User login
Time to rethink bioprosthetic valve guidelines?
Recent findings on the incidence and pathophysiology of bioprosthetic valve thrombosis require revisiting existing guidelines against routine echocardiography in the first 5 years after bioprosthetic valve replacement and a longer course of anticoagulation therapy than the current standard of 3 months, investigators from the Mayo Clinic said in an expert opinion article in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152;975-8).
In the expert commentary, Alexander C. Egbe, MBBS, of the departments of cardiovascular diseases and cardiovascular surgery at Mayo Clinic in Rochester, Minn., and coauthors explored the implications of their previous research, published in the Journal of the American College of Cardiology, that reported that bioprosthetic valve thrombosis (BPVT) is “not an uncommon cause of prosthetic valve dysfunction.” They identified BPVT in 46 of 397 (11%) bioprosthetic valves explanted at Mayo Clinic, and estimated the incidence of BPVT at 1% (J Am Coll Cardiol. 2015;66:2285-94), although Dr. Egbe and colleagues acknowledged the true incidence of BPVT is unknown, as is the time to occurrence. They noted that a different study design would be needed to determine that, along with the incidence of BPVT.
“The occurrence of BPVT is not restricted to surgically implanted bioprosthetic valves, but has also been observed after transcatheter aortic valve replacement (TAVR),” Dr. Egbe and colleagues said. They noted an association between BPVT and a lack of anticoagulation therapy in two earlier reports (N Engl J Med. 2015;373:2015-24; J Am Coll Cardiol. 2016;67:644-55). In their own study, 14 of 15 patients (93%) with diagnosed BPVT responded to anticoagulation therapy and avoided reoperation.
Dr. Egbe and coauthors did somewhat define the extent of the problem of misdiagnosis of BPVT. The diagnosis was considered in only 6 of 45 patients (13%) who had transesophageal echocardiography. “A significant proportion of the patients with BPVT were misdiagnosed as having structural failure and referred for reoperation,” Dr. Egbe and coauthors said. “This attests to the low level of awareness of the existence of BPVT and the lack of well-defined diagnostic criteria.”
They proposed a diagnostic model based on the echocardiography characteristics of three findings: a 50% increase in gradient within 5 years of implantation; increased cusp thickness; and abnormal cusp mobility. “The presence of all three echocardiographic features reliably diagnosed BPVT with a sensitivity of 72% and a specificity of 90%,” they said.
Their finding that 85% of BPVT cases occurred within 5 years of implantation flies in the face of clinical guidelines that state routine annual echocardiography is not recommended in that time frame (J Am So Echocardiogr. 2009;22;975-1014). But abnormal physical examination findings as a prerequisite for echocardiography may not be an effective method to diagnose BPVT. “In addition to transthoracic and transesophageal echocardiography, the use of other complementary imaging modalities, such as computed tomography, could be very effective in identifying subtle BPVT,” Dr. Egbe and colleagues said,
But preventing BPVT is more complicated. Clinical guidelines recommend anticoagulation of bioprosthetic valves for 3 months after implantation, but adhering to that guideline showed no protective effect against BPVT in their study, Dr. Egbe and coauthors said. Nor did antiplatelet therapy prove effective in preventing BPVT. However, a Danish study showed stopping anticoagulation within 6 months of surgical aortic valve replacement increased risk of thromboembolic complications and cardiovascular death (JAMA. 2012;308:2118-25). And the role of prosthesis type in BPVT “remains unclear.”
Dr. Egbe and coauthors acknowledged a number of questions persist with regard to BPVT in bioprosthetic valve dysfunction, including the true incidence, best screening method, risk factors, and the duration of anticoagulation, as well as the role of novel oral anticoagulants. “Answers to these questions will come from population-based prospective studies,” Dr. Egbe and colleagues said.
Dr. Egbe and his coauthors had no relationships to disclose.
Dr. Egbe and colleagues make a “provocative” case that it is the presence of thrombus on bioprosthetic valves, and not degeneration, that causes valve dysfunction, Clifford W. Barlow, MBBCh, DPhil, FRCS, of University Hospital Southampton (England) said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:978-80).
“This Expert Opinion is of particular interest because it relates to something commonly performed: conventional valve replacement,” Dr. Barlow said. Moreover, “BPVT is an under-recognized problem for which Dr. Egbe and colleagues concisely direct how future research should ascertain which diagnostic, preventive, and treatment strategies would improve long-term outcomes and avoid redo surgery.”
Dr. Egbe’s and colleagues’ recommendation of prolonged anticoagulation after bioprosthetic valve implantation complicates the selection of bioprosthetic valves – because cardiovascular surgeons frequently choose them to avoid anticoagulation, while accepting a higher risk of a reoperation because of valve degeneration, Dr. Barlow said.
And while Dr. Barlow noted this study found that porcine valves are not a predictor for BPVT, another Mayo Clinic study reported eight cases of BPVT, all in porcine valves (J Thorac Cardiovasc Surg. 2012;144:108-11). Nonetheless, the expert opinion by Dr. Egbe and colleagues is “relevant to much that is important – not only to improving outcomes with conventional valve replacement but also to these developing technologies,” Dr. Barlow said.
Dr. Egbe and colleagues make a “provocative” case that it is the presence of thrombus on bioprosthetic valves, and not degeneration, that causes valve dysfunction, Clifford W. Barlow, MBBCh, DPhil, FRCS, of University Hospital Southampton (England) said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:978-80).
“This Expert Opinion is of particular interest because it relates to something commonly performed: conventional valve replacement,” Dr. Barlow said. Moreover, “BPVT is an under-recognized problem for which Dr. Egbe and colleagues concisely direct how future research should ascertain which diagnostic, preventive, and treatment strategies would improve long-term outcomes and avoid redo surgery.”
Dr. Egbe’s and colleagues’ recommendation of prolonged anticoagulation after bioprosthetic valve implantation complicates the selection of bioprosthetic valves – because cardiovascular surgeons frequently choose them to avoid anticoagulation, while accepting a higher risk of a reoperation because of valve degeneration, Dr. Barlow said.
And while Dr. Barlow noted this study found that porcine valves are not a predictor for BPVT, another Mayo Clinic study reported eight cases of BPVT, all in porcine valves (J Thorac Cardiovasc Surg. 2012;144:108-11). Nonetheless, the expert opinion by Dr. Egbe and colleagues is “relevant to much that is important – not only to improving outcomes with conventional valve replacement but also to these developing technologies,” Dr. Barlow said.
Dr. Egbe and colleagues make a “provocative” case that it is the presence of thrombus on bioprosthetic valves, and not degeneration, that causes valve dysfunction, Clifford W. Barlow, MBBCh, DPhil, FRCS, of University Hospital Southampton (England) said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:978-80).
“This Expert Opinion is of particular interest because it relates to something commonly performed: conventional valve replacement,” Dr. Barlow said. Moreover, “BPVT is an under-recognized problem for which Dr. Egbe and colleagues concisely direct how future research should ascertain which diagnostic, preventive, and treatment strategies would improve long-term outcomes and avoid redo surgery.”
Dr. Egbe’s and colleagues’ recommendation of prolonged anticoagulation after bioprosthetic valve implantation complicates the selection of bioprosthetic valves – because cardiovascular surgeons frequently choose them to avoid anticoagulation, while accepting a higher risk of a reoperation because of valve degeneration, Dr. Barlow said.
And while Dr. Barlow noted this study found that porcine valves are not a predictor for BPVT, another Mayo Clinic study reported eight cases of BPVT, all in porcine valves (J Thorac Cardiovasc Surg. 2012;144:108-11). Nonetheless, the expert opinion by Dr. Egbe and colleagues is “relevant to much that is important – not only to improving outcomes with conventional valve replacement but also to these developing technologies,” Dr. Barlow said.
Recent findings on the incidence and pathophysiology of bioprosthetic valve thrombosis require revisiting existing guidelines against routine echocardiography in the first 5 years after bioprosthetic valve replacement and a longer course of anticoagulation therapy than the current standard of 3 months, investigators from the Mayo Clinic said in an expert opinion article in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152;975-8).
In the expert commentary, Alexander C. Egbe, MBBS, of the departments of cardiovascular diseases and cardiovascular surgery at Mayo Clinic in Rochester, Minn., and coauthors explored the implications of their previous research, published in the Journal of the American College of Cardiology, that reported that bioprosthetic valve thrombosis (BPVT) is “not an uncommon cause of prosthetic valve dysfunction.” They identified BPVT in 46 of 397 (11%) bioprosthetic valves explanted at Mayo Clinic, and estimated the incidence of BPVT at 1% (J Am Coll Cardiol. 2015;66:2285-94), although Dr. Egbe and colleagues acknowledged the true incidence of BPVT is unknown, as is the time to occurrence. They noted that a different study design would be needed to determine that, along with the incidence of BPVT.
“The occurrence of BPVT is not restricted to surgically implanted bioprosthetic valves, but has also been observed after transcatheter aortic valve replacement (TAVR),” Dr. Egbe and colleagues said. They noted an association between BPVT and a lack of anticoagulation therapy in two earlier reports (N Engl J Med. 2015;373:2015-24; J Am Coll Cardiol. 2016;67:644-55). In their own study, 14 of 15 patients (93%) with diagnosed BPVT responded to anticoagulation therapy and avoided reoperation.
Dr. Egbe and coauthors did somewhat define the extent of the problem of misdiagnosis of BPVT. The diagnosis was considered in only 6 of 45 patients (13%) who had transesophageal echocardiography. “A significant proportion of the patients with BPVT were misdiagnosed as having structural failure and referred for reoperation,” Dr. Egbe and coauthors said. “This attests to the low level of awareness of the existence of BPVT and the lack of well-defined diagnostic criteria.”
They proposed a diagnostic model based on the echocardiography characteristics of three findings: a 50% increase in gradient within 5 years of implantation; increased cusp thickness; and abnormal cusp mobility. “The presence of all three echocardiographic features reliably diagnosed BPVT with a sensitivity of 72% and a specificity of 90%,” they said.
Their finding that 85% of BPVT cases occurred within 5 years of implantation flies in the face of clinical guidelines that state routine annual echocardiography is not recommended in that time frame (J Am So Echocardiogr. 2009;22;975-1014). But abnormal physical examination findings as a prerequisite for echocardiography may not be an effective method to diagnose BPVT. “In addition to transthoracic and transesophageal echocardiography, the use of other complementary imaging modalities, such as computed tomography, could be very effective in identifying subtle BPVT,” Dr. Egbe and colleagues said,
But preventing BPVT is more complicated. Clinical guidelines recommend anticoagulation of bioprosthetic valves for 3 months after implantation, but adhering to that guideline showed no protective effect against BPVT in their study, Dr. Egbe and coauthors said. Nor did antiplatelet therapy prove effective in preventing BPVT. However, a Danish study showed stopping anticoagulation within 6 months of surgical aortic valve replacement increased risk of thromboembolic complications and cardiovascular death (JAMA. 2012;308:2118-25). And the role of prosthesis type in BPVT “remains unclear.”
Dr. Egbe and coauthors acknowledged a number of questions persist with regard to BPVT in bioprosthetic valve dysfunction, including the true incidence, best screening method, risk factors, and the duration of anticoagulation, as well as the role of novel oral anticoagulants. “Answers to these questions will come from population-based prospective studies,” Dr. Egbe and colleagues said.
Dr. Egbe and his coauthors had no relationships to disclose.
Recent findings on the incidence and pathophysiology of bioprosthetic valve thrombosis require revisiting existing guidelines against routine echocardiography in the first 5 years after bioprosthetic valve replacement and a longer course of anticoagulation therapy than the current standard of 3 months, investigators from the Mayo Clinic said in an expert opinion article in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152;975-8).
In the expert commentary, Alexander C. Egbe, MBBS, of the departments of cardiovascular diseases and cardiovascular surgery at Mayo Clinic in Rochester, Minn., and coauthors explored the implications of their previous research, published in the Journal of the American College of Cardiology, that reported that bioprosthetic valve thrombosis (BPVT) is “not an uncommon cause of prosthetic valve dysfunction.” They identified BPVT in 46 of 397 (11%) bioprosthetic valves explanted at Mayo Clinic, and estimated the incidence of BPVT at 1% (J Am Coll Cardiol. 2015;66:2285-94), although Dr. Egbe and colleagues acknowledged the true incidence of BPVT is unknown, as is the time to occurrence. They noted that a different study design would be needed to determine that, along with the incidence of BPVT.
“The occurrence of BPVT is not restricted to surgically implanted bioprosthetic valves, but has also been observed after transcatheter aortic valve replacement (TAVR),” Dr. Egbe and colleagues said. They noted an association between BPVT and a lack of anticoagulation therapy in two earlier reports (N Engl J Med. 2015;373:2015-24; J Am Coll Cardiol. 2016;67:644-55). In their own study, 14 of 15 patients (93%) with diagnosed BPVT responded to anticoagulation therapy and avoided reoperation.
Dr. Egbe and coauthors did somewhat define the extent of the problem of misdiagnosis of BPVT. The diagnosis was considered in only 6 of 45 patients (13%) who had transesophageal echocardiography. “A significant proportion of the patients with BPVT were misdiagnosed as having structural failure and referred for reoperation,” Dr. Egbe and coauthors said. “This attests to the low level of awareness of the existence of BPVT and the lack of well-defined diagnostic criteria.”
They proposed a diagnostic model based on the echocardiography characteristics of three findings: a 50% increase in gradient within 5 years of implantation; increased cusp thickness; and abnormal cusp mobility. “The presence of all three echocardiographic features reliably diagnosed BPVT with a sensitivity of 72% and a specificity of 90%,” they said.
Their finding that 85% of BPVT cases occurred within 5 years of implantation flies in the face of clinical guidelines that state routine annual echocardiography is not recommended in that time frame (J Am So Echocardiogr. 2009;22;975-1014). But abnormal physical examination findings as a prerequisite for echocardiography may not be an effective method to diagnose BPVT. “In addition to transthoracic and transesophageal echocardiography, the use of other complementary imaging modalities, such as computed tomography, could be very effective in identifying subtle BPVT,” Dr. Egbe and colleagues said,
But preventing BPVT is more complicated. Clinical guidelines recommend anticoagulation of bioprosthetic valves for 3 months after implantation, but adhering to that guideline showed no protective effect against BPVT in their study, Dr. Egbe and coauthors said. Nor did antiplatelet therapy prove effective in preventing BPVT. However, a Danish study showed stopping anticoagulation within 6 months of surgical aortic valve replacement increased risk of thromboembolic complications and cardiovascular death (JAMA. 2012;308:2118-25). And the role of prosthesis type in BPVT “remains unclear.”
Dr. Egbe and coauthors acknowledged a number of questions persist with regard to BPVT in bioprosthetic valve dysfunction, including the true incidence, best screening method, risk factors, and the duration of anticoagulation, as well as the role of novel oral anticoagulants. “Answers to these questions will come from population-based prospective studies,” Dr. Egbe and colleagues said.
Dr. Egbe and his coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Preoperative echocardiography can aid in the diagnosis of BPVT.
Major finding: Sixty-five percent of all reoperations for BPVT occurred more than a year after implantation and up to 15% of these reoperations occurred more than 5 years after the initial implantation.
Data source: Single-center retrospective study of 397 valve explants.
Disclosures: Dr. Egbe and his coauthors reported having no financial disclosures.
‘Stepping’ up to a better way to teach robotic lobectomy
Teaching minimally invasive robotic surgery to residents can be difficult in a health care environment obsessed with quality outcome measures and under scrutiny by hospital administrators and payers, but researchers at the University of Alabama at Birmingham may have devised a method to instruct residents in robotic lobectomy without compromising patient outcomes, according to a study published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:991-7).
Robert J. Cerfolio, MD, MBA, and his coauthors divided the procedure into 19 sequential, teachable steps and allowed residents to perform selected steps during operations that Dr. Cerfolio directed. “We then applied simulation training, coaching techniques, and video review of each step to help improve the steps that residents could not complete,” Dr. Cerfolio and his coauthors said.

Surgeons in academic centers face the challenge of teaching “the art and science of surgery,” Dr. Cerfolio and his colleagues said, while maintaining quality outcomes. “Teaching minimally invasive surgery, especially robotic surgery, is challenging given the risks and the limited availability of the robot.”
The researchers acknowledged that other groups have taken a similar approach to training, but this is the first study that included video review, coaching, and instruction tied to time constraints, they said. “A major concern is that while teaching robotic surgery, patients can be injured, care is worse, and metrics that are increasingly used as surrogates for quality outcomes suffer,” they noted.
They allotted each step in the procedure a set amount of time in which the resident had to complete it, totaling 80 minutes for all 19 steps and ranging from 1 minute to inspect the pleura after placing ports (9 minutes) to 20 minutes to close the five incisions. If the resident completed the task in the allotted time, it was recorded as “performed.”
Between February 2010 and December 2010 Dr. Cerfolio performed 520 robotic lobectomies, and over time the percentage of successful steps per resident improved. For example, in the first year, 50% of thoracic surgery residents completed the first five steps (mark and place ports, inspect pleura, resect the inferior pulmonary ligament, and remove three lymph nodes), but by the last year of the study 90% of them successfully completed the five steps.
Dr. Cerfolio and coauthors acknowledged “many flaws” in their study, but the study also had strengths: It involved only one operation and corroborated the database with each resident’s own surgical logs.
“Operations such as robotic lobectomy can be successfully taught by dividing them into a series of surgical maneuvers or steps,” the researchers noted. Recording what residents can and can’t do, reviewing video, and coaching contribute to the process to improve their skills. “Further studies that scientifically measure ‘ways to teach’ and ways to coach and mentor are needed,” they said.
Dr. Cerfolio disclosed relationships with Intuitive Surgical, Ethicon, Community Health Services, KCL, Bovie and C-SATS. Coauthor Douglas Minnich, MD, is a consultant to Medtronic. The other co-authors had no financial relationships to disclose.
Inderpal S. Sarkaria, MD, of the University of Pittsburgh acknowledged in his invited commentary how “metric-driven patient outcomes” have changed cardiothoracic surgical training (J Thorac Cardiovasc Surg. 2016;152:998).
But Dr. Sarkaria questioned the validity of using time performed as a metric in this study to evaluate a trainee’s competency. “Although ‘time’ is an important component, should not the primary focus be on ‘quality’ of the trainee’s work?” Dr. Sarkaria asked.

Despite these questions and the limitations of the study, he found the approach to surgical training “laudable.” Said Dr. Sarkaria: “It is arguable that the limitations of the study speak more to a common wisdom that certain aspects of surgical education remain an art to a greater or lesser extent, not easily amenable to our efforts to discretely compartmentalize and quantify the process.”
While the premise demands further study, Dr. Cerfolio and his coauthors “have laid a solid foundation on which further to build, explore, and potentially improve the science and art of teaching complex operations to our surgical residents,” Dr. Sarkaria said.
Dr. Sarkaria had no relationships to disclose.
Inderpal S. Sarkaria, MD, of the University of Pittsburgh acknowledged in his invited commentary how “metric-driven patient outcomes” have changed cardiothoracic surgical training (J Thorac Cardiovasc Surg. 2016;152:998).
But Dr. Sarkaria questioned the validity of using time performed as a metric in this study to evaluate a trainee’s competency. “Although ‘time’ is an important component, should not the primary focus be on ‘quality’ of the trainee’s work?” Dr. Sarkaria asked.
Despite these questions and the limitations of the study, he found the approach to surgical training “laudable.” Said Dr. Sarkaria: “It is arguable that the limitations of the study speak more to a common wisdom that certain aspects of surgical education remain an art to a greater or lesser extent, not easily amenable to our efforts to discretely compartmentalize and quantify the process.”
While the premise demands further study, Dr. Cerfolio and his coauthors “have laid a solid foundation on which further to build, explore, and potentially improve the science and art of teaching complex operations to our surgical residents,” Dr. Sarkaria said.
Dr. Sarkaria had no relationships to disclose.
Inderpal S. Sarkaria, MD, of the University of Pittsburgh acknowledged in his invited commentary how “metric-driven patient outcomes” have changed cardiothoracic surgical training (J Thorac Cardiovasc Surg. 2016;152:998).
But Dr. Sarkaria questioned the validity of using time performed as a metric in this study to evaluate a trainee’s competency. “Although ‘time’ is an important component, should not the primary focus be on ‘quality’ of the trainee’s work?” Dr. Sarkaria asked.
Despite these questions and the limitations of the study, he found the approach to surgical training “laudable.” Said Dr. Sarkaria: “It is arguable that the limitations of the study speak more to a common wisdom that certain aspects of surgical education remain an art to a greater or lesser extent, not easily amenable to our efforts to discretely compartmentalize and quantify the process.”
While the premise demands further study, Dr. Cerfolio and his coauthors “have laid a solid foundation on which further to build, explore, and potentially improve the science and art of teaching complex operations to our surgical residents,” Dr. Sarkaria said.
Dr. Sarkaria had no relationships to disclose.
Teaching minimally invasive robotic surgery to residents can be difficult in a health care environment obsessed with quality outcome measures and under scrutiny by hospital administrators and payers, but researchers at the University of Alabama at Birmingham may have devised a method to instruct residents in robotic lobectomy without compromising patient outcomes, according to a study published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:991-7).
Robert J. Cerfolio, MD, MBA, and his coauthors divided the procedure into 19 sequential, teachable steps and allowed residents to perform selected steps during operations that Dr. Cerfolio directed. “We then applied simulation training, coaching techniques, and video review of each step to help improve the steps that residents could not complete,” Dr. Cerfolio and his coauthors said.
Surgeons in academic centers face the challenge of teaching “the art and science of surgery,” Dr. Cerfolio and his colleagues said, while maintaining quality outcomes. “Teaching minimally invasive surgery, especially robotic surgery, is challenging given the risks and the limited availability of the robot.”
The researchers acknowledged that other groups have taken a similar approach to training, but this is the first study that included video review, coaching, and instruction tied to time constraints, they said. “A major concern is that while teaching robotic surgery, patients can be injured, care is worse, and metrics that are increasingly used as surrogates for quality outcomes suffer,” they noted.
They allotted each step in the procedure a set amount of time in which the resident had to complete it, totaling 80 minutes for all 19 steps and ranging from 1 minute to inspect the pleura after placing ports (9 minutes) to 20 minutes to close the five incisions. If the resident completed the task in the allotted time, it was recorded as “performed.”
Between February 2010 and December 2010 Dr. Cerfolio performed 520 robotic lobectomies, and over time the percentage of successful steps per resident improved. For example, in the first year, 50% of thoracic surgery residents completed the first five steps (mark and place ports, inspect pleura, resect the inferior pulmonary ligament, and remove three lymph nodes), but by the last year of the study 90% of them successfully completed the five steps.
Dr. Cerfolio and coauthors acknowledged “many flaws” in their study, but the study also had strengths: It involved only one operation and corroborated the database with each resident’s own surgical logs.
“Operations such as robotic lobectomy can be successfully taught by dividing them into a series of surgical maneuvers or steps,” the researchers noted. Recording what residents can and can’t do, reviewing video, and coaching contribute to the process to improve their skills. “Further studies that scientifically measure ‘ways to teach’ and ways to coach and mentor are needed,” they said.
Dr. Cerfolio disclosed relationships with Intuitive Surgical, Ethicon, Community Health Services, KCL, Bovie and C-SATS. Coauthor Douglas Minnich, MD, is a consultant to Medtronic. The other co-authors had no financial relationships to disclose.
Teaching minimally invasive robotic surgery to residents can be difficult in a health care environment obsessed with quality outcome measures and under scrutiny by hospital administrators and payers, but researchers at the University of Alabama at Birmingham may have devised a method to instruct residents in robotic lobectomy without compromising patient outcomes, according to a study published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:991-7).
Robert J. Cerfolio, MD, MBA, and his coauthors divided the procedure into 19 sequential, teachable steps and allowed residents to perform selected steps during operations that Dr. Cerfolio directed. “We then applied simulation training, coaching techniques, and video review of each step to help improve the steps that residents could not complete,” Dr. Cerfolio and his coauthors said.
Surgeons in academic centers face the challenge of teaching “the art and science of surgery,” Dr. Cerfolio and his colleagues said, while maintaining quality outcomes. “Teaching minimally invasive surgery, especially robotic surgery, is challenging given the risks and the limited availability of the robot.”
The researchers acknowledged that other groups have taken a similar approach to training, but this is the first study that included video review, coaching, and instruction tied to time constraints, they said. “A major concern is that while teaching robotic surgery, patients can be injured, care is worse, and metrics that are increasingly used as surrogates for quality outcomes suffer,” they noted.
They allotted each step in the procedure a set amount of time in which the resident had to complete it, totaling 80 minutes for all 19 steps and ranging from 1 minute to inspect the pleura after placing ports (9 minutes) to 20 minutes to close the five incisions. If the resident completed the task in the allotted time, it was recorded as “performed.”
Between February 2010 and December 2010 Dr. Cerfolio performed 520 robotic lobectomies, and over time the percentage of successful steps per resident improved. For example, in the first year, 50% of thoracic surgery residents completed the first five steps (mark and place ports, inspect pleura, resect the inferior pulmonary ligament, and remove three lymph nodes), but by the last year of the study 90% of them successfully completed the five steps.
Dr. Cerfolio and coauthors acknowledged “many flaws” in their study, but the study also had strengths: It involved only one operation and corroborated the database with each resident’s own surgical logs.
“Operations such as robotic lobectomy can be successfully taught by dividing them into a series of surgical maneuvers or steps,” the researchers noted. Recording what residents can and can’t do, reviewing video, and coaching contribute to the process to improve their skills. “Further studies that scientifically measure ‘ways to teach’ and ways to coach and mentor are needed,” they said.
Dr. Cerfolio disclosed relationships with Intuitive Surgical, Ethicon, Community Health Services, KCL, Bovie and C-SATS. Coauthor Douglas Minnich, MD, is a consultant to Medtronic. The other co-authors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Surgical residents learn and safely perform robotic lobectomy by dividing the procedure into a series of surgical maneuvers.
Major finding: The percentage of thoracic surgery residents who completed the first 5 of 19 procedural steps of the operation improved from 50% in the first year to 90% in the fifth year.
Data source: Single-center study of 520 consecutive lobectomies over 5 years by 35 general surgery residents and 7 cardiothoracic residents from February 2010 to December 2015.
Disclosures: Dr. Cerfolio disclosed relationships with Intuitive Surgical, Ethicon, Community Health Services, KCL, Bovie and C-SATS. Coauthor Douglas Minnich, MD, is a consultant to Medtronic. The other coauthors had no financial relationships to disclose.
Has mystery of exercise-intolerant chronic thromboembolic disease been solved?
The pathophysiology of exercise intolerance in chronic thromboembolic disease (CTED) and mechanism of improvement after pulmonary endarterectomy have not been well understood, but researchers in the Netherlands have identified those key clinical characteristics of exercise intolerance as well as the mechanisms to response of treatment.
This is the first study to identify the pathophysiology of the exercise intolerance—abnormal pulmonary vascular response—and the underlying mechanism for the pulmonary improvement, Coen van Kan, MD, of Our Lady’s Hospital in Amsterdam and colleagues at the University of Amsterdam reported in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152[3]:763-71).
“Our observations point to a hampered pulmonary vascular response and decreased ventilatory efficiency as underlying pathophysiological mechanisms to explain the exercise limitation observed in patients with CTED,” Dr. van Kan and colleagues wrote. “The clinically significant symptomatic improvement after surgery was shown to be related to significant improvements in both circulatory and ventilatory responses indicative for an improved right ventricle stroke volume during exercise and ventilatory efficiency.”
The researchers studied 14 patients with symptomatic CTED but with normal pulmonary pressures at rest. The patients underwent cardiopulmonary exercise testing (CPET) during right heart catheterization and then had noninvasive CPET 1 year later. During exercise the study subjects showed four features of abnormal pulmonary vascular responses:
• Steep mean pulmonary artery pressure/cardiac output (2.7 mm Hg/min per L).
• Low pulmonary vascular compliance (2.8 mL/mm Hg).
• Mean pulmonary artery pressure (mPAP)/cardiac output slope correlated with dead space ventilation (r = 0.586; P = .028).
• Ventilatory equivalents for carbon dioxide slope (r = 0.580; P = .030).
After screening for exercise-induced pulmonary hypertension, nine patients went on to have pulmonary endarterectomy (three patients had mPAP within normal limits during exercise and hence were not candidates, while two others declined surgery). All nine patients who had surgery survived, and a year afterward, their New York Heart Association functional class scores had improved from class II or II to class I in all patients. “Also, mean peak workload and mean oxygen consumption peak had increased, and the improvements observed tended to reach statistical significance,” Dr. van Kan and colleagues said.
After catheterization, improvement in exercise capacity was related to restoration of right ventricle stroke volume response, as measured by oxygen pulse improvement from 11.7 to 13.3 (P = .027) and heart rate response from 80.9 to 72 (P = .003); and a decrease in ventilatory equivalents for carbon dioxide slope from 38.2 to 32.8 (P = .014).
Dr. van Kan and coauthors had no financial relationships to disclose.
By studying subjects with symptomatic chronic thromboembolic disease and normal pulmonary pressures, Dr. van Kan and colleagues “cleverly opted to study an interesting group,” Robert B. Cameron, MD, of the University of California, Los Angeles, said in his invited commentary.

|
Dr. Robert B. Cameron |
“Logically, this patient group, representing potentially early pathophysiologic CTED, could reveal more pathophysiologic information about mechanisms active during the development of chronic thromboembolic pulmonary hypertension than would be seen in patients with more end-stage disease,” Dr. Cameron said (J Thorac Cardiovasc Surg. 2016;152[3]:771-2).
The early physiologic changes in patients with CTED that Dr. van Kan and colleagues reported on may make it possible to detect chronic thromboembolic pulmonary hypertension and intervene before advance disease sets in, Dr. Cameron said. “Surgical mortality may decrease to very-low levels simply from early surgical intervention,” he said.
Although the retrospective design is a limitation of the study, “these data improve our understanding of CTED and motivate all surgeons to promote prospective trials evaluating these findings and early intervention in a disease that is notoriously difficult to understand and treat,” Dr. Cameron said.
Dr. Cameron had no financial relationships to disclose.
By studying subjects with symptomatic chronic thromboembolic disease and normal pulmonary pressures, Dr. van Kan and colleagues “cleverly opted to study an interesting group,” Robert B. Cameron, MD, of the University of California, Los Angeles, said in his invited commentary.
|
|
Dr. Robert B. Cameron |
“Logically, this patient group, representing potentially early pathophysiologic CTED, could reveal more pathophysiologic information about mechanisms active during the development of chronic thromboembolic pulmonary hypertension than would be seen in patients with more end-stage disease,” Dr. Cameron said (J Thorac Cardiovasc Surg. 2016;152[3]:771-2).
The early physiologic changes in patients with CTED that Dr. van Kan and colleagues reported on may make it possible to detect chronic thromboembolic pulmonary hypertension and intervene before advance disease sets in, Dr. Cameron said. “Surgical mortality may decrease to very-low levels simply from early surgical intervention,” he said.
Although the retrospective design is a limitation of the study, “these data improve our understanding of CTED and motivate all surgeons to promote prospective trials evaluating these findings and early intervention in a disease that is notoriously difficult to understand and treat,” Dr. Cameron said.
Dr. Cameron had no financial relationships to disclose.
By studying subjects with symptomatic chronic thromboembolic disease and normal pulmonary pressures, Dr. van Kan and colleagues “cleverly opted to study an interesting group,” Robert B. Cameron, MD, of the University of California, Los Angeles, said in his invited commentary.
|
|
Dr. Robert B. Cameron |
“Logically, this patient group, representing potentially early pathophysiologic CTED, could reveal more pathophysiologic information about mechanisms active during the development of chronic thromboembolic pulmonary hypertension than would be seen in patients with more end-stage disease,” Dr. Cameron said (J Thorac Cardiovasc Surg. 2016;152[3]:771-2).
The early physiologic changes in patients with CTED that Dr. van Kan and colleagues reported on may make it possible to detect chronic thromboembolic pulmonary hypertension and intervene before advance disease sets in, Dr. Cameron said. “Surgical mortality may decrease to very-low levels simply from early surgical intervention,” he said.
Although the retrospective design is a limitation of the study, “these data improve our understanding of CTED and motivate all surgeons to promote prospective trials evaluating these findings and early intervention in a disease that is notoriously difficult to understand and treat,” Dr. Cameron said.
Dr. Cameron had no financial relationships to disclose.
The pathophysiology of exercise intolerance in chronic thromboembolic disease (CTED) and mechanism of improvement after pulmonary endarterectomy have not been well understood, but researchers in the Netherlands have identified those key clinical characteristics of exercise intolerance as well as the mechanisms to response of treatment.
This is the first study to identify the pathophysiology of the exercise intolerance—abnormal pulmonary vascular response—and the underlying mechanism for the pulmonary improvement, Coen van Kan, MD, of Our Lady’s Hospital in Amsterdam and colleagues at the University of Amsterdam reported in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152[3]:763-71).
“Our observations point to a hampered pulmonary vascular response and decreased ventilatory efficiency as underlying pathophysiological mechanisms to explain the exercise limitation observed in patients with CTED,” Dr. van Kan and colleagues wrote. “The clinically significant symptomatic improvement after surgery was shown to be related to significant improvements in both circulatory and ventilatory responses indicative for an improved right ventricle stroke volume during exercise and ventilatory efficiency.”
The researchers studied 14 patients with symptomatic CTED but with normal pulmonary pressures at rest. The patients underwent cardiopulmonary exercise testing (CPET) during right heart catheterization and then had noninvasive CPET 1 year later. During exercise the study subjects showed four features of abnormal pulmonary vascular responses:
• Steep mean pulmonary artery pressure/cardiac output (2.7 mm Hg/min per L).
• Low pulmonary vascular compliance (2.8 mL/mm Hg).
• Mean pulmonary artery pressure (mPAP)/cardiac output slope correlated with dead space ventilation (r = 0.586; P = .028).
• Ventilatory equivalents for carbon dioxide slope (r = 0.580; P = .030).
After screening for exercise-induced pulmonary hypertension, nine patients went on to have pulmonary endarterectomy (three patients had mPAP within normal limits during exercise and hence were not candidates, while two others declined surgery). All nine patients who had surgery survived, and a year afterward, their New York Heart Association functional class scores had improved from class II or II to class I in all patients. “Also, mean peak workload and mean oxygen consumption peak had increased, and the improvements observed tended to reach statistical significance,” Dr. van Kan and colleagues said.
After catheterization, improvement in exercise capacity was related to restoration of right ventricle stroke volume response, as measured by oxygen pulse improvement from 11.7 to 13.3 (P = .027) and heart rate response from 80.9 to 72 (P = .003); and a decrease in ventilatory equivalents for carbon dioxide slope from 38.2 to 32.8 (P = .014).
Dr. van Kan and coauthors had no financial relationships to disclose.
The pathophysiology of exercise intolerance in chronic thromboembolic disease (CTED) and mechanism of improvement after pulmonary endarterectomy have not been well understood, but researchers in the Netherlands have identified those key clinical characteristics of exercise intolerance as well as the mechanisms to response of treatment.
This is the first study to identify the pathophysiology of the exercise intolerance—abnormal pulmonary vascular response—and the underlying mechanism for the pulmonary improvement, Coen van Kan, MD, of Our Lady’s Hospital in Amsterdam and colleagues at the University of Amsterdam reported in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152[3]:763-71).
“Our observations point to a hampered pulmonary vascular response and decreased ventilatory efficiency as underlying pathophysiological mechanisms to explain the exercise limitation observed in patients with CTED,” Dr. van Kan and colleagues wrote. “The clinically significant symptomatic improvement after surgery was shown to be related to significant improvements in both circulatory and ventilatory responses indicative for an improved right ventricle stroke volume during exercise and ventilatory efficiency.”
The researchers studied 14 patients with symptomatic CTED but with normal pulmonary pressures at rest. The patients underwent cardiopulmonary exercise testing (CPET) during right heart catheterization and then had noninvasive CPET 1 year later. During exercise the study subjects showed four features of abnormal pulmonary vascular responses:
• Steep mean pulmonary artery pressure/cardiac output (2.7 mm Hg/min per L).
• Low pulmonary vascular compliance (2.8 mL/mm Hg).
• Mean pulmonary artery pressure (mPAP)/cardiac output slope correlated with dead space ventilation (r = 0.586; P = .028).
• Ventilatory equivalents for carbon dioxide slope (r = 0.580; P = .030).
After screening for exercise-induced pulmonary hypertension, nine patients went on to have pulmonary endarterectomy (three patients had mPAP within normal limits during exercise and hence were not candidates, while two others declined surgery). All nine patients who had surgery survived, and a year afterward, their New York Heart Association functional class scores had improved from class II or II to class I in all patients. “Also, mean peak workload and mean oxygen consumption peak had increased, and the improvements observed tended to reach statistical significance,” Dr. van Kan and colleagues said.
After catheterization, improvement in exercise capacity was related to restoration of right ventricle stroke volume response, as measured by oxygen pulse improvement from 11.7 to 13.3 (P = .027) and heart rate response from 80.9 to 72 (P = .003); and a decrease in ventilatory equivalents for carbon dioxide slope from 38.2 to 32.8 (P = .014).
Dr. van Kan and coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: This study identifies key clinical features of the pathophysiology of exercise intolerance in chronic thromboembolic disease (CTED) as well and the mechanisms of responses to treatment that have not been well understood .
Major finding: Exercise intolerance may result from an abnormal pulmonary vascular response and decreased ventilatory efficiency, while pulmonary endarterectomy restores right ventricle stroke volume response and ventilatory efficiency.
Data source: Fourteen subjects with exercise-intolerant CTED but normal pulmonary pressure underwent cardiopulmonary exercise testing (CPET) during right heart catheterization and noninvasive CPET 1 year later.
Disclosures: Dr. van Kan and coauthors had no financial relationships to disclose.

Survival shorter in extended-criteria lung recipients
The availability of lungs for transplant has been severely limited by usable donors, but organs from so-called extended criteria donors – those aged 65 years or older, had a 20 pack-years or more smoking history or history of diabetes mellitus, or were black – were found to be associated with shorter survival than lungs from standard donor lungs, and recipients with more severe lung disease had the lowest survival rates from extended-criteria organs, an analysis of the national donor database found.
“Matching donor quality to recipient severity is critical to achieve optimal outcomes in lung transplantation,” Matthew J. Mulligan, MD, and his colleagues from the University of Maryland, Baltimore, said in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:891-8). Dr. Mulligan previously presented the study results in April 2015 at the annual meeting of the American Association for Thoracic Surgery in Seattle.
The researchers analyzed 10,995 patients who received donor lungs between May 2005 and December 2012, 3,792 of whom received extended-criteria donor (ECD) organs. The study population was taken from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. Dr. Mulligan and his coauthors said this is the largest study examining ECD in lung transplants to date.
The goal of the study was to identify donor factors associated with reduced 1-year survival after transplantation, Dr. Mulligan and his colleagues said. “In the current literature, there is a paucity of data to guide the decision of matching donor quality to recipient severity,” the study authors said.
Recipients of extended-criteria lungs had a 41% increased risk of death, compared with recipients standard donor lungs, but individuals with more severe lung disease were at even greater risk with extended-criterial lungs, Dr. Mulligan and his colleagues said. Those who had a lung allocation score (LAS) less than 70 had a 1-year survival of 87% with standard donor lungs vs. 82% with extended-criteria lungs, while those who had a LAS of 70 or greater had survival rates of 80% and 72%, respectively.
Other donor factors that were inconsequential in recipient survival, Dr. Mulligan and his coauthors reported, included an abnormal chest x-ray, purulent secretions on bronchoscopy, blood type, mechanism of death (stroke, blunt trauma, gunshot, asphyxiation, and so on), or diagnosis of coronary artery disease and hypertension.
The researchers also did a Cox regression analysis, and found that recipients of extended-criteria lungs with a LAS greater than 70 had an 81% greater risk of death, compared with 37% for those with a LAS of 70 or greater who received standard-donor lungs, and 42% with a LAS of 70 or less and an extended-criteria donor lung.
These findings support the idea of not using ECD lungs in high-risk individuals with LAS greater than 70. “More important, ECD lungs were associated with the worst survival when transplanted into high-risk recipients,” Dr. Mulligan and his colleagues said.
The authors did acknowledge the inherent limitations of a retrospective analysis, but the large patient population is a redeeming factor of the study, Dr. Mulligan and his colleagues said. “Notwithstanding these limitations, the current study provides a rigorous analysis of a large number of lung transplants in the modern era, and the results reported will be useful to the lung transplant community,” the study authors said.
Dr. Mulligan and his coauthors had no relationships to disclose.
This study provides “greater clarity to the definition and significance of using lungs from an extended-criteria donor,” Benjamin Wei, MD, of the University of Alabama at Birmingham said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:899-900). “Now, we have more data about what constitutes an ECD for lung transplantation.”
The study also brought clarity on components of donor factors that do not affect survival – namely radiologic, bronchoscope, or laboratory criteria – Dr. Wei said. At the same time, the study raises questions about how transplant surgeons should use the findings. “Do we shy away from using donors with these high risk factors in low-risk recipients, high-risk recipients, neither, or both?” Dr. Wei asks. The study did not compare ECD lungs vs. no transplant, and becoming more selective in donors could cause more patients to die on the waiting list, he said.
A host of other questions also remain unanswered, Dr. Wei said, such as how a single standard-donor lung transplant compares with bilateral ECD transplants, or a single ECD lung vs. bilateral ECD lungs, and if use of ECD lungs by the criteria Dr. Mulligan and his coauthors outlined influences allograft patient survival.
“Of note, this study also did not include recipients receiving donor after cardiac death lungs or extracorporeal membrane oxygenation, both increasingly common situations,” he said. Nonetheless, the findings provide more information that transplant surgeons can base their decision-making on.
Dr. Wei had no financial relationships to disclose.
This study provides “greater clarity to the definition and significance of using lungs from an extended-criteria donor,” Benjamin Wei, MD, of the University of Alabama at Birmingham said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:899-900). “Now, we have more data about what constitutes an ECD for lung transplantation.”
The study also brought clarity on components of donor factors that do not affect survival – namely radiologic, bronchoscope, or laboratory criteria – Dr. Wei said. At the same time, the study raises questions about how transplant surgeons should use the findings. “Do we shy away from using donors with these high risk factors in low-risk recipients, high-risk recipients, neither, or both?” Dr. Wei asks. The study did not compare ECD lungs vs. no transplant, and becoming more selective in donors could cause more patients to die on the waiting list, he said.
A host of other questions also remain unanswered, Dr. Wei said, such as how a single standard-donor lung transplant compares with bilateral ECD transplants, or a single ECD lung vs. bilateral ECD lungs, and if use of ECD lungs by the criteria Dr. Mulligan and his coauthors outlined influences allograft patient survival.
“Of note, this study also did not include recipients receiving donor after cardiac death lungs or extracorporeal membrane oxygenation, both increasingly common situations,” he said. Nonetheless, the findings provide more information that transplant surgeons can base their decision-making on.
Dr. Wei had no financial relationships to disclose.
This study provides “greater clarity to the definition and significance of using lungs from an extended-criteria donor,” Benjamin Wei, MD, of the University of Alabama at Birmingham said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:899-900). “Now, we have more data about what constitutes an ECD for lung transplantation.”
The study also brought clarity on components of donor factors that do not affect survival – namely radiologic, bronchoscope, or laboratory criteria – Dr. Wei said. At the same time, the study raises questions about how transplant surgeons should use the findings. “Do we shy away from using donors with these high risk factors in low-risk recipients, high-risk recipients, neither, or both?” Dr. Wei asks. The study did not compare ECD lungs vs. no transplant, and becoming more selective in donors could cause more patients to die on the waiting list, he said.
A host of other questions also remain unanswered, Dr. Wei said, such as how a single standard-donor lung transplant compares with bilateral ECD transplants, or a single ECD lung vs. bilateral ECD lungs, and if use of ECD lungs by the criteria Dr. Mulligan and his coauthors outlined influences allograft patient survival.
“Of note, this study also did not include recipients receiving donor after cardiac death lungs or extracorporeal membrane oxygenation, both increasingly common situations,” he said. Nonetheless, the findings provide more information that transplant surgeons can base their decision-making on.
Dr. Wei had no financial relationships to disclose.
The availability of lungs for transplant has been severely limited by usable donors, but organs from so-called extended criteria donors – those aged 65 years or older, had a 20 pack-years or more smoking history or history of diabetes mellitus, or were black – were found to be associated with shorter survival than lungs from standard donor lungs, and recipients with more severe lung disease had the lowest survival rates from extended-criteria organs, an analysis of the national donor database found.
“Matching donor quality to recipient severity is critical to achieve optimal outcomes in lung transplantation,” Matthew J. Mulligan, MD, and his colleagues from the University of Maryland, Baltimore, said in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:891-8). Dr. Mulligan previously presented the study results in April 2015 at the annual meeting of the American Association for Thoracic Surgery in Seattle.
The researchers analyzed 10,995 patients who received donor lungs between May 2005 and December 2012, 3,792 of whom received extended-criteria donor (ECD) organs. The study population was taken from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. Dr. Mulligan and his coauthors said this is the largest study examining ECD in lung transplants to date.
The goal of the study was to identify donor factors associated with reduced 1-year survival after transplantation, Dr. Mulligan and his colleagues said. “In the current literature, there is a paucity of data to guide the decision of matching donor quality to recipient severity,” the study authors said.
Recipients of extended-criteria lungs had a 41% increased risk of death, compared with recipients standard donor lungs, but individuals with more severe lung disease were at even greater risk with extended-criterial lungs, Dr. Mulligan and his colleagues said. Those who had a lung allocation score (LAS) less than 70 had a 1-year survival of 87% with standard donor lungs vs. 82% with extended-criteria lungs, while those who had a LAS of 70 or greater had survival rates of 80% and 72%, respectively.
Other donor factors that were inconsequential in recipient survival, Dr. Mulligan and his coauthors reported, included an abnormal chest x-ray, purulent secretions on bronchoscopy, blood type, mechanism of death (stroke, blunt trauma, gunshot, asphyxiation, and so on), or diagnosis of coronary artery disease and hypertension.
The researchers also did a Cox regression analysis, and found that recipients of extended-criteria lungs with a LAS greater than 70 had an 81% greater risk of death, compared with 37% for those with a LAS of 70 or greater who received standard-donor lungs, and 42% with a LAS of 70 or less and an extended-criteria donor lung.
These findings support the idea of not using ECD lungs in high-risk individuals with LAS greater than 70. “More important, ECD lungs were associated with the worst survival when transplanted into high-risk recipients,” Dr. Mulligan and his colleagues said.
The authors did acknowledge the inherent limitations of a retrospective analysis, but the large patient population is a redeeming factor of the study, Dr. Mulligan and his colleagues said. “Notwithstanding these limitations, the current study provides a rigorous analysis of a large number of lung transplants in the modern era, and the results reported will be useful to the lung transplant community,” the study authors said.
Dr. Mulligan and his coauthors had no relationships to disclose.
The availability of lungs for transplant has been severely limited by usable donors, but organs from so-called extended criteria donors – those aged 65 years or older, had a 20 pack-years or more smoking history or history of diabetes mellitus, or were black – were found to be associated with shorter survival than lungs from standard donor lungs, and recipients with more severe lung disease had the lowest survival rates from extended-criteria organs, an analysis of the national donor database found.
“Matching donor quality to recipient severity is critical to achieve optimal outcomes in lung transplantation,” Matthew J. Mulligan, MD, and his colleagues from the University of Maryland, Baltimore, said in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:891-8). Dr. Mulligan previously presented the study results in April 2015 at the annual meeting of the American Association for Thoracic Surgery in Seattle.
The researchers analyzed 10,995 patients who received donor lungs between May 2005 and December 2012, 3,792 of whom received extended-criteria donor (ECD) organs. The study population was taken from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. Dr. Mulligan and his coauthors said this is the largest study examining ECD in lung transplants to date.
The goal of the study was to identify donor factors associated with reduced 1-year survival after transplantation, Dr. Mulligan and his colleagues said. “In the current literature, there is a paucity of data to guide the decision of matching donor quality to recipient severity,” the study authors said.
Recipients of extended-criteria lungs had a 41% increased risk of death, compared with recipients standard donor lungs, but individuals with more severe lung disease were at even greater risk with extended-criterial lungs, Dr. Mulligan and his colleagues said. Those who had a lung allocation score (LAS) less than 70 had a 1-year survival of 87% with standard donor lungs vs. 82% with extended-criteria lungs, while those who had a LAS of 70 or greater had survival rates of 80% and 72%, respectively.
Other donor factors that were inconsequential in recipient survival, Dr. Mulligan and his coauthors reported, included an abnormal chest x-ray, purulent secretions on bronchoscopy, blood type, mechanism of death (stroke, blunt trauma, gunshot, asphyxiation, and so on), or diagnosis of coronary artery disease and hypertension.
The researchers also did a Cox regression analysis, and found that recipients of extended-criteria lungs with a LAS greater than 70 had an 81% greater risk of death, compared with 37% for those with a LAS of 70 or greater who received standard-donor lungs, and 42% with a LAS of 70 or less and an extended-criteria donor lung.
These findings support the idea of not using ECD lungs in high-risk individuals with LAS greater than 70. “More important, ECD lungs were associated with the worst survival when transplanted into high-risk recipients,” Dr. Mulligan and his colleagues said.
The authors did acknowledge the inherent limitations of a retrospective analysis, but the large patient population is a redeeming factor of the study, Dr. Mulligan and his colleagues said. “Notwithstanding these limitations, the current study provides a rigorous analysis of a large number of lung transplants in the modern era, and the results reported will be useful to the lung transplant community,” the study authors said.
Dr. Mulligan and his coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Lung transplant recipients who received extended-criteria donor (ECD) lungs have lower rates of 1-year survival than recipients of standard donor lungs.
Major finding: Recipients of ECD lungs had a 41% higher risk of death than recipients of standard lungs, and those who had more severe lung disease had lower rates of 1-year survival after receiving ECD lungs, compared with standard donor lungs.
Data source: Retrospective analysis of 10,995 lung recipients, from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database, 3,792 of whom who received extended-criteria donor organs over 7.5 years.
Disclosures: Dr. Mulligan and his coauthors had no financial relationships to disclose.
Can TEE find septal defects in conotruncal repair?
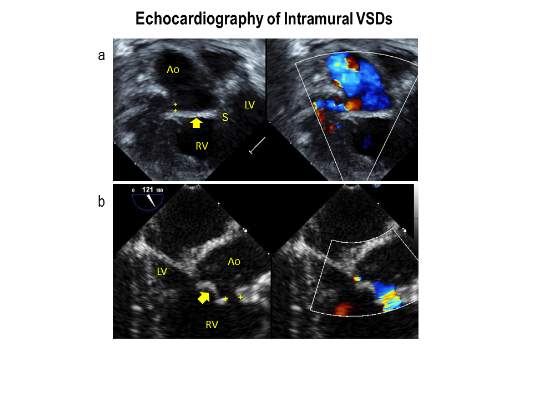
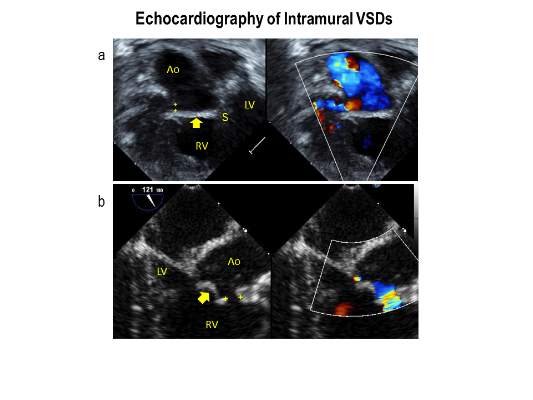
Intramural ventricular septal defects (VSD), residual defects that can occur after repair of conotruncal defects in newborns, increase the risk of complications and death if they’re not detected and closed during the index operation. While various methods have been tried to find these defects during surgery, researchers from Children’s Hospital of Philadelphia (CHOP) reported that the use of transesophageal echocardiography (TEE) has a good chance of finding VSDs and giving cardiac surgeons the opportunity to correct these residual defects.
“TEE has modest sensitivity but high specificity for identifying intramural VSDs and can identify most defects requiring reinterventions,” Jyoti Patel, MD, and her coauthors reported in a study published in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:688-95).
Previous studies have shown that intraoperative TEE is safe for evaluating operations in congenital heart disease, but this is the first study to evaluate the modality for detecting intramural VSDs, Dr. Patel and her colleagues said.
Dr. Patel and her coinvestigators analyzed results of TEE and postoperative transthoracic echocardiography (TTE) in patients who had biventricular repair of conotruncal anomalies at CHOP from January 2006 through June 2013. Intramural VSDs occurred in 34 of 337 patients who met the inclusion criteria out of a total population of 903. Actually, 462 patients had biventricular repairs of conotruncal defects involving baffle closure of a VSD, but 125 were excluded for various reasons, including 105 for inadequate intraoperative TEE.
TTE identified a total of 177 residual VSDs, 34 of which were intramural in nature. Among the evaluated procedures, both TEE at the end of the index operation and TTE detected VSD in 19 patients; TTE alone found VSD in 15. “Sensitivity was 56% and specificity was 100% for TEE to identify intramural VSDs,” Dr. Patel and her colleagues said.
What’s more, both TTE and TEE combined identified peripatch VSDs in 90 patients, while TTE only in 53 and TEE only in 15, “yielding a sensitivity of 63% and specificity of 92%,” Dr. Patel and her colleagues said.
Of the VSDs that required catheterization or reintervention during surgery, intraoperative TEE detected six of seven intramural VSDs and all five peripatch VSDs, the study found.
“In this study, TEE identified most intramural VSDs and all peripatch VSDs that required subsequent reintervention,” Dr. Patel and her colleagues said.
“This finding underscores the importance of adequate imaging of the superior aspect of the VSD patch during intraoperative TEE for conotruncal anomalies, given that many intramural defects may be repaired during the initial operation.”
Coauthor Andrew Glatz, MD, disclosed receiving consulting fees from Bristol-Myers Squibb, and coauthor Chitra Ravishankar, MD, disclosed lecture fees from Danone Medical. Dr. Patel and the remaining coauthors had no financial relationships to disclose.
Because of the clinical importance of intramural VSDs, cardiac surgeons need to be highly suspicious in any operation to repair conotruncal defects where the VSD margins are close to the trabeculae, Edward Buratto, MBBS, Philip Naimo, MD, and Igor Konstantinov, MD, PhD, of Royal Children’s Hospital at the University of Melbourne said in their invited commentary (J Thorac Cardiovasc Surg. 2016;152:696-7). “The best way to resolve the problem would be to prevent it,” they said.
While intraoperative TEE can detect VSDs preemptively, the imaging technique is “not without its flaws,” the commentators said, as evidenced by the 105 subjects the CHOP study excluded because of inadequate TEE imaging. Those excluded cases comprised patients aged 30 days and younger with lower body weight and higher early death rates. “It is these patients who would benefit most from intraoperative identification of intramural VSD,” the commentators said.
They also noted that TEE in detecting intramural and peripatch VSD in children aged 30 days and older “was not perfect either,” with sensitivities of 56% and 63%, respectively. In the CHOP study, TEE was more likely to detect intramural VSD in patients older than 30 days with higher body weight, Dr. Buratto and his colleagues said.
The favored approach at Royal Children’s Hospital in Melbourne is routine epicardial echocardiograms in conotruncal repair. This imaging technique provides “superb imaging quality,” they said. “This is of particular importance in small children.” They advocate closing a significant VSD once it’s identified.
“After all, failure to close intramural VSD occurs when surgeons do not realize how close they were to success when they gave up,” the commentators said. Precise echocardiographic guidance would “dramatically facilitate” that strategy.
Dr. Buratto, Dr. Naimo, and Dr. Konstantinov had no financial relationships to disclose.
Because of the clinical importance of intramural VSDs, cardiac surgeons need to be highly suspicious in any operation to repair conotruncal defects where the VSD margins are close to the trabeculae, Edward Buratto, MBBS, Philip Naimo, MD, and Igor Konstantinov, MD, PhD, of Royal Children’s Hospital at the University of Melbourne said in their invited commentary (J Thorac Cardiovasc Surg. 2016;152:696-7). “The best way to resolve the problem would be to prevent it,” they said.
While intraoperative TEE can detect VSDs preemptively, the imaging technique is “not without its flaws,” the commentators said, as evidenced by the 105 subjects the CHOP study excluded because of inadequate TEE imaging. Those excluded cases comprised patients aged 30 days and younger with lower body weight and higher early death rates. “It is these patients who would benefit most from intraoperative identification of intramural VSD,” the commentators said.
They also noted that TEE in detecting intramural and peripatch VSD in children aged 30 days and older “was not perfect either,” with sensitivities of 56% and 63%, respectively. In the CHOP study, TEE was more likely to detect intramural VSD in patients older than 30 days with higher body weight, Dr. Buratto and his colleagues said.
The favored approach at Royal Children’s Hospital in Melbourne is routine epicardial echocardiograms in conotruncal repair. This imaging technique provides “superb imaging quality,” they said. “This is of particular importance in small children.” They advocate closing a significant VSD once it’s identified.
“After all, failure to close intramural VSD occurs when surgeons do not realize how close they were to success when they gave up,” the commentators said. Precise echocardiographic guidance would “dramatically facilitate” that strategy.
Dr. Buratto, Dr. Naimo, and Dr. Konstantinov had no financial relationships to disclose.
Because of the clinical importance of intramural VSDs, cardiac surgeons need to be highly suspicious in any operation to repair conotruncal defects where the VSD margins are close to the trabeculae, Edward Buratto, MBBS, Philip Naimo, MD, and Igor Konstantinov, MD, PhD, of Royal Children’s Hospital at the University of Melbourne said in their invited commentary (J Thorac Cardiovasc Surg. 2016;152:696-7). “The best way to resolve the problem would be to prevent it,” they said.
While intraoperative TEE can detect VSDs preemptively, the imaging technique is “not without its flaws,” the commentators said, as evidenced by the 105 subjects the CHOP study excluded because of inadequate TEE imaging. Those excluded cases comprised patients aged 30 days and younger with lower body weight and higher early death rates. “It is these patients who would benefit most from intraoperative identification of intramural VSD,” the commentators said.
They also noted that TEE in detecting intramural and peripatch VSD in children aged 30 days and older “was not perfect either,” with sensitivities of 56% and 63%, respectively. In the CHOP study, TEE was more likely to detect intramural VSD in patients older than 30 days with higher body weight, Dr. Buratto and his colleagues said.
The favored approach at Royal Children’s Hospital in Melbourne is routine epicardial echocardiograms in conotruncal repair. This imaging technique provides “superb imaging quality,” they said. “This is of particular importance in small children.” They advocate closing a significant VSD once it’s identified.
“After all, failure to close intramural VSD occurs when surgeons do not realize how close they were to success when they gave up,” the commentators said. Precise echocardiographic guidance would “dramatically facilitate” that strategy.
Dr. Buratto, Dr. Naimo, and Dr. Konstantinov had no financial relationships to disclose.
Intramural ventricular septal defects (VSD), residual defects that can occur after repair of conotruncal defects in newborns, increase the risk of complications and death if they’re not detected and closed during the index operation. While various methods have been tried to find these defects during surgery, researchers from Children’s Hospital of Philadelphia (CHOP) reported that the use of transesophageal echocardiography (TEE) has a good chance of finding VSDs and giving cardiac surgeons the opportunity to correct these residual defects.
“TEE has modest sensitivity but high specificity for identifying intramural VSDs and can identify most defects requiring reinterventions,” Jyoti Patel, MD, and her coauthors reported in a study published in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:688-95).
Previous studies have shown that intraoperative TEE is safe for evaluating operations in congenital heart disease, but this is the first study to evaluate the modality for detecting intramural VSDs, Dr. Patel and her colleagues said.
Dr. Patel and her coinvestigators analyzed results of TEE and postoperative transthoracic echocardiography (TTE) in patients who had biventricular repair of conotruncal anomalies at CHOP from January 2006 through June 2013. Intramural VSDs occurred in 34 of 337 patients who met the inclusion criteria out of a total population of 903. Actually, 462 patients had biventricular repairs of conotruncal defects involving baffle closure of a VSD, but 125 were excluded for various reasons, including 105 for inadequate intraoperative TEE.
TTE identified a total of 177 residual VSDs, 34 of which were intramural in nature. Among the evaluated procedures, both TEE at the end of the index operation and TTE detected VSD in 19 patients; TTE alone found VSD in 15. “Sensitivity was 56% and specificity was 100% for TEE to identify intramural VSDs,” Dr. Patel and her colleagues said.
What’s more, both TTE and TEE combined identified peripatch VSDs in 90 patients, while TTE only in 53 and TEE only in 15, “yielding a sensitivity of 63% and specificity of 92%,” Dr. Patel and her colleagues said.
Of the VSDs that required catheterization or reintervention during surgery, intraoperative TEE detected six of seven intramural VSDs and all five peripatch VSDs, the study found.
“In this study, TEE identified most intramural VSDs and all peripatch VSDs that required subsequent reintervention,” Dr. Patel and her colleagues said.
“This finding underscores the importance of adequate imaging of the superior aspect of the VSD patch during intraoperative TEE for conotruncal anomalies, given that many intramural defects may be repaired during the initial operation.”
Coauthor Andrew Glatz, MD, disclosed receiving consulting fees from Bristol-Myers Squibb, and coauthor Chitra Ravishankar, MD, disclosed lecture fees from Danone Medical. Dr. Patel and the remaining coauthors had no financial relationships to disclose.
Intramural ventricular septal defects (VSD), residual defects that can occur after repair of conotruncal defects in newborns, increase the risk of complications and death if they’re not detected and closed during the index operation. While various methods have been tried to find these defects during surgery, researchers from Children’s Hospital of Philadelphia (CHOP) reported that the use of transesophageal echocardiography (TEE) has a good chance of finding VSDs and giving cardiac surgeons the opportunity to correct these residual defects.
“TEE has modest sensitivity but high specificity for identifying intramural VSDs and can identify most defects requiring reinterventions,” Jyoti Patel, MD, and her coauthors reported in a study published in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:688-95).
Previous studies have shown that intraoperative TEE is safe for evaluating operations in congenital heart disease, but this is the first study to evaluate the modality for detecting intramural VSDs, Dr. Patel and her colleagues said.
Dr. Patel and her coinvestigators analyzed results of TEE and postoperative transthoracic echocardiography (TTE) in patients who had biventricular repair of conotruncal anomalies at CHOP from January 2006 through June 2013. Intramural VSDs occurred in 34 of 337 patients who met the inclusion criteria out of a total population of 903. Actually, 462 patients had biventricular repairs of conotruncal defects involving baffle closure of a VSD, but 125 were excluded for various reasons, including 105 for inadequate intraoperative TEE.
TTE identified a total of 177 residual VSDs, 34 of which were intramural in nature. Among the evaluated procedures, both TEE at the end of the index operation and TTE detected VSD in 19 patients; TTE alone found VSD in 15. “Sensitivity was 56% and specificity was 100% for TEE to identify intramural VSDs,” Dr. Patel and her colleagues said.
What’s more, both TTE and TEE combined identified peripatch VSDs in 90 patients, while TTE only in 53 and TEE only in 15, “yielding a sensitivity of 63% and specificity of 92%,” Dr. Patel and her colleagues said.
Of the VSDs that required catheterization or reintervention during surgery, intraoperative TEE detected six of seven intramural VSDs and all five peripatch VSDs, the study found.
“In this study, TEE identified most intramural VSDs and all peripatch VSDs that required subsequent reintervention,” Dr. Patel and her colleagues said.
“This finding underscores the importance of adequate imaging of the superior aspect of the VSD patch during intraoperative TEE for conotruncal anomalies, given that many intramural defects may be repaired during the initial operation.”
Coauthor Andrew Glatz, MD, disclosed receiving consulting fees from Bristol-Myers Squibb, and coauthor Chitra Ravishankar, MD, disclosed lecture fees from Danone Medical. Dr. Patel and the remaining coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Intraoperative transesophageal echocardiography has modest sensitivity but high specificity for detecting ventricular septal defects after repair of conotruncal anomalies.
Major finding: TEE is useful for identifying most VSDs during the index operation, providing the opportunity to repair the defects during the index operation.
Data source: A single-institution database of 337 patients who had operations to repair conotruncal anomalies between January 2006 and June 2013.
Disclosures: Coauthor Andrew Glatz, MD, disclosed receiving consulting fees from Bristol-Myers Squibb, and coauthor Chitra Ravishankar, MD, disclosed lecture fees from Danone Medical. Dr. Patel and the remaining coauthors had no financial relationships to disclose.
Transcatheter mitral valve therapy at ‘event horizon’
As investigational transcatheter mitral valve therapies continue to explode onto the scene, cardiac surgeons must act now to seize and assert their place in the multidisciplinary team with interventional, imaging, and heart failure colleagues to deliver these treatments to people with complex mitral valve regurgitation, an expert opinion report in the August issue of the Journal of Thoracic and Cardiovascular Surgery states (J Thorac Cardiovasc Surg. 2016;152:330-6).
“There is a growing population of patients with primary and secondary mitral regurgitation underserved by surgical therapy because of comorbid risk,” Vinay Badhwar, MD, of West Virginia University and his colleagues said. “This has led to a tremendous activity of device development.”
With more than 25 different transcatheter mitral valve devices in development (MitraClip, Abbott Vascular, is the only FDA-approved transcatheter for primary mitral regurgitation [MR]), cardiac surgeons will soon have the tools to offer transcatheter mitral valve repair (TMVr) and transcatheter mitral valve replacement (TMVR) to more complex patients who have MR along with other health problems. Today about half of those patients do not get surgery because they are too frail, Dr. Badhwar and his colleagues said.
The authors used the astrophysical phrase “event horizon” to define the current state of transcatheter mitral valve therapies – “a point of no return.” They expect surgery to remain the treatment of choice for MR for the next 10 years. “However, as our patient cohorts become increasingly more complex and transcatheter mitral therapies more facile, the day when this will become a daily clinical reality will soon be upon us,” Dr. Badhwar and his colleagues said.
The multidisciplinary team approach will be integral in achieving the full potential of transcatheter mitral valve replacement or repair, Dr. Badhwar and his coauthors said. While surgery is the most effective treatment for primary MR, cardiac surgeons are challenged to introduce transcatheter treatments in patients who have other health problems. “The best way to adjudicate innovative surgical and interventional mitral therapies is through a robust collaboration within a well-functioning heart team that includes not only a cardiac surgeon and interventional cardiologist but also an imaging specialist,” the authors said.
The time to reach out to those other specialties is now, before those investigational devices start emerging from the development pipeline, Dr. Badhwar and his colleagues said. “This will soon enable the team-based mitral specialist to be facile in safely transitioning patients from open mitral surgery to TMVr or TMVR as most appropriate for durable long-term outcomes.”
Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign, and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
Channeling Bob Dylan’s “The Times They Are A-Changin’” in his invited commentary, W. Randolph Chitwood Jr., MD, of East Carolina University in Greenville, N.C., called Dr. Badhwar’s expert opinion “the clarion call for cardiac surgeons to become engaged in this rapidly evolving parade.”

|
Dr. W. Randolph Chitwood Jr. |
The evidence supporting the safety and efficacy of transcatheter aortic valve replacement (TAVR) is already strong, Dr. Chitwood noted. “It seems reasonable to suspect that the evolving pathway for the development of transcatheter mitral valve replacement (TMVR) could recapitulate the success of TAVR, with each generation having improved results,” he said (J Thorac Cardiovasc Surg. 2016;152:336-7).
Cardiac surgeons need to develop alternate access platforms and acquire the skills to use the new generation of transcatheter mitral devices, Dr. Chitwood said. The expert opinion “should encourage cardiac surgeons to become members of a heart team,” he said. “Guidewire skills are at the pinnacle of necessity to remain a player in this new world.”
Dr. Chitwood’s advice to colleagues: “Then you better start swimming or you’ll sink like a stone, For the times they are a-changin’.”
Dr. Chitwood disclosed he is a consultant to Direct Flow Medical and co-principal investigator for the Edwards Lifesciences Transform Trial.
Channeling Bob Dylan’s “The Times They Are A-Changin’” in his invited commentary, W. Randolph Chitwood Jr., MD, of East Carolina University in Greenville, N.C., called Dr. Badhwar’s expert opinion “the clarion call for cardiac surgeons to become engaged in this rapidly evolving parade.”
|
|
Dr. W. Randolph Chitwood Jr. |
The evidence supporting the safety and efficacy of transcatheter aortic valve replacement (TAVR) is already strong, Dr. Chitwood noted. “It seems reasonable to suspect that the evolving pathway for the development of transcatheter mitral valve replacement (TMVR) could recapitulate the success of TAVR, with each generation having improved results,” he said (J Thorac Cardiovasc Surg. 2016;152:336-7).
Cardiac surgeons need to develop alternate access platforms and acquire the skills to use the new generation of transcatheter mitral devices, Dr. Chitwood said. The expert opinion “should encourage cardiac surgeons to become members of a heart team,” he said. “Guidewire skills are at the pinnacle of necessity to remain a player in this new world.”
Dr. Chitwood’s advice to colleagues: “Then you better start swimming or you’ll sink like a stone, For the times they are a-changin’.”
Dr. Chitwood disclosed he is a consultant to Direct Flow Medical and co-principal investigator for the Edwards Lifesciences Transform Trial.
Channeling Bob Dylan’s “The Times They Are A-Changin’” in his invited commentary, W. Randolph Chitwood Jr., MD, of East Carolina University in Greenville, N.C., called Dr. Badhwar’s expert opinion “the clarion call for cardiac surgeons to become engaged in this rapidly evolving parade.”
|
|
Dr. W. Randolph Chitwood Jr. |
The evidence supporting the safety and efficacy of transcatheter aortic valve replacement (TAVR) is already strong, Dr. Chitwood noted. “It seems reasonable to suspect that the evolving pathway for the development of transcatheter mitral valve replacement (TMVR) could recapitulate the success of TAVR, with each generation having improved results,” he said (J Thorac Cardiovasc Surg. 2016;152:336-7).
Cardiac surgeons need to develop alternate access platforms and acquire the skills to use the new generation of transcatheter mitral devices, Dr. Chitwood said. The expert opinion “should encourage cardiac surgeons to become members of a heart team,” he said. “Guidewire skills are at the pinnacle of necessity to remain a player in this new world.”
Dr. Chitwood’s advice to colleagues: “Then you better start swimming or you’ll sink like a stone, For the times they are a-changin’.”
Dr. Chitwood disclosed he is a consultant to Direct Flow Medical and co-principal investigator for the Edwards Lifesciences Transform Trial.
As investigational transcatheter mitral valve therapies continue to explode onto the scene, cardiac surgeons must act now to seize and assert their place in the multidisciplinary team with interventional, imaging, and heart failure colleagues to deliver these treatments to people with complex mitral valve regurgitation, an expert opinion report in the August issue of the Journal of Thoracic and Cardiovascular Surgery states (J Thorac Cardiovasc Surg. 2016;152:330-6).
“There is a growing population of patients with primary and secondary mitral regurgitation underserved by surgical therapy because of comorbid risk,” Vinay Badhwar, MD, of West Virginia University and his colleagues said. “This has led to a tremendous activity of device development.”
With more than 25 different transcatheter mitral valve devices in development (MitraClip, Abbott Vascular, is the only FDA-approved transcatheter for primary mitral regurgitation [MR]), cardiac surgeons will soon have the tools to offer transcatheter mitral valve repair (TMVr) and transcatheter mitral valve replacement (TMVR) to more complex patients who have MR along with other health problems. Today about half of those patients do not get surgery because they are too frail, Dr. Badhwar and his colleagues said.
The authors used the astrophysical phrase “event horizon” to define the current state of transcatheter mitral valve therapies – “a point of no return.” They expect surgery to remain the treatment of choice for MR for the next 10 years. “However, as our patient cohorts become increasingly more complex and transcatheter mitral therapies more facile, the day when this will become a daily clinical reality will soon be upon us,” Dr. Badhwar and his colleagues said.
The multidisciplinary team approach will be integral in achieving the full potential of transcatheter mitral valve replacement or repair, Dr. Badhwar and his coauthors said. While surgery is the most effective treatment for primary MR, cardiac surgeons are challenged to introduce transcatheter treatments in patients who have other health problems. “The best way to adjudicate innovative surgical and interventional mitral therapies is through a robust collaboration within a well-functioning heart team that includes not only a cardiac surgeon and interventional cardiologist but also an imaging specialist,” the authors said.
The time to reach out to those other specialties is now, before those investigational devices start emerging from the development pipeline, Dr. Badhwar and his colleagues said. “This will soon enable the team-based mitral specialist to be facile in safely transitioning patients from open mitral surgery to TMVr or TMVR as most appropriate for durable long-term outcomes.”
Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign, and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
As investigational transcatheter mitral valve therapies continue to explode onto the scene, cardiac surgeons must act now to seize and assert their place in the multidisciplinary team with interventional, imaging, and heart failure colleagues to deliver these treatments to people with complex mitral valve regurgitation, an expert opinion report in the August issue of the Journal of Thoracic and Cardiovascular Surgery states (J Thorac Cardiovasc Surg. 2016;152:330-6).
“There is a growing population of patients with primary and secondary mitral regurgitation underserved by surgical therapy because of comorbid risk,” Vinay Badhwar, MD, of West Virginia University and his colleagues said. “This has led to a tremendous activity of device development.”
With more than 25 different transcatheter mitral valve devices in development (MitraClip, Abbott Vascular, is the only FDA-approved transcatheter for primary mitral regurgitation [MR]), cardiac surgeons will soon have the tools to offer transcatheter mitral valve repair (TMVr) and transcatheter mitral valve replacement (TMVR) to more complex patients who have MR along with other health problems. Today about half of those patients do not get surgery because they are too frail, Dr. Badhwar and his colleagues said.
The authors used the astrophysical phrase “event horizon” to define the current state of transcatheter mitral valve therapies – “a point of no return.” They expect surgery to remain the treatment of choice for MR for the next 10 years. “However, as our patient cohorts become increasingly more complex and transcatheter mitral therapies more facile, the day when this will become a daily clinical reality will soon be upon us,” Dr. Badhwar and his colleagues said.
The multidisciplinary team approach will be integral in achieving the full potential of transcatheter mitral valve replacement or repair, Dr. Badhwar and his coauthors said. While surgery is the most effective treatment for primary MR, cardiac surgeons are challenged to introduce transcatheter treatments in patients who have other health problems. “The best way to adjudicate innovative surgical and interventional mitral therapies is through a robust collaboration within a well-functioning heart team that includes not only a cardiac surgeon and interventional cardiologist but also an imaging specialist,” the authors said.
The time to reach out to those other specialties is now, before those investigational devices start emerging from the development pipeline, Dr. Badhwar and his colleagues said. “This will soon enable the team-based mitral specialist to be facile in safely transitioning patients from open mitral surgery to TMVr or TMVR as most appropriate for durable long-term outcomes.”
Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign, and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Transcatheter mitral valve repair and replacement technology has reached a critical point that requires cardiac surgeons to assume their place in a multidisciplinary team.
Major finding: One transcatheter device is commercially available in the United States and more than 25 companies have devices in development.
Data source: Review of 22 published reports on transcatheter mitral valve technology.
Disclosures: Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial, and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
Blacks found to have higher amputation rates than whites
COLUMBUS, OHIO – The disparity in amputation rates between blacks and non-Hispanic whites in Chicago was higher than the national average and up to five times greater on the predominantly black South Side than on the predominantly white North Side of the city.
The reasons for this disparity are unclear, but a recent study of white and black Chicagoans has shown that the rates at which the races self-report claudication do not differ, suggesting that better utilization of public health resources in the black community could potentially reduce this disparity.

Reporting at the annual meeting of the Midwestern Vascular Surgery Society, lead investigator Samantha Minc, MD, of Rush University in Chicago, said the difference in amputation rates may be traced to later recognition of disease in nonwhites.
“Possible reasons for late recognition of disease include lack of access to care, communication issues with doctors, education issues, or the patient and/or caregiver and primary care provider having difficulty accessing specialists,” Dr. Minc said. “Another often-cited explanation for the late recognition is the possibility of differences in disease symptom manifestations in nonwhites, which is what we chose to study.”
Investigators from Rush University analyzed data from a combined cohort of Chicago residents age 65 years and older from two studies of aging: The Rush Memory and Aging Project and the Minority Aging Research Study.
Because of the segregated nature of Chicago – the North Side is mostly white, the South Side mostly black and the West Side mostly Hispanic – prior research has coupled census data with the Illinois Department of Public Health database to analyze care patterns. This data showed that the disparity in amputation rates among groups in Chicago was higher than the national average and up to five times greater on the South Side, compared with the North, Dr. Minc said.
The latest study matched blacks and whites from both studies 1:2 based on age, education, gender, and length of follow-up. In all, a cohort of 2,487 subjects was generated: 801 blacks and 1,686 non-Hispanic whites. Among blacks, 6.5% reported claudication at baseline, compared with 5.9% of whites, and at any point of the study 19.5% of blacks and 19.6% of non-Hispanic whites reported claudication, differences that were not statistically significant.
Blacks did have higher rates of diabetes, 27% vs. 12.6%, were more likely to have used tobacco, more likely to be female, and were slightly younger on average, but other demographic factors – such as income or rates of congestive heart failure and coronary artery disease – were not significantly different, Dr. Minc said.
The study findings will inform the Chicago Department of Public Health’s Healthy Chicago 2.0 initiative to reduce the disparity in amputation rates between whites and blacks by 10% by 2020.
Dr. Minc acknowledged limitations of the study, among them that participants were volunteers, aged 65 years and older, and 72% female, that Hispanics were excluded, and that the use of the Modified Rose/World Health Organization questionnaire to detect claudication is “specific, but not very sensitive.”
“Our findings suggest that the delay in recognition in disease in nonwhites is not due to a racial differences in disease manifestation or symptomatology and that addressing socioeconomic issues, such as access to care, communication, and education may reduce the racial disparity in amputation rates,” Dr. Minc said. “Public health resources should focus on early recognition of the disease in higher-risk groups to decrease this disparity.”
Dr. Minc and her coauthors had no relationships to disclose.
COLUMBUS, OHIO – The disparity in amputation rates between blacks and non-Hispanic whites in Chicago was higher than the national average and up to five times greater on the predominantly black South Side than on the predominantly white North Side of the city.
The reasons for this disparity are unclear, but a recent study of white and black Chicagoans has shown that the rates at which the races self-report claudication do not differ, suggesting that better utilization of public health resources in the black community could potentially reduce this disparity.
Reporting at the annual meeting of the Midwestern Vascular Surgery Society, lead investigator Samantha Minc, MD, of Rush University in Chicago, said the difference in amputation rates may be traced to later recognition of disease in nonwhites.
“Possible reasons for late recognition of disease include lack of access to care, communication issues with doctors, education issues, or the patient and/or caregiver and primary care provider having difficulty accessing specialists,” Dr. Minc said. “Another often-cited explanation for the late recognition is the possibility of differences in disease symptom manifestations in nonwhites, which is what we chose to study.”
Investigators from Rush University analyzed data from a combined cohort of Chicago residents age 65 years and older from two studies of aging: The Rush Memory and Aging Project and the Minority Aging Research Study.
Because of the segregated nature of Chicago – the North Side is mostly white, the South Side mostly black and the West Side mostly Hispanic – prior research has coupled census data with the Illinois Department of Public Health database to analyze care patterns. This data showed that the disparity in amputation rates among groups in Chicago was higher than the national average and up to five times greater on the South Side, compared with the North, Dr. Minc said.
The latest study matched blacks and whites from both studies 1:2 based on age, education, gender, and length of follow-up. In all, a cohort of 2,487 subjects was generated: 801 blacks and 1,686 non-Hispanic whites. Among blacks, 6.5% reported claudication at baseline, compared with 5.9% of whites, and at any point of the study 19.5% of blacks and 19.6% of non-Hispanic whites reported claudication, differences that were not statistically significant.
Blacks did have higher rates of diabetes, 27% vs. 12.6%, were more likely to have used tobacco, more likely to be female, and were slightly younger on average, but other demographic factors – such as income or rates of congestive heart failure and coronary artery disease – were not significantly different, Dr. Minc said.
The study findings will inform the Chicago Department of Public Health’s Healthy Chicago 2.0 initiative to reduce the disparity in amputation rates between whites and blacks by 10% by 2020.
Dr. Minc acknowledged limitations of the study, among them that participants were volunteers, aged 65 years and older, and 72% female, that Hispanics were excluded, and that the use of the Modified Rose/World Health Organization questionnaire to detect claudication is “specific, but not very sensitive.”
“Our findings suggest that the delay in recognition in disease in nonwhites is not due to a racial differences in disease manifestation or symptomatology and that addressing socioeconomic issues, such as access to care, communication, and education may reduce the racial disparity in amputation rates,” Dr. Minc said. “Public health resources should focus on early recognition of the disease in higher-risk groups to decrease this disparity.”
Dr. Minc and her coauthors had no relationships to disclose.
COLUMBUS, OHIO – The disparity in amputation rates between blacks and non-Hispanic whites in Chicago was higher than the national average and up to five times greater on the predominantly black South Side than on the predominantly white North Side of the city.
The reasons for this disparity are unclear, but a recent study of white and black Chicagoans has shown that the rates at which the races self-report claudication do not differ, suggesting that better utilization of public health resources in the black community could potentially reduce this disparity.
Reporting at the annual meeting of the Midwestern Vascular Surgery Society, lead investigator Samantha Minc, MD, of Rush University in Chicago, said the difference in amputation rates may be traced to later recognition of disease in nonwhites.
“Possible reasons for late recognition of disease include lack of access to care, communication issues with doctors, education issues, or the patient and/or caregiver and primary care provider having difficulty accessing specialists,” Dr. Minc said. “Another often-cited explanation for the late recognition is the possibility of differences in disease symptom manifestations in nonwhites, which is what we chose to study.”
Investigators from Rush University analyzed data from a combined cohort of Chicago residents age 65 years and older from two studies of aging: The Rush Memory and Aging Project and the Minority Aging Research Study.
Because of the segregated nature of Chicago – the North Side is mostly white, the South Side mostly black and the West Side mostly Hispanic – prior research has coupled census data with the Illinois Department of Public Health database to analyze care patterns. This data showed that the disparity in amputation rates among groups in Chicago was higher than the national average and up to five times greater on the South Side, compared with the North, Dr. Minc said.
The latest study matched blacks and whites from both studies 1:2 based on age, education, gender, and length of follow-up. In all, a cohort of 2,487 subjects was generated: 801 blacks and 1,686 non-Hispanic whites. Among blacks, 6.5% reported claudication at baseline, compared with 5.9% of whites, and at any point of the study 19.5% of blacks and 19.6% of non-Hispanic whites reported claudication, differences that were not statistically significant.
Blacks did have higher rates of diabetes, 27% vs. 12.6%, were more likely to have used tobacco, more likely to be female, and were slightly younger on average, but other demographic factors – such as income or rates of congestive heart failure and coronary artery disease – were not significantly different, Dr. Minc said.
The study findings will inform the Chicago Department of Public Health’s Healthy Chicago 2.0 initiative to reduce the disparity in amputation rates between whites and blacks by 10% by 2020.
Dr. Minc acknowledged limitations of the study, among them that participants were volunteers, aged 65 years and older, and 72% female, that Hispanics were excluded, and that the use of the Modified Rose/World Health Organization questionnaire to detect claudication is “specific, but not very sensitive.”
“Our findings suggest that the delay in recognition in disease in nonwhites is not due to a racial differences in disease manifestation or symptomatology and that addressing socioeconomic issues, such as access to care, communication, and education may reduce the racial disparity in amputation rates,” Dr. Minc said. “Public health resources should focus on early recognition of the disease in higher-risk groups to decrease this disparity.”
Dr. Minc and her coauthors had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Amputation rates in Chicago were up to five times greater on the predominantly black South Side of the city than on the predominantly white North Side of the city.
Major finding: Disparities in amputation rates suggest a need to address access to care and improve communication and education with regard to amputation risks in the nonwhite communities.
Data source: 2,487 subjects from the Rush Memory and Aging Project and the Minority Aging Research Study.
Disclosures: Dr. Minc and her coauthors had no relationships to disclose.

Multiarterial grafting survival exceeds conventional CABG, PCI
A large, 16-year single-center study of patients with multivessel disease has determined that multivessel coronary artery bypass grafting achieved longer survival than not only percutaneous coronary interventions, but also conventional coronary artery bypass grafting, researchers from the Mayo Clinic reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:369-79).
Lead author Chaim Locker, MD, and his colleagues said the use of what they called MultiArt, for multivessel arterial grafting, also known as MAG, “must increase.”
The evolution of bare-metal and then drug-eluting stents may have favored percutaneous coronary interventions (PCI) over coronary artery bypass grafting (CABG), but, Dr. Locker and his coauthors said, “Evidence is accumulating that late outcome of surgical revascularization is improved when at least two arterial grafts are used.”
The study analyzed results of 12,615 patients who had either isolated primary CABG (6,667) or PCI (5,948) from 1993 to 2009. Among the CABG patients, 5,712 had the more conventional approach involving arterial grafts into the left internal thoracic artery/saphenous vein (ITA/SV) and 955 had MAG. Patients in the PCI group had three different procedures: balloon angioplasty (1,020), drug-eluting stent (1,686), or bare-metal stent (3,242). The study excluded patients who had revascularization procedures after a heart attack.
While the overall 15-year survival for patients with CABG was lower than it was for those who had PCI (36% vs. 46%), the survival for those who had MAG was significantly higher: 65% vs. 31% for those who had left ITA/SV revascularization. 8-year survival for the MAG subgroup was also significantly higher than all other subgroups: 87% vs. 69% for left ITA/SV, 75% for bare-metal stent, 73% for balloon angioplasty, and 70% for drug-eluting stent.
Propensity matching found similar survivability for balloon angioplasty and left ITA/SV when compared with MAG: 66% for MAG vs. 57% for the former; and 64% for MAG vs. 56% for the latter. The researchers also estimated the hazard ratio during the first 5 years of follow-up and found that those who had bare-metal stents had “significantly worse” survival, compared with MAG, but that survival evened out after that. Survival in the bare-metal stent group was similar to that of the left ITA/SV group, but “significantly worse” during the first 5 years for those who had balloon angioplasty.
Dr. Locker and his colleagues acknowledged that multiple randomized studies have compared CABG and PCI over the years, but they said that in most of those studies “the enrolled patients were highly selected and likely did not represent the broader population of patients with MVD [multivessel disease] undergoing revascularization.” With the exception of the SYNTAX trial (Synergy Between PCI With Taxus and Cardiac Surgery) (N Engl J Med. 2009;360:961-72; Lancet. 2013;381:629-38), those studies did not report on the frequency of MAG within the study population. The Mayo study, on the other hand, included all treated patients, excluding those who had a previous heart attack.
However, MAG is used infrequently, Dr. Locker and his colleagues said. The average annual rate of MAG in their Mayo practice was 15.2%, higher than the 5% annual rate the Society of Thoracic Surgeons National Cardiac Surgery Database (J Thorac Cardiovasc Surg. 2012;143:273-81) reported, and higher than the 12% rate in Europe (Eur J Cardiothorac Surg. 2006;29: 486-91). The SYNTAX trial reported an annual MAG rate of 27.6% for all CABG cases.
“It seems clear that use of MultiArt should be more frequent in patients with MVD undergoing CABG,” Dr. Locker and his coauthors said. “MultiArt can be used in most patients with MVD, including diabetic patients and elderly patients, and this strategy will improve outcomes of surgical revascularization.”
Dr. Locker and his coauthors had no financial relationships to disclose.
One might wonder about the validity of another retrospective, single-center study comparing revascularization techniques, but the study by Dr. Locker and his colleagues is “compelling” for two reasons, Paul Kurlansky, MD, of Columbia University, New York, pointed out in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:380-1).

|
Dr. Paul Kurlansky |
Dr. Kurlansky noted the finding of equivalent survival at up to 8 years among propensity-matched patients who had left coronary artery bypass grafting with the use of a single internal thoracic artery with supplemental vein grafts (left ITA/SV) and those who received drug-eluting stents was “a bit more provocative” than some of the expected study results; and the reversal of the survival benefit of left ITA/SV, compared with both balloon angioplasty and bare-metal stents after 7 to 10 years was “more perturbing for the surgical community.”
This study underscores that increased use of multiple arterial grafting is essential to give patients the best revascularization option, even in the age of growing percutaneous interventions, Dr. Kurlansky said.
“Limitations notwithstanding, the message for the surgical community is clear – if we wish to have the opportunity to treat patients with advanced, multivessel coronary artery disease, we will need to more fully embrace a strategy of MAG,” he said.
Dr. Kurlansky had no financial relationships to disclose.
One might wonder about the validity of another retrospective, single-center study comparing revascularization techniques, but the study by Dr. Locker and his colleagues is “compelling” for two reasons, Paul Kurlansky, MD, of Columbia University, New York, pointed out in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:380-1).
|
|
Dr. Paul Kurlansky |
Dr. Kurlansky noted the finding of equivalent survival at up to 8 years among propensity-matched patients who had left coronary artery bypass grafting with the use of a single internal thoracic artery with supplemental vein grafts (left ITA/SV) and those who received drug-eluting stents was “a bit more provocative” than some of the expected study results; and the reversal of the survival benefit of left ITA/SV, compared with both balloon angioplasty and bare-metal stents after 7 to 10 years was “more perturbing for the surgical community.”
This study underscores that increased use of multiple arterial grafting is essential to give patients the best revascularization option, even in the age of growing percutaneous interventions, Dr. Kurlansky said.
“Limitations notwithstanding, the message for the surgical community is clear – if we wish to have the opportunity to treat patients with advanced, multivessel coronary artery disease, we will need to more fully embrace a strategy of MAG,” he said.
Dr. Kurlansky had no financial relationships to disclose.
One might wonder about the validity of another retrospective, single-center study comparing revascularization techniques, but the study by Dr. Locker and his colleagues is “compelling” for two reasons, Paul Kurlansky, MD, of Columbia University, New York, pointed out in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:380-1).
|
|
Dr. Paul Kurlansky |
Dr. Kurlansky noted the finding of equivalent survival at up to 8 years among propensity-matched patients who had left coronary artery bypass grafting with the use of a single internal thoracic artery with supplemental vein grafts (left ITA/SV) and those who received drug-eluting stents was “a bit more provocative” than some of the expected study results; and the reversal of the survival benefit of left ITA/SV, compared with both balloon angioplasty and bare-metal stents after 7 to 10 years was “more perturbing for the surgical community.”
This study underscores that increased use of multiple arterial grafting is essential to give patients the best revascularization option, even in the age of growing percutaneous interventions, Dr. Kurlansky said.
“Limitations notwithstanding, the message for the surgical community is clear – if we wish to have the opportunity to treat patients with advanced, multivessel coronary artery disease, we will need to more fully embrace a strategy of MAG,” he said.
Dr. Kurlansky had no financial relationships to disclose.
A large, 16-year single-center study of patients with multivessel disease has determined that multivessel coronary artery bypass grafting achieved longer survival than not only percutaneous coronary interventions, but also conventional coronary artery bypass grafting, researchers from the Mayo Clinic reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:369-79).
Lead author Chaim Locker, MD, and his colleagues said the use of what they called MultiArt, for multivessel arterial grafting, also known as MAG, “must increase.”
The evolution of bare-metal and then drug-eluting stents may have favored percutaneous coronary interventions (PCI) over coronary artery bypass grafting (CABG), but, Dr. Locker and his coauthors said, “Evidence is accumulating that late outcome of surgical revascularization is improved when at least two arterial grafts are used.”
The study analyzed results of 12,615 patients who had either isolated primary CABG (6,667) or PCI (5,948) from 1993 to 2009. Among the CABG patients, 5,712 had the more conventional approach involving arterial grafts into the left internal thoracic artery/saphenous vein (ITA/SV) and 955 had MAG. Patients in the PCI group had three different procedures: balloon angioplasty (1,020), drug-eluting stent (1,686), or bare-metal stent (3,242). The study excluded patients who had revascularization procedures after a heart attack.
While the overall 15-year survival for patients with CABG was lower than it was for those who had PCI (36% vs. 46%), the survival for those who had MAG was significantly higher: 65% vs. 31% for those who had left ITA/SV revascularization. 8-year survival for the MAG subgroup was also significantly higher than all other subgroups: 87% vs. 69% for left ITA/SV, 75% for bare-metal stent, 73% for balloon angioplasty, and 70% for drug-eluting stent.
Propensity matching found similar survivability for balloon angioplasty and left ITA/SV when compared with MAG: 66% for MAG vs. 57% for the former; and 64% for MAG vs. 56% for the latter. The researchers also estimated the hazard ratio during the first 5 years of follow-up and found that those who had bare-metal stents had “significantly worse” survival, compared with MAG, but that survival evened out after that. Survival in the bare-metal stent group was similar to that of the left ITA/SV group, but “significantly worse” during the first 5 years for those who had balloon angioplasty.
Dr. Locker and his colleagues acknowledged that multiple randomized studies have compared CABG and PCI over the years, but they said that in most of those studies “the enrolled patients were highly selected and likely did not represent the broader population of patients with MVD [multivessel disease] undergoing revascularization.” With the exception of the SYNTAX trial (Synergy Between PCI With Taxus and Cardiac Surgery) (N Engl J Med. 2009;360:961-72; Lancet. 2013;381:629-38), those studies did not report on the frequency of MAG within the study population. The Mayo study, on the other hand, included all treated patients, excluding those who had a previous heart attack.
However, MAG is used infrequently, Dr. Locker and his colleagues said. The average annual rate of MAG in their Mayo practice was 15.2%, higher than the 5% annual rate the Society of Thoracic Surgeons National Cardiac Surgery Database (J Thorac Cardiovasc Surg. 2012;143:273-81) reported, and higher than the 12% rate in Europe (Eur J Cardiothorac Surg. 2006;29: 486-91). The SYNTAX trial reported an annual MAG rate of 27.6% for all CABG cases.
“It seems clear that use of MultiArt should be more frequent in patients with MVD undergoing CABG,” Dr. Locker and his coauthors said. “MultiArt can be used in most patients with MVD, including diabetic patients and elderly patients, and this strategy will improve outcomes of surgical revascularization.”
Dr. Locker and his coauthors had no financial relationships to disclose.
A large, 16-year single-center study of patients with multivessel disease has determined that multivessel coronary artery bypass grafting achieved longer survival than not only percutaneous coronary interventions, but also conventional coronary artery bypass grafting, researchers from the Mayo Clinic reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:369-79).
Lead author Chaim Locker, MD, and his colleagues said the use of what they called MultiArt, for multivessel arterial grafting, also known as MAG, “must increase.”
The evolution of bare-metal and then drug-eluting stents may have favored percutaneous coronary interventions (PCI) over coronary artery bypass grafting (CABG), but, Dr. Locker and his coauthors said, “Evidence is accumulating that late outcome of surgical revascularization is improved when at least two arterial grafts are used.”
The study analyzed results of 12,615 patients who had either isolated primary CABG (6,667) or PCI (5,948) from 1993 to 2009. Among the CABG patients, 5,712 had the more conventional approach involving arterial grafts into the left internal thoracic artery/saphenous vein (ITA/SV) and 955 had MAG. Patients in the PCI group had three different procedures: balloon angioplasty (1,020), drug-eluting stent (1,686), or bare-metal stent (3,242). The study excluded patients who had revascularization procedures after a heart attack.
While the overall 15-year survival for patients with CABG was lower than it was for those who had PCI (36% vs. 46%), the survival for those who had MAG was significantly higher: 65% vs. 31% for those who had left ITA/SV revascularization. 8-year survival for the MAG subgroup was also significantly higher than all other subgroups: 87% vs. 69% for left ITA/SV, 75% for bare-metal stent, 73% for balloon angioplasty, and 70% for drug-eluting stent.
Propensity matching found similar survivability for balloon angioplasty and left ITA/SV when compared with MAG: 66% for MAG vs. 57% for the former; and 64% for MAG vs. 56% for the latter. The researchers also estimated the hazard ratio during the first 5 years of follow-up and found that those who had bare-metal stents had “significantly worse” survival, compared with MAG, but that survival evened out after that. Survival in the bare-metal stent group was similar to that of the left ITA/SV group, but “significantly worse” during the first 5 years for those who had balloon angioplasty.
Dr. Locker and his colleagues acknowledged that multiple randomized studies have compared CABG and PCI over the years, but they said that in most of those studies “the enrolled patients were highly selected and likely did not represent the broader population of patients with MVD [multivessel disease] undergoing revascularization.” With the exception of the SYNTAX trial (Synergy Between PCI With Taxus and Cardiac Surgery) (N Engl J Med. 2009;360:961-72; Lancet. 2013;381:629-38), those studies did not report on the frequency of MAG within the study population. The Mayo study, on the other hand, included all treated patients, excluding those who had a previous heart attack.
However, MAG is used infrequently, Dr. Locker and his colleagues said. The average annual rate of MAG in their Mayo practice was 15.2%, higher than the 5% annual rate the Society of Thoracic Surgeons National Cardiac Surgery Database (J Thorac Cardiovasc Surg. 2012;143:273-81) reported, and higher than the 12% rate in Europe (Eur J Cardiothorac Surg. 2006;29: 486-91). The SYNTAX trial reported an annual MAG rate of 27.6% for all CABG cases.
“It seems clear that use of MultiArt should be more frequent in patients with MVD undergoing CABG,” Dr. Locker and his coauthors said. “MultiArt can be used in most patients with MVD, including diabetic patients and elderly patients, and this strategy will improve outcomes of surgical revascularization.”
Dr. Locker and his coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Cardiac surgeons should use multiple arterial coronary artery bypass grafting (MAG) more frequently because it achieves superior survival, compared with conventional bypass surgery or percutaneous coronary interventions.
Major finding: The overall 8-year survival of those who had MAG was 87% vs. 69% for conventional coronary bypass surgery and 70%-75% for percutaneous procedures.
Data source: Retrospective, single-institution study of 12,615 patients with multivessel disease who had revascularization procedures at the Mayo Clinic from 1993 to 2009.
Disclosures: Dr. Locker and his coauthors had no financial relationships to disclose.

Can anesthesia in infants affect IQ scores?
About 10,000 newborns receive general anesthesia for congenital heart defects every year, and the more exposure they have to inhaled anesthetic agents, the greater effect it may have on their neurologic development, investigators at Children’s Hospital of Philadelphia reported in a study of newborns with hypoplastic left heart syndrome.
While previous studies have linked worse neurodevelopment to patient factors like prematurity and genetics, this is the first study to show a consistent relationship between neurodevelopment outcomes and modifiable factors during cardiac surgery in infants, Laura K. Diaz, MD, and her colleagues reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:482-9).
They studied 96 patients with hypoplastic left heart syndrome (HLHS) or similar syndromes who received volatile anesthetic agents (VAA) at their institution from 1998 to 2003. The patients underwent a battery of neurodevelopmental tests between the ages of 4 and 5 years that included full-scale IQ (FSIQ), verbal IQ (VIQ), performance IQ (PIQ), and processing speed.
“This study provides evidence that in children undergoing staged reconstructive surgery for HLHS, increasing cumulative exposure to VAAs beginning in infancy is associated with worse performance for FSIQ and VIQ, suggesting that VAA exposure may be a modifiable risk factor for adverse neurodevelopment outcomes,” Dr. Diaz and her colleagues wrote.
While survival has improved significantly in recent years for infants with hypoplastic left heart syndrome, physicians have harbored concerns that these children encounter neurodevelopmental issues later on. Dr. Diaz and her colleagues acknowledged that previous studies have shown factors, such as the use of cardiopulmonary bypass (CPB) and hospital length of stay, that could affect neurodevelopment in these children, but the findings have been inconsistent. Instead, those studies have shown such patient-specific factors as birth weight, ethnicity, and hereditary disorders were strong determinants of neurodevelopment in infants who have cardiac surgery, Dr. Diaz and her coauthors pointed out.
Their own previous study of patients with single-ventricle congenital heart disease concurred with the findings of those other studies, but it did not evaluate exposure to anesthesia (J. Thorac. Cardiovasc. Surg. 2014;147:1276-82). That was the focus of their current study.
Among the study group, 94 patients had an initial operation with CPB in their first 30 days of life. All 96 infants in the study group had additional operations, whether cardiac or noncardiac. The study tracked all anesthetic exposures up until the neurodevelopment evaluation in February 2008. All but 2 patients had initial VAA exposure at less than 1 year of age, and 45 at less than 1 month of age. Deep hypothermic circulatory arrest was used uniformly for aortic arch reconstruction.
The study used four different generalized linear models to evaluate anesthesia exposure and neurodevelopment.
For both FSIQ and PIQ, total minimum alveolar concentration hours were deemed to be statistically significant factors for lower scores. For PIQ, birth weight and length of postoperative hospital stay were statistically significant. For processing speed, gestational age and length of hospital stay were statistically significant.
Dr. Diaz and her colleagues said their findings are preliminary and do not justify a change in practice. “Prospective randomized, controlled multicenter clinical trials are indicated to continue to clarify the effects of early and repetitive exposure to VAA in this and other pediatric populations,” the study authors concluded.
Dr. Diaz and the study authors had no financial relationships to disclose.
The study by Dr. Diaz and her colleagues makes all the more clear the need for a prospective randomized trial on the effect inhaled anesthetic agents in infants can have on their neurologic development, Richard A. Jonas, MD, of Children’s National Heart Institute, Children’s National Medical Center, Washington, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2016;152:490).

|
Dr. Richard A. Jonas |
However, besides the study limitations that Dr. Diaz and her colleagues pointed out in their study, another “problem” Dr. Jonas noted with the study subjects was that they had staged reconstruction for hypoplastic left heart syndrome. “Not only is this group of patients at risk for prenatal effects of their abnormal in utero circulation, but in addition, they all underwent additional cardiac or noncardiac procedures after their initial cardiac surgery,” he said. These factors, along with some degree of cyanosis in their formative years, may help explain why this study is an outlier in that it did not implicate nonoperative factors that other studies implicated, Dr. Jonas said.
Nonetheless, the study is “an important contribution that adds further evidence to the observation that volatile agents can affect neurodevelopmental outcome,” Dr. Jonas said. Hence the need for a prospective randomized trial.
Dr. Jonas had no financial relationships to disclose.
The study by Dr. Diaz and her colleagues makes all the more clear the need for a prospective randomized trial on the effect inhaled anesthetic agents in infants can have on their neurologic development, Richard A. Jonas, MD, of Children’s National Heart Institute, Children’s National Medical Center, Washington, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2016;152:490).
|
|
Dr. Richard A. Jonas |
However, besides the study limitations that Dr. Diaz and her colleagues pointed out in their study, another “problem” Dr. Jonas noted with the study subjects was that they had staged reconstruction for hypoplastic left heart syndrome. “Not only is this group of patients at risk for prenatal effects of their abnormal in utero circulation, but in addition, they all underwent additional cardiac or noncardiac procedures after their initial cardiac surgery,” he said. These factors, along with some degree of cyanosis in their formative years, may help explain why this study is an outlier in that it did not implicate nonoperative factors that other studies implicated, Dr. Jonas said.
Nonetheless, the study is “an important contribution that adds further evidence to the observation that volatile agents can affect neurodevelopmental outcome,” Dr. Jonas said. Hence the need for a prospective randomized trial.
Dr. Jonas had no financial relationships to disclose.
The study by Dr. Diaz and her colleagues makes all the more clear the need for a prospective randomized trial on the effect inhaled anesthetic agents in infants can have on their neurologic development, Richard A. Jonas, MD, of Children’s National Heart Institute, Children’s National Medical Center, Washington, said in his invited commentary (J. Thorac. Cardiovasc. Surg. 2016;152:490).
|
|
Dr. Richard A. Jonas |
However, besides the study limitations that Dr. Diaz and her colleagues pointed out in their study, another “problem” Dr. Jonas noted with the study subjects was that they had staged reconstruction for hypoplastic left heart syndrome. “Not only is this group of patients at risk for prenatal effects of their abnormal in utero circulation, but in addition, they all underwent additional cardiac or noncardiac procedures after their initial cardiac surgery,” he said. These factors, along with some degree of cyanosis in their formative years, may help explain why this study is an outlier in that it did not implicate nonoperative factors that other studies implicated, Dr. Jonas said.
Nonetheless, the study is “an important contribution that adds further evidence to the observation that volatile agents can affect neurodevelopmental outcome,” Dr. Jonas said. Hence the need for a prospective randomized trial.
Dr. Jonas had no financial relationships to disclose.
About 10,000 newborns receive general anesthesia for congenital heart defects every year, and the more exposure they have to inhaled anesthetic agents, the greater effect it may have on their neurologic development, investigators at Children’s Hospital of Philadelphia reported in a study of newborns with hypoplastic left heart syndrome.
While previous studies have linked worse neurodevelopment to patient factors like prematurity and genetics, this is the first study to show a consistent relationship between neurodevelopment outcomes and modifiable factors during cardiac surgery in infants, Laura K. Diaz, MD, and her colleagues reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:482-9).
They studied 96 patients with hypoplastic left heart syndrome (HLHS) or similar syndromes who received volatile anesthetic agents (VAA) at their institution from 1998 to 2003. The patients underwent a battery of neurodevelopmental tests between the ages of 4 and 5 years that included full-scale IQ (FSIQ), verbal IQ (VIQ), performance IQ (PIQ), and processing speed.
“This study provides evidence that in children undergoing staged reconstructive surgery for HLHS, increasing cumulative exposure to VAAs beginning in infancy is associated with worse performance for FSIQ and VIQ, suggesting that VAA exposure may be a modifiable risk factor for adverse neurodevelopment outcomes,” Dr. Diaz and her colleagues wrote.
While survival has improved significantly in recent years for infants with hypoplastic left heart syndrome, physicians have harbored concerns that these children encounter neurodevelopmental issues later on. Dr. Diaz and her colleagues acknowledged that previous studies have shown factors, such as the use of cardiopulmonary bypass (CPB) and hospital length of stay, that could affect neurodevelopment in these children, but the findings have been inconsistent. Instead, those studies have shown such patient-specific factors as birth weight, ethnicity, and hereditary disorders were strong determinants of neurodevelopment in infants who have cardiac surgery, Dr. Diaz and her coauthors pointed out.
Their own previous study of patients with single-ventricle congenital heart disease concurred with the findings of those other studies, but it did not evaluate exposure to anesthesia (J. Thorac. Cardiovasc. Surg. 2014;147:1276-82). That was the focus of their current study.
Among the study group, 94 patients had an initial operation with CPB in their first 30 days of life. All 96 infants in the study group had additional operations, whether cardiac or noncardiac. The study tracked all anesthetic exposures up until the neurodevelopment evaluation in February 2008. All but 2 patients had initial VAA exposure at less than 1 year of age, and 45 at less than 1 month of age. Deep hypothermic circulatory arrest was used uniformly for aortic arch reconstruction.
The study used four different generalized linear models to evaluate anesthesia exposure and neurodevelopment.
For both FSIQ and PIQ, total minimum alveolar concentration hours were deemed to be statistically significant factors for lower scores. For PIQ, birth weight and length of postoperative hospital stay were statistically significant. For processing speed, gestational age and length of hospital stay were statistically significant.
Dr. Diaz and her colleagues said their findings are preliminary and do not justify a change in practice. “Prospective randomized, controlled multicenter clinical trials are indicated to continue to clarify the effects of early and repetitive exposure to VAA in this and other pediatric populations,” the study authors concluded.
Dr. Diaz and the study authors had no financial relationships to disclose.
About 10,000 newborns receive general anesthesia for congenital heart defects every year, and the more exposure they have to inhaled anesthetic agents, the greater effect it may have on their neurologic development, investigators at Children’s Hospital of Philadelphia reported in a study of newborns with hypoplastic left heart syndrome.
While previous studies have linked worse neurodevelopment to patient factors like prematurity and genetics, this is the first study to show a consistent relationship between neurodevelopment outcomes and modifiable factors during cardiac surgery in infants, Laura K. Diaz, MD, and her colleagues reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:482-9).
They studied 96 patients with hypoplastic left heart syndrome (HLHS) or similar syndromes who received volatile anesthetic agents (VAA) at their institution from 1998 to 2003. The patients underwent a battery of neurodevelopmental tests between the ages of 4 and 5 years that included full-scale IQ (FSIQ), verbal IQ (VIQ), performance IQ (PIQ), and processing speed.
“This study provides evidence that in children undergoing staged reconstructive surgery for HLHS, increasing cumulative exposure to VAAs beginning in infancy is associated with worse performance for FSIQ and VIQ, suggesting that VAA exposure may be a modifiable risk factor for adverse neurodevelopment outcomes,” Dr. Diaz and her colleagues wrote.
While survival has improved significantly in recent years for infants with hypoplastic left heart syndrome, physicians have harbored concerns that these children encounter neurodevelopmental issues later on. Dr. Diaz and her colleagues acknowledged that previous studies have shown factors, such as the use of cardiopulmonary bypass (CPB) and hospital length of stay, that could affect neurodevelopment in these children, but the findings have been inconsistent. Instead, those studies have shown such patient-specific factors as birth weight, ethnicity, and hereditary disorders were strong determinants of neurodevelopment in infants who have cardiac surgery, Dr. Diaz and her coauthors pointed out.
Their own previous study of patients with single-ventricle congenital heart disease concurred with the findings of those other studies, but it did not evaluate exposure to anesthesia (J. Thorac. Cardiovasc. Surg. 2014;147:1276-82). That was the focus of their current study.
Among the study group, 94 patients had an initial operation with CPB in their first 30 days of life. All 96 infants in the study group had additional operations, whether cardiac or noncardiac. The study tracked all anesthetic exposures up until the neurodevelopment evaluation in February 2008. All but 2 patients had initial VAA exposure at less than 1 year of age, and 45 at less than 1 month of age. Deep hypothermic circulatory arrest was used uniformly for aortic arch reconstruction.
The study used four different generalized linear models to evaluate anesthesia exposure and neurodevelopment.
For both FSIQ and PIQ, total minimum alveolar concentration hours were deemed to be statistically significant factors for lower scores. For PIQ, birth weight and length of postoperative hospital stay were statistically significant. For processing speed, gestational age and length of hospital stay were statistically significant.
Dr. Diaz and her colleagues said their findings are preliminary and do not justify a change in practice. “Prospective randomized, controlled multicenter clinical trials are indicated to continue to clarify the effects of early and repetitive exposure to VAA in this and other pediatric populations,” the study authors concluded.
Dr. Diaz and the study authors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Volatile inhaled anesthesia may affect neurodevelopment in infants with hypoplastic left heart syndrome.
Major finding: Different generalized linear models determined an association between minimum alveolar concentration hours and hospital length of stay with lower IQ scores and processing speed.
Data source: Meta-analysis reviewed a subgroup of 96 patients with hypoplastic left heart syndrome who had neurodevelopmental testing at a single center between 1998 and 2003.
Disclosures: The authors have no financial relationships to disclose.
A dual Y-shaped stent can improve QOL with airway fistulas
Airway fistula is a rare but life-threatening complication of esophageal surgery, but an innovative technique using two custom-made, Y-shaped metallic stents can preserve airway patency, researchers at Zhengzhou University in China reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:557-63).
The study involved 10 patients who received Y-shaped stents to treat gastrotracheal or gastrobronchial fistulas (GTFs and GBFs, respectively) after esophageal surgery from 2010 through 2014. “Our patients tolerated the stents well and had good palliation of their symptoms,” wrote Teng-Fei Li, MD, and colleagues.
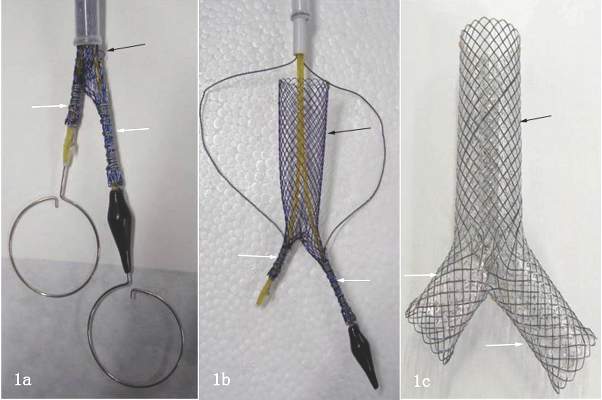
Six patients died within 8 months for unrelated reasons – either tumors (four patients), or hemoptysis or pulmonary infection (one each). In one patient, the carinal fistula enlarged 4 months after stenting, but the researchers successfully placed an additional small Y-shaped stent. At the publication of the paper, this patient and three others had survived, Dr. Li and colleagues said.
After esophagectomy, fistulas can form between the tracheobronchial tree and stomach for a variety of reasons. A metallic stent would seem the logical choice after fistula formation, but it can be problematic, Dr. Li and colleagues pointed out. “Most often the clinician faces a situation in which the esophageal stent should have a larger diameter on the gastric side, making stenting the alimentary side of the fistula insufficient,” they said. The risk of stent migration is high, and the bifurcated structure of the trachea and main bronchi can cause leakage and stent displacement.
The researchers noted that Y-shaped self-expanding stents have been used for sealing airway fistulas, but they don’t always fully seal large GTFs and GBFs. Their primary objective in studying the combined-type Y-shaped covered metallic stent was to determine the safety and feasibility of the technique; the secondary aim was to evaluate long-term patency and complication rates.
They designed a Y-shaped stent delivery system (Micro-Tech) and used a combined bundle-and-push to insert the main body of the stent. In all, they inserted 20 Y-shaped stents in the 10 patients, although two stents did not fully expand and were dilated with a balloon. The researchers reported resolution of coughing during eating, toleration of liquid or semiliquid diet, and no complications after insertion.
Dr. Li and colleagues also developed strategies to avoid complications of Y-shaped stents, which have been known to retain secretions because they hinder cilia function. “To avoid this, we provided sputum suction and administered continuous high-concentration oxygen during the procedure,” they noted. Also, speed and agility in placement are important. “The operation should be performed as rapidly and gently as possible to avoid irritation to the airway,” Dr. Li and colleagues wrote. The postoperative course involved IV expectorants and antiasthma agents and aerosol inhalation of terbutaline. Surveillance bronchoscopes and debridement of granulation tissue helped avoid stent obstruction.
Nonetheless, the researches acknowledged limitations of the retrospective study, namely its small sample size and lack of a control group.
Dr. Li and colleagues had no financial relationships to disclose.
The Zhengzhou University investigators provide an opportunity to “think outside the box” when managing complex airway fistulas, Waël C. Hanna, MDCM, of McMaster University and St. Joseph’s Healthcare in Hamilton, Ontario, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:564).

|
Dr. Waël Hanna |
Dr. Hanna credited a couple of innovations in their technique to overcome the challenge of Y stents that “remain notoriously difficult to position”: eliminating rigid bronchoscopy and using angiography-guided oral delivery; and developing the hybrid deployment mechanism.
Dr. Hanna also noted two “important nuances” of the technique: The stents are custom-made based on the length and location of the fistula; and the routine placement of two stents, with a limb of the smaller Y stent projecting through a limb of the larger Y stent to seal the entire airway. “This Y-en-Y technique using perfectly fitted stents is likely what caused the excellent outcomes that are reported in this series,” Dr. Hanna said.
But their approach may not be a practical solution to complex airway fistulas soon, he said. “Most of us who see the occasional case are unlikely to be able to commission custom-made Y stents,” he said. What’s more, the deployment mechanism is complicated, and the effect on patient quality of life is unclear.
Dr. Hanna had no financial relationships to disclose.
The Zhengzhou University investigators provide an opportunity to “think outside the box” when managing complex airway fistulas, Waël C. Hanna, MDCM, of McMaster University and St. Joseph’s Healthcare in Hamilton, Ontario, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:564).
|
|
Dr. Waël Hanna |
Dr. Hanna credited a couple of innovations in their technique to overcome the challenge of Y stents that “remain notoriously difficult to position”: eliminating rigid bronchoscopy and using angiography-guided oral delivery; and developing the hybrid deployment mechanism.
Dr. Hanna also noted two “important nuances” of the technique: The stents are custom-made based on the length and location of the fistula; and the routine placement of two stents, with a limb of the smaller Y stent projecting through a limb of the larger Y stent to seal the entire airway. “This Y-en-Y technique using perfectly fitted stents is likely what caused the excellent outcomes that are reported in this series,” Dr. Hanna said.
But their approach may not be a practical solution to complex airway fistulas soon, he said. “Most of us who see the occasional case are unlikely to be able to commission custom-made Y stents,” he said. What’s more, the deployment mechanism is complicated, and the effect on patient quality of life is unclear.
Dr. Hanna had no financial relationships to disclose.
The Zhengzhou University investigators provide an opportunity to “think outside the box” when managing complex airway fistulas, Waël C. Hanna, MDCM, of McMaster University and St. Joseph’s Healthcare in Hamilton, Ontario, said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:564).
|
|
Dr. Waël Hanna |
Dr. Hanna credited a couple of innovations in their technique to overcome the challenge of Y stents that “remain notoriously difficult to position”: eliminating rigid bronchoscopy and using angiography-guided oral delivery; and developing the hybrid deployment mechanism.
Dr. Hanna also noted two “important nuances” of the technique: The stents are custom-made based on the length and location of the fistula; and the routine placement of two stents, with a limb of the smaller Y stent projecting through a limb of the larger Y stent to seal the entire airway. “This Y-en-Y technique using perfectly fitted stents is likely what caused the excellent outcomes that are reported in this series,” Dr. Hanna said.
But their approach may not be a practical solution to complex airway fistulas soon, he said. “Most of us who see the occasional case are unlikely to be able to commission custom-made Y stents,” he said. What’s more, the deployment mechanism is complicated, and the effect on patient quality of life is unclear.
Dr. Hanna had no financial relationships to disclose.
Airway fistula is a rare but life-threatening complication of esophageal surgery, but an innovative technique using two custom-made, Y-shaped metallic stents can preserve airway patency, researchers at Zhengzhou University in China reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:557-63).
The study involved 10 patients who received Y-shaped stents to treat gastrotracheal or gastrobronchial fistulas (GTFs and GBFs, respectively) after esophageal surgery from 2010 through 2014. “Our patients tolerated the stents well and had good palliation of their symptoms,” wrote Teng-Fei Li, MD, and colleagues.
Six patients died within 8 months for unrelated reasons – either tumors (four patients), or hemoptysis or pulmonary infection (one each). In one patient, the carinal fistula enlarged 4 months after stenting, but the researchers successfully placed an additional small Y-shaped stent. At the publication of the paper, this patient and three others had survived, Dr. Li and colleagues said.
After esophagectomy, fistulas can form between the tracheobronchial tree and stomach for a variety of reasons. A metallic stent would seem the logical choice after fistula formation, but it can be problematic, Dr. Li and colleagues pointed out. “Most often the clinician faces a situation in which the esophageal stent should have a larger diameter on the gastric side, making stenting the alimentary side of the fistula insufficient,” they said. The risk of stent migration is high, and the bifurcated structure of the trachea and main bronchi can cause leakage and stent displacement.
The researchers noted that Y-shaped self-expanding stents have been used for sealing airway fistulas, but they don’t always fully seal large GTFs and GBFs. Their primary objective in studying the combined-type Y-shaped covered metallic stent was to determine the safety and feasibility of the technique; the secondary aim was to evaluate long-term patency and complication rates.
They designed a Y-shaped stent delivery system (Micro-Tech) and used a combined bundle-and-push to insert the main body of the stent. In all, they inserted 20 Y-shaped stents in the 10 patients, although two stents did not fully expand and were dilated with a balloon. The researchers reported resolution of coughing during eating, toleration of liquid or semiliquid diet, and no complications after insertion.
Dr. Li and colleagues also developed strategies to avoid complications of Y-shaped stents, which have been known to retain secretions because they hinder cilia function. “To avoid this, we provided sputum suction and administered continuous high-concentration oxygen during the procedure,” they noted. Also, speed and agility in placement are important. “The operation should be performed as rapidly and gently as possible to avoid irritation to the airway,” Dr. Li and colleagues wrote. The postoperative course involved IV expectorants and antiasthma agents and aerosol inhalation of terbutaline. Surveillance bronchoscopes and debridement of granulation tissue helped avoid stent obstruction.
Nonetheless, the researches acknowledged limitations of the retrospective study, namely its small sample size and lack of a control group.
Dr. Li and colleagues had no financial relationships to disclose.
Airway fistula is a rare but life-threatening complication of esophageal surgery, but an innovative technique using two custom-made, Y-shaped metallic stents can preserve airway patency, researchers at Zhengzhou University in China reported in the August issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2016;152:557-63).
The study involved 10 patients who received Y-shaped stents to treat gastrotracheal or gastrobronchial fistulas (GTFs and GBFs, respectively) after esophageal surgery from 2010 through 2014. “Our patients tolerated the stents well and had good palliation of their symptoms,” wrote Teng-Fei Li, MD, and colleagues.
Six patients died within 8 months for unrelated reasons – either tumors (four patients), or hemoptysis or pulmonary infection (one each). In one patient, the carinal fistula enlarged 4 months after stenting, but the researchers successfully placed an additional small Y-shaped stent. At the publication of the paper, this patient and three others had survived, Dr. Li and colleagues said.
After esophagectomy, fistulas can form between the tracheobronchial tree and stomach for a variety of reasons. A metallic stent would seem the logical choice after fistula formation, but it can be problematic, Dr. Li and colleagues pointed out. “Most often the clinician faces a situation in which the esophageal stent should have a larger diameter on the gastric side, making stenting the alimentary side of the fistula insufficient,” they said. The risk of stent migration is high, and the bifurcated structure of the trachea and main bronchi can cause leakage and stent displacement.
The researchers noted that Y-shaped self-expanding stents have been used for sealing airway fistulas, but they don’t always fully seal large GTFs and GBFs. Their primary objective in studying the combined-type Y-shaped covered metallic stent was to determine the safety and feasibility of the technique; the secondary aim was to evaluate long-term patency and complication rates.
They designed a Y-shaped stent delivery system (Micro-Tech) and used a combined bundle-and-push to insert the main body of the stent. In all, they inserted 20 Y-shaped stents in the 10 patients, although two stents did not fully expand and were dilated with a balloon. The researchers reported resolution of coughing during eating, toleration of liquid or semiliquid diet, and no complications after insertion.
Dr. Li and colleagues also developed strategies to avoid complications of Y-shaped stents, which have been known to retain secretions because they hinder cilia function. “To avoid this, we provided sputum suction and administered continuous high-concentration oxygen during the procedure,” they noted. Also, speed and agility in placement are important. “The operation should be performed as rapidly and gently as possible to avoid irritation to the airway,” Dr. Li and colleagues wrote. The postoperative course involved IV expectorants and antiasthma agents and aerosol inhalation of terbutaline. Surveillance bronchoscopes and debridement of granulation tissue helped avoid stent obstruction.
Nonetheless, the researches acknowledged limitations of the retrospective study, namely its small sample size and lack of a control group.
Dr. Li and colleagues had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: A combined type Y-shaped self-expandable coated metallic stent is a new approach for treatment of airway fistulas.
Major finding: Ten patients received the stents; all of them reported improved quality of life. Six died within 8 months because of unrelated factors.
Data source: Single-institution retrospective review of 10 patients with gastrotracheal or gastrobronchial fistulas who received the stent to reopen the airway.
Disclosures: Dr. Li and coauthors had no financial relationships to disclose. The study received support from the National High-Tech R&D Program of China.