User login
Official Newspaper of the American College of Surgeons
Statins might protect against rectal anastomotic leaks
SEATTLE – Statins appeared to decrease the risk of sepsis after colorectal surgery and of anastomotic leak after rectal resection in a review of 7,285 elective colorectal surgery patients at 64 Michigan hospitals.
Overall, 2,515 patients (34.5%) were on statins preoperatively and received at least one dose while in the hospital post op. Their outcomes were compared with those of the 4,770 patients (65.5%) who were not on statins.

Statin patients were older (mean, 68 vs. 59 years) with more comorbidities (mean, 2.4 vs. 1.1), including diabetes (34% vs.12%) and hypertension (78% vs. 41%). The majority of statin patients were American Society of Anesthesiologists class 3, and the majority of nonstatin patients were class 1 or 2. The investigators controlled for those and other confounders by multivariate logistic regression and propensity scoring.
“We believe that statin medications can reduce sepsis in the colorectal patient population and may improve anastomotic leak rates for rectal resections,” concluded investigators led by David Disbrow, MD, a colorectal surgery fellow at St. Joseph Mercy Hospital in Ann Arbor, Mich.
The immediate take-home from the study is to make sure that patients who should be on statins for hypercholesterolemia or other reasons are actually taking the drugs prior to colorectal surgery. It just might improve their surgical outcomes. “I think that would be a good way to start,” Dr. Disbrow said at the American Society of Colon and Rectal Surgeons annual meeting.
If statins truly do help reduce postop sepsis and rectal anastomotic leaks, he said, it’s probably because of their anti-inflammatory effects, which have been demonstrated in previous studies. New Zealand investigators, for instance, randomized 65 patients to 40 mg oral simvastatin for up to a week before elective colorectal resections or Hartmann’s procedure reversals and for 2 weeks afterwards; 67 patients were randomized to placebo. The simvastatin group had significantly lower postop plasma concentrations of IL-6, IL-8, and tumor necrosis factor–alpha (J Am Coll Surg. 2016 Aug;223[2]:308-20.e1).
Even so, there were no between-group differences in postoperative complications in that study, and, in general, the impact of statins on postop complications has been mixed in the literature. Some studies have shown benefits, others have suggested harm, and a few have shown nothing either way.
It’s the same situation with prior looks at anastomotic leaks. A Danish review of 2,766 patients who had colorectal anastomoses – 496 (19%) treated perioperatively with statins, some in high-dose – found no difference in leakage rates (OR, 1.31; 95% CI, 0.84-2.05; P = 0.23)(Dis Colon Rectum. 2013 Aug;56[8]:980-6). On the other hand, a more recent British review of 144 patients – 45 (39.4%) on preoperative statins – found that “although patients taking statins did not have a significantly reduced leak risk, compared to nonstatin users, high-risk patients taking statins had the same leak risk as non–high risk patients; therefore, it is plausible that statins normalize the risk of anastomotic leak in high-risk patients” (Gut. 2015;64:A162-3).
In the new Michigan study, there were no differences in surgical site infections or 30-day mortality between statin and nonstatin patients, but patients on statins were less likely to get pneumonia, which might help account for their lower sepsis risk, Dr. Disbrow said.
Data for the study came from the Michigan Surgical Quality Collaborative database.
Dr. Disbrow had no disclosures.
SEATTLE – Statins appeared to decrease the risk of sepsis after colorectal surgery and of anastomotic leak after rectal resection in a review of 7,285 elective colorectal surgery patients at 64 Michigan hospitals.
Overall, 2,515 patients (34.5%) were on statins preoperatively and received at least one dose while in the hospital post op. Their outcomes were compared with those of the 4,770 patients (65.5%) who were not on statins.
Statin patients were older (mean, 68 vs. 59 years) with more comorbidities (mean, 2.4 vs. 1.1), including diabetes (34% vs.12%) and hypertension (78% vs. 41%). The majority of statin patients were American Society of Anesthesiologists class 3, and the majority of nonstatin patients were class 1 or 2. The investigators controlled for those and other confounders by multivariate logistic regression and propensity scoring.
“We believe that statin medications can reduce sepsis in the colorectal patient population and may improve anastomotic leak rates for rectal resections,” concluded investigators led by David Disbrow, MD, a colorectal surgery fellow at St. Joseph Mercy Hospital in Ann Arbor, Mich.
The immediate take-home from the study is to make sure that patients who should be on statins for hypercholesterolemia or other reasons are actually taking the drugs prior to colorectal surgery. It just might improve their surgical outcomes. “I think that would be a good way to start,” Dr. Disbrow said at the American Society of Colon and Rectal Surgeons annual meeting.
If statins truly do help reduce postop sepsis and rectal anastomotic leaks, he said, it’s probably because of their anti-inflammatory effects, which have been demonstrated in previous studies. New Zealand investigators, for instance, randomized 65 patients to 40 mg oral simvastatin for up to a week before elective colorectal resections or Hartmann’s procedure reversals and for 2 weeks afterwards; 67 patients were randomized to placebo. The simvastatin group had significantly lower postop plasma concentrations of IL-6, IL-8, and tumor necrosis factor–alpha (J Am Coll Surg. 2016 Aug;223[2]:308-20.e1).
Even so, there were no between-group differences in postoperative complications in that study, and, in general, the impact of statins on postop complications has been mixed in the literature. Some studies have shown benefits, others have suggested harm, and a few have shown nothing either way.
It’s the same situation with prior looks at anastomotic leaks. A Danish review of 2,766 patients who had colorectal anastomoses – 496 (19%) treated perioperatively with statins, some in high-dose – found no difference in leakage rates (OR, 1.31; 95% CI, 0.84-2.05; P = 0.23)(Dis Colon Rectum. 2013 Aug;56[8]:980-6). On the other hand, a more recent British review of 144 patients – 45 (39.4%) on preoperative statins – found that “although patients taking statins did not have a significantly reduced leak risk, compared to nonstatin users, high-risk patients taking statins had the same leak risk as non–high risk patients; therefore, it is plausible that statins normalize the risk of anastomotic leak in high-risk patients” (Gut. 2015;64:A162-3).
In the new Michigan study, there were no differences in surgical site infections or 30-day mortality between statin and nonstatin patients, but patients on statins were less likely to get pneumonia, which might help account for their lower sepsis risk, Dr. Disbrow said.
Data for the study came from the Michigan Surgical Quality Collaborative database.
Dr. Disbrow had no disclosures.
SEATTLE – Statins appeared to decrease the risk of sepsis after colorectal surgery and of anastomotic leak after rectal resection in a review of 7,285 elective colorectal surgery patients at 64 Michigan hospitals.
Overall, 2,515 patients (34.5%) were on statins preoperatively and received at least one dose while in the hospital post op. Their outcomes were compared with those of the 4,770 patients (65.5%) who were not on statins.
Statin patients were older (mean, 68 vs. 59 years) with more comorbidities (mean, 2.4 vs. 1.1), including diabetes (34% vs.12%) and hypertension (78% vs. 41%). The majority of statin patients were American Society of Anesthesiologists class 3, and the majority of nonstatin patients were class 1 or 2. The investigators controlled for those and other confounders by multivariate logistic regression and propensity scoring.
“We believe that statin medications can reduce sepsis in the colorectal patient population and may improve anastomotic leak rates for rectal resections,” concluded investigators led by David Disbrow, MD, a colorectal surgery fellow at St. Joseph Mercy Hospital in Ann Arbor, Mich.
The immediate take-home from the study is to make sure that patients who should be on statins for hypercholesterolemia or other reasons are actually taking the drugs prior to colorectal surgery. It just might improve their surgical outcomes. “I think that would be a good way to start,” Dr. Disbrow said at the American Society of Colon and Rectal Surgeons annual meeting.
If statins truly do help reduce postop sepsis and rectal anastomotic leaks, he said, it’s probably because of their anti-inflammatory effects, which have been demonstrated in previous studies. New Zealand investigators, for instance, randomized 65 patients to 40 mg oral simvastatin for up to a week before elective colorectal resections or Hartmann’s procedure reversals and for 2 weeks afterwards; 67 patients were randomized to placebo. The simvastatin group had significantly lower postop plasma concentrations of IL-6, IL-8, and tumor necrosis factor–alpha (J Am Coll Surg. 2016 Aug;223[2]:308-20.e1).
Even so, there were no between-group differences in postoperative complications in that study, and, in general, the impact of statins on postop complications has been mixed in the literature. Some studies have shown benefits, others have suggested harm, and a few have shown nothing either way.
It’s the same situation with prior looks at anastomotic leaks. A Danish review of 2,766 patients who had colorectal anastomoses – 496 (19%) treated perioperatively with statins, some in high-dose – found no difference in leakage rates (OR, 1.31; 95% CI, 0.84-2.05; P = 0.23)(Dis Colon Rectum. 2013 Aug;56[8]:980-6). On the other hand, a more recent British review of 144 patients – 45 (39.4%) on preoperative statins – found that “although patients taking statins did not have a significantly reduced leak risk, compared to nonstatin users, high-risk patients taking statins had the same leak risk as non–high risk patients; therefore, it is plausible that statins normalize the risk of anastomotic leak in high-risk patients” (Gut. 2015;64:A162-3).
In the new Michigan study, there were no differences in surgical site infections or 30-day mortality between statin and nonstatin patients, but patients on statins were less likely to get pneumonia, which might help account for their lower sepsis risk, Dr. Disbrow said.
Data for the study came from the Michigan Surgical Quality Collaborative database.
Dr. Disbrow had no disclosures.
AT ASCRS 2017
Key clinical point:
Major finding: The statin group had a reduced risk of sepsis (OR, 0.712; 95% CI, 0.535-0.948; P = .020), and, while statins were not associated with a reduction in anastomotic leaks overall, they were protective in subgroup analysis of patients who had rectal resections, which are especially prone to leakage (OR, 0.260; 95% CI, 0.112-0.605, P = .002).
Data source: A review of 7,285 elective colorectal surgery patients.
Disclosures: The lead investigator had no disclosures.
Health IT: Cybercrime risks are real
Aging equipment, valuable data, and an improperly trained workforce make health care IT extraordinarily vulnerable to external malfeasance, as demonstrated by the WannaCry virus episode that occurred this spring in the United Kingdom.
Computer hackers used a weakness in the operating system employed by the U.K. National Health Service, allowing the WannaCry virus to spread quickly across connected systems. The ransomware attack locked clinicians out of patient records and diagnostic machines that were connected, bringing patient care to a near standstill.
The attack lasted 3 days until Marcus Hutchins, a 22-year-old security researcher, stumbled onto a way to slow the spread of the virus enough to manage it, but not before nearly 60 million attacks had been conducted, Salim Neino, CEO of Kryptos Logic, testified June 15 at a joint hearing of two subcommittees of the House Science, Space & Technology Committee. Mr. Hutchins is employed by Kryptos Logic.
U.S. officials are keenly aware that a similar attack could happen here. In June, the federally sponsored Health Care Industry Cybersecurity Task Force issued a report on their year-long look at the state of the health care IT in this country. The task force was mandated by the Cybersecurity Act of 2015and formed in March 2016.
Specifically, the task force recommended:
• Defining and streamlining leadership, governance, and expectations for health care industry cybersecurity.
• Increasing the security and resilience of medical devices and health IT.
• Developing the health care workforce capacity necessary to prioritize and ensure cybersecurity awareness and technical capabilities.
• Increasing health care industry readiness through improved cybersecurity awareness and education.
• Identifying mechanisms to protect research and development efforts and intellectual property from attacks or exposure.
• Improving information sharing of industry threats, weaknesses, and mitigations.
Health care cybercrime is a significant problem in the United States. In 2016, 328 U.S. health care firms reported data breaches, up from 268 in 2015, with a total of 16.6 million Americans affected, according to a report conducted by Bitglass (registration required), a security software company. In February 2016, a hospital in California was forced to pay about $17,000 in Bitcoin, an electronic currency that is known to be favored by cybercriminals, to access electronic health records (EHRs) that were held in a similar manner to last month’s attack on the NHS.
For physicians, this may seem like someone else’s problem; however, unsafe day-to-day interactions with connected devices and patient EHRs were among the task force’s primary concerns.
For many, creating a safe password or not giving out critical information may seem like common sense, but many physicians are not able or willing to take the time to make sure they are interacting with systems safely, or they are overconfident in their security system, according to task force member Mark Jarrett, MD, senior vice president and chief quality officer at Northwell Health in New York.
“Most physicians now will try to access medical records of their patients who have been in the hospital because that’s good care,” Dr. Jarrett said in an interview. But they have to recognize that “they cannot give these passwords to other people and they need to make these passwords complex.”
“Phishing” is another concern. In a phishing scam, cybercriminals will pose as a fraudulent institution or individual in order to trick a target into downloading a virus, sending additional valuable information, or even paying money directly to the criminals.
“Physicians checking their emails need to be aware of possible phishing episodes, because they could be infected, and then there is the possibility that infection could be introduced into the system, Dr. Jarrett said. “I think the disconnect is [that physicians] are not used to [cybersecurity]. It’s not part of their daily life and they also, up until recently, thought ‘it’s never going to happen to me.’ ”
While hospitals are not completely incapable of protecting themselves, experts are concerned about an overinflated sense of confidence among health care professionals.
“Health care workers often assume that the IT network and the devices they support function efficiently and that their level of cybersecurity vulnerability is low,” according to the task force report.
This can be a costly assumption, financially, as well for safety; the price per stolen EHR averaged at $380 in 2016-2017, according to the Ponemon Institute’s 2017 Cost of Data Breach Study, released in June. That is nearly triple the average cost of all breaches – $141– and higher than the price of $241 for information stolen from financial industries because, unlike a credit card number, patients’ data are unique and cannot be replaced.
Aging equipment is another concern. Legacy software and machine systems used in medical practices and hospitals are not equipped with the necessary security services needed to handle the growing risks of connectivity, despite being included in the network.
“Every CT machine, every x-ray machine today is connected online, on one consolidated Internet” cybersecurity expert Idan Udi Edry of Trustifi said in an interview. “The more comfortable we are with the digital edge coming into our lives, the more vulnerable we become and the more security we need to implement to protect ourselves.”
Some solutions already have been suggested to help health care professionals replace their outdated equipment, especially private practice physicians or smaller hospitals without much financial wiggle room,
The cybersecurity task force report recommended creating health IT version of Cash for Clunkers, an Obama administration program that offered rebates to consumers who traded in older, less fuel efficient cars when purchasing a new car.
While experts agree that the growing focus on connected health care will continue to create cybersecurity risks, with all members of the health care industry working together, it is possible to keep hospitals and patients safe from would-be criminals.
The next key step is creating regulations that would encourage a cohesive structure of cybersecurity guidelines. According to the task force report, “a priority for regulatory agencies should be to ensure consistency among various federal and state cybersecurity regulations so that health care providers can focus on deploying their resources appropriately between securing patient information and the quality, safety, and accessibility of patient care” rather than having to focus on statutory and regulatory inconsistencies.
[email protected]
On Twitter @eaztweets
When computer hackers took control of the United Kingdom’s National Health Service using a virus known as “WannaCry,” doctors and nurses were left helpless, blocked from the files they would need to treat their patients until they paid to get them those files back.
Doctors were forced to revert to older methods, slowing everything to a snail’s pace.
The media coverage of the event was dramatic, but there is no doubt the effects made it justifiably so.
NHS hospitals had not achieved their goal of being paperless; had they been, the service would have been completely unable to stop the attack.
It was not just software that was affected but medical devices as well. Physicians were unable to perform x-rays, and some hospitals found that the refrigerators used to store blood products were shut down.
While the NHS was particularly vulnerable to the WannaCry because of budget cuts, this cybercrime could have happened to any hospital, and its lessons are applicable far all.
Doctors do understand the value of patients records, but they seem to be unaware of the physical harm that could befall patients from a cyberattack.
This attack needs to serve as a wake-up call for health care professionals who are not invested in their facilities’ cybersecurity practices.
Underfunding left NHS hospitals terribly exposed and, if physicians continue to be complacent with how to handle this issue, the results are sure to be more severe.
Rachel Clarke, MD, is at Oxford (England) University Hospitals NHS Foundation Trust, and Taryn Youngstein, MD, is at Imperial College Healthcare NHS Trust, London. They reported having no relevant financial conflicts of interest. Their remarks were make in a perspective published in the New England Journal of Medicine (doi: 10.1056/NEJMp1706754).
When computer hackers took control of the United Kingdom’s National Health Service using a virus known as “WannaCry,” doctors and nurses were left helpless, blocked from the files they would need to treat their patients until they paid to get them those files back.
Doctors were forced to revert to older methods, slowing everything to a snail’s pace.
The media coverage of the event was dramatic, but there is no doubt the effects made it justifiably so.
NHS hospitals had not achieved their goal of being paperless; had they been, the service would have been completely unable to stop the attack.
It was not just software that was affected but medical devices as well. Physicians were unable to perform x-rays, and some hospitals found that the refrigerators used to store blood products were shut down.
While the NHS was particularly vulnerable to the WannaCry because of budget cuts, this cybercrime could have happened to any hospital, and its lessons are applicable far all.
Doctors do understand the value of patients records, but they seem to be unaware of the physical harm that could befall patients from a cyberattack.
This attack needs to serve as a wake-up call for health care professionals who are not invested in their facilities’ cybersecurity practices.
Underfunding left NHS hospitals terribly exposed and, if physicians continue to be complacent with how to handle this issue, the results are sure to be more severe.
Rachel Clarke, MD, is at Oxford (England) University Hospitals NHS Foundation Trust, and Taryn Youngstein, MD, is at Imperial College Healthcare NHS Trust, London. They reported having no relevant financial conflicts of interest. Their remarks were make in a perspective published in the New England Journal of Medicine (doi: 10.1056/NEJMp1706754).
When computer hackers took control of the United Kingdom’s National Health Service using a virus known as “WannaCry,” doctors and nurses were left helpless, blocked from the files they would need to treat their patients until they paid to get them those files back.
Doctors were forced to revert to older methods, slowing everything to a snail’s pace.
The media coverage of the event was dramatic, but there is no doubt the effects made it justifiably so.
NHS hospitals had not achieved their goal of being paperless; had they been, the service would have been completely unable to stop the attack.
It was not just software that was affected but medical devices as well. Physicians were unable to perform x-rays, and some hospitals found that the refrigerators used to store blood products were shut down.
While the NHS was particularly vulnerable to the WannaCry because of budget cuts, this cybercrime could have happened to any hospital, and its lessons are applicable far all.
Doctors do understand the value of patients records, but they seem to be unaware of the physical harm that could befall patients from a cyberattack.
This attack needs to serve as a wake-up call for health care professionals who are not invested in their facilities’ cybersecurity practices.
Underfunding left NHS hospitals terribly exposed and, if physicians continue to be complacent with how to handle this issue, the results are sure to be more severe.
Rachel Clarke, MD, is at Oxford (England) University Hospitals NHS Foundation Trust, and Taryn Youngstein, MD, is at Imperial College Healthcare NHS Trust, London. They reported having no relevant financial conflicts of interest. Their remarks were make in a perspective published in the New England Journal of Medicine (doi: 10.1056/NEJMp1706754).
Aging equipment, valuable data, and an improperly trained workforce make health care IT extraordinarily vulnerable to external malfeasance, as demonstrated by the WannaCry virus episode that occurred this spring in the United Kingdom.
Computer hackers used a weakness in the operating system employed by the U.K. National Health Service, allowing the WannaCry virus to spread quickly across connected systems. The ransomware attack locked clinicians out of patient records and diagnostic machines that were connected, bringing patient care to a near standstill.
The attack lasted 3 days until Marcus Hutchins, a 22-year-old security researcher, stumbled onto a way to slow the spread of the virus enough to manage it, but not before nearly 60 million attacks had been conducted, Salim Neino, CEO of Kryptos Logic, testified June 15 at a joint hearing of two subcommittees of the House Science, Space & Technology Committee. Mr. Hutchins is employed by Kryptos Logic.
U.S. officials are keenly aware that a similar attack could happen here. In June, the federally sponsored Health Care Industry Cybersecurity Task Force issued a report on their year-long look at the state of the health care IT in this country. The task force was mandated by the Cybersecurity Act of 2015and formed in March 2016.
Specifically, the task force recommended:
• Defining and streamlining leadership, governance, and expectations for health care industry cybersecurity.
• Increasing the security and resilience of medical devices and health IT.
• Developing the health care workforce capacity necessary to prioritize and ensure cybersecurity awareness and technical capabilities.
• Increasing health care industry readiness through improved cybersecurity awareness and education.
• Identifying mechanisms to protect research and development efforts and intellectual property from attacks or exposure.
• Improving information sharing of industry threats, weaknesses, and mitigations.
Health care cybercrime is a significant problem in the United States. In 2016, 328 U.S. health care firms reported data breaches, up from 268 in 2015, with a total of 16.6 million Americans affected, according to a report conducted by Bitglass (registration required), a security software company. In February 2016, a hospital in California was forced to pay about $17,000 in Bitcoin, an electronic currency that is known to be favored by cybercriminals, to access electronic health records (EHRs) that were held in a similar manner to last month’s attack on the NHS.
For physicians, this may seem like someone else’s problem; however, unsafe day-to-day interactions with connected devices and patient EHRs were among the task force’s primary concerns.
For many, creating a safe password or not giving out critical information may seem like common sense, but many physicians are not able or willing to take the time to make sure they are interacting with systems safely, or they are overconfident in their security system, according to task force member Mark Jarrett, MD, senior vice president and chief quality officer at Northwell Health in New York.
“Most physicians now will try to access medical records of their patients who have been in the hospital because that’s good care,” Dr. Jarrett said in an interview. But they have to recognize that “they cannot give these passwords to other people and they need to make these passwords complex.”
“Phishing” is another concern. In a phishing scam, cybercriminals will pose as a fraudulent institution or individual in order to trick a target into downloading a virus, sending additional valuable information, or even paying money directly to the criminals.
“Physicians checking their emails need to be aware of possible phishing episodes, because they could be infected, and then there is the possibility that infection could be introduced into the system, Dr. Jarrett said. “I think the disconnect is [that physicians] are not used to [cybersecurity]. It’s not part of their daily life and they also, up until recently, thought ‘it’s never going to happen to me.’ ”
While hospitals are not completely incapable of protecting themselves, experts are concerned about an overinflated sense of confidence among health care professionals.
“Health care workers often assume that the IT network and the devices they support function efficiently and that their level of cybersecurity vulnerability is low,” according to the task force report.
This can be a costly assumption, financially, as well for safety; the price per stolen EHR averaged at $380 in 2016-2017, according to the Ponemon Institute’s 2017 Cost of Data Breach Study, released in June. That is nearly triple the average cost of all breaches – $141– and higher than the price of $241 for information stolen from financial industries because, unlike a credit card number, patients’ data are unique and cannot be replaced.
Aging equipment is another concern. Legacy software and machine systems used in medical practices and hospitals are not equipped with the necessary security services needed to handle the growing risks of connectivity, despite being included in the network.
“Every CT machine, every x-ray machine today is connected online, on one consolidated Internet” cybersecurity expert Idan Udi Edry of Trustifi said in an interview. “The more comfortable we are with the digital edge coming into our lives, the more vulnerable we become and the more security we need to implement to protect ourselves.”
Some solutions already have been suggested to help health care professionals replace their outdated equipment, especially private practice physicians or smaller hospitals without much financial wiggle room,
The cybersecurity task force report recommended creating health IT version of Cash for Clunkers, an Obama administration program that offered rebates to consumers who traded in older, less fuel efficient cars when purchasing a new car.
While experts agree that the growing focus on connected health care will continue to create cybersecurity risks, with all members of the health care industry working together, it is possible to keep hospitals and patients safe from would-be criminals.
The next key step is creating regulations that would encourage a cohesive structure of cybersecurity guidelines. According to the task force report, “a priority for regulatory agencies should be to ensure consistency among various federal and state cybersecurity regulations so that health care providers can focus on deploying their resources appropriately between securing patient information and the quality, safety, and accessibility of patient care” rather than having to focus on statutory and regulatory inconsistencies.
[email protected]
On Twitter @eaztweets
Aging equipment, valuable data, and an improperly trained workforce make health care IT extraordinarily vulnerable to external malfeasance, as demonstrated by the WannaCry virus episode that occurred this spring in the United Kingdom.
Computer hackers used a weakness in the operating system employed by the U.K. National Health Service, allowing the WannaCry virus to spread quickly across connected systems. The ransomware attack locked clinicians out of patient records and diagnostic machines that were connected, bringing patient care to a near standstill.
The attack lasted 3 days until Marcus Hutchins, a 22-year-old security researcher, stumbled onto a way to slow the spread of the virus enough to manage it, but not before nearly 60 million attacks had been conducted, Salim Neino, CEO of Kryptos Logic, testified June 15 at a joint hearing of two subcommittees of the House Science, Space & Technology Committee. Mr. Hutchins is employed by Kryptos Logic.
U.S. officials are keenly aware that a similar attack could happen here. In June, the federally sponsored Health Care Industry Cybersecurity Task Force issued a report on their year-long look at the state of the health care IT in this country. The task force was mandated by the Cybersecurity Act of 2015and formed in March 2016.
Specifically, the task force recommended:
• Defining and streamlining leadership, governance, and expectations for health care industry cybersecurity.
• Increasing the security and resilience of medical devices and health IT.
• Developing the health care workforce capacity necessary to prioritize and ensure cybersecurity awareness and technical capabilities.
• Increasing health care industry readiness through improved cybersecurity awareness and education.
• Identifying mechanisms to protect research and development efforts and intellectual property from attacks or exposure.
• Improving information sharing of industry threats, weaknesses, and mitigations.
Health care cybercrime is a significant problem in the United States. In 2016, 328 U.S. health care firms reported data breaches, up from 268 in 2015, with a total of 16.6 million Americans affected, according to a report conducted by Bitglass (registration required), a security software company. In February 2016, a hospital in California was forced to pay about $17,000 in Bitcoin, an electronic currency that is known to be favored by cybercriminals, to access electronic health records (EHRs) that were held in a similar manner to last month’s attack on the NHS.
For physicians, this may seem like someone else’s problem; however, unsafe day-to-day interactions with connected devices and patient EHRs were among the task force’s primary concerns.
For many, creating a safe password or not giving out critical information may seem like common sense, but many physicians are not able or willing to take the time to make sure they are interacting with systems safely, or they are overconfident in their security system, according to task force member Mark Jarrett, MD, senior vice president and chief quality officer at Northwell Health in New York.
“Most physicians now will try to access medical records of their patients who have been in the hospital because that’s good care,” Dr. Jarrett said in an interview. But they have to recognize that “they cannot give these passwords to other people and they need to make these passwords complex.”
“Phishing” is another concern. In a phishing scam, cybercriminals will pose as a fraudulent institution or individual in order to trick a target into downloading a virus, sending additional valuable information, or even paying money directly to the criminals.
“Physicians checking their emails need to be aware of possible phishing episodes, because they could be infected, and then there is the possibility that infection could be introduced into the system, Dr. Jarrett said. “I think the disconnect is [that physicians] are not used to [cybersecurity]. It’s not part of their daily life and they also, up until recently, thought ‘it’s never going to happen to me.’ ”
While hospitals are not completely incapable of protecting themselves, experts are concerned about an overinflated sense of confidence among health care professionals.
“Health care workers often assume that the IT network and the devices they support function efficiently and that their level of cybersecurity vulnerability is low,” according to the task force report.
This can be a costly assumption, financially, as well for safety; the price per stolen EHR averaged at $380 in 2016-2017, according to the Ponemon Institute’s 2017 Cost of Data Breach Study, released in June. That is nearly triple the average cost of all breaches – $141– and higher than the price of $241 for information stolen from financial industries because, unlike a credit card number, patients’ data are unique and cannot be replaced.
Aging equipment is another concern. Legacy software and machine systems used in medical practices and hospitals are not equipped with the necessary security services needed to handle the growing risks of connectivity, despite being included in the network.
“Every CT machine, every x-ray machine today is connected online, on one consolidated Internet” cybersecurity expert Idan Udi Edry of Trustifi said in an interview. “The more comfortable we are with the digital edge coming into our lives, the more vulnerable we become and the more security we need to implement to protect ourselves.”
Some solutions already have been suggested to help health care professionals replace their outdated equipment, especially private practice physicians or smaller hospitals without much financial wiggle room,
The cybersecurity task force report recommended creating health IT version of Cash for Clunkers, an Obama administration program that offered rebates to consumers who traded in older, less fuel efficient cars when purchasing a new car.
While experts agree that the growing focus on connected health care will continue to create cybersecurity risks, with all members of the health care industry working together, it is possible to keep hospitals and patients safe from would-be criminals.
The next key step is creating regulations that would encourage a cohesive structure of cybersecurity guidelines. According to the task force report, “a priority for regulatory agencies should be to ensure consistency among various federal and state cybersecurity regulations so that health care providers can focus on deploying their resources appropriately between securing patient information and the quality, safety, and accessibility of patient care” rather than having to focus on statutory and regulatory inconsistencies.
[email protected]
On Twitter @eaztweets
Malpractice reform: House passes bill to cap damages
The House of Representatives has passed a bill that would cap damages in medical malpractice cases and impose a tighter time frame for legal challenges against physicians.
The House passed the Protecting Access to Care Act (H.R. 1215) on June 28 by a 218-210 vote. The bill, modeled after California’s Medical Injury Compensation Reform Act (MICRA), would limit noneconomic damages in medical malpractice cases to $250,000, restrict contingency fees charged by attorneys, and enforce a 3-year statute of limitations for liability lawsuits from the date of alleged injury. The legislation also includes a fair share rule in which defendants are liable only for the damages in direct proportion to their percentage of responsibility.
The American College of Physicians (ACP) praised the House for passing the bill, saying the time is ripe to develop and pass common-sense liability reforms.
“The American College of Physicians applauds the House of Representatives for its passage of a multifaceted approach to medical-liability reform,” Jack Ende, MD, ACP president, said in a statement. “ACP believes that any solution to improve the medical liability system in the U.S. should include a multifaceted approach, because no single program or law by itself is likely to achieve the goals of improving patient safety, ensuring fair compensation to patients, strengthening rather than undermining the patient-physician relationship, and reducing the economic costs associated with the current system.”
The American Association for Justice, a lobbying organization for plaintiffs’ attorneys, sent a letter to the House prior to the bill’s passage urging legislators to oppose the bill. More than 75 organizations signed the letter.
“Even if H.R. 1215 applied only to doctors and hospitals, recent studies clearly establish that its provisions would lead to more deaths and injuries, and increased health care costs due to a ‘broad relaxation of care,’ ” the letter stated. “... The latest statistics show that medical errors, most of which are preventable, are the third leading cause of death in America. This intolerable situation is perhaps all the more shocking because we already know about how to fix much of this problem. Congress should focus on improving patient safety and reducing deaths and injuries, not insulating negligent providers from accountability, harming patients, and saddling taxpayers with the cost.”
The legislation would apply to any patient who receives medical care provided via a federal program, such as Medicare or Medicaid, or via a subsidy or tax benefit, such as coverage purchased under the Affordable Care Act or a replacement. Medical care paid for via employer health plans also would fall under the legislation’s umbrella since insurance premiums receive federal tax exemptions. The bill would not preempt state medical malpractice laws that impose damage caps, whether higher or lower than $250,000, nor would the legislation affect the availability of economic damages, according to bill language.
As part of the H.R. 1215, courts could limit how much attorneys receive from a patient’s ultimate award. Specifically, courts would have the power to restrict payments from a plaintiff’s damage recovery to an attorney who claims a financial stake in the outcome by virtue of a contingent fee.
PIAA, a trade association representing medical liability insurers, said the House passage of the bill is a major victory for tort reform advocates. The bill is the first comprehensive medical liability reform legislation to be passed by either chamber of Congress in more than 5 years, according to PIAA.

H.R. 1215 now moves on to the Senate.
[email protected]
On Twitter @legal_med
The House of Representatives has passed a bill that would cap damages in medical malpractice cases and impose a tighter time frame for legal challenges against physicians.
The House passed the Protecting Access to Care Act (H.R. 1215) on June 28 by a 218-210 vote. The bill, modeled after California’s Medical Injury Compensation Reform Act (MICRA), would limit noneconomic damages in medical malpractice cases to $250,000, restrict contingency fees charged by attorneys, and enforce a 3-year statute of limitations for liability lawsuits from the date of alleged injury. The legislation also includes a fair share rule in which defendants are liable only for the damages in direct proportion to their percentage of responsibility.
The American College of Physicians (ACP) praised the House for passing the bill, saying the time is ripe to develop and pass common-sense liability reforms.
“The American College of Physicians applauds the House of Representatives for its passage of a multifaceted approach to medical-liability reform,” Jack Ende, MD, ACP president, said in a statement. “ACP believes that any solution to improve the medical liability system in the U.S. should include a multifaceted approach, because no single program or law by itself is likely to achieve the goals of improving patient safety, ensuring fair compensation to patients, strengthening rather than undermining the patient-physician relationship, and reducing the economic costs associated with the current system.”
The American Association for Justice, a lobbying organization for plaintiffs’ attorneys, sent a letter to the House prior to the bill’s passage urging legislators to oppose the bill. More than 75 organizations signed the letter.
“Even if H.R. 1215 applied only to doctors and hospitals, recent studies clearly establish that its provisions would lead to more deaths and injuries, and increased health care costs due to a ‘broad relaxation of care,’ ” the letter stated. “... The latest statistics show that medical errors, most of which are preventable, are the third leading cause of death in America. This intolerable situation is perhaps all the more shocking because we already know about how to fix much of this problem. Congress should focus on improving patient safety and reducing deaths and injuries, not insulating negligent providers from accountability, harming patients, and saddling taxpayers with the cost.”
The legislation would apply to any patient who receives medical care provided via a federal program, such as Medicare or Medicaid, or via a subsidy or tax benefit, such as coverage purchased under the Affordable Care Act or a replacement. Medical care paid for via employer health plans also would fall under the legislation’s umbrella since insurance premiums receive federal tax exemptions. The bill would not preempt state medical malpractice laws that impose damage caps, whether higher or lower than $250,000, nor would the legislation affect the availability of economic damages, according to bill language.
As part of the H.R. 1215, courts could limit how much attorneys receive from a patient’s ultimate award. Specifically, courts would have the power to restrict payments from a plaintiff’s damage recovery to an attorney who claims a financial stake in the outcome by virtue of a contingent fee.
PIAA, a trade association representing medical liability insurers, said the House passage of the bill is a major victory for tort reform advocates. The bill is the first comprehensive medical liability reform legislation to be passed by either chamber of Congress in more than 5 years, according to PIAA.
H.R. 1215 now moves on to the Senate.
[email protected]
On Twitter @legal_med
The House of Representatives has passed a bill that would cap damages in medical malpractice cases and impose a tighter time frame for legal challenges against physicians.
The House passed the Protecting Access to Care Act (H.R. 1215) on June 28 by a 218-210 vote. The bill, modeled after California’s Medical Injury Compensation Reform Act (MICRA), would limit noneconomic damages in medical malpractice cases to $250,000, restrict contingency fees charged by attorneys, and enforce a 3-year statute of limitations for liability lawsuits from the date of alleged injury. The legislation also includes a fair share rule in which defendants are liable only for the damages in direct proportion to their percentage of responsibility.
The American College of Physicians (ACP) praised the House for passing the bill, saying the time is ripe to develop and pass common-sense liability reforms.
“The American College of Physicians applauds the House of Representatives for its passage of a multifaceted approach to medical-liability reform,” Jack Ende, MD, ACP president, said in a statement. “ACP believes that any solution to improve the medical liability system in the U.S. should include a multifaceted approach, because no single program or law by itself is likely to achieve the goals of improving patient safety, ensuring fair compensation to patients, strengthening rather than undermining the patient-physician relationship, and reducing the economic costs associated with the current system.”
The American Association for Justice, a lobbying organization for plaintiffs’ attorneys, sent a letter to the House prior to the bill’s passage urging legislators to oppose the bill. More than 75 organizations signed the letter.
“Even if H.R. 1215 applied only to doctors and hospitals, recent studies clearly establish that its provisions would lead to more deaths and injuries, and increased health care costs due to a ‘broad relaxation of care,’ ” the letter stated. “... The latest statistics show that medical errors, most of which are preventable, are the third leading cause of death in America. This intolerable situation is perhaps all the more shocking because we already know about how to fix much of this problem. Congress should focus on improving patient safety and reducing deaths and injuries, not insulating negligent providers from accountability, harming patients, and saddling taxpayers with the cost.”
The legislation would apply to any patient who receives medical care provided via a federal program, such as Medicare or Medicaid, or via a subsidy or tax benefit, such as coverage purchased under the Affordable Care Act or a replacement. Medical care paid for via employer health plans also would fall under the legislation’s umbrella since insurance premiums receive federal tax exemptions. The bill would not preempt state medical malpractice laws that impose damage caps, whether higher or lower than $250,000, nor would the legislation affect the availability of economic damages, according to bill language.
As part of the H.R. 1215, courts could limit how much attorneys receive from a patient’s ultimate award. Specifically, courts would have the power to restrict payments from a plaintiff’s damage recovery to an attorney who claims a financial stake in the outcome by virtue of a contingent fee.
PIAA, a trade association representing medical liability insurers, said the House passage of the bill is a major victory for tort reform advocates. The bill is the first comprehensive medical liability reform legislation to be passed by either chamber of Congress in more than 5 years, according to PIAA.
H.R. 1215 now moves on to the Senate.
[email protected]
On Twitter @legal_med
Concomitant MIMV-TVS no worse than MIMV alone
NEW YORK – Concurrent mitral-tricuspid valve surgery has similar outcomes to isolated minimally invasive mitral valve surgery, according to results of a 12-year review reported at the 2017 Mitral Valve Conclave, sponsored by the American Association for Thoracic Surgery.
Indications for minimally invasive tricuspid valve surgery done at the same time of mitral valve surgery have not been well established, in part because the outcomes of such combined procedures have been underreported.

Dr. Kilic noted that patients who had concomitant TVS were typically higher risk at baseline. “The concomitant group was older, had a higher percentage of female patients, and higher rates of chronic lung disease and cerebrovascular disease as well,” Dr. Kilic said. In comparing the isolated MIMV surgery and MIMV-TVS groups in the unmatched analysis, 9% vs. 14% had chronic lung disease (P = .05), 12% vs. 16% had coronary artery disease (P = .15), 7% vs. 12% had cerebrovascular disease (P = .04), and 93% vs. 90% had elective surgery (P = .18). The majority of tricuspid repairs were for severe tricuspid regurgitation (TR) or moderate TR with a dilated annulus of 40 mm or greater.
The operative characteristics differed significantly between the two groups. “As one might expect, the cardiopulmonary bypass time and aortic occlusion times were longer in the concomitant group; and balloon aortic occlusion was used in more than 70% in each cohort,” Dr. Kilic said. Those differences were similar in the propensity-matched cohort: bypass times were 147.5 minutes for isolated MIMV surgery and 174.6 minutes for MIMV-TVS (P less than .001); and aortic occlusion time 104.8 vs. 128 minutes (P less than .001), respectively.
Operative mortality was 3% for isolated MIMV surgery and 4% for concurrent MIMV-TVS (P = .73), but the isolated MIMV surgery group required fewer permanent pacemakers, 1% vs. 6% (P = .03).
“Aside from permanent pacemaker implantation, the rates of every other complication were similar, including stoke, limb ischemia, atrial fibrillation, gastrointestinal complications, respiratory complications, blood product transfusions as well as discharge to home rates,” Dr. Kilic said. Median hospital length of stays were also similar: 7 days for isolated MIMV surgery vs. 8 days for MIMV-TVS (P = .13).
One limitation of the study Dr. Kilic pointed out was that the decision to perform concomitant MIMV-TVS was surgeon dependent.
Dr. Kilic reported having no financial disclosures.
NEW YORK – Concurrent mitral-tricuspid valve surgery has similar outcomes to isolated minimally invasive mitral valve surgery, according to results of a 12-year review reported at the 2017 Mitral Valve Conclave, sponsored by the American Association for Thoracic Surgery.
Indications for minimally invasive tricuspid valve surgery done at the same time of mitral valve surgery have not been well established, in part because the outcomes of such combined procedures have been underreported.
Dr. Kilic noted that patients who had concomitant TVS were typically higher risk at baseline. “The concomitant group was older, had a higher percentage of female patients, and higher rates of chronic lung disease and cerebrovascular disease as well,” Dr. Kilic said. In comparing the isolated MIMV surgery and MIMV-TVS groups in the unmatched analysis, 9% vs. 14% had chronic lung disease (P = .05), 12% vs. 16% had coronary artery disease (P = .15), 7% vs. 12% had cerebrovascular disease (P = .04), and 93% vs. 90% had elective surgery (P = .18). The majority of tricuspid repairs were for severe tricuspid regurgitation (TR) or moderate TR with a dilated annulus of 40 mm or greater.
The operative characteristics differed significantly between the two groups. “As one might expect, the cardiopulmonary bypass time and aortic occlusion times were longer in the concomitant group; and balloon aortic occlusion was used in more than 70% in each cohort,” Dr. Kilic said. Those differences were similar in the propensity-matched cohort: bypass times were 147.5 minutes for isolated MIMV surgery and 174.6 minutes for MIMV-TVS (P less than .001); and aortic occlusion time 104.8 vs. 128 minutes (P less than .001), respectively.
Operative mortality was 3% for isolated MIMV surgery and 4% for concurrent MIMV-TVS (P = .73), but the isolated MIMV surgery group required fewer permanent pacemakers, 1% vs. 6% (P = .03).
“Aside from permanent pacemaker implantation, the rates of every other complication were similar, including stoke, limb ischemia, atrial fibrillation, gastrointestinal complications, respiratory complications, blood product transfusions as well as discharge to home rates,” Dr. Kilic said. Median hospital length of stays were also similar: 7 days for isolated MIMV surgery vs. 8 days for MIMV-TVS (P = .13).
One limitation of the study Dr. Kilic pointed out was that the decision to perform concomitant MIMV-TVS was surgeon dependent.
Dr. Kilic reported having no financial disclosures.
NEW YORK – Concurrent mitral-tricuspid valve surgery has similar outcomes to isolated minimally invasive mitral valve surgery, according to results of a 12-year review reported at the 2017 Mitral Valve Conclave, sponsored by the American Association for Thoracic Surgery.
Indications for minimally invasive tricuspid valve surgery done at the same time of mitral valve surgery have not been well established, in part because the outcomes of such combined procedures have been underreported.
Dr. Kilic noted that patients who had concomitant TVS were typically higher risk at baseline. “The concomitant group was older, had a higher percentage of female patients, and higher rates of chronic lung disease and cerebrovascular disease as well,” Dr. Kilic said. In comparing the isolated MIMV surgery and MIMV-TVS groups in the unmatched analysis, 9% vs. 14% had chronic lung disease (P = .05), 12% vs. 16% had coronary artery disease (P = .15), 7% vs. 12% had cerebrovascular disease (P = .04), and 93% vs. 90% had elective surgery (P = .18). The majority of tricuspid repairs were for severe tricuspid regurgitation (TR) or moderate TR with a dilated annulus of 40 mm or greater.
The operative characteristics differed significantly between the two groups. “As one might expect, the cardiopulmonary bypass time and aortic occlusion times were longer in the concomitant group; and balloon aortic occlusion was used in more than 70% in each cohort,” Dr. Kilic said. Those differences were similar in the propensity-matched cohort: bypass times were 147.5 minutes for isolated MIMV surgery and 174.6 minutes for MIMV-TVS (P less than .001); and aortic occlusion time 104.8 vs. 128 minutes (P less than .001), respectively.
Operative mortality was 3% for isolated MIMV surgery and 4% for concurrent MIMV-TVS (P = .73), but the isolated MIMV surgery group required fewer permanent pacemakers, 1% vs. 6% (P = .03).
“Aside from permanent pacemaker implantation, the rates of every other complication were similar, including stoke, limb ischemia, atrial fibrillation, gastrointestinal complications, respiratory complications, blood product transfusions as well as discharge to home rates,” Dr. Kilic said. Median hospital length of stays were also similar: 7 days for isolated MIMV surgery vs. 8 days for MIMV-TVS (P = .13).
One limitation of the study Dr. Kilic pointed out was that the decision to perform concomitant MIMV-TVS was surgeon dependent.
Dr. Kilic reported having no financial disclosures.
AT THE 2017 MITRAL VALVE CONCLAVE
Key clinical point: Outcomes of isolated minimally invasive mitral valve surgery (MIMV) and MIMV with concomitant tricuspid valve surgery (TVS) are similar.
Major finding: Operative mortality was 3% for isolated MIMV and 4% for concurrent MIMV-TVS.
Data source: Single-center review of 1,158 patients who underwent either isolated MIMV or MIMV-TVS from 2002 to 2014, including a propensity-matched cohort.
Disclosures: Dr. Kilic reported having no financial disclosures.
Is female genital cosmetic surgery going mainstream?
Experts describe the field of female genital cosmetic surgery as the “Wild West,” but the lack of regulation and consensus has not kept it from exploding in recent years.
More than 10,000 labiaplasties were performed in 2016, a 23% jump over the previous year, and the procedures are offered by more than 35% of all plastic surgeons, according to data from the American Society for Aesthetic Plastic Surgery. As another indicator of increasing attention to the appearance of female genitalia, a 2013 survey of U.S. women revealed that more than 80% performed some sort of pubic hair grooming (JAMA Dermatol. 2016;152[10]:1106-13).

Dr. Iglesia recounted being contacted by a National Gallery of Art staff member, who, when confronted with Gustave Courbet’s L’Origine du Monde, an 1866 below-the-waist portrait of a nude woman, asked, “Is this normal? Do women have this much hair?” Dr. Iglesia said she reassured the staff member that the woman in the portrait did indeed have a normal female Tanner stage IV or V escutcheon. However, she said, social media and other images in the popular press have essentially erased female pubic hair from the public eye, even in explicit imagery that involves female nudity.
“This is an ideal that men and women are seeing in social media, in pornography, and even in the lay press.” And now, she said, “We’re in a new era of sex surgeries, with these ‘nips and tucks’ below the belt.”
Labiaplasty
The combination of a newly-hairless genital region, together with portrayals of adult women with a “Barbie doll” appearance, may contribute to women feeling self-conscious about labia minora protruding beyond the labia majora. Dr. Iglesia, who is section director for female pelvic medicine and reconstructive surgery at MedStar Washington Hospital Center, Washington, D.C., said this is true even though the normal length of labia minora can range from 7 mm to 5 cm.
That’s where labiaplasty comes in. The procedure, which can be performed with conventional surgical techniques or with a laser, is sometimes done for functional reasons.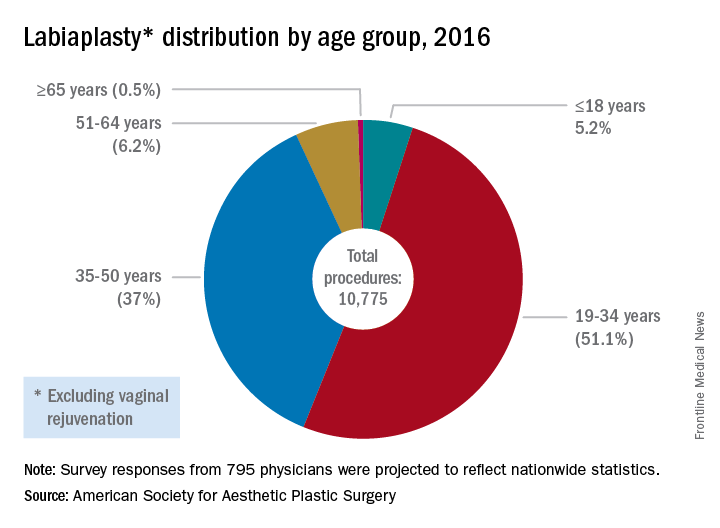
The waters are murkier when labiaplasty is performed for cosmetic reasons, to get that “Barbie doll” look, with some offices advertising the procedure as “designer lips,” Dr. Iglesia said.
In 2007, ACOG issued a committee opinion expressing concern about the lack of data and sometimes deceptive marketing practices surrounding a number of cosmetic vaginal surgeries (Obstet Gynecol 2007;110:737–8). The policy was reaffirmed in 2017.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/is-it-appropriate-to-perform-gynecologic-procedures-such-as-labiaplasty-for-cosmetic-reasons?iframe=1"}]Similarly, the Society of Obstetricians and Gynaecologists of Canada issued a 2013 statement about labiaplasty and other female genital cosmetic surgeries saying that “there is little evidence to support any of the female genital cosmetic surgeries in terms of improvement to sexual satisfaction or self-images. Physicians choosing to proceed with these cosmetic procedures should not promote these surgeries for the enhancement of sexual function and advertising of female genital cosmetic surgical procedures should be avoided.”
However, Mickey Karram, MD, who is director of the urogynecology program at Christ Hospital, Cincinnatti, said that informed consent is the key to dealing appropriately with these procedures.
“If a patient is physically bothered from a cosmetic standpoint that her labia are larger than she thinks they should be, and they are bothering her, is it appropriate or inappropriate to potentially discuss with her a labiaplasty?” Dr. Karram said at the ACOG meeting. For the patient who understands the risk and is also clear that the procedure is not medically necessary, he said he “feels strongly” that labiaplasty should be an option.
Fractional laser
The introduction of the fractional laser to gynecology is also adding to the debate about the appropriate integration of gynecologic procedures that may have nonmedical uses, such as vaginal “tightening.” Used primarily intravaginally, these devices have shallow penetration and are meant to stimulate collagen, proteoglycan, and hyaluronic acid synthesis with minimal tissue damage and downtime. One such device, the MonaLisa Touch, is marketed in the United States by Cynosure.
These energy sources hold great promise for the genitourinary syndrome of menopause (GSM) and other conditions, Dr. Karram said. “Many of these energy sources are being promoted for actual disease states, like vulvovaginal atrophy and lichen sclerosus,” he said.
Dr. Iglesia is not so sure: “This is not the fountain of youth.” She pointed out that the vasculature and innervation of the vagina and vulva are complex, with the outer one-eighth of the vagina being much more highly innervated. Laser treatment with a shallow penetration depth may not get at all of the issues that contribute to GSM.
“Is marketing ahead of the science? I would say yes,” she said. “There’s too much hype about this curing vaginal dryness and making your sex life better.”
Dr. Zahn also urged caution with the use of this technology. “The data are very limited, but, despite this, it’s become a very popular and highly-advertised approach. We need larger studies and more longitudinal data. This is especially true since one of the proposed ways this device works is by stimulating fibrosis. In every other body system, fibrosis stimulation may result in scarring. We have no idea if this is the case with this device. If it is, its application could result in worsening of bodily function, especially in regard to dyspareunia,” he said. “We clearly need more data.”
In 2016, ACOG issued a position statement about the fractional carbon dioxide and yttrium-aluminum-garnet laser systems that had received clearance from the Food and Drug Administration. The statement advised both ob.gyns. and patients that “this technology is, in fact, neither approved nor cleared by the FDA for the specific indication of treating vulvovaginal atrophy.”
Both Dr. Karram and Dr. Iglesia are investigators in an ongoing randomized, placebo- and sham-controlled trial comparing vaginal estrogen and laser therapy used both in conjunction and singly.
‘No-go’ procedures
Though Dr. Karram and Dr. Iglesia disagree on whether cosmetic labiaplasty is appropriate, they were in agreement that certain procedures are so untested, or have such potential risk with no proven benefit, that they should not be performed at all. The procedures on both physicians’ “no-go” lists included clitoral unhooding, G-spot amplification, “revirginification” in any form, vulval recontouring with autologous fat, and the so-called “O-shot,” injections of platelet-rich plasma that are touted as augmenting the sexual experience.
What’s to be done?
There is also agreement that a lack of common terminology is a significant problem. Step one, Dr. Karram said, is doing away with the term vaginal rejuvenation. “This is a terrible term. … There’s no real definition for this term.” He called for a multidisciplinary working group that would bring together gynecologists, plastic surgeons, and dermatologists to begin the work of terminology standardization.
From there, he proposed that the group develop a classification system that clarifies whether procedures are being done for cosmetic reasons, to enhance the sexual experience, or to address a specific disease state. Finally, he said, the group should recommend standardized outcome metrics that can be used to study the various interventions.
Dr. Zahn applauded this notion. “It’s a great point. I agree that multiple disciplines should be involved in examining outcomes, statistics, and criteria for evaluating procedures.”
And gynecologists should be leading this effort, Dr. Karram suggested. “Who knows this anatomy the best? We do.” He added, “If it’s going to be addressed, it should be addressed by us.”
But, Dr. Iglesia said she worries about vulnerable populations, such as adolescents and cancer survivors, who may undergo surgeries, for which the benefits may not outweigh the potential risks. For labiaplasty and laser resurfacing techniques, there have been a small number of studies on outcomes and patient satisfaction that have generally been conducted at single centers with no comparison arms and limited follow-up, she said.
“I also am concerned about pain, scarring, altered sensation, painful sex that could develop, wound complications, and what happens over time,” especially when these procedures may be performed on adolescents or women in their 20s or 30s who may later go on to have children, Dr. Iglesia said.
The question, she said, is not just whether gynecologists are better equipped than plastic surgeons or dermatologists to be performing female genital cosmetic surgery, “but should we be doing this at all?”
Dr. Zahn emphasized the need for evidence to guide decision making. “There has to be data that there is benefit and that the benefit outweighs the potential harm. There is no data on most cosmetic gynecologic procedures. If there are no data, they shouldn’t be done because we would not have the information necessary to appropriately counsel patients,” he said.
Dr. Karram has a financial relationship with Cynosure, which markets the MonaLisa Touch system in the United States. Dr. Iglesia reported that she had no relevant financial disclosures. Dr. Zahn is employed by ACOG.
[email protected]
On Twitter @karioakes
Experts describe the field of female genital cosmetic surgery as the “Wild West,” but the lack of regulation and consensus has not kept it from exploding in recent years.
More than 10,000 labiaplasties were performed in 2016, a 23% jump over the previous year, and the procedures are offered by more than 35% of all plastic surgeons, according to data from the American Society for Aesthetic Plastic Surgery. As another indicator of increasing attention to the appearance of female genitalia, a 2013 survey of U.S. women revealed that more than 80% performed some sort of pubic hair grooming (JAMA Dermatol. 2016;152[10]:1106-13).
Dr. Iglesia recounted being contacted by a National Gallery of Art staff member, who, when confronted with Gustave Courbet’s L’Origine du Monde, an 1866 below-the-waist portrait of a nude woman, asked, “Is this normal? Do women have this much hair?” Dr. Iglesia said she reassured the staff member that the woman in the portrait did indeed have a normal female Tanner stage IV or V escutcheon. However, she said, social media and other images in the popular press have essentially erased female pubic hair from the public eye, even in explicit imagery that involves female nudity.
“This is an ideal that men and women are seeing in social media, in pornography, and even in the lay press.” And now, she said, “We’re in a new era of sex surgeries, with these ‘nips and tucks’ below the belt.”
Labiaplasty
The combination of a newly-hairless genital region, together with portrayals of adult women with a “Barbie doll” appearance, may contribute to women feeling self-conscious about labia minora protruding beyond the labia majora. Dr. Iglesia, who is section director for female pelvic medicine and reconstructive surgery at MedStar Washington Hospital Center, Washington, D.C., said this is true even though the normal length of labia minora can range from 7 mm to 5 cm.
That’s where labiaplasty comes in. The procedure, which can be performed with conventional surgical techniques or with a laser, is sometimes done for functional reasons.
The waters are murkier when labiaplasty is performed for cosmetic reasons, to get that “Barbie doll” look, with some offices advertising the procedure as “designer lips,” Dr. Iglesia said.
In 2007, ACOG issued a committee opinion expressing concern about the lack of data and sometimes deceptive marketing practices surrounding a number of cosmetic vaginal surgeries (Obstet Gynecol 2007;110:737–8). The policy was reaffirmed in 2017.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/is-it-appropriate-to-perform-gynecologic-procedures-such-as-labiaplasty-for-cosmetic-reasons?iframe=1"}]Similarly, the Society of Obstetricians and Gynaecologists of Canada issued a 2013 statement about labiaplasty and other female genital cosmetic surgeries saying that “there is little evidence to support any of the female genital cosmetic surgeries in terms of improvement to sexual satisfaction or self-images. Physicians choosing to proceed with these cosmetic procedures should not promote these surgeries for the enhancement of sexual function and advertising of female genital cosmetic surgical procedures should be avoided.”
However, Mickey Karram, MD, who is director of the urogynecology program at Christ Hospital, Cincinnatti, said that informed consent is the key to dealing appropriately with these procedures.
“If a patient is physically bothered from a cosmetic standpoint that her labia are larger than she thinks they should be, and they are bothering her, is it appropriate or inappropriate to potentially discuss with her a labiaplasty?” Dr. Karram said at the ACOG meeting. For the patient who understands the risk and is also clear that the procedure is not medically necessary, he said he “feels strongly” that labiaplasty should be an option.
Fractional laser
The introduction of the fractional laser to gynecology is also adding to the debate about the appropriate integration of gynecologic procedures that may have nonmedical uses, such as vaginal “tightening.” Used primarily intravaginally, these devices have shallow penetration and are meant to stimulate collagen, proteoglycan, and hyaluronic acid synthesis with minimal tissue damage and downtime. One such device, the MonaLisa Touch, is marketed in the United States by Cynosure.
These energy sources hold great promise for the genitourinary syndrome of menopause (GSM) and other conditions, Dr. Karram said. “Many of these energy sources are being promoted for actual disease states, like vulvovaginal atrophy and lichen sclerosus,” he said.
Dr. Iglesia is not so sure: “This is not the fountain of youth.” She pointed out that the vasculature and innervation of the vagina and vulva are complex, with the outer one-eighth of the vagina being much more highly innervated. Laser treatment with a shallow penetration depth may not get at all of the issues that contribute to GSM.
“Is marketing ahead of the science? I would say yes,” she said. “There’s too much hype about this curing vaginal dryness and making your sex life better.”
Dr. Zahn also urged caution with the use of this technology. “The data are very limited, but, despite this, it’s become a very popular and highly-advertised approach. We need larger studies and more longitudinal data. This is especially true since one of the proposed ways this device works is by stimulating fibrosis. In every other body system, fibrosis stimulation may result in scarring. We have no idea if this is the case with this device. If it is, its application could result in worsening of bodily function, especially in regard to dyspareunia,” he said. “We clearly need more data.”
In 2016, ACOG issued a position statement about the fractional carbon dioxide and yttrium-aluminum-garnet laser systems that had received clearance from the Food and Drug Administration. The statement advised both ob.gyns. and patients that “this technology is, in fact, neither approved nor cleared by the FDA for the specific indication of treating vulvovaginal atrophy.”
Both Dr. Karram and Dr. Iglesia are investigators in an ongoing randomized, placebo- and sham-controlled trial comparing vaginal estrogen and laser therapy used both in conjunction and singly.
‘No-go’ procedures
Though Dr. Karram and Dr. Iglesia disagree on whether cosmetic labiaplasty is appropriate, they were in agreement that certain procedures are so untested, or have such potential risk with no proven benefit, that they should not be performed at all. The procedures on both physicians’ “no-go” lists included clitoral unhooding, G-spot amplification, “revirginification” in any form, vulval recontouring with autologous fat, and the so-called “O-shot,” injections of platelet-rich plasma that are touted as augmenting the sexual experience.
What’s to be done?
There is also agreement that a lack of common terminology is a significant problem. Step one, Dr. Karram said, is doing away with the term vaginal rejuvenation. “This is a terrible term. … There’s no real definition for this term.” He called for a multidisciplinary working group that would bring together gynecologists, plastic surgeons, and dermatologists to begin the work of terminology standardization.
From there, he proposed that the group develop a classification system that clarifies whether procedures are being done for cosmetic reasons, to enhance the sexual experience, or to address a specific disease state. Finally, he said, the group should recommend standardized outcome metrics that can be used to study the various interventions.
Dr. Zahn applauded this notion. “It’s a great point. I agree that multiple disciplines should be involved in examining outcomes, statistics, and criteria for evaluating procedures.”
And gynecologists should be leading this effort, Dr. Karram suggested. “Who knows this anatomy the best? We do.” He added, “If it’s going to be addressed, it should be addressed by us.”
But, Dr. Iglesia said she worries about vulnerable populations, such as adolescents and cancer survivors, who may undergo surgeries, for which the benefits may not outweigh the potential risks. For labiaplasty and laser resurfacing techniques, there have been a small number of studies on outcomes and patient satisfaction that have generally been conducted at single centers with no comparison arms and limited follow-up, she said.
“I also am concerned about pain, scarring, altered sensation, painful sex that could develop, wound complications, and what happens over time,” especially when these procedures may be performed on adolescents or women in their 20s or 30s who may later go on to have children, Dr. Iglesia said.
The question, she said, is not just whether gynecologists are better equipped than plastic surgeons or dermatologists to be performing female genital cosmetic surgery, “but should we be doing this at all?”
Dr. Zahn emphasized the need for evidence to guide decision making. “There has to be data that there is benefit and that the benefit outweighs the potential harm. There is no data on most cosmetic gynecologic procedures. If there are no data, they shouldn’t be done because we would not have the information necessary to appropriately counsel patients,” he said.
Dr. Karram has a financial relationship with Cynosure, which markets the MonaLisa Touch system in the United States. Dr. Iglesia reported that she had no relevant financial disclosures. Dr. Zahn is employed by ACOG.
[email protected]
On Twitter @karioakes
Experts describe the field of female genital cosmetic surgery as the “Wild West,” but the lack of regulation and consensus has not kept it from exploding in recent years.
More than 10,000 labiaplasties were performed in 2016, a 23% jump over the previous year, and the procedures are offered by more than 35% of all plastic surgeons, according to data from the American Society for Aesthetic Plastic Surgery. As another indicator of increasing attention to the appearance of female genitalia, a 2013 survey of U.S. women revealed that more than 80% performed some sort of pubic hair grooming (JAMA Dermatol. 2016;152[10]:1106-13).
Dr. Iglesia recounted being contacted by a National Gallery of Art staff member, who, when confronted with Gustave Courbet’s L’Origine du Monde, an 1866 below-the-waist portrait of a nude woman, asked, “Is this normal? Do women have this much hair?” Dr. Iglesia said she reassured the staff member that the woman in the portrait did indeed have a normal female Tanner stage IV or V escutcheon. However, she said, social media and other images in the popular press have essentially erased female pubic hair from the public eye, even in explicit imagery that involves female nudity.
“This is an ideal that men and women are seeing in social media, in pornography, and even in the lay press.” And now, she said, “We’re in a new era of sex surgeries, with these ‘nips and tucks’ below the belt.”
Labiaplasty
The combination of a newly-hairless genital region, together with portrayals of adult women with a “Barbie doll” appearance, may contribute to women feeling self-conscious about labia minora protruding beyond the labia majora. Dr. Iglesia, who is section director for female pelvic medicine and reconstructive surgery at MedStar Washington Hospital Center, Washington, D.C., said this is true even though the normal length of labia minora can range from 7 mm to 5 cm.
That’s where labiaplasty comes in. The procedure, which can be performed with conventional surgical techniques or with a laser, is sometimes done for functional reasons.
The waters are murkier when labiaplasty is performed for cosmetic reasons, to get that “Barbie doll” look, with some offices advertising the procedure as “designer lips,” Dr. Iglesia said.
In 2007, ACOG issued a committee opinion expressing concern about the lack of data and sometimes deceptive marketing practices surrounding a number of cosmetic vaginal surgeries (Obstet Gynecol 2007;110:737–8). The policy was reaffirmed in 2017.
[polldaddy:{"method":"iframe","type":"survey","src":"//newspolls2017.polldaddy.com/s/is-it-appropriate-to-perform-gynecologic-procedures-such-as-labiaplasty-for-cosmetic-reasons?iframe=1"}]Similarly, the Society of Obstetricians and Gynaecologists of Canada issued a 2013 statement about labiaplasty and other female genital cosmetic surgeries saying that “there is little evidence to support any of the female genital cosmetic surgeries in terms of improvement to sexual satisfaction or self-images. Physicians choosing to proceed with these cosmetic procedures should not promote these surgeries for the enhancement of sexual function and advertising of female genital cosmetic surgical procedures should be avoided.”
However, Mickey Karram, MD, who is director of the urogynecology program at Christ Hospital, Cincinnatti, said that informed consent is the key to dealing appropriately with these procedures.
“If a patient is physically bothered from a cosmetic standpoint that her labia are larger than she thinks they should be, and they are bothering her, is it appropriate or inappropriate to potentially discuss with her a labiaplasty?” Dr. Karram said at the ACOG meeting. For the patient who understands the risk and is also clear that the procedure is not medically necessary, he said he “feels strongly” that labiaplasty should be an option.
Fractional laser
The introduction of the fractional laser to gynecology is also adding to the debate about the appropriate integration of gynecologic procedures that may have nonmedical uses, such as vaginal “tightening.” Used primarily intravaginally, these devices have shallow penetration and are meant to stimulate collagen, proteoglycan, and hyaluronic acid synthesis with minimal tissue damage and downtime. One such device, the MonaLisa Touch, is marketed in the United States by Cynosure.
These energy sources hold great promise for the genitourinary syndrome of menopause (GSM) and other conditions, Dr. Karram said. “Many of these energy sources are being promoted for actual disease states, like vulvovaginal atrophy and lichen sclerosus,” he said.
Dr. Iglesia is not so sure: “This is not the fountain of youth.” She pointed out that the vasculature and innervation of the vagina and vulva are complex, with the outer one-eighth of the vagina being much more highly innervated. Laser treatment with a shallow penetration depth may not get at all of the issues that contribute to GSM.
“Is marketing ahead of the science? I would say yes,” she said. “There’s too much hype about this curing vaginal dryness and making your sex life better.”
Dr. Zahn also urged caution with the use of this technology. “The data are very limited, but, despite this, it’s become a very popular and highly-advertised approach. We need larger studies and more longitudinal data. This is especially true since one of the proposed ways this device works is by stimulating fibrosis. In every other body system, fibrosis stimulation may result in scarring. We have no idea if this is the case with this device. If it is, its application could result in worsening of bodily function, especially in regard to dyspareunia,” he said. “We clearly need more data.”
In 2016, ACOG issued a position statement about the fractional carbon dioxide and yttrium-aluminum-garnet laser systems that had received clearance from the Food and Drug Administration. The statement advised both ob.gyns. and patients that “this technology is, in fact, neither approved nor cleared by the FDA for the specific indication of treating vulvovaginal atrophy.”
Both Dr. Karram and Dr. Iglesia are investigators in an ongoing randomized, placebo- and sham-controlled trial comparing vaginal estrogen and laser therapy used both in conjunction and singly.
‘No-go’ procedures
Though Dr. Karram and Dr. Iglesia disagree on whether cosmetic labiaplasty is appropriate, they were in agreement that certain procedures are so untested, or have such potential risk with no proven benefit, that they should not be performed at all. The procedures on both physicians’ “no-go” lists included clitoral unhooding, G-spot amplification, “revirginification” in any form, vulval recontouring with autologous fat, and the so-called “O-shot,” injections of platelet-rich plasma that are touted as augmenting the sexual experience.
What’s to be done?
There is also agreement that a lack of common terminology is a significant problem. Step one, Dr. Karram said, is doing away with the term vaginal rejuvenation. “This is a terrible term. … There’s no real definition for this term.” He called for a multidisciplinary working group that would bring together gynecologists, plastic surgeons, and dermatologists to begin the work of terminology standardization.
From there, he proposed that the group develop a classification system that clarifies whether procedures are being done for cosmetic reasons, to enhance the sexual experience, or to address a specific disease state. Finally, he said, the group should recommend standardized outcome metrics that can be used to study the various interventions.
Dr. Zahn applauded this notion. “It’s a great point. I agree that multiple disciplines should be involved in examining outcomes, statistics, and criteria for evaluating procedures.”
And gynecologists should be leading this effort, Dr. Karram suggested. “Who knows this anatomy the best? We do.” He added, “If it’s going to be addressed, it should be addressed by us.”
But, Dr. Iglesia said she worries about vulnerable populations, such as adolescents and cancer survivors, who may undergo surgeries, for which the benefits may not outweigh the potential risks. For labiaplasty and laser resurfacing techniques, there have been a small number of studies on outcomes and patient satisfaction that have generally been conducted at single centers with no comparison arms and limited follow-up, she said.
“I also am concerned about pain, scarring, altered sensation, painful sex that could develop, wound complications, and what happens over time,” especially when these procedures may be performed on adolescents or women in their 20s or 30s who may later go on to have children, Dr. Iglesia said.
The question, she said, is not just whether gynecologists are better equipped than plastic surgeons or dermatologists to be performing female genital cosmetic surgery, “but should we be doing this at all?”
Dr. Zahn emphasized the need for evidence to guide decision making. “There has to be data that there is benefit and that the benefit outweighs the potential harm. There is no data on most cosmetic gynecologic procedures. If there are no data, they shouldn’t be done because we would not have the information necessary to appropriately counsel patients,” he said.
Dr. Karram has a financial relationship with Cynosure, which markets the MonaLisa Touch system in the United States. Dr. Iglesia reported that she had no relevant financial disclosures. Dr. Zahn is employed by ACOG.
[email protected]
On Twitter @karioakes
Imaging after bariatric surgery appears overdone
Nearly 70% of bariatric surgery patients received postoperative imaging, with more than one-third receiving CT imaging. This high level of screening resulted in symptom-related findings in only 23% of cases, and may be excessive, according to researchers who studied nearly 600 adults who underwent bariatric surgery.
As the volume of bariatric surgery has increased, so has the role of postoperative imaging, wrote Dana Haddad, MD, and her colleagues at Harlem Hospital Center, New York.
“However, there is a lack of well-defined postoperative imaging guidelines,” they said. “Detrimental aspects of postoperative imaging include the potential for false-positive findings leading to further and often unnecessary investigations, radiation exposure, and additional cost,” they added.
The primary outcomes were the numbers of initial postimaging studies and whether the findings supported subsequent studies.
The study population included 399 adults who underwent laparoscopic bypass and 144 who underwent sleeve gastrectomy. The average age of the patients was 41 years and 90% were women.
The researchers identified 907 imaging studies performed in 400 patients (69% of the study population). Of these, 38% were ultrasound, 36% were CT, 15% were x-ray, 6.6% were fluoroscopy, 3.3% were MRI, and .6% were nuclear medicine.
On review of the imaging findings, the researchers found that half (50%) were unremarkable, while 13% were either surgery related or symptom related, 6.8% were not related to surgery but might have explained patients’ symptoms, 4.3% were surgery-related but not likely to explain symptoms, and 26% were incidental. “Interestingly, no incidental findings were found to be of major clinical importance; all were benign,” according to the researchers.
However, incidental findings led to a total of 71 additional studies, and to 5 laparoscopic cholecystectomies.
A univariate analysis showed that the factors with a significant impact a patient’s odds of undergoing postoperative abdominal imaging included having a bypass procedure vs. a sleeve procedure, older age, and lower baseline body mass index. In addition, patients with a history of abdominal surgery or dyspepsia or those who had a routine postoperative upper gastrointestinal series were significantly more likely to undergo CT scans. Patients with history of ulcer or reflux were significantly less likely to undergo CT scans.
Although the study was limited by the retrospective design and lack of information about possible imaging of patients at other centers, “results suggest that nonroutine postoperative abdominal imaging in the bariatric population is common and requires streamlined protocols, with almost 70% of patients undergoing imaging and greater than 70% of findings being unrelated to symptoms or negative,” the researchers said.
A clinical algorithm for imaging of bariatric patients should be based on clinical parameters collected during a physical exam. “Once an algorithm is in place, further studies will be needed to validate its accuracy and efficiency,” the researchers stated.
Dr. Haddad and her colleagues had no financial conflicts to disclose.
Nearly 70% of bariatric surgery patients received postoperative imaging, with more than one-third receiving CT imaging. This high level of screening resulted in symptom-related findings in only 23% of cases, and may be excessive, according to researchers who studied nearly 600 adults who underwent bariatric surgery.
As the volume of bariatric surgery has increased, so has the role of postoperative imaging, wrote Dana Haddad, MD, and her colleagues at Harlem Hospital Center, New York.
“However, there is a lack of well-defined postoperative imaging guidelines,” they said. “Detrimental aspects of postoperative imaging include the potential for false-positive findings leading to further and often unnecessary investigations, radiation exposure, and additional cost,” they added.
The primary outcomes were the numbers of initial postimaging studies and whether the findings supported subsequent studies.
The study population included 399 adults who underwent laparoscopic bypass and 144 who underwent sleeve gastrectomy. The average age of the patients was 41 years and 90% were women.
The researchers identified 907 imaging studies performed in 400 patients (69% of the study population). Of these, 38% were ultrasound, 36% were CT, 15% were x-ray, 6.6% were fluoroscopy, 3.3% were MRI, and .6% were nuclear medicine.
On review of the imaging findings, the researchers found that half (50%) were unremarkable, while 13% were either surgery related or symptom related, 6.8% were not related to surgery but might have explained patients’ symptoms, 4.3% were surgery-related but not likely to explain symptoms, and 26% were incidental. “Interestingly, no incidental findings were found to be of major clinical importance; all were benign,” according to the researchers.
However, incidental findings led to a total of 71 additional studies, and to 5 laparoscopic cholecystectomies.
A univariate analysis showed that the factors with a significant impact a patient’s odds of undergoing postoperative abdominal imaging included having a bypass procedure vs. a sleeve procedure, older age, and lower baseline body mass index. In addition, patients with a history of abdominal surgery or dyspepsia or those who had a routine postoperative upper gastrointestinal series were significantly more likely to undergo CT scans. Patients with history of ulcer or reflux were significantly less likely to undergo CT scans.
Although the study was limited by the retrospective design and lack of information about possible imaging of patients at other centers, “results suggest that nonroutine postoperative abdominal imaging in the bariatric population is common and requires streamlined protocols, with almost 70% of patients undergoing imaging and greater than 70% of findings being unrelated to symptoms or negative,” the researchers said.
A clinical algorithm for imaging of bariatric patients should be based on clinical parameters collected during a physical exam. “Once an algorithm is in place, further studies will be needed to validate its accuracy and efficiency,” the researchers stated.
Dr. Haddad and her colleagues had no financial conflicts to disclose.
Nearly 70% of bariatric surgery patients received postoperative imaging, with more than one-third receiving CT imaging. This high level of screening resulted in symptom-related findings in only 23% of cases, and may be excessive, according to researchers who studied nearly 600 adults who underwent bariatric surgery.
As the volume of bariatric surgery has increased, so has the role of postoperative imaging, wrote Dana Haddad, MD, and her colleagues at Harlem Hospital Center, New York.
“However, there is a lack of well-defined postoperative imaging guidelines,” they said. “Detrimental aspects of postoperative imaging include the potential for false-positive findings leading to further and often unnecessary investigations, radiation exposure, and additional cost,” they added.
The primary outcomes were the numbers of initial postimaging studies and whether the findings supported subsequent studies.
The study population included 399 adults who underwent laparoscopic bypass and 144 who underwent sleeve gastrectomy. The average age of the patients was 41 years and 90% were women.
The researchers identified 907 imaging studies performed in 400 patients (69% of the study population). Of these, 38% were ultrasound, 36% were CT, 15% were x-ray, 6.6% were fluoroscopy, 3.3% were MRI, and .6% were nuclear medicine.
On review of the imaging findings, the researchers found that half (50%) were unremarkable, while 13% were either surgery related or symptom related, 6.8% were not related to surgery but might have explained patients’ symptoms, 4.3% were surgery-related but not likely to explain symptoms, and 26% were incidental. “Interestingly, no incidental findings were found to be of major clinical importance; all were benign,” according to the researchers.
However, incidental findings led to a total of 71 additional studies, and to 5 laparoscopic cholecystectomies.
A univariate analysis showed that the factors with a significant impact a patient’s odds of undergoing postoperative abdominal imaging included having a bypass procedure vs. a sleeve procedure, older age, and lower baseline body mass index. In addition, patients with a history of abdominal surgery or dyspepsia or those who had a routine postoperative upper gastrointestinal series were significantly more likely to undergo CT scans. Patients with history of ulcer or reflux were significantly less likely to undergo CT scans.
Although the study was limited by the retrospective design and lack of information about possible imaging of patients at other centers, “results suggest that nonroutine postoperative abdominal imaging in the bariatric population is common and requires streamlined protocols, with almost 70% of patients undergoing imaging and greater than 70% of findings being unrelated to symptoms or negative,” the researchers said.
A clinical algorithm for imaging of bariatric patients should be based on clinical parameters collected during a physical exam. “Once an algorithm is in place, further studies will be needed to validate its accuracy and efficiency,” the researchers stated.
Dr. Haddad and her colleagues had no financial conflicts to disclose.
FROM SURGERY FOR OBESITY AND RELATED DISEASES
Key clinical point: No well-defined guidelines exist for when to use postoperative imaging in bariatric surgery patients.
Major finding: Approximately 70% of postoperative imaging findings were not symptom related, and incidental findings led to 71 additional studies.
Data source: A review of 578 patients who underwent gastric bypass or sleeve gastrectomy.
Disclosures: The researchers had no financial conflicts to disclose.
Colonoscopy patients prefer propofol over fentanyl/midazolam
SEATTLE – As patient satisfaction becomes increasingly important for reimbursements, it might be a good idea to switch to propofol for colonoscopies.
The reason is because patients prefer propofol over standard-of-care fentanyl/midazolam as their anesthetic for outpatient colonoscopies, according to a randomized, blinded trial at a single center. Importantly, clinical assessment also showed that propofol outperformed fentanyl/midazolam in terms of hypoxia, pain, nausea, and procedural difficulties.
“Our study demonstrated the superiority of propofol over fentanyl/midazolam in an outpatient setting from both a patient satisfaction standpoint and from a provider prospective,” said lead investigator Anantha Padmanabhan, MD, a colorectal surgeon with Mount Carmel Health, Columbus, Ohio.
The short duration of action and quick turnaround time have led to an increase in the use of propofol for outpatient procedures. It’s been studied extensively for safety and efficacy, but patient preference has not been well documented. The investigators wanted to look into the issue because patient satisfaction has become an important metric for reimbursement, Dr. Padmanabhan said at the annual meeting of the American Society of Colon and Rectal Surgeons, where the study was presented.
Patients were randomly assigned to propofol or fentanyl/midazolam in the colonoscopy suite at the Taylor Station Surgical Center in Columbus. Anesthesia personnel administered the assigned anesthetic, and circulating nurses rated the difficulty of the procedure. Patients were surveyed after they came to, and again over the phone at least 24 hours after discharge.

Fewer propofol patients reported pain greater than zero during the procedure (2% versus 6%); fewer remembered being awake (2% versus 17%); and fewer had complications (2.7% versus 11.7%); 21 patients in the fentanyl/midazolam group had intraoperative hypoxia, versus 1 in the propofol group. Eleven fentanyl/midazolam patients had postprocedure nausea and vomiting, versus one propofol patient.
Nurses rated 26% of fentanyl/midazolam procedures as “difficult,” compared to 4.7% in the propofol group. Mean induction time was 2.1 minutes with propofol and 3.2 minutes with fentanyl/midazolam; mean procedure time was about 13 minutes in both groups. The cecal intubation rate was 100% in both groups, and there were no perforations.
Propofol patients reacted less during the procedure; an audience member wondered if the loss of feedback was a problem for Dr. Padmanabhan.
“We use propofol in a very light sedation, and sometimes we do get feedback, but more importantly we feel the technique of colonoscopy is as much by feel as it is by vision. If you feel that the scope is not going in correctly, you should pull back then try the loop reduction maneuvers,” he said.
The most common indication for colonoscopy was a history of polyps, followed by general colon screening. Patients in both groups were a mean of 61 years old, and about evenly split between the sexes. Body mass index was a mean of 30 kg/m2 in both groups. There were no between-group differences in comorbidities; hypertension and diabetes were the most common.
There was no external funding for the work, and the investigators had no disclosures.
SEATTLE – As patient satisfaction becomes increasingly important for reimbursements, it might be a good idea to switch to propofol for colonoscopies.
The reason is because patients prefer propofol over standard-of-care fentanyl/midazolam as their anesthetic for outpatient colonoscopies, according to a randomized, blinded trial at a single center. Importantly, clinical assessment also showed that propofol outperformed fentanyl/midazolam in terms of hypoxia, pain, nausea, and procedural difficulties.
“Our study demonstrated the superiority of propofol over fentanyl/midazolam in an outpatient setting from both a patient satisfaction standpoint and from a provider prospective,” said lead investigator Anantha Padmanabhan, MD, a colorectal surgeon with Mount Carmel Health, Columbus, Ohio.
The short duration of action and quick turnaround time have led to an increase in the use of propofol for outpatient procedures. It’s been studied extensively for safety and efficacy, but patient preference has not been well documented. The investigators wanted to look into the issue because patient satisfaction has become an important metric for reimbursement, Dr. Padmanabhan said at the annual meeting of the American Society of Colon and Rectal Surgeons, where the study was presented.
Patients were randomly assigned to propofol or fentanyl/midazolam in the colonoscopy suite at the Taylor Station Surgical Center in Columbus. Anesthesia personnel administered the assigned anesthetic, and circulating nurses rated the difficulty of the procedure. Patients were surveyed after they came to, and again over the phone at least 24 hours after discharge.
Fewer propofol patients reported pain greater than zero during the procedure (2% versus 6%); fewer remembered being awake (2% versus 17%); and fewer had complications (2.7% versus 11.7%); 21 patients in the fentanyl/midazolam group had intraoperative hypoxia, versus 1 in the propofol group. Eleven fentanyl/midazolam patients had postprocedure nausea and vomiting, versus one propofol patient.
Nurses rated 26% of fentanyl/midazolam procedures as “difficult,” compared to 4.7% in the propofol group. Mean induction time was 2.1 minutes with propofol and 3.2 minutes with fentanyl/midazolam; mean procedure time was about 13 minutes in both groups. The cecal intubation rate was 100% in both groups, and there were no perforations.
Propofol patients reacted less during the procedure; an audience member wondered if the loss of feedback was a problem for Dr. Padmanabhan.
“We use propofol in a very light sedation, and sometimes we do get feedback, but more importantly we feel the technique of colonoscopy is as much by feel as it is by vision. If you feel that the scope is not going in correctly, you should pull back then try the loop reduction maneuvers,” he said.
The most common indication for colonoscopy was a history of polyps, followed by general colon screening. Patients in both groups were a mean of 61 years old, and about evenly split between the sexes. Body mass index was a mean of 30 kg/m2 in both groups. There were no between-group differences in comorbidities; hypertension and diabetes were the most common.
There was no external funding for the work, and the investigators had no disclosures.
SEATTLE – As patient satisfaction becomes increasingly important for reimbursements, it might be a good idea to switch to propofol for colonoscopies.
The reason is because patients prefer propofol over standard-of-care fentanyl/midazolam as their anesthetic for outpatient colonoscopies, according to a randomized, blinded trial at a single center. Importantly, clinical assessment also showed that propofol outperformed fentanyl/midazolam in terms of hypoxia, pain, nausea, and procedural difficulties.
“Our study demonstrated the superiority of propofol over fentanyl/midazolam in an outpatient setting from both a patient satisfaction standpoint and from a provider prospective,” said lead investigator Anantha Padmanabhan, MD, a colorectal surgeon with Mount Carmel Health, Columbus, Ohio.
The short duration of action and quick turnaround time have led to an increase in the use of propofol for outpatient procedures. It’s been studied extensively for safety and efficacy, but patient preference has not been well documented. The investigators wanted to look into the issue because patient satisfaction has become an important metric for reimbursement, Dr. Padmanabhan said at the annual meeting of the American Society of Colon and Rectal Surgeons, where the study was presented.
Patients were randomly assigned to propofol or fentanyl/midazolam in the colonoscopy suite at the Taylor Station Surgical Center in Columbus. Anesthesia personnel administered the assigned anesthetic, and circulating nurses rated the difficulty of the procedure. Patients were surveyed after they came to, and again over the phone at least 24 hours after discharge.
Fewer propofol patients reported pain greater than zero during the procedure (2% versus 6%); fewer remembered being awake (2% versus 17%); and fewer had complications (2.7% versus 11.7%); 21 patients in the fentanyl/midazolam group had intraoperative hypoxia, versus 1 in the propofol group. Eleven fentanyl/midazolam patients had postprocedure nausea and vomiting, versus one propofol patient.
Nurses rated 26% of fentanyl/midazolam procedures as “difficult,” compared to 4.7% in the propofol group. Mean induction time was 2.1 minutes with propofol and 3.2 minutes with fentanyl/midazolam; mean procedure time was about 13 minutes in both groups. The cecal intubation rate was 100% in both groups, and there were no perforations.
Propofol patients reacted less during the procedure; an audience member wondered if the loss of feedback was a problem for Dr. Padmanabhan.
“We use propofol in a very light sedation, and sometimes we do get feedback, but more importantly we feel the technique of colonoscopy is as much by feel as it is by vision. If you feel that the scope is not going in correctly, you should pull back then try the loop reduction maneuvers,” he said.
The most common indication for colonoscopy was a history of polyps, followed by general colon screening. Patients in both groups were a mean of 61 years old, and about evenly split between the sexes. Body mass index was a mean of 30 kg/m2 in both groups. There were no between-group differences in comorbidities; hypertension and diabetes were the most common.
There was no external funding for the work, and the investigators had no disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point:
Major finding: The 300 patients randomized to propofol were more likely than were the 300 randomized to standard-of-care fentanyl/midazolam to state that they were “very satisfied” with their anesthesia during the procedure (86.3% versus 74%).
Data source: Randomized, blinded trial of 600 patients at a single center.
Disclosures: There was no external funding for the work, and the investigators had no disclosures.
Docs still don’t get MACRA
Seven months into the first year of the Quality Payment Program, the new value-based payment plan set up by the Medicare Access and CHIP Reauthorization Act (MACRA), and doctors’ knowledge of the program is still light.
“Physicians, especially those in small practices, need more help in preparing” for participation in QPP either through the Merit-Based Incentive Payment System (MIPS) or advanced Alternative Payment Models (APMs), according to a new report issued by the American Medical Association and consulting firm KPMG.
That said, about 70% of those surveyed responded that they have begun preparing to meet the requirements of the QPP in 2017. The survey did not make clear whether this meant meeting the minimum requirements to avoid any penalties or doing more to become eligible for potential bonus Medicare payments.
“Even those who feel prepared still don’t fully understand the financial ramifications of the program,” the report said. “In short, they may be prepared to ‘check the box’ of reporting requirements, but may lack the long-term strategic financial vision to succeed in 2018 and beyond,” noting that only 8% of the respondents said they are “very prepared” for long-term financial success. On the other side of the that spectrum, 26% said they are not at all prepared and 58% said they were slightly prepared.
Survey respondents indicated a number of areas where they need help:
• Time required to accurately capture and report performance data (66%)
• Understanding reporting requirements (58%)
• Understanding the overall MIPS scoring process (57%)
• Cost required to accurately capture and report performance data (53%)
• Organizational infrastructure needed to report performance (49%)
The report also noted the significant differences when it comes to practice size, although the differences were “not unexpected.” For example, solo practices, compared to those groups of 50 or more physicians, were “significantly more likely (56%) to view reporting requirements as very burdensome, ... significantly more like to feel ‘not at all prepared’ for long-term financial success, ... less likely to be participating in an advanced APM, [and] less likely to have begun preparing.”
Specialists, more so than primary care physicians were “slightly more likely to be deeply knowledgeable about MACRA/QPP, [and] more likely to expect to participate in MIPS (61% versus 48%) and less likely to participate in an advanced APM (15% versus 22%),” the report adds.
“Ongoing educational assistance from CMS, as well as those in the private sector, should focus on the areas where physicians need the most help: understanding requirements and potential financial impact, selection of quality measures, and clinical practice transformation strategies,” the report states.
The survey comes on the heels of CMS releasing its proposed update to the regulations surrounding the QPP for 2018. Comments on the proposed regulatory update are due to CMS on Aug. 21, 2017.
Seven months into the first year of the Quality Payment Program, the new value-based payment plan set up by the Medicare Access and CHIP Reauthorization Act (MACRA), and doctors’ knowledge of the program is still light.
“Physicians, especially those in small practices, need more help in preparing” for participation in QPP either through the Merit-Based Incentive Payment System (MIPS) or advanced Alternative Payment Models (APMs), according to a new report issued by the American Medical Association and consulting firm KPMG.
That said, about 70% of those surveyed responded that they have begun preparing to meet the requirements of the QPP in 2017. The survey did not make clear whether this meant meeting the minimum requirements to avoid any penalties or doing more to become eligible for potential bonus Medicare payments.
“Even those who feel prepared still don’t fully understand the financial ramifications of the program,” the report said. “In short, they may be prepared to ‘check the box’ of reporting requirements, but may lack the long-term strategic financial vision to succeed in 2018 and beyond,” noting that only 8% of the respondents said they are “very prepared” for long-term financial success. On the other side of the that spectrum, 26% said they are not at all prepared and 58% said they were slightly prepared.
Survey respondents indicated a number of areas where they need help:
• Time required to accurately capture and report performance data (66%)
• Understanding reporting requirements (58%)
• Understanding the overall MIPS scoring process (57%)
• Cost required to accurately capture and report performance data (53%)
• Organizational infrastructure needed to report performance (49%)
The report also noted the significant differences when it comes to practice size, although the differences were “not unexpected.” For example, solo practices, compared to those groups of 50 or more physicians, were “significantly more likely (56%) to view reporting requirements as very burdensome, ... significantly more like to feel ‘not at all prepared’ for long-term financial success, ... less likely to be participating in an advanced APM, [and] less likely to have begun preparing.”
Specialists, more so than primary care physicians were “slightly more likely to be deeply knowledgeable about MACRA/QPP, [and] more likely to expect to participate in MIPS (61% versus 48%) and less likely to participate in an advanced APM (15% versus 22%),” the report adds.
“Ongoing educational assistance from CMS, as well as those in the private sector, should focus on the areas where physicians need the most help: understanding requirements and potential financial impact, selection of quality measures, and clinical practice transformation strategies,” the report states.
The survey comes on the heels of CMS releasing its proposed update to the regulations surrounding the QPP for 2018. Comments on the proposed regulatory update are due to CMS on Aug. 21, 2017.
Seven months into the first year of the Quality Payment Program, the new value-based payment plan set up by the Medicare Access and CHIP Reauthorization Act (MACRA), and doctors’ knowledge of the program is still light.
“Physicians, especially those in small practices, need more help in preparing” for participation in QPP either through the Merit-Based Incentive Payment System (MIPS) or advanced Alternative Payment Models (APMs), according to a new report issued by the American Medical Association and consulting firm KPMG.
That said, about 70% of those surveyed responded that they have begun preparing to meet the requirements of the QPP in 2017. The survey did not make clear whether this meant meeting the minimum requirements to avoid any penalties or doing more to become eligible for potential bonus Medicare payments.
“Even those who feel prepared still don’t fully understand the financial ramifications of the program,” the report said. “In short, they may be prepared to ‘check the box’ of reporting requirements, but may lack the long-term strategic financial vision to succeed in 2018 and beyond,” noting that only 8% of the respondents said they are “very prepared” for long-term financial success. On the other side of the that spectrum, 26% said they are not at all prepared and 58% said they were slightly prepared.
Survey respondents indicated a number of areas where they need help:
• Time required to accurately capture and report performance data (66%)
• Understanding reporting requirements (58%)
• Understanding the overall MIPS scoring process (57%)
• Cost required to accurately capture and report performance data (53%)
• Organizational infrastructure needed to report performance (49%)
The report also noted the significant differences when it comes to practice size, although the differences were “not unexpected.” For example, solo practices, compared to those groups of 50 or more physicians, were “significantly more likely (56%) to view reporting requirements as very burdensome, ... significantly more like to feel ‘not at all prepared’ for long-term financial success, ... less likely to be participating in an advanced APM, [and] less likely to have begun preparing.”
Specialists, more so than primary care physicians were “slightly more likely to be deeply knowledgeable about MACRA/QPP, [and] more likely to expect to participate in MIPS (61% versus 48%) and less likely to participate in an advanced APM (15% versus 22%),” the report adds.
“Ongoing educational assistance from CMS, as well as those in the private sector, should focus on the areas where physicians need the most help: understanding requirements and potential financial impact, selection of quality measures, and clinical practice transformation strategies,” the report states.
The survey comes on the heels of CMS releasing its proposed update to the regulations surrounding the QPP for 2018. Comments on the proposed regulatory update are due to CMS on Aug. 21, 2017.
VIDEO: Hip, knee replacements fall in Danish RA patients
MADRID – The rates of both total hip and total knee replacement surgeries dropped among Danish patients with rheumatoid arthritis since the mid-1990s, reductions that were coincident with more widespread use of biologic drugs as well as with other improvements in care, according to analyses of Danish national health records.
“The introduction of guidelines [on biologic drug use] in 2002 and increasing use of biologic drugs [as a result] may have contributed to this positive development,” Lene Dreyer, MD, said at the European Congress of Rheumatology. Other factors that may have also contributed include widespread use of conventional disease-modifying antirheumatic drugs (DMARDs) and adoption of a treat-to-target strategy by many clinicians.
In 1996, the first year studied and before any biologic DMARDs were routinely used for rheumatoid arthritis, the rate of total knee replacement was nearly 6/1,000 person-years among RA patients, compared with a 0.42/1,000 person-years rate in the general adult Danish population, a roughly 14-fold excess among the RA patients, Dr. Dreyer reported. But by 2016, ”this gap had almost disappeared,” she said in a video interview. “It seems like rheumatologists in Denmark are doing a good job” treating RA patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
That may have been especially true subsequent to 2002, when the Danish Institute for Rational Pharmacotherapy issued recommendations that opened the door to wider use of biologic DMARDs, such as tumor necrosis factor inhibitors, to treat RA patients, noted Dr. Dreyer of Gentofte University Hospital, Copenhagen. During 2003-2011, use of total knee replacement surgery in RA patients fell by an average annualized rate of 0.2 surgeries/1,000 person-years. But among the general Danish population the average annualized rate of knee surgeries rose by 0.08/1,000 person-years.
“This is a very important finding,” commented Robert Landewé, MD, PhD, professor of rheumatology at the Academic Medical Center in Amsterdam. “It is extremely difficult to test the effect of the introduction of the [biologic DMARD] guidelines,” he cautioned. But he highlighted the positive finding that the excess of hip and knee replacement surgeries in patients with RA, compared with the general population, had recently narrowed.
Dr. Dreyer and her associates used records from the Danish National Patient Register to compare 29,427 patients with incident RA during 1996-2011 with more than 290,000 matched control individuals. All people studied had not undergone knee or hip replacement surgery prior to their entry into the study. The researchers used an “interrupted time series analysis” to examine the possible impact of the introduction of widespread access to biologic DMARDs starting in 2003.
The analysis showed that the rate of total hip replacements in 1996 was nearly 9 surgeries/1,000 person-years among RA patients and nearly 3/1,000 person-years in the general population, a threefold excess for RA patients. This rate fell by an average annual rate of 0.38/1,000 person-years among RA patients both before and after 2002, so that by 2011 the rate was roughly half the 1996 rate, about 4.5/1,000 patient-years. The rate in the general population rose during 1996-2011, and by 2011 was nearly 4/1,000 person-years and so nearly the same as RA patients. Wider availability of biologic DMARDs for RA patients starting in 2003 did not have an apparent impact on the rate of total hip replacement.
In contrast, wider use of biologic DMARDs appeared to have an effect on the rate of total knee surgeries among RA patients. During 1996-2001, the rate rose by an annual average of 0.19/1,000 person-years, very similar to the 0.21/1,000 person-years annual rise in the general Danish population. However, during 2003-2011, the average annual rate of total knee surgery fell by 0.20/1,000 person-years in the RA patients but continued to rise at an annual average rate of 0.08/1,000 person-years in the general population, Dr. Dreyer reported.
Additional Danish registry data exist for patients who received biologic DMARDs, and Dr. Dreyer said that she and her associates hope to use this to further examine the impact of these drugs on patient outcomes.
Dr. Dreyer has received lecture fees from Merck Sharp & Dohme and UCB. Dr. Landewé has received consulting fees from several drug companies.
[email protected]
On Twitter @mitchelzoler
MADRID – The rates of both total hip and total knee replacement surgeries dropped among Danish patients with rheumatoid arthritis since the mid-1990s, reductions that were coincident with more widespread use of biologic drugs as well as with other improvements in care, according to analyses of Danish national health records.
“The introduction of guidelines [on biologic drug use] in 2002 and increasing use of biologic drugs [as a result] may have contributed to this positive development,” Lene Dreyer, MD, said at the European Congress of Rheumatology. Other factors that may have also contributed include widespread use of conventional disease-modifying antirheumatic drugs (DMARDs) and adoption of a treat-to-target strategy by many clinicians.
In 1996, the first year studied and before any biologic DMARDs were routinely used for rheumatoid arthritis, the rate of total knee replacement was nearly 6/1,000 person-years among RA patients, compared with a 0.42/1,000 person-years rate in the general adult Danish population, a roughly 14-fold excess among the RA patients, Dr. Dreyer reported. But by 2016, ”this gap had almost disappeared,” she said in a video interview. “It seems like rheumatologists in Denmark are doing a good job” treating RA patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
That may have been especially true subsequent to 2002, when the Danish Institute for Rational Pharmacotherapy issued recommendations that opened the door to wider use of biologic DMARDs, such as tumor necrosis factor inhibitors, to treat RA patients, noted Dr. Dreyer of Gentofte University Hospital, Copenhagen. During 2003-2011, use of total knee replacement surgery in RA patients fell by an average annualized rate of 0.2 surgeries/1,000 person-years. But among the general Danish population the average annualized rate of knee surgeries rose by 0.08/1,000 person-years.
“This is a very important finding,” commented Robert Landewé, MD, PhD, professor of rheumatology at the Academic Medical Center in Amsterdam. “It is extremely difficult to test the effect of the introduction of the [biologic DMARD] guidelines,” he cautioned. But he highlighted the positive finding that the excess of hip and knee replacement surgeries in patients with RA, compared with the general population, had recently narrowed.
Dr. Dreyer and her associates used records from the Danish National Patient Register to compare 29,427 patients with incident RA during 1996-2011 with more than 290,000 matched control individuals. All people studied had not undergone knee or hip replacement surgery prior to their entry into the study. The researchers used an “interrupted time series analysis” to examine the possible impact of the introduction of widespread access to biologic DMARDs starting in 2003.
The analysis showed that the rate of total hip replacements in 1996 was nearly 9 surgeries/1,000 person-years among RA patients and nearly 3/1,000 person-years in the general population, a threefold excess for RA patients. This rate fell by an average annual rate of 0.38/1,000 person-years among RA patients both before and after 2002, so that by 2011 the rate was roughly half the 1996 rate, about 4.5/1,000 patient-years. The rate in the general population rose during 1996-2011, and by 2011 was nearly 4/1,000 person-years and so nearly the same as RA patients. Wider availability of biologic DMARDs for RA patients starting in 2003 did not have an apparent impact on the rate of total hip replacement.
In contrast, wider use of biologic DMARDs appeared to have an effect on the rate of total knee surgeries among RA patients. During 1996-2001, the rate rose by an annual average of 0.19/1,000 person-years, very similar to the 0.21/1,000 person-years annual rise in the general Danish population. However, during 2003-2011, the average annual rate of total knee surgery fell by 0.20/1,000 person-years in the RA patients but continued to rise at an annual average rate of 0.08/1,000 person-years in the general population, Dr. Dreyer reported.
Additional Danish registry data exist for patients who received biologic DMARDs, and Dr. Dreyer said that she and her associates hope to use this to further examine the impact of these drugs on patient outcomes.
Dr. Dreyer has received lecture fees from Merck Sharp & Dohme and UCB. Dr. Landewé has received consulting fees from several drug companies.
[email protected]
On Twitter @mitchelzoler
MADRID – The rates of both total hip and total knee replacement surgeries dropped among Danish patients with rheumatoid arthritis since the mid-1990s, reductions that were coincident with more widespread use of biologic drugs as well as with other improvements in care, according to analyses of Danish national health records.
“The introduction of guidelines [on biologic drug use] in 2002 and increasing use of biologic drugs [as a result] may have contributed to this positive development,” Lene Dreyer, MD, said at the European Congress of Rheumatology. Other factors that may have also contributed include widespread use of conventional disease-modifying antirheumatic drugs (DMARDs) and adoption of a treat-to-target strategy by many clinicians.
In 1996, the first year studied and before any biologic DMARDs were routinely used for rheumatoid arthritis, the rate of total knee replacement was nearly 6/1,000 person-years among RA patients, compared with a 0.42/1,000 person-years rate in the general adult Danish population, a roughly 14-fold excess among the RA patients, Dr. Dreyer reported. But by 2016, ”this gap had almost disappeared,” she said in a video interview. “It seems like rheumatologists in Denmark are doing a good job” treating RA patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
That may have been especially true subsequent to 2002, when the Danish Institute for Rational Pharmacotherapy issued recommendations that opened the door to wider use of biologic DMARDs, such as tumor necrosis factor inhibitors, to treat RA patients, noted Dr. Dreyer of Gentofte University Hospital, Copenhagen. During 2003-2011, use of total knee replacement surgery in RA patients fell by an average annualized rate of 0.2 surgeries/1,000 person-years. But among the general Danish population the average annualized rate of knee surgeries rose by 0.08/1,000 person-years.
“This is a very important finding,” commented Robert Landewé, MD, PhD, professor of rheumatology at the Academic Medical Center in Amsterdam. “It is extremely difficult to test the effect of the introduction of the [biologic DMARD] guidelines,” he cautioned. But he highlighted the positive finding that the excess of hip and knee replacement surgeries in patients with RA, compared with the general population, had recently narrowed.
Dr. Dreyer and her associates used records from the Danish National Patient Register to compare 29,427 patients with incident RA during 1996-2011 with more than 290,000 matched control individuals. All people studied had not undergone knee or hip replacement surgery prior to their entry into the study. The researchers used an “interrupted time series analysis” to examine the possible impact of the introduction of widespread access to biologic DMARDs starting in 2003.
The analysis showed that the rate of total hip replacements in 1996 was nearly 9 surgeries/1,000 person-years among RA patients and nearly 3/1,000 person-years in the general population, a threefold excess for RA patients. This rate fell by an average annual rate of 0.38/1,000 person-years among RA patients both before and after 2002, so that by 2011 the rate was roughly half the 1996 rate, about 4.5/1,000 patient-years. The rate in the general population rose during 1996-2011, and by 2011 was nearly 4/1,000 person-years and so nearly the same as RA patients. Wider availability of biologic DMARDs for RA patients starting in 2003 did not have an apparent impact on the rate of total hip replacement.
In contrast, wider use of biologic DMARDs appeared to have an effect on the rate of total knee surgeries among RA patients. During 1996-2001, the rate rose by an annual average of 0.19/1,000 person-years, very similar to the 0.21/1,000 person-years annual rise in the general Danish population. However, during 2003-2011, the average annual rate of total knee surgery fell by 0.20/1,000 person-years in the RA patients but continued to rise at an annual average rate of 0.08/1,000 person-years in the general population, Dr. Dreyer reported.
Additional Danish registry data exist for patients who received biologic DMARDs, and Dr. Dreyer said that she and her associates hope to use this to further examine the impact of these drugs on patient outcomes.
Dr. Dreyer has received lecture fees from Merck Sharp & Dohme and UCB. Dr. Landewé has received consulting fees from several drug companies.
[email protected]
On Twitter @mitchelzoler
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: RA patient hip replacements fell from nearly 9/1,000 person-years in 1996 to about 4.5/1,000 person-years in 2011.
Data source: Records from more than 300,000 people in the Danish National Patient Register.
Disclosures: Dr. Dreyer has received lecture fees from Merck Sharp & Dohme and UCB. Dr. Landewé has received consulting fees from several drug companies.

Medicaid expansion produced opposing cost effects
States that expanded Medicaid in 2014 both increased and decreased their Medicaid spending that year, compared with the nonexpansion states, according to an analysis from the Centers for Medicare & Medicaid Services.
The 26 states, along with the District of Columbia, that expanded Medicaid eligibility by the end of 2014 had an increase in total Medicaid spending of 12.3% over 2013, compared with an increase of 6.2% in nonexpansion states.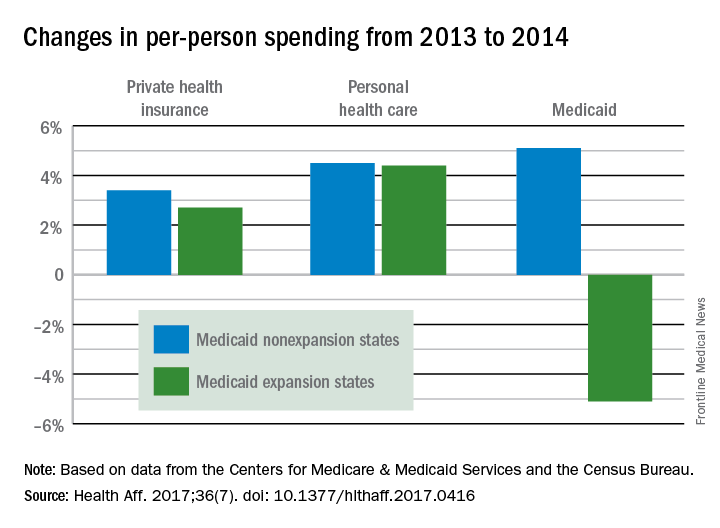
The expansion of coverage “increased the share of ... less expensive enrollees relative to the previous Medicaid beneficiary population mix,” the investigators said. Medicaid expansion brought in more relatively inexpensive adults – 43% of total enrollment in 2014, compared with 32% in 2013 – and reduced the proportion of disabled and aged enrollees, whose cost per person is much higher, they explained.
Private health insurance spending showed a different pattern: Nonexpansion states had larger increases in both higher per-person and overall costs than did expansion states. Per-person costs were up 3.4% for nonexpanders and 2.7% for expanders, and total costs rose 6.8% in nonexpansion states and 4.6% in the Medicaid expanders, Mr. Lassman and his associates said. Higher per-person spending growth for enrollees in the state and federal marketplaces, compared with nonmarketplace individual coverage, was partially responsible for this trend, they pointed out.
States that expanded Medicaid in 2014 both increased and decreased their Medicaid spending that year, compared with the nonexpansion states, according to an analysis from the Centers for Medicare & Medicaid Services.
The 26 states, along with the District of Columbia, that expanded Medicaid eligibility by the end of 2014 had an increase in total Medicaid spending of 12.3% over 2013, compared with an increase of 6.2% in nonexpansion states.
The expansion of coverage “increased the share of ... less expensive enrollees relative to the previous Medicaid beneficiary population mix,” the investigators said. Medicaid expansion brought in more relatively inexpensive adults – 43% of total enrollment in 2014, compared with 32% in 2013 – and reduced the proportion of disabled and aged enrollees, whose cost per person is much higher, they explained.
Private health insurance spending showed a different pattern: Nonexpansion states had larger increases in both higher per-person and overall costs than did expansion states. Per-person costs were up 3.4% for nonexpanders and 2.7% for expanders, and total costs rose 6.8% in nonexpansion states and 4.6% in the Medicaid expanders, Mr. Lassman and his associates said. Higher per-person spending growth for enrollees in the state and federal marketplaces, compared with nonmarketplace individual coverage, was partially responsible for this trend, they pointed out.
States that expanded Medicaid in 2014 both increased and decreased their Medicaid spending that year, compared with the nonexpansion states, according to an analysis from the Centers for Medicare & Medicaid Services.
The 26 states, along with the District of Columbia, that expanded Medicaid eligibility by the end of 2014 had an increase in total Medicaid spending of 12.3% over 2013, compared with an increase of 6.2% in nonexpansion states.
The expansion of coverage “increased the share of ... less expensive enrollees relative to the previous Medicaid beneficiary population mix,” the investigators said. Medicaid expansion brought in more relatively inexpensive adults – 43% of total enrollment in 2014, compared with 32% in 2013 – and reduced the proportion of disabled and aged enrollees, whose cost per person is much higher, they explained.
Private health insurance spending showed a different pattern: Nonexpansion states had larger increases in both higher per-person and overall costs than did expansion states. Per-person costs were up 3.4% for nonexpanders and 2.7% for expanders, and total costs rose 6.8% in nonexpansion states and 4.6% in the Medicaid expanders, Mr. Lassman and his associates said. Higher per-person spending growth for enrollees in the state and federal marketplaces, compared with nonmarketplace individual coverage, was partially responsible for this trend, they pointed out.
FROM HEALTH AFFAIRS