User login
Stimulants for kids with ADHD—how to proceed safely
› Complete a thorough, cardiac-focused history and physical examination before starting stimulants for attention deficit hyperactivity disorder (ADHD) in a child or adolescent. C
› Avoid using stimulants in children or adolescents with comorbid conditions associated with sudden cardiac death, including hypertrophic cardiomyopathy, long QT interval syndrome, and preexcitation syndromes such as Wolff-Parkinson-White syndrome. C
› Monitor all children and adolescents who are taking stimulants for tachycardia, hypertension, palpitations, and chest pain. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A young patient has been struggling in school. His worried mother, having had several conferences with the child’s teachers, brings him to the family physician (FP), where he is given a diagnosis of attention deficit hyperactivity disorder (ADHD). The FP considers prescribing a stimulant medication, but first plans on conducting a more thorough family history and exam. She also debates the merits of ordering an electrocardiogram (EKG) to screen for conditions that could lead to sudden cardiac death.
If you were caring for this patient, how would you proceed?
That’s a good question, given the debate that has surrounded this subject since the US Food and Drug Administration (FDA) first learned of 25 cases of sudden death that were linked to stimulant medications.1 The majority of the cases, which were reported to the FDA’s Adverse Event Reporting System between 1999 and 2003, involved amphetamines or methylphenidate in patients under the age of 19.1 In 2008, the American Heart Association (AHA) issued a scientific statement advocating that physicians perform a proper family history and physical exam that includes blood pressure (BP) and an EKG before prescribing a stimulant for children and adolescents.2 The inclusion of EKG screening was intended to increase the likelihood of identifying patients with potentially life-threatening conditions that could lead to sudden cardiac death (SCD).2
Not everyone, however, agreed.
Later that year, the American Academy of Pediatrics (AAP) challenged the routine use of EKGs in this screening process, citing a lack of evidence between stimulant use and the induction of potentially lethal arrhythmias.3 And in 2011, the European Guideline Group also concluded that there was no evidence to suggest an incremental benefit for routine EKG assessment of ADHD patients before initiation of medication.4
Underscoring the uncertainty surrounding the subject are the findings of a 2012 survey of 525 randomly selected US pediatricians.5 Nearly a quarter of the respondents expressed concerns over the risk for SCD in children receiving stimulants for ADHD, and a slightly higher number—30%—worried that the risks for legal liability were high enough to warrant cardiac assessment.5
So how should the prudent FP proceed? In this review, we will describe how to thoroughly screen children and adolescents for their risk of SCD before prescribing stimulants for ADHD. We’ll also summarize what the evidence tells us about whether—and when—you should order an EKG. But first, a word about the pharmacology of stimulants.
How stimulants might increase SCD risk
Stimulants have been used to treat ADHD for more than 40 years6 and are a first-line of therapy for children with ADHD. Stimulants increase attention span by releasing dopamine and norepinephrine at synapses in the frontal cortex, brain stem, and midbrain.
The effect on heart rate and BP. In clinical trials with small samples sizes, children and adolescents receiving stimulants to treat ADHD experienced a minimal rise in heart rate and BP. As measured by 24-hour ambulatory BP monitoring, 13 subjects in a double-blind, randomized, placebo/stimulant crossover trial had slightly elevated total diastolic BP (69.7 vs 65.8 mm Hg; P=.02), waking diastolic BP (75.5 vs 72.3 mm Hg; P=.03), and total heart rate (85.5 vs 79.9 beats per minutes [bpm]; P=.004) while receiving stimulants.7 Other investigators noted similar findings among 17 boys ages 7 to 11 years.8
Whether prolonged childhood exposure to stimulants increases the risk for developing hypertension or tachycardia is unknown. A 10-year follow-up study of 579 children between the ages of 7 to 9 years found stimulants had no effect on systolic or diastolic BP.9 Stimulants use did, however, lead to a higher heart rate (84.2±12.4 vs 79.1±12.0 bpm) during treatment.9 No stimulant-related QT interval changes—which some have proposed might explain SCD in ADHD patients—have been reported in pediatric patients.10 Researchers have noted small increases in mean QTc intervals in adults treated with stimulants for ADHD, but none were >480 msec.11
Steps you should always take before prescribing a stimulant
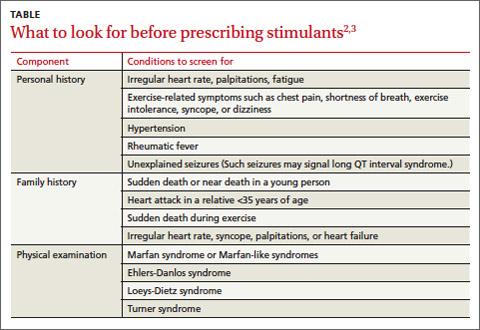
Before prescribing stimulants to children or adolescents with ADHD, complete an in-depth cardiac history and physical examination, as recommended by the AHA and AAP (TABLE),2,3 to identify conditions that increase the likelihood of SCD, such as hypertrophic cardiomyopathy (HCM), long QT interval syndrome (LQTS), and preexcitation syndromes such as Wolff-Parkinson-White syndrome (WPW).
Confirm, for instance, that your patient has a normal heart rate, rhythm, and BP, and no pathological murmurs. In a survey of families with a child or young adult who had sudden cardiac arrest, 72% reported the patient had at least one cardiovascular symptom within 19 to 71 months of SCD, and 27% reported having a family member with a history of SCD before age 50.12 For patients with no such complaints or family history, the news is good. Two large studies found that in the absence of any suspected or overt cardiac disease, children with ADHD who were receiving stimulant therapy had no increased risk of SCD.13,14
What about patients with this common heart problem? Physicians face a dilemma when a stimulant is needed and the patient has a common acyanotic congenital heart lesion, such as a small atrial or ventricular septal defect, which is considered nonlethal. Based on limited data, there is no evidence that the risk of SCD is higher when these patients take stimulants.15
Should you order that EKG—or not?
Currently, the AHA still favors an EKG, though in a correction to its original statement, it adjusted the language to say that EKG could be “useful,” in addition to an in-depth cardiac history and physical examination.16
Opposition to routine EKG screening in these patients stems from the procedure’s extremely low yield and relatively high false positive findings, which may result in higher financial and psychological burdens for patients and families. Thomas et al17 reported that at a single center, the number of EKGs ordered with an indication of “stimulant medication screening” quadrupled during 2009, the year after the AHA published its recommendations. Of 372 patients referred for EKG, 24 (6.4%) had abnormal findings and 18 were referred for further evaluation, but none were found to have cardiac disease. ADHD therapy was delayed in 6 patients because of the EKG.
In a similar evaluation of 1470 ADHD patients ages 21 years and younger, Mahle et al18 noted that 119 patients (8.1%) had an abnormal EKG, 78 of whom (65%) were already receiving stimulants. Five patients had cardiac disease, including 2 who had a preexcitation syndrome. Overall, the positive predictive value was low (4.2%).18 Other research, including a study lead by one of this article’s authors (SKM), has found similar increases in the number of EKGs ordered for patients with ADHD.19
Cost vs benefit. In the Mahle et al18 study described above, the mean cost of EKG screening, including further testing for patients with abnormal initial results, was $58 per child. The mean cost to identify a true-positive result was $17,162.18
In 2012, Leslie et al20 used simulation models to estimate the societal cost of routine EKG screening to prevent SCD in children with ADHD. Their findings: The cost would be high relative to its health benefits—approximately $91,000 to $204,000 per life year saved. Furthermore, these researchers found that ordering an EKG to screen for 3 common cardiac conditions linked to SCD (HCM, WPW, and LQTS) would add <2 days to a patient’s projected life expectancy.20
Our recommendations
We believe stimulants can safely be used in the treatment of children and adolescents with ADHD, given the evidence that suggests a low risk of SCD. That said, it is prudent to avoid prescribing stimulants for children who have an underlying condition that may deteriorate secondary to increased blood pressure or heart rate.
We agree with the current AHA and AAP recommendations that physicians should obtain an in-depth cardiac history and physical examination, with emphasis on screening for cardiac disorders that may put a child at risk for SCD, such as HCM, LQTS, and preexcitation syndromes. For instance, a history of a family member with palpitations should prompt an EKG, which may reveal familial preexcitation syndrome. Similarly, an EKG is in order if you suspect LQTS based on a parent’s description of a family member’s death after hearing a loud noise, such as fireworks.
It often takes active probing to uncover a history of sudden death in the family that a parent may not consider relevant. For example, one of the authors (SKM) cared for a 6-year-old boy who presented with a history of syncope after his hand got caught in a door jam. On further probing, his mother revealed that her father had died at age 30 while he was taking astemizole, an allergy drug known to prolong the QT interval. Subsequent EKGs revealed that both the boy and his mother had LQTS.
For patients already taking stimulants, we recommend monitoring BP and heart rate and ordering an EKG only if the patient exhibits cardiac symptoms or there are concerns based on follow-up history and physical examination. Should a patient develop palpitations while taking a therapeutic dose of stimulants, a detailed history of the onset and duration of symptoms is important. For example, tachycardia that has a gradual onset and occurs with exercise is suggestive of physiological sinus tachycardia. In our judgment, most patients who experience symptoms that suggest sinus tachycardia simply require downward readjustment of their medication or a switch to a nonstimulant.
However, if the patient or family history prompts you to suspect other arrhythmias such as ectopic beats or supraventricular tachycardia, immediate assessment either in an emergency department or in the physician’s office may be required, because obtaining an EKG during symptoms is crucial for the diagnosis. Similarly, unexplained exercise intolerance or the onset of chest pain associated with exercise, dizziness, syncope, seizures, or dyspnea requires immediate cardiovascular assessment.
And finally, whether your patient has just started taking medication for his or her ADHD or has been on the medication for some time, it’s important to periodically reassess the need to continue the stimulant therapy; ADHD symptoms may decrease during mid- to late adolescence and into adulthood.21
CASE › The FP completed a thorough physical exam and found no evidence of any conditions that would increase the likelihood of SCD in the young patient. There was no history of SCD in the boy’s family, either. Based on these findings, the FP opted to forgo an EKG. She prescribed lisdexamfetamine, starting with 20 mg/d (the lowest dose available) and then monitored his course by telephone. Eventually, 30 mg was found to be an effective dose. At a 6-week follow-up visit, the boy’s ADHD symptoms were substantially reduced, without any adverse effects—cardiac or otherwise.
CORRESPONDENCE
Sudhir Ken Mehta, Cleveland Clinic Children’s Hospital, 9500 Euclid Avenue, Cleveland, OH 44111; [email protected]
1. Safety review: Follow up review of AERS search identifying cases of sudden death occurring with drugs used for the treatment of Attention Deficit Hyperactivity Disorder (ADHD). US Food and Drug Administration Web site. Available at: http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4210b_07_01_safetyreview.pdf. Accessed January 17, 2014.
2. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation. 2008;117:2407-2423.
3. Perrin JM, Friedman RA, Knilans TK; Black Box Working Group; Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics. 2008;122:451-453.
4. Graham J, Banaschewski T, Buitelaar J, et al; European Guidelines Group. European guidelines on managing adverse effects of medication for ADHD. Eur Child Adolesc Psychiatry. 2011;20:17-37.
5. Leslie LK, Rodday AM, Saunders TS, et al. Cardiac screening prior to stimulant treatment of ADHD: a survey of US-based pediatricians. Pediatrics. 2012;129:222-230.
6. Conners CK. Symposium: behavior modification by drugs. II. Psychological effects of stimulant drugs in children with minimal brain dysfunction. Pediatrics. 1972;49:702-708.
7. Samuels JA, Franco K, Wan F, et al. Effect of stimulants on 24-h ambulatory blood pressure in children with ADHD: a double-blind, randomized, cross-over trial. Pediatr Nephrol. 2006;21:92-95.
8. Stowe CD, Gardner SF, Gist CC, et al. 24-hour ambulatory blood pressure monitoring in male children receiving stimulant therapy. Ann Pharmacother. 2002;36:1142-1149.
9. Vitiello B, Elliott GR, Swanson JM, et al. Blood pressure and heart rate over 10 years in the multimodal treatment study of children with ADHD. Am J Psychiatry. 2012;169:167-177.
10. Hammerness P, Wilens T, Mick E, et al. Cardiovascular effects of longer-term, high-dose OROS methylphenidate in adolescents with attention deficit hyperactivity disorder. J Pediatr. 2009;155:84-89,89.e1.
11. Weisler RH, Biederman J, Spencer TJ, et al. Long-term cardiovascular effects of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr. 2005;10(suppl 20):35-43.
12. Drezner JA, Fudge J, Harmon KG, et al. Warning symptoms and family history in children and young adults with sudden cardiac arrest. J Am Board Fam Med. 2012;25:408-415.
13. Cooper WO, Habel LA, Sox CM, et al. ADHD drugs and serious cardiovascular events in children and young adults. N Engl J Med. 2011;365:1896-1904.
14. Schelleman H, Bilker WB, Strom BL, et al. Cardiovascular events and death in children exposed and unexposed to ADHD agents. Pediatrics. 2011;127:1102-1110.
15. Winterstein AG, Gerhard T, Kubilis P, et al. Cardiovascular safety of central nervous system stimulants in children and adolescents: population based cohort study. BMJ. 2012;345:e4627.
16. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing [published correction appears in Circulation. 2009;120:e55-e59]. Circulation. 2008;117:2407-2423.
17. Thomas PE, Carlo WF, Decker JA, et al. Impact of the American Heart Association scientific statement on screening electrocardiograms and stimulant medications. Arch Pediatr Adolesc Med. 2011;165:166-170.
18. Mahle WT, Hebson C, Strieper MJ. Electrocardiographic screening in children with attention-deficit hyperactivity disorder. Am J Cardiol. 2009;104:1296-1299.
19. Mehta SK, Richards N, Jacobs I. Children and adolescents with attention deficit hyperactivity disorder in a pediatric cardiology office. Cardiol Young. 2010;20(suppl 3):167.
20. Leslie LK, Cohen JT, Newburger JW, et al. Costs and benefits of targeted screening for causes of sudden cardiac death in children and adolescents. Circulation. 2012;125:2621-2629.
21. Mannuzza S, Klein RG, Bessler A, et al. Adult psychiatric status of hyperactive boys grown up. Am J Psychiatry. 1998;155:493-488.
› Complete a thorough, cardiac-focused history and physical examination before starting stimulants for attention deficit hyperactivity disorder (ADHD) in a child or adolescent. C
› Avoid using stimulants in children or adolescents with comorbid conditions associated with sudden cardiac death, including hypertrophic cardiomyopathy, long QT interval syndrome, and preexcitation syndromes such as Wolff-Parkinson-White syndrome. C
› Monitor all children and adolescents who are taking stimulants for tachycardia, hypertension, palpitations, and chest pain. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A young patient has been struggling in school. His worried mother, having had several conferences with the child’s teachers, brings him to the family physician (FP), where he is given a diagnosis of attention deficit hyperactivity disorder (ADHD). The FP considers prescribing a stimulant medication, but first plans on conducting a more thorough family history and exam. She also debates the merits of ordering an electrocardiogram (EKG) to screen for conditions that could lead to sudden cardiac death.
If you were caring for this patient, how would you proceed?
That’s a good question, given the debate that has surrounded this subject since the US Food and Drug Administration (FDA) first learned of 25 cases of sudden death that were linked to stimulant medications.1 The majority of the cases, which were reported to the FDA’s Adverse Event Reporting System between 1999 and 2003, involved amphetamines or methylphenidate in patients under the age of 19.1 In 2008, the American Heart Association (AHA) issued a scientific statement advocating that physicians perform a proper family history and physical exam that includes blood pressure (BP) and an EKG before prescribing a stimulant for children and adolescents.2 The inclusion of EKG screening was intended to increase the likelihood of identifying patients with potentially life-threatening conditions that could lead to sudden cardiac death (SCD).2
Not everyone, however, agreed.
Later that year, the American Academy of Pediatrics (AAP) challenged the routine use of EKGs in this screening process, citing a lack of evidence between stimulant use and the induction of potentially lethal arrhythmias.3 And in 2011, the European Guideline Group also concluded that there was no evidence to suggest an incremental benefit for routine EKG assessment of ADHD patients before initiation of medication.4
Underscoring the uncertainty surrounding the subject are the findings of a 2012 survey of 525 randomly selected US pediatricians.5 Nearly a quarter of the respondents expressed concerns over the risk for SCD in children receiving stimulants for ADHD, and a slightly higher number—30%—worried that the risks for legal liability were high enough to warrant cardiac assessment.5
So how should the prudent FP proceed? In this review, we will describe how to thoroughly screen children and adolescents for their risk of SCD before prescribing stimulants for ADHD. We’ll also summarize what the evidence tells us about whether—and when—you should order an EKG. But first, a word about the pharmacology of stimulants.
How stimulants might increase SCD risk
Stimulants have been used to treat ADHD for more than 40 years6 and are a first-line of therapy for children with ADHD. Stimulants increase attention span by releasing dopamine and norepinephrine at synapses in the frontal cortex, brain stem, and midbrain.
The effect on heart rate and BP. In clinical trials with small samples sizes, children and adolescents receiving stimulants to treat ADHD experienced a minimal rise in heart rate and BP. As measured by 24-hour ambulatory BP monitoring, 13 subjects in a double-blind, randomized, placebo/stimulant crossover trial had slightly elevated total diastolic BP (69.7 vs 65.8 mm Hg; P=.02), waking diastolic BP (75.5 vs 72.3 mm Hg; P=.03), and total heart rate (85.5 vs 79.9 beats per minutes [bpm]; P=.004) while receiving stimulants.7 Other investigators noted similar findings among 17 boys ages 7 to 11 years.8
Whether prolonged childhood exposure to stimulants increases the risk for developing hypertension or tachycardia is unknown. A 10-year follow-up study of 579 children between the ages of 7 to 9 years found stimulants had no effect on systolic or diastolic BP.9 Stimulants use did, however, lead to a higher heart rate (84.2±12.4 vs 79.1±12.0 bpm) during treatment.9 No stimulant-related QT interval changes—which some have proposed might explain SCD in ADHD patients—have been reported in pediatric patients.10 Researchers have noted small increases in mean QTc intervals in adults treated with stimulants for ADHD, but none were >480 msec.11
Steps you should always take before prescribing a stimulant
Before prescribing stimulants to children or adolescents with ADHD, complete an in-depth cardiac history and physical examination, as recommended by the AHA and AAP (TABLE),2,3 to identify conditions that increase the likelihood of SCD, such as hypertrophic cardiomyopathy (HCM), long QT interval syndrome (LQTS), and preexcitation syndromes such as Wolff-Parkinson-White syndrome (WPW).
Confirm, for instance, that your patient has a normal heart rate, rhythm, and BP, and no pathological murmurs. In a survey of families with a child or young adult who had sudden cardiac arrest, 72% reported the patient had at least one cardiovascular symptom within 19 to 71 months of SCD, and 27% reported having a family member with a history of SCD before age 50.12 For patients with no such complaints or family history, the news is good. Two large studies found that in the absence of any suspected or overt cardiac disease, children with ADHD who were receiving stimulant therapy had no increased risk of SCD.13,14
What about patients with this common heart problem? Physicians face a dilemma when a stimulant is needed and the patient has a common acyanotic congenital heart lesion, such as a small atrial or ventricular septal defect, which is considered nonlethal. Based on limited data, there is no evidence that the risk of SCD is higher when these patients take stimulants.15
Should you order that EKG—or not?
Currently, the AHA still favors an EKG, though in a correction to its original statement, it adjusted the language to say that EKG could be “useful,” in addition to an in-depth cardiac history and physical examination.16
Opposition to routine EKG screening in these patients stems from the procedure’s extremely low yield and relatively high false positive findings, which may result in higher financial and psychological burdens for patients and families. Thomas et al17 reported that at a single center, the number of EKGs ordered with an indication of “stimulant medication screening” quadrupled during 2009, the year after the AHA published its recommendations. Of 372 patients referred for EKG, 24 (6.4%) had abnormal findings and 18 were referred for further evaluation, but none were found to have cardiac disease. ADHD therapy was delayed in 6 patients because of the EKG.
In a similar evaluation of 1470 ADHD patients ages 21 years and younger, Mahle et al18 noted that 119 patients (8.1%) had an abnormal EKG, 78 of whom (65%) were already receiving stimulants. Five patients had cardiac disease, including 2 who had a preexcitation syndrome. Overall, the positive predictive value was low (4.2%).18 Other research, including a study lead by one of this article’s authors (SKM), has found similar increases in the number of EKGs ordered for patients with ADHD.19
Cost vs benefit. In the Mahle et al18 study described above, the mean cost of EKG screening, including further testing for patients with abnormal initial results, was $58 per child. The mean cost to identify a true-positive result was $17,162.18
In 2012, Leslie et al20 used simulation models to estimate the societal cost of routine EKG screening to prevent SCD in children with ADHD. Their findings: The cost would be high relative to its health benefits—approximately $91,000 to $204,000 per life year saved. Furthermore, these researchers found that ordering an EKG to screen for 3 common cardiac conditions linked to SCD (HCM, WPW, and LQTS) would add <2 days to a patient’s projected life expectancy.20
Our recommendations
We believe stimulants can safely be used in the treatment of children and adolescents with ADHD, given the evidence that suggests a low risk of SCD. That said, it is prudent to avoid prescribing stimulants for children who have an underlying condition that may deteriorate secondary to increased blood pressure or heart rate.
We agree with the current AHA and AAP recommendations that physicians should obtain an in-depth cardiac history and physical examination, with emphasis on screening for cardiac disorders that may put a child at risk for SCD, such as HCM, LQTS, and preexcitation syndromes. For instance, a history of a family member with palpitations should prompt an EKG, which may reveal familial preexcitation syndrome. Similarly, an EKG is in order if you suspect LQTS based on a parent’s description of a family member’s death after hearing a loud noise, such as fireworks.
It often takes active probing to uncover a history of sudden death in the family that a parent may not consider relevant. For example, one of the authors (SKM) cared for a 6-year-old boy who presented with a history of syncope after his hand got caught in a door jam. On further probing, his mother revealed that her father had died at age 30 while he was taking astemizole, an allergy drug known to prolong the QT interval. Subsequent EKGs revealed that both the boy and his mother had LQTS.
For patients already taking stimulants, we recommend monitoring BP and heart rate and ordering an EKG only if the patient exhibits cardiac symptoms or there are concerns based on follow-up history and physical examination. Should a patient develop palpitations while taking a therapeutic dose of stimulants, a detailed history of the onset and duration of symptoms is important. For example, tachycardia that has a gradual onset and occurs with exercise is suggestive of physiological sinus tachycardia. In our judgment, most patients who experience symptoms that suggest sinus tachycardia simply require downward readjustment of their medication or a switch to a nonstimulant.
However, if the patient or family history prompts you to suspect other arrhythmias such as ectopic beats or supraventricular tachycardia, immediate assessment either in an emergency department or in the physician’s office may be required, because obtaining an EKG during symptoms is crucial for the diagnosis. Similarly, unexplained exercise intolerance or the onset of chest pain associated with exercise, dizziness, syncope, seizures, or dyspnea requires immediate cardiovascular assessment.
And finally, whether your patient has just started taking medication for his or her ADHD or has been on the medication for some time, it’s important to periodically reassess the need to continue the stimulant therapy; ADHD symptoms may decrease during mid- to late adolescence and into adulthood.21
CASE › The FP completed a thorough physical exam and found no evidence of any conditions that would increase the likelihood of SCD in the young patient. There was no history of SCD in the boy’s family, either. Based on these findings, the FP opted to forgo an EKG. She prescribed lisdexamfetamine, starting with 20 mg/d (the lowest dose available) and then monitored his course by telephone. Eventually, 30 mg was found to be an effective dose. At a 6-week follow-up visit, the boy’s ADHD symptoms were substantially reduced, without any adverse effects—cardiac or otherwise.
CORRESPONDENCE
Sudhir Ken Mehta, Cleveland Clinic Children’s Hospital, 9500 Euclid Avenue, Cleveland, OH 44111; [email protected]
› Complete a thorough, cardiac-focused history and physical examination before starting stimulants for attention deficit hyperactivity disorder (ADHD) in a child or adolescent. C
› Avoid using stimulants in children or adolescents with comorbid conditions associated with sudden cardiac death, including hypertrophic cardiomyopathy, long QT interval syndrome, and preexcitation syndromes such as Wolff-Parkinson-White syndrome. C
› Monitor all children and adolescents who are taking stimulants for tachycardia, hypertension, palpitations, and chest pain. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › A young patient has been struggling in school. His worried mother, having had several conferences with the child’s teachers, brings him to the family physician (FP), where he is given a diagnosis of attention deficit hyperactivity disorder (ADHD). The FP considers prescribing a stimulant medication, but first plans on conducting a more thorough family history and exam. She also debates the merits of ordering an electrocardiogram (EKG) to screen for conditions that could lead to sudden cardiac death.
If you were caring for this patient, how would you proceed?
That’s a good question, given the debate that has surrounded this subject since the US Food and Drug Administration (FDA) first learned of 25 cases of sudden death that were linked to stimulant medications.1 The majority of the cases, which were reported to the FDA’s Adverse Event Reporting System between 1999 and 2003, involved amphetamines or methylphenidate in patients under the age of 19.1 In 2008, the American Heart Association (AHA) issued a scientific statement advocating that physicians perform a proper family history and physical exam that includes blood pressure (BP) and an EKG before prescribing a stimulant for children and adolescents.2 The inclusion of EKG screening was intended to increase the likelihood of identifying patients with potentially life-threatening conditions that could lead to sudden cardiac death (SCD).2
Not everyone, however, agreed.
Later that year, the American Academy of Pediatrics (AAP) challenged the routine use of EKGs in this screening process, citing a lack of evidence between stimulant use and the induction of potentially lethal arrhythmias.3 And in 2011, the European Guideline Group also concluded that there was no evidence to suggest an incremental benefit for routine EKG assessment of ADHD patients before initiation of medication.4
Underscoring the uncertainty surrounding the subject are the findings of a 2012 survey of 525 randomly selected US pediatricians.5 Nearly a quarter of the respondents expressed concerns over the risk for SCD in children receiving stimulants for ADHD, and a slightly higher number—30%—worried that the risks for legal liability were high enough to warrant cardiac assessment.5
So how should the prudent FP proceed? In this review, we will describe how to thoroughly screen children and adolescents for their risk of SCD before prescribing stimulants for ADHD. We’ll also summarize what the evidence tells us about whether—and when—you should order an EKG. But first, a word about the pharmacology of stimulants.
How stimulants might increase SCD risk
Stimulants have been used to treat ADHD for more than 40 years6 and are a first-line of therapy for children with ADHD. Stimulants increase attention span by releasing dopamine and norepinephrine at synapses in the frontal cortex, brain stem, and midbrain.
The effect on heart rate and BP. In clinical trials with small samples sizes, children and adolescents receiving stimulants to treat ADHD experienced a minimal rise in heart rate and BP. As measured by 24-hour ambulatory BP monitoring, 13 subjects in a double-blind, randomized, placebo/stimulant crossover trial had slightly elevated total diastolic BP (69.7 vs 65.8 mm Hg; P=.02), waking diastolic BP (75.5 vs 72.3 mm Hg; P=.03), and total heart rate (85.5 vs 79.9 beats per minutes [bpm]; P=.004) while receiving stimulants.7 Other investigators noted similar findings among 17 boys ages 7 to 11 years.8
Whether prolonged childhood exposure to stimulants increases the risk for developing hypertension or tachycardia is unknown. A 10-year follow-up study of 579 children between the ages of 7 to 9 years found stimulants had no effect on systolic or diastolic BP.9 Stimulants use did, however, lead to a higher heart rate (84.2±12.4 vs 79.1±12.0 bpm) during treatment.9 No stimulant-related QT interval changes—which some have proposed might explain SCD in ADHD patients—have been reported in pediatric patients.10 Researchers have noted small increases in mean QTc intervals in adults treated with stimulants for ADHD, but none were >480 msec.11
Steps you should always take before prescribing a stimulant
Before prescribing stimulants to children or adolescents with ADHD, complete an in-depth cardiac history and physical examination, as recommended by the AHA and AAP (TABLE),2,3 to identify conditions that increase the likelihood of SCD, such as hypertrophic cardiomyopathy (HCM), long QT interval syndrome (LQTS), and preexcitation syndromes such as Wolff-Parkinson-White syndrome (WPW).
Confirm, for instance, that your patient has a normal heart rate, rhythm, and BP, and no pathological murmurs. In a survey of families with a child or young adult who had sudden cardiac arrest, 72% reported the patient had at least one cardiovascular symptom within 19 to 71 months of SCD, and 27% reported having a family member with a history of SCD before age 50.12 For patients with no such complaints or family history, the news is good. Two large studies found that in the absence of any suspected or overt cardiac disease, children with ADHD who were receiving stimulant therapy had no increased risk of SCD.13,14
What about patients with this common heart problem? Physicians face a dilemma when a stimulant is needed and the patient has a common acyanotic congenital heart lesion, such as a small atrial or ventricular septal defect, which is considered nonlethal. Based on limited data, there is no evidence that the risk of SCD is higher when these patients take stimulants.15
Should you order that EKG—or not?
Currently, the AHA still favors an EKG, though in a correction to its original statement, it adjusted the language to say that EKG could be “useful,” in addition to an in-depth cardiac history and physical examination.16
Opposition to routine EKG screening in these patients stems from the procedure’s extremely low yield and relatively high false positive findings, which may result in higher financial and psychological burdens for patients and families. Thomas et al17 reported that at a single center, the number of EKGs ordered with an indication of “stimulant medication screening” quadrupled during 2009, the year after the AHA published its recommendations. Of 372 patients referred for EKG, 24 (6.4%) had abnormal findings and 18 were referred for further evaluation, but none were found to have cardiac disease. ADHD therapy was delayed in 6 patients because of the EKG.
In a similar evaluation of 1470 ADHD patients ages 21 years and younger, Mahle et al18 noted that 119 patients (8.1%) had an abnormal EKG, 78 of whom (65%) were already receiving stimulants. Five patients had cardiac disease, including 2 who had a preexcitation syndrome. Overall, the positive predictive value was low (4.2%).18 Other research, including a study lead by one of this article’s authors (SKM), has found similar increases in the number of EKGs ordered for patients with ADHD.19
Cost vs benefit. In the Mahle et al18 study described above, the mean cost of EKG screening, including further testing for patients with abnormal initial results, was $58 per child. The mean cost to identify a true-positive result was $17,162.18
In 2012, Leslie et al20 used simulation models to estimate the societal cost of routine EKG screening to prevent SCD in children with ADHD. Their findings: The cost would be high relative to its health benefits—approximately $91,000 to $204,000 per life year saved. Furthermore, these researchers found that ordering an EKG to screen for 3 common cardiac conditions linked to SCD (HCM, WPW, and LQTS) would add <2 days to a patient’s projected life expectancy.20
Our recommendations
We believe stimulants can safely be used in the treatment of children and adolescents with ADHD, given the evidence that suggests a low risk of SCD. That said, it is prudent to avoid prescribing stimulants for children who have an underlying condition that may deteriorate secondary to increased blood pressure or heart rate.
We agree with the current AHA and AAP recommendations that physicians should obtain an in-depth cardiac history and physical examination, with emphasis on screening for cardiac disorders that may put a child at risk for SCD, such as HCM, LQTS, and preexcitation syndromes. For instance, a history of a family member with palpitations should prompt an EKG, which may reveal familial preexcitation syndrome. Similarly, an EKG is in order if you suspect LQTS based on a parent’s description of a family member’s death after hearing a loud noise, such as fireworks.
It often takes active probing to uncover a history of sudden death in the family that a parent may not consider relevant. For example, one of the authors (SKM) cared for a 6-year-old boy who presented with a history of syncope after his hand got caught in a door jam. On further probing, his mother revealed that her father had died at age 30 while he was taking astemizole, an allergy drug known to prolong the QT interval. Subsequent EKGs revealed that both the boy and his mother had LQTS.
For patients already taking stimulants, we recommend monitoring BP and heart rate and ordering an EKG only if the patient exhibits cardiac symptoms or there are concerns based on follow-up history and physical examination. Should a patient develop palpitations while taking a therapeutic dose of stimulants, a detailed history of the onset and duration of symptoms is important. For example, tachycardia that has a gradual onset and occurs with exercise is suggestive of physiological sinus tachycardia. In our judgment, most patients who experience symptoms that suggest sinus tachycardia simply require downward readjustment of their medication or a switch to a nonstimulant.
However, if the patient or family history prompts you to suspect other arrhythmias such as ectopic beats or supraventricular tachycardia, immediate assessment either in an emergency department or in the physician’s office may be required, because obtaining an EKG during symptoms is crucial for the diagnosis. Similarly, unexplained exercise intolerance or the onset of chest pain associated with exercise, dizziness, syncope, seizures, or dyspnea requires immediate cardiovascular assessment.
And finally, whether your patient has just started taking medication for his or her ADHD or has been on the medication for some time, it’s important to periodically reassess the need to continue the stimulant therapy; ADHD symptoms may decrease during mid- to late adolescence and into adulthood.21
CASE › The FP completed a thorough physical exam and found no evidence of any conditions that would increase the likelihood of SCD in the young patient. There was no history of SCD in the boy’s family, either. Based on these findings, the FP opted to forgo an EKG. She prescribed lisdexamfetamine, starting with 20 mg/d (the lowest dose available) and then monitored his course by telephone. Eventually, 30 mg was found to be an effective dose. At a 6-week follow-up visit, the boy’s ADHD symptoms were substantially reduced, without any adverse effects—cardiac or otherwise.
CORRESPONDENCE
Sudhir Ken Mehta, Cleveland Clinic Children’s Hospital, 9500 Euclid Avenue, Cleveland, OH 44111; [email protected]
1. Safety review: Follow up review of AERS search identifying cases of sudden death occurring with drugs used for the treatment of Attention Deficit Hyperactivity Disorder (ADHD). US Food and Drug Administration Web site. Available at: http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4210b_07_01_safetyreview.pdf. Accessed January 17, 2014.
2. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation. 2008;117:2407-2423.
3. Perrin JM, Friedman RA, Knilans TK; Black Box Working Group; Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics. 2008;122:451-453.
4. Graham J, Banaschewski T, Buitelaar J, et al; European Guidelines Group. European guidelines on managing adverse effects of medication for ADHD. Eur Child Adolesc Psychiatry. 2011;20:17-37.
5. Leslie LK, Rodday AM, Saunders TS, et al. Cardiac screening prior to stimulant treatment of ADHD: a survey of US-based pediatricians. Pediatrics. 2012;129:222-230.
6. Conners CK. Symposium: behavior modification by drugs. II. Psychological effects of stimulant drugs in children with minimal brain dysfunction. Pediatrics. 1972;49:702-708.
7. Samuels JA, Franco K, Wan F, et al. Effect of stimulants on 24-h ambulatory blood pressure in children with ADHD: a double-blind, randomized, cross-over trial. Pediatr Nephrol. 2006;21:92-95.
8. Stowe CD, Gardner SF, Gist CC, et al. 24-hour ambulatory blood pressure monitoring in male children receiving stimulant therapy. Ann Pharmacother. 2002;36:1142-1149.
9. Vitiello B, Elliott GR, Swanson JM, et al. Blood pressure and heart rate over 10 years in the multimodal treatment study of children with ADHD. Am J Psychiatry. 2012;169:167-177.
10. Hammerness P, Wilens T, Mick E, et al. Cardiovascular effects of longer-term, high-dose OROS methylphenidate in adolescents with attention deficit hyperactivity disorder. J Pediatr. 2009;155:84-89,89.e1.
11. Weisler RH, Biederman J, Spencer TJ, et al. Long-term cardiovascular effects of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr. 2005;10(suppl 20):35-43.
12. Drezner JA, Fudge J, Harmon KG, et al. Warning symptoms and family history in children and young adults with sudden cardiac arrest. J Am Board Fam Med. 2012;25:408-415.
13. Cooper WO, Habel LA, Sox CM, et al. ADHD drugs and serious cardiovascular events in children and young adults. N Engl J Med. 2011;365:1896-1904.
14. Schelleman H, Bilker WB, Strom BL, et al. Cardiovascular events and death in children exposed and unexposed to ADHD agents. Pediatrics. 2011;127:1102-1110.
15. Winterstein AG, Gerhard T, Kubilis P, et al. Cardiovascular safety of central nervous system stimulants in children and adolescents: population based cohort study. BMJ. 2012;345:e4627.
16. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing [published correction appears in Circulation. 2009;120:e55-e59]. Circulation. 2008;117:2407-2423.
17. Thomas PE, Carlo WF, Decker JA, et al. Impact of the American Heart Association scientific statement on screening electrocardiograms and stimulant medications. Arch Pediatr Adolesc Med. 2011;165:166-170.
18. Mahle WT, Hebson C, Strieper MJ. Electrocardiographic screening in children with attention-deficit hyperactivity disorder. Am J Cardiol. 2009;104:1296-1299.
19. Mehta SK, Richards N, Jacobs I. Children and adolescents with attention deficit hyperactivity disorder in a pediatric cardiology office. Cardiol Young. 2010;20(suppl 3):167.
20. Leslie LK, Cohen JT, Newburger JW, et al. Costs and benefits of targeted screening for causes of sudden cardiac death in children and adolescents. Circulation. 2012;125:2621-2629.
21. Mannuzza S, Klein RG, Bessler A, et al. Adult psychiatric status of hyperactive boys grown up. Am J Psychiatry. 1998;155:493-488.
1. Safety review: Follow up review of AERS search identifying cases of sudden death occurring with drugs used for the treatment of Attention Deficit Hyperactivity Disorder (ADHD). US Food and Drug Administration Web site. Available at: http://www.fda.gov/ohrms/dockets/ac/06/briefing/2006-4210b_07_01_safetyreview.pdf. Accessed January 17, 2014.
2. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing. Circulation. 2008;117:2407-2423.
3. Perrin JM, Friedman RA, Knilans TK; Black Box Working Group; Section on Cardiology and Cardiac Surgery. Cardiovascular monitoring and stimulant drugs for attention-deficit/hyperactivity disorder. Pediatrics. 2008;122:451-453.
4. Graham J, Banaschewski T, Buitelaar J, et al; European Guidelines Group. European guidelines on managing adverse effects of medication for ADHD. Eur Child Adolesc Psychiatry. 2011;20:17-37.
5. Leslie LK, Rodday AM, Saunders TS, et al. Cardiac screening prior to stimulant treatment of ADHD: a survey of US-based pediatricians. Pediatrics. 2012;129:222-230.
6. Conners CK. Symposium: behavior modification by drugs. II. Psychological effects of stimulant drugs in children with minimal brain dysfunction. Pediatrics. 1972;49:702-708.
7. Samuels JA, Franco K, Wan F, et al. Effect of stimulants on 24-h ambulatory blood pressure in children with ADHD: a double-blind, randomized, cross-over trial. Pediatr Nephrol. 2006;21:92-95.
8. Stowe CD, Gardner SF, Gist CC, et al. 24-hour ambulatory blood pressure monitoring in male children receiving stimulant therapy. Ann Pharmacother. 2002;36:1142-1149.
9. Vitiello B, Elliott GR, Swanson JM, et al. Blood pressure and heart rate over 10 years in the multimodal treatment study of children with ADHD. Am J Psychiatry. 2012;169:167-177.
10. Hammerness P, Wilens T, Mick E, et al. Cardiovascular effects of longer-term, high-dose OROS methylphenidate in adolescents with attention deficit hyperactivity disorder. J Pediatr. 2009;155:84-89,89.e1.
11. Weisler RH, Biederman J, Spencer TJ, et al. Long-term cardiovascular effects of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr. 2005;10(suppl 20):35-43.
12. Drezner JA, Fudge J, Harmon KG, et al. Warning symptoms and family history in children and young adults with sudden cardiac arrest. J Am Board Fam Med. 2012;25:408-415.
13. Cooper WO, Habel LA, Sox CM, et al. ADHD drugs and serious cardiovascular events in children and young adults. N Engl J Med. 2011;365:1896-1904.
14. Schelleman H, Bilker WB, Strom BL, et al. Cardiovascular events and death in children exposed and unexposed to ADHD agents. Pediatrics. 2011;127:1102-1110.
15. Winterstein AG, Gerhard T, Kubilis P, et al. Cardiovascular safety of central nervous system stimulants in children and adolescents: population based cohort study. BMJ. 2012;345:e4627.
16. Vetter VL, Elia J, Erickson C, et al. Cardiovascular monitoring of children and adolescents with heart disease receiving medications for attention deficit/hyperactivity disorder: a scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee and the Council on Cardiovascular Nursing [published correction appears in Circulation. 2009;120:e55-e59]. Circulation. 2008;117:2407-2423.
17. Thomas PE, Carlo WF, Decker JA, et al. Impact of the American Heart Association scientific statement on screening electrocardiograms and stimulant medications. Arch Pediatr Adolesc Med. 2011;165:166-170.
18. Mahle WT, Hebson C, Strieper MJ. Electrocardiographic screening in children with attention-deficit hyperactivity disorder. Am J Cardiol. 2009;104:1296-1299.
19. Mehta SK, Richards N, Jacobs I. Children and adolescents with attention deficit hyperactivity disorder in a pediatric cardiology office. Cardiol Young. 2010;20(suppl 3):167.
20. Leslie LK, Cohen JT, Newburger JW, et al. Costs and benefits of targeted screening for causes of sudden cardiac death in children and adolescents. Circulation. 2012;125:2621-2629.
21. Mannuzza S, Klein RG, Bessler A, et al. Adult psychiatric status of hyperactive boys grown up. Am J Psychiatry. 1998;155:493-488.

Urodynamic testing: Who needs it, and key pointers for a successful outcome
More than 300 attendees heard Dr. Mickey Karram address urodynamics and cystoscopy at the annual Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) in Las Vegas, December 12-14, 2013. Here, a key topic from his presentation.

Dr. Karram is Professor of OB/GYN and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio. He also is Course Director of the Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) and the Female Urology and Urogynecology Symposium (FUUS), both co-sponsored by OBG Management.
FUUS 2014: June 14-16, Aria, Las Vegas
Click here for more info.
More than 300 attendees heard Dr. Mickey Karram address urodynamics and cystoscopy at the annual Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) in Las Vegas, December 12-14, 2013. Here, a key topic from his presentation.
Dr. Karram is Professor of OB/GYN and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio. He also is Course Director of the Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) and the Female Urology and Urogynecology Symposium (FUUS), both co-sponsored by OBG Management.
FUUS 2014: June 14-16, Aria, Las Vegas
Click here for more info.
More than 300 attendees heard Dr. Mickey Karram address urodynamics and cystoscopy at the annual Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) in Las Vegas, December 12-14, 2013. Here, a key topic from his presentation.
Dr. Karram is Professor of OB/GYN and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio. He also is Course Director of the Pelvic Anatomy and Gynecologic Surgery Symposium (PAGS) and the Female Urology and Urogynecology Symposium (FUUS), both co-sponsored by OBG Management.
FUUS 2014: June 14-16, Aria, Las Vegas
Click here for more info.
Malaria screening program unsuccessful

blood cell; Credit: St Jude
Children’s Research Hospital
A school-based, intermittent screening and treatment program for malaria did not confer any benefits for children living in an area of low-to-moderate malaria transmission.
The program, which was implemented at schools in Kenya, did not significantly reduce the incidence of malaria infection or the prevalence of anemia.
Katherine Halliday, of the London School of Hygiene & Tropical Medicine in the UK, and her colleagues reported these results in PLOS Medicine.
The study included 5233 children, ages 5 to 20, studying at 101 government schools located on the south coast of Kenya. Fifty-one of the schools were randomized to the intermittent screening and treatment program.
Over 24 months, children in these schools underwent screening for malaria parasites once each term (a total of 5 times). And those who tested positive for malaria parasitemia (whether symptomatic or asymptomatic) received 6 cycles of treatment with the anti-malarial drug artemether-lumefantrine.
Eighty-four percent of the children were screened at 4 or more rounds, and 66.8% were screened at all 5 rounds. By the fifth round, 20% of children had been lost due to death, withdrawal, or migration.
The percentage of children who were positive for malaria at each screening ranged from 14.8% to 19.2%, and there was no distinct trend over time. Overall, 99.1% of the positive results led to treatment, and 92.6% of these were recorded as receiving the fully supervised, 6-dose treatment regimen.
The investigators followed a majority of the children in each group for an additional 24 months after the intervention ended. And the team found that the intervention had no significant impact on the prevalence of Plasmodium falciparum infection at 12 months or 24 months.
At 12 months, the prevalence of P falciparum (adjusted for age, sex, and stratification effects) was 10.7% in the intervention group and 14.3% in the control group (P=0.131). At 24 months, the prevalence of P falciparum was 11.8% in the intervention group and 8.5% in the control group (P=0.124).
Similarly, there was no significant difference between the 2 groups with regard to anemia.
At 12 months, the prevalence of anemia was 38.5% among controls and 40.1% in the intervention group (P=0.621). At 24 months, the prevalence was 39.5% among controls and 41.5% in the intervention group (P=0.953).
The investigators also evaluated education-related outcomes at 9 months and 24 months of follow-up. They found no significant difference between the study groups with regard to classroom attention.
However, younger children in the intervention group did not score as well as controls in spelling or arithmetic tests.
The team said this may be a chance finding, or it may indicate that apprehension about the finger prick needed for the diagnostic test had a negative effect on the children’s performance during educational tests.
In closing, the investigators said there are a number of possible reasons why this screening and treatment intervention proved unsuccesful.
These include geographical heterogeneity in transmission, a rapid rate of reinfection following treatment, the variable reliability of the diagnostic tests used, and the relative contribution of malaria to the etiology of anemia in this setting.
In a related perspective article, Lorenz von Seidlein, MD, PhD, of the Menzies School of Health Research in Casuarina, Australia, discusses these possibilities in more detail, as well as the wider issues involved in failure of screening and treating as a malaria elimination strategy. ![]()
blood cell; Credit: St Jude
Children’s Research Hospital
A school-based, intermittent screening and treatment program for malaria did not confer any benefits for children living in an area of low-to-moderate malaria transmission.
The program, which was implemented at schools in Kenya, did not significantly reduce the incidence of malaria infection or the prevalence of anemia.
Katherine Halliday, of the London School of Hygiene & Tropical Medicine in the UK, and her colleagues reported these results in PLOS Medicine.
The study included 5233 children, ages 5 to 20, studying at 101 government schools located on the south coast of Kenya. Fifty-one of the schools were randomized to the intermittent screening and treatment program.
Over 24 months, children in these schools underwent screening for malaria parasites once each term (a total of 5 times). And those who tested positive for malaria parasitemia (whether symptomatic or asymptomatic) received 6 cycles of treatment with the anti-malarial drug artemether-lumefantrine.
Eighty-four percent of the children were screened at 4 or more rounds, and 66.8% were screened at all 5 rounds. By the fifth round, 20% of children had been lost due to death, withdrawal, or migration.
The percentage of children who were positive for malaria at each screening ranged from 14.8% to 19.2%, and there was no distinct trend over time. Overall, 99.1% of the positive results led to treatment, and 92.6% of these were recorded as receiving the fully supervised, 6-dose treatment regimen.
The investigators followed a majority of the children in each group for an additional 24 months after the intervention ended. And the team found that the intervention had no significant impact on the prevalence of Plasmodium falciparum infection at 12 months or 24 months.
At 12 months, the prevalence of P falciparum (adjusted for age, sex, and stratification effects) was 10.7% in the intervention group and 14.3% in the control group (P=0.131). At 24 months, the prevalence of P falciparum was 11.8% in the intervention group and 8.5% in the control group (P=0.124).
Similarly, there was no significant difference between the 2 groups with regard to anemia.
At 12 months, the prevalence of anemia was 38.5% among controls and 40.1% in the intervention group (P=0.621). At 24 months, the prevalence was 39.5% among controls and 41.5% in the intervention group (P=0.953).
The investigators also evaluated education-related outcomes at 9 months and 24 months of follow-up. They found no significant difference between the study groups with regard to classroom attention.
However, younger children in the intervention group did not score as well as controls in spelling or arithmetic tests.
The team said this may be a chance finding, or it may indicate that apprehension about the finger prick needed for the diagnostic test had a negative effect on the children’s performance during educational tests.
In closing, the investigators said there are a number of possible reasons why this screening and treatment intervention proved unsuccesful.
These include geographical heterogeneity in transmission, a rapid rate of reinfection following treatment, the variable reliability of the diagnostic tests used, and the relative contribution of malaria to the etiology of anemia in this setting.
In a related perspective article, Lorenz von Seidlein, MD, PhD, of the Menzies School of Health Research in Casuarina, Australia, discusses these possibilities in more detail, as well as the wider issues involved in failure of screening and treating as a malaria elimination strategy. ![]()
blood cell; Credit: St Jude
Children’s Research Hospital
A school-based, intermittent screening and treatment program for malaria did not confer any benefits for children living in an area of low-to-moderate malaria transmission.
The program, which was implemented at schools in Kenya, did not significantly reduce the incidence of malaria infection or the prevalence of anemia.
Katherine Halliday, of the London School of Hygiene & Tropical Medicine in the UK, and her colleagues reported these results in PLOS Medicine.
The study included 5233 children, ages 5 to 20, studying at 101 government schools located on the south coast of Kenya. Fifty-one of the schools were randomized to the intermittent screening and treatment program.
Over 24 months, children in these schools underwent screening for malaria parasites once each term (a total of 5 times). And those who tested positive for malaria parasitemia (whether symptomatic or asymptomatic) received 6 cycles of treatment with the anti-malarial drug artemether-lumefantrine.
Eighty-four percent of the children were screened at 4 or more rounds, and 66.8% were screened at all 5 rounds. By the fifth round, 20% of children had been lost due to death, withdrawal, or migration.
The percentage of children who were positive for malaria at each screening ranged from 14.8% to 19.2%, and there was no distinct trend over time. Overall, 99.1% of the positive results led to treatment, and 92.6% of these were recorded as receiving the fully supervised, 6-dose treatment regimen.
The investigators followed a majority of the children in each group for an additional 24 months after the intervention ended. And the team found that the intervention had no significant impact on the prevalence of Plasmodium falciparum infection at 12 months or 24 months.
At 12 months, the prevalence of P falciparum (adjusted for age, sex, and stratification effects) was 10.7% in the intervention group and 14.3% in the control group (P=0.131). At 24 months, the prevalence of P falciparum was 11.8% in the intervention group and 8.5% in the control group (P=0.124).
Similarly, there was no significant difference between the 2 groups with regard to anemia.
At 12 months, the prevalence of anemia was 38.5% among controls and 40.1% in the intervention group (P=0.621). At 24 months, the prevalence was 39.5% among controls and 41.5% in the intervention group (P=0.953).
The investigators also evaluated education-related outcomes at 9 months and 24 months of follow-up. They found no significant difference between the study groups with regard to classroom attention.
However, younger children in the intervention group did not score as well as controls in spelling or arithmetic tests.
The team said this may be a chance finding, or it may indicate that apprehension about the finger prick needed for the diagnostic test had a negative effect on the children’s performance during educational tests.
In closing, the investigators said there are a number of possible reasons why this screening and treatment intervention proved unsuccesful.
These include geographical heterogeneity in transmission, a rapid rate of reinfection following treatment, the variable reliability of the diagnostic tests used, and the relative contribution of malaria to the etiology of anemia in this setting.
In a related perspective article, Lorenz von Seidlein, MD, PhD, of the Menzies School of Health Research in Casuarina, Australia, discusses these possibilities in more detail, as well as the wider issues involved in failure of screening and treating as a malaria elimination strategy. ![]()
Mouse model provides new insight into AML

Studies have suggested that mutations in isocitrate dehydrogenase-1 and 2 (IDH1 and IDH2) are present in approximately 20% of all acute myeloid leukemias (AMLs), and this implies that mutant IDH proteins are attractive drug targets.
With this in mind, a group of scientists generated a transgenic mouse model of the most common IDH2 mutation in human AML.
Experiments conducted with this model revealed that mutant IDH2 contributes to leukemia initiation and is required for the maintenance of leukemic cells in a living organism.
The researchers said these findings, published in Cell Stem Cell, confirm a potent oncogenic role for IDH2 and support its relevance as a therapeutic target for AML.
Furthermore, the model can be used to evaluate the pharmacological efficacy of IDH2 inhibitors, either alone or in combination with other compounds.
“The real hope is that we would one day be able to treat IDH2-mutant leukemia patients with a drug that targets this genetic abnormality,” said senior study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center (BIDMC) in Boston.
He and his colleagues knew that IDH1 and IDH2 proteins are critical enzymes in the TCA cycle, which is centrally important to many biochemical pathways. Mutated forms of these proteins gain a novel ability to produce 2-hydroxyglutarate (2HG), a metabolite that has been shown to accumulate at high levels in cancer patients.
“Our goal was to generate an animal model of mutant IDH that was both inducible and reversible,” said Markus Reschke, PhD, also of BIDMC.
“This enabled us to address an important unanswered question: Does inhibition of mutant IDH proteins in active disease have an effect on tumor maintenance or progression in a living organism?”
The researchers studied 2 different models: a retroviral transduction model and a genetically engineered model in which IDH mice were crossed with mice harboring other leukemia-relevant mutations.
In the first model, the IDH mutation was combined with the oncogenes HoxA9 and Meis1a, 2 downstream targets of numerous pathways that are deregulated in AML.
The results showed evidence of differentiation within 2 weeks of genetic deinduction of mutant IDH. And 2 weeks later, 6 of 8 animals showed complete remission with elimination of any detectable leukemic cells.
The researchers said these results were both surprising and encouraging, demonstrating a situation in which IDH mutation occurs as an early event, and leukemic transformation occurs as a result of subsequent genetic hits.
“The retroviral model enabled us to observe that mutant IDH2 is essential for the maintenance of HoxA9/Meis1a-induced AML,” said Lev Kats, PhD, of BIDMC. “But this was still a surrogate model. This isn’t what happens in human patients, per se.”
The researchers therefore went on to develop a transgenic model that more closely recapitulates the genetics of human AML.
“By crossing the mutant IDH2 animals with other leukemia-relevant mutations, including mutations in the FMS-like tyrosine kinase 3 [FLT3], we observed that compound-mutant animals developed acute leukemias,” Dr Reschke said. “This exciting finding told us that mutant IDH2 contributes to leukemia initiation in vivo.”
As with the retroviral transduction model, genetic deinduction of mutant IDH2 in the context of a cooperating FLT3 mutation resulted in reduced proliferation and/or differentiation of leukemic cells, further demonstrating that mutant IDH2 expression is required for leukemia maintenance.
“This model has validated mutant IDH proteins as very strong candidates for continued development of targeted anticancer therapeutics,” Dr Pandolfi said. “The model will also be of paramount importance to study mechanisms of resistance to treatment that may occur.” ![]()
Studies have suggested that mutations in isocitrate dehydrogenase-1 and 2 (IDH1 and IDH2) are present in approximately 20% of all acute myeloid leukemias (AMLs), and this implies that mutant IDH proteins are attractive drug targets.
With this in mind, a group of scientists generated a transgenic mouse model of the most common IDH2 mutation in human AML.
Experiments conducted with this model revealed that mutant IDH2 contributes to leukemia initiation and is required for the maintenance of leukemic cells in a living organism.
The researchers said these findings, published in Cell Stem Cell, confirm a potent oncogenic role for IDH2 and support its relevance as a therapeutic target for AML.
Furthermore, the model can be used to evaluate the pharmacological efficacy of IDH2 inhibitors, either alone or in combination with other compounds.
“The real hope is that we would one day be able to treat IDH2-mutant leukemia patients with a drug that targets this genetic abnormality,” said senior study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center (BIDMC) in Boston.
He and his colleagues knew that IDH1 and IDH2 proteins are critical enzymes in the TCA cycle, which is centrally important to many biochemical pathways. Mutated forms of these proteins gain a novel ability to produce 2-hydroxyglutarate (2HG), a metabolite that has been shown to accumulate at high levels in cancer patients.
“Our goal was to generate an animal model of mutant IDH that was both inducible and reversible,” said Markus Reschke, PhD, also of BIDMC.
“This enabled us to address an important unanswered question: Does inhibition of mutant IDH proteins in active disease have an effect on tumor maintenance or progression in a living organism?”
The researchers studied 2 different models: a retroviral transduction model and a genetically engineered model in which IDH mice were crossed with mice harboring other leukemia-relevant mutations.
In the first model, the IDH mutation was combined with the oncogenes HoxA9 and Meis1a, 2 downstream targets of numerous pathways that are deregulated in AML.
The results showed evidence of differentiation within 2 weeks of genetic deinduction of mutant IDH. And 2 weeks later, 6 of 8 animals showed complete remission with elimination of any detectable leukemic cells.
The researchers said these results were both surprising and encouraging, demonstrating a situation in which IDH mutation occurs as an early event, and leukemic transformation occurs as a result of subsequent genetic hits.
“The retroviral model enabled us to observe that mutant IDH2 is essential for the maintenance of HoxA9/Meis1a-induced AML,” said Lev Kats, PhD, of BIDMC. “But this was still a surrogate model. This isn’t what happens in human patients, per se.”
The researchers therefore went on to develop a transgenic model that more closely recapitulates the genetics of human AML.
“By crossing the mutant IDH2 animals with other leukemia-relevant mutations, including mutations in the FMS-like tyrosine kinase 3 [FLT3], we observed that compound-mutant animals developed acute leukemias,” Dr Reschke said. “This exciting finding told us that mutant IDH2 contributes to leukemia initiation in vivo.”
As with the retroviral transduction model, genetic deinduction of mutant IDH2 in the context of a cooperating FLT3 mutation resulted in reduced proliferation and/or differentiation of leukemic cells, further demonstrating that mutant IDH2 expression is required for leukemia maintenance.
“This model has validated mutant IDH proteins as very strong candidates for continued development of targeted anticancer therapeutics,” Dr Pandolfi said. “The model will also be of paramount importance to study mechanisms of resistance to treatment that may occur.” ![]()
Studies have suggested that mutations in isocitrate dehydrogenase-1 and 2 (IDH1 and IDH2) are present in approximately 20% of all acute myeloid leukemias (AMLs), and this implies that mutant IDH proteins are attractive drug targets.
With this in mind, a group of scientists generated a transgenic mouse model of the most common IDH2 mutation in human AML.
Experiments conducted with this model revealed that mutant IDH2 contributes to leukemia initiation and is required for the maintenance of leukemic cells in a living organism.
The researchers said these findings, published in Cell Stem Cell, confirm a potent oncogenic role for IDH2 and support its relevance as a therapeutic target for AML.
Furthermore, the model can be used to evaluate the pharmacological efficacy of IDH2 inhibitors, either alone or in combination with other compounds.
“The real hope is that we would one day be able to treat IDH2-mutant leukemia patients with a drug that targets this genetic abnormality,” said senior study author Pier Paolo Pandolfi, MD, PhD, of Beth Israel Deaconess Medical Center (BIDMC) in Boston.
He and his colleagues knew that IDH1 and IDH2 proteins are critical enzymes in the TCA cycle, which is centrally important to many biochemical pathways. Mutated forms of these proteins gain a novel ability to produce 2-hydroxyglutarate (2HG), a metabolite that has been shown to accumulate at high levels in cancer patients.
“Our goal was to generate an animal model of mutant IDH that was both inducible and reversible,” said Markus Reschke, PhD, also of BIDMC.
“This enabled us to address an important unanswered question: Does inhibition of mutant IDH proteins in active disease have an effect on tumor maintenance or progression in a living organism?”
The researchers studied 2 different models: a retroviral transduction model and a genetically engineered model in which IDH mice were crossed with mice harboring other leukemia-relevant mutations.
In the first model, the IDH mutation was combined with the oncogenes HoxA9 and Meis1a, 2 downstream targets of numerous pathways that are deregulated in AML.
The results showed evidence of differentiation within 2 weeks of genetic deinduction of mutant IDH. And 2 weeks later, 6 of 8 animals showed complete remission with elimination of any detectable leukemic cells.
The researchers said these results were both surprising and encouraging, demonstrating a situation in which IDH mutation occurs as an early event, and leukemic transformation occurs as a result of subsequent genetic hits.
“The retroviral model enabled us to observe that mutant IDH2 is essential for the maintenance of HoxA9/Meis1a-induced AML,” said Lev Kats, PhD, of BIDMC. “But this was still a surrogate model. This isn’t what happens in human patients, per se.”
The researchers therefore went on to develop a transgenic model that more closely recapitulates the genetics of human AML.
“By crossing the mutant IDH2 animals with other leukemia-relevant mutations, including mutations in the FMS-like tyrosine kinase 3 [FLT3], we observed that compound-mutant animals developed acute leukemias,” Dr Reschke said. “This exciting finding told us that mutant IDH2 contributes to leukemia initiation in vivo.”
As with the retroviral transduction model, genetic deinduction of mutant IDH2 in the context of a cooperating FLT3 mutation resulted in reduced proliferation and/or differentiation of leukemic cells, further demonstrating that mutant IDH2 expression is required for leukemia maintenance.
“This model has validated mutant IDH proteins as very strong candidates for continued development of targeted anticancer therapeutics,” Dr Pandolfi said. “The model will also be of paramount importance to study mechanisms of resistance to treatment that may occur.” ![]()
Analysis reveals effects of sponsorship on animal studies

A new analysis indicates that animal studies not funded by industry produce favorable results more often than animal studies that are industry-funded.
In other words, published reports of non-industry-sponsored studies were more likely to contain data suggesting a drug was effective.
However, reports of industry-funded studies were more likely to contain favorable conclusions, even though data were less favorable.
Investigators recounted these findings in PLOS Biology.
They analyzed 63 studies in which statins were tested in animal models. Forty-two of the studies had quantitative results and disclosed sponsorship.
Among these studies, industry-sponsored research was less likely to measure a benefit for the statins in slowing or preventing arterial disease. Favorable results were reported in 47% (9/19) of the industry-sponsored studies and 72% (18/25) of the studies not sponsored by industry.
“The interests of the pharmaceutical industry might be best served by underestimating efficacy prior to clinical trials and overestimating efficacy in clinical trials,” said study author Lisa Bero, PhD, of the University of California, San Francisco.
“By underestimating efficacy in preclinical studies, the pharmaceutical industry could reduce the money spent on clinical trials that did not lead to marketable products. Because demonstrating drug efficacy in human studies is linked to drug company profits, drug companies may have more incentive to publish favorable efficacy findings of human drug studies than animal studies.”
However, Dr Bero and her colleagues also found that favorable conclusions were more likely in industry-sponsored studies, even when data were less favorable. Study authors drew favorable conclusions in 94.7% (18/19) of industry-sponsored studies and 75% (21/28) of studies not funded by industry.
Other key findings of this analysis were that methodological problems were common in both types of studies, and harmful side effects were not investigated.
“Not a single animal study we looked at assessed adverse events following the statin intervention,” Dr Bero said. “As toxicity data from animal studies must be submitted to drug regulatory authorities before a compound can proceed to testing in humans, it is surprising that so little data on harm appear in the published scientific literature.”
The investigators also noted that about half of the studies analyzed were randomized, and about half were blinded. Inclusion and exclusion criteria were often not included in the published reports, and many studies failed to account properly for changes in the assigned treatment arm that occurred during the course of treatment.
Most of the studies in this analysis were conducted in rabbits and mice. To gauge atherosclerosis, targeted by statins, investigators quantified qualities such as the number of damaged blood vessels, blood-vessel diameter, plaque severity, blockage to coronary and other arteries, and plaque rupture. ![]()
A new analysis indicates that animal studies not funded by industry produce favorable results more often than animal studies that are industry-funded.
In other words, published reports of non-industry-sponsored studies were more likely to contain data suggesting a drug was effective.
However, reports of industry-funded studies were more likely to contain favorable conclusions, even though data were less favorable.
Investigators recounted these findings in PLOS Biology.
They analyzed 63 studies in which statins were tested in animal models. Forty-two of the studies had quantitative results and disclosed sponsorship.
Among these studies, industry-sponsored research was less likely to measure a benefit for the statins in slowing or preventing arterial disease. Favorable results were reported in 47% (9/19) of the industry-sponsored studies and 72% (18/25) of the studies not sponsored by industry.
“The interests of the pharmaceutical industry might be best served by underestimating efficacy prior to clinical trials and overestimating efficacy in clinical trials,” said study author Lisa Bero, PhD, of the University of California, San Francisco.
“By underestimating efficacy in preclinical studies, the pharmaceutical industry could reduce the money spent on clinical trials that did not lead to marketable products. Because demonstrating drug efficacy in human studies is linked to drug company profits, drug companies may have more incentive to publish favorable efficacy findings of human drug studies than animal studies.”
However, Dr Bero and her colleagues also found that favorable conclusions were more likely in industry-sponsored studies, even when data were less favorable. Study authors drew favorable conclusions in 94.7% (18/19) of industry-sponsored studies and 75% (21/28) of studies not funded by industry.
Other key findings of this analysis were that methodological problems were common in both types of studies, and harmful side effects were not investigated.
“Not a single animal study we looked at assessed adverse events following the statin intervention,” Dr Bero said. “As toxicity data from animal studies must be submitted to drug regulatory authorities before a compound can proceed to testing in humans, it is surprising that so little data on harm appear in the published scientific literature.”
The investigators also noted that about half of the studies analyzed were randomized, and about half were blinded. Inclusion and exclusion criteria were often not included in the published reports, and many studies failed to account properly for changes in the assigned treatment arm that occurred during the course of treatment.
Most of the studies in this analysis were conducted in rabbits and mice. To gauge atherosclerosis, targeted by statins, investigators quantified qualities such as the number of damaged blood vessels, blood-vessel diameter, plaque severity, blockage to coronary and other arteries, and plaque rupture. ![]()
A new analysis indicates that animal studies not funded by industry produce favorable results more often than animal studies that are industry-funded.
In other words, published reports of non-industry-sponsored studies were more likely to contain data suggesting a drug was effective.
However, reports of industry-funded studies were more likely to contain favorable conclusions, even though data were less favorable.
Investigators recounted these findings in PLOS Biology.
They analyzed 63 studies in which statins were tested in animal models. Forty-two of the studies had quantitative results and disclosed sponsorship.
Among these studies, industry-sponsored research was less likely to measure a benefit for the statins in slowing or preventing arterial disease. Favorable results were reported in 47% (9/19) of the industry-sponsored studies and 72% (18/25) of the studies not sponsored by industry.
“The interests of the pharmaceutical industry might be best served by underestimating efficacy prior to clinical trials and overestimating efficacy in clinical trials,” said study author Lisa Bero, PhD, of the University of California, San Francisco.
“By underestimating efficacy in preclinical studies, the pharmaceutical industry could reduce the money spent on clinical trials that did not lead to marketable products. Because demonstrating drug efficacy in human studies is linked to drug company profits, drug companies may have more incentive to publish favorable efficacy findings of human drug studies than animal studies.”
However, Dr Bero and her colleagues also found that favorable conclusions were more likely in industry-sponsored studies, even when data were less favorable. Study authors drew favorable conclusions in 94.7% (18/19) of industry-sponsored studies and 75% (21/28) of studies not funded by industry.
Other key findings of this analysis were that methodological problems were common in both types of studies, and harmful side effects were not investigated.
“Not a single animal study we looked at assessed adverse events following the statin intervention,” Dr Bero said. “As toxicity data from animal studies must be submitted to drug regulatory authorities before a compound can proceed to testing in humans, it is surprising that so little data on harm appear in the published scientific literature.”
The investigators also noted that about half of the studies analyzed were randomized, and about half were blinded. Inclusion and exclusion criteria were often not included in the published reports, and many studies failed to account properly for changes in the assigned treatment arm that occurred during the course of treatment.
Most of the studies in this analysis were conducted in rabbits and mice. To gauge atherosclerosis, targeted by statins, investigators quantified qualities such as the number of damaged blood vessels, blood-vessel diameter, plaque severity, blockage to coronary and other arteries, and plaque rupture. ![]()
TNFRII may play key role in CTCL, speaker says
SAN FRANCISCO—Researchers have found evidence to suggest that tumor necrosis factor receptor II (TNFRII) may be an important driver of cutaneous T-cell lymphomas (CTCLs).
The team discovered that a mutation in this receptor—TNFRII T377I—is present in patients with mycosis fungoides (MF) and those with Sézary syndrome (SS).
And previous research showed that the region encoding TNFRII on chromosome 1 is sometimes amplified in MF and SS patients.
So if, as these factors suggest, TNFRII does play a key role in CTCL, a number of currently available drugs—including proteasome inhibitors and MEK inhibitors—may be effective treatment options.
Alexander Ungewickell, MD, PhD, of Stanford University in California, discussed this possibility and the research supporting it at the 6th Annual T-cell Lymphoma Forum.
A novel mutation
Dr Ungewickell and his colleagues began this research by conducting transcriptome sequencing on samples from 3 patients with SS (Lee et al, Blood 2012). This revealed about 500 genes that were upregulated and about 500 that were downregulated in SS cells.
And pathway enrichment analysis showed that molecular mechanisms of cancer were the most significantly altered pathways. But the researchers also observed PI3 kinase signaling, T-cell receptor signaling, regulation of IL-2, and CD8 signaling.
To better understand the basis for these transcriptional changes, the team performed whole-exome sequencing in 11 CTCL-normal pairs. They uncovered an average of 46 mutations per exome, as well as pathways similar to those observed in the transcriptional analysis.
The researchers then used this information to generate a 245-gene capture reagent. And they used that to perform ultra-deep targeted resequencing on 83 samples from CTCL patients.
“Two things that stood out right away were that TNFRSF1B and KRAS had recurrent point mutations that suggested an activating phenotype,” Dr Ungewickell said. “It’s already known that KRAS is mutated in many human cancers, including CTCL. TNFRSF1B encodes TNFRII and was not previously associated with any malignancies.”
“We also found a smattering of other genes that were mutated, [but] we were most interested in the TNFRII mutation because of the novelty of the finding and also the potential for therapeutic intervention.”
Driving disease
Dr Ungewickell noted that TNFRII is expressed in CD4 and CD8 T lymphocytes but relatively few other cell types. TNFRII is activated by membrane-bound TNFα, which mediates the signal through TRAF proteins and CIAP proteins to activate the NF-κB-inducing kinase (NIK).
This activates the I kappa B kinase (IKK) complex to phosphorylate p100. When phosphorylated, it is processed in the proteasome and translocates to the nucleus. There, it interacts with RelB to mediate transcription that tends to cause T-cell activation and proliferation.
TNFRII also binds to TRAF2 and induces its degradation. The recurrent mutation the researchers identified in TNFRII (T377I) is in the TRAF2 regulatory domain in an evolutionarily conserved residue.
The ultra-deep targeted resequencing of 83 CTCL samples showed 4 mutations at that locus, all of which were acquired in the lymphoma.
This suggests TNFRII is important in CTCL. And the researchers hypothesized that, if that’s the case, TNFRII might be overexpressed in SS cells. So they looked at their transcriptome data and found TNFRII to be overexpressed in all 3 patients.
“Interestingly, the region that encodes TNFRII on chromosome 1 is also amplified in 1 of the 4 commonly used CTCL cell lines, suggesting that amplification may be another way of activating this pathway,” Dr Ungewickell said.
“And we were very interested by a study published by van Doorn et al a few years ago [Blood 2009], which showed that that region of chromosome 1 p36 is, in fact, amplified in 45% of cases of MF and 15% of cases of Sézary syndrome.”
“So we are currently doing FISH studies to confirm that this receptor is actually amplified in as many as half of cases of MF, suggesting that maybe, between mutation and amplification, this is an important driver of CTCL.”
Therapeutic possibilities
The researchers also thought that, if TNFRII is an important driver of CTCL, there would be some kind of transcriptional mark on the lymphoma cells. So they performed gene set enrichment analyses on 24 CTCL samples that had undergone 3-seq.
By comparing tumors expressing high levels of TNFRII and those expressing low levels of TNFRII, the team identified an expression signature that corresponds to the receptor’s known effects on RNA levels in T cells.
When they searched publicly available datasets, the researchers found this signature in 63 cases of MF (Shin et al, Blood 2007). And results of control experiments suggested the signature is specific to CTCL.
“If TNFRII is more active [in CTCL] and the mutation that we found is a hyperactivating mutation, we would expect this pathway to show increased activity downstream; namely, you would expect more processing of p100 to p52,” Dr Ungewickell said.
To investigate this possibility, the researchers generated Jurkat cells expressing empty vector, wild-type TNFRII, or mutant TNFRII and looked at NF-κB processing. They did see an increase in processing with the mutant receptor, compared to the wild-type receptor or empty vector.
“We also found, somewhat surprisingly, increases in phospho-ERK with the mutant receptor, as well as phospho-MEK,” Dr Ungewickell said.
“And to our knowledge, the RAS/MAP kinase pathway has not previously been linked to TNFRII signaling, suggesting that there is some kind of direct or indirect cross-talk between these pathways. We think it’s very interesting, since there are KRAS mutations that activate the RAS/MAP kinase pathway in a subset of these cases, suggesting some kind of synergy.”
Introducing the mutant receptor into primary CD4+ T cells had an effect similar to that observed in the Jurkat cells. The researchers did western blotting for NF-kB processing, and they saw an increase in p100 to p52 processing.
“This is a preliminary experiment, but we’re actually quite excited about this, since Jurkat cells have many abnormalities, due to the fact that they’re a leukemia line, and primary T cells will have the rest of the genome intact,” Dr Ungewickell said.
Now, he and his colleagues are conducting several studies to identify the changes that occur in primary T cells when mutant TNFRII is expressed. They also want to see if they can recapitulate CTCL and identify the transcriptional signature they previously found in patient biopsies and cells.
Lastly, the researchers are performing functional assays to evaluate proliferation, apoptosis, and pharmacological information, with the goal of identifying therapies that might be effective in patients with TNFRII mutation or amplification.
“Patients who have increased TNFRII signaling might respond to proteasome inhibitors, since p100 and p52 processing requires the proteasome,” Dr Ungewickell said. “And given that cross-talk with the RAS/MAP kinase signaling, as well as the KRAS mutations, we also think . . . that MEK inhibitors might be effective in the treatment of CTCL.” ![]()
SAN FRANCISCO—Researchers have found evidence to suggest that tumor necrosis factor receptor II (TNFRII) may be an important driver of cutaneous T-cell lymphomas (CTCLs).
The team discovered that a mutation in this receptor—TNFRII T377I—is present in patients with mycosis fungoides (MF) and those with Sézary syndrome (SS).
And previous research showed that the region encoding TNFRII on chromosome 1 is sometimes amplified in MF and SS patients.
So if, as these factors suggest, TNFRII does play a key role in CTCL, a number of currently available drugs—including proteasome inhibitors and MEK inhibitors—may be effective treatment options.
Alexander Ungewickell, MD, PhD, of Stanford University in California, discussed this possibility and the research supporting it at the 6th Annual T-cell Lymphoma Forum.
A novel mutation
Dr Ungewickell and his colleagues began this research by conducting transcriptome sequencing on samples from 3 patients with SS (Lee et al, Blood 2012). This revealed about 500 genes that were upregulated and about 500 that were downregulated in SS cells.
And pathway enrichment analysis showed that molecular mechanisms of cancer were the most significantly altered pathways. But the researchers also observed PI3 kinase signaling, T-cell receptor signaling, regulation of IL-2, and CD8 signaling.
To better understand the basis for these transcriptional changes, the team performed whole-exome sequencing in 11 CTCL-normal pairs. They uncovered an average of 46 mutations per exome, as well as pathways similar to those observed in the transcriptional analysis.
The researchers then used this information to generate a 245-gene capture reagent. And they used that to perform ultra-deep targeted resequencing on 83 samples from CTCL patients.
“Two things that stood out right away were that TNFRSF1B and KRAS had recurrent point mutations that suggested an activating phenotype,” Dr Ungewickell said. “It’s already known that KRAS is mutated in many human cancers, including CTCL. TNFRSF1B encodes TNFRII and was not previously associated with any malignancies.”
“We also found a smattering of other genes that were mutated, [but] we were most interested in the TNFRII mutation because of the novelty of the finding and also the potential for therapeutic intervention.”
Driving disease
Dr Ungewickell noted that TNFRII is expressed in CD4 and CD8 T lymphocytes but relatively few other cell types. TNFRII is activated by membrane-bound TNFα, which mediates the signal through TRAF proteins and CIAP proteins to activate the NF-κB-inducing kinase (NIK).
This activates the I kappa B kinase (IKK) complex to phosphorylate p100. When phosphorylated, it is processed in the proteasome and translocates to the nucleus. There, it interacts with RelB to mediate transcription that tends to cause T-cell activation and proliferation.
TNFRII also binds to TRAF2 and induces its degradation. The recurrent mutation the researchers identified in TNFRII (T377I) is in the TRAF2 regulatory domain in an evolutionarily conserved residue.
The ultra-deep targeted resequencing of 83 CTCL samples showed 4 mutations at that locus, all of which were acquired in the lymphoma.
This suggests TNFRII is important in CTCL. And the researchers hypothesized that, if that’s the case, TNFRII might be overexpressed in SS cells. So they looked at their transcriptome data and found TNFRII to be overexpressed in all 3 patients.
“Interestingly, the region that encodes TNFRII on chromosome 1 is also amplified in 1 of the 4 commonly used CTCL cell lines, suggesting that amplification may be another way of activating this pathway,” Dr Ungewickell said.
“And we were very interested by a study published by van Doorn et al a few years ago [Blood 2009], which showed that that region of chromosome 1 p36 is, in fact, amplified in 45% of cases of MF and 15% of cases of Sézary syndrome.”
“So we are currently doing FISH studies to confirm that this receptor is actually amplified in as many as half of cases of MF, suggesting that maybe, between mutation and amplification, this is an important driver of CTCL.”
Therapeutic possibilities
The researchers also thought that, if TNFRII is an important driver of CTCL, there would be some kind of transcriptional mark on the lymphoma cells. So they performed gene set enrichment analyses on 24 CTCL samples that had undergone 3-seq.
By comparing tumors expressing high levels of TNFRII and those expressing low levels of TNFRII, the team identified an expression signature that corresponds to the receptor’s known effects on RNA levels in T cells.
When they searched publicly available datasets, the researchers found this signature in 63 cases of MF (Shin et al, Blood 2007). And results of control experiments suggested the signature is specific to CTCL.
“If TNFRII is more active [in CTCL] and the mutation that we found is a hyperactivating mutation, we would expect this pathway to show increased activity downstream; namely, you would expect more processing of p100 to p52,” Dr Ungewickell said.
To investigate this possibility, the researchers generated Jurkat cells expressing empty vector, wild-type TNFRII, or mutant TNFRII and looked at NF-κB processing. They did see an increase in processing with the mutant receptor, compared to the wild-type receptor or empty vector.
“We also found, somewhat surprisingly, increases in phospho-ERK with the mutant receptor, as well as phospho-MEK,” Dr Ungewickell said.
“And to our knowledge, the RAS/MAP kinase pathway has not previously been linked to TNFRII signaling, suggesting that there is some kind of direct or indirect cross-talk between these pathways. We think it’s very interesting, since there are KRAS mutations that activate the RAS/MAP kinase pathway in a subset of these cases, suggesting some kind of synergy.”
Introducing the mutant receptor into primary CD4+ T cells had an effect similar to that observed in the Jurkat cells. The researchers did western blotting for NF-kB processing, and they saw an increase in p100 to p52 processing.
“This is a preliminary experiment, but we’re actually quite excited about this, since Jurkat cells have many abnormalities, due to the fact that they’re a leukemia line, and primary T cells will have the rest of the genome intact,” Dr Ungewickell said.
Now, he and his colleagues are conducting several studies to identify the changes that occur in primary T cells when mutant TNFRII is expressed. They also want to see if they can recapitulate CTCL and identify the transcriptional signature they previously found in patient biopsies and cells.
Lastly, the researchers are performing functional assays to evaluate proliferation, apoptosis, and pharmacological information, with the goal of identifying therapies that might be effective in patients with TNFRII mutation or amplification.
“Patients who have increased TNFRII signaling might respond to proteasome inhibitors, since p100 and p52 processing requires the proteasome,” Dr Ungewickell said. “And given that cross-talk with the RAS/MAP kinase signaling, as well as the KRAS mutations, we also think . . . that MEK inhibitors might be effective in the treatment of CTCL.” ![]()
SAN FRANCISCO—Researchers have found evidence to suggest that tumor necrosis factor receptor II (TNFRII) may be an important driver of cutaneous T-cell lymphomas (CTCLs).
The team discovered that a mutation in this receptor—TNFRII T377I—is present in patients with mycosis fungoides (MF) and those with Sézary syndrome (SS).
And previous research showed that the region encoding TNFRII on chromosome 1 is sometimes amplified in MF and SS patients.
So if, as these factors suggest, TNFRII does play a key role in CTCL, a number of currently available drugs—including proteasome inhibitors and MEK inhibitors—may be effective treatment options.
Alexander Ungewickell, MD, PhD, of Stanford University in California, discussed this possibility and the research supporting it at the 6th Annual T-cell Lymphoma Forum.
A novel mutation
Dr Ungewickell and his colleagues began this research by conducting transcriptome sequencing on samples from 3 patients with SS (Lee et al, Blood 2012). This revealed about 500 genes that were upregulated and about 500 that were downregulated in SS cells.
And pathway enrichment analysis showed that molecular mechanisms of cancer were the most significantly altered pathways. But the researchers also observed PI3 kinase signaling, T-cell receptor signaling, regulation of IL-2, and CD8 signaling.
To better understand the basis for these transcriptional changes, the team performed whole-exome sequencing in 11 CTCL-normal pairs. They uncovered an average of 46 mutations per exome, as well as pathways similar to those observed in the transcriptional analysis.
The researchers then used this information to generate a 245-gene capture reagent. And they used that to perform ultra-deep targeted resequencing on 83 samples from CTCL patients.
“Two things that stood out right away were that TNFRSF1B and KRAS had recurrent point mutations that suggested an activating phenotype,” Dr Ungewickell said. “It’s already known that KRAS is mutated in many human cancers, including CTCL. TNFRSF1B encodes TNFRII and was not previously associated with any malignancies.”
“We also found a smattering of other genes that were mutated, [but] we were most interested in the TNFRII mutation because of the novelty of the finding and also the potential for therapeutic intervention.”
Driving disease
Dr Ungewickell noted that TNFRII is expressed in CD4 and CD8 T lymphocytes but relatively few other cell types. TNFRII is activated by membrane-bound TNFα, which mediates the signal through TRAF proteins and CIAP proteins to activate the NF-κB-inducing kinase (NIK).
This activates the I kappa B kinase (IKK) complex to phosphorylate p100. When phosphorylated, it is processed in the proteasome and translocates to the nucleus. There, it interacts with RelB to mediate transcription that tends to cause T-cell activation and proliferation.
TNFRII also binds to TRAF2 and induces its degradation. The recurrent mutation the researchers identified in TNFRII (T377I) is in the TRAF2 regulatory domain in an evolutionarily conserved residue.
The ultra-deep targeted resequencing of 83 CTCL samples showed 4 mutations at that locus, all of which were acquired in the lymphoma.
This suggests TNFRII is important in CTCL. And the researchers hypothesized that, if that’s the case, TNFRII might be overexpressed in SS cells. So they looked at their transcriptome data and found TNFRII to be overexpressed in all 3 patients.
“Interestingly, the region that encodes TNFRII on chromosome 1 is also amplified in 1 of the 4 commonly used CTCL cell lines, suggesting that amplification may be another way of activating this pathway,” Dr Ungewickell said.
“And we were very interested by a study published by van Doorn et al a few years ago [Blood 2009], which showed that that region of chromosome 1 p36 is, in fact, amplified in 45% of cases of MF and 15% of cases of Sézary syndrome.”
“So we are currently doing FISH studies to confirm that this receptor is actually amplified in as many as half of cases of MF, suggesting that maybe, between mutation and amplification, this is an important driver of CTCL.”
Therapeutic possibilities
The researchers also thought that, if TNFRII is an important driver of CTCL, there would be some kind of transcriptional mark on the lymphoma cells. So they performed gene set enrichment analyses on 24 CTCL samples that had undergone 3-seq.
By comparing tumors expressing high levels of TNFRII and those expressing low levels of TNFRII, the team identified an expression signature that corresponds to the receptor’s known effects on RNA levels in T cells.
When they searched publicly available datasets, the researchers found this signature in 63 cases of MF (Shin et al, Blood 2007). And results of control experiments suggested the signature is specific to CTCL.
“If TNFRII is more active [in CTCL] and the mutation that we found is a hyperactivating mutation, we would expect this pathway to show increased activity downstream; namely, you would expect more processing of p100 to p52,” Dr Ungewickell said.
To investigate this possibility, the researchers generated Jurkat cells expressing empty vector, wild-type TNFRII, or mutant TNFRII and looked at NF-κB processing. They did see an increase in processing with the mutant receptor, compared to the wild-type receptor or empty vector.
“We also found, somewhat surprisingly, increases in phospho-ERK with the mutant receptor, as well as phospho-MEK,” Dr Ungewickell said.
“And to our knowledge, the RAS/MAP kinase pathway has not previously been linked to TNFRII signaling, suggesting that there is some kind of direct or indirect cross-talk between these pathways. We think it’s very interesting, since there are KRAS mutations that activate the RAS/MAP kinase pathway in a subset of these cases, suggesting some kind of synergy.”
Introducing the mutant receptor into primary CD4+ T cells had an effect similar to that observed in the Jurkat cells. The researchers did western blotting for NF-kB processing, and they saw an increase in p100 to p52 processing.
“This is a preliminary experiment, but we’re actually quite excited about this, since Jurkat cells have many abnormalities, due to the fact that they’re a leukemia line, and primary T cells will have the rest of the genome intact,” Dr Ungewickell said.
Now, he and his colleagues are conducting several studies to identify the changes that occur in primary T cells when mutant TNFRII is expressed. They also want to see if they can recapitulate CTCL and identify the transcriptional signature they previously found in patient biopsies and cells.
Lastly, the researchers are performing functional assays to evaluate proliferation, apoptosis, and pharmacological information, with the goal of identifying therapies that might be effective in patients with TNFRII mutation or amplification.
“Patients who have increased TNFRII signaling might respond to proteasome inhibitors, since p100 and p52 processing requires the proteasome,” Dr Ungewickell said. “And given that cross-talk with the RAS/MAP kinase signaling, as well as the KRAS mutations, we also think . . . that MEK inhibitors might be effective in the treatment of CTCL.” ![]()
Book review: Textbook is informative, comprehensive resource
Edited by Alan Michelson, MD
The textbook marketplace is crowded with many titles pertinent to the topic of hemostasis and thrombosis, and the field is becoming increasingly complex, with the addition of new antiplatelet medications and novel, target-specific therapeutic agents.
It has become incumbent for hematologists and oncologist-hematologists who care for or consult on patients with any disease process involving platelets to understand the pathophysiology and rationale of treatment of these disorders.
This third edition of Platelets is again an aggregation of the most prominent physicians, physician-scientists, and basic researchers in platelet biology and clinical hemostasis.
Very much an encyclopedia of platelet biology, Platelets is an informative tome that will serve as a comprehensive resource for the busy clinician, the academic hematologist preparing for lectures on platelet physiology and hemostasis, the basic scientist preparing a research grant, the house officer trying to understand treatment algorithms, the blood banker who runs a busy transfusion service, and the clinical pathologist who supervises a coagulation laboratory.
The foreword chapter by Dr Barry Coller sets the tone for the book, with a thoughtful, interesting, and easily readable overview of the platelet in health and disease.
Over the next 63 chapters and more than 1300 pages, the platelet is examined as an active organ that expresses mRNAs from one-quarter to one-third of the human genome; contains a highly adaptive proteome responsive to external signals of both healthy and pathological processes; and can then participate directly and indirectly as modulators of hemostasis, inflammation, immunology, atherogenesis, angiogenesis, carcinogenesis, etc.
The chapters on laboratory measurements of platelet function and interpretation thereof are very useful and provide practical information for the clinician and clinical laboratorian. The review of the new antiplatelet aggregating agents succinctly and comprehensively describes their pharmacology and their appropriate placement in therapeutic algorithms of many disease processes.
Similarly, the chapters on thrombopoietin and autoimmune thrombocytopenia provide critical insight on the appropriate use of and the potential complications associated with use of the new thrombopoietic agonists.
Finally, the chapters that concentrate on the blood banking aspects of platelet therapy and platelet disorders are particularly well-written and understandable. The chapters on the pathogenesis, diagnosis, and treatment of neonatal alloimmune thrombocytopenia and post-transfusion purpura are very helpful, and I found myself consulting them in my clinical practice, even as I was preparing this review on Platelets.
In summary, Platelets fills an important niche on the bookshelf of any academic hematologist. The user- friendly online access to the figures contained in the textbook will be especially useful for teaching purposes. Notwithstanding its considerable size and weight, this encyclopedia of the platelet contains critical information for physicians, educators, students, and research scientists.
Craig M. Kessler, MD, MACP
Lombardi Comprehensive Cancer Center
Georgetown University School of Medicine, Washington, DC ![]()
Edited by Alan Michelson, MD
The textbook marketplace is crowded with many titles pertinent to the topic of hemostasis and thrombosis, and the field is becoming increasingly complex, with the addition of new antiplatelet medications and novel, target-specific therapeutic agents.
It has become incumbent for hematologists and oncologist-hematologists who care for or consult on patients with any disease process involving platelets to understand the pathophysiology and rationale of treatment of these disorders.
This third edition of Platelets is again an aggregation of the most prominent physicians, physician-scientists, and basic researchers in platelet biology and clinical hemostasis.
Very much an encyclopedia of platelet biology, Platelets is an informative tome that will serve as a comprehensive resource for the busy clinician, the academic hematologist preparing for lectures on platelet physiology and hemostasis, the basic scientist preparing a research grant, the house officer trying to understand treatment algorithms, the blood banker who runs a busy transfusion service, and the clinical pathologist who supervises a coagulation laboratory.
The foreword chapter by Dr Barry Coller sets the tone for the book, with a thoughtful, interesting, and easily readable overview of the platelet in health and disease.
Over the next 63 chapters and more than 1300 pages, the platelet is examined as an active organ that expresses mRNAs from one-quarter to one-third of the human genome; contains a highly adaptive proteome responsive to external signals of both healthy and pathological processes; and can then participate directly and indirectly as modulators of hemostasis, inflammation, immunology, atherogenesis, angiogenesis, carcinogenesis, etc.
The chapters on laboratory measurements of platelet function and interpretation thereof are very useful and provide practical information for the clinician and clinical laboratorian. The review of the new antiplatelet aggregating agents succinctly and comprehensively describes their pharmacology and their appropriate placement in therapeutic algorithms of many disease processes.
Similarly, the chapters on thrombopoietin and autoimmune thrombocytopenia provide critical insight on the appropriate use of and the potential complications associated with use of the new thrombopoietic agonists.
Finally, the chapters that concentrate on the blood banking aspects of platelet therapy and platelet disorders are particularly well-written and understandable. The chapters on the pathogenesis, diagnosis, and treatment of neonatal alloimmune thrombocytopenia and post-transfusion purpura are very helpful, and I found myself consulting them in my clinical practice, even as I was preparing this review on Platelets.
In summary, Platelets fills an important niche on the bookshelf of any academic hematologist. The user- friendly online access to the figures contained in the textbook will be especially useful for teaching purposes. Notwithstanding its considerable size and weight, this encyclopedia of the platelet contains critical information for physicians, educators, students, and research scientists.
Craig M. Kessler, MD, MACP
Lombardi Comprehensive Cancer Center
Georgetown University School of Medicine, Washington, DC ![]()
Edited by Alan Michelson, MD
The textbook marketplace is crowded with many titles pertinent to the topic of hemostasis and thrombosis, and the field is becoming increasingly complex, with the addition of new antiplatelet medications and novel, target-specific therapeutic agents.
It has become incumbent for hematologists and oncologist-hematologists who care for or consult on patients with any disease process involving platelets to understand the pathophysiology and rationale of treatment of these disorders.
This third edition of Platelets is again an aggregation of the most prominent physicians, physician-scientists, and basic researchers in platelet biology and clinical hemostasis.
Very much an encyclopedia of platelet biology, Platelets is an informative tome that will serve as a comprehensive resource for the busy clinician, the academic hematologist preparing for lectures on platelet physiology and hemostasis, the basic scientist preparing a research grant, the house officer trying to understand treatment algorithms, the blood banker who runs a busy transfusion service, and the clinical pathologist who supervises a coagulation laboratory.
The foreword chapter by Dr Barry Coller sets the tone for the book, with a thoughtful, interesting, and easily readable overview of the platelet in health and disease.
Over the next 63 chapters and more than 1300 pages, the platelet is examined as an active organ that expresses mRNAs from one-quarter to one-third of the human genome; contains a highly adaptive proteome responsive to external signals of both healthy and pathological processes; and can then participate directly and indirectly as modulators of hemostasis, inflammation, immunology, atherogenesis, angiogenesis, carcinogenesis, etc.
The chapters on laboratory measurements of platelet function and interpretation thereof are very useful and provide practical information for the clinician and clinical laboratorian. The review of the new antiplatelet aggregating agents succinctly and comprehensively describes their pharmacology and their appropriate placement in therapeutic algorithms of many disease processes.
Similarly, the chapters on thrombopoietin and autoimmune thrombocytopenia provide critical insight on the appropriate use of and the potential complications associated with use of the new thrombopoietic agonists.
Finally, the chapters that concentrate on the blood banking aspects of platelet therapy and platelet disorders are particularly well-written and understandable. The chapters on the pathogenesis, diagnosis, and treatment of neonatal alloimmune thrombocytopenia and post-transfusion purpura are very helpful, and I found myself consulting them in my clinical practice, even as I was preparing this review on Platelets.
In summary, Platelets fills an important niche on the bookshelf of any academic hematologist. The user- friendly online access to the figures contained in the textbook will be especially useful for teaching purposes. Notwithstanding its considerable size and weight, this encyclopedia of the platelet contains critical information for physicians, educators, students, and research scientists.
Craig M. Kessler, MD, MACP
Lombardi Comprehensive Cancer Center
Georgetown University School of Medicine, Washington, DC ![]()
Vasovagal syncope, or something far worse?
Vasovagal syncope, or something far worse?
A 48-YEAR-OLD WOMAN with a history of syncopal events was brought to the emergency department (ED) by her daughter, following an episode in which the mother lost consciousness and vomited while driving. (The daughter was able to get the car safely to the shoulder of the road.) The episode occurred after the woman had eaten, and followed a week in which she’d experienced several episodes in which her left arm and chin briefly went numb. In fact, she experienced another chin/arm numbing episode while in the ED. The ED physician gave her a diagnosis of vasovagal syncope, instructed her to follow up with her primary care physician, and included “rule out transient ischemic attack (TIA)” on the discharge note.
The primary care physician subsequently established a differential diagnosis of “vasovagal vs hypoglycemia vs both or neurocardiogenic syncope” and referred the patient to an electrophysiologist, who concluded that she’d had a vasovagal syncope episode triggered by a gastrointestinal cause.
The patient continued to have arm/chin numbness but was unconcerned because her physicians didn’t seem worried. Months later, she sought treatment for low back pain, for which her primary care physician prescribed celecoxib; her numbness was not discussed with her physician. The next day, she suffered a stroke from an occluded right carotid artery. She had hemiparesis with little to no movement of her left shoulder, elbow, hand, hip, and ankle.
PLAINTIFF’S CLAIM The numbness and fainting were TIAs and an ultrasound should have been performed, which would have revealed the carotid artery occlusion and helped avoid the stroke.
THE DEFENSE The events the plaintiff experienced were not TIAs and there was no way to show whether, or to what degree, the carotid artery was occluded before the stroke. The plaintiff should have reported the continuing symptoms. Given that the patient had a long history of syncopal events—and a history of smoking—the diagnosis was reasonable.
VERDICT $1.6 million Wisconsin verdict.
COMMENT I think the lesson here is that physicians need to take focal neurological findings seriously and continue the evaluation until one has a reasonably certain diagnosis. The cause of this patient’s recurrent arm and chin numbness should have been pursued.
Failure to take full sexual history has devastating consequences
A MAN WITH A HISTORY OF ABNORMAL BLOOD TEST RESULTS sought treatment in the emergency department for extreme leg pain. He was given a diagnosis of sepsis and renal failure. A positive human immunodeficiency virus (HIV) test led to a diagnosis of acquired immunodeficiency syndrome (AIDS). The patient had been seeing his primary care physician for 10 years, but the doctor never asked about his sexual history. The patient survived, but suffers from AIDS-related kidney disease and must undergo peritoneal dialysis for the rest of his life.
PLAINTIFF’S CLAIM The physician should have tested for HIV much sooner to prevent the loss of kidney function. The physician’s questions were not specific enough to obtain proper information on whether the patient was having unprotected sex, if he had multiple partners, and what gender his partners were.
THE DEFENSE No information about the defense is available.
VERDICT $5.2 million Illinois verdict.
COMMENT I’m not sure the jury got this one right. Nonetheless, the Centers for Disease Control and Prevention now recommends HIV screening for all adults so it is worthwhile to offer it to all patients and to document refusal if a patient doesn’t want to be tested.
Vasovagal syncope, or something far worse?
A 48-YEAR-OLD WOMAN with a history of syncopal events was brought to the emergency department (ED) by her daughter, following an episode in which the mother lost consciousness and vomited while driving. (The daughter was able to get the car safely to the shoulder of the road.) The episode occurred after the woman had eaten, and followed a week in which she’d experienced several episodes in which her left arm and chin briefly went numb. In fact, she experienced another chin/arm numbing episode while in the ED. The ED physician gave her a diagnosis of vasovagal syncope, instructed her to follow up with her primary care physician, and included “rule out transient ischemic attack (TIA)” on the discharge note.
The primary care physician subsequently established a differential diagnosis of “vasovagal vs hypoglycemia vs both or neurocardiogenic syncope” and referred the patient to an electrophysiologist, who concluded that she’d had a vasovagal syncope episode triggered by a gastrointestinal cause.
The patient continued to have arm/chin numbness but was unconcerned because her physicians didn’t seem worried. Months later, she sought treatment for low back pain, for which her primary care physician prescribed celecoxib; her numbness was not discussed with her physician. The next day, she suffered a stroke from an occluded right carotid artery. She had hemiparesis with little to no movement of her left shoulder, elbow, hand, hip, and ankle.
PLAINTIFF’S CLAIM The numbness and fainting were TIAs and an ultrasound should have been performed, which would have revealed the carotid artery occlusion and helped avoid the stroke.
THE DEFENSE The events the plaintiff experienced were not TIAs and there was no way to show whether, or to what degree, the carotid artery was occluded before the stroke. The plaintiff should have reported the continuing symptoms. Given that the patient had a long history of syncopal events—and a history of smoking—the diagnosis was reasonable.
VERDICT $1.6 million Wisconsin verdict.
COMMENT I think the lesson here is that physicians need to take focal neurological findings seriously and continue the evaluation until one has a reasonably certain diagnosis. The cause of this patient’s recurrent arm and chin numbness should have been pursued.
Failure to take full sexual history has devastating consequences
A MAN WITH A HISTORY OF ABNORMAL BLOOD TEST RESULTS sought treatment in the emergency department for extreme leg pain. He was given a diagnosis of sepsis and renal failure. A positive human immunodeficiency virus (HIV) test led to a diagnosis of acquired immunodeficiency syndrome (AIDS). The patient had been seeing his primary care physician for 10 years, but the doctor never asked about his sexual history. The patient survived, but suffers from AIDS-related kidney disease and must undergo peritoneal dialysis for the rest of his life.
PLAINTIFF’S CLAIM The physician should have tested for HIV much sooner to prevent the loss of kidney function. The physician’s questions were not specific enough to obtain proper information on whether the patient was having unprotected sex, if he had multiple partners, and what gender his partners were.
THE DEFENSE No information about the defense is available.
VERDICT $5.2 million Illinois verdict.
COMMENT I’m not sure the jury got this one right. Nonetheless, the Centers for Disease Control and Prevention now recommends HIV screening for all adults so it is worthwhile to offer it to all patients and to document refusal if a patient doesn’t want to be tested.
Vasovagal syncope, or something far worse?
A 48-YEAR-OLD WOMAN with a history of syncopal events was brought to the emergency department (ED) by her daughter, following an episode in which the mother lost consciousness and vomited while driving. (The daughter was able to get the car safely to the shoulder of the road.) The episode occurred after the woman had eaten, and followed a week in which she’d experienced several episodes in which her left arm and chin briefly went numb. In fact, she experienced another chin/arm numbing episode while in the ED. The ED physician gave her a diagnosis of vasovagal syncope, instructed her to follow up with her primary care physician, and included “rule out transient ischemic attack (TIA)” on the discharge note.
The primary care physician subsequently established a differential diagnosis of “vasovagal vs hypoglycemia vs both or neurocardiogenic syncope” and referred the patient to an electrophysiologist, who concluded that she’d had a vasovagal syncope episode triggered by a gastrointestinal cause.
The patient continued to have arm/chin numbness but was unconcerned because her physicians didn’t seem worried. Months later, she sought treatment for low back pain, for which her primary care physician prescribed celecoxib; her numbness was not discussed with her physician. The next day, she suffered a stroke from an occluded right carotid artery. She had hemiparesis with little to no movement of her left shoulder, elbow, hand, hip, and ankle.
PLAINTIFF’S CLAIM The numbness and fainting were TIAs and an ultrasound should have been performed, which would have revealed the carotid artery occlusion and helped avoid the stroke.
THE DEFENSE The events the plaintiff experienced were not TIAs and there was no way to show whether, or to what degree, the carotid artery was occluded before the stroke. The plaintiff should have reported the continuing symptoms. Given that the patient had a long history of syncopal events—and a history of smoking—the diagnosis was reasonable.
VERDICT $1.6 million Wisconsin verdict.
COMMENT I think the lesson here is that physicians need to take focal neurological findings seriously and continue the evaluation until one has a reasonably certain diagnosis. The cause of this patient’s recurrent arm and chin numbness should have been pursued.
Failure to take full sexual history has devastating consequences
A MAN WITH A HISTORY OF ABNORMAL BLOOD TEST RESULTS sought treatment in the emergency department for extreme leg pain. He was given a diagnosis of sepsis and renal failure. A positive human immunodeficiency virus (HIV) test led to a diagnosis of acquired immunodeficiency syndrome (AIDS). The patient had been seeing his primary care physician for 10 years, but the doctor never asked about his sexual history. The patient survived, but suffers from AIDS-related kidney disease and must undergo peritoneal dialysis for the rest of his life.
PLAINTIFF’S CLAIM The physician should have tested for HIV much sooner to prevent the loss of kidney function. The physician’s questions were not specific enough to obtain proper information on whether the patient was having unprotected sex, if he had multiple partners, and what gender his partners were.
THE DEFENSE No information about the defense is available.
VERDICT $5.2 million Illinois verdict.
COMMENT I’m not sure the jury got this one right. Nonetheless, the Centers for Disease Control and Prevention now recommends HIV screening for all adults so it is worthwhile to offer it to all patients and to document refusal if a patient doesn’t want to be tested.
Inhibitor appears active in relapsed/refractory TCLs
SAN FRANCISCO—Preliminary results of a phase 1 trial suggest the PI3K-delta/gamma inhibitor IPI-145 is active in patients with relapsed or refractory T-cell lymphomas.
Among 26 evaluable patients, 9 experienced partial responses to treatment with IPI-145, and 1 achieved a complete response, for an overall response rate (ORR) of 38%.
The drug also appeared to be well-tolerated, although 30% of patients did experience treatment-related severe adverse events.
Steven Horwitz, MD, of Memorial Sloan-Kettering Cancer Center in New York, and his colleagues presented these results in a poster at the 6th Annual T-cell Lymphoma Forum, which took place January 23-25.
The study was sponsored by Infinity Pharmaceuticals, Inc., the company developing IPI-145.
Patient and treatment characteristics
The trial included 30 patients with peripheral T-cell lymphoma (PTCL) or cutaneous T-cell lymphoma (CTCL). Of the 17 CTCL patients, 16 had mycosis fungoides or Sezary syndrome, and 1 had primary cutaneous anaplastic large-cell lymphoma (ALCL).
Of the 13 patients with PTCL, 3 had angioimmunoblastic T-cell lymphoma (AITL), 3 had subcutaneous panniculitis-like T-cell lymphoma (SPTCL), 3 had PTCL-not otherwise specified, 2 had ALCL, 1 had enteropathy-associated T-cell lymphoma (EATL), and 1 had NK T-cell lymphoma (NKTL).
The patients had advanced disease, with a median of 5 prior systemic therapies (range, 1-11) and a median of 1 month from their last therapy to the first dose on study (range, 0.2-12).
Patients received IPI-145 in escalating doses, from 25 mg to 100 mg twice daily (n=10) and in an expansion cohort at 75 mg twice daily (n=20). All 30 patients were evaluable for the safety analysis, but only 26 were evaluable for clinical activity.
Response by disease type
The ORR for all 26 patients was 38% (1 complete and 9 partial responses).
Among the 11 evaluable PTCL patients, the ORR was 55%. One patient had a complete response, and 5 had partial responses.
Of the 15 evaluable CTCL patients, 4 had partial responses, for an ORR of 27%. In addition, 7 CTCL patients had stable disease.
The median time to response was 1.9 months (range, 1.5-2.7) for patients with PTCL and 2.4 months (range, 1.7-3.8) for patients with CTCL.
Four patients with PTCL and 3 patients with CTCL remain on treatment.
Adverse events
IPI-145 was generally well-tolerated, according to the researchers.
The most common adverse events of any grade were an increases in ALT/AST (47%), fatigue (37%), pyrexia (33%), diarrhea (30%), cough (27%), headache (27%), nausea (27%), rash (23%), increases in alkaline phosphatase (20%), increases in blood creatinine (17%), and weight loss (17%).
Grade 3 side effects included increased ALT/AST (33%), rash (13%), and fatigue (10%). One patient (3%) had grade 4 ALT/AST increases.
Forty percent of patients had severe adverse events, and 30% were treatment-related. Among CTCL patients, the severe events included ALT/AST increases (n=1), pneumonitis (n=1), HSV pneumonitis (n=1), lung infection (n=1), pyrexia (n=1), and staphylococcal sepsis (n=1).
Among PTCL patients, severe events included diarrhea (n=2), pneumonia (n=2), vomiting (n=2), cellulitis (n=1), colitis (n=1), dehydration (n=1), hypotension (n=1), pneumonia cytomegaloviral (n=1), pyrexia (n=1), and rash (macular papular; n=1).
Six CTCL patients and 3 PTCL patients discontinued treatment due to adverse events.
Pharmacodynamics
The data showed that treatment with IPI-145 led to decreases in serum levels of cytokines and chemokines known to play important roles in lymphocyte trafficking and function.
The researchers said this further supports the rationale that inhibiting PI3K-delta and PI3K-gamma has the potential to provide a therapeutic benefit for T-cell lymphomas and other hematologic malignancies.
For more details on this research, see the poster on Infinity’s website: http://www.infi.com/product-candidates-publications.asp. ![]()
SAN FRANCISCO—Preliminary results of a phase 1 trial suggest the PI3K-delta/gamma inhibitor IPI-145 is active in patients with relapsed or refractory T-cell lymphomas.
Among 26 evaluable patients, 9 experienced partial responses to treatment with IPI-145, and 1 achieved a complete response, for an overall response rate (ORR) of 38%.
The drug also appeared to be well-tolerated, although 30% of patients did experience treatment-related severe adverse events.
Steven Horwitz, MD, of Memorial Sloan-Kettering Cancer Center in New York, and his colleagues presented these results in a poster at the 6th Annual T-cell Lymphoma Forum, which took place January 23-25.
The study was sponsored by Infinity Pharmaceuticals, Inc., the company developing IPI-145.
Patient and treatment characteristics
The trial included 30 patients with peripheral T-cell lymphoma (PTCL) or cutaneous T-cell lymphoma (CTCL). Of the 17 CTCL patients, 16 had mycosis fungoides or Sezary syndrome, and 1 had primary cutaneous anaplastic large-cell lymphoma (ALCL).
Of the 13 patients with PTCL, 3 had angioimmunoblastic T-cell lymphoma (AITL), 3 had subcutaneous panniculitis-like T-cell lymphoma (SPTCL), 3 had PTCL-not otherwise specified, 2 had ALCL, 1 had enteropathy-associated T-cell lymphoma (EATL), and 1 had NK T-cell lymphoma (NKTL).
The patients had advanced disease, with a median of 5 prior systemic therapies (range, 1-11) and a median of 1 month from their last therapy to the first dose on study (range, 0.2-12).
Patients received IPI-145 in escalating doses, from 25 mg to 100 mg twice daily (n=10) and in an expansion cohort at 75 mg twice daily (n=20). All 30 patients were evaluable for the safety analysis, but only 26 were evaluable for clinical activity.
Response by disease type
The ORR for all 26 patients was 38% (1 complete and 9 partial responses).
Among the 11 evaluable PTCL patients, the ORR was 55%. One patient had a complete response, and 5 had partial responses.
Of the 15 evaluable CTCL patients, 4 had partial responses, for an ORR of 27%. In addition, 7 CTCL patients had stable disease.
The median time to response was 1.9 months (range, 1.5-2.7) for patients with PTCL and 2.4 months (range, 1.7-3.8) for patients with CTCL.
Four patients with PTCL and 3 patients with CTCL remain on treatment.
Adverse events
IPI-145 was generally well-tolerated, according to the researchers.
The most common adverse events of any grade were an increases in ALT/AST (47%), fatigue (37%), pyrexia (33%), diarrhea (30%), cough (27%), headache (27%), nausea (27%), rash (23%), increases in alkaline phosphatase (20%), increases in blood creatinine (17%), and weight loss (17%).
Grade 3 side effects included increased ALT/AST (33%), rash (13%), and fatigue (10%). One patient (3%) had grade 4 ALT/AST increases.
Forty percent of patients had severe adverse events, and 30% were treatment-related. Among CTCL patients, the severe events included ALT/AST increases (n=1), pneumonitis (n=1), HSV pneumonitis (n=1), lung infection (n=1), pyrexia (n=1), and staphylococcal sepsis (n=1).
Among PTCL patients, severe events included diarrhea (n=2), pneumonia (n=2), vomiting (n=2), cellulitis (n=1), colitis (n=1), dehydration (n=1), hypotension (n=1), pneumonia cytomegaloviral (n=1), pyrexia (n=1), and rash (macular papular; n=1).
Six CTCL patients and 3 PTCL patients discontinued treatment due to adverse events.
Pharmacodynamics
The data showed that treatment with IPI-145 led to decreases in serum levels of cytokines and chemokines known to play important roles in lymphocyte trafficking and function.
The researchers said this further supports the rationale that inhibiting PI3K-delta and PI3K-gamma has the potential to provide a therapeutic benefit for T-cell lymphomas and other hematologic malignancies.
For more details on this research, see the poster on Infinity’s website: http://www.infi.com/product-candidates-publications.asp. ![]()
SAN FRANCISCO—Preliminary results of a phase 1 trial suggest the PI3K-delta/gamma inhibitor IPI-145 is active in patients with relapsed or refractory T-cell lymphomas.
Among 26 evaluable patients, 9 experienced partial responses to treatment with IPI-145, and 1 achieved a complete response, for an overall response rate (ORR) of 38%.
The drug also appeared to be well-tolerated, although 30% of patients did experience treatment-related severe adverse events.
Steven Horwitz, MD, of Memorial Sloan-Kettering Cancer Center in New York, and his colleagues presented these results in a poster at the 6th Annual T-cell Lymphoma Forum, which took place January 23-25.
The study was sponsored by Infinity Pharmaceuticals, Inc., the company developing IPI-145.
Patient and treatment characteristics
The trial included 30 patients with peripheral T-cell lymphoma (PTCL) or cutaneous T-cell lymphoma (CTCL). Of the 17 CTCL patients, 16 had mycosis fungoides or Sezary syndrome, and 1 had primary cutaneous anaplastic large-cell lymphoma (ALCL).
Of the 13 patients with PTCL, 3 had angioimmunoblastic T-cell lymphoma (AITL), 3 had subcutaneous panniculitis-like T-cell lymphoma (SPTCL), 3 had PTCL-not otherwise specified, 2 had ALCL, 1 had enteropathy-associated T-cell lymphoma (EATL), and 1 had NK T-cell lymphoma (NKTL).
The patients had advanced disease, with a median of 5 prior systemic therapies (range, 1-11) and a median of 1 month from their last therapy to the first dose on study (range, 0.2-12).
Patients received IPI-145 in escalating doses, from 25 mg to 100 mg twice daily (n=10) and in an expansion cohort at 75 mg twice daily (n=20). All 30 patients were evaluable for the safety analysis, but only 26 were evaluable for clinical activity.
Response by disease type
The ORR for all 26 patients was 38% (1 complete and 9 partial responses).
Among the 11 evaluable PTCL patients, the ORR was 55%. One patient had a complete response, and 5 had partial responses.
Of the 15 evaluable CTCL patients, 4 had partial responses, for an ORR of 27%. In addition, 7 CTCL patients had stable disease.
The median time to response was 1.9 months (range, 1.5-2.7) for patients with PTCL and 2.4 months (range, 1.7-3.8) for patients with CTCL.
Four patients with PTCL and 3 patients with CTCL remain on treatment.
Adverse events
IPI-145 was generally well-tolerated, according to the researchers.
The most common adverse events of any grade were an increases in ALT/AST (47%), fatigue (37%), pyrexia (33%), diarrhea (30%), cough (27%), headache (27%), nausea (27%), rash (23%), increases in alkaline phosphatase (20%), increases in blood creatinine (17%), and weight loss (17%).
Grade 3 side effects included increased ALT/AST (33%), rash (13%), and fatigue (10%). One patient (3%) had grade 4 ALT/AST increases.
Forty percent of patients had severe adverse events, and 30% were treatment-related. Among CTCL patients, the severe events included ALT/AST increases (n=1), pneumonitis (n=1), HSV pneumonitis (n=1), lung infection (n=1), pyrexia (n=1), and staphylococcal sepsis (n=1).
Among PTCL patients, severe events included diarrhea (n=2), pneumonia (n=2), vomiting (n=2), cellulitis (n=1), colitis (n=1), dehydration (n=1), hypotension (n=1), pneumonia cytomegaloviral (n=1), pyrexia (n=1), and rash (macular papular; n=1).
Six CTCL patients and 3 PTCL patients discontinued treatment due to adverse events.
Pharmacodynamics
The data showed that treatment with IPI-145 led to decreases in serum levels of cytokines and chemokines known to play important roles in lymphocyte trafficking and function.
The researchers said this further supports the rationale that inhibiting PI3K-delta and PI3K-gamma has the potential to provide a therapeutic benefit for T-cell lymphomas and other hematologic malignancies.
For more details on this research, see the poster on Infinity’s website: http://www.infi.com/product-candidates-publications.asp. ![]()
Physical activity may cut death risk in male cancer survivors

Credit: Jason E. Miller
Physical activity may reduce the risk of mortality in male cancer survivors, according to research published in the Journal of Physical Activity & Health.
In a study of more than 1000 male cancer survivors, participants who were most active—expending more than 12,600 kilojoules per week in physical activity—cut their risk of death roughly in half.
This was in comparison to the least active cancer survivors—those who burned fewer than 2100 kilojoules per week.
Kathleen Y. Wolin, PhD, of Loyola University Chicago Stritch School of Medicine, and her colleagues conducted this research using data from the Harvard Alumni Health Study, an ongoing study of men who entered Harvard as undergraduates between 1916 and 1950.
The researchers looked at 1021 men, with an average age of 71, who had been diagnosed with cancers.
In 1988, the men completed questionnaires reporting their physical activities, including walking, stair-climbing, and participation in sports and recreational activities. Their physical activities were updated in 1993, and researchers followed the men until 2008.
In all, 777 of the men died—337 from cancer, 190 from cardiovascular disease, 228 from other causes, and 22 from unknown causes.
Compared with men who expended fewer than 2100 kilojoules per week in physical activity, men who expended more than 12,600 kilojoules per week were 48% less likely to die of any cause during the follow-up period. (Expending 12,600 kilojoules can be achieved with about 6 to 8 hours of moderate-intensity physical activity.)
This finding was adjusted for age, smoking habits, body mass index, early parental mortality, and dietary variables.
When the researchers tried to adjust for cancer severity and treatment, they were only able to collect data for 70 men. But the results were not very different from the prior analysis. The most active men were 49% less likely to die of any cause than the least active men.
The team also decided to analyze men who were diagnosed with cancer at least 5 years before baseline (n=421). And among these men, the most active were 52% less likely than the least active to die.
Similarly, among men diagnosed at least 10 years before baseline (n=262), the most active cancer survivors were 63% less likely to die of any cause than the least active survivors.
The researchers also obtained similar results when they assessed mortality from cancer and cardiovascular disease. The most physically active cancer survivors were 38% less likely to die of cancer and 49% less likely to die of cardiovascular disease during follow-up. ![]()
Credit: Jason E. Miller
Physical activity may reduce the risk of mortality in male cancer survivors, according to research published in the Journal of Physical Activity & Health.
In a study of more than 1000 male cancer survivors, participants who were most active—expending more than 12,600 kilojoules per week in physical activity—cut their risk of death roughly in half.
This was in comparison to the least active cancer survivors—those who burned fewer than 2100 kilojoules per week.
Kathleen Y. Wolin, PhD, of Loyola University Chicago Stritch School of Medicine, and her colleagues conducted this research using data from the Harvard Alumni Health Study, an ongoing study of men who entered Harvard as undergraduates between 1916 and 1950.
The researchers looked at 1021 men, with an average age of 71, who had been diagnosed with cancers.
In 1988, the men completed questionnaires reporting their physical activities, including walking, stair-climbing, and participation in sports and recreational activities. Their physical activities were updated in 1993, and researchers followed the men until 2008.
In all, 777 of the men died—337 from cancer, 190 from cardiovascular disease, 228 from other causes, and 22 from unknown causes.
Compared with men who expended fewer than 2100 kilojoules per week in physical activity, men who expended more than 12,600 kilojoules per week were 48% less likely to die of any cause during the follow-up period. (Expending 12,600 kilojoules can be achieved with about 6 to 8 hours of moderate-intensity physical activity.)
This finding was adjusted for age, smoking habits, body mass index, early parental mortality, and dietary variables.
When the researchers tried to adjust for cancer severity and treatment, they were only able to collect data for 70 men. But the results were not very different from the prior analysis. The most active men were 49% less likely to die of any cause than the least active men.
The team also decided to analyze men who were diagnosed with cancer at least 5 years before baseline (n=421). And among these men, the most active were 52% less likely than the least active to die.
Similarly, among men diagnosed at least 10 years before baseline (n=262), the most active cancer survivors were 63% less likely to die of any cause than the least active survivors.
The researchers also obtained similar results when they assessed mortality from cancer and cardiovascular disease. The most physically active cancer survivors were 38% less likely to die of cancer and 49% less likely to die of cardiovascular disease during follow-up. ![]()
Credit: Jason E. Miller
Physical activity may reduce the risk of mortality in male cancer survivors, according to research published in the Journal of Physical Activity & Health.
In a study of more than 1000 male cancer survivors, participants who were most active—expending more than 12,600 kilojoules per week in physical activity—cut their risk of death roughly in half.
This was in comparison to the least active cancer survivors—those who burned fewer than 2100 kilojoules per week.
Kathleen Y. Wolin, PhD, of Loyola University Chicago Stritch School of Medicine, and her colleagues conducted this research using data from the Harvard Alumni Health Study, an ongoing study of men who entered Harvard as undergraduates between 1916 and 1950.
The researchers looked at 1021 men, with an average age of 71, who had been diagnosed with cancers.
In 1988, the men completed questionnaires reporting their physical activities, including walking, stair-climbing, and participation in sports and recreational activities. Their physical activities were updated in 1993, and researchers followed the men until 2008.
In all, 777 of the men died—337 from cancer, 190 from cardiovascular disease, 228 from other causes, and 22 from unknown causes.
Compared with men who expended fewer than 2100 kilojoules per week in physical activity, men who expended more than 12,600 kilojoules per week were 48% less likely to die of any cause during the follow-up period. (Expending 12,600 kilojoules can be achieved with about 6 to 8 hours of moderate-intensity physical activity.)
This finding was adjusted for age, smoking habits, body mass index, early parental mortality, and dietary variables.
When the researchers tried to adjust for cancer severity and treatment, they were only able to collect data for 70 men. But the results were not very different from the prior analysis. The most active men were 49% less likely to die of any cause than the least active men.
The team also decided to analyze men who were diagnosed with cancer at least 5 years before baseline (n=421). And among these men, the most active were 52% less likely than the least active to die.
Similarly, among men diagnosed at least 10 years before baseline (n=262), the most active cancer survivors were 63% less likely to die of any cause than the least active survivors.
The researchers also obtained similar results when they assessed mortality from cancer and cardiovascular disease. The most physically active cancer survivors were 38% less likely to die of cancer and 49% less likely to die of cardiovascular disease during follow-up.