User login
A Rapidly Progressive Thoracic Tumor
Introduction
SMARCA4-deficient thoracic sarcomas are a rare entity, first described in 2015 in a study of 19 patients with a median age of 41 years who presented with large compressive masses with frequent infiltration into surrounding tissues [1]. This malignancy is more frequent in younger males (median 41-59 years) with an extensive smoking history and has an aggressive course with a median overall survival of 4-7 months [1-3]. There is currently no established treatment, but case reports show promise for immunotherapy and immuno- chemotherapy [4-8].
Case Report
We present the case of a 62 year old male with a 44 pack year smoking history who first presented to the emergency department (ED) with left shoulder pain in December 2020. He was initially treated with muscle relaxers but returned to the ED ten days later with hemoptysis and rapid weight loss. X-ray showed a 14.2 X 11.7 cm mass with rightward deviation of the trachea. PET scan showed extensive central necrosis with a surrounding pleural effusion and local pleural and nodal metastasis but no distant disease. He underwent thoracentesis which was negative for malignant cells. He underwent CT-guided biopsy in 1/2021, which showed predominantly discohesive small blue cells with pleomorphic cell contour and slightly plasmacytoid features. Extensive pathology review led to a diagnosis of SMARCA4 deficient thoracic sarcoma. On presentation to oncology clinic in 2/2021 his functional status had markedly deteriorated. He was started on ipilimumab/ nivolumab (ipi/nivo) and 1 week after his first cycle was admitted for severe left arm swelling and pain. Imaging showed significant progression of disease and new adrenal metastasis. He received cycle two of ipi/ nivo and was able to be discharged home on oxygen. By his follow-up appointment for cycle three of ipi/nivo in 3/2021, the patient was wheelchair bound with severe dyspnea. X-ray showed the mass now occupied the majority of the left hemi-thorax with worsening tracheal deviation. After discussion, the patient went home on hospice and died 8 days later. As demonstrated by this case, SMARCA4-deficient sarcoma requires high clinical suspicion with prompt diagnosis and treatment given its remarkably rapid progression and poor outcomes.
Introduction
SMARCA4-deficient thoracic sarcomas are a rare entity, first described in 2015 in a study of 19 patients with a median age of 41 years who presented with large compressive masses with frequent infiltration into surrounding tissues [1]. This malignancy is more frequent in younger males (median 41-59 years) with an extensive smoking history and has an aggressive course with a median overall survival of 4-7 months [1-3]. There is currently no established treatment, but case reports show promise for immunotherapy and immuno- chemotherapy [4-8].
Case Report
We present the case of a 62 year old male with a 44 pack year smoking history who first presented to the emergency department (ED) with left shoulder pain in December 2020. He was initially treated with muscle relaxers but returned to the ED ten days later with hemoptysis and rapid weight loss. X-ray showed a 14.2 X 11.7 cm mass with rightward deviation of the trachea. PET scan showed extensive central necrosis with a surrounding pleural effusion and local pleural and nodal metastasis but no distant disease. He underwent thoracentesis which was negative for malignant cells. He underwent CT-guided biopsy in 1/2021, which showed predominantly discohesive small blue cells with pleomorphic cell contour and slightly plasmacytoid features. Extensive pathology review led to a diagnosis of SMARCA4 deficient thoracic sarcoma. On presentation to oncology clinic in 2/2021 his functional status had markedly deteriorated. He was started on ipilimumab/ nivolumab (ipi/nivo) and 1 week after his first cycle was admitted for severe left arm swelling and pain. Imaging showed significant progression of disease and new adrenal metastasis. He received cycle two of ipi/ nivo and was able to be discharged home on oxygen. By his follow-up appointment for cycle three of ipi/nivo in 3/2021, the patient was wheelchair bound with severe dyspnea. X-ray showed the mass now occupied the majority of the left hemi-thorax with worsening tracheal deviation. After discussion, the patient went home on hospice and died 8 days later. As demonstrated by this case, SMARCA4-deficient sarcoma requires high clinical suspicion with prompt diagnosis and treatment given its remarkably rapid progression and poor outcomes.
Introduction
SMARCA4-deficient thoracic sarcomas are a rare entity, first described in 2015 in a study of 19 patients with a median age of 41 years who presented with large compressive masses with frequent infiltration into surrounding tissues [1]. This malignancy is more frequent in younger males (median 41-59 years) with an extensive smoking history and has an aggressive course with a median overall survival of 4-7 months [1-3]. There is currently no established treatment, but case reports show promise for immunotherapy and immuno- chemotherapy [4-8].
Case Report
We present the case of a 62 year old male with a 44 pack year smoking history who first presented to the emergency department (ED) with left shoulder pain in December 2020. He was initially treated with muscle relaxers but returned to the ED ten days later with hemoptysis and rapid weight loss. X-ray showed a 14.2 X 11.7 cm mass with rightward deviation of the trachea. PET scan showed extensive central necrosis with a surrounding pleural effusion and local pleural and nodal metastasis but no distant disease. He underwent thoracentesis which was negative for malignant cells. He underwent CT-guided biopsy in 1/2021, which showed predominantly discohesive small blue cells with pleomorphic cell contour and slightly plasmacytoid features. Extensive pathology review led to a diagnosis of SMARCA4 deficient thoracic sarcoma. On presentation to oncology clinic in 2/2021 his functional status had markedly deteriorated. He was started on ipilimumab/ nivolumab (ipi/nivo) and 1 week after his first cycle was admitted for severe left arm swelling and pain. Imaging showed significant progression of disease and new adrenal metastasis. He received cycle two of ipi/ nivo and was able to be discharged home on oxygen. By his follow-up appointment for cycle three of ipi/nivo in 3/2021, the patient was wheelchair bound with severe dyspnea. X-ray showed the mass now occupied the majority of the left hemi-thorax with worsening tracheal deviation. After discussion, the patient went home on hospice and died 8 days later. As demonstrated by this case, SMARCA4-deficient sarcoma requires high clinical suspicion with prompt diagnosis and treatment given its remarkably rapid progression and poor outcomes.
Antiviral Therapy Improves Hepatocellular Cancer Survival
Hepatocellular cancer (HCC) is the most common type of hepatic cancers, accounting for 65% of all hepatic cancers.1 Among all cancers, HCC is one of the fastest growing causes of death in the United States, and the rate of new HCC cases are on the rise over several decades.2 There are many risk factors leading to HCC, including alcohol use, obesity, and smoking. Infection with hepatitis C virus (HCV) poses a significant risk.1
The pathogenesis of HCV-induced carcinogenesis is mediated by a unique host-induced immunologic response. Viral replication induces production of inflammatory factors, such as tumor necrosis factor (TNF-α), interferon (IFN), and oxidative stress on hepatocytes, resulting in cell injury, death, and regeneration. Repetitive cycles of cellular death and regeneration induce fibrosis, which may lead to cirrhosis.3 Hence, early treatment of HCV infection and achieving sustained virologic response (SVR) may lead to decreased incidence and mortality associated with HCC.
Treatment of HCV infection has become more effective with the development of direct-acting antivirals (DAAs) leading to SVR in > 90% of patients compared with 40 to 50% with IFN-based treatment.4,5 DAAs have been proved safe and highly effective in eradicating HCV infection even in patients with advanced liver disease with decompensated cirrhosis.6 Although achieving SVR indicates a complete cure from chronic HCV infection, several studies have shown subsequent risk of developing HCC persists even after successful HCV treatment.7-9 Some studies show that using DAAs to achieve SVR in patients with HCV infection leads to a decreased relative risk of HCC development compared with patients who do not receive treatment.10-12 But data on HCC risk following DAA-induced SVR vs IFN-induced SVR are somewhat conflicting.
Much of the information regarding the association between SVR and HCC has been gleaned from large data banks without accounting for individual patient characteristics that can be obtained through full chart review. Due to small sample sizes in many chart review studies, the impact that SVR from DAA therapy has on the progression and severity of HCC is not entirely clear. The aim of our study is to evaluate the effect of HCV treatment and SVR status on overall survival (OS) in patients with HCC. Second, we aim to compare survival benefits, if any exist, among the 2 major HCV treatment modalities (IFN vs DAA).
Methods
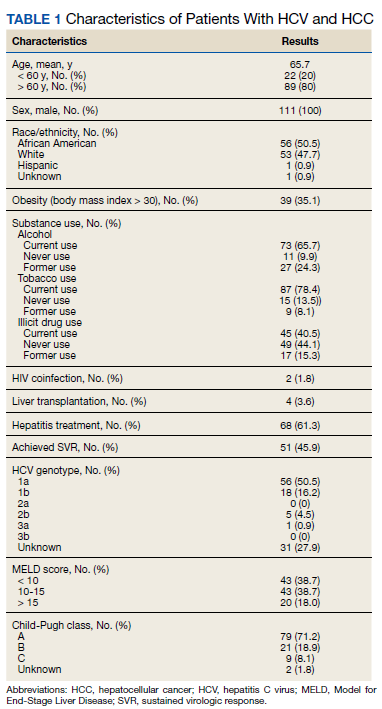
We performed a retrospective review of patients at Memphis Veterans Affairs Medical Center (VAMC) in Tennessee to determine whether treatment for HCV infection in general, and achieving SVR in particular, makes a difference in progression, recurrence, or OS among patients with HCV infection who develop HCC. We identified 111 patients with a diagnosis of both HCV and new or recurrent HCC lesions from November 2008 to March 2019 (Table 1). We divided these patients based on their HCV treatment status, SVR status, and treatment types (IFN vs DAA).
The inclusion criteria were patients aged > 18 years treated at the Memphis VAMC who have HCV infection and developed HCC. Exclusion criteria were patients who developed HCC from other causes such as alcoholic steatohepatitis, hepatitis B virus infection, hemochromatosis, patients without HCV infection, and patients who were not established at the Memphis VAMC. This protocol was approved by the Memphis VAMC Institutional Review Board.
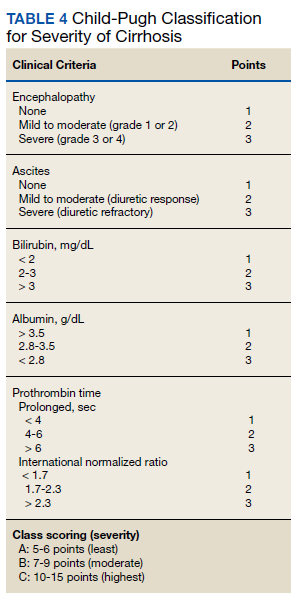
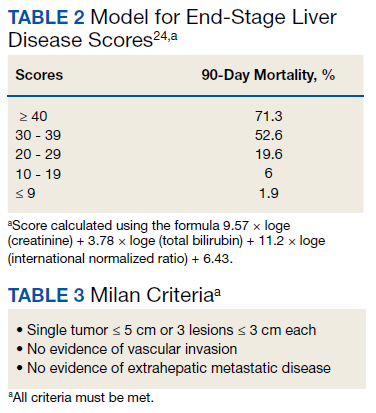
HCC diagnosis was determined using International Classification of Diseases codes (9th revision: 155 and 155.2; 10th revision: CD 22 and 22.9). We also used records of multidisciplinary gastrointestinal malignancy tumor conferences to identify patient who had been diagnosed and treated for HCV infection. We identified patients who were treated with DAA vs IFN as well as patients who had achieved SVR (classified as having negative HCV RNA tests at the end of DAA treatment). We were unable to evaluate Barcelona Clinic Liver Cancer staging since this required documented performance status that was not available in many patient records. We selected cases consistent with both treatment for HCV infection and subsequent development of HCC. Patient data included age; OS time; HIV status HCV genotype; time and status of progression to HCC; type and duration of treatment; and alcohol, tobacco, and drug use. Disease status was measured using the Model for End-Stage Liver Disease (MELD) score (Table 2), Milan criteria (Table 3), and Child-Pugh score (Table 4).
Statistical Analysis
OS was measured from the date of HCC diagnosis to the date of death or last follow-up. Progression-free survival (PFS) was defined from the date of HCC treatment initiation to the date of first HCC recurrence. We compared survival data for the SVR and non-SVR subgroups, the HCV treatment vs non-HCV treatment subgroups, and the IFN therapy vs DAA therapy subgroups, using the Kaplan-Meier method. The differences between subgroups were assessed using a log-rank test. Multivariate analysis using Cox proportional hazards regression model was used to identify factors that had significant impact on OS. Those factors included age; race; alcohol, tobacco, and illicit drug use; SVR status; HCV treatment status; IFN-based regimen vs DAA; MELD, and Child-Pugh scores. The results were expressed as hazard ratios (HRs) and 95% CI. Calculations were made using Statistical Analysis SAS and IBM SPSS software.
Results
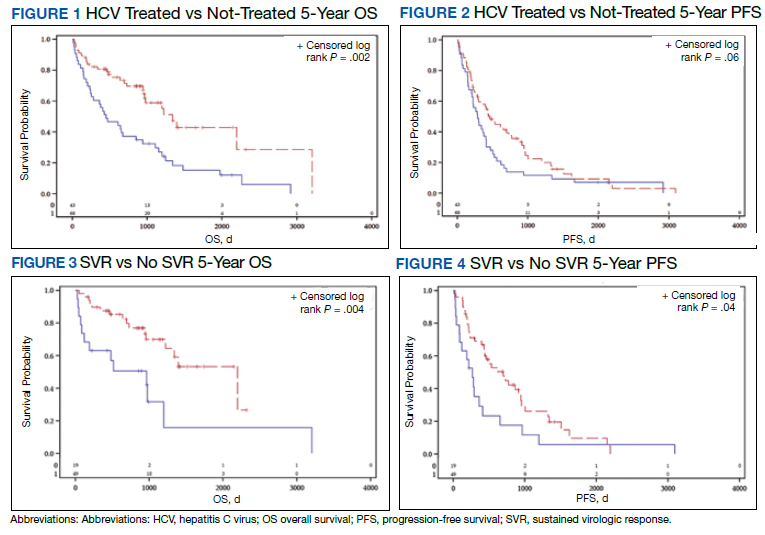
The study included 111 patients. The mean age was 65.7 years; all were male and half of were Black patients. The gender imbalance was due to the predominantly male patient population at Memphis VAMC. Among 111 patients with HCV infection and HCC, 68 patients were treated for HCV infection and had significantly improved OS and PFS compared with the nontreatment group. The median 5-year OS was 44.6 months (95% CI, 966-3202) in the treated HCV infection group compared with 15.1 months in the untreated HCV infection group with a Wilcoxon P = .0005 (Figure 1). Similarly, patients treated for HCV infection had a significantly better 5-year PFS of 15.3 months (95% CI, 294-726) compared with the nontreatment group 9.5 months (95% CI, 205-405) with a Wilcoxon P = .04 (Figure 2).
Among 68 patients treated for HCV infection, 51 achieved SVR, and 34 achieved SVR after the diagnosis of HCC. Patients who achieved SVR had an improved 5-year OS when compared with patients who did not achieve SVR (median 65.8 months [95% CI, 1222-NA] vs 15.7 months [95% CI, 242-853], Wilcoxon P < .001) (Figure 3). Similarly, patients with SVR had improved 5-year PFS when compared with the non-SVR group (median 20.5 months [95% CI, 431-914] vs 8.9 months [95% CI, 191-340], Wilcoxon P = .007 (Figure 4). Achievement of SVR after HCC diagnosis suggests a significantly improved OS (HR 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI, 0.23-1.82, P = .41)
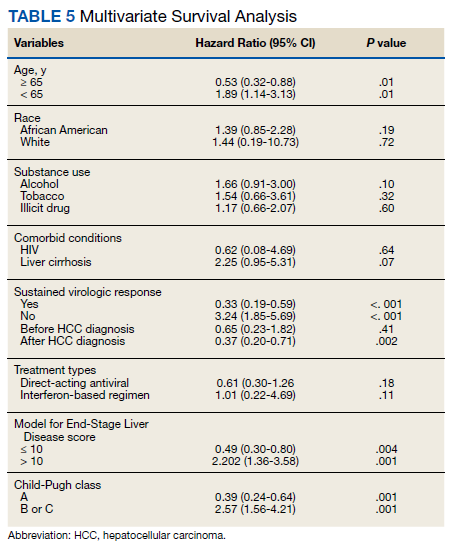
Multivariate Cox regression was used to determine factors with significant survival impact. Advanced age at diagnosis (aged ≥ 65 years) (HR, 0.53; 95% CI, 0.320-0.880; P = .01), SVR status (HR, 0.33; 95% CI, 0.190-0.587; P < .001), achieving SVR after HCC diagnosis (HR, 0.37; 95% CI, 0.20-0.71; P = .002), low MELD score (< 10) (HR, 0.49; 95% CI, 0.30-0.80; P = .004) and low Child-Pugh score (class A) (HR, 0.39; 95% CI, 0.24-0.64; P = .001) have a significant positive impact on OS. Survival was not significantly influenced by race, tobacco, drug use, HIV or cirrhosis status, or HCV treatment type. In addition, higher Child-Pugh class (B or C), higher MELD score (> 10), and younger age at diagnosis (< 65 years) have a negative impact on survival outcome (Table 5).
Discussion
The survival benefit of HCV eradication and achieving SVR status has been well established in patients with HCC.13 In a retrospective cohort study of 250 patients with HCV infection who had received curative treatment for HCC, multivariate analysis demonstrated that achieving SVR is an independent predictor of OS.14 The 3-year and 5-year OS rates were 97% and 94% for the SVR group, and 91% and 60% for the non‐SVR group, respectively (P < .001). Similarly, according to Sou and colleagues, of 122 patients with HCV-related HCC, patients with SVR had longer OS than patients with no SVR (P = .04).15 One of the hypotheses that could explain the survival benefit in patients who achieved SVR is the effect of achieving SVR in reducing persistent liver inflammation and associated liver mortality, and therefore lowering risks of complication in patients with HCC.16 In our study, multivariate analysis shows that achieving SVR is associated with significant improved OS (HR, 0.33). In contrast, patients with HCC who have not achieved SVR are associated with worse survival (HR, 3.24). This finding supports early treatment of HCV to obtain SVR in HCV-related patients with HCC, even after development of HCC.
Among 68 patients treated for HCV infection, 45 patients were treated after HCC diagnosis, and 34 patients achieved SVR after HCC diagnosis. The average time between HCV infection treatment after HCC diagnosis was 6 months. Our data suggested that achievement of SVR after HCC diagnosis suggests an improved OS (HR, 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI,0.23-1.82; P = .41). This lack of statistical significance is likely due to small sample size of patients achieving SVR prior to HCC diagnosis. Our results are consistent with the findings regarding the efficacy and timing of DAA treatment in patients with active HCC. According to Singal and colleagues, achieving SVR after DAA therapy may result in improved liver function and facilitate additional HCC-directed therapy, which potentially improves survival.17-19
Nagaoki and colleagues found that there was no significant difference in OS in patients with HCC between the DAA and IFN groups. According to the study, the 3-year and 5-year OS rates were 96% and 96% for DAA patients and 93% and 73% for IFN patients, respectively (P = .16).14 This finding is consistent with the results of our study. HCV treatment type (IFN vs DAA) was not found to be associated with either OS or PFS time, regardless of time period.
A higher MELD score (> 10) and a higher Child-Pugh class (B or C) score are associated with worse survival outcome regardless of SVR status. While patients with a low MELD score (≤ 10) have a better survival rate (HR 0.49), a higher MELD score has a significantly higher HR and therefore worse survival outcomes (HR, 2.20). Similarly, patients with Child-Pugh A (HR, 0.39) have a better survival outcome compared with those patients with Child-Pugh class B or C (HR, 2.57). This finding is consistent with results of multiple studies indicating that advanced liver disease, as measured by a high MELD score and Child-Pugh class score, can be used to predict the survival outcome in patients with HCV-related HCC.20-22
Unlike other studies that look at a single prognostic variable, our study evaluated prognostic impacts of multiple variables (age, SVR status, the order of SVR in relation to HCC development, HCV treatment type, MELD score and Child-Pugh class) in patients with HCC. The study included patients treated for HCV after development of HCC along with other multiple variables leading to OS benefit. It is one of the only studies in the United States that compared 5-year OS and PFS among patients with HCC treated for HCV and achieved SVR. The studies by Nagaoki and colleagues and Sou and colleagues were conducted in Japan, and some of their subset analyses were univariate. Among our study population of veterans, 50% were African American patients, suggesting that they may have similar OS benefit when compared to White patients with HCC and HCV treatment.
Limitations
Our findings were limited in that our study population is too small to conduct further subset analysis that would allow statistical significance of those subsets, such as the suggested benefit of SVR in patients who presented with HCC after antiviral therapy. Another limitation is the all-male population, likely a result of the older veteran population at the Memphis VAMC. The mean age at diagnosis was 65 years, which is slightly higher than the general population. Compared to the SEER database, HCC is most frequently diagnosed among people aged 55 to 64 years.23 The age difference was likely due to our aging veteran population.
Further studies are needed to determine the significance of SVR on HCC recurrence and treatment. Immunotherapy is now first-line treatment for patients with local advanced HCC. All the immunotherapy studies excluded patients with active HCV infection. Hence, we need more data on HCV treatment timing among patients scheduled to start treatment with immunotherapy.
Conclusions
In a population of older veterans, treatment of HCV infection leads to OS benefit among patients with HCC. In addition, patients with HCV infection who achieve SVR have an OS benefit over patients unable to achieve SVR. The type of treatment, DAA vs IFN-based regimen, did not show significant survival benefit.
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. Published 2017 May 29. doi:10.4103/jcar.JCar_9_16
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.21492
3. Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006;6(9):674-687. doi:10.1038/nrc1934
4. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis c virus infection: a systematic review. Ann Intern Med. 2017;166(9):637-648. doi:10.7326/M16-2575
5. Kouris G, Hydery T, Greenwood BC, et al. Effectiveness of Ledipasvir/Sofosbuvir and predictors of treatment failure in members with hepatitis C genotype 1 infection: a retrospective cohort study in a medicaid population. J Manag Care Spec Pharm. 2018;24(7):591-597. doi:10.18553/jmcp.2018.24.7.591
6. Jacobson IM, Lawitz E, Kwo PY, et al. Safety and efficacy of elbasvir/grazoprevir in patients with hepatitis c virus infection and compensated cirrhosis: an integrated analysis. Gastroenterology. 2017;152(6):1372-1382.e2. doi:10.1053/j.gastro.2017.01.050
7. Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155(5):1436-1450.e6. doi:10.1053/j.gastro.2018.07.01510.
8. Innes H, Barclay ST, Hayes PC, et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: role of the treatment regimen. J Hepatol. 2018;68(4):646-654. doi:10.1016/j.jhep.2017.10.033
9. Romano A, Angeli P, Piovesan S, et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: a prospective population study. J Hepatol. 2018;69(2):345-352. doi:10.1016/j.jhep.2018.03.009
10. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.e1. doi:10.1053/j.gastro.2017.06.0122
11. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):262-270. doi:10.1136/flgastro-2018-101017
12. Kuftinec G, Loehfelm T, Corwin M, et al. De novo hepatocellular carcinoma occurrence in hepatitis C cirrhotics treated with direct-acting antiviral agents. Hepat Oncol. 2018;5(1):HEP06. Published 2018 Jul 25. doi:10.2217/hep-2018-00033
13. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329-337. doi:10.7326/0003-4819-158-5-201303050-00005
14. Nagaoki Y, Imamura M, Nishida Y, et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: comparison with interferon-based therapy. J Med Virol. 2019;91(4):650-658. doi:10.1002/jmv.25352
15. Sou FM, Wu CK, Chang KC, et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J Formos Med Assoc. 2019;118(1 Pt 3):504-513. doi:10.1016/j.jfma.2018.10.017
16. Roche B, Coilly A, Duclos-Vallee JC, Samuel D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. 2018;38(suppl 1):139-145. doi:10.1111/liv.13659
17. Singal AG, Lim JK, Kanwal F. AGA clinical practice update on interaction between oral direct-acting antivirals for chronic hepatitis C infection and hepatocellular carcinoma: expert review. Gastroenterology. 2019;156(8):2149-2157. doi:10.1053/j.gastro.2019.02.046
18. Toyoda H, Kumada T, Hayashi K, et al. Characteristics and prognosis of hepatocellular carcinoma detected in sustained responders to interferon therapy for chronic hepatitis C. Cancer Detect Prev. 2003;27(6):498-502. doi:10.1016/j.cdp.2003.09.00719. Okamura Y, Sugiura T, Ito T, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis C virus-related hepatocellular carcinoma. Ann Surg Oncol. 2019; 26(13):4566-4575. doi:10.1245/s10434-019-07911-w
20. Wray CJ, Harvin JA, Silberfein EJ, Ko TC, Kao LS. Pilot prognostic model of extremely poor survival among high-risk hepatocellular carcinoma patients. Cancer. 2012;118(24):6118-6125. doi:10.1002/cncr.27649
21. Kim JH, Kim JH, Choi JH, et al. Value of the model for end-stage liver disease for predicting survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Scand J Gastroenterol. 2009;44(3):346-357. doi:10.1080/00365520802530838
22. Vogeler M, Mohr I, Pfeiffenberger J, et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(4):1033-1050. doi:10.1007/s00432-020-03135-8
23. National Institutes of Health, Surveillance, Epidemiology, and End Results. Cancer stat facts: cancer of the liver and intrahepatic bile duct. Accessed July 15, 2021. https://seer.cancer.gov/statfacts/html/livibd.html
24. Singal AK, Kamath PS. Model for End-stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
Hepatocellular cancer (HCC) is the most common type of hepatic cancers, accounting for 65% of all hepatic cancers.1 Among all cancers, HCC is one of the fastest growing causes of death in the United States, and the rate of new HCC cases are on the rise over several decades.2 There are many risk factors leading to HCC, including alcohol use, obesity, and smoking. Infection with hepatitis C virus (HCV) poses a significant risk.1
The pathogenesis of HCV-induced carcinogenesis is mediated by a unique host-induced immunologic response. Viral replication induces production of inflammatory factors, such as tumor necrosis factor (TNF-α), interferon (IFN), and oxidative stress on hepatocytes, resulting in cell injury, death, and regeneration. Repetitive cycles of cellular death and regeneration induce fibrosis, which may lead to cirrhosis.3 Hence, early treatment of HCV infection and achieving sustained virologic response (SVR) may lead to decreased incidence and mortality associated with HCC.
Treatment of HCV infection has become more effective with the development of direct-acting antivirals (DAAs) leading to SVR in > 90% of patients compared with 40 to 50% with IFN-based treatment.4,5 DAAs have been proved safe and highly effective in eradicating HCV infection even in patients with advanced liver disease with decompensated cirrhosis.6 Although achieving SVR indicates a complete cure from chronic HCV infection, several studies have shown subsequent risk of developing HCC persists even after successful HCV treatment.7-9 Some studies show that using DAAs to achieve SVR in patients with HCV infection leads to a decreased relative risk of HCC development compared with patients who do not receive treatment.10-12 But data on HCC risk following DAA-induced SVR vs IFN-induced SVR are somewhat conflicting.
Much of the information regarding the association between SVR and HCC has been gleaned from large data banks without accounting for individual patient characteristics that can be obtained through full chart review. Due to small sample sizes in many chart review studies, the impact that SVR from DAA therapy has on the progression and severity of HCC is not entirely clear. The aim of our study is to evaluate the effect of HCV treatment and SVR status on overall survival (OS) in patients with HCC. Second, we aim to compare survival benefits, if any exist, among the 2 major HCV treatment modalities (IFN vs DAA).
Methods
We performed a retrospective review of patients at Memphis Veterans Affairs Medical Center (VAMC) in Tennessee to determine whether treatment for HCV infection in general, and achieving SVR in particular, makes a difference in progression, recurrence, or OS among patients with HCV infection who develop HCC. We identified 111 patients with a diagnosis of both HCV and new or recurrent HCC lesions from November 2008 to March 2019 (Table 1). We divided these patients based on their HCV treatment status, SVR status, and treatment types (IFN vs DAA).
The inclusion criteria were patients aged > 18 years treated at the Memphis VAMC who have HCV infection and developed HCC. Exclusion criteria were patients who developed HCC from other causes such as alcoholic steatohepatitis, hepatitis B virus infection, hemochromatosis, patients without HCV infection, and patients who were not established at the Memphis VAMC. This protocol was approved by the Memphis VAMC Institutional Review Board.
HCC diagnosis was determined using International Classification of Diseases codes (9th revision: 155 and 155.2; 10th revision: CD 22 and 22.9). We also used records of multidisciplinary gastrointestinal malignancy tumor conferences to identify patient who had been diagnosed and treated for HCV infection. We identified patients who were treated with DAA vs IFN as well as patients who had achieved SVR (classified as having negative HCV RNA tests at the end of DAA treatment). We were unable to evaluate Barcelona Clinic Liver Cancer staging since this required documented performance status that was not available in many patient records. We selected cases consistent with both treatment for HCV infection and subsequent development of HCC. Patient data included age; OS time; HIV status HCV genotype; time and status of progression to HCC; type and duration of treatment; and alcohol, tobacco, and drug use. Disease status was measured using the Model for End-Stage Liver Disease (MELD) score (Table 2), Milan criteria (Table 3), and Child-Pugh score (Table 4).
Statistical Analysis
OS was measured from the date of HCC diagnosis to the date of death or last follow-up. Progression-free survival (PFS) was defined from the date of HCC treatment initiation to the date of first HCC recurrence. We compared survival data for the SVR and non-SVR subgroups, the HCV treatment vs non-HCV treatment subgroups, and the IFN therapy vs DAA therapy subgroups, using the Kaplan-Meier method. The differences between subgroups were assessed using a log-rank test. Multivariate analysis using Cox proportional hazards regression model was used to identify factors that had significant impact on OS. Those factors included age; race; alcohol, tobacco, and illicit drug use; SVR status; HCV treatment status; IFN-based regimen vs DAA; MELD, and Child-Pugh scores. The results were expressed as hazard ratios (HRs) and 95% CI. Calculations were made using Statistical Analysis SAS and IBM SPSS software.
Results
The study included 111 patients. The mean age was 65.7 years; all were male and half of were Black patients. The gender imbalance was due to the predominantly male patient population at Memphis VAMC. Among 111 patients with HCV infection and HCC, 68 patients were treated for HCV infection and had significantly improved OS and PFS compared with the nontreatment group. The median 5-year OS was 44.6 months (95% CI, 966-3202) in the treated HCV infection group compared with 15.1 months in the untreated HCV infection group with a Wilcoxon P = .0005 (Figure 1). Similarly, patients treated for HCV infection had a significantly better 5-year PFS of 15.3 months (95% CI, 294-726) compared with the nontreatment group 9.5 months (95% CI, 205-405) with a Wilcoxon P = .04 (Figure 2).
Among 68 patients treated for HCV infection, 51 achieved SVR, and 34 achieved SVR after the diagnosis of HCC. Patients who achieved SVR had an improved 5-year OS when compared with patients who did not achieve SVR (median 65.8 months [95% CI, 1222-NA] vs 15.7 months [95% CI, 242-853], Wilcoxon P < .001) (Figure 3). Similarly, patients with SVR had improved 5-year PFS when compared with the non-SVR group (median 20.5 months [95% CI, 431-914] vs 8.9 months [95% CI, 191-340], Wilcoxon P = .007 (Figure 4). Achievement of SVR after HCC diagnosis suggests a significantly improved OS (HR 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI, 0.23-1.82, P = .41)
Multivariate Cox regression was used to determine factors with significant survival impact. Advanced age at diagnosis (aged ≥ 65 years) (HR, 0.53; 95% CI, 0.320-0.880; P = .01), SVR status (HR, 0.33; 95% CI, 0.190-0.587; P < .001), achieving SVR after HCC diagnosis (HR, 0.37; 95% CI, 0.20-0.71; P = .002), low MELD score (< 10) (HR, 0.49; 95% CI, 0.30-0.80; P = .004) and low Child-Pugh score (class A) (HR, 0.39; 95% CI, 0.24-0.64; P = .001) have a significant positive impact on OS. Survival was not significantly influenced by race, tobacco, drug use, HIV or cirrhosis status, or HCV treatment type. In addition, higher Child-Pugh class (B or C), higher MELD score (> 10), and younger age at diagnosis (< 65 years) have a negative impact on survival outcome (Table 5).
Discussion
The survival benefit of HCV eradication and achieving SVR status has been well established in patients with HCC.13 In a retrospective cohort study of 250 patients with HCV infection who had received curative treatment for HCC, multivariate analysis demonstrated that achieving SVR is an independent predictor of OS.14 The 3-year and 5-year OS rates were 97% and 94% for the SVR group, and 91% and 60% for the non‐SVR group, respectively (P < .001). Similarly, according to Sou and colleagues, of 122 patients with HCV-related HCC, patients with SVR had longer OS than patients with no SVR (P = .04).15 One of the hypotheses that could explain the survival benefit in patients who achieved SVR is the effect of achieving SVR in reducing persistent liver inflammation and associated liver mortality, and therefore lowering risks of complication in patients with HCC.16 In our study, multivariate analysis shows that achieving SVR is associated with significant improved OS (HR, 0.33). In contrast, patients with HCC who have not achieved SVR are associated with worse survival (HR, 3.24). This finding supports early treatment of HCV to obtain SVR in HCV-related patients with HCC, even after development of HCC.
Among 68 patients treated for HCV infection, 45 patients were treated after HCC diagnosis, and 34 patients achieved SVR after HCC diagnosis. The average time between HCV infection treatment after HCC diagnosis was 6 months. Our data suggested that achievement of SVR after HCC diagnosis suggests an improved OS (HR, 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI,0.23-1.82; P = .41). This lack of statistical significance is likely due to small sample size of patients achieving SVR prior to HCC diagnosis. Our results are consistent with the findings regarding the efficacy and timing of DAA treatment in patients with active HCC. According to Singal and colleagues, achieving SVR after DAA therapy may result in improved liver function and facilitate additional HCC-directed therapy, which potentially improves survival.17-19
Nagaoki and colleagues found that there was no significant difference in OS in patients with HCC between the DAA and IFN groups. According to the study, the 3-year and 5-year OS rates were 96% and 96% for DAA patients and 93% and 73% for IFN patients, respectively (P = .16).14 This finding is consistent with the results of our study. HCV treatment type (IFN vs DAA) was not found to be associated with either OS or PFS time, regardless of time period.
A higher MELD score (> 10) and a higher Child-Pugh class (B or C) score are associated with worse survival outcome regardless of SVR status. While patients with a low MELD score (≤ 10) have a better survival rate (HR 0.49), a higher MELD score has a significantly higher HR and therefore worse survival outcomes (HR, 2.20). Similarly, patients with Child-Pugh A (HR, 0.39) have a better survival outcome compared with those patients with Child-Pugh class B or C (HR, 2.57). This finding is consistent with results of multiple studies indicating that advanced liver disease, as measured by a high MELD score and Child-Pugh class score, can be used to predict the survival outcome in patients with HCV-related HCC.20-22
Unlike other studies that look at a single prognostic variable, our study evaluated prognostic impacts of multiple variables (age, SVR status, the order of SVR in relation to HCC development, HCV treatment type, MELD score and Child-Pugh class) in patients with HCC. The study included patients treated for HCV after development of HCC along with other multiple variables leading to OS benefit. It is one of the only studies in the United States that compared 5-year OS and PFS among patients with HCC treated for HCV and achieved SVR. The studies by Nagaoki and colleagues and Sou and colleagues were conducted in Japan, and some of their subset analyses were univariate. Among our study population of veterans, 50% were African American patients, suggesting that they may have similar OS benefit when compared to White patients with HCC and HCV treatment.
Limitations
Our findings were limited in that our study population is too small to conduct further subset analysis that would allow statistical significance of those subsets, such as the suggested benefit of SVR in patients who presented with HCC after antiviral therapy. Another limitation is the all-male population, likely a result of the older veteran population at the Memphis VAMC. The mean age at diagnosis was 65 years, which is slightly higher than the general population. Compared to the SEER database, HCC is most frequently diagnosed among people aged 55 to 64 years.23 The age difference was likely due to our aging veteran population.
Further studies are needed to determine the significance of SVR on HCC recurrence and treatment. Immunotherapy is now first-line treatment for patients with local advanced HCC. All the immunotherapy studies excluded patients with active HCV infection. Hence, we need more data on HCV treatment timing among patients scheduled to start treatment with immunotherapy.
Conclusions
In a population of older veterans, treatment of HCV infection leads to OS benefit among patients with HCC. In addition, patients with HCV infection who achieve SVR have an OS benefit over patients unable to achieve SVR. The type of treatment, DAA vs IFN-based regimen, did not show significant survival benefit.
Hepatocellular cancer (HCC) is the most common type of hepatic cancers, accounting for 65% of all hepatic cancers.1 Among all cancers, HCC is one of the fastest growing causes of death in the United States, and the rate of new HCC cases are on the rise over several decades.2 There are many risk factors leading to HCC, including alcohol use, obesity, and smoking. Infection with hepatitis C virus (HCV) poses a significant risk.1
The pathogenesis of HCV-induced carcinogenesis is mediated by a unique host-induced immunologic response. Viral replication induces production of inflammatory factors, such as tumor necrosis factor (TNF-α), interferon (IFN), and oxidative stress on hepatocytes, resulting in cell injury, death, and regeneration. Repetitive cycles of cellular death and regeneration induce fibrosis, which may lead to cirrhosis.3 Hence, early treatment of HCV infection and achieving sustained virologic response (SVR) may lead to decreased incidence and mortality associated with HCC.
Treatment of HCV infection has become more effective with the development of direct-acting antivirals (DAAs) leading to SVR in > 90% of patients compared with 40 to 50% with IFN-based treatment.4,5 DAAs have been proved safe and highly effective in eradicating HCV infection even in patients with advanced liver disease with decompensated cirrhosis.6 Although achieving SVR indicates a complete cure from chronic HCV infection, several studies have shown subsequent risk of developing HCC persists even after successful HCV treatment.7-9 Some studies show that using DAAs to achieve SVR in patients with HCV infection leads to a decreased relative risk of HCC development compared with patients who do not receive treatment.10-12 But data on HCC risk following DAA-induced SVR vs IFN-induced SVR are somewhat conflicting.
Much of the information regarding the association between SVR and HCC has been gleaned from large data banks without accounting for individual patient characteristics that can be obtained through full chart review. Due to small sample sizes in many chart review studies, the impact that SVR from DAA therapy has on the progression and severity of HCC is not entirely clear. The aim of our study is to evaluate the effect of HCV treatment and SVR status on overall survival (OS) in patients with HCC. Second, we aim to compare survival benefits, if any exist, among the 2 major HCV treatment modalities (IFN vs DAA).
Methods
We performed a retrospective review of patients at Memphis Veterans Affairs Medical Center (VAMC) in Tennessee to determine whether treatment for HCV infection in general, and achieving SVR in particular, makes a difference in progression, recurrence, or OS among patients with HCV infection who develop HCC. We identified 111 patients with a diagnosis of both HCV and new or recurrent HCC lesions from November 2008 to March 2019 (Table 1). We divided these patients based on their HCV treatment status, SVR status, and treatment types (IFN vs DAA).
The inclusion criteria were patients aged > 18 years treated at the Memphis VAMC who have HCV infection and developed HCC. Exclusion criteria were patients who developed HCC from other causes such as alcoholic steatohepatitis, hepatitis B virus infection, hemochromatosis, patients without HCV infection, and patients who were not established at the Memphis VAMC. This protocol was approved by the Memphis VAMC Institutional Review Board.
HCC diagnosis was determined using International Classification of Diseases codes (9th revision: 155 and 155.2; 10th revision: CD 22 and 22.9). We also used records of multidisciplinary gastrointestinal malignancy tumor conferences to identify patient who had been diagnosed and treated for HCV infection. We identified patients who were treated with DAA vs IFN as well as patients who had achieved SVR (classified as having negative HCV RNA tests at the end of DAA treatment). We were unable to evaluate Barcelona Clinic Liver Cancer staging since this required documented performance status that was not available in many patient records. We selected cases consistent with both treatment for HCV infection and subsequent development of HCC. Patient data included age; OS time; HIV status HCV genotype; time and status of progression to HCC; type and duration of treatment; and alcohol, tobacco, and drug use. Disease status was measured using the Model for End-Stage Liver Disease (MELD) score (Table 2), Milan criteria (Table 3), and Child-Pugh score (Table 4).
Statistical Analysis
OS was measured from the date of HCC diagnosis to the date of death or last follow-up. Progression-free survival (PFS) was defined from the date of HCC treatment initiation to the date of first HCC recurrence. We compared survival data for the SVR and non-SVR subgroups, the HCV treatment vs non-HCV treatment subgroups, and the IFN therapy vs DAA therapy subgroups, using the Kaplan-Meier method. The differences between subgroups were assessed using a log-rank test. Multivariate analysis using Cox proportional hazards regression model was used to identify factors that had significant impact on OS. Those factors included age; race; alcohol, tobacco, and illicit drug use; SVR status; HCV treatment status; IFN-based regimen vs DAA; MELD, and Child-Pugh scores. The results were expressed as hazard ratios (HRs) and 95% CI. Calculations were made using Statistical Analysis SAS and IBM SPSS software.
Results
The study included 111 patients. The mean age was 65.7 years; all were male and half of were Black patients. The gender imbalance was due to the predominantly male patient population at Memphis VAMC. Among 111 patients with HCV infection and HCC, 68 patients were treated for HCV infection and had significantly improved OS and PFS compared with the nontreatment group. The median 5-year OS was 44.6 months (95% CI, 966-3202) in the treated HCV infection group compared with 15.1 months in the untreated HCV infection group with a Wilcoxon P = .0005 (Figure 1). Similarly, patients treated for HCV infection had a significantly better 5-year PFS of 15.3 months (95% CI, 294-726) compared with the nontreatment group 9.5 months (95% CI, 205-405) with a Wilcoxon P = .04 (Figure 2).
Among 68 patients treated for HCV infection, 51 achieved SVR, and 34 achieved SVR after the diagnosis of HCC. Patients who achieved SVR had an improved 5-year OS when compared with patients who did not achieve SVR (median 65.8 months [95% CI, 1222-NA] vs 15.7 months [95% CI, 242-853], Wilcoxon P < .001) (Figure 3). Similarly, patients with SVR had improved 5-year PFS when compared with the non-SVR group (median 20.5 months [95% CI, 431-914] vs 8.9 months [95% CI, 191-340], Wilcoxon P = .007 (Figure 4). Achievement of SVR after HCC diagnosis suggests a significantly improved OS (HR 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI, 0.23-1.82, P = .41)
Multivariate Cox regression was used to determine factors with significant survival impact. Advanced age at diagnosis (aged ≥ 65 years) (HR, 0.53; 95% CI, 0.320-0.880; P = .01), SVR status (HR, 0.33; 95% CI, 0.190-0.587; P < .001), achieving SVR after HCC diagnosis (HR, 0.37; 95% CI, 0.20-0.71; P = .002), low MELD score (< 10) (HR, 0.49; 95% CI, 0.30-0.80; P = .004) and low Child-Pugh score (class A) (HR, 0.39; 95% CI, 0.24-0.64; P = .001) have a significant positive impact on OS. Survival was not significantly influenced by race, tobacco, drug use, HIV or cirrhosis status, or HCV treatment type. In addition, higher Child-Pugh class (B or C), higher MELD score (> 10), and younger age at diagnosis (< 65 years) have a negative impact on survival outcome (Table 5).
Discussion
The survival benefit of HCV eradication and achieving SVR status has been well established in patients with HCC.13 In a retrospective cohort study of 250 patients with HCV infection who had received curative treatment for HCC, multivariate analysis demonstrated that achieving SVR is an independent predictor of OS.14 The 3-year and 5-year OS rates were 97% and 94% for the SVR group, and 91% and 60% for the non‐SVR group, respectively (P < .001). Similarly, according to Sou and colleagues, of 122 patients with HCV-related HCC, patients with SVR had longer OS than patients with no SVR (P = .04).15 One of the hypotheses that could explain the survival benefit in patients who achieved SVR is the effect of achieving SVR in reducing persistent liver inflammation and associated liver mortality, and therefore lowering risks of complication in patients with HCC.16 In our study, multivariate analysis shows that achieving SVR is associated with significant improved OS (HR, 0.33). In contrast, patients with HCC who have not achieved SVR are associated with worse survival (HR, 3.24). This finding supports early treatment of HCV to obtain SVR in HCV-related patients with HCC, even after development of HCC.
Among 68 patients treated for HCV infection, 45 patients were treated after HCC diagnosis, and 34 patients achieved SVR after HCC diagnosis. The average time between HCV infection treatment after HCC diagnosis was 6 months. Our data suggested that achievement of SVR after HCC diagnosis suggests an improved OS (HR, 0.37) compared with achievement prior to HCC diagnosis (HR, 0.65; 95% CI,0.23-1.82; P = .41). This lack of statistical significance is likely due to small sample size of patients achieving SVR prior to HCC diagnosis. Our results are consistent with the findings regarding the efficacy and timing of DAA treatment in patients with active HCC. According to Singal and colleagues, achieving SVR after DAA therapy may result in improved liver function and facilitate additional HCC-directed therapy, which potentially improves survival.17-19
Nagaoki and colleagues found that there was no significant difference in OS in patients with HCC between the DAA and IFN groups. According to the study, the 3-year and 5-year OS rates were 96% and 96% for DAA patients and 93% and 73% for IFN patients, respectively (P = .16).14 This finding is consistent with the results of our study. HCV treatment type (IFN vs DAA) was not found to be associated with either OS or PFS time, regardless of time period.
A higher MELD score (> 10) and a higher Child-Pugh class (B or C) score are associated with worse survival outcome regardless of SVR status. While patients with a low MELD score (≤ 10) have a better survival rate (HR 0.49), a higher MELD score has a significantly higher HR and therefore worse survival outcomes (HR, 2.20). Similarly, patients with Child-Pugh A (HR, 0.39) have a better survival outcome compared with those patients with Child-Pugh class B or C (HR, 2.57). This finding is consistent with results of multiple studies indicating that advanced liver disease, as measured by a high MELD score and Child-Pugh class score, can be used to predict the survival outcome in patients with HCV-related HCC.20-22
Unlike other studies that look at a single prognostic variable, our study evaluated prognostic impacts of multiple variables (age, SVR status, the order of SVR in relation to HCC development, HCV treatment type, MELD score and Child-Pugh class) in patients with HCC. The study included patients treated for HCV after development of HCC along with other multiple variables leading to OS benefit. It is one of the only studies in the United States that compared 5-year OS and PFS among patients with HCC treated for HCV and achieved SVR. The studies by Nagaoki and colleagues and Sou and colleagues were conducted in Japan, and some of their subset analyses were univariate. Among our study population of veterans, 50% were African American patients, suggesting that they may have similar OS benefit when compared to White patients with HCC and HCV treatment.
Limitations
Our findings were limited in that our study population is too small to conduct further subset analysis that would allow statistical significance of those subsets, such as the suggested benefit of SVR in patients who presented with HCC after antiviral therapy. Another limitation is the all-male population, likely a result of the older veteran population at the Memphis VAMC. The mean age at diagnosis was 65 years, which is slightly higher than the general population. Compared to the SEER database, HCC is most frequently diagnosed among people aged 55 to 64 years.23 The age difference was likely due to our aging veteran population.
Further studies are needed to determine the significance of SVR on HCC recurrence and treatment. Immunotherapy is now first-line treatment for patients with local advanced HCC. All the immunotherapy studies excluded patients with active HCV infection. Hence, we need more data on HCV treatment timing among patients scheduled to start treatment with immunotherapy.
Conclusions
In a population of older veterans, treatment of HCV infection leads to OS benefit among patients with HCC. In addition, patients with HCV infection who achieve SVR have an OS benefit over patients unable to achieve SVR. The type of treatment, DAA vs IFN-based regimen, did not show significant survival benefit.
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. Published 2017 May 29. doi:10.4103/jcar.JCar_9_16
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.21492
3. Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006;6(9):674-687. doi:10.1038/nrc1934
4. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis c virus infection: a systematic review. Ann Intern Med. 2017;166(9):637-648. doi:10.7326/M16-2575
5. Kouris G, Hydery T, Greenwood BC, et al. Effectiveness of Ledipasvir/Sofosbuvir and predictors of treatment failure in members with hepatitis C genotype 1 infection: a retrospective cohort study in a medicaid population. J Manag Care Spec Pharm. 2018;24(7):591-597. doi:10.18553/jmcp.2018.24.7.591
6. Jacobson IM, Lawitz E, Kwo PY, et al. Safety and efficacy of elbasvir/grazoprevir in patients with hepatitis c virus infection and compensated cirrhosis: an integrated analysis. Gastroenterology. 2017;152(6):1372-1382.e2. doi:10.1053/j.gastro.2017.01.050
7. Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155(5):1436-1450.e6. doi:10.1053/j.gastro.2018.07.01510.
8. Innes H, Barclay ST, Hayes PC, et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: role of the treatment regimen. J Hepatol. 2018;68(4):646-654. doi:10.1016/j.jhep.2017.10.033
9. Romano A, Angeli P, Piovesan S, et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: a prospective population study. J Hepatol. 2018;69(2):345-352. doi:10.1016/j.jhep.2018.03.009
10. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.e1. doi:10.1053/j.gastro.2017.06.0122
11. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):262-270. doi:10.1136/flgastro-2018-101017
12. Kuftinec G, Loehfelm T, Corwin M, et al. De novo hepatocellular carcinoma occurrence in hepatitis C cirrhotics treated with direct-acting antiviral agents. Hepat Oncol. 2018;5(1):HEP06. Published 2018 Jul 25. doi:10.2217/hep-2018-00033
13. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329-337. doi:10.7326/0003-4819-158-5-201303050-00005
14. Nagaoki Y, Imamura M, Nishida Y, et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: comparison with interferon-based therapy. J Med Virol. 2019;91(4):650-658. doi:10.1002/jmv.25352
15. Sou FM, Wu CK, Chang KC, et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J Formos Med Assoc. 2019;118(1 Pt 3):504-513. doi:10.1016/j.jfma.2018.10.017
16. Roche B, Coilly A, Duclos-Vallee JC, Samuel D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. 2018;38(suppl 1):139-145. doi:10.1111/liv.13659
17. Singal AG, Lim JK, Kanwal F. AGA clinical practice update on interaction between oral direct-acting antivirals for chronic hepatitis C infection and hepatocellular carcinoma: expert review. Gastroenterology. 2019;156(8):2149-2157. doi:10.1053/j.gastro.2019.02.046
18. Toyoda H, Kumada T, Hayashi K, et al. Characteristics and prognosis of hepatocellular carcinoma detected in sustained responders to interferon therapy for chronic hepatitis C. Cancer Detect Prev. 2003;27(6):498-502. doi:10.1016/j.cdp.2003.09.00719. Okamura Y, Sugiura T, Ito T, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis C virus-related hepatocellular carcinoma. Ann Surg Oncol. 2019; 26(13):4566-4575. doi:10.1245/s10434-019-07911-w
20. Wray CJ, Harvin JA, Silberfein EJ, Ko TC, Kao LS. Pilot prognostic model of extremely poor survival among high-risk hepatocellular carcinoma patients. Cancer. 2012;118(24):6118-6125. doi:10.1002/cncr.27649
21. Kim JH, Kim JH, Choi JH, et al. Value of the model for end-stage liver disease for predicting survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Scand J Gastroenterol. 2009;44(3):346-357. doi:10.1080/00365520802530838
22. Vogeler M, Mohr I, Pfeiffenberger J, et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(4):1033-1050. doi:10.1007/s00432-020-03135-8
23. National Institutes of Health, Surveillance, Epidemiology, and End Results. Cancer stat facts: cancer of the liver and intrahepatic bile duct. Accessed July 15, 2021. https://seer.cancer.gov/statfacts/html/livibd.html
24. Singal AK, Kamath PS. Model for End-stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
1. Ghouri YA, Mian I, Rowe JH. Review of hepatocellular carcinoma: epidemiology, etiology, and carcinogenesis. J Carcinog. 2017;16:1. Published 2017 May 29. doi:10.4103/jcar.JCar_9_16
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. doi:10.3322/caac.21492
3. Farazi PA, DePinho RA. Hepatocellular carcinoma pathogenesis: from genes to environment. Nat Rev Cancer. 2006;6(9):674-687. doi:10.1038/nrc1934
4. Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral direct-acting agent therapy for hepatitis c virus infection: a systematic review. Ann Intern Med. 2017;166(9):637-648. doi:10.7326/M16-2575
5. Kouris G, Hydery T, Greenwood BC, et al. Effectiveness of Ledipasvir/Sofosbuvir and predictors of treatment failure in members with hepatitis C genotype 1 infection: a retrospective cohort study in a medicaid population. J Manag Care Spec Pharm. 2018;24(7):591-597. doi:10.18553/jmcp.2018.24.7.591
6. Jacobson IM, Lawitz E, Kwo PY, et al. Safety and efficacy of elbasvir/grazoprevir in patients with hepatitis c virus infection and compensated cirrhosis: an integrated analysis. Gastroenterology. 2017;152(6):1372-1382.e2. doi:10.1053/j.gastro.2017.01.050
7. Nahon P, Layese R, Bourcier V, et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology. 2018;155(5):1436-1450.e6. doi:10.1053/j.gastro.2018.07.01510.
8. Innes H, Barclay ST, Hayes PC, et al. The risk of hepatocellular carcinoma in cirrhotic patients with hepatitis C and sustained viral response: role of the treatment regimen. J Hepatol. 2018;68(4):646-654. doi:10.1016/j.jhep.2017.10.033
9. Romano A, Angeli P, Piovesan S, et al. Newly diagnosed hepatocellular carcinoma in patients with advanced hepatitis C treated with DAAs: a prospective population study. J Hepatol. 2018;69(2):345-352. doi:10.1016/j.jhep.2018.03.009
10. Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.e1. doi:10.1053/j.gastro.2017.06.0122
11. Singh S, Nautiyal A, Loke YK. Oral direct-acting antivirals and the incidence or recurrence of hepatocellular carcinoma: a systematic review and meta-analysis. Frontline Gastroenterol. 2018;9(4):262-270. doi:10.1136/flgastro-2018-101017
12. Kuftinec G, Loehfelm T, Corwin M, et al. De novo hepatocellular carcinoma occurrence in hepatitis C cirrhotics treated with direct-acting antiviral agents. Hepat Oncol. 2018;5(1):HEP06. Published 2018 Jul 25. doi:10.2217/hep-2018-00033
13. Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158(5 Pt 1):329-337. doi:10.7326/0003-4819-158-5-201303050-00005
14. Nagaoki Y, Imamura M, Nishida Y, et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: comparison with interferon-based therapy. J Med Virol. 2019;91(4):650-658. doi:10.1002/jmv.25352
15. Sou FM, Wu CK, Chang KC, et al. Clinical characteristics and prognosis of HCC occurrence after antiviral therapy for HCV patients between sustained and non-sustained responders. J Formos Med Assoc. 2019;118(1 Pt 3):504-513. doi:10.1016/j.jfma.2018.10.017
16. Roche B, Coilly A, Duclos-Vallee JC, Samuel D. The impact of treatment of hepatitis C with DAAs on the occurrence of HCC. Liver Int. 2018;38(suppl 1):139-145. doi:10.1111/liv.13659
17. Singal AG, Lim JK, Kanwal F. AGA clinical practice update on interaction between oral direct-acting antivirals for chronic hepatitis C infection and hepatocellular carcinoma: expert review. Gastroenterology. 2019;156(8):2149-2157. doi:10.1053/j.gastro.2019.02.046
18. Toyoda H, Kumada T, Hayashi K, et al. Characteristics and prognosis of hepatocellular carcinoma detected in sustained responders to interferon therapy for chronic hepatitis C. Cancer Detect Prev. 2003;27(6):498-502. doi:10.1016/j.cdp.2003.09.00719. Okamura Y, Sugiura T, Ito T, et al. The achievement of a sustained virological response either before or after hepatectomy improves the prognosis of patients with primary hepatitis C virus-related hepatocellular carcinoma. Ann Surg Oncol. 2019; 26(13):4566-4575. doi:10.1245/s10434-019-07911-w
20. Wray CJ, Harvin JA, Silberfein EJ, Ko TC, Kao LS. Pilot prognostic model of extremely poor survival among high-risk hepatocellular carcinoma patients. Cancer. 2012;118(24):6118-6125. doi:10.1002/cncr.27649
21. Kim JH, Kim JH, Choi JH, et al. Value of the model for end-stage liver disease for predicting survival in hepatocellular carcinoma patients treated with transarterial chemoembolization. Scand J Gastroenterol. 2009;44(3):346-357. doi:10.1080/00365520802530838
22. Vogeler M, Mohr I, Pfeiffenberger J, et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2020;146(4):1033-1050. doi:10.1007/s00432-020-03135-8
23. National Institutes of Health, Surveillance, Epidemiology, and End Results. Cancer stat facts: cancer of the liver and intrahepatic bile duct. Accessed July 15, 2021. https://seer.cancer.gov/statfacts/html/livibd.html
24. Singal AK, Kamath PS. Model for End-stage Liver Disease. J Clin Exp Hepatol. 2013;3(1):50-60. doi:10.1016/j.jceh.2012.11.002
MS plus depression can increase risk of death, vascular disease
, a new study has found. “The effects of depression and MS on all-cause mortality are synergistic,” wrote lead author Raffaele Palladino, MD, PhD, research associate, faculty of medicine, Imperial College London.

The study was published in Neurology.
To assess the association between depression, vascular disease, and death in patients with MS, the researchers launched a population-based retrospective cohort study that reviewed English medical records from January 1987 to December 2018 and matched people with and without MS. Ultimately, 12,251 people with MS were matched with 72,572 controls. At baseline, 21% of the MS group (n = 2,535) and 9% of the controls (n = 6,278) had depression. Women were the majority in both cohorts and were more likely than men to be depressed.
People with both MS and depression had an all-cause mortality rate of 10.3 cases per 100,000 person-years (95% confidence interval, 9.17-11.57), compared with 10.6 for people with MS without depression (95% CI, 9.99-11.21), 3.6 for people with depression but not MS (95% CI, 3.18-4.05), and 2.5 for people with neither condition (95% CI, 2.42-2.64). Compared with controls without depression, the 10-year hazard of all-cause mortality was increasingly greater in controls with depression (hazard ratio, 1.75; 95% CI, 1.59-1.91), people with MS but not depression (HR, 3.88; 95% CI, 3.66-4.10), and people with MS and depression (HR, 5.43; 95% CI, 4.88-5.96). Overall, 14% of the observed effect on mortality was attributable to the interaction between MS status and depression.
As for vascular diseases, people with MS had an increased risk regardless of their depression status. That said, people with MS and depression (HR, 3.30; 95% CI, 2.37-4.23) had a notably higher risk than people with MS and no depression (HR, 1.48; 95% CI, 1.23-1.74). Women with MS and depression also had a greater risk of vascular disease than women with MS and no depression, while men with MS did not have significantly different risks of acute coronary syndrome or composite macrovascular disease than those in the control group who did not suffer from depression.
Does treating depression decrease the likelihood of vascular disease?
“The take-home message for me is the importance of treating depression in this population, in which we see it with great regularity,” Joseph Berger, MD, professor of neurology and associate chief of the multiple sclerosis division at the University of Pennsylvania, Philadelphia, said in an interview. “The question that I have is: If you treat depression in an individual with MS or an individual who is simply depressed and thus at risk for the subsequent development of vascular disease, does it decrease the likelihood of their subsequent development of vascular disease in comparison to had you not?
“I presume it does,” he added, noting that “the theories underlying why depression would increase one’s risk of subsequent vascular disease are enumerated by the authors, including such things as increased inflammation. Now, the inflammation may be contributing to the depression, or the depression may be contributing to the inflammation; it may be one of those chicken-and-egg scenarios. But if you decrease the depression, do you thereby decrease the inflammation, which has a pernicious effect on endothelial cells and increases one’s vascular risk?
“Alternatively, lifestyle in depressed patients is also altered,” he said. “They’re far less likely to engage in exercise, healthy habits, and healthy diets, and more likely perhaps to smoke. These all need to be addressed, but this study certainly gives you a greater impetus as a MS neurologist to address the issue of depression, realizing that there is also this comorbidity of vascular disease.”
Evaluating the biological interaction between MS and depression
Based on this and other studies, the joint effect of MS and depression on all-cause mortality may qualify as a biological interaction, Amber Salter, PhD, of the University of Texas Southwestern Medical Center, Dallas, wrote in an accompanying editorial.
“Biological interactions consider whether the joint effect of two factors follow an additive pattern, or the joint effect of two factors is greater than the sum of the individual effects for each factor alone,” she wrote. And though the interaction was not found to be present for vascular disease and cardiovascular mortality, it was for all-cause mortality.
“When warranted, the evaluation of biological interactions in future studies should be considered to provide insight on target subpopulations for interventions or test for potential mechanistic forms of interaction,” she added.
Dr. Salter highlighted the study’s strengths, including a large sample size and six controls matched to each MS patient. She also stated that the researchers’ inability to control for risk factors like body mass index and physical activity means the 14% increase in mortality “may not be a large absolute increase in mortality when other covariates cannot be considered.” In addition, their lack of data on suicide – and its association with depression – offers up the possibility that increases in mortality could be tied to a “potentially modifiable risk” as opposed to a biologically increased one.
In acknowledging their study’s limitations, the authors stated that body mass index, though an important vascular risk factor, has a “modest” association with mortality, and that the average annual suicide rate in the MS population – though higher than in the non-MS population – is still “relatively low.”
Two of the authors disclosed receiving support, including grants and research funding, from various institutions and organizations in the United Kingdom, the United States, and Canada, as well as several pharmaceutical companies. Dr. Salter reported no relevant disclosures.
, a new study has found. “The effects of depression and MS on all-cause mortality are synergistic,” wrote lead author Raffaele Palladino, MD, PhD, research associate, faculty of medicine, Imperial College London.
The study was published in Neurology.
To assess the association between depression, vascular disease, and death in patients with MS, the researchers launched a population-based retrospective cohort study that reviewed English medical records from January 1987 to December 2018 and matched people with and without MS. Ultimately, 12,251 people with MS were matched with 72,572 controls. At baseline, 21% of the MS group (n = 2,535) and 9% of the controls (n = 6,278) had depression. Women were the majority in both cohorts and were more likely than men to be depressed.
People with both MS and depression had an all-cause mortality rate of 10.3 cases per 100,000 person-years (95% confidence interval, 9.17-11.57), compared with 10.6 for people with MS without depression (95% CI, 9.99-11.21), 3.6 for people with depression but not MS (95% CI, 3.18-4.05), and 2.5 for people with neither condition (95% CI, 2.42-2.64). Compared with controls without depression, the 10-year hazard of all-cause mortality was increasingly greater in controls with depression (hazard ratio, 1.75; 95% CI, 1.59-1.91), people with MS but not depression (HR, 3.88; 95% CI, 3.66-4.10), and people with MS and depression (HR, 5.43; 95% CI, 4.88-5.96). Overall, 14% of the observed effect on mortality was attributable to the interaction between MS status and depression.
As for vascular diseases, people with MS had an increased risk regardless of their depression status. That said, people with MS and depression (HR, 3.30; 95% CI, 2.37-4.23) had a notably higher risk than people with MS and no depression (HR, 1.48; 95% CI, 1.23-1.74). Women with MS and depression also had a greater risk of vascular disease than women with MS and no depression, while men with MS did not have significantly different risks of acute coronary syndrome or composite macrovascular disease than those in the control group who did not suffer from depression.
Does treating depression decrease the likelihood of vascular disease?
“The take-home message for me is the importance of treating depression in this population, in which we see it with great regularity,” Joseph Berger, MD, professor of neurology and associate chief of the multiple sclerosis division at the University of Pennsylvania, Philadelphia, said in an interview. “The question that I have is: If you treat depression in an individual with MS or an individual who is simply depressed and thus at risk for the subsequent development of vascular disease, does it decrease the likelihood of their subsequent development of vascular disease in comparison to had you not?
“I presume it does,” he added, noting that “the theories underlying why depression would increase one’s risk of subsequent vascular disease are enumerated by the authors, including such things as increased inflammation. Now, the inflammation may be contributing to the depression, or the depression may be contributing to the inflammation; it may be one of those chicken-and-egg scenarios. But if you decrease the depression, do you thereby decrease the inflammation, which has a pernicious effect on endothelial cells and increases one’s vascular risk?
“Alternatively, lifestyle in depressed patients is also altered,” he said. “They’re far less likely to engage in exercise, healthy habits, and healthy diets, and more likely perhaps to smoke. These all need to be addressed, but this study certainly gives you a greater impetus as a MS neurologist to address the issue of depression, realizing that there is also this comorbidity of vascular disease.”
Evaluating the biological interaction between MS and depression
Based on this and other studies, the joint effect of MS and depression on all-cause mortality may qualify as a biological interaction, Amber Salter, PhD, of the University of Texas Southwestern Medical Center, Dallas, wrote in an accompanying editorial.
“Biological interactions consider whether the joint effect of two factors follow an additive pattern, or the joint effect of two factors is greater than the sum of the individual effects for each factor alone,” she wrote. And though the interaction was not found to be present for vascular disease and cardiovascular mortality, it was for all-cause mortality.
“When warranted, the evaluation of biological interactions in future studies should be considered to provide insight on target subpopulations for interventions or test for potential mechanistic forms of interaction,” she added.
Dr. Salter highlighted the study’s strengths, including a large sample size and six controls matched to each MS patient. She also stated that the researchers’ inability to control for risk factors like body mass index and physical activity means the 14% increase in mortality “may not be a large absolute increase in mortality when other covariates cannot be considered.” In addition, their lack of data on suicide – and its association with depression – offers up the possibility that increases in mortality could be tied to a “potentially modifiable risk” as opposed to a biologically increased one.
In acknowledging their study’s limitations, the authors stated that body mass index, though an important vascular risk factor, has a “modest” association with mortality, and that the average annual suicide rate in the MS population – though higher than in the non-MS population – is still “relatively low.”
Two of the authors disclosed receiving support, including grants and research funding, from various institutions and organizations in the United Kingdom, the United States, and Canada, as well as several pharmaceutical companies. Dr. Salter reported no relevant disclosures.
, a new study has found. “The effects of depression and MS on all-cause mortality are synergistic,” wrote lead author Raffaele Palladino, MD, PhD, research associate, faculty of medicine, Imperial College London.
The study was published in Neurology.
To assess the association between depression, vascular disease, and death in patients with MS, the researchers launched a population-based retrospective cohort study that reviewed English medical records from January 1987 to December 2018 and matched people with and without MS. Ultimately, 12,251 people with MS were matched with 72,572 controls. At baseline, 21% of the MS group (n = 2,535) and 9% of the controls (n = 6,278) had depression. Women were the majority in both cohorts and were more likely than men to be depressed.
People with both MS and depression had an all-cause mortality rate of 10.3 cases per 100,000 person-years (95% confidence interval, 9.17-11.57), compared with 10.6 for people with MS without depression (95% CI, 9.99-11.21), 3.6 for people with depression but not MS (95% CI, 3.18-4.05), and 2.5 for people with neither condition (95% CI, 2.42-2.64). Compared with controls without depression, the 10-year hazard of all-cause mortality was increasingly greater in controls with depression (hazard ratio, 1.75; 95% CI, 1.59-1.91), people with MS but not depression (HR, 3.88; 95% CI, 3.66-4.10), and people with MS and depression (HR, 5.43; 95% CI, 4.88-5.96). Overall, 14% of the observed effect on mortality was attributable to the interaction between MS status and depression.
As for vascular diseases, people with MS had an increased risk regardless of their depression status. That said, people with MS and depression (HR, 3.30; 95% CI, 2.37-4.23) had a notably higher risk than people with MS and no depression (HR, 1.48; 95% CI, 1.23-1.74). Women with MS and depression also had a greater risk of vascular disease than women with MS and no depression, while men with MS did not have significantly different risks of acute coronary syndrome or composite macrovascular disease than those in the control group who did not suffer from depression.
Does treating depression decrease the likelihood of vascular disease?
“The take-home message for me is the importance of treating depression in this population, in which we see it with great regularity,” Joseph Berger, MD, professor of neurology and associate chief of the multiple sclerosis division at the University of Pennsylvania, Philadelphia, said in an interview. “The question that I have is: If you treat depression in an individual with MS or an individual who is simply depressed and thus at risk for the subsequent development of vascular disease, does it decrease the likelihood of their subsequent development of vascular disease in comparison to had you not?
“I presume it does,” he added, noting that “the theories underlying why depression would increase one’s risk of subsequent vascular disease are enumerated by the authors, including such things as increased inflammation. Now, the inflammation may be contributing to the depression, or the depression may be contributing to the inflammation; it may be one of those chicken-and-egg scenarios. But if you decrease the depression, do you thereby decrease the inflammation, which has a pernicious effect on endothelial cells and increases one’s vascular risk?
“Alternatively, lifestyle in depressed patients is also altered,” he said. “They’re far less likely to engage in exercise, healthy habits, and healthy diets, and more likely perhaps to smoke. These all need to be addressed, but this study certainly gives you a greater impetus as a MS neurologist to address the issue of depression, realizing that there is also this comorbidity of vascular disease.”
Evaluating the biological interaction between MS and depression
Based on this and other studies, the joint effect of MS and depression on all-cause mortality may qualify as a biological interaction, Amber Salter, PhD, of the University of Texas Southwestern Medical Center, Dallas, wrote in an accompanying editorial.
“Biological interactions consider whether the joint effect of two factors follow an additive pattern, or the joint effect of two factors is greater than the sum of the individual effects for each factor alone,” she wrote. And though the interaction was not found to be present for vascular disease and cardiovascular mortality, it was for all-cause mortality.
“When warranted, the evaluation of biological interactions in future studies should be considered to provide insight on target subpopulations for interventions or test for potential mechanistic forms of interaction,” she added.
Dr. Salter highlighted the study’s strengths, including a large sample size and six controls matched to each MS patient. She also stated that the researchers’ inability to control for risk factors like body mass index and physical activity means the 14% increase in mortality “may not be a large absolute increase in mortality when other covariates cannot be considered.” In addition, their lack of data on suicide – and its association with depression – offers up the possibility that increases in mortality could be tied to a “potentially modifiable risk” as opposed to a biologically increased one.
In acknowledging their study’s limitations, the authors stated that body mass index, though an important vascular risk factor, has a “modest” association with mortality, and that the average annual suicide rate in the MS population – though higher than in the non-MS population – is still “relatively low.”
Two of the authors disclosed receiving support, including grants and research funding, from various institutions and organizations in the United Kingdom, the United States, and Canada, as well as several pharmaceutical companies. Dr. Salter reported no relevant disclosures.
FROM NEUROLOGY
Data sharing to improve AI used in breast-imaging research
The curated dataset, which consists of 22,032 DBT volumes associated with 5,610 studies from 5,060 patients, was published online in JAMA Network Open. The studies were divided into types: normal studies (91.4%), actionable studies that required additional imaging but no biopsy (5.0%), benign biopsied studies (2.0%), and studies that detected cancer (1.6%).
To develop and evaluate their deep-learning model for the detection of architectural distortions and masses, the researchers used a test set of 460 studies from 418 patients with cancer. Their algorithm reached a breast-based sensitivity of two false positives per DBT volume, or 65%.
“The main focus of this publication is on the dataset, rather than on a specific hypothesis,” said principal researcher Maciej A. Mazurowski, PhD, scientific director of the Duke Center for Artificial Intelligence in Radiology in Durham, N.C.
“We have publicly shared a large dataset of digital breast tomosynthesis images, which are sometimes referred to as 3D mammograms, for more than 5,000 patients. There are two purposes for sharing data like these. One is to improve research and development of machine-learning algorithms. You can train models with these data. The other reason, maybe even more important, is to provide a benchmark to test algorithms,” he said in an interview.
The large-scale sharing of data is a key step toward transparency in science, said Dr. Mazurowski. “It is about making sure results can be easily reproduced and setting benchmarks.”
The dataset includes masses and architectural distortions that were annotated by two experienced radiologists, but does not include annotations for calcifications and/or microcalcifications.
This lack of calcifications is a limitation of the study, said Jean Seely, MD, professor of radiology at the University of Ottawa, who is president of the Canadian Society of Breast Imaging and regional lead for the Ontario Breast Screening Program.
“About 45% of invasive breast cancers are diagnosed based on calcifications,” she explained.
Still, although the sensitivity of the AI algorithm was not high (65%) – the average sensitivity of 2D mammography is 85% – the researchers should be commended for releasing such a large dataset, said Dr. Seely.
“The fact that they have made it publicly available is very, very useful,” she said, adding that the dataset can be leveraged in future breast-imaging research.
Although DBT is much better at identifying breast cancers than mammography, DBT exams take about 30% more time to read.
“There’s a lot of work being done in artificial intelligence in breast imaging to not only improve the workflow for breast radiologists, but also to help with the diagnosis and detection,” she noted. “Anything that helps improve the confidence and the accuracy of the radiologist is really what we’re aiming for right now.”
The size and the content of this dataset will contribute to breast-imaging research, said Jaron Chong, MD, of the department of medical imaging at Western University in London, Ontario, who is chair of the AI Standing Committee at the Canadian Association of Radiologists.
“The contribution could be valuable in the long term because DBT is a rare dataset in comparison to conventional 2D mammography,” said Dr. Chong. “Most existing datasets have focused on two-dimensional imaging. We might see more research papers reference this dataset in the future, iterating and improving upon this article’s algorithm performance.”
Dr. Mazurowski reports serving as an adviser to Gradient Health. Dr. Seely is an unpaid principal investigator for the Ottawa site of the Tomosynthesis Mammographic Imaging Screening Trial (TMIST). Dr. Chong has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The curated dataset, which consists of 22,032 DBT volumes associated with 5,610 studies from 5,060 patients, was published online in JAMA Network Open. The studies were divided into types: normal studies (91.4%), actionable studies that required additional imaging but no biopsy (5.0%), benign biopsied studies (2.0%), and studies that detected cancer (1.6%).
To develop and evaluate their deep-learning model for the detection of architectural distortions and masses, the researchers used a test set of 460 studies from 418 patients with cancer. Their algorithm reached a breast-based sensitivity of two false positives per DBT volume, or 65%.
“The main focus of this publication is on the dataset, rather than on a specific hypothesis,” said principal researcher Maciej A. Mazurowski, PhD, scientific director of the Duke Center for Artificial Intelligence in Radiology in Durham, N.C.
“We have publicly shared a large dataset of digital breast tomosynthesis images, which are sometimes referred to as 3D mammograms, for more than 5,000 patients. There are two purposes for sharing data like these. One is to improve research and development of machine-learning algorithms. You can train models with these data. The other reason, maybe even more important, is to provide a benchmark to test algorithms,” he said in an interview.
The large-scale sharing of data is a key step toward transparency in science, said Dr. Mazurowski. “It is about making sure results can be easily reproduced and setting benchmarks.”
The dataset includes masses and architectural distortions that were annotated by two experienced radiologists, but does not include annotations for calcifications and/or microcalcifications.
This lack of calcifications is a limitation of the study, said Jean Seely, MD, professor of radiology at the University of Ottawa, who is president of the Canadian Society of Breast Imaging and regional lead for the Ontario Breast Screening Program.
“About 45% of invasive breast cancers are diagnosed based on calcifications,” she explained.
Still, although the sensitivity of the AI algorithm was not high (65%) – the average sensitivity of 2D mammography is 85% – the researchers should be commended for releasing such a large dataset, said Dr. Seely.
“The fact that they have made it publicly available is very, very useful,” she said, adding that the dataset can be leveraged in future breast-imaging research.
Although DBT is much better at identifying breast cancers than mammography, DBT exams take about 30% more time to read.
“There’s a lot of work being done in artificial intelligence in breast imaging to not only improve the workflow for breast radiologists, but also to help with the diagnosis and detection,” she noted. “Anything that helps improve the confidence and the accuracy of the radiologist is really what we’re aiming for right now.”
The size and the content of this dataset will contribute to breast-imaging research, said Jaron Chong, MD, of the department of medical imaging at Western University in London, Ontario, who is chair of the AI Standing Committee at the Canadian Association of Radiologists.
“The contribution could be valuable in the long term because DBT is a rare dataset in comparison to conventional 2D mammography,” said Dr. Chong. “Most existing datasets have focused on two-dimensional imaging. We might see more research papers reference this dataset in the future, iterating and improving upon this article’s algorithm performance.”
Dr. Mazurowski reports serving as an adviser to Gradient Health. Dr. Seely is an unpaid principal investigator for the Ottawa site of the Tomosynthesis Mammographic Imaging Screening Trial (TMIST). Dr. Chong has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The curated dataset, which consists of 22,032 DBT volumes associated with 5,610 studies from 5,060 patients, was published online in JAMA Network Open. The studies were divided into types: normal studies (91.4%), actionable studies that required additional imaging but no biopsy (5.0%), benign biopsied studies (2.0%), and studies that detected cancer (1.6%).
To develop and evaluate their deep-learning model for the detection of architectural distortions and masses, the researchers used a test set of 460 studies from 418 patients with cancer. Their algorithm reached a breast-based sensitivity of two false positives per DBT volume, or 65%.
“The main focus of this publication is on the dataset, rather than on a specific hypothesis,” said principal researcher Maciej A. Mazurowski, PhD, scientific director of the Duke Center for Artificial Intelligence in Radiology in Durham, N.C.
“We have publicly shared a large dataset of digital breast tomosynthesis images, which are sometimes referred to as 3D mammograms, for more than 5,000 patients. There are two purposes for sharing data like these. One is to improve research and development of machine-learning algorithms. You can train models with these data. The other reason, maybe even more important, is to provide a benchmark to test algorithms,” he said in an interview.
The large-scale sharing of data is a key step toward transparency in science, said Dr. Mazurowski. “It is about making sure results can be easily reproduced and setting benchmarks.”
The dataset includes masses and architectural distortions that were annotated by two experienced radiologists, but does not include annotations for calcifications and/or microcalcifications.
This lack of calcifications is a limitation of the study, said Jean Seely, MD, professor of radiology at the University of Ottawa, who is president of the Canadian Society of Breast Imaging and regional lead for the Ontario Breast Screening Program.
“About 45% of invasive breast cancers are diagnosed based on calcifications,” she explained.
Still, although the sensitivity of the AI algorithm was not high (65%) – the average sensitivity of 2D mammography is 85% – the researchers should be commended for releasing such a large dataset, said Dr. Seely.
“The fact that they have made it publicly available is very, very useful,” she said, adding that the dataset can be leveraged in future breast-imaging research.
Although DBT is much better at identifying breast cancers than mammography, DBT exams take about 30% more time to read.
“There’s a lot of work being done in artificial intelligence in breast imaging to not only improve the workflow for breast radiologists, but also to help with the diagnosis and detection,” she noted. “Anything that helps improve the confidence and the accuracy of the radiologist is really what we’re aiming for right now.”
The size and the content of this dataset will contribute to breast-imaging research, said Jaron Chong, MD, of the department of medical imaging at Western University in London, Ontario, who is chair of the AI Standing Committee at the Canadian Association of Radiologists.
“The contribution could be valuable in the long term because DBT is a rare dataset in comparison to conventional 2D mammography,” said Dr. Chong. “Most existing datasets have focused on two-dimensional imaging. We might see more research papers reference this dataset in the future, iterating and improving upon this article’s algorithm performance.”
Dr. Mazurowski reports serving as an adviser to Gradient Health. Dr. Seely is an unpaid principal investigator for the Ottawa site of the Tomosynthesis Mammographic Imaging Screening Trial (TMIST). Dr. Chong has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA warns again about robotic mastectomy, breaks new ground
The agency also called out robotically assisted surgical (RAS) device use in the United States that lacks proper federal oversight.
“The FDA is aware of allegations that clinical studies are being conducted” with RAS devices in breast cancer “without the FDA oversight required for such significant risk studies,” the agency said.
The new advisory comes 4 weeks after a Medscape Medical News exclusive story on a set of clinical trials recently underway using RAS devices for nipple-sparing mastectomy, both prophylactically and as a breast cancer treatment.
The report found that investigators are either not collecting cancer outcomes or not doing so as a primary measure – despite a stiff warning in 2019 from the FDA that those outcomes are important.
“Congratulations to the press on doing its job well and informing government. I think this [safety communication] is a direct result of Medscape following up on this issue,” said Hooman Noorchashm, MD, PhD, a patient advocate from Philadelphia. He is a former surgeon and faculty member at the University of Pennsylvania.
In reviewing the FDA’s new warning, Dr. Noorchashm pointed out that the agency also stated unequivocally – after previously hinting – that any study of robotic mastectomy “must include monitoring of long-term clinical outcomes” such as cancer recurrence, disease-free survival, and overall survival.
That’s a change in approach – previously the FDA has typically approved/cleared RAS devices for use in cancer surgery based on 30-day complication rates (compared with standards of care) and had no requirement for cancer-related outcomes data.
“This [new] advisory reiterates the need for a clear focus on primary oncologic outcomes to, at the very least, demonstrate the noninferiority of robotic assisted surgical devices for performing mastectomy procedures,” said Dr. Noorchashm.
In a 2019 warning about robotic mastectomy, the FDA suggested that it would require oncologic measures moving forward, saying that it “anticipates” that any evaluation of new use of robotic devices in women’s cancer “would be supported” by long-term cancer outcomes. But it stopped short of publicly saying so. The new advisory changes that.
Direct comparison with traditional mastectomy needed
There are safety concerns with robotic mastectomy. Experts question whether a surgeon can easily remove a breast tumor in one piece through the small incision (a selling point of the robot). If the tissue cannot be removed in one piece, cancer fragments may be left behind.
As a result, a randomized trial with traditional open mastectomy as a comparator is needed, Dr. Noorchashm stressed. The current batch of clinical trials in the United States are all single-arm studies and as such are “totally inappropriate,” he said.
Julie Margenthaler, MD, a breast surgeon at Washington University in St Louis, also noted the importance of a randomized trial.
“I feel strongly that robotic-assisted mastectomy should only be performed in the setting of a well-designed clinical trial and that oncologic outcomes should be a primary or secondary endpoint analysis as part of that trial,” she said in an email.
Intuitive Surgical, a California-based manufacturer of robotic devices in health care and a pioneer in robot-assisted surgery, is funding one of the current clinical trials of robotic mastectomy in the United States – a single-arm, five-center trial examining use in the prophylactic setting. The two primary outcomes are conversions to open mastectomy (efficacy measure) and the incidence of adverse events during surgery to 42 days after surgery (safety measure).
This news organization previously asked the company, which manufactures the market leader da Vinci robotic surgical equipment, if it planned to conduct a randomized trial.
“Any plans for use of da Vinci Xi surgical system in nipple-sparing mastectomy will be based on these [single-arm] study results as well as other data and evidence,” said a spokesperson, who did not confirm use of a randomized trial.
The new FDA requirement for long-term oncologic outcomes also in part arises from “diminished long-term survival” that was associated with robotic surgery and other minimally invasive surgery for hysterectomy related to cervical cancer.
A version of this article first appeared on Medscape.com.
The agency also called out robotically assisted surgical (RAS) device use in the United States that lacks proper federal oversight.
“The FDA is aware of allegations that clinical studies are being conducted” with RAS devices in breast cancer “without the FDA oversight required for such significant risk studies,” the agency said.
The new advisory comes 4 weeks after a Medscape Medical News exclusive story on a set of clinical trials recently underway using RAS devices for nipple-sparing mastectomy, both prophylactically and as a breast cancer treatment.
The report found that investigators are either not collecting cancer outcomes or not doing so as a primary measure – despite a stiff warning in 2019 from the FDA that those outcomes are important.
“Congratulations to the press on doing its job well and informing government. I think this [safety communication] is a direct result of Medscape following up on this issue,” said Hooman Noorchashm, MD, PhD, a patient advocate from Philadelphia. He is a former surgeon and faculty member at the University of Pennsylvania.
In reviewing the FDA’s new warning, Dr. Noorchashm pointed out that the agency also stated unequivocally – after previously hinting – that any study of robotic mastectomy “must include monitoring of long-term clinical outcomes” such as cancer recurrence, disease-free survival, and overall survival.
That’s a change in approach – previously the FDA has typically approved/cleared RAS devices for use in cancer surgery based on 30-day complication rates (compared with standards of care) and had no requirement for cancer-related outcomes data.
“This [new] advisory reiterates the need for a clear focus on primary oncologic outcomes to, at the very least, demonstrate the noninferiority of robotic assisted surgical devices for performing mastectomy procedures,” said Dr. Noorchashm.
In a 2019 warning about robotic mastectomy, the FDA suggested that it would require oncologic measures moving forward, saying that it “anticipates” that any evaluation of new use of robotic devices in women’s cancer “would be supported” by long-term cancer outcomes. But it stopped short of publicly saying so. The new advisory changes that.
Direct comparison with traditional mastectomy needed
There are safety concerns with robotic mastectomy. Experts question whether a surgeon can easily remove a breast tumor in one piece through the small incision (a selling point of the robot). If the tissue cannot be removed in one piece, cancer fragments may be left behind.
As a result, a randomized trial with traditional open mastectomy as a comparator is needed, Dr. Noorchashm stressed. The current batch of clinical trials in the United States are all single-arm studies and as such are “totally inappropriate,” he said.
Julie Margenthaler, MD, a breast surgeon at Washington University in St Louis, also noted the importance of a randomized trial.
“I feel strongly that robotic-assisted mastectomy should only be performed in the setting of a well-designed clinical trial and that oncologic outcomes should be a primary or secondary endpoint analysis as part of that trial,” she said in an email.
Intuitive Surgical, a California-based manufacturer of robotic devices in health care and a pioneer in robot-assisted surgery, is funding one of the current clinical trials of robotic mastectomy in the United States – a single-arm, five-center trial examining use in the prophylactic setting. The two primary outcomes are conversions to open mastectomy (efficacy measure) and the incidence of adverse events during surgery to 42 days after surgery (safety measure).
This news organization previously asked the company, which manufactures the market leader da Vinci robotic surgical equipment, if it planned to conduct a randomized trial.
“Any plans for use of da Vinci Xi surgical system in nipple-sparing mastectomy will be based on these [single-arm] study results as well as other data and evidence,” said a spokesperson, who did not confirm use of a randomized trial.
The new FDA requirement for long-term oncologic outcomes also in part arises from “diminished long-term survival” that was associated with robotic surgery and other minimally invasive surgery for hysterectomy related to cervical cancer.
A version of this article first appeared on Medscape.com.
The agency also called out robotically assisted surgical (RAS) device use in the United States that lacks proper federal oversight.
“The FDA is aware of allegations that clinical studies are being conducted” with RAS devices in breast cancer “without the FDA oversight required for such significant risk studies,” the agency said.
The new advisory comes 4 weeks after a Medscape Medical News exclusive story on a set of clinical trials recently underway using RAS devices for nipple-sparing mastectomy, both prophylactically and as a breast cancer treatment.
The report found that investigators are either not collecting cancer outcomes or not doing so as a primary measure – despite a stiff warning in 2019 from the FDA that those outcomes are important.
“Congratulations to the press on doing its job well and informing government. I think this [safety communication] is a direct result of Medscape following up on this issue,” said Hooman Noorchashm, MD, PhD, a patient advocate from Philadelphia. He is a former surgeon and faculty member at the University of Pennsylvania.
In reviewing the FDA’s new warning, Dr. Noorchashm pointed out that the agency also stated unequivocally – after previously hinting – that any study of robotic mastectomy “must include monitoring of long-term clinical outcomes” such as cancer recurrence, disease-free survival, and overall survival.
That’s a change in approach – previously the FDA has typically approved/cleared RAS devices for use in cancer surgery based on 30-day complication rates (compared with standards of care) and had no requirement for cancer-related outcomes data.
“This [new] advisory reiterates the need for a clear focus on primary oncologic outcomes to, at the very least, demonstrate the noninferiority of robotic assisted surgical devices for performing mastectomy procedures,” said Dr. Noorchashm.
In a 2019 warning about robotic mastectomy, the FDA suggested that it would require oncologic measures moving forward, saying that it “anticipates” that any evaluation of new use of robotic devices in women’s cancer “would be supported” by long-term cancer outcomes. But it stopped short of publicly saying so. The new advisory changes that.
Direct comparison with traditional mastectomy needed
There are safety concerns with robotic mastectomy. Experts question whether a surgeon can easily remove a breast tumor in one piece through the small incision (a selling point of the robot). If the tissue cannot be removed in one piece, cancer fragments may be left behind.
As a result, a randomized trial with traditional open mastectomy as a comparator is needed, Dr. Noorchashm stressed. The current batch of clinical trials in the United States are all single-arm studies and as such are “totally inappropriate,” he said.
Julie Margenthaler, MD, a breast surgeon at Washington University in St Louis, also noted the importance of a randomized trial.
“I feel strongly that robotic-assisted mastectomy should only be performed in the setting of a well-designed clinical trial and that oncologic outcomes should be a primary or secondary endpoint analysis as part of that trial,” she said in an email.
Intuitive Surgical, a California-based manufacturer of robotic devices in health care and a pioneer in robot-assisted surgery, is funding one of the current clinical trials of robotic mastectomy in the United States – a single-arm, five-center trial examining use in the prophylactic setting. The two primary outcomes are conversions to open mastectomy (efficacy measure) and the incidence of adverse events during surgery to 42 days after surgery (safety measure).
This news organization previously asked the company, which manufactures the market leader da Vinci robotic surgical equipment, if it planned to conduct a randomized trial.
“Any plans for use of da Vinci Xi surgical system in nipple-sparing mastectomy will be based on these [single-arm] study results as well as other data and evidence,” said a spokesperson, who did not confirm use of a randomized trial.
The new FDA requirement for long-term oncologic outcomes also in part arises from “diminished long-term survival” that was associated with robotic surgery and other minimally invasive surgery for hysterectomy related to cervical cancer.
A version of this article first appeared on Medscape.com.
A case is building for personalized, genome-based radiation dosing
A team of researchers from the Cleveland Clinic, the Moffitt Cancer Center in Tampa, and Case Western Reserve University in Cleveland is zeroing in on a way to personalize radiation therapy for cancer patients based on genomic profile, much as genomics is used to tailor oncologic drug therapy.
It’s called “genomic-adjusted radiation dose” (GARD), a dose tailored to a person’s radiosensitivity as determined by the expression of 10 genes, known as the radiosensitivity index (RSI), combined with a linear quadratic model to yield GARD, a prediction of risk and benefit at various radiation doses for a particular patient.
A recent report in The Lancet Oncology validated GARD in 1,615 patients with seven cancer types from 11 study cohorts. If it holds up in clinical trials set to start later this year, GARD should “allow us to predict the benefit of radiation for an individual patient and adjust their treatment strategy,” wrote the authors of an editorial that accompanied the study. “The efforts need to be applauded worldwide, because radiotherapy is considerably lagging, compared with the enormous progress done in the field of personalized medicine,” Orit Kaidar-Person, MD, a radiation oncologist at Sheba Medical Center in Ramat Gan, Israel, and colleagues wrote.
GARD was associated with time to first recurrence and overall survival for patients receiving radiotherapy and predicted radiotherapy benefit, while physical dose did not. The team found a relative 2% reduction in risk of first recurrence for each unit increase of GARD (P = .0017) and a relative 3% increase in overall survival for each unit increase in GARD (P = .0007), among those who got radiotherapy. Values of GARD run from 0 to over 100, with higher scores meaning more radiation benefit.
The radiosensitivity index, which was derived from genomic studies of cancer cell lines exposed to radiation, was previously validated by the team and other groups across several tumor types.
Currently, radiation dosing is generally uniform for a given disease site and stage, based on the assumption that a given dose of radiation results in the same clinical effect across patients. In fact, the biological effect of a given dose varies widely between individual patients. “Patients we treat uniformly do not have a uniform response” which is why a more personalized approach would help, said lead investigator and Cleveland Clinic radiation oncologist Jacob Scott, MD, DPhil.
One patient with a given tumor might benefit from 2 extra fractions, while the next might need an extra 15 for the same benefit. “You need to know about [a patient’s] tumor genomics to know how hard you have to work,” he said.
Dr. Scott and colleagues are working with a genomics company to commercialize the approach. The vision for now is that physicians would ship in biopsy samples to be analyzed; RSI and GARD would be calculated, and then a decision support report would be sent back to the treatment team outlining the risks and benefits of various doses for the patient.
Dr. Scott, who holds proprietary rights on the approach, is bullish. When asked if he anticipates GARD dosing to be standard of care in 10 years, he said that “I can’t imagine another world. Everything else in cancer is personalized. Why aren’t we? It just makes sense. I know there’s a better way” to prescribe radiation, “and I’m excited for the future when I can use it.”
When asked for comment, Brian Marples, PhD, a radiation oncology professor at the University of Rochester (N.Y.), said the data so far for GARD “seem very solid. I’m very excited by the concept.”
It’s been “the holy grail” of radiation researchers to find a biologic marker that predicts what dosages patients need and what can be given safely. “This strategy is a good way of doing that. Other groups are proposing similar strategies, but I think this group is ahead. I can see [GARD] being readily applied to the clinic because patients are [already] getting their tumors genomically characterized as part of care,” Dr. Marples said.
But many questions remain. For instance, the editorial writers questioned how GARD is “affected by tumor heterogeneity, response to systemic therapy, and changes in the tumor microenvironment.” Also, the approach is based on conventional 2 Gy fractions, but other fractionation regimens are becoming more common.
For Dr. Marples, the big caveat is that most cancer patients are treated with both radiation and chemotherapy. He said he would like to see GARD validated in patients who receive both.
They seven tumor types in the study included breast cancer, head and neck cancer, non–small cell lung cancer, pancreatic cancer, endometrial cancer, melanoma, and glioma. The majority of the subjects were treated with radiation, and each had the genomic data needed to calculate GARD.
Dr. Scott, senior author and Moffitt Center radiation oncologist Javier Torres-Roca, MD, and a third author hold intellectual property rights on RSI, GARD, and prescription dose base on RSI, plus equity in Cvergenx, a company that seeks to commercialize the approach. Dr. Torres-Roca and another author are cofounders. The editorial writers and Dr. Marples did not have any relevant disclosures.
A team of researchers from the Cleveland Clinic, the Moffitt Cancer Center in Tampa, and Case Western Reserve University in Cleveland is zeroing in on a way to personalize radiation therapy for cancer patients based on genomic profile, much as genomics is used to tailor oncologic drug therapy.
It’s called “genomic-adjusted radiation dose” (GARD), a dose tailored to a person’s radiosensitivity as determined by the expression of 10 genes, known as the radiosensitivity index (RSI), combined with a linear quadratic model to yield GARD, a prediction of risk and benefit at various radiation doses for a particular patient.
A recent report in The Lancet Oncology validated GARD in 1,615 patients with seven cancer types from 11 study cohorts. If it holds up in clinical trials set to start later this year, GARD should “allow us to predict the benefit of radiation for an individual patient and adjust their treatment strategy,” wrote the authors of an editorial that accompanied the study. “The efforts need to be applauded worldwide, because radiotherapy is considerably lagging, compared with the enormous progress done in the field of personalized medicine,” Orit Kaidar-Person, MD, a radiation oncologist at Sheba Medical Center in Ramat Gan, Israel, and colleagues wrote.
GARD was associated with time to first recurrence and overall survival for patients receiving radiotherapy and predicted radiotherapy benefit, while physical dose did not. The team found a relative 2% reduction in risk of first recurrence for each unit increase of GARD (P = .0017) and a relative 3% increase in overall survival for each unit increase in GARD (P = .0007), among those who got radiotherapy. Values of GARD run from 0 to over 100, with higher scores meaning more radiation benefit.
The radiosensitivity index, which was derived from genomic studies of cancer cell lines exposed to radiation, was previously validated by the team and other groups across several tumor types.
Currently, radiation dosing is generally uniform for a given disease site and stage, based on the assumption that a given dose of radiation results in the same clinical effect across patients. In fact, the biological effect of a given dose varies widely between individual patients. “Patients we treat uniformly do not have a uniform response” which is why a more personalized approach would help, said lead investigator and Cleveland Clinic radiation oncologist Jacob Scott, MD, DPhil.
One patient with a given tumor might benefit from 2 extra fractions, while the next might need an extra 15 for the same benefit. “You need to know about [a patient’s] tumor genomics to know how hard you have to work,” he said.
Dr. Scott and colleagues are working with a genomics company to commercialize the approach. The vision for now is that physicians would ship in biopsy samples to be analyzed; RSI and GARD would be calculated, and then a decision support report would be sent back to the treatment team outlining the risks and benefits of various doses for the patient.
Dr. Scott, who holds proprietary rights on the approach, is bullish. When asked if he anticipates GARD dosing to be standard of care in 10 years, he said that “I can’t imagine another world. Everything else in cancer is personalized. Why aren’t we? It just makes sense. I know there’s a better way” to prescribe radiation, “and I’m excited for the future when I can use it.”
When asked for comment, Brian Marples, PhD, a radiation oncology professor at the University of Rochester (N.Y.), said the data so far for GARD “seem very solid. I’m very excited by the concept.”
It’s been “the holy grail” of radiation researchers to find a biologic marker that predicts what dosages patients need and what can be given safely. “This strategy is a good way of doing that. Other groups are proposing similar strategies, but I think this group is ahead. I can see [GARD] being readily applied to the clinic because patients are [already] getting their tumors genomically characterized as part of care,” Dr. Marples said.
But many questions remain. For instance, the editorial writers questioned how GARD is “affected by tumor heterogeneity, response to systemic therapy, and changes in the tumor microenvironment.” Also, the approach is based on conventional 2 Gy fractions, but other fractionation regimens are becoming more common.
For Dr. Marples, the big caveat is that most cancer patients are treated with both radiation and chemotherapy. He said he would like to see GARD validated in patients who receive both.
They seven tumor types in the study included breast cancer, head and neck cancer, non–small cell lung cancer, pancreatic cancer, endometrial cancer, melanoma, and glioma. The majority of the subjects were treated with radiation, and each had the genomic data needed to calculate GARD.
Dr. Scott, senior author and Moffitt Center radiation oncologist Javier Torres-Roca, MD, and a third author hold intellectual property rights on RSI, GARD, and prescription dose base on RSI, plus equity in Cvergenx, a company that seeks to commercialize the approach. Dr. Torres-Roca and another author are cofounders. The editorial writers and Dr. Marples did not have any relevant disclosures.
A team of researchers from the Cleveland Clinic, the Moffitt Cancer Center in Tampa, and Case Western Reserve University in Cleveland is zeroing in on a way to personalize radiation therapy for cancer patients based on genomic profile, much as genomics is used to tailor oncologic drug therapy.
It’s called “genomic-adjusted radiation dose” (GARD), a dose tailored to a person’s radiosensitivity as determined by the expression of 10 genes, known as the radiosensitivity index (RSI), combined with a linear quadratic model to yield GARD, a prediction of risk and benefit at various radiation doses for a particular patient.
A recent report in The Lancet Oncology validated GARD in 1,615 patients with seven cancer types from 11 study cohorts. If it holds up in clinical trials set to start later this year, GARD should “allow us to predict the benefit of radiation for an individual patient and adjust their treatment strategy,” wrote the authors of an editorial that accompanied the study. “The efforts need to be applauded worldwide, because radiotherapy is considerably lagging, compared with the enormous progress done in the field of personalized medicine,” Orit Kaidar-Person, MD, a radiation oncologist at Sheba Medical Center in Ramat Gan, Israel, and colleagues wrote.
GARD was associated with time to first recurrence and overall survival for patients receiving radiotherapy and predicted radiotherapy benefit, while physical dose did not. The team found a relative 2% reduction in risk of first recurrence for each unit increase of GARD (P = .0017) and a relative 3% increase in overall survival for each unit increase in GARD (P = .0007), among those who got radiotherapy. Values of GARD run from 0 to over 100, with higher scores meaning more radiation benefit.
The radiosensitivity index, which was derived from genomic studies of cancer cell lines exposed to radiation, was previously validated by the team and other groups across several tumor types.
Currently, radiation dosing is generally uniform for a given disease site and stage, based on the assumption that a given dose of radiation results in the same clinical effect across patients. In fact, the biological effect of a given dose varies widely between individual patients. “Patients we treat uniformly do not have a uniform response” which is why a more personalized approach would help, said lead investigator and Cleveland Clinic radiation oncologist Jacob Scott, MD, DPhil.
One patient with a given tumor might benefit from 2 extra fractions, while the next might need an extra 15 for the same benefit. “You need to know about [a patient’s] tumor genomics to know how hard you have to work,” he said.
Dr. Scott and colleagues are working with a genomics company to commercialize the approach. The vision for now is that physicians would ship in biopsy samples to be analyzed; RSI and GARD would be calculated, and then a decision support report would be sent back to the treatment team outlining the risks and benefits of various doses for the patient.
Dr. Scott, who holds proprietary rights on the approach, is bullish. When asked if he anticipates GARD dosing to be standard of care in 10 years, he said that “I can’t imagine another world. Everything else in cancer is personalized. Why aren’t we? It just makes sense. I know there’s a better way” to prescribe radiation, “and I’m excited for the future when I can use it.”
When asked for comment, Brian Marples, PhD, a radiation oncology professor at the University of Rochester (N.Y.), said the data so far for GARD “seem very solid. I’m very excited by the concept.”
It’s been “the holy grail” of radiation researchers to find a biologic marker that predicts what dosages patients need and what can be given safely. “This strategy is a good way of doing that. Other groups are proposing similar strategies, but I think this group is ahead. I can see [GARD] being readily applied to the clinic because patients are [already] getting their tumors genomically characterized as part of care,” Dr. Marples said.
But many questions remain. For instance, the editorial writers questioned how GARD is “affected by tumor heterogeneity, response to systemic therapy, and changes in the tumor microenvironment.” Also, the approach is based on conventional 2 Gy fractions, but other fractionation regimens are becoming more common.
For Dr. Marples, the big caveat is that most cancer patients are treated with both radiation and chemotherapy. He said he would like to see GARD validated in patients who receive both.
They seven tumor types in the study included breast cancer, head and neck cancer, non–small cell lung cancer, pancreatic cancer, endometrial cancer, melanoma, and glioma. The majority of the subjects were treated with radiation, and each had the genomic data needed to calculate GARD.
Dr. Scott, senior author and Moffitt Center radiation oncologist Javier Torres-Roca, MD, and a third author hold intellectual property rights on RSI, GARD, and prescription dose base on RSI, plus equity in Cvergenx, a company that seeks to commercialize the approach. Dr. Torres-Roca and another author are cofounders. The editorial writers and Dr. Marples did not have any relevant disclosures.
FROM LANCET ONCOLOGY
Clinical Edge Journal Scan Commentary: Breast Cancer September 2021

Metastatic triple-negative breast cancer (TNBC) is a heterogeneous, biologically complex subtype, with continuing efforts to identify therapeutic targets. The PI3K/AKT signaling pathway plays a key role in cell proliferation, survival, invasion, and metabolism. In the phase II LOTUS trial (Dent et al) including 124 patients with advanced TNBC (no prior therapy for advanced disease), addition of the oral AKT inhibitor, ipatasertib, to paclitaxel led to a numerical improvement in OS that was not statistically significant. The median OS was 25.8 vs 16.9 months for the ipatasertib-paclitaxel vs placebo-paclitaxel, respectively (HR 0.80, 95% CI 0.50-1.28). Findings from cohort A of the phase III IPATunity130 trial showed that ipatasertib-paclitaxel did not lead to a statistically significant improvement in PFS vs placebo-paclitaxel in patients with PIK3CA/AKT1/PTEN-altered advanced TNBC in the first-line metastatic setting (mPFS 7.4 vs 6.1 months, respectively; HR 1.02, p=0.9237). These findings support further investigation into predictors of response and other molecular markers that may play a role in the diversity of mTNBC.
Endocrine therapy resistance remains a significant challenge in advanced HR+/HER2- breast cancer, and initial studies with the oral histone deacetylase inhibitor, etinostat, showed promise in this space. Unfortunately, these findings were not upheld in the phase III E2112 trial (Connolly et al), which failed to show an improvement in PFS or OS with exemestane-etinostat (EE) compared to exemestane-placebo (EP) among patients who had progressed on prior non-steroidal AI. Median PFS was 3.3 vs 3.1 months (HR 0.87; p=0.30) and median OS was 23.4 vs 21.7 months (HR 0.99; p=0.94) for the EE vs EP arms, respectively. The combination of an alternative HDAC inhibitor, tucidinostat, has been approved in China in combination with exemestane based on PFS benefit (3.6 months) in the phase III ACE trial. There are notable difference between E2112 and ACE trials, including patient population and design, and importantly OS has not been reported for the latter. The relatively short mPFS and low response rate (5-6%) in E2112 argues for more efficacious therapeutics. There is also value in correlative studies to help further elucidate if there is a role for HDAC inhibitors in this space.
Although adjuvant endocrine therapy has had a significantly beneficial effect on outcomes in early-stage HR+ breast cancer, late recurrences are characteristic of the luminal subtype, and have led to trials investigating extended adjuvant endocrine therapy. The phase III SALSA trial included 3484 women with early HR+ breast cancer who had received 5 years of adjuvant endocrine therapy with randomization to anastrozole for an additional 2 vs 5 years (comparing total of 7 vs 10 years). There was no significant difference in disease-free survival (DFS) at 8 years (73.6% vs 73.9% in the 2 vs 5-year groups, respectively; HR 0.99, p=0.90). Additionally, there was a lower risk of bone fracture in the 2 vs 5-year group (4.7% vs 6.3%; HR 1.35). It is essential to balance modest benefits with toxicities of prolonged AI use, and valuable to identify high-risk patients who may benefit from extended adjuvant endocrine therapy.
References:
Chan A, Moy B, Mansi J, et al; ExteNET Study Group. Final efficacy results of neratinib in HER2-positive hormone receptor-positive early-stage breast cancer from the phase III ExteNET trial. Clin Breast Cancer. 2021;21(1):80-91.e7.
von Minckwitz G, Huang CS, Mano MS, et al; KATHERINE Investigators. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Dent R, Kim SB, Oliveira M, et al. Double-blind placebo-controlled randomized phase III trial evaluating first-line ipatasertib combined with paclitaxel for PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer: primary results from IPATunity130 cohort A. Presented at: 2020 San Antonio Breast Cancer Symposium; December 8-11, 2020; Virtual. Oral GS3-04.
Jiang Z, Li W, Hu X, et al. Tucidinostat plus exemestane for postmenopausal patients with advanced, hormone receptor-positive breast cancer (ACE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(6):806-815.
Mamounas EP, Bandos H, Lembersky BC, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(1):88-99.
Metastatic triple-negative breast cancer (TNBC) is a heterogeneous, biologically complex subtype, with continuing efforts to identify therapeutic targets. The PI3K/AKT signaling pathway plays a key role in cell proliferation, survival, invasion, and metabolism. In the phase II LOTUS trial (Dent et al) including 124 patients with advanced TNBC (no prior therapy for advanced disease), addition of the oral AKT inhibitor, ipatasertib, to paclitaxel led to a numerical improvement in OS that was not statistically significant. The median OS was 25.8 vs 16.9 months for the ipatasertib-paclitaxel vs placebo-paclitaxel, respectively (HR 0.80, 95% CI 0.50-1.28). Findings from cohort A of the phase III IPATunity130 trial showed that ipatasertib-paclitaxel did not lead to a statistically significant improvement in PFS vs placebo-paclitaxel in patients with PIK3CA/AKT1/PTEN-altered advanced TNBC in the first-line metastatic setting (mPFS 7.4 vs 6.1 months, respectively; HR 1.02, p=0.9237). These findings support further investigation into predictors of response and other molecular markers that may play a role in the diversity of mTNBC.
Endocrine therapy resistance remains a significant challenge in advanced HR+/HER2- breast cancer, and initial studies with the oral histone deacetylase inhibitor, etinostat, showed promise in this space. Unfortunately, these findings were not upheld in the phase III E2112 trial (Connolly et al), which failed to show an improvement in PFS or OS with exemestane-etinostat (EE) compared to exemestane-placebo (EP) among patients who had progressed on prior non-steroidal AI. Median PFS was 3.3 vs 3.1 months (HR 0.87; p=0.30) and median OS was 23.4 vs 21.7 months (HR 0.99; p=0.94) for the EE vs EP arms, respectively. The combination of an alternative HDAC inhibitor, tucidinostat, has been approved in China in combination with exemestane based on PFS benefit (3.6 months) in the phase III ACE trial. There are notable difference between E2112 and ACE trials, including patient population and design, and importantly OS has not been reported for the latter. The relatively short mPFS and low response rate (5-6%) in E2112 argues for more efficacious therapeutics. There is also value in correlative studies to help further elucidate if there is a role for HDAC inhibitors in this space.
Although adjuvant endocrine therapy has had a significantly beneficial effect on outcomes in early-stage HR+ breast cancer, late recurrences are characteristic of the luminal subtype, and have led to trials investigating extended adjuvant endocrine therapy. The phase III SALSA trial included 3484 women with early HR+ breast cancer who had received 5 years of adjuvant endocrine therapy with randomization to anastrozole for an additional 2 vs 5 years (comparing total of 7 vs 10 years). There was no significant difference in disease-free survival (DFS) at 8 years (73.6% vs 73.9% in the 2 vs 5-year groups, respectively; HR 0.99, p=0.90). Additionally, there was a lower risk of bone fracture in the 2 vs 5-year group (4.7% vs 6.3%; HR 1.35). It is essential to balance modest benefits with toxicities of prolonged AI use, and valuable to identify high-risk patients who may benefit from extended adjuvant endocrine therapy.
References:
Chan A, Moy B, Mansi J, et al; ExteNET Study Group. Final efficacy results of neratinib in HER2-positive hormone receptor-positive early-stage breast cancer from the phase III ExteNET trial. Clin Breast Cancer. 2021;21(1):80-91.e7.
von Minckwitz G, Huang CS, Mano MS, et al; KATHERINE Investigators. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Dent R, Kim SB, Oliveira M, et al. Double-blind placebo-controlled randomized phase III trial evaluating first-line ipatasertib combined with paclitaxel for PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer: primary results from IPATunity130 cohort A. Presented at: 2020 San Antonio Breast Cancer Symposium; December 8-11, 2020; Virtual. Oral GS3-04.
Jiang Z, Li W, Hu X, et al. Tucidinostat plus exemestane for postmenopausal patients with advanced, hormone receptor-positive breast cancer (ACE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(6):806-815.
Mamounas EP, Bandos H, Lembersky BC, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(1):88-99.
Metastatic triple-negative breast cancer (TNBC) is a heterogeneous, biologically complex subtype, with continuing efforts to identify therapeutic targets. The PI3K/AKT signaling pathway plays a key role in cell proliferation, survival, invasion, and metabolism. In the phase II LOTUS trial (Dent et al) including 124 patients with advanced TNBC (no prior therapy for advanced disease), addition of the oral AKT inhibitor, ipatasertib, to paclitaxel led to a numerical improvement in OS that was not statistically significant. The median OS was 25.8 vs 16.9 months for the ipatasertib-paclitaxel vs placebo-paclitaxel, respectively (HR 0.80, 95% CI 0.50-1.28). Findings from cohort A of the phase III IPATunity130 trial showed that ipatasertib-paclitaxel did not lead to a statistically significant improvement in PFS vs placebo-paclitaxel in patients with PIK3CA/AKT1/PTEN-altered advanced TNBC in the first-line metastatic setting (mPFS 7.4 vs 6.1 months, respectively; HR 1.02, p=0.9237). These findings support further investigation into predictors of response and other molecular markers that may play a role in the diversity of mTNBC.
Endocrine therapy resistance remains a significant challenge in advanced HR+/HER2- breast cancer, and initial studies with the oral histone deacetylase inhibitor, etinostat, showed promise in this space. Unfortunately, these findings were not upheld in the phase III E2112 trial (Connolly et al), which failed to show an improvement in PFS or OS with exemestane-etinostat (EE) compared to exemestane-placebo (EP) among patients who had progressed on prior non-steroidal AI. Median PFS was 3.3 vs 3.1 months (HR 0.87; p=0.30) and median OS was 23.4 vs 21.7 months (HR 0.99; p=0.94) for the EE vs EP arms, respectively. The combination of an alternative HDAC inhibitor, tucidinostat, has been approved in China in combination with exemestane based on PFS benefit (3.6 months) in the phase III ACE trial. There are notable difference between E2112 and ACE trials, including patient population and design, and importantly OS has not been reported for the latter. The relatively short mPFS and low response rate (5-6%) in E2112 argues for more efficacious therapeutics. There is also value in correlative studies to help further elucidate if there is a role for HDAC inhibitors in this space.
Although adjuvant endocrine therapy has had a significantly beneficial effect on outcomes in early-stage HR+ breast cancer, late recurrences are characteristic of the luminal subtype, and have led to trials investigating extended adjuvant endocrine therapy. The phase III SALSA trial included 3484 women with early HR+ breast cancer who had received 5 years of adjuvant endocrine therapy with randomization to anastrozole for an additional 2 vs 5 years (comparing total of 7 vs 10 years). There was no significant difference in disease-free survival (DFS) at 8 years (73.6% vs 73.9% in the 2 vs 5-year groups, respectively; HR 0.99, p=0.90). Additionally, there was a lower risk of bone fracture in the 2 vs 5-year group (4.7% vs 6.3%; HR 1.35). It is essential to balance modest benefits with toxicities of prolonged AI use, and valuable to identify high-risk patients who may benefit from extended adjuvant endocrine therapy.
References:
Chan A, Moy B, Mansi J, et al; ExteNET Study Group. Final efficacy results of neratinib in HER2-positive hormone receptor-positive early-stage breast cancer from the phase III ExteNET trial. Clin Breast Cancer. 2021;21(1):80-91.e7.
von Minckwitz G, Huang CS, Mano MS, et al; KATHERINE Investigators. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2019;380(7):617-628.
Dent R, Kim SB, Oliveira M, et al. Double-blind placebo-controlled randomized phase III trial evaluating first-line ipatasertib combined with paclitaxel for PIK3CA/AKT1/PTEN-altered locally advanced unresectable or metastatic triple-negative breast cancer: primary results from IPATunity130 cohort A. Presented at: 2020 San Antonio Breast Cancer Symposium; December 8-11, 2020; Virtual. Oral GS3-04.
Jiang Z, Li W, Hu X, et al. Tucidinostat plus exemestane for postmenopausal patients with advanced, hormone receptor-positive breast cancer (ACE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(6):806-815.
Mamounas EP, Bandos H, Lembersky BC, et al. Use of letrozole after aromatase inhibitor-based therapy in postmenopausal breast cancer (NRG Oncology/NSABP B-42): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(1):88-99.
TNBC: Statin use is linked to survival benefit
Key clinical point: Initiation of statin treatment within 12 months of diagnosis improves survival in women with stage I-III triple-negative breast cancer (TNBC).
Major finding: Statin treatment was initiated in 2,281 patients within 12 months of diagnosis. In 1,534 patients with TNBC, statin use was associated with a significant improvement in breast cancer-specific survival (standardized hazard ratio [HR], 0.42; P = 0.022) and overall survival (HR, 0.70; P = 0.046). No significant association was observed between statin use and survival in patients without TNBC.
Study details: retrospective study of 23,192 patients with stage I-III breast cancer from the Surveillance, Epidemiology, and End Results-Medicare and Texas Cancer Registry-Medicare database between 2008 and 2015.
Disclosures: The study was supported by National Institutes of Health and Cancer Prevention Research Institute of Texas. The authors received grants, research funding, and personal fees outside this work.
Source: Nowakowska MK et al. Cancer. 2021 Aug 3. doi: 10.1002/cncr.33797.
Key clinical point: Initiation of statin treatment within 12 months of diagnosis improves survival in women with stage I-III triple-negative breast cancer (TNBC).
Major finding: Statin treatment was initiated in 2,281 patients within 12 months of diagnosis. In 1,534 patients with TNBC, statin use was associated with a significant improvement in breast cancer-specific survival (standardized hazard ratio [HR], 0.42; P = 0.022) and overall survival (HR, 0.70; P = 0.046). No significant association was observed between statin use and survival in patients without TNBC.
Study details: retrospective study of 23,192 patients with stage I-III breast cancer from the Surveillance, Epidemiology, and End Results-Medicare and Texas Cancer Registry-Medicare database between 2008 and 2015.
Disclosures: The study was supported by National Institutes of Health and Cancer Prevention Research Institute of Texas. The authors received grants, research funding, and personal fees outside this work.
Source: Nowakowska MK et al. Cancer. 2021 Aug 3. doi: 10.1002/cncr.33797.
Key clinical point: Initiation of statin treatment within 12 months of diagnosis improves survival in women with stage I-III triple-negative breast cancer (TNBC).
Major finding: Statin treatment was initiated in 2,281 patients within 12 months of diagnosis. In 1,534 patients with TNBC, statin use was associated with a significant improvement in breast cancer-specific survival (standardized hazard ratio [HR], 0.42; P = 0.022) and overall survival (HR, 0.70; P = 0.046). No significant association was observed between statin use and survival in patients without TNBC.
Study details: retrospective study of 23,192 patients with stage I-III breast cancer from the Surveillance, Epidemiology, and End Results-Medicare and Texas Cancer Registry-Medicare database between 2008 and 2015.
Disclosures: The study was supported by National Institutes of Health and Cancer Prevention Research Institute of Texas. The authors received grants, research funding, and personal fees outside this work.
Source: Nowakowska MK et al. Cancer. 2021 Aug 3. doi: 10.1002/cncr.33797.
Treatment trends in HR-positive, HER-negative breast cancer
Key clinical point: A survey-based study shows higher chemotherapy use in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with poor prognostic factors.
Major finding: At least 1 poor prognostic factor was reported in 63% of patients, with varying degrees of overlap between factors. The ability of patients to maintain usual activities was more common in patients without poor prognostic factors. Chemotherapy was prescribed more frequently in patients with poor prognostic factors, whereas endocrine therapy and nonopioid analgesic were more common in patients without poor prognostic factors.
Study details: Real-world data were derived from a large multinational Adelphi Real World Disease Specific Programme survey of 410 oncologists and 2,259 patients with HR-positive, HER-negative advanced breast cancer.
Disclosures: This study was supported by Eli Lilly and Company Ltd, Windlesham, UK. The authors were employees of or received consulting/advisory fees and/or honoraria from Eli Lilly and Company.
Source: Davie A et al. ESMO Open. 2021;6(4):10226 doi: 10.1016/j.esmoop.2021.100226.
Key clinical point: A survey-based study shows higher chemotherapy use in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with poor prognostic factors.
Major finding: At least 1 poor prognostic factor was reported in 63% of patients, with varying degrees of overlap between factors. The ability of patients to maintain usual activities was more common in patients without poor prognostic factors. Chemotherapy was prescribed more frequently in patients with poor prognostic factors, whereas endocrine therapy and nonopioid analgesic were more common in patients without poor prognostic factors.
Study details: Real-world data were derived from a large multinational Adelphi Real World Disease Specific Programme survey of 410 oncologists and 2,259 patients with HR-positive, HER-negative advanced breast cancer.
Disclosures: This study was supported by Eli Lilly and Company Ltd, Windlesham, UK. The authors were employees of or received consulting/advisory fees and/or honoraria from Eli Lilly and Company.
Source: Davie A et al. ESMO Open. 2021;6(4):10226 doi: 10.1016/j.esmoop.2021.100226.
Key clinical point: A survey-based study shows higher chemotherapy use in patients with hormone receptor (HR)-positive, human epidermal growth factor receptor 2 (HER2)-negative advanced breast cancer with poor prognostic factors.
Major finding: At least 1 poor prognostic factor was reported in 63% of patients, with varying degrees of overlap between factors. The ability of patients to maintain usual activities was more common in patients without poor prognostic factors. Chemotherapy was prescribed more frequently in patients with poor prognostic factors, whereas endocrine therapy and nonopioid analgesic were more common in patients without poor prognostic factors.
Study details: Real-world data were derived from a large multinational Adelphi Real World Disease Specific Programme survey of 410 oncologists and 2,259 patients with HR-positive, HER-negative advanced breast cancer.
Disclosures: This study was supported by Eli Lilly and Company Ltd, Windlesham, UK. The authors were employees of or received consulting/advisory fees and/or honoraria from Eli Lilly and Company.
Source: Davie A et al. ESMO Open. 2021;6(4):10226 doi: 10.1016/j.esmoop.2021.100226.
High risk for late-onset breast cancer in genetically predisposed women
Key clinical point: Women aged 65 years and above with pathogenic variants (PVs) in BRCA1/2, checkpoint kinase 2 (CHEK2), and partner and localizer of the BRCA2 (PALB2) genes are at an increased risk for breast cancer.
Major finding: The rate of PVs was 3.18% in women with breast cancer and 1.48% in those without. PVs in BRCA1 (odds ratio [OR], 3.37), BRCA2 (OR, 2.64), PALB2 (OR, 3.09), and CHEK2 (OR, 2.13) and were associated with moderate risk for breast cancer. The remaining lifetime risk was 18.4%, 18.7%, 15.9%, and 14.9% for BRCA1, BRCA2, PALB2, and CHEK2 PVs
Study details: This was a population-based study of 13,762 women with breast cancer (age, 65 years and above) and matched 12,945 women without cancer who were tested for PVs in germline predisposition genes.
Disclosures: The study was supported by the National Institutes of Health and Breast Cancer Research Foundation. The authors declared receiving grants, research funding, speaker/personal fees, and/or travel/accommodation/expenses and/or employment and stock ownership.
Source: Boddicker NJ et al. J Clin Oncol. 2021 Jul 22 (in press). doi: 10.1200/JCO.21.00531.
Key clinical point: Women aged 65 years and above with pathogenic variants (PVs) in BRCA1/2, checkpoint kinase 2 (CHEK2), and partner and localizer of the BRCA2 (PALB2) genes are at an increased risk for breast cancer.
Major finding: The rate of PVs was 3.18% in women with breast cancer and 1.48% in those without. PVs in BRCA1 (odds ratio [OR], 3.37), BRCA2 (OR, 2.64), PALB2 (OR, 3.09), and CHEK2 (OR, 2.13) and were associated with moderate risk for breast cancer. The remaining lifetime risk was 18.4%, 18.7%, 15.9%, and 14.9% for BRCA1, BRCA2, PALB2, and CHEK2 PVs
Study details: This was a population-based study of 13,762 women with breast cancer (age, 65 years and above) and matched 12,945 women without cancer who were tested for PVs in germline predisposition genes.
Disclosures: The study was supported by the National Institutes of Health and Breast Cancer Research Foundation. The authors declared receiving grants, research funding, speaker/personal fees, and/or travel/accommodation/expenses and/or employment and stock ownership.
Source: Boddicker NJ et al. J Clin Oncol. 2021 Jul 22 (in press). doi: 10.1200/JCO.21.00531.
Key clinical point: Women aged 65 years and above with pathogenic variants (PVs) in BRCA1/2, checkpoint kinase 2 (CHEK2), and partner and localizer of the BRCA2 (PALB2) genes are at an increased risk for breast cancer.
Major finding: The rate of PVs was 3.18% in women with breast cancer and 1.48% in those without. PVs in BRCA1 (odds ratio [OR], 3.37), BRCA2 (OR, 2.64), PALB2 (OR, 3.09), and CHEK2 (OR, 2.13) and were associated with moderate risk for breast cancer. The remaining lifetime risk was 18.4%, 18.7%, 15.9%, and 14.9% for BRCA1, BRCA2, PALB2, and CHEK2 PVs
Study details: This was a population-based study of 13,762 women with breast cancer (age, 65 years and above) and matched 12,945 women without cancer who were tested for PVs in germline predisposition genes.
Disclosures: The study was supported by the National Institutes of Health and Breast Cancer Research Foundation. The authors declared receiving grants, research funding, speaker/personal fees, and/or travel/accommodation/expenses and/or employment and stock ownership.
Source: Boddicker NJ et al. J Clin Oncol. 2021 Jul 22 (in press). doi: 10.1200/JCO.21.00531.