User login
Bevacizumab no better than placebo for epistaxis in HHT

of nasal spray
Bevacizumab nasal spray is no more effective than a placebo for reducing epistaxis caused by hereditary hemorrhagic telangiectasia (HHT), according to a study published in JAMA.
Researchers compared 3 different doses of bevacizumab to a sodium chloride placebo and found no significant difference between the treatment groups in the frequency or duration of epistaxis, the need for transfusion, or hemoglobin/ferritin levels.
Sophie Dupuis-Girod, MD, PhD, of the Hopital Femme-Mere-Enfants in Bron, France, and her colleagues conducted this trial, enrolling 80 patients with HHT and a history of epistaxis.
The patients were randomized to receive placebo (0.9% sodium chloride, n=21) or 1 of 3 doses of bevacizumab nasal spray.
Patients in the bevacizumab groups received 25 mg (n=20), 50 mg (n=20), or 75 mg (n=19) in 3 doses, 14 days apart, for a total treatment duration of 4 weeks, resulting in a total dose of 75 mg, 150 mg, or 225 mg.
Epistaxis duration
The researchers measured the mean monthly epistaxis duration at 3 months and found no significant difference between the placebo group and the bevacizumab groups (P=0.57). Likewise, there were no significant differences between the bevacizumab groups.
However, most of the groups experienced improvements in epistaxis duration after treatment.
The mean monthly epistaxis duration (in minutes) before treatment (from day −90 to day −1) and after treatment (from day 29 to day 118), respectively, was:
- 262.8 and 200.4 in the placebo group
- 285.5 and 259.2 in the 25 mg group
- 229.0 and 244.0 in the 50 mg group
- 272.9 and 215.0 in the 75 mg group.
Epistaxis frequency
There was no significant difference between the bevacizumab groups and the placebo group when it came to the number of epistaxis episodes (P=0.55). However, patients in all of the groups saw a reduction in episodes after treatment.
The mean number of epistaxis episodes before treatment (from day −90 to day −1) and after (from day 29 to day 118), respectively, were:
- 31.37 and 24.27 in the placebo group
- 30.99 and 23.13 in the 25 mg bevacizumab group
- 25.06 and 20.01 in the 50 mg bevacizumab group
- 27.84 and 24.35 in the 75 mg bevacizumab group.
Other outcomes
There was no significant difference between the bevacizumab groups and the placebo group regarding the number of red blood cell transfusions at 3 months (P=0.35) and 6 months (P=0.39), mean hemoglobin levels (P=0.66), and mean ferritin levels (P=0.86).
There were no adverse events (AEs) thought to be treatment-related. There were 161 AEs overall and no significant differences between the groups—47 AEs in the 25 mg bevacizumab group, 33 in the 50 mg bevacizumab group, 38 in the 75 mg bevacizumab group, and 43 in the placebo group.
After an interim analysis, an independent data monitoring committee recommended terminating this study early due to treatment futility. So the study was stopped before entering phase 3.
![]()
of nasal spray
Bevacizumab nasal spray is no more effective than a placebo for reducing epistaxis caused by hereditary hemorrhagic telangiectasia (HHT), according to a study published in JAMA.
Researchers compared 3 different doses of bevacizumab to a sodium chloride placebo and found no significant difference between the treatment groups in the frequency or duration of epistaxis, the need for transfusion, or hemoglobin/ferritin levels.
Sophie Dupuis-Girod, MD, PhD, of the Hopital Femme-Mere-Enfants in Bron, France, and her colleagues conducted this trial, enrolling 80 patients with HHT and a history of epistaxis.
The patients were randomized to receive placebo (0.9% sodium chloride, n=21) or 1 of 3 doses of bevacizumab nasal spray.
Patients in the bevacizumab groups received 25 mg (n=20), 50 mg (n=20), or 75 mg (n=19) in 3 doses, 14 days apart, for a total treatment duration of 4 weeks, resulting in a total dose of 75 mg, 150 mg, or 225 mg.
Epistaxis duration
The researchers measured the mean monthly epistaxis duration at 3 months and found no significant difference between the placebo group and the bevacizumab groups (P=0.57). Likewise, there were no significant differences between the bevacizumab groups.
However, most of the groups experienced improvements in epistaxis duration after treatment.
The mean monthly epistaxis duration (in minutes) before treatment (from day −90 to day −1) and after treatment (from day 29 to day 118), respectively, was:
- 262.8 and 200.4 in the placebo group
- 285.5 and 259.2 in the 25 mg group
- 229.0 and 244.0 in the 50 mg group
- 272.9 and 215.0 in the 75 mg group.
Epistaxis frequency
There was no significant difference between the bevacizumab groups and the placebo group when it came to the number of epistaxis episodes (P=0.55). However, patients in all of the groups saw a reduction in episodes after treatment.
The mean number of epistaxis episodes before treatment (from day −90 to day −1) and after (from day 29 to day 118), respectively, were:
- 31.37 and 24.27 in the placebo group
- 30.99 and 23.13 in the 25 mg bevacizumab group
- 25.06 and 20.01 in the 50 mg bevacizumab group
- 27.84 and 24.35 in the 75 mg bevacizumab group.
Other outcomes
There was no significant difference between the bevacizumab groups and the placebo group regarding the number of red blood cell transfusions at 3 months (P=0.35) and 6 months (P=0.39), mean hemoglobin levels (P=0.66), and mean ferritin levels (P=0.86).
There were no adverse events (AEs) thought to be treatment-related. There were 161 AEs overall and no significant differences between the groups—47 AEs in the 25 mg bevacizumab group, 33 in the 50 mg bevacizumab group, 38 in the 75 mg bevacizumab group, and 43 in the placebo group.
After an interim analysis, an independent data monitoring committee recommended terminating this study early due to treatment futility. So the study was stopped before entering phase 3.
![]()
of nasal spray
Bevacizumab nasal spray is no more effective than a placebo for reducing epistaxis caused by hereditary hemorrhagic telangiectasia (HHT), according to a study published in JAMA.
Researchers compared 3 different doses of bevacizumab to a sodium chloride placebo and found no significant difference between the treatment groups in the frequency or duration of epistaxis, the need for transfusion, or hemoglobin/ferritin levels.
Sophie Dupuis-Girod, MD, PhD, of the Hopital Femme-Mere-Enfants in Bron, France, and her colleagues conducted this trial, enrolling 80 patients with HHT and a history of epistaxis.
The patients were randomized to receive placebo (0.9% sodium chloride, n=21) or 1 of 3 doses of bevacizumab nasal spray.
Patients in the bevacizumab groups received 25 mg (n=20), 50 mg (n=20), or 75 mg (n=19) in 3 doses, 14 days apart, for a total treatment duration of 4 weeks, resulting in a total dose of 75 mg, 150 mg, or 225 mg.
Epistaxis duration
The researchers measured the mean monthly epistaxis duration at 3 months and found no significant difference between the placebo group and the bevacizumab groups (P=0.57). Likewise, there were no significant differences between the bevacizumab groups.
However, most of the groups experienced improvements in epistaxis duration after treatment.
The mean monthly epistaxis duration (in minutes) before treatment (from day −90 to day −1) and after treatment (from day 29 to day 118), respectively, was:
- 262.8 and 200.4 in the placebo group
- 285.5 and 259.2 in the 25 mg group
- 229.0 and 244.0 in the 50 mg group
- 272.9 and 215.0 in the 75 mg group.
Epistaxis frequency
There was no significant difference between the bevacizumab groups and the placebo group when it came to the number of epistaxis episodes (P=0.55). However, patients in all of the groups saw a reduction in episodes after treatment.
The mean number of epistaxis episodes before treatment (from day −90 to day −1) and after (from day 29 to day 118), respectively, were:
- 31.37 and 24.27 in the placebo group
- 30.99 and 23.13 in the 25 mg bevacizumab group
- 25.06 and 20.01 in the 50 mg bevacizumab group
- 27.84 and 24.35 in the 75 mg bevacizumab group.
Other outcomes
There was no significant difference between the bevacizumab groups and the placebo group regarding the number of red blood cell transfusions at 3 months (P=0.35) and 6 months (P=0.39), mean hemoglobin levels (P=0.66), and mean ferritin levels (P=0.86).
There were no adverse events (AEs) thought to be treatment-related. There were 161 AEs overall and no significant differences between the groups—47 AEs in the 25 mg bevacizumab group, 33 in the 50 mg bevacizumab group, 38 in the 75 mg bevacizumab group, and 43 in the placebo group.
After an interim analysis, an independent data monitoring committee recommended terminating this study early due to treatment futility. So the study was stopped before entering phase 3.
![]()
Improvements needed in SCD care, report says

Photo courtesy of St. Jude
Children’s Hospital
A new report suggests the current state of care for sickle cell disease (SCD) is inadequate, and improvements are needed.
The State of Sickle Cell Disease: 2016 Report outlines 4 main areas for improvement—SCD patients’ access to care, the training and education of healthcare professionals treating patients with SCD, research and clinical trials pertaining to SCD, and global health issues related to the disease.
The American Society of Hematology (ASH) published the report, with the endorsement of organizations in the SCD community.
The report includes statistics that highlight the need for improvements as well as future goals and recommended actions.
Access to care
The report states that more than 75% of adults with SCD who have frequent pain crises do not receive the recommended treatment, hydroxyurea.
One potential solution, according to the report, is to ensure that existing standard-of-care guidelines are being used. Another solution is to develop coordinated healthcare delivery models that ensure SCD patients can access quality care regardless of their age, location, and socioeconomic status.
“Not only are individuals with SCD burdened by the pain and disability that comes with a chronic condition, but they also have very few accessible treatment options due to our fragmented healthcare system,” said ASH President Charles S. Abrams, MD, of the University of Pennsylvania in Philadelphia.
Training and education
The report cites a national survey in which only 20.4% of family physicians said they felt comfortable treating SCD. And 69.4% of family physicians said clinical decision support tools would be useful for helping to guide their treatment decisions for SCD patients.
Therefore, the report recommends devising an “actionable plan” to educate healthcare providers about best practices in caring for SCD patients, developing clinical support tools, and encouraging medical trainees to pursue careers in SCD care, among other solutions.
“There are many unique challenges that people with SCD face,” said ASH Vice President Alexis Thompson, MD, of the Ann and Robert H. Lurie Children’s Hospital of Chicago in Illinois.
“For example, the transition from pediatric to adult care can be especially difficult, and many people struggle to find healthcare providers with comprehensive knowledge and expertise to provide proper care, especially in rural communities.”
Research and clinical trials
The report notes that hydroxyurea is the only drug approved by the US Food and Drug Administration to treat SCD. Therefore, research is needed to develop novel therapies, new drug delivery modes, and new agents that can be used in combination with hydroxyurea.
The report also highlights other areas where research is needed and recommends developing clinical trial networks to increase enrollment in trials.
Global issues
According to the report, roughly 1000 children in Africa are born with SCD every day, and more than half will die before they reach the age of 5. In addition, more than 90% of children with SCD who live in resource-poor countries do not survive to adulthood.
Therefore, the report recommends expanding newborn screening and early intervention programs, increasing SCD awareness and education, and improving access to quality care in developing regions.
Sickle Cell Disease Coalition
To address the aforementioned challenges, ASH and more than 20 other organizations launched the Sickle Cell Disease Coalition. The coalition is focused on promoting research, clinical care, education, training, and advocacy.
The aim of the coalition is to provide a platform to encourage stakeholders to work together to implement projects and activities that will ultimately help the SCD community and improve patient outcomes.
The coalition consists of leading patient advocacy groups, people with SCD and their families, researchers, clinicians, policymakers, industry stakeholders, and foundations with an interest in SCD. ![]()
Photo courtesy of St. Jude
Children’s Hospital
A new report suggests the current state of care for sickle cell disease (SCD) is inadequate, and improvements are needed.
The State of Sickle Cell Disease: 2016 Report outlines 4 main areas for improvement—SCD patients’ access to care, the training and education of healthcare professionals treating patients with SCD, research and clinical trials pertaining to SCD, and global health issues related to the disease.
The American Society of Hematology (ASH) published the report, with the endorsement of organizations in the SCD community.
The report includes statistics that highlight the need for improvements as well as future goals and recommended actions.
Access to care
The report states that more than 75% of adults with SCD who have frequent pain crises do not receive the recommended treatment, hydroxyurea.
One potential solution, according to the report, is to ensure that existing standard-of-care guidelines are being used. Another solution is to develop coordinated healthcare delivery models that ensure SCD patients can access quality care regardless of their age, location, and socioeconomic status.
“Not only are individuals with SCD burdened by the pain and disability that comes with a chronic condition, but they also have very few accessible treatment options due to our fragmented healthcare system,” said ASH President Charles S. Abrams, MD, of the University of Pennsylvania in Philadelphia.
Training and education
The report cites a national survey in which only 20.4% of family physicians said they felt comfortable treating SCD. And 69.4% of family physicians said clinical decision support tools would be useful for helping to guide their treatment decisions for SCD patients.
Therefore, the report recommends devising an “actionable plan” to educate healthcare providers about best practices in caring for SCD patients, developing clinical support tools, and encouraging medical trainees to pursue careers in SCD care, among other solutions.
“There are many unique challenges that people with SCD face,” said ASH Vice President Alexis Thompson, MD, of the Ann and Robert H. Lurie Children’s Hospital of Chicago in Illinois.
“For example, the transition from pediatric to adult care can be especially difficult, and many people struggle to find healthcare providers with comprehensive knowledge and expertise to provide proper care, especially in rural communities.”
Research and clinical trials
The report notes that hydroxyurea is the only drug approved by the US Food and Drug Administration to treat SCD. Therefore, research is needed to develop novel therapies, new drug delivery modes, and new agents that can be used in combination with hydroxyurea.
The report also highlights other areas where research is needed and recommends developing clinical trial networks to increase enrollment in trials.
Global issues
According to the report, roughly 1000 children in Africa are born with SCD every day, and more than half will die before they reach the age of 5. In addition, more than 90% of children with SCD who live in resource-poor countries do not survive to adulthood.
Therefore, the report recommends expanding newborn screening and early intervention programs, increasing SCD awareness and education, and improving access to quality care in developing regions.
Sickle Cell Disease Coalition
To address the aforementioned challenges, ASH and more than 20 other organizations launched the Sickle Cell Disease Coalition. The coalition is focused on promoting research, clinical care, education, training, and advocacy.
The aim of the coalition is to provide a platform to encourage stakeholders to work together to implement projects and activities that will ultimately help the SCD community and improve patient outcomes.
The coalition consists of leading patient advocacy groups, people with SCD and their families, researchers, clinicians, policymakers, industry stakeholders, and foundations with an interest in SCD. ![]()
Photo courtesy of St. Jude
Children’s Hospital
A new report suggests the current state of care for sickle cell disease (SCD) is inadequate, and improvements are needed.
The State of Sickle Cell Disease: 2016 Report outlines 4 main areas for improvement—SCD patients’ access to care, the training and education of healthcare professionals treating patients with SCD, research and clinical trials pertaining to SCD, and global health issues related to the disease.
The American Society of Hematology (ASH) published the report, with the endorsement of organizations in the SCD community.
The report includes statistics that highlight the need for improvements as well as future goals and recommended actions.
Access to care
The report states that more than 75% of adults with SCD who have frequent pain crises do not receive the recommended treatment, hydroxyurea.
One potential solution, according to the report, is to ensure that existing standard-of-care guidelines are being used. Another solution is to develop coordinated healthcare delivery models that ensure SCD patients can access quality care regardless of their age, location, and socioeconomic status.
“Not only are individuals with SCD burdened by the pain and disability that comes with a chronic condition, but they also have very few accessible treatment options due to our fragmented healthcare system,” said ASH President Charles S. Abrams, MD, of the University of Pennsylvania in Philadelphia.
Training and education
The report cites a national survey in which only 20.4% of family physicians said they felt comfortable treating SCD. And 69.4% of family physicians said clinical decision support tools would be useful for helping to guide their treatment decisions for SCD patients.
Therefore, the report recommends devising an “actionable plan” to educate healthcare providers about best practices in caring for SCD patients, developing clinical support tools, and encouraging medical trainees to pursue careers in SCD care, among other solutions.
“There are many unique challenges that people with SCD face,” said ASH Vice President Alexis Thompson, MD, of the Ann and Robert H. Lurie Children’s Hospital of Chicago in Illinois.
“For example, the transition from pediatric to adult care can be especially difficult, and many people struggle to find healthcare providers with comprehensive knowledge and expertise to provide proper care, especially in rural communities.”
Research and clinical trials
The report notes that hydroxyurea is the only drug approved by the US Food and Drug Administration to treat SCD. Therefore, research is needed to develop novel therapies, new drug delivery modes, and new agents that can be used in combination with hydroxyurea.
The report also highlights other areas where research is needed and recommends developing clinical trial networks to increase enrollment in trials.
Global issues
According to the report, roughly 1000 children in Africa are born with SCD every day, and more than half will die before they reach the age of 5. In addition, more than 90% of children with SCD who live in resource-poor countries do not survive to adulthood.
Therefore, the report recommends expanding newborn screening and early intervention programs, increasing SCD awareness and education, and improving access to quality care in developing regions.
Sickle Cell Disease Coalition
To address the aforementioned challenges, ASH and more than 20 other organizations launched the Sickle Cell Disease Coalition. The coalition is focused on promoting research, clinical care, education, training, and advocacy.
The aim of the coalition is to provide a platform to encourage stakeholders to work together to implement projects and activities that will ultimately help the SCD community and improve patient outcomes.
The coalition consists of leading patient advocacy groups, people with SCD and their families, researchers, clinicians, policymakers, industry stakeholders, and foundations with an interest in SCD. ![]()
Saline comparable to drug therapy for epistaxis in HHT

Photo courtesy of the
University of Utah
Health Sciences Center
Results of a phase 2 study suggest a saline nose spray may be as effective as 3 different medicated sprays for preventing epistaxis in patients with hemorrhagic telangiectasia (HHT).
The study was a comparison of bevacizumab, estriol, tranexamic acid, and saline.
The results showed no significant differences in the frequency or duration of epistaxis, and patients in all 4 groups reported improvements in Epistaxis Severity Scores (ESS).
“This research highlights that there could be a benefit even in the simplest of interventions,” said study author Kevin Whitehead, MD, of the University of Utah School of Medicine in Salt Lake City.
“No drug proved to be any better than the saline placebo, but the majority of patients improved over the course of treatment—even those using saline.”
Dr Whitehead and his colleagues reported these results in JAMA.
The study included 121 HHT patients who had experienced HHT-related epistaxis. They were randomized to twice-daily nose sprays with bevacizumab 1% (4 mg/day), estriol 0.1% (0.4 mg/day), tranexamic acid 10% (40 mg/day), or placebo (0.9% saline) for 12 weeks.
Safety
The investigators said nasal symptoms were the most common adverse events, and they occurred in all 4 treatment groups.
Gastrointestinal symptoms, including abdominal pain, nausea, and vomiting, were most common among patients receiving tranexamic acid.
There were no thrombotic complications, episodes of severe hypertension, serious drug-related adverse events, or deaths in any treatment group.
Efficacy
There was no significant difference in epistaxis frequency between the placebo group and the other treatment groups (P=0.97).
After 12 weeks of treatment, the median weekly number of bleeding episodes was 7.0 for patients in the bevacizumab group, 8.0 for the estriol group, 7.5 for the tranexamic acid group, and 8.0 for the placebo group. At baseline, the median weekly number of bleeding episodes was 10.0, 7.0, 7.8, and 7.0, respectively.
After 12 weeks of treatment, there was no significant difference in epistaxis duration between the placebo group and the other treatment groups (P=0.09).
The median duration of epistaxis per bleeding episode was 3.0 minutes for the bevacizumab group, 4.0 minutes for the estriol group, 6.2 minutes for the tranexamic acid group, and 5.0 minutes for the placebo group. (Bleeding duration was not recorded at baseline.)
After 12 weeks of treatment, there were no significant differences between the treatment groups when it came to hemoglobin levels (P=0.43), ferritin levels (P=0.10), treatment failure (P=0.08), the need for transfusion (P=0.42), or emergency department visits (P=0.72).
Patients in all 4 treatment groups experienced a significant decline in ESS from baseline to week 12 (P<0.001 for time effect).
The median ESS decreased from 5.71 to 3.74 in the placebo group, 5.16 to 3.54 in the bevacizumab group, 5.19 to 3.56 in the estriol group, and 5.43 to 4.06 in the tranexamic acid group. The investigators said the improvement in ESS was clinically significant.
However, the team also said they cannot completely rule out the possibility that symptoms may have improved because of a placebo effect.
What’s more, it could be that some of the drugs tested would work better if taken at a higher dose, or if applied as a gel or polymer that adheres better to the inside of the nasal cavity.
Nevertheless, the results from this trial were enough to convince Dr Whitehead and his colleagues to routinely recommend saline nasal spray to their patients with HHT.
“We stress the importance of hydration,” Dr Whitehead said. “We tell them that something as simple as a morning and night saline spray could offer them some benefit.” ![]()
Photo courtesy of the
University of Utah
Health Sciences Center
Results of a phase 2 study suggest a saline nose spray may be as effective as 3 different medicated sprays for preventing epistaxis in patients with hemorrhagic telangiectasia (HHT).
The study was a comparison of bevacizumab, estriol, tranexamic acid, and saline.
The results showed no significant differences in the frequency or duration of epistaxis, and patients in all 4 groups reported improvements in Epistaxis Severity Scores (ESS).
“This research highlights that there could be a benefit even in the simplest of interventions,” said study author Kevin Whitehead, MD, of the University of Utah School of Medicine in Salt Lake City.
“No drug proved to be any better than the saline placebo, but the majority of patients improved over the course of treatment—even those using saline.”
Dr Whitehead and his colleagues reported these results in JAMA.
The study included 121 HHT patients who had experienced HHT-related epistaxis. They were randomized to twice-daily nose sprays with bevacizumab 1% (4 mg/day), estriol 0.1% (0.4 mg/day), tranexamic acid 10% (40 mg/day), or placebo (0.9% saline) for 12 weeks.
Safety
The investigators said nasal symptoms were the most common adverse events, and they occurred in all 4 treatment groups.
Gastrointestinal symptoms, including abdominal pain, nausea, and vomiting, were most common among patients receiving tranexamic acid.
There were no thrombotic complications, episodes of severe hypertension, serious drug-related adverse events, or deaths in any treatment group.
Efficacy
There was no significant difference in epistaxis frequency between the placebo group and the other treatment groups (P=0.97).
After 12 weeks of treatment, the median weekly number of bleeding episodes was 7.0 for patients in the bevacizumab group, 8.0 for the estriol group, 7.5 for the tranexamic acid group, and 8.0 for the placebo group. At baseline, the median weekly number of bleeding episodes was 10.0, 7.0, 7.8, and 7.0, respectively.
After 12 weeks of treatment, there was no significant difference in epistaxis duration between the placebo group and the other treatment groups (P=0.09).
The median duration of epistaxis per bleeding episode was 3.0 minutes for the bevacizumab group, 4.0 minutes for the estriol group, 6.2 minutes for the tranexamic acid group, and 5.0 minutes for the placebo group. (Bleeding duration was not recorded at baseline.)
After 12 weeks of treatment, there were no significant differences between the treatment groups when it came to hemoglobin levels (P=0.43), ferritin levels (P=0.10), treatment failure (P=0.08), the need for transfusion (P=0.42), or emergency department visits (P=0.72).
Patients in all 4 treatment groups experienced a significant decline in ESS from baseline to week 12 (P<0.001 for time effect).
The median ESS decreased from 5.71 to 3.74 in the placebo group, 5.16 to 3.54 in the bevacizumab group, 5.19 to 3.56 in the estriol group, and 5.43 to 4.06 in the tranexamic acid group. The investigators said the improvement in ESS was clinically significant.
However, the team also said they cannot completely rule out the possibility that symptoms may have improved because of a placebo effect.
What’s more, it could be that some of the drugs tested would work better if taken at a higher dose, or if applied as a gel or polymer that adheres better to the inside of the nasal cavity.
Nevertheless, the results from this trial were enough to convince Dr Whitehead and his colleagues to routinely recommend saline nasal spray to their patients with HHT.
“We stress the importance of hydration,” Dr Whitehead said. “We tell them that something as simple as a morning and night saline spray could offer them some benefit.” ![]()
Photo courtesy of the
University of Utah
Health Sciences Center
Results of a phase 2 study suggest a saline nose spray may be as effective as 3 different medicated sprays for preventing epistaxis in patients with hemorrhagic telangiectasia (HHT).
The study was a comparison of bevacizumab, estriol, tranexamic acid, and saline.
The results showed no significant differences in the frequency or duration of epistaxis, and patients in all 4 groups reported improvements in Epistaxis Severity Scores (ESS).
“This research highlights that there could be a benefit even in the simplest of interventions,” said study author Kevin Whitehead, MD, of the University of Utah School of Medicine in Salt Lake City.
“No drug proved to be any better than the saline placebo, but the majority of patients improved over the course of treatment—even those using saline.”
Dr Whitehead and his colleagues reported these results in JAMA.
The study included 121 HHT patients who had experienced HHT-related epistaxis. They were randomized to twice-daily nose sprays with bevacizumab 1% (4 mg/day), estriol 0.1% (0.4 mg/day), tranexamic acid 10% (40 mg/day), or placebo (0.9% saline) for 12 weeks.
Safety
The investigators said nasal symptoms were the most common adverse events, and they occurred in all 4 treatment groups.
Gastrointestinal symptoms, including abdominal pain, nausea, and vomiting, were most common among patients receiving tranexamic acid.
There were no thrombotic complications, episodes of severe hypertension, serious drug-related adverse events, or deaths in any treatment group.
Efficacy
There was no significant difference in epistaxis frequency between the placebo group and the other treatment groups (P=0.97).
After 12 weeks of treatment, the median weekly number of bleeding episodes was 7.0 for patients in the bevacizumab group, 8.0 for the estriol group, 7.5 for the tranexamic acid group, and 8.0 for the placebo group. At baseline, the median weekly number of bleeding episodes was 10.0, 7.0, 7.8, and 7.0, respectively.
After 12 weeks of treatment, there was no significant difference in epistaxis duration between the placebo group and the other treatment groups (P=0.09).
The median duration of epistaxis per bleeding episode was 3.0 minutes for the bevacizumab group, 4.0 minutes for the estriol group, 6.2 minutes for the tranexamic acid group, and 5.0 minutes for the placebo group. (Bleeding duration was not recorded at baseline.)
After 12 weeks of treatment, there were no significant differences between the treatment groups when it came to hemoglobin levels (P=0.43), ferritin levels (P=0.10), treatment failure (P=0.08), the need for transfusion (P=0.42), or emergency department visits (P=0.72).
Patients in all 4 treatment groups experienced a significant decline in ESS from baseline to week 12 (P<0.001 for time effect).
The median ESS decreased from 5.71 to 3.74 in the placebo group, 5.16 to 3.54 in the bevacizumab group, 5.19 to 3.56 in the estriol group, and 5.43 to 4.06 in the tranexamic acid group. The investigators said the improvement in ESS was clinically significant.
However, the team also said they cannot completely rule out the possibility that symptoms may have improved because of a placebo effect.
What’s more, it could be that some of the drugs tested would work better if taken at a higher dose, or if applied as a gel or polymer that adheres better to the inside of the nasal cavity.
Nevertheless, the results from this trial were enough to convince Dr Whitehead and his colleagues to routinely recommend saline nasal spray to their patients with HHT.
“We stress the importance of hydration,” Dr Whitehead said. “We tell them that something as simple as a morning and night saline spray could offer them some benefit.” ![]()
FDA grants therapy orphan designation for hemophilia B

Image by Spencer Phillips
The US Food and Drug Administration (FDA) has granted orphan drug designation to SB-FIX, a zinc finger nuclease (ZFN)-mediated genome-editing product candidate for the treatment of hemophilia B.
SB-FIX is designed to be used as a one-time treatment that will provide stable, continuous production of factor IX (FIX) for the lifetime of the patient.
The ZFN-mediated in vivo genome-editing approach makes use of the albumin gene locus, a highly expressing and liver-specific genomic “safe-harbor site,” that can be edited with ZFNs to accept and express therapeutic genes.
The approach is designed is to enable the patient’s liver to permanently produce circulating therapeutic levels of a corrective protein product.
This differs from conventional adeno-associated virus complementary DNA gene therapy approaches, which are non-integrating and may “wash out” of the liver as cells divide and turn over.
Sangamo BioSciences, Inc., the company developing SB-FIX, expects to initiate a phase 1/2 trial of SB-FIX in adults with hemophilia B this year.
“We will enroll adult hemophilia patients into our first clinical trial. However, our goal is to move into pediatric patients, a population we believe could particularly benefit from a treatment that has the potential to provide life-long expression of therapeutic levels of factor IX protein,” said Geoff Nichol, MBChB, Sangamo’s executive vice president of research and development.
About orphan designation
The FDA grants orphan designation to drugs and biologics intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
Image by Spencer Phillips
The US Food and Drug Administration (FDA) has granted orphan drug designation to SB-FIX, a zinc finger nuclease (ZFN)-mediated genome-editing product candidate for the treatment of hemophilia B.
SB-FIX is designed to be used as a one-time treatment that will provide stable, continuous production of factor IX (FIX) for the lifetime of the patient.
The ZFN-mediated in vivo genome-editing approach makes use of the albumin gene locus, a highly expressing and liver-specific genomic “safe-harbor site,” that can be edited with ZFNs to accept and express therapeutic genes.
The approach is designed is to enable the patient’s liver to permanently produce circulating therapeutic levels of a corrective protein product.
This differs from conventional adeno-associated virus complementary DNA gene therapy approaches, which are non-integrating and may “wash out” of the liver as cells divide and turn over.
Sangamo BioSciences, Inc., the company developing SB-FIX, expects to initiate a phase 1/2 trial of SB-FIX in adults with hemophilia B this year.
“We will enroll adult hemophilia patients into our first clinical trial. However, our goal is to move into pediatric patients, a population we believe could particularly benefit from a treatment that has the potential to provide life-long expression of therapeutic levels of factor IX protein,” said Geoff Nichol, MBChB, Sangamo’s executive vice president of research and development.
About orphan designation
The FDA grants orphan designation to drugs and biologics intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
Image by Spencer Phillips
The US Food and Drug Administration (FDA) has granted orphan drug designation to SB-FIX, a zinc finger nuclease (ZFN)-mediated genome-editing product candidate for the treatment of hemophilia B.
SB-FIX is designed to be used as a one-time treatment that will provide stable, continuous production of factor IX (FIX) for the lifetime of the patient.
The ZFN-mediated in vivo genome-editing approach makes use of the albumin gene locus, a highly expressing and liver-specific genomic “safe-harbor site,” that can be edited with ZFNs to accept and express therapeutic genes.
The approach is designed is to enable the patient’s liver to permanently produce circulating therapeutic levels of a corrective protein product.
This differs from conventional adeno-associated virus complementary DNA gene therapy approaches, which are non-integrating and may “wash out” of the liver as cells divide and turn over.
Sangamo BioSciences, Inc., the company developing SB-FIX, expects to initiate a phase 1/2 trial of SB-FIX in adults with hemophilia B this year.
“We will enroll adult hemophilia patients into our first clinical trial. However, our goal is to move into pediatric patients, a population we believe could particularly benefit from a treatment that has the potential to provide life-long expression of therapeutic levels of factor IX protein,” said Geoff Nichol, MBChB, Sangamo’s executive vice president of research and development.
About orphan designation
The FDA grants orphan designation to drugs and biologics intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
Erratum
The article, Can the identification of an idle line facilitate its removal? published in the Journal of Hospital Medicine (J Hosp Med. 2016;11[7]: 489493; doi:
|
| IV access needs |
| Expected duration of IV antibiotics >6 days |
| Administration of TPN |
| Anticipated requirement of home IV medications |
| Requirement of IV medications with documented difficult access |
| Hemorrhage requiring blood transfusions |
| Requiring more than 3 infusions |
| Requiring more than 2 infusions and blood transfusions |
| Abnormal vitals |
| Diastolic blood pressure >120 mm Hg |
| Systolic blood pressure 90 mm Hg |
| Systolic blood pressure >200 mm Hg |
| Heart rate >120 beats per minute |
| Heart rate 50 beats per minute |
| Respiratory rate >30 breaths per minute |
| Respiratory rate 10 breaths per minute |
| Oxygen saturation 90% as measured by pulse oximetry |
| Meeting SIRS criteria (2 or more of the following present) |
| Temp >38C, Temp 36C, heart rate >90 beats per minute, respiratory rate >20 breaths per minute, WBC >12,000/mm3, WBC 4,000/mm3, bandemia >10% |
The article, Can the identification of an idle line facilitate its removal? published in the Journal of Hospital Medicine (J Hosp Med. 2016;11[7]: 489493; doi:
|
| IV access needs |
| Expected duration of IV antibiotics >6 days |
| Administration of TPN |
| Anticipated requirement of home IV medications |
| Requirement of IV medications with documented difficult access |
| Hemorrhage requiring blood transfusions |
| Requiring more than 3 infusions |
| Requiring more than 2 infusions and blood transfusions |
| Abnormal vitals |
| Diastolic blood pressure >120 mm Hg |
| Systolic blood pressure 90 mm Hg |
| Systolic blood pressure >200 mm Hg |
| Heart rate >120 beats per minute |
| Heart rate 50 beats per minute |
| Respiratory rate >30 breaths per minute |
| Respiratory rate 10 breaths per minute |
| Oxygen saturation 90% as measured by pulse oximetry |
| Meeting SIRS criteria (2 or more of the following present) |
| Temp >38C, Temp 36C, heart rate >90 beats per minute, respiratory rate >20 breaths per minute, WBC >12,000/mm3, WBC 4,000/mm3, bandemia >10% |
The article, Can the identification of an idle line facilitate its removal? published in the Journal of Hospital Medicine (J Hosp Med. 2016;11[7]: 489493; doi:
|
| IV access needs |
| Expected duration of IV antibiotics >6 days |
| Administration of TPN |
| Anticipated requirement of home IV medications |
| Requirement of IV medications with documented difficult access |
| Hemorrhage requiring blood transfusions |
| Requiring more than 3 infusions |
| Requiring more than 2 infusions and blood transfusions |
| Abnormal vitals |
| Diastolic blood pressure >120 mm Hg |
| Systolic blood pressure 90 mm Hg |
| Systolic blood pressure >200 mm Hg |
| Heart rate >120 beats per minute |
| Heart rate 50 beats per minute |
| Respiratory rate >30 breaths per minute |
| Respiratory rate 10 breaths per minute |
| Oxygen saturation 90% as measured by pulse oximetry |
| Meeting SIRS criteria (2 or more of the following present) |
| Temp >38C, Temp 36C, heart rate >90 beats per minute, respiratory rate >20 breaths per minute, WBC >12,000/mm3, WBC 4,000/mm3, bandemia >10% |
AAP report warns against early single-sport specialization
Delaying single-sport specialization until late adolescence not only minimizes the risks of overuse injuries and burnout, but it increases the likelihood of athletic success, according to a new clinical report from the American Academy of Pediatrics.
The new report gives pediatricians a current knowledge base to draw upon in well checks and sports injury visits, author Joel S. Brenner, MD, MPH, of the AAP’s Council on Sports Medicine and Fitness, said in an interview.

Specializing in a single sport at younger ages – and playing intensively year-round – has become increasingly common, and is often driven by aspirations for college scholarships or elite athletic status. Yet evidence suggests that early specialization may actually work against such goals.
Studies of top college athletes and reviews of other elite athletes and their specialization history show that “for the majority of sports, late specialization with early diversification [playing multiple sports early] is most likely to lead to elite status,” the report states (Pediatrics. 2016;138[3]:e20162148).
Youth who participate in a variety of sports until late adolescence (about 15-16 years of age) also have fewer injuries and a higher chance of remaining engaged in sports for the long term than do children who specialize early, according to the guideline. “Unfortunately, 70% of children drop out of organized sports by 13 years of age.”
If a young athlete has decided to specialize in a single sport, you should discuss his or her goals to determine if they are appropriate and realistic. A mere 1% of high school athletes receive athletic scholarships and only 3%-11% go on to compete at college level; of high school athletes, only 0.03%-0.5% proceed to the professional sports level, the report notes.
Having at least 1-2 days off per week from the focal sport can decrease the chance of injury, and taking 1 month off at least 3 times a year “will allow for athletes’ physical and psychological recovery.”
An estimated 50% of athletic injuries are related to overuse. The physiologic and psychological effects of intensive training in young athletes are detailed in other articles by the AAP (Pediatrics. 2007;119[6]:1242-5) and the American Medical Society for Sports Medicine (Clin J Sport Med. 2014;24[1]:3-20).
According to a 2008 report from the National Council of Youth Sports, 27% of the youth active in adult-led organized sports participated in only 1 sport. “There is increased pressure to participate at a high level, to specialize in one sport early, and to play year-round, often on multiple teams,” the guideline notes.
This clinical report replaces the academy’s 2000 policy statement on sports specialization and intensive training and provides “concrete guidance” for pediatricians, said Dr. Brenner, who is medical director of Children’s Hospital of the King’s Daughters’ sports medicine and adolescent medicine programs and the director of CHKD’s sports concussion program, in Norfolk, Va.
There was no external funding for this report and the authors had no relevant financial disclosures.
Delaying single-sport specialization until late adolescence not only minimizes the risks of overuse injuries and burnout, but it increases the likelihood of athletic success, according to a new clinical report from the American Academy of Pediatrics.
The new report gives pediatricians a current knowledge base to draw upon in well checks and sports injury visits, author Joel S. Brenner, MD, MPH, of the AAP’s Council on Sports Medicine and Fitness, said in an interview.
Specializing in a single sport at younger ages – and playing intensively year-round – has become increasingly common, and is often driven by aspirations for college scholarships or elite athletic status. Yet evidence suggests that early specialization may actually work against such goals.
Studies of top college athletes and reviews of other elite athletes and their specialization history show that “for the majority of sports, late specialization with early diversification [playing multiple sports early] is most likely to lead to elite status,” the report states (Pediatrics. 2016;138[3]:e20162148).
Youth who participate in a variety of sports until late adolescence (about 15-16 years of age) also have fewer injuries and a higher chance of remaining engaged in sports for the long term than do children who specialize early, according to the guideline. “Unfortunately, 70% of children drop out of organized sports by 13 years of age.”
If a young athlete has decided to specialize in a single sport, you should discuss his or her goals to determine if they are appropriate and realistic. A mere 1% of high school athletes receive athletic scholarships and only 3%-11% go on to compete at college level; of high school athletes, only 0.03%-0.5% proceed to the professional sports level, the report notes.
Having at least 1-2 days off per week from the focal sport can decrease the chance of injury, and taking 1 month off at least 3 times a year “will allow for athletes’ physical and psychological recovery.”
An estimated 50% of athletic injuries are related to overuse. The physiologic and psychological effects of intensive training in young athletes are detailed in other articles by the AAP (Pediatrics. 2007;119[6]:1242-5) and the American Medical Society for Sports Medicine (Clin J Sport Med. 2014;24[1]:3-20).
According to a 2008 report from the National Council of Youth Sports, 27% of the youth active in adult-led organized sports participated in only 1 sport. “There is increased pressure to participate at a high level, to specialize in one sport early, and to play year-round, often on multiple teams,” the guideline notes.
This clinical report replaces the academy’s 2000 policy statement on sports specialization and intensive training and provides “concrete guidance” for pediatricians, said Dr. Brenner, who is medical director of Children’s Hospital of the King’s Daughters’ sports medicine and adolescent medicine programs and the director of CHKD’s sports concussion program, in Norfolk, Va.
There was no external funding for this report and the authors had no relevant financial disclosures.
Delaying single-sport specialization until late adolescence not only minimizes the risks of overuse injuries and burnout, but it increases the likelihood of athletic success, according to a new clinical report from the American Academy of Pediatrics.
The new report gives pediatricians a current knowledge base to draw upon in well checks and sports injury visits, author Joel S. Brenner, MD, MPH, of the AAP’s Council on Sports Medicine and Fitness, said in an interview.
Specializing in a single sport at younger ages – and playing intensively year-round – has become increasingly common, and is often driven by aspirations for college scholarships or elite athletic status. Yet evidence suggests that early specialization may actually work against such goals.
Studies of top college athletes and reviews of other elite athletes and their specialization history show that “for the majority of sports, late specialization with early diversification [playing multiple sports early] is most likely to lead to elite status,” the report states (Pediatrics. 2016;138[3]:e20162148).
Youth who participate in a variety of sports until late adolescence (about 15-16 years of age) also have fewer injuries and a higher chance of remaining engaged in sports for the long term than do children who specialize early, according to the guideline. “Unfortunately, 70% of children drop out of organized sports by 13 years of age.”
If a young athlete has decided to specialize in a single sport, you should discuss his or her goals to determine if they are appropriate and realistic. A mere 1% of high school athletes receive athletic scholarships and only 3%-11% go on to compete at college level; of high school athletes, only 0.03%-0.5% proceed to the professional sports level, the report notes.
Having at least 1-2 days off per week from the focal sport can decrease the chance of injury, and taking 1 month off at least 3 times a year “will allow for athletes’ physical and psychological recovery.”
An estimated 50% of athletic injuries are related to overuse. The physiologic and psychological effects of intensive training in young athletes are detailed in other articles by the AAP (Pediatrics. 2007;119[6]:1242-5) and the American Medical Society for Sports Medicine (Clin J Sport Med. 2014;24[1]:3-20).
According to a 2008 report from the National Council of Youth Sports, 27% of the youth active in adult-led organized sports participated in only 1 sport. “There is increased pressure to participate at a high level, to specialize in one sport early, and to play year-round, often on multiple teams,” the guideline notes.
This clinical report replaces the academy’s 2000 policy statement on sports specialization and intensive training and provides “concrete guidance” for pediatricians, said Dr. Brenner, who is medical director of Children’s Hospital of the King’s Daughters’ sports medicine and adolescent medicine programs and the director of CHKD’s sports concussion program, in Norfolk, Va.
There was no external funding for this report and the authors had no relevant financial disclosures.
FROM PEDIATRICS

New biomarkers, standardization of AMA testing will improve PBC diagnosis
Standardization of liver diagnostic serology and clinical governance will improve understanding and diagnosis of primary biliary cholangitis (PBC), as will new biomarkers, according to a literature review from Nikolaos Gatselis, MD, PhD, and George Dalekos, MD, PhD, of the University of Thessaly, Greece.
Antimitochondrial antibodies are the most important diagnostic tool for the diagnosis of PBC, as AMA is seen in 90%-95% of patients with PBC. Indirect immunofluorescence assays using HEp-2 cells or cryostat sections of rat liver, kidney, and stomach remain the best way to detect AMA, but since the indirect immunofluorescence process cannot be fully automated, further analysis can be performed by immunoblotting. PBC-specific antinuclear antibodies are seen in 50%-70% of PBC cases, and are also important for the diagnosis of PBC.
Several new biomarkers have been proposed for improved diagnosis of PBC in recent years. The biomarkers include the autoantibodies KLHL12 and HK1, genetic markers in HLA regions, metabolomic profiling, miRNAs, and epigenetics.
“Development of clinical governance is of great importance in order to ensure that clinical standards are met, and that processes are in place to ensure continuing improvement and harmonization between laboratories. The guidance should include the whole testing process, beginning from the formulation of a reasonable clinical suspicion and the request of the most appropriate autoantibody test and continuing with handling of biological samples,” the investigators said.
Find the full review in Expert Review of Molecular Diagnostics (doi: 10.1080/14737159.2016.1217159).
Standardization of liver diagnostic serology and clinical governance will improve understanding and diagnosis of primary biliary cholangitis (PBC), as will new biomarkers, according to a literature review from Nikolaos Gatselis, MD, PhD, and George Dalekos, MD, PhD, of the University of Thessaly, Greece.
Antimitochondrial antibodies are the most important diagnostic tool for the diagnosis of PBC, as AMA is seen in 90%-95% of patients with PBC. Indirect immunofluorescence assays using HEp-2 cells or cryostat sections of rat liver, kidney, and stomach remain the best way to detect AMA, but since the indirect immunofluorescence process cannot be fully automated, further analysis can be performed by immunoblotting. PBC-specific antinuclear antibodies are seen in 50%-70% of PBC cases, and are also important for the diagnosis of PBC.
Several new biomarkers have been proposed for improved diagnosis of PBC in recent years. The biomarkers include the autoantibodies KLHL12 and HK1, genetic markers in HLA regions, metabolomic profiling, miRNAs, and epigenetics.
“Development of clinical governance is of great importance in order to ensure that clinical standards are met, and that processes are in place to ensure continuing improvement and harmonization between laboratories. The guidance should include the whole testing process, beginning from the formulation of a reasonable clinical suspicion and the request of the most appropriate autoantibody test and continuing with handling of biological samples,” the investigators said.
Find the full review in Expert Review of Molecular Diagnostics (doi: 10.1080/14737159.2016.1217159).
Standardization of liver diagnostic serology and clinical governance will improve understanding and diagnosis of primary biliary cholangitis (PBC), as will new biomarkers, according to a literature review from Nikolaos Gatselis, MD, PhD, and George Dalekos, MD, PhD, of the University of Thessaly, Greece.
Antimitochondrial antibodies are the most important diagnostic tool for the diagnosis of PBC, as AMA is seen in 90%-95% of patients with PBC. Indirect immunofluorescence assays using HEp-2 cells or cryostat sections of rat liver, kidney, and stomach remain the best way to detect AMA, but since the indirect immunofluorescence process cannot be fully automated, further analysis can be performed by immunoblotting. PBC-specific antinuclear antibodies are seen in 50%-70% of PBC cases, and are also important for the diagnosis of PBC.
Several new biomarkers have been proposed for improved diagnosis of PBC in recent years. The biomarkers include the autoantibodies KLHL12 and HK1, genetic markers in HLA regions, metabolomic profiling, miRNAs, and epigenetics.
“Development of clinical governance is of great importance in order to ensure that clinical standards are met, and that processes are in place to ensure continuing improvement and harmonization between laboratories. The guidance should include the whole testing process, beginning from the formulation of a reasonable clinical suspicion and the request of the most appropriate autoantibody test and continuing with handling of biological samples,” the investigators said.
Find the full review in Expert Review of Molecular Diagnostics (doi: 10.1080/14737159.2016.1217159).
FROM EXPERT REVIEW OF MOLECULAR DIAGNOSTICS
What’s Hot in Our National Organizations: A Follow-Up
In “What’s Hot and What’s Not in Our National Organizations, An Emergency Medicine Panel, Parts 1 and 2” (Emergency Medicine, April 2016 and May 2016, respectively), we published highlights from a panel discussion that took place at the annual retreat of the Association of Academic Chairs in Emergency Medicine in Tempe, Arizona in February 2016. That discussion included seven EM organizations: the American Academy of Emergency Medicine (AAEM), AAEM Resident and Student Association (AAEM/RSA), American Board of Emergency Medicine (ABEM), American College of Emergency Physicians (ACEP), Council of Residency Directors in Emergency Medicine (CORD), Emergency Medicine Residents’ Association (EMRA), and Society for Academic Emergency Medicine (SAEM). In this issue, we follow up with reports from the American College of Osteopathic Emergency Physicians (ACOEP) and the American Osteopathic Board of Emergency Medicine (AOBEM).
American College of Osteopathic Emergency Physicians
John C. Prestosh, DO, FACOEP-DPresident, ACOEP
Strategic Planning. The Board of Directors of ACOEP has recently adopted a revised mission statement and goals for the organization. The ACOEP “promotes patient-centric, holistic emergency care consistent with the osteopathic philosophy practiced by all emergency medicine professionals.” This statement is based on the belief that many non-osteopathic professionals practice aspects of holistic medicine, and will allow ACOEP to be a “home” for these practitioners. ACOEP’s goals are member engagement and value, advocacy and involvement, education and knowledge, improving awareness, and college strength and sustainability.
Workplace Issues. The ACOEP is aware of the issues emergency physicians (EPs) and professionals face every day. Therefore, we are including items for EPs on these issues in our educational programs. Upcoming events will include workshops on dealing with an active shooter scenario, ultrasound, and advanced airway management, which will be included in our Scientific Assembly in November.
The ACOEP is also a member of the White House Task Force addressing the opioid epidemic. Realizing there are times when opiates are necessary adjuncts to patient care, we also want to help educate physicians on the usage of alternative pain-relieving treatment plans when indicated.
Single Accreditation System and College Sustainability. Graduate medical education is undergoing an unprecedented change. The Single Accreditation System is currently being implemented with a target date of July 1, 2020 for all residency programs to fall under the jurisdiction of the Accreditation Council for Graduate Medical Education (ACGME) for accreditation. There is much anticipation regarding the changes that will occur.
We anticipate some American Osteopathic Association-accredited EM programs will become 3-year programs, thus precluding graduating residents from AOBEM certification. However, we expect a number of ACGME-accredited EM programs to establish “osteopathic-focused” tracks in which both DOs and MDs will learn osteopathic tenets and procedures to broaden their practice of EM. We anticipate this will allow residents to be certified by the AOBEM.
We believe the ACOEP can be a “home” for MD residents graduating from “osteopathic-focused” ACGME programs. Furthermore, the ACOEP is ready to amend its bylaws to offer active membership with full voting rights to MDs. We do not want to remain a closed organization, but are striving to have both DO and MD EPs belong to our College.
American Osteopathic Board of Emergency Medicine
Donald Phillips, DO, FACOEP-D, Executive Physician Director, AOBEM
Primary Certification News. The date for the 2017 Part I Examination (written examination) has been published. All candidates are advised that the examination has been moved from March to September beginning in 2017. Applications for Part I will be available on January 2, 2017. The deadline to submit the application is April 1, 2017. The examination will be administered at Prometric Testing Centers nationwide on September 12, 2017. Part II Examinations (oral examinations) are in March and November. Please refer to the AOBEM Web page at www.aobem.org for dates.
Subspecialty Certifications. AOBEM offers subspecialty certification opportunities to its diplomates in the following areas:
- Emergency medical services
- Hospice and palliative medicine
- Medical toxicology
- Sports medicine
- Undersea and hyperbaric medicine
- Internal medicine critical care
- Surgical critical care.
AOBEM and the American Osteopathic Board of Pediatrics are also engaged in the development of a pediatric EM subspecialty examination.
Osteopathic Continuous Certification (OCC). AOBEM continues to refine and evolve the OCC process. The Board has received approval to begin allowing group data for the Practice Performance Assessment portion of OCC. Diplomates may submit group data provided at least 30% of the charts reviewed are patients that the diplomate cared for personally. Diplomates may also submit unique projects that are not on the list of “preapproved” projects. It is recognized that many of our diplomates are involved in very advanced care systems. Many times, these systems have useful projects that will meet criteria for this component. If you wish to submit data for a unique project, they will be welcomed, but the Board asks that you contact us to have them approved before beginning the project.
Continuous Osteopathic Learning Assessments (COLAs) are a vital component. They demonstrate the diplomate is maintaining currency across the entire specialty of EM. We invite diplomates and candidates to submit journal articles they feel are significant to a topic for potential inclusion in the official list of COLA articles.
Candidates and diplomates are advised to keep apprised of important dates and announcements via the AOBEM Web page at www.aobem.org.
In “What’s Hot and What’s Not in Our National Organizations, An Emergency Medicine Panel, Parts 1 and 2” (Emergency Medicine, April 2016 and May 2016, respectively), we published highlights from a panel discussion that took place at the annual retreat of the Association of Academic Chairs in Emergency Medicine in Tempe, Arizona in February 2016. That discussion included seven EM organizations: the American Academy of Emergency Medicine (AAEM), AAEM Resident and Student Association (AAEM/RSA), American Board of Emergency Medicine (ABEM), American College of Emergency Physicians (ACEP), Council of Residency Directors in Emergency Medicine (CORD), Emergency Medicine Residents’ Association (EMRA), and Society for Academic Emergency Medicine (SAEM). In this issue, we follow up with reports from the American College of Osteopathic Emergency Physicians (ACOEP) and the American Osteopathic Board of Emergency Medicine (AOBEM).
American College of Osteopathic Emergency Physicians
John C. Prestosh, DO, FACOEP-DPresident, ACOEP
Strategic Planning. The Board of Directors of ACOEP has recently adopted a revised mission statement and goals for the organization. The ACOEP “promotes patient-centric, holistic emergency care consistent with the osteopathic philosophy practiced by all emergency medicine professionals.” This statement is based on the belief that many non-osteopathic professionals practice aspects of holistic medicine, and will allow ACOEP to be a “home” for these practitioners. ACOEP’s goals are member engagement and value, advocacy and involvement, education and knowledge, improving awareness, and college strength and sustainability.
Workplace Issues. The ACOEP is aware of the issues emergency physicians (EPs) and professionals face every day. Therefore, we are including items for EPs on these issues in our educational programs. Upcoming events will include workshops on dealing with an active shooter scenario, ultrasound, and advanced airway management, which will be included in our Scientific Assembly in November.
The ACOEP is also a member of the White House Task Force addressing the opioid epidemic. Realizing there are times when opiates are necessary adjuncts to patient care, we also want to help educate physicians on the usage of alternative pain-relieving treatment plans when indicated.
Single Accreditation System and College Sustainability. Graduate medical education is undergoing an unprecedented change. The Single Accreditation System is currently being implemented with a target date of July 1, 2020 for all residency programs to fall under the jurisdiction of the Accreditation Council for Graduate Medical Education (ACGME) for accreditation. There is much anticipation regarding the changes that will occur.
We anticipate some American Osteopathic Association-accredited EM programs will become 3-year programs, thus precluding graduating residents from AOBEM certification. However, we expect a number of ACGME-accredited EM programs to establish “osteopathic-focused” tracks in which both DOs and MDs will learn osteopathic tenets and procedures to broaden their practice of EM. We anticipate this will allow residents to be certified by the AOBEM.
We believe the ACOEP can be a “home” for MD residents graduating from “osteopathic-focused” ACGME programs. Furthermore, the ACOEP is ready to amend its bylaws to offer active membership with full voting rights to MDs. We do not want to remain a closed organization, but are striving to have both DO and MD EPs belong to our College.
American Osteopathic Board of Emergency Medicine
Donald Phillips, DO, FACOEP-D, Executive Physician Director, AOBEM
Primary Certification News. The date for the 2017 Part I Examination (written examination) has been published. All candidates are advised that the examination has been moved from March to September beginning in 2017. Applications for Part I will be available on January 2, 2017. The deadline to submit the application is April 1, 2017. The examination will be administered at Prometric Testing Centers nationwide on September 12, 2017. Part II Examinations (oral examinations) are in March and November. Please refer to the AOBEM Web page at www.aobem.org for dates.
Subspecialty Certifications. AOBEM offers subspecialty certification opportunities to its diplomates in the following areas:
- Emergency medical services
- Hospice and palliative medicine
- Medical toxicology
- Sports medicine
- Undersea and hyperbaric medicine
- Internal medicine critical care
- Surgical critical care.
AOBEM and the American Osteopathic Board of Pediatrics are also engaged in the development of a pediatric EM subspecialty examination.
Osteopathic Continuous Certification (OCC). AOBEM continues to refine and evolve the OCC process. The Board has received approval to begin allowing group data for the Practice Performance Assessment portion of OCC. Diplomates may submit group data provided at least 30% of the charts reviewed are patients that the diplomate cared for personally. Diplomates may also submit unique projects that are not on the list of “preapproved” projects. It is recognized that many of our diplomates are involved in very advanced care systems. Many times, these systems have useful projects that will meet criteria for this component. If you wish to submit data for a unique project, they will be welcomed, but the Board asks that you contact us to have them approved before beginning the project.
Continuous Osteopathic Learning Assessments (COLAs) are a vital component. They demonstrate the diplomate is maintaining currency across the entire specialty of EM. We invite diplomates and candidates to submit journal articles they feel are significant to a topic for potential inclusion in the official list of COLA articles.
Candidates and diplomates are advised to keep apprised of important dates and announcements via the AOBEM Web page at www.aobem.org.
In “What’s Hot and What’s Not in Our National Organizations, An Emergency Medicine Panel, Parts 1 and 2” (Emergency Medicine, April 2016 and May 2016, respectively), we published highlights from a panel discussion that took place at the annual retreat of the Association of Academic Chairs in Emergency Medicine in Tempe, Arizona in February 2016. That discussion included seven EM organizations: the American Academy of Emergency Medicine (AAEM), AAEM Resident and Student Association (AAEM/RSA), American Board of Emergency Medicine (ABEM), American College of Emergency Physicians (ACEP), Council of Residency Directors in Emergency Medicine (CORD), Emergency Medicine Residents’ Association (EMRA), and Society for Academic Emergency Medicine (SAEM). In this issue, we follow up with reports from the American College of Osteopathic Emergency Physicians (ACOEP) and the American Osteopathic Board of Emergency Medicine (AOBEM).
American College of Osteopathic Emergency Physicians
John C. Prestosh, DO, FACOEP-DPresident, ACOEP
Strategic Planning. The Board of Directors of ACOEP has recently adopted a revised mission statement and goals for the organization. The ACOEP “promotes patient-centric, holistic emergency care consistent with the osteopathic philosophy practiced by all emergency medicine professionals.” This statement is based on the belief that many non-osteopathic professionals practice aspects of holistic medicine, and will allow ACOEP to be a “home” for these practitioners. ACOEP’s goals are member engagement and value, advocacy and involvement, education and knowledge, improving awareness, and college strength and sustainability.
Workplace Issues. The ACOEP is aware of the issues emergency physicians (EPs) and professionals face every day. Therefore, we are including items for EPs on these issues in our educational programs. Upcoming events will include workshops on dealing with an active shooter scenario, ultrasound, and advanced airway management, which will be included in our Scientific Assembly in November.
The ACOEP is also a member of the White House Task Force addressing the opioid epidemic. Realizing there are times when opiates are necessary adjuncts to patient care, we also want to help educate physicians on the usage of alternative pain-relieving treatment plans when indicated.
Single Accreditation System and College Sustainability. Graduate medical education is undergoing an unprecedented change. The Single Accreditation System is currently being implemented with a target date of July 1, 2020 for all residency programs to fall under the jurisdiction of the Accreditation Council for Graduate Medical Education (ACGME) for accreditation. There is much anticipation regarding the changes that will occur.
We anticipate some American Osteopathic Association-accredited EM programs will become 3-year programs, thus precluding graduating residents from AOBEM certification. However, we expect a number of ACGME-accredited EM programs to establish “osteopathic-focused” tracks in which both DOs and MDs will learn osteopathic tenets and procedures to broaden their practice of EM. We anticipate this will allow residents to be certified by the AOBEM.
We believe the ACOEP can be a “home” for MD residents graduating from “osteopathic-focused” ACGME programs. Furthermore, the ACOEP is ready to amend its bylaws to offer active membership with full voting rights to MDs. We do not want to remain a closed organization, but are striving to have both DO and MD EPs belong to our College.
American Osteopathic Board of Emergency Medicine
Donald Phillips, DO, FACOEP-D, Executive Physician Director, AOBEM
Primary Certification News. The date for the 2017 Part I Examination (written examination) has been published. All candidates are advised that the examination has been moved from March to September beginning in 2017. Applications for Part I will be available on January 2, 2017. The deadline to submit the application is April 1, 2017. The examination will be administered at Prometric Testing Centers nationwide on September 12, 2017. Part II Examinations (oral examinations) are in March and November. Please refer to the AOBEM Web page at www.aobem.org for dates.
Subspecialty Certifications. AOBEM offers subspecialty certification opportunities to its diplomates in the following areas:
- Emergency medical services
- Hospice and palliative medicine
- Medical toxicology
- Sports medicine
- Undersea and hyperbaric medicine
- Internal medicine critical care
- Surgical critical care.
AOBEM and the American Osteopathic Board of Pediatrics are also engaged in the development of a pediatric EM subspecialty examination.
Osteopathic Continuous Certification (OCC). AOBEM continues to refine and evolve the OCC process. The Board has received approval to begin allowing group data for the Practice Performance Assessment portion of OCC. Diplomates may submit group data provided at least 30% of the charts reviewed are patients that the diplomate cared for personally. Diplomates may also submit unique projects that are not on the list of “preapproved” projects. It is recognized that many of our diplomates are involved in very advanced care systems. Many times, these systems have useful projects that will meet criteria for this component. If you wish to submit data for a unique project, they will be welcomed, but the Board asks that you contact us to have them approved before beginning the project.
Continuous Osteopathic Learning Assessments (COLAs) are a vital component. They demonstrate the diplomate is maintaining currency across the entire specialty of EM. We invite diplomates and candidates to submit journal articles they feel are significant to a topic for potential inclusion in the official list of COLA articles.
Candidates and diplomates are advised to keep apprised of important dates and announcements via the AOBEM Web page at www.aobem.org.

Intrauterine Device Migration
Although intrauterine devices (IUDs) are a mainstay of reversible contraception, they do carry the risk of complications, including septic abortion, abscess formation, ectopic pregnancy, bleeding, and uterine perforation.1 Although perforation is a relatively rare complication, occurring in 0.3 to 2.6 per 1,000 insertions for levonorgestrel-releasing intrauterine systems and 0.3 to 2.2 per 1,000 insertions for copper IUDs, it can lead to serious complications, including IUD migration to various sites.2 Most patients with uterine perforation and IUD migration present with abdominal pain and bleeding; however, 30% of patients are asymptomatic.3
This article presents the case of a young woman who was diagnosed with IUD migration into the abdominal cavity. I discuss the management of this uncommon complication, and stress the importance of adequate education for both patients and health care providers regarding proper surveillance.
Case
A 33-year-old woman (gravida 4, para 4, live 4) presented to our ED for evaluation of rectal bleeding that she had experienced intermittently over the past 2 years. She reported that the first occurrence had been 2 years ago, starting a few weeks after she had a cesarean delivery. The patient described the initial episode as bright red blood mixed with stool. She stated that subsequent episodes had been intermittent, felt as if she were “passing rocks” through her abdomen and rectum, and were accompanied by streaks of blood covering her stool. The day before the patient presented to the ED, she had experienced a second episode of a large bowel movement mixed with blood and accompanied by weakness, which prompted her to seek treatment.
A review of the patient’s symptoms revealed abdominal pain and weakness. She denied any bleeding disorders, fever, chills, sick contacts, anal trauma, presyncope, syncope, nausea, vomiting, diarrhea, or constipation. She further denied any prescription-medication use, illicit drug use, or smoking, but admitted to occasional alcohol use. Her last menstrual period had been 3 weeks prior to presentation. She denied any history of cancer or abnormal Pap smears. Her gynecologic history was significant for chlamydia and trichomoniasis, for which she had been treated. The patient’s surgical history was pertinent for umbilical hernia repair with surgical mesh.
On physical examination, the patient was mildly hypotensive (blood pressure, 97/78 mm Hg) but had a normal heart rate. She had mild conjunctival pallor. The abdominal examination exhibited normoactive bowel sounds with diffuse lower abdominal tenderness to deep palpation, but without rebound, guarding, or distension. Rectal examination revealed a small internal hemorrhoid at the 6 o’clock position (no active bleeding) and an external hemorrhoid with some tenderness to palpation; the external hemorrhoid was not thrombosed, had no signs of infection, and was the same color as the surrounding skin.
A fecal occult blood screen was negative, and a serum pregnancy test was also negative. Complete blood count, basic metabolic profile, and urinalysis were all unremarkable and within normal ranges. Abdominal X-ray revealed a nonobstructive stool pattern and a foreign body, likely in the abdominal cavity, which appeared to be an IUD (Figure 1). Computed tomography (CT) scans of the abdomen and pelvis without contrast were performed to accurately locate the foreign body and to assess for any complications. The CT scans revealed an IUD outside of the uterus, between loops of the transverse colon within the left midabdomen (Figure 2). There were no signs of infection, fluid, or free air. There were also findings of colonic diverticula and narrowed lumen, which were suggestive of diverticulosis.
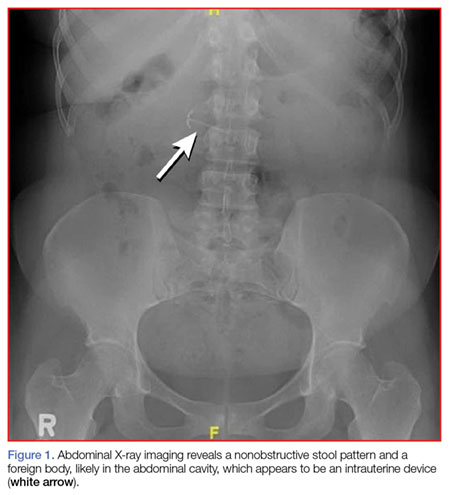
The patient stated that the IUD had been placed several months after the vaginal birth of her third child. She continued to have normal menstrual periods with the IUD in place. Seven years later, she became pregnant with her fourth child, who was delivered via cesarean, secondary to fetal malpositioning. The IUD was not removed during the cesarean delivery.
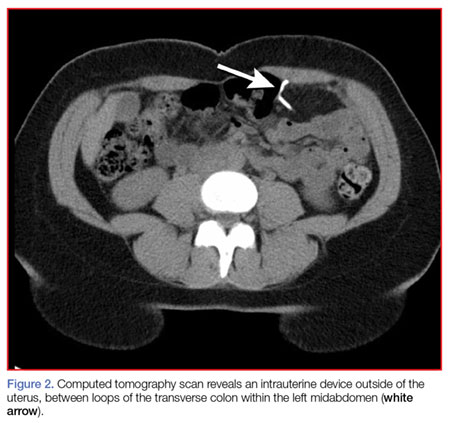
Based on the CT scan findings, gynecology services was consulted, and the gynecologist recommended immediate follow-up in a gynecology clinic. The patient was discharged on a bowel regimen. She was assessed in a gynecology clinic 4 days later, where she was found to have a mobile retroverted uterus without tenderness or signs of infection. She underwent exploratory laparoscopy, during which the IUD was removed from the omentum in the left upper abdomen without complications.
Discussion
The IUD has had great acceptance among women since the 1960s. According to the World Health Organization, approximately 14.3% of women used an IUD in 2009.4 Although complications are rare, the most serious are perforation of the uterus and migration of the IUD into adjacent organs.1
Risk factors of uterine perforation include clinician inexperience in IUD placement, an immobile uterus, a retroverted uterus, and the presence of a myometrial defect.4 Heinemann et al2 also suggested that breastfeeding and IUD placement soon after a delivery (≤36 weeks) are independent risk factors, and the presence of both factors has an additive increase in risk of perforation.
Primary rupture of the uterus has been reported at the time of IUD insertion, but secondary or delayed rupture is more common and seems to be due to the spasms of the uterus.5 Although 85% of perforations do not affect other organs, the remaining 15% lead to complications in the adjacent visceral organs.6 The most frequent sites of migration are to the omentum (26.7%), pouch of Douglas (21.5%), large bowel (10.4%), myometrium (7.4%), broad ligament (6.7%), abdominal cavity (5.2%), adhesion to ileal loop serosa (4.4%) or large bowel serosa (3.7%), and mesentery (3%).7 Rare sites are to the appendix, abdominal wall, ovary, and bladder.7
Intrauterine device migration should be suspected in patients who become pregnant after IUD placement (as was the case for our patient), when the “threads” or string cannot be located while attempting to remove an IUD, or when a patient has an “expulsed” IUD without observation of the device thereafter. Even though expulsion of the device happens in approximately 8 per 1,000 insertions, uterine perforation is also a possibility in the case of a “lost” IUD.8 When a lost IUD is suspected, a pelvic examination should be performed to assess for threads or string location. If unsuccessful, ultrasound or plain abdominal radiographic imaging may be used to locate the IUD. Once IUD migration has been confirmed, cross-sectional imaging such as CT scans or magnetic resonance imaging (MRI) is suggested to rule out adjacent organ involvement before considering surgical removal.4 If colonic involvement is suspected, colonoscopy can be used to confirm the diagnosis before operative removal.4
Although management of a migrated IUD in an asymptomatic patient is controversial, there appears to be a consensus that all extrauterine devices should be removed unless the patient’s surgical risk is excessive.1,5,9 Retrieval of an IUD can be performed by laparotomy or laparoscopy.10,11
To avoid these complications and interventions, IUDs should be inserted by an appropriately trained professional, after proper patient selection. These devices should be monitored by periodic examinations, either by medical professionals or by well-informed patients. This can be done by either checking for the threads or string in the cervical opening or by ultrasound imaging to confirm the location of the IUD.
Conclusion
Although many patients with uterine perforation and IUD migration present with symptoms, approximately 30% are asymptomatic.3 If a patient has a lost IUD and the threads or string is not visible during pelvic examination, appropriate work-up, including transvaginal or transabdominal ultrasound or radiographs, should be obtained to confirm the position of the IUD. If IUD migration is suspected, cross-sectional imaging, such as CT scans or MRI, is recommended to rule out adjacent organ involvement before considering surgical removal.4
Even though only 15% of migrated IUDs lead to complications in the adjacent visceral organs,6 surgical removal of the IUD is advised regardless of the presence of symptoms or identified complications. Importantly, to prevent the delayed diagnosis and morbidity of IUD migration, patients with IUDs should be educated about the possibility of migration and the importance of regular self-examination for missing threads or string.
1. Hoşcan MB, Koşar A, Gümüştaş U, Güney M. Intravesical migration of intrauterine device resulting in pregnancy. Int J Urol. 2006;13(3):301-302.
2. Heinemann K, Reed S, Moehner S, Minh TD. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European Active Surveillance Study on Intrauterine Devices. Contraception. 2015;91(4):274-279.
3. Singh SP, Mangla D, Chawan J, Haq AU. Asymptomatic presentation of silent uterine perforation by Cu-T 380A: a case report with review of literature. Int J Reprod Contracept Obstet Gynecol. 2014;3(4):1157-1159.
4. Akpinar F, Ozgur EN, Yilmaz S, Ustaoglu O. Sigmoid colon migration of an intrauterine device. Case Rep Obstet Gynecol. 2014;2014:207659.
5. Rahnemai-Azar AA, Apfel T, Naghshizadian R, Cosgrove JM, Farkas DT. Laparoscopic removal of migrated intrauterine device embedded in intestine. JSLS. 2014;18(3).
6. Zakin D, Stern WZ, Rosenblatt R. Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management. Obstet Gynecol Surv. 1981;36(8):401-417.
7. Gill RS, Mok D, Hudson M, Shi X, Birch DW, Karmali S. Laparoscopic removal of an intra-abdominal intrauterine device: case and systematic review. Contraception. 2012;85(1):15-18.
8. Paterson H, Ashton J, Harrison-Woolrych M. A nationwide cohort study of the use of the levonorgestrel intrauterine device in New Zealand adolescents. Contraception. 2009;79(6):433-438.
9. Gorsline JC, Osborne NG. Management of the missing intrauterine contraceptive device: report of a case. Am J Obstet Gynecol. 1985;153(2):228-229.
10. Mederos R, Humaran L, Minervini D. Surgical removal of an intrauterine device perforating the sigmoid colon: a case report. Int J Surg. 2008;6(6):e60-e62.
11. Chi E, Rosenfeld D, Sokol TP. Laparoscopic removal of an intrauterine device perforating the sigmoid colon: a case report and review of the literature. Am Surg. 2005;71(12):1055-1057.
Although intrauterine devices (IUDs) are a mainstay of reversible contraception, they do carry the risk of complications, including septic abortion, abscess formation, ectopic pregnancy, bleeding, and uterine perforation.1 Although perforation is a relatively rare complication, occurring in 0.3 to 2.6 per 1,000 insertions for levonorgestrel-releasing intrauterine systems and 0.3 to 2.2 per 1,000 insertions for copper IUDs, it can lead to serious complications, including IUD migration to various sites.2 Most patients with uterine perforation and IUD migration present with abdominal pain and bleeding; however, 30% of patients are asymptomatic.3
This article presents the case of a young woman who was diagnosed with IUD migration into the abdominal cavity. I discuss the management of this uncommon complication, and stress the importance of adequate education for both patients and health care providers regarding proper surveillance.
Case
A 33-year-old woman (gravida 4, para 4, live 4) presented to our ED for evaluation of rectal bleeding that she had experienced intermittently over the past 2 years. She reported that the first occurrence had been 2 years ago, starting a few weeks after she had a cesarean delivery. The patient described the initial episode as bright red blood mixed with stool. She stated that subsequent episodes had been intermittent, felt as if she were “passing rocks” through her abdomen and rectum, and were accompanied by streaks of blood covering her stool. The day before the patient presented to the ED, she had experienced a second episode of a large bowel movement mixed with blood and accompanied by weakness, which prompted her to seek treatment.
A review of the patient’s symptoms revealed abdominal pain and weakness. She denied any bleeding disorders, fever, chills, sick contacts, anal trauma, presyncope, syncope, nausea, vomiting, diarrhea, or constipation. She further denied any prescription-medication use, illicit drug use, or smoking, but admitted to occasional alcohol use. Her last menstrual period had been 3 weeks prior to presentation. She denied any history of cancer or abnormal Pap smears. Her gynecologic history was significant for chlamydia and trichomoniasis, for which she had been treated. The patient’s surgical history was pertinent for umbilical hernia repair with surgical mesh.
On physical examination, the patient was mildly hypotensive (blood pressure, 97/78 mm Hg) but had a normal heart rate. She had mild conjunctival pallor. The abdominal examination exhibited normoactive bowel sounds with diffuse lower abdominal tenderness to deep palpation, but without rebound, guarding, or distension. Rectal examination revealed a small internal hemorrhoid at the 6 o’clock position (no active bleeding) and an external hemorrhoid with some tenderness to palpation; the external hemorrhoid was not thrombosed, had no signs of infection, and was the same color as the surrounding skin.
A fecal occult blood screen was negative, and a serum pregnancy test was also negative. Complete blood count, basic metabolic profile, and urinalysis were all unremarkable and within normal ranges. Abdominal X-ray revealed a nonobstructive stool pattern and a foreign body, likely in the abdominal cavity, which appeared to be an IUD (Figure 1). Computed tomography (CT) scans of the abdomen and pelvis without contrast were performed to accurately locate the foreign body and to assess for any complications. The CT scans revealed an IUD outside of the uterus, between loops of the transverse colon within the left midabdomen (Figure 2). There were no signs of infection, fluid, or free air. There were also findings of colonic diverticula and narrowed lumen, which were suggestive of diverticulosis.
The patient stated that the IUD had been placed several months after the vaginal birth of her third child. She continued to have normal menstrual periods with the IUD in place. Seven years later, she became pregnant with her fourth child, who was delivered via cesarean, secondary to fetal malpositioning. The IUD was not removed during the cesarean delivery.
Based on the CT scan findings, gynecology services was consulted, and the gynecologist recommended immediate follow-up in a gynecology clinic. The patient was discharged on a bowel regimen. She was assessed in a gynecology clinic 4 days later, where she was found to have a mobile retroverted uterus without tenderness or signs of infection. She underwent exploratory laparoscopy, during which the IUD was removed from the omentum in the left upper abdomen without complications.
Discussion
The IUD has had great acceptance among women since the 1960s. According to the World Health Organization, approximately 14.3% of women used an IUD in 2009.4 Although complications are rare, the most serious are perforation of the uterus and migration of the IUD into adjacent organs.1
Risk factors of uterine perforation include clinician inexperience in IUD placement, an immobile uterus, a retroverted uterus, and the presence of a myometrial defect.4 Heinemann et al2 also suggested that breastfeeding and IUD placement soon after a delivery (≤36 weeks) are independent risk factors, and the presence of both factors has an additive increase in risk of perforation.
Primary rupture of the uterus has been reported at the time of IUD insertion, but secondary or delayed rupture is more common and seems to be due to the spasms of the uterus.5 Although 85% of perforations do not affect other organs, the remaining 15% lead to complications in the adjacent visceral organs.6 The most frequent sites of migration are to the omentum (26.7%), pouch of Douglas (21.5%), large bowel (10.4%), myometrium (7.4%), broad ligament (6.7%), abdominal cavity (5.2%), adhesion to ileal loop serosa (4.4%) or large bowel serosa (3.7%), and mesentery (3%).7 Rare sites are to the appendix, abdominal wall, ovary, and bladder.7
Intrauterine device migration should be suspected in patients who become pregnant after IUD placement (as was the case for our patient), when the “threads” or string cannot be located while attempting to remove an IUD, or when a patient has an “expulsed” IUD without observation of the device thereafter. Even though expulsion of the device happens in approximately 8 per 1,000 insertions, uterine perforation is also a possibility in the case of a “lost” IUD.8 When a lost IUD is suspected, a pelvic examination should be performed to assess for threads or string location. If unsuccessful, ultrasound or plain abdominal radiographic imaging may be used to locate the IUD. Once IUD migration has been confirmed, cross-sectional imaging such as CT scans or magnetic resonance imaging (MRI) is suggested to rule out adjacent organ involvement before considering surgical removal.4 If colonic involvement is suspected, colonoscopy can be used to confirm the diagnosis before operative removal.4
Although management of a migrated IUD in an asymptomatic patient is controversial, there appears to be a consensus that all extrauterine devices should be removed unless the patient’s surgical risk is excessive.1,5,9 Retrieval of an IUD can be performed by laparotomy or laparoscopy.10,11
To avoid these complications and interventions, IUDs should be inserted by an appropriately trained professional, after proper patient selection. These devices should be monitored by periodic examinations, either by medical professionals or by well-informed patients. This can be done by either checking for the threads or string in the cervical opening or by ultrasound imaging to confirm the location of the IUD.
Conclusion
Although many patients with uterine perforation and IUD migration present with symptoms, approximately 30% are asymptomatic.3 If a patient has a lost IUD and the threads or string is not visible during pelvic examination, appropriate work-up, including transvaginal or transabdominal ultrasound or radiographs, should be obtained to confirm the position of the IUD. If IUD migration is suspected, cross-sectional imaging, such as CT scans or MRI, is recommended to rule out adjacent organ involvement before considering surgical removal.4
Even though only 15% of migrated IUDs lead to complications in the adjacent visceral organs,6 surgical removal of the IUD is advised regardless of the presence of symptoms or identified complications. Importantly, to prevent the delayed diagnosis and morbidity of IUD migration, patients with IUDs should be educated about the possibility of migration and the importance of regular self-examination for missing threads or string.
Although intrauterine devices (IUDs) are a mainstay of reversible contraception, they do carry the risk of complications, including septic abortion, abscess formation, ectopic pregnancy, bleeding, and uterine perforation.1 Although perforation is a relatively rare complication, occurring in 0.3 to 2.6 per 1,000 insertions for levonorgestrel-releasing intrauterine systems and 0.3 to 2.2 per 1,000 insertions for copper IUDs, it can lead to serious complications, including IUD migration to various sites.2 Most patients with uterine perforation and IUD migration present with abdominal pain and bleeding; however, 30% of patients are asymptomatic.3
This article presents the case of a young woman who was diagnosed with IUD migration into the abdominal cavity. I discuss the management of this uncommon complication, and stress the importance of adequate education for both patients and health care providers regarding proper surveillance.
Case
A 33-year-old woman (gravida 4, para 4, live 4) presented to our ED for evaluation of rectal bleeding that she had experienced intermittently over the past 2 years. She reported that the first occurrence had been 2 years ago, starting a few weeks after she had a cesarean delivery. The patient described the initial episode as bright red blood mixed with stool. She stated that subsequent episodes had been intermittent, felt as if she were “passing rocks” through her abdomen and rectum, and were accompanied by streaks of blood covering her stool. The day before the patient presented to the ED, she had experienced a second episode of a large bowel movement mixed with blood and accompanied by weakness, which prompted her to seek treatment.
A review of the patient’s symptoms revealed abdominal pain and weakness. She denied any bleeding disorders, fever, chills, sick contacts, anal trauma, presyncope, syncope, nausea, vomiting, diarrhea, or constipation. She further denied any prescription-medication use, illicit drug use, or smoking, but admitted to occasional alcohol use. Her last menstrual period had been 3 weeks prior to presentation. She denied any history of cancer or abnormal Pap smears. Her gynecologic history was significant for chlamydia and trichomoniasis, for which she had been treated. The patient’s surgical history was pertinent for umbilical hernia repair with surgical mesh.
On physical examination, the patient was mildly hypotensive (blood pressure, 97/78 mm Hg) but had a normal heart rate. She had mild conjunctival pallor. The abdominal examination exhibited normoactive bowel sounds with diffuse lower abdominal tenderness to deep palpation, but without rebound, guarding, or distension. Rectal examination revealed a small internal hemorrhoid at the 6 o’clock position (no active bleeding) and an external hemorrhoid with some tenderness to palpation; the external hemorrhoid was not thrombosed, had no signs of infection, and was the same color as the surrounding skin.
A fecal occult blood screen was negative, and a serum pregnancy test was also negative. Complete blood count, basic metabolic profile, and urinalysis were all unremarkable and within normal ranges. Abdominal X-ray revealed a nonobstructive stool pattern and a foreign body, likely in the abdominal cavity, which appeared to be an IUD (Figure 1). Computed tomography (CT) scans of the abdomen and pelvis without contrast were performed to accurately locate the foreign body and to assess for any complications. The CT scans revealed an IUD outside of the uterus, between loops of the transverse colon within the left midabdomen (Figure 2). There were no signs of infection, fluid, or free air. There were also findings of colonic diverticula and narrowed lumen, which were suggestive of diverticulosis.
The patient stated that the IUD had been placed several months after the vaginal birth of her third child. She continued to have normal menstrual periods with the IUD in place. Seven years later, she became pregnant with her fourth child, who was delivered via cesarean, secondary to fetal malpositioning. The IUD was not removed during the cesarean delivery.
Based on the CT scan findings, gynecology services was consulted, and the gynecologist recommended immediate follow-up in a gynecology clinic. The patient was discharged on a bowel regimen. She was assessed in a gynecology clinic 4 days later, where she was found to have a mobile retroverted uterus without tenderness or signs of infection. She underwent exploratory laparoscopy, during which the IUD was removed from the omentum in the left upper abdomen without complications.
Discussion
The IUD has had great acceptance among women since the 1960s. According to the World Health Organization, approximately 14.3% of women used an IUD in 2009.4 Although complications are rare, the most serious are perforation of the uterus and migration of the IUD into adjacent organs.1
Risk factors of uterine perforation include clinician inexperience in IUD placement, an immobile uterus, a retroverted uterus, and the presence of a myometrial defect.4 Heinemann et al2 also suggested that breastfeeding and IUD placement soon after a delivery (≤36 weeks) are independent risk factors, and the presence of both factors has an additive increase in risk of perforation.
Primary rupture of the uterus has been reported at the time of IUD insertion, but secondary or delayed rupture is more common and seems to be due to the spasms of the uterus.5 Although 85% of perforations do not affect other organs, the remaining 15% lead to complications in the adjacent visceral organs.6 The most frequent sites of migration are to the omentum (26.7%), pouch of Douglas (21.5%), large bowel (10.4%), myometrium (7.4%), broad ligament (6.7%), abdominal cavity (5.2%), adhesion to ileal loop serosa (4.4%) or large bowel serosa (3.7%), and mesentery (3%).7 Rare sites are to the appendix, abdominal wall, ovary, and bladder.7
Intrauterine device migration should be suspected in patients who become pregnant after IUD placement (as was the case for our patient), when the “threads” or string cannot be located while attempting to remove an IUD, or when a patient has an “expulsed” IUD without observation of the device thereafter. Even though expulsion of the device happens in approximately 8 per 1,000 insertions, uterine perforation is also a possibility in the case of a “lost” IUD.8 When a lost IUD is suspected, a pelvic examination should be performed to assess for threads or string location. If unsuccessful, ultrasound or plain abdominal radiographic imaging may be used to locate the IUD. Once IUD migration has been confirmed, cross-sectional imaging such as CT scans or magnetic resonance imaging (MRI) is suggested to rule out adjacent organ involvement before considering surgical removal.4 If colonic involvement is suspected, colonoscopy can be used to confirm the diagnosis before operative removal.4
Although management of a migrated IUD in an asymptomatic patient is controversial, there appears to be a consensus that all extrauterine devices should be removed unless the patient’s surgical risk is excessive.1,5,9 Retrieval of an IUD can be performed by laparotomy or laparoscopy.10,11
To avoid these complications and interventions, IUDs should be inserted by an appropriately trained professional, after proper patient selection. These devices should be monitored by periodic examinations, either by medical professionals or by well-informed patients. This can be done by either checking for the threads or string in the cervical opening or by ultrasound imaging to confirm the location of the IUD.
Conclusion
Although many patients with uterine perforation and IUD migration present with symptoms, approximately 30% are asymptomatic.3 If a patient has a lost IUD and the threads or string is not visible during pelvic examination, appropriate work-up, including transvaginal or transabdominal ultrasound or radiographs, should be obtained to confirm the position of the IUD. If IUD migration is suspected, cross-sectional imaging, such as CT scans or MRI, is recommended to rule out adjacent organ involvement before considering surgical removal.4
Even though only 15% of migrated IUDs lead to complications in the adjacent visceral organs,6 surgical removal of the IUD is advised regardless of the presence of symptoms or identified complications. Importantly, to prevent the delayed diagnosis and morbidity of IUD migration, patients with IUDs should be educated about the possibility of migration and the importance of regular self-examination for missing threads or string.
1. Hoşcan MB, Koşar A, Gümüştaş U, Güney M. Intravesical migration of intrauterine device resulting in pregnancy. Int J Urol. 2006;13(3):301-302.
2. Heinemann K, Reed S, Moehner S, Minh TD. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European Active Surveillance Study on Intrauterine Devices. Contraception. 2015;91(4):274-279.
3. Singh SP, Mangla D, Chawan J, Haq AU. Asymptomatic presentation of silent uterine perforation by Cu-T 380A: a case report with review of literature. Int J Reprod Contracept Obstet Gynecol. 2014;3(4):1157-1159.
4. Akpinar F, Ozgur EN, Yilmaz S, Ustaoglu O. Sigmoid colon migration of an intrauterine device. Case Rep Obstet Gynecol. 2014;2014:207659.
5. Rahnemai-Azar AA, Apfel T, Naghshizadian R, Cosgrove JM, Farkas DT. Laparoscopic removal of migrated intrauterine device embedded in intestine. JSLS. 2014;18(3).
6. Zakin D, Stern WZ, Rosenblatt R. Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management. Obstet Gynecol Surv. 1981;36(8):401-417.
7. Gill RS, Mok D, Hudson M, Shi X, Birch DW, Karmali S. Laparoscopic removal of an intra-abdominal intrauterine device: case and systematic review. Contraception. 2012;85(1):15-18.
8. Paterson H, Ashton J, Harrison-Woolrych M. A nationwide cohort study of the use of the levonorgestrel intrauterine device in New Zealand adolescents. Contraception. 2009;79(6):433-438.
9. Gorsline JC, Osborne NG. Management of the missing intrauterine contraceptive device: report of a case. Am J Obstet Gynecol. 1985;153(2):228-229.
10. Mederos R, Humaran L, Minervini D. Surgical removal of an intrauterine device perforating the sigmoid colon: a case report. Int J Surg. 2008;6(6):e60-e62.
11. Chi E, Rosenfeld D, Sokol TP. Laparoscopic removal of an intrauterine device perforating the sigmoid colon: a case report and review of the literature. Am Surg. 2005;71(12):1055-1057.
1. Hoşcan MB, Koşar A, Gümüştaş U, Güney M. Intravesical migration of intrauterine device resulting in pregnancy. Int J Urol. 2006;13(3):301-302.
2. Heinemann K, Reed S, Moehner S, Minh TD. Risk of uterine perforation with levonorgestrel-releasing and copper intrauterine devices in the European Active Surveillance Study on Intrauterine Devices. Contraception. 2015;91(4):274-279.
3. Singh SP, Mangla D, Chawan J, Haq AU. Asymptomatic presentation of silent uterine perforation by Cu-T 380A: a case report with review of literature. Int J Reprod Contracept Obstet Gynecol. 2014;3(4):1157-1159.
4. Akpinar F, Ozgur EN, Yilmaz S, Ustaoglu O. Sigmoid colon migration of an intrauterine device. Case Rep Obstet Gynecol. 2014;2014:207659.
5. Rahnemai-Azar AA, Apfel T, Naghshizadian R, Cosgrove JM, Farkas DT. Laparoscopic removal of migrated intrauterine device embedded in intestine. JSLS. 2014;18(3).
6. Zakin D, Stern WZ, Rosenblatt R. Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management. Obstet Gynecol Surv. 1981;36(8):401-417.
7. Gill RS, Mok D, Hudson M, Shi X, Birch DW, Karmali S. Laparoscopic removal of an intra-abdominal intrauterine device: case and systematic review. Contraception. 2012;85(1):15-18.
8. Paterson H, Ashton J, Harrison-Woolrych M. A nationwide cohort study of the use of the levonorgestrel intrauterine device in New Zealand adolescents. Contraception. 2009;79(6):433-438.
9. Gorsline JC, Osborne NG. Management of the missing intrauterine contraceptive device: report of a case. Am J Obstet Gynecol. 1985;153(2):228-229.
10. Mederos R, Humaran L, Minervini D. Surgical removal of an intrauterine device perforating the sigmoid colon: a case report. Int J Surg. 2008;6(6):e60-e62.
11. Chi E, Rosenfeld D, Sokol TP. Laparoscopic removal of an intrauterine device perforating the sigmoid colon: a case report and review of the literature. Am Surg. 2005;71(12):1055-1057.

Emergency Ultrasound: Tips and Tricks for Imaging Digits
Clinicians familiar with point-of-care (POC) ultrasound know that structures such as the hands and feet require the use of the linear high-frequency transducer to obtain quality images. In reality, however, employing the standard technique (ie, applying gel to the probe surface and scanning the structure) can be challenging due to the uneven surfaces of the fingers and toes; therefore, obtaining good contact with the transducer is harder than it may seem at first glance. Additionally, since these structures are superficial, they are usually seen on the top half of the ultrasound display, while the focal zone of most ultrasound machines is located in the middle of the display and is nonadjustable.
We describe two simple adjuncts to POC ultrasound that can assist in visualizing digital structures with greater ease and improved image resolution: the water bath1,2 and standoff pad techniques.
Water Bath Technique
In the water bath technique, one fills a small basin with lukewarm water to a depth point where the extremity being studied (ie, hand or foot) is mostly—but not completely—submerged in the water bath. After the extremity is submerged, the high-frequency probe is then placed into the water bath (Figure 1). When employing this technique, the transducer does not need to make contact with the patient’s skin. Since the water acts as an excellent conduction medium for sound waves, no ultrasound gel is required. For a video demonstrating the use of the water bath technique to evaluate the distal tip of the finger, see below.

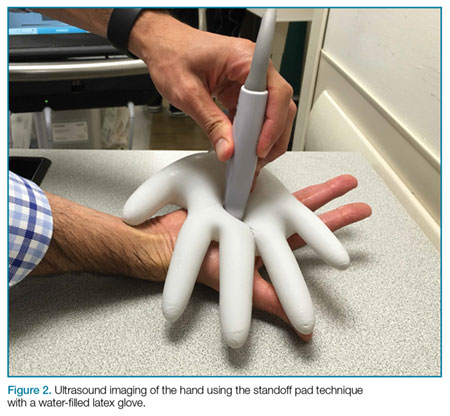
Standoff Pad
Another technique that enhances POC imaging of the digits involves a standoff pad. A variety of commercially available standoff pads can be used for this technique. Alternatively, the clinician can easily create a standoff pad using supplies that are readily available in the ED. One such method is to fill a latex glove with water, tie off the filled glove, and place it on top of the extremity to be imaged (Figure 2). The water in the glove will facilitate sound-wave transmission.

Pathology
The water bath and standoff pad techniques can facilitate visualization of several pathologies, including felons (Figure 3), flexor tenosynovitis, phalangeal and metacarpal/metatarsal fractures, and interphalangeal, metacarpophalangeal, and metatarsophalangeal joint effusions (Figure 4). In addition, these techniques also assist in visualizing digit tendons to evaluate for tears in these structures (Figure 5).

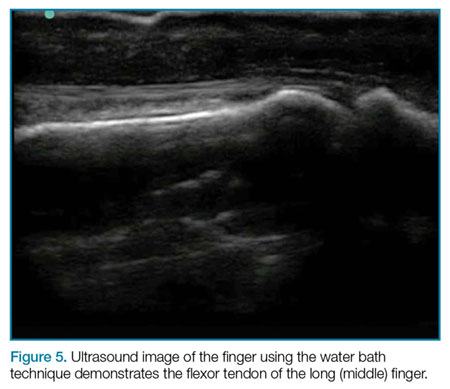
Summary
Point-of-care ultrasound imaging to evaluate superficial body parts such as hands or feet can be challenging due to the irregular shape and uneven surface of these structures. The employment of adjuncts such as the water bath or standoff pad techniques can mitigate these challenges, facilitating the acquisition of high-resolution images and providing easier identification of pathology.
1. Krishnamurthy R, Yoo JH, Thapa M, Callahan MJ. Water-bath method for sonographic evaluation of superficial structures of the extremities in children. Pediatr Radiol. 2013;4(Suppl 1):S41-S47. DOI:10.1007/s00247-012-2592-y.
2. Jeong HY, Krishnamurthy R. 1012: Water-bath method for sonographic evaluation of superficial structures of the extremities. Ultrasound Med Biol. 2009;35(8):S101-S102. doi:10.1016/j.ultrasmedbio.2009.06.394.
Clinicians familiar with point-of-care (POC) ultrasound know that structures such as the hands and feet require the use of the linear high-frequency transducer to obtain quality images. In reality, however, employing the standard technique (ie, applying gel to the probe surface and scanning the structure) can be challenging due to the uneven surfaces of the fingers and toes; therefore, obtaining good contact with the transducer is harder than it may seem at first glance. Additionally, since these structures are superficial, they are usually seen on the top half of the ultrasound display, while the focal zone of most ultrasound machines is located in the middle of the display and is nonadjustable.
We describe two simple adjuncts to POC ultrasound that can assist in visualizing digital structures with greater ease and improved image resolution: the water bath1,2 and standoff pad techniques.
Water Bath Technique
In the water bath technique, one fills a small basin with lukewarm water to a depth point where the extremity being studied (ie, hand or foot) is mostly—but not completely—submerged in the water bath. After the extremity is submerged, the high-frequency probe is then placed into the water bath (Figure 1). When employing this technique, the transducer does not need to make contact with the patient’s skin. Since the water acts as an excellent conduction medium for sound waves, no ultrasound gel is required. For a video demonstrating the use of the water bath technique to evaluate the distal tip of the finger, see below.
Standoff Pad
Another technique that enhances POC imaging of the digits involves a standoff pad. A variety of commercially available standoff pads can be used for this technique. Alternatively, the clinician can easily create a standoff pad using supplies that are readily available in the ED. One such method is to fill a latex glove with water, tie off the filled glove, and place it on top of the extremity to be imaged (Figure 2). The water in the glove will facilitate sound-wave transmission.
Pathology
The water bath and standoff pad techniques can facilitate visualization of several pathologies, including felons (Figure 3), flexor tenosynovitis, phalangeal and metacarpal/metatarsal fractures, and interphalangeal, metacarpophalangeal, and metatarsophalangeal joint effusions (Figure 4). In addition, these techniques also assist in visualizing digit tendons to evaluate for tears in these structures (Figure 5).
Summary
Point-of-care ultrasound imaging to evaluate superficial body parts such as hands or feet can be challenging due to the irregular shape and uneven surface of these structures. The employment of adjuncts such as the water bath or standoff pad techniques can mitigate these challenges, facilitating the acquisition of high-resolution images and providing easier identification of pathology.
Clinicians familiar with point-of-care (POC) ultrasound know that structures such as the hands and feet require the use of the linear high-frequency transducer to obtain quality images. In reality, however, employing the standard technique (ie, applying gel to the probe surface and scanning the structure) can be challenging due to the uneven surfaces of the fingers and toes; therefore, obtaining good contact with the transducer is harder than it may seem at first glance. Additionally, since these structures are superficial, they are usually seen on the top half of the ultrasound display, while the focal zone of most ultrasound machines is located in the middle of the display and is nonadjustable.
We describe two simple adjuncts to POC ultrasound that can assist in visualizing digital structures with greater ease and improved image resolution: the water bath1,2 and standoff pad techniques.
Water Bath Technique
In the water bath technique, one fills a small basin with lukewarm water to a depth point where the extremity being studied (ie, hand or foot) is mostly—but not completely—submerged in the water bath. After the extremity is submerged, the high-frequency probe is then placed into the water bath (Figure 1). When employing this technique, the transducer does not need to make contact with the patient’s skin. Since the water acts as an excellent conduction medium for sound waves, no ultrasound gel is required. For a video demonstrating the use of the water bath technique to evaluate the distal tip of the finger, see below.
Standoff Pad
Another technique that enhances POC imaging of the digits involves a standoff pad. A variety of commercially available standoff pads can be used for this technique. Alternatively, the clinician can easily create a standoff pad using supplies that are readily available in the ED. One such method is to fill a latex glove with water, tie off the filled glove, and place it on top of the extremity to be imaged (Figure 2). The water in the glove will facilitate sound-wave transmission.
Pathology
The water bath and standoff pad techniques can facilitate visualization of several pathologies, including felons (Figure 3), flexor tenosynovitis, phalangeal and metacarpal/metatarsal fractures, and interphalangeal, metacarpophalangeal, and metatarsophalangeal joint effusions (Figure 4). In addition, these techniques also assist in visualizing digit tendons to evaluate for tears in these structures (Figure 5).
Summary
Point-of-care ultrasound imaging to evaluate superficial body parts such as hands or feet can be challenging due to the irregular shape and uneven surface of these structures. The employment of adjuncts such as the water bath or standoff pad techniques can mitigate these challenges, facilitating the acquisition of high-resolution images and providing easier identification of pathology.
1. Krishnamurthy R, Yoo JH, Thapa M, Callahan MJ. Water-bath method for sonographic evaluation of superficial structures of the extremities in children. Pediatr Radiol. 2013;4(Suppl 1):S41-S47. DOI:10.1007/s00247-012-2592-y.
2. Jeong HY, Krishnamurthy R. 1012: Water-bath method for sonographic evaluation of superficial structures of the extremities. Ultrasound Med Biol. 2009;35(8):S101-S102. doi:10.1016/j.ultrasmedbio.2009.06.394.
1. Krishnamurthy R, Yoo JH, Thapa M, Callahan MJ. Water-bath method for sonographic evaluation of superficial structures of the extremities in children. Pediatr Radiol. 2013;4(Suppl 1):S41-S47. DOI:10.1007/s00247-012-2592-y.
2. Jeong HY, Krishnamurthy R. 1012: Water-bath method for sonographic evaluation of superficial structures of the extremities. Ultrasound Med Biol. 2009;35(8):S101-S102. doi:10.1016/j.ultrasmedbio.2009.06.394.
