User login
Four pillars of a successful practice: 3. Obtain and maintain physician referrals
READ THE REST OF THE SERIES
Pillar 1: Keep your current patients happy (March 2013)
Dr. Baum describes his number one strategy to retain patients (Audiocast, March 2013)
Pillar 2: Attract new patients (May 2013)
Pillar 4: Motivate your staff (August 2013)
Discussions of medical marketing often begin with the three As: availability, affability, and affordability. But most physicians already think of themselves as available, likeable, and offering appropriately priced services.
How do you differentiate yourself from the competition?
Fancy stationery; a slick, three-color brochure; a catchy logo; and a Web site will not do the trick. In fact, these are the last things you need.
One of the biggest misconceptions about marketing is that, to do it well, you must spend lots of money on peripherals. In truth, there are many other actions that are far more effective and essential to marketing than merely polishing your public relations image. The most essential element of your marketing plan is to make your practice user-friendly.
Nowhere is this need greater than when it comes to working with colleagues who are capable of referring patients to you—or are already doing so. In this article, I describe 10 strategies you can use to enhance your relationships with referring physicians.
1. WRITE AN EFFECTIVE REFERRAL LETTER
To obtain referrals from your colleagues, you need to ensure that your name crosses their mind and desk as frequently as possible—and in a positive fashion.
If you interview referring physicians, you will find that prompt communication is one of the most important reasons they refer a patient to a particular provider. According to the Annals of Family Medicine, more than 50% of physicians state that effective communication is the reason they select a doctor for referral (TABLE).1
| How primary care physicians select a doctor for referral | |
| Medical skill of the specialist | 87.5% |
| Access to the practice and acceptance of insurance | 59.0% |
| Previous experience with the specialist | 59.2% |
| Quality of communication | 52.5% |
| Board certification of the specialist | 33.9% |
| Medical school, residency | <1% |
Source: Kinchen et al1
Keep your referral letter short
The traditional referral letter is far too long, often 2 or 3 pages. It usually arrives 10 to 14 days after the patient was seen and is very expensive, costing a practice $12–$15 for each letter sent. The goal of an effective referral letter: Get it there before the patient returns to the primary care provider.
The key ingredients of an effective referral letter are:
diagnosis
medications you have prescribed for the patient
your treatment plan.
The referring doctor is not interested in the nuances of your history or physical exam. They just want the three ingredients listed above.
For example, let’s say that Dr. Bill Smith refers Jane Doe, who has an overactive bladder and cystocele. Her urinalysis is negative, so you prescribe an anticholinergic agent and schedule a follow-up visit in 1 month to check symptoms and to conduct a urodynamic study if she has not improved. Your letter to Dr. Smith would read as follows:
Now the letter can be faxed to the referring doctor, often before the patient leaves the office. That way you can be certain that the letter arrives before the patient calls the physician with questions or concerns.
This is the best way to keep the referring physician informed and to function as the captain of the patient’s health-care ship.
EHRs can smooth the referral process
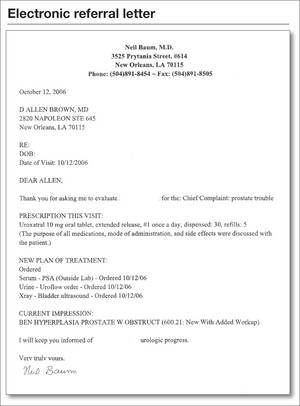
Most electronic health records (EHRs) have the capability to fax the entire note to the referring physician. However, if you were to ask a referring physician if she would like to read your entire note, the answer would probably be “No.” Most EHRs will allow you to select fields that contain the diagnosis, medications prescribed, and the treatment plan. A sample of this kind of letter appears in the FIGURE.
2. MAKE AN EFFORT TO PERSONALLY MEET EVERY PHYSICIAN WHO REFERS A PATIENT
Not only that, but try to meet all new physicians in your area. It is important to coddle your existing sources of referrals, but don’t forget to reach out to new physicians to let them know about your areas of interest or expertise.
3. REFER YOUR NEW PATIENTS TO REFERRING PHYSICIANS
Don’t refer to the same colleagues time after time. If a doctor starts sending new patients your way, it’s in your best interest to “reverse-refer” when a patient needs a primary care doctor, endocrinologist, or cardiologist.
You can be sure these referring doctors will appreciate your recommendations.
Related Article Complex atypical endometrial hyperplasia: When to refer
4. CREATE A LUNCH-AND-LEARN PROGRAM
You want other offices and medical staffs to get to know your staff and to be familiar with what you do. There’s no better way than to create a lunch-and-learn program in your office and extend an invitation to other offices in the area. At the program, have all of the staff members introduce themselves. Provide a tour of your office and give a 3- to 5-minute lecture on areas of your gynecologic interest and expertise.
5. ACKNOWLEDGE THE ACCOMPLISHMENTS OF REFERRING PHYSICIANS AND THEIR FAMILIES
If you see that one of your referring physicians has received an honor or award, send him a congratulatory note. If her children have been recognized for academic or athletic achievement, acknowledge this accomplishment with a note. You can be sure it will be one of the only acknowledgments they receive and will be deeply appreciated.
6. SHARE INFORMATION WITH A NO-MEETING JOURNAL CLUB
It’s very difficult to keep up with the medical literature. It’s challenging enough to keep up with the literature in your own specialty, let alone articles appearing in other specialty publications. One of the nicest gestures you can make is to copy any article that may be of interest to your colleagues and send it to them. Include a sticky note indicating where you would like them to look so that they don’t have to read the entire article.
7. SHARE NONMEDICAL INFORMATION, TOO
Your colleagues will appreciate it when you share nonmedical information to let them know you are thinking of them even when you are not discussing patient care. For example, one of my colleagues collects fine pens. When I saw an article about a very expensive pen made with diamonds, I sent the story to my friend, suggesting that he tell his wife what was on his wish list.
8. KEEP THE REFERRING DOCTOR IN THE MEDICAL LOOP
If you are caring for a patient and plan to discharge her from the hospital, make sure that you or someone in your office contacts the referring doctor to inform him that the patient is being discharged so he doesn’t make unnecessary rounds. Other times to notify the referring doctor:
upon admission of her patient to the hospital
after surgery or a procedure
when you receive a significant laboratory or pathology report.
9. BE USER-FRIENDLY
If you perform gynecologic surgery on a referred patient, be sure to dictate a discharge summary. If the patient is to be discharged with gynecologic medications, give the patient their names in writing. Another convenience for the patient: Arrange your follow-up appointment on the same day she is to return to see the referring physician.
10. DON’T FORGET NONPHYSICIAN REFERRAL SOURCES
Nurses, pharmacists, pharmaceutical representatives, social workers, lawyers, beauticians, and manicurists—all of these professionals are likely to refer patients to you if you keep them in the loop.
11. BOTTOM LINE
You can build a practice by word of mouth by doing a great job of caring for patients, hoping that they will tell others about their positive experience. However, there are other opportunities to enhance your practice—notably, by nurturing your relationship with referring physicians. Try a few of these ideas and you will certainly see your referrals increase significantly.

Neil H. Baum, MD
Dr. Baum practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
The author reports no financial relationships relevant to this article.
Neil H. Baum, MD
Dr. Baum practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
The author reports no financial relationships relevant to this article.
Neil H. Baum, MD
Dr. Baum practices urology in New Orleans, Louisiana. He is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans. He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, Louisiana. And he is the author of Marketing Your Clinical Practice: Ethically, Effectively, Economically (4th edition, 2009; Jones & Bartlett).
The author reports no financial relationships relevant to this article.
READ THE REST OF THE SERIES
Pillar 1: Keep your current patients happy (March 2013)
Dr. Baum describes his number one strategy to retain patients (Audiocast, March 2013)
Pillar 2: Attract new patients (May 2013)
Pillar 4: Motivate your staff (August 2013)
Discussions of medical marketing often begin with the three As: availability, affability, and affordability. But most physicians already think of themselves as available, likeable, and offering appropriately priced services.
How do you differentiate yourself from the competition?
Fancy stationery; a slick, three-color brochure; a catchy logo; and a Web site will not do the trick. In fact, these are the last things you need.
One of the biggest misconceptions about marketing is that, to do it well, you must spend lots of money on peripherals. In truth, there are many other actions that are far more effective and essential to marketing than merely polishing your public relations image. The most essential element of your marketing plan is to make your practice user-friendly.
Nowhere is this need greater than when it comes to working with colleagues who are capable of referring patients to you—or are already doing so. In this article, I describe 10 strategies you can use to enhance your relationships with referring physicians.
1. WRITE AN EFFECTIVE REFERRAL LETTER
To obtain referrals from your colleagues, you need to ensure that your name crosses their mind and desk as frequently as possible—and in a positive fashion.
If you interview referring physicians, you will find that prompt communication is one of the most important reasons they refer a patient to a particular provider. According to the Annals of Family Medicine, more than 50% of physicians state that effective communication is the reason they select a doctor for referral (TABLE).1
| How primary care physicians select a doctor for referral | |
| Medical skill of the specialist | 87.5% |
| Access to the practice and acceptance of insurance | 59.0% |
| Previous experience with the specialist | 59.2% |
| Quality of communication | 52.5% |
| Board certification of the specialist | 33.9% |
| Medical school, residency | <1% |
Source: Kinchen et al1
Keep your referral letter short
The traditional referral letter is far too long, often 2 or 3 pages. It usually arrives 10 to 14 days after the patient was seen and is very expensive, costing a practice $12–$15 for each letter sent. The goal of an effective referral letter: Get it there before the patient returns to the primary care provider.
The key ingredients of an effective referral letter are:
diagnosis
medications you have prescribed for the patient
your treatment plan.
The referring doctor is not interested in the nuances of your history or physical exam. They just want the three ingredients listed above.
For example, let’s say that Dr. Bill Smith refers Jane Doe, who has an overactive bladder and cystocele. Her urinalysis is negative, so you prescribe an anticholinergic agent and schedule a follow-up visit in 1 month to check symptoms and to conduct a urodynamic study if she has not improved. Your letter to Dr. Smith would read as follows:
Now the letter can be faxed to the referring doctor, often before the patient leaves the office. That way you can be certain that the letter arrives before the patient calls the physician with questions or concerns.
This is the best way to keep the referring physician informed and to function as the captain of the patient’s health-care ship.
EHRs can smooth the referral process
Most electronic health records (EHRs) have the capability to fax the entire note to the referring physician. However, if you were to ask a referring physician if she would like to read your entire note, the answer would probably be “No.” Most EHRs will allow you to select fields that contain the diagnosis, medications prescribed, and the treatment plan. A sample of this kind of letter appears in the FIGURE.
2. MAKE AN EFFORT TO PERSONALLY MEET EVERY PHYSICIAN WHO REFERS A PATIENT
Not only that, but try to meet all new physicians in your area. It is important to coddle your existing sources of referrals, but don’t forget to reach out to new physicians to let them know about your areas of interest or expertise.
3. REFER YOUR NEW PATIENTS TO REFERRING PHYSICIANS
Don’t refer to the same colleagues time after time. If a doctor starts sending new patients your way, it’s in your best interest to “reverse-refer” when a patient needs a primary care doctor, endocrinologist, or cardiologist.
You can be sure these referring doctors will appreciate your recommendations.
Related Article Complex atypical endometrial hyperplasia: When to refer
4. CREATE A LUNCH-AND-LEARN PROGRAM
You want other offices and medical staffs to get to know your staff and to be familiar with what you do. There’s no better way than to create a lunch-and-learn program in your office and extend an invitation to other offices in the area. At the program, have all of the staff members introduce themselves. Provide a tour of your office and give a 3- to 5-minute lecture on areas of your gynecologic interest and expertise.
5. ACKNOWLEDGE THE ACCOMPLISHMENTS OF REFERRING PHYSICIANS AND THEIR FAMILIES
If you see that one of your referring physicians has received an honor or award, send him a congratulatory note. If her children have been recognized for academic or athletic achievement, acknowledge this accomplishment with a note. You can be sure it will be one of the only acknowledgments they receive and will be deeply appreciated.
6. SHARE INFORMATION WITH A NO-MEETING JOURNAL CLUB
It’s very difficult to keep up with the medical literature. It’s challenging enough to keep up with the literature in your own specialty, let alone articles appearing in other specialty publications. One of the nicest gestures you can make is to copy any article that may be of interest to your colleagues and send it to them. Include a sticky note indicating where you would like them to look so that they don’t have to read the entire article.
7. SHARE NONMEDICAL INFORMATION, TOO
Your colleagues will appreciate it when you share nonmedical information to let them know you are thinking of them even when you are not discussing patient care. For example, one of my colleagues collects fine pens. When I saw an article about a very expensive pen made with diamonds, I sent the story to my friend, suggesting that he tell his wife what was on his wish list.
8. KEEP THE REFERRING DOCTOR IN THE MEDICAL LOOP
If you are caring for a patient and plan to discharge her from the hospital, make sure that you or someone in your office contacts the referring doctor to inform him that the patient is being discharged so he doesn’t make unnecessary rounds. Other times to notify the referring doctor:
upon admission of her patient to the hospital
after surgery or a procedure
when you receive a significant laboratory or pathology report.
9. BE USER-FRIENDLY
If you perform gynecologic surgery on a referred patient, be sure to dictate a discharge summary. If the patient is to be discharged with gynecologic medications, give the patient their names in writing. Another convenience for the patient: Arrange your follow-up appointment on the same day she is to return to see the referring physician.
10. DON’T FORGET NONPHYSICIAN REFERRAL SOURCES
Nurses, pharmacists, pharmaceutical representatives, social workers, lawyers, beauticians, and manicurists—all of these professionals are likely to refer patients to you if you keep them in the loop.
11. BOTTOM LINE
You can build a practice by word of mouth by doing a great job of caring for patients, hoping that they will tell others about their positive experience. However, there are other opportunities to enhance your practice—notably, by nurturing your relationship with referring physicians. Try a few of these ideas and you will certainly see your referrals increase significantly.
READ THE REST OF THE SERIES
Pillar 1: Keep your current patients happy (March 2013)
Dr. Baum describes his number one strategy to retain patients (Audiocast, March 2013)
Pillar 2: Attract new patients (May 2013)
Pillar 4: Motivate your staff (August 2013)
Discussions of medical marketing often begin with the three As: availability, affability, and affordability. But most physicians already think of themselves as available, likeable, and offering appropriately priced services.
How do you differentiate yourself from the competition?
Fancy stationery; a slick, three-color brochure; a catchy logo; and a Web site will not do the trick. In fact, these are the last things you need.
One of the biggest misconceptions about marketing is that, to do it well, you must spend lots of money on peripherals. In truth, there are many other actions that are far more effective and essential to marketing than merely polishing your public relations image. The most essential element of your marketing plan is to make your practice user-friendly.
Nowhere is this need greater than when it comes to working with colleagues who are capable of referring patients to you—or are already doing so. In this article, I describe 10 strategies you can use to enhance your relationships with referring physicians.
1. WRITE AN EFFECTIVE REFERRAL LETTER
To obtain referrals from your colleagues, you need to ensure that your name crosses their mind and desk as frequently as possible—and in a positive fashion.
If you interview referring physicians, you will find that prompt communication is one of the most important reasons they refer a patient to a particular provider. According to the Annals of Family Medicine, more than 50% of physicians state that effective communication is the reason they select a doctor for referral (TABLE).1
| How primary care physicians select a doctor for referral | |
| Medical skill of the specialist | 87.5% |
| Access to the practice and acceptance of insurance | 59.0% |
| Previous experience with the specialist | 59.2% |
| Quality of communication | 52.5% |
| Board certification of the specialist | 33.9% |
| Medical school, residency | <1% |
Source: Kinchen et al1
Keep your referral letter short
The traditional referral letter is far too long, often 2 or 3 pages. It usually arrives 10 to 14 days after the patient was seen and is very expensive, costing a practice $12–$15 for each letter sent. The goal of an effective referral letter: Get it there before the patient returns to the primary care provider.
The key ingredients of an effective referral letter are:
diagnosis
medications you have prescribed for the patient
your treatment plan.
The referring doctor is not interested in the nuances of your history or physical exam. They just want the three ingredients listed above.
For example, let’s say that Dr. Bill Smith refers Jane Doe, who has an overactive bladder and cystocele. Her urinalysis is negative, so you prescribe an anticholinergic agent and schedule a follow-up visit in 1 month to check symptoms and to conduct a urodynamic study if she has not improved. Your letter to Dr. Smith would read as follows:
Now the letter can be faxed to the referring doctor, often before the patient leaves the office. That way you can be certain that the letter arrives before the patient calls the physician with questions or concerns.
This is the best way to keep the referring physician informed and to function as the captain of the patient’s health-care ship.
EHRs can smooth the referral process
Most electronic health records (EHRs) have the capability to fax the entire note to the referring physician. However, if you were to ask a referring physician if she would like to read your entire note, the answer would probably be “No.” Most EHRs will allow you to select fields that contain the diagnosis, medications prescribed, and the treatment plan. A sample of this kind of letter appears in the FIGURE.
2. MAKE AN EFFORT TO PERSONALLY MEET EVERY PHYSICIAN WHO REFERS A PATIENT
Not only that, but try to meet all new physicians in your area. It is important to coddle your existing sources of referrals, but don’t forget to reach out to new physicians to let them know about your areas of interest or expertise.
3. REFER YOUR NEW PATIENTS TO REFERRING PHYSICIANS
Don’t refer to the same colleagues time after time. If a doctor starts sending new patients your way, it’s in your best interest to “reverse-refer” when a patient needs a primary care doctor, endocrinologist, or cardiologist.
You can be sure these referring doctors will appreciate your recommendations.
Related Article Complex atypical endometrial hyperplasia: When to refer
4. CREATE A LUNCH-AND-LEARN PROGRAM
You want other offices and medical staffs to get to know your staff and to be familiar with what you do. There’s no better way than to create a lunch-and-learn program in your office and extend an invitation to other offices in the area. At the program, have all of the staff members introduce themselves. Provide a tour of your office and give a 3- to 5-minute lecture on areas of your gynecologic interest and expertise.
5. ACKNOWLEDGE THE ACCOMPLISHMENTS OF REFERRING PHYSICIANS AND THEIR FAMILIES
If you see that one of your referring physicians has received an honor or award, send him a congratulatory note. If her children have been recognized for academic or athletic achievement, acknowledge this accomplishment with a note. You can be sure it will be one of the only acknowledgments they receive and will be deeply appreciated.
6. SHARE INFORMATION WITH A NO-MEETING JOURNAL CLUB
It’s very difficult to keep up with the medical literature. It’s challenging enough to keep up with the literature in your own specialty, let alone articles appearing in other specialty publications. One of the nicest gestures you can make is to copy any article that may be of interest to your colleagues and send it to them. Include a sticky note indicating where you would like them to look so that they don’t have to read the entire article.
7. SHARE NONMEDICAL INFORMATION, TOO
Your colleagues will appreciate it when you share nonmedical information to let them know you are thinking of them even when you are not discussing patient care. For example, one of my colleagues collects fine pens. When I saw an article about a very expensive pen made with diamonds, I sent the story to my friend, suggesting that he tell his wife what was on his wish list.
8. KEEP THE REFERRING DOCTOR IN THE MEDICAL LOOP
If you are caring for a patient and plan to discharge her from the hospital, make sure that you or someone in your office contacts the referring doctor to inform him that the patient is being discharged so he doesn’t make unnecessary rounds. Other times to notify the referring doctor:
upon admission of her patient to the hospital
after surgery or a procedure
when you receive a significant laboratory or pathology report.
9. BE USER-FRIENDLY
If you perform gynecologic surgery on a referred patient, be sure to dictate a discharge summary. If the patient is to be discharged with gynecologic medications, give the patient their names in writing. Another convenience for the patient: Arrange your follow-up appointment on the same day she is to return to see the referring physician.
10. DON’T FORGET NONPHYSICIAN REFERRAL SOURCES
Nurses, pharmacists, pharmaceutical representatives, social workers, lawyers, beauticians, and manicurists—all of these professionals are likely to refer patients to you if you keep them in the loop.
11. BOTTOM LINE
You can build a practice by word of mouth by doing a great job of caring for patients, hoping that they will tell others about their positive experience. However, there are other opportunities to enhance your practice—notably, by nurturing your relationship with referring physicians. Try a few of these ideas and you will certainly see your referrals increase significantly.

Grassroots Efforts to Improve Patient Care
When it joined with 15 other medical specialty societies at a Feb. 21 press conference to announce updates to the ABIM Foundation’s Choosing Wisely campaign to combat cost and waste reduction in healthcare , SHM leaders said they hoped the hospitalist-focused quality guidelines would trickle down from the national level to clinicians in the field (see “Stop! Think Twice Before You Order"). The lists of treatments adult and pediatric hospitalists should consider questioning in the absence of evidence or protocols include the urinary catheters, blood transfusions, telemetry monitoring outside of the ICU, and certain lab tests and medications for preventing stress ulcers.

Ian Jenkins, MD, a hospitalist at the University of California, San Diego, who presented during both Choosing Wisely sessions, said hospitalists are at the intersection of healthcare cost and quality improvement. “People recognize the moral imperatives,” he said.
Pre-course participants split into four teams and drilled deeper into questionable treatments and practices outlined by the campaign. SHM plans to make results of those small-group discussions available to its members, along with enhanced reference lists and best practices from the field. “We can contribute a bunch of stuff,” Dr. Jenkins told pre-course participants. “Tell us what you can contribute, and what you’d like to see from us.”
Hospitalist George Dimitriou, MD, of Allegheny General Hospital in Pittsburgh, said his hospital has spent the past couple of years working on several of the same hospital-focused quality issues outlined in the Choosing Wisely campaign.
“Our transfusion initiative was driven by the local blood bank, knowing we were over-transfusing,” he said. “We had an order set, but we recently put in place a more restrictive transfusion policy, following national guidelines.
“Our Foley catheter protocol was in response to the national recommendations to reduce urinary tract infections, mostly driven by our infectious disease department,” Dr. Dimitriou added. The hospital has not yet tackled the problem of overuse of telemetry services, “although that’s something I have wanted to do for a long time.”
Another hot-button issue, the daily ordering of lab tests, should be rectified by simply “taking it out of the electronic medical record as a default option.”
According to SHM staff, a Choosing Wisely case study competition will be held next year, with $10,000 in cash prizes awarded for adult and pediatric quality initiatives showing improvement in utilization, innovation, sustainability, and institutional commitment. An independent review panel will develop evaluation criteria, with a projected application deadline of Fall 2014. The competition is supported by a $50,000 grant from the ABIM Foundation. TH
Larry Beresford is a freelance writer in Oakland, Calif.
When it joined with 15 other medical specialty societies at a Feb. 21 press conference to announce updates to the ABIM Foundation’s Choosing Wisely campaign to combat cost and waste reduction in healthcare , SHM leaders said they hoped the hospitalist-focused quality guidelines would trickle down from the national level to clinicians in the field (see “Stop! Think Twice Before You Order"). The lists of treatments adult and pediatric hospitalists should consider questioning in the absence of evidence or protocols include the urinary catheters, blood transfusions, telemetry monitoring outside of the ICU, and certain lab tests and medications for preventing stress ulcers.
Ian Jenkins, MD, a hospitalist at the University of California, San Diego, who presented during both Choosing Wisely sessions, said hospitalists are at the intersection of healthcare cost and quality improvement. “People recognize the moral imperatives,” he said.
Pre-course participants split into four teams and drilled deeper into questionable treatments and practices outlined by the campaign. SHM plans to make results of those small-group discussions available to its members, along with enhanced reference lists and best practices from the field. “We can contribute a bunch of stuff,” Dr. Jenkins told pre-course participants. “Tell us what you can contribute, and what you’d like to see from us.”
Hospitalist George Dimitriou, MD, of Allegheny General Hospital in Pittsburgh, said his hospital has spent the past couple of years working on several of the same hospital-focused quality issues outlined in the Choosing Wisely campaign.
“Our transfusion initiative was driven by the local blood bank, knowing we were over-transfusing,” he said. “We had an order set, but we recently put in place a more restrictive transfusion policy, following national guidelines.
“Our Foley catheter protocol was in response to the national recommendations to reduce urinary tract infections, mostly driven by our infectious disease department,” Dr. Dimitriou added. The hospital has not yet tackled the problem of overuse of telemetry services, “although that’s something I have wanted to do for a long time.”
Another hot-button issue, the daily ordering of lab tests, should be rectified by simply “taking it out of the electronic medical record as a default option.”
According to SHM staff, a Choosing Wisely case study competition will be held next year, with $10,000 in cash prizes awarded for adult and pediatric quality initiatives showing improvement in utilization, innovation, sustainability, and institutional commitment. An independent review panel will develop evaluation criteria, with a projected application deadline of Fall 2014. The competition is supported by a $50,000 grant from the ABIM Foundation. TH
Larry Beresford is a freelance writer in Oakland, Calif.
When it joined with 15 other medical specialty societies at a Feb. 21 press conference to announce updates to the ABIM Foundation’s Choosing Wisely campaign to combat cost and waste reduction in healthcare , SHM leaders said they hoped the hospitalist-focused quality guidelines would trickle down from the national level to clinicians in the field (see “Stop! Think Twice Before You Order"). The lists of treatments adult and pediatric hospitalists should consider questioning in the absence of evidence or protocols include the urinary catheters, blood transfusions, telemetry monitoring outside of the ICU, and certain lab tests and medications for preventing stress ulcers.
Ian Jenkins, MD, a hospitalist at the University of California, San Diego, who presented during both Choosing Wisely sessions, said hospitalists are at the intersection of healthcare cost and quality improvement. “People recognize the moral imperatives,” he said.
Pre-course participants split into four teams and drilled deeper into questionable treatments and practices outlined by the campaign. SHM plans to make results of those small-group discussions available to its members, along with enhanced reference lists and best practices from the field. “We can contribute a bunch of stuff,” Dr. Jenkins told pre-course participants. “Tell us what you can contribute, and what you’d like to see from us.”
Hospitalist George Dimitriou, MD, of Allegheny General Hospital in Pittsburgh, said his hospital has spent the past couple of years working on several of the same hospital-focused quality issues outlined in the Choosing Wisely campaign.
“Our transfusion initiative was driven by the local blood bank, knowing we were over-transfusing,” he said. “We had an order set, but we recently put in place a more restrictive transfusion policy, following national guidelines.
“Our Foley catheter protocol was in response to the national recommendations to reduce urinary tract infections, mostly driven by our infectious disease department,” Dr. Dimitriou added. The hospital has not yet tackled the problem of overuse of telemetry services, “although that’s something I have wanted to do for a long time.”
Another hot-button issue, the daily ordering of lab tests, should be rectified by simply “taking it out of the electronic medical record as a default option.”
According to SHM staff, a Choosing Wisely case study competition will be held next year, with $10,000 in cash prizes awarded for adult and pediatric quality initiatives showing improvement in utilization, innovation, sustainability, and institutional commitment. An independent review panel will develop evaluation criteria, with a projected application deadline of Fall 2014. The competition is supported by a $50,000 grant from the ABIM Foundation. TH
Larry Beresford is a freelance writer in Oakland, Calif.

School nurses
When my children were in school and got head lice, I learned the full metaphorical scope of words like "lousy" and "nit-picking." I also learned that school nurses didn’t give a hoot for my opinions.
Despite my boards in pediatrics and dermatology, my protests against schools’ policies of dragging parents out of work to pick up a kid on whom the nurse found a nit, or thought she did, even after multiple treatments and fine-tooth combing (another nice, real-life metaphor) went unheard.
In vain did I cite policy statements by august professional organizations that no-nit policies were unnecessary. No sir – they find one dead egg case, and Johnny goes home. His parents are obviously irresponsible anyway, not to mention unhygienic. So I gave up, and my children grew up.
What reawakened these memories was my annual visit to Marcie, my eye doctor. "I really like your PA," she said. "Jared saw her when the school nurse sent him home with a rash. Your PA asked him why he was there. ‘The nurse sent me home,’ he said. ‘OK,’ said your PA, ‘now you can go back.’
"They once sent Jared home because of a chalazion," Marcie continued. "I called them up. ‘He’s on tobramycin,’ I told them. ‘And a chalazion isn’t contagious anyway.’ But they didn’t believe me!
"My husband called them. ‘My wife is an eye doctor,’ he said. ‘Oh,’ they said, ‘We didn’t know what kind of doctor she was.’ "
Probably the most egregious example of high-handed school medical behavior I have ever seen played out in my office just last month. The Hightowers brought in 4-year-old Jeffrey with an impetiginized rash. We started cephalexin, pending culture results. When these showed MRSA on Friday afternoon, we called the family to switch Jeffrey to trimethoprim-sulfamethoxazole.
Janice Hightower became very upset. "Should I call the school?" We suggested she use her discretion, because by Monday Jeffrey would no longer be contagious. "But I’m a teacher," she said. "I feel responsible." So she did.
The next day, Jeffrey’s dad, Brian Hightower, came to school to coach baseball (his kids stayed home). During the game, all the parents got text messages informing them: "Someone in the school is infected with MRSA, and school is closed until further notice." He then sat in stunned silence as the other parents commiserated with each other about what happens when their children have to hang around with other kids whose parents are irresponsible, dirty, and a lot of other unpleasant things.
On Monday, Brian Hightower brought Jeffrey’s older brother, Jason, to the office. Jason had no skin lesions at all. "My wife won’t let me go home without antibiotics for him," insisted Brian. We told him there was nothing to treat, and he left. Later, Janice Hightower called. "This is like ‘The Scarlet Letter,’ " she said. "We’ll never be able to show our faces in the community again."
We tried to reassure her (the MRSA culprit’s identity had mercifully not been divulged), but she pressed on. "When he grows up and kisses his first girl," she asked, "will he have to tell her about this?"
Things went downhill from there. Several days and many phone calls later, the Hightowers began to calm down. Jeffrey and Jason returned to school, which had somehow managed to reopen. I have no idea which medical authority authorized the reopening, any more than I know who told them to close it in the first place. Jeffrey hasn’t been sighted kissing any girls yet, other than possibly Aunt Susie.
What this episode says about how people judge and treat others who are ill, not to mention how ancient ideas about disease persist long after they are supposed to have been discarded, doesn’t need to be spelled out. Better to take polite notice and move on.
But it also says quite a lot about the limitations of our professional authority outside the spheres where we’re in charge. In the office, people may or may not listen to us, but at least they act as though they might.
But outside the office, in schools for instance, what we have to say often doesn’t count for much. Or anything.
Dr. Rockoff practices dermatology in Brookline, Mass. To respond to this column, e-mail him at our editorial offices at [email protected].
When my children were in school and got head lice, I learned the full metaphorical scope of words like "lousy" and "nit-picking." I also learned that school nurses didn’t give a hoot for my opinions.
Despite my boards in pediatrics and dermatology, my protests against schools’ policies of dragging parents out of work to pick up a kid on whom the nurse found a nit, or thought she did, even after multiple treatments and fine-tooth combing (another nice, real-life metaphor) went unheard.
In vain did I cite policy statements by august professional organizations that no-nit policies were unnecessary. No sir – they find one dead egg case, and Johnny goes home. His parents are obviously irresponsible anyway, not to mention unhygienic. So I gave up, and my children grew up.
What reawakened these memories was my annual visit to Marcie, my eye doctor. "I really like your PA," she said. "Jared saw her when the school nurse sent him home with a rash. Your PA asked him why he was there. ‘The nurse sent me home,’ he said. ‘OK,’ said your PA, ‘now you can go back.’
"They once sent Jared home because of a chalazion," Marcie continued. "I called them up. ‘He’s on tobramycin,’ I told them. ‘And a chalazion isn’t contagious anyway.’ But they didn’t believe me!
"My husband called them. ‘My wife is an eye doctor,’ he said. ‘Oh,’ they said, ‘We didn’t know what kind of doctor she was.’ "
Probably the most egregious example of high-handed school medical behavior I have ever seen played out in my office just last month. The Hightowers brought in 4-year-old Jeffrey with an impetiginized rash. We started cephalexin, pending culture results. When these showed MRSA on Friday afternoon, we called the family to switch Jeffrey to trimethoprim-sulfamethoxazole.
Janice Hightower became very upset. "Should I call the school?" We suggested she use her discretion, because by Monday Jeffrey would no longer be contagious. "But I’m a teacher," she said. "I feel responsible." So she did.
The next day, Jeffrey’s dad, Brian Hightower, came to school to coach baseball (his kids stayed home). During the game, all the parents got text messages informing them: "Someone in the school is infected with MRSA, and school is closed until further notice." He then sat in stunned silence as the other parents commiserated with each other about what happens when their children have to hang around with other kids whose parents are irresponsible, dirty, and a lot of other unpleasant things.
On Monday, Brian Hightower brought Jeffrey’s older brother, Jason, to the office. Jason had no skin lesions at all. "My wife won’t let me go home without antibiotics for him," insisted Brian. We told him there was nothing to treat, and he left. Later, Janice Hightower called. "This is like ‘The Scarlet Letter,’ " she said. "We’ll never be able to show our faces in the community again."
We tried to reassure her (the MRSA culprit’s identity had mercifully not been divulged), but she pressed on. "When he grows up and kisses his first girl," she asked, "will he have to tell her about this?"
Things went downhill from there. Several days and many phone calls later, the Hightowers began to calm down. Jeffrey and Jason returned to school, which had somehow managed to reopen. I have no idea which medical authority authorized the reopening, any more than I know who told them to close it in the first place. Jeffrey hasn’t been sighted kissing any girls yet, other than possibly Aunt Susie.
What this episode says about how people judge and treat others who are ill, not to mention how ancient ideas about disease persist long after they are supposed to have been discarded, doesn’t need to be spelled out. Better to take polite notice and move on.
But it also says quite a lot about the limitations of our professional authority outside the spheres where we’re in charge. In the office, people may or may not listen to us, but at least they act as though they might.
But outside the office, in schools for instance, what we have to say often doesn’t count for much. Or anything.
Dr. Rockoff practices dermatology in Brookline, Mass. To respond to this column, e-mail him at our editorial offices at [email protected].
When my children were in school and got head lice, I learned the full metaphorical scope of words like "lousy" and "nit-picking." I also learned that school nurses didn’t give a hoot for my opinions.
Despite my boards in pediatrics and dermatology, my protests against schools’ policies of dragging parents out of work to pick up a kid on whom the nurse found a nit, or thought she did, even after multiple treatments and fine-tooth combing (another nice, real-life metaphor) went unheard.
In vain did I cite policy statements by august professional organizations that no-nit policies were unnecessary. No sir – they find one dead egg case, and Johnny goes home. His parents are obviously irresponsible anyway, not to mention unhygienic. So I gave up, and my children grew up.
What reawakened these memories was my annual visit to Marcie, my eye doctor. "I really like your PA," she said. "Jared saw her when the school nurse sent him home with a rash. Your PA asked him why he was there. ‘The nurse sent me home,’ he said. ‘OK,’ said your PA, ‘now you can go back.’
"They once sent Jared home because of a chalazion," Marcie continued. "I called them up. ‘He’s on tobramycin,’ I told them. ‘And a chalazion isn’t contagious anyway.’ But they didn’t believe me!
"My husband called them. ‘My wife is an eye doctor,’ he said. ‘Oh,’ they said, ‘We didn’t know what kind of doctor she was.’ "
Probably the most egregious example of high-handed school medical behavior I have ever seen played out in my office just last month. The Hightowers brought in 4-year-old Jeffrey with an impetiginized rash. We started cephalexin, pending culture results. When these showed MRSA on Friday afternoon, we called the family to switch Jeffrey to trimethoprim-sulfamethoxazole.
Janice Hightower became very upset. "Should I call the school?" We suggested she use her discretion, because by Monday Jeffrey would no longer be contagious. "But I’m a teacher," she said. "I feel responsible." So she did.
The next day, Jeffrey’s dad, Brian Hightower, came to school to coach baseball (his kids stayed home). During the game, all the parents got text messages informing them: "Someone in the school is infected with MRSA, and school is closed until further notice." He then sat in stunned silence as the other parents commiserated with each other about what happens when their children have to hang around with other kids whose parents are irresponsible, dirty, and a lot of other unpleasant things.
On Monday, Brian Hightower brought Jeffrey’s older brother, Jason, to the office. Jason had no skin lesions at all. "My wife won’t let me go home without antibiotics for him," insisted Brian. We told him there was nothing to treat, and he left. Later, Janice Hightower called. "This is like ‘The Scarlet Letter,’ " she said. "We’ll never be able to show our faces in the community again."
We tried to reassure her (the MRSA culprit’s identity had mercifully not been divulged), but she pressed on. "When he grows up and kisses his first girl," she asked, "will he have to tell her about this?"
Things went downhill from there. Several days and many phone calls later, the Hightowers began to calm down. Jeffrey and Jason returned to school, which had somehow managed to reopen. I have no idea which medical authority authorized the reopening, any more than I know who told them to close it in the first place. Jeffrey hasn’t been sighted kissing any girls yet, other than possibly Aunt Susie.
What this episode says about how people judge and treat others who are ill, not to mention how ancient ideas about disease persist long after they are supposed to have been discarded, doesn’t need to be spelled out. Better to take polite notice and move on.
But it also says quite a lot about the limitations of our professional authority outside the spheres where we’re in charge. In the office, people may or may not listen to us, but at least they act as though they might.
But outside the office, in schools for instance, what we have to say often doesn’t count for much. Or anything.
Dr. Rockoff practices dermatology in Brookline, Mass. To respond to this column, e-mail him at our editorial offices at [email protected].

