User login
Young e-cigarette users graduating to the real thing
Children who use noncigarette forms of tobacco are significantly more likely to try cigarettes in the future, according to survey data from over 10,000 young people aged 12-17 years.
An initial survey (wave 1) was conducted as part of the nationally representative Population Assessment of Tobacco and Health (PATH) study, with a follow-up (wave 2) administered to participants a year later. The analysis by Shannon L. Watkins, PhD, of the University of California, San Francisco, and her associates was based on data for 10,384 respondents who reported never smoking a cigarette in wave 1 and whose later cigarette use, which occurred in less than 5% overall, was reported in wave 2.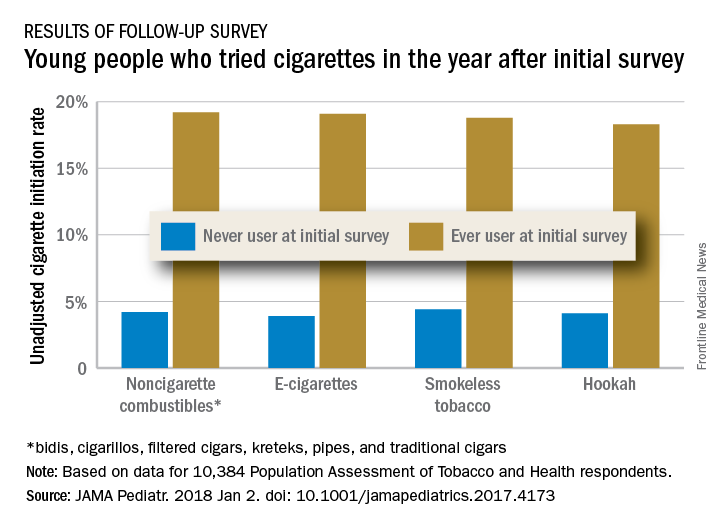
Those who used multiple noncigarette products were more likely than users of a single product to initiate cigarette use by wave 2. With never use of any tobacco as the reference, one model used by the investigators put the odds ratios of cigarette ever use at 4.98 for e-cigarettes only, 3.57 for combustibles only, and 8.57 for use of multiple products.
This study was supported by grants from the National Cancer Institute, Food and Drug Administration Center for Tobacco Products, National Institute on Drug Abuse, and National Center for Advancing Translational Sciences. No conflicts of interest were reported.
SOURCE: Watkins S et al. JAMA Pediatr. 2018 Jan 2. doi: 10.1001/jamapediatrics.2017.4173.
Children who use noncigarette forms of tobacco are significantly more likely to try cigarettes in the future, according to survey data from over 10,000 young people aged 12-17 years.
An initial survey (wave 1) was conducted as part of the nationally representative Population Assessment of Tobacco and Health (PATH) study, with a follow-up (wave 2) administered to participants a year later. The analysis by Shannon L. Watkins, PhD, of the University of California, San Francisco, and her associates was based on data for 10,384 respondents who reported never smoking a cigarette in wave 1 and whose later cigarette use, which occurred in less than 5% overall, was reported in wave 2.
Those who used multiple noncigarette products were more likely than users of a single product to initiate cigarette use by wave 2. With never use of any tobacco as the reference, one model used by the investigators put the odds ratios of cigarette ever use at 4.98 for e-cigarettes only, 3.57 for combustibles only, and 8.57 for use of multiple products.
This study was supported by grants from the National Cancer Institute, Food and Drug Administration Center for Tobacco Products, National Institute on Drug Abuse, and National Center for Advancing Translational Sciences. No conflicts of interest were reported.
SOURCE: Watkins S et al. JAMA Pediatr. 2018 Jan 2. doi: 10.1001/jamapediatrics.2017.4173.
Children who use noncigarette forms of tobacco are significantly more likely to try cigarettes in the future, according to survey data from over 10,000 young people aged 12-17 years.
An initial survey (wave 1) was conducted as part of the nationally representative Population Assessment of Tobacco and Health (PATH) study, with a follow-up (wave 2) administered to participants a year later. The analysis by Shannon L. Watkins, PhD, of the University of California, San Francisco, and her associates was based on data for 10,384 respondents who reported never smoking a cigarette in wave 1 and whose later cigarette use, which occurred in less than 5% overall, was reported in wave 2.
Those who used multiple noncigarette products were more likely than users of a single product to initiate cigarette use by wave 2. With never use of any tobacco as the reference, one model used by the investigators put the odds ratios of cigarette ever use at 4.98 for e-cigarettes only, 3.57 for combustibles only, and 8.57 for use of multiple products.
This study was supported by grants from the National Cancer Institute, Food and Drug Administration Center for Tobacco Products, National Institute on Drug Abuse, and National Center for Advancing Translational Sciences. No conflicts of interest were reported.
SOURCE: Watkins S et al. JAMA Pediatr. 2018 Jan 2. doi: 10.1001/jamapediatrics.2017.4173.
FROM JAMA PEDIATRICS
Innovative cholecystectomy grading scale could pay off for surgeons
ORLANDO – according to a study presented at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
As payment models shift toward bundled care, providers will be more closely evaluated on their postoperative outcomes, which can vary based on the difficulty of surgery, even for relatively common procedures.
“Gallbladder disease affects roughly 20 million people annually in the United States, with laparoscopic cholecystectomy being one of the most common operations performed by the typical surgeon,” said presenter Tarik Madni, MD, of the department of surgery, University of Texas Southwestern Medical Center, Dallas. “However not all cholecystectomies are created equal; increased inflammation can lead to increased operative times, increased conversion rates, as well as increased risk of complications.”
Given the increased scrutiny of surgical procedures, the current application of modifier 22, which allows surgeons to receive greater reimbursement for a more difficult surgery, is not enough, according to Dr. Madni.
To address this shortfall, investigators developed the Parkland grading scale, a five-tiered grading system that is designed to be easy to remember, limited in the number of grades, and correlated with clinical outcomes.
To determine the grades of the scale, Dr. Madni and his fellow investigators used 200 gallbladder images collected immediately before dissection and analyzed anatomy and inflammatory characteristics.
Gallbladders with a grade 1 would be relatively normal looking, while a grade 5 gallbladder would show perforation, necrosis, or not be clearly visible because of adhesions, according to Dr. Madni.
Between September 2016 and March 2017, investigators asked 11 acute care surgeons to prospectively grade gallbladders they saw before surgery using the Parkland scale and to fill out a questionnaire describing the difficulty of the procedure afterwards.
Of 667 gallbladders graded, 60 were assessed to be grade 1 (19%), 90 were grade 2 (28%), 102 were grade 3 (32%), 28 were grade 4 (9%), and 37 were grade 5 (12%) on the Parkland scale.
Grade 1 gallbladders had a mean procedure difficulty score of 1.43, while grade 5 gallbladders had a mean difficulty of 4.46. Grade 1 gallbladders also corresponded with the shortest mean surgery time of 63.31 minutes, compared with an average of 108.13 minutes for grade 5.
Acute cholecystitis diagnosis also increased by Parkland grade, from 36.7% in grade 1 gallbladders to 83.8% in grade 5 (P less than .0001), as did open conversion rates, from 0% to 21.6% (P less than .0001).
Mean length of stay rose fivefold between grade 1 and grade 5 procedures, from around 8 hours to 36 hours, respectively (P less than .0001).
Discussant Martin Zielinski, MD, FACS, director of medical trauma clinical research at the Mayo Clinic, Rochester, Minn., recognized the importance of having a grading scale but was curious why investigators did not analyze the American Association for the Surgery of Trauma’s (AAST) Emergency General Surgery anatomic grading scale, which is already in place.
“The AAST is a uniform, anatomic grading scale to measure the severity of diseases from the 16 most common [Emergency General Surgery] diseases,” Dr. Madni responded. “Unlike our operative-only finding scale, the AAST scale gives grades 1 through 5 definitions for four categories in each disease, not just operative, but clinical, imaging, operative, and pathologic categories.”
Comparatively, the Parkland scale is less cumbersome and covers a wider range of difficulty variation, according to Dr. Madni.
In the future, Dr. Madni and his colleagues will work to compare the Parkland scale to the AAST scale and look for ways to bridge the two.
Dr. Madni reported no relevant financial disclosures.
SOURCE: Madni T et al. EAST Scientific Assembly 2018 abstract #11.
ORLANDO – according to a study presented at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
As payment models shift toward bundled care, providers will be more closely evaluated on their postoperative outcomes, which can vary based on the difficulty of surgery, even for relatively common procedures.
“Gallbladder disease affects roughly 20 million people annually in the United States, with laparoscopic cholecystectomy being one of the most common operations performed by the typical surgeon,” said presenter Tarik Madni, MD, of the department of surgery, University of Texas Southwestern Medical Center, Dallas. “However not all cholecystectomies are created equal; increased inflammation can lead to increased operative times, increased conversion rates, as well as increased risk of complications.”
Given the increased scrutiny of surgical procedures, the current application of modifier 22, which allows surgeons to receive greater reimbursement for a more difficult surgery, is not enough, according to Dr. Madni.
To address this shortfall, investigators developed the Parkland grading scale, a five-tiered grading system that is designed to be easy to remember, limited in the number of grades, and correlated with clinical outcomes.
To determine the grades of the scale, Dr. Madni and his fellow investigators used 200 gallbladder images collected immediately before dissection and analyzed anatomy and inflammatory characteristics.
Gallbladders with a grade 1 would be relatively normal looking, while a grade 5 gallbladder would show perforation, necrosis, or not be clearly visible because of adhesions, according to Dr. Madni.
Between September 2016 and March 2017, investigators asked 11 acute care surgeons to prospectively grade gallbladders they saw before surgery using the Parkland scale and to fill out a questionnaire describing the difficulty of the procedure afterwards.
Of 667 gallbladders graded, 60 were assessed to be grade 1 (19%), 90 were grade 2 (28%), 102 were grade 3 (32%), 28 were grade 4 (9%), and 37 were grade 5 (12%) on the Parkland scale.
Grade 1 gallbladders had a mean procedure difficulty score of 1.43, while grade 5 gallbladders had a mean difficulty of 4.46. Grade 1 gallbladders also corresponded with the shortest mean surgery time of 63.31 minutes, compared with an average of 108.13 minutes for grade 5.
Acute cholecystitis diagnosis also increased by Parkland grade, from 36.7% in grade 1 gallbladders to 83.8% in grade 5 (P less than .0001), as did open conversion rates, from 0% to 21.6% (P less than .0001).
Mean length of stay rose fivefold between grade 1 and grade 5 procedures, from around 8 hours to 36 hours, respectively (P less than .0001).
Discussant Martin Zielinski, MD, FACS, director of medical trauma clinical research at the Mayo Clinic, Rochester, Minn., recognized the importance of having a grading scale but was curious why investigators did not analyze the American Association for the Surgery of Trauma’s (AAST) Emergency General Surgery anatomic grading scale, which is already in place.
“The AAST is a uniform, anatomic grading scale to measure the severity of diseases from the 16 most common [Emergency General Surgery] diseases,” Dr. Madni responded. “Unlike our operative-only finding scale, the AAST scale gives grades 1 through 5 definitions for four categories in each disease, not just operative, but clinical, imaging, operative, and pathologic categories.”
Comparatively, the Parkland scale is less cumbersome and covers a wider range of difficulty variation, according to Dr. Madni.
In the future, Dr. Madni and his colleagues will work to compare the Parkland scale to the AAST scale and look for ways to bridge the two.
Dr. Madni reported no relevant financial disclosures.
SOURCE: Madni T et al. EAST Scientific Assembly 2018 abstract #11.
ORLANDO – according to a study presented at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
As payment models shift toward bundled care, providers will be more closely evaluated on their postoperative outcomes, which can vary based on the difficulty of surgery, even for relatively common procedures.
“Gallbladder disease affects roughly 20 million people annually in the United States, with laparoscopic cholecystectomy being one of the most common operations performed by the typical surgeon,” said presenter Tarik Madni, MD, of the department of surgery, University of Texas Southwestern Medical Center, Dallas. “However not all cholecystectomies are created equal; increased inflammation can lead to increased operative times, increased conversion rates, as well as increased risk of complications.”
Given the increased scrutiny of surgical procedures, the current application of modifier 22, which allows surgeons to receive greater reimbursement for a more difficult surgery, is not enough, according to Dr. Madni.
To address this shortfall, investigators developed the Parkland grading scale, a five-tiered grading system that is designed to be easy to remember, limited in the number of grades, and correlated with clinical outcomes.
To determine the grades of the scale, Dr. Madni and his fellow investigators used 200 gallbladder images collected immediately before dissection and analyzed anatomy and inflammatory characteristics.
Gallbladders with a grade 1 would be relatively normal looking, while a grade 5 gallbladder would show perforation, necrosis, or not be clearly visible because of adhesions, according to Dr. Madni.
Between September 2016 and March 2017, investigators asked 11 acute care surgeons to prospectively grade gallbladders they saw before surgery using the Parkland scale and to fill out a questionnaire describing the difficulty of the procedure afterwards.
Of 667 gallbladders graded, 60 were assessed to be grade 1 (19%), 90 were grade 2 (28%), 102 were grade 3 (32%), 28 were grade 4 (9%), and 37 were grade 5 (12%) on the Parkland scale.
Grade 1 gallbladders had a mean procedure difficulty score of 1.43, while grade 5 gallbladders had a mean difficulty of 4.46. Grade 1 gallbladders also corresponded with the shortest mean surgery time of 63.31 minutes, compared with an average of 108.13 minutes for grade 5.
Acute cholecystitis diagnosis also increased by Parkland grade, from 36.7% in grade 1 gallbladders to 83.8% in grade 5 (P less than .0001), as did open conversion rates, from 0% to 21.6% (P less than .0001).
Mean length of stay rose fivefold between grade 1 and grade 5 procedures, from around 8 hours to 36 hours, respectively (P less than .0001).
Discussant Martin Zielinski, MD, FACS, director of medical trauma clinical research at the Mayo Clinic, Rochester, Minn., recognized the importance of having a grading scale but was curious why investigators did not analyze the American Association for the Surgery of Trauma’s (AAST) Emergency General Surgery anatomic grading scale, which is already in place.
“The AAST is a uniform, anatomic grading scale to measure the severity of diseases from the 16 most common [Emergency General Surgery] diseases,” Dr. Madni responded. “Unlike our operative-only finding scale, the AAST scale gives grades 1 through 5 definitions for four categories in each disease, not just operative, but clinical, imaging, operative, and pathologic categories.”
Comparatively, the Parkland scale is less cumbersome and covers a wider range of difficulty variation, according to Dr. Madni.
In the future, Dr. Madni and his colleagues will work to compare the Parkland scale to the AAST scale and look for ways to bridge the two.
Dr. Madni reported no relevant financial disclosures.
SOURCE: Madni T et al. EAST Scientific Assembly 2018 abstract #11.
REPORTING FROM EAST SCIENTIFIC ASSEMBLY
Key clinical point: A five-tiered grading system was developed to determine grades of cholecystectomy operative difficulty.
Major finding: Acute cholecystitis diagnosis also increased by Parkland grade, from 36.7% in grade 1 gallbladders to 83.8% in grade 5.
Study details: Eleven acute care surgeons graded gallbladders on initial view and then filled out a postoperative questionnaire.
Disclosures: The investigator reported no relevant financial disclosures.
Source: Madni T et al. EAST Scientifc Assembly 2018 abstract #11.
Behavioral issues, anorexia may presage celiac disease
The clinical challenges of celiac disease go beyond identifying the condition and helping families adjust to a child’s gluten-free diet. Behavioral problems and/or an eating disorder may predate celiac disease, according to Alex R. Kemper, MD, MPH, division chief of ambulatory pediatrics at Nationwide Children’s Hospital, Columbus, Ohio, and deputy editor of Pediatrics.
“We are learning more and more about celiac disease. The presentation and implication of celiac disease can involve more than the gastrointestinal tract,” Dr. Kemper noted. “Figuring out who to screen for celiac disease and how best to do so is complex, and we are always learning more about the best way to provide care after celiac disease is diagnosed.”
Impact of undiagnosed celiac disease on behavior
At the 2017 annual meeting of the American Academy of Pediatrics and, in a later interview, Dr. Kemper discussed a study that explored how behavior and celiac disease might be interrelated, particularly among children whose families don’t yet know their child has the condition.
“It’s challenging to assess the psychological impact of celiac disease autoimmunity when families aren’t aware a child has it, because prospective studies are difficult to do and recall bias can distort findings,” he noted.

Smith et al. used data from a prospective international study, The Environment Determinants of Diabetes in the Young (TEDDY), designed to learn about factors associated with type 1 diabetes and celiac disease over a 15-year follow-up period (Pediatrics. 2017 Mar. doi: 10.1542/peds.2016-2848).
TEDDY tracked 8,676 infants deemed at high risk for celiac autoimmunity based on their human leukocyte antigen (HLA) antigen status at birth. The investigators regularly measured celiac disease autoimmunity based on tissue transglutaminase antibodies (tTGA), beginning at age 2 years. They assessed the children’s behavior at ages 3.5 years and 4.5 years using the Achenbach System of Empirically Based Assessment. If a child was found to have celiac disease, the researchers revisited the earlier behavior scores reported by their mothers before their children’s status were known.
When the children were 3.5 years old, 66 had celiac disease that their mothers were not yet aware of and 440 children had diagnosed celiac disease. The 66 mothers unaware of their child’s condition reported more anxiety, depression, aggression, and sleep problems in their children than did the 440 mothers who knew their child’s diagnosis or the 3,651 mothers of children without celiac disease. The differences were subclinical but statistically significant.
“It is important to recognize that the magnitude of the psychological problems in the 3.5 year olds was small,” Dr. Kemper said in an interview. “Parents might not recognize these symptoms.”
When the researchers looked at child behavior reports only among the mothers who knew their children had celiac disease, no differences existed regardless of the children’s tTGA levels or whether they were following a gluten-free diet. Then, when the children were 4.5 years old and all mothers were aware of their child’s status, no significant differences in mothers’ reporting of child behavior existed across any of the groups.
“Perhaps the knowledge of the child’s celiac disease autoimmunity increases a parent’s sensitivity to physical discomforts of their child while providing an alternative explanation for any psychological symptoms the child exhibits,” the researchers offered.
“Pediatricians should be aware of this association and consider testing young children with a family history of celiac disease if there are concerns,” Dr. Kemper said in an interview. “Because the magnitude of change was subclinical, this study does not suggest the need for more extensive screening of all children.”
Link between celiac disease and anorexia nervosa
The eating disorders study Dr. Kemper discussed examined possible associations between celiac disease and anorexia nervosa (Pediatrics. 2017. doi: 10.1542/peds.2016-4367). Researchers compared 17,959 Swedish females diagnosed with celiac disease between 1969 and 2008, at a median 28 years old, to 89,379 controls matched by sex and age.
Anorexia occurred more often among those with celiac disease than those without: a rate of 27 girls per 100,000 with celiac disease developed anorexia per year, compared with 18 of 100,000 without celiac disease, for a hazard ratio for an anorexia nervosa diagnosis of 1.46 (95% confidence interval, 1.08-1.98). In addition, girls whose celiac disease had not yet been identified had more than double the odds of developing anorexia before diagnosis than did those without celiac disease (odds ratio, 2.13).
Females with celiac disease therefore were more likely to have anorexia both before and after their celiac diagnosis, although the authors noted that surveillance bias may have made it more likely for either of the patients’ conditions to be identified after the first was. Another possible explanation is shared genetic risk factors, the authors wrote.
Dr. Kemper also offered possible reasons, including one related to the child behavior study.
“It could be that girls with celiac disease might develop anorexia because of the need to focus on their diet,” he said in an interview. “Celiac disease has been associated with psychological problems, and so that could contribute.”
Until further research can shed light on the reasons for the associations, physicians simply should be aware of the study’s clinical implications.
“Pediatricians should be aware of the bidirectional association between celiac disease and anorexia nervosa in teens and young adult women, and be prepared to evaluate for celiac disease or treat anorexia,” Dr. Kemper said.
He noted the need for more research to learn “what pediatricians can do to help to either prevent these problems from developing in the first place, or identify and treat celiac disease or anorexia nervosa early to prevent long-term complications.”
Dr. Kemper reported having no relevant financial disclosures and no external funding. Ketil Stordal, MD, PhD, of the anorexia study received funding from the OAK foundation in Switzerland, and Cynthia M. Bulik, PhD, from the same study received funding from the Swedish Research Council, and has consulted for and received a grant from Shire. The remaining authors of the anorexia study had no relevant financial disclosures. The behavioral study was funded by the National Institutes of Health, the Juvenile Diabetes Research Foundation and the Centers for Disease Control and Prevention. The authors from the behavioral study had no relevant financial disclosures.
The clinical challenges of celiac disease go beyond identifying the condition and helping families adjust to a child’s gluten-free diet. Behavioral problems and/or an eating disorder may predate celiac disease, according to Alex R. Kemper, MD, MPH, division chief of ambulatory pediatrics at Nationwide Children’s Hospital, Columbus, Ohio, and deputy editor of Pediatrics.
“We are learning more and more about celiac disease. The presentation and implication of celiac disease can involve more than the gastrointestinal tract,” Dr. Kemper noted. “Figuring out who to screen for celiac disease and how best to do so is complex, and we are always learning more about the best way to provide care after celiac disease is diagnosed.”
Impact of undiagnosed celiac disease on behavior
At the 2017 annual meeting of the American Academy of Pediatrics and, in a later interview, Dr. Kemper discussed a study that explored how behavior and celiac disease might be interrelated, particularly among children whose families don’t yet know their child has the condition.
“It’s challenging to assess the psychological impact of celiac disease autoimmunity when families aren’t aware a child has it, because prospective studies are difficult to do and recall bias can distort findings,” he noted.
Smith et al. used data from a prospective international study, The Environment Determinants of Diabetes in the Young (TEDDY), designed to learn about factors associated with type 1 diabetes and celiac disease over a 15-year follow-up period (Pediatrics. 2017 Mar. doi: 10.1542/peds.2016-2848).
TEDDY tracked 8,676 infants deemed at high risk for celiac autoimmunity based on their human leukocyte antigen (HLA) antigen status at birth. The investigators regularly measured celiac disease autoimmunity based on tissue transglutaminase antibodies (tTGA), beginning at age 2 years. They assessed the children’s behavior at ages 3.5 years and 4.5 years using the Achenbach System of Empirically Based Assessment. If a child was found to have celiac disease, the researchers revisited the earlier behavior scores reported by their mothers before their children’s status were known.
When the children were 3.5 years old, 66 had celiac disease that their mothers were not yet aware of and 440 children had diagnosed celiac disease. The 66 mothers unaware of their child’s condition reported more anxiety, depression, aggression, and sleep problems in their children than did the 440 mothers who knew their child’s diagnosis or the 3,651 mothers of children without celiac disease. The differences were subclinical but statistically significant.
“It is important to recognize that the magnitude of the psychological problems in the 3.5 year olds was small,” Dr. Kemper said in an interview. “Parents might not recognize these symptoms.”
When the researchers looked at child behavior reports only among the mothers who knew their children had celiac disease, no differences existed regardless of the children’s tTGA levels or whether they were following a gluten-free diet. Then, when the children were 4.5 years old and all mothers were aware of their child’s status, no significant differences in mothers’ reporting of child behavior existed across any of the groups.
“Perhaps the knowledge of the child’s celiac disease autoimmunity increases a parent’s sensitivity to physical discomforts of their child while providing an alternative explanation for any psychological symptoms the child exhibits,” the researchers offered.
“Pediatricians should be aware of this association and consider testing young children with a family history of celiac disease if there are concerns,” Dr. Kemper said in an interview. “Because the magnitude of change was subclinical, this study does not suggest the need for more extensive screening of all children.”
Link between celiac disease and anorexia nervosa
The eating disorders study Dr. Kemper discussed examined possible associations between celiac disease and anorexia nervosa (Pediatrics. 2017. doi: 10.1542/peds.2016-4367). Researchers compared 17,959 Swedish females diagnosed with celiac disease between 1969 and 2008, at a median 28 years old, to 89,379 controls matched by sex and age.
Anorexia occurred more often among those with celiac disease than those without: a rate of 27 girls per 100,000 with celiac disease developed anorexia per year, compared with 18 of 100,000 without celiac disease, for a hazard ratio for an anorexia nervosa diagnosis of 1.46 (95% confidence interval, 1.08-1.98). In addition, girls whose celiac disease had not yet been identified had more than double the odds of developing anorexia before diagnosis than did those without celiac disease (odds ratio, 2.13).
Females with celiac disease therefore were more likely to have anorexia both before and after their celiac diagnosis, although the authors noted that surveillance bias may have made it more likely for either of the patients’ conditions to be identified after the first was. Another possible explanation is shared genetic risk factors, the authors wrote.
Dr. Kemper also offered possible reasons, including one related to the child behavior study.
“It could be that girls with celiac disease might develop anorexia because of the need to focus on their diet,” he said in an interview. “Celiac disease has been associated with psychological problems, and so that could contribute.”
Until further research can shed light on the reasons for the associations, physicians simply should be aware of the study’s clinical implications.
“Pediatricians should be aware of the bidirectional association between celiac disease and anorexia nervosa in teens and young adult women, and be prepared to evaluate for celiac disease or treat anorexia,” Dr. Kemper said.
He noted the need for more research to learn “what pediatricians can do to help to either prevent these problems from developing in the first place, or identify and treat celiac disease or anorexia nervosa early to prevent long-term complications.”
Dr. Kemper reported having no relevant financial disclosures and no external funding. Ketil Stordal, MD, PhD, of the anorexia study received funding from the OAK foundation in Switzerland, and Cynthia M. Bulik, PhD, from the same study received funding from the Swedish Research Council, and has consulted for and received a grant from Shire. The remaining authors of the anorexia study had no relevant financial disclosures. The behavioral study was funded by the National Institutes of Health, the Juvenile Diabetes Research Foundation and the Centers for Disease Control and Prevention. The authors from the behavioral study had no relevant financial disclosures.
The clinical challenges of celiac disease go beyond identifying the condition and helping families adjust to a child’s gluten-free diet. Behavioral problems and/or an eating disorder may predate celiac disease, according to Alex R. Kemper, MD, MPH, division chief of ambulatory pediatrics at Nationwide Children’s Hospital, Columbus, Ohio, and deputy editor of Pediatrics.
“We are learning more and more about celiac disease. The presentation and implication of celiac disease can involve more than the gastrointestinal tract,” Dr. Kemper noted. “Figuring out who to screen for celiac disease and how best to do so is complex, and we are always learning more about the best way to provide care after celiac disease is diagnosed.”
Impact of undiagnosed celiac disease on behavior
At the 2017 annual meeting of the American Academy of Pediatrics and, in a later interview, Dr. Kemper discussed a study that explored how behavior and celiac disease might be interrelated, particularly among children whose families don’t yet know their child has the condition.
“It’s challenging to assess the psychological impact of celiac disease autoimmunity when families aren’t aware a child has it, because prospective studies are difficult to do and recall bias can distort findings,” he noted.
Smith et al. used data from a prospective international study, The Environment Determinants of Diabetes in the Young (TEDDY), designed to learn about factors associated with type 1 diabetes and celiac disease over a 15-year follow-up period (Pediatrics. 2017 Mar. doi: 10.1542/peds.2016-2848).
TEDDY tracked 8,676 infants deemed at high risk for celiac autoimmunity based on their human leukocyte antigen (HLA) antigen status at birth. The investigators regularly measured celiac disease autoimmunity based on tissue transglutaminase antibodies (tTGA), beginning at age 2 years. They assessed the children’s behavior at ages 3.5 years and 4.5 years using the Achenbach System of Empirically Based Assessment. If a child was found to have celiac disease, the researchers revisited the earlier behavior scores reported by their mothers before their children’s status were known.
When the children were 3.5 years old, 66 had celiac disease that their mothers were not yet aware of and 440 children had diagnosed celiac disease. The 66 mothers unaware of their child’s condition reported more anxiety, depression, aggression, and sleep problems in their children than did the 440 mothers who knew their child’s diagnosis or the 3,651 mothers of children without celiac disease. The differences were subclinical but statistically significant.
“It is important to recognize that the magnitude of the psychological problems in the 3.5 year olds was small,” Dr. Kemper said in an interview. “Parents might not recognize these symptoms.”
When the researchers looked at child behavior reports only among the mothers who knew their children had celiac disease, no differences existed regardless of the children’s tTGA levels or whether they were following a gluten-free diet. Then, when the children were 4.5 years old and all mothers were aware of their child’s status, no significant differences in mothers’ reporting of child behavior existed across any of the groups.
“Perhaps the knowledge of the child’s celiac disease autoimmunity increases a parent’s sensitivity to physical discomforts of their child while providing an alternative explanation for any psychological symptoms the child exhibits,” the researchers offered.
“Pediatricians should be aware of this association and consider testing young children with a family history of celiac disease if there are concerns,” Dr. Kemper said in an interview. “Because the magnitude of change was subclinical, this study does not suggest the need for more extensive screening of all children.”
Link between celiac disease and anorexia nervosa
The eating disorders study Dr. Kemper discussed examined possible associations between celiac disease and anorexia nervosa (Pediatrics. 2017. doi: 10.1542/peds.2016-4367). Researchers compared 17,959 Swedish females diagnosed with celiac disease between 1969 and 2008, at a median 28 years old, to 89,379 controls matched by sex and age.
Anorexia occurred more often among those with celiac disease than those without: a rate of 27 girls per 100,000 with celiac disease developed anorexia per year, compared with 18 of 100,000 without celiac disease, for a hazard ratio for an anorexia nervosa diagnosis of 1.46 (95% confidence interval, 1.08-1.98). In addition, girls whose celiac disease had not yet been identified had more than double the odds of developing anorexia before diagnosis than did those without celiac disease (odds ratio, 2.13).
Females with celiac disease therefore were more likely to have anorexia both before and after their celiac diagnosis, although the authors noted that surveillance bias may have made it more likely for either of the patients’ conditions to be identified after the first was. Another possible explanation is shared genetic risk factors, the authors wrote.
Dr. Kemper also offered possible reasons, including one related to the child behavior study.
“It could be that girls with celiac disease might develop anorexia because of the need to focus on their diet,” he said in an interview. “Celiac disease has been associated with psychological problems, and so that could contribute.”
Until further research can shed light on the reasons for the associations, physicians simply should be aware of the study’s clinical implications.
“Pediatricians should be aware of the bidirectional association between celiac disease and anorexia nervosa in teens and young adult women, and be prepared to evaluate for celiac disease or treat anorexia,” Dr. Kemper said.
He noted the need for more research to learn “what pediatricians can do to help to either prevent these problems from developing in the first place, or identify and treat celiac disease or anorexia nervosa early to prevent long-term complications.”
Dr. Kemper reported having no relevant financial disclosures and no external funding. Ketil Stordal, MD, PhD, of the anorexia study received funding from the OAK foundation in Switzerland, and Cynthia M. Bulik, PhD, from the same study received funding from the Swedish Research Council, and has consulted for and received a grant from Shire. The remaining authors of the anorexia study had no relevant financial disclosures. The behavioral study was funded by the National Institutes of Health, the Juvenile Diabetes Research Foundation and the Centers for Disease Control and Prevention. The authors from the behavioral study had no relevant financial disclosures.
FVC deterioration signals increasing risk in rib fracture patients
ORLANDO – according to a study presented at the annual scientific assembly Eastern Association for the Surgery of Trauma.
Daily, easily conducted, bedside FVC monitoring can help identify the first signs of a worsening condition and lead to earlier intervention, according to presenter Rachel Warner, DO, a surgical resident at West Virginia University, Morgantown.
“Unplanned upgrades to the ICU have been associated with prolonged hospital stay, mechanical ventilation, and even higher risk of mortality when compared to planned upgrades,” Dr. Warner explained. “We aim to decrease these events by creating a system where early decline can be recognized by any member of the health care team.”
In a retrospective study, investigators analyzed 1,106 rib fracture patients enrolled in a rib fracture care pathway at a Level I trauma center during 2009-2014, all of whom were admitted with an FVC greater than 1 L. Patients’ FVCs were assessed with spirometry in the ED, and the results were then used to determine their care placement. Then FVC was continually monitored throughout each patient’s stay at the hospital. The investigators hypothesized that those patients whose FVC level deteriorated to lower than 1 L were at higher risk for complications.
Two groups of patients were analyzed: Group A was composed of patients whose initial FVC scores were greater than or equal to 1 but deteriorated over time to below 1, while Group B was composed of patients whose scores remained above 1. Group A patients were an average age 58 years and were majority male (61%); their had FVC scores initially averaged 1.3 but dropped to a low of 0.7. Patients in group B were on average younger, at 48 years, but also majority male (79%); they had a slightly higher initial average FVC of 1.6, with a low of 1.4.
Rate of complications among patients whose FVC scores dropped below 1 was 15%, compared with 3.2% in the other group (P less than .001).
Group A patients were significantly more likely than were Group B patients to develop pneumonia (9% vs. 4%, respectively), be upgraded to the intensive care unit (3.7% vs. 0.2%), require intubation (1.6% vs. 0.1%), or be readmitted (4% vs. 1%).
Average length of stay for patients whose FVC score dropped below 1 was 10 days, compared with 4 days among the patients who maintained a higher FVC. Mortality rates were also significantly higher at 3%, compared with 0.2%. Dr. Warner said that FVC levels can be the first indication of worsening clinical status and should be treated as an early warning sign for which patients may need to be preemptively moved to a higher level of care.
Dr. Warner and her colleagues were limited by the retrospective nature of their analysis, as well as not including other injuries into their analysis.
In a discussion of the study, Bryce R.H. Robinson, MD, FACS, of Harborview Medical Center, Seattle, Wash., supported using data such as FVC to help identify at-risk patients early. “I am encouraged to see others utilize easily obtainable, objective measures for those at risk for pulmonary decompensation with rib fractures,” said Dr. Robinson.
While keeping the cutoff at 1 L for FVC testing regardless of other factors, like sex or weight, would make it easy to train all members of the medical team, this may be oversimplifying FVC measurements, cautioned Dr. Robinson.
“While it is a little bit less specific to the patient, broad adaptation across the health care team is much more feasible with standard values,” responded Dr. Warner. “Given this, we do intentionally accept a level of overtriaged patients. We have found these patients generally make up the geriatric population and have confounding factors that would otherwise make them high risk for complications.”
Investigators reported no relevant financial disclosures.
SOURCE: Warner R et al. EAST Scientific Assembly 2018 abstract #9
ORLANDO – according to a study presented at the annual scientific assembly Eastern Association for the Surgery of Trauma.
Daily, easily conducted, bedside FVC monitoring can help identify the first signs of a worsening condition and lead to earlier intervention, according to presenter Rachel Warner, DO, a surgical resident at West Virginia University, Morgantown.
“Unplanned upgrades to the ICU have been associated with prolonged hospital stay, mechanical ventilation, and even higher risk of mortality when compared to planned upgrades,” Dr. Warner explained. “We aim to decrease these events by creating a system where early decline can be recognized by any member of the health care team.”
In a retrospective study, investigators analyzed 1,106 rib fracture patients enrolled in a rib fracture care pathway at a Level I trauma center during 2009-2014, all of whom were admitted with an FVC greater than 1 L. Patients’ FVCs were assessed with spirometry in the ED, and the results were then used to determine their care placement. Then FVC was continually monitored throughout each patient’s stay at the hospital. The investigators hypothesized that those patients whose FVC level deteriorated to lower than 1 L were at higher risk for complications.
Two groups of patients were analyzed: Group A was composed of patients whose initial FVC scores were greater than or equal to 1 but deteriorated over time to below 1, while Group B was composed of patients whose scores remained above 1. Group A patients were an average age 58 years and were majority male (61%); their had FVC scores initially averaged 1.3 but dropped to a low of 0.7. Patients in group B were on average younger, at 48 years, but also majority male (79%); they had a slightly higher initial average FVC of 1.6, with a low of 1.4.
Rate of complications among patients whose FVC scores dropped below 1 was 15%, compared with 3.2% in the other group (P less than .001).
Group A patients were significantly more likely than were Group B patients to develop pneumonia (9% vs. 4%, respectively), be upgraded to the intensive care unit (3.7% vs. 0.2%), require intubation (1.6% vs. 0.1%), or be readmitted (4% vs. 1%).
Average length of stay for patients whose FVC score dropped below 1 was 10 days, compared with 4 days among the patients who maintained a higher FVC. Mortality rates were also significantly higher at 3%, compared with 0.2%. Dr. Warner said that FVC levels can be the first indication of worsening clinical status and should be treated as an early warning sign for which patients may need to be preemptively moved to a higher level of care.
Dr. Warner and her colleagues were limited by the retrospective nature of their analysis, as well as not including other injuries into their analysis.
In a discussion of the study, Bryce R.H. Robinson, MD, FACS, of Harborview Medical Center, Seattle, Wash., supported using data such as FVC to help identify at-risk patients early. “I am encouraged to see others utilize easily obtainable, objective measures for those at risk for pulmonary decompensation with rib fractures,” said Dr. Robinson.
While keeping the cutoff at 1 L for FVC testing regardless of other factors, like sex or weight, would make it easy to train all members of the medical team, this may be oversimplifying FVC measurements, cautioned Dr. Robinson.
“While it is a little bit less specific to the patient, broad adaptation across the health care team is much more feasible with standard values,” responded Dr. Warner. “Given this, we do intentionally accept a level of overtriaged patients. We have found these patients generally make up the geriatric population and have confounding factors that would otherwise make them high risk for complications.”
Investigators reported no relevant financial disclosures.
SOURCE: Warner R et al. EAST Scientific Assembly 2018 abstract #9
ORLANDO – according to a study presented at the annual scientific assembly Eastern Association for the Surgery of Trauma.
Daily, easily conducted, bedside FVC monitoring can help identify the first signs of a worsening condition and lead to earlier intervention, according to presenter Rachel Warner, DO, a surgical resident at West Virginia University, Morgantown.
“Unplanned upgrades to the ICU have been associated with prolonged hospital stay, mechanical ventilation, and even higher risk of mortality when compared to planned upgrades,” Dr. Warner explained. “We aim to decrease these events by creating a system where early decline can be recognized by any member of the health care team.”
In a retrospective study, investigators analyzed 1,106 rib fracture patients enrolled in a rib fracture care pathway at a Level I trauma center during 2009-2014, all of whom were admitted with an FVC greater than 1 L. Patients’ FVCs were assessed with spirometry in the ED, and the results were then used to determine their care placement. Then FVC was continually monitored throughout each patient’s stay at the hospital. The investigators hypothesized that those patients whose FVC level deteriorated to lower than 1 L were at higher risk for complications.
Two groups of patients were analyzed: Group A was composed of patients whose initial FVC scores were greater than or equal to 1 but deteriorated over time to below 1, while Group B was composed of patients whose scores remained above 1. Group A patients were an average age 58 years and were majority male (61%); their had FVC scores initially averaged 1.3 but dropped to a low of 0.7. Patients in group B were on average younger, at 48 years, but also majority male (79%); they had a slightly higher initial average FVC of 1.6, with a low of 1.4.
Rate of complications among patients whose FVC scores dropped below 1 was 15%, compared with 3.2% in the other group (P less than .001).
Group A patients were significantly more likely than were Group B patients to develop pneumonia (9% vs. 4%, respectively), be upgraded to the intensive care unit (3.7% vs. 0.2%), require intubation (1.6% vs. 0.1%), or be readmitted (4% vs. 1%).
Average length of stay for patients whose FVC score dropped below 1 was 10 days, compared with 4 days among the patients who maintained a higher FVC. Mortality rates were also significantly higher at 3%, compared with 0.2%. Dr. Warner said that FVC levels can be the first indication of worsening clinical status and should be treated as an early warning sign for which patients may need to be preemptively moved to a higher level of care.
Dr. Warner and her colleagues were limited by the retrospective nature of their analysis, as well as not including other injuries into their analysis.
In a discussion of the study, Bryce R.H. Robinson, MD, FACS, of Harborview Medical Center, Seattle, Wash., supported using data such as FVC to help identify at-risk patients early. “I am encouraged to see others utilize easily obtainable, objective measures for those at risk for pulmonary decompensation with rib fractures,” said Dr. Robinson.
While keeping the cutoff at 1 L for FVC testing regardless of other factors, like sex or weight, would make it easy to train all members of the medical team, this may be oversimplifying FVC measurements, cautioned Dr. Robinson.
“While it is a little bit less specific to the patient, broad adaptation across the health care team is much more feasible with standard values,” responded Dr. Warner. “Given this, we do intentionally accept a level of overtriaged patients. We have found these patients generally make up the geriatric population and have confounding factors that would otherwise make them high risk for complications.”
Investigators reported no relevant financial disclosures.
SOURCE: Warner R et al. EAST Scientific Assembly 2018 abstract #9
REPORTING FROM EAST SCIENTIFIC ASSEMBLY
Key clinical point: Rib fracture patients with FVC below 1 are at higher risk for pulmonary complications.
Major finding: Rate of pulmonary complications was 15% among patients with FVC under 1, compared to 3% in patients with FVC above 1 (P less than .001).
Study details: Retrospective study of 1,106 patients enrolled at a Level I trauma center from 2009 through 2014.
Disclosures: Presenters reported no relevant financial disclosures.
Source: Warner R et al. EAST Scientific Assembly 2018 abstract #9.
Waiving Medicare coinsurance for positive colorectal screening likely beneficial
Currently, Medicare covers colorectal screening at no charge to the patient, but if a polyp is removed upon discovery during the procedure, the patient would then be subject to Medicare’s coinsurance payments for both the colonoscopy and the removal.
Researchers used the Microsimulation Screening Analysis-Colon model to estimate the cost-effectiveness of waiving coinsurance for every component of colorectal cancer screening. They estimated that, currently, using the colonoscopy regimen with coinsurance, 12.8 colorectal cancer deaths occurred per 1,000 people aged 65 years and 124.1 QALYs were gained per 1,000 people aged 65 years. The total number of procedures per 1,000 Medicare beneficiaries was 1,132, of which 410 (36%) were potentially subject to coinsurance requirements.
“We estimated that the total lifetime costs for [the Centers for Medicare & Medicaid], which included colorectal cancer screening, surveillance, and treatment with coinsurance, to be $2.675 million per 1,000 sixty-five-year-olds,” Ms. Peterse and her colleagues wrote.
Researchers noted that if the coinsurance was waived but there was no follow-on increase in the screening rate, the benefits of screening would not change but the total cost of screening and treatment would increase to $2.726 million per 1,000 people aged 65 years.
However, “an assumed 5-percentage-point increase in the rates of first colonoscopy screening and surveillance decreased the number of colorectal cancer deaths by 0.9 (6.4 percent), accompanied by an increase of $33,000 (1.2 percent) in total costs, with a cost per QALY gained (or cost-effectiveness ratio) of $4,086.”
They added that estimated screening benefits were similar when fecal testing was the primary screening method.
“In general, [fecal testing] screening was associated with lower number of procedures subject to coinsurance,” the researchers added. “If [fecal testing] screening becomes more popular in the United States, following trends observed in several settings, the costs of waiving coinsurance would be even lower.” The researchers also suggest that it could lead to reducing disparities of colorectal cancer in the United States as well.
AGA has been working for years to try to fix this issue, and supports the bipartisan Removing Barriers to Screening Act, which would correct this inequity for Medicare beneficiaries and remove the financial barriers that may prevent a patient from undergoing a screening. AGA is hopeful that the growing support for the legislation on both sides of the aisle will help get the bill passed this year. To learn more about this issue, visit http://www.gastro.org/take-action/top-issues/patient-cost-sharing-for-screening-colonoscopy. To help your patient understand this issue, AGA has created “What to Expect: Paying for Your Colonoscopy,” which can be downloaded at http://www.gastro.org/patient-care/procedures/Colonoscopy_CoPay_WhatToKnowFactSheet.pdf to be shared in your office. /p>
SOURCE: Peterse EFP et al. Health Affairs. 2017 Dec;36(12):2151-9.
Currently, Medicare covers colorectal screening at no charge to the patient, but if a polyp is removed upon discovery during the procedure, the patient would then be subject to Medicare’s coinsurance payments for both the colonoscopy and the removal.
Researchers used the Microsimulation Screening Analysis-Colon model to estimate the cost-effectiveness of waiving coinsurance for every component of colorectal cancer screening. They estimated that, currently, using the colonoscopy regimen with coinsurance, 12.8 colorectal cancer deaths occurred per 1,000 people aged 65 years and 124.1 QALYs were gained per 1,000 people aged 65 years. The total number of procedures per 1,000 Medicare beneficiaries was 1,132, of which 410 (36%) were potentially subject to coinsurance requirements.
“We estimated that the total lifetime costs for [the Centers for Medicare & Medicaid], which included colorectal cancer screening, surveillance, and treatment with coinsurance, to be $2.675 million per 1,000 sixty-five-year-olds,” Ms. Peterse and her colleagues wrote.
Researchers noted that if the coinsurance was waived but there was no follow-on increase in the screening rate, the benefits of screening would not change but the total cost of screening and treatment would increase to $2.726 million per 1,000 people aged 65 years.
However, “an assumed 5-percentage-point increase in the rates of first colonoscopy screening and surveillance decreased the number of colorectal cancer deaths by 0.9 (6.4 percent), accompanied by an increase of $33,000 (1.2 percent) in total costs, with a cost per QALY gained (or cost-effectiveness ratio) of $4,086.”
They added that estimated screening benefits were similar when fecal testing was the primary screening method.
“In general, [fecal testing] screening was associated with lower number of procedures subject to coinsurance,” the researchers added. “If [fecal testing] screening becomes more popular in the United States, following trends observed in several settings, the costs of waiving coinsurance would be even lower.” The researchers also suggest that it could lead to reducing disparities of colorectal cancer in the United States as well.
AGA has been working for years to try to fix this issue, and supports the bipartisan Removing Barriers to Screening Act, which would correct this inequity for Medicare beneficiaries and remove the financial barriers that may prevent a patient from undergoing a screening. AGA is hopeful that the growing support for the legislation on both sides of the aisle will help get the bill passed this year. To learn more about this issue, visit http://www.gastro.org/take-action/top-issues/patient-cost-sharing-for-screening-colonoscopy. To help your patient understand this issue, AGA has created “What to Expect: Paying for Your Colonoscopy,” which can be downloaded at http://www.gastro.org/patient-care/procedures/Colonoscopy_CoPay_WhatToKnowFactSheet.pdf to be shared in your office. /p>
SOURCE: Peterse EFP et al. Health Affairs. 2017 Dec;36(12):2151-9.
Currently, Medicare covers colorectal screening at no charge to the patient, but if a polyp is removed upon discovery during the procedure, the patient would then be subject to Medicare’s coinsurance payments for both the colonoscopy and the removal.
Researchers used the Microsimulation Screening Analysis-Colon model to estimate the cost-effectiveness of waiving coinsurance for every component of colorectal cancer screening. They estimated that, currently, using the colonoscopy regimen with coinsurance, 12.8 colorectal cancer deaths occurred per 1,000 people aged 65 years and 124.1 QALYs were gained per 1,000 people aged 65 years. The total number of procedures per 1,000 Medicare beneficiaries was 1,132, of which 410 (36%) were potentially subject to coinsurance requirements.
“We estimated that the total lifetime costs for [the Centers for Medicare & Medicaid], which included colorectal cancer screening, surveillance, and treatment with coinsurance, to be $2.675 million per 1,000 sixty-five-year-olds,” Ms. Peterse and her colleagues wrote.
Researchers noted that if the coinsurance was waived but there was no follow-on increase in the screening rate, the benefits of screening would not change but the total cost of screening and treatment would increase to $2.726 million per 1,000 people aged 65 years.
However, “an assumed 5-percentage-point increase in the rates of first colonoscopy screening and surveillance decreased the number of colorectal cancer deaths by 0.9 (6.4 percent), accompanied by an increase of $33,000 (1.2 percent) in total costs, with a cost per QALY gained (or cost-effectiveness ratio) of $4,086.”
They added that estimated screening benefits were similar when fecal testing was the primary screening method.
“In general, [fecal testing] screening was associated with lower number of procedures subject to coinsurance,” the researchers added. “If [fecal testing] screening becomes more popular in the United States, following trends observed in several settings, the costs of waiving coinsurance would be even lower.” The researchers also suggest that it could lead to reducing disparities of colorectal cancer in the United States as well.
AGA has been working for years to try to fix this issue, and supports the bipartisan Removing Barriers to Screening Act, which would correct this inequity for Medicare beneficiaries and remove the financial barriers that may prevent a patient from undergoing a screening. AGA is hopeful that the growing support for the legislation on both sides of the aisle will help get the bill passed this year. To learn more about this issue, visit http://www.gastro.org/take-action/top-issues/patient-cost-sharing-for-screening-colonoscopy. To help your patient understand this issue, AGA has created “What to Expect: Paying for Your Colonoscopy,” which can be downloaded at http://www.gastro.org/patient-care/procedures/Colonoscopy_CoPay_WhatToKnowFactSheet.pdf to be shared in your office. /p>
SOURCE: Peterse EFP et al. Health Affairs. 2017 Dec;36(12):2151-9.
FROM HEALTH AFFAIRS
Experience may not always the best teacher
“In medicine, a lack of experience may not actually be a bad thing.” The words leapt off my tablet, and my blood pressure hit the stratosphere. How could a 30-year-old physician who is still doing his cardiology fellowship have the nerve to take a cheap shot at one of the cornerstones of my identity? (“For Doctors, Age May Be More Than a Number,” by Haider Javed Warraich, The New York Times, Jan. 6, 2018.) My reputation as a skilled pediatrician was built on the breadth and depth of my clinical experience. In the first 30 years of my professional career, I had participated in more than 300,000 patient encounters. Wasn’t that effort good for something?

He wrote that in a study of hospitalists (BMJ. 2017;357:j1797), the patient death rate increased steadily from 10.8% for physicians younger than 40 years to 12.1% for those 6o years and older, except those physicians treating a high volume of patients. He also cites a study in which the authors analyzed 62 studies of quality of care. The investigators found that slightly more than half of the studies “report decreasing performance with increasing years in practice” (Ann Int Med. 2005 Feb 15;142[4]:260-73).
Still in a defensive mode, I decided to chase down the references and take a closer look. In the study demonstrating patient mortality increasing with physician age, we must consider that these physicians were hospitalists and the patients were elderly. The observations may not be applicable to those seeing younger patients in a primary care office setting.
Another caveat listed by the authors is that the association between increasing patient mortality with increasing physician age did not hold true “among physicians with high volumes of patients.” As a high-volume practitioner myself, I found this comforting. It may be that there is some threshold effect in which a little experience is a negative but a ton of experience is a plus. Experience can teach efficiency. But, of course, efficiency doesn’t always equate with quality.
The study citing a decline in quality of care with physician age is a bit more troublesome. However, it may be that, rightly or wrongly, older physicians who have seen the tide go in and out enough times are more hesitant to accept and adhere to “evidence-based” quality measures that they see as ephemeral.

After what for me was an inflammatory opening, Dr. Warraich’s article closes with the observation that “mentorship is a two-way street.” Any physician who has worked with medical students and inquisitive house officers realizes that our surplus of experience always can stand to gain a little refreshing from those who have little of their own.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
“In medicine, a lack of experience may not actually be a bad thing.” The words leapt off my tablet, and my blood pressure hit the stratosphere. How could a 30-year-old physician who is still doing his cardiology fellowship have the nerve to take a cheap shot at one of the cornerstones of my identity? (“For Doctors, Age May Be More Than a Number,” by Haider Javed Warraich, The New York Times, Jan. 6, 2018.) My reputation as a skilled pediatrician was built on the breadth and depth of my clinical experience. In the first 30 years of my professional career, I had participated in more than 300,000 patient encounters. Wasn’t that effort good for something?
He wrote that in a study of hospitalists (BMJ. 2017;357:j1797), the patient death rate increased steadily from 10.8% for physicians younger than 40 years to 12.1% for those 6o years and older, except those physicians treating a high volume of patients. He also cites a study in which the authors analyzed 62 studies of quality of care. The investigators found that slightly more than half of the studies “report decreasing performance with increasing years in practice” (Ann Int Med. 2005 Feb 15;142[4]:260-73).
Still in a defensive mode, I decided to chase down the references and take a closer look. In the study demonstrating patient mortality increasing with physician age, we must consider that these physicians were hospitalists and the patients were elderly. The observations may not be applicable to those seeing younger patients in a primary care office setting.
Another caveat listed by the authors is that the association between increasing patient mortality with increasing physician age did not hold true “among physicians with high volumes of patients.” As a high-volume practitioner myself, I found this comforting. It may be that there is some threshold effect in which a little experience is a negative but a ton of experience is a plus. Experience can teach efficiency. But, of course, efficiency doesn’t always equate with quality.
The study citing a decline in quality of care with physician age is a bit more troublesome. However, it may be that, rightly or wrongly, older physicians who have seen the tide go in and out enough times are more hesitant to accept and adhere to “evidence-based” quality measures that they see as ephemeral.
After what for me was an inflammatory opening, Dr. Warraich’s article closes with the observation that “mentorship is a two-way street.” Any physician who has worked with medical students and inquisitive house officers realizes that our surplus of experience always can stand to gain a little refreshing from those who have little of their own.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
“In medicine, a lack of experience may not actually be a bad thing.” The words leapt off my tablet, and my blood pressure hit the stratosphere. How could a 30-year-old physician who is still doing his cardiology fellowship have the nerve to take a cheap shot at one of the cornerstones of my identity? (“For Doctors, Age May Be More Than a Number,” by Haider Javed Warraich, The New York Times, Jan. 6, 2018.) My reputation as a skilled pediatrician was built on the breadth and depth of my clinical experience. In the first 30 years of my professional career, I had participated in more than 300,000 patient encounters. Wasn’t that effort good for something?
He wrote that in a study of hospitalists (BMJ. 2017;357:j1797), the patient death rate increased steadily from 10.8% for physicians younger than 40 years to 12.1% for those 6o years and older, except those physicians treating a high volume of patients. He also cites a study in which the authors analyzed 62 studies of quality of care. The investigators found that slightly more than half of the studies “report decreasing performance with increasing years in practice” (Ann Int Med. 2005 Feb 15;142[4]:260-73).
Still in a defensive mode, I decided to chase down the references and take a closer look. In the study demonstrating patient mortality increasing with physician age, we must consider that these physicians were hospitalists and the patients were elderly. The observations may not be applicable to those seeing younger patients in a primary care office setting.
Another caveat listed by the authors is that the association between increasing patient mortality with increasing physician age did not hold true “among physicians with high volumes of patients.” As a high-volume practitioner myself, I found this comforting. It may be that there is some threshold effect in which a little experience is a negative but a ton of experience is a plus. Experience can teach efficiency. But, of course, efficiency doesn’t always equate with quality.
The study citing a decline in quality of care with physician age is a bit more troublesome. However, it may be that, rightly or wrongly, older physicians who have seen the tide go in and out enough times are more hesitant to accept and adhere to “evidence-based” quality measures that they see as ephemeral.
After what for me was an inflammatory opening, Dr. Warraich’s article closes with the observation that “mentorship is a two-way street.” Any physician who has worked with medical students and inquisitive house officers realizes that our surplus of experience always can stand to gain a little refreshing from those who have little of their own.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
VIDEO: Lean body mass linked to atrial fib etiology
ORLANDO – Results from a large Danish epidemiologic study published in 2017 upended the traditional view that obesity directly contributes to new onset atrial fibrillation by instead fingering lean body mass as the key body-habitus culprit.
“It’s a very different way of thinking about obesity” and it’s relationship to the etiology of atrial fibrillation, Stanley Nattel, MD, said in a video interview at the annual International AF Symposium. “I wouldn’t qualify it yet as a complete shift,” because the results came from a single study, “but the results are quite persuasive and very interesting,” said Dr. Nattel, professor of medicine and director of the electrophysiology research program at the Montreal Heart Institute.
The study he cited tracked the incidence of atrial fibrillation during median of 17 years in more than 55,000 Danish people who were aged 50-64 years old at baseline, and showed that lean body mass was the predominant anthropometric risk factor for new-onset atrial fibrillation (J Am Coll Cardiol. 2017 May;69[20]:2488-97). When the article appeared, it was accompanied by an editorial written by Dr. Nattel (J Am Coll Cardiol. 2017 May;69[20]2498-501).
“People had not thought a lot in the past” about lean body mass and atrial fibrillation, he noted.
If the finding is confirmed, it might make sense to target screening for atrial fibrillation to people with higher levels of lean body mass, Dr. Nattel suggested.
ORLANDO – Results from a large Danish epidemiologic study published in 2017 upended the traditional view that obesity directly contributes to new onset atrial fibrillation by instead fingering lean body mass as the key body-habitus culprit.
“It’s a very different way of thinking about obesity” and it’s relationship to the etiology of atrial fibrillation, Stanley Nattel, MD, said in a video interview at the annual International AF Symposium. “I wouldn’t qualify it yet as a complete shift,” because the results came from a single study, “but the results are quite persuasive and very interesting,” said Dr. Nattel, professor of medicine and director of the electrophysiology research program at the Montreal Heart Institute.
The study he cited tracked the incidence of atrial fibrillation during median of 17 years in more than 55,000 Danish people who were aged 50-64 years old at baseline, and showed that lean body mass was the predominant anthropometric risk factor for new-onset atrial fibrillation (J Am Coll Cardiol. 2017 May;69[20]:2488-97). When the article appeared, it was accompanied by an editorial written by Dr. Nattel (J Am Coll Cardiol. 2017 May;69[20]2498-501).
“People had not thought a lot in the past” about lean body mass and atrial fibrillation, he noted.
If the finding is confirmed, it might make sense to target screening for atrial fibrillation to people with higher levels of lean body mass, Dr. Nattel suggested.
ORLANDO – Results from a large Danish epidemiologic study published in 2017 upended the traditional view that obesity directly contributes to new onset atrial fibrillation by instead fingering lean body mass as the key body-habitus culprit.
“It’s a very different way of thinking about obesity” and it’s relationship to the etiology of atrial fibrillation, Stanley Nattel, MD, said in a video interview at the annual International AF Symposium. “I wouldn’t qualify it yet as a complete shift,” because the results came from a single study, “but the results are quite persuasive and very interesting,” said Dr. Nattel, professor of medicine and director of the electrophysiology research program at the Montreal Heart Institute.
The study he cited tracked the incidence of atrial fibrillation during median of 17 years in more than 55,000 Danish people who were aged 50-64 years old at baseline, and showed that lean body mass was the predominant anthropometric risk factor for new-onset atrial fibrillation (J Am Coll Cardiol. 2017 May;69[20]:2488-97). When the article appeared, it was accompanied by an editorial written by Dr. Nattel (J Am Coll Cardiol. 2017 May;69[20]2498-501).
“People had not thought a lot in the past” about lean body mass and atrial fibrillation, he noted.
If the finding is confirmed, it might make sense to target screening for atrial fibrillation to people with higher levels of lean body mass, Dr. Nattel suggested.
EXPERT ANALYSIS FROM THE AF SYMPOSIUM 2018

Age at RRSO affects peritoneal cancer risk in BRCA mutation carriers
Carriers of the BRCA1/2 mutation who undergo risk-reducing salpingo-oophorectomy (RRSO) still face a risk of developing metachronous peritoneal carcinomatosis, according to new findings published in Cancer.
The risk was predominantly observed in BRCA1 mutation carriers, and disease development generally occurred within 5 years following RRSO. Women who underwent RRSO at an age older than that currently recommended also had a higher risk of developing peritoneal carcinoma.
Their median age was 52 years at the time they underwent surgery, and 60 years when they were diagnosed with peritoneal carcinomatosis. As compared with the control group, the patients were older at the time they underwent RRSO (P = .025).
In eight RRSO specimens that were obtained from women who subsequently developed peritoneal carcinomatosis, five (62.5%), had serous tubal intraepithelial carcinoma (STIC) and one had epithelial atypia.
“The findings of the current study can be used to refine gynecologic counseling for BRCA1/2 mutation carriers who consider risk-reducing surgery and to stress the importance of complete RRSO at the recommended ages,” wrote lead author Marline G. Harmsen, MD, PhD, of the Radboud University Medical Center, Nijmegen, the Netherlands.
BRCA1/2 mutation carriers face a higher risk of developing ovarian carcinoma, and RRSO can reduce that risk by 80%-96%. Surgery is recommended for carriers of BRCA1 mutations aged 35-40 years and for BRCA2 mutation carriers aged 40-45 years.
In this study, Dr. Harmsen and her colleagues conducted a literature search in order to collect and analyze clinical and pathological data from women with BRCA1/2 mutation who developed peritoneal carcinomatosis following RRSO. The cases that were identified were then compared with a cohort from a single institution.
Of the 36 cases that were identified, 86.1% were BRCA1 mutation carriers and the remaining 5 patients had a BRCA2 mutation. The median age at the time of surgery differed significantly between BRCA1 (51 years; range, 30-71 years) and BRCA2 mutation carriers (57 years; range, 56-65 years) (P = .006).
The majority of women had undergone salpingo-oophorectomy (31; 86.1%), and 16 (44.4%) had also had a hysterectomy.
The authors found that several statistically significant differences between the case studies and the control group: the median age surgery (52 vs. 46 years), percentage of BRCA1 mutation carriers (86.1% vs. 53.1%, P less than .001), and percentage of serous tubal intraepithelial carcinomas in the RRSO specimens (62.5% vs. 0%; P less than .001).
SOURCE: Hamsen MG et al. Cancer. 2018 Jan 9. doi: 10.1002/cncr.31211.
In an accompanying editorial, Christine S. Walsh, MD, of Cedars-Sinai Medical Center in Los Angeles, notes that the study authors have “done a commendable job in trying to shed light on a rare condition,” which occurs in about 1%-4% of women who undergo risk-reducing salpingo-oophorectomy (RRSO).
These findings can provide more information to clinicians, as they seek to guide and counsel women after they undergo RRSO, she wrote.
Dr. Walsh pointed out that National Comprehensive Cancer Network guidelines for genetic/familial high-risk assessment of breast and ovarian cancer specify the optimal ages when RRSO should be performed, but despite efforts to encourage this, occult gynecologic carcinomas still are found in approximately 4.5%-9% of women, with serous tubal intraepithelial carcinoma lesions developing in approximately 5%-8% of them.
“Ideally, the goal should be to intervene with a prophylactic surgery before the development of cancerous or precancerous pathology,” she wrote. Dr. Walsh had no disclosures.
In an accompanying editorial, Christine S. Walsh, MD, of Cedars-Sinai Medical Center in Los Angeles, notes that the study authors have “done a commendable job in trying to shed light on a rare condition,” which occurs in about 1%-4% of women who undergo risk-reducing salpingo-oophorectomy (RRSO).
These findings can provide more information to clinicians, as they seek to guide and counsel women after they undergo RRSO, she wrote.
Dr. Walsh pointed out that National Comprehensive Cancer Network guidelines for genetic/familial high-risk assessment of breast and ovarian cancer specify the optimal ages when RRSO should be performed, but despite efforts to encourage this, occult gynecologic carcinomas still are found in approximately 4.5%-9% of women, with serous tubal intraepithelial carcinoma lesions developing in approximately 5%-8% of them.
“Ideally, the goal should be to intervene with a prophylactic surgery before the development of cancerous or precancerous pathology,” she wrote. Dr. Walsh had no disclosures.
In an accompanying editorial, Christine S. Walsh, MD, of Cedars-Sinai Medical Center in Los Angeles, notes that the study authors have “done a commendable job in trying to shed light on a rare condition,” which occurs in about 1%-4% of women who undergo risk-reducing salpingo-oophorectomy (RRSO).
These findings can provide more information to clinicians, as they seek to guide and counsel women after they undergo RRSO, she wrote.
Dr. Walsh pointed out that National Comprehensive Cancer Network guidelines for genetic/familial high-risk assessment of breast and ovarian cancer specify the optimal ages when RRSO should be performed, but despite efforts to encourage this, occult gynecologic carcinomas still are found in approximately 4.5%-9% of women, with serous tubal intraepithelial carcinoma lesions developing in approximately 5%-8% of them.
“Ideally, the goal should be to intervene with a prophylactic surgery before the development of cancerous or precancerous pathology,” she wrote. Dr. Walsh had no disclosures.
Carriers of the BRCA1/2 mutation who undergo risk-reducing salpingo-oophorectomy (RRSO) still face a risk of developing metachronous peritoneal carcinomatosis, according to new findings published in Cancer.
The risk was predominantly observed in BRCA1 mutation carriers, and disease development generally occurred within 5 years following RRSO. Women who underwent RRSO at an age older than that currently recommended also had a higher risk of developing peritoneal carcinoma.
Their median age was 52 years at the time they underwent surgery, and 60 years when they were diagnosed with peritoneal carcinomatosis. As compared with the control group, the patients were older at the time they underwent RRSO (P = .025).
In eight RRSO specimens that were obtained from women who subsequently developed peritoneal carcinomatosis, five (62.5%), had serous tubal intraepithelial carcinoma (STIC) and one had epithelial atypia.
“The findings of the current study can be used to refine gynecologic counseling for BRCA1/2 mutation carriers who consider risk-reducing surgery and to stress the importance of complete RRSO at the recommended ages,” wrote lead author Marline G. Harmsen, MD, PhD, of the Radboud University Medical Center, Nijmegen, the Netherlands.
BRCA1/2 mutation carriers face a higher risk of developing ovarian carcinoma, and RRSO can reduce that risk by 80%-96%. Surgery is recommended for carriers of BRCA1 mutations aged 35-40 years and for BRCA2 mutation carriers aged 40-45 years.
In this study, Dr. Harmsen and her colleagues conducted a literature search in order to collect and analyze clinical and pathological data from women with BRCA1/2 mutation who developed peritoneal carcinomatosis following RRSO. The cases that were identified were then compared with a cohort from a single institution.
Of the 36 cases that were identified, 86.1% were BRCA1 mutation carriers and the remaining 5 patients had a BRCA2 mutation. The median age at the time of surgery differed significantly between BRCA1 (51 years; range, 30-71 years) and BRCA2 mutation carriers (57 years; range, 56-65 years) (P = .006).
The majority of women had undergone salpingo-oophorectomy (31; 86.1%), and 16 (44.4%) had also had a hysterectomy.
The authors found that several statistically significant differences between the case studies and the control group: the median age surgery (52 vs. 46 years), percentage of BRCA1 mutation carriers (86.1% vs. 53.1%, P less than .001), and percentage of serous tubal intraepithelial carcinomas in the RRSO specimens (62.5% vs. 0%; P less than .001).
SOURCE: Hamsen MG et al. Cancer. 2018 Jan 9. doi: 10.1002/cncr.31211.
Carriers of the BRCA1/2 mutation who undergo risk-reducing salpingo-oophorectomy (RRSO) still face a risk of developing metachronous peritoneal carcinomatosis, according to new findings published in Cancer.
The risk was predominantly observed in BRCA1 mutation carriers, and disease development generally occurred within 5 years following RRSO. Women who underwent RRSO at an age older than that currently recommended also had a higher risk of developing peritoneal carcinoma.
Their median age was 52 years at the time they underwent surgery, and 60 years when they were diagnosed with peritoneal carcinomatosis. As compared with the control group, the patients were older at the time they underwent RRSO (P = .025).
In eight RRSO specimens that were obtained from women who subsequently developed peritoneal carcinomatosis, five (62.5%), had serous tubal intraepithelial carcinoma (STIC) and one had epithelial atypia.
“The findings of the current study can be used to refine gynecologic counseling for BRCA1/2 mutation carriers who consider risk-reducing surgery and to stress the importance of complete RRSO at the recommended ages,” wrote lead author Marline G. Harmsen, MD, PhD, of the Radboud University Medical Center, Nijmegen, the Netherlands.
BRCA1/2 mutation carriers face a higher risk of developing ovarian carcinoma, and RRSO can reduce that risk by 80%-96%. Surgery is recommended for carriers of BRCA1 mutations aged 35-40 years and for BRCA2 mutation carriers aged 40-45 years.
In this study, Dr. Harmsen and her colleagues conducted a literature search in order to collect and analyze clinical and pathological data from women with BRCA1/2 mutation who developed peritoneal carcinomatosis following RRSO. The cases that were identified were then compared with a cohort from a single institution.
Of the 36 cases that were identified, 86.1% were BRCA1 mutation carriers and the remaining 5 patients had a BRCA2 mutation. The median age at the time of surgery differed significantly between BRCA1 (51 years; range, 30-71 years) and BRCA2 mutation carriers (57 years; range, 56-65 years) (P = .006).
The majority of women had undergone salpingo-oophorectomy (31; 86.1%), and 16 (44.4%) had also had a hysterectomy.
The authors found that several statistically significant differences between the case studies and the control group: the median age surgery (52 vs. 46 years), percentage of BRCA1 mutation carriers (86.1% vs. 53.1%, P less than .001), and percentage of serous tubal intraepithelial carcinomas in the RRSO specimens (62.5% vs. 0%; P less than .001).
SOURCE: Hamsen MG et al. Cancer. 2018 Jan 9. doi: 10.1002/cncr.31211.
FROM CANCER
Key clinical point: BRCA mutation carriers who undergo risk-reducing surgery at an older age have a higher risk of developing metachronous peritoneal carcinomatosis.
Major finding: Women with BRCA 1 were at a higher risk for developing peritoneal carcinomatosis, as were those who underwent surgery at an older age.
Data source: A literature search to identify patients with BRCA 1/2 mutations who had undergone risk-reducing surgery and developed peritoneal carcinomatosis; 36 cases were identified and compared with a control group from a single institution.
Disclosures: No specific funding was disclosed. The authors had no disclosures.
Source: Hamsen MG et al. Cancer. 2018 Jan 9. doi: 10.1002/cncr.31211.
FDA approves PARP inhibitor for BRCA+ advanced breast cancer
The Food and Drug Administration has approved the PARP inhibitor olaparib for the treatment of patients with germline BRCA-positive, HER2-negative metastatic breast cancer who have previously received chemotherapy.
This is the first PARP inhibitor approved to treat breast cancer and the first approval for treatment of patients with metastatic breast cancer who have a BRCA gene mutation, the FDA said in a press statement.
The FDA also expanded approval of the companion diagnostic, BRACAnalysis CDx, to include the detection of BRCA mutations in blood samples from patients with breast cancer.

A capsule form of olaparib (Lynparza) was first approved in 2014 for the treatment of patients with deleterious or suspected deleterious germline BRCA-mutated advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy. In August 2017, the FDA granted regular approval to olaparib tablets for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer, who are in a complete or partial response to platinum-based chemotherapy. Olaparib tablets and capsules are not interchangeable. Olaparib capsules are being phased out of the U.S. market and will be available only through the Lynparza Specialty Pharmacy Network, the FDA said.
Approval for the treatment of breast cancer was based on a 2.8 month improvement in progression-free survival with olaparib vs standard chemotherapy in the phase 3 OlympiAD trial of 302 previously treated patients with BRCA-positive, HER2-negative breast cancer. Results of the trial were presented at ASCO 2017 and simultaneously published in the New England Journal of Medicine (N Engl J Med. 2017 Jun 4. doi: 10.1056/NEJMoa1706450).
Common side effects of olaparib include anemia, neutropenia, leukopenia, nausea, fatigue, vomiting, nasopharyngitis, respiratory tract infection, influenza, diarrhea, arthralgia/myalgia, dysgeusia, headache, dyspepsia, decreased appetite, constipation and stomatitis.
Severe side effects include development of myelodysplastic syndrome/acute myeloid leukemia and pneumonitis. Women should be advised of the potential risk to the fetus and to use effective contraception, the FDA said.
The FDA granted the approval of olaparib to AstraZeneca Pharmaceuticals LP and the approval of the BRACAnalysis CDx to Myriad Genetic Laboratories, Inc.
The Food and Drug Administration has approved the PARP inhibitor olaparib for the treatment of patients with germline BRCA-positive, HER2-negative metastatic breast cancer who have previously received chemotherapy.
This is the first PARP inhibitor approved to treat breast cancer and the first approval for treatment of patients with metastatic breast cancer who have a BRCA gene mutation, the FDA said in a press statement.
The FDA also expanded approval of the companion diagnostic, BRACAnalysis CDx, to include the detection of BRCA mutations in blood samples from patients with breast cancer.
A capsule form of olaparib (Lynparza) was first approved in 2014 for the treatment of patients with deleterious or suspected deleterious germline BRCA-mutated advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy. In August 2017, the FDA granted regular approval to olaparib tablets for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer, who are in a complete or partial response to platinum-based chemotherapy. Olaparib tablets and capsules are not interchangeable. Olaparib capsules are being phased out of the U.S. market and will be available only through the Lynparza Specialty Pharmacy Network, the FDA said.
Approval for the treatment of breast cancer was based on a 2.8 month improvement in progression-free survival with olaparib vs standard chemotherapy in the phase 3 OlympiAD trial of 302 previously treated patients with BRCA-positive, HER2-negative breast cancer. Results of the trial were presented at ASCO 2017 and simultaneously published in the New England Journal of Medicine (N Engl J Med. 2017 Jun 4. doi: 10.1056/NEJMoa1706450).
Common side effects of olaparib include anemia, neutropenia, leukopenia, nausea, fatigue, vomiting, nasopharyngitis, respiratory tract infection, influenza, diarrhea, arthralgia/myalgia, dysgeusia, headache, dyspepsia, decreased appetite, constipation and stomatitis.
Severe side effects include development of myelodysplastic syndrome/acute myeloid leukemia and pneumonitis. Women should be advised of the potential risk to the fetus and to use effective contraception, the FDA said.
The FDA granted the approval of olaparib to AstraZeneca Pharmaceuticals LP and the approval of the BRACAnalysis CDx to Myriad Genetic Laboratories, Inc.
The Food and Drug Administration has approved the PARP inhibitor olaparib for the treatment of patients with germline BRCA-positive, HER2-negative metastatic breast cancer who have previously received chemotherapy.
This is the first PARP inhibitor approved to treat breast cancer and the first approval for treatment of patients with metastatic breast cancer who have a BRCA gene mutation, the FDA said in a press statement.
The FDA also expanded approval of the companion diagnostic, BRACAnalysis CDx, to include the detection of BRCA mutations in blood samples from patients with breast cancer.
A capsule form of olaparib (Lynparza) was first approved in 2014 for the treatment of patients with deleterious or suspected deleterious germline BRCA-mutated advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy. In August 2017, the FDA granted regular approval to olaparib tablets for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer, who are in a complete or partial response to platinum-based chemotherapy. Olaparib tablets and capsules are not interchangeable. Olaparib capsules are being phased out of the U.S. market and will be available only through the Lynparza Specialty Pharmacy Network, the FDA said.
Approval for the treatment of breast cancer was based on a 2.8 month improvement in progression-free survival with olaparib vs standard chemotherapy in the phase 3 OlympiAD trial of 302 previously treated patients with BRCA-positive, HER2-negative breast cancer. Results of the trial were presented at ASCO 2017 and simultaneously published in the New England Journal of Medicine (N Engl J Med. 2017 Jun 4. doi: 10.1056/NEJMoa1706450).
Common side effects of olaparib include anemia, neutropenia, leukopenia, nausea, fatigue, vomiting, nasopharyngitis, respiratory tract infection, influenza, diarrhea, arthralgia/myalgia, dysgeusia, headache, dyspepsia, decreased appetite, constipation and stomatitis.
Severe side effects include development of myelodysplastic syndrome/acute myeloid leukemia and pneumonitis. Women should be advised of the potential risk to the fetus and to use effective contraception, the FDA said.
The FDA granted the approval of olaparib to AstraZeneca Pharmaceuticals LP and the approval of the BRACAnalysis CDx to Myriad Genetic Laboratories, Inc.

Prescribe antibiotics wisely
Clinical question: What is the incidence of antibiotic-associated adverse drug events (ADEs) among adult inpatients?
Background: Antibiotics are used widely in the inpatient setting, although 20%-30% of inpatient antibiotic prescription are estimated to be unnecessary. Data are lacking on the rates of associated ADEs.
Study design: Retrospective cohort study.
Synopsis: Of the 5,579 patients admitted to four inpatient medicine services between September 2013 and June 2014, 1,488 (27%) received antibiotics for at least 24 hours. Patients were followed through admission and out to 90 days. A total of 324 unique antibiotic-associated ADEs occurred among 298 (20%) patients within 90 days of initial therapy. The overall rate of antibiotic-associated ADEs was 22.9/10,000 person-days. The investigators determined that 287 (19%) of antibiotic regimens were not clinically indicated, and among those, there were 56 (20%) ADEs. The most common 30-day ADEs were gastrointestinal, renal, and hematologic. The highest proportion of ADEs occurred with beta-lactams, fluoroquinolones, intravenous vancomycin, and trimethoprim-sulfamethoxazole, perhaps reflecting how commonly these agents are prescribed. Nearly all ADEs were considered clinically significant (97%). There were no deaths attributable to antibiotic-associated ADEs.
Bottom line: Antibiotic associated ADEs occur in about one in five inpatients, and about one in five antibiotic prescriptions may not be clinically indicated.
Citation: Tamma PD et al. Association of adverse events with antibiotic use in hospitalized patients. JAMA Intern Med. 2017 Sep 1;177(9):1308-15.
Dr. Anderson is an associate program director in the internal medicine residency training program at the University of Colorado School of Medicine and a hospitalist at the VA Eastern Colorado Health Care System in Denver.
Clinical question: What is the incidence of antibiotic-associated adverse drug events (ADEs) among adult inpatients?
Background: Antibiotics are used widely in the inpatient setting, although 20%-30% of inpatient antibiotic prescription are estimated to be unnecessary. Data are lacking on the rates of associated ADEs.
Study design: Retrospective cohort study.
Synopsis: Of the 5,579 patients admitted to four inpatient medicine services between September 2013 and June 2014, 1,488 (27%) received antibiotics for at least 24 hours. Patients were followed through admission and out to 90 days. A total of 324 unique antibiotic-associated ADEs occurred among 298 (20%) patients within 90 days of initial therapy. The overall rate of antibiotic-associated ADEs was 22.9/10,000 person-days. The investigators determined that 287 (19%) of antibiotic regimens were not clinically indicated, and among those, there were 56 (20%) ADEs. The most common 30-day ADEs were gastrointestinal, renal, and hematologic. The highest proportion of ADEs occurred with beta-lactams, fluoroquinolones, intravenous vancomycin, and trimethoprim-sulfamethoxazole, perhaps reflecting how commonly these agents are prescribed. Nearly all ADEs were considered clinically significant (97%). There were no deaths attributable to antibiotic-associated ADEs.
Bottom line: Antibiotic associated ADEs occur in about one in five inpatients, and about one in five antibiotic prescriptions may not be clinically indicated.
Citation: Tamma PD et al. Association of adverse events with antibiotic use in hospitalized patients. JAMA Intern Med. 2017 Sep 1;177(9):1308-15.
Dr. Anderson is an associate program director in the internal medicine residency training program at the University of Colorado School of Medicine and a hospitalist at the VA Eastern Colorado Health Care System in Denver.
Clinical question: What is the incidence of antibiotic-associated adverse drug events (ADEs) among adult inpatients?
Background: Antibiotics are used widely in the inpatient setting, although 20%-30% of inpatient antibiotic prescription are estimated to be unnecessary. Data are lacking on the rates of associated ADEs.
Study design: Retrospective cohort study.
Synopsis: Of the 5,579 patients admitted to four inpatient medicine services between September 2013 and June 2014, 1,488 (27%) received antibiotics for at least 24 hours. Patients were followed through admission and out to 90 days. A total of 324 unique antibiotic-associated ADEs occurred among 298 (20%) patients within 90 days of initial therapy. The overall rate of antibiotic-associated ADEs was 22.9/10,000 person-days. The investigators determined that 287 (19%) of antibiotic regimens were not clinically indicated, and among those, there were 56 (20%) ADEs. The most common 30-day ADEs were gastrointestinal, renal, and hematologic. The highest proportion of ADEs occurred with beta-lactams, fluoroquinolones, intravenous vancomycin, and trimethoprim-sulfamethoxazole, perhaps reflecting how commonly these agents are prescribed. Nearly all ADEs were considered clinically significant (97%). There were no deaths attributable to antibiotic-associated ADEs.
Bottom line: Antibiotic associated ADEs occur in about one in five inpatients, and about one in five antibiotic prescriptions may not be clinically indicated.
Citation: Tamma PD et al. Association of adverse events with antibiotic use in hospitalized patients. JAMA Intern Med. 2017 Sep 1;177(9):1308-15.
Dr. Anderson is an associate program director in the internal medicine residency training program at the University of Colorado School of Medicine and a hospitalist at the VA Eastern Colorado Health Care System in Denver.