User login
Intratumor heterogeneity drives need for multiple biopsies
BRUSSELS – When biopsying a primary breast cancer, once is probably not enough based on accumulating evidence of primary-tumor heterogeneity, but despite this evidence, taking multiple biopsies has not yet become routine practice.
"Intra-tumor heterogeneity is one of the causes of variation during genetic profiling" of tumors, Dr. Jorge S. Reis-Fiho said. "Taking multiple biopsies from a primary tumor and putting them all together may mitigate the effect of intra-tumor heterogeneity," but taking multiple biopsies has not yet become standard of care, he said at the conference, which was sponsored by the European Society for Medical Oncology.

"I think we should start to seriously consider taking more than one biopsy. Quite a few places already do it, and our radiologists will routinely take two or three biopsies," said Dr. Fiho, a surgical pathologist at Memorial Sloan-Kettering Cancer Center in New York. "With only a single, small biopsy of the primary tumor we may not have sufficient information to predict what the metastasis will respond to," he said in an interview.
Results from two studies reported at the meeting added to the evidence favoring multiple biopsies as a way to more precisely characterize primary tumors and target the best therapy.
In one study, Dr. Michal Jarzab and his associates took three core biopsies from the primary tumors of 26 patients and assessed them genetically for estrogen receptor, progesterone receptor, and HER2-receptor mutations. Their sample included some patients with early-stage disease and others with advanced-stage cancer. The results of the three individual biopsy tests showed significant heterogeneity in seven of the 26 tumors (27%), reported Dr. Jarzab, a researcher at the Maria Sklodowska-Curie Cancer Center and Institute of Oncology in Gliwice, Poland.
The intratumor heterogeneity in these seven patients "could negatively impact genomic assessment if done with one specimen," he said.
"If other studies report similar results" on intratumor heterogeneity, "then it could become common practice to evaluate prognostic or predictive breast cancer markers from more than one primary tumour area," Dr. Angelo Di Leo, chairman of oncology at Prato (Italy) Hospital, said in a written statement.
The second study looked at the impact of assessing one, two, or three biopsies on the variance in results from four different single- or multiple-genetic tests in biopsies collected from 51 breast cancer patients. The amount of variance depended on the gene or genes tested, but, overall, using three biopsy specimens rather than one substantially reduced the variance, reported Dr. Rosanna Lau, a researcher at the University of Texas M.D. Anderson Cancer Center in Houston.
"Pooling biopsies from a single tumor reduced outlier results and reduced variance more generally for certain genes," Dr. Lau said. "Pooling biopsies is usually preferable to a single biopsy." The results showed that "we can get a comprehensive picture of the genes being expressed in the tumor by sampling multiple areas of the tumor and pooling the samples together. This increases the precision of the assay and allows us to make more reliable predictions related to the disease," she said in a written statement.
Her study also looked at the scope of analytic variance – variance caused by technical issues – in the biopsies taken from a 20-patient subgroup and found that the extent of analytic variance also varied by gene and was generally of the same magnitude as intratumor heterogeneity. The analytic variance wasn’t helped by pooling multiple biopsies, but data-processing solutions such as normalizing and scaling reduced this part of the variance, Dr. Lau said.
Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.
BRUSSELS – When biopsying a primary breast cancer, once is probably not enough based on accumulating evidence of primary-tumor heterogeneity, but despite this evidence, taking multiple biopsies has not yet become routine practice.
"Intra-tumor heterogeneity is one of the causes of variation during genetic profiling" of tumors, Dr. Jorge S. Reis-Fiho said. "Taking multiple biopsies from a primary tumor and putting them all together may mitigate the effect of intra-tumor heterogeneity," but taking multiple biopsies has not yet become standard of care, he said at the conference, which was sponsored by the European Society for Medical Oncology.
"I think we should start to seriously consider taking more than one biopsy. Quite a few places already do it, and our radiologists will routinely take two or three biopsies," said Dr. Fiho, a surgical pathologist at Memorial Sloan-Kettering Cancer Center in New York. "With only a single, small biopsy of the primary tumor we may not have sufficient information to predict what the metastasis will respond to," he said in an interview.
Results from two studies reported at the meeting added to the evidence favoring multiple biopsies as a way to more precisely characterize primary tumors and target the best therapy.
In one study, Dr. Michal Jarzab and his associates took three core biopsies from the primary tumors of 26 patients and assessed them genetically for estrogen receptor, progesterone receptor, and HER2-receptor mutations. Their sample included some patients with early-stage disease and others with advanced-stage cancer. The results of the three individual biopsy tests showed significant heterogeneity in seven of the 26 tumors (27%), reported Dr. Jarzab, a researcher at the Maria Sklodowska-Curie Cancer Center and Institute of Oncology in Gliwice, Poland.
The intratumor heterogeneity in these seven patients "could negatively impact genomic assessment if done with one specimen," he said.
"If other studies report similar results" on intratumor heterogeneity, "then it could become common practice to evaluate prognostic or predictive breast cancer markers from more than one primary tumour area," Dr. Angelo Di Leo, chairman of oncology at Prato (Italy) Hospital, said in a written statement.
The second study looked at the impact of assessing one, two, or three biopsies on the variance in results from four different single- or multiple-genetic tests in biopsies collected from 51 breast cancer patients. The amount of variance depended on the gene or genes tested, but, overall, using three biopsy specimens rather than one substantially reduced the variance, reported Dr. Rosanna Lau, a researcher at the University of Texas M.D. Anderson Cancer Center in Houston.
"Pooling biopsies from a single tumor reduced outlier results and reduced variance more generally for certain genes," Dr. Lau said. "Pooling biopsies is usually preferable to a single biopsy." The results showed that "we can get a comprehensive picture of the genes being expressed in the tumor by sampling multiple areas of the tumor and pooling the samples together. This increases the precision of the assay and allows us to make more reliable predictions related to the disease," she said in a written statement.
Her study also looked at the scope of analytic variance – variance caused by technical issues – in the biopsies taken from a 20-patient subgroup and found that the extent of analytic variance also varied by gene and was generally of the same magnitude as intratumor heterogeneity. The analytic variance wasn’t helped by pooling multiple biopsies, but data-processing solutions such as normalizing and scaling reduced this part of the variance, Dr. Lau said.
Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.
BRUSSELS – When biopsying a primary breast cancer, once is probably not enough based on accumulating evidence of primary-tumor heterogeneity, but despite this evidence, taking multiple biopsies has not yet become routine practice.
"Intra-tumor heterogeneity is one of the causes of variation during genetic profiling" of tumors, Dr. Jorge S. Reis-Fiho said. "Taking multiple biopsies from a primary tumor and putting them all together may mitigate the effect of intra-tumor heterogeneity," but taking multiple biopsies has not yet become standard of care, he said at the conference, which was sponsored by the European Society for Medical Oncology.
"I think we should start to seriously consider taking more than one biopsy. Quite a few places already do it, and our radiologists will routinely take two or three biopsies," said Dr. Fiho, a surgical pathologist at Memorial Sloan-Kettering Cancer Center in New York. "With only a single, small biopsy of the primary tumor we may not have sufficient information to predict what the metastasis will respond to," he said in an interview.
Results from two studies reported at the meeting added to the evidence favoring multiple biopsies as a way to more precisely characterize primary tumors and target the best therapy.
In one study, Dr. Michal Jarzab and his associates took three core biopsies from the primary tumors of 26 patients and assessed them genetically for estrogen receptor, progesterone receptor, and HER2-receptor mutations. Their sample included some patients with early-stage disease and others with advanced-stage cancer. The results of the three individual biopsy tests showed significant heterogeneity in seven of the 26 tumors (27%), reported Dr. Jarzab, a researcher at the Maria Sklodowska-Curie Cancer Center and Institute of Oncology in Gliwice, Poland.
The intratumor heterogeneity in these seven patients "could negatively impact genomic assessment if done with one specimen," he said.
"If other studies report similar results" on intratumor heterogeneity, "then it could become common practice to evaluate prognostic or predictive breast cancer markers from more than one primary tumour area," Dr. Angelo Di Leo, chairman of oncology at Prato (Italy) Hospital, said in a written statement.
The second study looked at the impact of assessing one, two, or three biopsies on the variance in results from four different single- or multiple-genetic tests in biopsies collected from 51 breast cancer patients. The amount of variance depended on the gene or genes tested, but, overall, using three biopsy specimens rather than one substantially reduced the variance, reported Dr. Rosanna Lau, a researcher at the University of Texas M.D. Anderson Cancer Center in Houston.
"Pooling biopsies from a single tumor reduced outlier results and reduced variance more generally for certain genes," Dr. Lau said. "Pooling biopsies is usually preferable to a single biopsy." The results showed that "we can get a comprehensive picture of the genes being expressed in the tumor by sampling multiple areas of the tumor and pooling the samples together. This increases the precision of the assay and allows us to make more reliable predictions related to the disease," she said in a written statement.
Her study also looked at the scope of analytic variance – variance caused by technical issues – in the biopsies taken from a 20-patient subgroup and found that the extent of analytic variance also varied by gene and was generally of the same magnitude as intratumor heterogeneity. The analytic variance wasn’t helped by pooling multiple biopsies, but data-processing solutions such as normalizing and scaling reduced this part of the variance, Dr. Lau said.
Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.
AT IMPAKT 2013 BREAST CANCER CONFERENCE
Major finding: Significant intratumor heterogeneity occurred in the genetic-profile results from three individual biopsies for 27% of primary breast cancers tested.
Data source: Single-center study of 26 patients with either early- or advanced-stage breast cancer.
Disclosures: Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.

Ultralow-dose CT bests X-Ray for lung cancer follow-up, but is it enough?
MINNEAPOLIS – Minimal-dose computed tomography was superior to chest radiographs for surveillance after curative lung cancer resection in a randomized controlled trial involving over 300 patients.
"Minimal-dose CT should be the modality of choice for surveillance after resection of lung cancer," Dr. Waël Hanna said at the annual meeting of the American Association for Thoracic Surgery.

Repeated radiation exposure and a high false-positive rate have been stumbling blocks to national lung cancer screening with low-dose spiral CT, despite the technology demonstrating 20% fewer lung cancer deaths compared with chest x-ray in asymptomatic heavy smokers in the National Lung Cancer Screening Trial (NLST). Minimal-dose CT of the chest delivers a radiation dose of 0.2 mSv per scan, which is comparable to chest x-ray at 0.16 mSv and lower than a diagnostic CT or low-dose CT at roughly 8 mSv and 1.5 mSv, he said.
The 311 patients in the current study were prospectively enrolled after curative resection and underwent minimal-dose CT and chest x-ray at 3, 6, 12, 18, 24, 36, 48, and 60 months. A total of 1,137 pairs of chest X-ray and CT scans were analyzed by radiologists blinded to the other modality.
Minimal-dose CT detected 94.2% of the new or recurrent lung cancer, compared with 21.1% for chest x-ray (P value .0001), said Dr. Hanna, a thoracic surgery fellow at the University of Toronto.
The increased sensitivity came at a cost of significantly lower specificity (86% vs. 99.9%) and positive predictive value (25.1% vs. 91.6%; both P less than .0001). The negative predictive value for minimal-dose CT, however, was almost perfect (99.7% vs. 96.1%; P = .007).
More importantly, of the 63 patients diagnosed with new or recurrent cancer, 49 (78%) had asymptomatic disease detected only on minimal dose CT, Dr. Hanna said. Two-thirds of the asymptomatic patients were diagnosed within the first year of surveillance and 94% within 2 years of initial surgery.
"Why is this important? Because when you find it at an earlier stage, earlier in time, you can do something about it," he said.
Asymptomatic patients who were restaged and given curative surgery or radiation went on to live a median of 69 months (range, 12-76) after the initial operation, compared with a median survival of 25 months (range, 6-48) among asymptomatic patients given palliative treatment after restaging (P less than .001).
The 14 patients with symptomatic recurrent or new cancer had a median survival of only 15 months (range, 7-63) with palliative care.
"We are not saying that minimal-dose CT improves survival because these two patient populations are different," Dr. Hanna said. "The patient who presents with asymptomatic disease of the chest and is a candidate for surgery is clearly different from the patient who presents with brain metastases and is symptomatic. But follow-up with minimal-dose CT allows us to identify this cohort of patients in whom close surveillance after surgery is not futile, in whom close surveillance after surgery is amenable to intervention and treatment, and is associated with long survival."
Several prominent guidelines, including those from the AATS and National Comprehensive Cancer Network, have moved to include regular CT scans in the wake of the NLST, but evidence is lacking to suggest that earlier treatment of recurrence leads to better outcomes.
Invited discussant Dr. Michael Jaklitsch of Brigham and Women’s Hospital, Boston, said that the investigators were able to take a group of patients who would have had a 5-year survival of 50% and raise it to 75% through aggressive surveillance and show that they were "truly curing" these patients.
"Is this enough data to change our personal practices today," he posited. "For me personally, the answer is yes. This single paper presents me with enough data to say I will use minimal-dose CT scan as my sole method of screening for recurrence of early-stage lung cancer moving forward."
Dr. Jaklitsch questioned whether there were subpopulations in whom minimal-dose CT would not work, such as the obese or those with surgical clips. Dr. Hanna said that radiologists at his center are more comfortable using low-dose CT for surveillance because of the risk of scatter in either of these subgroups or in those with mediastinal involvement.
Dr. Hanna also noted that minimal-dose CT is not available everywhere, but Dr. Jaklitsch said that he took the specifications from the paper to his community hospital and they said they could be done. "So at least in the U.S., this will have dramatic penetrance," he added.

New AATS president David Sugarbaker, chief of thoracic surgery at Brigham and Women’s Hospital and the Richard E. Wilson Professor of Surgical Oncology at Harvard Medical School, Boston, was not convinced, and suggested that the study essentially describes the detection of new primary tumors following initial resection.
"It’s important to realize that what you’re really talking about is screening patients who’ve had lobar resection for lung cancer," Dr. Sugarbaker said.
"So, I’m not sure you’re conclusion about follow-up detection of metastatic disease is really an accurate description as to what you’ve done, particularly with the inability of minimal-dose CT to assess the mediastinal. Particularly in the larger lesions, where distant metastatic disease may be more frequent, I’m not sure that minimal dose CT is adequate for those patients, where again, mediastinal disease can be the real issue," he said.
Dr. Hanna said that they realize these patients are also at risk of mediastinal disease and that the future will include a more patient-centered approach to surveillance in which patients with a higher risk of distant recurrence will have some other test on top of minimal-dose CT.
Dr. Hanna and his coauthors reported having no study sponsorship or financial disclosures.
MINNEAPOLIS – Minimal-dose computed tomography was superior to chest radiographs for surveillance after curative lung cancer resection in a randomized controlled trial involving over 300 patients.
"Minimal-dose CT should be the modality of choice for surveillance after resection of lung cancer," Dr. Waël Hanna said at the annual meeting of the American Association for Thoracic Surgery.
Repeated radiation exposure and a high false-positive rate have been stumbling blocks to national lung cancer screening with low-dose spiral CT, despite the technology demonstrating 20% fewer lung cancer deaths compared with chest x-ray in asymptomatic heavy smokers in the National Lung Cancer Screening Trial (NLST). Minimal-dose CT of the chest delivers a radiation dose of 0.2 mSv per scan, which is comparable to chest x-ray at 0.16 mSv and lower than a diagnostic CT or low-dose CT at roughly 8 mSv and 1.5 mSv, he said.
The 311 patients in the current study were prospectively enrolled after curative resection and underwent minimal-dose CT and chest x-ray at 3, 6, 12, 18, 24, 36, 48, and 60 months. A total of 1,137 pairs of chest X-ray and CT scans were analyzed by radiologists blinded to the other modality.
Minimal-dose CT detected 94.2% of the new or recurrent lung cancer, compared with 21.1% for chest x-ray (P value .0001), said Dr. Hanna, a thoracic surgery fellow at the University of Toronto.
The increased sensitivity came at a cost of significantly lower specificity (86% vs. 99.9%) and positive predictive value (25.1% vs. 91.6%; both P less than .0001). The negative predictive value for minimal-dose CT, however, was almost perfect (99.7% vs. 96.1%; P = .007).
More importantly, of the 63 patients diagnosed with new or recurrent cancer, 49 (78%) had asymptomatic disease detected only on minimal dose CT, Dr. Hanna said. Two-thirds of the asymptomatic patients were diagnosed within the first year of surveillance and 94% within 2 years of initial surgery.
"Why is this important? Because when you find it at an earlier stage, earlier in time, you can do something about it," he said.
Asymptomatic patients who were restaged and given curative surgery or radiation went on to live a median of 69 months (range, 12-76) after the initial operation, compared with a median survival of 25 months (range, 6-48) among asymptomatic patients given palliative treatment after restaging (P less than .001).
The 14 patients with symptomatic recurrent or new cancer had a median survival of only 15 months (range, 7-63) with palliative care.
"We are not saying that minimal-dose CT improves survival because these two patient populations are different," Dr. Hanna said. "The patient who presents with asymptomatic disease of the chest and is a candidate for surgery is clearly different from the patient who presents with brain metastases and is symptomatic. But follow-up with minimal-dose CT allows us to identify this cohort of patients in whom close surveillance after surgery is not futile, in whom close surveillance after surgery is amenable to intervention and treatment, and is associated with long survival."
Several prominent guidelines, including those from the AATS and National Comprehensive Cancer Network, have moved to include regular CT scans in the wake of the NLST, but evidence is lacking to suggest that earlier treatment of recurrence leads to better outcomes.
Invited discussant Dr. Michael Jaklitsch of Brigham and Women’s Hospital, Boston, said that the investigators were able to take a group of patients who would have had a 5-year survival of 50% and raise it to 75% through aggressive surveillance and show that they were "truly curing" these patients.
"Is this enough data to change our personal practices today," he posited. "For me personally, the answer is yes. This single paper presents me with enough data to say I will use minimal-dose CT scan as my sole method of screening for recurrence of early-stage lung cancer moving forward."
Dr. Jaklitsch questioned whether there were subpopulations in whom minimal-dose CT would not work, such as the obese or those with surgical clips. Dr. Hanna said that radiologists at his center are more comfortable using low-dose CT for surveillance because of the risk of scatter in either of these subgroups or in those with mediastinal involvement.
Dr. Hanna also noted that minimal-dose CT is not available everywhere, but Dr. Jaklitsch said that he took the specifications from the paper to his community hospital and they said they could be done. "So at least in the U.S., this will have dramatic penetrance," he added.
New AATS president David Sugarbaker, chief of thoracic surgery at Brigham and Women’s Hospital and the Richard E. Wilson Professor of Surgical Oncology at Harvard Medical School, Boston, was not convinced, and suggested that the study essentially describes the detection of new primary tumors following initial resection.
"It’s important to realize that what you’re really talking about is screening patients who’ve had lobar resection for lung cancer," Dr. Sugarbaker said.
"So, I’m not sure you’re conclusion about follow-up detection of metastatic disease is really an accurate description as to what you’ve done, particularly with the inability of minimal-dose CT to assess the mediastinal. Particularly in the larger lesions, where distant metastatic disease may be more frequent, I’m not sure that minimal dose CT is adequate for those patients, where again, mediastinal disease can be the real issue," he said.
Dr. Hanna said that they realize these patients are also at risk of mediastinal disease and that the future will include a more patient-centered approach to surveillance in which patients with a higher risk of distant recurrence will have some other test on top of minimal-dose CT.
Dr. Hanna and his coauthors reported having no study sponsorship or financial disclosures.
MINNEAPOLIS – Minimal-dose computed tomography was superior to chest radiographs for surveillance after curative lung cancer resection in a randomized controlled trial involving over 300 patients.
"Minimal-dose CT should be the modality of choice for surveillance after resection of lung cancer," Dr. Waël Hanna said at the annual meeting of the American Association for Thoracic Surgery.
Repeated radiation exposure and a high false-positive rate have been stumbling blocks to national lung cancer screening with low-dose spiral CT, despite the technology demonstrating 20% fewer lung cancer deaths compared with chest x-ray in asymptomatic heavy smokers in the National Lung Cancer Screening Trial (NLST). Minimal-dose CT of the chest delivers a radiation dose of 0.2 mSv per scan, which is comparable to chest x-ray at 0.16 mSv and lower than a diagnostic CT or low-dose CT at roughly 8 mSv and 1.5 mSv, he said.
The 311 patients in the current study were prospectively enrolled after curative resection and underwent minimal-dose CT and chest x-ray at 3, 6, 12, 18, 24, 36, 48, and 60 months. A total of 1,137 pairs of chest X-ray and CT scans were analyzed by radiologists blinded to the other modality.
Minimal-dose CT detected 94.2% of the new or recurrent lung cancer, compared with 21.1% for chest x-ray (P value .0001), said Dr. Hanna, a thoracic surgery fellow at the University of Toronto.
The increased sensitivity came at a cost of significantly lower specificity (86% vs. 99.9%) and positive predictive value (25.1% vs. 91.6%; both P less than .0001). The negative predictive value for minimal-dose CT, however, was almost perfect (99.7% vs. 96.1%; P = .007).
More importantly, of the 63 patients diagnosed with new or recurrent cancer, 49 (78%) had asymptomatic disease detected only on minimal dose CT, Dr. Hanna said. Two-thirds of the asymptomatic patients were diagnosed within the first year of surveillance and 94% within 2 years of initial surgery.
"Why is this important? Because when you find it at an earlier stage, earlier in time, you can do something about it," he said.
Asymptomatic patients who were restaged and given curative surgery or radiation went on to live a median of 69 months (range, 12-76) after the initial operation, compared with a median survival of 25 months (range, 6-48) among asymptomatic patients given palliative treatment after restaging (P less than .001).
The 14 patients with symptomatic recurrent or new cancer had a median survival of only 15 months (range, 7-63) with palliative care.
"We are not saying that minimal-dose CT improves survival because these two patient populations are different," Dr. Hanna said. "The patient who presents with asymptomatic disease of the chest and is a candidate for surgery is clearly different from the patient who presents with brain metastases and is symptomatic. But follow-up with minimal-dose CT allows us to identify this cohort of patients in whom close surveillance after surgery is not futile, in whom close surveillance after surgery is amenable to intervention and treatment, and is associated with long survival."
Several prominent guidelines, including those from the AATS and National Comprehensive Cancer Network, have moved to include regular CT scans in the wake of the NLST, but evidence is lacking to suggest that earlier treatment of recurrence leads to better outcomes.
Invited discussant Dr. Michael Jaklitsch of Brigham and Women’s Hospital, Boston, said that the investigators were able to take a group of patients who would have had a 5-year survival of 50% and raise it to 75% through aggressive surveillance and show that they were "truly curing" these patients.
"Is this enough data to change our personal practices today," he posited. "For me personally, the answer is yes. This single paper presents me with enough data to say I will use minimal-dose CT scan as my sole method of screening for recurrence of early-stage lung cancer moving forward."
Dr. Jaklitsch questioned whether there were subpopulations in whom minimal-dose CT would not work, such as the obese or those with surgical clips. Dr. Hanna said that radiologists at his center are more comfortable using low-dose CT for surveillance because of the risk of scatter in either of these subgroups or in those with mediastinal involvement.
Dr. Hanna also noted that minimal-dose CT is not available everywhere, but Dr. Jaklitsch said that he took the specifications from the paper to his community hospital and they said they could be done. "So at least in the U.S., this will have dramatic penetrance," he added.
New AATS president David Sugarbaker, chief of thoracic surgery at Brigham and Women’s Hospital and the Richard E. Wilson Professor of Surgical Oncology at Harvard Medical School, Boston, was not convinced, and suggested that the study essentially describes the detection of new primary tumors following initial resection.
"It’s important to realize that what you’re really talking about is screening patients who’ve had lobar resection for lung cancer," Dr. Sugarbaker said.
"So, I’m not sure you’re conclusion about follow-up detection of metastatic disease is really an accurate description as to what you’ve done, particularly with the inability of minimal-dose CT to assess the mediastinal. Particularly in the larger lesions, where distant metastatic disease may be more frequent, I’m not sure that minimal dose CT is adequate for those patients, where again, mediastinal disease can be the real issue," he said.
Dr. Hanna said that they realize these patients are also at risk of mediastinal disease and that the future will include a more patient-centered approach to surveillance in which patients with a higher risk of distant recurrence will have some other test on top of minimal-dose CT.
Dr. Hanna and his coauthors reported having no study sponsorship or financial disclosures.
AT THE AATS ANNUAL MEETING
Major finding: Minimal-dose CT detected 94.2% of new or recurrent lung cancer, compared with 21.1% for chest x-ray.
Data source: Prospective study of 311 curative resection patients who underwent minimal-dose CT and chest x-ray at 3, 6, 12, 18, 24, 36, 48, and 60 months. A total of 1,137 pairs of chest x-ray and CT scans were analyzed.
Disclosures: The researchers reported having no study sponsorship or financial disclosures.

Postop surveillance sufficient for stage I testicular cancer
Surveillance is sufficient for most men with stage I seminoma after successful orchiectomy, according to the findings of the largest study ever performed to address the issue.
The 1,822 men followed only with surveillance in Denmark had an excellent disease-specific survival of 99.5%, Dr. Mette Saskø Mortensen said at a press briefing highlighting research to be presented at the upcoming American Society of Clinical Oncology annual meeting. Only 10 men died of testicular cancer or treatment-related causes during a median follow-up of 15.4 years.

This finding means that for every 1,000 men followed by a surveillance program, only 4 will die within 10 years, said incoming ASCO president Dr. Clifford Hudis, chief of breast cancer medicine service at Memorial Sloan-Kettering Cancer Center in New York.
He described the study as one of several recent reminders that sometimes "less is more" in patient care and noted that opting for surveillance spares patients from the harmful side effects of chemotherapy and radiation without diminishing their chances for long-term survival.
Seminoma is a relatively rare cancer, but it is the most common solid tumor among young men. Initial treatment is typically orchiectomy, but no standard postoperative management strategy has been established. The current results will likely accelerate the trend toward surveillance in the United States, where roughly 50% of men undergo either radiotherapy or chemotherapy with carboplatin after surgery.
Overall, 355 (19.5%) of the 1,822 men experienced a relapse during surveillance, said Dr. Mortensen, a PhD student in the oncology department at Copenhagen University Hospital.
The median time to relapse was 13.7 months, with the majority of patients (72.4%) relapsing within the first 2 years. Another 20.3% relapsed within years 2-5 and 7.3% after 5 years.
"With only 19.5% of the patients relapsing, the surveillance strategy spares the remaining 80% of patients from unnecessary treatment after orchiectomy," Dr. Mortensen said. "Surveillance is a safe strategy for stage I seminoma patients."
Surveillance has been the main follow-up strategy for stage I seminoma in Denmark since 1984, and consists of 5 years of scheduled clinical visits, computed tomography scans/chest x-rays, and blood measurements of tumor markers. Men in the analysis were diagnosed from 1984 to 2008, and their data were collected up to December 2012 from patient files and linked national registries.
As observed in other smaller studies, the risk for relapse was increased with elevated human chorionic gonadotropin levels of more than 200 IU/L, vascular invasion, and tumors larger than 4 cm, Dr. Mortensen said.
The study was supported in part by the Danish Cancer Society, Danish Research Foundation and the Preben and Anna Simonsen Foundation. Dr. Mortensen reported having no financial disclosures.
Surveillance is sufficient for most men with stage I seminoma after successful orchiectomy, according to the findings of the largest study ever performed to address the issue.
The 1,822 men followed only with surveillance in Denmark had an excellent disease-specific survival of 99.5%, Dr. Mette Saskø Mortensen said at a press briefing highlighting research to be presented at the upcoming American Society of Clinical Oncology annual meeting. Only 10 men died of testicular cancer or treatment-related causes during a median follow-up of 15.4 years.
This finding means that for every 1,000 men followed by a surveillance program, only 4 will die within 10 years, said incoming ASCO president Dr. Clifford Hudis, chief of breast cancer medicine service at Memorial Sloan-Kettering Cancer Center in New York.
He described the study as one of several recent reminders that sometimes "less is more" in patient care and noted that opting for surveillance spares patients from the harmful side effects of chemotherapy and radiation without diminishing their chances for long-term survival.
Seminoma is a relatively rare cancer, but it is the most common solid tumor among young men. Initial treatment is typically orchiectomy, but no standard postoperative management strategy has been established. The current results will likely accelerate the trend toward surveillance in the United States, where roughly 50% of men undergo either radiotherapy or chemotherapy with carboplatin after surgery.
Overall, 355 (19.5%) of the 1,822 men experienced a relapse during surveillance, said Dr. Mortensen, a PhD student in the oncology department at Copenhagen University Hospital.
The median time to relapse was 13.7 months, with the majority of patients (72.4%) relapsing within the first 2 years. Another 20.3% relapsed within years 2-5 and 7.3% after 5 years.
"With only 19.5% of the patients relapsing, the surveillance strategy spares the remaining 80% of patients from unnecessary treatment after orchiectomy," Dr. Mortensen said. "Surveillance is a safe strategy for stage I seminoma patients."
Surveillance has been the main follow-up strategy for stage I seminoma in Denmark since 1984, and consists of 5 years of scheduled clinical visits, computed tomography scans/chest x-rays, and blood measurements of tumor markers. Men in the analysis were diagnosed from 1984 to 2008, and their data were collected up to December 2012 from patient files and linked national registries.
As observed in other smaller studies, the risk for relapse was increased with elevated human chorionic gonadotropin levels of more than 200 IU/L, vascular invasion, and tumors larger than 4 cm, Dr. Mortensen said.
The study was supported in part by the Danish Cancer Society, Danish Research Foundation and the Preben and Anna Simonsen Foundation. Dr. Mortensen reported having no financial disclosures.
Surveillance is sufficient for most men with stage I seminoma after successful orchiectomy, according to the findings of the largest study ever performed to address the issue.
The 1,822 men followed only with surveillance in Denmark had an excellent disease-specific survival of 99.5%, Dr. Mette Saskø Mortensen said at a press briefing highlighting research to be presented at the upcoming American Society of Clinical Oncology annual meeting. Only 10 men died of testicular cancer or treatment-related causes during a median follow-up of 15.4 years.
This finding means that for every 1,000 men followed by a surveillance program, only 4 will die within 10 years, said incoming ASCO president Dr. Clifford Hudis, chief of breast cancer medicine service at Memorial Sloan-Kettering Cancer Center in New York.
He described the study as one of several recent reminders that sometimes "less is more" in patient care and noted that opting for surveillance spares patients from the harmful side effects of chemotherapy and radiation without diminishing their chances for long-term survival.
Seminoma is a relatively rare cancer, but it is the most common solid tumor among young men. Initial treatment is typically orchiectomy, but no standard postoperative management strategy has been established. The current results will likely accelerate the trend toward surveillance in the United States, where roughly 50% of men undergo either radiotherapy or chemotherapy with carboplatin after surgery.
Overall, 355 (19.5%) of the 1,822 men experienced a relapse during surveillance, said Dr. Mortensen, a PhD student in the oncology department at Copenhagen University Hospital.
The median time to relapse was 13.7 months, with the majority of patients (72.4%) relapsing within the first 2 years. Another 20.3% relapsed within years 2-5 and 7.3% after 5 years.
"With only 19.5% of the patients relapsing, the surveillance strategy spares the remaining 80% of patients from unnecessary treatment after orchiectomy," Dr. Mortensen said. "Surveillance is a safe strategy for stage I seminoma patients."
Surveillance has been the main follow-up strategy for stage I seminoma in Denmark since 1984, and consists of 5 years of scheduled clinical visits, computed tomography scans/chest x-rays, and blood measurements of tumor markers. Men in the analysis were diagnosed from 1984 to 2008, and their data were collected up to December 2012 from patient files and linked national registries.
As observed in other smaller studies, the risk for relapse was increased with elevated human chorionic gonadotropin levels of more than 200 IU/L, vascular invasion, and tumors larger than 4 cm, Dr. Mortensen said.
The study was supported in part by the Danish Cancer Society, Danish Research Foundation and the Preben and Anna Simonsen Foundation. Dr. Mortensen reported having no financial disclosures.
AT THE ASCO 2013 PRESSCAST
Major finding: The 10-year cancer-specific survival was 99.6%.
Data source: Retrospective, nationwide cohort study of surveillance in 1,822 men with stage I seminoma.
Disclosures: The study was supported in part by the Danish Cancer Society, Danish Research Foundation, and the Preben and Anna Simonsen Foundation. Dr. Mortensen reported having no financial disclosures.

Standard-dose radiation bests high-dose radiation in advanced NSCLC
Standard-dose radiation produced better overall survival and locoregional control than did high-dose radiation when given with concurrent chemotherapy in patients with newly diagnosed stage III non–small cell lung cancer in the phase III, randomized RTOG 0617 trial.
Patients on the high dose had a 56% greater risk of death than those on a standard 60 Gy dose. Median overall survival times were 18.5 months with high-dose radiation and 28.7 months with a standard dose (hazard ratio, 1.56; P = .0007).
The risk of local failure also was increased by 37% in the high-dose arm (HR, 1.37; P = .03).

"At this point, there is no clear reason for the poor outcome we experienced on the high-dose arm," lead author Dr. Jeffrey Bradley said in a press briefing highlighting studies to be presented at the upcoming annual meeting of the American Society of Clinical Oncology (ASCO).
The most likely culprit is unreported toxicities, although other possible explanations are increased heart dose, longer duration of therapy, or a combination of these factors, he said.
The results are surprising because conventional thinking has been that higher doses of radiation would more effectively kill the tumor and thereby improve survival.
A phase-III trial in the 1970s established the standard radiation dose of 60 Gy in this setting but, over time, several radiation dose-ranging phase-II studies have reported promising results and improved median survival times with radiation doses up to 74 Gy, explained Dr. Bradley, professor of radiation oncology and chief of the thoracic service at Washington University, St. Louis.
At the same time, improvements in technology such as three-dimensional radiation therapy (RT) and intensity-modulated RT techniques have made RT delivery more precise, allowing organs and tissues sensitive to radiation to receive less radiation while the tumor receives more. This technique was explored in Radiation Therapy Oncology Group (RTOG) 0617.
"This is a very surprising result, especially when using these special radiation techniques that were designed to be more precise, you would expect that the outcome would be better," ASCO president Sandra Swain, medical director of the Washington (D.C.) Cancer Institute, told reporters. "This should really put an end to higher-dose treatments, given the better outcomes in the standard-dose arms."
Dr. Bradley said, "A lot of phase-III trials turn out negative when phase-II trials look good, so I think it was good to do a phase-III trial and get this answered."
RTOG 0617 randomly assigned 464 patients with newly diagnosed, unresected stage-III non–small cell lung cancer to conformal RT to 60 Gy, five times per week for 6 weeks or to 74 Gy five times per week for 7.5 weeks. All patients received concurrent chemotherapy with weekly paclitaxel (Taxol) and carboplatin, with a second randomization for patients to receive consolidation chemotherapy with or without cetuximab (Erbitux).
Among the 419 patients available for analysis at 18 months, local failure rates were 25% with standard-dose RT and 34.3% with high-dose RT (P = .03, as noted above), Dr. Bradley reported.
Median 18-month overall survival rates were 67% with the standard radiation dose vs. 54% with the high dose.
Median overall survival times in both groups were higher than expected, but "the overall survival benefit of 60 Gy is independent of the cetuximab question," he said. Data from that portion of the trial are expected to be reported in 2014.
Finally, the only significant difference in physician-reported side effects was a slightly higher rate of esophagitis in the high-dose arms (21% vs. 7%).
Full details of RTOG 0617 (abstract 7501) will be reported 10:15 a.m. on June 4 at ASCO’s annual meeting in Chicago.
The study was supported by the National Cancer Institute. Dr. Bradley reported having no relevant financial disclosures. A coauthor reported research funding from the NCI.
Standard-dose radiation produced better overall survival and locoregional control than did high-dose radiation when given with concurrent chemotherapy in patients with newly diagnosed stage III non–small cell lung cancer in the phase III, randomized RTOG 0617 trial.
Patients on the high dose had a 56% greater risk of death than those on a standard 60 Gy dose. Median overall survival times were 18.5 months with high-dose radiation and 28.7 months with a standard dose (hazard ratio, 1.56; P = .0007).
The risk of local failure also was increased by 37% in the high-dose arm (HR, 1.37; P = .03).
"At this point, there is no clear reason for the poor outcome we experienced on the high-dose arm," lead author Dr. Jeffrey Bradley said in a press briefing highlighting studies to be presented at the upcoming annual meeting of the American Society of Clinical Oncology (ASCO).
The most likely culprit is unreported toxicities, although other possible explanations are increased heart dose, longer duration of therapy, or a combination of these factors, he said.
The results are surprising because conventional thinking has been that higher doses of radiation would more effectively kill the tumor and thereby improve survival.
A phase-III trial in the 1970s established the standard radiation dose of 60 Gy in this setting but, over time, several radiation dose-ranging phase-II studies have reported promising results and improved median survival times with radiation doses up to 74 Gy, explained Dr. Bradley, professor of radiation oncology and chief of the thoracic service at Washington University, St. Louis.
At the same time, improvements in technology such as three-dimensional radiation therapy (RT) and intensity-modulated RT techniques have made RT delivery more precise, allowing organs and tissues sensitive to radiation to receive less radiation while the tumor receives more. This technique was explored in Radiation Therapy Oncology Group (RTOG) 0617.
"This is a very surprising result, especially when using these special radiation techniques that were designed to be more precise, you would expect that the outcome would be better," ASCO president Sandra Swain, medical director of the Washington (D.C.) Cancer Institute, told reporters. "This should really put an end to higher-dose treatments, given the better outcomes in the standard-dose arms."
Dr. Bradley said, "A lot of phase-III trials turn out negative when phase-II trials look good, so I think it was good to do a phase-III trial and get this answered."
RTOG 0617 randomly assigned 464 patients with newly diagnosed, unresected stage-III non–small cell lung cancer to conformal RT to 60 Gy, five times per week for 6 weeks or to 74 Gy five times per week for 7.5 weeks. All patients received concurrent chemotherapy with weekly paclitaxel (Taxol) and carboplatin, with a second randomization for patients to receive consolidation chemotherapy with or without cetuximab (Erbitux).
Among the 419 patients available for analysis at 18 months, local failure rates were 25% with standard-dose RT and 34.3% with high-dose RT (P = .03, as noted above), Dr. Bradley reported.
Median 18-month overall survival rates were 67% with the standard radiation dose vs. 54% with the high dose.
Median overall survival times in both groups were higher than expected, but "the overall survival benefit of 60 Gy is independent of the cetuximab question," he said. Data from that portion of the trial are expected to be reported in 2014.
Finally, the only significant difference in physician-reported side effects was a slightly higher rate of esophagitis in the high-dose arms (21% vs. 7%).
Full details of RTOG 0617 (abstract 7501) will be reported 10:15 a.m. on June 4 at ASCO’s annual meeting in Chicago.
The study was supported by the National Cancer Institute. Dr. Bradley reported having no relevant financial disclosures. A coauthor reported research funding from the NCI.
Standard-dose radiation produced better overall survival and locoregional control than did high-dose radiation when given with concurrent chemotherapy in patients with newly diagnosed stage III non–small cell lung cancer in the phase III, randomized RTOG 0617 trial.
Patients on the high dose had a 56% greater risk of death than those on a standard 60 Gy dose. Median overall survival times were 18.5 months with high-dose radiation and 28.7 months with a standard dose (hazard ratio, 1.56; P = .0007).
The risk of local failure also was increased by 37% in the high-dose arm (HR, 1.37; P = .03).
"At this point, there is no clear reason for the poor outcome we experienced on the high-dose arm," lead author Dr. Jeffrey Bradley said in a press briefing highlighting studies to be presented at the upcoming annual meeting of the American Society of Clinical Oncology (ASCO).
The most likely culprit is unreported toxicities, although other possible explanations are increased heart dose, longer duration of therapy, or a combination of these factors, he said.
The results are surprising because conventional thinking has been that higher doses of radiation would more effectively kill the tumor and thereby improve survival.
A phase-III trial in the 1970s established the standard radiation dose of 60 Gy in this setting but, over time, several radiation dose-ranging phase-II studies have reported promising results and improved median survival times with radiation doses up to 74 Gy, explained Dr. Bradley, professor of radiation oncology and chief of the thoracic service at Washington University, St. Louis.
At the same time, improvements in technology such as three-dimensional radiation therapy (RT) and intensity-modulated RT techniques have made RT delivery more precise, allowing organs and tissues sensitive to radiation to receive less radiation while the tumor receives more. This technique was explored in Radiation Therapy Oncology Group (RTOG) 0617.
"This is a very surprising result, especially when using these special radiation techniques that were designed to be more precise, you would expect that the outcome would be better," ASCO president Sandra Swain, medical director of the Washington (D.C.) Cancer Institute, told reporters. "This should really put an end to higher-dose treatments, given the better outcomes in the standard-dose arms."
Dr. Bradley said, "A lot of phase-III trials turn out negative when phase-II trials look good, so I think it was good to do a phase-III trial and get this answered."
RTOG 0617 randomly assigned 464 patients with newly diagnosed, unresected stage-III non–small cell lung cancer to conformal RT to 60 Gy, five times per week for 6 weeks or to 74 Gy five times per week for 7.5 weeks. All patients received concurrent chemotherapy with weekly paclitaxel (Taxol) and carboplatin, with a second randomization for patients to receive consolidation chemotherapy with or without cetuximab (Erbitux).
Among the 419 patients available for analysis at 18 months, local failure rates were 25% with standard-dose RT and 34.3% with high-dose RT (P = .03, as noted above), Dr. Bradley reported.
Median 18-month overall survival rates were 67% with the standard radiation dose vs. 54% with the high dose.
Median overall survival times in both groups were higher than expected, but "the overall survival benefit of 60 Gy is independent of the cetuximab question," he said. Data from that portion of the trial are expected to be reported in 2014.
Finally, the only significant difference in physician-reported side effects was a slightly higher rate of esophagitis in the high-dose arms (21% vs. 7%).
Full details of RTOG 0617 (abstract 7501) will be reported 10:15 a.m. on June 4 at ASCO’s annual meeting in Chicago.
The study was supported by the National Cancer Institute. Dr. Bradley reported having no relevant financial disclosures. A coauthor reported research funding from the NCI.
FROM THE ASCO 2013 PRESSCAST
Major finding: Patients with stage-III non–small cell lung cancer who received high-dose radiation had a 56% greater risk of death than those on a standard 60 Gy dose.
Data source: Phase-III randomized trial in 464 patients with stage-III non–small cell lung cancer.
Disclosures: The study was supported by the National Cancer Institute. Dr. Bradley reported having no relevant financial disclosures. A coauthor reported research funding from the NCI.

FDA approves radiotherapy for metastatic prostate cancer
Radium-223 dichloride, an alpha-particle–emitting radioactive agent, has been approved for treating men with castration-resistant prostate cancer that has spread to the bones, the Food and Drug Administration announced on May 15.
The agent "binds with minerals in the bone to deliver radiation directly to bone tumors," Dr. Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, noted in the statement.

Ra-223 is the second drug for prostate cancer approved by the FDA in the last year that has been shown to extend the survival of men with metastatic prostate cancer, Dr. Pazdur noted. Enzalutamide (Xtandi), an androgen receptor inhibitor, was approved in August 2012 for treating men with metastatic castration-resistant prostate cancer who were previously treated with docetaxel.
Approval of the radium-223 treatment, which will be marketed as Xofigo by Bayer Pharmaceuticals, was based on a phase III study of men with symptomatic castration-resistant prostate cancer with symptomatic bone metastases, and no other metastases, randomized to treatment with radium 233 (541 men) every 4 weeks for six cycles or placebo (268 men). All patients received best standard of care, which included external-beam radiation therapy, corticosteroids, antiandrogens, estrogens, estramustine, or ketoconazole.
In an interim analysis, overall survival, the primary endpoint, was a median of 14 months among those in the radiotherapy arm, compared with 11.2 months among those on placebo, a highly statistically significant improvement, with a hazard ratio of 0.695. An updated exploratory analysis conducted later in the trial "confirmed Xofigo’s ability to extend overall survival," the FDA statement noted.
(The prescribing information states that in the updated analysis, median survival was 14.9 months vs. 11.3 months among those on placebo, with a hazard ratio of 0.695).
The most common side effects reported during clinical trials in men receiving the treatment, in 10% or more of patients, were nausea, diarrhea, vomiting and peripheral edema. The most common laboratory abnormalities detected, in 10% or more of patients, were anemia, lymphocytopenia, leukopenia, thrombocytopenia, and neutropenia.
Xofigo comes in a solution and is administered at 4-week intervals for six injection cycles; it is slowly administered intravenously over 1 minute. Safety and efficacy of more than six injections has not been studied, according to the prescribing information.
Radium-223 dichloride, an alpha-particle–emitting radioactive agent, has been approved for treating men with castration-resistant prostate cancer that has spread to the bones, the Food and Drug Administration announced on May 15.
The agent "binds with minerals in the bone to deliver radiation directly to bone tumors," Dr. Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, noted in the statement.
Ra-223 is the second drug for prostate cancer approved by the FDA in the last year that has been shown to extend the survival of men with metastatic prostate cancer, Dr. Pazdur noted. Enzalutamide (Xtandi), an androgen receptor inhibitor, was approved in August 2012 for treating men with metastatic castration-resistant prostate cancer who were previously treated with docetaxel.
Approval of the radium-223 treatment, which will be marketed as Xofigo by Bayer Pharmaceuticals, was based on a phase III study of men with symptomatic castration-resistant prostate cancer with symptomatic bone metastases, and no other metastases, randomized to treatment with radium 233 (541 men) every 4 weeks for six cycles or placebo (268 men). All patients received best standard of care, which included external-beam radiation therapy, corticosteroids, antiandrogens, estrogens, estramustine, or ketoconazole.
In an interim analysis, overall survival, the primary endpoint, was a median of 14 months among those in the radiotherapy arm, compared with 11.2 months among those on placebo, a highly statistically significant improvement, with a hazard ratio of 0.695. An updated exploratory analysis conducted later in the trial "confirmed Xofigo’s ability to extend overall survival," the FDA statement noted.
(The prescribing information states that in the updated analysis, median survival was 14.9 months vs. 11.3 months among those on placebo, with a hazard ratio of 0.695).
The most common side effects reported during clinical trials in men receiving the treatment, in 10% or more of patients, were nausea, diarrhea, vomiting and peripheral edema. The most common laboratory abnormalities detected, in 10% or more of patients, were anemia, lymphocytopenia, leukopenia, thrombocytopenia, and neutropenia.
Xofigo comes in a solution and is administered at 4-week intervals for six injection cycles; it is slowly administered intravenously over 1 minute. Safety and efficacy of more than six injections has not been studied, according to the prescribing information.
Radium-223 dichloride, an alpha-particle–emitting radioactive agent, has been approved for treating men with castration-resistant prostate cancer that has spread to the bones, the Food and Drug Administration announced on May 15.
The agent "binds with minerals in the bone to deliver radiation directly to bone tumors," Dr. Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, noted in the statement.
Ra-223 is the second drug for prostate cancer approved by the FDA in the last year that has been shown to extend the survival of men with metastatic prostate cancer, Dr. Pazdur noted. Enzalutamide (Xtandi), an androgen receptor inhibitor, was approved in August 2012 for treating men with metastatic castration-resistant prostate cancer who were previously treated with docetaxel.
Approval of the radium-223 treatment, which will be marketed as Xofigo by Bayer Pharmaceuticals, was based on a phase III study of men with symptomatic castration-resistant prostate cancer with symptomatic bone metastases, and no other metastases, randomized to treatment with radium 233 (541 men) every 4 weeks for six cycles or placebo (268 men). All patients received best standard of care, which included external-beam radiation therapy, corticosteroids, antiandrogens, estrogens, estramustine, or ketoconazole.
In an interim analysis, overall survival, the primary endpoint, was a median of 14 months among those in the radiotherapy arm, compared with 11.2 months among those on placebo, a highly statistically significant improvement, with a hazard ratio of 0.695. An updated exploratory analysis conducted later in the trial "confirmed Xofigo’s ability to extend overall survival," the FDA statement noted.
(The prescribing information states that in the updated analysis, median survival was 14.9 months vs. 11.3 months among those on placebo, with a hazard ratio of 0.695).
The most common side effects reported during clinical trials in men receiving the treatment, in 10% or more of patients, were nausea, diarrhea, vomiting and peripheral edema. The most common laboratory abnormalities detected, in 10% or more of patients, were anemia, lymphocytopenia, leukopenia, thrombocytopenia, and neutropenia.
Xofigo comes in a solution and is administered at 4-week intervals for six injection cycles; it is slowly administered intravenously over 1 minute. Safety and efficacy of more than six injections has not been studied, according to the prescribing information.

Genetic tests gauge breast-cancer recurrence risk
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.

But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.

All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.

|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.
But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.
All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.
But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.
All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
AT IMPAKT 2013 BREAST CANCER CONFERENCE
Major finding: Low-risk patients by the PAM50 test had 97.6% 15-year disease-free survival compared with 82.5% in high-risk patients.
Data source: A retrospective analysis of 1,478 women enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial.
Disclosures: Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.

Esophagectomy cases rising steadily
INDIANAPOLIS – Transthoracic esophagectomy for esophageal cancer provides significantly lower in-hospital mortality and major morbidity rates than does transhiatal esophagectomy, according to an analysis of a large multiyear national database.
Further, in-hospital outcomes of esophagectomy didn’t differ significantly between high-volume centers – in this study, defined as those doing 10 or more cases per year – and low-volume centers, Dr. Mehraneh D. Jafari reported at the annual meeting of the American Surgical Association.

That finding was met with skepticism, and discussants were quick to argue that study limitations make it difficult to draw any meaningful conclusions from the data. For one thing, speakers contended that defining a high-volume center based upon an institutional threshold of 10 or more cases per year sets the bar far too low given that a single dedicated esophageal surgery specialist might easily perform 50 or more esophagectomies annually.
Dr. Jafari presented an analysis of 11,473 transthoracic and 3,717 transhiatal esophagectomies performed for esophageal cancer. The data came from the Nationwide Inpatient Sample (NIS) during 2001-2010. The NIS records data on in-hospital outcomes for a nationally representative sample composed of roughly 20% of the country’s hospital discharges each year.
The number of esophagectomies rose steadily by an average of 4% annually during the study years, reflecting the substantial national increase in cases of esophageal cancer. The growing case count, expected to reach an estimated 18,000 cases of esophageal cancer nationwide in 2013, has been attributed to rising rates of gastroesophageal reflux disease, Barrett’s esophagus, and obesity. Transthoracic esophagectomy, used in 76% of cases, remained the preferred operative strategy throughout the study years.
In-hospital outcomes were markedly better in patients who had transthoracic esophagectomy. After adjustment for potential confounding variables in a multivariate analysis, transhiatal esophagectomy recipients had a 67% increased risk of in-hospital mortality and a 39% greater risk of serious complications, including a 37% increased risk of pulmonary complications. However, anastomotic leak rates were similar with both operations, according to Dr. Jafari of the University of California, Irvine.
Of note, the referral rate to high-volume esophagectomy centers climbed steadily over time, rising from 22% of all cases in 2001 to 58% in 2010.

The 35 high-volume centers performed an average of 16 cases per year. In contrast, the 484 low-volume centers averaged 2 cases per year. In-hospital mortality among the 9,386 patients treated in low-volume centers averaged 7.6% compared with 4.3% for patients in high-volume centers. Overall in-hospital serious morbidity rates were greater in the low-volume centers as well: 47% versus 41%. While these raw differences were statistically significant, a risk-adjusted multivariate analysis found no significant outcome differences between low- and high-volume centers.
Discussant Dr. Michael J. Zinner noted that in an earlier study he and his coworkers showed that an institutional threshold of roughly 30 esophagectomies per year is required to discriminate between low- and high-volume centers in terms of in-hospital mortality. So why define high-volume centers as those doing a mere 10 cases per year? asked Dr. Zinner, chairman of the department of surgery at Brigham and Women’s Hospital and professor of surgery at Harvard Medical School, Boston.
"The problem here is if you establish 30 cases per year as the threshold for a high-volume center, I can tell you there are probably less than 20 centers in the whole U.S. capable of doing that volume. That’s a real issue, because then how are patients who live in a remote region going to get care at one of those centers?" replied Dr. Jafari’s senior coauthor Dr. Ninh T. Nguyen, professor and vice-chair of surgery at UC Irvine.
"I think instead we should try to lift all boats: develop a national esophageal center network to identify the qualities reflective of better outcomes in the high-volume centers and introduce those factors at low-volume centers. This way we’re not impeding access to care for our patients," he continued.
Dr. Nguyen said that in-hospital surgical morbidity rates in the NIS need to be taken with a grain of salt, as the accuracy of coding for complications is "rather low." The development of minimally invasive techniques for intrathoracic anastomosis has transformed transthoracic esophagectomy into a procedure with an improved complication profile.
"I switched to transthoracic esophagectomy 5 years ago. One reason was development of the minimally invasive approach. As a result, we’re not scared of a chest anastomosis like we used to be. When patients undergoing transthoracic esophagectomy with thoracotomy had a leak in the chest they had a very high risk for mortality. That’s not the case anymore. We have not observed any mortality associated with a leak in the chest for many, many years now," he said.
The investigators reported having no conflicts of interest.
Dr. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
I have major problems with this study, stemming from inherent limitations in the Nationwide Inpatient Sample. It’s an administrative database set up chiefly to track costs, utilization, and length of stay. It contains no information at all on key clinical outcomes such as 30- and 90-day mortality, discharge disposition, or 30-day readmission rates.

|
|
In addition, the accuracy of the quoted in-hospital morbidity rates is suspect, probably because data entry isn’t performed by trained researchers. For example, the 8% incidence of renal failure in esophagectomy patients cited in this study sounds too high to be right.
And there’s another major problem with this database: The superior outcomes reported for transthoracic esophagectomy recipients in this study fly in the face of earlier, well-conducted meta-analyses that reached the opposite conclusion. The most likely explanation for the discordant findings lies in the fact that the NIS doesn’t show whether a transthoracic esophagectomy was performed via open thoracotomy in the old-school manner or with an intrathoracic anastomosis created using contemporary minimally invasive techniques which, while complex, have been associated with better outcomes.
Dr. James D. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
I have major problems with this study, stemming from inherent limitations in the Nationwide Inpatient Sample. It’s an administrative database set up chiefly to track costs, utilization, and length of stay. It contains no information at all on key clinical outcomes such as 30- and 90-day mortality, discharge disposition, or 30-day readmission rates.
|
|
|
In addition, the accuracy of the quoted in-hospital morbidity rates is suspect, probably because data entry isn’t performed by trained researchers. For example, the 8% incidence of renal failure in esophagectomy patients cited in this study sounds too high to be right.
And there’s another major problem with this database: The superior outcomes reported for transthoracic esophagectomy recipients in this study fly in the face of earlier, well-conducted meta-analyses that reached the opposite conclusion. The most likely explanation for the discordant findings lies in the fact that the NIS doesn’t show whether a transthoracic esophagectomy was performed via open thoracotomy in the old-school manner or with an intrathoracic anastomosis created using contemporary minimally invasive techniques which, while complex, have been associated with better outcomes.
Dr. James D. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
I have major problems with this study, stemming from inherent limitations in the Nationwide Inpatient Sample. It’s an administrative database set up chiefly to track costs, utilization, and length of stay. It contains no information at all on key clinical outcomes such as 30- and 90-day mortality, discharge disposition, or 30-day readmission rates.
|
|
|
In addition, the accuracy of the quoted in-hospital morbidity rates is suspect, probably because data entry isn’t performed by trained researchers. For example, the 8% incidence of renal failure in esophagectomy patients cited in this study sounds too high to be right.
And there’s another major problem with this database: The superior outcomes reported for transthoracic esophagectomy recipients in this study fly in the face of earlier, well-conducted meta-analyses that reached the opposite conclusion. The most likely explanation for the discordant findings lies in the fact that the NIS doesn’t show whether a transthoracic esophagectomy was performed via open thoracotomy in the old-school manner or with an intrathoracic anastomosis created using contemporary minimally invasive techniques which, while complex, have been associated with better outcomes.
Dr. James D. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
INDIANAPOLIS – Transthoracic esophagectomy for esophageal cancer provides significantly lower in-hospital mortality and major morbidity rates than does transhiatal esophagectomy, according to an analysis of a large multiyear national database.
Further, in-hospital outcomes of esophagectomy didn’t differ significantly between high-volume centers – in this study, defined as those doing 10 or more cases per year – and low-volume centers, Dr. Mehraneh D. Jafari reported at the annual meeting of the American Surgical Association.
That finding was met with skepticism, and discussants were quick to argue that study limitations make it difficult to draw any meaningful conclusions from the data. For one thing, speakers contended that defining a high-volume center based upon an institutional threshold of 10 or more cases per year sets the bar far too low given that a single dedicated esophageal surgery specialist might easily perform 50 or more esophagectomies annually.
Dr. Jafari presented an analysis of 11,473 transthoracic and 3,717 transhiatal esophagectomies performed for esophageal cancer. The data came from the Nationwide Inpatient Sample (NIS) during 2001-2010. The NIS records data on in-hospital outcomes for a nationally representative sample composed of roughly 20% of the country’s hospital discharges each year.
The number of esophagectomies rose steadily by an average of 4% annually during the study years, reflecting the substantial national increase in cases of esophageal cancer. The growing case count, expected to reach an estimated 18,000 cases of esophageal cancer nationwide in 2013, has been attributed to rising rates of gastroesophageal reflux disease, Barrett’s esophagus, and obesity. Transthoracic esophagectomy, used in 76% of cases, remained the preferred operative strategy throughout the study years.
In-hospital outcomes were markedly better in patients who had transthoracic esophagectomy. After adjustment for potential confounding variables in a multivariate analysis, transhiatal esophagectomy recipients had a 67% increased risk of in-hospital mortality and a 39% greater risk of serious complications, including a 37% increased risk of pulmonary complications. However, anastomotic leak rates were similar with both operations, according to Dr. Jafari of the University of California, Irvine.
Of note, the referral rate to high-volume esophagectomy centers climbed steadily over time, rising from 22% of all cases in 2001 to 58% in 2010.
The 35 high-volume centers performed an average of 16 cases per year. In contrast, the 484 low-volume centers averaged 2 cases per year. In-hospital mortality among the 9,386 patients treated in low-volume centers averaged 7.6% compared with 4.3% for patients in high-volume centers. Overall in-hospital serious morbidity rates were greater in the low-volume centers as well: 47% versus 41%. While these raw differences were statistically significant, a risk-adjusted multivariate analysis found no significant outcome differences between low- and high-volume centers.
Discussant Dr. Michael J. Zinner noted that in an earlier study he and his coworkers showed that an institutional threshold of roughly 30 esophagectomies per year is required to discriminate between low- and high-volume centers in terms of in-hospital mortality. So why define high-volume centers as those doing a mere 10 cases per year? asked Dr. Zinner, chairman of the department of surgery at Brigham and Women’s Hospital and professor of surgery at Harvard Medical School, Boston.
"The problem here is if you establish 30 cases per year as the threshold for a high-volume center, I can tell you there are probably less than 20 centers in the whole U.S. capable of doing that volume. That’s a real issue, because then how are patients who live in a remote region going to get care at one of those centers?" replied Dr. Jafari’s senior coauthor Dr. Ninh T. Nguyen, professor and vice-chair of surgery at UC Irvine.
"I think instead we should try to lift all boats: develop a national esophageal center network to identify the qualities reflective of better outcomes in the high-volume centers and introduce those factors at low-volume centers. This way we’re not impeding access to care for our patients," he continued.
Dr. Nguyen said that in-hospital surgical morbidity rates in the NIS need to be taken with a grain of salt, as the accuracy of coding for complications is "rather low." The development of minimally invasive techniques for intrathoracic anastomosis has transformed transthoracic esophagectomy into a procedure with an improved complication profile.
"I switched to transthoracic esophagectomy 5 years ago. One reason was development of the minimally invasive approach. As a result, we’re not scared of a chest anastomosis like we used to be. When patients undergoing transthoracic esophagectomy with thoracotomy had a leak in the chest they had a very high risk for mortality. That’s not the case anymore. We have not observed any mortality associated with a leak in the chest for many, many years now," he said.
The investigators reported having no conflicts of interest.
Dr. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
INDIANAPOLIS – Transthoracic esophagectomy for esophageal cancer provides significantly lower in-hospital mortality and major morbidity rates than does transhiatal esophagectomy, according to an analysis of a large multiyear national database.
Further, in-hospital outcomes of esophagectomy didn’t differ significantly between high-volume centers – in this study, defined as those doing 10 or more cases per year – and low-volume centers, Dr. Mehraneh D. Jafari reported at the annual meeting of the American Surgical Association.
That finding was met with skepticism, and discussants were quick to argue that study limitations make it difficult to draw any meaningful conclusions from the data. For one thing, speakers contended that defining a high-volume center based upon an institutional threshold of 10 or more cases per year sets the bar far too low given that a single dedicated esophageal surgery specialist might easily perform 50 or more esophagectomies annually.
Dr. Jafari presented an analysis of 11,473 transthoracic and 3,717 transhiatal esophagectomies performed for esophageal cancer. The data came from the Nationwide Inpatient Sample (NIS) during 2001-2010. The NIS records data on in-hospital outcomes for a nationally representative sample composed of roughly 20% of the country’s hospital discharges each year.
The number of esophagectomies rose steadily by an average of 4% annually during the study years, reflecting the substantial national increase in cases of esophageal cancer. The growing case count, expected to reach an estimated 18,000 cases of esophageal cancer nationwide in 2013, has been attributed to rising rates of gastroesophageal reflux disease, Barrett’s esophagus, and obesity. Transthoracic esophagectomy, used in 76% of cases, remained the preferred operative strategy throughout the study years.
In-hospital outcomes were markedly better in patients who had transthoracic esophagectomy. After adjustment for potential confounding variables in a multivariate analysis, transhiatal esophagectomy recipients had a 67% increased risk of in-hospital mortality and a 39% greater risk of serious complications, including a 37% increased risk of pulmonary complications. However, anastomotic leak rates were similar with both operations, according to Dr. Jafari of the University of California, Irvine.
Of note, the referral rate to high-volume esophagectomy centers climbed steadily over time, rising from 22% of all cases in 2001 to 58% in 2010.
The 35 high-volume centers performed an average of 16 cases per year. In contrast, the 484 low-volume centers averaged 2 cases per year. In-hospital mortality among the 9,386 patients treated in low-volume centers averaged 7.6% compared with 4.3% for patients in high-volume centers. Overall in-hospital serious morbidity rates were greater in the low-volume centers as well: 47% versus 41%. While these raw differences were statistically significant, a risk-adjusted multivariate analysis found no significant outcome differences between low- and high-volume centers.
Discussant Dr. Michael J. Zinner noted that in an earlier study he and his coworkers showed that an institutional threshold of roughly 30 esophagectomies per year is required to discriminate between low- and high-volume centers in terms of in-hospital mortality. So why define high-volume centers as those doing a mere 10 cases per year? asked Dr. Zinner, chairman of the department of surgery at Brigham and Women’s Hospital and professor of surgery at Harvard Medical School, Boston.
"The problem here is if you establish 30 cases per year as the threshold for a high-volume center, I can tell you there are probably less than 20 centers in the whole U.S. capable of doing that volume. That’s a real issue, because then how are patients who live in a remote region going to get care at one of those centers?" replied Dr. Jafari’s senior coauthor Dr. Ninh T. Nguyen, professor and vice-chair of surgery at UC Irvine.
"I think instead we should try to lift all boats: develop a national esophageal center network to identify the qualities reflective of better outcomes in the high-volume centers and introduce those factors at low-volume centers. This way we’re not impeding access to care for our patients," he continued.
Dr. Nguyen said that in-hospital surgical morbidity rates in the NIS need to be taken with a grain of salt, as the accuracy of coding for complications is "rather low." The development of minimally invasive techniques for intrathoracic anastomosis has transformed transthoracic esophagectomy into a procedure with an improved complication profile.
"I switched to transthoracic esophagectomy 5 years ago. One reason was development of the minimally invasive approach. As a result, we’re not scared of a chest anastomosis like we used to be. When patients undergoing transthoracic esophagectomy with thoracotomy had a leak in the chest they had a very high risk for mortality. That’s not the case anymore. We have not observed any mortality associated with a leak in the chest for many, many years now," he said.
The investigators reported having no conflicts of interest.
Dr. Luketich is professor of surgery and chief of the Heart, Lung, and Esophageal Surgery Institute at the University of Pittsburgh. He was the designated discussant of the study at the meeting.
AT THE ASA ANNUAL MEETING
Major finding: In-hospital mortality occurred nationally in 5.8% of esophageal cancer patients who underwent transthoracic esophagectomy compared with 8.3% of transhiatal esophagectomy recipients.
Data source: A retrospective study of more than 15,000 patients who underwent esophagectomy for esophageal cancer during 2001-2010 and were Included in the Nationwide Inpatient Sample, a database sponsored by the Agency for Healthcare Research and Quality.
Disclosures: The study presenters reported having no financial conflicts.
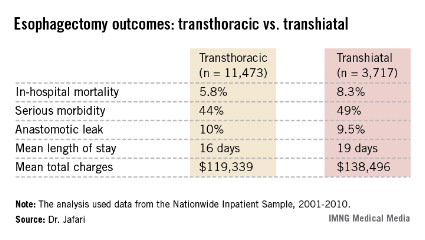
Sequential laser therapy clears basal cell carcinomas
BOSTON – Sequential application of pulsed dye and Nd:YAG lasers is safe and effective for treating small basal cell carcinomas, based on data from a prospective study of patients with nodular and superficial BCC subtypes on the trunk and extremities.
The findings were presented at the annual meeting of the American Society for Laser Medicine and Surgery.

In a study of 10 patients with BCC, 7 of the 12 lesions treated with pulsed dye laser followed by Nd:YAG laser showed completed clinical and histologic clearance, said Dr. H. Ray Jalian of Massachusetts General Hospital in Boston.
"Targeting the microvasculature of BCC offers a promising new treatment approach. These tumors have large caliber feeding vessels; oftentimes these vessels are larger than the surrounding stroma," he said.
Data from a previous study (Lasers Surg. Med. 2009;41:417-42) showed a 92% regression rate of BCC lesions smaller than 1.5 cm treated with a 595 nm pulsed dye laser, Dr. Jalian noted.
The rationale for the sequential laser therapy is that pulsed dye laser energy is well absorbed by hemoglobin, which generates methemoglobin that in turn absorbs 1064 nm Nd:YAG energy, allowing the energy to penetrate to deep vessels.
"We hypothesized that targeting the vasculature of basal cells at two levels may be able to selectively destroy deeper vessels and perhaps achieve a higher cure rate," he said.
The investigators conducted a prospective study with 10 patients who had a total of 13 BCC of nodular and superficial subtypes on the trunk and extremities (1 patient with a single lesion was not available for follow-up).
The treated lesions were less than 2 cm with clearly visible margins that would be suitable for treatment with standard surgical excision. Patients with scars or infections in the area to be treated were excluded, as were those who were immunocompromised or pregnant.
The participants underwent four laser treatments 2-4 weeks apart with a 585-nm PDL set for a 7-mm spot size, 8-J/cm2, 2-ms pulse duration, followed by a 1064-nm Nd:YAG laser set with a 7-mm spot, 40-J/cm2, 15-ms pulse duration.
A total of 7 of the 12 lesions available for follow-up were completely cleared on both clinical and histologic evaluation. Of the eight tumors under 1 cm in size, six were completely cleared by sequential laser therapy,
Of the four patients with 5 lesions with residual disease after four laser sessions, three were on anticoagulation therapy with aspirin, and one with warfarin.
"We did see a clearance of the nodular component in most cases, but there was persistent residual superficial BCC in these patients," Dr. Jalian said.
Anticoagulation may hamper the laser effect by reducing laser-induced vascular injury, he noted.
Treatment-related side effects included erythema, scarring, and hyperpigmentation. Erythema and scarring decreased from the first treatment to the last follow-up visit, while hyperpigmentation increased slightly from the first to the third treatment, and then plateaued.
Biopsy scars improved with sequential treatments, Dr. Jalian noted.
Possible explanations for the lower success rate treating BCC compared to previous studies include the use of a slightly lower wavelength laser (585 vs. 595), and lower energy settings (8 J/cm2 for 2 ms, vs. 15 J/cm2 for 3 ms), and by mix of histologic subtypes, said Dr. Jalian.
"Superficial subtypes present in residual lesions suggest there may be a different vascular pattern in these lesions."
The findings also suggest that anticoagulation therapy may need to be suspended before treatment with pulsed dye, Nd:YAG, and other vascular-specific lasers, he added.
The study was internally supported. Dr. Jalian reported having no financial disclosures.
BOSTON – Sequential application of pulsed dye and Nd:YAG lasers is safe and effective for treating small basal cell carcinomas, based on data from a prospective study of patients with nodular and superficial BCC subtypes on the trunk and extremities.
The findings were presented at the annual meeting of the American Society for Laser Medicine and Surgery.
In a study of 10 patients with BCC, 7 of the 12 lesions treated with pulsed dye laser followed by Nd:YAG laser showed completed clinical and histologic clearance, said Dr. H. Ray Jalian of Massachusetts General Hospital in Boston.
"Targeting the microvasculature of BCC offers a promising new treatment approach. These tumors have large caliber feeding vessels; oftentimes these vessels are larger than the surrounding stroma," he said.
Data from a previous study (Lasers Surg. Med. 2009;41:417-42) showed a 92% regression rate of BCC lesions smaller than 1.5 cm treated with a 595 nm pulsed dye laser, Dr. Jalian noted.
The rationale for the sequential laser therapy is that pulsed dye laser energy is well absorbed by hemoglobin, which generates methemoglobin that in turn absorbs 1064 nm Nd:YAG energy, allowing the energy to penetrate to deep vessels.
"We hypothesized that targeting the vasculature of basal cells at two levels may be able to selectively destroy deeper vessels and perhaps achieve a higher cure rate," he said.
The investigators conducted a prospective study with 10 patients who had a total of 13 BCC of nodular and superficial subtypes on the trunk and extremities (1 patient with a single lesion was not available for follow-up).
The treated lesions were less than 2 cm with clearly visible margins that would be suitable for treatment with standard surgical excision. Patients with scars or infections in the area to be treated were excluded, as were those who were immunocompromised or pregnant.
The participants underwent four laser treatments 2-4 weeks apart with a 585-nm PDL set for a 7-mm spot size, 8-J/cm2, 2-ms pulse duration, followed by a 1064-nm Nd:YAG laser set with a 7-mm spot, 40-J/cm2, 15-ms pulse duration.
A total of 7 of the 12 lesions available for follow-up were completely cleared on both clinical and histologic evaluation. Of the eight tumors under 1 cm in size, six were completely cleared by sequential laser therapy,
Of the four patients with 5 lesions with residual disease after four laser sessions, three were on anticoagulation therapy with aspirin, and one with warfarin.
"We did see a clearance of the nodular component in most cases, but there was persistent residual superficial BCC in these patients," Dr. Jalian said.
Anticoagulation may hamper the laser effect by reducing laser-induced vascular injury, he noted.
Treatment-related side effects included erythema, scarring, and hyperpigmentation. Erythema and scarring decreased from the first treatment to the last follow-up visit, while hyperpigmentation increased slightly from the first to the third treatment, and then plateaued.
Biopsy scars improved with sequential treatments, Dr. Jalian noted.
Possible explanations for the lower success rate treating BCC compared to previous studies include the use of a slightly lower wavelength laser (585 vs. 595), and lower energy settings (8 J/cm2 for 2 ms, vs. 15 J/cm2 for 3 ms), and by mix of histologic subtypes, said Dr. Jalian.
"Superficial subtypes present in residual lesions suggest there may be a different vascular pattern in these lesions."
The findings also suggest that anticoagulation therapy may need to be suspended before treatment with pulsed dye, Nd:YAG, and other vascular-specific lasers, he added.
The study was internally supported. Dr. Jalian reported having no financial disclosures.
BOSTON – Sequential application of pulsed dye and Nd:YAG lasers is safe and effective for treating small basal cell carcinomas, based on data from a prospective study of patients with nodular and superficial BCC subtypes on the trunk and extremities.
The findings were presented at the annual meeting of the American Society for Laser Medicine and Surgery.
In a study of 10 patients with BCC, 7 of the 12 lesions treated with pulsed dye laser followed by Nd:YAG laser showed completed clinical and histologic clearance, said Dr. H. Ray Jalian of Massachusetts General Hospital in Boston.
"Targeting the microvasculature of BCC offers a promising new treatment approach. These tumors have large caliber feeding vessels; oftentimes these vessels are larger than the surrounding stroma," he said.
Data from a previous study (Lasers Surg. Med. 2009;41:417-42) showed a 92% regression rate of BCC lesions smaller than 1.5 cm treated with a 595 nm pulsed dye laser, Dr. Jalian noted.
The rationale for the sequential laser therapy is that pulsed dye laser energy is well absorbed by hemoglobin, which generates methemoglobin that in turn absorbs 1064 nm Nd:YAG energy, allowing the energy to penetrate to deep vessels.
"We hypothesized that targeting the vasculature of basal cells at two levels may be able to selectively destroy deeper vessels and perhaps achieve a higher cure rate," he said.
The investigators conducted a prospective study with 10 patients who had a total of 13 BCC of nodular and superficial subtypes on the trunk and extremities (1 patient with a single lesion was not available for follow-up).
The treated lesions were less than 2 cm with clearly visible margins that would be suitable for treatment with standard surgical excision. Patients with scars or infections in the area to be treated were excluded, as were those who were immunocompromised or pregnant.
The participants underwent four laser treatments 2-4 weeks apart with a 585-nm PDL set for a 7-mm spot size, 8-J/cm2, 2-ms pulse duration, followed by a 1064-nm Nd:YAG laser set with a 7-mm spot, 40-J/cm2, 15-ms pulse duration.
A total of 7 of the 12 lesions available for follow-up were completely cleared on both clinical and histologic evaluation. Of the eight tumors under 1 cm in size, six were completely cleared by sequential laser therapy,
Of the four patients with 5 lesions with residual disease after four laser sessions, three were on anticoagulation therapy with aspirin, and one with warfarin.
"We did see a clearance of the nodular component in most cases, but there was persistent residual superficial BCC in these patients," Dr. Jalian said.
Anticoagulation may hamper the laser effect by reducing laser-induced vascular injury, he noted.
Treatment-related side effects included erythema, scarring, and hyperpigmentation. Erythema and scarring decreased from the first treatment to the last follow-up visit, while hyperpigmentation increased slightly from the first to the third treatment, and then plateaued.
Biopsy scars improved with sequential treatments, Dr. Jalian noted.
Possible explanations for the lower success rate treating BCC compared to previous studies include the use of a slightly lower wavelength laser (585 vs. 595), and lower energy settings (8 J/cm2 for 2 ms, vs. 15 J/cm2 for 3 ms), and by mix of histologic subtypes, said Dr. Jalian.
"Superficial subtypes present in residual lesions suggest there may be a different vascular pattern in these lesions."
The findings also suggest that anticoagulation therapy may need to be suspended before treatment with pulsed dye, Nd:YAG, and other vascular-specific lasers, he added.
The study was internally supported. Dr. Jalian reported having no financial disclosures.
AT LASER 2013
Major finding: Seven of 12 basal cell carcinomas treated with sequential lasers showed complete clinical and histologic clearance.
Data source: Prospective case series of 10 patients with 13 BCC lesions.
Disclosures: The study was internally supported. Dr. Jalian reported having no financial disclosures.

'Slow Mohs' advised for lentigo maligna
MAUI, HAWAII – "Slow Mohs" has gained near-universal acceptance among skin cancer specialists as a definitive surgical technique for complete removal of lentigo maligna melanoma while simultaneously sparing normal tissue, according to Dr. Ellen Marmur of Mount Sinai School of Medicine, New York.
The big advantage that slow Mohs has over standard wide local excision with 0.5- to 1-cm margins is a 5-year cure rate approaching 100%. In contrast, standard excision has a recurrence rate of up to 20%, she said at the Hawaii Dermatology Seminar, sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.

Slow Mohs is a modified form of Mohs micrographic surgery. The surgery compares with conventional Mohs: It is staged, margin-controlled excision. But in slow Mohs, rush permanent sections are sent off to the pathologist rather than the frozen sections integral to conventional Mohs.
Dr. Marmur relies upon slow Mohs, with "bread-loafing" of the central tumor by the pathologist, because the permanent sections better preserve the tumor’s microscopic features. Interpreting atypical melanocytes in frozen sections can be quite a challenge. However, she added, some Mohs surgeons have found that using rapid immunostains also markedly improves the sensitivity and specificity of frozen sections in lentigo maligna surgery.
Slow Mohs takes place over the course of days, she said. "Basically, you do your Wood’s lamp to define the lesion diameter, you measure out your margins, you excise the tumor, pack the area with a bandage, and send the patient home. You rush your pathology, and you don’t do any reconstruction until you get the margins clear."
A pathology report that comes back stating narrow margins are present is "a heart stopper," she added.
"You have the option of observing the area if the margin is clear but the tumor was close to the margin. That’s a good approach for an elderly patient or when the lentigo maligna was in a cosmetically important area."
Lentigo maligna melanoma accounts for 4% of all cases of melanoma. It typically arises on sun-damaged skin in individuals in their 70s or older. Common sites include the malar area, forehead, nose, and temple. The differential diagnosis includes seborrheic keratosis, pigmented actinic keratosis, and pigmented nevus.
Lentigo maligna becomes lentigo maligna melanoma when malignant melanoma cells invade the dermis and deeper appendages. Roughly 5% of lentigo malignas eventually progress to invasive melanoma, according to Dr. Marmur. Typically, a lentigo maligna undergoes extended gradual horizontal growth before beginning a vertical growth phase.
"It spreads like an oil slick for many years," Dr. Marmur said at the seminar.
Established treatment modalities for patients who aren’t surgical candidates include cryotherapy, radiotherapy, and topical imiquimod 5%. All have disadvantages, including high 5-year recurrence rates.
Dr. Marmur noted that a newer nonsurgical therapy drawing considerable interest involves off-label use of topical combination therapy with imiquimod and tazarotene gel. The concept is to use the topical retinoid to disrupt the stratum corneum in order to enhance imiquimod penetration, thereby achieving a greater inflammatory response than possible with imiquimod alone.
Initial data have been published by researchers at the University of Utah, Salt Lake City. They randomized 90 patients with 91 lentigo malignas to imiquimod 5% cream applied 5 days per week for 3 months or to the imiquimod regimen plus tazarotene 0.1% gel on the other 2 days per week. After 3 months of topical therapy, patients underwent conservative staged excision with frozen section analysis with Melan A immunostaining to confirm negative margins.
Of those treated with dual topical therapy for 3 months, 29 of 37 lesions (78%) had complete responses with no residual lentigo maligna at the time of staged excision. So did 27 of 42 (64%) treated with imiquimod alone (Arch. Dermatol. 2012;148:592-6).
The modest difference in outcome was not significant (P = .17). Nevertheless, the Utah investigators wrote that topical pretreatment appears to reduce surgical defect sizes, an important consideration in lentigo maligna because the lesions are often large and located on cosmetically sensitive facial sites. At the patient’s first visit, the researchers saucerize the entire tumor to remove all visible evidence of lentigo maligna and nip in the bud any invasive element that might be present. One month later, after the wound has healed by secondary intention, the patient begins topical imiquimod therapy 5 days per week. If no inflammation is observed, tazarotene gel is added on the other 2 days per week. After 3 months of topical therapy, the patient goes off treatment for 2 months so the inflammatory response can subside. Then a staged excision is performed with 2-mm margins around the perimeter of the original tumor outline.
"This is an interesting thought, but it’s still not considered standard of care," Dr. Marmur commented in describing the Utah research.

Session chair Dr. Allan C. Halpern, chief of the dermatology service at Memorial Sloan-Kettering Cancer Center in New York, said he and his colleagues, like the Utah group, are using a lot of topical imiquimod as adjunctive therapy for lentigo maligna.
"Because we’re a referral center, we see all those patients whose melanomas unfortunately do recur at the edge of large surgeries. We see a lot of patients whose local surgeons have chased around their faces for a certain amount of time. So I think the general concept of the cure rates of surgery is a bit overstated. I’m not trying to sell an off-label use of a drug, but I think sometimes imiquimod can be very helpful," Dr. Halpern said.
He offered a clinical pearl in diagnosing lentigo maligna: Consider a broad shave biopsy of a suspicious lesion rather than a deeper, smaller-diameter biopsy.
"Sampling errors are a real problem with lentigo maligna. We learned early on that if you take a large lentigo maligna and do multiple biopsies of the same lesion and send them to what we think are our very expert pathologists, on average, we get two or three back that were melanoma and two or three back that were pigmented actinic keratoses. The sampling error tends to be more in the horizontal than in the depth for these very early lesions," according to Dr. Halpern.
Dr. Marmur and Dr. Halpern reported having no relevant financial interests. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – "Slow Mohs" has gained near-universal acceptance among skin cancer specialists as a definitive surgical technique for complete removal of lentigo maligna melanoma while simultaneously sparing normal tissue, according to Dr. Ellen Marmur of Mount Sinai School of Medicine, New York.
The big advantage that slow Mohs has over standard wide local excision with 0.5- to 1-cm margins is a 5-year cure rate approaching 100%. In contrast, standard excision has a recurrence rate of up to 20%, she said at the Hawaii Dermatology Seminar, sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Slow Mohs is a modified form of Mohs micrographic surgery. The surgery compares with conventional Mohs: It is staged, margin-controlled excision. But in slow Mohs, rush permanent sections are sent off to the pathologist rather than the frozen sections integral to conventional Mohs.
Dr. Marmur relies upon slow Mohs, with "bread-loafing" of the central tumor by the pathologist, because the permanent sections better preserve the tumor’s microscopic features. Interpreting atypical melanocytes in frozen sections can be quite a challenge. However, she added, some Mohs surgeons have found that using rapid immunostains also markedly improves the sensitivity and specificity of frozen sections in lentigo maligna surgery.
Slow Mohs takes place over the course of days, she said. "Basically, you do your Wood’s lamp to define the lesion diameter, you measure out your margins, you excise the tumor, pack the area with a bandage, and send the patient home. You rush your pathology, and you don’t do any reconstruction until you get the margins clear."
A pathology report that comes back stating narrow margins are present is "a heart stopper," she added.
"You have the option of observing the area if the margin is clear but the tumor was close to the margin. That’s a good approach for an elderly patient or when the lentigo maligna was in a cosmetically important area."
Lentigo maligna melanoma accounts for 4% of all cases of melanoma. It typically arises on sun-damaged skin in individuals in their 70s or older. Common sites include the malar area, forehead, nose, and temple. The differential diagnosis includes seborrheic keratosis, pigmented actinic keratosis, and pigmented nevus.
Lentigo maligna becomes lentigo maligna melanoma when malignant melanoma cells invade the dermis and deeper appendages. Roughly 5% of lentigo malignas eventually progress to invasive melanoma, according to Dr. Marmur. Typically, a lentigo maligna undergoes extended gradual horizontal growth before beginning a vertical growth phase.
"It spreads like an oil slick for many years," Dr. Marmur said at the seminar.
Established treatment modalities for patients who aren’t surgical candidates include cryotherapy, radiotherapy, and topical imiquimod 5%. All have disadvantages, including high 5-year recurrence rates.
Dr. Marmur noted that a newer nonsurgical therapy drawing considerable interest involves off-label use of topical combination therapy with imiquimod and tazarotene gel. The concept is to use the topical retinoid to disrupt the stratum corneum in order to enhance imiquimod penetration, thereby achieving a greater inflammatory response than possible with imiquimod alone.
Initial data have been published by researchers at the University of Utah, Salt Lake City. They randomized 90 patients with 91 lentigo malignas to imiquimod 5% cream applied 5 days per week for 3 months or to the imiquimod regimen plus tazarotene 0.1% gel on the other 2 days per week. After 3 months of topical therapy, patients underwent conservative staged excision with frozen section analysis with Melan A immunostaining to confirm negative margins.
Of those treated with dual topical therapy for 3 months, 29 of 37 lesions (78%) had complete responses with no residual lentigo maligna at the time of staged excision. So did 27 of 42 (64%) treated with imiquimod alone (Arch. Dermatol. 2012;148:592-6).
The modest difference in outcome was not significant (P = .17). Nevertheless, the Utah investigators wrote that topical pretreatment appears to reduce surgical defect sizes, an important consideration in lentigo maligna because the lesions are often large and located on cosmetically sensitive facial sites. At the patient’s first visit, the researchers saucerize the entire tumor to remove all visible evidence of lentigo maligna and nip in the bud any invasive element that might be present. One month later, after the wound has healed by secondary intention, the patient begins topical imiquimod therapy 5 days per week. If no inflammation is observed, tazarotene gel is added on the other 2 days per week. After 3 months of topical therapy, the patient goes off treatment for 2 months so the inflammatory response can subside. Then a staged excision is performed with 2-mm margins around the perimeter of the original tumor outline.
"This is an interesting thought, but it’s still not considered standard of care," Dr. Marmur commented in describing the Utah research.
Session chair Dr. Allan C. Halpern, chief of the dermatology service at Memorial Sloan-Kettering Cancer Center in New York, said he and his colleagues, like the Utah group, are using a lot of topical imiquimod as adjunctive therapy for lentigo maligna.
"Because we’re a referral center, we see all those patients whose melanomas unfortunately do recur at the edge of large surgeries. We see a lot of patients whose local surgeons have chased around their faces for a certain amount of time. So I think the general concept of the cure rates of surgery is a bit overstated. I’m not trying to sell an off-label use of a drug, but I think sometimes imiquimod can be very helpful," Dr. Halpern said.
He offered a clinical pearl in diagnosing lentigo maligna: Consider a broad shave biopsy of a suspicious lesion rather than a deeper, smaller-diameter biopsy.
"Sampling errors are a real problem with lentigo maligna. We learned early on that if you take a large lentigo maligna and do multiple biopsies of the same lesion and send them to what we think are our very expert pathologists, on average, we get two or three back that were melanoma and two or three back that were pigmented actinic keratoses. The sampling error tends to be more in the horizontal than in the depth for these very early lesions," according to Dr. Halpern.
Dr. Marmur and Dr. Halpern reported having no relevant financial interests. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – "Slow Mohs" has gained near-universal acceptance among skin cancer specialists as a definitive surgical technique for complete removal of lentigo maligna melanoma while simultaneously sparing normal tissue, according to Dr. Ellen Marmur of Mount Sinai School of Medicine, New York.
The big advantage that slow Mohs has over standard wide local excision with 0.5- to 1-cm margins is a 5-year cure rate approaching 100%. In contrast, standard excision has a recurrence rate of up to 20%, she said at the Hawaii Dermatology Seminar, sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Slow Mohs is a modified form of Mohs micrographic surgery. The surgery compares with conventional Mohs: It is staged, margin-controlled excision. But in slow Mohs, rush permanent sections are sent off to the pathologist rather than the frozen sections integral to conventional Mohs.
Dr. Marmur relies upon slow Mohs, with "bread-loafing" of the central tumor by the pathologist, because the permanent sections better preserve the tumor’s microscopic features. Interpreting atypical melanocytes in frozen sections can be quite a challenge. However, she added, some Mohs surgeons have found that using rapid immunostains also markedly improves the sensitivity and specificity of frozen sections in lentigo maligna surgery.
Slow Mohs takes place over the course of days, she said. "Basically, you do your Wood’s lamp to define the lesion diameter, you measure out your margins, you excise the tumor, pack the area with a bandage, and send the patient home. You rush your pathology, and you don’t do any reconstruction until you get the margins clear."
A pathology report that comes back stating narrow margins are present is "a heart stopper," she added.
"You have the option of observing the area if the margin is clear but the tumor was close to the margin. That’s a good approach for an elderly patient or when the lentigo maligna was in a cosmetically important area."
Lentigo maligna melanoma accounts for 4% of all cases of melanoma. It typically arises on sun-damaged skin in individuals in their 70s or older. Common sites include the malar area, forehead, nose, and temple. The differential diagnosis includes seborrheic keratosis, pigmented actinic keratosis, and pigmented nevus.
Lentigo maligna becomes lentigo maligna melanoma when malignant melanoma cells invade the dermis and deeper appendages. Roughly 5% of lentigo malignas eventually progress to invasive melanoma, according to Dr. Marmur. Typically, a lentigo maligna undergoes extended gradual horizontal growth before beginning a vertical growth phase.
"It spreads like an oil slick for many years," Dr. Marmur said at the seminar.
Established treatment modalities for patients who aren’t surgical candidates include cryotherapy, radiotherapy, and topical imiquimod 5%. All have disadvantages, including high 5-year recurrence rates.
Dr. Marmur noted that a newer nonsurgical therapy drawing considerable interest involves off-label use of topical combination therapy with imiquimod and tazarotene gel. The concept is to use the topical retinoid to disrupt the stratum corneum in order to enhance imiquimod penetration, thereby achieving a greater inflammatory response than possible with imiquimod alone.
Initial data have been published by researchers at the University of Utah, Salt Lake City. They randomized 90 patients with 91 lentigo malignas to imiquimod 5% cream applied 5 days per week for 3 months or to the imiquimod regimen plus tazarotene 0.1% gel on the other 2 days per week. After 3 months of topical therapy, patients underwent conservative staged excision with frozen section analysis with Melan A immunostaining to confirm negative margins.
Of those treated with dual topical therapy for 3 months, 29 of 37 lesions (78%) had complete responses with no residual lentigo maligna at the time of staged excision. So did 27 of 42 (64%) treated with imiquimod alone (Arch. Dermatol. 2012;148:592-6).
The modest difference in outcome was not significant (P = .17). Nevertheless, the Utah investigators wrote that topical pretreatment appears to reduce surgical defect sizes, an important consideration in lentigo maligna because the lesions are often large and located on cosmetically sensitive facial sites. At the patient’s first visit, the researchers saucerize the entire tumor to remove all visible evidence of lentigo maligna and nip in the bud any invasive element that might be present. One month later, after the wound has healed by secondary intention, the patient begins topical imiquimod therapy 5 days per week. If no inflammation is observed, tazarotene gel is added on the other 2 days per week. After 3 months of topical therapy, the patient goes off treatment for 2 months so the inflammatory response can subside. Then a staged excision is performed with 2-mm margins around the perimeter of the original tumor outline.
"This is an interesting thought, but it’s still not considered standard of care," Dr. Marmur commented in describing the Utah research.
Session chair Dr. Allan C. Halpern, chief of the dermatology service at Memorial Sloan-Kettering Cancer Center in New York, said he and his colleagues, like the Utah group, are using a lot of topical imiquimod as adjunctive therapy for lentigo maligna.
"Because we’re a referral center, we see all those patients whose melanomas unfortunately do recur at the edge of large surgeries. We see a lot of patients whose local surgeons have chased around their faces for a certain amount of time. So I think the general concept of the cure rates of surgery is a bit overstated. I’m not trying to sell an off-label use of a drug, but I think sometimes imiquimod can be very helpful," Dr. Halpern said.
He offered a clinical pearl in diagnosing lentigo maligna: Consider a broad shave biopsy of a suspicious lesion rather than a deeper, smaller-diameter biopsy.
"Sampling errors are a real problem with lentigo maligna. We learned early on that if you take a large lentigo maligna and do multiple biopsies of the same lesion and send them to what we think are our very expert pathologists, on average, we get two or three back that were melanoma and two or three back that were pigmented actinic keratoses. The sampling error tends to be more in the horizontal than in the depth for these very early lesions," according to Dr. Halpern.
Dr. Marmur and Dr. Halpern reported having no relevant financial interests. SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR

FDA advisory panel nixes approval of drug-device for liver metastases
SILVER SPRING, MD. – The risks outweigh any possible benefits of treatment with a drug-device combination that delivers melphalan directly to the livers of patients with liver metastases from ocular melanoma, a Food and Drug Administration advisory panel concluded in a 16-0 vote.
At a meeting of the FDA’s Oncologic Drugs Advisory Committee, several panelists said that the treatment was promising but should remain investigational, given its marked toxicity and lack of effect on overall survival.
The Melblez Kit is a combination of melphalan and the Delcath Hepatic Delivery System, which includes two catheters and an extracorporeal hemofiltration component. The catheter is used to administer high doses of the chemotherapy drug directly to the liver via the hepatic artery, and the hemofiltration component lowers the drug level before the blood is returned to the systemic circulation, according to the manufacturer, Delcath Systems. Patients are hospitalized for about 4 days for the procedure, which takes about 3 hours and is performed at 4-week intervals under general anesthesia.
There are no FDA-approved treatments for patients with unresectable metastatic ocular melanoma to the liver, which is the indication under FDA review.
Treatment with the kit was associated with antitumor activity, but it also was associated with fatal and life-threatening adverse reactions. There was a trend towards a detrimental effect on survival, and the risk evaluation and mitigation strategy (REMS) proposed by the company to address those risks "will not improve the observed benefit-risk profile," Dr. Geoffrey Kim, a medical officer in the FDA’s office of hematology and oncology products, told the panel.
In an open-label, randomized multicenter phase-III study conducted between 2006 and 2010 in the United States, the device was used to treat 44 patients. Their outcomes were compared with those of 49 matched patients given the best alternative care (BAC). All patients had surgically unresectable hepatic-dominant metastatic ocular or cutaneous melanoma (89% had ocular melanoma, and almost half were treated at the National Cancer Institute). Subjects were treated until their hepatic disease progressed. The dose administered with the Melblez Kit was 3.0 mg/kg for a median of three treatment cycles and a median of 120 days; best alternative care included systemic chemotherapy in 49% of patients and intrahepatic chemotherapy in 22%.
The primary end point, median hepatic progression-free survival (hPFS) was 7 months among those on the device, compared with 1.6 months among those on BAC, a statistically significant difference that represented a 61% reduction in risk (hazard ratio, 0.39), according to the company. The median overall PFS was 4.8 months among those treated with the device, compared with 1.6 months among those on BAC, also a statistically significant difference.
Overall survival was comparable: 9.8 months in the device-treated group and 9.9 months in those on best alternative care. Further, almost 80% of patients in the Melblez Kit arm had a serious adverse event and almost 70% had a grade-4 adverse event. With best alternative care, the rate of serious adverse events was 16% and the rate of grade-4 events was 2%. No patients on best alternative care died because of an adverse event. Three patients treated with the drug-device died from adverse events.
The adverse reactions in a combined population of 121 patients in the phase-III and phase-II studies and in 28 patients in the BAC arm who crossed over to treatment with the device included toxic deaths in 7% (including cases of hepatic failure, streptococcal sepsis, and GI hemorrhage), cerebral infarction in 4%, MI in 2%, and grade-4 bone marrow suppression with a median time to recovery of more than 1 week in more than 70%. About half had to be rehospitalized for an adverse event.
For a cancer treatment, this safety profile "is unprecedented, in terms of the toxicity," Dr. Richard Pazdur, director of the FDA’s office of hematology and oncology products, remarked.
After the vote, panel member Dr. Louis Diehl, professor of medicine at Duke University, Durham, N.C., said that progression-free survival is valued in studies as an indicator of improved quality of life and it can be an early marker of increased survival. "Unfortunately, this treatment has an increase in morbidity and an increase in mortality and I can’t see from the survival curve that it will ever translate into an improvement in survival."
Delcath did not issue a response after the panel’s vote.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may occasionally be given a waiver. At this meeting, two panelists who had expertise in the topic were given waivers (one panelist is the principal investigator in a study of a competing device and the other works at a medical center where a study of a competing device is being conducted).
About 2,000 cases of ocular melanoma are diagnosed annually in the United States and about 50% metastasize, most often to the liver, according to Delcath. In Europe and Australia, the company markets the device for a broad range of liver metastases, not just those caused by ocular melanoma, according to the company.
SILVER SPRING, MD. – The risks outweigh any possible benefits of treatment with a drug-device combination that delivers melphalan directly to the livers of patients with liver metastases from ocular melanoma, a Food and Drug Administration advisory panel concluded in a 16-0 vote.
At a meeting of the FDA’s Oncologic Drugs Advisory Committee, several panelists said that the treatment was promising but should remain investigational, given its marked toxicity and lack of effect on overall survival.
The Melblez Kit is a combination of melphalan and the Delcath Hepatic Delivery System, which includes two catheters and an extracorporeal hemofiltration component. The catheter is used to administer high doses of the chemotherapy drug directly to the liver via the hepatic artery, and the hemofiltration component lowers the drug level before the blood is returned to the systemic circulation, according to the manufacturer, Delcath Systems. Patients are hospitalized for about 4 days for the procedure, which takes about 3 hours and is performed at 4-week intervals under general anesthesia.
There are no FDA-approved treatments for patients with unresectable metastatic ocular melanoma to the liver, which is the indication under FDA review.
Treatment with the kit was associated with antitumor activity, but it also was associated with fatal and life-threatening adverse reactions. There was a trend towards a detrimental effect on survival, and the risk evaluation and mitigation strategy (REMS) proposed by the company to address those risks "will not improve the observed benefit-risk profile," Dr. Geoffrey Kim, a medical officer in the FDA’s office of hematology and oncology products, told the panel.
In an open-label, randomized multicenter phase-III study conducted between 2006 and 2010 in the United States, the device was used to treat 44 patients. Their outcomes were compared with those of 49 matched patients given the best alternative care (BAC). All patients had surgically unresectable hepatic-dominant metastatic ocular or cutaneous melanoma (89% had ocular melanoma, and almost half were treated at the National Cancer Institute). Subjects were treated until their hepatic disease progressed. The dose administered with the Melblez Kit was 3.0 mg/kg for a median of three treatment cycles and a median of 120 days; best alternative care included systemic chemotherapy in 49% of patients and intrahepatic chemotherapy in 22%.
The primary end point, median hepatic progression-free survival (hPFS) was 7 months among those on the device, compared with 1.6 months among those on BAC, a statistically significant difference that represented a 61% reduction in risk (hazard ratio, 0.39), according to the company. The median overall PFS was 4.8 months among those treated with the device, compared with 1.6 months among those on BAC, also a statistically significant difference.
Overall survival was comparable: 9.8 months in the device-treated group and 9.9 months in those on best alternative care. Further, almost 80% of patients in the Melblez Kit arm had a serious adverse event and almost 70% had a grade-4 adverse event. With best alternative care, the rate of serious adverse events was 16% and the rate of grade-4 events was 2%. No patients on best alternative care died because of an adverse event. Three patients treated with the drug-device died from adverse events.
The adverse reactions in a combined population of 121 patients in the phase-III and phase-II studies and in 28 patients in the BAC arm who crossed over to treatment with the device included toxic deaths in 7% (including cases of hepatic failure, streptococcal sepsis, and GI hemorrhage), cerebral infarction in 4%, MI in 2%, and grade-4 bone marrow suppression with a median time to recovery of more than 1 week in more than 70%. About half had to be rehospitalized for an adverse event.
For a cancer treatment, this safety profile "is unprecedented, in terms of the toxicity," Dr. Richard Pazdur, director of the FDA’s office of hematology and oncology products, remarked.
After the vote, panel member Dr. Louis Diehl, professor of medicine at Duke University, Durham, N.C., said that progression-free survival is valued in studies as an indicator of improved quality of life and it can be an early marker of increased survival. "Unfortunately, this treatment has an increase in morbidity and an increase in mortality and I can’t see from the survival curve that it will ever translate into an improvement in survival."
Delcath did not issue a response after the panel’s vote.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may occasionally be given a waiver. At this meeting, two panelists who had expertise in the topic were given waivers (one panelist is the principal investigator in a study of a competing device and the other works at a medical center where a study of a competing device is being conducted).
About 2,000 cases of ocular melanoma are diagnosed annually in the United States and about 50% metastasize, most often to the liver, according to Delcath. In Europe and Australia, the company markets the device for a broad range of liver metastases, not just those caused by ocular melanoma, according to the company.
SILVER SPRING, MD. – The risks outweigh any possible benefits of treatment with a drug-device combination that delivers melphalan directly to the livers of patients with liver metastases from ocular melanoma, a Food and Drug Administration advisory panel concluded in a 16-0 vote.
At a meeting of the FDA’s Oncologic Drugs Advisory Committee, several panelists said that the treatment was promising but should remain investigational, given its marked toxicity and lack of effect on overall survival.
The Melblez Kit is a combination of melphalan and the Delcath Hepatic Delivery System, which includes two catheters and an extracorporeal hemofiltration component. The catheter is used to administer high doses of the chemotherapy drug directly to the liver via the hepatic artery, and the hemofiltration component lowers the drug level before the blood is returned to the systemic circulation, according to the manufacturer, Delcath Systems. Patients are hospitalized for about 4 days for the procedure, which takes about 3 hours and is performed at 4-week intervals under general anesthesia.
There are no FDA-approved treatments for patients with unresectable metastatic ocular melanoma to the liver, which is the indication under FDA review.
Treatment with the kit was associated with antitumor activity, but it also was associated with fatal and life-threatening adverse reactions. There was a trend towards a detrimental effect on survival, and the risk evaluation and mitigation strategy (REMS) proposed by the company to address those risks "will not improve the observed benefit-risk profile," Dr. Geoffrey Kim, a medical officer in the FDA’s office of hematology and oncology products, told the panel.
In an open-label, randomized multicenter phase-III study conducted between 2006 and 2010 in the United States, the device was used to treat 44 patients. Their outcomes were compared with those of 49 matched patients given the best alternative care (BAC). All patients had surgically unresectable hepatic-dominant metastatic ocular or cutaneous melanoma (89% had ocular melanoma, and almost half were treated at the National Cancer Institute). Subjects were treated until their hepatic disease progressed. The dose administered with the Melblez Kit was 3.0 mg/kg for a median of three treatment cycles and a median of 120 days; best alternative care included systemic chemotherapy in 49% of patients and intrahepatic chemotherapy in 22%.
The primary end point, median hepatic progression-free survival (hPFS) was 7 months among those on the device, compared with 1.6 months among those on BAC, a statistically significant difference that represented a 61% reduction in risk (hazard ratio, 0.39), according to the company. The median overall PFS was 4.8 months among those treated with the device, compared with 1.6 months among those on BAC, also a statistically significant difference.
Overall survival was comparable: 9.8 months in the device-treated group and 9.9 months in those on best alternative care. Further, almost 80% of patients in the Melblez Kit arm had a serious adverse event and almost 70% had a grade-4 adverse event. With best alternative care, the rate of serious adverse events was 16% and the rate of grade-4 events was 2%. No patients on best alternative care died because of an adverse event. Three patients treated with the drug-device died from adverse events.
The adverse reactions in a combined population of 121 patients in the phase-III and phase-II studies and in 28 patients in the BAC arm who crossed over to treatment with the device included toxic deaths in 7% (including cases of hepatic failure, streptococcal sepsis, and GI hemorrhage), cerebral infarction in 4%, MI in 2%, and grade-4 bone marrow suppression with a median time to recovery of more than 1 week in more than 70%. About half had to be rehospitalized for an adverse event.
For a cancer treatment, this safety profile "is unprecedented, in terms of the toxicity," Dr. Richard Pazdur, director of the FDA’s office of hematology and oncology products, remarked.
After the vote, panel member Dr. Louis Diehl, professor of medicine at Duke University, Durham, N.C., said that progression-free survival is valued in studies as an indicator of improved quality of life and it can be an early marker of increased survival. "Unfortunately, this treatment has an increase in morbidity and an increase in mortality and I can’t see from the survival curve that it will ever translate into an improvement in survival."
Delcath did not issue a response after the panel’s vote.
The FDA usually follows the recommendations of its advisory panels. Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although a panelist may occasionally be given a waiver. At this meeting, two panelists who had expertise in the topic were given waivers (one panelist is the principal investigator in a study of a competing device and the other works at a medical center where a study of a competing device is being conducted).
About 2,000 cases of ocular melanoma are diagnosed annually in the United States and about 50% metastasize, most often to the liver, according to Delcath. In Europe and Australia, the company markets the device for a broad range of liver metastases, not just those caused by ocular melanoma, according to the company.
AT AN FDA ADVISORY PANEL MEETING