User login
Do oral contraceptives put women with a family history of breast cancer at increased risk?
No. Modern combined oral contraceptive pills (OCPs) don’t increase breast cancer risk in women with a family history (strength of recommendation [SOR]: B, systematic review of cohort, case-control studies). However, older, higher-dose OCPs (in use before 1975) did increase breast cancer risk in these women (SOR: C, case-control study).
Similarly, modern OCPs don’t raise breast cancer risk in women with BRCA1/2 mutations, although higher-dose, pre-1975 OCPs did (SOR: B and C, a meta-analysis of cohort and case-control studies).
EVIDENCE SUMMARY
A systematic review of the effect of combined OCPs on women with a family history of breast cancer found no additional increase in risk.1 Investigators identified 3 retrospective cohort studies (N=66,500, with 8500 cases) and 7 case-control studies (total 10,500 cases) from the past 40 years, most including women from the United States and Canada, but one including women from 5 continents.
In most trials, women of reproductive age using combined OCPs had 1 or more first-degree female relatives with breast cancer, although a few trials also included second-degree relatives. Women ranged in age from 20 to 79 years at diagnosis, and most trials controlled for age, parity, menstrual and menopausal history, duration of OCP exposure, and age at first use. Follow-up intervals for the retrospective cohort studies ranged from 5 to 16 years. Investigators were unable to combine results because of heterogenous populations.
Three of the cohort studies found no significant difference in breast cancer risk between OCP users and nonusers, regardless of age or duration of use. One cohort study found an increased risk in women taking older, higher-dose OCPs from before 1975 (relative risk [RR]=3.3; 95% confidence interval [CI], 1.5-7.2). All of the case-control studies found no significant difference in breast cancer risk for any age of starting, duration of OCP use, or degree of relative with breast cancer.
A meta-analysis of 54 case-control studies (6757 cases), comprising approximately 90% of the epidemiologic information on this topic, also found no significant difference in breast cancer risk related to OCP use among women with one or more first-degree relatives with breast cancer.2 Investigators found that neither recent OCP use (<10 years, RR=0.77; 95% CI, 0.54-1.11) nor past OCP use (>10 years, RR=1.01; 95% CI, 0.80-1.28) affected risk of developing breast cancer.
Three additional case-control studies involving women with a family history of breast cancer also found no significant association for breast cancer incidence among OCP users compared with nonusers.3-5
Modern combined OCPs don’t raise risk in women with BRCA1/2 mutations
A meta-analysis of 5 studies (one retrospective cohort, 4 case-control, with a total of 2855 breast cancer cases and 2944 controls) evaluated whether combined OCPs increased the risk of breast cancer in women, all of whom were carrying BRCA1/2 mutations.6
Using modern combined OCPs didn’t raise the risk of breast cancer in BRCA1/2 carriers overall (RR=1.13; 95% CI, 0.88-1.45) or separately in BRCA1 carriers (5 studies, RR=1.09; 95% CI, 0.77-1.54) or BRCA2 carriers (3 studies, RR=1.15; 95% CI, 0.88-1.45).
However, pre-1975 (higher dose) combined OCPs produced significantly increased risk (RR=1.47; 95% CI, 1.06-2.04). Similarly, women who had used combined OCPs >10 years before the study (older women, likely to have been using pre-1975 OCPs) also had significantly increased risk (RR=1.46; 95% CI, 1.07-2.07).
A bit of good news: Combined OCPs reduce ovarian cancer risk
The analysis also determined that combined OCPs significantly reduced the risk of ovarian cancer in women carrying BRCA1/2 mutations (RR=0.50; 95% CI, 0.33-0.75), with an additional linear decrease in risk for each 10 years of OCP use (RR=0.64; 95% CI, 0.53-0.78).
RECOMMENDATIONS
The World Health Organization guidelines outlining criteria for contraceptive use state that OCPs don’t alter the risk of breast cancer among women with either a family history of breast cancer or breast cancer susceptibility genes.7
The American College of Obstetricians and Gynecologists (ACOG) says that a positive family history of breast cancer shouldn’t be regarded as a contraindication to OCP use.8 ACOG also says that women with the BRCA1 mutation have an increased risk of breast cancer if they used OCPs for longer than 5 years before age 30, but this risk may be more than balanced by the benefit of a greatly reduced risk of ovarian cancer.
1. Gaffield ME, Culwell KR, Ravi A. Oral contraceptives and family history of breast cancer. Contraception. 2009;80:372-380.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative re-analysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet. 1996;347:1713-1727.
3. Jernström H, Loman N, Johannsson OT, et al. Impact of teenage oral contraceptive use in a population-based series of early-onset breast cancer cases who have undergone BRCA mutation testing. Eur J Cancer. 2005;41:2312-2320.
4. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Human Reprod Update. 2010;16: 631-650.
5. Long-term oral contraceptive use and the risk of breast cancer. The Centers for Disease Control Cancer and Steroid Hormone Study. JAMA. 1983;249:1591-1595.
6. Iodice S, Barile M, Rotmensz N, et al. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer. 2010;46:2275-2284.
7. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. 4th ed. Geneva, Switzerland: World Health Organization; 2009. World Health Organization Web site. Available at: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed September 24, 2013.
8. ACOG Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107:1453-1472.
No. Modern combined oral contraceptive pills (OCPs) don’t increase breast cancer risk in women with a family history (strength of recommendation [SOR]: B, systematic review of cohort, case-control studies). However, older, higher-dose OCPs (in use before 1975) did increase breast cancer risk in these women (SOR: C, case-control study).
Similarly, modern OCPs don’t raise breast cancer risk in women with BRCA1/2 mutations, although higher-dose, pre-1975 OCPs did (SOR: B and C, a meta-analysis of cohort and case-control studies).
EVIDENCE SUMMARY
A systematic review of the effect of combined OCPs on women with a family history of breast cancer found no additional increase in risk.1 Investigators identified 3 retrospective cohort studies (N=66,500, with 8500 cases) and 7 case-control studies (total 10,500 cases) from the past 40 years, most including women from the United States and Canada, but one including women from 5 continents.
In most trials, women of reproductive age using combined OCPs had 1 or more first-degree female relatives with breast cancer, although a few trials also included second-degree relatives. Women ranged in age from 20 to 79 years at diagnosis, and most trials controlled for age, parity, menstrual and menopausal history, duration of OCP exposure, and age at first use. Follow-up intervals for the retrospective cohort studies ranged from 5 to 16 years. Investigators were unable to combine results because of heterogenous populations.
Three of the cohort studies found no significant difference in breast cancer risk between OCP users and nonusers, regardless of age or duration of use. One cohort study found an increased risk in women taking older, higher-dose OCPs from before 1975 (relative risk [RR]=3.3; 95% confidence interval [CI], 1.5-7.2). All of the case-control studies found no significant difference in breast cancer risk for any age of starting, duration of OCP use, or degree of relative with breast cancer.
A meta-analysis of 54 case-control studies (6757 cases), comprising approximately 90% of the epidemiologic information on this topic, also found no significant difference in breast cancer risk related to OCP use among women with one or more first-degree relatives with breast cancer.2 Investigators found that neither recent OCP use (<10 years, RR=0.77; 95% CI, 0.54-1.11) nor past OCP use (>10 years, RR=1.01; 95% CI, 0.80-1.28) affected risk of developing breast cancer.
Three additional case-control studies involving women with a family history of breast cancer also found no significant association for breast cancer incidence among OCP users compared with nonusers.3-5
Modern combined OCPs don’t raise risk in women with BRCA1/2 mutations
A meta-analysis of 5 studies (one retrospective cohort, 4 case-control, with a total of 2855 breast cancer cases and 2944 controls) evaluated whether combined OCPs increased the risk of breast cancer in women, all of whom were carrying BRCA1/2 mutations.6
Using modern combined OCPs didn’t raise the risk of breast cancer in BRCA1/2 carriers overall (RR=1.13; 95% CI, 0.88-1.45) or separately in BRCA1 carriers (5 studies, RR=1.09; 95% CI, 0.77-1.54) or BRCA2 carriers (3 studies, RR=1.15; 95% CI, 0.88-1.45).
However, pre-1975 (higher dose) combined OCPs produced significantly increased risk (RR=1.47; 95% CI, 1.06-2.04). Similarly, women who had used combined OCPs >10 years before the study (older women, likely to have been using pre-1975 OCPs) also had significantly increased risk (RR=1.46; 95% CI, 1.07-2.07).
A bit of good news: Combined OCPs reduce ovarian cancer risk
The analysis also determined that combined OCPs significantly reduced the risk of ovarian cancer in women carrying BRCA1/2 mutations (RR=0.50; 95% CI, 0.33-0.75), with an additional linear decrease in risk for each 10 years of OCP use (RR=0.64; 95% CI, 0.53-0.78).
RECOMMENDATIONS
The World Health Organization guidelines outlining criteria for contraceptive use state that OCPs don’t alter the risk of breast cancer among women with either a family history of breast cancer or breast cancer susceptibility genes.7
The American College of Obstetricians and Gynecologists (ACOG) says that a positive family history of breast cancer shouldn’t be regarded as a contraindication to OCP use.8 ACOG also says that women with the BRCA1 mutation have an increased risk of breast cancer if they used OCPs for longer than 5 years before age 30, but this risk may be more than balanced by the benefit of a greatly reduced risk of ovarian cancer.
No. Modern combined oral contraceptive pills (OCPs) don’t increase breast cancer risk in women with a family history (strength of recommendation [SOR]: B, systematic review of cohort, case-control studies). However, older, higher-dose OCPs (in use before 1975) did increase breast cancer risk in these women (SOR: C, case-control study).
Similarly, modern OCPs don’t raise breast cancer risk in women with BRCA1/2 mutations, although higher-dose, pre-1975 OCPs did (SOR: B and C, a meta-analysis of cohort and case-control studies).
EVIDENCE SUMMARY
A systematic review of the effect of combined OCPs on women with a family history of breast cancer found no additional increase in risk.1 Investigators identified 3 retrospective cohort studies (N=66,500, with 8500 cases) and 7 case-control studies (total 10,500 cases) from the past 40 years, most including women from the United States and Canada, but one including women from 5 continents.
In most trials, women of reproductive age using combined OCPs had 1 or more first-degree female relatives with breast cancer, although a few trials also included second-degree relatives. Women ranged in age from 20 to 79 years at diagnosis, and most trials controlled for age, parity, menstrual and menopausal history, duration of OCP exposure, and age at first use. Follow-up intervals for the retrospective cohort studies ranged from 5 to 16 years. Investigators were unable to combine results because of heterogenous populations.
Three of the cohort studies found no significant difference in breast cancer risk between OCP users and nonusers, regardless of age or duration of use. One cohort study found an increased risk in women taking older, higher-dose OCPs from before 1975 (relative risk [RR]=3.3; 95% confidence interval [CI], 1.5-7.2). All of the case-control studies found no significant difference in breast cancer risk for any age of starting, duration of OCP use, or degree of relative with breast cancer.
A meta-analysis of 54 case-control studies (6757 cases), comprising approximately 90% of the epidemiologic information on this topic, also found no significant difference in breast cancer risk related to OCP use among women with one or more first-degree relatives with breast cancer.2 Investigators found that neither recent OCP use (<10 years, RR=0.77; 95% CI, 0.54-1.11) nor past OCP use (>10 years, RR=1.01; 95% CI, 0.80-1.28) affected risk of developing breast cancer.
Three additional case-control studies involving women with a family history of breast cancer also found no significant association for breast cancer incidence among OCP users compared with nonusers.3-5
Modern combined OCPs don’t raise risk in women with BRCA1/2 mutations
A meta-analysis of 5 studies (one retrospective cohort, 4 case-control, with a total of 2855 breast cancer cases and 2944 controls) evaluated whether combined OCPs increased the risk of breast cancer in women, all of whom were carrying BRCA1/2 mutations.6
Using modern combined OCPs didn’t raise the risk of breast cancer in BRCA1/2 carriers overall (RR=1.13; 95% CI, 0.88-1.45) or separately in BRCA1 carriers (5 studies, RR=1.09; 95% CI, 0.77-1.54) or BRCA2 carriers (3 studies, RR=1.15; 95% CI, 0.88-1.45).
However, pre-1975 (higher dose) combined OCPs produced significantly increased risk (RR=1.47; 95% CI, 1.06-2.04). Similarly, women who had used combined OCPs >10 years before the study (older women, likely to have been using pre-1975 OCPs) also had significantly increased risk (RR=1.46; 95% CI, 1.07-2.07).
A bit of good news: Combined OCPs reduce ovarian cancer risk
The analysis also determined that combined OCPs significantly reduced the risk of ovarian cancer in women carrying BRCA1/2 mutations (RR=0.50; 95% CI, 0.33-0.75), with an additional linear decrease in risk for each 10 years of OCP use (RR=0.64; 95% CI, 0.53-0.78).
RECOMMENDATIONS
The World Health Organization guidelines outlining criteria for contraceptive use state that OCPs don’t alter the risk of breast cancer among women with either a family history of breast cancer or breast cancer susceptibility genes.7
The American College of Obstetricians and Gynecologists (ACOG) says that a positive family history of breast cancer shouldn’t be regarded as a contraindication to OCP use.8 ACOG also says that women with the BRCA1 mutation have an increased risk of breast cancer if they used OCPs for longer than 5 years before age 30, but this risk may be more than balanced by the benefit of a greatly reduced risk of ovarian cancer.
1. Gaffield ME, Culwell KR, Ravi A. Oral contraceptives and family history of breast cancer. Contraception. 2009;80:372-380.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative re-analysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet. 1996;347:1713-1727.
3. Jernström H, Loman N, Johannsson OT, et al. Impact of teenage oral contraceptive use in a population-based series of early-onset breast cancer cases who have undergone BRCA mutation testing. Eur J Cancer. 2005;41:2312-2320.
4. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Human Reprod Update. 2010;16: 631-650.
5. Long-term oral contraceptive use and the risk of breast cancer. The Centers for Disease Control Cancer and Steroid Hormone Study. JAMA. 1983;249:1591-1595.
6. Iodice S, Barile M, Rotmensz N, et al. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer. 2010;46:2275-2284.
7. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. 4th ed. Geneva, Switzerland: World Health Organization; 2009. World Health Organization Web site. Available at: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed September 24, 2013.
8. ACOG Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107:1453-1472.
1. Gaffield ME, Culwell KR, Ravi A. Oral contraceptives and family history of breast cancer. Contraception. 2009;80:372-380.
2. Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative re-analysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet. 1996;347:1713-1727.
3. Jernström H, Loman N, Johannsson OT, et al. Impact of teenage oral contraceptive use in a population-based series of early-onset breast cancer cases who have undergone BRCA mutation testing. Eur J Cancer. 2005;41:2312-2320.
4. Cibula D, Gompel A, Mueck AO, et al. Hormonal contraception and risk of cancer. Human Reprod Update. 2010;16: 631-650.
5. Long-term oral contraceptive use and the risk of breast cancer. The Centers for Disease Control Cancer and Steroid Hormone Study. JAMA. 1983;249:1591-1595.
6. Iodice S, Barile M, Rotmensz N, et al. Oral contraceptive use and breast or ovarian cancer risk in BRCA1/2 carriers: a meta-analysis. Eur J Cancer. 2010;46:2275-2284.
7. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. 4th ed. Geneva, Switzerland: World Health Organization; 2009. World Health Organization Web site. Available at: http://whqlibdoc.who.int/publications/2010/9789241563888_eng.pdf. Accessed September 24, 2013.
8. ACOG Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin. No. 73: Use of hormonal contraception in women with coexisting medical conditions. Obstet Gynecol. 2006;107:1453-1472.
Evidence-based answers from the Family Physicians Inquiries Network
LISTEN NOW: Mark Williams, MD, MHM, Discusses SHM's Mentored Implementation Programs
Click here to listen to excerpts of our interview with Dr. Williams
Click here to listen to excerpts of our interview with Dr. Williams
Click here to listen to excerpts of our interview with Dr. Williams
Surgery for persistent knee pain? Not so fast
Do not refer patients with a degenerative medial meniscus tear for arthroscopic partial meniscectomy because outcomes are no better than those of conservative treatment.1
Strength of recommendation
B: Based on a single high-quality randomized control trial.
Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
Illustrative case
A 40-year-old man comes to your office for follow-up of medial left knee pain he’s had for 3 months that hasn’t responded to conservative treatment. The pain developed gradually, without a history of trauma. The patient has no signs of degenerative joint disease on x-ray but magnetic resonance imaging (MRI) reveals a tear of the medial meniscus. Should you refer him for meniscectomy?
Patients and doctors alike tend to look for a treatment that will “fix” the problem, which may be why we have continued to use arthroscopic partial meniscectomy to attempt to relieve symptoms of meniscal tears despite a lack of evidence to support the practice.
Guidelines from the American Academy of Orthopaedic Surgeons state that the evidence for medial meniscectomy in patients with a torn meniscus and osteoarthritis (OA) is inconclusive; the organization offers no guidelines for patients with a torn meniscus who don’t have OA.2 The American College of Occupational and Environmental Medicine states that there is insufficient evidence to support arthroscopic partial meniscectomy for symptomatic, torn medial menisci for select patients and “the vast majority of patients [with medial meniscal tears] do not require surgery.”3 Previous studies have concluded that arthroscopic surgery for OA of the knee provides no additional benefit to optimized physical and medical therapy.4 Furthermore, research by Katz et al5 shows that meniscectomy provides no benefit over conservative treatment in functional status at 6 months in patients with OA and a medial meniscal tear.
That said, arthroscopic partial meniscectomy is still the most common orthopedic procedure in the United States.1 Although its use has decreased over the last 15 years, it is performed nearly 700,000 times annually at a cost of approximately $4 billion.1,6,7 Like any surgical procedure, meniscectomy carries a risk of complications. In the double-blind, randomized trial reported on here, Sihvonen et al1 compared meniscectomy to a sham procedure for patients with knee pain, but not OA.
STUDY SUMMARY: Meniscectomy and sham surgery are equally effective
Sihvonen et al1 conducted a randomized, double-blind, sham-controlled trial at 5 orthopedic clinics in Finland. Patients ages 35 to 65 years were enrolled if they had clinical findings of a medial meniscus tear and knee pain for >3 months that wasn’t relieved by conservative treatment. The trial excluded patients who had an obvious traumatic onset of symptoms; clinical or radiological evidence of knee OA; a locked knee that could not be straightened; knee instability or decreased range of motion; previous surgery on the affected knee; fracture within the past 12 months on the affected limb; or other notable pathology on MRI or during arthroscopy.
Before randomization, 160 patients underwent diagnostic arthroscopy. Fourteen patients were excluded: 6 because they did not actually have a medial meniscal tear, one because he also had a lateral meniscus tear, 3 due to a major chondral flap, 2 who had already undergone meniscal repair, and 2 due to an osteochondral microfracture.
At the end of the diagnostic arthroscopy, each patient was blindly randomized to arthroscopic partial meniscectomy or sham surgery. To simulate the meniscectomy procedure, the surgeon similarly manipulated the knee, made comparable noise and vibration using tools and suction, and ensured that the patient was kept in the operating room (OR) for a comparable time. Only the orthopedic surgeon and OR staff were aware of which surgery the patient underwent, and these staff members were not included in further treatment or follow-up. After the procedure, all patients received the same walking aids and instructions for a graduated exercise program.
The 70 patients in the meniscectomy group and the 76 in the sham surgery group were similar in age (mean: 52 years), sex, body mass index, and duration of pain (mean: 10 months). Patients in both groups also had similar tears noted on arthroscopy.
Three primary outcomes were measured before surgery and at 12 months: knee pain, knee symptoms and function, and quality of life. Knee pain after exercise was evaluated on a 0 to 10 scale, with 0 indicating no pain. The validated Lysholm knee score was used to assess knee symptoms and function and the Western Ontario Meniscal Evaluation Tool (WOMET) was utilized to evaluate quality of life; both are 100-point scales in which lower scores indicate more severe symptoms.
Both groups had marked improvement in pain and function from baseline to 12 months, and there was no significant difference between the 2 groups. Knee pain scores improved by 3.1 in the meniscectomy group and 3.3 in the sham surgery group.
Lysholm symptom and function scores improved 21.7 points in the meniscectomy group and 23.3 points in the sham surgery group (a change of 11.5 points would have been considered clinically significant). The mean between-group difference was -1.6 points (95% confidence interval [CI], -7.2 to 4.0).
WOMET quality of life scores improved 24.6 points in the meniscectomy group and 27.1 points in the sham surgery (a change of 15.5 points would have been considered clinically significant). The mean between-group difference was -2.5 points (95% CI, -9.2 to 4.1).
There were no significant between-group differences in serious adverse events or number of patients who required subsequent knee surgery. Similar proportions in each group thought they had sham surgery, which confirmed the effectiveness of the blinding. Ninety-six percent of patients in the sham procedure group and 93% in the meniscectomy group reported they would be willing to repeat the procedure.
WHAT'S NEW: Recommend physical therapy, exercise instead of surgery
Previous studies of arthroscopic partial meniscectomy to treat degenerative meniscal tears in patients with knee OA found no benefit.6,8 This study specifically examined patients without OA and found arthroscopic partial meniscectomy offered no benefit over sham surgery.
In addition to fewer referrals for meniscectomy, these findings could lead to another change in practice: Physicians may be less likely to order an MRI to confirm the diagnosis of a medial meniscal tear, since doing so will not change their therapeutic approach. This approach centers on recommending that patients with a degenerative meniscal tear start and stick with physical therapy and their designated exercise regimen.
CAVEATS: Surgery might be effective for more active patients
This study, as well as previous research, did not look at surgery for an acute medial meniscus tear following a traumatic incident, such as a fall or direct blow. Additionally, these results are based on improved outcomes in activities of daily living, and may not extend to patients who engage in high-level functioning, such as sports or strenuous work. The sham surgery group received lavage, which could be considered an active treatment, although a previous trial found lavage had no benefit over conservative treatment in patients with knee OA.4
CHALLENGES TO IMPLEMENTATION: It might be hard to convince patients they don’t need surgery
Some patients expect immediate intervention with surgery. It may be difficult to convince such patients that active participation in physical therapy can lead to the same outcomes as surgery. Spending time with your patient to explain the injury, what happens during surgery, and the evidence that shows a lack of difference in outcomes can lead to fewer surgeries. Most patients and physicians will want to do an MRI after 3 months of persistent pain to determine the diagnosis, although some may be comfortable with continuing conservative treatment.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
2. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
3. Knee disorders. In: Hegmann KT, ed. Occupational Medicine Practice Guidelines. Evaluation and Management of Common Health Problems and Functional Recovery in Workers. 3rd ed. Elk Grove Village, IL: American College of Occupational and Environmental Medicine; 2011:1-503.
4. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial for arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359:1097-1107.
5. Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368:1675-1684.
6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health State Report. 2009;11:1-25.
7. Salzler MJ, Lin A, Miller CD, et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014;42:292-296.
8. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347:81-88.
Do not refer patients with a degenerative medial meniscus tear for arthroscopic partial meniscectomy because outcomes are no better than those of conservative treatment.1
Strength of recommendation
B: Based on a single high-quality randomized control trial.
Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
Illustrative case
A 40-year-old man comes to your office for follow-up of medial left knee pain he’s had for 3 months that hasn’t responded to conservative treatment. The pain developed gradually, without a history of trauma. The patient has no signs of degenerative joint disease on x-ray but magnetic resonance imaging (MRI) reveals a tear of the medial meniscus. Should you refer him for meniscectomy?
Patients and doctors alike tend to look for a treatment that will “fix” the problem, which may be why we have continued to use arthroscopic partial meniscectomy to attempt to relieve symptoms of meniscal tears despite a lack of evidence to support the practice.
Guidelines from the American Academy of Orthopaedic Surgeons state that the evidence for medial meniscectomy in patients with a torn meniscus and osteoarthritis (OA) is inconclusive; the organization offers no guidelines for patients with a torn meniscus who don’t have OA.2 The American College of Occupational and Environmental Medicine states that there is insufficient evidence to support arthroscopic partial meniscectomy for symptomatic, torn medial menisci for select patients and “the vast majority of patients [with medial meniscal tears] do not require surgery.”3 Previous studies have concluded that arthroscopic surgery for OA of the knee provides no additional benefit to optimized physical and medical therapy.4 Furthermore, research by Katz et al5 shows that meniscectomy provides no benefit over conservative treatment in functional status at 6 months in patients with OA and a medial meniscal tear.
That said, arthroscopic partial meniscectomy is still the most common orthopedic procedure in the United States.1 Although its use has decreased over the last 15 years, it is performed nearly 700,000 times annually at a cost of approximately $4 billion.1,6,7 Like any surgical procedure, meniscectomy carries a risk of complications. In the double-blind, randomized trial reported on here, Sihvonen et al1 compared meniscectomy to a sham procedure for patients with knee pain, but not OA.
STUDY SUMMARY: Meniscectomy and sham surgery are equally effective
Sihvonen et al1 conducted a randomized, double-blind, sham-controlled trial at 5 orthopedic clinics in Finland. Patients ages 35 to 65 years were enrolled if they had clinical findings of a medial meniscus tear and knee pain for >3 months that wasn’t relieved by conservative treatment. The trial excluded patients who had an obvious traumatic onset of symptoms; clinical or radiological evidence of knee OA; a locked knee that could not be straightened; knee instability or decreased range of motion; previous surgery on the affected knee; fracture within the past 12 months on the affected limb; or other notable pathology on MRI or during arthroscopy.
Before randomization, 160 patients underwent diagnostic arthroscopy. Fourteen patients were excluded: 6 because they did not actually have a medial meniscal tear, one because he also had a lateral meniscus tear, 3 due to a major chondral flap, 2 who had already undergone meniscal repair, and 2 due to an osteochondral microfracture.
At the end of the diagnostic arthroscopy, each patient was blindly randomized to arthroscopic partial meniscectomy or sham surgery. To simulate the meniscectomy procedure, the surgeon similarly manipulated the knee, made comparable noise and vibration using tools and suction, and ensured that the patient was kept in the operating room (OR) for a comparable time. Only the orthopedic surgeon and OR staff were aware of which surgery the patient underwent, and these staff members were not included in further treatment or follow-up. After the procedure, all patients received the same walking aids and instructions for a graduated exercise program.
The 70 patients in the meniscectomy group and the 76 in the sham surgery group were similar in age (mean: 52 years), sex, body mass index, and duration of pain (mean: 10 months). Patients in both groups also had similar tears noted on arthroscopy.
Three primary outcomes were measured before surgery and at 12 months: knee pain, knee symptoms and function, and quality of life. Knee pain after exercise was evaluated on a 0 to 10 scale, with 0 indicating no pain. The validated Lysholm knee score was used to assess knee symptoms and function and the Western Ontario Meniscal Evaluation Tool (WOMET) was utilized to evaluate quality of life; both are 100-point scales in which lower scores indicate more severe symptoms.
Both groups had marked improvement in pain and function from baseline to 12 months, and there was no significant difference between the 2 groups. Knee pain scores improved by 3.1 in the meniscectomy group and 3.3 in the sham surgery group.
Lysholm symptom and function scores improved 21.7 points in the meniscectomy group and 23.3 points in the sham surgery group (a change of 11.5 points would have been considered clinically significant). The mean between-group difference was -1.6 points (95% confidence interval [CI], -7.2 to 4.0).
WOMET quality of life scores improved 24.6 points in the meniscectomy group and 27.1 points in the sham surgery (a change of 15.5 points would have been considered clinically significant). The mean between-group difference was -2.5 points (95% CI, -9.2 to 4.1).
There were no significant between-group differences in serious adverse events or number of patients who required subsequent knee surgery. Similar proportions in each group thought they had sham surgery, which confirmed the effectiveness of the blinding. Ninety-six percent of patients in the sham procedure group and 93% in the meniscectomy group reported they would be willing to repeat the procedure.
WHAT'S NEW: Recommend physical therapy, exercise instead of surgery
Previous studies of arthroscopic partial meniscectomy to treat degenerative meniscal tears in patients with knee OA found no benefit.6,8 This study specifically examined patients without OA and found arthroscopic partial meniscectomy offered no benefit over sham surgery.
In addition to fewer referrals for meniscectomy, these findings could lead to another change in practice: Physicians may be less likely to order an MRI to confirm the diagnosis of a medial meniscal tear, since doing so will not change their therapeutic approach. This approach centers on recommending that patients with a degenerative meniscal tear start and stick with physical therapy and their designated exercise regimen.
CAVEATS: Surgery might be effective for more active patients
This study, as well as previous research, did not look at surgery for an acute medial meniscus tear following a traumatic incident, such as a fall or direct blow. Additionally, these results are based on improved outcomes in activities of daily living, and may not extend to patients who engage in high-level functioning, such as sports or strenuous work. The sham surgery group received lavage, which could be considered an active treatment, although a previous trial found lavage had no benefit over conservative treatment in patients with knee OA.4
CHALLENGES TO IMPLEMENTATION: It might be hard to convince patients they don’t need surgery
Some patients expect immediate intervention with surgery. It may be difficult to convince such patients that active participation in physical therapy can lead to the same outcomes as surgery. Spending time with your patient to explain the injury, what happens during surgery, and the evidence that shows a lack of difference in outcomes can lead to fewer surgeries. Most patients and physicians will want to do an MRI after 3 months of persistent pain to determine the diagnosis, although some may be comfortable with continuing conservative treatment.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Do not refer patients with a degenerative medial meniscus tear for arthroscopic partial meniscectomy because outcomes are no better than those of conservative treatment.1
Strength of recommendation
B: Based on a single high-quality randomized control trial.
Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
Illustrative case
A 40-year-old man comes to your office for follow-up of medial left knee pain he’s had for 3 months that hasn’t responded to conservative treatment. The pain developed gradually, without a history of trauma. The patient has no signs of degenerative joint disease on x-ray but magnetic resonance imaging (MRI) reveals a tear of the medial meniscus. Should you refer him for meniscectomy?
Patients and doctors alike tend to look for a treatment that will “fix” the problem, which may be why we have continued to use arthroscopic partial meniscectomy to attempt to relieve symptoms of meniscal tears despite a lack of evidence to support the practice.
Guidelines from the American Academy of Orthopaedic Surgeons state that the evidence for medial meniscectomy in patients with a torn meniscus and osteoarthritis (OA) is inconclusive; the organization offers no guidelines for patients with a torn meniscus who don’t have OA.2 The American College of Occupational and Environmental Medicine states that there is insufficient evidence to support arthroscopic partial meniscectomy for symptomatic, torn medial menisci for select patients and “the vast majority of patients [with medial meniscal tears] do not require surgery.”3 Previous studies have concluded that arthroscopic surgery for OA of the knee provides no additional benefit to optimized physical and medical therapy.4 Furthermore, research by Katz et al5 shows that meniscectomy provides no benefit over conservative treatment in functional status at 6 months in patients with OA and a medial meniscal tear.
That said, arthroscopic partial meniscectomy is still the most common orthopedic procedure in the United States.1 Although its use has decreased over the last 15 years, it is performed nearly 700,000 times annually at a cost of approximately $4 billion.1,6,7 Like any surgical procedure, meniscectomy carries a risk of complications. In the double-blind, randomized trial reported on here, Sihvonen et al1 compared meniscectomy to a sham procedure for patients with knee pain, but not OA.
STUDY SUMMARY: Meniscectomy and sham surgery are equally effective
Sihvonen et al1 conducted a randomized, double-blind, sham-controlled trial at 5 orthopedic clinics in Finland. Patients ages 35 to 65 years were enrolled if they had clinical findings of a medial meniscus tear and knee pain for >3 months that wasn’t relieved by conservative treatment. The trial excluded patients who had an obvious traumatic onset of symptoms; clinical or radiological evidence of knee OA; a locked knee that could not be straightened; knee instability or decreased range of motion; previous surgery on the affected knee; fracture within the past 12 months on the affected limb; or other notable pathology on MRI or during arthroscopy.
Before randomization, 160 patients underwent diagnostic arthroscopy. Fourteen patients were excluded: 6 because they did not actually have a medial meniscal tear, one because he also had a lateral meniscus tear, 3 due to a major chondral flap, 2 who had already undergone meniscal repair, and 2 due to an osteochondral microfracture.
At the end of the diagnostic arthroscopy, each patient was blindly randomized to arthroscopic partial meniscectomy or sham surgery. To simulate the meniscectomy procedure, the surgeon similarly manipulated the knee, made comparable noise and vibration using tools and suction, and ensured that the patient was kept in the operating room (OR) for a comparable time. Only the orthopedic surgeon and OR staff were aware of which surgery the patient underwent, and these staff members were not included in further treatment or follow-up. After the procedure, all patients received the same walking aids and instructions for a graduated exercise program.
The 70 patients in the meniscectomy group and the 76 in the sham surgery group were similar in age (mean: 52 years), sex, body mass index, and duration of pain (mean: 10 months). Patients in both groups also had similar tears noted on arthroscopy.
Three primary outcomes were measured before surgery and at 12 months: knee pain, knee symptoms and function, and quality of life. Knee pain after exercise was evaluated on a 0 to 10 scale, with 0 indicating no pain. The validated Lysholm knee score was used to assess knee symptoms and function and the Western Ontario Meniscal Evaluation Tool (WOMET) was utilized to evaluate quality of life; both are 100-point scales in which lower scores indicate more severe symptoms.
Both groups had marked improvement in pain and function from baseline to 12 months, and there was no significant difference between the 2 groups. Knee pain scores improved by 3.1 in the meniscectomy group and 3.3 in the sham surgery group.
Lysholm symptom and function scores improved 21.7 points in the meniscectomy group and 23.3 points in the sham surgery group (a change of 11.5 points would have been considered clinically significant). The mean between-group difference was -1.6 points (95% confidence interval [CI], -7.2 to 4.0).
WOMET quality of life scores improved 24.6 points in the meniscectomy group and 27.1 points in the sham surgery (a change of 15.5 points would have been considered clinically significant). The mean between-group difference was -2.5 points (95% CI, -9.2 to 4.1).
There were no significant between-group differences in serious adverse events or number of patients who required subsequent knee surgery. Similar proportions in each group thought they had sham surgery, which confirmed the effectiveness of the blinding. Ninety-six percent of patients in the sham procedure group and 93% in the meniscectomy group reported they would be willing to repeat the procedure.
WHAT'S NEW: Recommend physical therapy, exercise instead of surgery
Previous studies of arthroscopic partial meniscectomy to treat degenerative meniscal tears in patients with knee OA found no benefit.6,8 This study specifically examined patients without OA and found arthroscopic partial meniscectomy offered no benefit over sham surgery.
In addition to fewer referrals for meniscectomy, these findings could lead to another change in practice: Physicians may be less likely to order an MRI to confirm the diagnosis of a medial meniscal tear, since doing so will not change their therapeutic approach. This approach centers on recommending that patients with a degenerative meniscal tear start and stick with physical therapy and their designated exercise regimen.
CAVEATS: Surgery might be effective for more active patients
This study, as well as previous research, did not look at surgery for an acute medial meniscus tear following a traumatic incident, such as a fall or direct blow. Additionally, these results are based on improved outcomes in activities of daily living, and may not extend to patients who engage in high-level functioning, such as sports or strenuous work. The sham surgery group received lavage, which could be considered an active treatment, although a previous trial found lavage had no benefit over conservative treatment in patients with knee OA.4
CHALLENGES TO IMPLEMENTATION: It might be hard to convince patients they don’t need surgery
Some patients expect immediate intervention with surgery. It may be difficult to convince such patients that active participation in physical therapy can lead to the same outcomes as surgery. Spending time with your patient to explain the injury, what happens during surgery, and the evidence that shows a lack of difference in outcomes can lead to fewer surgeries. Most patients and physicians will want to do an MRI after 3 months of persistent pain to determine the diagnosis, although some may be comfortable with continuing conservative treatment.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
2. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
3. Knee disorders. In: Hegmann KT, ed. Occupational Medicine Practice Guidelines. Evaluation and Management of Common Health Problems and Functional Recovery in Workers. 3rd ed. Elk Grove Village, IL: American College of Occupational and Environmental Medicine; 2011:1-503.
4. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial for arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359:1097-1107.
5. Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368:1675-1684.
6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health State Report. 2009;11:1-25.
7. Salzler MJ, Lin A, Miller CD, et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014;42:292-296.
8. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347:81-88.
1. Sihvonen R, Paavola M, Malmivaara A, et al; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013;369:2515-2524.
2. American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis of the Knee. Evidence-Based Guideline. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2013.
3. Knee disorders. In: Hegmann KT, ed. Occupational Medicine Practice Guidelines. Evaluation and Management of Common Health Problems and Functional Recovery in Workers. 3rd ed. Elk Grove Village, IL: American College of Occupational and Environmental Medicine; 2011:1-503.
4. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial for arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2008;359:1097-1107.
5. Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013;368:1675-1684.
6. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health State Report. 2009;11:1-25.
7. Salzler MJ, Lin A, Miller CD, et al. Complications after arthroscopic knee surgery. Am J Sports Med. 2014;42:292-296.
8. Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347:81-88.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
LISTEN NOW: Highlights of the September 2014 issue of The Hospitalist newsmagazine
In the September issue of The Hospitalist, we look at SHM’s award-winning quality improvement (QI) programs in our cover story, “Mentored Implementation.” Dr. Mark Williams, professor of medicine at the University of Kentucky and principal investigator for SHM’s Project BOOST, outlines what mentored implementation really means and explains how site visits became a central feature. Dr. Gregory Maynard, director of the UC San Diego Center for Innovation and Improvement Science and senior vice president of SHM’s Center for Hospital Innovation and Improvement, talks about how mentored implementation of QI programs works. Also featured in this issue, we recap key sessions from the 2014 Pediatric Hospital Medicine conference held last month, and launch into part one of our two-part series on using electronic health record systems to reduce readmissions. This issue also features a write-up on The Hospitalist’s latest editorial award: an APEX Grand Award for Magazines, Journals, and Tabloids!
In the September issue of The Hospitalist, we look at SHM’s award-winning quality improvement (QI) programs in our cover story, “Mentored Implementation.” Dr. Mark Williams, professor of medicine at the University of Kentucky and principal investigator for SHM’s Project BOOST, outlines what mentored implementation really means and explains how site visits became a central feature. Dr. Gregory Maynard, director of the UC San Diego Center for Innovation and Improvement Science and senior vice president of SHM’s Center for Hospital Innovation and Improvement, talks about how mentored implementation of QI programs works. Also featured in this issue, we recap key sessions from the 2014 Pediatric Hospital Medicine conference held last month, and launch into part one of our two-part series on using electronic health record systems to reduce readmissions. This issue also features a write-up on The Hospitalist’s latest editorial award: an APEX Grand Award for Magazines, Journals, and Tabloids!
In the September issue of The Hospitalist, we look at SHM’s award-winning quality improvement (QI) programs in our cover story, “Mentored Implementation.” Dr. Mark Williams, professor of medicine at the University of Kentucky and principal investigator for SHM’s Project BOOST, outlines what mentored implementation really means and explains how site visits became a central feature. Dr. Gregory Maynard, director of the UC San Diego Center for Innovation and Improvement Science and senior vice president of SHM’s Center for Hospital Innovation and Improvement, talks about how mentored implementation of QI programs works. Also featured in this issue, we recap key sessions from the 2014 Pediatric Hospital Medicine conference held last month, and launch into part one of our two-part series on using electronic health record systems to reduce readmissions. This issue also features a write-up on The Hospitalist’s latest editorial award: an APEX Grand Award for Magazines, Journals, and Tabloids!
The 2014-2015 influenza season: What you need to know
As physicians and the Centers for Disease Control and Prevention (CDC) prepare for the upcoming influenza season, many of the recommendations remain unchanged from last season. Vaccination continues to be recommended for everyone 6 months of age and older. However, for the first time, a specific vaccine is preferred for children ages 2 through 8 years. Here’s what you need to know about this change, as well as how to handle vaccination in patients who are, or might be, allergic to eggs.
Use LAIV for kids ages 2 through 8 (if available)
For the first time, the CDC’s Advisory Committee on Immunization Practices (ACIP) has stated a preference for a specific influenza vaccine for a specific age group. It recommends using the live attenuated influenza vaccine (LAIV), which is a nasal spray, for children ages 2 through 8 years.1
A systematic review found evidence of increased efficacy of LAIV compared to inactivated influenza vaccine (IIV) in this age group; both types of vaccine have similar rates of adverse reactions.2 This increased effectiveness results in 46 fewer cases of confirmed influenza per 1000 children vaccinated (number needed to treat=24). Although the evidence of LAIV’s increased effectiveness was found for children ages 2 to 6 years, ACIP extended this recommendation through age 8 because this is the age through which physicians need to consider 2 doses of vaccine for a child previously unvaccinated with the influenza vaccine. Children younger than age 2 should receive IIV3 or IIV4.3
ACIP realizes that due to programmatic constraints it would be difficult to vaccinate all children with LAIV this year and is emphasizing that it should be implemented when feasible this year but no later than the 2015 to 2016 influenza season. IIV is effective in children and should be given if LAIV is not available or is contraindicated. Vaccine should not be delayed in the hopes of receiving LAIV if IIV is available.1
LAIV should not be used in children <2 years or adults >49. This vaccine is contraindicated in children and adolescents who are taking chronic aspirin therapy, pregnant women, those who are immunosuppressed, those with a history of egg allergy, or those who have taken influenza antiviral medications in the past 48 hours.1 LAIV also is not recommended for children ages 2 through 4 years who have asthma or had a wheezing episode in the past 12 months.1
There are precautions for the use of LAIV in patients with chronic medical conditions that can place them at high risk for complications from influenza, such as chronic lung, heart, renal, neurologic, liver, blood, or metabolic disorders, including asthma and diabetes.1
Which vaccine for patients who are allergic to eggs?
Two influenza vaccines are now available that are not prepared in embryonated eggs: recombinant influenza vaccine (RIV3) and cell culture-based inactivated influenza vaccine (ccIIV3). Both are trivalent products that contain antigens from 2 influenza A viruses and one influenza B virus and were introduced in time for the 2013 to 2014 flu season. The RIV3 is considered egg-free but ccIIV3 is not, although the amount of egg protein in it is miniscule, estimated at 5 × 10-8 mcg/0.5 mL dose.1 Neither product is licensed for children younger than 18 years and RIV3 is licensed only for those ages 18 through 49 years.
Patients who experience only hives after egg exposure can receive any of the flu vaccines except LAIV, and only because of a lack of data on this product, not because it has been shown to be less safe than the other vaccines. Patients who are unsure if they have an egg allergy or only get hives when they eat eggs should be observed for at least 30 minutes1 following injection as a precaution. Those ages 18 through 49 who have a history of severe reactions to eggs should receive RIV3. Patients younger than 18 years of age and older than 49 years of age can receive IIV vaccines approved for their specific age group. Any patient who is severely allergic and who cannot receive an egg-free vaccine should be vaccinated by a physician with experience managing severe allergic conditions.
Although severe, anaphylactic reactions to influenza vaccine are very rare, physicians should be equipped and prepared to respond to a severe allergic reaction after providing influenza vaccine to anyone with a history of an egg allergy.
Additional tips and resources
In addition to the LAIV, RIV3, and ccIIV3 vaccines described here, 10 other vaccines are available, including 5 egg-based IIV3 products in standard-dose form, 1 IIV3 vaccine for intradermal use, 1 high-dose IIV3 product for patients ages 65 or older, and 3 standard-dose IIV4 products. More details on each of these vaccines are available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6207a1.htm?_%20cid=rr6207a1_w#Tab1.
Regardless of which type of flu vaccine they receive, children 6 months through 8 years should receive 2 doses, at least 4 weeks apart, unless they received:
- 1 dose in 2013 to 2014, or
- 2 or more doses of seasonal influenza vaccine since July 2010, or
- 2 or more doses of seasonal influenza vaccine before July 2010 and ≥1 dose of monovalent H1N1 vaccine, or
- at least 1 dose of seasonal influenza vaccine prior to July 2010 and ≥1 after.
Vaccine effectiveness. The CDC estimated that vaccine effectiveness during the 2013 to 2014 flu season was 66%.3 While this degree of effectiveness is important for minimizing the morbidity and mortality from influenza each year, it’s important to appreciate the limitations of the vaccine and not rely on it as the only prevention intervention.
Other forms of prevention. We need to advise and practice good respiratory hygiene, frequent hand washing, self-isolation when sick, effective infection control practices at health care facilities, targeted early treatment with antivirals, and targeted pre- and post-exposure antiviral chemoprevention. Details on each of these interventions, including recommendations on the use of antiviral medications, can be found on the CDC Web site at http://www.cdc.gov/flu.
1. Grohskopf LA, Olsen SJ, Sokolow LZ, et al; Influenza Division, National Center for Immunization and Respiratory Diseases, CDC. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States 2014-2015 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63:691-697.
2. Grohskopf L, Olsen S, Sokolow L. Effectiveness of live-attenuated vs inactivated influenza vaccines for healthy children. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/05-Flu-Grohskopf.pdf. Accessed August 6, 2014.
3. Flannery B. Interim estimates of 2013-14 seasonal influenza vaccine effectiveness. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/04-Flu-Flannery.pdf. Accessed August 6, 2014.
As physicians and the Centers for Disease Control and Prevention (CDC) prepare for the upcoming influenza season, many of the recommendations remain unchanged from last season. Vaccination continues to be recommended for everyone 6 months of age and older. However, for the first time, a specific vaccine is preferred for children ages 2 through 8 years. Here’s what you need to know about this change, as well as how to handle vaccination in patients who are, or might be, allergic to eggs.
Use LAIV for kids ages 2 through 8 (if available)
For the first time, the CDC’s Advisory Committee on Immunization Practices (ACIP) has stated a preference for a specific influenza vaccine for a specific age group. It recommends using the live attenuated influenza vaccine (LAIV), which is a nasal spray, for children ages 2 through 8 years.1
A systematic review found evidence of increased efficacy of LAIV compared to inactivated influenza vaccine (IIV) in this age group; both types of vaccine have similar rates of adverse reactions.2 This increased effectiveness results in 46 fewer cases of confirmed influenza per 1000 children vaccinated (number needed to treat=24). Although the evidence of LAIV’s increased effectiveness was found for children ages 2 to 6 years, ACIP extended this recommendation through age 8 because this is the age through which physicians need to consider 2 doses of vaccine for a child previously unvaccinated with the influenza vaccine. Children younger than age 2 should receive IIV3 or IIV4.3
ACIP realizes that due to programmatic constraints it would be difficult to vaccinate all children with LAIV this year and is emphasizing that it should be implemented when feasible this year but no later than the 2015 to 2016 influenza season. IIV is effective in children and should be given if LAIV is not available or is contraindicated. Vaccine should not be delayed in the hopes of receiving LAIV if IIV is available.1
LAIV should not be used in children <2 years or adults >49. This vaccine is contraindicated in children and adolescents who are taking chronic aspirin therapy, pregnant women, those who are immunosuppressed, those with a history of egg allergy, or those who have taken influenza antiviral medications in the past 48 hours.1 LAIV also is not recommended for children ages 2 through 4 years who have asthma or had a wheezing episode in the past 12 months.1
There are precautions for the use of LAIV in patients with chronic medical conditions that can place them at high risk for complications from influenza, such as chronic lung, heart, renal, neurologic, liver, blood, or metabolic disorders, including asthma and diabetes.1
Which vaccine for patients who are allergic to eggs?
Two influenza vaccines are now available that are not prepared in embryonated eggs: recombinant influenza vaccine (RIV3) and cell culture-based inactivated influenza vaccine (ccIIV3). Both are trivalent products that contain antigens from 2 influenza A viruses and one influenza B virus and were introduced in time for the 2013 to 2014 flu season. The RIV3 is considered egg-free but ccIIV3 is not, although the amount of egg protein in it is miniscule, estimated at 5 × 10-8 mcg/0.5 mL dose.1 Neither product is licensed for children younger than 18 years and RIV3 is licensed only for those ages 18 through 49 years.
Patients who experience only hives after egg exposure can receive any of the flu vaccines except LAIV, and only because of a lack of data on this product, not because it has been shown to be less safe than the other vaccines. Patients who are unsure if they have an egg allergy or only get hives when they eat eggs should be observed for at least 30 minutes1 following injection as a precaution. Those ages 18 through 49 who have a history of severe reactions to eggs should receive RIV3. Patients younger than 18 years of age and older than 49 years of age can receive IIV vaccines approved for their specific age group. Any patient who is severely allergic and who cannot receive an egg-free vaccine should be vaccinated by a physician with experience managing severe allergic conditions.
Although severe, anaphylactic reactions to influenza vaccine are very rare, physicians should be equipped and prepared to respond to a severe allergic reaction after providing influenza vaccine to anyone with a history of an egg allergy.
Additional tips and resources
In addition to the LAIV, RIV3, and ccIIV3 vaccines described here, 10 other vaccines are available, including 5 egg-based IIV3 products in standard-dose form, 1 IIV3 vaccine for intradermal use, 1 high-dose IIV3 product for patients ages 65 or older, and 3 standard-dose IIV4 products. More details on each of these vaccines are available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6207a1.htm?_%20cid=rr6207a1_w#Tab1.
Regardless of which type of flu vaccine they receive, children 6 months through 8 years should receive 2 doses, at least 4 weeks apart, unless they received:
- 1 dose in 2013 to 2014, or
- 2 or more doses of seasonal influenza vaccine since July 2010, or
- 2 or more doses of seasonal influenza vaccine before July 2010 and ≥1 dose of monovalent H1N1 vaccine, or
- at least 1 dose of seasonal influenza vaccine prior to July 2010 and ≥1 after.
Vaccine effectiveness. The CDC estimated that vaccine effectiveness during the 2013 to 2014 flu season was 66%.3 While this degree of effectiveness is important for minimizing the morbidity and mortality from influenza each year, it’s important to appreciate the limitations of the vaccine and not rely on it as the only prevention intervention.
Other forms of prevention. We need to advise and practice good respiratory hygiene, frequent hand washing, self-isolation when sick, effective infection control practices at health care facilities, targeted early treatment with antivirals, and targeted pre- and post-exposure antiviral chemoprevention. Details on each of these interventions, including recommendations on the use of antiviral medications, can be found on the CDC Web site at http://www.cdc.gov/flu.
As physicians and the Centers for Disease Control and Prevention (CDC) prepare for the upcoming influenza season, many of the recommendations remain unchanged from last season. Vaccination continues to be recommended for everyone 6 months of age and older. However, for the first time, a specific vaccine is preferred for children ages 2 through 8 years. Here’s what you need to know about this change, as well as how to handle vaccination in patients who are, or might be, allergic to eggs.
Use LAIV for kids ages 2 through 8 (if available)
For the first time, the CDC’s Advisory Committee on Immunization Practices (ACIP) has stated a preference for a specific influenza vaccine for a specific age group. It recommends using the live attenuated influenza vaccine (LAIV), which is a nasal spray, for children ages 2 through 8 years.1
A systematic review found evidence of increased efficacy of LAIV compared to inactivated influenza vaccine (IIV) in this age group; both types of vaccine have similar rates of adverse reactions.2 This increased effectiveness results in 46 fewer cases of confirmed influenza per 1000 children vaccinated (number needed to treat=24). Although the evidence of LAIV’s increased effectiveness was found for children ages 2 to 6 years, ACIP extended this recommendation through age 8 because this is the age through which physicians need to consider 2 doses of vaccine for a child previously unvaccinated with the influenza vaccine. Children younger than age 2 should receive IIV3 or IIV4.3
ACIP realizes that due to programmatic constraints it would be difficult to vaccinate all children with LAIV this year and is emphasizing that it should be implemented when feasible this year but no later than the 2015 to 2016 influenza season. IIV is effective in children and should be given if LAIV is not available or is contraindicated. Vaccine should not be delayed in the hopes of receiving LAIV if IIV is available.1
LAIV should not be used in children <2 years or adults >49. This vaccine is contraindicated in children and adolescents who are taking chronic aspirin therapy, pregnant women, those who are immunosuppressed, those with a history of egg allergy, or those who have taken influenza antiviral medications in the past 48 hours.1 LAIV also is not recommended for children ages 2 through 4 years who have asthma or had a wheezing episode in the past 12 months.1
There are precautions for the use of LAIV in patients with chronic medical conditions that can place them at high risk for complications from influenza, such as chronic lung, heart, renal, neurologic, liver, blood, or metabolic disorders, including asthma and diabetes.1
Which vaccine for patients who are allergic to eggs?
Two influenza vaccines are now available that are not prepared in embryonated eggs: recombinant influenza vaccine (RIV3) and cell culture-based inactivated influenza vaccine (ccIIV3). Both are trivalent products that contain antigens from 2 influenza A viruses and one influenza B virus and were introduced in time for the 2013 to 2014 flu season. The RIV3 is considered egg-free but ccIIV3 is not, although the amount of egg protein in it is miniscule, estimated at 5 × 10-8 mcg/0.5 mL dose.1 Neither product is licensed for children younger than 18 years and RIV3 is licensed only for those ages 18 through 49 years.
Patients who experience only hives after egg exposure can receive any of the flu vaccines except LAIV, and only because of a lack of data on this product, not because it has been shown to be less safe than the other vaccines. Patients who are unsure if they have an egg allergy or only get hives when they eat eggs should be observed for at least 30 minutes1 following injection as a precaution. Those ages 18 through 49 who have a history of severe reactions to eggs should receive RIV3. Patients younger than 18 years of age and older than 49 years of age can receive IIV vaccines approved for their specific age group. Any patient who is severely allergic and who cannot receive an egg-free vaccine should be vaccinated by a physician with experience managing severe allergic conditions.
Although severe, anaphylactic reactions to influenza vaccine are very rare, physicians should be equipped and prepared to respond to a severe allergic reaction after providing influenza vaccine to anyone with a history of an egg allergy.
Additional tips and resources
In addition to the LAIV, RIV3, and ccIIV3 vaccines described here, 10 other vaccines are available, including 5 egg-based IIV3 products in standard-dose form, 1 IIV3 vaccine for intradermal use, 1 high-dose IIV3 product for patients ages 65 or older, and 3 standard-dose IIV4 products. More details on each of these vaccines are available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6207a1.htm?_%20cid=rr6207a1_w#Tab1.
Regardless of which type of flu vaccine they receive, children 6 months through 8 years should receive 2 doses, at least 4 weeks apart, unless they received:
- 1 dose in 2013 to 2014, or
- 2 or more doses of seasonal influenza vaccine since July 2010, or
- 2 or more doses of seasonal influenza vaccine before July 2010 and ≥1 dose of monovalent H1N1 vaccine, or
- at least 1 dose of seasonal influenza vaccine prior to July 2010 and ≥1 after.
Vaccine effectiveness. The CDC estimated that vaccine effectiveness during the 2013 to 2014 flu season was 66%.3 While this degree of effectiveness is important for minimizing the morbidity and mortality from influenza each year, it’s important to appreciate the limitations of the vaccine and not rely on it as the only prevention intervention.
Other forms of prevention. We need to advise and practice good respiratory hygiene, frequent hand washing, self-isolation when sick, effective infection control practices at health care facilities, targeted early treatment with antivirals, and targeted pre- and post-exposure antiviral chemoprevention. Details on each of these interventions, including recommendations on the use of antiviral medications, can be found on the CDC Web site at http://www.cdc.gov/flu.
1. Grohskopf LA, Olsen SJ, Sokolow LZ, et al; Influenza Division, National Center for Immunization and Respiratory Diseases, CDC. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States 2014-2015 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63:691-697.
2. Grohskopf L, Olsen S, Sokolow L. Effectiveness of live-attenuated vs inactivated influenza vaccines for healthy children. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/05-Flu-Grohskopf.pdf. Accessed August 6, 2014.
3. Flannery B. Interim estimates of 2013-14 seasonal influenza vaccine effectiveness. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/04-Flu-Flannery.pdf. Accessed August 6, 2014.
1. Grohskopf LA, Olsen SJ, Sokolow LZ, et al; Influenza Division, National Center for Immunization and Respiratory Diseases, CDC. Prevention and control of seasonal influenza with vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP)—United States 2014-2015 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63:691-697.
2. Grohskopf L, Olsen S, Sokolow L. Effectiveness of live-attenuated vs inactivated influenza vaccines for healthy children. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/05-Flu-Grohskopf.pdf. Accessed August 6, 2014.
3. Flannery B. Interim estimates of 2013-14 seasonal influenza vaccine effectiveness. PowerPoint presented at: Meeting of the Advisory Committee on Immunization Practices; February 26, 2014; Atlanta, GA. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2014-02/04-Flu-Flannery.pdf. Accessed August 6, 2014.
Reticulated erythematous patch on teenager’s foot
An 18-year-old Caucasian male sought care for an ill-defined reticulated patch on his right plantar arch (FIGURE 1). The patient said that the lesion had gradually appeared 2 years earlier, had grown slowly, and was occasionally itchy. Physical exam revealed a lacy violaceous, hyperpigmented, reticulated patch that was blanchable and nontender to palpation.
Our patient denied having a history of trauma to the area or a coagulation or connective tissue disorder. The lesion didn’t vary with temperature or season, and there were no known triggers. The patient’s left plantar arch was unchanged.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Erythema ab igne
Upon further questioning, the patient acknowledged that he occasionally rested his bare feet around a portable heater under his desk while using his computer for a few hours each day (FIGURE 2). He often kept his right foot on the heater while he let his left foot rest on the ground. A punch biopsy was performed; the findings, when combined with the patient’s report of having exposed his foot to heat, supported the diagnosis of erythema ab igne (EAI).

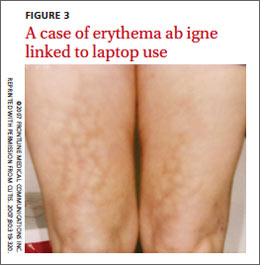
EAI commonly presents as an asymptomatic reticulated erythematous to violaceous patch in an area of the body that has been in contact with heat.1 It originally was described on the bilateral anterior lower extremities after prolonged exposure to burning stoves or open fires.1 With the advent of central heating, these presentations have decreased, but there has been a resurgence of EAI with atypical distributions as a result of evolving technology and new heating sources. Reported causes of EAI include heating pads,1,2 laptop computers3 (FIGURE 3), car seat heaters,4 hot water bottles, popcorn bags, cell phones,5 and space heaters that have resulted in patches on the breast, thighs, arms, and, in our patient, foot.1-5
Blood work, biopsy can help narrow the differential
The differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectasia. Livedo reticularis can be associated with autoimmune conditions and coagulopathies. Livedo racemosa is a typical sign of Sneddon’s syndrome and can be seen in up to 70% of patients with antiphospholipid-antibody syndrome and systemic lupus erythematosus. Diagnosis of these conditions is confirmed by elevated coagulation factors, presence of autoimmune antibodies, or history of cerebrovascular accident.6 These tests would be normal in EAI.
Histopathologic changes observed in EAI include an atrophic epidermis with an interface dermatitis, vasodilation, and dermal pigmentation. Necrotic keratinocytes and focal hyperkeratosis can be noted, along with squamous atypia. Although these changes are nonspecific, they can be used to confirm an EAI diagnosis in patients for whom the affected area has been exposed to a heat source.
Histologically, EAI is similar to actinic keratosis, with epidermal changes showing squamous atypia.2 Due to the similarities, these lesions are sometimes referred to as “thermal keratosis.” Some researchers have suggested that the thermal heat may induce epithelial changes in the same way that ultraviolet light produces epithelial changes.7
Rarely, EAI can turn into cancer. There have been a few reported cases of EAI transforming into squamous cell carcinoma or Merkel cell carcinoma; squamous cell carcinoma is more common, and tends to occur after a long latent period (up to 30 years).7-9 EAI lesions often begin as a chronic ulcer and tend not to heal. If the lesion continues to evolve (ie, ulcerate), a biopsy may be warranted to rule out a malignant transformation.
Eliminate heat exposure, consider a topical treatment
Treatment of acute EAI involves eliminating the offending heat source. The hyperpigmentation will slowly resolve over months to years.4 Persistent exposure to heat sources can lead to chronic EAI, which is more difficult to eliminate.
Because hyperpigmentation can be visually unappealing and emotionally distressing, some patients prefer active treatment. EAI has been effectively treated with 4% hydroquinone topical cream twice a day and tretinoin topical cream at night.2,10,11 Lesions that have epithelial atypia have improved with 5-fluorouracil topical cream.7
EAI also has been successfully treated with laser therapy with the 1064-nm Q-switched Nd:YAG laser with low fluence at 2-week intervals.9
Our patient declined topical therapy. He improved after a few months of avoiding the heater under his desk.
CORRESPONDENCE
Megan Morrison, DO, 5333 McAuley Drive Suite R-5003, Ypsilanti, MI 48197; [email protected]
1. Huynh N, Sarma D, Huerter C. Erythema ab igne: a case report and review of the literature. Cutis. 2011;88:290-292.
2. Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
3. Fu LW, Vender R. Erythema ab igne caused by laptop computer gaming—a case report. Int J Dermatol. 2012;51:716-717.
4. Brodell D, Mostow EN. Automobile seat heater-induced erythema ab igne. Arch Dermtol. 2012;148:264-265.
5. Dela Rosa K, Satter EK. Erythematous patches on the chest. Arch Dermatol. 2012;148:113-118.
6. Uthman IW, Khamashta MA. Livedo racemosa: a striking dermatological sign for antiphospholipid syndrome. J Rheumatol. 2006;33:2379-2382.
7. Bilic M, Adams B. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973-974.
8. Jones CS, Tyring SK, Lee PC, et al. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Arch Dermatol. 1998;124:110-113.
9. Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011;37:551-553.
10. Cardona LFC, Parsons AC, Sangueza OP. Erythematous lesions on the back of a man: challenge. Erythema ab igne. Am J Dermatopathol. 2011;33:185,199.
11. Sahl WJ, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. J Am Acad Dermatol. 1992;27:109-110.
An 18-year-old Caucasian male sought care for an ill-defined reticulated patch on his right plantar arch (FIGURE 1). The patient said that the lesion had gradually appeared 2 years earlier, had grown slowly, and was occasionally itchy. Physical exam revealed a lacy violaceous, hyperpigmented, reticulated patch that was blanchable and nontender to palpation.
Our patient denied having a history of trauma to the area or a coagulation or connective tissue disorder. The lesion didn’t vary with temperature or season, and there were no known triggers. The patient’s left plantar arch was unchanged.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Erythema ab igne
Upon further questioning, the patient acknowledged that he occasionally rested his bare feet around a portable heater under his desk while using his computer for a few hours each day (FIGURE 2). He often kept his right foot on the heater while he let his left foot rest on the ground. A punch biopsy was performed; the findings, when combined with the patient’s report of having exposed his foot to heat, supported the diagnosis of erythema ab igne (EAI).
EAI commonly presents as an asymptomatic reticulated erythematous to violaceous patch in an area of the body that has been in contact with heat.1 It originally was described on the bilateral anterior lower extremities after prolonged exposure to burning stoves or open fires.1 With the advent of central heating, these presentations have decreased, but there has been a resurgence of EAI with atypical distributions as a result of evolving technology and new heating sources. Reported causes of EAI include heating pads,1,2 laptop computers3 (FIGURE 3), car seat heaters,4 hot water bottles, popcorn bags, cell phones,5 and space heaters that have resulted in patches on the breast, thighs, arms, and, in our patient, foot.1-5
Blood work, biopsy can help narrow the differential
The differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectasia. Livedo reticularis can be associated with autoimmune conditions and coagulopathies. Livedo racemosa is a typical sign of Sneddon’s syndrome and can be seen in up to 70% of patients with antiphospholipid-antibody syndrome and systemic lupus erythematosus. Diagnosis of these conditions is confirmed by elevated coagulation factors, presence of autoimmune antibodies, or history of cerebrovascular accident.6 These tests would be normal in EAI.
Histopathologic changes observed in EAI include an atrophic epidermis with an interface dermatitis, vasodilation, and dermal pigmentation. Necrotic keratinocytes and focal hyperkeratosis can be noted, along with squamous atypia. Although these changes are nonspecific, they can be used to confirm an EAI diagnosis in patients for whom the affected area has been exposed to a heat source.
Histologically, EAI is similar to actinic keratosis, with epidermal changes showing squamous atypia.2 Due to the similarities, these lesions are sometimes referred to as “thermal keratosis.” Some researchers have suggested that the thermal heat may induce epithelial changes in the same way that ultraviolet light produces epithelial changes.7
Rarely, EAI can turn into cancer. There have been a few reported cases of EAI transforming into squamous cell carcinoma or Merkel cell carcinoma; squamous cell carcinoma is more common, and tends to occur after a long latent period (up to 30 years).7-9 EAI lesions often begin as a chronic ulcer and tend not to heal. If the lesion continues to evolve (ie, ulcerate), a biopsy may be warranted to rule out a malignant transformation.
Eliminate heat exposure, consider a topical treatment
Treatment of acute EAI involves eliminating the offending heat source. The hyperpigmentation will slowly resolve over months to years.4 Persistent exposure to heat sources can lead to chronic EAI, which is more difficult to eliminate.
Because hyperpigmentation can be visually unappealing and emotionally distressing, some patients prefer active treatment. EAI has been effectively treated with 4% hydroquinone topical cream twice a day and tretinoin topical cream at night.2,10,11 Lesions that have epithelial atypia have improved with 5-fluorouracil topical cream.7
EAI also has been successfully treated with laser therapy with the 1064-nm Q-switched Nd:YAG laser with low fluence at 2-week intervals.9
Our patient declined topical therapy. He improved after a few months of avoiding the heater under his desk.
CORRESPONDENCE
Megan Morrison, DO, 5333 McAuley Drive Suite R-5003, Ypsilanti, MI 48197; [email protected]
An 18-year-old Caucasian male sought care for an ill-defined reticulated patch on his right plantar arch (FIGURE 1). The patient said that the lesion had gradually appeared 2 years earlier, had grown slowly, and was occasionally itchy. Physical exam revealed a lacy violaceous, hyperpigmented, reticulated patch that was blanchable and nontender to palpation.
Our patient denied having a history of trauma to the area or a coagulation or connective tissue disorder. The lesion didn’t vary with temperature or season, and there were no known triggers. The patient’s left plantar arch was unchanged.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Erythema ab igne
Upon further questioning, the patient acknowledged that he occasionally rested his bare feet around a portable heater under his desk while using his computer for a few hours each day (FIGURE 2). He often kept his right foot on the heater while he let his left foot rest on the ground. A punch biopsy was performed; the findings, when combined with the patient’s report of having exposed his foot to heat, supported the diagnosis of erythema ab igne (EAI).
EAI commonly presents as an asymptomatic reticulated erythematous to violaceous patch in an area of the body that has been in contact with heat.1 It originally was described on the bilateral anterior lower extremities after prolonged exposure to burning stoves or open fires.1 With the advent of central heating, these presentations have decreased, but there has been a resurgence of EAI with atypical distributions as a result of evolving technology and new heating sources. Reported causes of EAI include heating pads,1,2 laptop computers3 (FIGURE 3), car seat heaters,4 hot water bottles, popcorn bags, cell phones,5 and space heaters that have resulted in patches on the breast, thighs, arms, and, in our patient, foot.1-5
Blood work, biopsy can help narrow the differential
The differential for EAI includes livedo reticularis, livedo racemosa, cutis marmorata, and cutis marmorata telangiectasia. Livedo reticularis can be associated with autoimmune conditions and coagulopathies. Livedo racemosa is a typical sign of Sneddon’s syndrome and can be seen in up to 70% of patients with antiphospholipid-antibody syndrome and systemic lupus erythematosus. Diagnosis of these conditions is confirmed by elevated coagulation factors, presence of autoimmune antibodies, or history of cerebrovascular accident.6 These tests would be normal in EAI.
Histopathologic changes observed in EAI include an atrophic epidermis with an interface dermatitis, vasodilation, and dermal pigmentation. Necrotic keratinocytes and focal hyperkeratosis can be noted, along with squamous atypia. Although these changes are nonspecific, they can be used to confirm an EAI diagnosis in patients for whom the affected area has been exposed to a heat source.
Histologically, EAI is similar to actinic keratosis, with epidermal changes showing squamous atypia.2 Due to the similarities, these lesions are sometimes referred to as “thermal keratosis.” Some researchers have suggested that the thermal heat may induce epithelial changes in the same way that ultraviolet light produces epithelial changes.7
Rarely, EAI can turn into cancer. There have been a few reported cases of EAI transforming into squamous cell carcinoma or Merkel cell carcinoma; squamous cell carcinoma is more common, and tends to occur after a long latent period (up to 30 years).7-9 EAI lesions often begin as a chronic ulcer and tend not to heal. If the lesion continues to evolve (ie, ulcerate), a biopsy may be warranted to rule out a malignant transformation.
Eliminate heat exposure, consider a topical treatment
Treatment of acute EAI involves eliminating the offending heat source. The hyperpigmentation will slowly resolve over months to years.4 Persistent exposure to heat sources can lead to chronic EAI, which is more difficult to eliminate.
Because hyperpigmentation can be visually unappealing and emotionally distressing, some patients prefer active treatment. EAI has been effectively treated with 4% hydroquinone topical cream twice a day and tretinoin topical cream at night.2,10,11 Lesions that have epithelial atypia have improved with 5-fluorouracil topical cream.7
EAI also has been successfully treated with laser therapy with the 1064-nm Q-switched Nd:YAG laser with low fluence at 2-week intervals.9
Our patient declined topical therapy. He improved after a few months of avoiding the heater under his desk.
CORRESPONDENCE
Megan Morrison, DO, 5333 McAuley Drive Suite R-5003, Ypsilanti, MI 48197; [email protected]
1. Huynh N, Sarma D, Huerter C. Erythema ab igne: a case report and review of the literature. Cutis. 2011;88:290-292.
2. Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
3. Fu LW, Vender R. Erythema ab igne caused by laptop computer gaming—a case report. Int J Dermatol. 2012;51:716-717.
4. Brodell D, Mostow EN. Automobile seat heater-induced erythema ab igne. Arch Dermtol. 2012;148:264-265.
5. Dela Rosa K, Satter EK. Erythematous patches on the chest. Arch Dermatol. 2012;148:113-118.
6. Uthman IW, Khamashta MA. Livedo racemosa: a striking dermatological sign for antiphospholipid syndrome. J Rheumatol. 2006;33:2379-2382.
7. Bilic M, Adams B. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973-974.
8. Jones CS, Tyring SK, Lee PC, et al. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Arch Dermatol. 1998;124:110-113.
9. Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011;37:551-553.
10. Cardona LFC, Parsons AC, Sangueza OP. Erythematous lesions on the back of a man: challenge. Erythema ab igne. Am J Dermatopathol. 2011;33:185,199.
11. Sahl WJ, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. J Am Acad Dermatol. 1992;27:109-110.
1. Huynh N, Sarma D, Huerter C. Erythema ab igne: a case report and review of the literature. Cutis. 2011;88:290-292.
2. Tan S, Bertucci V. Erythema ab igne: an old condition new again. CMAJ. 2000;162:77-78.
3. Fu LW, Vender R. Erythema ab igne caused by laptop computer gaming—a case report. Int J Dermatol. 2012;51:716-717.
4. Brodell D, Mostow EN. Automobile seat heater-induced erythema ab igne. Arch Dermtol. 2012;148:264-265.
5. Dela Rosa K, Satter EK. Erythematous patches on the chest. Arch Dermatol. 2012;148:113-118.
6. Uthman IW, Khamashta MA. Livedo racemosa: a striking dermatological sign for antiphospholipid syndrome. J Rheumatol. 2006;33:2379-2382.
7. Bilic M, Adams B. Erythema ab igne induced by a laptop computer. J Am Acad Dermatol. 2004;50:973-974.
8. Jones CS, Tyring SK, Lee PC, et al. Development of neuroendocrine (Merkel cell) carcinoma mixed with squamous cell carcinoma in erythema ab igne. Arch Dermatol. 1998;124:110-113.
9. Cho S, Jung JY, Lee JH. Erythema ab igne successfully treated using 1,064-nm Q-switched neodymium-doped yttrium aluminum garnet laser with low fluence. Dermatol Surg. 2011;37:551-553.
10. Cardona LFC, Parsons AC, Sangueza OP. Erythematous lesions on the back of a man: challenge. Erythema ab igne. Am J Dermatopathol. 2011;33:185,199.
11. Sahl WJ, Taira JW. Erythema ab igne: treatment with 5-fluorouracil cream. J Am Acad Dermatol. 1992;27:109-110.

Fever, wet cough, rash—Dx?
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
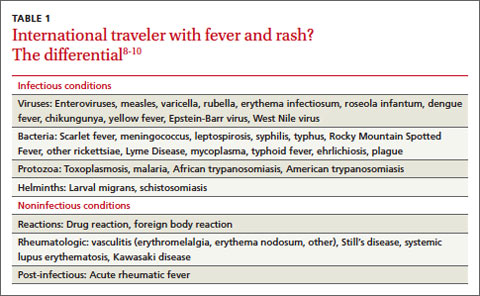
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
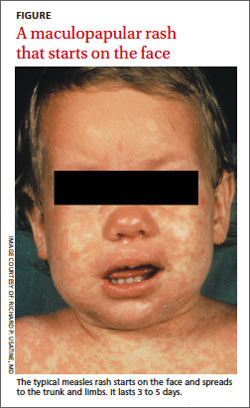
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness

Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness
Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness
Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
Unhealthy drug use: How to screen, when to intervene

› Implement screening and brief intervention (SBI) for unhealthy drug use among adults in primary care. C
› Consult the National Institute on Drug Abuse’s Screening for Drug Use in General Medical Settings Resource Guide for step-by-step recommendations for implementing a drug SBI. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Joe M, age 54, comes to your office for his annual physical examination. As part of your routine screening, you ask him, “In the past year, how often have you used alcohol, tobacco, prescription drugs for nonmedical reasons, or illegal drugs?” Mr. M replies that he does not use tobacco and has not used prescription drugs for nonmedical reasons, but drinks alcohol weekly and uses cannabis and cocaine monthly.
If Mr. M were your patient, what would your next steps be?
One promising approach to alleviate substance use problems is screening and brief intervention (SBI), and—when appropriate—referral to an addiction treatment program. With strong evidence of efficacy, alcohol and tobacco SBIs have become recommended “usual” care for adults in primary care settings.1,2 Strategies for applying SBI to unhealthy drug use (“drug” SBI) in primary care have been a natural extension of the evidence that supports alcohol and tobacco SBIs.
Screening for unhealthy drug use consists of a quick risk appraisal, typically via a brief questionnaire.3-5 Patients with a positive screen then receive a more detailed assessment to estimate the extent of their substance use and severity of its consequences. If appropriate, this is followed with a brief intervention (BI), which is a time-limited, patient-centered counseling session designed to reduce substance use and/or related harm.4-6
So how can you make use of a drug SBI in your office setting?
Drug screening: What the evidence says
Currently, evidence on drug SBI is limited. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against universal drug SBI.4,7,8 The scarcity of validated screening and assessment tools that are brief enough to be used in primary care, patients’ use of multiple drugs, and confidentiality concerns likely contribute to the relative lack of research in this area.3,6,9
To our knowledge, results of only 5 randomized controlled trials (RCTs) of drug SBI that included universal screening have been published in English. Here is what these researchers found:
Bernstein et al10 investigated the efficacy of SBI for cocaine and heroin use among 23,699 adults in urgent care, women’s health, and homeless clinic settings. They randomized 1175 patients who screened positive on the Drug Abuse Screening Test11 to receive a single BI session or a handout. At 6 months, patients in the BI group were 1.5 times more likely than controls to be abstinent from cocaine (22% vs 17%; P=.045) and heroin (40% vs 31%; P=.050).
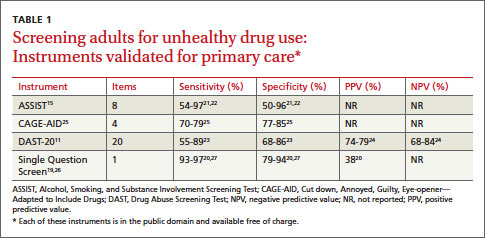
Zahradnik et al12 examined the efficacy of SBI in reducing the use of potentially addictive prescription drugs by hospitalized patients. After researchers screened 6000 inpatients, 126 patients who used, abused, or were dependent on prescription medications were randomized to receive 2 BI sessions or an information booklet. At 3 months, 52% of patients in the BI group had a ≥25% reduction in their daily doses of prescription drugs, compared to 30% in the control group (P=.017),12 However, this difference was not maintained at 12 months.13
Humeniuk et al14 evaluated the efficacy of SBI among primary care patients ages 16 to 62 years in Australia, Brazil, India, and the United States who used cannabis, cocaine, amphetamines, or opioids. Patients were screened and assessed using the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST).15 Patients whose scores indicated they had a moderate risk for problem use (N=731) were randomly assigned to receive a BI or usual care. At 3 months, patients in the BI group reported a reduction in total score for “illicit substance involvement” compared to controls (P<.001). However, country-specific analyses found that BI did not have a statistically significant effect on drug use by those in the United States (N=218), possibly due to protocol differences and a greater exposure to previous substance use treatment among US patients.14
Saitz et al16 investigated the efficacy of drug SBI among primary care patients (N=528) who had been screened using the ASSIST. The most commonly used drugs were marijuana (63% of patients), cocaine (19%), and opioids (17%). Patients were randomly assigned to a 10- to 15-minute BI, a 30- to 45-minute intervention, or no intervention. BI did not show efficacy for decreasing drug use at 6-month follow-up.
Roy-Byrne et al17 screened 10,337 primary care patients of “safety net” clinics serving low-income populations. Of 1621 patients who screened positive for problem drug use, 868 were enrolled and randomly assigned to either a BI group (one-time BI using motivational interviewing, a telephone booster session, and a handout, which included relevant drug-use related information and a list of substance abuse resources) or enhanced care as usual (usual care plus a handout). Over 12 months of follow-up, there were no differences between groups in drug use or related consequences. However, a subgroup analysis suggested that compared to enhanced usual care, BI may help reduce emergency department use and increase admissions to specialized drug treatment programs among those with severe drug problems.
In addition to these 5 RCTs, a large, prospective, uncontrolled trial looked at the efficacy of drug BI among 459,599 patients from various medical settings, including primary care.18 Twenty-three percent of patients screened positive for illicit drug use and were recommended BI (16%), brief treatment (3%) or specialty treatment (4%). At a 6-month follow-up, drug use among these patients decreased by 68% and heavy alcohol use decreased by 39% (P<.001). In addition, general health, mental health, employment, housing status, and criminal behavior improved among patients recommended for brief or specialty treatments (P<.001). Although this trial lent support for the efficacy of drug SBI in primary care, it was limited by the lack of a control group and low follow-up rates at some sites.
A step-by-step approach to drug screening
Although a variety of instruments can be used to screen and assess patients for unhealthy drug use, few have been validated in primary care (TABLE 1).11,15,19-27 Despite limited evidence, multiple professional organizations, including the American Academy of Family Physicians28 and the American Psychiatric Association,26 support routine implementation of drug SBI in primary care.
The National Institute on Drug Abuse (NIDA)’s Screening for Drug Use in General Medical Settings Resource Guide19 provides a step-by-step approach to drug SBI in primary care and other general medical settings. Primarily focused on drug SBI in adults, the NIDA guide details the use of the NIDA Quick Screen and the NIDA-Modified ASSIST (NM ASSIST). These tools are available as a PDF that you can print out and complete manually (http://www.drugabuse.gov/sites/default/ files/pdf/nmassist.pdf) or as a series of forms you can complete online (http://www.drugabuse.gov/nmassist). The NIDA guide also conveniently incorporates links to alcohol and tobacco SBI recommendations.
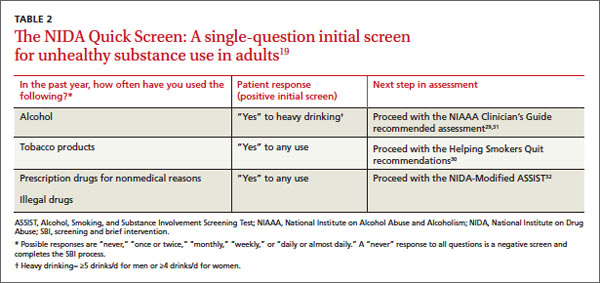
What to ask first. Following the NIDA algorithm, first screen patients with the Quick Screen, which consists of a single question about substance use: “In the past year, how often have you used alcohol, tobacco products, prescription drugs for nonmedical reasons, or illegal drugs?" (TABLE 2).19,29-32
A negative Quick Screen (a “never” response for all substances) completes the process. Patients with a negative screen should be praised and encouraged to continue their healthy lifestyle, then rescreened annually.
For patients who respond “Yes” to heavy drinking or any tobacco use, the NIDA guide recommends proceeding with an alcohol29 or tobacco30 SBI, respectively, and provides links to appropriate resources (TABLE 2).19,29-32 Those who screen positive for drugs (“Yes” to any drug use in the past year) should receive a detailed assessment using the NM ASSIST32 to determine their risk level for developing a substance use disorder. The NM ASSIST includes 8 questions about the patient’s desire for, use of, and problems related to the use of a wide range of drugs, including cannabis, cocaine, methamphetamine, hallucinogens, and other substances (eg, “In the past 3 months, how often have you used the following substances?” “How often have you had a strong desire or urge to use this substance?” “How often has your use of this substance led to health, social, legal or financial problems?”). The score on the NM ASSIST is used to calculate the patient’s risk level as low, moderate, or high.
For patients who use more than one drug, this risk level is scored separately for each drug and may differ from drug to drug. Multi-drug assessment can become time-consuming and may not be appropriate in some patients, especially if time is an issue (eg, the patient would like to focus on other concerns) or the patient is not interested in addressing certain drugs. In general, the decision about which substances to address should be clinically-driven, tailored to the needs of an individual patient. Focusing on the substance with the highest risk score or associated with the patient’s expressed greatest motivation to change may produce the best results.
CASE › Based on Mr. M’s response to your Quick Screen indicating he drinks alcohol and uses illicit drugs, you administer the NM ASSIST to perform a detailed assessment. His answer to a screening question for problematic alcohol use is negative (In the past year, he has not had >4 drinks in a day). Next, you calculate his NM ASSIST-based risk scores for cannabis and cocaine, and determine he is at moderate risk for developing problems due to cannabis use and at high risk for developing problems based on his use of cocaine. You also note Mr. M’s blood pressure (BP) is elevated (155/90 mm hg).
Conducting a brief intervention
Depending on the patient’s risk level for developing a substance use disorder, he or she should receive either brief advice (for those at low risk) or a BI (for those at moderate or high risk) and, if needed, a referral to treatment. Two popular approaches are FRAMES (Feedback, Responsibility, Advice, Menu of Strategies, Empathy, Self-efficacy) and the NIDA-recommended 5 As intervention. The latter approach entails Asking the patient about his drug use (via the Quick Screen); Advising the patient about his drug use by providing specific medical advice on why he should stop or cut down, and how; Assessing the patient’s readiness to quit or reduce use; Assisting the patient in making a change by creating a plan with specific goals; and Arranging a follow-up visit or specialty assessment and treatment by making referrals as appropriate.19
What about children and adolescents? Implementing a drug SBI in young patients often entails overcoming unique challenges and ethical dilemmas. Although the American Academy of Pediatrics recommends SBI for unhealthy drug and alcohol use among children and adolescents,33,34 the USPSTF did not find sufficient evidence to recommend the practice.1,8,35 Screening for drug use in minors often is complicated by questions about the age at which to start routine screening and issues related to confidentiality and parental involvement. The Center for Adolescent Health and the Law and the National Institute on Alcohol Abuse and Alcoholism provide useful resources related to youth SBI, including guidance on when to consider breeching a child’s confidentiality by engaging parents or guardians (TABLE 3).
TABLE 3
Resources
NIDA Resource Guide NIDA-Modified ASSIST Coding for SBI reimbursement SAMHSA’s Treatment Services Locator NIDA’s List of Community Treatment Programs SAMHSA Opioid Overdose Toolkit Buprenorphine training program Center for Adolescent Health and the Law NIAAA Alcohol Screening and Brief Intervention for Youth |
Help is available for securing treatment, reimbursement
In addition to NIDA, many other organizations offer resources to assist clinicians in using drug SBI and helping patients obtain treatment (TABLE 3). For reimbursement, the Centers for Medicare and Medicaid Services has adopted billing codes for SBI services.36,37 The Substance Abuse and Mental Health Services Administration (SAMHSA)’s Behavioral Health Treatment Services Locator and NIDA’s National Drug Abuse Treatment Clinical Trials Network List of Associated Community Treatment Programs can assist clinicians and patients in finding specialty treatment programs. Self-help groups such as Narcotics Anonymous, Alcoholic Anonymous, or Self-Managment and Recovery Training may help alleviate problems related to insurance coverage, location, and/or timing of services.
SAMHSA’s Opioid Overdose Toolkit provides guidance to clinicians and patients on ways to reduce the risk of overdose. Physicians also can complete a short training program in office-based buprenorphine maintenance therapy to provide evidence-based care to patients with opioid dependence; more details about this program are available from http://www.buppractice.com.
CASE › You decide to use the 5 as intervention with Mr. M. You explain to him that he is at high risk of developing a substance use disorder. You also discuss his elevated BP and the possible negative effects of drug use, especially cocaine, on BP. You advise him that medically it is in his best interest to stop using cocaine and stop or reduce using cannabis. When you ask Mr. M about his readiness to change his drug use, he expresses moderate interest in stopping cocaine but is not willing to reduce his cannabis use. At this time, he is not willing to discuss these issues further (“I’ll think about that”) or create a specific plan. You assure him of your ongoing support, provide him with resources on specialty treatment programs should he wish to consider those, and schedule a follow-up visit in 2 weeks to address BP and, if the patient agrees, drug use.
CORRESPONDENCE
Aleksandra Zgierska, MD, Phd, Department of Family Medicine, University of Wisconsin School of Medicine and Public Health, 1100 Delaplaine Court, Madison, WI 53715-1896; [email protected]
1. US Preventive Services Task Force. Screening and behavioral counseling interventions in primary care to reduce alcohol misuse. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/ uspsdrin.htm. Accessed March 4, 2013.
2. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspstbac2.htm. Accessed March 4, 2014.
3. Saitz R, Alford DP, Bernstein J, et al. Screening and brief intervention for unhealthy drug use in primary care settings: randomized clinical trials are needed. J Addict Med. 2010;4: 123-130.
4. Pilowsky DJ, Wu LT. Screening for alcohol and drug use disorders among adults in primary care: a review. Subst Abuse Rehabil. 2012;3:25-34.
5. Substance Abuse and Mental Health Services Administration. Screening, Brief Intervention, and Referral to Treatment (SBIRT). Substance Abuse and Mental Health Services Administration Web site. Available at: http://www.samhsa.gov/ prevention/sbirt/. Accessed March 4, 2014.
6. Squires LE, Alford DP, Bernstein J, et al. Clinical case discussion: screening and brief intervention for drug use in primary care. J Addict Med. 2010;4:131-136.
7. Krupski A, Joesch JM, Dunn C, et al. Testing the effects of brief intervention in primary care for problem drug use in a randomized controlled trial: rationale, design, and methods. Addict Sci Clin Pract. 2012;7:27.
8. US Preventive Services Task Force. Screening for illicit drug use. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsdrug.htm. Accessed March 4, 2014.
9. Lanier D, Ko S. Screening in Primary Care Settings for Illicit Drug Use: Assessment of Screening Instruments—A Supplemental Evidence Update for the U.S. Preventive Services Task Force. AHRQ Publication No. 08-05108-EF-2. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
10. Bernstein J, Bernstein E, Tassiopoulos K, et al. Brief motivational intervention at a clinic visit reduces cocaine and heroin use. Drug Alcohol Depend. 2005;77:49-59.
11. Skinner HA. The drug abuse screening test. Addict Behav. 1982;7:363-371.
12. Zahradnik A, Otto C, Crackau B, et al. Randomized controlled trial of a brief intervention for problematic prescription drug use in non-treatment-seeking patients. Addiction. 2009;104:109-117.
13. Otto C, Crackau B, Löhrmann I, et al. Brief intervention in general hospital for problematic prescription drug use: 12-month outcome. Drug Alcohol Depend. 2009;105:221-226.
14. Humeniuk R, Ali R, Babor T, et al. A randomized controlled trial of a brief intervention for illicit drugs linked to the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in clients recruited from primary health-care settings in four countries. Addiction. 2012;107:957-966.
15. WHO ASSIST Working Group. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction. 2002;97:1183-1194.
16. Saitz R, Palfai TP, Cheng DM, et al. Screening and brief intervention for drug use in primary care: the Assessing Screening Plus brief Intervention’s Resulting Efficacy to stop drug use (ASPIRE) randomized trial. Addict Sci Clin Pract. 2013;8(suppl 1):A61.
17. Roy-Byrne P, Bumgardner K, Krupski A, et al. Brief intervention for problem drug use in safety-net primary care settings: a randomized clinical trial. JAMA. 2014;312(5):492-501.
18. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99:280-295.
19. National Institute on Drug Abuse. Resource guide: Screening for drug use in general medical settings. National Institute on Drug Abuse Web site. Available at: http://www.drugabuse. gov/publications/resource-guide. Accessed March 8, 2014.
20. Saitz R, Cheng DM, Allensworth-Davies D, et al. The ability of single screening questions for unhealthy alcohol and other drug use to identify substance dependence in primary care. J Stud Alcohol Drugs. 2014;75:153-157.
21. Newcombe DA, Humeniuk RE, Ali R. Validation of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): report of results from the Australian site. Drug Alcohol Rev. 2005;24:217-226.
22. Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking And Substance Involvement Screening Test (ASSIST). Addiction. 2008;103:1039-1047.
23. Mdege ND, Lang J. Screening instruments for detecting illicit drug use/abuse that could be useful in general hospital wards: a systematic review. Addict Behav. 2011;36:1111-1119.
24. Cassidy CM, Schmitz N, Malla A. Validation of the alcohol use disorders identification test and the drug abuse screening test in first episode psychosis. Can J Psychiatry. 2008;53:26-33.
25. Brown RL, Rounds LA. Conjoint screening questionnaires for alcohol and other drug abuse: criterion validity in a primary care practice. Wis Med J. 1995;94:135-140.
26. American Psychiatric Association. Position statement on substance use disorders. American Psychiatric Association Web site. Available at: http://www.psychiatry.org/File%20Library/Advocacy%20and%20Newsroom/Position%20Statements/ps2012_Substance.pdf. Accessed March 4, 2014.
27. Smith PC, Schmidt SM, Allensworth-Davies D, et al. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170:1155-1160.
28. American Academy of Family Physicians. Substance abuse and addiction. American Academy of Family Physicians Web site. Available at: http://www.aafp.org/about/policies/all/substance-abuse.html. Accessed March 4, 2014.
29. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: A clinician’s guide. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed March 4, 2014.
30. US Department of Health and Human Services Public Health Service. Helping smokers quit: A guide for clinicians. US Department of Health and Human Services Public Health Service Web site. Available at: http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/tobacco/clinicians//clinhlpsmkqt/. Accessed March 4, 2014.
31. National Institute on Alcohol Abuse and Alcoholism. A Pocket Guide for Alcohol Screening and Brief Intervention. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/pocketguide/pocket_guide.htm. Accessed July 30, 2014.
32. National Institute on Drug Abuse. NIDA-Quick Screen V1.0. National Institute on Drug Abuse Web site. Available at: http://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf. Accessed March 4, 2014.
33. Committee on Substance Abuse, Levy SJ, Kokotailo PK. Substance use screening, brief intervention, and referral to treatment for pediatricians. Pediatrics. 2011;128:e1330-e1340.
34. Kulig JW; American Academy of Pediatrics Committee on Substance Abuse. Tobacco, alcohol, and other drugs: the role of the pediatrician in prevention, identification, and management of substance abuse. Pediatrics. 2005;115:816-821.
35. US Preventive Services Task Force. Primary care behavioral interventions to reduce the nonmedical use of drugs in children and adolescents. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsnonmed.htm. Accessed March 4, 2014.
36. Centers for Medicare & Medicaid Services. Screening, Brief Intervention, and Referral to Treatment (SBIRT) services. Centers for Medicare & Medicaid Services Web site. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/sbirt_factsheet_icn904084.pdf. Accessed March 4, 2014.
37. Substance Abuse and Mental Health Services Administration. Coding for screening and brief intervention reimbursement. Substance Abuse and Mental Health Services Administration Web site. Available at: http://beta.samhsa.gov/sbirt/coding-reimbursement. Accessed August 4, 2014.
› Implement screening and brief intervention (SBI) for unhealthy drug use among adults in primary care. C
› Consult the National Institute on Drug Abuse’s Screening for Drug Use in General Medical Settings Resource Guide for step-by-step recommendations for implementing a drug SBI. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Joe M, age 54, comes to your office for his annual physical examination. As part of your routine screening, you ask him, “In the past year, how often have you used alcohol, tobacco, prescription drugs for nonmedical reasons, or illegal drugs?” Mr. M replies that he does not use tobacco and has not used prescription drugs for nonmedical reasons, but drinks alcohol weekly and uses cannabis and cocaine monthly.
If Mr. M were your patient, what would your next steps be?
One promising approach to alleviate substance use problems is screening and brief intervention (SBI), and—when appropriate—referral to an addiction treatment program. With strong evidence of efficacy, alcohol and tobacco SBIs have become recommended “usual” care for adults in primary care settings.1,2 Strategies for applying SBI to unhealthy drug use (“drug” SBI) in primary care have been a natural extension of the evidence that supports alcohol and tobacco SBIs.
Screening for unhealthy drug use consists of a quick risk appraisal, typically via a brief questionnaire.3-5 Patients with a positive screen then receive a more detailed assessment to estimate the extent of their substance use and severity of its consequences. If appropriate, this is followed with a brief intervention (BI), which is a time-limited, patient-centered counseling session designed to reduce substance use and/or related harm.4-6
So how can you make use of a drug SBI in your office setting?
Drug screening: What the evidence says
Currently, evidence on drug SBI is limited. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against universal drug SBI.4,7,8 The scarcity of validated screening and assessment tools that are brief enough to be used in primary care, patients’ use of multiple drugs, and confidentiality concerns likely contribute to the relative lack of research in this area.3,6,9
To our knowledge, results of only 5 randomized controlled trials (RCTs) of drug SBI that included universal screening have been published in English. Here is what these researchers found:
Bernstein et al10 investigated the efficacy of SBI for cocaine and heroin use among 23,699 adults in urgent care, women’s health, and homeless clinic settings. They randomized 1175 patients who screened positive on the Drug Abuse Screening Test11 to receive a single BI session or a handout. At 6 months, patients in the BI group were 1.5 times more likely than controls to be abstinent from cocaine (22% vs 17%; P=.045) and heroin (40% vs 31%; P=.050).
Zahradnik et al12 examined the efficacy of SBI in reducing the use of potentially addictive prescription drugs by hospitalized patients. After researchers screened 6000 inpatients, 126 patients who used, abused, or were dependent on prescription medications were randomized to receive 2 BI sessions or an information booklet. At 3 months, 52% of patients in the BI group had a ≥25% reduction in their daily doses of prescription drugs, compared to 30% in the control group (P=.017),12 However, this difference was not maintained at 12 months.13
Humeniuk et al14 evaluated the efficacy of SBI among primary care patients ages 16 to 62 years in Australia, Brazil, India, and the United States who used cannabis, cocaine, amphetamines, or opioids. Patients were screened and assessed using the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST).15 Patients whose scores indicated they had a moderate risk for problem use (N=731) were randomly assigned to receive a BI or usual care. At 3 months, patients in the BI group reported a reduction in total score for “illicit substance involvement” compared to controls (P<.001). However, country-specific analyses found that BI did not have a statistically significant effect on drug use by those in the United States (N=218), possibly due to protocol differences and a greater exposure to previous substance use treatment among US patients.14
Saitz et al16 investigated the efficacy of drug SBI among primary care patients (N=528) who had been screened using the ASSIST. The most commonly used drugs were marijuana (63% of patients), cocaine (19%), and opioids (17%). Patients were randomly assigned to a 10- to 15-minute BI, a 30- to 45-minute intervention, or no intervention. BI did not show efficacy for decreasing drug use at 6-month follow-up.
Roy-Byrne et al17 screened 10,337 primary care patients of “safety net” clinics serving low-income populations. Of 1621 patients who screened positive for problem drug use, 868 were enrolled and randomly assigned to either a BI group (one-time BI using motivational interviewing, a telephone booster session, and a handout, which included relevant drug-use related information and a list of substance abuse resources) or enhanced care as usual (usual care plus a handout). Over 12 months of follow-up, there were no differences between groups in drug use or related consequences. However, a subgroup analysis suggested that compared to enhanced usual care, BI may help reduce emergency department use and increase admissions to specialized drug treatment programs among those with severe drug problems.
In addition to these 5 RCTs, a large, prospective, uncontrolled trial looked at the efficacy of drug BI among 459,599 patients from various medical settings, including primary care.18 Twenty-three percent of patients screened positive for illicit drug use and were recommended BI (16%), brief treatment (3%) or specialty treatment (4%). At a 6-month follow-up, drug use among these patients decreased by 68% and heavy alcohol use decreased by 39% (P<.001). In addition, general health, mental health, employment, housing status, and criminal behavior improved among patients recommended for brief or specialty treatments (P<.001). Although this trial lent support for the efficacy of drug SBI in primary care, it was limited by the lack of a control group and low follow-up rates at some sites.
A step-by-step approach to drug screening
Although a variety of instruments can be used to screen and assess patients for unhealthy drug use, few have been validated in primary care (TABLE 1).11,15,19-27 Despite limited evidence, multiple professional organizations, including the American Academy of Family Physicians28 and the American Psychiatric Association,26 support routine implementation of drug SBI in primary care.
The National Institute on Drug Abuse (NIDA)’s Screening for Drug Use in General Medical Settings Resource Guide19 provides a step-by-step approach to drug SBI in primary care and other general medical settings. Primarily focused on drug SBI in adults, the NIDA guide details the use of the NIDA Quick Screen and the NIDA-Modified ASSIST (NM ASSIST). These tools are available as a PDF that you can print out and complete manually (http://www.drugabuse.gov/sites/default/ files/pdf/nmassist.pdf) or as a series of forms you can complete online (http://www.drugabuse.gov/nmassist). The NIDA guide also conveniently incorporates links to alcohol and tobacco SBI recommendations.
What to ask first. Following the NIDA algorithm, first screen patients with the Quick Screen, which consists of a single question about substance use: “In the past year, how often have you used alcohol, tobacco products, prescription drugs for nonmedical reasons, or illegal drugs?" (TABLE 2).19,29-32
A negative Quick Screen (a “never” response for all substances) completes the process. Patients with a negative screen should be praised and encouraged to continue their healthy lifestyle, then rescreened annually.
For patients who respond “Yes” to heavy drinking or any tobacco use, the NIDA guide recommends proceeding with an alcohol29 or tobacco30 SBI, respectively, and provides links to appropriate resources (TABLE 2).19,29-32 Those who screen positive for drugs (“Yes” to any drug use in the past year) should receive a detailed assessment using the NM ASSIST32 to determine their risk level for developing a substance use disorder. The NM ASSIST includes 8 questions about the patient’s desire for, use of, and problems related to the use of a wide range of drugs, including cannabis, cocaine, methamphetamine, hallucinogens, and other substances (eg, “In the past 3 months, how often have you used the following substances?” “How often have you had a strong desire or urge to use this substance?” “How often has your use of this substance led to health, social, legal or financial problems?”). The score on the NM ASSIST is used to calculate the patient’s risk level as low, moderate, or high.
For patients who use more than one drug, this risk level is scored separately for each drug and may differ from drug to drug. Multi-drug assessment can become time-consuming and may not be appropriate in some patients, especially if time is an issue (eg, the patient would like to focus on other concerns) or the patient is not interested in addressing certain drugs. In general, the decision about which substances to address should be clinically-driven, tailored to the needs of an individual patient. Focusing on the substance with the highest risk score or associated with the patient’s expressed greatest motivation to change may produce the best results.
CASE › Based on Mr. M’s response to your Quick Screen indicating he drinks alcohol and uses illicit drugs, you administer the NM ASSIST to perform a detailed assessment. His answer to a screening question for problematic alcohol use is negative (In the past year, he has not had >4 drinks in a day). Next, you calculate his NM ASSIST-based risk scores for cannabis and cocaine, and determine he is at moderate risk for developing problems due to cannabis use and at high risk for developing problems based on his use of cocaine. You also note Mr. M’s blood pressure (BP) is elevated (155/90 mm hg).
Conducting a brief intervention
Depending on the patient’s risk level for developing a substance use disorder, he or she should receive either brief advice (for those at low risk) or a BI (for those at moderate or high risk) and, if needed, a referral to treatment. Two popular approaches are FRAMES (Feedback, Responsibility, Advice, Menu of Strategies, Empathy, Self-efficacy) and the NIDA-recommended 5 As intervention. The latter approach entails Asking the patient about his drug use (via the Quick Screen); Advising the patient about his drug use by providing specific medical advice on why he should stop or cut down, and how; Assessing the patient’s readiness to quit or reduce use; Assisting the patient in making a change by creating a plan with specific goals; and Arranging a follow-up visit or specialty assessment and treatment by making referrals as appropriate.19
What about children and adolescents? Implementing a drug SBI in young patients often entails overcoming unique challenges and ethical dilemmas. Although the American Academy of Pediatrics recommends SBI for unhealthy drug and alcohol use among children and adolescents,33,34 the USPSTF did not find sufficient evidence to recommend the practice.1,8,35 Screening for drug use in minors often is complicated by questions about the age at which to start routine screening and issues related to confidentiality and parental involvement. The Center for Adolescent Health and the Law and the National Institute on Alcohol Abuse and Alcoholism provide useful resources related to youth SBI, including guidance on when to consider breeching a child’s confidentiality by engaging parents or guardians (TABLE 3).
TABLE 3
Resources
NIDA Resource Guide NIDA-Modified ASSIST Coding for SBI reimbursement SAMHSA’s Treatment Services Locator NIDA’s List of Community Treatment Programs SAMHSA Opioid Overdose Toolkit Buprenorphine training program Center for Adolescent Health and the Law NIAAA Alcohol Screening and Brief Intervention for Youth |
Help is available for securing treatment, reimbursement
In addition to NIDA, many other organizations offer resources to assist clinicians in using drug SBI and helping patients obtain treatment (TABLE 3). For reimbursement, the Centers for Medicare and Medicaid Services has adopted billing codes for SBI services.36,37 The Substance Abuse and Mental Health Services Administration (SAMHSA)’s Behavioral Health Treatment Services Locator and NIDA’s National Drug Abuse Treatment Clinical Trials Network List of Associated Community Treatment Programs can assist clinicians and patients in finding specialty treatment programs. Self-help groups such as Narcotics Anonymous, Alcoholic Anonymous, or Self-Managment and Recovery Training may help alleviate problems related to insurance coverage, location, and/or timing of services.
SAMHSA’s Opioid Overdose Toolkit provides guidance to clinicians and patients on ways to reduce the risk of overdose. Physicians also can complete a short training program in office-based buprenorphine maintenance therapy to provide evidence-based care to patients with opioid dependence; more details about this program are available from http://www.buppractice.com.
CASE › You decide to use the 5 as intervention with Mr. M. You explain to him that he is at high risk of developing a substance use disorder. You also discuss his elevated BP and the possible negative effects of drug use, especially cocaine, on BP. You advise him that medically it is in his best interest to stop using cocaine and stop or reduce using cannabis. When you ask Mr. M about his readiness to change his drug use, he expresses moderate interest in stopping cocaine but is not willing to reduce his cannabis use. At this time, he is not willing to discuss these issues further (“I’ll think about that”) or create a specific plan. You assure him of your ongoing support, provide him with resources on specialty treatment programs should he wish to consider those, and schedule a follow-up visit in 2 weeks to address BP and, if the patient agrees, drug use.
CORRESPONDENCE
Aleksandra Zgierska, MD, Phd, Department of Family Medicine, University of Wisconsin School of Medicine and Public Health, 1100 Delaplaine Court, Madison, WI 53715-1896; [email protected]
› Implement screening and brief intervention (SBI) for unhealthy drug use among adults in primary care. C
› Consult the National Institute on Drug Abuse’s Screening for Drug Use in General Medical Settings Resource Guide for step-by-step recommendations for implementing a drug SBI. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Joe M, age 54, comes to your office for his annual physical examination. As part of your routine screening, you ask him, “In the past year, how often have you used alcohol, tobacco, prescription drugs for nonmedical reasons, or illegal drugs?” Mr. M replies that he does not use tobacco and has not used prescription drugs for nonmedical reasons, but drinks alcohol weekly and uses cannabis and cocaine monthly.
If Mr. M were your patient, what would your next steps be?
One promising approach to alleviate substance use problems is screening and brief intervention (SBI), and—when appropriate—referral to an addiction treatment program. With strong evidence of efficacy, alcohol and tobacco SBIs have become recommended “usual” care for adults in primary care settings.1,2 Strategies for applying SBI to unhealthy drug use (“drug” SBI) in primary care have been a natural extension of the evidence that supports alcohol and tobacco SBIs.
Screening for unhealthy drug use consists of a quick risk appraisal, typically via a brief questionnaire.3-5 Patients with a positive screen then receive a more detailed assessment to estimate the extent of their substance use and severity of its consequences. If appropriate, this is followed with a brief intervention (BI), which is a time-limited, patient-centered counseling session designed to reduce substance use and/or related harm.4-6
So how can you make use of a drug SBI in your office setting?
Drug screening: What the evidence says
Currently, evidence on drug SBI is limited. The US Preventive Services Task Force (USPSTF) found insufficient evidence to recommend for or against universal drug SBI.4,7,8 The scarcity of validated screening and assessment tools that are brief enough to be used in primary care, patients’ use of multiple drugs, and confidentiality concerns likely contribute to the relative lack of research in this area.3,6,9
To our knowledge, results of only 5 randomized controlled trials (RCTs) of drug SBI that included universal screening have been published in English. Here is what these researchers found:
Bernstein et al10 investigated the efficacy of SBI for cocaine and heroin use among 23,699 adults in urgent care, women’s health, and homeless clinic settings. They randomized 1175 patients who screened positive on the Drug Abuse Screening Test11 to receive a single BI session or a handout. At 6 months, patients in the BI group were 1.5 times more likely than controls to be abstinent from cocaine (22% vs 17%; P=.045) and heroin (40% vs 31%; P=.050).
Zahradnik et al12 examined the efficacy of SBI in reducing the use of potentially addictive prescription drugs by hospitalized patients. After researchers screened 6000 inpatients, 126 patients who used, abused, or were dependent on prescription medications were randomized to receive 2 BI sessions or an information booklet. At 3 months, 52% of patients in the BI group had a ≥25% reduction in their daily doses of prescription drugs, compared to 30% in the control group (P=.017),12 However, this difference was not maintained at 12 months.13
Humeniuk et al14 evaluated the efficacy of SBI among primary care patients ages 16 to 62 years in Australia, Brazil, India, and the United States who used cannabis, cocaine, amphetamines, or opioids. Patients were screened and assessed using the World Health Organization Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST).15 Patients whose scores indicated they had a moderate risk for problem use (N=731) were randomly assigned to receive a BI or usual care. At 3 months, patients in the BI group reported a reduction in total score for “illicit substance involvement” compared to controls (P<.001). However, country-specific analyses found that BI did not have a statistically significant effect on drug use by those in the United States (N=218), possibly due to protocol differences and a greater exposure to previous substance use treatment among US patients.14
Saitz et al16 investigated the efficacy of drug SBI among primary care patients (N=528) who had been screened using the ASSIST. The most commonly used drugs were marijuana (63% of patients), cocaine (19%), and opioids (17%). Patients were randomly assigned to a 10- to 15-minute BI, a 30- to 45-minute intervention, or no intervention. BI did not show efficacy for decreasing drug use at 6-month follow-up.
Roy-Byrne et al17 screened 10,337 primary care patients of “safety net” clinics serving low-income populations. Of 1621 patients who screened positive for problem drug use, 868 were enrolled and randomly assigned to either a BI group (one-time BI using motivational interviewing, a telephone booster session, and a handout, which included relevant drug-use related information and a list of substance abuse resources) or enhanced care as usual (usual care plus a handout). Over 12 months of follow-up, there were no differences between groups in drug use or related consequences. However, a subgroup analysis suggested that compared to enhanced usual care, BI may help reduce emergency department use and increase admissions to specialized drug treatment programs among those with severe drug problems.
In addition to these 5 RCTs, a large, prospective, uncontrolled trial looked at the efficacy of drug BI among 459,599 patients from various medical settings, including primary care.18 Twenty-three percent of patients screened positive for illicit drug use and were recommended BI (16%), brief treatment (3%) or specialty treatment (4%). At a 6-month follow-up, drug use among these patients decreased by 68% and heavy alcohol use decreased by 39% (P<.001). In addition, general health, mental health, employment, housing status, and criminal behavior improved among patients recommended for brief or specialty treatments (P<.001). Although this trial lent support for the efficacy of drug SBI in primary care, it was limited by the lack of a control group and low follow-up rates at some sites.
A step-by-step approach to drug screening
Although a variety of instruments can be used to screen and assess patients for unhealthy drug use, few have been validated in primary care (TABLE 1).11,15,19-27 Despite limited evidence, multiple professional organizations, including the American Academy of Family Physicians28 and the American Psychiatric Association,26 support routine implementation of drug SBI in primary care.
The National Institute on Drug Abuse (NIDA)’s Screening for Drug Use in General Medical Settings Resource Guide19 provides a step-by-step approach to drug SBI in primary care and other general medical settings. Primarily focused on drug SBI in adults, the NIDA guide details the use of the NIDA Quick Screen and the NIDA-Modified ASSIST (NM ASSIST). These tools are available as a PDF that you can print out and complete manually (http://www.drugabuse.gov/sites/default/ files/pdf/nmassist.pdf) or as a series of forms you can complete online (http://www.drugabuse.gov/nmassist). The NIDA guide also conveniently incorporates links to alcohol and tobacco SBI recommendations.
What to ask first. Following the NIDA algorithm, first screen patients with the Quick Screen, which consists of a single question about substance use: “In the past year, how often have you used alcohol, tobacco products, prescription drugs for nonmedical reasons, or illegal drugs?" (TABLE 2).19,29-32
A negative Quick Screen (a “never” response for all substances) completes the process. Patients with a negative screen should be praised and encouraged to continue their healthy lifestyle, then rescreened annually.
For patients who respond “Yes” to heavy drinking or any tobacco use, the NIDA guide recommends proceeding with an alcohol29 or tobacco30 SBI, respectively, and provides links to appropriate resources (TABLE 2).19,29-32 Those who screen positive for drugs (“Yes” to any drug use in the past year) should receive a detailed assessment using the NM ASSIST32 to determine their risk level for developing a substance use disorder. The NM ASSIST includes 8 questions about the patient’s desire for, use of, and problems related to the use of a wide range of drugs, including cannabis, cocaine, methamphetamine, hallucinogens, and other substances (eg, “In the past 3 months, how often have you used the following substances?” “How often have you had a strong desire or urge to use this substance?” “How often has your use of this substance led to health, social, legal or financial problems?”). The score on the NM ASSIST is used to calculate the patient’s risk level as low, moderate, or high.
For patients who use more than one drug, this risk level is scored separately for each drug and may differ from drug to drug. Multi-drug assessment can become time-consuming and may not be appropriate in some patients, especially if time is an issue (eg, the patient would like to focus on other concerns) or the patient is not interested in addressing certain drugs. In general, the decision about which substances to address should be clinically-driven, tailored to the needs of an individual patient. Focusing on the substance with the highest risk score or associated with the patient’s expressed greatest motivation to change may produce the best results.
CASE › Based on Mr. M’s response to your Quick Screen indicating he drinks alcohol and uses illicit drugs, you administer the NM ASSIST to perform a detailed assessment. His answer to a screening question for problematic alcohol use is negative (In the past year, he has not had >4 drinks in a day). Next, you calculate his NM ASSIST-based risk scores for cannabis and cocaine, and determine he is at moderate risk for developing problems due to cannabis use and at high risk for developing problems based on his use of cocaine. You also note Mr. M’s blood pressure (BP) is elevated (155/90 mm hg).
Conducting a brief intervention
Depending on the patient’s risk level for developing a substance use disorder, he or she should receive either brief advice (for those at low risk) or a BI (for those at moderate or high risk) and, if needed, a referral to treatment. Two popular approaches are FRAMES (Feedback, Responsibility, Advice, Menu of Strategies, Empathy, Self-efficacy) and the NIDA-recommended 5 As intervention. The latter approach entails Asking the patient about his drug use (via the Quick Screen); Advising the patient about his drug use by providing specific medical advice on why he should stop or cut down, and how; Assessing the patient’s readiness to quit or reduce use; Assisting the patient in making a change by creating a plan with specific goals; and Arranging a follow-up visit or specialty assessment and treatment by making referrals as appropriate.19
What about children and adolescents? Implementing a drug SBI in young patients often entails overcoming unique challenges and ethical dilemmas. Although the American Academy of Pediatrics recommends SBI for unhealthy drug and alcohol use among children and adolescents,33,34 the USPSTF did not find sufficient evidence to recommend the practice.1,8,35 Screening for drug use in minors often is complicated by questions about the age at which to start routine screening and issues related to confidentiality and parental involvement. The Center for Adolescent Health and the Law and the National Institute on Alcohol Abuse and Alcoholism provide useful resources related to youth SBI, including guidance on when to consider breeching a child’s confidentiality by engaging parents or guardians (TABLE 3).
TABLE 3
Resources
NIDA Resource Guide NIDA-Modified ASSIST Coding for SBI reimbursement SAMHSA’s Treatment Services Locator NIDA’s List of Community Treatment Programs SAMHSA Opioid Overdose Toolkit Buprenorphine training program Center for Adolescent Health and the Law NIAAA Alcohol Screening and Brief Intervention for Youth |
Help is available for securing treatment, reimbursement
In addition to NIDA, many other organizations offer resources to assist clinicians in using drug SBI and helping patients obtain treatment (TABLE 3). For reimbursement, the Centers for Medicare and Medicaid Services has adopted billing codes for SBI services.36,37 The Substance Abuse and Mental Health Services Administration (SAMHSA)’s Behavioral Health Treatment Services Locator and NIDA’s National Drug Abuse Treatment Clinical Trials Network List of Associated Community Treatment Programs can assist clinicians and patients in finding specialty treatment programs. Self-help groups such as Narcotics Anonymous, Alcoholic Anonymous, or Self-Managment and Recovery Training may help alleviate problems related to insurance coverage, location, and/or timing of services.
SAMHSA’s Opioid Overdose Toolkit provides guidance to clinicians and patients on ways to reduce the risk of overdose. Physicians also can complete a short training program in office-based buprenorphine maintenance therapy to provide evidence-based care to patients with opioid dependence; more details about this program are available from http://www.buppractice.com.
CASE › You decide to use the 5 as intervention with Mr. M. You explain to him that he is at high risk of developing a substance use disorder. You also discuss his elevated BP and the possible negative effects of drug use, especially cocaine, on BP. You advise him that medically it is in his best interest to stop using cocaine and stop or reduce using cannabis. When you ask Mr. M about his readiness to change his drug use, he expresses moderate interest in stopping cocaine but is not willing to reduce his cannabis use. At this time, he is not willing to discuss these issues further (“I’ll think about that”) or create a specific plan. You assure him of your ongoing support, provide him with resources on specialty treatment programs should he wish to consider those, and schedule a follow-up visit in 2 weeks to address BP and, if the patient agrees, drug use.
CORRESPONDENCE
Aleksandra Zgierska, MD, Phd, Department of Family Medicine, University of Wisconsin School of Medicine and Public Health, 1100 Delaplaine Court, Madison, WI 53715-1896; [email protected]
1. US Preventive Services Task Force. Screening and behavioral counseling interventions in primary care to reduce alcohol misuse. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/ uspsdrin.htm. Accessed March 4, 2013.
2. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspstbac2.htm. Accessed March 4, 2014.
3. Saitz R, Alford DP, Bernstein J, et al. Screening and brief intervention for unhealthy drug use in primary care settings: randomized clinical trials are needed. J Addict Med. 2010;4: 123-130.
4. Pilowsky DJ, Wu LT. Screening for alcohol and drug use disorders among adults in primary care: a review. Subst Abuse Rehabil. 2012;3:25-34.
5. Substance Abuse and Mental Health Services Administration. Screening, Brief Intervention, and Referral to Treatment (SBIRT). Substance Abuse and Mental Health Services Administration Web site. Available at: http://www.samhsa.gov/ prevention/sbirt/. Accessed March 4, 2014.
6. Squires LE, Alford DP, Bernstein J, et al. Clinical case discussion: screening and brief intervention for drug use in primary care. J Addict Med. 2010;4:131-136.
7. Krupski A, Joesch JM, Dunn C, et al. Testing the effects of brief intervention in primary care for problem drug use in a randomized controlled trial: rationale, design, and methods. Addict Sci Clin Pract. 2012;7:27.
8. US Preventive Services Task Force. Screening for illicit drug use. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsdrug.htm. Accessed March 4, 2014.
9. Lanier D, Ko S. Screening in Primary Care Settings for Illicit Drug Use: Assessment of Screening Instruments—A Supplemental Evidence Update for the U.S. Preventive Services Task Force. AHRQ Publication No. 08-05108-EF-2. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
10. Bernstein J, Bernstein E, Tassiopoulos K, et al. Brief motivational intervention at a clinic visit reduces cocaine and heroin use. Drug Alcohol Depend. 2005;77:49-59.
11. Skinner HA. The drug abuse screening test. Addict Behav. 1982;7:363-371.
12. Zahradnik A, Otto C, Crackau B, et al. Randomized controlled trial of a brief intervention for problematic prescription drug use in non-treatment-seeking patients. Addiction. 2009;104:109-117.
13. Otto C, Crackau B, Löhrmann I, et al. Brief intervention in general hospital for problematic prescription drug use: 12-month outcome. Drug Alcohol Depend. 2009;105:221-226.
14. Humeniuk R, Ali R, Babor T, et al. A randomized controlled trial of a brief intervention for illicit drugs linked to the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in clients recruited from primary health-care settings in four countries. Addiction. 2012;107:957-966.
15. WHO ASSIST Working Group. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction. 2002;97:1183-1194.
16. Saitz R, Palfai TP, Cheng DM, et al. Screening and brief intervention for drug use in primary care: the Assessing Screening Plus brief Intervention’s Resulting Efficacy to stop drug use (ASPIRE) randomized trial. Addict Sci Clin Pract. 2013;8(suppl 1):A61.
17. Roy-Byrne P, Bumgardner K, Krupski A, et al. Brief intervention for problem drug use in safety-net primary care settings: a randomized clinical trial. JAMA. 2014;312(5):492-501.
18. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99:280-295.
19. National Institute on Drug Abuse. Resource guide: Screening for drug use in general medical settings. National Institute on Drug Abuse Web site. Available at: http://www.drugabuse. gov/publications/resource-guide. Accessed March 8, 2014.
20. Saitz R, Cheng DM, Allensworth-Davies D, et al. The ability of single screening questions for unhealthy alcohol and other drug use to identify substance dependence in primary care. J Stud Alcohol Drugs. 2014;75:153-157.
21. Newcombe DA, Humeniuk RE, Ali R. Validation of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): report of results from the Australian site. Drug Alcohol Rev. 2005;24:217-226.
22. Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking And Substance Involvement Screening Test (ASSIST). Addiction. 2008;103:1039-1047.
23. Mdege ND, Lang J. Screening instruments for detecting illicit drug use/abuse that could be useful in general hospital wards: a systematic review. Addict Behav. 2011;36:1111-1119.
24. Cassidy CM, Schmitz N, Malla A. Validation of the alcohol use disorders identification test and the drug abuse screening test in first episode psychosis. Can J Psychiatry. 2008;53:26-33.
25. Brown RL, Rounds LA. Conjoint screening questionnaires for alcohol and other drug abuse: criterion validity in a primary care practice. Wis Med J. 1995;94:135-140.
26. American Psychiatric Association. Position statement on substance use disorders. American Psychiatric Association Web site. Available at: http://www.psychiatry.org/File%20Library/Advocacy%20and%20Newsroom/Position%20Statements/ps2012_Substance.pdf. Accessed March 4, 2014.
27. Smith PC, Schmidt SM, Allensworth-Davies D, et al. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170:1155-1160.
28. American Academy of Family Physicians. Substance abuse and addiction. American Academy of Family Physicians Web site. Available at: http://www.aafp.org/about/policies/all/substance-abuse.html. Accessed March 4, 2014.
29. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: A clinician’s guide. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed March 4, 2014.
30. US Department of Health and Human Services Public Health Service. Helping smokers quit: A guide for clinicians. US Department of Health and Human Services Public Health Service Web site. Available at: http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/tobacco/clinicians//clinhlpsmkqt/. Accessed March 4, 2014.
31. National Institute on Alcohol Abuse and Alcoholism. A Pocket Guide for Alcohol Screening and Brief Intervention. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/pocketguide/pocket_guide.htm. Accessed July 30, 2014.
32. National Institute on Drug Abuse. NIDA-Quick Screen V1.0. National Institute on Drug Abuse Web site. Available at: http://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf. Accessed March 4, 2014.
33. Committee on Substance Abuse, Levy SJ, Kokotailo PK. Substance use screening, brief intervention, and referral to treatment for pediatricians. Pediatrics. 2011;128:e1330-e1340.
34. Kulig JW; American Academy of Pediatrics Committee on Substance Abuse. Tobacco, alcohol, and other drugs: the role of the pediatrician in prevention, identification, and management of substance abuse. Pediatrics. 2005;115:816-821.
35. US Preventive Services Task Force. Primary care behavioral interventions to reduce the nonmedical use of drugs in children and adolescents. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsnonmed.htm. Accessed March 4, 2014.
36. Centers for Medicare & Medicaid Services. Screening, Brief Intervention, and Referral to Treatment (SBIRT) services. Centers for Medicare & Medicaid Services Web site. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/sbirt_factsheet_icn904084.pdf. Accessed March 4, 2014.
37. Substance Abuse and Mental Health Services Administration. Coding for screening and brief intervention reimbursement. Substance Abuse and Mental Health Services Administration Web site. Available at: http://beta.samhsa.gov/sbirt/coding-reimbursement. Accessed August 4, 2014.
1. US Preventive Services Task Force. Screening and behavioral counseling interventions in primary care to reduce alcohol misuse. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/ uspsdrin.htm. Accessed March 4, 2013.
2. US Preventive Services Task Force. Counseling and interventions to prevent tobacco use and tobacco-caused disease in adults and pregnant women. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspstbac2.htm. Accessed March 4, 2014.
3. Saitz R, Alford DP, Bernstein J, et al. Screening and brief intervention for unhealthy drug use in primary care settings: randomized clinical trials are needed. J Addict Med. 2010;4: 123-130.
4. Pilowsky DJ, Wu LT. Screening for alcohol and drug use disorders among adults in primary care: a review. Subst Abuse Rehabil. 2012;3:25-34.
5. Substance Abuse and Mental Health Services Administration. Screening, Brief Intervention, and Referral to Treatment (SBIRT). Substance Abuse and Mental Health Services Administration Web site. Available at: http://www.samhsa.gov/ prevention/sbirt/. Accessed March 4, 2014.
6. Squires LE, Alford DP, Bernstein J, et al. Clinical case discussion: screening and brief intervention for drug use in primary care. J Addict Med. 2010;4:131-136.
7. Krupski A, Joesch JM, Dunn C, et al. Testing the effects of brief intervention in primary care for problem drug use in a randomized controlled trial: rationale, design, and methods. Addict Sci Clin Pract. 2012;7:27.
8. US Preventive Services Task Force. Screening for illicit drug use. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsdrug.htm. Accessed March 4, 2014.
9. Lanier D, Ko S. Screening in Primary Care Settings for Illicit Drug Use: Assessment of Screening Instruments—A Supplemental Evidence Update for the U.S. Preventive Services Task Force. AHRQ Publication No. 08-05108-EF-2. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
10. Bernstein J, Bernstein E, Tassiopoulos K, et al. Brief motivational intervention at a clinic visit reduces cocaine and heroin use. Drug Alcohol Depend. 2005;77:49-59.
11. Skinner HA. The drug abuse screening test. Addict Behav. 1982;7:363-371.
12. Zahradnik A, Otto C, Crackau B, et al. Randomized controlled trial of a brief intervention for problematic prescription drug use in non-treatment-seeking patients. Addiction. 2009;104:109-117.
13. Otto C, Crackau B, Löhrmann I, et al. Brief intervention in general hospital for problematic prescription drug use: 12-month outcome. Drug Alcohol Depend. 2009;105:221-226.
14. Humeniuk R, Ali R, Babor T, et al. A randomized controlled trial of a brief intervention for illicit drugs linked to the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in clients recruited from primary health-care settings in four countries. Addiction. 2012;107:957-966.
15. WHO ASSIST Working Group. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction. 2002;97:1183-1194.
16. Saitz R, Palfai TP, Cheng DM, et al. Screening and brief intervention for drug use in primary care: the Assessing Screening Plus brief Intervention’s Resulting Efficacy to stop drug use (ASPIRE) randomized trial. Addict Sci Clin Pract. 2013;8(suppl 1):A61.
17. Roy-Byrne P, Bumgardner K, Krupski A, et al. Brief intervention for problem drug use in safety-net primary care settings: a randomized clinical trial. JAMA. 2014;312(5):492-501.
18. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99:280-295.
19. National Institute on Drug Abuse. Resource guide: Screening for drug use in general medical settings. National Institute on Drug Abuse Web site. Available at: http://www.drugabuse. gov/publications/resource-guide. Accessed March 8, 2014.
20. Saitz R, Cheng DM, Allensworth-Davies D, et al. The ability of single screening questions for unhealthy alcohol and other drug use to identify substance dependence in primary care. J Stud Alcohol Drugs. 2014;75:153-157.
21. Newcombe DA, Humeniuk RE, Ali R. Validation of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): report of results from the Australian site. Drug Alcohol Rev. 2005;24:217-226.
22. Humeniuk R, Ali R, Babor TF, et al. Validation of the Alcohol, Smoking And Substance Involvement Screening Test (ASSIST). Addiction. 2008;103:1039-1047.
23. Mdege ND, Lang J. Screening instruments for detecting illicit drug use/abuse that could be useful in general hospital wards: a systematic review. Addict Behav. 2011;36:1111-1119.
24. Cassidy CM, Schmitz N, Malla A. Validation of the alcohol use disorders identification test and the drug abuse screening test in first episode psychosis. Can J Psychiatry. 2008;53:26-33.
25. Brown RL, Rounds LA. Conjoint screening questionnaires for alcohol and other drug abuse: criterion validity in a primary care practice. Wis Med J. 1995;94:135-140.
26. American Psychiatric Association. Position statement on substance use disorders. American Psychiatric Association Web site. Available at: http://www.psychiatry.org/File%20Library/Advocacy%20and%20Newsroom/Position%20Statements/ps2012_Substance.pdf. Accessed March 4, 2014.
27. Smith PC, Schmidt SM, Allensworth-Davies D, et al. A single-question screening test for drug use in primary care. Arch Intern Med. 2010;170:1155-1160.
28. American Academy of Family Physicians. Substance abuse and addiction. American Academy of Family Physicians Web site. Available at: http://www.aafp.org/about/policies/all/substance-abuse.html. Accessed March 4, 2014.
29. National Institute on Alcohol Abuse and Alcoholism. Helping patients who drink too much: A clinician’s guide. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/CliniciansGuide2005/clinicians_guide.htm. Accessed March 4, 2014.
30. US Department of Health and Human Services Public Health Service. Helping smokers quit: A guide for clinicians. US Department of Health and Human Services Public Health Service Web site. Available at: http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/tobacco/clinicians//clinhlpsmkqt/. Accessed March 4, 2014.
31. National Institute on Alcohol Abuse and Alcoholism. A Pocket Guide for Alcohol Screening and Brief Intervention. National Institute on Alcohol Abuse and Alcoholism Web site. Available at: http://pubs.niaaa.nih.gov/publications/Practitioner/pocketguide/pocket_guide.htm. Accessed July 30, 2014.
32. National Institute on Drug Abuse. NIDA-Quick Screen V1.0. National Institute on Drug Abuse Web site. Available at: http://www.drugabuse.gov/sites/default/files/pdf/nmassist.pdf. Accessed March 4, 2014.
33. Committee on Substance Abuse, Levy SJ, Kokotailo PK. Substance use screening, brief intervention, and referral to treatment for pediatricians. Pediatrics. 2011;128:e1330-e1340.
34. Kulig JW; American Academy of Pediatrics Committee on Substance Abuse. Tobacco, alcohol, and other drugs: the role of the pediatrician in prevention, identification, and management of substance abuse. Pediatrics. 2005;115:816-821.
35. US Preventive Services Task Force. Primary care behavioral interventions to reduce the nonmedical use of drugs in children and adolescents. US Preventive Services Task Force Web site. Available at: http://www.uspreventiveservicestaskforce.org/uspstf/uspsnonmed.htm. Accessed March 4, 2014.
36. Centers for Medicare & Medicaid Services. Screening, Brief Intervention, and Referral to Treatment (SBIRT) services. Centers for Medicare & Medicaid Services Web site. Available at: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/sbirt_factsheet_icn904084.pdf. Accessed March 4, 2014.
37. Substance Abuse and Mental Health Services Administration. Coding for screening and brief intervention reimbursement. Substance Abuse and Mental Health Services Administration Web site. Available at: http://beta.samhsa.gov/sbirt/coding-reimbursement. Accessed August 4, 2014.

Why celiac disease is so easy to miss
› Do not rely on symptoms or symptom response to
a gluten-free diet alone
to diagnose celiac disease (CD); this approach does not differentiate CD from non-celiac gluten sensitivity. B
› Use HLA-DQ2 and -DQ8 genotype testing to effectively rule out the disease in selected clinical situations. B
› Test for CD in any
patient who has unexplained elevated serum aminotransferase levels, even in the absence of CD symptoms. A
› Screen all first-degree relatives of patients with
CD by testing for immunoglobulin A (IgA) tissue transglutaminase antibodies and serum IgA levels. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › It was a clinical conundrum. A 2011 case study1 described a 33-year-old woman with a 10-year history of progressive, debilitating pain and weakness. The patient had not received a unifying diagnosis or effective treatment despite multiple diagnostic tests and different recommendations from multiple specialists. The diagnosis remained elusive until a rheumatologist agreed to reexamine the case.
While reviewing the woman’s thick chart, the rheumatologist noted a series of negative results from upper and lower endoscopies and abdominal scans. Further investigation revealed an almost obfuscated clue—blood tests performed 2 years earlier that were positive for celiac disease (CD). However, a small intestine biopsy, which normally is done to confirm the diagnosis, was never performed.
The rheumatologist made a tentative diagnosis of CD and referred her to a nutritionist, who recommended the patient adhere to a strict gluten-free diet. Within 3 months, the patient experienced marked improvement and returned to work.
CD is an often-missed diagnosis. According to a study based on National Health and Nutrition Examination Survey data, only 17% of patients with CD are aware they have the disease.2 As such, it is imperative that primary care physicians familiarize themselves with CD’s myriad clinical presentations, diagnosis, and treatment.3-6
Gluten triggers an immune response in genetically susceptible patients
CD initially was known as “celiac sprue” because it shares characteristics with tropical sprue—diarrhea, malabsorption, and emaciation. It is a unique T-cell autoimmune enteropathy that is precipitated in genetically susceptible individuals by the ingestion of gluten, the major storage protein of wheat, barley, and rye.3,7
Upon ingestion, gluten breaks down to gliadin, which provokes an immune response in the intestinal mucosa of patients with CD. This response results in an inflammatory reaction, primarily in the upper small intestine, that destroys the absorption surface and causes villous atrophy, leading to nutrient malabsorption and chronic diarrhea.8 CD is associated with significant morbidity due to an abnormal excretion of fat (steatorrhea) and varying degrees of malabsorption of vitamins A, D, and K, as well as B complex vitamins including B12 and folate; carbohydrates; protein; water; and minerals such as magnesium, calcium, and iron.9
CD develops only in individuals who possess alleles that encode for HLA-DQ2 or HLA-DQ8 proteins, products of 2 of the HLA genes. And while 30% of Caucasians carry the HLA-DQ2 allele and virtually 100% consume wheat, only 1 in 100 will develop CD.3,10,11 Although the genes are necessary, it is the interplay between genes (both HLA and non-HLA associated) and environment (ie, gluten) that leads to the intestinal mucosa damage typical of the disease. The HLA-DQ region also is associated with increased risk of type 1 diabetes, which might explain the correlation of CD to a host of other autoimmune disorders, including Graves’ disease and rheumatoid arthritis.8,10,11
Increased prevalence reflects better recognition of celiac disease
CD affects .6% to 1% of the population worldwide, with wide regional variation.3 Before the development of serologic assays in the 1970s, CD was a clinical diagnosis based on classic symptoms. With the advent of assays for immunoglobulin A (IgA) antibodies, the prevalence of CD has drastically increased to the current estimates of 1:250 to 1:500.4,5 The prevalence will continue to increase as clinicians become more aware of the different presentations of the disease, which are described below.
CD runs in families. Most patients with CD have a family history of the disease based on inheritance of the HLA alleles. A US study determined that the prevalence of CD was 1:22 in first-degree relatives and 1:39 in second-degree relatives of patients with biopsy-proven CD.12
Less than half of patients have GI symptoms
The classic presentation of CD involves a constellation of signs and symptoms of malabsorption: diarrhea, muscle wasting, and weight loss. Other typical gastrointestinal (GI) symptoms include bloating, flatulence, and abdominal pain.
Recognizing CD can be challenging, however, because <50% of patients diagnosed with CD present with these classic GI symptoms.3 About 50% of CD patients present with extra-intestinal symptoms, such as iron deficiency anemia, aphthous stomatitis, chronic fatigue, osteopenia, and dental enamel hypoplasia.3,8,13 Other possible non-GI symptoms include abnormal liver function test results and skin disorders such as dermatitis herpetiformis, a pruritic rash with cutaneous IgA deposits.3,8 In addition, many patients are asymptomatic.14 This highly variable clinical picture is due to the genetic and immunologic basis of the disease, extent of mucosal injury, and patients’ dietary habits, gender, and age of onset.15 A common clue that suggests a patient may have CD is unexplained iron deficiency anemia that does not improve with oral iron supplementation.4,13
Because symptoms may be intermittent, a patient may delay seeking care until he or she develops secondary manifestations, which often are debilitating and overshadow the GI complaints. Chronic complications of untreated CD include lymphoma and adenocarcinomas of the jejunum, recurrent miscarriages, neurologic disorders, osteoporosis, and hyposplenism.3,4,8
Since CD can manifest with widely varying symptoms, some researchers believe the disease should be classified into 3 categories based on presentation: classic CD, which presents with diarrhea, weight loss, malabsorption, and vitamin deficiency; atypical CD, which presents with minimal GI symptoms but can include anemia, neurologic symptoms, arthritis, or infertility; and asymptomatic CD, which typically displays no symptoms but usually is identified on incidental screening.3,8,16 Non-celiac gluten sensitivity is a distinct condition in which the body reacts adversely to gluten; it is not an autoimmune disease with an inflammatory response.
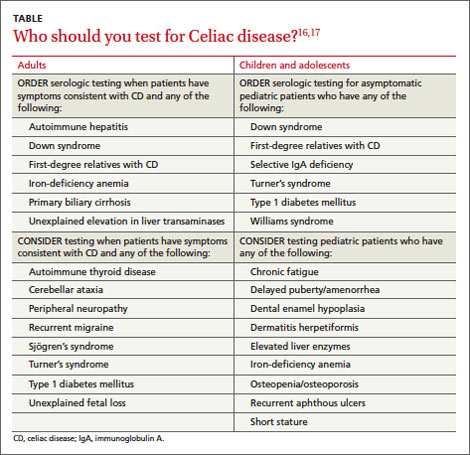
Order serologic testing for at-risk patients
Because CD remains underdiagnosed,16 taking a thorough family history and dietary history and making sure to at least consider CD as a part of a differential diagnosis is important. Although population-based screening has been proposed, its benefits and cost-effectiveness remain unproven. As a result, serologic testing of at-risk groups—individuals with conditions known to be associated with CD—remains the current standard.3 The TABLE lists groups for whom serologic testing for CD is indicated.16,17
In addition, the American College of Gastroenterology (ACG) and the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) provide guidance on the diagnosis and treatment of adults and children with CD. (An ACG diagnostic algorithm is available at http://www.nature.com/ajg/journal/v108/n5/pdf/ajg201379a.pdf.)
Adults. For patients who are consuming a diet that includes gluten and have symptoms that suggest CD, the ACG guidelines recommend initial testing for IgA tissue transglutaminase (tTG) antibodies.16 The IgA tTG has a sensitivity and specificity >95%.16 An alternative test, the IgA endomysial (IgA EMA) test, has similar sensitivity but is time-consuming and its accuracy depends on the experience and skill of the laboratory technician. A negative result for either test has a high negative predictive value for CD.3,16
IgA deficiency is much more common in patients with CD than in the general population and can result in a false negative test for tTG and EMA. Therefore, consider taking a baseline IgA measurement first. If the patient has an IgA deficiency, the test you’ll use next will change: The preferred test for CD is either immunoglobulin G (IgG) tTG or IgG deamidated gliadin peptides (DGP).3,16
If a patient is already gluten-free... To rule out CD in patients who are already consuming a gluten-free diet, order HLA-DQ2 and HLA-DQ8 testing because these markers have a specificity >99%; if the HLA test is negative, the disease is excluded.8,16
Children. NASPGHAN recommends taking a baseline IgA measurement in children at risk for CD and then testing for IgA tTG antibodies, but not until patients are 3 years old and have been on a diet that includes gluten for at least 1 year.17 Repeat testing at a later date it is recommended for those with negative results because some evidence suggests that in certain patients, later serologic testing will be positive. Alternatively, you may offer HLA testing. If the HLA test is negative, CD can be excluded >99% of the time.
Diagnosis usually is confirmed by intestinal biopsy
Positive results on serologic testing should be confirmed with a biopsy of the small bowel; findings characteristic of CD include an increased number of intraepithelial lymphocytes (>25 per 100 enterocytes), elongation of the crypts, and partial to total villous atrophy.4 Final confirmation of CD is resolution of symptoms by consuming a gluten-free diet.3,8
Alternate approaches to confirming the diagnosis. Although intestinal biopsy has long been considered the gold standard for diagnosis of CD, this may change. In 2012, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition proposed that the biopsy may not be necessary in children with the following 3 characteristics: classic intestinal symptoms of CD, IgA tTG levels >10 times higher than normal, and a positive HLA-DQ2.18
Catassi and Fasano19 have proposed shifting from relying on algorithms and intestinal biopsy to a quantitative approach. They suggest using the “4 out of 5” rule, meaning the diagnosis of CD can be confirmed if at least 4 of the following 5 criteria are satisfied: typical CD symptoms, a positive IgA tTG, a positive HLA-DQ2 or -DQ8, celiac enteropathy on small bowel biopsy, and response to a gluten-free diet.19
The only proven treatment: A gluten-free diet
Lifelong adherence to a gluten-free diet is the only effective treatment for CD.14,16 Previously, patients with CD were advised to also avoid oats, but most evidence supports the safety of oats (<2 oz/d), provided there is no cross-contamination with gluten.14 Adhering to a strict gluten-free diet can be challenging because cereal flours are ubiquitous in western foods, and some foods may be cross-contaminated. The Celiac Disease Foundation (http://www.celiac.org) offers guidance on maintaining a gluten-free diet.
Because avoiding gluten has become popular even among people who don’t have CD, product labeling that includes information on gluten content has become pervasive. However, determining which items contain gluten depends on accurate labeling, a standard that often is not met in many countries; in the United States, such labeling began to be phased in starting in July 2014.20 As a result, CD patients may unwittingly be exposed to gluten over the long term, which can result in greater morbidity and mortality. Unless a food is labeled “gluten-free," it is best to check with the manufacturer.
Compliance with a gluten-free diet can be monitored by following IgA tTG titers every 1 to 2 years, as these values normalize after a patient has been adhering to the diet for 6 to 24 months.3,16
In addition to lifelong adherence to a gluten-free diet, a National Institutes of Health Consensus Development Conference recommended that management of patients with CD should include21:
- consultation with a skilled dietitian
- education about the disease
- continuous long-term follow-up by a multidisciplinary team
- identification and follow-up of abnormalities found at baseline, such as abnormal liver function test results
- treatment of nutritional deficiencies.
The ACG also recommends that CD patients receive a dual energy x-ray scan for follow-up of osteopenia and a pneumococcal vaccine because functional hyposplenism is associated with CD, and pneumonia is a common complication of hyposplenism.16,18
Compared to infants who are breastfed and don’t receive gluten until ages 4 to 6 months, infants who are fed gluten in their first 3 months have a significantly increased risk of developing antibodies that are associated with celiac disease (CD).22 Recent studies suggest that the effects of breast milk on the microbiota composition of the intestine may help explain this difference. Breast milk selectively stimulates the growth of specific bacteria, including bifidobacteria, which are relatively depleted in children with CD.23,24 Researchers believe breastfeeding and delaying introduction of gluten-containing foods until 4 to 6 months of age might protect against CD.25
Should you recommend a gluten-free diet for other patients? Because avoiding gluten is now popular and many gluten-free products are marketed as “health food,” physicians may be reluctant to recommend a gluten-free diet for patients who have vague abdominal symptoms but negative CD test results. Despite the current popularity of “going gluten-free,” the reality is that in addition to CD, many other diseases may be helped by a gluten-free diet, such as dermatitis herpetiformis, irritable bowel syndrome, and neurologic diseases such as gluten-sensitive ataxia.19 In the end, whether to adopt a gluten-free diet is a decision that you and your patient will need to make together.
Researchers are searching for additional treatments
Because many patients find it difficult to adhere to a gluten-free diet, researchers are investigating several alternative treatments, including a derivative from cholera toxin that inhibits the opening of intestinal epithelial junctions, thereby reducing the resultant inflammatory response, and a desensitizing vaccine.19,22,23 Another intriguing approach involves using the parasite Necator americanus to modulate the immune response to gluten.18 Finally, certain infant feeding practices, including breastfeeding and delaying introduction of gluten to the diet, may minimize the risk of developing CD. (See "A link between infant feeding practices and the risk of CD?" above.22-25)
CORRESPONDENCE
Patrick T. Dowling, MD, MPH, Department of Family Medicine, 50-078 Center for Health Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095-1683; [email protected]
1. Sanders L. Hurt all over. New York Times Sunday Magazine. November 11, 2011:MM22.
2. Rubio-Tapia A, Ludvigsson JF, Brantner TL, et al. The prevalence of celiac disease in the United States. Am J Gastroenterol. 2012;107:1538-1544.
3. Fasano A, Catassi C. Clinical practice. Celiac disease. N Engl J Med. 2012;367:2419-2426.
4. Green PH, Cellier C. Celiac disease. N Engl J Med. 2007;357: 1731-1743.
5. Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163:286-292.
6. Mustalahti K, Catassi C, Reunanen A, et al; Coeliac EU Cluster, Project Epidemiology. The prevalence of celiac disease in Europe: results of centralized, international mass screening project. Ann Med. 2010;42:587-595.
7. Farrel R, Kelly C. Celiac disease and refractory celiac disease. In: Feldman M, Friedman LS, Brandt LJ. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia, PA: Saunders; 2010: 1797-1820.
8. Gujral N, Freeman HJ, Thomson Ab. Celiac disease: prevalence, diagnosis, pathogenesis and treatment. World J Gastroenterol. 2012;18:6036-6059.
9. Sleisenger MH. Diseases of malabsorption. In: Beeson PB, McDermott W. Cecil-Loeb Textbook of Medicine. 13th ed. Philadelphia, PA: WB Saunders Company; 1971:1285-1291.
10. Reilly NR, Green PH. Epidemiology and clinical presentations of celiac disease. Sem Immunopathol. 2012;34:473-478.
11. Kagnoff MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components. Gastroenterol Clin North Am. 1992;21:405-425.
12. Riddle MS, Murray JA, Porter CK. The incidence and risk of celiac disease in a healthy US adult population. Am J Gastroenterol. 2012;107:1248-1255.
13. Rampertab SD, Pooran N, Brar P, et al. Trends in the presentation of celiac disease. Am J Med. 2006;119:355.e9-355.e14.
14. Pietzak M. Celiac disease, wheat allergy, and gluten sensitivity: when gluten free is not a fad. JPEN J Parenter Enteral Nutr. 2012;36(1 suppl):68S-75S.
15. Sapone A, Bai JC, Ciacci C, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med. 2012;10:13.
16. Rubio-Tapia A, Hill ID, Kelly CP, et al; American College of Gastroenterology. ACG clinical guidelines: diagnosis and management celiac disease. Am J Gastroenterol. 2013;108:656-676.
17. Hill ID, Dirks MH, Liptak GS, et al; North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Guidelines for the diagnosis and treatment of celiac disease in children: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroentertol Nutr. 2005;40:1-19.
18. Husby S, Koletsko S, Korponay-Szabó IR, et al; ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastoenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. European Society for Pediatric Gastroenterology, Hepatology and Nutrition Guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136-160.
19. Catassi C, Fasano A. Celiac disease diagnosis: simple rules are better than complicated algorithms. Am J Med. 2010;123:691-693.
20. US Food and Drug Administration. Foods labeled gluten-free must now meet FDA's definition. Available at: http://www.fda. gov/Food/NewsEvents/ConstituentUpdates/ucm407867.htm. Accessed August 13, 2014.
21. National Institutes of Health Consensus Development Conference on Celiac Disease. National Institutes of Health Consensus Development Conference Statement. Available at: http://consensus.nih.gov/2004/2004celiacdisease118html.htm. Accessed August 13, 2014.
22. Norris JM, Barriga K, Hoffenberg EJ, et al. Risk of celiac disease autoimmunity and timing of gluten introduction in the diet of infants at increased risk of disease. JAMA. 2005;293:2343-2351.
23. Pozo-Rubio T, Olivares M, Nova E, et al. Immune development and intestinal microbiota in celiac disease. Clin Dev Immunol. 2012;2012:654143
24. Ivarsson A, Myléus A, Norström F, et al. Prevalence of childhood celiac disease and changes in infant feeding. Pediatrics. 2013;131:687-694.
25. Cataldo F, Montalto G. Celiac disease in the developing countries: a new and challenging public health problem. World J Gastroenterol. 2007;13:2153-2159.
› Do not rely on symptoms or symptom response to
a gluten-free diet alone
to diagnose celiac disease (CD); this approach does not differentiate CD from non-celiac gluten sensitivity. B
› Use HLA-DQ2 and -DQ8 genotype testing to effectively rule out the disease in selected clinical situations. B
› Test for CD in any
patient who has unexplained elevated serum aminotransferase levels, even in the absence of CD symptoms. A
› Screen all first-degree relatives of patients with
CD by testing for immunoglobulin A (IgA) tissue transglutaminase antibodies and serum IgA levels. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › It was a clinical conundrum. A 2011 case study1 described a 33-year-old woman with a 10-year history of progressive, debilitating pain and weakness. The patient had not received a unifying diagnosis or effective treatment despite multiple diagnostic tests and different recommendations from multiple specialists. The diagnosis remained elusive until a rheumatologist agreed to reexamine the case.
While reviewing the woman’s thick chart, the rheumatologist noted a series of negative results from upper and lower endoscopies and abdominal scans. Further investigation revealed an almost obfuscated clue—blood tests performed 2 years earlier that were positive for celiac disease (CD). However, a small intestine biopsy, which normally is done to confirm the diagnosis, was never performed.
The rheumatologist made a tentative diagnosis of CD and referred her to a nutritionist, who recommended the patient adhere to a strict gluten-free diet. Within 3 months, the patient experienced marked improvement and returned to work.
CD is an often-missed diagnosis. According to a study based on National Health and Nutrition Examination Survey data, only 17% of patients with CD are aware they have the disease.2 As such, it is imperative that primary care physicians familiarize themselves with CD’s myriad clinical presentations, diagnosis, and treatment.3-6
Gluten triggers an immune response in genetically susceptible patients
CD initially was known as “celiac sprue” because it shares characteristics with tropical sprue—diarrhea, malabsorption, and emaciation. It is a unique T-cell autoimmune enteropathy that is precipitated in genetically susceptible individuals by the ingestion of gluten, the major storage protein of wheat, barley, and rye.3,7
Upon ingestion, gluten breaks down to gliadin, which provokes an immune response in the intestinal mucosa of patients with CD. This response results in an inflammatory reaction, primarily in the upper small intestine, that destroys the absorption surface and causes villous atrophy, leading to nutrient malabsorption and chronic diarrhea.8 CD is associated with significant morbidity due to an abnormal excretion of fat (steatorrhea) and varying degrees of malabsorption of vitamins A, D, and K, as well as B complex vitamins including B12 and folate; carbohydrates; protein; water; and minerals such as magnesium, calcium, and iron.9
CD develops only in individuals who possess alleles that encode for HLA-DQ2 or HLA-DQ8 proteins, products of 2 of the HLA genes. And while 30% of Caucasians carry the HLA-DQ2 allele and virtually 100% consume wheat, only 1 in 100 will develop CD.3,10,11 Although the genes are necessary, it is the interplay between genes (both HLA and non-HLA associated) and environment (ie, gluten) that leads to the intestinal mucosa damage typical of the disease. The HLA-DQ region also is associated with increased risk of type 1 diabetes, which might explain the correlation of CD to a host of other autoimmune disorders, including Graves’ disease and rheumatoid arthritis.8,10,11
Increased prevalence reflects better recognition of celiac disease
CD affects .6% to 1% of the population worldwide, with wide regional variation.3 Before the development of serologic assays in the 1970s, CD was a clinical diagnosis based on classic symptoms. With the advent of assays for immunoglobulin A (IgA) antibodies, the prevalence of CD has drastically increased to the current estimates of 1:250 to 1:500.4,5 The prevalence will continue to increase as clinicians become more aware of the different presentations of the disease, which are described below.
CD runs in families. Most patients with CD have a family history of the disease based on inheritance of the HLA alleles. A US study determined that the prevalence of CD was 1:22 in first-degree relatives and 1:39 in second-degree relatives of patients with biopsy-proven CD.12
Less than half of patients have GI symptoms
The classic presentation of CD involves a constellation of signs and symptoms of malabsorption: diarrhea, muscle wasting, and weight loss. Other typical gastrointestinal (GI) symptoms include bloating, flatulence, and abdominal pain.
Recognizing CD can be challenging, however, because <50% of patients diagnosed with CD present with these classic GI symptoms.3 About 50% of CD patients present with extra-intestinal symptoms, such as iron deficiency anemia, aphthous stomatitis, chronic fatigue, osteopenia, and dental enamel hypoplasia.3,8,13 Other possible non-GI symptoms include abnormal liver function test results and skin disorders such as dermatitis herpetiformis, a pruritic rash with cutaneous IgA deposits.3,8 In addition, many patients are asymptomatic.14 This highly variable clinical picture is due to the genetic and immunologic basis of the disease, extent of mucosal injury, and patients’ dietary habits, gender, and age of onset.15 A common clue that suggests a patient may have CD is unexplained iron deficiency anemia that does not improve with oral iron supplementation.4,13
Because symptoms may be intermittent, a patient may delay seeking care until he or she develops secondary manifestations, which often are debilitating and overshadow the GI complaints. Chronic complications of untreated CD include lymphoma and adenocarcinomas of the jejunum, recurrent miscarriages, neurologic disorders, osteoporosis, and hyposplenism.3,4,8
Since CD can manifest with widely varying symptoms, some researchers believe the disease should be classified into 3 categories based on presentation: classic CD, which presents with diarrhea, weight loss, malabsorption, and vitamin deficiency; atypical CD, which presents with minimal GI symptoms but can include anemia, neurologic symptoms, arthritis, or infertility; and asymptomatic CD, which typically displays no symptoms but usually is identified on incidental screening.3,8,16 Non-celiac gluten sensitivity is a distinct condition in which the body reacts adversely to gluten; it is not an autoimmune disease with an inflammatory response.
Order serologic testing for at-risk patients
Because CD remains underdiagnosed,16 taking a thorough family history and dietary history and making sure to at least consider CD as a part of a differential diagnosis is important. Although population-based screening has been proposed, its benefits and cost-effectiveness remain unproven. As a result, serologic testing of at-risk groups—individuals with conditions known to be associated with CD—remains the current standard.3 The TABLE lists groups for whom serologic testing for CD is indicated.16,17
In addition, the American College of Gastroenterology (ACG) and the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) provide guidance on the diagnosis and treatment of adults and children with CD. (An ACG diagnostic algorithm is available at http://www.nature.com/ajg/journal/v108/n5/pdf/ajg201379a.pdf.)
Adults. For patients who are consuming a diet that includes gluten and have symptoms that suggest CD, the ACG guidelines recommend initial testing for IgA tissue transglutaminase (tTG) antibodies.16 The IgA tTG has a sensitivity and specificity >95%.16 An alternative test, the IgA endomysial (IgA EMA) test, has similar sensitivity but is time-consuming and its accuracy depends on the experience and skill of the laboratory technician. A negative result for either test has a high negative predictive value for CD.3,16
IgA deficiency is much more common in patients with CD than in the general population and can result in a false negative test for tTG and EMA. Therefore, consider taking a baseline IgA measurement first. If the patient has an IgA deficiency, the test you’ll use next will change: The preferred test for CD is either immunoglobulin G (IgG) tTG or IgG deamidated gliadin peptides (DGP).3,16
If a patient is already gluten-free... To rule out CD in patients who are already consuming a gluten-free diet, order HLA-DQ2 and HLA-DQ8 testing because these markers have a specificity >99%; if the HLA test is negative, the disease is excluded.8,16
Children. NASPGHAN recommends taking a baseline IgA measurement in children at risk for CD and then testing for IgA tTG antibodies, but not until patients are 3 years old and have been on a diet that includes gluten for at least 1 year.17 Repeat testing at a later date it is recommended for those with negative results because some evidence suggests that in certain patients, later serologic testing will be positive. Alternatively, you may offer HLA testing. If the HLA test is negative, CD can be excluded >99% of the time.
Diagnosis usually is confirmed by intestinal biopsy
Positive results on serologic testing should be confirmed with a biopsy of the small bowel; findings characteristic of CD include an increased number of intraepithelial lymphocytes (>25 per 100 enterocytes), elongation of the crypts, and partial to total villous atrophy.4 Final confirmation of CD is resolution of symptoms by consuming a gluten-free diet.3,8
Alternate approaches to confirming the diagnosis. Although intestinal biopsy has long been considered the gold standard for diagnosis of CD, this may change. In 2012, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition proposed that the biopsy may not be necessary in children with the following 3 characteristics: classic intestinal symptoms of CD, IgA tTG levels >10 times higher than normal, and a positive HLA-DQ2.18
Catassi and Fasano19 have proposed shifting from relying on algorithms and intestinal biopsy to a quantitative approach. They suggest using the “4 out of 5” rule, meaning the diagnosis of CD can be confirmed if at least 4 of the following 5 criteria are satisfied: typical CD symptoms, a positive IgA tTG, a positive HLA-DQ2 or -DQ8, celiac enteropathy on small bowel biopsy, and response to a gluten-free diet.19
The only proven treatment: A gluten-free diet
Lifelong adherence to a gluten-free diet is the only effective treatment for CD.14,16 Previously, patients with CD were advised to also avoid oats, but most evidence supports the safety of oats (<2 oz/d), provided there is no cross-contamination with gluten.14 Adhering to a strict gluten-free diet can be challenging because cereal flours are ubiquitous in western foods, and some foods may be cross-contaminated. The Celiac Disease Foundation (http://www.celiac.org) offers guidance on maintaining a gluten-free diet.
Because avoiding gluten has become popular even among people who don’t have CD, product labeling that includes information on gluten content has become pervasive. However, determining which items contain gluten depends on accurate labeling, a standard that often is not met in many countries; in the United States, such labeling began to be phased in starting in July 2014.20 As a result, CD patients may unwittingly be exposed to gluten over the long term, which can result in greater morbidity and mortality. Unless a food is labeled “gluten-free," it is best to check with the manufacturer.
Compliance with a gluten-free diet can be monitored by following IgA tTG titers every 1 to 2 years, as these values normalize after a patient has been adhering to the diet for 6 to 24 months.3,16
In addition to lifelong adherence to a gluten-free diet, a National Institutes of Health Consensus Development Conference recommended that management of patients with CD should include21:
- consultation with a skilled dietitian
- education about the disease
- continuous long-term follow-up by a multidisciplinary team
- identification and follow-up of abnormalities found at baseline, such as abnormal liver function test results
- treatment of nutritional deficiencies.
The ACG also recommends that CD patients receive a dual energy x-ray scan for follow-up of osteopenia and a pneumococcal vaccine because functional hyposplenism is associated with CD, and pneumonia is a common complication of hyposplenism.16,18
Compared to infants who are breastfed and don’t receive gluten until ages 4 to 6 months, infants who are fed gluten in their first 3 months have a significantly increased risk of developing antibodies that are associated with celiac disease (CD).22 Recent studies suggest that the effects of breast milk on the microbiota composition of the intestine may help explain this difference. Breast milk selectively stimulates the growth of specific bacteria, including bifidobacteria, which are relatively depleted in children with CD.23,24 Researchers believe breastfeeding and delaying introduction of gluten-containing foods until 4 to 6 months of age might protect against CD.25
Should you recommend a gluten-free diet for other patients? Because avoiding gluten is now popular and many gluten-free products are marketed as “health food,” physicians may be reluctant to recommend a gluten-free diet for patients who have vague abdominal symptoms but negative CD test results. Despite the current popularity of “going gluten-free,” the reality is that in addition to CD, many other diseases may be helped by a gluten-free diet, such as dermatitis herpetiformis, irritable bowel syndrome, and neurologic diseases such as gluten-sensitive ataxia.19 In the end, whether to adopt a gluten-free diet is a decision that you and your patient will need to make together.
Researchers are searching for additional treatments
Because many patients find it difficult to adhere to a gluten-free diet, researchers are investigating several alternative treatments, including a derivative from cholera toxin that inhibits the opening of intestinal epithelial junctions, thereby reducing the resultant inflammatory response, and a desensitizing vaccine.19,22,23 Another intriguing approach involves using the parasite Necator americanus to modulate the immune response to gluten.18 Finally, certain infant feeding practices, including breastfeeding and delaying introduction of gluten to the diet, may minimize the risk of developing CD. (See "A link between infant feeding practices and the risk of CD?" above.22-25)
CORRESPONDENCE
Patrick T. Dowling, MD, MPH, Department of Family Medicine, 50-078 Center for Health Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095-1683; [email protected]
› Do not rely on symptoms or symptom response to
a gluten-free diet alone
to diagnose celiac disease (CD); this approach does not differentiate CD from non-celiac gluten sensitivity. B
› Use HLA-DQ2 and -DQ8 genotype testing to effectively rule out the disease in selected clinical situations. B
› Test for CD in any
patient who has unexplained elevated serum aminotransferase levels, even in the absence of CD symptoms. A
› Screen all first-degree relatives of patients with
CD by testing for immunoglobulin A (IgA) tissue transglutaminase antibodies and serum IgA levels. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › It was a clinical conundrum. A 2011 case study1 described a 33-year-old woman with a 10-year history of progressive, debilitating pain and weakness. The patient had not received a unifying diagnosis or effective treatment despite multiple diagnostic tests and different recommendations from multiple specialists. The diagnosis remained elusive until a rheumatologist agreed to reexamine the case.
While reviewing the woman’s thick chart, the rheumatologist noted a series of negative results from upper and lower endoscopies and abdominal scans. Further investigation revealed an almost obfuscated clue—blood tests performed 2 years earlier that were positive for celiac disease (CD). However, a small intestine biopsy, which normally is done to confirm the diagnosis, was never performed.
The rheumatologist made a tentative diagnosis of CD and referred her to a nutritionist, who recommended the patient adhere to a strict gluten-free diet. Within 3 months, the patient experienced marked improvement and returned to work.
CD is an often-missed diagnosis. According to a study based on National Health and Nutrition Examination Survey data, only 17% of patients with CD are aware they have the disease.2 As such, it is imperative that primary care physicians familiarize themselves with CD’s myriad clinical presentations, diagnosis, and treatment.3-6
Gluten triggers an immune response in genetically susceptible patients
CD initially was known as “celiac sprue” because it shares characteristics with tropical sprue—diarrhea, malabsorption, and emaciation. It is a unique T-cell autoimmune enteropathy that is precipitated in genetically susceptible individuals by the ingestion of gluten, the major storage protein of wheat, barley, and rye.3,7
Upon ingestion, gluten breaks down to gliadin, which provokes an immune response in the intestinal mucosa of patients with CD. This response results in an inflammatory reaction, primarily in the upper small intestine, that destroys the absorption surface and causes villous atrophy, leading to nutrient malabsorption and chronic diarrhea.8 CD is associated with significant morbidity due to an abnormal excretion of fat (steatorrhea) and varying degrees of malabsorption of vitamins A, D, and K, as well as B complex vitamins including B12 and folate; carbohydrates; protein; water; and minerals such as magnesium, calcium, and iron.9
CD develops only in individuals who possess alleles that encode for HLA-DQ2 or HLA-DQ8 proteins, products of 2 of the HLA genes. And while 30% of Caucasians carry the HLA-DQ2 allele and virtually 100% consume wheat, only 1 in 100 will develop CD.3,10,11 Although the genes are necessary, it is the interplay between genes (both HLA and non-HLA associated) and environment (ie, gluten) that leads to the intestinal mucosa damage typical of the disease. The HLA-DQ region also is associated with increased risk of type 1 diabetes, which might explain the correlation of CD to a host of other autoimmune disorders, including Graves’ disease and rheumatoid arthritis.8,10,11
Increased prevalence reflects better recognition of celiac disease
CD affects .6% to 1% of the population worldwide, with wide regional variation.3 Before the development of serologic assays in the 1970s, CD was a clinical diagnosis based on classic symptoms. With the advent of assays for immunoglobulin A (IgA) antibodies, the prevalence of CD has drastically increased to the current estimates of 1:250 to 1:500.4,5 The prevalence will continue to increase as clinicians become more aware of the different presentations of the disease, which are described below.
CD runs in families. Most patients with CD have a family history of the disease based on inheritance of the HLA alleles. A US study determined that the prevalence of CD was 1:22 in first-degree relatives and 1:39 in second-degree relatives of patients with biopsy-proven CD.12
Less than half of patients have GI symptoms
The classic presentation of CD involves a constellation of signs and symptoms of malabsorption: diarrhea, muscle wasting, and weight loss. Other typical gastrointestinal (GI) symptoms include bloating, flatulence, and abdominal pain.
Recognizing CD can be challenging, however, because <50% of patients diagnosed with CD present with these classic GI symptoms.3 About 50% of CD patients present with extra-intestinal symptoms, such as iron deficiency anemia, aphthous stomatitis, chronic fatigue, osteopenia, and dental enamel hypoplasia.3,8,13 Other possible non-GI symptoms include abnormal liver function test results and skin disorders such as dermatitis herpetiformis, a pruritic rash with cutaneous IgA deposits.3,8 In addition, many patients are asymptomatic.14 This highly variable clinical picture is due to the genetic and immunologic basis of the disease, extent of mucosal injury, and patients’ dietary habits, gender, and age of onset.15 A common clue that suggests a patient may have CD is unexplained iron deficiency anemia that does not improve with oral iron supplementation.4,13
Because symptoms may be intermittent, a patient may delay seeking care until he or she develops secondary manifestations, which often are debilitating and overshadow the GI complaints. Chronic complications of untreated CD include lymphoma and adenocarcinomas of the jejunum, recurrent miscarriages, neurologic disorders, osteoporosis, and hyposplenism.3,4,8
Since CD can manifest with widely varying symptoms, some researchers believe the disease should be classified into 3 categories based on presentation: classic CD, which presents with diarrhea, weight loss, malabsorption, and vitamin deficiency; atypical CD, which presents with minimal GI symptoms but can include anemia, neurologic symptoms, arthritis, or infertility; and asymptomatic CD, which typically displays no symptoms but usually is identified on incidental screening.3,8,16 Non-celiac gluten sensitivity is a distinct condition in which the body reacts adversely to gluten; it is not an autoimmune disease with an inflammatory response.
Order serologic testing for at-risk patients
Because CD remains underdiagnosed,16 taking a thorough family history and dietary history and making sure to at least consider CD as a part of a differential diagnosis is important. Although population-based screening has been proposed, its benefits and cost-effectiveness remain unproven. As a result, serologic testing of at-risk groups—individuals with conditions known to be associated with CD—remains the current standard.3 The TABLE lists groups for whom serologic testing for CD is indicated.16,17
In addition, the American College of Gastroenterology (ACG) and the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) provide guidance on the diagnosis and treatment of adults and children with CD. (An ACG diagnostic algorithm is available at http://www.nature.com/ajg/journal/v108/n5/pdf/ajg201379a.pdf.)
Adults. For patients who are consuming a diet that includes gluten and have symptoms that suggest CD, the ACG guidelines recommend initial testing for IgA tissue transglutaminase (tTG) antibodies.16 The IgA tTG has a sensitivity and specificity >95%.16 An alternative test, the IgA endomysial (IgA EMA) test, has similar sensitivity but is time-consuming and its accuracy depends on the experience and skill of the laboratory technician. A negative result for either test has a high negative predictive value for CD.3,16
IgA deficiency is much more common in patients with CD than in the general population and can result in a false negative test for tTG and EMA. Therefore, consider taking a baseline IgA measurement first. If the patient has an IgA deficiency, the test you’ll use next will change: The preferred test for CD is either immunoglobulin G (IgG) tTG or IgG deamidated gliadin peptides (DGP).3,16
If a patient is already gluten-free... To rule out CD in patients who are already consuming a gluten-free diet, order HLA-DQ2 and HLA-DQ8 testing because these markers have a specificity >99%; if the HLA test is negative, the disease is excluded.8,16
Children. NASPGHAN recommends taking a baseline IgA measurement in children at risk for CD and then testing for IgA tTG antibodies, but not until patients are 3 years old and have been on a diet that includes gluten for at least 1 year.17 Repeat testing at a later date it is recommended for those with negative results because some evidence suggests that in certain patients, later serologic testing will be positive. Alternatively, you may offer HLA testing. If the HLA test is negative, CD can be excluded >99% of the time.
Diagnosis usually is confirmed by intestinal biopsy
Positive results on serologic testing should be confirmed with a biopsy of the small bowel; findings characteristic of CD include an increased number of intraepithelial lymphocytes (>25 per 100 enterocytes), elongation of the crypts, and partial to total villous atrophy.4 Final confirmation of CD is resolution of symptoms by consuming a gluten-free diet.3,8
Alternate approaches to confirming the diagnosis. Although intestinal biopsy has long been considered the gold standard for diagnosis of CD, this may change. In 2012, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition proposed that the biopsy may not be necessary in children with the following 3 characteristics: classic intestinal symptoms of CD, IgA tTG levels >10 times higher than normal, and a positive HLA-DQ2.18
Catassi and Fasano19 have proposed shifting from relying on algorithms and intestinal biopsy to a quantitative approach. They suggest using the “4 out of 5” rule, meaning the diagnosis of CD can be confirmed if at least 4 of the following 5 criteria are satisfied: typical CD symptoms, a positive IgA tTG, a positive HLA-DQ2 or -DQ8, celiac enteropathy on small bowel biopsy, and response to a gluten-free diet.19
The only proven treatment: A gluten-free diet
Lifelong adherence to a gluten-free diet is the only effective treatment for CD.14,16 Previously, patients with CD were advised to also avoid oats, but most evidence supports the safety of oats (<2 oz/d), provided there is no cross-contamination with gluten.14 Adhering to a strict gluten-free diet can be challenging because cereal flours are ubiquitous in western foods, and some foods may be cross-contaminated. The Celiac Disease Foundation (http://www.celiac.org) offers guidance on maintaining a gluten-free diet.
Because avoiding gluten has become popular even among people who don’t have CD, product labeling that includes information on gluten content has become pervasive. However, determining which items contain gluten depends on accurate labeling, a standard that often is not met in many countries; in the United States, such labeling began to be phased in starting in July 2014.20 As a result, CD patients may unwittingly be exposed to gluten over the long term, which can result in greater morbidity and mortality. Unless a food is labeled “gluten-free," it is best to check with the manufacturer.
Compliance with a gluten-free diet can be monitored by following IgA tTG titers every 1 to 2 years, as these values normalize after a patient has been adhering to the diet for 6 to 24 months.3,16
In addition to lifelong adherence to a gluten-free diet, a National Institutes of Health Consensus Development Conference recommended that management of patients with CD should include21:
- consultation with a skilled dietitian
- education about the disease
- continuous long-term follow-up by a multidisciplinary team
- identification and follow-up of abnormalities found at baseline, such as abnormal liver function test results
- treatment of nutritional deficiencies.
The ACG also recommends that CD patients receive a dual energy x-ray scan for follow-up of osteopenia and a pneumococcal vaccine because functional hyposplenism is associated with CD, and pneumonia is a common complication of hyposplenism.16,18
Compared to infants who are breastfed and don’t receive gluten until ages 4 to 6 months, infants who are fed gluten in their first 3 months have a significantly increased risk of developing antibodies that are associated with celiac disease (CD).22 Recent studies suggest that the effects of breast milk on the microbiota composition of the intestine may help explain this difference. Breast milk selectively stimulates the growth of specific bacteria, including bifidobacteria, which are relatively depleted in children with CD.23,24 Researchers believe breastfeeding and delaying introduction of gluten-containing foods until 4 to 6 months of age might protect against CD.25
Should you recommend a gluten-free diet for other patients? Because avoiding gluten is now popular and many gluten-free products are marketed as “health food,” physicians may be reluctant to recommend a gluten-free diet for patients who have vague abdominal symptoms but negative CD test results. Despite the current popularity of “going gluten-free,” the reality is that in addition to CD, many other diseases may be helped by a gluten-free diet, such as dermatitis herpetiformis, irritable bowel syndrome, and neurologic diseases such as gluten-sensitive ataxia.19 In the end, whether to adopt a gluten-free diet is a decision that you and your patient will need to make together.
Researchers are searching for additional treatments
Because many patients find it difficult to adhere to a gluten-free diet, researchers are investigating several alternative treatments, including a derivative from cholera toxin that inhibits the opening of intestinal epithelial junctions, thereby reducing the resultant inflammatory response, and a desensitizing vaccine.19,22,23 Another intriguing approach involves using the parasite Necator americanus to modulate the immune response to gluten.18 Finally, certain infant feeding practices, including breastfeeding and delaying introduction of gluten to the diet, may minimize the risk of developing CD. (See "A link between infant feeding practices and the risk of CD?" above.22-25)
CORRESPONDENCE
Patrick T. Dowling, MD, MPH, Department of Family Medicine, 50-078 Center for Health Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095-1683; [email protected]
1. Sanders L. Hurt all over. New York Times Sunday Magazine. November 11, 2011:MM22.
2. Rubio-Tapia A, Ludvigsson JF, Brantner TL, et al. The prevalence of celiac disease in the United States. Am J Gastroenterol. 2012;107:1538-1544.
3. Fasano A, Catassi C. Clinical practice. Celiac disease. N Engl J Med. 2012;367:2419-2426.
4. Green PH, Cellier C. Celiac disease. N Engl J Med. 2007;357: 1731-1743.
5. Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163:286-292.
6. Mustalahti K, Catassi C, Reunanen A, et al; Coeliac EU Cluster, Project Epidemiology. The prevalence of celiac disease in Europe: results of centralized, international mass screening project. Ann Med. 2010;42:587-595.
7. Farrel R, Kelly C. Celiac disease and refractory celiac disease. In: Feldman M, Friedman LS, Brandt LJ. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia, PA: Saunders; 2010: 1797-1820.
8. Gujral N, Freeman HJ, Thomson Ab. Celiac disease: prevalence, diagnosis, pathogenesis and treatment. World J Gastroenterol. 2012;18:6036-6059.
9. Sleisenger MH. Diseases of malabsorption. In: Beeson PB, McDermott W. Cecil-Loeb Textbook of Medicine. 13th ed. Philadelphia, PA: WB Saunders Company; 1971:1285-1291.
10. Reilly NR, Green PH. Epidemiology and clinical presentations of celiac disease. Sem Immunopathol. 2012;34:473-478.
11. Kagnoff MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components. Gastroenterol Clin North Am. 1992;21:405-425.
12. Riddle MS, Murray JA, Porter CK. The incidence and risk of celiac disease in a healthy US adult population. Am J Gastroenterol. 2012;107:1248-1255.
13. Rampertab SD, Pooran N, Brar P, et al. Trends in the presentation of celiac disease. Am J Med. 2006;119:355.e9-355.e14.
14. Pietzak M. Celiac disease, wheat allergy, and gluten sensitivity: when gluten free is not a fad. JPEN J Parenter Enteral Nutr. 2012;36(1 suppl):68S-75S.
15. Sapone A, Bai JC, Ciacci C, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med. 2012;10:13.
16. Rubio-Tapia A, Hill ID, Kelly CP, et al; American College of Gastroenterology. ACG clinical guidelines: diagnosis and management celiac disease. Am J Gastroenterol. 2013;108:656-676.
17. Hill ID, Dirks MH, Liptak GS, et al; North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Guidelines for the diagnosis and treatment of celiac disease in children: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroentertol Nutr. 2005;40:1-19.
18. Husby S, Koletsko S, Korponay-Szabó IR, et al; ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastoenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. European Society for Pediatric Gastroenterology, Hepatology and Nutrition Guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136-160.
19. Catassi C, Fasano A. Celiac disease diagnosis: simple rules are better than complicated algorithms. Am J Med. 2010;123:691-693.
20. US Food and Drug Administration. Foods labeled gluten-free must now meet FDA's definition. Available at: http://www.fda. gov/Food/NewsEvents/ConstituentUpdates/ucm407867.htm. Accessed August 13, 2014.
21. National Institutes of Health Consensus Development Conference on Celiac Disease. National Institutes of Health Consensus Development Conference Statement. Available at: http://consensus.nih.gov/2004/2004celiacdisease118html.htm. Accessed August 13, 2014.
22. Norris JM, Barriga K, Hoffenberg EJ, et al. Risk of celiac disease autoimmunity and timing of gluten introduction in the diet of infants at increased risk of disease. JAMA. 2005;293:2343-2351.
23. Pozo-Rubio T, Olivares M, Nova E, et al. Immune development and intestinal microbiota in celiac disease. Clin Dev Immunol. 2012;2012:654143
24. Ivarsson A, Myléus A, Norström F, et al. Prevalence of childhood celiac disease and changes in infant feeding. Pediatrics. 2013;131:687-694.
25. Cataldo F, Montalto G. Celiac disease in the developing countries: a new and challenging public health problem. World J Gastroenterol. 2007;13:2153-2159.
1. Sanders L. Hurt all over. New York Times Sunday Magazine. November 11, 2011:MM22.
2. Rubio-Tapia A, Ludvigsson JF, Brantner TL, et al. The prevalence of celiac disease in the United States. Am J Gastroenterol. 2012;107:1538-1544.
3. Fasano A, Catassi C. Clinical practice. Celiac disease. N Engl J Med. 2012;367:2419-2426.
4. Green PH, Cellier C. Celiac disease. N Engl J Med. 2007;357: 1731-1743.
5. Fasano A, Berti I, Gerarduzzi T, et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med. 2003;163:286-292.
6. Mustalahti K, Catassi C, Reunanen A, et al; Coeliac EU Cluster, Project Epidemiology. The prevalence of celiac disease in Europe: results of centralized, international mass screening project. Ann Med. 2010;42:587-595.
7. Farrel R, Kelly C. Celiac disease and refractory celiac disease. In: Feldman M, Friedman LS, Brandt LJ. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia, PA: Saunders; 2010: 1797-1820.
8. Gujral N, Freeman HJ, Thomson Ab. Celiac disease: prevalence, diagnosis, pathogenesis and treatment. World J Gastroenterol. 2012;18:6036-6059.
9. Sleisenger MH. Diseases of malabsorption. In: Beeson PB, McDermott W. Cecil-Loeb Textbook of Medicine. 13th ed. Philadelphia, PA: WB Saunders Company; 1971:1285-1291.
10. Reilly NR, Green PH. Epidemiology and clinical presentations of celiac disease. Sem Immunopathol. 2012;34:473-478.
11. Kagnoff MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components. Gastroenterol Clin North Am. 1992;21:405-425.
12. Riddle MS, Murray JA, Porter CK. The incidence and risk of celiac disease in a healthy US adult population. Am J Gastroenterol. 2012;107:1248-1255.
13. Rampertab SD, Pooran N, Brar P, et al. Trends in the presentation of celiac disease. Am J Med. 2006;119:355.e9-355.e14.
14. Pietzak M. Celiac disease, wheat allergy, and gluten sensitivity: when gluten free is not a fad. JPEN J Parenter Enteral Nutr. 2012;36(1 suppl):68S-75S.
15. Sapone A, Bai JC, Ciacci C, et al. Spectrum of gluten-related disorders: consensus on new nomenclature and classification. BMC Med. 2012;10:13.
16. Rubio-Tapia A, Hill ID, Kelly CP, et al; American College of Gastroenterology. ACG clinical guidelines: diagnosis and management celiac disease. Am J Gastroenterol. 2013;108:656-676.
17. Hill ID, Dirks MH, Liptak GS, et al; North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Guidelines for the diagnosis and treatment of celiac disease in children: recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroentertol Nutr. 2005;40:1-19.
18. Husby S, Koletsko S, Korponay-Szabó IR, et al; ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastoenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. European Society for Pediatric Gastroenterology, Hepatology and Nutrition Guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012;54:136-160.
19. Catassi C, Fasano A. Celiac disease diagnosis: simple rules are better than complicated algorithms. Am J Med. 2010;123:691-693.
20. US Food and Drug Administration. Foods labeled gluten-free must now meet FDA's definition. Available at: http://www.fda. gov/Food/NewsEvents/ConstituentUpdates/ucm407867.htm. Accessed August 13, 2014.
21. National Institutes of Health Consensus Development Conference on Celiac Disease. National Institutes of Health Consensus Development Conference Statement. Available at: http://consensus.nih.gov/2004/2004celiacdisease118html.htm. Accessed August 13, 2014.
22. Norris JM, Barriga K, Hoffenberg EJ, et al. Risk of celiac disease autoimmunity and timing of gluten introduction in the diet of infants at increased risk of disease. JAMA. 2005;293:2343-2351.
23. Pozo-Rubio T, Olivares M, Nova E, et al. Immune development and intestinal microbiota in celiac disease. Clin Dev Immunol. 2012;2012:654143
24. Ivarsson A, Myléus A, Norström F, et al. Prevalence of childhood celiac disease and changes in infant feeding. Pediatrics. 2013;131:687-694.
25. Cataldo F, Montalto G. Celiac disease in the developing countries: a new and challenging public health problem. World J Gastroenterol. 2007;13:2153-2159.

Stress testing
To the Editor: I was delighted to see an article addressing the overuse of stress tests in asymptomatic individuals.1 I still think, however, that one could really look at the issue a little further. In truly asymptomatic individuals, even those with established coronary heart disease, what is the value of the “annual stress echocardiogram,” often done in cardiologist’s offices? I was perturbed a bit by the statement, “a physician may consider ordering exercise electrocardiography in asymptomatic adults at intermediate risk of coronary heart disease.” Are there data to suggest the number needed to treat or the number needed to harm? I was sobered by the results of the Detection of Ischemia in Asymptomatic Diabetics trial,2 which showed no benefit in screening patients with type 2 diabetes with stress myocardial perfusion imaging (a technique probably more costly but more accurate than stress echocardiography).
I understand that bold statements about the lack of usefulness of the stress test in asymptomatic individuals might be misinterpreted by payers as a justification for denying coverage, but it would provide more help for those of us in primary care who are trying to dissuade patients from inappropriate and potentially harmful testing.
- Smith CD, Alguire PC. Is cardiac stress testing appropriate in asymptomatic adults at low risk? Cleve Clin J Med 2014; 81:405–406.
- Young LH, Wackers FJ, Chyun DA, et al; DIAD Investigators. Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes: the DIAD study: a randomized controlled trial. JAMA 2009; 301:1547–1555.
To the Editor: I was delighted to see an article addressing the overuse of stress tests in asymptomatic individuals.1 I still think, however, that one could really look at the issue a little further. In truly asymptomatic individuals, even those with established coronary heart disease, what is the value of the “annual stress echocardiogram,” often done in cardiologist’s offices? I was perturbed a bit by the statement, “a physician may consider ordering exercise electrocardiography in asymptomatic adults at intermediate risk of coronary heart disease.” Are there data to suggest the number needed to treat or the number needed to harm? I was sobered by the results of the Detection of Ischemia in Asymptomatic Diabetics trial,2 which showed no benefit in screening patients with type 2 diabetes with stress myocardial perfusion imaging (a technique probably more costly but more accurate than stress echocardiography).
I understand that bold statements about the lack of usefulness of the stress test in asymptomatic individuals might be misinterpreted by payers as a justification for denying coverage, but it would provide more help for those of us in primary care who are trying to dissuade patients from inappropriate and potentially harmful testing.
To the Editor: I was delighted to see an article addressing the overuse of stress tests in asymptomatic individuals.1 I still think, however, that one could really look at the issue a little further. In truly asymptomatic individuals, even those with established coronary heart disease, what is the value of the “annual stress echocardiogram,” often done in cardiologist’s offices? I was perturbed a bit by the statement, “a physician may consider ordering exercise electrocardiography in asymptomatic adults at intermediate risk of coronary heart disease.” Are there data to suggest the number needed to treat or the number needed to harm? I was sobered by the results of the Detection of Ischemia in Asymptomatic Diabetics trial,2 which showed no benefit in screening patients with type 2 diabetes with stress myocardial perfusion imaging (a technique probably more costly but more accurate than stress echocardiography).
I understand that bold statements about the lack of usefulness of the stress test in asymptomatic individuals might be misinterpreted by payers as a justification for denying coverage, but it would provide more help for those of us in primary care who are trying to dissuade patients from inappropriate and potentially harmful testing.
- Smith CD, Alguire PC. Is cardiac stress testing appropriate in asymptomatic adults at low risk? Cleve Clin J Med 2014; 81:405–406.
- Young LH, Wackers FJ, Chyun DA, et al; DIAD Investigators. Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes: the DIAD study: a randomized controlled trial. JAMA 2009; 301:1547–1555.
- Smith CD, Alguire PC. Is cardiac stress testing appropriate in asymptomatic adults at low risk? Cleve Clin J Med 2014; 81:405–406.
- Young LH, Wackers FJ, Chyun DA, et al; DIAD Investigators. Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes: the DIAD study: a randomized controlled trial. JAMA 2009; 301:1547–1555.