User login
Fertility and Fertility Preservation: Scripts to Support Oncology Nurses in Discussions with Adolescent and Young Adult Patients
From the Moffitt Cancer Center, Tampa, FL (Dr. Vadaparampil, Ms. Bowman, Ms. Sehovic, Dr. Quinn), Memorial Sloan Kettering Cancer Center, New York, NY (Ms. Kelvin), and Edward Via College of Osteopathic Medicine, Auburn, AL (Ms. Murphy).
Abstract
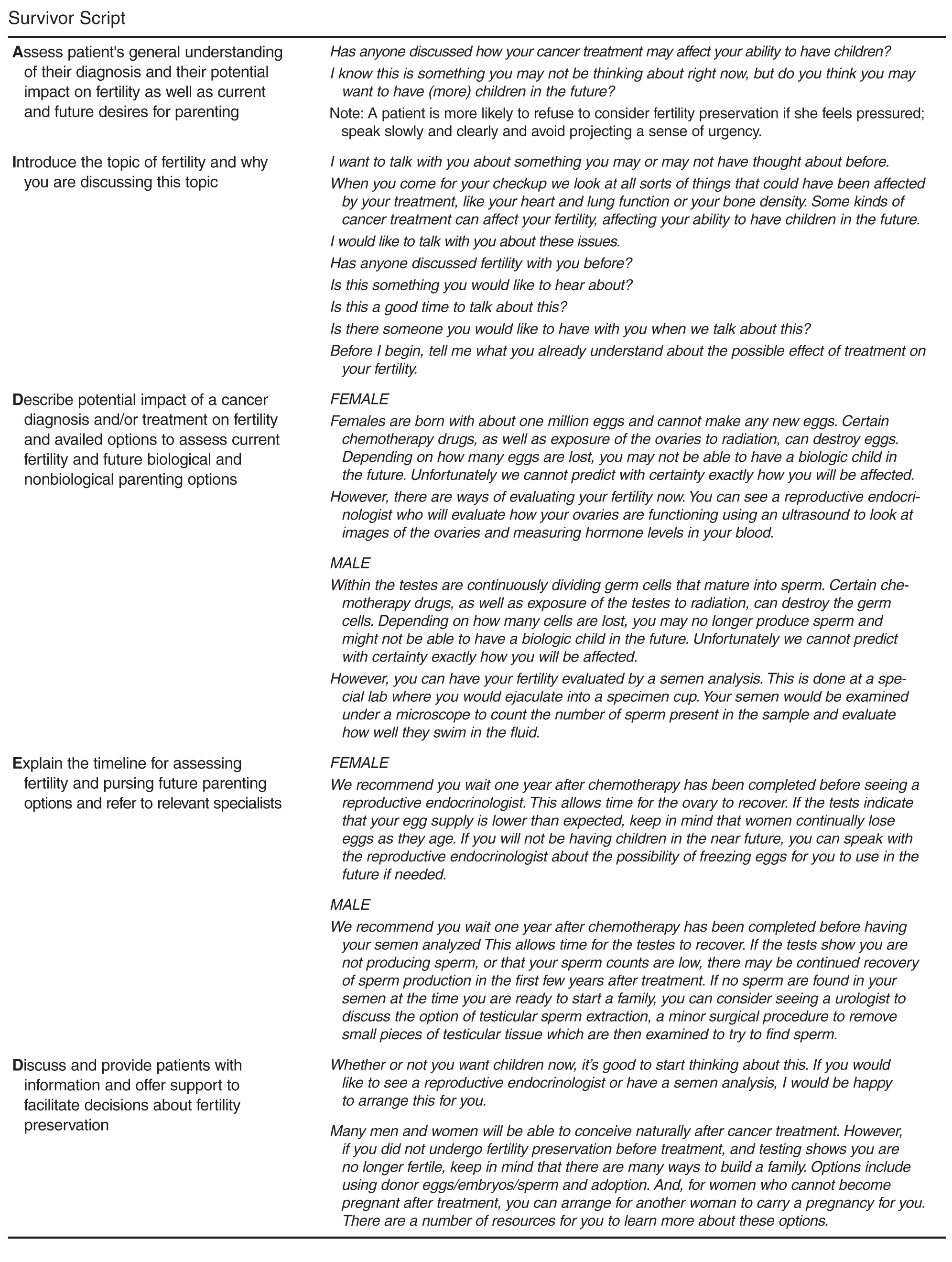
- Objective: To describe a script-based approach to assist oncology nurses in fertility discussions with their adolescent and young adult (AYA) patients.
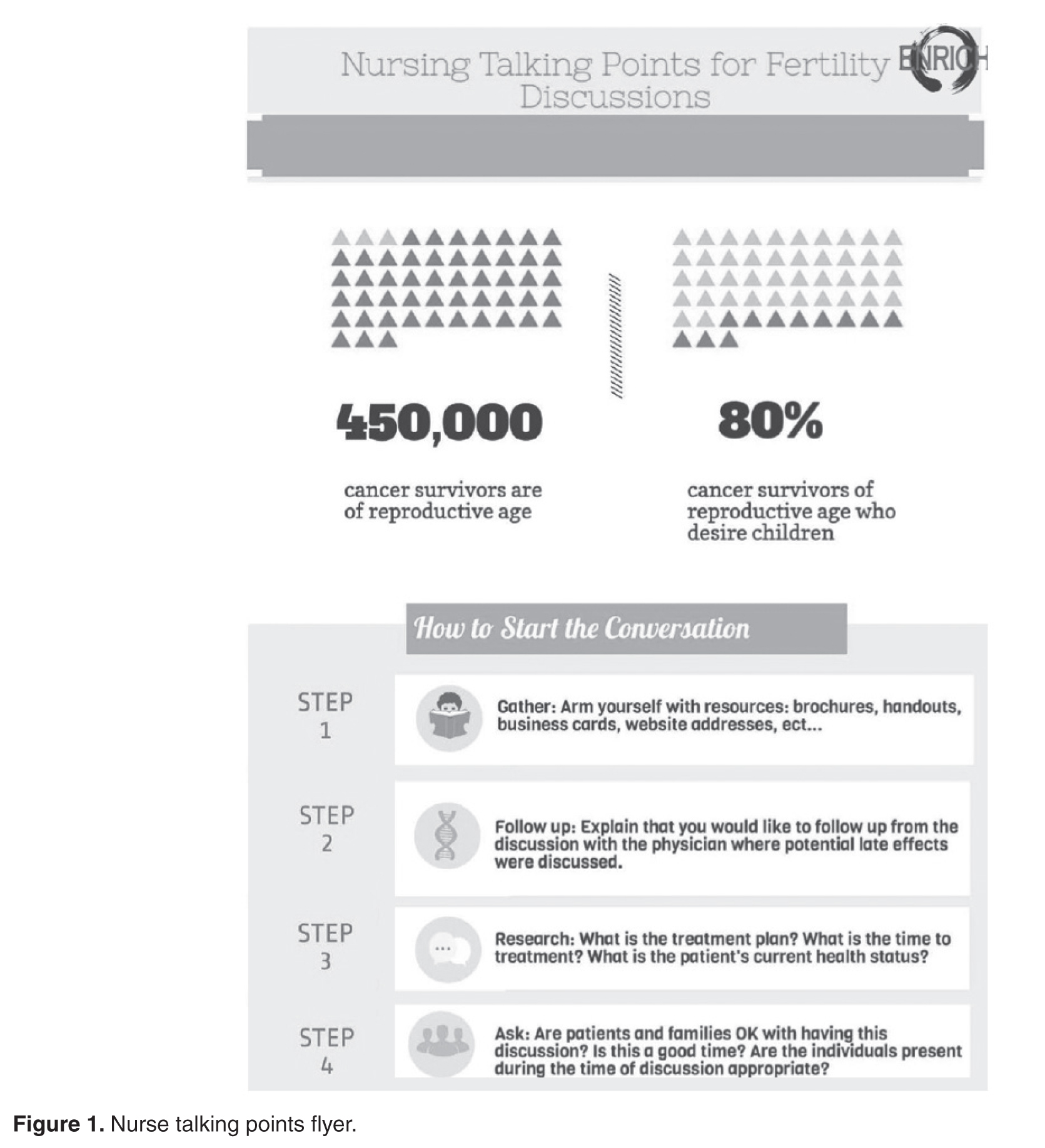
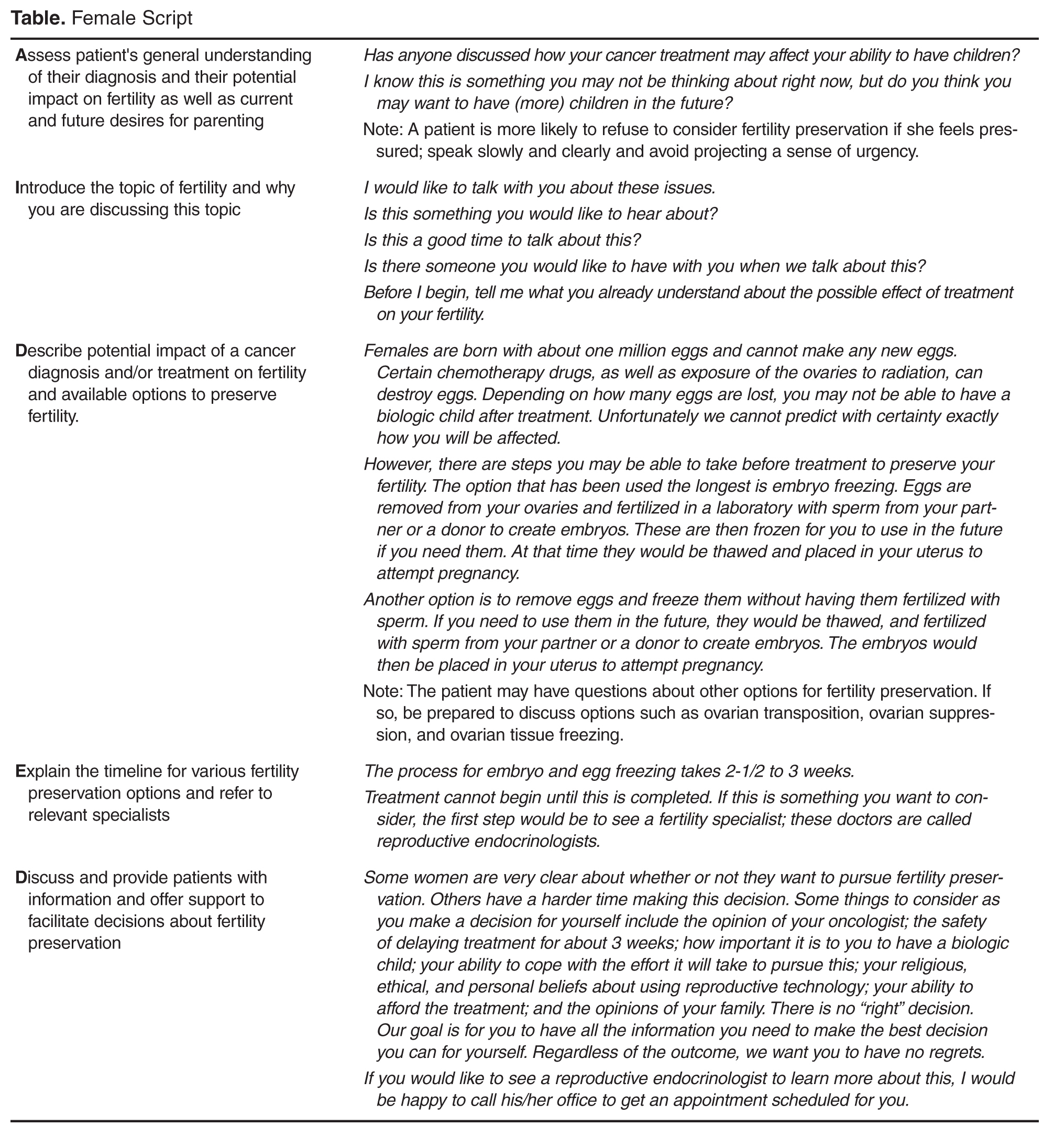
- Methods: Scripts were developed by a team that included experts in fertility and reproductive health, health education, health communication, and clinical care of AYA patients. Individual scripts for females, males, and survivors were created and accompanied by a flyer and frequently asked questions sheet. The script and supplementary materials were then vetted by oncology nurses who participated in the Educating Nurses about Reproductive Health Issues in Cancer Healthcare (ENRICH) training program.
- Results: The scripts were rated as helpful and socially appropriate with minor concerns noted about awkward wording and medical jargon.
- Conclusion: The updated scripts provide one approach for nurses to become more adept at discussing the topic of infertility and FP with AYA oncology patients and survivors.
In the United States, over 70,000 adolescents and young adults (AYAs) are diagnosed with cancer each year [1,2]. Treatments are available that are associated with improved survival for these cancers. Unfortunately, cancer treatment may significantly impact AYA survivors’ future fertility. Infertility or premature ovarian failure can occur during or after cancer treatment (eg, chemotherapy, radiation) for females, and males may be temporarily or permanently azoospermic [3]. There are a number of established methods of fertility preservation (FP) that are available; these include oocyte and embryo cryopreservation and ovarian transposition for females and sperm banking for males [3]. Experimental options for males include testicular tissue freezing and for females ovarian tissue cryopreservation.
The American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network [4,5] recommend discussing FP with patients of reproductive age, ideally before initiation of treatment. In 2013, ASCO updated guidelines extending the responsibility for discussion and referral for FP beyond the medical oncologist to explicitly include other physician specialties, nurses, and allied health care professionals in the oncology care setting [3]. However, multiple publications, including patient surveys and interviews, physician surveys, and medical record abstraction studies suggest these discussions do not consistently take place. In an analysis of 156 practice groups submitting data as part of ASCO's Quality Oncology Practice Initiative, only ~15%–20% of practices routinely discussed infertility risks and FP options [6]. A recent review of medical charts of patients aged 18–45 treated in 2011 at 1 of 4 large U.S. cancer care institutions found that documentation of discussions for infertility risk was 26%, 24% for FP option discussion, and 13% for fertility specialist referral [7].
Oncology nurses play a key role in patients’ care and, compared to other health care providers, are more likely to have multiple interactions with patients prior to the initiation of treatment [8]. They are often attuned to the medical and psychosocial needs of the patient and family and can advocate for their needs and desires [9]. However, existing research finds few oncology nurses discuss this topic with AYA patients. Studies examining barriers have identified factors that may hinder discussions about infertility and FP with AYA oncology patients. These barriers include lack of knowledge about cancer related infertility and available FP procedures; access to reproductive endocrinologists or sperm banking clinics; time constraints in busy clinics and concerns about delaying treatment; discomforts discussing reproductive health; patient’s ability to afford FP; bias about the suitability of FP for young or unpartnered or LGBT patients or those with a poor prognosis; and personal religious or moral values about the use of assisted reproductive technologies [10–15].
Equipping nurses with content-specific communication may overcome some of the barriers described. A method often used in nursing education and communication interventions is scripting [16–18]. Scripting provides precise key words that ensure consistency in the message, no matter the messenger [19]. This paper reports on the development and refinement of a series of scripts to guide discussions about FP for male and female AYA patients and survivors.
Script Development
In 2003 Studer developed the AIDET (Acknowledge, Introduce, Duration, Explanation, and Thank you) model of communication for health professionals [19]. AIDET is an effective tool in facilitating communication practices among nurses and physicians in adult and pediatric settings [20–24]. The AIDET model was adapted by our team to develop AIDED: Assess, Introduce, Decide, Explain, and Discuss, a script-based approach to assist oncology nurses in fertility discussions with their AYA patients. Our team included experts in fertility and reproductive health, health education, health communication, as well as clinical and psychosocial care of AYA patients.
Educating Nurses 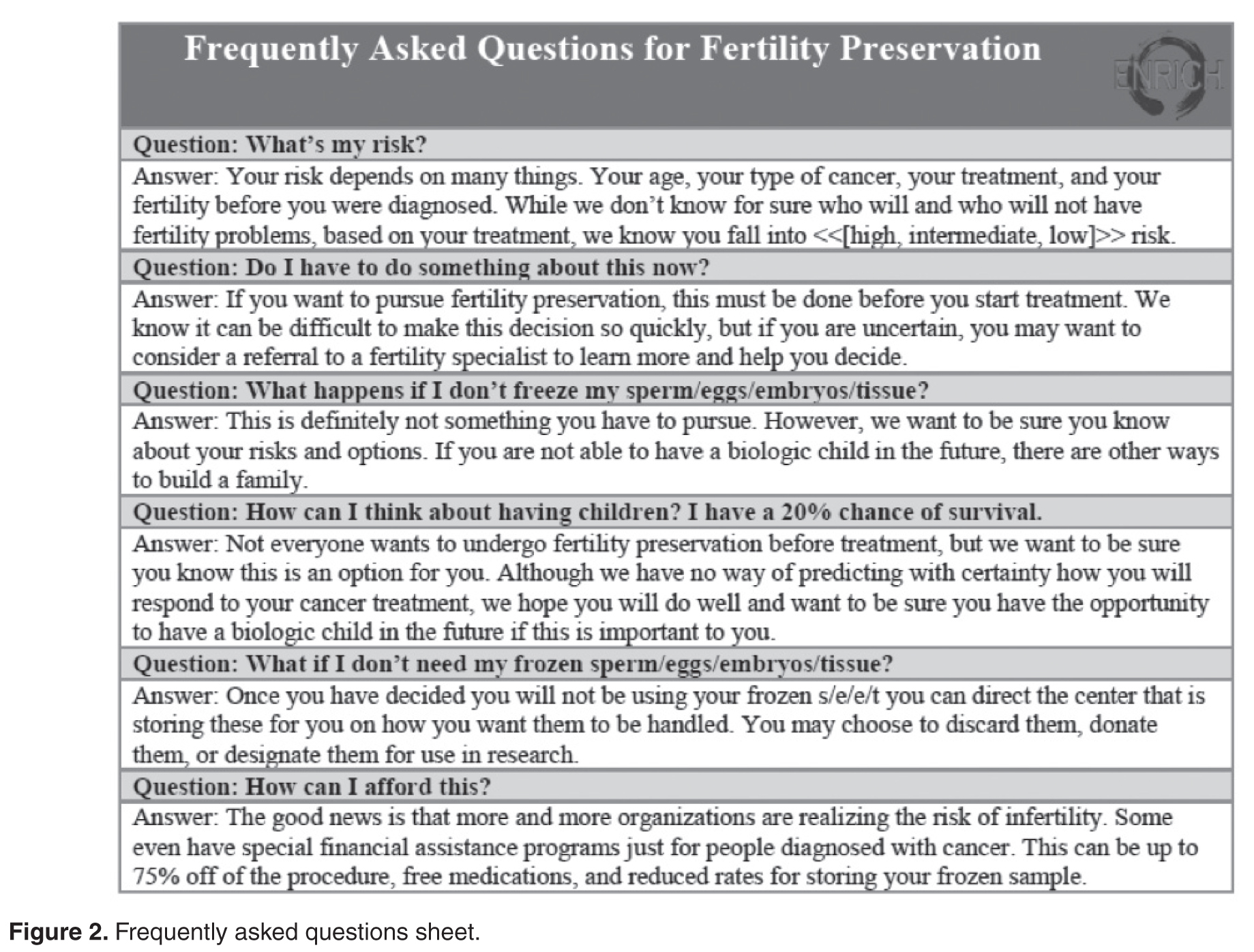
Benefits of Scripts
Communication difficulties may present an obstacle for oncology nurses to address the infertility, FP information, and supportive care needs of AYA cancer patients [15]. While guidelines from leading health and professional organizations support the need to discuss these issues with patients, implementation requires providing practical tools that meet the needs of nurses’ practice setting and patient population [26].
The use of scripts has a long history in the 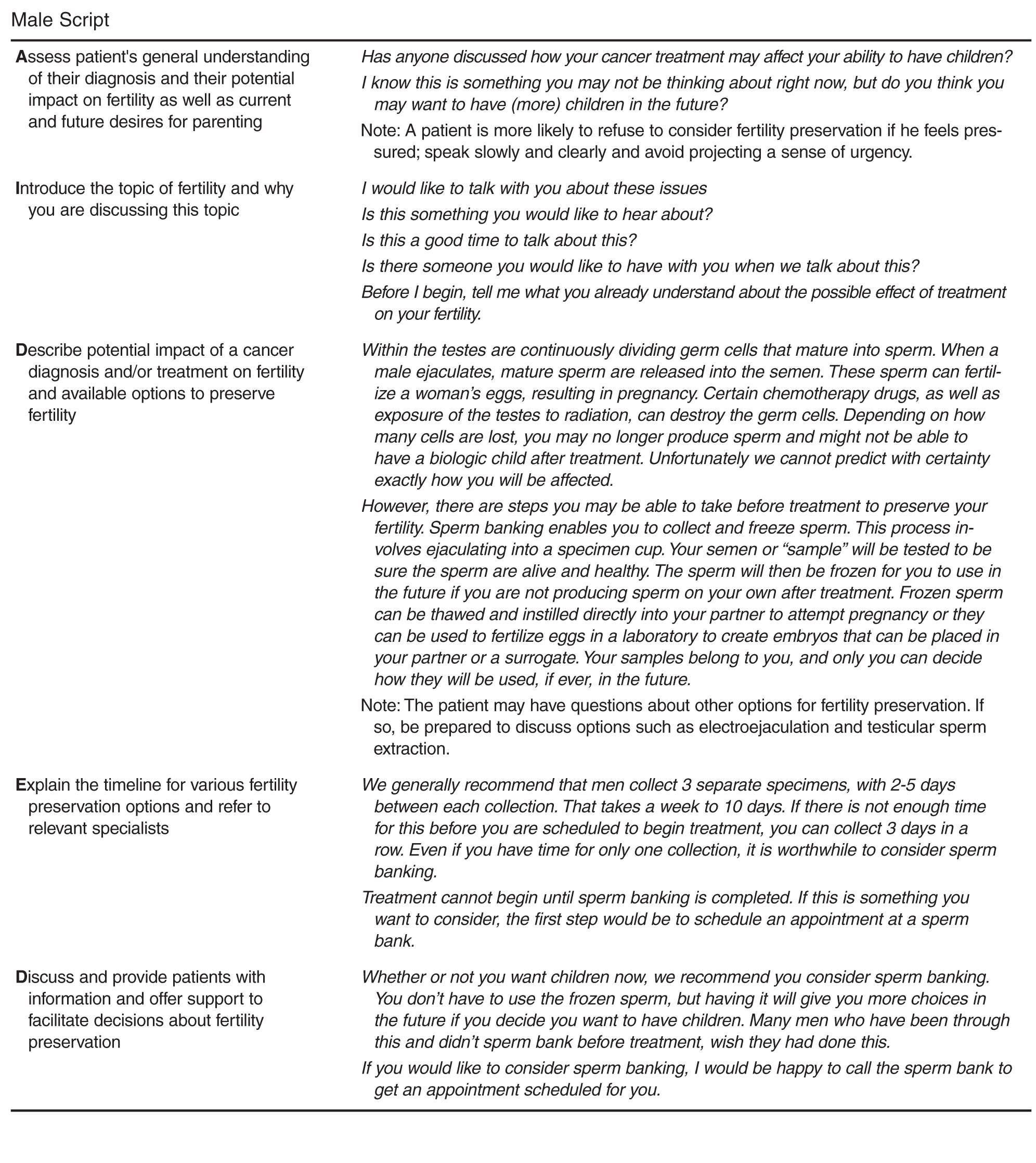
Conclusion

These scripts provide one approach for nurses to become more adept at discussing the topic of FP with AYA oncology patients. We will continue to update and refine these scripts and ultimately test their efficacy in improving psychosocial and behavioral outcomes for AYA patients. While scripts are effective, they must be updated to reflect relevant advances in clinical care. In addition, it is important to identify local resources to facilitate discussion and referral for those who seek additional information and or services related to FP. Such resources include psychosocial support, reproductive endocrinologists with expertise in the unique needs of AYA oncology patients, providers who accept pediatric patients (if needed), and financial assistance.
Corresponding author: Susan T. Vadaparampil, PhD, MPH, 12902 Magnolia Dr., MRC CANCONT, Tampa, FL 33612, [email protected].
Funding/support: ENRICH is funded by a National Cancer Institute R25 Training Grant: #5R25CA142519-05.
Financial disclosures: None.
1. Bleyer AOLM, O’Leary M, Barr L, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. Bethesda, MD: National Cancer Institute; 2006.
2. Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 2014;64: 83–103.
3. Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013;31:2500–10.
4. Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
5. Coccia P, Altman J, Bhatia S, et al. Adolescent and young adult (AYA) oncology version 1.2012. National Comprehensive Cancer Network; 2012.
6. Neuss MN, Malin JL, Chan S, et al. Measuring the improving quality of outpatient care in medical oncology practices in the United States. J Clin Oncol 2013;31:1471–7.
7. Quinn GP, Block RG, Clayman ML, et al. If you did not document it, it did not happen: rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J Oncol Pract 2015;11: 137–44.
8. Cope D. Patients’ and physicians’ experinces with sperm banking and infertility issues related to cancer treatment. Clin J Oncol Nurs 2002;6:293–5.
9. Vaartio-Rajalin H, Leino-Kilpi H. Nurses as patient advocates in oncology care: activities based on literature. Clin J Oncol Nurs. 2011;15:526–32.
10. King LM, Quinn GP, Vadaparampil ST, et al. Oncology nurses’ perceptions of barriers to discussion of fertility preservation with patients with cancer. Clin J Oncol Nurs 2008; 12:467–76.
11. Clayton HB, Vadaparampil ST, Quinn GP, et al. Trends in clinical practice and nurses’ attitudes about fertility preservation for pediatric patients with cancer. Oncol Nurs Forum 2008;35:449–55.
12. Vadaparampil ST, Clayton H, Quinn GP, et al. Pediatric oncology nurses’ attitudes related to discussing fertility preservation with pediatric cancer patients and their families. J Pediatr Oncol Nurs 2007;24:255–63.
13. Kotronoulas G, Papadopoulou C, Patiraki E. Nurses’ knowledge, attitudes, and practices regarding provision of sexual health care in patients with cancer: critical review of the evidence. Support Care Cancer 2009;17:479–501.
14. Reebals JF, Brown R, Buckner EB. Nurse practice issues regarding sperm banking in adolescent male cancer patients. J Pediatr Oncol Nurs 2006;23:182–8.
15. Goossens J, Delbaere I, Beeckman D, et al. Communication difficulties and the experience of loneliness in patients with cancer dealing with fertility issues: a qualitative study. Oncol Nurs Forum 2015;42:34–43.
16. Mustard LW. Improving patient satisfaction through the consistent use of scripting by the nursing staff. JONAS Healthc Law Ethics Regul 2003;5:68–72.
17. Kuiper RA. Integration of innovative clinical reasoning pedagogies into a baccalaureate nursing curriculum. Creat Nurs 2013;19:128–39.
18. Handel DA, Fu R, Daya M, et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med 2010; 17:495–500.
19. Studer Q. Hardwiring excellence: purpose, worthwhile work, making a difference. Gulf Breeze, FL: Fire Starter Publishing; 2003.
20. Katona A, Kunkel E, Arfaa J, et al. Methodology for delivering feedback to neurology house staff on communication skills using AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You). Neurology 2014;82(10 Suppl):P1–328.
21. Prestia A , Dyess S. Maximizing caring relationships between nursing assistants and patients: Care partners. J Nurs Admin 2012;42:144–7.
22. Fisher MJ. A brief intervention to improve emotion-focused communication between newly licensed pediatric nurses and parents [dissertation]. Indianapolis: Indiana University; 2012.
23. Baker SJ. Key words: a prescriptive approach to reducing patient anxiety and improving safety. J Emerg Nurs 2011; 37:571–4.
24. Shupe R. Using skills validation and verification techniques to hardwire staff behaviors. J Emerg Nurs 2013;39:364–8.
25. Vadaparampil ST, Hutchins NM, Quinn GP. Reproductive health in the adolescent and young adult cancer patient: an innovative training program for oncology nurses. J Cancer Educ 2013;28:197–208.
26. Shekelle P, Woolf S, Grimshaw JM, et al. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci 2012;7:62.
27. Clayton JM, Adler JL, O’Callaghan A, et al. Intensive communication skills teaching for specialist training in palliative medicine: development and evaluation of an experiential workshop. J Palliat Med 2012;15:585–91.
28. Hymes DH. On communicative competence. In: Pride JB, Holmes J, editors. Sociolinguistics: selected readings. Harmondsworth: Penguin; 1972:269–93.
29. Asnani MR. Patient-physician communication. West Indian Med J 2009;58:357–61.
30. Clark PA. Medical practices’ sensitivity to patients’ needs: Opportunities and practices for improvement. J Ambulat Care Manage 2003;26:110–23.
31. Wanzer MB, Booth-Butterfield M, Gruber K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Care Commun 2004;16:363–84.
From the Moffitt Cancer Center, Tampa, FL (Dr. Vadaparampil, Ms. Bowman, Ms. Sehovic, Dr. Quinn), Memorial Sloan Kettering Cancer Center, New York, NY (Ms. Kelvin), and Edward Via College of Osteopathic Medicine, Auburn, AL (Ms. Murphy).
Abstract
- Objective: To describe a script-based approach to assist oncology nurses in fertility discussions with their adolescent and young adult (AYA) patients.
- Methods: Scripts were developed by a team that included experts in fertility and reproductive health, health education, health communication, and clinical care of AYA patients. Individual scripts for females, males, and survivors were created and accompanied by a flyer and frequently asked questions sheet. The script and supplementary materials were then vetted by oncology nurses who participated in the Educating Nurses about Reproductive Health Issues in Cancer Healthcare (ENRICH) training program.
- Results: The scripts were rated as helpful and socially appropriate with minor concerns noted about awkward wording and medical jargon.
- Conclusion: The updated scripts provide one approach for nurses to become more adept at discussing the topic of infertility and FP with AYA oncology patients and survivors.
In the United States, over 70,000 adolescents and young adults (AYAs) are diagnosed with cancer each year [1,2]. Treatments are available that are associated with improved survival for these cancers. Unfortunately, cancer treatment may significantly impact AYA survivors’ future fertility. Infertility or premature ovarian failure can occur during or after cancer treatment (eg, chemotherapy, radiation) for females, and males may be temporarily or permanently azoospermic [3]. There are a number of established methods of fertility preservation (FP) that are available; these include oocyte and embryo cryopreservation and ovarian transposition for females and sperm banking for males [3]. Experimental options for males include testicular tissue freezing and for females ovarian tissue cryopreservation.
The American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network [4,5] recommend discussing FP with patients of reproductive age, ideally before initiation of treatment. In 2013, ASCO updated guidelines extending the responsibility for discussion and referral for FP beyond the medical oncologist to explicitly include other physician specialties, nurses, and allied health care professionals in the oncology care setting [3]. However, multiple publications, including patient surveys and interviews, physician surveys, and medical record abstraction studies suggest these discussions do not consistently take place. In an analysis of 156 practice groups submitting data as part of ASCO's Quality Oncology Practice Initiative, only ~15%–20% of practices routinely discussed infertility risks and FP options [6]. A recent review of medical charts of patients aged 18–45 treated in 2011 at 1 of 4 large U.S. cancer care institutions found that documentation of discussions for infertility risk was 26%, 24% for FP option discussion, and 13% for fertility specialist referral [7].
Oncology nurses play a key role in patients’ care and, compared to other health care providers, are more likely to have multiple interactions with patients prior to the initiation of treatment [8]. They are often attuned to the medical and psychosocial needs of the patient and family and can advocate for their needs and desires [9]. However, existing research finds few oncology nurses discuss this topic with AYA patients. Studies examining barriers have identified factors that may hinder discussions about infertility and FP with AYA oncology patients. These barriers include lack of knowledge about cancer related infertility and available FP procedures; access to reproductive endocrinologists or sperm banking clinics; time constraints in busy clinics and concerns about delaying treatment; discomforts discussing reproductive health; patient’s ability to afford FP; bias about the suitability of FP for young or unpartnered or LGBT patients or those with a poor prognosis; and personal religious or moral values about the use of assisted reproductive technologies [10–15].
Equipping nurses with content-specific communication may overcome some of the barriers described. A method often used in nursing education and communication interventions is scripting [16–18]. Scripting provides precise key words that ensure consistency in the message, no matter the messenger [19]. This paper reports on the development and refinement of a series of scripts to guide discussions about FP for male and female AYA patients and survivors.
Script Development
In 2003 Studer developed the AIDET (Acknowledge, Introduce, Duration, Explanation, and Thank you) model of communication for health professionals [19]. AIDET is an effective tool in facilitating communication practices among nurses and physicians in adult and pediatric settings [20–24]. The AIDET model was adapted by our team to develop AIDED: Assess, Introduce, Decide, Explain, and Discuss, a script-based approach to assist oncology nurses in fertility discussions with their AYA patients. Our team included experts in fertility and reproductive health, health education, health communication, as well as clinical and psychosocial care of AYA patients.
Educating Nurses
Benefits of Scripts
Communication difficulties may present an obstacle for oncology nurses to address the infertility, FP information, and supportive care needs of AYA cancer patients [15]. While guidelines from leading health and professional organizations support the need to discuss these issues with patients, implementation requires providing practical tools that meet the needs of nurses’ practice setting and patient population [26].
The use of scripts has a long history in the
Conclusion
These scripts provide one approach for nurses to become more adept at discussing the topic of FP with AYA oncology patients. We will continue to update and refine these scripts and ultimately test their efficacy in improving psychosocial and behavioral outcomes for AYA patients. While scripts are effective, they must be updated to reflect relevant advances in clinical care. In addition, it is important to identify local resources to facilitate discussion and referral for those who seek additional information and or services related to FP. Such resources include psychosocial support, reproductive endocrinologists with expertise in the unique needs of AYA oncology patients, providers who accept pediatric patients (if needed), and financial assistance.
Corresponding author: Susan T. Vadaparampil, PhD, MPH, 12902 Magnolia Dr., MRC CANCONT, Tampa, FL 33612, [email protected].
Funding/support: ENRICH is funded by a National Cancer Institute R25 Training Grant: #5R25CA142519-05.
Financial disclosures: None.
From the Moffitt Cancer Center, Tampa, FL (Dr. Vadaparampil, Ms. Bowman, Ms. Sehovic, Dr. Quinn), Memorial Sloan Kettering Cancer Center, New York, NY (Ms. Kelvin), and Edward Via College of Osteopathic Medicine, Auburn, AL (Ms. Murphy).
Abstract
- Objective: To describe a script-based approach to assist oncology nurses in fertility discussions with their adolescent and young adult (AYA) patients.
- Methods: Scripts were developed by a team that included experts in fertility and reproductive health, health education, health communication, and clinical care of AYA patients. Individual scripts for females, males, and survivors were created and accompanied by a flyer and frequently asked questions sheet. The script and supplementary materials were then vetted by oncology nurses who participated in the Educating Nurses about Reproductive Health Issues in Cancer Healthcare (ENRICH) training program.
- Results: The scripts were rated as helpful and socially appropriate with minor concerns noted about awkward wording and medical jargon.
- Conclusion: The updated scripts provide one approach for nurses to become more adept at discussing the topic of infertility and FP with AYA oncology patients and survivors.
In the United States, over 70,000 adolescents and young adults (AYAs) are diagnosed with cancer each year [1,2]. Treatments are available that are associated with improved survival for these cancers. Unfortunately, cancer treatment may significantly impact AYA survivors’ future fertility. Infertility or premature ovarian failure can occur during or after cancer treatment (eg, chemotherapy, radiation) for females, and males may be temporarily or permanently azoospermic [3]. There are a number of established methods of fertility preservation (FP) that are available; these include oocyte and embryo cryopreservation and ovarian transposition for females and sperm banking for males [3]. Experimental options for males include testicular tissue freezing and for females ovarian tissue cryopreservation.
The American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network [4,5] recommend discussing FP with patients of reproductive age, ideally before initiation of treatment. In 2013, ASCO updated guidelines extending the responsibility for discussion and referral for FP beyond the medical oncologist to explicitly include other physician specialties, nurses, and allied health care professionals in the oncology care setting [3]. However, multiple publications, including patient surveys and interviews, physician surveys, and medical record abstraction studies suggest these discussions do not consistently take place. In an analysis of 156 practice groups submitting data as part of ASCO's Quality Oncology Practice Initiative, only ~15%–20% of practices routinely discussed infertility risks and FP options [6]. A recent review of medical charts of patients aged 18–45 treated in 2011 at 1 of 4 large U.S. cancer care institutions found that documentation of discussions for infertility risk was 26%, 24% for FP option discussion, and 13% for fertility specialist referral [7].
Oncology nurses play a key role in patients’ care and, compared to other health care providers, are more likely to have multiple interactions with patients prior to the initiation of treatment [8]. They are often attuned to the medical and psychosocial needs of the patient and family and can advocate for their needs and desires [9]. However, existing research finds few oncology nurses discuss this topic with AYA patients. Studies examining barriers have identified factors that may hinder discussions about infertility and FP with AYA oncology patients. These barriers include lack of knowledge about cancer related infertility and available FP procedures; access to reproductive endocrinologists or sperm banking clinics; time constraints in busy clinics and concerns about delaying treatment; discomforts discussing reproductive health; patient’s ability to afford FP; bias about the suitability of FP for young or unpartnered or LGBT patients or those with a poor prognosis; and personal religious or moral values about the use of assisted reproductive technologies [10–15].
Equipping nurses with content-specific communication may overcome some of the barriers described. A method often used in nursing education and communication interventions is scripting [16–18]. Scripting provides precise key words that ensure consistency in the message, no matter the messenger [19]. This paper reports on the development and refinement of a series of scripts to guide discussions about FP for male and female AYA patients and survivors.
Script Development
In 2003 Studer developed the AIDET (Acknowledge, Introduce, Duration, Explanation, and Thank you) model of communication for health professionals [19]. AIDET is an effective tool in facilitating communication practices among nurses and physicians in adult and pediatric settings [20–24]. The AIDET model was adapted by our team to develop AIDED: Assess, Introduce, Decide, Explain, and Discuss, a script-based approach to assist oncology nurses in fertility discussions with their AYA patients. Our team included experts in fertility and reproductive health, health education, health communication, as well as clinical and psychosocial care of AYA patients.
Educating Nurses
Benefits of Scripts
Communication difficulties may present an obstacle for oncology nurses to address the infertility, FP information, and supportive care needs of AYA cancer patients [15]. While guidelines from leading health and professional organizations support the need to discuss these issues with patients, implementation requires providing practical tools that meet the needs of nurses’ practice setting and patient population [26].
The use of scripts has a long history in the
Conclusion
These scripts provide one approach for nurses to become more adept at discussing the topic of FP with AYA oncology patients. We will continue to update and refine these scripts and ultimately test their efficacy in improving psychosocial and behavioral outcomes for AYA patients. While scripts are effective, they must be updated to reflect relevant advances in clinical care. In addition, it is important to identify local resources to facilitate discussion and referral for those who seek additional information and or services related to FP. Such resources include psychosocial support, reproductive endocrinologists with expertise in the unique needs of AYA oncology patients, providers who accept pediatric patients (if needed), and financial assistance.
Corresponding author: Susan T. Vadaparampil, PhD, MPH, 12902 Magnolia Dr., MRC CANCONT, Tampa, FL 33612, [email protected].
Funding/support: ENRICH is funded by a National Cancer Institute R25 Training Grant: #5R25CA142519-05.
Financial disclosures: None.
1. Bleyer AOLM, O’Leary M, Barr L, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. Bethesda, MD: National Cancer Institute; 2006.
2. Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 2014;64: 83–103.
3. Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013;31:2500–10.
4. Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
5. Coccia P, Altman J, Bhatia S, et al. Adolescent and young adult (AYA) oncology version 1.2012. National Comprehensive Cancer Network; 2012.
6. Neuss MN, Malin JL, Chan S, et al. Measuring the improving quality of outpatient care in medical oncology practices in the United States. J Clin Oncol 2013;31:1471–7.
7. Quinn GP, Block RG, Clayman ML, et al. If you did not document it, it did not happen: rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J Oncol Pract 2015;11: 137–44.
8. Cope D. Patients’ and physicians’ experinces with sperm banking and infertility issues related to cancer treatment. Clin J Oncol Nurs 2002;6:293–5.
9. Vaartio-Rajalin H, Leino-Kilpi H. Nurses as patient advocates in oncology care: activities based on literature. Clin J Oncol Nurs. 2011;15:526–32.
10. King LM, Quinn GP, Vadaparampil ST, et al. Oncology nurses’ perceptions of barriers to discussion of fertility preservation with patients with cancer. Clin J Oncol Nurs 2008; 12:467–76.
11. Clayton HB, Vadaparampil ST, Quinn GP, et al. Trends in clinical practice and nurses’ attitudes about fertility preservation for pediatric patients with cancer. Oncol Nurs Forum 2008;35:449–55.
12. Vadaparampil ST, Clayton H, Quinn GP, et al. Pediatric oncology nurses’ attitudes related to discussing fertility preservation with pediatric cancer patients and their families. J Pediatr Oncol Nurs 2007;24:255–63.
13. Kotronoulas G, Papadopoulou C, Patiraki E. Nurses’ knowledge, attitudes, and practices regarding provision of sexual health care in patients with cancer: critical review of the evidence. Support Care Cancer 2009;17:479–501.
14. Reebals JF, Brown R, Buckner EB. Nurse practice issues regarding sperm banking in adolescent male cancer patients. J Pediatr Oncol Nurs 2006;23:182–8.
15. Goossens J, Delbaere I, Beeckman D, et al. Communication difficulties and the experience of loneliness in patients with cancer dealing with fertility issues: a qualitative study. Oncol Nurs Forum 2015;42:34–43.
16. Mustard LW. Improving patient satisfaction through the consistent use of scripting by the nursing staff. JONAS Healthc Law Ethics Regul 2003;5:68–72.
17. Kuiper RA. Integration of innovative clinical reasoning pedagogies into a baccalaureate nursing curriculum. Creat Nurs 2013;19:128–39.
18. Handel DA, Fu R, Daya M, et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med 2010; 17:495–500.
19. Studer Q. Hardwiring excellence: purpose, worthwhile work, making a difference. Gulf Breeze, FL: Fire Starter Publishing; 2003.
20. Katona A, Kunkel E, Arfaa J, et al. Methodology for delivering feedback to neurology house staff on communication skills using AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You). Neurology 2014;82(10 Suppl):P1–328.
21. Prestia A , Dyess S. Maximizing caring relationships between nursing assistants and patients: Care partners. J Nurs Admin 2012;42:144–7.
22. Fisher MJ. A brief intervention to improve emotion-focused communication between newly licensed pediatric nurses and parents [dissertation]. Indianapolis: Indiana University; 2012.
23. Baker SJ. Key words: a prescriptive approach to reducing patient anxiety and improving safety. J Emerg Nurs 2011; 37:571–4.
24. Shupe R. Using skills validation and verification techniques to hardwire staff behaviors. J Emerg Nurs 2013;39:364–8.
25. Vadaparampil ST, Hutchins NM, Quinn GP. Reproductive health in the adolescent and young adult cancer patient: an innovative training program for oncology nurses. J Cancer Educ 2013;28:197–208.
26. Shekelle P, Woolf S, Grimshaw JM, et al. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci 2012;7:62.
27. Clayton JM, Adler JL, O’Callaghan A, et al. Intensive communication skills teaching for specialist training in palliative medicine: development and evaluation of an experiential workshop. J Palliat Med 2012;15:585–91.
28. Hymes DH. On communicative competence. In: Pride JB, Holmes J, editors. Sociolinguistics: selected readings. Harmondsworth: Penguin; 1972:269–93.
29. Asnani MR. Patient-physician communication. West Indian Med J 2009;58:357–61.
30. Clark PA. Medical practices’ sensitivity to patients’ needs: Opportunities and practices for improvement. J Ambulat Care Manage 2003;26:110–23.
31. Wanzer MB, Booth-Butterfield M, Gruber K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Care Commun 2004;16:363–84.
1. Bleyer AOLM, O’Leary M, Barr L, Ries LAG. Cancer epidemiology in older adolescents and young adults 15 to 29 years of age, including SEER incidence and survival: 1975–2000. Bethesda, MD: National Cancer Institute; 2006.
2. Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 2014;64: 83–103.
3. Loren AW, Mangu PB, Beck LN, et al. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013;31:2500–10.
4. Lee SJ, Schover LR, Partridge AH, et al. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol 2006;24:2917–31.
5. Coccia P, Altman J, Bhatia S, et al. Adolescent and young adult (AYA) oncology version 1.2012. National Comprehensive Cancer Network; 2012.
6. Neuss MN, Malin JL, Chan S, et al. Measuring the improving quality of outpatient care in medical oncology practices in the United States. J Clin Oncol 2013;31:1471–7.
7. Quinn GP, Block RG, Clayman ML, et al. If you did not document it, it did not happen: rates of documentation of discussion of infertility risk in adolescent and young adult oncology patients’ medical records. J Oncol Pract 2015;11: 137–44.
8. Cope D. Patients’ and physicians’ experinces with sperm banking and infertility issues related to cancer treatment. Clin J Oncol Nurs 2002;6:293–5.
9. Vaartio-Rajalin H, Leino-Kilpi H. Nurses as patient advocates in oncology care: activities based on literature. Clin J Oncol Nurs. 2011;15:526–32.
10. King LM, Quinn GP, Vadaparampil ST, et al. Oncology nurses’ perceptions of barriers to discussion of fertility preservation with patients with cancer. Clin J Oncol Nurs 2008; 12:467–76.
11. Clayton HB, Vadaparampil ST, Quinn GP, et al. Trends in clinical practice and nurses’ attitudes about fertility preservation for pediatric patients with cancer. Oncol Nurs Forum 2008;35:449–55.
12. Vadaparampil ST, Clayton H, Quinn GP, et al. Pediatric oncology nurses’ attitudes related to discussing fertility preservation with pediatric cancer patients and their families. J Pediatr Oncol Nurs 2007;24:255–63.
13. Kotronoulas G, Papadopoulou C, Patiraki E. Nurses’ knowledge, attitudes, and practices regarding provision of sexual health care in patients with cancer: critical review of the evidence. Support Care Cancer 2009;17:479–501.
14. Reebals JF, Brown R, Buckner EB. Nurse practice issues regarding sperm banking in adolescent male cancer patients. J Pediatr Oncol Nurs 2006;23:182–8.
15. Goossens J, Delbaere I, Beeckman D, et al. Communication difficulties and the experience of loneliness in patients with cancer dealing with fertility issues: a qualitative study. Oncol Nurs Forum 2015;42:34–43.
16. Mustard LW. Improving patient satisfaction through the consistent use of scripting by the nursing staff. JONAS Healthc Law Ethics Regul 2003;5:68–72.
17. Kuiper RA. Integration of innovative clinical reasoning pedagogies into a baccalaureate nursing curriculum. Creat Nurs 2013;19:128–39.
18. Handel DA, Fu R, Daya M, et al. The use of scripting at triage and its impact on elopements. Acad Emerg Med 2010; 17:495–500.
19. Studer Q. Hardwiring excellence: purpose, worthwhile work, making a difference. Gulf Breeze, FL: Fire Starter Publishing; 2003.
20. Katona A, Kunkel E, Arfaa J, et al. Methodology for delivering feedback to neurology house staff on communication skills using AIDET (Acknowledge, Introduce, Duration, Explanation, Thank You). Neurology 2014;82(10 Suppl):P1–328.
21. Prestia A , Dyess S. Maximizing caring relationships between nursing assistants and patients: Care partners. J Nurs Admin 2012;42:144–7.
22. Fisher MJ. A brief intervention to improve emotion-focused communication between newly licensed pediatric nurses and parents [dissertation]. Indianapolis: Indiana University; 2012.
23. Baker SJ. Key words: a prescriptive approach to reducing patient anxiety and improving safety. J Emerg Nurs 2011; 37:571–4.
24. Shupe R. Using skills validation and verification techniques to hardwire staff behaviors. J Emerg Nurs 2013;39:364–8.
25. Vadaparampil ST, Hutchins NM, Quinn GP. Reproductive health in the adolescent and young adult cancer patient: an innovative training program for oncology nurses. J Cancer Educ 2013;28:197–208.
26. Shekelle P, Woolf S, Grimshaw JM, et al. Developing clinical practice guidelines: reviewing, reporting, and publishing guidelines; updating guidelines; and the emerging issues of enhancing guideline implementability and accounting for comorbid conditions in guideline development. Implement Sci 2012;7:62.
27. Clayton JM, Adler JL, O’Callaghan A, et al. Intensive communication skills teaching for specialist training in palliative medicine: development and evaluation of an experiential workshop. J Palliat Med 2012;15:585–91.
28. Hymes DH. On communicative competence. In: Pride JB, Holmes J, editors. Sociolinguistics: selected readings. Harmondsworth: Penguin; 1972:269–93.
29. Asnani MR. Patient-physician communication. West Indian Med J 2009;58:357–61.
30. Clark PA. Medical practices’ sensitivity to patients’ needs: Opportunities and practices for improvement. J Ambulat Care Manage 2003;26:110–23.
31. Wanzer MB, Booth-Butterfield M, Gruber K. Perceptions of health care providers’ communication: Relationships between patient-centered communication and satisfaction. Health Care Commun 2004;16:363–84.
Laboring in the Shadow of the Media: Care and Perceptions of Care in the VA
Just over 2 years ago, I finished a psychiatry residency at the Mayo Clinic, turned down an offer to stay on staff, and topped it off by taking a position at the VA. Not one of my brighter moments—or so one of my friends thought. “Are you off your rocker? Don’t you know that the VA is terrible? Why would you go work there?” he jabbed incredulously. I cringed, knowing that I had passed up an opportunity to stay in arguably the best hospital system in the nation, possibly the world, to work at what some (maybe even a lot) view as a corpulent and recalcitrant bastion of ineptitude bound by the dictates of a fickle Congress.
In the wake of the Phoenix wait-time scandal (and no, it’s not like Disneyland), the suicide by self-immolation of Charles Richard Ingram III outside a VA facility in New Jersey, the new data on veteran suicide showing progress but continued significant concern, and the ongoing VA privatization discussion, the prevailing discourse about the VA is largely negative.1,2 And in a high-voltage election cycle where public outrage can serve as an efficient tool to garner support, the VA risks getting pummeled.
Add to this the shocking research that shows nearly half of VA psychiatrists are considering leaving the VA within the next 2 years, and it’s clear that dissatisfaction within and outside the VA is high.3 This does not bode well for veterans at a time when suicide and mental health care needs are so critically important. But while the bureaucracy of the VA is often the focus of negative press, it also filters down and unfortunately has the potential to directly affect VA practitioners and veterans. When we lose sight of what the VA does well, we risk being caught up in a vortex of negativity and a profound sense of inadequacy and helplessness. More attention to what is already being done well can help us as a nation more realistically chart a path forward rather than being fueled by negative rhetoric and rage.
Despite the challenges, the VA is currently succeeding in a number of areas that deserve recognition:
Medical school and resident education and collaboration with VA. In 2014, > 41,000 medical residents and nearly 23,000 medical students had some or all of their training in a VA setting. More than 95% of allopathic medical schools and nearly 90% of osteopathic medical schools had affiliation agreements with the VA in 2014.4 Suffice it to say, if the educational endeavors of the VA were curtailed, there would be an unholy scramble to provide well-trained physicians for our nation. (This does not include the dentists, psychologists, pharmacists, social workers, nurses, and other health care professionals whose training involves the VA in some capacity.) In addition, the VA often provides loan repayment assistance, which is very important given that many young professionals carry substantial school debt after completing training.
Mental health and primary care integration. Medical care overall is changing, and there is an increasing shift away from volume-based, fee-for-service care to integrated, team-based models. The VA is one of several successful leaders at a time when most U.S. health care providers are being scrutinized for their use of health care dollars and overall national health outcomes.5 In addition to primary care integration, the VA uses home-based primary care and mental health intensive case management teams for vulnerable veterans, adding flexibility, continuity, and access for many.
Overall excellent mental health care. A recent study by Watkins and colleagues found that when comparing quality measures for medication evaluation and management for schizophrenia, bipolar disorder, posttraumatic stress disorder, depression, and substance use disorders, “In every case, VA performance was superior to that of the private sector by more than 30%.”6 This is not an aberration and not limited to mental health care. It is a consistent finding about which books have been written.7 However, the availability of evidence-based care may not be consistent across all VA facilities nationally, depending on demand and staffing.
Despite the rumors, VA has high customer satisfaction. According to the American Customer Satisfaction Index, the VA has consistently performed well in measures of customer satisfaction compared with those of the private sector health care providers.8 Let’s not ignore what veterans have actually said and continue to say about their care.
Once in, you’re in! I recently missed an initial appointment with a private sector pediatrician for one of my sons. I was tersely invited to find another doctor. This seemed scandalous since I have become accustomed in my role as a VA physician to reaching out, sometimes incessantly, to patients who do not come in for either a new or follow-up appointment. Yes, I call my patients; personally, directly, and often. In many clinics, patients receive reminder letters about upcoming appointments and then phone calls and sometimes letters when appointments are missed. My colleagues and I have jokingly referred to this practice as “benign stalking.”
Further, if a veteran is dissatisfied with care, there is a process to review and make adjustments if necessary, including transfer to a different doctor. Additionally, and sometimes alarmingly, veterans are not “fired” (and actually can’t be) for bad behavior (including direct threats to VA staff). Time, place, and manner of care can be tailored based on assessed risk, and VA police may be involved, but veterans continue to get care. I can assure you that if I made a threat to one of my doctors in private practice, I would very quickly be searching for a new doctor and answering some tough questions from law enforcement. Unlike many patients in private care, veterans have consistent access via phone (though admittedly not always user-friendly), walk-in appointments, after-hours availability in some locations, and secure messaging.
Electronic medical record and telehealth initiatives. The VA Computerized Patient Record System, has been around for some time and provides an excellent (although not perfect) system for documenting patient care. Each VA is linked to other VAs across the nation so patients don’t have to reinvent their story when they move and can actually get down to the business of being treated. Prior interventions, hospitalizations, medication trials, diagnostic impressions, imaging, lab work, etc, are all available at the touch of a button! And the VA’s telehealth initiative is all about access.
Veteran suicide prevention and opioid prescribing. Suicide is disproportionately high among veterans in the U.S. Recent data show that in 2014, an average of 20 veterans died by suicide per day.1 This accounted for 18% of all U.S. adult suicide deaths, even though veterans represent only 8.5% of the population. And while these recent statistics represent some improvement over prior research, prevention and care coordination remain major priorities in the VA. Veterans have access to same-day care (at least in Boise, Idaho) and a 24-hour crisis line that gives feedback to the patient’s local VA and can help coordinate follow-up care. The VA has specialized suicide prevention coordinators who attend to the needs of patients assessed to be at high risk for suicide and also disseminate training to providers in a variety of disciplines. All of this as the VA moves to ensure that suicide prevention remains a priority across disciplines and treatment sites.
Additionally, the VA is directly addressing the nationwide crisis of overprescription of opioids, beginning with education for both patients and staff and systemic encouragement of responsible prescribing via the national Opioid Safety Initiative and increased emphasis on providing at-risk veterans with naloxone kits.9
Research. VA research endeavors are wide ranging. The VA has been involved in pioneering clinical research in a substantial way since at least the 1920s and has contributed to important innovations in treatment, ranging from prosthetics to imaging, neuromodulation to medication intervention for a broad array of pathology.10
Drawing in professionals who want to work with veterans. The reason that many health care providers work at the VA is the veterans themselves. Veterans by and large represent a segment of our population who have demonstrated dedication, commitment to a shared goal, and the willingness to sacrifice their health or their lives for a greater good. The veteran identity and sacrifice has drawn many of us to want to serve them. My father’s and cousin’s service are truly inspirational on a personal level. I am not alone in this.
I recently had a veteran in my office who, once seated, pulled his chair closer to mine than I ordinarily prefer. He then gave me a penetrating stare, moved well within the comfort zone of even the closest of close-talkers, and began to scream about the wrongs he had heard about in the VA system. When he finished screaming (and once the other clinicians in the building realized that I wasn’t being physically attacked), he freely acknowledged that he had never actually experienced any of the VA shortcomings personally but, nonetheless, learned how reprehensible the VA is through the media. Our veterans deserve the best care that we as a nation can provide, and they also deserve to know the truth about the quality of VA care. But too often the negative media attention does not tell the whole story that directly impacts the well-being of our veterans.
I sit on the disruptive behavior committee at the Boise VAMC and see firsthand the stress that our veterans and staff are under. We review reports of veterans who disrupt the environment, sometimes by direct threats to shoot or in some way physically harm those taking care of them. Some of this is over pain medications or other specific health care issues. Some is due to frustration in trying to navigate an increasingly complex and nonintuitive system as the VA scrambles to implement congressional directives that sometimes clash with what is clinically appropriate and evidence-based. Some of the disruptive behavior, however, is fueled by the negative national discourse against the political establishment and its nearest representative—in this case, the VA. And again, this is often fueled, in my opinion, by incomplete media coverage.
The VA has problems. It would be delusional to argue otherwise. It is rightly open to public scrutiny as a tax-funded governmental agency, and lives are literally at stake as we grapple nationally with how best to deliver on Lincoln’s promise to “care for those who have borne the battle.”
As I reflect on my friend’s skepticism at my taking a VA position, I can answer that yes, the VA needs work. It has some major issues. But I no longer feel the need to cringe, because I now know firsthand the kind of care that is being delivered (at least to the veterans in Boise).
Wherever you stand on the quality of VA care, the movement to privatize, or the politicizing inevitable during an election year, to indiscriminately excoriate the VA is to risk marginalizing the superlative care that many currently receive by the thousands of physicians and other health care providers and administrators throughout the VA. Our veterans are a national treasure that deserve excellent care and real solutions to the problems that exist in the VA, not overwhelming negative rhetoric.
1. U.S. Department of Veterans Affairs, Office of Suicide Prevention. Suicide Among Veterans and Other Americans 2001-2014. http://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published August 3, 2016. Accessed August 10, 2016.
2. Longman P, Gordon S. A conversation about the commission on care and the future of the VA. Washington Monthly. http://washingtonmonthly.com/2016/07/14/a-conversation-about-the-commission-on-care-and-the-future-of-the-va/. Published July 14, 2016. Accessed August 4, 2016.
3. Garcia HA, McGeary CA, Finley EP, Ketchum NS, McGeary DD, Peterson AL. Burnout among psychiatrists in the Veterans Health Administration. Burnout Research. 2015;2(4):108-114.
4. U.S. Department of Veterans Affairs, Office of Academic Affiliations. Medical and dental education program. http://www.va.gov/oaa/GME_default.asp. Updated December 9, 2015. Accessed August 4, 2016.
5. Katzelnick DJ, Williams MD. Large-scale dissemination of collaborative care and implications for psychiatry. Psychiatr Serv. 2015;66(9):904-906.
6. Watkins KE, Smith B, Akincigil A, et al. The quality of medication treatment for mental disorders in the Department of Veterans Affairs and in private-sector plans. Psychiatr Serv. 2016;67(4):391-396.
7. Longman P. Best Care Anywhere: Why VA Health Care Would Work Better for Everyone. 3rd ed. San Francisco, CA: Berrett-Koehler; 2012.
8. U.S. Department of Veterans Affairs, Veterans Health Administration. American customer satisfaction index 2013 customer satisfaction outpatient survey. http://www.va.gov/health/docs/VA2013OutpatientACSI.pdf. Published March 2014. Accessed August 10, 2016.
9. U.S. Department of Veterans Affairs. VHA pain management, Opioid Safety Initiative (OSI). http://www.va.gov/PAINMANAGEMENT/Opioid_Safety_Initiative_OSI.asp. Updated June 17, 2015. Accessed August 4, 2016.
10. U.S. Department of Veterans Affairs. Office of Research and Development. http://www.research.va.gov. Updated July 21, 2016. Accessed August 4, 2016.
Just over 2 years ago, I finished a psychiatry residency at the Mayo Clinic, turned down an offer to stay on staff, and topped it off by taking a position at the VA. Not one of my brighter moments—or so one of my friends thought. “Are you off your rocker? Don’t you know that the VA is terrible? Why would you go work there?” he jabbed incredulously. I cringed, knowing that I had passed up an opportunity to stay in arguably the best hospital system in the nation, possibly the world, to work at what some (maybe even a lot) view as a corpulent and recalcitrant bastion of ineptitude bound by the dictates of a fickle Congress.
In the wake of the Phoenix wait-time scandal (and no, it’s not like Disneyland), the suicide by self-immolation of Charles Richard Ingram III outside a VA facility in New Jersey, the new data on veteran suicide showing progress but continued significant concern, and the ongoing VA privatization discussion, the prevailing discourse about the VA is largely negative.1,2 And in a high-voltage election cycle where public outrage can serve as an efficient tool to garner support, the VA risks getting pummeled.
Add to this the shocking research that shows nearly half of VA psychiatrists are considering leaving the VA within the next 2 years, and it’s clear that dissatisfaction within and outside the VA is high.3 This does not bode well for veterans at a time when suicide and mental health care needs are so critically important. But while the bureaucracy of the VA is often the focus of negative press, it also filters down and unfortunately has the potential to directly affect VA practitioners and veterans. When we lose sight of what the VA does well, we risk being caught up in a vortex of negativity and a profound sense of inadequacy and helplessness. More attention to what is already being done well can help us as a nation more realistically chart a path forward rather than being fueled by negative rhetoric and rage.
Despite the challenges, the VA is currently succeeding in a number of areas that deserve recognition:
Medical school and resident education and collaboration with VA. In 2014, > 41,000 medical residents and nearly 23,000 medical students had some or all of their training in a VA setting. More than 95% of allopathic medical schools and nearly 90% of osteopathic medical schools had affiliation agreements with the VA in 2014.4 Suffice it to say, if the educational endeavors of the VA were curtailed, there would be an unholy scramble to provide well-trained physicians for our nation. (This does not include the dentists, psychologists, pharmacists, social workers, nurses, and other health care professionals whose training involves the VA in some capacity.) In addition, the VA often provides loan repayment assistance, which is very important given that many young professionals carry substantial school debt after completing training.
Mental health and primary care integration. Medical care overall is changing, and there is an increasing shift away from volume-based, fee-for-service care to integrated, team-based models. The VA is one of several successful leaders at a time when most U.S. health care providers are being scrutinized for their use of health care dollars and overall national health outcomes.5 In addition to primary care integration, the VA uses home-based primary care and mental health intensive case management teams for vulnerable veterans, adding flexibility, continuity, and access for many.
Overall excellent mental health care. A recent study by Watkins and colleagues found that when comparing quality measures for medication evaluation and management for schizophrenia, bipolar disorder, posttraumatic stress disorder, depression, and substance use disorders, “In every case, VA performance was superior to that of the private sector by more than 30%.”6 This is not an aberration and not limited to mental health care. It is a consistent finding about which books have been written.7 However, the availability of evidence-based care may not be consistent across all VA facilities nationally, depending on demand and staffing.
Despite the rumors, VA has high customer satisfaction. According to the American Customer Satisfaction Index, the VA has consistently performed well in measures of customer satisfaction compared with those of the private sector health care providers.8 Let’s not ignore what veterans have actually said and continue to say about their care.
Once in, you’re in! I recently missed an initial appointment with a private sector pediatrician for one of my sons. I was tersely invited to find another doctor. This seemed scandalous since I have become accustomed in my role as a VA physician to reaching out, sometimes incessantly, to patients who do not come in for either a new or follow-up appointment. Yes, I call my patients; personally, directly, and often. In many clinics, patients receive reminder letters about upcoming appointments and then phone calls and sometimes letters when appointments are missed. My colleagues and I have jokingly referred to this practice as “benign stalking.”
Further, if a veteran is dissatisfied with care, there is a process to review and make adjustments if necessary, including transfer to a different doctor. Additionally, and sometimes alarmingly, veterans are not “fired” (and actually can’t be) for bad behavior (including direct threats to VA staff). Time, place, and manner of care can be tailored based on assessed risk, and VA police may be involved, but veterans continue to get care. I can assure you that if I made a threat to one of my doctors in private practice, I would very quickly be searching for a new doctor and answering some tough questions from law enforcement. Unlike many patients in private care, veterans have consistent access via phone (though admittedly not always user-friendly), walk-in appointments, after-hours availability in some locations, and secure messaging.
Electronic medical record and telehealth initiatives. The VA Computerized Patient Record System, has been around for some time and provides an excellent (although not perfect) system for documenting patient care. Each VA is linked to other VAs across the nation so patients don’t have to reinvent their story when they move and can actually get down to the business of being treated. Prior interventions, hospitalizations, medication trials, diagnostic impressions, imaging, lab work, etc, are all available at the touch of a button! And the VA’s telehealth initiative is all about access.
Veteran suicide prevention and opioid prescribing. Suicide is disproportionately high among veterans in the U.S. Recent data show that in 2014, an average of 20 veterans died by suicide per day.1 This accounted for 18% of all U.S. adult suicide deaths, even though veterans represent only 8.5% of the population. And while these recent statistics represent some improvement over prior research, prevention and care coordination remain major priorities in the VA. Veterans have access to same-day care (at least in Boise, Idaho) and a 24-hour crisis line that gives feedback to the patient’s local VA and can help coordinate follow-up care. The VA has specialized suicide prevention coordinators who attend to the needs of patients assessed to be at high risk for suicide and also disseminate training to providers in a variety of disciplines. All of this as the VA moves to ensure that suicide prevention remains a priority across disciplines and treatment sites.
Additionally, the VA is directly addressing the nationwide crisis of overprescription of opioids, beginning with education for both patients and staff and systemic encouragement of responsible prescribing via the national Opioid Safety Initiative and increased emphasis on providing at-risk veterans with naloxone kits.9
Research. VA research endeavors are wide ranging. The VA has been involved in pioneering clinical research in a substantial way since at least the 1920s and has contributed to important innovations in treatment, ranging from prosthetics to imaging, neuromodulation to medication intervention for a broad array of pathology.10
Drawing in professionals who want to work with veterans. The reason that many health care providers work at the VA is the veterans themselves. Veterans by and large represent a segment of our population who have demonstrated dedication, commitment to a shared goal, and the willingness to sacrifice their health or their lives for a greater good. The veteran identity and sacrifice has drawn many of us to want to serve them. My father’s and cousin’s service are truly inspirational on a personal level. I am not alone in this.
I recently had a veteran in my office who, once seated, pulled his chair closer to mine than I ordinarily prefer. He then gave me a penetrating stare, moved well within the comfort zone of even the closest of close-talkers, and began to scream about the wrongs he had heard about in the VA system. When he finished screaming (and once the other clinicians in the building realized that I wasn’t being physically attacked), he freely acknowledged that he had never actually experienced any of the VA shortcomings personally but, nonetheless, learned how reprehensible the VA is through the media. Our veterans deserve the best care that we as a nation can provide, and they also deserve to know the truth about the quality of VA care. But too often the negative media attention does not tell the whole story that directly impacts the well-being of our veterans.
I sit on the disruptive behavior committee at the Boise VAMC and see firsthand the stress that our veterans and staff are under. We review reports of veterans who disrupt the environment, sometimes by direct threats to shoot or in some way physically harm those taking care of them. Some of this is over pain medications or other specific health care issues. Some is due to frustration in trying to navigate an increasingly complex and nonintuitive system as the VA scrambles to implement congressional directives that sometimes clash with what is clinically appropriate and evidence-based. Some of the disruptive behavior, however, is fueled by the negative national discourse against the political establishment and its nearest representative—in this case, the VA. And again, this is often fueled, in my opinion, by incomplete media coverage.
The VA has problems. It would be delusional to argue otherwise. It is rightly open to public scrutiny as a tax-funded governmental agency, and lives are literally at stake as we grapple nationally with how best to deliver on Lincoln’s promise to “care for those who have borne the battle.”
As I reflect on my friend’s skepticism at my taking a VA position, I can answer that yes, the VA needs work. It has some major issues. But I no longer feel the need to cringe, because I now know firsthand the kind of care that is being delivered (at least to the veterans in Boise).
Wherever you stand on the quality of VA care, the movement to privatize, or the politicizing inevitable during an election year, to indiscriminately excoriate the VA is to risk marginalizing the superlative care that many currently receive by the thousands of physicians and other health care providers and administrators throughout the VA. Our veterans are a national treasure that deserve excellent care and real solutions to the problems that exist in the VA, not overwhelming negative rhetoric.
Just over 2 years ago, I finished a psychiatry residency at the Mayo Clinic, turned down an offer to stay on staff, and topped it off by taking a position at the VA. Not one of my brighter moments—or so one of my friends thought. “Are you off your rocker? Don’t you know that the VA is terrible? Why would you go work there?” he jabbed incredulously. I cringed, knowing that I had passed up an opportunity to stay in arguably the best hospital system in the nation, possibly the world, to work at what some (maybe even a lot) view as a corpulent and recalcitrant bastion of ineptitude bound by the dictates of a fickle Congress.
In the wake of the Phoenix wait-time scandal (and no, it’s not like Disneyland), the suicide by self-immolation of Charles Richard Ingram III outside a VA facility in New Jersey, the new data on veteran suicide showing progress but continued significant concern, and the ongoing VA privatization discussion, the prevailing discourse about the VA is largely negative.1,2 And in a high-voltage election cycle where public outrage can serve as an efficient tool to garner support, the VA risks getting pummeled.
Add to this the shocking research that shows nearly half of VA psychiatrists are considering leaving the VA within the next 2 years, and it’s clear that dissatisfaction within and outside the VA is high.3 This does not bode well for veterans at a time when suicide and mental health care needs are so critically important. But while the bureaucracy of the VA is often the focus of negative press, it also filters down and unfortunately has the potential to directly affect VA practitioners and veterans. When we lose sight of what the VA does well, we risk being caught up in a vortex of negativity and a profound sense of inadequacy and helplessness. More attention to what is already being done well can help us as a nation more realistically chart a path forward rather than being fueled by negative rhetoric and rage.
Despite the challenges, the VA is currently succeeding in a number of areas that deserve recognition:
Medical school and resident education and collaboration with VA. In 2014, > 41,000 medical residents and nearly 23,000 medical students had some or all of their training in a VA setting. More than 95% of allopathic medical schools and nearly 90% of osteopathic medical schools had affiliation agreements with the VA in 2014.4 Suffice it to say, if the educational endeavors of the VA were curtailed, there would be an unholy scramble to provide well-trained physicians for our nation. (This does not include the dentists, psychologists, pharmacists, social workers, nurses, and other health care professionals whose training involves the VA in some capacity.) In addition, the VA often provides loan repayment assistance, which is very important given that many young professionals carry substantial school debt after completing training.
Mental health and primary care integration. Medical care overall is changing, and there is an increasing shift away from volume-based, fee-for-service care to integrated, team-based models. The VA is one of several successful leaders at a time when most U.S. health care providers are being scrutinized for their use of health care dollars and overall national health outcomes.5 In addition to primary care integration, the VA uses home-based primary care and mental health intensive case management teams for vulnerable veterans, adding flexibility, continuity, and access for many.
Overall excellent mental health care. A recent study by Watkins and colleagues found that when comparing quality measures for medication evaluation and management for schizophrenia, bipolar disorder, posttraumatic stress disorder, depression, and substance use disorders, “In every case, VA performance was superior to that of the private sector by more than 30%.”6 This is not an aberration and not limited to mental health care. It is a consistent finding about which books have been written.7 However, the availability of evidence-based care may not be consistent across all VA facilities nationally, depending on demand and staffing.
Despite the rumors, VA has high customer satisfaction. According to the American Customer Satisfaction Index, the VA has consistently performed well in measures of customer satisfaction compared with those of the private sector health care providers.8 Let’s not ignore what veterans have actually said and continue to say about their care.
Once in, you’re in! I recently missed an initial appointment with a private sector pediatrician for one of my sons. I was tersely invited to find another doctor. This seemed scandalous since I have become accustomed in my role as a VA physician to reaching out, sometimes incessantly, to patients who do not come in for either a new or follow-up appointment. Yes, I call my patients; personally, directly, and often. In many clinics, patients receive reminder letters about upcoming appointments and then phone calls and sometimes letters when appointments are missed. My colleagues and I have jokingly referred to this practice as “benign stalking.”
Further, if a veteran is dissatisfied with care, there is a process to review and make adjustments if necessary, including transfer to a different doctor. Additionally, and sometimes alarmingly, veterans are not “fired” (and actually can’t be) for bad behavior (including direct threats to VA staff). Time, place, and manner of care can be tailored based on assessed risk, and VA police may be involved, but veterans continue to get care. I can assure you that if I made a threat to one of my doctors in private practice, I would very quickly be searching for a new doctor and answering some tough questions from law enforcement. Unlike many patients in private care, veterans have consistent access via phone (though admittedly not always user-friendly), walk-in appointments, after-hours availability in some locations, and secure messaging.
Electronic medical record and telehealth initiatives. The VA Computerized Patient Record System, has been around for some time and provides an excellent (although not perfect) system for documenting patient care. Each VA is linked to other VAs across the nation so patients don’t have to reinvent their story when they move and can actually get down to the business of being treated. Prior interventions, hospitalizations, medication trials, diagnostic impressions, imaging, lab work, etc, are all available at the touch of a button! And the VA’s telehealth initiative is all about access.
Veteran suicide prevention and opioid prescribing. Suicide is disproportionately high among veterans in the U.S. Recent data show that in 2014, an average of 20 veterans died by suicide per day.1 This accounted for 18% of all U.S. adult suicide deaths, even though veterans represent only 8.5% of the population. And while these recent statistics represent some improvement over prior research, prevention and care coordination remain major priorities in the VA. Veterans have access to same-day care (at least in Boise, Idaho) and a 24-hour crisis line that gives feedback to the patient’s local VA and can help coordinate follow-up care. The VA has specialized suicide prevention coordinators who attend to the needs of patients assessed to be at high risk for suicide and also disseminate training to providers in a variety of disciplines. All of this as the VA moves to ensure that suicide prevention remains a priority across disciplines and treatment sites.
Additionally, the VA is directly addressing the nationwide crisis of overprescription of opioids, beginning with education for both patients and staff and systemic encouragement of responsible prescribing via the national Opioid Safety Initiative and increased emphasis on providing at-risk veterans with naloxone kits.9
Research. VA research endeavors are wide ranging. The VA has been involved in pioneering clinical research in a substantial way since at least the 1920s and has contributed to important innovations in treatment, ranging from prosthetics to imaging, neuromodulation to medication intervention for a broad array of pathology.10
Drawing in professionals who want to work with veterans. The reason that many health care providers work at the VA is the veterans themselves. Veterans by and large represent a segment of our population who have demonstrated dedication, commitment to a shared goal, and the willingness to sacrifice their health or their lives for a greater good. The veteran identity and sacrifice has drawn many of us to want to serve them. My father’s and cousin’s service are truly inspirational on a personal level. I am not alone in this.
I recently had a veteran in my office who, once seated, pulled his chair closer to mine than I ordinarily prefer. He then gave me a penetrating stare, moved well within the comfort zone of even the closest of close-talkers, and began to scream about the wrongs he had heard about in the VA system. When he finished screaming (and once the other clinicians in the building realized that I wasn’t being physically attacked), he freely acknowledged that he had never actually experienced any of the VA shortcomings personally but, nonetheless, learned how reprehensible the VA is through the media. Our veterans deserve the best care that we as a nation can provide, and they also deserve to know the truth about the quality of VA care. But too often the negative media attention does not tell the whole story that directly impacts the well-being of our veterans.
I sit on the disruptive behavior committee at the Boise VAMC and see firsthand the stress that our veterans and staff are under. We review reports of veterans who disrupt the environment, sometimes by direct threats to shoot or in some way physically harm those taking care of them. Some of this is over pain medications or other specific health care issues. Some is due to frustration in trying to navigate an increasingly complex and nonintuitive system as the VA scrambles to implement congressional directives that sometimes clash with what is clinically appropriate and evidence-based. Some of the disruptive behavior, however, is fueled by the negative national discourse against the political establishment and its nearest representative—in this case, the VA. And again, this is often fueled, in my opinion, by incomplete media coverage.
The VA has problems. It would be delusional to argue otherwise. It is rightly open to public scrutiny as a tax-funded governmental agency, and lives are literally at stake as we grapple nationally with how best to deliver on Lincoln’s promise to “care for those who have borne the battle.”
As I reflect on my friend’s skepticism at my taking a VA position, I can answer that yes, the VA needs work. It has some major issues. But I no longer feel the need to cringe, because I now know firsthand the kind of care that is being delivered (at least to the veterans in Boise).
Wherever you stand on the quality of VA care, the movement to privatize, or the politicizing inevitable during an election year, to indiscriminately excoriate the VA is to risk marginalizing the superlative care that many currently receive by the thousands of physicians and other health care providers and administrators throughout the VA. Our veterans are a national treasure that deserve excellent care and real solutions to the problems that exist in the VA, not overwhelming negative rhetoric.
1. U.S. Department of Veterans Affairs, Office of Suicide Prevention. Suicide Among Veterans and Other Americans 2001-2014. http://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published August 3, 2016. Accessed August 10, 2016.
2. Longman P, Gordon S. A conversation about the commission on care and the future of the VA. Washington Monthly. http://washingtonmonthly.com/2016/07/14/a-conversation-about-the-commission-on-care-and-the-future-of-the-va/. Published July 14, 2016. Accessed August 4, 2016.
3. Garcia HA, McGeary CA, Finley EP, Ketchum NS, McGeary DD, Peterson AL. Burnout among psychiatrists in the Veterans Health Administration. Burnout Research. 2015;2(4):108-114.
4. U.S. Department of Veterans Affairs, Office of Academic Affiliations. Medical and dental education program. http://www.va.gov/oaa/GME_default.asp. Updated December 9, 2015. Accessed August 4, 2016.
5. Katzelnick DJ, Williams MD. Large-scale dissemination of collaborative care and implications for psychiatry. Psychiatr Serv. 2015;66(9):904-906.
6. Watkins KE, Smith B, Akincigil A, et al. The quality of medication treatment for mental disorders in the Department of Veterans Affairs and in private-sector plans. Psychiatr Serv. 2016;67(4):391-396.
7. Longman P. Best Care Anywhere: Why VA Health Care Would Work Better for Everyone. 3rd ed. San Francisco, CA: Berrett-Koehler; 2012.
8. U.S. Department of Veterans Affairs, Veterans Health Administration. American customer satisfaction index 2013 customer satisfaction outpatient survey. http://www.va.gov/health/docs/VA2013OutpatientACSI.pdf. Published March 2014. Accessed August 10, 2016.
9. U.S. Department of Veterans Affairs. VHA pain management, Opioid Safety Initiative (OSI). http://www.va.gov/PAINMANAGEMENT/Opioid_Safety_Initiative_OSI.asp. Updated June 17, 2015. Accessed August 4, 2016.
10. U.S. Department of Veterans Affairs. Office of Research and Development. http://www.research.va.gov. Updated July 21, 2016. Accessed August 4, 2016.
1. U.S. Department of Veterans Affairs, Office of Suicide Prevention. Suicide Among Veterans and Other Americans 2001-2014. http://www.mentalhealth.va.gov/docs/2016suicidedatareport.pdf. Published August 3, 2016. Accessed August 10, 2016.
2. Longman P, Gordon S. A conversation about the commission on care and the future of the VA. Washington Monthly. http://washingtonmonthly.com/2016/07/14/a-conversation-about-the-commission-on-care-and-the-future-of-the-va/. Published July 14, 2016. Accessed August 4, 2016.
3. Garcia HA, McGeary CA, Finley EP, Ketchum NS, McGeary DD, Peterson AL. Burnout among psychiatrists in the Veterans Health Administration. Burnout Research. 2015;2(4):108-114.
4. U.S. Department of Veterans Affairs, Office of Academic Affiliations. Medical and dental education program. http://www.va.gov/oaa/GME_default.asp. Updated December 9, 2015. Accessed August 4, 2016.
5. Katzelnick DJ, Williams MD. Large-scale dissemination of collaborative care and implications for psychiatry. Psychiatr Serv. 2015;66(9):904-906.
6. Watkins KE, Smith B, Akincigil A, et al. The quality of medication treatment for mental disorders in the Department of Veterans Affairs and in private-sector plans. Psychiatr Serv. 2016;67(4):391-396.
7. Longman P. Best Care Anywhere: Why VA Health Care Would Work Better for Everyone. 3rd ed. San Francisco, CA: Berrett-Koehler; 2012.
8. U.S. Department of Veterans Affairs, Veterans Health Administration. American customer satisfaction index 2013 customer satisfaction outpatient survey. http://www.va.gov/health/docs/VA2013OutpatientACSI.pdf. Published March 2014. Accessed August 10, 2016.
9. U.S. Department of Veterans Affairs. VHA pain management, Opioid Safety Initiative (OSI). http://www.va.gov/PAINMANAGEMENT/Opioid_Safety_Initiative_OSI.asp. Updated June 17, 2015. Accessed August 4, 2016.
10. U.S. Department of Veterans Affairs. Office of Research and Development. http://www.research.va.gov. Updated July 21, 2016. Accessed August 4, 2016.
The Burden of Cardiac Complications in Patients with Community-Acquired Pneumonia
From the Division of Infectious Diseases, School of Medicine, University of Louisville, Louisville, KY.
Abstract
- Objective: To summarize the published literature on cardiac complications in patients with community-acquired pneumonia (CAP) as well as provide a historical context for the topic; and to provide recommendations concerning preventing and anticipating cardiac complications in patients with CAP.
- Methods: Literature review.
- Results: CAP patients are at increased risk for arrhythmias (~5%), myocardial infarction (~5%), and congestive heart failure (~14%). Oxygenation, the level of heart conditioning, local (pulmonary) and systemic (cytokines) inflammation, and medication all contribute to the pathophysiology of cardiac complications in CAP patients. A high Pneumonia Severity Index (PSI) can be used to screen for risk of cardiac complications in CAP patients; however, a new but less studied clinical rule developed to risk stratify patient hospitalized for CAP was shown to outperform the PSI. A troponin test and ECG should be obtained in all patients admitted for CAP while a cardiac echocardiogram may be reserved for higher-risk patients.
- Conclusions: Cardiac complications, including arrhythmias, myocardial infarctions, and congestive heart failure, are a significant burden among patients hospitalized for CAP. Influenza and pneumococcal vaccination should be emphasized among appropriate patients. Preliminary data suggest that those with CAP may be helped if they are already on aspirin or a statin. Early recognition of cardiac complications and treatment may improve clinical outcomes for patients with CAP.
Community-acquired pneumonia (CAP) is a common condition in the United States and a leading cause of morbidity and mortality [1,2], with medical costs exceeding $10 billion in 2011 [3]. The mortality rate is much higher for those aged 65 years and older [4]. Men have a higher death rate than women (18.6 vs. 13.9 per 100,000 population), and death rate varies based on ethnicity, with mortality rates for American Indian/Alaska natives at 19.2, blacks at 17.1, whites at 15.9, Asian/Pacific Islanders at 15.0, and Hispanics at 13.1 (all rates per 100,000) [2]. CAP causes considerable worldwide mortality, with differences in mortality varying according to world region [5].
Cardiovascular complications and death from other comorbidities cause a substantial proportion of CAP-associated mortality. In Mortensen et al’s study, among patients with CAP who died, at least one third had a cardiac complication, and 13% had a cardiac-related cause of death [6]. One study showed that hospitalized patients with CAP complicated by heart disease were 30% more likely to die than patients hospitalized with CAP alone [7]. In this article, we discuss the burden of cardiac complications in adults with CAP, including underlying pathophysiological processes and strategies to prevent their occurence.
Pathophysiological Processes of Heart Disease Caused by CAP
The pathophysiology of cardiac complications as a result of CAP is made up of several hypotheses, including (1) declining oxygen provision by the lungs in the face of increasing demand by the heart, (2) a lack of reserve for stress because of cardiac comorbidities and (3) localized (pulmonary) inflammation leading to systemic (including cardiac) complications by the release of cytokines or other chemicals. Any of these may result in cardiac complications occurring before, during, or after a patient has been hospitalized for CAP. Antimicrobial treatment, specifically azithromycin, has also been implicated in myocardial adverse effects. Although azithromycin is most noted for causing QT prolongation, it was associated with myocardial infarction (MI) in a study of 73,690 patients with pneumonia [8]. A higher proportion of those who received azithromycin had an MI compared to those who did not (5.1% vs 4.4%; OR 1.17; 95% CI, 1.08–1.25), but there was no statistical difference in cardiac arrhythmias, and the 90-day mortality was actually better in the azithromycin group (17.4% vs 22.3%; odds ratio [OR], 0.73; 95% CI, 0.70–0.76).
Systemic inflammation is the result of several molecules, such as cytokines, chemokines and reactive oxidant species. Reactive oxidant species may determine oxidation of proteins, lipids and DNA, which leads to cell death. The hypothesis also purports that they also cause destabilization of atherosclerotic plaques leading to MIs. Other reactions as a result of inflammation lead to arrhythmias with or without compromised cardiac function, causing congestive heart failure (CHF). For this reason, some authors have approached the pathophysiology of cardiac complications by considering them to be either plaque-related or plaque-unrelated events [9].
A few studies have linked specific inflammatory molecules to cardiac toxicity. NOX2 is chemically unstable and may provoke cellular damage, thus maintaining a certain redox balance is crucial for cardiomyocyte health. In 248 patients with CAP, an elevated troponin T was present in 135 patients and among those, NOX2 correlated with the troponin T values (OR 1.13, 95% CI 1.08–1.17; P < 0.001) [10]. Both disrupting the equilibrium of the redox balance by upregulating NOX2, and finding NOX2 to be associated with troponin T suggest that oxidative stress is implicated in damage to the myocardium during CAP. In another study of 432 patients with CAP, 41 developed atrial fibrillation within 24 to 72 hours of admission and showed higher blood levels of NOX2 than those who had CAP without atrial fibrillation [11]. Oxidative stress has been shown to cause hypertrophy, dysfunction, apoptotic cell death, and fibrosis in the myocardium [12].
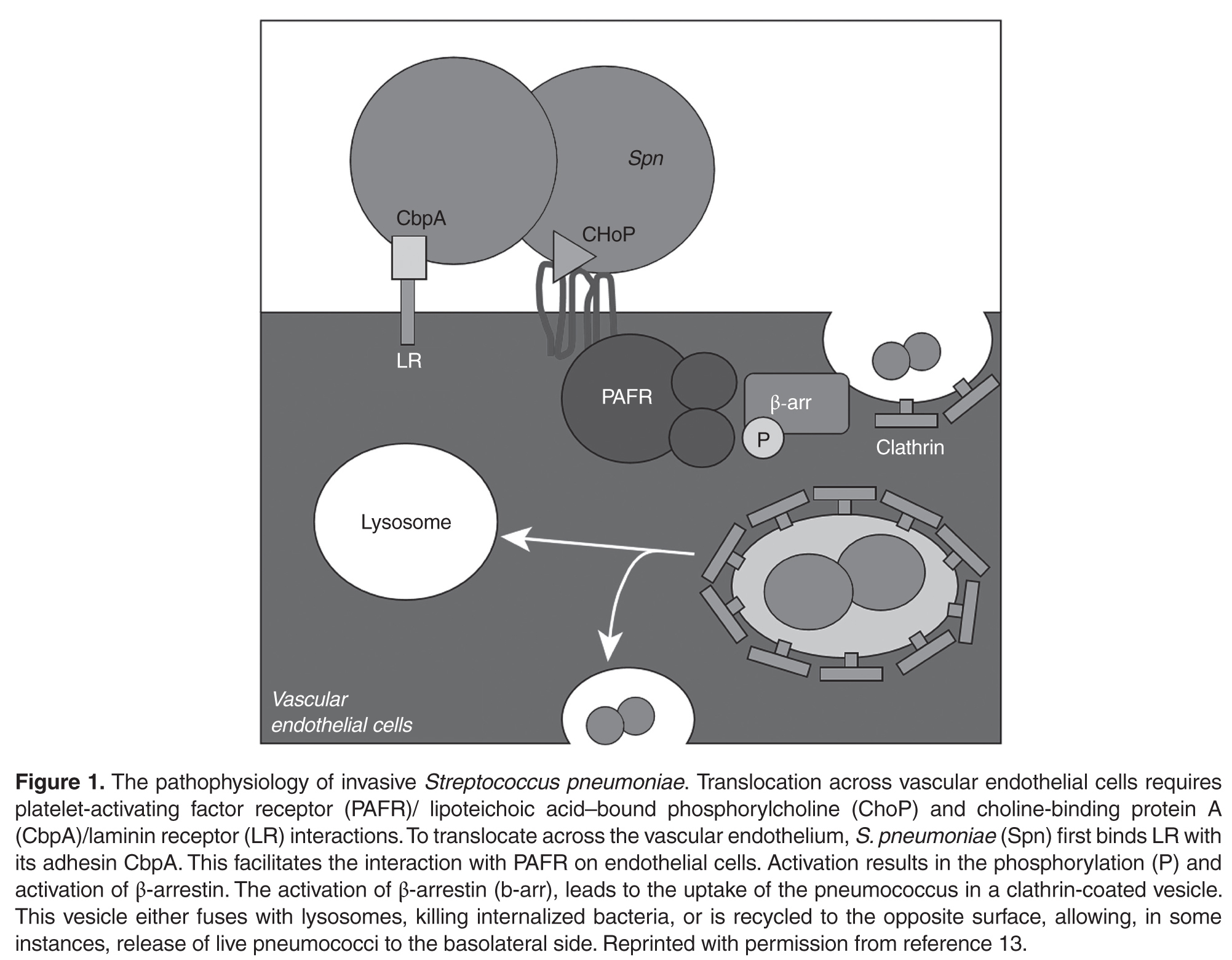
There is likely a high level of variability in how individual patients respond to a predisposing factor for a cardiac complication. For example, one patient may tolerate a mild hypoxia while another is sensitive. The association of inflammatory markers with the presence of cardiac markers, however, would support that once there are systemic reactions, the complications increase. Macrolides, however, were not found to contribute to long-term mortality due to cardiac complications.
Cardiac Complications of CAP
After the H1N1 influenza outbreak of 1918, it was noted that all-cause mortality increased during the outbreak as did influenza-related deaths. This prompted inquiry as to whether there was an actual association between the outbreak and increased overall mortality, or whether the 2 occurrences were simply coincidental [14]. Near that time, arrhythmias in CAP patients were studied. T-wave changes were found to be associated with CAP [15]. Among 92 patients studied, 449 electrocardiograms (ECGs) were reviewed. T-wave changes were the most common ECG changes. They were found in 5 of 10 of the patients who died, and in 35 of the 82 patients who lived. Twelve living patients had persistent ECG changes, and although they were all thought to have had underlying myocardial disease, 2 of them certainly did as they each had an acute MI (and the ECG was included as a figure for one of them).
A study in the 1980s that reported 3 of 38 CAP patients with CHF interrupted the paucity of data at the time that showed that having a cardiac complication during CAP was a known entity [16]. By the end of the 20th century, Meier et al noted that among case patients who had an MI, an acute respiratory tract infection preceded the MI in 2.8% while in only 0.9% of control patients [17]. They also noted that patients who had an acute respiratory tract infection were 2.7 times more likely to have an MI in the following 10 days than control patients.
 Further study by Musher et al revealed that MI was associated with pneumococcal pneumonia in 12 (7%) of 170 veteran patients [18]. An MI was defined on the basis of ECG abnormalities (Q waves or ST segment elevation or depression) with troponin I levels ≥ 0.5 ng/mL. They also evaluated arrhythmias and CHF. They included atrial fibrillation or flutter and ventricular tachycardia while excluding terminal arrhythmias. An arrhythmia was found in 8 (5%) patients. CHF was based on Framingham criteria (Table 1) [19]. New or worsening CHF was determined by comparing physical findings, laboratory values, chest radiograph, and echocardiogram reports in medical records. CHF was found in 13 (19%) patients. Ramirez et al found that MI was associated with CAP in 29 (5.8%) of 500 similar veteran patients [20].
Further study by Musher et al revealed that MI was associated with pneumococcal pneumonia in 12 (7%) of 170 veteran patients [18]. An MI was defined on the basis of ECG abnormalities (Q waves or ST segment elevation or depression) with troponin I levels ≥ 0.5 ng/mL. They also evaluated arrhythmias and CHF. They included atrial fibrillation or flutter and ventricular tachycardia while excluding terminal arrhythmias. An arrhythmia was found in 8 (5%) patients. CHF was based on Framingham criteria (Table 1) [19]. New or worsening CHF was determined by comparing physical findings, laboratory values, chest radiograph, and echocardiogram reports in medical records. CHF was found in 13 (19%) patients. Ramirez et al found that MI was associated with CAP in 29 (5.8%) of 500 similar veteran patients [20].
Corrales-Medina et al reported cardiac complications in CAP patients in the Pneumonia Patient Outcomes Team cohort study [21]. They defined MI as the presence of 2 of 3 criteria: ECG abnormalities, elevated cardiac enzymes, and chest pain. They found 43 (3.2%) of 1343 patients with an MI. Arrhythmias included atrial fibrillation or flutter, multifocal atrial tachycardia, supraventricular tachycardia, ventricular tachycardia (≥ 3 beat run) or ventricular fibrillation. With the more inclusive list, they found a greater proportion, 137 (10%) patients affected. They defined CHF with physical examination findings plus a radiographic abnormality, and found 279 (21%) patients affected. A meta-analysis of 17 studies had pooled incidences for an MI of 5.3%, an arrhythmia of 4.7% and CHF of 14.1% [22].
In summary, the most prominent cardiac complications in patients with CAP have been found to be CHF, MI, and arrhythmia.
Timing of Cardiac Complications in Relation to CAP
While a patient is still in the community, cardiac complications may occur with the onset of CAP, or afterwards. For these patients, the primary goal is to identify the complication and manage it as soon as the patient is admitted for CAP, rather than allowing the complications to worsen only to be recognized later. Cardiac complications are rare in outpatients overall. A study of 944 outpatients found heart failure in 1.4%, arrhythmias in 1.0% and MI in 0.1% [21].
For patients who are admitted with CAP but who do not have a cardiac complication, the goals are either to prevent any complication or to recognize and manage a complication early. This also applies to patients who have been discharged after an admission for CAP. Cardiac complications have been recorded shortly after (within 30 days), and late (up to 1 year) after discharge. A study of over 50,000 veterans who were admitted for CAP were followed for any cardiovascular complication in the next 90 days. Approximately 7500 veterans were found to have a cardiac complication, including (in order of highest to lowest frequency) CHF, arrhythmia, MI, stroke and angina [23]. More than 75% of the complications were found on the day of hospitalization, but events were still measured at 30 days and 90 days.
Two other studies sought to determine an association between CAP and cardiac complications differently; not by following CAP patients prospectively for complications but by retrospectively evaluating patients for a respiratory infection among those who were admitted for a cardiovascular complication (MI or stroke). A study of over 35,000 first-time admissions for either an MI or a stroke were evaluated for a respiratory infection within the previous 90 days [24]. The incidence rates were statistically significant for every time period up to 90 days. The preceding 3 days was the time period with the highest frequency for a respiratory infection preceding an event. When the event was an MI, the incident rate was 4.95 (95% CI, 4.43–5.53). A similar study of over 20,000 first-time admissions for either an MI or stroke were evaluated for a preceding primary care visit for a respiratory infection [25]. An infection preceded 2.9% of patients with an MI and 2.8% of patients with a stroke. Statistical significance was found for the group of patients who had a respiratory infection within 7 days preceding an MI (OR 2.10 [95% CI 1.38–3.21]) or preceding a stroke (OR 1.92 [95% CI 1.24–2.97]). In fact, every time period analyzed for both complications (MI and stroke) was significant up to 1 year. Because the timing of a cardiac complication varies and can occur up to 90 days or even a year after acute infection, physicians should maintain vigilance in suspecting and screening for them.
Predictors of Cardiac Complications During CAP
Recently, Cangemi et al reviewed mortality in 301 patients admitted for CAP 6 to 60 months after they were discharged [26]. Mortality was compared between patients who experienced a cardiac complication—atrial fibrillation or an ST- or non-ST-elevation MI—during their admission and those who did not. A total of 55 (18%) patients had a cardiac complication while hospitalized. During the follow-up, 90 (30%) of the 301 patients died. Death occurred in more patients who had had a cardiac complication while hospitalized than in those who did not (32% vs 13%; P < 0.001). The study also showed that age and the pneumonia severity index (PSI) predicted death in addition to intra-hospital complication. A Cox regression analysis showed that intrahospital cardiac complications (hazard ratio [HR] 1.76 [95% CI 1.10–2.82]; P = 0.019), age (HR 1.05 [95% CI 1.03–1.08]; P < 0.001) and the PSI (HR 1.01 [95% CI 1.00–1.02] P = 0.012) independently predicted death after adjusting for possible confounders [26].
The PSI score was published in 1997, and it instructed that patients with a risk class of I or II (low risk) should be managed as outpatients. Data eventually showed that there is a portion of the population with a risk class of I or II whose hospital admission is justified [4]. Among the reasons found was “comorbidity,” including MI and other cardiac complications. The PSI prediction rule was found to be useful in novel ways, and being associated with a risk of MI in patients with CAP was one of them. The propensity-adjusted association between the PSI score and MI was significant (P < 0.05) in an observational study of the CAP Organization (CAPO) [20]. Knowing that a PSI of 80 is in the middle of risk class III (71–90), it was noted that below 80 the risk for MI was zero to 2.5%, while above 80 the risk rose from 2.5% to 12.5%. A later study using the same statistical method showed a correlation between the PSI score and cardiac complications (MI, arrhythmias and CHF) with a P value of < 0.01 [21]. Determining the probability for the combination of complications, rather than just an MI, yielded an unsurprisingly higher range of risk for the PSI below 80, which was zero to 17.5%, while risk for a PSI above 80 was 17.5% to 80%.
In a study to determine risk factors for cardiac complications among 3068 patients with CAP, Griffin et al applied a purposeful selection algorithm to a list of factors with reasonable potential to be associated with the 376 patients who actually had a cardiac complication [27]. After multivariate logistic regression analysis, hyperlipidemia, an infection with Staphlococcus aureus or Klebsiella pneumoniae, and the PSI were found to be statistically significant. In contrast, statin therapy was associated with a lower risk of an event.
In 2014, a validated score similar to the PSI and using the same database was derived to predict short-term risk for cardiac events in hospitalized patients with CAP [28]. It attributes points for age, 3 preexisting conditions, 2 vital signs and 7 radiological and laboratory values, with a point scoring system that defines 4 risk stratification classes. In the derivation cohort, the incidence of cardiac complications across the risk classes increased linearly (3%, 18%, 35%, and 72%, respectively). The score was validated in the original publication with a separate database but has not been evaluated since. The score outperformed the PSI score in predicting cardiac complications in the validation cohort (proportion of patients correctly reclassified by the new score, 44%). Potentially, the rule could help identify high-risk patients upon admission and could assist clinicians in their decision making.
Strategies to Prevent Cardiac Complications During CAP
 It is now well established that there is a heavy burden of long-lasting cardiac complications among patients with CAP; therefore, preventing CAP should be a priority. This can be accomplished by counseling patients to refrain from alcohol and smoking and by administering influenza (Table 2) and pneumococcal vaccines (Figure 2). Since the 7-valent protein-polysaccharide conjugate pneumococcal vaccine (PCV-7) was released for children in 2000, there have been fewer hospitalizations in the United States [27] and improved outcomes globally;
It is now well established that there is a heavy burden of long-lasting cardiac complications among patients with CAP; therefore, preventing CAP should be a priority. This can be accomplished by counseling patients to refrain from alcohol and smoking and by administering influenza (Table 2) and pneumococcal vaccines (Figure 2). Since the 7-valent protein-polysaccharide conjugate pneumococcal vaccine (PCV-7) was released for children in 2000, there have been fewer hospitalizations in the United States [27] and improved outcomes globally;  for instance, fewer hospitalizations among children < 14 years of age in Uruguay [29], and decreased invasive pneumococcal disease among children < 5 years of age in Taiwan [30]. Furthermore, a decrease in invasive pneumococcal disease by 18% in persons aged > 65 years in the US and Canada decreased with the introduction of PCV-7 to children. Although this showed a beneficial indirect effect (herd immunity) in unvaccinated populations [31,32], there have been no randomized controlled trials in adults demonstrating a decrease in pneumococcal pneumonia or invasive pneumococcal disease which were vaccinated with PCV-13. The Food and Drug Administration approved PCV-13 for children in 2010 and for adults in 2012. Although it included fewer serotypes, it did include serotype 6A, which has a high pathogenicity and is not in 23-valent pneumococcal polysaccharide vaccine (PPSV-23). The criteria for vaccinating adults for pneumococcal infection were recently published [33]. A study of patients with invasive pneumococcal disease, which also determined pneumococcal serotypes, included 5 patients who had CAP as well [34]. Those patients had serotypes 6A, 7C, 14, and 23F (2 patients). The patient who had serotype 14 (higher pathogenicity) died and the other 4 lived. Serotypes 14 and 23F are in both vaccines while serotype 7C is in neither. Vaccination status was not provided in the study. At this time, there is evidence to support vaccinating patients for both S. pneumoniae and influenza virus.
for instance, fewer hospitalizations among children < 14 years of age in Uruguay [29], and decreased invasive pneumococcal disease among children < 5 years of age in Taiwan [30]. Furthermore, a decrease in invasive pneumococcal disease by 18% in persons aged > 65 years in the US and Canada decreased with the introduction of PCV-7 to children. Although this showed a beneficial indirect effect (herd immunity) in unvaccinated populations [31,32], there have been no randomized controlled trials in adults demonstrating a decrease in pneumococcal pneumonia or invasive pneumococcal disease which were vaccinated with PCV-13. The Food and Drug Administration approved PCV-13 for children in 2010 and for adults in 2012. Although it included fewer serotypes, it did include serotype 6A, which has a high pathogenicity and is not in 23-valent pneumococcal polysaccharide vaccine (PPSV-23). The criteria for vaccinating adults for pneumococcal infection were recently published [33]. A study of patients with invasive pneumococcal disease, which also determined pneumococcal serotypes, included 5 patients who had CAP as well [34]. Those patients had serotypes 6A, 7C, 14, and 23F (2 patients). The patient who had serotype 14 (higher pathogenicity) died and the other 4 lived. Serotypes 14 and 23F are in both vaccines while serotype 7C is in neither. Vaccination status was not provided in the study. At this time, there is evidence to support vaccinating patients for both S. pneumoniae and influenza virus.
Two methods used to prevent cardiac complications in general have been administration of aspirin and statins. The anticlotting properties of aspirin help to maintain blood flow in arteries narrowed by atherosclerosis. A meta-analysis of 10 randomized controlled trials found a statistically significant association between aspirin and a benefit on nonfatal myocardial infarctions/coronary events [35]. The associations were found with doses of 100 mg or less daily, and benefits were seen within 1 to 5 years. Statins have also been found to reduce all-cause mortality, cardiac-related mortality, and myocardial infarction [36]. A statin may stabilize coronary artery plaques that otherwise may rupture and cause myocardial ischemia or an infarct. But statins have also been found to be associated with a decreased risk of CAP. A comprehensive systematic review and meta-analysis found a decreased risk of CAP (OR 0.84; 95% CI, 0.74– 0.95) and decreased short-term mortality in patients with CAP (OR 0.68; 95% CI, 0.56–0.78) as a result of statin therapy [37]. The studies included any of 8 available statins. A prospective observational study found that patients who had been on a statin prior to being admitted for CAP had lower mortality, a lower incidence of complicated pneumonia and a lower C-reactive protein [38]. The lower C-reactive protein identifies decreased inflammation, which translates into improved endothelial function, modulated antioxidant effects, and a reduction in pro-inflammatory cytokines, hence its association with less severe CAP. Further study may reveal that a certain patient population should receive a statin to prevent CAP and improve outcomes. Overall, data support taking aspirin to prevent cardiac events regardless of CAP; further investigation of the benefits of statins to prevent cardiac complications in CAP patients is needed.
Clinical Applications
There are several implications of knowing the relationship between cardiac complications and CAP. First, physicians can better inform their patients about risks once they have been diagnosed with pneumonia. Second, physicians may be more likely to recognize a complication early and provide appropriate intervention. Third, physicians can risk stratify patients using the prediction score for cardiac complications in CAP patients [28]. In 1931 Master et al found that some patients with CAP also had PR interval or T-wave changes present for about 3 days, so they recommended obtaining an ECG to determine when a patient might be able to be discharged or declared “cured” [39]. Now, we are similarly recommending obtaining an ECG in CAP patients, but upon admission, in order to identify those who may get ischemic changes, arrhythmias or QTc prolongations. Pro-brain natriuretic peptide and troponins may be obtained independently of ECG results, and a cardiac echocardiogram may be reserved for those with a high risk of complications [40]. Finally, we recommend screening all patients for need for influenza and pneumococcal vaccines and administering according to the Advisory Committee on Immunization Practices of the Centers for Disease and Prevention [33].
Research Implications
The fact that cardiac complications in CAP patients is a well-defined entity with a significant degree of morbidity and mortality should prompt attentiona and resources to be directed to this area. The prediction score created specifically for this subpopulation of patients [28] can improve research by allowing adequate risk stratification to efficiently design and execute studies. Studies may be designed with fewer patients required to be enrolled while maintaining statistical power by limiting subject inclusion criteria to certain risk classes. Specific areas of future investigation should include the mechanisms of pathophysiology, which are not completely understood, and other complications, such as pulmonary edema, infectious endocarditis and pericarditis. Finally, cost has not been studied in this area or the potential savings of recognizing and preventing cardiac complications.
Summary
Cardiac complications, including arrhythmias, MI, and CHF are a significant burden among patients hospitalized for CAP. Influenza and pneumococcal vaccination should be emphasized among appropriate patients. The cardiac complication prediction score may be used to screen patients once admitted. A troponin and ECG should be obtained in all patients admitted for CAP while a cardiac echocardiogram may be reserved in higher-risk patients. Future research may be directed towards the subjects of pathophysiology other complications and cost.
Acknowledgment: We appreciate the critical review by Jessica Lynn Petrey, MSLS, Clinical Librarian, Kornhauser Health Sciences Library, University of Louisville, Louisville, KY.
Corresponding author: Dr. Forest Arnold, 501 E. Broadway, Suite 140 B, Louisville, KY 40202, [email protected]
Financial disclosures: None.
1. Pfuntner A, Wier LM, Stocks C. HCUP statistical brief #162. Agency for Healthcare Research and Quality; Rockville, MD: 2013. Most frequent conditions in U.S. hospitals, 2011. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf..
2. FastStats deaths and mortality. Centers for Disease Control and Prevention. Accessed 14 Oct 2015 at www.cdc.gov/nchs/fastats/deaths.htm.
3. Pfuntner A, Wier LM, Steiner C. HCUP statistical brief #168. Agency for Healthcare Research and Quality; Rockville, MD: 2013. Costs for hospital stays in the United States, 2011. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-United-States-2011.pdf.
4. American Lung Association. Trends in pneumonia and influenza morbidity and mortality. November 2015. Available at
www.lung.org/assets/documents/research/pi-trend-report.pdf.
5. Arnold FW, Wiemken TL, Peyrani P, et al. Mortality differences among hospitalized patients with community-acquired pneumonia in three world regions: results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort Study. Respir Med 2013;107:1101–11.
6. Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med 2002;162:1059–64.
7. Bordon J, Wiemken T, Peyrani P, et al. Decrease in long-term survival for hospitalized patients with community-acquired pneumonia. Chest 2010;138:279–83.
8. Mortensen EM, Halm EA, Pugh MJ, et al. Association of azithromycin with mortality and cardiovascular events among older patients hospitalized with pneumonia. JAMA 2014;311:2199–208.
9. Aliberti S, Ramirez JA. Cardiac diseases complicating community-acquired pneumonia. Curr Opin Infect Dis 2014;27:295–301.
10. Cangemi R, Calvieri C, Bucci T, et al. Is NOX2 upregulation implicated in myocardial injury in patients with pneumonia? Antioxid Redox Signal 2014;20:2949–54.
11. Violi F, Carnevale R, Calvieri C, et al. Nox2 up-regulation is associated with an enhanced risk of atrial fibrillation in patients with pneumonia. Thorax 2015;70:961–6.
12. Zhang Y, Tocchetti CG, Krieg T, Moens AL. Oxidative and nitrosative stress in the maintenance of myocardial function. Free Radic Biol Med 2012;53:1531–40.
13. Brown AO, Millett ER, Quint JK, Orihuela CJ. Cardiotoxicity during invasive pneumococcal disease. Am J Respir Crit Care Med 2015;191:739–45.
14. Collins SD. Excess mortality from causes other than influenza and pneumonia during influenza epidemics. Pub Health Rep 1932;47:2159–79.
15. Thomson KJ, Rustein DD, et al. Electrocardiographic studies during and after pneumococcus pneumonia. Am Heart J 1946;31:565–79.
16. Esposito AL. Community-acquired bacteremic pneumococcal pneumonia. Effect of age on manifestations and outcome. Arch Intern Med 1984;144:945–8.
17. Meier CR, Jick SS, Derby LE, et al. Acute respiratory-tract infections and risk of first-time acute myocardial infarction. Lancet 1998;351(9114):1467–71.
18. Musher DM, Rueda AM, Kaka AS, Mapara SM. The association between pneumococcal pneumonia and acute cardiac events. Clin Infect Dis 2007;45:158–65.
19. McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med 1971;285:1441–6.
20. Ramirez J, Aliberti S, Mirsaeidi M, et al. Acute myocardial infarction in hospitalized patients with community-acquired pneumonia. Clin Infect Dis 2008;47:182–7.
21. Corrales-Medina VF, Musher DM, Wells GA, et al. Cardiac complications in patients with community-acquired pneumonia: incidence, timing, risk factors, and association with short-term mortality. Circulation 2012;125:773–81.
22. Corrales-Medina VF, Suh KN, Rose G, et al. Cardiac complications in patients with community-acquired pneumonia: a systematic review and meta-analysis of observational studies. PLoS Med 2011;8(6):e1001048.
23. Perry TW, Pugh MJ, Waterer GW, et al. Incidence of cardiovascular events after hospital admission for pneumonia. Am J Med 2011;124:244–51.
24. Smeeth L, Thomas SL, Hall AJ, et al. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med 2004;351:2611–8.
25. Clayton TC, Thompson M, Meade TW. Recent respiratory infection and risk of cardiovascular disease: case-control study through a general practice database. Eur Heart J 2008;29:96–103.
26. Cangemi R, Calvieri C, Falcone M, et al. Relation of cardiac complications in the early phase of community-acquired pneumonia to long-term mortality and cardiovascular events. Am J Cardiol 2015;116:647–51.
27. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med 2013;369:155–63.
28. Corrales-Medina VF, Taljaard M, Fine MJ, et al. Risk stratification for cardiac complications in patients hospitalized for community-acquired pneumonia. Mayo Clin Proc 2014;89:60–8.
29. Pirez MC, Algorta G, Cedres A, et al. Impact of universal pneumococcal vaccination on hospitalizations for pneumonia and meningitis in children in Montevideo, Uruguay. Pediatr Infect Dis J 2011;30:669–74.
30. Liao WH, Lin SH, Lai CC, et al. Impact of pneumococcal vaccines on invasive pneumococcal disease in Taiwan. Eur J Clin Microbiol Infect Dis 2010;29:489–92.
31. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med 2003;348:1737–46.
32. Kellner JD, Church DL, MacDonald J, et al. Progress in the prevention of pneumococcal infection. CMAJ 2005;173:1149–51.
33. Kim DK, Bridges CB, Harriman KH, Advisory Committee on Immunization Practices. Recommended immunization schedule for adults aged 19 years or older: United States, 2016. Ann Intern Med 2016;164:184–94.
34. Kan B, Ries J, Normark BH, et al. Endocarditis and pericarditis complicating pneumococcal bacteraemia, with special reference to the adhesive abilities of pneumococci: results from a prospective study. Clin Microbiol Infect 2006;12:338–44.
35. Guirguis-Blake JM, Evans CV, Senger CA, et al. Aspirin for the primary prevention of cardiovascular events: a systematic evidence review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 131. Rockville, MD: Agency for Healthcare Research and Quality; 2015.
36. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267–78.
37. Khan AR, Riaz M, Bin Abdulhak AA, et al. The role of statins in prevention and treatment of community acquired pneumonia: a systematic review and meta-analysis. PLoS One 2013;8:e52929.
38. Chalmers JD, Singanayagam A, Murray MP, Hill AT. Prior statin use is associated with improved outcomes in community-acquired pneumonia. Am J Med 2008;121:1002–7 e1.
39. Master AM, Romanoff A, Jaffe H. Electrocardiographic changes in pneumonia. Am Heart J 1931;6:696–709.
40. Corrales-Medina VF, Musher DM, Shachkina S, Chirinos JA. Acute pneumonia and the cardiovascular system. Lancet 2015;381:496–505.
From the Division of Infectious Diseases, School of Medicine, University of Louisville, Louisville, KY.
Abstract
- Objective: To summarize the published literature on cardiac complications in patients with community-acquired pneumonia (CAP) as well as provide a historical context for the topic; and to provide recommendations concerning preventing and anticipating cardiac complications in patients with CAP.
- Methods: Literature review.
- Results: CAP patients are at increased risk for arrhythmias (~5%), myocardial infarction (~5%), and congestive heart failure (~14%). Oxygenation, the level of heart conditioning, local (pulmonary) and systemic (cytokines) inflammation, and medication all contribute to the pathophysiology of cardiac complications in CAP patients. A high Pneumonia Severity Index (PSI) can be used to screen for risk of cardiac complications in CAP patients; however, a new but less studied clinical rule developed to risk stratify patient hospitalized for CAP was shown to outperform the PSI. A troponin test and ECG should be obtained in all patients admitted for CAP while a cardiac echocardiogram may be reserved for higher-risk patients.
- Conclusions: Cardiac complications, including arrhythmias, myocardial infarctions, and congestive heart failure, are a significant burden among patients hospitalized for CAP. Influenza and pneumococcal vaccination should be emphasized among appropriate patients. Preliminary data suggest that those with CAP may be helped if they are already on aspirin or a statin. Early recognition of cardiac complications and treatment may improve clinical outcomes for patients with CAP.
Community-acquired pneumonia (CAP) is a common condition in the United States and a leading cause of morbidity and mortality [1,2], with medical costs exceeding $10 billion in 2011 [3]. The mortality rate is much higher for those aged 65 years and older [4]. Men have a higher death rate than women (18.6 vs. 13.9 per 100,000 population), and death rate varies based on ethnicity, with mortality rates for American Indian/Alaska natives at 19.2, blacks at 17.1, whites at 15.9, Asian/Pacific Islanders at 15.0, and Hispanics at 13.1 (all rates per 100,000) [2]. CAP causes considerable worldwide mortality, with differences in mortality varying according to world region [5].
Cardiovascular complications and death from other comorbidities cause a substantial proportion of CAP-associated mortality. In Mortensen et al’s study, among patients with CAP who died, at least one third had a cardiac complication, and 13% had a cardiac-related cause of death [6]. One study showed that hospitalized patients with CAP complicated by heart disease were 30% more likely to die than patients hospitalized with CAP alone [7]. In this article, we discuss the burden of cardiac complications in adults with CAP, including underlying pathophysiological processes and strategies to prevent their occurence.
Pathophysiological Processes of Heart Disease Caused by CAP
The pathophysiology of cardiac complications as a result of CAP is made up of several hypotheses, including (1) declining oxygen provision by the lungs in the face of increasing demand by the heart, (2) a lack of reserve for stress because of cardiac comorbidities and (3) localized (pulmonary) inflammation leading to systemic (including cardiac) complications by the release of cytokines or other chemicals. Any of these may result in cardiac complications occurring before, during, or after a patient has been hospitalized for CAP. Antimicrobial treatment, specifically azithromycin, has also been implicated in myocardial adverse effects. Although azithromycin is most noted for causing QT prolongation, it was associated with myocardial infarction (MI) in a study of 73,690 patients with pneumonia [8]. A higher proportion of those who received azithromycin had an MI compared to those who did not (5.1% vs 4.4%; OR 1.17; 95% CI, 1.08–1.25), but there was no statistical difference in cardiac arrhythmias, and the 90-day mortality was actually better in the azithromycin group (17.4% vs 22.3%; odds ratio [OR], 0.73; 95% CI, 0.70–0.76).
Systemic inflammation is the result of several molecules, such as cytokines, chemokines and reactive oxidant species. Reactive oxidant species may determine oxidation of proteins, lipids and DNA, which leads to cell death. The hypothesis also purports that they also cause destabilization of atherosclerotic plaques leading to MIs. Other reactions as a result of inflammation lead to arrhythmias with or without compromised cardiac function, causing congestive heart failure (CHF). For this reason, some authors have approached the pathophysiology of cardiac complications by considering them to be either plaque-related or plaque-unrelated events [9].
A few studies have linked specific inflammatory molecules to cardiac toxicity. NOX2 is chemically unstable and may provoke cellular damage, thus maintaining a certain redox balance is crucial for cardiomyocyte health. In 248 patients with CAP, an elevated troponin T was present in 135 patients and among those, NOX2 correlated with the troponin T values (OR 1.13, 95% CI 1.08–1.17; P < 0.001) [10]. Both disrupting the equilibrium of the redox balance by upregulating NOX2, and finding NOX2 to be associated with troponin T suggest that oxidative stress is implicated in damage to the myocardium during CAP. In another study of 432 patients with CAP, 41 developed atrial fibrillation within 24 to 72 hours of admission and showed higher blood levels of NOX2 than those who had CAP without atrial fibrillation [11]. Oxidative stress has been shown to cause hypertrophy, dysfunction, apoptotic cell death, and fibrosis in the myocardium [12].
There is likely a high level of variability in how individual patients respond to a predisposing factor for a cardiac complication. For example, one patient may tolerate a mild hypoxia while another is sensitive. The association of inflammatory markers with the presence of cardiac markers, however, would support that once there are systemic reactions, the complications increase. Macrolides, however, were not found to contribute to long-term mortality due to cardiac complications.
Cardiac Complications of CAP
After the H1N1 influenza outbreak of 1918, it was noted that all-cause mortality increased during the outbreak as did influenza-related deaths. This prompted inquiry as to whether there was an actual association between the outbreak and increased overall mortality, or whether the 2 occurrences were simply coincidental [14]. Near that time, arrhythmias in CAP patients were studied. T-wave changes were found to be associated with CAP [15]. Among 92 patients studied, 449 electrocardiograms (ECGs) were reviewed. T-wave changes were the most common ECG changes. They were found in 5 of 10 of the patients who died, and in 35 of the 82 patients who lived. Twelve living patients had persistent ECG changes, and although they were all thought to have had underlying myocardial disease, 2 of them certainly did as they each had an acute MI (and the ECG was included as a figure for one of them).
A study in the 1980s that reported 3 of 38 CAP patients with CHF interrupted the paucity of data at the time that showed that having a cardiac complication during CAP was a known entity [16]. By the end of the 20th century, Meier et al noted that among case patients who had an MI, an acute respiratory tract infection preceded the MI in 2.8% while in only 0.9% of control patients [17]. They also noted that patients who had an acute respiratory tract infection were 2.7 times more likely to have an MI in the following 10 days than control patients.
Further study by Musher et al revealed that MI was associated with pneumococcal pneumonia in 12 (7%) of 170 veteran patients [18]. An MI was defined on the basis of ECG abnormalities (Q waves or ST segment elevation or depression) with troponin I levels ≥ 0.5 ng/mL. They also evaluated arrhythmias and CHF. They included atrial fibrillation or flutter and ventricular tachycardia while excluding terminal arrhythmias. An arrhythmia was found in 8 (5%) patients. CHF was based on Framingham criteria (Table 1) [19]. New or worsening CHF was determined by comparing physical findings, laboratory values, chest radiograph, and echocardiogram reports in medical records. CHF was found in 13 (19%) patients. Ramirez et al found that MI was associated with CAP in 29 (5.8%) of 500 similar veteran patients [20].
Corrales-Medina et al reported cardiac complications in CAP patients in the Pneumonia Patient Outcomes Team cohort study [21]. They defined MI as the presence of 2 of 3 criteria: ECG abnormalities, elevated cardiac enzymes, and chest pain. They found 43 (3.2%) of 1343 patients with an MI. Arrhythmias included atrial fibrillation or flutter, multifocal atrial tachycardia, supraventricular tachycardia, ventricular tachycardia (≥ 3 beat run) or ventricular fibrillation. With the more inclusive list, they found a greater proportion, 137 (10%) patients affected. They defined CHF with physical examination findings plus a radiographic abnormality, and found 279 (21%) patients affected. A meta-analysis of 17 studies had pooled incidences for an MI of 5.3%, an arrhythmia of 4.7% and CHF of 14.1% [22].
In summary, the most prominent cardiac complications in patients with CAP have been found to be CHF, MI, and arrhythmia.
Timing of Cardiac Complications in Relation to CAP
While a patient is still in the community, cardiac complications may occur with the onset of CAP, or afterwards. For these patients, the primary goal is to identify the complication and manage it as soon as the patient is admitted for CAP, rather than allowing the complications to worsen only to be recognized later. Cardiac complications are rare in outpatients overall. A study of 944 outpatients found heart failure in 1.4%, arrhythmias in 1.0% and MI in 0.1% [21].
For patients who are admitted with CAP but who do not have a cardiac complication, the goals are either to prevent any complication or to recognize and manage a complication early. This also applies to patients who have been discharged after an admission for CAP. Cardiac complications have been recorded shortly after (within 30 days), and late (up to 1 year) after discharge. A study of over 50,000 veterans who were admitted for CAP were followed for any cardiovascular complication in the next 90 days. Approximately 7500 veterans were found to have a cardiac complication, including (in order of highest to lowest frequency) CHF, arrhythmia, MI, stroke and angina [23]. More than 75% of the complications were found on the day of hospitalization, but events were still measured at 30 days and 90 days.
Two other studies sought to determine an association between CAP and cardiac complications differently; not by following CAP patients prospectively for complications but by retrospectively evaluating patients for a respiratory infection among those who were admitted for a cardiovascular complication (MI or stroke). A study of over 35,000 first-time admissions for either an MI or a stroke were evaluated for a respiratory infection within the previous 90 days [24]. The incidence rates were statistically significant for every time period up to 90 days. The preceding 3 days was the time period with the highest frequency for a respiratory infection preceding an event. When the event was an MI, the incident rate was 4.95 (95% CI, 4.43–5.53). A similar study of over 20,000 first-time admissions for either an MI or stroke were evaluated for a preceding primary care visit for a respiratory infection [25]. An infection preceded 2.9% of patients with an MI and 2.8% of patients with a stroke. Statistical significance was found for the group of patients who had a respiratory infection within 7 days preceding an MI (OR 2.10 [95% CI 1.38–3.21]) or preceding a stroke (OR 1.92 [95% CI 1.24–2.97]). In fact, every time period analyzed for both complications (MI and stroke) was significant up to 1 year. Because the timing of a cardiac complication varies and can occur up to 90 days or even a year after acute infection, physicians should maintain vigilance in suspecting and screening for them.
Predictors of Cardiac Complications During CAP
Recently, Cangemi et al reviewed mortality in 301 patients admitted for CAP 6 to 60 months after they were discharged [26]. Mortality was compared between patients who experienced a cardiac complication—atrial fibrillation or an ST- or non-ST-elevation MI—during their admission and those who did not. A total of 55 (18%) patients had a cardiac complication while hospitalized. During the follow-up, 90 (30%) of the 301 patients died. Death occurred in more patients who had had a cardiac complication while hospitalized than in those who did not (32% vs 13%; P < 0.001). The study also showed that age and the pneumonia severity index (PSI) predicted death in addition to intra-hospital complication. A Cox regression analysis showed that intrahospital cardiac complications (hazard ratio [HR] 1.76 [95% CI 1.10–2.82]; P = 0.019), age (HR 1.05 [95% CI 1.03–1.08]; P < 0.001) and the PSI (HR 1.01 [95% CI 1.00–1.02] P = 0.012) independently predicted death after adjusting for possible confounders [26].
The PSI score was published in 1997, and it instructed that patients with a risk class of I or II (low risk) should be managed as outpatients. Data eventually showed that there is a portion of the population with a risk class of I or II whose hospital admission is justified [4]. Among the reasons found was “comorbidity,” including MI and other cardiac complications. The PSI prediction rule was found to be useful in novel ways, and being associated with a risk of MI in patients with CAP was one of them. The propensity-adjusted association between the PSI score and MI was significant (P < 0.05) in an observational study of the CAP Organization (CAPO) [20]. Knowing that a PSI of 80 is in the middle of risk class III (71–90), it was noted that below 80 the risk for MI was zero to 2.5%, while above 80 the risk rose from 2.5% to 12.5%. A later study using the same statistical method showed a correlation between the PSI score and cardiac complications (MI, arrhythmias and CHF) with a P value of < 0.01 [21]. Determining the probability for the combination of complications, rather than just an MI, yielded an unsurprisingly higher range of risk for the PSI below 80, which was zero to 17.5%, while risk for a PSI above 80 was 17.5% to 80%.
In a study to determine risk factors for cardiac complications among 3068 patients with CAP, Griffin et al applied a purposeful selection algorithm to a list of factors with reasonable potential to be associated with the 376 patients who actually had a cardiac complication [27]. After multivariate logistic regression analysis, hyperlipidemia, an infection with Staphlococcus aureus or Klebsiella pneumoniae, and the PSI were found to be statistically significant. In contrast, statin therapy was associated with a lower risk of an event.
In 2014, a validated score similar to the PSI and using the same database was derived to predict short-term risk for cardiac events in hospitalized patients with CAP [28]. It attributes points for age, 3 preexisting conditions, 2 vital signs and 7 radiological and laboratory values, with a point scoring system that defines 4 risk stratification classes. In the derivation cohort, the incidence of cardiac complications across the risk classes increased linearly (3%, 18%, 35%, and 72%, respectively). The score was validated in the original publication with a separate database but has not been evaluated since. The score outperformed the PSI score in predicting cardiac complications in the validation cohort (proportion of patients correctly reclassified by the new score, 44%). Potentially, the rule could help identify high-risk patients upon admission and could assist clinicians in their decision making.
Strategies to Prevent Cardiac Complications During CAP
It is now well established that there is a heavy burden of long-lasting cardiac complications among patients with CAP; therefore, preventing CAP should be a priority. This can be accomplished by counseling patients to refrain from alcohol and smoking and by administering influenza (Table 2) and pneumococcal vaccines (Figure 2). Since the 7-valent protein-polysaccharide conjugate pneumococcal vaccine (PCV-7) was released for children in 2000, there have been fewer hospitalizations in the United States [27] and improved outcomes globally; for instance, fewer hospitalizations among children < 14 years of age in Uruguay [29], and decreased invasive pneumococcal disease among children < 5 years of age in Taiwan [30]. Furthermore, a decrease in invasive pneumococcal disease by 18% in persons aged > 65 years in the US and Canada decreased with the introduction of PCV-7 to children. Although this showed a beneficial indirect effect (herd immunity) in unvaccinated populations [31,32], there have been no randomized controlled trials in adults demonstrating a decrease in pneumococcal pneumonia or invasive pneumococcal disease which were vaccinated with PCV-13. The Food and Drug Administration approved PCV-13 for children in 2010 and for adults in 2012. Although it included fewer serotypes, it did include serotype 6A, which has a high pathogenicity and is not in 23-valent pneumococcal polysaccharide vaccine (PPSV-23). The criteria for vaccinating adults for pneumococcal infection were recently published [33]. A study of patients with invasive pneumococcal disease, which also determined pneumococcal serotypes, included 5 patients who had CAP as well [34]. Those patients had serotypes 6A, 7C, 14, and 23F (2 patients). The patient who had serotype 14 (higher pathogenicity) died and the other 4 lived. Serotypes 14 and 23F are in both vaccines while serotype 7C is in neither. Vaccination status was not provided in the study. At this time, there is evidence to support vaccinating patients for both S. pneumoniae and influenza virus.
Two methods used to prevent cardiac complications in general have been administration of aspirin and statins. The anticlotting properties of aspirin help to maintain blood flow in arteries narrowed by atherosclerosis. A meta-analysis of 10 randomized controlled trials found a statistically significant association between aspirin and a benefit on nonfatal myocardial infarctions/coronary events [35]. The associations were found with doses of 100 mg or less daily, and benefits were seen within 1 to 5 years. Statins have also been found to reduce all-cause mortality, cardiac-related mortality, and myocardial infarction [36]. A statin may stabilize coronary artery plaques that otherwise may rupture and cause myocardial ischemia or an infarct. But statins have also been found to be associated with a decreased risk of CAP. A comprehensive systematic review and meta-analysis found a decreased risk of CAP (OR 0.84; 95% CI, 0.74– 0.95) and decreased short-term mortality in patients with CAP (OR 0.68; 95% CI, 0.56–0.78) as a result of statin therapy [37]. The studies included any of 8 available statins. A prospective observational study found that patients who had been on a statin prior to being admitted for CAP had lower mortality, a lower incidence of complicated pneumonia and a lower C-reactive protein [38]. The lower C-reactive protein identifies decreased inflammation, which translates into improved endothelial function, modulated antioxidant effects, and a reduction in pro-inflammatory cytokines, hence its association with less severe CAP. Further study may reveal that a certain patient population should receive a statin to prevent CAP and improve outcomes. Overall, data support taking aspirin to prevent cardiac events regardless of CAP; further investigation of the benefits of statins to prevent cardiac complications in CAP patients is needed.
Clinical Applications
There are several implications of knowing the relationship between cardiac complications and CAP. First, physicians can better inform their patients about risks once they have been diagnosed with pneumonia. Second, physicians may be more likely to recognize a complication early and provide appropriate intervention. Third, physicians can risk stratify patients using the prediction score for cardiac complications in CAP patients [28]. In 1931 Master et al found that some patients with CAP also had PR interval or T-wave changes present for about 3 days, so they recommended obtaining an ECG to determine when a patient might be able to be discharged or declared “cured” [39]. Now, we are similarly recommending obtaining an ECG in CAP patients, but upon admission, in order to identify those who may get ischemic changes, arrhythmias or QTc prolongations. Pro-brain natriuretic peptide and troponins may be obtained independently of ECG results, and a cardiac echocardiogram may be reserved for those with a high risk of complications [40]. Finally, we recommend screening all patients for need for influenza and pneumococcal vaccines and administering according to the Advisory Committee on Immunization Practices of the Centers for Disease and Prevention [33].
Research Implications
The fact that cardiac complications in CAP patients is a well-defined entity with a significant degree of morbidity and mortality should prompt attentiona and resources to be directed to this area. The prediction score created specifically for this subpopulation of patients [28] can improve research by allowing adequate risk stratification to efficiently design and execute studies. Studies may be designed with fewer patients required to be enrolled while maintaining statistical power by limiting subject inclusion criteria to certain risk classes. Specific areas of future investigation should include the mechanisms of pathophysiology, which are not completely understood, and other complications, such as pulmonary edema, infectious endocarditis and pericarditis. Finally, cost has not been studied in this area or the potential savings of recognizing and preventing cardiac complications.
Summary
Cardiac complications, including arrhythmias, MI, and CHF are a significant burden among patients hospitalized for CAP. Influenza and pneumococcal vaccination should be emphasized among appropriate patients. The cardiac complication prediction score may be used to screen patients once admitted. A troponin and ECG should be obtained in all patients admitted for CAP while a cardiac echocardiogram may be reserved in higher-risk patients. Future research may be directed towards the subjects of pathophysiology other complications and cost.
Acknowledgment: We appreciate the critical review by Jessica Lynn Petrey, MSLS, Clinical Librarian, Kornhauser Health Sciences Library, University of Louisville, Louisville, KY.
Corresponding author: Dr. Forest Arnold, 501 E. Broadway, Suite 140 B, Louisville, KY 40202, [email protected]
Financial disclosures: None.
From the Division of Infectious Diseases, School of Medicine, University of Louisville, Louisville, KY.
Abstract
- Objective: To summarize the published literature on cardiac complications in patients with community-acquired pneumonia (CAP) as well as provide a historical context for the topic; and to provide recommendations concerning preventing and anticipating cardiac complications in patients with CAP.
- Methods: Literature review.
- Results: CAP patients are at increased risk for arrhythmias (~5%), myocardial infarction (~5%), and congestive heart failure (~14%). Oxygenation, the level of heart conditioning, local (pulmonary) and systemic (cytokines) inflammation, and medication all contribute to the pathophysiology of cardiac complications in CAP patients. A high Pneumonia Severity Index (PSI) can be used to screen for risk of cardiac complications in CAP patients; however, a new but less studied clinical rule developed to risk stratify patient hospitalized for CAP was shown to outperform the PSI. A troponin test and ECG should be obtained in all patients admitted for CAP while a cardiac echocardiogram may be reserved for higher-risk patients.
- Conclusions: Cardiac complications, including arrhythmias, myocardial infarctions, and congestive heart failure, are a significant burden among patients hospitalized for CAP. Influenza and pneumococcal vaccination should be emphasized among appropriate patients. Preliminary data suggest that those with CAP may be helped if they are already on aspirin or a statin. Early recognition of cardiac complications and treatment may improve clinical outcomes for patients with CAP.
Community-acquired pneumonia (CAP) is a common condition in the United States and a leading cause of morbidity and mortality [1,2], with medical costs exceeding $10 billion in 2011 [3]. The mortality rate is much higher for those aged 65 years and older [4]. Men have a higher death rate than women (18.6 vs. 13.9 per 100,000 population), and death rate varies based on ethnicity, with mortality rates for American Indian/Alaska natives at 19.2, blacks at 17.1, whites at 15.9, Asian/Pacific Islanders at 15.0, and Hispanics at 13.1 (all rates per 100,000) [2]. CAP causes considerable worldwide mortality, with differences in mortality varying according to world region [5].
Cardiovascular complications and death from other comorbidities cause a substantial proportion of CAP-associated mortality. In Mortensen et al’s study, among patients with CAP who died, at least one third had a cardiac complication, and 13% had a cardiac-related cause of death [6]. One study showed that hospitalized patients with CAP complicated by heart disease were 30% more likely to die than patients hospitalized with CAP alone [7]. In this article, we discuss the burden of cardiac complications in adults with CAP, including underlying pathophysiological processes and strategies to prevent their occurence.
Pathophysiological Processes of Heart Disease Caused by CAP
The pathophysiology of cardiac complications as a result of CAP is made up of several hypotheses, including (1) declining oxygen provision by the lungs in the face of increasing demand by the heart, (2) a lack of reserve for stress because of cardiac comorbidities and (3) localized (pulmonary) inflammation leading to systemic (including cardiac) complications by the release of cytokines or other chemicals. Any of these may result in cardiac complications occurring before, during, or after a patient has been hospitalized for CAP. Antimicrobial treatment, specifically azithromycin, has also been implicated in myocardial adverse effects. Although azithromycin is most noted for causing QT prolongation, it was associated with myocardial infarction (MI) in a study of 73,690 patients with pneumonia [8]. A higher proportion of those who received azithromycin had an MI compared to those who did not (5.1% vs 4.4%; OR 1.17; 95% CI, 1.08–1.25), but there was no statistical difference in cardiac arrhythmias, and the 90-day mortality was actually better in the azithromycin group (17.4% vs 22.3%; odds ratio [OR], 0.73; 95% CI, 0.70–0.76).
Systemic inflammation is the result of several molecules, such as cytokines, chemokines and reactive oxidant species. Reactive oxidant species may determine oxidation of proteins, lipids and DNA, which leads to cell death. The hypothesis also purports that they also cause destabilization of atherosclerotic plaques leading to MIs. Other reactions as a result of inflammation lead to arrhythmias with or without compromised cardiac function, causing congestive heart failure (CHF). For this reason, some authors have approached the pathophysiology of cardiac complications by considering them to be either plaque-related or plaque-unrelated events [9].
A few studies have linked specific inflammatory molecules to cardiac toxicity. NOX2 is chemically unstable and may provoke cellular damage, thus maintaining a certain redox balance is crucial for cardiomyocyte health. In 248 patients with CAP, an elevated troponin T was present in 135 patients and among those, NOX2 correlated with the troponin T values (OR 1.13, 95% CI 1.08–1.17; P < 0.001) [10]. Both disrupting the equilibrium of the redox balance by upregulating NOX2, and finding NOX2 to be associated with troponin T suggest that oxidative stress is implicated in damage to the myocardium during CAP. In another study of 432 patients with CAP, 41 developed atrial fibrillation within 24 to 72 hours of admission and showed higher blood levels of NOX2 than those who had CAP without atrial fibrillation [11]. Oxidative stress has been shown to cause hypertrophy, dysfunction, apoptotic cell death, and fibrosis in the myocardium [12].
There is likely a high level of variability in how individual patients respond to a predisposing factor for a cardiac complication. For example, one patient may tolerate a mild hypoxia while another is sensitive. The association of inflammatory markers with the presence of cardiac markers, however, would support that once there are systemic reactions, the complications increase. Macrolides, however, were not found to contribute to long-term mortality due to cardiac complications.
Cardiac Complications of CAP
After the H1N1 influenza outbreak of 1918, it was noted that all-cause mortality increased during the outbreak as did influenza-related deaths. This prompted inquiry as to whether there was an actual association between the outbreak and increased overall mortality, or whether the 2 occurrences were simply coincidental [14]. Near that time, arrhythmias in CAP patients were studied. T-wave changes were found to be associated with CAP [15]. Among 92 patients studied, 449 electrocardiograms (ECGs) were reviewed. T-wave changes were the most common ECG changes. They were found in 5 of 10 of the patients who died, and in 35 of the 82 patients who lived. Twelve living patients had persistent ECG changes, and although they were all thought to have had underlying myocardial disease, 2 of them certainly did as they each had an acute MI (and the ECG was included as a figure for one of them).
A study in the 1980s that reported 3 of 38 CAP patients with CHF interrupted the paucity of data at the time that showed that having a cardiac complication during CAP was a known entity [16]. By the end of the 20th century, Meier et al noted that among case patients who had an MI, an acute respiratory tract infection preceded the MI in 2.8% while in only 0.9% of control patients [17]. They also noted that patients who had an acute respiratory tract infection were 2.7 times more likely to have an MI in the following 10 days than control patients.
Further study by Musher et al revealed that MI was associated with pneumococcal pneumonia in 12 (7%) of 170 veteran patients [18]. An MI was defined on the basis of ECG abnormalities (Q waves or ST segment elevation or depression) with troponin I levels ≥ 0.5 ng/mL. They also evaluated arrhythmias and CHF. They included atrial fibrillation or flutter and ventricular tachycardia while excluding terminal arrhythmias. An arrhythmia was found in 8 (5%) patients. CHF was based on Framingham criteria (Table 1) [19]. New or worsening CHF was determined by comparing physical findings, laboratory values, chest radiograph, and echocardiogram reports in medical records. CHF was found in 13 (19%) patients. Ramirez et al found that MI was associated with CAP in 29 (5.8%) of 500 similar veteran patients [20].
Corrales-Medina et al reported cardiac complications in CAP patients in the Pneumonia Patient Outcomes Team cohort study [21]. They defined MI as the presence of 2 of 3 criteria: ECG abnormalities, elevated cardiac enzymes, and chest pain. They found 43 (3.2%) of 1343 patients with an MI. Arrhythmias included atrial fibrillation or flutter, multifocal atrial tachycardia, supraventricular tachycardia, ventricular tachycardia (≥ 3 beat run) or ventricular fibrillation. With the more inclusive list, they found a greater proportion, 137 (10%) patients affected. They defined CHF with physical examination findings plus a radiographic abnormality, and found 279 (21%) patients affected. A meta-analysis of 17 studies had pooled incidences for an MI of 5.3%, an arrhythmia of 4.7% and CHF of 14.1% [22].
In summary, the most prominent cardiac complications in patients with CAP have been found to be CHF, MI, and arrhythmia.
Timing of Cardiac Complications in Relation to CAP
While a patient is still in the community, cardiac complications may occur with the onset of CAP, or afterwards. For these patients, the primary goal is to identify the complication and manage it as soon as the patient is admitted for CAP, rather than allowing the complications to worsen only to be recognized later. Cardiac complications are rare in outpatients overall. A study of 944 outpatients found heart failure in 1.4%, arrhythmias in 1.0% and MI in 0.1% [21].
For patients who are admitted with CAP but who do not have a cardiac complication, the goals are either to prevent any complication or to recognize and manage a complication early. This also applies to patients who have been discharged after an admission for CAP. Cardiac complications have been recorded shortly after (within 30 days), and late (up to 1 year) after discharge. A study of over 50,000 veterans who were admitted for CAP were followed for any cardiovascular complication in the next 90 days. Approximately 7500 veterans were found to have a cardiac complication, including (in order of highest to lowest frequency) CHF, arrhythmia, MI, stroke and angina [23]. More than 75% of the complications were found on the day of hospitalization, but events were still measured at 30 days and 90 days.
Two other studies sought to determine an association between CAP and cardiac complications differently; not by following CAP patients prospectively for complications but by retrospectively evaluating patients for a respiratory infection among those who were admitted for a cardiovascular complication (MI or stroke). A study of over 35,000 first-time admissions for either an MI or a stroke were evaluated for a respiratory infection within the previous 90 days [24]. The incidence rates were statistically significant for every time period up to 90 days. The preceding 3 days was the time period with the highest frequency for a respiratory infection preceding an event. When the event was an MI, the incident rate was 4.95 (95% CI, 4.43–5.53). A similar study of over 20,000 first-time admissions for either an MI or stroke were evaluated for a preceding primary care visit for a respiratory infection [25]. An infection preceded 2.9% of patients with an MI and 2.8% of patients with a stroke. Statistical significance was found for the group of patients who had a respiratory infection within 7 days preceding an MI (OR 2.10 [95% CI 1.38–3.21]) or preceding a stroke (OR 1.92 [95% CI 1.24–2.97]). In fact, every time period analyzed for both complications (MI and stroke) was significant up to 1 year. Because the timing of a cardiac complication varies and can occur up to 90 days or even a year after acute infection, physicians should maintain vigilance in suspecting and screening for them.
Predictors of Cardiac Complications During CAP
Recently, Cangemi et al reviewed mortality in 301 patients admitted for CAP 6 to 60 months after they were discharged [26]. Mortality was compared between patients who experienced a cardiac complication—atrial fibrillation or an ST- or non-ST-elevation MI—during their admission and those who did not. A total of 55 (18%) patients had a cardiac complication while hospitalized. During the follow-up, 90 (30%) of the 301 patients died. Death occurred in more patients who had had a cardiac complication while hospitalized than in those who did not (32% vs 13%; P < 0.001). The study also showed that age and the pneumonia severity index (PSI) predicted death in addition to intra-hospital complication. A Cox regression analysis showed that intrahospital cardiac complications (hazard ratio [HR] 1.76 [95% CI 1.10–2.82]; P = 0.019), age (HR 1.05 [95% CI 1.03–1.08]; P < 0.001) and the PSI (HR 1.01 [95% CI 1.00–1.02] P = 0.012) independently predicted death after adjusting for possible confounders [26].
The PSI score was published in 1997, and it instructed that patients with a risk class of I or II (low risk) should be managed as outpatients. Data eventually showed that there is a portion of the population with a risk class of I or II whose hospital admission is justified [4]. Among the reasons found was “comorbidity,” including MI and other cardiac complications. The PSI prediction rule was found to be useful in novel ways, and being associated with a risk of MI in patients with CAP was one of them. The propensity-adjusted association between the PSI score and MI was significant (P < 0.05) in an observational study of the CAP Organization (CAPO) [20]. Knowing that a PSI of 80 is in the middle of risk class III (71–90), it was noted that below 80 the risk for MI was zero to 2.5%, while above 80 the risk rose from 2.5% to 12.5%. A later study using the same statistical method showed a correlation between the PSI score and cardiac complications (MI, arrhythmias and CHF) with a P value of < 0.01 [21]. Determining the probability for the combination of complications, rather than just an MI, yielded an unsurprisingly higher range of risk for the PSI below 80, which was zero to 17.5%, while risk for a PSI above 80 was 17.5% to 80%.
In a study to determine risk factors for cardiac complications among 3068 patients with CAP, Griffin et al applied a purposeful selection algorithm to a list of factors with reasonable potential to be associated with the 376 patients who actually had a cardiac complication [27]. After multivariate logistic regression analysis, hyperlipidemia, an infection with Staphlococcus aureus or Klebsiella pneumoniae, and the PSI were found to be statistically significant. In contrast, statin therapy was associated with a lower risk of an event.
In 2014, a validated score similar to the PSI and using the same database was derived to predict short-term risk for cardiac events in hospitalized patients with CAP [28]. It attributes points for age, 3 preexisting conditions, 2 vital signs and 7 radiological and laboratory values, with a point scoring system that defines 4 risk stratification classes. In the derivation cohort, the incidence of cardiac complications across the risk classes increased linearly (3%, 18%, 35%, and 72%, respectively). The score was validated in the original publication with a separate database but has not been evaluated since. The score outperformed the PSI score in predicting cardiac complications in the validation cohort (proportion of patients correctly reclassified by the new score, 44%). Potentially, the rule could help identify high-risk patients upon admission and could assist clinicians in their decision making.
Strategies to Prevent Cardiac Complications During CAP
It is now well established that there is a heavy burden of long-lasting cardiac complications among patients with CAP; therefore, preventing CAP should be a priority. This can be accomplished by counseling patients to refrain from alcohol and smoking and by administering influenza (Table 2) and pneumococcal vaccines (Figure 2). Since the 7-valent protein-polysaccharide conjugate pneumococcal vaccine (PCV-7) was released for children in 2000, there have been fewer hospitalizations in the United States [27] and improved outcomes globally; for instance, fewer hospitalizations among children < 14 years of age in Uruguay [29], and decreased invasive pneumococcal disease among children < 5 years of age in Taiwan [30]. Furthermore, a decrease in invasive pneumococcal disease by 18% in persons aged > 65 years in the US and Canada decreased with the introduction of PCV-7 to children. Although this showed a beneficial indirect effect (herd immunity) in unvaccinated populations [31,32], there have been no randomized controlled trials in adults demonstrating a decrease in pneumococcal pneumonia or invasive pneumococcal disease which were vaccinated with PCV-13. The Food and Drug Administration approved PCV-13 for children in 2010 and for adults in 2012. Although it included fewer serotypes, it did include serotype 6A, which has a high pathogenicity and is not in 23-valent pneumococcal polysaccharide vaccine (PPSV-23). The criteria for vaccinating adults for pneumococcal infection were recently published [33]. A study of patients with invasive pneumococcal disease, which also determined pneumococcal serotypes, included 5 patients who had CAP as well [34]. Those patients had serotypes 6A, 7C, 14, and 23F (2 patients). The patient who had serotype 14 (higher pathogenicity) died and the other 4 lived. Serotypes 14 and 23F are in both vaccines while serotype 7C is in neither. Vaccination status was not provided in the study. At this time, there is evidence to support vaccinating patients for both S. pneumoniae and influenza virus.
Two methods used to prevent cardiac complications in general have been administration of aspirin and statins. The anticlotting properties of aspirin help to maintain blood flow in arteries narrowed by atherosclerosis. A meta-analysis of 10 randomized controlled trials found a statistically significant association between aspirin and a benefit on nonfatal myocardial infarctions/coronary events [35]. The associations were found with doses of 100 mg or less daily, and benefits were seen within 1 to 5 years. Statins have also been found to reduce all-cause mortality, cardiac-related mortality, and myocardial infarction [36]. A statin may stabilize coronary artery plaques that otherwise may rupture and cause myocardial ischemia or an infarct. But statins have also been found to be associated with a decreased risk of CAP. A comprehensive systematic review and meta-analysis found a decreased risk of CAP (OR 0.84; 95% CI, 0.74– 0.95) and decreased short-term mortality in patients with CAP (OR 0.68; 95% CI, 0.56–0.78) as a result of statin therapy [37]. The studies included any of 8 available statins. A prospective observational study found that patients who had been on a statin prior to being admitted for CAP had lower mortality, a lower incidence of complicated pneumonia and a lower C-reactive protein [38]. The lower C-reactive protein identifies decreased inflammation, which translates into improved endothelial function, modulated antioxidant effects, and a reduction in pro-inflammatory cytokines, hence its association with less severe CAP. Further study may reveal that a certain patient population should receive a statin to prevent CAP and improve outcomes. Overall, data support taking aspirin to prevent cardiac events regardless of CAP; further investigation of the benefits of statins to prevent cardiac complications in CAP patients is needed.
Clinical Applications
There are several implications of knowing the relationship between cardiac complications and CAP. First, physicians can better inform their patients about risks once they have been diagnosed with pneumonia. Second, physicians may be more likely to recognize a complication early and provide appropriate intervention. Third, physicians can risk stratify patients using the prediction score for cardiac complications in CAP patients [28]. In 1931 Master et al found that some patients with CAP also had PR interval or T-wave changes present for about 3 days, so they recommended obtaining an ECG to determine when a patient might be able to be discharged or declared “cured” [39]. Now, we are similarly recommending obtaining an ECG in CAP patients, but upon admission, in order to identify those who may get ischemic changes, arrhythmias or QTc prolongations. Pro-brain natriuretic peptide and troponins may be obtained independently of ECG results, and a cardiac echocardiogram may be reserved for those with a high risk of complications [40]. Finally, we recommend screening all patients for need for influenza and pneumococcal vaccines and administering according to the Advisory Committee on Immunization Practices of the Centers for Disease and Prevention [33].
Research Implications
The fact that cardiac complications in CAP patients is a well-defined entity with a significant degree of morbidity and mortality should prompt attentiona and resources to be directed to this area. The prediction score created specifically for this subpopulation of patients [28] can improve research by allowing adequate risk stratification to efficiently design and execute studies. Studies may be designed with fewer patients required to be enrolled while maintaining statistical power by limiting subject inclusion criteria to certain risk classes. Specific areas of future investigation should include the mechanisms of pathophysiology, which are not completely understood, and other complications, such as pulmonary edema, infectious endocarditis and pericarditis. Finally, cost has not been studied in this area or the potential savings of recognizing and preventing cardiac complications.
Summary
Cardiac complications, including arrhythmias, MI, and CHF are a significant burden among patients hospitalized for CAP. Influenza and pneumococcal vaccination should be emphasized among appropriate patients. The cardiac complication prediction score may be used to screen patients once admitted. A troponin and ECG should be obtained in all patients admitted for CAP while a cardiac echocardiogram may be reserved in higher-risk patients. Future research may be directed towards the subjects of pathophysiology other complications and cost.
Acknowledgment: We appreciate the critical review by Jessica Lynn Petrey, MSLS, Clinical Librarian, Kornhauser Health Sciences Library, University of Louisville, Louisville, KY.
Corresponding author: Dr. Forest Arnold, 501 E. Broadway, Suite 140 B, Louisville, KY 40202, [email protected]
Financial disclosures: None.
1. Pfuntner A, Wier LM, Stocks C. HCUP statistical brief #162. Agency for Healthcare Research and Quality; Rockville, MD: 2013. Most frequent conditions in U.S. hospitals, 2011. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf..
2. FastStats deaths and mortality. Centers for Disease Control and Prevention. Accessed 14 Oct 2015 at www.cdc.gov/nchs/fastats/deaths.htm.
3. Pfuntner A, Wier LM, Steiner C. HCUP statistical brief #168. Agency for Healthcare Research and Quality; Rockville, MD: 2013. Costs for hospital stays in the United States, 2011. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-United-States-2011.pdf.
4. American Lung Association. Trends in pneumonia and influenza morbidity and mortality. November 2015. Available at
www.lung.org/assets/documents/research/pi-trend-report.pdf.
5. Arnold FW, Wiemken TL, Peyrani P, et al. Mortality differences among hospitalized patients with community-acquired pneumonia in three world regions: results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort Study. Respir Med 2013;107:1101–11.
6. Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med 2002;162:1059–64.
7. Bordon J, Wiemken T, Peyrani P, et al. Decrease in long-term survival for hospitalized patients with community-acquired pneumonia. Chest 2010;138:279–83.
8. Mortensen EM, Halm EA, Pugh MJ, et al. Association of azithromycin with mortality and cardiovascular events among older patients hospitalized with pneumonia. JAMA 2014;311:2199–208.
9. Aliberti S, Ramirez JA. Cardiac diseases complicating community-acquired pneumonia. Curr Opin Infect Dis 2014;27:295–301.
10. Cangemi R, Calvieri C, Bucci T, et al. Is NOX2 upregulation implicated in myocardial injury in patients with pneumonia? Antioxid Redox Signal 2014;20:2949–54.
11. Violi F, Carnevale R, Calvieri C, et al. Nox2 up-regulation is associated with an enhanced risk of atrial fibrillation in patients with pneumonia. Thorax 2015;70:961–6.
12. Zhang Y, Tocchetti CG, Krieg T, Moens AL. Oxidative and nitrosative stress in the maintenance of myocardial function. Free Radic Biol Med 2012;53:1531–40.
13. Brown AO, Millett ER, Quint JK, Orihuela CJ. Cardiotoxicity during invasive pneumococcal disease. Am J Respir Crit Care Med 2015;191:739–45.
14. Collins SD. Excess mortality from causes other than influenza and pneumonia during influenza epidemics. Pub Health Rep 1932;47:2159–79.
15. Thomson KJ, Rustein DD, et al. Electrocardiographic studies during and after pneumococcus pneumonia. Am Heart J 1946;31:565–79.
16. Esposito AL. Community-acquired bacteremic pneumococcal pneumonia. Effect of age on manifestations and outcome. Arch Intern Med 1984;144:945–8.
17. Meier CR, Jick SS, Derby LE, et al. Acute respiratory-tract infections and risk of first-time acute myocardial infarction. Lancet 1998;351(9114):1467–71.
18. Musher DM, Rueda AM, Kaka AS, Mapara SM. The association between pneumococcal pneumonia and acute cardiac events. Clin Infect Dis 2007;45:158–65.
19. McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med 1971;285:1441–6.
20. Ramirez J, Aliberti S, Mirsaeidi M, et al. Acute myocardial infarction in hospitalized patients with community-acquired pneumonia. Clin Infect Dis 2008;47:182–7.
21. Corrales-Medina VF, Musher DM, Wells GA, et al. Cardiac complications in patients with community-acquired pneumonia: incidence, timing, risk factors, and association with short-term mortality. Circulation 2012;125:773–81.
22. Corrales-Medina VF, Suh KN, Rose G, et al. Cardiac complications in patients with community-acquired pneumonia: a systematic review and meta-analysis of observational studies. PLoS Med 2011;8(6):e1001048.
23. Perry TW, Pugh MJ, Waterer GW, et al. Incidence of cardiovascular events after hospital admission for pneumonia. Am J Med 2011;124:244–51.
24. Smeeth L, Thomas SL, Hall AJ, et al. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med 2004;351:2611–8.
25. Clayton TC, Thompson M, Meade TW. Recent respiratory infection and risk of cardiovascular disease: case-control study through a general practice database. Eur Heart J 2008;29:96–103.
26. Cangemi R, Calvieri C, Falcone M, et al. Relation of cardiac complications in the early phase of community-acquired pneumonia to long-term mortality and cardiovascular events. Am J Cardiol 2015;116:647–51.
27. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med 2013;369:155–63.
28. Corrales-Medina VF, Taljaard M, Fine MJ, et al. Risk stratification for cardiac complications in patients hospitalized for community-acquired pneumonia. Mayo Clin Proc 2014;89:60–8.
29. Pirez MC, Algorta G, Cedres A, et al. Impact of universal pneumococcal vaccination on hospitalizations for pneumonia and meningitis in children in Montevideo, Uruguay. Pediatr Infect Dis J 2011;30:669–74.
30. Liao WH, Lin SH, Lai CC, et al. Impact of pneumococcal vaccines on invasive pneumococcal disease in Taiwan. Eur J Clin Microbiol Infect Dis 2010;29:489–92.
31. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med 2003;348:1737–46.
32. Kellner JD, Church DL, MacDonald J, et al. Progress in the prevention of pneumococcal infection. CMAJ 2005;173:1149–51.
33. Kim DK, Bridges CB, Harriman KH, Advisory Committee on Immunization Practices. Recommended immunization schedule for adults aged 19 years or older: United States, 2016. Ann Intern Med 2016;164:184–94.
34. Kan B, Ries J, Normark BH, et al. Endocarditis and pericarditis complicating pneumococcal bacteraemia, with special reference to the adhesive abilities of pneumococci: results from a prospective study. Clin Microbiol Infect 2006;12:338–44.
35. Guirguis-Blake JM, Evans CV, Senger CA, et al. Aspirin for the primary prevention of cardiovascular events: a systematic evidence review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 131. Rockville, MD: Agency for Healthcare Research and Quality; 2015.
36. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267–78.
37. Khan AR, Riaz M, Bin Abdulhak AA, et al. The role of statins in prevention and treatment of community acquired pneumonia: a systematic review and meta-analysis. PLoS One 2013;8:e52929.
38. Chalmers JD, Singanayagam A, Murray MP, Hill AT. Prior statin use is associated with improved outcomes in community-acquired pneumonia. Am J Med 2008;121:1002–7 e1.
39. Master AM, Romanoff A, Jaffe H. Electrocardiographic changes in pneumonia. Am Heart J 1931;6:696–709.
40. Corrales-Medina VF, Musher DM, Shachkina S, Chirinos JA. Acute pneumonia and the cardiovascular system. Lancet 2015;381:496–505.
1. Pfuntner A, Wier LM, Stocks C. HCUP statistical brief #162. Agency for Healthcare Research and Quality; Rockville, MD: 2013. Most frequent conditions in U.S. hospitals, 2011. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf..
2. FastStats deaths and mortality. Centers for Disease Control and Prevention. Accessed 14 Oct 2015 at www.cdc.gov/nchs/fastats/deaths.htm.
3. Pfuntner A, Wier LM, Steiner C. HCUP statistical brief #168. Agency for Healthcare Research and Quality; Rockville, MD: 2013. Costs for hospital stays in the United States, 2011. Available at www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-United-States-2011.pdf.
4. American Lung Association. Trends in pneumonia and influenza morbidity and mortality. November 2015. Available at
www.lung.org/assets/documents/research/pi-trend-report.pdf.
5. Arnold FW, Wiemken TL, Peyrani P, et al. Mortality differences among hospitalized patients with community-acquired pneumonia in three world regions: results from the Community-Acquired Pneumonia Organization (CAPO) International Cohort Study. Respir Med 2013;107:1101–11.
6. Mortensen EM, Coley CM, Singer DE, et al. Causes of death for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team cohort study. Arch Intern Med 2002;162:1059–64.
7. Bordon J, Wiemken T, Peyrani P, et al. Decrease in long-term survival for hospitalized patients with community-acquired pneumonia. Chest 2010;138:279–83.
8. Mortensen EM, Halm EA, Pugh MJ, et al. Association of azithromycin with mortality and cardiovascular events among older patients hospitalized with pneumonia. JAMA 2014;311:2199–208.
9. Aliberti S, Ramirez JA. Cardiac diseases complicating community-acquired pneumonia. Curr Opin Infect Dis 2014;27:295–301.
10. Cangemi R, Calvieri C, Bucci T, et al. Is NOX2 upregulation implicated in myocardial injury in patients with pneumonia? Antioxid Redox Signal 2014;20:2949–54.
11. Violi F, Carnevale R, Calvieri C, et al. Nox2 up-regulation is associated with an enhanced risk of atrial fibrillation in patients with pneumonia. Thorax 2015;70:961–6.
12. Zhang Y, Tocchetti CG, Krieg T, Moens AL. Oxidative and nitrosative stress in the maintenance of myocardial function. Free Radic Biol Med 2012;53:1531–40.
13. Brown AO, Millett ER, Quint JK, Orihuela CJ. Cardiotoxicity during invasive pneumococcal disease. Am J Respir Crit Care Med 2015;191:739–45.
14. Collins SD. Excess mortality from causes other than influenza and pneumonia during influenza epidemics. Pub Health Rep 1932;47:2159–79.
15. Thomson KJ, Rustein DD, et al. Electrocardiographic studies during and after pneumococcus pneumonia. Am Heart J 1946;31:565–79.
16. Esposito AL. Community-acquired bacteremic pneumococcal pneumonia. Effect of age on manifestations and outcome. Arch Intern Med 1984;144:945–8.
17. Meier CR, Jick SS, Derby LE, et al. Acute respiratory-tract infections and risk of first-time acute myocardial infarction. Lancet 1998;351(9114):1467–71.
18. Musher DM, Rueda AM, Kaka AS, Mapara SM. The association between pneumococcal pneumonia and acute cardiac events. Clin Infect Dis 2007;45:158–65.
19. McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: the Framingham study. N Engl J Med 1971;285:1441–6.
20. Ramirez J, Aliberti S, Mirsaeidi M, et al. Acute myocardial infarction in hospitalized patients with community-acquired pneumonia. Clin Infect Dis 2008;47:182–7.
21. Corrales-Medina VF, Musher DM, Wells GA, et al. Cardiac complications in patients with community-acquired pneumonia: incidence, timing, risk factors, and association with short-term mortality. Circulation 2012;125:773–81.
22. Corrales-Medina VF, Suh KN, Rose G, et al. Cardiac complications in patients with community-acquired pneumonia: a systematic review and meta-analysis of observational studies. PLoS Med 2011;8(6):e1001048.
23. Perry TW, Pugh MJ, Waterer GW, et al. Incidence of cardiovascular events after hospital admission for pneumonia. Am J Med 2011;124:244–51.
24. Smeeth L, Thomas SL, Hall AJ, et al. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med 2004;351:2611–8.
25. Clayton TC, Thompson M, Meade TW. Recent respiratory infection and risk of cardiovascular disease: case-control study through a general practice database. Eur Heart J 2008;29:96–103.
26. Cangemi R, Calvieri C, Falcone M, et al. Relation of cardiac complications in the early phase of community-acquired pneumonia to long-term mortality and cardiovascular events. Am J Cardiol 2015;116:647–51.
27. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med 2013;369:155–63.
28. Corrales-Medina VF, Taljaard M, Fine MJ, et al. Risk stratification for cardiac complications in patients hospitalized for community-acquired pneumonia. Mayo Clin Proc 2014;89:60–8.
29. Pirez MC, Algorta G, Cedres A, et al. Impact of universal pneumococcal vaccination on hospitalizations for pneumonia and meningitis in children in Montevideo, Uruguay. Pediatr Infect Dis J 2011;30:669–74.
30. Liao WH, Lin SH, Lai CC, et al. Impact of pneumococcal vaccines on invasive pneumococcal disease in Taiwan. Eur J Clin Microbiol Infect Dis 2010;29:489–92.
31. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med 2003;348:1737–46.
32. Kellner JD, Church DL, MacDonald J, et al. Progress in the prevention of pneumococcal infection. CMAJ 2005;173:1149–51.
33. Kim DK, Bridges CB, Harriman KH, Advisory Committee on Immunization Practices. Recommended immunization schedule for adults aged 19 years or older: United States, 2016. Ann Intern Med 2016;164:184–94.
34. Kan B, Ries J, Normark BH, et al. Endocarditis and pericarditis complicating pneumococcal bacteraemia, with special reference to the adhesive abilities of pneumococci: results from a prospective study. Clin Microbiol Infect 2006;12:338–44.
35. Guirguis-Blake JM, Evans CV, Senger CA, et al. Aspirin for the primary prevention of cardiovascular events: a systematic evidence review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 131. Rockville, MD: Agency for Healthcare Research and Quality; 2015.
36. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005;366:1267–78.
37. Khan AR, Riaz M, Bin Abdulhak AA, et al. The role of statins in prevention and treatment of community acquired pneumonia: a systematic review and meta-analysis. PLoS One 2013;8:e52929.
38. Chalmers JD, Singanayagam A, Murray MP, Hill AT. Prior statin use is associated with improved outcomes in community-acquired pneumonia. Am J Med 2008;121:1002–7 e1.
39. Master AM, Romanoff A, Jaffe H. Electrocardiographic changes in pneumonia. Am Heart J 1931;6:696–709.
40. Corrales-Medina VF, Musher DM, Shachkina S, Chirinos JA. Acute pneumonia and the cardiovascular system. Lancet 2015;381:496–505.
Rash on left hand, feet

The FP diagnosed this patient with two foot one hand syndrome, which is a fungal infection involving both feet and one hand. To be sure of the diagnosis, the FP performed a potassium hydroxide (KOH) preparation from the scale on the left hand and found typical branching hyphae caused by a dermatophyte. (See video on how to perform a KOH preparation.) The dermatophyte was most likely Trichophyton rubrum, but it wasn’t necessary to determine the exact species in order to treat this condition.
Two foot one hand syndrome is not rare, but it is somewhat puzzling as to why it involves only one hand while involving both feet. Also, it does not preferentially involve the dominant hand. In this case, the patient’s 2 large toenails had visible onychomycosis and 3 of the nails on his left hand had fungal changes (his dominant right hand was not affected). Tinea pedis was seen between the toes in a moccasin distribution, as well.
Treatment for this condition usually requires an oral antifungal agent. (If, however, the nails were not involved and there were contraindications to an oral antifungal, then a topical antifungal cream could be tried first.)
The patient described here had no history of liver disease or alcohol abuse. So the FP prescribed terbinafine 250 mg daily for one month to fully clear the skin infection and a follow-up appointment was set for 4 weeks. At that appointment, the FP planned to discuss continuing oral treatment for 2 additional months to clear the fungal infection from the nails. If ongoing oral terbinafine was needed, liver function tests could be performed at that time.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Fungal overview. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill;2013:771-776.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP diagnosed this patient with two foot one hand syndrome, which is a fungal infection involving both feet and one hand. To be sure of the diagnosis, the FP performed a potassium hydroxide (KOH) preparation from the scale on the left hand and found typical branching hyphae caused by a dermatophyte. (See video on how to perform a KOH preparation.) The dermatophyte was most likely Trichophyton rubrum, but it wasn’t necessary to determine the exact species in order to treat this condition.
Two foot one hand syndrome is not rare, but it is somewhat puzzling as to why it involves only one hand while involving both feet. Also, it does not preferentially involve the dominant hand. In this case, the patient’s 2 large toenails had visible onychomycosis and 3 of the nails on his left hand had fungal changes (his dominant right hand was not affected). Tinea pedis was seen between the toes in a moccasin distribution, as well.
Treatment for this condition usually requires an oral antifungal agent. (If, however, the nails were not involved and there were contraindications to an oral antifungal, then a topical antifungal cream could be tried first.)
The patient described here had no history of liver disease or alcohol abuse. So the FP prescribed terbinafine 250 mg daily for one month to fully clear the skin infection and a follow-up appointment was set for 4 weeks. At that appointment, the FP planned to discuss continuing oral treatment for 2 additional months to clear the fungal infection from the nails. If ongoing oral terbinafine was needed, liver function tests could be performed at that time.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Fungal overview. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill;2013:771-776.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP diagnosed this patient with two foot one hand syndrome, which is a fungal infection involving both feet and one hand. To be sure of the diagnosis, the FP performed a potassium hydroxide (KOH) preparation from the scale on the left hand and found typical branching hyphae caused by a dermatophyte. (See video on how to perform a KOH preparation.) The dermatophyte was most likely Trichophyton rubrum, but it wasn’t necessary to determine the exact species in order to treat this condition.
Two foot one hand syndrome is not rare, but it is somewhat puzzling as to why it involves only one hand while involving both feet. Also, it does not preferentially involve the dominant hand. In this case, the patient’s 2 large toenails had visible onychomycosis and 3 of the nails on his left hand had fungal changes (his dominant right hand was not affected). Tinea pedis was seen between the toes in a moccasin distribution, as well.
Treatment for this condition usually requires an oral antifungal agent. (If, however, the nails were not involved and there were contraindications to an oral antifungal, then a topical antifungal cream could be tried first.)
The patient described here had no history of liver disease or alcohol abuse. So the FP prescribed terbinafine 250 mg daily for one month to fully clear the skin infection and a follow-up appointment was set for 4 weeks. At that appointment, the FP planned to discuss continuing oral treatment for 2 additional months to clear the fungal infection from the nails. If ongoing oral terbinafine was needed, liver function tests could be performed at that time.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Usatine R. Fungal overview. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill;2013:771-776.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

The Complement System in Refractory Myasthenia Gravis

Click here to read the supplement.
Click here to read the supplement.
Click here to read the supplement.

LETTER: Engaging the Next Generation: Hospital Medicine Student Interest Groups

Since the inception of hospital medicine, we are seeing unprecedented levels of reliance on hospitalists for educating and leading the next generation of physicians toward better care. A 2008 survey of internal medicine programs reported that learners gave hospitalists higher scores in the areas of attending rounds quality and the teaching of cost-effective care, in addition to providing an overall better learning experience as compared with non-hospitalist attendings.1
As successful educators, the development of mentorship programs has been shown to improve professional satisfaction and academic productivity in hospitalist communities.2, 3 Unfortunately, most of these programs failed to consider medical schools as valuable targets for outreach, education and support. By limiting vertical integration of training and mentorship, the hospitalist community is keeping itself from realizing its potential in building a pipeline for shaping the leaders of tomorrow’s healthcare sector.
A Hospital Medicine Student Interest Group (HM-SIG) is an organization composed of medical, nurse practitioner or physician assistant students interested in exploring future careers in hospital medicine. The goals of an HM-SIG are multidimensional: (1) introduce students to, or cultivate prior interest in, a career in hospital medicine, (2) provide opportunities for mentorship with faculty, (3) develop a community of future hospitalists, and (4) facilitate student involvement in institutional, local, regional and national hospital medicine projects on patient safety, high-value care and quality improvement.
Since starting the first medical school HM-SIG chapter in 2015, our efforts have led to significant changes in the way students are exposed not only to hospital medicine as a career, but to the tools and the mindset of hospitalists for improving care as well. In the fall of 2015, after brief discussions on the merits of and opportunities in hospital medicine, we selected a dedicated group of individuals and built our executive board. We collectively defined our goals and designed an 18-month plan to create student-led programming, coordinate mentorship opportunities with faculty and build a research pipeline for future medical students to have easier access to quality improvement work within the Loyola University Stritch School of Medicine. Within the first 6 months, we hosted a panel discussion with our hospitalist faculty, facilitated a quality improvement workshop to teach the lean methodology and rolled out a shadowing program that has given students deeper insight into the day in the life of a hospitalist. We’ve also developed a lecture series that has guided curriculum changes in quality improvement, and organized a student-led regional hospital medicine conference for nurse practitioners, physician assistants, medical students and internal medicine residents.
Without any representation from within the medical student community, student exposure to the hospitalist career is entirely dependent on the resources and availability of the affiliate hospital’s department of hospital medicine. With an investment in hospital medicine student interest groups at medical schools, SHM will equip students to become articulate advocates for the profession and SHM as a community.
References
- Goldenberg J, Glasheen JJ. Hospitalist educators: future of inpatient internal medicine training. Mt Sinai J Med 2008;75:430-5.
2. Pane LA, Davis AB, Ottolini MC. Career satisfaction and the role of mentorship: a survey of pediatric hospitalists. Hosp Pediatr. 2012;2(3):141-8.
3. Leary JC, Schainker EG, Leyenaar JK. The unwritten rules of mentorship: Facilitators of and barriers to effective mentorship in pediatric hospital medicine. Hospital Pediatrics. 2016;6(4):219-225; DOI: 10.1542/hpeds.2015-0108
Since the inception of hospital medicine, we are seeing unprecedented levels of reliance on hospitalists for educating and leading the next generation of physicians toward better care. A 2008 survey of internal medicine programs reported that learners gave hospitalists higher scores in the areas of attending rounds quality and the teaching of cost-effective care, in addition to providing an overall better learning experience as compared with non-hospitalist attendings.1
As successful educators, the development of mentorship programs has been shown to improve professional satisfaction and academic productivity in hospitalist communities.2, 3 Unfortunately, most of these programs failed to consider medical schools as valuable targets for outreach, education and support. By limiting vertical integration of training and mentorship, the hospitalist community is keeping itself from realizing its potential in building a pipeline for shaping the leaders of tomorrow’s healthcare sector.
A Hospital Medicine Student Interest Group (HM-SIG) is an organization composed of medical, nurse practitioner or physician assistant students interested in exploring future careers in hospital medicine. The goals of an HM-SIG are multidimensional: (1) introduce students to, or cultivate prior interest in, a career in hospital medicine, (2) provide opportunities for mentorship with faculty, (3) develop a community of future hospitalists, and (4) facilitate student involvement in institutional, local, regional and national hospital medicine projects on patient safety, high-value care and quality improvement.
Since starting the first medical school HM-SIG chapter in 2015, our efforts have led to significant changes in the way students are exposed not only to hospital medicine as a career, but to the tools and the mindset of hospitalists for improving care as well. In the fall of 2015, after brief discussions on the merits of and opportunities in hospital medicine, we selected a dedicated group of individuals and built our executive board. We collectively defined our goals and designed an 18-month plan to create student-led programming, coordinate mentorship opportunities with faculty and build a research pipeline for future medical students to have easier access to quality improvement work within the Loyola University Stritch School of Medicine. Within the first 6 months, we hosted a panel discussion with our hospitalist faculty, facilitated a quality improvement workshop to teach the lean methodology and rolled out a shadowing program that has given students deeper insight into the day in the life of a hospitalist. We’ve also developed a lecture series that has guided curriculum changes in quality improvement, and organized a student-led regional hospital medicine conference for nurse practitioners, physician assistants, medical students and internal medicine residents.
Without any representation from within the medical student community, student exposure to the hospitalist career is entirely dependent on the resources and availability of the affiliate hospital’s department of hospital medicine. With an investment in hospital medicine student interest groups at medical schools, SHM will equip students to become articulate advocates for the profession and SHM as a community.
References
- Goldenberg J, Glasheen JJ. Hospitalist educators: future of inpatient internal medicine training. Mt Sinai J Med 2008;75:430-5.
2. Pane LA, Davis AB, Ottolini MC. Career satisfaction and the role of mentorship: a survey of pediatric hospitalists. Hosp Pediatr. 2012;2(3):141-8.
3. Leary JC, Schainker EG, Leyenaar JK. The unwritten rules of mentorship: Facilitators of and barriers to effective mentorship in pediatric hospital medicine. Hospital Pediatrics. 2016;6(4):219-225; DOI: 10.1542/hpeds.2015-0108
Since the inception of hospital medicine, we are seeing unprecedented levels of reliance on hospitalists for educating and leading the next generation of physicians toward better care. A 2008 survey of internal medicine programs reported that learners gave hospitalists higher scores in the areas of attending rounds quality and the teaching of cost-effective care, in addition to providing an overall better learning experience as compared with non-hospitalist attendings.1
As successful educators, the development of mentorship programs has been shown to improve professional satisfaction and academic productivity in hospitalist communities.2, 3 Unfortunately, most of these programs failed to consider medical schools as valuable targets for outreach, education and support. By limiting vertical integration of training and mentorship, the hospitalist community is keeping itself from realizing its potential in building a pipeline for shaping the leaders of tomorrow’s healthcare sector.
A Hospital Medicine Student Interest Group (HM-SIG) is an organization composed of medical, nurse practitioner or physician assistant students interested in exploring future careers in hospital medicine. The goals of an HM-SIG are multidimensional: (1) introduce students to, or cultivate prior interest in, a career in hospital medicine, (2) provide opportunities for mentorship with faculty, (3) develop a community of future hospitalists, and (4) facilitate student involvement in institutional, local, regional and national hospital medicine projects on patient safety, high-value care and quality improvement.
Since starting the first medical school HM-SIG chapter in 2015, our efforts have led to significant changes in the way students are exposed not only to hospital medicine as a career, but to the tools and the mindset of hospitalists for improving care as well. In the fall of 2015, after brief discussions on the merits of and opportunities in hospital medicine, we selected a dedicated group of individuals and built our executive board. We collectively defined our goals and designed an 18-month plan to create student-led programming, coordinate mentorship opportunities with faculty and build a research pipeline for future medical students to have easier access to quality improvement work within the Loyola University Stritch School of Medicine. Within the first 6 months, we hosted a panel discussion with our hospitalist faculty, facilitated a quality improvement workshop to teach the lean methodology and rolled out a shadowing program that has given students deeper insight into the day in the life of a hospitalist. We’ve also developed a lecture series that has guided curriculum changes in quality improvement, and organized a student-led regional hospital medicine conference for nurse practitioners, physician assistants, medical students and internal medicine residents.
Without any representation from within the medical student community, student exposure to the hospitalist career is entirely dependent on the resources and availability of the affiliate hospital’s department of hospital medicine. With an investment in hospital medicine student interest groups at medical schools, SHM will equip students to become articulate advocates for the profession and SHM as a community.
References
- Goldenberg J, Glasheen JJ. Hospitalist educators: future of inpatient internal medicine training. Mt Sinai J Med 2008;75:430-5.
2. Pane LA, Davis AB, Ottolini MC. Career satisfaction and the role of mentorship: a survey of pediatric hospitalists. Hosp Pediatr. 2012;2(3):141-8.
3. Leary JC, Schainker EG, Leyenaar JK. The unwritten rules of mentorship: Facilitators of and barriers to effective mentorship in pediatric hospital medicine. Hospital Pediatrics. 2016;6(4):219-225; DOI: 10.1542/hpeds.2015-0108
CBT may be best option for pts with MRD, doc says

Photo courtesy of NHS
A cord blood transplant (CBT) may be the best option for patients with acute leukemia or myelodysplastic syndrome who have minimal residual disease (MRD) and no related donor, according to the senior author of a study published in NEJM.
This retrospective study showed that patients with MRD at the time of transplant were less likely to relapse if they received CBT rather than a graft from an unrelated adult donor, whether HLA-matched or mismatched.
In addition, the risk of death was significantly higher for patients with a mismatched donor than for CBT recipients, although there was no significant difference between those with a matched donor and CBT recipients.
Among patients without MRD, there were no significant differences between the transplant types for the risk of relapse or death.
“This paper shows that if you’ve got high-risk disease and are at high risk for relapse post-transplant, transplant with a cord blood donor may be the best option,” said Colleen Delaney, MD, of Fred Hutchinson Cancer Research Center in Seattle, Washington.
Dr Delaney and her colleagues analyzed data on 582 patients—300 with acute myeloid leukemia, 185 with acute lymphoblastic leukemia, and 97 with myelodysplastic syndromes.
Most patients received a transplant from an HLA-matched unrelated donor (n=344), 140 received a CBT from an unrelated donor, and 98 received a transplant from an HLA-mismatched unrelated donor.
The researchers calculated the relative risks of death and relapse for each transplant group, and they found that a patient’s MRD status prior to transplant played a role.
Presence of MRD
Among patients with MRD, the risk of death was significantly higher for recipients of mismatched grafts than for CBT recipients, with a hazard ratio (HR) of 2.92 (P=0.001).
However, the risk of death was not significantly different for recipients of matched grafts compared to CBT recipients. The HR was 1.69 (P=0.08).
The risk of relapse was about 3 times higher for recipients of mismatched grafts (HR=3.01, P=0.02) or matched grafts (HR=2.92, P=0.007) than for CBT recipients.
No MRD
Among patients without MRD, there was no significant difference in the risk of death for recipients of CBT, mismatched grafts (HR=1.36, P=0.30), or matched grafts (HR=0.78, P=0.33).
And there was no significant difference in the risk of relapse for recipients of CBT, mismatched grafts (HR=1.28, P=0.60), or matched grafts (HR=1.30, P=0.46).
“This brings home the point that cord blood shouldn’t be called an alternative donor,” Dr Delaney said. “The outcomes are the same as a conventional donor.” ![]()
Photo courtesy of NHS
A cord blood transplant (CBT) may be the best option for patients with acute leukemia or myelodysplastic syndrome who have minimal residual disease (MRD) and no related donor, according to the senior author of a study published in NEJM.
This retrospective study showed that patients with MRD at the time of transplant were less likely to relapse if they received CBT rather than a graft from an unrelated adult donor, whether HLA-matched or mismatched.
In addition, the risk of death was significantly higher for patients with a mismatched donor than for CBT recipients, although there was no significant difference between those with a matched donor and CBT recipients.
Among patients without MRD, there were no significant differences between the transplant types for the risk of relapse or death.
“This paper shows that if you’ve got high-risk disease and are at high risk for relapse post-transplant, transplant with a cord blood donor may be the best option,” said Colleen Delaney, MD, of Fred Hutchinson Cancer Research Center in Seattle, Washington.
Dr Delaney and her colleagues analyzed data on 582 patients—300 with acute myeloid leukemia, 185 with acute lymphoblastic leukemia, and 97 with myelodysplastic syndromes.
Most patients received a transplant from an HLA-matched unrelated donor (n=344), 140 received a CBT from an unrelated donor, and 98 received a transplant from an HLA-mismatched unrelated donor.
The researchers calculated the relative risks of death and relapse for each transplant group, and they found that a patient’s MRD status prior to transplant played a role.
Presence of MRD
Among patients with MRD, the risk of death was significantly higher for recipients of mismatched grafts than for CBT recipients, with a hazard ratio (HR) of 2.92 (P=0.001).
However, the risk of death was not significantly different for recipients of matched grafts compared to CBT recipients. The HR was 1.69 (P=0.08).
The risk of relapse was about 3 times higher for recipients of mismatched grafts (HR=3.01, P=0.02) or matched grafts (HR=2.92, P=0.007) than for CBT recipients.
No MRD
Among patients without MRD, there was no significant difference in the risk of death for recipients of CBT, mismatched grafts (HR=1.36, P=0.30), or matched grafts (HR=0.78, P=0.33).
And there was no significant difference in the risk of relapse for recipients of CBT, mismatched grafts (HR=1.28, P=0.60), or matched grafts (HR=1.30, P=0.46).
“This brings home the point that cord blood shouldn’t be called an alternative donor,” Dr Delaney said. “The outcomes are the same as a conventional donor.” ![]()
Photo courtesy of NHS
A cord blood transplant (CBT) may be the best option for patients with acute leukemia or myelodysplastic syndrome who have minimal residual disease (MRD) and no related donor, according to the senior author of a study published in NEJM.
This retrospective study showed that patients with MRD at the time of transplant were less likely to relapse if they received CBT rather than a graft from an unrelated adult donor, whether HLA-matched or mismatched.
In addition, the risk of death was significantly higher for patients with a mismatched donor than for CBT recipients, although there was no significant difference between those with a matched donor and CBT recipients.
Among patients without MRD, there were no significant differences between the transplant types for the risk of relapse or death.
“This paper shows that if you’ve got high-risk disease and are at high risk for relapse post-transplant, transplant with a cord blood donor may be the best option,” said Colleen Delaney, MD, of Fred Hutchinson Cancer Research Center in Seattle, Washington.
Dr Delaney and her colleagues analyzed data on 582 patients—300 with acute myeloid leukemia, 185 with acute lymphoblastic leukemia, and 97 with myelodysplastic syndromes.
Most patients received a transplant from an HLA-matched unrelated donor (n=344), 140 received a CBT from an unrelated donor, and 98 received a transplant from an HLA-mismatched unrelated donor.
The researchers calculated the relative risks of death and relapse for each transplant group, and they found that a patient’s MRD status prior to transplant played a role.
Presence of MRD
Among patients with MRD, the risk of death was significantly higher for recipients of mismatched grafts than for CBT recipients, with a hazard ratio (HR) of 2.92 (P=0.001).
However, the risk of death was not significantly different for recipients of matched grafts compared to CBT recipients. The HR was 1.69 (P=0.08).
The risk of relapse was about 3 times higher for recipients of mismatched grafts (HR=3.01, P=0.02) or matched grafts (HR=2.92, P=0.007) than for CBT recipients.
No MRD
Among patients without MRD, there was no significant difference in the risk of death for recipients of CBT, mismatched grafts (HR=1.36, P=0.30), or matched grafts (HR=0.78, P=0.33).
And there was no significant difference in the risk of relapse for recipients of CBT, mismatched grafts (HR=1.28, P=0.60), or matched grafts (HR=1.30, P=0.46).
“This brings home the point that cord blood shouldn’t be called an alternative donor,” Dr Delaney said. “The outcomes are the same as a conventional donor.” ![]()
Risk factors for early death in older pts with DLBCL

Photo courtesy of CDC
A retrospective study has uncovered potential risk factors for early death in older patients with diffuse large B-cell lymphoma (DLBCL).
Researchers examined electronic health record data for roughly 5500 DLBCL patients over the age of 65 who received contemporary immunochemotherapy.
This revealed 7 factors that were significantly associated with the risk of death within 30 days of treatment initiation.
“The first month of treatment, when patients are compromised both by active lymphoma and toxicities of chemotherapy, is a period of particular concern, as nearly 1 in 4 patients were hospitalized during that time,” said study author Adam J. Olszewski, MD, of Rhode Island Hospital in Providence.
“While comprehensive geriatric assessment remains the gold standard for risk assessment, our study suggests that readily available data from electronic medical records can help identify the high-risk factors in practice.”
Dr Olszewski and his colleagues described their study in JNCCN.
The researchers looked at Medicare claims linked to Surveillance, Epidemiology and End Results registry data for 5530 DLBCL patients who had a median age of 76.
The patients were treated with rituximab, cyclophosphamide, and vincristine in combination with doxorubicin, mitoxantrone, or etoposide from 2003 to 2012.
The cumulative incidence of death at 30 days was 2.2%. The most common causes of death were lymphoma (72%), heart disease (9%), septicemia (3%), and cerebrovascular events (3%).
The researchers created a prediction model based on 7 factors that were significantly associated with early death in multivariate analysis. These include:
- B symptoms
- Chronic kidney disease
- Poor performance status
- Prior use of walking aids or wheelchairs
- Prior hospitalization within the past 12 months
- Upper endoscopy within the past 12 months
- Age 75 or older.
Patients with 0 to 1 of these risk factors were considered low-risk, with a 0.6% chance of early death. Fifty-six percent of the patients studied fit this definition.
Patients with 2 to 3 of the risk factors were intermediate-risk, with a 3.2% chance of early death. Thirty-eight percent of the patients studied fell into this category.
Only 6% of the patients studied were considered high-risk. These patients had 4 or more risk factors and an 8.3% chance of early death.
The researchers also found the administration of prophylactic granulocyte-colony stimulating factor (G-CSF) was associated with lower probability of early death in the high-risk group.
They noted that prophylactic G-CSF was given to 66% of patients in this study, which suggests an opportunity for preventing early deaths.
“It is equally important to realize that a majority of older patients without risk factors can safely receive curative immunochemotherapy,” Dr Olszewski said. “Enhanced supportive care and monitoring should be provided for high-risk groups.” ![]()
Photo courtesy of CDC
A retrospective study has uncovered potential risk factors for early death in older patients with diffuse large B-cell lymphoma (DLBCL).
Researchers examined electronic health record data for roughly 5500 DLBCL patients over the age of 65 who received contemporary immunochemotherapy.
This revealed 7 factors that were significantly associated with the risk of death within 30 days of treatment initiation.
“The first month of treatment, when patients are compromised both by active lymphoma and toxicities of chemotherapy, is a period of particular concern, as nearly 1 in 4 patients were hospitalized during that time,” said study author Adam J. Olszewski, MD, of Rhode Island Hospital in Providence.
“While comprehensive geriatric assessment remains the gold standard for risk assessment, our study suggests that readily available data from electronic medical records can help identify the high-risk factors in practice.”
Dr Olszewski and his colleagues described their study in JNCCN.
The researchers looked at Medicare claims linked to Surveillance, Epidemiology and End Results registry data for 5530 DLBCL patients who had a median age of 76.
The patients were treated with rituximab, cyclophosphamide, and vincristine in combination with doxorubicin, mitoxantrone, or etoposide from 2003 to 2012.
The cumulative incidence of death at 30 days was 2.2%. The most common causes of death were lymphoma (72%), heart disease (9%), septicemia (3%), and cerebrovascular events (3%).
The researchers created a prediction model based on 7 factors that were significantly associated with early death in multivariate analysis. These include:
- B symptoms
- Chronic kidney disease
- Poor performance status
- Prior use of walking aids or wheelchairs
- Prior hospitalization within the past 12 months
- Upper endoscopy within the past 12 months
- Age 75 or older.
Patients with 0 to 1 of these risk factors were considered low-risk, with a 0.6% chance of early death. Fifty-six percent of the patients studied fit this definition.
Patients with 2 to 3 of the risk factors were intermediate-risk, with a 3.2% chance of early death. Thirty-eight percent of the patients studied fell into this category.
Only 6% of the patients studied were considered high-risk. These patients had 4 or more risk factors and an 8.3% chance of early death.
The researchers also found the administration of prophylactic granulocyte-colony stimulating factor (G-CSF) was associated with lower probability of early death in the high-risk group.
They noted that prophylactic G-CSF was given to 66% of patients in this study, which suggests an opportunity for preventing early deaths.
“It is equally important to realize that a majority of older patients without risk factors can safely receive curative immunochemotherapy,” Dr Olszewski said. “Enhanced supportive care and monitoring should be provided for high-risk groups.” ![]()
Photo courtesy of CDC
A retrospective study has uncovered potential risk factors for early death in older patients with diffuse large B-cell lymphoma (DLBCL).
Researchers examined electronic health record data for roughly 5500 DLBCL patients over the age of 65 who received contemporary immunochemotherapy.
This revealed 7 factors that were significantly associated with the risk of death within 30 days of treatment initiation.
“The first month of treatment, when patients are compromised both by active lymphoma and toxicities of chemotherapy, is a period of particular concern, as nearly 1 in 4 patients were hospitalized during that time,” said study author Adam J. Olszewski, MD, of Rhode Island Hospital in Providence.
“While comprehensive geriatric assessment remains the gold standard for risk assessment, our study suggests that readily available data from electronic medical records can help identify the high-risk factors in practice.”
Dr Olszewski and his colleagues described their study in JNCCN.
The researchers looked at Medicare claims linked to Surveillance, Epidemiology and End Results registry data for 5530 DLBCL patients who had a median age of 76.
The patients were treated with rituximab, cyclophosphamide, and vincristine in combination with doxorubicin, mitoxantrone, or etoposide from 2003 to 2012.
The cumulative incidence of death at 30 days was 2.2%. The most common causes of death were lymphoma (72%), heart disease (9%), septicemia (3%), and cerebrovascular events (3%).
The researchers created a prediction model based on 7 factors that were significantly associated with early death in multivariate analysis. These include:
- B symptoms
- Chronic kidney disease
- Poor performance status
- Prior use of walking aids or wheelchairs
- Prior hospitalization within the past 12 months
- Upper endoscopy within the past 12 months
- Age 75 or older.
Patients with 0 to 1 of these risk factors were considered low-risk, with a 0.6% chance of early death. Fifty-six percent of the patients studied fit this definition.
Patients with 2 to 3 of the risk factors were intermediate-risk, with a 3.2% chance of early death. Thirty-eight percent of the patients studied fell into this category.
Only 6% of the patients studied were considered high-risk. These patients had 4 or more risk factors and an 8.3% chance of early death.
The researchers also found the administration of prophylactic granulocyte-colony stimulating factor (G-CSF) was associated with lower probability of early death in the high-risk group.
They noted that prophylactic G-CSF was given to 66% of patients in this study, which suggests an opportunity for preventing early deaths.
“It is equally important to realize that a majority of older patients without risk factors can safely receive curative immunochemotherapy,” Dr Olszewski said. “Enhanced supportive care and monitoring should be provided for high-risk groups.” ![]()
Gene therapy effective against SCD in mice

blood cells from a mouse
Image courtesy of
University of Michigan
Preclinical research suggests a novel gene therapy may be effective against sickle cell disease (SCD).
The therapy is designed to selectively inhibit the fetal hemoglobin repressor BCL11A in erythroid cells.
Researchers found this was sufficient to increase fetal hemoglobin production and reverse the effects of SCD in vivo, without presenting the same problems as ubiquitous BCL11A knockdown.
The team reported these findings in The Journal of Clinical Investigation.
Previous research showed that suppressing BCL11A can replace the defective beta
hemoglobin that causes sickling with healthy fetal hemoglobin.
“BCL11A represses fetal hemoglobin, which does not lead to sickling, and also activates beta hemoglobin, which is affected by the sickle cell mutation,” explained study author David A. Williams, MD, of Boston Children’s Hospital in Massachusetts.
“So when you knock BCL11A down, you simultaneously increase fetal hemoglobin and repress sickling hemoglobin, which is why we think this is the best approach to gene therapy in sickle cell disease.”
However, Dr Williams and his colleagues found that ubiquitous knockdown of BCL11A impaired the engraftment of human and murine hematopoietic stem cells (HSCs).
To circumvent this problem, the researchers set out to silence BCL11A only in erythroid cells.
Selectively knocking down BCL11A involved several layers of engineering. As the core of their gene therapy vector, the researchers used a short hairpin RNA that inactivates BCL11A. To get it into cells, they embedded the short hairpin RNA in a microRNA that cells generally recognize and process.
To make this assembly work in the right place at the right time, the team hooked it to a promoter of beta hemoglobin expression, together with regulatory elements active only in erythroid cells. Finally, they inserted the whole package into a lentivirus.
HSCs from mice and SCD patients were then exposed to the manipulated virus, taking up the new genetic material. The resulting genetically engineered erythroid cells began producing fetal hemoglobin rather than the mutated beta hemoglobin.
When HSCs treated with this gene therapy were transplanted into mice with SCD, the cells engrafted successfully and reduced signs of SCD—namely, hemolytic anemia and increased numbers
of reticulocytes.
Dr Williams believes this approach could substantially increase the ratio of non-sickling to sickling hemoglobin in SCD. He also said the approach could be beneficial in beta-thalassemia. ![]()
blood cells from a mouse
Image courtesy of
University of Michigan
Preclinical research suggests a novel gene therapy may be effective against sickle cell disease (SCD).
The therapy is designed to selectively inhibit the fetal hemoglobin repressor BCL11A in erythroid cells.
Researchers found this was sufficient to increase fetal hemoglobin production and reverse the effects of SCD in vivo, without presenting the same problems as ubiquitous BCL11A knockdown.
The team reported these findings in The Journal of Clinical Investigation.
Previous research showed that suppressing BCL11A can replace the defective beta
hemoglobin that causes sickling with healthy fetal hemoglobin.
“BCL11A represses fetal hemoglobin, which does not lead to sickling, and also activates beta hemoglobin, which is affected by the sickle cell mutation,” explained study author David A. Williams, MD, of Boston Children’s Hospital in Massachusetts.
“So when you knock BCL11A down, you simultaneously increase fetal hemoglobin and repress sickling hemoglobin, which is why we think this is the best approach to gene therapy in sickle cell disease.”
However, Dr Williams and his colleagues found that ubiquitous knockdown of BCL11A impaired the engraftment of human and murine hematopoietic stem cells (HSCs).
To circumvent this problem, the researchers set out to silence BCL11A only in erythroid cells.
Selectively knocking down BCL11A involved several layers of engineering. As the core of their gene therapy vector, the researchers used a short hairpin RNA that inactivates BCL11A. To get it into cells, they embedded the short hairpin RNA in a microRNA that cells generally recognize and process.
To make this assembly work in the right place at the right time, the team hooked it to a promoter of beta hemoglobin expression, together with regulatory elements active only in erythroid cells. Finally, they inserted the whole package into a lentivirus.
HSCs from mice and SCD patients were then exposed to the manipulated virus, taking up the new genetic material. The resulting genetically engineered erythroid cells began producing fetal hemoglobin rather than the mutated beta hemoglobin.
When HSCs treated with this gene therapy were transplanted into mice with SCD, the cells engrafted successfully and reduced signs of SCD—namely, hemolytic anemia and increased numbers
of reticulocytes.
Dr Williams believes this approach could substantially increase the ratio of non-sickling to sickling hemoglobin in SCD. He also said the approach could be beneficial in beta-thalassemia. ![]()
blood cells from a mouse
Image courtesy of
University of Michigan
Preclinical research suggests a novel gene therapy may be effective against sickle cell disease (SCD).
The therapy is designed to selectively inhibit the fetal hemoglobin repressor BCL11A in erythroid cells.
Researchers found this was sufficient to increase fetal hemoglobin production and reverse the effects of SCD in vivo, without presenting the same problems as ubiquitous BCL11A knockdown.
The team reported these findings in The Journal of Clinical Investigation.
Previous research showed that suppressing BCL11A can replace the defective beta
hemoglobin that causes sickling with healthy fetal hemoglobin.
“BCL11A represses fetal hemoglobin, which does not lead to sickling, and also activates beta hemoglobin, which is affected by the sickle cell mutation,” explained study author David A. Williams, MD, of Boston Children’s Hospital in Massachusetts.
“So when you knock BCL11A down, you simultaneously increase fetal hemoglobin and repress sickling hemoglobin, which is why we think this is the best approach to gene therapy in sickle cell disease.”
However, Dr Williams and his colleagues found that ubiquitous knockdown of BCL11A impaired the engraftment of human and murine hematopoietic stem cells (HSCs).
To circumvent this problem, the researchers set out to silence BCL11A only in erythroid cells.
Selectively knocking down BCL11A involved several layers of engineering. As the core of their gene therapy vector, the researchers used a short hairpin RNA that inactivates BCL11A. To get it into cells, they embedded the short hairpin RNA in a microRNA that cells generally recognize and process.
To make this assembly work in the right place at the right time, the team hooked it to a promoter of beta hemoglobin expression, together with regulatory elements active only in erythroid cells. Finally, they inserted the whole package into a lentivirus.
HSCs from mice and SCD patients were then exposed to the manipulated virus, taking up the new genetic material. The resulting genetically engineered erythroid cells began producing fetal hemoglobin rather than the mutated beta hemoglobin.
When HSCs treated with this gene therapy were transplanted into mice with SCD, the cells engrafted successfully and reduced signs of SCD—namely, hemolytic anemia and increased numbers
of reticulocytes.
Dr Williams believes this approach could substantially increase the ratio of non-sickling to sickling hemoglobin in SCD. He also said the approach could be beneficial in beta-thalassemia. ![]()
Optimizing CAR T-cell therapy in NHL

Photo from Fred Hutchinson
Cancer Research Center
Results from a phase 1 study have provided insights that may help researchers optimize treatment with JCAR014, a chimeric antigen receptor (CAR) T-cell therapy, in patients with advanced non-Hodgkin lymphoma (NHL).
Researchers said they identified a lymphodepleting regimen that improved the likelihood of complete response (CR) to JCAR014.
Although the regimen also increased the risk of severe cytokine release syndrome (CRS) and neurotoxicity, the researchers discovered biomarkers that might allow them to identify patients who have a high risk of these events and could potentially benefit from early interventions.
The researchers reported these findings in Science Translational Medicine. The trial (NCT01865617) was funded, in part, by Juno Therapeutics, the company developing JCAR014.
Previous results from this trial, in patients with acute lymphoblastic leukemia, were published in The Journal of Clinical Investigation.
About JCAR014
JCAR014 is a CD19-directed CAR T-cell therapy in which CD4+ and CD8+ cells are administered in equal proportions.
“The idea . . . is that by [controlling the ratio of T cells], we would get more reproducible data around the effects of the cells—both beneficial effects against the cancer and also any side effects they might cause the patient,” said study author Stanley Riddell, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington.
“And then, by adjusting the dose, we could improve what we call the therapeutic index—the benefit against the tumor—without too much toxicity.”
Patients and treatment
Dr Riddell and his colleagues reported results with JCAR014, following lymphodepleting chemotherapy, in 32 patients with NHL who had a median age of 58 (range, 36-70).
The patients had de novo large B-cell lymphoma (n=11), transformed de novo large B-cell lymphoma (n=11), mantle cell lymphoma (n=4), and follicular lymphoma (n=6).
They had received a median of 5 prior treatment regimens (range, 2 to 11), including autologous
(n=14) and allogeneic (n=4) transplant. All patients had measurable disease (≥ 2 cm) in the lymph nodes or other extramedullary sites at baseline.
The patients received JCAR014 at 1 of 3 dose levels, given 36 to 96 hours after lymphodepleting chemotherapy.
Twelve patients received cyclophosphamide (Cy) alone or Cy and etoposide (E), and 20 received Cy plus fludarabine (Flu). Five patients received 2 × 105 CAR T cells/kg, 18 received 2 × 106 CAR T cells/kg, and 9 received 2 × 107 CAR T cells/kg.
Efficacy
In the 30 evaluable patients, the overall response rate (ORR) was 63% (n=19), and the CR rate was 33% (n=10).
Among patients who received Cy or Cy/E, the ORR was 50% (n=6), and the CR rate was 8% (n=1). Among patients who received Cy/Flu, the ORR was 72% (n=13), and the CR rate was 50% (n=9).
The patients who received Cy/Flu had better CAR T-cell expansion and persistence than patients who received Cy or Cy/E, which was reflected in the higher response rates.
Higher response rates were also observed in patients who received 2 × 106 CAR T cells/kg rather than the other 2 dose levels.
The researchers noted that, although follow-up is short, patients who received CAR T cells at ≤ 2 × 106/kg after Cy/Flu had better progression-free survival (P=0.008) than patients who received CAR T cells at ≤ 2 × 106/kg after Cy or Cy/E.
Of the 9 patients who achieved a CR after Cy/Flu and JCAR014, 1 has relapsed, with follow-up ranging from 2.3 months to 11.2 months. (Seven of these 9 patients had received 2 × 106 CAR T cells/kg, and 1 patient each had received the other 2 doses.)
“The main message is that you can treat patients with non-Hodgkin’s lymphoma with CAR T cells and get very good response rates with optimization of the CAR T-cell dose and lymphodepletion,” said study author Cameron Turtle, MBBS, PhD, of the Fred Hutchinson Cancer Research Center.
“Strategies like modifying the lymphodepletion in conjunction with suitable CAR T-cell dosing can have a big impact on clinical outcome.”
Safety
Two patients who were treated with the highest CAR T-cell dose (2 × 107 cells/kg) died—1 of pontine hemorrhage and 1 of gastrointestinal hemorrhage associated with a known gastrointestinal invasive lymphomatous mass.
This dose was also associated with an increased risk of severe CRS and neurotoxicity, as was the Cy/Flu regimen.
Twenty patients (62.5%) developed CRS, and 4 (12.5%) had severe CRS. All 4 of these patients had received Cy/Flu.
Nine patients (28%) developed severe neurotoxicity (grade 3 or higher), 7 of whom had received Cy/Flu.
Three of the 6 patients (50%) treated at 2 × 107 CAR-T cells/kg after Cy/Flu developed severe CRS, and 4 of the 6 patients (67%) developed severe neurotoxicity.
The researchers looked for biomarkers of toxicity in serum collected 1 day after CAR T-cell infusion.
They found that high IL-6, IL-8, IL-10, IL-15, and IFN-γ concentrations were associated with subsequent severe CRS and neurotoxicity, and low TGF-Β concentration was associated with neurotoxicity.
The team said these findings provide an opportunity for studying the use of serum cytokine concentrations to identify patients at the highest risk of toxicity who might benefit from early interventions. ![]()
Photo from Fred Hutchinson
Cancer Research Center
Results from a phase 1 study have provided insights that may help researchers optimize treatment with JCAR014, a chimeric antigen receptor (CAR) T-cell therapy, in patients with advanced non-Hodgkin lymphoma (NHL).
Researchers said they identified a lymphodepleting regimen that improved the likelihood of complete response (CR) to JCAR014.
Although the regimen also increased the risk of severe cytokine release syndrome (CRS) and neurotoxicity, the researchers discovered biomarkers that might allow them to identify patients who have a high risk of these events and could potentially benefit from early interventions.
The researchers reported these findings in Science Translational Medicine. The trial (NCT01865617) was funded, in part, by Juno Therapeutics, the company developing JCAR014.
Previous results from this trial, in patients with acute lymphoblastic leukemia, were published in The Journal of Clinical Investigation.
About JCAR014
JCAR014 is a CD19-directed CAR T-cell therapy in which CD4+ and CD8+ cells are administered in equal proportions.
“The idea . . . is that by [controlling the ratio of T cells], we would get more reproducible data around the effects of the cells—both beneficial effects against the cancer and also any side effects they might cause the patient,” said study author Stanley Riddell, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington.
“And then, by adjusting the dose, we could improve what we call the therapeutic index—the benefit against the tumor—without too much toxicity.”
Patients and treatment
Dr Riddell and his colleagues reported results with JCAR014, following lymphodepleting chemotherapy, in 32 patients with NHL who had a median age of 58 (range, 36-70).
The patients had de novo large B-cell lymphoma (n=11), transformed de novo large B-cell lymphoma (n=11), mantle cell lymphoma (n=4), and follicular lymphoma (n=6).
They had received a median of 5 prior treatment regimens (range, 2 to 11), including autologous
(n=14) and allogeneic (n=4) transplant. All patients had measurable disease (≥ 2 cm) in the lymph nodes or other extramedullary sites at baseline.
The patients received JCAR014 at 1 of 3 dose levels, given 36 to 96 hours after lymphodepleting chemotherapy.
Twelve patients received cyclophosphamide (Cy) alone or Cy and etoposide (E), and 20 received Cy plus fludarabine (Flu). Five patients received 2 × 105 CAR T cells/kg, 18 received 2 × 106 CAR T cells/kg, and 9 received 2 × 107 CAR T cells/kg.
Efficacy
In the 30 evaluable patients, the overall response rate (ORR) was 63% (n=19), and the CR rate was 33% (n=10).
Among patients who received Cy or Cy/E, the ORR was 50% (n=6), and the CR rate was 8% (n=1). Among patients who received Cy/Flu, the ORR was 72% (n=13), and the CR rate was 50% (n=9).
The patients who received Cy/Flu had better CAR T-cell expansion and persistence than patients who received Cy or Cy/E, which was reflected in the higher response rates.
Higher response rates were also observed in patients who received 2 × 106 CAR T cells/kg rather than the other 2 dose levels.
The researchers noted that, although follow-up is short, patients who received CAR T cells at ≤ 2 × 106/kg after Cy/Flu had better progression-free survival (P=0.008) than patients who received CAR T cells at ≤ 2 × 106/kg after Cy or Cy/E.
Of the 9 patients who achieved a CR after Cy/Flu and JCAR014, 1 has relapsed, with follow-up ranging from 2.3 months to 11.2 months. (Seven of these 9 patients had received 2 × 106 CAR T cells/kg, and 1 patient each had received the other 2 doses.)
“The main message is that you can treat patients with non-Hodgkin’s lymphoma with CAR T cells and get very good response rates with optimization of the CAR T-cell dose and lymphodepletion,” said study author Cameron Turtle, MBBS, PhD, of the Fred Hutchinson Cancer Research Center.
“Strategies like modifying the lymphodepletion in conjunction with suitable CAR T-cell dosing can have a big impact on clinical outcome.”
Safety
Two patients who were treated with the highest CAR T-cell dose (2 × 107 cells/kg) died—1 of pontine hemorrhage and 1 of gastrointestinal hemorrhage associated with a known gastrointestinal invasive lymphomatous mass.
This dose was also associated with an increased risk of severe CRS and neurotoxicity, as was the Cy/Flu regimen.
Twenty patients (62.5%) developed CRS, and 4 (12.5%) had severe CRS. All 4 of these patients had received Cy/Flu.
Nine patients (28%) developed severe neurotoxicity (grade 3 or higher), 7 of whom had received Cy/Flu.
Three of the 6 patients (50%) treated at 2 × 107 CAR-T cells/kg after Cy/Flu developed severe CRS, and 4 of the 6 patients (67%) developed severe neurotoxicity.
The researchers looked for biomarkers of toxicity in serum collected 1 day after CAR T-cell infusion.
They found that high IL-6, IL-8, IL-10, IL-15, and IFN-γ concentrations were associated with subsequent severe CRS and neurotoxicity, and low TGF-Β concentration was associated with neurotoxicity.
The team said these findings provide an opportunity for studying the use of serum cytokine concentrations to identify patients at the highest risk of toxicity who might benefit from early interventions. ![]()
Photo from Fred Hutchinson
Cancer Research Center
Results from a phase 1 study have provided insights that may help researchers optimize treatment with JCAR014, a chimeric antigen receptor (CAR) T-cell therapy, in patients with advanced non-Hodgkin lymphoma (NHL).
Researchers said they identified a lymphodepleting regimen that improved the likelihood of complete response (CR) to JCAR014.
Although the regimen also increased the risk of severe cytokine release syndrome (CRS) and neurotoxicity, the researchers discovered biomarkers that might allow them to identify patients who have a high risk of these events and could potentially benefit from early interventions.
The researchers reported these findings in Science Translational Medicine. The trial (NCT01865617) was funded, in part, by Juno Therapeutics, the company developing JCAR014.
Previous results from this trial, in patients with acute lymphoblastic leukemia, were published in The Journal of Clinical Investigation.
About JCAR014
JCAR014 is a CD19-directed CAR T-cell therapy in which CD4+ and CD8+ cells are administered in equal proportions.
“The idea . . . is that by [controlling the ratio of T cells], we would get more reproducible data around the effects of the cells—both beneficial effects against the cancer and also any side effects they might cause the patient,” said study author Stanley Riddell, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington.
“And then, by adjusting the dose, we could improve what we call the therapeutic index—the benefit against the tumor—without too much toxicity.”
Patients and treatment
Dr Riddell and his colleagues reported results with JCAR014, following lymphodepleting chemotherapy, in 32 patients with NHL who had a median age of 58 (range, 36-70).
The patients had de novo large B-cell lymphoma (n=11), transformed de novo large B-cell lymphoma (n=11), mantle cell lymphoma (n=4), and follicular lymphoma (n=6).
They had received a median of 5 prior treatment regimens (range, 2 to 11), including autologous
(n=14) and allogeneic (n=4) transplant. All patients had measurable disease (≥ 2 cm) in the lymph nodes or other extramedullary sites at baseline.
The patients received JCAR014 at 1 of 3 dose levels, given 36 to 96 hours after lymphodepleting chemotherapy.
Twelve patients received cyclophosphamide (Cy) alone or Cy and etoposide (E), and 20 received Cy plus fludarabine (Flu). Five patients received 2 × 105 CAR T cells/kg, 18 received 2 × 106 CAR T cells/kg, and 9 received 2 × 107 CAR T cells/kg.
Efficacy
In the 30 evaluable patients, the overall response rate (ORR) was 63% (n=19), and the CR rate was 33% (n=10).
Among patients who received Cy or Cy/E, the ORR was 50% (n=6), and the CR rate was 8% (n=1). Among patients who received Cy/Flu, the ORR was 72% (n=13), and the CR rate was 50% (n=9).
The patients who received Cy/Flu had better CAR T-cell expansion and persistence than patients who received Cy or Cy/E, which was reflected in the higher response rates.
Higher response rates were also observed in patients who received 2 × 106 CAR T cells/kg rather than the other 2 dose levels.
The researchers noted that, although follow-up is short, patients who received CAR T cells at ≤ 2 × 106/kg after Cy/Flu had better progression-free survival (P=0.008) than patients who received CAR T cells at ≤ 2 × 106/kg after Cy or Cy/E.
Of the 9 patients who achieved a CR after Cy/Flu and JCAR014, 1 has relapsed, with follow-up ranging from 2.3 months to 11.2 months. (Seven of these 9 patients had received 2 × 106 CAR T cells/kg, and 1 patient each had received the other 2 doses.)
“The main message is that you can treat patients with non-Hodgkin’s lymphoma with CAR T cells and get very good response rates with optimization of the CAR T-cell dose and lymphodepletion,” said study author Cameron Turtle, MBBS, PhD, of the Fred Hutchinson Cancer Research Center.
“Strategies like modifying the lymphodepletion in conjunction with suitable CAR T-cell dosing can have a big impact on clinical outcome.”
Safety
Two patients who were treated with the highest CAR T-cell dose (2 × 107 cells/kg) died—1 of pontine hemorrhage and 1 of gastrointestinal hemorrhage associated with a known gastrointestinal invasive lymphomatous mass.
This dose was also associated with an increased risk of severe CRS and neurotoxicity, as was the Cy/Flu regimen.
Twenty patients (62.5%) developed CRS, and 4 (12.5%) had severe CRS. All 4 of these patients had received Cy/Flu.
Nine patients (28%) developed severe neurotoxicity (grade 3 or higher), 7 of whom had received Cy/Flu.
Three of the 6 patients (50%) treated at 2 × 107 CAR-T cells/kg after Cy/Flu developed severe CRS, and 4 of the 6 patients (67%) developed severe neurotoxicity.
The researchers looked for biomarkers of toxicity in serum collected 1 day after CAR T-cell infusion.
They found that high IL-6, IL-8, IL-10, IL-15, and IFN-γ concentrations were associated with subsequent severe CRS and neurotoxicity, and low TGF-Β concentration was associated with neurotoxicity.
The team said these findings provide an opportunity for studying the use of serum cytokine concentrations to identify patients at the highest risk of toxicity who might benefit from early interventions. ![]()