User login
“Triple Rule Outs” for Chest Pain: A Tool to Evaluate the Coronaries but Not Pulmonary Embolism or Aortic Dissection
Clinical question: How does “triple rule out” (TRO) computed tomographic (CT) angiography compare to other imaging modalities in evaluating coronary and other life-threatening etiologies of chest pain, such as pulmonary embolism (PE) and aortic dissection?
Background: TRO CT angiography is a noninvasive technology that evaluates the coronary arteries, thoracic aorta, and pulmonary vasculature simultaneously. Comparison with other tests in the diagnosis of common clinical conditions is useful information for clinical practice.
Study design: Systematic review and meta-analysis.
Setting: Systematic review of 11 studies (one randomized, 10 observational).
Synopsis: Using an enrolled population of 3,539 patients, TRO CT was compared to other imaging modalities on the basis of image quality, diagnostic accuracy, radiation, and contrast volume. When TRO CT was compared to dedicated CT scans, no significant imaging difference was discovered. TRO CT detected CAD with a sensitivity of 94.3% (95% CI, 89.1% to 97.5%, I2=58.2%) and specificity of 97.4% (95% CI, 96.1% to 98.5%, I2=91.2%).
An insufficient number of patients with PE or aortic dissection were studied to generate diagnostic accuracy for these conditions. TRO CT involved greater radiation exposure and contrast exposure than non-TRO CT.
This study reports high accuracy of TRO CT in the diagnosis of coronary artery disease. Due to the low prevalence of patients with PE or aortic dissection (<1%), the data cannot be extrapolated to these conditions.
Bottom line: Although TRO CT is highly accurate for detecting coronary artery disease, there is insufficient data to recommend its use for the diagnosis of PE or aortic dissection.
Citation: Ayaram D, Bellolio MF, Murad MH, et al. Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis. Acad Emerg Med. 2013;20(9):861-871.
Clinical question: How does “triple rule out” (TRO) computed tomographic (CT) angiography compare to other imaging modalities in evaluating coronary and other life-threatening etiologies of chest pain, such as pulmonary embolism (PE) and aortic dissection?
Background: TRO CT angiography is a noninvasive technology that evaluates the coronary arteries, thoracic aorta, and pulmonary vasculature simultaneously. Comparison with other tests in the diagnosis of common clinical conditions is useful information for clinical practice.
Study design: Systematic review and meta-analysis.
Setting: Systematic review of 11 studies (one randomized, 10 observational).
Synopsis: Using an enrolled population of 3,539 patients, TRO CT was compared to other imaging modalities on the basis of image quality, diagnostic accuracy, radiation, and contrast volume. When TRO CT was compared to dedicated CT scans, no significant imaging difference was discovered. TRO CT detected CAD with a sensitivity of 94.3% (95% CI, 89.1% to 97.5%, I2=58.2%) and specificity of 97.4% (95% CI, 96.1% to 98.5%, I2=91.2%).
An insufficient number of patients with PE or aortic dissection were studied to generate diagnostic accuracy for these conditions. TRO CT involved greater radiation exposure and contrast exposure than non-TRO CT.
This study reports high accuracy of TRO CT in the diagnosis of coronary artery disease. Due to the low prevalence of patients with PE or aortic dissection (<1%), the data cannot be extrapolated to these conditions.
Bottom line: Although TRO CT is highly accurate for detecting coronary artery disease, there is insufficient data to recommend its use for the diagnosis of PE or aortic dissection.
Citation: Ayaram D, Bellolio MF, Murad MH, et al. Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis. Acad Emerg Med. 2013;20(9):861-871.
Clinical question: How does “triple rule out” (TRO) computed tomographic (CT) angiography compare to other imaging modalities in evaluating coronary and other life-threatening etiologies of chest pain, such as pulmonary embolism (PE) and aortic dissection?
Background: TRO CT angiography is a noninvasive technology that evaluates the coronary arteries, thoracic aorta, and pulmonary vasculature simultaneously. Comparison with other tests in the diagnosis of common clinical conditions is useful information for clinical practice.
Study design: Systematic review and meta-analysis.
Setting: Systematic review of 11 studies (one randomized, 10 observational).
Synopsis: Using an enrolled population of 3,539 patients, TRO CT was compared to other imaging modalities on the basis of image quality, diagnostic accuracy, radiation, and contrast volume. When TRO CT was compared to dedicated CT scans, no significant imaging difference was discovered. TRO CT detected CAD with a sensitivity of 94.3% (95% CI, 89.1% to 97.5%, I2=58.2%) and specificity of 97.4% (95% CI, 96.1% to 98.5%, I2=91.2%).
An insufficient number of patients with PE or aortic dissection were studied to generate diagnostic accuracy for these conditions. TRO CT involved greater radiation exposure and contrast exposure than non-TRO CT.
This study reports high accuracy of TRO CT in the diagnosis of coronary artery disease. Due to the low prevalence of patients with PE or aortic dissection (<1%), the data cannot be extrapolated to these conditions.
Bottom line: Although TRO CT is highly accurate for detecting coronary artery disease, there is insufficient data to recommend its use for the diagnosis of PE or aortic dissection.
Citation: Ayaram D, Bellolio MF, Murad MH, et al. Triple rule-out computed tomographic angiography for chest pain: a diagnostic systematic review and meta-analysis. Acad Emerg Med. 2013;20(9):861-871.
Hippocampus-sparing brain radiotherapy preserves memory, QOL
For cancer patients who have multiple brain metastases, tailoring whole-brain radiotherapy so that it avoids the hippocampus preserves memory and quality of life for at least 6 months, according to a report published online Oct. 27 in the Journal of Clinical Oncology.
Injury to the compartment of neural stem cells located in the subgranular zone of the hippocampal dentate gyrus is thought to suppress the formation of new memory and to impair recall, and injury to this region by relatively low doses of radiotherapy is thought to account for radiation-induced early cognitive decline. Researchers performed a multicenter phase II trial to determine whether sparing this region would prevent such cognitive decline. They assessed 100 patients who had brain metastases of nonhematopoietic malignancies and underwent irradiation of the whole-brain parenchyma minus the “hippocampal avoidance regions” that had been designated using advanced imaging techniques, said Dr. Vinai Gondi of the Cadence Brain Tumor Center and CDH Proton Center, Warrenville, Ill., and his associates.
The study participants underwent cognitive assessment at baseline and at regular intervals following radiotherapy, as well as assessment of health-related quality of life. Their results were compared with those of 208 historical control subjects who had received standard whole-brain radiotherapy without hippocampal avoidance in an unrelated clinical trial. The radiation-sparing technique, which reduced the mean dose to the neural stem compartment by an estimated 80%, produced significant memory preservation that persisted for up to 6 months of follow-up. The mean probability of cognitive deterioration at 4 months was only 7%, compared with 30% in the historical control group.
The hippocampal-sparing technique also preserved physical, social/family, emotional, and functional well-being, as assessed by the patient and his or her family, the investigators said (J. Clin. Oncol. 2014 Oct. 27 [doi:10.1200/JCO.2014.57.2909]).
The risk that metastases would develop in the nonradiated hippocampus was considered low, as only three patients (4.5%) developed such metastases. Previously, investigators have predicted that the risk would be closer to 10%, but they appear to have overestimated the actual risk, Dr. Gondi and his associates said.
These promising results require further validation in phase III trials. Studies are now underway to assess whether further reducing the radiation dose to the hippocampal area may improve outcomes even more, and future studies also are being planned to assess whether hippocampal avoidance prevents longer-term cognitive decline, beyond the 6-month mark established in this study, the investigators added.
This study was supported by the National Cancer Institute’s Radiation Therapy Oncology Group and Community Clinical Oncology Program. Dr. Gondi reported having no financial disclosures; his associates reported numerous ties to industry sources.
The findings of this phase II study need to be replicated and expanded upon before this innovative treatment approach can be offered to patients.
To justify the increased cost, time, and effort involved in hippocampal-avoidance whole-brain radiotherapy, it may be necessary to prove that the technique improves survival, not just QOL. And the influence of factors such as the number and size of brain metastases, extracranial disease status, and prognostic assessment scores should be addressed in future studies, to narrow down which patients will benefit most from the therapy.
Dr. John H. Suh is in the department of radiation oncology at the Cleveland Clinic. He reported receiving honoraria and serving as a consultant or adviser to Varian Medical Systems. Dr. Suh made these remarks in an editorial accompanying Dr. Gondi’s report (J. Clin. Oncol. 2014 Oct. 27 [doi:10.1200/JCO.2014.58.4367]).
The findings of this phase II study need to be replicated and expanded upon before this innovative treatment approach can be offered to patients.
To justify the increased cost, time, and effort involved in hippocampal-avoidance whole-brain radiotherapy, it may be necessary to prove that the technique improves survival, not just QOL. And the influence of factors such as the number and size of brain metastases, extracranial disease status, and prognostic assessment scores should be addressed in future studies, to narrow down which patients will benefit most from the therapy.
Dr. John H. Suh is in the department of radiation oncology at the Cleveland Clinic. He reported receiving honoraria and serving as a consultant or adviser to Varian Medical Systems. Dr. Suh made these remarks in an editorial accompanying Dr. Gondi’s report (J. Clin. Oncol. 2014 Oct. 27 [doi:10.1200/JCO.2014.58.4367]).
The findings of this phase II study need to be replicated and expanded upon before this innovative treatment approach can be offered to patients.
To justify the increased cost, time, and effort involved in hippocampal-avoidance whole-brain radiotherapy, it may be necessary to prove that the technique improves survival, not just QOL. And the influence of factors such as the number and size of brain metastases, extracranial disease status, and prognostic assessment scores should be addressed in future studies, to narrow down which patients will benefit most from the therapy.
Dr. John H. Suh is in the department of radiation oncology at the Cleveland Clinic. He reported receiving honoraria and serving as a consultant or adviser to Varian Medical Systems. Dr. Suh made these remarks in an editorial accompanying Dr. Gondi’s report (J. Clin. Oncol. 2014 Oct. 27 [doi:10.1200/JCO.2014.58.4367]).
For cancer patients who have multiple brain metastases, tailoring whole-brain radiotherapy so that it avoids the hippocampus preserves memory and quality of life for at least 6 months, according to a report published online Oct. 27 in the Journal of Clinical Oncology.
Injury to the compartment of neural stem cells located in the subgranular zone of the hippocampal dentate gyrus is thought to suppress the formation of new memory and to impair recall, and injury to this region by relatively low doses of radiotherapy is thought to account for radiation-induced early cognitive decline. Researchers performed a multicenter phase II trial to determine whether sparing this region would prevent such cognitive decline. They assessed 100 patients who had brain metastases of nonhematopoietic malignancies and underwent irradiation of the whole-brain parenchyma minus the “hippocampal avoidance regions” that had been designated using advanced imaging techniques, said Dr. Vinai Gondi of the Cadence Brain Tumor Center and CDH Proton Center, Warrenville, Ill., and his associates.
The study participants underwent cognitive assessment at baseline and at regular intervals following radiotherapy, as well as assessment of health-related quality of life. Their results were compared with those of 208 historical control subjects who had received standard whole-brain radiotherapy without hippocampal avoidance in an unrelated clinical trial. The radiation-sparing technique, which reduced the mean dose to the neural stem compartment by an estimated 80%, produced significant memory preservation that persisted for up to 6 months of follow-up. The mean probability of cognitive deterioration at 4 months was only 7%, compared with 30% in the historical control group.
The hippocampal-sparing technique also preserved physical, social/family, emotional, and functional well-being, as assessed by the patient and his or her family, the investigators said (J. Clin. Oncol. 2014 Oct. 27 [doi:10.1200/JCO.2014.57.2909]).
The risk that metastases would develop in the nonradiated hippocampus was considered low, as only three patients (4.5%) developed such metastases. Previously, investigators have predicted that the risk would be closer to 10%, but they appear to have overestimated the actual risk, Dr. Gondi and his associates said.
These promising results require further validation in phase III trials. Studies are now underway to assess whether further reducing the radiation dose to the hippocampal area may improve outcomes even more, and future studies also are being planned to assess whether hippocampal avoidance prevents longer-term cognitive decline, beyond the 6-month mark established in this study, the investigators added.
This study was supported by the National Cancer Institute’s Radiation Therapy Oncology Group and Community Clinical Oncology Program. Dr. Gondi reported having no financial disclosures; his associates reported numerous ties to industry sources.
For cancer patients who have multiple brain metastases, tailoring whole-brain radiotherapy so that it avoids the hippocampus preserves memory and quality of life for at least 6 months, according to a report published online Oct. 27 in the Journal of Clinical Oncology.
Injury to the compartment of neural stem cells located in the subgranular zone of the hippocampal dentate gyrus is thought to suppress the formation of new memory and to impair recall, and injury to this region by relatively low doses of radiotherapy is thought to account for radiation-induced early cognitive decline. Researchers performed a multicenter phase II trial to determine whether sparing this region would prevent such cognitive decline. They assessed 100 patients who had brain metastases of nonhematopoietic malignancies and underwent irradiation of the whole-brain parenchyma minus the “hippocampal avoidance regions” that had been designated using advanced imaging techniques, said Dr. Vinai Gondi of the Cadence Brain Tumor Center and CDH Proton Center, Warrenville, Ill., and his associates.
The study participants underwent cognitive assessment at baseline and at regular intervals following radiotherapy, as well as assessment of health-related quality of life. Their results were compared with those of 208 historical control subjects who had received standard whole-brain radiotherapy without hippocampal avoidance in an unrelated clinical trial. The radiation-sparing technique, which reduced the mean dose to the neural stem compartment by an estimated 80%, produced significant memory preservation that persisted for up to 6 months of follow-up. The mean probability of cognitive deterioration at 4 months was only 7%, compared with 30% in the historical control group.
The hippocampal-sparing technique also preserved physical, social/family, emotional, and functional well-being, as assessed by the patient and his or her family, the investigators said (J. Clin. Oncol. 2014 Oct. 27 [doi:10.1200/JCO.2014.57.2909]).
The risk that metastases would develop in the nonradiated hippocampus was considered low, as only three patients (4.5%) developed such metastases. Previously, investigators have predicted that the risk would be closer to 10%, but they appear to have overestimated the actual risk, Dr. Gondi and his associates said.
These promising results require further validation in phase III trials. Studies are now underway to assess whether further reducing the radiation dose to the hippocampal area may improve outcomes even more, and future studies also are being planned to assess whether hippocampal avoidance prevents longer-term cognitive decline, beyond the 6-month mark established in this study, the investigators added.
This study was supported by the National Cancer Institute’s Radiation Therapy Oncology Group and Community Clinical Oncology Program. Dr. Gondi reported having no financial disclosures; his associates reported numerous ties to industry sources.
Key clinical point: Whole-brain radiotherapy that spares the hippocampal neural stem cell compartment preserves memory and QOL in cancer patients with brain metastases.
Major finding: The mean probability of cognitive deterioration at 4 months was only 7% in patients who underwent hippocampus-sparing brain radiotherapy, compared with 30% in a historical control group.
Data source: A multicenter phase II study comparing cognitive function and QOL between 100 patients with brain metastases who had hippocampus-sparing radiotherapy and 208 historical control subjects who had standard whole-brain radiotherapy.
Disclosures: This study was supported by the National Cancer Institute’s Radiation Therapy Oncology Group and Community Clinical Oncology Program. Dr. Gondi reported having no financial disclosures; his associates reported numerous ties to industry sources.
Patients Prefer Inpatient Boarding to Emergency Department Boarding
Clinical question: Do patients who experience overcrowding and long waits in the emergency department (ED) prefer boarding within ED hallways or within inpatient medical unit hallways?
Background: Boarding of admitted patients in EDs can be problematic, especially with regard to patient safety and patient satisfaction. Patient satisfaction data comparing boarding in the ED versus boarding in an inpatient unit hallway is limited.
Study design: Post-discharge, structured, telephone satisfaction survey.
Setting: Suburban, university-based teaching hospital.
Synopsis: A group of patients who experienced hallway boarding in the ED and then hallway boarding on the inpatient medical unit were identified. They were contacted by phone and asked to take a survey on their experience; 105 of 110 patients identified agreed. Patients were asked to rate their location preference with regard to various aspects of care. A five-point Likert scale consisting of the following answers was used: ED hallway much better, ED hallway better, no preference, inpatient hallway better, and inpatient hallway much better.
The inpatient hallway was the overall preferred location in 85% of respondents. Respondents preferred inpatient boarding with regard to multiple other parameters: rest, 85%; safety, 83%; confidentiality, 82%; treatment, 78%; comfort, 79%; quiet, 84%; staff availability, 84%; and privacy, 84%. For no item was there a preference for boarding in the ED.
Patient demographics in this hospital may differ from other settings and should be considered when applying the results. With Hospital Consumer Assessment of Healthcare Providers and Systems scores and ED throughput being publicly reported, further studies in this area would be valuable.
Bottom line: In a post-discharge telephone survey, patients preferred boarding in inpatient unit hallways rather than boarding in the ED.
Citation: Viccellio P, Zito JA, Sayage V, et al. Patients overwhelmingly prefer inpatient boarding to emergency department boarding. J Emerg Med. 2013;45(6):942-946.
Clinical question: Do patients who experience overcrowding and long waits in the emergency department (ED) prefer boarding within ED hallways or within inpatient medical unit hallways?
Background: Boarding of admitted patients in EDs can be problematic, especially with regard to patient safety and patient satisfaction. Patient satisfaction data comparing boarding in the ED versus boarding in an inpatient unit hallway is limited.
Study design: Post-discharge, structured, telephone satisfaction survey.
Setting: Suburban, university-based teaching hospital.
Synopsis: A group of patients who experienced hallway boarding in the ED and then hallway boarding on the inpatient medical unit were identified. They were contacted by phone and asked to take a survey on their experience; 105 of 110 patients identified agreed. Patients were asked to rate their location preference with regard to various aspects of care. A five-point Likert scale consisting of the following answers was used: ED hallway much better, ED hallway better, no preference, inpatient hallway better, and inpatient hallway much better.
The inpatient hallway was the overall preferred location in 85% of respondents. Respondents preferred inpatient boarding with regard to multiple other parameters: rest, 85%; safety, 83%; confidentiality, 82%; treatment, 78%; comfort, 79%; quiet, 84%; staff availability, 84%; and privacy, 84%. For no item was there a preference for boarding in the ED.
Patient demographics in this hospital may differ from other settings and should be considered when applying the results. With Hospital Consumer Assessment of Healthcare Providers and Systems scores and ED throughput being publicly reported, further studies in this area would be valuable.
Bottom line: In a post-discharge telephone survey, patients preferred boarding in inpatient unit hallways rather than boarding in the ED.
Citation: Viccellio P, Zito JA, Sayage V, et al. Patients overwhelmingly prefer inpatient boarding to emergency department boarding. J Emerg Med. 2013;45(6):942-946.
Clinical question: Do patients who experience overcrowding and long waits in the emergency department (ED) prefer boarding within ED hallways or within inpatient medical unit hallways?
Background: Boarding of admitted patients in EDs can be problematic, especially with regard to patient safety and patient satisfaction. Patient satisfaction data comparing boarding in the ED versus boarding in an inpatient unit hallway is limited.
Study design: Post-discharge, structured, telephone satisfaction survey.
Setting: Suburban, university-based teaching hospital.
Synopsis: A group of patients who experienced hallway boarding in the ED and then hallway boarding on the inpatient medical unit were identified. They were contacted by phone and asked to take a survey on their experience; 105 of 110 patients identified agreed. Patients were asked to rate their location preference with regard to various aspects of care. A five-point Likert scale consisting of the following answers was used: ED hallway much better, ED hallway better, no preference, inpatient hallway better, and inpatient hallway much better.
The inpatient hallway was the overall preferred location in 85% of respondents. Respondents preferred inpatient boarding with regard to multiple other parameters: rest, 85%; safety, 83%; confidentiality, 82%; treatment, 78%; comfort, 79%; quiet, 84%; staff availability, 84%; and privacy, 84%. For no item was there a preference for boarding in the ED.
Patient demographics in this hospital may differ from other settings and should be considered when applying the results. With Hospital Consumer Assessment of Healthcare Providers and Systems scores and ED throughput being publicly reported, further studies in this area would be valuable.
Bottom line: In a post-discharge telephone survey, patients preferred boarding in inpatient unit hallways rather than boarding in the ED.
Citation: Viccellio P, Zito JA, Sayage V, et al. Patients overwhelmingly prefer inpatient boarding to emergency department boarding. J Emerg Med. 2013;45(6):942-946.
Benefit of Therapeutic Hypothermia after Cardiac Arrest Unclear
Clinical question: Does targeted hypothermia (33°C) after cardiac arrest confer benefits compared with targeted temperature management at 36°C?
Background: Therapeutic hypothermia is a current recommendation in resuscitation guidelines after cardiac arrest. Fever develops in many patients after arrest, and it is unclear if the treatment benefit is due to hypothermia or due to the prevention of fever.
Study design: RCT.
Setting: ICUs in Europe and Australia.
Synopsis: The study authors randomized 950 patients who experienced out-of-hospital cardiac arrest to targeted temperature management at either 36°C or 33°C. The goal of this trial was to prevent fever in both groups during the first 36 hours after cardiac arrest. No statistically significant difference in outcomes between these two approaches was found. In the 33°C group, 54% died or had poor neurologic function, compared with 52% in the 36°C group (risk ratio 1.02; 95% CI 0.88 to 1.16; P=0.78).
Given the wide confidence interval, a trial with either more participants or more events might be able to determine whether a true difference in these management approaches exists.
Bottom line: Therapeutic hypothermia at 33°C after out-of-hospital cardiac arrest did not confer a benefit compared with targeted temperature management at 36°C.
Citation: Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369(23):2197-2206.
Clinical question: Does targeted hypothermia (33°C) after cardiac arrest confer benefits compared with targeted temperature management at 36°C?
Background: Therapeutic hypothermia is a current recommendation in resuscitation guidelines after cardiac arrest. Fever develops in many patients after arrest, and it is unclear if the treatment benefit is due to hypothermia or due to the prevention of fever.
Study design: RCT.
Setting: ICUs in Europe and Australia.
Synopsis: The study authors randomized 950 patients who experienced out-of-hospital cardiac arrest to targeted temperature management at either 36°C or 33°C. The goal of this trial was to prevent fever in both groups during the first 36 hours after cardiac arrest. No statistically significant difference in outcomes between these two approaches was found. In the 33°C group, 54% died or had poor neurologic function, compared with 52% in the 36°C group (risk ratio 1.02; 95% CI 0.88 to 1.16; P=0.78).
Given the wide confidence interval, a trial with either more participants or more events might be able to determine whether a true difference in these management approaches exists.
Bottom line: Therapeutic hypothermia at 33°C after out-of-hospital cardiac arrest did not confer a benefit compared with targeted temperature management at 36°C.
Citation: Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369(23):2197-2206.
Clinical question: Does targeted hypothermia (33°C) after cardiac arrest confer benefits compared with targeted temperature management at 36°C?
Background: Therapeutic hypothermia is a current recommendation in resuscitation guidelines after cardiac arrest. Fever develops in many patients after arrest, and it is unclear if the treatment benefit is due to hypothermia or due to the prevention of fever.
Study design: RCT.
Setting: ICUs in Europe and Australia.
Synopsis: The study authors randomized 950 patients who experienced out-of-hospital cardiac arrest to targeted temperature management at either 36°C or 33°C. The goal of this trial was to prevent fever in both groups during the first 36 hours after cardiac arrest. No statistically significant difference in outcomes between these two approaches was found. In the 33°C group, 54% died or had poor neurologic function, compared with 52% in the 36°C group (risk ratio 1.02; 95% CI 0.88 to 1.16; P=0.78).
Given the wide confidence interval, a trial with either more participants or more events might be able to determine whether a true difference in these management approaches exists.
Bottom line: Therapeutic hypothermia at 33°C after out-of-hospital cardiac arrest did not confer a benefit compared with targeted temperature management at 36°C.
Citation: Nielsen N, Wetterslev J, Cronberg T, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369(23):2197-2206.
Pre-Operative Beta Blockers May Benefit Some Cardiac Patients
Clinical question: In patients with ischemic heart disease (IHD) undergoing non-cardiac surgery, do pre-operative beta blockers reduce post-operative major cardiovascular events (MACE) or mortality at 30 days?
Background: Peri-operative beta blocker use has become more restricted, as evidence about which patients derive benefit has become clearer. Opinions and practice vary regarding whether all patients with IHD, or only certain populations within this group, benefit from peri-operative beta blockers.
Study design: Retrospective, national registry-based cohort study.
Setting: Denmark, 2004-2009.
Synopsis: No benefit was found for the overall cohort of 28,263 patients. Patients with IHD and heart failure (n=7990) had lower risk of MACE (HR=0.75, 95% CI, 0.70-0.87) and mortality (HR=0.80, 95% CI, 0.70-0.92). Patients with IHD and myocardial infarction within two years (n=1664) had lower risk of MACE (HR=0.54, 95% CI, 0.37-0.78) but not mortality.
Beta blocker dose and compliance were unknown. Whether patients had symptoms or inducible ischemia was not clear.
This study supports the concept that higher-risk patients benefit more from peri-operative beta blockers, but it is not high-grade evidence.
Bottom line: Not all patients with IHD benefit from pre-operative beta blockers; those with concomitant heart failure or recent MI have a lower risk of MACE and/or mortality at 30 days with beta blockers.
Citation: Andersson C, Merie C, Jorgensen M, et al. Association of ß-blocker therapy with risks of adverse cardiovascular events and deaths in patients with ischemic heart disease undergoing non-cardiac surgery: a Danish nationwide cohort study. JAMA Intern Med. 2014;174(3):336-344.
Clinical question: In patients with ischemic heart disease (IHD) undergoing non-cardiac surgery, do pre-operative beta blockers reduce post-operative major cardiovascular events (MACE) or mortality at 30 days?
Background: Peri-operative beta blocker use has become more restricted, as evidence about which patients derive benefit has become clearer. Opinions and practice vary regarding whether all patients with IHD, or only certain populations within this group, benefit from peri-operative beta blockers.
Study design: Retrospective, national registry-based cohort study.
Setting: Denmark, 2004-2009.
Synopsis: No benefit was found for the overall cohort of 28,263 patients. Patients with IHD and heart failure (n=7990) had lower risk of MACE (HR=0.75, 95% CI, 0.70-0.87) and mortality (HR=0.80, 95% CI, 0.70-0.92). Patients with IHD and myocardial infarction within two years (n=1664) had lower risk of MACE (HR=0.54, 95% CI, 0.37-0.78) but not mortality.
Beta blocker dose and compliance were unknown. Whether patients had symptoms or inducible ischemia was not clear.
This study supports the concept that higher-risk patients benefit more from peri-operative beta blockers, but it is not high-grade evidence.
Bottom line: Not all patients with IHD benefit from pre-operative beta blockers; those with concomitant heart failure or recent MI have a lower risk of MACE and/or mortality at 30 days with beta blockers.
Citation: Andersson C, Merie C, Jorgensen M, et al. Association of ß-blocker therapy with risks of adverse cardiovascular events and deaths in patients with ischemic heart disease undergoing non-cardiac surgery: a Danish nationwide cohort study. JAMA Intern Med. 2014;174(3):336-344.
Clinical question: In patients with ischemic heart disease (IHD) undergoing non-cardiac surgery, do pre-operative beta blockers reduce post-operative major cardiovascular events (MACE) or mortality at 30 days?
Background: Peri-operative beta blocker use has become more restricted, as evidence about which patients derive benefit has become clearer. Opinions and practice vary regarding whether all patients with IHD, or only certain populations within this group, benefit from peri-operative beta blockers.
Study design: Retrospective, national registry-based cohort study.
Setting: Denmark, 2004-2009.
Synopsis: No benefit was found for the overall cohort of 28,263 patients. Patients with IHD and heart failure (n=7990) had lower risk of MACE (HR=0.75, 95% CI, 0.70-0.87) and mortality (HR=0.80, 95% CI, 0.70-0.92). Patients with IHD and myocardial infarction within two years (n=1664) had lower risk of MACE (HR=0.54, 95% CI, 0.37-0.78) but not mortality.
Beta blocker dose and compliance were unknown. Whether patients had symptoms or inducible ischemia was not clear.
This study supports the concept that higher-risk patients benefit more from peri-operative beta blockers, but it is not high-grade evidence.
Bottom line: Not all patients with IHD benefit from pre-operative beta blockers; those with concomitant heart failure or recent MI have a lower risk of MACE and/or mortality at 30 days with beta blockers.
Citation: Andersson C, Merie C, Jorgensen M, et al. Association of ß-blocker therapy with risks of adverse cardiovascular events and deaths in patients with ischemic heart disease undergoing non-cardiac surgery: a Danish nationwide cohort study. JAMA Intern Med. 2014;174(3):336-344.
Facecards Improve Familiarity with Physician Names but Not Satisfaction
Clinical question: Do facecards improve patients’ familiarity with physicians and increase satisfaction, trust, and agreement with physicians?
Background: Facecards can improve patients’ knowledge of names and roles of physicians, but their impact on other outcomes is unclear. This pilot trial was designed to assess facecards’ impact on patient satisfaction, trust, or agreement with physicians.
Study design: Cluster, randomized controlled trial (RCT).
Setting: A large teaching hospital in the United States.
Synopsis: Patients (n=138) were randomized to receive either facecards with the name and picture of their hospitalists, as well as a brief description of the hospitalist’s role (n=66), or to receive traditional communication (n=72). There were no significant differences in patient age, sex, or race.
Patients who received a facecard were more likely to correctly identify their hospital physician (89.1% vs. 51.1%; P< 0.01) and were more likely to correctly identify the role of their hospital physician than those in the control group (67.4% vs. 16.3%; P<0.01).
Patients who received a facecard rated satisfaction, trust, and agreement slightly higher compared with those who had not received a card, but the results were not statistically significant (P values 0.27, 0.32, 0.37, respectively.) The authors note that larger studies may be needed to see a difference in these areas.
Bottom line: Facecards improve patients’ knowledge of the names and roles of hospital physicians but have no clear impact on satisfaction with, trust of, or agreement with physicians.
Citation: Simons Y, Caprio T, Furiasse N, Kriss, M, Williams MV, O’Leary KJ. The impact of facecards on patients’ knowledge, satisfaction, trust, and agreement with hospitalist physicians: a pilot study. J Hosp Med. 2014;9(3):137-141.
Clinical question: Do facecards improve patients’ familiarity with physicians and increase satisfaction, trust, and agreement with physicians?
Background: Facecards can improve patients’ knowledge of names and roles of physicians, but their impact on other outcomes is unclear. This pilot trial was designed to assess facecards’ impact on patient satisfaction, trust, or agreement with physicians.
Study design: Cluster, randomized controlled trial (RCT).
Setting: A large teaching hospital in the United States.
Synopsis: Patients (n=138) were randomized to receive either facecards with the name and picture of their hospitalists, as well as a brief description of the hospitalist’s role (n=66), or to receive traditional communication (n=72). There were no significant differences in patient age, sex, or race.
Patients who received a facecard were more likely to correctly identify their hospital physician (89.1% vs. 51.1%; P< 0.01) and were more likely to correctly identify the role of their hospital physician than those in the control group (67.4% vs. 16.3%; P<0.01).
Patients who received a facecard rated satisfaction, trust, and agreement slightly higher compared with those who had not received a card, but the results were not statistically significant (P values 0.27, 0.32, 0.37, respectively.) The authors note that larger studies may be needed to see a difference in these areas.
Bottom line: Facecards improve patients’ knowledge of the names and roles of hospital physicians but have no clear impact on satisfaction with, trust of, or agreement with physicians.
Citation: Simons Y, Caprio T, Furiasse N, Kriss, M, Williams MV, O’Leary KJ. The impact of facecards on patients’ knowledge, satisfaction, trust, and agreement with hospitalist physicians: a pilot study. J Hosp Med. 2014;9(3):137-141.
Clinical question: Do facecards improve patients’ familiarity with physicians and increase satisfaction, trust, and agreement with physicians?
Background: Facecards can improve patients’ knowledge of names and roles of physicians, but their impact on other outcomes is unclear. This pilot trial was designed to assess facecards’ impact on patient satisfaction, trust, or agreement with physicians.
Study design: Cluster, randomized controlled trial (RCT).
Setting: A large teaching hospital in the United States.
Synopsis: Patients (n=138) were randomized to receive either facecards with the name and picture of their hospitalists, as well as a brief description of the hospitalist’s role (n=66), or to receive traditional communication (n=72). There were no significant differences in patient age, sex, or race.
Patients who received a facecard were more likely to correctly identify their hospital physician (89.1% vs. 51.1%; P< 0.01) and were more likely to correctly identify the role of their hospital physician than those in the control group (67.4% vs. 16.3%; P<0.01).
Patients who received a facecard rated satisfaction, trust, and agreement slightly higher compared with those who had not received a card, but the results were not statistically significant (P values 0.27, 0.32, 0.37, respectively.) The authors note that larger studies may be needed to see a difference in these areas.
Bottom line: Facecards improve patients’ knowledge of the names and roles of hospital physicians but have no clear impact on satisfaction with, trust of, or agreement with physicians.
Citation: Simons Y, Caprio T, Furiasse N, Kriss, M, Williams MV, O’Leary KJ. The impact of facecards on patients’ knowledge, satisfaction, trust, and agreement with hospitalist physicians: a pilot study. J Hosp Med. 2014;9(3):137-141.
New Oral Anticoagulants Safe and Effective for Atrial Fibrillation Treatment
Clinical question: Is there a difference in efficacy and safety among new oral anticoagulants compared to warfarin in subgroups of patients with atrial fibrillation (Afib)?
Background: Studies of new oral anticoagulants have demonstrated that these agents are at least as safe and effective as warfarin for prevention of stroke and systemic embolism in Afib. This study was designed to look at available phase 3 randomized trials, with the goal of subgroup analysis for both efficacy and bleeding risks.
Study design: Meta-analysis.
Setting: Phase 3 randomized controlled trials of patients with Afib.
Synopsis: The analysis included four trials of Afib patients randomized to receive warfarin or a novel oral anticoagulant (NOAC), including dabigatran, rivaroxaban, apixaban, and edoxaban. In total, 42,411 patients received an NOAC and 29,272 patients received warfarin. Separate analyses were performed for high-dose and low-dose NOACs.
The high-dose NOAC demonstrated a 19% reduction in stroke and systemic embolic events as compared to warfarin, largely due to the reduction of hemorrhagic strokes by the NOAC. The low-dose NOAC showed similar efficacy to warfarin for reduction of stroke and systemic embolic events, with an increase noted in the subset of ischemic stroke in low-dose NOAC. Both doses of NOAC demonstrated a significant reduction in all-cause mortality. NOAC showed a non-significant reduction in bleeding compared to warfarin; however, subset analysis demonstrated an increase in gastrointestinal bleeding with high-dose NOAC and a significant reduction in intracranial hemorrhage with low-dose NOAC.
A notable limitation of the study is that it only included clinical trials in the analysis.
Bottom line: In relation to stroke, systemic embolic events, and all-cause mortality, new oral anticoagulants showed a favorable efficacy and safety profile as compared to warfarin in Afib patients.
Citation: Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962.
Clinical question: Is there a difference in efficacy and safety among new oral anticoagulants compared to warfarin in subgroups of patients with atrial fibrillation (Afib)?
Background: Studies of new oral anticoagulants have demonstrated that these agents are at least as safe and effective as warfarin for prevention of stroke and systemic embolism in Afib. This study was designed to look at available phase 3 randomized trials, with the goal of subgroup analysis for both efficacy and bleeding risks.
Study design: Meta-analysis.
Setting: Phase 3 randomized controlled trials of patients with Afib.
Synopsis: The analysis included four trials of Afib patients randomized to receive warfarin or a novel oral anticoagulant (NOAC), including dabigatran, rivaroxaban, apixaban, and edoxaban. In total, 42,411 patients received an NOAC and 29,272 patients received warfarin. Separate analyses were performed for high-dose and low-dose NOACs.
The high-dose NOAC demonstrated a 19% reduction in stroke and systemic embolic events as compared to warfarin, largely due to the reduction of hemorrhagic strokes by the NOAC. The low-dose NOAC showed similar efficacy to warfarin for reduction of stroke and systemic embolic events, with an increase noted in the subset of ischemic stroke in low-dose NOAC. Both doses of NOAC demonstrated a significant reduction in all-cause mortality. NOAC showed a non-significant reduction in bleeding compared to warfarin; however, subset analysis demonstrated an increase in gastrointestinal bleeding with high-dose NOAC and a significant reduction in intracranial hemorrhage with low-dose NOAC.
A notable limitation of the study is that it only included clinical trials in the analysis.
Bottom line: In relation to stroke, systemic embolic events, and all-cause mortality, new oral anticoagulants showed a favorable efficacy and safety profile as compared to warfarin in Afib patients.
Citation: Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962.
Clinical question: Is there a difference in efficacy and safety among new oral anticoagulants compared to warfarin in subgroups of patients with atrial fibrillation (Afib)?
Background: Studies of new oral anticoagulants have demonstrated that these agents are at least as safe and effective as warfarin for prevention of stroke and systemic embolism in Afib. This study was designed to look at available phase 3 randomized trials, with the goal of subgroup analysis for both efficacy and bleeding risks.
Study design: Meta-analysis.
Setting: Phase 3 randomized controlled trials of patients with Afib.
Synopsis: The analysis included four trials of Afib patients randomized to receive warfarin or a novel oral anticoagulant (NOAC), including dabigatran, rivaroxaban, apixaban, and edoxaban. In total, 42,411 patients received an NOAC and 29,272 patients received warfarin. Separate analyses were performed for high-dose and low-dose NOACs.
The high-dose NOAC demonstrated a 19% reduction in stroke and systemic embolic events as compared to warfarin, largely due to the reduction of hemorrhagic strokes by the NOAC. The low-dose NOAC showed similar efficacy to warfarin for reduction of stroke and systemic embolic events, with an increase noted in the subset of ischemic stroke in low-dose NOAC. Both doses of NOAC demonstrated a significant reduction in all-cause mortality. NOAC showed a non-significant reduction in bleeding compared to warfarin; however, subset analysis demonstrated an increase in gastrointestinal bleeding with high-dose NOAC and a significant reduction in intracranial hemorrhage with low-dose NOAC.
A notable limitation of the study is that it only included clinical trials in the analysis.
Bottom line: In relation to stroke, systemic embolic events, and all-cause mortality, new oral anticoagulants showed a favorable efficacy and safety profile as compared to warfarin in Afib patients.
Citation: Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962.
Sepsis Diagnoses Are Common in ED, but Many Septic Patients in the ED Do Not Receive Antibiotics
Clinical question: Has the frequency of sepsis rates, along with administration of antibiotics in U.S. emergency departments (EDs), changed over time?
Background: Prior studies reviewing discharge data from hospitals suggest an increase of sepsis over time; however, little epidemiological research has evaluated the diagnosis of sepsis and antibiotic use in ED settings.
Study design: Retrospective, four-stage probability sample.
Setting: National Hospital Ambulatory Medical Care Survey (NHAMCS).
Synopsis: The NHAMCS includes a sample of all U.S. ED visits, except federal, military, and VA hospitals. According to NHAMCS data, an estimated 1.3 billion visits by adults to U.S. EDs occurred from 1994-2009, or approximately 81 million visits per year. Explicit sepsis was defined by the presence of the following, with ICD-9 codes: septicemia (038), sepsis (995.91), severe sepsis (995.92), or septic shock (785.52). Implicit sepsis was defined as a code indicating infection plus a code indicting organ dysfunction.
In U.S. EDs, explicit sepsis did not become more prevalent from 1994-2009; however, implicitly diagnosed sepsis increased by 7% every two years. There were 260,000 explicit sepsis-related ED visits per year, or 1.23 visits per 1,000 U.S. population. In-hospital mortality was 17% and 9% for the explicit and implicit diagnosis groups, respectively. On review of the explicit sepsis group, only 61% of the patients were found to have received antibiotics in the ED. The rate did increase over the time studied, from 52% in 1994-1997 to 69% in 2006-2009.
The study was limited by the retrospective analysis of data not designed to track sepsis or antibiotic use.
Bottom Line: Explicitly recognized sepsis remained stable in the ED setting from 1994-2009, and early antibiotic use has improved during this time, but there is still much opportunity for improvement.
Citation: Filbin MR, Arias SA, Camargo CA Jr, Barche A, Pallin DJ. Sepsis visits and antibiotic utilization in the U.S. emergency departments. Crit Care Med. 2014;42(3):528-535.
Clinical question: Has the frequency of sepsis rates, along with administration of antibiotics in U.S. emergency departments (EDs), changed over time?
Background: Prior studies reviewing discharge data from hospitals suggest an increase of sepsis over time; however, little epidemiological research has evaluated the diagnosis of sepsis and antibiotic use in ED settings.
Study design: Retrospective, four-stage probability sample.
Setting: National Hospital Ambulatory Medical Care Survey (NHAMCS).
Synopsis: The NHAMCS includes a sample of all U.S. ED visits, except federal, military, and VA hospitals. According to NHAMCS data, an estimated 1.3 billion visits by adults to U.S. EDs occurred from 1994-2009, or approximately 81 million visits per year. Explicit sepsis was defined by the presence of the following, with ICD-9 codes: septicemia (038), sepsis (995.91), severe sepsis (995.92), or septic shock (785.52). Implicit sepsis was defined as a code indicating infection plus a code indicting organ dysfunction.
In U.S. EDs, explicit sepsis did not become more prevalent from 1994-2009; however, implicitly diagnosed sepsis increased by 7% every two years. There were 260,000 explicit sepsis-related ED visits per year, or 1.23 visits per 1,000 U.S. population. In-hospital mortality was 17% and 9% for the explicit and implicit diagnosis groups, respectively. On review of the explicit sepsis group, only 61% of the patients were found to have received antibiotics in the ED. The rate did increase over the time studied, from 52% in 1994-1997 to 69% in 2006-2009.
The study was limited by the retrospective analysis of data not designed to track sepsis or antibiotic use.
Bottom Line: Explicitly recognized sepsis remained stable in the ED setting from 1994-2009, and early antibiotic use has improved during this time, but there is still much opportunity for improvement.
Citation: Filbin MR, Arias SA, Camargo CA Jr, Barche A, Pallin DJ. Sepsis visits and antibiotic utilization in the U.S. emergency departments. Crit Care Med. 2014;42(3):528-535.
Clinical question: Has the frequency of sepsis rates, along with administration of antibiotics in U.S. emergency departments (EDs), changed over time?
Background: Prior studies reviewing discharge data from hospitals suggest an increase of sepsis over time; however, little epidemiological research has evaluated the diagnosis of sepsis and antibiotic use in ED settings.
Study design: Retrospective, four-stage probability sample.
Setting: National Hospital Ambulatory Medical Care Survey (NHAMCS).
Synopsis: The NHAMCS includes a sample of all U.S. ED visits, except federal, military, and VA hospitals. According to NHAMCS data, an estimated 1.3 billion visits by adults to U.S. EDs occurred from 1994-2009, or approximately 81 million visits per year. Explicit sepsis was defined by the presence of the following, with ICD-9 codes: septicemia (038), sepsis (995.91), severe sepsis (995.92), or septic shock (785.52). Implicit sepsis was defined as a code indicating infection plus a code indicting organ dysfunction.
In U.S. EDs, explicit sepsis did not become more prevalent from 1994-2009; however, implicitly diagnosed sepsis increased by 7% every two years. There were 260,000 explicit sepsis-related ED visits per year, or 1.23 visits per 1,000 U.S. population. In-hospital mortality was 17% and 9% for the explicit and implicit diagnosis groups, respectively. On review of the explicit sepsis group, only 61% of the patients were found to have received antibiotics in the ED. The rate did increase over the time studied, from 52% in 1994-1997 to 69% in 2006-2009.
The study was limited by the retrospective analysis of data not designed to track sepsis or antibiotic use.
Bottom Line: Explicitly recognized sepsis remained stable in the ED setting from 1994-2009, and early antibiotic use has improved during this time, but there is still much opportunity for improvement.
Citation: Filbin MR, Arias SA, Camargo CA Jr, Barche A, Pallin DJ. Sepsis visits and antibiotic utilization in the U.S. emergency departments. Crit Care Med. 2014;42(3):528-535.
Multifaceted Discharge Interventions Reduce Rates of Pediatric Readmission and Post-Hospital ED Utilization
Clinical question: Do interventions at discharge reduce the rate of readmissions and post-hospitalization ED visits among pediatric patients?
Background: Readmissions are a high-priority quality measure in both the adult and pediatric settings. Although a broadening body of literature is evaluating the impact of interventions on readmissions in adult populations, the literature does not contain a similar breadth of assessments of interventions in the pediatric setting.
Study design: Systematic review.
Setting: English-language articles studying pediatric inpatient discharge interventions.
Synopsis: A total of 1,296 unique articles were identified from PubMed and the Cumulative Index to Nursing and Allied Health Literature. Additional articles were identified on review of references, yielding 14 articles that met inclusion criteria. Included studies evaluated the effect of pediatric discharge interventions on the primary outcomes of hospital readmission or post-hospitalization ED visits. Interventions focused on three main patient populations: asthma, cancer, and prematurity.
Six studies demonstrated statistically significant reductions in readmissions and/or ED visits, while two studies actually demonstrated an increase in post-discharge utilization. All successful interventions began in the inpatient setting and were multifaceted, with four of six studies including an educational component and a post-discharge follow-up component.
While all of the studies evaluated sought to enhance the transitional care from the inpatient to outpatient setting, only the interventions that included one responsible party (individual or team) with expertise in the medical condition providing oversight and support were successful in reducing the specified outcomes. A significant limitation was that many of the studies identified were not sufficiently powered to detect either outcome of interest.
Bottom line: A multifaceted intervention involving educational and post-discharge follow-up components with an experienced individual or team supporting the transition is associated with a reduction in hospital readmissions and post-discharge ED utilization.
Citation: Auger KA, Kenyon CC, Feudtner C, Davis MM. Pediatric hospital discharge interventions to reduce subsequent utilization: a systematic review [published online ahead of print December 20, 2013]. J Hosp Med.
Clinical question: Do interventions at discharge reduce the rate of readmissions and post-hospitalization ED visits among pediatric patients?
Background: Readmissions are a high-priority quality measure in both the adult and pediatric settings. Although a broadening body of literature is evaluating the impact of interventions on readmissions in adult populations, the literature does not contain a similar breadth of assessments of interventions in the pediatric setting.
Study design: Systematic review.
Setting: English-language articles studying pediatric inpatient discharge interventions.
Synopsis: A total of 1,296 unique articles were identified from PubMed and the Cumulative Index to Nursing and Allied Health Literature. Additional articles were identified on review of references, yielding 14 articles that met inclusion criteria. Included studies evaluated the effect of pediatric discharge interventions on the primary outcomes of hospital readmission or post-hospitalization ED visits. Interventions focused on three main patient populations: asthma, cancer, and prematurity.
Six studies demonstrated statistically significant reductions in readmissions and/or ED visits, while two studies actually demonstrated an increase in post-discharge utilization. All successful interventions began in the inpatient setting and were multifaceted, with four of six studies including an educational component and a post-discharge follow-up component.
While all of the studies evaluated sought to enhance the transitional care from the inpatient to outpatient setting, only the interventions that included one responsible party (individual or team) with expertise in the medical condition providing oversight and support were successful in reducing the specified outcomes. A significant limitation was that many of the studies identified were not sufficiently powered to detect either outcome of interest.
Bottom line: A multifaceted intervention involving educational and post-discharge follow-up components with an experienced individual or team supporting the transition is associated with a reduction in hospital readmissions and post-discharge ED utilization.
Citation: Auger KA, Kenyon CC, Feudtner C, Davis MM. Pediatric hospital discharge interventions to reduce subsequent utilization: a systematic review [published online ahead of print December 20, 2013]. J Hosp Med.
Clinical question: Do interventions at discharge reduce the rate of readmissions and post-hospitalization ED visits among pediatric patients?
Background: Readmissions are a high-priority quality measure in both the adult and pediatric settings. Although a broadening body of literature is evaluating the impact of interventions on readmissions in adult populations, the literature does not contain a similar breadth of assessments of interventions in the pediatric setting.
Study design: Systematic review.
Setting: English-language articles studying pediatric inpatient discharge interventions.
Synopsis: A total of 1,296 unique articles were identified from PubMed and the Cumulative Index to Nursing and Allied Health Literature. Additional articles were identified on review of references, yielding 14 articles that met inclusion criteria. Included studies evaluated the effect of pediatric discharge interventions on the primary outcomes of hospital readmission or post-hospitalization ED visits. Interventions focused on three main patient populations: asthma, cancer, and prematurity.
Six studies demonstrated statistically significant reductions in readmissions and/or ED visits, while two studies actually demonstrated an increase in post-discharge utilization. All successful interventions began in the inpatient setting and were multifaceted, with four of six studies including an educational component and a post-discharge follow-up component.
While all of the studies evaluated sought to enhance the transitional care from the inpatient to outpatient setting, only the interventions that included one responsible party (individual or team) with expertise in the medical condition providing oversight and support were successful in reducing the specified outcomes. A significant limitation was that many of the studies identified were not sufficiently powered to detect either outcome of interest.
Bottom line: A multifaceted intervention involving educational and post-discharge follow-up components with an experienced individual or team supporting the transition is associated with a reduction in hospital readmissions and post-discharge ED utilization.
Citation: Auger KA, Kenyon CC, Feudtner C, Davis MM. Pediatric hospital discharge interventions to reduce subsequent utilization: a systematic review [published online ahead of print December 20, 2013]. J Hosp Med.
Woman, 66, With Persistent Abdominal and Back Pain
A 66-year-old Latin American woman presented to the emergency department (ED) with persistent abdominal and back pain of about one month’s duration. She had visited another ED eight days earlier for similar symptoms and was discharged home with a mild opioid pain medication and a proton pump inhibitor. However, she said that she had received neither a diagnosis nor an explanation for her symptoms.
Medical history, obtained with the assistance of an interpreter because the patient was not fluent in English, included hypertension, coronary artery disease, and hyperlipidemia; these had gone untreated for at least two years. She denied any personal or family history of cancer or endocrine disorders. Surgical history included a cholecystectomy and a percutaneous coronary intervention for an unknown coronary artery lesion.
She had a 14-pack-year history of cigarette smoking. Her medications included only ibuprofen and hydrocodone, and she had no known drug allergies. The patient denied use of herbal preparations or vitamin supplements and unusual dietary practices.
Review of systems revealed occasional dizziness, constipation, decreased appetite, and some mild confusion noted by family members, but no fever, chills, palpitations, chest pain, shortness of breath, muscle spasm, or weakness. Vital signs were normal. Physical examination was remarkable for tenderness of the upper quadrants of the abdomen with deep palpation, without guarding or rebound. Bony tenderness at the right anterior costal margin of the rib cage was also noted.
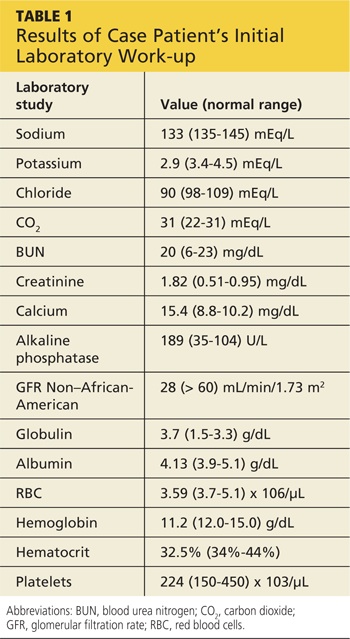
Laboratory work-up revealed marked hypercalcemia (15.4 mg/dL), electrolyte abnormalities, anemia, impaired renal function, and elevated alkaline phosphatase and globulin levels (see Table 1). In addition, a plain abdominal x-ray series was negative for acute findings, but x-rays of the right ribs revealed a fracture of the sixth rib and osteopenia.
Continued >>
The patient was admitted to the hospital for treatment of hypercalcemia and hypokalemia and for work-up of elevated alkaline phosphatase and abdominal pain. Upon admission, serum ionized calcium measurement confirmed true hypercalcemia. Additional diagnostic tests were then ordered to help differentiate between parathyroid hormone (PTH)–mediated and non-PTH–mediated causes for the hypercalcemia (see Table 2).
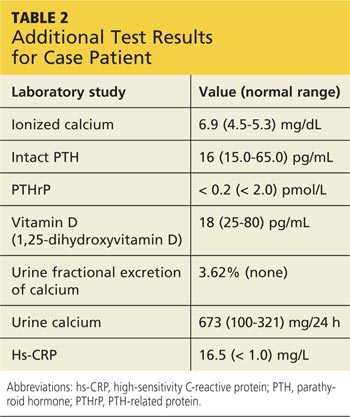
The patient’s PTH level was normal and the urine fractional excretion of calcium level was high, ruling out familial hypocalciuric hypercalcemia (FHH), in which urine calcium level is low. A measurement of PTH-related protein (PTHrP), secreted by some cancers, was normal, suggesting exclusion of solid tumor malignancy. Vitamin D toxicity was ruled out because the patient’s 1,25-dihydroxyvitamin D level was low.

The patient continued to experience vague abdominal, back, and rib pain that seemed to migrate daily and worsened with movement. A skeletal x-ray was performed and revealed numerous lytic lesions of the skull (Figure 1), midright humerus (Figure 2), and distal left radius.

Continue for discussion >>
DISCUSSION
Hypercalcemia is a relatively common presentation in primary care. The most frequent causes are primary hyperparathyroidism and malignancy.1 One in 500 patients will be diagnosed incidentally with asymptomatic hypercalcemia caused by underlying hyperparathyroidism.1
Clinical manifestations of hypercalcemia can range from no symptoms to multisystem disease. Fatigue, nausea, vomiting, constipation, bone pain, osteoporosis, nephrolithiasis, mental status changes, hypertension, anemia, elevated creatinine, and cardiac arrhythmias are among the more common clinical conditions associated with hypercalcemia (hence the mnemonic “stones, bones, abdominal moans, and psychic groans” for its signs and symptoms).1
Diagnostic overview
Causes of hypercalcemia are numerous and can be broken down into two categories: PTH-mediated and non-PTH–mediated. PTH-mediated causes include primary and secondary hyperparathyroidism and FHH. Non-PTH–mediated causes include vitamin D toxicity, solid tumor malignancy with or without metastasis, multiple myeloma (MM) and other plasma cell dyscrasias, granulomatous disease such as sarcoid, and some medications.1
The differential diagnosis for hypercalcemia begins with measurement of the patient’s intact PTH level. An elevated or high-normal result indicates a PTH-mediated cause, so 24-hour measurement of excretion of urinary calcium is the next step. A low or low-normal PTH level (< 20 pg/mL), however, suggests the cause is non-PTH-mediated.2 The diagnostic approach in this situation is more challenging because testing to exclude or confirm various potential causes can be expensive and time-consuming. The degree of hypercalcemia, however, can aid in the diagnosis: Primary hyperparathyroidism is often associated with borderline or mild hypercalcemia, while calcium values > 13 mg/dL are more common in patients with malignancies.2
PTH elevates calcium levels in the blood when ionized (free) calcium levels are low by increasing gastrointestinal absorption, decreasing urinary excretion, and increasing bone resorption.3 With malignant tumors such as lung, breast, and renal cell, osteolytic metastases can destroy the bone, resulting in release of calcium. In other cases, solid-tumor cancers produce PTHrP, which increases serum calcium. This latter situation is referred to as humoral hypercalcemia of malignancy.3 Lymphoma and granulomatous disease, such as sarcoid, can be associated with excess production of 1,25-dihydroxyvitamin D.2 If vitamin D is elevated but PTH and PTHrP are normal, a chest x-ray should be obtained to evaluate the patient for sarcoid or lymphoma.
Hypercalcemia work-up
The work-up for suspected hypercalcemia begins with measurement of the patient’s calcium level. Because calcium is bound to albumin in the blood, the standard serum calcium test may not reflect the true calcium level. (If albumin is high, the calcium level will be high, and vice versa.)1 The true (serum ionized) calcium level (also known as corrected calcium level) should always be calculated to confirm true hypercalcemia. A formula commonly used to calculate the corrected calcium level is
Corrected calcium (mg/dL) = (measured calcium [mg/dL]) + 0.8 (4.0 – serum albumin [mg/dL])
Direct measurement of the serum ionized calcium level is not affected by the albumin level and can also confirm true hypercalcemia.4
Once hypercalcemia is confirmed, the next step is to measure the patient’s intact PTH level.
If intact PTH is elevated or high normal, consider primary hyperparathyroidism or FHH and confirm by obtaining the urine calcium level.
• If urine calcium level is high (> 200 mg/24 h), the diagnosis is primary hyperparathyroidism.
• If urine calcium level is low (< 100 mg/24 h), the diagnosis is FHH.
If intact PTH is low, consider non–PTH-mediated causes and confirm by obtaining PTHrP and vitamin D levels.
• If PTHrP level is elevated, scan for malignancy.
• If 1,25-dihydroxyvitamin D level is elevated, order a chest x-ray to rule out sarcoid or lymphoma.
• If both PTHrP and vitamin D levels are normal, order both serum protein electrophoresis (SPEP) and urine protein electrophoresis (UPEP) with immunofixation to rule out MM.
• If vitamin D level is elevated, check vitamin and herbal supplement use for excessive vitamin D intake.
Treatment of symptomatic hypercalcemia
The goals of treatment of symptomatic hypercalcemia are to reduce the serum calcium level to the normal range and to treat the underlying cause.1 Mild hypercalcemia (calcium level, 10-12 mg/dL) is typically asymptomatic and does not need to be treated. Moderate hypercalcemia (calcium level, 12-14 mg/dL) may not require treatment unless the patient is symptomatic and/or has had an acute rise in calcium level.1 In mild to moderate hypercalcemia, the serum calcium level should be monitored to establish a trend.
Treatment for symptomatic moderate and severe hypercalcemia (calcium level, > 14 mg/dL) typically involves a similar regimen:
• Volume expansion with isotonic saline at an initial rate of 2 to 4 L/d, which is then adjusted to achieve 200 mL/h of continuous urine output. IV furosemide can be used with caution (10-20 mg IV as needed) to promote diuresis if volume overload is a concern (furosemide promotes renal excretion of calcium).
• Administration of subcutaneous calcitonin (4-8 IU/kg, repeated every 6 h for 24 h). Calcitonin works rapidly to lower calcium levels in 4 to 6 h.
• Concurrent administration of IV bisphosphonate (zoledronic acid [4 mg over 15 min] or pamidronate [60-90 mg over 4 h]). Pamidronate is superior for reversal of malignancy-related hypercalcemia.1
Hypercalcemia and multiple myeloma
MM is a malignant neoplasm of plasma cells that accounts for approximately 1% of all cancers and about 10% of hematologic malignancies in the United States, with a median patient age of 70 at diagnosis.5-7 In MM, myeloma cells induce the secretion of cytokines and growth factors that alter plasma cells, activate osteoclasts, suppress osteoblasts, cause abnormal interactions between plasma cells and bone marrow, and stimulate aberrant angiogenesis.8 Osteoclastic bone resorption produces hypercalcemia as well as the lytic lesions seen on x-ray.7
Approximately 74% of patients present with typical MM symptoms of calcium elevation in the blood, renal insufficiency, anemia, and bone lesions, known as CRAB symptoms, but other myeloma-related manifestations may be present.9
Diagnostic criteria for MM include the following (all three must be present):10
• Monoclonal bone marrow plasma cells ≥ 10% and/or a biopsy-proven plasmacytoma
• Monoclonal protein in the serum and/or urine (if none is detected, disease is nonsecretory and diagnosis requires ≥ 30% bone marrow plasma cells and/or biopsy-proven plasmacytoma)
• Myeloma-related organ dysfunction, indicated by at least one of the CRAB symptoms.
In the absence of CRAB symptoms, an asymptomatic patient may have an MM precursor syndrome: monoclonal gammopathy of undetermined significance or smoldering (or indolent) MM.10
Treatment of multiple myeloma
In recent years, the use of induction therapy followed by autologous stem cell transplantation and the development of novel therapeutic agents have extended overall survival for patients with MM. These agents include proteasome inhibitors (bortezomib and the second-generation carfilzomib)11 and immunomodulators (thalidomide and the second-generation lenalidomide). Early diagnosis and treatment can improve progression-free survival as well as overall survival, including recovery of renal function for patients with renal failure.12 With survival ranging from one year or less—with aggressive disease—to 10 years or more for patients with responsive disease,7 there remains no cure for MM.
Outcome for the case patient >>
OUTCOME FOR THE CASE PATIENT
Further work-up included SPEP and UPEP with immunofixation, which revealed marked IgG free λ light chains with an M (monoclonal) component, making MM a very likely diagnosis. Confirmation by means of bone marrow biopsy was indicated, but the patient refused the procedure.
The patient’s hypercalcemia was treated by IV administration of calcitonin with isotonic saline. This reduced the serum calcium level from 15.4 mg/dL to 10.6 mg/dL within 48 hours. One dose of ergocalciferol (vitamin D2) was then administered to promote intestinal absorption of calcium and support bone mineralization, further lowering the patient’s serum calcium level to a normal 8.9 mg/dL. Hypokalemia was treated with oral potassium supplementation.
The patient, now stable, was referred to the hematology/oncology and bone mineral metabolism clinics and was discharged from the hospital. She did not keep those appointments and was lost to follow-up.
CONCLUSION
The most common causes of hypercalcemia are hyperparathyroidism and malignancy. Most cases do not require treatment unless the calcium level is >14 mg/dL and/or the patient is symptomatic. Red flag symptoms include weakness, abdominal pain, mental status changes, and coma.4 Primary care clinicians should suspect MM in older patients with laboratory findings of hypercalcemia, anemia, and renal dysfunction, with lytic lesions on x-ray.
REFERENCES
1. Carroll MF, Schade DS. A practical approach to hypercalcemia. Am Fam Physician. 2003;67(9):1959-1966.
2. Endres DB. Investigation of hypercalcemia. Clin Biochem. 2012;45(12):
954-963.
3. Moe SM. Disorders involving calcium, phosphorus, and magnesium. Prim Care. 2008;35(2):215-237.
4. Sharma B, Misicko NE. How should you evaluate elevated calcium in an asymptomatic patient? J Fam Pract. 2008;57(4):267-269.
5. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11-30.
6. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33.
7. Shaheen SP, Talwalkar SS, Medeiros LJ. Multiple myeloma and immunosecretory disorders: an update. Adv Anat Pathol. 2008;15(4):196-210.
8. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11): 1046-1060.
9. Talamo G, Farooq U, Zangari M, et al. Beyond the CRAB symptoms: a study of presenting clinical manifestations of multiple myeloma. Clin Lymphoma Myeloma Leuk. 2010;10(6):464-468.
10. Palumbo A, Sezer O, Kyle R, et al. International Myeloma Working Group guidelines for the management of multiple myeloma patients ineligible for standard high-dose chemotherapy with autologous stem cell transportation. Leukemia. 2009;23(10):1716-1730.
11. Kyprolis [package insert]. South San Francisco, CA: Onyx Pharmaceuticals, Inc; 2012.
12. Suyani E, Sucak GT, Erten Y, et al. Evaluation of multiple myeloma patients presenting with renal failure in a university hospital in the year 2010. Ren Fail. 2012;34(2):257-262.
A 66-year-old Latin American woman presented to the emergency department (ED) with persistent abdominal and back pain of about one month’s duration. She had visited another ED eight days earlier for similar symptoms and was discharged home with a mild opioid pain medication and a proton pump inhibitor. However, she said that she had received neither a diagnosis nor an explanation for her symptoms.
Medical history, obtained with the assistance of an interpreter because the patient was not fluent in English, included hypertension, coronary artery disease, and hyperlipidemia; these had gone untreated for at least two years. She denied any personal or family history of cancer or endocrine disorders. Surgical history included a cholecystectomy and a percutaneous coronary intervention for an unknown coronary artery lesion.
She had a 14-pack-year history of cigarette smoking. Her medications included only ibuprofen and hydrocodone, and she had no known drug allergies. The patient denied use of herbal preparations or vitamin supplements and unusual dietary practices.
Review of systems revealed occasional dizziness, constipation, decreased appetite, and some mild confusion noted by family members, but no fever, chills, palpitations, chest pain, shortness of breath, muscle spasm, or weakness. Vital signs were normal. Physical examination was remarkable for tenderness of the upper quadrants of the abdomen with deep palpation, without guarding or rebound. Bony tenderness at the right anterior costal margin of the rib cage was also noted.
Laboratory work-up revealed marked hypercalcemia (15.4 mg/dL), electrolyte abnormalities, anemia, impaired renal function, and elevated alkaline phosphatase and globulin levels (see Table 1). In addition, a plain abdominal x-ray series was negative for acute findings, but x-rays of the right ribs revealed a fracture of the sixth rib and osteopenia.
Continued >>
The patient was admitted to the hospital for treatment of hypercalcemia and hypokalemia and for work-up of elevated alkaline phosphatase and abdominal pain. Upon admission, serum ionized calcium measurement confirmed true hypercalcemia. Additional diagnostic tests were then ordered to help differentiate between parathyroid hormone (PTH)–mediated and non-PTH–mediated causes for the hypercalcemia (see Table 2).
The patient’s PTH level was normal and the urine fractional excretion of calcium level was high, ruling out familial hypocalciuric hypercalcemia (FHH), in which urine calcium level is low. A measurement of PTH-related protein (PTHrP), secreted by some cancers, was normal, suggesting exclusion of solid tumor malignancy. Vitamin D toxicity was ruled out because the patient’s 1,25-dihydroxyvitamin D level was low.
The patient continued to experience vague abdominal, back, and rib pain that seemed to migrate daily and worsened with movement. A skeletal x-ray was performed and revealed numerous lytic lesions of the skull (Figure 1), midright humerus (Figure 2), and distal left radius.
Continue for discussion >>
DISCUSSION
Hypercalcemia is a relatively common presentation in primary care. The most frequent causes are primary hyperparathyroidism and malignancy.1 One in 500 patients will be diagnosed incidentally with asymptomatic hypercalcemia caused by underlying hyperparathyroidism.1
Clinical manifestations of hypercalcemia can range from no symptoms to multisystem disease. Fatigue, nausea, vomiting, constipation, bone pain, osteoporosis, nephrolithiasis, mental status changes, hypertension, anemia, elevated creatinine, and cardiac arrhythmias are among the more common clinical conditions associated with hypercalcemia (hence the mnemonic “stones, bones, abdominal moans, and psychic groans” for its signs and symptoms).1
Diagnostic overview
Causes of hypercalcemia are numerous and can be broken down into two categories: PTH-mediated and non-PTH–mediated. PTH-mediated causes include primary and secondary hyperparathyroidism and FHH. Non-PTH–mediated causes include vitamin D toxicity, solid tumor malignancy with or without metastasis, multiple myeloma (MM) and other plasma cell dyscrasias, granulomatous disease such as sarcoid, and some medications.1
The differential diagnosis for hypercalcemia begins with measurement of the patient’s intact PTH level. An elevated or high-normal result indicates a PTH-mediated cause, so 24-hour measurement of excretion of urinary calcium is the next step. A low or low-normal PTH level (< 20 pg/mL), however, suggests the cause is non-PTH-mediated.2 The diagnostic approach in this situation is more challenging because testing to exclude or confirm various potential causes can be expensive and time-consuming. The degree of hypercalcemia, however, can aid in the diagnosis: Primary hyperparathyroidism is often associated with borderline or mild hypercalcemia, while calcium values > 13 mg/dL are more common in patients with malignancies.2
PTH elevates calcium levels in the blood when ionized (free) calcium levels are low by increasing gastrointestinal absorption, decreasing urinary excretion, and increasing bone resorption.3 With malignant tumors such as lung, breast, and renal cell, osteolytic metastases can destroy the bone, resulting in release of calcium. In other cases, solid-tumor cancers produce PTHrP, which increases serum calcium. This latter situation is referred to as humoral hypercalcemia of malignancy.3 Lymphoma and granulomatous disease, such as sarcoid, can be associated with excess production of 1,25-dihydroxyvitamin D.2 If vitamin D is elevated but PTH and PTHrP are normal, a chest x-ray should be obtained to evaluate the patient for sarcoid or lymphoma.
Hypercalcemia work-up
The work-up for suspected hypercalcemia begins with measurement of the patient’s calcium level. Because calcium is bound to albumin in the blood, the standard serum calcium test may not reflect the true calcium level. (If albumin is high, the calcium level will be high, and vice versa.)1 The true (serum ionized) calcium level (also known as corrected calcium level) should always be calculated to confirm true hypercalcemia. A formula commonly used to calculate the corrected calcium level is
Corrected calcium (mg/dL) = (measured calcium [mg/dL]) + 0.8 (4.0 – serum albumin [mg/dL])
Direct measurement of the serum ionized calcium level is not affected by the albumin level and can also confirm true hypercalcemia.4
Once hypercalcemia is confirmed, the next step is to measure the patient’s intact PTH level.
If intact PTH is elevated or high normal, consider primary hyperparathyroidism or FHH and confirm by obtaining the urine calcium level.
• If urine calcium level is high (> 200 mg/24 h), the diagnosis is primary hyperparathyroidism.
• If urine calcium level is low (< 100 mg/24 h), the diagnosis is FHH.
If intact PTH is low, consider non–PTH-mediated causes and confirm by obtaining PTHrP and vitamin D levels.
• If PTHrP level is elevated, scan for malignancy.
• If 1,25-dihydroxyvitamin D level is elevated, order a chest x-ray to rule out sarcoid or lymphoma.
• If both PTHrP and vitamin D levels are normal, order both serum protein electrophoresis (SPEP) and urine protein electrophoresis (UPEP) with immunofixation to rule out MM.
• If vitamin D level is elevated, check vitamin and herbal supplement use for excessive vitamin D intake.
Treatment of symptomatic hypercalcemia
The goals of treatment of symptomatic hypercalcemia are to reduce the serum calcium level to the normal range and to treat the underlying cause.1 Mild hypercalcemia (calcium level, 10-12 mg/dL) is typically asymptomatic and does not need to be treated. Moderate hypercalcemia (calcium level, 12-14 mg/dL) may not require treatment unless the patient is symptomatic and/or has had an acute rise in calcium level.1 In mild to moderate hypercalcemia, the serum calcium level should be monitored to establish a trend.
Treatment for symptomatic moderate and severe hypercalcemia (calcium level, > 14 mg/dL) typically involves a similar regimen:
• Volume expansion with isotonic saline at an initial rate of 2 to 4 L/d, which is then adjusted to achieve 200 mL/h of continuous urine output. IV furosemide can be used with caution (10-20 mg IV as needed) to promote diuresis if volume overload is a concern (furosemide promotes renal excretion of calcium).
• Administration of subcutaneous calcitonin (4-8 IU/kg, repeated every 6 h for 24 h). Calcitonin works rapidly to lower calcium levels in 4 to 6 h.
• Concurrent administration of IV bisphosphonate (zoledronic acid [4 mg over 15 min] or pamidronate [60-90 mg over 4 h]). Pamidronate is superior for reversal of malignancy-related hypercalcemia.1
Hypercalcemia and multiple myeloma
MM is a malignant neoplasm of plasma cells that accounts for approximately 1% of all cancers and about 10% of hematologic malignancies in the United States, with a median patient age of 70 at diagnosis.5-7 In MM, myeloma cells induce the secretion of cytokines and growth factors that alter plasma cells, activate osteoclasts, suppress osteoblasts, cause abnormal interactions between plasma cells and bone marrow, and stimulate aberrant angiogenesis.8 Osteoclastic bone resorption produces hypercalcemia as well as the lytic lesions seen on x-ray.7
Approximately 74% of patients present with typical MM symptoms of calcium elevation in the blood, renal insufficiency, anemia, and bone lesions, known as CRAB symptoms, but other myeloma-related manifestations may be present.9
Diagnostic criteria for MM include the following (all three must be present):10
• Monoclonal bone marrow plasma cells ≥ 10% and/or a biopsy-proven plasmacytoma
• Monoclonal protein in the serum and/or urine (if none is detected, disease is nonsecretory and diagnosis requires ≥ 30% bone marrow plasma cells and/or biopsy-proven plasmacytoma)
• Myeloma-related organ dysfunction, indicated by at least one of the CRAB symptoms.
In the absence of CRAB symptoms, an asymptomatic patient may have an MM precursor syndrome: monoclonal gammopathy of undetermined significance or smoldering (or indolent) MM.10
Treatment of multiple myeloma
In recent years, the use of induction therapy followed by autologous stem cell transplantation and the development of novel therapeutic agents have extended overall survival for patients with MM. These agents include proteasome inhibitors (bortezomib and the second-generation carfilzomib)11 and immunomodulators (thalidomide and the second-generation lenalidomide). Early diagnosis and treatment can improve progression-free survival as well as overall survival, including recovery of renal function for patients with renal failure.12 With survival ranging from one year or less—with aggressive disease—to 10 years or more for patients with responsive disease,7 there remains no cure for MM.
Outcome for the case patient >>
OUTCOME FOR THE CASE PATIENT
Further work-up included SPEP and UPEP with immunofixation, which revealed marked IgG free λ light chains with an M (monoclonal) component, making MM a very likely diagnosis. Confirmation by means of bone marrow biopsy was indicated, but the patient refused the procedure.
The patient’s hypercalcemia was treated by IV administration of calcitonin with isotonic saline. This reduced the serum calcium level from 15.4 mg/dL to 10.6 mg/dL within 48 hours. One dose of ergocalciferol (vitamin D2) was then administered to promote intestinal absorption of calcium and support bone mineralization, further lowering the patient’s serum calcium level to a normal 8.9 mg/dL. Hypokalemia was treated with oral potassium supplementation.
The patient, now stable, was referred to the hematology/oncology and bone mineral metabolism clinics and was discharged from the hospital. She did not keep those appointments and was lost to follow-up.
CONCLUSION
The most common causes of hypercalcemia are hyperparathyroidism and malignancy. Most cases do not require treatment unless the calcium level is >14 mg/dL and/or the patient is symptomatic. Red flag symptoms include weakness, abdominal pain, mental status changes, and coma.4 Primary care clinicians should suspect MM in older patients with laboratory findings of hypercalcemia, anemia, and renal dysfunction, with lytic lesions on x-ray.
REFERENCES
1. Carroll MF, Schade DS. A practical approach to hypercalcemia. Am Fam Physician. 2003;67(9):1959-1966.
2. Endres DB. Investigation of hypercalcemia. Clin Biochem. 2012;45(12):
954-963.
3. Moe SM. Disorders involving calcium, phosphorus, and magnesium. Prim Care. 2008;35(2):215-237.
4. Sharma B, Misicko NE. How should you evaluate elevated calcium in an asymptomatic patient? J Fam Pract. 2008;57(4):267-269.
5. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11-30.
6. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33.
7. Shaheen SP, Talwalkar SS, Medeiros LJ. Multiple myeloma and immunosecretory disorders: an update. Adv Anat Pathol. 2008;15(4):196-210.
8. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11): 1046-1060.
9. Talamo G, Farooq U, Zangari M, et al. Beyond the CRAB symptoms: a study of presenting clinical manifestations of multiple myeloma. Clin Lymphoma Myeloma Leuk. 2010;10(6):464-468.
10. Palumbo A, Sezer O, Kyle R, et al. International Myeloma Working Group guidelines for the management of multiple myeloma patients ineligible for standard high-dose chemotherapy with autologous stem cell transportation. Leukemia. 2009;23(10):1716-1730.
11. Kyprolis [package insert]. South San Francisco, CA: Onyx Pharmaceuticals, Inc; 2012.
12. Suyani E, Sucak GT, Erten Y, et al. Evaluation of multiple myeloma patients presenting with renal failure in a university hospital in the year 2010. Ren Fail. 2012;34(2):257-262.
A 66-year-old Latin American woman presented to the emergency department (ED) with persistent abdominal and back pain of about one month’s duration. She had visited another ED eight days earlier for similar symptoms and was discharged home with a mild opioid pain medication and a proton pump inhibitor. However, she said that she had received neither a diagnosis nor an explanation for her symptoms.
Medical history, obtained with the assistance of an interpreter because the patient was not fluent in English, included hypertension, coronary artery disease, and hyperlipidemia; these had gone untreated for at least two years. She denied any personal or family history of cancer or endocrine disorders. Surgical history included a cholecystectomy and a percutaneous coronary intervention for an unknown coronary artery lesion.
She had a 14-pack-year history of cigarette smoking. Her medications included only ibuprofen and hydrocodone, and she had no known drug allergies. The patient denied use of herbal preparations or vitamin supplements and unusual dietary practices.
Review of systems revealed occasional dizziness, constipation, decreased appetite, and some mild confusion noted by family members, but no fever, chills, palpitations, chest pain, shortness of breath, muscle spasm, or weakness. Vital signs were normal. Physical examination was remarkable for tenderness of the upper quadrants of the abdomen with deep palpation, without guarding or rebound. Bony tenderness at the right anterior costal margin of the rib cage was also noted.
Laboratory work-up revealed marked hypercalcemia (15.4 mg/dL), electrolyte abnormalities, anemia, impaired renal function, and elevated alkaline phosphatase and globulin levels (see Table 1). In addition, a plain abdominal x-ray series was negative for acute findings, but x-rays of the right ribs revealed a fracture of the sixth rib and osteopenia.
Continued >>
The patient was admitted to the hospital for treatment of hypercalcemia and hypokalemia and for work-up of elevated alkaline phosphatase and abdominal pain. Upon admission, serum ionized calcium measurement confirmed true hypercalcemia. Additional diagnostic tests were then ordered to help differentiate between parathyroid hormone (PTH)–mediated and non-PTH–mediated causes for the hypercalcemia (see Table 2).
The patient’s PTH level was normal and the urine fractional excretion of calcium level was high, ruling out familial hypocalciuric hypercalcemia (FHH), in which urine calcium level is low. A measurement of PTH-related protein (PTHrP), secreted by some cancers, was normal, suggesting exclusion of solid tumor malignancy. Vitamin D toxicity was ruled out because the patient’s 1,25-dihydroxyvitamin D level was low.
The patient continued to experience vague abdominal, back, and rib pain that seemed to migrate daily and worsened with movement. A skeletal x-ray was performed and revealed numerous lytic lesions of the skull (Figure 1), midright humerus (Figure 2), and distal left radius.
Continue for discussion >>
DISCUSSION
Hypercalcemia is a relatively common presentation in primary care. The most frequent causes are primary hyperparathyroidism and malignancy.1 One in 500 patients will be diagnosed incidentally with asymptomatic hypercalcemia caused by underlying hyperparathyroidism.1
Clinical manifestations of hypercalcemia can range from no symptoms to multisystem disease. Fatigue, nausea, vomiting, constipation, bone pain, osteoporosis, nephrolithiasis, mental status changes, hypertension, anemia, elevated creatinine, and cardiac arrhythmias are among the more common clinical conditions associated with hypercalcemia (hence the mnemonic “stones, bones, abdominal moans, and psychic groans” for its signs and symptoms).1
Diagnostic overview
Causes of hypercalcemia are numerous and can be broken down into two categories: PTH-mediated and non-PTH–mediated. PTH-mediated causes include primary and secondary hyperparathyroidism and FHH. Non-PTH–mediated causes include vitamin D toxicity, solid tumor malignancy with or without metastasis, multiple myeloma (MM) and other plasma cell dyscrasias, granulomatous disease such as sarcoid, and some medications.1
The differential diagnosis for hypercalcemia begins with measurement of the patient’s intact PTH level. An elevated or high-normal result indicates a PTH-mediated cause, so 24-hour measurement of excretion of urinary calcium is the next step. A low or low-normal PTH level (< 20 pg/mL), however, suggests the cause is non-PTH-mediated.2 The diagnostic approach in this situation is more challenging because testing to exclude or confirm various potential causes can be expensive and time-consuming. The degree of hypercalcemia, however, can aid in the diagnosis: Primary hyperparathyroidism is often associated with borderline or mild hypercalcemia, while calcium values > 13 mg/dL are more common in patients with malignancies.2
PTH elevates calcium levels in the blood when ionized (free) calcium levels are low by increasing gastrointestinal absorption, decreasing urinary excretion, and increasing bone resorption.3 With malignant tumors such as lung, breast, and renal cell, osteolytic metastases can destroy the bone, resulting in release of calcium. In other cases, solid-tumor cancers produce PTHrP, which increases serum calcium. This latter situation is referred to as humoral hypercalcemia of malignancy.3 Lymphoma and granulomatous disease, such as sarcoid, can be associated with excess production of 1,25-dihydroxyvitamin D.2 If vitamin D is elevated but PTH and PTHrP are normal, a chest x-ray should be obtained to evaluate the patient for sarcoid or lymphoma.
Hypercalcemia work-up
The work-up for suspected hypercalcemia begins with measurement of the patient’s calcium level. Because calcium is bound to albumin in the blood, the standard serum calcium test may not reflect the true calcium level. (If albumin is high, the calcium level will be high, and vice versa.)1 The true (serum ionized) calcium level (also known as corrected calcium level) should always be calculated to confirm true hypercalcemia. A formula commonly used to calculate the corrected calcium level is
Corrected calcium (mg/dL) = (measured calcium [mg/dL]) + 0.8 (4.0 – serum albumin [mg/dL])
Direct measurement of the serum ionized calcium level is not affected by the albumin level and can also confirm true hypercalcemia.4
Once hypercalcemia is confirmed, the next step is to measure the patient’s intact PTH level.
If intact PTH is elevated or high normal, consider primary hyperparathyroidism or FHH and confirm by obtaining the urine calcium level.
• If urine calcium level is high (> 200 mg/24 h), the diagnosis is primary hyperparathyroidism.
• If urine calcium level is low (< 100 mg/24 h), the diagnosis is FHH.
If intact PTH is low, consider non–PTH-mediated causes and confirm by obtaining PTHrP and vitamin D levels.
• If PTHrP level is elevated, scan for malignancy.
• If 1,25-dihydroxyvitamin D level is elevated, order a chest x-ray to rule out sarcoid or lymphoma.
• If both PTHrP and vitamin D levels are normal, order both serum protein electrophoresis (SPEP) and urine protein electrophoresis (UPEP) with immunofixation to rule out MM.
• If vitamin D level is elevated, check vitamin and herbal supplement use for excessive vitamin D intake.
Treatment of symptomatic hypercalcemia
The goals of treatment of symptomatic hypercalcemia are to reduce the serum calcium level to the normal range and to treat the underlying cause.1 Mild hypercalcemia (calcium level, 10-12 mg/dL) is typically asymptomatic and does not need to be treated. Moderate hypercalcemia (calcium level, 12-14 mg/dL) may not require treatment unless the patient is symptomatic and/or has had an acute rise in calcium level.1 In mild to moderate hypercalcemia, the serum calcium level should be monitored to establish a trend.
Treatment for symptomatic moderate and severe hypercalcemia (calcium level, > 14 mg/dL) typically involves a similar regimen:
• Volume expansion with isotonic saline at an initial rate of 2 to 4 L/d, which is then adjusted to achieve 200 mL/h of continuous urine output. IV furosemide can be used with caution (10-20 mg IV as needed) to promote diuresis if volume overload is a concern (furosemide promotes renal excretion of calcium).
• Administration of subcutaneous calcitonin (4-8 IU/kg, repeated every 6 h for 24 h). Calcitonin works rapidly to lower calcium levels in 4 to 6 h.
• Concurrent administration of IV bisphosphonate (zoledronic acid [4 mg over 15 min] or pamidronate [60-90 mg over 4 h]). Pamidronate is superior for reversal of malignancy-related hypercalcemia.1
Hypercalcemia and multiple myeloma
MM is a malignant neoplasm of plasma cells that accounts for approximately 1% of all cancers and about 10% of hematologic malignancies in the United States, with a median patient age of 70 at diagnosis.5-7 In MM, myeloma cells induce the secretion of cytokines and growth factors that alter plasma cells, activate osteoclasts, suppress osteoblasts, cause abnormal interactions between plasma cells and bone marrow, and stimulate aberrant angiogenesis.8 Osteoclastic bone resorption produces hypercalcemia as well as the lytic lesions seen on x-ray.7
Approximately 74% of patients present with typical MM symptoms of calcium elevation in the blood, renal insufficiency, anemia, and bone lesions, known as CRAB symptoms, but other myeloma-related manifestations may be present.9
Diagnostic criteria for MM include the following (all three must be present):10
• Monoclonal bone marrow plasma cells ≥ 10% and/or a biopsy-proven plasmacytoma
• Monoclonal protein in the serum and/or urine (if none is detected, disease is nonsecretory and diagnosis requires ≥ 30% bone marrow plasma cells and/or biopsy-proven plasmacytoma)
• Myeloma-related organ dysfunction, indicated by at least one of the CRAB symptoms.
In the absence of CRAB symptoms, an asymptomatic patient may have an MM precursor syndrome: monoclonal gammopathy of undetermined significance or smoldering (or indolent) MM.10
Treatment of multiple myeloma
In recent years, the use of induction therapy followed by autologous stem cell transplantation and the development of novel therapeutic agents have extended overall survival for patients with MM. These agents include proteasome inhibitors (bortezomib and the second-generation carfilzomib)11 and immunomodulators (thalidomide and the second-generation lenalidomide). Early diagnosis and treatment can improve progression-free survival as well as overall survival, including recovery of renal function for patients with renal failure.12 With survival ranging from one year or less—with aggressive disease—to 10 years or more for patients with responsive disease,7 there remains no cure for MM.
Outcome for the case patient >>
OUTCOME FOR THE CASE PATIENT
Further work-up included SPEP and UPEP with immunofixation, which revealed marked IgG free λ light chains with an M (monoclonal) component, making MM a very likely diagnosis. Confirmation by means of bone marrow biopsy was indicated, but the patient refused the procedure.
The patient’s hypercalcemia was treated by IV administration of calcitonin with isotonic saline. This reduced the serum calcium level from 15.4 mg/dL to 10.6 mg/dL within 48 hours. One dose of ergocalciferol (vitamin D2) was then administered to promote intestinal absorption of calcium and support bone mineralization, further lowering the patient’s serum calcium level to a normal 8.9 mg/dL. Hypokalemia was treated with oral potassium supplementation.
The patient, now stable, was referred to the hematology/oncology and bone mineral metabolism clinics and was discharged from the hospital. She did not keep those appointments and was lost to follow-up.
CONCLUSION
The most common causes of hypercalcemia are hyperparathyroidism and malignancy. Most cases do not require treatment unless the calcium level is >14 mg/dL and/or the patient is symptomatic. Red flag symptoms include weakness, abdominal pain, mental status changes, and coma.4 Primary care clinicians should suspect MM in older patients with laboratory findings of hypercalcemia, anemia, and renal dysfunction, with lytic lesions on x-ray.
REFERENCES
1. Carroll MF, Schade DS. A practical approach to hypercalcemia. Am Fam Physician. 2003;67(9):1959-1966.
2. Endres DB. Investigation of hypercalcemia. Clin Biochem. 2012;45(12):
954-963.
3. Moe SM. Disorders involving calcium, phosphorus, and magnesium. Prim Care. 2008;35(2):215-237.
4. Sharma B, Misicko NE. How should you evaluate elevated calcium in an asymptomatic patient? J Fam Pract. 2008;57(4):267-269.
5. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11-30.
6. Kyle RA, Gertz MA, Witzig TE, et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin Proc. 2003;78(1):21-33.
7. Shaheen SP, Talwalkar SS, Medeiros LJ. Multiple myeloma and immunosecretory disorders: an update. Adv Anat Pathol. 2008;15(4):196-210.
8. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11): 1046-1060.
9. Talamo G, Farooq U, Zangari M, et al. Beyond the CRAB symptoms: a study of presenting clinical manifestations of multiple myeloma. Clin Lymphoma Myeloma Leuk. 2010;10(6):464-468.
10. Palumbo A, Sezer O, Kyle R, et al. International Myeloma Working Group guidelines for the management of multiple myeloma patients ineligible for standard high-dose chemotherapy with autologous stem cell transportation. Leukemia. 2009;23(10):1716-1730.
11. Kyprolis [package insert]. South San Francisco, CA: Onyx Pharmaceuticals, Inc; 2012.
12. Suyani E, Sucak GT, Erten Y, et al. Evaluation of multiple myeloma patients presenting with renal failure in a university hospital in the year 2010. Ren Fail. 2012;34(2):257-262.