User login
Medicare Program to Reduce Hospital-Acquired Conditions Could Be Better

Hospitals with the highest rates of preventable adverse events will soon see their Medicare reimbursements cut by 1%.
The Centers for Medicare and Medicaid Services (CMS) Hospital-Acquired Condition Reduction Program (HACRP) is a product of the Affordable Care Act, implemented to tackle the high number of patients who experience avoidable, adverse—and too often fatal—medical events in the hospital; however, while patient safety has been a crucial issue for years, and one largely ignored by Congress until recently, some experts say the new metrics used to evaluate safety and penalize the bottom 25% of hospitals are imprecise and stand to punish those that serve the sickest patients and those that are among the most diligent about tracking patient safety.
“The biggest surprise was how big of a difference there was between academic medical centers and safety-net hospitals and everybody else,” says Ashish Jha, MD, MPH, hospitalist at the VA Boston Healthcare System, professor of health policy at the Harvard School of Public Health, and part of a team that recently used the CMS measures—patient safety indicators (PSI), central line-associated bloodstream infections (CLABSI), and catheter-associated urinary tract infections (CAUTI)—to evaluate where the nation’s hospitals might fall under HACRP.
In its analysis, Dr. Jha’s team found that major teaching hospitals are 2.9% more likely to be penalized under the program than nonteaching hospitals. Large, urban, public, teaching hospitals in the Northeast, with lots of poor patients, have a 62% chance of being penalized, compared to just a 9% chance for small, rural, for-profit, nonteaching hospitals in the South.
In 1998, the Institutes of Medicine estimated that nearly 100,000 patients die every year due to preventable medical errors. A recent estimate in the Journal of Patient Safety says this number may now be as high as 440,000.
In 2012, CMS reported that one in eight Medicare patients incurred a potentially avoidable complication while in the hospital, a 9% reduction from the previous baseline in 2010.
Patient safety clearly is an issue in the United States. But whether all of the HACRP metrics decided upon by CMS are appropriate is up for debate.
“PSI scores…were initially developed to look at healthcare trends broadly and not for comparing institutional performance,” says Ken Sands, MD, MPH, senior vice president of healthcare quality and chief quality officer at Beth Israel Deaconess Medical Center. “They were hijacked for that purpose, and a lot of the measures are based on administrative data.”
Dr. Sands, like Dr. Jha, is concerned that variation in the way hospitals code can influence the rate of adverse events reported through PSIs—which scan billing codes for hospital complications—without a clearly defined set of rules and without clearly defined language. Hospitals vary in how hard they look for complications and in how diligently they code, Dr. Jha says. Hospitals looking for safety issues are more likely to find and code for them, compared to less attentive institutions.
“It’s an inexpensive way to collect data nationally,” Dr. Sands says. “But whether we’re discriminating on quality is not that clear.”
Beth Israel ranks better than most U.S. hospitals on measures of mortality yet falls to the bottom quartile of the hospital-acquired condition (HAC) measures. The medical center may be penalized starting in October.
Although Dr. Sands says his colleagues continue to work to improve their CAUTI rates, an endeavor that preceded the CMS program, he is seeking better training for his coding staff and is working within the medical center’s electronic health record (EHR) to ensure accurate and consistent reporting.
At small, rural Nanticoke Memorial Hospital in southern Delaware, which is not at risk of HAC penalties next year, chief operating officer and chief nursing officer Penny Short says the hospital is currently adopting a “pretty robust” EHR to assist clinicians with early identification of sepsis and other risks. She says there is a lot more that EHRs can do to assist in patient safety, and hospitalists at her institution have been at the helm, driving progress.
It’s an approach Dr. Jha advocates for moving the needle forward in identifying better patient safety metrics. Meaningful use of EHRs provides clinically based, high quality metrics that can be captured far more effectively than the billing record, he says, offering an “automated approach as a routine part of the delivery of health care for tracking and potentially identifying adverse events.”
It’s up to physician leaders, Dr. Jha says—indeed, it is their moral responsibility—to encourage their CEOs to make these investments. And it’s something he believes CMS should get behind as well.
“Is this going to be cheap and easy? No,” Dr. Jha says. “Does CMS have the capacity to say hospitals have to invest? I think they do.
“I think we can do so much better. The opportunity to do so much better is right now.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Hospitals with the highest rates of preventable adverse events will soon see their Medicare reimbursements cut by 1%.
The Centers for Medicare and Medicaid Services (CMS) Hospital-Acquired Condition Reduction Program (HACRP) is a product of the Affordable Care Act, implemented to tackle the high number of patients who experience avoidable, adverse—and too often fatal—medical events in the hospital; however, while patient safety has been a crucial issue for years, and one largely ignored by Congress until recently, some experts say the new metrics used to evaluate safety and penalize the bottom 25% of hospitals are imprecise and stand to punish those that serve the sickest patients and those that are among the most diligent about tracking patient safety.
“The biggest surprise was how big of a difference there was between academic medical centers and safety-net hospitals and everybody else,” says Ashish Jha, MD, MPH, hospitalist at the VA Boston Healthcare System, professor of health policy at the Harvard School of Public Health, and part of a team that recently used the CMS measures—patient safety indicators (PSI), central line-associated bloodstream infections (CLABSI), and catheter-associated urinary tract infections (CAUTI)—to evaluate where the nation’s hospitals might fall under HACRP.
In its analysis, Dr. Jha’s team found that major teaching hospitals are 2.9% more likely to be penalized under the program than nonteaching hospitals. Large, urban, public, teaching hospitals in the Northeast, with lots of poor patients, have a 62% chance of being penalized, compared to just a 9% chance for small, rural, for-profit, nonteaching hospitals in the South.
In 1998, the Institutes of Medicine estimated that nearly 100,000 patients die every year due to preventable medical errors. A recent estimate in the Journal of Patient Safety says this number may now be as high as 440,000.
In 2012, CMS reported that one in eight Medicare patients incurred a potentially avoidable complication while in the hospital, a 9% reduction from the previous baseline in 2010.
Patient safety clearly is an issue in the United States. But whether all of the HACRP metrics decided upon by CMS are appropriate is up for debate.
“PSI scores…were initially developed to look at healthcare trends broadly and not for comparing institutional performance,” says Ken Sands, MD, MPH, senior vice president of healthcare quality and chief quality officer at Beth Israel Deaconess Medical Center. “They were hijacked for that purpose, and a lot of the measures are based on administrative data.”
Dr. Sands, like Dr. Jha, is concerned that variation in the way hospitals code can influence the rate of adverse events reported through PSIs—which scan billing codes for hospital complications—without a clearly defined set of rules and without clearly defined language. Hospitals vary in how hard they look for complications and in how diligently they code, Dr. Jha says. Hospitals looking for safety issues are more likely to find and code for them, compared to less attentive institutions.
“It’s an inexpensive way to collect data nationally,” Dr. Sands says. “But whether we’re discriminating on quality is not that clear.”
Beth Israel ranks better than most U.S. hospitals on measures of mortality yet falls to the bottom quartile of the hospital-acquired condition (HAC) measures. The medical center may be penalized starting in October.
Although Dr. Sands says his colleagues continue to work to improve their CAUTI rates, an endeavor that preceded the CMS program, he is seeking better training for his coding staff and is working within the medical center’s electronic health record (EHR) to ensure accurate and consistent reporting.
At small, rural Nanticoke Memorial Hospital in southern Delaware, which is not at risk of HAC penalties next year, chief operating officer and chief nursing officer Penny Short says the hospital is currently adopting a “pretty robust” EHR to assist clinicians with early identification of sepsis and other risks. She says there is a lot more that EHRs can do to assist in patient safety, and hospitalists at her institution have been at the helm, driving progress.
It’s an approach Dr. Jha advocates for moving the needle forward in identifying better patient safety metrics. Meaningful use of EHRs provides clinically based, high quality metrics that can be captured far more effectively than the billing record, he says, offering an “automated approach as a routine part of the delivery of health care for tracking and potentially identifying adverse events.”
It’s up to physician leaders, Dr. Jha says—indeed, it is their moral responsibility—to encourage their CEOs to make these investments. And it’s something he believes CMS should get behind as well.
“Is this going to be cheap and easy? No,” Dr. Jha says. “Does CMS have the capacity to say hospitals have to invest? I think they do.
“I think we can do so much better. The opportunity to do so much better is right now.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Hospitals with the highest rates of preventable adverse events will soon see their Medicare reimbursements cut by 1%.
The Centers for Medicare and Medicaid Services (CMS) Hospital-Acquired Condition Reduction Program (HACRP) is a product of the Affordable Care Act, implemented to tackle the high number of patients who experience avoidable, adverse—and too often fatal—medical events in the hospital; however, while patient safety has been a crucial issue for years, and one largely ignored by Congress until recently, some experts say the new metrics used to evaluate safety and penalize the bottom 25% of hospitals are imprecise and stand to punish those that serve the sickest patients and those that are among the most diligent about tracking patient safety.
“The biggest surprise was how big of a difference there was between academic medical centers and safety-net hospitals and everybody else,” says Ashish Jha, MD, MPH, hospitalist at the VA Boston Healthcare System, professor of health policy at the Harvard School of Public Health, and part of a team that recently used the CMS measures—patient safety indicators (PSI), central line-associated bloodstream infections (CLABSI), and catheter-associated urinary tract infections (CAUTI)—to evaluate where the nation’s hospitals might fall under HACRP.
In its analysis, Dr. Jha’s team found that major teaching hospitals are 2.9% more likely to be penalized under the program than nonteaching hospitals. Large, urban, public, teaching hospitals in the Northeast, with lots of poor patients, have a 62% chance of being penalized, compared to just a 9% chance for small, rural, for-profit, nonteaching hospitals in the South.
In 1998, the Institutes of Medicine estimated that nearly 100,000 patients die every year due to preventable medical errors. A recent estimate in the Journal of Patient Safety says this number may now be as high as 440,000.
In 2012, CMS reported that one in eight Medicare patients incurred a potentially avoidable complication while in the hospital, a 9% reduction from the previous baseline in 2010.
Patient safety clearly is an issue in the United States. But whether all of the HACRP metrics decided upon by CMS are appropriate is up for debate.
“PSI scores…were initially developed to look at healthcare trends broadly and not for comparing institutional performance,” says Ken Sands, MD, MPH, senior vice president of healthcare quality and chief quality officer at Beth Israel Deaconess Medical Center. “They were hijacked for that purpose, and a lot of the measures are based on administrative data.”
Dr. Sands, like Dr. Jha, is concerned that variation in the way hospitals code can influence the rate of adverse events reported through PSIs—which scan billing codes for hospital complications—without a clearly defined set of rules and without clearly defined language. Hospitals vary in how hard they look for complications and in how diligently they code, Dr. Jha says. Hospitals looking for safety issues are more likely to find and code for them, compared to less attentive institutions.
“It’s an inexpensive way to collect data nationally,” Dr. Sands says. “But whether we’re discriminating on quality is not that clear.”
Beth Israel ranks better than most U.S. hospitals on measures of mortality yet falls to the bottom quartile of the hospital-acquired condition (HAC) measures. The medical center may be penalized starting in October.
Although Dr. Sands says his colleagues continue to work to improve their CAUTI rates, an endeavor that preceded the CMS program, he is seeking better training for his coding staff and is working within the medical center’s electronic health record (EHR) to ensure accurate and consistent reporting.
At small, rural Nanticoke Memorial Hospital in southern Delaware, which is not at risk of HAC penalties next year, chief operating officer and chief nursing officer Penny Short says the hospital is currently adopting a “pretty robust” EHR to assist clinicians with early identification of sepsis and other risks. She says there is a lot more that EHRs can do to assist in patient safety, and hospitalists at her institution have been at the helm, driving progress.
It’s an approach Dr. Jha advocates for moving the needle forward in identifying better patient safety metrics. Meaningful use of EHRs provides clinically based, high quality metrics that can be captured far more effectively than the billing record, he says, offering an “automated approach as a routine part of the delivery of health care for tracking and potentially identifying adverse events.”
It’s up to physician leaders, Dr. Jha says—indeed, it is their moral responsibility—to encourage their CEOs to make these investments. And it’s something he believes CMS should get behind as well.
“Is this going to be cheap and easy? No,” Dr. Jha says. “Does CMS have the capacity to say hospitals have to invest? I think they do.
“I think we can do so much better. The opportunity to do so much better is right now.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
When Should You Decolonize Methicillin-Resistant Staphylococcus aureus (MRSA) in Hospitalized Patients?
Case
A 45-year-old previously healthy female was admitted to the ICU with sepsis caused by community-acquired pneumonia. Per hospital policy, all patients admitted to the ICU are screened for MRSA colonization. If the nasal screen is positive, contact isolation is initiated and the hospital’s MRSA decolonization protocol is implemented. Her nasal screen was positive for MRSA.
Overview
MRSA infections are associated with significant morbidity and mortality, and death occurs in almost 5% of patients who develop a MRSA infection. In 2005, invasive MRSA was responsible for approximately 278,000 hospitalizations and 19,000 deaths. MRSA is a common cause of healthcare-associated infections (HAIs) and is the most common pathogen in surgical site infections (SSIs) and ventilator-associated pneumonias. The cost of treating MRSA infections is substantial; in 2003, $14.5 billion was spent on MRSA-related hospitalizations.
It is well known that MRSA colonization is a risk factor for the subsequent development of a MRSA infection. This risk persists over time, and approximately 25% of individuals who are colonized with MRSA for more than one year will develop a late-onset MRSA infection.1 It is estimated that between 0.8% and 6% of people in the U.S. are asymptomatically colonized with MRSA.
One infection control strategy for reducing the transmission of MRSA among hospitalized patients involves screening for the presence of this organism and then placing colonized and/or infected patients in isolation; however, there is considerable controversy about which patients should be screened.
An additional element of many infection control strategies involves MRSA decolonization, but there is uncertainty about which patients benefit from it and significant variability in its reported success rates.2 Additionally, several studies have indicated that MRSA decolonization is only temporary and that patients become recolonized over time.
Treatment
It is estimated that 10% to 20% of MRSA carriers will develop an infection while they are hospitalized. Furthermore, even after they have been discharged from the hospital, their risk for developing a MRSA infection persists.
Most patients who develop a MRSA infection have been colonized prior to infection, and these patients usually develop an infection caused by the same strain as the colonization. In view of this fact, a primary goal of decolonization is reducing the likelihood of “auto-infection.” Another goal of decolonization is reducing the transmission of MRSA to other patients.
In order to determine whether MRSA colonization is present, patients undergo screening, and specimens are collected from the nares using nasal swabs. Specimens from extranasal sites, such as the groin, are sometimes also obtained for screening. These screening tests are usually done with either cultures or polymerase chain reaction testing.
There is significant variability in the details of screening and decolonization protocols among different healthcare facilities. Typically, the screening test costs more than the agents used for decolonization. Partly for this reason, some facilities forego screening altogether, instead treating all patients with a decolonization regimen; however, there is concern that administering decolonizing medications to all patients would lead to the unnecessary treatment of large numbers of patients. Such widespread use of the decolonizing agents might promote the development of resistance to these medications.
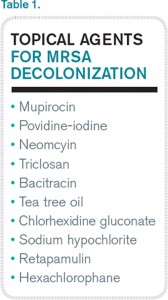
Medications. Decolonization typically involves the use of a topical antibiotic, most commonly mupirocin, which is applied to the nares. This may be used in conjunction with an oral antimicrobial agent. While the nares are the anatomical locations most commonly colonized by MRSA, extranasal colonization occurs in 50% of those who are nasally colonized.
Of the topical medications available for decolonization, mupirocin has the highest efficacy, with eradication of MRSA and methicillin-sensitive Staphylococcus aureus (MSSA) colonization ranging from 81% to 93%. To increase the likelihood of successful decolonization, an antiseptic agent, such as chlorhexidine gluconate, may also be applied to the skin. Chlorhexidine gluconate is also commonly used to prevent other HAIs.
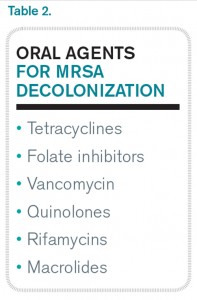
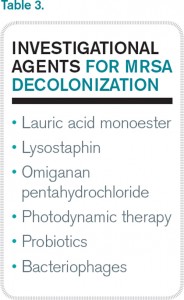
Neomycin is sometimes used for decolonization, but its efficacy for this purpose is questionable. There are also concerns about resistance, but it may be an option in cases of documented mupirocin resistance. Preparations that contain tea tree oil appear to be more effective for decolonization of skin sites than for nasal decolonization. Table 1 lists the topical antibiotics and antiseptics that may be utilized for decolonization, while Table 2 lists the oral medications that can be used for this purpose. Table 3 lists investigational agents being evaluated for their ability to decolonize patients.
It has been suggested that the patients who might derive the most benefit from decolonization are those at increased risk for developing a MRSA infection during a specific time interval. This would include patients who are admitted to the ICU for an acute illness and cardiothoracic surgery patients. A benefit from decolonization has also been observed in hemodialysis patients, who have an incidence of invasive MRSA infections 100 times greater than the general population. Otherwise, there are no data to support the routine use of decolonization in nonsurgical patients.
It is not uncommon for hospitals to screen patients admitted to the ICU for MRSA nasal colonization; in fact, screening is mandatory in nine states. If the nasal screen is positive, contact precautions are instituted. The decision about whether or not to initiate a decolonization protocol varies among different ICUs, but most do not carry out universal decolonization.
Some studies show decolonization is beneficial for ICU patients. These studies include a large cluster-randomized trial called REDUCE MRSA,3 which took place in 43 hospitals and involved 74,256 patients in 74 ICUs. The study showed that universal (i.e., without screening) decolonization using mupirocin and chlorhexidine was effective in reducing rates of MRSA clinical isolates, as well as bloodstream infection from any pathogen. Other studies have demonstrated benefits from the decolonization of ICU patients.4,5
Surgical Site Infections. Meanwhile, SSIs are often associated with increased mortality rates and substantial healthcare costs, including increased hospital lengths of stay and readmission rates. Staphylococcus aureus is the pathogen most commonly isolated from SSIs. In surgical patients, colonization with MRSA is associated with an elevated rate of MRSA SSIs. The goal of decolonization in surgical patients is not to permanently eliminate MRSA but to prevent SSIs by suppressing the presence of this organism for a relatively brief duration.
There is evidence that decolonization reduces SSIs for cardiothoracic surgeries.6 For these patients, it is cost effective to screen for nasal carriage of MRSA and then treat carriers with a combination of pre-operative mupirocin and chlorhexidine. It may be reasonable to delay cardiothoracic surgery in colonized patients who will require implantation of prosthetic material until they complete MRSA decolonization.
In addition to reducing the risk of auto-infection, another goal of decolonization is limiting the possibility of transmission of MRSA from a colonized patient to a susceptible individual; however, there are only limited data available that measure the efficacy of decolonization for preventing transmission.
Concerns about the potential hazards of decolonization therapy have impacted its widespread implementation. The biggest concern is that patients may develop resistance to the antimicrobial agents used for decolonization, particularly if they are used at increased frequency. Mupirocin resistance monitoring is valuable, but, unfortunately, the susceptibility of Staphylococcus aureus to mupirocin is not routinely evaluated, so the prevalence of mupirocin resistance in local strains is often unknown. Another concern about decolonization is the cost of screening and decolonizing patients.
Back to the Case
The patient in this case required admission to an ICU and, based on the results of the REDUCE MRSA clinical trial, she would likely benefit from undergoing decolonization to reduce her risk of both MRSA-positive clinical cultures and bloodstream infections caused by any pathogen.
Bottom Line
Decolonization is beneficial for patients at increased risk of developing a MRSA infection during a specific period, such as patients admitted to the ICU and those undergoing cardiothoracic surgery.
Dr. Clarke is assistant professor in the division of hospital medicine at Emory University Hospital and a faculty member in the Emory University Department of Medicine, both in Atlanta.
References
- Dow G, Field D, Mancuso M, Allard J. Decolonization of methicillin-resistant Staphylococcus aureus during routine hospital care: Efficacy and long-term follow-up. Can J Infect Dis Med Microbiol. 2010;21(1):38-44.
- Simor AE. Staphylococcal decolonisation: An effective strategy for prevention of infection? Lancet Infect Dis. 2011;11(12):952-962.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255-2265.
- Fraser T, Fatica C, Scarpelli M, et al. Decrease in Staphylococcus aureus colonization and hospital-acquired infection in a medical intensive care unit after institution of an active surveillance and decolonization program. Infect Control Hosp Epidemiol. 2010;31(8):779-783.
- Robotham J, Graves N, Cookson B, et al. Screening, isolation, and decolonisation strategies in the control of methicillin-resistant Staphylococcus aureus in intensive care units: Cost effectiveness evaluation. BMJ. 2011;343:d5694.
- Schweizer M, Perencevich E, McDanel J, et al. Effectiveness of a bundled intervention of decolonization and prophylaxis to decrease Gram positive surgical site infections after cardiac or orthopedic surgery: Systematic review and meta-analysis. BMJ. 2013;346:f2743.
Case
A 45-year-old previously healthy female was admitted to the ICU with sepsis caused by community-acquired pneumonia. Per hospital policy, all patients admitted to the ICU are screened for MRSA colonization. If the nasal screen is positive, contact isolation is initiated and the hospital’s MRSA decolonization protocol is implemented. Her nasal screen was positive for MRSA.
Overview
MRSA infections are associated with significant morbidity and mortality, and death occurs in almost 5% of patients who develop a MRSA infection. In 2005, invasive MRSA was responsible for approximately 278,000 hospitalizations and 19,000 deaths. MRSA is a common cause of healthcare-associated infections (HAIs) and is the most common pathogen in surgical site infections (SSIs) and ventilator-associated pneumonias. The cost of treating MRSA infections is substantial; in 2003, $14.5 billion was spent on MRSA-related hospitalizations.
It is well known that MRSA colonization is a risk factor for the subsequent development of a MRSA infection. This risk persists over time, and approximately 25% of individuals who are colonized with MRSA for more than one year will develop a late-onset MRSA infection.1 It is estimated that between 0.8% and 6% of people in the U.S. are asymptomatically colonized with MRSA.
One infection control strategy for reducing the transmission of MRSA among hospitalized patients involves screening for the presence of this organism and then placing colonized and/or infected patients in isolation; however, there is considerable controversy about which patients should be screened.
An additional element of many infection control strategies involves MRSA decolonization, but there is uncertainty about which patients benefit from it and significant variability in its reported success rates.2 Additionally, several studies have indicated that MRSA decolonization is only temporary and that patients become recolonized over time.
Treatment
It is estimated that 10% to 20% of MRSA carriers will develop an infection while they are hospitalized. Furthermore, even after they have been discharged from the hospital, their risk for developing a MRSA infection persists.
Most patients who develop a MRSA infection have been colonized prior to infection, and these patients usually develop an infection caused by the same strain as the colonization. In view of this fact, a primary goal of decolonization is reducing the likelihood of “auto-infection.” Another goal of decolonization is reducing the transmission of MRSA to other patients.
In order to determine whether MRSA colonization is present, patients undergo screening, and specimens are collected from the nares using nasal swabs. Specimens from extranasal sites, such as the groin, are sometimes also obtained for screening. These screening tests are usually done with either cultures or polymerase chain reaction testing.
There is significant variability in the details of screening and decolonization protocols among different healthcare facilities. Typically, the screening test costs more than the agents used for decolonization. Partly for this reason, some facilities forego screening altogether, instead treating all patients with a decolonization regimen; however, there is concern that administering decolonizing medications to all patients would lead to the unnecessary treatment of large numbers of patients. Such widespread use of the decolonizing agents might promote the development of resistance to these medications.
Medications. Decolonization typically involves the use of a topical antibiotic, most commonly mupirocin, which is applied to the nares. This may be used in conjunction with an oral antimicrobial agent. While the nares are the anatomical locations most commonly colonized by MRSA, extranasal colonization occurs in 50% of those who are nasally colonized.
Of the topical medications available for decolonization, mupirocin has the highest efficacy, with eradication of MRSA and methicillin-sensitive Staphylococcus aureus (MSSA) colonization ranging from 81% to 93%. To increase the likelihood of successful decolonization, an antiseptic agent, such as chlorhexidine gluconate, may also be applied to the skin. Chlorhexidine gluconate is also commonly used to prevent other HAIs.
Neomycin is sometimes used for decolonization, but its efficacy for this purpose is questionable. There are also concerns about resistance, but it may be an option in cases of documented mupirocin resistance. Preparations that contain tea tree oil appear to be more effective for decolonization of skin sites than for nasal decolonization. Table 1 lists the topical antibiotics and antiseptics that may be utilized for decolonization, while Table 2 lists the oral medications that can be used for this purpose. Table 3 lists investigational agents being evaluated for their ability to decolonize patients.
It has been suggested that the patients who might derive the most benefit from decolonization are those at increased risk for developing a MRSA infection during a specific time interval. This would include patients who are admitted to the ICU for an acute illness and cardiothoracic surgery patients. A benefit from decolonization has also been observed in hemodialysis patients, who have an incidence of invasive MRSA infections 100 times greater than the general population. Otherwise, there are no data to support the routine use of decolonization in nonsurgical patients.
It is not uncommon for hospitals to screen patients admitted to the ICU for MRSA nasal colonization; in fact, screening is mandatory in nine states. If the nasal screen is positive, contact precautions are instituted. The decision about whether or not to initiate a decolonization protocol varies among different ICUs, but most do not carry out universal decolonization.
Some studies show decolonization is beneficial for ICU patients. These studies include a large cluster-randomized trial called REDUCE MRSA,3 which took place in 43 hospitals and involved 74,256 patients in 74 ICUs. The study showed that universal (i.e., without screening) decolonization using mupirocin and chlorhexidine was effective in reducing rates of MRSA clinical isolates, as well as bloodstream infection from any pathogen. Other studies have demonstrated benefits from the decolonization of ICU patients.4,5
Surgical Site Infections. Meanwhile, SSIs are often associated with increased mortality rates and substantial healthcare costs, including increased hospital lengths of stay and readmission rates. Staphylococcus aureus is the pathogen most commonly isolated from SSIs. In surgical patients, colonization with MRSA is associated with an elevated rate of MRSA SSIs. The goal of decolonization in surgical patients is not to permanently eliminate MRSA but to prevent SSIs by suppressing the presence of this organism for a relatively brief duration.
There is evidence that decolonization reduces SSIs for cardiothoracic surgeries.6 For these patients, it is cost effective to screen for nasal carriage of MRSA and then treat carriers with a combination of pre-operative mupirocin and chlorhexidine. It may be reasonable to delay cardiothoracic surgery in colonized patients who will require implantation of prosthetic material until they complete MRSA decolonization.
In addition to reducing the risk of auto-infection, another goal of decolonization is limiting the possibility of transmission of MRSA from a colonized patient to a susceptible individual; however, there are only limited data available that measure the efficacy of decolonization for preventing transmission.
Concerns about the potential hazards of decolonization therapy have impacted its widespread implementation. The biggest concern is that patients may develop resistance to the antimicrobial agents used for decolonization, particularly if they are used at increased frequency. Mupirocin resistance monitoring is valuable, but, unfortunately, the susceptibility of Staphylococcus aureus to mupirocin is not routinely evaluated, so the prevalence of mupirocin resistance in local strains is often unknown. Another concern about decolonization is the cost of screening and decolonizing patients.
Back to the Case
The patient in this case required admission to an ICU and, based on the results of the REDUCE MRSA clinical trial, she would likely benefit from undergoing decolonization to reduce her risk of both MRSA-positive clinical cultures and bloodstream infections caused by any pathogen.
Bottom Line
Decolonization is beneficial for patients at increased risk of developing a MRSA infection during a specific period, such as patients admitted to the ICU and those undergoing cardiothoracic surgery.
Dr. Clarke is assistant professor in the division of hospital medicine at Emory University Hospital and a faculty member in the Emory University Department of Medicine, both in Atlanta.
References
- Dow G, Field D, Mancuso M, Allard J. Decolonization of methicillin-resistant Staphylococcus aureus during routine hospital care: Efficacy and long-term follow-up. Can J Infect Dis Med Microbiol. 2010;21(1):38-44.
- Simor AE. Staphylococcal decolonisation: An effective strategy for prevention of infection? Lancet Infect Dis. 2011;11(12):952-962.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255-2265.
- Fraser T, Fatica C, Scarpelli M, et al. Decrease in Staphylococcus aureus colonization and hospital-acquired infection in a medical intensive care unit after institution of an active surveillance and decolonization program. Infect Control Hosp Epidemiol. 2010;31(8):779-783.
- Robotham J, Graves N, Cookson B, et al. Screening, isolation, and decolonisation strategies in the control of methicillin-resistant Staphylococcus aureus in intensive care units: Cost effectiveness evaluation. BMJ. 2011;343:d5694.
- Schweizer M, Perencevich E, McDanel J, et al. Effectiveness of a bundled intervention of decolonization and prophylaxis to decrease Gram positive surgical site infections after cardiac or orthopedic surgery: Systematic review and meta-analysis. BMJ. 2013;346:f2743.
Case
A 45-year-old previously healthy female was admitted to the ICU with sepsis caused by community-acquired pneumonia. Per hospital policy, all patients admitted to the ICU are screened for MRSA colonization. If the nasal screen is positive, contact isolation is initiated and the hospital’s MRSA decolonization protocol is implemented. Her nasal screen was positive for MRSA.
Overview
MRSA infections are associated with significant morbidity and mortality, and death occurs in almost 5% of patients who develop a MRSA infection. In 2005, invasive MRSA was responsible for approximately 278,000 hospitalizations and 19,000 deaths. MRSA is a common cause of healthcare-associated infections (HAIs) and is the most common pathogen in surgical site infections (SSIs) and ventilator-associated pneumonias. The cost of treating MRSA infections is substantial; in 2003, $14.5 billion was spent on MRSA-related hospitalizations.
It is well known that MRSA colonization is a risk factor for the subsequent development of a MRSA infection. This risk persists over time, and approximately 25% of individuals who are colonized with MRSA for more than one year will develop a late-onset MRSA infection.1 It is estimated that between 0.8% and 6% of people in the U.S. are asymptomatically colonized with MRSA.
One infection control strategy for reducing the transmission of MRSA among hospitalized patients involves screening for the presence of this organism and then placing colonized and/or infected patients in isolation; however, there is considerable controversy about which patients should be screened.
An additional element of many infection control strategies involves MRSA decolonization, but there is uncertainty about which patients benefit from it and significant variability in its reported success rates.2 Additionally, several studies have indicated that MRSA decolonization is only temporary and that patients become recolonized over time.
Treatment
It is estimated that 10% to 20% of MRSA carriers will develop an infection while they are hospitalized. Furthermore, even after they have been discharged from the hospital, their risk for developing a MRSA infection persists.
Most patients who develop a MRSA infection have been colonized prior to infection, and these patients usually develop an infection caused by the same strain as the colonization. In view of this fact, a primary goal of decolonization is reducing the likelihood of “auto-infection.” Another goal of decolonization is reducing the transmission of MRSA to other patients.
In order to determine whether MRSA colonization is present, patients undergo screening, and specimens are collected from the nares using nasal swabs. Specimens from extranasal sites, such as the groin, are sometimes also obtained for screening. These screening tests are usually done with either cultures or polymerase chain reaction testing.
There is significant variability in the details of screening and decolonization protocols among different healthcare facilities. Typically, the screening test costs more than the agents used for decolonization. Partly for this reason, some facilities forego screening altogether, instead treating all patients with a decolonization regimen; however, there is concern that administering decolonizing medications to all patients would lead to the unnecessary treatment of large numbers of patients. Such widespread use of the decolonizing agents might promote the development of resistance to these medications.
Medications. Decolonization typically involves the use of a topical antibiotic, most commonly mupirocin, which is applied to the nares. This may be used in conjunction with an oral antimicrobial agent. While the nares are the anatomical locations most commonly colonized by MRSA, extranasal colonization occurs in 50% of those who are nasally colonized.
Of the topical medications available for decolonization, mupirocin has the highest efficacy, with eradication of MRSA and methicillin-sensitive Staphylococcus aureus (MSSA) colonization ranging from 81% to 93%. To increase the likelihood of successful decolonization, an antiseptic agent, such as chlorhexidine gluconate, may also be applied to the skin. Chlorhexidine gluconate is also commonly used to prevent other HAIs.
Neomycin is sometimes used for decolonization, but its efficacy for this purpose is questionable. There are also concerns about resistance, but it may be an option in cases of documented mupirocin resistance. Preparations that contain tea tree oil appear to be more effective for decolonization of skin sites than for nasal decolonization. Table 1 lists the topical antibiotics and antiseptics that may be utilized for decolonization, while Table 2 lists the oral medications that can be used for this purpose. Table 3 lists investigational agents being evaluated for their ability to decolonize patients.
It has been suggested that the patients who might derive the most benefit from decolonization are those at increased risk for developing a MRSA infection during a specific time interval. This would include patients who are admitted to the ICU for an acute illness and cardiothoracic surgery patients. A benefit from decolonization has also been observed in hemodialysis patients, who have an incidence of invasive MRSA infections 100 times greater than the general population. Otherwise, there are no data to support the routine use of decolonization in nonsurgical patients.
It is not uncommon for hospitals to screen patients admitted to the ICU for MRSA nasal colonization; in fact, screening is mandatory in nine states. If the nasal screen is positive, contact precautions are instituted. The decision about whether or not to initiate a decolonization protocol varies among different ICUs, but most do not carry out universal decolonization.
Some studies show decolonization is beneficial for ICU patients. These studies include a large cluster-randomized trial called REDUCE MRSA,3 which took place in 43 hospitals and involved 74,256 patients in 74 ICUs. The study showed that universal (i.e., without screening) decolonization using mupirocin and chlorhexidine was effective in reducing rates of MRSA clinical isolates, as well as bloodstream infection from any pathogen. Other studies have demonstrated benefits from the decolonization of ICU patients.4,5
Surgical Site Infections. Meanwhile, SSIs are often associated with increased mortality rates and substantial healthcare costs, including increased hospital lengths of stay and readmission rates. Staphylococcus aureus is the pathogen most commonly isolated from SSIs. In surgical patients, colonization with MRSA is associated with an elevated rate of MRSA SSIs. The goal of decolonization in surgical patients is not to permanently eliminate MRSA but to prevent SSIs by suppressing the presence of this organism for a relatively brief duration.
There is evidence that decolonization reduces SSIs for cardiothoracic surgeries.6 For these patients, it is cost effective to screen for nasal carriage of MRSA and then treat carriers with a combination of pre-operative mupirocin and chlorhexidine. It may be reasonable to delay cardiothoracic surgery in colonized patients who will require implantation of prosthetic material until they complete MRSA decolonization.
In addition to reducing the risk of auto-infection, another goal of decolonization is limiting the possibility of transmission of MRSA from a colonized patient to a susceptible individual; however, there are only limited data available that measure the efficacy of decolonization for preventing transmission.
Concerns about the potential hazards of decolonization therapy have impacted its widespread implementation. The biggest concern is that patients may develop resistance to the antimicrobial agents used for decolonization, particularly if they are used at increased frequency. Mupirocin resistance monitoring is valuable, but, unfortunately, the susceptibility of Staphylococcus aureus to mupirocin is not routinely evaluated, so the prevalence of mupirocin resistance in local strains is often unknown. Another concern about decolonization is the cost of screening and decolonizing patients.
Back to the Case
The patient in this case required admission to an ICU and, based on the results of the REDUCE MRSA clinical trial, she would likely benefit from undergoing decolonization to reduce her risk of both MRSA-positive clinical cultures and bloodstream infections caused by any pathogen.
Bottom Line
Decolonization is beneficial for patients at increased risk of developing a MRSA infection during a specific period, such as patients admitted to the ICU and those undergoing cardiothoracic surgery.
Dr. Clarke is assistant professor in the division of hospital medicine at Emory University Hospital and a faculty member in the Emory University Department of Medicine, both in Atlanta.
References
- Dow G, Field D, Mancuso M, Allard J. Decolonization of methicillin-resistant Staphylococcus aureus during routine hospital care: Efficacy and long-term follow-up. Can J Infect Dis Med Microbiol. 2010;21(1):38-44.
- Simor AE. Staphylococcal decolonisation: An effective strategy for prevention of infection? Lancet Infect Dis. 2011;11(12):952-962.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368(24):2255-2265.
- Fraser T, Fatica C, Scarpelli M, et al. Decrease in Staphylococcus aureus colonization and hospital-acquired infection in a medical intensive care unit after institution of an active surveillance and decolonization program. Infect Control Hosp Epidemiol. 2010;31(8):779-783.
- Robotham J, Graves N, Cookson B, et al. Screening, isolation, and decolonisation strategies in the control of methicillin-resistant Staphylococcus aureus in intensive care units: Cost effectiveness evaluation. BMJ. 2011;343:d5694.
- Schweizer M, Perencevich E, McDanel J, et al. Effectiveness of a bundled intervention of decolonization and prophylaxis to decrease Gram positive surgical site infections after cardiac or orthopedic surgery: Systematic review and meta-analysis. BMJ. 2013;346:f2743.
State of Hospital Medicine Report an Evaluation Tool for Hospital Medicine Groups
I think my team of hospitalists is probably tired of hearing my sports analogies. But as I look at the State of Hospital Medicine 2014 report (SOHM), I cannot help but see relationships to athletics.
When you think about football, you automatically contemplate the scope of a particular team and the context of the upcoming season. What are the strengths of the team—do we emphasize offense or defense or special teams? How about the variety of formations or the scheduling and strength of opponents? How about the depth of our roster—what is the talent level available? How do we compare to other teams?
How in the world does this relate to the SOHM? It gives us a chance to evaluate our own hospital medicine groups (HMGs) in the context of the other HMGs across the country. When I look at scope of services and, particularly, the data from Figure 3.1, I am struck with the breadth of the range of services in which HMGs engage. Certainly, our core identity as hospitalists includes admitting referral patients and unassigned patients, but, as of 2014, nearly 90% of hospitalist groups are also managing and co-managing surgical and medical subspecialty patients. To my eyes, the big change since 2012 is the 20% increase in the number of HMGs medically co-managing medical subspecialty patients.
There are some newcomers to our roster, as well—the palliative care and post-acute care work being done by 15% and 25% of our groups, respectively. Particularly striking is the fact that one quarter of HMGs are involved in post-acute care, follow-up clinics, nursing homes, and the like.
My take on this is that factors such as increased complexity of hospitalized patients with lean length of stay and higher acuity needs at discharge transition are driving the need for a measure of continuity and expertise post discharge that may best be provided by HMGs. The trending of the post-acute care challenges/opportunities will certainly be worth watching—sort of like a rookie player who is having a big impact.

As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution.
—William A. Landis, MD, FHM
Not surprisingly, nighttime admissions work continues to gain traction. Nearly 60% of HMGs are performing nighttime admissions.
In my regional chapter, we recently heard a presentation on “nocturnists.” An interesting contention that caught my attention was that the nocturnist viewed herself as providing expert clinical care during off-hours—particularly at night—and that she was looking to increase the value and not just “put her finger in the dike,” so to speak, until the cavalry arrived at daybreak. As HMG responsibilities increase during the off-hours, I am thinking that my colleague is right: We are going to have to increase our depth and strength at this particular position so that we might actually become known as the “nighttime experts.” I look for this trend to continue.
Finally, I am drawn to the data on care of patients in the ICU, a number that continues to rise—almost 70% of HMGs now. Meanwhile, procedures have dipped to 33% from 53% in the last report. At first, it seemed a little bit puzzling to me that as involvement in the ICUs seemed to increase, procedures diminished. My anecdotal experience is that most of my procedures occurred on patients who had intensive care requirements. Nonetheless, many hospitalists I have talked to seem to believe that the requirement/expectation of imaging in the performance of more and more invasive procedures—now a standard of care— has increasingly driven procedures to specialized areas of the hospital such as imaging/radiology departments. There may also be a net decrease in the number of procedures performed as more noninvasive diagnostic modalities provide satisfactory information.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution. It may make sense for others to be doing procedures. Whatever the cause, my guess is these two trends may continue.
Diving deeper into the granularity of the report will lead the reader to discover subtle differences and trends. Academics, pediatric hospitalists, and independent HMGs all have some nuances, not to mention regional variation. You will have to dig into the report yourself to explore.
Just as there is a freshness to every new sports season, there is a freshness to reviewing the information from the SOHM reports, and evaluating the scope of service is always an exciting moment.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
I think my team of hospitalists is probably tired of hearing my sports analogies. But as I look at the State of Hospital Medicine 2014 report (SOHM), I cannot help but see relationships to athletics.
When you think about football, you automatically contemplate the scope of a particular team and the context of the upcoming season. What are the strengths of the team—do we emphasize offense or defense or special teams? How about the variety of formations or the scheduling and strength of opponents? How about the depth of our roster—what is the talent level available? How do we compare to other teams?
How in the world does this relate to the SOHM? It gives us a chance to evaluate our own hospital medicine groups (HMGs) in the context of the other HMGs across the country. When I look at scope of services and, particularly, the data from Figure 3.1, I am struck with the breadth of the range of services in which HMGs engage. Certainly, our core identity as hospitalists includes admitting referral patients and unassigned patients, but, as of 2014, nearly 90% of hospitalist groups are also managing and co-managing surgical and medical subspecialty patients. To my eyes, the big change since 2012 is the 20% increase in the number of HMGs medically co-managing medical subspecialty patients.
There are some newcomers to our roster, as well—the palliative care and post-acute care work being done by 15% and 25% of our groups, respectively. Particularly striking is the fact that one quarter of HMGs are involved in post-acute care, follow-up clinics, nursing homes, and the like.
My take on this is that factors such as increased complexity of hospitalized patients with lean length of stay and higher acuity needs at discharge transition are driving the need for a measure of continuity and expertise post discharge that may best be provided by HMGs. The trending of the post-acute care challenges/opportunities will certainly be worth watching—sort of like a rookie player who is having a big impact.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution.
—William A. Landis, MD, FHM
Not surprisingly, nighttime admissions work continues to gain traction. Nearly 60% of HMGs are performing nighttime admissions.
In my regional chapter, we recently heard a presentation on “nocturnists.” An interesting contention that caught my attention was that the nocturnist viewed herself as providing expert clinical care during off-hours—particularly at night—and that she was looking to increase the value and not just “put her finger in the dike,” so to speak, until the cavalry arrived at daybreak. As HMG responsibilities increase during the off-hours, I am thinking that my colleague is right: We are going to have to increase our depth and strength at this particular position so that we might actually become known as the “nighttime experts.” I look for this trend to continue.
Finally, I am drawn to the data on care of patients in the ICU, a number that continues to rise—almost 70% of HMGs now. Meanwhile, procedures have dipped to 33% from 53% in the last report. At first, it seemed a little bit puzzling to me that as involvement in the ICUs seemed to increase, procedures diminished. My anecdotal experience is that most of my procedures occurred on patients who had intensive care requirements. Nonetheless, many hospitalists I have talked to seem to believe that the requirement/expectation of imaging in the performance of more and more invasive procedures—now a standard of care— has increasingly driven procedures to specialized areas of the hospital such as imaging/radiology departments. There may also be a net decrease in the number of procedures performed as more noninvasive diagnostic modalities provide satisfactory information.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution. It may make sense for others to be doing procedures. Whatever the cause, my guess is these two trends may continue.
Diving deeper into the granularity of the report will lead the reader to discover subtle differences and trends. Academics, pediatric hospitalists, and independent HMGs all have some nuances, not to mention regional variation. You will have to dig into the report yourself to explore.
Just as there is a freshness to every new sports season, there is a freshness to reviewing the information from the SOHM reports, and evaluating the scope of service is always an exciting moment.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
I think my team of hospitalists is probably tired of hearing my sports analogies. But as I look at the State of Hospital Medicine 2014 report (SOHM), I cannot help but see relationships to athletics.
When you think about football, you automatically contemplate the scope of a particular team and the context of the upcoming season. What are the strengths of the team—do we emphasize offense or defense or special teams? How about the variety of formations or the scheduling and strength of opponents? How about the depth of our roster—what is the talent level available? How do we compare to other teams?
How in the world does this relate to the SOHM? It gives us a chance to evaluate our own hospital medicine groups (HMGs) in the context of the other HMGs across the country. When I look at scope of services and, particularly, the data from Figure 3.1, I am struck with the breadth of the range of services in which HMGs engage. Certainly, our core identity as hospitalists includes admitting referral patients and unassigned patients, but, as of 2014, nearly 90% of hospitalist groups are also managing and co-managing surgical and medical subspecialty patients. To my eyes, the big change since 2012 is the 20% increase in the number of HMGs medically co-managing medical subspecialty patients.
There are some newcomers to our roster, as well—the palliative care and post-acute care work being done by 15% and 25% of our groups, respectively. Particularly striking is the fact that one quarter of HMGs are involved in post-acute care, follow-up clinics, nursing homes, and the like.
My take on this is that factors such as increased complexity of hospitalized patients with lean length of stay and higher acuity needs at discharge transition are driving the need for a measure of continuity and expertise post discharge that may best be provided by HMGs. The trending of the post-acute care challenges/opportunities will certainly be worth watching—sort of like a rookie player who is having a big impact.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution.
—William A. Landis, MD, FHM
Not surprisingly, nighttime admissions work continues to gain traction. Nearly 60% of HMGs are performing nighttime admissions.
In my regional chapter, we recently heard a presentation on “nocturnists.” An interesting contention that caught my attention was that the nocturnist viewed herself as providing expert clinical care during off-hours—particularly at night—and that she was looking to increase the value and not just “put her finger in the dike,” so to speak, until the cavalry arrived at daybreak. As HMG responsibilities increase during the off-hours, I am thinking that my colleague is right: We are going to have to increase our depth and strength at this particular position so that we might actually become known as the “nighttime experts.” I look for this trend to continue.
Finally, I am drawn to the data on care of patients in the ICU, a number that continues to rise—almost 70% of HMGs now. Meanwhile, procedures have dipped to 33% from 53% in the last report. At first, it seemed a little bit puzzling to me that as involvement in the ICUs seemed to increase, procedures diminished. My anecdotal experience is that most of my procedures occurred on patients who had intensive care requirements. Nonetheless, many hospitalists I have talked to seem to believe that the requirement/expectation of imaging in the performance of more and more invasive procedures—now a standard of care— has increasingly driven procedures to specialized areas of the hospital such as imaging/radiology departments. There may also be a net decrease in the number of procedures performed as more noninvasive diagnostic modalities provide satisfactory information.
As hospitalists may become focused on throughput (admissions discharges and transfers), the interruption to perform procedures may decrease the net value of the hospitalist to the institution. It may make sense for others to be doing procedures. Whatever the cause, my guess is these two trends may continue.
Diving deeper into the granularity of the report will lead the reader to discover subtle differences and trends. Academics, pediatric hospitalists, and independent HMGs all have some nuances, not to mention regional variation. You will have to dig into the report yourself to explore.
Just as there is a freshness to every new sports season, there is a freshness to reviewing the information from the SOHM reports, and evaluating the scope of service is always an exciting moment.
Dr. Landis is medical director of Wellspan Hospitalists in York, Pa., and a member of SHM’s Practice Analysis Committee.
Veterans Health Administration Will Pilot New Health Information Technology Platform
The Veterans Health Administration (VHA) aggressively reorganized its infrastructure in the mid-1990s, undergoing a dramatic transformation from a stagnant “hospital system” to a model “healthcare system” characterized by patient-centered quality care. Central to these efforts was an enterprise-wide update of its existing health information technology (HIT), known as VistA (Veterans Health Information Systems and Technology Architecture), with the rollout of a graphical user interface familiar to most U.S. trainees, the computerized patient record system (CPRS). Although many U.S. hospitals are struggling to meet the national directive related to electronic health records (EHR), the VA boasts a comprehensive electronic records system that has been utilized across all its major clinical sites and units for over 15 years.
In light of the high price tag usually attached to HIT implementation, cost-conscious readers should be able to appreciate the magnitude of the VHA’s accomplishment in rolling out a CPRS in a cost-neutral fashion. Despite a 75% increase in the overall number of patients treated at the VA from 1996 to 2004 (2.8 million to 4.9 million), the VA witnessed a startling net decrease in cost per patient during the same time period—compare $5,058 spent per patient per year in 1996 to $5,048 per patient in 2004. Even more striking was the measurable impact on quality and efficiency in care delivery, particularly in preventive services and chronic disease management and outcomes. In a separate cost-benefit analysis of the VA’s HIT investment and implementation, a staggering benefit of $3.09 billion was found. It is not surprising that the VHA advanced to the top of the leaderboard compared to other U.S. health systems.
In a recent Medscape Electronic Health Records survey of more than 18,500 physicians in a variety of practice situations between April and June of 2014, VA-CPRS received the highest marks for user satisfaction, outshining other popular systems, including Practice Fusion, Epic Systems, and Amazing Charts. It is no wonder that international observers have praised VistA as “the gold standard in clinical informatics.”
What distinguishes the VA’s EHR from any “off-the-shelf” software available is the continued dynamic partnership that exists between frontline end users and supportive programmers. This relationship has resulted in 26 discreet versions of CPRS customized to enhance the capabilities and meet the local needs of VHA clinicians. Emphasis is placed on end user value-added functionality with the vision to optimize workflow rather than requiring physicians to align their clinical processes to a pre-scripted system.
The VA’s transformation has not ground to a halt. Rather, the successor to CPRS, known as the Health Management Platform (HMP), is already being piloted. Built as a groundbreaking, browser-based tool designed to further modernize patient care, the HMP shifts the focus away from a single-provider, single patient-chart model to a patient-centered team-based approach that better reflects and supports the way healthcare teams actually provide care. VA clinicians will be able to customize their own interface to support their workflow, communicate with other healthcare providers using secure internal instant messaging, and access built-in guideline-driven support tools that can assist clinical decision making.
Veterans will be able to input personal information using mobile devices and have complete access to their patient record, patient-provider communication tools, and consumer-friendly disease management information.
Administrators will have the ability to extract population-based data in real time to provide prompt feedback to frontline clinicians and identify specific gaps in healthcare delivery. The new HMP opens doors for improved interactions with system and developer partners worldwide.
Clearly the VA is not content to mimic the advancements of others, but once again is poised to revolutionize the arena of healthcare informatics.
Dr. Hazelrigg is section chief of hospital medicine at McGuire VAMC in Richmond, VA. Dr. Kwan is a hospitalist at the VA in San Diego, CA. Both are members of SHM's VA Task Force.
The Veterans Health Administration (VHA) aggressively reorganized its infrastructure in the mid-1990s, undergoing a dramatic transformation from a stagnant “hospital system” to a model “healthcare system” characterized by patient-centered quality care. Central to these efforts was an enterprise-wide update of its existing health information technology (HIT), known as VistA (Veterans Health Information Systems and Technology Architecture), with the rollout of a graphical user interface familiar to most U.S. trainees, the computerized patient record system (CPRS). Although many U.S. hospitals are struggling to meet the national directive related to electronic health records (EHR), the VA boasts a comprehensive electronic records system that has been utilized across all its major clinical sites and units for over 15 years.
In light of the high price tag usually attached to HIT implementation, cost-conscious readers should be able to appreciate the magnitude of the VHA’s accomplishment in rolling out a CPRS in a cost-neutral fashion. Despite a 75% increase in the overall number of patients treated at the VA from 1996 to 2004 (2.8 million to 4.9 million), the VA witnessed a startling net decrease in cost per patient during the same time period—compare $5,058 spent per patient per year in 1996 to $5,048 per patient in 2004. Even more striking was the measurable impact on quality and efficiency in care delivery, particularly in preventive services and chronic disease management and outcomes. In a separate cost-benefit analysis of the VA’s HIT investment and implementation, a staggering benefit of $3.09 billion was found. It is not surprising that the VHA advanced to the top of the leaderboard compared to other U.S. health systems.
In a recent Medscape Electronic Health Records survey of more than 18,500 physicians in a variety of practice situations between April and June of 2014, VA-CPRS received the highest marks for user satisfaction, outshining other popular systems, including Practice Fusion, Epic Systems, and Amazing Charts. It is no wonder that international observers have praised VistA as “the gold standard in clinical informatics.”
What distinguishes the VA’s EHR from any “off-the-shelf” software available is the continued dynamic partnership that exists between frontline end users and supportive programmers. This relationship has resulted in 26 discreet versions of CPRS customized to enhance the capabilities and meet the local needs of VHA clinicians. Emphasis is placed on end user value-added functionality with the vision to optimize workflow rather than requiring physicians to align their clinical processes to a pre-scripted system.
The VA’s transformation has not ground to a halt. Rather, the successor to CPRS, known as the Health Management Platform (HMP), is already being piloted. Built as a groundbreaking, browser-based tool designed to further modernize patient care, the HMP shifts the focus away from a single-provider, single patient-chart model to a patient-centered team-based approach that better reflects and supports the way healthcare teams actually provide care. VA clinicians will be able to customize their own interface to support their workflow, communicate with other healthcare providers using secure internal instant messaging, and access built-in guideline-driven support tools that can assist clinical decision making.
Veterans will be able to input personal information using mobile devices and have complete access to their patient record, patient-provider communication tools, and consumer-friendly disease management information.
Administrators will have the ability to extract population-based data in real time to provide prompt feedback to frontline clinicians and identify specific gaps in healthcare delivery. The new HMP opens doors for improved interactions with system and developer partners worldwide.
Clearly the VA is not content to mimic the advancements of others, but once again is poised to revolutionize the arena of healthcare informatics.
Dr. Hazelrigg is section chief of hospital medicine at McGuire VAMC in Richmond, VA. Dr. Kwan is a hospitalist at the VA in San Diego, CA. Both are members of SHM's VA Task Force.
The Veterans Health Administration (VHA) aggressively reorganized its infrastructure in the mid-1990s, undergoing a dramatic transformation from a stagnant “hospital system” to a model “healthcare system” characterized by patient-centered quality care. Central to these efforts was an enterprise-wide update of its existing health information technology (HIT), known as VistA (Veterans Health Information Systems and Technology Architecture), with the rollout of a graphical user interface familiar to most U.S. trainees, the computerized patient record system (CPRS). Although many U.S. hospitals are struggling to meet the national directive related to electronic health records (EHR), the VA boasts a comprehensive electronic records system that has been utilized across all its major clinical sites and units for over 15 years.
In light of the high price tag usually attached to HIT implementation, cost-conscious readers should be able to appreciate the magnitude of the VHA’s accomplishment in rolling out a CPRS in a cost-neutral fashion. Despite a 75% increase in the overall number of patients treated at the VA from 1996 to 2004 (2.8 million to 4.9 million), the VA witnessed a startling net decrease in cost per patient during the same time period—compare $5,058 spent per patient per year in 1996 to $5,048 per patient in 2004. Even more striking was the measurable impact on quality and efficiency in care delivery, particularly in preventive services and chronic disease management and outcomes. In a separate cost-benefit analysis of the VA’s HIT investment and implementation, a staggering benefit of $3.09 billion was found. It is not surprising that the VHA advanced to the top of the leaderboard compared to other U.S. health systems.
In a recent Medscape Electronic Health Records survey of more than 18,500 physicians in a variety of practice situations between April and June of 2014, VA-CPRS received the highest marks for user satisfaction, outshining other popular systems, including Practice Fusion, Epic Systems, and Amazing Charts. It is no wonder that international observers have praised VistA as “the gold standard in clinical informatics.”
What distinguishes the VA’s EHR from any “off-the-shelf” software available is the continued dynamic partnership that exists between frontline end users and supportive programmers. This relationship has resulted in 26 discreet versions of CPRS customized to enhance the capabilities and meet the local needs of VHA clinicians. Emphasis is placed on end user value-added functionality with the vision to optimize workflow rather than requiring physicians to align their clinical processes to a pre-scripted system.
The VA’s transformation has not ground to a halt. Rather, the successor to CPRS, known as the Health Management Platform (HMP), is already being piloted. Built as a groundbreaking, browser-based tool designed to further modernize patient care, the HMP shifts the focus away from a single-provider, single patient-chart model to a patient-centered team-based approach that better reflects and supports the way healthcare teams actually provide care. VA clinicians will be able to customize their own interface to support their workflow, communicate with other healthcare providers using secure internal instant messaging, and access built-in guideline-driven support tools that can assist clinical decision making.
Veterans will be able to input personal information using mobile devices and have complete access to their patient record, patient-provider communication tools, and consumer-friendly disease management information.
Administrators will have the ability to extract population-based data in real time to provide prompt feedback to frontline clinicians and identify specific gaps in healthcare delivery. The new HMP opens doors for improved interactions with system and developer partners worldwide.
Clearly the VA is not content to mimic the advancements of others, but once again is poised to revolutionize the arena of healthcare informatics.
Dr. Hazelrigg is section chief of hospital medicine at McGuire VAMC in Richmond, VA. Dr. Kwan is a hospitalist at the VA in San Diego, CA. Both are members of SHM's VA Task Force.
Society of Hospital Medicine Event Dates, Deadlines
December 17
Masters Deadline for Nominations
Do you know someone who has earned a place in the “Hall of Fame” for hospital medicine? Nominations for the Master in Hospital Medicine are due next month.
December 31
Membership Ambassadors
Now through Dec. 31, all active SHM members can earn 2015-2016 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
January 9, 2015
SFHM and FHM Deadline for Submission
Don’t wait until the last minute to submit your application for the Fellow or Senior Fellow in Hospital Medicine designation. Start now and submit ahead of time.
May 7-9, 2015
Quality and Safety Educators Academy
Quality improvement and patient safety are no longer just electives for trainees; they are part of the core education. That’s why educators everywhere need to learn from SHM’s Quality and Safety Educators Academy.
December 17
Masters Deadline for Nominations
Do you know someone who has earned a place in the “Hall of Fame” for hospital medicine? Nominations for the Master in Hospital Medicine are due next month.
December 31
Membership Ambassadors
Now through Dec. 31, all active SHM members can earn 2015-2016 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
January 9, 2015
SFHM and FHM Deadline for Submission
Don’t wait until the last minute to submit your application for the Fellow or Senior Fellow in Hospital Medicine designation. Start now and submit ahead of time.
May 7-9, 2015
Quality and Safety Educators Academy
Quality improvement and patient safety are no longer just electives for trainees; they are part of the core education. That’s why educators everywhere need to learn from SHM’s Quality and Safety Educators Academy.
December 17
Masters Deadline for Nominations
Do you know someone who has earned a place in the “Hall of Fame” for hospital medicine? Nominations for the Master in Hospital Medicine are due next month.
December 31
Membership Ambassadors
Now through Dec. 31, all active SHM members can earn 2015-2016 dues credits and special recognition for recruiting new physician, physician assistant, nurse practitioner, pharmacist, or affiliate members.
January 9, 2015
SFHM and FHM Deadline for Submission
Don’t wait until the last minute to submit your application for the Fellow or Senior Fellow in Hospital Medicine designation. Start now and submit ahead of time.
May 7-9, 2015
Quality and Safety Educators Academy
Quality improvement and patient safety are no longer just electives for trainees; they are part of the core education. That’s why educators everywhere need to learn from SHM’s Quality and Safety Educators Academy.
Medication Reconciliation Toolkit Updated, Available to Hospitalists
Adverse drug events and medication errors are unfortunately all too common within hospitals, but hospitalists can now take the lead in preventing them using SHM’s MARQUIS [Multi-Center Medication Reconciliation Quality Improvement Study] toolkit.
The authors of the new toolkit outline the hospitalist’s role in reducing medication errors as:
- Take responsibility for the accuracy of the medication reconciliation process for each patient under your care;
- Lead, coordinate, or participate in medication reconciliation quality improvement (QI) efforts with other key team members on the “front lines” to inform the hospital QI team on key interventions that would lead to improved patient outcomes;
- Become trained in taking the “best possible medication history” and in using effective discharge medication counseling; and
- Identify patients who are at high risk for a medication reconciliation error and would benefit from a more intensive medication reconciliation process.
“The MARQUIS study is important because it shows the potential of a mentored implementation effort, working with local hospitalist leaders and a QI toolkit, to improve medication safety related to the medication reconciliation process,” says MARQUIS principal investigator Jeff Schnipper, MD, MPH, FHM.
“It also shows the importance of institutional commitment to the success of these efforts. Lastly, hospitalists need to realize that medication reconciliation is not just some external regulatory requirement—it’s about the safety of the medications they order—and, therefore, that they need to ensure the quality of the process for the patients they care for and to lead efforts to improve the process across their hospitals.”
For more information, visit www.hospitalmedicine.org/marquis.
Adverse drug events and medication errors are unfortunately all too common within hospitals, but hospitalists can now take the lead in preventing them using SHM’s MARQUIS [Multi-Center Medication Reconciliation Quality Improvement Study] toolkit.
The authors of the new toolkit outline the hospitalist’s role in reducing medication errors as:
- Take responsibility for the accuracy of the medication reconciliation process for each patient under your care;
- Lead, coordinate, or participate in medication reconciliation quality improvement (QI) efforts with other key team members on the “front lines” to inform the hospital QI team on key interventions that would lead to improved patient outcomes;
- Become trained in taking the “best possible medication history” and in using effective discharge medication counseling; and
- Identify patients who are at high risk for a medication reconciliation error and would benefit from a more intensive medication reconciliation process.
“The MARQUIS study is important because it shows the potential of a mentored implementation effort, working with local hospitalist leaders and a QI toolkit, to improve medication safety related to the medication reconciliation process,” says MARQUIS principal investigator Jeff Schnipper, MD, MPH, FHM.
“It also shows the importance of institutional commitment to the success of these efforts. Lastly, hospitalists need to realize that medication reconciliation is not just some external regulatory requirement—it’s about the safety of the medications they order—and, therefore, that they need to ensure the quality of the process for the patients they care for and to lead efforts to improve the process across their hospitals.”
For more information, visit www.hospitalmedicine.org/marquis.
Adverse drug events and medication errors are unfortunately all too common within hospitals, but hospitalists can now take the lead in preventing them using SHM’s MARQUIS [Multi-Center Medication Reconciliation Quality Improvement Study] toolkit.
The authors of the new toolkit outline the hospitalist’s role in reducing medication errors as:
- Take responsibility for the accuracy of the medication reconciliation process for each patient under your care;
- Lead, coordinate, or participate in medication reconciliation quality improvement (QI) efforts with other key team members on the “front lines” to inform the hospital QI team on key interventions that would lead to improved patient outcomes;
- Become trained in taking the “best possible medication history” and in using effective discharge medication counseling; and
- Identify patients who are at high risk for a medication reconciliation error and would benefit from a more intensive medication reconciliation process.
“The MARQUIS study is important because it shows the potential of a mentored implementation effort, working with local hospitalist leaders and a QI toolkit, to improve medication safety related to the medication reconciliation process,” says MARQUIS principal investigator Jeff Schnipper, MD, MPH, FHM.
“It also shows the importance of institutional commitment to the success of these efforts. Lastly, hospitalists need to realize that medication reconciliation is not just some external regulatory requirement—it’s about the safety of the medications they order—and, therefore, that they need to ensure the quality of the process for the patients they care for and to lead efforts to improve the process across their hospitals.”
For more information, visit www.hospitalmedicine.org/marquis.
Post-Acute Care Transitions Toolkit Available to Hospitalists
Hospitalists know that many hospitalizations aren’t like those on TV. Instead of being discharged to their homes, many patients are discharged to post-acute care facilities for further care. And those transitions from hospital to post-acute care can be just as challenging as—if not more than—discharges to home care.
Making those transitions safer, smoother, and more effective can not only help an individual patient, but it can have a broader impact, according to the lead author of SHM’s new Post-Acute Care Transitions Toolkit, now available at www.hospitalmedicine.org/pact.
“Post-acute care transitions is an important area where hospitalists can contribute to improving the population health of their community,” says hospitalist Robert Young, MD, of Northwestern University in Chicago.
Both Dr. Young and the new toolkit recommend that hospitalists partner with the post-acute providers to make sure that communication between settings is complete during transitioning and open for ongoing questions as they arise. “Developing a relationship with your post-acute providers to work on these transitions issues provides the opportunity for ongoing quality and process improvement vital to our patients’ care,” Dr. Young says.
Hospitalists know that many hospitalizations aren’t like those on TV. Instead of being discharged to their homes, many patients are discharged to post-acute care facilities for further care. And those transitions from hospital to post-acute care can be just as challenging as—if not more than—discharges to home care.
Making those transitions safer, smoother, and more effective can not only help an individual patient, but it can have a broader impact, according to the lead author of SHM’s new Post-Acute Care Transitions Toolkit, now available at www.hospitalmedicine.org/pact.
“Post-acute care transitions is an important area where hospitalists can contribute to improving the population health of their community,” says hospitalist Robert Young, MD, of Northwestern University in Chicago.
Both Dr. Young and the new toolkit recommend that hospitalists partner with the post-acute providers to make sure that communication between settings is complete during transitioning and open for ongoing questions as they arise. “Developing a relationship with your post-acute providers to work on these transitions issues provides the opportunity for ongoing quality and process improvement vital to our patients’ care,” Dr. Young says.
Hospitalists know that many hospitalizations aren’t like those on TV. Instead of being discharged to their homes, many patients are discharged to post-acute care facilities for further care. And those transitions from hospital to post-acute care can be just as challenging as—if not more than—discharges to home care.
Making those transitions safer, smoother, and more effective can not only help an individual patient, but it can have a broader impact, according to the lead author of SHM’s new Post-Acute Care Transitions Toolkit, now available at www.hospitalmedicine.org/pact.
“Post-acute care transitions is an important area where hospitalists can contribute to improving the population health of their community,” says hospitalist Robert Young, MD, of Northwestern University in Chicago.
Both Dr. Young and the new toolkit recommend that hospitalists partner with the post-acute providers to make sure that communication between settings is complete during transitioning and open for ongoing questions as they arise. “Developing a relationship with your post-acute providers to work on these transitions issues provides the opportunity for ongoing quality and process improvement vital to our patients’ care,” Dr. Young says.
Society of Hospital Medicine's Online Learning Portal Hosts New Content
If you haven’t checked out SHM’s online Learning Portal, now is the time. SHM will be introducing new content for pediatric hospitalists and more information on the use of anticoagulants. Access to the SHM Learning Portal is free for members: www.shmlearningportal.org.
If you haven’t checked out SHM’s online Learning Portal, now is the time. SHM will be introducing new content for pediatric hospitalists and more information on the use of anticoagulants. Access to the SHM Learning Portal is free for members: www.shmlearningportal.org.
If you haven’t checked out SHM’s online Learning Portal, now is the time. SHM will be introducing new content for pediatric hospitalists and more information on the use of anticoagulants. Access to the SHM Learning Portal is free for members: www.shmlearningportal.org.
HM15 to Feature Exclusive Content for Medical Students, Residents, Early Career Hospitalists
As the HM movement continues to grow, more medical students, residents, and hospitalists in the first few years of their new career are looking to answer some of the fundamental questions about a career in the specialty: How can I get involved in quality improvement?
How do I find a career mentor and approach him or her? How can I build a CV that reflects my career path and aspirations?
Many of those topics—and lots of others—will be addressed comprehensively for the first time ever at Hospital Medicine 2015 during a daylong track for young physicians. Courses on Monday, March 30, will include:
- Career Pathways in Hospital Medicine
- How to Stand Out: Being the Best Applicant
You Can Be
- Getting to the Top of the Pile: Writing Your CV
- Quality and Safety for Residents and Students
- Time Management
- Making the Most of Your Mentoring Relationships
Registration discounts apply for residents and medical students. For more information, visit www.hospitalmedicine2015.org.
As the HM movement continues to grow, more medical students, residents, and hospitalists in the first few years of their new career are looking to answer some of the fundamental questions about a career in the specialty: How can I get involved in quality improvement?
How do I find a career mentor and approach him or her? How can I build a CV that reflects my career path and aspirations?
Many of those topics—and lots of others—will be addressed comprehensively for the first time ever at Hospital Medicine 2015 during a daylong track for young physicians. Courses on Monday, March 30, will include:
- Career Pathways in Hospital Medicine
- How to Stand Out: Being the Best Applicant
You Can Be
- Getting to the Top of the Pile: Writing Your CV
- Quality and Safety for Residents and Students
- Time Management
- Making the Most of Your Mentoring Relationships
Registration discounts apply for residents and medical students. For more information, visit www.hospitalmedicine2015.org.
As the HM movement continues to grow, more medical students, residents, and hospitalists in the first few years of their new career are looking to answer some of the fundamental questions about a career in the specialty: How can I get involved in quality improvement?
How do I find a career mentor and approach him or her? How can I build a CV that reflects my career path and aspirations?
Many of those topics—and lots of others—will be addressed comprehensively for the first time ever at Hospital Medicine 2015 during a daylong track for young physicians. Courses on Monday, March 30, will include:
- Career Pathways in Hospital Medicine
- How to Stand Out: Being the Best Applicant
You Can Be
- Getting to the Top of the Pile: Writing Your CV
- Quality and Safety for Residents and Students
- Time Management
- Making the Most of Your Mentoring Relationships
Registration discounts apply for residents and medical students. For more information, visit www.hospitalmedicine2015.org.
Tips, Tools to Control Diabetes, Hyperglycemia in Hospitalized Patients
Controlling diabetes in the hospital is one of the most predominant challenges hospitalists face. In addition to the condition’s increased prevalence among the general population, patients with diabetes are commonly admitted to the hospital multiple times. And the treatment of diabetes can make the treatment of other conditions more difficult.
In fact, a 2014 study conducted in California by the UCLA Center for Health Policy Research and the California Center for Public Health Advocacy revealed that one-third of hospitalized patients older than 34 in California have diabetes.
For hospitalists ready to tackle a condition like diabetes—increasingly common and challenging to treat—SHM now has more resources than ever. And hospitalists can start to take advantage of them today.
Glycemic Control Implementation Toolkit
SHM’s Glycemic Control Implementation Toolkit gives hospitalists the first advantages in treating hyperglycemia in the hospital. Using SHM’s proven approach to quality improvement, including personal experience and evidence-based medicine, the toolkit enables hospitalists to implement effective regimens and protocols that optimize glycemic control and minimize hypoglycemia.
The toolkit (www.hospitalmedicine.org/gcmi) is easy to use and includes step-by-step instructions, from first steps to performance tracking to continuing improvement.
Hospital Medicine 2015
Ready to learn directly from the experts in inpatient glycemic control and share experiences with thousands of other hospitalists? HM15 will feature the most current information and research from the leading authorities on glycemic control.
For more information and to register online, visit www.hospitalmedicine2015.org.
Glycemic Control Mentored Implementation
SHM’s signature mentored implementation model helps hospitals create and implement programs that make a difference. The Glycemic Control Mentored Implementation (GCMI) Program links hospitals with national leaders in the field for a mentored relationship, critical data benchmarking, and collaboration with peers.
GCMI has now moved to a rolling acceptance model, so hospitals can now apply any time to start preventing hypoglycemia and better managing their inpatients with hyperglycemia and diabetes. For more information, visit www.hospitalmedicine.org/gcmi.
Brendon Shank is SHM’s associate vice president of communications.
Controlling diabetes in the hospital is one of the most predominant challenges hospitalists face. In addition to the condition’s increased prevalence among the general population, patients with diabetes are commonly admitted to the hospital multiple times. And the treatment of diabetes can make the treatment of other conditions more difficult.
In fact, a 2014 study conducted in California by the UCLA Center for Health Policy Research and the California Center for Public Health Advocacy revealed that one-third of hospitalized patients older than 34 in California have diabetes.
For hospitalists ready to tackle a condition like diabetes—increasingly common and challenging to treat—SHM now has more resources than ever. And hospitalists can start to take advantage of them today.
Glycemic Control Implementation Toolkit
SHM’s Glycemic Control Implementation Toolkit gives hospitalists the first advantages in treating hyperglycemia in the hospital. Using SHM’s proven approach to quality improvement, including personal experience and evidence-based medicine, the toolkit enables hospitalists to implement effective regimens and protocols that optimize glycemic control and minimize hypoglycemia.
The toolkit (www.hospitalmedicine.org/gcmi) is easy to use and includes step-by-step instructions, from first steps to performance tracking to continuing improvement.
Hospital Medicine 2015
Ready to learn directly from the experts in inpatient glycemic control and share experiences with thousands of other hospitalists? HM15 will feature the most current information and research from the leading authorities on glycemic control.
For more information and to register online, visit www.hospitalmedicine2015.org.
Glycemic Control Mentored Implementation
SHM’s signature mentored implementation model helps hospitals create and implement programs that make a difference. The Glycemic Control Mentored Implementation (GCMI) Program links hospitals with national leaders in the field for a mentored relationship, critical data benchmarking, and collaboration with peers.
GCMI has now moved to a rolling acceptance model, so hospitals can now apply any time to start preventing hypoglycemia and better managing their inpatients with hyperglycemia and diabetes. For more information, visit www.hospitalmedicine.org/gcmi.
Brendon Shank is SHM’s associate vice president of communications.
Controlling diabetes in the hospital is one of the most predominant challenges hospitalists face. In addition to the condition’s increased prevalence among the general population, patients with diabetes are commonly admitted to the hospital multiple times. And the treatment of diabetes can make the treatment of other conditions more difficult.
In fact, a 2014 study conducted in California by the UCLA Center for Health Policy Research and the California Center for Public Health Advocacy revealed that one-third of hospitalized patients older than 34 in California have diabetes.
For hospitalists ready to tackle a condition like diabetes—increasingly common and challenging to treat—SHM now has more resources than ever. And hospitalists can start to take advantage of them today.
Glycemic Control Implementation Toolkit
SHM’s Glycemic Control Implementation Toolkit gives hospitalists the first advantages in treating hyperglycemia in the hospital. Using SHM’s proven approach to quality improvement, including personal experience and evidence-based medicine, the toolkit enables hospitalists to implement effective regimens and protocols that optimize glycemic control and minimize hypoglycemia.
The toolkit (www.hospitalmedicine.org/gcmi) is easy to use and includes step-by-step instructions, from first steps to performance tracking to continuing improvement.
Hospital Medicine 2015
Ready to learn directly from the experts in inpatient glycemic control and share experiences with thousands of other hospitalists? HM15 will feature the most current information and research from the leading authorities on glycemic control.
For more information and to register online, visit www.hospitalmedicine2015.org.
Glycemic Control Mentored Implementation
SHM’s signature mentored implementation model helps hospitals create and implement programs that make a difference. The Glycemic Control Mentored Implementation (GCMI) Program links hospitals with national leaders in the field for a mentored relationship, critical data benchmarking, and collaboration with peers.
GCMI has now moved to a rolling acceptance model, so hospitals can now apply any time to start preventing hypoglycemia and better managing their inpatients with hyperglycemia and diabetes. For more information, visit www.hospitalmedicine.org/gcmi.
Brendon Shank is SHM’s associate vice president of communications.