the University of the West of England, Bristol, England, was not.
“There is quite a large literature to show that nursing care is often superior to physician-led patient management in the appropriate circumstances,” Mr. Ndosi said. In this specific instance of gout management, he said that the treatment target is clear, and nurses are often able to devote more time to a specific goal, like T2T, than clinicians balancing more priorities.
“In this trial, the care was administered by nurse specialists who presumably are skilled in this disease and know their limitations if a consultation with a physician is needed,” he said.
Mr. Ndosi, like Mr. Larsen, considers it likely that nurse-led programs for a T2T gout protocol will be implemented elsewhere. Mr. Ndosi pointed out that patients who are concerned about the quality of nurse-led care are generally convinced of its merits over time.
Because of factors such as nurses’ ability to spend more clinical time with patients and greater willingness to engage in resolving obstacles to self-care, compared with physicians, “there are many studies to show that patients are often more satisfied with care provided by nurses,” he said.
Mr. Larsen and Mr. Ndosi reported no potential conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
Low Hydroxychloroquine Levels in Early Pregnancy Tied to Greater Flares in SLE
TOPLINE:
A study reveals that hydroxychloroquine levels during the first trimester in pregnant women with systemic lupus erythematosus (SLE) are linked to severe maternal flares but not to adverse pregnancy outcomes.
METHODOLOGY:
- Researchers included pregnant women with SLE (median age, 32.1 years; median duration of disease, 8.3 years) who were enrolled in an ongoing French prospective observational study and were receiving hydroxychloroquine.
- The study assessed hydroxychloroquine blood levels during the first trimester. It defined severe nonadherence as having levels < 200 ng/mL and classified levels < 500 ng/mL as subtherapeutic.
- Primary outcomes were maternal flares during pregnancy and adverse pregnancy outcomes, including fetal/neonatal death and preterm delivery.
TAKEAWAY:
- Overall, 32 women experienced at least one flare during the second and third trimester; four had severe flares.
- The rates of severe maternal SLE flares were significantly associated with hydroxychloroquine levels in the first trimester that were classified as subtherapeutic (8.8% vs 0.7% with above subtherapeutic levels, P = .02) and severely nonadherent (13.3% vs 1.3% with above severely nonadherent levels, P = .04).
- There was no significant difference in adverse pregnancy outcomes by hydroxychloroquine level, suggesting its specific effect on maternal health rather than fetal health.
IN PRACTICE:
According to the authors, “this study supports hydroxychloroquine blood level assessment in pregnant women with SLE, as a predictor of severe maternal disease activity in pregnancy.”
SOURCE:
The study was led by Gelsomina Alle, MD, Assistance Publique-Hôpitaux de Paris, Paris, France. It was published online in Rheumatology.
LIMITATIONS:
The study’s sample size limited the ability to perform multivariate analyses for severe flares. Patients had to have an ongoing pregnancy at 12 weeks to be included, potentially excluding those with early pregnancy loss. The study only observed first-trimester hydroxychloroquine levels, not accounting for adherence variations throughout pregnancy.
DISCLOSURES:
The study funding source was not disclosed. Several authors declared financial relationships with pharmaceutical companies, including research support and consulting fees.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A study reveals that hydroxychloroquine levels during the first trimester in pregnant women with systemic lupus erythematosus (SLE) are linked to severe maternal flares but not to adverse pregnancy outcomes.
METHODOLOGY:
- Researchers included pregnant women with SLE (median age, 32.1 years; median duration of disease, 8.3 years) who were enrolled in an ongoing French prospective observational study and were receiving hydroxychloroquine.
- The study assessed hydroxychloroquine blood levels during the first trimester. It defined severe nonadherence as having levels < 200 ng/mL and classified levels < 500 ng/mL as subtherapeutic.
- Primary outcomes were maternal flares during pregnancy and adverse pregnancy outcomes, including fetal/neonatal death and preterm delivery.
TAKEAWAY:
- Overall, 32 women experienced at least one flare during the second and third trimester; four had severe flares.
- The rates of severe maternal SLE flares were significantly associated with hydroxychloroquine levels in the first trimester that were classified as subtherapeutic (8.8% vs 0.7% with above subtherapeutic levels, P = .02) and severely nonadherent (13.3% vs 1.3% with above severely nonadherent levels, P = .04).
- There was no significant difference in adverse pregnancy outcomes by hydroxychloroquine level, suggesting its specific effect on maternal health rather than fetal health.
IN PRACTICE:
According to the authors, “this study supports hydroxychloroquine blood level assessment in pregnant women with SLE, as a predictor of severe maternal disease activity in pregnancy.”
SOURCE:
The study was led by Gelsomina Alle, MD, Assistance Publique-Hôpitaux de Paris, Paris, France. It was published online in Rheumatology.
LIMITATIONS:
The study’s sample size limited the ability to perform multivariate analyses for severe flares. Patients had to have an ongoing pregnancy at 12 weeks to be included, potentially excluding those with early pregnancy loss. The study only observed first-trimester hydroxychloroquine levels, not accounting for adherence variations throughout pregnancy.
DISCLOSURES:
The study funding source was not disclosed. Several authors declared financial relationships with pharmaceutical companies, including research support and consulting fees.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
A study reveals that hydroxychloroquine levels during the first trimester in pregnant women with systemic lupus erythematosus (SLE) are linked to severe maternal flares but not to adverse pregnancy outcomes.
METHODOLOGY:
- Researchers included pregnant women with SLE (median age, 32.1 years; median duration of disease, 8.3 years) who were enrolled in an ongoing French prospective observational study and were receiving hydroxychloroquine.
- The study assessed hydroxychloroquine blood levels during the first trimester. It defined severe nonadherence as having levels < 200 ng/mL and classified levels < 500 ng/mL as subtherapeutic.
- Primary outcomes were maternal flares during pregnancy and adverse pregnancy outcomes, including fetal/neonatal death and preterm delivery.
TAKEAWAY:
- Overall, 32 women experienced at least one flare during the second and third trimester; four had severe flares.
- The rates of severe maternal SLE flares were significantly associated with hydroxychloroquine levels in the first trimester that were classified as subtherapeutic (8.8% vs 0.7% with above subtherapeutic levels, P = .02) and severely nonadherent (13.3% vs 1.3% with above severely nonadherent levels, P = .04).
- There was no significant difference in adverse pregnancy outcomes by hydroxychloroquine level, suggesting its specific effect on maternal health rather than fetal health.
IN PRACTICE:
According to the authors, “this study supports hydroxychloroquine blood level assessment in pregnant women with SLE, as a predictor of severe maternal disease activity in pregnancy.”
SOURCE:
The study was led by Gelsomina Alle, MD, Assistance Publique-Hôpitaux de Paris, Paris, France. It was published online in Rheumatology.
LIMITATIONS:
The study’s sample size limited the ability to perform multivariate analyses for severe flares. Patients had to have an ongoing pregnancy at 12 weeks to be included, potentially excluding those with early pregnancy loss. The study only observed first-trimester hydroxychloroquine levels, not accounting for adherence variations throughout pregnancy.
DISCLOSURES:
The study funding source was not disclosed. Several authors declared financial relationships with pharmaceutical companies, including research support and consulting fees.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Sex-Related Differences Found in IgG4-Related Disease Epidemiology
TOPLINE:
Men with immunoglobulin G4 (IgG4)-related disease exhibit significantly lower serum lipase levels and a greater likelihood of organ involvement than women, highlighting significant sex-dependent differences in disease manifestations.
METHODOLOGY:
- Researchers conducted a retrospective study of 328 patients (69% men) diagnosed with IgG4-related disease at the Massachusetts General Hospital – Rheumatology Clinic, Boston, who met the American College of Rheumatology–European Alliance of Associations for Rheumatology (ACR-EULAR) classification criteria between January 2008 and May 2023.
- Among the 328 patients, 69% were men and 31% were women, with a significant male-to-female ratio of 2.2:1.0. Men were typically older at diagnosis (median age, 63.7 vs 58.2 years).
- Data on serum lipase levels, renal involvement, and other clinical and laboratory parameters were collected.
TAKEAWAY:
- Men had higher baseline ACR-EULAR scores, indicating more severe disease (median score of 35.0 vs 29.5; P = .0010).
- Male patients demonstrated a median baseline serum lipase concentration of 24.5 U/L, significantly lower than the 33.5 U/L observed in women.
- Pancreatic (50% vs 26%) or renal (36% vs 18%) involvement was more common in men.
- Men exhibited higher IgG4 levels (P = .0050) and active B-cell responses in the blood (P = .0095).
IN PRACTICE:
According to the authors, this work confirms “the impression of an important sex disparity among patients with IgG4-related disease, with most patients being male, and male patients demonstrating strong tendencies toward more severe disease than female patients.”
SOURCE:
The study was led by Isha Jha, MD, Massachusetts General Hospital, Boston. It was published online on May 30, 2024, in The Lancet Rheumatology.
LIMITATIONS:
The study’s retrospective design may limit the ability to establish causality between sex differences and IgG4-related disease manifestations. A relatively small percentage of patients were assessed before receiving any immunosuppressive treatment, potentially influencing the observed clinical parameters.
DISCLOSURES:
This work was supported by the National Institutes of Health/National Institute of Allergy and Infectious Diseases, the Rheumatology Research Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Some authors declared financial ties outside this work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Men with immunoglobulin G4 (IgG4)-related disease exhibit significantly lower serum lipase levels and a greater likelihood of organ involvement than women, highlighting significant sex-dependent differences in disease manifestations.
METHODOLOGY:
- Researchers conducted a retrospective study of 328 patients (69% men) diagnosed with IgG4-related disease at the Massachusetts General Hospital – Rheumatology Clinic, Boston, who met the American College of Rheumatology–European Alliance of Associations for Rheumatology (ACR-EULAR) classification criteria between January 2008 and May 2023.
- Among the 328 patients, 69% were men and 31% were women, with a significant male-to-female ratio of 2.2:1.0. Men were typically older at diagnosis (median age, 63.7 vs 58.2 years).
- Data on serum lipase levels, renal involvement, and other clinical and laboratory parameters were collected.
TAKEAWAY:
- Men had higher baseline ACR-EULAR scores, indicating more severe disease (median score of 35.0 vs 29.5; P = .0010).
- Male patients demonstrated a median baseline serum lipase concentration of 24.5 U/L, significantly lower than the 33.5 U/L observed in women.
- Pancreatic (50% vs 26%) or renal (36% vs 18%) involvement was more common in men.
- Men exhibited higher IgG4 levels (P = .0050) and active B-cell responses in the blood (P = .0095).
IN PRACTICE:
According to the authors, this work confirms “the impression of an important sex disparity among patients with IgG4-related disease, with most patients being male, and male patients demonstrating strong tendencies toward more severe disease than female patients.”
SOURCE:
The study was led by Isha Jha, MD, Massachusetts General Hospital, Boston. It was published online on May 30, 2024, in The Lancet Rheumatology.
LIMITATIONS:
The study’s retrospective design may limit the ability to establish causality between sex differences and IgG4-related disease manifestations. A relatively small percentage of patients were assessed before receiving any immunosuppressive treatment, potentially influencing the observed clinical parameters.
DISCLOSURES:
This work was supported by the National Institutes of Health/National Institute of Allergy and Infectious Diseases, the Rheumatology Research Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Some authors declared financial ties outside this work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Men with immunoglobulin G4 (IgG4)-related disease exhibit significantly lower serum lipase levels and a greater likelihood of organ involvement than women, highlighting significant sex-dependent differences in disease manifestations.
METHODOLOGY:
- Researchers conducted a retrospective study of 328 patients (69% men) diagnosed with IgG4-related disease at the Massachusetts General Hospital – Rheumatology Clinic, Boston, who met the American College of Rheumatology–European Alliance of Associations for Rheumatology (ACR-EULAR) classification criteria between January 2008 and May 2023.
- Among the 328 patients, 69% were men and 31% were women, with a significant male-to-female ratio of 2.2:1.0. Men were typically older at diagnosis (median age, 63.7 vs 58.2 years).
- Data on serum lipase levels, renal involvement, and other clinical and laboratory parameters were collected.
TAKEAWAY:
- Men had higher baseline ACR-EULAR scores, indicating more severe disease (median score of 35.0 vs 29.5; P = .0010).
- Male patients demonstrated a median baseline serum lipase concentration of 24.5 U/L, significantly lower than the 33.5 U/L observed in women.
- Pancreatic (50% vs 26%) or renal (36% vs 18%) involvement was more common in men.
- Men exhibited higher IgG4 levels (P = .0050) and active B-cell responses in the blood (P = .0095).
IN PRACTICE:
According to the authors, this work confirms “the impression of an important sex disparity among patients with IgG4-related disease, with most patients being male, and male patients demonstrating strong tendencies toward more severe disease than female patients.”
SOURCE:
The study was led by Isha Jha, MD, Massachusetts General Hospital, Boston. It was published online on May 30, 2024, in The Lancet Rheumatology.
LIMITATIONS:
The study’s retrospective design may limit the ability to establish causality between sex differences and IgG4-related disease manifestations. A relatively small percentage of patients were assessed before receiving any immunosuppressive treatment, potentially influencing the observed clinical parameters.
DISCLOSURES:
This work was supported by the National Institutes of Health/National Institute of Allergy and Infectious Diseases, the Rheumatology Research Foundation, and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Some authors declared financial ties outside this work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
Why Do Investigational OA Drugs Need Better Trial Endpoints? Lorecivivint Serves as an Example
VIENNA — The hypothesis that pivotal clinical trials for osteoarthritis (OA)-modifying therapies are not using appropriate designs or endpoints appears to be consistent with the recent failure of the phase 3 trial of the investigational agent lorecivivint, according to experts tackling this issue.
For the elusive target of disease-modifying OA drugs (DMOADs), “there have been a lot of developments in the last few years but so far a lot of disappointments,” said Francis Berenbaum, MD, PhD, head of the department of rheumatology, Saint-Antoine Hospital, Paris, France.
Disagreement on the target most likely to favorably alter the natural history of disease might be the key issue. Dr. Berenbaum considers it essential to determine which changes in the joint signify a favorable drug effect and will lead to what regulatory agencies consider a clinically meaningful benefit. These include improved function and long-term preservation of the joint, as well as symptom control.
Of primary targets to modify the course of OA, cartilage is not one of them, according to Dr. Berenbaum, who spoke in a session on DMOADs and regenerative OA therapies at the annual European Congress of Rheumatology.
OA Is Not a Cartilage-Only Disease
“There is now a big consensus that osteoarthritis is not a cartilage-only disease,” he said. Rather, he addressed the inadequate appreciation of the “whole joint” pathology that underlies OA. He called for a fundamental “paradigm change” to work toward a disease-modifying effect that produces benefit on a hard endpoint.
There are multiple steps needed to work toward this goal after a consensus is reached on a meaningful surrogate endpoint, Dr. Berenbaum said. While symptom reduction is a good start, he called for evidence of disease attenuation or a regenerative effect on an important surrogate such as improved integrity of synovial tissue and improved bone health. Such surrogates are necessary to guide DMOAD development but not sufficient. The proof that a therapy is a DMOAD depends on a favorable effect on a hard endpoint. In the case of the knee, freedom from joint replacement is an example, Dr. Berenbaum said.
Philip G. Conaghan, MBBS, PhD, director of rheumatic and musculoskeletal medicine, University of Leeds, England, agreed with this general premise. Speaking just before Dr. Berenbaum in the same session, Dr. Conaghan traced this history of the effort to create DMOADs and updated those in clinical trials.

In his talk, he listed some of the many disappointments, including those which have targeted cartilage thickness, before updating the numerous ongoing development programs. There are many targets that appear viable, but none are in final stages of testing.
In remarks to this news organization, he said he generally agreed with Dr. Berenbaum about the need for greater rigor for developing drugs to meet regulatory criteria for disease-modifying effects.
Of the drugs he reviewed, Dr. Conaghan identified lorecivivint, an intra-articular CLK/DYRK inhibitor that’s thought to modulate Wnt and inflammatory pathways, as the only drug with DMOAD potential to go to a multicenter phase 3 trial so far. The drug’s negative outcome in phase 3 was particularly disappointing after the substantial promise shown in a phase 2b study published in 2021.
In the phase 3 study, lorecivivint, relative to placebo, did not achieve a significant improvement in the primary endpoint of improved medial joint space width (JSW) in the target knee as assessed at the end of a 48-week, double-blind trial.
New Follow-Up Data Support DMOAD Activity
Yet, additional extension data from the phase 3 lorecivivint trial presented in the EULAR DMOAD session challenge the conclusion even if they do not change the results.
The new data presented at EULAR is the second of two sets of extension data. The first, reported earlier, involved an analysis at 96 weeks or 48 weeks after the double-blind trial. At the beginning of this extension, lorecivivint-start patients had received a second intraarticular injection of 0.07 mg, while placebo patients were crossed over to receive their first injection.
Over the course of this first extension, the gradual loss in medial JSW observed from baseline to the end of the initial 48 weeks had plateaued in those treated with lorecivivint, but the decline continued in the placebo group. As a result, the lorecivivint-start patients had a numerical but not a statistically significant advantage for medial JSW over the placebo-switch group, according to Yusuf Yazici, MD, chief medical officer of Biosplice Therapeutics, San Diego, which developed lorecivivint.
In a second open-label extension described by Dr. Yazici at EULAR 2024, a third injection was administered to the lorecivivint-start patients and a second injection to the placebo-start patients. After 52 more weeks of follow-up, there were now 3 years of follow-up in the lorecivivint-start group and 2 years of follow-up in the placebo-start group.
At the end of this second extension, lorecivivint-start patients had a median increase in JSW that was approaching the baseline level at study entry. Although the placebo-start group had experienced a decline in the medial JSW at the end of the first extension when they had received one injection, JSW had also improved in the direction of baseline after a second injection with 2 years of follow-up. The advantage of three injections of lorecivivint over 3 years had now reached statistical significance (P = .031) despite the improvement seen in the placebo-start group following two injections over 2 years.
At 3 Years, Benefit Is Finally Potentially Significant
If placebo-treated patients had not received a second shot of lorecivivint and progressed at the rate seen before their second shot, the hypothetical trajectory would have provided lorecivivint with a highly statistically significant advantage (P < .001), said Dr. Yazici, displaying a hypothetical graph.
Along with improvements in pain and function associated with lorecivivint relative to placebo at 6 months, 12 months, and 24 months, the structural improvements in 3 years now suggest that “long-term treatment with lorecivivint has the potential to be a DMOAD for knee OA,” Dr. Yazici said.
While Dr. Berenbaum did not comment on this speculation, he did note the potential need for long-term studies to prove a disease-modifying effect in OA. This is the rationale for identifying surrogates.
To illustrate this point, Dr. Berenbaum made an analogy between OA and cardiovascular disease. In cardiovascular disease, surrogates of disease-modifying therapies, such as control of hypertension or hyperlipidemia, are accepted by regulatory agencies on the basis of their proven association with hard endpoints, such as myocardial infarction, stroke, or cardiovascular death. Like joint failure, these events can take years or decades to arise.
“For trials in OA, we need to agree on these surrogates,” Dr. Berenbaum said, although he acknowledged that they would then have to be validated. Noting that the US Food and Drug Administration has now identified OA as a serious disease for which accelerated drug approvals will be considered to address an unmet need, Dr. Berenbaum suggested there is an even greater impetus for improving strategies for DMOAD development.
Dr. Berenbaum reported financial relationships with Grünenthal, GlaxoSmithKline, Eli Lilly, Novartis, Pfizer, and Servier. Dr. Conaghan reported financial relationships with AbbVie, AstraZeneca, Eli Lilly, Galapagos, GlaxoSmithKline, Grünenthal, Janssen, Levicept, Merck, Novartis, Pfizer, Regeneron, Stryker, and UCB. Dr. Yazici is an employee of Biosplice Therapeutics, which provided funding for the OAS-07 trial.
A version of this article first appeared on Medscape.com.
VIENNA — The hypothesis that pivotal clinical trials for osteoarthritis (OA)-modifying therapies are not using appropriate designs or endpoints appears to be consistent with the recent failure of the phase 3 trial of the investigational agent lorecivivint, according to experts tackling this issue.
For the elusive target of disease-modifying OA drugs (DMOADs), “there have been a lot of developments in the last few years but so far a lot of disappointments,” said Francis Berenbaum, MD, PhD, head of the department of rheumatology, Saint-Antoine Hospital, Paris, France.
Disagreement on the target most likely to favorably alter the natural history of disease might be the key issue. Dr. Berenbaum considers it essential to determine which changes in the joint signify a favorable drug effect and will lead to what regulatory agencies consider a clinically meaningful benefit. These include improved function and long-term preservation of the joint, as well as symptom control.
Of primary targets to modify the course of OA, cartilage is not one of them, according to Dr. Berenbaum, who spoke in a session on DMOADs and regenerative OA therapies at the annual European Congress of Rheumatology.
OA Is Not a Cartilage-Only Disease
“There is now a big consensus that osteoarthritis is not a cartilage-only disease,” he said. Rather, he addressed the inadequate appreciation of the “whole joint” pathology that underlies OA. He called for a fundamental “paradigm change” to work toward a disease-modifying effect that produces benefit on a hard endpoint.
There are multiple steps needed to work toward this goal after a consensus is reached on a meaningful surrogate endpoint, Dr. Berenbaum said. While symptom reduction is a good start, he called for evidence of disease attenuation or a regenerative effect on an important surrogate such as improved integrity of synovial tissue and improved bone health. Such surrogates are necessary to guide DMOAD development but not sufficient. The proof that a therapy is a DMOAD depends on a favorable effect on a hard endpoint. In the case of the knee, freedom from joint replacement is an example, Dr. Berenbaum said.
Philip G. Conaghan, MBBS, PhD, director of rheumatic and musculoskeletal medicine, University of Leeds, England, agreed with this general premise. Speaking just before Dr. Berenbaum in the same session, Dr. Conaghan traced this history of the effort to create DMOADs and updated those in clinical trials.
In his talk, he listed some of the many disappointments, including those which have targeted cartilage thickness, before updating the numerous ongoing development programs. There are many targets that appear viable, but none are in final stages of testing.
In remarks to this news organization, he said he generally agreed with Dr. Berenbaum about the need for greater rigor for developing drugs to meet regulatory criteria for disease-modifying effects.
Of the drugs he reviewed, Dr. Conaghan identified lorecivivint, an intra-articular CLK/DYRK inhibitor that’s thought to modulate Wnt and inflammatory pathways, as the only drug with DMOAD potential to go to a multicenter phase 3 trial so far. The drug’s negative outcome in phase 3 was particularly disappointing after the substantial promise shown in a phase 2b study published in 2021.
In the phase 3 study, lorecivivint, relative to placebo, did not achieve a significant improvement in the primary endpoint of improved medial joint space width (JSW) in the target knee as assessed at the end of a 48-week, double-blind trial.
New Follow-Up Data Support DMOAD Activity
Yet, additional extension data from the phase 3 lorecivivint trial presented in the EULAR DMOAD session challenge the conclusion even if they do not change the results.
The new data presented at EULAR is the second of two sets of extension data. The first, reported earlier, involved an analysis at 96 weeks or 48 weeks after the double-blind trial. At the beginning of this extension, lorecivivint-start patients had received a second intraarticular injection of 0.07 mg, while placebo patients were crossed over to receive their first injection.
Over the course of this first extension, the gradual loss in medial JSW observed from baseline to the end of the initial 48 weeks had plateaued in those treated with lorecivivint, but the decline continued in the placebo group. As a result, the lorecivivint-start patients had a numerical but not a statistically significant advantage for medial JSW over the placebo-switch group, according to Yusuf Yazici, MD, chief medical officer of Biosplice Therapeutics, San Diego, which developed lorecivivint.
In a second open-label extension described by Dr. Yazici at EULAR 2024, a third injection was administered to the lorecivivint-start patients and a second injection to the placebo-start patients. After 52 more weeks of follow-up, there were now 3 years of follow-up in the lorecivivint-start group and 2 years of follow-up in the placebo-start group.
At the end of this second extension, lorecivivint-start patients had a median increase in JSW that was approaching the baseline level at study entry. Although the placebo-start group had experienced a decline in the medial JSW at the end of the first extension when they had received one injection, JSW had also improved in the direction of baseline after a second injection with 2 years of follow-up. The advantage of three injections of lorecivivint over 3 years had now reached statistical significance (P = .031) despite the improvement seen in the placebo-start group following two injections over 2 years.
At 3 Years, Benefit Is Finally Potentially Significant
If placebo-treated patients had not received a second shot of lorecivivint and progressed at the rate seen before their second shot, the hypothetical trajectory would have provided lorecivivint with a highly statistically significant advantage (P < .001), said Dr. Yazici, displaying a hypothetical graph.
Along with improvements in pain and function associated with lorecivivint relative to placebo at 6 months, 12 months, and 24 months, the structural improvements in 3 years now suggest that “long-term treatment with lorecivivint has the potential to be a DMOAD for knee OA,” Dr. Yazici said.
While Dr. Berenbaum did not comment on this speculation, he did note the potential need for long-term studies to prove a disease-modifying effect in OA. This is the rationale for identifying surrogates.
To illustrate this point, Dr. Berenbaum made an analogy between OA and cardiovascular disease. In cardiovascular disease, surrogates of disease-modifying therapies, such as control of hypertension or hyperlipidemia, are accepted by regulatory agencies on the basis of their proven association with hard endpoints, such as myocardial infarction, stroke, or cardiovascular death. Like joint failure, these events can take years or decades to arise.
“For trials in OA, we need to agree on these surrogates,” Dr. Berenbaum said, although he acknowledged that they would then have to be validated. Noting that the US Food and Drug Administration has now identified OA as a serious disease for which accelerated drug approvals will be considered to address an unmet need, Dr. Berenbaum suggested there is an even greater impetus for improving strategies for DMOAD development.
Dr. Berenbaum reported financial relationships with Grünenthal, GlaxoSmithKline, Eli Lilly, Novartis, Pfizer, and Servier. Dr. Conaghan reported financial relationships with AbbVie, AstraZeneca, Eli Lilly, Galapagos, GlaxoSmithKline, Grünenthal, Janssen, Levicept, Merck, Novartis, Pfizer, Regeneron, Stryker, and UCB. Dr. Yazici is an employee of Biosplice Therapeutics, which provided funding for the OAS-07 trial.
A version of this article first appeared on Medscape.com.
VIENNA — The hypothesis that pivotal clinical trials for osteoarthritis (OA)-modifying therapies are not using appropriate designs or endpoints appears to be consistent with the recent failure of the phase 3 trial of the investigational agent lorecivivint, according to experts tackling this issue.
For the elusive target of disease-modifying OA drugs (DMOADs), “there have been a lot of developments in the last few years but so far a lot of disappointments,” said Francis Berenbaum, MD, PhD, head of the department of rheumatology, Saint-Antoine Hospital, Paris, France.
Disagreement on the target most likely to favorably alter the natural history of disease might be the key issue. Dr. Berenbaum considers it essential to determine which changes in the joint signify a favorable drug effect and will lead to what regulatory agencies consider a clinically meaningful benefit. These include improved function and long-term preservation of the joint, as well as symptom control.
Of primary targets to modify the course of OA, cartilage is not one of them, according to Dr. Berenbaum, who spoke in a session on DMOADs and regenerative OA therapies at the annual European Congress of Rheumatology.
OA Is Not a Cartilage-Only Disease
“There is now a big consensus that osteoarthritis is not a cartilage-only disease,” he said. Rather, he addressed the inadequate appreciation of the “whole joint” pathology that underlies OA. He called for a fundamental “paradigm change” to work toward a disease-modifying effect that produces benefit on a hard endpoint.
There are multiple steps needed to work toward this goal after a consensus is reached on a meaningful surrogate endpoint, Dr. Berenbaum said. While symptom reduction is a good start, he called for evidence of disease attenuation or a regenerative effect on an important surrogate such as improved integrity of synovial tissue and improved bone health. Such surrogates are necessary to guide DMOAD development but not sufficient. The proof that a therapy is a DMOAD depends on a favorable effect on a hard endpoint. In the case of the knee, freedom from joint replacement is an example, Dr. Berenbaum said.
Philip G. Conaghan, MBBS, PhD, director of rheumatic and musculoskeletal medicine, University of Leeds, England, agreed with this general premise. Speaking just before Dr. Berenbaum in the same session, Dr. Conaghan traced this history of the effort to create DMOADs and updated those in clinical trials.
In his talk, he listed some of the many disappointments, including those which have targeted cartilage thickness, before updating the numerous ongoing development programs. There are many targets that appear viable, but none are in final stages of testing.
In remarks to this news organization, he said he generally agreed with Dr. Berenbaum about the need for greater rigor for developing drugs to meet regulatory criteria for disease-modifying effects.
Of the drugs he reviewed, Dr. Conaghan identified lorecivivint, an intra-articular CLK/DYRK inhibitor that’s thought to modulate Wnt and inflammatory pathways, as the only drug with DMOAD potential to go to a multicenter phase 3 trial so far. The drug’s negative outcome in phase 3 was particularly disappointing after the substantial promise shown in a phase 2b study published in 2021.
In the phase 3 study, lorecivivint, relative to placebo, did not achieve a significant improvement in the primary endpoint of improved medial joint space width (JSW) in the target knee as assessed at the end of a 48-week, double-blind trial.
New Follow-Up Data Support DMOAD Activity
Yet, additional extension data from the phase 3 lorecivivint trial presented in the EULAR DMOAD session challenge the conclusion even if they do not change the results.
The new data presented at EULAR is the second of two sets of extension data. The first, reported earlier, involved an analysis at 96 weeks or 48 weeks after the double-blind trial. At the beginning of this extension, lorecivivint-start patients had received a second intraarticular injection of 0.07 mg, while placebo patients were crossed over to receive their first injection.
Over the course of this first extension, the gradual loss in medial JSW observed from baseline to the end of the initial 48 weeks had plateaued in those treated with lorecivivint, but the decline continued in the placebo group. As a result, the lorecivivint-start patients had a numerical but not a statistically significant advantage for medial JSW over the placebo-switch group, according to Yusuf Yazici, MD, chief medical officer of Biosplice Therapeutics, San Diego, which developed lorecivivint.
In a second open-label extension described by Dr. Yazici at EULAR 2024, a third injection was administered to the lorecivivint-start patients and a second injection to the placebo-start patients. After 52 more weeks of follow-up, there were now 3 years of follow-up in the lorecivivint-start group and 2 years of follow-up in the placebo-start group.
At the end of this second extension, lorecivivint-start patients had a median increase in JSW that was approaching the baseline level at study entry. Although the placebo-start group had experienced a decline in the medial JSW at the end of the first extension when they had received one injection, JSW had also improved in the direction of baseline after a second injection with 2 years of follow-up. The advantage of three injections of lorecivivint over 3 years had now reached statistical significance (P = .031) despite the improvement seen in the placebo-start group following two injections over 2 years.
At 3 Years, Benefit Is Finally Potentially Significant
If placebo-treated patients had not received a second shot of lorecivivint and progressed at the rate seen before their second shot, the hypothetical trajectory would have provided lorecivivint with a highly statistically significant advantage (P < .001), said Dr. Yazici, displaying a hypothetical graph.
Along with improvements in pain and function associated with lorecivivint relative to placebo at 6 months, 12 months, and 24 months, the structural improvements in 3 years now suggest that “long-term treatment with lorecivivint has the potential to be a DMOAD for knee OA,” Dr. Yazici said.
While Dr. Berenbaum did not comment on this speculation, he did note the potential need for long-term studies to prove a disease-modifying effect in OA. This is the rationale for identifying surrogates.
To illustrate this point, Dr. Berenbaum made an analogy between OA and cardiovascular disease. In cardiovascular disease, surrogates of disease-modifying therapies, such as control of hypertension or hyperlipidemia, are accepted by regulatory agencies on the basis of their proven association with hard endpoints, such as myocardial infarction, stroke, or cardiovascular death. Like joint failure, these events can take years or decades to arise.
“For trials in OA, we need to agree on these surrogates,” Dr. Berenbaum said, although he acknowledged that they would then have to be validated. Noting that the US Food and Drug Administration has now identified OA as a serious disease for which accelerated drug approvals will be considered to address an unmet need, Dr. Berenbaum suggested there is an even greater impetus for improving strategies for DMOAD development.
Dr. Berenbaum reported financial relationships with Grünenthal, GlaxoSmithKline, Eli Lilly, Novartis, Pfizer, and Servier. Dr. Conaghan reported financial relationships with AbbVie, AstraZeneca, Eli Lilly, Galapagos, GlaxoSmithKline, Grünenthal, Janssen, Levicept, Merck, Novartis, Pfizer, Regeneron, Stryker, and UCB. Dr. Yazici is an employee of Biosplice Therapeutics, which provided funding for the OAS-07 trial.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
VEXAS Syndrome: Study Highlights Cutaneous Symptoms
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
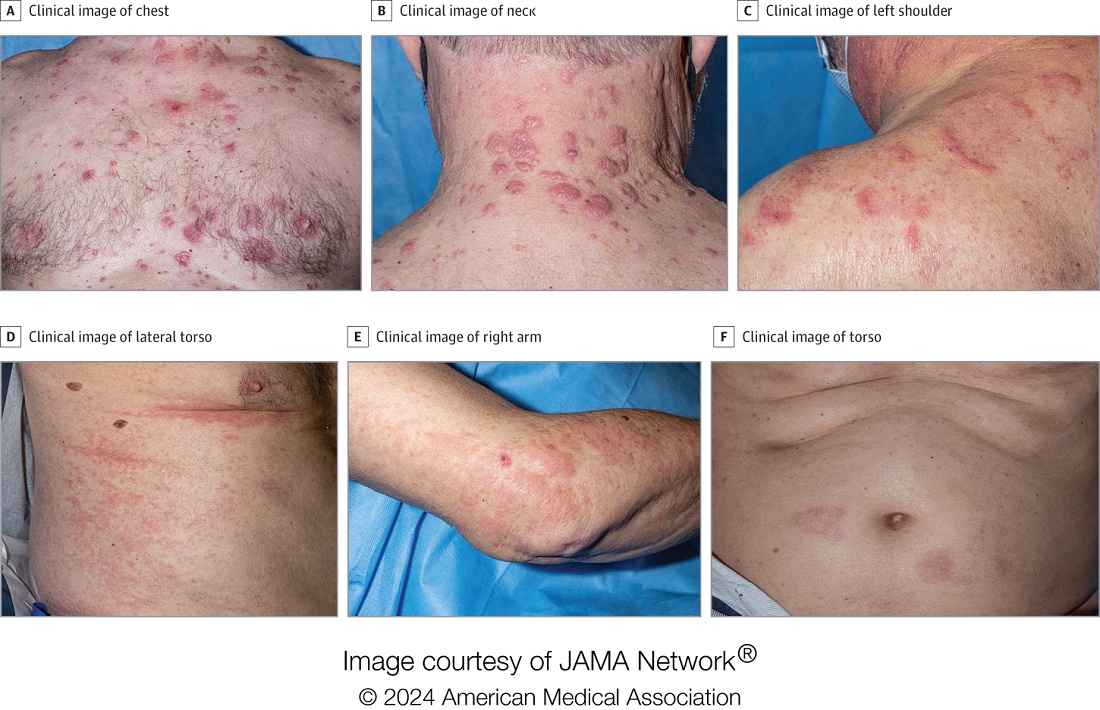
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
Additionally, the most common histologic findings include leukocytoclastic vasculitis, neutrophilic dermatosis, and perivascular dermatitis; different variants in the UBA1 gene are associated with specific skin manifestations.
Those are key findings from a cohort study of 112 patients with VEXAS published online in JAMA Dermatology. The study, conducted by researchers at the National Institutes of Health (NIH) and several other institutions, aimed to define the spectrum of cutaneous manifestations in VEXAS in association with genetic, histologic, and other clinical findings.
First described in 2020, VEXAS syndrome is an adult-onset multisystem disease that can pose a diagnostic challenge to clinicians, the study’s corresponding author, Edward W. Cowen, MD, MHSc, of the dermatology branch at the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), said in an interview. The disease is caused by pathogenic variants in the UBA1 gene, located on the X chromosome. Affected individuals exhibit a wide range of manifestations, including cytopenia/myelodysplasia, multiorgan systemic inflammation, and cutaneous involvement.
“Patients may present to a variety of disease specialists depending on their symptoms and providers may not immediately consider a genetic etiology in an older individual,” Dr. Cowen said in an interview. “Although skin involvement occurs in more than 80% of patients, it is pleomorphic and may resemble a variety of other conditions such as vasculitis and Sweet syndrome.”
To better understand the cutaneous manifestations of VEXAS syndrome, the researchers evaluated data from 112 patients with VEXAS-defining genetic variants in the UBA1 gene between 2019 and 2023. Of the 112 patients, 73 underwent medical record review only, and 39 were prospectively evaluated at NIH. All but one of the patients were men, 94% were White individuals, and their mean age was 64 years. Skin involvement occurred in 83% of cases and was the most common presenting feature of VEXAS in 61% of cases.
Of the 64 histopathologic reports available from 60 patients, the main skin histopathologic findings were leukocytoclastic vasculitis in 23 patients (36%), neutrophilic dermatosis in 22 patients (34%), and perivascular dermatitis in 19 patients (30%). According to Dr. Cowen, one key histologic finding was a distinct pattern of “histiocytoid” dermal neutrophilic inflammation, which was present in 13 of 15 specimens (86%) that underwent central re-review. “This pattern can occasionally also be seen in patients with Sweet syndrome, unrelated to VEXAS, but was a hallmark feature found in the majority of skin biopsies of patients with VEXAS,” he said.
“Together with another pathologic finding, leukocytoclasia, these features can be useful clues to alert the pathologist to a potential diagnosis of VEXAS. This myeloid predominant pattern of skin inflammation was also most strongly associated with the leucine pathogenic variant of the UBA1 gene.” In contrast, cutaneous vasculitis was most strongly associated with the valine pathogenic variant of UBA1. “This is important because the valine variant has been previously independently linked to decreased survival,” he said.
In findings related to pathogenic genetic variants, the researchers observed that the p.Met41Leu variant was most frequently associated with neutrophilic dermal infiltrates in 14 of 17 patients (82%) with this variant and often resembled histiocytoid Sweet syndrome. In addition, the p.Met41Val variant was associated with vasculitic lesions in 11 of 20 patients (55%) with this variant and with a mixed leukocytic infiltrate in 17 of these 20 patients (85%).
Treatment Outcomes
In the realm of therapies, skin manifestations improved in 67 of 73 patients (92%) treated with oral prednisone, while treatment with the interleukin-1 receptor antagonist anakinra improved cutaneous disease in 9 of the 16 (56%) who received it. However, 12 (75%) of those who received anakinra developed severe injection-site reactions, including ulceration in two patients and abscess formation in one patient.
Dr. Cowen noted that VEXAS is associated with high mortality (22% in this cohort), and a high degree of suspicion is required to diagnose patients with VEXAS before significant end organ damage has occurred. “This diagnosis should be considered in all older male patients who present with neutrophilic dermatosis — particularly histiocytoid Sweet syndrome, vasculitis, or leukocytoclasia without vasculitis. Patients who appear to have isolated skin involvement may have cytopenias and acute phase reactants. Therefore, complete blood count with differential and ESR and CRP should be considered to investigate for macrocytosis, cytopenias, and systemic inflammation.”
He acknowledged certain limitations of the study, including the fact that many patients were first evaluated at the NIH after having disease symptoms for many months or years. “It is possible that patients with VEXAS referred to the NIH, either for genetic testing or in person evaluation, represent a population with more aggressive disease.”
Christine Ko, MD, professor of dermatology and pathology at Yale University, New Haven, Connecticut, who was asked to comment on the study, emphasized the importance of the UBA1 mutation in the diagnosis of this complex syndrome. “Dermatologists should be aware of VEXAS syndrome as the majority of patients present with skin lesions, which can range from urticarial to Sweet syndrome–like to palpable purpura,” Dr. Ko said.
“Chondritis and periorbital edema, sometimes unilateral, are also associated. Histopathologic clues include a predominantly histiocytoid infiltrate,” she noted. In addition, “the prominent myxoid stroma around blood vessels and adnexal structures as a clue to VEXAS syndrome surprised me; I had not read that before.”
The study was supported by the Intramural Research Program of NIAMS. One of the study authors reported personal fees from Alexion, Novartis, and Sobi outside of the submitted work. No other disclosures were reported. Dr. Ko reported having no disclosures.
A version of this article appeared on Medscape.com .
FROM JAMA DERMATOLOGY
Long-Term OA, RA Symptom Improvement Seen with Plant-Based Diet, Lifestyle Changes
VIENNA — An intervention consisting of a plant-based diet, exercise, and sleep and stress advice improved pain, stiffness, and physical function in people with knee and/or hip osteoarthritis (OA) and metabolic syndrome, while in patients with rheumatoid arthritis (RA), disease activity improved significantly, and medication use was reduced.
At the annual European Congress of Rheumatology, Carlijn Wagenaar, MD, a PhD candidate in Clinical Immunology and Rheumatology at Amsterdam University Medical Center, presented 2-year extension study results for OA and RA and an overview of the possible biological mechanisms underpinning the plant-based intervention in RA.
“At 2 years, RA patients on the PFJ [Plants for Joints] intervention resulted in a significant improvement in disease activity of RA, and these outcomes were maintained 2 years after program end,” Dr. Wagenaar reported.
“Some initial improvements in body composition and metabolic outcomes were also maintained at the end of the 2-year extension phase, and there was a net decrease in antirheumatic medication use,” she continued.
In the patients with OA, Dr. Wagenaar said the PFJ intervention improved pain, stiffness, and physical function in people with knee and/or hip OA and metabolic syndrome. “In the 2-year extension study, these effects were maintained, and we saw lasting body composition changes and a decrease in cholesterol-lowering medications. There was also high acceptability of the program; the study shows long-term maintenance of clinically relevant effects.”
Significant Improvement in OA Pain, Stiffness, Physical Function
In the OA randomized controlled trial, 64 people with hip and/or knee OA and metabolic syndrome were randomized to the PFJ intervention or usual care (waitlist control group). A total of 62 participants (including those in the control group previously) entered the long-term effectiveness study, and 44 had 2 years of follow-up data for analysis. Twenty participants dropped out, with most being unreachable or too busy.
“The PFJ program is a theoretical and practical program where people learn about and follow a whole food, plant-based diet, and receive advice on sleep and stress management and exercise,” said Dr. Wagenaar.
The program lasted 16 weeks with group sessions of 6-12 participants. The diet was a plant-based version of the Dutch dietary guidelines with a focus on unprocessed food. It was rich in whole grains, legumes, nuts, seeds, fruit, and vegetables, but without calorie restrictions and participants had one-to-one contact with a dietitian. The exercise advice followed the Dutch exercise guidelines, which advise 150 minutes of moderate to intense exercise per week, as well as twice-weekly muscle strength exercises, noted Dr. Wagenaar.
The 2-year follow-up study involved twice-yearly visits and six adherence-promoting webinars per year, as well as monthly newsletters. Researchers also monitored changes in medication intensity (classified as “increased,” “stable,” or “decreased/stopped”) between the start of the PFJ intervention and end of the 2-year extension study, and they were grouped into medications for pain, blood pressure, glucose, and cholesterol.
Participants were encouraged to try to avoid making changes to medication during the intervention phase, but they could do so during the 2-year extension study, said Dr. Wagenaar. In fact, the researchers actively monitored and quantified medication changes between the start of the PFJ intervention and end of the 2-year follow-up period.
Patients in the 16-week trial had an average age of 64 years, 84% were women, and their mean body mass index (BMI) was 33 kg/m2. A total of 73% had knee OA and 78% hip OA, and their mean WOMAC score was 38.2, indicative of moderate to severe OA.
In participants who completed the 2-year extension study, the primary outcome (WOMAC score for mean stiffness and physical function) showed a significant improvement of −9.1 (95% CI, −12.8 to −5.3; P < .0001) compared with the start of the PFJ intervention.
“Looking at individual components of the WOMAC score — pain, stiffness, and physical function — we found these also all significantly improved at the end of the 2-year extension phase,” reported Dr. Wagenaar.
She added that after 2 years, there were significant improvements in weight loss (from 94.9 to 92.1 kg), BMI (from 33.3 to 32 kg/m2), and waist circumference (from 110 to 106.7 cm).
By the end of the trial and at 1 year of the extension study, there were significant improvements in A1c, fasting blood glucose, and low-density lipoprotein cholesterol, but at 2 years, these were no longer significant.
Regarding medications use, Dr. Wagenaar reported that, overall, there was no net change in use of pain, glucose-lowering, or hypertension medications, but 44% of patients using cholesterol-lowering medications were able to lower their dose or stop them.
Disease Activity Improvement and Medication Reduction in RA
Turning to the study of the intervention in patients with RA, 77 people (DAS28 ≥ 2.6 and ≤ 5.1, mild to moderate disease) were randomized to receive either the PFJ intervention in addition to usual care or only usual care (control group). Of these, 48 (62%) from both the intervention and control groups also completed the 2-year follow-up. The details of the PFJ intervention and the extension study for RA were the same as for the OA patient group.
Dr. Wagenaar commented on how they tried to individualize the exercise part of the program. “We noticed many of the RA patients asked too much of their body, while in contrast, those with OA were too hesitant,” she said. “We decided to focus on people’s own physical barriers, and we wanted to protect these. Sometimes, people needed to move more, and at other times, we had to tell people to slow down. Often, we advised people to move more by integrating exercise into their daily life.”
Similar to the OA study, patients were asked to try to avoid changing their medications in the 16-week study. “In the extension study, they were encouraged to reduce their medication in collaboration with their rheumatologist,” explained Wagenaar, who monitored any changes.
Differences were quantified according to medication groups comprising rheumatic medications, as well as pain, blood pressure, glucose-lowering, and cholesterol medications, and changes were categorized as increased, stable, or decreased/stopped.
Again, participants were mostly women (92%) with an average age of 55 years, BMI of 26 kg/m2, and DAS28 of 3.85 at baseline. Dropout reasons were similar to those for OA, and over 85% of participants were on medications.
During the 16-week trial period, the DAS28 changed more in the intervention participants than in the controls, and after 2 years of follow-up, DAS28 was significantly lower than baseline with a mean difference of −0.9 (95% CI, −1.2 to −0.6; P < .0001).
“Comparing with the literature, the drop in DAS28 was similar to that seen with medication, so it’s a very significant reduction,” remarked Dr. Wagenaar.
Mean tender joint count dropped from 3 to 0, and general health components of the DAS28 improved significantly over the intervention and over the 2-year follow-up, whereas there was no significant difference in the already low erythrocyte sedimentation rate and swollen joint count compared with baseline. C-reactive protein (CRP) changed from 3.2 to 1.3 mg/L over the 2-year follow-up. High-density lipoprotein increased from 1.6 to 1.8 mmol/L.
A total of 44% of people using antirheumatic medication decreased or stopped them after the 2-year extension.
Dr. Wagenaar went on to say that focus group findings suggested that “participants were very enthusiastic about the program despite it largely involving lifestyle change, and this is reflected in our low dropout rates after the trial and 1-year extension [20% for OA and RA].” There were more dropouts in year 2 of the extension.
In an interview, Dr. Wagenaar explained why she felt the program had been so well received. “People in the program felt like they had more control over their disease, and they felt listened to.”
Mechanisms Underpinning PFJ
Dr. Wagenaar and colleagues also sought to determine the possible mechanisms underlying the clinical effects of the plant-based diet on RA. “With RA, we have the mucosal origins hypothesis, which suggests RA is triggered at the mucosal site [of the gut] in genetically predisposed individuals, and this consequently transfers to the synovial [fluid in] joints,” she said.
“On top of this, we know that fiber protects our gut barrier and therefore reduces inflammation. The PFJ intervention is a very high-fiber program, so our hypothesis is that it might help [strengthen] the barrier,” she explained.
Dr. Wagenaar and colleagues collected fecal samples from patients and measured the albumin and calprotectin in them, which are both indicators of the gut barrier function. The researchers analyzed metabolomic data and found that fecal albumin — considered a gut barrier integrity marker — decreased significantly in the intervention group. In patients with RA, this improvement corresponded with an improvement in DAS28, the researchers reported in a poster at the meeting.
“Patients who had the greatest improvement in their gut barrier function also showed the greatest improvement in the DAS28 score, suggestive of a possible link between gut barrier improvement and clinical effects.”
They did not identify any change in calprotectin, an inflammation marker, but Dr. Wagenaar said this might change later. “We found that in those on the intervention, at 4 months, the CRP wasn’t reduced, but 1 year later it was.”
The metabolite lenticin, a lentil intake biomarker considered protective against inflammation and osteoclastic differentiation, also increased. Tryptophan was also reduced in people on the PFJ intervention.
Fernando Estevez-Lopez, PhD, a sports scientist at Harvard T.H. Chan School of Public Health, Boston, who specializes in physical activity and behavioral change in rheumatology patients, co-moderated the session and remarked that, “In this study, they did a brilliant job with encouraging participants to follow the program. The design and methods were really good — the sample size was good, and they followed people up. Also, these researchers come from Reade [a medical research center in Amsterdam University Medical Center] where they are well known for applying their research findings to the clinic,” he said.
“In terms of physical activity, we really mean increasing the time spent moving, for example, gentle activity such as walking, or changing behaviors in people with OA and RA. We don’t want them to have more pain the next day.”
Dr. Wagenaar reported receiving a grant from ZonMw (The Netherlands Organization for Health Research and Development). She and colleagues hold shares in Plants for Health, a limited liability company. Dr. Estevez-Lopez reported having no relevant disclosures.
A version of this article appeared on Medscape.com.
VIENNA — An intervention consisting of a plant-based diet, exercise, and sleep and stress advice improved pain, stiffness, and physical function in people with knee and/or hip osteoarthritis (OA) and metabolic syndrome, while in patients with rheumatoid arthritis (RA), disease activity improved significantly, and medication use was reduced.
At the annual European Congress of Rheumatology, Carlijn Wagenaar, MD, a PhD candidate in Clinical Immunology and Rheumatology at Amsterdam University Medical Center, presented 2-year extension study results for OA and RA and an overview of the possible biological mechanisms underpinning the plant-based intervention in RA.
“At 2 years, RA patients on the PFJ [Plants for Joints] intervention resulted in a significant improvement in disease activity of RA, and these outcomes were maintained 2 years after program end,” Dr. Wagenaar reported.
“Some initial improvements in body composition and metabolic outcomes were also maintained at the end of the 2-year extension phase, and there was a net decrease in antirheumatic medication use,” she continued.
In the patients with OA, Dr. Wagenaar said the PFJ intervention improved pain, stiffness, and physical function in people with knee and/or hip OA and metabolic syndrome. “In the 2-year extension study, these effects were maintained, and we saw lasting body composition changes and a decrease in cholesterol-lowering medications. There was also high acceptability of the program; the study shows long-term maintenance of clinically relevant effects.”
Significant Improvement in OA Pain, Stiffness, Physical Function
In the OA randomized controlled trial, 64 people with hip and/or knee OA and metabolic syndrome were randomized to the PFJ intervention or usual care (waitlist control group). A total of 62 participants (including those in the control group previously) entered the long-term effectiveness study, and 44 had 2 years of follow-up data for analysis. Twenty participants dropped out, with most being unreachable or too busy.
“The PFJ program is a theoretical and practical program where people learn about and follow a whole food, plant-based diet, and receive advice on sleep and stress management and exercise,” said Dr. Wagenaar.
The program lasted 16 weeks with group sessions of 6-12 participants. The diet was a plant-based version of the Dutch dietary guidelines with a focus on unprocessed food. It was rich in whole grains, legumes, nuts, seeds, fruit, and vegetables, but without calorie restrictions and participants had one-to-one contact with a dietitian. The exercise advice followed the Dutch exercise guidelines, which advise 150 minutes of moderate to intense exercise per week, as well as twice-weekly muscle strength exercises, noted Dr. Wagenaar.
The 2-year follow-up study involved twice-yearly visits and six adherence-promoting webinars per year, as well as monthly newsletters. Researchers also monitored changes in medication intensity (classified as “increased,” “stable,” or “decreased/stopped”) between the start of the PFJ intervention and end of the 2-year extension study, and they were grouped into medications for pain, blood pressure, glucose, and cholesterol.
Participants were encouraged to try to avoid making changes to medication during the intervention phase, but they could do so during the 2-year extension study, said Dr. Wagenaar. In fact, the researchers actively monitored and quantified medication changes between the start of the PFJ intervention and end of the 2-year follow-up period.
Patients in the 16-week trial had an average age of 64 years, 84% were women, and their mean body mass index (BMI) was 33 kg/m2. A total of 73% had knee OA and 78% hip OA, and their mean WOMAC score was 38.2, indicative of moderate to severe OA.
In participants who completed the 2-year extension study, the primary outcome (WOMAC score for mean stiffness and physical function) showed a significant improvement of −9.1 (95% CI, −12.8 to −5.3; P < .0001) compared with the start of the PFJ intervention.
“Looking at individual components of the WOMAC score — pain, stiffness, and physical function — we found these also all significantly improved at the end of the 2-year extension phase,” reported Dr. Wagenaar.
She added that after 2 years, there were significant improvements in weight loss (from 94.9 to 92.1 kg), BMI (from 33.3 to 32 kg/m2), and waist circumference (from 110 to 106.7 cm).
By the end of the trial and at 1 year of the extension study, there were significant improvements in A1c, fasting blood glucose, and low-density lipoprotein cholesterol, but at 2 years, these were no longer significant.
Regarding medications use, Dr. Wagenaar reported that, overall, there was no net change in use of pain, glucose-lowering, or hypertension medications, but 44% of patients using cholesterol-lowering medications were able to lower their dose or stop them.
Disease Activity Improvement and Medication Reduction in RA
Turning to the study of the intervention in patients with RA, 77 people (DAS28 ≥ 2.6 and ≤ 5.1, mild to moderate disease) were randomized to receive either the PFJ intervention in addition to usual care or only usual care (control group). Of these, 48 (62%) from both the intervention and control groups also completed the 2-year follow-up. The details of the PFJ intervention and the extension study for RA were the same as for the OA patient group.
Dr. Wagenaar commented on how they tried to individualize the exercise part of the program. “We noticed many of the RA patients asked too much of their body, while in contrast, those with OA were too hesitant,” she said. “We decided to focus on people’s own physical barriers, and we wanted to protect these. Sometimes, people needed to move more, and at other times, we had to tell people to slow down. Often, we advised people to move more by integrating exercise into their daily life.”
Similar to the OA study, patients were asked to try to avoid changing their medications in the 16-week study. “In the extension study, they were encouraged to reduce their medication in collaboration with their rheumatologist,” explained Wagenaar, who monitored any changes.
Differences were quantified according to medication groups comprising rheumatic medications, as well as pain, blood pressure, glucose-lowering, and cholesterol medications, and changes were categorized as increased, stable, or decreased/stopped.
Again, participants were mostly women (92%) with an average age of 55 years, BMI of 26 kg/m2, and DAS28 of 3.85 at baseline. Dropout reasons were similar to those for OA, and over 85% of participants were on medications.
During the 16-week trial period, the DAS28 changed more in the intervention participants than in the controls, and after 2 years of follow-up, DAS28 was significantly lower than baseline with a mean difference of −0.9 (95% CI, −1.2 to −0.6; P < .0001).
“Comparing with the literature, the drop in DAS28 was similar to that seen with medication, so it’s a very significant reduction,” remarked Dr. Wagenaar.
Mean tender joint count dropped from 3 to 0, and general health components of the DAS28 improved significantly over the intervention and over the 2-year follow-up, whereas there was no significant difference in the already low erythrocyte sedimentation rate and swollen joint count compared with baseline. C-reactive protein (CRP) changed from 3.2 to 1.3 mg/L over the 2-year follow-up. High-density lipoprotein increased from 1.6 to 1.8 mmol/L.
A total of 44% of people using antirheumatic medication decreased or stopped them after the 2-year extension.
Dr. Wagenaar went on to say that focus group findings suggested that “participants were very enthusiastic about the program despite it largely involving lifestyle change, and this is reflected in our low dropout rates after the trial and 1-year extension [20% for OA and RA].” There were more dropouts in year 2 of the extension.
In an interview, Dr. Wagenaar explained why she felt the program had been so well received. “People in the program felt like they had more control over their disease, and they felt listened to.”
Mechanisms Underpinning PFJ
Dr. Wagenaar and colleagues also sought to determine the possible mechanisms underlying the clinical effects of the plant-based diet on RA. “With RA, we have the mucosal origins hypothesis, which suggests RA is triggered at the mucosal site [of the gut] in genetically predisposed individuals, and this consequently transfers to the synovial [fluid in] joints,” she said.
“On top of this, we know that fiber protects our gut barrier and therefore reduces inflammation. The PFJ intervention is a very high-fiber program, so our hypothesis is that it might help [strengthen] the barrier,” she explained.
Dr. Wagenaar and colleagues collected fecal samples from patients and measured the albumin and calprotectin in them, which are both indicators of the gut barrier function. The researchers analyzed metabolomic data and found that fecal albumin — considered a gut barrier integrity marker — decreased significantly in the intervention group. In patients with RA, this improvement corresponded with an improvement in DAS28, the researchers reported in a poster at the meeting.
“Patients who had the greatest improvement in their gut barrier function also showed the greatest improvement in the DAS28 score, suggestive of a possible link between gut barrier improvement and clinical effects.”
They did not identify any change in calprotectin, an inflammation marker, but Dr. Wagenaar said this might change later. “We found that in those on the intervention, at 4 months, the CRP wasn’t reduced, but 1 year later it was.”
The metabolite lenticin, a lentil intake biomarker considered protective against inflammation and osteoclastic differentiation, also increased. Tryptophan was also reduced in people on the PFJ intervention.
Fernando Estevez-Lopez, PhD, a sports scientist at Harvard T.H. Chan School of Public Health, Boston, who specializes in physical activity and behavioral change in rheumatology patients, co-moderated the session and remarked that, “In this study, they did a brilliant job with encouraging participants to follow the program. The design and methods were really good — the sample size was good, and they followed people up. Also, these researchers come from Reade [a medical research center in Amsterdam University Medical Center] where they are well known for applying their research findings to the clinic,” he said.
“In terms of physical activity, we really mean increasing the time spent moving, for example, gentle activity such as walking, or changing behaviors in people with OA and RA. We don’t want them to have more pain the next day.”
Dr. Wagenaar reported receiving a grant from ZonMw (The Netherlands Organization for Health Research and Development). She and colleagues hold shares in Plants for Health, a limited liability company. Dr. Estevez-Lopez reported having no relevant disclosures.
A version of this article appeared on Medscape.com.
VIENNA — An intervention consisting of a plant-based diet, exercise, and sleep and stress advice improved pain, stiffness, and physical function in people with knee and/or hip osteoarthritis (OA) and metabolic syndrome, while in patients with rheumatoid arthritis (RA), disease activity improved significantly, and medication use was reduced.
At the annual European Congress of Rheumatology, Carlijn Wagenaar, MD, a PhD candidate in Clinical Immunology and Rheumatology at Amsterdam University Medical Center, presented 2-year extension study results for OA and RA and an overview of the possible biological mechanisms underpinning the plant-based intervention in RA.
“At 2 years, RA patients on the PFJ [Plants for Joints] intervention resulted in a significant improvement in disease activity of RA, and these outcomes were maintained 2 years after program end,” Dr. Wagenaar reported.
“Some initial improvements in body composition and metabolic outcomes were also maintained at the end of the 2-year extension phase, and there was a net decrease in antirheumatic medication use,” she continued.
In the patients with OA, Dr. Wagenaar said the PFJ intervention improved pain, stiffness, and physical function in people with knee and/or hip OA and metabolic syndrome. “In the 2-year extension study, these effects were maintained, and we saw lasting body composition changes and a decrease in cholesterol-lowering medications. There was also high acceptability of the program; the study shows long-term maintenance of clinically relevant effects.”
Significant Improvement in OA Pain, Stiffness, Physical Function
In the OA randomized controlled trial, 64 people with hip and/or knee OA and metabolic syndrome were randomized to the PFJ intervention or usual care (waitlist control group). A total of 62 participants (including those in the control group previously) entered the long-term effectiveness study, and 44 had 2 years of follow-up data for analysis. Twenty participants dropped out, with most being unreachable or too busy.
“The PFJ program is a theoretical and practical program where people learn about and follow a whole food, plant-based diet, and receive advice on sleep and stress management and exercise,” said Dr. Wagenaar.
The program lasted 16 weeks with group sessions of 6-12 participants. The diet was a plant-based version of the Dutch dietary guidelines with a focus on unprocessed food. It was rich in whole grains, legumes, nuts, seeds, fruit, and vegetables, but without calorie restrictions and participants had one-to-one contact with a dietitian. The exercise advice followed the Dutch exercise guidelines, which advise 150 minutes of moderate to intense exercise per week, as well as twice-weekly muscle strength exercises, noted Dr. Wagenaar.
The 2-year follow-up study involved twice-yearly visits and six adherence-promoting webinars per year, as well as monthly newsletters. Researchers also monitored changes in medication intensity (classified as “increased,” “stable,” or “decreased/stopped”) between the start of the PFJ intervention and end of the 2-year extension study, and they were grouped into medications for pain, blood pressure, glucose, and cholesterol.
Participants were encouraged to try to avoid making changes to medication during the intervention phase, but they could do so during the 2-year extension study, said Dr. Wagenaar. In fact, the researchers actively monitored and quantified medication changes between the start of the PFJ intervention and end of the 2-year follow-up period.
Patients in the 16-week trial had an average age of 64 years, 84% were women, and their mean body mass index (BMI) was 33 kg/m2. A total of 73% had knee OA and 78% hip OA, and their mean WOMAC score was 38.2, indicative of moderate to severe OA.
In participants who completed the 2-year extension study, the primary outcome (WOMAC score for mean stiffness and physical function) showed a significant improvement of −9.1 (95% CI, −12.8 to −5.3; P < .0001) compared with the start of the PFJ intervention.
“Looking at individual components of the WOMAC score — pain, stiffness, and physical function — we found these also all significantly improved at the end of the 2-year extension phase,” reported Dr. Wagenaar.
She added that after 2 years, there were significant improvements in weight loss (from 94.9 to 92.1 kg), BMI (from 33.3 to 32 kg/m2), and waist circumference (from 110 to 106.7 cm).
By the end of the trial and at 1 year of the extension study, there were significant improvements in A1c, fasting blood glucose, and low-density lipoprotein cholesterol, but at 2 years, these were no longer significant.
Regarding medications use, Dr. Wagenaar reported that, overall, there was no net change in use of pain, glucose-lowering, or hypertension medications, but 44% of patients using cholesterol-lowering medications were able to lower their dose or stop them.
Disease Activity Improvement and Medication Reduction in RA
Turning to the study of the intervention in patients with RA, 77 people (DAS28 ≥ 2.6 and ≤ 5.1, mild to moderate disease) were randomized to receive either the PFJ intervention in addition to usual care or only usual care (control group). Of these, 48 (62%) from both the intervention and control groups also completed the 2-year follow-up. The details of the PFJ intervention and the extension study for RA were the same as for the OA patient group.
Dr. Wagenaar commented on how they tried to individualize the exercise part of the program. “We noticed many of the RA patients asked too much of their body, while in contrast, those with OA were too hesitant,” she said. “We decided to focus on people’s own physical barriers, and we wanted to protect these. Sometimes, people needed to move more, and at other times, we had to tell people to slow down. Often, we advised people to move more by integrating exercise into their daily life.”
Similar to the OA study, patients were asked to try to avoid changing their medications in the 16-week study. “In the extension study, they were encouraged to reduce their medication in collaboration with their rheumatologist,” explained Wagenaar, who monitored any changes.
Differences were quantified according to medication groups comprising rheumatic medications, as well as pain, blood pressure, glucose-lowering, and cholesterol medications, and changes were categorized as increased, stable, or decreased/stopped.
Again, participants were mostly women (92%) with an average age of 55 years, BMI of 26 kg/m2, and DAS28 of 3.85 at baseline. Dropout reasons were similar to those for OA, and over 85% of participants were on medications.
During the 16-week trial period, the DAS28 changed more in the intervention participants than in the controls, and after 2 years of follow-up, DAS28 was significantly lower than baseline with a mean difference of −0.9 (95% CI, −1.2 to −0.6; P < .0001).
“Comparing with the literature, the drop in DAS28 was similar to that seen with medication, so it’s a very significant reduction,” remarked Dr. Wagenaar.
Mean tender joint count dropped from 3 to 0, and general health components of the DAS28 improved significantly over the intervention and over the 2-year follow-up, whereas there was no significant difference in the already low erythrocyte sedimentation rate and swollen joint count compared with baseline. C-reactive protein (CRP) changed from 3.2 to 1.3 mg/L over the 2-year follow-up. High-density lipoprotein increased from 1.6 to 1.8 mmol/L.
A total of 44% of people using antirheumatic medication decreased or stopped them after the 2-year extension.
Dr. Wagenaar went on to say that focus group findings suggested that “participants were very enthusiastic about the program despite it largely involving lifestyle change, and this is reflected in our low dropout rates after the trial and 1-year extension [20% for OA and RA].” There were more dropouts in year 2 of the extension.
In an interview, Dr. Wagenaar explained why she felt the program had been so well received. “People in the program felt like they had more control over their disease, and they felt listened to.”
Mechanisms Underpinning PFJ
Dr. Wagenaar and colleagues also sought to determine the possible mechanisms underlying the clinical effects of the plant-based diet on RA. “With RA, we have the mucosal origins hypothesis, which suggests RA is triggered at the mucosal site [of the gut] in genetically predisposed individuals, and this consequently transfers to the synovial [fluid in] joints,” she said.
“On top of this, we know that fiber protects our gut barrier and therefore reduces inflammation. The PFJ intervention is a very high-fiber program, so our hypothesis is that it might help [strengthen] the barrier,” she explained.
Dr. Wagenaar and colleagues collected fecal samples from patients and measured the albumin and calprotectin in them, which are both indicators of the gut barrier function. The researchers analyzed metabolomic data and found that fecal albumin — considered a gut barrier integrity marker — decreased significantly in the intervention group. In patients with RA, this improvement corresponded with an improvement in DAS28, the researchers reported in a poster at the meeting.
“Patients who had the greatest improvement in their gut barrier function also showed the greatest improvement in the DAS28 score, suggestive of a possible link between gut barrier improvement and clinical effects.”
They did not identify any change in calprotectin, an inflammation marker, but Dr. Wagenaar said this might change later. “We found that in those on the intervention, at 4 months, the CRP wasn’t reduced, but 1 year later it was.”
The metabolite lenticin, a lentil intake biomarker considered protective against inflammation and osteoclastic differentiation, also increased. Tryptophan was also reduced in people on the PFJ intervention.
Fernando Estevez-Lopez, PhD, a sports scientist at Harvard T.H. Chan School of Public Health, Boston, who specializes in physical activity and behavioral change in rheumatology patients, co-moderated the session and remarked that, “In this study, they did a brilliant job with encouraging participants to follow the program. The design and methods were really good — the sample size was good, and they followed people up. Also, these researchers come from Reade [a medical research center in Amsterdam University Medical Center] where they are well known for applying their research findings to the clinic,” he said.
“In terms of physical activity, we really mean increasing the time spent moving, for example, gentle activity such as walking, or changing behaviors in people with OA and RA. We don’t want them to have more pain the next day.”
Dr. Wagenaar reported receiving a grant from ZonMw (The Netherlands Organization for Health Research and Development). She and colleagues hold shares in Plants for Health, a limited liability company. Dr. Estevez-Lopez reported having no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM EULAR 2024
Trial Confirms Treating Gout Based on Uric Acid Level, Not Symptoms
UPDATED July 8, 2024 // Editor's note: This article has been revised to give a more nuanced view from Yael Klionsky, MD, about the need for more accurate and consistent gout management guidelines for busy primary care clinicians who often rely on them in clinical practice.
VIENNA — The first multicenter randomized trial in gout to compare treat-to-target (T2T) and treat for symptom avoidance (T2S) strategies has finally generated data to make the guideline-recommended practice of T2T evidence-based.
The T2T strategy may be guideline-endorsed, but it has never been validated, contended Anusha Moses, MSc, a researcher and PhD candidate at the University of Twente, Enschede, the Netherlands. She argued that this controlled trial fills an evidence gap.
T2T is defined as maintaining a serum uric acid (sUA) level below the physiologic threshold level of 36 mmol/L (< 6 mg/dL). T2S, in contrast, is a strategy of symptom control, typically basing therapy on suppression of symptoms independent of sUA, Dr. Moses explained.
Both the American College of Rheumatology and European Alliance of Associations for Rheumatology (EULAR) have already endorsed T2T, but other organizations, such as the American College of Physicians (ACP), still accept symptom-based treatment in its gout clinical practice guideline, according to Dr. Moses.
The results of the trial were not surprising based on the pathophysiology of gout. Elevated sUA is considered the driver of both flares and the complications of gout. This well-established association led to endorsement of T2T in guidelines from organizations such as EULAR, but Dr. Moses said a controlled trial allows this to be declared as evidence based.
To provide proof that T2T is superior, 308 gout patients at eight centers were randomized to one of the two strategies in a trial called GO TEST OVERTURE. In the T2T arm, commonly used therapies, such as allopurinol, benzbromarone, and febuxostat were employed to achieve and maintain a target sUA of < 0.36 mmol/L. In the T2S comparator arm, the same drugs were offered to control symptoms and prevent recurrences, but sUA levels were not used to guide treatment.
The 1-year results of a planned 2-year study were presented in an oral abstract session at the annual European Congress of Rheumatology. For this analysis, outcomes were compared in the last 6 months prior to the 1-year data analysis. When assessed at 2 years, the comparison will again be made in the prior 6 months of the study.
For the primary endpoint of flares defined by the validated Gallo criteria, the mean rates were 1.3 for T2T and 1.85 for T2S (P < .001), Dr. Moses reported.
The reduced risk for flares correlated with the greater proportion of patients with sUA < 0.36 mmol/L. These proportions were 72% and 26% (P < .001) for the T2T and T2S groups, respectively. The mean sUA levels were 0.31 mmol/L and 0.42 mmol/L (P < .001), respectively.
At the 1-year mark, none of the secondary endpoints reached statistical significance. These included mean numeric rating pain scale (2.46 vs 2.41), the proportion of patients in remission (8% vs 5.7%), and the mean Health Assessment Questionnaire-Disability Index score (0.65 vs 0.62), according to Dr. Moses, who said all of these endpoints will continue to be followed in the planned second year of the study.
At baseline, there were no differences in any of the variables evaluated, including age (about 62.5 years in both groups), proportion of patients with a body mass index > 30 kg/m2 (about 62%), sUA (about 0.5 mmol/L), or estimated glomerular filtration rate (about 70 mL/min/1.73 m2).
Nonspecialists Should Heed the Results
According to Yael Klionsky, MD, a clinical assistant professor of rheumatology and immunology at Wake Forest University School of Medicine, Winston-Salem, North Carolina, these data are not a surprise.
Even before this trial was completed, the message for clinicians is that they “should be focused on maintaining serum uric acid levels below physiological levels to improve outcomes” in patients with recurrent flares, said Klionsky, citing the validated EULAR and ACR guidelines.
While the ACP does still consider T2S acceptable as a strategy for chronic gout management, Klionsky pointed out that those guidelines have not been updated recently. Specialists in the treatment of gout do not need any more evidence that the T2T approach leads to better outcomes.
However, she agreed with the principle that non-rheumatologists need to be reached with better guidance in regard to gout management. While she expects the ACP to endorse T2T the next time their guidelines are updated, she hopes that primary care physicians recognize that T2T should now be a standard.
“In a 10- to 20-minute visit, managing multiple chronic conditions can be a challenge in primary care,” Klionsky said. “Many clinicians rely on guidelines so it is important to have consistent and accurate information.”
There is currently some distance between specialists and primary care physicians regarding the goals of gout management, according to a study that Klionsky presented at EULAR 2024. In a survey, nonspecialists and specialists did not perceive treatment priorities in the same way.
In this survey, which elicited responses from 151 rheumatologists, 150 nephrologists, and 102 primary care physicians, there was general agreement that preventing flares is a priority, but only 30% of primary care physicians and 35% of nephrologists vs 64% of rheumatologists identified the T2T target of < 0.36 mmol/L as a key step in reaching this goal.
Conversely, 58% of primary care physicians and 42% of nephrologists vs only 34% of rheumatologists considered absence of gout pain to be in the top three criteria.
In addition to the fact that primary care physicians differ from specialists in their goals for gout treatment, these data “highlight the need for the importance of a standardized definition of gout remission that includes serum uric acid control,” Dr. Klionsky said. She further thinks that this type of guidance should be disseminated to nonspecialists.
Dr. Moses reported no potential conflicts of interest. Dr. Klionsky reported financial relationships with Amgen, AstraZeneca, Eli Lilly, and MedIQ.
A version of this article appeared on Medscape.com.
UPDATED July 8, 2024 // Editor's note: This article has been revised to give a more nuanced view from Yael Klionsky, MD, about the need for more accurate and consistent gout management guidelines for busy primary care clinicians who often rely on them in clinical practice.
VIENNA — The first multicenter randomized trial in gout to compare treat-to-target (T2T) and treat for symptom avoidance (T2S) strategies has finally generated data to make the guideline-recommended practice of T2T evidence-based.
The T2T strategy may be guideline-endorsed, but it has never been validated, contended Anusha Moses, MSc, a researcher and PhD candidate at the University of Twente, Enschede, the Netherlands. She argued that this controlled trial fills an evidence gap.
T2T is defined as maintaining a serum uric acid (sUA) level below the physiologic threshold level of 36 mmol/L (< 6 mg/dL). T2S, in contrast, is a strategy of symptom control, typically basing therapy on suppression of symptoms independent of sUA, Dr. Moses explained.
Both the American College of Rheumatology and European Alliance of Associations for Rheumatology (EULAR) have already endorsed T2T, but other organizations, such as the American College of Physicians (ACP), still accept symptom-based treatment in its gout clinical practice guideline, according to Dr. Moses.
The results of the trial were not surprising based on the pathophysiology of gout. Elevated sUA is considered the driver of both flares and the complications of gout. This well-established association led to endorsement of T2T in guidelines from organizations such as EULAR, but Dr. Moses said a controlled trial allows this to be declared as evidence based.
To provide proof that T2T is superior, 308 gout patients at eight centers were randomized to one of the two strategies in a trial called GO TEST OVERTURE. In the T2T arm, commonly used therapies, such as allopurinol, benzbromarone, and febuxostat were employed to achieve and maintain a target sUA of < 0.36 mmol/L. In the T2S comparator arm, the same drugs were offered to control symptoms and prevent recurrences, but sUA levels were not used to guide treatment.
The 1-year results of a planned 2-year study were presented in an oral abstract session at the annual European Congress of Rheumatology. For this analysis, outcomes were compared in the last 6 months prior to the 1-year data analysis. When assessed at 2 years, the comparison will again be made in the prior 6 months of the study.
For the primary endpoint of flares defined by the validated Gallo criteria, the mean rates were 1.3 for T2T and 1.85 for T2S (P < .001), Dr. Moses reported.
The reduced risk for flares correlated with the greater proportion of patients with sUA < 0.36 mmol/L. These proportions were 72% and 26% (P < .001) for the T2T and T2S groups, respectively. The mean sUA levels were 0.31 mmol/L and 0.42 mmol/L (P < .001), respectively.
At the 1-year mark, none of the secondary endpoints reached statistical significance. These included mean numeric rating pain scale (2.46 vs 2.41), the proportion of patients in remission (8% vs 5.7%), and the mean Health Assessment Questionnaire-Disability Index score (0.65 vs 0.62), according to Dr. Moses, who said all of these endpoints will continue to be followed in the planned second year of the study.
At baseline, there were no differences in any of the variables evaluated, including age (about 62.5 years in both groups), proportion of patients with a body mass index > 30 kg/m2 (about 62%), sUA (about 0.5 mmol/L), or estimated glomerular filtration rate (about 70 mL/min/1.73 m2).
Nonspecialists Should Heed the Results
According to Yael Klionsky, MD, a clinical assistant professor of rheumatology and immunology at Wake Forest University School of Medicine, Winston-Salem, North Carolina, these data are not a surprise.
Even before this trial was completed, the message for clinicians is that they “should be focused on maintaining serum uric acid levels below physiological levels to improve outcomes” in patients with recurrent flares, said Klionsky, citing the validated EULAR and ACR guidelines.
While the ACP does still consider T2S acceptable as a strategy for chronic gout management, Klionsky pointed out that those guidelines have not been updated recently. Specialists in the treatment of gout do not need any more evidence that the T2T approach leads to better outcomes.
However, she agreed with the principle that non-rheumatologists need to be reached with better guidance in regard to gout management. While she expects the ACP to endorse T2T the next time their guidelines are updated, she hopes that primary care physicians recognize that T2T should now be a standard.
“In a 10- to 20-minute visit, managing multiple chronic conditions can be a challenge in primary care,” Klionsky said. “Many clinicians rely on guidelines so it is important to have consistent and accurate information.”
There is currently some distance between specialists and primary care physicians regarding the goals of gout management, according to a study that Klionsky presented at EULAR 2024. In a survey, nonspecialists and specialists did not perceive treatment priorities in the same way.
In this survey, which elicited responses from 151 rheumatologists, 150 nephrologists, and 102 primary care physicians, there was general agreement that preventing flares is a priority, but only 30% of primary care physicians and 35% of nephrologists vs 64% of rheumatologists identified the T2T target of < 0.36 mmol/L as a key step in reaching this goal.
Conversely, 58% of primary care physicians and 42% of nephrologists vs only 34% of rheumatologists considered absence of gout pain to be in the top three criteria.
In addition to the fact that primary care physicians differ from specialists in their goals for gout treatment, these data “highlight the need for the importance of a standardized definition of gout remission that includes serum uric acid control,” Dr. Klionsky said. She further thinks that this type of guidance should be disseminated to nonspecialists.
Dr. Moses reported no potential conflicts of interest. Dr. Klionsky reported financial relationships with Amgen, AstraZeneca, Eli Lilly, and MedIQ.
A version of this article appeared on Medscape.com.
UPDATED July 8, 2024 // Editor's note: This article has been revised to give a more nuanced view from Yael Klionsky, MD, about the need for more accurate and consistent gout management guidelines for busy primary care clinicians who often rely on them in clinical practice.
VIENNA — The first multicenter randomized trial in gout to compare treat-to-target (T2T) and treat for symptom avoidance (T2S) strategies has finally generated data to make the guideline-recommended practice of T2T evidence-based.
The T2T strategy may be guideline-endorsed, but it has never been validated, contended Anusha Moses, MSc, a researcher and PhD candidate at the University of Twente, Enschede, the Netherlands. She argued that this controlled trial fills an evidence gap.
T2T is defined as maintaining a serum uric acid (sUA) level below the physiologic threshold level of 36 mmol/L (< 6 mg/dL). T2S, in contrast, is a strategy of symptom control, typically basing therapy on suppression of symptoms independent of sUA, Dr. Moses explained.
Both the American College of Rheumatology and European Alliance of Associations for Rheumatology (EULAR) have already endorsed T2T, but other organizations, such as the American College of Physicians (ACP), still accept symptom-based treatment in its gout clinical practice guideline, according to Dr. Moses.
The results of the trial were not surprising based on the pathophysiology of gout. Elevated sUA is considered the driver of both flares and the complications of gout. This well-established association led to endorsement of T2T in guidelines from organizations such as EULAR, but Dr. Moses said a controlled trial allows this to be declared as evidence based.
To provide proof that T2T is superior, 308 gout patients at eight centers were randomized to one of the two strategies in a trial called GO TEST OVERTURE. In the T2T arm, commonly used therapies, such as allopurinol, benzbromarone, and febuxostat were employed to achieve and maintain a target sUA of < 0.36 mmol/L. In the T2S comparator arm, the same drugs were offered to control symptoms and prevent recurrences, but sUA levels were not used to guide treatment.
The 1-year results of a planned 2-year study were presented in an oral abstract session at the annual European Congress of Rheumatology. For this analysis, outcomes were compared in the last 6 months prior to the 1-year data analysis. When assessed at 2 years, the comparison will again be made in the prior 6 months of the study.
For the primary endpoint of flares defined by the validated Gallo criteria, the mean rates were 1.3 for T2T and 1.85 for T2S (P < .001), Dr. Moses reported.
The reduced risk for flares correlated with the greater proportion of patients with sUA < 0.36 mmol/L. These proportions were 72% and 26% (P < .001) for the T2T and T2S groups, respectively. The mean sUA levels were 0.31 mmol/L and 0.42 mmol/L (P < .001), respectively.
At the 1-year mark, none of the secondary endpoints reached statistical significance. These included mean numeric rating pain scale (2.46 vs 2.41), the proportion of patients in remission (8% vs 5.7%), and the mean Health Assessment Questionnaire-Disability Index score (0.65 vs 0.62), according to Dr. Moses, who said all of these endpoints will continue to be followed in the planned second year of the study.
At baseline, there were no differences in any of the variables evaluated, including age (about 62.5 years in both groups), proportion of patients with a body mass index > 30 kg/m2 (about 62%), sUA (about 0.5 mmol/L), or estimated glomerular filtration rate (about 70 mL/min/1.73 m2).
Nonspecialists Should Heed the Results
According to Yael Klionsky, MD, a clinical assistant professor of rheumatology and immunology at Wake Forest University School of Medicine, Winston-Salem, North Carolina, these data are not a surprise.
Even before this trial was completed, the message for clinicians is that they “should be focused on maintaining serum uric acid levels below physiological levels to improve outcomes” in patients with recurrent flares, said Klionsky, citing the validated EULAR and ACR guidelines.
While the ACP does still consider T2S acceptable as a strategy for chronic gout management, Klionsky pointed out that those guidelines have not been updated recently. Specialists in the treatment of gout do not need any more evidence that the T2T approach leads to better outcomes.
However, she agreed with the principle that non-rheumatologists need to be reached with better guidance in regard to gout management. While she expects the ACP to endorse T2T the next time their guidelines are updated, she hopes that primary care physicians recognize that T2T should now be a standard.
“In a 10- to 20-minute visit, managing multiple chronic conditions can be a challenge in primary care,” Klionsky said. “Many clinicians rely on guidelines so it is important to have consistent and accurate information.”
There is currently some distance between specialists and primary care physicians regarding the goals of gout management, according to a study that Klionsky presented at EULAR 2024. In a survey, nonspecialists and specialists did not perceive treatment priorities in the same way.
In this survey, which elicited responses from 151 rheumatologists, 150 nephrologists, and 102 primary care physicians, there was general agreement that preventing flares is a priority, but only 30% of primary care physicians and 35% of nephrologists vs 64% of rheumatologists identified the T2T target of < 0.36 mmol/L as a key step in reaching this goal.
Conversely, 58% of primary care physicians and 42% of nephrologists vs only 34% of rheumatologists considered absence of gout pain to be in the top three criteria.
In addition to the fact that primary care physicians differ from specialists in their goals for gout treatment, these data “highlight the need for the importance of a standardized definition of gout remission that includes serum uric acid control,” Dr. Klionsky said. She further thinks that this type of guidance should be disseminated to nonspecialists.
Dr. Moses reported no potential conflicts of interest. Dr. Klionsky reported financial relationships with Amgen, AstraZeneca, Eli Lilly, and MedIQ.
A version of this article appeared on Medscape.com.
FROM EULAR 2024