User login
Over-the-counter Topical Musculoskeletal Pain Relievers Used With a Heat Source: A Dangerous Combination
To the Editor:
The combination of menthol and methyl salicylate found in a variety of over-the-counter (OTC) creams in conjunction with a heat source such as a heating pad used for musculoskeletal symptoms can be a dire combination due to increased systemic absorption with associated toxicity and localized effects ranging from contact dermatitis or irritation to burn or necrosis.1-6 We present a case of localized burn due a combination of topical methyl salicylate and heating pad use. We also discuss 2 commonly encountered side effects in the literature—localized burns and systemic toxicity associated with percutaneous absorption—and provide specific considerations related to the geriatric and pediatric populations.
A 62-year-old woman with a history of eczematous dermatitis and osteoarthritis with pain of the left shoulder presented to the dermatology clinic with painful skin-related changes on the left arm of 1 week’s duration. She was prescribed acetaminophen and ibuprofen. However, she self-medicated the left shoulder pain with 2 OTC products containing topical menthol and/or methyl salicylate in combination with a heating pad and likely fell asleep with this combination therapy applied. She noticed the burn the next morning. On examination, the left arm exhibited a geometric, irregularly shaped, erythematous, scaly plaque with a sharp transverse linear demarcation proximally and numerous erythematous linear scaly plaques oriented in an axial orientation with less-defined borders distally (Figure). The patient was diagnosed with burn secondary to combination of topical methyl salicylate and heating pad use. The patient was advised to discontinue the topical medication and to use caution with the heating pad in the future. She was prescribed pramoxine-hydrocortisone lotion to be applied to the affected area twice daily up to 5 days weekly until resolution. Subsequent evaluations revealed progressive improvement with only mild postinflammatory hyperpigmentation noted at 6 months after the burn.

The US Food and Drug Administration (FDA) released statements in 2012 regarding concern for burns related to use of OTC musculoskeletal pain relievers, with 43 cases of burns reported due to methyl salicylate and menthol from 2004 to 2010. Most of the second- and third-degree burns occurred following topical applications of products containing either menthol monotherapy or a combination of methyl salicylate and menthol.1,2 In 2006, the FDA had already ordered 5 firms to stop compounding topical pain relief formulations containing these ingredients, with concerns that it puts patients at increased risk because the compounded formulations had not received FDA approval.3 Despite package warnings, patients may not be aware of the concerning side effects and risks associated with use of OTC creams, especially in combination with occlusion or heating pad use. Our case highlights the importance of ongoing patient education and physician counseling when encountering patients with arthritis or musculoskeletal pain who may often try various OTC self-treatments for pain relief.7
In 2012, the FDA reports stated that the cases of mild to serious burns were associated with methyl salicylate and menthol usage, in some cases 24 hours after first usage. Typically, these effects occur when concentrations are more than either 3% menthol alone or a combination of more than 3% menthol and more than 10% methyl salicylate.1,2 In our case, the patient had been using 2 different OTC products that may have contained as much as 11% menthol and/or 30% methyl salicylate. Electronic resources are available that disclose safety instructions including not to occlude the site, not to use on wounds, and not to be used in conjunction with a heating pad.8,9 Skin breakdown and vasodilation are more likely to occur in a setting of heat and occlusion, which allows for more absorption and localized side effects.4,10 Localized reactions may range from contact dermatitis4 to muscle necrosis.5
The most noteworthy case of localized destruction described a 62-year-old man who had applied topical methyl salicylate and menthol to the forearms, calves, and thighs, then intermittently used a heating pad for 15 to 20 minutes (total duration).5 He subsequently developed erythema and numerous 7.62- to 10.16-cm bullae, which was thought to be consistent with contact dermatitis. Three days later, he was found to have full-thickness cutaneous, fascial, and muscle necrosis in a linear pattern. He was hospitalized for approximately 1 year and treated with extensive debridement and a skin graft. His serum creatinine level increased from 0.7 mg per 100 mL to 2.7 mg per 100 mL (reference range, 0.6–1.2 mg/dL) with evidence of toxic nephrosis and persistent interstitial nephritis, demonstrating the severity of localized destruction that may result when combining these products with direct heat and potential subsequent systemic consequences of this combination.5
The systemic absorption of OTC formulations also has been studied. Morra et al10 studied 12 volunteers (6 women, 6 men) who applied either 5 g of methyl salicylate ointment 12.5% twice daily for 4 days to an area on the thigh (approximately equal to 567 mg salicylate) or trolamine cream 10% twice for 1 day. The participants underwent a break for 7 days and then switched to the alternate treatment. They found that 0.31 to 0.91 mg/L methyl salicylate was detected in the serum 1 hour after applying the ointment consisting of methyl salicylate, and 2 to 6 mg/L methyl salicylate was detected on day 4. Therapeutic serum salicylate levels are 150 to 300 mg/L. They found that approximately 22% of the methyl salicylate also was found in urine samples on day 4. Although these figures may appear small, this study was prompted when a 62-year-old man presented to the emergency department with symptoms of salicylate toxicity and a serum concentration of 518 mg/L from twice-daily use of an OTC formulation containing methyl salicylate over the course of multiple weeks.10 Additionally, those who have aspirin hypersensitivity should be cautious when using such products due to the risk for reported angioedema.4
Providers must exercise extreme caution while caring for geriatric patients, especially if patients are taking warfarin. The combined effects of warfarin and methyl salicylate have previously caused cutaneous purpura, gastrointestinal bleeding, and elevated international normalized ratio values.4,10 Older individuals also have increased skin fragility, allowing microtraumatic insult to easily develop. This fragility, along with an overall decreased intactness of the skin barrier, may lead to increased skin absorption. Furthermore, the addition of applying any heat source places the geriatric patient at greater risk for adverse events.10
In considering the limits of age, the pediatric population also has been studied regarding salicylate toxicity. Most commonly, oral ingestion has caused fatalities, as oil of wintergreen has been cited as extremely dangerous for children if swallowed; doses as small as a teaspoon (5 mL: 7000 mg salicylate) have resulted in fatalities.4,6 Although the consumption of a large amount of a cream- or ointment-based product is unlikely due to the consistency of the medication,6 the thought does merit consideration in the inquisitive toddler age group. For a 15-kg toddler, 150 mg/kg of aspirin or 2250 mg of aspirin, is considered the toxic level, which upon conversion to methyl salicylate levels using a 1.4 factor equates to 1607 mg of methyl salicylate to reach toxicity.6 If using a product with methyl salicylate 30% composition, 1 g of the product contains 300 mg of methyl salicylate; therefore if the toddler consumed approximately 5.3 g of the product (1607 mg methyl salicylate [toxic level] divided by 300 mg methyl salicylate per 1 g of product), he/she would reach toxic levels.6,11 To put this into perspective, a 2-oz tube contains 57 g (approximately 10 times the toxic dose) of the product.8 Thus, although there is less concern overall for consumption of cream- or ointment-based methyl salicylate, there still is potential for harm if a small child were to ingest such a product containing higher percentages of methyl salicylate.6
There also have been reports of pediatric toxicity related to percutaneous absorption, even leading to pediatric fatality.4,6 In particular, there was a case of a young boy hospitalized with ichthyosis who received escalating doses of percutaneous salicylate, which resulted in toxicity; when therapy was discontinued, he experienced full recovery.12 In 2007, a 17-year-old adolescent girl died from methyl salicylate toxicity after numerous applications of salicylate-containing products in conjunction with medicated pads.7
Although the FDA has drawn attention and encouraged caution with use of OTC topical musculoskeletal pain relievers, the importance of ensuring patients are fully aware of potential burns, permanent skin or muscle damage, and even death if used inappropriately cannot be overstated. The FDA consumer health information website has 2 patient-directed handouts2,3 that may be useful to post in patient waiting areas to increase overall understanding of the risks associated with OTC products containing methyl salicylate and menthol ingredients. Fortunately, our patient suffered only mild postinflammatory hyperpigmentation without substantial sustained consequences.
- US Food and Drug Administration. FDA Drug Safety Communication: rare cases of serious burns with the use of over-the-counter topical muscle and joint pain relievers. http://www.fda.gov/Drugs/DrugSafety/ucm318858.htm. Published September 13, 2012. Updated February 11, 2016. Accessed October 31, 2017.
- US Food and Drug Administration. Topical pain relievers may cause burns. http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm318674.htm. Published September 13, 2012. Updated November 5, 2015. Accessed October 31, 2017.
- US Food and Drug Administration. Use caution with over-the-counter creams, ointments. http://www.fda.gov/forconsumers/consumerupdates/ucm049367.htm. Updated October 17, 2017. Accessed October 31, 2017.
- Chan TY. Potential dangers from topical preparations containing methyl salicylate. Hum Exp Toxicol. 1996;15:747-750.
- Heng MC. Local necrosis and interstitial nephritis due to topical methyl salicylate and menthol. Cutis. 1987;39:442-444.
- Davis JE. Are one or two dangerous? methyl salicylate exposure in toddlers. J Emerg Med. 2007;32:63-69.
- Associated Press. Sports cream warnings urged after teen’s death: track star’s overdose points to risks of popular muscle salve. NBC News. http://www.nbcnews.com/id/19208195. Updated June 13, 2007. Accessed October 31, 2017.
- Ultra Strength Bengay Cream. Bengay website. http://www.bengay.com/bengay-ultra-strength-cream. Accessed November 1, 2017.
- Tiger Balm Arthritis Rub. Tiger Balm website. http://www.tigerbalm.com/us/pages/tb_product?product_id=6. Accessed November 1, 2017.
- Morra P, Bartle WR, Walker SE, et al. Serum concentrations of salicylic acid following topically applied salicylate derivatives. Ann Pharmacother. 1996;9:935-940.
- US National Library of Medicine. Bengay Ultra Strength non greasy pain relieving- camphor (synthetic), menthol, and methyl salicylate cream. Daily Med website. http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=5aa265f8-ab45-47b2-b5ab-d4df54daed01. Updated November 3, 2016. Accessed November 1, 2017.
- Aspinall JB, Goel KM. Salicylate poisoning in dermatological therapy. Br Med J. 1978;2:1373.
To the Editor:
The combination of menthol and methyl salicylate found in a variety of over-the-counter (OTC) creams in conjunction with a heat source such as a heating pad used for musculoskeletal symptoms can be a dire combination due to increased systemic absorption with associated toxicity and localized effects ranging from contact dermatitis or irritation to burn or necrosis.1-6 We present a case of localized burn due a combination of topical methyl salicylate and heating pad use. We also discuss 2 commonly encountered side effects in the literature—localized burns and systemic toxicity associated with percutaneous absorption—and provide specific considerations related to the geriatric and pediatric populations.
A 62-year-old woman with a history of eczematous dermatitis and osteoarthritis with pain of the left shoulder presented to the dermatology clinic with painful skin-related changes on the left arm of 1 week’s duration. She was prescribed acetaminophen and ibuprofen. However, she self-medicated the left shoulder pain with 2 OTC products containing topical menthol and/or methyl salicylate in combination with a heating pad and likely fell asleep with this combination therapy applied. She noticed the burn the next morning. On examination, the left arm exhibited a geometric, irregularly shaped, erythematous, scaly plaque with a sharp transverse linear demarcation proximally and numerous erythematous linear scaly plaques oriented in an axial orientation with less-defined borders distally (Figure). The patient was diagnosed with burn secondary to combination of topical methyl salicylate and heating pad use. The patient was advised to discontinue the topical medication and to use caution with the heating pad in the future. She was prescribed pramoxine-hydrocortisone lotion to be applied to the affected area twice daily up to 5 days weekly until resolution. Subsequent evaluations revealed progressive improvement with only mild postinflammatory hyperpigmentation noted at 6 months after the burn.
The US Food and Drug Administration (FDA) released statements in 2012 regarding concern for burns related to use of OTC musculoskeletal pain relievers, with 43 cases of burns reported due to methyl salicylate and menthol from 2004 to 2010. Most of the second- and third-degree burns occurred following topical applications of products containing either menthol monotherapy or a combination of methyl salicylate and menthol.1,2 In 2006, the FDA had already ordered 5 firms to stop compounding topical pain relief formulations containing these ingredients, with concerns that it puts patients at increased risk because the compounded formulations had not received FDA approval.3 Despite package warnings, patients may not be aware of the concerning side effects and risks associated with use of OTC creams, especially in combination with occlusion or heating pad use. Our case highlights the importance of ongoing patient education and physician counseling when encountering patients with arthritis or musculoskeletal pain who may often try various OTC self-treatments for pain relief.7
In 2012, the FDA reports stated that the cases of mild to serious burns were associated with methyl salicylate and menthol usage, in some cases 24 hours after first usage. Typically, these effects occur when concentrations are more than either 3% menthol alone or a combination of more than 3% menthol and more than 10% methyl salicylate.1,2 In our case, the patient had been using 2 different OTC products that may have contained as much as 11% menthol and/or 30% methyl salicylate. Electronic resources are available that disclose safety instructions including not to occlude the site, not to use on wounds, and not to be used in conjunction with a heating pad.8,9 Skin breakdown and vasodilation are more likely to occur in a setting of heat and occlusion, which allows for more absorption and localized side effects.4,10 Localized reactions may range from contact dermatitis4 to muscle necrosis.5
The most noteworthy case of localized destruction described a 62-year-old man who had applied topical methyl salicylate and menthol to the forearms, calves, and thighs, then intermittently used a heating pad for 15 to 20 minutes (total duration).5 He subsequently developed erythema and numerous 7.62- to 10.16-cm bullae, which was thought to be consistent with contact dermatitis. Three days later, he was found to have full-thickness cutaneous, fascial, and muscle necrosis in a linear pattern. He was hospitalized for approximately 1 year and treated with extensive debridement and a skin graft. His serum creatinine level increased from 0.7 mg per 100 mL to 2.7 mg per 100 mL (reference range, 0.6–1.2 mg/dL) with evidence of toxic nephrosis and persistent interstitial nephritis, demonstrating the severity of localized destruction that may result when combining these products with direct heat and potential subsequent systemic consequences of this combination.5
The systemic absorption of OTC formulations also has been studied. Morra et al10 studied 12 volunteers (6 women, 6 men) who applied either 5 g of methyl salicylate ointment 12.5% twice daily for 4 days to an area on the thigh (approximately equal to 567 mg salicylate) or trolamine cream 10% twice for 1 day. The participants underwent a break for 7 days and then switched to the alternate treatment. They found that 0.31 to 0.91 mg/L methyl salicylate was detected in the serum 1 hour after applying the ointment consisting of methyl salicylate, and 2 to 6 mg/L methyl salicylate was detected on day 4. Therapeutic serum salicylate levels are 150 to 300 mg/L. They found that approximately 22% of the methyl salicylate also was found in urine samples on day 4. Although these figures may appear small, this study was prompted when a 62-year-old man presented to the emergency department with symptoms of salicylate toxicity and a serum concentration of 518 mg/L from twice-daily use of an OTC formulation containing methyl salicylate over the course of multiple weeks.10 Additionally, those who have aspirin hypersensitivity should be cautious when using such products due to the risk for reported angioedema.4
Providers must exercise extreme caution while caring for geriatric patients, especially if patients are taking warfarin. The combined effects of warfarin and methyl salicylate have previously caused cutaneous purpura, gastrointestinal bleeding, and elevated international normalized ratio values.4,10 Older individuals also have increased skin fragility, allowing microtraumatic insult to easily develop. This fragility, along with an overall decreased intactness of the skin barrier, may lead to increased skin absorption. Furthermore, the addition of applying any heat source places the geriatric patient at greater risk for adverse events.10
In considering the limits of age, the pediatric population also has been studied regarding salicylate toxicity. Most commonly, oral ingestion has caused fatalities, as oil of wintergreen has been cited as extremely dangerous for children if swallowed; doses as small as a teaspoon (5 mL: 7000 mg salicylate) have resulted in fatalities.4,6 Although the consumption of a large amount of a cream- or ointment-based product is unlikely due to the consistency of the medication,6 the thought does merit consideration in the inquisitive toddler age group. For a 15-kg toddler, 150 mg/kg of aspirin or 2250 mg of aspirin, is considered the toxic level, which upon conversion to methyl salicylate levels using a 1.4 factor equates to 1607 mg of methyl salicylate to reach toxicity.6 If using a product with methyl salicylate 30% composition, 1 g of the product contains 300 mg of methyl salicylate; therefore if the toddler consumed approximately 5.3 g of the product (1607 mg methyl salicylate [toxic level] divided by 300 mg methyl salicylate per 1 g of product), he/she would reach toxic levels.6,11 To put this into perspective, a 2-oz tube contains 57 g (approximately 10 times the toxic dose) of the product.8 Thus, although there is less concern overall for consumption of cream- or ointment-based methyl salicylate, there still is potential for harm if a small child were to ingest such a product containing higher percentages of methyl salicylate.6
There also have been reports of pediatric toxicity related to percutaneous absorption, even leading to pediatric fatality.4,6 In particular, there was a case of a young boy hospitalized with ichthyosis who received escalating doses of percutaneous salicylate, which resulted in toxicity; when therapy was discontinued, he experienced full recovery.12 In 2007, a 17-year-old adolescent girl died from methyl salicylate toxicity after numerous applications of salicylate-containing products in conjunction with medicated pads.7
Although the FDA has drawn attention and encouraged caution with use of OTC topical musculoskeletal pain relievers, the importance of ensuring patients are fully aware of potential burns, permanent skin or muscle damage, and even death if used inappropriately cannot be overstated. The FDA consumer health information website has 2 patient-directed handouts2,3 that may be useful to post in patient waiting areas to increase overall understanding of the risks associated with OTC products containing methyl salicylate and menthol ingredients. Fortunately, our patient suffered only mild postinflammatory hyperpigmentation without substantial sustained consequences.
To the Editor:
The combination of menthol and methyl salicylate found in a variety of over-the-counter (OTC) creams in conjunction with a heat source such as a heating pad used for musculoskeletal symptoms can be a dire combination due to increased systemic absorption with associated toxicity and localized effects ranging from contact dermatitis or irritation to burn or necrosis.1-6 We present a case of localized burn due a combination of topical methyl salicylate and heating pad use. We also discuss 2 commonly encountered side effects in the literature—localized burns and systemic toxicity associated with percutaneous absorption—and provide specific considerations related to the geriatric and pediatric populations.
A 62-year-old woman with a history of eczematous dermatitis and osteoarthritis with pain of the left shoulder presented to the dermatology clinic with painful skin-related changes on the left arm of 1 week’s duration. She was prescribed acetaminophen and ibuprofen. However, she self-medicated the left shoulder pain with 2 OTC products containing topical menthol and/or methyl salicylate in combination with a heating pad and likely fell asleep with this combination therapy applied. She noticed the burn the next morning. On examination, the left arm exhibited a geometric, irregularly shaped, erythematous, scaly plaque with a sharp transverse linear demarcation proximally and numerous erythematous linear scaly plaques oriented in an axial orientation with less-defined borders distally (Figure). The patient was diagnosed with burn secondary to combination of topical methyl salicylate and heating pad use. The patient was advised to discontinue the topical medication and to use caution with the heating pad in the future. She was prescribed pramoxine-hydrocortisone lotion to be applied to the affected area twice daily up to 5 days weekly until resolution. Subsequent evaluations revealed progressive improvement with only mild postinflammatory hyperpigmentation noted at 6 months after the burn.
The US Food and Drug Administration (FDA) released statements in 2012 regarding concern for burns related to use of OTC musculoskeletal pain relievers, with 43 cases of burns reported due to methyl salicylate and menthol from 2004 to 2010. Most of the second- and third-degree burns occurred following topical applications of products containing either menthol monotherapy or a combination of methyl salicylate and menthol.1,2 In 2006, the FDA had already ordered 5 firms to stop compounding topical pain relief formulations containing these ingredients, with concerns that it puts patients at increased risk because the compounded formulations had not received FDA approval.3 Despite package warnings, patients may not be aware of the concerning side effects and risks associated with use of OTC creams, especially in combination with occlusion or heating pad use. Our case highlights the importance of ongoing patient education and physician counseling when encountering patients with arthritis or musculoskeletal pain who may often try various OTC self-treatments for pain relief.7
In 2012, the FDA reports stated that the cases of mild to serious burns were associated with methyl salicylate and menthol usage, in some cases 24 hours after first usage. Typically, these effects occur when concentrations are more than either 3% menthol alone or a combination of more than 3% menthol and more than 10% methyl salicylate.1,2 In our case, the patient had been using 2 different OTC products that may have contained as much as 11% menthol and/or 30% methyl salicylate. Electronic resources are available that disclose safety instructions including not to occlude the site, not to use on wounds, and not to be used in conjunction with a heating pad.8,9 Skin breakdown and vasodilation are more likely to occur in a setting of heat and occlusion, which allows for more absorption and localized side effects.4,10 Localized reactions may range from contact dermatitis4 to muscle necrosis.5
The most noteworthy case of localized destruction described a 62-year-old man who had applied topical methyl salicylate and menthol to the forearms, calves, and thighs, then intermittently used a heating pad for 15 to 20 minutes (total duration).5 He subsequently developed erythema and numerous 7.62- to 10.16-cm bullae, which was thought to be consistent with contact dermatitis. Three days later, he was found to have full-thickness cutaneous, fascial, and muscle necrosis in a linear pattern. He was hospitalized for approximately 1 year and treated with extensive debridement and a skin graft. His serum creatinine level increased from 0.7 mg per 100 mL to 2.7 mg per 100 mL (reference range, 0.6–1.2 mg/dL) with evidence of toxic nephrosis and persistent interstitial nephritis, demonstrating the severity of localized destruction that may result when combining these products with direct heat and potential subsequent systemic consequences of this combination.5
The systemic absorption of OTC formulations also has been studied. Morra et al10 studied 12 volunteers (6 women, 6 men) who applied either 5 g of methyl salicylate ointment 12.5% twice daily for 4 days to an area on the thigh (approximately equal to 567 mg salicylate) or trolamine cream 10% twice for 1 day. The participants underwent a break for 7 days and then switched to the alternate treatment. They found that 0.31 to 0.91 mg/L methyl salicylate was detected in the serum 1 hour after applying the ointment consisting of methyl salicylate, and 2 to 6 mg/L methyl salicylate was detected on day 4. Therapeutic serum salicylate levels are 150 to 300 mg/L. They found that approximately 22% of the methyl salicylate also was found in urine samples on day 4. Although these figures may appear small, this study was prompted when a 62-year-old man presented to the emergency department with symptoms of salicylate toxicity and a serum concentration of 518 mg/L from twice-daily use of an OTC formulation containing methyl salicylate over the course of multiple weeks.10 Additionally, those who have aspirin hypersensitivity should be cautious when using such products due to the risk for reported angioedema.4
Providers must exercise extreme caution while caring for geriatric patients, especially if patients are taking warfarin. The combined effects of warfarin and methyl salicylate have previously caused cutaneous purpura, gastrointestinal bleeding, and elevated international normalized ratio values.4,10 Older individuals also have increased skin fragility, allowing microtraumatic insult to easily develop. This fragility, along with an overall decreased intactness of the skin barrier, may lead to increased skin absorption. Furthermore, the addition of applying any heat source places the geriatric patient at greater risk for adverse events.10
In considering the limits of age, the pediatric population also has been studied regarding salicylate toxicity. Most commonly, oral ingestion has caused fatalities, as oil of wintergreen has been cited as extremely dangerous for children if swallowed; doses as small as a teaspoon (5 mL: 7000 mg salicylate) have resulted in fatalities.4,6 Although the consumption of a large amount of a cream- or ointment-based product is unlikely due to the consistency of the medication,6 the thought does merit consideration in the inquisitive toddler age group. For a 15-kg toddler, 150 mg/kg of aspirin or 2250 mg of aspirin, is considered the toxic level, which upon conversion to methyl salicylate levels using a 1.4 factor equates to 1607 mg of methyl salicylate to reach toxicity.6 If using a product with methyl salicylate 30% composition, 1 g of the product contains 300 mg of methyl salicylate; therefore if the toddler consumed approximately 5.3 g of the product (1607 mg methyl salicylate [toxic level] divided by 300 mg methyl salicylate per 1 g of product), he/she would reach toxic levels.6,11 To put this into perspective, a 2-oz tube contains 57 g (approximately 10 times the toxic dose) of the product.8 Thus, although there is less concern overall for consumption of cream- or ointment-based methyl salicylate, there still is potential for harm if a small child were to ingest such a product containing higher percentages of methyl salicylate.6
There also have been reports of pediatric toxicity related to percutaneous absorption, even leading to pediatric fatality.4,6 In particular, there was a case of a young boy hospitalized with ichthyosis who received escalating doses of percutaneous salicylate, which resulted in toxicity; when therapy was discontinued, he experienced full recovery.12 In 2007, a 17-year-old adolescent girl died from methyl salicylate toxicity after numerous applications of salicylate-containing products in conjunction with medicated pads.7
Although the FDA has drawn attention and encouraged caution with use of OTC topical musculoskeletal pain relievers, the importance of ensuring patients are fully aware of potential burns, permanent skin or muscle damage, and even death if used inappropriately cannot be overstated. The FDA consumer health information website has 2 patient-directed handouts2,3 that may be useful to post in patient waiting areas to increase overall understanding of the risks associated with OTC products containing methyl salicylate and menthol ingredients. Fortunately, our patient suffered only mild postinflammatory hyperpigmentation without substantial sustained consequences.
- US Food and Drug Administration. FDA Drug Safety Communication: rare cases of serious burns with the use of over-the-counter topical muscle and joint pain relievers. http://www.fda.gov/Drugs/DrugSafety/ucm318858.htm. Published September 13, 2012. Updated February 11, 2016. Accessed October 31, 2017.
- US Food and Drug Administration. Topical pain relievers may cause burns. http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm318674.htm. Published September 13, 2012. Updated November 5, 2015. Accessed October 31, 2017.
- US Food and Drug Administration. Use caution with over-the-counter creams, ointments. http://www.fda.gov/forconsumers/consumerupdates/ucm049367.htm. Updated October 17, 2017. Accessed October 31, 2017.
- Chan TY. Potential dangers from topical preparations containing methyl salicylate. Hum Exp Toxicol. 1996;15:747-750.
- Heng MC. Local necrosis and interstitial nephritis due to topical methyl salicylate and menthol. Cutis. 1987;39:442-444.
- Davis JE. Are one or two dangerous? methyl salicylate exposure in toddlers. J Emerg Med. 2007;32:63-69.
- Associated Press. Sports cream warnings urged after teen’s death: track star’s overdose points to risks of popular muscle salve. NBC News. http://www.nbcnews.com/id/19208195. Updated June 13, 2007. Accessed October 31, 2017.
- Ultra Strength Bengay Cream. Bengay website. http://www.bengay.com/bengay-ultra-strength-cream. Accessed November 1, 2017.
- Tiger Balm Arthritis Rub. Tiger Balm website. http://www.tigerbalm.com/us/pages/tb_product?product_id=6. Accessed November 1, 2017.
- Morra P, Bartle WR, Walker SE, et al. Serum concentrations of salicylic acid following topically applied salicylate derivatives. Ann Pharmacother. 1996;9:935-940.
- US National Library of Medicine. Bengay Ultra Strength non greasy pain relieving- camphor (synthetic), menthol, and methyl salicylate cream. Daily Med website. http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=5aa265f8-ab45-47b2-b5ab-d4df54daed01. Updated November 3, 2016. Accessed November 1, 2017.
- Aspinall JB, Goel KM. Salicylate poisoning in dermatological therapy. Br Med J. 1978;2:1373.
- US Food and Drug Administration. FDA Drug Safety Communication: rare cases of serious burns with the use of over-the-counter topical muscle and joint pain relievers. http://www.fda.gov/Drugs/DrugSafety/ucm318858.htm. Published September 13, 2012. Updated February 11, 2016. Accessed October 31, 2017.
- US Food and Drug Administration. Topical pain relievers may cause burns. http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm318674.htm. Published September 13, 2012. Updated November 5, 2015. Accessed October 31, 2017.
- US Food and Drug Administration. Use caution with over-the-counter creams, ointments. http://www.fda.gov/forconsumers/consumerupdates/ucm049367.htm. Updated October 17, 2017. Accessed October 31, 2017.
- Chan TY. Potential dangers from topical preparations containing methyl salicylate. Hum Exp Toxicol. 1996;15:747-750.
- Heng MC. Local necrosis and interstitial nephritis due to topical methyl salicylate and menthol. Cutis. 1987;39:442-444.
- Davis JE. Are one or two dangerous? methyl salicylate exposure in toddlers. J Emerg Med. 2007;32:63-69.
- Associated Press. Sports cream warnings urged after teen’s death: track star’s overdose points to risks of popular muscle salve. NBC News. http://www.nbcnews.com/id/19208195. Updated June 13, 2007. Accessed October 31, 2017.
- Ultra Strength Bengay Cream. Bengay website. http://www.bengay.com/bengay-ultra-strength-cream. Accessed November 1, 2017.
- Tiger Balm Arthritis Rub. Tiger Balm website. http://www.tigerbalm.com/us/pages/tb_product?product_id=6. Accessed November 1, 2017.
- Morra P, Bartle WR, Walker SE, et al. Serum concentrations of salicylic acid following topically applied salicylate derivatives. Ann Pharmacother. 1996;9:935-940.
- US National Library of Medicine. Bengay Ultra Strength non greasy pain relieving- camphor (synthetic), menthol, and methyl salicylate cream. Daily Med website. http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=5aa265f8-ab45-47b2-b5ab-d4df54daed01. Updated November 3, 2016. Accessed November 1, 2017.
- Aspinall JB, Goel KM. Salicylate poisoning in dermatological therapy. Br Med J. 1978;2:1373.
Practice Points
- Recognize the potential complication of burn from use of over-the-counter (OTC) musculoskeletal relievers in combination with a heat source.
- Screen for OTC product use as well as device application when evaluating an atypically patterned cutaneous eruption.
- Recognize potential toxicity associated with both topical application and accidental ingestion in the pediatric population.
- Physicians should become familiar with resources available, including patient handouts that describe risks associated with use of OTC musculoskeletal relievers containing methyl salicylate and menthol ingredients.

Pediatricians urge focus on human trafficking victims
For pediatricians to better help victims of human trafficking, it is critical that there be improvements in research, medical education, advocacy, and community collaborations, according to a policy statement issued by the American Academy of Pediatrics (AAP) Committee on Child Abuse and Neglect, Section on International Child Health.
The full effects of human trafficking are still very much hidden in shadows, leading the AAP to add human trafficking education to its list of top 10 priorities at the 2014 AAP Annual Leadership Forum.
The policy statement is the latest step in the AAP’s effort to involve medical professionals more heavily in combating child sex and labor trafficking, which the AAP asserts is a critical role for pediatricians. Even with the limited information available, the United Nations Office of Drugs and Crime 2016 report found 33% of the 40,000 trafficking victims reported were children, an indication of the vulnerability of younger populations.
“We wanted to give not just background information on trafficking, but we also wanted to give some guidance for academy members in regard to how we can increase awareness of human trafficking, how we can start to implement it into medical education for medical trainees and practicing pediatricians,” Nia Bodrick, MD, MPH, coauthor of the statement and a member of the AAP Section on International Child Health, said in an interview. “Due to the very narrow amount of evidence-based research that is available on this issue, there is a call to look more deeply into the topic.”
Currently, many health care professionals may be more exposed to child trafficking than they think because of a lack knowledge on how to recognize it. Victims can pass unnoticed.
“Most victims and survivors of human trafficking have had some sort of interaction with the health care setting at some point before they escape their situation,” said Dr. Bodrick. “So whether we as pediatricians realize it or not, we are more than likely interacting with young people who are in these situations.”
There are not enough data to list definitive characteristics of trafficking victims; however, there are certain signs associated with those who have been identified as victims so far. While history of neglect, homelessness, substance abuse, mental disorder, and identifying as a member of the LGBTQ community are more common among trafficking victims, many doctors are not equipped to handle confronting patients about the possibility of sex or labor trafficking, nor do they know what resources are available.
The AAP emphasized a need to expand the current scope of knowledge medical professionals have regarding such victims to create better, evidence-based care programs and protective policies.
An influx of information would help pediatricians understand the prevalence of trafficking, the extent of physical and emotional harm victims experience, and the effectiveness of psychological and mental health interventions, according to the statement (Pediatrics. 2017 November. doi: 10.1542/peds.2017-3138).
It also may help shed light on male trafficking victims, which Dr. Bodrick and coauthor Jordan Greenbaum, MD, of the Stephanie V. Blank Center for Safe and Healthy Children at Children’s Healthcare of Atlanta, assert are highly underrepresented.
Separating human trafficking from other types of violence and exploitation in the International Classification of Diseases codes may improve research initiatives, according to Dr. Bodrick.
There is also a need to delve deeper into the social determinants of health to better predict what makes victims more vulnerable.
While improving the number of studies on trafficking is essential, the results are more long term, which means in the mean time other actions can, and should, be made, according to the statement.
One of the best things pediatricians can do is gather as much knowledge on the topic as they can, according to Dr. Bodrick.
“For the average pediatrician, one of the first things one could do is educate oneself on the topic,” she explained. “Look for CME associated with your local AAP chapter or even on a national level online or even if you just have a couple hours for lunch, to become aware of what’s happening.”
The AAP also is encouraging physicians to advocate for legislative policies that will help improve victim care and to create partnerships within the community.
“In DC, in our local AAP chapter, we have opportunities to go to the Hill and advocate for bills, and while not everyone can do that, there are always local legislators that pediatricians can push to do more,” said Dr. Bodrick. “If you have a local paper, you could write an op-ed about the topic, you could educate your local schools about the topic by talking to the school board, or you could even engage in interviews on a local radio or television station.”
While many states have laws protecting victims of sex trafficking from being prosecuted for performing illegal acts, many have not passed such legislation.
Pediatricians can see what protections their states have through the National Conference of State Legislatures’ web page, as well as review current human trafficking laws.
Dr. Greenbaum and Dr. Bodrick reported no relevant financial disclosures.
[email protected]
On Twitter@eaztweets
This statement does a good job bringing the health aspects of human trafficking into the open. Human trafficking has become a significant issue in the United States, and this document serves as a way to open the door for discussion on how pediatricians can become a part of the solution.

Armed with a clearer idea of the issues of child trafficking, pediatricians should take this document as a call to increase their – and their colleagues’ – awareness on this issue. Whether that involves a deeper focus on the social environmental determinants of health or political advocacy, education is key to developing a better role as a pediatrician as we work together to help those who have experienced trafficking first hand.
Francis Rushton Jr., MD, practiced pediatrics in Beaufort, S.C. for 32 years. He also is a member of the Pediatric News editorial advisory board.
This statement does a good job bringing the health aspects of human trafficking into the open. Human trafficking has become a significant issue in the United States, and this document serves as a way to open the door for discussion on how pediatricians can become a part of the solution.
Armed with a clearer idea of the issues of child trafficking, pediatricians should take this document as a call to increase their – and their colleagues’ – awareness on this issue. Whether that involves a deeper focus on the social environmental determinants of health or political advocacy, education is key to developing a better role as a pediatrician as we work together to help those who have experienced trafficking first hand.
Francis Rushton Jr., MD, practiced pediatrics in Beaufort, S.C. for 32 years. He also is a member of the Pediatric News editorial advisory board.
This statement does a good job bringing the health aspects of human trafficking into the open. Human trafficking has become a significant issue in the United States, and this document serves as a way to open the door for discussion on how pediatricians can become a part of the solution.
Armed with a clearer idea of the issues of child trafficking, pediatricians should take this document as a call to increase their – and their colleagues’ – awareness on this issue. Whether that involves a deeper focus on the social environmental determinants of health or political advocacy, education is key to developing a better role as a pediatrician as we work together to help those who have experienced trafficking first hand.
Francis Rushton Jr., MD, practiced pediatrics in Beaufort, S.C. for 32 years. He also is a member of the Pediatric News editorial advisory board.
For pediatricians to better help victims of human trafficking, it is critical that there be improvements in research, medical education, advocacy, and community collaborations, according to a policy statement issued by the American Academy of Pediatrics (AAP) Committee on Child Abuse and Neglect, Section on International Child Health.
The full effects of human trafficking are still very much hidden in shadows, leading the AAP to add human trafficking education to its list of top 10 priorities at the 2014 AAP Annual Leadership Forum.
The policy statement is the latest step in the AAP’s effort to involve medical professionals more heavily in combating child sex and labor trafficking, which the AAP asserts is a critical role for pediatricians. Even with the limited information available, the United Nations Office of Drugs and Crime 2016 report found 33% of the 40,000 trafficking victims reported were children, an indication of the vulnerability of younger populations.
“We wanted to give not just background information on trafficking, but we also wanted to give some guidance for academy members in regard to how we can increase awareness of human trafficking, how we can start to implement it into medical education for medical trainees and practicing pediatricians,” Nia Bodrick, MD, MPH, coauthor of the statement and a member of the AAP Section on International Child Health, said in an interview. “Due to the very narrow amount of evidence-based research that is available on this issue, there is a call to look more deeply into the topic.”
Currently, many health care professionals may be more exposed to child trafficking than they think because of a lack knowledge on how to recognize it. Victims can pass unnoticed.
“Most victims and survivors of human trafficking have had some sort of interaction with the health care setting at some point before they escape their situation,” said Dr. Bodrick. “So whether we as pediatricians realize it or not, we are more than likely interacting with young people who are in these situations.”
There are not enough data to list definitive characteristics of trafficking victims; however, there are certain signs associated with those who have been identified as victims so far. While history of neglect, homelessness, substance abuse, mental disorder, and identifying as a member of the LGBTQ community are more common among trafficking victims, many doctors are not equipped to handle confronting patients about the possibility of sex or labor trafficking, nor do they know what resources are available.
The AAP emphasized a need to expand the current scope of knowledge medical professionals have regarding such victims to create better, evidence-based care programs and protective policies.
An influx of information would help pediatricians understand the prevalence of trafficking, the extent of physical and emotional harm victims experience, and the effectiveness of psychological and mental health interventions, according to the statement (Pediatrics. 2017 November. doi: 10.1542/peds.2017-3138).
It also may help shed light on male trafficking victims, which Dr. Bodrick and coauthor Jordan Greenbaum, MD, of the Stephanie V. Blank Center for Safe and Healthy Children at Children’s Healthcare of Atlanta, assert are highly underrepresented.
Separating human trafficking from other types of violence and exploitation in the International Classification of Diseases codes may improve research initiatives, according to Dr. Bodrick.
There is also a need to delve deeper into the social determinants of health to better predict what makes victims more vulnerable.
While improving the number of studies on trafficking is essential, the results are more long term, which means in the mean time other actions can, and should, be made, according to the statement.
One of the best things pediatricians can do is gather as much knowledge on the topic as they can, according to Dr. Bodrick.
“For the average pediatrician, one of the first things one could do is educate oneself on the topic,” she explained. “Look for CME associated with your local AAP chapter or even on a national level online or even if you just have a couple hours for lunch, to become aware of what’s happening.”
The AAP also is encouraging physicians to advocate for legislative policies that will help improve victim care and to create partnerships within the community.
“In DC, in our local AAP chapter, we have opportunities to go to the Hill and advocate for bills, and while not everyone can do that, there are always local legislators that pediatricians can push to do more,” said Dr. Bodrick. “If you have a local paper, you could write an op-ed about the topic, you could educate your local schools about the topic by talking to the school board, or you could even engage in interviews on a local radio or television station.”
While many states have laws protecting victims of sex trafficking from being prosecuted for performing illegal acts, many have not passed such legislation.
Pediatricians can see what protections their states have through the National Conference of State Legislatures’ web page, as well as review current human trafficking laws.
Dr. Greenbaum and Dr. Bodrick reported no relevant financial disclosures.
[email protected]
On Twitter@eaztweets
For pediatricians to better help victims of human trafficking, it is critical that there be improvements in research, medical education, advocacy, and community collaborations, according to a policy statement issued by the American Academy of Pediatrics (AAP) Committee on Child Abuse and Neglect, Section on International Child Health.
The full effects of human trafficking are still very much hidden in shadows, leading the AAP to add human trafficking education to its list of top 10 priorities at the 2014 AAP Annual Leadership Forum.
The policy statement is the latest step in the AAP’s effort to involve medical professionals more heavily in combating child sex and labor trafficking, which the AAP asserts is a critical role for pediatricians. Even with the limited information available, the United Nations Office of Drugs and Crime 2016 report found 33% of the 40,000 trafficking victims reported were children, an indication of the vulnerability of younger populations.
“We wanted to give not just background information on trafficking, but we also wanted to give some guidance for academy members in regard to how we can increase awareness of human trafficking, how we can start to implement it into medical education for medical trainees and practicing pediatricians,” Nia Bodrick, MD, MPH, coauthor of the statement and a member of the AAP Section on International Child Health, said in an interview. “Due to the very narrow amount of evidence-based research that is available on this issue, there is a call to look more deeply into the topic.”
Currently, many health care professionals may be more exposed to child trafficking than they think because of a lack knowledge on how to recognize it. Victims can pass unnoticed.
“Most victims and survivors of human trafficking have had some sort of interaction with the health care setting at some point before they escape their situation,” said Dr. Bodrick. “So whether we as pediatricians realize it or not, we are more than likely interacting with young people who are in these situations.”
There are not enough data to list definitive characteristics of trafficking victims; however, there are certain signs associated with those who have been identified as victims so far. While history of neglect, homelessness, substance abuse, mental disorder, and identifying as a member of the LGBTQ community are more common among trafficking victims, many doctors are not equipped to handle confronting patients about the possibility of sex or labor trafficking, nor do they know what resources are available.
The AAP emphasized a need to expand the current scope of knowledge medical professionals have regarding such victims to create better, evidence-based care programs and protective policies.
An influx of information would help pediatricians understand the prevalence of trafficking, the extent of physical and emotional harm victims experience, and the effectiveness of psychological and mental health interventions, according to the statement (Pediatrics. 2017 November. doi: 10.1542/peds.2017-3138).
It also may help shed light on male trafficking victims, which Dr. Bodrick and coauthor Jordan Greenbaum, MD, of the Stephanie V. Blank Center for Safe and Healthy Children at Children’s Healthcare of Atlanta, assert are highly underrepresented.
Separating human trafficking from other types of violence and exploitation in the International Classification of Diseases codes may improve research initiatives, according to Dr. Bodrick.
There is also a need to delve deeper into the social determinants of health to better predict what makes victims more vulnerable.
While improving the number of studies on trafficking is essential, the results are more long term, which means in the mean time other actions can, and should, be made, according to the statement.
One of the best things pediatricians can do is gather as much knowledge on the topic as they can, according to Dr. Bodrick.
“For the average pediatrician, one of the first things one could do is educate oneself on the topic,” she explained. “Look for CME associated with your local AAP chapter or even on a national level online or even if you just have a couple hours for lunch, to become aware of what’s happening.”
The AAP also is encouraging physicians to advocate for legislative policies that will help improve victim care and to create partnerships within the community.
“In DC, in our local AAP chapter, we have opportunities to go to the Hill and advocate for bills, and while not everyone can do that, there are always local legislators that pediatricians can push to do more,” said Dr. Bodrick. “If you have a local paper, you could write an op-ed about the topic, you could educate your local schools about the topic by talking to the school board, or you could even engage in interviews on a local radio or television station.”
While many states have laws protecting victims of sex trafficking from being prosecuted for performing illegal acts, many have not passed such legislation.
Pediatricians can see what protections their states have through the National Conference of State Legislatures’ web page, as well as review current human trafficking laws.
Dr. Greenbaum and Dr. Bodrick reported no relevant financial disclosures.
[email protected]
On Twitter@eaztweets
FROM PEDIATRICS
Cellular Versus Acellular Grafts for Diabetic Foot Ulcers: Altering the Protocol to Improve Recruitment to a Comparative Efficacy Trial
Chronic diabetic foot ulcers (DFUs) remain a serious therapeutic challenge worldwide.1-2 Patients with DFUs are at higher risk for infections, which may lead to limb loss.1-5 In fact, 1 in 6 patients with DFUs will undergo an amputation.6 The long-term consequences of DFUs are numerous and can severely affect patients’ quality of life, including loss of productivity.7 The current standard of care for DFUs consists of debridement of the necrotic tissue, application of a moist dressing, and use of an off-loading device that protects the wound from pressure or trauma related to ambulation and other acts of daily living.4-6,8 Unfortunately, studies have shown that the best standard of care (SOC) only heals 30% of DFUs after 20 weeks of therapy.9 With the estimated cost per episode of care approaching $40,000, DFUs remain a costly and important problem.10
The altered extracellular matrix (ECM) in DFUs has been a target for the development of new therapeutic devices that provide a new matrix that is either devoid of cells or can be enriched with fibroblasts.8,11 These bioengineered skin substitutes stimulate the growth of new vessels and generate cytokines essential for tissue repair. In 2013, Lev-Tov et al12 published this study protocol (Dermagraft Oasis Longitudinal Comparative Efficacy [DOLCE] trial) to compare the effectiveness of 2 advanced wound care devices, specifically to evaluate the clinical efficacy of a cellular matrix versus an acellular matrix, which we have amended. The cellular matrix used in the study is a dermal substitute composed of viable newborn foreskin fibroblasts seeded onto a bioabsorbable polyglactin mesh on which fibroblasts generate an ECM.13,14 It is supplied frozen and requires specific thawing steps prior to application. The recommended regimen for treatment of DFUs for this cellular matrix is 8 weekly applications.13,14 In 2016, the cost of the product was reported as $1411 per 5.0×7.5-cm sheet.15 The acellular matrix product used in the study is a bioabsorbable ECM that is derived from porcine small intestinal submucosa.16,17 It is stored at room temperature and has a long shelf life, with a current price of $112.6 for a 3.0×3.5-cm single-layer fenestrated sheet ($1126.60 per box of 10 sheets). The industry-supported randomized controlled trials for each of these devices have reported a 20% added benefit in the rate of wound closure at week 12 compared to SOC.14,17
This article provides the interim report of the trial (registered at www.clinicaltrials.gov with the identifier NCT01450943) described in the published protocol and initiated in 2011,12 focusing on elements that required modification during the trial’s duration.
Methods
Study Protocol
The clinical trial was approved by the Veterans’ Affairs Institutional Research and Development Committee and their institutional review board. This study was funded by the Veteran’s Administration Merit Award (#10554640), which was awarded to 2 of the investigators (S.E.D. and R.R.I.). Eligible veterans were recruited from all 7 sites of the VA Northern California Healthcare System. This trial is a randomized, single-blinded, 3-armed, controlled clinical equivalence trial comparing the effectiveness of an SOC treatment, cellular ECM, and acellular ECM.
Study Products
The SOC dressing applied in the clinical trial included a sterile antimicrobial gel, a nonadherent dressing, and gauze.12 The SOC dressing also was used as a secondary dressing for the active treatment arms. Bacitracin antibiotic ointment was used as an alternative for patients with allergy to iodine.12
Randomization
The inclusion and exclusion criteria were previously outlined.12 After a 2-week screening phase to exclude rapid healers, patients were randomized into a treatment arm and entered the active phase for 12 weeks.
Primary and Secondary Outcomes
The primary outcome was complete wound closure by week 12.12 Complete healing was defined as full reepithelialization with no drainage or dressing requirement. The secondary outcomes included healing at 28 weeks, rate of healing, ulcer recurrence at week 20, association of wound healing with ulcer characteristics or patients’ characteristic, incidence of adverse events, and cost-effectiveness of each treatment compared to the SOC arm.12
Statistical Analysis
To detect a 25% difference in the incidence of ulcer closure between the 2 study groups and the SOC group, the estimation of the sample size was based on 80% power with a significance level of 0.05. Specifically, it was expected that 50% of the cellular and acellular matrix groups and 25% of the SOC group would reach complete wound closure. The protocol indicated that 57 participants would be enrolled in each arm (total of 171 participants). Lev-Tov et al12 discussed the statistical analysis in more detail.
Results
Study Protocol Amendments
Given the number of diabetic patients in the US veteran population, we anticipated that there would be enough participants meeting the inclusion and exclusion criteria; however, because of the difficulty with recruitment, the initial study criteria were modified. The study was initially designed to incorporate DFUs with a minimum size of 1.0 cm2.12
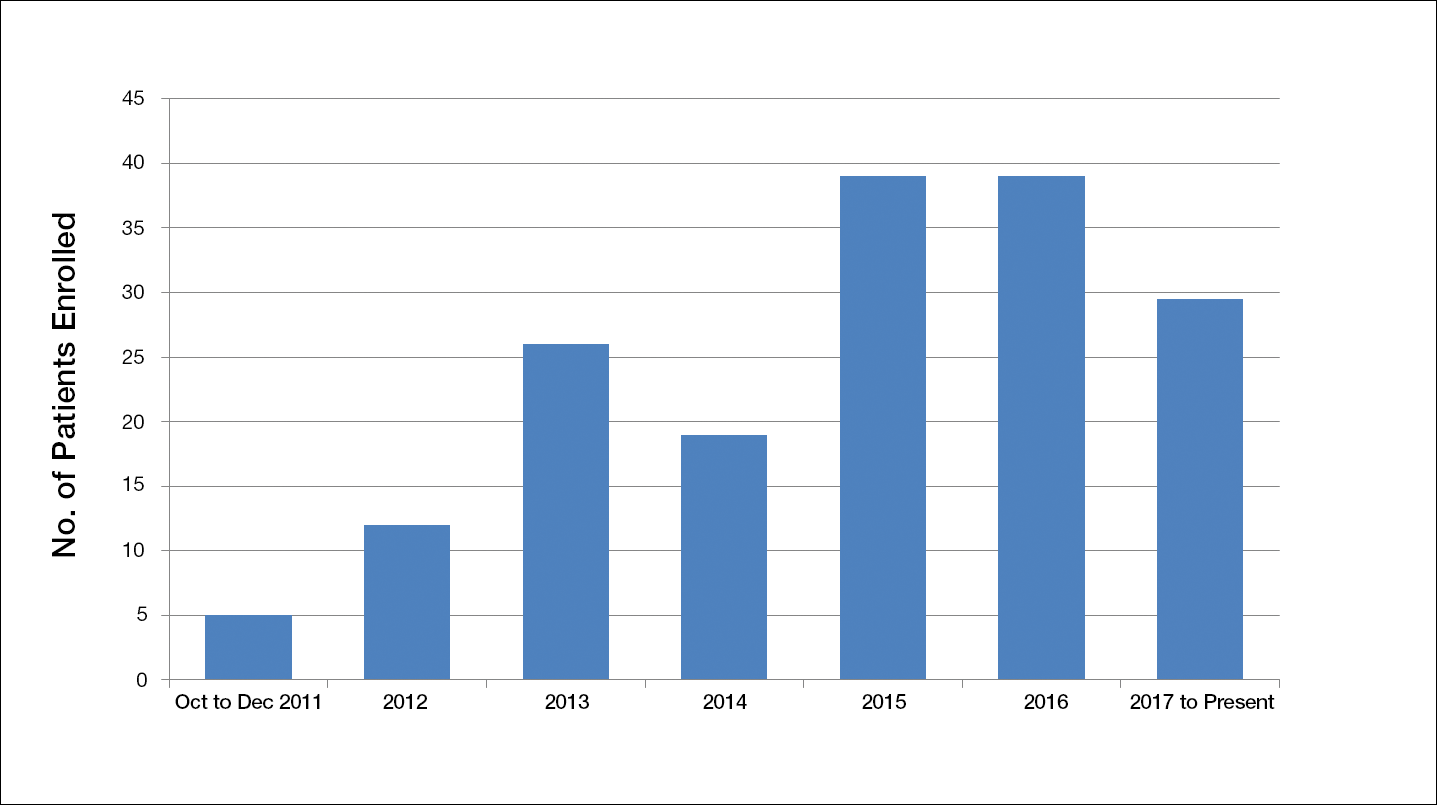
Another limiting criterion was the percentage of total hemoglobin level for hemoglobin A1C (HbA1C). The study was originally established to include participants with an HbA1C level of 10% of total hemoglobin or below.12 Unfortunately, the majority of the potential participants had values substantially higher, and thus could not be enrolled in the trial, requiring another amendment to the study protocol in 2014, which was approved to include patients with an HbA1C level less than 12% of total hemoglobin. This change contributed considerably to the noted increase in enrollment rates in 2015, which almost doubled relative to enrollment under the original exclusion criteria (Figure).
The study has screened more than 600 patients. Among them, 137 were assessed for eligibility; 71 were excluded for various reasons, including screen failure (eg, decrease in wound size by >40% during the 2-week screening phase), loss to follow-up, and adverse events. Sixty-six participants reached the primary outcome at week 12, while 55 participants completed the study (19 in the SOC group; 18 in the cellular matrix group; 18 in the acellular matrix group).
We have stopped enrolling patients from all sites and the community, as we have reached our target enrollment.
Comment
One of the challenges of clinical trials is the recruitment of an adequate number of participants within an appropriate time frame, which is explained by Lasagna’s Law,18 a well-described phenomenon whereby the investigator overestimates the number of potential participants available to meet the inclusion criteria. This so-called funnel-effect was partly encountered in our selection process. A review of the veteran population with DFUs seemed to be more than adequate to fulfill the sample size; however, some important participant-related factors also played a substantial role.
In addition, the Veterans’ Affairs network centralizes health information, making it readily available to all providers participating in their care. As a result, patients with diabetes mellitus typically are seen by a primary care physician along with an endocrinologist, a diabetic nurse, and/or a dietician. Despite the collaboration with an interdisciplinary team, the glycemic control of the participants remains an issue along with other psychosocial factors that are deterrents in patient compliance. As a result, patients with poorly controlled diabetes and an HbA1C level above 10% (and less than 12%) of total hemoglobin who were initially excluded from the study were reincluded after modifying the inclusion criteria. Some patients were interested in joining the study, but physical limitations (eg, impaired mobility) prompted their decision not to join the trial, even though they met all the inclusion criteria.
As far as research-related factors that could affect participation, it is notable that most of the patients were retired; thus, the interventions did not cause additional burden of taking time off from work or loss of productivity. Although randomization could be a deterrent in many clinical trials, the majority of patients were willing to participate without demanding to be assigned to a particular treatment group.
There are many factors that are intertwined and can lead to enrollment and/or attrition rates. It was critical for our team to make some adjustment without compromising the controlled nature of a randomized trial.
Acknowledgment
The authors wish to acknowledge Huong Le, DPM, MPH, who was the coauthor of the study protocol.
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771.
- Gurtner GC, Werner S, Barrandon Y, et al. Wound repair and regeneration. Nature. 2008;453:314-321.
- Falanga V. Wound healing and its impairment in the diabetic foot. Lancet. 2005;366:1736-1743.
- Boulton AJ. The diabetic foot: grand overview, epidemiology and pathogenesis. Diabetes Metab Res Rev. 2008;24(suppl 1):S3-S6.
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293:217-228.
- Vuorisalo S, Venermo M, Lepäntalo M. Treatment of diabetic foot ulcers. J Cardiovasc Surg (Torino). 2009;50:275-291.
- Meijer JW, Trip J, Jaegers SM, et al. Quality of life in patients with diabetic foot ulcers. Disabil Rehabil. 2001;23:336-340.
- Santema TB, Poyck PP, Ubbink DT. Skin grafting and tissue replacement for treating foot ulcers in people with diabetes. Cochrane Database Syst Rev. 2016;2:CD011255.
- Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. a meta-analysis. Diabetes Care. 1999;22:692-695.
- Cavanagh P, Attinger C, Abbas Z, et al. Cost of treating diabetic foot ulcers in five different countries. Diabetes Metab Res Rev. 2012;2(suppl 1):107-111.
- Panuncialman J, Falanga V. The science of wound bed preparation. Surg Clin North Am. 2009;89:611-626.
- Lev-Tov H, Li CS, Dahle S, et al. Cellular versus acellular matrix devices in treatment of diabetic foot ulcers: study protocol for a comparative efficacy randomized controlled trial. Trials. 2013;14:8.
- Gentzkow GD, Iwasaki SD, Hershon KS, et al. Use of dermagraft, a cultured human dermis, to treat diabetic foot ulcers. Diabetes Care. 1996;19:350-354.
- Marston WA, Hanft J, Norwood P, et al; Dermagraft Diabetic Foot Ulcer Study Group. The efficacy and safety of Dermagraft in improving the healing of chronic diabetic foot ulcers: results of a prospective randomized trial. Diabetes Care. 2003;26:1701-1705.
- 2016 Dermagraft® Medicare Product and Related Procedure Payment. http://www.dermagraft.com/wp-content/uploads/sites/1/Dermagraft_Hotsheet%202016%20Q1%20HOSPITAL_FINAL.pdf. Accessed November 23, 2017.
- Oasis® Wound Matrix. http://www.oasiswoundmatrix.com/aboutowm. Accessed November 23, 2017.
- Niezgoda JA, Van Gils CC, Frykberg RG, et al. Randomized clinical trial comparing OASIS Wound Matrix to Regranex Gel for diabetic ulcers. Adv Skin Wound Care. 2005;18(5, pt 1):258-266.
- Torgerson JS, Arlinger K, Käppi M, et al. Principles for enhanced recruitment of subjects in a large clinical trial. the XENDOS (XENical in the prevention of Diabetes in Obese Subjects) study experience. Controlled Clin Trials. 2001;22:515-525.
Chronic diabetic foot ulcers (DFUs) remain a serious therapeutic challenge worldwide.1-2 Patients with DFUs are at higher risk for infections, which may lead to limb loss.1-5 In fact, 1 in 6 patients with DFUs will undergo an amputation.6 The long-term consequences of DFUs are numerous and can severely affect patients’ quality of life, including loss of productivity.7 The current standard of care for DFUs consists of debridement of the necrotic tissue, application of a moist dressing, and use of an off-loading device that protects the wound from pressure or trauma related to ambulation and other acts of daily living.4-6,8 Unfortunately, studies have shown that the best standard of care (SOC) only heals 30% of DFUs after 20 weeks of therapy.9 With the estimated cost per episode of care approaching $40,000, DFUs remain a costly and important problem.10
The altered extracellular matrix (ECM) in DFUs has been a target for the development of new therapeutic devices that provide a new matrix that is either devoid of cells or can be enriched with fibroblasts.8,11 These bioengineered skin substitutes stimulate the growth of new vessels and generate cytokines essential for tissue repair. In 2013, Lev-Tov et al12 published this study protocol (Dermagraft Oasis Longitudinal Comparative Efficacy [DOLCE] trial) to compare the effectiveness of 2 advanced wound care devices, specifically to evaluate the clinical efficacy of a cellular matrix versus an acellular matrix, which we have amended. The cellular matrix used in the study is a dermal substitute composed of viable newborn foreskin fibroblasts seeded onto a bioabsorbable polyglactin mesh on which fibroblasts generate an ECM.13,14 It is supplied frozen and requires specific thawing steps prior to application. The recommended regimen for treatment of DFUs for this cellular matrix is 8 weekly applications.13,14 In 2016, the cost of the product was reported as $1411 per 5.0×7.5-cm sheet.15 The acellular matrix product used in the study is a bioabsorbable ECM that is derived from porcine small intestinal submucosa.16,17 It is stored at room temperature and has a long shelf life, with a current price of $112.6 for a 3.0×3.5-cm single-layer fenestrated sheet ($1126.60 per box of 10 sheets). The industry-supported randomized controlled trials for each of these devices have reported a 20% added benefit in the rate of wound closure at week 12 compared to SOC.14,17
This article provides the interim report of the trial (registered at www.clinicaltrials.gov with the identifier NCT01450943) described in the published protocol and initiated in 2011,12 focusing on elements that required modification during the trial’s duration.
Methods
Study Protocol
The clinical trial was approved by the Veterans’ Affairs Institutional Research and Development Committee and their institutional review board. This study was funded by the Veteran’s Administration Merit Award (#10554640), which was awarded to 2 of the investigators (S.E.D. and R.R.I.). Eligible veterans were recruited from all 7 sites of the VA Northern California Healthcare System. This trial is a randomized, single-blinded, 3-armed, controlled clinical equivalence trial comparing the effectiveness of an SOC treatment, cellular ECM, and acellular ECM.
Study Products
The SOC dressing applied in the clinical trial included a sterile antimicrobial gel, a nonadherent dressing, and gauze.12 The SOC dressing also was used as a secondary dressing for the active treatment arms. Bacitracin antibiotic ointment was used as an alternative for patients with allergy to iodine.12
Randomization
The inclusion and exclusion criteria were previously outlined.12 After a 2-week screening phase to exclude rapid healers, patients were randomized into a treatment arm and entered the active phase for 12 weeks.
Primary and Secondary Outcomes
The primary outcome was complete wound closure by week 12.12 Complete healing was defined as full reepithelialization with no drainage or dressing requirement. The secondary outcomes included healing at 28 weeks, rate of healing, ulcer recurrence at week 20, association of wound healing with ulcer characteristics or patients’ characteristic, incidence of adverse events, and cost-effectiveness of each treatment compared to the SOC arm.12
Statistical Analysis
To detect a 25% difference in the incidence of ulcer closure between the 2 study groups and the SOC group, the estimation of the sample size was based on 80% power with a significance level of 0.05. Specifically, it was expected that 50% of the cellular and acellular matrix groups and 25% of the SOC group would reach complete wound closure. The protocol indicated that 57 participants would be enrolled in each arm (total of 171 participants). Lev-Tov et al12 discussed the statistical analysis in more detail.
Results
Study Protocol Amendments
Given the number of diabetic patients in the US veteran population, we anticipated that there would be enough participants meeting the inclusion and exclusion criteria; however, because of the difficulty with recruitment, the initial study criteria were modified. The study was initially designed to incorporate DFUs with a minimum size of 1.0 cm2.12
Another limiting criterion was the percentage of total hemoglobin level for hemoglobin A1C (HbA1C). The study was originally established to include participants with an HbA1C level of 10% of total hemoglobin or below.12 Unfortunately, the majority of the potential participants had values substantially higher, and thus could not be enrolled in the trial, requiring another amendment to the study protocol in 2014, which was approved to include patients with an HbA1C level less than 12% of total hemoglobin. This change contributed considerably to the noted increase in enrollment rates in 2015, which almost doubled relative to enrollment under the original exclusion criteria (Figure).
The study has screened more than 600 patients. Among them, 137 were assessed for eligibility; 71 were excluded for various reasons, including screen failure (eg, decrease in wound size by >40% during the 2-week screening phase), loss to follow-up, and adverse events. Sixty-six participants reached the primary outcome at week 12, while 55 participants completed the study (19 in the SOC group; 18 in the cellular matrix group; 18 in the acellular matrix group).
We have stopped enrolling patients from all sites and the community, as we have reached our target enrollment.
Comment
One of the challenges of clinical trials is the recruitment of an adequate number of participants within an appropriate time frame, which is explained by Lasagna’s Law,18 a well-described phenomenon whereby the investigator overestimates the number of potential participants available to meet the inclusion criteria. This so-called funnel-effect was partly encountered in our selection process. A review of the veteran population with DFUs seemed to be more than adequate to fulfill the sample size; however, some important participant-related factors also played a substantial role.
In addition, the Veterans’ Affairs network centralizes health information, making it readily available to all providers participating in their care. As a result, patients with diabetes mellitus typically are seen by a primary care physician along with an endocrinologist, a diabetic nurse, and/or a dietician. Despite the collaboration with an interdisciplinary team, the glycemic control of the participants remains an issue along with other psychosocial factors that are deterrents in patient compliance. As a result, patients with poorly controlled diabetes and an HbA1C level above 10% (and less than 12%) of total hemoglobin who were initially excluded from the study were reincluded after modifying the inclusion criteria. Some patients were interested in joining the study, but physical limitations (eg, impaired mobility) prompted their decision not to join the trial, even though they met all the inclusion criteria.
As far as research-related factors that could affect participation, it is notable that most of the patients were retired; thus, the interventions did not cause additional burden of taking time off from work or loss of productivity. Although randomization could be a deterrent in many clinical trials, the majority of patients were willing to participate without demanding to be assigned to a particular treatment group.
There are many factors that are intertwined and can lead to enrollment and/or attrition rates. It was critical for our team to make some adjustment without compromising the controlled nature of a randomized trial.
Acknowledgment
The authors wish to acknowledge Huong Le, DPM, MPH, who was the coauthor of the study protocol.
Chronic diabetic foot ulcers (DFUs) remain a serious therapeutic challenge worldwide.1-2 Patients with DFUs are at higher risk for infections, which may lead to limb loss.1-5 In fact, 1 in 6 patients with DFUs will undergo an amputation.6 The long-term consequences of DFUs are numerous and can severely affect patients’ quality of life, including loss of productivity.7 The current standard of care for DFUs consists of debridement of the necrotic tissue, application of a moist dressing, and use of an off-loading device that protects the wound from pressure or trauma related to ambulation and other acts of daily living.4-6,8 Unfortunately, studies have shown that the best standard of care (SOC) only heals 30% of DFUs after 20 weeks of therapy.9 With the estimated cost per episode of care approaching $40,000, DFUs remain a costly and important problem.10
The altered extracellular matrix (ECM) in DFUs has been a target for the development of new therapeutic devices that provide a new matrix that is either devoid of cells or can be enriched with fibroblasts.8,11 These bioengineered skin substitutes stimulate the growth of new vessels and generate cytokines essential for tissue repair. In 2013, Lev-Tov et al12 published this study protocol (Dermagraft Oasis Longitudinal Comparative Efficacy [DOLCE] trial) to compare the effectiveness of 2 advanced wound care devices, specifically to evaluate the clinical efficacy of a cellular matrix versus an acellular matrix, which we have amended. The cellular matrix used in the study is a dermal substitute composed of viable newborn foreskin fibroblasts seeded onto a bioabsorbable polyglactin mesh on which fibroblasts generate an ECM.13,14 It is supplied frozen and requires specific thawing steps prior to application. The recommended regimen for treatment of DFUs for this cellular matrix is 8 weekly applications.13,14 In 2016, the cost of the product was reported as $1411 per 5.0×7.5-cm sheet.15 The acellular matrix product used in the study is a bioabsorbable ECM that is derived from porcine small intestinal submucosa.16,17 It is stored at room temperature and has a long shelf life, with a current price of $112.6 for a 3.0×3.5-cm single-layer fenestrated sheet ($1126.60 per box of 10 sheets). The industry-supported randomized controlled trials for each of these devices have reported a 20% added benefit in the rate of wound closure at week 12 compared to SOC.14,17
This article provides the interim report of the trial (registered at www.clinicaltrials.gov with the identifier NCT01450943) described in the published protocol and initiated in 2011,12 focusing on elements that required modification during the trial’s duration.
Methods
Study Protocol
The clinical trial was approved by the Veterans’ Affairs Institutional Research and Development Committee and their institutional review board. This study was funded by the Veteran’s Administration Merit Award (#10554640), which was awarded to 2 of the investigators (S.E.D. and R.R.I.). Eligible veterans were recruited from all 7 sites of the VA Northern California Healthcare System. This trial is a randomized, single-blinded, 3-armed, controlled clinical equivalence trial comparing the effectiveness of an SOC treatment, cellular ECM, and acellular ECM.
Study Products
The SOC dressing applied in the clinical trial included a sterile antimicrobial gel, a nonadherent dressing, and gauze.12 The SOC dressing also was used as a secondary dressing for the active treatment arms. Bacitracin antibiotic ointment was used as an alternative for patients with allergy to iodine.12
Randomization
The inclusion and exclusion criteria were previously outlined.12 After a 2-week screening phase to exclude rapid healers, patients were randomized into a treatment arm and entered the active phase for 12 weeks.
Primary and Secondary Outcomes
The primary outcome was complete wound closure by week 12.12 Complete healing was defined as full reepithelialization with no drainage or dressing requirement. The secondary outcomes included healing at 28 weeks, rate of healing, ulcer recurrence at week 20, association of wound healing with ulcer characteristics or patients’ characteristic, incidence of adverse events, and cost-effectiveness of each treatment compared to the SOC arm.12
Statistical Analysis
To detect a 25% difference in the incidence of ulcer closure between the 2 study groups and the SOC group, the estimation of the sample size was based on 80% power with a significance level of 0.05. Specifically, it was expected that 50% of the cellular and acellular matrix groups and 25% of the SOC group would reach complete wound closure. The protocol indicated that 57 participants would be enrolled in each arm (total of 171 participants). Lev-Tov et al12 discussed the statistical analysis in more detail.
Results
Study Protocol Amendments
Given the number of diabetic patients in the US veteran population, we anticipated that there would be enough participants meeting the inclusion and exclusion criteria; however, because of the difficulty with recruitment, the initial study criteria were modified. The study was initially designed to incorporate DFUs with a minimum size of 1.0 cm2.12
Another limiting criterion was the percentage of total hemoglobin level for hemoglobin A1C (HbA1C). The study was originally established to include participants with an HbA1C level of 10% of total hemoglobin or below.12 Unfortunately, the majority of the potential participants had values substantially higher, and thus could not be enrolled in the trial, requiring another amendment to the study protocol in 2014, which was approved to include patients with an HbA1C level less than 12% of total hemoglobin. This change contributed considerably to the noted increase in enrollment rates in 2015, which almost doubled relative to enrollment under the original exclusion criteria (Figure).
The study has screened more than 600 patients. Among them, 137 were assessed for eligibility; 71 were excluded for various reasons, including screen failure (eg, decrease in wound size by >40% during the 2-week screening phase), loss to follow-up, and adverse events. Sixty-six participants reached the primary outcome at week 12, while 55 participants completed the study (19 in the SOC group; 18 in the cellular matrix group; 18 in the acellular matrix group).
We have stopped enrolling patients from all sites and the community, as we have reached our target enrollment.
Comment
One of the challenges of clinical trials is the recruitment of an adequate number of participants within an appropriate time frame, which is explained by Lasagna’s Law,18 a well-described phenomenon whereby the investigator overestimates the number of potential participants available to meet the inclusion criteria. This so-called funnel-effect was partly encountered in our selection process. A review of the veteran population with DFUs seemed to be more than adequate to fulfill the sample size; however, some important participant-related factors also played a substantial role.
In addition, the Veterans’ Affairs network centralizes health information, making it readily available to all providers participating in their care. As a result, patients with diabetes mellitus typically are seen by a primary care physician along with an endocrinologist, a diabetic nurse, and/or a dietician. Despite the collaboration with an interdisciplinary team, the glycemic control of the participants remains an issue along with other psychosocial factors that are deterrents in patient compliance. As a result, patients with poorly controlled diabetes and an HbA1C level above 10% (and less than 12%) of total hemoglobin who were initially excluded from the study were reincluded after modifying the inclusion criteria. Some patients were interested in joining the study, but physical limitations (eg, impaired mobility) prompted their decision not to join the trial, even though they met all the inclusion criteria.
As far as research-related factors that could affect participation, it is notable that most of the patients were retired; thus, the interventions did not cause additional burden of taking time off from work or loss of productivity. Although randomization could be a deterrent in many clinical trials, the majority of patients were willing to participate without demanding to be assigned to a particular treatment group.
There are many factors that are intertwined and can lead to enrollment and/or attrition rates. It was critical for our team to make some adjustment without compromising the controlled nature of a randomized trial.
Acknowledgment
The authors wish to acknowledge Huong Le, DPM, MPH, who was the coauthor of the study protocol.
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771.
- Gurtner GC, Werner S, Barrandon Y, et al. Wound repair and regeneration. Nature. 2008;453:314-321.
- Falanga V. Wound healing and its impairment in the diabetic foot. Lancet. 2005;366:1736-1743.
- Boulton AJ. The diabetic foot: grand overview, epidemiology and pathogenesis. Diabetes Metab Res Rev. 2008;24(suppl 1):S3-S6.
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293:217-228.
- Vuorisalo S, Venermo M, Lepäntalo M. Treatment of diabetic foot ulcers. J Cardiovasc Surg (Torino). 2009;50:275-291.
- Meijer JW, Trip J, Jaegers SM, et al. Quality of life in patients with diabetic foot ulcers. Disabil Rehabil. 2001;23:336-340.
- Santema TB, Poyck PP, Ubbink DT. Skin grafting and tissue replacement for treating foot ulcers in people with diabetes. Cochrane Database Syst Rev. 2016;2:CD011255.
- Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. a meta-analysis. Diabetes Care. 1999;22:692-695.
- Cavanagh P, Attinger C, Abbas Z, et al. Cost of treating diabetic foot ulcers in five different countries. Diabetes Metab Res Rev. 2012;2(suppl 1):107-111.
- Panuncialman J, Falanga V. The science of wound bed preparation. Surg Clin North Am. 2009;89:611-626.
- Lev-Tov H, Li CS, Dahle S, et al. Cellular versus acellular matrix devices in treatment of diabetic foot ulcers: study protocol for a comparative efficacy randomized controlled trial. Trials. 2013;14:8.
- Gentzkow GD, Iwasaki SD, Hershon KS, et al. Use of dermagraft, a cultured human dermis, to treat diabetic foot ulcers. Diabetes Care. 1996;19:350-354.
- Marston WA, Hanft J, Norwood P, et al; Dermagraft Diabetic Foot Ulcer Study Group. The efficacy and safety of Dermagraft in improving the healing of chronic diabetic foot ulcers: results of a prospective randomized trial. Diabetes Care. 2003;26:1701-1705.
- 2016 Dermagraft® Medicare Product and Related Procedure Payment. http://www.dermagraft.com/wp-content/uploads/sites/1/Dermagraft_Hotsheet%202016%20Q1%20HOSPITAL_FINAL.pdf. Accessed November 23, 2017.
- Oasis® Wound Matrix. http://www.oasiswoundmatrix.com/aboutowm. Accessed November 23, 2017.
- Niezgoda JA, Van Gils CC, Frykberg RG, et al. Randomized clinical trial comparing OASIS Wound Matrix to Regranex Gel for diabetic ulcers. Adv Skin Wound Care. 2005;18(5, pt 1):258-266.
- Torgerson JS, Arlinger K, Käppi M, et al. Principles for enhanced recruitment of subjects in a large clinical trial. the XENDOS (XENical in the prevention of Diabetes in Obese Subjects) study experience. Controlled Clin Trials. 2001;22:515-525.
- Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17:763-771.
- Gurtner GC, Werner S, Barrandon Y, et al. Wound repair and regeneration. Nature. 2008;453:314-321.
- Falanga V. Wound healing and its impairment in the diabetic foot. Lancet. 2005;366:1736-1743.
- Boulton AJ. The diabetic foot: grand overview, epidemiology and pathogenesis. Diabetes Metab Res Rev. 2008;24(suppl 1):S3-S6.
- Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293:217-228.
- Vuorisalo S, Venermo M, Lepäntalo M. Treatment of diabetic foot ulcers. J Cardiovasc Surg (Torino). 2009;50:275-291.
- Meijer JW, Trip J, Jaegers SM, et al. Quality of life in patients with diabetic foot ulcers. Disabil Rehabil. 2001;23:336-340.
- Santema TB, Poyck PP, Ubbink DT. Skin grafting and tissue replacement for treating foot ulcers in people with diabetes. Cochrane Database Syst Rev. 2016;2:CD011255.
- Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. a meta-analysis. Diabetes Care. 1999;22:692-695.
- Cavanagh P, Attinger C, Abbas Z, et al. Cost of treating diabetic foot ulcers in five different countries. Diabetes Metab Res Rev. 2012;2(suppl 1):107-111.
- Panuncialman J, Falanga V. The science of wound bed preparation. Surg Clin North Am. 2009;89:611-626.
- Lev-Tov H, Li CS, Dahle S, et al. Cellular versus acellular matrix devices in treatment of diabetic foot ulcers: study protocol for a comparative efficacy randomized controlled trial. Trials. 2013;14:8.
- Gentzkow GD, Iwasaki SD, Hershon KS, et al. Use of dermagraft, a cultured human dermis, to treat diabetic foot ulcers. Diabetes Care. 1996;19:350-354.
- Marston WA, Hanft J, Norwood P, et al; Dermagraft Diabetic Foot Ulcer Study Group. The efficacy and safety of Dermagraft in improving the healing of chronic diabetic foot ulcers: results of a prospective randomized trial. Diabetes Care. 2003;26:1701-1705.
- 2016 Dermagraft® Medicare Product and Related Procedure Payment. http://www.dermagraft.com/wp-content/uploads/sites/1/Dermagraft_Hotsheet%202016%20Q1%20HOSPITAL_FINAL.pdf. Accessed November 23, 2017.
- Oasis® Wound Matrix. http://www.oasiswoundmatrix.com/aboutowm. Accessed November 23, 2017.
- Niezgoda JA, Van Gils CC, Frykberg RG, et al. Randomized clinical trial comparing OASIS Wound Matrix to Regranex Gel for diabetic ulcers. Adv Skin Wound Care. 2005;18(5, pt 1):258-266.
- Torgerson JS, Arlinger K, Käppi M, et al. Principles for enhanced recruitment of subjects in a large clinical trial. the XENDOS (XENical in the prevention of Diabetes in Obese Subjects) study experience. Controlled Clin Trials. 2001;22:515-525.
Resident Pearl
- Deciding on the appropriate wound care regimen for diabetic foot ulcers is difficult given the vast amount of wound products on the market. This head-to-head clinical trial compared the use of an expensive cellular matrix and an inexpensive acellular matrix relative to the standard of care. We hope that this study will help to guide therapy based on cost-effectiveness of wound adjuncts without compromising patient care.

Eating disorders over the holidays
For many, the holiday season is a time to celebrate, relax, and enjoy the company of family. Much of this celebrating centers on eating and food. Historically, eating disorders were associated with young, straight, cisgender, white females. Data collected over the past 15 years suggest that eating disorders can affect youth of all ethnicities and genders.

Below are some tips from the National Eating Disorder Association that may be helpful for youth struggling with an eating disorder over the holiday season:
• Eat regularly and in a consistent pattern. Avoid skipping meals or restricting intake in preparation for a holiday meal.
• Discuss any anticipated struggles around food or family with your parents, therapist, health care provider, dietitian, or other members of your support group. This can allow you to plan ahead for any challenges that may arise, and could prevent potential negative or harmful coping behaviors

• Consider choosing a loved one to be your “reality check” with food, to either help fix a plate for you or to give you sound feedback on the food portion sizes you make for yourself.
• Have a game plan before you go to a holiday event. Know who your support people are and how you’ll recognize when it may be time to make a quick exit and get connected with needed support.
• Avoid overextending yourself. A lower stress level can decrease the need to turn to eating-disordered behaviors or other unhelpful coping strategies.
• Work on being flexible in your thoughts. Learn to be flexible when setting guidelines for yourself and expectations of yourself and others. Strive to be flexible in what you can eat during the holidays. Take a holiday from self-imposed criticism, rigidity, and perfectionism.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus. She said she had no relevant financial disclosures. Email her at [email protected].
Resources
National Eating Disorders Association: www.nationaleatingdisorders.org
“Body image and eating disorders among lesbian, gay, bisexual, and transgender youth” (Pediatr Clin North Am. 2016 Dec;63[6]:1079-90.
References
1. Prev Chronic Dis. 2008 Oct;5(4):A114.
2. Arch Gen Psychiatry. 2011 Jul;68(7):714-23.
3. Pediatr Clin North Am. 2016 Dec;63(6):1079-90.
4. Curr Psychiatry Rep. 2012 Aug;14(4):391-7.
5. J Adolesc Health. 2015 Aug;57(2):144-9.
6. Am J Public Health. 2013 Feb;103(2):e16-22.
7. J Adolesc Health. 2009 Sep;45(3):238-45.
For many, the holiday season is a time to celebrate, relax, and enjoy the company of family. Much of this celebrating centers on eating and food. Historically, eating disorders were associated with young, straight, cisgender, white females. Data collected over the past 15 years suggest that eating disorders can affect youth of all ethnicities and genders.
Below are some tips from the National Eating Disorder Association that may be helpful for youth struggling with an eating disorder over the holiday season:
• Eat regularly and in a consistent pattern. Avoid skipping meals or restricting intake in preparation for a holiday meal.
• Discuss any anticipated struggles around food or family with your parents, therapist, health care provider, dietitian, or other members of your support group. This can allow you to plan ahead for any challenges that may arise, and could prevent potential negative or harmful coping behaviors
• Consider choosing a loved one to be your “reality check” with food, to either help fix a plate for you or to give you sound feedback on the food portion sizes you make for yourself.
• Have a game plan before you go to a holiday event. Know who your support people are and how you’ll recognize when it may be time to make a quick exit and get connected with needed support.
• Avoid overextending yourself. A lower stress level can decrease the need to turn to eating-disordered behaviors or other unhelpful coping strategies.
• Work on being flexible in your thoughts. Learn to be flexible when setting guidelines for yourself and expectations of yourself and others. Strive to be flexible in what you can eat during the holidays. Take a holiday from self-imposed criticism, rigidity, and perfectionism.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus. She said she had no relevant financial disclosures. Email her at [email protected].
Resources
National Eating Disorders Association: www.nationaleatingdisorders.org
“Body image and eating disorders among lesbian, gay, bisexual, and transgender youth” (Pediatr Clin North Am. 2016 Dec;63[6]:1079-90.
References
1. Prev Chronic Dis. 2008 Oct;5(4):A114.
2. Arch Gen Psychiatry. 2011 Jul;68(7):714-23.
3. Pediatr Clin North Am. 2016 Dec;63(6):1079-90.
4. Curr Psychiatry Rep. 2012 Aug;14(4):391-7.
5. J Adolesc Health. 2015 Aug;57(2):144-9.
6. Am J Public Health. 2013 Feb;103(2):e16-22.
7. J Adolesc Health. 2009 Sep;45(3):238-45.
For many, the holiday season is a time to celebrate, relax, and enjoy the company of family. Much of this celebrating centers on eating and food. Historically, eating disorders were associated with young, straight, cisgender, white females. Data collected over the past 15 years suggest that eating disorders can affect youth of all ethnicities and genders.
Below are some tips from the National Eating Disorder Association that may be helpful for youth struggling with an eating disorder over the holiday season:
• Eat regularly and in a consistent pattern. Avoid skipping meals or restricting intake in preparation for a holiday meal.
• Discuss any anticipated struggles around food or family with your parents, therapist, health care provider, dietitian, or other members of your support group. This can allow you to plan ahead for any challenges that may arise, and could prevent potential negative or harmful coping behaviors
• Consider choosing a loved one to be your “reality check” with food, to either help fix a plate for you or to give you sound feedback on the food portion sizes you make for yourself.
• Have a game plan before you go to a holiday event. Know who your support people are and how you’ll recognize when it may be time to make a quick exit and get connected with needed support.
• Avoid overextending yourself. A lower stress level can decrease the need to turn to eating-disordered behaviors or other unhelpful coping strategies.
• Work on being flexible in your thoughts. Learn to be flexible when setting guidelines for yourself and expectations of yourself and others. Strive to be flexible in what you can eat during the holidays. Take a holiday from self-imposed criticism, rigidity, and perfectionism.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus. She said she had no relevant financial disclosures. Email her at [email protected].
Resources
National Eating Disorders Association: www.nationaleatingdisorders.org
“Body image and eating disorders among lesbian, gay, bisexual, and transgender youth” (Pediatr Clin North Am. 2016 Dec;63[6]:1079-90.
References
1. Prev Chronic Dis. 2008 Oct;5(4):A114.
2. Arch Gen Psychiatry. 2011 Jul;68(7):714-23.
3. Pediatr Clin North Am. 2016 Dec;63(6):1079-90.
4. Curr Psychiatry Rep. 2012 Aug;14(4):391-7.
5. J Adolesc Health. 2015 Aug;57(2):144-9.
6. Am J Public Health. 2013 Feb;103(2):e16-22.
7. J Adolesc Health. 2009 Sep;45(3):238-45.
Double Vision From a Rare Gastrointestinal Tumor
A 78-year-old man with a history of benign prostatic hyperplasia had double vision for 7 weeks. He also had pain in the right side of the face, altered taste, headaches that were worse when he was lying down, and lower abdominal lymphadenopathy.
His clinicians, at Brigham and Women’s Hospital in Boston, Massachusetts, say neurological examination revealed palsies of the right V, VI, VII, and XII cranial nerves. Magnetic resonance imaging revealed a clival mass and multiple lesions in the vertebrae. Radionuclide studies showed extensive tumor burden in the patient’s liver and peritoneum.
Because it is the most common cause of clival metastases, the clinicians initially suspected prostate cancer was the source of the symptoms. Moreover, the patient’s prostate-specific antigen was modestly elevated, a finding the clinicians called a red herring. The patient was instead diagnosed with a clival tumor, which is extremely rare—and made even more rare due to upper gastrointestinal (GI), the clinicians say. Only 5 cases have been reported of upper GI malignancy with clival metastasis.
Related: Cancer Prevention and Gastrointestinal Risk
The clivus is a bony structure located where the occipital and sphenoid bones meet, close to the long course of the abducens nerve. Double vision, caused by palsy at that nerve, is a prominent sign of a clival lesion, seen in > 40% of cases, the clinicians note. They suggest considering clival pathology as the cause of an abducens palsy or multiple cranial neuropathies.
The patient underwent several cycles of radiation therapy but ultimately decided on hospice care.
Source:
Lee C, Thon JM, Dhand A. BMJ Case Rep. 2017;2017: pii: bcr-2017-222725
doi: 10.1136/bcr-2017-222725.
A 78-year-old man with a history of benign prostatic hyperplasia had double vision for 7 weeks. He also had pain in the right side of the face, altered taste, headaches that were worse when he was lying down, and lower abdominal lymphadenopathy.
His clinicians, at Brigham and Women’s Hospital in Boston, Massachusetts, say neurological examination revealed palsies of the right V, VI, VII, and XII cranial nerves. Magnetic resonance imaging revealed a clival mass and multiple lesions in the vertebrae. Radionuclide studies showed extensive tumor burden in the patient’s liver and peritoneum.
Because it is the most common cause of clival metastases, the clinicians initially suspected prostate cancer was the source of the symptoms. Moreover, the patient’s prostate-specific antigen was modestly elevated, a finding the clinicians called a red herring. The patient was instead diagnosed with a clival tumor, which is extremely rare—and made even more rare due to upper gastrointestinal (GI), the clinicians say. Only 5 cases have been reported of upper GI malignancy with clival metastasis.
Related: Cancer Prevention and Gastrointestinal Risk
The clivus is a bony structure located where the occipital and sphenoid bones meet, close to the long course of the abducens nerve. Double vision, caused by palsy at that nerve, is a prominent sign of a clival lesion, seen in > 40% of cases, the clinicians note. They suggest considering clival pathology as the cause of an abducens palsy or multiple cranial neuropathies.
The patient underwent several cycles of radiation therapy but ultimately decided on hospice care.
Source:
Lee C, Thon JM, Dhand A. BMJ Case Rep. 2017;2017: pii: bcr-2017-222725
doi: 10.1136/bcr-2017-222725.
A 78-year-old man with a history of benign prostatic hyperplasia had double vision for 7 weeks. He also had pain in the right side of the face, altered taste, headaches that were worse when he was lying down, and lower abdominal lymphadenopathy.
His clinicians, at Brigham and Women’s Hospital in Boston, Massachusetts, say neurological examination revealed palsies of the right V, VI, VII, and XII cranial nerves. Magnetic resonance imaging revealed a clival mass and multiple lesions in the vertebrae. Radionuclide studies showed extensive tumor burden in the patient’s liver and peritoneum.
Because it is the most common cause of clival metastases, the clinicians initially suspected prostate cancer was the source of the symptoms. Moreover, the patient’s prostate-specific antigen was modestly elevated, a finding the clinicians called a red herring. The patient was instead diagnosed with a clival tumor, which is extremely rare—and made even more rare due to upper gastrointestinal (GI), the clinicians say. Only 5 cases have been reported of upper GI malignancy with clival metastasis.
Related: Cancer Prevention and Gastrointestinal Risk
The clivus is a bony structure located where the occipital and sphenoid bones meet, close to the long course of the abducens nerve. Double vision, caused by palsy at that nerve, is a prominent sign of a clival lesion, seen in > 40% of cases, the clinicians note. They suggest considering clival pathology as the cause of an abducens palsy or multiple cranial neuropathies.
The patient underwent several cycles of radiation therapy but ultimately decided on hospice care.
Source:
Lee C, Thon JM, Dhand A. BMJ Case Rep. 2017;2017: pii: bcr-2017-222725
doi: 10.1136/bcr-2017-222725.
Study reveals potential target for AML treatment

New research has revealed a potential therapeutic target for acute myeloid leukemia (AML)—the methyl transferase enzyme METTL3.
Researchers found that inhibiting METTL3 destroys human and mouse AML cells without harming non-leukemic blood cells.
The team also discovered why METTL3 is required for AML cell survival by deciphering the mechanism it uses to regulate several other leukemia genes.
The researchers described this work in Nature.
“New treatments for AML are desperately needed, and we have been looking for genes that would be good drug targets,” said study author Tony Kouzarides, PhD, of University of Cambridge in the UK.
“We identified the methyl transferase enzyme METTL3 as a highly viable target against AML. Our study will inspire pharmaceutical efforts to find drugs that specifically inhibit METTL3 to treat AML.”
In their attempt to find therapeutic targets for AML, Dr Kouzarides and his colleagues used CRISPR-Cas9 to screen AML cells for vulnerable points.
The researchers created mouse leukemia cells with mutations in genes that may be targeted in human AML cells and systematically tested each gene, finding which were essential for AML survival.
The team ended up with 46 likely candidate genes, many of which produce proteins that could modify RNA. Among these, METTL3 was one of the genes with the strongest effect.
Experiments revealed that METTL3 was essential for the survival of AML cells, but it was not required for healthy blood cells.
Having found a potential target in METTL3, the researchers investigated how it worked.
They discovered that the protein produced by METTL3 bound to the beginning of 126 different genes, including several required for AML cell survival.
As RNAs were produced, the METTL3 protein added methyl groups to their middle section, something which had not been previously observed. These middle methyl groups increased the ability of the RNAs to be translated into proteins.
The researchers then found that when METTL3 was inhibited, no methyl groups were added to the RNA. This prevented the production of their essential proteins, so the AML cells started dying.
“This study uncovered an entirely new mechanism of gene regulation in AML that operates through modifications of RNA,” said study author Konstantinos Tzelepis, PhD, of Wellcome Trust Sanger Institute in Cambridge, UK.
“We discovered that inhibiting the methyl transferase activity of METTL3 would stop the translation of a whole set of proteins that the leukemia needs. This mechanism shows that a drug to inhibit methylation could be effective against AML without affecting normal cells.” ![]()
New research has revealed a potential therapeutic target for acute myeloid leukemia (AML)—the methyl transferase enzyme METTL3.
Researchers found that inhibiting METTL3 destroys human and mouse AML cells without harming non-leukemic blood cells.
The team also discovered why METTL3 is required for AML cell survival by deciphering the mechanism it uses to regulate several other leukemia genes.
The researchers described this work in Nature.
“New treatments for AML are desperately needed, and we have been looking for genes that would be good drug targets,” said study author Tony Kouzarides, PhD, of University of Cambridge in the UK.
“We identified the methyl transferase enzyme METTL3 as a highly viable target against AML. Our study will inspire pharmaceutical efforts to find drugs that specifically inhibit METTL3 to treat AML.”
In their attempt to find therapeutic targets for AML, Dr Kouzarides and his colleagues used CRISPR-Cas9 to screen AML cells for vulnerable points.
The researchers created mouse leukemia cells with mutations in genes that may be targeted in human AML cells and systematically tested each gene, finding which were essential for AML survival.
The team ended up with 46 likely candidate genes, many of which produce proteins that could modify RNA. Among these, METTL3 was one of the genes with the strongest effect.
Experiments revealed that METTL3 was essential for the survival of AML cells, but it was not required for healthy blood cells.
Having found a potential target in METTL3, the researchers investigated how it worked.
They discovered that the protein produced by METTL3 bound to the beginning of 126 different genes, including several required for AML cell survival.
As RNAs were produced, the METTL3 protein added methyl groups to their middle section, something which had not been previously observed. These middle methyl groups increased the ability of the RNAs to be translated into proteins.
The researchers then found that when METTL3 was inhibited, no methyl groups were added to the RNA. This prevented the production of their essential proteins, so the AML cells started dying.
“This study uncovered an entirely new mechanism of gene regulation in AML that operates through modifications of RNA,” said study author Konstantinos Tzelepis, PhD, of Wellcome Trust Sanger Institute in Cambridge, UK.
“We discovered that inhibiting the methyl transferase activity of METTL3 would stop the translation of a whole set of proteins that the leukemia needs. This mechanism shows that a drug to inhibit methylation could be effective against AML without affecting normal cells.” ![]()
New research has revealed a potential therapeutic target for acute myeloid leukemia (AML)—the methyl transferase enzyme METTL3.
Researchers found that inhibiting METTL3 destroys human and mouse AML cells without harming non-leukemic blood cells.
The team also discovered why METTL3 is required for AML cell survival by deciphering the mechanism it uses to regulate several other leukemia genes.
The researchers described this work in Nature.
“New treatments for AML are desperately needed, and we have been looking for genes that would be good drug targets,” said study author Tony Kouzarides, PhD, of University of Cambridge in the UK.
“We identified the methyl transferase enzyme METTL3 as a highly viable target against AML. Our study will inspire pharmaceutical efforts to find drugs that specifically inhibit METTL3 to treat AML.”
In their attempt to find therapeutic targets for AML, Dr Kouzarides and his colleagues used CRISPR-Cas9 to screen AML cells for vulnerable points.
The researchers created mouse leukemia cells with mutations in genes that may be targeted in human AML cells and systematically tested each gene, finding which were essential for AML survival.
The team ended up with 46 likely candidate genes, many of which produce proteins that could modify RNA. Among these, METTL3 was one of the genes with the strongest effect.
Experiments revealed that METTL3 was essential for the survival of AML cells, but it was not required for healthy blood cells.
Having found a potential target in METTL3, the researchers investigated how it worked.
They discovered that the protein produced by METTL3 bound to the beginning of 126 different genes, including several required for AML cell survival.
As RNAs were produced, the METTL3 protein added methyl groups to their middle section, something which had not been previously observed. These middle methyl groups increased the ability of the RNAs to be translated into proteins.
The researchers then found that when METTL3 was inhibited, no methyl groups were added to the RNA. This prevented the production of their essential proteins, so the AML cells started dying.
“This study uncovered an entirely new mechanism of gene regulation in AML that operates through modifications of RNA,” said study author Konstantinos Tzelepis, PhD, of Wellcome Trust Sanger Institute in Cambridge, UK.
“We discovered that inhibiting the methyl transferase activity of METTL3 would stop the translation of a whole set of proteins that the leukemia needs. This mechanism shows that a drug to inhibit methylation could be effective against AML without affecting normal cells.” ![]()
Inhibitor exhibits activity against range of lymphomas

Preclinical research suggests the dual PI3K/mTOR inhibitor PQR309 has activity against several types of lymphoma and works well in combination with other agents.
PQR309 exhibited anti-lymphoma activity as a single agent and in combination with venetoclax, panobinostat, ibrutinib, lenalidomide, ARV-825, marizomib, and rituximab.
PQR309 demonstrated greater activity against B-cell lymphoma than T-cell lymphoma, and the inhibitor was able to overcome both primary and acquired resistance to idelalisib.
Francesco Bertoni, MD, of the Institute of Oncology Research in Bellinzona, Switzerland, and his colleagues conducted this research and reported the results in Clinical Cancer Research.
The work was funded by PIQUR Therapeutics AG, the company developing PQR309, and some study authors are PIQUR employees.
The researchers tested PQR309 in 49 human lymphoma cell lines—7 activated B-cell-like (ABC) diffuse large B-cell lymphoma (DLBCL), 18 germinal center B-cell (GCB) DLBCL, 10 mantle cell lymphoma (MCL), 3 splenic marginal zone lymphoma (SMZL), 2 chronic lymphocytic leukemia (CLL), 4 Hodgkin lymphoma, and 5 anaplastic large-cell lymphoma (ALCL).
In most cell lines, PQR309 halted proliferation, mainly due to cell-cycle arrest with a block in G1. However, PQR309 induced apoptosis in 2 cell lines tested—SU-DHL-4 and TMD8.
The researchers noted that PQR309 was significantly more active in the B-cell lymphoma cell lines (DLBCL, MCL, CLL, and SMZL) than in the T-cell lymphoma cell line ALCL (P=0.028).
PQR309 exhibited similar activity in ABC and GCB DLBCL cell lines, de novo DLBCL, and DLBCL derived from transformed follicular lymphoma. TP53, MYC, and BCL2 status also had no significant effect on PQR309 activity.
The researchers compared cell lines that were very sensitive to PQR309 to those with low sensitivity to the drug and identified differences.
The team said that transcripts preferentially expressed in PQR309-sensitive cell lines were significantly enriched of genes involved in BCR pathway/signaling and BLIMP1 targets. Transcripts associated with less sensitive cell lines were enriched of members of proteasome pathway, response to unfolded proteins, MYC targets, XBP1 targets, genes downregulated by mTOR inhibitors, and genes involved in oxidative phosphorylation.
PQR309 demonstrated synergistic effects when combined with the BTK inhibitor ibrutinib, the immunomodulatory drug lenalidomide, the anti-CD20 monoclonal antibody rituximab, and the proteasome inhibitor marizomib.
PQR309 demonstrated synergistic or additive effects when combined with the BCL2 inhibitor venetoclax, the HDAC inhibitor panobinostat, and the PROTAC BET inhibitor ARV-825.
In addition, PQR309 was active in lymphoma cell lines with primary and secondary resistance to the PI3K inhibitor idelalisib.
The researchers believe the results of this study, together with ongoing clinical studies of PQR309, can lead to better treatments for lymphoma patients and better understanding of the mechanisms of anti-lymphoma agents. ![]()
Preclinical research suggests the dual PI3K/mTOR inhibitor PQR309 has activity against several types of lymphoma and works well in combination with other agents.
PQR309 exhibited anti-lymphoma activity as a single agent and in combination with venetoclax, panobinostat, ibrutinib, lenalidomide, ARV-825, marizomib, and rituximab.
PQR309 demonstrated greater activity against B-cell lymphoma than T-cell lymphoma, and the inhibitor was able to overcome both primary and acquired resistance to idelalisib.
Francesco Bertoni, MD, of the Institute of Oncology Research in Bellinzona, Switzerland, and his colleagues conducted this research and reported the results in Clinical Cancer Research.
The work was funded by PIQUR Therapeutics AG, the company developing PQR309, and some study authors are PIQUR employees.
The researchers tested PQR309 in 49 human lymphoma cell lines—7 activated B-cell-like (ABC) diffuse large B-cell lymphoma (DLBCL), 18 germinal center B-cell (GCB) DLBCL, 10 mantle cell lymphoma (MCL), 3 splenic marginal zone lymphoma (SMZL), 2 chronic lymphocytic leukemia (CLL), 4 Hodgkin lymphoma, and 5 anaplastic large-cell lymphoma (ALCL).
In most cell lines, PQR309 halted proliferation, mainly due to cell-cycle arrest with a block in G1. However, PQR309 induced apoptosis in 2 cell lines tested—SU-DHL-4 and TMD8.
The researchers noted that PQR309 was significantly more active in the B-cell lymphoma cell lines (DLBCL, MCL, CLL, and SMZL) than in the T-cell lymphoma cell line ALCL (P=0.028).
PQR309 exhibited similar activity in ABC and GCB DLBCL cell lines, de novo DLBCL, and DLBCL derived from transformed follicular lymphoma. TP53, MYC, and BCL2 status also had no significant effect on PQR309 activity.
The researchers compared cell lines that were very sensitive to PQR309 to those with low sensitivity to the drug and identified differences.
The team said that transcripts preferentially expressed in PQR309-sensitive cell lines were significantly enriched of genes involved in BCR pathway/signaling and BLIMP1 targets. Transcripts associated with less sensitive cell lines were enriched of members of proteasome pathway, response to unfolded proteins, MYC targets, XBP1 targets, genes downregulated by mTOR inhibitors, and genes involved in oxidative phosphorylation.
PQR309 demonstrated synergistic effects when combined with the BTK inhibitor ibrutinib, the immunomodulatory drug lenalidomide, the anti-CD20 monoclonal antibody rituximab, and the proteasome inhibitor marizomib.
PQR309 demonstrated synergistic or additive effects when combined with the BCL2 inhibitor venetoclax, the HDAC inhibitor panobinostat, and the PROTAC BET inhibitor ARV-825.
In addition, PQR309 was active in lymphoma cell lines with primary and secondary resistance to the PI3K inhibitor idelalisib.
The researchers believe the results of this study, together with ongoing clinical studies of PQR309, can lead to better treatments for lymphoma patients and better understanding of the mechanisms of anti-lymphoma agents. ![]()
Preclinical research suggests the dual PI3K/mTOR inhibitor PQR309 has activity against several types of lymphoma and works well in combination with other agents.
PQR309 exhibited anti-lymphoma activity as a single agent and in combination with venetoclax, panobinostat, ibrutinib, lenalidomide, ARV-825, marizomib, and rituximab.
PQR309 demonstrated greater activity against B-cell lymphoma than T-cell lymphoma, and the inhibitor was able to overcome both primary and acquired resistance to idelalisib.
Francesco Bertoni, MD, of the Institute of Oncology Research in Bellinzona, Switzerland, and his colleagues conducted this research and reported the results in Clinical Cancer Research.
The work was funded by PIQUR Therapeutics AG, the company developing PQR309, and some study authors are PIQUR employees.
The researchers tested PQR309 in 49 human lymphoma cell lines—7 activated B-cell-like (ABC) diffuse large B-cell lymphoma (DLBCL), 18 germinal center B-cell (GCB) DLBCL, 10 mantle cell lymphoma (MCL), 3 splenic marginal zone lymphoma (SMZL), 2 chronic lymphocytic leukemia (CLL), 4 Hodgkin lymphoma, and 5 anaplastic large-cell lymphoma (ALCL).
In most cell lines, PQR309 halted proliferation, mainly due to cell-cycle arrest with a block in G1. However, PQR309 induced apoptosis in 2 cell lines tested—SU-DHL-4 and TMD8.
The researchers noted that PQR309 was significantly more active in the B-cell lymphoma cell lines (DLBCL, MCL, CLL, and SMZL) than in the T-cell lymphoma cell line ALCL (P=0.028).
PQR309 exhibited similar activity in ABC and GCB DLBCL cell lines, de novo DLBCL, and DLBCL derived from transformed follicular lymphoma. TP53, MYC, and BCL2 status also had no significant effect on PQR309 activity.
The researchers compared cell lines that were very sensitive to PQR309 to those with low sensitivity to the drug and identified differences.
The team said that transcripts preferentially expressed in PQR309-sensitive cell lines were significantly enriched of genes involved in BCR pathway/signaling and BLIMP1 targets. Transcripts associated with less sensitive cell lines were enriched of members of proteasome pathway, response to unfolded proteins, MYC targets, XBP1 targets, genes downregulated by mTOR inhibitors, and genes involved in oxidative phosphorylation.
PQR309 demonstrated synergistic effects when combined with the BTK inhibitor ibrutinib, the immunomodulatory drug lenalidomide, the anti-CD20 monoclonal antibody rituximab, and the proteasome inhibitor marizomib.
PQR309 demonstrated synergistic or additive effects when combined with the BCL2 inhibitor venetoclax, the HDAC inhibitor panobinostat, and the PROTAC BET inhibitor ARV-825.
In addition, PQR309 was active in lymphoma cell lines with primary and secondary resistance to the PI3K inhibitor idelalisib.
The researchers believe the results of this study, together with ongoing clinical studies of PQR309, can lead to better treatments for lymphoma patients and better understanding of the mechanisms of anti-lymphoma agents. ![]()
FDA grants drug orphan designation for AML, MDS

The US Food and Drug Administration (FDA) has granted orphan drug designation to AMV564, a CD33/CD3 bispecific antibody, for the treatment of acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS).
AMV564 is a T-cell engager, derived from human protein sequences, that binds both CD33 and CD3 to mediate T-cell directed lysis of CD33-positive cancer cells.
Amphivena Therapeutics Inc., is currently conducting a phase 1 trial of AMV564 in relapsed or refractory AML. The company plans to launch a phase 1 trial in patients with MDS in early 2018.
According to Amphivena, AMV564 has demonstrated “potent activity” in AML patient samples, and that activity was independent of CD33 expression level, disease stage, and cytogenetic risk.
AMV564 also eliminated nearly all blasts from the bone marrow and spleen in a stringent AML patient-derived xenograft murine model.
In addition, Amphivena established a therapeutic window for AMV564 in cynomolgus monkeys, with rapid and sustained elimination of CD33-expressing cells during AMV564 dosing and rapid hematopoietic recovery following dosing.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to AMV564, a CD33/CD3 bispecific antibody, for the treatment of acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS).
AMV564 is a T-cell engager, derived from human protein sequences, that binds both CD33 and CD3 to mediate T-cell directed lysis of CD33-positive cancer cells.
Amphivena Therapeutics Inc., is currently conducting a phase 1 trial of AMV564 in relapsed or refractory AML. The company plans to launch a phase 1 trial in patients with MDS in early 2018.
According to Amphivena, AMV564 has demonstrated “potent activity” in AML patient samples, and that activity was independent of CD33 expression level, disease stage, and cytogenetic risk.
AMV564 also eliminated nearly all blasts from the bone marrow and spleen in a stringent AML patient-derived xenograft murine model.
In addition, Amphivena established a therapeutic window for AMV564 in cynomolgus monkeys, with rapid and sustained elimination of CD33-expressing cells during AMV564 dosing and rapid hematopoietic recovery following dosing.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to AMV564, a CD33/CD3 bispecific antibody, for the treatment of acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS).
AMV564 is a T-cell engager, derived from human protein sequences, that binds both CD33 and CD3 to mediate T-cell directed lysis of CD33-positive cancer cells.
Amphivena Therapeutics Inc., is currently conducting a phase 1 trial of AMV564 in relapsed or refractory AML. The company plans to launch a phase 1 trial in patients with MDS in early 2018.
According to Amphivena, AMV564 has demonstrated “potent activity” in AML patient samples, and that activity was independent of CD33 expression level, disease stage, and cytogenetic risk.
AMV564 also eliminated nearly all blasts from the bone marrow and spleen in a stringent AML patient-derived xenograft murine model.
In addition, Amphivena established a therapeutic window for AMV564 in cynomolgus monkeys, with rapid and sustained elimination of CD33-expressing cells during AMV564 dosing and rapid hematopoietic recovery following dosing.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
Prenatal vitamin D supplementation plagued by lack of evidence
Prenatal vitamin D supplementation may reduce the risk of small for gestational age and early wheeze in infants, but most of the evidence comes from small, low-quality trials, according to a systematic review and meta-analysis.
Researchers reported on a meta-analysis of 43 randomized controlled trials, involving 8,406 participants, which examined the effects of vitamin D supplementation during pregnancy (BMJ. 2017;359:j5237. doi: 10.1136/bmj.j5237).
The most commonly reported outcomes involved fetal growth and preterm birth. A pooling of 37 comparisons suggested that vitamin D supplementation increased mean birth weight by an average of 58 g, compared with low-dose vitamin D, no vitamin D, or placebo.
Two high-quality trials using a regular dose of vitamin D, which were conducted in high-income countries, found a 19% reduction in the risk of persistent/recurrent wheeze by age 3, which the authors said was consistent with other data suggesting a beneficial effect of vitamin D in adults with asthma. However, there were no other respiratory effects, such as on the risk of upper or lower respiratory tract infections.
There were few studies that reported on maternal clinical outcomes, and those that did showed no evidence of benefit.
“Though some observational studies have shown associations between maternal vitamin D deficiency and gestational diabetes and preeclampsia, we did not find robust corroborating evidence from randomised controlled trials,” wrote Daniel E. Roth, MD, and his colleagues at the Hospital for Sick Children, Toronto, and the University of Toronto.
They did report significantly higher maternal and cord blood concentrations of 25-hydroxyvitamin D in the intervention groups, compared with controls.
The median sample size of the studies was 133, and the researchers found that only 8 of the 43 trials had an overall low risk of bias. They also noted that there were wide variations in baseline maternal vitamin D levels.
“Though trials of prenatal vitamin D supplementation are being published at an accelerating pace, randomised controlled trials published up to 2017 were generally small, low quality, and rarely designed to examine clinical outcomes,” the researchers wrote.
The study was supported by the Hospital for Sick Children. No conflicts of interest were declared.
Prenatal vitamin D supplementation may reduce the risk of small for gestational age and early wheeze in infants, but most of the evidence comes from small, low-quality trials, according to a systematic review and meta-analysis.
Researchers reported on a meta-analysis of 43 randomized controlled trials, involving 8,406 participants, which examined the effects of vitamin D supplementation during pregnancy (BMJ. 2017;359:j5237. doi: 10.1136/bmj.j5237).
The most commonly reported outcomes involved fetal growth and preterm birth. A pooling of 37 comparisons suggested that vitamin D supplementation increased mean birth weight by an average of 58 g, compared with low-dose vitamin D, no vitamin D, or placebo.
Two high-quality trials using a regular dose of vitamin D, which were conducted in high-income countries, found a 19% reduction in the risk of persistent/recurrent wheeze by age 3, which the authors said was consistent with other data suggesting a beneficial effect of vitamin D in adults with asthma. However, there were no other respiratory effects, such as on the risk of upper or lower respiratory tract infections.
There were few studies that reported on maternal clinical outcomes, and those that did showed no evidence of benefit.
“Though some observational studies have shown associations between maternal vitamin D deficiency and gestational diabetes and preeclampsia, we did not find robust corroborating evidence from randomised controlled trials,” wrote Daniel E. Roth, MD, and his colleagues at the Hospital for Sick Children, Toronto, and the University of Toronto.
They did report significantly higher maternal and cord blood concentrations of 25-hydroxyvitamin D in the intervention groups, compared with controls.
The median sample size of the studies was 133, and the researchers found that only 8 of the 43 trials had an overall low risk of bias. They also noted that there were wide variations in baseline maternal vitamin D levels.
“Though trials of prenatal vitamin D supplementation are being published at an accelerating pace, randomised controlled trials published up to 2017 were generally small, low quality, and rarely designed to examine clinical outcomes,” the researchers wrote.
The study was supported by the Hospital for Sick Children. No conflicts of interest were declared.
Prenatal vitamin D supplementation may reduce the risk of small for gestational age and early wheeze in infants, but most of the evidence comes from small, low-quality trials, according to a systematic review and meta-analysis.
Researchers reported on a meta-analysis of 43 randomized controlled trials, involving 8,406 participants, which examined the effects of vitamin D supplementation during pregnancy (BMJ. 2017;359:j5237. doi: 10.1136/bmj.j5237).
The most commonly reported outcomes involved fetal growth and preterm birth. A pooling of 37 comparisons suggested that vitamin D supplementation increased mean birth weight by an average of 58 g, compared with low-dose vitamin D, no vitamin D, or placebo.
Two high-quality trials using a regular dose of vitamin D, which were conducted in high-income countries, found a 19% reduction in the risk of persistent/recurrent wheeze by age 3, which the authors said was consistent with other data suggesting a beneficial effect of vitamin D in adults with asthma. However, there were no other respiratory effects, such as on the risk of upper or lower respiratory tract infections.
There were few studies that reported on maternal clinical outcomes, and those that did showed no evidence of benefit.
“Though some observational studies have shown associations between maternal vitamin D deficiency and gestational diabetes and preeclampsia, we did not find robust corroborating evidence from randomised controlled trials,” wrote Daniel E. Roth, MD, and his colleagues at the Hospital for Sick Children, Toronto, and the University of Toronto.
They did report significantly higher maternal and cord blood concentrations of 25-hydroxyvitamin D in the intervention groups, compared with controls.
The median sample size of the studies was 133, and the researchers found that only 8 of the 43 trials had an overall low risk of bias. They also noted that there were wide variations in baseline maternal vitamin D levels.
“Though trials of prenatal vitamin D supplementation are being published at an accelerating pace, randomised controlled trials published up to 2017 were generally small, low quality, and rarely designed to examine clinical outcomes,” the researchers wrote.
The study was supported by the Hospital for Sick Children. No conflicts of interest were declared.
FROM BMJ
Key clinical point:
Major finding: Prenatal vitamin D supplementation is associated with a 40% reduction in the risk of having an SGA infant.
Data source: A systematic review and meta-analysis of 43 randomized controlled trials.
Disclosures: The study was supported by the Hospital for Sick Children, Toronto. No conflicts of interest were declared.
Drug prices a key focus of Senate HELP examination of Azar nomination
WASHINGTON Escalating drug prices topped the agenda as members of the Senate Health, Education, Labor & Pensions Committee interviewed Alex Azar regarding his nomination as secretary of the Department of Health & Human Services.
Mr. Azar, a former HHS deputy secretary and general counsel during the Bush Administration and a former president of Eli Lilly’s U.S. operations, outlined his priorities to the Senate HELP committee during the Nov. 29 hearing.

Drug prices were the focus of many senators’ questions, and while many contentious questions came from panel Democrats, Sen. Rand Paul (R-Ky.) signaled he was not yet on board with his approval for Mr. Azar’s nomination.
“I think many [Americans] perceive [that drug companies use] their economic might to manipulate the system to maximize profits,” Sen. Paul said. “It’s not like they are selling a cheaper product to more people. They are using government to maximize their profits. Do you acknowledge that, under the current system, Big Pharma uses their economic clout to manipulate the patent system to increase drug prices?”
“There are clearly abuses, Senator, in the system, and that is why one of the steps that I mentioned ... that I believe we have to go after, is the gaming of that,” Mr. Azar responded. He suggested that although Hatch-Waxman rules give innovators a time frame to exclusively sell products “there should be a certain moment” when full generic competition should begin.
Sen. Paul also challenged Mr. Azar on the notion of drug importation.
There has not been a successful path to certify that drugs being imported are “safe and reliable,” Mr. Azar noted.
Sen. Paul countered that “you would have to sit there and say that the European Union has unsafe drugs. It would be unsafe for Americans to buy drugs from the European Union or from Canada or Australia. It’s just frankly not true.”
Sen. Paul told Mr. Azar that if he cannot come up with a way to reimport drugs as a means of addressing the high cost of pharmaceuticals in the United States, “I can’t support you.”
Sen. Paul continued that a lot of people have talked about how they are going to change the system, particularly patent issues that stand in the way of generic competition, and “you’ve got some convincing to make me believe that you are going to represent the American people and not Big Pharma, and I know that’s insulting, and I don’t mean it to be because I am sure you are an honest and upright person. But we all have our doubts because Big Pharma manipulates the system to keep prices high. ... We’ve got to fix it. We can’t tepidly go at it. We have to really fix it, and you need to convince those of us who are skeptical that you will be part of fixing it and won’t be beholden to Big Pharma.”
Regarding his other priorities, Mr. Azar noted that, through his “experience helping to implement [Medicare] Part D and with my extensive knowledge of how insurance, manufacturers, pharmacy, and government programs work together, I believe I can bring the skills and experiences to the table that can help us address these issues, while still encouraging discovery so Americans have access to high-quality care.”
He called for making health care “more affordable, more available, and more tailored to what individuals want and need. … Under the status quo, premiums have been skyrocketing year after year, and choices have been dwindling. We must address these challenges for those who have insurance coverage and for those who have been pushed out or left out of the insurance market by the Affordable Care Act.”
Mr. Azar signaled that he will continue the push toward value-based care and will use the power of Medicare to lead the rest of the health care delivery system to follow suit.
“We can better channel the power of health information technology and leverage what is best in our programs and in the private competitive marketplace to ensure the individual patient is the center of decision making and his or her needs are being met with greater transparency and accountability.”
Regarding the opioid crisis, Mr. Azar said that “we must heed President Trump’s call to action and tackle the scourge of the opioid epidemic that is destroying so many individuals, families, and communities. We need aggressive prevention, education, regulatory, and enforcement efforts to stop overprescribing and overuse of these legal and illegal drugs. And we need compassionate treatment for those suffering from dependence and addiction.”
Mr. Azar also was challenged on women’s health issues, particularly the ability of employers to exclude health insurance coverage of contraception because of religious objections. He noted that there needs to be a balance between the medical needs of the patient and the rights of an organization to follow its conscience.
When queried about making contraception available over the counter, he noted that the regulations regarding OTC conversion are outdated, and he was encouraged that FDA Commissioner Scott Gottlieb, MD, is looking into that.
Mr. Azar also committed during the hearing to working with improving interoperability of electronic health records as well as working with physicians to reduce the associated documentation burden.
He voiced his support of reforming the Affordable Care Act, adding that, “if it remains the law, my goal is to implement a way that leads to affordable insurance, leads to choice of insurance that leads to real access and not a meaningless insurance care, and insurance that has the benefits that people want, not what we say in D.C. for them.”
He also expressed support for the use of block grants to help fund Medicaid.
Mr. Azar’s appearance before the HELP committee was a courtesy as the Senate Finance Committee holds jurisdiction over his nomination. No confirmation hearing had been scheduled at press time.
WASHINGTON Escalating drug prices topped the agenda as members of the Senate Health, Education, Labor & Pensions Committee interviewed Alex Azar regarding his nomination as secretary of the Department of Health & Human Services.
Mr. Azar, a former HHS deputy secretary and general counsel during the Bush Administration and a former president of Eli Lilly’s U.S. operations, outlined his priorities to the Senate HELP committee during the Nov. 29 hearing.
Drug prices were the focus of many senators’ questions, and while many contentious questions came from panel Democrats, Sen. Rand Paul (R-Ky.) signaled he was not yet on board with his approval for Mr. Azar’s nomination.
“I think many [Americans] perceive [that drug companies use] their economic might to manipulate the system to maximize profits,” Sen. Paul said. “It’s not like they are selling a cheaper product to more people. They are using government to maximize their profits. Do you acknowledge that, under the current system, Big Pharma uses their economic clout to manipulate the patent system to increase drug prices?”
“There are clearly abuses, Senator, in the system, and that is why one of the steps that I mentioned ... that I believe we have to go after, is the gaming of that,” Mr. Azar responded. He suggested that although Hatch-Waxman rules give innovators a time frame to exclusively sell products “there should be a certain moment” when full generic competition should begin.
Sen. Paul also challenged Mr. Azar on the notion of drug importation.
There has not been a successful path to certify that drugs being imported are “safe and reliable,” Mr. Azar noted.
Sen. Paul countered that “you would have to sit there and say that the European Union has unsafe drugs. It would be unsafe for Americans to buy drugs from the European Union or from Canada or Australia. It’s just frankly not true.”
Sen. Paul told Mr. Azar that if he cannot come up with a way to reimport drugs as a means of addressing the high cost of pharmaceuticals in the United States, “I can’t support you.”
Sen. Paul continued that a lot of people have talked about how they are going to change the system, particularly patent issues that stand in the way of generic competition, and “you’ve got some convincing to make me believe that you are going to represent the American people and not Big Pharma, and I know that’s insulting, and I don’t mean it to be because I am sure you are an honest and upright person. But we all have our doubts because Big Pharma manipulates the system to keep prices high. ... We’ve got to fix it. We can’t tepidly go at it. We have to really fix it, and you need to convince those of us who are skeptical that you will be part of fixing it and won’t be beholden to Big Pharma.”
Regarding his other priorities, Mr. Azar noted that, through his “experience helping to implement [Medicare] Part D and with my extensive knowledge of how insurance, manufacturers, pharmacy, and government programs work together, I believe I can bring the skills and experiences to the table that can help us address these issues, while still encouraging discovery so Americans have access to high-quality care.”
He called for making health care “more affordable, more available, and more tailored to what individuals want and need. … Under the status quo, premiums have been skyrocketing year after year, and choices have been dwindling. We must address these challenges for those who have insurance coverage and for those who have been pushed out or left out of the insurance market by the Affordable Care Act.”
Mr. Azar signaled that he will continue the push toward value-based care and will use the power of Medicare to lead the rest of the health care delivery system to follow suit.
“We can better channel the power of health information technology and leverage what is best in our programs and in the private competitive marketplace to ensure the individual patient is the center of decision making and his or her needs are being met with greater transparency and accountability.”
Regarding the opioid crisis, Mr. Azar said that “we must heed President Trump’s call to action and tackle the scourge of the opioid epidemic that is destroying so many individuals, families, and communities. We need aggressive prevention, education, regulatory, and enforcement efforts to stop overprescribing and overuse of these legal and illegal drugs. And we need compassionate treatment for those suffering from dependence and addiction.”
Mr. Azar also was challenged on women’s health issues, particularly the ability of employers to exclude health insurance coverage of contraception because of religious objections. He noted that there needs to be a balance between the medical needs of the patient and the rights of an organization to follow its conscience.
When queried about making contraception available over the counter, he noted that the regulations regarding OTC conversion are outdated, and he was encouraged that FDA Commissioner Scott Gottlieb, MD, is looking into that.
Mr. Azar also committed during the hearing to working with improving interoperability of electronic health records as well as working with physicians to reduce the associated documentation burden.
He voiced his support of reforming the Affordable Care Act, adding that, “if it remains the law, my goal is to implement a way that leads to affordable insurance, leads to choice of insurance that leads to real access and not a meaningless insurance care, and insurance that has the benefits that people want, not what we say in D.C. for them.”
He also expressed support for the use of block grants to help fund Medicaid.
Mr. Azar’s appearance before the HELP committee was a courtesy as the Senate Finance Committee holds jurisdiction over his nomination. No confirmation hearing had been scheduled at press time.
WASHINGTON Escalating drug prices topped the agenda as members of the Senate Health, Education, Labor & Pensions Committee interviewed Alex Azar regarding his nomination as secretary of the Department of Health & Human Services.
Mr. Azar, a former HHS deputy secretary and general counsel during the Bush Administration and a former president of Eli Lilly’s U.S. operations, outlined his priorities to the Senate HELP committee during the Nov. 29 hearing.
Drug prices were the focus of many senators’ questions, and while many contentious questions came from panel Democrats, Sen. Rand Paul (R-Ky.) signaled he was not yet on board with his approval for Mr. Azar’s nomination.
“I think many [Americans] perceive [that drug companies use] their economic might to manipulate the system to maximize profits,” Sen. Paul said. “It’s not like they are selling a cheaper product to more people. They are using government to maximize their profits. Do you acknowledge that, under the current system, Big Pharma uses their economic clout to manipulate the patent system to increase drug prices?”
“There are clearly abuses, Senator, in the system, and that is why one of the steps that I mentioned ... that I believe we have to go after, is the gaming of that,” Mr. Azar responded. He suggested that although Hatch-Waxman rules give innovators a time frame to exclusively sell products “there should be a certain moment” when full generic competition should begin.
Sen. Paul also challenged Mr. Azar on the notion of drug importation.
There has not been a successful path to certify that drugs being imported are “safe and reliable,” Mr. Azar noted.
Sen. Paul countered that “you would have to sit there and say that the European Union has unsafe drugs. It would be unsafe for Americans to buy drugs from the European Union or from Canada or Australia. It’s just frankly not true.”
Sen. Paul told Mr. Azar that if he cannot come up with a way to reimport drugs as a means of addressing the high cost of pharmaceuticals in the United States, “I can’t support you.”
Sen. Paul continued that a lot of people have talked about how they are going to change the system, particularly patent issues that stand in the way of generic competition, and “you’ve got some convincing to make me believe that you are going to represent the American people and not Big Pharma, and I know that’s insulting, and I don’t mean it to be because I am sure you are an honest and upright person. But we all have our doubts because Big Pharma manipulates the system to keep prices high. ... We’ve got to fix it. We can’t tepidly go at it. We have to really fix it, and you need to convince those of us who are skeptical that you will be part of fixing it and won’t be beholden to Big Pharma.”
Regarding his other priorities, Mr. Azar noted that, through his “experience helping to implement [Medicare] Part D and with my extensive knowledge of how insurance, manufacturers, pharmacy, and government programs work together, I believe I can bring the skills and experiences to the table that can help us address these issues, while still encouraging discovery so Americans have access to high-quality care.”
He called for making health care “more affordable, more available, and more tailored to what individuals want and need. … Under the status quo, premiums have been skyrocketing year after year, and choices have been dwindling. We must address these challenges for those who have insurance coverage and for those who have been pushed out or left out of the insurance market by the Affordable Care Act.”
Mr. Azar signaled that he will continue the push toward value-based care and will use the power of Medicare to lead the rest of the health care delivery system to follow suit.
“We can better channel the power of health information technology and leverage what is best in our programs and in the private competitive marketplace to ensure the individual patient is the center of decision making and his or her needs are being met with greater transparency and accountability.”
Regarding the opioid crisis, Mr. Azar said that “we must heed President Trump’s call to action and tackle the scourge of the opioid epidemic that is destroying so many individuals, families, and communities. We need aggressive prevention, education, regulatory, and enforcement efforts to stop overprescribing and overuse of these legal and illegal drugs. And we need compassionate treatment for those suffering from dependence and addiction.”
Mr. Azar also was challenged on women’s health issues, particularly the ability of employers to exclude health insurance coverage of contraception because of religious objections. He noted that there needs to be a balance between the medical needs of the patient and the rights of an organization to follow its conscience.
When queried about making contraception available over the counter, he noted that the regulations regarding OTC conversion are outdated, and he was encouraged that FDA Commissioner Scott Gottlieb, MD, is looking into that.
Mr. Azar also committed during the hearing to working with improving interoperability of electronic health records as well as working with physicians to reduce the associated documentation burden.
He voiced his support of reforming the Affordable Care Act, adding that, “if it remains the law, my goal is to implement a way that leads to affordable insurance, leads to choice of insurance that leads to real access and not a meaningless insurance care, and insurance that has the benefits that people want, not what we say in D.C. for them.”
He also expressed support for the use of block grants to help fund Medicaid.
Mr. Azar’s appearance before the HELP committee was a courtesy as the Senate Finance Committee holds jurisdiction over his nomination. No confirmation hearing had been scheduled at press time.
AT A SENATE HELP COMMITTEE HEARING