User login
Hospitalists Share Strategies to Overcome Career-Related Struggles
LAS VEGAS—If she said it once, Patience Reich, MD, SFHM, said it a half-dozen times during SHM’s annual meeting: “Let it go.”
“You can’t be Martha Stewart and a perfect doctor. Just let it go,” said Dr. Reich, associate professor of internal medicine and associate faculty for the Office of Women in Medicine and Science at the Wake Forest School of Medicine in Winston-Salem, N.C., told about 75 female hospitalists during a two-hour workshop focused on women’s issues at the Mandalay Bay Resort and Casino. “Even in 2014, there are trade-offs to be made.
.jpg)
Dr. Reich and Rachel George, MD, MBA, CPE, SFHM, of Cogent Healthcare, have been moderating the workshop at SHM meetings for several years. They said the issues they encounter among hospitalists around the country, which are no different today than they were in years past, include gender bias, career advancement challenges, and the guilt some feel spending time away from their children or communicating with their stay-at-home husbands.
At HM14, workshop attendees searched for solutions to common struggles.
“Don’t pretend you can have it all,” Dr. George said. “It’s a myth ruining womankind. There’s nothing that says you have to be June Cleaver and Marcus Welby all rolled into one. We have to stop thinking that we have to do it.”
Dr. George told the workshop attendees that cooking and cleaning are so far down on her priority list that “they practically don’t exist.”
“It’s OK. My kids are happy and healthy,” she said. “It doesn’t matter if they come home to a dirty house or if they eat pizza. They’re going to survive. I think women put all that guilt on themselves. Some of it society does, but a lot of women put the guilt on themselves just because they don’t cook a three-course meal every night.”
Open Forum
The issues were much the same during a Special Interest Group attended by nearly 35 hospitalists and moderated by Melissa Mattison, MD, FACP, SFHM, of Beth Israel Deaconess Medical Center in Boston. Topics ranged from personal experiences with workplace discrimination to apprehension in pursuing leadership roles to “partner envy” and dealing with the “guilt” of being a working parent.
One hospitalist wondered how others dealt with harassment from patients. “I’m young, petite, and a minority,” she said. “I get ‘sweetie’ and ‘honey’ all the time from my patients.”
Another explained the difficulty of working full time while taking care of an elderly parent. Yet another admitted her desire for a role model, “as there are none in my area.”
“Men seem to have an innate drive to be the breadwinner,” one attendee said. “No matter how much help you have at home, it doesn’t take away the guilt I feel.”
Another said, “I think about all of these issues constantly.”
Dr. Mattison, a member of the annual meeting committee, left the 45-minute open forum with four action items:
- Increase the exposure of programming for issues related to work-life balance at annual meeting;
- Suggest keynote speakers who are not men;
- Create a toolkit for HM leaders and department of medicine leaders to help them understand work-life issues; and
- Create a community on the HMX portal to discuss work-life issues, “whether they are related to being a mother or father, juggling work and home, or whatever issues come up.”
The Key: Flex Schedules
Many physicians who choose a career in HM do it because of the work-life balance the specialty affords, and many of the challenges women hospitalists face at the local level revolve around the schedule. That’s how Zenobia JonesFoster, MD, MPH, a hospitalist at Wellstar Health in Atlanta, views it.
“I think it’s very facility-dependent. I think when we look for a job and decide where we want to go, we really need to understand the culture and how people advance within that culture,” said Dr. JonesFoster, who attended the women’s issues workshop. “The academic environment has a lot more deferred policy and bureaucracy versus a private institution, but you’re going to find that anywhere.”
A hospitalist for a little more than two years, Dr. JonesFoster has two young children, ages one and three, and works in a group with 30 full-time hospitalists and 10 nurse practitioners and physician assistants. Her husband is a businessman, so schedules and work-life balance are a major concern.
“If I was given a job opportunity Monday through Friday, regular work hours, there’s no way I would take it because of the flexibility of hospital medicine hours, with the seven-on seven-off schedule,” she said. “The time I have off, I get to just be a mom and not think about work. But when I’m at work, I love it.”
Dr. JonesFoster’s group has seen an increase in patient census recently and just went live with a new hospital-wide electronic health records system, which has opened up more shifts and moonlighting opportunities. Attending her first annual meeting, she was most interested in learning the pros and cons of leadership positions, because her health system “offers a lot of opportunity for advancement” and is “talking about adding a residency program.”
“Another thing I wanted to learn about was mentorship,” she said. “I wanted to meet women who have done this before, who have had children, who are working full-time trying to do a little bit of everything. I wanted to see how they did it and try and learn from their experiences.”
From all accounts, mission accomplished.
Richard Quinn is a freelance writer in New Jersey.
LAS VEGAS—If she said it once, Patience Reich, MD, SFHM, said it a half-dozen times during SHM’s annual meeting: “Let it go.”
“You can’t be Martha Stewart and a perfect doctor. Just let it go,” said Dr. Reich, associate professor of internal medicine and associate faculty for the Office of Women in Medicine and Science at the Wake Forest School of Medicine in Winston-Salem, N.C., told about 75 female hospitalists during a two-hour workshop focused on women’s issues at the Mandalay Bay Resort and Casino. “Even in 2014, there are trade-offs to be made.
Dr. Reich and Rachel George, MD, MBA, CPE, SFHM, of Cogent Healthcare, have been moderating the workshop at SHM meetings for several years. They said the issues they encounter among hospitalists around the country, which are no different today than they were in years past, include gender bias, career advancement challenges, and the guilt some feel spending time away from their children or communicating with their stay-at-home husbands.
At HM14, workshop attendees searched for solutions to common struggles.
“Don’t pretend you can have it all,” Dr. George said. “It’s a myth ruining womankind. There’s nothing that says you have to be June Cleaver and Marcus Welby all rolled into one. We have to stop thinking that we have to do it.”
Dr. George told the workshop attendees that cooking and cleaning are so far down on her priority list that “they practically don’t exist.”
“It’s OK. My kids are happy and healthy,” she said. “It doesn’t matter if they come home to a dirty house or if they eat pizza. They’re going to survive. I think women put all that guilt on themselves. Some of it society does, but a lot of women put the guilt on themselves just because they don’t cook a three-course meal every night.”
Open Forum
The issues were much the same during a Special Interest Group attended by nearly 35 hospitalists and moderated by Melissa Mattison, MD, FACP, SFHM, of Beth Israel Deaconess Medical Center in Boston. Topics ranged from personal experiences with workplace discrimination to apprehension in pursuing leadership roles to “partner envy” and dealing with the “guilt” of being a working parent.
One hospitalist wondered how others dealt with harassment from patients. “I’m young, petite, and a minority,” she said. “I get ‘sweetie’ and ‘honey’ all the time from my patients.”
Another explained the difficulty of working full time while taking care of an elderly parent. Yet another admitted her desire for a role model, “as there are none in my area.”
“Men seem to have an innate drive to be the breadwinner,” one attendee said. “No matter how much help you have at home, it doesn’t take away the guilt I feel.”
Another said, “I think about all of these issues constantly.”
Dr. Mattison, a member of the annual meeting committee, left the 45-minute open forum with four action items:
- Increase the exposure of programming for issues related to work-life balance at annual meeting;
- Suggest keynote speakers who are not men;
- Create a toolkit for HM leaders and department of medicine leaders to help them understand work-life issues; and
- Create a community on the HMX portal to discuss work-life issues, “whether they are related to being a mother or father, juggling work and home, or whatever issues come up.”
The Key: Flex Schedules
Many physicians who choose a career in HM do it because of the work-life balance the specialty affords, and many of the challenges women hospitalists face at the local level revolve around the schedule. That’s how Zenobia JonesFoster, MD, MPH, a hospitalist at Wellstar Health in Atlanta, views it.
“I think it’s very facility-dependent. I think when we look for a job and decide where we want to go, we really need to understand the culture and how people advance within that culture,” said Dr. JonesFoster, who attended the women’s issues workshop. “The academic environment has a lot more deferred policy and bureaucracy versus a private institution, but you’re going to find that anywhere.”
A hospitalist for a little more than two years, Dr. JonesFoster has two young children, ages one and three, and works in a group with 30 full-time hospitalists and 10 nurse practitioners and physician assistants. Her husband is a businessman, so schedules and work-life balance are a major concern.
“If I was given a job opportunity Monday through Friday, regular work hours, there’s no way I would take it because of the flexibility of hospital medicine hours, with the seven-on seven-off schedule,” she said. “The time I have off, I get to just be a mom and not think about work. But when I’m at work, I love it.”
Dr. JonesFoster’s group has seen an increase in patient census recently and just went live with a new hospital-wide electronic health records system, which has opened up more shifts and moonlighting opportunities. Attending her first annual meeting, she was most interested in learning the pros and cons of leadership positions, because her health system “offers a lot of opportunity for advancement” and is “talking about adding a residency program.”
“Another thing I wanted to learn about was mentorship,” she said. “I wanted to meet women who have done this before, who have had children, who are working full-time trying to do a little bit of everything. I wanted to see how they did it and try and learn from their experiences.”
From all accounts, mission accomplished.
Richard Quinn is a freelance writer in New Jersey.
LAS VEGAS—If she said it once, Patience Reich, MD, SFHM, said it a half-dozen times during SHM’s annual meeting: “Let it go.”
“You can’t be Martha Stewart and a perfect doctor. Just let it go,” said Dr. Reich, associate professor of internal medicine and associate faculty for the Office of Women in Medicine and Science at the Wake Forest School of Medicine in Winston-Salem, N.C., told about 75 female hospitalists during a two-hour workshop focused on women’s issues at the Mandalay Bay Resort and Casino. “Even in 2014, there are trade-offs to be made.
Dr. Reich and Rachel George, MD, MBA, CPE, SFHM, of Cogent Healthcare, have been moderating the workshop at SHM meetings for several years. They said the issues they encounter among hospitalists around the country, which are no different today than they were in years past, include gender bias, career advancement challenges, and the guilt some feel spending time away from their children or communicating with their stay-at-home husbands.
At HM14, workshop attendees searched for solutions to common struggles.
“Don’t pretend you can have it all,” Dr. George said. “It’s a myth ruining womankind. There’s nothing that says you have to be June Cleaver and Marcus Welby all rolled into one. We have to stop thinking that we have to do it.”
Dr. George told the workshop attendees that cooking and cleaning are so far down on her priority list that “they practically don’t exist.”
“It’s OK. My kids are happy and healthy,” she said. “It doesn’t matter if they come home to a dirty house or if they eat pizza. They’re going to survive. I think women put all that guilt on themselves. Some of it society does, but a lot of women put the guilt on themselves just because they don’t cook a three-course meal every night.”
Open Forum
The issues were much the same during a Special Interest Group attended by nearly 35 hospitalists and moderated by Melissa Mattison, MD, FACP, SFHM, of Beth Israel Deaconess Medical Center in Boston. Topics ranged from personal experiences with workplace discrimination to apprehension in pursuing leadership roles to “partner envy” and dealing with the “guilt” of being a working parent.
One hospitalist wondered how others dealt with harassment from patients. “I’m young, petite, and a minority,” she said. “I get ‘sweetie’ and ‘honey’ all the time from my patients.”
Another explained the difficulty of working full time while taking care of an elderly parent. Yet another admitted her desire for a role model, “as there are none in my area.”
“Men seem to have an innate drive to be the breadwinner,” one attendee said. “No matter how much help you have at home, it doesn’t take away the guilt I feel.”
Another said, “I think about all of these issues constantly.”
Dr. Mattison, a member of the annual meeting committee, left the 45-minute open forum with four action items:
- Increase the exposure of programming for issues related to work-life balance at annual meeting;
- Suggest keynote speakers who are not men;
- Create a toolkit for HM leaders and department of medicine leaders to help them understand work-life issues; and
- Create a community on the HMX portal to discuss work-life issues, “whether they are related to being a mother or father, juggling work and home, or whatever issues come up.”
The Key: Flex Schedules
Many physicians who choose a career in HM do it because of the work-life balance the specialty affords, and many of the challenges women hospitalists face at the local level revolve around the schedule. That’s how Zenobia JonesFoster, MD, MPH, a hospitalist at Wellstar Health in Atlanta, views it.
“I think it’s very facility-dependent. I think when we look for a job and decide where we want to go, we really need to understand the culture and how people advance within that culture,” said Dr. JonesFoster, who attended the women’s issues workshop. “The academic environment has a lot more deferred policy and bureaucracy versus a private institution, but you’re going to find that anywhere.”
A hospitalist for a little more than two years, Dr. JonesFoster has two young children, ages one and three, and works in a group with 30 full-time hospitalists and 10 nurse practitioners and physician assistants. Her husband is a businessman, so schedules and work-life balance are a major concern.
“If I was given a job opportunity Monday through Friday, regular work hours, there’s no way I would take it because of the flexibility of hospital medicine hours, with the seven-on seven-off schedule,” she said. “The time I have off, I get to just be a mom and not think about work. But when I’m at work, I love it.”
Dr. JonesFoster’s group has seen an increase in patient census recently and just went live with a new hospital-wide electronic health records system, which has opened up more shifts and moonlighting opportunities. Attending her first annual meeting, she was most interested in learning the pros and cons of leadership positions, because her health system “offers a lot of opportunity for advancement” and is “talking about adding a residency program.”
“Another thing I wanted to learn about was mentorship,” she said. “I wanted to meet women who have done this before, who have had children, who are working full-time trying to do a little bit of everything. I wanted to see how they did it and try and learn from their experiences.”
From all accounts, mission accomplished.
Richard Quinn is a freelance writer in New Jersey.

Open Surgical Dislocation Versus Arthroscopic Treatment of Femoroacetabular Impingement
Analysis of Intermediate Outcomes of Glenoid Bone Grafting in Revision Shoulder Arthroplasty
The Applications of Biologics in Orthopedic Surgery
As orthopedic surgeons, we have done a great job continually trying to improve the outcomes of our patients. During the first decade of the 21st century, many of these advances centered on strengthening the biomechanics of constructs used to repair patients’ pathologies. Trauma surgeons incorporated minimally invasive osteosynthesis with locked plates; shoulder surgeons began using double-row and transosseous-equivalent rotator cuff repairs. As a result of these shifts in treatment methods, healing rates and outcomes have improved. Unfortunately, to take rotator cuff repair as an example, healing rates have still not achieved 100%. To reach this goal in the future, biologic manipulation of the healing milieu will play a critical role.
This issue of The American Journal of Orthopedics features an article on the “Analysis of Intermediate Outcomes of Glenoid Bone Grafting in Revision Shoulder Arthroplasty” by Dr. Schubkegel and colleagues. While not as cutting edge or in vogue as growth factors or stem cells, bone graft is one of the original biologics used by orthopedic surgeons. The authors review the midterm results of glenoid bone grafting secondary to failed total shoulder arthroplasty and find that bone grafting resulted in good functional outcomes. Studies such as this one highlight the important role that biologics play, particularly in challenging or revision cases.
Platelet-rich plasma (PRP) is another biologic that is presently available for use. Reviewing its use as it pertains to orthopedics highlights both the potential benefits
as well as the difficulties associated with incorporating biologics into everyday practice. In 2006, Mishra and colleagues1 published one of the first studies that looked at the potential benefits of using PRP to treat lateral epicondylitis. While, from a purist’s standpoint, it wasn’t the best-designed study, it did provide cause for optimism with regard to a novel treatment option for an age-old problem. Since that time, hundreds of studies have been done on PRP looking at its potential treatment uses in everything from tennis elbow to rotator cuff repairs.
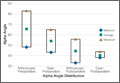
Study designs have improved, and with that, so have our indications for using PRP. Interestingly though, the more we study PRP (and other exogenous growth factors), it almost seems as if more questions are raised than answered. For instance, preparing PRP from a given patient will result in different concentrations of the PRP depending on what time of the day the patient’s blood is drawn. What is the ideal time to prepare the PRP? Additionally, PRP prepared using different companies’ systems results in different concentrations of growth factors. So, not only is a given patient’s PRP different at different times of day, but these differences get magnified by using different preparation systems.
One of the main issues with tendon healing is that the tissue heals via reactive scar formation instead of truly regenerating new tendon. In this scenario, it is possible that adding PRP or other growth factors to the repair construct may only increase scar formation. Along these lines, newer work is focusing on cellular solutions to healing problems. Stem cells, which are undifferentiated, unspecialized cells, have shown potential to improve healing when added to injury/repair sites. Thus far, unfortunately, there is very little clinical data pertaining to their use in orthopedic surgery. Compounding this problem are the US Food and Drug Administration’s regulations on manipulating stem cells.
In the future, it is likely that growth factors, cytokines, PRP, and cellular approaches will be used to enhance healing. For now, a significant amount of preclinical work is being done to figure out the most advantageous ways to use such adjuvants. This is an extremely exciting field with ample opportunities to
answer well-designed research questions. Future issues of this journal will likely highlight such studies. ◾
Reference
1. Mishra A, Pavelko T. Treatment of chronic elbow tendinosis with buffered
platelet-rich plasma. Am J Sports Med. 2006;34(11):1774-1778.
As orthopedic surgeons, we have done a great job continually trying to improve the outcomes of our patients. During the first decade of the 21st century, many of these advances centered on strengthening the biomechanics of constructs used to repair patients’ pathologies. Trauma surgeons incorporated minimally invasive osteosynthesis with locked plates; shoulder surgeons began using double-row and transosseous-equivalent rotator cuff repairs. As a result of these shifts in treatment methods, healing rates and outcomes have improved. Unfortunately, to take rotator cuff repair as an example, healing rates have still not achieved 100%. To reach this goal in the future, biologic manipulation of the healing milieu will play a critical role.
This issue of The American Journal of Orthopedics features an article on the “Analysis of Intermediate Outcomes of Glenoid Bone Grafting in Revision Shoulder Arthroplasty” by Dr. Schubkegel and colleagues. While not as cutting edge or in vogue as growth factors or stem cells, bone graft is one of the original biologics used by orthopedic surgeons. The authors review the midterm results of glenoid bone grafting secondary to failed total shoulder arthroplasty and find that bone grafting resulted in good functional outcomes. Studies such as this one highlight the important role that biologics play, particularly in challenging or revision cases.
Platelet-rich plasma (PRP) is another biologic that is presently available for use. Reviewing its use as it pertains to orthopedics highlights both the potential benefits
as well as the difficulties associated with incorporating biologics into everyday practice. In 2006, Mishra and colleagues1 published one of the first studies that looked at the potential benefits of using PRP to treat lateral epicondylitis. While, from a purist’s standpoint, it wasn’t the best-designed study, it did provide cause for optimism with regard to a novel treatment option for an age-old problem. Since that time, hundreds of studies have been done on PRP looking at its potential treatment uses in everything from tennis elbow to rotator cuff repairs.
Study designs have improved, and with that, so have our indications for using PRP. Interestingly though, the more we study PRP (and other exogenous growth factors), it almost seems as if more questions are raised than answered. For instance, preparing PRP from a given patient will result in different concentrations of the PRP depending on what time of the day the patient’s blood is drawn. What is the ideal time to prepare the PRP? Additionally, PRP prepared using different companies’ systems results in different concentrations of growth factors. So, not only is a given patient’s PRP different at different times of day, but these differences get magnified by using different preparation systems.
One of the main issues with tendon healing is that the tissue heals via reactive scar formation instead of truly regenerating new tendon. In this scenario, it is possible that adding PRP or other growth factors to the repair construct may only increase scar formation. Along these lines, newer work is focusing on cellular solutions to healing problems. Stem cells, which are undifferentiated, unspecialized cells, have shown potential to improve healing when added to injury/repair sites. Thus far, unfortunately, there is very little clinical data pertaining to their use in orthopedic surgery. Compounding this problem are the US Food and Drug Administration’s regulations on manipulating stem cells.
In the future, it is likely that growth factors, cytokines, PRP, and cellular approaches will be used to enhance healing. For now, a significant amount of preclinical work is being done to figure out the most advantageous ways to use such adjuvants. This is an extremely exciting field with ample opportunities to
answer well-designed research questions. Future issues of this journal will likely highlight such studies. ◾
Reference
1. Mishra A, Pavelko T. Treatment of chronic elbow tendinosis with buffered
platelet-rich plasma. Am J Sports Med. 2006;34(11):1774-1778.
As orthopedic surgeons, we have done a great job continually trying to improve the outcomes of our patients. During the first decade of the 21st century, many of these advances centered on strengthening the biomechanics of constructs used to repair patients’ pathologies. Trauma surgeons incorporated minimally invasive osteosynthesis with locked plates; shoulder surgeons began using double-row and transosseous-equivalent rotator cuff repairs. As a result of these shifts in treatment methods, healing rates and outcomes have improved. Unfortunately, to take rotator cuff repair as an example, healing rates have still not achieved 100%. To reach this goal in the future, biologic manipulation of the healing milieu will play a critical role.
This issue of The American Journal of Orthopedics features an article on the “Analysis of Intermediate Outcomes of Glenoid Bone Grafting in Revision Shoulder Arthroplasty” by Dr. Schubkegel and colleagues. While not as cutting edge or in vogue as growth factors or stem cells, bone graft is one of the original biologics used by orthopedic surgeons. The authors review the midterm results of glenoid bone grafting secondary to failed total shoulder arthroplasty and find that bone grafting resulted in good functional outcomes. Studies such as this one highlight the important role that biologics play, particularly in challenging or revision cases.
Platelet-rich plasma (PRP) is another biologic that is presently available for use. Reviewing its use as it pertains to orthopedics highlights both the potential benefits
as well as the difficulties associated with incorporating biologics into everyday practice. In 2006, Mishra and colleagues1 published one of the first studies that looked at the potential benefits of using PRP to treat lateral epicondylitis. While, from a purist’s standpoint, it wasn’t the best-designed study, it did provide cause for optimism with regard to a novel treatment option for an age-old problem. Since that time, hundreds of studies have been done on PRP looking at its potential treatment uses in everything from tennis elbow to rotator cuff repairs.
Study designs have improved, and with that, so have our indications for using PRP. Interestingly though, the more we study PRP (and other exogenous growth factors), it almost seems as if more questions are raised than answered. For instance, preparing PRP from a given patient will result in different concentrations of the PRP depending on what time of the day the patient’s blood is drawn. What is the ideal time to prepare the PRP? Additionally, PRP prepared using different companies’ systems results in different concentrations of growth factors. So, not only is a given patient’s PRP different at different times of day, but these differences get magnified by using different preparation systems.
One of the main issues with tendon healing is that the tissue heals via reactive scar formation instead of truly regenerating new tendon. In this scenario, it is possible that adding PRP or other growth factors to the repair construct may only increase scar formation. Along these lines, newer work is focusing on cellular solutions to healing problems. Stem cells, which are undifferentiated, unspecialized cells, have shown potential to improve healing when added to injury/repair sites. Thus far, unfortunately, there is very little clinical data pertaining to their use in orthopedic surgery. Compounding this problem are the US Food and Drug Administration’s regulations on manipulating stem cells.
In the future, it is likely that growth factors, cytokines, PRP, and cellular approaches will be used to enhance healing. For now, a significant amount of preclinical work is being done to figure out the most advantageous ways to use such adjuvants. This is an extremely exciting field with ample opportunities to
answer well-designed research questions. Future issues of this journal will likely highlight such studies. ◾
Reference
1. Mishra A, Pavelko T. Treatment of chronic elbow tendinosis with buffered
platelet-rich plasma. Am J Sports Med. 2006;34(11):1774-1778.

Vomiting, abdominal pain, compulsive bathing—Dx?
THE CASE
A 33-year-old multiparous pregnant woman at 7 weeks gestation came to our clinic after 3 days of vomiting. She had been vomiting up to 7 times a day and had right lower quadrant pain radiating into her flank. She described the pain as continuous, severe, and “crampy” in nature. The patient also complained of a loss of appetite, nonbloody diarrhea, fever, chills, night sweats, and urinary urgency. She’d tried acetaminophen without relief and repeatedly took hot showers—for up to 6 hours each day—which she said temporarily improved her symptoms.
At presentation, the patient’s vital signs were normal, with no orthostatic changes in blood pressure or heart rate. A physical and pelvic examination revealed tenderness in her right lower quadrant and flank and a mildly tender uterus. Chlamydia culture was positive. Pelvic ultrasound showed a normal intrauterine pregnancy, a surgically absent right ovary and tube, and a normal left ovary and tube. Her appendix was not visualized. Laboratory results, including a basic metabolic panel, complete blood count, liver function tests, amylase test, lipase test, and urinalysis were normal.
On admission, the patient received intravenous (IV) fluids, oral ondansetron 4 mg every 6 hours and IV hydromorphone 2 mg every 3 to 6 hours. Because her symptoms did not respond to initial therapy, we administered IV metoclopramide 10 mg every 6 to 8 hours and promethazine 12.5 mg rectally 3 times daily. After a discussion of the risks associated with benzodiazepine use during pregnancy, the patient agreed to treatment with IV lorazepam 2 mg. She was also informed of the risks of radiation during pregnancy,1 and opted to undergo an abdominal computed tomography (CT) scan and ultrasound. No abnormalities were found.
The patient said that in prior pregnancies, she had experienced nausea and vomiting during the first trimester, but that her current symptoms were much worse. She also said she’d been smoking cannabis twice a day for a year.
THE DIAGNOSIS
Based on our patient’s symptoms, her history of daily cannabis use, and the lack of improvement from antiemetics and analgesics, we concluded that she was suffering from cannabinoid hyperemesis. By Day 3, her symptoms improved and she could tolerate oral fluids. We advised her to stop using cannabis and discharged her.
One week later, the patient reported that she had not smoked cannabis since she’d been admitted to the hospital and that her symptoms, including her compulsive bathing, continued to improve. The patient subsequently delivered a healthy newborn at term.
DISCUSSION
A drug sometimes used to relieve nausea may make it much worse
First described in 2004, cannabinoid hyperemesis is a triad of vomiting, abdominal pain, and compulsive bathing in patients with chronic cannabis use.2 Other symptoms include subjective fevers, chills, and diaphoresis. Symptoms of cannabinoid hyperemesis may persist for weeks and spontaneously remit for weeks to months. The syndrome can lead to serious complications, including volume depletion, weight loss of 5 to 10 kg per episode, burns caused by frequent hot showers, and esophageal rupture.2-4 The frequent hot baths or showers associated with cannabinoid hyperemesis are potentially harmful to the fetus—hyperthermia during early gestation can cause fetal mental deficiency, seizures, and neural tube defects.5-8
The association between cannabinoid hyperemesis and pregnancy is unknown. However, because 11% of pregnant women use cannabis,9 many women may be at risk for the condition. Pregnant women may use cannabis recreationally or to combat morning sickness. The high rate of cannabis use in this population may be due in part to a lack of perceived risk to the fetus, although prenatal cannabis exposure is associated with reduced fetal growth.10
Active component of cannabis may trigger vomiting, pain
While chronic cannabis use causes cannabinoid hyperemesis, the pathogenesis and pathophysiology of the disease remain unknown. Delta-9-tetrahydrocannabinol (THC), the active ingredient in cannabis, appears to be to blame.11-15
THC is lipophilic and accumulates in the body with chronic cannabis use. At higher accumulated levels, THC binds to cannabinoid receptors in the intestinal nerve plexus, causing lower esophageal sphincter relaxation and gastrointestinal motility inhibition.11,12 At high concentrations, THC also binds to CB1 receptors in the hypothalamus, which is responsible for integrating satiety, thirst, digestive function, and thermoregulation.13-15 This causes hypothalamic dysregulation that may be temporarily relieved by hot showers.2
Possible causes of our patient’s signs and symptoms included appendicitis, pyelonephritis, nephrolithiasis, ectopic pregnancy, and pelvic inflammatory disease. Our patient’s normal laboratory and imaging studies made these diagnoses less likely. Her lack of a fallopian tube or ovary on the right side prompted us to quickly rule out a right-sided ectopic implantation.
We considered our patient’s chlamydial infection as the source of her symptoms. However, she had experienced no vaginal discharge or bleeding, and her nausea and abdominal pain did not improve with a therapeutic dose of azithromycin. Imaging showed no evidence of chlamydia-associated complications, such as pelvic inflammatory disease or tubo-ovarian abscess, both of which are uncommon in pregnancy.
THE TAKEAWAY
Consider cannabinoid hyperemesis in patients who are experiencing vomiting and abdominal pain that are temporarily relieved by bathing in hot water. Ask such patients about their cannabis use, and strongly encourage them to discontinue the drug. Counsel pregnant women about the maternal and fetal risks of cannabis use and the potential teratogenicity of hot water bathing. Provide IV fluids to ensure adequate hydration and a benzodiazepine as appropriate for anxiety and cannabis withdrawal symptoms.16 Advise patients that their symptoms may return within weeks to months if they resume using cannabis.2,17
1. ACOG Committee on Obstetric Practice. ACOG Committee Opinion. Number 299, September 2004 (replaces No. 158, September 1995). Guidelines for diagnostic imaging during pregnancy. Obstet Gynecol. 2004;104:647-651.
2. Allen JH, de Moore GM, Heddle R, et al. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut. 2004;53:1566-1570.
3. Sontineni SP, Chaudhary S, Sontineni V, et al. Cannabinoid hyperemesis syndrome: clinical diagnosis of an underrecognised manifestation of chronic cannabis abuse. World J Gastroenterol. 2009;15:1264-1266.
4. de Moore GM, Baker J, Bui T. Psychogenic vomiting complicated by marijuana abuse and spontaneous pneumomediastinum. Aust N Z J Psychiatry. 1996;30:290-294.
5. Smith DW, Clarren SK, Harvey MA. Hyperthermia as a possible teratogenic agent. J Pediatr. 1978;92:878-883.
6. Shiota K. Neural tube defects and maternal hyperthermia in early pregnancy: epidemiology in a human embryo population. Am J Med Genet. 1982;12:281-288.
7. Milunsky A, Ulcickas M, Rothman K, et al. Maternal heat exposure and neural tube defects. JAMA. 1992;268:882-885.
8. Miller P, Smith DW, Shepard TH. Maternal hyperthermia as a possible cause of anencephaly. Lancet. 1978;11:1519-1521.
9. Substance Abuse and Mental Health Services Administration Web site. Results from the 2008 National Survey on Drug Use and Health: national findings. Available at: http://www.samhsa.gov/data/nsduh/2k8nsduh/2k8Results.htm. Accessed December 15, 2011.
10. Gray TR, Eiden RD, Leonard KD, et al. Identifying prenatal cannabis exposure and effects of concurrent tobacco exposure on neonatal growth. Clin Chem. 2010;56:1442-1450.
11. Izzo AA, Coutts AA. Cannabinoids and the digestive tract. Handb Exp Pharmacol. 2005;(168):573-598.
12. McCallum RW, Soykan I, Sridhar KR, et al. Delta-9-tetrahydrocannabinol delays the gastric emptying of solid food in humans: a double-blind, randomized study. Aliment Pharmacol Ther. 1999;13:77-80.
13. Pertwee RG. Pharmacology of cannabinoid CB1 and CB2 receptors. Pharmacol Ther. 1997;74:129-180.
14. Childers SR, Breivogel CS. Cannabis and endogenous cannabinoid systems. Drug Alcohol Dependence. 1998;51:173-187.
15. Herkenham M, Lynn AB, Little MD, et al. Cannabinoid receptor localization in brain. Proc Natl Acad Sci. 1990;87:1932-1936.
16. Bergman U, Rosa FW, Baum C, et al. Effects of exposure to benzodiazepine during fetal life. Lancet. 1992;340:694-696.
17. Wallace D, Martin AL, Park B. Cannabinoid hyperemesis: marijuana puts patients in hot water. Australas Psychiatry. 2007;15:156-158.
THE CASE
A 33-year-old multiparous pregnant woman at 7 weeks gestation came to our clinic after 3 days of vomiting. She had been vomiting up to 7 times a day and had right lower quadrant pain radiating into her flank. She described the pain as continuous, severe, and “crampy” in nature. The patient also complained of a loss of appetite, nonbloody diarrhea, fever, chills, night sweats, and urinary urgency. She’d tried acetaminophen without relief and repeatedly took hot showers—for up to 6 hours each day—which she said temporarily improved her symptoms.
At presentation, the patient’s vital signs were normal, with no orthostatic changes in blood pressure or heart rate. A physical and pelvic examination revealed tenderness in her right lower quadrant and flank and a mildly tender uterus. Chlamydia culture was positive. Pelvic ultrasound showed a normal intrauterine pregnancy, a surgically absent right ovary and tube, and a normal left ovary and tube. Her appendix was not visualized. Laboratory results, including a basic metabolic panel, complete blood count, liver function tests, amylase test, lipase test, and urinalysis were normal.
On admission, the patient received intravenous (IV) fluids, oral ondansetron 4 mg every 6 hours and IV hydromorphone 2 mg every 3 to 6 hours. Because her symptoms did not respond to initial therapy, we administered IV metoclopramide 10 mg every 6 to 8 hours and promethazine 12.5 mg rectally 3 times daily. After a discussion of the risks associated with benzodiazepine use during pregnancy, the patient agreed to treatment with IV lorazepam 2 mg. She was also informed of the risks of radiation during pregnancy,1 and opted to undergo an abdominal computed tomography (CT) scan and ultrasound. No abnormalities were found.
The patient said that in prior pregnancies, she had experienced nausea and vomiting during the first trimester, but that her current symptoms were much worse. She also said she’d been smoking cannabis twice a day for a year.
THE DIAGNOSIS
Based on our patient’s symptoms, her history of daily cannabis use, and the lack of improvement from antiemetics and analgesics, we concluded that she was suffering from cannabinoid hyperemesis. By Day 3, her symptoms improved and she could tolerate oral fluids. We advised her to stop using cannabis and discharged her.
One week later, the patient reported that she had not smoked cannabis since she’d been admitted to the hospital and that her symptoms, including her compulsive bathing, continued to improve. The patient subsequently delivered a healthy newborn at term.
DISCUSSION
A drug sometimes used to relieve nausea may make it much worse
First described in 2004, cannabinoid hyperemesis is a triad of vomiting, abdominal pain, and compulsive bathing in patients with chronic cannabis use.2 Other symptoms include subjective fevers, chills, and diaphoresis. Symptoms of cannabinoid hyperemesis may persist for weeks and spontaneously remit for weeks to months. The syndrome can lead to serious complications, including volume depletion, weight loss of 5 to 10 kg per episode, burns caused by frequent hot showers, and esophageal rupture.2-4 The frequent hot baths or showers associated with cannabinoid hyperemesis are potentially harmful to the fetus—hyperthermia during early gestation can cause fetal mental deficiency, seizures, and neural tube defects.5-8
The association between cannabinoid hyperemesis and pregnancy is unknown. However, because 11% of pregnant women use cannabis,9 many women may be at risk for the condition. Pregnant women may use cannabis recreationally or to combat morning sickness. The high rate of cannabis use in this population may be due in part to a lack of perceived risk to the fetus, although prenatal cannabis exposure is associated with reduced fetal growth.10
Active component of cannabis may trigger vomiting, pain
While chronic cannabis use causes cannabinoid hyperemesis, the pathogenesis and pathophysiology of the disease remain unknown. Delta-9-tetrahydrocannabinol (THC), the active ingredient in cannabis, appears to be to blame.11-15
THC is lipophilic and accumulates in the body with chronic cannabis use. At higher accumulated levels, THC binds to cannabinoid receptors in the intestinal nerve plexus, causing lower esophageal sphincter relaxation and gastrointestinal motility inhibition.11,12 At high concentrations, THC also binds to CB1 receptors in the hypothalamus, which is responsible for integrating satiety, thirst, digestive function, and thermoregulation.13-15 This causes hypothalamic dysregulation that may be temporarily relieved by hot showers.2
Possible causes of our patient’s signs and symptoms included appendicitis, pyelonephritis, nephrolithiasis, ectopic pregnancy, and pelvic inflammatory disease. Our patient’s normal laboratory and imaging studies made these diagnoses less likely. Her lack of a fallopian tube or ovary on the right side prompted us to quickly rule out a right-sided ectopic implantation.
We considered our patient’s chlamydial infection as the source of her symptoms. However, she had experienced no vaginal discharge or bleeding, and her nausea and abdominal pain did not improve with a therapeutic dose of azithromycin. Imaging showed no evidence of chlamydia-associated complications, such as pelvic inflammatory disease or tubo-ovarian abscess, both of which are uncommon in pregnancy.
THE TAKEAWAY
Consider cannabinoid hyperemesis in patients who are experiencing vomiting and abdominal pain that are temporarily relieved by bathing in hot water. Ask such patients about their cannabis use, and strongly encourage them to discontinue the drug. Counsel pregnant women about the maternal and fetal risks of cannabis use and the potential teratogenicity of hot water bathing. Provide IV fluids to ensure adequate hydration and a benzodiazepine as appropriate for anxiety and cannabis withdrawal symptoms.16 Advise patients that their symptoms may return within weeks to months if they resume using cannabis.2,17
THE CASE
A 33-year-old multiparous pregnant woman at 7 weeks gestation came to our clinic after 3 days of vomiting. She had been vomiting up to 7 times a day and had right lower quadrant pain radiating into her flank. She described the pain as continuous, severe, and “crampy” in nature. The patient also complained of a loss of appetite, nonbloody diarrhea, fever, chills, night sweats, and urinary urgency. She’d tried acetaminophen without relief and repeatedly took hot showers—for up to 6 hours each day—which she said temporarily improved her symptoms.
At presentation, the patient’s vital signs were normal, with no orthostatic changes in blood pressure or heart rate. A physical and pelvic examination revealed tenderness in her right lower quadrant and flank and a mildly tender uterus. Chlamydia culture was positive. Pelvic ultrasound showed a normal intrauterine pregnancy, a surgically absent right ovary and tube, and a normal left ovary and tube. Her appendix was not visualized. Laboratory results, including a basic metabolic panel, complete blood count, liver function tests, amylase test, lipase test, and urinalysis were normal.
On admission, the patient received intravenous (IV) fluids, oral ondansetron 4 mg every 6 hours and IV hydromorphone 2 mg every 3 to 6 hours. Because her symptoms did not respond to initial therapy, we administered IV metoclopramide 10 mg every 6 to 8 hours and promethazine 12.5 mg rectally 3 times daily. After a discussion of the risks associated with benzodiazepine use during pregnancy, the patient agreed to treatment with IV lorazepam 2 mg. She was also informed of the risks of radiation during pregnancy,1 and opted to undergo an abdominal computed tomography (CT) scan and ultrasound. No abnormalities were found.
The patient said that in prior pregnancies, she had experienced nausea and vomiting during the first trimester, but that her current symptoms were much worse. She also said she’d been smoking cannabis twice a day for a year.
THE DIAGNOSIS
Based on our patient’s symptoms, her history of daily cannabis use, and the lack of improvement from antiemetics and analgesics, we concluded that she was suffering from cannabinoid hyperemesis. By Day 3, her symptoms improved and she could tolerate oral fluids. We advised her to stop using cannabis and discharged her.
One week later, the patient reported that she had not smoked cannabis since she’d been admitted to the hospital and that her symptoms, including her compulsive bathing, continued to improve. The patient subsequently delivered a healthy newborn at term.
DISCUSSION
A drug sometimes used to relieve nausea may make it much worse
First described in 2004, cannabinoid hyperemesis is a triad of vomiting, abdominal pain, and compulsive bathing in patients with chronic cannabis use.2 Other symptoms include subjective fevers, chills, and diaphoresis. Symptoms of cannabinoid hyperemesis may persist for weeks and spontaneously remit for weeks to months. The syndrome can lead to serious complications, including volume depletion, weight loss of 5 to 10 kg per episode, burns caused by frequent hot showers, and esophageal rupture.2-4 The frequent hot baths or showers associated with cannabinoid hyperemesis are potentially harmful to the fetus—hyperthermia during early gestation can cause fetal mental deficiency, seizures, and neural tube defects.5-8
The association between cannabinoid hyperemesis and pregnancy is unknown. However, because 11% of pregnant women use cannabis,9 many women may be at risk for the condition. Pregnant women may use cannabis recreationally or to combat morning sickness. The high rate of cannabis use in this population may be due in part to a lack of perceived risk to the fetus, although prenatal cannabis exposure is associated with reduced fetal growth.10
Active component of cannabis may trigger vomiting, pain
While chronic cannabis use causes cannabinoid hyperemesis, the pathogenesis and pathophysiology of the disease remain unknown. Delta-9-tetrahydrocannabinol (THC), the active ingredient in cannabis, appears to be to blame.11-15
THC is lipophilic and accumulates in the body with chronic cannabis use. At higher accumulated levels, THC binds to cannabinoid receptors in the intestinal nerve plexus, causing lower esophageal sphincter relaxation and gastrointestinal motility inhibition.11,12 At high concentrations, THC also binds to CB1 receptors in the hypothalamus, which is responsible for integrating satiety, thirst, digestive function, and thermoregulation.13-15 This causes hypothalamic dysregulation that may be temporarily relieved by hot showers.2
Possible causes of our patient’s signs and symptoms included appendicitis, pyelonephritis, nephrolithiasis, ectopic pregnancy, and pelvic inflammatory disease. Our patient’s normal laboratory and imaging studies made these diagnoses less likely. Her lack of a fallopian tube or ovary on the right side prompted us to quickly rule out a right-sided ectopic implantation.
We considered our patient’s chlamydial infection as the source of her symptoms. However, she had experienced no vaginal discharge or bleeding, and her nausea and abdominal pain did not improve with a therapeutic dose of azithromycin. Imaging showed no evidence of chlamydia-associated complications, such as pelvic inflammatory disease or tubo-ovarian abscess, both of which are uncommon in pregnancy.
THE TAKEAWAY
Consider cannabinoid hyperemesis in patients who are experiencing vomiting and abdominal pain that are temporarily relieved by bathing in hot water. Ask such patients about their cannabis use, and strongly encourage them to discontinue the drug. Counsel pregnant women about the maternal and fetal risks of cannabis use and the potential teratogenicity of hot water bathing. Provide IV fluids to ensure adequate hydration and a benzodiazepine as appropriate for anxiety and cannabis withdrawal symptoms.16 Advise patients that their symptoms may return within weeks to months if they resume using cannabis.2,17
1. ACOG Committee on Obstetric Practice. ACOG Committee Opinion. Number 299, September 2004 (replaces No. 158, September 1995). Guidelines for diagnostic imaging during pregnancy. Obstet Gynecol. 2004;104:647-651.
2. Allen JH, de Moore GM, Heddle R, et al. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut. 2004;53:1566-1570.
3. Sontineni SP, Chaudhary S, Sontineni V, et al. Cannabinoid hyperemesis syndrome: clinical diagnosis of an underrecognised manifestation of chronic cannabis abuse. World J Gastroenterol. 2009;15:1264-1266.
4. de Moore GM, Baker J, Bui T. Psychogenic vomiting complicated by marijuana abuse and spontaneous pneumomediastinum. Aust N Z J Psychiatry. 1996;30:290-294.
5. Smith DW, Clarren SK, Harvey MA. Hyperthermia as a possible teratogenic agent. J Pediatr. 1978;92:878-883.
6. Shiota K. Neural tube defects and maternal hyperthermia in early pregnancy: epidemiology in a human embryo population. Am J Med Genet. 1982;12:281-288.
7. Milunsky A, Ulcickas M, Rothman K, et al. Maternal heat exposure and neural tube defects. JAMA. 1992;268:882-885.
8. Miller P, Smith DW, Shepard TH. Maternal hyperthermia as a possible cause of anencephaly. Lancet. 1978;11:1519-1521.
9. Substance Abuse and Mental Health Services Administration Web site. Results from the 2008 National Survey on Drug Use and Health: national findings. Available at: http://www.samhsa.gov/data/nsduh/2k8nsduh/2k8Results.htm. Accessed December 15, 2011.
10. Gray TR, Eiden RD, Leonard KD, et al. Identifying prenatal cannabis exposure and effects of concurrent tobacco exposure on neonatal growth. Clin Chem. 2010;56:1442-1450.
11. Izzo AA, Coutts AA. Cannabinoids and the digestive tract. Handb Exp Pharmacol. 2005;(168):573-598.
12. McCallum RW, Soykan I, Sridhar KR, et al. Delta-9-tetrahydrocannabinol delays the gastric emptying of solid food in humans: a double-blind, randomized study. Aliment Pharmacol Ther. 1999;13:77-80.
13. Pertwee RG. Pharmacology of cannabinoid CB1 and CB2 receptors. Pharmacol Ther. 1997;74:129-180.
14. Childers SR, Breivogel CS. Cannabis and endogenous cannabinoid systems. Drug Alcohol Dependence. 1998;51:173-187.
15. Herkenham M, Lynn AB, Little MD, et al. Cannabinoid receptor localization in brain. Proc Natl Acad Sci. 1990;87:1932-1936.
16. Bergman U, Rosa FW, Baum C, et al. Effects of exposure to benzodiazepine during fetal life. Lancet. 1992;340:694-696.
17. Wallace D, Martin AL, Park B. Cannabinoid hyperemesis: marijuana puts patients in hot water. Australas Psychiatry. 2007;15:156-158.
1. ACOG Committee on Obstetric Practice. ACOG Committee Opinion. Number 299, September 2004 (replaces No. 158, September 1995). Guidelines for diagnostic imaging during pregnancy. Obstet Gynecol. 2004;104:647-651.
2. Allen JH, de Moore GM, Heddle R, et al. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut. 2004;53:1566-1570.
3. Sontineni SP, Chaudhary S, Sontineni V, et al. Cannabinoid hyperemesis syndrome: clinical diagnosis of an underrecognised manifestation of chronic cannabis abuse. World J Gastroenterol. 2009;15:1264-1266.
4. de Moore GM, Baker J, Bui T. Psychogenic vomiting complicated by marijuana abuse and spontaneous pneumomediastinum. Aust N Z J Psychiatry. 1996;30:290-294.
5. Smith DW, Clarren SK, Harvey MA. Hyperthermia as a possible teratogenic agent. J Pediatr. 1978;92:878-883.
6. Shiota K. Neural tube defects and maternal hyperthermia in early pregnancy: epidemiology in a human embryo population. Am J Med Genet. 1982;12:281-288.
7. Milunsky A, Ulcickas M, Rothman K, et al. Maternal heat exposure and neural tube defects. JAMA. 1992;268:882-885.
8. Miller P, Smith DW, Shepard TH. Maternal hyperthermia as a possible cause of anencephaly. Lancet. 1978;11:1519-1521.
9. Substance Abuse and Mental Health Services Administration Web site. Results from the 2008 National Survey on Drug Use and Health: national findings. Available at: http://www.samhsa.gov/data/nsduh/2k8nsduh/2k8Results.htm. Accessed December 15, 2011.
10. Gray TR, Eiden RD, Leonard KD, et al. Identifying prenatal cannabis exposure and effects of concurrent tobacco exposure on neonatal growth. Clin Chem. 2010;56:1442-1450.
11. Izzo AA, Coutts AA. Cannabinoids and the digestive tract. Handb Exp Pharmacol. 2005;(168):573-598.
12. McCallum RW, Soykan I, Sridhar KR, et al. Delta-9-tetrahydrocannabinol delays the gastric emptying of solid food in humans: a double-blind, randomized study. Aliment Pharmacol Ther. 1999;13:77-80.
13. Pertwee RG. Pharmacology of cannabinoid CB1 and CB2 receptors. Pharmacol Ther. 1997;74:129-180.
14. Childers SR, Breivogel CS. Cannabis and endogenous cannabinoid systems. Drug Alcohol Dependence. 1998;51:173-187.
15. Herkenham M, Lynn AB, Little MD, et al. Cannabinoid receptor localization in brain. Proc Natl Acad Sci. 1990;87:1932-1936.
16. Bergman U, Rosa FW, Baum C, et al. Effects of exposure to benzodiazepine during fetal life. Lancet. 1992;340:694-696.
17. Wallace D, Martin AL, Park B. Cannabinoid hyperemesis: marijuana puts patients in hot water. Australas Psychiatry. 2007;15:156-158.

A simple way to reduce catheter-associated UTIs
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk of urinary tract infections (UTIs).1
Strength of recommendation
B: Based on a meta-analysis.
Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
Illustrative case
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and his urinary catheter soon will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2 Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species make up the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. Centers for Disease Control and Prevention (CDC) guidelines published in 2009 outline which patients are appropriate for catheterization, but do not recommend routine use of antibiotics to prevent CAUTIs.2 The 2014 Infectious Diseases Society of America guidelines, which came out before the study reported on here was published, state the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY: Meta-analysis shows prophylactic antibiotics reduce UTI ris
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed 7 studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of 2 surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including 2 that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to 3 days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics vs 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17 (95% confidence interval [CI], 12-30), with a risk ratio (RR) of .45 (95% CI, .28-.72). The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial, and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the 2 studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT'S NEW: We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
CAVEATS: Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk of attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION: Which antibiotics to use, and for how long, remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for 3 days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administering antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. Available at: http://www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed April 15, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk of urinary tract infections (UTIs).1
Strength of recommendation
B: Based on a meta-analysis.
Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
Illustrative case
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and his urinary catheter soon will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2 Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species make up the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. Centers for Disease Control and Prevention (CDC) guidelines published in 2009 outline which patients are appropriate for catheterization, but do not recommend routine use of antibiotics to prevent CAUTIs.2 The 2014 Infectious Diseases Society of America guidelines, which came out before the study reported on here was published, state the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY: Meta-analysis shows prophylactic antibiotics reduce UTI ris
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed 7 studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of 2 surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including 2 that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to 3 days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics vs 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17 (95% confidence interval [CI], 12-30), with a risk ratio (RR) of .45 (95% CI, .28-.72). The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial, and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the 2 studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT'S NEW: We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
CAVEATS: Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk of attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION: Which antibiotics to use, and for how long, remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for 3 days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administering antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Ensure that antibiotics are administered to surgical patients when their urinary catheter is removed to reduce the risk of urinary tract infections (UTIs).1
Strength of recommendation
B: Based on a meta-analysis.
Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
Illustrative case
A 49-year-old man was admitted to the hospital for resection of a vertebral mass. He is almost ready for discharge, and his urinary catheter soon will be removed. Should he be given an antibiotic when his catheter is removed to prevent a UTI?
Approximately 15% to 25% of hospitalized patients receive a urinary catheter, typically during the perioperative period.2 UTIs are the most common hospital-acquired infections, and virtually all of these UTIs are caused by instrumentation of the urinary tract, primarily by catheters.2 Although the mortality rate among patients with catheter-associated UTIs (CAUTIs) is just 2.3%, CAUTIs are the leading cause of hospital-acquired bacteremia, which increases morbidity and length of stay.2 The most common pathogens for CAUTIs are Escherichia coli (21.4%), Candida species (21%), and Enterococcus species (14.9%).2Pseudomonas aeruginosa, Klebsiella, and Enterobacter species make up the bulk of the remainder.2
Support for antibiotic prophylaxis has historically been equivocal
Until now, no data clearly supported routine use of prophylactic antibiotics after urinary catheterization. Centers for Disease Control and Prevention (CDC) guidelines published in 2009 outline which patients are appropriate for catheterization, but do not recommend routine use of antibiotics to prevent CAUTIs.2 The 2014 Infectious Diseases Society of America guidelines, which came out before the study reported on here was published, state the benefit of antibiotics at the time of catheter removal is an unresolved issue.3
STUDY SUMMARY: Meta-analysis shows prophylactic antibiotics reduce UTI ris
Marschall et al1 searched multiple databases for studies published between 1947 and 2012 that evaluated prophylactic use of antibiotics at the time of urinary catheter removal. The endpoint for their analysis was symptomatic UTI, which they defined as bacteriuria plus at least one clinical symptom. Trials were excluded if patients had suprapubic catheters or if antibiotics were started shortly after the catheter was inserted.
The authors analyzed 7 studies. Six were randomized controlled trials, of which one was unpublished. The seventh trial was a nonrandomized study that compared outcomes of patients of 2 surgeons, one of whom used prophylactic antibiotics and one who did not. Five studies enrolled surgical patients exclusively, including 2 that focused on urology patients. In all of the studies, patients had a urinary catheter in place for fewer than 15 days. The duration of antibiotic treatment varied from a single dose to 3 days. The antibiotics used included trimethoprim/sulfamethoxazole, nitrofurantoin, ciprofloxacin, and a cephalosporin.
Antibiotic prophylaxis significantly reduced the rate of CAUTIs. The absolute risk reduction was 5.8%; the rate of CAUTIs was 4.7% in the group treated with antibiotics vs 10.5% in the control group. The number needed to treat to prevent one CAUTI was 17 (95% confidence interval [CI], 12-30), with a risk ratio (RR) of .45 (95% CI, .28-.72). The RR varied only slightly (.36) when the researchers repeated their analysis but excluded the unpublished trial, and remained at .45 when they analyzed only studies of surgical patients.
The reduction in CAUTIs remained consistent despite varying lengths of antibiotic administration and choice of antimicrobial agents. However, when the authors looked at pooled results just from the 2 studies that included both surgical and medical patients, they found no decrease in CAUTIs.
WHAT'S NEW: We now have an effective way to reduce CAUTIs
Prophylactic use of antibiotics when a urinary catheter is removed appears to reduce the rate of CAUTIs by more than 50% in surgical patients. The 2009 CDC guidelines on CAUTI prevention emphasize the use of appropriate infection control measures and limiting the duration of urinary catheter use.2 Now there are data showing a reduction in the incidence of CAUTIs when prophylactic antibiotics are given during catheter removal.
CAVEATS: Results may not apply to nonsurgical patients
This meta-analysis does not provide enough information to identify which patients are most likely to benefit from antibiotic prophylaxis. Most patients (92%) in this analysis had undergone surgery, but urinary catheterization is common among medically hospitalized patients. Studies of antibiotic prophylaxis at the time of catheter removal in nonsurgical patients are needed to strengthen the recommendation of this practice for all patients.
Some of the studies analyzed may have been biased. The authors determined that most of the studies in their meta-analysis were at high risk of attrition bias because there was potential for systematic differences in withdrawals between the treatment and control groups. In addition, in most studies, the randomization and allocation appeared to be inadequate, which increased the risk for selection bias.
CHALLENGES TO IMPLEMENTATION: Which antibiotics to use, and for how long, remains unclear
Antibiotic choice depends upon institutional policies and local resistance patterns, which complicates making universal recommendations. The optimal duration of treatment also is unknown, although this meta-analysis suggests that prophylaxis for 3 days or less can reduce CAUTI risk.
Catheters impregnated with antimicrobials or with microbial resistance barriers may be an alternative to administering antibiotics at catheter removal, but in preliminary studies, these devices have not been shown to reduce the incidence of CAUTIs.4,5 Increasing antimicrobial resistance also complicates the widespread use of prophylaxis.
Acknowledgement
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. Available at: http://www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed April 15, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
1. Marschall J, Carpenter CR, Fowler S, et al; CDC Prevention Epicenters Program. Antibiotic prophylaxis for urinary tract infections after removal of urinary catheter: meta-analysis. BMJ. 2013;346:f3147.
2. Gould CV, Umscheid CA, Agarwal RK, et al. Guideline for prevention of catheter-associated urinary tract infections 2009. Available at: http://www.cdc.gov/hicpac/pdf/cauti/cautiguideline2009final.pdf. Accessed April 15, 2014.
3. Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:464-479.
4. Pickard R, Lam T, Maclennan G, et al. Types of urethral catheter for reducing symptomatic urinary tract infections in hospitalised adults requiring short-term catheterisation: multicentre randomised controlled trial and economic evaluation of antimicrobial- and antiseptic-impregnated urethral catheters (the CATHETER trial). Health Technol Assess. 2012;16:1-197.
5. Pickard R, Lam T, MacLennan G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-1935.
Copyright © 2014 Family Physicians Inquiries Network. All rights reserved.
Baby severely handicapped after premature labor: $42.9M verdict

BABY SEVERELY HANDICAPPED AFTER PREMATURE LABOR: $42.9M VERDICT
A 27-year-old mother had a normal prenatal ultrasonography (US) result in March 2007. In July, she went to the emergency department (ED) with pelvic pressure. A maternal-fetal medicine (MFM) specialist noted that the patient’s cervix had shortened to 1.3 cm. US showed that excessive amniotic fluid was causing uterine distention. The patient was monitored by an on-call ObGyn for 3.5 hours before being discharged home on pelvic and modified bed rest.
Two days later, the mother reported frequent contractions to her ObGyn. The baby was born the next day by emergency cesarean delivery at 25 weeks’ gestation. The newborn had seizures and a brain hemorrhage. The child has mental disabilities, blindness, spastic quadriparesis, cerebral palsy, gastroesophageal reflux, and complex feeding disorder.
PARENTS’ CLAIM The on-call ObGyn did not give the patient specific instructions for pelvic and bed rest upon discharge. The MFM specialist and on-call ObGyn failed to admit the patient to the hospital, and failed to administer intravenous steroids (betamethasone) to protect the fetal brain and induce respiratory development.
DEFENDANTS’ DEFENSE There was no indication during the MFM specialist’s examination that delivery was imminent. The use of betamethasone would not have prevented or inhibited premature labor. The infant’s problems were due to prematurity and low birth weight.
VERDICT A $42.9 million Pennsylvania verdict was returned against the MFM specialist; the on-call ObGyn and hospital were vindicated.
PELVIC LYMPH NODES NOT SAMPLED
When a 68-year-old woman reported vaginal spotting to her gynecologist (Dr. A) in March 2006, the results of an endometrial biopsy were negative. She saw another gynecologist (Dr. B) for a second opinion when bleeding continued. After dilation and curettage, grade 1B endometrial cancer was identified. The patient underwent a hysterectomy and bilateral salpingo-oophorectomy. She received a diagnosis of metastatic cancer of the pelvis and pelvic and para-aortic lymph nodes 18 months later. After additional surgery, the patient died in March 2008.
ESTATE’S CLAIM Dr. A was negligent in failing to diagnose the cancer in March 2006. Dr. B should have performed pelvic lymphadenectomy at hysterectomy; a lymphadenectomy would have accurately staged metastatic cancer.
DEFENDANTS’ DEFENSE Care and treatment were appropriate. Performing a lymphadenectomy would have exposed the patient to a significant risk of morbidity.
VERDICT A $750,000 California verdict was reduced to $250,000 under the state cap.
LARGE BABY: ERB’S PALSY
Shoulder dystocia was encountered when a 38-year-old woman gave birth. The child later received a diagnosis of Erb’s palsy, and has had several operations. At trial, the child had loss of function of the affected arm and wore a brace.
PARENTS’ CLAIM A vaginal delivery should not have been performed because the mother had gestational diabetes and the baby weighed 8 lb 8 oz at birth. Cesarean delivery was never offered.
DEFENDANTS’ DEFENSE Labor appeared normal. Proper delivery techniques were used when shoulder dystocia was encountered.
VERDICT A $12.9 million Michigan verdict was reduced to $4 million under the state cap.
Related articles:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
STOP all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Ronald T. Burkman, MD (Stop/Start; March 2013)
The natural history of obstetric brachial plexus injury Robert L. Barbieri, MD (Editorial, February 2013)
SPINAL CORD INJURY
During anesthesia administration before cesarean delivery, a mother’s spinal cord was injured, resulting in irritation of multiple nerve roots. She has chronic nerve pain syndrome.
PATIENT’S CLAIM The anesthesiologist was negligent in how he administered the spinal block.
PHYSICIAN’S DEFENSE There was no negligence. The injury is a known complication of the procedure.
VERDICT An Indiana defense verdict was returned.

AORTA PUNCTURED: $4M VERDICT
A 35-year-old woman underwent laparoscopic cystectomy on her left ovary performed by her gynecologist. During the procedure, the patient’s aorta was punctured, and she lost more than half her blood volume. After immediate surgery to repair the aorta, she was hospitalized for 5 days.
PATIENT’S CLAIM The injury was due to improper insertion of the laparoscopic instruments; the trocars were improperly angled and too forcefully inserted. The injury was a known risk of the procedure for obese patients, but she is not obese. She has a residual scar and is at increased risk of developing adhesions.
PHYSICIAN’S DEFENSE The instruments were properly inserted. The injury is a known risk of the procedure.
VERDICT A $4 million New York verdict was returned.
RESUSCITATION TOOK 22 MINUTES
At 40 6/7 weeks’ gestation, a mother went to the ED after her membranes spontaneously ruptured. The child was delivered by vacuum extraction 30 hours later.
At birth, the baby was blue and limp with Apgar scores of 2, 3, and 7, at 1, 5, and 10 minutes, respectively. The infant required 22 minutes of resuscitation. The neonatal record included metabolic acidosis, respiratory distress, possible sepsis, shoulder dystocia, and seizure activity. The child suffered hypoxic ischemic encephalopathy and permanent neurologic injury.
PARENTS’ CLAIM Cesarean delivery should have been performed due to repetitive decelerations, fetal tachycardia, and increasingly long uterine contractions. Continued use of oxytocin contributed to the infant’s injuries.
DEFENDANTS’ DEFENSE Fetal heart-rate tracings were reassuring during labor. Decreased variability, rising fetal heart rate, and late decelerations are normal during labor and delivery. The infant’s blood gas did not fall below 7.0 pH. The use of oxytocin was proper. There was no way to determine cephalopelvic disproportion or the baby’s size at 6 days postterm. The mother was opposed to a cesarean delivery and requested vaginal delivery (although no such request was included in the medical records).
VERDICT A $55 million Pennsylvania verdict was returned.
INJURY DURING OVARIAN REMNANT RESECTION
A woman in her 40s reported lower left quadrant pain. A previous oophorectomy report indicated that ovarian tissue attached to the bowel had not been removed. Thinking the pain might be related to residual ovarian tissue, her gynecologist recommended resection. During surgery, the patient’s bowel was injured. Four additional operations were required, including bowel resection with colostomy, and then colostomy reversal 5 months later.
PATIENT’S CLAIM The gynecologist was negligent in failing to properly perform surgery. The surgeon’s report from the oophorectomy indicated that there were extensive adhesions, which increased the risk of complications from surgery to remove the remnant. Ovarian remnant syndrome could have been treated with medication to induce menopause.
PHYSICIAN’S DEFENSE The patient might have suffered injury from medication-induced menopause. Surgery was appropriate; the injury is a known risk of the procedure.
VERDICT A $200,000 New York verdict was returned.
SEVERE INFECTION AFTER BIRTH
A 32-year-old woman left the hospital within hours of giving birth because her mother was ill. Before discharge, she reported severe abdominal pain and was examined by a first-year resident. The patient returned to the hospital 6 hours later with a severe uterine infection. She was hospitalized for a month.
PATIENT’S CLAIM The resident failed to properly assess her symptom reports, failed to order testing, and was negligent in allowing her to leave the hospital.
DEFENDANTS’ DEFENSE The patient left the hospital against medical recommendations. She might have acquired the infection after leaving the hospital.
VERDICT A $285,000 Michigan verdict was returned. The patient was found to be 40% at fault.

TERMINAL BRADYCARDIA: $12M VERDICT WITH MIXED FAULT
Four days after her due date, a mother’s blood pressure was elevated, and labor was induced. Two days after oxytocin was started, decelerations occurred. The ObGyn was called after the second deceleration, and witnessed the fourth deceleration about an hour later. After six decelerations, the fetal heart rate dropped to 70 bpm and did not return to baseline. A cesarean delivery was performed 26 minutes later. The child was born with a severe brain injury.
PARENTS’ CLAIM The nurses and ObGyn failed to recognize, report, and address nonreassuring fetal heart signs, and did not discontinue oxytocin after the second deceleration. Hospital protocols were ignored. An earlier cesarean delivery would have avoided injury; the fetus was without oxygen from the sixth deceleration until delivery.
DEFENDANTS’ DEFENSE There was no causation between the alleged violation of hospital protocols and the outcome. The ObGyn was appropriately notified. The injury was caused by terminal bradycardia during a prolonged deceleration that resulted from cord compression; it was unpredictable.
The ObGyn claimed earlier delivery was not indicated. Decelerations did not predict a bradycardic event from which the fetus would not recover nor indicate a need to stop oxytocin. The fetal heart rate had always recovered until the final deceleration. Bradycardia is unpredictable.
VERDICT A $12.165 million Hawaii verdict was returned, with the ObGyn 35% at fault, and the hospital 65% at fault.
Related article: Stop staring at that Category-II fetal heart-rate tracing… Robert L. Barbieri, MD (Editorial, April 2011)
BREAST BIOPSY MIXUP; SHE DIDN’T HAVE CANCER
A 53-year-old woman reported right breast pain. Mammography revealed scattered fibroglandular elements. Targeted US showed a solid nodule that could be an intramammary lymph node or small fibroadenoma. After an office-based biopsy, the breast surgeon (Dr. A) told the patient that she had breast cancer.
Because Dr. A was not in her health insurance plan, the patient took her imaging studies and biopsy results to Dr. B, another surgeon. Dr. B performed a mastectomy with lymphadenectomy. There was no evidence of malignancy in the pathologic review of breast and lymph tissue.
PATIENT’S CLAIM Dr. A performed biopsies on several women that same day; all were sent to the same laboratory for analysis. Dr. A and the laboratory failed to properly label and handle the biopsy specimens. Incorrect diagnosis caused her to undergo unnecessary mastectomy, lymph node biopsy, and a long, complicated breast reconstruction.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $1,780,000 Virginia settlement was reached.
Related article: Does screening mammography save lives? Janelle Yates (April 2014)
CLUES MISSED; BABY HAS CP, OTHER INJURIES
A 19-year-old mother had regular prenatal care. In early June, she weighed 221 lb and had a fundal height of 36 cm. The certified nurse midwife (CNM) noted little fetal movement, was uncertain of the fetal position, and made a note to check the amniotic fluid at the next visit. A week later, US did not indicate a decrease in amniotic fluid. Records do not indicate that the amniotic fluid index was checked at the next visit (38 weeks’ gestation).
Two days later, the patient reported decreased fetal movement. At the ED, nonreassuring fetal heart tracings were recorded. Fifteen minutes later, the fetal heart rate fell to 50 bpm and did not recover. The on-call ObGyn artificially ruptured the membranes and placed a direct fetal lead. An emergency cesarean delivery was performed in 15 minutes through thick meconium.
Apgar scores were 0, 2, and 4 at 1, 5, and 10 minutes, respectively. The baby weighed 4 lb 4 oz, and was transferred to a children’s hospital, where she stayed for 6 weeks. She suffered seizures and was tube fed. The child has cerebral palsy and profound neurologic impairment. At age 7, she is unable to speak.
PATIENT’S CLAIM The CNM was negligent for not being more proactive when she questioned the amniotic fluid index and noted reduced fetal movement in early June and at subsequent visits. The presence of meconium at birth attested that the fetus had been in distress.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $2 million Massachusetts settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state.
Stay in touch! Your feedback is important to us!
BABY SEVERELY HANDICAPPED AFTER PREMATURE LABOR: $42.9M VERDICT
A 27-year-old mother had a normal prenatal ultrasonography (US) result in March 2007. In July, she went to the emergency department (ED) with pelvic pressure. A maternal-fetal medicine (MFM) specialist noted that the patient’s cervix had shortened to 1.3 cm. US showed that excessive amniotic fluid was causing uterine distention. The patient was monitored by an on-call ObGyn for 3.5 hours before being discharged home on pelvic and modified bed rest.
Two days later, the mother reported frequent contractions to her ObGyn. The baby was born the next day by emergency cesarean delivery at 25 weeks’ gestation. The newborn had seizures and a brain hemorrhage. The child has mental disabilities, blindness, spastic quadriparesis, cerebral palsy, gastroesophageal reflux, and complex feeding disorder.
PARENTS’ CLAIM The on-call ObGyn did not give the patient specific instructions for pelvic and bed rest upon discharge. The MFM specialist and on-call ObGyn failed to admit the patient to the hospital, and failed to administer intravenous steroids (betamethasone) to protect the fetal brain and induce respiratory development.
DEFENDANTS’ DEFENSE There was no indication during the MFM specialist’s examination that delivery was imminent. The use of betamethasone would not have prevented or inhibited premature labor. The infant’s problems were due to prematurity and low birth weight.
VERDICT A $42.9 million Pennsylvania verdict was returned against the MFM specialist; the on-call ObGyn and hospital were vindicated.
PELVIC LYMPH NODES NOT SAMPLED
When a 68-year-old woman reported vaginal spotting to her gynecologist (Dr. A) in March 2006, the results of an endometrial biopsy were negative. She saw another gynecologist (Dr. B) for a second opinion when bleeding continued. After dilation and curettage, grade 1B endometrial cancer was identified. The patient underwent a hysterectomy and bilateral salpingo-oophorectomy. She received a diagnosis of metastatic cancer of the pelvis and pelvic and para-aortic lymph nodes 18 months later. After additional surgery, the patient died in March 2008.
ESTATE’S CLAIM Dr. A was negligent in failing to diagnose the cancer in March 2006. Dr. B should have performed pelvic lymphadenectomy at hysterectomy; a lymphadenectomy would have accurately staged metastatic cancer.
DEFENDANTS’ DEFENSE Care and treatment were appropriate. Performing a lymphadenectomy would have exposed the patient to a significant risk of morbidity.
VERDICT A $750,000 California verdict was reduced to $250,000 under the state cap.
LARGE BABY: ERB’S PALSY
Shoulder dystocia was encountered when a 38-year-old woman gave birth. The child later received a diagnosis of Erb’s palsy, and has had several operations. At trial, the child had loss of function of the affected arm and wore a brace.
PARENTS’ CLAIM A vaginal delivery should not have been performed because the mother had gestational diabetes and the baby weighed 8 lb 8 oz at birth. Cesarean delivery was never offered.
DEFENDANTS’ DEFENSE Labor appeared normal. Proper delivery techniques were used when shoulder dystocia was encountered.
VERDICT A $12.9 million Michigan verdict was reduced to $4 million under the state cap.
Related articles:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
STOP all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Ronald T. Burkman, MD (Stop/Start; March 2013)
The natural history of obstetric brachial plexus injury Robert L. Barbieri, MD (Editorial, February 2013)
SPINAL CORD INJURY
During anesthesia administration before cesarean delivery, a mother’s spinal cord was injured, resulting in irritation of multiple nerve roots. She has chronic nerve pain syndrome.
PATIENT’S CLAIM The anesthesiologist was negligent in how he administered the spinal block.
PHYSICIAN’S DEFENSE There was no negligence. The injury is a known complication of the procedure.
VERDICT An Indiana defense verdict was returned.
AORTA PUNCTURED: $4M VERDICT
A 35-year-old woman underwent laparoscopic cystectomy on her left ovary performed by her gynecologist. During the procedure, the patient’s aorta was punctured, and she lost more than half her blood volume. After immediate surgery to repair the aorta, she was hospitalized for 5 days.
PATIENT’S CLAIM The injury was due to improper insertion of the laparoscopic instruments; the trocars were improperly angled and too forcefully inserted. The injury was a known risk of the procedure for obese patients, but she is not obese. She has a residual scar and is at increased risk of developing adhesions.
PHYSICIAN’S DEFENSE The instruments were properly inserted. The injury is a known risk of the procedure.
VERDICT A $4 million New York verdict was returned.
RESUSCITATION TOOK 22 MINUTES
At 40 6/7 weeks’ gestation, a mother went to the ED after her membranes spontaneously ruptured. The child was delivered by vacuum extraction 30 hours later.
At birth, the baby was blue and limp with Apgar scores of 2, 3, and 7, at 1, 5, and 10 minutes, respectively. The infant required 22 minutes of resuscitation. The neonatal record included metabolic acidosis, respiratory distress, possible sepsis, shoulder dystocia, and seizure activity. The child suffered hypoxic ischemic encephalopathy and permanent neurologic injury.
PARENTS’ CLAIM Cesarean delivery should have been performed due to repetitive decelerations, fetal tachycardia, and increasingly long uterine contractions. Continued use of oxytocin contributed to the infant’s injuries.
DEFENDANTS’ DEFENSE Fetal heart-rate tracings were reassuring during labor. Decreased variability, rising fetal heart rate, and late decelerations are normal during labor and delivery. The infant’s blood gas did not fall below 7.0 pH. The use of oxytocin was proper. There was no way to determine cephalopelvic disproportion or the baby’s size at 6 days postterm. The mother was opposed to a cesarean delivery and requested vaginal delivery (although no such request was included in the medical records).
VERDICT A $55 million Pennsylvania verdict was returned.
INJURY DURING OVARIAN REMNANT RESECTION
A woman in her 40s reported lower left quadrant pain. A previous oophorectomy report indicated that ovarian tissue attached to the bowel had not been removed. Thinking the pain might be related to residual ovarian tissue, her gynecologist recommended resection. During surgery, the patient’s bowel was injured. Four additional operations were required, including bowel resection with colostomy, and then colostomy reversal 5 months later.
PATIENT’S CLAIM The gynecologist was negligent in failing to properly perform surgery. The surgeon’s report from the oophorectomy indicated that there were extensive adhesions, which increased the risk of complications from surgery to remove the remnant. Ovarian remnant syndrome could have been treated with medication to induce menopause.
PHYSICIAN’S DEFENSE The patient might have suffered injury from medication-induced menopause. Surgery was appropriate; the injury is a known risk of the procedure.
VERDICT A $200,000 New York verdict was returned.
SEVERE INFECTION AFTER BIRTH
A 32-year-old woman left the hospital within hours of giving birth because her mother was ill. Before discharge, she reported severe abdominal pain and was examined by a first-year resident. The patient returned to the hospital 6 hours later with a severe uterine infection. She was hospitalized for a month.
PATIENT’S CLAIM The resident failed to properly assess her symptom reports, failed to order testing, and was negligent in allowing her to leave the hospital.
DEFENDANTS’ DEFENSE The patient left the hospital against medical recommendations. She might have acquired the infection after leaving the hospital.
VERDICT A $285,000 Michigan verdict was returned. The patient was found to be 40% at fault.
TERMINAL BRADYCARDIA: $12M VERDICT WITH MIXED FAULT
Four days after her due date, a mother’s blood pressure was elevated, and labor was induced. Two days after oxytocin was started, decelerations occurred. The ObGyn was called after the second deceleration, and witnessed the fourth deceleration about an hour later. After six decelerations, the fetal heart rate dropped to 70 bpm and did not return to baseline. A cesarean delivery was performed 26 minutes later. The child was born with a severe brain injury.
PARENTS’ CLAIM The nurses and ObGyn failed to recognize, report, and address nonreassuring fetal heart signs, and did not discontinue oxytocin after the second deceleration. Hospital protocols were ignored. An earlier cesarean delivery would have avoided injury; the fetus was without oxygen from the sixth deceleration until delivery.
DEFENDANTS’ DEFENSE There was no causation between the alleged violation of hospital protocols and the outcome. The ObGyn was appropriately notified. The injury was caused by terminal bradycardia during a prolonged deceleration that resulted from cord compression; it was unpredictable.
The ObGyn claimed earlier delivery was not indicated. Decelerations did not predict a bradycardic event from which the fetus would not recover nor indicate a need to stop oxytocin. The fetal heart rate had always recovered until the final deceleration. Bradycardia is unpredictable.
VERDICT A $12.165 million Hawaii verdict was returned, with the ObGyn 35% at fault, and the hospital 65% at fault.
Related article: Stop staring at that Category-II fetal heart-rate tracing… Robert L. Barbieri, MD (Editorial, April 2011)
BREAST BIOPSY MIXUP; SHE DIDN’T HAVE CANCER
A 53-year-old woman reported right breast pain. Mammography revealed scattered fibroglandular elements. Targeted US showed a solid nodule that could be an intramammary lymph node or small fibroadenoma. After an office-based biopsy, the breast surgeon (Dr. A) told the patient that she had breast cancer.
Because Dr. A was not in her health insurance plan, the patient took her imaging studies and biopsy results to Dr. B, another surgeon. Dr. B performed a mastectomy with lymphadenectomy. There was no evidence of malignancy in the pathologic review of breast and lymph tissue.
PATIENT’S CLAIM Dr. A performed biopsies on several women that same day; all were sent to the same laboratory for analysis. Dr. A and the laboratory failed to properly label and handle the biopsy specimens. Incorrect diagnosis caused her to undergo unnecessary mastectomy, lymph node biopsy, and a long, complicated breast reconstruction.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $1,780,000 Virginia settlement was reached.
Related article: Does screening mammography save lives? Janelle Yates (April 2014)
CLUES MISSED; BABY HAS CP, OTHER INJURIES
A 19-year-old mother had regular prenatal care. In early June, she weighed 221 lb and had a fundal height of 36 cm. The certified nurse midwife (CNM) noted little fetal movement, was uncertain of the fetal position, and made a note to check the amniotic fluid at the next visit. A week later, US did not indicate a decrease in amniotic fluid. Records do not indicate that the amniotic fluid index was checked at the next visit (38 weeks’ gestation).
Two days later, the patient reported decreased fetal movement. At the ED, nonreassuring fetal heart tracings were recorded. Fifteen minutes later, the fetal heart rate fell to 50 bpm and did not recover. The on-call ObGyn artificially ruptured the membranes and placed a direct fetal lead. An emergency cesarean delivery was performed in 15 minutes through thick meconium.
Apgar scores were 0, 2, and 4 at 1, 5, and 10 minutes, respectively. The baby weighed 4 lb 4 oz, and was transferred to a children’s hospital, where she stayed for 6 weeks. She suffered seizures and was tube fed. The child has cerebral palsy and profound neurologic impairment. At age 7, she is unable to speak.
PATIENT’S CLAIM The CNM was negligent for not being more proactive when she questioned the amniotic fluid index and noted reduced fetal movement in early June and at subsequent visits. The presence of meconium at birth attested that the fetus had been in distress.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $2 million Massachusetts settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state.
Stay in touch! Your feedback is important to us!
BABY SEVERELY HANDICAPPED AFTER PREMATURE LABOR: $42.9M VERDICT
A 27-year-old mother had a normal prenatal ultrasonography (US) result in March 2007. In July, she went to the emergency department (ED) with pelvic pressure. A maternal-fetal medicine (MFM) specialist noted that the patient’s cervix had shortened to 1.3 cm. US showed that excessive amniotic fluid was causing uterine distention. The patient was monitored by an on-call ObGyn for 3.5 hours before being discharged home on pelvic and modified bed rest.
Two days later, the mother reported frequent contractions to her ObGyn. The baby was born the next day by emergency cesarean delivery at 25 weeks’ gestation. The newborn had seizures and a brain hemorrhage. The child has mental disabilities, blindness, spastic quadriparesis, cerebral palsy, gastroesophageal reflux, and complex feeding disorder.
PARENTS’ CLAIM The on-call ObGyn did not give the patient specific instructions for pelvic and bed rest upon discharge. The MFM specialist and on-call ObGyn failed to admit the patient to the hospital, and failed to administer intravenous steroids (betamethasone) to protect the fetal brain and induce respiratory development.
DEFENDANTS’ DEFENSE There was no indication during the MFM specialist’s examination that delivery was imminent. The use of betamethasone would not have prevented or inhibited premature labor. The infant’s problems were due to prematurity and low birth weight.
VERDICT A $42.9 million Pennsylvania verdict was returned against the MFM specialist; the on-call ObGyn and hospital were vindicated.
PELVIC LYMPH NODES NOT SAMPLED
When a 68-year-old woman reported vaginal spotting to her gynecologist (Dr. A) in March 2006, the results of an endometrial biopsy were negative. She saw another gynecologist (Dr. B) for a second opinion when bleeding continued. After dilation and curettage, grade 1B endometrial cancer was identified. The patient underwent a hysterectomy and bilateral salpingo-oophorectomy. She received a diagnosis of metastatic cancer of the pelvis and pelvic and para-aortic lymph nodes 18 months later. After additional surgery, the patient died in March 2008.
ESTATE’S CLAIM Dr. A was negligent in failing to diagnose the cancer in March 2006. Dr. B should have performed pelvic lymphadenectomy at hysterectomy; a lymphadenectomy would have accurately staged metastatic cancer.
DEFENDANTS’ DEFENSE Care and treatment were appropriate. Performing a lymphadenectomy would have exposed the patient to a significant risk of morbidity.
VERDICT A $750,000 California verdict was reduced to $250,000 under the state cap.
LARGE BABY: ERB’S PALSY
Shoulder dystocia was encountered when a 38-year-old woman gave birth. The child later received a diagnosis of Erb’s palsy, and has had several operations. At trial, the child had loss of function of the affected arm and wore a brace.
PARENTS’ CLAIM A vaginal delivery should not have been performed because the mother had gestational diabetes and the baby weighed 8 lb 8 oz at birth. Cesarean delivery was never offered.
DEFENDANTS’ DEFENSE Labor appeared normal. Proper delivery techniques were used when shoulder dystocia was encountered.
VERDICT A $12.9 million Michigan verdict was reduced to $4 million under the state cap.
Related articles:
You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial; May 2013)
STOP all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia Ronald T. Burkman, MD (Stop/Start; March 2013)
The natural history of obstetric brachial plexus injury Robert L. Barbieri, MD (Editorial, February 2013)
SPINAL CORD INJURY
During anesthesia administration before cesarean delivery, a mother’s spinal cord was injured, resulting in irritation of multiple nerve roots. She has chronic nerve pain syndrome.
PATIENT’S CLAIM The anesthesiologist was negligent in how he administered the spinal block.
PHYSICIAN’S DEFENSE There was no negligence. The injury is a known complication of the procedure.
VERDICT An Indiana defense verdict was returned.
AORTA PUNCTURED: $4M VERDICT
A 35-year-old woman underwent laparoscopic cystectomy on her left ovary performed by her gynecologist. During the procedure, the patient’s aorta was punctured, and she lost more than half her blood volume. After immediate surgery to repair the aorta, she was hospitalized for 5 days.
PATIENT’S CLAIM The injury was due to improper insertion of the laparoscopic instruments; the trocars were improperly angled and too forcefully inserted. The injury was a known risk of the procedure for obese patients, but she is not obese. She has a residual scar and is at increased risk of developing adhesions.
PHYSICIAN’S DEFENSE The instruments were properly inserted. The injury is a known risk of the procedure.
VERDICT A $4 million New York verdict was returned.
RESUSCITATION TOOK 22 MINUTES
At 40 6/7 weeks’ gestation, a mother went to the ED after her membranes spontaneously ruptured. The child was delivered by vacuum extraction 30 hours later.
At birth, the baby was blue and limp with Apgar scores of 2, 3, and 7, at 1, 5, and 10 minutes, respectively. The infant required 22 minutes of resuscitation. The neonatal record included metabolic acidosis, respiratory distress, possible sepsis, shoulder dystocia, and seizure activity. The child suffered hypoxic ischemic encephalopathy and permanent neurologic injury.
PARENTS’ CLAIM Cesarean delivery should have been performed due to repetitive decelerations, fetal tachycardia, and increasingly long uterine contractions. Continued use of oxytocin contributed to the infant’s injuries.
DEFENDANTS’ DEFENSE Fetal heart-rate tracings were reassuring during labor. Decreased variability, rising fetal heart rate, and late decelerations are normal during labor and delivery. The infant’s blood gas did not fall below 7.0 pH. The use of oxytocin was proper. There was no way to determine cephalopelvic disproportion or the baby’s size at 6 days postterm. The mother was opposed to a cesarean delivery and requested vaginal delivery (although no such request was included in the medical records).
VERDICT A $55 million Pennsylvania verdict was returned.
INJURY DURING OVARIAN REMNANT RESECTION
A woman in her 40s reported lower left quadrant pain. A previous oophorectomy report indicated that ovarian tissue attached to the bowel had not been removed. Thinking the pain might be related to residual ovarian tissue, her gynecologist recommended resection. During surgery, the patient’s bowel was injured. Four additional operations were required, including bowel resection with colostomy, and then colostomy reversal 5 months later.
PATIENT’S CLAIM The gynecologist was negligent in failing to properly perform surgery. The surgeon’s report from the oophorectomy indicated that there were extensive adhesions, which increased the risk of complications from surgery to remove the remnant. Ovarian remnant syndrome could have been treated with medication to induce menopause.
PHYSICIAN’S DEFENSE The patient might have suffered injury from medication-induced menopause. Surgery was appropriate; the injury is a known risk of the procedure.
VERDICT A $200,000 New York verdict was returned.
SEVERE INFECTION AFTER BIRTH
A 32-year-old woman left the hospital within hours of giving birth because her mother was ill. Before discharge, she reported severe abdominal pain and was examined by a first-year resident. The patient returned to the hospital 6 hours later with a severe uterine infection. She was hospitalized for a month.
PATIENT’S CLAIM The resident failed to properly assess her symptom reports, failed to order testing, and was negligent in allowing her to leave the hospital.
DEFENDANTS’ DEFENSE The patient left the hospital against medical recommendations. She might have acquired the infection after leaving the hospital.
VERDICT A $285,000 Michigan verdict was returned. The patient was found to be 40% at fault.
TERMINAL BRADYCARDIA: $12M VERDICT WITH MIXED FAULT
Four days after her due date, a mother’s blood pressure was elevated, and labor was induced. Two days after oxytocin was started, decelerations occurred. The ObGyn was called after the second deceleration, and witnessed the fourth deceleration about an hour later. After six decelerations, the fetal heart rate dropped to 70 bpm and did not return to baseline. A cesarean delivery was performed 26 minutes later. The child was born with a severe brain injury.
PARENTS’ CLAIM The nurses and ObGyn failed to recognize, report, and address nonreassuring fetal heart signs, and did not discontinue oxytocin after the second deceleration. Hospital protocols were ignored. An earlier cesarean delivery would have avoided injury; the fetus was without oxygen from the sixth deceleration until delivery.
DEFENDANTS’ DEFENSE There was no causation between the alleged violation of hospital protocols and the outcome. The ObGyn was appropriately notified. The injury was caused by terminal bradycardia during a prolonged deceleration that resulted from cord compression; it was unpredictable.
The ObGyn claimed earlier delivery was not indicated. Decelerations did not predict a bradycardic event from which the fetus would not recover nor indicate a need to stop oxytocin. The fetal heart rate had always recovered until the final deceleration. Bradycardia is unpredictable.
VERDICT A $12.165 million Hawaii verdict was returned, with the ObGyn 35% at fault, and the hospital 65% at fault.
Related article: Stop staring at that Category-II fetal heart-rate tracing… Robert L. Barbieri, MD (Editorial, April 2011)
BREAST BIOPSY MIXUP; SHE DIDN’T HAVE CANCER
A 53-year-old woman reported right breast pain. Mammography revealed scattered fibroglandular elements. Targeted US showed a solid nodule that could be an intramammary lymph node or small fibroadenoma. After an office-based biopsy, the breast surgeon (Dr. A) told the patient that she had breast cancer.
Because Dr. A was not in her health insurance plan, the patient took her imaging studies and biopsy results to Dr. B, another surgeon. Dr. B performed a mastectomy with lymphadenectomy. There was no evidence of malignancy in the pathologic review of breast and lymph tissue.
PATIENT’S CLAIM Dr. A performed biopsies on several women that same day; all were sent to the same laboratory for analysis. Dr. A and the laboratory failed to properly label and handle the biopsy specimens. Incorrect diagnosis caused her to undergo unnecessary mastectomy, lymph node biopsy, and a long, complicated breast reconstruction.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $1,780,000 Virginia settlement was reached.
Related article: Does screening mammography save lives? Janelle Yates (April 2014)
CLUES MISSED; BABY HAS CP, OTHER INJURIES
A 19-year-old mother had regular prenatal care. In early June, she weighed 221 lb and had a fundal height of 36 cm. The certified nurse midwife (CNM) noted little fetal movement, was uncertain of the fetal position, and made a note to check the amniotic fluid at the next visit. A week later, US did not indicate a decrease in amniotic fluid. Records do not indicate that the amniotic fluid index was checked at the next visit (38 weeks’ gestation).
Two days later, the patient reported decreased fetal movement. At the ED, nonreassuring fetal heart tracings were recorded. Fifteen minutes later, the fetal heart rate fell to 50 bpm and did not recover. The on-call ObGyn artificially ruptured the membranes and placed a direct fetal lead. An emergency cesarean delivery was performed in 15 minutes through thick meconium.
Apgar scores were 0, 2, and 4 at 1, 5, and 10 minutes, respectively. The baby weighed 4 lb 4 oz, and was transferred to a children’s hospital, where she stayed for 6 weeks. She suffered seizures and was tube fed. The child has cerebral palsy and profound neurologic impairment. At age 7, she is unable to speak.
PATIENT’S CLAIM The CNM was negligent for not being more proactive when she questioned the amniotic fluid index and noted reduced fetal movement in early June and at subsequent visits. The presence of meconium at birth attested that the fetus had been in distress.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $2 million Massachusetts settlement was reached.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
TELL US WHAT YOU THINK!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected] Please include your name, city and state.
Stay in touch! Your feedback is important to us!

Team overcomes problem with new lab on a chip

Credit: Rhoda Baer
Chemists say they have overcome one of the main obstacles in creating effective lab-on-a-chip devices, and the device they’ve invented has many potential applications, such as screening biological molecules.
To create their device, the team developed a technique that involves printing droplets of a special solvent onto a gold-coated or glass surface.
“We use a class of ‘green’ solvents called ionic liquids, which are salts that are liquid at room temperature,” said study author Chuan Zhao, PhD, of The University of New South Wales in Sydney, Australia.
“They are non-volatile, so this overcomes one of the main problems in making useful miniaturized devices—rapid evaporation of the solvents on the chip.”
Dr Zhao and his colleagues described this research in Nature Communications.
Lab-on-a-chip devices, where chemical reactions are carried out on a miniature scale, are under intensive development because they offer the promise of faster reaction times, reduced use of materials, and high yields of product.
However, the evaporation of solvents on the chip is a problem because it can affect the concentration of substances and disrupt the reactions.
Researchers have attempted to overcome the problem by containing the solvents within tiny channels, or “walls,” and having reservoirs to store extra solvent on the chip.
Dr Zhao and his colleagues said their “wall-less” design—using non-volatile ionic liquids as solvents to fabricate a microarray of droplets chemically anchored to the chip—has several advantages.
“Ionic liquids are designer solvents and have wide application,” Dr Zhao said. “We can now carry out many reactions or analytical procedures in ionic liquids at the micro-scale on a chip with enhanced yields and efficiency.”
“These microarray chips can be easily produced in high numbers and are very stable. They can survive being turned upside down and heated to 50 degrees, and some can even survive being immersed in another liquid. These properties will be important for commercial applications, including storage and transportation of microchips.”
The droplets of ionic liquid are about 50 µm across and 10 µm high. The researchers showed these tiny droplets can act as rapid, sensitive monitors of the presence of a gas, due to their small volume.
Metal salts dissolved in the droplets could be electrically deposited as microstructures, a technique that could be of use in the fabrication of integrated circuits.
And some biological molecules added to the droplets remained stable and active, opening up the possibility of using the microarrays for diagnostic purposes.
“The versatility of our chips means they could have a wide range of prospective functions,” Dr Zhao said, “such as for use in fast and accurate hand-held sensors for environmental monitoring, medical diagnosis, and process control in manufacturing.” ![]()
Credit: Rhoda Baer
Chemists say they have overcome one of the main obstacles in creating effective lab-on-a-chip devices, and the device they’ve invented has many potential applications, such as screening biological molecules.
To create their device, the team developed a technique that involves printing droplets of a special solvent onto a gold-coated or glass surface.
“We use a class of ‘green’ solvents called ionic liquids, which are salts that are liquid at room temperature,” said study author Chuan Zhao, PhD, of The University of New South Wales in Sydney, Australia.
“They are non-volatile, so this overcomes one of the main problems in making useful miniaturized devices—rapid evaporation of the solvents on the chip.”
Dr Zhao and his colleagues described this research in Nature Communications.
Lab-on-a-chip devices, where chemical reactions are carried out on a miniature scale, are under intensive development because they offer the promise of faster reaction times, reduced use of materials, and high yields of product.
However, the evaporation of solvents on the chip is a problem because it can affect the concentration of substances and disrupt the reactions.
Researchers have attempted to overcome the problem by containing the solvents within tiny channels, or “walls,” and having reservoirs to store extra solvent on the chip.
Dr Zhao and his colleagues said their “wall-less” design—using non-volatile ionic liquids as solvents to fabricate a microarray of droplets chemically anchored to the chip—has several advantages.
“Ionic liquids are designer solvents and have wide application,” Dr Zhao said. “We can now carry out many reactions or analytical procedures in ionic liquids at the micro-scale on a chip with enhanced yields and efficiency.”
“These microarray chips can be easily produced in high numbers and are very stable. They can survive being turned upside down and heated to 50 degrees, and some can even survive being immersed in another liquid. These properties will be important for commercial applications, including storage and transportation of microchips.”
The droplets of ionic liquid are about 50 µm across and 10 µm high. The researchers showed these tiny droplets can act as rapid, sensitive monitors of the presence of a gas, due to their small volume.
Metal salts dissolved in the droplets could be electrically deposited as microstructures, a technique that could be of use in the fabrication of integrated circuits.
And some biological molecules added to the droplets remained stable and active, opening up the possibility of using the microarrays for diagnostic purposes.
“The versatility of our chips means they could have a wide range of prospective functions,” Dr Zhao said, “such as for use in fast and accurate hand-held sensors for environmental monitoring, medical diagnosis, and process control in manufacturing.” ![]()
Credit: Rhoda Baer
Chemists say they have overcome one of the main obstacles in creating effective lab-on-a-chip devices, and the device they’ve invented has many potential applications, such as screening biological molecules.
To create their device, the team developed a technique that involves printing droplets of a special solvent onto a gold-coated or glass surface.
“We use a class of ‘green’ solvents called ionic liquids, which are salts that are liquid at room temperature,” said study author Chuan Zhao, PhD, of The University of New South Wales in Sydney, Australia.
“They are non-volatile, so this overcomes one of the main problems in making useful miniaturized devices—rapid evaporation of the solvents on the chip.”
Dr Zhao and his colleagues described this research in Nature Communications.
Lab-on-a-chip devices, where chemical reactions are carried out on a miniature scale, are under intensive development because they offer the promise of faster reaction times, reduced use of materials, and high yields of product.
However, the evaporation of solvents on the chip is a problem because it can affect the concentration of substances and disrupt the reactions.
Researchers have attempted to overcome the problem by containing the solvents within tiny channels, or “walls,” and having reservoirs to store extra solvent on the chip.
Dr Zhao and his colleagues said their “wall-less” design—using non-volatile ionic liquids as solvents to fabricate a microarray of droplets chemically anchored to the chip—has several advantages.
“Ionic liquids are designer solvents and have wide application,” Dr Zhao said. “We can now carry out many reactions or analytical procedures in ionic liquids at the micro-scale on a chip with enhanced yields and efficiency.”
“These microarray chips can be easily produced in high numbers and are very stable. They can survive being turned upside down and heated to 50 degrees, and some can even survive being immersed in another liquid. These properties will be important for commercial applications, including storage and transportation of microchips.”
The droplets of ionic liquid are about 50 µm across and 10 µm high. The researchers showed these tiny droplets can act as rapid, sensitive monitors of the presence of a gas, due to their small volume.
Metal salts dissolved in the droplets could be electrically deposited as microstructures, a technique that could be of use in the fabrication of integrated circuits.
And some biological molecules added to the droplets remained stable and active, opening up the possibility of using the microarrays for diagnostic purposes.
“The versatility of our chips means they could have a wide range of prospective functions,” Dr Zhao said, “such as for use in fast and accurate hand-held sensors for environmental monitoring, medical diagnosis, and process control in manufacturing.” ![]()
FDA allows importation of more saline

In response to the ongoing shortage of normal saline (0.9% sodium chloride injection), the US Food and Drug Administration (FDA) is allowing a company to import product manufactured in Spain.
Baxter Healthcare Corp. will be allowed to temporarily distribute sodium chloride 0.9% injection solution for intravenous infusion in VIAFLO
non-polyvinyl chloride containers, which is manufactured at the company’s Bieffe Medital, Sabinanigo, Spain facility.
This is the second time in recent months that the FDA has allowed the importation of saline. Last month, the agency announced it would allow Fresenius Kabi USA to import saline products manufactured in Norway.
As with the Norway plant, the FDA has inspected Baxter’s Spain facility to ensure it meets FDA standards.
Baxter will import sodium chloride 0.9% intravenous infusion in VIAFLO containers in the following volumes and quantities: 250 mL (30 bags per carton), 500 mL (20 bags per carton), and 1 L (10 bags per carton).
The FDA is asking that healthcare professionals contact Baxter directly to obtain the product. To place an order, contact Baxter’s Center for Service at 1-888-229-0001.
For more information on the products, see Baxter’s “Dear Healthcare Professional” letter, visit the company’s website, or contact Baxter’s Medical Information Service at 1-800-933-0303.
In addition to the imported saline, US-based manufacturers—B.Braun Medical Inc., Hospira Inc., and Baxter Healthcare Corp.—are producing and releasing normal saline. (Baxter’s saline product from Spain will be distributed in addition to Baxter’s FDA-approved version that is manufactured in the US.)
The FDA noted that, although the aforementioned shipments will help reduce current disruptions, they will not resolve the shortage of 0.9% sodium chloride injection. So the agency will continue working to alleviate the shortage. ![]()
In response to the ongoing shortage of normal saline (0.9% sodium chloride injection), the US Food and Drug Administration (FDA) is allowing a company to import product manufactured in Spain.
Baxter Healthcare Corp. will be allowed to temporarily distribute sodium chloride 0.9% injection solution for intravenous infusion in VIAFLO
non-polyvinyl chloride containers, which is manufactured at the company’s Bieffe Medital, Sabinanigo, Spain facility.
This is the second time in recent months that the FDA has allowed the importation of saline. Last month, the agency announced it would allow Fresenius Kabi USA to import saline products manufactured in Norway.
As with the Norway plant, the FDA has inspected Baxter’s Spain facility to ensure it meets FDA standards.
Baxter will import sodium chloride 0.9% intravenous infusion in VIAFLO containers in the following volumes and quantities: 250 mL (30 bags per carton), 500 mL (20 bags per carton), and 1 L (10 bags per carton).
The FDA is asking that healthcare professionals contact Baxter directly to obtain the product. To place an order, contact Baxter’s Center for Service at 1-888-229-0001.
For more information on the products, see Baxter’s “Dear Healthcare Professional” letter, visit the company’s website, or contact Baxter’s Medical Information Service at 1-800-933-0303.
In addition to the imported saline, US-based manufacturers—B.Braun Medical Inc., Hospira Inc., and Baxter Healthcare Corp.—are producing and releasing normal saline. (Baxter’s saline product from Spain will be distributed in addition to Baxter’s FDA-approved version that is manufactured in the US.)
The FDA noted that, although the aforementioned shipments will help reduce current disruptions, they will not resolve the shortage of 0.9% sodium chloride injection. So the agency will continue working to alleviate the shortage. ![]()
In response to the ongoing shortage of normal saline (0.9% sodium chloride injection), the US Food and Drug Administration (FDA) is allowing a company to import product manufactured in Spain.
Baxter Healthcare Corp. will be allowed to temporarily distribute sodium chloride 0.9% injection solution for intravenous infusion in VIAFLO
non-polyvinyl chloride containers, which is manufactured at the company’s Bieffe Medital, Sabinanigo, Spain facility.
This is the second time in recent months that the FDA has allowed the importation of saline. Last month, the agency announced it would allow Fresenius Kabi USA to import saline products manufactured in Norway.
As with the Norway plant, the FDA has inspected Baxter’s Spain facility to ensure it meets FDA standards.
Baxter will import sodium chloride 0.9% intravenous infusion in VIAFLO containers in the following volumes and quantities: 250 mL (30 bags per carton), 500 mL (20 bags per carton), and 1 L (10 bags per carton).
The FDA is asking that healthcare professionals contact Baxter directly to obtain the product. To place an order, contact Baxter’s Center for Service at 1-888-229-0001.
For more information on the products, see Baxter’s “Dear Healthcare Professional” letter, visit the company’s website, or contact Baxter’s Medical Information Service at 1-800-933-0303.
In addition to the imported saline, US-based manufacturers—B.Braun Medical Inc., Hospira Inc., and Baxter Healthcare Corp.—are producing and releasing normal saline. (Baxter’s saline product from Spain will be distributed in addition to Baxter’s FDA-approved version that is manufactured in the US.)
The FDA noted that, although the aforementioned shipments will help reduce current disruptions, they will not resolve the shortage of 0.9% sodium chloride injection. So the agency will continue working to alleviate the shortage. ![]()
Protein is key to HSC recovery after chemo, radiation

in the bone marrow
The protein beta-catenin plays a critical role in promoting the recovery of hematopoietic stem cells (HSCs) after exposure to radiation or chemotherapy, according to preclinical research published in Genes & Development.
The study provides new insight into the impact of radiation and chemotherapy on cellular and molecular processes.
And it points to possibilities for improving HSC regeneration in cancer patients who have undergone these treatments.
Study investigators first used mouse models to show that exposure to radiation triggers activation of the Wnt signaling pathway in hematopoietic stem and progenitor cells.
“The Wnt pathway and its key mediator, beta catenin, are critical for embryonic development and establishment of the body plan,” explained Tannishtha Reya, PhD, of the University of California, San Diego.
“In addition, the Wnt pathway is activated in stem cells from many tissues and is needed for their continued maintenance.”
Dr Reya and her colleagues then found that mice deficient in beta-catenin lacked the ability to activate canonical Wnt signaling. They also suffered from impaired HSC regeneration and bone marrow recovery after radiation or chemotherapy.
Mouse HSCs without beta-catenin could not suppress the production of reactive oxygen species or resolve DNA double-strand breaks. As a result, they could not recover effectively after radiation exposure or treatment with the chemotherapeutic agent fluorouracil.
“Our work shows that Wnt signaling is important in the mammalian hematopoietic system and is critical for recovery from chemotherapy and radiation,” Dr Reya said. “There are 2 major reasons why accelerating regeneration is important clinically.”
“One is that, after cancer patients are irradiated and transplanted with stem cells, the rate and extent of recovery is often not sufficient to protect the patient from anemia or infections . . . . Identifying signals that can boost regeneration after the bone marrow is severely damaged may help improve outcomes after transplantation.”
“Second, doses of chemotherapy and radiation used to treat cancer are often limited by the collateral damage they cause to normal tissues. If we can improve and accelerate recovery, we might be able to use higher doses of radiation or chemotherapy and reduce the risk of cancer relapse.”
Dr Reya added that this research suggests HSC regeneration could be accelerated by modulating the Wnt pathway, either by delivering additional Wnt proteins directly to patients or through drugs that activate the pathway. ![]()
in the bone marrow
The protein beta-catenin plays a critical role in promoting the recovery of hematopoietic stem cells (HSCs) after exposure to radiation or chemotherapy, according to preclinical research published in Genes & Development.
The study provides new insight into the impact of radiation and chemotherapy on cellular and molecular processes.
And it points to possibilities for improving HSC regeneration in cancer patients who have undergone these treatments.
Study investigators first used mouse models to show that exposure to radiation triggers activation of the Wnt signaling pathway in hematopoietic stem and progenitor cells.
“The Wnt pathway and its key mediator, beta catenin, are critical for embryonic development and establishment of the body plan,” explained Tannishtha Reya, PhD, of the University of California, San Diego.
“In addition, the Wnt pathway is activated in stem cells from many tissues and is needed for their continued maintenance.”
Dr Reya and her colleagues then found that mice deficient in beta-catenin lacked the ability to activate canonical Wnt signaling. They also suffered from impaired HSC regeneration and bone marrow recovery after radiation or chemotherapy.
Mouse HSCs without beta-catenin could not suppress the production of reactive oxygen species or resolve DNA double-strand breaks. As a result, they could not recover effectively after radiation exposure or treatment with the chemotherapeutic agent fluorouracil.
“Our work shows that Wnt signaling is important in the mammalian hematopoietic system and is critical for recovery from chemotherapy and radiation,” Dr Reya said. “There are 2 major reasons why accelerating regeneration is important clinically.”
“One is that, after cancer patients are irradiated and transplanted with stem cells, the rate and extent of recovery is often not sufficient to protect the patient from anemia or infections . . . . Identifying signals that can boost regeneration after the bone marrow is severely damaged may help improve outcomes after transplantation.”
“Second, doses of chemotherapy and radiation used to treat cancer are often limited by the collateral damage they cause to normal tissues. If we can improve and accelerate recovery, we might be able to use higher doses of radiation or chemotherapy and reduce the risk of cancer relapse.”
Dr Reya added that this research suggests HSC regeneration could be accelerated by modulating the Wnt pathway, either by delivering additional Wnt proteins directly to patients or through drugs that activate the pathway. ![]()
in the bone marrow
The protein beta-catenin plays a critical role in promoting the recovery of hematopoietic stem cells (HSCs) after exposure to radiation or chemotherapy, according to preclinical research published in Genes & Development.
The study provides new insight into the impact of radiation and chemotherapy on cellular and molecular processes.
And it points to possibilities for improving HSC regeneration in cancer patients who have undergone these treatments.
Study investigators first used mouse models to show that exposure to radiation triggers activation of the Wnt signaling pathway in hematopoietic stem and progenitor cells.
“The Wnt pathway and its key mediator, beta catenin, are critical for embryonic development and establishment of the body plan,” explained Tannishtha Reya, PhD, of the University of California, San Diego.
“In addition, the Wnt pathway is activated in stem cells from many tissues and is needed for their continued maintenance.”
Dr Reya and her colleagues then found that mice deficient in beta-catenin lacked the ability to activate canonical Wnt signaling. They also suffered from impaired HSC regeneration and bone marrow recovery after radiation or chemotherapy.
Mouse HSCs without beta-catenin could not suppress the production of reactive oxygen species or resolve DNA double-strand breaks. As a result, they could not recover effectively after radiation exposure or treatment with the chemotherapeutic agent fluorouracil.
“Our work shows that Wnt signaling is important in the mammalian hematopoietic system and is critical for recovery from chemotherapy and radiation,” Dr Reya said. “There are 2 major reasons why accelerating regeneration is important clinically.”
“One is that, after cancer patients are irradiated and transplanted with stem cells, the rate and extent of recovery is often not sufficient to protect the patient from anemia or infections . . . . Identifying signals that can boost regeneration after the bone marrow is severely damaged may help improve outcomes after transplantation.”
“Second, doses of chemotherapy and radiation used to treat cancer are often limited by the collateral damage they cause to normal tissues. If we can improve and accelerate recovery, we might be able to use higher doses of radiation or chemotherapy and reduce the risk of cancer relapse.”
Dr Reya added that this research suggests HSC regeneration could be accelerated by modulating the Wnt pathway, either by delivering additional Wnt proteins directly to patients or through drugs that activate the pathway. ![]()