User login
Temozolomide + RT boosts survival in elderly with glioblastoma
CHICAGO – Adding concomitant and adjuvant temozolomide to a shorter course of radiotherapy (RT) for elderly patients with glioblastoma improves progression-free survival, according to a phase III study presented at the annual meeting of the American Society of Clinical Oncology.
Both patients with and without MGMT methylated promoters in their tumors benefited, with the greatest benefit accruing to patients with promoter methylation, reported Dr. James Perry, head of the division of neurology at Sunnybrook Health Sciences Centre, Toronto.

The age of peak incidence of glioblastoma is 64 years, and the incidence is increasing. Best practice has been surgical resection and 6 weeks of radiation combined with oral temozolomide. A pivotal trial just over 10 years ago was restricted to patients younger than age 70 years and included few patients older than 65 years. It showed decreasing benefit of temozolomide with increasing age. Furthermore, trials in the elderly have compared only head-to-head radiation schedules or radiation alone with temozolomide alone. There has been no evidence on which to base practice for combining radiotherapy with temozolomide, Dr. Perry said.
To address this deficiency, Dr. Perry and his colleagues randomly assigned patients 65 years or older with newly diagnosed glioblastoma either to a short course of RT, consisting of 40 Gy in 15 fractions over 3 weeks or to the same radiotherapy plus 3 weeks of concomitant temozolomide and then adjuvant temozolomide for 12 months or until progression.
Patients (n = 562; 281 in each arm) averaged 73 years (range, 65-90 years), 77% had Eastern Cooperative Oncology Group performance score (PS) 0/1 and the rest PS 2, and 58% had had tumor resection.
Median overall survival was 9.3 months with the combined therapy and 7.6 months with radiation alone. Median progression-free survival was 5.3 vs. 3.9 months, respectively, with a hazard ratio of 0.50 (P less than .0001).
MGMT promoter methylation is a predictive marker for benefit from chemotherapy and a prognostic factor for survival. Forty-six percent of the tumors had this promoter methylation.
Temozolomide use added relatively more benefit if promoters were methylated. Patients with methylated promoters had an overall survival of 7.7 months with radiation alone and 13.5 months with combined radiation and temozolomide (HR, 0.53; P = .0001). For unmethylated promoters, overall survival with radiation alone was 7.9 months and was 10.0 months when temozolomide was added (HR, 0.75; P = .055), suggesting some benefit from temozolomide, although not as great as with tumors with methylated promoters.
“The advantage of this combined treatment with chemoradiation was achieved with minimal side effects,” Dr. Perry reported. Mild nausea and vomiting occurred mostly in the first weeks of therapy, and a slight increase in grade 3/4 hematologic toxicity was seen but occurred in less than 5% of patients. No differences in quality of life were reported between the treatment arms.
Most patients could easily complete the treatment plan, with 97% adherence to the 3 weeks of chemoradiation. “This is quite important because the elderly often have difficulties with mobility, distance from treatment centers, and sometimes don’t have caregivers [who] are able to bring them back and forth for treatment,” Dr. Perry said. He suggested that the shorter course of radiotherapy may have been one factor in the high adherence rate.
Based on these results of higher efficacy using concomitant and adjuvant temozolomide with manageable toxicities and no sacrifice in quality of life, “oncologists now have evidence to consider radiation with chemotherapy in all newly diagnosed elderly patients with glioblastoma,” he said.
Dr. Julie Vose, president of the American Society of Clinical Oncology, said the study was important because it compared the treatments in the appropriate patient population, that is, in the elderly who have the highest incidence of glioblastoma.
CHICAGO – Adding concomitant and adjuvant temozolomide to a shorter course of radiotherapy (RT) for elderly patients with glioblastoma improves progression-free survival, according to a phase III study presented at the annual meeting of the American Society of Clinical Oncology.
Both patients with and without MGMT methylated promoters in their tumors benefited, with the greatest benefit accruing to patients with promoter methylation, reported Dr. James Perry, head of the division of neurology at Sunnybrook Health Sciences Centre, Toronto.
The age of peak incidence of glioblastoma is 64 years, and the incidence is increasing. Best practice has been surgical resection and 6 weeks of radiation combined with oral temozolomide. A pivotal trial just over 10 years ago was restricted to patients younger than age 70 years and included few patients older than 65 years. It showed decreasing benefit of temozolomide with increasing age. Furthermore, trials in the elderly have compared only head-to-head radiation schedules or radiation alone with temozolomide alone. There has been no evidence on which to base practice for combining radiotherapy with temozolomide, Dr. Perry said.
To address this deficiency, Dr. Perry and his colleagues randomly assigned patients 65 years or older with newly diagnosed glioblastoma either to a short course of RT, consisting of 40 Gy in 15 fractions over 3 weeks or to the same radiotherapy plus 3 weeks of concomitant temozolomide and then adjuvant temozolomide for 12 months or until progression.
Patients (n = 562; 281 in each arm) averaged 73 years (range, 65-90 years), 77% had Eastern Cooperative Oncology Group performance score (PS) 0/1 and the rest PS 2, and 58% had had tumor resection.
Median overall survival was 9.3 months with the combined therapy and 7.6 months with radiation alone. Median progression-free survival was 5.3 vs. 3.9 months, respectively, with a hazard ratio of 0.50 (P less than .0001).
MGMT promoter methylation is a predictive marker for benefit from chemotherapy and a prognostic factor for survival. Forty-six percent of the tumors had this promoter methylation.
Temozolomide use added relatively more benefit if promoters were methylated. Patients with methylated promoters had an overall survival of 7.7 months with radiation alone and 13.5 months with combined radiation and temozolomide (HR, 0.53; P = .0001). For unmethylated promoters, overall survival with radiation alone was 7.9 months and was 10.0 months when temozolomide was added (HR, 0.75; P = .055), suggesting some benefit from temozolomide, although not as great as with tumors with methylated promoters.
“The advantage of this combined treatment with chemoradiation was achieved with minimal side effects,” Dr. Perry reported. Mild nausea and vomiting occurred mostly in the first weeks of therapy, and a slight increase in grade 3/4 hematologic toxicity was seen but occurred in less than 5% of patients. No differences in quality of life were reported between the treatment arms.
Most patients could easily complete the treatment plan, with 97% adherence to the 3 weeks of chemoradiation. “This is quite important because the elderly often have difficulties with mobility, distance from treatment centers, and sometimes don’t have caregivers [who] are able to bring them back and forth for treatment,” Dr. Perry said. He suggested that the shorter course of radiotherapy may have been one factor in the high adherence rate.
Based on these results of higher efficacy using concomitant and adjuvant temozolomide with manageable toxicities and no sacrifice in quality of life, “oncologists now have evidence to consider radiation with chemotherapy in all newly diagnosed elderly patients with glioblastoma,” he said.
Dr. Julie Vose, president of the American Society of Clinical Oncology, said the study was important because it compared the treatments in the appropriate patient population, that is, in the elderly who have the highest incidence of glioblastoma.
CHICAGO – Adding concomitant and adjuvant temozolomide to a shorter course of radiotherapy (RT) for elderly patients with glioblastoma improves progression-free survival, according to a phase III study presented at the annual meeting of the American Society of Clinical Oncology.
Both patients with and without MGMT methylated promoters in their tumors benefited, with the greatest benefit accruing to patients with promoter methylation, reported Dr. James Perry, head of the division of neurology at Sunnybrook Health Sciences Centre, Toronto.
The age of peak incidence of glioblastoma is 64 years, and the incidence is increasing. Best practice has been surgical resection and 6 weeks of radiation combined with oral temozolomide. A pivotal trial just over 10 years ago was restricted to patients younger than age 70 years and included few patients older than 65 years. It showed decreasing benefit of temozolomide with increasing age. Furthermore, trials in the elderly have compared only head-to-head radiation schedules or radiation alone with temozolomide alone. There has been no evidence on which to base practice for combining radiotherapy with temozolomide, Dr. Perry said.
To address this deficiency, Dr. Perry and his colleagues randomly assigned patients 65 years or older with newly diagnosed glioblastoma either to a short course of RT, consisting of 40 Gy in 15 fractions over 3 weeks or to the same radiotherapy plus 3 weeks of concomitant temozolomide and then adjuvant temozolomide for 12 months or until progression.
Patients (n = 562; 281 in each arm) averaged 73 years (range, 65-90 years), 77% had Eastern Cooperative Oncology Group performance score (PS) 0/1 and the rest PS 2, and 58% had had tumor resection.
Median overall survival was 9.3 months with the combined therapy and 7.6 months with radiation alone. Median progression-free survival was 5.3 vs. 3.9 months, respectively, with a hazard ratio of 0.50 (P less than .0001).
MGMT promoter methylation is a predictive marker for benefit from chemotherapy and a prognostic factor for survival. Forty-six percent of the tumors had this promoter methylation.
Temozolomide use added relatively more benefit if promoters were methylated. Patients with methylated promoters had an overall survival of 7.7 months with radiation alone and 13.5 months with combined radiation and temozolomide (HR, 0.53; P = .0001). For unmethylated promoters, overall survival with radiation alone was 7.9 months and was 10.0 months when temozolomide was added (HR, 0.75; P = .055), suggesting some benefit from temozolomide, although not as great as with tumors with methylated promoters.
“The advantage of this combined treatment with chemoradiation was achieved with minimal side effects,” Dr. Perry reported. Mild nausea and vomiting occurred mostly in the first weeks of therapy, and a slight increase in grade 3/4 hematologic toxicity was seen but occurred in less than 5% of patients. No differences in quality of life were reported between the treatment arms.
Most patients could easily complete the treatment plan, with 97% adherence to the 3 weeks of chemoradiation. “This is quite important because the elderly often have difficulties with mobility, distance from treatment centers, and sometimes don’t have caregivers [who] are able to bring them back and forth for treatment,” Dr. Perry said. He suggested that the shorter course of radiotherapy may have been one factor in the high adherence rate.
Based on these results of higher efficacy using concomitant and adjuvant temozolomide with manageable toxicities and no sacrifice in quality of life, “oncologists now have evidence to consider radiation with chemotherapy in all newly diagnosed elderly patients with glioblastoma,” he said.
Dr. Julie Vose, president of the American Society of Clinical Oncology, said the study was important because it compared the treatments in the appropriate patient population, that is, in the elderly who have the highest incidence of glioblastoma.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Combining temozolomide with radiotherapy prolongs survival for elderly with glioblastoma.
Major finding: Combining temozolomide with radiotherapy increased survival by 33% vs. radiation alone.
Data source: Global phase III study of 562 elderly patients with newly diagnosed glioblastoma randomized to temozolomide plus radiation vs radiation alone.
Disclosures: Dr. Perry reported stock or other ownership interests in DelMar Pharmaceuticals and VBL Therapeutics. Dr. Vose reported receiving honoraria from Sanofi-Aventis and Seattle Genetics; consulting for Bio Connections; and receiving research funding to her institution from Acerta, Bristol-Myers Squibb, Celgene, Genentech, GlaxoSmithKline, Incyte, Janssen Biotech, Kite Pharma, Pharmacyclics, and Spectrum Pharmaceuticals.

Tandem beats single ASCT for childhood neuroblastoma
CHICAGO – More children treated for high-risk neuroblastoma who received a second autologous stem cell transplant in consolidation after induction chemotherapy were alive after 3 years compared with children getting a single transplant, Dr. Julie R. Park reported at the annual meeting of the American Society of Clinical Oncology.
Neuroblastoma (NB) is the most common extracranial tumor of childhood and arises in the sympathetic nervous system of very young children. Fewer than 50% of children with high-risk NB survive 5 years following today’s multiagent, aggressive therapy. Single autologous hematopoietic stem cell transplant (ASCT) has improved outcomes, and in pilot studies, tandem ASCT appeared tolerable with better efficacy as consolidation therapy for high-risk NB.

The present trial enrolled 665 patients (mean age 3.1 years), who received an induction regimen of six cycles of chemotherapy, with harvest of peripheral blood stem cells after the first two cycles and surgery after five cycles. Patients with adequate stem cell collection, adequate organ function, and no evidence of disease progression were randomized to either standard therapy with a single ASCT with carboplatin, etoposide, melphalan and local radiotherapy (n = 179); or to a double (tandem) ASCT with cyclophosphamide and thiotepa prior to the first ASCT followed 6 weeks later by a dose-modified regimen of carboplatin, etoposide, melphalan and radiotherapy prior to a second ASCT (n = 176). The two transplants were separated by 6-8 weeks.
About 70% of patients in each arm received dinutuximab plus cytokine immunotherapy after their transplants. Dinutuximab is an antibody directed against GD2, an antigen present on neuroblastoma cells. About 38% of patients had high-risk tumors based on the presence of MYCN gene amplification.
The children who were randomized to receive a tandem transplant had a statistically significant, improved event-free survival, with a 3-year event-free survival of 61%, compared to those children receiving a single transplant, with a 3-year event-free survival of 48% (P = .0081), reported Dr. Park, professor of pediatrics at the University of Washington, Seattle.
Three-year overall survival did not differ between the two groups, at 74% for the tandem transplant group and 69% for the single transplant group (P = .185). The study was powered to see a difference in event-free survival, and the study was probably not long enough to detect a difference in overall survival, Dr. Park said.
Anti-GD2 immunotherapy improved both event-free and overall survival for both the tandem and single ASCT groups. At 3 years from the time of the patients’ receiving immunotherapy, event-free survival was 73.7% and 56%, respectively (P = .0033), and overall survival was 83.7% and 74.4% (P = .0322), respectively.
The benefit of tandem transplant occurred without an increase in toxicity or regimen-related mortality. The rates of severe toxicities were similar in the two arms. Two patients receiving a tandem ASCT died, compared with eight receiving a single ASCT.
“This finding will change the way we treat children with high-risk neuroblastoma in North America, which still claims many young lives and is in urgent need of better treatments,” Dr. Park said in a press release.
Dr. Park noted that most NB recurrences happen within 2-3 years from diagnosis and that patients who have not had a recurrence by 3 years have a better chance of long-term survival. Patients in this study will continue to be followed for 10 years.
Dr. Park disclosed ties with Roche. Dr. Hunger reported ties with Merck, Sigma Tau, Jazz Pharmaceuticals, and Spectrum Pharmaceuticals.
CHICAGO – More children treated for high-risk neuroblastoma who received a second autologous stem cell transplant in consolidation after induction chemotherapy were alive after 3 years compared with children getting a single transplant, Dr. Julie R. Park reported at the annual meeting of the American Society of Clinical Oncology.
Neuroblastoma (NB) is the most common extracranial tumor of childhood and arises in the sympathetic nervous system of very young children. Fewer than 50% of children with high-risk NB survive 5 years following today’s multiagent, aggressive therapy. Single autologous hematopoietic stem cell transplant (ASCT) has improved outcomes, and in pilot studies, tandem ASCT appeared tolerable with better efficacy as consolidation therapy for high-risk NB.
The present trial enrolled 665 patients (mean age 3.1 years), who received an induction regimen of six cycles of chemotherapy, with harvest of peripheral blood stem cells after the first two cycles and surgery after five cycles. Patients with adequate stem cell collection, adequate organ function, and no evidence of disease progression were randomized to either standard therapy with a single ASCT with carboplatin, etoposide, melphalan and local radiotherapy (n = 179); or to a double (tandem) ASCT with cyclophosphamide and thiotepa prior to the first ASCT followed 6 weeks later by a dose-modified regimen of carboplatin, etoposide, melphalan and radiotherapy prior to a second ASCT (n = 176). The two transplants were separated by 6-8 weeks.
About 70% of patients in each arm received dinutuximab plus cytokine immunotherapy after their transplants. Dinutuximab is an antibody directed against GD2, an antigen present on neuroblastoma cells. About 38% of patients had high-risk tumors based on the presence of MYCN gene amplification.
The children who were randomized to receive a tandem transplant had a statistically significant, improved event-free survival, with a 3-year event-free survival of 61%, compared to those children receiving a single transplant, with a 3-year event-free survival of 48% (P = .0081), reported Dr. Park, professor of pediatrics at the University of Washington, Seattle.
Three-year overall survival did not differ between the two groups, at 74% for the tandem transplant group and 69% for the single transplant group (P = .185). The study was powered to see a difference in event-free survival, and the study was probably not long enough to detect a difference in overall survival, Dr. Park said.
Anti-GD2 immunotherapy improved both event-free and overall survival for both the tandem and single ASCT groups. At 3 years from the time of the patients’ receiving immunotherapy, event-free survival was 73.7% and 56%, respectively (P = .0033), and overall survival was 83.7% and 74.4% (P = .0322), respectively.
The benefit of tandem transplant occurred without an increase in toxicity or regimen-related mortality. The rates of severe toxicities were similar in the two arms. Two patients receiving a tandem ASCT died, compared with eight receiving a single ASCT.
“This finding will change the way we treat children with high-risk neuroblastoma in North America, which still claims many young lives and is in urgent need of better treatments,” Dr. Park said in a press release.
Dr. Park noted that most NB recurrences happen within 2-3 years from diagnosis and that patients who have not had a recurrence by 3 years have a better chance of long-term survival. Patients in this study will continue to be followed for 10 years.
Dr. Park disclosed ties with Roche. Dr. Hunger reported ties with Merck, Sigma Tau, Jazz Pharmaceuticals, and Spectrum Pharmaceuticals.
CHICAGO – More children treated for high-risk neuroblastoma who received a second autologous stem cell transplant in consolidation after induction chemotherapy were alive after 3 years compared with children getting a single transplant, Dr. Julie R. Park reported at the annual meeting of the American Society of Clinical Oncology.
Neuroblastoma (NB) is the most common extracranial tumor of childhood and arises in the sympathetic nervous system of very young children. Fewer than 50% of children with high-risk NB survive 5 years following today’s multiagent, aggressive therapy. Single autologous hematopoietic stem cell transplant (ASCT) has improved outcomes, and in pilot studies, tandem ASCT appeared tolerable with better efficacy as consolidation therapy for high-risk NB.
The present trial enrolled 665 patients (mean age 3.1 years), who received an induction regimen of six cycles of chemotherapy, with harvest of peripheral blood stem cells after the first two cycles and surgery after five cycles. Patients with adequate stem cell collection, adequate organ function, and no evidence of disease progression were randomized to either standard therapy with a single ASCT with carboplatin, etoposide, melphalan and local radiotherapy (n = 179); or to a double (tandem) ASCT with cyclophosphamide and thiotepa prior to the first ASCT followed 6 weeks later by a dose-modified regimen of carboplatin, etoposide, melphalan and radiotherapy prior to a second ASCT (n = 176). The two transplants were separated by 6-8 weeks.
About 70% of patients in each arm received dinutuximab plus cytokine immunotherapy after their transplants. Dinutuximab is an antibody directed against GD2, an antigen present on neuroblastoma cells. About 38% of patients had high-risk tumors based on the presence of MYCN gene amplification.
The children who were randomized to receive a tandem transplant had a statistically significant, improved event-free survival, with a 3-year event-free survival of 61%, compared to those children receiving a single transplant, with a 3-year event-free survival of 48% (P = .0081), reported Dr. Park, professor of pediatrics at the University of Washington, Seattle.
Three-year overall survival did not differ between the two groups, at 74% for the tandem transplant group and 69% for the single transplant group (P = .185). The study was powered to see a difference in event-free survival, and the study was probably not long enough to detect a difference in overall survival, Dr. Park said.
Anti-GD2 immunotherapy improved both event-free and overall survival for both the tandem and single ASCT groups. At 3 years from the time of the patients’ receiving immunotherapy, event-free survival was 73.7% and 56%, respectively (P = .0033), and overall survival was 83.7% and 74.4% (P = .0322), respectively.
The benefit of tandem transplant occurred without an increase in toxicity or regimen-related mortality. The rates of severe toxicities were similar in the two arms. Two patients receiving a tandem ASCT died, compared with eight receiving a single ASCT.
“This finding will change the way we treat children with high-risk neuroblastoma in North America, which still claims many young lives and is in urgent need of better treatments,” Dr. Park said in a press release.
Dr. Park noted that most NB recurrences happen within 2-3 years from diagnosis and that patients who have not had a recurrence by 3 years have a better chance of long-term survival. Patients in this study will continue to be followed for 10 years.
Dr. Park disclosed ties with Roche. Dr. Hunger reported ties with Merck, Sigma Tau, Jazz Pharmaceuticals, and Spectrum Pharmaceuticals.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Neuroblastoma event-free survival was better with tandem than with single ASCT.
Major finding: Event-free survival was 61% with tandem vs. 48% with single ASCT.
Data source: Randomized phase III trial of 355 patients assigned equally to single vs. tandem autologous stem cell transplant.
Disclosures: Dr. Park disclosed ties with Roche. Dr. Hunger reported ties with Merck, Sigma Tau, Jazz Pharmaceuticals, and Spectrum Pharmaceuticals.

Enlist appropriate psychological consults for gender dysphoria
ORLANDO – Old notions about transgender and transsexual individuals are changing, driven by the emergence of transgender identity, scientific evidence, political activism in those communities, and the gay and lesbian rights movement, as well as patients demanding to be part of the decision-making process.
The terminology has evolved as well. What was called transsexualism in the DSM-III in 1980 became gender identity disorder in the DSM-IV (1994; 2000), and in the current DSM-5 is gender dysphoria. Terminology is still in flux with the possibility that terminology may evolve to “gender incongruence.”

The umbrella term “transgender” now covers transsexual, crossdressing, bigender, drag queen/king, female/male impersonator, and gender queer, and probably more, according to Eli Coleman, Ph.D., professor and director of the program in human sexuality at the University of Minnesota, Minneapolis. “Probably the most proper term you hear now is ‘trans,’ ” he said during a session on transgender medicine at the annual meeting of the American Association of Clinical Endocrinologists.
The DSM-5 criteria for gender dysphoria include a marked incongruence between one’s experienced/expressed gender and the assigned gender for at least 6 months with at least two of the following: an incongruence between one’s felt gender identity and one’s primary and secondary sex characteristics, a strong desire to be rid of one’s gender, a strong desire for the primary and/or secondary sex characteristics of the other gender, a strong desire to be of the other gender (or an alternative gender from the assigned one), a strong desire to be treated as such, and a strong conviction that one has the typical feeling and reactions of the other gender. Dr. Coleman said a further criterion of the DSM-5 is that “the condition is associated with clinically significant distress or impairment in social, occupational, or other areas of functioning.”
A new view of trans
There is now an awareness of a spectrum of gender identity and an affirmation of the right of individuals to express that identity as they would like. Many treatment options exist, and it is up to the individual to decide which way and how far they want to go. Dr. Coleman quoted the late Virginia Prince, a transvestite and a pioneering transgender activist: “If you get on a train in Los Angeles bound for New York, you don’t have to go all the way to New York. If you want, you can get off in Chicago.” So even if a person wants to undergo medical transitioning, hormone therapy does not necessarily have to be followed by sex-reassignment surgery.
Dr. Coleman is past president of the World Professional Association for Transgender Health (WPATH, www.wpath.org), which has published “Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People,” Version 7, a set of guidelines for health care providers. The guidelines are designed help patients achieve comfort with their gendered selves, maximize their overall health and psychological well-being, and achieve self-fulfillment. If untreated or undertreated, gender dysphoria is associated with increased morbidity and mortality, according to WPATH. Hormone treatment may reduce gender dysphoria symptoms by reducing the characteristics of the original sex and inducing ones of the opposite sex. Hormones can be used before or after sex-reassignment surgery, or on their own for patients not seeking surgery who “want [to] … get off in Chicago,” Dr. Coleman said.
Gender nonconformity is not pathological
“Gender nonconformity is not pathological, yet gender dysphoria is a specific distress that can be alleviated through medically necessary treatment,” Dr. Coleman said. “Gender dysphoria may be classified as a mental disorder [but] not necessarily a lifetime diagnosis.” It is the stress of the dysphoria that may be diagnosable and treated, but being gender nonconforming in itself is not the target of treatment. He said mental health professionals therefore have an important role in addressing the negative effects of stigma and helping the individuals become comfortable with a form of gender expression that suits them. This role requires a mental health professional who is skilled in this area.
Treatments to try to change gender identity and expression to become congruent with the sex assigned at birth have failed in the past and are no longer considered ethical, he said. Dr. Coleman suggested that intervening with medical treatments early to suppress puberty and then offering feminizing or masculinizing hormone therapy at the appropriate time may be the best course of action to avoid or alleviate gender dysphoria. He said studies have shown that sex-reassignment surgery can provide “an undeniable effect” on outcomes such as “subjective well-being, cosmesis, and sexual function.”
He recommended that health care professionals become familiar with transgender health care issues, examine their own attitudes and beliefs about these issues, seek out educational opportunities, and get to know and consult with experts in transgender health care. But that is not enough.
“You’ll never understand the condition if you just listen to your patients in the office,” he said. “You’ve got to get into a car and talk to somebody or have coffee with them and really get to know them outside of the office.” That includes meeting with transgender people several years after they have transitioned, who can give insights into the process that are not apparent from just seeing patients in the office in the midst of their gender dysphoria.
The knowledge gained must also be imbued in the health care professional’s staff as well. “You’ve got to have the right attitudes, but you’ve got to train your whole staff about this … that [patients] cannot be treated badly at all,” he said.
ORLANDO – Old notions about transgender and transsexual individuals are changing, driven by the emergence of transgender identity, scientific evidence, political activism in those communities, and the gay and lesbian rights movement, as well as patients demanding to be part of the decision-making process.
The terminology has evolved as well. What was called transsexualism in the DSM-III in 1980 became gender identity disorder in the DSM-IV (1994; 2000), and in the current DSM-5 is gender dysphoria. Terminology is still in flux with the possibility that terminology may evolve to “gender incongruence.”
The umbrella term “transgender” now covers transsexual, crossdressing, bigender, drag queen/king, female/male impersonator, and gender queer, and probably more, according to Eli Coleman, Ph.D., professor and director of the program in human sexuality at the University of Minnesota, Minneapolis. “Probably the most proper term you hear now is ‘trans,’ ” he said during a session on transgender medicine at the annual meeting of the American Association of Clinical Endocrinologists.
The DSM-5 criteria for gender dysphoria include a marked incongruence between one’s experienced/expressed gender and the assigned gender for at least 6 months with at least two of the following: an incongruence between one’s felt gender identity and one’s primary and secondary sex characteristics, a strong desire to be rid of one’s gender, a strong desire for the primary and/or secondary sex characteristics of the other gender, a strong desire to be of the other gender (or an alternative gender from the assigned one), a strong desire to be treated as such, and a strong conviction that one has the typical feeling and reactions of the other gender. Dr. Coleman said a further criterion of the DSM-5 is that “the condition is associated with clinically significant distress or impairment in social, occupational, or other areas of functioning.”
A new view of trans
There is now an awareness of a spectrum of gender identity and an affirmation of the right of individuals to express that identity as they would like. Many treatment options exist, and it is up to the individual to decide which way and how far they want to go. Dr. Coleman quoted the late Virginia Prince, a transvestite and a pioneering transgender activist: “If you get on a train in Los Angeles bound for New York, you don’t have to go all the way to New York. If you want, you can get off in Chicago.” So even if a person wants to undergo medical transitioning, hormone therapy does not necessarily have to be followed by sex-reassignment surgery.
Dr. Coleman is past president of the World Professional Association for Transgender Health (WPATH, www.wpath.org), which has published “Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People,” Version 7, a set of guidelines for health care providers. The guidelines are designed help patients achieve comfort with their gendered selves, maximize their overall health and psychological well-being, and achieve self-fulfillment. If untreated or undertreated, gender dysphoria is associated with increased morbidity and mortality, according to WPATH. Hormone treatment may reduce gender dysphoria symptoms by reducing the characteristics of the original sex and inducing ones of the opposite sex. Hormones can be used before or after sex-reassignment surgery, or on their own for patients not seeking surgery who “want [to] … get off in Chicago,” Dr. Coleman said.
Gender nonconformity is not pathological
“Gender nonconformity is not pathological, yet gender dysphoria is a specific distress that can be alleviated through medically necessary treatment,” Dr. Coleman said. “Gender dysphoria may be classified as a mental disorder [but] not necessarily a lifetime diagnosis.” It is the stress of the dysphoria that may be diagnosable and treated, but being gender nonconforming in itself is not the target of treatment. He said mental health professionals therefore have an important role in addressing the negative effects of stigma and helping the individuals become comfortable with a form of gender expression that suits them. This role requires a mental health professional who is skilled in this area.
Treatments to try to change gender identity and expression to become congruent with the sex assigned at birth have failed in the past and are no longer considered ethical, he said. Dr. Coleman suggested that intervening with medical treatments early to suppress puberty and then offering feminizing or masculinizing hormone therapy at the appropriate time may be the best course of action to avoid or alleviate gender dysphoria. He said studies have shown that sex-reassignment surgery can provide “an undeniable effect” on outcomes such as “subjective well-being, cosmesis, and sexual function.”
He recommended that health care professionals become familiar with transgender health care issues, examine their own attitudes and beliefs about these issues, seek out educational opportunities, and get to know and consult with experts in transgender health care. But that is not enough.
“You’ll never understand the condition if you just listen to your patients in the office,” he said. “You’ve got to get into a car and talk to somebody or have coffee with them and really get to know them outside of the office.” That includes meeting with transgender people several years after they have transitioned, who can give insights into the process that are not apparent from just seeing patients in the office in the midst of their gender dysphoria.
The knowledge gained must also be imbued in the health care professional’s staff as well. “You’ve got to have the right attitudes, but you’ve got to train your whole staff about this … that [patients] cannot be treated badly at all,” he said.
ORLANDO – Old notions about transgender and transsexual individuals are changing, driven by the emergence of transgender identity, scientific evidence, political activism in those communities, and the gay and lesbian rights movement, as well as patients demanding to be part of the decision-making process.
The terminology has evolved as well. What was called transsexualism in the DSM-III in 1980 became gender identity disorder in the DSM-IV (1994; 2000), and in the current DSM-5 is gender dysphoria. Terminology is still in flux with the possibility that terminology may evolve to “gender incongruence.”
The umbrella term “transgender” now covers transsexual, crossdressing, bigender, drag queen/king, female/male impersonator, and gender queer, and probably more, according to Eli Coleman, Ph.D., professor and director of the program in human sexuality at the University of Minnesota, Minneapolis. “Probably the most proper term you hear now is ‘trans,’ ” he said during a session on transgender medicine at the annual meeting of the American Association of Clinical Endocrinologists.
The DSM-5 criteria for gender dysphoria include a marked incongruence between one’s experienced/expressed gender and the assigned gender for at least 6 months with at least two of the following: an incongruence between one’s felt gender identity and one’s primary and secondary sex characteristics, a strong desire to be rid of one’s gender, a strong desire for the primary and/or secondary sex characteristics of the other gender, a strong desire to be of the other gender (or an alternative gender from the assigned one), a strong desire to be treated as such, and a strong conviction that one has the typical feeling and reactions of the other gender. Dr. Coleman said a further criterion of the DSM-5 is that “the condition is associated with clinically significant distress or impairment in social, occupational, or other areas of functioning.”
A new view of trans
There is now an awareness of a spectrum of gender identity and an affirmation of the right of individuals to express that identity as they would like. Many treatment options exist, and it is up to the individual to decide which way and how far they want to go. Dr. Coleman quoted the late Virginia Prince, a transvestite and a pioneering transgender activist: “If you get on a train in Los Angeles bound for New York, you don’t have to go all the way to New York. If you want, you can get off in Chicago.” So even if a person wants to undergo medical transitioning, hormone therapy does not necessarily have to be followed by sex-reassignment surgery.
Dr. Coleman is past president of the World Professional Association for Transgender Health (WPATH, www.wpath.org), which has published “Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People,” Version 7, a set of guidelines for health care providers. The guidelines are designed help patients achieve comfort with their gendered selves, maximize their overall health and psychological well-being, and achieve self-fulfillment. If untreated or undertreated, gender dysphoria is associated with increased morbidity and mortality, according to WPATH. Hormone treatment may reduce gender dysphoria symptoms by reducing the characteristics of the original sex and inducing ones of the opposite sex. Hormones can be used before or after sex-reassignment surgery, or on their own for patients not seeking surgery who “want [to] … get off in Chicago,” Dr. Coleman said.
Gender nonconformity is not pathological
“Gender nonconformity is not pathological, yet gender dysphoria is a specific distress that can be alleviated through medically necessary treatment,” Dr. Coleman said. “Gender dysphoria may be classified as a mental disorder [but] not necessarily a lifetime diagnosis.” It is the stress of the dysphoria that may be diagnosable and treated, but being gender nonconforming in itself is not the target of treatment. He said mental health professionals therefore have an important role in addressing the negative effects of stigma and helping the individuals become comfortable with a form of gender expression that suits them. This role requires a mental health professional who is skilled in this area.
Treatments to try to change gender identity and expression to become congruent with the sex assigned at birth have failed in the past and are no longer considered ethical, he said. Dr. Coleman suggested that intervening with medical treatments early to suppress puberty and then offering feminizing or masculinizing hormone therapy at the appropriate time may be the best course of action to avoid or alleviate gender dysphoria. He said studies have shown that sex-reassignment surgery can provide “an undeniable effect” on outcomes such as “subjective well-being, cosmesis, and sexual function.”
He recommended that health care professionals become familiar with transgender health care issues, examine their own attitudes and beliefs about these issues, seek out educational opportunities, and get to know and consult with experts in transgender health care. But that is not enough.
“You’ll never understand the condition if you just listen to your patients in the office,” he said. “You’ve got to get into a car and talk to somebody or have coffee with them and really get to know them outside of the office.” That includes meeting with transgender people several years after they have transitioned, who can give insights into the process that are not apparent from just seeing patients in the office in the midst of their gender dysphoria.
The knowledge gained must also be imbued in the health care professional’s staff as well. “You’ve got to have the right attitudes, but you’ve got to train your whole staff about this … that [patients] cannot be treated badly at all,” he said.
EXPERT ANALYSIS FROM AACE 2016

IL-2 adds only toxicity to neuroblastoma antibody tx
CHICAGO – Adding the cytokine IL-2 to front-line therapy with the anti-GD2 antibody ch14.18/CHO provided no additional survival benefit and only added to toxicity in the treatment of pediatric patients with high-risk neuroblastoma (NB), Dr. Ruth Ladenstein reported at the annual meeting of the American Society of Clinical Oncology.
A form of the antibody (dinutuximab) is approved for use in combination with granulocyte-macrophage colony stimulating factor, IL-2, and 13-cis-retinoic acid (RA) to treat high risk NB. A previous study (N Engl J Med. 2010;363:1324-34) showed that a combination of ch14.18 and the cytokines improved event free survival to 66% at 2 years, but the role of cytokines in this context remained unclear. Dr. Ladenstein and associates therefore performed a phase III trial that randomized patients to the antibody with or without subcutaneous (sc) IL-2.

High-risk NB was defined as patients with International Neuroblastoma Staging System stage 4 disease 1 year old or older, stage 4 less than 1 year old with MYCN amplification, or stage 2,3 patients up to age 21 years with MYCN amplification. Patients underwent a rapid induction therapy, followed by peripheral stem cell harvest, local control with complete tumor resection, myeloablative therapy with peripheral stem cell transplant, local control with radiotherapy, and then ch14.18 anti-GD2 monoclonal immunotherapy with RA, with or without sc IL-2.
Inclusion criteria were a complete response or partial response with three or fewer skeletal metastatic spots and no positive bone marrow biopsies on two aspirates. Randomization occurred between day 60 and 90 post stem cell infusion. RA was given on days 1-14 post randomization. For the arm receiving IL-2, it was given as 5 daily injections of 6 x 106 IU/m2 per day over 8 hours on days 15-19. IL-2 was repeated on days 22-26. Both groups also received the ch14.18 antibody on days 22-26. All patients received high-dose morphine for pain management.
For event free survival (EFS), the primary endpoint of the trial, “if we look at 3 years, we see with antibody alone it’s 57%. With IL-2, it’s 60%. It’s completely clear that there’s no superiority for the IL-2 arm,” said Dr. Ladenstein, professor of pediatrics at the Children’s Cancer Research Institute, Austria.
At 5 years, the EFS was no different for the two treatment arms, at 51% for antibody alone and 56% for antibody plus IL-2 (P = .561). There were 199/200 patients in the antibody-alone arm with follow-up after randomization and 203/206 in the antibody plus IL-2 arm. The same was true for the secondary endpoint of overall survival, with 66% survival with antibody-alone and 58% in the antibody plus IL-2 at 5 years.
The EFS for patients with a complete response prior to immunotherapy was 66% at 3 years and was 50% for patients with less than a complete response, a significant difference (P = .003) in favor of those with a complete response. IL-2 administration had no effect on the EFS of the patients with a complete response if it was given with the immunotherapy. Similarly, IL-2 made no difference for patients who had had a very good partial response or a partial response prior to immunotherapy. For complete, very good partial, or partial responses prior to immunotherapy, the overall response to immunotherapy was 51%.
“However, feasibility is a concern, particularly in the IL-2 arm. Only 61% of the cycles were completed whereas it was 85% in the antibody-only arm, and the interruptions are definitely related mainly to the IL-2 component,” Dr. Ladenstein said.
Toxicity was higher for those patients receiving IL-2 compared to those getting antibody alone: Lansky performance status of 30% or less was 41% vs. 17%, early termination of therapy was 39% vs. 15%, and Common Terminology Criteria grade 3/4 fever was 41% vs. 14%, respectively (all P less than .001). There were also significantly more grade 3/4 allergic reactions and incidences of capillary leak, as well as diarrhea, hypotension, central nervous toxicity, and pain with IL-2.
The outcomes were favorable with antibody immunotherapy alone, but the higher toxicity with IL-2 shows that “a less toxic treatment schedule therefore is needed for this late treatment phase,” Dr. Ladenstein said.
Commenting on the trial, Dr. Barbara Hero of University Children’s Hospital in Cologne, Germany, asked whether cytokines are a useful part of the regimen “because we know the cytokines add quite a lot of toxicity to the regimens.” Even if they are potentially useful, researchers still do not know which cytokines, route of administration, and at what doses and timing would be best. Also, it is not known if a different induction regimen or antibody treatment could make a difference in using cytokines.
Another question is whether cytokines may be of benefit in patients with a higher tumor burden, e.g., more than three skeletal spots, used as the eligibility cut-off in this trial, Dr. Hero said.
CHICAGO – Adding the cytokine IL-2 to front-line therapy with the anti-GD2 antibody ch14.18/CHO provided no additional survival benefit and only added to toxicity in the treatment of pediatric patients with high-risk neuroblastoma (NB), Dr. Ruth Ladenstein reported at the annual meeting of the American Society of Clinical Oncology.
A form of the antibody (dinutuximab) is approved for use in combination with granulocyte-macrophage colony stimulating factor, IL-2, and 13-cis-retinoic acid (RA) to treat high risk NB. A previous study (N Engl J Med. 2010;363:1324-34) showed that a combination of ch14.18 and the cytokines improved event free survival to 66% at 2 years, but the role of cytokines in this context remained unclear. Dr. Ladenstein and associates therefore performed a phase III trial that randomized patients to the antibody with or without subcutaneous (sc) IL-2.
High-risk NB was defined as patients with International Neuroblastoma Staging System stage 4 disease 1 year old or older, stage 4 less than 1 year old with MYCN amplification, or stage 2,3 patients up to age 21 years with MYCN amplification. Patients underwent a rapid induction therapy, followed by peripheral stem cell harvest, local control with complete tumor resection, myeloablative therapy with peripheral stem cell transplant, local control with radiotherapy, and then ch14.18 anti-GD2 monoclonal immunotherapy with RA, with or without sc IL-2.
Inclusion criteria were a complete response or partial response with three or fewer skeletal metastatic spots and no positive bone marrow biopsies on two aspirates. Randomization occurred between day 60 and 90 post stem cell infusion. RA was given on days 1-14 post randomization. For the arm receiving IL-2, it was given as 5 daily injections of 6 x 106 IU/m2 per day over 8 hours on days 15-19. IL-2 was repeated on days 22-26. Both groups also received the ch14.18 antibody on days 22-26. All patients received high-dose morphine for pain management.
For event free survival (EFS), the primary endpoint of the trial, “if we look at 3 years, we see with antibody alone it’s 57%. With IL-2, it’s 60%. It’s completely clear that there’s no superiority for the IL-2 arm,” said Dr. Ladenstein, professor of pediatrics at the Children’s Cancer Research Institute, Austria.
At 5 years, the EFS was no different for the two treatment arms, at 51% for antibody alone and 56% for antibody plus IL-2 (P = .561). There were 199/200 patients in the antibody-alone arm with follow-up after randomization and 203/206 in the antibody plus IL-2 arm. The same was true for the secondary endpoint of overall survival, with 66% survival with antibody-alone and 58% in the antibody plus IL-2 at 5 years.
The EFS for patients with a complete response prior to immunotherapy was 66% at 3 years and was 50% for patients with less than a complete response, a significant difference (P = .003) in favor of those with a complete response. IL-2 administration had no effect on the EFS of the patients with a complete response if it was given with the immunotherapy. Similarly, IL-2 made no difference for patients who had had a very good partial response or a partial response prior to immunotherapy. For complete, very good partial, or partial responses prior to immunotherapy, the overall response to immunotherapy was 51%.
“However, feasibility is a concern, particularly in the IL-2 arm. Only 61% of the cycles were completed whereas it was 85% in the antibody-only arm, and the interruptions are definitely related mainly to the IL-2 component,” Dr. Ladenstein said.
Toxicity was higher for those patients receiving IL-2 compared to those getting antibody alone: Lansky performance status of 30% or less was 41% vs. 17%, early termination of therapy was 39% vs. 15%, and Common Terminology Criteria grade 3/4 fever was 41% vs. 14%, respectively (all P less than .001). There were also significantly more grade 3/4 allergic reactions and incidences of capillary leak, as well as diarrhea, hypotension, central nervous toxicity, and pain with IL-2.
The outcomes were favorable with antibody immunotherapy alone, but the higher toxicity with IL-2 shows that “a less toxic treatment schedule therefore is needed for this late treatment phase,” Dr. Ladenstein said.
Commenting on the trial, Dr. Barbara Hero of University Children’s Hospital in Cologne, Germany, asked whether cytokines are a useful part of the regimen “because we know the cytokines add quite a lot of toxicity to the regimens.” Even if they are potentially useful, researchers still do not know which cytokines, route of administration, and at what doses and timing would be best. Also, it is not known if a different induction regimen or antibody treatment could make a difference in using cytokines.
Another question is whether cytokines may be of benefit in patients with a higher tumor burden, e.g., more than three skeletal spots, used as the eligibility cut-off in this trial, Dr. Hero said.
CHICAGO – Adding the cytokine IL-2 to front-line therapy with the anti-GD2 antibody ch14.18/CHO provided no additional survival benefit and only added to toxicity in the treatment of pediatric patients with high-risk neuroblastoma (NB), Dr. Ruth Ladenstein reported at the annual meeting of the American Society of Clinical Oncology.
A form of the antibody (dinutuximab) is approved for use in combination with granulocyte-macrophage colony stimulating factor, IL-2, and 13-cis-retinoic acid (RA) to treat high risk NB. A previous study (N Engl J Med. 2010;363:1324-34) showed that a combination of ch14.18 and the cytokines improved event free survival to 66% at 2 years, but the role of cytokines in this context remained unclear. Dr. Ladenstein and associates therefore performed a phase III trial that randomized patients to the antibody with or without subcutaneous (sc) IL-2.
High-risk NB was defined as patients with International Neuroblastoma Staging System stage 4 disease 1 year old or older, stage 4 less than 1 year old with MYCN amplification, or stage 2,3 patients up to age 21 years with MYCN amplification. Patients underwent a rapid induction therapy, followed by peripheral stem cell harvest, local control with complete tumor resection, myeloablative therapy with peripheral stem cell transplant, local control with radiotherapy, and then ch14.18 anti-GD2 monoclonal immunotherapy with RA, with or without sc IL-2.
Inclusion criteria were a complete response or partial response with three or fewer skeletal metastatic spots and no positive bone marrow biopsies on two aspirates. Randomization occurred between day 60 and 90 post stem cell infusion. RA was given on days 1-14 post randomization. For the arm receiving IL-2, it was given as 5 daily injections of 6 x 106 IU/m2 per day over 8 hours on days 15-19. IL-2 was repeated on days 22-26. Both groups also received the ch14.18 antibody on days 22-26. All patients received high-dose morphine for pain management.
For event free survival (EFS), the primary endpoint of the trial, “if we look at 3 years, we see with antibody alone it’s 57%. With IL-2, it’s 60%. It’s completely clear that there’s no superiority for the IL-2 arm,” said Dr. Ladenstein, professor of pediatrics at the Children’s Cancer Research Institute, Austria.
At 5 years, the EFS was no different for the two treatment arms, at 51% for antibody alone and 56% for antibody plus IL-2 (P = .561). There were 199/200 patients in the antibody-alone arm with follow-up after randomization and 203/206 in the antibody plus IL-2 arm. The same was true for the secondary endpoint of overall survival, with 66% survival with antibody-alone and 58% in the antibody plus IL-2 at 5 years.
The EFS for patients with a complete response prior to immunotherapy was 66% at 3 years and was 50% for patients with less than a complete response, a significant difference (P = .003) in favor of those with a complete response. IL-2 administration had no effect on the EFS of the patients with a complete response if it was given with the immunotherapy. Similarly, IL-2 made no difference for patients who had had a very good partial response or a partial response prior to immunotherapy. For complete, very good partial, or partial responses prior to immunotherapy, the overall response to immunotherapy was 51%.
“However, feasibility is a concern, particularly in the IL-2 arm. Only 61% of the cycles were completed whereas it was 85% in the antibody-only arm, and the interruptions are definitely related mainly to the IL-2 component,” Dr. Ladenstein said.
Toxicity was higher for those patients receiving IL-2 compared to those getting antibody alone: Lansky performance status of 30% or less was 41% vs. 17%, early termination of therapy was 39% vs. 15%, and Common Terminology Criteria grade 3/4 fever was 41% vs. 14%, respectively (all P less than .001). There were also significantly more grade 3/4 allergic reactions and incidences of capillary leak, as well as diarrhea, hypotension, central nervous toxicity, and pain with IL-2.
The outcomes were favorable with antibody immunotherapy alone, but the higher toxicity with IL-2 shows that “a less toxic treatment schedule therefore is needed for this late treatment phase,” Dr. Ladenstein said.
Commenting on the trial, Dr. Barbara Hero of University Children’s Hospital in Cologne, Germany, asked whether cytokines are a useful part of the regimen “because we know the cytokines add quite a lot of toxicity to the regimens.” Even if they are potentially useful, researchers still do not know which cytokines, route of administration, and at what doses and timing would be best. Also, it is not known if a different induction regimen or antibody treatment could make a difference in using cytokines.
Another question is whether cytokines may be of benefit in patients with a higher tumor burden, e.g., more than three skeletal spots, used as the eligibility cut-off in this trial, Dr. Hero said.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: IL-2 adds no benefit, only toxicity, to neuroblastoma antibody therapy.
Major finding: Only 61% of treatment cycles were completed with IL-2.
Data source: Phase III, randomized, two-arm study of 402 pediatric/adolescent neuroblastoma patients.
Disclosures: Dr. Ladenstein has received honoraria and has had a consulting or advisory role with Apeiron Biologics and Boehringer Ingelheim, and has research funding from, patents with, has provided expert testimony for, and has received travel expenses from Apeiron. Dr. Hero had no disclosures.

Most people who undergo gender reassignment surgery appreciate the results
ORLANDO – Gender reassignment surgery is the most extreme step for those transgender individuals who wish to complete the transformation to the opposite sex. While many transgender people do not opt to take this step, it may be an option for people who still have gender dysphoria after a thorough diagnostic work-up by a mental health professional, hormonal treatment, and having lived in the desired gender role as a “real-life test.”
Dr. Stan Monstrey, of Ghent University Hospital, Belgium, is an experienced gender reassignment surgeon and reported at the annual meeting of the American Academy of Clinical Endocrinology that between 1995 and 2005, he saw about 20-30 new patients a year. But now, he said, “We operate on a weekly basis between a minimum of three and sometimes six or seven transsexuals, so ... in our practice, probably between 90% and 95% are still going the whole way, still want what was called initially binary surgery.”

Transwomen: Male to female
The transformation procedure for male to female begins with feminizing aesthetic procedures, such as reducing the Adam’s apple (laryngeal prominence of the thyroid cartilage) and chin, frontal boss of the forehead, and possibly other facial work such as rhinoplasty. “Sometimes minor changes can have a huge effect on the face of the patient,” Dr. Monstrey said. “This is becoming, in our opinion, increasingly important for transwomen.”
Then, in about 75% of cases, Dr. Monstrey performs at least two surgeries under the same anesthesia – breast augmentation and perineal transformation. He said even after years of hormone therapy, most such patients have only a limited amount of breast tissue but want more prominent breasts. Implants can be placed behind or in front of the pectoralis muscle via inframammary, transaxillary, or occasionally periareolar approaches. Results are immediate, and complications are rare.
Another technique, which has become very popular over the past 5-10 years, is lipofilling to fill defects and depressions in the breasts. Stem cells contained in the fat may help soften scars. But when faced with a patient who had a BRCA1 mutation, the surgeons would not use lipofilling, fearing the potential for breast cancer, and would use prostheses instead (J Sex Med. 2014 Oct;11:2496-9). Still, questions remain about even using hormone treatments in such a patient.
Dr. Monstrey mentioned that in Belgium, breast augmentation for transwomen is considered reconstructive surgery and is always reimbursed whereas it is considered aesthetic surgery and never reimbursed for non-transwomen who want larger breasts. (For transmen, breast amputation is similarly reimbursed.)
The second operation is genital transformation. Basically, the interior of the penis is removed and the skin is invaginated to form a vagina of 8-18.5 cm and a scrotal flap, along with castration and removal of the penile bulb erectile tissue (corpus spongiosum) posteriorly. It is important to protect the rectal wall, which is not very strong. The foreskin becomes the new clitoral hood and inner side of the labia minora, and the clitoris is formed by reducing and transposing the penile glans. If the patient had a small penis and not enough tissue for the reconstruction, skin flaps from various other sites can be used.
Among more than 1,200 patients, 92% could achieve orgasm. Rectovaginal fistulas occurred in 4 patients, 19 needed repositioning of the urethra, 21 needed an operation to lengthen the vagina, and 95 needed aesthetic correction of the vulva. Dr. Monstrey said many patients have asked him when they should tell their new boyfriends about their transformation, meaning that the surgery was quite convincing even with penetrative sex.
If the first operation does not work, another technique is to use an isolated piece of colon or sigmoid bowel, which has been performed completely laparoscopically by a very skilled gastroenterologic surgeon at the hospital in Ghent.
Speaking to a roomful of endocrinologists, Dr. Monstrey told them, “I’ll be the first one to agree with you that indeed puberty blockers are a very good thing. However, we as surgeons are not so enthusiastic about them because … it is impossible to create a normal vagina” because of a lack of available tissue from the underdeveloped penis.
Transmen: Female to male
“Transmen react much better to hormonal therapy than do transwomen,” he said. “If they hide their breasts they really look like men. The disadvantage is that the surgical treatment is much more complex.” The most important operation for them is subcutaneous mastectomy and male contouring. A small, semiareolar incision leaves almost no scar. Most patients still require excision of redundant skin of the breasts.
Phalloplasty is a complex operation aimed at giving the patient an aesthetic phallus, a normal scrotum, the ability to void while standing, and to perform sexual intercourse, all while protecting erogenous sensation, with minimal morbidity and mortality. Dr. Monstrey reported that he has performed 600-700 phalloplasties.
The most common technique has been to use a free vascularized flap from another bodily site with the artery, vein, and nerves to reconnect at the phalloplasty site. Because the skin is very thin on the inner forearm, it is often used and allows forming an inner tube for the urethra and an outer tube for the penis. The surgery may have to be done in three or four stages for the best results. From pictures that Dr. Monstrey showed, it was obvious that the constructed penises were not absolutely natural in appearance, but he said most patients were “rather happy” with them, despite many of these patients being quite demanding. A scrotum is constructed from transposition of the labia minora.
Unfortunately, voiding while standing is often a problem, with 197 out of 562 patients (35%) having a fistula and urine leakage, but this issue frequently corrects itself. “More difficult to treat are the strictures with stenosis, which can be a problem voiding,” he said (occurring in 78/562). Other complications were 5 complete and 43 partial flap failures, 4 cases of compression syndrome, 58 cases of delayed wound healing, and 15 cases of transient ischemia. Flap failures occurred mainly in smokers, “so we don’t operate on smokers anymore,” he said.
One year after the constructive surgery, a penile prosthesis is implanted for those who want it, allowing sexual intercourse. Most individuals had orgasmic function, not because of reconnected nerves in the flap, but, Dr. Monstrey said he believes, because the clitoris, placed beneath the phallus, is denuded and stimulated during sexual activity. He said the problem is that the prostheses are usually intended for elderly men “who have sex a couple of times a month and who have a normal anatomy.” Young transmen may engage in more sexual activity, “so we have a lot of problems with exposure [of the prosthesis], infection, technical defects, and so on,” he said.
A technique gaining popularity is to use a skin flap from the groin area to make a urethra and one from the thigh to construct a penis. Although a penile transplant has recently been performed for a patient who had lost his penis to cancer, transplants are not being considered at this point, both for surgical technical reasons and because of a need for lifelong immunosuppressive drugs.
Proper referrals and counseling
The World Professional Association for Transgender Health in its Standard of Care guidelines 7 recommends one mental health professional referral for the breast surgery and two such referrals for genital surgery. The issue of possible parenthood should be discussed with patients, along with early counseling about fertility options. The age of majority and consent in different countries is important. Dr. Monstrey said genital surgery may be possible before the age of 18 years if all members of a multidisciplinary team of health professionals agree on a case by case basis that the adolescent can understand the risks, benefits, and alternatives to the surgery with the same degree of competence as someone 18 years of age or older.
Dr. Monstrey reported having no financial disclosures.
ORLANDO – Gender reassignment surgery is the most extreme step for those transgender individuals who wish to complete the transformation to the opposite sex. While many transgender people do not opt to take this step, it may be an option for people who still have gender dysphoria after a thorough diagnostic work-up by a mental health professional, hormonal treatment, and having lived in the desired gender role as a “real-life test.”
Dr. Stan Monstrey, of Ghent University Hospital, Belgium, is an experienced gender reassignment surgeon and reported at the annual meeting of the American Academy of Clinical Endocrinology that between 1995 and 2005, he saw about 20-30 new patients a year. But now, he said, “We operate on a weekly basis between a minimum of three and sometimes six or seven transsexuals, so ... in our practice, probably between 90% and 95% are still going the whole way, still want what was called initially binary surgery.”
Transwomen: Male to female
The transformation procedure for male to female begins with feminizing aesthetic procedures, such as reducing the Adam’s apple (laryngeal prominence of the thyroid cartilage) and chin, frontal boss of the forehead, and possibly other facial work such as rhinoplasty. “Sometimes minor changes can have a huge effect on the face of the patient,” Dr. Monstrey said. “This is becoming, in our opinion, increasingly important for transwomen.”
Then, in about 75% of cases, Dr. Monstrey performs at least two surgeries under the same anesthesia – breast augmentation and perineal transformation. He said even after years of hormone therapy, most such patients have only a limited amount of breast tissue but want more prominent breasts. Implants can be placed behind or in front of the pectoralis muscle via inframammary, transaxillary, or occasionally periareolar approaches. Results are immediate, and complications are rare.
Another technique, which has become very popular over the past 5-10 years, is lipofilling to fill defects and depressions in the breasts. Stem cells contained in the fat may help soften scars. But when faced with a patient who had a BRCA1 mutation, the surgeons would not use lipofilling, fearing the potential for breast cancer, and would use prostheses instead (J Sex Med. 2014 Oct;11:2496-9). Still, questions remain about even using hormone treatments in such a patient.
Dr. Monstrey mentioned that in Belgium, breast augmentation for transwomen is considered reconstructive surgery and is always reimbursed whereas it is considered aesthetic surgery and never reimbursed for non-transwomen who want larger breasts. (For transmen, breast amputation is similarly reimbursed.)
The second operation is genital transformation. Basically, the interior of the penis is removed and the skin is invaginated to form a vagina of 8-18.5 cm and a scrotal flap, along with castration and removal of the penile bulb erectile tissue (corpus spongiosum) posteriorly. It is important to protect the rectal wall, which is not very strong. The foreskin becomes the new clitoral hood and inner side of the labia minora, and the clitoris is formed by reducing and transposing the penile glans. If the patient had a small penis and not enough tissue for the reconstruction, skin flaps from various other sites can be used.
Among more than 1,200 patients, 92% could achieve orgasm. Rectovaginal fistulas occurred in 4 patients, 19 needed repositioning of the urethra, 21 needed an operation to lengthen the vagina, and 95 needed aesthetic correction of the vulva. Dr. Monstrey said many patients have asked him when they should tell their new boyfriends about their transformation, meaning that the surgery was quite convincing even with penetrative sex.
If the first operation does not work, another technique is to use an isolated piece of colon or sigmoid bowel, which has been performed completely laparoscopically by a very skilled gastroenterologic surgeon at the hospital in Ghent.
Speaking to a roomful of endocrinologists, Dr. Monstrey told them, “I’ll be the first one to agree with you that indeed puberty blockers are a very good thing. However, we as surgeons are not so enthusiastic about them because … it is impossible to create a normal vagina” because of a lack of available tissue from the underdeveloped penis.
Transmen: Female to male
“Transmen react much better to hormonal therapy than do transwomen,” he said. “If they hide their breasts they really look like men. The disadvantage is that the surgical treatment is much more complex.” The most important operation for them is subcutaneous mastectomy and male contouring. A small, semiareolar incision leaves almost no scar. Most patients still require excision of redundant skin of the breasts.
Phalloplasty is a complex operation aimed at giving the patient an aesthetic phallus, a normal scrotum, the ability to void while standing, and to perform sexual intercourse, all while protecting erogenous sensation, with minimal morbidity and mortality. Dr. Monstrey reported that he has performed 600-700 phalloplasties.
The most common technique has been to use a free vascularized flap from another bodily site with the artery, vein, and nerves to reconnect at the phalloplasty site. Because the skin is very thin on the inner forearm, it is often used and allows forming an inner tube for the urethra and an outer tube for the penis. The surgery may have to be done in three or four stages for the best results. From pictures that Dr. Monstrey showed, it was obvious that the constructed penises were not absolutely natural in appearance, but he said most patients were “rather happy” with them, despite many of these patients being quite demanding. A scrotum is constructed from transposition of the labia minora.
Unfortunately, voiding while standing is often a problem, with 197 out of 562 patients (35%) having a fistula and urine leakage, but this issue frequently corrects itself. “More difficult to treat are the strictures with stenosis, which can be a problem voiding,” he said (occurring in 78/562). Other complications were 5 complete and 43 partial flap failures, 4 cases of compression syndrome, 58 cases of delayed wound healing, and 15 cases of transient ischemia. Flap failures occurred mainly in smokers, “so we don’t operate on smokers anymore,” he said.
One year after the constructive surgery, a penile prosthesis is implanted for those who want it, allowing sexual intercourse. Most individuals had orgasmic function, not because of reconnected nerves in the flap, but, Dr. Monstrey said he believes, because the clitoris, placed beneath the phallus, is denuded and stimulated during sexual activity. He said the problem is that the prostheses are usually intended for elderly men “who have sex a couple of times a month and who have a normal anatomy.” Young transmen may engage in more sexual activity, “so we have a lot of problems with exposure [of the prosthesis], infection, technical defects, and so on,” he said.
A technique gaining popularity is to use a skin flap from the groin area to make a urethra and one from the thigh to construct a penis. Although a penile transplant has recently been performed for a patient who had lost his penis to cancer, transplants are not being considered at this point, both for surgical technical reasons and because of a need for lifelong immunosuppressive drugs.
Proper referrals and counseling
The World Professional Association for Transgender Health in its Standard of Care guidelines 7 recommends one mental health professional referral for the breast surgery and two such referrals for genital surgery. The issue of possible parenthood should be discussed with patients, along with early counseling about fertility options. The age of majority and consent in different countries is important. Dr. Monstrey said genital surgery may be possible before the age of 18 years if all members of a multidisciplinary team of health professionals agree on a case by case basis that the adolescent can understand the risks, benefits, and alternatives to the surgery with the same degree of competence as someone 18 years of age or older.
Dr. Monstrey reported having no financial disclosures.
ORLANDO – Gender reassignment surgery is the most extreme step for those transgender individuals who wish to complete the transformation to the opposite sex. While many transgender people do not opt to take this step, it may be an option for people who still have gender dysphoria after a thorough diagnostic work-up by a mental health professional, hormonal treatment, and having lived in the desired gender role as a “real-life test.”
Dr. Stan Monstrey, of Ghent University Hospital, Belgium, is an experienced gender reassignment surgeon and reported at the annual meeting of the American Academy of Clinical Endocrinology that between 1995 and 2005, he saw about 20-30 new patients a year. But now, he said, “We operate on a weekly basis between a minimum of three and sometimes six or seven transsexuals, so ... in our practice, probably between 90% and 95% are still going the whole way, still want what was called initially binary surgery.”
Transwomen: Male to female
The transformation procedure for male to female begins with feminizing aesthetic procedures, such as reducing the Adam’s apple (laryngeal prominence of the thyroid cartilage) and chin, frontal boss of the forehead, and possibly other facial work such as rhinoplasty. “Sometimes minor changes can have a huge effect on the face of the patient,” Dr. Monstrey said. “This is becoming, in our opinion, increasingly important for transwomen.”
Then, in about 75% of cases, Dr. Monstrey performs at least two surgeries under the same anesthesia – breast augmentation and perineal transformation. He said even after years of hormone therapy, most such patients have only a limited amount of breast tissue but want more prominent breasts. Implants can be placed behind or in front of the pectoralis muscle via inframammary, transaxillary, or occasionally periareolar approaches. Results are immediate, and complications are rare.
Another technique, which has become very popular over the past 5-10 years, is lipofilling to fill defects and depressions in the breasts. Stem cells contained in the fat may help soften scars. But when faced with a patient who had a BRCA1 mutation, the surgeons would not use lipofilling, fearing the potential for breast cancer, and would use prostheses instead (J Sex Med. 2014 Oct;11:2496-9). Still, questions remain about even using hormone treatments in such a patient.
Dr. Monstrey mentioned that in Belgium, breast augmentation for transwomen is considered reconstructive surgery and is always reimbursed whereas it is considered aesthetic surgery and never reimbursed for non-transwomen who want larger breasts. (For transmen, breast amputation is similarly reimbursed.)
The second operation is genital transformation. Basically, the interior of the penis is removed and the skin is invaginated to form a vagina of 8-18.5 cm and a scrotal flap, along with castration and removal of the penile bulb erectile tissue (corpus spongiosum) posteriorly. It is important to protect the rectal wall, which is not very strong. The foreskin becomes the new clitoral hood and inner side of the labia minora, and the clitoris is formed by reducing and transposing the penile glans. If the patient had a small penis and not enough tissue for the reconstruction, skin flaps from various other sites can be used.
Among more than 1,200 patients, 92% could achieve orgasm. Rectovaginal fistulas occurred in 4 patients, 19 needed repositioning of the urethra, 21 needed an operation to lengthen the vagina, and 95 needed aesthetic correction of the vulva. Dr. Monstrey said many patients have asked him when they should tell their new boyfriends about their transformation, meaning that the surgery was quite convincing even with penetrative sex.
If the first operation does not work, another technique is to use an isolated piece of colon or sigmoid bowel, which has been performed completely laparoscopically by a very skilled gastroenterologic surgeon at the hospital in Ghent.
Speaking to a roomful of endocrinologists, Dr. Monstrey told them, “I’ll be the first one to agree with you that indeed puberty blockers are a very good thing. However, we as surgeons are not so enthusiastic about them because … it is impossible to create a normal vagina” because of a lack of available tissue from the underdeveloped penis.
Transmen: Female to male
“Transmen react much better to hormonal therapy than do transwomen,” he said. “If they hide their breasts they really look like men. The disadvantage is that the surgical treatment is much more complex.” The most important operation for them is subcutaneous mastectomy and male contouring. A small, semiareolar incision leaves almost no scar. Most patients still require excision of redundant skin of the breasts.
Phalloplasty is a complex operation aimed at giving the patient an aesthetic phallus, a normal scrotum, the ability to void while standing, and to perform sexual intercourse, all while protecting erogenous sensation, with minimal morbidity and mortality. Dr. Monstrey reported that he has performed 600-700 phalloplasties.
The most common technique has been to use a free vascularized flap from another bodily site with the artery, vein, and nerves to reconnect at the phalloplasty site. Because the skin is very thin on the inner forearm, it is often used and allows forming an inner tube for the urethra and an outer tube for the penis. The surgery may have to be done in three or four stages for the best results. From pictures that Dr. Monstrey showed, it was obvious that the constructed penises were not absolutely natural in appearance, but he said most patients were “rather happy” with them, despite many of these patients being quite demanding. A scrotum is constructed from transposition of the labia minora.
Unfortunately, voiding while standing is often a problem, with 197 out of 562 patients (35%) having a fistula and urine leakage, but this issue frequently corrects itself. “More difficult to treat are the strictures with stenosis, which can be a problem voiding,” he said (occurring in 78/562). Other complications were 5 complete and 43 partial flap failures, 4 cases of compression syndrome, 58 cases of delayed wound healing, and 15 cases of transient ischemia. Flap failures occurred mainly in smokers, “so we don’t operate on smokers anymore,” he said.
One year after the constructive surgery, a penile prosthesis is implanted for those who want it, allowing sexual intercourse. Most individuals had orgasmic function, not because of reconnected nerves in the flap, but, Dr. Monstrey said he believes, because the clitoris, placed beneath the phallus, is denuded and stimulated during sexual activity. He said the problem is that the prostheses are usually intended for elderly men “who have sex a couple of times a month and who have a normal anatomy.” Young transmen may engage in more sexual activity, “so we have a lot of problems with exposure [of the prosthesis], infection, technical defects, and so on,” he said.
A technique gaining popularity is to use a skin flap from the groin area to make a urethra and one from the thigh to construct a penis. Although a penile transplant has recently been performed for a patient who had lost his penis to cancer, transplants are not being considered at this point, both for surgical technical reasons and because of a need for lifelong immunosuppressive drugs.
Proper referrals and counseling
The World Professional Association for Transgender Health in its Standard of Care guidelines 7 recommends one mental health professional referral for the breast surgery and two such referrals for genital surgery. The issue of possible parenthood should be discussed with patients, along with early counseling about fertility options. The age of majority and consent in different countries is important. Dr. Monstrey said genital surgery may be possible before the age of 18 years if all members of a multidisciplinary team of health professionals agree on a case by case basis that the adolescent can understand the risks, benefits, and alternatives to the surgery with the same degree of competence as someone 18 years of age or older.
Dr. Monstrey reported having no financial disclosures.
AACE 2016

Expert simplifies diagnosis of endocrine hypertension
ORLANDO – The diagnosis of hypertension with its origin in the endocrine system may appear complex, but it does not have to be. Primary aldosteronism may be underappreciated and underdiagnosed. On the other hand, catecholamine-secreting tumors are rare, but they often come to mind in making a diagnosis of endocrine hypertension. Dr. William Young Jr., professor of medicine at the Mayo Clinic, Rochester, Minn., presented cases in a lively session of audience participation at the annual meeting of the America Association of Clinical Endocrinologists. Later, Dr. Young summarized some of the key points in an interview, which has been edited for brevity.
Frontline Medical News: What is the endocrinologist’s role in working up the patient who has hypertension of suspected endocrine origin?
Dr. William Young Jr.: The first is knowing when to suspect endocrine hypertension. The most common form of endocrine hypertension is primary aldosteronism. So this is the adrenal-dependent autonomous production of aldosterone, which leads to high blood pressure, volume expansion, and sometimes hypokalemia. One of the concepts that many clinicians forget is that only about 30% of patients with primary aldosteronism present with hypokalemia. So 70% of patients with this disorder don’t have hypokalemia. They look like any other person with high blood pressure.

So when should we look for primary aldosteronism? Onset of high blood pressure at a young age, for example, less than age 30, drug resistant hypertension – so three drugs [with] poor control. Twenty percent of those patients will prove to have primary aldosteronism. Simply poorly controlled hypertension is another group; [or] family history of primary aldosteronism, so all first degree relatives should be tested. Or a patient who has hypertension and has had an incidental discovery of an adrenal mass should also be tested for primary aldosteronism.
Unfortunately, most primary care providers ... think that this is a complicated and dense endocrine disorder, and they frequently will not look for it, but it’s actually very simple. Some of the complexities are historical in nature in that when this disorder was first described, several rules were made for what medications a patient could be on, for example. And it’s difficult to comply with those rules. For example, if you have a patient who’s on five drugs and has poor control, you’re not going to switch him to the two drugs that are recommended because they are weak antihypertensives. It wouldn’t be ethical to do so. [The two drug classes are the calcium channel blocker verapamil and the alpha-1 antagonists doxazosin (Cardura) and terazosin (Hytrin).]
So the best thing to do regardless of what drugs the patient is on – it doesn’t matter if they’re on ACE inhibitors or angiotensin-receptor blockers or diuretics – just get a morning blood sample as your aldosterone and plasma renin activity. If aldosterone is high or generous, greater than 15 ng/dL, if the plasma renin activity is less than 1 ng/mL per hour, that’s a positive case detection test.
That doesn’t prove the patient has primary aldosteronism. The sensitivity/specificity of aldosterone and renin case detection testing is about 75%. So most patients need confirmatory testing, which would either be the saline infusion test or the 24-hour urine for aldosterone on a high-sodium diet. And once primary aldosteronism is confirmed, then we would do an adrenal-directed CT scan.
The problem with the findings in the adrenal glands on CT is that the prevalence of adrenal nodularity increases with age. So people in their 60s and 70s can have adrenal nodules that have nothing to do with aldosterone production. So whereas if the patient is less than age 35 and CT shows a unilateral macroadenoma, the contralateral adrenal is perfectly normal appearing, and the patient has a marked primary aldosteronism – so spontaneous hypokalemia, plasma aldosterone over 30 ng/dL – that subset of patients could go straight to surgery and skip adrenal vein sampling. However, everyone else over age 35 if they want to pursue the surgical option, adrenal vein sampling is a key test.
FMN: Is there anything that rules out primary aldosteronism?
Dr. Young: If the plasma aldosterone level is less than 10 ng/dL it makes primary aldosteronism very unlikely, and if the renin level is higher than 1 ng/mL per hour, that makes primary aldosteronism very unlikely.
FMN: What about working up pheochromocytoma?
Dr. Young: Clinicians, unlike with primary aldosteronism, where they don’t look for it enough, for pheochromocytoma they look for it a lot, and it’s really rare. Between 0.1 and 0.01% of the hypertensive population will prove to have pheochromocytoma.
The false positive rate with our case detection testing of plasma metanephrines about 15%. So based on how rare pheochromocytoma is and a 15% false positive rate with plasma metanephrines, 97% of patients with elevated plasma normetanephrines do not have pheochromocytoma.
So we have a real problem with case detection testing. The 24-hour urine metanephrines and catecholamines using appropriate reference ranges are probably a better way to do case detection testing for pheochromocytoma, but there’s still a false positive rate with urinary normetanephrine.
Never mistake a benign adrenal adenoma for a pheo. In terms of the imaging phenotype, pheos are dense and vascular. As they enlarge, they get cystic hemorrhagic areas within them.
FMN: What goes on with other paragangliomas?
Dr. Young: Pheochromocytoma is the term we use when you have a catecholamine-secreting tumor in the adrenal gland itself. It develops in the adrenal medulla. Paraganglioma is an identical tumor, but it’s outside of the adrenal gland. It’s somewhere in the pelvis, could be in the chest, could be in the skull base, or neck. Most commonly it’s in the abdomen. So the case detection testing is the same.
But patients we should consider testing for pheochromocytoma and paraganglioma are those with paroxysmal symptoms like episodes of pounding heartbeat, sweating, headache, tremor, and pallor. Young people with new onset hypertension, hypertension that’s poorly controlled, and vascular adrenal masses should also be tested for pheochromocytoma.
FMN: Are there things that can confound any of these tests we discussed or any drugs that should be noted that could get in the way?
Dr. Young: For pheochromocytoma, the good news is now that most reference labs use tandem mass spectrometry technology, the hypertension drugs that potentially interfered in the past like labetalol and sotalol no longer interfere. So these days the clinician doesn’t need to stop any blood pressure–related medications.
The medications that can cause false positive testing are primarily tricyclic antidepressants. Flexeril, which is cyclobenzaprine, is commonly used to treat fibromyalgia, and that is a tricyclic antidepressant, and that will cause false positive testing ... with norepinephrine and normetanephrine. Tricyclic antidepressants can increase those levels three, four, or fivefold. Levodopa, which is in Sinemet, can cause false positive testing. Antipsychotics can cause false positive testing, and MAO inhibitors ... So the clinician shouldn’t worry about blood pressure medications but should worry about the other medications the patient is taking.
FMN: When someone looks at laboratory values, should you be comparing these values to people with hypertension who do not have these conditions, and do labs have adjusted values?
Dr. Young: That’s a good question, and in the Mayo medical lab, our reference range that we use is based on patients who were tested for pheochromocytoma [and] proved not to have it. So our cutoffs are 50% to 100% higher than some other reference labs.
These other reference labs use normal laboratory volunteers who have normal blood pressure and who are taking no medications, and I’ve never tested such a patient for pheochromocytoma, so why would we use that group of people to determine our reference range? So we should use reference ranges based on patients tested for pheo but who prove to not have pheo. And that leads to higher accuracy of our case detection tests.
FMN: What are the treatments for these conditions and follow-up? I take it if there’s an adrenal mass, you get a surgeon, and I think you also noted that you need an experienced endocrine surgeon.
Dr. Young: For primary aldosteronism, if the patient has a unilateral aldosterone-producing adenoma, the outstanding treatment is laparoscopic adrenalectomy. Patients are in the hospital one night, [and] they’re back at work in 7-10 days, but that does require an expert laparoscopic adrenal surgeon. And in the United States we have a 1-year endocrine surgery program. It’s optimal that patients are referred to surgeons who have done that unique training.
For pheochromocytoma less than 8-9 cm, laparoscopic adrenalectomy with an experienced endocrine surgeon is an excellent treatment option. When the adrenal pheochromocytoma is larger than 8 or 9 cm, especially if it’s cystic, the surgeon may want to do it as open [surgery] because it’s critical that the capsule of the pheochromocytoma is not ruptured intraoperatively. If it is ruptured, a benign pheochromocytoma has just been transformed to malignant, incurable disease.
If it’s a paraganglioma, typically that requires an open operation whether it’s in the neck or the chest or the pelvis or lower abdomen.
FMN: What is the follow-up to any of these conditions?
Dr. Young: The follow-up once you’ve resected an adrenal pheochromocytoma depends on whether there is a germline mutation. If there is a germline mutation, for example, succinate dehydrogenase mutation [SDH], these patients are at higher risk for developing recurrent pheochromocytoma or paraganglioma, and they’re at risk for developing malignant pheochromocytoma or paraganglioma.
One of our challenges is when we resect a pheochromocytoma or paraganglioma, the pathologist doesn’t have the tools to tell us if it’s benign or malignant ... So all patients need lifelong biochemical follow-up, basically a 24-hour urine for metanephrines and catecholamines annually or plasma metanephrines for life.
If the patients have an underlying mutation like succinate dehydrogenase, they’re at risk for developing nonfunctioning paragangliomas. So these patients need periodic imaging in addition to the annual biochemical testing. For example, if a patient had an abdominal paraganglioma with an SDHB [succinate dehydrogenase complex iron sulfur subunit B], we would do abdominal MRI scans every 1-2 years. That would include the pelvis. We would screen for paragangliomas elsewhere with MRI of the skull base and neck and the chest every 3-5 years, and a total body scan every 5 years or so, either FDG-PET [18F-fluorodeoxyglucose positron emission tomography] scan or 123I-MIBG [metaiodobenzyl-guanidine] scan.
FMN: Is there anything that is particularly new in the past couple of years?
Dr. Young: Some of the innovations lately have been in the area of metastatic pheochromocytoma and paraganglioma. These are in patients who have limited metastatic disease that’s localized to bone or to liver, and we’ve been using ablative therapies. This includes cryoablation ... and radiofrequency ablation, which is killing the tumor with hot temperature, and that’s very effective for patients who have limited metastatic lesions in the bone or liver.
For patients with complex tumors in difficult areas of the body, for example, in the mediastinum or surrounding the heart, we’ve been using 3D printer technology to print [a replica of the structures and] the tumor preoperatively, and this assists in surgical planning.
FMN: And what do you see coming?
Dr. Young: I think we’re getting close to something near curative for patients with malignant pheochromocytoma and paraganglioma. We’re understanding the basic biology better [and] pathophysiology, and I think that’s going to lead to some novel treatments.
Also, what I see coming is that we’ll be able to use germline mutation information and somatic tumor mutation information to guide us on specific imaging modalities, to guide us on forms of preventative therapy so that we prevent the paraganglioma from ever developing and also provide us with additional treatment options.
ORLANDO – The diagnosis of hypertension with its origin in the endocrine system may appear complex, but it does not have to be. Primary aldosteronism may be underappreciated and underdiagnosed. On the other hand, catecholamine-secreting tumors are rare, but they often come to mind in making a diagnosis of endocrine hypertension. Dr. William Young Jr., professor of medicine at the Mayo Clinic, Rochester, Minn., presented cases in a lively session of audience participation at the annual meeting of the America Association of Clinical Endocrinologists. Later, Dr. Young summarized some of the key points in an interview, which has been edited for brevity.
Frontline Medical News: What is the endocrinologist’s role in working up the patient who has hypertension of suspected endocrine origin?
Dr. William Young Jr.: The first is knowing when to suspect endocrine hypertension. The most common form of endocrine hypertension is primary aldosteronism. So this is the adrenal-dependent autonomous production of aldosterone, which leads to high blood pressure, volume expansion, and sometimes hypokalemia. One of the concepts that many clinicians forget is that only about 30% of patients with primary aldosteronism present with hypokalemia. So 70% of patients with this disorder don’t have hypokalemia. They look like any other person with high blood pressure.
So when should we look for primary aldosteronism? Onset of high blood pressure at a young age, for example, less than age 30, drug resistant hypertension – so three drugs [with] poor control. Twenty percent of those patients will prove to have primary aldosteronism. Simply poorly controlled hypertension is another group; [or] family history of primary aldosteronism, so all first degree relatives should be tested. Or a patient who has hypertension and has had an incidental discovery of an adrenal mass should also be tested for primary aldosteronism.
Unfortunately, most primary care providers ... think that this is a complicated and dense endocrine disorder, and they frequently will not look for it, but it’s actually very simple. Some of the complexities are historical in nature in that when this disorder was first described, several rules were made for what medications a patient could be on, for example. And it’s difficult to comply with those rules. For example, if you have a patient who’s on five drugs and has poor control, you’re not going to switch him to the two drugs that are recommended because they are weak antihypertensives. It wouldn’t be ethical to do so. [The two drug classes are the calcium channel blocker verapamil and the alpha-1 antagonists doxazosin (Cardura) and terazosin (Hytrin).]
So the best thing to do regardless of what drugs the patient is on – it doesn’t matter if they’re on ACE inhibitors or angiotensin-receptor blockers or diuretics – just get a morning blood sample as your aldosterone and plasma renin activity. If aldosterone is high or generous, greater than 15 ng/dL, if the plasma renin activity is less than 1 ng/mL per hour, that’s a positive case detection test.
That doesn’t prove the patient has primary aldosteronism. The sensitivity/specificity of aldosterone and renin case detection testing is about 75%. So most patients need confirmatory testing, which would either be the saline infusion test or the 24-hour urine for aldosterone on a high-sodium diet. And once primary aldosteronism is confirmed, then we would do an adrenal-directed CT scan.
The problem with the findings in the adrenal glands on CT is that the prevalence of adrenal nodularity increases with age. So people in their 60s and 70s can have adrenal nodules that have nothing to do with aldosterone production. So whereas if the patient is less than age 35 and CT shows a unilateral macroadenoma, the contralateral adrenal is perfectly normal appearing, and the patient has a marked primary aldosteronism – so spontaneous hypokalemia, plasma aldosterone over 30 ng/dL – that subset of patients could go straight to surgery and skip adrenal vein sampling. However, everyone else over age 35 if they want to pursue the surgical option, adrenal vein sampling is a key test.
FMN: Is there anything that rules out primary aldosteronism?
Dr. Young: If the plasma aldosterone level is less than 10 ng/dL it makes primary aldosteronism very unlikely, and if the renin level is higher than 1 ng/mL per hour, that makes primary aldosteronism very unlikely.
FMN: What about working up pheochromocytoma?
Dr. Young: Clinicians, unlike with primary aldosteronism, where they don’t look for it enough, for pheochromocytoma they look for it a lot, and it’s really rare. Between 0.1 and 0.01% of the hypertensive population will prove to have pheochromocytoma.
The false positive rate with our case detection testing of plasma metanephrines about 15%. So based on how rare pheochromocytoma is and a 15% false positive rate with plasma metanephrines, 97% of patients with elevated plasma normetanephrines do not have pheochromocytoma.
So we have a real problem with case detection testing. The 24-hour urine metanephrines and catecholamines using appropriate reference ranges are probably a better way to do case detection testing for pheochromocytoma, but there’s still a false positive rate with urinary normetanephrine.
Never mistake a benign adrenal adenoma for a pheo. In terms of the imaging phenotype, pheos are dense and vascular. As they enlarge, they get cystic hemorrhagic areas within them.
FMN: What goes on with other paragangliomas?
Dr. Young: Pheochromocytoma is the term we use when you have a catecholamine-secreting tumor in the adrenal gland itself. It develops in the adrenal medulla. Paraganglioma is an identical tumor, but it’s outside of the adrenal gland. It’s somewhere in the pelvis, could be in the chest, could be in the skull base, or neck. Most commonly it’s in the abdomen. So the case detection testing is the same.
But patients we should consider testing for pheochromocytoma and paraganglioma are those with paroxysmal symptoms like episodes of pounding heartbeat, sweating, headache, tremor, and pallor. Young people with new onset hypertension, hypertension that’s poorly controlled, and vascular adrenal masses should also be tested for pheochromocytoma.
FMN: Are there things that can confound any of these tests we discussed or any drugs that should be noted that could get in the way?
Dr. Young: For pheochromocytoma, the good news is now that most reference labs use tandem mass spectrometry technology, the hypertension drugs that potentially interfered in the past like labetalol and sotalol no longer interfere. So these days the clinician doesn’t need to stop any blood pressure–related medications.
The medications that can cause false positive testing are primarily tricyclic antidepressants. Flexeril, which is cyclobenzaprine, is commonly used to treat fibromyalgia, and that is a tricyclic antidepressant, and that will cause false positive testing ... with norepinephrine and normetanephrine. Tricyclic antidepressants can increase those levels three, four, or fivefold. Levodopa, which is in Sinemet, can cause false positive testing. Antipsychotics can cause false positive testing, and MAO inhibitors ... So the clinician shouldn’t worry about blood pressure medications but should worry about the other medications the patient is taking.
FMN: When someone looks at laboratory values, should you be comparing these values to people with hypertension who do not have these conditions, and do labs have adjusted values?
Dr. Young: That’s a good question, and in the Mayo medical lab, our reference range that we use is based on patients who were tested for pheochromocytoma [and] proved not to have it. So our cutoffs are 50% to 100% higher than some other reference labs.
These other reference labs use normal laboratory volunteers who have normal blood pressure and who are taking no medications, and I’ve never tested such a patient for pheochromocytoma, so why would we use that group of people to determine our reference range? So we should use reference ranges based on patients tested for pheo but who prove to not have pheo. And that leads to higher accuracy of our case detection tests.
FMN: What are the treatments for these conditions and follow-up? I take it if there’s an adrenal mass, you get a surgeon, and I think you also noted that you need an experienced endocrine surgeon.
Dr. Young: For primary aldosteronism, if the patient has a unilateral aldosterone-producing adenoma, the outstanding treatment is laparoscopic adrenalectomy. Patients are in the hospital one night, [and] they’re back at work in 7-10 days, but that does require an expert laparoscopic adrenal surgeon. And in the United States we have a 1-year endocrine surgery program. It’s optimal that patients are referred to surgeons who have done that unique training.
For pheochromocytoma less than 8-9 cm, laparoscopic adrenalectomy with an experienced endocrine surgeon is an excellent treatment option. When the adrenal pheochromocytoma is larger than 8 or 9 cm, especially if it’s cystic, the surgeon may want to do it as open [surgery] because it’s critical that the capsule of the pheochromocytoma is not ruptured intraoperatively. If it is ruptured, a benign pheochromocytoma has just been transformed to malignant, incurable disease.
If it’s a paraganglioma, typically that requires an open operation whether it’s in the neck or the chest or the pelvis or lower abdomen.
FMN: What is the follow-up to any of these conditions?
Dr. Young: The follow-up once you’ve resected an adrenal pheochromocytoma depends on whether there is a germline mutation. If there is a germline mutation, for example, succinate dehydrogenase mutation [SDH], these patients are at higher risk for developing recurrent pheochromocytoma or paraganglioma, and they’re at risk for developing malignant pheochromocytoma or paraganglioma.
One of our challenges is when we resect a pheochromocytoma or paraganglioma, the pathologist doesn’t have the tools to tell us if it’s benign or malignant ... So all patients need lifelong biochemical follow-up, basically a 24-hour urine for metanephrines and catecholamines annually or plasma metanephrines for life.
If the patients have an underlying mutation like succinate dehydrogenase, they’re at risk for developing nonfunctioning paragangliomas. So these patients need periodic imaging in addition to the annual biochemical testing. For example, if a patient had an abdominal paraganglioma with an SDHB [succinate dehydrogenase complex iron sulfur subunit B], we would do abdominal MRI scans every 1-2 years. That would include the pelvis. We would screen for paragangliomas elsewhere with MRI of the skull base and neck and the chest every 3-5 years, and a total body scan every 5 years or so, either FDG-PET [18F-fluorodeoxyglucose positron emission tomography] scan or 123I-MIBG [metaiodobenzyl-guanidine] scan.
FMN: Is there anything that is particularly new in the past couple of years?
Dr. Young: Some of the innovations lately have been in the area of metastatic pheochromocytoma and paraganglioma. These are in patients who have limited metastatic disease that’s localized to bone or to liver, and we’ve been using ablative therapies. This includes cryoablation ... and radiofrequency ablation, which is killing the tumor with hot temperature, and that’s very effective for patients who have limited metastatic lesions in the bone or liver.
For patients with complex tumors in difficult areas of the body, for example, in the mediastinum or surrounding the heart, we’ve been using 3D printer technology to print [a replica of the structures and] the tumor preoperatively, and this assists in surgical planning.
FMN: And what do you see coming?
Dr. Young: I think we’re getting close to something near curative for patients with malignant pheochromocytoma and paraganglioma. We’re understanding the basic biology better [and] pathophysiology, and I think that’s going to lead to some novel treatments.
Also, what I see coming is that we’ll be able to use germline mutation information and somatic tumor mutation information to guide us on specific imaging modalities, to guide us on forms of preventative therapy so that we prevent the paraganglioma from ever developing and also provide us with additional treatment options.
ORLANDO – The diagnosis of hypertension with its origin in the endocrine system may appear complex, but it does not have to be. Primary aldosteronism may be underappreciated and underdiagnosed. On the other hand, catecholamine-secreting tumors are rare, but they often come to mind in making a diagnosis of endocrine hypertension. Dr. William Young Jr., professor of medicine at the Mayo Clinic, Rochester, Minn., presented cases in a lively session of audience participation at the annual meeting of the America Association of Clinical Endocrinologists. Later, Dr. Young summarized some of the key points in an interview, which has been edited for brevity.
Frontline Medical News: What is the endocrinologist’s role in working up the patient who has hypertension of suspected endocrine origin?
Dr. William Young Jr.: The first is knowing when to suspect endocrine hypertension. The most common form of endocrine hypertension is primary aldosteronism. So this is the adrenal-dependent autonomous production of aldosterone, which leads to high blood pressure, volume expansion, and sometimes hypokalemia. One of the concepts that many clinicians forget is that only about 30% of patients with primary aldosteronism present with hypokalemia. So 70% of patients with this disorder don’t have hypokalemia. They look like any other person with high blood pressure.
So when should we look for primary aldosteronism? Onset of high blood pressure at a young age, for example, less than age 30, drug resistant hypertension – so three drugs [with] poor control. Twenty percent of those patients will prove to have primary aldosteronism. Simply poorly controlled hypertension is another group; [or] family history of primary aldosteronism, so all first degree relatives should be tested. Or a patient who has hypertension and has had an incidental discovery of an adrenal mass should also be tested for primary aldosteronism.
Unfortunately, most primary care providers ... think that this is a complicated and dense endocrine disorder, and they frequently will not look for it, but it’s actually very simple. Some of the complexities are historical in nature in that when this disorder was first described, several rules were made for what medications a patient could be on, for example. And it’s difficult to comply with those rules. For example, if you have a patient who’s on five drugs and has poor control, you’re not going to switch him to the two drugs that are recommended because they are weak antihypertensives. It wouldn’t be ethical to do so. [The two drug classes are the calcium channel blocker verapamil and the alpha-1 antagonists doxazosin (Cardura) and terazosin (Hytrin).]
So the best thing to do regardless of what drugs the patient is on – it doesn’t matter if they’re on ACE inhibitors or angiotensin-receptor blockers or diuretics – just get a morning blood sample as your aldosterone and plasma renin activity. If aldosterone is high or generous, greater than 15 ng/dL, if the plasma renin activity is less than 1 ng/mL per hour, that’s a positive case detection test.
That doesn’t prove the patient has primary aldosteronism. The sensitivity/specificity of aldosterone and renin case detection testing is about 75%. So most patients need confirmatory testing, which would either be the saline infusion test or the 24-hour urine for aldosterone on a high-sodium diet. And once primary aldosteronism is confirmed, then we would do an adrenal-directed CT scan.
The problem with the findings in the adrenal glands on CT is that the prevalence of adrenal nodularity increases with age. So people in their 60s and 70s can have adrenal nodules that have nothing to do with aldosterone production. So whereas if the patient is less than age 35 and CT shows a unilateral macroadenoma, the contralateral adrenal is perfectly normal appearing, and the patient has a marked primary aldosteronism – so spontaneous hypokalemia, plasma aldosterone over 30 ng/dL – that subset of patients could go straight to surgery and skip adrenal vein sampling. However, everyone else over age 35 if they want to pursue the surgical option, adrenal vein sampling is a key test.
FMN: Is there anything that rules out primary aldosteronism?
Dr. Young: If the plasma aldosterone level is less than 10 ng/dL it makes primary aldosteronism very unlikely, and if the renin level is higher than 1 ng/mL per hour, that makes primary aldosteronism very unlikely.
FMN: What about working up pheochromocytoma?
Dr. Young: Clinicians, unlike with primary aldosteronism, where they don’t look for it enough, for pheochromocytoma they look for it a lot, and it’s really rare. Between 0.1 and 0.01% of the hypertensive population will prove to have pheochromocytoma.
The false positive rate with our case detection testing of plasma metanephrines about 15%. So based on how rare pheochromocytoma is and a 15% false positive rate with plasma metanephrines, 97% of patients with elevated plasma normetanephrines do not have pheochromocytoma.
So we have a real problem with case detection testing. The 24-hour urine metanephrines and catecholamines using appropriate reference ranges are probably a better way to do case detection testing for pheochromocytoma, but there’s still a false positive rate with urinary normetanephrine.
Never mistake a benign adrenal adenoma for a pheo. In terms of the imaging phenotype, pheos are dense and vascular. As they enlarge, they get cystic hemorrhagic areas within them.
FMN: What goes on with other paragangliomas?
Dr. Young: Pheochromocytoma is the term we use when you have a catecholamine-secreting tumor in the adrenal gland itself. It develops in the adrenal medulla. Paraganglioma is an identical tumor, but it’s outside of the adrenal gland. It’s somewhere in the pelvis, could be in the chest, could be in the skull base, or neck. Most commonly it’s in the abdomen. So the case detection testing is the same.
But patients we should consider testing for pheochromocytoma and paraganglioma are those with paroxysmal symptoms like episodes of pounding heartbeat, sweating, headache, tremor, and pallor. Young people with new onset hypertension, hypertension that’s poorly controlled, and vascular adrenal masses should also be tested for pheochromocytoma.
FMN: Are there things that can confound any of these tests we discussed or any drugs that should be noted that could get in the way?
Dr. Young: For pheochromocytoma, the good news is now that most reference labs use tandem mass spectrometry technology, the hypertension drugs that potentially interfered in the past like labetalol and sotalol no longer interfere. So these days the clinician doesn’t need to stop any blood pressure–related medications.
The medications that can cause false positive testing are primarily tricyclic antidepressants. Flexeril, which is cyclobenzaprine, is commonly used to treat fibromyalgia, and that is a tricyclic antidepressant, and that will cause false positive testing ... with norepinephrine and normetanephrine. Tricyclic antidepressants can increase those levels three, four, or fivefold. Levodopa, which is in Sinemet, can cause false positive testing. Antipsychotics can cause false positive testing, and MAO inhibitors ... So the clinician shouldn’t worry about blood pressure medications but should worry about the other medications the patient is taking.
FMN: When someone looks at laboratory values, should you be comparing these values to people with hypertension who do not have these conditions, and do labs have adjusted values?
Dr. Young: That’s a good question, and in the Mayo medical lab, our reference range that we use is based on patients who were tested for pheochromocytoma [and] proved not to have it. So our cutoffs are 50% to 100% higher than some other reference labs.
These other reference labs use normal laboratory volunteers who have normal blood pressure and who are taking no medications, and I’ve never tested such a patient for pheochromocytoma, so why would we use that group of people to determine our reference range? So we should use reference ranges based on patients tested for pheo but who prove to not have pheo. And that leads to higher accuracy of our case detection tests.
FMN: What are the treatments for these conditions and follow-up? I take it if there’s an adrenal mass, you get a surgeon, and I think you also noted that you need an experienced endocrine surgeon.
Dr. Young: For primary aldosteronism, if the patient has a unilateral aldosterone-producing adenoma, the outstanding treatment is laparoscopic adrenalectomy. Patients are in the hospital one night, [and] they’re back at work in 7-10 days, but that does require an expert laparoscopic adrenal surgeon. And in the United States we have a 1-year endocrine surgery program. It’s optimal that patients are referred to surgeons who have done that unique training.
For pheochromocytoma less than 8-9 cm, laparoscopic adrenalectomy with an experienced endocrine surgeon is an excellent treatment option. When the adrenal pheochromocytoma is larger than 8 or 9 cm, especially if it’s cystic, the surgeon may want to do it as open [surgery] because it’s critical that the capsule of the pheochromocytoma is not ruptured intraoperatively. If it is ruptured, a benign pheochromocytoma has just been transformed to malignant, incurable disease.
If it’s a paraganglioma, typically that requires an open operation whether it’s in the neck or the chest or the pelvis or lower abdomen.
FMN: What is the follow-up to any of these conditions?
Dr. Young: The follow-up once you’ve resected an adrenal pheochromocytoma depends on whether there is a germline mutation. If there is a germline mutation, for example, succinate dehydrogenase mutation [SDH], these patients are at higher risk for developing recurrent pheochromocytoma or paraganglioma, and they’re at risk for developing malignant pheochromocytoma or paraganglioma.
One of our challenges is when we resect a pheochromocytoma or paraganglioma, the pathologist doesn’t have the tools to tell us if it’s benign or malignant ... So all patients need lifelong biochemical follow-up, basically a 24-hour urine for metanephrines and catecholamines annually or plasma metanephrines for life.
If the patients have an underlying mutation like succinate dehydrogenase, they’re at risk for developing nonfunctioning paragangliomas. So these patients need periodic imaging in addition to the annual biochemical testing. For example, if a patient had an abdominal paraganglioma with an SDHB [succinate dehydrogenase complex iron sulfur subunit B], we would do abdominal MRI scans every 1-2 years. That would include the pelvis. We would screen for paragangliomas elsewhere with MRI of the skull base and neck and the chest every 3-5 years, and a total body scan every 5 years or so, either FDG-PET [18F-fluorodeoxyglucose positron emission tomography] scan or 123I-MIBG [metaiodobenzyl-guanidine] scan.
FMN: Is there anything that is particularly new in the past couple of years?
Dr. Young: Some of the innovations lately have been in the area of metastatic pheochromocytoma and paraganglioma. These are in patients who have limited metastatic disease that’s localized to bone or to liver, and we’ve been using ablative therapies. This includes cryoablation ... and radiofrequency ablation, which is killing the tumor with hot temperature, and that’s very effective for patients who have limited metastatic lesions in the bone or liver.
For patients with complex tumors in difficult areas of the body, for example, in the mediastinum or surrounding the heart, we’ve been using 3D printer technology to print [a replica of the structures and] the tumor preoperatively, and this assists in surgical planning.
FMN: And what do you see coming?
Dr. Young: I think we’re getting close to something near curative for patients with malignant pheochromocytoma and paraganglioma. We’re understanding the basic biology better [and] pathophysiology, and I think that’s going to lead to some novel treatments.
Also, what I see coming is that we’ll be able to use germline mutation information and somatic tumor mutation information to guide us on specific imaging modalities, to guide us on forms of preventative therapy so that we prevent the paraganglioma from ever developing and also provide us with additional treatment options.
EXPERT ANALYSIS AT AACE 2016

High-tech pills help increase medication adherence
orlando – A digital device that patients swallow every time they take a medication may be an answer to improving compliance and disease control. An aim of this digital health system is to encourage patient engagement and provider interaction. Despite available and efficacious medicines, only slightly more than half of patients with type 2 diabetes mellitus have glycated hemoglobin (HbA1c), hypertension, or LDL cholesterol under good control. One study showed only 17% had all three under control (Endocr Pract. 2016;22:689-98).
“Important in this are the facts of medication nonadherence by the patient, poor patient engagement frequently in their care, as well as from a clinician perspective, therapeutic inertia,” said Dr. Juan Frias at the annual meeting of the American Association of Clinical Endocrinologists. Approximately half of patients with chronic diseases do not take their medications as prescribed (Circulation. 2013;128:29-41).

To improve treatment adherence, diagnose the reasons for a patient not reaching therapeutic goals, address those issues with patient education or counseling or changes in medication, and engage with the patient to reinforce adherence goals. A digital system called Proteus Discover has been designed to assist patients and clinicians with all these tasks.
Proteus uses ingestible sensor-detectable medications. Each medication and dose of medication has a unique marker. A compounding pharmacy co-encapsulates a tiny detectable chip about the size of a grain of sand with a medication as prescribed by a physician. The patient wears a Band-Aid sized skin patch sensor that transmits to a mobile device that uploads to a secure cloud server. The sensor can tell if a medication has been taken and also serves as a pedometer and activity gauge.
The information is available to the patient, who can gain insight into medication taking, activity, and rest, along with other health parameters that are entered into the system. Entering the system through a provider portal and with the patient’s permission, the clinician can see patient behavior patterns outside of the clinic, including medication adherence, which helps to determine the best treatment for that patient. The system provides a report to the clinician that can be a point of discussion when the patient visits the clinic.
Trial demonstrates better medication adherence and goal attainment
Dr. Frias, CEO and principal investigator of National Research Institute in Los Angeles, described a 12 week multicenter cluster-randomized pilot study involving 90 patients with uncontrolled hypertension and type 2 diabetes to investigate the effect of Proteus on blood pressure, HbA1c, and LDL cholesterol reduction. Other goals of the trial were to promote medication adherence and physical activity and alert providers to a need to make more medical decisions.
Cluster randomization meant that each of the 16 trial sites randomized patients to one of three treatment arms within that site. The arms were: Proteus Discover for 4 or 12 weeks or usual care. Patients had to have systolic blood pressure of 140 mm Hg or greater, have failed therapy with 2 or more antihypertensive agents, and have HbA1c at 7% or greater on metformin or a sulfonylurea. Two-thirds of the subjects also had dyslipidemia and were treated with statins. Subjects were excluded if they had a history of acute or chronic dermatitis, had a skin allergy or sensitivity to adhesive medical tape, or had secondary causes for uncontrolled hypertension or type 2 diabetes.
Usual care consisted of all standard interventions, including medication titrations, patient education, and lifestyle coaching. All subjects took medications for 12 weeks and were followed for 12 weeks after enrollment. Available medications were various doses of lisinopril, losartan, hydrochlorothiazide, amlodipine, atorvastatin, metformin, and glipizide.
All the arms were fairly well balanced as to age (58-62 years), ethnicity, employment, education, and income. About one quarter had incomes in the $20,000-$40,000 range, and about half had incomes of $20,000 or less. Body mass index was 32 kg/m2 in the Proteus and usual care arms. Total cholesterol was similar for the Proteus and usual care groups at 173-177 mg/dL, but LDL was slightly higher in the Proteus arms (103 vs. 95 mg/dL).
Better adherence and outcomes for patients using Proteus
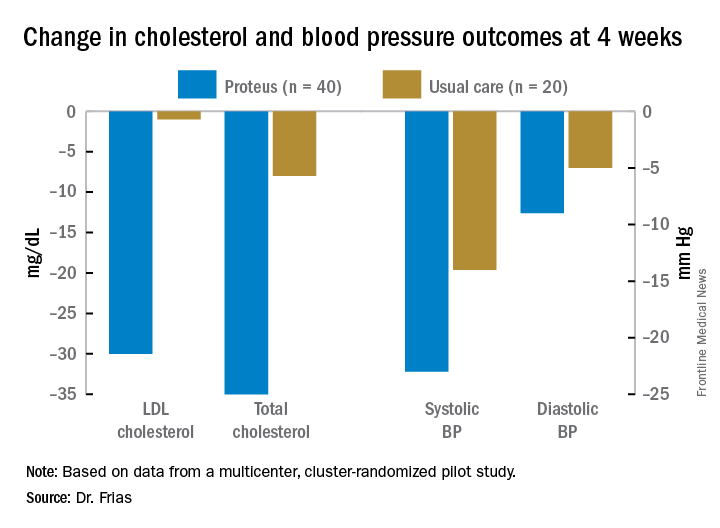
Dr. Frias presented 4-week results for blood pressure and cholesterol reduction. The 4- and 12-week Proteus arms were combined for this analysis, since up to 4 weeks they received the same intervention. Blood pressure, LDL cholesterol, and total cholesterol were all significantly reduced in the Proteus group, compared with the usual care group. At week 4, 83% of the subjects in the Proteus group had reached a blood pressure goal of less than 140/90 mm Hg vs. 33% in the usual care arm (difference of 50%; 95% confidence interval, 24%, 76%). Across all 11 medications/doses, the adherence was between 80% and 89% for every one.
The system spurred clinicians to make more treatment decisions for their patients. Providers made more changes to treatment for the Proteus patients, compared with the usual care providers (50% vs. 36%), gave more adherence counseling (28% vs. 0%), and provided more patient education (42% vs. 9%). Patients using the Proteus Discover system expressed high levels of satisfaction and acceptance of the technology (83%-100%), including ease of use in one’s daily routine, learning to use it, motivation to manage one’s health, better discussions with providers, understanding their care plan, seeing how they take their medications, and applying and wearing the sensor patch.
Safety was excellent. Twenty-seven adverse effects occurred in the Proteus arms, none of them serious, and about half were attributed to the device, mostly self-limited rashes. Seven adverse effects were attributed to the medications, mostly gastrointestinal side effects. There were four adverse effects in the usual care group, two of them serious.
Overall, compared with about 50% typical medication adherence, Proteus users had 84% adherence, which was associated with better blood pressure and LDL cholesterol control, compared with usual care.

Session moderator Dr. David Lieb, associate professor of medicine at Eastern Virginia Medical School in Norfolk, said the Proteus system may be very helpful for patients who are taking multiple medications to prompt them when to take them. “I could easily see somebody who has this system in place where they’re also able to measure their blood pressure and get that information to their provider and for their provider to make changes in their medicine dose,” he said.
This research study of 90 patients was quite manageable, but “what about when you have 300 people on this therapy and all those data are starting to come in? Who’s going to manage those data... and look at it all?” Dr. Lieb wondered. Patients may have to be taught to understand the data and make changes on their own to their medication behavior, exercise, and other factors within their control.
Half the patients in the study made $20,000 or less a year. “If you could help underserved patients with their compliance and all those other things... that would be fantastic. It’s a huge area of need,” he said. People will need internet access to upload their data to the cloud server.
Another question is how the data can interface with the various electronic health records in use and generate reports.
Proteus Discover is approved by the U.S. Food and Drug Administration and is available now.
orlando – A digital device that patients swallow every time they take a medication may be an answer to improving compliance and disease control. An aim of this digital health system is to encourage patient engagement and provider interaction. Despite available and efficacious medicines, only slightly more than half of patients with type 2 diabetes mellitus have glycated hemoglobin (HbA1c), hypertension, or LDL cholesterol under good control. One study showed only 17% had all three under control (Endocr Pract. 2016;22:689-98).
“Important in this are the facts of medication nonadherence by the patient, poor patient engagement frequently in their care, as well as from a clinician perspective, therapeutic inertia,” said Dr. Juan Frias at the annual meeting of the American Association of Clinical Endocrinologists. Approximately half of patients with chronic diseases do not take their medications as prescribed (Circulation. 2013;128:29-41).
To improve treatment adherence, diagnose the reasons for a patient not reaching therapeutic goals, address those issues with patient education or counseling or changes in medication, and engage with the patient to reinforce adherence goals. A digital system called Proteus Discover has been designed to assist patients and clinicians with all these tasks.
Proteus uses ingestible sensor-detectable medications. Each medication and dose of medication has a unique marker. A compounding pharmacy co-encapsulates a tiny detectable chip about the size of a grain of sand with a medication as prescribed by a physician. The patient wears a Band-Aid sized skin patch sensor that transmits to a mobile device that uploads to a secure cloud server. The sensor can tell if a medication has been taken and also serves as a pedometer and activity gauge.
The information is available to the patient, who can gain insight into medication taking, activity, and rest, along with other health parameters that are entered into the system. Entering the system through a provider portal and with the patient’s permission, the clinician can see patient behavior patterns outside of the clinic, including medication adherence, which helps to determine the best treatment for that patient. The system provides a report to the clinician that can be a point of discussion when the patient visits the clinic.
Trial demonstrates better medication adherence and goal attainment
Dr. Frias, CEO and principal investigator of National Research Institute in Los Angeles, described a 12 week multicenter cluster-randomized pilot study involving 90 patients with uncontrolled hypertension and type 2 diabetes to investigate the effect of Proteus on blood pressure, HbA1c, and LDL cholesterol reduction. Other goals of the trial were to promote medication adherence and physical activity and alert providers to a need to make more medical decisions.
Cluster randomization meant that each of the 16 trial sites randomized patients to one of three treatment arms within that site. The arms were: Proteus Discover for 4 or 12 weeks or usual care. Patients had to have systolic blood pressure of 140 mm Hg or greater, have failed therapy with 2 or more antihypertensive agents, and have HbA1c at 7% or greater on metformin or a sulfonylurea. Two-thirds of the subjects also had dyslipidemia and were treated with statins. Subjects were excluded if they had a history of acute or chronic dermatitis, had a skin allergy or sensitivity to adhesive medical tape, or had secondary causes for uncontrolled hypertension or type 2 diabetes.
Usual care consisted of all standard interventions, including medication titrations, patient education, and lifestyle coaching. All subjects took medications for 12 weeks and were followed for 12 weeks after enrollment. Available medications were various doses of lisinopril, losartan, hydrochlorothiazide, amlodipine, atorvastatin, metformin, and glipizide.
All the arms were fairly well balanced as to age (58-62 years), ethnicity, employment, education, and income. About one quarter had incomes in the $20,000-$40,000 range, and about half had incomes of $20,000 or less. Body mass index was 32 kg/m2 in the Proteus and usual care arms. Total cholesterol was similar for the Proteus and usual care groups at 173-177 mg/dL, but LDL was slightly higher in the Proteus arms (103 vs. 95 mg/dL).
Better adherence and outcomes for patients using Proteus
Dr. Frias presented 4-week results for blood pressure and cholesterol reduction. The 4- and 12-week Proteus arms were combined for this analysis, since up to 4 weeks they received the same intervention. Blood pressure, LDL cholesterol, and total cholesterol were all significantly reduced in the Proteus group, compared with the usual care group. At week 4, 83% of the subjects in the Proteus group had reached a blood pressure goal of less than 140/90 mm Hg vs. 33% in the usual care arm (difference of 50%; 95% confidence interval, 24%, 76%). Across all 11 medications/doses, the adherence was between 80% and 89% for every one.
The system spurred clinicians to make more treatment decisions for their patients. Providers made more changes to treatment for the Proteus patients, compared with the usual care providers (50% vs. 36%), gave more adherence counseling (28% vs. 0%), and provided more patient education (42% vs. 9%). Patients using the Proteus Discover system expressed high levels of satisfaction and acceptance of the technology (83%-100%), including ease of use in one’s daily routine, learning to use it, motivation to manage one’s health, better discussions with providers, understanding their care plan, seeing how they take their medications, and applying and wearing the sensor patch.
Safety was excellent. Twenty-seven adverse effects occurred in the Proteus arms, none of them serious, and about half were attributed to the device, mostly self-limited rashes. Seven adverse effects were attributed to the medications, mostly gastrointestinal side effects. There were four adverse effects in the usual care group, two of them serious.
Overall, compared with about 50% typical medication adherence, Proteus users had 84% adherence, which was associated with better blood pressure and LDL cholesterol control, compared with usual care.
Session moderator Dr. David Lieb, associate professor of medicine at Eastern Virginia Medical School in Norfolk, said the Proteus system may be very helpful for patients who are taking multiple medications to prompt them when to take them. “I could easily see somebody who has this system in place where they’re also able to measure their blood pressure and get that information to their provider and for their provider to make changes in their medicine dose,” he said.
This research study of 90 patients was quite manageable, but “what about when you have 300 people on this therapy and all those data are starting to come in? Who’s going to manage those data... and look at it all?” Dr. Lieb wondered. Patients may have to be taught to understand the data and make changes on their own to their medication behavior, exercise, and other factors within their control.
Half the patients in the study made $20,000 or less a year. “If you could help underserved patients with their compliance and all those other things... that would be fantastic. It’s a huge area of need,” he said. People will need internet access to upload their data to the cloud server.
Another question is how the data can interface with the various electronic health records in use and generate reports.
Proteus Discover is approved by the U.S. Food and Drug Administration and is available now.
orlando – A digital device that patients swallow every time they take a medication may be an answer to improving compliance and disease control. An aim of this digital health system is to encourage patient engagement and provider interaction. Despite available and efficacious medicines, only slightly more than half of patients with type 2 diabetes mellitus have glycated hemoglobin (HbA1c), hypertension, or LDL cholesterol under good control. One study showed only 17% had all three under control (Endocr Pract. 2016;22:689-98).
“Important in this are the facts of medication nonadherence by the patient, poor patient engagement frequently in their care, as well as from a clinician perspective, therapeutic inertia,” said Dr. Juan Frias at the annual meeting of the American Association of Clinical Endocrinologists. Approximately half of patients with chronic diseases do not take their medications as prescribed (Circulation. 2013;128:29-41).
To improve treatment adherence, diagnose the reasons for a patient not reaching therapeutic goals, address those issues with patient education or counseling or changes in medication, and engage with the patient to reinforce adherence goals. A digital system called Proteus Discover has been designed to assist patients and clinicians with all these tasks.
Proteus uses ingestible sensor-detectable medications. Each medication and dose of medication has a unique marker. A compounding pharmacy co-encapsulates a tiny detectable chip about the size of a grain of sand with a medication as prescribed by a physician. The patient wears a Band-Aid sized skin patch sensor that transmits to a mobile device that uploads to a secure cloud server. The sensor can tell if a medication has been taken and also serves as a pedometer and activity gauge.
The information is available to the patient, who can gain insight into medication taking, activity, and rest, along with other health parameters that are entered into the system. Entering the system through a provider portal and with the patient’s permission, the clinician can see patient behavior patterns outside of the clinic, including medication adherence, which helps to determine the best treatment for that patient. The system provides a report to the clinician that can be a point of discussion when the patient visits the clinic.
Trial demonstrates better medication adherence and goal attainment
Dr. Frias, CEO and principal investigator of National Research Institute in Los Angeles, described a 12 week multicenter cluster-randomized pilot study involving 90 patients with uncontrolled hypertension and type 2 diabetes to investigate the effect of Proteus on blood pressure, HbA1c, and LDL cholesterol reduction. Other goals of the trial were to promote medication adherence and physical activity and alert providers to a need to make more medical decisions.
Cluster randomization meant that each of the 16 trial sites randomized patients to one of three treatment arms within that site. The arms were: Proteus Discover for 4 or 12 weeks or usual care. Patients had to have systolic blood pressure of 140 mm Hg or greater, have failed therapy with 2 or more antihypertensive agents, and have HbA1c at 7% or greater on metformin or a sulfonylurea. Two-thirds of the subjects also had dyslipidemia and were treated with statins. Subjects were excluded if they had a history of acute or chronic dermatitis, had a skin allergy or sensitivity to adhesive medical tape, or had secondary causes for uncontrolled hypertension or type 2 diabetes.
Usual care consisted of all standard interventions, including medication titrations, patient education, and lifestyle coaching. All subjects took medications for 12 weeks and were followed for 12 weeks after enrollment. Available medications were various doses of lisinopril, losartan, hydrochlorothiazide, amlodipine, atorvastatin, metformin, and glipizide.
All the arms were fairly well balanced as to age (58-62 years), ethnicity, employment, education, and income. About one quarter had incomes in the $20,000-$40,000 range, and about half had incomes of $20,000 or less. Body mass index was 32 kg/m2 in the Proteus and usual care arms. Total cholesterol was similar for the Proteus and usual care groups at 173-177 mg/dL, but LDL was slightly higher in the Proteus arms (103 vs. 95 mg/dL).
Better adherence and outcomes for patients using Proteus
Dr. Frias presented 4-week results for blood pressure and cholesterol reduction. The 4- and 12-week Proteus arms were combined for this analysis, since up to 4 weeks they received the same intervention. Blood pressure, LDL cholesterol, and total cholesterol were all significantly reduced in the Proteus group, compared with the usual care group. At week 4, 83% of the subjects in the Proteus group had reached a blood pressure goal of less than 140/90 mm Hg vs. 33% in the usual care arm (difference of 50%; 95% confidence interval, 24%, 76%). Across all 11 medications/doses, the adherence was between 80% and 89% for every one.
The system spurred clinicians to make more treatment decisions for their patients. Providers made more changes to treatment for the Proteus patients, compared with the usual care providers (50% vs. 36%), gave more adherence counseling (28% vs. 0%), and provided more patient education (42% vs. 9%). Patients using the Proteus Discover system expressed high levels of satisfaction and acceptance of the technology (83%-100%), including ease of use in one’s daily routine, learning to use it, motivation to manage one’s health, better discussions with providers, understanding their care plan, seeing how they take their medications, and applying and wearing the sensor patch.
Safety was excellent. Twenty-seven adverse effects occurred in the Proteus arms, none of them serious, and about half were attributed to the device, mostly self-limited rashes. Seven adverse effects were attributed to the medications, mostly gastrointestinal side effects. There were four adverse effects in the usual care group, two of them serious.
Overall, compared with about 50% typical medication adherence, Proteus users had 84% adherence, which was associated with better blood pressure and LDL cholesterol control, compared with usual care.
Session moderator Dr. David Lieb, associate professor of medicine at Eastern Virginia Medical School in Norfolk, said the Proteus system may be very helpful for patients who are taking multiple medications to prompt them when to take them. “I could easily see somebody who has this system in place where they’re also able to measure their blood pressure and get that information to their provider and for their provider to make changes in their medicine dose,” he said.
This research study of 90 patients was quite manageable, but “what about when you have 300 people on this therapy and all those data are starting to come in? Who’s going to manage those data... and look at it all?” Dr. Lieb wondered. Patients may have to be taught to understand the data and make changes on their own to their medication behavior, exercise, and other factors within their control.
Half the patients in the study made $20,000 or less a year. “If you could help underserved patients with their compliance and all those other things... that would be fantastic. It’s a huge area of need,” he said. People will need internet access to upload their data to the cloud server.
Another question is how the data can interface with the various electronic health records in use and generate reports.
Proteus Discover is approved by the U.S. Food and Drug Administration and is available now.
AT AACE 2016
Key clinical point: Feedback from a system of digital-enabled pills enhanced medication adherence.
Major finding: Patients using Proteus had 84% adherence and better risk control.
Data source: Randomized unblinded study of 90 patients.
Disclosures: Dr. Frias has study grants from AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Johnson & Johnson, Merck, Novo Nordisk, Pfizer, and Sanofi and has consulting relationships with Proteus Digital Health, Johnson & Johnson, AstraZeneca, CeQur, and Sanofi.

Anticlaudin antibody increases survival in advanced gastric cancer
CHICAGO – The novel antibody IMAB362 extended survival of patients with advanced gastric cancer when added to chemotherapy, according to a phase II trial presented at the annual meeting of the Society of Clinical Oncology.
IMAB362 is a first-in-class monoclonal antibody targeting claudin18.2, a protein component of cellular tight junctions abundant in gastric tumors, as well as tumors of the pancreas, lung, esophagus, and ovaries.
IMAB362 significantly extended median overall survival (OS) when added to standard chemotherapy (13.2 vs. 8.4 months, hazard ratio [HR] = 0.51, P = .0001). Patients with the highest levels of claudin18.2 had an even longer median overall survival (16.7 vs. 9.0 months, HR = 0.45, P less than .0005).
The FAST (Phase II First-Line Therapy in Patients With Advanced CLDN18.2+ Gastric and Gastroesophageal Junction Adenocarcinoma) trial included patients who had no prior chemotherapy for locally advanced or metastatic disease. Tumors had to have 2+/3+ CLDN18.2 expression in 40% or more of tumor cells, and patients had an Eastern Cooperative Oncology Group performance status of 0-1.
Patients with tumors that expressed higher levels of claudin18,2, the target antigen, did better than the overall cohort in terms of progression-free survival (PFS), the primary endpoint.

“The FAST trial clearly met its primary endpoint, and there is a significant improvement in PFS and OS in the entire cohort and also in the higher expressers,” lead author Dr. Salah-Eddin Al-Batran, medical director of the Institute of Clinical Cancer Research, Nordwest Hospital in Frankfurst am Main, Germany, said in a news conference at the meeting.
The IMAB362 monoclonal antibody is highly specific for CLDN18.2 and works through antibody-dependent cellular cytotoxicity and complement-dependent cytotoxicity. In combination with chemotherapy, by binding to tumor debris, it is an immunomodulator of the tumor microenvironment.
About 50% of gastric tumors express CLDN18.2. After screening, the investigators randomized 246 patients to three treatment arms: epirubicin/oxaliplatin/capecitabine (EOX), n = 84; EOX + IMAB362 at a loading dose of 800 mg/m2, then 600 mg/m2 on day 1 every 3 weeks, n = 77; or a higher dose of IMAB362 with EOX, n = 85. Dr. Al-Batran reported results of the first two arms and will present results for the third arm at a later time.
Median progression-free survival was 4.8 months with EOX and 7.9 months with EOX plus IMAB362 (HR = .47; P = .0001).
If 70% or more of the tumor cells expressed CLDN18.2, IMAB362 improved the median PFS from 5.6 months for EOX alone to 7.2 months (HR = 0.36, P less than .0005), and OS improved from 9 months to 16.7 months (HR = 0.45, P less than .0005).
Response rates were also better with the addition of IMAB362. The objective response rate by RECIST criteria was 39.0% with EOX + IMAB362 vs. 25.0% with EOX alone. Most of the responses were partial (28.6% vs. 21.4%, respectively) or stable disease (44.2% vs. 51.2%, respectively). There were only 10.4% complete responses with IMAB362 and 3.6% with EOX alone. About 12% of the patients in each arm were not evaluable, or the data were missing.
Both treatments were well tolerated, with most adverse effects being grade 1/2. However, there was more grade 3/4 neutropenia with the combination (32.5% vs. 21.4% for EOX alone) as well as grade 3/4 vomiting (10.4% vs. 3.6%, respectively). Grade 1/2 vomiting was common in both arms, with about one-third of patients receiving EOX alone and just over half of patients on EOX + IMAB362 being affected.

Dr. Al-Batran said that there may have been more vomiting with IMAB362 because tight junction proteins, including claudin, are present in the gastric mucosa. Diarrhea was largely grade 1/2, affected about one-third of patients receiving EOX alone, and was only about half as common among patients receiving the combination.
Dr. Al-Batran said this trial “provides a strong rationale for a confirmatory phase III trial.”
Press conference moderator Dr. Smitha Krishnamurthi said the study is important because it documents the activity of a first-in-class antibody in patients with advanced gastric and gastroesophageal junction cancers. Since CLDN18.2 is expressed in about 50% of these cancers, “this treatment could apply to many patients,” she said.
The study was initiated and sponsored by Ganymed Pharmaceuticals. Dr. Al-Batran has had a consulting or advisory role with Merck, Roche, Celgene, and Lilly; has been on the speakers bureau of Lilly, Roche, Celgene, and Nordic Bioscience; and has received research funding from Celgene, Roche Pharma, Lilly, Novartis, Vfor Pharma, Medac, and Hospira.
On Twitter @OncologyPractic
CHICAGO – The novel antibody IMAB362 extended survival of patients with advanced gastric cancer when added to chemotherapy, according to a phase II trial presented at the annual meeting of the Society of Clinical Oncology.
IMAB362 is a first-in-class monoclonal antibody targeting claudin18.2, a protein component of cellular tight junctions abundant in gastric tumors, as well as tumors of the pancreas, lung, esophagus, and ovaries.
IMAB362 significantly extended median overall survival (OS) when added to standard chemotherapy (13.2 vs. 8.4 months, hazard ratio [HR] = 0.51, P = .0001). Patients with the highest levels of claudin18.2 had an even longer median overall survival (16.7 vs. 9.0 months, HR = 0.45, P less than .0005).
The FAST (Phase II First-Line Therapy in Patients With Advanced CLDN18.2+ Gastric and Gastroesophageal Junction Adenocarcinoma) trial included patients who had no prior chemotherapy for locally advanced or metastatic disease. Tumors had to have 2+/3+ CLDN18.2 expression in 40% or more of tumor cells, and patients had an Eastern Cooperative Oncology Group performance status of 0-1.
Patients with tumors that expressed higher levels of claudin18,2, the target antigen, did better than the overall cohort in terms of progression-free survival (PFS), the primary endpoint.
“The FAST trial clearly met its primary endpoint, and there is a significant improvement in PFS and OS in the entire cohort and also in the higher expressers,” lead author Dr. Salah-Eddin Al-Batran, medical director of the Institute of Clinical Cancer Research, Nordwest Hospital in Frankfurst am Main, Germany, said in a news conference at the meeting.
The IMAB362 monoclonal antibody is highly specific for CLDN18.2 and works through antibody-dependent cellular cytotoxicity and complement-dependent cytotoxicity. In combination with chemotherapy, by binding to tumor debris, it is an immunomodulator of the tumor microenvironment.
About 50% of gastric tumors express CLDN18.2. After screening, the investigators randomized 246 patients to three treatment arms: epirubicin/oxaliplatin/capecitabine (EOX), n = 84; EOX + IMAB362 at a loading dose of 800 mg/m2, then 600 mg/m2 on day 1 every 3 weeks, n = 77; or a higher dose of IMAB362 with EOX, n = 85. Dr. Al-Batran reported results of the first two arms and will present results for the third arm at a later time.
Median progression-free survival was 4.8 months with EOX and 7.9 months with EOX plus IMAB362 (HR = .47; P = .0001).
If 70% or more of the tumor cells expressed CLDN18.2, IMAB362 improved the median PFS from 5.6 months for EOX alone to 7.2 months (HR = 0.36, P less than .0005), and OS improved from 9 months to 16.7 months (HR = 0.45, P less than .0005).
Response rates were also better with the addition of IMAB362. The objective response rate by RECIST criteria was 39.0% with EOX + IMAB362 vs. 25.0% with EOX alone. Most of the responses were partial (28.6% vs. 21.4%, respectively) or stable disease (44.2% vs. 51.2%, respectively). There were only 10.4% complete responses with IMAB362 and 3.6% with EOX alone. About 12% of the patients in each arm were not evaluable, or the data were missing.
Both treatments were well tolerated, with most adverse effects being grade 1/2. However, there was more grade 3/4 neutropenia with the combination (32.5% vs. 21.4% for EOX alone) as well as grade 3/4 vomiting (10.4% vs. 3.6%, respectively). Grade 1/2 vomiting was common in both arms, with about one-third of patients receiving EOX alone and just over half of patients on EOX + IMAB362 being affected.
Dr. Al-Batran said that there may have been more vomiting with IMAB362 because tight junction proteins, including claudin, are present in the gastric mucosa. Diarrhea was largely grade 1/2, affected about one-third of patients receiving EOX alone, and was only about half as common among patients receiving the combination.
Dr. Al-Batran said this trial “provides a strong rationale for a confirmatory phase III trial.”
Press conference moderator Dr. Smitha Krishnamurthi said the study is important because it documents the activity of a first-in-class antibody in patients with advanced gastric and gastroesophageal junction cancers. Since CLDN18.2 is expressed in about 50% of these cancers, “this treatment could apply to many patients,” she said.
The study was initiated and sponsored by Ganymed Pharmaceuticals. Dr. Al-Batran has had a consulting or advisory role with Merck, Roche, Celgene, and Lilly; has been on the speakers bureau of Lilly, Roche, Celgene, and Nordic Bioscience; and has received research funding from Celgene, Roche Pharma, Lilly, Novartis, Vfor Pharma, Medac, and Hospira.
On Twitter @OncologyPractic
CHICAGO – The novel antibody IMAB362 extended survival of patients with advanced gastric cancer when added to chemotherapy, according to a phase II trial presented at the annual meeting of the Society of Clinical Oncology.
IMAB362 is a first-in-class monoclonal antibody targeting claudin18.2, a protein component of cellular tight junctions abundant in gastric tumors, as well as tumors of the pancreas, lung, esophagus, and ovaries.
IMAB362 significantly extended median overall survival (OS) when added to standard chemotherapy (13.2 vs. 8.4 months, hazard ratio [HR] = 0.51, P = .0001). Patients with the highest levels of claudin18.2 had an even longer median overall survival (16.7 vs. 9.0 months, HR = 0.45, P less than .0005).
The FAST (Phase II First-Line Therapy in Patients With Advanced CLDN18.2+ Gastric and Gastroesophageal Junction Adenocarcinoma) trial included patients who had no prior chemotherapy for locally advanced or metastatic disease. Tumors had to have 2+/3+ CLDN18.2 expression in 40% or more of tumor cells, and patients had an Eastern Cooperative Oncology Group performance status of 0-1.
Patients with tumors that expressed higher levels of claudin18,2, the target antigen, did better than the overall cohort in terms of progression-free survival (PFS), the primary endpoint.
“The FAST trial clearly met its primary endpoint, and there is a significant improvement in PFS and OS in the entire cohort and also in the higher expressers,” lead author Dr. Salah-Eddin Al-Batran, medical director of the Institute of Clinical Cancer Research, Nordwest Hospital in Frankfurst am Main, Germany, said in a news conference at the meeting.
The IMAB362 monoclonal antibody is highly specific for CLDN18.2 and works through antibody-dependent cellular cytotoxicity and complement-dependent cytotoxicity. In combination with chemotherapy, by binding to tumor debris, it is an immunomodulator of the tumor microenvironment.
About 50% of gastric tumors express CLDN18.2. After screening, the investigators randomized 246 patients to three treatment arms: epirubicin/oxaliplatin/capecitabine (EOX), n = 84; EOX + IMAB362 at a loading dose of 800 mg/m2, then 600 mg/m2 on day 1 every 3 weeks, n = 77; or a higher dose of IMAB362 with EOX, n = 85. Dr. Al-Batran reported results of the first two arms and will present results for the third arm at a later time.
Median progression-free survival was 4.8 months with EOX and 7.9 months with EOX plus IMAB362 (HR = .47; P = .0001).
If 70% or more of the tumor cells expressed CLDN18.2, IMAB362 improved the median PFS from 5.6 months for EOX alone to 7.2 months (HR = 0.36, P less than .0005), and OS improved from 9 months to 16.7 months (HR = 0.45, P less than .0005).
Response rates were also better with the addition of IMAB362. The objective response rate by RECIST criteria was 39.0% with EOX + IMAB362 vs. 25.0% with EOX alone. Most of the responses were partial (28.6% vs. 21.4%, respectively) or stable disease (44.2% vs. 51.2%, respectively). There were only 10.4% complete responses with IMAB362 and 3.6% with EOX alone. About 12% of the patients in each arm were not evaluable, or the data were missing.
Both treatments were well tolerated, with most adverse effects being grade 1/2. However, there was more grade 3/4 neutropenia with the combination (32.5% vs. 21.4% for EOX alone) as well as grade 3/4 vomiting (10.4% vs. 3.6%, respectively). Grade 1/2 vomiting was common in both arms, with about one-third of patients receiving EOX alone and just over half of patients on EOX + IMAB362 being affected.
Dr. Al-Batran said that there may have been more vomiting with IMAB362 because tight junction proteins, including claudin, are present in the gastric mucosa. Diarrhea was largely grade 1/2, affected about one-third of patients receiving EOX alone, and was only about half as common among patients receiving the combination.
Dr. Al-Batran said this trial “provides a strong rationale for a confirmatory phase III trial.”
Press conference moderator Dr. Smitha Krishnamurthi said the study is important because it documents the activity of a first-in-class antibody in patients with advanced gastric and gastroesophageal junction cancers. Since CLDN18.2 is expressed in about 50% of these cancers, “this treatment could apply to many patients,” she said.
The study was initiated and sponsored by Ganymed Pharmaceuticals. Dr. Al-Batran has had a consulting or advisory role with Merck, Roche, Celgene, and Lilly; has been on the speakers bureau of Lilly, Roche, Celgene, and Nordic Bioscience; and has received research funding from Celgene, Roche Pharma, Lilly, Novartis, Vfor Pharma, Medac, and Hospira.
On Twitter @OncologyPractic
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: A novel monoclonal antibody in combination with chemotherapy increased overall and progression-free survival in advanced gastric cancer, compared with chemotherapy alone.
Major finding: IMAB362 added to chemotherapy extended median overall survival from 8.4 months to 13.2 months over chemotherapy alone.
Data source: A phase II, randomized, active controlled study of 161 patients.
Disclosures: The study was initiated and sponsored by Ganymed Pharmaceuticals. Dr. Al-Batran has had a consulting or advisory role with Merck, Roche, Celgene, and Lilly; has been on the speakers bureau of Lilly, Roche, Celgene, and Nordic Bioscience; and has received research funding from Celgene, Roche Pharma, Lilly, Novartis, Vfor Pharma, Medac, and Hospira.

Ethnic groups differ in BRCA risk management
Chicago – Young black women with breast cancer are much less likely than white or Hispanic women to undergo testing for BRCA gene mutations, which puts them also at risk for ovarian cancer. And if they carry a BRCA mutation, they are much less likely to undergo removal of their ovaries and fallopian tubes.
Carriers of BRCA mutations have a high lifetime risk of breast and ovarian cancers – up to 60%-70% risk of developing breast cancer, up to 44% risk for ovarian cancer, and a 50% or greater risk for a secondary breast cancer after a first breast cancer diagnosis. Breast cancer risk management may consist of periodic screening or prophylactic mastectomy. But because there are no reliable screening methods for ovarian cancer, the main option for risk management is surgical.At the American Society of Clinical Oncology annual meeting, Dr. Tuya Pal said, “It is very important to think about the benefits of detecting a BRCA mutation. It’s not really about getting them tested, but the health benefit arises from doing something with that information.”
For a population-based, cross-sectional study to investigate women’s receipt of BRCA testing and the uptake of preventive surgery among BRCA mutation carriers, she recruited 440 black, 284 Hispanic, and 897 non-Hispanic white breast cancer survivors through the Florida State Cancer Registry. The study included women who had been diagnosed with invasive breast cancer at up to age 50 years between 2009 and 2012, who completed a baseline survey.
“Among our black women, 36% had received BRCA testing at the time of study recruitment compared with 62% of the Hispanic women and 65% of the non-Hispanic white women,” said Dr. Pal, a clinical geneticist at the H. Lee Moffitt Cancer Center & Research Institute in Tampa, Fla. Even after controlling for meeting high-risk criteria based on national practice guidelines, socioeconomic status variables, and provider referral patterns, there were still significant disparities in BRCA testing (P = .025) for black women, compared with the other two groups.
Of the 1,621 women in the study, 917 (57%) reported BRCA testing, of whom 92 (10%) tested positive for the mutation (28 Black, 13 Hispanic, and 51 non-Hispanic White).
The pattern of ethnic disparity persisted for cancer risk management practices among women with the gene mutation, with 68% of black women opting for bilateral mastectomy vs. 85% of Hispanic women and 94% of non-Hispanic whites. Because mastectomy is not the only form of risk management, Dr. Pal also looked at the rates of breast cancer screening in these women.
“That brought us up to 86% with the black women, 100% among Hispanic women, and 98% among the white women,” she said. However, three out of four of the Black women who did not use any risk management techniques were still in treatment, so it was too early to see what they would do.
For salpingo-oophorectomy, the rates were 32% of black, 85% of Hispanic, and 71% of non-Hispanic white women. After controlling for age at enrollment, time since diagnosis, income, family medical history, and insurance status, there were still disparities between black women and Hispanic women (P = .01) and between black and white women (P = .02).
Even in light of these findings that black women are much less likely to have BRCA testing and to undergo salpingo-oophorectomy if they carry a BRCA mutation, Dr. Pal offers some caveats. First, the findings require confirmation given the limited number of mutation carriers in the study. Second, as a cross-sectional study, it is only a snapshot in time. Third, BRCA testing and the options for risk management are a choice, and many factors enter into the choice, Dr. Pal pointed out.
They include patient preference, cultural factors, information and communication, economic factors, and provider recommendations. “We really need to understand the reasons that these women are making these decisions. Are they being given the opportunity to make an informed decision, or are there other factors that are playing into it where they’re not getting information that they need?” she asked. She said the study highlights the need to design strategies to overcome the reasons for the disparities and to ensure access to testing and cancer risk management practices across all populations.
Session moderator Dr. Patricia Ganz, director of Cancer Prevention and Control Research at the Jonsson Comprehensive Cancer Center of the University of California, Los Angeles, said recruiting from a cancer registry gave the investigators a population-based snapshot of the situation at that time. But the women in the study had their cancer diagnoses between 2009 and 2012, and “a lot of things have happened since then,” she said.
Angelina Jolie was found to have a BRCA mutation and publicly announced her decision to have major risk-reduction surgery. “That led to a lot of public awareness… so,many more women are much more aware,” Dr. Ganz said. “They’re going to ask their doctors about testing if they have a breast cancer diagnosis.”
Also, guidelines have changed, and rather than looking only at family history, clinicians are testing almost any breast cancer patient under age 50 for BRCA. “So I would suggest that perhaps temporal trends may have alleviated some of this disparity,” she said, “and it will be very interesting if Dr. Pal or others recruit a more contemporary sample [and] if we see some shift in this kind of difference in testing and decision making.”
Another factor affecting contemporary BRCA testing is the U.S. Supreme Court’s rejection in 2013 of the patents on the original test, resulting in about a 90% reduction in the cost of the test, making it more affordable for more women. Finally, because a breast cancer diagnosis is devastating to many women, they may choose to pursue breast cancer treatment and risk reduction strategies before addressing their ovarian cancer risk. Therefore, it may be worthwhile to conduct follow up studies to track these women’s cancer risk management choices over time.
The study received funding from the Bankhead Coley Cancer Research Program and the American Cancer Society. Dr. Pal reported no financial disclosures. Patricia Ganz, MD reported stock and other ownership interest in Abbott Laboratories, GlaxoSmithKline, Johnson & Johnson, Merck, Novartis, Pfizer, and Teva.
Chicago – Young black women with breast cancer are much less likely than white or Hispanic women to undergo testing for BRCA gene mutations, which puts them also at risk for ovarian cancer. And if they carry a BRCA mutation, they are much less likely to undergo removal of their ovaries and fallopian tubes.
Carriers of BRCA mutations have a high lifetime risk of breast and ovarian cancers – up to 60%-70% risk of developing breast cancer, up to 44% risk for ovarian cancer, and a 50% or greater risk for a secondary breast cancer after a first breast cancer diagnosis. Breast cancer risk management may consist of periodic screening or prophylactic mastectomy. But because there are no reliable screening methods for ovarian cancer, the main option for risk management is surgical.At the American Society of Clinical Oncology annual meeting, Dr. Tuya Pal said, “It is very important to think about the benefits of detecting a BRCA mutation. It’s not really about getting them tested, but the health benefit arises from doing something with that information.”
For a population-based, cross-sectional study to investigate women’s receipt of BRCA testing and the uptake of preventive surgery among BRCA mutation carriers, she recruited 440 black, 284 Hispanic, and 897 non-Hispanic white breast cancer survivors through the Florida State Cancer Registry. The study included women who had been diagnosed with invasive breast cancer at up to age 50 years between 2009 and 2012, who completed a baseline survey.
“Among our black women, 36% had received BRCA testing at the time of study recruitment compared with 62% of the Hispanic women and 65% of the non-Hispanic white women,” said Dr. Pal, a clinical geneticist at the H. Lee Moffitt Cancer Center & Research Institute in Tampa, Fla. Even after controlling for meeting high-risk criteria based on national practice guidelines, socioeconomic status variables, and provider referral patterns, there were still significant disparities in BRCA testing (P = .025) for black women, compared with the other two groups.
Of the 1,621 women in the study, 917 (57%) reported BRCA testing, of whom 92 (10%) tested positive for the mutation (28 Black, 13 Hispanic, and 51 non-Hispanic White).
The pattern of ethnic disparity persisted for cancer risk management practices among women with the gene mutation, with 68% of black women opting for bilateral mastectomy vs. 85% of Hispanic women and 94% of non-Hispanic whites. Because mastectomy is not the only form of risk management, Dr. Pal also looked at the rates of breast cancer screening in these women.
“That brought us up to 86% with the black women, 100% among Hispanic women, and 98% among the white women,” she said. However, three out of four of the Black women who did not use any risk management techniques were still in treatment, so it was too early to see what they would do.
For salpingo-oophorectomy, the rates were 32% of black, 85% of Hispanic, and 71% of non-Hispanic white women. After controlling for age at enrollment, time since diagnosis, income, family medical history, and insurance status, there were still disparities between black women and Hispanic women (P = .01) and between black and white women (P = .02).
Even in light of these findings that black women are much less likely to have BRCA testing and to undergo salpingo-oophorectomy if they carry a BRCA mutation, Dr. Pal offers some caveats. First, the findings require confirmation given the limited number of mutation carriers in the study. Second, as a cross-sectional study, it is only a snapshot in time. Third, BRCA testing and the options for risk management are a choice, and many factors enter into the choice, Dr. Pal pointed out.
They include patient preference, cultural factors, information and communication, economic factors, and provider recommendations. “We really need to understand the reasons that these women are making these decisions. Are they being given the opportunity to make an informed decision, or are there other factors that are playing into it where they’re not getting information that they need?” she asked. She said the study highlights the need to design strategies to overcome the reasons for the disparities and to ensure access to testing and cancer risk management practices across all populations.
Session moderator Dr. Patricia Ganz, director of Cancer Prevention and Control Research at the Jonsson Comprehensive Cancer Center of the University of California, Los Angeles, said recruiting from a cancer registry gave the investigators a population-based snapshot of the situation at that time. But the women in the study had their cancer diagnoses between 2009 and 2012, and “a lot of things have happened since then,” she said.
Angelina Jolie was found to have a BRCA mutation and publicly announced her decision to have major risk-reduction surgery. “That led to a lot of public awareness… so,many more women are much more aware,” Dr. Ganz said. “They’re going to ask their doctors about testing if they have a breast cancer diagnosis.”
Also, guidelines have changed, and rather than looking only at family history, clinicians are testing almost any breast cancer patient under age 50 for BRCA. “So I would suggest that perhaps temporal trends may have alleviated some of this disparity,” she said, “and it will be very interesting if Dr. Pal or others recruit a more contemporary sample [and] if we see some shift in this kind of difference in testing and decision making.”
Another factor affecting contemporary BRCA testing is the U.S. Supreme Court’s rejection in 2013 of the patents on the original test, resulting in about a 90% reduction in the cost of the test, making it more affordable for more women. Finally, because a breast cancer diagnosis is devastating to many women, they may choose to pursue breast cancer treatment and risk reduction strategies before addressing their ovarian cancer risk. Therefore, it may be worthwhile to conduct follow up studies to track these women’s cancer risk management choices over time.
The study received funding from the Bankhead Coley Cancer Research Program and the American Cancer Society. Dr. Pal reported no financial disclosures. Patricia Ganz, MD reported stock and other ownership interest in Abbott Laboratories, GlaxoSmithKline, Johnson & Johnson, Merck, Novartis, Pfizer, and Teva.
Chicago – Young black women with breast cancer are much less likely than white or Hispanic women to undergo testing for BRCA gene mutations, which puts them also at risk for ovarian cancer. And if they carry a BRCA mutation, they are much less likely to undergo removal of their ovaries and fallopian tubes.
Carriers of BRCA mutations have a high lifetime risk of breast and ovarian cancers – up to 60%-70% risk of developing breast cancer, up to 44% risk for ovarian cancer, and a 50% or greater risk for a secondary breast cancer after a first breast cancer diagnosis. Breast cancer risk management may consist of periodic screening or prophylactic mastectomy. But because there are no reliable screening methods for ovarian cancer, the main option for risk management is surgical.At the American Society of Clinical Oncology annual meeting, Dr. Tuya Pal said, “It is very important to think about the benefits of detecting a BRCA mutation. It’s not really about getting them tested, but the health benefit arises from doing something with that information.”
For a population-based, cross-sectional study to investigate women’s receipt of BRCA testing and the uptake of preventive surgery among BRCA mutation carriers, she recruited 440 black, 284 Hispanic, and 897 non-Hispanic white breast cancer survivors through the Florida State Cancer Registry. The study included women who had been diagnosed with invasive breast cancer at up to age 50 years between 2009 and 2012, who completed a baseline survey.
“Among our black women, 36% had received BRCA testing at the time of study recruitment compared with 62% of the Hispanic women and 65% of the non-Hispanic white women,” said Dr. Pal, a clinical geneticist at the H. Lee Moffitt Cancer Center & Research Institute in Tampa, Fla. Even after controlling for meeting high-risk criteria based on national practice guidelines, socioeconomic status variables, and provider referral patterns, there were still significant disparities in BRCA testing (P = .025) for black women, compared with the other two groups.
Of the 1,621 women in the study, 917 (57%) reported BRCA testing, of whom 92 (10%) tested positive for the mutation (28 Black, 13 Hispanic, and 51 non-Hispanic White).
The pattern of ethnic disparity persisted for cancer risk management practices among women with the gene mutation, with 68% of black women opting for bilateral mastectomy vs. 85% of Hispanic women and 94% of non-Hispanic whites. Because mastectomy is not the only form of risk management, Dr. Pal also looked at the rates of breast cancer screening in these women.
“That brought us up to 86% with the black women, 100% among Hispanic women, and 98% among the white women,” she said. However, three out of four of the Black women who did not use any risk management techniques were still in treatment, so it was too early to see what they would do.
For salpingo-oophorectomy, the rates were 32% of black, 85% of Hispanic, and 71% of non-Hispanic white women. After controlling for age at enrollment, time since diagnosis, income, family medical history, and insurance status, there were still disparities between black women and Hispanic women (P = .01) and between black and white women (P = .02).
Even in light of these findings that black women are much less likely to have BRCA testing and to undergo salpingo-oophorectomy if they carry a BRCA mutation, Dr. Pal offers some caveats. First, the findings require confirmation given the limited number of mutation carriers in the study. Second, as a cross-sectional study, it is only a snapshot in time. Third, BRCA testing and the options for risk management are a choice, and many factors enter into the choice, Dr. Pal pointed out.
They include patient preference, cultural factors, information and communication, economic factors, and provider recommendations. “We really need to understand the reasons that these women are making these decisions. Are they being given the opportunity to make an informed decision, or are there other factors that are playing into it where they’re not getting information that they need?” she asked. She said the study highlights the need to design strategies to overcome the reasons for the disparities and to ensure access to testing and cancer risk management practices across all populations.
Session moderator Dr. Patricia Ganz, director of Cancer Prevention and Control Research at the Jonsson Comprehensive Cancer Center of the University of California, Los Angeles, said recruiting from a cancer registry gave the investigators a population-based snapshot of the situation at that time. But the women in the study had their cancer diagnoses between 2009 and 2012, and “a lot of things have happened since then,” she said.
Angelina Jolie was found to have a BRCA mutation and publicly announced her decision to have major risk-reduction surgery. “That led to a lot of public awareness… so,many more women are much more aware,” Dr. Ganz said. “They’re going to ask their doctors about testing if they have a breast cancer diagnosis.”
Also, guidelines have changed, and rather than looking only at family history, clinicians are testing almost any breast cancer patient under age 50 for BRCA. “So I would suggest that perhaps temporal trends may have alleviated some of this disparity,” she said, “and it will be very interesting if Dr. Pal or others recruit a more contemporary sample [and] if we see some shift in this kind of difference in testing and decision making.”
Another factor affecting contemporary BRCA testing is the U.S. Supreme Court’s rejection in 2013 of the patents on the original test, resulting in about a 90% reduction in the cost of the test, making it more affordable for more women. Finally, because a breast cancer diagnosis is devastating to many women, they may choose to pursue breast cancer treatment and risk reduction strategies before addressing their ovarian cancer risk. Therefore, it may be worthwhile to conduct follow up studies to track these women’s cancer risk management choices over time.
The study received funding from the Bankhead Coley Cancer Research Program and the American Cancer Society. Dr. Pal reported no financial disclosures. Patricia Ganz, MD reported stock and other ownership interest in Abbott Laboratories, GlaxoSmithKline, Johnson & Johnson, Merck, Novartis, Pfizer, and Teva.
AT THE 2016 ASCO MEETING
Key clinical point: Black, Hispanic, and white women differ in BRCA risk management.
Major finding: Half as many at-risk black female patients get BRCA tests vs. Hispanic/white female patients.
Data source: Population-based, cross-sectional study of 1,621 women in a cancer registry.
Disclosures: The study received funding from the Bankhead Coley Cancer Research Program and the American Cancer Society. Dr. Pal reported no financial disclosures. Dr. Patricia Ganz reported stock and other ownership interest in Abbott Laboratories, GlaxoSmithKline, Johnson & Johnson, Merck, Novartis, Pfizer, and Teva.
Adjuvant temozolomide increases survival in rare anaplastic glioma
CHICAGO – Adjuvant temozolomide given after radiation therapy improves survival of patients with a form of anaplastic glioma, a rare brain tumor. The patients had anaplastic glioma without 1p/19q co-deletion.
This co-deletion – the short arm of chromosome 1 and the long arm of chromosome 19 – is a favorable marker in the tumor, and patients without the deletion have traditionally done worse than those with the deletion. Until this study, no one knew if temozolomide would improve outcomes of patients without the co-deletion.
The four-arm, Phase III Trial on Concurrent and Adjuvant Temozolomide [TMZ] Chemotherapy in NON-1p/19q Deleted Anaplastic Glioma: The CATNON Intergroup Trial (EORTC 26053-22054), still ongoing, is testing radiotherapy, radiotherapy plus concurrent TMZ, radiotherapy plus 12 months of adjuvant TMZ, or radiotherapy plus concurrent TMZ plus 12 months of adjuvant TMZ. Adjuvant TMZ was given in 12 cycles.
Given the rarity of the tumor, the trial involved 118 institutions on three continents and ran for eight years between 2007 and 2015. From 1407 patients 18 years or older with World Health Organization performance status 0-2 screened, 751 were confirmed to have grade III anaplastic gliomas that were intact for 1p/19q (ie, no deletions). After radiation therapy with 59.4 Gy in 33 fractions, these patients were randomly assigned to one of the four treatment arms.
The trial asked two questions: Does adjuvant chemotherapy after radiotherapy improve outcome, and does chemotherapy concurrent with radiotherapy improve outcomes?

Just after enrollment was completed, a data monitoring committee recommended, based on an interim analysis in October 2015, that the data for the adjuvant arm be released, reported Dr. Martin van den Bent, professor of neuro-oncology at Erasmus MC Cancer Center in Rotterdam, The Netherlands. “It completely came as a surprise,” he said at a press conference at the annual meeting of the American Society of Clinical Oncology.
Comparing radiation with or without concurrent TMZ followed by adjuvant TMZ to treatment without adjuvant therapy, the overall survival at five years increased from 44% without any TMZ or with TMZ concurrent with radiation (n = 372) to 56% with adjuvant temozolomide (n = 373). “This corresponds to a hazard ratio of 0.67, a highly statistically significant increment,” Dr. van den Bent said.
Adjuvant TMZ was also associated with a statistically significant increase in median progression free survival from 19 months without adjuvant therapy to almost 43 months with it.
When patients were stratified by O6-methyl-guanine DNA methyltransferase (MGMT) promoter methylation status, the researchers found that MGMT methylation was prognostic for overall survival but not predictive of improved outcome to adjuvant TMZ.
For the nonadjuvant group, the median overall survival was 41 months (95% CI, 37-61 months), but the groups receiving adjuvant TMZ had not yet reached a median overall survival. “We know now that temozolomide given after radiation therapy improves survival in this disease,” Dr. van den Bent said.
A trial of such a rare disease requires many collaborating centers and oncology groups and a long duration to show improvements in outcome. Collaborating oncology groups across many countries “have shown the capacity to answer important clinical questions in orphan diseases,” he said.
Press conference moderator Dr. Don Dizon of Massachusetts General Hospital, Boston, said, “I think this illustrates… the theme of this year’s meeting, which is Collective Wisdom, and even more than that it illustrates that even with a rare tumor type and using standard chemotherapy it’s very important, and we can select patients who are most likely to benefit from treatment and at the same time potentially spare patients from the toxicities of therapy that they’re unlikely to benefit from.”
Results from the arm of the trial testing temozolomide given only at the time of radiation therapy are not yet available and are expected in 2020. In addition, investigators plan to assess genetic abnormalities that are known to affect prognosis in the disease, specifically MGMT promoter methylation and IDH (isocitrate dehydrogenase) mutation.
Common toxicities with temozolomide were mainly low platelet and white cell counts with severe toxicity in 5-10% of patients.
CHICAGO – Adjuvant temozolomide given after radiation therapy improves survival of patients with a form of anaplastic glioma, a rare brain tumor. The patients had anaplastic glioma without 1p/19q co-deletion.
This co-deletion – the short arm of chromosome 1 and the long arm of chromosome 19 – is a favorable marker in the tumor, and patients without the deletion have traditionally done worse than those with the deletion. Until this study, no one knew if temozolomide would improve outcomes of patients without the co-deletion.
The four-arm, Phase III Trial on Concurrent and Adjuvant Temozolomide [TMZ] Chemotherapy in NON-1p/19q Deleted Anaplastic Glioma: The CATNON Intergroup Trial (EORTC 26053-22054), still ongoing, is testing radiotherapy, radiotherapy plus concurrent TMZ, radiotherapy plus 12 months of adjuvant TMZ, or radiotherapy plus concurrent TMZ plus 12 months of adjuvant TMZ. Adjuvant TMZ was given in 12 cycles.
Given the rarity of the tumor, the trial involved 118 institutions on three continents and ran for eight years between 2007 and 2015. From 1407 patients 18 years or older with World Health Organization performance status 0-2 screened, 751 were confirmed to have grade III anaplastic gliomas that were intact for 1p/19q (ie, no deletions). After radiation therapy with 59.4 Gy in 33 fractions, these patients were randomly assigned to one of the four treatment arms.
The trial asked two questions: Does adjuvant chemotherapy after radiotherapy improve outcome, and does chemotherapy concurrent with radiotherapy improve outcomes?
Just after enrollment was completed, a data monitoring committee recommended, based on an interim analysis in October 2015, that the data for the adjuvant arm be released, reported Dr. Martin van den Bent, professor of neuro-oncology at Erasmus MC Cancer Center in Rotterdam, The Netherlands. “It completely came as a surprise,” he said at a press conference at the annual meeting of the American Society of Clinical Oncology.
Comparing radiation with or without concurrent TMZ followed by adjuvant TMZ to treatment without adjuvant therapy, the overall survival at five years increased from 44% without any TMZ or with TMZ concurrent with radiation (n = 372) to 56% with adjuvant temozolomide (n = 373). “This corresponds to a hazard ratio of 0.67, a highly statistically significant increment,” Dr. van den Bent said.
Adjuvant TMZ was also associated with a statistically significant increase in median progression free survival from 19 months without adjuvant therapy to almost 43 months with it.
When patients were stratified by O6-methyl-guanine DNA methyltransferase (MGMT) promoter methylation status, the researchers found that MGMT methylation was prognostic for overall survival but not predictive of improved outcome to adjuvant TMZ.
For the nonadjuvant group, the median overall survival was 41 months (95% CI, 37-61 months), but the groups receiving adjuvant TMZ had not yet reached a median overall survival. “We know now that temozolomide given after radiation therapy improves survival in this disease,” Dr. van den Bent said.
A trial of such a rare disease requires many collaborating centers and oncology groups and a long duration to show improvements in outcome. Collaborating oncology groups across many countries “have shown the capacity to answer important clinical questions in orphan diseases,” he said.
Press conference moderator Dr. Don Dizon of Massachusetts General Hospital, Boston, said, “I think this illustrates… the theme of this year’s meeting, which is Collective Wisdom, and even more than that it illustrates that even with a rare tumor type and using standard chemotherapy it’s very important, and we can select patients who are most likely to benefit from treatment and at the same time potentially spare patients from the toxicities of therapy that they’re unlikely to benefit from.”
Results from the arm of the trial testing temozolomide given only at the time of radiation therapy are not yet available and are expected in 2020. In addition, investigators plan to assess genetic abnormalities that are known to affect prognosis in the disease, specifically MGMT promoter methylation and IDH (isocitrate dehydrogenase) mutation.
Common toxicities with temozolomide were mainly low platelet and white cell counts with severe toxicity in 5-10% of patients.
CHICAGO – Adjuvant temozolomide given after radiation therapy improves survival of patients with a form of anaplastic glioma, a rare brain tumor. The patients had anaplastic glioma without 1p/19q co-deletion.
This co-deletion – the short arm of chromosome 1 and the long arm of chromosome 19 – is a favorable marker in the tumor, and patients without the deletion have traditionally done worse than those with the deletion. Until this study, no one knew if temozolomide would improve outcomes of patients without the co-deletion.
The four-arm, Phase III Trial on Concurrent and Adjuvant Temozolomide [TMZ] Chemotherapy in NON-1p/19q Deleted Anaplastic Glioma: The CATNON Intergroup Trial (EORTC 26053-22054), still ongoing, is testing radiotherapy, radiotherapy plus concurrent TMZ, radiotherapy plus 12 months of adjuvant TMZ, or radiotherapy plus concurrent TMZ plus 12 months of adjuvant TMZ. Adjuvant TMZ was given in 12 cycles.
Given the rarity of the tumor, the trial involved 118 institutions on three continents and ran for eight years between 2007 and 2015. From 1407 patients 18 years or older with World Health Organization performance status 0-2 screened, 751 were confirmed to have grade III anaplastic gliomas that were intact for 1p/19q (ie, no deletions). After radiation therapy with 59.4 Gy in 33 fractions, these patients were randomly assigned to one of the four treatment arms.
The trial asked two questions: Does adjuvant chemotherapy after radiotherapy improve outcome, and does chemotherapy concurrent with radiotherapy improve outcomes?
Just after enrollment was completed, a data monitoring committee recommended, based on an interim analysis in October 2015, that the data for the adjuvant arm be released, reported Dr. Martin van den Bent, professor of neuro-oncology at Erasmus MC Cancer Center in Rotterdam, The Netherlands. “It completely came as a surprise,” he said at a press conference at the annual meeting of the American Society of Clinical Oncology.
Comparing radiation with or without concurrent TMZ followed by adjuvant TMZ to treatment without adjuvant therapy, the overall survival at five years increased from 44% without any TMZ or with TMZ concurrent with radiation (n = 372) to 56% with adjuvant temozolomide (n = 373). “This corresponds to a hazard ratio of 0.67, a highly statistically significant increment,” Dr. van den Bent said.
Adjuvant TMZ was also associated with a statistically significant increase in median progression free survival from 19 months without adjuvant therapy to almost 43 months with it.
When patients were stratified by O6-methyl-guanine DNA methyltransferase (MGMT) promoter methylation status, the researchers found that MGMT methylation was prognostic for overall survival but not predictive of improved outcome to adjuvant TMZ.
For the nonadjuvant group, the median overall survival was 41 months (95% CI, 37-61 months), but the groups receiving adjuvant TMZ had not yet reached a median overall survival. “We know now that temozolomide given after radiation therapy improves survival in this disease,” Dr. van den Bent said.
A trial of such a rare disease requires many collaborating centers and oncology groups and a long duration to show improvements in outcome. Collaborating oncology groups across many countries “have shown the capacity to answer important clinical questions in orphan diseases,” he said.
Press conference moderator Dr. Don Dizon of Massachusetts General Hospital, Boston, said, “I think this illustrates… the theme of this year’s meeting, which is Collective Wisdom, and even more than that it illustrates that even with a rare tumor type and using standard chemotherapy it’s very important, and we can select patients who are most likely to benefit from treatment and at the same time potentially spare patients from the toxicities of therapy that they’re unlikely to benefit from.”
Results from the arm of the trial testing temozolomide given only at the time of radiation therapy are not yet available and are expected in 2020. In addition, investigators plan to assess genetic abnormalities that are known to affect prognosis in the disease, specifically MGMT promoter methylation and IDH (isocitrate dehydrogenase) mutation.
Common toxicities with temozolomide were mainly low platelet and white cell counts with severe toxicity in 5-10% of patients.
AT THE 2016 ASCO ANNUAL MEETING
Key clinical point: Adjuvant temozolomide post-radiation improves survival in non-1p/19q-deleted anaplastic glioma.
Major finding: Adjuvant temozolomide improved overall survival to 56% from 44%.
Data source: Randomized, 4-arm trial of adjuvant temozolomide or not among 751 patients with non-1p/19q-deleted anaplastic glioma.
Disclosures: Schering Plough/MSD provided an unrestricted grant for the research and supplied temozolomide. Dr. van den Bent has consulting or advisory roles with Merck, Roche, Celldex, Novocure, Abbvie, and Amgen; has received honoraria from Roche, Actelion, Celldex, Bristol-Myers Squibb, Merck, Abbvie, and Novocure; and has research funding from Abbvie and Roche.
