User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Everything We Say and Do
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Each article will focus on how the contributor applies one or more of the “key communication” tactics in practice to maintain provider accountability for “everything we say and do that affects our patients’ thoughts, feelings, and well-being.”
What I say and do
I inform my patients that I have reviewed their chart and that I am familiar with their diagnosis.
Why I do it
In the hospital setting, in particular, patients are concerned about communication between their various healthcare professionals. Many times, the patient’s primary-care provider works strictly in the outpatient setting, so the hospitalist is the person who assumes total care of the patient throughout hospitalization. This understandably creates anxiety for patients and families because they wonder if the hospitalist really knows their medical history. One way to alleviate this anxiety is to review your patients’ charts prior to speaking with them and to verbally let your patients know you are familiar with their diagnoses.
How I do it
Step 1: Before entering the room, I review my patient’s chart. If I am taking over the service from my colleague, I review all notes from the current hospitalization to ensure I understand everything that has happened. I also review tests, procedures, and radiographic studies. To gain a better understanding of my patient, I read the most recent discharge summary and outpatient clinic note. Likewise, if I am admitting a new patient to the hospital, before entering the room to do the history and physical examination, I review recent hospitalizations, clinic notes, and emergency department visits.
I also like to review the chart to see if I have taken care of the patient before. Patients often remember me even though I may not remember them, so reviewing my prior notes may be helpful. Thankfully, my electronic health record (EHR) has a search function where I can enter my name or any other keyword and it searches for patient records based on this keyword.
Step 2: Even though reading the chart and being informed about my patient is important, it is only the first step. The next step is to let my patient and family know that I have read the chart and that I am up-to-date on my patient’s diagnosis. I feel it is very important for me to verbalize that I have read the chart because without doing this, my patients never really know that I took the time prior to entering the room to learn about them.
I might say:
- “I was reviewing your chart before I came in, and I saw that your daughter brought you to the hospital for chest pain.”
- “I read your chart and saw that you have been to the emergency room twice in the last week.”
- “I read your primary-care doctor’s note, and I saw that she recently treated you for pneumonia.”
- “I read your chart, and I wanted to confirm a few things I read to ensure we are on the same page.”
There are many different ways you can phrase this, but the important point is to make sure your patients know you read the chart by specifically referencing something you learned. This helps your patients feel more confident that you know their medical history.
I know some of the doctors reading this column see patients in the outpatient setting. One way to help yourself remember pertinent facts about a patient’s medical history is to include these facts in a specific place in your clinic note. That way, prior to seeing the patient, you can always review your last note and know the important information about your patient’s medical history will always be in the same place in each note. Another tip is to use your EHR’s note function. My EHR has “sticky notes,” and they provide a place for the PCP to store information about the patient without it becoming part of the permanent medical record.
These notes allow the PCP to record important events that happen between one clinic visit and the next. Thus, when the patient returns to the clinic, the PCP opens the chart, reviews the sticky note, and enters the exam room prepared to discuss significant events in the patient’s recent medical history.
In the end, it does not matter which technique you use. It simply matters that you take time to review your patient’s chart prior to entering the room and that you verbalize what you have learned. In patients, this inspires confidence and trust and helps alleviate concerns that the physician does not know important information in their medical history.
Dr. Dorrah is regional medical director for quality and the patient experience at Baylor Scott & White Health in Round Rock, Tex. She is a member of SHM’s Patient Experience Committee.
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Each article will focus on how the contributor applies one or more of the “key communication” tactics in practice to maintain provider accountability for “everything we say and do that affects our patients’ thoughts, feelings, and well-being.”
What I say and do
I inform my patients that I have reviewed their chart and that I am familiar with their diagnosis.
Why I do it
In the hospital setting, in particular, patients are concerned about communication between their various healthcare professionals. Many times, the patient’s primary-care provider works strictly in the outpatient setting, so the hospitalist is the person who assumes total care of the patient throughout hospitalization. This understandably creates anxiety for patients and families because they wonder if the hospitalist really knows their medical history. One way to alleviate this anxiety is to review your patients’ charts prior to speaking with them and to verbally let your patients know you are familiar with their diagnoses.
How I do it
Step 1: Before entering the room, I review my patient’s chart. If I am taking over the service from my colleague, I review all notes from the current hospitalization to ensure I understand everything that has happened. I also review tests, procedures, and radiographic studies. To gain a better understanding of my patient, I read the most recent discharge summary and outpatient clinic note. Likewise, if I am admitting a new patient to the hospital, before entering the room to do the history and physical examination, I review recent hospitalizations, clinic notes, and emergency department visits.
I also like to review the chart to see if I have taken care of the patient before. Patients often remember me even though I may not remember them, so reviewing my prior notes may be helpful. Thankfully, my electronic health record (EHR) has a search function where I can enter my name or any other keyword and it searches for patient records based on this keyword.
Step 2: Even though reading the chart and being informed about my patient is important, it is only the first step. The next step is to let my patient and family know that I have read the chart and that I am up-to-date on my patient’s diagnosis. I feel it is very important for me to verbalize that I have read the chart because without doing this, my patients never really know that I took the time prior to entering the room to learn about them.
I might say:
- “I was reviewing your chart before I came in, and I saw that your daughter brought you to the hospital for chest pain.”
- “I read your chart and saw that you have been to the emergency room twice in the last week.”
- “I read your primary-care doctor’s note, and I saw that she recently treated you for pneumonia.”
- “I read your chart, and I wanted to confirm a few things I read to ensure we are on the same page.”
There are many different ways you can phrase this, but the important point is to make sure your patients know you read the chart by specifically referencing something you learned. This helps your patients feel more confident that you know their medical history.
I know some of the doctors reading this column see patients in the outpatient setting. One way to help yourself remember pertinent facts about a patient’s medical history is to include these facts in a specific place in your clinic note. That way, prior to seeing the patient, you can always review your last note and know the important information about your patient’s medical history will always be in the same place in each note. Another tip is to use your EHR’s note function. My EHR has “sticky notes,” and they provide a place for the PCP to store information about the patient without it becoming part of the permanent medical record.
These notes allow the PCP to record important events that happen between one clinic visit and the next. Thus, when the patient returns to the clinic, the PCP opens the chart, reviews the sticky note, and enters the exam room prepared to discuss significant events in the patient’s recent medical history.
In the end, it does not matter which technique you use. It simply matters that you take time to review your patient’s chart prior to entering the room and that you verbalize what you have learned. In patients, this inspires confidence and trust and helps alleviate concerns that the physician does not know important information in their medical history.
Dr. Dorrah is regional medical director for quality and the patient experience at Baylor Scott & White Health in Round Rock, Tex. She is a member of SHM’s Patient Experience Committee.
Editor’s note: “Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Each article will focus on how the contributor applies one or more of the “key communication” tactics in practice to maintain provider accountability for “everything we say and do that affects our patients’ thoughts, feelings, and well-being.”
What I say and do
I inform my patients that I have reviewed their chart and that I am familiar with their diagnosis.
Why I do it
In the hospital setting, in particular, patients are concerned about communication between their various healthcare professionals. Many times, the patient’s primary-care provider works strictly in the outpatient setting, so the hospitalist is the person who assumes total care of the patient throughout hospitalization. This understandably creates anxiety for patients and families because they wonder if the hospitalist really knows their medical history. One way to alleviate this anxiety is to review your patients’ charts prior to speaking with them and to verbally let your patients know you are familiar with their diagnoses.
How I do it
Step 1: Before entering the room, I review my patient’s chart. If I am taking over the service from my colleague, I review all notes from the current hospitalization to ensure I understand everything that has happened. I also review tests, procedures, and radiographic studies. To gain a better understanding of my patient, I read the most recent discharge summary and outpatient clinic note. Likewise, if I am admitting a new patient to the hospital, before entering the room to do the history and physical examination, I review recent hospitalizations, clinic notes, and emergency department visits.
I also like to review the chart to see if I have taken care of the patient before. Patients often remember me even though I may not remember them, so reviewing my prior notes may be helpful. Thankfully, my electronic health record (EHR) has a search function where I can enter my name or any other keyword and it searches for patient records based on this keyword.
Step 2: Even though reading the chart and being informed about my patient is important, it is only the first step. The next step is to let my patient and family know that I have read the chart and that I am up-to-date on my patient’s diagnosis. I feel it is very important for me to verbalize that I have read the chart because without doing this, my patients never really know that I took the time prior to entering the room to learn about them.
I might say:
- “I was reviewing your chart before I came in, and I saw that your daughter brought you to the hospital for chest pain.”
- “I read your chart and saw that you have been to the emergency room twice in the last week.”
- “I read your primary-care doctor’s note, and I saw that she recently treated you for pneumonia.”
- “I read your chart, and I wanted to confirm a few things I read to ensure we are on the same page.”
There are many different ways you can phrase this, but the important point is to make sure your patients know you read the chart by specifically referencing something you learned. This helps your patients feel more confident that you know their medical history.
I know some of the doctors reading this column see patients in the outpatient setting. One way to help yourself remember pertinent facts about a patient’s medical history is to include these facts in a specific place in your clinic note. That way, prior to seeing the patient, you can always review your last note and know the important information about your patient’s medical history will always be in the same place in each note. Another tip is to use your EHR’s note function. My EHR has “sticky notes,” and they provide a place for the PCP to store information about the patient without it becoming part of the permanent medical record.
These notes allow the PCP to record important events that happen between one clinic visit and the next. Thus, when the patient returns to the clinic, the PCP opens the chart, reviews the sticky note, and enters the exam room prepared to discuss significant events in the patient’s recent medical history.
In the end, it does not matter which technique you use. It simply matters that you take time to review your patient’s chart prior to entering the room and that you verbalize what you have learned. In patients, this inspires confidence and trust and helps alleviate concerns that the physician does not know important information in their medical history.
Dr. Dorrah is regional medical director for quality and the patient experience at Baylor Scott & White Health in Round Rock, Tex. She is a member of SHM’s Patient Experience Committee.

Idle intravenous catheters are associated with preventable complications
Intravenous catheters (ICs) are common and necessary for inpatient care. However, peripheral and especially central venous catheters (CVCs) are associated with increased risk for local and systemic complications, including bloodstream infections and endocarditis.

Prevention of these complications is important and should be a major focus of infection control and patient safety practices. There are three main points of focus on infection prevention with regard to ICs – proper insertion techniques, proper care of the catheter, and prompt removal when it is no longer necessary.
We focused our review, published in the American Journal of Infection Control (2016 Oct. doi: 10.1016/j.ajic.2016.03.073), on the final point – determining the prevalence, risk factors, and outcomes related to idle intravenous catheters. To accomplish this, we conducted an integrative review of published studies related to idle catheters, excluding reviews, abstracts, and commentaries. Thirteen studies met the inclusion criteria and four of these focused on CVCs.
Generally, an idle catheter is one that remains in place even though it is not being used for patient care. However, the definition of an “idle” catheter varied amongst the reviewed studies, as did the unit of measure, especially for peripheral catheters. Central venous catheter-focused studies were more consistent in using “idle catheter days” and “catheter days.”
Studies of peripheral catheters revealed that 16%-50% of patients had an idle catheter of some type. For the studies focused on CVCs, the percentage of patients with idle catheters ranged from 2.7% in one intensive care unit to 26.2% in a different study. Interestingly, in the study with 2.7% idle CVCs in the ICU, there was a higher percentage of idle CVCs outside of the ICU in the same hospital.
The major reasons for leaving catheters in place in studies where reasons were noted were convenience, future intention to use intravenous medication, and inappropriate use of intravenous medications when oral could be used.
Although data are scarce, complications in the reviewed studies were relatively common with idle peripheral catheters, where 9%-12% suffered thrombophlebitis. Obviously, the risk for catheter-related bloodstream infection increases as the number of catheter days increases – this is especially important with regard to idle CVCs.
Decreasing the prevalence of idle catheters is likely to decrease the risk for infection and improve patient safety. Based on our review of the data, a standardized definition of an “idle catheter” is needed. At the very least, a standard definition should be developed at each institution. This would allow an individual hospital the ability to identify and track the presence of these lines, and implement targeted interventions to decrease the proportion of idle lines. Ideally, a common definition would be created and validated so that data and interventions could be comparable across institutions and guidelines could be developed.
The goal of targeted interventions should be zero idle lines. Prevention of idle peripheral catheters should also be pursued, but because CVC-related complications are often more serious, these lines are often the focus of efforts. Use of peripherally inserted central catheters (PICCs) has increased and while these catheters in some settings may have decreased complication risk, compared with femoral/internal jugular/subclavian CVCs, prevention of idle catheter days is paramount for these catheters as well.
Many ICUs, including at our own institution, have instituted programs to closely monitor for ongoing need for CVCs. This increased focus on the CVC likely explains the lower rates of idle catheters in ICUs noted in the reviewed studies. This close surveillance can be done outside of the ICU as well, and could include peripheral catheters.
At our own institution, the need for catheters is reviewed on some units as part of formalized patient safety rounds. Another potential group of interventions could focus on electronic medical record (EMR)-based changes such as limits on the duration of the order, requirement for renewal of the order, or on-screen reminders of the presence of a catheter. This sort of intervention could possibly be expanded as EMR use becomes more common and robust. For instance, if intravenous medications have not been ordered or given in a certain amount of time, an alert might be triggered. Another EMR-based mechanism could be to require an indication for ongoing catheter use.
Education about the potential adverse outcomes of idle catheters is important. Promoting a team-based approach to interventions, where all involved team members can discuss patient safety issues on equal ground is paramount to successfully decreasing idle catheters and improving patient care and safety in general. As with other hospital-wide initiatives, engagement of hospital administration is important to decrease barriers to implementation.
Intravenous catheter use will remain an integral part of patient care, but efforts should be made to create standardization around the definition of an idle catheter, standardize units of measure, and institute programs to prevent idle catheters.
Daniel Shirley, MD, MS, is assistant professor in the division of infectious disease at the University of Wisconsin–Madison School of Medicine and Public Health and the William S. Middleton Memorial Veterans Hospital. Nasia Safdar, MD, PhD, is associate professor in the division of infectious disease at the University of Wisconsin–Madison School of Medicine and Public Health and the William S. Middleton Memorial Veterans Hospital.
Intravenous catheters (ICs) are common and necessary for inpatient care. However, peripheral and especially central venous catheters (CVCs) are associated with increased risk for local and systemic complications, including bloodstream infections and endocarditis.
Prevention of these complications is important and should be a major focus of infection control and patient safety practices. There are three main points of focus on infection prevention with regard to ICs – proper insertion techniques, proper care of the catheter, and prompt removal when it is no longer necessary.
We focused our review, published in the American Journal of Infection Control (2016 Oct. doi: 10.1016/j.ajic.2016.03.073), on the final point – determining the prevalence, risk factors, and outcomes related to idle intravenous catheters. To accomplish this, we conducted an integrative review of published studies related to idle catheters, excluding reviews, abstracts, and commentaries. Thirteen studies met the inclusion criteria and four of these focused on CVCs.
Generally, an idle catheter is one that remains in place even though it is not being used for patient care. However, the definition of an “idle” catheter varied amongst the reviewed studies, as did the unit of measure, especially for peripheral catheters. Central venous catheter-focused studies were more consistent in using “idle catheter days” and “catheter days.”
Studies of peripheral catheters revealed that 16%-50% of patients had an idle catheter of some type. For the studies focused on CVCs, the percentage of patients with idle catheters ranged from 2.7% in one intensive care unit to 26.2% in a different study. Interestingly, in the study with 2.7% idle CVCs in the ICU, there was a higher percentage of idle CVCs outside of the ICU in the same hospital.
The major reasons for leaving catheters in place in studies where reasons were noted were convenience, future intention to use intravenous medication, and inappropriate use of intravenous medications when oral could be used.
Although data are scarce, complications in the reviewed studies were relatively common with idle peripheral catheters, where 9%-12% suffered thrombophlebitis. Obviously, the risk for catheter-related bloodstream infection increases as the number of catheter days increases – this is especially important with regard to idle CVCs.
Decreasing the prevalence of idle catheters is likely to decrease the risk for infection and improve patient safety. Based on our review of the data, a standardized definition of an “idle catheter” is needed. At the very least, a standard definition should be developed at each institution. This would allow an individual hospital the ability to identify and track the presence of these lines, and implement targeted interventions to decrease the proportion of idle lines. Ideally, a common definition would be created and validated so that data and interventions could be comparable across institutions and guidelines could be developed.
The goal of targeted interventions should be zero idle lines. Prevention of idle peripheral catheters should also be pursued, but because CVC-related complications are often more serious, these lines are often the focus of efforts. Use of peripherally inserted central catheters (PICCs) has increased and while these catheters in some settings may have decreased complication risk, compared with femoral/internal jugular/subclavian CVCs, prevention of idle catheter days is paramount for these catheters as well.
Many ICUs, including at our own institution, have instituted programs to closely monitor for ongoing need for CVCs. This increased focus on the CVC likely explains the lower rates of idle catheters in ICUs noted in the reviewed studies. This close surveillance can be done outside of the ICU as well, and could include peripheral catheters.
At our own institution, the need for catheters is reviewed on some units as part of formalized patient safety rounds. Another potential group of interventions could focus on electronic medical record (EMR)-based changes such as limits on the duration of the order, requirement for renewal of the order, or on-screen reminders of the presence of a catheter. This sort of intervention could possibly be expanded as EMR use becomes more common and robust. For instance, if intravenous medications have not been ordered or given in a certain amount of time, an alert might be triggered. Another EMR-based mechanism could be to require an indication for ongoing catheter use.
Education about the potential adverse outcomes of idle catheters is important. Promoting a team-based approach to interventions, where all involved team members can discuss patient safety issues on equal ground is paramount to successfully decreasing idle catheters and improving patient care and safety in general. As with other hospital-wide initiatives, engagement of hospital administration is important to decrease barriers to implementation.
Intravenous catheter use will remain an integral part of patient care, but efforts should be made to create standardization around the definition of an idle catheter, standardize units of measure, and institute programs to prevent idle catheters.
Daniel Shirley, MD, MS, is assistant professor in the division of infectious disease at the University of Wisconsin–Madison School of Medicine and Public Health and the William S. Middleton Memorial Veterans Hospital. Nasia Safdar, MD, PhD, is associate professor in the division of infectious disease at the University of Wisconsin–Madison School of Medicine and Public Health and the William S. Middleton Memorial Veterans Hospital.
Intravenous catheters (ICs) are common and necessary for inpatient care. However, peripheral and especially central venous catheters (CVCs) are associated with increased risk for local and systemic complications, including bloodstream infections and endocarditis.
Prevention of these complications is important and should be a major focus of infection control and patient safety practices. There are three main points of focus on infection prevention with regard to ICs – proper insertion techniques, proper care of the catheter, and prompt removal when it is no longer necessary.
We focused our review, published in the American Journal of Infection Control (2016 Oct. doi: 10.1016/j.ajic.2016.03.073), on the final point – determining the prevalence, risk factors, and outcomes related to idle intravenous catheters. To accomplish this, we conducted an integrative review of published studies related to idle catheters, excluding reviews, abstracts, and commentaries. Thirteen studies met the inclusion criteria and four of these focused on CVCs.
Generally, an idle catheter is one that remains in place even though it is not being used for patient care. However, the definition of an “idle” catheter varied amongst the reviewed studies, as did the unit of measure, especially for peripheral catheters. Central venous catheter-focused studies were more consistent in using “idle catheter days” and “catheter days.”
Studies of peripheral catheters revealed that 16%-50% of patients had an idle catheter of some type. For the studies focused on CVCs, the percentage of patients with idle catheters ranged from 2.7% in one intensive care unit to 26.2% in a different study. Interestingly, in the study with 2.7% idle CVCs in the ICU, there was a higher percentage of idle CVCs outside of the ICU in the same hospital.
The major reasons for leaving catheters in place in studies where reasons were noted were convenience, future intention to use intravenous medication, and inappropriate use of intravenous medications when oral could be used.
Although data are scarce, complications in the reviewed studies were relatively common with idle peripheral catheters, where 9%-12% suffered thrombophlebitis. Obviously, the risk for catheter-related bloodstream infection increases as the number of catheter days increases – this is especially important with regard to idle CVCs.
Decreasing the prevalence of idle catheters is likely to decrease the risk for infection and improve patient safety. Based on our review of the data, a standardized definition of an “idle catheter” is needed. At the very least, a standard definition should be developed at each institution. This would allow an individual hospital the ability to identify and track the presence of these lines, and implement targeted interventions to decrease the proportion of idle lines. Ideally, a common definition would be created and validated so that data and interventions could be comparable across institutions and guidelines could be developed.
The goal of targeted interventions should be zero idle lines. Prevention of idle peripheral catheters should also be pursued, but because CVC-related complications are often more serious, these lines are often the focus of efforts. Use of peripherally inserted central catheters (PICCs) has increased and while these catheters in some settings may have decreased complication risk, compared with femoral/internal jugular/subclavian CVCs, prevention of idle catheter days is paramount for these catheters as well.
Many ICUs, including at our own institution, have instituted programs to closely monitor for ongoing need for CVCs. This increased focus on the CVC likely explains the lower rates of idle catheters in ICUs noted in the reviewed studies. This close surveillance can be done outside of the ICU as well, and could include peripheral catheters.
At our own institution, the need for catheters is reviewed on some units as part of formalized patient safety rounds. Another potential group of interventions could focus on electronic medical record (EMR)-based changes such as limits on the duration of the order, requirement for renewal of the order, or on-screen reminders of the presence of a catheter. This sort of intervention could possibly be expanded as EMR use becomes more common and robust. For instance, if intravenous medications have not been ordered or given in a certain amount of time, an alert might be triggered. Another EMR-based mechanism could be to require an indication for ongoing catheter use.
Education about the potential adverse outcomes of idle catheters is important. Promoting a team-based approach to interventions, where all involved team members can discuss patient safety issues on equal ground is paramount to successfully decreasing idle catheters and improving patient care and safety in general. As with other hospital-wide initiatives, engagement of hospital administration is important to decrease barriers to implementation.
Intravenous catheter use will remain an integral part of patient care, but efforts should be made to create standardization around the definition of an idle catheter, standardize units of measure, and institute programs to prevent idle catheters.
Daniel Shirley, MD, MS, is assistant professor in the division of infectious disease at the University of Wisconsin–Madison School of Medicine and Public Health and the William S. Middleton Memorial Veterans Hospital. Nasia Safdar, MD, PhD, is associate professor in the division of infectious disease at the University of Wisconsin–Madison School of Medicine and Public Health and the William S. Middleton Memorial Veterans Hospital.
Seeing the Future of Hospital Medicine
Hospitalists touch the lives of patients and shape health systems’ practices and health policy on a national and international scale according to an editorial titled “The Next 20 Years of Hospital Medicine: Continuing to Foster the Mind, Heart, and Soul of Our Field.”1
“This editorial was my reflection on the ‘Year of the Hospitalist’ and where I think the field needs to go in terms of its professionalism, patient-centeredness, and science,” says author Andrew D. Auerbach, MD, MPH, SFHM, who has worked as a hospitalist for more than 20 years. “We’ve grown extraordinarily fast, but some important aspects of our work need to be fleshed out.”
One example: Hospital medicine has been growing research capacity at a rate that is slower than the field overall, a problem due in part to funding limitations for fellowships and early-career awards, which has restricted the pipeline of young researchers. “Slow growth may also be a result of an emphasis on health systems rather than diseases,” Dr. Auerbach says.
Dr. Auerbach also is concerned about making sure the field of hospital medicine is attractive and sustainable as a career.
“A large amount of burnout can be attributed to things like EHRs, billing, etc., that are real dissatisfiers, but another broad area is in reconnecting with our professional/personal reasons for becoming physicians,” he says. “That needs to be reinvigorated. I also feel very strongly that we need to develop our own research agenda and grow research networks, but even those will need to be reconnected to patient needs more directly.”
Reference
- Auerbach AD. The next 20 years of hospital medicine: continuing to foster the mind, heart, and soul of our field [published online ahead of print July 4, 2016]. J Hosp Med. doi:10.1002/jhm.2631.
Hospitalists touch the lives of patients and shape health systems’ practices and health policy on a national and international scale according to an editorial titled “The Next 20 Years of Hospital Medicine: Continuing to Foster the Mind, Heart, and Soul of Our Field.”1
“This editorial was my reflection on the ‘Year of the Hospitalist’ and where I think the field needs to go in terms of its professionalism, patient-centeredness, and science,” says author Andrew D. Auerbach, MD, MPH, SFHM, who has worked as a hospitalist for more than 20 years. “We’ve grown extraordinarily fast, but some important aspects of our work need to be fleshed out.”
One example: Hospital medicine has been growing research capacity at a rate that is slower than the field overall, a problem due in part to funding limitations for fellowships and early-career awards, which has restricted the pipeline of young researchers. “Slow growth may also be a result of an emphasis on health systems rather than diseases,” Dr. Auerbach says.
Dr. Auerbach also is concerned about making sure the field of hospital medicine is attractive and sustainable as a career.
“A large amount of burnout can be attributed to things like EHRs, billing, etc., that are real dissatisfiers, but another broad area is in reconnecting with our professional/personal reasons for becoming physicians,” he says. “That needs to be reinvigorated. I also feel very strongly that we need to develop our own research agenda and grow research networks, but even those will need to be reconnected to patient needs more directly.”
Reference
- Auerbach AD. The next 20 years of hospital medicine: continuing to foster the mind, heart, and soul of our field [published online ahead of print July 4, 2016]. J Hosp Med. doi:10.1002/jhm.2631.
Hospitalists touch the lives of patients and shape health systems’ practices and health policy on a national and international scale according to an editorial titled “The Next 20 Years of Hospital Medicine: Continuing to Foster the Mind, Heart, and Soul of Our Field.”1
“This editorial was my reflection on the ‘Year of the Hospitalist’ and where I think the field needs to go in terms of its professionalism, patient-centeredness, and science,” says author Andrew D. Auerbach, MD, MPH, SFHM, who has worked as a hospitalist for more than 20 years. “We’ve grown extraordinarily fast, but some important aspects of our work need to be fleshed out.”
One example: Hospital medicine has been growing research capacity at a rate that is slower than the field overall, a problem due in part to funding limitations for fellowships and early-career awards, which has restricted the pipeline of young researchers. “Slow growth may also be a result of an emphasis on health systems rather than diseases,” Dr. Auerbach says.
Dr. Auerbach also is concerned about making sure the field of hospital medicine is attractive and sustainable as a career.
“A large amount of burnout can be attributed to things like EHRs, billing, etc., that are real dissatisfiers, but another broad area is in reconnecting with our professional/personal reasons for becoming physicians,” he says. “That needs to be reinvigorated. I also feel very strongly that we need to develop our own research agenda and grow research networks, but even those will need to be reconnected to patient needs more directly.”
Reference
- Auerbach AD. The next 20 years of hospital medicine: continuing to foster the mind, heart, and soul of our field [published online ahead of print July 4, 2016]. J Hosp Med. doi:10.1002/jhm.2631.
Promoting the Health of Healthcare Employees
Provisions in the Affordable Care Act (ACA) encourage hospitals to work with their communities to improve population health. Like so many things, these efforts can and should begin at home—in this case, the hospital itself. Health and wellness programs for healthcare workers need to be emphasized, according to “Health and Wellness Programs for Hospital Employees: Results from a 2015 American Hospital Association Survey.”1
Such efforts allow healthcare workers to lead by example.
“To help create a culture of health, hospitals and health systems can provide leadership, and hospital employees can be role models, for health and wellness in their communities,” according to the report. “Developing health and wellness strategies and programs at hospitals will help establish an environment that provides the support, resources, and incentives for hospital employees to serve as such role models.”
Developing health and wellness programs can also help hospitals achieve the public health goals of the Healthy People 2020 initiative from the Office of Disease Prevention and Health Promotion.
To find out how hospitals are doing in this work, the 26-question survey was done in 2010 and again in 2015 and sent to approximately 6,000 hospitals in the United States. Response rate was 15% in 2010 and 18% in 2015. Some of the findings include:
- About the same number of hospitals have a health and wellness program or other initiative(s) for employees (86% in 2010 and 87% in 2015); however, the types of health and wellness programs and benefits that hospitals offer to their employees increased.
- The number of hospitals with 70% to 90% or more of employees participating in health and wellness programs increased from 19% in 2010 to 31% in 2015.
- The number of hospitals offering health and wellness programs to people in the community increased from 19% in 2010 to 66% in 2015.
- The number of hospitals offering incentives for participating in health and wellness programs increased as did the value of incentives, with more hospitals giving $500 or more to employees (7% in 2010 and 29% in 2015).
Reference
- Health Research & Educational Trust. Health and wellness programs for hospital employees: results from a 2015 American Hospital Association survey. Hospitals in Pursuit of Excellence website.
Provisions in the Affordable Care Act (ACA) encourage hospitals to work with their communities to improve population health. Like so many things, these efforts can and should begin at home—in this case, the hospital itself. Health and wellness programs for healthcare workers need to be emphasized, according to “Health and Wellness Programs for Hospital Employees: Results from a 2015 American Hospital Association Survey.”1
Such efforts allow healthcare workers to lead by example.
“To help create a culture of health, hospitals and health systems can provide leadership, and hospital employees can be role models, for health and wellness in their communities,” according to the report. “Developing health and wellness strategies and programs at hospitals will help establish an environment that provides the support, resources, and incentives for hospital employees to serve as such role models.”
Developing health and wellness programs can also help hospitals achieve the public health goals of the Healthy People 2020 initiative from the Office of Disease Prevention and Health Promotion.
To find out how hospitals are doing in this work, the 26-question survey was done in 2010 and again in 2015 and sent to approximately 6,000 hospitals in the United States. Response rate was 15% in 2010 and 18% in 2015. Some of the findings include:
- About the same number of hospitals have a health and wellness program or other initiative(s) for employees (86% in 2010 and 87% in 2015); however, the types of health and wellness programs and benefits that hospitals offer to their employees increased.
- The number of hospitals with 70% to 90% or more of employees participating in health and wellness programs increased from 19% in 2010 to 31% in 2015.
- The number of hospitals offering health and wellness programs to people in the community increased from 19% in 2010 to 66% in 2015.
- The number of hospitals offering incentives for participating in health and wellness programs increased as did the value of incentives, with more hospitals giving $500 or more to employees (7% in 2010 and 29% in 2015).
Reference
- Health Research & Educational Trust. Health and wellness programs for hospital employees: results from a 2015 American Hospital Association survey. Hospitals in Pursuit of Excellence website.
Provisions in the Affordable Care Act (ACA) encourage hospitals to work with their communities to improve population health. Like so many things, these efforts can and should begin at home—in this case, the hospital itself. Health and wellness programs for healthcare workers need to be emphasized, according to “Health and Wellness Programs for Hospital Employees: Results from a 2015 American Hospital Association Survey.”1
Such efforts allow healthcare workers to lead by example.
“To help create a culture of health, hospitals and health systems can provide leadership, and hospital employees can be role models, for health and wellness in their communities,” according to the report. “Developing health and wellness strategies and programs at hospitals will help establish an environment that provides the support, resources, and incentives for hospital employees to serve as such role models.”
Developing health and wellness programs can also help hospitals achieve the public health goals of the Healthy People 2020 initiative from the Office of Disease Prevention and Health Promotion.
To find out how hospitals are doing in this work, the 26-question survey was done in 2010 and again in 2015 and sent to approximately 6,000 hospitals in the United States. Response rate was 15% in 2010 and 18% in 2015. Some of the findings include:
- About the same number of hospitals have a health and wellness program or other initiative(s) for employees (86% in 2010 and 87% in 2015); however, the types of health and wellness programs and benefits that hospitals offer to their employees increased.
- The number of hospitals with 70% to 90% or more of employees participating in health and wellness programs increased from 19% in 2010 to 31% in 2015.
- The number of hospitals offering health and wellness programs to people in the community increased from 19% in 2010 to 66% in 2015.
- The number of hospitals offering incentives for participating in health and wellness programs increased as did the value of incentives, with more hospitals giving $500 or more to employees (7% in 2010 and 29% in 2015).
Reference
- Health Research & Educational Trust. Health and wellness programs for hospital employees: results from a 2015 American Hospital Association survey. Hospitals in Pursuit of Excellence website.
Republicans Envision Their Healthcare Plan for the Future
On November 8, 2016, the fate of the Affordable Care Act (ACA) was all but sealed.
In a sweep of the legislative branch, Republicans maintained majorities in the House and Senate, and Donald Trump became the 45th president, running on the popular Republican refrain to “repeal and replace Obamacare.”
“Now, the real onus is going to be on them if they do move to repeal it in its entirety,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee. “It’s going to be a real burden to replace it with something meaningful and not something that’s recycled from six or eight years ago when the conversation first started.”
In the days following the election, President-elect Trump appeared to be backing off his campaign promises to repeal President Barack Obama’s landmark health reform law, acknowledging that at least some of its provisions should remain intact, including maintaining the ban on insurance companies denying coverage based on preexisting conditions and allowing dependent children to remain on their parents’ health insurance until age 26.
These ideas are also part of House Majority Leader Paul Ryan’s healthcare plan, called A Better Way. However, at least on the campaign trail, Trump and GOP leaders like Rep. Ryan did not see eye-to-eye on all aspects of health reform, including how to deal with Medicare and on issues of pharmaceutical regulation, leaving uncertainty over which platforms will be adopted.
What Comes Next?
“There is a lot of rhetoric out there and a lot of promises to replace the Affordable Care Act, which clearly is an important objective for Republicans, but as sort of a consolation, as [health economist] Stuart Altman used to say before the Affordable Care Act was passed, ‘Everybody’s number-one choice is universal health reform the way they want it, and the second is the status quo,’” says Sherry Glied, MA, PhD, health policy expert and dean of New York University’s Robert F. Wagner Graduate School of Public Service.
But the status quo is no longer an option. Passage of the ACA was driven by high healthcare costs in the U.S. and, in part, around access to coverage. Healthcare spending slowed after passage of the ACA, and while it cannot be fully attributed to the law, cost remains an issue.
The Congressional Budget Office (CBO) estimates that repeal of the ACA would increase the federal deficit by $137 billion to $353 billion between 2016 and 2025, growing even more after 2025.1 And without a mechanism to cover the 20 million people who have gained coverage through Medicaid expansion and private insurance coverage on state exchanges, scores of people could rejoin the ranks of the uninsured.
A Series of Small Cuts
“Whatever system replaces it, don’t expect in Trump’s first week in office Congress will hand him a bill to repeal and replace Obamacare. They’ve tried to do that a number of times in the past, and what they’ve come up with has been a little lackluster. And that’s being generous,” says Dr. Lenchus, who overall supports President-elect Trump’s economic plans and is optimistic about what they could mean for health reform.
Most likely, the ACA will not be repealed in “one fell swoop,” says Glied, who also served under President Obama in the Department of Health and Human Services from 2010 to 2012 and was a senior economist for health care and labor market policy under Presidents George H.W. Bush and Bill Clinton. Rather, lawmakers are likely faced with having to “demolish it through a series of small cuts.”
What that will look like remains unknown. To fully repeal the ACA, Republicans would need 60 filibuster-proof votes in the Senate. However, Republicans have just 51 seats to the Democrats’ 45 after the GOP lost two seats in the November election.
House Republicans can push through a bill using a legislative maneuver called reconciliation, but it requires a majority vote in both chambers and would be restricted to changes that have an impact on the federal budget. At a minimum, Republicans would need a budget before they could attempt this strategy.
They achieved this in late 2015, drafting a bill (H.R. 3762) that would have eliminated Medicaid expansion and the subsidies that currently help 83% of enrollees on the ACA exchange afford their premiums. President Obama vetoed the bill; President-elect Trump is unlikely to do the same.
However, he and Republican party leaders must first come to agreement over what their version of health reform should look like. In general, Republicans have called for a healthcare system rooted in the free market, with more individual responsibility, less regulation, and more flexibility.
For instance, Rep. Ryan’s planwould restrict insurers from denying patients with preexisting conditions but only if individuals maintain continuous coverage, with a one-time open-enrollment opportunity.
Campaign Promises Versus President-Elect Promises
While campaigning, President-elect Trump proposed a seven-point plan that included lifting restrictions on tax-free health savings accounts, providing tax deductions for health insurance premiums, allowing the sale of health insurance across state lines, requiring physicians and hospitals to be transparent about pricing, and eliminating the individual mandate to purchase health insurance. He also proposed converting Medicaid into block grants to states and vowed not to change Medicare.
As president-elect, he has pledged, with few details, to challenge abortion access, further research and development, provide “flexibility” to Medicaid, “modernize” Medicare, and reestablish high-risk pools for sick patients with traditionally high premiums. 1 The ACA does not currently allow insurers to charge sick patients higher rates than healthy ones.
While block grants are one option for attempting to control costs in Medicaid by providing states a fixed sum to administer the entitlement program, Rep. Ryan’s plan calls for another option: per-capita limits on enrollees on Medicaid. He has not detailed what those limits would be. What will happen in states that expanded Medicaid through the ACA relative to those that did not is also unknown.
“Frankly, I think that what this election showed is a complete disdain for the general establishment,” says Dr. Lenchus. “If they do give money to state legislatures, I don’t know if I trust them any more to manage that money than the feds, where they could be robbing that block grant for general revenue.”
While President-elect Trump has not yet provided more information about his plans for Medicare, Republicans in the past, including Rep. Ryan, have proposed offering premium support to beneficiaries (sometimes called a voucher or defined contribution), a fixed sum given to Medicare participants to use toward premiums under traditional Medicare or Medicare Advantage plans.
While this could reduce beneficiaries’ out-of-pocket costs, according to the CBO, spending could also increase and beneficiaries may pay variable out-of-pocket costs. Direct spending, meanwhile, would increase by $879 billion over the next decade if all the ACA and its changes to Medicare are eliminated, hastening depletion of the Medicare trust fund.2
“Frankly, I would not be opposed to seeing a sort of sliding scale for Medicare,” says Dr. Lenchus. “If you’re Warren Buffet taking $150 a month for Medicare, do you need to do that? That $150 spread to three other people who are barely making ends meet could make the difference for them taking a lifesaving medication that month.”
Day-to-Day Medicine
What should and will likely be maintained, both Glied and Dr. Lenchus say, are changes to the delivery of and payment models for healthcare. Medicine has been moving toward higher-quality care and away from fee-for-service for years, and “everybody would agree that’s probably not the correct incentive in medicine,” Dr. Lenchus adds.
With a shift toward more state-level responsibility, Glied says the GOP may also encourage states to innovate around healthcare so long as costs are well-managed. Incidentally, under the ACA, 2017 marks the start of Section 1332 waivers, which provide structure for states to develop their own approaches to healthcare.
However, “changes in the practice of medicine are not going to come out of government,” Glied says. “They’re going to come out of improvements in health IT technology, through changes in the use of midlevel professionals who eventually slide into practice as new residents come out of training.”
Though the election all but guaranteed continued uncertainty moving forward, Dr. Lenchus does not believe it will mean much change in his day-to-day practice of medicine. His safety-net hospital, however, may see an uptick in uncompensated care once more while also trying to survive with cuts to reimbursement made through the ACA.
““I don’t think anyone’s getting the hospitals back that money,” Glied says.
The experts say Congress has its work cut out, particularly as it shapes the future of healthcare in the U.S. based on conservative principles while also taking into account the potential number of newly uninsured patients upon repeal of the ACA.
“The problem is people don’t have coverage because they don’t have money. … Healthcare is expensive, and people are poor,” says Glied. “There is a lots of space to move left in healthcare. It’s hard to see where it can move right.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- President Elect Donald J. Trump. https://www.greatagain.gov/policy/healthcare.html
Accessed November 22, 2016
- Budgetary and economic effects of repealing the Affordable Care Act. Congressional Budget Office website. Accessed November 15, 2016.
On November 8, 2016, the fate of the Affordable Care Act (ACA) was all but sealed.
In a sweep of the legislative branch, Republicans maintained majorities in the House and Senate, and Donald Trump became the 45th president, running on the popular Republican refrain to “repeal and replace Obamacare.”
“Now, the real onus is going to be on them if they do move to repeal it in its entirety,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee. “It’s going to be a real burden to replace it with something meaningful and not something that’s recycled from six or eight years ago when the conversation first started.”
In the days following the election, President-elect Trump appeared to be backing off his campaign promises to repeal President Barack Obama’s landmark health reform law, acknowledging that at least some of its provisions should remain intact, including maintaining the ban on insurance companies denying coverage based on preexisting conditions and allowing dependent children to remain on their parents’ health insurance until age 26.
These ideas are also part of House Majority Leader Paul Ryan’s healthcare plan, called A Better Way. However, at least on the campaign trail, Trump and GOP leaders like Rep. Ryan did not see eye-to-eye on all aspects of health reform, including how to deal with Medicare and on issues of pharmaceutical regulation, leaving uncertainty over which platforms will be adopted.
What Comes Next?
“There is a lot of rhetoric out there and a lot of promises to replace the Affordable Care Act, which clearly is an important objective for Republicans, but as sort of a consolation, as [health economist] Stuart Altman used to say before the Affordable Care Act was passed, ‘Everybody’s number-one choice is universal health reform the way they want it, and the second is the status quo,’” says Sherry Glied, MA, PhD, health policy expert and dean of New York University’s Robert F. Wagner Graduate School of Public Service.
But the status quo is no longer an option. Passage of the ACA was driven by high healthcare costs in the U.S. and, in part, around access to coverage. Healthcare spending slowed after passage of the ACA, and while it cannot be fully attributed to the law, cost remains an issue.
The Congressional Budget Office (CBO) estimates that repeal of the ACA would increase the federal deficit by $137 billion to $353 billion between 2016 and 2025, growing even more after 2025.1 And without a mechanism to cover the 20 million people who have gained coverage through Medicaid expansion and private insurance coverage on state exchanges, scores of people could rejoin the ranks of the uninsured.
A Series of Small Cuts
“Whatever system replaces it, don’t expect in Trump’s first week in office Congress will hand him a bill to repeal and replace Obamacare. They’ve tried to do that a number of times in the past, and what they’ve come up with has been a little lackluster. And that’s being generous,” says Dr. Lenchus, who overall supports President-elect Trump’s economic plans and is optimistic about what they could mean for health reform.
Most likely, the ACA will not be repealed in “one fell swoop,” says Glied, who also served under President Obama in the Department of Health and Human Services from 2010 to 2012 and was a senior economist for health care and labor market policy under Presidents George H.W. Bush and Bill Clinton. Rather, lawmakers are likely faced with having to “demolish it through a series of small cuts.”
What that will look like remains unknown. To fully repeal the ACA, Republicans would need 60 filibuster-proof votes in the Senate. However, Republicans have just 51 seats to the Democrats’ 45 after the GOP lost two seats in the November election.
House Republicans can push through a bill using a legislative maneuver called reconciliation, but it requires a majority vote in both chambers and would be restricted to changes that have an impact on the federal budget. At a minimum, Republicans would need a budget before they could attempt this strategy.
They achieved this in late 2015, drafting a bill (H.R. 3762) that would have eliminated Medicaid expansion and the subsidies that currently help 83% of enrollees on the ACA exchange afford their premiums. President Obama vetoed the bill; President-elect Trump is unlikely to do the same.
However, he and Republican party leaders must first come to agreement over what their version of health reform should look like. In general, Republicans have called for a healthcare system rooted in the free market, with more individual responsibility, less regulation, and more flexibility.
For instance, Rep. Ryan’s planwould restrict insurers from denying patients with preexisting conditions but only if individuals maintain continuous coverage, with a one-time open-enrollment opportunity.
Campaign Promises Versus President-Elect Promises
While campaigning, President-elect Trump proposed a seven-point plan that included lifting restrictions on tax-free health savings accounts, providing tax deductions for health insurance premiums, allowing the sale of health insurance across state lines, requiring physicians and hospitals to be transparent about pricing, and eliminating the individual mandate to purchase health insurance. He also proposed converting Medicaid into block grants to states and vowed not to change Medicare.
As president-elect, he has pledged, with few details, to challenge abortion access, further research and development, provide “flexibility” to Medicaid, “modernize” Medicare, and reestablish high-risk pools for sick patients with traditionally high premiums. 1 The ACA does not currently allow insurers to charge sick patients higher rates than healthy ones.
While block grants are one option for attempting to control costs in Medicaid by providing states a fixed sum to administer the entitlement program, Rep. Ryan’s plan calls for another option: per-capita limits on enrollees on Medicaid. He has not detailed what those limits would be. What will happen in states that expanded Medicaid through the ACA relative to those that did not is also unknown.
“Frankly, I think that what this election showed is a complete disdain for the general establishment,” says Dr. Lenchus. “If they do give money to state legislatures, I don’t know if I trust them any more to manage that money than the feds, where they could be robbing that block grant for general revenue.”
While President-elect Trump has not yet provided more information about his plans for Medicare, Republicans in the past, including Rep. Ryan, have proposed offering premium support to beneficiaries (sometimes called a voucher or defined contribution), a fixed sum given to Medicare participants to use toward premiums under traditional Medicare or Medicare Advantage plans.
While this could reduce beneficiaries’ out-of-pocket costs, according to the CBO, spending could also increase and beneficiaries may pay variable out-of-pocket costs. Direct spending, meanwhile, would increase by $879 billion over the next decade if all the ACA and its changes to Medicare are eliminated, hastening depletion of the Medicare trust fund.2
“Frankly, I would not be opposed to seeing a sort of sliding scale for Medicare,” says Dr. Lenchus. “If you’re Warren Buffet taking $150 a month for Medicare, do you need to do that? That $150 spread to three other people who are barely making ends meet could make the difference for them taking a lifesaving medication that month.”
Day-to-Day Medicine
What should and will likely be maintained, both Glied and Dr. Lenchus say, are changes to the delivery of and payment models for healthcare. Medicine has been moving toward higher-quality care and away from fee-for-service for years, and “everybody would agree that’s probably not the correct incentive in medicine,” Dr. Lenchus adds.
With a shift toward more state-level responsibility, Glied says the GOP may also encourage states to innovate around healthcare so long as costs are well-managed. Incidentally, under the ACA, 2017 marks the start of Section 1332 waivers, which provide structure for states to develop their own approaches to healthcare.
However, “changes in the practice of medicine are not going to come out of government,” Glied says. “They’re going to come out of improvements in health IT technology, through changes in the use of midlevel professionals who eventually slide into practice as new residents come out of training.”
Though the election all but guaranteed continued uncertainty moving forward, Dr. Lenchus does not believe it will mean much change in his day-to-day practice of medicine. His safety-net hospital, however, may see an uptick in uncompensated care once more while also trying to survive with cuts to reimbursement made through the ACA.
““I don’t think anyone’s getting the hospitals back that money,” Glied says.
The experts say Congress has its work cut out, particularly as it shapes the future of healthcare in the U.S. based on conservative principles while also taking into account the potential number of newly uninsured patients upon repeal of the ACA.
“The problem is people don’t have coverage because they don’t have money. … Healthcare is expensive, and people are poor,” says Glied. “There is a lots of space to move left in healthcare. It’s hard to see where it can move right.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- President Elect Donald J. Trump. https://www.greatagain.gov/policy/healthcare.html
Accessed November 22, 2016
- Budgetary and economic effects of repealing the Affordable Care Act. Congressional Budget Office website. Accessed November 15, 2016.
On November 8, 2016, the fate of the Affordable Care Act (ACA) was all but sealed.
In a sweep of the legislative branch, Republicans maintained majorities in the House and Senate, and Donald Trump became the 45th president, running on the popular Republican refrain to “repeal and replace Obamacare.”
“Now, the real onus is going to be on them if they do move to repeal it in its entirety,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee. “It’s going to be a real burden to replace it with something meaningful and not something that’s recycled from six or eight years ago when the conversation first started.”
In the days following the election, President-elect Trump appeared to be backing off his campaign promises to repeal President Barack Obama’s landmark health reform law, acknowledging that at least some of its provisions should remain intact, including maintaining the ban on insurance companies denying coverage based on preexisting conditions and allowing dependent children to remain on their parents’ health insurance until age 26.
These ideas are also part of House Majority Leader Paul Ryan’s healthcare plan, called A Better Way. However, at least on the campaign trail, Trump and GOP leaders like Rep. Ryan did not see eye-to-eye on all aspects of health reform, including how to deal with Medicare and on issues of pharmaceutical regulation, leaving uncertainty over which platforms will be adopted.
What Comes Next?
“There is a lot of rhetoric out there and a lot of promises to replace the Affordable Care Act, which clearly is an important objective for Republicans, but as sort of a consolation, as [health economist] Stuart Altman used to say before the Affordable Care Act was passed, ‘Everybody’s number-one choice is universal health reform the way they want it, and the second is the status quo,’” says Sherry Glied, MA, PhD, health policy expert and dean of New York University’s Robert F. Wagner Graduate School of Public Service.
But the status quo is no longer an option. Passage of the ACA was driven by high healthcare costs in the U.S. and, in part, around access to coverage. Healthcare spending slowed after passage of the ACA, and while it cannot be fully attributed to the law, cost remains an issue.
The Congressional Budget Office (CBO) estimates that repeal of the ACA would increase the federal deficit by $137 billion to $353 billion between 2016 and 2025, growing even more after 2025.1 And without a mechanism to cover the 20 million people who have gained coverage through Medicaid expansion and private insurance coverage on state exchanges, scores of people could rejoin the ranks of the uninsured.
A Series of Small Cuts
“Whatever system replaces it, don’t expect in Trump’s first week in office Congress will hand him a bill to repeal and replace Obamacare. They’ve tried to do that a number of times in the past, and what they’ve come up with has been a little lackluster. And that’s being generous,” says Dr. Lenchus, who overall supports President-elect Trump’s economic plans and is optimistic about what they could mean for health reform.
Most likely, the ACA will not be repealed in “one fell swoop,” says Glied, who also served under President Obama in the Department of Health and Human Services from 2010 to 2012 and was a senior economist for health care and labor market policy under Presidents George H.W. Bush and Bill Clinton. Rather, lawmakers are likely faced with having to “demolish it through a series of small cuts.”
What that will look like remains unknown. To fully repeal the ACA, Republicans would need 60 filibuster-proof votes in the Senate. However, Republicans have just 51 seats to the Democrats’ 45 after the GOP lost two seats in the November election.
House Republicans can push through a bill using a legislative maneuver called reconciliation, but it requires a majority vote in both chambers and would be restricted to changes that have an impact on the federal budget. At a minimum, Republicans would need a budget before they could attempt this strategy.
They achieved this in late 2015, drafting a bill (H.R. 3762) that would have eliminated Medicaid expansion and the subsidies that currently help 83% of enrollees on the ACA exchange afford their premiums. President Obama vetoed the bill; President-elect Trump is unlikely to do the same.
However, he and Republican party leaders must first come to agreement over what their version of health reform should look like. In general, Republicans have called for a healthcare system rooted in the free market, with more individual responsibility, less regulation, and more flexibility.
For instance, Rep. Ryan’s planwould restrict insurers from denying patients with preexisting conditions but only if individuals maintain continuous coverage, with a one-time open-enrollment opportunity.
Campaign Promises Versus President-Elect Promises
While campaigning, President-elect Trump proposed a seven-point plan that included lifting restrictions on tax-free health savings accounts, providing tax deductions for health insurance premiums, allowing the sale of health insurance across state lines, requiring physicians and hospitals to be transparent about pricing, and eliminating the individual mandate to purchase health insurance. He also proposed converting Medicaid into block grants to states and vowed not to change Medicare.
As president-elect, he has pledged, with few details, to challenge abortion access, further research and development, provide “flexibility” to Medicaid, “modernize” Medicare, and reestablish high-risk pools for sick patients with traditionally high premiums. 1 The ACA does not currently allow insurers to charge sick patients higher rates than healthy ones.
While block grants are one option for attempting to control costs in Medicaid by providing states a fixed sum to administer the entitlement program, Rep. Ryan’s plan calls for another option: per-capita limits on enrollees on Medicaid. He has not detailed what those limits would be. What will happen in states that expanded Medicaid through the ACA relative to those that did not is also unknown.
“Frankly, I think that what this election showed is a complete disdain for the general establishment,” says Dr. Lenchus. “If they do give money to state legislatures, I don’t know if I trust them any more to manage that money than the feds, where they could be robbing that block grant for general revenue.”
While President-elect Trump has not yet provided more information about his plans for Medicare, Republicans in the past, including Rep. Ryan, have proposed offering premium support to beneficiaries (sometimes called a voucher or defined contribution), a fixed sum given to Medicare participants to use toward premiums under traditional Medicare or Medicare Advantage plans.
While this could reduce beneficiaries’ out-of-pocket costs, according to the CBO, spending could also increase and beneficiaries may pay variable out-of-pocket costs. Direct spending, meanwhile, would increase by $879 billion over the next decade if all the ACA and its changes to Medicare are eliminated, hastening depletion of the Medicare trust fund.2
“Frankly, I would not be opposed to seeing a sort of sliding scale for Medicare,” says Dr. Lenchus. “If you’re Warren Buffet taking $150 a month for Medicare, do you need to do that? That $150 spread to three other people who are barely making ends meet could make the difference for them taking a lifesaving medication that month.”
Day-to-Day Medicine
What should and will likely be maintained, both Glied and Dr. Lenchus say, are changes to the delivery of and payment models for healthcare. Medicine has been moving toward higher-quality care and away from fee-for-service for years, and “everybody would agree that’s probably not the correct incentive in medicine,” Dr. Lenchus adds.
With a shift toward more state-level responsibility, Glied says the GOP may also encourage states to innovate around healthcare so long as costs are well-managed. Incidentally, under the ACA, 2017 marks the start of Section 1332 waivers, which provide structure for states to develop their own approaches to healthcare.
However, “changes in the practice of medicine are not going to come out of government,” Glied says. “They’re going to come out of improvements in health IT technology, through changes in the use of midlevel professionals who eventually slide into practice as new residents come out of training.”
Though the election all but guaranteed continued uncertainty moving forward, Dr. Lenchus does not believe it will mean much change in his day-to-day practice of medicine. His safety-net hospital, however, may see an uptick in uncompensated care once more while also trying to survive with cuts to reimbursement made through the ACA.
““I don’t think anyone’s getting the hospitals back that money,” Glied says.
The experts say Congress has its work cut out, particularly as it shapes the future of healthcare in the U.S. based on conservative principles while also taking into account the potential number of newly uninsured patients upon repeal of the ACA.
“The problem is people don’t have coverage because they don’t have money. … Healthcare is expensive, and people are poor,” says Glied. “There is a lots of space to move left in healthcare. It’s hard to see where it can move right.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- President Elect Donald J. Trump. https://www.greatagain.gov/policy/healthcare.html
Accessed November 22, 2016
- Budgetary and economic effects of repealing the Affordable Care Act. Congressional Budget Office website. Accessed November 15, 2016.
Trump administration to focus on ACA reform, tort reform
Look for three things from the Trump administration: significant changes to the Affordable Care Act, few changes to MACRA’s Quality Payment Program, and a conservative swing in the courts.
Republicans have had their sights on the Affordable Care Act since its passage in 2010; with majorities in both the House and the Senate, the question is not if, but when President Obama’s signature piece of legislation will be dismantled.
President-elect Donald Trump ran on the promise of ACA repeal. Health policy priorities on his transition website focus on greater use of health savings accounts, the ability to purchase insurance across state lines, and the reestablishment of high-risk pools.
Health policy experts differ in how they see ACA reform coming about, with some predicting a quick repeal coupled with an immediate legislative replacement, while others envision repeal with more time to craft replacement legislation. Reform also could come as a series of smaller bills rather than one comprehensive package.
Using budget reconciliation would not allow for full ACA repeal since only provisions that involve revenue generation or spending could be altered. However, since budget reconciliation bills cannot be filibustered, only a simple majority is needed for Senate passage. With their razor-thin majority – 51 seats – Republicans will need some support from outside of their own party.
“Twenty-some Democrats, many in very-deep ‘red states’ including North Dakota, are up for reelection in 2018,” Ms. Turner said. “They saw what happened to the candidates who supported Obamacare in 2016 – many of them went down. It happened with Evan Bayh in Indiana, who was running again to reclaim the Senate seat he left in 2010. And the Republican candidate [Todd Young] reminded the voters over and over that Evan Bayh voted for Obamacare. Same thing happened in Wisconsin with [Republican] Sen. Ron Johnson being challenged by Russ Feingold, who also was in the Senate when Obamacare passed. Feingold went down to defeat again. I think the lot of Democratic senators are going to be looking at what happened to those people and think ‘Maybe I better participate in coming up with a more sensible solution.’ ”
More importantly, the GOP may be looking for bipartisan support, especially since the ACA passed on a strict party-line vote. To that end, it could make more sense to delay reform efforts until a broader coalition can be formed and simultaneous repeal/replace package could be brought to both the House and the Senate floors.

In the new Congress, Senate Republicans might face some of the same obstructionist tactics they used during the Obama administration, which could complicate efforts to get bipartisan support.
“When you have people like Sen. [Bernie] Sanders (I-Vt.) and Sen. [Elizabeth] Warren (D-Mass.) saying they are going to adapt a scorched earth approach going forward, they and their followers don’t have any intention of doing anything that would in any way appear to cooperate with the Republicans,” Dr. Wilensky said. “Of course, there are other Democrats, especially some of the ones who will be up in 2018, who might not be quite so adamant.”

“Repeal without a clear idea of what the replacement would be would really throw that market into chaos, where right now we are at a place where the markets are relatively stable,” Dr. Collins said in an interview.“The best way to think about the ACA, and particularly on the marketplaces and what repeal means, is this image of the three-legged stool. The individual market is the seat and the legs include consumer protections, particularly guaranteed issue; the individual requirement to have insurance; and the subsidies to make that coverage affordable – Medicaid expansion is part of that as well. If you start to remove any one of those legs, the market becomes extremely unstable.”
Repealing the individual mandate is problematic as it goes hand in hand with the ban on coverage denial because of preexisting conditions, something President-elect Trump has signaled he is looking to maintain, Ms. Turner said, adding that free market solutions with appropriate incentives could be a different way to encourage healthy people to get coverage to help generate premium revenue to cover patients with preexisting conditions.
While the ACA will be in the crosshairs, experts expect MACRA to remain more or less intact, maybe with some minor tweaks, at least early on.
While the Medicare Access and CHIP Reauthorization Act of 2015 passed with overwhelming support from both parties, “the [implementing regulations] are just a nightmare and I think the Trump administration is going to have to take a look at them,” Ms. Turner said. She added that physicians are weary of the ever-growing federal administrative hassles. “You do not want doctors to leave private practice in droves, and they are looking at this cost of compliance.”
“I think that [MACRA] is just way too much of an in-the-weeds policy thing for the Trump administration to have addressed yet,” Ms. Turner continued. “But this certainly is going to have to be on the agenda because they are going to hear from a lot of doctors that this is not acceptable.”

Mr. Trump also has called for Medicaid reform, with block grants to the states.
“Everyone keeps talking about a block grant, but that is a clumsy way of doing it,” Ms. Turner said, suggesting the program be even more refined to cover people in different baskets, including dual-eligibles, healthy adults that were part of the ACA Medicaid expansion, mothers and infants, and disabled individuals. “A capitated allotment [allows the government to provide more support to] the people who need it.”
Dr. Wilensky suggested that the Trump administration could revisit the 1332 waiver process, another provision of the ACA.
“The current administration has taken a very-rigid view on that you have to keep savings from Medicaid and the ACA separate and any changes have to be budget neutral to each, which is an extremely rigid set of requirements,” she said. Instead “Medicaid and ACA savings could count together and it just needs to be budget neutral over a 3- or 5-year period. That would then allow states to come in and request a lot of flexibility that the current administration hasn’t been inclined to give them.”
Likewise, the Children’s Health Insurance Plan (CHIP) is up for reauthorization. While the program remains relatively popular, it could be due for some reforms as well. Dr. Wilensky said it might be time for the program to go away, though doing that would face resistance from congressional Democrats.
Likewise, Ms. Turner suggested it could be time to fold CHIP into another program like Medicaid.
“Does it really make sense for a mother who is overwhelmed, maybe even with two jobs, to have her kids on a different health insurance program than she’s on?” Ms. Turner said. “It just adds to the burden and the paperwork. Would it make more sense to blend some of these programs together, making sure the people get the health coverage they need, but without all these artificial silos that really make it much more difficult for the user at the other end. I think they are going to take a look at that.”
Whether the ACA is amended or repealed may affect some – but not all – of the ACA-related cases lingering in the courts.
Zubik v. Burwell for instance, may become irrelevant if President-elect Trump eliminates the ACA’s birth control mandate or its accommodation clause. Zubik centers on an exception to the birth control mandate for organizations that oppose coverage for contraceptives but are not exempted entities, such as churches. The plaintiffs argue that the government’s opt-out process makes them complicit in offering contraception coverage indirectly.

The Trump administration could choose to broaden the mandate’s exemption to include the religious organizations, thus satisfying the plaintiffs, said Timothy S. Jost, a health law professor at Washington and Lee University in Lexington, Va., who added that the case would become moot if the ACA is repealed wholesale.
“Millions of women [currently] get access to birth control without cost sharing through the Affordable Care Act,” he said in an interview. “That’s an issue [the new administration] is going to have to confront.”
In March, U.S. Supreme Court justices requested that both sides provide new briefs that outlined how contraception could be provided without requiring notice on the part of the suing employers. Then, in light of the briefs, the high court vacated the lower court rulings related to Zubik and remanded the case to the four appeals courts that had originally ruled on the issue.
If the case makes its way back to the Supreme Court, the ultimate ruling will largely depend on the makeup of the court at the time, said Eric D. Fader, a New York–based health law attorney.
“As long as we have a 4-4 Supreme Court, everything is up in the air,” Mr. Fader said in an interview. “As soon as that ninth slot is filled, I think we’re going to see some decisions that are going to be in line with traditional Republican conservative positions.”
However, a set of ACA-related cases that involve payments to insurers will continue litigating, regardless of actions by the new administration, analysts said. A half-dozen health insurers have sued the Health & Human Services department over alleged underpayments under the ACA’s risk corridor program.
“Even if you do away with the ACA, these cases all pertain to conduct that has already occurred, so they’re not going to be automatically moot,” Mr. Fader said in an interview. “They may struggle along for a while.”
The cases stem from the ACA’s risk corridor program, which requires HHS to collect funds from excessively profitable insurers that offer qualified health plans under the exchanges, while paying out funds to QHP insurers that have excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
The plaintiffs allege they’ve been shortchanged and that the government must reimburse them full payments for 2014. The Department of Justice (DOJ) argues the cases are premature because the full amount owed under the program is not due until 2016, after the program runs its course.
The Trump administration may surrender another ACA-linked challenge that questions billions in payments made to insurers, Mr. Jost said in an interview. In House v. Burwell, the House of Representatives accuses HHS of wrongly spending billions to repay insurers for health insurance provided to certain low-income patients under the ACA. The House claims HHS is illegally spending monies that Congress never appropriated. HHS argues that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements. In May, the U.S. District Court for the District of Columbia decided in favor of the House, ruling that Congress never appropriated money for the payments and that no public money can be spent without an appropriation.
There is speculation that the Trump administration may not pursue an appeal, Mr. Jost said. “I think they better think long and hard about that because I don’t know why any president would want court precedent saying one house of Congress can sue the president whenever it disagrees,” he said. “If the Trump administration would give in on the lawsuit or the House would win … there would be some very large losses and some very large premium increases next year. There could be some very significant disruption of insurance markets.”
Again, if the ACA is repealed, the case may become irrelevant, Mr. Fader said. “If you get rid of the ACA and eliminate the cost sharing structure, than House v. Burwell is going to just be moot.”

“We have seen a substantial uptick in antitrust enforcement activity in health care over the last several years,” he said in an interview. “The Trump administration has said that one of its themes is reducing the regulatory burden on businesses. People will be watching to see if that means an attempt to back off of some of the more-aggressive antitrust enforcement activities in health care and other industries.”
The Obama administration is currently fighting to block two mega-mergers among four of the largest health insurers in the nation. The DOJ filed legal challenges earlier this year seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers by limiting price competition, reducing benefits, and lowering quality of care. A majority of physician associations and patient groups oppose the mergers. But experts said the new administration could drop the challenges.
Similarly, the Trump administration could be more lax in its enforcement of the Stark Law. “You could certainly say if the administration is committed to reducing regulatory burden, one thing the administration might push forward is reducing some of the enforcement with respect to technical violations of Stark,” Mr. Horton said, noting that the Senate recently questioned if the government is going too far in regulating physician relationships under Stark. “If your theme is ‘Let’s cut back on regulation,’ that would be an area that you would think the administration would look at.”

Meanwhile, stronger medical malpractice reforms could be on the horizon in light of a Republican-controlled Congress. Tort reform advocates have a good chance at passing federal medical liability reforms that were left out of the ACA’s passage in 2010, said Dennis A. Cardoza, public affairs director and cochair of the federal public affairs practice at a national health law firm.
Earlier versions of the ACA included amendments that mandated lawsuits go through a state or federal alternative dispute resolution system prior to being filed in court. Another provision that failed would have provided federal grants to states that created special health courts for medical malpractice claims. The amendment would have allowed states to create expert panels, administrative health care tribunals, or a combination of the two.
“There’s much stronger support for tort reform among the Republicans in Congress,” Mr. Cardoza said in an interview. “There’s a shot [now]. If the reforms don’t go too far where they would penalize injured patients, I think they could get additional support and be well received by the Congress.”
Tougher abortion restrictions are likely under the Trump administration, experts said. President-elect Trump has said he is committed to nominating a ninth Supreme Court justice who opposes Roe v. Wade.

Vice President-elect Mike Pence, who is considered a strong voice for the religious right, will likely influence who Mr. Trump nominates for the high court, said Rep-elect Raskin, who added that if ever there was time that abortion rights are in jeopardy, it’s now.
“This really puts the Republicans to the test,” he said in an interview. “For decades now, they have been calling for the overruling of Roe v. Wade. The religious right will never forgive them if it doesn’t happen now. [Republicans] control the House, the Senate, and the White House. They have it within their reach to create a five-justice majority on the court.”
[email protected]
[email protected]
On Twitter @legal_med
Look for three things from the Trump administration: significant changes to the Affordable Care Act, few changes to MACRA’s Quality Payment Program, and a conservative swing in the courts.
Republicans have had their sights on the Affordable Care Act since its passage in 2010; with majorities in both the House and the Senate, the question is not if, but when President Obama’s signature piece of legislation will be dismantled.
President-elect Donald Trump ran on the promise of ACA repeal. Health policy priorities on his transition website focus on greater use of health savings accounts, the ability to purchase insurance across state lines, and the reestablishment of high-risk pools.
Health policy experts differ in how they see ACA reform coming about, with some predicting a quick repeal coupled with an immediate legislative replacement, while others envision repeal with more time to craft replacement legislation. Reform also could come as a series of smaller bills rather than one comprehensive package.
Using budget reconciliation would not allow for full ACA repeal since only provisions that involve revenue generation or spending could be altered. However, since budget reconciliation bills cannot be filibustered, only a simple majority is needed for Senate passage. With their razor-thin majority – 51 seats – Republicans will need some support from outside of their own party.
“Twenty-some Democrats, many in very-deep ‘red states’ including North Dakota, are up for reelection in 2018,” Ms. Turner said. “They saw what happened to the candidates who supported Obamacare in 2016 – many of them went down. It happened with Evan Bayh in Indiana, who was running again to reclaim the Senate seat he left in 2010. And the Republican candidate [Todd Young] reminded the voters over and over that Evan Bayh voted for Obamacare. Same thing happened in Wisconsin with [Republican] Sen. Ron Johnson being challenged by Russ Feingold, who also was in the Senate when Obamacare passed. Feingold went down to defeat again. I think the lot of Democratic senators are going to be looking at what happened to those people and think ‘Maybe I better participate in coming up with a more sensible solution.’ ”
More importantly, the GOP may be looking for bipartisan support, especially since the ACA passed on a strict party-line vote. To that end, it could make more sense to delay reform efforts until a broader coalition can be formed and simultaneous repeal/replace package could be brought to both the House and the Senate floors.
In the new Congress, Senate Republicans might face some of the same obstructionist tactics they used during the Obama administration, which could complicate efforts to get bipartisan support.
“When you have people like Sen. [Bernie] Sanders (I-Vt.) and Sen. [Elizabeth] Warren (D-Mass.) saying they are going to adapt a scorched earth approach going forward, they and their followers don’t have any intention of doing anything that would in any way appear to cooperate with the Republicans,” Dr. Wilensky said. “Of course, there are other Democrats, especially some of the ones who will be up in 2018, who might not be quite so adamant.”
“Repeal without a clear idea of what the replacement would be would really throw that market into chaos, where right now we are at a place where the markets are relatively stable,” Dr. Collins said in an interview.“The best way to think about the ACA, and particularly on the marketplaces and what repeal means, is this image of the three-legged stool. The individual market is the seat and the legs include consumer protections, particularly guaranteed issue; the individual requirement to have insurance; and the subsidies to make that coverage affordable – Medicaid expansion is part of that as well. If you start to remove any one of those legs, the market becomes extremely unstable.”
Repealing the individual mandate is problematic as it goes hand in hand with the ban on coverage denial because of preexisting conditions, something President-elect Trump has signaled he is looking to maintain, Ms. Turner said, adding that free market solutions with appropriate incentives could be a different way to encourage healthy people to get coverage to help generate premium revenue to cover patients with preexisting conditions.
While the ACA will be in the crosshairs, experts expect MACRA to remain more or less intact, maybe with some minor tweaks, at least early on.
While the Medicare Access and CHIP Reauthorization Act of 2015 passed with overwhelming support from both parties, “the [implementing regulations] are just a nightmare and I think the Trump administration is going to have to take a look at them,” Ms. Turner said. She added that physicians are weary of the ever-growing federal administrative hassles. “You do not want doctors to leave private practice in droves, and they are looking at this cost of compliance.”
“I think that [MACRA] is just way too much of an in-the-weeds policy thing for the Trump administration to have addressed yet,” Ms. Turner continued. “But this certainly is going to have to be on the agenda because they are going to hear from a lot of doctors that this is not acceptable.”
Mr. Trump also has called for Medicaid reform, with block grants to the states.
“Everyone keeps talking about a block grant, but that is a clumsy way of doing it,” Ms. Turner said, suggesting the program be even more refined to cover people in different baskets, including dual-eligibles, healthy adults that were part of the ACA Medicaid expansion, mothers and infants, and disabled individuals. “A capitated allotment [allows the government to provide more support to] the people who need it.”
Dr. Wilensky suggested that the Trump administration could revisit the 1332 waiver process, another provision of the ACA.
“The current administration has taken a very-rigid view on that you have to keep savings from Medicaid and the ACA separate and any changes have to be budget neutral to each, which is an extremely rigid set of requirements,” she said. Instead “Medicaid and ACA savings could count together and it just needs to be budget neutral over a 3- or 5-year period. That would then allow states to come in and request a lot of flexibility that the current administration hasn’t been inclined to give them.”
Likewise, the Children’s Health Insurance Plan (CHIP) is up for reauthorization. While the program remains relatively popular, it could be due for some reforms as well. Dr. Wilensky said it might be time for the program to go away, though doing that would face resistance from congressional Democrats.
Likewise, Ms. Turner suggested it could be time to fold CHIP into another program like Medicaid.
“Does it really make sense for a mother who is overwhelmed, maybe even with two jobs, to have her kids on a different health insurance program than she’s on?” Ms. Turner said. “It just adds to the burden and the paperwork. Would it make more sense to blend some of these programs together, making sure the people get the health coverage they need, but without all these artificial silos that really make it much more difficult for the user at the other end. I think they are going to take a look at that.”
Whether the ACA is amended or repealed may affect some – but not all – of the ACA-related cases lingering in the courts.
Zubik v. Burwell for instance, may become irrelevant if President-elect Trump eliminates the ACA’s birth control mandate or its accommodation clause. Zubik centers on an exception to the birth control mandate for organizations that oppose coverage for contraceptives but are not exempted entities, such as churches. The plaintiffs argue that the government’s opt-out process makes them complicit in offering contraception coverage indirectly.
The Trump administration could choose to broaden the mandate’s exemption to include the religious organizations, thus satisfying the plaintiffs, said Timothy S. Jost, a health law professor at Washington and Lee University in Lexington, Va., who added that the case would become moot if the ACA is repealed wholesale.
“Millions of women [currently] get access to birth control without cost sharing through the Affordable Care Act,” he said in an interview. “That’s an issue [the new administration] is going to have to confront.”
In March, U.S. Supreme Court justices requested that both sides provide new briefs that outlined how contraception could be provided without requiring notice on the part of the suing employers. Then, in light of the briefs, the high court vacated the lower court rulings related to Zubik and remanded the case to the four appeals courts that had originally ruled on the issue.
If the case makes its way back to the Supreme Court, the ultimate ruling will largely depend on the makeup of the court at the time, said Eric D. Fader, a New York–based health law attorney.
“As long as we have a 4-4 Supreme Court, everything is up in the air,” Mr. Fader said in an interview. “As soon as that ninth slot is filled, I think we’re going to see some decisions that are going to be in line with traditional Republican conservative positions.”
However, a set of ACA-related cases that involve payments to insurers will continue litigating, regardless of actions by the new administration, analysts said. A half-dozen health insurers have sued the Health & Human Services department over alleged underpayments under the ACA’s risk corridor program.
“Even if you do away with the ACA, these cases all pertain to conduct that has already occurred, so they’re not going to be automatically moot,” Mr. Fader said in an interview. “They may struggle along for a while.”
The cases stem from the ACA’s risk corridor program, which requires HHS to collect funds from excessively profitable insurers that offer qualified health plans under the exchanges, while paying out funds to QHP insurers that have excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
The plaintiffs allege they’ve been shortchanged and that the government must reimburse them full payments for 2014. The Department of Justice (DOJ) argues the cases are premature because the full amount owed under the program is not due until 2016, after the program runs its course.
The Trump administration may surrender another ACA-linked challenge that questions billions in payments made to insurers, Mr. Jost said in an interview. In House v. Burwell, the House of Representatives accuses HHS of wrongly spending billions to repay insurers for health insurance provided to certain low-income patients under the ACA. The House claims HHS is illegally spending monies that Congress never appropriated. HHS argues that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements. In May, the U.S. District Court for the District of Columbia decided in favor of the House, ruling that Congress never appropriated money for the payments and that no public money can be spent without an appropriation.
There is speculation that the Trump administration may not pursue an appeal, Mr. Jost said. “I think they better think long and hard about that because I don’t know why any president would want court precedent saying one house of Congress can sue the president whenever it disagrees,” he said. “If the Trump administration would give in on the lawsuit or the House would win … there would be some very large losses and some very large premium increases next year. There could be some very significant disruption of insurance markets.”
Again, if the ACA is repealed, the case may become irrelevant, Mr. Fader said. “If you get rid of the ACA and eliminate the cost sharing structure, than House v. Burwell is going to just be moot.”
“We have seen a substantial uptick in antitrust enforcement activity in health care over the last several years,” he said in an interview. “The Trump administration has said that one of its themes is reducing the regulatory burden on businesses. People will be watching to see if that means an attempt to back off of some of the more-aggressive antitrust enforcement activities in health care and other industries.”
The Obama administration is currently fighting to block two mega-mergers among four of the largest health insurers in the nation. The DOJ filed legal challenges earlier this year seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers by limiting price competition, reducing benefits, and lowering quality of care. A majority of physician associations and patient groups oppose the mergers. But experts said the new administration could drop the challenges.
Similarly, the Trump administration could be more lax in its enforcement of the Stark Law. “You could certainly say if the administration is committed to reducing regulatory burden, one thing the administration might push forward is reducing some of the enforcement with respect to technical violations of Stark,” Mr. Horton said, noting that the Senate recently questioned if the government is going too far in regulating physician relationships under Stark. “If your theme is ‘Let’s cut back on regulation,’ that would be an area that you would think the administration would look at.”
Meanwhile, stronger medical malpractice reforms could be on the horizon in light of a Republican-controlled Congress. Tort reform advocates have a good chance at passing federal medical liability reforms that were left out of the ACA’s passage in 2010, said Dennis A. Cardoza, public affairs director and cochair of the federal public affairs practice at a national health law firm.
Earlier versions of the ACA included amendments that mandated lawsuits go through a state or federal alternative dispute resolution system prior to being filed in court. Another provision that failed would have provided federal grants to states that created special health courts for medical malpractice claims. The amendment would have allowed states to create expert panels, administrative health care tribunals, or a combination of the two.
“There’s much stronger support for tort reform among the Republicans in Congress,” Mr. Cardoza said in an interview. “There’s a shot [now]. If the reforms don’t go too far where they would penalize injured patients, I think they could get additional support and be well received by the Congress.”
Tougher abortion restrictions are likely under the Trump administration, experts said. President-elect Trump has said he is committed to nominating a ninth Supreme Court justice who opposes Roe v. Wade.
Vice President-elect Mike Pence, who is considered a strong voice for the religious right, will likely influence who Mr. Trump nominates for the high court, said Rep-elect Raskin, who added that if ever there was time that abortion rights are in jeopardy, it’s now.
“This really puts the Republicans to the test,” he said in an interview. “For decades now, they have been calling for the overruling of Roe v. Wade. The religious right will never forgive them if it doesn’t happen now. [Republicans] control the House, the Senate, and the White House. They have it within their reach to create a five-justice majority on the court.”
[email protected]
[email protected]
On Twitter @legal_med
Look for three things from the Trump administration: significant changes to the Affordable Care Act, few changes to MACRA’s Quality Payment Program, and a conservative swing in the courts.
Republicans have had their sights on the Affordable Care Act since its passage in 2010; with majorities in both the House and the Senate, the question is not if, but when President Obama’s signature piece of legislation will be dismantled.
President-elect Donald Trump ran on the promise of ACA repeal. Health policy priorities on his transition website focus on greater use of health savings accounts, the ability to purchase insurance across state lines, and the reestablishment of high-risk pools.
Health policy experts differ in how they see ACA reform coming about, with some predicting a quick repeal coupled with an immediate legislative replacement, while others envision repeal with more time to craft replacement legislation. Reform also could come as a series of smaller bills rather than one comprehensive package.
Using budget reconciliation would not allow for full ACA repeal since only provisions that involve revenue generation or spending could be altered. However, since budget reconciliation bills cannot be filibustered, only a simple majority is needed for Senate passage. With their razor-thin majority – 51 seats – Republicans will need some support from outside of their own party.
“Twenty-some Democrats, many in very-deep ‘red states’ including North Dakota, are up for reelection in 2018,” Ms. Turner said. “They saw what happened to the candidates who supported Obamacare in 2016 – many of them went down. It happened with Evan Bayh in Indiana, who was running again to reclaim the Senate seat he left in 2010. And the Republican candidate [Todd Young] reminded the voters over and over that Evan Bayh voted for Obamacare. Same thing happened in Wisconsin with [Republican] Sen. Ron Johnson being challenged by Russ Feingold, who also was in the Senate when Obamacare passed. Feingold went down to defeat again. I think the lot of Democratic senators are going to be looking at what happened to those people and think ‘Maybe I better participate in coming up with a more sensible solution.’ ”
More importantly, the GOP may be looking for bipartisan support, especially since the ACA passed on a strict party-line vote. To that end, it could make more sense to delay reform efforts until a broader coalition can be formed and simultaneous repeal/replace package could be brought to both the House and the Senate floors.
In the new Congress, Senate Republicans might face some of the same obstructionist tactics they used during the Obama administration, which could complicate efforts to get bipartisan support.
“When you have people like Sen. [Bernie] Sanders (I-Vt.) and Sen. [Elizabeth] Warren (D-Mass.) saying they are going to adapt a scorched earth approach going forward, they and their followers don’t have any intention of doing anything that would in any way appear to cooperate with the Republicans,” Dr. Wilensky said. “Of course, there are other Democrats, especially some of the ones who will be up in 2018, who might not be quite so adamant.”
“Repeal without a clear idea of what the replacement would be would really throw that market into chaos, where right now we are at a place where the markets are relatively stable,” Dr. Collins said in an interview.“The best way to think about the ACA, and particularly on the marketplaces and what repeal means, is this image of the three-legged stool. The individual market is the seat and the legs include consumer protections, particularly guaranteed issue; the individual requirement to have insurance; and the subsidies to make that coverage affordable – Medicaid expansion is part of that as well. If you start to remove any one of those legs, the market becomes extremely unstable.”
Repealing the individual mandate is problematic as it goes hand in hand with the ban on coverage denial because of preexisting conditions, something President-elect Trump has signaled he is looking to maintain, Ms. Turner said, adding that free market solutions with appropriate incentives could be a different way to encourage healthy people to get coverage to help generate premium revenue to cover patients with preexisting conditions.
While the ACA will be in the crosshairs, experts expect MACRA to remain more or less intact, maybe with some minor tweaks, at least early on.
While the Medicare Access and CHIP Reauthorization Act of 2015 passed with overwhelming support from both parties, “the [implementing regulations] are just a nightmare and I think the Trump administration is going to have to take a look at them,” Ms. Turner said. She added that physicians are weary of the ever-growing federal administrative hassles. “You do not want doctors to leave private practice in droves, and they are looking at this cost of compliance.”
“I think that [MACRA] is just way too much of an in-the-weeds policy thing for the Trump administration to have addressed yet,” Ms. Turner continued. “But this certainly is going to have to be on the agenda because they are going to hear from a lot of doctors that this is not acceptable.”
Mr. Trump also has called for Medicaid reform, with block grants to the states.
“Everyone keeps talking about a block grant, but that is a clumsy way of doing it,” Ms. Turner said, suggesting the program be even more refined to cover people in different baskets, including dual-eligibles, healthy adults that were part of the ACA Medicaid expansion, mothers and infants, and disabled individuals. “A capitated allotment [allows the government to provide more support to] the people who need it.”
Dr. Wilensky suggested that the Trump administration could revisit the 1332 waiver process, another provision of the ACA.
“The current administration has taken a very-rigid view on that you have to keep savings from Medicaid and the ACA separate and any changes have to be budget neutral to each, which is an extremely rigid set of requirements,” she said. Instead “Medicaid and ACA savings could count together and it just needs to be budget neutral over a 3- or 5-year period. That would then allow states to come in and request a lot of flexibility that the current administration hasn’t been inclined to give them.”
Likewise, the Children’s Health Insurance Plan (CHIP) is up for reauthorization. While the program remains relatively popular, it could be due for some reforms as well. Dr. Wilensky said it might be time for the program to go away, though doing that would face resistance from congressional Democrats.
Likewise, Ms. Turner suggested it could be time to fold CHIP into another program like Medicaid.
“Does it really make sense for a mother who is overwhelmed, maybe even with two jobs, to have her kids on a different health insurance program than she’s on?” Ms. Turner said. “It just adds to the burden and the paperwork. Would it make more sense to blend some of these programs together, making sure the people get the health coverage they need, but without all these artificial silos that really make it much more difficult for the user at the other end. I think they are going to take a look at that.”
Whether the ACA is amended or repealed may affect some – but not all – of the ACA-related cases lingering in the courts.
Zubik v. Burwell for instance, may become irrelevant if President-elect Trump eliminates the ACA’s birth control mandate or its accommodation clause. Zubik centers on an exception to the birth control mandate for organizations that oppose coverage for contraceptives but are not exempted entities, such as churches. The plaintiffs argue that the government’s opt-out process makes them complicit in offering contraception coverage indirectly.
The Trump administration could choose to broaden the mandate’s exemption to include the religious organizations, thus satisfying the plaintiffs, said Timothy S. Jost, a health law professor at Washington and Lee University in Lexington, Va., who added that the case would become moot if the ACA is repealed wholesale.
“Millions of women [currently] get access to birth control without cost sharing through the Affordable Care Act,” he said in an interview. “That’s an issue [the new administration] is going to have to confront.”
In March, U.S. Supreme Court justices requested that both sides provide new briefs that outlined how contraception could be provided without requiring notice on the part of the suing employers. Then, in light of the briefs, the high court vacated the lower court rulings related to Zubik and remanded the case to the four appeals courts that had originally ruled on the issue.
If the case makes its way back to the Supreme Court, the ultimate ruling will largely depend on the makeup of the court at the time, said Eric D. Fader, a New York–based health law attorney.
“As long as we have a 4-4 Supreme Court, everything is up in the air,” Mr. Fader said in an interview. “As soon as that ninth slot is filled, I think we’re going to see some decisions that are going to be in line with traditional Republican conservative positions.”
However, a set of ACA-related cases that involve payments to insurers will continue litigating, regardless of actions by the new administration, analysts said. A half-dozen health insurers have sued the Health & Human Services department over alleged underpayments under the ACA’s risk corridor program.
“Even if you do away with the ACA, these cases all pertain to conduct that has already occurred, so they’re not going to be automatically moot,” Mr. Fader said in an interview. “They may struggle along for a while.”
The cases stem from the ACA’s risk corridor program, which requires HHS to collect funds from excessively profitable insurers that offer qualified health plans under the exchanges, while paying out funds to QHP insurers that have excessive losses. Collections from profitable insurers under the program fell short in 2014 and again in 2015, resulting in HHS paying about 12 cents on the dollar in payments to insurers.
The plaintiffs allege they’ve been shortchanged and that the government must reimburse them full payments for 2014. The Department of Justice (DOJ) argues the cases are premature because the full amount owed under the program is not due until 2016, after the program runs its course.
The Trump administration may surrender another ACA-linked challenge that questions billions in payments made to insurers, Mr. Jost said in an interview. In House v. Burwell, the House of Representatives accuses HHS of wrongly spending billions to repay insurers for health insurance provided to certain low-income patients under the ACA. The House claims HHS is illegally spending monies that Congress never appropriated. HHS argues that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements. In May, the U.S. District Court for the District of Columbia decided in favor of the House, ruling that Congress never appropriated money for the payments and that no public money can be spent without an appropriation.
There is speculation that the Trump administration may not pursue an appeal, Mr. Jost said. “I think they better think long and hard about that because I don’t know why any president would want court precedent saying one house of Congress can sue the president whenever it disagrees,” he said. “If the Trump administration would give in on the lawsuit or the House would win … there would be some very large losses and some very large premium increases next year. There could be some very significant disruption of insurance markets.”
Again, if the ACA is repealed, the case may become irrelevant, Mr. Fader said. “If you get rid of the ACA and eliminate the cost sharing structure, than House v. Burwell is going to just be moot.”
“We have seen a substantial uptick in antitrust enforcement activity in health care over the last several years,” he said in an interview. “The Trump administration has said that one of its themes is reducing the regulatory burden on businesses. People will be watching to see if that means an attempt to back off of some of the more-aggressive antitrust enforcement activities in health care and other industries.”
The Obama administration is currently fighting to block two mega-mergers among four of the largest health insurers in the nation. The DOJ filed legal challenges earlier this year seeking to ban Anthem’s proposed acquisition of Cigna and Aetna’s proposed acquisition of Humana. The lawsuits allege the mergers – valued at $54 billion and $37 billion respectively – would negatively affect doctors, patients, and employers by limiting price competition, reducing benefits, and lowering quality of care. A majority of physician associations and patient groups oppose the mergers. But experts said the new administration could drop the challenges.
Similarly, the Trump administration could be more lax in its enforcement of the Stark Law. “You could certainly say if the administration is committed to reducing regulatory burden, one thing the administration might push forward is reducing some of the enforcement with respect to technical violations of Stark,” Mr. Horton said, noting that the Senate recently questioned if the government is going too far in regulating physician relationships under Stark. “If your theme is ‘Let’s cut back on regulation,’ that would be an area that you would think the administration would look at.”
Meanwhile, stronger medical malpractice reforms could be on the horizon in light of a Republican-controlled Congress. Tort reform advocates have a good chance at passing federal medical liability reforms that were left out of the ACA’s passage in 2010, said Dennis A. Cardoza, public affairs director and cochair of the federal public affairs practice at a national health law firm.
Earlier versions of the ACA included amendments that mandated lawsuits go through a state or federal alternative dispute resolution system prior to being filed in court. Another provision that failed would have provided federal grants to states that created special health courts for medical malpractice claims. The amendment would have allowed states to create expert panels, administrative health care tribunals, or a combination of the two.
“There’s much stronger support for tort reform among the Republicans in Congress,” Mr. Cardoza said in an interview. “There’s a shot [now]. If the reforms don’t go too far where they would penalize injured patients, I think they could get additional support and be well received by the Congress.”
Tougher abortion restrictions are likely under the Trump administration, experts said. President-elect Trump has said he is committed to nominating a ninth Supreme Court justice who opposes Roe v. Wade.
Vice President-elect Mike Pence, who is considered a strong voice for the religious right, will likely influence who Mr. Trump nominates for the high court, said Rep-elect Raskin, who added that if ever there was time that abortion rights are in jeopardy, it’s now.
“This really puts the Republicans to the test,” he said in an interview. “For decades now, they have been calling for the overruling of Roe v. Wade. The religious right will never forgive them if it doesn’t happen now. [Republicans] control the House, the Senate, and the White House. They have it within their reach to create a five-justice majority on the court.”
[email protected]
[email protected]
On Twitter @legal_med
Miguel Angel Villagra Brings Management Skills to The Hospitalist's Volunteer Editorial Advisory Board
Some have called this the “Year of the Hospitalist,” as it’s the 20th anniversary of the New England Journal of Medicine paper by Dr. Robert Wachter and Dr. Lee Goldman that first used the term “hospitalist” to describe physicians who care for hospitalized patients.

But the paper was more than just that to Miguel Angel Villagra, MD.
He saw it four years ago while training in internal medicine at Texas Tech University Health Sciences Center in El Paso, Texas.
“I was very intrigued,” Dr. Villagra says. “I asked a few of my mentors. They were very skeptical on following a hospitalist career, [but] I saw opportunities for improvement and professional growth in the field, so I decided to jump in. And after four years, I don’t regret my decision of becoming a full-time hospitalist.”

The field doesn’t regret it either. Dr. Villagra was promoted last fall to hospitalist department program medical director at White River Medical Center in Batesville, Ark. And this year, he was named one of eight new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory board.
Question: Why did you choose a career in medicine?
Answer: At age 11 and after an emergent appendectomy, I decided that I wanted to become a physician. That was one of the best decisions of my life. It is a great combination of art and science, and you get to help people in difficult moments of their life.
Q: Tell us more about your background.
A: I went to medical school in my country of origin at Universidad Autonóma de Nicaragua of Managua, and I did an internal medicine residency at Hospital Militar Escuela Dr. Alejandro Dávila Bolaños. I came to the U.S. for internal medicine residency training at Texas Tech of El Paso. I enjoy learning new skills and this power of knowledge that can help your patients in desperate moments. Most of my challenges during my training involved how to manage stress and sleep deprivation.
Q: Did you have a mentor during your training or early career? If so, who was the mentor, and what were most important lessons you learned from them?
A: Dr. Jorge Cuadra [from Hospital Militar in Nicaragua] and Dr. Manuel Rivera [from Texas Tech], both pulmonologists. They taught me that medicine is a changing field that requires everyday reading. You never end learning new things and approaches. Taking full advantage of your interaction with your patients always improves your clinical skills.
Q: What do you like most about working as a hospitalist?
A: It is an evolving field; we are still trying to “figure it out.” That creates challenges but also opportunities for growth and career development, [for example], how to tackle the readmission problem, how to improve quality at lower cost while keeping patient satisfaction, how to face the burnout challenge and improve physician engagement, just to name a few.
Q: What do you dislike most?
A: In the beginning of my career as a hospitalist, I was exposed constantly to high patient loads that were more than I should have. I also dislike the difficulties at times of electronic medical records. You have to spend excessive time sitting in front of a monitor.
Q: You note the challenges the field of HM is facing. How exciting is it to hopefully be part of the solutions?
A: I feel pumped having been part of this amazing movement of hospital medicine. I think we are leading the change from the acute-care setting front line, helping to take better care of our patients. The current healthcare changes create multiple challenges and, along with that, endless opportunities for professional growth and career development.
Q: You’ve said you see being a chief quality officer in the future. Why? What appeals about those C-suite positions?
A: I think that physicians as leaders are in a great position to drive the change within a healthcare organization toward high-value care. We are at the front line, at the bedside taking care of patients. That gives us firsthand information on what needs to be done. With appropriate training, we can be the executives the institution needs. When I started my role as medical director, initially I focused mainly on managing the group, but rapidly I was involved in several quality projects and academic activities. And soon I realized that I can have a broader impact on what I was doing, going beyond the bedside where you try to offer the best care possible for your patients to an organizational level of change.
Q: How has your journey from Nicaragua to the U.S. shaped you, and how has it shaped the way you practice medicine?
A: Certainly it shaped what I am today, coming from a country that struggles with poverty. During medical school, you lack advances in technology and depend mainly on your desire to excel and be better for the benefit of your patients. You build strong clinical skills from history to physical exam. When you move to the U.S. and have access to so many technological advances, from new diagnostic tests to top-of the-line imaging studies, you combine the best of both worlds, and [that] makes you a better physician. I am very proud of my heritage, and definitely I wouldn’t change anything on my path thus far. I believe the more you overcome difficulties and adversities, the more you appreciate what you accomplished.
Q: As a group leader, why is it important for you to continue seeing patients?
A: We lead our teams by example, and that requires treating patients. I am also a clinician, and I love my profession, so I don’t foresee myself only in an administrative role. Finding the sweet spot of clinician-administrative time is very difficult, and I am still working on it.
Q: What’s the best advice you ever received?
A: Read and learn every day, be good to people, and also dream big.
Q: What’s the worst advice you ever received?
A: Never get married. I didn’t listen.
Richard Quinn is a freelance writer in New Jersey.
Some have called this the “Year of the Hospitalist,” as it’s the 20th anniversary of the New England Journal of Medicine paper by Dr. Robert Wachter and Dr. Lee Goldman that first used the term “hospitalist” to describe physicians who care for hospitalized patients.
But the paper was more than just that to Miguel Angel Villagra, MD.
He saw it four years ago while training in internal medicine at Texas Tech University Health Sciences Center in El Paso, Texas.
“I was very intrigued,” Dr. Villagra says. “I asked a few of my mentors. They were very skeptical on following a hospitalist career, [but] I saw opportunities for improvement and professional growth in the field, so I decided to jump in. And after four years, I don’t regret my decision of becoming a full-time hospitalist.”
The field doesn’t regret it either. Dr. Villagra was promoted last fall to hospitalist department program medical director at White River Medical Center in Batesville, Ark. And this year, he was named one of eight new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory board.
Question: Why did you choose a career in medicine?
Answer: At age 11 and after an emergent appendectomy, I decided that I wanted to become a physician. That was one of the best decisions of my life. It is a great combination of art and science, and you get to help people in difficult moments of their life.
Q: Tell us more about your background.
A: I went to medical school in my country of origin at Universidad Autonóma de Nicaragua of Managua, and I did an internal medicine residency at Hospital Militar Escuela Dr. Alejandro Dávila Bolaños. I came to the U.S. for internal medicine residency training at Texas Tech of El Paso. I enjoy learning new skills and this power of knowledge that can help your patients in desperate moments. Most of my challenges during my training involved how to manage stress and sleep deprivation.
Q: Did you have a mentor during your training or early career? If so, who was the mentor, and what were most important lessons you learned from them?
A: Dr. Jorge Cuadra [from Hospital Militar in Nicaragua] and Dr. Manuel Rivera [from Texas Tech], both pulmonologists. They taught me that medicine is a changing field that requires everyday reading. You never end learning new things and approaches. Taking full advantage of your interaction with your patients always improves your clinical skills.
Q: What do you like most about working as a hospitalist?
A: It is an evolving field; we are still trying to “figure it out.” That creates challenges but also opportunities for growth and career development, [for example], how to tackle the readmission problem, how to improve quality at lower cost while keeping patient satisfaction, how to face the burnout challenge and improve physician engagement, just to name a few.
Q: What do you dislike most?
A: In the beginning of my career as a hospitalist, I was exposed constantly to high patient loads that were more than I should have. I also dislike the difficulties at times of electronic medical records. You have to spend excessive time sitting in front of a monitor.
Q: You note the challenges the field of HM is facing. How exciting is it to hopefully be part of the solutions?
A: I feel pumped having been part of this amazing movement of hospital medicine. I think we are leading the change from the acute-care setting front line, helping to take better care of our patients. The current healthcare changes create multiple challenges and, along with that, endless opportunities for professional growth and career development.
Q: You’ve said you see being a chief quality officer in the future. Why? What appeals about those C-suite positions?
A: I think that physicians as leaders are in a great position to drive the change within a healthcare organization toward high-value care. We are at the front line, at the bedside taking care of patients. That gives us firsthand information on what needs to be done. With appropriate training, we can be the executives the institution needs. When I started my role as medical director, initially I focused mainly on managing the group, but rapidly I was involved in several quality projects and academic activities. And soon I realized that I can have a broader impact on what I was doing, going beyond the bedside where you try to offer the best care possible for your patients to an organizational level of change.
Q: How has your journey from Nicaragua to the U.S. shaped you, and how has it shaped the way you practice medicine?
A: Certainly it shaped what I am today, coming from a country that struggles with poverty. During medical school, you lack advances in technology and depend mainly on your desire to excel and be better for the benefit of your patients. You build strong clinical skills from history to physical exam. When you move to the U.S. and have access to so many technological advances, from new diagnostic tests to top-of the-line imaging studies, you combine the best of both worlds, and [that] makes you a better physician. I am very proud of my heritage, and definitely I wouldn’t change anything on my path thus far. I believe the more you overcome difficulties and adversities, the more you appreciate what you accomplished.
Q: As a group leader, why is it important for you to continue seeing patients?
A: We lead our teams by example, and that requires treating patients. I am also a clinician, and I love my profession, so I don’t foresee myself only in an administrative role. Finding the sweet spot of clinician-administrative time is very difficult, and I am still working on it.
Q: What’s the best advice you ever received?
A: Read and learn every day, be good to people, and also dream big.
Q: What’s the worst advice you ever received?
A: Never get married. I didn’t listen.
Richard Quinn is a freelance writer in New Jersey.
Some have called this the “Year of the Hospitalist,” as it’s the 20th anniversary of the New England Journal of Medicine paper by Dr. Robert Wachter and Dr. Lee Goldman that first used the term “hospitalist” to describe physicians who care for hospitalized patients.
But the paper was more than just that to Miguel Angel Villagra, MD.
He saw it four years ago while training in internal medicine at Texas Tech University Health Sciences Center in El Paso, Texas.
“I was very intrigued,” Dr. Villagra says. “I asked a few of my mentors. They were very skeptical on following a hospitalist career, [but] I saw opportunities for improvement and professional growth in the field, so I decided to jump in. And after four years, I don’t regret my decision of becoming a full-time hospitalist.”
The field doesn’t regret it either. Dr. Villagra was promoted last fall to hospitalist department program medical director at White River Medical Center in Batesville, Ark. And this year, he was named one of eight new members of Team Hospitalist, The Hospitalist’s volunteer editorial advisory board.
Question: Why did you choose a career in medicine?
Answer: At age 11 and after an emergent appendectomy, I decided that I wanted to become a physician. That was one of the best decisions of my life. It is a great combination of art and science, and you get to help people in difficult moments of their life.
Q: Tell us more about your background.
A: I went to medical school in my country of origin at Universidad Autonóma de Nicaragua of Managua, and I did an internal medicine residency at Hospital Militar Escuela Dr. Alejandro Dávila Bolaños. I came to the U.S. for internal medicine residency training at Texas Tech of El Paso. I enjoy learning new skills and this power of knowledge that can help your patients in desperate moments. Most of my challenges during my training involved how to manage stress and sleep deprivation.
Q: Did you have a mentor during your training or early career? If so, who was the mentor, and what were most important lessons you learned from them?
A: Dr. Jorge Cuadra [from Hospital Militar in Nicaragua] and Dr. Manuel Rivera [from Texas Tech], both pulmonologists. They taught me that medicine is a changing field that requires everyday reading. You never end learning new things and approaches. Taking full advantage of your interaction with your patients always improves your clinical skills.
Q: What do you like most about working as a hospitalist?
A: It is an evolving field; we are still trying to “figure it out.” That creates challenges but also opportunities for growth and career development, [for example], how to tackle the readmission problem, how to improve quality at lower cost while keeping patient satisfaction, how to face the burnout challenge and improve physician engagement, just to name a few.
Q: What do you dislike most?
A: In the beginning of my career as a hospitalist, I was exposed constantly to high patient loads that were more than I should have. I also dislike the difficulties at times of electronic medical records. You have to spend excessive time sitting in front of a monitor.
Q: You note the challenges the field of HM is facing. How exciting is it to hopefully be part of the solutions?
A: I feel pumped having been part of this amazing movement of hospital medicine. I think we are leading the change from the acute-care setting front line, helping to take better care of our patients. The current healthcare changes create multiple challenges and, along with that, endless opportunities for professional growth and career development.
Q: You’ve said you see being a chief quality officer in the future. Why? What appeals about those C-suite positions?
A: I think that physicians as leaders are in a great position to drive the change within a healthcare organization toward high-value care. We are at the front line, at the bedside taking care of patients. That gives us firsthand information on what needs to be done. With appropriate training, we can be the executives the institution needs. When I started my role as medical director, initially I focused mainly on managing the group, but rapidly I was involved in several quality projects and academic activities. And soon I realized that I can have a broader impact on what I was doing, going beyond the bedside where you try to offer the best care possible for your patients to an organizational level of change.
Q: How has your journey from Nicaragua to the U.S. shaped you, and how has it shaped the way you practice medicine?
A: Certainly it shaped what I am today, coming from a country that struggles with poverty. During medical school, you lack advances in technology and depend mainly on your desire to excel and be better for the benefit of your patients. You build strong clinical skills from history to physical exam. When you move to the U.S. and have access to so many technological advances, from new diagnostic tests to top-of the-line imaging studies, you combine the best of both worlds, and [that] makes you a better physician. I am very proud of my heritage, and definitely I wouldn’t change anything on my path thus far. I believe the more you overcome difficulties and adversities, the more you appreciate what you accomplished.
Q: As a group leader, why is it important for you to continue seeing patients?
A: We lead our teams by example, and that requires treating patients. I am also a clinician, and I love my profession, so I don’t foresee myself only in an administrative role. Finding the sweet spot of clinician-administrative time is very difficult, and I am still working on it.
Q: What’s the best advice you ever received?
A: Read and learn every day, be good to people, and also dream big.
Q: What’s the worst advice you ever received?
A: Never get married. I didn’t listen.
Richard Quinn is a freelance writer in New Jersey.
How NPs and PAs Work with HM Groups
While the role of nurse practitioners (NPs) and physician assistants (PAs) in hospital medicine is far from uniform, data from the 2016 State of Hospital Medicine Report show that a majority of hospital medicine groups utilize NPs or PAs. Over the past decade, the percentage of hospital medicine groups that include NPs or PAs has grown from about 20% in 20051 to 65% in 2015.2

I suspect a large part of this growth is fueled by demand continuing to outstrip supply for hospitalist physicians and continued increases in hospitalist salaries. In academic institutions, restrictions in house staff duty hours over the past decade no doubt also contributed to the growth of NP and PA utilization.
How Should HM Groups Use NPs and PAs?
In addition to obtaining group buy-in prior to deploying NPs or PAs in a hospital medicine group, a thoughtful consideration about the role of NPs or PAs in providing care is perhaps most important. Even with careful planning, groups should expect implementation of an NP or PA model to require lead-in and training time.
The fact that NPs and PAs have been adopted by so many groups suggests that practices have found increased value; however, models vary widely. In some practices, NPs or PAs work side by side with hospitalists, assisting with documentation, meeting with patients and families, and implementing an agreed-upon management plan. In this model, NPs and PAs may also add value by helping with time-consuming discharges, freeing hospitalists to attend to other patients and thus improving productivity, bed flow, and perhaps also job sustainability.
Other groups have found niche roles for NPs or PAs, including but not limited to providing cross-coverage, performing procedures, triaging admissions, staffing observation units, and developing expertise in a specific clinical area such as consultative medicine or orthopedics.
How to Bill
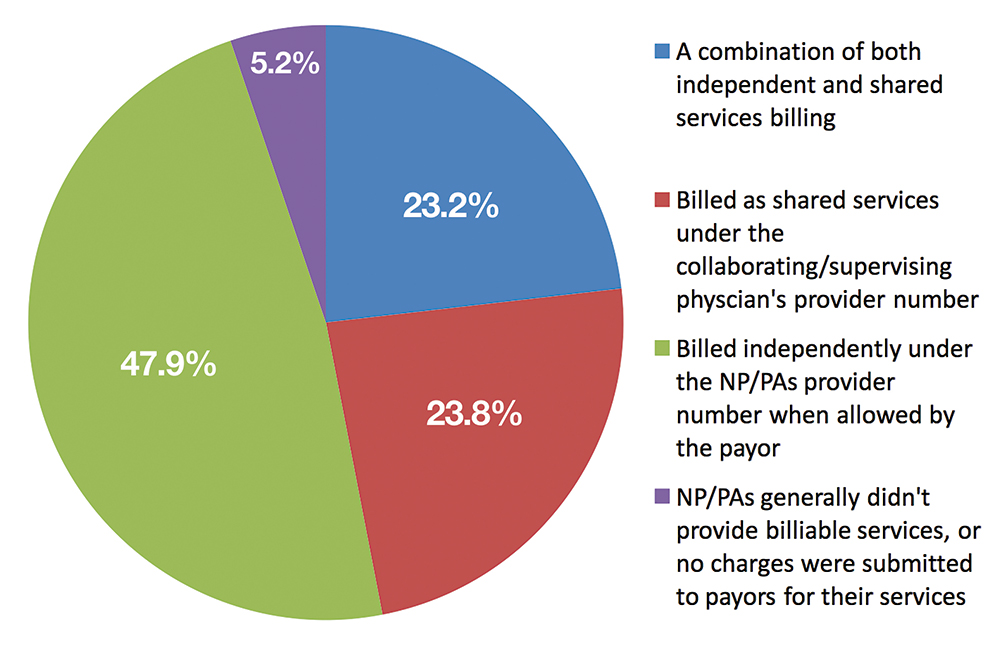
Depending on the model adopted, groups must also decide whether it is advantageous for NPs or PAs to bill for services independently versus as shared services under the supervising physician’s provider number. The Centers for Medicare & Medicaid Services reimburses NPs and PAs who bill independently at 85% of the physician rate. Nonetheless, some groups may find it more cost-effective for NPs or PAs to bill independently given the substantial salary differential compared to hospitalists. Data published in the 2016 State of Hospital Medicine Report show that NPs and PAs bill independently 47.9% of the time (see Figure 1).
At the University of California, San Diego, we’ve found that our PAs added the most value when working one-on-one with a single hospitalist rather than with multiple physicians. Specifically, our PAs have added to the capacity of our non-teaching service, typically implementing a plan of care developed cooperatively with the hospitalist but also managing a select cohort of patients independently during times of excess volume. By increasing capacity, our PAs have also allowed us to avoid calling in a backup hospitalist during high census periods.
References
- Society of Hospital Medicine. 2006 State of Hospital Medicine Report.
- 2016 State of Hospital Medicine Report. Society of Hospital Medicine website. Accessed October 23, 2016.
While the role of nurse practitioners (NPs) and physician assistants (PAs) in hospital medicine is far from uniform, data from the 2016 State of Hospital Medicine Report show that a majority of hospital medicine groups utilize NPs or PAs. Over the past decade, the percentage of hospital medicine groups that include NPs or PAs has grown from about 20% in 20051 to 65% in 2015.2
I suspect a large part of this growth is fueled by demand continuing to outstrip supply for hospitalist physicians and continued increases in hospitalist salaries. In academic institutions, restrictions in house staff duty hours over the past decade no doubt also contributed to the growth of NP and PA utilization.
How Should HM Groups Use NPs and PAs?
In addition to obtaining group buy-in prior to deploying NPs or PAs in a hospital medicine group, a thoughtful consideration about the role of NPs or PAs in providing care is perhaps most important. Even with careful planning, groups should expect implementation of an NP or PA model to require lead-in and training time.
The fact that NPs and PAs have been adopted by so many groups suggests that practices have found increased value; however, models vary widely. In some practices, NPs or PAs work side by side with hospitalists, assisting with documentation, meeting with patients and families, and implementing an agreed-upon management plan. In this model, NPs and PAs may also add value by helping with time-consuming discharges, freeing hospitalists to attend to other patients and thus improving productivity, bed flow, and perhaps also job sustainability.
Other groups have found niche roles for NPs or PAs, including but not limited to providing cross-coverage, performing procedures, triaging admissions, staffing observation units, and developing expertise in a specific clinical area such as consultative medicine or orthopedics.
How to Bill
Depending on the model adopted, groups must also decide whether it is advantageous for NPs or PAs to bill for services independently versus as shared services under the supervising physician’s provider number. The Centers for Medicare & Medicaid Services reimburses NPs and PAs who bill independently at 85% of the physician rate. Nonetheless, some groups may find it more cost-effective for NPs or PAs to bill independently given the substantial salary differential compared to hospitalists. Data published in the 2016 State of Hospital Medicine Report show that NPs and PAs bill independently 47.9% of the time (see Figure 1).
At the University of California, San Diego, we’ve found that our PAs added the most value when working one-on-one with a single hospitalist rather than with multiple physicians. Specifically, our PAs have added to the capacity of our non-teaching service, typically implementing a plan of care developed cooperatively with the hospitalist but also managing a select cohort of patients independently during times of excess volume. By increasing capacity, our PAs have also allowed us to avoid calling in a backup hospitalist during high census periods.
References
- Society of Hospital Medicine. 2006 State of Hospital Medicine Report.
- 2016 State of Hospital Medicine Report. Society of Hospital Medicine website. Accessed October 23, 2016.
While the role of nurse practitioners (NPs) and physician assistants (PAs) in hospital medicine is far from uniform, data from the 2016 State of Hospital Medicine Report show that a majority of hospital medicine groups utilize NPs or PAs. Over the past decade, the percentage of hospital medicine groups that include NPs or PAs has grown from about 20% in 20051 to 65% in 2015.2
I suspect a large part of this growth is fueled by demand continuing to outstrip supply for hospitalist physicians and continued increases in hospitalist salaries. In academic institutions, restrictions in house staff duty hours over the past decade no doubt also contributed to the growth of NP and PA utilization.
How Should HM Groups Use NPs and PAs?
In addition to obtaining group buy-in prior to deploying NPs or PAs in a hospital medicine group, a thoughtful consideration about the role of NPs or PAs in providing care is perhaps most important. Even with careful planning, groups should expect implementation of an NP or PA model to require lead-in and training time.
The fact that NPs and PAs have been adopted by so many groups suggests that practices have found increased value; however, models vary widely. In some practices, NPs or PAs work side by side with hospitalists, assisting with documentation, meeting with patients and families, and implementing an agreed-upon management plan. In this model, NPs and PAs may also add value by helping with time-consuming discharges, freeing hospitalists to attend to other patients and thus improving productivity, bed flow, and perhaps also job sustainability.
Other groups have found niche roles for NPs or PAs, including but not limited to providing cross-coverage, performing procedures, triaging admissions, staffing observation units, and developing expertise in a specific clinical area such as consultative medicine or orthopedics.
How to Bill
Depending on the model adopted, groups must also decide whether it is advantageous for NPs or PAs to bill for services independently versus as shared services under the supervising physician’s provider number. The Centers for Medicare & Medicaid Services reimburses NPs and PAs who bill independently at 85% of the physician rate. Nonetheless, some groups may find it more cost-effective for NPs or PAs to bill independently given the substantial salary differential compared to hospitalists. Data published in the 2016 State of Hospital Medicine Report show that NPs and PAs bill independently 47.9% of the time (see Figure 1).
At the University of California, San Diego, we’ve found that our PAs added the most value when working one-on-one with a single hospitalist rather than with multiple physicians. Specifically, our PAs have added to the capacity of our non-teaching service, typically implementing a plan of care developed cooperatively with the hospitalist but also managing a select cohort of patients independently during times of excess volume. By increasing capacity, our PAs have also allowed us to avoid calling in a backup hospitalist during high census periods.
References
- Society of Hospital Medicine. 2006 State of Hospital Medicine Report.
- 2016 State of Hospital Medicine Report. Society of Hospital Medicine website. Accessed October 23, 2016.
SHM Commits to Help Hospitals with Judicious Opioid Prescribing
SHM recently enrolled 10 hospitals in the United States in a one-year mentored implementation program to reduce adverse events associated with opioid prescribing. Each hospital will have an assigned physician mentor to guide them through:

- A needs assessment.
- Formal selection of data collection measures.
- Outcome and process data collection on intervention units.
- Design and implementation of key interventions to enhance safety for patients in the hospital who are prescribed opioid medications.
The one-year program includes monthly calls, a site visit with the SHM physician mentor, and a formal assessment of the program’s implementation.
Visit www.hospitalmedicine.org/RADEO to view the online toolkit or download the Reducing Adverse Drug Events Related to Opioids (RADEO) Implementation Guide.
SHM recently enrolled 10 hospitals in the United States in a one-year mentored implementation program to reduce adverse events associated with opioid prescribing. Each hospital will have an assigned physician mentor to guide them through:
- A needs assessment.
- Formal selection of data collection measures.
- Outcome and process data collection on intervention units.
- Design and implementation of key interventions to enhance safety for patients in the hospital who are prescribed opioid medications.
The one-year program includes monthly calls, a site visit with the SHM physician mentor, and a formal assessment of the program’s implementation.
Visit www.hospitalmedicine.org/RADEO to view the online toolkit or download the Reducing Adverse Drug Events Related to Opioids (RADEO) Implementation Guide.
SHM recently enrolled 10 hospitals in the United States in a one-year mentored implementation program to reduce adverse events associated with opioid prescribing. Each hospital will have an assigned physician mentor to guide them through:
- A needs assessment.
- Formal selection of data collection measures.
- Outcome and process data collection on intervention units.
- Design and implementation of key interventions to enhance safety for patients in the hospital who are prescribed opioid medications.
The one-year program includes monthly calls, a site visit with the SHM physician mentor, and a formal assessment of the program’s implementation.
Visit www.hospitalmedicine.org/RADEO to view the online toolkit or download the Reducing Adverse Drug Events Related to Opioids (RADEO) Implementation Guide.
Track List Available for Hospital Medicine 2017

Looking for more? Seize the opportunity to learn from an elite group of experts. Earn additional CME credits, broaden your skills, and fine-tune your practice. Immerse yourself in a day of learning by enrolling in one six pre-courses on May 1. Visit www.hospitalmedicine2017.org/precourse to view course topics, agendas, faculty, and more.
Looking for more? Seize the opportunity to learn from an elite group of experts. Earn additional CME credits, broaden your skills, and fine-tune your practice. Immerse yourself in a day of learning by enrolling in one six pre-courses on May 1. Visit www.hospitalmedicine2017.org/precourse to view course topics, agendas, faculty, and more.
Looking for more? Seize the opportunity to learn from an elite group of experts. Earn additional CME credits, broaden your skills, and fine-tune your practice. Immerse yourself in a day of learning by enrolling in one six pre-courses on May 1. Visit www.hospitalmedicine2017.org/precourse to view course topics, agendas, faculty, and more.