User login
Do any folk remedies or herbals help induce labor?
Yes, some do. Breast stimulation and electroacupuncture help, while other common remedies that have been studied are ineffective, possibly unsafe, or both. Unilateral breast stimulation shortens the time until the onset of labor in women at term (strength of recommendation [SOR]: A, systematic review). Electroacupuncture also may stimulate the onset of labor (SOR: C, observational studies).
Sexual intercourse doesn’t appear to ripen the cervix or stimulate labor (SOR: C, 1 observational study). Castor oil universally produces nausea and doesn’t promote labor (SOR: C, low-quality case-control study). Red raspberry leaf is likely safe but ineffective (SOR: B, 1 small randomized controlled trial); evening primrose oil is ineffective and possibly unsafe (SOR: B, 1 small retrospective cohort study); black cohosh and blue cohosh lack evidence of efficacy and may be unsafe (SOR: C, expert opinion and case reports).
Evidence summary
Breast stimulation works
A systematic review of 6 trials with a total of 719 participants compared unilateral breast stimulation with no intervention to induce labor in women at term.1 In 2 trials, the 300 participants stimulated 1 breast for 1 hour a day for 3 days; in the other 4 trials, 419 women stimulated either breast alternately for 3 hours a day.
Breast stimulation significantly reduced the number of women who hadn’t gone into labor at 72 hours compared with nonintervention (62.7% vs 93.6%; relative risk [RR]=0.67; 95% confidence interval [CI], 0.60-0.74; number needed to treat [NNT]=3.2). This result remained significant when primiparous and multiparous women were analyzed separately, but not in the 1 trial (37 participants) that reported on women with an unfavorable cervix.1 Breast stimulation also reduced postpartum hemorrhage (0.7% vs 6%; RR=0.16; 95% CI, 0.03-0.87; NNT=18.8).
None of the trials documented uterine hyperstimulation or meconium-stained fluid, and they didn’t find significant differences in the rates of cesarean section (9% vs 10%; RR=0.90; 95% CI, 0.38-2.12). One trial reported 4 perinatal deaths in a high-risk population—3 in the breast stimulation group and 1 in the control group—but this finding was not replicated in any other trials.1
Acupuncture may also help
A Cochrane systematic review evaluating acupuncture for inducing labor identified 1 randomized trial with methodologic flaws (allowing no conclusion), 3 case series, and 2 nonrandomized trials. The first case series used electroacupuncture at 38 to 42 weeks to successfully induce labor in 21 of 31 women. The second series, using acupuncture with and without electrical stimulation, induced labor in 10 of 12 women at 19 to 43 weeks. The third study induced labor with electroacupuncture in 78% of 41 women—34 term and postterm patients and 7 with a fetal demise.
In the first nonrandomized trial, 20 of 27 women at term who received electroacupuncture gave birth between 39 weeks 3 days and 40 weeks, compared with 47 of 102 women in the control group. In the second study, 31 of 35 women who received electroacupuncture reported increased intensity of contractions compared with none of the 35 women in the control group.2
Sexual intercourse induces pregnancy, not labor
A Cochrane systematic review found 1 observational study of the effect of sexual intercourse on cervical ripening and induction of labor among 28 women at term. The study evaluated cervical Bishop scores after sexual intercourse with intravaginal semen deposition for 3 consecutive nights compared with no intercourse. The difference in Bishop score was not significant (1.0 with coitus vs 0.5 controls; P>.05) and no difference in the number of women who delivered within 3 days was noted in the 2 groups (RR=0.99; 95% CI, 0.45-2.20).3
Castor oil made women nauseous
A Cochrane systematic review included 1 study of women at term with intact membranes who received 1 dose of castor oil to induce labor (n=52) compared with no treatment (n=48). All women who received castor oil felt nauseous, but no other differences were noted between the castor oil group and controls in rates of cesarean section, meconium-stained fluid, or Apgar scores less than 7 at 5 minutes.4
Herbal preparations raise many questions—and some concerns
A prospective controlled trial that randomized 192 women to receive either red raspberry leaf tablets (1.2 g twice daily beginning at 32 weeks) or placebo found no significant differences in duration of the first stage of labor or birth outcomes. Symptom surveys of 108 women revealed no adverse effects.5

A retrospective cohort study compared pregnancy outcomes in 54 women who took evening primrose oil (500 mg 3 times a day beginning at 37 weeks) with a matched group of 54 women who did not take it. The study found no significant differences between the groups in maternal age, Apgar scores, or days of gestation. However, the women taking evening primrose oil tended to have protracted active phase of labor, prolonged rupture of membranes, arrest of descent, and oxytocin augmentation (none of which were statistically significant).6
A systematic review of the literature on black cohosh in pregnancy found no trials that evaluated its efficacy for inducing labor.7 A review of herbal preparations used by midwives reported a case of an infant with low Apgar scores after black cohosh use.8 Both articles described black cohosh as potentially unsafe because of the lack of trials demonstrating safety and possible deleterious estrogenic effects.
A systematic review of the literature on blue cohosh found only in vitro studies of efficacy (increased estradiol-induced transcription in estrogen-responsive cells and increased tone in excised guinea pig uteri) and 3 case reports of maternal adverse events after ingestion (perinatal stroke, congestive heart failure with shock, and multiorgan hypoxic injury).9 In vitro evidence presented in the review suggests that blue cohosh may have teratogenic, embryotoxic, and oxytocic effects.
Recommendations
We found no recommendations from professional organizations regarding folk methods to stimulate labor. The authors of a survey of herbal preparations used by midwives do not advocate their use in pregnancy because of unknown risks to the fetus, although “raspberry leaf tea does not seem to have any significant pharmacologic activity and is probably safe.”8
1. Kavanagh J, Kelly AJ, Thomas J. Breast stimulation for cervical ripening and induction of labour. Cochrane Database Syst Rev. 2005;(3):CD003392.-
2. Smith CA, Crowther CA. Acupuncture for induction of labour. Cochrane Database Syst Rev. 2004;(1):CD002962.-
3. Kavanagh J, Kelly AJ, Thomas J. Sexual intercourse for cervical ripening and induction of labor. Cochrane Database Syst Rev. 2001;(2):CD003093.-
4. Kelly AJ, Kavanagh J, Thomas J. Castor oil, bath and/or enema for cervical priming and induction of labour. Cochrane Database Syst Rev. 2001;(2):CD003099.-
5. Simpson M, Parsons M, Greenwood J, Wade K. Raspberry leaf in pregnancy: its safety and efficacy in labor. J Midwifery Womens Health. 2001;46:51-59.
6. Dove D, Johnson P. Oral evening primrose oil: its effect on length of pregnancy and selected intrapartum outcomes in low-risk nulliparous women. J Nurse Midwifery. 1999;44:320-324.
7. Dugoua JJ, Seely D, Perri D, Koren G, Mills E. Safety and efficacy of black cohosh (Cimicifuga racemosa) during pregnancy and lactation. Can J Clin Pharmacol. 2006;13:e257-e261.
8. McFarlin BL, Gibson MH, O’Rear J, Harman P. A national survey of herbal preparation use by nurse-midwives for labor stimulation. Review of the literature and recommendations for practice. J Nurse Midwifery. 1999;44:205-216.
9. Dugoua JJ, Perri D, Seely D, Mills E, Koren G. Safety and efficacy of blue cohosh (Caulophyllum thalictroides) during pregnancy and lactation. Can J Clin Pharmacol. 2008;15:e66-e73.
Yes, some do. Breast stimulation and electroacupuncture help, while other common remedies that have been studied are ineffective, possibly unsafe, or both. Unilateral breast stimulation shortens the time until the onset of labor in women at term (strength of recommendation [SOR]: A, systematic review). Electroacupuncture also may stimulate the onset of labor (SOR: C, observational studies).
Sexual intercourse doesn’t appear to ripen the cervix or stimulate labor (SOR: C, 1 observational study). Castor oil universally produces nausea and doesn’t promote labor (SOR: C, low-quality case-control study). Red raspberry leaf is likely safe but ineffective (SOR: B, 1 small randomized controlled trial); evening primrose oil is ineffective and possibly unsafe (SOR: B, 1 small retrospective cohort study); black cohosh and blue cohosh lack evidence of efficacy and may be unsafe (SOR: C, expert opinion and case reports).
Evidence summary
Breast stimulation works
A systematic review of 6 trials with a total of 719 participants compared unilateral breast stimulation with no intervention to induce labor in women at term.1 In 2 trials, the 300 participants stimulated 1 breast for 1 hour a day for 3 days; in the other 4 trials, 419 women stimulated either breast alternately for 3 hours a day.
Breast stimulation significantly reduced the number of women who hadn’t gone into labor at 72 hours compared with nonintervention (62.7% vs 93.6%; relative risk [RR]=0.67; 95% confidence interval [CI], 0.60-0.74; number needed to treat [NNT]=3.2). This result remained significant when primiparous and multiparous women were analyzed separately, but not in the 1 trial (37 participants) that reported on women with an unfavorable cervix.1 Breast stimulation also reduced postpartum hemorrhage (0.7% vs 6%; RR=0.16; 95% CI, 0.03-0.87; NNT=18.8).
None of the trials documented uterine hyperstimulation or meconium-stained fluid, and they didn’t find significant differences in the rates of cesarean section (9% vs 10%; RR=0.90; 95% CI, 0.38-2.12). One trial reported 4 perinatal deaths in a high-risk population—3 in the breast stimulation group and 1 in the control group—but this finding was not replicated in any other trials.1
Acupuncture may also help
A Cochrane systematic review evaluating acupuncture for inducing labor identified 1 randomized trial with methodologic flaws (allowing no conclusion), 3 case series, and 2 nonrandomized trials. The first case series used electroacupuncture at 38 to 42 weeks to successfully induce labor in 21 of 31 women. The second series, using acupuncture with and without electrical stimulation, induced labor in 10 of 12 women at 19 to 43 weeks. The third study induced labor with electroacupuncture in 78% of 41 women—34 term and postterm patients and 7 with a fetal demise.
In the first nonrandomized trial, 20 of 27 women at term who received electroacupuncture gave birth between 39 weeks 3 days and 40 weeks, compared with 47 of 102 women in the control group. In the second study, 31 of 35 women who received electroacupuncture reported increased intensity of contractions compared with none of the 35 women in the control group.2
Sexual intercourse induces pregnancy, not labor
A Cochrane systematic review found 1 observational study of the effect of sexual intercourse on cervical ripening and induction of labor among 28 women at term. The study evaluated cervical Bishop scores after sexual intercourse with intravaginal semen deposition for 3 consecutive nights compared with no intercourse. The difference in Bishop score was not significant (1.0 with coitus vs 0.5 controls; P>.05) and no difference in the number of women who delivered within 3 days was noted in the 2 groups (RR=0.99; 95% CI, 0.45-2.20).3
Castor oil made women nauseous
A Cochrane systematic review included 1 study of women at term with intact membranes who received 1 dose of castor oil to induce labor (n=52) compared with no treatment (n=48). All women who received castor oil felt nauseous, but no other differences were noted between the castor oil group and controls in rates of cesarean section, meconium-stained fluid, or Apgar scores less than 7 at 5 minutes.4
Herbal preparations raise many questions—and some concerns
A prospective controlled trial that randomized 192 women to receive either red raspberry leaf tablets (1.2 g twice daily beginning at 32 weeks) or placebo found no significant differences in duration of the first stage of labor or birth outcomes. Symptom surveys of 108 women revealed no adverse effects.5
A retrospective cohort study compared pregnancy outcomes in 54 women who took evening primrose oil (500 mg 3 times a day beginning at 37 weeks) with a matched group of 54 women who did not take it. The study found no significant differences between the groups in maternal age, Apgar scores, or days of gestation. However, the women taking evening primrose oil tended to have protracted active phase of labor, prolonged rupture of membranes, arrest of descent, and oxytocin augmentation (none of which were statistically significant).6
A systematic review of the literature on black cohosh in pregnancy found no trials that evaluated its efficacy for inducing labor.7 A review of herbal preparations used by midwives reported a case of an infant with low Apgar scores after black cohosh use.8 Both articles described black cohosh as potentially unsafe because of the lack of trials demonstrating safety and possible deleterious estrogenic effects.
A systematic review of the literature on blue cohosh found only in vitro studies of efficacy (increased estradiol-induced transcription in estrogen-responsive cells and increased tone in excised guinea pig uteri) and 3 case reports of maternal adverse events after ingestion (perinatal stroke, congestive heart failure with shock, and multiorgan hypoxic injury).9 In vitro evidence presented in the review suggests that blue cohosh may have teratogenic, embryotoxic, and oxytocic effects.
Recommendations
We found no recommendations from professional organizations regarding folk methods to stimulate labor. The authors of a survey of herbal preparations used by midwives do not advocate their use in pregnancy because of unknown risks to the fetus, although “raspberry leaf tea does not seem to have any significant pharmacologic activity and is probably safe.”8
Yes, some do. Breast stimulation and electroacupuncture help, while other common remedies that have been studied are ineffective, possibly unsafe, or both. Unilateral breast stimulation shortens the time until the onset of labor in women at term (strength of recommendation [SOR]: A, systematic review). Electroacupuncture also may stimulate the onset of labor (SOR: C, observational studies).
Sexual intercourse doesn’t appear to ripen the cervix or stimulate labor (SOR: C, 1 observational study). Castor oil universally produces nausea and doesn’t promote labor (SOR: C, low-quality case-control study). Red raspberry leaf is likely safe but ineffective (SOR: B, 1 small randomized controlled trial); evening primrose oil is ineffective and possibly unsafe (SOR: B, 1 small retrospective cohort study); black cohosh and blue cohosh lack evidence of efficacy and may be unsafe (SOR: C, expert opinion and case reports).
Evidence summary
Breast stimulation works
A systematic review of 6 trials with a total of 719 participants compared unilateral breast stimulation with no intervention to induce labor in women at term.1 In 2 trials, the 300 participants stimulated 1 breast for 1 hour a day for 3 days; in the other 4 trials, 419 women stimulated either breast alternately for 3 hours a day.
Breast stimulation significantly reduced the number of women who hadn’t gone into labor at 72 hours compared with nonintervention (62.7% vs 93.6%; relative risk [RR]=0.67; 95% confidence interval [CI], 0.60-0.74; number needed to treat [NNT]=3.2). This result remained significant when primiparous and multiparous women were analyzed separately, but not in the 1 trial (37 participants) that reported on women with an unfavorable cervix.1 Breast stimulation also reduced postpartum hemorrhage (0.7% vs 6%; RR=0.16; 95% CI, 0.03-0.87; NNT=18.8).
None of the trials documented uterine hyperstimulation or meconium-stained fluid, and they didn’t find significant differences in the rates of cesarean section (9% vs 10%; RR=0.90; 95% CI, 0.38-2.12). One trial reported 4 perinatal deaths in a high-risk population—3 in the breast stimulation group and 1 in the control group—but this finding was not replicated in any other trials.1
Acupuncture may also help
A Cochrane systematic review evaluating acupuncture for inducing labor identified 1 randomized trial with methodologic flaws (allowing no conclusion), 3 case series, and 2 nonrandomized trials. The first case series used electroacupuncture at 38 to 42 weeks to successfully induce labor in 21 of 31 women. The second series, using acupuncture with and without electrical stimulation, induced labor in 10 of 12 women at 19 to 43 weeks. The third study induced labor with electroacupuncture in 78% of 41 women—34 term and postterm patients and 7 with a fetal demise.
In the first nonrandomized trial, 20 of 27 women at term who received electroacupuncture gave birth between 39 weeks 3 days and 40 weeks, compared with 47 of 102 women in the control group. In the second study, 31 of 35 women who received electroacupuncture reported increased intensity of contractions compared with none of the 35 women in the control group.2
Sexual intercourse induces pregnancy, not labor
A Cochrane systematic review found 1 observational study of the effect of sexual intercourse on cervical ripening and induction of labor among 28 women at term. The study evaluated cervical Bishop scores after sexual intercourse with intravaginal semen deposition for 3 consecutive nights compared with no intercourse. The difference in Bishop score was not significant (1.0 with coitus vs 0.5 controls; P>.05) and no difference in the number of women who delivered within 3 days was noted in the 2 groups (RR=0.99; 95% CI, 0.45-2.20).3
Castor oil made women nauseous
A Cochrane systematic review included 1 study of women at term with intact membranes who received 1 dose of castor oil to induce labor (n=52) compared with no treatment (n=48). All women who received castor oil felt nauseous, but no other differences were noted between the castor oil group and controls in rates of cesarean section, meconium-stained fluid, or Apgar scores less than 7 at 5 minutes.4
Herbal preparations raise many questions—and some concerns
A prospective controlled trial that randomized 192 women to receive either red raspberry leaf tablets (1.2 g twice daily beginning at 32 weeks) or placebo found no significant differences in duration of the first stage of labor or birth outcomes. Symptom surveys of 108 women revealed no adverse effects.5
A retrospective cohort study compared pregnancy outcomes in 54 women who took evening primrose oil (500 mg 3 times a day beginning at 37 weeks) with a matched group of 54 women who did not take it. The study found no significant differences between the groups in maternal age, Apgar scores, or days of gestation. However, the women taking evening primrose oil tended to have protracted active phase of labor, prolonged rupture of membranes, arrest of descent, and oxytocin augmentation (none of which were statistically significant).6
A systematic review of the literature on black cohosh in pregnancy found no trials that evaluated its efficacy for inducing labor.7 A review of herbal preparations used by midwives reported a case of an infant with low Apgar scores after black cohosh use.8 Both articles described black cohosh as potentially unsafe because of the lack of trials demonstrating safety and possible deleterious estrogenic effects.
A systematic review of the literature on blue cohosh found only in vitro studies of efficacy (increased estradiol-induced transcription in estrogen-responsive cells and increased tone in excised guinea pig uteri) and 3 case reports of maternal adverse events after ingestion (perinatal stroke, congestive heart failure with shock, and multiorgan hypoxic injury).9 In vitro evidence presented in the review suggests that blue cohosh may have teratogenic, embryotoxic, and oxytocic effects.
Recommendations
We found no recommendations from professional organizations regarding folk methods to stimulate labor. The authors of a survey of herbal preparations used by midwives do not advocate their use in pregnancy because of unknown risks to the fetus, although “raspberry leaf tea does not seem to have any significant pharmacologic activity and is probably safe.”8
1. Kavanagh J, Kelly AJ, Thomas J. Breast stimulation for cervical ripening and induction of labour. Cochrane Database Syst Rev. 2005;(3):CD003392.-
2. Smith CA, Crowther CA. Acupuncture for induction of labour. Cochrane Database Syst Rev. 2004;(1):CD002962.-
3. Kavanagh J, Kelly AJ, Thomas J. Sexual intercourse for cervical ripening and induction of labor. Cochrane Database Syst Rev. 2001;(2):CD003093.-
4. Kelly AJ, Kavanagh J, Thomas J. Castor oil, bath and/or enema for cervical priming and induction of labour. Cochrane Database Syst Rev. 2001;(2):CD003099.-
5. Simpson M, Parsons M, Greenwood J, Wade K. Raspberry leaf in pregnancy: its safety and efficacy in labor. J Midwifery Womens Health. 2001;46:51-59.
6. Dove D, Johnson P. Oral evening primrose oil: its effect on length of pregnancy and selected intrapartum outcomes in low-risk nulliparous women. J Nurse Midwifery. 1999;44:320-324.
7. Dugoua JJ, Seely D, Perri D, Koren G, Mills E. Safety and efficacy of black cohosh (Cimicifuga racemosa) during pregnancy and lactation. Can J Clin Pharmacol. 2006;13:e257-e261.
8. McFarlin BL, Gibson MH, O’Rear J, Harman P. A national survey of herbal preparation use by nurse-midwives for labor stimulation. Review of the literature and recommendations for practice. J Nurse Midwifery. 1999;44:205-216.
9. Dugoua JJ, Perri D, Seely D, Mills E, Koren G. Safety and efficacy of blue cohosh (Caulophyllum thalictroides) during pregnancy and lactation. Can J Clin Pharmacol. 2008;15:e66-e73.
1. Kavanagh J, Kelly AJ, Thomas J. Breast stimulation for cervical ripening and induction of labour. Cochrane Database Syst Rev. 2005;(3):CD003392.-
2. Smith CA, Crowther CA. Acupuncture for induction of labour. Cochrane Database Syst Rev. 2004;(1):CD002962.-
3. Kavanagh J, Kelly AJ, Thomas J. Sexual intercourse for cervical ripening and induction of labor. Cochrane Database Syst Rev. 2001;(2):CD003093.-
4. Kelly AJ, Kavanagh J, Thomas J. Castor oil, bath and/or enema for cervical priming and induction of labour. Cochrane Database Syst Rev. 2001;(2):CD003099.-
5. Simpson M, Parsons M, Greenwood J, Wade K. Raspberry leaf in pregnancy: its safety and efficacy in labor. J Midwifery Womens Health. 2001;46:51-59.
6. Dove D, Johnson P. Oral evening primrose oil: its effect on length of pregnancy and selected intrapartum outcomes in low-risk nulliparous women. J Nurse Midwifery. 1999;44:320-324.
7. Dugoua JJ, Seely D, Perri D, Koren G, Mills E. Safety and efficacy of black cohosh (Cimicifuga racemosa) during pregnancy and lactation. Can J Clin Pharmacol. 2006;13:e257-e261.
8. McFarlin BL, Gibson MH, O’Rear J, Harman P. A national survey of herbal preparation use by nurse-midwives for labor stimulation. Review of the literature and recommendations for practice. J Nurse Midwifery. 1999;44:205-216.
9. Dugoua JJ, Perri D, Seely D, Mills E, Koren G. Safety and efficacy of blue cohosh (Caulophyllum thalictroides) during pregnancy and lactation. Can J Clin Pharmacol. 2008;15:e66-e73.
Evidence-based answers from the Family Physicians Inquiries Network
Which patients undergoing noncardiac surgery benefit from perioperative beta-blockers?
Patients with moderate to high cardiac risk (a Revised Cardiac Risk Index [RCRI] score of 2 or higher [TABLE]) have a reduced risk of in-hospital death following perioperative beta-blocker therapy (strength of recommendation [SOR]: B, based on a large retrospective cohort study). There is, however, no proven benefit to perioperative beta-blocker therapy without prior cardiac risk stratification (SOR: A, based on systematic reviews).
Perioperative beta-blockers reduce cardiovascular risk even more when a long-acting beta-blocker (atenolol) is chosen over a shorter-acting one (metoprolol) (SOR: B, based on a retrospective cohort study), and when this therapy is titrated to a target heart rate of <65 BPM (SOR: B, based on cohort studies).
Perioperative beta-blocker therapy is most effective when initiated at least 30 days before surgery and continued throughout the hospital stay (SOR: C, expert opinion extrapolated from systematic review). Patients already on beta-blockers before surgery should continue at least through the perioperative period (SOR: C, expert opinion).
Who better than you to reduce your patient’s risk?
Vincent Lo, MD
San Joaquin Family Residency, French Camp, Calif
Family physicians are in an excellent position to assess and reduce their patients’ risks of complications from elective surgery.
While perioperative beta-blockers do not benefit every surgical patient, they do benefit certain high-risk patients. In fact, these same high-risk patients are often candidates for chronic beta-blocker therapy, according to current ACC/AHA guidelines. Thus, an upcoming surgery gives us another opportunity to identify these patients and get them treated.
Evidence summary
Studies without risk stratification find little benefit from beta-blockers
A systematic review including 25 randomized controlled trials (RCTs) evaluated perioperative beta-blocker therapy for noncardiac surgery in a total of 2722 patients who were not stratified according to cardiac risk status.1
Perioperative beta-blockers produced no significant effect on:
- all-cause mortality (odds ratio [OR]=0.78; 95% confidence interval [CI], 0.33–1.87),
- acute myocardial infarction (OR=0.59; 95% CI, 0.25–1.39),
- atrial fibrillation/flutter and other supraventricular arrhythmias (OR=0.43; 95% CI, 0.14–1.37), or
- length of hospital stay (weighted mean difference, –5.6 days; 95% CI, –12.2, 1.04).
However, in this review perioperative beta-blocker therapy reduced perioperative myocardial ischemia (OR=0.38; 95% CI, 0.21–0.69), and increased 2 adverse outcomes: hemodynamically significant bradycardia (OR=1.98; 95% CI, 1.08– 3.66) and hypotension requiring treatment (OR=2.52; 95% CI, 1.94–3.28).1 This study was limited by the inconsistent definition and assessment of outcomes among the individual trials.
No effect on total mortality, but a benefit in a composite outcome. An earlier systematic review with 22 RCTs and 2437 total patients, that was also not stratified according to cardiac risk status, found no effect from perioperative beta-blockers on total mortality or cardiovascular mortality alone. However, it did demonstrate a composite outcome of reduced cardiovascular mortality, reduced nonfatal myocardial infarction, and reduced nonfatal cardiac arrest (relative risk [RR]=0.44; 95% CI, 0.20–0.97) 30 days after surgery.2
Beta-blockers benefit certain high-risk patients
A retrospective cohort study evaluated the effect of perioperative beta-blocker therapy on perioperative mortality, according to preoperative RCRI assessment.3 The study population included 663,635 adults (mean age, 62 years) undergoing major noncardiac surgery at 329 US hospitals. Researchers calculated individual RCRI scores (TABLE).4 Half the patients had an RCRI of 0, 38% had an RCRI of 1, 10% had an RCRI of 2, and only 2% had an RCRI of 3 or greater.
Be wary of beta-blockers in low-risk patients. In the 580,665 patients with low cardiac risk, perioperative beta-blocker therapy increased the risk of in-hospital death: for all patients with an RCRI of 0: OR=1.36 (95% CI, 1.27–1.45); number needed to harm (NNH)=208; for all patients with an RCRI of 1: OR=1.09 (95% CI, 1.01–1.19); NNH=504).
A different story for high-risk cardiac patients. Perioperative beta-blocker therapy reduced the risk of in-hospital death in patients with an RCRI of 2 (OR=0.88; 95% CI, 0.80–0.98; number needed to treat [NNT]=227), an RCRI of 3 (OR=0.71; 95% CI, 0.63–0.80; NNT=62), or an RCRI of 4 or more (OR=0.58; 95% CI, 0.50–0.67; NNT=33).
TABLE
Before surgery, calculate your patient’s cardiac risk
| Assign 1 point for each of the following, and total: | ||
| ||
| POINTS | CLASS | RISK OF MAJOR CARDIAC EVENT* |
| 0 | I | 0.4% |
| 1 | II | 0.9% |
| 2 | III | 6.6% |
| 3+ | IV | 11% |
| *Major cardiac event includes myocardial infarction, pulmonary edema, ventricular fibrillation, primary cardiac arrest, and complete heart block. | ||
| Source: Lee et al, 1999.4 | ||
Long-acting beta-blockers=fewer MIs
A population-based, retrospective cohort analysis with 37,151 patients over 65 years of age compared perioperative beta-blocker therapy using atenolol (a long-acting beta-blocker) with metoprolol (a shorter-acting beta-blocker) for elective surgery.5 Investigators excluded patients with symptomatic coronary disease.
Patients taking atenolol had fewer MIs (1.6% vs 2.0%, P=.004) and fewer deaths (1.2% vs 1.6%, P=.007) when compared with metoprolol. Atenolol produced a 13% relative risk reduction over metoprolol for MI or death after adjusting for age, sex, type of surgery, and use of furosemide, calcium-channel blockers, angiotensin-converting enzyme inhibitors, and statins (comparative NNT=165).
Dose titration by heart rate
An observational cohort study with 272 patients undergoing elective major vascular surgery (mean age 67.4 years, 80% male) evaluated whether higher doses of beta-blockers and tight heart rate control reduced perioperative myocardial ischemia and troponin T release.6 Patients with higher beta-blocker doses, lower heart rates, and lower absolute change in heart rate during the perioperative period had significantly less perioperative myocardial ischemia and troponin T release (P<.0001).
The DECREASE-II trial, a prospective cohort study with 1476 patients undergoing elective open abdominal aortic or infrainguinal arterial reconstruction also found that patients with heart rates <65 beats per minute had a significantly lower risk of cardiac death or MI at 30 days postoperatively (1.3% vs 5.2%, OR=0.24; 95% CI, 0.09–0.66).7
Begin therapy 30 days before surgery
Authors of a systematic review including 5 RCTs (586 total patients) evaluating perioperative beta-blocker therapy in noncardiac surgery concluded that beta-blocker therapy should begin as long as 30 days prior to surgery to allow for titration of dose to the target heart rate and continue at least throughout hospitalization (longer if adequate medical follow-up can be arranged postoperatively).8
Recommendations from others
The American College of Cardiology/American Heart Association Task Force on Practice Guidelines9 recommends:
- continuing beta-blockers for patients already receiving them to treat angina, symptomatic arrhythmias, and hypertension before their surgical risk evaluation.
- initiating perioperative beta-blocker therapy for patients undergoing vascular surgery if they are at high cardiac risk, as evidenced by ischemia on preoperative testing.
- considering perioperative beta-blocker therapy for patients undergoing intermediate-to high-risk procedures if preoperative risk assessment identifies them as having intermediate or higher cardiac risk, and for patients undergoing vascular surgery who are at low cardiac risk.
1. Wiesbauer F, Schlager O, Domanovits H, et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity: A systematic review and meta-analysis. Anesth Analg 2007;104:27-41.
2. Devereaux PJ, Beattie WS, Choi PT, et al. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials. BMJ 2005;331:313-321.
3. Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med 2005;353:349-361.
4. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100:1043-1049.
5. Redelmeier D, Scales D, Kopp A. Beta blockers for elective surgery in elderly patients: population based, retrospective cohort study. BMJ 2005;331:932.-Epub 2005 Oct 6.
6. Feringa HH, Bax JJ, Boersma E, et al. High-dose beta-blockers and tight heart rate control reduce myocardial ischemia and troponin T release in vascular surgery patients. Circulation 2006;114:I344-I349.
7. Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol 2006;48:964-969.
8. Auerbach AD, Goldman L. Beta-blockers and reduction of cardiac events in noncardiac surgery: scientific review. JAMA 2002;287:1435-1444.
9. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guideline update on perioperative cardiovascular evaluation for noncardiac surgery: focused update on perioperative beta-blocker therapy: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2006;113:2662-2674.
Patients with moderate to high cardiac risk (a Revised Cardiac Risk Index [RCRI] score of 2 or higher [TABLE]) have a reduced risk of in-hospital death following perioperative beta-blocker therapy (strength of recommendation [SOR]: B, based on a large retrospective cohort study). There is, however, no proven benefit to perioperative beta-blocker therapy without prior cardiac risk stratification (SOR: A, based on systematic reviews).
Perioperative beta-blockers reduce cardiovascular risk even more when a long-acting beta-blocker (atenolol) is chosen over a shorter-acting one (metoprolol) (SOR: B, based on a retrospective cohort study), and when this therapy is titrated to a target heart rate of <65 BPM (SOR: B, based on cohort studies).
Perioperative beta-blocker therapy is most effective when initiated at least 30 days before surgery and continued throughout the hospital stay (SOR: C, expert opinion extrapolated from systematic review). Patients already on beta-blockers before surgery should continue at least through the perioperative period (SOR: C, expert opinion).
Who better than you to reduce your patient’s risk?
Vincent Lo, MD
San Joaquin Family Residency, French Camp, Calif
Family physicians are in an excellent position to assess and reduce their patients’ risks of complications from elective surgery.
While perioperative beta-blockers do not benefit every surgical patient, they do benefit certain high-risk patients. In fact, these same high-risk patients are often candidates for chronic beta-blocker therapy, according to current ACC/AHA guidelines. Thus, an upcoming surgery gives us another opportunity to identify these patients and get them treated.
Evidence summary
Studies without risk stratification find little benefit from beta-blockers
A systematic review including 25 randomized controlled trials (RCTs) evaluated perioperative beta-blocker therapy for noncardiac surgery in a total of 2722 patients who were not stratified according to cardiac risk status.1
Perioperative beta-blockers produced no significant effect on:
- all-cause mortality (odds ratio [OR]=0.78; 95% confidence interval [CI], 0.33–1.87),
- acute myocardial infarction (OR=0.59; 95% CI, 0.25–1.39),
- atrial fibrillation/flutter and other supraventricular arrhythmias (OR=0.43; 95% CI, 0.14–1.37), or
- length of hospital stay (weighted mean difference, –5.6 days; 95% CI, –12.2, 1.04).
However, in this review perioperative beta-blocker therapy reduced perioperative myocardial ischemia (OR=0.38; 95% CI, 0.21–0.69), and increased 2 adverse outcomes: hemodynamically significant bradycardia (OR=1.98; 95% CI, 1.08– 3.66) and hypotension requiring treatment (OR=2.52; 95% CI, 1.94–3.28).1 This study was limited by the inconsistent definition and assessment of outcomes among the individual trials.
No effect on total mortality, but a benefit in a composite outcome. An earlier systematic review with 22 RCTs and 2437 total patients, that was also not stratified according to cardiac risk status, found no effect from perioperative beta-blockers on total mortality or cardiovascular mortality alone. However, it did demonstrate a composite outcome of reduced cardiovascular mortality, reduced nonfatal myocardial infarction, and reduced nonfatal cardiac arrest (relative risk [RR]=0.44; 95% CI, 0.20–0.97) 30 days after surgery.2
Beta-blockers benefit certain high-risk patients
A retrospective cohort study evaluated the effect of perioperative beta-blocker therapy on perioperative mortality, according to preoperative RCRI assessment.3 The study population included 663,635 adults (mean age, 62 years) undergoing major noncardiac surgery at 329 US hospitals. Researchers calculated individual RCRI scores (TABLE).4 Half the patients had an RCRI of 0, 38% had an RCRI of 1, 10% had an RCRI of 2, and only 2% had an RCRI of 3 or greater.
Be wary of beta-blockers in low-risk patients. In the 580,665 patients with low cardiac risk, perioperative beta-blocker therapy increased the risk of in-hospital death: for all patients with an RCRI of 0: OR=1.36 (95% CI, 1.27–1.45); number needed to harm (NNH)=208; for all patients with an RCRI of 1: OR=1.09 (95% CI, 1.01–1.19); NNH=504).
A different story for high-risk cardiac patients. Perioperative beta-blocker therapy reduced the risk of in-hospital death in patients with an RCRI of 2 (OR=0.88; 95% CI, 0.80–0.98; number needed to treat [NNT]=227), an RCRI of 3 (OR=0.71; 95% CI, 0.63–0.80; NNT=62), or an RCRI of 4 or more (OR=0.58; 95% CI, 0.50–0.67; NNT=33).
TABLE
Before surgery, calculate your patient’s cardiac risk
| Assign 1 point for each of the following, and total: | ||
| ||
| POINTS | CLASS | RISK OF MAJOR CARDIAC EVENT* |
| 0 | I | 0.4% |
| 1 | II | 0.9% |
| 2 | III | 6.6% |
| 3+ | IV | 11% |
| *Major cardiac event includes myocardial infarction, pulmonary edema, ventricular fibrillation, primary cardiac arrest, and complete heart block. | ||
| Source: Lee et al, 1999.4 | ||
Long-acting beta-blockers=fewer MIs
A population-based, retrospective cohort analysis with 37,151 patients over 65 years of age compared perioperative beta-blocker therapy using atenolol (a long-acting beta-blocker) with metoprolol (a shorter-acting beta-blocker) for elective surgery.5 Investigators excluded patients with symptomatic coronary disease.
Patients taking atenolol had fewer MIs (1.6% vs 2.0%, P=.004) and fewer deaths (1.2% vs 1.6%, P=.007) when compared with metoprolol. Atenolol produced a 13% relative risk reduction over metoprolol for MI or death after adjusting for age, sex, type of surgery, and use of furosemide, calcium-channel blockers, angiotensin-converting enzyme inhibitors, and statins (comparative NNT=165).
Dose titration by heart rate
An observational cohort study with 272 patients undergoing elective major vascular surgery (mean age 67.4 years, 80% male) evaluated whether higher doses of beta-blockers and tight heart rate control reduced perioperative myocardial ischemia and troponin T release.6 Patients with higher beta-blocker doses, lower heart rates, and lower absolute change in heart rate during the perioperative period had significantly less perioperative myocardial ischemia and troponin T release (P<.0001).
The DECREASE-II trial, a prospective cohort study with 1476 patients undergoing elective open abdominal aortic or infrainguinal arterial reconstruction also found that patients with heart rates <65 beats per minute had a significantly lower risk of cardiac death or MI at 30 days postoperatively (1.3% vs 5.2%, OR=0.24; 95% CI, 0.09–0.66).7
Begin therapy 30 days before surgery
Authors of a systematic review including 5 RCTs (586 total patients) evaluating perioperative beta-blocker therapy in noncardiac surgery concluded that beta-blocker therapy should begin as long as 30 days prior to surgery to allow for titration of dose to the target heart rate and continue at least throughout hospitalization (longer if adequate medical follow-up can be arranged postoperatively).8
Recommendations from others
The American College of Cardiology/American Heart Association Task Force on Practice Guidelines9 recommends:
- continuing beta-blockers for patients already receiving them to treat angina, symptomatic arrhythmias, and hypertension before their surgical risk evaluation.
- initiating perioperative beta-blocker therapy for patients undergoing vascular surgery if they are at high cardiac risk, as evidenced by ischemia on preoperative testing.
- considering perioperative beta-blocker therapy for patients undergoing intermediate-to high-risk procedures if preoperative risk assessment identifies them as having intermediate or higher cardiac risk, and for patients undergoing vascular surgery who are at low cardiac risk.
Patients with moderate to high cardiac risk (a Revised Cardiac Risk Index [RCRI] score of 2 or higher [TABLE]) have a reduced risk of in-hospital death following perioperative beta-blocker therapy (strength of recommendation [SOR]: B, based on a large retrospective cohort study). There is, however, no proven benefit to perioperative beta-blocker therapy without prior cardiac risk stratification (SOR: A, based on systematic reviews).
Perioperative beta-blockers reduce cardiovascular risk even more when a long-acting beta-blocker (atenolol) is chosen over a shorter-acting one (metoprolol) (SOR: B, based on a retrospective cohort study), and when this therapy is titrated to a target heart rate of <65 BPM (SOR: B, based on cohort studies).
Perioperative beta-blocker therapy is most effective when initiated at least 30 days before surgery and continued throughout the hospital stay (SOR: C, expert opinion extrapolated from systematic review). Patients already on beta-blockers before surgery should continue at least through the perioperative period (SOR: C, expert opinion).
Who better than you to reduce your patient’s risk?
Vincent Lo, MD
San Joaquin Family Residency, French Camp, Calif
Family physicians are in an excellent position to assess and reduce their patients’ risks of complications from elective surgery.
While perioperative beta-blockers do not benefit every surgical patient, they do benefit certain high-risk patients. In fact, these same high-risk patients are often candidates for chronic beta-blocker therapy, according to current ACC/AHA guidelines. Thus, an upcoming surgery gives us another opportunity to identify these patients and get them treated.
Evidence summary
Studies without risk stratification find little benefit from beta-blockers
A systematic review including 25 randomized controlled trials (RCTs) evaluated perioperative beta-blocker therapy for noncardiac surgery in a total of 2722 patients who were not stratified according to cardiac risk status.1
Perioperative beta-blockers produced no significant effect on:
- all-cause mortality (odds ratio [OR]=0.78; 95% confidence interval [CI], 0.33–1.87),
- acute myocardial infarction (OR=0.59; 95% CI, 0.25–1.39),
- atrial fibrillation/flutter and other supraventricular arrhythmias (OR=0.43; 95% CI, 0.14–1.37), or
- length of hospital stay (weighted mean difference, –5.6 days; 95% CI, –12.2, 1.04).
However, in this review perioperative beta-blocker therapy reduced perioperative myocardial ischemia (OR=0.38; 95% CI, 0.21–0.69), and increased 2 adverse outcomes: hemodynamically significant bradycardia (OR=1.98; 95% CI, 1.08– 3.66) and hypotension requiring treatment (OR=2.52; 95% CI, 1.94–3.28).1 This study was limited by the inconsistent definition and assessment of outcomes among the individual trials.
No effect on total mortality, but a benefit in a composite outcome. An earlier systematic review with 22 RCTs and 2437 total patients, that was also not stratified according to cardiac risk status, found no effect from perioperative beta-blockers on total mortality or cardiovascular mortality alone. However, it did demonstrate a composite outcome of reduced cardiovascular mortality, reduced nonfatal myocardial infarction, and reduced nonfatal cardiac arrest (relative risk [RR]=0.44; 95% CI, 0.20–0.97) 30 days after surgery.2
Beta-blockers benefit certain high-risk patients
A retrospective cohort study evaluated the effect of perioperative beta-blocker therapy on perioperative mortality, according to preoperative RCRI assessment.3 The study population included 663,635 adults (mean age, 62 years) undergoing major noncardiac surgery at 329 US hospitals. Researchers calculated individual RCRI scores (TABLE).4 Half the patients had an RCRI of 0, 38% had an RCRI of 1, 10% had an RCRI of 2, and only 2% had an RCRI of 3 or greater.
Be wary of beta-blockers in low-risk patients. In the 580,665 patients with low cardiac risk, perioperative beta-blocker therapy increased the risk of in-hospital death: for all patients with an RCRI of 0: OR=1.36 (95% CI, 1.27–1.45); number needed to harm (NNH)=208; for all patients with an RCRI of 1: OR=1.09 (95% CI, 1.01–1.19); NNH=504).
A different story for high-risk cardiac patients. Perioperative beta-blocker therapy reduced the risk of in-hospital death in patients with an RCRI of 2 (OR=0.88; 95% CI, 0.80–0.98; number needed to treat [NNT]=227), an RCRI of 3 (OR=0.71; 95% CI, 0.63–0.80; NNT=62), or an RCRI of 4 or more (OR=0.58; 95% CI, 0.50–0.67; NNT=33).
TABLE
Before surgery, calculate your patient’s cardiac risk
| Assign 1 point for each of the following, and total: | ||
| ||
| POINTS | CLASS | RISK OF MAJOR CARDIAC EVENT* |
| 0 | I | 0.4% |
| 1 | II | 0.9% |
| 2 | III | 6.6% |
| 3+ | IV | 11% |
| *Major cardiac event includes myocardial infarction, pulmonary edema, ventricular fibrillation, primary cardiac arrest, and complete heart block. | ||
| Source: Lee et al, 1999.4 | ||
Long-acting beta-blockers=fewer MIs
A population-based, retrospective cohort analysis with 37,151 patients over 65 years of age compared perioperative beta-blocker therapy using atenolol (a long-acting beta-blocker) with metoprolol (a shorter-acting beta-blocker) for elective surgery.5 Investigators excluded patients with symptomatic coronary disease.
Patients taking atenolol had fewer MIs (1.6% vs 2.0%, P=.004) and fewer deaths (1.2% vs 1.6%, P=.007) when compared with metoprolol. Atenolol produced a 13% relative risk reduction over metoprolol for MI or death after adjusting for age, sex, type of surgery, and use of furosemide, calcium-channel blockers, angiotensin-converting enzyme inhibitors, and statins (comparative NNT=165).
Dose titration by heart rate
An observational cohort study with 272 patients undergoing elective major vascular surgery (mean age 67.4 years, 80% male) evaluated whether higher doses of beta-blockers and tight heart rate control reduced perioperative myocardial ischemia and troponin T release.6 Patients with higher beta-blocker doses, lower heart rates, and lower absolute change in heart rate during the perioperative period had significantly less perioperative myocardial ischemia and troponin T release (P<.0001).
The DECREASE-II trial, a prospective cohort study with 1476 patients undergoing elective open abdominal aortic or infrainguinal arterial reconstruction also found that patients with heart rates <65 beats per minute had a significantly lower risk of cardiac death or MI at 30 days postoperatively (1.3% vs 5.2%, OR=0.24; 95% CI, 0.09–0.66).7
Begin therapy 30 days before surgery
Authors of a systematic review including 5 RCTs (586 total patients) evaluating perioperative beta-blocker therapy in noncardiac surgery concluded that beta-blocker therapy should begin as long as 30 days prior to surgery to allow for titration of dose to the target heart rate and continue at least throughout hospitalization (longer if adequate medical follow-up can be arranged postoperatively).8
Recommendations from others
The American College of Cardiology/American Heart Association Task Force on Practice Guidelines9 recommends:
- continuing beta-blockers for patients already receiving them to treat angina, symptomatic arrhythmias, and hypertension before their surgical risk evaluation.
- initiating perioperative beta-blocker therapy for patients undergoing vascular surgery if they are at high cardiac risk, as evidenced by ischemia on preoperative testing.
- considering perioperative beta-blocker therapy for patients undergoing intermediate-to high-risk procedures if preoperative risk assessment identifies them as having intermediate or higher cardiac risk, and for patients undergoing vascular surgery who are at low cardiac risk.
1. Wiesbauer F, Schlager O, Domanovits H, et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity: A systematic review and meta-analysis. Anesth Analg 2007;104:27-41.
2. Devereaux PJ, Beattie WS, Choi PT, et al. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials. BMJ 2005;331:313-321.
3. Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med 2005;353:349-361.
4. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100:1043-1049.
5. Redelmeier D, Scales D, Kopp A. Beta blockers for elective surgery in elderly patients: population based, retrospective cohort study. BMJ 2005;331:932.-Epub 2005 Oct 6.
6. Feringa HH, Bax JJ, Boersma E, et al. High-dose beta-blockers and tight heart rate control reduce myocardial ischemia and troponin T release in vascular surgery patients. Circulation 2006;114:I344-I349.
7. Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol 2006;48:964-969.
8. Auerbach AD, Goldman L. Beta-blockers and reduction of cardiac events in noncardiac surgery: scientific review. JAMA 2002;287:1435-1444.
9. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guideline update on perioperative cardiovascular evaluation for noncardiac surgery: focused update on perioperative beta-blocker therapy: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2006;113:2662-2674.
1. Wiesbauer F, Schlager O, Domanovits H, et al. Perioperative beta-blockers for preventing surgery-related mortality and morbidity: A systematic review and meta-analysis. Anesth Analg 2007;104:27-41.
2. Devereaux PJ, Beattie WS, Choi PT, et al. How strong is the evidence for the use of perioperative beta blockers in non-cardiac surgery? Systematic review and meta-analysis of randomised controlled trials. BMJ 2005;331:313-321.
3. Lindenauer PK, Pekow P, Wang K, Mamidi DK, Gutierrez B, Benjamin EM, et al. Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med 2005;353:349-361.
4. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999;100:1043-1049.
5. Redelmeier D, Scales D, Kopp A. Beta blockers for elective surgery in elderly patients: population based, retrospective cohort study. BMJ 2005;331:932.-Epub 2005 Oct 6.
6. Feringa HH, Bax JJ, Boersma E, et al. High-dose beta-blockers and tight heart rate control reduce myocardial ischemia and troponin T release in vascular surgery patients. Circulation 2006;114:I344-I349.
7. Poldermans D, Bax JJ, Schouten O, et al. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol 2006;48:964-969.
8. Auerbach AD, Goldman L. Beta-blockers and reduction of cardiac events in noncardiac surgery: scientific review. JAMA 2002;287:1435-1444.
9. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2006 guideline update on perioperative cardiovascular evaluation for noncardiac surgery: focused update on perioperative beta-blocker therapy: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2006;113:2662-2674.
Evidence-based answers from the Family Physicians Inquiries Network
What is the role of combination therapy (insulin plus oral medication) in type 2 diabetes?
Combination therapy using insulin plus metformin (Glucophage), a sulfonylurea, or both produces glycemic control comparable with using insulin alone, but there is less weight gain when metformin is used (strength of recommendation [SOR]: B, based on systematic review of randomized controlled trials [RCTs] with some heterogeneity). Combination therapy using insulin and pioglitazone (Actos) reduces glycosylated hemoglobin (HbA1c) more than either insulin alone or adding pioglitazone to a sulfonylurea, but results in more weight gain (SOR: A, based on RCT). Using insulin glargine (Lantus) in combination therapy produces fewer nocturnal hypoglycemic events than using neutral protamine Hagedorn (NPH) insulin, while producing equivalent HbA1c reduction (SOR: B, based on RCT).
When the HbA1c is high (above 9.0% to 9.5%) on 1 or 2 oral agents, beginning combination therapy is more effective than adding another oral agent (SOR: B, based on subpopulation analysis in RCTs).
Educate patients from the time of diagnosis that insulin is not a failure
Vincent Lo, MD
San Joaquin General Hospital, French Camp, Calif
Combination therapy for patients with type 2 diabetes is a safe and effective stepping stone between oral therapy and insulin therapy. Unfortunately, significant barriers remain to getting insulin started when oral agents alone are insufficient. Patients often do not understand the common need for insulin therapy as type 2 diabetes advances, and some physicians continue to use the threat of insulin as a punitive incentive to promote patient compliance. It is little wonder that many patients perceive a physician’s eventual recommendation for insulin therapy as a personal failure. Patients are also concerned about the discomfort, inconvenience, and risk of insulin injections. Physicians should focus on educating their patients from the time of diagnosis that insulin is not a failure, but just another tool that will help them achieve their blood sugar goals.
Evidence summary
A systematic review evaluated beginning combination therapy (adding insulin to oral medication) compared with switching to insulin alone in patients with type 2 diabetes mellitus with inadequate glycemic control on oral medication.1 Twenty RCTs studied a total of 1811 patients; glycemic control was the primary outcome measure. Oral medication comprised either sulfonylureas (75%), metformin (4%), or both (21%). Individual studies used different insulin dosing schedules and statistical measures. However, overall, combination therapy provided glucose control comparable with insulin alone. In only 1 small, low-quality study did insulin plus metformin reduce HbA1c more than other combination therapy regimens or insulin alone. Ten studies reported a trend toward less weight gain with combination therapy that included metformin. Fourteen studies found the same incidence of hypoglycemic episodes in combination therapy and insulin alone.
Three later RCTs of overweight patients with inadequate control on oral agents (HbA1c >7% on a sulfonylurea, metformin, or both) also compared beginning combination therapy with switching to insulin alone (with 70/30 or NPH insulin twice daily). In one study with 64 patients followed for 12 months, HbA1c fell by 0.14% less (nonsignificant) in the combination therapy group (bedtime NPH plus sulfonylurea and metformin) than in the insulin alone group (70/30 twice daily).2 The combination therapy group gained significantly less weight than the insulin-alone group (1.3 kg vs 4.2 kg; P=.01).
In the second study of 261 patients, the combination therapy group (glimepiride [Amaryl] plus bedtime NPH) had a significantly higher HbA1c after 9 months than 2 groups using insulin alone (twice daily 70/30, and twice daily NPH insulin) (8.9% vs 8.3% and 8.4%).3 Mean weight gain was similar in all 3 groups but only a minority of patients reached a target HbA1c of 6.5%. In the final study of only 16 patients, HbA1c after 6 months improved significantly and equally in both groups (baseline: 8.3%, combination therapy final: 6.8%; insulin alone final: 7.0%). However, the combination therapy group gained significantly less weight.4
An open-label RCT with 341 patients who were inadequately controlled on metformin compared beginning combination therapy (biphasic insulin aspart 30/70 [Novolog Mix 70/30] and metformin) with switching to insulin alone (biphasic insulin aspart 30/70).5 A third group added a second oral medication (sulfonylurea and metformin). After 16 weeks, patients taking combination therapy had a significantly lower HbA1c than those on insulin alone (treatment difference 0.39%, P=.007).
Overall, combination therapy and 2 oral medications reduced HbA1c by the same amount, but combination therapy reduced HbA1c more in a subpopulation of patients with HbA1c >9.0% at baseline (treatment difference 0.46%, P=.027). The group on insulin alone weighed significantly more (4.6 kg, P<.001) at the end of the trial than the group taking 2 oral medications.
An open-label RCT of 756 patients with inadequate glycemic control (HbA1c >7.5%, mean 8.6%) on either 1 or 2 oral agents (70% taking both metformin and a sulfonylurea) compared combination therapy using bedtime insulin glargine with combination therapy using morning NPH.6 Each group titrated insulin doses to achieve a target fasting glucose ≤100. By 24 weeks, both groups had equivalently reduced HbA1c (mean HbA1c=6.96% with glargine, and 6.97% with NPH; P=NS), but fewer patients experienced nocturnal hypoglycemia with glargine than with NPH (33.2% vs 26.7%, P<.05).
Another open-label RCT evaluated 281 patients with at least 3 months of inadequate glycemic control (HbA1c=7.4%–14.7%) on a sulfonylurea.7 Patients were randomized to a) switching to a combination of biphasic insulin aspart 30/70 plus pioglitazone, b) adding pioglitazone to the sulfonylurea, or c) switching to insulin alone (biphasic insulin aspart 30/70). After 18 weeks, insulin plus pioglitazone reduced HbA1c significantly more than either glyburide plus pioglitazone (P=.005) or insulin alone (P=.005). However, the insulin plus pioglitazone group had the most weight gain (mean 4 kg, similar to other pioglitazone trials). There were no major hypoglycemic events.
Another open-label RCT evaluated 217 patients inadequately controlled (HbA1c=7.5%–11%) on a 2-drug oral regimen (metformin and a sulfonylurea, each drug dosed at ≥50% of the recommended maximum), randomized to add either insulin glargine or rosiglitazone (Avandia).8 Both groups reduced HbA1c equivalently after 24 weeks (–1.7% for glargine vs –1.5% for rosiglitazone). However, in patients with a baseline HbA1c >9.5%, adding insulin glargine reduced HbA1c significantly more than rosiglitazone.
Recommendations from others
A comparative analysis of guidelines on diabetes from 13 different countries (including the US) found general agreement in the recommendation to add a second oral agent to maximum doses of an initial agent in patients with poor glycemic control.9 However, no consensus was reached on the value or indications of combination therapy with oral agents and insulin.
The European Diabetes Policy Group recommends adding a second oral agent when the maximum dose of a single agent is reached, and using triple therapy when targets are not reached on maximum tolerated doses of 2 agents. Continued therapy with oral agents is advised when initiating insulin.10
1. Goudswaard AN, Furlong NJ, Rutten GE, Stolk RP, Valk GD. Insulin monotherapy versus combinations of insulin with oral hypoglycaemic agents in patients with type 2 diabetes mellitus. ochrane Database Syst Rev 2004;(4):CD003418.-
2. Goudswaard AN, Stolk RP, Zuithoff P, de Valk HW, Rutten GE. Starting insulin in type 2 diabetes: continue oral hypoglycemic agents? A randomized trial in primary care. J Fam Pract 2004;53:393-399.
3. Stehouwer MHA, DeVries JH, Lumeij JA, et al. Combined bedtime insulin-daytime sulphonylurea regimen compared with two different daily insulin regimens in type 2 diabetes: effects on HbA1c and hypoglycemia rate-a randomized trial . Diabetes Metab Res Rev 2003;19:148-152.
4. Olsson PO, Lindstrom T. Combination-therapy with bedtime NPH insulin and sulphonylureas gives similar glycaemic control but lower weight gain than insulin twice daily in patients with type 2 diabetes. Diabetes Metab 2002;28(4 Pt 1):272-277.
5. Kvapil M, Swatko A, Hilberg C, Shestakova M. Biphasic insulin aspart 30 plus metformin: an effective combination in type 2 diabetes. Diabetes Obes Metab 2006;8:39-48.
6. Riddle MC, Rosenstock J, Gerich J. The Insulin Glargine 4002 Study Investigators. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003;26:3080-3086.
7. Raz I, Stranks S, Filipczak R, et al. Efficacy and safety of biphasic insulin aspart 30 combined with pioglitazone in type 2 diabetes poorly controlled on glibenclamide (glyburide) monotherapy or combination therapy: an 18 week, randomized, open-label study. Clin Ther 2005;27:1432-1443.
8. Rosenstock J, Sugimoto D, Strange P, Stewart JA, SoltesRak E, Dailey G. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naïve patients. Diabetes Care 2006;29:554-559.
9. Burgers JS, Grol R, Klazinga NS, et al. Inside guidelines: comparative analysis of recommendations and evidence in diabetes guidelines from 13 countries. Diabetes Care 2002;25:1933-1939.
10. European Diabetes Policy Group 1999. A desktop guide to Type 2 diabetes mellitus. Diabet Med 1999;16:716-730.
Combination therapy using insulin plus metformin (Glucophage), a sulfonylurea, or both produces glycemic control comparable with using insulin alone, but there is less weight gain when metformin is used (strength of recommendation [SOR]: B, based on systematic review of randomized controlled trials [RCTs] with some heterogeneity). Combination therapy using insulin and pioglitazone (Actos) reduces glycosylated hemoglobin (HbA1c) more than either insulin alone or adding pioglitazone to a sulfonylurea, but results in more weight gain (SOR: A, based on RCT). Using insulin glargine (Lantus) in combination therapy produces fewer nocturnal hypoglycemic events than using neutral protamine Hagedorn (NPH) insulin, while producing equivalent HbA1c reduction (SOR: B, based on RCT).
When the HbA1c is high (above 9.0% to 9.5%) on 1 or 2 oral agents, beginning combination therapy is more effective than adding another oral agent (SOR: B, based on subpopulation analysis in RCTs).
Educate patients from the time of diagnosis that insulin is not a failure
Vincent Lo, MD
San Joaquin General Hospital, French Camp, Calif
Combination therapy for patients with type 2 diabetes is a safe and effective stepping stone between oral therapy and insulin therapy. Unfortunately, significant barriers remain to getting insulin started when oral agents alone are insufficient. Patients often do not understand the common need for insulin therapy as type 2 diabetes advances, and some physicians continue to use the threat of insulin as a punitive incentive to promote patient compliance. It is little wonder that many patients perceive a physician’s eventual recommendation for insulin therapy as a personal failure. Patients are also concerned about the discomfort, inconvenience, and risk of insulin injections. Physicians should focus on educating their patients from the time of diagnosis that insulin is not a failure, but just another tool that will help them achieve their blood sugar goals.
Evidence summary
A systematic review evaluated beginning combination therapy (adding insulin to oral medication) compared with switching to insulin alone in patients with type 2 diabetes mellitus with inadequate glycemic control on oral medication.1 Twenty RCTs studied a total of 1811 patients; glycemic control was the primary outcome measure. Oral medication comprised either sulfonylureas (75%), metformin (4%), or both (21%). Individual studies used different insulin dosing schedules and statistical measures. However, overall, combination therapy provided glucose control comparable with insulin alone. In only 1 small, low-quality study did insulin plus metformin reduce HbA1c more than other combination therapy regimens or insulin alone. Ten studies reported a trend toward less weight gain with combination therapy that included metformin. Fourteen studies found the same incidence of hypoglycemic episodes in combination therapy and insulin alone.
Three later RCTs of overweight patients with inadequate control on oral agents (HbA1c >7% on a sulfonylurea, metformin, or both) also compared beginning combination therapy with switching to insulin alone (with 70/30 or NPH insulin twice daily). In one study with 64 patients followed for 12 months, HbA1c fell by 0.14% less (nonsignificant) in the combination therapy group (bedtime NPH plus sulfonylurea and metformin) than in the insulin alone group (70/30 twice daily).2 The combination therapy group gained significantly less weight than the insulin-alone group (1.3 kg vs 4.2 kg; P=.01).
In the second study of 261 patients, the combination therapy group (glimepiride [Amaryl] plus bedtime NPH) had a significantly higher HbA1c after 9 months than 2 groups using insulin alone (twice daily 70/30, and twice daily NPH insulin) (8.9% vs 8.3% and 8.4%).3 Mean weight gain was similar in all 3 groups but only a minority of patients reached a target HbA1c of 6.5%. In the final study of only 16 patients, HbA1c after 6 months improved significantly and equally in both groups (baseline: 8.3%, combination therapy final: 6.8%; insulin alone final: 7.0%). However, the combination therapy group gained significantly less weight.4
An open-label RCT with 341 patients who were inadequately controlled on metformin compared beginning combination therapy (biphasic insulin aspart 30/70 [Novolog Mix 70/30] and metformin) with switching to insulin alone (biphasic insulin aspart 30/70).5 A third group added a second oral medication (sulfonylurea and metformin). After 16 weeks, patients taking combination therapy had a significantly lower HbA1c than those on insulin alone (treatment difference 0.39%, P=.007).
Overall, combination therapy and 2 oral medications reduced HbA1c by the same amount, but combination therapy reduced HbA1c more in a subpopulation of patients with HbA1c >9.0% at baseline (treatment difference 0.46%, P=.027). The group on insulin alone weighed significantly more (4.6 kg, P<.001) at the end of the trial than the group taking 2 oral medications.
An open-label RCT of 756 patients with inadequate glycemic control (HbA1c >7.5%, mean 8.6%) on either 1 or 2 oral agents (70% taking both metformin and a sulfonylurea) compared combination therapy using bedtime insulin glargine with combination therapy using morning NPH.6 Each group titrated insulin doses to achieve a target fasting glucose ≤100. By 24 weeks, both groups had equivalently reduced HbA1c (mean HbA1c=6.96% with glargine, and 6.97% with NPH; P=NS), but fewer patients experienced nocturnal hypoglycemia with glargine than with NPH (33.2% vs 26.7%, P<.05).
Another open-label RCT evaluated 281 patients with at least 3 months of inadequate glycemic control (HbA1c=7.4%–14.7%) on a sulfonylurea.7 Patients were randomized to a) switching to a combination of biphasic insulin aspart 30/70 plus pioglitazone, b) adding pioglitazone to the sulfonylurea, or c) switching to insulin alone (biphasic insulin aspart 30/70). After 18 weeks, insulin plus pioglitazone reduced HbA1c significantly more than either glyburide plus pioglitazone (P=.005) or insulin alone (P=.005). However, the insulin plus pioglitazone group had the most weight gain (mean 4 kg, similar to other pioglitazone trials). There were no major hypoglycemic events.
Another open-label RCT evaluated 217 patients inadequately controlled (HbA1c=7.5%–11%) on a 2-drug oral regimen (metformin and a sulfonylurea, each drug dosed at ≥50% of the recommended maximum), randomized to add either insulin glargine or rosiglitazone (Avandia).8 Both groups reduced HbA1c equivalently after 24 weeks (–1.7% for glargine vs –1.5% for rosiglitazone). However, in patients with a baseline HbA1c >9.5%, adding insulin glargine reduced HbA1c significantly more than rosiglitazone.
Recommendations from others
A comparative analysis of guidelines on diabetes from 13 different countries (including the US) found general agreement in the recommendation to add a second oral agent to maximum doses of an initial agent in patients with poor glycemic control.9 However, no consensus was reached on the value or indications of combination therapy with oral agents and insulin.
The European Diabetes Policy Group recommends adding a second oral agent when the maximum dose of a single agent is reached, and using triple therapy when targets are not reached on maximum tolerated doses of 2 agents. Continued therapy with oral agents is advised when initiating insulin.10
Combination therapy using insulin plus metformin (Glucophage), a sulfonylurea, or both produces glycemic control comparable with using insulin alone, but there is less weight gain when metformin is used (strength of recommendation [SOR]: B, based on systematic review of randomized controlled trials [RCTs] with some heterogeneity). Combination therapy using insulin and pioglitazone (Actos) reduces glycosylated hemoglobin (HbA1c) more than either insulin alone or adding pioglitazone to a sulfonylurea, but results in more weight gain (SOR: A, based on RCT). Using insulin glargine (Lantus) in combination therapy produces fewer nocturnal hypoglycemic events than using neutral protamine Hagedorn (NPH) insulin, while producing equivalent HbA1c reduction (SOR: B, based on RCT).
When the HbA1c is high (above 9.0% to 9.5%) on 1 or 2 oral agents, beginning combination therapy is more effective than adding another oral agent (SOR: B, based on subpopulation analysis in RCTs).
Educate patients from the time of diagnosis that insulin is not a failure
Vincent Lo, MD
San Joaquin General Hospital, French Camp, Calif
Combination therapy for patients with type 2 diabetes is a safe and effective stepping stone between oral therapy and insulin therapy. Unfortunately, significant barriers remain to getting insulin started when oral agents alone are insufficient. Patients often do not understand the common need for insulin therapy as type 2 diabetes advances, and some physicians continue to use the threat of insulin as a punitive incentive to promote patient compliance. It is little wonder that many patients perceive a physician’s eventual recommendation for insulin therapy as a personal failure. Patients are also concerned about the discomfort, inconvenience, and risk of insulin injections. Physicians should focus on educating their patients from the time of diagnosis that insulin is not a failure, but just another tool that will help them achieve their blood sugar goals.
Evidence summary
A systematic review evaluated beginning combination therapy (adding insulin to oral medication) compared with switching to insulin alone in patients with type 2 diabetes mellitus with inadequate glycemic control on oral medication.1 Twenty RCTs studied a total of 1811 patients; glycemic control was the primary outcome measure. Oral medication comprised either sulfonylureas (75%), metformin (4%), or both (21%). Individual studies used different insulin dosing schedules and statistical measures. However, overall, combination therapy provided glucose control comparable with insulin alone. In only 1 small, low-quality study did insulin plus metformin reduce HbA1c more than other combination therapy regimens or insulin alone. Ten studies reported a trend toward less weight gain with combination therapy that included metformin. Fourteen studies found the same incidence of hypoglycemic episodes in combination therapy and insulin alone.
Three later RCTs of overweight patients with inadequate control on oral agents (HbA1c >7% on a sulfonylurea, metformin, or both) also compared beginning combination therapy with switching to insulin alone (with 70/30 or NPH insulin twice daily). In one study with 64 patients followed for 12 months, HbA1c fell by 0.14% less (nonsignificant) in the combination therapy group (bedtime NPH plus sulfonylurea and metformin) than in the insulin alone group (70/30 twice daily).2 The combination therapy group gained significantly less weight than the insulin-alone group (1.3 kg vs 4.2 kg; P=.01).
In the second study of 261 patients, the combination therapy group (glimepiride [Amaryl] plus bedtime NPH) had a significantly higher HbA1c after 9 months than 2 groups using insulin alone (twice daily 70/30, and twice daily NPH insulin) (8.9% vs 8.3% and 8.4%).3 Mean weight gain was similar in all 3 groups but only a minority of patients reached a target HbA1c of 6.5%. In the final study of only 16 patients, HbA1c after 6 months improved significantly and equally in both groups (baseline: 8.3%, combination therapy final: 6.8%; insulin alone final: 7.0%). However, the combination therapy group gained significantly less weight.4
An open-label RCT with 341 patients who were inadequately controlled on metformin compared beginning combination therapy (biphasic insulin aspart 30/70 [Novolog Mix 70/30] and metformin) with switching to insulin alone (biphasic insulin aspart 30/70).5 A third group added a second oral medication (sulfonylurea and metformin). After 16 weeks, patients taking combination therapy had a significantly lower HbA1c than those on insulin alone (treatment difference 0.39%, P=.007).
Overall, combination therapy and 2 oral medications reduced HbA1c by the same amount, but combination therapy reduced HbA1c more in a subpopulation of patients with HbA1c >9.0% at baseline (treatment difference 0.46%, P=.027). The group on insulin alone weighed significantly more (4.6 kg, P<.001) at the end of the trial than the group taking 2 oral medications.
An open-label RCT of 756 patients with inadequate glycemic control (HbA1c >7.5%, mean 8.6%) on either 1 or 2 oral agents (70% taking both metformin and a sulfonylurea) compared combination therapy using bedtime insulin glargine with combination therapy using morning NPH.6 Each group titrated insulin doses to achieve a target fasting glucose ≤100. By 24 weeks, both groups had equivalently reduced HbA1c (mean HbA1c=6.96% with glargine, and 6.97% with NPH; P=NS), but fewer patients experienced nocturnal hypoglycemia with glargine than with NPH (33.2% vs 26.7%, P<.05).
Another open-label RCT evaluated 281 patients with at least 3 months of inadequate glycemic control (HbA1c=7.4%–14.7%) on a sulfonylurea.7 Patients were randomized to a) switching to a combination of biphasic insulin aspart 30/70 plus pioglitazone, b) adding pioglitazone to the sulfonylurea, or c) switching to insulin alone (biphasic insulin aspart 30/70). After 18 weeks, insulin plus pioglitazone reduced HbA1c significantly more than either glyburide plus pioglitazone (P=.005) or insulin alone (P=.005). However, the insulin plus pioglitazone group had the most weight gain (mean 4 kg, similar to other pioglitazone trials). There were no major hypoglycemic events.
Another open-label RCT evaluated 217 patients inadequately controlled (HbA1c=7.5%–11%) on a 2-drug oral regimen (metformin and a sulfonylurea, each drug dosed at ≥50% of the recommended maximum), randomized to add either insulin glargine or rosiglitazone (Avandia).8 Both groups reduced HbA1c equivalently after 24 weeks (–1.7% for glargine vs –1.5% for rosiglitazone). However, in patients with a baseline HbA1c >9.5%, adding insulin glargine reduced HbA1c significantly more than rosiglitazone.
Recommendations from others
A comparative analysis of guidelines on diabetes from 13 different countries (including the US) found general agreement in the recommendation to add a second oral agent to maximum doses of an initial agent in patients with poor glycemic control.9 However, no consensus was reached on the value or indications of combination therapy with oral agents and insulin.
The European Diabetes Policy Group recommends adding a second oral agent when the maximum dose of a single agent is reached, and using triple therapy when targets are not reached on maximum tolerated doses of 2 agents. Continued therapy with oral agents is advised when initiating insulin.10
1. Goudswaard AN, Furlong NJ, Rutten GE, Stolk RP, Valk GD. Insulin monotherapy versus combinations of insulin with oral hypoglycaemic agents in patients with type 2 diabetes mellitus. ochrane Database Syst Rev 2004;(4):CD003418.-
2. Goudswaard AN, Stolk RP, Zuithoff P, de Valk HW, Rutten GE. Starting insulin in type 2 diabetes: continue oral hypoglycemic agents? A randomized trial in primary care. J Fam Pract 2004;53:393-399.
3. Stehouwer MHA, DeVries JH, Lumeij JA, et al. Combined bedtime insulin-daytime sulphonylurea regimen compared with two different daily insulin regimens in type 2 diabetes: effects on HbA1c and hypoglycemia rate-a randomized trial . Diabetes Metab Res Rev 2003;19:148-152.
4. Olsson PO, Lindstrom T. Combination-therapy with bedtime NPH insulin and sulphonylureas gives similar glycaemic control but lower weight gain than insulin twice daily in patients with type 2 diabetes. Diabetes Metab 2002;28(4 Pt 1):272-277.
5. Kvapil M, Swatko A, Hilberg C, Shestakova M. Biphasic insulin aspart 30 plus metformin: an effective combination in type 2 diabetes. Diabetes Obes Metab 2006;8:39-48.
6. Riddle MC, Rosenstock J, Gerich J. The Insulin Glargine 4002 Study Investigators. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003;26:3080-3086.
7. Raz I, Stranks S, Filipczak R, et al. Efficacy and safety of biphasic insulin aspart 30 combined with pioglitazone in type 2 diabetes poorly controlled on glibenclamide (glyburide) monotherapy or combination therapy: an 18 week, randomized, open-label study. Clin Ther 2005;27:1432-1443.
8. Rosenstock J, Sugimoto D, Strange P, Stewart JA, SoltesRak E, Dailey G. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naïve patients. Diabetes Care 2006;29:554-559.
9. Burgers JS, Grol R, Klazinga NS, et al. Inside guidelines: comparative analysis of recommendations and evidence in diabetes guidelines from 13 countries. Diabetes Care 2002;25:1933-1939.
10. European Diabetes Policy Group 1999. A desktop guide to Type 2 diabetes mellitus. Diabet Med 1999;16:716-730.
1. Goudswaard AN, Furlong NJ, Rutten GE, Stolk RP, Valk GD. Insulin monotherapy versus combinations of insulin with oral hypoglycaemic agents in patients with type 2 diabetes mellitus. ochrane Database Syst Rev 2004;(4):CD003418.-
2. Goudswaard AN, Stolk RP, Zuithoff P, de Valk HW, Rutten GE. Starting insulin in type 2 diabetes: continue oral hypoglycemic agents? A randomized trial in primary care. J Fam Pract 2004;53:393-399.
3. Stehouwer MHA, DeVries JH, Lumeij JA, et al. Combined bedtime insulin-daytime sulphonylurea regimen compared with two different daily insulin regimens in type 2 diabetes: effects on HbA1c and hypoglycemia rate-a randomized trial . Diabetes Metab Res Rev 2003;19:148-152.
4. Olsson PO, Lindstrom T. Combination-therapy with bedtime NPH insulin and sulphonylureas gives similar glycaemic control but lower weight gain than insulin twice daily in patients with type 2 diabetes. Diabetes Metab 2002;28(4 Pt 1):272-277.
5. Kvapil M, Swatko A, Hilberg C, Shestakova M. Biphasic insulin aspart 30 plus metformin: an effective combination in type 2 diabetes. Diabetes Obes Metab 2006;8:39-48.
6. Riddle MC, Rosenstock J, Gerich J. The Insulin Glargine 4002 Study Investigators. The treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003;26:3080-3086.
7. Raz I, Stranks S, Filipczak R, et al. Efficacy and safety of biphasic insulin aspart 30 combined with pioglitazone in type 2 diabetes poorly controlled on glibenclamide (glyburide) monotherapy or combination therapy: an 18 week, randomized, open-label study. Clin Ther 2005;27:1432-1443.
8. Rosenstock J, Sugimoto D, Strange P, Stewart JA, SoltesRak E, Dailey G. Triple therapy in type 2 diabetes: insulin glargine or rosiglitazone added to combination therapy of sulfonylurea plus metformin in insulin-naïve patients. Diabetes Care 2006;29:554-559.
9. Burgers JS, Grol R, Klazinga NS, et al. Inside guidelines: comparative analysis of recommendations and evidence in diabetes guidelines from 13 countries. Diabetes Care 2002;25:1933-1939.
10. European Diabetes Policy Group 1999. A desktop guide to Type 2 diabetes mellitus. Diabet Med 1999;16:716-730.
Evidence-based answers from the Family Physicians Inquiries Network
What is the risk of adverse outcomes in a woman who develops mild hypertension from OCs?
Women who take oral contraceptives (OCs) have an increased risk of developing new hypertension, which returns to baseline within 1 to 3 months of OC cessation (strength of recommendation [SOR]: A, based on cohort studies).
Among large populations of women with hypertension from all causes, risk of adverse cardiovascular outcomes is increased (SOR: B, based on Framingham data). Women with pre-existing hypertension who take OCs have an increased risk of stroke and myocardial infarction (MI) when compared with hypertensive women who do not (SOR: B, based on case-control studies).
Is an increase of 178 per million woman-years of CV events clinically significant?
Sarina Schrager, MD
University of Wisconsin
In clinical practice, we continually balance the risks and benefits of any treatment. Oral contraceptive pills are the most commonly used reversible form of contraception in the United States. Although this review documents an increased risk of reversible new hypertension for women on OCs and a possibly significant increase in cardiovascular events, the clinical meaning of these data is unclear. Is an increase of 178 per million woman-years of CV events clinically significant? It would be a shame to limit the availability of this effective contraception method to otherwise young and healthy women because of this very rare event.
Evidence summary
No studies specifically examine the risk of adverse outcomes for women who have mild elevations in blood pressure as a result of taking OCs. However, for the general population cardiovascular risk increases 30% for each 10 mm Hg rise in systolic pressure.1
A prospective cohort study found an increased incidence of new hypertension developing among women taking OCs. The study, conducted in the US, included 68,297 female nurses aged 25 to 42 years without a previous diagnosis of hypertension, diabetes, coronary heart disease, stroke, or cancer, who were followed for 4 years. Women were excluded from the study if they had not had a physical exam in the last 2 years or were taking antihypertensive medication at study inception. The nurses self-reported their blood pressure readings via questionnaire; medical records were sampled to validate the accuracy of self-reports. After adjusting for risk factors, current oral contraceptive use increased the risk of developing hypertension (relative risk [RR]=1.8; 95% confidence interval [CI], 1.5–2.3; corresponding to 41.5 new cases of hypertension per 10,000 person-years).2
A systematic review of 8 case control studies (with 4907 cases and 13,443 controls) found an increased risk of stroke and MI among hypertensive women taking combined type OCs vs those not taking OCs. Women with hypertension aged 20 to 24 years had an estimated CV event risk of 312 per million woman-years while taking OCs vs 134 per million woman-years not taking OCs. Among hypertensive women aged 40 to 44 years, the estimated risks were 1213 vs 529 per million woman-years, respectively. Primary endpoints varied across the studies and statistical significance was not given.3
Three studies showed that blood pressure elevations due to taking oral contraceptives returned to baseline with discontinuation of the medication. A prospective cohort study followed 13,358 women who were neither pregnant nor postpartum between the ages of 15 and 60. Women who either initiated or resumed using OCs experienced a statistically significant rise of about 4 mm Hg in the systolic pressure and 1 mm Hg in the diastolic pressure. Women who stopped using OCs experienced significant decreases in both systolic and diastolic components (about 5 mm Hg and 1.5 mm Hg, respectively).1
Similarly, a survey study of 461 women attending family planning clinics found that mean blood pressures were significantly higher for those taking OCs than for those using nonhormonal contraception. Elevated blood pressures correlated with duration of current use of OCs but returned to normal soon after stopping OCs. The mean pressures of those who had stopped OCs more than a month were similar to those of women who had never taken an OC and significantly lower than those of women who were currently taking OCs.4
Finally, a prospective study which followed 32 women who had taken combined OCs for 1 to 3 years and then stopped found that blood pressures returned to pretreatment levels at 3 months. Systolic pressure fell by 9.7 mm Hg and diastolic by 2.9 mm Hg compared with measurements made 1 month before stopping. No cardiovascular complications were reported among women during this study.5
Recommendations from others
The American College of Obstetricians and Gynecologists says that women with well-controlled and monitored hypertension aged 35 years and younger are appropriate candidates for a trial of combination OCs, provided they are otherwise healthy, have no evidence of end-organ vascular disease, and do not smoke cigarettes.6 If blood pressure remains well controlled with careful monitoring several months after initiating OCs, use can be continued.
1. Fisch IR, Frank J. Oral contraceptives and blood pressure. JAMA 1977;237:2499-2503.
2. Chasen-Taber L, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996;94:483-489.
3. Curtis K, et al. Contraception for women in selected circumstances. Obstet Gynecol 2002;6:1100-1112.
4. Khaw K-T, Peart WS. Blood pressure and contraceptive use. Br Med J 1982;285:403-407.
5. Weir RJ, Briggs E, Mack A, Naismith L, Taylor L, Wilson E. Blood pressure in women taking oral contraceptives. Br Med J 1974;1:533-535.
6. American College of Obstetricians and Gynecologists (ACOG). The use of hormonal contraception in women with coexisting medical conditions. Washington, DC: American College of Obstetricians and Gynecologists (ACOG); 2006 June. 20 p. (ACOG practice bulletin; no. 73).
Women who take oral contraceptives (OCs) have an increased risk of developing new hypertension, which returns to baseline within 1 to 3 months of OC cessation (strength of recommendation [SOR]: A, based on cohort studies).
Among large populations of women with hypertension from all causes, risk of adverse cardiovascular outcomes is increased (SOR: B, based on Framingham data). Women with pre-existing hypertension who take OCs have an increased risk of stroke and myocardial infarction (MI) when compared with hypertensive women who do not (SOR: B, based on case-control studies).
Is an increase of 178 per million woman-years of CV events clinically significant?
Sarina Schrager, MD
University of Wisconsin
In clinical practice, we continually balance the risks and benefits of any treatment. Oral contraceptive pills are the most commonly used reversible form of contraception in the United States. Although this review documents an increased risk of reversible new hypertension for women on OCs and a possibly significant increase in cardiovascular events, the clinical meaning of these data is unclear. Is an increase of 178 per million woman-years of CV events clinically significant? It would be a shame to limit the availability of this effective contraception method to otherwise young and healthy women because of this very rare event.
Evidence summary
No studies specifically examine the risk of adverse outcomes for women who have mild elevations in blood pressure as a result of taking OCs. However, for the general population cardiovascular risk increases 30% for each 10 mm Hg rise in systolic pressure.1
A prospective cohort study found an increased incidence of new hypertension developing among women taking OCs. The study, conducted in the US, included 68,297 female nurses aged 25 to 42 years without a previous diagnosis of hypertension, diabetes, coronary heart disease, stroke, or cancer, who were followed for 4 years. Women were excluded from the study if they had not had a physical exam in the last 2 years or were taking antihypertensive medication at study inception. The nurses self-reported their blood pressure readings via questionnaire; medical records were sampled to validate the accuracy of self-reports. After adjusting for risk factors, current oral contraceptive use increased the risk of developing hypertension (relative risk [RR]=1.8; 95% confidence interval [CI], 1.5–2.3; corresponding to 41.5 new cases of hypertension per 10,000 person-years).2
A systematic review of 8 case control studies (with 4907 cases and 13,443 controls) found an increased risk of stroke and MI among hypertensive women taking combined type OCs vs those not taking OCs. Women with hypertension aged 20 to 24 years had an estimated CV event risk of 312 per million woman-years while taking OCs vs 134 per million woman-years not taking OCs. Among hypertensive women aged 40 to 44 years, the estimated risks were 1213 vs 529 per million woman-years, respectively. Primary endpoints varied across the studies and statistical significance was not given.3
Three studies showed that blood pressure elevations due to taking oral contraceptives returned to baseline with discontinuation of the medication. A prospective cohort study followed 13,358 women who were neither pregnant nor postpartum between the ages of 15 and 60. Women who either initiated or resumed using OCs experienced a statistically significant rise of about 4 mm Hg in the systolic pressure and 1 mm Hg in the diastolic pressure. Women who stopped using OCs experienced significant decreases in both systolic and diastolic components (about 5 mm Hg and 1.5 mm Hg, respectively).1
Similarly, a survey study of 461 women attending family planning clinics found that mean blood pressures were significantly higher for those taking OCs than for those using nonhormonal contraception. Elevated blood pressures correlated with duration of current use of OCs but returned to normal soon after stopping OCs. The mean pressures of those who had stopped OCs more than a month were similar to those of women who had never taken an OC and significantly lower than those of women who were currently taking OCs.4
Finally, a prospective study which followed 32 women who had taken combined OCs for 1 to 3 years and then stopped found that blood pressures returned to pretreatment levels at 3 months. Systolic pressure fell by 9.7 mm Hg and diastolic by 2.9 mm Hg compared with measurements made 1 month before stopping. No cardiovascular complications were reported among women during this study.5
Recommendations from others
The American College of Obstetricians and Gynecologists says that women with well-controlled and monitored hypertension aged 35 years and younger are appropriate candidates for a trial of combination OCs, provided they are otherwise healthy, have no evidence of end-organ vascular disease, and do not smoke cigarettes.6 If blood pressure remains well controlled with careful monitoring several months after initiating OCs, use can be continued.
Women who take oral contraceptives (OCs) have an increased risk of developing new hypertension, which returns to baseline within 1 to 3 months of OC cessation (strength of recommendation [SOR]: A, based on cohort studies).
Among large populations of women with hypertension from all causes, risk of adverse cardiovascular outcomes is increased (SOR: B, based on Framingham data). Women with pre-existing hypertension who take OCs have an increased risk of stroke and myocardial infarction (MI) when compared with hypertensive women who do not (SOR: B, based on case-control studies).
Is an increase of 178 per million woman-years of CV events clinically significant?
Sarina Schrager, MD
University of Wisconsin
In clinical practice, we continually balance the risks and benefits of any treatment. Oral contraceptive pills are the most commonly used reversible form of contraception in the United States. Although this review documents an increased risk of reversible new hypertension for women on OCs and a possibly significant increase in cardiovascular events, the clinical meaning of these data is unclear. Is an increase of 178 per million woman-years of CV events clinically significant? It would be a shame to limit the availability of this effective contraception method to otherwise young and healthy women because of this very rare event.
Evidence summary
No studies specifically examine the risk of adverse outcomes for women who have mild elevations in blood pressure as a result of taking OCs. However, for the general population cardiovascular risk increases 30% for each 10 mm Hg rise in systolic pressure.1
A prospective cohort study found an increased incidence of new hypertension developing among women taking OCs. The study, conducted in the US, included 68,297 female nurses aged 25 to 42 years without a previous diagnosis of hypertension, diabetes, coronary heart disease, stroke, or cancer, who were followed for 4 years. Women were excluded from the study if they had not had a physical exam in the last 2 years or were taking antihypertensive medication at study inception. The nurses self-reported their blood pressure readings via questionnaire; medical records were sampled to validate the accuracy of self-reports. After adjusting for risk factors, current oral contraceptive use increased the risk of developing hypertension (relative risk [RR]=1.8; 95% confidence interval [CI], 1.5–2.3; corresponding to 41.5 new cases of hypertension per 10,000 person-years).2
A systematic review of 8 case control studies (with 4907 cases and 13,443 controls) found an increased risk of stroke and MI among hypertensive women taking combined type OCs vs those not taking OCs. Women with hypertension aged 20 to 24 years had an estimated CV event risk of 312 per million woman-years while taking OCs vs 134 per million woman-years not taking OCs. Among hypertensive women aged 40 to 44 years, the estimated risks were 1213 vs 529 per million woman-years, respectively. Primary endpoints varied across the studies and statistical significance was not given.3
Three studies showed that blood pressure elevations due to taking oral contraceptives returned to baseline with discontinuation of the medication. A prospective cohort study followed 13,358 women who were neither pregnant nor postpartum between the ages of 15 and 60. Women who either initiated or resumed using OCs experienced a statistically significant rise of about 4 mm Hg in the systolic pressure and 1 mm Hg in the diastolic pressure. Women who stopped using OCs experienced significant decreases in both systolic and diastolic components (about 5 mm Hg and 1.5 mm Hg, respectively).1
Similarly, a survey study of 461 women attending family planning clinics found that mean blood pressures were significantly higher for those taking OCs than for those using nonhormonal contraception. Elevated blood pressures correlated with duration of current use of OCs but returned to normal soon after stopping OCs. The mean pressures of those who had stopped OCs more than a month were similar to those of women who had never taken an OC and significantly lower than those of women who were currently taking OCs.4
Finally, a prospective study which followed 32 women who had taken combined OCs for 1 to 3 years and then stopped found that blood pressures returned to pretreatment levels at 3 months. Systolic pressure fell by 9.7 mm Hg and diastolic by 2.9 mm Hg compared with measurements made 1 month before stopping. No cardiovascular complications were reported among women during this study.5
Recommendations from others
The American College of Obstetricians and Gynecologists says that women with well-controlled and monitored hypertension aged 35 years and younger are appropriate candidates for a trial of combination OCs, provided they are otherwise healthy, have no evidence of end-organ vascular disease, and do not smoke cigarettes.6 If blood pressure remains well controlled with careful monitoring several months after initiating OCs, use can be continued.
1. Fisch IR, Frank J. Oral contraceptives and blood pressure. JAMA 1977;237:2499-2503.
2. Chasen-Taber L, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996;94:483-489.
3. Curtis K, et al. Contraception for women in selected circumstances. Obstet Gynecol 2002;6:1100-1112.
4. Khaw K-T, Peart WS. Blood pressure and contraceptive use. Br Med J 1982;285:403-407.
5. Weir RJ, Briggs E, Mack A, Naismith L, Taylor L, Wilson E. Blood pressure in women taking oral contraceptives. Br Med J 1974;1:533-535.
6. American College of Obstetricians and Gynecologists (ACOG). The use of hormonal contraception in women with coexisting medical conditions. Washington, DC: American College of Obstetricians and Gynecologists (ACOG); 2006 June. 20 p. (ACOG practice bulletin; no. 73).
1. Fisch IR, Frank J. Oral contraceptives and blood pressure. JAMA 1977;237:2499-2503.
2. Chasen-Taber L, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996;94:483-489.
3. Curtis K, et al. Contraception for women in selected circumstances. Obstet Gynecol 2002;6:1100-1112.
4. Khaw K-T, Peart WS. Blood pressure and contraceptive use. Br Med J 1982;285:403-407.
5. Weir RJ, Briggs E, Mack A, Naismith L, Taylor L, Wilson E. Blood pressure in women taking oral contraceptives. Br Med J 1974;1:533-535.
6. American College of Obstetricians and Gynecologists (ACOG). The use of hormonal contraception in women with coexisting medical conditions. Washington, DC: American College of Obstetricians and Gynecologists (ACOG); 2006 June. 20 p. (ACOG practice bulletin; no. 73).
Evidence-based answers from the Family Physicians Inquiries Network
What are effective treatments for oppositional defiant behaviors in adolescents?
Psychological interventions for the family—such as parenting skills training and behavioral therapy for the child, the parents, or the whole family—reduce conflict behaviors in adolescents with oppositional defiant disorder (ODD) (strength of recommendation [SOR]: C, based on extrapolation from systematic reviews of younger children with ODD and adolescents with conduct disorder).
ODD most commonly does not occur as a solitary diagnosis. When ODD is associated with attention deficit/hyperactivity disorder (ADHD) or other medication-responsive comorbid conditions, medical treatment reduces overall symptoms (SOR: B, based on a meta-analysis of adolescent and younger children with both ODD and ADHD).
Model good parenting skills, educate parents about basic behavioral tools, provide referral as resources allow
Elizabeth A. Rulon, MD
Family Medicine Residency of Idaho, Boise
It can be challenging to distinguish oppositional defiant behaviors from variations of normal development as adolescents try to become “independent” from their parents. However, adolescents may engage in many dangerous risk-taking behaviors during this period, so timely diagnosis and interventions are important. Affected adolescents often have a difficult home life, with parents who may have very poor social support and coping skills. Typically, such parents must be convinced that the oppositional and defiant behaviors are a family problem requiring a family solution with no quick fix. Significant financial barriers to counseling and other resources are also common in many of these families. At a minimum, the family doctor can model good parenting skills in the exam room, educate parents about basic behavioral tools to use when interacting with their adolescents, and provide referral as resources allow.
Evidence summary
No studies specifically evaluate effective treatments for ODD (distinguished by chronic argumentativeness and refusal to comply with adult requests) for adolescent patients. However, there are treatment studies of younger children with ODD and studies of adolescents with the more disruptive behavior problem of conduct disorder (distinguished by a persistent pattern of violating other’s rights, aggression, and illegal acts).
A Clinical Inquiry summarized 8 well-done systematic reviews of ODD treatments of preadolescent children and found improved behavior with parenting interventions and behavioral therapy.1 Each of the systematic reviews assessed multiple randomized controlled trials (RCTs) using a variety of parenting and behavioral therapy interventions. The most rigorous systematic review (which included 16 RCTs), compared group-based parenting skills training with untreated wait-list controls and found decreased aggression, noncompliance, and temper tantrums by children aged 3 to 10 years (total number of subjects not given) by an average effect size of 0.6 to 2.9. (Effect size is the difference between the means of the experimental and control groups expressed in standard deviations. An effect size of 0.2 is considered small, 0.5 is medium, and 0.8 is moderate to large.) Behavioral therapy (cognitive-behavioral therapy, social problem-solving skills training, parent management training), comprising 12 to 25 sessions with either the child alone or with teachers or parents, decreased disruptive or aggressive behaviors by 20% to 30%.
A 2-year case-control study2 of 158 self-referred families with young adolescents (11 to 14 years old) without a formal ODD diagnosis but with reported problem behaviors (defined as smoking, negative engagement in family problem solving, and parental ratings of unpleasant events) found significant improvements (P<.01) with parent-only, teen-only, and parent-teen behavioral interventions for negative engagement behaviors (average of 30% reduction in scores), and with parent and teen interventions for unpleasant events (average of 9% reduction in scores). Interventions comprised 12 weekly 90-minute sessions, with the parent-only group targeting family management practices and communication skills, the teen-only group targeting adolescent self-regulation and pro-social behavior, and the parent-teen group following a structured curriculum.
A meta-analysis3 of 8 RCTs (with a total of 749 children) of various behavioral treatments for conduct disorder and juvenile delinquency among children aged 10 to 17 years found significant reductions in rearrest rates (relative risk [RR]=0.66; 95% confidence interval [CI], 0.44–0.98; number needed to treat [NNT] to prevent 1 rearrest=3.7) and time spent in institutions (mean difference, 51 days) with family and parenting interventions (comprising 1 to 6 months of individual and group parenting training, short and long-term family therapy, and individual and group adolescent interventions).
ODD comorbid with other psychiatric conditions
Approximately half to two-thirds of adolescents with ODD also have ADHD.4 A meta-analysis5 evaluated 28 studies of stimulant medication (methylphenidate, amphetamine, or pemoline) for children with comorbid ADHD and ODD. A total of 683 patients aged 8 to 18 years were included. Stimulants reduced aggression-related behaviors in these children by an effect size of 0.84 for overt aggression and 0.69 for covert aggression. Stimulants typically reduce aggressive behaviors by similar effect sizes when prescribed for children with ADD alone. The study groups did not separate children with ADHD and ODD from those with ADHD and conduct disorder; they also grouped adolescents together with younger children.
An RCT6 of different doses of atomoxetine (Strattera) treatment vs placebo for children ages 8 to 18 (mean age=11) with ADHD alone (N=178) and children with both ADHD and ODD (N=115) found significant effect sizes for atomoxetine in both groups. Two dosages of atomoxetine (1.2 and 1.8 mg/kg/d) produced equivalent effect sizes in the ADHD-only group (0.55 and 0.56); however, the higher dosage had a greater effect size (0.49 vs 0.69) in the group with ODD comorbid with ADHD.
A double-blind crossover RCT7 evaluated divalproex (Depakote) vs placebo for 20 children (aged 10 to 18 years) with explosive temper and mood lability who also met DSM-IV criteria for either ODD or conduct disorder. Patients with significant medical problems, such as bipolar disorder, major depression, or mental retardation, were excluded. Divalproex significantly (P=.003) reduced aggressive behaviors and anger-hostility items by approximately 33% as reported by child, parent, school, and clinician on 2 standardized scales.
Experts say antidepressant medications may be helpful in treating children with conduct disorder and comorbid major depression.8
Recommendations by others
An international consensus statement on ADHD and disruptive behavior disorders (comprising ODD, conduct disorder, and disruptive behavior not otherwise specified) says that psychopharmacologic treatment would not be appropriate for cases of ODD in the absence of psychiatric comorbidity, unless severe aggression or destructive behavior persisted despite attempts at psychosocial interventions of established efficacy.4
1. Farley SE, Adams JS, Lutton ME, Scoville C, Fulkerson RC, Webb AR. What are effective treatments for oppositional and defiant behaviors in preadolescents? J Fam Pract 2005;54:162-165.
2. Dishion TJ, Andrews DW. Preventing escalation of problem behaviors with high-risk young adolescents: immediate and 1-year outcomes. J Consult Clin Psychol 1995;63:538-548.
3. Woolfenden SR, Williams K, Peat JK. Family and parenting interventions for conduct disorder and delinquency: a meta-analysis of randomized controlled trials. Arch Dis Child 2002;86:251-256.
4. Kutcher S, Aman M, Brooks SJ, et al. International consensus statement on attention-deficit/hyperactivity disorder (ADHD) and disruptive behaviour disorders (DBDs): clinical implications and treatment practice suggestions. Eur Neuropsychopharmacol 2004;14:11-28.
5. Connor DF, Glatt SJ, Lopez ID, Jackson D, Melloni RH, Jr. Psychopharmacology and aggression. I: a meta-analysis of stimulant effects on overt/covert aggression-related behaviors in ADHD. J Am Acad Child Adolesc Psychiatry 2002;41:253-261.
6. Newcorn JH, Spencer TJ, Biederman J, Milton DR, Michelson D. Atomoxetine treatment in children and adolescents with attention deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry 2005;44:240-248.
7. Donovan SJ, Stewart JW, Nunes EV, et al. Divalproex treatment for youth with explosive temper and mood lability: a double-blind, placebo-controlled crossover design. Am J Psychiatry 2000;157:818-820.
8. Searight HR, Rottneck F, Abby SL. Conduct disorder: diagnosis and treatment in primary care. Am Fam Physician 2001;63:1579-1592.
Psychological interventions for the family—such as parenting skills training and behavioral therapy for the child, the parents, or the whole family—reduce conflict behaviors in adolescents with oppositional defiant disorder (ODD) (strength of recommendation [SOR]: C, based on extrapolation from systematic reviews of younger children with ODD and adolescents with conduct disorder).
ODD most commonly does not occur as a solitary diagnosis. When ODD is associated with attention deficit/hyperactivity disorder (ADHD) or other medication-responsive comorbid conditions, medical treatment reduces overall symptoms (SOR: B, based on a meta-analysis of adolescent and younger children with both ODD and ADHD).
Model good parenting skills, educate parents about basic behavioral tools, provide referral as resources allow
Elizabeth A. Rulon, MD
Family Medicine Residency of Idaho, Boise
It can be challenging to distinguish oppositional defiant behaviors from variations of normal development as adolescents try to become “independent” from their parents. However, adolescents may engage in many dangerous risk-taking behaviors during this period, so timely diagnosis and interventions are important. Affected adolescents often have a difficult home life, with parents who may have very poor social support and coping skills. Typically, such parents must be convinced that the oppositional and defiant behaviors are a family problem requiring a family solution with no quick fix. Significant financial barriers to counseling and other resources are also common in many of these families. At a minimum, the family doctor can model good parenting skills in the exam room, educate parents about basic behavioral tools to use when interacting with their adolescents, and provide referral as resources allow.
Evidence summary
No studies specifically evaluate effective treatments for ODD (distinguished by chronic argumentativeness and refusal to comply with adult requests) for adolescent patients. However, there are treatment studies of younger children with ODD and studies of adolescents with the more disruptive behavior problem of conduct disorder (distinguished by a persistent pattern of violating other’s rights, aggression, and illegal acts).
A Clinical Inquiry summarized 8 well-done systematic reviews of ODD treatments of preadolescent children and found improved behavior with parenting interventions and behavioral therapy.1 Each of the systematic reviews assessed multiple randomized controlled trials (RCTs) using a variety of parenting and behavioral therapy interventions. The most rigorous systematic review (which included 16 RCTs), compared group-based parenting skills training with untreated wait-list controls and found decreased aggression, noncompliance, and temper tantrums by children aged 3 to 10 years (total number of subjects not given) by an average effect size of 0.6 to 2.9. (Effect size is the difference between the means of the experimental and control groups expressed in standard deviations. An effect size of 0.2 is considered small, 0.5 is medium, and 0.8 is moderate to large.) Behavioral therapy (cognitive-behavioral therapy, social problem-solving skills training, parent management training), comprising 12 to 25 sessions with either the child alone or with teachers or parents, decreased disruptive or aggressive behaviors by 20% to 30%.
A 2-year case-control study2 of 158 self-referred families with young adolescents (11 to 14 years old) without a formal ODD diagnosis but with reported problem behaviors (defined as smoking, negative engagement in family problem solving, and parental ratings of unpleasant events) found significant improvements (P<.01) with parent-only, teen-only, and parent-teen behavioral interventions for negative engagement behaviors (average of 30% reduction in scores), and with parent and teen interventions for unpleasant events (average of 9% reduction in scores). Interventions comprised 12 weekly 90-minute sessions, with the parent-only group targeting family management practices and communication skills, the teen-only group targeting adolescent self-regulation and pro-social behavior, and the parent-teen group following a structured curriculum.
A meta-analysis3 of 8 RCTs (with a total of 749 children) of various behavioral treatments for conduct disorder and juvenile delinquency among children aged 10 to 17 years found significant reductions in rearrest rates (relative risk [RR]=0.66; 95% confidence interval [CI], 0.44–0.98; number needed to treat [NNT] to prevent 1 rearrest=3.7) and time spent in institutions (mean difference, 51 days) with family and parenting interventions (comprising 1 to 6 months of individual and group parenting training, short and long-term family therapy, and individual and group adolescent interventions).
ODD comorbid with other psychiatric conditions
Approximately half to two-thirds of adolescents with ODD also have ADHD.4 A meta-analysis5 evaluated 28 studies of stimulant medication (methylphenidate, amphetamine, or pemoline) for children with comorbid ADHD and ODD. A total of 683 patients aged 8 to 18 years were included. Stimulants reduced aggression-related behaviors in these children by an effect size of 0.84 for overt aggression and 0.69 for covert aggression. Stimulants typically reduce aggressive behaviors by similar effect sizes when prescribed for children with ADD alone. The study groups did not separate children with ADHD and ODD from those with ADHD and conduct disorder; they also grouped adolescents together with younger children.
An RCT6 of different doses of atomoxetine (Strattera) treatment vs placebo for children ages 8 to 18 (mean age=11) with ADHD alone (N=178) and children with both ADHD and ODD (N=115) found significant effect sizes for atomoxetine in both groups. Two dosages of atomoxetine (1.2 and 1.8 mg/kg/d) produced equivalent effect sizes in the ADHD-only group (0.55 and 0.56); however, the higher dosage had a greater effect size (0.49 vs 0.69) in the group with ODD comorbid with ADHD.
A double-blind crossover RCT7 evaluated divalproex (Depakote) vs placebo for 20 children (aged 10 to 18 years) with explosive temper and mood lability who also met DSM-IV criteria for either ODD or conduct disorder. Patients with significant medical problems, such as bipolar disorder, major depression, or mental retardation, were excluded. Divalproex significantly (P=.003) reduced aggressive behaviors and anger-hostility items by approximately 33% as reported by child, parent, school, and clinician on 2 standardized scales.
Experts say antidepressant medications may be helpful in treating children with conduct disorder and comorbid major depression.8
Recommendations by others
An international consensus statement on ADHD and disruptive behavior disorders (comprising ODD, conduct disorder, and disruptive behavior not otherwise specified) says that psychopharmacologic treatment would not be appropriate for cases of ODD in the absence of psychiatric comorbidity, unless severe aggression or destructive behavior persisted despite attempts at psychosocial interventions of established efficacy.4
Psychological interventions for the family—such as parenting skills training and behavioral therapy for the child, the parents, or the whole family—reduce conflict behaviors in adolescents with oppositional defiant disorder (ODD) (strength of recommendation [SOR]: C, based on extrapolation from systematic reviews of younger children with ODD and adolescents with conduct disorder).
ODD most commonly does not occur as a solitary diagnosis. When ODD is associated with attention deficit/hyperactivity disorder (ADHD) or other medication-responsive comorbid conditions, medical treatment reduces overall symptoms (SOR: B, based on a meta-analysis of adolescent and younger children with both ODD and ADHD).
Model good parenting skills, educate parents about basic behavioral tools, provide referral as resources allow
Elizabeth A. Rulon, MD
Family Medicine Residency of Idaho, Boise
It can be challenging to distinguish oppositional defiant behaviors from variations of normal development as adolescents try to become “independent” from their parents. However, adolescents may engage in many dangerous risk-taking behaviors during this period, so timely diagnosis and interventions are important. Affected adolescents often have a difficult home life, with parents who may have very poor social support and coping skills. Typically, such parents must be convinced that the oppositional and defiant behaviors are a family problem requiring a family solution with no quick fix. Significant financial barriers to counseling and other resources are also common in many of these families. At a minimum, the family doctor can model good parenting skills in the exam room, educate parents about basic behavioral tools to use when interacting with their adolescents, and provide referral as resources allow.
Evidence summary
No studies specifically evaluate effective treatments for ODD (distinguished by chronic argumentativeness and refusal to comply with adult requests) for adolescent patients. However, there are treatment studies of younger children with ODD and studies of adolescents with the more disruptive behavior problem of conduct disorder (distinguished by a persistent pattern of violating other’s rights, aggression, and illegal acts).
A Clinical Inquiry summarized 8 well-done systematic reviews of ODD treatments of preadolescent children and found improved behavior with parenting interventions and behavioral therapy.1 Each of the systematic reviews assessed multiple randomized controlled trials (RCTs) using a variety of parenting and behavioral therapy interventions. The most rigorous systematic review (which included 16 RCTs), compared group-based parenting skills training with untreated wait-list controls and found decreased aggression, noncompliance, and temper tantrums by children aged 3 to 10 years (total number of subjects not given) by an average effect size of 0.6 to 2.9. (Effect size is the difference between the means of the experimental and control groups expressed in standard deviations. An effect size of 0.2 is considered small, 0.5 is medium, and 0.8 is moderate to large.) Behavioral therapy (cognitive-behavioral therapy, social problem-solving skills training, parent management training), comprising 12 to 25 sessions with either the child alone or with teachers or parents, decreased disruptive or aggressive behaviors by 20% to 30%.
A 2-year case-control study2 of 158 self-referred families with young adolescents (11 to 14 years old) without a formal ODD diagnosis but with reported problem behaviors (defined as smoking, negative engagement in family problem solving, and parental ratings of unpleasant events) found significant improvements (P<.01) with parent-only, teen-only, and parent-teen behavioral interventions for negative engagement behaviors (average of 30% reduction in scores), and with parent and teen interventions for unpleasant events (average of 9% reduction in scores). Interventions comprised 12 weekly 90-minute sessions, with the parent-only group targeting family management practices and communication skills, the teen-only group targeting adolescent self-regulation and pro-social behavior, and the parent-teen group following a structured curriculum.
A meta-analysis3 of 8 RCTs (with a total of 749 children) of various behavioral treatments for conduct disorder and juvenile delinquency among children aged 10 to 17 years found significant reductions in rearrest rates (relative risk [RR]=0.66; 95% confidence interval [CI], 0.44–0.98; number needed to treat [NNT] to prevent 1 rearrest=3.7) and time spent in institutions (mean difference, 51 days) with family and parenting interventions (comprising 1 to 6 months of individual and group parenting training, short and long-term family therapy, and individual and group adolescent interventions).
ODD comorbid with other psychiatric conditions
Approximately half to two-thirds of adolescents with ODD also have ADHD.4 A meta-analysis5 evaluated 28 studies of stimulant medication (methylphenidate, amphetamine, or pemoline) for children with comorbid ADHD and ODD. A total of 683 patients aged 8 to 18 years were included. Stimulants reduced aggression-related behaviors in these children by an effect size of 0.84 for overt aggression and 0.69 for covert aggression. Stimulants typically reduce aggressive behaviors by similar effect sizes when prescribed for children with ADD alone. The study groups did not separate children with ADHD and ODD from those with ADHD and conduct disorder; they also grouped adolescents together with younger children.
An RCT6 of different doses of atomoxetine (Strattera) treatment vs placebo for children ages 8 to 18 (mean age=11) with ADHD alone (N=178) and children with both ADHD and ODD (N=115) found significant effect sizes for atomoxetine in both groups. Two dosages of atomoxetine (1.2 and 1.8 mg/kg/d) produced equivalent effect sizes in the ADHD-only group (0.55 and 0.56); however, the higher dosage had a greater effect size (0.49 vs 0.69) in the group with ODD comorbid with ADHD.
A double-blind crossover RCT7 evaluated divalproex (Depakote) vs placebo for 20 children (aged 10 to 18 years) with explosive temper and mood lability who also met DSM-IV criteria for either ODD or conduct disorder. Patients with significant medical problems, such as bipolar disorder, major depression, or mental retardation, were excluded. Divalproex significantly (P=.003) reduced aggressive behaviors and anger-hostility items by approximately 33% as reported by child, parent, school, and clinician on 2 standardized scales.
Experts say antidepressant medications may be helpful in treating children with conduct disorder and comorbid major depression.8
Recommendations by others
An international consensus statement on ADHD and disruptive behavior disorders (comprising ODD, conduct disorder, and disruptive behavior not otherwise specified) says that psychopharmacologic treatment would not be appropriate for cases of ODD in the absence of psychiatric comorbidity, unless severe aggression or destructive behavior persisted despite attempts at psychosocial interventions of established efficacy.4
1. Farley SE, Adams JS, Lutton ME, Scoville C, Fulkerson RC, Webb AR. What are effective treatments for oppositional and defiant behaviors in preadolescents? J Fam Pract 2005;54:162-165.
2. Dishion TJ, Andrews DW. Preventing escalation of problem behaviors with high-risk young adolescents: immediate and 1-year outcomes. J Consult Clin Psychol 1995;63:538-548.
3. Woolfenden SR, Williams K, Peat JK. Family and parenting interventions for conduct disorder and delinquency: a meta-analysis of randomized controlled trials. Arch Dis Child 2002;86:251-256.
4. Kutcher S, Aman M, Brooks SJ, et al. International consensus statement on attention-deficit/hyperactivity disorder (ADHD) and disruptive behaviour disorders (DBDs): clinical implications and treatment practice suggestions. Eur Neuropsychopharmacol 2004;14:11-28.
5. Connor DF, Glatt SJ, Lopez ID, Jackson D, Melloni RH, Jr. Psychopharmacology and aggression. I: a meta-analysis of stimulant effects on overt/covert aggression-related behaviors in ADHD. J Am Acad Child Adolesc Psychiatry 2002;41:253-261.
6. Newcorn JH, Spencer TJ, Biederman J, Milton DR, Michelson D. Atomoxetine treatment in children and adolescents with attention deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry 2005;44:240-248.
7. Donovan SJ, Stewart JW, Nunes EV, et al. Divalproex treatment for youth with explosive temper and mood lability: a double-blind, placebo-controlled crossover design. Am J Psychiatry 2000;157:818-820.
8. Searight HR, Rottneck F, Abby SL. Conduct disorder: diagnosis and treatment in primary care. Am Fam Physician 2001;63:1579-1592.
1. Farley SE, Adams JS, Lutton ME, Scoville C, Fulkerson RC, Webb AR. What are effective treatments for oppositional and defiant behaviors in preadolescents? J Fam Pract 2005;54:162-165.
2. Dishion TJ, Andrews DW. Preventing escalation of problem behaviors with high-risk young adolescents: immediate and 1-year outcomes. J Consult Clin Psychol 1995;63:538-548.
3. Woolfenden SR, Williams K, Peat JK. Family and parenting interventions for conduct disorder and delinquency: a meta-analysis of randomized controlled trials. Arch Dis Child 2002;86:251-256.
4. Kutcher S, Aman M, Brooks SJ, et al. International consensus statement on attention-deficit/hyperactivity disorder (ADHD) and disruptive behaviour disorders (DBDs): clinical implications and treatment practice suggestions. Eur Neuropsychopharmacol 2004;14:11-28.
5. Connor DF, Glatt SJ, Lopez ID, Jackson D, Melloni RH, Jr. Psychopharmacology and aggression. I: a meta-analysis of stimulant effects on overt/covert aggression-related behaviors in ADHD. J Am Acad Child Adolesc Psychiatry 2002;41:253-261.
6. Newcorn JH, Spencer TJ, Biederman J, Milton DR, Michelson D. Atomoxetine treatment in children and adolescents with attention deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry 2005;44:240-248.
7. Donovan SJ, Stewart JW, Nunes EV, et al. Divalproex treatment for youth with explosive temper and mood lability: a double-blind, placebo-controlled crossover design. Am J Psychiatry 2000;157:818-820.
8. Searight HR, Rottneck F, Abby SL. Conduct disorder: diagnosis and treatment in primary care. Am Fam Physician 2001;63:1579-1592.
Evidence-based answers from the Family Physicians Inquiries Network
What is the prognostic value of stress echocardiography for patients with atypical chest pain?
Patients with atypical chest pain and no history of cardiovascular events (coronary artery disease, unstable angina, or history of percutaneous transthoracic coronary angioplasty [PTCA]) and a negative stress echocardiography test are unlikely to experience a cardiovascular event in the next 1 to 4 years. However, the positive predictive value of the test in this population is low, indicating that a positive stress echocardiography is less useful for prognostic purposes (strength of recommendation: B, based on multiple cohort studies).
Using stress echocardiography reduces need for diagnostic cardiac catheterization for atypical chest pain
Timothy Huber, MD
Oroville, Calif
Patients presenting to emergency and urgent care departments with atypical chest pain are a dilemma whenever their ECG and biomarkers are nondiagnostic. Graded exercise stress testing to further define risk is not effective in many patient populations: including some women, patients with mobility problems, and patients with underlying conduction issues such as pre-excitation syndromes, left bundle branch blocks, and ventricular pacemakers. Stress echocardiography is a reasonable alternative for such patients. While physicians may take a negative test at face value in this clinical setting, a positive test is not diagnostic and will often necessitate further workup. Using stress echocardiography therefore reduces but does not eliminate the need for diagnostic cardiac catheterization for atypical chest pain.
Evidence summary
A prospective cohort study1 evaluated dobutamine or dipyridamole pharmacologic stress echocardiography among 904 primary care patients with either typical or atypical chest pain. Patients were enrolled into the study if they had normal resting wall motion, sinus rhythm, and had no history of coronary artery disease, unstable angina, or PTCA. Patients (average age 61 years, 42% men) were followed for an average of 44 months for primary cardiovascular endpoints (fatal or nonfatal myocardial infarction [MI], unstable angina, PTCA, or cardiac death). A negative or positive stress echocardiography is defined as the absence or presence of abnormal cardiac wall motion on either exercise or pharmacologic stress echocardiography. Eighteen percent of patients had a positive pharmacologic stress echocardiography. Over the length of the study, 81 of 904 patients (9%) suffered a cardiovascular event. Patients with a negative pharmacologic stress echocardiography had a mean annual probability of a cardiovascular event of 0.8% vs 8.5% with a positive pharmacologic stress echocardiography (P<0001). The 4-year infarct-free negative predictive value (NPV) of pharmacologic stress echocardiography was 97%, and the positive predictive value (PPV) was 70%.
A similar prospective cohort study2 evaluated 105 patients (50% men) with atypical chest pain in an emergency department setting with either exercise or dobutamine/atropine stress echocardiography. The average patient age was 55 years and follow-up was 2.8 years. Patients were clinically stable, had normal or nondiagnostic electrocardiogram (ECG), normal cardiac enzymes, normal left ventricular function, and no history of coronary artery disease or unstable angina. Cardiovascular endpoints included fatal or nonfatal MI, unstable angina, PTCA, or cardiac death. A total of 7 patients (7%) suffered a cardiovascular event during the follow-up period. Positive stress echocardiography results occurred for 9% of patients. The NPV was 99% and the PPV was 75%.
Three other cohort studies3-5 evaluated exercise or dobutamine/atropine stress echocardiography for a total of 615 patients (48%–67% men, average age 56–58 years) presenting to an emergency department with classical cardiac or atypical chest pain. Patients had normal or nondiagnostic ECG, negative cardiac enzymes, and either no history of coronary artery disease3,4 or known coronary artery disease of unknown significance.5 A positive stress echocardiography was obtained for 4.8% to 42% of patients in the cohorts. During 6 months of follow-up, cardiovascular events occurred in 4 of 145 patients (3%),3 22 of 227 patients (6%),4 and in 11 of 80 patients (14%).5 At 6-month follow-up, exercise stress echocardiography had a NPV of 99.3% and a PPV of 43%.3 Dobutamine/atropine stress echocardiography had a NPV of 95% to 96% and a PPV of 25% to 31%.4,5
One retrospective review6 evaluated exercise and dobutamine/atropine stress echocardiography and stress ECG for 661 low-risk outpatients (48% men, average age 58 years) with atypical chest pain. All patients had normal left ventricular function and no history of coronary artery disease and were followed for an average of 23 months. A positive stress echocardiography test occurred among 16% of the patient population.
During follow-up, 41 of 661 patients (6%) suffered a cardiovascular event. For either exercise or dobutamine/atropine stress echocardiography, the NPV was 99% at 12 months and 96% at 30 months. Patients with a positive stress echocardiography test and a negative stress ECG had a 66% event-free survival rate. Event-free survival rate for patients with a negative stress echocardiography and a positive or negative stress ECG was 97% and 96%, respectively.
Recommendations from others
The American College of Cardiology7 gives a Class I recommendation (tests for which there is evidence or general agreement that a given procedure or treatment is useful and effective) for standard echocardiogram for evaluation of chest pain for patients with suspected acute myocardial ischemia (when baseline ECG and other laboratory markers are nondiagnostic and when the study can be obtained during pain or within minutes after its abatement).
It gives a Class IIa recommendation (tests for which there is conflicting evidence or divergence of opinion, but favoring usefulness) to stress echocardiography for the detection of myocardial ischemia for women with an intermediate pretest likelihood of coronary artery disease. It also gives a Class IIa recommendation to stress echocardiography for determining the prognosis of myocardial ischemia among patients for whom ECG assessment is less reliable. This group comprises patients with the following ECG abnormalities: pre-excitation syndrome (such as Wolff-Parkinson-White), electronically paced ventricular rhythm, more than 1 mm of ST depression at rest, and complete left bundle branch block.
1. Amici E, Cortigiani L, Coletta C, et al. Usefulness of pharmacologic stress echocardiography for the long-term prognostic assessment of patients with typical versus atypical chest pain. Am J Cardiol 2003;91:440-442.
2. Colon PJ, 3rd, Cheirif J. Long-term value of stress echocardiography in the triage of patients with atypical chest pain presenting to the emergency department. Echocardiography 1999;16:171-177.
3. Buchsbaum M, Marshall E, Levine B, et al. Emergency department evaluation of chest pain using exercise stress echocardiography. Acad Emerg Med 2001;8:196-199.
4. Bholasingh R, Cornel JH, Kamp O, et al. Prognostic value of predischarge dobutamine stress echocardiography in chest pain patients with a negative cardiac troponin T. J Am Coll Cardiol 2003;41:596-602.
5. Geleijnse ML, Elhendy A, Kasprzak JD, et al. Safety and prognostic value of early dobutamine-atropine stress echocardiography in patients with spontaneous chest pain and a nondiagnostic electrocardiogram. Eur Heart J 2000;21:397-406.
6. Colon PJ, 3rd, Mobarek SK, Milani RV, et al. Prognostic value of stress echocardiography in the evaluation of atypical chest pain patients without known coronary artery disease. Am J Cardiol 1998;81:545-551.
7. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. (ACC/AHA/ASE Committee to update the 1997 guidelines for the clinical application of echocardiography.) Available at: www.acc.org/qualityandscience/clinical/guidelines/echo/index_clean.pdf. Accessed on September 6, 2006.
Patients with atypical chest pain and no history of cardiovascular events (coronary artery disease, unstable angina, or history of percutaneous transthoracic coronary angioplasty [PTCA]) and a negative stress echocardiography test are unlikely to experience a cardiovascular event in the next 1 to 4 years. However, the positive predictive value of the test in this population is low, indicating that a positive stress echocardiography is less useful for prognostic purposes (strength of recommendation: B, based on multiple cohort studies).
Using stress echocardiography reduces need for diagnostic cardiac catheterization for atypical chest pain
Timothy Huber, MD
Oroville, Calif
Patients presenting to emergency and urgent care departments with atypical chest pain are a dilemma whenever their ECG and biomarkers are nondiagnostic. Graded exercise stress testing to further define risk is not effective in many patient populations: including some women, patients with mobility problems, and patients with underlying conduction issues such as pre-excitation syndromes, left bundle branch blocks, and ventricular pacemakers. Stress echocardiography is a reasonable alternative for such patients. While physicians may take a negative test at face value in this clinical setting, a positive test is not diagnostic and will often necessitate further workup. Using stress echocardiography therefore reduces but does not eliminate the need for diagnostic cardiac catheterization for atypical chest pain.
Evidence summary
A prospective cohort study1 evaluated dobutamine or dipyridamole pharmacologic stress echocardiography among 904 primary care patients with either typical or atypical chest pain. Patients were enrolled into the study if they had normal resting wall motion, sinus rhythm, and had no history of coronary artery disease, unstable angina, or PTCA. Patients (average age 61 years, 42% men) were followed for an average of 44 months for primary cardiovascular endpoints (fatal or nonfatal myocardial infarction [MI], unstable angina, PTCA, or cardiac death). A negative or positive stress echocardiography is defined as the absence or presence of abnormal cardiac wall motion on either exercise or pharmacologic stress echocardiography. Eighteen percent of patients had a positive pharmacologic stress echocardiography. Over the length of the study, 81 of 904 patients (9%) suffered a cardiovascular event. Patients with a negative pharmacologic stress echocardiography had a mean annual probability of a cardiovascular event of 0.8% vs 8.5% with a positive pharmacologic stress echocardiography (P<0001). The 4-year infarct-free negative predictive value (NPV) of pharmacologic stress echocardiography was 97%, and the positive predictive value (PPV) was 70%.
A similar prospective cohort study2 evaluated 105 patients (50% men) with atypical chest pain in an emergency department setting with either exercise or dobutamine/atropine stress echocardiography. The average patient age was 55 years and follow-up was 2.8 years. Patients were clinically stable, had normal or nondiagnostic electrocardiogram (ECG), normal cardiac enzymes, normal left ventricular function, and no history of coronary artery disease or unstable angina. Cardiovascular endpoints included fatal or nonfatal MI, unstable angina, PTCA, or cardiac death. A total of 7 patients (7%) suffered a cardiovascular event during the follow-up period. Positive stress echocardiography results occurred for 9% of patients. The NPV was 99% and the PPV was 75%.
Three other cohort studies3-5 evaluated exercise or dobutamine/atropine stress echocardiography for a total of 615 patients (48%–67% men, average age 56–58 years) presenting to an emergency department with classical cardiac or atypical chest pain. Patients had normal or nondiagnostic ECG, negative cardiac enzymes, and either no history of coronary artery disease3,4 or known coronary artery disease of unknown significance.5 A positive stress echocardiography was obtained for 4.8% to 42% of patients in the cohorts. During 6 months of follow-up, cardiovascular events occurred in 4 of 145 patients (3%),3 22 of 227 patients (6%),4 and in 11 of 80 patients (14%).5 At 6-month follow-up, exercise stress echocardiography had a NPV of 99.3% and a PPV of 43%.3 Dobutamine/atropine stress echocardiography had a NPV of 95% to 96% and a PPV of 25% to 31%.4,5
One retrospective review6 evaluated exercise and dobutamine/atropine stress echocardiography and stress ECG for 661 low-risk outpatients (48% men, average age 58 years) with atypical chest pain. All patients had normal left ventricular function and no history of coronary artery disease and were followed for an average of 23 months. A positive stress echocardiography test occurred among 16% of the patient population.
During follow-up, 41 of 661 patients (6%) suffered a cardiovascular event. For either exercise or dobutamine/atropine stress echocardiography, the NPV was 99% at 12 months and 96% at 30 months. Patients with a positive stress echocardiography test and a negative stress ECG had a 66% event-free survival rate. Event-free survival rate for patients with a negative stress echocardiography and a positive or negative stress ECG was 97% and 96%, respectively.
Recommendations from others
The American College of Cardiology7 gives a Class I recommendation (tests for which there is evidence or general agreement that a given procedure or treatment is useful and effective) for standard echocardiogram for evaluation of chest pain for patients with suspected acute myocardial ischemia (when baseline ECG and other laboratory markers are nondiagnostic and when the study can be obtained during pain or within minutes after its abatement).
It gives a Class IIa recommendation (tests for which there is conflicting evidence or divergence of opinion, but favoring usefulness) to stress echocardiography for the detection of myocardial ischemia for women with an intermediate pretest likelihood of coronary artery disease. It also gives a Class IIa recommendation to stress echocardiography for determining the prognosis of myocardial ischemia among patients for whom ECG assessment is less reliable. This group comprises patients with the following ECG abnormalities: pre-excitation syndrome (such as Wolff-Parkinson-White), electronically paced ventricular rhythm, more than 1 mm of ST depression at rest, and complete left bundle branch block.
Patients with atypical chest pain and no history of cardiovascular events (coronary artery disease, unstable angina, or history of percutaneous transthoracic coronary angioplasty [PTCA]) and a negative stress echocardiography test are unlikely to experience a cardiovascular event in the next 1 to 4 years. However, the positive predictive value of the test in this population is low, indicating that a positive stress echocardiography is less useful for prognostic purposes (strength of recommendation: B, based on multiple cohort studies).
Using stress echocardiography reduces need for diagnostic cardiac catheterization for atypical chest pain
Timothy Huber, MD
Oroville, Calif
Patients presenting to emergency and urgent care departments with atypical chest pain are a dilemma whenever their ECG and biomarkers are nondiagnostic. Graded exercise stress testing to further define risk is not effective in many patient populations: including some women, patients with mobility problems, and patients with underlying conduction issues such as pre-excitation syndromes, left bundle branch blocks, and ventricular pacemakers. Stress echocardiography is a reasonable alternative for such patients. While physicians may take a negative test at face value in this clinical setting, a positive test is not diagnostic and will often necessitate further workup. Using stress echocardiography therefore reduces but does not eliminate the need for diagnostic cardiac catheterization for atypical chest pain.
Evidence summary
A prospective cohort study1 evaluated dobutamine or dipyridamole pharmacologic stress echocardiography among 904 primary care patients with either typical or atypical chest pain. Patients were enrolled into the study if they had normal resting wall motion, sinus rhythm, and had no history of coronary artery disease, unstable angina, or PTCA. Patients (average age 61 years, 42% men) were followed for an average of 44 months for primary cardiovascular endpoints (fatal or nonfatal myocardial infarction [MI], unstable angina, PTCA, or cardiac death). A negative or positive stress echocardiography is defined as the absence or presence of abnormal cardiac wall motion on either exercise or pharmacologic stress echocardiography. Eighteen percent of patients had a positive pharmacologic stress echocardiography. Over the length of the study, 81 of 904 patients (9%) suffered a cardiovascular event. Patients with a negative pharmacologic stress echocardiography had a mean annual probability of a cardiovascular event of 0.8% vs 8.5% with a positive pharmacologic stress echocardiography (P<0001). The 4-year infarct-free negative predictive value (NPV) of pharmacologic stress echocardiography was 97%, and the positive predictive value (PPV) was 70%.
A similar prospective cohort study2 evaluated 105 patients (50% men) with atypical chest pain in an emergency department setting with either exercise or dobutamine/atropine stress echocardiography. The average patient age was 55 years and follow-up was 2.8 years. Patients were clinically stable, had normal or nondiagnostic electrocardiogram (ECG), normal cardiac enzymes, normal left ventricular function, and no history of coronary artery disease or unstable angina. Cardiovascular endpoints included fatal or nonfatal MI, unstable angina, PTCA, or cardiac death. A total of 7 patients (7%) suffered a cardiovascular event during the follow-up period. Positive stress echocardiography results occurred for 9% of patients. The NPV was 99% and the PPV was 75%.
Three other cohort studies3-5 evaluated exercise or dobutamine/atropine stress echocardiography for a total of 615 patients (48%–67% men, average age 56–58 years) presenting to an emergency department with classical cardiac or atypical chest pain. Patients had normal or nondiagnostic ECG, negative cardiac enzymes, and either no history of coronary artery disease3,4 or known coronary artery disease of unknown significance.5 A positive stress echocardiography was obtained for 4.8% to 42% of patients in the cohorts. During 6 months of follow-up, cardiovascular events occurred in 4 of 145 patients (3%),3 22 of 227 patients (6%),4 and in 11 of 80 patients (14%).5 At 6-month follow-up, exercise stress echocardiography had a NPV of 99.3% and a PPV of 43%.3 Dobutamine/atropine stress echocardiography had a NPV of 95% to 96% and a PPV of 25% to 31%.4,5
One retrospective review6 evaluated exercise and dobutamine/atropine stress echocardiography and stress ECG for 661 low-risk outpatients (48% men, average age 58 years) with atypical chest pain. All patients had normal left ventricular function and no history of coronary artery disease and were followed for an average of 23 months. A positive stress echocardiography test occurred among 16% of the patient population.
During follow-up, 41 of 661 patients (6%) suffered a cardiovascular event. For either exercise or dobutamine/atropine stress echocardiography, the NPV was 99% at 12 months and 96% at 30 months. Patients with a positive stress echocardiography test and a negative stress ECG had a 66% event-free survival rate. Event-free survival rate for patients with a negative stress echocardiography and a positive or negative stress ECG was 97% and 96%, respectively.
Recommendations from others
The American College of Cardiology7 gives a Class I recommendation (tests for which there is evidence or general agreement that a given procedure or treatment is useful and effective) for standard echocardiogram for evaluation of chest pain for patients with suspected acute myocardial ischemia (when baseline ECG and other laboratory markers are nondiagnostic and when the study can be obtained during pain or within minutes after its abatement).
It gives a Class IIa recommendation (tests for which there is conflicting evidence or divergence of opinion, but favoring usefulness) to stress echocardiography for the detection of myocardial ischemia for women with an intermediate pretest likelihood of coronary artery disease. It also gives a Class IIa recommendation to stress echocardiography for determining the prognosis of myocardial ischemia among patients for whom ECG assessment is less reliable. This group comprises patients with the following ECG abnormalities: pre-excitation syndrome (such as Wolff-Parkinson-White), electronically paced ventricular rhythm, more than 1 mm of ST depression at rest, and complete left bundle branch block.
1. Amici E, Cortigiani L, Coletta C, et al. Usefulness of pharmacologic stress echocardiography for the long-term prognostic assessment of patients with typical versus atypical chest pain. Am J Cardiol 2003;91:440-442.
2. Colon PJ, 3rd, Cheirif J. Long-term value of stress echocardiography in the triage of patients with atypical chest pain presenting to the emergency department. Echocardiography 1999;16:171-177.
3. Buchsbaum M, Marshall E, Levine B, et al. Emergency department evaluation of chest pain using exercise stress echocardiography. Acad Emerg Med 2001;8:196-199.
4. Bholasingh R, Cornel JH, Kamp O, et al. Prognostic value of predischarge dobutamine stress echocardiography in chest pain patients with a negative cardiac troponin T. J Am Coll Cardiol 2003;41:596-602.
5. Geleijnse ML, Elhendy A, Kasprzak JD, et al. Safety and prognostic value of early dobutamine-atropine stress echocardiography in patients with spontaneous chest pain and a nondiagnostic electrocardiogram. Eur Heart J 2000;21:397-406.
6. Colon PJ, 3rd, Mobarek SK, Milani RV, et al. Prognostic value of stress echocardiography in the evaluation of atypical chest pain patients without known coronary artery disease. Am J Cardiol 1998;81:545-551.
7. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. (ACC/AHA/ASE Committee to update the 1997 guidelines for the clinical application of echocardiography.) Available at: www.acc.org/qualityandscience/clinical/guidelines/echo/index_clean.pdf. Accessed on September 6, 2006.
1. Amici E, Cortigiani L, Coletta C, et al. Usefulness of pharmacologic stress echocardiography for the long-term prognostic assessment of patients with typical versus atypical chest pain. Am J Cardiol 2003;91:440-442.
2. Colon PJ, 3rd, Cheirif J. Long-term value of stress echocardiography in the triage of patients with atypical chest pain presenting to the emergency department. Echocardiography 1999;16:171-177.
3. Buchsbaum M, Marshall E, Levine B, et al. Emergency department evaluation of chest pain using exercise stress echocardiography. Acad Emerg Med 2001;8:196-199.
4. Bholasingh R, Cornel JH, Kamp O, et al. Prognostic value of predischarge dobutamine stress echocardiography in chest pain patients with a negative cardiac troponin T. J Am Coll Cardiol 2003;41:596-602.
5. Geleijnse ML, Elhendy A, Kasprzak JD, et al. Safety and prognostic value of early dobutamine-atropine stress echocardiography in patients with spontaneous chest pain and a nondiagnostic electrocardiogram. Eur Heart J 2000;21:397-406.
6. Colon PJ, 3rd, Mobarek SK, Milani RV, et al. Prognostic value of stress echocardiography in the evaluation of atypical chest pain patients without known coronary artery disease. Am J Cardiol 1998;81:545-551.
7. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. (ACC/AHA/ASE Committee to update the 1997 guidelines for the clinical application of echocardiography.) Available at: www.acc.org/qualityandscience/clinical/guidelines/echo/index_clean.pdf. Accessed on September 6, 2006.
Evidence-based answers from the Family Physicians Inquiries Network
When should a child with an undescended testis be referred to a urologist?
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism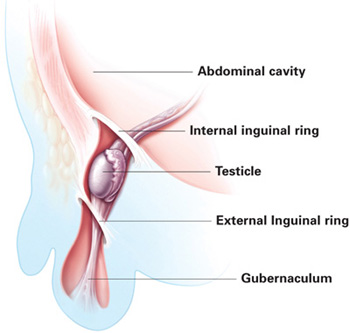
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
Infants with an undescended testis should be referred between ages 6 and 15 months, since almost all who experience spontaneous descent do so by 6 months (strength of recommendation [SOR]: A, extrapolation from cohort studies).
The incidence of germ cell aplasia in undescended testes begins to rise at 15 months (SOR: C, extrapolation of observational studies); however, evidence is inconclusive that orchiopexy at this age results in higher rates of paternity success (SOR: B, retrospective cohort study).
Orchiopexy may allow earlier detection of testicular tumors (SOR: C, expert opinion), but it has not been shown to reduce the risk of testicular cancer (SOR: B, retrospective cohort study) or improve 5-year survival rates for those patients diagnosed with testicular cancer (SOR: B, retrospective cohort study).
Periodically evaluate a newborn’s scrotum for either an undescended or reascended testicle
Danny Thomason, DO
Oklahoma State University, Tulsa
This Inquiry highlights 2 important considerations regarding the child with a cryptorchid testis. First, periodically evaluate the newborn and infant patient’s scrotum for either an undescended or reascended testicle. In my practice at Oklahoma State University Family Medicine Residency, I ask residents to perform the scrotal examination at birth, at every well-child visit up to 1 year of age, and then yearly thereafter. During puberty, these exams serve as opportunities to educate patients about testicular self-examination.
Secondly, as the authors indicate, there is some disagreement in the literature as to the risk of testicular cancer following orchiopexy for cryptorchidism. However, surgical repair is likely to facilitate regular testicular self-examination, which could increase the likelihood of detection of cancer during young adulthood.
Evidence summary
Three large cohort studies determined that cryptorchidism (FIGURE) is present at birth in approximately 3% of term infants (higher in preterm infants), with spontaneous descent occurring in two thirds of cases by age 3 to 6 months. One study1 of 10,730 consecutive male term infants found cryptorchidism at birth in 2.7%, dropping to 1.22% by 6 months of age, but without further change at 1 year. A similar study2 followed 6935 infant boys, finding cryptorchidism at birth in 3.7%, which decreased to 1% at 3 months and remained unchanged at 1 year. A third study3 found cryptorchidism at birth in 90 of 6414 (2.7%) infant boys. At follow-up, 45 of 90 had testicular descent at 1 month, 60 of 90 at 3 months, 67 of 90 at 9 months and at 1 year.
The 2 main indications for orchiopexy are potential avoidance of infertility and early detection and treatment of testicular cancer. A literature review4 of fertility after orchiopexy for undescended testis found inconclusive results. While epidemiological and pathological data (testicular biopsy, hormonal analysis, and sperm counts performed after orchiopexy) predict diminished fertility potential for men with unilaterally undescended testes, studies evaluating paternity find no difference from normal men. Biopsy studies of undescended testes at the time of orchiopexy show increased incidence of germ cell aplasia with older age at surgery (0.5%, 2%, 20%, and 45% at 6, 12, 24, and 48 months, respectively).4 A retrospective cohort study5 found 87% successful paternity after orchiopexy for 24 patients with unilateral undescended testis and 33% success for 9 with bilateral undescended testes but there was no normal control group. The boys were aged 1 to 14 years (mean, 7 years) at surgery, and there was no relationship between timing of orchiopexy and paternity success.5
The benefits of orchiopexy for testicular cancer are also unclear; expert opinion suggests that orchiopexy may allow earlier detection of testicular tumors.6 A cohort study7 of boys with cryptorchidism showed an increased risk of testicular cancer (relative risk=5.2). However, risk did not decrease after orchiopexy in early childhood. A retrospective cohort study8 of 137 men with cryptorchidism who developed testicular cancer found no difference in 5-year survival between those who had orchiopexy (at ages 2 to 42) and those who had not (61% vs 63%, respectively).
FIGURE
Cryptorchidism
In most cases of cryptorchidism, the testis will be inguinal or prescrotal. A smaller number of cases are ectopic (have left the inguinal ring), abdominal, or absent. ILLUSTRATION BY RICH LaROCCO
Recommendations from others
The American Academy of Pediatrics policy section on urology says that spontaneous descent after 6 months is unlikely and recommends orchiopexy by 1 year of age.9
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
1. Ghirri P, Ciulli C, Vuerich M, et al. Incidence at birth and natural history of cryptorchidism: a study of 10,730 consecutive male infants. J Endocrinol Invest 2002;25:709-715.
2. Berkowitz GS, Lapinski RH, Dolgin MD, et al. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-49.
3. Scorer CG. The descent of the testis. Arch Dis Childhood 1964;39:605-609.
4. Husmann DA. Cryptorchidism. In: Belman AB, King LR, Kramer SA, eds. Clinical Pediatric Urology. 4th ed. London, UK: Martin Dunitz Ltd.; 2002: 1125–1154.
5. Cendron M, Keating MA, Huff DS, Koop CE, Snyder HM, 3rd, Duckett JW. Cryptorchidism, orchiopexy and infertility: a critical long-term retrospective analysis. J Urol 1989;142(2 pt 2):559-562.
6. Docimo SG, Silver RI, Cromie W. The undescended testicle: diagnosis and management. Am Fam Physician 2000;62:2037-2048.
7. Prener A, Engholm G, Jensen OM. Genital anomalies and risk for testicular cancer in Danish men. Epidemiology 1996;7:14-19.
8. Batata MA, Chu FC, Hilaris BS, Whitmore WF, Golbey RB. Testicular cancer in cryptorchids. Cancer 1982;49:1023-1030.
9. American Academy of Pediatrics Policy Statement. Timing of elective surgery on the genitalia of male children with particular reference to the risks, benefits, and psychological effects of surgery and anesthesia. Pediatrics 1996;97:590-594.
Evidence-based answers from the Family Physicians Inquiries Network
What treatments prevent miscarriage after recurrent pregnancy loss?
Progesterone produces a small but significant decrease in miscarriage among pregnant women with 3 or more unexplained pregnancy losses (strength of recommendation [SOR]: A, based on a meta-analysis of 3 small randomized controlled trials [RCTs] with wide confidence intervals). Human chorionic gonadotropin (HCG) reduces the rate of recurrent pregnancy loss among women with 2 or more unexplained pregnancy losses (SOR: B, based on a meta-analysis of 4 RCTs with significant methodologic weaknesses).
Four types of immunotherapy are ineffective for preventing miscarriage (SOR: A, based on RCTs and systematic reviews of RCTs). Aspirin therapy is ineffective for preventing recurrent miscarriage for women who do not have an autoimmune explanation for previous pregnancy losses (SOR: A, based on RCTs).
Document your patient’s understanding of the risks and benefits
Beth Damitz, MD
Medical College of Wisconsin
When discussing future childbearing with a woman who has had multiple miscarriages, there are several important issues to address. First, ask what concerns she might have about becoming pregnant again. Second, ascertain how significant another pregnancy loss would be to her. Third, outline the therapeutic options, clearly stating that they alter loss rates but do not guarantee successful delivery. Finally, fully document her understanding of the risks and benefits, including the possibility of treatment failure. Remember, even if the miscarriage rate is reduced from 25% to 20% with treatment, should your patient miscarry, her miscarriage rate is 100%!
Evidence summary
Progesterone. A Cochrane meta-analysis on the use of progesterone to prevent pregnancy loss looked at a subset of 3 small RCTs that evaluated women with 3 or more pregnancy losses. Patients with primary recurrent spontaneous abortion (RSA) (no prior live births), were not differentiated from those with secondary RSA (previous live birth with subsequent miscarriages).
Progesterone administration resulted in a significant reduction in miscarriage compared with placebo (odds ratio [OR]=0.37; 95% confidence interval [CI], 0.17–0.91), independent of administration routes (oral, vaginal, or intramuscular). This benefit was lost in the larger meta-analysis when studies containing women with fewer than 3 pregnancy losses were included.1
Human choriogonadotropin. A meta-analysis reviewed 4 trials (n=180 total) of varying methodological quality, which were constructed to determine if women, with at least 2 consecutive miscarriages of unknown cause, derive any protective effect when they receive HCG during the first trimester. Although the overall outcome favored the use of HCG (OR=0.26 compared with placebo; 95% CI, 0.14–0.52), the trials contained major methodological weaknesses (poor description of methods, no power calculations, selection and unclear randomization techniques).2
Immunotherapy. A systematic review of 22 RCTs evaluating 4 different types of immunotherapy for recurrent miscarriage found no significant improvement in live birth rates. All studies were of high quality with a low level of bias. Only one lacked double-blinding.
Immunotherapy types included: paternal leukocyte immunization (PLI) (11 trials, 596 women) (OR=1.05; 95% CI, 0.75–1.47); intravenous immune globulin (IVIG) (OR=0.98; 95% CI, 0.61–1.58); third-party donor cell immunization (3 trials, 156 women) (OR=1.39; 95% CI, 0.68–2.82); and trophoblast membrane infusion (1 trial, 37 women) (OR=0.40; 95% CI, 0.11–1.45).3
A subsequent RCT comparing PLI with placebo among 79 women with primary RSA of unknown cause again found no significant difference in live birth rates (89% vs 71%, respectively).4 However, an additional RCT evaluating PLI (32 patients) vs placebo (19 patients) among women with unexplained primary RSA did find significantly higher birth rates with PLI (84% vs 25%; P=.001). This small study used different techniques than previous PLI studies.5
A later meta-analysis of 5 RCTs including a total of 246 patients also found that IVIG did not improve the subsequent live birth rate for women with a history of primary or secondary RSA (OR=0.98; 95% CI, 0.45–2.13).6
Aspirin. An RCT involving 54 pregnant women (mean age 32.7 years) with a history of primary RSA of unknown cause (negative standard workup) evaluated 50 mg of aspirin daily (n=27) vs placebo (n=27).7 The method of blinding was not reported.
The live birth rate was identical for the 2 groups (88%). A second (unblinded) trial randomized 805 women from a large referral center (mean age 34 years) with a history of first-trimester RSA (not differentiated between primary and secondary RSA) of unknown cause to either 75 mg of aspirin daily or no treatment.8 There was no significant difference in the live birth rate between those who took aspirin (251/367; 68.4%) and those who did not (278/438; 63.5%; OR=1.24; 95% CI, 0.93–1.67).
Recommendations from others
The American College of Obstetricians and Gynecologists (ACOG) states that “it has not been shown conclusively that progesterone treatment or corpus luteum support (HCG) influences pregnancy outcome for women with recurrent spontaneous abortion.”9 ACOG does not recommend immunotherapy, citing a lack of demonstrated efficacy (IVIG and PLI), a lack of standards for cell storage and administration, and a risk profile similar to that of blood transfusion (PLI). They recommend “couples with otherwise unexplained recurrent pregnancy loss should be counseled regarding the potential for successful pregnancy without treatment.”
1. Oates-Whitehead RM, Haas DM, Carrier JA. Progestogen for preventing miscarriage. Cochrane Database Syst Rev 2003;(4):CD003511.-
2. Scott JR, Pattison N. Human chorionic gonadotrophin for recurrent miscarriage. Cochrane Database Syst Rev 2000;(2):CD000101.-
3. Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev 2003;(1):CD000112.-
4. Ramhorst R, Agriello E, Zittermann S, et al. Is the paternal mononuclear cells’ immunization a successful treatment for recurrent spontaneous abortion? Am J Reprod Immunol 2000;44:129-135.
5. Pandey MK, Agrawal S. Induction of MLR-Bf and protection of fetal loss: a current double blind randomized trial of paternal lymphocyte immunization for women with recurrent spontaneous abortion. Int Immunopharmacol 2004;4:289-298.
6. Practice Committee of the American Society for Reproductive Medicine. Intravenous immunoglobulin (IVIG) and recurrent spontaneous pregnancy loss. Fertil Steril 2004;82 Suppl 1:S199-S200.
7. Tulppala M, Marttunen M. Soderstrom-Anttila V, et al. Low-dose aspirin in prevention of miscarriage in women with unexplained or autoimmune related recurrent miscarriage: effect on prostacyclin and thromboxane A2 production. Hum Reprod 1997;12:1567-1572.
8. Rai R, Backos M, Baxter N, Chilcott I, Regan L. Recurrent miscarriage-an aspirin a day? Hum Reprod 2000;15:2220-2223.
9. American College of Obstetricians and Gynecologists. ACOG practice bulletin. Management of recurrent pregnancy loss. Number 24, February 2001. (Replaces Technical Bulletin Number 212, September 1995). American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet 2002;78:179-190.
Progesterone produces a small but significant decrease in miscarriage among pregnant women with 3 or more unexplained pregnancy losses (strength of recommendation [SOR]: A, based on a meta-analysis of 3 small randomized controlled trials [RCTs] with wide confidence intervals). Human chorionic gonadotropin (HCG) reduces the rate of recurrent pregnancy loss among women with 2 or more unexplained pregnancy losses (SOR: B, based on a meta-analysis of 4 RCTs with significant methodologic weaknesses).
Four types of immunotherapy are ineffective for preventing miscarriage (SOR: A, based on RCTs and systematic reviews of RCTs). Aspirin therapy is ineffective for preventing recurrent miscarriage for women who do not have an autoimmune explanation for previous pregnancy losses (SOR: A, based on RCTs).
Document your patient’s understanding of the risks and benefits
Beth Damitz, MD
Medical College of Wisconsin
When discussing future childbearing with a woman who has had multiple miscarriages, there are several important issues to address. First, ask what concerns she might have about becoming pregnant again. Second, ascertain how significant another pregnancy loss would be to her. Third, outline the therapeutic options, clearly stating that they alter loss rates but do not guarantee successful delivery. Finally, fully document her understanding of the risks and benefits, including the possibility of treatment failure. Remember, even if the miscarriage rate is reduced from 25% to 20% with treatment, should your patient miscarry, her miscarriage rate is 100%!
Evidence summary
Progesterone. A Cochrane meta-analysis on the use of progesterone to prevent pregnancy loss looked at a subset of 3 small RCTs that evaluated women with 3 or more pregnancy losses. Patients with primary recurrent spontaneous abortion (RSA) (no prior live births), were not differentiated from those with secondary RSA (previous live birth with subsequent miscarriages).
Progesterone administration resulted in a significant reduction in miscarriage compared with placebo (odds ratio [OR]=0.37; 95% confidence interval [CI], 0.17–0.91), independent of administration routes (oral, vaginal, or intramuscular). This benefit was lost in the larger meta-analysis when studies containing women with fewer than 3 pregnancy losses were included.1
Human choriogonadotropin. A meta-analysis reviewed 4 trials (n=180 total) of varying methodological quality, which were constructed to determine if women, with at least 2 consecutive miscarriages of unknown cause, derive any protective effect when they receive HCG during the first trimester. Although the overall outcome favored the use of HCG (OR=0.26 compared with placebo; 95% CI, 0.14–0.52), the trials contained major methodological weaknesses (poor description of methods, no power calculations, selection and unclear randomization techniques).2
Immunotherapy. A systematic review of 22 RCTs evaluating 4 different types of immunotherapy for recurrent miscarriage found no significant improvement in live birth rates. All studies were of high quality with a low level of bias. Only one lacked double-blinding.
Immunotherapy types included: paternal leukocyte immunization (PLI) (11 trials, 596 women) (OR=1.05; 95% CI, 0.75–1.47); intravenous immune globulin (IVIG) (OR=0.98; 95% CI, 0.61–1.58); third-party donor cell immunization (3 trials, 156 women) (OR=1.39; 95% CI, 0.68–2.82); and trophoblast membrane infusion (1 trial, 37 women) (OR=0.40; 95% CI, 0.11–1.45).3
A subsequent RCT comparing PLI with placebo among 79 women with primary RSA of unknown cause again found no significant difference in live birth rates (89% vs 71%, respectively).4 However, an additional RCT evaluating PLI (32 patients) vs placebo (19 patients) among women with unexplained primary RSA did find significantly higher birth rates with PLI (84% vs 25%; P=.001). This small study used different techniques than previous PLI studies.5
A later meta-analysis of 5 RCTs including a total of 246 patients also found that IVIG did not improve the subsequent live birth rate for women with a history of primary or secondary RSA (OR=0.98; 95% CI, 0.45–2.13).6
Aspirin. An RCT involving 54 pregnant women (mean age 32.7 years) with a history of primary RSA of unknown cause (negative standard workup) evaluated 50 mg of aspirin daily (n=27) vs placebo (n=27).7 The method of blinding was not reported.
The live birth rate was identical for the 2 groups (88%). A second (unblinded) trial randomized 805 women from a large referral center (mean age 34 years) with a history of first-trimester RSA (not differentiated between primary and secondary RSA) of unknown cause to either 75 mg of aspirin daily or no treatment.8 There was no significant difference in the live birth rate between those who took aspirin (251/367; 68.4%) and those who did not (278/438; 63.5%; OR=1.24; 95% CI, 0.93–1.67).
Recommendations from others
The American College of Obstetricians and Gynecologists (ACOG) states that “it has not been shown conclusively that progesterone treatment or corpus luteum support (HCG) influences pregnancy outcome for women with recurrent spontaneous abortion.”9 ACOG does not recommend immunotherapy, citing a lack of demonstrated efficacy (IVIG and PLI), a lack of standards for cell storage and administration, and a risk profile similar to that of blood transfusion (PLI). They recommend “couples with otherwise unexplained recurrent pregnancy loss should be counseled regarding the potential for successful pregnancy without treatment.”
Progesterone produces a small but significant decrease in miscarriage among pregnant women with 3 or more unexplained pregnancy losses (strength of recommendation [SOR]: A, based on a meta-analysis of 3 small randomized controlled trials [RCTs] with wide confidence intervals). Human chorionic gonadotropin (HCG) reduces the rate of recurrent pregnancy loss among women with 2 or more unexplained pregnancy losses (SOR: B, based on a meta-analysis of 4 RCTs with significant methodologic weaknesses).
Four types of immunotherapy are ineffective for preventing miscarriage (SOR: A, based on RCTs and systematic reviews of RCTs). Aspirin therapy is ineffective for preventing recurrent miscarriage for women who do not have an autoimmune explanation for previous pregnancy losses (SOR: A, based on RCTs).
Document your patient’s understanding of the risks and benefits
Beth Damitz, MD
Medical College of Wisconsin
When discussing future childbearing with a woman who has had multiple miscarriages, there are several important issues to address. First, ask what concerns she might have about becoming pregnant again. Second, ascertain how significant another pregnancy loss would be to her. Third, outline the therapeutic options, clearly stating that they alter loss rates but do not guarantee successful delivery. Finally, fully document her understanding of the risks and benefits, including the possibility of treatment failure. Remember, even if the miscarriage rate is reduced from 25% to 20% with treatment, should your patient miscarry, her miscarriage rate is 100%!
Evidence summary
Progesterone. A Cochrane meta-analysis on the use of progesterone to prevent pregnancy loss looked at a subset of 3 small RCTs that evaluated women with 3 or more pregnancy losses. Patients with primary recurrent spontaneous abortion (RSA) (no prior live births), were not differentiated from those with secondary RSA (previous live birth with subsequent miscarriages).
Progesterone administration resulted in a significant reduction in miscarriage compared with placebo (odds ratio [OR]=0.37; 95% confidence interval [CI], 0.17–0.91), independent of administration routes (oral, vaginal, or intramuscular). This benefit was lost in the larger meta-analysis when studies containing women with fewer than 3 pregnancy losses were included.1
Human choriogonadotropin. A meta-analysis reviewed 4 trials (n=180 total) of varying methodological quality, which were constructed to determine if women, with at least 2 consecutive miscarriages of unknown cause, derive any protective effect when they receive HCG during the first trimester. Although the overall outcome favored the use of HCG (OR=0.26 compared with placebo; 95% CI, 0.14–0.52), the trials contained major methodological weaknesses (poor description of methods, no power calculations, selection and unclear randomization techniques).2
Immunotherapy. A systematic review of 22 RCTs evaluating 4 different types of immunotherapy for recurrent miscarriage found no significant improvement in live birth rates. All studies were of high quality with a low level of bias. Only one lacked double-blinding.
Immunotherapy types included: paternal leukocyte immunization (PLI) (11 trials, 596 women) (OR=1.05; 95% CI, 0.75–1.47); intravenous immune globulin (IVIG) (OR=0.98; 95% CI, 0.61–1.58); third-party donor cell immunization (3 trials, 156 women) (OR=1.39; 95% CI, 0.68–2.82); and trophoblast membrane infusion (1 trial, 37 women) (OR=0.40; 95% CI, 0.11–1.45).3
A subsequent RCT comparing PLI with placebo among 79 women with primary RSA of unknown cause again found no significant difference in live birth rates (89% vs 71%, respectively).4 However, an additional RCT evaluating PLI (32 patients) vs placebo (19 patients) among women with unexplained primary RSA did find significantly higher birth rates with PLI (84% vs 25%; P=.001). This small study used different techniques than previous PLI studies.5
A later meta-analysis of 5 RCTs including a total of 246 patients also found that IVIG did not improve the subsequent live birth rate for women with a history of primary or secondary RSA (OR=0.98; 95% CI, 0.45–2.13).6
Aspirin. An RCT involving 54 pregnant women (mean age 32.7 years) with a history of primary RSA of unknown cause (negative standard workup) evaluated 50 mg of aspirin daily (n=27) vs placebo (n=27).7 The method of blinding was not reported.
The live birth rate was identical for the 2 groups (88%). A second (unblinded) trial randomized 805 women from a large referral center (mean age 34 years) with a history of first-trimester RSA (not differentiated between primary and secondary RSA) of unknown cause to either 75 mg of aspirin daily or no treatment.8 There was no significant difference in the live birth rate between those who took aspirin (251/367; 68.4%) and those who did not (278/438; 63.5%; OR=1.24; 95% CI, 0.93–1.67).
Recommendations from others
The American College of Obstetricians and Gynecologists (ACOG) states that “it has not been shown conclusively that progesterone treatment or corpus luteum support (HCG) influences pregnancy outcome for women with recurrent spontaneous abortion.”9 ACOG does not recommend immunotherapy, citing a lack of demonstrated efficacy (IVIG and PLI), a lack of standards for cell storage and administration, and a risk profile similar to that of blood transfusion (PLI). They recommend “couples with otherwise unexplained recurrent pregnancy loss should be counseled regarding the potential for successful pregnancy without treatment.”
1. Oates-Whitehead RM, Haas DM, Carrier JA. Progestogen for preventing miscarriage. Cochrane Database Syst Rev 2003;(4):CD003511.-
2. Scott JR, Pattison N. Human chorionic gonadotrophin for recurrent miscarriage. Cochrane Database Syst Rev 2000;(2):CD000101.-
3. Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev 2003;(1):CD000112.-
4. Ramhorst R, Agriello E, Zittermann S, et al. Is the paternal mononuclear cells’ immunization a successful treatment for recurrent spontaneous abortion? Am J Reprod Immunol 2000;44:129-135.
5. Pandey MK, Agrawal S. Induction of MLR-Bf and protection of fetal loss: a current double blind randomized trial of paternal lymphocyte immunization for women with recurrent spontaneous abortion. Int Immunopharmacol 2004;4:289-298.
6. Practice Committee of the American Society for Reproductive Medicine. Intravenous immunoglobulin (IVIG) and recurrent spontaneous pregnancy loss. Fertil Steril 2004;82 Suppl 1:S199-S200.
7. Tulppala M, Marttunen M. Soderstrom-Anttila V, et al. Low-dose aspirin in prevention of miscarriage in women with unexplained or autoimmune related recurrent miscarriage: effect on prostacyclin and thromboxane A2 production. Hum Reprod 1997;12:1567-1572.
8. Rai R, Backos M, Baxter N, Chilcott I, Regan L. Recurrent miscarriage-an aspirin a day? Hum Reprod 2000;15:2220-2223.
9. American College of Obstetricians and Gynecologists. ACOG practice bulletin. Management of recurrent pregnancy loss. Number 24, February 2001. (Replaces Technical Bulletin Number 212, September 1995). American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet 2002;78:179-190.
1. Oates-Whitehead RM, Haas DM, Carrier JA. Progestogen for preventing miscarriage. Cochrane Database Syst Rev 2003;(4):CD003511.-
2. Scott JR, Pattison N. Human chorionic gonadotrophin for recurrent miscarriage. Cochrane Database Syst Rev 2000;(2):CD000101.-
3. Scott JR. Immunotherapy for recurrent miscarriage. Cochrane Database Syst Rev 2003;(1):CD000112.-
4. Ramhorst R, Agriello E, Zittermann S, et al. Is the paternal mononuclear cells’ immunization a successful treatment for recurrent spontaneous abortion? Am J Reprod Immunol 2000;44:129-135.
5. Pandey MK, Agrawal S. Induction of MLR-Bf and protection of fetal loss: a current double blind randomized trial of paternal lymphocyte immunization for women with recurrent spontaneous abortion. Int Immunopharmacol 2004;4:289-298.
6. Practice Committee of the American Society for Reproductive Medicine. Intravenous immunoglobulin (IVIG) and recurrent spontaneous pregnancy loss. Fertil Steril 2004;82 Suppl 1:S199-S200.
7. Tulppala M, Marttunen M. Soderstrom-Anttila V, et al. Low-dose aspirin in prevention of miscarriage in women with unexplained or autoimmune related recurrent miscarriage: effect on prostacyclin and thromboxane A2 production. Hum Reprod 1997;12:1567-1572.
8. Rai R, Backos M, Baxter N, Chilcott I, Regan L. Recurrent miscarriage-an aspirin a day? Hum Reprod 2000;15:2220-2223.
9. American College of Obstetricians and Gynecologists. ACOG practice bulletin. Management of recurrent pregnancy loss. Number 24, February 2001. (Replaces Technical Bulletin Number 212, September 1995). American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet 2002;78:179-190.
Evidence-based answers from the Family Physicians Inquiries Network
How long is expectant management safe in first-trimester miscarriage?
More than 80% of women with a first-trimester spontaneous abortion have complete natural passage of tissue within 2 to 6 weeks with no higher complication rate than that from surgical intervention (strength of recommendation [SOR]: A, based on multiple randomized controlled trials [RCTs] and cohort studies). Expectant management is successful within 2 to 6 weeks without increased complications in 80% to 90% of women with first-trimester incomplete spontaneous abortion and 65% to 75% of women with first-trimester missed abortion or anembryonic gestation (presenting with spotting or bleeding and ultrasound evidence of fetal demise) (SOR: B, based on multiple cohort studies). There is no difference in short-term psychological outcomes between expectant and surgical management (SOR: B, based on RCT). Women experiencing spontaneous abortion with unstable vital signs, uncontrolled bleeding, or evidence of infection should be considered for surgical evacuation (SOR: C, expert opinion).
FPs should empathize, explain, and expedite
Paul Crawford, MD
USAF-Eglin Family Practice Residency, Eglin Air Force Base, Eglin, Fla
A spontaneous abortion can be a very distressing event for a woman and her family; and helping a patient through the complex medical and emotional issues that arise due to the miscarriage stretches the skills of a compassionate clinician. Fortunately, family physicians are ideally positioned to empathize with families, explain treatment options, and expedite medical procedures. This evidence summary gives clear information on outcomes that physicians can share with their patients; however, most women quickly know what they want regarding retained products of conception. Adoption of a wait-and-see approach is common, but a substantial minority wants closure and presses for surgical therapy. Now both groups can be reassured that their choices are equally safe, and physicians can comfortably comply with their patients’ wishes.
Evidence summary
A systematic review of 18 studies, including 3 RCTs, compared outcomes for expectant management (545 women) vs surgical evacuation (1408 women) for first-trimester spontaneous abortion.1 A successful first-trimester spontaneous abortion was defined as vaginal bleeding for 3 weeks or less, fully expelled products of conception by 14 days, and no complications (infection, transfusion, uterine perforation, hospitalization, or death). Expectant management was successful in 93% overall, and 80% using only the data from RCTs.
An observational study evaluated 1096 consecutive patients with suspected first-trimester abortion, classified by ultrasound as complete, incomplete, missed, or anembryonic.2 In the latter 3 categories, patients chose expectant management (478) or immediate surgical evacuation (208). Those choosing expectant management were monitored weekly and offered surgical evacuation if their abortion was incomplete after 1 month (TABLE). Complications arose in 6 of 451 patients (1%) managed expectantly for up to 46 days, and in 5 of 208 patients (2%) managed surgically (not statistically significant). One patient in the expectant group had emergency surgery and blood transfusion.2
A smaller observational study evaluated 108 women with first-trimester missed abortions or anembryonic pregnancies who chose either expectant (85 women) or surgical management. They were followed with weekly ultrasound (including color Doppler imaging) and serum β-hCG for up to 1 month. Fifty-three (62%) completed a spontaneous abortion at 14 days and 71 (84%) at 28 days. There were no significant differences in the rate of complications.3
A prospective trial compared psychological morbidity for 86 women with ultrasound-confirmed first-trimester missed abortions, randomized to expectant or surgical management. At 2 weeks, a self-administered questionnaire about the experience of pregnancy loss found no significant difference in psychological reactions. No increase was seen in anxiety or depression symptoms between women who had miscarried and healthy nonpregnant working women aged 19 to 39 years.4
Expert opinion recommends that women with spontaneous abortion beyond 13 weeks, a temperature >100.4° F, unstable blood pressure, uncontrolled vaginal bleeding, or evidence of endometritis or pelvic inflammatory disease should have surgical evacuation.2
TABLE
Completed abortions with expectant management by type2
| TYPE OF ABORTION | TOTAL PATIENTS | ABORTION COMPLETE BY… | ||
|---|---|---|---|---|
| 7 DAYS | 14 DAYS | 46 DAYS | ||
| Incomplete | 221 (49%) | 117 (53%) | 185 (84%) | 201 (91%) |
| Missed | 138 (31%) | 41 (30%) | 81 (59%) | 105 (76%) |
| Anembryonic | 92 (20%) | 23 (25%) | 48 (52%) | 61 (66%) |
| Total | 451 (100%) | 181 (40%) | 314 (70%) | 367 (81%) |
Recommendations from others
UpToDate recommends expectant management for stable women who do not want any medical or surgical intervention, and are willing to wait for expulsion to occur. Surgical evacuation is recommended for women who are not stable because of bleeding or infection or for those who want immediate, definitive treatment of the nonviable pregnancy.5
1. Geyman JP, Oliver LM, Sullivan SD. Expectant, medical, or surgical treatment of spontaneous abortion in the first trimester of pregnancy? A pooled quantitative literature evaluation. J Am Board Fam Pract 1999;12:55-64.
2. Luise C, Jermy K, May C, Costello G, Collins WP, Bourne TH. Outcome of expectant management of spontaneous first trimester miscarriage: observational study. BMJ 2002;324:873-875.
3. Schwarzler P, Holden D, Neilsen S, Hahlin M, Sladkevicius P, Bourne TH. The conservative management of first trimester miscarriages and the use of colour Doppler sonography for patient selection. Hum Reprod 1999;14:1341-1345.
4. Nielsen S, Hahlin M, Moller A, Grandberg S. Bereavement, grieving and psychological morbidity after first trimester spontaneous abortion: comparing expectant management with surgical evacuation. Human Reproduction 1996;8:1767-1770.
5. Al-Fozan H, Tulandi T. Spontaneous abortion: management summary and recommendations. UpToDate [database]. Waltham, Mass: UpToDate; 2005.
More than 80% of women with a first-trimester spontaneous abortion have complete natural passage of tissue within 2 to 6 weeks with no higher complication rate than that from surgical intervention (strength of recommendation [SOR]: A, based on multiple randomized controlled trials [RCTs] and cohort studies). Expectant management is successful within 2 to 6 weeks without increased complications in 80% to 90% of women with first-trimester incomplete spontaneous abortion and 65% to 75% of women with first-trimester missed abortion or anembryonic gestation (presenting with spotting or bleeding and ultrasound evidence of fetal demise) (SOR: B, based on multiple cohort studies). There is no difference in short-term psychological outcomes between expectant and surgical management (SOR: B, based on RCT). Women experiencing spontaneous abortion with unstable vital signs, uncontrolled bleeding, or evidence of infection should be considered for surgical evacuation (SOR: C, expert opinion).
FPs should empathize, explain, and expedite
Paul Crawford, MD
USAF-Eglin Family Practice Residency, Eglin Air Force Base, Eglin, Fla
A spontaneous abortion can be a very distressing event for a woman and her family; and helping a patient through the complex medical and emotional issues that arise due to the miscarriage stretches the skills of a compassionate clinician. Fortunately, family physicians are ideally positioned to empathize with families, explain treatment options, and expedite medical procedures. This evidence summary gives clear information on outcomes that physicians can share with their patients; however, most women quickly know what they want regarding retained products of conception. Adoption of a wait-and-see approach is common, but a substantial minority wants closure and presses for surgical therapy. Now both groups can be reassured that their choices are equally safe, and physicians can comfortably comply with their patients’ wishes.
Evidence summary
A systematic review of 18 studies, including 3 RCTs, compared outcomes for expectant management (545 women) vs surgical evacuation (1408 women) for first-trimester spontaneous abortion.1 A successful first-trimester spontaneous abortion was defined as vaginal bleeding for 3 weeks or less, fully expelled products of conception by 14 days, and no complications (infection, transfusion, uterine perforation, hospitalization, or death). Expectant management was successful in 93% overall, and 80% using only the data from RCTs.
An observational study evaluated 1096 consecutive patients with suspected first-trimester abortion, classified by ultrasound as complete, incomplete, missed, or anembryonic.2 In the latter 3 categories, patients chose expectant management (478) or immediate surgical evacuation (208). Those choosing expectant management were monitored weekly and offered surgical evacuation if their abortion was incomplete after 1 month (TABLE). Complications arose in 6 of 451 patients (1%) managed expectantly for up to 46 days, and in 5 of 208 patients (2%) managed surgically (not statistically significant). One patient in the expectant group had emergency surgery and blood transfusion.2
A smaller observational study evaluated 108 women with first-trimester missed abortions or anembryonic pregnancies who chose either expectant (85 women) or surgical management. They were followed with weekly ultrasound (including color Doppler imaging) and serum β-hCG for up to 1 month. Fifty-three (62%) completed a spontaneous abortion at 14 days and 71 (84%) at 28 days. There were no significant differences in the rate of complications.3
A prospective trial compared psychological morbidity for 86 women with ultrasound-confirmed first-trimester missed abortions, randomized to expectant or surgical management. At 2 weeks, a self-administered questionnaire about the experience of pregnancy loss found no significant difference in psychological reactions. No increase was seen in anxiety or depression symptoms between women who had miscarried and healthy nonpregnant working women aged 19 to 39 years.4
Expert opinion recommends that women with spontaneous abortion beyond 13 weeks, a temperature >100.4° F, unstable blood pressure, uncontrolled vaginal bleeding, or evidence of endometritis or pelvic inflammatory disease should have surgical evacuation.2
TABLE
Completed abortions with expectant management by type2
| TYPE OF ABORTION | TOTAL PATIENTS | ABORTION COMPLETE BY… | ||
|---|---|---|---|---|
| 7 DAYS | 14 DAYS | 46 DAYS | ||
| Incomplete | 221 (49%) | 117 (53%) | 185 (84%) | 201 (91%) |
| Missed | 138 (31%) | 41 (30%) | 81 (59%) | 105 (76%) |
| Anembryonic | 92 (20%) | 23 (25%) | 48 (52%) | 61 (66%) |
| Total | 451 (100%) | 181 (40%) | 314 (70%) | 367 (81%) |
Recommendations from others
UpToDate recommends expectant management for stable women who do not want any medical or surgical intervention, and are willing to wait for expulsion to occur. Surgical evacuation is recommended for women who are not stable because of bleeding or infection or for those who want immediate, definitive treatment of the nonviable pregnancy.5
More than 80% of women with a first-trimester spontaneous abortion have complete natural passage of tissue within 2 to 6 weeks with no higher complication rate than that from surgical intervention (strength of recommendation [SOR]: A, based on multiple randomized controlled trials [RCTs] and cohort studies). Expectant management is successful within 2 to 6 weeks without increased complications in 80% to 90% of women with first-trimester incomplete spontaneous abortion and 65% to 75% of women with first-trimester missed abortion or anembryonic gestation (presenting with spotting or bleeding and ultrasound evidence of fetal demise) (SOR: B, based on multiple cohort studies). There is no difference in short-term psychological outcomes between expectant and surgical management (SOR: B, based on RCT). Women experiencing spontaneous abortion with unstable vital signs, uncontrolled bleeding, or evidence of infection should be considered for surgical evacuation (SOR: C, expert opinion).
FPs should empathize, explain, and expedite
Paul Crawford, MD
USAF-Eglin Family Practice Residency, Eglin Air Force Base, Eglin, Fla
A spontaneous abortion can be a very distressing event for a woman and her family; and helping a patient through the complex medical and emotional issues that arise due to the miscarriage stretches the skills of a compassionate clinician. Fortunately, family physicians are ideally positioned to empathize with families, explain treatment options, and expedite medical procedures. This evidence summary gives clear information on outcomes that physicians can share with their patients; however, most women quickly know what they want regarding retained products of conception. Adoption of a wait-and-see approach is common, but a substantial minority wants closure and presses for surgical therapy. Now both groups can be reassured that their choices are equally safe, and physicians can comfortably comply with their patients’ wishes.
Evidence summary
A systematic review of 18 studies, including 3 RCTs, compared outcomes for expectant management (545 women) vs surgical evacuation (1408 women) for first-trimester spontaneous abortion.1 A successful first-trimester spontaneous abortion was defined as vaginal bleeding for 3 weeks or less, fully expelled products of conception by 14 days, and no complications (infection, transfusion, uterine perforation, hospitalization, or death). Expectant management was successful in 93% overall, and 80% using only the data from RCTs.
An observational study evaluated 1096 consecutive patients with suspected first-trimester abortion, classified by ultrasound as complete, incomplete, missed, or anembryonic.2 In the latter 3 categories, patients chose expectant management (478) or immediate surgical evacuation (208). Those choosing expectant management were monitored weekly and offered surgical evacuation if their abortion was incomplete after 1 month (TABLE). Complications arose in 6 of 451 patients (1%) managed expectantly for up to 46 days, and in 5 of 208 patients (2%) managed surgically (not statistically significant). One patient in the expectant group had emergency surgery and blood transfusion.2
A smaller observational study evaluated 108 women with first-trimester missed abortions or anembryonic pregnancies who chose either expectant (85 women) or surgical management. They were followed with weekly ultrasound (including color Doppler imaging) and serum β-hCG for up to 1 month. Fifty-three (62%) completed a spontaneous abortion at 14 days and 71 (84%) at 28 days. There were no significant differences in the rate of complications.3
A prospective trial compared psychological morbidity for 86 women with ultrasound-confirmed first-trimester missed abortions, randomized to expectant or surgical management. At 2 weeks, a self-administered questionnaire about the experience of pregnancy loss found no significant difference in psychological reactions. No increase was seen in anxiety or depression symptoms between women who had miscarried and healthy nonpregnant working women aged 19 to 39 years.4
Expert opinion recommends that women with spontaneous abortion beyond 13 weeks, a temperature >100.4° F, unstable blood pressure, uncontrolled vaginal bleeding, or evidence of endometritis or pelvic inflammatory disease should have surgical evacuation.2
TABLE
Completed abortions with expectant management by type2
| TYPE OF ABORTION | TOTAL PATIENTS | ABORTION COMPLETE BY… | ||
|---|---|---|---|---|
| 7 DAYS | 14 DAYS | 46 DAYS | ||
| Incomplete | 221 (49%) | 117 (53%) | 185 (84%) | 201 (91%) |
| Missed | 138 (31%) | 41 (30%) | 81 (59%) | 105 (76%) |
| Anembryonic | 92 (20%) | 23 (25%) | 48 (52%) | 61 (66%) |
| Total | 451 (100%) | 181 (40%) | 314 (70%) | 367 (81%) |
Recommendations from others
UpToDate recommends expectant management for stable women who do not want any medical or surgical intervention, and are willing to wait for expulsion to occur. Surgical evacuation is recommended for women who are not stable because of bleeding or infection or for those who want immediate, definitive treatment of the nonviable pregnancy.5
1. Geyman JP, Oliver LM, Sullivan SD. Expectant, medical, or surgical treatment of spontaneous abortion in the first trimester of pregnancy? A pooled quantitative literature evaluation. J Am Board Fam Pract 1999;12:55-64.
2. Luise C, Jermy K, May C, Costello G, Collins WP, Bourne TH. Outcome of expectant management of spontaneous first trimester miscarriage: observational study. BMJ 2002;324:873-875.
3. Schwarzler P, Holden D, Neilsen S, Hahlin M, Sladkevicius P, Bourne TH. The conservative management of first trimester miscarriages and the use of colour Doppler sonography for patient selection. Hum Reprod 1999;14:1341-1345.
4. Nielsen S, Hahlin M, Moller A, Grandberg S. Bereavement, grieving and psychological morbidity after first trimester spontaneous abortion: comparing expectant management with surgical evacuation. Human Reproduction 1996;8:1767-1770.
5. Al-Fozan H, Tulandi T. Spontaneous abortion: management summary and recommendations. UpToDate [database]. Waltham, Mass: UpToDate; 2005.
1. Geyman JP, Oliver LM, Sullivan SD. Expectant, medical, or surgical treatment of spontaneous abortion in the first trimester of pregnancy? A pooled quantitative literature evaluation. J Am Board Fam Pract 1999;12:55-64.
2. Luise C, Jermy K, May C, Costello G, Collins WP, Bourne TH. Outcome of expectant management of spontaneous first trimester miscarriage: observational study. BMJ 2002;324:873-875.
3. Schwarzler P, Holden D, Neilsen S, Hahlin M, Sladkevicius P, Bourne TH. The conservative management of first trimester miscarriages and the use of colour Doppler sonography for patient selection. Hum Reprod 1999;14:1341-1345.
4. Nielsen S, Hahlin M, Moller A, Grandberg S. Bereavement, grieving and psychological morbidity after first trimester spontaneous abortion: comparing expectant management with surgical evacuation. Human Reproduction 1996;8:1767-1770.
5. Al-Fozan H, Tulandi T. Spontaneous abortion: management summary and recommendations. UpToDate [database]. Waltham, Mass: UpToDate; 2005.
Evidence-based answers from the Family Physicians Inquiries Network
What is the initial work-up in the diagnosis of hypertension?
Patients with a new diagnosis of hypertension should be evaluated with a history and physical exam and the following initial studies: serum potassium and creatinine, fasting serum glucose and lipid panel, hematocrit, urinalysis, and electrocardiogram (strength of recommendation [SOR]: C, based on a consensus of expert opinion). Consensus is lacking for measuring serum sodium, calcium, and uric acid.
Testing for microalbuminuria is optional in the work-up for a patient without diabetes (SOR: C, expert consensus). Some expert panels list limited echocardiography as another option.
Not all recommendations for working-up hypertensive patients are cost-effective
Brian Crownover, MD, FAAFP
96th Medical Group, Family Medicine Residency, Eglin Air Force Base, Eglin, Fla
There is obvious enthusiasm among the expert panels for a detailed workup of patients with hypertension. But are the recommendations cost-effective? Annual urine dipstick testing beginning at age 30 for hypertensive patients is highly cost-effective. Identification of proteinuria and treatment with an ACE inhibitor or angiotensin receptor blocker prevents the progression of renal disease at a quality-adjusted life-year cost of $15,484 to $26,320, depending on the age group.1 Unfortunately, evaluation for secondary causes of hypertension, screening for LVH, and ruling out comorbidities have not been explicitly evaluated for cost-effectiveness.
Evidence summary
There are currently no large outcome studies evaluating the initial work-up of hypertension; however, 4 international expert panels have published recommendations.2-5 These panels advise 3 initial objectives: 1) assess lifestyle and identify other cardiovascular risk factors or concomitant disorders that may affect prognosis and guide treatment; 2) search for treatable causes of high blood pressure; and 3) assess for the presence of target organ damage that would change the management of the patient (such as chronic kidney disease or heart disease).
In addition to a thorough history and physical, the following studies are recommended for patients with newly diagnosed hypertension:
Serum potassium and creatinine. All 4 panels recommend measuring serum potassium and creatinine in order to: 1) monitor the effects of diuretics and angiotensin-converting enzyme (ACE) inhibitors used in hypertension therapy, 2) screen for unexplained hypokalemia that may indicate a low-renin form of hypertension, 3) calculate baseline creatinine clearance, and 4) screen for chronic kidney disease.
Fasting blood glucose. All 4 panels recommend measuring a fasting glucose level to screen for diabetes. An abnormal glucose level may also reveal glucose intolerance, one of the diagnostic criteria of metabolic syndrome. Up to 60% of patients with diabetes also have hypertension.6
Fasting lipid panel. All 4 expert panels recommend screening for dyslipidemia with a fasting lipid panel to assess cardiovascular risk. A cohort study evaluating 356,222 men aged 35 to 57 years found a continuous, positive, graded correlation between plasma cholesterol levels and coronary risk.7
Hematocrit. All 4 panels recommend a hematocrit to screen for anemia, which may be due to chronic kidney disease.
Urinalysis. All 4 panels recommend a urinalysis to screen for renal disease.
Electrocardiogram (ECG). All 4 panels recommend an ECG to screen for findings associated with hypertension, including left ventricular hypertrophy (LVH), myocardial infarction, and rhythm abnormalities. A cohort study followed 2363 patients for 14 years who had untreated hypertension and were without pre-existing cardiovascular disease. After controlling for age, sex, diabetes, and mean blood pressure, LVH by ECG conferred a significant increased risk for cerebrovascular events (relative risk=1.79; 95% confidence interval [CI], 1.17–2.76).8 However, in a cohort of 4684 subjects from the Framingham Heart Study, ECG had a sensitivity of only 6.9% for the detection of LVH (specificity 98.8%; positive likelihood ratio=5.3; negative likelihood ratio=0.94).8
Echocardiography. Two panels3,4 and an online text10 recommend echocardiography, preferably limited echo, as an optional study. A systematic review of studies comparing the sensitivities and specificities of ECG and echo found that each was highly specific for the detection of LVH (77%–97%), but the sensitivity of echocardiography (88%–93%) exceeded that of ECG (21%–54%). However, LVH detected by ECG is a better predictor of cardiovascular complications.11 Because echocardiography may help assess disease duration and guide management, both panels recommend it for patients with severe or refractory hypertension but without other target organ damage.
Microalbuminuria. All panels listed microalbuminuria testing as an optional study for patients without diabetes because of its association with an increased incidence of cerebrovascular disease.12 It is unclear whether microalbuminuria results from the increased intraglomerular pressure in hypertension or if it represents glomerular damage.13
Sodium, calcium, uric acid. There is no consensus on the routine inclusion of several studies: serum sodium (recommended by 2 panels and an online text4,5,10 ), serum calcium (recommended by 1 panel and the text2,10), and uric acid (1 panel3 recommends it while the text10 lists it as optional).
Recommendations from others
Recommendations from major organizations are included in Evidence Summary, above.
Acknowledgments
The opinions and assertions contained herein are the private views of the author and are not to be construed as official, or as reflecting the views of the US Air Force Medical Service or the US Air Force at large.
1. Boulware LE, Jaar BG, Tarver-Carr ME, Brancati FL, Powe NR. Screening for proteinuria in US adults. A cost-effective analysis. JAMA 2003;290:3101-3114.
2. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42:1206-1252.
3. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens 2003;21:1011-1053.
4. Hemmelgarn BR, Zarnke KB, Campbell NRC, et al. The 2004 Canadian Hypertension Education Program recommendations for the management of hypertension: Part I—Blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol 2004;20:31-40.
5. Institute for Clinical Systems Improvement (ICSI). Hypertension Diagnosis and Treatment. Bloomington, Minn: ICSI; 2004.
6. Arauz-Pacheco C, Parrott MA, Raskin P. The treatment of hypertension in adult patients with diabetes. Diabetes Care 2002;25:134-147.
7. Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in the 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986;256:2823-2828.
8. Verdecchia P, Porcellati C, Ambrosio G, et al. Left Ventricular Hypertrophy as an independent predictor of acute cerebrovascular events inessential hypertension. Circulation 2001;104:2039-2044.
9. Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP. Determinants of sensitivity and specificity of electrocardiographic criteria for left ventricular hypertrophy. Circulation 1990;81:815-820.
10. Kaplan NM. Initial evaluation of the hypertensive patient. UpToDate Monograph. Available at www.uptodate.com.
11. Dijkstra RF, van Schayck CP, Bakx JC, Thien T, Verheugt FW, Mokkink HG. Left ventricular hypertrophy; differences in the diagnostic and prognostic value of electrocardiography and echocardiography. Ned Tijdschr Geneeskd 1997;141:1969-1972.
12. Gerstein HC, Mann JF, Yi Q, Yusuf S, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA 2001;286:421-426.
13. Rosa TT, Palatini P. Clinical value of microalbuminuria in hypertension. J Hypertens 2000;18:645-654.
Patients with a new diagnosis of hypertension should be evaluated with a history and physical exam and the following initial studies: serum potassium and creatinine, fasting serum glucose and lipid panel, hematocrit, urinalysis, and electrocardiogram (strength of recommendation [SOR]: C, based on a consensus of expert opinion). Consensus is lacking for measuring serum sodium, calcium, and uric acid.
Testing for microalbuminuria is optional in the work-up for a patient without diabetes (SOR: C, expert consensus). Some expert panels list limited echocardiography as another option.
Not all recommendations for working-up hypertensive patients are cost-effective
Brian Crownover, MD, FAAFP
96th Medical Group, Family Medicine Residency, Eglin Air Force Base, Eglin, Fla
There is obvious enthusiasm among the expert panels for a detailed workup of patients with hypertension. But are the recommendations cost-effective? Annual urine dipstick testing beginning at age 30 for hypertensive patients is highly cost-effective. Identification of proteinuria and treatment with an ACE inhibitor or angiotensin receptor blocker prevents the progression of renal disease at a quality-adjusted life-year cost of $15,484 to $26,320, depending on the age group.1 Unfortunately, evaluation for secondary causes of hypertension, screening for LVH, and ruling out comorbidities have not been explicitly evaluated for cost-effectiveness.
Evidence summary
There are currently no large outcome studies evaluating the initial work-up of hypertension; however, 4 international expert panels have published recommendations.2-5 These panels advise 3 initial objectives: 1) assess lifestyle and identify other cardiovascular risk factors or concomitant disorders that may affect prognosis and guide treatment; 2) search for treatable causes of high blood pressure; and 3) assess for the presence of target organ damage that would change the management of the patient (such as chronic kidney disease or heart disease).
In addition to a thorough history and physical, the following studies are recommended for patients with newly diagnosed hypertension:
Serum potassium and creatinine. All 4 panels recommend measuring serum potassium and creatinine in order to: 1) monitor the effects of diuretics and angiotensin-converting enzyme (ACE) inhibitors used in hypertension therapy, 2) screen for unexplained hypokalemia that may indicate a low-renin form of hypertension, 3) calculate baseline creatinine clearance, and 4) screen for chronic kidney disease.
Fasting blood glucose. All 4 panels recommend measuring a fasting glucose level to screen for diabetes. An abnormal glucose level may also reveal glucose intolerance, one of the diagnostic criteria of metabolic syndrome. Up to 60% of patients with diabetes also have hypertension.6
Fasting lipid panel. All 4 expert panels recommend screening for dyslipidemia with a fasting lipid panel to assess cardiovascular risk. A cohort study evaluating 356,222 men aged 35 to 57 years found a continuous, positive, graded correlation between plasma cholesterol levels and coronary risk.7
Hematocrit. All 4 panels recommend a hematocrit to screen for anemia, which may be due to chronic kidney disease.
Urinalysis. All 4 panels recommend a urinalysis to screen for renal disease.
Electrocardiogram (ECG). All 4 panels recommend an ECG to screen for findings associated with hypertension, including left ventricular hypertrophy (LVH), myocardial infarction, and rhythm abnormalities. A cohort study followed 2363 patients for 14 years who had untreated hypertension and were without pre-existing cardiovascular disease. After controlling for age, sex, diabetes, and mean blood pressure, LVH by ECG conferred a significant increased risk for cerebrovascular events (relative risk=1.79; 95% confidence interval [CI], 1.17–2.76).8 However, in a cohort of 4684 subjects from the Framingham Heart Study, ECG had a sensitivity of only 6.9% for the detection of LVH (specificity 98.8%; positive likelihood ratio=5.3; negative likelihood ratio=0.94).8
Echocardiography. Two panels3,4 and an online text10 recommend echocardiography, preferably limited echo, as an optional study. A systematic review of studies comparing the sensitivities and specificities of ECG and echo found that each was highly specific for the detection of LVH (77%–97%), but the sensitivity of echocardiography (88%–93%) exceeded that of ECG (21%–54%). However, LVH detected by ECG is a better predictor of cardiovascular complications.11 Because echocardiography may help assess disease duration and guide management, both panels recommend it for patients with severe or refractory hypertension but without other target organ damage.
Microalbuminuria. All panels listed microalbuminuria testing as an optional study for patients without diabetes because of its association with an increased incidence of cerebrovascular disease.12 It is unclear whether microalbuminuria results from the increased intraglomerular pressure in hypertension or if it represents glomerular damage.13
Sodium, calcium, uric acid. There is no consensus on the routine inclusion of several studies: serum sodium (recommended by 2 panels and an online text4,5,10 ), serum calcium (recommended by 1 panel and the text2,10), and uric acid (1 panel3 recommends it while the text10 lists it as optional).
Recommendations from others
Recommendations from major organizations are included in Evidence Summary, above.
Acknowledgments
The opinions and assertions contained herein are the private views of the author and are not to be construed as official, or as reflecting the views of the US Air Force Medical Service or the US Air Force at large.
Patients with a new diagnosis of hypertension should be evaluated with a history and physical exam and the following initial studies: serum potassium and creatinine, fasting serum glucose and lipid panel, hematocrit, urinalysis, and electrocardiogram (strength of recommendation [SOR]: C, based on a consensus of expert opinion). Consensus is lacking for measuring serum sodium, calcium, and uric acid.
Testing for microalbuminuria is optional in the work-up for a patient without diabetes (SOR: C, expert consensus). Some expert panels list limited echocardiography as another option.
Not all recommendations for working-up hypertensive patients are cost-effective
Brian Crownover, MD, FAAFP
96th Medical Group, Family Medicine Residency, Eglin Air Force Base, Eglin, Fla
There is obvious enthusiasm among the expert panels for a detailed workup of patients with hypertension. But are the recommendations cost-effective? Annual urine dipstick testing beginning at age 30 for hypertensive patients is highly cost-effective. Identification of proteinuria and treatment with an ACE inhibitor or angiotensin receptor blocker prevents the progression of renal disease at a quality-adjusted life-year cost of $15,484 to $26,320, depending on the age group.1 Unfortunately, evaluation for secondary causes of hypertension, screening for LVH, and ruling out comorbidities have not been explicitly evaluated for cost-effectiveness.
Evidence summary
There are currently no large outcome studies evaluating the initial work-up of hypertension; however, 4 international expert panels have published recommendations.2-5 These panels advise 3 initial objectives: 1) assess lifestyle and identify other cardiovascular risk factors or concomitant disorders that may affect prognosis and guide treatment; 2) search for treatable causes of high blood pressure; and 3) assess for the presence of target organ damage that would change the management of the patient (such as chronic kidney disease or heart disease).
In addition to a thorough history and physical, the following studies are recommended for patients with newly diagnosed hypertension:
Serum potassium and creatinine. All 4 panels recommend measuring serum potassium and creatinine in order to: 1) monitor the effects of diuretics and angiotensin-converting enzyme (ACE) inhibitors used in hypertension therapy, 2) screen for unexplained hypokalemia that may indicate a low-renin form of hypertension, 3) calculate baseline creatinine clearance, and 4) screen for chronic kidney disease.
Fasting blood glucose. All 4 panels recommend measuring a fasting glucose level to screen for diabetes. An abnormal glucose level may also reveal glucose intolerance, one of the diagnostic criteria of metabolic syndrome. Up to 60% of patients with diabetes also have hypertension.6
Fasting lipid panel. All 4 expert panels recommend screening for dyslipidemia with a fasting lipid panel to assess cardiovascular risk. A cohort study evaluating 356,222 men aged 35 to 57 years found a continuous, positive, graded correlation between plasma cholesterol levels and coronary risk.7
Hematocrit. All 4 panels recommend a hematocrit to screen for anemia, which may be due to chronic kidney disease.
Urinalysis. All 4 panels recommend a urinalysis to screen for renal disease.
Electrocardiogram (ECG). All 4 panels recommend an ECG to screen for findings associated with hypertension, including left ventricular hypertrophy (LVH), myocardial infarction, and rhythm abnormalities. A cohort study followed 2363 patients for 14 years who had untreated hypertension and were without pre-existing cardiovascular disease. After controlling for age, sex, diabetes, and mean blood pressure, LVH by ECG conferred a significant increased risk for cerebrovascular events (relative risk=1.79; 95% confidence interval [CI], 1.17–2.76).8 However, in a cohort of 4684 subjects from the Framingham Heart Study, ECG had a sensitivity of only 6.9% for the detection of LVH (specificity 98.8%; positive likelihood ratio=5.3; negative likelihood ratio=0.94).8
Echocardiography. Two panels3,4 and an online text10 recommend echocardiography, preferably limited echo, as an optional study. A systematic review of studies comparing the sensitivities and specificities of ECG and echo found that each was highly specific for the detection of LVH (77%–97%), but the sensitivity of echocardiography (88%–93%) exceeded that of ECG (21%–54%). However, LVH detected by ECG is a better predictor of cardiovascular complications.11 Because echocardiography may help assess disease duration and guide management, both panels recommend it for patients with severe or refractory hypertension but without other target organ damage.
Microalbuminuria. All panels listed microalbuminuria testing as an optional study for patients without diabetes because of its association with an increased incidence of cerebrovascular disease.12 It is unclear whether microalbuminuria results from the increased intraglomerular pressure in hypertension or if it represents glomerular damage.13
Sodium, calcium, uric acid. There is no consensus on the routine inclusion of several studies: serum sodium (recommended by 2 panels and an online text4,5,10 ), serum calcium (recommended by 1 panel and the text2,10), and uric acid (1 panel3 recommends it while the text10 lists it as optional).
Recommendations from others
Recommendations from major organizations are included in Evidence Summary, above.
Acknowledgments
The opinions and assertions contained herein are the private views of the author and are not to be construed as official, or as reflecting the views of the US Air Force Medical Service or the US Air Force at large.
1. Boulware LE, Jaar BG, Tarver-Carr ME, Brancati FL, Powe NR. Screening for proteinuria in US adults. A cost-effective analysis. JAMA 2003;290:3101-3114.
2. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42:1206-1252.
3. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens 2003;21:1011-1053.
4. Hemmelgarn BR, Zarnke KB, Campbell NRC, et al. The 2004 Canadian Hypertension Education Program recommendations for the management of hypertension: Part I—Blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol 2004;20:31-40.
5. Institute for Clinical Systems Improvement (ICSI). Hypertension Diagnosis and Treatment. Bloomington, Minn: ICSI; 2004.
6. Arauz-Pacheco C, Parrott MA, Raskin P. The treatment of hypertension in adult patients with diabetes. Diabetes Care 2002;25:134-147.
7. Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in the 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986;256:2823-2828.
8. Verdecchia P, Porcellati C, Ambrosio G, et al. Left Ventricular Hypertrophy as an independent predictor of acute cerebrovascular events inessential hypertension. Circulation 2001;104:2039-2044.
9. Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP. Determinants of sensitivity and specificity of electrocardiographic criteria for left ventricular hypertrophy. Circulation 1990;81:815-820.
10. Kaplan NM. Initial evaluation of the hypertensive patient. UpToDate Monograph. Available at www.uptodate.com.
11. Dijkstra RF, van Schayck CP, Bakx JC, Thien T, Verheugt FW, Mokkink HG. Left ventricular hypertrophy; differences in the diagnostic and prognostic value of electrocardiography and echocardiography. Ned Tijdschr Geneeskd 1997;141:1969-1972.
12. Gerstein HC, Mann JF, Yi Q, Yusuf S, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA 2001;286:421-426.
13. Rosa TT, Palatini P. Clinical value of microalbuminuria in hypertension. J Hypertens 2000;18:645-654.
1. Boulware LE, Jaar BG, Tarver-Carr ME, Brancati FL, Powe NR. Screening for proteinuria in US adults. A cost-effective analysis. JAMA 2003;290:3101-3114.
2. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42:1206-1252.
3. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens 2003;21:1011-1053.
4. Hemmelgarn BR, Zarnke KB, Campbell NRC, et al. The 2004 Canadian Hypertension Education Program recommendations for the management of hypertension: Part I—Blood pressure measurement, diagnosis and assessment of risk. Can J Cardiol 2004;20:31-40.
5. Institute for Clinical Systems Improvement (ICSI). Hypertension Diagnosis and Treatment. Bloomington, Minn: ICSI; 2004.
6. Arauz-Pacheco C, Parrott MA, Raskin P. The treatment of hypertension in adult patients with diabetes. Diabetes Care 2002;25:134-147.
7. Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in the 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986;256:2823-2828.
8. Verdecchia P, Porcellati C, Ambrosio G, et al. Left Ventricular Hypertrophy as an independent predictor of acute cerebrovascular events inessential hypertension. Circulation 2001;104:2039-2044.
9. Levy D, Labib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP. Determinants of sensitivity and specificity of electrocardiographic criteria for left ventricular hypertrophy. Circulation 1990;81:815-820.
10. Kaplan NM. Initial evaluation of the hypertensive patient. UpToDate Monograph. Available at www.uptodate.com.
11. Dijkstra RF, van Schayck CP, Bakx JC, Thien T, Verheugt FW, Mokkink HG. Left ventricular hypertrophy; differences in the diagnostic and prognostic value of electrocardiography and echocardiography. Ned Tijdschr Geneeskd 1997;141:1969-1972.
12. Gerstein HC, Mann JF, Yi Q, Yusuf S, et al. Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA 2001;286:421-426.
13. Rosa TT, Palatini P. Clinical value of microalbuminuria in hypertension. J Hypertens 2000;18:645-654.
Evidence-based answers from the Family Physicians Inquiries Network