User login
Tool identifies optimal TKI for cancers

Photo courtesy of the
University of Colorado
Researchers say they have developed a tool that allows us to determine which tyrosine kinase inhibitor (TKI) will be most effective against a certain type of cancer.
The tool, known as the Kinase Addiction Ranker (KAR), predicts the genetic abnormalities that are driving the cancer in any population of cells and chooses the best TKI or combination of TKIs to target these abnormalities.
The researchers described the tool in Bioinformatics.
“A lot of [TKIs] inhibit a lot more than what they’re supposed to inhibit,” said study author Aik Choon Tan, PhD, of the University of Colorado Anschutz Medical Campus in Aurora.
“Maybe drug A was designed to inhibit kinase B, but it also inhibits kinase C and D as well. Our approach centers on exploiting the promiscuity of these drugs, the ‘drug spillover.’”
For each TKI, there is a signature describing the kinases each drug fully or partially inhibits. Dr Tan and his colleagues combined these kinase inhibition signatures with the results of high-throughput screening. They used the Genomics of Drug Sensitivity in Cancer database to determine which TKIs have already proven active against which cancer cell lines.
The result is KAR, which does 2 things. For any cancer cell line, the program ranks the kinases that are most important to the growth of the disease. Then, the program recommends the combination of existing TKIs that is likely to do the most good against the implicated kinases.
Dr Tan and his colleagues tested KAR using samples from 151 leukemia patients and found that, among the kinases analyzed, FLT3 had the highest variance in sensitivity to TKIs.
But EPHA5, EPHA3, and BTK were the kinases most commonly associated with drug sensitivity. They had significant associations in 72%, 58%, and 54% of the patient samples, respectively.
The researchers said the frequency of BTK dependence they observed is interesting given the fact that the BTK inhibitor ibrutinib produced favorable results in a phase 1b/2 trial of patients with chronic lymphocytic leukemia (CLL). The progression-free survival rate at 26 months was 75% in that trial.
Dr Tan and his colleagues said this was consistent with their findings, which showed that 70% of CLL patient data had a significant association between BTK inhibition and drug sensitivity.
The researchers also found that KAR could predict TKI sensitivity in 21 lung cancer cell lines. In addition, the tool was able to recommend a combination of TKIs that hindered proliferation in the lung cancer cell line H1581. KAR suggested ponatinib and the experimental anticancer agent AZD8055, and experiments showed that these drugs synergistically reduced proliferation in H1581.
KAR is available for download on the Tan lab’s website. ![]()
Photo courtesy of the
University of Colorado
Researchers say they have developed a tool that allows us to determine which tyrosine kinase inhibitor (TKI) will be most effective against a certain type of cancer.
The tool, known as the Kinase Addiction Ranker (KAR), predicts the genetic abnormalities that are driving the cancer in any population of cells and chooses the best TKI or combination of TKIs to target these abnormalities.
The researchers described the tool in Bioinformatics.
“A lot of [TKIs] inhibit a lot more than what they’re supposed to inhibit,” said study author Aik Choon Tan, PhD, of the University of Colorado Anschutz Medical Campus in Aurora.
“Maybe drug A was designed to inhibit kinase B, but it also inhibits kinase C and D as well. Our approach centers on exploiting the promiscuity of these drugs, the ‘drug spillover.’”
For each TKI, there is a signature describing the kinases each drug fully or partially inhibits. Dr Tan and his colleagues combined these kinase inhibition signatures with the results of high-throughput screening. They used the Genomics of Drug Sensitivity in Cancer database to determine which TKIs have already proven active against which cancer cell lines.
The result is KAR, which does 2 things. For any cancer cell line, the program ranks the kinases that are most important to the growth of the disease. Then, the program recommends the combination of existing TKIs that is likely to do the most good against the implicated kinases.
Dr Tan and his colleagues tested KAR using samples from 151 leukemia patients and found that, among the kinases analyzed, FLT3 had the highest variance in sensitivity to TKIs.
But EPHA5, EPHA3, and BTK were the kinases most commonly associated with drug sensitivity. They had significant associations in 72%, 58%, and 54% of the patient samples, respectively.
The researchers said the frequency of BTK dependence they observed is interesting given the fact that the BTK inhibitor ibrutinib produced favorable results in a phase 1b/2 trial of patients with chronic lymphocytic leukemia (CLL). The progression-free survival rate at 26 months was 75% in that trial.
Dr Tan and his colleagues said this was consistent with their findings, which showed that 70% of CLL patient data had a significant association between BTK inhibition and drug sensitivity.
The researchers also found that KAR could predict TKI sensitivity in 21 lung cancer cell lines. In addition, the tool was able to recommend a combination of TKIs that hindered proliferation in the lung cancer cell line H1581. KAR suggested ponatinib and the experimental anticancer agent AZD8055, and experiments showed that these drugs synergistically reduced proliferation in H1581.
KAR is available for download on the Tan lab’s website. ![]()
Photo courtesy of the
University of Colorado
Researchers say they have developed a tool that allows us to determine which tyrosine kinase inhibitor (TKI) will be most effective against a certain type of cancer.
The tool, known as the Kinase Addiction Ranker (KAR), predicts the genetic abnormalities that are driving the cancer in any population of cells and chooses the best TKI or combination of TKIs to target these abnormalities.
The researchers described the tool in Bioinformatics.
“A lot of [TKIs] inhibit a lot more than what they’re supposed to inhibit,” said study author Aik Choon Tan, PhD, of the University of Colorado Anschutz Medical Campus in Aurora.
“Maybe drug A was designed to inhibit kinase B, but it also inhibits kinase C and D as well. Our approach centers on exploiting the promiscuity of these drugs, the ‘drug spillover.’”
For each TKI, there is a signature describing the kinases each drug fully or partially inhibits. Dr Tan and his colleagues combined these kinase inhibition signatures with the results of high-throughput screening. They used the Genomics of Drug Sensitivity in Cancer database to determine which TKIs have already proven active against which cancer cell lines.
The result is KAR, which does 2 things. For any cancer cell line, the program ranks the kinases that are most important to the growth of the disease. Then, the program recommends the combination of existing TKIs that is likely to do the most good against the implicated kinases.
Dr Tan and his colleagues tested KAR using samples from 151 leukemia patients and found that, among the kinases analyzed, FLT3 had the highest variance in sensitivity to TKIs.
But EPHA5, EPHA3, and BTK were the kinases most commonly associated with drug sensitivity. They had significant associations in 72%, 58%, and 54% of the patient samples, respectively.
The researchers said the frequency of BTK dependence they observed is interesting given the fact that the BTK inhibitor ibrutinib produced favorable results in a phase 1b/2 trial of patients with chronic lymphocytic leukemia (CLL). The progression-free survival rate at 26 months was 75% in that trial.
Dr Tan and his colleagues said this was consistent with their findings, which showed that 70% of CLL patient data had a significant association between BTK inhibition and drug sensitivity.
The researchers also found that KAR could predict TKI sensitivity in 21 lung cancer cell lines. In addition, the tool was able to recommend a combination of TKIs that hindered proliferation in the lung cancer cell line H1581. KAR suggested ponatinib and the experimental anticancer agent AZD8055, and experiments showed that these drugs synergistically reduced proliferation in H1581.
KAR is available for download on the Tan lab’s website. ![]()
Analysis reveals ‘distinctive biology’ of CTCL
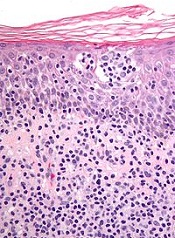
New research suggests cutaneous T-cell lymphoma (CTCL) is driven by a plethora of genetic mutations.
Investigators conducted a genomic analysis of normal and cancer cells from patients with CTCL and identified mutations in 17 genes that are implicated in CTCL pathogenesis.
They also found that somatic copy number variants (SCNVs) driving CTCL outnumbered somatic single-nucleotide variants (SSNVs) by more than 10 to 1.
The team reported these findings in Nature Genetics.
They performed exome and whole-genome DNA sequencing and RNA sequencing on purified CTCL cells and matched normal cells. And they identified genes implicated in CTCL pathogenesis by looking for:
- Genes with recurrent SSNVs altering the same amino acid more often than expected by chance
- Genes with SSNVs previously identified as recurrent mutations in other cancers
- Genes having a significantly increased burden of protein-altering SSNVs
- SCNVs that occurred more often than expected by chance.
This revealed mutations in 17 genes that are implicated in CTCL pathogenesis—TP53, ZEB1, ARID1A, DNMT3A, CDKN2A, FAS, NFKB2, CD28, RHOA, PLCG1, STAT5B, BRAF, ATM, CTCF, TNFAIP3, PRKCQ, and IRF4.
The investigators noted that these are genes involved in T-cell activation, apoptosis, NF-κB signaling, chromatin remodeling, and DNA damage response.
The team also discovered “a striking bias” for SCNVs as drivers of CTCL. They identified 12 statistically significant chromosome-arm SCNVs and 36 significant focal SCNVs.
Collectively, these SCNVs occurred 473 times in the CTCL samples analyzed—a mean of 7.5 focal deletions, 1.6 broad deletions, 1.0 focal amplification, and 1.8 broad amplifications per CTCL.
On the other hand, there were 38 SSNVs in CTCL driver genes—1.0 per tumor.
So, according to these data, SCNVs comprise 92% of all driver mutations in CTCL—a mean of 11.8 pathogenic SCNVs vs 1.0 SSNV per CTCL.
“This cancer has a very distinctive biology,” said Jaehyuk Choi, MD, PhD, of the Yale School of Medicine in New Haven, Connecticut.
And decoding this biology has revealed potential treatment approaches, according to Dr Choi and his colleagues.
For example, the presence of mutations activating the NF-κB pathway suggests NF-κB inhibitors such as bortezomib may have therapeutic potential in CTCL, and the presence of CD28 mutations suggests inhibitors such as abatacept may be effective against the disease. ![]()
New research suggests cutaneous T-cell lymphoma (CTCL) is driven by a plethora of genetic mutations.
Investigators conducted a genomic analysis of normal and cancer cells from patients with CTCL and identified mutations in 17 genes that are implicated in CTCL pathogenesis.
They also found that somatic copy number variants (SCNVs) driving CTCL outnumbered somatic single-nucleotide variants (SSNVs) by more than 10 to 1.
The team reported these findings in Nature Genetics.
They performed exome and whole-genome DNA sequencing and RNA sequencing on purified CTCL cells and matched normal cells. And they identified genes implicated in CTCL pathogenesis by looking for:
- Genes with recurrent SSNVs altering the same amino acid more often than expected by chance
- Genes with SSNVs previously identified as recurrent mutations in other cancers
- Genes having a significantly increased burden of protein-altering SSNVs
- SCNVs that occurred more often than expected by chance.
This revealed mutations in 17 genes that are implicated in CTCL pathogenesis—TP53, ZEB1, ARID1A, DNMT3A, CDKN2A, FAS, NFKB2, CD28, RHOA, PLCG1, STAT5B, BRAF, ATM, CTCF, TNFAIP3, PRKCQ, and IRF4.
The investigators noted that these are genes involved in T-cell activation, apoptosis, NF-κB signaling, chromatin remodeling, and DNA damage response.
The team also discovered “a striking bias” for SCNVs as drivers of CTCL. They identified 12 statistically significant chromosome-arm SCNVs and 36 significant focal SCNVs.
Collectively, these SCNVs occurred 473 times in the CTCL samples analyzed—a mean of 7.5 focal deletions, 1.6 broad deletions, 1.0 focal amplification, and 1.8 broad amplifications per CTCL.
On the other hand, there were 38 SSNVs in CTCL driver genes—1.0 per tumor.
So, according to these data, SCNVs comprise 92% of all driver mutations in CTCL—a mean of 11.8 pathogenic SCNVs vs 1.0 SSNV per CTCL.
“This cancer has a very distinctive biology,” said Jaehyuk Choi, MD, PhD, of the Yale School of Medicine in New Haven, Connecticut.
And decoding this biology has revealed potential treatment approaches, according to Dr Choi and his colleagues.
For example, the presence of mutations activating the NF-κB pathway suggests NF-κB inhibitors such as bortezomib may have therapeutic potential in CTCL, and the presence of CD28 mutations suggests inhibitors such as abatacept may be effective against the disease. ![]()
New research suggests cutaneous T-cell lymphoma (CTCL) is driven by a plethora of genetic mutations.
Investigators conducted a genomic analysis of normal and cancer cells from patients with CTCL and identified mutations in 17 genes that are implicated in CTCL pathogenesis.
They also found that somatic copy number variants (SCNVs) driving CTCL outnumbered somatic single-nucleotide variants (SSNVs) by more than 10 to 1.
The team reported these findings in Nature Genetics.
They performed exome and whole-genome DNA sequencing and RNA sequencing on purified CTCL cells and matched normal cells. And they identified genes implicated in CTCL pathogenesis by looking for:
- Genes with recurrent SSNVs altering the same amino acid more often than expected by chance
- Genes with SSNVs previously identified as recurrent mutations in other cancers
- Genes having a significantly increased burden of protein-altering SSNVs
- SCNVs that occurred more often than expected by chance.
This revealed mutations in 17 genes that are implicated in CTCL pathogenesis—TP53, ZEB1, ARID1A, DNMT3A, CDKN2A, FAS, NFKB2, CD28, RHOA, PLCG1, STAT5B, BRAF, ATM, CTCF, TNFAIP3, PRKCQ, and IRF4.
The investigators noted that these are genes involved in T-cell activation, apoptosis, NF-κB signaling, chromatin remodeling, and DNA damage response.
The team also discovered “a striking bias” for SCNVs as drivers of CTCL. They identified 12 statistically significant chromosome-arm SCNVs and 36 significant focal SCNVs.
Collectively, these SCNVs occurred 473 times in the CTCL samples analyzed—a mean of 7.5 focal deletions, 1.6 broad deletions, 1.0 focal amplification, and 1.8 broad amplifications per CTCL.
On the other hand, there were 38 SSNVs in CTCL driver genes—1.0 per tumor.
So, according to these data, SCNVs comprise 92% of all driver mutations in CTCL—a mean of 11.8 pathogenic SCNVs vs 1.0 SSNV per CTCL.
“This cancer has a very distinctive biology,” said Jaehyuk Choi, MD, PhD, of the Yale School of Medicine in New Haven, Connecticut.
And decoding this biology has revealed potential treatment approaches, according to Dr Choi and his colleagues.
For example, the presence of mutations activating the NF-κB pathway suggests NF-κB inhibitors such as bortezomib may have therapeutic potential in CTCL, and the presence of CD28 mutations suggests inhibitors such as abatacept may be effective against the disease. ![]()
Drones can transport blood samples

Robert Chalmers launch drone
Photo courtesy of
Johns Hopkins Medicine
Small drones can safely transport blood samples, according to a study published in PLOS ONE.
Investigators found that 40 minutes of travel on hobby-sized drones did not affect the results of common and routine blood tests.
The team said that’s promising news for people living in rural and economically impoverished areas that lack passable roads because drones can give healthcare workers quick access to lab tests needed for diagnoses and treatments.
“Biological samples can be very sensitive and fragile,” said study author Timothy Amukele, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
That sensitivity makes even the pneumatic tube systems used by many hospitals, for example, unsuitable for transporting blood for certain purposes.
Of particular concern related to the use of drones, Dr Amukele noted, is the sudden acceleration that marks the launch of the vehicle and the jostling when the drone lands on its belly.
“Such movements could have destroyed blood cells or prompted blood to coagulate, and I thought all kinds of blood tests might be affected, but our study shows they weren’t . . . ,” he said.
For the study, which Dr Amukele believes is the first rigorous examination of the impact of drone transport on biological samples, his team collected 6 blood samples from each of 56 healthy adult volunteers at The Johns Hopkins Hospital.
The samples were then driven to a flight site an hour’s drive from the hospital on days when the temperature was in the 70s. There, half of the samples were packaged for flight, with a view to protecting them for the in-flight environment and preventing leakage.
Those samples were then loaded into a hand-launched, fixed-wing drone and flown around for periods of 6 to 38 minutes. Owing to Federal Aviation Administration rules, the flights were conducted in an unpopulated area, stayed below 100 meters (328 feet) and were in the line of sight of the certified pilot.
The other samples were driven back from the drone flight field to The Johns Hopkins Hospital’s Core Laboratory, where they underwent the 33 most common laboratory tests that account for around 80% of all such tests done. A few of the tests performed were for sodium, glucose, and red blood cell count.
Comparing lab results of the flown versus nonflown blood samples, the investigators found that the flight did not have a significant impact.
Dr Amukele and his team noted that one blood test—the bicarbonate test—did yield different results for some of the flown versus nonflown samples. Dr Amukele said the team isn’t sure why, but the reason could be because the blood sat around for up to 8 hours before being tested.
There were no consistent differences between flown versus nonflown blood, he said, and it’s unknown whether the out-of-range results were due to the time lag or because of the drone transport.
“The ideal way to test that would be to fly the blood around immediately after drawing it, but neither the FAA nor Johns Hopkins would like drones flying around the hospital,” he said.
Given the successful results of this proof-of-concept study, Dr Amukele said the likely next step is a pilot study in a location in Africa where healthcare clinics are sometimes 60 or more miles away from labs.
“A drone could go 100 kilometers in 40 minutes,” he noted. “They’re less expensive than motorcycles and are not subject to traffic delays, and the technology already exists for the drone to be programmed to home to certain GPS coordinates, like a carrier pigeon.”
Drones have already been tested as carriers of medicines to clinics in remote areas, but whether and how drones will be used in flights over populated areas will depend on laws and regulations. ![]()
Robert Chalmers launch drone
Photo courtesy of
Johns Hopkins Medicine
Small drones can safely transport blood samples, according to a study published in PLOS ONE.
Investigators found that 40 minutes of travel on hobby-sized drones did not affect the results of common and routine blood tests.
The team said that’s promising news for people living in rural and economically impoverished areas that lack passable roads because drones can give healthcare workers quick access to lab tests needed for diagnoses and treatments.
“Biological samples can be very sensitive and fragile,” said study author Timothy Amukele, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
That sensitivity makes even the pneumatic tube systems used by many hospitals, for example, unsuitable for transporting blood for certain purposes.
Of particular concern related to the use of drones, Dr Amukele noted, is the sudden acceleration that marks the launch of the vehicle and the jostling when the drone lands on its belly.
“Such movements could have destroyed blood cells or prompted blood to coagulate, and I thought all kinds of blood tests might be affected, but our study shows they weren’t . . . ,” he said.
For the study, which Dr Amukele believes is the first rigorous examination of the impact of drone transport on biological samples, his team collected 6 blood samples from each of 56 healthy adult volunteers at The Johns Hopkins Hospital.
The samples were then driven to a flight site an hour’s drive from the hospital on days when the temperature was in the 70s. There, half of the samples were packaged for flight, with a view to protecting them for the in-flight environment and preventing leakage.
Those samples were then loaded into a hand-launched, fixed-wing drone and flown around for periods of 6 to 38 minutes. Owing to Federal Aviation Administration rules, the flights were conducted in an unpopulated area, stayed below 100 meters (328 feet) and were in the line of sight of the certified pilot.
The other samples were driven back from the drone flight field to The Johns Hopkins Hospital’s Core Laboratory, where they underwent the 33 most common laboratory tests that account for around 80% of all such tests done. A few of the tests performed were for sodium, glucose, and red blood cell count.
Comparing lab results of the flown versus nonflown blood samples, the investigators found that the flight did not have a significant impact.
Dr Amukele and his team noted that one blood test—the bicarbonate test—did yield different results for some of the flown versus nonflown samples. Dr Amukele said the team isn’t sure why, but the reason could be because the blood sat around for up to 8 hours before being tested.
There were no consistent differences between flown versus nonflown blood, he said, and it’s unknown whether the out-of-range results were due to the time lag or because of the drone transport.
“The ideal way to test that would be to fly the blood around immediately after drawing it, but neither the FAA nor Johns Hopkins would like drones flying around the hospital,” he said.
Given the successful results of this proof-of-concept study, Dr Amukele said the likely next step is a pilot study in a location in Africa where healthcare clinics are sometimes 60 or more miles away from labs.
“A drone could go 100 kilometers in 40 minutes,” he noted. “They’re less expensive than motorcycles and are not subject to traffic delays, and the technology already exists for the drone to be programmed to home to certain GPS coordinates, like a carrier pigeon.”
Drones have already been tested as carriers of medicines to clinics in remote areas, but whether and how drones will be used in flights over populated areas will depend on laws and regulations. ![]()
Robert Chalmers launch drone
Photo courtesy of
Johns Hopkins Medicine
Small drones can safely transport blood samples, according to a study published in PLOS ONE.
Investigators found that 40 minutes of travel on hobby-sized drones did not affect the results of common and routine blood tests.
The team said that’s promising news for people living in rural and economically impoverished areas that lack passable roads because drones can give healthcare workers quick access to lab tests needed for diagnoses and treatments.
“Biological samples can be very sensitive and fragile,” said study author Timothy Amukele, MD, PhD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
That sensitivity makes even the pneumatic tube systems used by many hospitals, for example, unsuitable for transporting blood for certain purposes.
Of particular concern related to the use of drones, Dr Amukele noted, is the sudden acceleration that marks the launch of the vehicle and the jostling when the drone lands on its belly.
“Such movements could have destroyed blood cells or prompted blood to coagulate, and I thought all kinds of blood tests might be affected, but our study shows they weren’t . . . ,” he said.
For the study, which Dr Amukele believes is the first rigorous examination of the impact of drone transport on biological samples, his team collected 6 blood samples from each of 56 healthy adult volunteers at The Johns Hopkins Hospital.
The samples were then driven to a flight site an hour’s drive from the hospital on days when the temperature was in the 70s. There, half of the samples were packaged for flight, with a view to protecting them for the in-flight environment and preventing leakage.
Those samples were then loaded into a hand-launched, fixed-wing drone and flown around for periods of 6 to 38 minutes. Owing to Federal Aviation Administration rules, the flights were conducted in an unpopulated area, stayed below 100 meters (328 feet) and were in the line of sight of the certified pilot.
The other samples were driven back from the drone flight field to The Johns Hopkins Hospital’s Core Laboratory, where they underwent the 33 most common laboratory tests that account for around 80% of all such tests done. A few of the tests performed were for sodium, glucose, and red blood cell count.
Comparing lab results of the flown versus nonflown blood samples, the investigators found that the flight did not have a significant impact.
Dr Amukele and his team noted that one blood test—the bicarbonate test—did yield different results for some of the flown versus nonflown samples. Dr Amukele said the team isn’t sure why, but the reason could be because the blood sat around for up to 8 hours before being tested.
There were no consistent differences between flown versus nonflown blood, he said, and it’s unknown whether the out-of-range results were due to the time lag or because of the drone transport.
“The ideal way to test that would be to fly the blood around immediately after drawing it, but neither the FAA nor Johns Hopkins would like drones flying around the hospital,” he said.
Given the successful results of this proof-of-concept study, Dr Amukele said the likely next step is a pilot study in a location in Africa where healthcare clinics are sometimes 60 or more miles away from labs.
“A drone could go 100 kilometers in 40 minutes,” he noted. “They’re less expensive than motorcycles and are not subject to traffic delays, and the technology already exists for the drone to be programmed to home to certain GPS coordinates, like a carrier pigeon.”
Drones have already been tested as carriers of medicines to clinics in remote areas, but whether and how drones will be used in flights over populated areas will depend on laws and regulations. ![]()
10 Tips for Hospitalists to Achieve an Effective Medical Consult
A medical consult is an amazing way to learn. Consultation challenges us to practice our best medicine while also exposing us to innovations in other specialties. It can forge new and productive relationships with physicians from all specialties. At its best, it is the purest of medicine or, as some put it, “medicine without the drama.”
As hospitalists, we are increasingly asked to be medical consultants and co-managers. Yet most training programs spend very little time educating residents on what makes a high-quality consultation. One of the first articles written on this subject was by Lee Goldman and colleagues in 1983. In this article, Goldman sets out 10 commandments for effective consultation.1
Many of the lessons in these 10 commandments continue to ring true today. As primary providers, we know that consulting another service can run the gamut from being pleasant, helpful, and enlightening to being the most frustrating, slam-the-phone-down experience of the day. In this article, we update these commandments to create five golden rules for medical consultations that ensure that your referring providers’ experiences are purely positive.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
Five Golden Rules
1 Listen and determine the needs of your customer.
Understanding the needs of your requesting physician is paramount to being an effective consultant, and the first step is to determine the physician’s question. Some referring providers want the bird’s eye view of a general medicine consult, whereas others have just one specific question. In one study stratified by specialty, 59% of surgeons preferred a general medicine consult, while most non-surgeons preferred a focused consult.2
Next, establish the timeframe: Is it emergent, urgent, or routine? One rule of thumb is that all consults should be seen within 24 hours. But many consults need to be seen more quickly, or even immediately. For example, you may be correct to assume that a patient is stable enough to wait for your consult, but perhaps the lack of pre-operative medical assessment will cause her to lose her spot on the OR schedule. The orthopedic surgeon now operates late into the night. Truly understanding the needs of your referring provider might have avoided that scenario.
There are of course times when you really can’t get to a consult expeditiously, but you must let the referring provider know. Ultimately, once you agree upon the urgency, all parties, including the patient, will know when to expect the consultant at the bedside.
2 Look for yourself, and do it yourself.
We practice in an age in which we spend more time in front of computers than in front of patients. As Lee and colleagues write, “A consultant should not expect to make brilliant diagnostic conclusions based on an assessment of data that are already in the chart. Usually, if the answer could be deduced from this information, the consultations would not have been called.”1 Effective consultants always obtain their own history and physical—your special expertise may allow you to extract overlooked information.
In addition, simply leaving recommendations to repeat tests or obtain records often delays care. If you feel the information is vital, take it upon yourself to obtain it. This may include contacting outside primary care providers or medicine subspecialists, or getting outside records.
Although we are not the primary provider, our goal must always be to do what is best for our patients.
3 Make brief, detailed plans with contingencies.
Recommendations can easily be lost in the deluge of information bombarding the primary care team. Our goal is not only to make recommendations, but also to have them followed.
In a study looking at which aspects of a consultation lead to increased compliance, researchers noted that if dose and duration of therapy were not specified, 64% of recommendations were implemented.3 When only one was specified, implementation increased to 85%, and when both were specified, implementation rates increased to 100%. Sadly, only 15% of over 200 consults had both duration and dose in their recommendations. Another study on compliance found that when five or fewer recommendations were specified, compliance increased from 79% to 96%.4
Contingency plans are a way of life for hospitalists when we sign out. Consultations are no different. Patients we consult on are often critically ill, and their status is dynamic. Anticipating problems and giving recommendations if those problems arise can save valuable time later for both you and your colleagues.
As consultants, we often feel compelled to “do something,” yet we know as primary providers how frustrating it is to have a consultant ask for a battery of tests or treatments that don’t address the big picture. Never be afraid to recommend continuing current management if it is appropriate or even to recommend stopping treatment or avoiding additional testing when it does not help the patient.
In summary, consults are most effective when they are brief (five or fewer recommendations), are detailed, and provide contingency plans. What good is a great consultation if it is not followed?
4 Communicate, communicate, communicate.
When 323 surgeons and non-surgeons were surveyed, both groups agreed that initial recommendations should be discussed verbally. Direct verbal communication allows the primary team to provide important information that you may have missed. In addition, discussing recommendations improves compliance and allows everyone to agree on the next plan of action and provide a unified plan to the patient, improving patient satisfaction and adherence.
Lastly and most importantly, opening the lines of communication between consultant and requesting physician creates effective consulting relationships.
Developing this relationship with other services may mean that the next time you call them for a consult, you will already have good rapport to build on.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
5 Follow up.
Several studies have shown that follow-up notes improve compliance with recommendations.3,5 Follow-up is also important to ensure that critical recommendations are followed and that any changes in patient status can be addressed. Furthermore, following up can provide valuable feedback on your own initial clinical judgment. Finally, it is bad practice to recommend testing and then sign off before these tests are completed. Either you feel they are important to patient care and worth obtaining, or they are not needed.
Following these five golden rules can ensure that you are the consultant who gives other physicians the satisfying experience of an effective and great consult. If it’s done right, the experience of a general medicine consult is the purest of medicine.
Dr. Chang is assistant professor, inpatient medicine clerkship director, and director of education in the division of hospital medicine at Mount Sinai Medical Center in New York City. Dr. Gabriel is assistant professor and director of medicine consult preoperative services in the division of hospital medicine at Mount Sinai.
References
- Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755.
- Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275.
- Horwitz RI, Henes CG, Horwitz SM. Developing strategies for improving the diagnostic and management efficacy of medical consultations. J Chron Dis. 1983;36(2):213-218.
- Sears CL, Charlson ME. The effectiveness of a consultation: compliance with initial recommendations. Am J Med. 1983;74(5):870-876.
- MacKenzie TB, Popkin MK, Callies AL, Jorgensen CR, Cohn JN. The effectiveness of cardiology consultations. Concordance with diagnostic and drug recommendations. Chest. 1981;79(1):16-22.
A medical consult is an amazing way to learn. Consultation challenges us to practice our best medicine while also exposing us to innovations in other specialties. It can forge new and productive relationships with physicians from all specialties. At its best, it is the purest of medicine or, as some put it, “medicine without the drama.”
As hospitalists, we are increasingly asked to be medical consultants and co-managers. Yet most training programs spend very little time educating residents on what makes a high-quality consultation. One of the first articles written on this subject was by Lee Goldman and colleagues in 1983. In this article, Goldman sets out 10 commandments for effective consultation.1
Many of the lessons in these 10 commandments continue to ring true today. As primary providers, we know that consulting another service can run the gamut from being pleasant, helpful, and enlightening to being the most frustrating, slam-the-phone-down experience of the day. In this article, we update these commandments to create five golden rules for medical consultations that ensure that your referring providers’ experiences are purely positive.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
Five Golden Rules
1 Listen and determine the needs of your customer.
Understanding the needs of your requesting physician is paramount to being an effective consultant, and the first step is to determine the physician’s question. Some referring providers want the bird’s eye view of a general medicine consult, whereas others have just one specific question. In one study stratified by specialty, 59% of surgeons preferred a general medicine consult, while most non-surgeons preferred a focused consult.2
Next, establish the timeframe: Is it emergent, urgent, or routine? One rule of thumb is that all consults should be seen within 24 hours. But many consults need to be seen more quickly, or even immediately. For example, you may be correct to assume that a patient is stable enough to wait for your consult, but perhaps the lack of pre-operative medical assessment will cause her to lose her spot on the OR schedule. The orthopedic surgeon now operates late into the night. Truly understanding the needs of your referring provider might have avoided that scenario.
There are of course times when you really can’t get to a consult expeditiously, but you must let the referring provider know. Ultimately, once you agree upon the urgency, all parties, including the patient, will know when to expect the consultant at the bedside.
2 Look for yourself, and do it yourself.
We practice in an age in which we spend more time in front of computers than in front of patients. As Lee and colleagues write, “A consultant should not expect to make brilliant diagnostic conclusions based on an assessment of data that are already in the chart. Usually, if the answer could be deduced from this information, the consultations would not have been called.”1 Effective consultants always obtain their own history and physical—your special expertise may allow you to extract overlooked information.
In addition, simply leaving recommendations to repeat tests or obtain records often delays care. If you feel the information is vital, take it upon yourself to obtain it. This may include contacting outside primary care providers or medicine subspecialists, or getting outside records.
Although we are not the primary provider, our goal must always be to do what is best for our patients.
3 Make brief, detailed plans with contingencies.
Recommendations can easily be lost in the deluge of information bombarding the primary care team. Our goal is not only to make recommendations, but also to have them followed.
In a study looking at which aspects of a consultation lead to increased compliance, researchers noted that if dose and duration of therapy were not specified, 64% of recommendations were implemented.3 When only one was specified, implementation increased to 85%, and when both were specified, implementation rates increased to 100%. Sadly, only 15% of over 200 consults had both duration and dose in their recommendations. Another study on compliance found that when five or fewer recommendations were specified, compliance increased from 79% to 96%.4
Contingency plans are a way of life for hospitalists when we sign out. Consultations are no different. Patients we consult on are often critically ill, and their status is dynamic. Anticipating problems and giving recommendations if those problems arise can save valuable time later for both you and your colleagues.
As consultants, we often feel compelled to “do something,” yet we know as primary providers how frustrating it is to have a consultant ask for a battery of tests or treatments that don’t address the big picture. Never be afraid to recommend continuing current management if it is appropriate or even to recommend stopping treatment or avoiding additional testing when it does not help the patient.
In summary, consults are most effective when they are brief (five or fewer recommendations), are detailed, and provide contingency plans. What good is a great consultation if it is not followed?
4 Communicate, communicate, communicate.
When 323 surgeons and non-surgeons were surveyed, both groups agreed that initial recommendations should be discussed verbally. Direct verbal communication allows the primary team to provide important information that you may have missed. In addition, discussing recommendations improves compliance and allows everyone to agree on the next plan of action and provide a unified plan to the patient, improving patient satisfaction and adherence.
Lastly and most importantly, opening the lines of communication between consultant and requesting physician creates effective consulting relationships.
Developing this relationship with other services may mean that the next time you call them for a consult, you will already have good rapport to build on.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
5 Follow up.
Several studies have shown that follow-up notes improve compliance with recommendations.3,5 Follow-up is also important to ensure that critical recommendations are followed and that any changes in patient status can be addressed. Furthermore, following up can provide valuable feedback on your own initial clinical judgment. Finally, it is bad practice to recommend testing and then sign off before these tests are completed. Either you feel they are important to patient care and worth obtaining, or they are not needed.
Following these five golden rules can ensure that you are the consultant who gives other physicians the satisfying experience of an effective and great consult. If it’s done right, the experience of a general medicine consult is the purest of medicine.
Dr. Chang is assistant professor, inpatient medicine clerkship director, and director of education in the division of hospital medicine at Mount Sinai Medical Center in New York City. Dr. Gabriel is assistant professor and director of medicine consult preoperative services in the division of hospital medicine at Mount Sinai.
References
- Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755.
- Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275.
- Horwitz RI, Henes CG, Horwitz SM. Developing strategies for improving the diagnostic and management efficacy of medical consultations. J Chron Dis. 1983;36(2):213-218.
- Sears CL, Charlson ME. The effectiveness of a consultation: compliance with initial recommendations. Am J Med. 1983;74(5):870-876.
- MacKenzie TB, Popkin MK, Callies AL, Jorgensen CR, Cohn JN. The effectiveness of cardiology consultations. Concordance with diagnostic and drug recommendations. Chest. 1981;79(1):16-22.
A medical consult is an amazing way to learn. Consultation challenges us to practice our best medicine while also exposing us to innovations in other specialties. It can forge new and productive relationships with physicians from all specialties. At its best, it is the purest of medicine or, as some put it, “medicine without the drama.”
As hospitalists, we are increasingly asked to be medical consultants and co-managers. Yet most training programs spend very little time educating residents on what makes a high-quality consultation. One of the first articles written on this subject was by Lee Goldman and colleagues in 1983. In this article, Goldman sets out 10 commandments for effective consultation.1
Many of the lessons in these 10 commandments continue to ring true today. As primary providers, we know that consulting another service can run the gamut from being pleasant, helpful, and enlightening to being the most frustrating, slam-the-phone-down experience of the day. In this article, we update these commandments to create five golden rules for medical consultations that ensure that your referring providers’ experiences are purely positive.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
Five Golden Rules
1 Listen and determine the needs of your customer.
Understanding the needs of your requesting physician is paramount to being an effective consultant, and the first step is to determine the physician’s question. Some referring providers want the bird’s eye view of a general medicine consult, whereas others have just one specific question. In one study stratified by specialty, 59% of surgeons preferred a general medicine consult, while most non-surgeons preferred a focused consult.2
Next, establish the timeframe: Is it emergent, urgent, or routine? One rule of thumb is that all consults should be seen within 24 hours. But many consults need to be seen more quickly, or even immediately. For example, you may be correct to assume that a patient is stable enough to wait for your consult, but perhaps the lack of pre-operative medical assessment will cause her to lose her spot on the OR schedule. The orthopedic surgeon now operates late into the night. Truly understanding the needs of your referring provider might have avoided that scenario.
There are of course times when you really can’t get to a consult expeditiously, but you must let the referring provider know. Ultimately, once you agree upon the urgency, all parties, including the patient, will know when to expect the consultant at the bedside.
2 Look for yourself, and do it yourself.
We practice in an age in which we spend more time in front of computers than in front of patients. As Lee and colleagues write, “A consultant should not expect to make brilliant diagnostic conclusions based on an assessment of data that are already in the chart. Usually, if the answer could be deduced from this information, the consultations would not have been called.”1 Effective consultants always obtain their own history and physical—your special expertise may allow you to extract overlooked information.
In addition, simply leaving recommendations to repeat tests or obtain records often delays care. If you feel the information is vital, take it upon yourself to obtain it. This may include contacting outside primary care providers or medicine subspecialists, or getting outside records.
Although we are not the primary provider, our goal must always be to do what is best for our patients.
3 Make brief, detailed plans with contingencies.
Recommendations can easily be lost in the deluge of information bombarding the primary care team. Our goal is not only to make recommendations, but also to have them followed.
In a study looking at which aspects of a consultation lead to increased compliance, researchers noted that if dose and duration of therapy were not specified, 64% of recommendations were implemented.3 When only one was specified, implementation increased to 85%, and when both were specified, implementation rates increased to 100%. Sadly, only 15% of over 200 consults had both duration and dose in their recommendations. Another study on compliance found that when five or fewer recommendations were specified, compliance increased from 79% to 96%.4
Contingency plans are a way of life for hospitalists when we sign out. Consultations are no different. Patients we consult on are often critically ill, and their status is dynamic. Anticipating problems and giving recommendations if those problems arise can save valuable time later for both you and your colleagues.
As consultants, we often feel compelled to “do something,” yet we know as primary providers how frustrating it is to have a consultant ask for a battery of tests or treatments that don’t address the big picture. Never be afraid to recommend continuing current management if it is appropriate or even to recommend stopping treatment or avoiding additional testing when it does not help the patient.
In summary, consults are most effective when they are brief (five or fewer recommendations), are detailed, and provide contingency plans. What good is a great consultation if it is not followed?
4 Communicate, communicate, communicate.
When 323 surgeons and non-surgeons were surveyed, both groups agreed that initial recommendations should be discussed verbally. Direct verbal communication allows the primary team to provide important information that you may have missed. In addition, discussing recommendations improves compliance and allows everyone to agree on the next plan of action and provide a unified plan to the patient, improving patient satisfaction and adherence.
Lastly and most importantly, opening the lines of communication between consultant and requesting physician creates effective consulting relationships.
Developing this relationship with other services may mean that the next time you call them for a consult, you will already have good rapport to build on.
One warning about communication: If you do not agree with the primary team’s plan of care, make sure you discuss these concerns instead of just writing them in the chart. Any teaching moments should be reserved for those who are open to that discussion, not forced on providers who are not receptive to it at that time.
5 Follow up.
Several studies have shown that follow-up notes improve compliance with recommendations.3,5 Follow-up is also important to ensure that critical recommendations are followed and that any changes in patient status can be addressed. Furthermore, following up can provide valuable feedback on your own initial clinical judgment. Finally, it is bad practice to recommend testing and then sign off before these tests are completed. Either you feel they are important to patient care and worth obtaining, or they are not needed.
Following these five golden rules can ensure that you are the consultant who gives other physicians the satisfying experience of an effective and great consult. If it’s done right, the experience of a general medicine consult is the purest of medicine.
Dr. Chang is assistant professor, inpatient medicine clerkship director, and director of education in the division of hospital medicine at Mount Sinai Medical Center in New York City. Dr. Gabriel is assistant professor and director of medicine consult preoperative services in the division of hospital medicine at Mount Sinai.
References
- Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755.
- Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275.
- Horwitz RI, Henes CG, Horwitz SM. Developing strategies for improving the diagnostic and management efficacy of medical consultations. J Chron Dis. 1983;36(2):213-218.
- Sears CL, Charlson ME. The effectiveness of a consultation: compliance with initial recommendations. Am J Med. 1983;74(5):870-876.
- MacKenzie TB, Popkin MK, Callies AL, Jorgensen CR, Cohn JN. The effectiveness of cardiology consultations. Concordance with diagnostic and drug recommendations. Chest. 1981;79(1):16-22.
New Bill Hopes to Increase Residency Medicare Slots after Two Previous Bills Failed

Two federal bills introduced in 2013, the Resident Physician Shortage Reduction Act and the Training Tomorrow’s Doctors Today Act, would have increased the number of Medicare-funded residency slots by 15,000 over five years. The latter bill also would have required each teaching hospital to release annual reports on the costs of training residents and of running specialized services, and it would have tied 2% to 3% of IME funding to quality measures, such as how well an institution trains providers to work in teams and in different settings. (In 2010, the Medicare Payment Advisory Commission, also known as MedPAC, instead recommended redirecting more than half of Medicare’s IME funding to performance-based incentives.)
After both bills died in the House of Representatives, supporters resurrected some key features and incorporated them into the Resident Physician Shortage Reduction Act of 2015 (H.R. 2124), reintroduced this spring in both the House and the Senate. The new version again seeks to increase Medicare residency slots by 15,000 over five years, while attempting to identify physician shortage specialties and increase the workforce diversity.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and a member of the IOM committee that recommended a significant GME overhaul, says requirements to increase the transparency of actual training costs would be a step in the right direction if implemented appropriately. She is less enthusiastic about tying a small percentage of funding to quality measures without moving to a robust system that ties funding to residency education in a meaningful way. The IOM report concluded that overall reform of the system is needed, she says, “not tweaking at the edges.”
A bold overhaul may be a tough sell, however, and she acknowledges that the committee’s own recommendations have gained little traction so far.
Vikas Parekh, MD, FACP, SFHM, chair of the SHM Academic Hospitalist Committee, says putting 2% or 3% of a hospital’s total Medicare money at risk is more in line with what the agency is doing in other quality improvement programs.
“So far,” he says, “the indications are that that’s enough money for most big academic medical centers to pay attention to it.”
Two federal bills introduced in 2013, the Resident Physician Shortage Reduction Act and the Training Tomorrow’s Doctors Today Act, would have increased the number of Medicare-funded residency slots by 15,000 over five years. The latter bill also would have required each teaching hospital to release annual reports on the costs of training residents and of running specialized services, and it would have tied 2% to 3% of IME funding to quality measures, such as how well an institution trains providers to work in teams and in different settings. (In 2010, the Medicare Payment Advisory Commission, also known as MedPAC, instead recommended redirecting more than half of Medicare’s IME funding to performance-based incentives.)
After both bills died in the House of Representatives, supporters resurrected some key features and incorporated them into the Resident Physician Shortage Reduction Act of 2015 (H.R. 2124), reintroduced this spring in both the House and the Senate. The new version again seeks to increase Medicare residency slots by 15,000 over five years, while attempting to identify physician shortage specialties and increase the workforce diversity.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and a member of the IOM committee that recommended a significant GME overhaul, says requirements to increase the transparency of actual training costs would be a step in the right direction if implemented appropriately. She is less enthusiastic about tying a small percentage of funding to quality measures without moving to a robust system that ties funding to residency education in a meaningful way. The IOM report concluded that overall reform of the system is needed, she says, “not tweaking at the edges.”
A bold overhaul may be a tough sell, however, and she acknowledges that the committee’s own recommendations have gained little traction so far.
Vikas Parekh, MD, FACP, SFHM, chair of the SHM Academic Hospitalist Committee, says putting 2% or 3% of a hospital’s total Medicare money at risk is more in line with what the agency is doing in other quality improvement programs.
“So far,” he says, “the indications are that that’s enough money for most big academic medical centers to pay attention to it.”
Two federal bills introduced in 2013, the Resident Physician Shortage Reduction Act and the Training Tomorrow’s Doctors Today Act, would have increased the number of Medicare-funded residency slots by 15,000 over five years. The latter bill also would have required each teaching hospital to release annual reports on the costs of training residents and of running specialized services, and it would have tied 2% to 3% of IME funding to quality measures, such as how well an institution trains providers to work in teams and in different settings. (In 2010, the Medicare Payment Advisory Commission, also known as MedPAC, instead recommended redirecting more than half of Medicare’s IME funding to performance-based incentives.)
After both bills died in the House of Representatives, supporters resurrected some key features and incorporated them into the Resident Physician Shortage Reduction Act of 2015 (H.R. 2124), reintroduced this spring in both the House and the Senate. The new version again seeks to increase Medicare residency slots by 15,000 over five years, while attempting to identify physician shortage specialties and increase the workforce diversity.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and a member of the IOM committee that recommended a significant GME overhaul, says requirements to increase the transparency of actual training costs would be a step in the right direction if implemented appropriately. She is less enthusiastic about tying a small percentage of funding to quality measures without moving to a robust system that ties funding to residency education in a meaningful way. The IOM report concluded that overall reform of the system is needed, she says, “not tweaking at the edges.”
A bold overhaul may be a tough sell, however, and she acknowledges that the committee’s own recommendations have gained little traction so far.
Vikas Parekh, MD, FACP, SFHM, chair of the SHM Academic Hospitalist Committee, says putting 2% or 3% of a hospital’s total Medicare money at risk is more in line with what the agency is doing in other quality improvement programs.
“So far,” he says, “the indications are that that’s enough money for most big academic medical centers to pay attention to it.”
Hospitalist Hopes to Build Website Featuring Stories about Delivering Babies in the 1950s

When Ruth Ann Crystal, MD, performed her residency at Stanford University Medical Center more than 15 years ago, she often worked side by side in the operating room with one of her favorite professors, Bert Johnson, MD, a skilled surgeon and obstetrician. While performing vaginal hysterectomies, Dr. Johnson would often share stories of when he was a resident back in the 1950s at the Chicago Maternity Center (CMC) and delivered babies for poor families on Chicago’s south side.
One of the stories Dr. Johnson told was about a time when he and another medical student were called to a home to “turn a baby that was stuck,” recalls Dr. Crystal, now a hospitalist at El Camino Hospital, which supports two campuses in Mountain View, Calif., and Los Gatos, Calif. They were going to administer ether, which is highly flammable, to the young mother to relax the uterus and help turn the baby, but then realized that a wood fire was burning. As the woman writhed in pain, they doused the flames with water.
“He said it was like Dante’s Inferno as smoke filled the room,” Dr. Crystal says. “It was quite the scene.”
Stories told by Dr. Johnson and other physicians who worked at the CMC during medical school or residency in the 1950s are legendary. They reflect a time in medicine when doctors not only made house calls, but also stayed in the family’s home until the baby was delivered, getting glimpses into the life of the poor. In an effort to preserve these stories, Dr. Crystal wanted to produce a one-hour PBS documentary called Catch the Baby. But financial realities set in, and she now plans to convert the stories into short vignettes that will be posted on a website by the same name for medical humanities classes.
“I thought, ‘Wow, this is an amazing part of history that shouldn’t be lost,’” says Dr. Crystal, who also supports a private practice. “The Chicago Maternity Center was an incredible place that, for almost 80 years, taught medical students how to be self-sufficient.
They learned “to count on their own skills and [find] ways of solving problems in very real situations when being sent out to these deliveries.”
Big Plans, No Budget
During her residency, Dr. Crystal videotaped approximately seven hours of interviews with Dr. Johnson about his experiences at CMC. She planned to write a book about the 80-something-year-old doctor, who still owns a ranch, ropes cattle, and, at one time, headed the California Beef Council; however, her job, growing family, and well, life, simply got in the way.
Then, in 2009, roughly a decade later, one of her patients mentioned that she knew a film crew who produced documentaries for PBS. Dr. Crystal asked for an introduction.
Members of the film crew were excited about the project. Their first task was to create a trailer for the documentary. They spent an entire day filming Dr. Johnson at his ranch telling stories about kitchen table deliveries in the slums and doing activities around the ranch, like roping cattle with a fellow cowboy—someone he actually delivered as a baby years ago. More film was later shot at the Santa Clara Valley Medical Center of Dr. Johnson performing a C-section and vaginal delivery with a resident and medical student.
The four-minute and 20-second trailer cost $37,000, she says, explaining that the money was mostly raised through donations from Dr. Johnson’s “cowboy friends” who also owned ranches in the area. It is still posted on the original website Dr. Crystal created: www.CatchTheBaby.com.
–Dr. Crystal
Now came the hard part—fundraising.
“I found out that I would have to raise between $650,000 and $700,000 to make a one-hour film,” Dr. Crystal says. “I tried, but I’m a doctor and don’t like asking people for money. I realized that probably wasn’t going to happen.”
But she wasn’t willing to abandon the project. So she turned her attention to YouTube, which, by then, had been online for four years. At the time, shorter videos were popular. Dr. Crystal had to develop a new plan.
Her current goal is to build a website that would highlight the CMC stories, which would be part of a medical humanities course at medical schools across the country. Medical students, residents, and other doctors could learn about the history of medicine and obstetrics. She says there are many lessons to be learned that don’t involve medical procedures, such as the impact of social and cultural issues on a physician’s ability to deliver healthcare.

“We need to look back on the important lessons the medical students learned at the CMC,” she says. “Not about how to do specific procedures, but how to interact with patients who may be very different from themselves.”
There seems to be plenty of interest in the topic; Dr. Crystal has since built a Twitter following of 5,700 people who read articles she tweets about medicine’s past, present, and future (@CatchTheBaby).
Still, she needs to build the website, edit the hours of film into short films, and then post them on the website with a study guide. The cost, she says, could run anywhere between $35,000 and $65,000.
“I don’t necessarily have to work with people who are PBS documentarians,” she says, adding that over recent years she has contacted several university film professors and students who turned down the project because it was too much to tackle. “I’d like to use a crowd-funding [platform like] Kickstarter or Indiegogo to raise the money, so I could edit the film.”
Meanwhile, Dr. Johnson is getting older and would enjoy seeing this project completed. So would his friends who helped pay for the trailer and original filming, says Dr. Crystal. Besides, she believes these stories can help new doctors better balance their focus between technology and face time with patients.
“Medical school education is changing quite a bit,” she says. “Despite advances in technology, we can’t forget we’re treating a human being first.”
Carol Patton is a freelance writer in Las Vegas.
When Ruth Ann Crystal, MD, performed her residency at Stanford University Medical Center more than 15 years ago, she often worked side by side in the operating room with one of her favorite professors, Bert Johnson, MD, a skilled surgeon and obstetrician. While performing vaginal hysterectomies, Dr. Johnson would often share stories of when he was a resident back in the 1950s at the Chicago Maternity Center (CMC) and delivered babies for poor families on Chicago’s south side.
One of the stories Dr. Johnson told was about a time when he and another medical student were called to a home to “turn a baby that was stuck,” recalls Dr. Crystal, now a hospitalist at El Camino Hospital, which supports two campuses in Mountain View, Calif., and Los Gatos, Calif. They were going to administer ether, which is highly flammable, to the young mother to relax the uterus and help turn the baby, but then realized that a wood fire was burning. As the woman writhed in pain, they doused the flames with water.
“He said it was like Dante’s Inferno as smoke filled the room,” Dr. Crystal says. “It was quite the scene.”
Stories told by Dr. Johnson and other physicians who worked at the CMC during medical school or residency in the 1950s are legendary. They reflect a time in medicine when doctors not only made house calls, but also stayed in the family’s home until the baby was delivered, getting glimpses into the life of the poor. In an effort to preserve these stories, Dr. Crystal wanted to produce a one-hour PBS documentary called Catch the Baby. But financial realities set in, and she now plans to convert the stories into short vignettes that will be posted on a website by the same name for medical humanities classes.
“I thought, ‘Wow, this is an amazing part of history that shouldn’t be lost,’” says Dr. Crystal, who also supports a private practice. “The Chicago Maternity Center was an incredible place that, for almost 80 years, taught medical students how to be self-sufficient.
They learned “to count on their own skills and [find] ways of solving problems in very real situations when being sent out to these deliveries.”
Big Plans, No Budget
During her residency, Dr. Crystal videotaped approximately seven hours of interviews with Dr. Johnson about his experiences at CMC. She planned to write a book about the 80-something-year-old doctor, who still owns a ranch, ropes cattle, and, at one time, headed the California Beef Council; however, her job, growing family, and well, life, simply got in the way.
Then, in 2009, roughly a decade later, one of her patients mentioned that she knew a film crew who produced documentaries for PBS. Dr. Crystal asked for an introduction.
Members of the film crew were excited about the project. Their first task was to create a trailer for the documentary. They spent an entire day filming Dr. Johnson at his ranch telling stories about kitchen table deliveries in the slums and doing activities around the ranch, like roping cattle with a fellow cowboy—someone he actually delivered as a baby years ago. More film was later shot at the Santa Clara Valley Medical Center of Dr. Johnson performing a C-section and vaginal delivery with a resident and medical student.
The four-minute and 20-second trailer cost $37,000, she says, explaining that the money was mostly raised through donations from Dr. Johnson’s “cowboy friends” who also owned ranches in the area. It is still posted on the original website Dr. Crystal created: www.CatchTheBaby.com.
–Dr. Crystal
Now came the hard part—fundraising.
“I found out that I would have to raise between $650,000 and $700,000 to make a one-hour film,” Dr. Crystal says. “I tried, but I’m a doctor and don’t like asking people for money. I realized that probably wasn’t going to happen.”
But she wasn’t willing to abandon the project. So she turned her attention to YouTube, which, by then, had been online for four years. At the time, shorter videos were popular. Dr. Crystal had to develop a new plan.
Her current goal is to build a website that would highlight the CMC stories, which would be part of a medical humanities course at medical schools across the country. Medical students, residents, and other doctors could learn about the history of medicine and obstetrics. She says there are many lessons to be learned that don’t involve medical procedures, such as the impact of social and cultural issues on a physician’s ability to deliver healthcare.
“We need to look back on the important lessons the medical students learned at the CMC,” she says. “Not about how to do specific procedures, but how to interact with patients who may be very different from themselves.”
There seems to be plenty of interest in the topic; Dr. Crystal has since built a Twitter following of 5,700 people who read articles she tweets about medicine’s past, present, and future (@CatchTheBaby).
Still, she needs to build the website, edit the hours of film into short films, and then post them on the website with a study guide. The cost, she says, could run anywhere between $35,000 and $65,000.
“I don’t necessarily have to work with people who are PBS documentarians,” she says, adding that over recent years she has contacted several university film professors and students who turned down the project because it was too much to tackle. “I’d like to use a crowd-funding [platform like] Kickstarter or Indiegogo to raise the money, so I could edit the film.”
Meanwhile, Dr. Johnson is getting older and would enjoy seeing this project completed. So would his friends who helped pay for the trailer and original filming, says Dr. Crystal. Besides, she believes these stories can help new doctors better balance their focus between technology and face time with patients.
“Medical school education is changing quite a bit,” she says. “Despite advances in technology, we can’t forget we’re treating a human being first.”
Carol Patton is a freelance writer in Las Vegas.
When Ruth Ann Crystal, MD, performed her residency at Stanford University Medical Center more than 15 years ago, she often worked side by side in the operating room with one of her favorite professors, Bert Johnson, MD, a skilled surgeon and obstetrician. While performing vaginal hysterectomies, Dr. Johnson would often share stories of when he was a resident back in the 1950s at the Chicago Maternity Center (CMC) and delivered babies for poor families on Chicago’s south side.
One of the stories Dr. Johnson told was about a time when he and another medical student were called to a home to “turn a baby that was stuck,” recalls Dr. Crystal, now a hospitalist at El Camino Hospital, which supports two campuses in Mountain View, Calif., and Los Gatos, Calif. They were going to administer ether, which is highly flammable, to the young mother to relax the uterus and help turn the baby, but then realized that a wood fire was burning. As the woman writhed in pain, they doused the flames with water.
“He said it was like Dante’s Inferno as smoke filled the room,” Dr. Crystal says. “It was quite the scene.”
Stories told by Dr. Johnson and other physicians who worked at the CMC during medical school or residency in the 1950s are legendary. They reflect a time in medicine when doctors not only made house calls, but also stayed in the family’s home until the baby was delivered, getting glimpses into the life of the poor. In an effort to preserve these stories, Dr. Crystal wanted to produce a one-hour PBS documentary called Catch the Baby. But financial realities set in, and she now plans to convert the stories into short vignettes that will be posted on a website by the same name for medical humanities classes.
“I thought, ‘Wow, this is an amazing part of history that shouldn’t be lost,’” says Dr. Crystal, who also supports a private practice. “The Chicago Maternity Center was an incredible place that, for almost 80 years, taught medical students how to be self-sufficient.
They learned “to count on their own skills and [find] ways of solving problems in very real situations when being sent out to these deliveries.”
Big Plans, No Budget
During her residency, Dr. Crystal videotaped approximately seven hours of interviews with Dr. Johnson about his experiences at CMC. She planned to write a book about the 80-something-year-old doctor, who still owns a ranch, ropes cattle, and, at one time, headed the California Beef Council; however, her job, growing family, and well, life, simply got in the way.
Then, in 2009, roughly a decade later, one of her patients mentioned that she knew a film crew who produced documentaries for PBS. Dr. Crystal asked for an introduction.
Members of the film crew were excited about the project. Their first task was to create a trailer for the documentary. They spent an entire day filming Dr. Johnson at his ranch telling stories about kitchen table deliveries in the slums and doing activities around the ranch, like roping cattle with a fellow cowboy—someone he actually delivered as a baby years ago. More film was later shot at the Santa Clara Valley Medical Center of Dr. Johnson performing a C-section and vaginal delivery with a resident and medical student.
The four-minute and 20-second trailer cost $37,000, she says, explaining that the money was mostly raised through donations from Dr. Johnson’s “cowboy friends” who also owned ranches in the area. It is still posted on the original website Dr. Crystal created: www.CatchTheBaby.com.
–Dr. Crystal
Now came the hard part—fundraising.
“I found out that I would have to raise between $650,000 and $700,000 to make a one-hour film,” Dr. Crystal says. “I tried, but I’m a doctor and don’t like asking people for money. I realized that probably wasn’t going to happen.”
But she wasn’t willing to abandon the project. So she turned her attention to YouTube, which, by then, had been online for four years. At the time, shorter videos were popular. Dr. Crystal had to develop a new plan.
Her current goal is to build a website that would highlight the CMC stories, which would be part of a medical humanities course at medical schools across the country. Medical students, residents, and other doctors could learn about the history of medicine and obstetrics. She says there are many lessons to be learned that don’t involve medical procedures, such as the impact of social and cultural issues on a physician’s ability to deliver healthcare.
“We need to look back on the important lessons the medical students learned at the CMC,” she says. “Not about how to do specific procedures, but how to interact with patients who may be very different from themselves.”
There seems to be plenty of interest in the topic; Dr. Crystal has since built a Twitter following of 5,700 people who read articles she tweets about medicine’s past, present, and future (@CatchTheBaby).
Still, she needs to build the website, edit the hours of film into short films, and then post them on the website with a study guide. The cost, she says, could run anywhere between $35,000 and $65,000.
“I don’t necessarily have to work with people who are PBS documentarians,” she says, adding that over recent years she has contacted several university film professors and students who turned down the project because it was too much to tackle. “I’d like to use a crowd-funding [platform like] Kickstarter or Indiegogo to raise the money, so I could edit the film.”
Meanwhile, Dr. Johnson is getting older and would enjoy seeing this project completed. So would his friends who helped pay for the trailer and original filming, says Dr. Crystal. Besides, she believes these stories can help new doctors better balance their focus between technology and face time with patients.
“Medical school education is changing quite a bit,” she says. “Despite advances in technology, we can’t forget we’re treating a human being first.”
Carol Patton is a freelance writer in Las Vegas.
Most Important Elements of End-of-Life Care

An Australian team conducted a literature review of expected deaths in the hospital—where the majority of deaths in the developed world occur—and identified elements of end-of-life care that are important to patients and families.1 Published in the British journal Palliative Medicine, the review of nine electronic data bases and 1859 articles released between 1990 and 2014 identified eight quantitative studies that met inclusion criteria.
The authors, led by Claudia Virdun, RN, of the faculty of health at the University of Technology in Sydney, found four end-of-life domains that were most important to both patients and families:
- Effective communication and shared decision-making;
- Expert care;
- Respectful and compassionate care; and
- Trust and confidence in clinicians.
Not all patients dying in hospitals receive best evidence-based palliative care, the authors note, adding that the “challenge for healthcare services is to act on this evidence, reconfigure care systems accordingly and ensure universal access to optimal end-of-life care within hospitals.”
Reference
- Virdun C, Luckett T, Davidson PM, Phillips J. Dying in the hospital setting: A systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important [published online ahead of print April 28, 2015]. Palliat Med.
An Australian team conducted a literature review of expected deaths in the hospital—where the majority of deaths in the developed world occur—and identified elements of end-of-life care that are important to patients and families.1 Published in the British journal Palliative Medicine, the review of nine electronic data bases and 1859 articles released between 1990 and 2014 identified eight quantitative studies that met inclusion criteria.
The authors, led by Claudia Virdun, RN, of the faculty of health at the University of Technology in Sydney, found four end-of-life domains that were most important to both patients and families:
- Effective communication and shared decision-making;
- Expert care;
- Respectful and compassionate care; and
- Trust and confidence in clinicians.
Not all patients dying in hospitals receive best evidence-based palliative care, the authors note, adding that the “challenge for healthcare services is to act on this evidence, reconfigure care systems accordingly and ensure universal access to optimal end-of-life care within hospitals.”
Reference
- Virdun C, Luckett T, Davidson PM, Phillips J. Dying in the hospital setting: A systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important [published online ahead of print April 28, 2015]. Palliat Med.
An Australian team conducted a literature review of expected deaths in the hospital—where the majority of deaths in the developed world occur—and identified elements of end-of-life care that are important to patients and families.1 Published in the British journal Palliative Medicine, the review of nine electronic data bases and 1859 articles released between 1990 and 2014 identified eight quantitative studies that met inclusion criteria.
The authors, led by Claudia Virdun, RN, of the faculty of health at the University of Technology in Sydney, found four end-of-life domains that were most important to both patients and families:
- Effective communication and shared decision-making;
- Expert care;
- Respectful and compassionate care; and
- Trust and confidence in clinicians.
Not all patients dying in hospitals receive best evidence-based palliative care, the authors note, adding that the “challenge for healthcare services is to act on this evidence, reconfigure care systems accordingly and ensure universal access to optimal end-of-life care within hospitals.”
Reference
- Virdun C, Luckett T, Davidson PM, Phillips J. Dying in the hospital setting: A systematic review of quantitative studies identifying the elements of end-of-life care that patients and their families rank as being most important [published online ahead of print April 28, 2015]. Palliat Med.
Highest-Volume Hospitals Linked with Lower Risk for Some Procedures
An estimated 11,000 deaths could have been prevented between 2010 and 2012, if patients who went to the U.S. hospitals with the lowest patient volumes for five common procedures and conditions had gone instead to the highest-volume hospitals, according to analysis presented in U.S. News and World Report’s “Best Hospitals for Common Care.”1
For example, one small rural hospital’s relative risk for death from elective knee replacement was 24 times the national average.”1
Reference
- Sternberg S, Dougherty G. Risks are high at low-volume hospitals. May 18, 2015. U.S. News & World Report. Accessed July 2, 2015.
An estimated 11,000 deaths could have been prevented between 2010 and 2012, if patients who went to the U.S. hospitals with the lowest patient volumes for five common procedures and conditions had gone instead to the highest-volume hospitals, according to analysis presented in U.S. News and World Report’s “Best Hospitals for Common Care.”1
For example, one small rural hospital’s relative risk for death from elective knee replacement was 24 times the national average.”1
Reference
- Sternberg S, Dougherty G. Risks are high at low-volume hospitals. May 18, 2015. U.S. News & World Report. Accessed July 2, 2015.
An estimated 11,000 deaths could have been prevented between 2010 and 2012, if patients who went to the U.S. hospitals with the lowest patient volumes for five common procedures and conditions had gone instead to the highest-volume hospitals, according to analysis presented in U.S. News and World Report’s “Best Hospitals for Common Care.”1
For example, one small rural hospital’s relative risk for death from elective knee replacement was 24 times the national average.”1
Reference
- Sternberg S, Dougherty G. Risks are high at low-volume hospitals. May 18, 2015. U.S. News & World Report. Accessed July 2, 2015.
Clinical Variables Predict Debridement Failure in Septic Arthritis
Clinical question: What risk factors predict septic arthritis surgical debridement failure?
Background: Standard treatment of septic arthritis is debridement and antibiotics. Unfortunately, 23%-48% of patients fail single debridement. Data is limited on what factors correlate with treatment failure.
Study design: Retrospective, logistic regression analysis.
Setting: Billing database query of one academic medical center from 2000-2011.
Synopsis: After excluding patients with orthopedic comorbidities, multivariate logistic regression was performed on 128 patients greater than 18 years of age and treated operatively for septic arthritis, 38% of whom had failed a single debridement. Five significant independent clinical variables were identified as predictors for failure of a single surgical debridement:
- History of inflammatory arthropathy (OR, 7.3; 95% CI, 2.4 to 22.6; P<0.001);
- Involvement of a large joint (knee, shoulder, or hip; OR 7.0; 95% CI, 1.2-37.5; P=0.02);
- Synovial fluid nucleated cell count >85.0 x 109 cells/L (OR, 4.7; 95% CI, 1.8-17.7; P=0.002);
- S. aureus as an isolate (OR, 4.6; 95% CI, 1.8 to 11.9; P=0.002); and
- History of diabetes (OR, 2.6; 95% CI, 1.1 to 6.2; P=0.04).
Using these variables, a prognostic model was created with an ROC curve of 0.79.
The study’s limitations include its retrospective nature, reliance on coding and documentation, small sample size, and the fact that all patients were treated at a single center.
Bottom line: Risk factors for failing single debridement in septic arthritis include inflammatory arthropathy, large joint involvement, more than 85.0 x 109 nucleated cells, S. aureus infection, and history of diabetes.
Citation: Hunter JG, Gross JM, Dahl JD, Amsdell SL, Gorczyca JT. Risk factors for failure of a single surgical debridement in adults with acute septic arthritis. J Bone Joint Surg Am. 2015;97(7):558-564.
Clinical question: What risk factors predict septic arthritis surgical debridement failure?
Background: Standard treatment of septic arthritis is debridement and antibiotics. Unfortunately, 23%-48% of patients fail single debridement. Data is limited on what factors correlate with treatment failure.
Study design: Retrospective, logistic regression analysis.
Setting: Billing database query of one academic medical center from 2000-2011.
Synopsis: After excluding patients with orthopedic comorbidities, multivariate logistic regression was performed on 128 patients greater than 18 years of age and treated operatively for septic arthritis, 38% of whom had failed a single debridement. Five significant independent clinical variables were identified as predictors for failure of a single surgical debridement:
- History of inflammatory arthropathy (OR, 7.3; 95% CI, 2.4 to 22.6; P<0.001);
- Involvement of a large joint (knee, shoulder, or hip; OR 7.0; 95% CI, 1.2-37.5; P=0.02);
- Synovial fluid nucleated cell count >85.0 x 109 cells/L (OR, 4.7; 95% CI, 1.8-17.7; P=0.002);
- S. aureus as an isolate (OR, 4.6; 95% CI, 1.8 to 11.9; P=0.002); and
- History of diabetes (OR, 2.6; 95% CI, 1.1 to 6.2; P=0.04).
Using these variables, a prognostic model was created with an ROC curve of 0.79.
The study’s limitations include its retrospective nature, reliance on coding and documentation, small sample size, and the fact that all patients were treated at a single center.
Bottom line: Risk factors for failing single debridement in septic arthritis include inflammatory arthropathy, large joint involvement, more than 85.0 x 109 nucleated cells, S. aureus infection, and history of diabetes.
Citation: Hunter JG, Gross JM, Dahl JD, Amsdell SL, Gorczyca JT. Risk factors for failure of a single surgical debridement in adults with acute septic arthritis. J Bone Joint Surg Am. 2015;97(7):558-564.
Clinical question: What risk factors predict septic arthritis surgical debridement failure?
Background: Standard treatment of septic arthritis is debridement and antibiotics. Unfortunately, 23%-48% of patients fail single debridement. Data is limited on what factors correlate with treatment failure.
Study design: Retrospective, logistic regression analysis.
Setting: Billing database query of one academic medical center from 2000-2011.
Synopsis: After excluding patients with orthopedic comorbidities, multivariate logistic regression was performed on 128 patients greater than 18 years of age and treated operatively for septic arthritis, 38% of whom had failed a single debridement. Five significant independent clinical variables were identified as predictors for failure of a single surgical debridement:
- History of inflammatory arthropathy (OR, 7.3; 95% CI, 2.4 to 22.6; P<0.001);
- Involvement of a large joint (knee, shoulder, or hip; OR 7.0; 95% CI, 1.2-37.5; P=0.02);
- Synovial fluid nucleated cell count >85.0 x 109 cells/L (OR, 4.7; 95% CI, 1.8-17.7; P=0.002);
- S. aureus as an isolate (OR, 4.6; 95% CI, 1.8 to 11.9; P=0.002); and
- History of diabetes (OR, 2.6; 95% CI, 1.1 to 6.2; P=0.04).
Using these variables, a prognostic model was created with an ROC curve of 0.79.
The study’s limitations include its retrospective nature, reliance on coding and documentation, small sample size, and the fact that all patients were treated at a single center.
Bottom line: Risk factors for failing single debridement in septic arthritis include inflammatory arthropathy, large joint involvement, more than 85.0 x 109 nucleated cells, S. aureus infection, and history of diabetes.
Citation: Hunter JG, Gross JM, Dahl JD, Amsdell SL, Gorczyca JT. Risk factors for failure of a single surgical debridement in adults with acute septic arthritis. J Bone Joint Surg Am. 2015;97(7):558-564.
Prednisolone or Pentoxifylline Show No Mortality Benefit in Alcoholic Hepatitis
Clinical question: Does administration of prednisolone or pentoxifylline reduce mortality in patients hospitalized with severe alcoholic hepatitis?
Background: Alcoholic hepatitis is associated with high mortality. Studies have shown unclear mortality benefit with prednisolone and pentoxifylline. Despite multiple studies and meta-analyses, controversy about the use of these medications persists.
Study Design: Multicenter, double-blind, randomized trial with 2-by-2 design.
Setting: Sixty-five hospitals across the United Kingdom.
Synopsis: Approximately 1,100 patients with a clinical diagnosis of alcoholic hepatitis were randomized to four groups: placebo + placebo; prednisolone + pentoxifylline-matched placebo; prednisolone-matched placebo + pentoxifylline; or prednisolone + pentoxifylline. Groups received 28 days of treatment. The primary endpoint was 28-day mortality. Secondary endpoints were mortality or liver transplantation at 90 days and one year.
Neither intervention showed a significant reduction in 28-day mortality. Secondary analysis with adjustments for risk showed a reduction in 28-day mortality in the prednisolone groups. There was no difference between groups for mortality or liver transplantation at 90 days or one year.
Adverse events of death, infection, and acute kidney injury were reported in 42% of patients. Infection rates were higher in the prednisolone groups; however, attributable deaths were no different between groups.
Patients in this trial were younger, with a lower incidence of encephalopathy, infection, and acute kidney injury than those seen in similar trials, which could affect the rates of mortality seen here. Also, liver biopsy was not used, so patients may have been incorrectly included.
Bottom line: No difference was found in mortality or liver transplantation at 90 days and one year for prednisolone or pentoxifylline, although subanalysis showed there may be short-term benefit with prednisolone.
Citation: Thursz MR, Richardson P, Allison M, et al. Prednisolone or pentoxifylline for alcoholic hepatitis. New Engl J Med. 2015;372(17):1619-1628.
Clinical question: Does administration of prednisolone or pentoxifylline reduce mortality in patients hospitalized with severe alcoholic hepatitis?
Background: Alcoholic hepatitis is associated with high mortality. Studies have shown unclear mortality benefit with prednisolone and pentoxifylline. Despite multiple studies and meta-analyses, controversy about the use of these medications persists.
Study Design: Multicenter, double-blind, randomized trial with 2-by-2 design.
Setting: Sixty-five hospitals across the United Kingdom.
Synopsis: Approximately 1,100 patients with a clinical diagnosis of alcoholic hepatitis were randomized to four groups: placebo + placebo; prednisolone + pentoxifylline-matched placebo; prednisolone-matched placebo + pentoxifylline; or prednisolone + pentoxifylline. Groups received 28 days of treatment. The primary endpoint was 28-day mortality. Secondary endpoints were mortality or liver transplantation at 90 days and one year.
Neither intervention showed a significant reduction in 28-day mortality. Secondary analysis with adjustments for risk showed a reduction in 28-day mortality in the prednisolone groups. There was no difference between groups for mortality or liver transplantation at 90 days or one year.
Adverse events of death, infection, and acute kidney injury were reported in 42% of patients. Infection rates were higher in the prednisolone groups; however, attributable deaths were no different between groups.
Patients in this trial were younger, with a lower incidence of encephalopathy, infection, and acute kidney injury than those seen in similar trials, which could affect the rates of mortality seen here. Also, liver biopsy was not used, so patients may have been incorrectly included.
Bottom line: No difference was found in mortality or liver transplantation at 90 days and one year for prednisolone or pentoxifylline, although subanalysis showed there may be short-term benefit with prednisolone.
Citation: Thursz MR, Richardson P, Allison M, et al. Prednisolone or pentoxifylline for alcoholic hepatitis. New Engl J Med. 2015;372(17):1619-1628.
Clinical question: Does administration of prednisolone or pentoxifylline reduce mortality in patients hospitalized with severe alcoholic hepatitis?
Background: Alcoholic hepatitis is associated with high mortality. Studies have shown unclear mortality benefit with prednisolone and pentoxifylline. Despite multiple studies and meta-analyses, controversy about the use of these medications persists.
Study Design: Multicenter, double-blind, randomized trial with 2-by-2 design.
Setting: Sixty-five hospitals across the United Kingdom.
Synopsis: Approximately 1,100 patients with a clinical diagnosis of alcoholic hepatitis were randomized to four groups: placebo + placebo; prednisolone + pentoxifylline-matched placebo; prednisolone-matched placebo + pentoxifylline; or prednisolone + pentoxifylline. Groups received 28 days of treatment. The primary endpoint was 28-day mortality. Secondary endpoints were mortality or liver transplantation at 90 days and one year.
Neither intervention showed a significant reduction in 28-day mortality. Secondary analysis with adjustments for risk showed a reduction in 28-day mortality in the prednisolone groups. There was no difference between groups for mortality or liver transplantation at 90 days or one year.
Adverse events of death, infection, and acute kidney injury were reported in 42% of patients. Infection rates were higher in the prednisolone groups; however, attributable deaths were no different between groups.
Patients in this trial were younger, with a lower incidence of encephalopathy, infection, and acute kidney injury than those seen in similar trials, which could affect the rates of mortality seen here. Also, liver biopsy was not used, so patients may have been incorrectly included.
Bottom line: No difference was found in mortality or liver transplantation at 90 days and one year for prednisolone or pentoxifylline, although subanalysis showed there may be short-term benefit with prednisolone.
Citation: Thursz MR, Richardson P, Allison M, et al. Prednisolone or pentoxifylline for alcoholic hepatitis. New Engl J Med. 2015;372(17):1619-1628.