User login
Families are essential partners in treating substance use disorders
Addiction used to be considered a moral failing, and the family was blamed for keeping the relative with addictions sick, through behaviors labeled “codependency” and “enabling.” The opioid epidemic can take credit for putting a serious dent in these destructive and stigmatizing notions. When psychiatrists actively include families as educated treatment partners, fatalities are less likely, and the havoc created by addiction on families is mitigated.

Genes and addiction
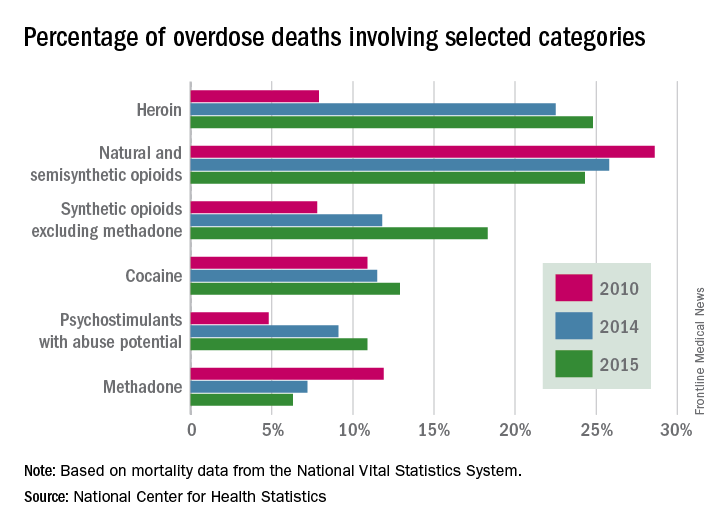
What causes addiction? Statistics show that Native Americans fare the worst of all minority groups, with death by opiates in whites and Native Americans double or triple the rates of African Americans and Latinos. Reasons put forward for Native American deaths are their vulnerability related to systemic racism, intergenerational trauma, and lack of access to health care. These “reasons” are well known to contribute to poor overall health status of impoverished communities.
Among impoverished white communities, the Monongahela Valley of Pennsylvania has been studied by Katherine McLean, PhD, as an example of postindustrial decay (Int J Drug Policy. 2016;[29]:19-26). Once a global center of steel production, the exodus of jobs, residents, and businesses since the early 1980s is thought to contribute to the high numbers of opioid deaths. A qualitative study of the people with addiction in the deteriorating mill city of McKeesport, Pa., characterized a risk environment hidden behind closed doors, and populated by unprepared, ambivalent overdose “assistants.” These people are “co-drug” users who themselves are reluctant to step forward because of fear of getting in trouble. The participants described the hopelessness and lack of opportunity as driving the use of heroin, with many stating that jobs and community reinvestment are needed to reduce fatalities. This certainly resonates with the Native American experience.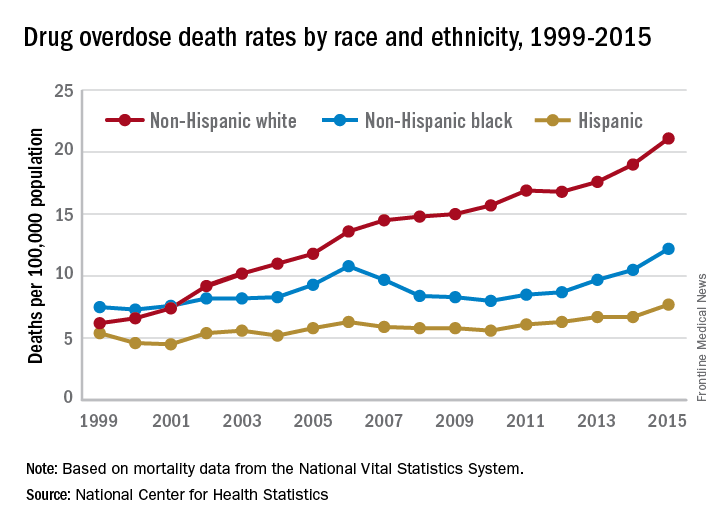
People with the AA variant of OXTR also have been shown to have less secure adult attachment and more social anxiety (World J Biol Psychiatry. 2016;17[1]:76-83). Comparing people with OXTR variants, the AA genotype was associated with a perceived negative social environment and significantly increased PTSD symptoms, whereas the GG genotype was protective.
However, for many decades, psychological theories about the defects of individuals and their moral failing have prevailed. In the family, aspersions have been cast on the family’s deficits in terms of setting limits and their enabling behaviors, mostly focusing on wives and mothers. The social mantra has been that since not all people get addicted, the strong resist and the weak succumb. Psychiatry has focused on providing psychotherapy to correct the personal deficits of the weak and addicted and, from a family perspective, on correcting negative personality traits in the caregivers, classified as codependency.
Roots of codependency
The concept of codependency began as a grassroots idea in the 1960s to describe family members, usually wives or mothers, who were deemed excessive in their caring for their husband or son with addiction. The term was used to describe women who had an overresponsibility for relationships, rather than a responsibility to self. Support groups for codependency, such as Co-Dependents Anonymous, Al-Anon/Alateen, Nar-Anon, and Adult Children of Alcoholics, based on the 12-step program model of Alcoholics Anonymous, were established. Codependents were negatively labeled as rescuers, supporters, and confidantes of their family member with substance use disorder. These helpers were described as dependent on the other person’s poor functioning to satisfy their own emotional needs.
In these early descriptions, there was a lack of discussion about possible deeper family dynamics: Inequality in financial independence of each partner, the desire for family stability focusing on the welfare of children, the real possibility that disrupting a relationship might result in violence if the woman was more assertive. Women were blamed for trying to love their spouse out of the addiction. One aspect of codependency is self-sacrifice, which used to be considered an important trait of the good wife but became a negative trait in the 1960s. Recovery from codependence was considered achieved when the wife or mother expressed healthy self-assertiveness. Some scholars did state, however, that they believed that codependency was not a negative trait, but rather a healthy personality trait taken to excess. In most studies, women with high codependency ratings have tended to be unemployed and with lower educations. Their behavior had been considered worthy of a DSM inclusion as a personality disorder, but luckily, this was thwarted.
A family is forced to make some accounting when an individual develops a substance use disorder. If the family tries to maintain equilibrium and keeps things as stable as possible for the sake of maintaining the family unit or the stability of the lives of the children, accommodation will be required. Accommodation minimizes the impact of the addiction: the sober spouse stepping up to complete the roles of the ill relative and in all ways reducing the impact of dysfunction on the family. If you swap out the illness and consider the ill family member as having cancer or respiratory distress, then you reframe the spouse’s “codependence” as the behavior of a caring spouse.
This long preamble is intended to illustrate how little family dynamics have to do with the etiology of addiction. Addiction is a chronic neurobiological disease, and like all diseases, individuals, and couples and families have the option of learning to cope well. We, as psychiatrists, must move away from blaming people (usually women who have less-than-optimal coping skills) and consider how best to engage partners and families in optimal programs.*
Families can benefit from specialist treatment and thus contribute to the recovery process. One example is a telepsychiatry program that aimed to improve family coping skills to cope with relatives who have substance use disorders. The Tele-intervention Model and Monitoring of Families of Drug Users is based on motivational interviewing and stages of change. Families were randomized into the intervention group (n = 163) or the usual treatment (n = 162). After 6 months of follow-up, the family members of the telepsychiatry group were twice as likely to modify their behavior (odds ratio; 2.08; 95% confidence interval, 1.18-3.65) (J Sub Use Misuse. 2017 Jan 28;52[2]:164-74). This model was organized so that each of nine calls had a specific goal to stimulate the family members in their process of change.
Family change and engagement also can occur through Alanon (Subst Use Misuse. 2015; 50[1]:62-71) and the use of the Arise program of Judith Landau, MD, (Landau J et al. Am J Drug Alcohol Abuse. 2000;26[3]:379-98).
In summary, the family can be engaged in treatment and can develop family coping skills to support their relative with this chronic neurobiological disease.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
*Updated on January 12, 2018.
Addiction used to be considered a moral failing, and the family was blamed for keeping the relative with addictions sick, through behaviors labeled “codependency” and “enabling.” The opioid epidemic can take credit for putting a serious dent in these destructive and stigmatizing notions. When psychiatrists actively include families as educated treatment partners, fatalities are less likely, and the havoc created by addiction on families is mitigated.
Genes and addiction
What causes addiction? Statistics show that Native Americans fare the worst of all minority groups, with death by opiates in whites and Native Americans double or triple the rates of African Americans and Latinos. Reasons put forward for Native American deaths are their vulnerability related to systemic racism, intergenerational trauma, and lack of access to health care. These “reasons” are well known to contribute to poor overall health status of impoverished communities.
Among impoverished white communities, the Monongahela Valley of Pennsylvania has been studied by Katherine McLean, PhD, as an example of postindustrial decay (Int J Drug Policy. 2016;[29]:19-26). Once a global center of steel production, the exodus of jobs, residents, and businesses since the early 1980s is thought to contribute to the high numbers of opioid deaths. A qualitative study of the people with addiction in the deteriorating mill city of McKeesport, Pa., characterized a risk environment hidden behind closed doors, and populated by unprepared, ambivalent overdose “assistants.” These people are “co-drug” users who themselves are reluctant to step forward because of fear of getting in trouble. The participants described the hopelessness and lack of opportunity as driving the use of heroin, with many stating that jobs and community reinvestment are needed to reduce fatalities. This certainly resonates with the Native American experience.
People with the AA variant of OXTR also have been shown to have less secure adult attachment and more social anxiety (World J Biol Psychiatry. 2016;17[1]:76-83). Comparing people with OXTR variants, the AA genotype was associated with a perceived negative social environment and significantly increased PTSD symptoms, whereas the GG genotype was protective.
However, for many decades, psychological theories about the defects of individuals and their moral failing have prevailed. In the family, aspersions have been cast on the family’s deficits in terms of setting limits and their enabling behaviors, mostly focusing on wives and mothers. The social mantra has been that since not all people get addicted, the strong resist and the weak succumb. Psychiatry has focused on providing psychotherapy to correct the personal deficits of the weak and addicted and, from a family perspective, on correcting negative personality traits in the caregivers, classified as codependency.
Roots of codependency
The concept of codependency began as a grassroots idea in the 1960s to describe family members, usually wives or mothers, who were deemed excessive in their caring for their husband or son with addiction. The term was used to describe women who had an overresponsibility for relationships, rather than a responsibility to self. Support groups for codependency, such as Co-Dependents Anonymous, Al-Anon/Alateen, Nar-Anon, and Adult Children of Alcoholics, based on the 12-step program model of Alcoholics Anonymous, were established. Codependents were negatively labeled as rescuers, supporters, and confidantes of their family member with substance use disorder. These helpers were described as dependent on the other person’s poor functioning to satisfy their own emotional needs.
In these early descriptions, there was a lack of discussion about possible deeper family dynamics: Inequality in financial independence of each partner, the desire for family stability focusing on the welfare of children, the real possibility that disrupting a relationship might result in violence if the woman was more assertive. Women were blamed for trying to love their spouse out of the addiction. One aspect of codependency is self-sacrifice, which used to be considered an important trait of the good wife but became a negative trait in the 1960s. Recovery from codependence was considered achieved when the wife or mother expressed healthy self-assertiveness. Some scholars did state, however, that they believed that codependency was not a negative trait, but rather a healthy personality trait taken to excess. In most studies, women with high codependency ratings have tended to be unemployed and with lower educations. Their behavior had been considered worthy of a DSM inclusion as a personality disorder, but luckily, this was thwarted.
A family is forced to make some accounting when an individual develops a substance use disorder. If the family tries to maintain equilibrium and keeps things as stable as possible for the sake of maintaining the family unit or the stability of the lives of the children, accommodation will be required. Accommodation minimizes the impact of the addiction: the sober spouse stepping up to complete the roles of the ill relative and in all ways reducing the impact of dysfunction on the family. If you swap out the illness and consider the ill family member as having cancer or respiratory distress, then you reframe the spouse’s “codependence” as the behavior of a caring spouse.
This long preamble is intended to illustrate how little family dynamics have to do with the etiology of addiction. Addiction is a chronic neurobiological disease, and like all diseases, individuals, and couples and families have the option of learning to cope well. We, as psychiatrists, must move away from blaming people (usually women who have less-than-optimal coping skills) and consider how best to engage partners and families in optimal programs.*
Families can benefit from specialist treatment and thus contribute to the recovery process. One example is a telepsychiatry program that aimed to improve family coping skills to cope with relatives who have substance use disorders. The Tele-intervention Model and Monitoring of Families of Drug Users is based on motivational interviewing and stages of change. Families were randomized into the intervention group (n = 163) or the usual treatment (n = 162). After 6 months of follow-up, the family members of the telepsychiatry group were twice as likely to modify their behavior (odds ratio; 2.08; 95% confidence interval, 1.18-3.65) (J Sub Use Misuse. 2017 Jan 28;52[2]:164-74). This model was organized so that each of nine calls had a specific goal to stimulate the family members in their process of change.
Family change and engagement also can occur through Alanon (Subst Use Misuse. 2015; 50[1]:62-71) and the use of the Arise program of Judith Landau, MD, (Landau J et al. Am J Drug Alcohol Abuse. 2000;26[3]:379-98).
In summary, the family can be engaged in treatment and can develop family coping skills to support their relative with this chronic neurobiological disease.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
*Updated on January 12, 2018.
Addiction used to be considered a moral failing, and the family was blamed for keeping the relative with addictions sick, through behaviors labeled “codependency” and “enabling.” The opioid epidemic can take credit for putting a serious dent in these destructive and stigmatizing notions. When psychiatrists actively include families as educated treatment partners, fatalities are less likely, and the havoc created by addiction on families is mitigated.
Genes and addiction
What causes addiction? Statistics show that Native Americans fare the worst of all minority groups, with death by opiates in whites and Native Americans double or triple the rates of African Americans and Latinos. Reasons put forward for Native American deaths are their vulnerability related to systemic racism, intergenerational trauma, and lack of access to health care. These “reasons” are well known to contribute to poor overall health status of impoverished communities.
Among impoverished white communities, the Monongahela Valley of Pennsylvania has been studied by Katherine McLean, PhD, as an example of postindustrial decay (Int J Drug Policy. 2016;[29]:19-26). Once a global center of steel production, the exodus of jobs, residents, and businesses since the early 1980s is thought to contribute to the high numbers of opioid deaths. A qualitative study of the people with addiction in the deteriorating mill city of McKeesport, Pa., characterized a risk environment hidden behind closed doors, and populated by unprepared, ambivalent overdose “assistants.” These people are “co-drug” users who themselves are reluctant to step forward because of fear of getting in trouble. The participants described the hopelessness and lack of opportunity as driving the use of heroin, with many stating that jobs and community reinvestment are needed to reduce fatalities. This certainly resonates with the Native American experience.
People with the AA variant of OXTR also have been shown to have less secure adult attachment and more social anxiety (World J Biol Psychiatry. 2016;17[1]:76-83). Comparing people with OXTR variants, the AA genotype was associated with a perceived negative social environment and significantly increased PTSD symptoms, whereas the GG genotype was protective.
However, for many decades, psychological theories about the defects of individuals and their moral failing have prevailed. In the family, aspersions have been cast on the family’s deficits in terms of setting limits and their enabling behaviors, mostly focusing on wives and mothers. The social mantra has been that since not all people get addicted, the strong resist and the weak succumb. Psychiatry has focused on providing psychotherapy to correct the personal deficits of the weak and addicted and, from a family perspective, on correcting negative personality traits in the caregivers, classified as codependency.
Roots of codependency
The concept of codependency began as a grassroots idea in the 1960s to describe family members, usually wives or mothers, who were deemed excessive in their caring for their husband or son with addiction. The term was used to describe women who had an overresponsibility for relationships, rather than a responsibility to self. Support groups for codependency, such as Co-Dependents Anonymous, Al-Anon/Alateen, Nar-Anon, and Adult Children of Alcoholics, based on the 12-step program model of Alcoholics Anonymous, were established. Codependents were negatively labeled as rescuers, supporters, and confidantes of their family member with substance use disorder. These helpers were described as dependent on the other person’s poor functioning to satisfy their own emotional needs.
In these early descriptions, there was a lack of discussion about possible deeper family dynamics: Inequality in financial independence of each partner, the desire for family stability focusing on the welfare of children, the real possibility that disrupting a relationship might result in violence if the woman was more assertive. Women were blamed for trying to love their spouse out of the addiction. One aspect of codependency is self-sacrifice, which used to be considered an important trait of the good wife but became a negative trait in the 1960s. Recovery from codependence was considered achieved when the wife or mother expressed healthy self-assertiveness. Some scholars did state, however, that they believed that codependency was not a negative trait, but rather a healthy personality trait taken to excess. In most studies, women with high codependency ratings have tended to be unemployed and with lower educations. Their behavior had been considered worthy of a DSM inclusion as a personality disorder, but luckily, this was thwarted.
A family is forced to make some accounting when an individual develops a substance use disorder. If the family tries to maintain equilibrium and keeps things as stable as possible for the sake of maintaining the family unit or the stability of the lives of the children, accommodation will be required. Accommodation minimizes the impact of the addiction: the sober spouse stepping up to complete the roles of the ill relative and in all ways reducing the impact of dysfunction on the family. If you swap out the illness and consider the ill family member as having cancer or respiratory distress, then you reframe the spouse’s “codependence” as the behavior of a caring spouse.
This long preamble is intended to illustrate how little family dynamics have to do with the etiology of addiction. Addiction is a chronic neurobiological disease, and like all diseases, individuals, and couples and families have the option of learning to cope well. We, as psychiatrists, must move away from blaming people (usually women who have less-than-optimal coping skills) and consider how best to engage partners and families in optimal programs.*
Families can benefit from specialist treatment and thus contribute to the recovery process. One example is a telepsychiatry program that aimed to improve family coping skills to cope with relatives who have substance use disorders. The Tele-intervention Model and Monitoring of Families of Drug Users is based on motivational interviewing and stages of change. Families were randomized into the intervention group (n = 163) or the usual treatment (n = 162). After 6 months of follow-up, the family members of the telepsychiatry group were twice as likely to modify their behavior (odds ratio; 2.08; 95% confidence interval, 1.18-3.65) (J Sub Use Misuse. 2017 Jan 28;52[2]:164-74). This model was organized so that each of nine calls had a specific goal to stimulate the family members in their process of change.
Family change and engagement also can occur through Alanon (Subst Use Misuse. 2015; 50[1]:62-71) and the use of the Arise program of Judith Landau, MD, (Landau J et al. Am J Drug Alcohol Abuse. 2000;26[3]:379-98).
In summary, the family can be engaged in treatment and can develop family coping skills to support their relative with this chronic neurobiological disease.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest to disclose.
*Updated on January 12, 2018.
Common food additive makes C. difficile more virulent
, a study showed.
“Out of several carbon sources identified that supported CD2015 growth [epidemic RT027 isolate], we found the disaccharide trehalose increased the growth yield of CD2015 by approximately fivefold, compared with a non-RT027 strain,” according to James Collins, PhD, of Baylor University, Houston, and his colleagues. The increased growth of the epidemic strain of C. difficile observed by Dr. Collins and his team demonstrates that trehalose is a robust carbon source for C. difficile bacterium.

In one experiment, mice with humanized microbiota were infected with two strains of RT027, either R20291 (n = 27) or R20291-delta treA (n = 28), a phosphotrehalase enzyme (TreA) deletion mutant that cannot metabolize trehalose. Mice were then given 5 mM of trehalose ad libitum in their drinking water. Researchers observed that the mice infected with R20291-delta treA had much lower mortality rates than the R20291 group (33.3% vs.78.6%). These findings were then reinforced with a second experiment using mice with humanized microbiota, in which trehalose addition increased mortality in RT027 mice, compared with RT027-infected mice that were not given dietary trehalose.
While Dr. Collins and his team demonstrated the effect of trehalose on C. difficile in mice, they also conducted a limited analysis of ileostomy effluent from three human donors. The researchers found that in two of three samples, treA was strongly induced in CD2015, but not in another ribotype, CD2048. This demonstrates that amounts of trehalose found in food are high enough to be metabolized by certain epidemic strains of C. difficile in humans.
Prior to 2000, trehalose use was limited by a relatively high cost of production, approximately $700 per kilogram. A production innovation that utilized a novel enzymatic method that yielded trehalose from starch brought the price of trehalose to approximately $3 per kilogram, making it a commercially viable food supplement. After being considered “generally recognized as safe” by the U.S. Food and Drug Administration in 2000 and approved for use in Europe, the trehalose concentrations in food skyrocketed from around 2% to 11.25%, and trehalose became widely used in several foods, including ice cream, pasta, and ground beef.
Dr. Collins and his associates said that there is considerable evidence that the widespread use of dietary trehalose has contributed to the spread of epidemic C. difficile ribotypes. First, strains RT027 and RT078 have always had the ability to metabolize trehalose, as evidenced by outbreaks of nonepidemic C. difficile in the 1980s. But no epidemic outbreaks were reported until after 2003, several years after trehalose was approved by the FDA. Second, RT027 and RT078 are phylogenetically distant, but independently evolved the ability to metabolize low levels of trehalose. Third, increased severity of the RT027 strain, which metabolizes trehalose in mice, is consistent with increased virulence of RT078 and RT027 in human patients. Fourth, a competitive advantage is conferred to C. difficile being able to metabolize trehalose in low concentrations in a diverse intestinal setting. Finally, the levels of trehalose in ileostomy fluid from patients who eat a normal diet are high enough to be utilized by RT027 strains.
“On the basis of these observations, we propose that the widespread adoption and use of the disaccharide trehalose in the human diet has played a significant role in the emergence of these epidemic and hypervirulent strains,” Dr. Collins and his colleagues wrote in their article in Nature.
The authors of the study had no relevant financial disclosures to report.
SOURCE: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Fecal microbiota transplantation (FMT) is a promising new treatment for recurring C. diff infections. The AGA FMT National Registry — conducted in collaboration with the Crohn’s and Colitis Foundation, the Infectious Diseases Society of America, and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition — will allow physicians and patients to report back on outcomes of the FMT procedure. This data will help answer critical questions about the longer-term health effects of FMT and guide future use. Learn more at www.gastro.org/FMTRegistry.
, a study showed.
“Out of several carbon sources identified that supported CD2015 growth [epidemic RT027 isolate], we found the disaccharide trehalose increased the growth yield of CD2015 by approximately fivefold, compared with a non-RT027 strain,” according to James Collins, PhD, of Baylor University, Houston, and his colleagues. The increased growth of the epidemic strain of C. difficile observed by Dr. Collins and his team demonstrates that trehalose is a robust carbon source for C. difficile bacterium.
In one experiment, mice with humanized microbiota were infected with two strains of RT027, either R20291 (n = 27) or R20291-delta treA (n = 28), a phosphotrehalase enzyme (TreA) deletion mutant that cannot metabolize trehalose. Mice were then given 5 mM of trehalose ad libitum in their drinking water. Researchers observed that the mice infected with R20291-delta treA had much lower mortality rates than the R20291 group (33.3% vs.78.6%). These findings were then reinforced with a second experiment using mice with humanized microbiota, in which trehalose addition increased mortality in RT027 mice, compared with RT027-infected mice that were not given dietary trehalose.
While Dr. Collins and his team demonstrated the effect of trehalose on C. difficile in mice, they also conducted a limited analysis of ileostomy effluent from three human donors. The researchers found that in two of three samples, treA was strongly induced in CD2015, but not in another ribotype, CD2048. This demonstrates that amounts of trehalose found in food are high enough to be metabolized by certain epidemic strains of C. difficile in humans.
Prior to 2000, trehalose use was limited by a relatively high cost of production, approximately $700 per kilogram. A production innovation that utilized a novel enzymatic method that yielded trehalose from starch brought the price of trehalose to approximately $3 per kilogram, making it a commercially viable food supplement. After being considered “generally recognized as safe” by the U.S. Food and Drug Administration in 2000 and approved for use in Europe, the trehalose concentrations in food skyrocketed from around 2% to 11.25%, and trehalose became widely used in several foods, including ice cream, pasta, and ground beef.
Dr. Collins and his associates said that there is considerable evidence that the widespread use of dietary trehalose has contributed to the spread of epidemic C. difficile ribotypes. First, strains RT027 and RT078 have always had the ability to metabolize trehalose, as evidenced by outbreaks of nonepidemic C. difficile in the 1980s. But no epidemic outbreaks were reported until after 2003, several years after trehalose was approved by the FDA. Second, RT027 and RT078 are phylogenetically distant, but independently evolved the ability to metabolize low levels of trehalose. Third, increased severity of the RT027 strain, which metabolizes trehalose in mice, is consistent with increased virulence of RT078 and RT027 in human patients. Fourth, a competitive advantage is conferred to C. difficile being able to metabolize trehalose in low concentrations in a diverse intestinal setting. Finally, the levels of trehalose in ileostomy fluid from patients who eat a normal diet are high enough to be utilized by RT027 strains.
“On the basis of these observations, we propose that the widespread adoption and use of the disaccharide trehalose in the human diet has played a significant role in the emergence of these epidemic and hypervirulent strains,” Dr. Collins and his colleagues wrote in their article in Nature.
The authors of the study had no relevant financial disclosures to report.
SOURCE: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Fecal microbiota transplantation (FMT) is a promising new treatment for recurring C. diff infections. The AGA FMT National Registry — conducted in collaboration with the Crohn’s and Colitis Foundation, the Infectious Diseases Society of America, and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition — will allow physicians and patients to report back on outcomes of the FMT procedure. This data will help answer critical questions about the longer-term health effects of FMT and guide future use. Learn more at www.gastro.org/FMTRegistry.
, a study showed.
“Out of several carbon sources identified that supported CD2015 growth [epidemic RT027 isolate], we found the disaccharide trehalose increased the growth yield of CD2015 by approximately fivefold, compared with a non-RT027 strain,” according to James Collins, PhD, of Baylor University, Houston, and his colleagues. The increased growth of the epidemic strain of C. difficile observed by Dr. Collins and his team demonstrates that trehalose is a robust carbon source for C. difficile bacterium.
In one experiment, mice with humanized microbiota were infected with two strains of RT027, either R20291 (n = 27) or R20291-delta treA (n = 28), a phosphotrehalase enzyme (TreA) deletion mutant that cannot metabolize trehalose. Mice were then given 5 mM of trehalose ad libitum in their drinking water. Researchers observed that the mice infected with R20291-delta treA had much lower mortality rates than the R20291 group (33.3% vs.78.6%). These findings were then reinforced with a second experiment using mice with humanized microbiota, in which trehalose addition increased mortality in RT027 mice, compared with RT027-infected mice that were not given dietary trehalose.
While Dr. Collins and his team demonstrated the effect of trehalose on C. difficile in mice, they also conducted a limited analysis of ileostomy effluent from three human donors. The researchers found that in two of three samples, treA was strongly induced in CD2015, but not in another ribotype, CD2048. This demonstrates that amounts of trehalose found in food are high enough to be metabolized by certain epidemic strains of C. difficile in humans.
Prior to 2000, trehalose use was limited by a relatively high cost of production, approximately $700 per kilogram. A production innovation that utilized a novel enzymatic method that yielded trehalose from starch brought the price of trehalose to approximately $3 per kilogram, making it a commercially viable food supplement. After being considered “generally recognized as safe” by the U.S. Food and Drug Administration in 2000 and approved for use in Europe, the trehalose concentrations in food skyrocketed from around 2% to 11.25%, and trehalose became widely used in several foods, including ice cream, pasta, and ground beef.
Dr. Collins and his associates said that there is considerable evidence that the widespread use of dietary trehalose has contributed to the spread of epidemic C. difficile ribotypes. First, strains RT027 and RT078 have always had the ability to metabolize trehalose, as evidenced by outbreaks of nonepidemic C. difficile in the 1980s. But no epidemic outbreaks were reported until after 2003, several years after trehalose was approved by the FDA. Second, RT027 and RT078 are phylogenetically distant, but independently evolved the ability to metabolize low levels of trehalose. Third, increased severity of the RT027 strain, which metabolizes trehalose in mice, is consistent with increased virulence of RT078 and RT027 in human patients. Fourth, a competitive advantage is conferred to C. difficile being able to metabolize trehalose in low concentrations in a diverse intestinal setting. Finally, the levels of trehalose in ileostomy fluid from patients who eat a normal diet are high enough to be utilized by RT027 strains.
“On the basis of these observations, we propose that the widespread adoption and use of the disaccharide trehalose in the human diet has played a significant role in the emergence of these epidemic and hypervirulent strains,” Dr. Collins and his colleagues wrote in their article in Nature.
The authors of the study had no relevant financial disclosures to report.
SOURCE: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Fecal microbiota transplantation (FMT) is a promising new treatment for recurring C. diff infections. The AGA FMT National Registry — conducted in collaboration with the Crohn’s and Colitis Foundation, the Infectious Diseases Society of America, and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition — will allow physicians and patients to report back on outcomes of the FMT procedure. This data will help answer critical questions about the longer-term health effects of FMT and guide future use. Learn more at www.gastro.org/FMTRegistry.
FROM NATURE
Key clinical point: Metabolizing trehalose increases the virulence and mortality of C. difficile ribotype 027 (RT027).
Major finding: The ability to metabolize trehalose with the phosphotrehalase enzyme (TreA) increases mortality in RT027.
Study details: Experimental mouse models and an analysis of ileostomy effluent from three anonymous donors.
Disclosures: All authors had no financial disclosures to report.
Source: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Acronym Alert: EVAR is Now EVR
Recent references to "EVR" coding changes weren't typos. We really meant "EVR" and not the "EVAR" with which we are all familiar. That's because there's been a change in vascular surgery acronyms. EVAR – Endovascular Aneurysm Repair – has become EVR – Endovascular Repair. The change was made by the CPT (Current Procedural Terminology) Editorial Panel and the SVS Coding Committee, as recent treatment strategies are not confined to the aorta.
We know EVR doesn't flow as trippingly off the tongue. Still, as the telephone operator used to say when informing a caller of a change in a phone number, "Please ... make a note of it."
Recent references to "EVR" coding changes weren't typos. We really meant "EVR" and not the "EVAR" with which we are all familiar. That's because there's been a change in vascular surgery acronyms. EVAR – Endovascular Aneurysm Repair – has become EVR – Endovascular Repair. The change was made by the CPT (Current Procedural Terminology) Editorial Panel and the SVS Coding Committee, as recent treatment strategies are not confined to the aorta.
We know EVR doesn't flow as trippingly off the tongue. Still, as the telephone operator used to say when informing a caller of a change in a phone number, "Please ... make a note of it."
Recent references to "EVR" coding changes weren't typos. We really meant "EVR" and not the "EVAR" with which we are all familiar. That's because there's been a change in vascular surgery acronyms. EVAR – Endovascular Aneurysm Repair – has become EVR – Endovascular Repair. The change was made by the CPT (Current Procedural Terminology) Editorial Panel and the SVS Coding Committee, as recent treatment strategies are not confined to the aorta.
We know EVR doesn't flow as trippingly off the tongue. Still, as the telephone operator used to say when informing a caller of a change in a phone number, "Please ... make a note of it."
Two VAM Scholarship, Fellowship deadlines are Feb. 1
- VAM travel scholarships (Feb. 1): The scholarships (General Surgery Resident/Medical Student Travel Scholarship and Diversity Medical Student Travel Scholarship) are for medical students and residents for the Vascular Annual Meeting. Recipients will be able to meet other students and residents plus talk with members and leaders of the vascular surgical community. Applicants get complimentary meeting registration plus financial resources to help defray travel costs.
- Student Research Fellowship (Feb. 1): Sponsored by the SVS Foundation, this award seeks to introduce the student to the application of rigorous scientific methods to clinical problems and underlying biologic processes important to patients with vascular disease.
- VAM travel scholarships (Feb. 1): The scholarships (General Surgery Resident/Medical Student Travel Scholarship and Diversity Medical Student Travel Scholarship) are for medical students and residents for the Vascular Annual Meeting. Recipients will be able to meet other students and residents plus talk with members and leaders of the vascular surgical community. Applicants get complimentary meeting registration plus financial resources to help defray travel costs.
- Student Research Fellowship (Feb. 1): Sponsored by the SVS Foundation, this award seeks to introduce the student to the application of rigorous scientific methods to clinical problems and underlying biologic processes important to patients with vascular disease.
- VAM travel scholarships (Feb. 1): The scholarships (General Surgery Resident/Medical Student Travel Scholarship and Diversity Medical Student Travel Scholarship) are for medical students and residents for the Vascular Annual Meeting. Recipients will be able to meet other students and residents plus talk with members and leaders of the vascular surgical community. Applicants get complimentary meeting registration plus financial resources to help defray travel costs.
- Student Research Fellowship (Feb. 1): Sponsored by the SVS Foundation, this award seeks to introduce the student to the application of rigorous scientific methods to clinical problems and underlying biologic processes important to patients with vascular disease.
Two Important VAM Deadlines are Wednesday
The deadline is Wednesday, Jan. 17, for two important research endeavors related to the 2018 Vascular Annual Meeting: abstract submissions and the Resident Research Award. This year's VAM will be June 20 to 23 at the Hynes Convention Center in Boston. Following a full day of programming on Wednesday, June 20, plenary sessions are set for June 21-23. Exhibits will be June 21-22. VAM registration and housing are scheduled to open in early March 2018.
Abstract Submission: Abstracts must be submitted by 3 p.m. Wednesday (CST), Jan. 17.
Resident Research Award (Jan. 17): The recipient will showcase his or her work at the 2018 Vascular Annual Meeting. This award is an excellent opportunity for surgical trainees in vascular research laboratories to be recognized and rewarded for their research efforts. The winner receives a $5,000 award and the VAM presentation opportunity.
The deadline is Wednesday, Jan. 17, for two important research endeavors related to the 2018 Vascular Annual Meeting: abstract submissions and the Resident Research Award. This year's VAM will be June 20 to 23 at the Hynes Convention Center in Boston. Following a full day of programming on Wednesday, June 20, plenary sessions are set for June 21-23. Exhibits will be June 21-22. VAM registration and housing are scheduled to open in early March 2018.
Abstract Submission: Abstracts must be submitted by 3 p.m. Wednesday (CST), Jan. 17.
Resident Research Award (Jan. 17): The recipient will showcase his or her work at the 2018 Vascular Annual Meeting. This award is an excellent opportunity for surgical trainees in vascular research laboratories to be recognized and rewarded for their research efforts. The winner receives a $5,000 award and the VAM presentation opportunity.
The deadline is Wednesday, Jan. 17, for two important research endeavors related to the 2018 Vascular Annual Meeting: abstract submissions and the Resident Research Award. This year's VAM will be June 20 to 23 at the Hynes Convention Center in Boston. Following a full day of programming on Wednesday, June 20, plenary sessions are set for June 21-23. Exhibits will be June 21-22. VAM registration and housing are scheduled to open in early March 2018.
Abstract Submission: Abstracts must be submitted by 3 p.m. Wednesday (CST), Jan. 17.
Resident Research Award (Jan. 17): The recipient will showcase his or her work at the 2018 Vascular Annual Meeting. This award is an excellent opportunity for surgical trainees in vascular research laboratories to be recognized and rewarded for their research efforts. The winner receives a $5,000 award and the VAM presentation opportunity.
Trump administration clears way to require work for some Medicaid enrollees
The Trump administration early on Jan. 11 initiated a pivotal change in the Medicaid program, announcing that
The announcement came in a 10-page memo with detailed directions about how states can reshape the federal-state health program for low-income people.
The document says who should be excluded from the new work requirements – including children and people being treated for opioid abuse – and offers suggestions as to what counts as “work.” Besides employment, it can include job training, volunteering, or caring for a close relative.
“Medicaid needs to be more flexible so that states can best address the needs of this population,” Seema Verma, administrator of the Centers for Medicare & Medicaid Services, said in a press release. “Our fundamental goal is to make a positive and lasting difference in the health and wellness of our beneficiaries.”
Adding a work requirement to Medicaid would mark one of the biggest changes to the program since its inception in 1966. It is likely to prompt a lawsuit from patient advocacy groups, which claim the requirement is inconsistent with Medicaid’s objectives and would require an act of Congress.
Republicans have been pushing for the change since the Affordable Care Act added millions of so called “able-bodied” adults to Medicaid. It allowed states to provide coverage to anyone earning up to 138% of the federal poverty level (about $16,600 for an individual).
The Obama administration turned down several state requests to add a work requirement.
Ten states have applied for a federal waiver to add a work requirement – Arizona, Arkansas, Indiana, Kansas, Kentucky, Maine, New Hampshire, North Carolina, Utah and Wisconsin. Officials in several other states have said they are interested in the idea.
An HHS official, who spoke on the condition of anonymity because the official had not been authorized to discuss the developments, said the agency may approve Kentucky’s request as early asJan. 12. Gov. Matt Bevin, a Republican, first sought to add such a provision in 2016. The current request would require able-bodied adults without dependents to work at least 20 hours a week.
Kentucky, which has some of the poorest counties in the country, has seen its Medicaid enrollment double in the past 3 years after the state expanded eligibility under the ACA.
While more than 74 million people are enrolled in Medicaid, only a small fraction would be affected by the work requirement. That’s because children – who make up nearly half of Medicaid enrollees – are excluded. So are the more than 10 million people on Medicaid because they have a disability.
More than 4 in 10 adults with Medicaid coverage already work full time, and most others either go to school, take care of a relative, or are too sick to work.
Still, critics fear a work requirement could have a chilling effect on people signing up for Medicaid or make it harder for people to get coverage.
But work requirements have strong public backing. About 70% of Americans say they support states imposing a work requirement on non-disabled adults, according to a Kaiser Family Foundation poll last year.
The Trump administration, along with many Republican leaders in Congress, has long supported such a move. The failed efforts in the House to replace Obamacare included a work requirement for Medicaid.
In its guidance to states, CMS said they should consider how some communities have high unemployment rates and whether enrollees need to care for young children and elderly families.
CMS also advised states to make work requirements for Medicaid similar than those used with food stamps to “reduce the burden on both states and beneficiaries.”
“This new guidance paves the way for states to demonstrate how their ideas will improve the health of Medicaid beneficiaries, as well as potentially improve their economic well-being,” Brian Neale, CMS deputy administrator and director for the Center for Medicaid and CHIP Services, said in the press release.
Ms. Verma, who has said she doesn’t think Medicaid should become a way of life for people who are not disabled, said the new guidance shows how the administration is trying to give states more flexibility in running Medicaid.
“Our policy guidance was in response to states that asked us for the flexibility they need to improve their programs and to help people in achieving greater well-being and self-sufficiency,” she said.
Ms. Verma, who worked with Kentucky and Indiana on their work requirement waivers as a health consultant before joining the Trump administration, recused herself from the decision on those states’ waiver requests.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The Trump administration early on Jan. 11 initiated a pivotal change in the Medicaid program, announcing that
The announcement came in a 10-page memo with detailed directions about how states can reshape the federal-state health program for low-income people.
The document says who should be excluded from the new work requirements – including children and people being treated for opioid abuse – and offers suggestions as to what counts as “work.” Besides employment, it can include job training, volunteering, or caring for a close relative.
“Medicaid needs to be more flexible so that states can best address the needs of this population,” Seema Verma, administrator of the Centers for Medicare & Medicaid Services, said in a press release. “Our fundamental goal is to make a positive and lasting difference in the health and wellness of our beneficiaries.”
Adding a work requirement to Medicaid would mark one of the biggest changes to the program since its inception in 1966. It is likely to prompt a lawsuit from patient advocacy groups, which claim the requirement is inconsistent with Medicaid’s objectives and would require an act of Congress.
Republicans have been pushing for the change since the Affordable Care Act added millions of so called “able-bodied” adults to Medicaid. It allowed states to provide coverage to anyone earning up to 138% of the federal poverty level (about $16,600 for an individual).
The Obama administration turned down several state requests to add a work requirement.
Ten states have applied for a federal waiver to add a work requirement – Arizona, Arkansas, Indiana, Kansas, Kentucky, Maine, New Hampshire, North Carolina, Utah and Wisconsin. Officials in several other states have said they are interested in the idea.
An HHS official, who spoke on the condition of anonymity because the official had not been authorized to discuss the developments, said the agency may approve Kentucky’s request as early asJan. 12. Gov. Matt Bevin, a Republican, first sought to add such a provision in 2016. The current request would require able-bodied adults without dependents to work at least 20 hours a week.
Kentucky, which has some of the poorest counties in the country, has seen its Medicaid enrollment double in the past 3 years after the state expanded eligibility under the ACA.
While more than 74 million people are enrolled in Medicaid, only a small fraction would be affected by the work requirement. That’s because children – who make up nearly half of Medicaid enrollees – are excluded. So are the more than 10 million people on Medicaid because they have a disability.
More than 4 in 10 adults with Medicaid coverage already work full time, and most others either go to school, take care of a relative, or are too sick to work.
Still, critics fear a work requirement could have a chilling effect on people signing up for Medicaid or make it harder for people to get coverage.
But work requirements have strong public backing. About 70% of Americans say they support states imposing a work requirement on non-disabled adults, according to a Kaiser Family Foundation poll last year.
The Trump administration, along with many Republican leaders in Congress, has long supported such a move. The failed efforts in the House to replace Obamacare included a work requirement for Medicaid.
In its guidance to states, CMS said they should consider how some communities have high unemployment rates and whether enrollees need to care for young children and elderly families.
CMS also advised states to make work requirements for Medicaid similar than those used with food stamps to “reduce the burden on both states and beneficiaries.”
“This new guidance paves the way for states to demonstrate how their ideas will improve the health of Medicaid beneficiaries, as well as potentially improve their economic well-being,” Brian Neale, CMS deputy administrator and director for the Center for Medicaid and CHIP Services, said in the press release.
Ms. Verma, who has said she doesn’t think Medicaid should become a way of life for people who are not disabled, said the new guidance shows how the administration is trying to give states more flexibility in running Medicaid.
“Our policy guidance was in response to states that asked us for the flexibility they need to improve their programs and to help people in achieving greater well-being and self-sufficiency,” she said.
Ms. Verma, who worked with Kentucky and Indiana on their work requirement waivers as a health consultant before joining the Trump administration, recused herself from the decision on those states’ waiver requests.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The Trump administration early on Jan. 11 initiated a pivotal change in the Medicaid program, announcing that
The announcement came in a 10-page memo with detailed directions about how states can reshape the federal-state health program for low-income people.
The document says who should be excluded from the new work requirements – including children and people being treated for opioid abuse – and offers suggestions as to what counts as “work.” Besides employment, it can include job training, volunteering, or caring for a close relative.
“Medicaid needs to be more flexible so that states can best address the needs of this population,” Seema Verma, administrator of the Centers for Medicare & Medicaid Services, said in a press release. “Our fundamental goal is to make a positive and lasting difference in the health and wellness of our beneficiaries.”
Adding a work requirement to Medicaid would mark one of the biggest changes to the program since its inception in 1966. It is likely to prompt a lawsuit from patient advocacy groups, which claim the requirement is inconsistent with Medicaid’s objectives and would require an act of Congress.
Republicans have been pushing for the change since the Affordable Care Act added millions of so called “able-bodied” adults to Medicaid. It allowed states to provide coverage to anyone earning up to 138% of the federal poverty level (about $16,600 for an individual).
The Obama administration turned down several state requests to add a work requirement.
Ten states have applied for a federal waiver to add a work requirement – Arizona, Arkansas, Indiana, Kansas, Kentucky, Maine, New Hampshire, North Carolina, Utah and Wisconsin. Officials in several other states have said they are interested in the idea.
An HHS official, who spoke on the condition of anonymity because the official had not been authorized to discuss the developments, said the agency may approve Kentucky’s request as early asJan. 12. Gov. Matt Bevin, a Republican, first sought to add such a provision in 2016. The current request would require able-bodied adults without dependents to work at least 20 hours a week.
Kentucky, which has some of the poorest counties in the country, has seen its Medicaid enrollment double in the past 3 years after the state expanded eligibility under the ACA.
While more than 74 million people are enrolled in Medicaid, only a small fraction would be affected by the work requirement. That’s because children – who make up nearly half of Medicaid enrollees – are excluded. So are the more than 10 million people on Medicaid because they have a disability.
More than 4 in 10 adults with Medicaid coverage already work full time, and most others either go to school, take care of a relative, or are too sick to work.
Still, critics fear a work requirement could have a chilling effect on people signing up for Medicaid or make it harder for people to get coverage.
But work requirements have strong public backing. About 70% of Americans say they support states imposing a work requirement on non-disabled adults, according to a Kaiser Family Foundation poll last year.
The Trump administration, along with many Republican leaders in Congress, has long supported such a move. The failed efforts in the House to replace Obamacare included a work requirement for Medicaid.
In its guidance to states, CMS said they should consider how some communities have high unemployment rates and whether enrollees need to care for young children and elderly families.
CMS also advised states to make work requirements for Medicaid similar than those used with food stamps to “reduce the burden on both states and beneficiaries.”
“This new guidance paves the way for states to demonstrate how their ideas will improve the health of Medicaid beneficiaries, as well as potentially improve their economic well-being,” Brian Neale, CMS deputy administrator and director for the Center for Medicaid and CHIP Services, said in the press release.
Ms. Verma, who has said she doesn’t think Medicaid should become a way of life for people who are not disabled, said the new guidance shows how the administration is trying to give states more flexibility in running Medicaid.
“Our policy guidance was in response to states that asked us for the flexibility they need to improve their programs and to help people in achieving greater well-being and self-sufficiency,” she said.
Ms. Verma, who worked with Kentucky and Indiana on their work requirement waivers as a health consultant before joining the Trump administration, recused herself from the decision on those states’ waiver requests.
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Does maternal sleep position affect risk of stillbirth?
WHAT DOES THIS MEAN FOR PRACTICE?
Encourage pregnant patients to not go to sleep in the supine position, especially those who:
- are obese
- have medical complications of pregnancy
- have a history of prior stillbirth
- smoke
- are of advanced maternal age

Normal prepregnancy weight becoming less normal
according to the Centers for Disease Control and Prevention.
The overall prevalence of normal prepregnancy weight declined from 47.3% to 45.1% over that period in 36 states, the District of Columbia, and New York City, which reports natality data separately from New York state. The decreases were statistically significant in 26 states and New York City, the CDC investigators reported (MMWR. 2018 Jan 5;66[51-2]:1402-7).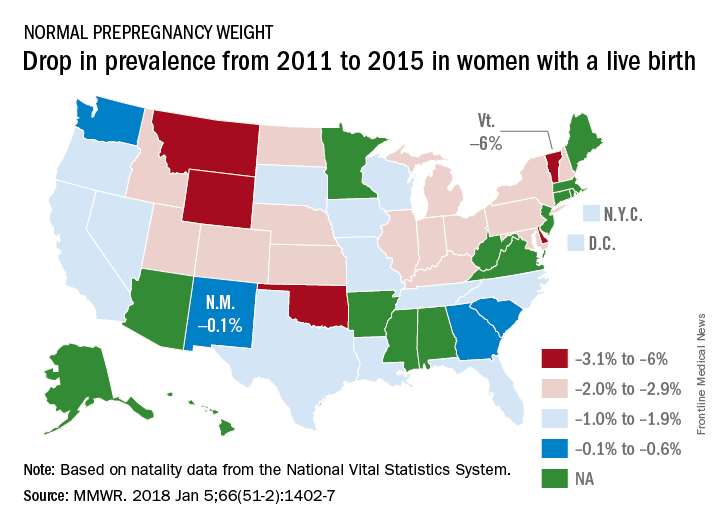
Based on data from 48 states, D.C., and New York City, the distribution of prevalence for the BMI categories in 2015 was 3.6% underweight, 45% normal weight, 25.8% overweight, and 25.6% obese, the investigators said.
The CDC analysis was based on natality data from the National Vital Statistics System. The standard birth certificate was revised in 2003 to include maternal height and prepregnancy weight, but only 38 jurisdictions were using it by 2011. By 2015, all states except Connecticut and New Jersey had adopted its use.
according to the Centers for Disease Control and Prevention.
The overall prevalence of normal prepregnancy weight declined from 47.3% to 45.1% over that period in 36 states, the District of Columbia, and New York City, which reports natality data separately from New York state. The decreases were statistically significant in 26 states and New York City, the CDC investigators reported (MMWR. 2018 Jan 5;66[51-2]:1402-7).
Based on data from 48 states, D.C., and New York City, the distribution of prevalence for the BMI categories in 2015 was 3.6% underweight, 45% normal weight, 25.8% overweight, and 25.6% obese, the investigators said.
The CDC analysis was based on natality data from the National Vital Statistics System. The standard birth certificate was revised in 2003 to include maternal height and prepregnancy weight, but only 38 jurisdictions were using it by 2011. By 2015, all states except Connecticut and New Jersey had adopted its use.
according to the Centers for Disease Control and Prevention.
The overall prevalence of normal prepregnancy weight declined from 47.3% to 45.1% over that period in 36 states, the District of Columbia, and New York City, which reports natality data separately from New York state. The decreases were statistically significant in 26 states and New York City, the CDC investigators reported (MMWR. 2018 Jan 5;66[51-2]:1402-7).
Based on data from 48 states, D.C., and New York City, the distribution of prevalence for the BMI categories in 2015 was 3.6% underweight, 45% normal weight, 25.8% overweight, and 25.6% obese, the investigators said.
The CDC analysis was based on natality data from the National Vital Statistics System. The standard birth certificate was revised in 2003 to include maternal height and prepregnancy weight, but only 38 jurisdictions were using it by 2011. By 2015, all states except Connecticut and New Jersey had adopted its use.
FROM MMWR
Role of Obstructive Sleep Apnea in HTN
Heart disease and stroke are leading causes of death and disability. High blood pressure (BP) is a major risk factor for both.
The 2017 guidelines regarding “Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure” (JNC 7) were recently published, which is an update incorporating new information from studies regarding BP-related risk of cardiovascular disease (CVD) and strategies to improve hypertension (HTN) treatment and control.
Screening for secondary causes of HTN is necessary for new-onset or uncontrolled HTN in adults, including drug-resistant HTN. Screening includes testing for obstructive sleep apnea, which is highly prevalent in this population.
Obstructive sleep apnea is a common chronic condition characterized by recurrent collapse of upper airways during sleep, inducing intermittent episodes of apnea/hypopnea, hypoxemia, and sleep disruption (Pedrosa RP, et al. Chest. 2013;144[5]:1487).
It is estimated to affect 17% of US adults but is overwhelmingly underrecognized and untreated (JAMA. 2012;307[20]:2169). The prevalence is higher in men than women. The major risk factors for OSA are obesity, male sex, and advancing age. Since these conditions oftentimes predispose to and are concomitant with HTN, it can be challenging to determine the independent effects of OSA on the development of HTN.
The relationship between obstructive sleep apnea (OSA) and HTN has been a point of interest for decades, with untreated OSA being associated with an increased risk for developing new-onset HTN (JAMA. 2012;307[20]:2169).
There have been several landmark trials that have sought to determine the extent of a causal relationship between OSAS and HTN. Sleep Heart Health Study (Sleep. 2006;29;1009) was one such study, which was limited by the inability to prove that OSA preceded the onset of HTN.
Wisconsin Sleep Cohort (N Engl J Med. 2000;342:1378) was another landmark prospective longitudinal study that implicates OSA as a possible causal factor in HTN. The notable limitation of the study was the presence of HTN after initial assessment was found to be dependent upon the severity of OSA at baseline.
While these two cohort studies found an association between OSA and HTN, the Vitoria Sleep Cohort out of Spain (Am J Respir Crit Care Med. 2011;184[11]:1299), the third and most recent longitudinal cohort study, looked at younger and thinner patients than the SHHS and the Wisconsin Sleep Cohort, failed to show a significant association between OSA and incident HTN. Methodologic differences may help to explain the disparity in results.
NREM sleep has normal circadian variation of BP, causing “dipping” of both systolic and diastolic BP at night due to decreased sympathetic and increased parasympathetic activity. REM sleep has predominant sympathetic activity and transient nocturnal BP surges.

OSA results in hypoxemia, which causes nocturnal catecholamine surges, resulting in nocturnal increase in heart rate and BP that is most prominent during post-apneic hyperventilation.
Reduced nocturnal BP (nondipping) or even higher nocturnal BP than daytime BP is an undoubted risk factor for hypertensive patients due to the end-organ damage and subsequent cardiovascular events. With sleep apnea, sleep quality is decreased due to frequent arousal from sleep (Hypertension. 2006;47[5]:833).
Sleep duration of less than or equal to 5 hours per night was shown to significantly increase risk for HTN in patients less than or equal to 60 years of age, even after controlling for obesity and diabetes.
Sleep Heart Health Study suggests that sleep duration above or below a median of 7 to 8 hours per night is associated with a higher prevalence of HTN (Sleep. 2006;29:1009). Thus, improving duration and quality of sleep in sleep apnea patients may help decrease the risk of developing HTN.
Key question: Will treatment of OSA appreciably alter BP?
Continuous positive airway pressure (CPAP) is an efficacious treatment of choice for OSA. Interventional trials, though limited by issues related to compliance, have shown CPAP to acutely reduce sympathetic drive and BP during sleep. However, this improvement in BP control is not entirely consistent in all patients with the data being less clear-cut regarding nighttime CPAP therapy and impact on daytime BP.
A randomized controlled trial from Barbe et al suggests that normotensive subjects with severe OSA but without demonstrable daytime sleepiness are immune to the BP-reducing effects of CPAP (Ann Intern Med. 2001;134:1015); those who were objectively sleepy had a more robust response to the BP lowering effects of CPAP with better cardiovascular outcomes among patients who were adherent to CPAP therapy (≥4 hours per night).
Sleep Apnea Cardiovascular Endpoints (SAVE) study looked at CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea (N Engl J Med. 2016;375:919). CPAP significantly reduced snoring and daytime sleepiness and improved health-related quality of life and mood, but the risk of serious cardiovascular events was not lower among patients who received treatment with CPAP in addition to usual care compared with usual care alone. This study was not powered to provide definitive answers regarding the effects of CPAP on secondary cardiovascular end points, and the use of PAP was less than 4 hours.
A recent systematic review and meta-analysis looked at “Association of Positive Airway Pressure with Cardiovascular Events and Death in Adults with Sleep Apnea” (JAMA. 2017;318(2):156). No significant associations between PAP treatment and a range of cardiovascular events were noted in this meta-analysis.

It is possible that the limited adherence to therapy in many trials was insufficient to drive protection, along with short follow-up duration of most trials that may have given insufficient time for PAP to have affected vascular outcomes.
In a cross-over study of valsartan and CPAP, combining drug treatment with CPAP appeared to have a more synergistic effect in reducing BP than either agent alone (Am J Respir Crit Care Med. 2010;182:954).
The beneficial effect of CPAP remains an open question. Considering the multifactorial pathophysiology of OSA-associated HTN, proven therapies, such as BP lowering, lipid lowering, and antiplatelet therapy, along with PAP therapy, should be utilized. This combination strategy is likely to be more effective in improving both nocturnal and daytime BP control in OSA.
Dr. Singh is Director, Sleep Disorder and Research Center, Michael E. DeBakey VA Medical Center; and Dr. Singh is Assistant Professor and Dr. Velamuri is Associate Professor, Pulmonary, Critical Care and Sleep Medicine, Baylor College of Medicine. Houston, Texas.
Heart disease and stroke are leading causes of death and disability. High blood pressure (BP) is a major risk factor for both.
The 2017 guidelines regarding “Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure” (JNC 7) were recently published, which is an update incorporating new information from studies regarding BP-related risk of cardiovascular disease (CVD) and strategies to improve hypertension (HTN) treatment and control.
Screening for secondary causes of HTN is necessary for new-onset or uncontrolled HTN in adults, including drug-resistant HTN. Screening includes testing for obstructive sleep apnea, which is highly prevalent in this population.
Obstructive sleep apnea is a common chronic condition characterized by recurrent collapse of upper airways during sleep, inducing intermittent episodes of apnea/hypopnea, hypoxemia, and sleep disruption (Pedrosa RP, et al. Chest. 2013;144[5]:1487).
It is estimated to affect 17% of US adults but is overwhelmingly underrecognized and untreated (JAMA. 2012;307[20]:2169). The prevalence is higher in men than women. The major risk factors for OSA are obesity, male sex, and advancing age. Since these conditions oftentimes predispose to and are concomitant with HTN, it can be challenging to determine the independent effects of OSA on the development of HTN.
The relationship between obstructive sleep apnea (OSA) and HTN has been a point of interest for decades, with untreated OSA being associated with an increased risk for developing new-onset HTN (JAMA. 2012;307[20]:2169).
There have been several landmark trials that have sought to determine the extent of a causal relationship between OSAS and HTN. Sleep Heart Health Study (Sleep. 2006;29;1009) was one such study, which was limited by the inability to prove that OSA preceded the onset of HTN.
Wisconsin Sleep Cohort (N Engl J Med. 2000;342:1378) was another landmark prospective longitudinal study that implicates OSA as a possible causal factor in HTN. The notable limitation of the study was the presence of HTN after initial assessment was found to be dependent upon the severity of OSA at baseline.
While these two cohort studies found an association between OSA and HTN, the Vitoria Sleep Cohort out of Spain (Am J Respir Crit Care Med. 2011;184[11]:1299), the third and most recent longitudinal cohort study, looked at younger and thinner patients than the SHHS and the Wisconsin Sleep Cohort, failed to show a significant association between OSA and incident HTN. Methodologic differences may help to explain the disparity in results.
NREM sleep has normal circadian variation of BP, causing “dipping” of both systolic and diastolic BP at night due to decreased sympathetic and increased parasympathetic activity. REM sleep has predominant sympathetic activity and transient nocturnal BP surges.
OSA results in hypoxemia, which causes nocturnal catecholamine surges, resulting in nocturnal increase in heart rate and BP that is most prominent during post-apneic hyperventilation.
Reduced nocturnal BP (nondipping) or even higher nocturnal BP than daytime BP is an undoubted risk factor for hypertensive patients due to the end-organ damage and subsequent cardiovascular events. With sleep apnea, sleep quality is decreased due to frequent arousal from sleep (Hypertension. 2006;47[5]:833).
Sleep duration of less than or equal to 5 hours per night was shown to significantly increase risk for HTN in patients less than or equal to 60 years of age, even after controlling for obesity and diabetes.
Sleep Heart Health Study suggests that sleep duration above or below a median of 7 to 8 hours per night is associated with a higher prevalence of HTN (Sleep. 2006;29:1009). Thus, improving duration and quality of sleep in sleep apnea patients may help decrease the risk of developing HTN.
Key question: Will treatment of OSA appreciably alter BP?
Continuous positive airway pressure (CPAP) is an efficacious treatment of choice for OSA. Interventional trials, though limited by issues related to compliance, have shown CPAP to acutely reduce sympathetic drive and BP during sleep. However, this improvement in BP control is not entirely consistent in all patients with the data being less clear-cut regarding nighttime CPAP therapy and impact on daytime BP.
A randomized controlled trial from Barbe et al suggests that normotensive subjects with severe OSA but without demonstrable daytime sleepiness are immune to the BP-reducing effects of CPAP (Ann Intern Med. 2001;134:1015); those who were objectively sleepy had a more robust response to the BP lowering effects of CPAP with better cardiovascular outcomes among patients who were adherent to CPAP therapy (≥4 hours per night).
Sleep Apnea Cardiovascular Endpoints (SAVE) study looked at CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea (N Engl J Med. 2016;375:919). CPAP significantly reduced snoring and daytime sleepiness and improved health-related quality of life and mood, but the risk of serious cardiovascular events was not lower among patients who received treatment with CPAP in addition to usual care compared with usual care alone. This study was not powered to provide definitive answers regarding the effects of CPAP on secondary cardiovascular end points, and the use of PAP was less than 4 hours.
A recent systematic review and meta-analysis looked at “Association of Positive Airway Pressure with Cardiovascular Events and Death in Adults with Sleep Apnea” (JAMA. 2017;318(2):156). No significant associations between PAP treatment and a range of cardiovascular events were noted in this meta-analysis.
It is possible that the limited adherence to therapy in many trials was insufficient to drive protection, along with short follow-up duration of most trials that may have given insufficient time for PAP to have affected vascular outcomes.
In a cross-over study of valsartan and CPAP, combining drug treatment with CPAP appeared to have a more synergistic effect in reducing BP than either agent alone (Am J Respir Crit Care Med. 2010;182:954).
The beneficial effect of CPAP remains an open question. Considering the multifactorial pathophysiology of OSA-associated HTN, proven therapies, such as BP lowering, lipid lowering, and antiplatelet therapy, along with PAP therapy, should be utilized. This combination strategy is likely to be more effective in improving both nocturnal and daytime BP control in OSA.
Dr. Singh is Director, Sleep Disorder and Research Center, Michael E. DeBakey VA Medical Center; and Dr. Singh is Assistant Professor and Dr. Velamuri is Associate Professor, Pulmonary, Critical Care and Sleep Medicine, Baylor College of Medicine. Houston, Texas.
Heart disease and stroke are leading causes of death and disability. High blood pressure (BP) is a major risk factor for both.
The 2017 guidelines regarding “Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure” (JNC 7) were recently published, which is an update incorporating new information from studies regarding BP-related risk of cardiovascular disease (CVD) and strategies to improve hypertension (HTN) treatment and control.
Screening for secondary causes of HTN is necessary for new-onset or uncontrolled HTN in adults, including drug-resistant HTN. Screening includes testing for obstructive sleep apnea, which is highly prevalent in this population.
Obstructive sleep apnea is a common chronic condition characterized by recurrent collapse of upper airways during sleep, inducing intermittent episodes of apnea/hypopnea, hypoxemia, and sleep disruption (Pedrosa RP, et al. Chest. 2013;144[5]:1487).
It is estimated to affect 17% of US adults but is overwhelmingly underrecognized and untreated (JAMA. 2012;307[20]:2169). The prevalence is higher in men than women. The major risk factors for OSA are obesity, male sex, and advancing age. Since these conditions oftentimes predispose to and are concomitant with HTN, it can be challenging to determine the independent effects of OSA on the development of HTN.
The relationship between obstructive sleep apnea (OSA) and HTN has been a point of interest for decades, with untreated OSA being associated with an increased risk for developing new-onset HTN (JAMA. 2012;307[20]:2169).
There have been several landmark trials that have sought to determine the extent of a causal relationship between OSAS and HTN. Sleep Heart Health Study (Sleep. 2006;29;1009) was one such study, which was limited by the inability to prove that OSA preceded the onset of HTN.
Wisconsin Sleep Cohort (N Engl J Med. 2000;342:1378) was another landmark prospective longitudinal study that implicates OSA as a possible causal factor in HTN. The notable limitation of the study was the presence of HTN after initial assessment was found to be dependent upon the severity of OSA at baseline.
While these two cohort studies found an association between OSA and HTN, the Vitoria Sleep Cohort out of Spain (Am J Respir Crit Care Med. 2011;184[11]:1299), the third and most recent longitudinal cohort study, looked at younger and thinner patients than the SHHS and the Wisconsin Sleep Cohort, failed to show a significant association between OSA and incident HTN. Methodologic differences may help to explain the disparity in results.
NREM sleep has normal circadian variation of BP, causing “dipping” of both systolic and diastolic BP at night due to decreased sympathetic and increased parasympathetic activity. REM sleep has predominant sympathetic activity and transient nocturnal BP surges.
OSA results in hypoxemia, which causes nocturnal catecholamine surges, resulting in nocturnal increase in heart rate and BP that is most prominent during post-apneic hyperventilation.
Reduced nocturnal BP (nondipping) or even higher nocturnal BP than daytime BP is an undoubted risk factor for hypertensive patients due to the end-organ damage and subsequent cardiovascular events. With sleep apnea, sleep quality is decreased due to frequent arousal from sleep (Hypertension. 2006;47[5]:833).
Sleep duration of less than or equal to 5 hours per night was shown to significantly increase risk for HTN in patients less than or equal to 60 years of age, even after controlling for obesity and diabetes.
Sleep Heart Health Study suggests that sleep duration above or below a median of 7 to 8 hours per night is associated with a higher prevalence of HTN (Sleep. 2006;29:1009). Thus, improving duration and quality of sleep in sleep apnea patients may help decrease the risk of developing HTN.
Key question: Will treatment of OSA appreciably alter BP?
Continuous positive airway pressure (CPAP) is an efficacious treatment of choice for OSA. Interventional trials, though limited by issues related to compliance, have shown CPAP to acutely reduce sympathetic drive and BP during sleep. However, this improvement in BP control is not entirely consistent in all patients with the data being less clear-cut regarding nighttime CPAP therapy and impact on daytime BP.
A randomized controlled trial from Barbe et al suggests that normotensive subjects with severe OSA but without demonstrable daytime sleepiness are immune to the BP-reducing effects of CPAP (Ann Intern Med. 2001;134:1015); those who were objectively sleepy had a more robust response to the BP lowering effects of CPAP with better cardiovascular outcomes among patients who were adherent to CPAP therapy (≥4 hours per night).
Sleep Apnea Cardiovascular Endpoints (SAVE) study looked at CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea (N Engl J Med. 2016;375:919). CPAP significantly reduced snoring and daytime sleepiness and improved health-related quality of life and mood, but the risk of serious cardiovascular events was not lower among patients who received treatment with CPAP in addition to usual care compared with usual care alone. This study was not powered to provide definitive answers regarding the effects of CPAP on secondary cardiovascular end points, and the use of PAP was less than 4 hours.
A recent systematic review and meta-analysis looked at “Association of Positive Airway Pressure with Cardiovascular Events and Death in Adults with Sleep Apnea” (JAMA. 2017;318(2):156). No significant associations between PAP treatment and a range of cardiovascular events were noted in this meta-analysis.
It is possible that the limited adherence to therapy in many trials was insufficient to drive protection, along with short follow-up duration of most trials that may have given insufficient time for PAP to have affected vascular outcomes.
In a cross-over study of valsartan and CPAP, combining drug treatment with CPAP appeared to have a more synergistic effect in reducing BP than either agent alone (Am J Respir Crit Care Med. 2010;182:954).
The beneficial effect of CPAP remains an open question. Considering the multifactorial pathophysiology of OSA-associated HTN, proven therapies, such as BP lowering, lipid lowering, and antiplatelet therapy, along with PAP therapy, should be utilized. This combination strategy is likely to be more effective in improving both nocturnal and daytime BP control in OSA.
Dr. Singh is Director, Sleep Disorder and Research Center, Michael E. DeBakey VA Medical Center; and Dr. Singh is Assistant Professor and Dr. Velamuri is Associate Professor, Pulmonary, Critical Care and Sleep Medicine, Baylor College of Medicine. Houston, Texas.
Check orthostatic vital signs within 1 minute
Clinical question: What is the relationship between timing of measurement of postural blood pressure (BP) and adverse clinical outcomes?
Background: Guidelines recommend measuring postural BP after 3 minutes of standing to avoid potentially false-positive readings obtained before that interval. In SPRINT, orthostatic hypotension (OH) determined at 1 minute was associated with higher risk of emergency department visits for OH and syncope. Whether that finding was because of the shortened interval of measurement is uncertain.
Setting: Four U.S. communities over 2 decades.
Synopsis: In a cohort of 11,429 middle-aged patients, upright BP was measured every 25 seconds over a 5-minute interval after participants had been supine for 20 minutes. About 2-3 seconds elapsed between the end of one BP measurement and the initiation of the next. OH was defined as a 20–mm Hg drop in systolic BP. After researchers adjusted for covariates, OH at 30 seconds and 1 minute were associated with higher odds of dizziness, fracture, syncope, death, and motor vehicle crashes recorded over a median follow-up of 23 years. Measurements after 1 minute were not reliably associated with any adverse outcomes.
Bottom line: Measuring OH at 30 seconds and 1 minute reliably identifies patients at risk for associated adverse clinical outcomes.
Citation: Juraschek SP et al. Association of history of dizziness and long-term adverse outcomes with early vs. later orthostatic hypotension times in middle-aged adults. JAMA Intern Med. 2017 Sep 1;177(9):1316-23.
Dr. Anderson is an associate program director in the internal medicine residency training program at the University of Colorado School of Medicine and a hospitalist at the VA Eastern Colorado Health Care System in Denver.
Clinical question: What is the relationship between timing of measurement of postural blood pressure (BP) and adverse clinical outcomes?
Background: Guidelines recommend measuring postural BP after 3 minutes of standing to avoid potentially false-positive readings obtained before that interval. In SPRINT, orthostatic hypotension (OH) determined at 1 minute was associated with higher risk of emergency department visits for OH and syncope. Whether that finding was because of the shortened interval of measurement is uncertain.
Setting: Four U.S. communities over 2 decades.
Synopsis: In a cohort of 11,429 middle-aged patients, upright BP was measured every 25 seconds over a 5-minute interval after participants had been supine for 20 minutes. About 2-3 seconds elapsed between the end of one BP measurement and the initiation of the next. OH was defined as a 20–mm Hg drop in systolic BP. After researchers adjusted for covariates, OH at 30 seconds and 1 minute were associated with higher odds of dizziness, fracture, syncope, death, and motor vehicle crashes recorded over a median follow-up of 23 years. Measurements after 1 minute were not reliably associated with any adverse outcomes.
Bottom line: Measuring OH at 30 seconds and 1 minute reliably identifies patients at risk for associated adverse clinical outcomes.
Citation: Juraschek SP et al. Association of history of dizziness and long-term adverse outcomes with early vs. later orthostatic hypotension times in middle-aged adults. JAMA Intern Med. 2017 Sep 1;177(9):1316-23.
Dr. Anderson is an associate program director in the internal medicine residency training program at the University of Colorado School of Medicine and a hospitalist at the VA Eastern Colorado Health Care System in Denver.
Clinical question: What is the relationship between timing of measurement of postural blood pressure (BP) and adverse clinical outcomes?
Background: Guidelines recommend measuring postural BP after 3 minutes of standing to avoid potentially false-positive readings obtained before that interval. In SPRINT, orthostatic hypotension (OH) determined at 1 minute was associated with higher risk of emergency department visits for OH and syncope. Whether that finding was because of the shortened interval of measurement is uncertain.
Setting: Four U.S. communities over 2 decades.
Synopsis: In a cohort of 11,429 middle-aged patients, upright BP was measured every 25 seconds over a 5-minute interval after participants had been supine for 20 minutes. About 2-3 seconds elapsed between the end of one BP measurement and the initiation of the next. OH was defined as a 20–mm Hg drop in systolic BP. After researchers adjusted for covariates, OH at 30 seconds and 1 minute were associated with higher odds of dizziness, fracture, syncope, death, and motor vehicle crashes recorded over a median follow-up of 23 years. Measurements after 1 minute were not reliably associated with any adverse outcomes.
Bottom line: Measuring OH at 30 seconds and 1 minute reliably identifies patients at risk for associated adverse clinical outcomes.
Citation: Juraschek SP et al. Association of history of dizziness and long-term adverse outcomes with early vs. later orthostatic hypotension times in middle-aged adults. JAMA Intern Med. 2017 Sep 1;177(9):1316-23.
Dr. Anderson is an associate program director in the internal medicine residency training program at the University of Colorado School of Medicine and a hospitalist at the VA Eastern Colorado Health Care System in Denver.
