User login
Test Your Knowledge: Generalized Pustular Psoriasis Quiz
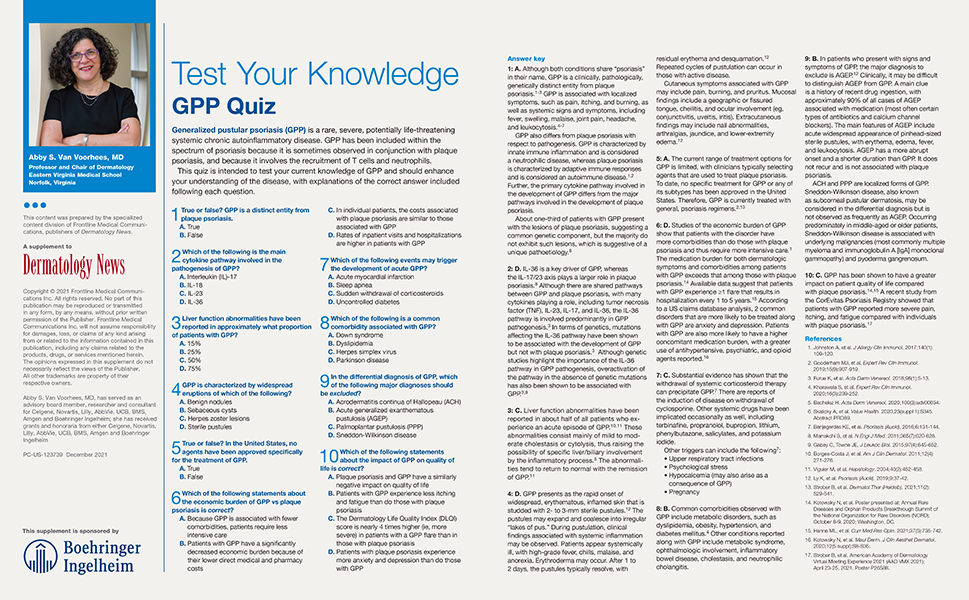
In this quiz to Dermatology News, test your current knowledge of Generalized Pustular Psoriasis. Join Abby S. Van Voorhees, MD, as she shares insights on GPP and understanding the disorder.
PC-US-123740 December 2021
In this quiz to Dermatology News, test your current knowledge of Generalized Pustular Psoriasis. Join Abby S. Van Voorhees, MD, as she shares insights on GPP and understanding the disorder.
PC-US-123740 December 2021
In this quiz to Dermatology News, test your current knowledge of Generalized Pustular Psoriasis. Join Abby S. Van Voorhees, MD, as she shares insights on GPP and understanding the disorder.
PC-US-123740 December 2021
Supporting clinician wellbeing and organizational resilience

In a 2020 report, the National Academy of Medicine advocated for “fixing the workplace,” rather than “fixing the worker,” as a more sustainable mechanism to advance physician wellbeing and foster organizational resilience. According to the report, “A resilient organization, or one that has matched job demands with job resources for its workers and that has created a culture of connection, transparency, and improvement, is better positioned to achieve organizational objectives during ordinary times and also to weather challenges during times of crisis” (Sinsky CA et al. “Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being.” National Academy of Medicine. Nov. 2, 2020.
The report highlights six domains of evidence-based practices to support organizational resilience and improve clinician well-being: organizational commitment, workforce assessment (such as measurement of physician wellbeing and burnout); leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer), policy (such as eliminating and/or re-envisioning policies and practices that interfere with clinicians’ ability to provide high-quality patient care), (5) efficiency (such as minimizing administrative tasks to allow clinicians to focus on patient care), and (6) support (such as providing resources and/or policies to support work-life balance, fostering a culture of connection at work). While many organizations (including both academic and community practices) already have begun to invest in this transformation, I urge you to think creatively about whether there is more your practice can do at an organizational level to support and sustain clinician wellbeing and prevent burnout.
In this month’s issue of GIHN, we highlight AGA’s new Clinical Practice Guideline on Coagulation in Cirrhosis, as well as results from a study confirming the benefits of coffee for liver health (welcome news to the caffeine-lovers among us!). We also report on a novel text-based patient-education intervention that aims to connect patients newly diagnosed with colorectal cancer to valuable resources and support.
Thank you for your dedicated readership – we look forward to continuing to bring you engaging, clinically-relevant content in 2022!
Megan A. Adams, MD, JD, MSc
Editor in Chief
In a 2020 report, the National Academy of Medicine advocated for “fixing the workplace,” rather than “fixing the worker,” as a more sustainable mechanism to advance physician wellbeing and foster organizational resilience. According to the report, “A resilient organization, or one that has matched job demands with job resources for its workers and that has created a culture of connection, transparency, and improvement, is better positioned to achieve organizational objectives during ordinary times and also to weather challenges during times of crisis” (Sinsky CA et al. “Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being.” National Academy of Medicine. Nov. 2, 2020.
The report highlights six domains of evidence-based practices to support organizational resilience and improve clinician well-being: organizational commitment, workforce assessment (such as measurement of physician wellbeing and burnout); leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer), policy (such as eliminating and/or re-envisioning policies and practices that interfere with clinicians’ ability to provide high-quality patient care), (5) efficiency (such as minimizing administrative tasks to allow clinicians to focus on patient care), and (6) support (such as providing resources and/or policies to support work-life balance, fostering a culture of connection at work). While many organizations (including both academic and community practices) already have begun to invest in this transformation, I urge you to think creatively about whether there is more your practice can do at an organizational level to support and sustain clinician wellbeing and prevent burnout.
In this month’s issue of GIHN, we highlight AGA’s new Clinical Practice Guideline on Coagulation in Cirrhosis, as well as results from a study confirming the benefits of coffee for liver health (welcome news to the caffeine-lovers among us!). We also report on a novel text-based patient-education intervention that aims to connect patients newly diagnosed with colorectal cancer to valuable resources and support.
Thank you for your dedicated readership – we look forward to continuing to bring you engaging, clinically-relevant content in 2022!
Megan A. Adams, MD, JD, MSc
Editor in Chief
In a 2020 report, the National Academy of Medicine advocated for “fixing the workplace,” rather than “fixing the worker,” as a more sustainable mechanism to advance physician wellbeing and foster organizational resilience. According to the report, “A resilient organization, or one that has matched job demands with job resources for its workers and that has created a culture of connection, transparency, and improvement, is better positioned to achieve organizational objectives during ordinary times and also to weather challenges during times of crisis” (Sinsky CA et al. “Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being.” National Academy of Medicine. Nov. 2, 2020.
The report highlights six domains of evidence-based practices to support organizational resilience and improve clinician well-being: organizational commitment, workforce assessment (such as measurement of physician wellbeing and burnout); leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer), policy (such as eliminating and/or re-envisioning policies and practices that interfere with clinicians’ ability to provide high-quality patient care), (5) efficiency (such as minimizing administrative tasks to allow clinicians to focus on patient care), and (6) support (such as providing resources and/or policies to support work-life balance, fostering a culture of connection at work). While many organizations (including both academic and community practices) already have begun to invest in this transformation, I urge you to think creatively about whether there is more your practice can do at an organizational level to support and sustain clinician wellbeing and prevent burnout.
In this month’s issue of GIHN, we highlight AGA’s new Clinical Practice Guideline on Coagulation in Cirrhosis, as well as results from a study confirming the benefits of coffee for liver health (welcome news to the caffeine-lovers among us!). We also report on a novel text-based patient-education intervention that aims to connect patients newly diagnosed with colorectal cancer to valuable resources and support.
Thank you for your dedicated readership – we look forward to continuing to bring you engaging, clinically-relevant content in 2022!
Megan A. Adams, MD, JD, MSc
Editor in Chief
Top case
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. Here’s a preview of a recent popular clinical discussion:
Robert Herman, MD, wrote in “Rectal lesion”:
A 42-year-old healthy female was seen by me for symptoms of non-ulcer dyspepsia that was unresponsive to H2 Blockers and for assessment for screening colonoscopy. Her father had developed colon cancer at the age of 50. She denied changes in bowel habits, pattern, rectal bleeding, or melena. An EGD revealed a medium sized hiatal hernia and LA Grade B esophagitis that responded well to an OTC PPI qd.
A colonoscopy was performed and revealed a 4-cm anterior rectal “bulge” just above the hemorrhoidal plexus, appearing somewhat firm and mobile on probing the lesion with a closed biopsy forceps, and a 1 cm sessile IC valve adenomatous polyp.
And then the endoscopic medical assistant made a comment that changed everything. Read the full case discussion: https://community.gastro.org/posts/25568.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. Here’s a preview of a recent popular clinical discussion:
Robert Herman, MD, wrote in “Rectal lesion”:
A 42-year-old healthy female was seen by me for symptoms of non-ulcer dyspepsia that was unresponsive to H2 Blockers and for assessment for screening colonoscopy. Her father had developed colon cancer at the age of 50. She denied changes in bowel habits, pattern, rectal bleeding, or melena. An EGD revealed a medium sized hiatal hernia and LA Grade B esophagitis that responded well to an OTC PPI qd.
A colonoscopy was performed and revealed a 4-cm anterior rectal “bulge” just above the hemorrhoidal plexus, appearing somewhat firm and mobile on probing the lesion with a closed biopsy forceps, and a 1 cm sessile IC valve adenomatous polyp.
And then the endoscopic medical assistant made a comment that changed everything. Read the full case discussion: https://community.gastro.org/posts/25568.
Physicians with difficult patient scenarios regularly bring their questions to the AGA Community (https://community.gastro.org) to seek advice from colleagues about therapy and disease management options, best practices, and diagnoses. Here’s a preview of a recent popular clinical discussion:
Robert Herman, MD, wrote in “Rectal lesion”:
A 42-year-old healthy female was seen by me for symptoms of non-ulcer dyspepsia that was unresponsive to H2 Blockers and for assessment for screening colonoscopy. Her father had developed colon cancer at the age of 50. She denied changes in bowel habits, pattern, rectal bleeding, or melena. An EGD revealed a medium sized hiatal hernia and LA Grade B esophagitis that responded well to an OTC PPI qd.
A colonoscopy was performed and revealed a 4-cm anterior rectal “bulge” just above the hemorrhoidal plexus, appearing somewhat firm and mobile on probing the lesion with a closed biopsy forceps, and a 1 cm sessile IC valve adenomatous polyp.
And then the endoscopic medical assistant made a comment that changed everything. Read the full case discussion: https://community.gastro.org/posts/25568.
Serum vitamin D level inversely tied to severe sarcopenia in females with RA
Key clinical point: Vitamin D status was inversely associated with severe sarcopenia, impaired physical performance, and decreased skeletal muscle mass in females with rheumatoid arthritis (RA), highlighting the need to investigate vitamin D supplementation as a therapeutic strategy for sarcopenic patients with RA.
Major finding: Low 25-hydroxyvitamin D (25[OH])D status (16.0 ng/mL or lower) was significantly associated with a high prevalence of severe sarcopenia (adjusted odds ratio [aOR], 6.00; P = .0006) in females with RA. Low physical performance (aOR, 2.65; P = .0043) and skeletal muscle mass (aOR, 2.54; P = .027) were the major components of sarcopenia linked with a low serum 25(OH)D level.
Study details: This was a cross-sectional study involving 156 female outpatients with RA.
Disclosures: This study was funded by AMED and Daiichi Sankyo Co. Ltd. Several authors reported receiving research grants and speaker’s fees from various sources including Daiichi Sankyo. Some of the authors including the lead author declared no conflict of interests.
Source: Minamino H et al. Sci Rep. 2021 Oct 14. doi: 10.1038/s41598-021-99894-6.
Key clinical point: Vitamin D status was inversely associated with severe sarcopenia, impaired physical performance, and decreased skeletal muscle mass in females with rheumatoid arthritis (RA), highlighting the need to investigate vitamin D supplementation as a therapeutic strategy for sarcopenic patients with RA.
Major finding: Low 25-hydroxyvitamin D (25[OH])D status (16.0 ng/mL or lower) was significantly associated with a high prevalence of severe sarcopenia (adjusted odds ratio [aOR], 6.00; P = .0006) in females with RA. Low physical performance (aOR, 2.65; P = .0043) and skeletal muscle mass (aOR, 2.54; P = .027) were the major components of sarcopenia linked with a low serum 25(OH)D level.
Study details: This was a cross-sectional study involving 156 female outpatients with RA.
Disclosures: This study was funded by AMED and Daiichi Sankyo Co. Ltd. Several authors reported receiving research grants and speaker’s fees from various sources including Daiichi Sankyo. Some of the authors including the lead author declared no conflict of interests.
Source: Minamino H et al. Sci Rep. 2021 Oct 14. doi: 10.1038/s41598-021-99894-6.
Key clinical point: Vitamin D status was inversely associated with severe sarcopenia, impaired physical performance, and decreased skeletal muscle mass in females with rheumatoid arthritis (RA), highlighting the need to investigate vitamin D supplementation as a therapeutic strategy for sarcopenic patients with RA.
Major finding: Low 25-hydroxyvitamin D (25[OH])D status (16.0 ng/mL or lower) was significantly associated with a high prevalence of severe sarcopenia (adjusted odds ratio [aOR], 6.00; P = .0006) in females with RA. Low physical performance (aOR, 2.65; P = .0043) and skeletal muscle mass (aOR, 2.54; P = .027) were the major components of sarcopenia linked with a low serum 25(OH)D level.
Study details: This was a cross-sectional study involving 156 female outpatients with RA.
Disclosures: This study was funded by AMED and Daiichi Sankyo Co. Ltd. Several authors reported receiving research grants and speaker’s fees from various sources including Daiichi Sankyo. Some of the authors including the lead author declared no conflict of interests.
Source: Minamino H et al. Sci Rep. 2021 Oct 14. doi: 10.1038/s41598-021-99894-6.
No impact of anti-inflammatory diet on health-related quality of life in RA
Key clinical point: The anti-inflammatory diet did not enhance health-related quality of life in patients with rheumatoid arthritis (RA) compared with a control diet. However, physical functioning improved significantly, particularly in patients who did not alter antirheumatic medication.
Major finding: The Health Assessment Questionnaire was not significantly different between the intervention and control diet periods (P = .503); however, the physical functioning improved significantly during intervention diet vs. control diet period (mean, 5.791; 95% CI, 1.576-10.005), particularly in patients without pharmacological treatment changes (mean, 7.898; P = .036).
Study details: Findings are from the ADIRA trial, a controlled crossover trial including 50 patients with RA who were randomly assigned to either an intervention diet including foods with suggested anti-inflammatory properties and promising effects on RA symptoms (n=24) or control diet (usual Swedish diet; n=26) for 10 weeks before switching to the other diet.
Disclosures: This study received grants from the Swedish government, Swedish Research Council for Health, Working Life and Welfare, and others. No conflict of interests was reported.
Source: Turesson Wadell A et al. PLoS One. 2021 Oct 14. doi: 10.1371/journal.pone.0258716.
Key clinical point: The anti-inflammatory diet did not enhance health-related quality of life in patients with rheumatoid arthritis (RA) compared with a control diet. However, physical functioning improved significantly, particularly in patients who did not alter antirheumatic medication.
Major finding: The Health Assessment Questionnaire was not significantly different between the intervention and control diet periods (P = .503); however, the physical functioning improved significantly during intervention diet vs. control diet period (mean, 5.791; 95% CI, 1.576-10.005), particularly in patients without pharmacological treatment changes (mean, 7.898; P = .036).
Study details: Findings are from the ADIRA trial, a controlled crossover trial including 50 patients with RA who were randomly assigned to either an intervention diet including foods with suggested anti-inflammatory properties and promising effects on RA symptoms (n=24) or control diet (usual Swedish diet; n=26) for 10 weeks before switching to the other diet.
Disclosures: This study received grants from the Swedish government, Swedish Research Council for Health, Working Life and Welfare, and others. No conflict of interests was reported.
Source: Turesson Wadell A et al. PLoS One. 2021 Oct 14. doi: 10.1371/journal.pone.0258716.
Key clinical point: The anti-inflammatory diet did not enhance health-related quality of life in patients with rheumatoid arthritis (RA) compared with a control diet. However, physical functioning improved significantly, particularly in patients who did not alter antirheumatic medication.
Major finding: The Health Assessment Questionnaire was not significantly different between the intervention and control diet periods (P = .503); however, the physical functioning improved significantly during intervention diet vs. control diet period (mean, 5.791; 95% CI, 1.576-10.005), particularly in patients without pharmacological treatment changes (mean, 7.898; P = .036).
Study details: Findings are from the ADIRA trial, a controlled crossover trial including 50 patients with RA who were randomly assigned to either an intervention diet including foods with suggested anti-inflammatory properties and promising effects on RA symptoms (n=24) or control diet (usual Swedish diet; n=26) for 10 weeks before switching to the other diet.
Disclosures: This study received grants from the Swedish government, Swedish Research Council for Health, Working Life and Welfare, and others. No conflict of interests was reported.
Source: Turesson Wadell A et al. PLoS One. 2021 Oct 14. doi: 10.1371/journal.pone.0258716.
Sinusitis and upper respiratory tract diseases may increase the risk for rheumatoid arthritis
Key clinical point: Sinusitis, pharyngitis, and acute respiratory burden all raised the likelihood of developing rheumatoid arthritis (RA).
Major finding: Acute sinusitis (odds ratio [OR], 1.61; 95% CI, 1.05-2.45), chronic sinusitis (OR, 2.16; 95% CI, 1.39-3.35), asthma (OR, 1.39; 95% CI, 1.03-1.87), and burden of acute respiratory tract disease during the preindex exposure period (OR, 1.30 per 10 codes; 95% CI, 1.08-1.55) were associated with an elevated risk for RA. Acute pharyngitis was associated with seronegative RA (OR, 1.68; 95% CI, 1.02-2.74), whereas chronic rhinitis/pharyngitis was associated with seropositive RA (OR, 2.46; 95% CI, 1.01-5.99).
Study details: This was a case-control study involving 741 patients with RA matched with 2,223 healthy controls.
Disclosures: The National Institute of Arthritis and Musculoskeletal and Skin Diseases and Rheumatology Research Foundation funded this research. No conflict of interests was reported.
Source: Kronzer VL et al. J Rheumatol. 2021 Oct 15. doi: 10.3899/jrheum.210580.
Key clinical point: Sinusitis, pharyngitis, and acute respiratory burden all raised the likelihood of developing rheumatoid arthritis (RA).
Major finding: Acute sinusitis (odds ratio [OR], 1.61; 95% CI, 1.05-2.45), chronic sinusitis (OR, 2.16; 95% CI, 1.39-3.35), asthma (OR, 1.39; 95% CI, 1.03-1.87), and burden of acute respiratory tract disease during the preindex exposure period (OR, 1.30 per 10 codes; 95% CI, 1.08-1.55) were associated with an elevated risk for RA. Acute pharyngitis was associated with seronegative RA (OR, 1.68; 95% CI, 1.02-2.74), whereas chronic rhinitis/pharyngitis was associated with seropositive RA (OR, 2.46; 95% CI, 1.01-5.99).
Study details: This was a case-control study involving 741 patients with RA matched with 2,223 healthy controls.
Disclosures: The National Institute of Arthritis and Musculoskeletal and Skin Diseases and Rheumatology Research Foundation funded this research. No conflict of interests was reported.
Source: Kronzer VL et al. J Rheumatol. 2021 Oct 15. doi: 10.3899/jrheum.210580.
Key clinical point: Sinusitis, pharyngitis, and acute respiratory burden all raised the likelihood of developing rheumatoid arthritis (RA).
Major finding: Acute sinusitis (odds ratio [OR], 1.61; 95% CI, 1.05-2.45), chronic sinusitis (OR, 2.16; 95% CI, 1.39-3.35), asthma (OR, 1.39; 95% CI, 1.03-1.87), and burden of acute respiratory tract disease during the preindex exposure period (OR, 1.30 per 10 codes; 95% CI, 1.08-1.55) were associated with an elevated risk for RA. Acute pharyngitis was associated with seronegative RA (OR, 1.68; 95% CI, 1.02-2.74), whereas chronic rhinitis/pharyngitis was associated with seropositive RA (OR, 2.46; 95% CI, 1.01-5.99).
Study details: This was a case-control study involving 741 patients with RA matched with 2,223 healthy controls.
Disclosures: The National Institute of Arthritis and Musculoskeletal and Skin Diseases and Rheumatology Research Foundation funded this research. No conflict of interests was reported.
Source: Kronzer VL et al. J Rheumatol. 2021 Oct 15. doi: 10.3899/jrheum.210580.
Similar long-term safety/tolerability of filgotinib 100 mg and 200 mg in moderate-to-severe RA
Key clinical point: Filgotinib 200 mg (FIL200) and 100 mg (FIL100) showed similar safety/tolerability in patients with moderate-to-severe rheumatoid arthritis (RA) with over a median of 1.6 years and maximum of 5.6 years of exposure, with FIL200 showing a lower infection rate in the long term.
Major finding: Treatment-emergent adverse events (TEAEs) were similar between FIL200 (exposure-adjusted incidence rate [EAIR], 195.4 per 100 patient-years of exposure [100 PYE]), FIL100 (176.3 per 100 PYE), and placebo (175.9 per 100 PYE) during the 12-week period. During long-term exposure, EAIR for grade ≥3 TEAEs were 6.4 and 7.6 per 100 PYE for FIL200 and FIL100, respectively, but serious infectious AEs were lower with FIL200 vs. FIL100 (EAIR, 1.6 vs. 3.1 per 100 PYE).
Study details: Data come from integrated analysis of 7 clinical trials including patients with moderate-to-severe RA who received ≥1 dose of FIL200, FIL100, or placebo.
Disclosures: This study was funded by Gilead Sciences, Inc. Some investigators including the lead author reported receiving grants, honoraria, consultancy/speaker’s fees, and being an employee of or shareholder of various sources including Gilead Sciences.
Source: Winthrop KL et al. Ann Rheum Dis. 2021 Nov 5. doi: 10.1136/annrheumdis-2021-221051.
Key clinical point: Filgotinib 200 mg (FIL200) and 100 mg (FIL100) showed similar safety/tolerability in patients with moderate-to-severe rheumatoid arthritis (RA) with over a median of 1.6 years and maximum of 5.6 years of exposure, with FIL200 showing a lower infection rate in the long term.
Major finding: Treatment-emergent adverse events (TEAEs) were similar between FIL200 (exposure-adjusted incidence rate [EAIR], 195.4 per 100 patient-years of exposure [100 PYE]), FIL100 (176.3 per 100 PYE), and placebo (175.9 per 100 PYE) during the 12-week period. During long-term exposure, EAIR for grade ≥3 TEAEs were 6.4 and 7.6 per 100 PYE for FIL200 and FIL100, respectively, but serious infectious AEs were lower with FIL200 vs. FIL100 (EAIR, 1.6 vs. 3.1 per 100 PYE).
Study details: Data come from integrated analysis of 7 clinical trials including patients with moderate-to-severe RA who received ≥1 dose of FIL200, FIL100, or placebo.
Disclosures: This study was funded by Gilead Sciences, Inc. Some investigators including the lead author reported receiving grants, honoraria, consultancy/speaker’s fees, and being an employee of or shareholder of various sources including Gilead Sciences.
Source: Winthrop KL et al. Ann Rheum Dis. 2021 Nov 5. doi: 10.1136/annrheumdis-2021-221051.
Key clinical point: Filgotinib 200 mg (FIL200) and 100 mg (FIL100) showed similar safety/tolerability in patients with moderate-to-severe rheumatoid arthritis (RA) with over a median of 1.6 years and maximum of 5.6 years of exposure, with FIL200 showing a lower infection rate in the long term.
Major finding: Treatment-emergent adverse events (TEAEs) were similar between FIL200 (exposure-adjusted incidence rate [EAIR], 195.4 per 100 patient-years of exposure [100 PYE]), FIL100 (176.3 per 100 PYE), and placebo (175.9 per 100 PYE) during the 12-week period. During long-term exposure, EAIR for grade ≥3 TEAEs were 6.4 and 7.6 per 100 PYE for FIL200 and FIL100, respectively, but serious infectious AEs were lower with FIL200 vs. FIL100 (EAIR, 1.6 vs. 3.1 per 100 PYE).
Study details: Data come from integrated analysis of 7 clinical trials including patients with moderate-to-severe RA who received ≥1 dose of FIL200, FIL100, or placebo.
Disclosures: This study was funded by Gilead Sciences, Inc. Some investigators including the lead author reported receiving grants, honoraria, consultancy/speaker’s fees, and being an employee of or shareholder of various sources including Gilead Sciences.
Source: Winthrop KL et al. Ann Rheum Dis. 2021 Nov 5. doi: 10.1136/annrheumdis-2021-221051.
Obesity, depression, anxiety, and illness beliefs influence remission, pain, and fatigue in RA
Key clinical point: Obesity, anxiety, depression, and illness perception at baseline were associated with treatment outcomes, pain, and fatigue in patients with rheumatoid arthritis (RA).
Major finding: At 12 months, obesity vs. normal weight was associated with a lower likelihood of remission (adjusted odds ratio [aOR], 0.33; P=.005). Obesity and illness perception were significantly associated with pain (aOR, 8.16; P = .002 and aOR, 0.62; P < .001, respectively) and fatigue (aOR, 5.66; P = .049 and aOR, 0.51; P = .001, respectively) with patients with severe vs. no anxiety having higher pain (aOR, 9.60; P = .010) and those with severe (aOR, 17.07; P < .001) and moderate (aOR, 10.13; P = .001) depression having higher fatigue.
Study details: This secondary analysis of the TITRATE trial included 335 patients with RA treated with intensive management (n=168) or standard care (n=167).
Disclosures: This study was funded by the National Institute for Health Research. E Nikiphorou received speaker fees and served on advisory boards for various sources. Other authors declared no competing interest.
Source: Lee SY et al. Arthritis Res Ther. 2021 Nov 4. doi: 10.1186/s13075-021-02653-1.
Key clinical point: Obesity, anxiety, depression, and illness perception at baseline were associated with treatment outcomes, pain, and fatigue in patients with rheumatoid arthritis (RA).
Major finding: At 12 months, obesity vs. normal weight was associated with a lower likelihood of remission (adjusted odds ratio [aOR], 0.33; P=.005). Obesity and illness perception were significantly associated with pain (aOR, 8.16; P = .002 and aOR, 0.62; P < .001, respectively) and fatigue (aOR, 5.66; P = .049 and aOR, 0.51; P = .001, respectively) with patients with severe vs. no anxiety having higher pain (aOR, 9.60; P = .010) and those with severe (aOR, 17.07; P < .001) and moderate (aOR, 10.13; P = .001) depression having higher fatigue.
Study details: This secondary analysis of the TITRATE trial included 335 patients with RA treated with intensive management (n=168) or standard care (n=167).
Disclosures: This study was funded by the National Institute for Health Research. E Nikiphorou received speaker fees and served on advisory boards for various sources. Other authors declared no competing interest.
Source: Lee SY et al. Arthritis Res Ther. 2021 Nov 4. doi: 10.1186/s13075-021-02653-1.
Key clinical point: Obesity, anxiety, depression, and illness perception at baseline were associated with treatment outcomes, pain, and fatigue in patients with rheumatoid arthritis (RA).
Major finding: At 12 months, obesity vs. normal weight was associated with a lower likelihood of remission (adjusted odds ratio [aOR], 0.33; P=.005). Obesity and illness perception were significantly associated with pain (aOR, 8.16; P = .002 and aOR, 0.62; P < .001, respectively) and fatigue (aOR, 5.66; P = .049 and aOR, 0.51; P = .001, respectively) with patients with severe vs. no anxiety having higher pain (aOR, 9.60; P = .010) and those with severe (aOR, 17.07; P < .001) and moderate (aOR, 10.13; P = .001) depression having higher fatigue.
Study details: This secondary analysis of the TITRATE trial included 335 patients with RA treated with intensive management (n=168) or standard care (n=167).
Disclosures: This study was funded by the National Institute for Health Research. E Nikiphorou received speaker fees and served on advisory boards for various sources. Other authors declared no competing interest.
Source: Lee SY et al. Arthritis Res Ther. 2021 Nov 4. doi: 10.1186/s13075-021-02653-1.
Certolizumab seems effective as monotherapy in RA patients with failure to csDMARDs
Key clinical point: Certolizumab (CTZ) monotherapy seemed as effective as combination therapy with methotrexate (MTX) or leflunomide (LFN) or MTX+LFN in patients with rheumatoid arthritis (RA) who failed previous conventional synthetic disease-modifying antirheumatic drugs (csDMARD) therapy.
Major finding: Overall, 63% of patients were in remission or showed low disease activity (LDA) within 3 months of follow-up, with no difference between groups (P = .080). Most patients maintained response at 12 months, with remission or LDA achieved by 94.4%, 81.8%, 80.5%, and 51.4% of patients receiving CTZ monotherapy, CTZ+MTX, CTZ+LFN, and MTX+LFN, respectively (P = .001).
Study details: This was a retrospective cohort study of 181 patients with RA who were treated for a minimum of 3 months with certolizumab as monotherapy (n=24) or in combination with MTX (n=62), LFN (n=47) or MTX+LFN (n=48).
Disclosures: No information on funding was provided. P Santos-Moreno and A Rojas-Villarrage received fees for conferences, counseling, advisory boards, or travel expenses and research grants from various sources.
Source: Santos-Moreno P et al. Biologics. 2021 Oct 22. doi: 10.2147/BTT.S322860.
Key clinical point: Certolizumab (CTZ) monotherapy seemed as effective as combination therapy with methotrexate (MTX) or leflunomide (LFN) or MTX+LFN in patients with rheumatoid arthritis (RA) who failed previous conventional synthetic disease-modifying antirheumatic drugs (csDMARD) therapy.
Major finding: Overall, 63% of patients were in remission or showed low disease activity (LDA) within 3 months of follow-up, with no difference between groups (P = .080). Most patients maintained response at 12 months, with remission or LDA achieved by 94.4%, 81.8%, 80.5%, and 51.4% of patients receiving CTZ monotherapy, CTZ+MTX, CTZ+LFN, and MTX+LFN, respectively (P = .001).
Study details: This was a retrospective cohort study of 181 patients with RA who were treated for a minimum of 3 months with certolizumab as monotherapy (n=24) or in combination with MTX (n=62), LFN (n=47) or MTX+LFN (n=48).
Disclosures: No information on funding was provided. P Santos-Moreno and A Rojas-Villarrage received fees for conferences, counseling, advisory boards, or travel expenses and research grants from various sources.
Source: Santos-Moreno P et al. Biologics. 2021 Oct 22. doi: 10.2147/BTT.S322860.
Key clinical point: Certolizumab (CTZ) monotherapy seemed as effective as combination therapy with methotrexate (MTX) or leflunomide (LFN) or MTX+LFN in patients with rheumatoid arthritis (RA) who failed previous conventional synthetic disease-modifying antirheumatic drugs (csDMARD) therapy.
Major finding: Overall, 63% of patients were in remission or showed low disease activity (LDA) within 3 months of follow-up, with no difference between groups (P = .080). Most patients maintained response at 12 months, with remission or LDA achieved by 94.4%, 81.8%, 80.5%, and 51.4% of patients receiving CTZ monotherapy, CTZ+MTX, CTZ+LFN, and MTX+LFN, respectively (P = .001).
Study details: This was a retrospective cohort study of 181 patients with RA who were treated for a minimum of 3 months with certolizumab as monotherapy (n=24) or in combination with MTX (n=62), LFN (n=47) or MTX+LFN (n=48).
Disclosures: No information on funding was provided. P Santos-Moreno and A Rojas-Villarrage received fees for conferences, counseling, advisory boards, or travel expenses and research grants from various sources.
Source: Santos-Moreno P et al. Biologics. 2021 Oct 22. doi: 10.2147/BTT.S322860.
T-helper cell derangements tied to atrial fibrillation in RA
Key clinical point: Elevated T helper (Th)1, Th17, or Th1/T-regulatory (Treg) cell frequencies in the peripheral blood were significantly associated with the development of atrial fibrillation (AF) in patients with rheumatoid arthritis (RA).
Major finding: The percentage of Th1 cells (adjusted odds ratio [aOR], 1.05; P = .0027], absolute number of Th17 cells (aOR, 1.11; P = .0046), and ratio of Th1/Treg (aOR, 1.08; P = .0374) were significantly associated with AF development in RA.
Study details: This was a retrospective case-control study of 40 patients with RA and AF who were propensity matched (1:3) with 120 control patients with RA.
Disclosures: This work was supported by the National Natural Science Foundation of China and the Excellent Youth Foundation of Shanxi Province. No conflict of interests was reported.
Source: Wang X et al. Front Immunol. 2021 Oct 15. doi: 10.3389/fimmu.2021.744254.
Key clinical point: Elevated T helper (Th)1, Th17, or Th1/T-regulatory (Treg) cell frequencies in the peripheral blood were significantly associated with the development of atrial fibrillation (AF) in patients with rheumatoid arthritis (RA).
Major finding: The percentage of Th1 cells (adjusted odds ratio [aOR], 1.05; P = .0027], absolute number of Th17 cells (aOR, 1.11; P = .0046), and ratio of Th1/Treg (aOR, 1.08; P = .0374) were significantly associated with AF development in RA.
Study details: This was a retrospective case-control study of 40 patients with RA and AF who were propensity matched (1:3) with 120 control patients with RA.
Disclosures: This work was supported by the National Natural Science Foundation of China and the Excellent Youth Foundation of Shanxi Province. No conflict of interests was reported.
Source: Wang X et al. Front Immunol. 2021 Oct 15. doi: 10.3389/fimmu.2021.744254.
Key clinical point: Elevated T helper (Th)1, Th17, or Th1/T-regulatory (Treg) cell frequencies in the peripheral blood were significantly associated with the development of atrial fibrillation (AF) in patients with rheumatoid arthritis (RA).
Major finding: The percentage of Th1 cells (adjusted odds ratio [aOR], 1.05; P = .0027], absolute number of Th17 cells (aOR, 1.11; P = .0046), and ratio of Th1/Treg (aOR, 1.08; P = .0374) were significantly associated with AF development in RA.
Study details: This was a retrospective case-control study of 40 patients with RA and AF who were propensity matched (1:3) with 120 control patients with RA.
Disclosures: This work was supported by the National Natural Science Foundation of China and the Excellent Youth Foundation of Shanxi Province. No conflict of interests was reported.
Source: Wang X et al. Front Immunol. 2021 Oct 15. doi: 10.3389/fimmu.2021.744254.