User login
Calcium Hydroxylapatite Filler Foreign Body Granulomas: A Case Report of a Rare Occurrence and Review of the Literature
CEA vs. stenting in the elderly: The debate continues
For elderly patients with carotid disease, carotid endarterectomy carries a lower risk of perioperative stroke or transient ischemic attack, the same risk of perioperative MI, and a slightly higher risk of perioperative death compared with carotid artery stenting, according to a meta-analysis.
However, the individual elderly patient’s vascular anatomy plays a crucial role in determining perioperative risk, as does his or her overall health and clinical profile.
"The results of [our] analysis suggest that careful consideration of a constellation of clinical and anatomic factors is required before an appropriate treatment of carotid disease in elderly patients is selected. The cardiovascular disease burden and general health of the individual patient should be meticulously evaluated before interventional instead of optimal medical treatment is applied," said Dr. George A. Antoniou of the department of vascular surgery, Hellenic Red Cross Hospital, Athens, and his associates.
Which treatment is the most appropriate for elderly patients with carotid disease is still much debated. Dr. Antoniou and his colleagues performed a comprehensive review of the medical literature since 1986 and a meta-analysis of 44 articles that directly compared outcomes in elderly patients with those of younger patients after carotid endarterectomy (39 studies) or carotid stenting (18 articles).
"Elderly" was defined as older than 80 years in most of these studies, and as older than 75 years in many, but there was great variability among the studies, and some even considered "older than 65 years" to be elderly.
Overall, the meta-analysis included 269,596 endarterectomies in elderly patients against 243,089 in younger patients, and 38,751 carotid stenting procedures in elderly patients against 36,450 in younger patients.
For endarterectomy, the rate of perioperative stroke was not significantly different between elderly (0.9%) and younger (1.2%) patients, nor was the rate of TIA (1.9% vs 1.8%, respectively). However, perioperative mortality was significantly higher in elderly (0.5%) than in younger (0.4%) patients.
In contrast, for carotid stenting, the rate of perioperative stroke was significantly higher for elderly patients (2.4%) than for younger patients (1.7%), as was the rate of TIA (3.6% vs 2.1%). And mortality was not significantly different between elderly patients (0.6%) and younger patients (0.7%), the researchers wrote (JAMA Surg. 2013 Oct. 23 [doi:10.1001/jamasurg.2013.4135]).
Both procedures were associated with an increased rate of perioperative MI in elderly patients, compared with younger patients. These rates were 2.2% in elderly patients, compared with 1.4% in younger patients undergoing endarterectomy; and 2.3% in elderly patients, compared with 1.5% in younger patients undergoing carotid stenting.
These findings remained robust in sensitivity analyses.
"It seems that endarterectomy is associated with improved neurologic outcomes compared with carotid stenting in elderly patients, at the expense of increased perioperative mortality." However, the small increase in mortality seen with endarterectomy – one-tenth of 1% – may not be clinically significant, Dr. Antoniou and his associates said.
Moreover, neurologic risk is closely tied to vascular anatomy. Elderly patients tend to have more unfavorable anatomy than do younger patients, but should be assessed on an individual basis. Unfavorable traits include heavily calcified and tortuous supra-aortic branches, as well as adverse morphology of the aortic arch such as elongation, distortion, and stenosis.
Manipulating the stenting instruments through such features may in itself raise the risk of neurologic sequelae. It also makes the procedure more technically difficult, which increases the risk of endothelial trauma, thrombus dislodgment, and thromboembolic events.
"In addition, elderly patients with significant extracranial atherosclerotic disease are likely to have a compromised cerebrovascular reserve, which makes them more susceptible to ischemic events from cerebral microembolization," the researchers said.
They reported having no conflicts.
This study’s conclusions are not surprising, given that most clinicians have already seen them both in randomized prospective studies and in their own practices, said Dr. R. Clement Darling III.
However, the variation in the definition of "elderly" among the trials in this meta-analysis is a real concern: 64% used 80 years as the cutoff, 31% used 75 years, and some used 70 or even 65 years as the cutoff.
"The bottom line is, carotid endarterectomy and carotid stenting seem to work equally well in younger patients, in expert hands. However, in the ‘elderly’ (at any age), endarterectomy has better outcomes with low morbidity, mortality, and stroke rate, and it remains the standard of care."
Dr. Darling of the Vascular Group, Albany, N.Y., made these remarks in an invited commentary (JAMA Surgery 2013 Oct. 23 [doi:10.1001/jamasurg.2013.4160]). He reported no financial conflicts of interest.
This study’s conclusions are not surprising, given that most clinicians have already seen them both in randomized prospective studies and in their own practices, said Dr. R. Clement Darling III.
However, the variation in the definition of "elderly" among the trials in this meta-analysis is a real concern: 64% used 80 years as the cutoff, 31% used 75 years, and some used 70 or even 65 years as the cutoff.
"The bottom line is, carotid endarterectomy and carotid stenting seem to work equally well in younger patients, in expert hands. However, in the ‘elderly’ (at any age), endarterectomy has better outcomes with low morbidity, mortality, and stroke rate, and it remains the standard of care."
Dr. Darling of the Vascular Group, Albany, N.Y., made these remarks in an invited commentary (JAMA Surgery 2013 Oct. 23 [doi:10.1001/jamasurg.2013.4160]). He reported no financial conflicts of interest.
This study’s conclusions are not surprising, given that most clinicians have already seen them both in randomized prospective studies and in their own practices, said Dr. R. Clement Darling III.
However, the variation in the definition of "elderly" among the trials in this meta-analysis is a real concern: 64% used 80 years as the cutoff, 31% used 75 years, and some used 70 or even 65 years as the cutoff.
"The bottom line is, carotid endarterectomy and carotid stenting seem to work equally well in younger patients, in expert hands. However, in the ‘elderly’ (at any age), endarterectomy has better outcomes with low morbidity, mortality, and stroke rate, and it remains the standard of care."
Dr. Darling of the Vascular Group, Albany, N.Y., made these remarks in an invited commentary (JAMA Surgery 2013 Oct. 23 [doi:10.1001/jamasurg.2013.4160]). He reported no financial conflicts of interest.
For elderly patients with carotid disease, carotid endarterectomy carries a lower risk of perioperative stroke or transient ischemic attack, the same risk of perioperative MI, and a slightly higher risk of perioperative death compared with carotid artery stenting, according to a meta-analysis.
However, the individual elderly patient’s vascular anatomy plays a crucial role in determining perioperative risk, as does his or her overall health and clinical profile.
"The results of [our] analysis suggest that careful consideration of a constellation of clinical and anatomic factors is required before an appropriate treatment of carotid disease in elderly patients is selected. The cardiovascular disease burden and general health of the individual patient should be meticulously evaluated before interventional instead of optimal medical treatment is applied," said Dr. George A. Antoniou of the department of vascular surgery, Hellenic Red Cross Hospital, Athens, and his associates.
Which treatment is the most appropriate for elderly patients with carotid disease is still much debated. Dr. Antoniou and his colleagues performed a comprehensive review of the medical literature since 1986 and a meta-analysis of 44 articles that directly compared outcomes in elderly patients with those of younger patients after carotid endarterectomy (39 studies) or carotid stenting (18 articles).
"Elderly" was defined as older than 80 years in most of these studies, and as older than 75 years in many, but there was great variability among the studies, and some even considered "older than 65 years" to be elderly.
Overall, the meta-analysis included 269,596 endarterectomies in elderly patients against 243,089 in younger patients, and 38,751 carotid stenting procedures in elderly patients against 36,450 in younger patients.
For endarterectomy, the rate of perioperative stroke was not significantly different between elderly (0.9%) and younger (1.2%) patients, nor was the rate of TIA (1.9% vs 1.8%, respectively). However, perioperative mortality was significantly higher in elderly (0.5%) than in younger (0.4%) patients.
In contrast, for carotid stenting, the rate of perioperative stroke was significantly higher for elderly patients (2.4%) than for younger patients (1.7%), as was the rate of TIA (3.6% vs 2.1%). And mortality was not significantly different between elderly patients (0.6%) and younger patients (0.7%), the researchers wrote (JAMA Surg. 2013 Oct. 23 [doi:10.1001/jamasurg.2013.4135]).
Both procedures were associated with an increased rate of perioperative MI in elderly patients, compared with younger patients. These rates were 2.2% in elderly patients, compared with 1.4% in younger patients undergoing endarterectomy; and 2.3% in elderly patients, compared with 1.5% in younger patients undergoing carotid stenting.
These findings remained robust in sensitivity analyses.
"It seems that endarterectomy is associated with improved neurologic outcomes compared with carotid stenting in elderly patients, at the expense of increased perioperative mortality." However, the small increase in mortality seen with endarterectomy – one-tenth of 1% – may not be clinically significant, Dr. Antoniou and his associates said.
Moreover, neurologic risk is closely tied to vascular anatomy. Elderly patients tend to have more unfavorable anatomy than do younger patients, but should be assessed on an individual basis. Unfavorable traits include heavily calcified and tortuous supra-aortic branches, as well as adverse morphology of the aortic arch such as elongation, distortion, and stenosis.
Manipulating the stenting instruments through such features may in itself raise the risk of neurologic sequelae. It also makes the procedure more technically difficult, which increases the risk of endothelial trauma, thrombus dislodgment, and thromboembolic events.
"In addition, elderly patients with significant extracranial atherosclerotic disease are likely to have a compromised cerebrovascular reserve, which makes them more susceptible to ischemic events from cerebral microembolization," the researchers said.
They reported having no conflicts.
For elderly patients with carotid disease, carotid endarterectomy carries a lower risk of perioperative stroke or transient ischemic attack, the same risk of perioperative MI, and a slightly higher risk of perioperative death compared with carotid artery stenting, according to a meta-analysis.
However, the individual elderly patient’s vascular anatomy plays a crucial role in determining perioperative risk, as does his or her overall health and clinical profile.
"The results of [our] analysis suggest that careful consideration of a constellation of clinical and anatomic factors is required before an appropriate treatment of carotid disease in elderly patients is selected. The cardiovascular disease burden and general health of the individual patient should be meticulously evaluated before interventional instead of optimal medical treatment is applied," said Dr. George A. Antoniou of the department of vascular surgery, Hellenic Red Cross Hospital, Athens, and his associates.
Which treatment is the most appropriate for elderly patients with carotid disease is still much debated. Dr. Antoniou and his colleagues performed a comprehensive review of the medical literature since 1986 and a meta-analysis of 44 articles that directly compared outcomes in elderly patients with those of younger patients after carotid endarterectomy (39 studies) or carotid stenting (18 articles).
"Elderly" was defined as older than 80 years in most of these studies, and as older than 75 years in many, but there was great variability among the studies, and some even considered "older than 65 years" to be elderly.
Overall, the meta-analysis included 269,596 endarterectomies in elderly patients against 243,089 in younger patients, and 38,751 carotid stenting procedures in elderly patients against 36,450 in younger patients.
For endarterectomy, the rate of perioperative stroke was not significantly different between elderly (0.9%) and younger (1.2%) patients, nor was the rate of TIA (1.9% vs 1.8%, respectively). However, perioperative mortality was significantly higher in elderly (0.5%) than in younger (0.4%) patients.
In contrast, for carotid stenting, the rate of perioperative stroke was significantly higher for elderly patients (2.4%) than for younger patients (1.7%), as was the rate of TIA (3.6% vs 2.1%). And mortality was not significantly different between elderly patients (0.6%) and younger patients (0.7%), the researchers wrote (JAMA Surg. 2013 Oct. 23 [doi:10.1001/jamasurg.2013.4135]).
Both procedures were associated with an increased rate of perioperative MI in elderly patients, compared with younger patients. These rates were 2.2% in elderly patients, compared with 1.4% in younger patients undergoing endarterectomy; and 2.3% in elderly patients, compared with 1.5% in younger patients undergoing carotid stenting.
These findings remained robust in sensitivity analyses.
"It seems that endarterectomy is associated with improved neurologic outcomes compared with carotid stenting in elderly patients, at the expense of increased perioperative mortality." However, the small increase in mortality seen with endarterectomy – one-tenth of 1% – may not be clinically significant, Dr. Antoniou and his associates said.
Moreover, neurologic risk is closely tied to vascular anatomy. Elderly patients tend to have more unfavorable anatomy than do younger patients, but should be assessed on an individual basis. Unfavorable traits include heavily calcified and tortuous supra-aortic branches, as well as adverse morphology of the aortic arch such as elongation, distortion, and stenosis.
Manipulating the stenting instruments through such features may in itself raise the risk of neurologic sequelae. It also makes the procedure more technically difficult, which increases the risk of endothelial trauma, thrombus dislodgment, and thromboembolic events.
"In addition, elderly patients with significant extracranial atherosclerotic disease are likely to have a compromised cerebrovascular reserve, which makes them more susceptible to ischemic events from cerebral microembolization," the researchers said.
They reported having no conflicts.
Ibrutinib trial stopped early

Credit: Steven Harbour
The phase 3 RESONATE study has been stopped early due to positive results in patients receiving ibrutinib.
In this trial, researchers compared the BTK inhibitor ibrutinib to the CD20-directed antibody ofatumumab in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL).
The study has ended early because 2 key endpoints were met—namely, ibrutinib significantly improved progression-free and overall survival rates.
The RESONATE study enrolled 391 patients with relapsed or refractory CLL or SLL with measurable nodal disease who were not eligible for treatment with purine-analog-based therapy. Patients had received at least 1 prior therapy.
The researchers randomized patients to receive 420 mg of ibrutinib orally once daily or intravenous doses of ofatumumab over the course of 24 weeks until disease progression or unacceptable toxicity.
At the planned interim analysis, ibrutinib had significantly improved progression-free survival (the primary endpoint) and overall survival (a secondary endpoint).
And the safety profile of ibrutinib was acceptable, according to the companies developing the drug (Pharmacyclics, Inc. and Janssen Research and Development, LLC).
Based on these results, an independent data monitoring committee recommended that patients in the ofatumumab arm be given access to ibrutinib.
Pharmacyclics has informed the US Food and Drug Administration of this recommendation, and Janssen has informed the European Medicines Agency. Both companies are in talks with the health authorities to define the next regulatory steps.
Pharmacyclics has said detailed data from the RESONATE study will be presented at an upcoming oncology conference.
Ibrutinib was recently approved by the US Food and Drug Administration to treat mantle cell lymphoma. ![]()
Credit: Steven Harbour
The phase 3 RESONATE study has been stopped early due to positive results in patients receiving ibrutinib.
In this trial, researchers compared the BTK inhibitor ibrutinib to the CD20-directed antibody ofatumumab in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL).
The study has ended early because 2 key endpoints were met—namely, ibrutinib significantly improved progression-free and overall survival rates.
The RESONATE study enrolled 391 patients with relapsed or refractory CLL or SLL with measurable nodal disease who were not eligible for treatment with purine-analog-based therapy. Patients had received at least 1 prior therapy.
The researchers randomized patients to receive 420 mg of ibrutinib orally once daily or intravenous doses of ofatumumab over the course of 24 weeks until disease progression or unacceptable toxicity.
At the planned interim analysis, ibrutinib had significantly improved progression-free survival (the primary endpoint) and overall survival (a secondary endpoint).
And the safety profile of ibrutinib was acceptable, according to the companies developing the drug (Pharmacyclics, Inc. and Janssen Research and Development, LLC).
Based on these results, an independent data monitoring committee recommended that patients in the ofatumumab arm be given access to ibrutinib.
Pharmacyclics has informed the US Food and Drug Administration of this recommendation, and Janssen has informed the European Medicines Agency. Both companies are in talks with the health authorities to define the next regulatory steps.
Pharmacyclics has said detailed data from the RESONATE study will be presented at an upcoming oncology conference.
Ibrutinib was recently approved by the US Food and Drug Administration to treat mantle cell lymphoma. ![]()
Credit: Steven Harbour
The phase 3 RESONATE study has been stopped early due to positive results in patients receiving ibrutinib.
In this trial, researchers compared the BTK inhibitor ibrutinib to the CD20-directed antibody ofatumumab in patients with relapsed or refractory chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL).
The study has ended early because 2 key endpoints were met—namely, ibrutinib significantly improved progression-free and overall survival rates.
The RESONATE study enrolled 391 patients with relapsed or refractory CLL or SLL with measurable nodal disease who were not eligible for treatment with purine-analog-based therapy. Patients had received at least 1 prior therapy.
The researchers randomized patients to receive 420 mg of ibrutinib orally once daily or intravenous doses of ofatumumab over the course of 24 weeks until disease progression or unacceptable toxicity.
At the planned interim analysis, ibrutinib had significantly improved progression-free survival (the primary endpoint) and overall survival (a secondary endpoint).
And the safety profile of ibrutinib was acceptable, according to the companies developing the drug (Pharmacyclics, Inc. and Janssen Research and Development, LLC).
Based on these results, an independent data monitoring committee recommended that patients in the ofatumumab arm be given access to ibrutinib.
Pharmacyclics has informed the US Food and Drug Administration of this recommendation, and Janssen has informed the European Medicines Agency. Both companies are in talks with the health authorities to define the next regulatory steps.
Pharmacyclics has said detailed data from the RESONATE study will be presented at an upcoming oncology conference.
Ibrutinib was recently approved by the US Food and Drug Administration to treat mantle cell lymphoma. ![]()
Music therapy helps AYAs undergoing HSCT
![]()
Credit: Chad McNeeley
A music therapy intervention can help adolescents and young adults (AYAs) cope with cancer and its treatment, according to research published in the journal Cancer.
The intervention consisted of writing song lyrics and producing music videos.
It helped AYA cancer patients communicate their feelings about their disease and its treatment, hematopoietic stem cell transplant (HSCT).
The program also had positive effects on patients’ social integration and family environment.
About the intervention
The therapeutic music video (TMV) intervention was designed to improve resilience in AYA cancer patients undergoing HSCT. Resilience is the process of positively adjusting to stressors.
“Adolescents and young adults who are resilient have the ability to rise above their illness, gain a sense of mastery and confidence in how they have dealt with their cancer, and demonstrate a desire to reach out and help others,” said study author Joan Haase, PhD, RN, of the Indiana University School of Nursing.
Dr Haase and her colleagues wanted to use the TMV intervention to help AYAs explore and express thoughts and emotions about their disease and treatment that might otherwise go unspoken.
The patients did this by writing song lyrics and producing videos with the help of a board-certified music therapist. As they moved through phases of the intervention—making sound recordings, collecting video images, and storyboarding—patients had opportunities to involve family, friends, and healthcare providers in their project.
Results of the study
To test the intervention, Dr Haase and her colleagues enrolled 113 cancer patients (aged 11 to 24 years) who were undergoing HSCT.
The patients were randomized to the TMV intervention group or a control group that received audiobooks. All patients completed 6 sessions over 3 weeks.
After the intervention, the TMV group reported significantly better courageous coping. And at 100 days after HSCT, the TMV group reported significantly better social integration and family environments.
Parents reported that the videos gave them insight into their children’s cancer experiences. However, parents needed help to initiate and sustain conversations about messages shared through their children’s videos.
The investigators said these findings provide evidence supporting the use of a music-based intervention delivered by a music therapist to help AYAs cope with high-risk, high-intensity cancer treatments.
“The availability of music therapy services from a board-certified music therapist in the United States has become more widespread, and, through studies like this one, we hope to see increased availability and access to this important allied health service,” said study author Sheri L. Robb, PhD, also of the Indiana University School of Nursing.
“One of our team’s next steps is to disseminate findings, train professional music therapists on this intervention, and then conduct an implementation study to examine how the intervention may change as it moves into the standard care setting and whether, in the presence of these changes, patient benefits are maintained.” ![]()
![]()
Credit: Chad McNeeley
A music therapy intervention can help adolescents and young adults (AYAs) cope with cancer and its treatment, according to research published in the journal Cancer.
The intervention consisted of writing song lyrics and producing music videos.
It helped AYA cancer patients communicate their feelings about their disease and its treatment, hematopoietic stem cell transplant (HSCT).
The program also had positive effects on patients’ social integration and family environment.
About the intervention
The therapeutic music video (TMV) intervention was designed to improve resilience in AYA cancer patients undergoing HSCT. Resilience is the process of positively adjusting to stressors.
“Adolescents and young adults who are resilient have the ability to rise above their illness, gain a sense of mastery and confidence in how they have dealt with their cancer, and demonstrate a desire to reach out and help others,” said study author Joan Haase, PhD, RN, of the Indiana University School of Nursing.
Dr Haase and her colleagues wanted to use the TMV intervention to help AYAs explore and express thoughts and emotions about their disease and treatment that might otherwise go unspoken.
The patients did this by writing song lyrics and producing videos with the help of a board-certified music therapist. As they moved through phases of the intervention—making sound recordings, collecting video images, and storyboarding—patients had opportunities to involve family, friends, and healthcare providers in their project.
Results of the study
To test the intervention, Dr Haase and her colleagues enrolled 113 cancer patients (aged 11 to 24 years) who were undergoing HSCT.
The patients were randomized to the TMV intervention group or a control group that received audiobooks. All patients completed 6 sessions over 3 weeks.
After the intervention, the TMV group reported significantly better courageous coping. And at 100 days after HSCT, the TMV group reported significantly better social integration and family environments.
Parents reported that the videos gave them insight into their children’s cancer experiences. However, parents needed help to initiate and sustain conversations about messages shared through their children’s videos.
The investigators said these findings provide evidence supporting the use of a music-based intervention delivered by a music therapist to help AYAs cope with high-risk, high-intensity cancer treatments.
“The availability of music therapy services from a board-certified music therapist in the United States has become more widespread, and, through studies like this one, we hope to see increased availability and access to this important allied health service,” said study author Sheri L. Robb, PhD, also of the Indiana University School of Nursing.
“One of our team’s next steps is to disseminate findings, train professional music therapists on this intervention, and then conduct an implementation study to examine how the intervention may change as it moves into the standard care setting and whether, in the presence of these changes, patient benefits are maintained.” ![]()
![]()
Credit: Chad McNeeley
A music therapy intervention can help adolescents and young adults (AYAs) cope with cancer and its treatment, according to research published in the journal Cancer.
The intervention consisted of writing song lyrics and producing music videos.
It helped AYA cancer patients communicate their feelings about their disease and its treatment, hematopoietic stem cell transplant (HSCT).
The program also had positive effects on patients’ social integration and family environment.
About the intervention
The therapeutic music video (TMV) intervention was designed to improve resilience in AYA cancer patients undergoing HSCT. Resilience is the process of positively adjusting to stressors.
“Adolescents and young adults who are resilient have the ability to rise above their illness, gain a sense of mastery and confidence in how they have dealt with their cancer, and demonstrate a desire to reach out and help others,” said study author Joan Haase, PhD, RN, of the Indiana University School of Nursing.
Dr Haase and her colleagues wanted to use the TMV intervention to help AYAs explore and express thoughts and emotions about their disease and treatment that might otherwise go unspoken.
The patients did this by writing song lyrics and producing videos with the help of a board-certified music therapist. As they moved through phases of the intervention—making sound recordings, collecting video images, and storyboarding—patients had opportunities to involve family, friends, and healthcare providers in their project.
Results of the study
To test the intervention, Dr Haase and her colleagues enrolled 113 cancer patients (aged 11 to 24 years) who were undergoing HSCT.
The patients were randomized to the TMV intervention group or a control group that received audiobooks. All patients completed 6 sessions over 3 weeks.
After the intervention, the TMV group reported significantly better courageous coping. And at 100 days after HSCT, the TMV group reported significantly better social integration and family environments.
Parents reported that the videos gave them insight into their children’s cancer experiences. However, parents needed help to initiate and sustain conversations about messages shared through their children’s videos.
The investigators said these findings provide evidence supporting the use of a music-based intervention delivered by a music therapist to help AYAs cope with high-risk, high-intensity cancer treatments.
“The availability of music therapy services from a board-certified music therapist in the United States has become more widespread, and, through studies like this one, we hope to see increased availability and access to this important allied health service,” said study author Sheri L. Robb, PhD, also of the Indiana University School of Nursing.
“One of our team’s next steps is to disseminate findings, train professional music therapists on this intervention, and then conduct an implementation study to examine how the intervention may change as it moves into the standard care setting and whether, in the presence of these changes, patient benefits are maintained.” ![]()
Does vaginal prolapse repair using synthetic mesh confer long-term benefit over native-tissue colpopexy?
This is the third report from Gutman and colleagues on the outcomes of a double-blind, multicenter, randomized, controlled trial of vaginal prolapse repair using synthetic mesh versus native-tissue colpopexy in women with significant vaginal prolapse.
The trial involved 33 women who underwent mesh repair and 32 who underwent repair without mesh. (The mesh-free repair consisted primarily of uterosacral suspension and concurrent colporrhaphy.) It was halted when it reached a predetermined threshold for discontinuation, which was a mesh erosion rate of 15% or more.
Investigators found no difference in long-term cure rates between the mesh and no-mesh groups, regardless of the definition of cure (ie, anatomic, symptomatic, or combined). Nor was there a difference in the overall recurrence rate.
Summary of earlier reports
Three-month outcomes. The first report from this trial described 3-month objective treatment outcomes, with success described as prolapse no greater than stage 1.1 It found a high erosion rate (15.6%) for vaginal mesh, with no differences between groups in overall subjective or objective cure rates, with an overall recurrence rate of 59.4% (19 cases) in the mesh group versus 70.4% (24 cases) in the no-mesh group (P = .28), with recurrence defined as prolapse beyond stage 1 in any compartment. Investigators also observed potential benefit in the mesh group in the anterior vaginal wall at point Ba at a median of 9.7 months after surgery.
Related Article: Stop using synthetic mesh for routine repair of pelvic organ prolapse Cheryl B. Iglesia, MD (Stop/Start, April 2013)
One-year outcomes. The second report described 1-year objective and functional outcomes in all participants of the trial.2 It found comparable objective and subjective cure rates between groups but a higher reoperation rate for mesh repairs. Prolapse recurred in the anterior department in 46.9% of women in the mesh group versus 60.6% in the no-mesh group (P = .40).
Subjective quality-of-life assessments continued to reflect significant improvement in symptoms from baseline. Vaginal bulging was relieved in 96.2% of women in the mesh group, compared with 90.9% in the no-mesh group (P = .62).
More women in the mesh group required reoperation for recurrent prolapse or mesh exposure (5 in the mesh group vs 0 in the no-mesh group; P = .017).
Strengths and limitations of the trial
Gutman and colleagues are to be congratulated for continuing to monitor longer-term outcomes of vaginal prolapse repairs augmented with synthetic mesh, as data are sorely needed on both early complications and those more remote from surgery. However, it is regrettable that continued attrition in this trial led to minimal power to compare outcomes between groups.
Cure rates were assessed three ways: anatomically, by virtue of symptoms, and by a combination of the two measures. Participants had documentation of at least 2-year anatomic outcomes and 3-year subjective outcomes using validated measures.
Forty-one (63%) of the original 65 women in the trial had anatomic outcomes (20 in the mesh group vs 21 in the no-mesh group), and 51 (78%) of the original 65 women had evaluable subjective outcomes (25 in the mesh group vs 26 in the no-mesh group).
Women who underwent reoperation for recurrent prolapse were removed from any outcomes analysis and considered to have failed composite outcomes measures (anatomic and subjective assessment and whether reoperation or a pessary was required for recurrent prolapse).
The length of follow-up was similar between groups (median, 3 years; interquartile range, 2.97–3.15), and both groups demonstrated significant anatomic and subjective improvement from baseline.
No difference was observed between groups in the original primary anatomic outcome, which was a POP-Q stage no greater than 1 (45% in the mesh group vs 43% in the no-mesh group; P >.99). Nor was there a difference between groups in any other anatomic outcome, including POP-Q point Ba (median, –1.5 for mesh [range, –2.5, 1.0] vs –0.5 [range, –3.0, 4.0] for the no-mesh group; P = .21) and bulge symptoms (92% for the mesh group vs 81% for the no-mesh group; relative risk, 1.4; 95% confidence interval, 0.91–1.42).
Despite small numbers and markedly reduced comparative validity (readily acknowledged by the investigators), these longer-term outcomes were assessed by examiners blinded to treatment and using validated objective and subjective outcome measures.
The only other randomized trial of mesh versus native-tissue repair with 3-year outcomes had a much larger sample size and follow-up but addressed only anterior-compartment prolapse.3
What this evidence means for practice
The 3-year data presented by Gutman and colleagues should be viewed with caution, owing to the trial’s reduced sample size and power. However, they may be useful in designing future trials.
In the meantime, given the limited longer-term outcomes data available at present, I would recommend continued individualized use of mesh versus native-tissue repair in women presenting with prolapse, including educating patients about the risks and benefits of both approaches. It also is important that outcomes be followed in all of our patients in a robust, unbiased fashion. The new American Urogynecologic Society Pelvic Floor Disorders Registry provides the opportunity for this.
Holly E. Richter, PhD, MD
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
- Iglesia CB, Sokol AI, Sokol ER, et al. Vaginal mesh for prolapse: A randomized controlled trial. Obstet Gynecol. 2010;116(2 Pt 1):293–303.
- Sokol AI, Iglesia CB, Kudish BI, et al. One-year objective and functional outcomes of a randomized clinical trial of vaginal mesh for prolapse. Am J Obstet Gynecol. 2012;206(1):86.e1–e9.
- Nieminen K, Hiltunen R, Takala T, et al. Outcomes after anterior vaginal wall repair with mesh: A randomized, controlled trial with a 3-year follow-up. Am J Obstet Gynecol. 2010;203(3):235.e1–e8.
This is the third report from Gutman and colleagues on the outcomes of a double-blind, multicenter, randomized, controlled trial of vaginal prolapse repair using synthetic mesh versus native-tissue colpopexy in women with significant vaginal prolapse.
The trial involved 33 women who underwent mesh repair and 32 who underwent repair without mesh. (The mesh-free repair consisted primarily of uterosacral suspension and concurrent colporrhaphy.) It was halted when it reached a predetermined threshold for discontinuation, which was a mesh erosion rate of 15% or more.
Investigators found no difference in long-term cure rates between the mesh and no-mesh groups, regardless of the definition of cure (ie, anatomic, symptomatic, or combined). Nor was there a difference in the overall recurrence rate.
Summary of earlier reports
Three-month outcomes. The first report from this trial described 3-month objective treatment outcomes, with success described as prolapse no greater than stage 1.1 It found a high erosion rate (15.6%) for vaginal mesh, with no differences between groups in overall subjective or objective cure rates, with an overall recurrence rate of 59.4% (19 cases) in the mesh group versus 70.4% (24 cases) in the no-mesh group (P = .28), with recurrence defined as prolapse beyond stage 1 in any compartment. Investigators also observed potential benefit in the mesh group in the anterior vaginal wall at point Ba at a median of 9.7 months after surgery.
Related Article: Stop using synthetic mesh for routine repair of pelvic organ prolapse Cheryl B. Iglesia, MD (Stop/Start, April 2013)
One-year outcomes. The second report described 1-year objective and functional outcomes in all participants of the trial.2 It found comparable objective and subjective cure rates between groups but a higher reoperation rate for mesh repairs. Prolapse recurred in the anterior department in 46.9% of women in the mesh group versus 60.6% in the no-mesh group (P = .40).
Subjective quality-of-life assessments continued to reflect significant improvement in symptoms from baseline. Vaginal bulging was relieved in 96.2% of women in the mesh group, compared with 90.9% in the no-mesh group (P = .62).
More women in the mesh group required reoperation for recurrent prolapse or mesh exposure (5 in the mesh group vs 0 in the no-mesh group; P = .017).
Strengths and limitations of the trial
Gutman and colleagues are to be congratulated for continuing to monitor longer-term outcomes of vaginal prolapse repairs augmented with synthetic mesh, as data are sorely needed on both early complications and those more remote from surgery. However, it is regrettable that continued attrition in this trial led to minimal power to compare outcomes between groups.
Cure rates were assessed three ways: anatomically, by virtue of symptoms, and by a combination of the two measures. Participants had documentation of at least 2-year anatomic outcomes and 3-year subjective outcomes using validated measures.
Forty-one (63%) of the original 65 women in the trial had anatomic outcomes (20 in the mesh group vs 21 in the no-mesh group), and 51 (78%) of the original 65 women had evaluable subjective outcomes (25 in the mesh group vs 26 in the no-mesh group).
Women who underwent reoperation for recurrent prolapse were removed from any outcomes analysis and considered to have failed composite outcomes measures (anatomic and subjective assessment and whether reoperation or a pessary was required for recurrent prolapse).
The length of follow-up was similar between groups (median, 3 years; interquartile range, 2.97–3.15), and both groups demonstrated significant anatomic and subjective improvement from baseline.
No difference was observed between groups in the original primary anatomic outcome, which was a POP-Q stage no greater than 1 (45% in the mesh group vs 43% in the no-mesh group; P >.99). Nor was there a difference between groups in any other anatomic outcome, including POP-Q point Ba (median, –1.5 for mesh [range, –2.5, 1.0] vs –0.5 [range, –3.0, 4.0] for the no-mesh group; P = .21) and bulge symptoms (92% for the mesh group vs 81% for the no-mesh group; relative risk, 1.4; 95% confidence interval, 0.91–1.42).
Despite small numbers and markedly reduced comparative validity (readily acknowledged by the investigators), these longer-term outcomes were assessed by examiners blinded to treatment and using validated objective and subjective outcome measures.
The only other randomized trial of mesh versus native-tissue repair with 3-year outcomes had a much larger sample size and follow-up but addressed only anterior-compartment prolapse.3
What this evidence means for practice
The 3-year data presented by Gutman and colleagues should be viewed with caution, owing to the trial’s reduced sample size and power. However, they may be useful in designing future trials.
In the meantime, given the limited longer-term outcomes data available at present, I would recommend continued individualized use of mesh versus native-tissue repair in women presenting with prolapse, including educating patients about the risks and benefits of both approaches. It also is important that outcomes be followed in all of our patients in a robust, unbiased fashion. The new American Urogynecologic Society Pelvic Floor Disorders Registry provides the opportunity for this.
Holly E. Richter, PhD, MD
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
This is the third report from Gutman and colleagues on the outcomes of a double-blind, multicenter, randomized, controlled trial of vaginal prolapse repair using synthetic mesh versus native-tissue colpopexy in women with significant vaginal prolapse.
The trial involved 33 women who underwent mesh repair and 32 who underwent repair without mesh. (The mesh-free repair consisted primarily of uterosacral suspension and concurrent colporrhaphy.) It was halted when it reached a predetermined threshold for discontinuation, which was a mesh erosion rate of 15% or more.
Investigators found no difference in long-term cure rates between the mesh and no-mesh groups, regardless of the definition of cure (ie, anatomic, symptomatic, or combined). Nor was there a difference in the overall recurrence rate.
Summary of earlier reports
Three-month outcomes. The first report from this trial described 3-month objective treatment outcomes, with success described as prolapse no greater than stage 1.1 It found a high erosion rate (15.6%) for vaginal mesh, with no differences between groups in overall subjective or objective cure rates, with an overall recurrence rate of 59.4% (19 cases) in the mesh group versus 70.4% (24 cases) in the no-mesh group (P = .28), with recurrence defined as prolapse beyond stage 1 in any compartment. Investigators also observed potential benefit in the mesh group in the anterior vaginal wall at point Ba at a median of 9.7 months after surgery.
Related Article: Stop using synthetic mesh for routine repair of pelvic organ prolapse Cheryl B. Iglesia, MD (Stop/Start, April 2013)
One-year outcomes. The second report described 1-year objective and functional outcomes in all participants of the trial.2 It found comparable objective and subjective cure rates between groups but a higher reoperation rate for mesh repairs. Prolapse recurred in the anterior department in 46.9% of women in the mesh group versus 60.6% in the no-mesh group (P = .40).
Subjective quality-of-life assessments continued to reflect significant improvement in symptoms from baseline. Vaginal bulging was relieved in 96.2% of women in the mesh group, compared with 90.9% in the no-mesh group (P = .62).
More women in the mesh group required reoperation for recurrent prolapse or mesh exposure (5 in the mesh group vs 0 in the no-mesh group; P = .017).
Strengths and limitations of the trial
Gutman and colleagues are to be congratulated for continuing to monitor longer-term outcomes of vaginal prolapse repairs augmented with synthetic mesh, as data are sorely needed on both early complications and those more remote from surgery. However, it is regrettable that continued attrition in this trial led to minimal power to compare outcomes between groups.
Cure rates were assessed three ways: anatomically, by virtue of symptoms, and by a combination of the two measures. Participants had documentation of at least 2-year anatomic outcomes and 3-year subjective outcomes using validated measures.
Forty-one (63%) of the original 65 women in the trial had anatomic outcomes (20 in the mesh group vs 21 in the no-mesh group), and 51 (78%) of the original 65 women had evaluable subjective outcomes (25 in the mesh group vs 26 in the no-mesh group).
Women who underwent reoperation for recurrent prolapse were removed from any outcomes analysis and considered to have failed composite outcomes measures (anatomic and subjective assessment and whether reoperation or a pessary was required for recurrent prolapse).
The length of follow-up was similar between groups (median, 3 years; interquartile range, 2.97–3.15), and both groups demonstrated significant anatomic and subjective improvement from baseline.
No difference was observed between groups in the original primary anatomic outcome, which was a POP-Q stage no greater than 1 (45% in the mesh group vs 43% in the no-mesh group; P >.99). Nor was there a difference between groups in any other anatomic outcome, including POP-Q point Ba (median, –1.5 for mesh [range, –2.5, 1.0] vs –0.5 [range, –3.0, 4.0] for the no-mesh group; P = .21) and bulge symptoms (92% for the mesh group vs 81% for the no-mesh group; relative risk, 1.4; 95% confidence interval, 0.91–1.42).
Despite small numbers and markedly reduced comparative validity (readily acknowledged by the investigators), these longer-term outcomes were assessed by examiners blinded to treatment and using validated objective and subjective outcome measures.
The only other randomized trial of mesh versus native-tissue repair with 3-year outcomes had a much larger sample size and follow-up but addressed only anterior-compartment prolapse.3
What this evidence means for practice
The 3-year data presented by Gutman and colleagues should be viewed with caution, owing to the trial’s reduced sample size and power. However, they may be useful in designing future trials.
In the meantime, given the limited longer-term outcomes data available at present, I would recommend continued individualized use of mesh versus native-tissue repair in women presenting with prolapse, including educating patients about the risks and benefits of both approaches. It also is important that outcomes be followed in all of our patients in a robust, unbiased fashion. The new American Urogynecologic Society Pelvic Floor Disorders Registry provides the opportunity for this.
Holly E. Richter, PhD, MD
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
- Iglesia CB, Sokol AI, Sokol ER, et al. Vaginal mesh for prolapse: A randomized controlled trial. Obstet Gynecol. 2010;116(2 Pt 1):293–303.
- Sokol AI, Iglesia CB, Kudish BI, et al. One-year objective and functional outcomes of a randomized clinical trial of vaginal mesh for prolapse. Am J Obstet Gynecol. 2012;206(1):86.e1–e9.
- Nieminen K, Hiltunen R, Takala T, et al. Outcomes after anterior vaginal wall repair with mesh: A randomized, controlled trial with a 3-year follow-up. Am J Obstet Gynecol. 2010;203(3):235.e1–e8.
- Iglesia CB, Sokol AI, Sokol ER, et al. Vaginal mesh for prolapse: A randomized controlled trial. Obstet Gynecol. 2010;116(2 Pt 1):293–303.
- Sokol AI, Iglesia CB, Kudish BI, et al. One-year objective and functional outcomes of a randomized clinical trial of vaginal mesh for prolapse. Am J Obstet Gynecol. 2012;206(1):86.e1–e9.
- Nieminen K, Hiltunen R, Takala T, et al. Outcomes after anterior vaginal wall repair with mesh: A randomized, controlled trial with a 3-year follow-up. Am J Obstet Gynecol. 2010;203(3):235.e1–e8.

Circumcision accident: $1.3M verdict

CIRCUMCISION ACCIDENT: $1.3M VERDICT
A newborn underwent circumcision when 12 hours old. The ObGyn removed adhesions present between the foreskin and glans. After locking the Mogen clamp, the ObGyn amputated a 9-mm by 8-mm portion of the top of the penis along with the foreskin. The newborn was rushed to a children’s hospital where a pediatric urologist surgically reattached the amputated glans. The child’s penis is not cosmetically normal, with permanent scars and disfigurement. He has altered nerve sensation at and above the area of the amputation.
PARENTS’ CLAIM The ObGyn improperly performed the circumcision. He failed to remove a sufficient amount of adhesions, pulled too much into the clamp, and amputated 30% of the distal portion of the glans.
PHYSICIAN’S DEFENSE The ObGyn circumcised this child the same way he had performed more than 1,000 circumcisions. Multiple dense adhesions between the glans and foreskin caused the top of the penis to be inadvertently pulled through the clamp. Amputation is a known risk of the procedure.
VERDICT A $1,357,901 Illinois verdict was returned.
WHAT CAUSED CHILD’S KIDNEY DISEASE?
At 36 weeks’ gestation, a mother came to the emergency department (ED) with abdominal pain. She had proteinuria, elevated liver enzymes, and a low-normal platelet count. An ObGyn determined that the fetus was normal, and discharged her.
The patient returned 2 days later with internal bleeding and placental abruption. She was diagnosed with hemolysis, elevated liver enzymes, and low platelet count (HELLP syndrome). The child, born by cesarean delivery, had kidney failure that caused growth retardation. The child has received a kidney transplant.
PARENTS’ CLAIM The mother should not have been discharged from the hospital with abnormal findings.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million New Jersey settlement was reached, of which $100,000 was provided to the mother.
Related Article: A stepwise approach to managing eclampsia and other hypertensive emergencies Baha M. Sibai, MD (October 2013)
EXCESSIVE FORCE BLAMED FOR ERB’S PALSY
Shoulder dystocia was encountered during delivery. The child suffered a brachial plexus injury with Erb’s palsy. She received botulinum toxin injections and underwent nerve-graft surgery to restore some function. She has limited use of her right arm and a protruding right elbow.
PARENTS’ CLAIM The ObGyn used excessive force in response to shoulder dystocia.
PHYSICIAN’S DEFENSE The case was settled at trial.
VERDICT A $1 million New Jersey settlement was placed in a structured payment fund to provide a net $1.78 million over the child’s lifetime.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
WAS WOMAN UNLAWFULLY SEEKING DRUGS?
A 30-year-old woman went to an ED with pelvic pain and vaginal discharge. An ED physician conducted a physical exam. Blood tests indicated the patient had taken barbiturates, but the patient could not explain the findings. Determining no cause for her symptoms, the ED physician discharged the patient.
Just after she left, the ED physician found that the patient had several narcotics prescriptions and called the police. The patient was arrested and charged with unlawfully seeking drugs at the hospital. Criminal charges were later dismissed.
PATIENT’S CLAIM The ED physician did not properly examine her; she was found to have endometriosis and underwent surgery a few weeks later. The ED physician was negligent for divulging her personal information to police.
The ED physician had had his physician’s license suspended due to substance abuse and had also been arrested for driving under the influence after his license was restored.
PHYSICIAN’S DEFENSE The ED physician’s examination and treatment were proper. The phone call to police was not part of treatment. The patient had a malicious prosecution basis for any claims.
VERDICT A $125,000 Kentucky verdict was returned.

CASCADING PROBLEMS: MOTHER AND BABY DIE
A pregnant woman was admitted to an ED, where the on-call physician determined that she had pneumonia. The patient’s ObGyn, 45 miles away, refused to come to the hospital or arrange for another ObGyn to take the case.
Several hours later, after the mother was found to have fulminant preeclampsia, the ObGyn demanded the patient be moved to the hospital’s internal medicine (IM) service. However, the IM service refused to admit the patient because she needed obstetric care. The ObGyn tried to transfer the patient to a maternal-fetal medicine (MFM) specialist at a tertiary care center; transfer was refused because the patient was too unstable and needed an emergency cesarean delivery. The ObGyn continued to refuse to relinquish care to another ObGyn.
The ED physician decided to transfer the patient to another hospital 50 miles away even though she was now in active labor. An MFM specialist accepted transfer. After 5 hours in the ED, the mother left by ambulance, but, during transport, she suffered placental abruption and internal hemorrhaging. She was in critical condition upon arrival. An emergency cesarean delivery was performed, but the mother died. The baby, born with severe brain damage, also died.
ESTATES’ CLAIM The ED physician failed to properly and timely determine that the mother had preeclampsia; no treatment for hypertension was provided. The ED physician withheld critical information, including the patient’s severe hypertension, proteinurea, and edema, when speaking to the MFM specialist who accepted transfer. The ED physician did not evaluate the mother before departure and certified the transfer although the patient was highly unstable.
The ObGyn was negligent in not transferring care to another ObGyn and not coming to the hospital. The ObGyn did not inform the ED physician of the rejected attempt to transfer the patient or of the first MFM specialist’s recommendation for emergency cesarean. Both mother and baby could have survived with proper treatment.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $900,000 Michigan settlement was reached.
FECAL INCONTINENCE AFTER EPISIOTOMY
A 26-year-old woman gave birth after her ObGyn created an episiotomy to facilitate delivery. The incision was repaired and the ObGyn prescribed docusate (Colace) to soften her stools.
A month later, the patient report-ed fecal incontinence. The ObGyn determined that the incontinence was related to the episiotomy, but did not feel that immediate attention was needed. When the condition did not improve, the patient saw a colorectal surgeon, who diagnosed a significant sphincter defect. The patient underwent a sphincteroplasty, with minor improvement.
PATIENT’S CLAIM The ObGyn failed to properly manage episiotomy healing. The patient remembers being told to stop docusate after she had passed one stool after delivery. A 10-day regimen of docusate and a diet to reduce defecation frequency should have been prescribed. Incontinence should have prompted an immediate referral to a colorectal surgeon.
PHYSICIAN’S DEFENSE Prompt surgical intervention was not necessary. Sphincteroplasty can be delayed until conservative methods have been tried. Episiotomy healing was properly addressed. Permanent incontinence is a known risk of the procedure.
VERDICT A $6 million New York verdict was returned.
Related Article: Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery? Errol R. Norwitz, MD, PhD (Examining the Evidence, August 2012)
MECONIUM ASPIRATION SYNDROME
A baby stayed in hospital for 3 weeks postdelivery due to meconium aspiration syndrome.
PARENTS’ CLAIM The resident who followed the mother during her pregnancy was negligent in allowing the pregnancy to progress to 46 weeks’ gestation before delivery.
DEFENDANTS’ DEFENSE The estimated date of conception was disputed. The resident claimed that the baby was born at 42 weeks’ gestation. An attending physician reviewed all prenatal visits with the resident. The mother’s cervix was never ripe before induction of labor. Aspiration occurred despite aggressive suctioning. The child has had no further respiratory issues since her neonatal discharge.
VERDICT An Illinois defense verdict was returned.
BOWEL INJURY AFTER HYSTERECTOMY
A woman underwent laparoscopic-assisted vaginal hysterectomy and was discharged the following day. Two days later, she went to an ED in acute distress. A bowel perforation was found during emergency surgery, and her colon was repaired. She made a full recovery.
PATIENT’S CLAIM The ObGyn was negligent in failing to properly evaluate the patient after surgery. The ObGyn also failed to explain the signs of a possible perforation to the patient before she left the hospital.
PHYSICIAN’S DEFENSE The patient’s postoperative course was normal while she was hospitalized. Bowel perforation is a known complication of the procedure. The patient had been informed of all the signs and symptoms of a bowel perforation and had been instructed to call the ObGyn or return to the hospital if she began to have any symptoms.
VERDICT A South Carolina defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
CIRCUMCISION ACCIDENT: $1.3M VERDICT
A newborn underwent circumcision when 12 hours old. The ObGyn removed adhesions present between the foreskin and glans. After locking the Mogen clamp, the ObGyn amputated a 9-mm by 8-mm portion of the top of the penis along with the foreskin. The newborn was rushed to a children’s hospital where a pediatric urologist surgically reattached the amputated glans. The child’s penis is not cosmetically normal, with permanent scars and disfigurement. He has altered nerve sensation at and above the area of the amputation.
PARENTS’ CLAIM The ObGyn improperly performed the circumcision. He failed to remove a sufficient amount of adhesions, pulled too much into the clamp, and amputated 30% of the distal portion of the glans.
PHYSICIAN’S DEFENSE The ObGyn circumcised this child the same way he had performed more than 1,000 circumcisions. Multiple dense adhesions between the glans and foreskin caused the top of the penis to be inadvertently pulled through the clamp. Amputation is a known risk of the procedure.
VERDICT A $1,357,901 Illinois verdict was returned.
WHAT CAUSED CHILD’S KIDNEY DISEASE?
At 36 weeks’ gestation, a mother came to the emergency department (ED) with abdominal pain. She had proteinuria, elevated liver enzymes, and a low-normal platelet count. An ObGyn determined that the fetus was normal, and discharged her.
The patient returned 2 days later with internal bleeding and placental abruption. She was diagnosed with hemolysis, elevated liver enzymes, and low platelet count (HELLP syndrome). The child, born by cesarean delivery, had kidney failure that caused growth retardation. The child has received a kidney transplant.
PARENTS’ CLAIM The mother should not have been discharged from the hospital with abnormal findings.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million New Jersey settlement was reached, of which $100,000 was provided to the mother.
Related Article: A stepwise approach to managing eclampsia and other hypertensive emergencies Baha M. Sibai, MD (October 2013)
EXCESSIVE FORCE BLAMED FOR ERB’S PALSY
Shoulder dystocia was encountered during delivery. The child suffered a brachial plexus injury with Erb’s palsy. She received botulinum toxin injections and underwent nerve-graft surgery to restore some function. She has limited use of her right arm and a protruding right elbow.
PARENTS’ CLAIM The ObGyn used excessive force in response to shoulder dystocia.
PHYSICIAN’S DEFENSE The case was settled at trial.
VERDICT A $1 million New Jersey settlement was placed in a structured payment fund to provide a net $1.78 million over the child’s lifetime.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
WAS WOMAN UNLAWFULLY SEEKING DRUGS?
A 30-year-old woman went to an ED with pelvic pain and vaginal discharge. An ED physician conducted a physical exam. Blood tests indicated the patient had taken barbiturates, but the patient could not explain the findings. Determining no cause for her symptoms, the ED physician discharged the patient.
Just after she left, the ED physician found that the patient had several narcotics prescriptions and called the police. The patient was arrested and charged with unlawfully seeking drugs at the hospital. Criminal charges were later dismissed.
PATIENT’S CLAIM The ED physician did not properly examine her; she was found to have endometriosis and underwent surgery a few weeks later. The ED physician was negligent for divulging her personal information to police.
The ED physician had had his physician’s license suspended due to substance abuse and had also been arrested for driving under the influence after his license was restored.
PHYSICIAN’S DEFENSE The ED physician’s examination and treatment were proper. The phone call to police was not part of treatment. The patient had a malicious prosecution basis for any claims.
VERDICT A $125,000 Kentucky verdict was returned.
CASCADING PROBLEMS: MOTHER AND BABY DIE
A pregnant woman was admitted to an ED, where the on-call physician determined that she had pneumonia. The patient’s ObGyn, 45 miles away, refused to come to the hospital or arrange for another ObGyn to take the case.
Several hours later, after the mother was found to have fulminant preeclampsia, the ObGyn demanded the patient be moved to the hospital’s internal medicine (IM) service. However, the IM service refused to admit the patient because she needed obstetric care. The ObGyn tried to transfer the patient to a maternal-fetal medicine (MFM) specialist at a tertiary care center; transfer was refused because the patient was too unstable and needed an emergency cesarean delivery. The ObGyn continued to refuse to relinquish care to another ObGyn.
The ED physician decided to transfer the patient to another hospital 50 miles away even though she was now in active labor. An MFM specialist accepted transfer. After 5 hours in the ED, the mother left by ambulance, but, during transport, she suffered placental abruption and internal hemorrhaging. She was in critical condition upon arrival. An emergency cesarean delivery was performed, but the mother died. The baby, born with severe brain damage, also died.
ESTATES’ CLAIM The ED physician failed to properly and timely determine that the mother had preeclampsia; no treatment for hypertension was provided. The ED physician withheld critical information, including the patient’s severe hypertension, proteinurea, and edema, when speaking to the MFM specialist who accepted transfer. The ED physician did not evaluate the mother before departure and certified the transfer although the patient was highly unstable.
The ObGyn was negligent in not transferring care to another ObGyn and not coming to the hospital. The ObGyn did not inform the ED physician of the rejected attempt to transfer the patient or of the first MFM specialist’s recommendation for emergency cesarean. Both mother and baby could have survived with proper treatment.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $900,000 Michigan settlement was reached.
FECAL INCONTINENCE AFTER EPISIOTOMY
A 26-year-old woman gave birth after her ObGyn created an episiotomy to facilitate delivery. The incision was repaired and the ObGyn prescribed docusate (Colace) to soften her stools.
A month later, the patient report-ed fecal incontinence. The ObGyn determined that the incontinence was related to the episiotomy, but did not feel that immediate attention was needed. When the condition did not improve, the patient saw a colorectal surgeon, who diagnosed a significant sphincter defect. The patient underwent a sphincteroplasty, with minor improvement.
PATIENT’S CLAIM The ObGyn failed to properly manage episiotomy healing. The patient remembers being told to stop docusate after she had passed one stool after delivery. A 10-day regimen of docusate and a diet to reduce defecation frequency should have been prescribed. Incontinence should have prompted an immediate referral to a colorectal surgeon.
PHYSICIAN’S DEFENSE Prompt surgical intervention was not necessary. Sphincteroplasty can be delayed until conservative methods have been tried. Episiotomy healing was properly addressed. Permanent incontinence is a known risk of the procedure.
VERDICT A $6 million New York verdict was returned.
Related Article: Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery? Errol R. Norwitz, MD, PhD (Examining the Evidence, August 2012)
MECONIUM ASPIRATION SYNDROME
A baby stayed in hospital for 3 weeks postdelivery due to meconium aspiration syndrome.
PARENTS’ CLAIM The resident who followed the mother during her pregnancy was negligent in allowing the pregnancy to progress to 46 weeks’ gestation before delivery.
DEFENDANTS’ DEFENSE The estimated date of conception was disputed. The resident claimed that the baby was born at 42 weeks’ gestation. An attending physician reviewed all prenatal visits with the resident. The mother’s cervix was never ripe before induction of labor. Aspiration occurred despite aggressive suctioning. The child has had no further respiratory issues since her neonatal discharge.
VERDICT An Illinois defense verdict was returned.
BOWEL INJURY AFTER HYSTERECTOMY
A woman underwent laparoscopic-assisted vaginal hysterectomy and was discharged the following day. Two days later, she went to an ED in acute distress. A bowel perforation was found during emergency surgery, and her colon was repaired. She made a full recovery.
PATIENT’S CLAIM The ObGyn was negligent in failing to properly evaluate the patient after surgery. The ObGyn also failed to explain the signs of a possible perforation to the patient before she left the hospital.
PHYSICIAN’S DEFENSE The patient’s postoperative course was normal while she was hospitalized. Bowel perforation is a known complication of the procedure. The patient had been informed of all the signs and symptoms of a bowel perforation and had been instructed to call the ObGyn or return to the hospital if she began to have any symptoms.
VERDICT A South Carolina defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
CIRCUMCISION ACCIDENT: $1.3M VERDICT
A newborn underwent circumcision when 12 hours old. The ObGyn removed adhesions present between the foreskin and glans. After locking the Mogen clamp, the ObGyn amputated a 9-mm by 8-mm portion of the top of the penis along with the foreskin. The newborn was rushed to a children’s hospital where a pediatric urologist surgically reattached the amputated glans. The child’s penis is not cosmetically normal, with permanent scars and disfigurement. He has altered nerve sensation at and above the area of the amputation.
PARENTS’ CLAIM The ObGyn improperly performed the circumcision. He failed to remove a sufficient amount of adhesions, pulled too much into the clamp, and amputated 30% of the distal portion of the glans.
PHYSICIAN’S DEFENSE The ObGyn circumcised this child the same way he had performed more than 1,000 circumcisions. Multiple dense adhesions between the glans and foreskin caused the top of the penis to be inadvertently pulled through the clamp. Amputation is a known risk of the procedure.
VERDICT A $1,357,901 Illinois verdict was returned.
WHAT CAUSED CHILD’S KIDNEY DISEASE?
At 36 weeks’ gestation, a mother came to the emergency department (ED) with abdominal pain. She had proteinuria, elevated liver enzymes, and a low-normal platelet count. An ObGyn determined that the fetus was normal, and discharged her.
The patient returned 2 days later with internal bleeding and placental abruption. She was diagnosed with hemolysis, elevated liver enzymes, and low platelet count (HELLP syndrome). The child, born by cesarean delivery, had kidney failure that caused growth retardation. The child has received a kidney transplant.
PARENTS’ CLAIM The mother should not have been discharged from the hospital with abnormal findings.
DEFENDANTS’ DEFENSE The case was settled during trial.
VERDICT A $1 million New Jersey settlement was reached, of which $100,000 was provided to the mother.
Related Article: A stepwise approach to managing eclampsia and other hypertensive emergencies Baha M. Sibai, MD (October 2013)
EXCESSIVE FORCE BLAMED FOR ERB’S PALSY
Shoulder dystocia was encountered during delivery. The child suffered a brachial plexus injury with Erb’s palsy. She received botulinum toxin injections and underwent nerve-graft surgery to restore some function. She has limited use of her right arm and a protruding right elbow.
PARENTS’ CLAIM The ObGyn used excessive force in response to shoulder dystocia.
PHYSICIAN’S DEFENSE The case was settled at trial.
VERDICT A $1 million New Jersey settlement was placed in a structured payment fund to provide a net $1.78 million over the child’s lifetime.
Related Article: You are the second responder to a shoulder dystocia emergency. What do you do first? Robert L. Barbieri, MD (Editorial, May 2013)
WAS WOMAN UNLAWFULLY SEEKING DRUGS?
A 30-year-old woman went to an ED with pelvic pain and vaginal discharge. An ED physician conducted a physical exam. Blood tests indicated the patient had taken barbiturates, but the patient could not explain the findings. Determining no cause for her symptoms, the ED physician discharged the patient.
Just after she left, the ED physician found that the patient had several narcotics prescriptions and called the police. The patient was arrested and charged with unlawfully seeking drugs at the hospital. Criminal charges were later dismissed.
PATIENT’S CLAIM The ED physician did not properly examine her; she was found to have endometriosis and underwent surgery a few weeks later. The ED physician was negligent for divulging her personal information to police.
The ED physician had had his physician’s license suspended due to substance abuse and had also been arrested for driving under the influence after his license was restored.
PHYSICIAN’S DEFENSE The ED physician’s examination and treatment were proper. The phone call to police was not part of treatment. The patient had a malicious prosecution basis for any claims.
VERDICT A $125,000 Kentucky verdict was returned.
CASCADING PROBLEMS: MOTHER AND BABY DIE
A pregnant woman was admitted to an ED, where the on-call physician determined that she had pneumonia. The patient’s ObGyn, 45 miles away, refused to come to the hospital or arrange for another ObGyn to take the case.
Several hours later, after the mother was found to have fulminant preeclampsia, the ObGyn demanded the patient be moved to the hospital’s internal medicine (IM) service. However, the IM service refused to admit the patient because she needed obstetric care. The ObGyn tried to transfer the patient to a maternal-fetal medicine (MFM) specialist at a tertiary care center; transfer was refused because the patient was too unstable and needed an emergency cesarean delivery. The ObGyn continued to refuse to relinquish care to another ObGyn.
The ED physician decided to transfer the patient to another hospital 50 miles away even though she was now in active labor. An MFM specialist accepted transfer. After 5 hours in the ED, the mother left by ambulance, but, during transport, she suffered placental abruption and internal hemorrhaging. She was in critical condition upon arrival. An emergency cesarean delivery was performed, but the mother died. The baby, born with severe brain damage, also died.
ESTATES’ CLAIM The ED physician failed to properly and timely determine that the mother had preeclampsia; no treatment for hypertension was provided. The ED physician withheld critical information, including the patient’s severe hypertension, proteinurea, and edema, when speaking to the MFM specialist who accepted transfer. The ED physician did not evaluate the mother before departure and certified the transfer although the patient was highly unstable.
The ObGyn was negligent in not transferring care to another ObGyn and not coming to the hospital. The ObGyn did not inform the ED physician of the rejected attempt to transfer the patient or of the first MFM specialist’s recommendation for emergency cesarean. Both mother and baby could have survived with proper treatment.
DEFENDANTS’ DEFENSE The case was settled at trial.
VERDICT A $900,000 Michigan settlement was reached.
FECAL INCONTINENCE AFTER EPISIOTOMY
A 26-year-old woman gave birth after her ObGyn created an episiotomy to facilitate delivery. The incision was repaired and the ObGyn prescribed docusate (Colace) to soften her stools.
A month later, the patient report-ed fecal incontinence. The ObGyn determined that the incontinence was related to the episiotomy, but did not feel that immediate attention was needed. When the condition did not improve, the patient saw a colorectal surgeon, who diagnosed a significant sphincter defect. The patient underwent a sphincteroplasty, with minor improvement.
PATIENT’S CLAIM The ObGyn failed to properly manage episiotomy healing. The patient remembers being told to stop docusate after she had passed one stool after delivery. A 10-day regimen of docusate and a diet to reduce defecation frequency should have been prescribed. Incontinence should have prompted an immediate referral to a colorectal surgeon.
PHYSICIAN’S DEFENSE Prompt surgical intervention was not necessary. Sphincteroplasty can be delayed until conservative methods have been tried. Episiotomy healing was properly addressed. Permanent incontinence is a known risk of the procedure.
VERDICT A $6 million New York verdict was returned.
Related Article: Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery? Errol R. Norwitz, MD, PhD (Examining the Evidence, August 2012)
MECONIUM ASPIRATION SYNDROME
A baby stayed in hospital for 3 weeks postdelivery due to meconium aspiration syndrome.
PARENTS’ CLAIM The resident who followed the mother during her pregnancy was negligent in allowing the pregnancy to progress to 46 weeks’ gestation before delivery.
DEFENDANTS’ DEFENSE The estimated date of conception was disputed. The resident claimed that the baby was born at 42 weeks’ gestation. An attending physician reviewed all prenatal visits with the resident. The mother’s cervix was never ripe before induction of labor. Aspiration occurred despite aggressive suctioning. The child has had no further respiratory issues since her neonatal discharge.
VERDICT An Illinois defense verdict was returned.
BOWEL INJURY AFTER HYSTERECTOMY
A woman underwent laparoscopic-assisted vaginal hysterectomy and was discharged the following day. Two days later, she went to an ED in acute distress. A bowel perforation was found during emergency surgery, and her colon was repaired. She made a full recovery.
PATIENT’S CLAIM The ObGyn was negligent in failing to properly evaluate the patient after surgery. The ObGyn also failed to explain the signs of a possible perforation to the patient before she left the hospital.
PHYSICIAN’S DEFENSE The patient’s postoperative course was normal while she was hospitalized. Bowel perforation is a known complication of the procedure. The patient had been informed of all the signs and symptoms of a bowel perforation and had been instructed to call the ObGyn or return to the hospital if she began to have any symptoms.
VERDICT A South Carolina defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]

Mutation could be target for MDS/AML treatment
Scientists have found evidence to suggest that a genetic alteration in osteoblasts can induce acute myeloid leukemia (AML).
And this provides a potential therapeutic target for AML and myelodysplastic syndromes (MDS).
Stavroula Kousteni, PhD, of Columbia University Medical Center in New York, and her colleagues described these findings in Nature.
The researchers discovered that an activating mutation of beta-catenin in mouse osteoblasts induces AML.
This mutation leads to cancer in adjacent hematopoietic stem cells (HSCs) through a series of events. First, the mutated beta-catenin protein moves from its normal location on the exterior of the osteoblast to the cell’s nucleus, where it activates production of the protein jagged1.
Jagged1 proteins are then shipped to the osteoblast’s exterior membrane, where they can bind to Notch proteins—which activate signaling pathways—on neighboring HSCs. When this happens, Notch transmits signals inside the HSCs that enable leukemic transformation.
To confirm the role of jagged1 in AML development, the investigators removed 1 allele of jagged1 in osteoblasts. This decreased Notch signaling in Lin-Sca+c-Kit+ cells, rescued anemia and deregulation of HSC lineage differentiation, and prevented AML development.
The researchers then evaluated the effects of blocking Notch signaling using a gamma-secretase inhibitor. The treatment reversed hematopoietic deregulation and myeloid expansion in the blood, marrow, and spleens of the mice and reversed their AML.
“If the [process] works the same way in humans, our study suggests practical ways that we may be able to intervene with a drug or an antibody,” Dr Kousteni said.
With this in mind, she and her colleagues analyzed cells from 107 patients with AML or MDS. About 38% of the patients had changes in beta-catenin, jagged1, and Notch signaling that mirrored the changes in the mice. But none of the 56 healthy control subjects studied had these changes.
The investigators therefore concluded that these findings provide new insight into AML/MDS pathogenesis and may have implications for treatment. ![]()
Scientists have found evidence to suggest that a genetic alteration in osteoblasts can induce acute myeloid leukemia (AML).
And this provides a potential therapeutic target for AML and myelodysplastic syndromes (MDS).
Stavroula Kousteni, PhD, of Columbia University Medical Center in New York, and her colleagues described these findings in Nature.
The researchers discovered that an activating mutation of beta-catenin in mouse osteoblasts induces AML.
This mutation leads to cancer in adjacent hematopoietic stem cells (HSCs) through a series of events. First, the mutated beta-catenin protein moves from its normal location on the exterior of the osteoblast to the cell’s nucleus, where it activates production of the protein jagged1.
Jagged1 proteins are then shipped to the osteoblast’s exterior membrane, where they can bind to Notch proteins—which activate signaling pathways—on neighboring HSCs. When this happens, Notch transmits signals inside the HSCs that enable leukemic transformation.
To confirm the role of jagged1 in AML development, the investigators removed 1 allele of jagged1 in osteoblasts. This decreased Notch signaling in Lin-Sca+c-Kit+ cells, rescued anemia and deregulation of HSC lineage differentiation, and prevented AML development.
The researchers then evaluated the effects of blocking Notch signaling using a gamma-secretase inhibitor. The treatment reversed hematopoietic deregulation and myeloid expansion in the blood, marrow, and spleens of the mice and reversed their AML.
“If the [process] works the same way in humans, our study suggests practical ways that we may be able to intervene with a drug or an antibody,” Dr Kousteni said.
With this in mind, she and her colleagues analyzed cells from 107 patients with AML or MDS. About 38% of the patients had changes in beta-catenin, jagged1, and Notch signaling that mirrored the changes in the mice. But none of the 56 healthy control subjects studied had these changes.
The investigators therefore concluded that these findings provide new insight into AML/MDS pathogenesis and may have implications for treatment. ![]()
Scientists have found evidence to suggest that a genetic alteration in osteoblasts can induce acute myeloid leukemia (AML).
And this provides a potential therapeutic target for AML and myelodysplastic syndromes (MDS).
Stavroula Kousteni, PhD, of Columbia University Medical Center in New York, and her colleagues described these findings in Nature.
The researchers discovered that an activating mutation of beta-catenin in mouse osteoblasts induces AML.
This mutation leads to cancer in adjacent hematopoietic stem cells (HSCs) through a series of events. First, the mutated beta-catenin protein moves from its normal location on the exterior of the osteoblast to the cell’s nucleus, where it activates production of the protein jagged1.
Jagged1 proteins are then shipped to the osteoblast’s exterior membrane, where they can bind to Notch proteins—which activate signaling pathways—on neighboring HSCs. When this happens, Notch transmits signals inside the HSCs that enable leukemic transformation.
To confirm the role of jagged1 in AML development, the investigators removed 1 allele of jagged1 in osteoblasts. This decreased Notch signaling in Lin-Sca+c-Kit+ cells, rescued anemia and deregulation of HSC lineage differentiation, and prevented AML development.
The researchers then evaluated the effects of blocking Notch signaling using a gamma-secretase inhibitor. The treatment reversed hematopoietic deregulation and myeloid expansion in the blood, marrow, and spleens of the mice and reversed their AML.
“If the [process] works the same way in humans, our study suggests practical ways that we may be able to intervene with a drug or an antibody,” Dr Kousteni said.
With this in mind, she and her colleagues analyzed cells from 107 patients with AML or MDS. About 38% of the patients had changes in beta-catenin, jagged1, and Notch signaling that mirrored the changes in the mice. But none of the 56 healthy control subjects studied had these changes.
The investigators therefore concluded that these findings provide new insight into AML/MDS pathogenesis and may have implications for treatment. ![]()
Sickle cell trait affects need for ESAs

Researchers may have discovered why African Americans on dialysis sometimes require higher doses of erythropoietin-stimulating agents (ESAs) than dialysis patients of other ethnicities.
The team found that sickle cell trait was more common in African Americans on dialysis than in the general African American population.
And patients with sickle cell trait required higher ESA doses than other African American dialysis patients to reach the same hemoglobin level.
The researchers reported these findings in the Journal of the American Society of Nephrology.
The team noted that kidney abnormalities have been reported in some individuals with sickle cell trait. And studies have shown that African Americans with kidney failure require higher doses of ESAs to treat anemia during dialysis. So researchers wondered if there was a correlation.
To find out, Vimal Derebail, MD, of the University of North Carolina at Chapel Hill, and his colleagues examined laboratory and clinical data concerning 5319 adult African American hemodialysis patients.
But the researchers looked at the presence of hemoglobin C trait as well as sickle cell trait.
In the entire study cohort, 542 (10.2%) patients had sickle cell trait, and 129 (2.4%) had hemoglobin C trait. There were no other hemoglobinopathy traits present.
Sickle cell trait was more common among dialysis patients than the general African American population—10.2% and 6.5%-8.7%, respectively (P<0.05).
Among the 5002 patients receiving ESAs, 10.3% had sickle cell trait and 2.4% had hemoglobin C trait.
The patients with hemoglobinopathy traits received higher median ESA doses than patients with normal traits—4737.4 units/treatment and 4364.1 units/treatment, respectively (P=0.02).
Having either hemoglobinopathy trait was associated with a 13.2% increase in ESA dose (P=0.001). And patients with either trait had a 30% increased risk of falling into the highest quartile of ESA dosing.
There was no significant difference in the dose increase according to trait type (P=0.10).
The researchers therefore said these findings suggest the presence of hemoglobinopathy traits, particularly sickle cell trait, may explain why greater ESA doses are administered to African American dialysis patients relative to Caucasian patients.
“While we don’t know whether there are any adverse consequences to this higher dose of medication yet, further policies and decisions regarding management of anemia in dialysis patients should take into account these findings,” Dr Derebail said.
He added that future research should also explore whether sickle cell trait is more common in dialysis patients because it contributes to kidney disease. ![]()
Researchers may have discovered why African Americans on dialysis sometimes require higher doses of erythropoietin-stimulating agents (ESAs) than dialysis patients of other ethnicities.
The team found that sickle cell trait was more common in African Americans on dialysis than in the general African American population.
And patients with sickle cell trait required higher ESA doses than other African American dialysis patients to reach the same hemoglobin level.
The researchers reported these findings in the Journal of the American Society of Nephrology.
The team noted that kidney abnormalities have been reported in some individuals with sickle cell trait. And studies have shown that African Americans with kidney failure require higher doses of ESAs to treat anemia during dialysis. So researchers wondered if there was a correlation.
To find out, Vimal Derebail, MD, of the University of North Carolina at Chapel Hill, and his colleagues examined laboratory and clinical data concerning 5319 adult African American hemodialysis patients.
But the researchers looked at the presence of hemoglobin C trait as well as sickle cell trait.
In the entire study cohort, 542 (10.2%) patients had sickle cell trait, and 129 (2.4%) had hemoglobin C trait. There were no other hemoglobinopathy traits present.
Sickle cell trait was more common among dialysis patients than the general African American population—10.2% and 6.5%-8.7%, respectively (P<0.05).
Among the 5002 patients receiving ESAs, 10.3% had sickle cell trait and 2.4% had hemoglobin C trait.
The patients with hemoglobinopathy traits received higher median ESA doses than patients with normal traits—4737.4 units/treatment and 4364.1 units/treatment, respectively (P=0.02).
Having either hemoglobinopathy trait was associated with a 13.2% increase in ESA dose (P=0.001). And patients with either trait had a 30% increased risk of falling into the highest quartile of ESA dosing.
There was no significant difference in the dose increase according to trait type (P=0.10).
The researchers therefore said these findings suggest the presence of hemoglobinopathy traits, particularly sickle cell trait, may explain why greater ESA doses are administered to African American dialysis patients relative to Caucasian patients.
“While we don’t know whether there are any adverse consequences to this higher dose of medication yet, further policies and decisions regarding management of anemia in dialysis patients should take into account these findings,” Dr Derebail said.
He added that future research should also explore whether sickle cell trait is more common in dialysis patients because it contributes to kidney disease. ![]()
Researchers may have discovered why African Americans on dialysis sometimes require higher doses of erythropoietin-stimulating agents (ESAs) than dialysis patients of other ethnicities.
The team found that sickle cell trait was more common in African Americans on dialysis than in the general African American population.
And patients with sickle cell trait required higher ESA doses than other African American dialysis patients to reach the same hemoglobin level.
The researchers reported these findings in the Journal of the American Society of Nephrology.
The team noted that kidney abnormalities have been reported in some individuals with sickle cell trait. And studies have shown that African Americans with kidney failure require higher doses of ESAs to treat anemia during dialysis. So researchers wondered if there was a correlation.
To find out, Vimal Derebail, MD, of the University of North Carolina at Chapel Hill, and his colleagues examined laboratory and clinical data concerning 5319 adult African American hemodialysis patients.
But the researchers looked at the presence of hemoglobin C trait as well as sickle cell trait.
In the entire study cohort, 542 (10.2%) patients had sickle cell trait, and 129 (2.4%) had hemoglobin C trait. There were no other hemoglobinopathy traits present.
Sickle cell trait was more common among dialysis patients than the general African American population—10.2% and 6.5%-8.7%, respectively (P<0.05).
Among the 5002 patients receiving ESAs, 10.3% had sickle cell trait and 2.4% had hemoglobin C trait.
The patients with hemoglobinopathy traits received higher median ESA doses than patients with normal traits—4737.4 units/treatment and 4364.1 units/treatment, respectively (P=0.02).
Having either hemoglobinopathy trait was associated with a 13.2% increase in ESA dose (P=0.001). And patients with either trait had a 30% increased risk of falling into the highest quartile of ESA dosing.
There was no significant difference in the dose increase according to trait type (P=0.10).
The researchers therefore said these findings suggest the presence of hemoglobinopathy traits, particularly sickle cell trait, may explain why greater ESA doses are administered to African American dialysis patients relative to Caucasian patients.
“While we don’t know whether there are any adverse consequences to this higher dose of medication yet, further policies and decisions regarding management of anemia in dialysis patients should take into account these findings,” Dr Derebail said.
He added that future research should also explore whether sickle cell trait is more common in dialysis patients because it contributes to kidney disease. ![]()
High-volume centers better for severe sepsis patients

Credit: CDC
A new study suggests that “practice makes perfect” when it comes to caring for patients with severe sepsis.
Researchers found that patients admitted to academic medical centers with a higher volume of severe sepsis patients had significantly lower mortality rates than patients treated at centers with lower volumes of sepsis patients.
And the superior outcomes did not come at a greater cost.
Allan J. Walkey, MD, of the Boston University School of Medicine in Massachusetts, and his colleagues reported these findings in the American Journal of Respiratory and Critical Care Medicine.
The researchers noted that processes of care can influence outcomes in patients with severe sepsis. However, it hasn’t been clear whether a hospital’s level of experience in caring for patients with severe sepsis affects patient outcomes.
So Dr Walkey and his colleagues conducted a large, retrospective study to find out. The team analyzed data from academic hospitals across the US, provided by the University HealthSystem Consortium.
They identified 56,997 patients with severe sepsis who were admitted to 124 academic medical centers in 2011.
The patients’ median length of stay was 12.5 days, the median direct cost for each patient was $26,304, and the average hospital mortality was 25.6 ± 5.3%.
Hospitals caring for more sepsis patients had a 7% lower mortality rate than hospitals with lower volumes.
The high-volume medical centers (604-977 cases) had a 22.2% adjusted mortality rate, and the lower-volume hospitals (30-317) had a 29.2% adjusted mortality rate (P<0.01).
There was no significant difference in direct costs between the low-volume and high-volume centers (P=0.79).
“Given the lack of new drugs to treat severe sepsis, medical professionals must look at other ways to increase patient safety and positive outcomes, including the process of how we deliver care,” Dr Walkey said.
“Our study results demonstrate that hospitals with more experience caring for patients with severe sepsis were able to achieve better outcomes than hospitals with less experience with sepsis, possibly due to better processes of care for patients with sepsis.” ![]()
Credit: CDC
A new study suggests that “practice makes perfect” when it comes to caring for patients with severe sepsis.
Researchers found that patients admitted to academic medical centers with a higher volume of severe sepsis patients had significantly lower mortality rates than patients treated at centers with lower volumes of sepsis patients.
And the superior outcomes did not come at a greater cost.
Allan J. Walkey, MD, of the Boston University School of Medicine in Massachusetts, and his colleagues reported these findings in the American Journal of Respiratory and Critical Care Medicine.
The researchers noted that processes of care can influence outcomes in patients with severe sepsis. However, it hasn’t been clear whether a hospital’s level of experience in caring for patients with severe sepsis affects patient outcomes.
So Dr Walkey and his colleagues conducted a large, retrospective study to find out. The team analyzed data from academic hospitals across the US, provided by the University HealthSystem Consortium.
They identified 56,997 patients with severe sepsis who were admitted to 124 academic medical centers in 2011.
The patients’ median length of stay was 12.5 days, the median direct cost for each patient was $26,304, and the average hospital mortality was 25.6 ± 5.3%.
Hospitals caring for more sepsis patients had a 7% lower mortality rate than hospitals with lower volumes.
The high-volume medical centers (604-977 cases) had a 22.2% adjusted mortality rate, and the lower-volume hospitals (30-317) had a 29.2% adjusted mortality rate (P<0.01).
There was no significant difference in direct costs between the low-volume and high-volume centers (P=0.79).
“Given the lack of new drugs to treat severe sepsis, medical professionals must look at other ways to increase patient safety and positive outcomes, including the process of how we deliver care,” Dr Walkey said.
“Our study results demonstrate that hospitals with more experience caring for patients with severe sepsis were able to achieve better outcomes than hospitals with less experience with sepsis, possibly due to better processes of care for patients with sepsis.” ![]()
Credit: CDC
A new study suggests that “practice makes perfect” when it comes to caring for patients with severe sepsis.
Researchers found that patients admitted to academic medical centers with a higher volume of severe sepsis patients had significantly lower mortality rates than patients treated at centers with lower volumes of sepsis patients.
And the superior outcomes did not come at a greater cost.
Allan J. Walkey, MD, of the Boston University School of Medicine in Massachusetts, and his colleagues reported these findings in the American Journal of Respiratory and Critical Care Medicine.
The researchers noted that processes of care can influence outcomes in patients with severe sepsis. However, it hasn’t been clear whether a hospital’s level of experience in caring for patients with severe sepsis affects patient outcomes.
So Dr Walkey and his colleagues conducted a large, retrospective study to find out. The team analyzed data from academic hospitals across the US, provided by the University HealthSystem Consortium.
They identified 56,997 patients with severe sepsis who were admitted to 124 academic medical centers in 2011.
The patients’ median length of stay was 12.5 days, the median direct cost for each patient was $26,304, and the average hospital mortality was 25.6 ± 5.3%.
Hospitals caring for more sepsis patients had a 7% lower mortality rate than hospitals with lower volumes.
The high-volume medical centers (604-977 cases) had a 22.2% adjusted mortality rate, and the lower-volume hospitals (30-317) had a 29.2% adjusted mortality rate (P<0.01).
There was no significant difference in direct costs between the low-volume and high-volume centers (P=0.79).
“Given the lack of new drugs to treat severe sepsis, medical professionals must look at other ways to increase patient safety and positive outcomes, including the process of how we deliver care,” Dr Walkey said.
“Our study results demonstrate that hospitals with more experience caring for patients with severe sepsis were able to achieve better outcomes than hospitals with less experience with sepsis, possibly due to better processes of care for patients with sepsis.” ![]()
Outcomes of ESBL‐EK UTI
Community‐onset urinary tract infection (UTI) is a common bacterial infection encountered in hospital medicine, accounting for >350,000 hospital admissions and $3.4 billion in healthcare costs annually.[1] High proportions of these infections are caused by Enterobacteriaceae, primarily Escherichia coli and Klebsiella species.[2] The prevalence of hospitalized patients with UTI caused by multidrug‐resistant E coli and Klebsiella species has increased.[3, 4, 5] Enterobacteriaceae can produce hydrolytic enzymes, specifically extended‐spectrum ‐lactamases (ESBL), which result in high rates of bacterial resistance to frequently used agents.[6] Global rates vary widely by region, and recent surveillance data showed increasing rates of clinical isolates in North America are ESBL producers.[7, 8, 9, 10] More alarming is the emergence of these resistant organisms in the community.[11]
In addition to ‐lactams, ESBL production is associated with resistance to other antibiotic classes (fluoroquinolones, aminoglycosides, and sulfonamides), and has become an important cause of failed therapy.[12, 13] Consequently, providing adequate and timely antibiotics can become convoluted due to fewer remaining treatment options. Therefore, carbapenems, which are less susceptible to hydrolysis by these enzymes, have become the preferred therapy for infection with ESBL‐producing pathogens.[3, 13, 14]
The consequences of ESBL production, mainly in bloodstream infection (BSI), are well characterized, including notable delays in receipt of appropriate antibiotic therapy, prolonged length of stay (LOS), and increased cost of care.[15, 16] Importantly, others have found higher rates of mortality.[17, 18, 19, 20, 21] However, the impact on outcomes specifically in UTI remains unclear. As a result of the prevalence of UTI admissions to the hospital, the increasing incidence of ESBLs, and the potential impact on the clinical course of care, additional study is required to support best practices for this common diagnosis.
PATIENTS AND METHODS
Study Subjects and Design
This was a retrospective, matched‐cohort analysis of patients admitted to the hospital with UTI (International Classification of Diseases, 9th Revision‐Clinical Modification code 599.0) caused by extended‐spectrum b‐lactamase‐producing Escherichia coli and Klebsiella species (ESBL‐EK). Patients admitted to Hartford Hospital from September 1, 2011 through August 31, 2012 with UTI present on admission (48 hours) were evaluated. Cases were patients 18 years of age, with a positive urine culture (104 CFU/mL) for an ESBL‐producing organism (48 hours of admission), who received antibiotic treatment directed at the positive culture for 48 hours, and beginning prior to availability of in vitro susceptibility results. Cases were identified by a detailed search of the microbiology department database of ESBL‐EK cultures. Only the first positive (index) culture for each patient was included. Bacteremia was defined as isolation of a blood culture organism identical to the one isolated from the urine culture. Patients were excluded if they were discharged, died, or placed on palliative care prior to or on the date of urine collection. Controls (patients admitted with UTI on admission caused by nonESBL‐EK) were matched to cases in a 1:1 fashion on the basis of isolated urinary pathogen, age (5 years), sex, and race. ESBL‐producing organisms were identified and classified according to the Clinical and Laboratory Standards Institute guidelines.[22]
Data Collection
Once patients were identified, the following information was collected from the patient's medical record by 2 investigators using a standardized case report form: demographic characteristics, comorbid conditions and severity of comorbidities using the Charlson comorbidity index, recent patient medical history, and clinical and economic attributes.[23]
The study was approved by the institutional review board of Hartford Hospital. An informed consent waiver was granted as all data were currently in existence and no patient‐specific interventions were conducted for the study. The collection of data was in compliance with the Health Insurance Portability and Accountability Act of 1996.
Outcomes and Definitions
Onset of UTI was defined as the date/time of the index culture collection. An initial antibiotic treatment was a course of therapy initiated empirically (prior to availability of in vitro susceptibility) and that continued for 48 hours. An appropriate empiric antibiotic was defined as an initial antibiotic that ultimately possessed in vitro activity against the isolated pathogen.
The primary clinical outcomes were initial antibiotic response and clinical response. Initial antibiotic response was defined as failure if there was lack of clinical improvement, as evident by a switch to an alternative antibiotic (excluding switches to similar/narrower‐spectrum agents and courses begun at discharge) or infection‐related mortality while receiving the initial antibiotic. Patients were deemed clinical success if they were clinically stable at discharge or end of therapy, whichever occurred first, with resolution of signs and symptoms of infection. Clinical failures were patients with (1) infection‐related mortality or (2) readmission to hospital with UTI within 30 days of discharge. Clinical response was chosen as a primary outcome because significant mortality attributed to UTI was not anticipated. Secondary clinical outcomes included: time to appropriate antibiotic therapy, mortality (all cause and infection related), and 30‐day readmission (all cause and UTI related). Patients were considered to have received appropriate antibiotic therapy when they had received their first dose of antibiotic with activity against the isolated pathogen based on the patient‐specific in vitro susceptibility results. Time to appropriate antibiotics was defined as the elapsed time (hours) between the index culture collection and the initial dose of appropriate antibiotic therapy. All‐cause mortality was defined as any cause of death at the end of hospitalization, whereas infection‐related mortality was defined as death occurring while receiving antibiotics for the index infection, without any other obvious cause of death.
The primary economic outcomes were hospital LOS, costs, and reimbursement. Antibiotic costs were calculated for each patient according to acquisition costs. Additional economic outcomes evaluated were net hospital reimbursement and primary payor. Net hospital reimbursement was calculated as the difference between hospital reimbursement and hospital costs for each patient. Hospital costs were calculated as the direct plus indirect hospitalization costs for each patient, as determined by our institutional accounting department. All economic values were reported in United States dollars.
Statistical Analysis
Statistical comparisons were performed between cases and controls using a paired t test or Wilcoxon signed rank test for continuous variables, where appropriate. Dichotomous variables were compared using the McNemar test. Multivariate logistic regression was performed to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to determine independent risk factors for ESBL‐EK, including all pertinent variables with a P value <0.1 in univariate analyses. All data were analyzed using SigmaStat version 2.03 (IBM/SPSS, Armonk, NY). A P value of 0.05 was considered statistically significant.
RESULTS
Patient Population
Between September 2011 and August 2012, there were 220 specimens of ESBL‐related infection and 2345 patients admitted with a UTI on admission. Eighty‐four were confirmed ESBL‐EK cases (3.6%), and 55 met criteria for inclusion. Twenty‐nine of these cases were excluded because the index culture was polymicrobial, for which the response to antibiotics for ESBL‐EK could not be elicited (n=22); they had incomplete medical records (n=4); or they did not have a matched control patient (n=3). Fifty‐five matched control patients were identified, resulting in 110 patients overall.
Patient demographics and baseline characteristics are shown in Table 1. Patients with ESBL‐EK UTI were more likely to have diabetes mellitus, chronic obstructive pulmonary disorder, and a history of recurrent UTIs. They were more likely to have recently received antibiotics, been hospitalized, or had isolation of an ESBL‐producing organism. No significant differences in Charlson comorbidity index, recent immunosuppressive therapy, or urinary catheterization were observed. Compared with controls, patients with ESBL‐EK UTI were more frequently transferred from another healthcare facility, although the difference was not statistically significant (P=0.06). In the multivariate regression model, diabetes mellitus (OR: 4.4, 95% CI: 1.711.5; P=0.002), history of recurrent UTIs (OR: 4.4, 95% CI: 1.810.9; P=0.001), and transfer from another healthcare facility (OR: 2.38, 95% CI: 1.05.7; P=0.05) were independently associated with ESBL‐EK UTI. Previous isolation of an ESBL‐producing organism (P<0.001) was unable to be included in the multivariate logistic regression model because only patients with UTI caused by ESBL‐EK were positive for this variable. However, as noted in Table 1, 27.2% of cases had isolation of an ESBL‐producing organism in the previous year.
| ESBL Positive, n=55 | ESBL Negative, n=55 | Pa | |
|---|---|---|---|
| |||
| Demographics | |||
| Age, y, median (IQR) | 77 (6785) | 77 (6685) | 0.83b |
| Female | 36 (65.4) | 36 (65.4) | 1.00 |
| White | 42 (76.4) | 42 (76.4) | 1.00 |
| Black | 5 (9.1) | 5 (9.1) | 1.00 |
| Hispanic/Latino | 6 (10.9) | 6 (10.9) | 1.00 |
| Other | 2 (3.6) | 2 (3.6) | 1.00 |
| Comorbidities | |||
| Diabetes mellitus | 25 (45.5) | 10 (18.1) | 0.004 |
| COPD | 15 (27.2) | 6 (10.9) | 0.04 |
| Liver disease | 2 (3.6) | 1 (1.8) | 1.00 |
| Hemodialysis | 9 (16.4) | 6 (10.9) | 0.58 |
| Hematological malignancy | 3 (5.5) | 2 (3.6) | 1.00 |
| Solid malignancy | 13 (23.6) | 9 (16.4) | 0.45 |
| HIV/AIDS | 0 | 1 (1.8) | 1.00 |
| Age >65 years | 44 (80.0) | 43 (78.2) | 1.00 |
| Urinary abnormality | 15 (27.2) | 15 (27.2) | 1.00 |
| Charlson comorbidity index, median (IQR) | 3 (24) | 2 (13.8) | 0.19 |
| History | |||
| Previous hospitalizationc | 38 (69.1) | 24 (43.6) | 0.01 |
| Previous antibioticsd | 23 (41.8) | 12 (21.8) | 0.04 |
| Recent immunosuppressive therapye | 9 (16.4) | 3 (5.5) | 0.11 |
| History of recurrent UTIsf | 29 (52.7) | 12 (21.8) | 0.001 |
| History of urinary catheterizationg | 18 (32.7) | 14 (25.4) | 0.45 |
| Previous genitourinary procedure/surgery | 10 (18.2) | 6 (10.9) | 0.39 |
| Previous ESBL‐producing organismh | 15 (27.2) | 0 | <0.001 |
| Clinical features | |||
| Transfer from another healthcare facility | 27 (49.1) | 17 (21.0) | 0.06 |
| ICU admission | 12 (21.8) | 7 (12.7) | 0.33 |
| Bacteremia | 7 (12.7) | 5 (9.1) | 0.75 |
| Infectious Diseases consulted | 39 (70.1) | 16 (29.1) | <0.001 |
| Empiric ‐lactam (noncarbapenem) | 35 (63.6) | 50 (90.9) | 0.001 |
Isolate Characteristics
The distribution of causative pathogens in each cohort was: 44 (80%) Escherichia coli, 8 (14.5%) Klebsiella pneumoniae, and 3 (5.5%) Klebsiella oxytoca. In vitro nonsusceptibility profiles of the 55 ESBL‐EK cases are characterized in Figure 1. The most active agents were carbapenems, with 98.2% susceptibility to the entire isolate profile, whereas <10% of isolates were susceptible to the fluoroquinolones. All ESBL‐producing isolates were resistant to cefepime.
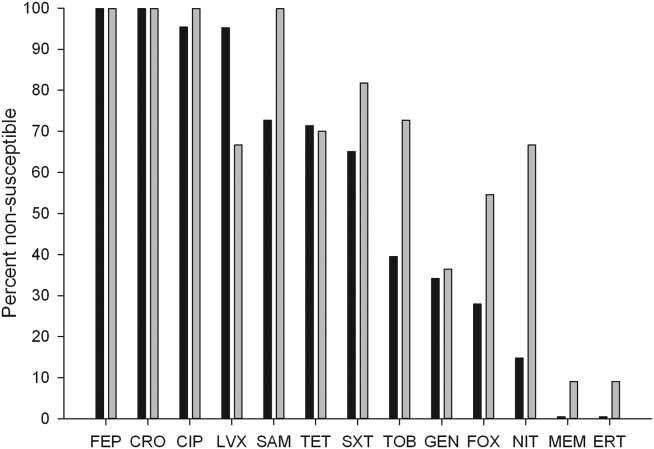
Failure on Initial Antibiotic Regimen
Initial antibiotic therapy is shown in Table 2. A majority of patients (87.2%) were initially treated with a ‐lactam. Empiric carbapenem use was greater in ESBL‐EK cases (18.1% vs 0%; P<0.001), and there were no other significant differences in the distribution of initial antibiotic therapy between cohorts. Less than one‐quarter of ESBL‐EK patients (23.6%) received appropriate initial therapy, whereas 98.2% of controls were initially treated appropriately (P<0.001).
| Initial Antibiotic | ESBL Positive, n=55 | ESBL Negative, n=55 | Pa |
|---|---|---|---|
| |||
| Ceftriaxone | 21 (38.1) | 32 (58.1) | 0.06 |
| Cefepime | 10 (18.2) | 12 (21.8) | 0.81 |
| Ertapenem | 7 (12.7) | 0 | 0.02 |
| Levofloxacin | 6 (10.9) | 4 (7.3) | 0.74 |
| Cefazolin | 0 | 4 (7.3) | 0.13 |
| Piperacillin‐tazobactam | 3 (5.5) | 0 | 0.24 |
| Ciprofloxacin | 2 (3.6) | 1 (1.8) | 1.00 |
| Doripenem | 2 (3.6) | 0 | 0.48 |
| Trimethoprim‐sulfamethoxazole | 2 (3.6) | 0 | 0.48 |
| Meropenem | 1 (1.8) | 0 | 1.00 |
| Cephalexin | 1 (1.8) | 0 | 1.00 |
| Aztreonam | 0 | 2 (3.6) | 0.48 |
Compared with controls, failure of initial antibiotic therapy was more common in patients with ESBL‐EK UTI, resulting in a significantly longer time to appropriate antibiotics (Table 3). Among ESBL‐EK UTI cases, failure of initial antibiotic therapy was greater for patients who received noncarbapenem ‐lactams (85.7%) as compared to those who empirically received a carbapenem (0%) (P<0.001). Antibiotic failure (>2 patients treated) in ESBL‐EK was highest with the following antibiotics: cefepime (100% [10/10]), piperacillin‐tazobactam (100% [3/3]), and ceftriaxone (76.2% [16/21]).
| ESBL Positive, n=55 | ESBL Negative, n=55 | Pa | |
|---|---|---|---|
| |||
| Clinical parameter | |||
| Initial antibiotic failure | 34 (61.8) | 3 (5.5) | <0.001 |
| Escalation to an alternative antibiotic | 33 (60.0) | 3 (5.5) | <0.001 |
| Time to appropriate antibiotics, h, median (IQR) | 51 (32.560.8) | 2.5 (1.07.2) | <0.001b |
| Appropriate empiric antibiotics | 13 (23.6) | 54 (98.2) | <0.001 |
| Clinical success | 47 (85.5) | 52 (94.5) | 0.23 |
| All‐cause mortality | 5 (9.1) | 1 (1.8) | 0.21 |
| Infection‐related mortality | 4 (7.2) | 1 (1.8) | 0.37 |
| All‐cause 30‐day readmission | 12 (21.8) | 15 (27.2) | 0.63 |
| UTI‐related 30‐day readmission | 4 (7.2) | 2 (3.6) | 0.68 |
| Economic parameterb | |||
| Length of stay, d, median (IQR) | 6 (48) | 4 (36) | 0.02 |
| Total hospital cost, median (IQR)c | 10,741 (684615,819) | 7,083 (566711,652) | 0.02 |
| Bed cost, % total cost, median (IQR) | 57.5 (51.666.0) | 63.8 (51.973.5) | 0.21 |
| Antibiotic cost, % total cost, median (IQR) | 0.5 (0.12.0) | 0.1(0.030.2) | <0.001 |
| Primary payor, n (%) | |||
| Medicare | 44 (80) | 44 (80) | 1.00 |
| Medicaid | 7 (12.7) | 3 (5.4) | 0.32 |
| Private insurance | 2 (3.6) | 2 (3.6) | 0.61 |
| Managed care | 2 (3.6) | 6 (10.9) | 0.27 |
Clinical Outcomes
There were no significant differences in clinical success, mortality, or 30‐day readmission between cohorts (Table 3). Among ESBL‐EK patients, those who received appropriate antibiotics within 48 hours were significantly more likely to achieve treatment success (100% vs 77.1%; P=0.04). All 8 ESBL‐EK treatment failures (4 infection‐related mortality and 4 UTI readmitted with the same ESBL pathogen) failed to receive appropriate antibiotics within 48 hours of culture collection.
More ESBL‐EK patients required a switch in their antibiotics. Within the subgroup of ESBL‐EK patients with an escalation in antibiotics, ertapenem was added to 19 of 33 (57.6%) cases.
Economic Outcomes
ESBL‐EK patients who received inappropriate initial therapy received longer antibiotic treatment courses than those empirically treated with a carbapenem (meanstandard deviation, 8.93.7 vs 6.23.2 days, respectively; P=0.04). When compared to non‐ESBL infection, ESBL‐EK patients required more days of antibiotic therapy (median 8 vs 5 days; P=0.03). The median LOS was significantly longer and total hospital costs were significantly greater for ESBL cases. Antibiotic costs contributed minimally to the overall cost, accounting for <1% (0.5% for cases vs 0.1% for controls), regardless of ESBL status. A comparison of economic outcomes is presented in Table 3. LOS among ESBL cases was not different between those discharged with and without continued antimicrobial therapy. Moreover, for those discharged on antimicrobial therapy, the utilization of either the oral or intravenous route did not delay discharge (data not shown).
The payor mix was similar between cases and controls. Given the predominately elderly population, Medicare was the primary payor for a majority of patients. Median differences in cost and reimbursement between cohorts (ESBL‐EK vs nonESBL‐EK) were $3658 (P=0.02) and $469 (P=0.56), respectively. As a result, median loss per patient with ESBL‐EK infection was $3189 when compared with controls.
Bacteremia
All cases of bacteremia were present on admission. Bacteremic UTI due to ESBL‐EK was associated with initial antibiotic failure (85.7% [6/7] vs 0% [0/5]; P=0.015), delayed appropriate therapy (median, 56 vs 2 hours; P=0.003), longer median hospital stays (11 vs 5 days; P=0.05), and higher median cost ($27,671 vs $5898; P=0.03) as compared with bacteremic UTI due to non‐ESBL‐EK. Infection‐related mortality occurred in 2 ESBL‐EK bacteremic patients, but no mortality was observed among the nonESBL‐EK bacteremic UTI cohort (28.6% [2/7] vs 0% [0/5]; P=0.47].
DISCUSSION
This matched cohort analysis revealed that ESBL‐EK has detrimental effects on the outcomes of patients admitted to the hospital with UTI. While matching for demographics and infecting pathogen, patients with ESBL‐EK UTI had diminished initial antibiotic response and considerably longer time to appropriate antibiotic therapy (48 hours longer) than their non‐ESBL comparator. Despite significant delays in appropriate therapy, we saw no attributable difference in clinical outcome and mortality; however, numerical trends toward increased risk were observed in ESBL‐EK patients. Although clinical response was largely unchanged, prolonged hospitals stays and increased cost of care were endured by ESBL‐EK patients.
Antimicrobial resistance, a primary factor in the postponement of appropriate antibiotic therapy, is a worrisome occurrence with meaningful clinical implications.16[21, 24] In BSI, delayed appropriate therapy due to ESBLs has been associated with prolonged LOS, increased costs, and increased mortality.[20, 25] However, the clinical significance of ESBL production on patient outcomes in UTI remains equivocal. To the best of our knowledge, this is the first matched control analysis evaluating the clinical and economic impact of ESBL specifically in UTI. We saw a 50% increase in the median LOS (from 4 to 6 days) and cost of care (additional $3658 per patient) in the ESBL‐EK UTI cohort. Albeit as small subpopulation, patients with bacteremic UTI due to ESBL‐EK had significantly longer hospital stays and increased cost of care as compared with nonESBL‐EK bacteremic UTI. These economic findings are consistent with data from other investigations. For example, a matched case‐control study of infection (51.5% UTI) due to ESBL‐producing E coli and K pneumoniae by Lautenbach and colleagues found an additional 60‐hour (72 vs 11.5 hours, P<0.001) delay in time to appropriate antibiotics for case patients, resulting in significantly longer LOS (1.8 times) and increased hospital charges (2.9 times).[17] With respect to costs, a matched case‐control analysis of ESBL‐EK in non‐UTI saw a 70% increase in cost ($41,353 vs $24,902).[26] Moreover, the increased cost in that study, like this one, was driven primarily by LOS (additional 9.7 days) and not drug utilization, with antibiotic costs representing <2% of the total hospitalization cost. Tumbarello and colleagues observed an approximate 50% increase in LOS and hospital costs in patients with BSI caused by ESBL‐producing E coli.[20]
Distinctive from those studies, we investigated the significance of ESBL production on hospital reimbursement. Despite the additional healthcare resource utilization (50% greater), we saw no appreciable increase (<5%) in median hospital reimbursement. Given that the primary payors between cohorts were comparable, infection with ESBL‐producing bacteria may result in a potential loss of income if optimal treatment is not initiated on admission.
The risk factors for development of UTI due to ESBL‐EK are well defined.[27, 28, 29, 30, 31, 32] Two scoring systems, an Italian and a Duke model, have identified patients at increased risk of harboring ESBL‐producing organisms on hospital admission.[33, 34] The features of each model center on established risk factors for ESBL‐EK UTI. In our study population, these scoring model features were more common in ESBL‐EK patients, supporting their potential application in UTI. However, because of our study design (infected controls) and matching criteria, only 2 features (recent antibiotics and previous hospitalization) achieved statistical significance as detectable risk factors in our population. Regardless, these data, coupled with increasing prevalence of UTI with ESBL‐producing bacteria, provide justification and advocacy for the empiric use of ESBL active antibiotics (ie, carbapenems) in certain high‐risk individuals, particularly those patients with a previous history of ESBL or those with multiple risk factors identified in our study as well as others (previous hospitalization, recent antibiotic exposure). Importantly, an aggressive de‐escalation strategy should be used to temper collateral damage for patients with non‐ESBL infections. Moreover, the utilization of oral therapies beyond the fluoroquinolones and trimethoprim‐sulfamethoxazole, such as fosfomycin and nitrofurantoin, coupled with coordinated transitions of care, may alleviate the demand for intravenous access in patients prepared for discharge.[35, 36]
This study is not without limitations. As only a distinct period in time was studied, we are unable to determine the implications of previous episodes of UTI on the current admission. Although the Charlson comorbidity score was not significantly different between the 2 patient cohorts, ESBL‐EK patients were more likely to have several demographic features (ie, diabetes mellitus, recurrent UTIs, previous hospitalization, and recent antibiotic exposure), which are to be expected in the ESBL population.[37, 38] Although these differences have been observed as expected, we believe the driver of prolonged LOS and increased costs of care stem from inappropriate initial antibiotic therapy as evident by the initial clinical failure observed in ESBL‐EK patients. It should also be noted that we defined antibiotics as appropriate based on the laboratory criteria for susceptibility, as such agents that have high concentration in the urinary tract (ie, fluoroquinolones) may be effective despite these laboratory definitions.[17] For instance, 10 of our ESBL‐EK patients never received appropriate antibiotics (3 fluoroquinolones, 7 noncarbapenem ‐lactams) as defined by laboratory‐based susceptibility testing, 8 of whom experienced clinical success. Previous studies have shown discordance between phenotypic ESBL‐related resistance profiles and outcomes.[17, 18, 19, 20, 21, 25, 39, 40]
In summary, recent increases in antimicrobial resistance present ongoing challenges in the treatment of hospitalized patients, as appropriate treatment options are extremely limited. Our findings strengthen the consortium of data stating that antimicrobial resistance unfavorably impacts patient outcomes.[41, 42] ESBL‐EK in UTI is associated with high rates of failure of initial antibiotic therapy, prolonged LOS, and increased cost of care. Furthermore, the added cost associated with UTI due to ESBL‐EK is not recognized in hospital reimbursement, as evident by a $3200 net loss relative to reimbursement. This loss appears to be solely due to the increased LOS, as antibiotic costs were <1% of cost of care. Moreover, these negative consequences could be even more pronounced at institutions with a higher prevalence of ESBL infection. A multidisciplinary approach (infection control, microbiology) using these data as a benchmark, may enhance the detection, treatment, and prevention of these ESBL‐producing organisms. With high levels of coresistance to noncarbapenem ‐lactams and fluoroquinolones, providers should be cognizant of organisms capable of producing ESBL when selecting initial antibiotic therapy in high‐risk populations. Early recognition and timely initiation of appropriate antibiotic therapy appear paramount to minimizing the burden of ESBL‐EK in patients admitted to the hospital with a UTI.
Acknowledgements
The authors thank Gilbert Fotunato for his assistance with administrative data retrieval.
Disclosures
This work is supported by a grant from Merck & Co., Inc. D.P.N. reports having received grant support and honorarium from Merck & Co., Inc. S.H.M and L.O.T report no conflicts of interest relevant to this article.
- , , , et al. Urologic diseases in America project: analytical methods and principal findings. J Urol. 2005;173(3):933–937.
- . Urinary tract pathogens in complicated infection and in elderly individuals. J Infect Dis. 2001;183(suppl 1):S5–S8.
- , , , , . Antimicrobial susceptibility of global inpatient urinary tract isolates of Escherichia coli: results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) program: 2009–2010. Diagn Microbiol Infect Dis. 2011;70(4):507–511.
- , . Extended‐spectrum β‐lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657–686.
- , , . Extended‐spectrum β‐lactamase producing Escherichia coli: changing epidemiology and clinical impact. Curr Opin Infect Dis. 2010;23(4):320–326.
- . Defining an extended‐spectrum beta‐lactamase. Clin Microbiol Infect. 2008;14(suppl 5):3–10.
- , , , , , . Antimicrobial susceptibility among organisms from the Asia/Pacific Rim, Europe and Latin and North America collected as part of TEST and the in vitro activity of tigecycline. J Antimicrob Chemother. 2007;60(5):1018–1029.
- , , , . Variations in the prevalence of strains expressing an extended‐spectrum β‐lactamase phenotype and characterization of isolates from Europe, the Americas, and the Western Pacific region. Clin Infect Dis. 2001;32(suppl 2):S94–S103.
- National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004. Am J Infect Control. 2004;32(8):470–485.
- , . Prevalence and antimicrobial susceptibility data for extended‐spectrum β‐lactamase‐ and AmpC‐producing Enterobacteriaceae from the MYSTIC Program in Europe and the United States (1997–2004). Diagn Microbiol Infect Dis. 2005;53(4):257–264.
- , , , . Emergence of Enterobacteriaceae producing extended‐spectrum b‐lactamases (ESBLs) in the community. J Antimicrob Chemother. 2005;56(1):52–59.
- , , , et al. Epidemiology of ciprofloxacin resistance and its relationship to extended‐spectrum B‐lactamase production in Klebsiella pneumoniae isolates causing bacteremia. Clin Infect Dis. 2000;30(4):473–478.
- , , , , , Epidemiological investigation of fluoroquinolone resistance in infections due to extended‐spectrum‐β‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae. Clin Infect Dis. 2001;33(8):1288–1294.
- , , , . High levels of antimicrobial coresistance among extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae. Antimicrob Agents Chemother. 2005;49(5):2137–2139.
- . Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31(suppl 4):S131–S138.
- . The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin Infect Dis. 2006;42(suppl 2):S82–S89.
- , , , , , Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes. Clin Infect Dis. 2001:32(8):1162–1171.
- , , , et al. Predictors of mortality in patients with bloodstream infections caused by extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae: importance of inadequate initial antimicrobial treatment. Antimicrob Agents Chemother. 2007;51(6):1987–1994.
- , . Mortality and delay in effective therapy associated with extended‐spectrum β lactamase production in Enterobacteriaceae bacteraemia: a systematic review and meta‐analysis. J Antimicrob Chemother. 2007;60(5):913–920.
- , , , et al. Costs of bloodstream infections caused by Escherichia coli and influence of extended‐spectrum‐β‐lactamase production and inadequate initial antibiotic therapy. Antimicrob Agents Chemother. 2010;54(10):4085–4091.
- , , . Effects of confounders and intermediates on the association of bacteraemia caused by extended‐spectrum β‐lactamase‐producing Enterobacteriaceae and patient outcome: a meta‐analysis. J Antimicrob Chemother. 2012;67(6):1311–1320.
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: 21st informational supplement. M100‐S20. Wayne, PA: Clinical and Laboratory Standards Institute; 2010.
- , , , . A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
- , , , et al. Bloodstream infections caused by antibiotic‐resistant gram‐negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother. 2005;49(2):760–766.
- , , , , . Clinical implications of extended‐spectrum beta‐lactamase‐producing Klebsiella pneumoniae bacteraemia. J Hosp Infect. 2002;52(2):99–106.
- , , , , . Impact of extended‐spectrum β‐lactamase‐producing Escherichia coli and Klebsiella species on clinical outcomes and hospital costs: a matched cohort study. Infect Control Hosp Epidemiol. 2006;27(11):1226–1232.
- , , , et al. Risk factors for community‐onset urinary tract infections due to Escherichia coli harbouring extended‐spectrum‐β‐lactamases. J Antimicrob Chemother. 2006:57(4):780–783.
- , , , et al. Community infections caused extended‐spectrum‐β‐lactamase‐producing Escherichia coli. Arch Intern Med. 2008;168(17):1897–1902.
- , , . Prevalence and risk factors for extended spectrum‐β‐lactamase‐producing uropathogens in urinary tract infection. Korean J Urol. 2010;51(7):492–497.
- , , , , . Extended‐spectrum β‐lactamase‐producing gram‐negative pathogens in community‐acquired urinary tract infections: an increasing challenge for antimicrobial therapy. Infection. 2011;39(4):333–340.
- , , , et al. Epidemiology and genetic characteristics of extended‐spectrum‐β‐lactamase‐producing gram‐negative bacteria causing urinary tract infections in long‐term care facilities. J Antimicrob Chemother. 2012;67(12):2982–2987.
- , , , et al. Epidemiology, risk factors and comorbidity for urinary tract infections caused by extended‐spectrum beta‐lactamase (ESBL)‐producing enterobacteria. Int J Clin Pract. 2012;66(9):891–896.
- , , , et al. Identifying patients harboring extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae on hospital admission: derivation and validation of a scoring system. Antimicrob Agents Chemother. 2011;55(7):3485–3490.
- , , , . Utility of a clinical risk factor scoring model in predicting infection with extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae on hospital admission. Infect Control Hosp Epidemiol. 2013;34(4):385–392.
- , , , , , . Fosfomycin in the treatment of extended spectrum beta‐lactamase‐producing Escherichia coli‐related lower urinary tract infections. Int J Amtimicrob Agents. 2007;29(1):62–65.
- , , , , . Nitrofurantoin in the treatment of extended‐spectrum beta‐lactamase‐producing Escherichia coli‐related lower urinary tract infection. Int J Antimicrob Agents. 2012;40:554–556.
- , , , et al. Epidemiology and clinical features of infections caused by extended‐spectrum beta‐lactamase‐producing Escherichia coli in nonhospitalized patients. J Clin Microb. 2004;42(3):1089–1094.
- , , , et al. Community infections caused by extended‐spectrum β‐lactamase‐producing Escherichia coli. Arch Intern Med. 2008:168(17):1897–1902.
- , , , et al. Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae bloodstream infection: risk factors and clinical outcome. Intensive Care Med. 2002;28(12):1718–1723.
- , , , et al. Ceftazidime‐resistant Klebsiella pneumoniae and Escherichia coli bloodstream infection: a case‐control and molecular epidemiologic investigation. J Infect Dis. 1996;174(3):529–536.
- , . The impact of antimicrobial resistance on health and economic outcomes. Clin Infect Dis. 2003;36(11):1433–1437.
- . Clinical implications of antimicrobial resistance for therapy. J Antimicrob Chemother. 2008;62(suppl 2):ii105–ii114.
Community‐onset urinary tract infection (UTI) is a common bacterial infection encountered in hospital medicine, accounting for >350,000 hospital admissions and $3.4 billion in healthcare costs annually.[1] High proportions of these infections are caused by Enterobacteriaceae, primarily Escherichia coli and Klebsiella species.[2] The prevalence of hospitalized patients with UTI caused by multidrug‐resistant E coli and Klebsiella species has increased.[3, 4, 5] Enterobacteriaceae can produce hydrolytic enzymes, specifically extended‐spectrum ‐lactamases (ESBL), which result in high rates of bacterial resistance to frequently used agents.[6] Global rates vary widely by region, and recent surveillance data showed increasing rates of clinical isolates in North America are ESBL producers.[7, 8, 9, 10] More alarming is the emergence of these resistant organisms in the community.[11]
In addition to ‐lactams, ESBL production is associated with resistance to other antibiotic classes (fluoroquinolones, aminoglycosides, and sulfonamides), and has become an important cause of failed therapy.[12, 13] Consequently, providing adequate and timely antibiotics can become convoluted due to fewer remaining treatment options. Therefore, carbapenems, which are less susceptible to hydrolysis by these enzymes, have become the preferred therapy for infection with ESBL‐producing pathogens.[3, 13, 14]
The consequences of ESBL production, mainly in bloodstream infection (BSI), are well characterized, including notable delays in receipt of appropriate antibiotic therapy, prolonged length of stay (LOS), and increased cost of care.[15, 16] Importantly, others have found higher rates of mortality.[17, 18, 19, 20, 21] However, the impact on outcomes specifically in UTI remains unclear. As a result of the prevalence of UTI admissions to the hospital, the increasing incidence of ESBLs, and the potential impact on the clinical course of care, additional study is required to support best practices for this common diagnosis.
PATIENTS AND METHODS
Study Subjects and Design
This was a retrospective, matched‐cohort analysis of patients admitted to the hospital with UTI (International Classification of Diseases, 9th Revision‐Clinical Modification code 599.0) caused by extended‐spectrum b‐lactamase‐producing Escherichia coli and Klebsiella species (ESBL‐EK). Patients admitted to Hartford Hospital from September 1, 2011 through August 31, 2012 with UTI present on admission (48 hours) were evaluated. Cases were patients 18 years of age, with a positive urine culture (104 CFU/mL) for an ESBL‐producing organism (48 hours of admission), who received antibiotic treatment directed at the positive culture for 48 hours, and beginning prior to availability of in vitro susceptibility results. Cases were identified by a detailed search of the microbiology department database of ESBL‐EK cultures. Only the first positive (index) culture for each patient was included. Bacteremia was defined as isolation of a blood culture organism identical to the one isolated from the urine culture. Patients were excluded if they were discharged, died, or placed on palliative care prior to or on the date of urine collection. Controls (patients admitted with UTI on admission caused by nonESBL‐EK) were matched to cases in a 1:1 fashion on the basis of isolated urinary pathogen, age (5 years), sex, and race. ESBL‐producing organisms were identified and classified according to the Clinical and Laboratory Standards Institute guidelines.[22]
Data Collection
Once patients were identified, the following information was collected from the patient's medical record by 2 investigators using a standardized case report form: demographic characteristics, comorbid conditions and severity of comorbidities using the Charlson comorbidity index, recent patient medical history, and clinical and economic attributes.[23]
The study was approved by the institutional review board of Hartford Hospital. An informed consent waiver was granted as all data were currently in existence and no patient‐specific interventions were conducted for the study. The collection of data was in compliance with the Health Insurance Portability and Accountability Act of 1996.
Outcomes and Definitions
Onset of UTI was defined as the date/time of the index culture collection. An initial antibiotic treatment was a course of therapy initiated empirically (prior to availability of in vitro susceptibility) and that continued for 48 hours. An appropriate empiric antibiotic was defined as an initial antibiotic that ultimately possessed in vitro activity against the isolated pathogen.
The primary clinical outcomes were initial antibiotic response and clinical response. Initial antibiotic response was defined as failure if there was lack of clinical improvement, as evident by a switch to an alternative antibiotic (excluding switches to similar/narrower‐spectrum agents and courses begun at discharge) or infection‐related mortality while receiving the initial antibiotic. Patients were deemed clinical success if they were clinically stable at discharge or end of therapy, whichever occurred first, with resolution of signs and symptoms of infection. Clinical failures were patients with (1) infection‐related mortality or (2) readmission to hospital with UTI within 30 days of discharge. Clinical response was chosen as a primary outcome because significant mortality attributed to UTI was not anticipated. Secondary clinical outcomes included: time to appropriate antibiotic therapy, mortality (all cause and infection related), and 30‐day readmission (all cause and UTI related). Patients were considered to have received appropriate antibiotic therapy when they had received their first dose of antibiotic with activity against the isolated pathogen based on the patient‐specific in vitro susceptibility results. Time to appropriate antibiotics was defined as the elapsed time (hours) between the index culture collection and the initial dose of appropriate antibiotic therapy. All‐cause mortality was defined as any cause of death at the end of hospitalization, whereas infection‐related mortality was defined as death occurring while receiving antibiotics for the index infection, without any other obvious cause of death.
The primary economic outcomes were hospital LOS, costs, and reimbursement. Antibiotic costs were calculated for each patient according to acquisition costs. Additional economic outcomes evaluated were net hospital reimbursement and primary payor. Net hospital reimbursement was calculated as the difference between hospital reimbursement and hospital costs for each patient. Hospital costs were calculated as the direct plus indirect hospitalization costs for each patient, as determined by our institutional accounting department. All economic values were reported in United States dollars.
Statistical Analysis
Statistical comparisons were performed between cases and controls using a paired t test or Wilcoxon signed rank test for continuous variables, where appropriate. Dichotomous variables were compared using the McNemar test. Multivariate logistic regression was performed to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to determine independent risk factors for ESBL‐EK, including all pertinent variables with a P value <0.1 in univariate analyses. All data were analyzed using SigmaStat version 2.03 (IBM/SPSS, Armonk, NY). A P value of 0.05 was considered statistically significant.
RESULTS
Patient Population
Between September 2011 and August 2012, there were 220 specimens of ESBL‐related infection and 2345 patients admitted with a UTI on admission. Eighty‐four were confirmed ESBL‐EK cases (3.6%), and 55 met criteria for inclusion. Twenty‐nine of these cases were excluded because the index culture was polymicrobial, for which the response to antibiotics for ESBL‐EK could not be elicited (n=22); they had incomplete medical records (n=4); or they did not have a matched control patient (n=3). Fifty‐five matched control patients were identified, resulting in 110 patients overall.
Patient demographics and baseline characteristics are shown in Table 1. Patients with ESBL‐EK UTI were more likely to have diabetes mellitus, chronic obstructive pulmonary disorder, and a history of recurrent UTIs. They were more likely to have recently received antibiotics, been hospitalized, or had isolation of an ESBL‐producing organism. No significant differences in Charlson comorbidity index, recent immunosuppressive therapy, or urinary catheterization were observed. Compared with controls, patients with ESBL‐EK UTI were more frequently transferred from another healthcare facility, although the difference was not statistically significant (P=0.06). In the multivariate regression model, diabetes mellitus (OR: 4.4, 95% CI: 1.711.5; P=0.002), history of recurrent UTIs (OR: 4.4, 95% CI: 1.810.9; P=0.001), and transfer from another healthcare facility (OR: 2.38, 95% CI: 1.05.7; P=0.05) were independently associated with ESBL‐EK UTI. Previous isolation of an ESBL‐producing organism (P<0.001) was unable to be included in the multivariate logistic regression model because only patients with UTI caused by ESBL‐EK were positive for this variable. However, as noted in Table 1, 27.2% of cases had isolation of an ESBL‐producing organism in the previous year.
| ESBL Positive, n=55 | ESBL Negative, n=55 | Pa | |
|---|---|---|---|
| |||
| Demographics | |||
| Age, y, median (IQR) | 77 (6785) | 77 (6685) | 0.83b |
| Female | 36 (65.4) | 36 (65.4) | 1.00 |
| White | 42 (76.4) | 42 (76.4) | 1.00 |
| Black | 5 (9.1) | 5 (9.1) | 1.00 |
| Hispanic/Latino | 6 (10.9) | 6 (10.9) | 1.00 |
| Other | 2 (3.6) | 2 (3.6) | 1.00 |
| Comorbidities | |||
| Diabetes mellitus | 25 (45.5) | 10 (18.1) | 0.004 |
| COPD | 15 (27.2) | 6 (10.9) | 0.04 |
| Liver disease | 2 (3.6) | 1 (1.8) | 1.00 |
| Hemodialysis | 9 (16.4) | 6 (10.9) | 0.58 |
| Hematological malignancy | 3 (5.5) | 2 (3.6) | 1.00 |
| Solid malignancy | 13 (23.6) | 9 (16.4) | 0.45 |
| HIV/AIDS | 0 | 1 (1.8) | 1.00 |
| Age >65 years | 44 (80.0) | 43 (78.2) | 1.00 |
| Urinary abnormality | 15 (27.2) | 15 (27.2) | 1.00 |
| Charlson comorbidity index, median (IQR) | 3 (24) | 2 (13.8) | 0.19 |
| History | |||
| Previous hospitalizationc | 38 (69.1) | 24 (43.6) | 0.01 |
| Previous antibioticsd | 23 (41.8) | 12 (21.8) | 0.04 |
| Recent immunosuppressive therapye | 9 (16.4) | 3 (5.5) | 0.11 |
| History of recurrent UTIsf | 29 (52.7) | 12 (21.8) | 0.001 |
| History of urinary catheterizationg | 18 (32.7) | 14 (25.4) | 0.45 |
| Previous genitourinary procedure/surgery | 10 (18.2) | 6 (10.9) | 0.39 |
| Previous ESBL‐producing organismh | 15 (27.2) | 0 | <0.001 |
| Clinical features | |||
| Transfer from another healthcare facility | 27 (49.1) | 17 (21.0) | 0.06 |
| ICU admission | 12 (21.8) | 7 (12.7) | 0.33 |
| Bacteremia | 7 (12.7) | 5 (9.1) | 0.75 |
| Infectious Diseases consulted | 39 (70.1) | 16 (29.1) | <0.001 |
| Empiric ‐lactam (noncarbapenem) | 35 (63.6) | 50 (90.9) | 0.001 |
Isolate Characteristics
The distribution of causative pathogens in each cohort was: 44 (80%) Escherichia coli, 8 (14.5%) Klebsiella pneumoniae, and 3 (5.5%) Klebsiella oxytoca. In vitro nonsusceptibility profiles of the 55 ESBL‐EK cases are characterized in Figure 1. The most active agents were carbapenems, with 98.2% susceptibility to the entire isolate profile, whereas <10% of isolates were susceptible to the fluoroquinolones. All ESBL‐producing isolates were resistant to cefepime.
Failure on Initial Antibiotic Regimen
Initial antibiotic therapy is shown in Table 2. A majority of patients (87.2%) were initially treated with a ‐lactam. Empiric carbapenem use was greater in ESBL‐EK cases (18.1% vs 0%; P<0.001), and there were no other significant differences in the distribution of initial antibiotic therapy between cohorts. Less than one‐quarter of ESBL‐EK patients (23.6%) received appropriate initial therapy, whereas 98.2% of controls were initially treated appropriately (P<0.001).
| Initial Antibiotic | ESBL Positive, n=55 | ESBL Negative, n=55 | Pa |
|---|---|---|---|
| |||
| Ceftriaxone | 21 (38.1) | 32 (58.1) | 0.06 |
| Cefepime | 10 (18.2) | 12 (21.8) | 0.81 |
| Ertapenem | 7 (12.7) | 0 | 0.02 |
| Levofloxacin | 6 (10.9) | 4 (7.3) | 0.74 |
| Cefazolin | 0 | 4 (7.3) | 0.13 |
| Piperacillin‐tazobactam | 3 (5.5) | 0 | 0.24 |
| Ciprofloxacin | 2 (3.6) | 1 (1.8) | 1.00 |
| Doripenem | 2 (3.6) | 0 | 0.48 |
| Trimethoprim‐sulfamethoxazole | 2 (3.6) | 0 | 0.48 |
| Meropenem | 1 (1.8) | 0 | 1.00 |
| Cephalexin | 1 (1.8) | 0 | 1.00 |
| Aztreonam | 0 | 2 (3.6) | 0.48 |
Compared with controls, failure of initial antibiotic therapy was more common in patients with ESBL‐EK UTI, resulting in a significantly longer time to appropriate antibiotics (Table 3). Among ESBL‐EK UTI cases, failure of initial antibiotic therapy was greater for patients who received noncarbapenem ‐lactams (85.7%) as compared to those who empirically received a carbapenem (0%) (P<0.001). Antibiotic failure (>2 patients treated) in ESBL‐EK was highest with the following antibiotics: cefepime (100% [10/10]), piperacillin‐tazobactam (100% [3/3]), and ceftriaxone (76.2% [16/21]).
| ESBL Positive, n=55 | ESBL Negative, n=55 | Pa | |
|---|---|---|---|
| |||
| Clinical parameter | |||
| Initial antibiotic failure | 34 (61.8) | 3 (5.5) | <0.001 |
| Escalation to an alternative antibiotic | 33 (60.0) | 3 (5.5) | <0.001 |
| Time to appropriate antibiotics, h, median (IQR) | 51 (32.560.8) | 2.5 (1.07.2) | <0.001b |
| Appropriate empiric antibiotics | 13 (23.6) | 54 (98.2) | <0.001 |
| Clinical success | 47 (85.5) | 52 (94.5) | 0.23 |
| All‐cause mortality | 5 (9.1) | 1 (1.8) | 0.21 |
| Infection‐related mortality | 4 (7.2) | 1 (1.8) | 0.37 |
| All‐cause 30‐day readmission | 12 (21.8) | 15 (27.2) | 0.63 |
| UTI‐related 30‐day readmission | 4 (7.2) | 2 (3.6) | 0.68 |
| Economic parameterb | |||
| Length of stay, d, median (IQR) | 6 (48) | 4 (36) | 0.02 |
| Total hospital cost, median (IQR)c | 10,741 (684615,819) | 7,083 (566711,652) | 0.02 |
| Bed cost, % total cost, median (IQR) | 57.5 (51.666.0) | 63.8 (51.973.5) | 0.21 |
| Antibiotic cost, % total cost, median (IQR) | 0.5 (0.12.0) | 0.1(0.030.2) | <0.001 |
| Primary payor, n (%) | |||
| Medicare | 44 (80) | 44 (80) | 1.00 |
| Medicaid | 7 (12.7) | 3 (5.4) | 0.32 |
| Private insurance | 2 (3.6) | 2 (3.6) | 0.61 |
| Managed care | 2 (3.6) | 6 (10.9) | 0.27 |
Clinical Outcomes
There were no significant differences in clinical success, mortality, or 30‐day readmission between cohorts (Table 3). Among ESBL‐EK patients, those who received appropriate antibiotics within 48 hours were significantly more likely to achieve treatment success (100% vs 77.1%; P=0.04). All 8 ESBL‐EK treatment failures (4 infection‐related mortality and 4 UTI readmitted with the same ESBL pathogen) failed to receive appropriate antibiotics within 48 hours of culture collection.
More ESBL‐EK patients required a switch in their antibiotics. Within the subgroup of ESBL‐EK patients with an escalation in antibiotics, ertapenem was added to 19 of 33 (57.6%) cases.
Economic Outcomes
ESBL‐EK patients who received inappropriate initial therapy received longer antibiotic treatment courses than those empirically treated with a carbapenem (meanstandard deviation, 8.93.7 vs 6.23.2 days, respectively; P=0.04). When compared to non‐ESBL infection, ESBL‐EK patients required more days of antibiotic therapy (median 8 vs 5 days; P=0.03). The median LOS was significantly longer and total hospital costs were significantly greater for ESBL cases. Antibiotic costs contributed minimally to the overall cost, accounting for <1% (0.5% for cases vs 0.1% for controls), regardless of ESBL status. A comparison of economic outcomes is presented in Table 3. LOS among ESBL cases was not different between those discharged with and without continued antimicrobial therapy. Moreover, for those discharged on antimicrobial therapy, the utilization of either the oral or intravenous route did not delay discharge (data not shown).
The payor mix was similar between cases and controls. Given the predominately elderly population, Medicare was the primary payor for a majority of patients. Median differences in cost and reimbursement between cohorts (ESBL‐EK vs nonESBL‐EK) were $3658 (P=0.02) and $469 (P=0.56), respectively. As a result, median loss per patient with ESBL‐EK infection was $3189 when compared with controls.
Bacteremia
All cases of bacteremia were present on admission. Bacteremic UTI due to ESBL‐EK was associated with initial antibiotic failure (85.7% [6/7] vs 0% [0/5]; P=0.015), delayed appropriate therapy (median, 56 vs 2 hours; P=0.003), longer median hospital stays (11 vs 5 days; P=0.05), and higher median cost ($27,671 vs $5898; P=0.03) as compared with bacteremic UTI due to non‐ESBL‐EK. Infection‐related mortality occurred in 2 ESBL‐EK bacteremic patients, but no mortality was observed among the nonESBL‐EK bacteremic UTI cohort (28.6% [2/7] vs 0% [0/5]; P=0.47].
DISCUSSION
This matched cohort analysis revealed that ESBL‐EK has detrimental effects on the outcomes of patients admitted to the hospital with UTI. While matching for demographics and infecting pathogen, patients with ESBL‐EK UTI had diminished initial antibiotic response and considerably longer time to appropriate antibiotic therapy (48 hours longer) than their non‐ESBL comparator. Despite significant delays in appropriate therapy, we saw no attributable difference in clinical outcome and mortality; however, numerical trends toward increased risk were observed in ESBL‐EK patients. Although clinical response was largely unchanged, prolonged hospitals stays and increased cost of care were endured by ESBL‐EK patients.
Antimicrobial resistance, a primary factor in the postponement of appropriate antibiotic therapy, is a worrisome occurrence with meaningful clinical implications.16[21, 24] In BSI, delayed appropriate therapy due to ESBLs has been associated with prolonged LOS, increased costs, and increased mortality.[20, 25] However, the clinical significance of ESBL production on patient outcomes in UTI remains equivocal. To the best of our knowledge, this is the first matched control analysis evaluating the clinical and economic impact of ESBL specifically in UTI. We saw a 50% increase in the median LOS (from 4 to 6 days) and cost of care (additional $3658 per patient) in the ESBL‐EK UTI cohort. Albeit as small subpopulation, patients with bacteremic UTI due to ESBL‐EK had significantly longer hospital stays and increased cost of care as compared with nonESBL‐EK bacteremic UTI. These economic findings are consistent with data from other investigations. For example, a matched case‐control study of infection (51.5% UTI) due to ESBL‐producing E coli and K pneumoniae by Lautenbach and colleagues found an additional 60‐hour (72 vs 11.5 hours, P<0.001) delay in time to appropriate antibiotics for case patients, resulting in significantly longer LOS (1.8 times) and increased hospital charges (2.9 times).[17] With respect to costs, a matched case‐control analysis of ESBL‐EK in non‐UTI saw a 70% increase in cost ($41,353 vs $24,902).[26] Moreover, the increased cost in that study, like this one, was driven primarily by LOS (additional 9.7 days) and not drug utilization, with antibiotic costs representing <2% of the total hospitalization cost. Tumbarello and colleagues observed an approximate 50% increase in LOS and hospital costs in patients with BSI caused by ESBL‐producing E coli.[20]
Distinctive from those studies, we investigated the significance of ESBL production on hospital reimbursement. Despite the additional healthcare resource utilization (50% greater), we saw no appreciable increase (<5%) in median hospital reimbursement. Given that the primary payors between cohorts were comparable, infection with ESBL‐producing bacteria may result in a potential loss of income if optimal treatment is not initiated on admission.
The risk factors for development of UTI due to ESBL‐EK are well defined.[27, 28, 29, 30, 31, 32] Two scoring systems, an Italian and a Duke model, have identified patients at increased risk of harboring ESBL‐producing organisms on hospital admission.[33, 34] The features of each model center on established risk factors for ESBL‐EK UTI. In our study population, these scoring model features were more common in ESBL‐EK patients, supporting their potential application in UTI. However, because of our study design (infected controls) and matching criteria, only 2 features (recent antibiotics and previous hospitalization) achieved statistical significance as detectable risk factors in our population. Regardless, these data, coupled with increasing prevalence of UTI with ESBL‐producing bacteria, provide justification and advocacy for the empiric use of ESBL active antibiotics (ie, carbapenems) in certain high‐risk individuals, particularly those patients with a previous history of ESBL or those with multiple risk factors identified in our study as well as others (previous hospitalization, recent antibiotic exposure). Importantly, an aggressive de‐escalation strategy should be used to temper collateral damage for patients with non‐ESBL infections. Moreover, the utilization of oral therapies beyond the fluoroquinolones and trimethoprim‐sulfamethoxazole, such as fosfomycin and nitrofurantoin, coupled with coordinated transitions of care, may alleviate the demand for intravenous access in patients prepared for discharge.[35, 36]
This study is not without limitations. As only a distinct period in time was studied, we are unable to determine the implications of previous episodes of UTI on the current admission. Although the Charlson comorbidity score was not significantly different between the 2 patient cohorts, ESBL‐EK patients were more likely to have several demographic features (ie, diabetes mellitus, recurrent UTIs, previous hospitalization, and recent antibiotic exposure), which are to be expected in the ESBL population.[37, 38] Although these differences have been observed as expected, we believe the driver of prolonged LOS and increased costs of care stem from inappropriate initial antibiotic therapy as evident by the initial clinical failure observed in ESBL‐EK patients. It should also be noted that we defined antibiotics as appropriate based on the laboratory criteria for susceptibility, as such agents that have high concentration in the urinary tract (ie, fluoroquinolones) may be effective despite these laboratory definitions.[17] For instance, 10 of our ESBL‐EK patients never received appropriate antibiotics (3 fluoroquinolones, 7 noncarbapenem ‐lactams) as defined by laboratory‐based susceptibility testing, 8 of whom experienced clinical success. Previous studies have shown discordance between phenotypic ESBL‐related resistance profiles and outcomes.[17, 18, 19, 20, 21, 25, 39, 40]
In summary, recent increases in antimicrobial resistance present ongoing challenges in the treatment of hospitalized patients, as appropriate treatment options are extremely limited. Our findings strengthen the consortium of data stating that antimicrobial resistance unfavorably impacts patient outcomes.[41, 42] ESBL‐EK in UTI is associated with high rates of failure of initial antibiotic therapy, prolonged LOS, and increased cost of care. Furthermore, the added cost associated with UTI due to ESBL‐EK is not recognized in hospital reimbursement, as evident by a $3200 net loss relative to reimbursement. This loss appears to be solely due to the increased LOS, as antibiotic costs were <1% of cost of care. Moreover, these negative consequences could be even more pronounced at institutions with a higher prevalence of ESBL infection. A multidisciplinary approach (infection control, microbiology) using these data as a benchmark, may enhance the detection, treatment, and prevention of these ESBL‐producing organisms. With high levels of coresistance to noncarbapenem ‐lactams and fluoroquinolones, providers should be cognizant of organisms capable of producing ESBL when selecting initial antibiotic therapy in high‐risk populations. Early recognition and timely initiation of appropriate antibiotic therapy appear paramount to minimizing the burden of ESBL‐EK in patients admitted to the hospital with a UTI.
Acknowledgements
The authors thank Gilbert Fotunato for his assistance with administrative data retrieval.
Disclosures
This work is supported by a grant from Merck & Co., Inc. D.P.N. reports having received grant support and honorarium from Merck & Co., Inc. S.H.M and L.O.T report no conflicts of interest relevant to this article.
Community‐onset urinary tract infection (UTI) is a common bacterial infection encountered in hospital medicine, accounting for >350,000 hospital admissions and $3.4 billion in healthcare costs annually.[1] High proportions of these infections are caused by Enterobacteriaceae, primarily Escherichia coli and Klebsiella species.[2] The prevalence of hospitalized patients with UTI caused by multidrug‐resistant E coli and Klebsiella species has increased.[3, 4, 5] Enterobacteriaceae can produce hydrolytic enzymes, specifically extended‐spectrum ‐lactamases (ESBL), which result in high rates of bacterial resistance to frequently used agents.[6] Global rates vary widely by region, and recent surveillance data showed increasing rates of clinical isolates in North America are ESBL producers.[7, 8, 9, 10] More alarming is the emergence of these resistant organisms in the community.[11]
In addition to ‐lactams, ESBL production is associated with resistance to other antibiotic classes (fluoroquinolones, aminoglycosides, and sulfonamides), and has become an important cause of failed therapy.[12, 13] Consequently, providing adequate and timely antibiotics can become convoluted due to fewer remaining treatment options. Therefore, carbapenems, which are less susceptible to hydrolysis by these enzymes, have become the preferred therapy for infection with ESBL‐producing pathogens.[3, 13, 14]
The consequences of ESBL production, mainly in bloodstream infection (BSI), are well characterized, including notable delays in receipt of appropriate antibiotic therapy, prolonged length of stay (LOS), and increased cost of care.[15, 16] Importantly, others have found higher rates of mortality.[17, 18, 19, 20, 21] However, the impact on outcomes specifically in UTI remains unclear. As a result of the prevalence of UTI admissions to the hospital, the increasing incidence of ESBLs, and the potential impact on the clinical course of care, additional study is required to support best practices for this common diagnosis.
PATIENTS AND METHODS
Study Subjects and Design
This was a retrospective, matched‐cohort analysis of patients admitted to the hospital with UTI (International Classification of Diseases, 9th Revision‐Clinical Modification code 599.0) caused by extended‐spectrum b‐lactamase‐producing Escherichia coli and Klebsiella species (ESBL‐EK). Patients admitted to Hartford Hospital from September 1, 2011 through August 31, 2012 with UTI present on admission (48 hours) were evaluated. Cases were patients 18 years of age, with a positive urine culture (104 CFU/mL) for an ESBL‐producing organism (48 hours of admission), who received antibiotic treatment directed at the positive culture for 48 hours, and beginning prior to availability of in vitro susceptibility results. Cases were identified by a detailed search of the microbiology department database of ESBL‐EK cultures. Only the first positive (index) culture for each patient was included. Bacteremia was defined as isolation of a blood culture organism identical to the one isolated from the urine culture. Patients were excluded if they were discharged, died, or placed on palliative care prior to or on the date of urine collection. Controls (patients admitted with UTI on admission caused by nonESBL‐EK) were matched to cases in a 1:1 fashion on the basis of isolated urinary pathogen, age (5 years), sex, and race. ESBL‐producing organisms were identified and classified according to the Clinical and Laboratory Standards Institute guidelines.[22]
Data Collection
Once patients were identified, the following information was collected from the patient's medical record by 2 investigators using a standardized case report form: demographic characteristics, comorbid conditions and severity of comorbidities using the Charlson comorbidity index, recent patient medical history, and clinical and economic attributes.[23]
The study was approved by the institutional review board of Hartford Hospital. An informed consent waiver was granted as all data were currently in existence and no patient‐specific interventions were conducted for the study. The collection of data was in compliance with the Health Insurance Portability and Accountability Act of 1996.
Outcomes and Definitions
Onset of UTI was defined as the date/time of the index culture collection. An initial antibiotic treatment was a course of therapy initiated empirically (prior to availability of in vitro susceptibility) and that continued for 48 hours. An appropriate empiric antibiotic was defined as an initial antibiotic that ultimately possessed in vitro activity against the isolated pathogen.
The primary clinical outcomes were initial antibiotic response and clinical response. Initial antibiotic response was defined as failure if there was lack of clinical improvement, as evident by a switch to an alternative antibiotic (excluding switches to similar/narrower‐spectrum agents and courses begun at discharge) or infection‐related mortality while receiving the initial antibiotic. Patients were deemed clinical success if they were clinically stable at discharge or end of therapy, whichever occurred first, with resolution of signs and symptoms of infection. Clinical failures were patients with (1) infection‐related mortality or (2) readmission to hospital with UTI within 30 days of discharge. Clinical response was chosen as a primary outcome because significant mortality attributed to UTI was not anticipated. Secondary clinical outcomes included: time to appropriate antibiotic therapy, mortality (all cause and infection related), and 30‐day readmission (all cause and UTI related). Patients were considered to have received appropriate antibiotic therapy when they had received their first dose of antibiotic with activity against the isolated pathogen based on the patient‐specific in vitro susceptibility results. Time to appropriate antibiotics was defined as the elapsed time (hours) between the index culture collection and the initial dose of appropriate antibiotic therapy. All‐cause mortality was defined as any cause of death at the end of hospitalization, whereas infection‐related mortality was defined as death occurring while receiving antibiotics for the index infection, without any other obvious cause of death.
The primary economic outcomes were hospital LOS, costs, and reimbursement. Antibiotic costs were calculated for each patient according to acquisition costs. Additional economic outcomes evaluated were net hospital reimbursement and primary payor. Net hospital reimbursement was calculated as the difference between hospital reimbursement and hospital costs for each patient. Hospital costs were calculated as the direct plus indirect hospitalization costs for each patient, as determined by our institutional accounting department. All economic values were reported in United States dollars.
Statistical Analysis
Statistical comparisons were performed between cases and controls using a paired t test or Wilcoxon signed rank test for continuous variables, where appropriate. Dichotomous variables were compared using the McNemar test. Multivariate logistic regression was performed to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to determine independent risk factors for ESBL‐EK, including all pertinent variables with a P value <0.1 in univariate analyses. All data were analyzed using SigmaStat version 2.03 (IBM/SPSS, Armonk, NY). A P value of 0.05 was considered statistically significant.
RESULTS
Patient Population
Between September 2011 and August 2012, there were 220 specimens of ESBL‐related infection and 2345 patients admitted with a UTI on admission. Eighty‐four were confirmed ESBL‐EK cases (3.6%), and 55 met criteria for inclusion. Twenty‐nine of these cases were excluded because the index culture was polymicrobial, for which the response to antibiotics for ESBL‐EK could not be elicited (n=22); they had incomplete medical records (n=4); or they did not have a matched control patient (n=3). Fifty‐five matched control patients were identified, resulting in 110 patients overall.
Patient demographics and baseline characteristics are shown in Table 1. Patients with ESBL‐EK UTI were more likely to have diabetes mellitus, chronic obstructive pulmonary disorder, and a history of recurrent UTIs. They were more likely to have recently received antibiotics, been hospitalized, or had isolation of an ESBL‐producing organism. No significant differences in Charlson comorbidity index, recent immunosuppressive therapy, or urinary catheterization were observed. Compared with controls, patients with ESBL‐EK UTI were more frequently transferred from another healthcare facility, although the difference was not statistically significant (P=0.06). In the multivariate regression model, diabetes mellitus (OR: 4.4, 95% CI: 1.711.5; P=0.002), history of recurrent UTIs (OR: 4.4, 95% CI: 1.810.9; P=0.001), and transfer from another healthcare facility (OR: 2.38, 95% CI: 1.05.7; P=0.05) were independently associated with ESBL‐EK UTI. Previous isolation of an ESBL‐producing organism (P<0.001) was unable to be included in the multivariate logistic regression model because only patients with UTI caused by ESBL‐EK were positive for this variable. However, as noted in Table 1, 27.2% of cases had isolation of an ESBL‐producing organism in the previous year.
| ESBL Positive, n=55 | ESBL Negative, n=55 | Pa | |
|---|---|---|---|
| |||
| Demographics | |||
| Age, y, median (IQR) | 77 (6785) | 77 (6685) | 0.83b |
| Female | 36 (65.4) | 36 (65.4) | 1.00 |
| White | 42 (76.4) | 42 (76.4) | 1.00 |
| Black | 5 (9.1) | 5 (9.1) | 1.00 |
| Hispanic/Latino | 6 (10.9) | 6 (10.9) | 1.00 |
| Other | 2 (3.6) | 2 (3.6) | 1.00 |
| Comorbidities | |||
| Diabetes mellitus | 25 (45.5) | 10 (18.1) | 0.004 |
| COPD | 15 (27.2) | 6 (10.9) | 0.04 |
| Liver disease | 2 (3.6) | 1 (1.8) | 1.00 |
| Hemodialysis | 9 (16.4) | 6 (10.9) | 0.58 |
| Hematological malignancy | 3 (5.5) | 2 (3.6) | 1.00 |
| Solid malignancy | 13 (23.6) | 9 (16.4) | 0.45 |
| HIV/AIDS | 0 | 1 (1.8) | 1.00 |
| Age >65 years | 44 (80.0) | 43 (78.2) | 1.00 |
| Urinary abnormality | 15 (27.2) | 15 (27.2) | 1.00 |
| Charlson comorbidity index, median (IQR) | 3 (24) | 2 (13.8) | 0.19 |
| History | |||
| Previous hospitalizationc | 38 (69.1) | 24 (43.6) | 0.01 |
| Previous antibioticsd | 23 (41.8) | 12 (21.8) | 0.04 |
| Recent immunosuppressive therapye | 9 (16.4) | 3 (5.5) | 0.11 |
| History of recurrent UTIsf | 29 (52.7) | 12 (21.8) | 0.001 |
| History of urinary catheterizationg | 18 (32.7) | 14 (25.4) | 0.45 |
| Previous genitourinary procedure/surgery | 10 (18.2) | 6 (10.9) | 0.39 |
| Previous ESBL‐producing organismh | 15 (27.2) | 0 | <0.001 |
| Clinical features | |||
| Transfer from another healthcare facility | 27 (49.1) | 17 (21.0) | 0.06 |
| ICU admission | 12 (21.8) | 7 (12.7) | 0.33 |
| Bacteremia | 7 (12.7) | 5 (9.1) | 0.75 |
| Infectious Diseases consulted | 39 (70.1) | 16 (29.1) | <0.001 |
| Empiric ‐lactam (noncarbapenem) | 35 (63.6) | 50 (90.9) | 0.001 |
Isolate Characteristics
The distribution of causative pathogens in each cohort was: 44 (80%) Escherichia coli, 8 (14.5%) Klebsiella pneumoniae, and 3 (5.5%) Klebsiella oxytoca. In vitro nonsusceptibility profiles of the 55 ESBL‐EK cases are characterized in Figure 1. The most active agents were carbapenems, with 98.2% susceptibility to the entire isolate profile, whereas <10% of isolates were susceptible to the fluoroquinolones. All ESBL‐producing isolates were resistant to cefepime.
Failure on Initial Antibiotic Regimen
Initial antibiotic therapy is shown in Table 2. A majority of patients (87.2%) were initially treated with a ‐lactam. Empiric carbapenem use was greater in ESBL‐EK cases (18.1% vs 0%; P<0.001), and there were no other significant differences in the distribution of initial antibiotic therapy between cohorts. Less than one‐quarter of ESBL‐EK patients (23.6%) received appropriate initial therapy, whereas 98.2% of controls were initially treated appropriately (P<0.001).
| Initial Antibiotic | ESBL Positive, n=55 | ESBL Negative, n=55 | Pa |
|---|---|---|---|
| |||
| Ceftriaxone | 21 (38.1) | 32 (58.1) | 0.06 |
| Cefepime | 10 (18.2) | 12 (21.8) | 0.81 |
| Ertapenem | 7 (12.7) | 0 | 0.02 |
| Levofloxacin | 6 (10.9) | 4 (7.3) | 0.74 |
| Cefazolin | 0 | 4 (7.3) | 0.13 |
| Piperacillin‐tazobactam | 3 (5.5) | 0 | 0.24 |
| Ciprofloxacin | 2 (3.6) | 1 (1.8) | 1.00 |
| Doripenem | 2 (3.6) | 0 | 0.48 |
| Trimethoprim‐sulfamethoxazole | 2 (3.6) | 0 | 0.48 |
| Meropenem | 1 (1.8) | 0 | 1.00 |
| Cephalexin | 1 (1.8) | 0 | 1.00 |
| Aztreonam | 0 | 2 (3.6) | 0.48 |
Compared with controls, failure of initial antibiotic therapy was more common in patients with ESBL‐EK UTI, resulting in a significantly longer time to appropriate antibiotics (Table 3). Among ESBL‐EK UTI cases, failure of initial antibiotic therapy was greater for patients who received noncarbapenem ‐lactams (85.7%) as compared to those who empirically received a carbapenem (0%) (P<0.001). Antibiotic failure (>2 patients treated) in ESBL‐EK was highest with the following antibiotics: cefepime (100% [10/10]), piperacillin‐tazobactam (100% [3/3]), and ceftriaxone (76.2% [16/21]).
| ESBL Positive, n=55 | ESBL Negative, n=55 | Pa | |
|---|---|---|---|
| |||
| Clinical parameter | |||
| Initial antibiotic failure | 34 (61.8) | 3 (5.5) | <0.001 |
| Escalation to an alternative antibiotic | 33 (60.0) | 3 (5.5) | <0.001 |
| Time to appropriate antibiotics, h, median (IQR) | 51 (32.560.8) | 2.5 (1.07.2) | <0.001b |
| Appropriate empiric antibiotics | 13 (23.6) | 54 (98.2) | <0.001 |
| Clinical success | 47 (85.5) | 52 (94.5) | 0.23 |
| All‐cause mortality | 5 (9.1) | 1 (1.8) | 0.21 |
| Infection‐related mortality | 4 (7.2) | 1 (1.8) | 0.37 |
| All‐cause 30‐day readmission | 12 (21.8) | 15 (27.2) | 0.63 |
| UTI‐related 30‐day readmission | 4 (7.2) | 2 (3.6) | 0.68 |
| Economic parameterb | |||
| Length of stay, d, median (IQR) | 6 (48) | 4 (36) | 0.02 |
| Total hospital cost, median (IQR)c | 10,741 (684615,819) | 7,083 (566711,652) | 0.02 |
| Bed cost, % total cost, median (IQR) | 57.5 (51.666.0) | 63.8 (51.973.5) | 0.21 |
| Antibiotic cost, % total cost, median (IQR) | 0.5 (0.12.0) | 0.1(0.030.2) | <0.001 |
| Primary payor, n (%) | |||
| Medicare | 44 (80) | 44 (80) | 1.00 |
| Medicaid | 7 (12.7) | 3 (5.4) | 0.32 |
| Private insurance | 2 (3.6) | 2 (3.6) | 0.61 |
| Managed care | 2 (3.6) | 6 (10.9) | 0.27 |
Clinical Outcomes
There were no significant differences in clinical success, mortality, or 30‐day readmission between cohorts (Table 3). Among ESBL‐EK patients, those who received appropriate antibiotics within 48 hours were significantly more likely to achieve treatment success (100% vs 77.1%; P=0.04). All 8 ESBL‐EK treatment failures (4 infection‐related mortality and 4 UTI readmitted with the same ESBL pathogen) failed to receive appropriate antibiotics within 48 hours of culture collection.
More ESBL‐EK patients required a switch in their antibiotics. Within the subgroup of ESBL‐EK patients with an escalation in antibiotics, ertapenem was added to 19 of 33 (57.6%) cases.
Economic Outcomes
ESBL‐EK patients who received inappropriate initial therapy received longer antibiotic treatment courses than those empirically treated with a carbapenem (meanstandard deviation, 8.93.7 vs 6.23.2 days, respectively; P=0.04). When compared to non‐ESBL infection, ESBL‐EK patients required more days of antibiotic therapy (median 8 vs 5 days; P=0.03). The median LOS was significantly longer and total hospital costs were significantly greater for ESBL cases. Antibiotic costs contributed minimally to the overall cost, accounting for <1% (0.5% for cases vs 0.1% for controls), regardless of ESBL status. A comparison of economic outcomes is presented in Table 3. LOS among ESBL cases was not different between those discharged with and without continued antimicrobial therapy. Moreover, for those discharged on antimicrobial therapy, the utilization of either the oral or intravenous route did not delay discharge (data not shown).
The payor mix was similar between cases and controls. Given the predominately elderly population, Medicare was the primary payor for a majority of patients. Median differences in cost and reimbursement between cohorts (ESBL‐EK vs nonESBL‐EK) were $3658 (P=0.02) and $469 (P=0.56), respectively. As a result, median loss per patient with ESBL‐EK infection was $3189 when compared with controls.
Bacteremia
All cases of bacteremia were present on admission. Bacteremic UTI due to ESBL‐EK was associated with initial antibiotic failure (85.7% [6/7] vs 0% [0/5]; P=0.015), delayed appropriate therapy (median, 56 vs 2 hours; P=0.003), longer median hospital stays (11 vs 5 days; P=0.05), and higher median cost ($27,671 vs $5898; P=0.03) as compared with bacteremic UTI due to non‐ESBL‐EK. Infection‐related mortality occurred in 2 ESBL‐EK bacteremic patients, but no mortality was observed among the nonESBL‐EK bacteremic UTI cohort (28.6% [2/7] vs 0% [0/5]; P=0.47].
DISCUSSION
This matched cohort analysis revealed that ESBL‐EK has detrimental effects on the outcomes of patients admitted to the hospital with UTI. While matching for demographics and infecting pathogen, patients with ESBL‐EK UTI had diminished initial antibiotic response and considerably longer time to appropriate antibiotic therapy (48 hours longer) than their non‐ESBL comparator. Despite significant delays in appropriate therapy, we saw no attributable difference in clinical outcome and mortality; however, numerical trends toward increased risk were observed in ESBL‐EK patients. Although clinical response was largely unchanged, prolonged hospitals stays and increased cost of care were endured by ESBL‐EK patients.
Antimicrobial resistance, a primary factor in the postponement of appropriate antibiotic therapy, is a worrisome occurrence with meaningful clinical implications.16[21, 24] In BSI, delayed appropriate therapy due to ESBLs has been associated with prolonged LOS, increased costs, and increased mortality.[20, 25] However, the clinical significance of ESBL production on patient outcomes in UTI remains equivocal. To the best of our knowledge, this is the first matched control analysis evaluating the clinical and economic impact of ESBL specifically in UTI. We saw a 50% increase in the median LOS (from 4 to 6 days) and cost of care (additional $3658 per patient) in the ESBL‐EK UTI cohort. Albeit as small subpopulation, patients with bacteremic UTI due to ESBL‐EK had significantly longer hospital stays and increased cost of care as compared with nonESBL‐EK bacteremic UTI. These economic findings are consistent with data from other investigations. For example, a matched case‐control study of infection (51.5% UTI) due to ESBL‐producing E coli and K pneumoniae by Lautenbach and colleagues found an additional 60‐hour (72 vs 11.5 hours, P<0.001) delay in time to appropriate antibiotics for case patients, resulting in significantly longer LOS (1.8 times) and increased hospital charges (2.9 times).[17] With respect to costs, a matched case‐control analysis of ESBL‐EK in non‐UTI saw a 70% increase in cost ($41,353 vs $24,902).[26] Moreover, the increased cost in that study, like this one, was driven primarily by LOS (additional 9.7 days) and not drug utilization, with antibiotic costs representing <2% of the total hospitalization cost. Tumbarello and colleagues observed an approximate 50% increase in LOS and hospital costs in patients with BSI caused by ESBL‐producing E coli.[20]
Distinctive from those studies, we investigated the significance of ESBL production on hospital reimbursement. Despite the additional healthcare resource utilization (50% greater), we saw no appreciable increase (<5%) in median hospital reimbursement. Given that the primary payors between cohorts were comparable, infection with ESBL‐producing bacteria may result in a potential loss of income if optimal treatment is not initiated on admission.
The risk factors for development of UTI due to ESBL‐EK are well defined.[27, 28, 29, 30, 31, 32] Two scoring systems, an Italian and a Duke model, have identified patients at increased risk of harboring ESBL‐producing organisms on hospital admission.[33, 34] The features of each model center on established risk factors for ESBL‐EK UTI. In our study population, these scoring model features were more common in ESBL‐EK patients, supporting their potential application in UTI. However, because of our study design (infected controls) and matching criteria, only 2 features (recent antibiotics and previous hospitalization) achieved statistical significance as detectable risk factors in our population. Regardless, these data, coupled with increasing prevalence of UTI with ESBL‐producing bacteria, provide justification and advocacy for the empiric use of ESBL active antibiotics (ie, carbapenems) in certain high‐risk individuals, particularly those patients with a previous history of ESBL or those with multiple risk factors identified in our study as well as others (previous hospitalization, recent antibiotic exposure). Importantly, an aggressive de‐escalation strategy should be used to temper collateral damage for patients with non‐ESBL infections. Moreover, the utilization of oral therapies beyond the fluoroquinolones and trimethoprim‐sulfamethoxazole, such as fosfomycin and nitrofurantoin, coupled with coordinated transitions of care, may alleviate the demand for intravenous access in patients prepared for discharge.[35, 36]
This study is not without limitations. As only a distinct period in time was studied, we are unable to determine the implications of previous episodes of UTI on the current admission. Although the Charlson comorbidity score was not significantly different between the 2 patient cohorts, ESBL‐EK patients were more likely to have several demographic features (ie, diabetes mellitus, recurrent UTIs, previous hospitalization, and recent antibiotic exposure), which are to be expected in the ESBL population.[37, 38] Although these differences have been observed as expected, we believe the driver of prolonged LOS and increased costs of care stem from inappropriate initial antibiotic therapy as evident by the initial clinical failure observed in ESBL‐EK patients. It should also be noted that we defined antibiotics as appropriate based on the laboratory criteria for susceptibility, as such agents that have high concentration in the urinary tract (ie, fluoroquinolones) may be effective despite these laboratory definitions.[17] For instance, 10 of our ESBL‐EK patients never received appropriate antibiotics (3 fluoroquinolones, 7 noncarbapenem ‐lactams) as defined by laboratory‐based susceptibility testing, 8 of whom experienced clinical success. Previous studies have shown discordance between phenotypic ESBL‐related resistance profiles and outcomes.[17, 18, 19, 20, 21, 25, 39, 40]
In summary, recent increases in antimicrobial resistance present ongoing challenges in the treatment of hospitalized patients, as appropriate treatment options are extremely limited. Our findings strengthen the consortium of data stating that antimicrobial resistance unfavorably impacts patient outcomes.[41, 42] ESBL‐EK in UTI is associated with high rates of failure of initial antibiotic therapy, prolonged LOS, and increased cost of care. Furthermore, the added cost associated with UTI due to ESBL‐EK is not recognized in hospital reimbursement, as evident by a $3200 net loss relative to reimbursement. This loss appears to be solely due to the increased LOS, as antibiotic costs were <1% of cost of care. Moreover, these negative consequences could be even more pronounced at institutions with a higher prevalence of ESBL infection. A multidisciplinary approach (infection control, microbiology) using these data as a benchmark, may enhance the detection, treatment, and prevention of these ESBL‐producing organisms. With high levels of coresistance to noncarbapenem ‐lactams and fluoroquinolones, providers should be cognizant of organisms capable of producing ESBL when selecting initial antibiotic therapy in high‐risk populations. Early recognition and timely initiation of appropriate antibiotic therapy appear paramount to minimizing the burden of ESBL‐EK in patients admitted to the hospital with a UTI.
Acknowledgements
The authors thank Gilbert Fotunato for his assistance with administrative data retrieval.
Disclosures
This work is supported by a grant from Merck & Co., Inc. D.P.N. reports having received grant support and honorarium from Merck & Co., Inc. S.H.M and L.O.T report no conflicts of interest relevant to this article.
- , , , et al. Urologic diseases in America project: analytical methods and principal findings. J Urol. 2005;173(3):933–937.
- . Urinary tract pathogens in complicated infection and in elderly individuals. J Infect Dis. 2001;183(suppl 1):S5–S8.
- , , , , . Antimicrobial susceptibility of global inpatient urinary tract isolates of Escherichia coli: results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) program: 2009–2010. Diagn Microbiol Infect Dis. 2011;70(4):507–511.
- , . Extended‐spectrum β‐lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657–686.
- , , . Extended‐spectrum β‐lactamase producing Escherichia coli: changing epidemiology and clinical impact. Curr Opin Infect Dis. 2010;23(4):320–326.
- . Defining an extended‐spectrum beta‐lactamase. Clin Microbiol Infect. 2008;14(suppl 5):3–10.
- , , , , , . Antimicrobial susceptibility among organisms from the Asia/Pacific Rim, Europe and Latin and North America collected as part of TEST and the in vitro activity of tigecycline. J Antimicrob Chemother. 2007;60(5):1018–1029.
- , , , . Variations in the prevalence of strains expressing an extended‐spectrum β‐lactamase phenotype and characterization of isolates from Europe, the Americas, and the Western Pacific region. Clin Infect Dis. 2001;32(suppl 2):S94–S103.
- National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004. Am J Infect Control. 2004;32(8):470–485.
- , . Prevalence and antimicrobial susceptibility data for extended‐spectrum β‐lactamase‐ and AmpC‐producing Enterobacteriaceae from the MYSTIC Program in Europe and the United States (1997–2004). Diagn Microbiol Infect Dis. 2005;53(4):257–264.
- , , , . Emergence of Enterobacteriaceae producing extended‐spectrum b‐lactamases (ESBLs) in the community. J Antimicrob Chemother. 2005;56(1):52–59.
- , , , et al. Epidemiology of ciprofloxacin resistance and its relationship to extended‐spectrum B‐lactamase production in Klebsiella pneumoniae isolates causing bacteremia. Clin Infect Dis. 2000;30(4):473–478.
- , , , , , Epidemiological investigation of fluoroquinolone resistance in infections due to extended‐spectrum‐β‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae. Clin Infect Dis. 2001;33(8):1288–1294.
- , , , . High levels of antimicrobial coresistance among extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae. Antimicrob Agents Chemother. 2005;49(5):2137–2139.
- . Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31(suppl 4):S131–S138.
- . The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin Infect Dis. 2006;42(suppl 2):S82–S89.
- , , , , , Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes. Clin Infect Dis. 2001:32(8):1162–1171.
- , , , et al. Predictors of mortality in patients with bloodstream infections caused by extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae: importance of inadequate initial antimicrobial treatment. Antimicrob Agents Chemother. 2007;51(6):1987–1994.
- , . Mortality and delay in effective therapy associated with extended‐spectrum β lactamase production in Enterobacteriaceae bacteraemia: a systematic review and meta‐analysis. J Antimicrob Chemother. 2007;60(5):913–920.
- , , , et al. Costs of bloodstream infections caused by Escherichia coli and influence of extended‐spectrum‐β‐lactamase production and inadequate initial antibiotic therapy. Antimicrob Agents Chemother. 2010;54(10):4085–4091.
- , , . Effects of confounders and intermediates on the association of bacteraemia caused by extended‐spectrum β‐lactamase‐producing Enterobacteriaceae and patient outcome: a meta‐analysis. J Antimicrob Chemother. 2012;67(6):1311–1320.
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: 21st informational supplement. M100‐S20. Wayne, PA: Clinical and Laboratory Standards Institute; 2010.
- , , , . A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
- , , , et al. Bloodstream infections caused by antibiotic‐resistant gram‐negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother. 2005;49(2):760–766.
- , , , , . Clinical implications of extended‐spectrum beta‐lactamase‐producing Klebsiella pneumoniae bacteraemia. J Hosp Infect. 2002;52(2):99–106.
- , , , , . Impact of extended‐spectrum β‐lactamase‐producing Escherichia coli and Klebsiella species on clinical outcomes and hospital costs: a matched cohort study. Infect Control Hosp Epidemiol. 2006;27(11):1226–1232.
- , , , et al. Risk factors for community‐onset urinary tract infections due to Escherichia coli harbouring extended‐spectrum‐β‐lactamases. J Antimicrob Chemother. 2006:57(4):780–783.
- , , , et al. Community infections caused extended‐spectrum‐β‐lactamase‐producing Escherichia coli. Arch Intern Med. 2008;168(17):1897–1902.
- , , . Prevalence and risk factors for extended spectrum‐β‐lactamase‐producing uropathogens in urinary tract infection. Korean J Urol. 2010;51(7):492–497.
- , , , , . Extended‐spectrum β‐lactamase‐producing gram‐negative pathogens in community‐acquired urinary tract infections: an increasing challenge for antimicrobial therapy. Infection. 2011;39(4):333–340.
- , , , et al. Epidemiology and genetic characteristics of extended‐spectrum‐β‐lactamase‐producing gram‐negative bacteria causing urinary tract infections in long‐term care facilities. J Antimicrob Chemother. 2012;67(12):2982–2987.
- , , , et al. Epidemiology, risk factors and comorbidity for urinary tract infections caused by extended‐spectrum beta‐lactamase (ESBL)‐producing enterobacteria. Int J Clin Pract. 2012;66(9):891–896.
- , , , et al. Identifying patients harboring extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae on hospital admission: derivation and validation of a scoring system. Antimicrob Agents Chemother. 2011;55(7):3485–3490.
- , , , . Utility of a clinical risk factor scoring model in predicting infection with extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae on hospital admission. Infect Control Hosp Epidemiol. 2013;34(4):385–392.
- , , , , , . Fosfomycin in the treatment of extended spectrum beta‐lactamase‐producing Escherichia coli‐related lower urinary tract infections. Int J Amtimicrob Agents. 2007;29(1):62–65.
- , , , , . Nitrofurantoin in the treatment of extended‐spectrum beta‐lactamase‐producing Escherichia coli‐related lower urinary tract infection. Int J Antimicrob Agents. 2012;40:554–556.
- , , , et al. Epidemiology and clinical features of infections caused by extended‐spectrum beta‐lactamase‐producing Escherichia coli in nonhospitalized patients. J Clin Microb. 2004;42(3):1089–1094.
- , , , et al. Community infections caused by extended‐spectrum β‐lactamase‐producing Escherichia coli. Arch Intern Med. 2008:168(17):1897–1902.
- , , , et al. Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae bloodstream infection: risk factors and clinical outcome. Intensive Care Med. 2002;28(12):1718–1723.
- , , , et al. Ceftazidime‐resistant Klebsiella pneumoniae and Escherichia coli bloodstream infection: a case‐control and molecular epidemiologic investigation. J Infect Dis. 1996;174(3):529–536.
- , . The impact of antimicrobial resistance on health and economic outcomes. Clin Infect Dis. 2003;36(11):1433–1437.
- . Clinical implications of antimicrobial resistance for therapy. J Antimicrob Chemother. 2008;62(suppl 2):ii105–ii114.
- , , , et al. Urologic diseases in America project: analytical methods and principal findings. J Urol. 2005;173(3):933–937.
- . Urinary tract pathogens in complicated infection and in elderly individuals. J Infect Dis. 2001;183(suppl 1):S5–S8.
- , , , , . Antimicrobial susceptibility of global inpatient urinary tract isolates of Escherichia coli: results from the Study for Monitoring Antimicrobial Resistance Trends (SMART) program: 2009–2010. Diagn Microbiol Infect Dis. 2011;70(4):507–511.
- , . Extended‐spectrum β‐lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657–686.
- , , . Extended‐spectrum β‐lactamase producing Escherichia coli: changing epidemiology and clinical impact. Curr Opin Infect Dis. 2010;23(4):320–326.
- . Defining an extended‐spectrum beta‐lactamase. Clin Microbiol Infect. 2008;14(suppl 5):3–10.
- , , , , , . Antimicrobial susceptibility among organisms from the Asia/Pacific Rim, Europe and Latin and North America collected as part of TEST and the in vitro activity of tigecycline. J Antimicrob Chemother. 2007;60(5):1018–1029.
- , , , . Variations in the prevalence of strains expressing an extended‐spectrum β‐lactamase phenotype and characterization of isolates from Europe, the Americas, and the Western Pacific region. Clin Infect Dis. 2001;32(suppl 2):S94–S103.
- National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004. Am J Infect Control. 2004;32(8):470–485.
- , . Prevalence and antimicrobial susceptibility data for extended‐spectrum β‐lactamase‐ and AmpC‐producing Enterobacteriaceae from the MYSTIC Program in Europe and the United States (1997–2004). Diagn Microbiol Infect Dis. 2005;53(4):257–264.
- , , , . Emergence of Enterobacteriaceae producing extended‐spectrum b‐lactamases (ESBLs) in the community. J Antimicrob Chemother. 2005;56(1):52–59.
- , , , et al. Epidemiology of ciprofloxacin resistance and its relationship to extended‐spectrum B‐lactamase production in Klebsiella pneumoniae isolates causing bacteremia. Clin Infect Dis. 2000;30(4):473–478.
- , , , , , Epidemiological investigation of fluoroquinolone resistance in infections due to extended‐spectrum‐β‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae. Clin Infect Dis. 2001;33(8):1288–1294.
- , , , . High levels of antimicrobial coresistance among extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae. Antimicrob Agents Chemother. 2005;49(5):2137–2139.
- . Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis. 2000;31(suppl 4):S131–S138.
- . The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin Infect Dis. 2006;42(suppl 2):S82–S89.
- , , , , , Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes. Clin Infect Dis. 2001:32(8):1162–1171.
- , , , et al. Predictors of mortality in patients with bloodstream infections caused by extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae: importance of inadequate initial antimicrobial treatment. Antimicrob Agents Chemother. 2007;51(6):1987–1994.
- , . Mortality and delay in effective therapy associated with extended‐spectrum β lactamase production in Enterobacteriaceae bacteraemia: a systematic review and meta‐analysis. J Antimicrob Chemother. 2007;60(5):913–920.
- , , , et al. Costs of bloodstream infections caused by Escherichia coli and influence of extended‐spectrum‐β‐lactamase production and inadequate initial antibiotic therapy. Antimicrob Agents Chemother. 2010;54(10):4085–4091.
- , , . Effects of confounders and intermediates on the association of bacteraemia caused by extended‐spectrum β‐lactamase‐producing Enterobacteriaceae and patient outcome: a meta‐analysis. J Antimicrob Chemother. 2012;67(6):1311–1320.
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: 21st informational supplement. M100‐S20. Wayne, PA: Clinical and Laboratory Standards Institute; 2010.
- , , , . A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383.
- , , , et al. Bloodstream infections caused by antibiotic‐resistant gram‐negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother. 2005;49(2):760–766.
- , , , , . Clinical implications of extended‐spectrum beta‐lactamase‐producing Klebsiella pneumoniae bacteraemia. J Hosp Infect. 2002;52(2):99–106.
- , , , , . Impact of extended‐spectrum β‐lactamase‐producing Escherichia coli and Klebsiella species on clinical outcomes and hospital costs: a matched cohort study. Infect Control Hosp Epidemiol. 2006;27(11):1226–1232.
- , , , et al. Risk factors for community‐onset urinary tract infections due to Escherichia coli harbouring extended‐spectrum‐β‐lactamases. J Antimicrob Chemother. 2006:57(4):780–783.
- , , , et al. Community infections caused extended‐spectrum‐β‐lactamase‐producing Escherichia coli. Arch Intern Med. 2008;168(17):1897–1902.
- , , . Prevalence and risk factors for extended spectrum‐β‐lactamase‐producing uropathogens in urinary tract infection. Korean J Urol. 2010;51(7):492–497.
- , , , , . Extended‐spectrum β‐lactamase‐producing gram‐negative pathogens in community‐acquired urinary tract infections: an increasing challenge for antimicrobial therapy. Infection. 2011;39(4):333–340.
- , , , et al. Epidemiology and genetic characteristics of extended‐spectrum‐β‐lactamase‐producing gram‐negative bacteria causing urinary tract infections in long‐term care facilities. J Antimicrob Chemother. 2012;67(12):2982–2987.
- , , , et al. Epidemiology, risk factors and comorbidity for urinary tract infections caused by extended‐spectrum beta‐lactamase (ESBL)‐producing enterobacteria. Int J Clin Pract. 2012;66(9):891–896.
- , , , et al. Identifying patients harboring extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae on hospital admission: derivation and validation of a scoring system. Antimicrob Agents Chemother. 2011;55(7):3485–3490.
- , , , . Utility of a clinical risk factor scoring model in predicting infection with extended‐spectrum‐β‐lactamase‐producing Enterobacteriaceae on hospital admission. Infect Control Hosp Epidemiol. 2013;34(4):385–392.
- , , , , , . Fosfomycin in the treatment of extended spectrum beta‐lactamase‐producing Escherichia coli‐related lower urinary tract infections. Int J Amtimicrob Agents. 2007;29(1):62–65.
- , , , , . Nitrofurantoin in the treatment of extended‐spectrum beta‐lactamase‐producing Escherichia coli‐related lower urinary tract infection. Int J Antimicrob Agents. 2012;40:554–556.
- , , , et al. Epidemiology and clinical features of infections caused by extended‐spectrum beta‐lactamase‐producing Escherichia coli in nonhospitalized patients. J Clin Microb. 2004;42(3):1089–1094.
- , , , et al. Community infections caused by extended‐spectrum β‐lactamase‐producing Escherichia coli. Arch Intern Med. 2008:168(17):1897–1902.
- , , , et al. Extended‐spectrum beta‐lactamase‐producing Escherichia coli and Klebsiella pneumoniae bloodstream infection: risk factors and clinical outcome. Intensive Care Med. 2002;28(12):1718–1723.
- , , , et al. Ceftazidime‐resistant Klebsiella pneumoniae and Escherichia coli bloodstream infection: a case‐control and molecular epidemiologic investigation. J Infect Dis. 1996;174(3):529–536.
- , . The impact of antimicrobial resistance on health and economic outcomes. Clin Infect Dis. 2003;36(11):1433–1437.
- . Clinical implications of antimicrobial resistance for therapy. J Antimicrob Chemother. 2008;62(suppl 2):ii105–ii114.
© 2014 Society of Hospital Medicine