User login
Fewer nocturnal hypoglycemia episodes with insulin degludec
PHOENIX – Patients with type 1 diabetes who received high doses of once-daily insulin degludec had fewer episodes of nocturnal hypoglycemia compared with those who received a similar dose of insulin glargine, a meta-analysis of two randomized trials has shown.
"The issue is of particular concern in patients with high BMIs," said Dr. Helena Rodbard, who presented the unpublished study at the annual meeting of the American Association of Clinical Endocrinologists.

Insulin degludec is a new basal insulin with an ultralong and stable glucose-lowering effect. A previous prospective meta-analysis of phase IIIa trials comparing insulin degludec with insulin glargine showed that patients with type 1 diabetes who were on degludec had a statistically significant, 17% lower rate of nocturnal hypoglycemia across the entire treatment period and a 25% lower rate during the maintenance period (16 weeks onward), compared with those who took glargine (Diabetes Obes. Metab. 2013;15:175-84).
In their post-hoc meta-analysis, Dr. Rodbard and her colleagues compared the hypoglycemia rates for a subset of type 1 diabetes patients who required high doses of either degludec or glargine in two published trials (Lancet 2012;379:1489-97; J. Clin. Endocrinol. Metab. 2013;98:1154-62).
Nearly 25% of the patients – 235 out of a total of 950 patients in the two trials – received an end-of-trial basal insulin dose of more than 0.45 U/kg and were included in the meta-analysis.
The results showed that compared with glargine, degludec was associated with significantly lower rates of nocturnal confirmed hypoglycemia, by 36% in the full trial period (risk ratio [RR], 0.64) and by 44% in the maintenance period (RR, 0.56).
"Since patients taking higher doses of basal insulin have a longer duration of action than that seen in patients taking small doses of basal insulin, it is apparent that duration of action does not explain the benefit observed with insulin degludec," said Dr. Alan J. Garber, professor of medicine, biochemistry and molecular biology, and molecular and cellular biology at Baylor College of Medicine, Houston, and the immediate past president of the AACE. "Instead, the other dose-related characteristic of basal insulin, namely the [maximum serum concentration] of insulin, seems to explain this finding. Thus, if one basal insulin has a greater peak effect than another, it will have a greater hypoglycemic potential at higher as compared to lower doses. That is what we saw here and therefore explains the finding, owing most likely to the more definable peak of glargine compared to degludec." Dr. Garber was not involved in the study.

Meanwhile, the mean end-of-trial basal insulin dose was similar for degludec (0.63 U/kg) and glargine (0.65 U/kg). Patients also had similar mean end-of-trial hemoglobin A1c values with degludec and glargine, at 7.41% and 7.55%, respectively.
The mean end-of-trial fasting plasma glucose levels were comparable between degludec (133 mg/dL) and glargine (136 mg/dL), at 133 mg/dL and 136 mg/dL. Also, rates of overall confirmed hypoglycemia (plasma glucose less than 56 mg/dL) did not differ significantly between the two insulins in either the full trial period or the maintenance period.
"These findings are consistent with results for the overall study population, confirming that [insulin degludec] is a well tolerated and effective basal insulin choice for patients with [type 1 diabetes] across the spectrum of insulin requirements," said Dr. Rodbard.
Dr. Rodbard is an adviser and speaker for, and has receiving research support from, several companies including AstraZeneca, Blondel, Eli Lily, Merck, Novo Nordisk, and Sanofi. Dr. Garber is a consultant/advisory board member, and/or is on the speakers bureaus, for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
PHOENIX – Patients with type 1 diabetes who received high doses of once-daily insulin degludec had fewer episodes of nocturnal hypoglycemia compared with those who received a similar dose of insulin glargine, a meta-analysis of two randomized trials has shown.
"The issue is of particular concern in patients with high BMIs," said Dr. Helena Rodbard, who presented the unpublished study at the annual meeting of the American Association of Clinical Endocrinologists.
Insulin degludec is a new basal insulin with an ultralong and stable glucose-lowering effect. A previous prospective meta-analysis of phase IIIa trials comparing insulin degludec with insulin glargine showed that patients with type 1 diabetes who were on degludec had a statistically significant, 17% lower rate of nocturnal hypoglycemia across the entire treatment period and a 25% lower rate during the maintenance period (16 weeks onward), compared with those who took glargine (Diabetes Obes. Metab. 2013;15:175-84).
In their post-hoc meta-analysis, Dr. Rodbard and her colleagues compared the hypoglycemia rates for a subset of type 1 diabetes patients who required high doses of either degludec or glargine in two published trials (Lancet 2012;379:1489-97; J. Clin. Endocrinol. Metab. 2013;98:1154-62).
Nearly 25% of the patients – 235 out of a total of 950 patients in the two trials – received an end-of-trial basal insulin dose of more than 0.45 U/kg and were included in the meta-analysis.
The results showed that compared with glargine, degludec was associated with significantly lower rates of nocturnal confirmed hypoglycemia, by 36% in the full trial period (risk ratio [RR], 0.64) and by 44% in the maintenance period (RR, 0.56).
"Since patients taking higher doses of basal insulin have a longer duration of action than that seen in patients taking small doses of basal insulin, it is apparent that duration of action does not explain the benefit observed with insulin degludec," said Dr. Alan J. Garber, professor of medicine, biochemistry and molecular biology, and molecular and cellular biology at Baylor College of Medicine, Houston, and the immediate past president of the AACE. "Instead, the other dose-related characteristic of basal insulin, namely the [maximum serum concentration] of insulin, seems to explain this finding. Thus, if one basal insulin has a greater peak effect than another, it will have a greater hypoglycemic potential at higher as compared to lower doses. That is what we saw here and therefore explains the finding, owing most likely to the more definable peak of glargine compared to degludec." Dr. Garber was not involved in the study.
Meanwhile, the mean end-of-trial basal insulin dose was similar for degludec (0.63 U/kg) and glargine (0.65 U/kg). Patients also had similar mean end-of-trial hemoglobin A1c values with degludec and glargine, at 7.41% and 7.55%, respectively.
The mean end-of-trial fasting plasma glucose levels were comparable between degludec (133 mg/dL) and glargine (136 mg/dL), at 133 mg/dL and 136 mg/dL. Also, rates of overall confirmed hypoglycemia (plasma glucose less than 56 mg/dL) did not differ significantly between the two insulins in either the full trial period or the maintenance period.
"These findings are consistent with results for the overall study population, confirming that [insulin degludec] is a well tolerated and effective basal insulin choice for patients with [type 1 diabetes] across the spectrum of insulin requirements," said Dr. Rodbard.
Dr. Rodbard is an adviser and speaker for, and has receiving research support from, several companies including AstraZeneca, Blondel, Eli Lily, Merck, Novo Nordisk, and Sanofi. Dr. Garber is a consultant/advisory board member, and/or is on the speakers bureaus, for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
PHOENIX – Patients with type 1 diabetes who received high doses of once-daily insulin degludec had fewer episodes of nocturnal hypoglycemia compared with those who received a similar dose of insulin glargine, a meta-analysis of two randomized trials has shown.
"The issue is of particular concern in patients with high BMIs," said Dr. Helena Rodbard, who presented the unpublished study at the annual meeting of the American Association of Clinical Endocrinologists.
Insulin degludec is a new basal insulin with an ultralong and stable glucose-lowering effect. A previous prospective meta-analysis of phase IIIa trials comparing insulin degludec with insulin glargine showed that patients with type 1 diabetes who were on degludec had a statistically significant, 17% lower rate of nocturnal hypoglycemia across the entire treatment period and a 25% lower rate during the maintenance period (16 weeks onward), compared with those who took glargine (Diabetes Obes. Metab. 2013;15:175-84).
In their post-hoc meta-analysis, Dr. Rodbard and her colleagues compared the hypoglycemia rates for a subset of type 1 diabetes patients who required high doses of either degludec or glargine in two published trials (Lancet 2012;379:1489-97; J. Clin. Endocrinol. Metab. 2013;98:1154-62).
Nearly 25% of the patients – 235 out of a total of 950 patients in the two trials – received an end-of-trial basal insulin dose of more than 0.45 U/kg and were included in the meta-analysis.
The results showed that compared with glargine, degludec was associated with significantly lower rates of nocturnal confirmed hypoglycemia, by 36% in the full trial period (risk ratio [RR], 0.64) and by 44% in the maintenance period (RR, 0.56).
"Since patients taking higher doses of basal insulin have a longer duration of action than that seen in patients taking small doses of basal insulin, it is apparent that duration of action does not explain the benefit observed with insulin degludec," said Dr. Alan J. Garber, professor of medicine, biochemistry and molecular biology, and molecular and cellular biology at Baylor College of Medicine, Houston, and the immediate past president of the AACE. "Instead, the other dose-related characteristic of basal insulin, namely the [maximum serum concentration] of insulin, seems to explain this finding. Thus, if one basal insulin has a greater peak effect than another, it will have a greater hypoglycemic potential at higher as compared to lower doses. That is what we saw here and therefore explains the finding, owing most likely to the more definable peak of glargine compared to degludec." Dr. Garber was not involved in the study.
Meanwhile, the mean end-of-trial basal insulin dose was similar for degludec (0.63 U/kg) and glargine (0.65 U/kg). Patients also had similar mean end-of-trial hemoglobin A1c values with degludec and glargine, at 7.41% and 7.55%, respectively.
The mean end-of-trial fasting plasma glucose levels were comparable between degludec (133 mg/dL) and glargine (136 mg/dL), at 133 mg/dL and 136 mg/dL. Also, rates of overall confirmed hypoglycemia (plasma glucose less than 56 mg/dL) did not differ significantly between the two insulins in either the full trial period or the maintenance period.
"These findings are consistent with results for the overall study population, confirming that [insulin degludec] is a well tolerated and effective basal insulin choice for patients with [type 1 diabetes] across the spectrum of insulin requirements," said Dr. Rodbard.
Dr. Rodbard is an adviser and speaker for, and has receiving research support from, several companies including AstraZeneca, Blondel, Eli Lily, Merck, Novo Nordisk, and Sanofi. Dr. Garber is a consultant/advisory board member, and/or is on the speakers bureaus, for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
AT THE AACE ANNUAL MEETING
Major finding: Compared with insulin glargine, insulin degludec was associated with significantly lower rates of nocturnal confirmed hypoglycemia – by 36% in the full trial period and by 44% in the maintenance period.
Data source: A post-hoc meta-analysis of two published trials comparing the hypoglycemia rates of a subset of type 1 diabetes patients who required high doses of either insulin degludec or insulin glargine.
Disclosures: Dr. Rodbard is an adviser and speaker for, and has received research support from, several companies including AstraZeneka, Blondel, Eli Lily, Merck, Novo Nordisk, and Sanofi. Dr. Garber is a consultant/advisory board member, and/or is on the speakers bureaus, for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.

Newcomer canagliflozin improves beta-cell function in type 2 diabetes
PHOENIX – The recently approved diabetes drug canagliflozin improved beta-cell function in patients with advanced type 2 diabetes inadequately controlled with metformin plus sulfonylurea, according to a phase III study.
Although some of the changes did not reach statistical significance, the mean value of all calculated measures of beta-cell function increased with two different canagliflozin doses, compared with placebo, the randomized, double-blind placebo-controlled study showed.
The finding is promising, said David Polidori, Ph.D., an employee of Janssen Research and Development, who presented the abstract at the annual meeting of the American Association of Clinical Endocrinologists.
Canagliflozin is a sodium glucose cotransporter 2 (SGLT2) inhibitor, which lowers plasma glucose by a renal mechanism. It also reduces the fasting and postprandial glucose hemoglobin A1c levels.

Several animal studies have shown beneficial effects of SGLT2 inhibition on beta-cell mass or function. Other clinical studies have shown improvements in measures of beta-cell function with canagliflozin, including a 26-week phase III study with the drug as monotherapy, said Dr. Polidori. But it is not clear exactly how canagliflozin improves beta-cell function. "It may be due to the glucose toxicity. Or it may also be due to reducing the load on beta cells, the so-called unloading," he said.
The improvement in beta-cell function is worthwhile, said Dr. Alan Garber, outgoing AACE president, and professor of medicine, biochemistry, and molecular biology and molecular and cellular biology at Baylor College, Houston. "But it’s not unique to this drug."
Although both canagliflozin doses were generally well tolerated, patients in treatment groups reported higher rates of genital mycotic infections, urinary tract infections, and adverse events related to osmotic diuresis, compared with placebo. The adverse events led to few study discontinuations, said Dr. Polidori.
The SGLT2 class of drugs has been included in the recently updated AACE diabetes management algorithm, but with a note to use with caution. Dr. Garber, chair of the algorithm task force, said that the 10% risk of vulvovaginitis in women and 1% balanitis in men are not minor concerns to some patients, especially those at risk of recurrence. For men, balanitis means a trip to the emergency department, he said, "So a 1% risk requires a little bit of forethought on the part of the clinician before prescribing in at-risk patients for recurrence."
To assess the effect of canagliflozin on beta-cell function as an add-on therapy in patients with type 2 diabetes on metformin plus sulfonylurea, researchers conducted a 26-week study comparing patients on 100 mg and 300 mg of daily canaglifozin with placebo.
The study included 469 patients. A subset of them (168 patients) was given a meal tolerance test on day 1 and week 26. Their liquid meal contained 700 kcal and 100 g of glucose. Patients had a mean age of 57 years, an average HbA1c level of 8%, a body mass index of 33 kg/m2, and type 2 diabetes for an average of 10 years.
Their plasma glucose and serum C-peptide levels were measured at seven time points over a period of 3 hours.
Results showed that the mean ratio of C-peptide area under the curve (AUCc) to glucose (AUCg) increased by a mean of roughly 20% from a baseline of 132 with the 100-mg dosage and 123 with the 300-mg dosage to 160 and 152, respectively, at week 26. There was a small decrease of 3.4% in the placebo group. There was a roughly 27% difference between the canagliflozin and placebo groups that did not reach statistical significance (100 mg, P = .051; 300 mg, P = .056)
The mean insulin secretion rate at 9 mM glucose at week 26 increased significantly in the treatment groups, compared with a 12.2% decrease in the placebo group. There was a 55% difference from placebo in the 100-mg canagliflozin group (P = .02) and a 70% difference in the 300-mg (P = .007) canagliflozin group.
The mean beta-cell glucose sensitivity increased by roughly 20% from baseline in both treatment groups, but the increases were not statistically significant.
"This is 26-week data. It will be interesting to see longer-term data, and to see if this type of treatment can better prolong beta-cell function and hopefully slow the rate of progression of type 2 diabetes," said Dr. Polidori.
Dr. Polidori is an employee of Janssen Research and Development, which funded and supported the study. Dr. Garber is a consultant/advisory board member and/or is on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
PHOENIX – The recently approved diabetes drug canagliflozin improved beta-cell function in patients with advanced type 2 diabetes inadequately controlled with metformin plus sulfonylurea, according to a phase III study.
Although some of the changes did not reach statistical significance, the mean value of all calculated measures of beta-cell function increased with two different canagliflozin doses, compared with placebo, the randomized, double-blind placebo-controlled study showed.
The finding is promising, said David Polidori, Ph.D., an employee of Janssen Research and Development, who presented the abstract at the annual meeting of the American Association of Clinical Endocrinologists.
Canagliflozin is a sodium glucose cotransporter 2 (SGLT2) inhibitor, which lowers plasma glucose by a renal mechanism. It also reduces the fasting and postprandial glucose hemoglobin A1c levels.
Several animal studies have shown beneficial effects of SGLT2 inhibition on beta-cell mass or function. Other clinical studies have shown improvements in measures of beta-cell function with canagliflozin, including a 26-week phase III study with the drug as monotherapy, said Dr. Polidori. But it is not clear exactly how canagliflozin improves beta-cell function. "It may be due to the glucose toxicity. Or it may also be due to reducing the load on beta cells, the so-called unloading," he said.
The improvement in beta-cell function is worthwhile, said Dr. Alan Garber, outgoing AACE president, and professor of medicine, biochemistry, and molecular biology and molecular and cellular biology at Baylor College, Houston. "But it’s not unique to this drug."
Although both canagliflozin doses were generally well tolerated, patients in treatment groups reported higher rates of genital mycotic infections, urinary tract infections, and adverse events related to osmotic diuresis, compared with placebo. The adverse events led to few study discontinuations, said Dr. Polidori.
The SGLT2 class of drugs has been included in the recently updated AACE diabetes management algorithm, but with a note to use with caution. Dr. Garber, chair of the algorithm task force, said that the 10% risk of vulvovaginitis in women and 1% balanitis in men are not minor concerns to some patients, especially those at risk of recurrence. For men, balanitis means a trip to the emergency department, he said, "So a 1% risk requires a little bit of forethought on the part of the clinician before prescribing in at-risk patients for recurrence."
To assess the effect of canagliflozin on beta-cell function as an add-on therapy in patients with type 2 diabetes on metformin plus sulfonylurea, researchers conducted a 26-week study comparing patients on 100 mg and 300 mg of daily canaglifozin with placebo.
The study included 469 patients. A subset of them (168 patients) was given a meal tolerance test on day 1 and week 26. Their liquid meal contained 700 kcal and 100 g of glucose. Patients had a mean age of 57 years, an average HbA1c level of 8%, a body mass index of 33 kg/m2, and type 2 diabetes for an average of 10 years.
Their plasma glucose and serum C-peptide levels were measured at seven time points over a period of 3 hours.
Results showed that the mean ratio of C-peptide area under the curve (AUCc) to glucose (AUCg) increased by a mean of roughly 20% from a baseline of 132 with the 100-mg dosage and 123 with the 300-mg dosage to 160 and 152, respectively, at week 26. There was a small decrease of 3.4% in the placebo group. There was a roughly 27% difference between the canagliflozin and placebo groups that did not reach statistical significance (100 mg, P = .051; 300 mg, P = .056)
The mean insulin secretion rate at 9 mM glucose at week 26 increased significantly in the treatment groups, compared with a 12.2% decrease in the placebo group. There was a 55% difference from placebo in the 100-mg canagliflozin group (P = .02) and a 70% difference in the 300-mg (P = .007) canagliflozin group.
The mean beta-cell glucose sensitivity increased by roughly 20% from baseline in both treatment groups, but the increases were not statistically significant.
"This is 26-week data. It will be interesting to see longer-term data, and to see if this type of treatment can better prolong beta-cell function and hopefully slow the rate of progression of type 2 diabetes," said Dr. Polidori.
Dr. Polidori is an employee of Janssen Research and Development, which funded and supported the study. Dr. Garber is a consultant/advisory board member and/or is on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
PHOENIX – The recently approved diabetes drug canagliflozin improved beta-cell function in patients with advanced type 2 diabetes inadequately controlled with metformin plus sulfonylurea, according to a phase III study.
Although some of the changes did not reach statistical significance, the mean value of all calculated measures of beta-cell function increased with two different canagliflozin doses, compared with placebo, the randomized, double-blind placebo-controlled study showed.
The finding is promising, said David Polidori, Ph.D., an employee of Janssen Research and Development, who presented the abstract at the annual meeting of the American Association of Clinical Endocrinologists.
Canagliflozin is a sodium glucose cotransporter 2 (SGLT2) inhibitor, which lowers plasma glucose by a renal mechanism. It also reduces the fasting and postprandial glucose hemoglobin A1c levels.
Several animal studies have shown beneficial effects of SGLT2 inhibition on beta-cell mass or function. Other clinical studies have shown improvements in measures of beta-cell function with canagliflozin, including a 26-week phase III study with the drug as monotherapy, said Dr. Polidori. But it is not clear exactly how canagliflozin improves beta-cell function. "It may be due to the glucose toxicity. Or it may also be due to reducing the load on beta cells, the so-called unloading," he said.
The improvement in beta-cell function is worthwhile, said Dr. Alan Garber, outgoing AACE president, and professor of medicine, biochemistry, and molecular biology and molecular and cellular biology at Baylor College, Houston. "But it’s not unique to this drug."
Although both canagliflozin doses were generally well tolerated, patients in treatment groups reported higher rates of genital mycotic infections, urinary tract infections, and adverse events related to osmotic diuresis, compared with placebo. The adverse events led to few study discontinuations, said Dr. Polidori.
The SGLT2 class of drugs has been included in the recently updated AACE diabetes management algorithm, but with a note to use with caution. Dr. Garber, chair of the algorithm task force, said that the 10% risk of vulvovaginitis in women and 1% balanitis in men are not minor concerns to some patients, especially those at risk of recurrence. For men, balanitis means a trip to the emergency department, he said, "So a 1% risk requires a little bit of forethought on the part of the clinician before prescribing in at-risk patients for recurrence."
To assess the effect of canagliflozin on beta-cell function as an add-on therapy in patients with type 2 diabetes on metformin plus sulfonylurea, researchers conducted a 26-week study comparing patients on 100 mg and 300 mg of daily canaglifozin with placebo.
The study included 469 patients. A subset of them (168 patients) was given a meal tolerance test on day 1 and week 26. Their liquid meal contained 700 kcal and 100 g of glucose. Patients had a mean age of 57 years, an average HbA1c level of 8%, a body mass index of 33 kg/m2, and type 2 diabetes for an average of 10 years.
Their plasma glucose and serum C-peptide levels were measured at seven time points over a period of 3 hours.
Results showed that the mean ratio of C-peptide area under the curve (AUCc) to glucose (AUCg) increased by a mean of roughly 20% from a baseline of 132 with the 100-mg dosage and 123 with the 300-mg dosage to 160 and 152, respectively, at week 26. There was a small decrease of 3.4% in the placebo group. There was a roughly 27% difference between the canagliflozin and placebo groups that did not reach statistical significance (100 mg, P = .051; 300 mg, P = .056)
The mean insulin secretion rate at 9 mM glucose at week 26 increased significantly in the treatment groups, compared with a 12.2% decrease in the placebo group. There was a 55% difference from placebo in the 100-mg canagliflozin group (P = .02) and a 70% difference in the 300-mg (P = .007) canagliflozin group.
The mean beta-cell glucose sensitivity increased by roughly 20% from baseline in both treatment groups, but the increases were not statistically significant.
"This is 26-week data. It will be interesting to see longer-term data, and to see if this type of treatment can better prolong beta-cell function and hopefully slow the rate of progression of type 2 diabetes," said Dr. Polidori.
Dr. Polidori is an employee of Janssen Research and Development, which funded and supported the study. Dr. Garber is a consultant/advisory board member and/or is on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
AT THE AACE ANNUAL MEETING
Major Finding: The mean ratio of C-peptide to glucose area under the curve increased by a mean of roughly 20% from a baseline of 132 for canagliflozin 100 mg and 123 for 300 mg to 160 and 152, respectively, at week 26.
Data Source: A randomized, double-blind placebo-controlled study of a subset of 168 patients.
Disclosures: Dr. Polidori is an employee of Janssen Research and Development, which funded and supported the study. Dr. Garber is a consultant/advisory board member and/or is on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.

Hypoglycemia associated with daily variation in blood glucose
PHOENIX – Patients who had higher rates of confirmed hypoglycemia also had greater daily variations in fasting blood glucose, regardless of diabetes type or insulin drug, according to a meta-analysis of seven trials on two long-acting basal insulin drugs.
"The data clearly show that the variation in plasma glucose is associated with hypoglycemia," said Dr. Bruce W. Bode, who presented the study at the annual meeting of the American Association of Clinical Endocrinologists.
Previous studies have shown that patients whose fasting blood glucose changes daily, due to pharmacokinetics and pharmacodynamics of basal insulin, have a difficult time adjusting their insulin dose. This, in turn, can put them at an increased risk of a hypoglycemic event. "We also need to look at what patients do and what they eat. We should look at what causes hypoglycemia in them," said Dr. Bode, a diabetes specialist at Atlanta Diabetes Associates.
The study analyzed data from seven open-label, randomized, treat-to-target published phase IIIa trials, which had compared once-daily insulin degludec (Novo Nordisk) and insulin glargine (Sanofi-Aventis).
Two trials included individuals with type 1 diabetes and five trials included those with type 2 diabetes. The trials had a 26- or 52-week duration. Daily within-subject variability (coefficient variance [CV%]) in self-measured prebreakfast plasma glucose was determined from three consecutive daily measurements made in the final week of each trial. The analysis did not compare degludec with glargine.
The CV% was compared between individuals with the highest rate of confirmed hypoglycemic events (top 25%) and those outside of this range (bottom 75%), using a linear mixed model.
Results showed that, in individuals with type 1 diabetes, the CV% ratio (top 25%/bottom 75%) was 1.33 for degludec and 1.25 for glargine, Dr. Bode said.
In insulin-experienced patients with type 2 diabetes receiving basal insulin plus oral antidiabetic therapy, the ratio was 1.33 for degludec and 1.46 for glargine, he said.
For insulin-naive patients with type 2 diabetes in whom basal insulin plus oral antidiabetic therapy was initiated in the trials, the ratios were 1.33 for degludec and 1.49 for glargine. Patients with type 2 diabetes on basal-bolus therapy had identical ratios of 1.65.
In the pooled data from type 2 diabetes trials, the ratio was 1.50 for degludec and 1.46 for glargine.
With both insulins, estimated day-to-day variability in prebreakfast plasma glucose was significantly higher for patients with the highest rates of confirmed hypoglycemia than for those with lower rates, regardless of diabetes type, type 2 diabetes treatment history, or insulin type (P less than .05), Dr. Bode reported.
Dr. Alan Garber, the outgoing AACE president and session moderator, said that "it will be interesting to go back and analyze the data to see what patient characteristics, irrespective of the type of insulin, predict great risk of variability."
Dr. Bode has been a speaker, consultant, and advisory board member for, and has received research funding from several companies, including Novo Nordisk, SanofiAventis, Eli Lily, and Medtronic. Dr. Garber is a consultant/advisory board member and/or on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
PHOENIX – Patients who had higher rates of confirmed hypoglycemia also had greater daily variations in fasting blood glucose, regardless of diabetes type or insulin drug, according to a meta-analysis of seven trials on two long-acting basal insulin drugs.
"The data clearly show that the variation in plasma glucose is associated with hypoglycemia," said Dr. Bruce W. Bode, who presented the study at the annual meeting of the American Association of Clinical Endocrinologists.
Previous studies have shown that patients whose fasting blood glucose changes daily, due to pharmacokinetics and pharmacodynamics of basal insulin, have a difficult time adjusting their insulin dose. This, in turn, can put them at an increased risk of a hypoglycemic event. "We also need to look at what patients do and what they eat. We should look at what causes hypoglycemia in them," said Dr. Bode, a diabetes specialist at Atlanta Diabetes Associates.
The study analyzed data from seven open-label, randomized, treat-to-target published phase IIIa trials, which had compared once-daily insulin degludec (Novo Nordisk) and insulin glargine (Sanofi-Aventis).
Two trials included individuals with type 1 diabetes and five trials included those with type 2 diabetes. The trials had a 26- or 52-week duration. Daily within-subject variability (coefficient variance [CV%]) in self-measured prebreakfast plasma glucose was determined from three consecutive daily measurements made in the final week of each trial. The analysis did not compare degludec with glargine.
The CV% was compared between individuals with the highest rate of confirmed hypoglycemic events (top 25%) and those outside of this range (bottom 75%), using a linear mixed model.
Results showed that, in individuals with type 1 diabetes, the CV% ratio (top 25%/bottom 75%) was 1.33 for degludec and 1.25 for glargine, Dr. Bode said.
In insulin-experienced patients with type 2 diabetes receiving basal insulin plus oral antidiabetic therapy, the ratio was 1.33 for degludec and 1.46 for glargine, he said.
For insulin-naive patients with type 2 diabetes in whom basal insulin plus oral antidiabetic therapy was initiated in the trials, the ratios were 1.33 for degludec and 1.49 for glargine. Patients with type 2 diabetes on basal-bolus therapy had identical ratios of 1.65.
In the pooled data from type 2 diabetes trials, the ratio was 1.50 for degludec and 1.46 for glargine.
With both insulins, estimated day-to-day variability in prebreakfast plasma glucose was significantly higher for patients with the highest rates of confirmed hypoglycemia than for those with lower rates, regardless of diabetes type, type 2 diabetes treatment history, or insulin type (P less than .05), Dr. Bode reported.
Dr. Alan Garber, the outgoing AACE president and session moderator, said that "it will be interesting to go back and analyze the data to see what patient characteristics, irrespective of the type of insulin, predict great risk of variability."
Dr. Bode has been a speaker, consultant, and advisory board member for, and has received research funding from several companies, including Novo Nordisk, SanofiAventis, Eli Lily, and Medtronic. Dr. Garber is a consultant/advisory board member and/or on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
PHOENIX – Patients who had higher rates of confirmed hypoglycemia also had greater daily variations in fasting blood glucose, regardless of diabetes type or insulin drug, according to a meta-analysis of seven trials on two long-acting basal insulin drugs.
"The data clearly show that the variation in plasma glucose is associated with hypoglycemia," said Dr. Bruce W. Bode, who presented the study at the annual meeting of the American Association of Clinical Endocrinologists.
Previous studies have shown that patients whose fasting blood glucose changes daily, due to pharmacokinetics and pharmacodynamics of basal insulin, have a difficult time adjusting their insulin dose. This, in turn, can put them at an increased risk of a hypoglycemic event. "We also need to look at what patients do and what they eat. We should look at what causes hypoglycemia in them," said Dr. Bode, a diabetes specialist at Atlanta Diabetes Associates.
The study analyzed data from seven open-label, randomized, treat-to-target published phase IIIa trials, which had compared once-daily insulin degludec (Novo Nordisk) and insulin glargine (Sanofi-Aventis).
Two trials included individuals with type 1 diabetes and five trials included those with type 2 diabetes. The trials had a 26- or 52-week duration. Daily within-subject variability (coefficient variance [CV%]) in self-measured prebreakfast plasma glucose was determined from three consecutive daily measurements made in the final week of each trial. The analysis did not compare degludec with glargine.
The CV% was compared between individuals with the highest rate of confirmed hypoglycemic events (top 25%) and those outside of this range (bottom 75%), using a linear mixed model.
Results showed that, in individuals with type 1 diabetes, the CV% ratio (top 25%/bottom 75%) was 1.33 for degludec and 1.25 for glargine, Dr. Bode said.
In insulin-experienced patients with type 2 diabetes receiving basal insulin plus oral antidiabetic therapy, the ratio was 1.33 for degludec and 1.46 for glargine, he said.
For insulin-naive patients with type 2 diabetes in whom basal insulin plus oral antidiabetic therapy was initiated in the trials, the ratios were 1.33 for degludec and 1.49 for glargine. Patients with type 2 diabetes on basal-bolus therapy had identical ratios of 1.65.
In the pooled data from type 2 diabetes trials, the ratio was 1.50 for degludec and 1.46 for glargine.
With both insulins, estimated day-to-day variability in prebreakfast plasma glucose was significantly higher for patients with the highest rates of confirmed hypoglycemia than for those with lower rates, regardless of diabetes type, type 2 diabetes treatment history, or insulin type (P less than .05), Dr. Bode reported.
Dr. Alan Garber, the outgoing AACE president and session moderator, said that "it will be interesting to go back and analyze the data to see what patient characteristics, irrespective of the type of insulin, predict great risk of variability."
Dr. Bode has been a speaker, consultant, and advisory board member for, and has received research funding from several companies, including Novo Nordisk, SanofiAventis, Eli Lily, and Medtronic. Dr. Garber is a consultant/advisory board member and/or on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
On Twitter @NaseemSMiller
At THE AACE ANNUAL MEETING
Major finding: With both insulin degludec and insulin glargine, estimated day-to-day variability in prebreakfast plasma glucose was significantly higher for patients with the highest rates of confirmed hypoglycemia than for those with lower rates, regardless of diabetes type, type 2 diabetes treatment history, or insulin type.
Data source: A meta-analysis of seven open-label, randomized, treat-to-target published phase IIIa trials comparing once-daily insulin degludec with insulin glargine.
Disclosures: Dr. Bode has been a speaker, consultant, and advisory board member for, and has received research funding from, several companies, including Novo Nordisk, SanofiAventis, Eli Lily, and Medtronic. Dr. Garber is a consultant/advisory board member and/or on the speakers bureaus for Novo Nordisk, Daiichi Sankyo, Merck, Takeda, LipoScience, Boehringer Ingelheim, Sekris, and Lexicon.
Case Report: Chronic marijuana use potential cause for hypopituitarism
PHOENIX – Chronic marijuana use can be a potential cause for hypopituitarism, according to an unpublished case report, which relied on existing data about the effect of cannabis on the hypothalamic-pituitary-gonadal axis.
The case hints at a largely underrepresented problem, researchers said, especially as various states contemplate legalizing marijuana, which is currently the most commonly used illicit drug in the nation, said Dr. Richard Pinsker at the annual meeting of the American Association of Clinical Endocrinologists.
The 37-year-old man arrived at the emergency department of Jamaica (N.Y.) Hospital Medical Center in Queens in late 2012 complaining of shortness of breath, increasing fatigue, and loss of libido. The patient had low blood pressure, and physical examination revealed gynecomastia, bilateral atrophied testis, and bibasilar rales. He disclosed that he had used marijuana daily for 15 years.
After ruling out hemochromatosis, conducting a battery of hormonal tests, and an MRI, Dr. Pinsker and his colleagues diagnosed the patient with hypopituitarism. The culprit? Chronic marijuana use, they concluded after finding no other potential cause.
"I think it’s a thought-provoking study," said Dr. R. Mack Harrell, who will be the president-elect of the AACE this year. "We’ve known for many years, if you use a lot of cannabis, it suppresses the gonadal axis, and it’s been assumed that [cannabis’] only effect was on the gonadal axis. This poster poses the question of whether other pituitary hormones may be affected, and whether every pituitary hormone is at risk, so it’s hypothesis generating."
Dr. Pinsker, who is a practicing endocrinologist and the internal medicine residency program director at Jamaica Hospital Medical Center, said that the finding – and high rate of marijuana use – call for further research on the effect of chronic marijuana use on the endocrine system. He added that that physicians need to do a better job of obtaining a social history from their patients.
Tetrahydrocannabinol, or THC, which is the psychoactive ingredient of marijuana, can alter the hypothalamic-pituitary-gonadal axis either by acting directly on the hypothalamus and altering the gonadotropin-releasing hormone (GnRH) or by altering neural transmitters in the central nervous system, which affect the hypothalamus. The result is lowered luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which lead to reduced testosterone production by Leydig cells of the testis.
Studies have shown cannabis exposure can result in impaired cortisol response to stress. Animal studies have shown that cannabinoids can suppress several hypothalamic-pituitary pathways, including the growth hormone, and the thyroid hormone, reported Dr. Hineshkumar Upadhyay, coauthor of the report.
Meanwhile, THC, which is lipid soluble, can remain stored in the fatty tissue and re-enter the blood stream at very low levels. This pharmacokinetics can cause chronic effect on organ systems even though it is used occasionally, researchers said.
In the case of the 37-year-old patient, researchers first suspected hemochromatosis, which they ruled out by iron studies and echocardiography. Hypopituitarism is rare in young people.
The patient had low levels of LH (0.2 mIU/mL), FSH (1.8 mIU/mL), and testosterone (22 ng/dL). His prolactin levels were high (53 ng/mL), an increase that confirms trouble in the hypothalamic-pituitary axis, said Dr. Pinsker.
Further endocrine chemistry showed that he had adrenocorticotropic hormone (ACTH) of 6 pg/mL and cortisol at 0 mcg/dL. At 60 minutes, following administration of cosyntropin, the levels changed to 6.4 pg/mL and 9.3 mcg/dL, respectively.
Additional tests revealed low levels of total T3 (30 ng/dL), high T3 resin reuptake (49%), low total T4 (3.94 mcg/dL), normal free T4 (0.97 ng/dL), and low TSH (0.22 mcIU/mL). Growth hormone was within normal limits (5.0 ng/mL), and insulinlike growth factor-1 was low (75 ng/mL; Z-score of –1.3).
MRI showed that the protuberant pituitary gland was slightly larger than the expected size, but there was no identified mass lesion, researchers reported.
Researchers started the patient on replacement hormones – 25 mg cortisone in the morning and 12.5 mg at bedtime, with 25 mcg levothyroxine daily. The patient’s fatigue and edema improved dramatically, they reported. As with other patients who abuse substances, they advised him to stop using marijuana.
Dr. Pinsker, who is also a colonel in the U.S. Army Reserve Medical Corps, said he was planning on collecting more cases before publishing the findings. He added the same mechanism could affect women as well. "We just haven’t looked at it," he said.
"I think it’ll be frightening if the use goes up" as more states make the drug legal "and the awareness does not follow it," he said.
Dr. Pinsker and Dr. Upadhyay had no disclosures.
On Twitter @NaseemSMiller
PHOENIX – Chronic marijuana use can be a potential cause for hypopituitarism, according to an unpublished case report, which relied on existing data about the effect of cannabis on the hypothalamic-pituitary-gonadal axis.
The case hints at a largely underrepresented problem, researchers said, especially as various states contemplate legalizing marijuana, which is currently the most commonly used illicit drug in the nation, said Dr. Richard Pinsker at the annual meeting of the American Association of Clinical Endocrinologists.
The 37-year-old man arrived at the emergency department of Jamaica (N.Y.) Hospital Medical Center in Queens in late 2012 complaining of shortness of breath, increasing fatigue, and loss of libido. The patient had low blood pressure, and physical examination revealed gynecomastia, bilateral atrophied testis, and bibasilar rales. He disclosed that he had used marijuana daily for 15 years.
After ruling out hemochromatosis, conducting a battery of hormonal tests, and an MRI, Dr. Pinsker and his colleagues diagnosed the patient with hypopituitarism. The culprit? Chronic marijuana use, they concluded after finding no other potential cause.
"I think it’s a thought-provoking study," said Dr. R. Mack Harrell, who will be the president-elect of the AACE this year. "We’ve known for many years, if you use a lot of cannabis, it suppresses the gonadal axis, and it’s been assumed that [cannabis’] only effect was on the gonadal axis. This poster poses the question of whether other pituitary hormones may be affected, and whether every pituitary hormone is at risk, so it’s hypothesis generating."
Dr. Pinsker, who is a practicing endocrinologist and the internal medicine residency program director at Jamaica Hospital Medical Center, said that the finding – and high rate of marijuana use – call for further research on the effect of chronic marijuana use on the endocrine system. He added that that physicians need to do a better job of obtaining a social history from their patients.
Tetrahydrocannabinol, or THC, which is the psychoactive ingredient of marijuana, can alter the hypothalamic-pituitary-gonadal axis either by acting directly on the hypothalamus and altering the gonadotropin-releasing hormone (GnRH) or by altering neural transmitters in the central nervous system, which affect the hypothalamus. The result is lowered luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which lead to reduced testosterone production by Leydig cells of the testis.
Studies have shown cannabis exposure can result in impaired cortisol response to stress. Animal studies have shown that cannabinoids can suppress several hypothalamic-pituitary pathways, including the growth hormone, and the thyroid hormone, reported Dr. Hineshkumar Upadhyay, coauthor of the report.
Meanwhile, THC, which is lipid soluble, can remain stored in the fatty tissue and re-enter the blood stream at very low levels. This pharmacokinetics can cause chronic effect on organ systems even though it is used occasionally, researchers said.
In the case of the 37-year-old patient, researchers first suspected hemochromatosis, which they ruled out by iron studies and echocardiography. Hypopituitarism is rare in young people.
The patient had low levels of LH (0.2 mIU/mL), FSH (1.8 mIU/mL), and testosterone (22 ng/dL). His prolactin levels were high (53 ng/mL), an increase that confirms trouble in the hypothalamic-pituitary axis, said Dr. Pinsker.
Further endocrine chemistry showed that he had adrenocorticotropic hormone (ACTH) of 6 pg/mL and cortisol at 0 mcg/dL. At 60 minutes, following administration of cosyntropin, the levels changed to 6.4 pg/mL and 9.3 mcg/dL, respectively.
Additional tests revealed low levels of total T3 (30 ng/dL), high T3 resin reuptake (49%), low total T4 (3.94 mcg/dL), normal free T4 (0.97 ng/dL), and low TSH (0.22 mcIU/mL). Growth hormone was within normal limits (5.0 ng/mL), and insulinlike growth factor-1 was low (75 ng/mL; Z-score of –1.3).
MRI showed that the protuberant pituitary gland was slightly larger than the expected size, but there was no identified mass lesion, researchers reported.
Researchers started the patient on replacement hormones – 25 mg cortisone in the morning and 12.5 mg at bedtime, with 25 mcg levothyroxine daily. The patient’s fatigue and edema improved dramatically, they reported. As with other patients who abuse substances, they advised him to stop using marijuana.
Dr. Pinsker, who is also a colonel in the U.S. Army Reserve Medical Corps, said he was planning on collecting more cases before publishing the findings. He added the same mechanism could affect women as well. "We just haven’t looked at it," he said.
"I think it’ll be frightening if the use goes up" as more states make the drug legal "and the awareness does not follow it," he said.
Dr. Pinsker and Dr. Upadhyay had no disclosures.
On Twitter @NaseemSMiller
PHOENIX – Chronic marijuana use can be a potential cause for hypopituitarism, according to an unpublished case report, which relied on existing data about the effect of cannabis on the hypothalamic-pituitary-gonadal axis.
The case hints at a largely underrepresented problem, researchers said, especially as various states contemplate legalizing marijuana, which is currently the most commonly used illicit drug in the nation, said Dr. Richard Pinsker at the annual meeting of the American Association of Clinical Endocrinologists.
The 37-year-old man arrived at the emergency department of Jamaica (N.Y.) Hospital Medical Center in Queens in late 2012 complaining of shortness of breath, increasing fatigue, and loss of libido. The patient had low blood pressure, and physical examination revealed gynecomastia, bilateral atrophied testis, and bibasilar rales. He disclosed that he had used marijuana daily for 15 years.
After ruling out hemochromatosis, conducting a battery of hormonal tests, and an MRI, Dr. Pinsker and his colleagues diagnosed the patient with hypopituitarism. The culprit? Chronic marijuana use, they concluded after finding no other potential cause.
"I think it’s a thought-provoking study," said Dr. R. Mack Harrell, who will be the president-elect of the AACE this year. "We’ve known for many years, if you use a lot of cannabis, it suppresses the gonadal axis, and it’s been assumed that [cannabis’] only effect was on the gonadal axis. This poster poses the question of whether other pituitary hormones may be affected, and whether every pituitary hormone is at risk, so it’s hypothesis generating."
Dr. Pinsker, who is a practicing endocrinologist and the internal medicine residency program director at Jamaica Hospital Medical Center, said that the finding – and high rate of marijuana use – call for further research on the effect of chronic marijuana use on the endocrine system. He added that that physicians need to do a better job of obtaining a social history from their patients.
Tetrahydrocannabinol, or THC, which is the psychoactive ingredient of marijuana, can alter the hypothalamic-pituitary-gonadal axis either by acting directly on the hypothalamus and altering the gonadotropin-releasing hormone (GnRH) or by altering neural transmitters in the central nervous system, which affect the hypothalamus. The result is lowered luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which lead to reduced testosterone production by Leydig cells of the testis.
Studies have shown cannabis exposure can result in impaired cortisol response to stress. Animal studies have shown that cannabinoids can suppress several hypothalamic-pituitary pathways, including the growth hormone, and the thyroid hormone, reported Dr. Hineshkumar Upadhyay, coauthor of the report.
Meanwhile, THC, which is lipid soluble, can remain stored in the fatty tissue and re-enter the blood stream at very low levels. This pharmacokinetics can cause chronic effect on organ systems even though it is used occasionally, researchers said.
In the case of the 37-year-old patient, researchers first suspected hemochromatosis, which they ruled out by iron studies and echocardiography. Hypopituitarism is rare in young people.
The patient had low levels of LH (0.2 mIU/mL), FSH (1.8 mIU/mL), and testosterone (22 ng/dL). His prolactin levels were high (53 ng/mL), an increase that confirms trouble in the hypothalamic-pituitary axis, said Dr. Pinsker.
Further endocrine chemistry showed that he had adrenocorticotropic hormone (ACTH) of 6 pg/mL and cortisol at 0 mcg/dL. At 60 minutes, following administration of cosyntropin, the levels changed to 6.4 pg/mL and 9.3 mcg/dL, respectively.
Additional tests revealed low levels of total T3 (30 ng/dL), high T3 resin reuptake (49%), low total T4 (3.94 mcg/dL), normal free T4 (0.97 ng/dL), and low TSH (0.22 mcIU/mL). Growth hormone was within normal limits (5.0 ng/mL), and insulinlike growth factor-1 was low (75 ng/mL; Z-score of –1.3).
MRI showed that the protuberant pituitary gland was slightly larger than the expected size, but there was no identified mass lesion, researchers reported.
Researchers started the patient on replacement hormones – 25 mg cortisone in the morning and 12.5 mg at bedtime, with 25 mcg levothyroxine daily. The patient’s fatigue and edema improved dramatically, they reported. As with other patients who abuse substances, they advised him to stop using marijuana.
Dr. Pinsker, who is also a colonel in the U.S. Army Reserve Medical Corps, said he was planning on collecting more cases before publishing the findings. He added the same mechanism could affect women as well. "We just haven’t looked at it," he said.
"I think it’ll be frightening if the use goes up" as more states make the drug legal "and the awareness does not follow it," he said.
Dr. Pinsker and Dr. Upadhyay had no disclosures.
On Twitter @NaseemSMiller
AT AACE ANNUAL MEETING
Case Report: Chronic marijuana use potential cause for hypopituitarism
PHOENIX – Chronic marijuana use can be a potential cause for hypopituitarism, according to an unpublished case report, which relied on existing data about the effect of cannabis on the hypothalamic-pituitary-gonadal axis.
The case hints at a largely underrepresented problem, researchers said, especially as various states contemplate legalizing marijuana, which is currently the most commonly used illicit drug in the nation, said Dr. Richard Pinsker at the annual meeting of the American Association of Clinical Endocrinologists.
The 37-year-old man arrived at the emergency department of Jamaica (N.Y.) Hospital Medical Center in Queens in late 2012 complaining of shortness of breath, increasing fatigue, and loss of libido. The patient had low blood pressure, and physical examination revealed gynecomastia, bilateral atrophied testis, and bibasilar rales. He disclosed that he had used marijuana daily for 15 years.
After ruling out hemochromatosis, conducting a battery of hormonal tests, and an MRI, Dr. Pinsker and his colleagues diagnosed the patient with hypopituitarism. The culprit? Chronic marijuana use, they concluded after finding no other potential cause.
"I think it’s a thought-provoking study," said Dr. R. Mack Harrell, who will be the president-elect of the AACE this year. "We’ve known for many years, if you use a lot of cannabis, it suppresses the gonadal axis, and it’s been assumed that [cannabis’] only effect was on the gonadal axis. This poster poses the question of whether other pituitary hormones may be affected, and whether every pituitary hormone is at risk, so it’s hypothesis generating."
Dr. Pinsker, who is a practicing endocrinologist and the internal medicine residency program director at Jamaica Hospital Medical Center, said that the finding – and high rate of marijuana use – call for further research on the effect of chronic marijuana use on the endocrine system. He added that that physicians need to do a better job of obtaining a social history from their patients.
Tetrahydrocannabinol, or THC, which is the psychoactive ingredient of marijuana, can alter the hypothalamic-pituitary-gonadal axis either by acting directly on the hypothalamus and altering the gonadotropin-releasing hormone (GnRH) or by altering neural transmitters in the central nervous system, which affect the hypothalamus. The result is lowered luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which lead to reduced testosterone production by Leydig cells of the testis.
Studies have shown cannabis exposure can result in impaired cortisol response to stress. Animal studies have shown that cannabinoids can suppress several hypothalamic-pituitary pathways, including the growth hormone, and the thyroid hormone, reported Dr. Hineshkumar Upadhyay, coauthor of the report.
Meanwhile, THC, which is lipid soluble, can remain stored in the fatty tissue and re-enter the blood stream at very low levels. This pharmacokinetics can cause chronic effect on organ systems even though it is used occasionally, researchers said.
In the case of the 37-year-old patient, researchers first suspected hemochromatosis, which they ruled out by iron studies and echocardiography. Hypopituitarism is rare in young people.
The patient had low levels of LH (0.2 mIU/mL), FSH (1.8 mIU/mL), and testosterone (22 ng/dL). His prolactin levels were high (53 ng/mL), an increase that confirms trouble in the hypothalamic-pituitary axis, said Dr. Pinsker.
Further endocrine chemistry showed that he had adrenocorticotropic hormone (ACTH) of 6 pg/mL and cortisol at 0 mcg/dL. At 60 minutes, following administration of cosyntropin, the levels changed to 6.4 pg/mL and 9.3 mcg/dL, respectively.
Additional tests revealed low levels of total T3 (30 ng/dL), high T3 resin reuptake (49%), low total T4 (3.94 mcg/dL), normal free T4 (0.97 ng/dL), and low TSH (0.22 mcIU/mL). Growth hormone was within normal limits (5.0 ng/mL), and insulinlike growth factor-1 was low (75 ng/mL; Z-score of –1.3).
MRI showed that the protuberant pituitary gland was slightly larger than the expected size, but there was no identified mass lesion, researchers reported.
Researchers started the patient on replacement hormones – 25 mg cortisone in the morning and 12.5 mg at bedtime, with 25 mcg levothyroxine daily. The patient’s fatigue and edema improved dramatically, they reported. As with other patients who abuse substances, they advised him to stop using marijuana.
Dr. Pinsker, who is also a colonel in the U.S. Army Reserve Medical Corps, said he was planning on collecting more cases before publishing the findings. He added the same mechanism could affect women as well. "We just haven’t looked at it," he said.
"I think it’ll be frightening if the use goes up" as more states make the drug legal "and the awareness does not follow it," he said.
Dr. Pinsker and Dr. Upadhyay had no disclosures.
On Twitter @NaseemSMiller
PHOENIX – Chronic marijuana use can be a potential cause for hypopituitarism, according to an unpublished case report, which relied on existing data about the effect of cannabis on the hypothalamic-pituitary-gonadal axis.
The case hints at a largely underrepresented problem, researchers said, especially as various states contemplate legalizing marijuana, which is currently the most commonly used illicit drug in the nation, said Dr. Richard Pinsker at the annual meeting of the American Association of Clinical Endocrinologists.
The 37-year-old man arrived at the emergency department of Jamaica (N.Y.) Hospital Medical Center in Queens in late 2012 complaining of shortness of breath, increasing fatigue, and loss of libido. The patient had low blood pressure, and physical examination revealed gynecomastia, bilateral atrophied testis, and bibasilar rales. He disclosed that he had used marijuana daily for 15 years.
After ruling out hemochromatosis, conducting a battery of hormonal tests, and an MRI, Dr. Pinsker and his colleagues diagnosed the patient with hypopituitarism. The culprit? Chronic marijuana use, they concluded after finding no other potential cause.
"I think it’s a thought-provoking study," said Dr. R. Mack Harrell, who will be the president-elect of the AACE this year. "We’ve known for many years, if you use a lot of cannabis, it suppresses the gonadal axis, and it’s been assumed that [cannabis’] only effect was on the gonadal axis. This poster poses the question of whether other pituitary hormones may be affected, and whether every pituitary hormone is at risk, so it’s hypothesis generating."
Dr. Pinsker, who is a practicing endocrinologist and the internal medicine residency program director at Jamaica Hospital Medical Center, said that the finding – and high rate of marijuana use – call for further research on the effect of chronic marijuana use on the endocrine system. He added that that physicians need to do a better job of obtaining a social history from their patients.
Tetrahydrocannabinol, or THC, which is the psychoactive ingredient of marijuana, can alter the hypothalamic-pituitary-gonadal axis either by acting directly on the hypothalamus and altering the gonadotropin-releasing hormone (GnRH) or by altering neural transmitters in the central nervous system, which affect the hypothalamus. The result is lowered luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which lead to reduced testosterone production by Leydig cells of the testis.
Studies have shown cannabis exposure can result in impaired cortisol response to stress. Animal studies have shown that cannabinoids can suppress several hypothalamic-pituitary pathways, including the growth hormone, and the thyroid hormone, reported Dr. Hineshkumar Upadhyay, coauthor of the report.
Meanwhile, THC, which is lipid soluble, can remain stored in the fatty tissue and re-enter the blood stream at very low levels. This pharmacokinetics can cause chronic effect on organ systems even though it is used occasionally, researchers said.
In the case of the 37-year-old patient, researchers first suspected hemochromatosis, which they ruled out by iron studies and echocardiography. Hypopituitarism is rare in young people.
The patient had low levels of LH (0.2 mIU/mL), FSH (1.8 mIU/mL), and testosterone (22 ng/dL). His prolactin levels were high (53 ng/mL), an increase that confirms trouble in the hypothalamic-pituitary axis, said Dr. Pinsker.
Further endocrine chemistry showed that he had adrenocorticotropic hormone (ACTH) of 6 pg/mL and cortisol at 0 mcg/dL. At 60 minutes, following administration of cosyntropin, the levels changed to 6.4 pg/mL and 9.3 mcg/dL, respectively.
Additional tests revealed low levels of total T3 (30 ng/dL), high T3 resin reuptake (49%), low total T4 (3.94 mcg/dL), normal free T4 (0.97 ng/dL), and low TSH (0.22 mcIU/mL). Growth hormone was within normal limits (5.0 ng/mL), and insulinlike growth factor-1 was low (75 ng/mL; Z-score of –1.3).
MRI showed that the protuberant pituitary gland was slightly larger than the expected size, but there was no identified mass lesion, researchers reported.
Researchers started the patient on replacement hormones – 25 mg cortisone in the morning and 12.5 mg at bedtime, with 25 mcg levothyroxine daily. The patient’s fatigue and edema improved dramatically, they reported. As with other patients who abuse substances, they advised him to stop using marijuana.
Dr. Pinsker, who is also a colonel in the U.S. Army Reserve Medical Corps, said he was planning on collecting more cases before publishing the findings. He added the same mechanism could affect women as well. "We just haven’t looked at it," he said.
"I think it’ll be frightening if the use goes up" as more states make the drug legal "and the awareness does not follow it," he said.
Dr. Pinsker and Dr. Upadhyay had no disclosures.
On Twitter @NaseemSMiller
PHOENIX – Chronic marijuana use can be a potential cause for hypopituitarism, according to an unpublished case report, which relied on existing data about the effect of cannabis on the hypothalamic-pituitary-gonadal axis.
The case hints at a largely underrepresented problem, researchers said, especially as various states contemplate legalizing marijuana, which is currently the most commonly used illicit drug in the nation, said Dr. Richard Pinsker at the annual meeting of the American Association of Clinical Endocrinologists.
The 37-year-old man arrived at the emergency department of Jamaica (N.Y.) Hospital Medical Center in Queens in late 2012 complaining of shortness of breath, increasing fatigue, and loss of libido. The patient had low blood pressure, and physical examination revealed gynecomastia, bilateral atrophied testis, and bibasilar rales. He disclosed that he had used marijuana daily for 15 years.
After ruling out hemochromatosis, conducting a battery of hormonal tests, and an MRI, Dr. Pinsker and his colleagues diagnosed the patient with hypopituitarism. The culprit? Chronic marijuana use, they concluded after finding no other potential cause.
"I think it’s a thought-provoking study," said Dr. R. Mack Harrell, who will be the president-elect of the AACE this year. "We’ve known for many years, if you use a lot of cannabis, it suppresses the gonadal axis, and it’s been assumed that [cannabis’] only effect was on the gonadal axis. This poster poses the question of whether other pituitary hormones may be affected, and whether every pituitary hormone is at risk, so it’s hypothesis generating."
Dr. Pinsker, who is a practicing endocrinologist and the internal medicine residency program director at Jamaica Hospital Medical Center, said that the finding – and high rate of marijuana use – call for further research on the effect of chronic marijuana use on the endocrine system. He added that that physicians need to do a better job of obtaining a social history from their patients.
Tetrahydrocannabinol, or THC, which is the psychoactive ingredient of marijuana, can alter the hypothalamic-pituitary-gonadal axis either by acting directly on the hypothalamus and altering the gonadotropin-releasing hormone (GnRH) or by altering neural transmitters in the central nervous system, which affect the hypothalamus. The result is lowered luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which lead to reduced testosterone production by Leydig cells of the testis.
Studies have shown cannabis exposure can result in impaired cortisol response to stress. Animal studies have shown that cannabinoids can suppress several hypothalamic-pituitary pathways, including the growth hormone, and the thyroid hormone, reported Dr. Hineshkumar Upadhyay, coauthor of the report.
Meanwhile, THC, which is lipid soluble, can remain stored in the fatty tissue and re-enter the blood stream at very low levels. This pharmacokinetics can cause chronic effect on organ systems even though it is used occasionally, researchers said.
In the case of the 37-year-old patient, researchers first suspected hemochromatosis, which they ruled out by iron studies and echocardiography. Hypopituitarism is rare in young people.
The patient had low levels of LH (0.2 mIU/mL), FSH (1.8 mIU/mL), and testosterone (22 ng/dL). His prolactin levels were high (53 ng/mL), an increase that confirms trouble in the hypothalamic-pituitary axis, said Dr. Pinsker.
Further endocrine chemistry showed that he had adrenocorticotropic hormone (ACTH) of 6 pg/mL and cortisol at 0 mcg/dL. At 60 minutes, following administration of cosyntropin, the levels changed to 6.4 pg/mL and 9.3 mcg/dL, respectively.
Additional tests revealed low levels of total T3 (30 ng/dL), high T3 resin reuptake (49%), low total T4 (3.94 mcg/dL), normal free T4 (0.97 ng/dL), and low TSH (0.22 mcIU/mL). Growth hormone was within normal limits (5.0 ng/mL), and insulinlike growth factor-1 was low (75 ng/mL; Z-score of –1.3).
MRI showed that the protuberant pituitary gland was slightly larger than the expected size, but there was no identified mass lesion, researchers reported.
Researchers started the patient on replacement hormones – 25 mg cortisone in the morning and 12.5 mg at bedtime, with 25 mcg levothyroxine daily. The patient’s fatigue and edema improved dramatically, they reported. As with other patients who abuse substances, they advised him to stop using marijuana.
Dr. Pinsker, who is also a colonel in the U.S. Army Reserve Medical Corps, said he was planning on collecting more cases before publishing the findings. He added the same mechanism could affect women as well. "We just haven’t looked at it," he said.
"I think it’ll be frightening if the use goes up" as more states make the drug legal "and the awareness does not follow it," he said.
Dr. Pinsker and Dr. Upadhyay had no disclosures.
On Twitter @NaseemSMiller
AT AACE ANNUAL MEETING

Eight principles for safe opioid prescribing
FORT LAUDERDALE, FLA. – Opioids aren’t always appropriate for treating pain, and if they have to be prescribed, they must be used cautiously and at the lowest effective dosage, Dr. Lynn R. Webster advised.
Misuse and abuse of pharmaceuticals including opioids rank high among the nation’s public health concerns. Emergency department visits involving these drugs increased from 627,000 in 2004 to nearly 1,430,000 in 2011, according to the latest data from the Substance Abuse and Mental Health Services Administration. Narcotic pain relievers were among the most commonly misused or abused drug (134.8 ED visits per 100,000 population).

And while the majority of overdose deaths due to opioids occur in people who obtain them illegally, "there’s a subset that physicians are responsible for," Dr. Webster, president of the American Academy of Pain Medicine, said at the academy’s annual meeting.
For the past 8 years, since Utah’s medical examiner was quoted on the front page of a local newspaper saying that there was an epidemic of overdose deaths from prescription drugs, Dr. Webster has been on a mission to establish easy-to-follow, evidence-based principles for safe opioid prescribing in outpatient settings.
Various guidelines on safe opioid prescribing are currently available, "and they are all useful and helpful, but, in my view, not specific-enough to have an immediate impact," Dr. Webster said in an interview. "They address grander, larger problems. But these eight principles are specifically targeted to prevent deaths."
For easy recall, the principles are summed up in the trademarked acronym: RELIABLE – Respiratory, Experience, Long term, Initiating methadone, Apnea, Benzodiazepine, Look for comorbidities, and Exercise caution with switching. They’re now part of the AAPM’s Safe Opioid Prescribing Initiative:
• Respiratory: If you have a patient who is on long-term opioids and develops a respiratory condition (asthma, pneumonia, flu), reduce the opioid dose by 20%-30%.
• Experience: Assess the patient before prescribing opioids. Find out what the biologic, social, and psychiatric risk factors are.
• Long term: Extended-release opioids should not be used for acute pain. "And that’s the bottom line," said Dr. Webster.
• Initiating methadone: "Never start anybody on more than 15 mg a day," Dr. Webster advised, adding that the wrong starting dose for methadone can be lethal. "There are reported deaths of people on 30 mg a day."
• Apnea: Screen for obstructive and central sleep apnea. Screen for hypoxemia. "Patients that are on 150 mg morphine-equivalent, people who are very overweight, people who are infirm and elderly people, we need to make sure that opioids are safe for them, and we need to do sleep studies."
• Benzodiazepines: "Should be avoided if at all possible when you are prescribing opioids," because in the face of benzodiazepines, the toxicity of opioids is significantly enhanced. "If a benzo is used, reduce the dose of opioids. And look for an alternative (to benzodiazepines) if you have to prescribe an opioid."
• Look for comorbidities: Find out if patients have a history of bipolar disorder, posttraumatic stress disorder, depression, stress, "and particularly general anxiety disorder." Patients will often misuse the medications for their mental health disorder instead of their pain.
• Exercise caution with rotation: "Conversion tables and equal analgesic tables should not be used to determine the starting dose of opioids. You have to assume that everybody is opioid naive, and start on a low dose, and titrate slowly to a level that you think is the maximum dose you think you can safely prescribe.
"Physicians can have an impact in reducing the number of overdose deaths, but it’s going to require a little bit of effort to learn these eight principles, and if we all do this, I think we’ll see a dramatic reduction in overdose deaths," Dr. Webster said.
The principles are likely to be published soon, he said, and they will be available on the AAPM’s website in the near future.
Dr. Webster said he had received honoraria/travel support from AstraZeneca, Covidien Mallinckrodt, Jazz Pharmaceuticals, Medtronic, Nektar Therapeutics, Pfizer, and Salix.
On Twitter @NaseemSMiller
FORT LAUDERDALE, FLA. – Opioids aren’t always appropriate for treating pain, and if they have to be prescribed, they must be used cautiously and at the lowest effective dosage, Dr. Lynn R. Webster advised.
Misuse and abuse of pharmaceuticals including opioids rank high among the nation’s public health concerns. Emergency department visits involving these drugs increased from 627,000 in 2004 to nearly 1,430,000 in 2011, according to the latest data from the Substance Abuse and Mental Health Services Administration. Narcotic pain relievers were among the most commonly misused or abused drug (134.8 ED visits per 100,000 population).
And while the majority of overdose deaths due to opioids occur in people who obtain them illegally, "there’s a subset that physicians are responsible for," Dr. Webster, president of the American Academy of Pain Medicine, said at the academy’s annual meeting.
For the past 8 years, since Utah’s medical examiner was quoted on the front page of a local newspaper saying that there was an epidemic of overdose deaths from prescription drugs, Dr. Webster has been on a mission to establish easy-to-follow, evidence-based principles for safe opioid prescribing in outpatient settings.
Various guidelines on safe opioid prescribing are currently available, "and they are all useful and helpful, but, in my view, not specific-enough to have an immediate impact," Dr. Webster said in an interview. "They address grander, larger problems. But these eight principles are specifically targeted to prevent deaths."
For easy recall, the principles are summed up in the trademarked acronym: RELIABLE – Respiratory, Experience, Long term, Initiating methadone, Apnea, Benzodiazepine, Look for comorbidities, and Exercise caution with switching. They’re now part of the AAPM’s Safe Opioid Prescribing Initiative:
• Respiratory: If you have a patient who is on long-term opioids and develops a respiratory condition (asthma, pneumonia, flu), reduce the opioid dose by 20%-30%.
• Experience: Assess the patient before prescribing opioids. Find out what the biologic, social, and psychiatric risk factors are.
• Long term: Extended-release opioids should not be used for acute pain. "And that’s the bottom line," said Dr. Webster.
• Initiating methadone: "Never start anybody on more than 15 mg a day," Dr. Webster advised, adding that the wrong starting dose for methadone can be lethal. "There are reported deaths of people on 30 mg a day."
• Apnea: Screen for obstructive and central sleep apnea. Screen for hypoxemia. "Patients that are on 150 mg morphine-equivalent, people who are very overweight, people who are infirm and elderly people, we need to make sure that opioids are safe for them, and we need to do sleep studies."
• Benzodiazepines: "Should be avoided if at all possible when you are prescribing opioids," because in the face of benzodiazepines, the toxicity of opioids is significantly enhanced. "If a benzo is used, reduce the dose of opioids. And look for an alternative (to benzodiazepines) if you have to prescribe an opioid."
• Look for comorbidities: Find out if patients have a history of bipolar disorder, posttraumatic stress disorder, depression, stress, "and particularly general anxiety disorder." Patients will often misuse the medications for their mental health disorder instead of their pain.
• Exercise caution with rotation: "Conversion tables and equal analgesic tables should not be used to determine the starting dose of opioids. You have to assume that everybody is opioid naive, and start on a low dose, and titrate slowly to a level that you think is the maximum dose you think you can safely prescribe.
"Physicians can have an impact in reducing the number of overdose deaths, but it’s going to require a little bit of effort to learn these eight principles, and if we all do this, I think we’ll see a dramatic reduction in overdose deaths," Dr. Webster said.
The principles are likely to be published soon, he said, and they will be available on the AAPM’s website in the near future.
Dr. Webster said he had received honoraria/travel support from AstraZeneca, Covidien Mallinckrodt, Jazz Pharmaceuticals, Medtronic, Nektar Therapeutics, Pfizer, and Salix.
On Twitter @NaseemSMiller
FORT LAUDERDALE, FLA. – Opioids aren’t always appropriate for treating pain, and if they have to be prescribed, they must be used cautiously and at the lowest effective dosage, Dr. Lynn R. Webster advised.
Misuse and abuse of pharmaceuticals including opioids rank high among the nation’s public health concerns. Emergency department visits involving these drugs increased from 627,000 in 2004 to nearly 1,430,000 in 2011, according to the latest data from the Substance Abuse and Mental Health Services Administration. Narcotic pain relievers were among the most commonly misused or abused drug (134.8 ED visits per 100,000 population).
And while the majority of overdose deaths due to opioids occur in people who obtain them illegally, "there’s a subset that physicians are responsible for," Dr. Webster, president of the American Academy of Pain Medicine, said at the academy’s annual meeting.
For the past 8 years, since Utah’s medical examiner was quoted on the front page of a local newspaper saying that there was an epidemic of overdose deaths from prescription drugs, Dr. Webster has been on a mission to establish easy-to-follow, evidence-based principles for safe opioid prescribing in outpatient settings.
Various guidelines on safe opioid prescribing are currently available, "and they are all useful and helpful, but, in my view, not specific-enough to have an immediate impact," Dr. Webster said in an interview. "They address grander, larger problems. But these eight principles are specifically targeted to prevent deaths."
For easy recall, the principles are summed up in the trademarked acronym: RELIABLE – Respiratory, Experience, Long term, Initiating methadone, Apnea, Benzodiazepine, Look for comorbidities, and Exercise caution with switching. They’re now part of the AAPM’s Safe Opioid Prescribing Initiative:
• Respiratory: If you have a patient who is on long-term opioids and develops a respiratory condition (asthma, pneumonia, flu), reduce the opioid dose by 20%-30%.
• Experience: Assess the patient before prescribing opioids. Find out what the biologic, social, and psychiatric risk factors are.
• Long term: Extended-release opioids should not be used for acute pain. "And that’s the bottom line," said Dr. Webster.
• Initiating methadone: "Never start anybody on more than 15 mg a day," Dr. Webster advised, adding that the wrong starting dose for methadone can be lethal. "There are reported deaths of people on 30 mg a day."
• Apnea: Screen for obstructive and central sleep apnea. Screen for hypoxemia. "Patients that are on 150 mg morphine-equivalent, people who are very overweight, people who are infirm and elderly people, we need to make sure that opioids are safe for them, and we need to do sleep studies."
• Benzodiazepines: "Should be avoided if at all possible when you are prescribing opioids," because in the face of benzodiazepines, the toxicity of opioids is significantly enhanced. "If a benzo is used, reduce the dose of opioids. And look for an alternative (to benzodiazepines) if you have to prescribe an opioid."
• Look for comorbidities: Find out if patients have a history of bipolar disorder, posttraumatic stress disorder, depression, stress, "and particularly general anxiety disorder." Patients will often misuse the medications for their mental health disorder instead of their pain.
• Exercise caution with rotation: "Conversion tables and equal analgesic tables should not be used to determine the starting dose of opioids. You have to assume that everybody is opioid naive, and start on a low dose, and titrate slowly to a level that you think is the maximum dose you think you can safely prescribe.
"Physicians can have an impact in reducing the number of overdose deaths, but it’s going to require a little bit of effort to learn these eight principles, and if we all do this, I think we’ll see a dramatic reduction in overdose deaths," Dr. Webster said.
The principles are likely to be published soon, he said, and they will be available on the AAPM’s website in the near future.
Dr. Webster said he had received honoraria/travel support from AstraZeneca, Covidien Mallinckrodt, Jazz Pharmaceuticals, Medtronic, Nektar Therapeutics, Pfizer, and Salix.
On Twitter @NaseemSMiller
AT THE AAPM ANNUAL MEETING

Technique is key for filler injection in darker skin
MIAMI BEACH – When considering dermal fillers for skin of color patients, remember that fewer injections can help reduce the risk of keloid formation and pigmentary changes, Dr. Valerie D. Callender said at the annual meeting of the American Academy of Dermatology.
People with skin of color made up 20% of the patient population seeking cosmetic procedures in 2011, and they are the fastest-growing demographic group in the U.S. population, Dr. Callender said. Dermatologists can expect to see more patients with ethnic skin in their practices, and it’s important for them to remember that not all aging skin is created equal, and that different techniques come into play for different skin types, she added.

Aging in ethnic facial skin differs from aging in lighter skin, mainly because of the photoprotective effect of melanin against UV radiation, said Dr. Callender. The effects of photodamage usually appear 10-20 years later in skin of color patients and with less severity.
"Your typical skin of color patient is 45 years old, has some volume loss, some infraorbital hollowing, and is definitely concerned about laugh lines," said Dr. Callender.
"The No. 1 tip is to minimize the number of injections to minimize the risk of postinflammatory hyperpigmentation," she emphasized. "If there is erythema, apply a topical corticosteroid."
Hyaluronic acid fillers are among the top five nonsurgical cosmetic procedures in the United States, but there is a paucity of published studies in skin of color patients, said Dr. Callender of Howard University, Washington. The population included in large, pivotal clinical studies is composed mainly of white patients, and even if these studies include a subset of skin of color patients, they don’t specifically report on treatment and safety outcomes in those patients, Dr. Callender said.
Dr. Callender listed several published and unpublished studies including data on the use of fillers in patients with Fitzpatrick Skin Types IV to VI. The products studied included Restylane, Perlane, Juvéderm Ultra and Ultra Plus, Hylaform, Hylaform Plus, Captique, Belotero Balance, and Radiesse.
Pigmentary changes were common throughout the studies, but they did not affected more than 9% of the study population, according to Dr. Callender. In the Radiesse study, the authors concluded that lack of pigmentary changes may have occurred from a deeper injection level, compared with HA fillers, she noted. No keloids or scarring were reported at 6 months’ follow-up and the investigators used a 25- to 27-gauge needle (Dermatol. Surg. 2009; 35:1641-5).
There have been no formal clinical trials evaluating safety of Sculptra in skin of color patients, said Dr. Callender, director of Callender Dermatology & Cosmetic Center, Glenn Dale, Md. However, the investigators in a 2010 study advised clinicians to lower the injection time, use proper product reconstitution and proper produce placement, perform immediate and postoperative massage, and avoid Sculptra on patients with a history of keloids in order to reduce the risk of adverse events (J. Drugs Dermatol. 2010;9:451-6).
Dr. Callender has been a consultant and investigator for Allergan, Galderma, Medicis, and Merz.
On Twitter @NaseemSMiller
MIAMI BEACH – When considering dermal fillers for skin of color patients, remember that fewer injections can help reduce the risk of keloid formation and pigmentary changes, Dr. Valerie D. Callender said at the annual meeting of the American Academy of Dermatology.
People with skin of color made up 20% of the patient population seeking cosmetic procedures in 2011, and they are the fastest-growing demographic group in the U.S. population, Dr. Callender said. Dermatologists can expect to see more patients with ethnic skin in their practices, and it’s important for them to remember that not all aging skin is created equal, and that different techniques come into play for different skin types, she added.
Aging in ethnic facial skin differs from aging in lighter skin, mainly because of the photoprotective effect of melanin against UV radiation, said Dr. Callender. The effects of photodamage usually appear 10-20 years later in skin of color patients and with less severity.
"Your typical skin of color patient is 45 years old, has some volume loss, some infraorbital hollowing, and is definitely concerned about laugh lines," said Dr. Callender.
"The No. 1 tip is to minimize the number of injections to minimize the risk of postinflammatory hyperpigmentation," she emphasized. "If there is erythema, apply a topical corticosteroid."
Hyaluronic acid fillers are among the top five nonsurgical cosmetic procedures in the United States, but there is a paucity of published studies in skin of color patients, said Dr. Callender of Howard University, Washington. The population included in large, pivotal clinical studies is composed mainly of white patients, and even if these studies include a subset of skin of color patients, they don’t specifically report on treatment and safety outcomes in those patients, Dr. Callender said.
Dr. Callender listed several published and unpublished studies including data on the use of fillers in patients with Fitzpatrick Skin Types IV to VI. The products studied included Restylane, Perlane, Juvéderm Ultra and Ultra Plus, Hylaform, Hylaform Plus, Captique, Belotero Balance, and Radiesse.
Pigmentary changes were common throughout the studies, but they did not affected more than 9% of the study population, according to Dr. Callender. In the Radiesse study, the authors concluded that lack of pigmentary changes may have occurred from a deeper injection level, compared with HA fillers, she noted. No keloids or scarring were reported at 6 months’ follow-up and the investigators used a 25- to 27-gauge needle (Dermatol. Surg. 2009; 35:1641-5).
There have been no formal clinical trials evaluating safety of Sculptra in skin of color patients, said Dr. Callender, director of Callender Dermatology & Cosmetic Center, Glenn Dale, Md. However, the investigators in a 2010 study advised clinicians to lower the injection time, use proper product reconstitution and proper produce placement, perform immediate and postoperative massage, and avoid Sculptra on patients with a history of keloids in order to reduce the risk of adverse events (J. Drugs Dermatol. 2010;9:451-6).
Dr. Callender has been a consultant and investigator for Allergan, Galderma, Medicis, and Merz.
On Twitter @NaseemSMiller
MIAMI BEACH – When considering dermal fillers for skin of color patients, remember that fewer injections can help reduce the risk of keloid formation and pigmentary changes, Dr. Valerie D. Callender said at the annual meeting of the American Academy of Dermatology.
People with skin of color made up 20% of the patient population seeking cosmetic procedures in 2011, and they are the fastest-growing demographic group in the U.S. population, Dr. Callender said. Dermatologists can expect to see more patients with ethnic skin in their practices, and it’s important for them to remember that not all aging skin is created equal, and that different techniques come into play for different skin types, she added.
Aging in ethnic facial skin differs from aging in lighter skin, mainly because of the photoprotective effect of melanin against UV radiation, said Dr. Callender. The effects of photodamage usually appear 10-20 years later in skin of color patients and with less severity.
"Your typical skin of color patient is 45 years old, has some volume loss, some infraorbital hollowing, and is definitely concerned about laugh lines," said Dr. Callender.
"The No. 1 tip is to minimize the number of injections to minimize the risk of postinflammatory hyperpigmentation," she emphasized. "If there is erythema, apply a topical corticosteroid."
Hyaluronic acid fillers are among the top five nonsurgical cosmetic procedures in the United States, but there is a paucity of published studies in skin of color patients, said Dr. Callender of Howard University, Washington. The population included in large, pivotal clinical studies is composed mainly of white patients, and even if these studies include a subset of skin of color patients, they don’t specifically report on treatment and safety outcomes in those patients, Dr. Callender said.
Dr. Callender listed several published and unpublished studies including data on the use of fillers in patients with Fitzpatrick Skin Types IV to VI. The products studied included Restylane, Perlane, Juvéderm Ultra and Ultra Plus, Hylaform, Hylaform Plus, Captique, Belotero Balance, and Radiesse.
Pigmentary changes were common throughout the studies, but they did not affected more than 9% of the study population, according to Dr. Callender. In the Radiesse study, the authors concluded that lack of pigmentary changes may have occurred from a deeper injection level, compared with HA fillers, she noted. No keloids or scarring were reported at 6 months’ follow-up and the investigators used a 25- to 27-gauge needle (Dermatol. Surg. 2009; 35:1641-5).
There have been no formal clinical trials evaluating safety of Sculptra in skin of color patients, said Dr. Callender, director of Callender Dermatology & Cosmetic Center, Glenn Dale, Md. However, the investigators in a 2010 study advised clinicians to lower the injection time, use proper product reconstitution and proper produce placement, perform immediate and postoperative massage, and avoid Sculptra on patients with a history of keloids in order to reduce the risk of adverse events (J. Drugs Dermatol. 2010;9:451-6).
Dr. Callender has been a consultant and investigator for Allergan, Galderma, Medicis, and Merz.
On Twitter @NaseemSMiller
EXPERT ANALYSIS FROM THE AAD ANNUAL MEETING

Small arteries show change in women with preeclampsia history
ORLANDO – Women with a history of severe preeclampsia show signs of small artery dysfunction as early as 2 years after delivery, an indication of cardiovascular disease later in life if not addressed by ob.gyns. and cardiologists early on, according to a small, unpublished study.
Researchers led by Dr. Karolina Kublickiene found that in women with a history of preeclampsia, endothelium-dependent dilation to flow was reduced, a change that could be due to nitric oxide contribution deficiency. The small arteries seen in the study group also exhibited increased myogenic tone, with enhanced sensitivity to the vasoconstrictor norepinephrine.
Dr. Louise Kenny, who moderated the session at the annual meeting of the Society for Gynecologic Investigation, said the study was "exquisitely executed."
"This is very basic science, but has massive clinical implications," said Dr. Kenny, a professor of obstetrics at the University College Cork, Ireland.
Several studies have shown that a history of preeclampsia is a risk factor for developing cardiovascular disease (Circulation 2012;125:1367-80). However, many women with preeclampsia go back to the community without proper follow-up with a cardiologist.
"I’m a high-risk maternal medicine obstetrician, and I’m very well aware that the long-term follow-up for women with preeclampsia is quite patchy," said Dr. Kenny. "We have a complete disconnect at several levels, and it is time to act."
Researchers hypothesized that functional and structural abnormalities in peripheral arteries are present as early as 2 years after delivery in mothers who had a pregnancy complicated by early-onset and severe preeclampsia.
They selected 15 women with a history of severe preeclampsia who had delivered between 2007 and 2011 at Karolinska University Hospital in Stockholm. They selected 15 closely matched controls who had normal pregnancies and gave birth during the same period. The women were on average 35 years old.
The investigators defined severe preeclampsia as systolic blood pressure of more than 160 mm Hg and/or diastolic blood pressure of more than 110 mm Hg on two occasions, at least 6 hours apart, and/or proteinuria of more than 5 g in a 24-hour period and/or organ damage.
The preeclampsia group and the control group were closely matched with regard to several biochemical characteristics, including the low-density lipoprotein to high-density lipoprotein (LDL/HDL) ratio (1.9 and 1.6, respectively). However, women in the preeclampsia group had higher blood pressure, insulin levels, and hemostatic model assessment index than did controls: The average diastolic blood pressure in the preeclampsia group was 74 mm Hg, versus 66 mm Hg in the control group. The average fasting insulin level in the preeclampsia group was almost twice as high as that of the control group (83 pmol/L vs. 44 pmol/L). Neither group showed evidence of early renal damage.
Researchers took subcutaneous fat biopsies from the women. They used pressure myography to compare the structure and function of the isolated small subcutaneous resistance arteries. They used immunostaining to compare endothelial nitric oxide synthase (eNOS) and lectin-like oxidized LDL receptor-1 (LOX-1) expression.
The arteries in both groups had similar diameters, wall thickness, wall-lumen ratio, and cross-sectional area.
Results showed that eNOS expression was similar in both groups, but LOX-1 expression was significantly enhanced in the study group. Inhibition of NOS had no effect on either group.
Myogenic tone was enhanced in the arteries of women with a history of preeclampsia, and was positively correlated with the LDL/HDL ratio, a change characterizing small artery dysfunction.
Basal tone in the study group also was positively correlated with the LDL/HDL ratio, triglycerides, glycated hemoglobin, and high-sensitivity C-reactive protein, and was negatively correlated with HDL. Basal tone at 60 mm Hg was 8 in the preeclampsia group, compared with 5 in the control group (P = .07).
Meanwhile, the study group had higher sensitivity to norepinephrine and angiotensin II, and showed reduced distensibility. Distensibility was negatively correlated with homocysteine level, which has been associated with cardiovascular disease, in the study group only.
"The changes in passive properties of vascular wall are characterized by reduced distensibility that will affect stiffness of the arteries in women with a history of preeclampsia," said Dr. Kublickiene, an associate professor of obstetrics and gynecology and senior researcher at the Karolinska Institute Hospital-Huddinge in Stockholm. She also leads the Center for Gender Medicine at the institute.
Endothelium-dependent dilation to bradykinin (BK) and NO donor compounds were similar between the two groups. But endothelium-dependent response to flow was significantly attenuated in the study group, which could mean possible impairment of flow detection and signaling, according to Dr. Kublickiene.
"Preserved relaxation and the contribution of NO to BK-induced responses to NO donor and eNOS expression between the groups further support the specific importance of NO deficiency in flow-mediated dilation," she said.
"The observed changes will contribute to an increased peripheral resistance and blood pressure, which are of critical importance for long-term women’s cardiovascular health," she said. Counseling following a preeclamptic pregnancy and preterm delivery should include a discussion about reproduction and cardiovascular risks, she said.
And, she emphasized, "Let’s work with cardiologists."
A 2012 study that focused on a different group of women showed that collaboration between cardiologists and ob.gyns. is indeed possible.
Dr. Kublickiene said that several questions remain: What are the appropriate preventive strategies? What screening schedules should be recommended? What are the clinical targets? And, what are the treatment regimens?
"I think now clinical trials of statins and other early interventions in these women are warranted," said Dr. Kenny.
Dr. Kublickiene and Dr. Kenny said they had no disclosures. The study was funded by the Center for Gender Medicine at the Karolinska Institute, by the Karolinska Institute, and by the ALF fund of the Stockholm County Council.
On Twitter @NaseemSMiller
ORLANDO – Women with a history of severe preeclampsia show signs of small artery dysfunction as early as 2 years after delivery, an indication of cardiovascular disease later in life if not addressed by ob.gyns. and cardiologists early on, according to a small, unpublished study.
Researchers led by Dr. Karolina Kublickiene found that in women with a history of preeclampsia, endothelium-dependent dilation to flow was reduced, a change that could be due to nitric oxide contribution deficiency. The small arteries seen in the study group also exhibited increased myogenic tone, with enhanced sensitivity to the vasoconstrictor norepinephrine.
Dr. Louise Kenny, who moderated the session at the annual meeting of the Society for Gynecologic Investigation, said the study was "exquisitely executed."
"This is very basic science, but has massive clinical implications," said Dr. Kenny, a professor of obstetrics at the University College Cork, Ireland.
Several studies have shown that a history of preeclampsia is a risk factor for developing cardiovascular disease (Circulation 2012;125:1367-80). However, many women with preeclampsia go back to the community without proper follow-up with a cardiologist.
"I’m a high-risk maternal medicine obstetrician, and I’m very well aware that the long-term follow-up for women with preeclampsia is quite patchy," said Dr. Kenny. "We have a complete disconnect at several levels, and it is time to act."
Researchers hypothesized that functional and structural abnormalities in peripheral arteries are present as early as 2 years after delivery in mothers who had a pregnancy complicated by early-onset and severe preeclampsia.
They selected 15 women with a history of severe preeclampsia who had delivered between 2007 and 2011 at Karolinska University Hospital in Stockholm. They selected 15 closely matched controls who had normal pregnancies and gave birth during the same period. The women were on average 35 years old.
The investigators defined severe preeclampsia as systolic blood pressure of more than 160 mm Hg and/or diastolic blood pressure of more than 110 mm Hg on two occasions, at least 6 hours apart, and/or proteinuria of more than 5 g in a 24-hour period and/or organ damage.
The preeclampsia group and the control group were closely matched with regard to several biochemical characteristics, including the low-density lipoprotein to high-density lipoprotein (LDL/HDL) ratio (1.9 and 1.6, respectively). However, women in the preeclampsia group had higher blood pressure, insulin levels, and hemostatic model assessment index than did controls: The average diastolic blood pressure in the preeclampsia group was 74 mm Hg, versus 66 mm Hg in the control group. The average fasting insulin level in the preeclampsia group was almost twice as high as that of the control group (83 pmol/L vs. 44 pmol/L). Neither group showed evidence of early renal damage.
Researchers took subcutaneous fat biopsies from the women. They used pressure myography to compare the structure and function of the isolated small subcutaneous resistance arteries. They used immunostaining to compare endothelial nitric oxide synthase (eNOS) and lectin-like oxidized LDL receptor-1 (LOX-1) expression.
The arteries in both groups had similar diameters, wall thickness, wall-lumen ratio, and cross-sectional area.
Results showed that eNOS expression was similar in both groups, but LOX-1 expression was significantly enhanced in the study group. Inhibition of NOS had no effect on either group.
Myogenic tone was enhanced in the arteries of women with a history of preeclampsia, and was positively correlated with the LDL/HDL ratio, a change characterizing small artery dysfunction.
Basal tone in the study group also was positively correlated with the LDL/HDL ratio, triglycerides, glycated hemoglobin, and high-sensitivity C-reactive protein, and was negatively correlated with HDL. Basal tone at 60 mm Hg was 8 in the preeclampsia group, compared with 5 in the control group (P = .07).
Meanwhile, the study group had higher sensitivity to norepinephrine and angiotensin II, and showed reduced distensibility. Distensibility was negatively correlated with homocysteine level, which has been associated with cardiovascular disease, in the study group only.
"The changes in passive properties of vascular wall are characterized by reduced distensibility that will affect stiffness of the arteries in women with a history of preeclampsia," said Dr. Kublickiene, an associate professor of obstetrics and gynecology and senior researcher at the Karolinska Institute Hospital-Huddinge in Stockholm. She also leads the Center for Gender Medicine at the institute.
Endothelium-dependent dilation to bradykinin (BK) and NO donor compounds were similar between the two groups. But endothelium-dependent response to flow was significantly attenuated in the study group, which could mean possible impairment of flow detection and signaling, according to Dr. Kublickiene.
"Preserved relaxation and the contribution of NO to BK-induced responses to NO donor and eNOS expression between the groups further support the specific importance of NO deficiency in flow-mediated dilation," she said.
"The observed changes will contribute to an increased peripheral resistance and blood pressure, which are of critical importance for long-term women’s cardiovascular health," she said. Counseling following a preeclamptic pregnancy and preterm delivery should include a discussion about reproduction and cardiovascular risks, she said.
And, she emphasized, "Let’s work with cardiologists."
A 2012 study that focused on a different group of women showed that collaboration between cardiologists and ob.gyns. is indeed possible.
Dr. Kublickiene said that several questions remain: What are the appropriate preventive strategies? What screening schedules should be recommended? What are the clinical targets? And, what are the treatment regimens?
"I think now clinical trials of statins and other early interventions in these women are warranted," said Dr. Kenny.
Dr. Kublickiene and Dr. Kenny said they had no disclosures. The study was funded by the Center for Gender Medicine at the Karolinska Institute, by the Karolinska Institute, and by the ALF fund of the Stockholm County Council.
On Twitter @NaseemSMiller
ORLANDO – Women with a history of severe preeclampsia show signs of small artery dysfunction as early as 2 years after delivery, an indication of cardiovascular disease later in life if not addressed by ob.gyns. and cardiologists early on, according to a small, unpublished study.
Researchers led by Dr. Karolina Kublickiene found that in women with a history of preeclampsia, endothelium-dependent dilation to flow was reduced, a change that could be due to nitric oxide contribution deficiency. The small arteries seen in the study group also exhibited increased myogenic tone, with enhanced sensitivity to the vasoconstrictor norepinephrine.
Dr. Louise Kenny, who moderated the session at the annual meeting of the Society for Gynecologic Investigation, said the study was "exquisitely executed."
"This is very basic science, but has massive clinical implications," said Dr. Kenny, a professor of obstetrics at the University College Cork, Ireland.
Several studies have shown that a history of preeclampsia is a risk factor for developing cardiovascular disease (Circulation 2012;125:1367-80). However, many women with preeclampsia go back to the community without proper follow-up with a cardiologist.
"I’m a high-risk maternal medicine obstetrician, and I’m very well aware that the long-term follow-up for women with preeclampsia is quite patchy," said Dr. Kenny. "We have a complete disconnect at several levels, and it is time to act."
Researchers hypothesized that functional and structural abnormalities in peripheral arteries are present as early as 2 years after delivery in mothers who had a pregnancy complicated by early-onset and severe preeclampsia.
They selected 15 women with a history of severe preeclampsia who had delivered between 2007 and 2011 at Karolinska University Hospital in Stockholm. They selected 15 closely matched controls who had normal pregnancies and gave birth during the same period. The women were on average 35 years old.
The investigators defined severe preeclampsia as systolic blood pressure of more than 160 mm Hg and/or diastolic blood pressure of more than 110 mm Hg on two occasions, at least 6 hours apart, and/or proteinuria of more than 5 g in a 24-hour period and/or organ damage.
The preeclampsia group and the control group were closely matched with regard to several biochemical characteristics, including the low-density lipoprotein to high-density lipoprotein (LDL/HDL) ratio (1.9 and 1.6, respectively). However, women in the preeclampsia group had higher blood pressure, insulin levels, and hemostatic model assessment index than did controls: The average diastolic blood pressure in the preeclampsia group was 74 mm Hg, versus 66 mm Hg in the control group. The average fasting insulin level in the preeclampsia group was almost twice as high as that of the control group (83 pmol/L vs. 44 pmol/L). Neither group showed evidence of early renal damage.
Researchers took subcutaneous fat biopsies from the women. They used pressure myography to compare the structure and function of the isolated small subcutaneous resistance arteries. They used immunostaining to compare endothelial nitric oxide synthase (eNOS) and lectin-like oxidized LDL receptor-1 (LOX-1) expression.
The arteries in both groups had similar diameters, wall thickness, wall-lumen ratio, and cross-sectional area.
Results showed that eNOS expression was similar in both groups, but LOX-1 expression was significantly enhanced in the study group. Inhibition of NOS had no effect on either group.
Myogenic tone was enhanced in the arteries of women with a history of preeclampsia, and was positively correlated with the LDL/HDL ratio, a change characterizing small artery dysfunction.
Basal tone in the study group also was positively correlated with the LDL/HDL ratio, triglycerides, glycated hemoglobin, and high-sensitivity C-reactive protein, and was negatively correlated with HDL. Basal tone at 60 mm Hg was 8 in the preeclampsia group, compared with 5 in the control group (P = .07).
Meanwhile, the study group had higher sensitivity to norepinephrine and angiotensin II, and showed reduced distensibility. Distensibility was negatively correlated with homocysteine level, which has been associated with cardiovascular disease, in the study group only.
"The changes in passive properties of vascular wall are characterized by reduced distensibility that will affect stiffness of the arteries in women with a history of preeclampsia," said Dr. Kublickiene, an associate professor of obstetrics and gynecology and senior researcher at the Karolinska Institute Hospital-Huddinge in Stockholm. She also leads the Center for Gender Medicine at the institute.
Endothelium-dependent dilation to bradykinin (BK) and NO donor compounds were similar between the two groups. But endothelium-dependent response to flow was significantly attenuated in the study group, which could mean possible impairment of flow detection and signaling, according to Dr. Kublickiene.
"Preserved relaxation and the contribution of NO to BK-induced responses to NO donor and eNOS expression between the groups further support the specific importance of NO deficiency in flow-mediated dilation," she said.
"The observed changes will contribute to an increased peripheral resistance and blood pressure, which are of critical importance for long-term women’s cardiovascular health," she said. Counseling following a preeclamptic pregnancy and preterm delivery should include a discussion about reproduction and cardiovascular risks, she said.
And, she emphasized, "Let’s work with cardiologists."
A 2012 study that focused on a different group of women showed that collaboration between cardiologists and ob.gyns. is indeed possible.
Dr. Kublickiene said that several questions remain: What are the appropriate preventive strategies? What screening schedules should be recommended? What are the clinical targets? And, what are the treatment regimens?
"I think now clinical trials of statins and other early interventions in these women are warranted," said Dr. Kenny.
Dr. Kublickiene and Dr. Kenny said they had no disclosures. The study was funded by the Center for Gender Medicine at the Karolinska Institute, by the Karolinska Institute, and by the ALF fund of the Stockholm County Council.
On Twitter @NaseemSMiller
AT THE SGI ANNUAL MEETING
Major finding: Basal tone in the preeclampsia group was positively correlated with LDL/HDL ratio, triglycerides, glycated hemoglobin, and high-sensitivity C-reactive protein, and was negatively correlated with HDL. Basal tone at 60 mm Hg was 8 in the preeclampsia group, compared with 5 in the control group (P = .07).
Data source: A study of 15 women with a history of severe preeclampsia who had delivered between 2007 and 2011 at Karolinska University Hospital in Stockholm, compared with 15 women who had normal pregnancies.
Disclosures: Dr. Kublickiene and Dr. Kenny said they had no disclosures. The study was funded by the Center for Gender Medicine at the Karolinska Institute, by the Karolinska Institute, and by the ALF fund of the Stockholm County Council.
Most pain apps lack physician input
FORT LAUDERDALE, FLA. – An evaluation of 222 pain-related smartphone apps showed that many were developed without the input of a health professional, some had inaccurate information, and some of their features weren’t as robust as they could be.
"Many of them were giving advice and offering coping strategies, but we don’t know if they’re effective," said Lorraine S. Wallace, Ph.D., who led the study. In addition, the apps could potentially be dangerous for users if the coping strategy – for instance, exercise – isn’t right for them, she said.
Experts have begun studying the safety and efficacy of health-related smartphone apps, many of which are aimed at patients for managing various diseases and conditions.
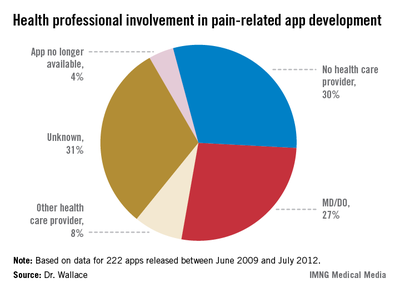
Dr. Wallace said that, ideally, app developers, physicians, and patients should collaborate to create the apps. "And there needs to be a list of good apps. I always get asked ‘show us a good app,’ so there are definitely some features that we should look at, and that should be driven by health care professionals to determine what a pain app should look like," she said. She advised physicians to be aware of the apps that are currently available to patients.
Dr. Wallace said her study was modeled after a 2011 British study of 111 pain-related apps. The authors of that study also concluded, "Pain apps appear to be able to promise pain relief without any concern for the effectiveness of the product, or for possible adverse effects of product use. In a population often desperate for a solution to distressing and debilitating pain conditions, there is considerable risk of individuals being misled" (J. Telemed. Telecare. 2011;17:308-12).

Dr. Wallace of the department of family medicine and director of research at the Ohio State University in Columbus said that in her evaluation, she didn’t find an ideal pain-related app. "There were certain ones that had better features such as pain diaries or other characteristics, but most of them were not that comprehensive."
Dr. Wallace and her colleagues searched Apple, Android, and Blackberry app stores for the word "pain." They chose 222 apps, and evaluated certain information such as cost, purpose, and key features and documentation of medical professional involvement in design and/or content.
The apps were released between June 2009 and July 2012, with an average cost of $4.99 or less (only seven apps cost more than $9.99). Researchers didn’t purchase any of the apps.
Pain diaries, exercises, and coping strategies were the most common app features. Many apps focused on general pain (93), 57 addressed back and/or neck pain, and 21 dealt with migraine/headache pain. Researchers found one app for muscle pain and one for pain from each of the following conditions: fibromyalgia, menstruation, injury, patellar tendonitis, rheumatism, and sciatica.
But, "the key finding was that in 30% of the apps, there was no evidence of a health provider input," said Dr. Wallace, who presented her findings in a poster at the annual meeting of the American Academy of Pain Medicine. In another 30%, the developer was unknown, and researchers couldn’t determine whether a health provider was involved in developing the app. In only 27% of the apps was there a clear involvement of an MD or DO.
Dr. Wallace and her team are working to get the study published and are planning to do a more extensive review of the apps this year. "We’re also planning on connecting some of the studies and looking at what percentages of physicians are recommending these apps and under what circumstances."
Dr. Wallace said she had no relevant financial disclosures.
On Twitter @NaseemSMiller
FORT LAUDERDALE, FLA. – An evaluation of 222 pain-related smartphone apps showed that many were developed without the input of a health professional, some had inaccurate information, and some of their features weren’t as robust as they could be.
"Many of them were giving advice and offering coping strategies, but we don’t know if they’re effective," said Lorraine S. Wallace, Ph.D., who led the study. In addition, the apps could potentially be dangerous for users if the coping strategy – for instance, exercise – isn’t right for them, she said.
Experts have begun studying the safety and efficacy of health-related smartphone apps, many of which are aimed at patients for managing various diseases and conditions.
Dr. Wallace said that, ideally, app developers, physicians, and patients should collaborate to create the apps. "And there needs to be a list of good apps. I always get asked ‘show us a good app,’ so there are definitely some features that we should look at, and that should be driven by health care professionals to determine what a pain app should look like," she said. She advised physicians to be aware of the apps that are currently available to patients.
Dr. Wallace said her study was modeled after a 2011 British study of 111 pain-related apps. The authors of that study also concluded, "Pain apps appear to be able to promise pain relief without any concern for the effectiveness of the product, or for possible adverse effects of product use. In a population often desperate for a solution to distressing and debilitating pain conditions, there is considerable risk of individuals being misled" (J. Telemed. Telecare. 2011;17:308-12).
Dr. Wallace of the department of family medicine and director of research at the Ohio State University in Columbus said that in her evaluation, she didn’t find an ideal pain-related app. "There were certain ones that had better features such as pain diaries or other characteristics, but most of them were not that comprehensive."
Dr. Wallace and her colleagues searched Apple, Android, and Blackberry app stores for the word "pain." They chose 222 apps, and evaluated certain information such as cost, purpose, and key features and documentation of medical professional involvement in design and/or content.
The apps were released between June 2009 and July 2012, with an average cost of $4.99 or less (only seven apps cost more than $9.99). Researchers didn’t purchase any of the apps.
Pain diaries, exercises, and coping strategies were the most common app features. Many apps focused on general pain (93), 57 addressed back and/or neck pain, and 21 dealt with migraine/headache pain. Researchers found one app for muscle pain and one for pain from each of the following conditions: fibromyalgia, menstruation, injury, patellar tendonitis, rheumatism, and sciatica.
But, "the key finding was that in 30% of the apps, there was no evidence of a health provider input," said Dr. Wallace, who presented her findings in a poster at the annual meeting of the American Academy of Pain Medicine. In another 30%, the developer was unknown, and researchers couldn’t determine whether a health provider was involved in developing the app. In only 27% of the apps was there a clear involvement of an MD or DO.
Dr. Wallace and her team are working to get the study published and are planning to do a more extensive review of the apps this year. "We’re also planning on connecting some of the studies and looking at what percentages of physicians are recommending these apps and under what circumstances."
Dr. Wallace said she had no relevant financial disclosures.
On Twitter @NaseemSMiller
FORT LAUDERDALE, FLA. – An evaluation of 222 pain-related smartphone apps showed that many were developed without the input of a health professional, some had inaccurate information, and some of their features weren’t as robust as they could be.
"Many of them were giving advice and offering coping strategies, but we don’t know if they’re effective," said Lorraine S. Wallace, Ph.D., who led the study. In addition, the apps could potentially be dangerous for users if the coping strategy – for instance, exercise – isn’t right for them, she said.
Experts have begun studying the safety and efficacy of health-related smartphone apps, many of which are aimed at patients for managing various diseases and conditions.
Dr. Wallace said that, ideally, app developers, physicians, and patients should collaborate to create the apps. "And there needs to be a list of good apps. I always get asked ‘show us a good app,’ so there are definitely some features that we should look at, and that should be driven by health care professionals to determine what a pain app should look like," she said. She advised physicians to be aware of the apps that are currently available to patients.
Dr. Wallace said her study was modeled after a 2011 British study of 111 pain-related apps. The authors of that study also concluded, "Pain apps appear to be able to promise pain relief without any concern for the effectiveness of the product, or for possible adverse effects of product use. In a population often desperate for a solution to distressing and debilitating pain conditions, there is considerable risk of individuals being misled" (J. Telemed. Telecare. 2011;17:308-12).
Dr. Wallace of the department of family medicine and director of research at the Ohio State University in Columbus said that in her evaluation, she didn’t find an ideal pain-related app. "There were certain ones that had better features such as pain diaries or other characteristics, but most of them were not that comprehensive."
Dr. Wallace and her colleagues searched Apple, Android, and Blackberry app stores for the word "pain." They chose 222 apps, and evaluated certain information such as cost, purpose, and key features and documentation of medical professional involvement in design and/or content.
The apps were released between June 2009 and July 2012, with an average cost of $4.99 or less (only seven apps cost more than $9.99). Researchers didn’t purchase any of the apps.
Pain diaries, exercises, and coping strategies were the most common app features. Many apps focused on general pain (93), 57 addressed back and/or neck pain, and 21 dealt with migraine/headache pain. Researchers found one app for muscle pain and one for pain from each of the following conditions: fibromyalgia, menstruation, injury, patellar tendonitis, rheumatism, and sciatica.
But, "the key finding was that in 30% of the apps, there was no evidence of a health provider input," said Dr. Wallace, who presented her findings in a poster at the annual meeting of the American Academy of Pain Medicine. In another 30%, the developer was unknown, and researchers couldn’t determine whether a health provider was involved in developing the app. In only 27% of the apps was there a clear involvement of an MD or DO.
Dr. Wallace and her team are working to get the study published and are planning to do a more extensive review of the apps this year. "We’re also planning on connecting some of the studies and looking at what percentages of physicians are recommending these apps and under what circumstances."
Dr. Wallace said she had no relevant financial disclosures.
On Twitter @NaseemSMiller
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PAIN MEDICINE
Major finding: In more than 60% of the apps, there was no clear indication that a health care professional was involved in the development process.
Data source: Researchers selected 222 apps by searching for the word "pain" in Apple, Android, and Blackberry app stores.
Disclosures: Dr. Wallace said she had no relevant financial disclosures.
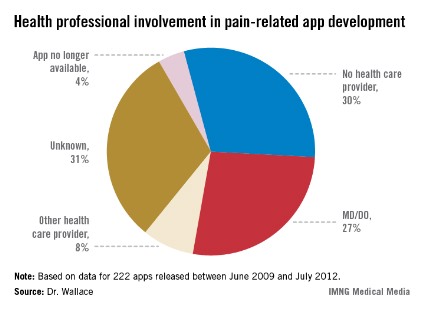
Fatty acid ratio may be associated with IVF success
ORLANDO – A higher ratio of serum omega-6 to omega-3 fatty acids was associated with an improved chance of pregnancy through in vitro fertilization, according to a prospective cohort study.
The study, which investigated the relationship between serum levels of polyunsaturated fatty acids (PUFAs) and embryo implantation in women undergoing IVF, found no association between IVF success and any of the PUFAs alone, or total fatty acid levels.

"While interesting, our findings should not be interpreted to influence current clinical practice, as they were not the result of a clinical trial," said Antonina I. Frolova, an M.D./Ph.D. student in the department of obstetrics and gynecology at Washington University, St. Louis.
"Our study suggests that PUFAs may also play a role in endometrial receptivity, but again, to our knowledge there is no clinical trial data to guide clinicians in counseling women on their intake of specific PUFAs to improve pregnancy rates in IVF," Ms. Frolova said in an interview. She presented the study at the annual meeting of the Society for Gynecologic Investigation.
The measurement of PUFA levels is currently not a part of standard assisted reproductive technology (ART) practice, said Dr. Vasiliki A. Moragianni, a reproductive endocrinologist at Beth Israel Deaconess Medical Center in Boston, who moderated the session.
The study "certainly adds a valuable piece of information and can be used as a springboard for more targeted investigations," Dr. Moragianni said in an interview. Once strong evidence and more data become available, "we will be able to make specific dietary recommendations and/or measure certain markers that can help improve couples’ fertility," she said.
Using the Women and Infants Health Specimen Consortium, Ms. Frolova and her colleagues measured the fasting serum levels of PUFAs in 200 women undergoing IVF. The women were divided into two groups: those who conceived and those who did not.
PUFA measurements included levels of linoleic acid (LA), alpha-linoleic acid (ALA), eicosapentaenoic acid (EPA), arachidonic acid (AA), and docosahexaenoic acid (DHA).
Researchers used standard regression to find out if any of the serum PUFAs was associated with pregnancy. They also analyzed the relationship between omega-6 to omega-3 ratios (LA:ALA) and (AA:EPA) and the odds of pregnancy
Although they found no association between individual PUFAs and the odds of pregnancy through IVF, they found a significant difference in LA:ALA ratios between women who conceived after their IVF cycle and those who did not (14.5 vs. 13.8, respectively; P = .03).
Women in the highest tertile of LA:ALA ratios had the highest chance of pregnancy compared with women with the lowest LA:ALA ratios (odds ratio, 2.5).
Embryo implantation was also weakly associated with LA:ALA ratios (P = .003), the researchers reported in the abstract.
There was no association between pregnancy and AA:EPA in this study, Ms. Frolova said. However, AA:EPA was positively correlated with the LA:ALA ratio (r = 0.4, P less than .001).
"Our findings are significant, as they suggest dietary intake of specific PUFAs may be altered to benefit women undergoing IVF," Ms. Frolova said. "Specifically, the study suggests that omega-3 and omega-6 PUFAs may have opposing effects in the endometrium, similar to other tissues."
She noted that further studies are needed to elucidate this mechanism, adding, "Prior to making any clinical recommendations, however, we would like to see a clinical trial investigating supplementation of certain PUFAs and pregnancy outcomes after IVF."
Ms. Frolova and Dr. Moragianni said they had no disclosures.
On Twitter @naseemsmiller
ORLANDO – A higher ratio of serum omega-6 to omega-3 fatty acids was associated with an improved chance of pregnancy through in vitro fertilization, according to a prospective cohort study.
The study, which investigated the relationship between serum levels of polyunsaturated fatty acids (PUFAs) and embryo implantation in women undergoing IVF, found no association between IVF success and any of the PUFAs alone, or total fatty acid levels.
"While interesting, our findings should not be interpreted to influence current clinical practice, as they were not the result of a clinical trial," said Antonina I. Frolova, an M.D./Ph.D. student in the department of obstetrics and gynecology at Washington University, St. Louis.
"Our study suggests that PUFAs may also play a role in endometrial receptivity, but again, to our knowledge there is no clinical trial data to guide clinicians in counseling women on their intake of specific PUFAs to improve pregnancy rates in IVF," Ms. Frolova said in an interview. She presented the study at the annual meeting of the Society for Gynecologic Investigation.
The measurement of PUFA levels is currently not a part of standard assisted reproductive technology (ART) practice, said Dr. Vasiliki A. Moragianni, a reproductive endocrinologist at Beth Israel Deaconess Medical Center in Boston, who moderated the session.
The study "certainly adds a valuable piece of information and can be used as a springboard for more targeted investigations," Dr. Moragianni said in an interview. Once strong evidence and more data become available, "we will be able to make specific dietary recommendations and/or measure certain markers that can help improve couples’ fertility," she said.
Using the Women and Infants Health Specimen Consortium, Ms. Frolova and her colleagues measured the fasting serum levels of PUFAs in 200 women undergoing IVF. The women were divided into two groups: those who conceived and those who did not.
PUFA measurements included levels of linoleic acid (LA), alpha-linoleic acid (ALA), eicosapentaenoic acid (EPA), arachidonic acid (AA), and docosahexaenoic acid (DHA).
Researchers used standard regression to find out if any of the serum PUFAs was associated with pregnancy. They also analyzed the relationship between omega-6 to omega-3 ratios (LA:ALA) and (AA:EPA) and the odds of pregnancy
Although they found no association between individual PUFAs and the odds of pregnancy through IVF, they found a significant difference in LA:ALA ratios between women who conceived after their IVF cycle and those who did not (14.5 vs. 13.8, respectively; P = .03).
Women in the highest tertile of LA:ALA ratios had the highest chance of pregnancy compared with women with the lowest LA:ALA ratios (odds ratio, 2.5).
Embryo implantation was also weakly associated with LA:ALA ratios (P = .003), the researchers reported in the abstract.
There was no association between pregnancy and AA:EPA in this study, Ms. Frolova said. However, AA:EPA was positively correlated with the LA:ALA ratio (r = 0.4, P less than .001).
"Our findings are significant, as they suggest dietary intake of specific PUFAs may be altered to benefit women undergoing IVF," Ms. Frolova said. "Specifically, the study suggests that omega-3 and omega-6 PUFAs may have opposing effects in the endometrium, similar to other tissues."
She noted that further studies are needed to elucidate this mechanism, adding, "Prior to making any clinical recommendations, however, we would like to see a clinical trial investigating supplementation of certain PUFAs and pregnancy outcomes after IVF."
Ms. Frolova and Dr. Moragianni said they had no disclosures.
On Twitter @naseemsmiller
ORLANDO – A higher ratio of serum omega-6 to omega-3 fatty acids was associated with an improved chance of pregnancy through in vitro fertilization, according to a prospective cohort study.
The study, which investigated the relationship between serum levels of polyunsaturated fatty acids (PUFAs) and embryo implantation in women undergoing IVF, found no association between IVF success and any of the PUFAs alone, or total fatty acid levels.
"While interesting, our findings should not be interpreted to influence current clinical practice, as they were not the result of a clinical trial," said Antonina I. Frolova, an M.D./Ph.D. student in the department of obstetrics and gynecology at Washington University, St. Louis.
"Our study suggests that PUFAs may also play a role in endometrial receptivity, but again, to our knowledge there is no clinical trial data to guide clinicians in counseling women on their intake of specific PUFAs to improve pregnancy rates in IVF," Ms. Frolova said in an interview. She presented the study at the annual meeting of the Society for Gynecologic Investigation.
The measurement of PUFA levels is currently not a part of standard assisted reproductive technology (ART) practice, said Dr. Vasiliki A. Moragianni, a reproductive endocrinologist at Beth Israel Deaconess Medical Center in Boston, who moderated the session.
The study "certainly adds a valuable piece of information and can be used as a springboard for more targeted investigations," Dr. Moragianni said in an interview. Once strong evidence and more data become available, "we will be able to make specific dietary recommendations and/or measure certain markers that can help improve couples’ fertility," she said.
Using the Women and Infants Health Specimen Consortium, Ms. Frolova and her colleagues measured the fasting serum levels of PUFAs in 200 women undergoing IVF. The women were divided into two groups: those who conceived and those who did not.
PUFA measurements included levels of linoleic acid (LA), alpha-linoleic acid (ALA), eicosapentaenoic acid (EPA), arachidonic acid (AA), and docosahexaenoic acid (DHA).
Researchers used standard regression to find out if any of the serum PUFAs was associated with pregnancy. They also analyzed the relationship between omega-6 to omega-3 ratios (LA:ALA) and (AA:EPA) and the odds of pregnancy
Although they found no association between individual PUFAs and the odds of pregnancy through IVF, they found a significant difference in LA:ALA ratios between women who conceived after their IVF cycle and those who did not (14.5 vs. 13.8, respectively; P = .03).
Women in the highest tertile of LA:ALA ratios had the highest chance of pregnancy compared with women with the lowest LA:ALA ratios (odds ratio, 2.5).
Embryo implantation was also weakly associated with LA:ALA ratios (P = .003), the researchers reported in the abstract.
There was no association between pregnancy and AA:EPA in this study, Ms. Frolova said. However, AA:EPA was positively correlated with the LA:ALA ratio (r = 0.4, P less than .001).
"Our findings are significant, as they suggest dietary intake of specific PUFAs may be altered to benefit women undergoing IVF," Ms. Frolova said. "Specifically, the study suggests that omega-3 and omega-6 PUFAs may have opposing effects in the endometrium, similar to other tissues."
She noted that further studies are needed to elucidate this mechanism, adding, "Prior to making any clinical recommendations, however, we would like to see a clinical trial investigating supplementation of certain PUFAs and pregnancy outcomes after IVF."
Ms. Frolova and Dr. Moragianni said they had no disclosures.
On Twitter @naseemsmiller
AT THE SGI ANNUAL MEETING
Major Finding: There was a significant difference in LA:ALA ratios between women who conceived after their IVF cycle and those who did not (14.5 vs. 13.8, respectively; P = .03).
Data Source: Measurement of the fasting serum levels of PUFAs in 200 women undergoing IVF, registered in the Women and Infants Health Specimen Consortium.
Disclosures: Ms. Frolova and Dr. Moragianni had no disclosures.
