User login
Expanding High Blood Pressure Screening to the Nonprimary Care Setting to Improve Early Recognition
Study Overview
Objective. To identify the prevalence and characteristics of patients identified with high blood pressure (BP) in nonprimary care compared with primary care visits.
Design. Longitudinal population-based study.
Setting and participants. This study was conducted at Kaiser Permanente Southern California (KPSC) after implementation of a system-wide change to improve hypertension care, which included comprehensive decision support tools embedded in the EHR system, including BP measurement flag alerts. Patient eligible for the study were normotensive members (BP < 140/90 mm Hg), older than 18 years, and enrolled in a KPSC health plan for at least 12 months on January of 2009. A gap of < 3 months in health care coverage in the year prior was allowed. Excluded were patients with a history of elevated BP during an outpatient visit, an inpatient or outpatient diagnosis code for hypertension, prescription for any antihypertensive medication within 24 months prior to 1 January 2009, missing BP information or whose only BP measurements were from a visit indicating fever or in preparation for a surgery or pain management. Pregnant patients, patients with missing sex information, and missing visit specialty information were also excluded. The study period was from January 2009 to March 2011.
Measurement. BP was measured routinely at the beginning of almost every primary and nonprimary outpatient visit. Nurses and medical assistants were trained according to a standard KPSC protocol using automated sphygmomanometer digital devices. According to the study protocol, in cases in which BP was elevated (≥ 140/90 mm Hg), a second measurement was obtained. At KPSC, all staff members including those in primary and nonprimary care are certified in BP measurement during their initial staff orientation and recertified annually.
Main outcome measure. An initial BP ≥ 140/90 mm Hg during a primary or nonprimary care outpatient visit.
Results. The mean ages of patients at baseline and at end of follow-up for the primary outcome were 39.7 (SD, 13.9) and 41.5 (SD, 14.0) years, respectively. The total cohort (n = 1,075,522) was nearly equally representative of both men (48.6%) and women (51.4%). The majority of the patients (91.7%) were younger than 60 years. A large proportion of the cohort belonged to racial/ethnic minorities with 33.1% Hispanic, 6.5% black, and 8.4% Asian/Pacific Islander.
The total cohort had 4,903,200 office visits, of which 3,996,190 were primary care visits, 901,275 nonprimary care visits, and 5735 visits of unknown specialty. During a mean follow-up of 1.6 years (SD, 0.8) 111,996 patients had a BP measurement ≥ 140/90 mm Hg. Of these, 92,577 (82.7%) were measured during primary care visits and 19,419 (17.3%) during nonprimary care visits. Of 15,356 patients with confirmed high BP, 12,587 (82%) were measured during primary care visits and 2769 (18.0%) patients during nonprimary care visits. Patients with a BP ≥ 140/90 mm Hg measured during nonprimary care visits were older, more likely to be male and non-Hispanic white, less likely to be obese, but more likely to smoke or have a Framingham risk score ≥ 20%. Ophthalmology/optometry, neurology, and dermatology were the main specialties to identify a first BP ≥ 140/90 mm Hg.
The follow-up after a first elevated BP was marginally higher in patients identified in nonprimary care than in primary care. Among patients with a first BP ≥ 140/90 mm Hg measured during a primary care visit, 60.6% had a follow-up BP within 3 months of the first high BP, 22.9% after 3 months or more, and 16.5% did not have a follow-up BP. Among individuals with a first BP ≥ 140/90 mm Hg measured during a nonprimary care visit, 64.7% had a follow-up BP within 3 months of the first high BP, 22.6% after 3 months or more, and 12.7% did not have a follow-up BP measurement.
The proportion of false-positives, defined as individuals with an initial BP ≥ 140/90 mm Hg who had a follow-up visit with a normal BP within 3 months, was the same for patients identified in primary and nonprimary care. False-positives were most frequent in individuals identified during visits in other specialty care, rheuma-tology, and neurology fields.
Conclusion. Expanding screening for hypertension to nonprimary care settings may improve the detection of hypertension and may contribute to better hypertension control. However, an effective system to ensure appropriate follow-up if high BP is detected is needed. Elderly, non-Hispanic, white male patients and those with very high BP are more likely to benefit from this screening.
Commentary
Hypertension is a common and costly health problem [1]. BP screening can identify adults with hypertension, who are at increased risk of cardiovascular and other diseases. Effective treatments are available to control high BP and reduce associated morbidity and mortality [2], but the first step is to identify patients with this largely asymptomatic disorder.
BP measurement is standard practice in primary care. However, many people do not regularly see a primary care clinician. In this study, researchers aimed to identify the prevalence and characteristics of patients identified with high BP in nonprimary care compared with primary care visits in a large integrated health care system that had implemented a system-level, multifaceted quality improvement program to improve hypertension care. Of the patients who were found to have high BP, 83% were diagnosed in a primary care setting and 17% in a specialty care setting, and the number of false-positive results were comparable.
In general, the study was well conducted and a strength of the study was the large sample size. Limitations included the fact that the study was conducted as part of a quality improvement project in an integrated health system, and there were no control clinics.
The authors noted that a high BP reading requires adequate follow-up, and nonprimary care detected elevated BP patients had lower follow-up rates. Also, some specialties had higher false-positive rates. Quality of measurement can be maximized with regular staff training.
Applications for Clinical Practice
Expanding routine screening for hypertension to non-primary care can potentially improve rates of detection, capturing patients who might otherwise have been missed. An effective system to ensure appropriate follow-up attention if high BP is detected is essential, and it is important that staff be well trained in using standard technique to minimize false-positives, which could lead to unnecessary resource use.
—Paloma Cesar de Sales, BN, RN, MS
1. American Heart Association. High blood pressure: statistical fact sheet 2013 update. Available at www.heart.org/idc/groups/heartpublic/@wcm/@sop/@smd/documents/downloadable/ucm_319587.pdf.
2. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014;311:507–20.
Study Overview
Objective. To identify the prevalence and characteristics of patients identified with high blood pressure (BP) in nonprimary care compared with primary care visits.
Design. Longitudinal population-based study.
Setting and participants. This study was conducted at Kaiser Permanente Southern California (KPSC) after implementation of a system-wide change to improve hypertension care, which included comprehensive decision support tools embedded in the EHR system, including BP measurement flag alerts. Patient eligible for the study were normotensive members (BP < 140/90 mm Hg), older than 18 years, and enrolled in a KPSC health plan for at least 12 months on January of 2009. A gap of < 3 months in health care coverage in the year prior was allowed. Excluded were patients with a history of elevated BP during an outpatient visit, an inpatient or outpatient diagnosis code for hypertension, prescription for any antihypertensive medication within 24 months prior to 1 January 2009, missing BP information or whose only BP measurements were from a visit indicating fever or in preparation for a surgery or pain management. Pregnant patients, patients with missing sex information, and missing visit specialty information were also excluded. The study period was from January 2009 to March 2011.
Measurement. BP was measured routinely at the beginning of almost every primary and nonprimary outpatient visit. Nurses and medical assistants were trained according to a standard KPSC protocol using automated sphygmomanometer digital devices. According to the study protocol, in cases in which BP was elevated (≥ 140/90 mm Hg), a second measurement was obtained. At KPSC, all staff members including those in primary and nonprimary care are certified in BP measurement during their initial staff orientation and recertified annually.
Main outcome measure. An initial BP ≥ 140/90 mm Hg during a primary or nonprimary care outpatient visit.
Results. The mean ages of patients at baseline and at end of follow-up for the primary outcome were 39.7 (SD, 13.9) and 41.5 (SD, 14.0) years, respectively. The total cohort (n = 1,075,522) was nearly equally representative of both men (48.6%) and women (51.4%). The majority of the patients (91.7%) were younger than 60 years. A large proportion of the cohort belonged to racial/ethnic minorities with 33.1% Hispanic, 6.5% black, and 8.4% Asian/Pacific Islander.
The total cohort had 4,903,200 office visits, of which 3,996,190 were primary care visits, 901,275 nonprimary care visits, and 5735 visits of unknown specialty. During a mean follow-up of 1.6 years (SD, 0.8) 111,996 patients had a BP measurement ≥ 140/90 mm Hg. Of these, 92,577 (82.7%) were measured during primary care visits and 19,419 (17.3%) during nonprimary care visits. Of 15,356 patients with confirmed high BP, 12,587 (82%) were measured during primary care visits and 2769 (18.0%) patients during nonprimary care visits. Patients with a BP ≥ 140/90 mm Hg measured during nonprimary care visits were older, more likely to be male and non-Hispanic white, less likely to be obese, but more likely to smoke or have a Framingham risk score ≥ 20%. Ophthalmology/optometry, neurology, and dermatology were the main specialties to identify a first BP ≥ 140/90 mm Hg.
The follow-up after a first elevated BP was marginally higher in patients identified in nonprimary care than in primary care. Among patients with a first BP ≥ 140/90 mm Hg measured during a primary care visit, 60.6% had a follow-up BP within 3 months of the first high BP, 22.9% after 3 months or more, and 16.5% did not have a follow-up BP. Among individuals with a first BP ≥ 140/90 mm Hg measured during a nonprimary care visit, 64.7% had a follow-up BP within 3 months of the first high BP, 22.6% after 3 months or more, and 12.7% did not have a follow-up BP measurement.
The proportion of false-positives, defined as individuals with an initial BP ≥ 140/90 mm Hg who had a follow-up visit with a normal BP within 3 months, was the same for patients identified in primary and nonprimary care. False-positives were most frequent in individuals identified during visits in other specialty care, rheuma-tology, and neurology fields.
Conclusion. Expanding screening for hypertension to nonprimary care settings may improve the detection of hypertension and may contribute to better hypertension control. However, an effective system to ensure appropriate follow-up if high BP is detected is needed. Elderly, non-Hispanic, white male patients and those with very high BP are more likely to benefit from this screening.
Commentary
Hypertension is a common and costly health problem [1]. BP screening can identify adults with hypertension, who are at increased risk of cardiovascular and other diseases. Effective treatments are available to control high BP and reduce associated morbidity and mortality [2], but the first step is to identify patients with this largely asymptomatic disorder.
BP measurement is standard practice in primary care. However, many people do not regularly see a primary care clinician. In this study, researchers aimed to identify the prevalence and characteristics of patients identified with high BP in nonprimary care compared with primary care visits in a large integrated health care system that had implemented a system-level, multifaceted quality improvement program to improve hypertension care. Of the patients who were found to have high BP, 83% were diagnosed in a primary care setting and 17% in a specialty care setting, and the number of false-positive results were comparable.
In general, the study was well conducted and a strength of the study was the large sample size. Limitations included the fact that the study was conducted as part of a quality improvement project in an integrated health system, and there were no control clinics.
The authors noted that a high BP reading requires adequate follow-up, and nonprimary care detected elevated BP patients had lower follow-up rates. Also, some specialties had higher false-positive rates. Quality of measurement can be maximized with regular staff training.
Applications for Clinical Practice
Expanding routine screening for hypertension to non-primary care can potentially improve rates of detection, capturing patients who might otherwise have been missed. An effective system to ensure appropriate follow-up attention if high BP is detected is essential, and it is important that staff be well trained in using standard technique to minimize false-positives, which could lead to unnecessary resource use.
—Paloma Cesar de Sales, BN, RN, MS
Study Overview
Objective. To identify the prevalence and characteristics of patients identified with high blood pressure (BP) in nonprimary care compared with primary care visits.
Design. Longitudinal population-based study.
Setting and participants. This study was conducted at Kaiser Permanente Southern California (KPSC) after implementation of a system-wide change to improve hypertension care, which included comprehensive decision support tools embedded in the EHR system, including BP measurement flag alerts. Patient eligible for the study were normotensive members (BP < 140/90 mm Hg), older than 18 years, and enrolled in a KPSC health plan for at least 12 months on January of 2009. A gap of < 3 months in health care coverage in the year prior was allowed. Excluded were patients with a history of elevated BP during an outpatient visit, an inpatient or outpatient diagnosis code for hypertension, prescription for any antihypertensive medication within 24 months prior to 1 January 2009, missing BP information or whose only BP measurements were from a visit indicating fever or in preparation for a surgery or pain management. Pregnant patients, patients with missing sex information, and missing visit specialty information were also excluded. The study period was from January 2009 to March 2011.
Measurement. BP was measured routinely at the beginning of almost every primary and nonprimary outpatient visit. Nurses and medical assistants were trained according to a standard KPSC protocol using automated sphygmomanometer digital devices. According to the study protocol, in cases in which BP was elevated (≥ 140/90 mm Hg), a second measurement was obtained. At KPSC, all staff members including those in primary and nonprimary care are certified in BP measurement during their initial staff orientation and recertified annually.
Main outcome measure. An initial BP ≥ 140/90 mm Hg during a primary or nonprimary care outpatient visit.
Results. The mean ages of patients at baseline and at end of follow-up for the primary outcome were 39.7 (SD, 13.9) and 41.5 (SD, 14.0) years, respectively. The total cohort (n = 1,075,522) was nearly equally representative of both men (48.6%) and women (51.4%). The majority of the patients (91.7%) were younger than 60 years. A large proportion of the cohort belonged to racial/ethnic minorities with 33.1% Hispanic, 6.5% black, and 8.4% Asian/Pacific Islander.
The total cohort had 4,903,200 office visits, of which 3,996,190 were primary care visits, 901,275 nonprimary care visits, and 5735 visits of unknown specialty. During a mean follow-up of 1.6 years (SD, 0.8) 111,996 patients had a BP measurement ≥ 140/90 mm Hg. Of these, 92,577 (82.7%) were measured during primary care visits and 19,419 (17.3%) during nonprimary care visits. Of 15,356 patients with confirmed high BP, 12,587 (82%) were measured during primary care visits and 2769 (18.0%) patients during nonprimary care visits. Patients with a BP ≥ 140/90 mm Hg measured during nonprimary care visits were older, more likely to be male and non-Hispanic white, less likely to be obese, but more likely to smoke or have a Framingham risk score ≥ 20%. Ophthalmology/optometry, neurology, and dermatology were the main specialties to identify a first BP ≥ 140/90 mm Hg.
The follow-up after a first elevated BP was marginally higher in patients identified in nonprimary care than in primary care. Among patients with a first BP ≥ 140/90 mm Hg measured during a primary care visit, 60.6% had a follow-up BP within 3 months of the first high BP, 22.9% after 3 months or more, and 16.5% did not have a follow-up BP. Among individuals with a first BP ≥ 140/90 mm Hg measured during a nonprimary care visit, 64.7% had a follow-up BP within 3 months of the first high BP, 22.6% after 3 months or more, and 12.7% did not have a follow-up BP measurement.
The proportion of false-positives, defined as individuals with an initial BP ≥ 140/90 mm Hg who had a follow-up visit with a normal BP within 3 months, was the same for patients identified in primary and nonprimary care. False-positives were most frequent in individuals identified during visits in other specialty care, rheuma-tology, and neurology fields.
Conclusion. Expanding screening for hypertension to nonprimary care settings may improve the detection of hypertension and may contribute to better hypertension control. However, an effective system to ensure appropriate follow-up if high BP is detected is needed. Elderly, non-Hispanic, white male patients and those with very high BP are more likely to benefit from this screening.
Commentary
Hypertension is a common and costly health problem [1]. BP screening can identify adults with hypertension, who are at increased risk of cardiovascular and other diseases. Effective treatments are available to control high BP and reduce associated morbidity and mortality [2], but the first step is to identify patients with this largely asymptomatic disorder.
BP measurement is standard practice in primary care. However, many people do not regularly see a primary care clinician. In this study, researchers aimed to identify the prevalence and characteristics of patients identified with high BP in nonprimary care compared with primary care visits in a large integrated health care system that had implemented a system-level, multifaceted quality improvement program to improve hypertension care. Of the patients who were found to have high BP, 83% were diagnosed in a primary care setting and 17% in a specialty care setting, and the number of false-positive results were comparable.
In general, the study was well conducted and a strength of the study was the large sample size. Limitations included the fact that the study was conducted as part of a quality improvement project in an integrated health system, and there were no control clinics.
The authors noted that a high BP reading requires adequate follow-up, and nonprimary care detected elevated BP patients had lower follow-up rates. Also, some specialties had higher false-positive rates. Quality of measurement can be maximized with regular staff training.
Applications for Clinical Practice
Expanding routine screening for hypertension to non-primary care can potentially improve rates of detection, capturing patients who might otherwise have been missed. An effective system to ensure appropriate follow-up attention if high BP is detected is essential, and it is important that staff be well trained in using standard technique to minimize false-positives, which could lead to unnecessary resource use.
—Paloma Cesar de Sales, BN, RN, MS
1. American Heart Association. High blood pressure: statistical fact sheet 2013 update. Available at www.heart.org/idc/groups/heartpublic/@wcm/@sop/@smd/documents/downloadable/ucm_319587.pdf.
2. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014;311:507–20.
1. American Heart Association. High blood pressure: statistical fact sheet 2013 update. Available at www.heart.org/idc/groups/heartpublic/@wcm/@sop/@smd/documents/downloadable/ucm_319587.pdf.
2. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014;311:507–20.
Impact of Standardized Screening Protocols for Cystic Fibrosis–Related Diabetes in a Pediatric Population
From Children’s Hospitals and Clinics of Minnesota, and Children’s Respiratory and Critical Care Specialists, Minneapolis, MN.
Abstract
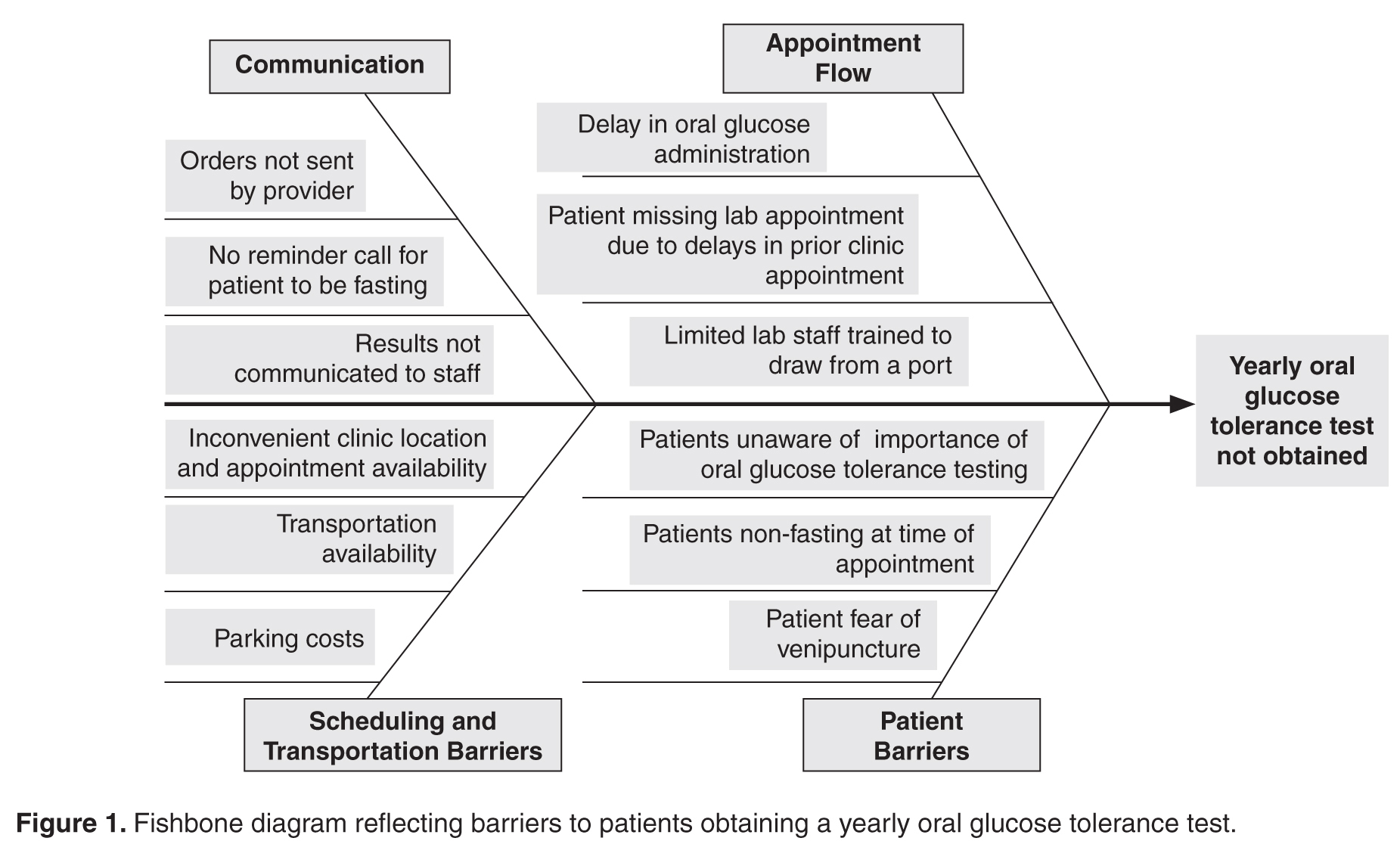
- Objective: In an effort to improve our pediatric center’s processes for screening, identifying, and treating cystic fibrosis–related diabetes (CFRD), we aimed to create outpatient and inpatient CFRD screening protocols.
- Methods: We identified barriers in our existing screening processes. The lab protocol for outpatients receiving oral glucose tolerance tests was streamlined. Inpatient screening order sets were developed. Interdisciplinary communication between pulmonary and endocrine care teams was improved. A protocol was developed for endocrinology consultation and follow-up for CFRD patients. Staff and families received additional education.
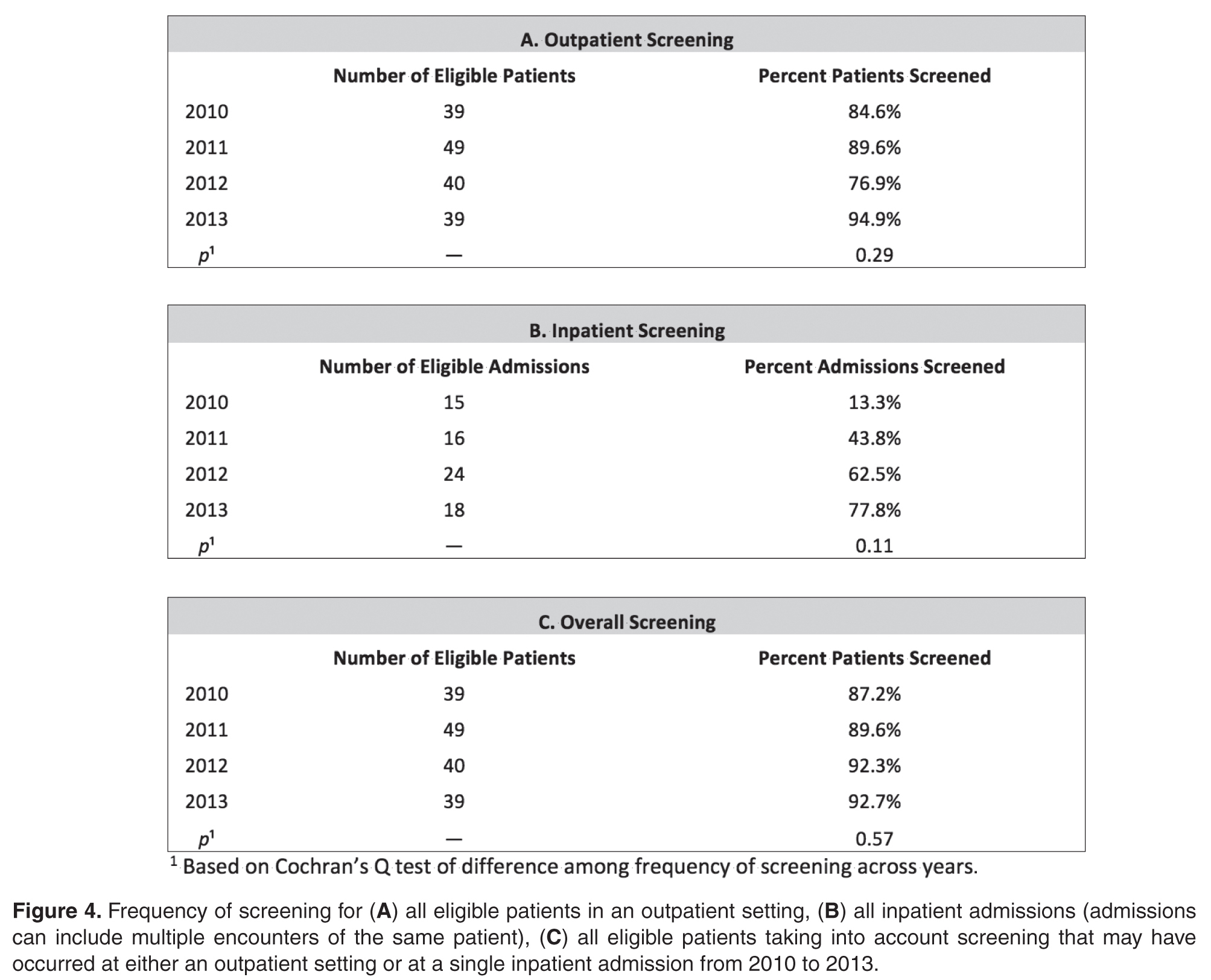
- Results: Outpatient screening was 85% in 2010, 90% in 2011, 77% in 2012, and 95% in 2013 (P = 0.29). Inpatient screening was 13% in 2010, 44% in 2011, 63% in 2012, and 78% 2013 (P = 0.11). Therefore, the combined screening protocols improved overall screening from 87% in 2010 to 90% in 2011, 92% in 2012, and 93% in 2013 (P = 0.57).
- Conclusion: Development of screening protocols improved identification of patients with CFRD.
The most prevalent comorbidity of cystic fibrosis (CF) is cystic fibrosis–related diabetes (CFRD) [1]. The incidence of CFRD increases with age and disease progression. In 2009, Moran et al noted a CFRD prevalence of approximately 20% in adolescents and 40% to 50% in adults [1]. An early diagnosis is especially important due to the correlation of an insulin-deficient state with pulmonary decline, increased pulmonary exacerbations, nutritional impairment, and increased mortality [2–6].
In 2009, the CF Foundation (CFF), the American Diabetes Association, and the Pediatric Endocrine Society updated the clinical care guidelines for the screening, diagnosis, and medical management of CFRD [7]. Soon after, the CFF, the Pediatric Endocrine Society, and the Dartmouth Institute Microsystem Academy sponsored a Learning and Leadership Collaborative (LLC) focusing on CFRD with the purpose of standardizing evidence-based clinical care processes to improve outcomes for patients with CF [8]. Our institution was selected to participate in this endeavor along with 6 other accredited CF centers in the United States.
We report how our pediatric institution established CFRD screening processes in the areas of outpatient care and inpatient care, thereby increasing screening rates.
Methods
Context
Our center cares for approximately 140 pediatric patients with CF. Our CF multidisciplinary program provides outpatient care within a private practice as well as inpatient hospital care within an independent, not-for-profit health care system. The clinic and hospital collaboratively provide services for our patients. Our center has a comprehensive annual clinic day for each child including annual laboratory tests, x-rays, pulmonary function tests, and interaction with the multidisciplinary CF team.
This year-long CFRD screening project was conducted from 2011 to 2012. We began this project with an outpatient screening rate of 85% in 2010. While this rate is high, we identified room for improvement in our screening processes for both outpatients and inpatients. The LLC provided tools and coaching during the project. Locally, we received support and leadership from our institution.
Reflecting on our initial high outpatient screening rate, we identified 2 pre-existing elements:
- As the affiliate center of the University of Minnesota, we have been influenced by their leadership in the field of CFRD. Accordingly, we have made screening for CFRD a priority, which included integrating an endocrinologist into our CF team.
- A review of our established annual patient standard-of-care laboratory results demonstrated 75% of patients in 2010 were completing laboratory testing. Therefore, the timing of the oral glucose tolerance test (OGTT) was changed from an unscheduled basis to becoming part of the outpatient annual lab protocol in an effort to screen the majority of patients.
Target Patient Population
The 2010 CFF guidelines recommend screening patients for CFRD beginning at age 10 years; however, it has been our practice to initiate screening beginning at age 8 years. For the purpose of this project and to increase generalizability for other centers, our results were adapted to include only patients 10 years of age and older.
Definitions
Successful outpatient screening was defined as completion of a 2-hour OGTT obtained by the following process: 1) The patient fasted for 8 hours, 2) a venous blood sample was drawn for a fasting serum glucose, 3) the patient consumed an oral glucose dose of 75 g within 5 minutes of the fasting blood draw, 4) a venous blood sample was drawn 2 hours after glucose administration for the postprandial serum glucose [9]. Patients weighing less than 43 kg received 1.75 g/kg of oral glucose. Outpatients eligible for screening were 10 years of age or older at their first quarterly visit of the year when annual laboratory tests including serum glucose are drawn.
Inpatient screening parameters were determined with guidance from the clinical care guidelines for cystic fibrosis-related diabetes [7], which recommends “monitoring fasting and 2-hour postprandial plasma glucose levels for the first 48 hours.” As this recommendation leaves room for interpretation as far as the quantity and interval of testing, we elected to define a successful screening as completion of one 2-hour postprandial plasma glucose level within 24 hours of admission plus one fasting glucose level within 48 hours of admission. If a patient was identified as having a fasting level ≥ 125 mg/dL or a 2-hour postprandial ≥ 200 mg/dL, additional glucose testing continued beyond 48 hours. However, for the purpose of identifying a successful screening, only the criteria of completing one 2-hour postprandial glucose plus one fasting glucose was considered. Successful screening for inpatients who received a course of steroids was defined as completion of three 2-hour postprandial plasma glucose levels within 24, 48, and 72 hours of admission or initiation of steroids. Inpatients eligible for screening were ten years of age or older at the time of admission.
Patients were not included if they were lost to follow-up for longer than 1 year or were seen for 2 or more quarterly visits at another CF center. Additionally, patients were not eligible if they had been previously diagnosed with CFRD.
Ethical Considerations
Ethical approval for this project was provided by Children’s Hospitals and Clinics of Minnesota Institutional Review Board.
Strategy for Change
We applied the principles of clinical microsystems and conducted numerous tests of change following the Plan-Do-Study-Act (PDSA) technique [10,11]. We organized a core team consisting of 6 individuals: our CF center director (pulmonologist); a hospital-employed pediatric endocrinologist; an outpatient CF clinic nurse coordinator; the hospital’s CF coordinator (pediatric nurse practitioner); a hospital-employed, certified diabetes educator (nurse); and the hospital’s CF dietitian. The core team met weekly throughout the year-long project and ensured other CF care providers were kept up-to-date on the changes implemented with the project.
Interventions
Outpatient Screening
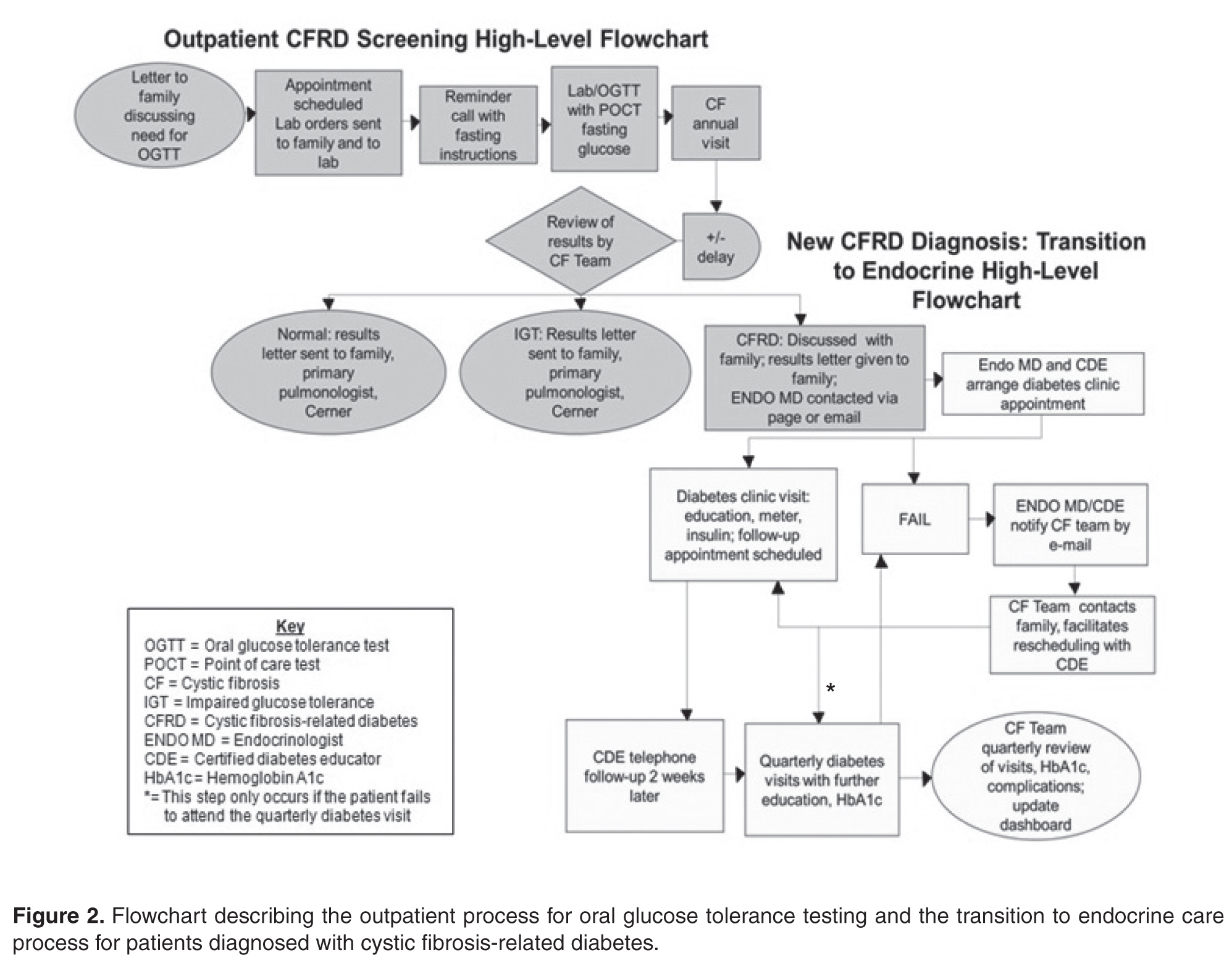
The OGTT was added to a previously established protocol for all patients to complete their annual labs at their first visit of the year. We stressed the importance and rationale for the OGTT in an annual clinic letter sent to families. The family was also sent a reminder letter with fasting instructions, a copy of the annual lab orders, and a reminder telephone call before the appointment. Based on family input regarding delays in the turn-around time for venous blood samples, a point of care (POC) glucose protocol was implemented. Laboratory personnel drew annual blood work, completed a POC blood glucose (in addition to the serum glucose), and administered the oral glucose load if the POC glucose was < 200 mg/dL.
Subsequent to completion of our project, we learned that our lab had inadvertently administered a 37.5-g dose for the OGTT instead of the recommended 75-g dose. To identify patients who may have had CFRD but were not diagnosed due to the low oral glucose dose, we have screened all patients with the corrected dose since January 2013.
To improve communication between the pulmonary and endocrine teams, weekly meetings were scheduled. The teams reviewed patients who had recently completed their annual laboratory tests or recently saw an endocrinology provider. After review of lab values, the patient families were mailed letters informing them of their child’s glucose test results which were categorized as normal, impaired, or abnormal suggesting CFRD. If the patient did not complete the OGTT, the family was mailed a letter reiterating the importance of screening. In the event of an abnormal OGTT suggesting CFRD, the results were discussed with the family during a clinic appointment. The endocrinologist and diabetes educator were subsequently notified, and an endocrine clinic appointment was arranged with the family to discuss the results and care plan. An electronic dashboard (spreadsheet) was created to track lab values and clinic visits for patients with impaired blood glucose tolerance as well as CFRD. The dashboard was reviewed and updated on a quarterly basis.
Inpatient Screening
To improve screening of hospitalized patients with CF not known to have CFRD, 4 standardized order sets detailing blood glucose testing schedules were developed in our electronic medical record as listed below. Our team educated physicians and nurses on the standardized order sets as well as patient families about the additional testing needed during hospitalization. An endocrine nurse practitioner conducted daily rounds on weekdays. All glucose results were verified by the laboratory. If a patient was identified to have a fasting blood glucose ≥ 125 mg/dL or 2-hour postprandial ≥ 200 mg/dL, the endocrine service was notified, and additional glucose testing was ordered. If the patient’s glucose levels persisted at high levels, meeting the criteria for a diagnosis of CFRD, further education was provided for the family and follow-up care was arranged.
Order Sets
1) Not receiving G-tube feedings
Day 1: 2-hour postprandial
Day 2: Fasting
2) Receiving G-tube feedings
Day 1: 2-hour postprandial, 2-hours after start of
G-tube feeds and at end of G-tube feeds
3) Receiving low-dose steroid therapy (IV methylprednisolone up to 4 mg/kg per day, administered every 6 hours and oral prednisolone 1 mg/kg twice per day for 5 days) [12]
Day 1: 2-hour postprandial
Day 2: Fasting and 2-hour postprandial
Day 3: 2-hour postprandial
4) Receiving high-dose steroid therapy per the allergic bronchopulmonary aspergillosis protocol (IV methylprednisolone 10–15 mg/kg once per day for 3 days) [12]
Days 1-4: Point of care prior to every meal, at bedtime, and at 0200 hours
Analysis
All patients with CF who are seen at our clinic were included in this project. Approximately 96% of our patients have consented to be part of the CFF supported patient registry, PortCF [13]. Data are entered by the CF clinic nurse coordinator for these patients to document clinic visits, hospital admissions, medications, lab values, and other parameters. We retrieved data from PortCF documenting the number of patients eligible for the OGTT and the number of patients diagnosed with CFRD. Individual medical records were cross-referenced with these results and also reviewed for patients who do not participate in PortCF. We retrieved data reports from our hospital informatics department to identify the number of patients with CF who were hospitalized each year and to obtain all glucose levels obtained during hospitalization. From these data, we calculated screening rates and the annual number of patients diagnosed with CFRD. We used the Cochran’s Q test to compare the differences in frequency of screening across years.
Results
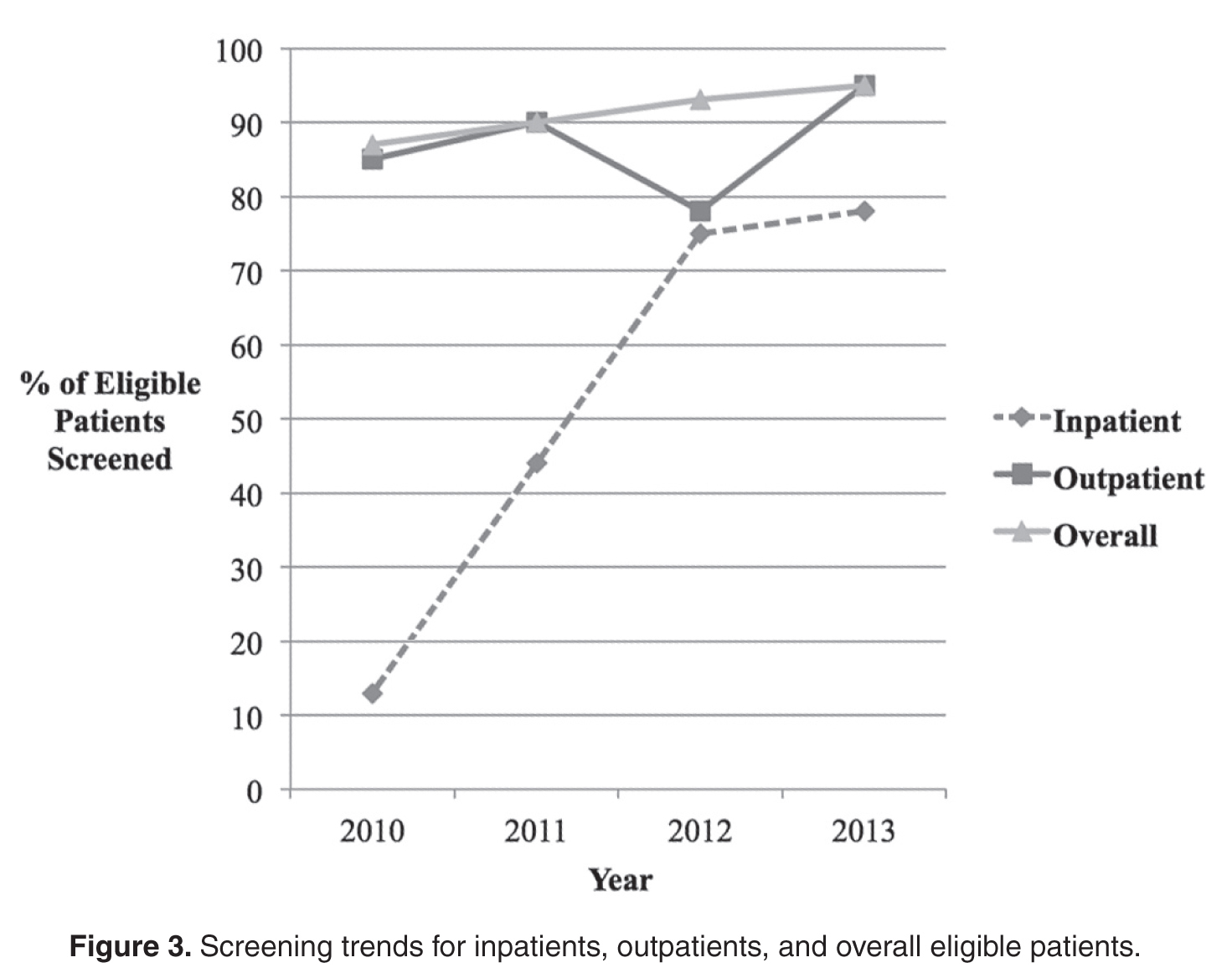
The newly implemented inpatient protocol, formally instituted in the third quarter of 2011, yielded a 43.8% screening rate in 2011 compared to a rate of 13.3% in 2010. Inpatient screening rates improved to 62.5% in 2012, and 77.8% in 2013 (Figures 3 and 4).
In 2011, 10 patients with CFRD were identified: 6 patients were diagnosed retrospectively based on a review of glucose levels collected in 2010 prior to the release of the new guidelines; 1 was diagnosed via inpatient screening; 3 were diagnosed via outpatient screening. In 2012, 5 patients with CFRD were identified: 4 were diagnosed via inpatient screening and one was diagnosed via outpatient screening. In 2013, 5 patients were identified: 1 diagnosed via inpatient screening and 4 diagnosed via outpatient screening. All diagnosed patients met the criteria of having a fasting blood sugar ≥ 126 mg/dL or a 2-hour postprandial ≥ 200 mg/dL that persisted for more than 48 hours.
Discussion
This collaborative initiative resulted in the development of structured screening protocols leading to overall screening improvement. A standardized screening protocol is fundamental to the identification and subsequent treatment of a patient with CFRD. Patients with CFRD may have decreased mortality when diagnosed early and treated aggressively, underscoring the necessity for CF centers to improve screening protocols [1,6].
Determining the best methods for implementation may vary from center to center, but the key factors we have identified from this project include strong leadership and team commitment—elements that have previously been identified as being predictive of positive quality improvement outcomes [14].
Education of staff, families, and patients is also an important factor. Education played a significant role during the inpatient screening PDSA cycles. For example, a time intensive but worthwhile training was conducted for the physicians and nurses on the order sets. Education for the patients and families during inpatient stays led to a better understanding of the rationale for, and support of, the additional blood draws.
The importance of family involvement was evident as we refined our outpatient protocol. Input from the phone surveys allowed us to identify barriers in our process that led us to establish more efficient clinic visits with reduced time in the lab, improved clinic flow and increased patient satisfaction. Other important factors were co-location of the endocrine and pulmonary clinics and flexibility of scheduling to facilitate seeing patients in both clinics on the same day.
Although we uncovered an error in oral glucose dosing, we were able to appropriately screen the majority of these patients within the next year. At the conclusion of 2013, our outpatient protocol had facilitated a screening rate of 95%, surpassing the 2012 rate of 77%. Interestingly, 2 of the patients diagnosed with CFRD in 2011 were diagnosed by HbA1c criteria, with normal OGTT results, perhaps due to the substandard glucose dose. Only 5 additional patients screened positive for CFRD at the end of 2013, which is the same number identified in 2012. It is unclear whether they would have been diagnosed earlier with the recommended dose of oral glucose or if they developed CFRD due to the progression of their disease.
A limitation of this project may be its reproducibility at other institutions. It is likely that the success of this project was due to the strong relationship between the endocrinology and pulmonary teams, committed leadership, institutional support for co-location of the clinics, and the team’s competency in quality improvement techniques with guidance from the LLC. The process of developing, implementing, and sustaining screening protocols was time-intensive and may be difficult to replicate in another center without similar resources available.
A strong motivation behind this project was the LLC, and while other centers may not have the same opportunity, the CFRD Evidence-Based Practice and Smart Change Idea Compendium was published as result of the LLC to serve as a guide for other centers [8]. Kern et al successfully demonstrated that a process based on the ideas from this compendium can help achieve higher OGTT outpatient screening rates in a CF center [15]. Kern et al’s project was similar to ours although the duration was shorter (< 1 year) and it began with a 47% screening rate prior to implementation. Our center extended the efforts of Kern et al by implementing our initiative over the course of 3 years, but unlike Kern et al, we included patients with failed or rescheduled appointments. Kern et al defined, identified, and excluded patients with moderate or severe pulmonary exacerbation from their eligible screening pool. We included all patients over the course of our year-long screening periods, as we have created an opportunity to screen ill patients at subsequent visits or as inpatients.
As with any quality improvement project, there is the risk of not sustaining improvements. In 2012 our outpatient screening rates were lower than the previous year. However, the coordination of the outpatient and inpatient protocols helped us achieve an improved overall screening rate of 92% in 2012. One possible explanation for the decrease in 2012 outpatient screening is that several patients eligible for screening in 2012 were less adherent with attending clinic visits. Five of these patients transitioned to an adult center or were diagnosed with CFRD in 2013. With this shift in the eligibility pool, our outpatient screening rate for 2013 surpassed our rate from 2012. In an attempt to sustain our gains, members of our team continue to review patient screening and endocrine referrals at monthly meetings. The decrease in outpatient screening demonstrates the importance of ongoing evaluation and monitoring of quality improvement projects after the initial objectives have been achieved.
Typically, our less adherent patients are only seen in clinic when experiencing an exacerbation when we cannot administer the OGTT. As a result, these patients are generally admitted for treatment of their exacerbation, and we are able to screen them during their hospitalization. Of the 9 patients not screened as outpatients in 2012, 7 were screened as inpatients. Three patients were unscreened that year: 1 patient failed to fast, another refused the test, and the last patient was inadvertently missed. While our intention is to screen all patients as an outpatient with OGTT, we have found that the only opportunity we have for screening less adherent patients is often while hospitalized, emphasizing the importance of a dual screening approach. This approach has allowed us to screen the majority of our patients as reflected in our overall screening rate.
One of our major challenges moving forward is to help the patients diagnosed with CFRD and their families accept yet another diagnosis and the burden of care associated with it. Our focus has shifted now to determine the best methods to motivate patients with CFRD to regularly attend endocrine clinic appointments, recognizing the challenges of additional clinic visits, monitoring, and medications. It is interesting to speculate whether improved CFRD clinical outcomes may correlate with improved screening rates. In 2012 our patients had a median HbA1c of 5.7 when the national average is 6.6 [16]. Further research is needed to delineate a possible relationship between an effective screening protocol and favorable clinical outcome measures.
Conclusion
The use of a structured process developed by a multidisciplinary team resulted in improved CFRD screening rates. In addition to outpatient protocols, it is critical to develop inpatient glucose testing protocols in order to capture patients who are only seen at times of exacerbation. Even in this era of treatment at a cellular level with correctors and potentiators, early detection and treatment of CFRD is essential for optimal clinical outcomes [1,5,17]. The next step for us is to sustain our gains and to improve endocrine care facilitation. We hope this report may guide other teams and institutional leadership in their efforts to improve identification of individuals with CFRD.
Acknowledgments: We would like to acknowledge Gautham Suresh, MD, Jennifer Abuzzahab, MD, Robert Payne, MD, and Andrew Flood, PhD, for their assistance in the preparation of our manuscript. We also acknowledge John Nash, MSW, LMSW, who provided us tools and coaching throughout the Learning and Leadership Collaborative.
Corresponding author: Lisa Read, MPH, 2525 Chicago Ave. South, MS 17-750, Minneapolis, MN 55404, [email protected].
Funding/support. This work was supported by a grant from the Cystic Fibrosis Foundation for the Learning and Leadership Collaborative: Cystic Fibrosis-Related Diabetes Care (MCNAMA11Q10, to Dr. McNamara).
1. Moran A, Dunitz J, Nathan B, et al. Cystic fibrosis–related diabetes: current trends in prevalence, incidence, and mortality. Diabetes Care 2009;32:1626–31.
2. Cawood TJ, McKenna MJ, Gallagher CG, et al. Cystic fibrosis-related diabetes in adults. Ir Med J 2006;99:83–6.
3. Koch C, Rainisio M, Madessani U, et al. Investigators of the European Epidemiologic Registry of Cystic Fibrosis. Presence of cystic fibrosis-related diabetes mellitus tightly linked to poor lung function in patients with cystic fibrosis: data from the European Epidemiologic Registry of Cystic Fibrosis. Pediatr Pulmonol 2001;32:343–50.
4. Marshall BC, Butler SM, Stoddard M, et al. Epidemiology of cystic fibrosis-related diabetes. J Pediatr 2005;146:681–7.
5. Milla CE, Billings J, Moran A. Diabetes is associated with dramatically decreased survival in female but not male subjects with cystic fibrosis. Diabetes Care 2005;28:2141–4.
6. Lewis C, Blackman SM, Nelson A, et al. Diabetes-related mortality in adults with cystic fibrosis. Role of genotype and sex. Am J Respir Crit Care Med 2015;191:194–200.
7. Moran A, Brunzell C, Cohen, RC, et al. Clinical Care guidelines for cystic fibrosis–related diabetes. A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care 2010;33:2697–708.
8. Nash J, Messier R, Casella SJ, et al. Learning and Leadership Collaborative: CFRD. Cystic fibrosis related diabetes (CFRD) evidence-based practice and smart change idea compendium 2012. Bethesda, MD: Cystic Fibrosis Foundation; McLean, VA: Pediatric Endocrine Society; Lebanon, NH: Dartmouth Institute Microsystem Academy; May 2012.
9. WHO Expert Committee on Diabetes Mellitus: Second Report of the WHO Expert Committee on Diabetes Mellitus. Geneva: World Health Organization; 1980 (Tech. Rep. Ser no. 646).
10. Cystic Fibrosis Foundation, Dartmouth Medical School: Center for the Evaluative Clinical Sciences, Dartmouth/Hitchcock Medical Center. Action guide for accelerating improvement in cystic fibrosis care: clinical microsystems. 2006.
11. Langley GJ, Nolan KM, Nolan TW, et al. The improvement guide: a practical approach to enhancing organizational performance. San Francisco, CA: Jossey-Bass; 1996.
12. Cohen-Cymberknoh M, Blau H, Shoseyov D, et al. Intravenous monthly pulse methylprednisolone treatment for ABPA in patients with cystic fibrosis. J Cyst Fibros 2009;8:253–7.
13. Center Specific Patient Registry Report for 2011. Bethesda, MD: Cystic Fibrosis Foundation; 2012.
14. Parker VA, Wubbenhorst WH, Young GJ, et al. Implementing quality improvement in hospitals: The role of leadership and culture. Am J Med Qual 1999; 14:64–9.
15. Kern AS, Prestridge AL. Improving screening for cystic fibrosis-related diabetes at a pediatric cystic fibrosis program. Pediatrics 2013;132:e512–8.
16. Center Specific Patient Registry Report for 2012. Bethesda, MD: Cystic Fibrosis Foundation; 2013.
17. Schwarzenberg SJ, Thomas W, Olsen TW, et al. Microvascular complications in cystic fibrosis-related diabetes. Diabetes Care 2007;30:1056–61.
From Children’s Hospitals and Clinics of Minnesota, and Children’s Respiratory and Critical Care Specialists, Minneapolis, MN.
Abstract
- Objective: In an effort to improve our pediatric center’s processes for screening, identifying, and treating cystic fibrosis–related diabetes (CFRD), we aimed to create outpatient and inpatient CFRD screening protocols.
- Methods: We identified barriers in our existing screening processes. The lab protocol for outpatients receiving oral glucose tolerance tests was streamlined. Inpatient screening order sets were developed. Interdisciplinary communication between pulmonary and endocrine care teams was improved. A protocol was developed for endocrinology consultation and follow-up for CFRD patients. Staff and families received additional education.
- Results: Outpatient screening was 85% in 2010, 90% in 2011, 77% in 2012, and 95% in 2013 (P = 0.29). Inpatient screening was 13% in 2010, 44% in 2011, 63% in 2012, and 78% 2013 (P = 0.11). Therefore, the combined screening protocols improved overall screening from 87% in 2010 to 90% in 2011, 92% in 2012, and 93% in 2013 (P = 0.57).
- Conclusion: Development of screening protocols improved identification of patients with CFRD.
The most prevalent comorbidity of cystic fibrosis (CF) is cystic fibrosis–related diabetes (CFRD) [1]. The incidence of CFRD increases with age and disease progression. In 2009, Moran et al noted a CFRD prevalence of approximately 20% in adolescents and 40% to 50% in adults [1]. An early diagnosis is especially important due to the correlation of an insulin-deficient state with pulmonary decline, increased pulmonary exacerbations, nutritional impairment, and increased mortality [2–6].
In 2009, the CF Foundation (CFF), the American Diabetes Association, and the Pediatric Endocrine Society updated the clinical care guidelines for the screening, diagnosis, and medical management of CFRD [7]. Soon after, the CFF, the Pediatric Endocrine Society, and the Dartmouth Institute Microsystem Academy sponsored a Learning and Leadership Collaborative (LLC) focusing on CFRD with the purpose of standardizing evidence-based clinical care processes to improve outcomes for patients with CF [8]. Our institution was selected to participate in this endeavor along with 6 other accredited CF centers in the United States.
We report how our pediatric institution established CFRD screening processes in the areas of outpatient care and inpatient care, thereby increasing screening rates.
Methods
Context
Our center cares for approximately 140 pediatric patients with CF. Our CF multidisciplinary program provides outpatient care within a private practice as well as inpatient hospital care within an independent, not-for-profit health care system. The clinic and hospital collaboratively provide services for our patients. Our center has a comprehensive annual clinic day for each child including annual laboratory tests, x-rays, pulmonary function tests, and interaction with the multidisciplinary CF team.
This year-long CFRD screening project was conducted from 2011 to 2012. We began this project with an outpatient screening rate of 85% in 2010. While this rate is high, we identified room for improvement in our screening processes for both outpatients and inpatients. The LLC provided tools and coaching during the project. Locally, we received support and leadership from our institution.
Reflecting on our initial high outpatient screening rate, we identified 2 pre-existing elements:
- As the affiliate center of the University of Minnesota, we have been influenced by their leadership in the field of CFRD. Accordingly, we have made screening for CFRD a priority, which included integrating an endocrinologist into our CF team.
- A review of our established annual patient standard-of-care laboratory results demonstrated 75% of patients in 2010 were completing laboratory testing. Therefore, the timing of the oral glucose tolerance test (OGTT) was changed from an unscheduled basis to becoming part of the outpatient annual lab protocol in an effort to screen the majority of patients.
Target Patient Population
The 2010 CFF guidelines recommend screening patients for CFRD beginning at age 10 years; however, it has been our practice to initiate screening beginning at age 8 years. For the purpose of this project and to increase generalizability for other centers, our results were adapted to include only patients 10 years of age and older.
Definitions
Successful outpatient screening was defined as completion of a 2-hour OGTT obtained by the following process: 1) The patient fasted for 8 hours, 2) a venous blood sample was drawn for a fasting serum glucose, 3) the patient consumed an oral glucose dose of 75 g within 5 minutes of the fasting blood draw, 4) a venous blood sample was drawn 2 hours after glucose administration for the postprandial serum glucose [9]. Patients weighing less than 43 kg received 1.75 g/kg of oral glucose. Outpatients eligible for screening were 10 years of age or older at their first quarterly visit of the year when annual laboratory tests including serum glucose are drawn.
Inpatient screening parameters were determined with guidance from the clinical care guidelines for cystic fibrosis-related diabetes [7], which recommends “monitoring fasting and 2-hour postprandial plasma glucose levels for the first 48 hours.” As this recommendation leaves room for interpretation as far as the quantity and interval of testing, we elected to define a successful screening as completion of one 2-hour postprandial plasma glucose level within 24 hours of admission plus one fasting glucose level within 48 hours of admission. If a patient was identified as having a fasting level ≥ 125 mg/dL or a 2-hour postprandial ≥ 200 mg/dL, additional glucose testing continued beyond 48 hours. However, for the purpose of identifying a successful screening, only the criteria of completing one 2-hour postprandial glucose plus one fasting glucose was considered. Successful screening for inpatients who received a course of steroids was defined as completion of three 2-hour postprandial plasma glucose levels within 24, 48, and 72 hours of admission or initiation of steroids. Inpatients eligible for screening were ten years of age or older at the time of admission.
Patients were not included if they were lost to follow-up for longer than 1 year or were seen for 2 or more quarterly visits at another CF center. Additionally, patients were not eligible if they had been previously diagnosed with CFRD.
Ethical Considerations
Ethical approval for this project was provided by Children’s Hospitals and Clinics of Minnesota Institutional Review Board.
Strategy for Change
We applied the principles of clinical microsystems and conducted numerous tests of change following the Plan-Do-Study-Act (PDSA) technique [10,11]. We organized a core team consisting of 6 individuals: our CF center director (pulmonologist); a hospital-employed pediatric endocrinologist; an outpatient CF clinic nurse coordinator; the hospital’s CF coordinator (pediatric nurse practitioner); a hospital-employed, certified diabetes educator (nurse); and the hospital’s CF dietitian. The core team met weekly throughout the year-long project and ensured other CF care providers were kept up-to-date on the changes implemented with the project.
Interventions
Outpatient Screening
The OGTT was added to a previously established protocol for all patients to complete their annual labs at their first visit of the year. We stressed the importance and rationale for the OGTT in an annual clinic letter sent to families. The family was also sent a reminder letter with fasting instructions, a copy of the annual lab orders, and a reminder telephone call before the appointment. Based on family input regarding delays in the turn-around time for venous blood samples, a point of care (POC) glucose protocol was implemented. Laboratory personnel drew annual blood work, completed a POC blood glucose (in addition to the serum glucose), and administered the oral glucose load if the POC glucose was < 200 mg/dL.
Subsequent to completion of our project, we learned that our lab had inadvertently administered a 37.5-g dose for the OGTT instead of the recommended 75-g dose. To identify patients who may have had CFRD but were not diagnosed due to the low oral glucose dose, we have screened all patients with the corrected dose since January 2013.
To improve communication between the pulmonary and endocrine teams, weekly meetings were scheduled. The teams reviewed patients who had recently completed their annual laboratory tests or recently saw an endocrinology provider. After review of lab values, the patient families were mailed letters informing them of their child’s glucose test results which were categorized as normal, impaired, or abnormal suggesting CFRD. If the patient did not complete the OGTT, the family was mailed a letter reiterating the importance of screening. In the event of an abnormal OGTT suggesting CFRD, the results were discussed with the family during a clinic appointment. The endocrinologist and diabetes educator were subsequently notified, and an endocrine clinic appointment was arranged with the family to discuss the results and care plan. An electronic dashboard (spreadsheet) was created to track lab values and clinic visits for patients with impaired blood glucose tolerance as well as CFRD. The dashboard was reviewed and updated on a quarterly basis.
Inpatient Screening
To improve screening of hospitalized patients with CF not known to have CFRD, 4 standardized order sets detailing blood glucose testing schedules were developed in our electronic medical record as listed below. Our team educated physicians and nurses on the standardized order sets as well as patient families about the additional testing needed during hospitalization. An endocrine nurse practitioner conducted daily rounds on weekdays. All glucose results were verified by the laboratory. If a patient was identified to have a fasting blood glucose ≥ 125 mg/dL or 2-hour postprandial ≥ 200 mg/dL, the endocrine service was notified, and additional glucose testing was ordered. If the patient’s glucose levels persisted at high levels, meeting the criteria for a diagnosis of CFRD, further education was provided for the family and follow-up care was arranged.
Order Sets
1) Not receiving G-tube feedings
Day 1: 2-hour postprandial
Day 2: Fasting
2) Receiving G-tube feedings
Day 1: 2-hour postprandial, 2-hours after start of
G-tube feeds and at end of G-tube feeds
3) Receiving low-dose steroid therapy (IV methylprednisolone up to 4 mg/kg per day, administered every 6 hours and oral prednisolone 1 mg/kg twice per day for 5 days) [12]
Day 1: 2-hour postprandial
Day 2: Fasting and 2-hour postprandial
Day 3: 2-hour postprandial
4) Receiving high-dose steroid therapy per the allergic bronchopulmonary aspergillosis protocol (IV methylprednisolone 10–15 mg/kg once per day for 3 days) [12]
Days 1-4: Point of care prior to every meal, at bedtime, and at 0200 hours
Analysis
All patients with CF who are seen at our clinic were included in this project. Approximately 96% of our patients have consented to be part of the CFF supported patient registry, PortCF [13]. Data are entered by the CF clinic nurse coordinator for these patients to document clinic visits, hospital admissions, medications, lab values, and other parameters. We retrieved data from PortCF documenting the number of patients eligible for the OGTT and the number of patients diagnosed with CFRD. Individual medical records were cross-referenced with these results and also reviewed for patients who do not participate in PortCF. We retrieved data reports from our hospital informatics department to identify the number of patients with CF who were hospitalized each year and to obtain all glucose levels obtained during hospitalization. From these data, we calculated screening rates and the annual number of patients diagnosed with CFRD. We used the Cochran’s Q test to compare the differences in frequency of screening across years.
Results
The newly implemented inpatient protocol, formally instituted in the third quarter of 2011, yielded a 43.8% screening rate in 2011 compared to a rate of 13.3% in 2010. Inpatient screening rates improved to 62.5% in 2012, and 77.8% in 2013 (Figures 3 and 4).
In 2011, 10 patients with CFRD were identified: 6 patients were diagnosed retrospectively based on a review of glucose levels collected in 2010 prior to the release of the new guidelines; 1 was diagnosed via inpatient screening; 3 were diagnosed via outpatient screening. In 2012, 5 patients with CFRD were identified: 4 were diagnosed via inpatient screening and one was diagnosed via outpatient screening. In 2013, 5 patients were identified: 1 diagnosed via inpatient screening and 4 diagnosed via outpatient screening. All diagnosed patients met the criteria of having a fasting blood sugar ≥ 126 mg/dL or a 2-hour postprandial ≥ 200 mg/dL that persisted for more than 48 hours.
Discussion
This collaborative initiative resulted in the development of structured screening protocols leading to overall screening improvement. A standardized screening protocol is fundamental to the identification and subsequent treatment of a patient with CFRD. Patients with CFRD may have decreased mortality when diagnosed early and treated aggressively, underscoring the necessity for CF centers to improve screening protocols [1,6].
Determining the best methods for implementation may vary from center to center, but the key factors we have identified from this project include strong leadership and team commitment—elements that have previously been identified as being predictive of positive quality improvement outcomes [14].
Education of staff, families, and patients is also an important factor. Education played a significant role during the inpatient screening PDSA cycles. For example, a time intensive but worthwhile training was conducted for the physicians and nurses on the order sets. Education for the patients and families during inpatient stays led to a better understanding of the rationale for, and support of, the additional blood draws.
The importance of family involvement was evident as we refined our outpatient protocol. Input from the phone surveys allowed us to identify barriers in our process that led us to establish more efficient clinic visits with reduced time in the lab, improved clinic flow and increased patient satisfaction. Other important factors were co-location of the endocrine and pulmonary clinics and flexibility of scheduling to facilitate seeing patients in both clinics on the same day.
Although we uncovered an error in oral glucose dosing, we were able to appropriately screen the majority of these patients within the next year. At the conclusion of 2013, our outpatient protocol had facilitated a screening rate of 95%, surpassing the 2012 rate of 77%. Interestingly, 2 of the patients diagnosed with CFRD in 2011 were diagnosed by HbA1c criteria, with normal OGTT results, perhaps due to the substandard glucose dose. Only 5 additional patients screened positive for CFRD at the end of 2013, which is the same number identified in 2012. It is unclear whether they would have been diagnosed earlier with the recommended dose of oral glucose or if they developed CFRD due to the progression of their disease.
A limitation of this project may be its reproducibility at other institutions. It is likely that the success of this project was due to the strong relationship between the endocrinology and pulmonary teams, committed leadership, institutional support for co-location of the clinics, and the team’s competency in quality improvement techniques with guidance from the LLC. The process of developing, implementing, and sustaining screening protocols was time-intensive and may be difficult to replicate in another center without similar resources available.
A strong motivation behind this project was the LLC, and while other centers may not have the same opportunity, the CFRD Evidence-Based Practice and Smart Change Idea Compendium was published as result of the LLC to serve as a guide for other centers [8]. Kern et al successfully demonstrated that a process based on the ideas from this compendium can help achieve higher OGTT outpatient screening rates in a CF center [15]. Kern et al’s project was similar to ours although the duration was shorter (< 1 year) and it began with a 47% screening rate prior to implementation. Our center extended the efforts of Kern et al by implementing our initiative over the course of 3 years, but unlike Kern et al, we included patients with failed or rescheduled appointments. Kern et al defined, identified, and excluded patients with moderate or severe pulmonary exacerbation from their eligible screening pool. We included all patients over the course of our year-long screening periods, as we have created an opportunity to screen ill patients at subsequent visits or as inpatients.
As with any quality improvement project, there is the risk of not sustaining improvements. In 2012 our outpatient screening rates were lower than the previous year. However, the coordination of the outpatient and inpatient protocols helped us achieve an improved overall screening rate of 92% in 2012. One possible explanation for the decrease in 2012 outpatient screening is that several patients eligible for screening in 2012 were less adherent with attending clinic visits. Five of these patients transitioned to an adult center or were diagnosed with CFRD in 2013. With this shift in the eligibility pool, our outpatient screening rate for 2013 surpassed our rate from 2012. In an attempt to sustain our gains, members of our team continue to review patient screening and endocrine referrals at monthly meetings. The decrease in outpatient screening demonstrates the importance of ongoing evaluation and monitoring of quality improvement projects after the initial objectives have been achieved.
Typically, our less adherent patients are only seen in clinic when experiencing an exacerbation when we cannot administer the OGTT. As a result, these patients are generally admitted for treatment of their exacerbation, and we are able to screen them during their hospitalization. Of the 9 patients not screened as outpatients in 2012, 7 were screened as inpatients. Three patients were unscreened that year: 1 patient failed to fast, another refused the test, and the last patient was inadvertently missed. While our intention is to screen all patients as an outpatient with OGTT, we have found that the only opportunity we have for screening less adherent patients is often while hospitalized, emphasizing the importance of a dual screening approach. This approach has allowed us to screen the majority of our patients as reflected in our overall screening rate.
One of our major challenges moving forward is to help the patients diagnosed with CFRD and their families accept yet another diagnosis and the burden of care associated with it. Our focus has shifted now to determine the best methods to motivate patients with CFRD to regularly attend endocrine clinic appointments, recognizing the challenges of additional clinic visits, monitoring, and medications. It is interesting to speculate whether improved CFRD clinical outcomes may correlate with improved screening rates. In 2012 our patients had a median HbA1c of 5.7 when the national average is 6.6 [16]. Further research is needed to delineate a possible relationship between an effective screening protocol and favorable clinical outcome measures.
Conclusion
The use of a structured process developed by a multidisciplinary team resulted in improved CFRD screening rates. In addition to outpatient protocols, it is critical to develop inpatient glucose testing protocols in order to capture patients who are only seen at times of exacerbation. Even in this era of treatment at a cellular level with correctors and potentiators, early detection and treatment of CFRD is essential for optimal clinical outcomes [1,5,17]. The next step for us is to sustain our gains and to improve endocrine care facilitation. We hope this report may guide other teams and institutional leadership in their efforts to improve identification of individuals with CFRD.
Acknowledgments: We would like to acknowledge Gautham Suresh, MD, Jennifer Abuzzahab, MD, Robert Payne, MD, and Andrew Flood, PhD, for their assistance in the preparation of our manuscript. We also acknowledge John Nash, MSW, LMSW, who provided us tools and coaching throughout the Learning and Leadership Collaborative.
Corresponding author: Lisa Read, MPH, 2525 Chicago Ave. South, MS 17-750, Minneapolis, MN 55404, [email protected].
Funding/support. This work was supported by a grant from the Cystic Fibrosis Foundation for the Learning and Leadership Collaborative: Cystic Fibrosis-Related Diabetes Care (MCNAMA11Q10, to Dr. McNamara).
From Children’s Hospitals and Clinics of Minnesota, and Children’s Respiratory and Critical Care Specialists, Minneapolis, MN.
Abstract
- Objective: In an effort to improve our pediatric center’s processes for screening, identifying, and treating cystic fibrosis–related diabetes (CFRD), we aimed to create outpatient and inpatient CFRD screening protocols.
- Methods: We identified barriers in our existing screening processes. The lab protocol for outpatients receiving oral glucose tolerance tests was streamlined. Inpatient screening order sets were developed. Interdisciplinary communication between pulmonary and endocrine care teams was improved. A protocol was developed for endocrinology consultation and follow-up for CFRD patients. Staff and families received additional education.
- Results: Outpatient screening was 85% in 2010, 90% in 2011, 77% in 2012, and 95% in 2013 (P = 0.29). Inpatient screening was 13% in 2010, 44% in 2011, 63% in 2012, and 78% 2013 (P = 0.11). Therefore, the combined screening protocols improved overall screening from 87% in 2010 to 90% in 2011, 92% in 2012, and 93% in 2013 (P = 0.57).
- Conclusion: Development of screening protocols improved identification of patients with CFRD.
The most prevalent comorbidity of cystic fibrosis (CF) is cystic fibrosis–related diabetes (CFRD) [1]. The incidence of CFRD increases with age and disease progression. In 2009, Moran et al noted a CFRD prevalence of approximately 20% in adolescents and 40% to 50% in adults [1]. An early diagnosis is especially important due to the correlation of an insulin-deficient state with pulmonary decline, increased pulmonary exacerbations, nutritional impairment, and increased mortality [2–6].
In 2009, the CF Foundation (CFF), the American Diabetes Association, and the Pediatric Endocrine Society updated the clinical care guidelines for the screening, diagnosis, and medical management of CFRD [7]. Soon after, the CFF, the Pediatric Endocrine Society, and the Dartmouth Institute Microsystem Academy sponsored a Learning and Leadership Collaborative (LLC) focusing on CFRD with the purpose of standardizing evidence-based clinical care processes to improve outcomes for patients with CF [8]. Our institution was selected to participate in this endeavor along with 6 other accredited CF centers in the United States.
We report how our pediatric institution established CFRD screening processes in the areas of outpatient care and inpatient care, thereby increasing screening rates.
Methods
Context
Our center cares for approximately 140 pediatric patients with CF. Our CF multidisciplinary program provides outpatient care within a private practice as well as inpatient hospital care within an independent, not-for-profit health care system. The clinic and hospital collaboratively provide services for our patients. Our center has a comprehensive annual clinic day for each child including annual laboratory tests, x-rays, pulmonary function tests, and interaction with the multidisciplinary CF team.
This year-long CFRD screening project was conducted from 2011 to 2012. We began this project with an outpatient screening rate of 85% in 2010. While this rate is high, we identified room for improvement in our screening processes for both outpatients and inpatients. The LLC provided tools and coaching during the project. Locally, we received support and leadership from our institution.
Reflecting on our initial high outpatient screening rate, we identified 2 pre-existing elements:
- As the affiliate center of the University of Minnesota, we have been influenced by their leadership in the field of CFRD. Accordingly, we have made screening for CFRD a priority, which included integrating an endocrinologist into our CF team.
- A review of our established annual patient standard-of-care laboratory results demonstrated 75% of patients in 2010 were completing laboratory testing. Therefore, the timing of the oral glucose tolerance test (OGTT) was changed from an unscheduled basis to becoming part of the outpatient annual lab protocol in an effort to screen the majority of patients.
Target Patient Population
The 2010 CFF guidelines recommend screening patients for CFRD beginning at age 10 years; however, it has been our practice to initiate screening beginning at age 8 years. For the purpose of this project and to increase generalizability for other centers, our results were adapted to include only patients 10 years of age and older.
Definitions
Successful outpatient screening was defined as completion of a 2-hour OGTT obtained by the following process: 1) The patient fasted for 8 hours, 2) a venous blood sample was drawn for a fasting serum glucose, 3) the patient consumed an oral glucose dose of 75 g within 5 minutes of the fasting blood draw, 4) a venous blood sample was drawn 2 hours after glucose administration for the postprandial serum glucose [9]. Patients weighing less than 43 kg received 1.75 g/kg of oral glucose. Outpatients eligible for screening were 10 years of age or older at their first quarterly visit of the year when annual laboratory tests including serum glucose are drawn.
Inpatient screening parameters were determined with guidance from the clinical care guidelines for cystic fibrosis-related diabetes [7], which recommends “monitoring fasting and 2-hour postprandial plasma glucose levels for the first 48 hours.” As this recommendation leaves room for interpretation as far as the quantity and interval of testing, we elected to define a successful screening as completion of one 2-hour postprandial plasma glucose level within 24 hours of admission plus one fasting glucose level within 48 hours of admission. If a patient was identified as having a fasting level ≥ 125 mg/dL or a 2-hour postprandial ≥ 200 mg/dL, additional glucose testing continued beyond 48 hours. However, for the purpose of identifying a successful screening, only the criteria of completing one 2-hour postprandial glucose plus one fasting glucose was considered. Successful screening for inpatients who received a course of steroids was defined as completion of three 2-hour postprandial plasma glucose levels within 24, 48, and 72 hours of admission or initiation of steroids. Inpatients eligible for screening were ten years of age or older at the time of admission.
Patients were not included if they were lost to follow-up for longer than 1 year or were seen for 2 or more quarterly visits at another CF center. Additionally, patients were not eligible if they had been previously diagnosed with CFRD.
Ethical Considerations
Ethical approval for this project was provided by Children’s Hospitals and Clinics of Minnesota Institutional Review Board.
Strategy for Change
We applied the principles of clinical microsystems and conducted numerous tests of change following the Plan-Do-Study-Act (PDSA) technique [10,11]. We organized a core team consisting of 6 individuals: our CF center director (pulmonologist); a hospital-employed pediatric endocrinologist; an outpatient CF clinic nurse coordinator; the hospital’s CF coordinator (pediatric nurse practitioner); a hospital-employed, certified diabetes educator (nurse); and the hospital’s CF dietitian. The core team met weekly throughout the year-long project and ensured other CF care providers were kept up-to-date on the changes implemented with the project.
Interventions
Outpatient Screening
The OGTT was added to a previously established protocol for all patients to complete their annual labs at their first visit of the year. We stressed the importance and rationale for the OGTT in an annual clinic letter sent to families. The family was also sent a reminder letter with fasting instructions, a copy of the annual lab orders, and a reminder telephone call before the appointment. Based on family input regarding delays in the turn-around time for venous blood samples, a point of care (POC) glucose protocol was implemented. Laboratory personnel drew annual blood work, completed a POC blood glucose (in addition to the serum glucose), and administered the oral glucose load if the POC glucose was < 200 mg/dL.
Subsequent to completion of our project, we learned that our lab had inadvertently administered a 37.5-g dose for the OGTT instead of the recommended 75-g dose. To identify patients who may have had CFRD but were not diagnosed due to the low oral glucose dose, we have screened all patients with the corrected dose since January 2013.
To improve communication between the pulmonary and endocrine teams, weekly meetings were scheduled. The teams reviewed patients who had recently completed their annual laboratory tests or recently saw an endocrinology provider. After review of lab values, the patient families were mailed letters informing them of their child’s glucose test results which were categorized as normal, impaired, or abnormal suggesting CFRD. If the patient did not complete the OGTT, the family was mailed a letter reiterating the importance of screening. In the event of an abnormal OGTT suggesting CFRD, the results were discussed with the family during a clinic appointment. The endocrinologist and diabetes educator were subsequently notified, and an endocrine clinic appointment was arranged with the family to discuss the results and care plan. An electronic dashboard (spreadsheet) was created to track lab values and clinic visits for patients with impaired blood glucose tolerance as well as CFRD. The dashboard was reviewed and updated on a quarterly basis.
Inpatient Screening
To improve screening of hospitalized patients with CF not known to have CFRD, 4 standardized order sets detailing blood glucose testing schedules were developed in our electronic medical record as listed below. Our team educated physicians and nurses on the standardized order sets as well as patient families about the additional testing needed during hospitalization. An endocrine nurse practitioner conducted daily rounds on weekdays. All glucose results were verified by the laboratory. If a patient was identified to have a fasting blood glucose ≥ 125 mg/dL or 2-hour postprandial ≥ 200 mg/dL, the endocrine service was notified, and additional glucose testing was ordered. If the patient’s glucose levels persisted at high levels, meeting the criteria for a diagnosis of CFRD, further education was provided for the family and follow-up care was arranged.
Order Sets
1) Not receiving G-tube feedings
Day 1: 2-hour postprandial
Day 2: Fasting
2) Receiving G-tube feedings
Day 1: 2-hour postprandial, 2-hours after start of
G-tube feeds and at end of G-tube feeds
3) Receiving low-dose steroid therapy (IV methylprednisolone up to 4 mg/kg per day, administered every 6 hours and oral prednisolone 1 mg/kg twice per day for 5 days) [12]
Day 1: 2-hour postprandial
Day 2: Fasting and 2-hour postprandial
Day 3: 2-hour postprandial
4) Receiving high-dose steroid therapy per the allergic bronchopulmonary aspergillosis protocol (IV methylprednisolone 10–15 mg/kg once per day for 3 days) [12]
Days 1-4: Point of care prior to every meal, at bedtime, and at 0200 hours
Analysis
All patients with CF who are seen at our clinic were included in this project. Approximately 96% of our patients have consented to be part of the CFF supported patient registry, PortCF [13]. Data are entered by the CF clinic nurse coordinator for these patients to document clinic visits, hospital admissions, medications, lab values, and other parameters. We retrieved data from PortCF documenting the number of patients eligible for the OGTT and the number of patients diagnosed with CFRD. Individual medical records were cross-referenced with these results and also reviewed for patients who do not participate in PortCF. We retrieved data reports from our hospital informatics department to identify the number of patients with CF who were hospitalized each year and to obtain all glucose levels obtained during hospitalization. From these data, we calculated screening rates and the annual number of patients diagnosed with CFRD. We used the Cochran’s Q test to compare the differences in frequency of screening across years.
Results
The newly implemented inpatient protocol, formally instituted in the third quarter of 2011, yielded a 43.8% screening rate in 2011 compared to a rate of 13.3% in 2010. Inpatient screening rates improved to 62.5% in 2012, and 77.8% in 2013 (Figures 3 and 4).
In 2011, 10 patients with CFRD were identified: 6 patients were diagnosed retrospectively based on a review of glucose levels collected in 2010 prior to the release of the new guidelines; 1 was diagnosed via inpatient screening; 3 were diagnosed via outpatient screening. In 2012, 5 patients with CFRD were identified: 4 were diagnosed via inpatient screening and one was diagnosed via outpatient screening. In 2013, 5 patients were identified: 1 diagnosed via inpatient screening and 4 diagnosed via outpatient screening. All diagnosed patients met the criteria of having a fasting blood sugar ≥ 126 mg/dL or a 2-hour postprandial ≥ 200 mg/dL that persisted for more than 48 hours.
Discussion
This collaborative initiative resulted in the development of structured screening protocols leading to overall screening improvement. A standardized screening protocol is fundamental to the identification and subsequent treatment of a patient with CFRD. Patients with CFRD may have decreased mortality when diagnosed early and treated aggressively, underscoring the necessity for CF centers to improve screening protocols [1,6].
Determining the best methods for implementation may vary from center to center, but the key factors we have identified from this project include strong leadership and team commitment—elements that have previously been identified as being predictive of positive quality improvement outcomes [14].
Education of staff, families, and patients is also an important factor. Education played a significant role during the inpatient screening PDSA cycles. For example, a time intensive but worthwhile training was conducted for the physicians and nurses on the order sets. Education for the patients and families during inpatient stays led to a better understanding of the rationale for, and support of, the additional blood draws.
The importance of family involvement was evident as we refined our outpatient protocol. Input from the phone surveys allowed us to identify barriers in our process that led us to establish more efficient clinic visits with reduced time in the lab, improved clinic flow and increased patient satisfaction. Other important factors were co-location of the endocrine and pulmonary clinics and flexibility of scheduling to facilitate seeing patients in both clinics on the same day.
Although we uncovered an error in oral glucose dosing, we were able to appropriately screen the majority of these patients within the next year. At the conclusion of 2013, our outpatient protocol had facilitated a screening rate of 95%, surpassing the 2012 rate of 77%. Interestingly, 2 of the patients diagnosed with CFRD in 2011 were diagnosed by HbA1c criteria, with normal OGTT results, perhaps due to the substandard glucose dose. Only 5 additional patients screened positive for CFRD at the end of 2013, which is the same number identified in 2012. It is unclear whether they would have been diagnosed earlier with the recommended dose of oral glucose or if they developed CFRD due to the progression of their disease.
A limitation of this project may be its reproducibility at other institutions. It is likely that the success of this project was due to the strong relationship between the endocrinology and pulmonary teams, committed leadership, institutional support for co-location of the clinics, and the team’s competency in quality improvement techniques with guidance from the LLC. The process of developing, implementing, and sustaining screening protocols was time-intensive and may be difficult to replicate in another center without similar resources available.
A strong motivation behind this project was the LLC, and while other centers may not have the same opportunity, the CFRD Evidence-Based Practice and Smart Change Idea Compendium was published as result of the LLC to serve as a guide for other centers [8]. Kern et al successfully demonstrated that a process based on the ideas from this compendium can help achieve higher OGTT outpatient screening rates in a CF center [15]. Kern et al’s project was similar to ours although the duration was shorter (< 1 year) and it began with a 47% screening rate prior to implementation. Our center extended the efforts of Kern et al by implementing our initiative over the course of 3 years, but unlike Kern et al, we included patients with failed or rescheduled appointments. Kern et al defined, identified, and excluded patients with moderate or severe pulmonary exacerbation from their eligible screening pool. We included all patients over the course of our year-long screening periods, as we have created an opportunity to screen ill patients at subsequent visits or as inpatients.
As with any quality improvement project, there is the risk of not sustaining improvements. In 2012 our outpatient screening rates were lower than the previous year. However, the coordination of the outpatient and inpatient protocols helped us achieve an improved overall screening rate of 92% in 2012. One possible explanation for the decrease in 2012 outpatient screening is that several patients eligible for screening in 2012 were less adherent with attending clinic visits. Five of these patients transitioned to an adult center or were diagnosed with CFRD in 2013. With this shift in the eligibility pool, our outpatient screening rate for 2013 surpassed our rate from 2012. In an attempt to sustain our gains, members of our team continue to review patient screening and endocrine referrals at monthly meetings. The decrease in outpatient screening demonstrates the importance of ongoing evaluation and monitoring of quality improvement projects after the initial objectives have been achieved.
Typically, our less adherent patients are only seen in clinic when experiencing an exacerbation when we cannot administer the OGTT. As a result, these patients are generally admitted for treatment of their exacerbation, and we are able to screen them during their hospitalization. Of the 9 patients not screened as outpatients in 2012, 7 were screened as inpatients. Three patients were unscreened that year: 1 patient failed to fast, another refused the test, and the last patient was inadvertently missed. While our intention is to screen all patients as an outpatient with OGTT, we have found that the only opportunity we have for screening less adherent patients is often while hospitalized, emphasizing the importance of a dual screening approach. This approach has allowed us to screen the majority of our patients as reflected in our overall screening rate.
One of our major challenges moving forward is to help the patients diagnosed with CFRD and their families accept yet another diagnosis and the burden of care associated with it. Our focus has shifted now to determine the best methods to motivate patients with CFRD to regularly attend endocrine clinic appointments, recognizing the challenges of additional clinic visits, monitoring, and medications. It is interesting to speculate whether improved CFRD clinical outcomes may correlate with improved screening rates. In 2012 our patients had a median HbA1c of 5.7 when the national average is 6.6 [16]. Further research is needed to delineate a possible relationship between an effective screening protocol and favorable clinical outcome measures.
Conclusion
The use of a structured process developed by a multidisciplinary team resulted in improved CFRD screening rates. In addition to outpatient protocols, it is critical to develop inpatient glucose testing protocols in order to capture patients who are only seen at times of exacerbation. Even in this era of treatment at a cellular level with correctors and potentiators, early detection and treatment of CFRD is essential for optimal clinical outcomes [1,5,17]. The next step for us is to sustain our gains and to improve endocrine care facilitation. We hope this report may guide other teams and institutional leadership in their efforts to improve identification of individuals with CFRD.
Acknowledgments: We would like to acknowledge Gautham Suresh, MD, Jennifer Abuzzahab, MD, Robert Payne, MD, and Andrew Flood, PhD, for their assistance in the preparation of our manuscript. We also acknowledge John Nash, MSW, LMSW, who provided us tools and coaching throughout the Learning and Leadership Collaborative.
Corresponding author: Lisa Read, MPH, 2525 Chicago Ave. South, MS 17-750, Minneapolis, MN 55404, [email protected].
Funding/support. This work was supported by a grant from the Cystic Fibrosis Foundation for the Learning and Leadership Collaborative: Cystic Fibrosis-Related Diabetes Care (MCNAMA11Q10, to Dr. McNamara).
1. Moran A, Dunitz J, Nathan B, et al. Cystic fibrosis–related diabetes: current trends in prevalence, incidence, and mortality. Diabetes Care 2009;32:1626–31.
2. Cawood TJ, McKenna MJ, Gallagher CG, et al. Cystic fibrosis-related diabetes in adults. Ir Med J 2006;99:83–6.
3. Koch C, Rainisio M, Madessani U, et al. Investigators of the European Epidemiologic Registry of Cystic Fibrosis. Presence of cystic fibrosis-related diabetes mellitus tightly linked to poor lung function in patients with cystic fibrosis: data from the European Epidemiologic Registry of Cystic Fibrosis. Pediatr Pulmonol 2001;32:343–50.
4. Marshall BC, Butler SM, Stoddard M, et al. Epidemiology of cystic fibrosis-related diabetes. J Pediatr 2005;146:681–7.
5. Milla CE, Billings J, Moran A. Diabetes is associated with dramatically decreased survival in female but not male subjects with cystic fibrosis. Diabetes Care 2005;28:2141–4.
6. Lewis C, Blackman SM, Nelson A, et al. Diabetes-related mortality in adults with cystic fibrosis. Role of genotype and sex. Am J Respir Crit Care Med 2015;191:194–200.
7. Moran A, Brunzell C, Cohen, RC, et al. Clinical Care guidelines for cystic fibrosis–related diabetes. A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care 2010;33:2697–708.
8. Nash J, Messier R, Casella SJ, et al. Learning and Leadership Collaborative: CFRD. Cystic fibrosis related diabetes (CFRD) evidence-based practice and smart change idea compendium 2012. Bethesda, MD: Cystic Fibrosis Foundation; McLean, VA: Pediatric Endocrine Society; Lebanon, NH: Dartmouth Institute Microsystem Academy; May 2012.
9. WHO Expert Committee on Diabetes Mellitus: Second Report of the WHO Expert Committee on Diabetes Mellitus. Geneva: World Health Organization; 1980 (Tech. Rep. Ser no. 646).
10. Cystic Fibrosis Foundation, Dartmouth Medical School: Center for the Evaluative Clinical Sciences, Dartmouth/Hitchcock Medical Center. Action guide for accelerating improvement in cystic fibrosis care: clinical microsystems. 2006.
11. Langley GJ, Nolan KM, Nolan TW, et al. The improvement guide: a practical approach to enhancing organizational performance. San Francisco, CA: Jossey-Bass; 1996.
12. Cohen-Cymberknoh M, Blau H, Shoseyov D, et al. Intravenous monthly pulse methylprednisolone treatment for ABPA in patients with cystic fibrosis. J Cyst Fibros 2009;8:253–7.
13. Center Specific Patient Registry Report for 2011. Bethesda, MD: Cystic Fibrosis Foundation; 2012.
14. Parker VA, Wubbenhorst WH, Young GJ, et al. Implementing quality improvement in hospitals: The role of leadership and culture. Am J Med Qual 1999; 14:64–9.
15. Kern AS, Prestridge AL. Improving screening for cystic fibrosis-related diabetes at a pediatric cystic fibrosis program. Pediatrics 2013;132:e512–8.
16. Center Specific Patient Registry Report for 2012. Bethesda, MD: Cystic Fibrosis Foundation; 2013.
17. Schwarzenberg SJ, Thomas W, Olsen TW, et al. Microvascular complications in cystic fibrosis-related diabetes. Diabetes Care 2007;30:1056–61.
1. Moran A, Dunitz J, Nathan B, et al. Cystic fibrosis–related diabetes: current trends in prevalence, incidence, and mortality. Diabetes Care 2009;32:1626–31.
2. Cawood TJ, McKenna MJ, Gallagher CG, et al. Cystic fibrosis-related diabetes in adults. Ir Med J 2006;99:83–6.
3. Koch C, Rainisio M, Madessani U, et al. Investigators of the European Epidemiologic Registry of Cystic Fibrosis. Presence of cystic fibrosis-related diabetes mellitus tightly linked to poor lung function in patients with cystic fibrosis: data from the European Epidemiologic Registry of Cystic Fibrosis. Pediatr Pulmonol 2001;32:343–50.
4. Marshall BC, Butler SM, Stoddard M, et al. Epidemiology of cystic fibrosis-related diabetes. J Pediatr 2005;146:681–7.
5. Milla CE, Billings J, Moran A. Diabetes is associated with dramatically decreased survival in female but not male subjects with cystic fibrosis. Diabetes Care 2005;28:2141–4.
6. Lewis C, Blackman SM, Nelson A, et al. Diabetes-related mortality in adults with cystic fibrosis. Role of genotype and sex. Am J Respir Crit Care Med 2015;191:194–200.
7. Moran A, Brunzell C, Cohen, RC, et al. Clinical Care guidelines for cystic fibrosis–related diabetes. A position statement of the American Diabetes Association and a clinical practice guideline of the Cystic Fibrosis Foundation, endorsed by the Pediatric Endocrine Society. Diabetes Care 2010;33:2697–708.
8. Nash J, Messier R, Casella SJ, et al. Learning and Leadership Collaborative: CFRD. Cystic fibrosis related diabetes (CFRD) evidence-based practice and smart change idea compendium 2012. Bethesda, MD: Cystic Fibrosis Foundation; McLean, VA: Pediatric Endocrine Society; Lebanon, NH: Dartmouth Institute Microsystem Academy; May 2012.
9. WHO Expert Committee on Diabetes Mellitus: Second Report of the WHO Expert Committee on Diabetes Mellitus. Geneva: World Health Organization; 1980 (Tech. Rep. Ser no. 646).
10. Cystic Fibrosis Foundation, Dartmouth Medical School: Center for the Evaluative Clinical Sciences, Dartmouth/Hitchcock Medical Center. Action guide for accelerating improvement in cystic fibrosis care: clinical microsystems. 2006.
11. Langley GJ, Nolan KM, Nolan TW, et al. The improvement guide: a practical approach to enhancing organizational performance. San Francisco, CA: Jossey-Bass; 1996.
12. Cohen-Cymberknoh M, Blau H, Shoseyov D, et al. Intravenous monthly pulse methylprednisolone treatment for ABPA in patients with cystic fibrosis. J Cyst Fibros 2009;8:253–7.
13. Center Specific Patient Registry Report for 2011. Bethesda, MD: Cystic Fibrosis Foundation; 2012.
14. Parker VA, Wubbenhorst WH, Young GJ, et al. Implementing quality improvement in hospitals: The role of leadership and culture. Am J Med Qual 1999; 14:64–9.
15. Kern AS, Prestridge AL. Improving screening for cystic fibrosis-related diabetes at a pediatric cystic fibrosis program. Pediatrics 2013;132:e512–8.
16. Center Specific Patient Registry Report for 2012. Bethesda, MD: Cystic Fibrosis Foundation; 2013.
17. Schwarzenberg SJ, Thomas W, Olsen TW, et al. Microvascular complications in cystic fibrosis-related diabetes. Diabetes Care 2007;30:1056–61.
Evaluation of a Diabetes Care Coordination Program for African-American Women Living in Public Housing
From the University of Kansas Work Group for Community Health and Development, Lawrence, KS (Hassaballa, Schultz, Hunter-Skidmore, Fawcett, Watson-Thompson) and Whittier Street Health Center, Boston, MA (Ebekozien, Ogungbadero, Williams)
Abstract
- Objective: To examine the implementation of the Diabetes Care Coordination Program (DCCP) and its effects on diabetes-related clinical health outcomes.
- Methods: Program participants were African American women (n = 148) with type 2 diabetes who lived in public housing in Boston’s Roxbury neighborhood. Through the DCCP, Whittier Street Health Center’s clinical team provided diabetes self-management education, support, and comprehensive diabetes care using the patient-centered medical home model and Diabetes Health Ambassadors as mediators for program delivery. Core intervention components of the DCCP included: 1) diabetes self-management education, 2) support for managing diabetes and distress, 3) enhancing access and linkage to care, 4) improving quality of care, 5) community organization, mobilization, and advocacy, and 6) health system and community transformation. A participatory monitoring and evaluation system was used to document and systematically reflect on program implementation.
- Results: DCCP implementation was associated with modest improvements in diabetes-related clinical health outcomes for program participants. Results showed statistically significant improvements in HbA1c (P = 0.016), weight (P = 0.021) and diastolic blood pressure (P = 0.027).
- Conclusion: Using neighborhood Diabetes Health Ambassadors for program delivery has implications for assuring access to quality diabetes care for populations experiencing health disparities.
The growing prevalence of type 2 diabetes, with its high morbidity and excess mortality, is imposing a heavy burden on the U.S. health care system [1–3]. It has been recognized that adoption of self-management skills by the person with diabetes is necessary in order to manage their diabetes. Diabetes self-management education and support (DSME/S) provides the foundation to help people with diabetes to navigate these decisions and activities and has been shown to improve health outcomes.
Compared to the general population, African Americans are disproportionately affected by diabetes. African Americans are also less likely to seek diabetes care and have routine diabetes-related visits with a health care professional [4,5]. African Americans have higher HbA1c levels, which contribute to the increased mortality and morbidity rates among this population [6]. Furthermore, African-American women have the poorest HbA1c control as compared to other groups [4]. Concentrated poverty and lower socioeconomic status are social determinants associated with higher prevalence of diabetes [7]. Economic barriers, living conditions, and the built environment play a significant role in contributing to this health disparity [8].
In 2010, the Bristol-Myers Squibb (BMS) Foundation launched the Together on Diabetes initiative to improve the health outcomes of adult populations disproportionately affected by type 2 diabetes. In November 2010, Together on Diabetes issued a request for proposals to encourage, identify, and promote new and evidence-based approaches to empower African-American women to control their diabetes [9–11], taking into account the opportunity these women have to influence the health of their families and communities. Whittier Street Health Center in Boston received a grant to implement a program that would connect African-American women living in public housing in the Roxbury neighborhood with comprehensive diabetes management, including health education by a certified diabetes educator, nutritional counseling by a dietitian, and a tailored program of physical activity.
In this article, we describe the project and effects on diabetes-related clinical health outcomes.
Methods
Setting
Whittier Street Health Center (WSHC) is a federally qualified community health center that serves over 25,000 patients annually. The WSHC is situated in the heart of Boston’s Roxbury neighborhood, close to 5 public housing developments; 83% of WSHC patients live in public housing units. Roxbury is an underserved neighborhood with high rates of poverty, violence, and disease [12]. African Americans comprise the majority of residents living in Roxbury, making up 55.6% of the total population [13].
Diabetes Care Coordination Program
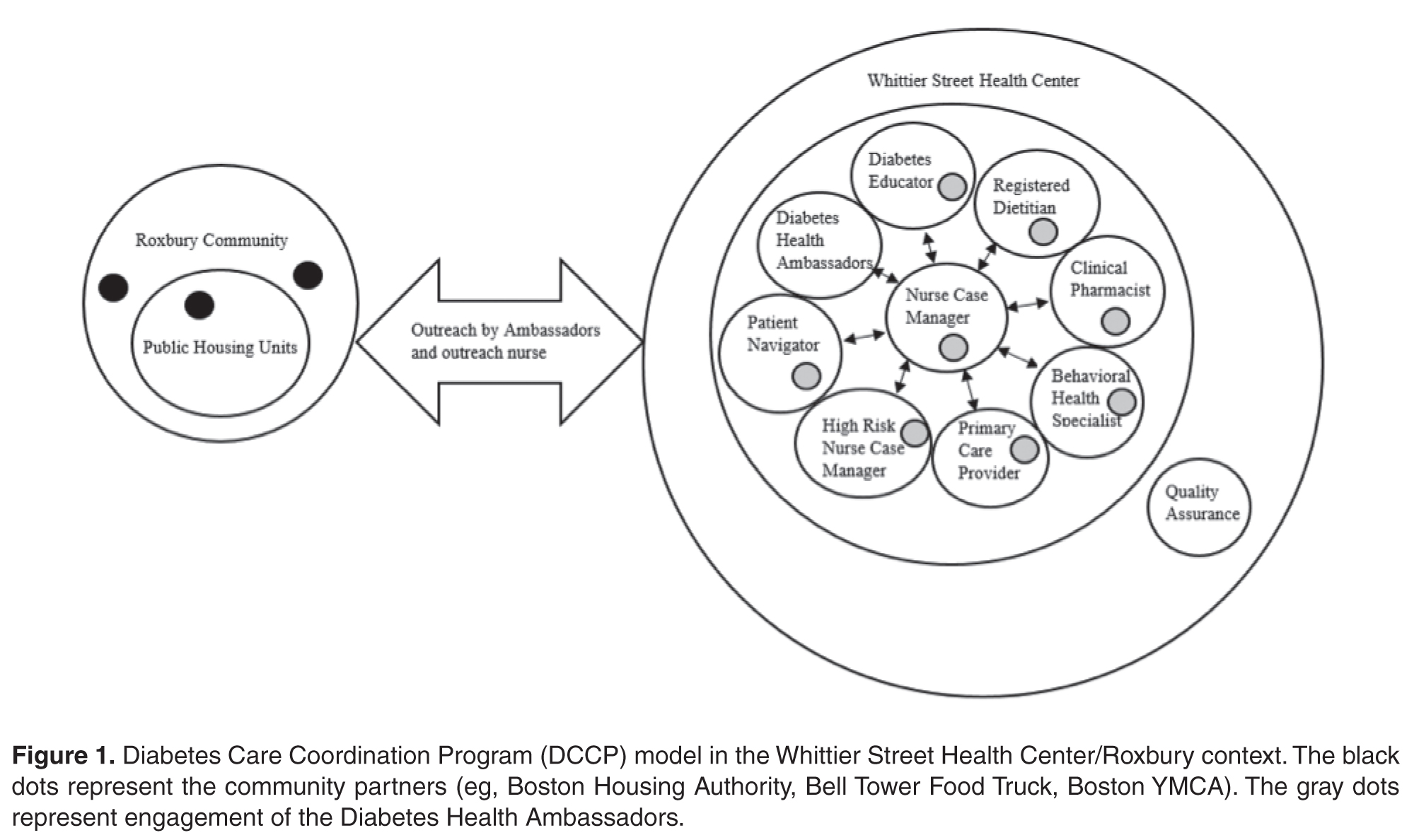
Ambassadors
Diabetes Health Ambassadors, a key component of the program, were hired to engage community members in managing their own health. Five Ambassadors were recruited and retained throughout the project period. Ambassadors were referred by their primary care provider at WSHC and interviewed for the job by the patient navigator. Ambassadors were required to be African-American women with type 2 diabetes living in a public housing unit within the Roxbury neighborhood. In addition, they were required to have their diabetes under control as defined by the WSHC clinical team (HbA1c of 8.0 or below). They also had to want to help other women control their diabetes and be able to deliver motivational presentations as well as have knowledge of available community resources.
Ambassadors received 30 hours of paid training from the certified diabetes educator. During training, they learned the definition, risk factors, and causes of diabetes, how it is controlled, and how to explain this information at a fifth-grade level. Modeling and feedback was used to assure that the information each Ambassador presented was accurate. Ambassadors were also trained on how to measure blood pressure and blood glucose levels and how to respectfully deliver the results. Additionally, Ambassadors received training on cultural competence. Ambassadors were engaged in community outreach and patient support for 20 hours per week and were compensated for their time with stipends.
Participant Recruitment and Outreach
A rolling enrollment for the DCCP began January 2012. The outreach team from the WSHC attended coffee hours at the public housing units and other community events where they conducted onsite blood pressure and glucose screenings as well as educated community members on healthy eating and active lifestyle to reduce the risks for diabetes. Mobile kits were used for testing, so participants received the test results immediately. Two Ambassadors, the outreach nurse, and the patient navigator conducted the outreach events. The set up included two tables, 6 chairs, education materials, and blood pressure and blood sugar screening materials.
Screenings were offered in the public housing units 3 times a week (twice during the week and once during the weekend). Posters in the neighborhood notifed women of the time and location of the screenings. Other settings for services such as screenings and referrals to primary care and health insurance applications included churches, mosques, community festivals, farmers markets, parks, and hair salons.
Women who had elevated glucose readings were invited to enroll in the DCCP program and an appointment at the WSHC was made for those who signed up.
During the period January 2012 to June 2013, 980 African-American women were screened for diabetes. Most screenings took place in the public housing units. Among those screened, 340 had an elevated blood glucose and were referred to WSHC for services. Of those, 175 women were recruited and enrolled into the DCCP. At the WSHC, a standardized protocol was used to measure HbA1c to confirm a diagnosis of diabetes once patients attended their first appointment. Age of participants ranged from 40 to 49. Most women were unemployed and had many competing responsibilities and stressors. Completed preassessment questionaires indicated that participants did not engage in healthy eating or physical activity as part of their daily routines prior to enrollment.
Program Components
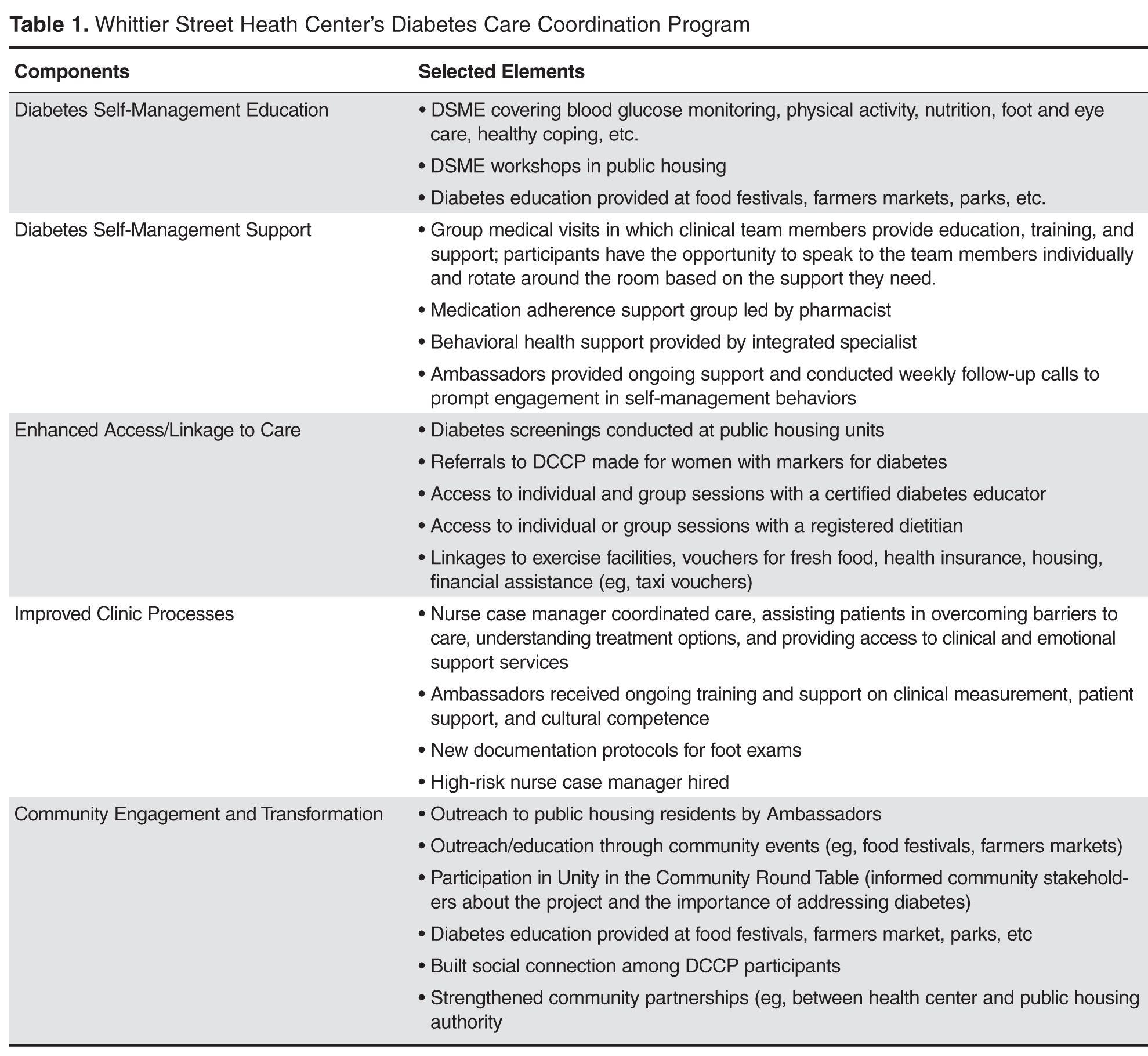
At the Center, Ambassadors spoke with program participants and inquired about their barriers to diabetes care (eg, access to food [15], health insurance, etc.) using a standardized list. Ambassadors linked program participants to community support services as needed, including health insurance enrollment, financial support, and housing support. Services were also provided in collaboration with community organizations. For example, subsidized gym memberships were available at the local YMCA and a local fitness studio, and there was an instructor at the YMCA to guide the women through physical activity routines.
Participants could attend DSME group sessions provided by the certified diabetes educator. The course met twice a week for 2 hours for a period of 6 weeks. The course was interactive and included hands-on training in blood glucose measurement and food preparation. Healthy food was offered after each session, which provided a further opportunity for participants to engage in peer-to-peer support. After the completion of the DSME course, bi-weekly support group sessions were held until program completion (June 2013). All clinical team members were present at the support group sessions, with patients rotating to speak to them to ask questions or discuss concerns related to self-management.
A part of DSME, the registered dietitian provided nutrition information and healthy cooking demonstrations for program participants within group sessions. The primary care physician met the patient once a month and kept track of clinical changes over time. Patients with HbA1c ≥ 9% were referred to the high-risk nurse case manager who worked one-on-one with program participants to help them avoid serious diabetes complications.
Ambassadors were a part of all the course and support group sessions, and when needed they attended indivdual sessions, such as doctor visits and meetings with the high-risk nurse case manager. Ambassadors accompanied program participants during visits with clinical staff to provide additional support when requested.
The manager of quality assurance assured the safety of intervention procedures and employed performance improvement methods. Program participants provided informed consent, and had the right to withdraw at any time. The Quality Assurance Committee at WSHC protected the rights of participants, assured the safety of intervention procedures, and assured the quality of care received by each participant.
Evaluation
The Work Group for Community Health and Development at the University of Kansas was selected by the BMS Foundation to evaluate the implementation and related clinical outcomes of the program using a participatory evaluation framework [16–18]. A similarly funded study used the same study approach [19]. Clinical health outcomes were analyzed through a pre-post test comparison using STATA Version 12. Paired t tests were used to examine within-patient health outcome changes. The mean interval between the pre and post measurements was 16 months. A 0.05 level of significance was used. Using a one-sided t test, Cohen’s d was computed to measure effect size.
Results
Services
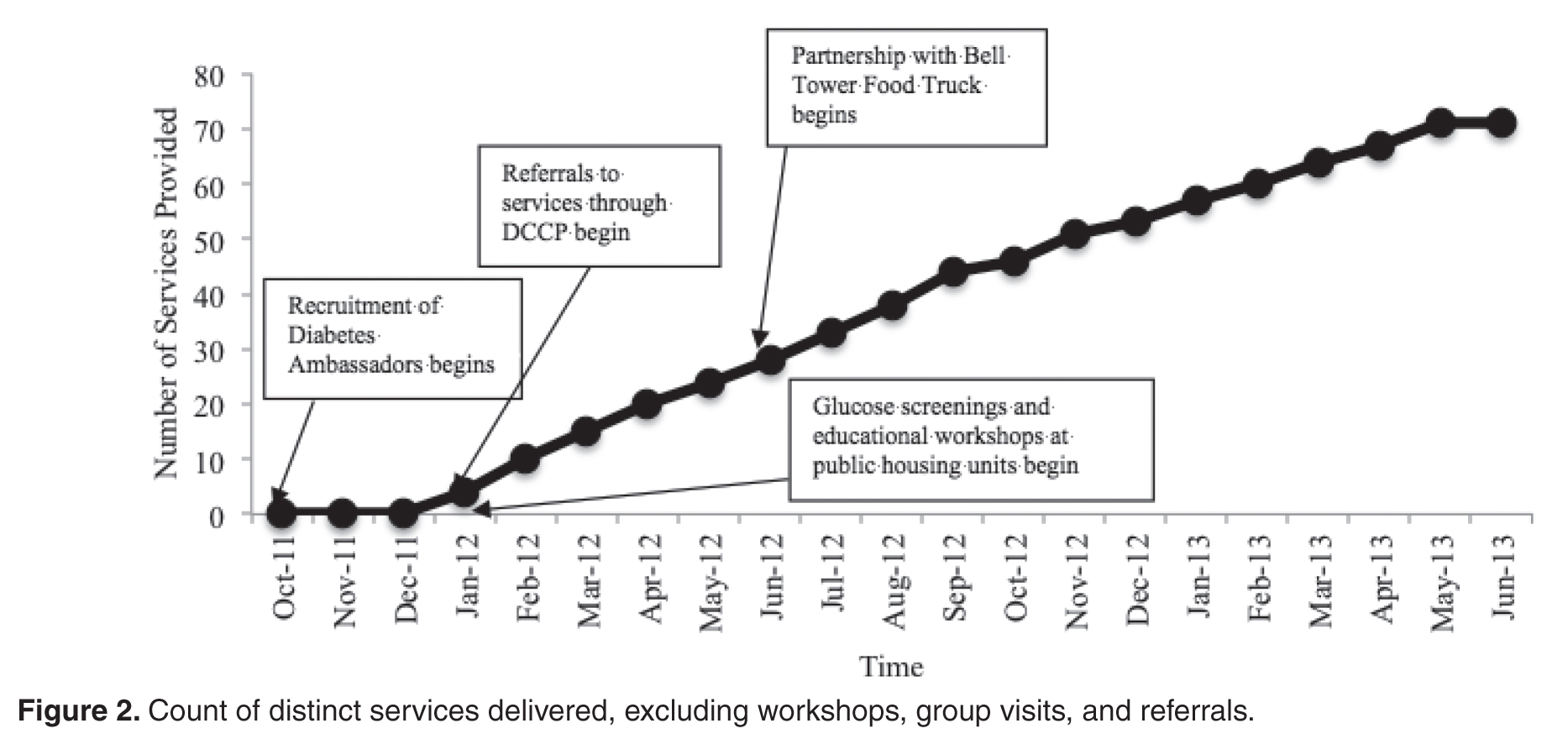
Clinical Outcomes
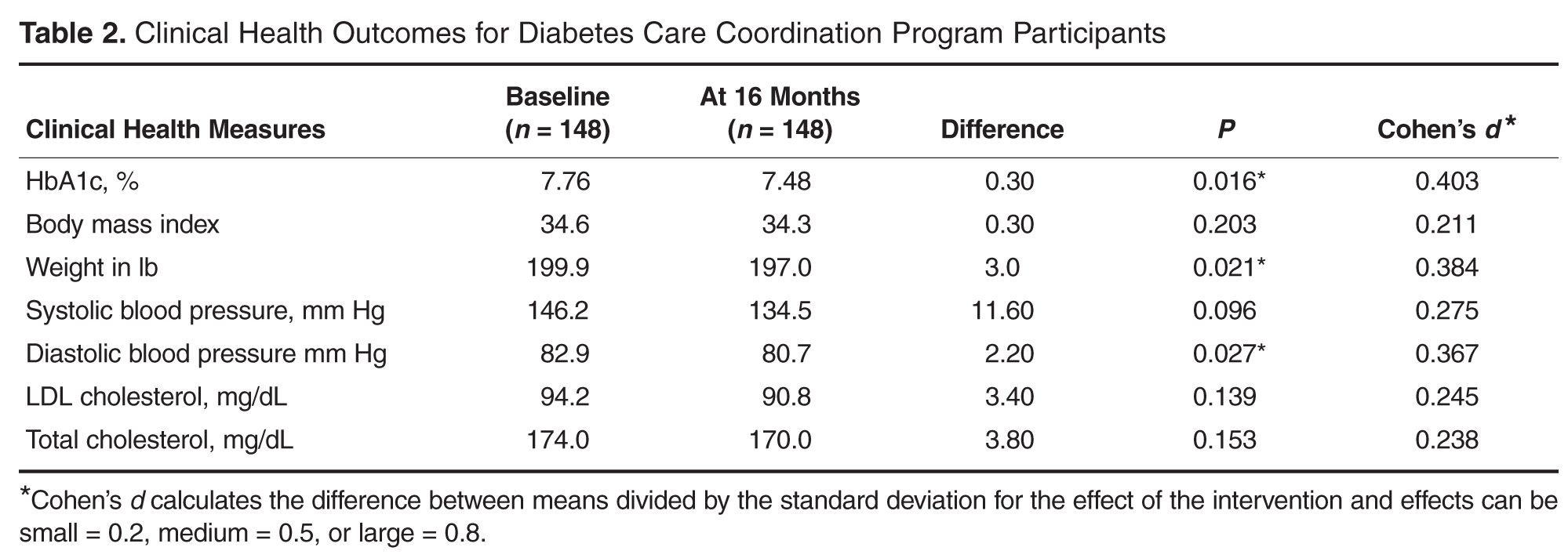
Discussion
This empirical case study examined the implementation of the Diabetes Care Coordination Program (DCCP) and its effects on diabetes-related clinical health outcomes for program participants. The program’ glucose screenings and educational workshops at public housing units provided enhanced access to diabetes care services for community members. Referrals to WSHC allowed for the provision of clinical health services through a comprehensive care model. Modest improvements in diabetes-related clinical health indicators were seen.
Some challenges were noted during implementation of the DCCP and addressed as part of a quality improvement process. First, Diabetes Health Ambassadors originally went door to door and had difficulty recruiting participants. Holding screening events in public spaces within housing units addressed this problem. Second, the WSHC team found that women needed more behavioral health support than was being provided, with some of the women reporting to their case managers that it was difficult for them to handle the stresses of life and at the same time manage their diabetes. In response, an integrated behavioral health specialist was hired to provide guidance on how to manage life stressors and how to increase health behaviors despite physical, social, and financial barriers.
Third, women reported a lack of access to fresh fruits and vegetables. In response, WSHC implemented a formal collaboration with a mobile food truck (June 2012) that sold subsidized fresh food 3 days a week to public housing residents. Fourth, participants reported some barriers related to transportation for scheduled appointments at the WSHC. The team addressed this issue by providing taxi vouchers for those who lacked adequate access to transportation. Finally, the coordinated team noticed that medication adherence was a barrier to care for many program participants. Consequently, they developed a medication management support group led by the clinical pharmacist to address barriers related to medication adherence.
There were several methodological challenges confronted in carrying out this study. First, the dose of services that were provided for each individual participant was difficult to ascertain. For example, some of those enrolled in the DCCP earlier may not have had the full set of services that were available towards the end of the program. Second, although group data were available, data on individual level outcomes were not; this made it difficult to assess whether there was change in behavior on the part of particular individuals. Third, a case study design, without a comparison group, does not control for threats to internal validity (eg, history, maturation, and attrition) that might have accounted for improvements in clinical outcomes. Finally, despite the comprehensive documentation, there could have been program elements that were implemented but not documented. Despite these methodological limitations, the case study design facilitated learning about associations between program implementation and changes in clinical health outcomes in a context of health disparities [20].
A particular strength of the program was use of Diabetes Health Ambassadors as mediators for DCCP service delivery. Ambassadors increased diabetes awareness within the community and also played a key role in building rapport and trust in the diabetes program among community members.
Lessons Learned
As part of a qualitative component, key informant interviews with WSHC staff were used to examine lessons learned during project implementation. First, an identified positive outcome was that the Ambassadors gained new insights into the management of their own diabetes and adopted additional lifestyle changes along with program participants. Second, the WSHC team affirmed that African-American women act as gatekeepers for their families, and that teaching and serving one woman allowed for teaching and serving the entire family. Program participants reported that their own lifestyle changes had an impact on other family members. For example, one participant reported she stopped purchasing soda beverages for her family. Another participant began using healthier cooking strategies, such as using olive oil instead of butter. Third, consistent with another study, the coordinated care model helped to assure comprehensive diabetes care [21]. Staff noted that “it takes a village” (a coordinated team) to address the diverse array of clinical issues needed for diabetes control. Fourth, self-management education was helpful, especially when coupled with social support from peers and family members. Fifth, working collaboratively with partners in non-health sectors was helpful in achieving the conditions needed for improved diabetes care [22].
Recommendations for Future Research and Practice
There are several recommendations for future research and practice. First, to achieve stronger clinical health outcomes, the DCCP would need to be enhanced by assuring lower caseloads for the WSHC clinical team. Second, to expand the evidence base, stronger experimental designs are needed to draw firmer conclusions about causal relationships. For instance, a multiple-baseline design across similar federally qualified heath centers could enable a better understanding of the effects of this community-based DCCP intervention in urban contexts. Third, research and practice would benefit from further testing of the model using community health workers for delivery of DSME and DSMS services. Fourth, implementation science can aid in enhancing the role of Ambassadors by providing tools/frameworks for improved delivery of services such as the core implementation components of selection and training [23]. Finally, the use of behavioral science methods can help extend the evidence base for the effects of the DCCP intervention on behavior change at the individual and the community levels [24,25].
Conclusion
This empirical case study adds to our understanding of delivering community-based diabetes care in a public housing context. This study examined the implementation and effects of a diabetes program for African-American women experiencing health disparities. The delivery of diabetes services by Diabetes Health Ambassadors was effective in engaging women with diabetes who lived in low-income housing. This study provided further evidence that coordinated diabetes care, with a focus on culturally and contextually appropriate service delivery, can have positive health outcomes. Further research is needed to examine effects of the DCCP intervention at the individual, clinic, family, and community levels.
Addressing the rapidly increasing prevalence of diabetes is a huge challenge, especially among vulnerable populations at disproportionate risk for adverse health outcomes. These patients face physical, emotional, and financial burdens. We need to assure that community health workers and coordinated clinical teams are prepared to support patients’ acquisition and maintenance of self-care behaviors. Eliminating diabetes-related disparities requires modifying the health system and the broader community environment [26]. Addressing the barriers to medical and self-care that vulnerable populations with type 2 diabetes face will provide them with greater opportunities for health and well-being.
Acknowledgments: The authors thank the many community partners throughout Boston that made this project possible.
Corresponding author: Ithar Hassaballa, KU Work Group for Community Health and Development, University of Kansas, 1000 Sunnyside Ave, 4082 Dole Center, Lawrence, KS 66045, [email protected].
Funding/support: Funding for the Whittier Street Health Center’s Diabetes Care Coordination Program and for the evaluation of the Together on Diabetes initiative was provided by the Bristol-Myers Squibb Foundation.
Financial disclosures: None.
1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047–53.
2. Centers for Disease Control and Prevention. National diabetes statistics report: estimates of diabetes and its burden in the United States, 2014. Atlanta: U.S. Department of Health and Human Services; 2014.
3. Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S., 2005-2050. Diabetes Care 2006;29:2114–6.
4. Tang TS, Brown MB, Funnell MM, Anderson RM. Social support, quality of life, and self-care behaviors among African Americans with type 2 diabetes. Diabetes Educ 2008;34:266-76.
5. Crabtree K, Sherrer N, Rushton T, Willig A, Agne A, Shelton T, Cherrington A. Diabetes connect: African American men's preferences for a community-based diabetes management program. Diabetes Educ 2015;41:118-26.
6. Kirk JK, D'Agostino RB Jr, Bell RA, Passmore LV, Bonds DE, Karter AJ, Narayan KM. Disparities in HbA1c levels between African-American and non-Hispanic white adults with diabetes: a meta-analysis. Diabetes Care 2006;29:2130–6.
7. Batts ML, Gary TL, Huss K, Hill MN, Bone L, Brancati FL. Patient priorities and needs for diabetes care among urban African American adults. Diabetes Educ 2001;27:405–12.
8. Horowitz CR, Colson KA, Hebert PL, Lancaster K. Barriers to buying healthy foods for people with diabetes: evidence of environmental disparities. Am J Public Health 2004;94:1549–54.
9. Haas L, Maryniuk M, Beck J, et al; 2012 Standards Revision Task Force. National standards for diabetes self-management education and support. Diabetes Care 2013;36 Suppl 1:S100–8.
10. Cené CW, Haymore LB, Ellis D, Whitaker S, Henderson S, Lin FC, Corbie-Smith G. Implementation of the power to prevent diabetes prevention educational curriculum into rural African American communities: a feasibility study. Diabetes Educ 2013;39:776–85.
11. Feathers JT, Kieffer EC, Palmisano G, et al. The development, implementation, and process evaluation of the REACH Detroit Partnership's Diabetes Lifestyle Intervention. Diabetes Educ 2007;33:509–20.
12. Rahman S, Hu H, McNeely E, et al. Social and environmental risk factors for hypertension in African Americans. Fla Public Health Rev 2008;5:64–72.
13. US Bureau of the Census. Available at www.cityofboston.gov/dnd/PDR/Maps_and_Neighborhood_Profiles.asp.
14. Reid RJ, Coleman K, Johnson EA, Fishman PA, Hsu C, Soman MP, Trescott CE, Erikson M, Larson EB. The Group Health medical home at year two: cost savings, higher patient satisfaction, and less burnout for providers. Health Aff (Millwood) 2010;29:835–43.
15. Fulp RS, McManus KD, Johnson PA. Barriers to purchasing foods for a high-quality, healthy diet in a low-income African American community. Fam Community Health 2009;32:206–17.
16. Fawcett SB, Schultz JA. Supporting participatory evaluation using the Community Tool Box online documentation system. Community-Based Participatory Research for Health. San Francisco: Jossey-Bass; 2008: 419–23.
17. Collie-Akers V, Schultz JA, Carson V, Fawcett SB, Ronan M. REACH 2010: Kansas City, Missouri evaluating mobilization strategies with neighborhood and faith organizations to reduce risk for health disparities. Health Prom Pract 2009;10(Suppl 2):118S–127S.
18. Fawcett SB, Boothroyd R, Schultz JA, Francisco VT, Carson V, Bremby R. Building capacity for participatory evaluation within community initiatives. J Prev Interven Comm 2003;26:21–36.
19. Sepers CE Jr, Fawcett SB, Lipman R, Schultz J, Colie-Akers V, Perez A. Measuring the implementation and effects of a coordinated care model featuring diabetes self-management education within four patient-centered medical homes. Diabetes Educ 2015;41:328–42.
20. Yin RK. Case study research: Design and methods. Sage; 2013.
21. Mead H, Andres E, Regenstein M. Underserved patients' perspectives on patient-centered primary care: does the patient-centered medical home model meet their needs? Med Care Res Rev 2014;71:61–84.
22. Fawcett S, Schultz J, Watson-Thompson J, Fox M, Bremby R. Building multisectoral partnerships for population health and health equity. Prev Chronic Disease 2010;7:A118. Epub 2010 Oct 15.
23. Fixsen DL, Blase KA, Naoom SF, Wallace F. Core implementation components. Res Soc Work Prac 2009; 19:531–540.
24. Cooper JO, Heron TE, Heward WL. Applied behavior analysis. 2nd ed. Pearson; 2007.
25. Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health 2010;31:399–418.
26. Jack L, Jack NH, Hayes SC. Social determinants of health in minority populations: a call for multidisciplinary approaches to eliminate diabetes-related health disparities. Diabetes Spectrum 2012;25:9–13.
From the University of Kansas Work Group for Community Health and Development, Lawrence, KS (Hassaballa, Schultz, Hunter-Skidmore, Fawcett, Watson-Thompson) and Whittier Street Health Center, Boston, MA (Ebekozien, Ogungbadero, Williams)
Abstract
- Objective: To examine the implementation of the Diabetes Care Coordination Program (DCCP) and its effects on diabetes-related clinical health outcomes.
- Methods: Program participants were African American women (n = 148) with type 2 diabetes who lived in public housing in Boston’s Roxbury neighborhood. Through the DCCP, Whittier Street Health Center’s clinical team provided diabetes self-management education, support, and comprehensive diabetes care using the patient-centered medical home model and Diabetes Health Ambassadors as mediators for program delivery. Core intervention components of the DCCP included: 1) diabetes self-management education, 2) support for managing diabetes and distress, 3) enhancing access and linkage to care, 4) improving quality of care, 5) community organization, mobilization, and advocacy, and 6) health system and community transformation. A participatory monitoring and evaluation system was used to document and systematically reflect on program implementation.
- Results: DCCP implementation was associated with modest improvements in diabetes-related clinical health outcomes for program participants. Results showed statistically significant improvements in HbA1c (P = 0.016), weight (P = 0.021) and diastolic blood pressure (P = 0.027).
- Conclusion: Using neighborhood Diabetes Health Ambassadors for program delivery has implications for assuring access to quality diabetes care for populations experiencing health disparities.
The growing prevalence of type 2 diabetes, with its high morbidity and excess mortality, is imposing a heavy burden on the U.S. health care system [1–3]. It has been recognized that adoption of self-management skills by the person with diabetes is necessary in order to manage their diabetes. Diabetes self-management education and support (DSME/S) provides the foundation to help people with diabetes to navigate these decisions and activities and has been shown to improve health outcomes.
Compared to the general population, African Americans are disproportionately affected by diabetes. African Americans are also less likely to seek diabetes care and have routine diabetes-related visits with a health care professional [4,5]. African Americans have higher HbA1c levels, which contribute to the increased mortality and morbidity rates among this population [6]. Furthermore, African-American women have the poorest HbA1c control as compared to other groups [4]. Concentrated poverty and lower socioeconomic status are social determinants associated with higher prevalence of diabetes [7]. Economic barriers, living conditions, and the built environment play a significant role in contributing to this health disparity [8].
In 2010, the Bristol-Myers Squibb (BMS) Foundation launched the Together on Diabetes initiative to improve the health outcomes of adult populations disproportionately affected by type 2 diabetes. In November 2010, Together on Diabetes issued a request for proposals to encourage, identify, and promote new and evidence-based approaches to empower African-American women to control their diabetes [9–11], taking into account the opportunity these women have to influence the health of their families and communities. Whittier Street Health Center in Boston received a grant to implement a program that would connect African-American women living in public housing in the Roxbury neighborhood with comprehensive diabetes management, including health education by a certified diabetes educator, nutritional counseling by a dietitian, and a tailored program of physical activity.
In this article, we describe the project and effects on diabetes-related clinical health outcomes.
Methods
Setting
Whittier Street Health Center (WSHC) is a federally qualified community health center that serves over 25,000 patients annually. The WSHC is situated in the heart of Boston’s Roxbury neighborhood, close to 5 public housing developments; 83% of WSHC patients live in public housing units. Roxbury is an underserved neighborhood with high rates of poverty, violence, and disease [12]. African Americans comprise the majority of residents living in Roxbury, making up 55.6% of the total population [13].
Diabetes Care Coordination Program
Ambassadors
Diabetes Health Ambassadors, a key component of the program, were hired to engage community members in managing their own health. Five Ambassadors were recruited and retained throughout the project period. Ambassadors were referred by their primary care provider at WSHC and interviewed for the job by the patient navigator. Ambassadors were required to be African-American women with type 2 diabetes living in a public housing unit within the Roxbury neighborhood. In addition, they were required to have their diabetes under control as defined by the WSHC clinical team (HbA1c of 8.0 or below). They also had to want to help other women control their diabetes and be able to deliver motivational presentations as well as have knowledge of available community resources.
Ambassadors received 30 hours of paid training from the certified diabetes educator. During training, they learned the definition, risk factors, and causes of diabetes, how it is controlled, and how to explain this information at a fifth-grade level. Modeling and feedback was used to assure that the information each Ambassador presented was accurate. Ambassadors were also trained on how to measure blood pressure and blood glucose levels and how to respectfully deliver the results. Additionally, Ambassadors received training on cultural competence. Ambassadors were engaged in community outreach and patient support for 20 hours per week and were compensated for their time with stipends.
Participant Recruitment and Outreach
A rolling enrollment for the DCCP began January 2012. The outreach team from the WSHC attended coffee hours at the public housing units and other community events where they conducted onsite blood pressure and glucose screenings as well as educated community members on healthy eating and active lifestyle to reduce the risks for diabetes. Mobile kits were used for testing, so participants received the test results immediately. Two Ambassadors, the outreach nurse, and the patient navigator conducted the outreach events. The set up included two tables, 6 chairs, education materials, and blood pressure and blood sugar screening materials.
Screenings were offered in the public housing units 3 times a week (twice during the week and once during the weekend). Posters in the neighborhood notifed women of the time and location of the screenings. Other settings for services such as screenings and referrals to primary care and health insurance applications included churches, mosques, community festivals, farmers markets, parks, and hair salons.
Women who had elevated glucose readings were invited to enroll in the DCCP program and an appointment at the WSHC was made for those who signed up.
During the period January 2012 to June 2013, 980 African-American women were screened for diabetes. Most screenings took place in the public housing units. Among those screened, 340 had an elevated blood glucose and were referred to WSHC for services. Of those, 175 women were recruited and enrolled into the DCCP. At the WSHC, a standardized protocol was used to measure HbA1c to confirm a diagnosis of diabetes once patients attended their first appointment. Age of participants ranged from 40 to 49. Most women were unemployed and had many competing responsibilities and stressors. Completed preassessment questionaires indicated that participants did not engage in healthy eating or physical activity as part of their daily routines prior to enrollment.
Program Components
At the Center, Ambassadors spoke with program participants and inquired about their barriers to diabetes care (eg, access to food [15], health insurance, etc.) using a standardized list. Ambassadors linked program participants to community support services as needed, including health insurance enrollment, financial support, and housing support. Services were also provided in collaboration with community organizations. For example, subsidized gym memberships were available at the local YMCA and a local fitness studio, and there was an instructor at the YMCA to guide the women through physical activity routines.
Participants could attend DSME group sessions provided by the certified diabetes educator. The course met twice a week for 2 hours for a period of 6 weeks. The course was interactive and included hands-on training in blood glucose measurement and food preparation. Healthy food was offered after each session, which provided a further opportunity for participants to engage in peer-to-peer support. After the completion of the DSME course, bi-weekly support group sessions were held until program completion (June 2013). All clinical team members were present at the support group sessions, with patients rotating to speak to them to ask questions or discuss concerns related to self-management.
A part of DSME, the registered dietitian provided nutrition information and healthy cooking demonstrations for program participants within group sessions. The primary care physician met the patient once a month and kept track of clinical changes over time. Patients with HbA1c ≥ 9% were referred to the high-risk nurse case manager who worked one-on-one with program participants to help them avoid serious diabetes complications.
Ambassadors were a part of all the course and support group sessions, and when needed they attended indivdual sessions, such as doctor visits and meetings with the high-risk nurse case manager. Ambassadors accompanied program participants during visits with clinical staff to provide additional support when requested.
The manager of quality assurance assured the safety of intervention procedures and employed performance improvement methods. Program participants provided informed consent, and had the right to withdraw at any time. The Quality Assurance Committee at WSHC protected the rights of participants, assured the safety of intervention procedures, and assured the quality of care received by each participant.
Evaluation
The Work Group for Community Health and Development at the University of Kansas was selected by the BMS Foundation to evaluate the implementation and related clinical outcomes of the program using a participatory evaluation framework [16–18]. A similarly funded study used the same study approach [19]. Clinical health outcomes were analyzed through a pre-post test comparison using STATA Version 12. Paired t tests were used to examine within-patient health outcome changes. The mean interval between the pre and post measurements was 16 months. A 0.05 level of significance was used. Using a one-sided t test, Cohen’s d was computed to measure effect size.
Results
Services
Clinical Outcomes
Discussion
This empirical case study examined the implementation of the Diabetes Care Coordination Program (DCCP) and its effects on diabetes-related clinical health outcomes for program participants. The program’ glucose screenings and educational workshops at public housing units provided enhanced access to diabetes care services for community members. Referrals to WSHC allowed for the provision of clinical health services through a comprehensive care model. Modest improvements in diabetes-related clinical health indicators were seen.
Some challenges were noted during implementation of the DCCP and addressed as part of a quality improvement process. First, Diabetes Health Ambassadors originally went door to door and had difficulty recruiting participants. Holding screening events in public spaces within housing units addressed this problem. Second, the WSHC team found that women needed more behavioral health support than was being provided, with some of the women reporting to their case managers that it was difficult for them to handle the stresses of life and at the same time manage their diabetes. In response, an integrated behavioral health specialist was hired to provide guidance on how to manage life stressors and how to increase health behaviors despite physical, social, and financial barriers.
Third, women reported a lack of access to fresh fruits and vegetables. In response, WSHC implemented a formal collaboration with a mobile food truck (June 2012) that sold subsidized fresh food 3 days a week to public housing residents. Fourth, participants reported some barriers related to transportation for scheduled appointments at the WSHC. The team addressed this issue by providing taxi vouchers for those who lacked adequate access to transportation. Finally, the coordinated team noticed that medication adherence was a barrier to care for many program participants. Consequently, they developed a medication management support group led by the clinical pharmacist to address barriers related to medication adherence.
There were several methodological challenges confronted in carrying out this study. First, the dose of services that were provided for each individual participant was difficult to ascertain. For example, some of those enrolled in the DCCP earlier may not have had the full set of services that were available towards the end of the program. Second, although group data were available, data on individual level outcomes were not; this made it difficult to assess whether there was change in behavior on the part of particular individuals. Third, a case study design, without a comparison group, does not control for threats to internal validity (eg, history, maturation, and attrition) that might have accounted for improvements in clinical outcomes. Finally, despite the comprehensive documentation, there could have been program elements that were implemented but not documented. Despite these methodological limitations, the case study design facilitated learning about associations between program implementation and changes in clinical health outcomes in a context of health disparities [20].
A particular strength of the program was use of Diabetes Health Ambassadors as mediators for DCCP service delivery. Ambassadors increased diabetes awareness within the community and also played a key role in building rapport and trust in the diabetes program among community members.
Lessons Learned
As part of a qualitative component, key informant interviews with WSHC staff were used to examine lessons learned during project implementation. First, an identified positive outcome was that the Ambassadors gained new insights into the management of their own diabetes and adopted additional lifestyle changes along with program participants. Second, the WSHC team affirmed that African-American women act as gatekeepers for their families, and that teaching and serving one woman allowed for teaching and serving the entire family. Program participants reported that their own lifestyle changes had an impact on other family members. For example, one participant reported she stopped purchasing soda beverages for her family. Another participant began using healthier cooking strategies, such as using olive oil instead of butter. Third, consistent with another study, the coordinated care model helped to assure comprehensive diabetes care [21]. Staff noted that “it takes a village” (a coordinated team) to address the diverse array of clinical issues needed for diabetes control. Fourth, self-management education was helpful, especially when coupled with social support from peers and family members. Fifth, working collaboratively with partners in non-health sectors was helpful in achieving the conditions needed for improved diabetes care [22].
Recommendations for Future Research and Practice
There are several recommendations for future research and practice. First, to achieve stronger clinical health outcomes, the DCCP would need to be enhanced by assuring lower caseloads for the WSHC clinical team. Second, to expand the evidence base, stronger experimental designs are needed to draw firmer conclusions about causal relationships. For instance, a multiple-baseline design across similar federally qualified heath centers could enable a better understanding of the effects of this community-based DCCP intervention in urban contexts. Third, research and practice would benefit from further testing of the model using community health workers for delivery of DSME and DSMS services. Fourth, implementation science can aid in enhancing the role of Ambassadors by providing tools/frameworks for improved delivery of services such as the core implementation components of selection and training [23]. Finally, the use of behavioral science methods can help extend the evidence base for the effects of the DCCP intervention on behavior change at the individual and the community levels [24,25].
Conclusion
This empirical case study adds to our understanding of delivering community-based diabetes care in a public housing context. This study examined the implementation and effects of a diabetes program for African-American women experiencing health disparities. The delivery of diabetes services by Diabetes Health Ambassadors was effective in engaging women with diabetes who lived in low-income housing. This study provided further evidence that coordinated diabetes care, with a focus on culturally and contextually appropriate service delivery, can have positive health outcomes. Further research is needed to examine effects of the DCCP intervention at the individual, clinic, family, and community levels.
Addressing the rapidly increasing prevalence of diabetes is a huge challenge, especially among vulnerable populations at disproportionate risk for adverse health outcomes. These patients face physical, emotional, and financial burdens. We need to assure that community health workers and coordinated clinical teams are prepared to support patients’ acquisition and maintenance of self-care behaviors. Eliminating diabetes-related disparities requires modifying the health system and the broader community environment [26]. Addressing the barriers to medical and self-care that vulnerable populations with type 2 diabetes face will provide them with greater opportunities for health and well-being.
Acknowledgments: The authors thank the many community partners throughout Boston that made this project possible.
Corresponding author: Ithar Hassaballa, KU Work Group for Community Health and Development, University of Kansas, 1000 Sunnyside Ave, 4082 Dole Center, Lawrence, KS 66045, [email protected].
Funding/support: Funding for the Whittier Street Health Center’s Diabetes Care Coordination Program and for the evaluation of the Together on Diabetes initiative was provided by the Bristol-Myers Squibb Foundation.
Financial disclosures: None.
From the University of Kansas Work Group for Community Health and Development, Lawrence, KS (Hassaballa, Schultz, Hunter-Skidmore, Fawcett, Watson-Thompson) and Whittier Street Health Center, Boston, MA (Ebekozien, Ogungbadero, Williams)
Abstract
- Objective: To examine the implementation of the Diabetes Care Coordination Program (DCCP) and its effects on diabetes-related clinical health outcomes.
- Methods: Program participants were African American women (n = 148) with type 2 diabetes who lived in public housing in Boston’s Roxbury neighborhood. Through the DCCP, Whittier Street Health Center’s clinical team provided diabetes self-management education, support, and comprehensive diabetes care using the patient-centered medical home model and Diabetes Health Ambassadors as mediators for program delivery. Core intervention components of the DCCP included: 1) diabetes self-management education, 2) support for managing diabetes and distress, 3) enhancing access and linkage to care, 4) improving quality of care, 5) community organization, mobilization, and advocacy, and 6) health system and community transformation. A participatory monitoring and evaluation system was used to document and systematically reflect on program implementation.
- Results: DCCP implementation was associated with modest improvements in diabetes-related clinical health outcomes for program participants. Results showed statistically significant improvements in HbA1c (P = 0.016), weight (P = 0.021) and diastolic blood pressure (P = 0.027).
- Conclusion: Using neighborhood Diabetes Health Ambassadors for program delivery has implications for assuring access to quality diabetes care for populations experiencing health disparities.
The growing prevalence of type 2 diabetes, with its high morbidity and excess mortality, is imposing a heavy burden on the U.S. health care system [1–3]. It has been recognized that adoption of self-management skills by the person with diabetes is necessary in order to manage their diabetes. Diabetes self-management education and support (DSME/S) provides the foundation to help people with diabetes to navigate these decisions and activities and has been shown to improve health outcomes.
Compared to the general population, African Americans are disproportionately affected by diabetes. African Americans are also less likely to seek diabetes care and have routine diabetes-related visits with a health care professional [4,5]. African Americans have higher HbA1c levels, which contribute to the increased mortality and morbidity rates among this population [6]. Furthermore, African-American women have the poorest HbA1c control as compared to other groups [4]. Concentrated poverty and lower socioeconomic status are social determinants associated with higher prevalence of diabetes [7]. Economic barriers, living conditions, and the built environment play a significant role in contributing to this health disparity [8].
In 2010, the Bristol-Myers Squibb (BMS) Foundation launched the Together on Diabetes initiative to improve the health outcomes of adult populations disproportionately affected by type 2 diabetes. In November 2010, Together on Diabetes issued a request for proposals to encourage, identify, and promote new and evidence-based approaches to empower African-American women to control their diabetes [9–11], taking into account the opportunity these women have to influence the health of their families and communities. Whittier Street Health Center in Boston received a grant to implement a program that would connect African-American women living in public housing in the Roxbury neighborhood with comprehensive diabetes management, including health education by a certified diabetes educator, nutritional counseling by a dietitian, and a tailored program of physical activity.
In this article, we describe the project and effects on diabetes-related clinical health outcomes.
Methods
Setting
Whittier Street Health Center (WSHC) is a federally qualified community health center that serves over 25,000 patients annually. The WSHC is situated in the heart of Boston’s Roxbury neighborhood, close to 5 public housing developments; 83% of WSHC patients live in public housing units. Roxbury is an underserved neighborhood with high rates of poverty, violence, and disease [12]. African Americans comprise the majority of residents living in Roxbury, making up 55.6% of the total population [13].
Diabetes Care Coordination Program
Ambassadors
Diabetes Health Ambassadors, a key component of the program, were hired to engage community members in managing their own health. Five Ambassadors were recruited and retained throughout the project period. Ambassadors were referred by their primary care provider at WSHC and interviewed for the job by the patient navigator. Ambassadors were required to be African-American women with type 2 diabetes living in a public housing unit within the Roxbury neighborhood. In addition, they were required to have their diabetes under control as defined by the WSHC clinical team (HbA1c of 8.0 or below). They also had to want to help other women control their diabetes and be able to deliver motivational presentations as well as have knowledge of available community resources.
Ambassadors received 30 hours of paid training from the certified diabetes educator. During training, they learned the definition, risk factors, and causes of diabetes, how it is controlled, and how to explain this information at a fifth-grade level. Modeling and feedback was used to assure that the information each Ambassador presented was accurate. Ambassadors were also trained on how to measure blood pressure and blood glucose levels and how to respectfully deliver the results. Additionally, Ambassadors received training on cultural competence. Ambassadors were engaged in community outreach and patient support for 20 hours per week and were compensated for their time with stipends.
Participant Recruitment and Outreach
A rolling enrollment for the DCCP began January 2012. The outreach team from the WSHC attended coffee hours at the public housing units and other community events where they conducted onsite blood pressure and glucose screenings as well as educated community members on healthy eating and active lifestyle to reduce the risks for diabetes. Mobile kits were used for testing, so participants received the test results immediately. Two Ambassadors, the outreach nurse, and the patient navigator conducted the outreach events. The set up included two tables, 6 chairs, education materials, and blood pressure and blood sugar screening materials.
Screenings were offered in the public housing units 3 times a week (twice during the week and once during the weekend). Posters in the neighborhood notifed women of the time and location of the screenings. Other settings for services such as screenings and referrals to primary care and health insurance applications included churches, mosques, community festivals, farmers markets, parks, and hair salons.
Women who had elevated glucose readings were invited to enroll in the DCCP program and an appointment at the WSHC was made for those who signed up.
During the period January 2012 to June 2013, 980 African-American women were screened for diabetes. Most screenings took place in the public housing units. Among those screened, 340 had an elevated blood glucose and were referred to WSHC for services. Of those, 175 women were recruited and enrolled into the DCCP. At the WSHC, a standardized protocol was used to measure HbA1c to confirm a diagnosis of diabetes once patients attended their first appointment. Age of participants ranged from 40 to 49. Most women were unemployed and had many competing responsibilities and stressors. Completed preassessment questionaires indicated that participants did not engage in healthy eating or physical activity as part of their daily routines prior to enrollment.
Program Components
At the Center, Ambassadors spoke with program participants and inquired about their barriers to diabetes care (eg, access to food [15], health insurance, etc.) using a standardized list. Ambassadors linked program participants to community support services as needed, including health insurance enrollment, financial support, and housing support. Services were also provided in collaboration with community organizations. For example, subsidized gym memberships were available at the local YMCA and a local fitness studio, and there was an instructor at the YMCA to guide the women through physical activity routines.
Participants could attend DSME group sessions provided by the certified diabetes educator. The course met twice a week for 2 hours for a period of 6 weeks. The course was interactive and included hands-on training in blood glucose measurement and food preparation. Healthy food was offered after each session, which provided a further opportunity for participants to engage in peer-to-peer support. After the completion of the DSME course, bi-weekly support group sessions were held until program completion (June 2013). All clinical team members were present at the support group sessions, with patients rotating to speak to them to ask questions or discuss concerns related to self-management.
A part of DSME, the registered dietitian provided nutrition information and healthy cooking demonstrations for program participants within group sessions. The primary care physician met the patient once a month and kept track of clinical changes over time. Patients with HbA1c ≥ 9% were referred to the high-risk nurse case manager who worked one-on-one with program participants to help them avoid serious diabetes complications.
Ambassadors were a part of all the course and support group sessions, and when needed they attended indivdual sessions, such as doctor visits and meetings with the high-risk nurse case manager. Ambassadors accompanied program participants during visits with clinical staff to provide additional support when requested.
The manager of quality assurance assured the safety of intervention procedures and employed performance improvement methods. Program participants provided informed consent, and had the right to withdraw at any time. The Quality Assurance Committee at WSHC protected the rights of participants, assured the safety of intervention procedures, and assured the quality of care received by each participant.
Evaluation
The Work Group for Community Health and Development at the University of Kansas was selected by the BMS Foundation to evaluate the implementation and related clinical outcomes of the program using a participatory evaluation framework [16–18]. A similarly funded study used the same study approach [19]. Clinical health outcomes were analyzed through a pre-post test comparison using STATA Version 12. Paired t tests were used to examine within-patient health outcome changes. The mean interval between the pre and post measurements was 16 months. A 0.05 level of significance was used. Using a one-sided t test, Cohen’s d was computed to measure effect size.
Results
Services
Clinical Outcomes
Discussion
This empirical case study examined the implementation of the Diabetes Care Coordination Program (DCCP) and its effects on diabetes-related clinical health outcomes for program participants. The program’ glucose screenings and educational workshops at public housing units provided enhanced access to diabetes care services for community members. Referrals to WSHC allowed for the provision of clinical health services through a comprehensive care model. Modest improvements in diabetes-related clinical health indicators were seen.
Some challenges were noted during implementation of the DCCP and addressed as part of a quality improvement process. First, Diabetes Health Ambassadors originally went door to door and had difficulty recruiting participants. Holding screening events in public spaces within housing units addressed this problem. Second, the WSHC team found that women needed more behavioral health support than was being provided, with some of the women reporting to their case managers that it was difficult for them to handle the stresses of life and at the same time manage their diabetes. In response, an integrated behavioral health specialist was hired to provide guidance on how to manage life stressors and how to increase health behaviors despite physical, social, and financial barriers.
Third, women reported a lack of access to fresh fruits and vegetables. In response, WSHC implemented a formal collaboration with a mobile food truck (June 2012) that sold subsidized fresh food 3 days a week to public housing residents. Fourth, participants reported some barriers related to transportation for scheduled appointments at the WSHC. The team addressed this issue by providing taxi vouchers for those who lacked adequate access to transportation. Finally, the coordinated team noticed that medication adherence was a barrier to care for many program participants. Consequently, they developed a medication management support group led by the clinical pharmacist to address barriers related to medication adherence.
There were several methodological challenges confronted in carrying out this study. First, the dose of services that were provided for each individual participant was difficult to ascertain. For example, some of those enrolled in the DCCP earlier may not have had the full set of services that were available towards the end of the program. Second, although group data were available, data on individual level outcomes were not; this made it difficult to assess whether there was change in behavior on the part of particular individuals. Third, a case study design, without a comparison group, does not control for threats to internal validity (eg, history, maturation, and attrition) that might have accounted for improvements in clinical outcomes. Finally, despite the comprehensive documentation, there could have been program elements that were implemented but not documented. Despite these methodological limitations, the case study design facilitated learning about associations between program implementation and changes in clinical health outcomes in a context of health disparities [20].
A particular strength of the program was use of Diabetes Health Ambassadors as mediators for DCCP service delivery. Ambassadors increased diabetes awareness within the community and also played a key role in building rapport and trust in the diabetes program among community members.
Lessons Learned
As part of a qualitative component, key informant interviews with WSHC staff were used to examine lessons learned during project implementation. First, an identified positive outcome was that the Ambassadors gained new insights into the management of their own diabetes and adopted additional lifestyle changes along with program participants. Second, the WSHC team affirmed that African-American women act as gatekeepers for their families, and that teaching and serving one woman allowed for teaching and serving the entire family. Program participants reported that their own lifestyle changes had an impact on other family members. For example, one participant reported she stopped purchasing soda beverages for her family. Another participant began using healthier cooking strategies, such as using olive oil instead of butter. Third, consistent with another study, the coordinated care model helped to assure comprehensive diabetes care [21]. Staff noted that “it takes a village” (a coordinated team) to address the diverse array of clinical issues needed for diabetes control. Fourth, self-management education was helpful, especially when coupled with social support from peers and family members. Fifth, working collaboratively with partners in non-health sectors was helpful in achieving the conditions needed for improved diabetes care [22].
Recommendations for Future Research and Practice
There are several recommendations for future research and practice. First, to achieve stronger clinical health outcomes, the DCCP would need to be enhanced by assuring lower caseloads for the WSHC clinical team. Second, to expand the evidence base, stronger experimental designs are needed to draw firmer conclusions about causal relationships. For instance, a multiple-baseline design across similar federally qualified heath centers could enable a better understanding of the effects of this community-based DCCP intervention in urban contexts. Third, research and practice would benefit from further testing of the model using community health workers for delivery of DSME and DSMS services. Fourth, implementation science can aid in enhancing the role of Ambassadors by providing tools/frameworks for improved delivery of services such as the core implementation components of selection and training [23]. Finally, the use of behavioral science methods can help extend the evidence base for the effects of the DCCP intervention on behavior change at the individual and the community levels [24,25].
Conclusion
This empirical case study adds to our understanding of delivering community-based diabetes care in a public housing context. This study examined the implementation and effects of a diabetes program for African-American women experiencing health disparities. The delivery of diabetes services by Diabetes Health Ambassadors was effective in engaging women with diabetes who lived in low-income housing. This study provided further evidence that coordinated diabetes care, with a focus on culturally and contextually appropriate service delivery, can have positive health outcomes. Further research is needed to examine effects of the DCCP intervention at the individual, clinic, family, and community levels.
Addressing the rapidly increasing prevalence of diabetes is a huge challenge, especially among vulnerable populations at disproportionate risk for adverse health outcomes. These patients face physical, emotional, and financial burdens. We need to assure that community health workers and coordinated clinical teams are prepared to support patients’ acquisition and maintenance of self-care behaviors. Eliminating diabetes-related disparities requires modifying the health system and the broader community environment [26]. Addressing the barriers to medical and self-care that vulnerable populations with type 2 diabetes face will provide them with greater opportunities for health and well-being.
Acknowledgments: The authors thank the many community partners throughout Boston that made this project possible.
Corresponding author: Ithar Hassaballa, KU Work Group for Community Health and Development, University of Kansas, 1000 Sunnyside Ave, 4082 Dole Center, Lawrence, KS 66045, [email protected].
Funding/support: Funding for the Whittier Street Health Center’s Diabetes Care Coordination Program and for the evaluation of the Together on Diabetes initiative was provided by the Bristol-Myers Squibb Foundation.
Financial disclosures: None.
1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047–53.
2. Centers for Disease Control and Prevention. National diabetes statistics report: estimates of diabetes and its burden in the United States, 2014. Atlanta: U.S. Department of Health and Human Services; 2014.
3. Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S., 2005-2050. Diabetes Care 2006;29:2114–6.
4. Tang TS, Brown MB, Funnell MM, Anderson RM. Social support, quality of life, and self-care behaviors among African Americans with type 2 diabetes. Diabetes Educ 2008;34:266-76.
5. Crabtree K, Sherrer N, Rushton T, Willig A, Agne A, Shelton T, Cherrington A. Diabetes connect: African American men's preferences for a community-based diabetes management program. Diabetes Educ 2015;41:118-26.
6. Kirk JK, D'Agostino RB Jr, Bell RA, Passmore LV, Bonds DE, Karter AJ, Narayan KM. Disparities in HbA1c levels between African-American and non-Hispanic white adults with diabetes: a meta-analysis. Diabetes Care 2006;29:2130–6.
7. Batts ML, Gary TL, Huss K, Hill MN, Bone L, Brancati FL. Patient priorities and needs for diabetes care among urban African American adults. Diabetes Educ 2001;27:405–12.
8. Horowitz CR, Colson KA, Hebert PL, Lancaster K. Barriers to buying healthy foods for people with diabetes: evidence of environmental disparities. Am J Public Health 2004;94:1549–54.
9. Haas L, Maryniuk M, Beck J, et al; 2012 Standards Revision Task Force. National standards for diabetes self-management education and support. Diabetes Care 2013;36 Suppl 1:S100–8.
10. Cené CW, Haymore LB, Ellis D, Whitaker S, Henderson S, Lin FC, Corbie-Smith G. Implementation of the power to prevent diabetes prevention educational curriculum into rural African American communities: a feasibility study. Diabetes Educ 2013;39:776–85.
11. Feathers JT, Kieffer EC, Palmisano G, et al. The development, implementation, and process evaluation of the REACH Detroit Partnership's Diabetes Lifestyle Intervention. Diabetes Educ 2007;33:509–20.
12. Rahman S, Hu H, McNeely E, et al. Social and environmental risk factors for hypertension in African Americans. Fla Public Health Rev 2008;5:64–72.
13. US Bureau of the Census. Available at www.cityofboston.gov/dnd/PDR/Maps_and_Neighborhood_Profiles.asp.
14. Reid RJ, Coleman K, Johnson EA, Fishman PA, Hsu C, Soman MP, Trescott CE, Erikson M, Larson EB. The Group Health medical home at year two: cost savings, higher patient satisfaction, and less burnout for providers. Health Aff (Millwood) 2010;29:835–43.
15. Fulp RS, McManus KD, Johnson PA. Barriers to purchasing foods for a high-quality, healthy diet in a low-income African American community. Fam Community Health 2009;32:206–17.
16. Fawcett SB, Schultz JA. Supporting participatory evaluation using the Community Tool Box online documentation system. Community-Based Participatory Research for Health. San Francisco: Jossey-Bass; 2008: 419–23.
17. Collie-Akers V, Schultz JA, Carson V, Fawcett SB, Ronan M. REACH 2010: Kansas City, Missouri evaluating mobilization strategies with neighborhood and faith organizations to reduce risk for health disparities. Health Prom Pract 2009;10(Suppl 2):118S–127S.
18. Fawcett SB, Boothroyd R, Schultz JA, Francisco VT, Carson V, Bremby R. Building capacity for participatory evaluation within community initiatives. J Prev Interven Comm 2003;26:21–36.
19. Sepers CE Jr, Fawcett SB, Lipman R, Schultz J, Colie-Akers V, Perez A. Measuring the implementation and effects of a coordinated care model featuring diabetes self-management education within four patient-centered medical homes. Diabetes Educ 2015;41:328–42.
20. Yin RK. Case study research: Design and methods. Sage; 2013.
21. Mead H, Andres E, Regenstein M. Underserved patients' perspectives on patient-centered primary care: does the patient-centered medical home model meet their needs? Med Care Res Rev 2014;71:61–84.
22. Fawcett S, Schultz J, Watson-Thompson J, Fox M, Bremby R. Building multisectoral partnerships for population health and health equity. Prev Chronic Disease 2010;7:A118. Epub 2010 Oct 15.
23. Fixsen DL, Blase KA, Naoom SF, Wallace F. Core implementation components. Res Soc Work Prac 2009; 19:531–540.
24. Cooper JO, Heron TE, Heward WL. Applied behavior analysis. 2nd ed. Pearson; 2007.
25. Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health 2010;31:399–418.
26. Jack L, Jack NH, Hayes SC. Social determinants of health in minority populations: a call for multidisciplinary approaches to eliminate diabetes-related health disparities. Diabetes Spectrum 2012;25:9–13.
1. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047–53.
2. Centers for Disease Control and Prevention. National diabetes statistics report: estimates of diabetes and its burden in the United States, 2014. Atlanta: U.S. Department of Health and Human Services; 2014.
3. Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: U.S., 2005-2050. Diabetes Care 2006;29:2114–6.
4. Tang TS, Brown MB, Funnell MM, Anderson RM. Social support, quality of life, and self-care behaviors among African Americans with type 2 diabetes. Diabetes Educ 2008;34:266-76.
5. Crabtree K, Sherrer N, Rushton T, Willig A, Agne A, Shelton T, Cherrington A. Diabetes connect: African American men's preferences for a community-based diabetes management program. Diabetes Educ 2015;41:118-26.
6. Kirk JK, D'Agostino RB Jr, Bell RA, Passmore LV, Bonds DE, Karter AJ, Narayan KM. Disparities in HbA1c levels between African-American and non-Hispanic white adults with diabetes: a meta-analysis. Diabetes Care 2006;29:2130–6.
7. Batts ML, Gary TL, Huss K, Hill MN, Bone L, Brancati FL. Patient priorities and needs for diabetes care among urban African American adults. Diabetes Educ 2001;27:405–12.
8. Horowitz CR, Colson KA, Hebert PL, Lancaster K. Barriers to buying healthy foods for people with diabetes: evidence of environmental disparities. Am J Public Health 2004;94:1549–54.
9. Haas L, Maryniuk M, Beck J, et al; 2012 Standards Revision Task Force. National standards for diabetes self-management education and support. Diabetes Care 2013;36 Suppl 1:S100–8.
10. Cené CW, Haymore LB, Ellis D, Whitaker S, Henderson S, Lin FC, Corbie-Smith G. Implementation of the power to prevent diabetes prevention educational curriculum into rural African American communities: a feasibility study. Diabetes Educ 2013;39:776–85.
11. Feathers JT, Kieffer EC, Palmisano G, et al. The development, implementation, and process evaluation of the REACH Detroit Partnership's Diabetes Lifestyle Intervention. Diabetes Educ 2007;33:509–20.
12. Rahman S, Hu H, McNeely E, et al. Social and environmental risk factors for hypertension in African Americans. Fla Public Health Rev 2008;5:64–72.
13. US Bureau of the Census. Available at www.cityofboston.gov/dnd/PDR/Maps_and_Neighborhood_Profiles.asp.
14. Reid RJ, Coleman K, Johnson EA, Fishman PA, Hsu C, Soman MP, Trescott CE, Erikson M, Larson EB. The Group Health medical home at year two: cost savings, higher patient satisfaction, and less burnout for providers. Health Aff (Millwood) 2010;29:835–43.
15. Fulp RS, McManus KD, Johnson PA. Barriers to purchasing foods for a high-quality, healthy diet in a low-income African American community. Fam Community Health 2009;32:206–17.
16. Fawcett SB, Schultz JA. Supporting participatory evaluation using the Community Tool Box online documentation system. Community-Based Participatory Research for Health. San Francisco: Jossey-Bass; 2008: 419–23.
17. Collie-Akers V, Schultz JA, Carson V, Fawcett SB, Ronan M. REACH 2010: Kansas City, Missouri evaluating mobilization strategies with neighborhood and faith organizations to reduce risk for health disparities. Health Prom Pract 2009;10(Suppl 2):118S–127S.
18. Fawcett SB, Boothroyd R, Schultz JA, Francisco VT, Carson V, Bremby R. Building capacity for participatory evaluation within community initiatives. J Prev Interven Comm 2003;26:21–36.
19. Sepers CE Jr, Fawcett SB, Lipman R, Schultz J, Colie-Akers V, Perez A. Measuring the implementation and effects of a coordinated care model featuring diabetes self-management education within four patient-centered medical homes. Diabetes Educ 2015;41:328–42.
20. Yin RK. Case study research: Design and methods. Sage; 2013.
21. Mead H, Andres E, Regenstein M. Underserved patients' perspectives on patient-centered primary care: does the patient-centered medical home model meet their needs? Med Care Res Rev 2014;71:61–84.
22. Fawcett S, Schultz J, Watson-Thompson J, Fox M, Bremby R. Building multisectoral partnerships for population health and health equity. Prev Chronic Disease 2010;7:A118. Epub 2010 Oct 15.
23. Fixsen DL, Blase KA, Naoom SF, Wallace F. Core implementation components. Res Soc Work Prac 2009; 19:531–540.
24. Cooper JO, Heron TE, Heward WL. Applied behavior analysis. 2nd ed. Pearson; 2007.
25. Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health 2010;31:399–418.
26. Jack L, Jack NH, Hayes SC. Social determinants of health in minority populations: a call for multidisciplinary approaches to eliminate diabetes-related health disparities. Diabetes Spectrum 2012;25:9–13.
Society of Hospital Medicine Launches Med Student Scholarship Program
The Society of Hospital Medicine has launched a new scholarship program to bring the "best and brightest" medical students into the specialty.
The Student Hospitalist Scholar Grant program awards eligible students a $5,000 summer stipend for scholarly work on a project related to patient safety, quality improvement (QI), or other areas relevant to the field of hospital medicine. The program also provides up to $1,500 in travel-related reimbursement for students to attend the SHM annual meeting.
This summer's inaugural class has three students, all going into their second year of medical school: Frank Zadravecz Jr. of the University of Illinois College of Medicine at Chicago, Miriam Zander of Touro College of Osteopathic Medicine in New York City, and Monica Shah of Wayne State University School of Medicine in Detroit.
"Getting medical students involved is important for us," says hospitalist Darlene Tad-y, MD, an assistant professor of medicine at the University of Colorado in Denver and chair of SHM's Physicians in Training Committee. It means "the future of medicine will have people who know how to do this work, people who will be more skilled and effective at this work."
Dr. Tad-y says it makes sense to merge efforts to recruit the "best and brightest" medical students to HM with QI research. This year's projects include examinations of post-hospital syndrome and physiologic alarm responses.
The program drew about a dozen applicants in its first year. Over the next few years, SHM hopes to award 10 scholarships each summer.
"QI work is really only getting off the ground broadly with people who've been in the field for a really long time," Dr. Tad-y says. "To have that many students early on in their medical school career already understand some of these concepts and be aware that this is going on, for us, it's really exciting." TH
Visit our website for more information on engaging young physicians in HM.
The Society of Hospital Medicine has launched a new scholarship program to bring the "best and brightest" medical students into the specialty.
The Student Hospitalist Scholar Grant program awards eligible students a $5,000 summer stipend for scholarly work on a project related to patient safety, quality improvement (QI), or other areas relevant to the field of hospital medicine. The program also provides up to $1,500 in travel-related reimbursement for students to attend the SHM annual meeting.
This summer's inaugural class has three students, all going into their second year of medical school: Frank Zadravecz Jr. of the University of Illinois College of Medicine at Chicago, Miriam Zander of Touro College of Osteopathic Medicine in New York City, and Monica Shah of Wayne State University School of Medicine in Detroit.
"Getting medical students involved is important for us," says hospitalist Darlene Tad-y, MD, an assistant professor of medicine at the University of Colorado in Denver and chair of SHM's Physicians in Training Committee. It means "the future of medicine will have people who know how to do this work, people who will be more skilled and effective at this work."
Dr. Tad-y says it makes sense to merge efforts to recruit the "best and brightest" medical students to HM with QI research. This year's projects include examinations of post-hospital syndrome and physiologic alarm responses.
The program drew about a dozen applicants in its first year. Over the next few years, SHM hopes to award 10 scholarships each summer.
"QI work is really only getting off the ground broadly with people who've been in the field for a really long time," Dr. Tad-y says. "To have that many students early on in their medical school career already understand some of these concepts and be aware that this is going on, for us, it's really exciting." TH
Visit our website for more information on engaging young physicians in HM.
The Society of Hospital Medicine has launched a new scholarship program to bring the "best and brightest" medical students into the specialty.
The Student Hospitalist Scholar Grant program awards eligible students a $5,000 summer stipend for scholarly work on a project related to patient safety, quality improvement (QI), or other areas relevant to the field of hospital medicine. The program also provides up to $1,500 in travel-related reimbursement for students to attend the SHM annual meeting.
This summer's inaugural class has three students, all going into their second year of medical school: Frank Zadravecz Jr. of the University of Illinois College of Medicine at Chicago, Miriam Zander of Touro College of Osteopathic Medicine in New York City, and Monica Shah of Wayne State University School of Medicine in Detroit.
"Getting medical students involved is important for us," says hospitalist Darlene Tad-y, MD, an assistant professor of medicine at the University of Colorado in Denver and chair of SHM's Physicians in Training Committee. It means "the future of medicine will have people who know how to do this work, people who will be more skilled and effective at this work."
Dr. Tad-y says it makes sense to merge efforts to recruit the "best and brightest" medical students to HM with QI research. This year's projects include examinations of post-hospital syndrome and physiologic alarm responses.
The program drew about a dozen applicants in its first year. Over the next few years, SHM hopes to award 10 scholarships each summer.
"QI work is really only getting off the ground broadly with people who've been in the field for a really long time," Dr. Tad-y says. "To have that many students early on in their medical school career already understand some of these concepts and be aware that this is going on, for us, it's really exciting." TH
Visit our website for more information on engaging young physicians in HM.
Single-session psychiatry at 11,000 feet
The woman sitting across from me talked, through two translators (Quechua to Spanish to English) about how sad she had been since the death of her husband last year. “I eat alone,” she said, and my Spanish translator, a native Peruvian, explained the cultural significance of such a phrase to me. Eating alone is not a good thing; sometimes it’s how people are shunned. The woman talked about her adult children and how little contact she had with them, a continual disappointment in a poor rural area where the younger generation often flocked to the city and the hope of a better life.

She was in her 60s and dressed in the traditional attire of the indigenous people of the Andes: a high bowler hat, layers of sweaters, a long skirt, and woolen stockings. Her long black braids remained ageless in a land where somehow hair does not turn gray, but her bronze skin was leathery from generations in the sun. Her problems – grief and loneliness – are universal issues, and while she had moments where she longed for death, she felt her animals, and her cow in particular, needed her now.
Months ago, a friend – an internist – asked if my husband and I would join him, his wife, and some other families we knew on a volunteer medical mission to Peru. Hands Across the Americas is an organization founded by Jennifer Diamond and it has sent 27 medical and surgical missions to Latin America to serve those with limited access to medical treatments. I hesitated when I heard the request, and in case I wasn’t entranced by the idea of spending a week addressing the mental health needs of indigenous people in remote Andean villages, he added that another friend of ours, Patricia Poppe, a native of Peru and an expert on health communications at the Johns Hopkins School of Public Health, was eager to show our group of friends around her homeland before we all joined the mission. With this, I was sold on the whole adventure. I will spare you the details of our wonderful vacation, but will share with you, instead, what I learned about psychiatry in the Andes.
The mission orientation began in Cusco, Peru’s second-largest city and a way station for travelers headed to Machu Picchu. The tourist district of Cusco is a beautiful and fascinating city that reflects both Incan and pre-Incan Latin America and the heavy Spanish influence brought by the 16th- century conquistadors. While the city is beautiful, and the worlds have intertwined over the centuries, it remains a land where there is tension between the different cultures.

At just over 11,000 feet, the air is thin and visitors get easily winded just walking the hills. The villages we worked in were all about an hour outside of Cusco. They were impoverished and dilapidated, with some of the homes still constructed of bricks made from mud and straw. Dogs and farm animals roamed the streets. July is midwinter there, and it’s the dry season, so everything – and everyone – was covered in a layer of Andean grit. By the end of each day, we were as well.
I wish I could say that I wasn’t anxious about the work, but I was. What can a psychiatrist do in a single visit, much less a single session that requires one, and occasionally two, translators, in a population where I had no knowledge of their culture or resources? I didn’t know what types of patients I might see, if using medication would be reasonable, or if follow-up of any kind would be feasible. In the 27 missions of Hands Across the Americas, I was to be the first psychiatrist.
Four years earlier, a psychologist, Dr. David Doolittle, had gone with another psychologist, and when we spoke on the phone, he was very enthusiastic. He told me that this had been one of the best experiences of his professional life, and he was pleased to hear that mental health would continue to be a part of the agenda.
Finally, I should add that despite my hesitation about how helpful I might be as part of a medical team offering one-time services, I did have a similar experience in a different setting; In 2005, I volunteered for 2 weeks with the Substance Abuse and Mental Health Services Administration’s Katrina Assistance Project, and while I wondered then if my efforts were helpful to those I was trying to serve, I walked away feeling that I personally had gotten a great deal from the experience. I decided I would go to Peru with limited expectations and one simple agenda: I would try to be helpful.
The mission started with a brief orientation in Cusco, and it didn’t escape me when the medical director announced that patients could be seen by internal medicine, pediatrics, ENT, gynecology, and optometry. Psychiatry was strangely missing from the list, and when I pointed this out, he told me he had a special job for me: to run the pharmacy. While I was happy to help dispense medications, I had the sense that this population might have unmet mental health needs and suggested that it could be worthwhile to offer psychiatry as a specialty as well!
While the group came with an extensive supply of medications, vitamins, reading glasses, toothbrushes, and some wheelchairs, canes, and walkers, there were no psychotropic medications in the stash. I spoke with a local doctor who served as a liaison, and learned that he was familiar only with diazepam and alprazolam. Psychiatric patients were referred to doctors in Cusco, and local doctors did not prescribe antidepressants. For complex issues that required medical or surgical subspecialization, the referrals were even more complex: Patients traveled 18 hours by bus to be treated in Lima.
On the morning of our first clinic, I was given a small supply of fluoxetine (per my request) and alprazolam. Over 5 days we worked in three sites. On the first day, we were at the municipal center in Huarocondo, a little more than an hour outside of Cusco. Tents were set up inside the building, with the waiting room, triage, and pharmacy all stationed outside on the dirt. Inside, there was very little light, and like the other places we’d set up, no heat. My tent had a table and two chairs meant for primary school children, and I absconded with an adult-sized plastic chair for my interpreter. We had no access to medical records, no labs or radiographic equipment, and no clear place to send anyone for follow-up – this was true across all specialties, though the ENT who was working with us had come with suitcases full of his own equipment. Patients didn’t know what a psychiatrist or psychologist was, and some responded to questions about depression by saying that their blood pressure was just fine. Triage resorted to asking people if they felt sad and wanted to talk to a doctor about it.
The next 2 days, we worked in medical clinics in Ancahuasi and Anta, and while the conditions were more conducive to providing medical care, there was still no heat, the lighting was poor, and the buildings had not seen new coats of paint or furniture in many years. The clinics did not have psychiatrists, but they did each have a psychologist, and a couple of the people I saw had been seen. I was also told that fluoxetine could be obtained in Anta.

Hundreds of patients came each day, and all told, more than a thousand patients were seen by nine doctors in those 5 days. My official psychiatry tally was 79, but my personal count was less – I imagine some people became impatient with the long line and left without being seen – I recorded visits with 8-15 people each day.
First, let me say that I was surprised at the lack of pure psychopathology; the issues were more reactions to tremendous deprivation, violence, loneliness, medical and developmental disorders, and chronic struggles. I saw only two adult men, the rest of the patients were women and a few children. No one I saw had ever seen a psychiatrist before, and no one had taken psychotropic medications (not even the diazepam or alprazolam, which I was told could be obtained), and in fact, very few were on any medications of any kind. No one had ever been in a psychiatric hospital. Poverty was rampant, as was domestic violence: Men beat their wives, parents beat their children, and there seemed to be no societal means to interrupt this. One bruised woman said her husband had been released from jail in a day, and several women spoke of living in fear for their lives; still, their families encouraged them to stay with men who were abusive or unfaithful. I was told that the statistic for spousal abuse in Peru was 60%, in Cusco it was 75%; I suspect it was even higher in these outlying villages. Families were fractured; employment was physically very difficult; and stress was extreme. Low mood and poor sleep were pervasive, but given the fact that I was unsure if people could get follow-up or even afford to refill medications, I gave out very little in the way of medications, and used the fluoxetine only for a few people where I felt their mood and circumstances were so dire that perhaps it would help – and it seemed unlikely to hurt. I was able to hospitalize one 18-year-old mother who was suicidal and said she had tried to hang herself, though she was released early the next morning before she was ever seen by a doctor; she did note she felt much better and was grateful for the help.
Despite tremendous stresses and limited access to care, the suicide rate in Peru are quite low at 3.2 per 100,000 (as compared with nearly 14 per 100,000 in the United States), and despite the fact that some of the patients I saw had considered it, most said that their children or animals needed them, and there are religious prohibitions.
At moments, I wondered what I could possibly offer. One woman came in with a 5-year-old child with Down syndrome strapped to her, and another, older, developmentally delayed child in tow. There were other children at home, and while many women noted that their husbands beat them while they were drunk, this woman said her husband was calmer when he was drinking; he beat her when he was sober. I asked her what would help, and she said she needed money. Feeling I had nothing else to offer, I did something I have never done in my years as a psychiatrist: I gave her money. I hoped that she would spend it on something that might provide a moment of relief from her anguished life.
For the most part, it was interesting work, and often, it felt useful to make psychological interventions, to validate the distress the patients felt and to reorient them to seeing their own strengths. The people talked of holding their problems close, and of a relief and ease that came with sharing their difficulties.
In the end, I did feel helpful for at least some of the patients some of the time. At the very least, I felt appreciated – in one clinic, we were greeted by the mayor and a band – and patients expressed their thanks to both me and my cadre of interpreters, sometimes profusely. In the end, it was an adventure, from the vacation with 16 people to Lima, the Sacred Valley, and Machu Picchu, to my foray into high-volume, single-session psychiatry in a culture so vastly different from my own.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: Johns Hopkins University Press, 2011).
The woman sitting across from me talked, through two translators (Quechua to Spanish to English) about how sad she had been since the death of her husband last year. “I eat alone,” she said, and my Spanish translator, a native Peruvian, explained the cultural significance of such a phrase to me. Eating alone is not a good thing; sometimes it’s how people are shunned. The woman talked about her adult children and how little contact she had with them, a continual disappointment in a poor rural area where the younger generation often flocked to the city and the hope of a better life.
She was in her 60s and dressed in the traditional attire of the indigenous people of the Andes: a high bowler hat, layers of sweaters, a long skirt, and woolen stockings. Her long black braids remained ageless in a land where somehow hair does not turn gray, but her bronze skin was leathery from generations in the sun. Her problems – grief and loneliness – are universal issues, and while she had moments where she longed for death, she felt her animals, and her cow in particular, needed her now.
Months ago, a friend – an internist – asked if my husband and I would join him, his wife, and some other families we knew on a volunteer medical mission to Peru. Hands Across the Americas is an organization founded by Jennifer Diamond and it has sent 27 medical and surgical missions to Latin America to serve those with limited access to medical treatments. I hesitated when I heard the request, and in case I wasn’t entranced by the idea of spending a week addressing the mental health needs of indigenous people in remote Andean villages, he added that another friend of ours, Patricia Poppe, a native of Peru and an expert on health communications at the Johns Hopkins School of Public Health, was eager to show our group of friends around her homeland before we all joined the mission. With this, I was sold on the whole adventure. I will spare you the details of our wonderful vacation, but will share with you, instead, what I learned about psychiatry in the Andes.
The mission orientation began in Cusco, Peru’s second-largest city and a way station for travelers headed to Machu Picchu. The tourist district of Cusco is a beautiful and fascinating city that reflects both Incan and pre-Incan Latin America and the heavy Spanish influence brought by the 16th- century conquistadors. While the city is beautiful, and the worlds have intertwined over the centuries, it remains a land where there is tension between the different cultures.
At just over 11,000 feet, the air is thin and visitors get easily winded just walking the hills. The villages we worked in were all about an hour outside of Cusco. They were impoverished and dilapidated, with some of the homes still constructed of bricks made from mud and straw. Dogs and farm animals roamed the streets. July is midwinter there, and it’s the dry season, so everything – and everyone – was covered in a layer of Andean grit. By the end of each day, we were as well.
I wish I could say that I wasn’t anxious about the work, but I was. What can a psychiatrist do in a single visit, much less a single session that requires one, and occasionally two, translators, in a population where I had no knowledge of their culture or resources? I didn’t know what types of patients I might see, if using medication would be reasonable, or if follow-up of any kind would be feasible. In the 27 missions of Hands Across the Americas, I was to be the first psychiatrist.
Four years earlier, a psychologist, Dr. David Doolittle, had gone with another psychologist, and when we spoke on the phone, he was very enthusiastic. He told me that this had been one of the best experiences of his professional life, and he was pleased to hear that mental health would continue to be a part of the agenda.
Finally, I should add that despite my hesitation about how helpful I might be as part of a medical team offering one-time services, I did have a similar experience in a different setting; In 2005, I volunteered for 2 weeks with the Substance Abuse and Mental Health Services Administration’s Katrina Assistance Project, and while I wondered then if my efforts were helpful to those I was trying to serve, I walked away feeling that I personally had gotten a great deal from the experience. I decided I would go to Peru with limited expectations and one simple agenda: I would try to be helpful.
The mission started with a brief orientation in Cusco, and it didn’t escape me when the medical director announced that patients could be seen by internal medicine, pediatrics, ENT, gynecology, and optometry. Psychiatry was strangely missing from the list, and when I pointed this out, he told me he had a special job for me: to run the pharmacy. While I was happy to help dispense medications, I had the sense that this population might have unmet mental health needs and suggested that it could be worthwhile to offer psychiatry as a specialty as well!
While the group came with an extensive supply of medications, vitamins, reading glasses, toothbrushes, and some wheelchairs, canes, and walkers, there were no psychotropic medications in the stash. I spoke with a local doctor who served as a liaison, and learned that he was familiar only with diazepam and alprazolam. Psychiatric patients were referred to doctors in Cusco, and local doctors did not prescribe antidepressants. For complex issues that required medical or surgical subspecialization, the referrals were even more complex: Patients traveled 18 hours by bus to be treated in Lima.
On the morning of our first clinic, I was given a small supply of fluoxetine (per my request) and alprazolam. Over 5 days we worked in three sites. On the first day, we were at the municipal center in Huarocondo, a little more than an hour outside of Cusco. Tents were set up inside the building, with the waiting room, triage, and pharmacy all stationed outside on the dirt. Inside, there was very little light, and like the other places we’d set up, no heat. My tent had a table and two chairs meant for primary school children, and I absconded with an adult-sized plastic chair for my interpreter. We had no access to medical records, no labs or radiographic equipment, and no clear place to send anyone for follow-up – this was true across all specialties, though the ENT who was working with us had come with suitcases full of his own equipment. Patients didn’t know what a psychiatrist or psychologist was, and some responded to questions about depression by saying that their blood pressure was just fine. Triage resorted to asking people if they felt sad and wanted to talk to a doctor about it.
The next 2 days, we worked in medical clinics in Ancahuasi and Anta, and while the conditions were more conducive to providing medical care, there was still no heat, the lighting was poor, and the buildings had not seen new coats of paint or furniture in many years. The clinics did not have psychiatrists, but they did each have a psychologist, and a couple of the people I saw had been seen. I was also told that fluoxetine could be obtained in Anta.
Hundreds of patients came each day, and all told, more than a thousand patients were seen by nine doctors in those 5 days. My official psychiatry tally was 79, but my personal count was less – I imagine some people became impatient with the long line and left without being seen – I recorded visits with 8-15 people each day.
First, let me say that I was surprised at the lack of pure psychopathology; the issues were more reactions to tremendous deprivation, violence, loneliness, medical and developmental disorders, and chronic struggles. I saw only two adult men, the rest of the patients were women and a few children. No one I saw had ever seen a psychiatrist before, and no one had taken psychotropic medications (not even the diazepam or alprazolam, which I was told could be obtained), and in fact, very few were on any medications of any kind. No one had ever been in a psychiatric hospital. Poverty was rampant, as was domestic violence: Men beat their wives, parents beat their children, and there seemed to be no societal means to interrupt this. One bruised woman said her husband had been released from jail in a day, and several women spoke of living in fear for their lives; still, their families encouraged them to stay with men who were abusive or unfaithful. I was told that the statistic for spousal abuse in Peru was 60%, in Cusco it was 75%; I suspect it was even higher in these outlying villages. Families were fractured; employment was physically very difficult; and stress was extreme. Low mood and poor sleep were pervasive, but given the fact that I was unsure if people could get follow-up or even afford to refill medications, I gave out very little in the way of medications, and used the fluoxetine only for a few people where I felt their mood and circumstances were so dire that perhaps it would help – and it seemed unlikely to hurt. I was able to hospitalize one 18-year-old mother who was suicidal and said she had tried to hang herself, though she was released early the next morning before she was ever seen by a doctor; she did note she felt much better and was grateful for the help.
Despite tremendous stresses and limited access to care, the suicide rate in Peru are quite low at 3.2 per 100,000 (as compared with nearly 14 per 100,000 in the United States), and despite the fact that some of the patients I saw had considered it, most said that their children or animals needed them, and there are religious prohibitions.
At moments, I wondered what I could possibly offer. One woman came in with a 5-year-old child with Down syndrome strapped to her, and another, older, developmentally delayed child in tow. There were other children at home, and while many women noted that their husbands beat them while they were drunk, this woman said her husband was calmer when he was drinking; he beat her when he was sober. I asked her what would help, and she said she needed money. Feeling I had nothing else to offer, I did something I have never done in my years as a psychiatrist: I gave her money. I hoped that she would spend it on something that might provide a moment of relief from her anguished life.
For the most part, it was interesting work, and often, it felt useful to make psychological interventions, to validate the distress the patients felt and to reorient them to seeing their own strengths. The people talked of holding their problems close, and of a relief and ease that came with sharing their difficulties.
In the end, I did feel helpful for at least some of the patients some of the time. At the very least, I felt appreciated – in one clinic, we were greeted by the mayor and a band – and patients expressed their thanks to both me and my cadre of interpreters, sometimes profusely. In the end, it was an adventure, from the vacation with 16 people to Lima, the Sacred Valley, and Machu Picchu, to my foray into high-volume, single-session psychiatry in a culture so vastly different from my own.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: Johns Hopkins University Press, 2011).
The woman sitting across from me talked, through two translators (Quechua to Spanish to English) about how sad she had been since the death of her husband last year. “I eat alone,” she said, and my Spanish translator, a native Peruvian, explained the cultural significance of such a phrase to me. Eating alone is not a good thing; sometimes it’s how people are shunned. The woman talked about her adult children and how little contact she had with them, a continual disappointment in a poor rural area where the younger generation often flocked to the city and the hope of a better life.
She was in her 60s and dressed in the traditional attire of the indigenous people of the Andes: a high bowler hat, layers of sweaters, a long skirt, and woolen stockings. Her long black braids remained ageless in a land where somehow hair does not turn gray, but her bronze skin was leathery from generations in the sun. Her problems – grief and loneliness – are universal issues, and while she had moments where she longed for death, she felt her animals, and her cow in particular, needed her now.
Months ago, a friend – an internist – asked if my husband and I would join him, his wife, and some other families we knew on a volunteer medical mission to Peru. Hands Across the Americas is an organization founded by Jennifer Diamond and it has sent 27 medical and surgical missions to Latin America to serve those with limited access to medical treatments. I hesitated when I heard the request, and in case I wasn’t entranced by the idea of spending a week addressing the mental health needs of indigenous people in remote Andean villages, he added that another friend of ours, Patricia Poppe, a native of Peru and an expert on health communications at the Johns Hopkins School of Public Health, was eager to show our group of friends around her homeland before we all joined the mission. With this, I was sold on the whole adventure. I will spare you the details of our wonderful vacation, but will share with you, instead, what I learned about psychiatry in the Andes.
The mission orientation began in Cusco, Peru’s second-largest city and a way station for travelers headed to Machu Picchu. The tourist district of Cusco is a beautiful and fascinating city that reflects both Incan and pre-Incan Latin America and the heavy Spanish influence brought by the 16th- century conquistadors. While the city is beautiful, and the worlds have intertwined over the centuries, it remains a land where there is tension between the different cultures.
At just over 11,000 feet, the air is thin and visitors get easily winded just walking the hills. The villages we worked in were all about an hour outside of Cusco. They were impoverished and dilapidated, with some of the homes still constructed of bricks made from mud and straw. Dogs and farm animals roamed the streets. July is midwinter there, and it’s the dry season, so everything – and everyone – was covered in a layer of Andean grit. By the end of each day, we were as well.
I wish I could say that I wasn’t anxious about the work, but I was. What can a psychiatrist do in a single visit, much less a single session that requires one, and occasionally two, translators, in a population where I had no knowledge of their culture or resources? I didn’t know what types of patients I might see, if using medication would be reasonable, or if follow-up of any kind would be feasible. In the 27 missions of Hands Across the Americas, I was to be the first psychiatrist.
Four years earlier, a psychologist, Dr. David Doolittle, had gone with another psychologist, and when we spoke on the phone, he was very enthusiastic. He told me that this had been one of the best experiences of his professional life, and he was pleased to hear that mental health would continue to be a part of the agenda.
Finally, I should add that despite my hesitation about how helpful I might be as part of a medical team offering one-time services, I did have a similar experience in a different setting; In 2005, I volunteered for 2 weeks with the Substance Abuse and Mental Health Services Administration’s Katrina Assistance Project, and while I wondered then if my efforts were helpful to those I was trying to serve, I walked away feeling that I personally had gotten a great deal from the experience. I decided I would go to Peru with limited expectations and one simple agenda: I would try to be helpful.
The mission started with a brief orientation in Cusco, and it didn’t escape me when the medical director announced that patients could be seen by internal medicine, pediatrics, ENT, gynecology, and optometry. Psychiatry was strangely missing from the list, and when I pointed this out, he told me he had a special job for me: to run the pharmacy. While I was happy to help dispense medications, I had the sense that this population might have unmet mental health needs and suggested that it could be worthwhile to offer psychiatry as a specialty as well!
While the group came with an extensive supply of medications, vitamins, reading glasses, toothbrushes, and some wheelchairs, canes, and walkers, there were no psychotropic medications in the stash. I spoke with a local doctor who served as a liaison, and learned that he was familiar only with diazepam and alprazolam. Psychiatric patients were referred to doctors in Cusco, and local doctors did not prescribe antidepressants. For complex issues that required medical or surgical subspecialization, the referrals were even more complex: Patients traveled 18 hours by bus to be treated in Lima.
On the morning of our first clinic, I was given a small supply of fluoxetine (per my request) and alprazolam. Over 5 days we worked in three sites. On the first day, we were at the municipal center in Huarocondo, a little more than an hour outside of Cusco. Tents were set up inside the building, with the waiting room, triage, and pharmacy all stationed outside on the dirt. Inside, there was very little light, and like the other places we’d set up, no heat. My tent had a table and two chairs meant for primary school children, and I absconded with an adult-sized plastic chair for my interpreter. We had no access to medical records, no labs or radiographic equipment, and no clear place to send anyone for follow-up – this was true across all specialties, though the ENT who was working with us had come with suitcases full of his own equipment. Patients didn’t know what a psychiatrist or psychologist was, and some responded to questions about depression by saying that their blood pressure was just fine. Triage resorted to asking people if they felt sad and wanted to talk to a doctor about it.
The next 2 days, we worked in medical clinics in Ancahuasi and Anta, and while the conditions were more conducive to providing medical care, there was still no heat, the lighting was poor, and the buildings had not seen new coats of paint or furniture in many years. The clinics did not have psychiatrists, but they did each have a psychologist, and a couple of the people I saw had been seen. I was also told that fluoxetine could be obtained in Anta.
Hundreds of patients came each day, and all told, more than a thousand patients were seen by nine doctors in those 5 days. My official psychiatry tally was 79, but my personal count was less – I imagine some people became impatient with the long line and left without being seen – I recorded visits with 8-15 people each day.
First, let me say that I was surprised at the lack of pure psychopathology; the issues were more reactions to tremendous deprivation, violence, loneliness, medical and developmental disorders, and chronic struggles. I saw only two adult men, the rest of the patients were women and a few children. No one I saw had ever seen a psychiatrist before, and no one had taken psychotropic medications (not even the diazepam or alprazolam, which I was told could be obtained), and in fact, very few were on any medications of any kind. No one had ever been in a psychiatric hospital. Poverty was rampant, as was domestic violence: Men beat their wives, parents beat their children, and there seemed to be no societal means to interrupt this. One bruised woman said her husband had been released from jail in a day, and several women spoke of living in fear for their lives; still, their families encouraged them to stay with men who were abusive or unfaithful. I was told that the statistic for spousal abuse in Peru was 60%, in Cusco it was 75%; I suspect it was even higher in these outlying villages. Families were fractured; employment was physically very difficult; and stress was extreme. Low mood and poor sleep were pervasive, but given the fact that I was unsure if people could get follow-up or even afford to refill medications, I gave out very little in the way of medications, and used the fluoxetine only for a few people where I felt their mood and circumstances were so dire that perhaps it would help – and it seemed unlikely to hurt. I was able to hospitalize one 18-year-old mother who was suicidal and said she had tried to hang herself, though she was released early the next morning before she was ever seen by a doctor; she did note she felt much better and was grateful for the help.
Despite tremendous stresses and limited access to care, the suicide rate in Peru are quite low at 3.2 per 100,000 (as compared with nearly 14 per 100,000 in the United States), and despite the fact that some of the patients I saw had considered it, most said that their children or animals needed them, and there are religious prohibitions.
At moments, I wondered what I could possibly offer. One woman came in with a 5-year-old child with Down syndrome strapped to her, and another, older, developmentally delayed child in tow. There were other children at home, and while many women noted that their husbands beat them while they were drunk, this woman said her husband was calmer when he was drinking; he beat her when he was sober. I asked her what would help, and she said she needed money. Feeling I had nothing else to offer, I did something I have never done in my years as a psychiatrist: I gave her money. I hoped that she would spend it on something that might provide a moment of relief from her anguished life.
For the most part, it was interesting work, and often, it felt useful to make psychological interventions, to validate the distress the patients felt and to reorient them to seeing their own strengths. The people talked of holding their problems close, and of a relief and ease that came with sharing their difficulties.
In the end, I did feel helpful for at least some of the patients some of the time. At the very least, I felt appreciated – in one clinic, we were greeted by the mayor and a band – and patients expressed their thanks to both me and my cadre of interpreters, sometimes profusely. In the end, it was an adventure, from the vacation with 16 people to Lima, the Sacred Valley, and Machu Picchu, to my foray into high-volume, single-session psychiatry in a culture so vastly different from my own.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: Johns Hopkins University Press, 2011).

CMS Proposes Major Initiative for Hip and Knee Replacements
In an attempt to reduce the rate and cost of complications following hip and knee replacements among Medicare beneficiaries, the Centers for Medicare & Medicaid Services (CMS) announced a new Comprehensive Care for Joint Replacement payment model. With this new measure, the CMS proposes to hold hospitals accountable for the quality of care they deliver to Medicare fee-for-service beneficiaries for hip and knee replacements from surgery through recovery.
“We are committed to changing our health care system to pay for quality over quantity, so that we spend our dollars more wisely and improve care for patients,” said Sylvia M. Burwell, Secretary of Health and Human Services.

Through the proposed 5-year payment model, health care providers in 75 geographic areas would continue to be paid under existing Medicare payment systems. However, the hospital where the hip or knee replacement is performed would be held liable for the quality and costs of care for the duration of care, from the time of the surgery through 90 days after discharge.
Depending on the hospital’s quality and cost performance during the episode, the hospital may receive an additional payment or be required to repay Medicare for a portion of the episode costs. As a result, hospitals would have an incentive to work with physicians, home health agencies, and nursing facilities to ensure that beneficiaries receive the coordinated care they need, with the goal of reducing avoidable hospitalizations and complications. Hospitals would receive tools, such as spending and utilization data and sharing of best practices, to improve the effectiveness of care coordination.
These bundled payments for joint replacement surgeries would build upon successful demonstration programs already underway in Medicare. This model is also consistent with the private sector, where major employers and leading providers and care systems are moving towards bundled payments for orthopedic services.
“Today, we are taking another important step to improve the quality of care for the hundreds of thousands of Americans who have hip and knee replacements through Medicare every year. By focusing on episodes of care, rather than a piecemeal system, hospitals and physicians have an incentive to work together to deliver more effective and efficient care. This model will incentivize providing patients with the right care the first time and finding better ways to help them recover successfully. It will reward providers and doctors for helping patients get and stay healthy, ” stated Ms. Burwell.
In an attempt to reduce the rate and cost of complications following hip and knee replacements among Medicare beneficiaries, the Centers for Medicare & Medicaid Services (CMS) announced a new Comprehensive Care for Joint Replacement payment model. With this new measure, the CMS proposes to hold hospitals accountable for the quality of care they deliver to Medicare fee-for-service beneficiaries for hip and knee replacements from surgery through recovery.
“We are committed to changing our health care system to pay for quality over quantity, so that we spend our dollars more wisely and improve care for patients,” said Sylvia M. Burwell, Secretary of Health and Human Services.
Through the proposed 5-year payment model, health care providers in 75 geographic areas would continue to be paid under existing Medicare payment systems. However, the hospital where the hip or knee replacement is performed would be held liable for the quality and costs of care for the duration of care, from the time of the surgery through 90 days after discharge.
Depending on the hospital’s quality and cost performance during the episode, the hospital may receive an additional payment or be required to repay Medicare for a portion of the episode costs. As a result, hospitals would have an incentive to work with physicians, home health agencies, and nursing facilities to ensure that beneficiaries receive the coordinated care they need, with the goal of reducing avoidable hospitalizations and complications. Hospitals would receive tools, such as spending and utilization data and sharing of best practices, to improve the effectiveness of care coordination.
These bundled payments for joint replacement surgeries would build upon successful demonstration programs already underway in Medicare. This model is also consistent with the private sector, where major employers and leading providers and care systems are moving towards bundled payments for orthopedic services.
“Today, we are taking another important step to improve the quality of care for the hundreds of thousands of Americans who have hip and knee replacements through Medicare every year. By focusing on episodes of care, rather than a piecemeal system, hospitals and physicians have an incentive to work together to deliver more effective and efficient care. This model will incentivize providing patients with the right care the first time and finding better ways to help them recover successfully. It will reward providers and doctors for helping patients get and stay healthy, ” stated Ms. Burwell.
In an attempt to reduce the rate and cost of complications following hip and knee replacements among Medicare beneficiaries, the Centers for Medicare & Medicaid Services (CMS) announced a new Comprehensive Care for Joint Replacement payment model. With this new measure, the CMS proposes to hold hospitals accountable for the quality of care they deliver to Medicare fee-for-service beneficiaries for hip and knee replacements from surgery through recovery.
“We are committed to changing our health care system to pay for quality over quantity, so that we spend our dollars more wisely and improve care for patients,” said Sylvia M. Burwell, Secretary of Health and Human Services.
Through the proposed 5-year payment model, health care providers in 75 geographic areas would continue to be paid under existing Medicare payment systems. However, the hospital where the hip or knee replacement is performed would be held liable for the quality and costs of care for the duration of care, from the time of the surgery through 90 days after discharge.
Depending on the hospital’s quality and cost performance during the episode, the hospital may receive an additional payment or be required to repay Medicare for a portion of the episode costs. As a result, hospitals would have an incentive to work with physicians, home health agencies, and nursing facilities to ensure that beneficiaries receive the coordinated care they need, with the goal of reducing avoidable hospitalizations and complications. Hospitals would receive tools, such as spending and utilization data and sharing of best practices, to improve the effectiveness of care coordination.
These bundled payments for joint replacement surgeries would build upon successful demonstration programs already underway in Medicare. This model is also consistent with the private sector, where major employers and leading providers and care systems are moving towards bundled payments for orthopedic services.
“Today, we are taking another important step to improve the quality of care for the hundreds of thousands of Americans who have hip and knee replacements through Medicare every year. By focusing on episodes of care, rather than a piecemeal system, hospitals and physicians have an incentive to work together to deliver more effective and efficient care. This model will incentivize providing patients with the right care the first time and finding better ways to help them recover successfully. It will reward providers and doctors for helping patients get and stay healthy, ” stated Ms. Burwell.

PHM15: Challenging Diagnoses, Ethical Dilemmas in Pediatric Immigrant, Refugee Patient Cases
Presenters: Nichole Chandler MD, Suresh Nagappan MD MSPH, Angela Hartsell MD MPH, and Emily Hodnett MD
This workshop focused on interactive cases to highlight healthcare issues specific to the population of refugee/immigrant children in the US. It was an interactive format with small groups to allow the participants to work through the diagnoses by discovery. The cases included a Burmese infant with macrocephaly due to congenital toxoplasmosis and a school-age Eritrean child with abdominal pain due to Plasmodium vivax malaria. In addition to discussing the clinical presentation and work up of the patients, there were accompanying ethical dilemmas that were a part of taking care these patients. The presenters emphasized the importance of culturally sensitive communication and seeking competent translation for key clinical discussions. At the end, they supplied a list of resources for more information on refugees in the US and refugee healthcare.
Bethany Hodge MD MPH
Just for Kids Pediatric Hospitalists, Kosair Children’s Hospital
Assistant professor, Department of Pediatrics
Director of the Distinction in Global Health Track
University of Louisville School of Medicine
Presenters: Nichole Chandler MD, Suresh Nagappan MD MSPH, Angela Hartsell MD MPH, and Emily Hodnett MD
This workshop focused on interactive cases to highlight healthcare issues specific to the population of refugee/immigrant children in the US. It was an interactive format with small groups to allow the participants to work through the diagnoses by discovery. The cases included a Burmese infant with macrocephaly due to congenital toxoplasmosis and a school-age Eritrean child with abdominal pain due to Plasmodium vivax malaria. In addition to discussing the clinical presentation and work up of the patients, there were accompanying ethical dilemmas that were a part of taking care these patients. The presenters emphasized the importance of culturally sensitive communication and seeking competent translation for key clinical discussions. At the end, they supplied a list of resources for more information on refugees in the US and refugee healthcare.
Bethany Hodge MD MPH
Just for Kids Pediatric Hospitalists, Kosair Children’s Hospital
Assistant professor, Department of Pediatrics
Director of the Distinction in Global Health Track
University of Louisville School of Medicine
Presenters: Nichole Chandler MD, Suresh Nagappan MD MSPH, Angela Hartsell MD MPH, and Emily Hodnett MD
This workshop focused on interactive cases to highlight healthcare issues specific to the population of refugee/immigrant children in the US. It was an interactive format with small groups to allow the participants to work through the diagnoses by discovery. The cases included a Burmese infant with macrocephaly due to congenital toxoplasmosis and a school-age Eritrean child with abdominal pain due to Plasmodium vivax malaria. In addition to discussing the clinical presentation and work up of the patients, there were accompanying ethical dilemmas that were a part of taking care these patients. The presenters emphasized the importance of culturally sensitive communication and seeking competent translation for key clinical discussions. At the end, they supplied a list of resources for more information on refugees in the US and refugee healthcare.
Bethany Hodge MD MPH
Just for Kids Pediatric Hospitalists, Kosair Children’s Hospital
Assistant professor, Department of Pediatrics
Director of the Distinction in Global Health Track
University of Louisville School of Medicine
New hope for treating fatal subtype of ALL

Photo by Aaron Logan
Preclinical research has revealed potential therapeutic options for TCF3-HLF-positive acute lymphoblastic leukemia (ALL).
Investigators discovered a range of mutations in this subtype of ALL and identified features that appear to contribute to treatment resistance.
However, the team also found that TCF3-HLF-positive ALL is sensitive to treatment with glucocorticoids, anthracyclines, and certain agents in clinical development.
The BCL2-specific inhibitor venetoclax (ABT-199) proved particularly active against the disease.
Jean-Pierre Bourquin, MD, PhD, of the University Children’s Hospital Zurich in Switzerland, and his colleagues reported these findings in Nature Genetics.
The investigators sequenced samples from patients with TCF3-HLF-positive ALL and found a range of mutations. Most samples (67%) had deletions in PAX5, and most of the samples without PAX5 deletions had deletions in VPREB1.
The team also found recurrent mutations of TCF3, a new fusion gene (KHDRBS1-LCK), and activating mutations in RAS signaling pathway genes (NRAS, KRAS, and PTPN11), among other mutations.
After additional investigation, Dr Bourquin and his colleagues hypothesized that the initiating TCF3-HLF fusion in this disease occurs in a B-cell progenitor, and the specific lineage context is constrained further in a restricted developmental stage by additional mutations.
The investigators also tested various treatments in mouse models of TCF3-HLF-positive ALL. They observed resistance to dasatinib, nucleotide analogs, mitotic spindle inhibitors, and polo-like and aurora kinase inhibitors.
On the other hand, the disease was sensitive to glucocorticoids, mTOR inhibitors, anthracyclines, bortezomib, the HSP90 inhibitor AUY922, and panobinostat.
The team also found evidence suggesting that BCL2 might promote leukemic cell survival and constitute a druggable target in TCF3-HLF-positive ALL. So they tested the BCL2 inhibitor venetoclax in the mice.
A 2-week course of daily venetoclax significantly delayed leukemia progression, and xenografts from relapsed patients and those with minimal residual disease remained sensitive to venetoclax. The drug also exhibited synergistic effects when combined with vincristine or dexamethasone.
“Further studies are now needed to test how the results of our study might be used for therapeutic possibilities,” Dr Bourquin concluded. ![]()
Photo by Aaron Logan
Preclinical research has revealed potential therapeutic options for TCF3-HLF-positive acute lymphoblastic leukemia (ALL).
Investigators discovered a range of mutations in this subtype of ALL and identified features that appear to contribute to treatment resistance.
However, the team also found that TCF3-HLF-positive ALL is sensitive to treatment with glucocorticoids, anthracyclines, and certain agents in clinical development.
The BCL2-specific inhibitor venetoclax (ABT-199) proved particularly active against the disease.
Jean-Pierre Bourquin, MD, PhD, of the University Children’s Hospital Zurich in Switzerland, and his colleagues reported these findings in Nature Genetics.
The investigators sequenced samples from patients with TCF3-HLF-positive ALL and found a range of mutations. Most samples (67%) had deletions in PAX5, and most of the samples without PAX5 deletions had deletions in VPREB1.
The team also found recurrent mutations of TCF3, a new fusion gene (KHDRBS1-LCK), and activating mutations in RAS signaling pathway genes (NRAS, KRAS, and PTPN11), among other mutations.
After additional investigation, Dr Bourquin and his colleagues hypothesized that the initiating TCF3-HLF fusion in this disease occurs in a B-cell progenitor, and the specific lineage context is constrained further in a restricted developmental stage by additional mutations.
The investigators also tested various treatments in mouse models of TCF3-HLF-positive ALL. They observed resistance to dasatinib, nucleotide analogs, mitotic spindle inhibitors, and polo-like and aurora kinase inhibitors.
On the other hand, the disease was sensitive to glucocorticoids, mTOR inhibitors, anthracyclines, bortezomib, the HSP90 inhibitor AUY922, and panobinostat.
The team also found evidence suggesting that BCL2 might promote leukemic cell survival and constitute a druggable target in TCF3-HLF-positive ALL. So they tested the BCL2 inhibitor venetoclax in the mice.
A 2-week course of daily venetoclax significantly delayed leukemia progression, and xenografts from relapsed patients and those with minimal residual disease remained sensitive to venetoclax. The drug also exhibited synergistic effects when combined with vincristine or dexamethasone.
“Further studies are now needed to test how the results of our study might be used for therapeutic possibilities,” Dr Bourquin concluded. ![]()
Photo by Aaron Logan
Preclinical research has revealed potential therapeutic options for TCF3-HLF-positive acute lymphoblastic leukemia (ALL).
Investigators discovered a range of mutations in this subtype of ALL and identified features that appear to contribute to treatment resistance.
However, the team also found that TCF3-HLF-positive ALL is sensitive to treatment with glucocorticoids, anthracyclines, and certain agents in clinical development.
The BCL2-specific inhibitor venetoclax (ABT-199) proved particularly active against the disease.
Jean-Pierre Bourquin, MD, PhD, of the University Children’s Hospital Zurich in Switzerland, and his colleagues reported these findings in Nature Genetics.
The investigators sequenced samples from patients with TCF3-HLF-positive ALL and found a range of mutations. Most samples (67%) had deletions in PAX5, and most of the samples without PAX5 deletions had deletions in VPREB1.
The team also found recurrent mutations of TCF3, a new fusion gene (KHDRBS1-LCK), and activating mutations in RAS signaling pathway genes (NRAS, KRAS, and PTPN11), among other mutations.
After additional investigation, Dr Bourquin and his colleagues hypothesized that the initiating TCF3-HLF fusion in this disease occurs in a B-cell progenitor, and the specific lineage context is constrained further in a restricted developmental stage by additional mutations.
The investigators also tested various treatments in mouse models of TCF3-HLF-positive ALL. They observed resistance to dasatinib, nucleotide analogs, mitotic spindle inhibitors, and polo-like and aurora kinase inhibitors.
On the other hand, the disease was sensitive to glucocorticoids, mTOR inhibitors, anthracyclines, bortezomib, the HSP90 inhibitor AUY922, and panobinostat.
The team also found evidence suggesting that BCL2 might promote leukemic cell survival and constitute a druggable target in TCF3-HLF-positive ALL. So they tested the BCL2 inhibitor venetoclax in the mice.
A 2-week course of daily venetoclax significantly delayed leukemia progression, and xenografts from relapsed patients and those with minimal residual disease remained sensitive to venetoclax. The drug also exhibited synergistic effects when combined with vincristine or dexamethasone.
“Further studies are now needed to test how the results of our study might be used for therapeutic possibilities,” Dr Bourquin concluded. ![]()
Corrected iPSCs fight hemophilia A in mice

Image from the Salk Institute
Researchers say they have found a way to correct the chromosomal inversions that can cause severe hemophilia A.
The team used CRISPR-Cas9 RNA-guided engineered nucleases (RGENs) to correct the inversions and reverse factor VIII (FVIII) deficiency in patient-specific induced pluripotent stem cells (iPSCs).
Once the iPSCs had matured into endothelial cells, the group transplanted those cells into mice with hemophilia A.
This increased FVIII activity in the mice without any off-target effects.
The researchers described this work in Cell Stem Cell.
“We used CRISPR RGENs to repair two recurrent, large chromosomal inversions responsible for almost half of all severe hemophilia A cases,” said Jin-Soo Kim, PhD, of the Institute for Basic Science in Seoul, Korea.
The inversions involve the FVIII intron 1 homolog (responsible for about 5% of severe hemophilia A cases) and the intron 22 homolog (responsible for about 40% of cases).
The researchers first collected urinary cells from patients with these inversions, using the cells to generate iPSCs. The team then applied CRISPR-Cas9 RGENs.
The gene-editing technique effectively repaired the FVIII gene in iPSCs that had harbored either inversion. The researchers then forced the corrected iPSCs to differentiate into mature endothelial cells and found these cells successfully expressed the FVIII protein.
To verify that the endothelial cells could reverse FVIII deficiency, the team transplanted the cells into mice with hemophilia A.
The mice soon began producing FVIII on their own, although the FVIII activity in these mice was 10% that of wild-type mice. The activity was higher than FVIII activity in control mice with hemophilia A (3.3% of wild-type mice), but the difference was not statistically significant.
“To the best of our knowledge, this report is the first demonstration that chromosomal inversions or other large rearrangements can be corrected using RGENs or any other programmable nuclease in patient iPSCs,” said Dong-Wook Kim, PhD, of Yonsei University College of Medicine in Seoul, Korea.
The researchers also noted that there was no evidence of off-target mutations with the 3 RGENS used in this study. ![]()
Image from the Salk Institute
Researchers say they have found a way to correct the chromosomal inversions that can cause severe hemophilia A.
The team used CRISPR-Cas9 RNA-guided engineered nucleases (RGENs) to correct the inversions and reverse factor VIII (FVIII) deficiency in patient-specific induced pluripotent stem cells (iPSCs).
Once the iPSCs had matured into endothelial cells, the group transplanted those cells into mice with hemophilia A.
This increased FVIII activity in the mice without any off-target effects.
The researchers described this work in Cell Stem Cell.
“We used CRISPR RGENs to repair two recurrent, large chromosomal inversions responsible for almost half of all severe hemophilia A cases,” said Jin-Soo Kim, PhD, of the Institute for Basic Science in Seoul, Korea.
The inversions involve the FVIII intron 1 homolog (responsible for about 5% of severe hemophilia A cases) and the intron 22 homolog (responsible for about 40% of cases).
The researchers first collected urinary cells from patients with these inversions, using the cells to generate iPSCs. The team then applied CRISPR-Cas9 RGENs.
The gene-editing technique effectively repaired the FVIII gene in iPSCs that had harbored either inversion. The researchers then forced the corrected iPSCs to differentiate into mature endothelial cells and found these cells successfully expressed the FVIII protein.
To verify that the endothelial cells could reverse FVIII deficiency, the team transplanted the cells into mice with hemophilia A.
The mice soon began producing FVIII on their own, although the FVIII activity in these mice was 10% that of wild-type mice. The activity was higher than FVIII activity in control mice with hemophilia A (3.3% of wild-type mice), but the difference was not statistically significant.
“To the best of our knowledge, this report is the first demonstration that chromosomal inversions or other large rearrangements can be corrected using RGENs or any other programmable nuclease in patient iPSCs,” said Dong-Wook Kim, PhD, of Yonsei University College of Medicine in Seoul, Korea.
The researchers also noted that there was no evidence of off-target mutations with the 3 RGENS used in this study. ![]()
Image from the Salk Institute
Researchers say they have found a way to correct the chromosomal inversions that can cause severe hemophilia A.
The team used CRISPR-Cas9 RNA-guided engineered nucleases (RGENs) to correct the inversions and reverse factor VIII (FVIII) deficiency in patient-specific induced pluripotent stem cells (iPSCs).
Once the iPSCs had matured into endothelial cells, the group transplanted those cells into mice with hemophilia A.
This increased FVIII activity in the mice without any off-target effects.
The researchers described this work in Cell Stem Cell.
“We used CRISPR RGENs to repair two recurrent, large chromosomal inversions responsible for almost half of all severe hemophilia A cases,” said Jin-Soo Kim, PhD, of the Institute for Basic Science in Seoul, Korea.
The inversions involve the FVIII intron 1 homolog (responsible for about 5% of severe hemophilia A cases) and the intron 22 homolog (responsible for about 40% of cases).
The researchers first collected urinary cells from patients with these inversions, using the cells to generate iPSCs. The team then applied CRISPR-Cas9 RGENs.
The gene-editing technique effectively repaired the FVIII gene in iPSCs that had harbored either inversion. The researchers then forced the corrected iPSCs to differentiate into mature endothelial cells and found these cells successfully expressed the FVIII protein.
To verify that the endothelial cells could reverse FVIII deficiency, the team transplanted the cells into mice with hemophilia A.
The mice soon began producing FVIII on their own, although the FVIII activity in these mice was 10% that of wild-type mice. The activity was higher than FVIII activity in control mice with hemophilia A (3.3% of wild-type mice), but the difference was not statistically significant.
“To the best of our knowledge, this report is the first demonstration that chromosomal inversions or other large rearrangements can be corrected using RGENs or any other programmable nuclease in patient iPSCs,” said Dong-Wook Kim, PhD, of Yonsei University College of Medicine in Seoul, Korea.
The researchers also noted that there was no evidence of off-target mutations with the 3 RGENS used in this study. ![]()
Some AEs not reported according to regulations

Photo courtesy of the FDA
A new study indicates that drug manufacturers fail to report about 10% of serious and unexpected adverse events (AEs) within the timeframe set out in federal regulations.
Manufacturers are required to report a serious AE (death, hospitalization, disability, etc.) or unexpected AE (anything not listed in the drug’s label) to the US Food and Drug Administration (FDA) within 15 calendar days of learning about the event.
But an analysis of more than 1.6 million AE reports showed that manufacturers failed to meet this requirement for nearly 10% of AEs.
Pinar Karaca-Mandic, PhD, of the University of Minnesota School of Public Health in Minneapolis, and her colleagues conducted the analysis and detailed the results in JAMA Internal Medicine.
The team examined data from the FDA Adverse Event Reporting System for AE reports made from January 2004 through June 2014. The final study sample included only reports that were subject to the regulation requiring submission within 15 days—a total of 1,613,079 reports.
The researchers found that 9.94% of reports were not received by the FDA within the 15-day timeframe. This was a total of 160,383 reports—40,464 cases in which patients died and 119,919 in which they did not.
So 90.06% of reports (n=1,452,696) were reported within 15 days, 5.28% (n=85,161) were reported within 16 to 90 days, 2.19% (n=35,392) were reported within 91 to 180 days, and 2.47% (n=39,830) were reported after 180 days.
Multivariate analysis revealed that patient death was positively associated with delayed AE reporting. About 91% (90.71%) of AEs that did not involve death were reported within 15 days, compared to 88.25% of AEs that did involve death.
The percentage of reports received within 16 to 90 days was 5.19% for AEs without death and 6.42% for AEs with death. The percentage of reports received within 91 to 180 days was 1.98% and 2.53%, respectively. And the percentage of reports received after 180 days was 2.12% and 2.80%, respectively.
The researchers said perhaps manufacturers spend additional time verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.
In a related Editor’s Note, Rita F. Redberg, MD, editor of JAMA Internal Medicine, wrote that delays in reporting AEs should never occur because they mean exposing patients to serious harm, including death, that could potentially be avoided.
“One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer . . . ,” she wrote. “Physicians and their patients must be knowledgeable of benefits, harms, and alternatives for a wide choice of treatments, especially those recently approved for which clinical experience is limited.” ![]()
Photo courtesy of the FDA
A new study indicates that drug manufacturers fail to report about 10% of serious and unexpected adverse events (AEs) within the timeframe set out in federal regulations.
Manufacturers are required to report a serious AE (death, hospitalization, disability, etc.) or unexpected AE (anything not listed in the drug’s label) to the US Food and Drug Administration (FDA) within 15 calendar days of learning about the event.
But an analysis of more than 1.6 million AE reports showed that manufacturers failed to meet this requirement for nearly 10% of AEs.
Pinar Karaca-Mandic, PhD, of the University of Minnesota School of Public Health in Minneapolis, and her colleagues conducted the analysis and detailed the results in JAMA Internal Medicine.
The team examined data from the FDA Adverse Event Reporting System for AE reports made from January 2004 through June 2014. The final study sample included only reports that were subject to the regulation requiring submission within 15 days—a total of 1,613,079 reports.
The researchers found that 9.94% of reports were not received by the FDA within the 15-day timeframe. This was a total of 160,383 reports—40,464 cases in which patients died and 119,919 in which they did not.
So 90.06% of reports (n=1,452,696) were reported within 15 days, 5.28% (n=85,161) were reported within 16 to 90 days, 2.19% (n=35,392) were reported within 91 to 180 days, and 2.47% (n=39,830) were reported after 180 days.
Multivariate analysis revealed that patient death was positively associated with delayed AE reporting. About 91% (90.71%) of AEs that did not involve death were reported within 15 days, compared to 88.25% of AEs that did involve death.
The percentage of reports received within 16 to 90 days was 5.19% for AEs without death and 6.42% for AEs with death. The percentage of reports received within 91 to 180 days was 1.98% and 2.53%, respectively. And the percentage of reports received after 180 days was 2.12% and 2.80%, respectively.
The researchers said perhaps manufacturers spend additional time verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.
In a related Editor’s Note, Rita F. Redberg, MD, editor of JAMA Internal Medicine, wrote that delays in reporting AEs should never occur because they mean exposing patients to serious harm, including death, that could potentially be avoided.
“One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer . . . ,” she wrote. “Physicians and their patients must be knowledgeable of benefits, harms, and alternatives for a wide choice of treatments, especially those recently approved for which clinical experience is limited.” ![]()
Photo courtesy of the FDA
A new study indicates that drug manufacturers fail to report about 10% of serious and unexpected adverse events (AEs) within the timeframe set out in federal regulations.
Manufacturers are required to report a serious AE (death, hospitalization, disability, etc.) or unexpected AE (anything not listed in the drug’s label) to the US Food and Drug Administration (FDA) within 15 calendar days of learning about the event.
But an analysis of more than 1.6 million AE reports showed that manufacturers failed to meet this requirement for nearly 10% of AEs.
Pinar Karaca-Mandic, PhD, of the University of Minnesota School of Public Health in Minneapolis, and her colleagues conducted the analysis and detailed the results in JAMA Internal Medicine.
The team examined data from the FDA Adverse Event Reporting System for AE reports made from January 2004 through June 2014. The final study sample included only reports that were subject to the regulation requiring submission within 15 days—a total of 1,613,079 reports.
The researchers found that 9.94% of reports were not received by the FDA within the 15-day timeframe. This was a total of 160,383 reports—40,464 cases in which patients died and 119,919 in which they did not.
So 90.06% of reports (n=1,452,696) were reported within 15 days, 5.28% (n=85,161) were reported within 16 to 90 days, 2.19% (n=35,392) were reported within 91 to 180 days, and 2.47% (n=39,830) were reported after 180 days.
Multivariate analysis revealed that patient death was positively associated with delayed AE reporting. About 91% (90.71%) of AEs that did not involve death were reported within 15 days, compared to 88.25% of AEs that did involve death.
The percentage of reports received within 16 to 90 days was 5.19% for AEs without death and 6.42% for AEs with death. The percentage of reports received within 91 to 180 days was 1.98% and 2.53%, respectively. And the percentage of reports received after 180 days was 2.12% and 2.80%, respectively.
The researchers said perhaps manufacturers spend additional time verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.
In a related Editor’s Note, Rita F. Redberg, MD, editor of JAMA Internal Medicine, wrote that delays in reporting AEs should never occur because they mean exposing patients to serious harm, including death, that could potentially be avoided.
“One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer . . . ,” she wrote. “Physicians and their patients must be knowledgeable of benefits, harms, and alternatives for a wide choice of treatments, especially those recently approved for which clinical experience is limited.” ![]()