User login
Comorbidities may cut effectiveness of psoriasis biologics
PARIS – in response to biologic therapy, according to the results of the prospective observational PSO-BIO-REAL study.
The clinical importance of this finding lies in the fact that comorbidities are highly prevalent among patients with moderate to severe psoriasis. Indeed, fully 64% of the 846 participants in PSO-BIO-REAL had at least one major comorbid condition at baseline, Finn Ziegler said at the annual congress of the European Academy of Dermatology and Venereology.
“I think this reflects a picture that has been seen in other studies,” noted Mr. Ziegler, director of global patient access at Leo Pharma in Ballerup, Denmark.
The purpose of the 12-month PSO-BIO-REAL (PSOriasis treated with BIOlogics in REAL life) study was to assess the effectiveness of a variety of biologic agents in a real-world population typical of patients encountered in routine clinical practice, as opposed to more restrictive format of often-cited randomized trials, which generally feature a lengthy list of exclusions. One-third of participants were from the United States, with the rest drawn from four Western European countries. Their mean age was 47 years, with an 18.4-year history of psoriasis and a baseline Psoriasis Area and Severity Index (PASI) score of 14.3.
Sixty percent of participants were starting treatment with a biologic agent for the first time. The other 40% had prior biologic experience. At physician discretion, 61% of enrollees were put on a tumor necrosis factor inhibitor, either etanercept (Enbrel), adalimumab (Humira), or infliximab (Remicade); 30% initiated treatment with the interleukin-12/23 inhibitor ustekinumab (Stelara); and 9% received secukinumab (Cosentyx), an interleukin-17 inhibitor.
The five most common comorbid conditions present at baseline were hypertension, present in 33.5% of participants; psoriatic arthritis (PsA), present in 28.1%; hyperlipidemia, 20.9%; diabetes, 13.9%, and depression, present in 13.7% of the psoriasis patients.
Baseline comorbidities were significantly more common among the biologic-experienced patients. For example, their prevalence of hypertension was 42%, compared with 28% in the biologic-naive group. PsA was present in 35% of the biologic-experienced and 23% of the biologic-naive patients. Nineteen percent of biologic-experienced patients had diabetes at baseline, as did 11% of the biologic-naive group.
During the 12-month study, 3.7% of patients developed a new comorbidity, the most common being anxiety, hypertension, PsA, depression, and hyperlipidemia.
The primary outcome in the study was the complete clearance rate – a PASI 100 response – at 6 months. It ranged from a high of 31% in patients with no baseline comorbid conditions to a low of 16.5% in those with three or more. The results were similar at 12 months.
Conversely, an inadequate therapeutic response as defined by a PASI 50 or less at 6 months occurred in 15% of psoriasis patients with no baseline comorbidities, 27% with one, 35% with two comorbid conditions, and 28% with three or more.
The major caveat regarding this study is that the observed association between comorbid conditions and complete clearance rates doesn’t prove causality, Mr. Ziegler noted.
The PSO-BIO-REAL study was sponsored by Amgen, AstraZeneca, and Leo Pharma. Mr. Ziegler is a Leo executive.
SOURCE: Ziegler F. EADV Congress, Abstract FC04.01.
PARIS – in response to biologic therapy, according to the results of the prospective observational PSO-BIO-REAL study.
The clinical importance of this finding lies in the fact that comorbidities are highly prevalent among patients with moderate to severe psoriasis. Indeed, fully 64% of the 846 participants in PSO-BIO-REAL had at least one major comorbid condition at baseline, Finn Ziegler said at the annual congress of the European Academy of Dermatology and Venereology.
“I think this reflects a picture that has been seen in other studies,” noted Mr. Ziegler, director of global patient access at Leo Pharma in Ballerup, Denmark.
The purpose of the 12-month PSO-BIO-REAL (PSOriasis treated with BIOlogics in REAL life) study was to assess the effectiveness of a variety of biologic agents in a real-world population typical of patients encountered in routine clinical practice, as opposed to more restrictive format of often-cited randomized trials, which generally feature a lengthy list of exclusions. One-third of participants were from the United States, with the rest drawn from four Western European countries. Their mean age was 47 years, with an 18.4-year history of psoriasis and a baseline Psoriasis Area and Severity Index (PASI) score of 14.3.
Sixty percent of participants were starting treatment with a biologic agent for the first time. The other 40% had prior biologic experience. At physician discretion, 61% of enrollees were put on a tumor necrosis factor inhibitor, either etanercept (Enbrel), adalimumab (Humira), or infliximab (Remicade); 30% initiated treatment with the interleukin-12/23 inhibitor ustekinumab (Stelara); and 9% received secukinumab (Cosentyx), an interleukin-17 inhibitor.
The five most common comorbid conditions present at baseline were hypertension, present in 33.5% of participants; psoriatic arthritis (PsA), present in 28.1%; hyperlipidemia, 20.9%; diabetes, 13.9%, and depression, present in 13.7% of the psoriasis patients.
Baseline comorbidities were significantly more common among the biologic-experienced patients. For example, their prevalence of hypertension was 42%, compared with 28% in the biologic-naive group. PsA was present in 35% of the biologic-experienced and 23% of the biologic-naive patients. Nineteen percent of biologic-experienced patients had diabetes at baseline, as did 11% of the biologic-naive group.
During the 12-month study, 3.7% of patients developed a new comorbidity, the most common being anxiety, hypertension, PsA, depression, and hyperlipidemia.
The primary outcome in the study was the complete clearance rate – a PASI 100 response – at 6 months. It ranged from a high of 31% in patients with no baseline comorbid conditions to a low of 16.5% in those with three or more. The results were similar at 12 months.
Conversely, an inadequate therapeutic response as defined by a PASI 50 or less at 6 months occurred in 15% of psoriasis patients with no baseline comorbidities, 27% with one, 35% with two comorbid conditions, and 28% with three or more.
The major caveat regarding this study is that the observed association between comorbid conditions and complete clearance rates doesn’t prove causality, Mr. Ziegler noted.
The PSO-BIO-REAL study was sponsored by Amgen, AstraZeneca, and Leo Pharma. Mr. Ziegler is a Leo executive.
SOURCE: Ziegler F. EADV Congress, Abstract FC04.01.
PARIS – in response to biologic therapy, according to the results of the prospective observational PSO-BIO-REAL study.
The clinical importance of this finding lies in the fact that comorbidities are highly prevalent among patients with moderate to severe psoriasis. Indeed, fully 64% of the 846 participants in PSO-BIO-REAL had at least one major comorbid condition at baseline, Finn Ziegler said at the annual congress of the European Academy of Dermatology and Venereology.
“I think this reflects a picture that has been seen in other studies,” noted Mr. Ziegler, director of global patient access at Leo Pharma in Ballerup, Denmark.
The purpose of the 12-month PSO-BIO-REAL (PSOriasis treated with BIOlogics in REAL life) study was to assess the effectiveness of a variety of biologic agents in a real-world population typical of patients encountered in routine clinical practice, as opposed to more restrictive format of often-cited randomized trials, which generally feature a lengthy list of exclusions. One-third of participants were from the United States, with the rest drawn from four Western European countries. Their mean age was 47 years, with an 18.4-year history of psoriasis and a baseline Psoriasis Area and Severity Index (PASI) score of 14.3.
Sixty percent of participants were starting treatment with a biologic agent for the first time. The other 40% had prior biologic experience. At physician discretion, 61% of enrollees were put on a tumor necrosis factor inhibitor, either etanercept (Enbrel), adalimumab (Humira), or infliximab (Remicade); 30% initiated treatment with the interleukin-12/23 inhibitor ustekinumab (Stelara); and 9% received secukinumab (Cosentyx), an interleukin-17 inhibitor.
The five most common comorbid conditions present at baseline were hypertension, present in 33.5% of participants; psoriatic arthritis (PsA), present in 28.1%; hyperlipidemia, 20.9%; diabetes, 13.9%, and depression, present in 13.7% of the psoriasis patients.
Baseline comorbidities were significantly more common among the biologic-experienced patients. For example, their prevalence of hypertension was 42%, compared with 28% in the biologic-naive group. PsA was present in 35% of the biologic-experienced and 23% of the biologic-naive patients. Nineteen percent of biologic-experienced patients had diabetes at baseline, as did 11% of the biologic-naive group.
During the 12-month study, 3.7% of patients developed a new comorbidity, the most common being anxiety, hypertension, PsA, depression, and hyperlipidemia.
The primary outcome in the study was the complete clearance rate – a PASI 100 response – at 6 months. It ranged from a high of 31% in patients with no baseline comorbid conditions to a low of 16.5% in those with three or more. The results were similar at 12 months.
Conversely, an inadequate therapeutic response as defined by a PASI 50 or less at 6 months occurred in 15% of psoriasis patients with no baseline comorbidities, 27% with one, 35% with two comorbid conditions, and 28% with three or more.
The major caveat regarding this study is that the observed association between comorbid conditions and complete clearance rates doesn’t prove causality, Mr. Ziegler noted.
The PSO-BIO-REAL study was sponsored by Amgen, AstraZeneca, and Leo Pharma. Mr. Ziegler is a Leo executive.
SOURCE: Ziegler F. EADV Congress, Abstract FC04.01.
REPORTING FROM THE EADV CONGRESS
Key clinical point: As the number of baseline comorbid conditions increases, the complete clearance rate in response to biologic agents for psoriasis falls.
Major finding: The complete clearance rate after 6 months of biologic therapy ranged from a high of 31% in patients with no baseline comorbid conditions to a low of 16.5% in those with three or more.
Study details: This multinational, prospective, observational, 12-month study included 846 patients initiating biologic therapy for moderate to severe psoriasis.
Disclosures: The PSO-BIO-REAL study was sponsored by Amgen, AstraZeneca, and Leo Pharma and was presented by a Leo executive.
Source: Ziegler F. EADV Congress, Abstract FC04.01.
Uninterrupted ibrutinib with CAR T could improve CLL outcomes
SAN DIEGO – Ibrutinib treatment continued before, during, and after infusion of the CD19-specific chimeric antigen receptor (CAR) T-cell therapy JCAR014 in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) appears to improve patient responses and decrease the risk of severe cytokine release syndrome.

The findings come from a comparison of sequential cohorts from a phase 1/2 study.
At 4 weeks after infusion, the approach was highly efficacious; overall response rates by 2008 International Workshop on CLL (IWCLL) criteria were 83% in 24 patients who received the uninterrupted ibrutinib regimen along with the JCAR014 therapy – a combination of CD4 and CD8 T cells – and 65% in 19 patients from a prior cohort who did not receive continuous ibrutinib, Jordan Gauthier, MD, reported at the annual meeting of the American Society of Hematology.
Concurrent ibrutinib was generally well tolerated, with 13 of 19 patients in the ibrutinib cohort receiving treatment as planned without discontinuation. The rates of grade 1 or higher cytokine release syndrome (CRS) were statistically similar in the ibrutinib and no-ibrutinib cohorts (74% and 92%, respectively). However, the rates of severe CRS (grade 3 or higher) were, strikingly, 0% and 25%, respectively, said Dr. Gauthier, a senior fellow in the Turtle Lab at Fred Hutchinson Cancer Center, Seattle.
Neurotoxicity occurred in 32% and 42% of patients in the groups; severe neurotoxicity occurred in 26% and 29%, respectively.
In the ibrutinib cohort, one patient with grade 2 CRS developed fatal presumed cardiac arrhythmia; in the no-ibrutinib cohort, one patient died from a CAR T cell–related toxicity.
Notably, a trend toward better expansion of CD8 CAR T cells and a significantly greater expansion of CD4 CAR T cells was observed in the ibrutinib cohort, he said.
The study was designed to assess JCAR014, and based on the initial cohort findings published in 2017, established a regimen of cyclophosphamide and fludarabine (Cy/Flu) lymphodepletion followed by JCAR014 infusion at 2 x 106 CAR T cells/kg. The study was not a randomized, head-to-head comparison but the groups were similar with respect to both patient and disease characteristics, Dr. Gauthier noted.
The outcomes in the first cohort were then compared retrospectively with those from the subsequent cohort of patients who received Cy/Flu with 2 x 106 CAR T cells/kg with concurrent ibrutinib administered at 420 mg per day from at least 2 weeks prior to leukapheresis until at least 3 months after JCAR014 infusion.
The rationale for uninterrupted ibrutinib in relapsed/refractory CLL patients receiving JCAR014 included potential prevention of tumor flare, mobilization of CLL cells into the blood from the lymph nodes, improvement of CAR T-cell function, and a decrease in CAR T-cell related toxicity, he said.
The concurrent administration of ibrutinib and JCAR014 was feasible for most patients. “[It] induced high response rates and deep responses early on at 4 weeks, and it was associated with higher in vivo expansion of CD4 CAR T cells and with lower rates of severe toxicity,” Dr. Gauthier said. “The next step is to hopefully validate these findings in a prospective phase 1/2 study.”
Dr. Gauthier reported having no financial disclosures.
SOURCE: Gauthier J et al. ASH 18, Abstract 299.
SAN DIEGO – Ibrutinib treatment continued before, during, and after infusion of the CD19-specific chimeric antigen receptor (CAR) T-cell therapy JCAR014 in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) appears to improve patient responses and decrease the risk of severe cytokine release syndrome.
The findings come from a comparison of sequential cohorts from a phase 1/2 study.
At 4 weeks after infusion, the approach was highly efficacious; overall response rates by 2008 International Workshop on CLL (IWCLL) criteria were 83% in 24 patients who received the uninterrupted ibrutinib regimen along with the JCAR014 therapy – a combination of CD4 and CD8 T cells – and 65% in 19 patients from a prior cohort who did not receive continuous ibrutinib, Jordan Gauthier, MD, reported at the annual meeting of the American Society of Hematology.
Concurrent ibrutinib was generally well tolerated, with 13 of 19 patients in the ibrutinib cohort receiving treatment as planned without discontinuation. The rates of grade 1 or higher cytokine release syndrome (CRS) were statistically similar in the ibrutinib and no-ibrutinib cohorts (74% and 92%, respectively). However, the rates of severe CRS (grade 3 or higher) were, strikingly, 0% and 25%, respectively, said Dr. Gauthier, a senior fellow in the Turtle Lab at Fred Hutchinson Cancer Center, Seattle.
Neurotoxicity occurred in 32% and 42% of patients in the groups; severe neurotoxicity occurred in 26% and 29%, respectively.
In the ibrutinib cohort, one patient with grade 2 CRS developed fatal presumed cardiac arrhythmia; in the no-ibrutinib cohort, one patient died from a CAR T cell–related toxicity.
Notably, a trend toward better expansion of CD8 CAR T cells and a significantly greater expansion of CD4 CAR T cells was observed in the ibrutinib cohort, he said.
The study was designed to assess JCAR014, and based on the initial cohort findings published in 2017, established a regimen of cyclophosphamide and fludarabine (Cy/Flu) lymphodepletion followed by JCAR014 infusion at 2 x 106 CAR T cells/kg. The study was not a randomized, head-to-head comparison but the groups were similar with respect to both patient and disease characteristics, Dr. Gauthier noted.
The outcomes in the first cohort were then compared retrospectively with those from the subsequent cohort of patients who received Cy/Flu with 2 x 106 CAR T cells/kg with concurrent ibrutinib administered at 420 mg per day from at least 2 weeks prior to leukapheresis until at least 3 months after JCAR014 infusion.
The rationale for uninterrupted ibrutinib in relapsed/refractory CLL patients receiving JCAR014 included potential prevention of tumor flare, mobilization of CLL cells into the blood from the lymph nodes, improvement of CAR T-cell function, and a decrease in CAR T-cell related toxicity, he said.
The concurrent administration of ibrutinib and JCAR014 was feasible for most patients. “[It] induced high response rates and deep responses early on at 4 weeks, and it was associated with higher in vivo expansion of CD4 CAR T cells and with lower rates of severe toxicity,” Dr. Gauthier said. “The next step is to hopefully validate these findings in a prospective phase 1/2 study.”
Dr. Gauthier reported having no financial disclosures.
SOURCE: Gauthier J et al. ASH 18, Abstract 299.
SAN DIEGO – Ibrutinib treatment continued before, during, and after infusion of the CD19-specific chimeric antigen receptor (CAR) T-cell therapy JCAR014 in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) appears to improve patient responses and decrease the risk of severe cytokine release syndrome.
The findings come from a comparison of sequential cohorts from a phase 1/2 study.
At 4 weeks after infusion, the approach was highly efficacious; overall response rates by 2008 International Workshop on CLL (IWCLL) criteria were 83% in 24 patients who received the uninterrupted ibrutinib regimen along with the JCAR014 therapy – a combination of CD4 and CD8 T cells – and 65% in 19 patients from a prior cohort who did not receive continuous ibrutinib, Jordan Gauthier, MD, reported at the annual meeting of the American Society of Hematology.
Concurrent ibrutinib was generally well tolerated, with 13 of 19 patients in the ibrutinib cohort receiving treatment as planned without discontinuation. The rates of grade 1 or higher cytokine release syndrome (CRS) were statistically similar in the ibrutinib and no-ibrutinib cohorts (74% and 92%, respectively). However, the rates of severe CRS (grade 3 or higher) were, strikingly, 0% and 25%, respectively, said Dr. Gauthier, a senior fellow in the Turtle Lab at Fred Hutchinson Cancer Center, Seattle.
Neurotoxicity occurred in 32% and 42% of patients in the groups; severe neurotoxicity occurred in 26% and 29%, respectively.
In the ibrutinib cohort, one patient with grade 2 CRS developed fatal presumed cardiac arrhythmia; in the no-ibrutinib cohort, one patient died from a CAR T cell–related toxicity.
Notably, a trend toward better expansion of CD8 CAR T cells and a significantly greater expansion of CD4 CAR T cells was observed in the ibrutinib cohort, he said.
The study was designed to assess JCAR014, and based on the initial cohort findings published in 2017, established a regimen of cyclophosphamide and fludarabine (Cy/Flu) lymphodepletion followed by JCAR014 infusion at 2 x 106 CAR T cells/kg. The study was not a randomized, head-to-head comparison but the groups were similar with respect to both patient and disease characteristics, Dr. Gauthier noted.
The outcomes in the first cohort were then compared retrospectively with those from the subsequent cohort of patients who received Cy/Flu with 2 x 106 CAR T cells/kg with concurrent ibrutinib administered at 420 mg per day from at least 2 weeks prior to leukapheresis until at least 3 months after JCAR014 infusion.
The rationale for uninterrupted ibrutinib in relapsed/refractory CLL patients receiving JCAR014 included potential prevention of tumor flare, mobilization of CLL cells into the blood from the lymph nodes, improvement of CAR T-cell function, and a decrease in CAR T-cell related toxicity, he said.
The concurrent administration of ibrutinib and JCAR014 was feasible for most patients. “[It] induced high response rates and deep responses early on at 4 weeks, and it was associated with higher in vivo expansion of CD4 CAR T cells and with lower rates of severe toxicity,” Dr. Gauthier said. “The next step is to hopefully validate these findings in a prospective phase 1/2 study.”
Dr. Gauthier reported having no financial disclosures.
SOURCE: Gauthier J et al. ASH 18, Abstract 299.
REPORTING FROM ASH 2018
Key clinical point:
Major finding: Severe cytokine release syndrome occurred in 0% versus 25% of patients in the ibrutinib and no-ibrutinib cohorts, respectively.
Study details: A retrospective comparison of 43 patients in two cohorts from a phase 1/2 study.
Disclosures: Dr. Gauthier reported having no financial disclosures.
Source: Gauthier J et al. ASH 2018, Abstract 299.
Strategic planning for physicians
1) You are probably never going to be reimbursed better than you are today.
“Wait,” you say, “Don’t we get occasional Medicare updates?”
Yes, but these never keep up with inflation, just as any unlikely increases from private insurers always lag behind the cost of providing the service and have been grinding down toward Medicare rates – or even below them – for years. Any other sweeping insurance proposals, such as Medicare for All, include a hefty cut to physician reimbursement. One exception might be allowing those under age 55 years to buy into the existing Medicare program, which would be beneficial in areas where current private insurers and Medicare Advantage plans pay less than Medicare. It is also possible that you could see some increase if you are on the right side of bundled payments, although this has been more of a threat of penalty rather than a reward so far.
2) Don’t expect an imminent repeal of the ACA
The Affordable Care Act (ACA) favors large groups, and it is still the law, and it’s likely to remain the law for at least the next 5-10 years. Republicans could not repeal it when they held both the Senate and House, as well as the presidency, and certainly Democrats won’t repeal it.

There are myriad regulations and rules that only allow larger groups to reap the benefits from the ACA. Recall President Obama visiting the Cleveland Clinic and touting it and the Geisinger Clinic as examples of the way American medicine should be practiced.
Participation in alternative payment models that bypass many of the onerous requirements of “quality improvement,” and may even allow shared cost savings, are only practical for large groups. A notable exception is the recently proposed “site neutrality of payment” rule proposed by the current administration. This reduces by 50% or so the premium paid to large physician/hospital groups that are not located on the hospital campus to the prevailing rate of pay in the community. No more $3,000echocardiograms that used to cost $300.
Still, this does not increase the overall payments to physicians. Possibly, the proposed new telemedicine reimbursement rules may allow you to more efficiently manage patients without dramatically increasing your overhead.
3) Medicare recipients are going to grow exponentially.
An estimated 10,000 Baby Boomers are turning age 65 years every day. This ensures an increasing supply of patients, but also strains a federal government that has overpromised on Medicare and Social Security benefits. Recall that on average every Medicare recipient takes out far more than what they put into the program.
It is pay-up time, and the IOUs in the lockbox are unredeemable. This makes inflation and cutting reimbursements the easiest way to cope with older voters and a looming budget crisis.
4) Physicians are the weakest leg of the health care chair.
Hospitals, pharma, and insurers all have more powerful lobbying groups, donate more, and are better organized than physician groups. In our system of government, that means they will be favored in health care–related legislation. Physicians are the easiest to cut, although we account for only 15.9% of expenditures, according to 2014 data from the AMA.
The hospitals can close, insurers can refuse to write policies, and pharma can refuse to develop new drugs or manufacture generic ones. Big money (for example, Amazon, Berkshire Hathaway, and JPMorgan Chase) wants to consolidate health care and vertically integrate it. Most physicians cannot even unionize.
So what cheerful conclusions can we draw? If you go to work for a big group, try to negotiate the least restrictive practice covenant possible – or at least one that is not applicable if you are terminated without “cause.” The big group may have to disgorge you someday, and it could be disastrous to have to move or not be able to practice. If you opt for a small group or private practice, keep it small and lean. Build no palaces. There are special small practice situations that will survive or even prosper. Tightly managing your overhead is the key to survival.
Young physicians should recognize that the opportunity costs of an extensive residency after medical school may not be worth it. In fact, considering tuition that results in huge debt, lost income, and lost years of practice, high school graduates aspiring to a career in health care may do better from an economic perspective by pursuing a career as a nurse practitioner or physician assistant than one as a physician. The ACA, with its favoritism to large groups, will not be repealed anytime soon, and the regulations favoring larger groups are not even under discussion. This makes even hospital management more attractive as a career choice.
5. You’ll be doing more with less.
With a projected shortage of more than 100,000 physicians in the next 11 years, prepare for a high volume of patients, less pay for each encounter, and responsibility for multiple extenders. Practice will be much more stressful and difficult than simply managing your own panel of patients. Expect physician networks so narrow that they include only primary care physicians, with all other physicians having moved, died, or retired. It is much easier for insurers to save money by not receiving bills. Start thinking about integrating telemedicine into your practice because this may be a lifeline considering the most recent Medicare final rule that provides for payment for several new telehealth codes.
That all said, I must quote a lawmaker who, when discussing the ACA, told me “Well, you doctors are awfully late to the punch bowl” to which I replied, “Without doctors, there is no punch in the punch bowl.”
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
1) You are probably never going to be reimbursed better than you are today.
“Wait,” you say, “Don’t we get occasional Medicare updates?”
Yes, but these never keep up with inflation, just as any unlikely increases from private insurers always lag behind the cost of providing the service and have been grinding down toward Medicare rates – or even below them – for years. Any other sweeping insurance proposals, such as Medicare for All, include a hefty cut to physician reimbursement. One exception might be allowing those under age 55 years to buy into the existing Medicare program, which would be beneficial in areas where current private insurers and Medicare Advantage plans pay less than Medicare. It is also possible that you could see some increase if you are on the right side of bundled payments, although this has been more of a threat of penalty rather than a reward so far.
2) Don’t expect an imminent repeal of the ACA
The Affordable Care Act (ACA) favors large groups, and it is still the law, and it’s likely to remain the law for at least the next 5-10 years. Republicans could not repeal it when they held both the Senate and House, as well as the presidency, and certainly Democrats won’t repeal it.
There are myriad regulations and rules that only allow larger groups to reap the benefits from the ACA. Recall President Obama visiting the Cleveland Clinic and touting it and the Geisinger Clinic as examples of the way American medicine should be practiced.
Participation in alternative payment models that bypass many of the onerous requirements of “quality improvement,” and may even allow shared cost savings, are only practical for large groups. A notable exception is the recently proposed “site neutrality of payment” rule proposed by the current administration. This reduces by 50% or so the premium paid to large physician/hospital groups that are not located on the hospital campus to the prevailing rate of pay in the community. No more $3,000echocardiograms that used to cost $300.
Still, this does not increase the overall payments to physicians. Possibly, the proposed new telemedicine reimbursement rules may allow you to more efficiently manage patients without dramatically increasing your overhead.
3) Medicare recipients are going to grow exponentially.
An estimated 10,000 Baby Boomers are turning age 65 years every day. This ensures an increasing supply of patients, but also strains a federal government that has overpromised on Medicare and Social Security benefits. Recall that on average every Medicare recipient takes out far more than what they put into the program.
It is pay-up time, and the IOUs in the lockbox are unredeemable. This makes inflation and cutting reimbursements the easiest way to cope with older voters and a looming budget crisis.
4) Physicians are the weakest leg of the health care chair.
Hospitals, pharma, and insurers all have more powerful lobbying groups, donate more, and are better organized than physician groups. In our system of government, that means they will be favored in health care–related legislation. Physicians are the easiest to cut, although we account for only 15.9% of expenditures, according to 2014 data from the AMA.
The hospitals can close, insurers can refuse to write policies, and pharma can refuse to develop new drugs or manufacture generic ones. Big money (for example, Amazon, Berkshire Hathaway, and JPMorgan Chase) wants to consolidate health care and vertically integrate it. Most physicians cannot even unionize.
So what cheerful conclusions can we draw? If you go to work for a big group, try to negotiate the least restrictive practice covenant possible – or at least one that is not applicable if you are terminated without “cause.” The big group may have to disgorge you someday, and it could be disastrous to have to move or not be able to practice. If you opt for a small group or private practice, keep it small and lean. Build no palaces. There are special small practice situations that will survive or even prosper. Tightly managing your overhead is the key to survival.
Young physicians should recognize that the opportunity costs of an extensive residency after medical school may not be worth it. In fact, considering tuition that results in huge debt, lost income, and lost years of practice, high school graduates aspiring to a career in health care may do better from an economic perspective by pursuing a career as a nurse practitioner or physician assistant than one as a physician. The ACA, with its favoritism to large groups, will not be repealed anytime soon, and the regulations favoring larger groups are not even under discussion. This makes even hospital management more attractive as a career choice.
5. You’ll be doing more with less.
With a projected shortage of more than 100,000 physicians in the next 11 years, prepare for a high volume of patients, less pay for each encounter, and responsibility for multiple extenders. Practice will be much more stressful and difficult than simply managing your own panel of patients. Expect physician networks so narrow that they include only primary care physicians, with all other physicians having moved, died, or retired. It is much easier for insurers to save money by not receiving bills. Start thinking about integrating telemedicine into your practice because this may be a lifeline considering the most recent Medicare final rule that provides for payment for several new telehealth codes.
That all said, I must quote a lawmaker who, when discussing the ACA, told me “Well, you doctors are awfully late to the punch bowl” to which I replied, “Without doctors, there is no punch in the punch bowl.”
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
1) You are probably never going to be reimbursed better than you are today.
“Wait,” you say, “Don’t we get occasional Medicare updates?”
Yes, but these never keep up with inflation, just as any unlikely increases from private insurers always lag behind the cost of providing the service and have been grinding down toward Medicare rates – or even below them – for years. Any other sweeping insurance proposals, such as Medicare for All, include a hefty cut to physician reimbursement. One exception might be allowing those under age 55 years to buy into the existing Medicare program, which would be beneficial in areas where current private insurers and Medicare Advantage plans pay less than Medicare. It is also possible that you could see some increase if you are on the right side of bundled payments, although this has been more of a threat of penalty rather than a reward so far.
2) Don’t expect an imminent repeal of the ACA
The Affordable Care Act (ACA) favors large groups, and it is still the law, and it’s likely to remain the law for at least the next 5-10 years. Republicans could not repeal it when they held both the Senate and House, as well as the presidency, and certainly Democrats won’t repeal it.
There are myriad regulations and rules that only allow larger groups to reap the benefits from the ACA. Recall President Obama visiting the Cleveland Clinic and touting it and the Geisinger Clinic as examples of the way American medicine should be practiced.
Participation in alternative payment models that bypass many of the onerous requirements of “quality improvement,” and may even allow shared cost savings, are only practical for large groups. A notable exception is the recently proposed “site neutrality of payment” rule proposed by the current administration. This reduces by 50% or so the premium paid to large physician/hospital groups that are not located on the hospital campus to the prevailing rate of pay in the community. No more $3,000echocardiograms that used to cost $300.
Still, this does not increase the overall payments to physicians. Possibly, the proposed new telemedicine reimbursement rules may allow you to more efficiently manage patients without dramatically increasing your overhead.
3) Medicare recipients are going to grow exponentially.
An estimated 10,000 Baby Boomers are turning age 65 years every day. This ensures an increasing supply of patients, but also strains a federal government that has overpromised on Medicare and Social Security benefits. Recall that on average every Medicare recipient takes out far more than what they put into the program.
It is pay-up time, and the IOUs in the lockbox are unredeemable. This makes inflation and cutting reimbursements the easiest way to cope with older voters and a looming budget crisis.
4) Physicians are the weakest leg of the health care chair.
Hospitals, pharma, and insurers all have more powerful lobbying groups, donate more, and are better organized than physician groups. In our system of government, that means they will be favored in health care–related legislation. Physicians are the easiest to cut, although we account for only 15.9% of expenditures, according to 2014 data from the AMA.
The hospitals can close, insurers can refuse to write policies, and pharma can refuse to develop new drugs or manufacture generic ones. Big money (for example, Amazon, Berkshire Hathaway, and JPMorgan Chase) wants to consolidate health care and vertically integrate it. Most physicians cannot even unionize.
So what cheerful conclusions can we draw? If you go to work for a big group, try to negotiate the least restrictive practice covenant possible – or at least one that is not applicable if you are terminated without “cause.” The big group may have to disgorge you someday, and it could be disastrous to have to move or not be able to practice. If you opt for a small group or private practice, keep it small and lean. Build no palaces. There are special small practice situations that will survive or even prosper. Tightly managing your overhead is the key to survival.
Young physicians should recognize that the opportunity costs of an extensive residency after medical school may not be worth it. In fact, considering tuition that results in huge debt, lost income, and lost years of practice, high school graduates aspiring to a career in health care may do better from an economic perspective by pursuing a career as a nurse practitioner or physician assistant than one as a physician. The ACA, with its favoritism to large groups, will not be repealed anytime soon, and the regulations favoring larger groups are not even under discussion. This makes even hospital management more attractive as a career choice.
5. You’ll be doing more with less.
With a projected shortage of more than 100,000 physicians in the next 11 years, prepare for a high volume of patients, less pay for each encounter, and responsibility for multiple extenders. Practice will be much more stressful and difficult than simply managing your own panel of patients. Expect physician networks so narrow that they include only primary care physicians, with all other physicians having moved, died, or retired. It is much easier for insurers to save money by not receiving bills. Start thinking about integrating telemedicine into your practice because this may be a lifeline considering the most recent Medicare final rule that provides for payment for several new telehealth codes.
That all said, I must quote a lawmaker who, when discussing the ACA, told me “Well, you doctors are awfully late to the punch bowl” to which I replied, “Without doctors, there is no punch in the punch bowl.”
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at [email protected].
Prescribed opioids and pneumonia risk
Also today, evidence of herd immunity with the HPV vaccine, COPD is linked to higher in-hosptial death rates in peripheral arterial disease, and discussions of actinic keratoses need to include the word cancer.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, evidence of herd immunity with the HPV vaccine, COPD is linked to higher in-hosptial death rates in peripheral arterial disease, and discussions of actinic keratoses need to include the word cancer.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, evidence of herd immunity with the HPV vaccine, COPD is linked to higher in-hosptial death rates in peripheral arterial disease, and discussions of actinic keratoses need to include the word cancer.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Diagnosing Anemia
This clinical puzzle is based on O’Neil. Diagnosing and classifying anemia in adult primary care. Clinician Reviews. 2017; 27(8):28-35.
For the best mobile experience, rotate screen to landscape mode.
Have feedback on our new crossword puzzle? Share your thoughts at [email protected].
This clinical puzzle is based on O’Neil. Diagnosing and classifying anemia in adult primary care. Clinician Reviews. 2017; 27(8):28-35.
For the best mobile experience, rotate screen to landscape mode.
Have feedback on our new crossword puzzle? Share your thoughts at [email protected].
This clinical puzzle is based on O’Neil. Diagnosing and classifying anemia in adult primary care. Clinician Reviews. 2017; 27(8):28-35.
For the best mobile experience, rotate screen to landscape mode.
Have feedback on our new crossword puzzle? Share your thoughts at [email protected].

Age of migraine onset may affect stroke risk
The age at which a patient develops migraine with aura may be an important factor in assessing stroke risk, according to a prospective cohort study published in Headache.

Patients who had onset of migraine with visual aura after age 50 years had an increased risk of ischemic stroke, compared with patients with no headache, the researchers found. Patients with longer exposure to migraine with visual aura – that is, onset before age 50 years – did not have significantly increased ischemic stroke risk, said X. Michelle Androulakis, MD, of the department of neurology at the University of South Carolina in Columbia, and her colleagues.
“Migraine, especially migraine with aura, is associated with increased risk of ischemic stroke,” but whether age of migraine onset affects the risk of cardiovascular disease has been unclear, the researchers said.
To examine the risk of ischemic stroke in migraineurs with and without aura with onset before and after age 50 years, the investigators conducted a post hoc analysis of data from the ongoing Atherosclerosis Risk in Communities (ARIC) study. The researchers adjusted for potential confounders, including diabetes, body mass index, hypertension, and hyperlipidemia.
In ARIC, participants completed a questionnaire about their migraine history at their third study visit (1993-1995) and were followed for ischemic stroke incidence over 20 years.
Of the 11,592 ARIC participants included in the analysis (mean age, 61 years; 76.5% white; and 55.3% female), 447 had migraine with aura, and 1,128 had migraine without aura. Onset of migraine with aura at age 50 years or older (average duration, 4.75 years) was associated with more than twofold greater risk of ischemic stroke, compared with no headache (multivariable adjusted hazard ratio = 2.17). Onset of migraine with aura before age 50 years (average duration, 28.17 years) was not significantly associated with stroke. A logistic regression model yielded consistent results.
In addition, patients with migraine without aura did not have an increased risk of stroke, regardless of the age of onset. The absolute risk for stroke in migraine with aura was 8.27%, and the absolute risk in migraine without aura was 4.25%.
“We found unexpected results suggesting that the onset of migraine with aura before age 50 is not associated with ischemic stroke. ... These results are specific to first-time ischemic stroke incidents that occurred in mid- to late life; therefore, it cannot be generalized to stroke in younger patients,” the authors wrote.
It could be that migraine with aura symptoms that start at a later age are a red flag for paradoxical emboli from a patent foramen ovale or microemboli, Dr. Androulakis and her colleagues noted. It also is possible that the degree of cortical spreading depression required to induce migraine with aura symptoms is different later in life versus earlier in life.
“This study underscores the importance of MA symptoms onset in evaluation of ischemic stroke risk in late life,” the researchers concluded.
The authors had no relevant conflicts of interest. ARIC has been funded by the National Heart, Lung, and Blood Institute.
SOURCE: Androulakis XM et al. Headache. 2019 Jan 21. doi: 10.1111/head.13468.
The age at which a patient develops migraine with aura may be an important factor in assessing stroke risk, according to a prospective cohort study published in Headache.
Patients who had onset of migraine with visual aura after age 50 years had an increased risk of ischemic stroke, compared with patients with no headache, the researchers found. Patients with longer exposure to migraine with visual aura – that is, onset before age 50 years – did not have significantly increased ischemic stroke risk, said X. Michelle Androulakis, MD, of the department of neurology at the University of South Carolina in Columbia, and her colleagues.
“Migraine, especially migraine with aura, is associated with increased risk of ischemic stroke,” but whether age of migraine onset affects the risk of cardiovascular disease has been unclear, the researchers said.
To examine the risk of ischemic stroke in migraineurs with and without aura with onset before and after age 50 years, the investigators conducted a post hoc analysis of data from the ongoing Atherosclerosis Risk in Communities (ARIC) study. The researchers adjusted for potential confounders, including diabetes, body mass index, hypertension, and hyperlipidemia.
In ARIC, participants completed a questionnaire about their migraine history at their third study visit (1993-1995) and were followed for ischemic stroke incidence over 20 years.
Of the 11,592 ARIC participants included in the analysis (mean age, 61 years; 76.5% white; and 55.3% female), 447 had migraine with aura, and 1,128 had migraine without aura. Onset of migraine with aura at age 50 years or older (average duration, 4.75 years) was associated with more than twofold greater risk of ischemic stroke, compared with no headache (multivariable adjusted hazard ratio = 2.17). Onset of migraine with aura before age 50 years (average duration, 28.17 years) was not significantly associated with stroke. A logistic regression model yielded consistent results.
In addition, patients with migraine without aura did not have an increased risk of stroke, regardless of the age of onset. The absolute risk for stroke in migraine with aura was 8.27%, and the absolute risk in migraine without aura was 4.25%.
“We found unexpected results suggesting that the onset of migraine with aura before age 50 is not associated with ischemic stroke. ... These results are specific to first-time ischemic stroke incidents that occurred in mid- to late life; therefore, it cannot be generalized to stroke in younger patients,” the authors wrote.
It could be that migraine with aura symptoms that start at a later age are a red flag for paradoxical emboli from a patent foramen ovale or microemboli, Dr. Androulakis and her colleagues noted. It also is possible that the degree of cortical spreading depression required to induce migraine with aura symptoms is different later in life versus earlier in life.
“This study underscores the importance of MA symptoms onset in evaluation of ischemic stroke risk in late life,” the researchers concluded.
The authors had no relevant conflicts of interest. ARIC has been funded by the National Heart, Lung, and Blood Institute.
SOURCE: Androulakis XM et al. Headache. 2019 Jan 21. doi: 10.1111/head.13468.
The age at which a patient develops migraine with aura may be an important factor in assessing stroke risk, according to a prospective cohort study published in Headache.
Patients who had onset of migraine with visual aura after age 50 years had an increased risk of ischemic stroke, compared with patients with no headache, the researchers found. Patients with longer exposure to migraine with visual aura – that is, onset before age 50 years – did not have significantly increased ischemic stroke risk, said X. Michelle Androulakis, MD, of the department of neurology at the University of South Carolina in Columbia, and her colleagues.
“Migraine, especially migraine with aura, is associated with increased risk of ischemic stroke,” but whether age of migraine onset affects the risk of cardiovascular disease has been unclear, the researchers said.
To examine the risk of ischemic stroke in migraineurs with and without aura with onset before and after age 50 years, the investigators conducted a post hoc analysis of data from the ongoing Atherosclerosis Risk in Communities (ARIC) study. The researchers adjusted for potential confounders, including diabetes, body mass index, hypertension, and hyperlipidemia.
In ARIC, participants completed a questionnaire about their migraine history at their third study visit (1993-1995) and were followed for ischemic stroke incidence over 20 years.
Of the 11,592 ARIC participants included in the analysis (mean age, 61 years; 76.5% white; and 55.3% female), 447 had migraine with aura, and 1,128 had migraine without aura. Onset of migraine with aura at age 50 years or older (average duration, 4.75 years) was associated with more than twofold greater risk of ischemic stroke, compared with no headache (multivariable adjusted hazard ratio = 2.17). Onset of migraine with aura before age 50 years (average duration, 28.17 years) was not significantly associated with stroke. A logistic regression model yielded consistent results.
In addition, patients with migraine without aura did not have an increased risk of stroke, regardless of the age of onset. The absolute risk for stroke in migraine with aura was 8.27%, and the absolute risk in migraine without aura was 4.25%.
“We found unexpected results suggesting that the onset of migraine with aura before age 50 is not associated with ischemic stroke. ... These results are specific to first-time ischemic stroke incidents that occurred in mid- to late life; therefore, it cannot be generalized to stroke in younger patients,” the authors wrote.
It could be that migraine with aura symptoms that start at a later age are a red flag for paradoxical emboli from a patent foramen ovale or microemboli, Dr. Androulakis and her colleagues noted. It also is possible that the degree of cortical spreading depression required to induce migraine with aura symptoms is different later in life versus earlier in life.
“This study underscores the importance of MA symptoms onset in evaluation of ischemic stroke risk in late life,” the researchers concluded.
The authors had no relevant conflicts of interest. ARIC has been funded by the National Heart, Lung, and Blood Institute.
SOURCE: Androulakis XM et al. Headache. 2019 Jan 21. doi: 10.1111/head.13468.
FROM HEADACHE
Key clinical point: Age of migraine onset may be an important factor in assessing stroke risk.
Major finding: (multivariable adjusted hazard ratio = 2.17).
Study details: A post hoc analysis of data from more than 11,500 participants in the Atherosclerosis Risk in Communities (ARIC) study.
Disclosures: The authors had no relevant conflicts of interest. ARIC has been funded by the National Heart, Lung, and Blood Institute.
Source: Androulakis XM et al. Headache. 2019 Jan 21. doi: 10.1111/head.13468.
Survey: Americans support Medicare for all
A majority of Americans support the concept of Medicare for all, but “larger majorities favor more incremental changes to the health care system,” according to a new survey by the Kaiser Family Foundation.
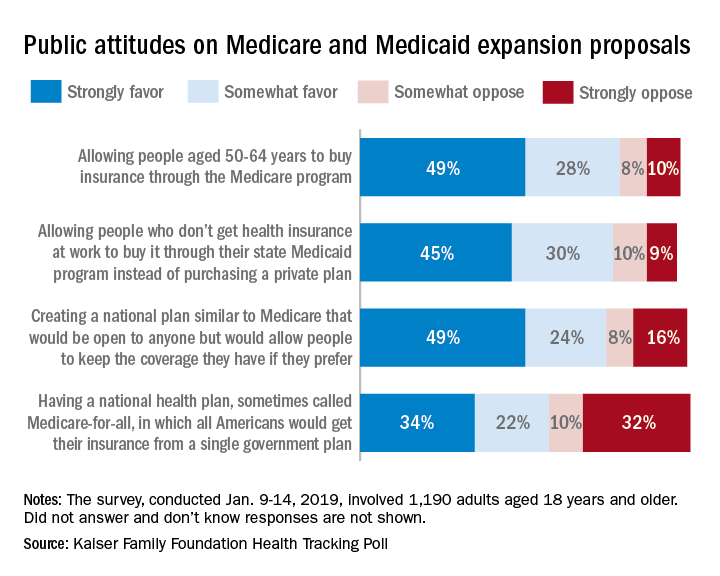
Support for a Medicare-for-all health care system came in at 56% (strongly favor, 34%; somewhat favor, 22%) among the 1,190 respondents to the latest KFF Health Tracking Poll, which was conducted Jan. 9-14, 2019. That support came largely from Democrats, 81% of whom favored the plan, compared with only 23% of Republicans, the Kaiser investigators said Jan. 23.
A Medicare buy-in plan for Americans aged 50-64 years also was highly popular, receiving support from 77% of all respondents – 85% of Democrats, 75% of Independents, and 69% of Republicans. Support by party identification was similar for a proposal to enable all those who don’t have employer-based insurance to get coverage through state Medicaid programs, which received 75% support overall, they reported.
Just behind those proposals at 74% support was a federally administered health plan that would be open to anyone but would allow people to keep the coverage they have. It was the most popular proposal among Democrats (91%) but did not garner a majority among Republicans (47%), the investigators said.
Support for the Medicare-for-all plan varied considerably, depending on number of arguments presented to respondents. When told that such a proposal would guarantee insurance as a right for all Americans, 71% favored it, and when they heard that it would eliminate health insurance premiums and reduce out-of-pockets costs, 67% of respondents expressed support. Favorable responses, however, were in the minority when people were told that Medicare-for-all would eliminate private health insurance companies (37%), threaten the current Medicare program (32%), and lead to some delayed medical tests and treatments (26%), according to the Kaiser report.
A majority of Americans support the concept of Medicare for all, but “larger majorities favor more incremental changes to the health care system,” according to a new survey by the Kaiser Family Foundation.
Support for a Medicare-for-all health care system came in at 56% (strongly favor, 34%; somewhat favor, 22%) among the 1,190 respondents to the latest KFF Health Tracking Poll, which was conducted Jan. 9-14, 2019. That support came largely from Democrats, 81% of whom favored the plan, compared with only 23% of Republicans, the Kaiser investigators said Jan. 23.
A Medicare buy-in plan for Americans aged 50-64 years also was highly popular, receiving support from 77% of all respondents – 85% of Democrats, 75% of Independents, and 69% of Republicans. Support by party identification was similar for a proposal to enable all those who don’t have employer-based insurance to get coverage through state Medicaid programs, which received 75% support overall, they reported.
Just behind those proposals at 74% support was a federally administered health plan that would be open to anyone but would allow people to keep the coverage they have. It was the most popular proposal among Democrats (91%) but did not garner a majority among Republicans (47%), the investigators said.
Support for the Medicare-for-all plan varied considerably, depending on number of arguments presented to respondents. When told that such a proposal would guarantee insurance as a right for all Americans, 71% favored it, and when they heard that it would eliminate health insurance premiums and reduce out-of-pockets costs, 67% of respondents expressed support. Favorable responses, however, were in the minority when people were told that Medicare-for-all would eliminate private health insurance companies (37%), threaten the current Medicare program (32%), and lead to some delayed medical tests and treatments (26%), according to the Kaiser report.
A majority of Americans support the concept of Medicare for all, but “larger majorities favor more incremental changes to the health care system,” according to a new survey by the Kaiser Family Foundation.
Support for a Medicare-for-all health care system came in at 56% (strongly favor, 34%; somewhat favor, 22%) among the 1,190 respondents to the latest KFF Health Tracking Poll, which was conducted Jan. 9-14, 2019. That support came largely from Democrats, 81% of whom favored the plan, compared with only 23% of Republicans, the Kaiser investigators said Jan. 23.
A Medicare buy-in plan for Americans aged 50-64 years also was highly popular, receiving support from 77% of all respondents – 85% of Democrats, 75% of Independents, and 69% of Republicans. Support by party identification was similar for a proposal to enable all those who don’t have employer-based insurance to get coverage through state Medicaid programs, which received 75% support overall, they reported.
Just behind those proposals at 74% support was a federally administered health plan that would be open to anyone but would allow people to keep the coverage they have. It was the most popular proposal among Democrats (91%) but did not garner a majority among Republicans (47%), the investigators said.
Support for the Medicare-for-all plan varied considerably, depending on number of arguments presented to respondents. When told that such a proposal would guarantee insurance as a right for all Americans, 71% favored it, and when they heard that it would eliminate health insurance premiums and reduce out-of-pockets costs, 67% of respondents expressed support. Favorable responses, however, were in the minority when people were told that Medicare-for-all would eliminate private health insurance companies (37%), threaten the current Medicare program (32%), and lead to some delayed medical tests and treatments (26%), according to the Kaiser report.
Rheumatology News Best of 2018 – The RA Report: Top News Highlights

The ideas and opinions expressed in Best of 2018 – The RA Report: Top News Highlights do not necessarily reflect those of the publisher. Frontline Medical Communications will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein.
The ideas and opinions expressed in Best of 2018 – The RA Report: Top News Highlights do not necessarily reflect those of the publisher. Frontline Medical Communications will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein.
The ideas and opinions expressed in Best of 2018 – The RA Report: Top News Highlights do not necessarily reflect those of the publisher. Frontline Medical Communications will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein.
FDA: Benefits still outweigh risks from paclitaxel-coated devices for PAD
This week, the FDA weighs in on concerning reports about paclitaxel-coated stents, and it approves a device to treat patent ductus arteriosus in infants weighing as little as 2 pounds. Also, a treat-to-target approach for CVD risk factors decreased atherosclerosis in rheumatoid arthritis patients, and ezetimibe was effective for primary prevention in elderly patients.
Subscribe to Cardiocast wherever you get your podcasts.
Amazon Alexa
Apple Podcasts
This week, the FDA weighs in on concerning reports about paclitaxel-coated stents, and it approves a device to treat patent ductus arteriosus in infants weighing as little as 2 pounds. Also, a treat-to-target approach for CVD risk factors decreased atherosclerosis in rheumatoid arthritis patients, and ezetimibe was effective for primary prevention in elderly patients.
Subscribe to Cardiocast wherever you get your podcasts.
Amazon Alexa
Apple Podcasts
This week, the FDA weighs in on concerning reports about paclitaxel-coated stents, and it approves a device to treat patent ductus arteriosus in infants weighing as little as 2 pounds. Also, a treat-to-target approach for CVD risk factors decreased atherosclerosis in rheumatoid arthritis patients, and ezetimibe was effective for primary prevention in elderly patients.
Subscribe to Cardiocast wherever you get your podcasts.
Amazon Alexa
Apple Podcasts

Meta-analysis supports aspirin to reduce cardiovascular events
Aspirin use is associated with a reduced risk of cardiovascular events among adults without cardiovascular disease, but this protection comes with a similarly increased risk for bleeding, according to data from a meta-analysis that included more than 1 million participant-years of follow-up.

“The uncertain role of aspirin in primary prevention of cardiovascular events is reflected in contrasting recommendations offered by guideline bodies,” and has led to a decline in prescribing aspirin for primary prevention of such events, wrote Sean L. Zheng, MRCP, of Imperial College London (England) and his colleagues.
In a systematic review and meta-analysis published in JAMA, the researchers examined 13 randomized trials altogether including 164,225 participants and 1,050,511 participant-years of follow-up.
Overall, aspirin use significantly reduced a composite of cardiovascular outcomes, compared with no aspirin (hazard ratio, 0.89). The composite outcome included cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke, and it occurred in 57.1 per 10,000 participant-years in aspirin users versus 61.4 per 10,000 participant-years among individuals who did not use aspirin. The absolute risk reduction was 0.38%.
The median age of the study participants was 62 years, and roughly half (47%) were male.
However, the risk of major bleeding events was significantly higher among aspirin users, compared with nonusers (23.1 per 10,000 participant-years and 16.4 per 10,000 participant-years, respectively), with a HR of 1.43 and an absolute risk increase of 0.47%.
Aspirin use was not associated with several secondary outcomes, including reductions in all-cause mortality or cardiovascular mortality, compared with no aspirin, but it was associated with a reduced risk specifically of myocardial infarction and ischemic stroke. Few deaths related to bleeding were reported.
The number needed to treat (265) and the number needed to harm (210) were similar, which emphasizes the need for an individual approach to treatment, the researchers noted.
“Consequently, the decision to use aspirin for primary prevention may need to be made on an individual basis, accounting for the patient’s risk of bleeding and their views on the balance of risk vs. benefit,” they concluded.
The researchers had no financial conflicts to disclose.
SOURCE: Zheng SL et al. JAMA. 2019;321(3):277-87.
Aspirin remains an important tool for the primary prevention of atherothrombotic vascular events, wrote J. Michael Gaziano, MD, in an accompanying editorial.
Historically, some guidelines have recommended against using aspirin for primary prevention of cardiovascular events because of the potential for harm, Dr. Gaziano noted, so a personalized approach to aspirin based on risk assessment is warranted. Dr. Gaziano also commented that risk is fluid; for example, patients who take action to improve their health and reduce risk by stopping smoking, eating differently, or exercising can reduce their risk for future CVD events.
“Because weighing the risks and benefits of aspirin in primary prevention is complicated, it should involve a shared decision-making discussion between the patient and the clinician,” he wrote. The current meta-analysis shows the consistency of recent trials with older studies, he remarked, noting that aspirin could be even more important as a cost-effective intervention in certain parts of the world where cardiovascular disease is on the rise and other treatments for CVD may be limited.
“Aspirin remains an important medication for acute management of vascular events; for use after certain procedures; for secondary prevention; and, after careful selection of the right patients, for primary prevention,” he concluded (JAMA. 2019;321[3]:253-5).
Dr. Gaziano is affiliated with Brigham and Women’s Hospital in Boston. He disclosed serving on the executive committee of the ARRIVE trial and serving as a consultant and receiving honoraria for speaking for Bayer.
Aspirin remains an important tool for the primary prevention of atherothrombotic vascular events, wrote J. Michael Gaziano, MD, in an accompanying editorial.
Historically, some guidelines have recommended against using aspirin for primary prevention of cardiovascular events because of the potential for harm, Dr. Gaziano noted, so a personalized approach to aspirin based on risk assessment is warranted. Dr. Gaziano also commented that risk is fluid; for example, patients who take action to improve their health and reduce risk by stopping smoking, eating differently, or exercising can reduce their risk for future CVD events.
“Because weighing the risks and benefits of aspirin in primary prevention is complicated, it should involve a shared decision-making discussion between the patient and the clinician,” he wrote. The current meta-analysis shows the consistency of recent trials with older studies, he remarked, noting that aspirin could be even more important as a cost-effective intervention in certain parts of the world where cardiovascular disease is on the rise and other treatments for CVD may be limited.
“Aspirin remains an important medication for acute management of vascular events; for use after certain procedures; for secondary prevention; and, after careful selection of the right patients, for primary prevention,” he concluded (JAMA. 2019;321[3]:253-5).
Dr. Gaziano is affiliated with Brigham and Women’s Hospital in Boston. He disclosed serving on the executive committee of the ARRIVE trial and serving as a consultant and receiving honoraria for speaking for Bayer.
Aspirin remains an important tool for the primary prevention of atherothrombotic vascular events, wrote J. Michael Gaziano, MD, in an accompanying editorial.
Historically, some guidelines have recommended against using aspirin for primary prevention of cardiovascular events because of the potential for harm, Dr. Gaziano noted, so a personalized approach to aspirin based on risk assessment is warranted. Dr. Gaziano also commented that risk is fluid; for example, patients who take action to improve their health and reduce risk by stopping smoking, eating differently, or exercising can reduce their risk for future CVD events.
“Because weighing the risks and benefits of aspirin in primary prevention is complicated, it should involve a shared decision-making discussion between the patient and the clinician,” he wrote. The current meta-analysis shows the consistency of recent trials with older studies, he remarked, noting that aspirin could be even more important as a cost-effective intervention in certain parts of the world where cardiovascular disease is on the rise and other treatments for CVD may be limited.
“Aspirin remains an important medication for acute management of vascular events; for use after certain procedures; for secondary prevention; and, after careful selection of the right patients, for primary prevention,” he concluded (JAMA. 2019;321[3]:253-5).
Dr. Gaziano is affiliated with Brigham and Women’s Hospital in Boston. He disclosed serving on the executive committee of the ARRIVE trial and serving as a consultant and receiving honoraria for speaking for Bayer.
Aspirin use is associated with a reduced risk of cardiovascular events among adults without cardiovascular disease, but this protection comes with a similarly increased risk for bleeding, according to data from a meta-analysis that included more than 1 million participant-years of follow-up.
“The uncertain role of aspirin in primary prevention of cardiovascular events is reflected in contrasting recommendations offered by guideline bodies,” and has led to a decline in prescribing aspirin for primary prevention of such events, wrote Sean L. Zheng, MRCP, of Imperial College London (England) and his colleagues.
In a systematic review and meta-analysis published in JAMA, the researchers examined 13 randomized trials altogether including 164,225 participants and 1,050,511 participant-years of follow-up.
Overall, aspirin use significantly reduced a composite of cardiovascular outcomes, compared with no aspirin (hazard ratio, 0.89). The composite outcome included cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke, and it occurred in 57.1 per 10,000 participant-years in aspirin users versus 61.4 per 10,000 participant-years among individuals who did not use aspirin. The absolute risk reduction was 0.38%.
The median age of the study participants was 62 years, and roughly half (47%) were male.
However, the risk of major bleeding events was significantly higher among aspirin users, compared with nonusers (23.1 per 10,000 participant-years and 16.4 per 10,000 participant-years, respectively), with a HR of 1.43 and an absolute risk increase of 0.47%.
Aspirin use was not associated with several secondary outcomes, including reductions in all-cause mortality or cardiovascular mortality, compared with no aspirin, but it was associated with a reduced risk specifically of myocardial infarction and ischemic stroke. Few deaths related to bleeding were reported.
The number needed to treat (265) and the number needed to harm (210) were similar, which emphasizes the need for an individual approach to treatment, the researchers noted.
“Consequently, the decision to use aspirin for primary prevention may need to be made on an individual basis, accounting for the patient’s risk of bleeding and their views on the balance of risk vs. benefit,” they concluded.
The researchers had no financial conflicts to disclose.
SOURCE: Zheng SL et al. JAMA. 2019;321(3):277-87.
Aspirin use is associated with a reduced risk of cardiovascular events among adults without cardiovascular disease, but this protection comes with a similarly increased risk for bleeding, according to data from a meta-analysis that included more than 1 million participant-years of follow-up.
“The uncertain role of aspirin in primary prevention of cardiovascular events is reflected in contrasting recommendations offered by guideline bodies,” and has led to a decline in prescribing aspirin for primary prevention of such events, wrote Sean L. Zheng, MRCP, of Imperial College London (England) and his colleagues.
In a systematic review and meta-analysis published in JAMA, the researchers examined 13 randomized trials altogether including 164,225 participants and 1,050,511 participant-years of follow-up.
Overall, aspirin use significantly reduced a composite of cardiovascular outcomes, compared with no aspirin (hazard ratio, 0.89). The composite outcome included cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke, and it occurred in 57.1 per 10,000 participant-years in aspirin users versus 61.4 per 10,000 participant-years among individuals who did not use aspirin. The absolute risk reduction was 0.38%.
The median age of the study participants was 62 years, and roughly half (47%) were male.
However, the risk of major bleeding events was significantly higher among aspirin users, compared with nonusers (23.1 per 10,000 participant-years and 16.4 per 10,000 participant-years, respectively), with a HR of 1.43 and an absolute risk increase of 0.47%.
Aspirin use was not associated with several secondary outcomes, including reductions in all-cause mortality or cardiovascular mortality, compared with no aspirin, but it was associated with a reduced risk specifically of myocardial infarction and ischemic stroke. Few deaths related to bleeding were reported.
The number needed to treat (265) and the number needed to harm (210) were similar, which emphasizes the need for an individual approach to treatment, the researchers noted.
“Consequently, the decision to use aspirin for primary prevention may need to be made on an individual basis, accounting for the patient’s risk of bleeding and their views on the balance of risk vs. benefit,” they concluded.
The researchers had no financial conflicts to disclose.
SOURCE: Zheng SL et al. JAMA. 2019;321(3):277-87.
FROM JAMA
Key clinical point:
Major finding: The absolute risk reduction was 0.38% for a composite of cardiovascular events among aspirin users versus nonusers.
Study details: The data come from a meta-analysis of 13 randomized trials altogether including 1,050,511 participants-years of follow-up.
Disclosures: The researchers had no financial conflicts to disclose.
Source: Zheng SL et al. JAMA. 2019;321(3):277-87.