User login
Team Hospitalist Seats Nine New Members

Jairy C. Hunter, MD, MBA, SFHM
Associate executive medical director for case management and care transitions, Medical University of South Carolina, Charleston
QUOTABLE: “Hospital medicine is at the forefront of the changes to the way our country approaches healthcare delivery. In my view, hospitalists will play a pivotal role, through innovation, to ensure our patients receive the care they deserve in a safe and efficient manner. We should view this time as an opportunity to demonstrate the value of our expertise.”

Gregory Harlan, MD, MPH
Director of medical affairs, IPC: The Hospitalist Company, North Hollywood, Calif.; clinical instructor, University of Southern California Medical School; pediatric hospitalist, Children’s Hospital of Los Angeles
QUOTABLE: “Hospitalist medicine is defining the next iteration of acute- and post-acute care at a systems level. Hospitalists are innovative and working within their facilities to enact change. I have worked in various settings: as an academic, medical director, PCP, and acute hospitalist. I appreciate the complexity of health care today.”

Klaus Suehler, MD, FHMHospitalist, Midwest Internal Medicine Hospitalists, Mercy Hospital, Coon Rapids, Minn.
QUOTABLE: “Being a hospitalist is both a challenging and rewarding way to practice medicine. We are the patient’s advocate at a time of acute and often life-threatening illness.”

Anand Kartha, MD, MSc
Hospitalist, VA Boston Healthcare System; assistant professor of medicine, Boston University; lecturer in medicine, Harvard Medical School
QUOTABLE: “Being a hospitalist gives me the wonderful opportunity to help people in their time of acute need. Taking care of veterans in particular allows me the privilege of caring for those who help keep us safe.”

Midori Larrabee, MD
Hospitalist medical director, Valley General Hospital, Monroe, Wash.
QUOTABLE: “Hospital medicine allows me the time and flexibility to both practice clinical medicine and advocate for my patients as a physician leader.”

Bryan Weiss, MBA
Director, consulting services practice, MedSynergies, Irving, Texas
QUOTABLE: “I am passionate and believe in hospital medicine.”

James O’Callaghan, MD, FAAP, FHM
Regional pediatric hospitalist, Evergreen (Wash.) Hospital; medical hospitalist, Seattle Children’s Hospital
QUOTABLE: “As a pediatric hospitalist, I am privileged to work with patients and families during what is typically the most stressful event of their lives, and to help them successfully navigate the complexities of modern U.S. health care.”

Julie L. Fedderson, MD
Assistant professor of medicine and internal-medicine chief quality and outcomes officer, The Nebraska Medical Center, Omaha
QUOTABLE: “Being a hospitalist has provided me daily challenges and forces me
to think outside the box to obtain the best outcomes for my patients. The ability to truly steer standardization of care and evidence-based medicine is amazing. This unique opportunity to care for patients on the individual level, and still provide insight into population management, epitomizes what our goals as hospitalists should be.”

Julianna Lindsey, MD, MBA, FHM
COO and strategist, Synergy Surgicalists; lead consultant, Asynd Consulting, Nashville, Tenn.
QUOTABLE: “Being a hospitalist is the best job in medicine. Hospitalists have the satisfaction of delivering care to patients at the bedside, in addition to the opportunity to drive patient quality, safety, and satisfaction initiatives on a larger scale. It’s the best place in medicine, in my opinion.”
Jairy C. Hunter, MD, MBA, SFHM
Associate executive medical director for case management and care transitions, Medical University of South Carolina, Charleston
QUOTABLE: “Hospital medicine is at the forefront of the changes to the way our country approaches healthcare delivery. In my view, hospitalists will play a pivotal role, through innovation, to ensure our patients receive the care they deserve in a safe and efficient manner. We should view this time as an opportunity to demonstrate the value of our expertise.”
Gregory Harlan, MD, MPH
Director of medical affairs, IPC: The Hospitalist Company, North Hollywood, Calif.; clinical instructor, University of Southern California Medical School; pediatric hospitalist, Children’s Hospital of Los Angeles
QUOTABLE: “Hospitalist medicine is defining the next iteration of acute- and post-acute care at a systems level. Hospitalists are innovative and working within their facilities to enact change. I have worked in various settings: as an academic, medical director, PCP, and acute hospitalist. I appreciate the complexity of health care today.”
Klaus Suehler, MD, FHMHospitalist, Midwest Internal Medicine Hospitalists, Mercy Hospital, Coon Rapids, Minn.
QUOTABLE: “Being a hospitalist is both a challenging and rewarding way to practice medicine. We are the patient’s advocate at a time of acute and often life-threatening illness.”
Anand Kartha, MD, MSc
Hospitalist, VA Boston Healthcare System; assistant professor of medicine, Boston University; lecturer in medicine, Harvard Medical School
QUOTABLE: “Being a hospitalist gives me the wonderful opportunity to help people in their time of acute need. Taking care of veterans in particular allows me the privilege of caring for those who help keep us safe.”
Midori Larrabee, MD
Hospitalist medical director, Valley General Hospital, Monroe, Wash.
QUOTABLE: “Hospital medicine allows me the time and flexibility to both practice clinical medicine and advocate for my patients as a physician leader.”
Bryan Weiss, MBA
Director, consulting services practice, MedSynergies, Irving, Texas
QUOTABLE: “I am passionate and believe in hospital medicine.”
James O’Callaghan, MD, FAAP, FHM
Regional pediatric hospitalist, Evergreen (Wash.) Hospital; medical hospitalist, Seattle Children’s Hospital
QUOTABLE: “As a pediatric hospitalist, I am privileged to work with patients and families during what is typically the most stressful event of their lives, and to help them successfully navigate the complexities of modern U.S. health care.”
Julie L. Fedderson, MD
Assistant professor of medicine and internal-medicine chief quality and outcomes officer, The Nebraska Medical Center, Omaha
QUOTABLE: “Being a hospitalist has provided me daily challenges and forces me
to think outside the box to obtain the best outcomes for my patients. The ability to truly steer standardization of care and evidence-based medicine is amazing. This unique opportunity to care for patients on the individual level, and still provide insight into population management, epitomizes what our goals as hospitalists should be.”
Julianna Lindsey, MD, MBA, FHM
COO and strategist, Synergy Surgicalists; lead consultant, Asynd Consulting, Nashville, Tenn.
QUOTABLE: “Being a hospitalist is the best job in medicine. Hospitalists have the satisfaction of delivering care to patients at the bedside, in addition to the opportunity to drive patient quality, safety, and satisfaction initiatives on a larger scale. It’s the best place in medicine, in my opinion.”
Jairy C. Hunter, MD, MBA, SFHM
Associate executive medical director for case management and care transitions, Medical University of South Carolina, Charleston
QUOTABLE: “Hospital medicine is at the forefront of the changes to the way our country approaches healthcare delivery. In my view, hospitalists will play a pivotal role, through innovation, to ensure our patients receive the care they deserve in a safe and efficient manner. We should view this time as an opportunity to demonstrate the value of our expertise.”
Gregory Harlan, MD, MPH
Director of medical affairs, IPC: The Hospitalist Company, North Hollywood, Calif.; clinical instructor, University of Southern California Medical School; pediatric hospitalist, Children’s Hospital of Los Angeles
QUOTABLE: “Hospitalist medicine is defining the next iteration of acute- and post-acute care at a systems level. Hospitalists are innovative and working within their facilities to enact change. I have worked in various settings: as an academic, medical director, PCP, and acute hospitalist. I appreciate the complexity of health care today.”
Klaus Suehler, MD, FHMHospitalist, Midwest Internal Medicine Hospitalists, Mercy Hospital, Coon Rapids, Minn.
QUOTABLE: “Being a hospitalist is both a challenging and rewarding way to practice medicine. We are the patient’s advocate at a time of acute and often life-threatening illness.”
Anand Kartha, MD, MSc
Hospitalist, VA Boston Healthcare System; assistant professor of medicine, Boston University; lecturer in medicine, Harvard Medical School
QUOTABLE: “Being a hospitalist gives me the wonderful opportunity to help people in their time of acute need. Taking care of veterans in particular allows me the privilege of caring for those who help keep us safe.”
Midori Larrabee, MD
Hospitalist medical director, Valley General Hospital, Monroe, Wash.
QUOTABLE: “Hospital medicine allows me the time and flexibility to both practice clinical medicine and advocate for my patients as a physician leader.”
Bryan Weiss, MBA
Director, consulting services practice, MedSynergies, Irving, Texas
QUOTABLE: “I am passionate and believe in hospital medicine.”
James O’Callaghan, MD, FAAP, FHM
Regional pediatric hospitalist, Evergreen (Wash.) Hospital; medical hospitalist, Seattle Children’s Hospital
QUOTABLE: “As a pediatric hospitalist, I am privileged to work with patients and families during what is typically the most stressful event of their lives, and to help them successfully navigate the complexities of modern U.S. health care.”
Julie L. Fedderson, MD
Assistant professor of medicine and internal-medicine chief quality and outcomes officer, The Nebraska Medical Center, Omaha
QUOTABLE: “Being a hospitalist has provided me daily challenges and forces me
to think outside the box to obtain the best outcomes for my patients. The ability to truly steer standardization of care and evidence-based medicine is amazing. This unique opportunity to care for patients on the individual level, and still provide insight into population management, epitomizes what our goals as hospitalists should be.”
Julianna Lindsey, MD, MBA, FHM
COO and strategist, Synergy Surgicalists; lead consultant, Asynd Consulting, Nashville, Tenn.
QUOTABLE: “Being a hospitalist is the best job in medicine. Hospitalists have the satisfaction of delivering care to patients at the bedside, in addition to the opportunity to drive patient quality, safety, and satisfaction initiatives on a larger scale. It’s the best place in medicine, in my opinion.”
Movers and Shakers in Hospital Medicine

Mark Shapiro, MD, has been appointed chief of medicine at Sharp Memorial Hospital in San Diego. A hospitalist with Sharp Rees-Stealy Medical Group since 2006, Dr. Shapiro recently began work as a physician collaborator with PracticingExcellence.com, a Web-based physician-learning platform expected to launch this fall.
John Davidyock, MD, SFHM, is the new section chief of hospital medicine at Temple University Hospital in Philadelphia. Dr. Davidyock also is vice chair of patient safety and quality improvement, and assistant professor of medicine at the Temple University School of Medicine. Dr. Davidyock has been a Senior Fellow of Hospital Medicine since 2012.
Rana Tan, MD, chief hospitalist at Harrison Medical Center in Bremerton, Wash., recently received the 2013 Summit Award for excellence in hospital medicine from Tacoma, Wash.-based Sound Physicians. Dr. Tan has served as chief hospitalist at Harrison Medical Center since 2010 and has been with Sound Physicians since 2005. She oversees 16 hospitalists on her team at Harrison.
Gary J. Carver, MD, is the new director of hospital medicine at Coshocton (Ohio) Hospital. He previously worked as Coshocton Hospital’s chief of staff and sat on the board of trustees.

Thomas McIlraith, MD, SFHM, CLHM, received SHM’s Certificate of Leadership in Hospital Medicine at HM13 in May. Dr. McIlraith is chairman of hospital medicine at Mercy Medical Group in Sacramento, Calif. He is responsible for 24/7 operations at four hospitals and a department of 60 hospitalist physicians. In addition, he is a member of the Mercy Medical Group board of directors. He also is a clinical instructor at the University of California at Davis.
Sameh Naseib, MD, SFHM, CLHM, also received SHM’s Certificate of Leadership in Hospital Medicine at HM13 in May. Dr. Naseib is inpatient medical director at Beaver Medical Group in Redlands, Calif., where he supervises the hospitalist programs at San Gorgonio Memorial and Redlands Community hospitals.
Business Moves

Sound Physicians has announced new contracts for hospitalist services at San Joaquin Community Hospital, a 254-bed facility in Bakersfield, Calif., and at Kona Community Hospital, a 94-bed hospital in Kealakekua, Hawaii.
Emeryville, Calif.–based CEP America, a private physician-staffing firm, is providing hospitalist services at both Palomar Medical Center in Escondido, Calif., and Pomerado Hospital in Poway, Calif. CEP’s added services are in addition to the emergency medicine services the group has provided at the two hospitals for more than a decade.
Apollo Medical Holdings Inc. (ApolloMed), based in Glendale, Calif., is providing hospitalist services to Pacifica Hospital of the Valley in Sun Valley, Calif. Pacifica is a 242-bed acute-care hospital that serves several communities throughout the San Fernando Valley. ApolloMed provides physician services at 29 hospitals throughout southern and central California.
Michael O'Neal is a freelance writer in New York.
Mark Shapiro, MD, has been appointed chief of medicine at Sharp Memorial Hospital in San Diego. A hospitalist with Sharp Rees-Stealy Medical Group since 2006, Dr. Shapiro recently began work as a physician collaborator with PracticingExcellence.com, a Web-based physician-learning platform expected to launch this fall.
John Davidyock, MD, SFHM, is the new section chief of hospital medicine at Temple University Hospital in Philadelphia. Dr. Davidyock also is vice chair of patient safety and quality improvement, and assistant professor of medicine at the Temple University School of Medicine. Dr. Davidyock has been a Senior Fellow of Hospital Medicine since 2012.
Rana Tan, MD, chief hospitalist at Harrison Medical Center in Bremerton, Wash., recently received the 2013 Summit Award for excellence in hospital medicine from Tacoma, Wash.-based Sound Physicians. Dr. Tan has served as chief hospitalist at Harrison Medical Center since 2010 and has been with Sound Physicians since 2005. She oversees 16 hospitalists on her team at Harrison.
Gary J. Carver, MD, is the new director of hospital medicine at Coshocton (Ohio) Hospital. He previously worked as Coshocton Hospital’s chief of staff and sat on the board of trustees.
Thomas McIlraith, MD, SFHM, CLHM, received SHM’s Certificate of Leadership in Hospital Medicine at HM13 in May. Dr. McIlraith is chairman of hospital medicine at Mercy Medical Group in Sacramento, Calif. He is responsible for 24/7 operations at four hospitals and a department of 60 hospitalist physicians. In addition, he is a member of the Mercy Medical Group board of directors. He also is a clinical instructor at the University of California at Davis.
Sameh Naseib, MD, SFHM, CLHM, also received SHM’s Certificate of Leadership in Hospital Medicine at HM13 in May. Dr. Naseib is inpatient medical director at Beaver Medical Group in Redlands, Calif., where he supervises the hospitalist programs at San Gorgonio Memorial and Redlands Community hospitals.
Business Moves
Sound Physicians has announced new contracts for hospitalist services at San Joaquin Community Hospital, a 254-bed facility in Bakersfield, Calif., and at Kona Community Hospital, a 94-bed hospital in Kealakekua, Hawaii.
Emeryville, Calif.–based CEP America, a private physician-staffing firm, is providing hospitalist services at both Palomar Medical Center in Escondido, Calif., and Pomerado Hospital in Poway, Calif. CEP’s added services are in addition to the emergency medicine services the group has provided at the two hospitals for more than a decade.
Apollo Medical Holdings Inc. (ApolloMed), based in Glendale, Calif., is providing hospitalist services to Pacifica Hospital of the Valley in Sun Valley, Calif. Pacifica is a 242-bed acute-care hospital that serves several communities throughout the San Fernando Valley. ApolloMed provides physician services at 29 hospitals throughout southern and central California.
Michael O'Neal is a freelance writer in New York.
Mark Shapiro, MD, has been appointed chief of medicine at Sharp Memorial Hospital in San Diego. A hospitalist with Sharp Rees-Stealy Medical Group since 2006, Dr. Shapiro recently began work as a physician collaborator with PracticingExcellence.com, a Web-based physician-learning platform expected to launch this fall.
John Davidyock, MD, SFHM, is the new section chief of hospital medicine at Temple University Hospital in Philadelphia. Dr. Davidyock also is vice chair of patient safety and quality improvement, and assistant professor of medicine at the Temple University School of Medicine. Dr. Davidyock has been a Senior Fellow of Hospital Medicine since 2012.
Rana Tan, MD, chief hospitalist at Harrison Medical Center in Bremerton, Wash., recently received the 2013 Summit Award for excellence in hospital medicine from Tacoma, Wash.-based Sound Physicians. Dr. Tan has served as chief hospitalist at Harrison Medical Center since 2010 and has been with Sound Physicians since 2005. She oversees 16 hospitalists on her team at Harrison.
Gary J. Carver, MD, is the new director of hospital medicine at Coshocton (Ohio) Hospital. He previously worked as Coshocton Hospital’s chief of staff and sat on the board of trustees.
Thomas McIlraith, MD, SFHM, CLHM, received SHM’s Certificate of Leadership in Hospital Medicine at HM13 in May. Dr. McIlraith is chairman of hospital medicine at Mercy Medical Group in Sacramento, Calif. He is responsible for 24/7 operations at four hospitals and a department of 60 hospitalist physicians. In addition, he is a member of the Mercy Medical Group board of directors. He also is a clinical instructor at the University of California at Davis.
Sameh Naseib, MD, SFHM, CLHM, also received SHM’s Certificate of Leadership in Hospital Medicine at HM13 in May. Dr. Naseib is inpatient medical director at Beaver Medical Group in Redlands, Calif., where he supervises the hospitalist programs at San Gorgonio Memorial and Redlands Community hospitals.
Business Moves
Sound Physicians has announced new contracts for hospitalist services at San Joaquin Community Hospital, a 254-bed facility in Bakersfield, Calif., and at Kona Community Hospital, a 94-bed hospital in Kealakekua, Hawaii.
Emeryville, Calif.–based CEP America, a private physician-staffing firm, is providing hospitalist services at both Palomar Medical Center in Escondido, Calif., and Pomerado Hospital in Poway, Calif. CEP’s added services are in addition to the emergency medicine services the group has provided at the two hospitals for more than a decade.
Apollo Medical Holdings Inc. (ApolloMed), based in Glendale, Calif., is providing hospitalist services to Pacifica Hospital of the Valley in Sun Valley, Calif. Pacifica is a 242-bed acute-care hospital that serves several communities throughout the San Fernando Valley. ApolloMed provides physician services at 29 hospitals throughout southern and central California.
Michael O'Neal is a freelance writer in New York.
SHM’s Awards of Excellence Honor the Best in Hospital Medicine

SHM presented its annual Awards of Excellence to five hospitalists and one hospital care team at its annual meeting May 18 just outside Washington, D.C. The awards honor the best practices in the growing specialty in such fields as quality improvement (QI), research, teaching, and teamwork.
“We are thrilled to honor this year’s award winners. Not only do they exemplify the very best in hospital medicine, they are also leading the way for thousands of other of hospitalists across the country,” says Jack Percelay, MD, SFHM, MPH, FAAP, chair of SHM’s Awards Committee. “These are not just personal achievements, they are achievements for the entire specialty—and they are a great representation of the depth and diversity of hospital medicine.”
The 2013 SHM Awards of Excellence recipients are:

Award for Clinical Excellence: Tierza M. Stephan, MD, FACP, SFHM, of Allina Health, for her work in creating new models for improving clinical practices for hospitalists. She has played a vital role in the development and maintenance of a number of tools designed to make a significant impact on the patient experience, including a “Top 10 List to Improve Communication with Patients,” and a monthly patient experience newsletter.

Award for Excellence in Research: Jeffrey Schnipper, MD, MPH, FHM of Harvard Medical School and Brigham & Women’s Hospital, for his track record in uniting the often separate worlds of quality improvement (QI) and clinical trial research. In addition to earning eight Awards of Excellence from Partners Heatlhcare, he has been an investigator on 24 funded studies and served as the Principal Investigator SHM’s first large federal research grant, a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ).

Award for Excellence in Teaching: Bradley Sharpe, MD, FACP, SFHM, of the University of California at San Francisco (UCSF). Dr. Sharpe earned this year’s award for his continued role in teaching at national meetings, presentations at the Academic Hospitalist Academy, multiple peer-reviewed publications, and scholarly work. He has also been recognized with the UCSF Academic Senate Distinction in Teaching Award.
Award for Outstanding Service in Hospital Medicine: Patrick J. Torcson, MD, MMM, SFHM, of St. Tammany Parish Hospital in Covington, La., for his advocacy on behalf of hospitalists and hospitals for quality and performance in health care. Dr. Torcson has distinguished himself as a national leader in hospital value-based purchasing and helped hospitalists better understand the concept through SHM’s Value-Based Toolkit.

Award for Excellence in Hospital Medicine for Nonphysicians: Jeanette Kalupa, DNP, ACNP-BC, APNP, of Hospitalists of Northern Michigan, for her work in improving outcomes for patients and implementing best-practice models in hospitalist programs. Those best-practice models have re-engineered patient-care processes, and her dedication to hospital medicine has paved the way for many other nonphysician providers in the specialty.
Award for Excellence in Teamwork in Quality Improvement: The INTERdisciplinary Approaches to Communication and Teamwork (INTERACT) team at Northwestern Memorial Hospital in Chicago, for improving teamwork among physicians, nurses, and other healthcare providers. The INTERACT team focuses on one of the most common sites of hospital care: medical surgical units, where effective communication is critical but can be difficult.
SHM is accepting nominations for its 2014 Awards of Excellence, which will be presented at the 2014 annual meeting in Las Vegas. For more information, visit www.hospitalmedicine.org/awards.
Brendon Shank is SHM’s associate vice president of communications.
SHM presented its annual Awards of Excellence to five hospitalists and one hospital care team at its annual meeting May 18 just outside Washington, D.C. The awards honor the best practices in the growing specialty in such fields as quality improvement (QI), research, teaching, and teamwork.
“We are thrilled to honor this year’s award winners. Not only do they exemplify the very best in hospital medicine, they are also leading the way for thousands of other of hospitalists across the country,” says Jack Percelay, MD, SFHM, MPH, FAAP, chair of SHM’s Awards Committee. “These are not just personal achievements, they are achievements for the entire specialty—and they are a great representation of the depth and diversity of hospital medicine.”
The 2013 SHM Awards of Excellence recipients are:
Award for Clinical Excellence: Tierza M. Stephan, MD, FACP, SFHM, of Allina Health, for her work in creating new models for improving clinical practices for hospitalists. She has played a vital role in the development and maintenance of a number of tools designed to make a significant impact on the patient experience, including a “Top 10 List to Improve Communication with Patients,” and a monthly patient experience newsletter.
Award for Excellence in Research: Jeffrey Schnipper, MD, MPH, FHM of Harvard Medical School and Brigham & Women’s Hospital, for his track record in uniting the often separate worlds of quality improvement (QI) and clinical trial research. In addition to earning eight Awards of Excellence from Partners Heatlhcare, he has been an investigator on 24 funded studies and served as the Principal Investigator SHM’s first large federal research grant, a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ).
Award for Excellence in Teaching: Bradley Sharpe, MD, FACP, SFHM, of the University of California at San Francisco (UCSF). Dr. Sharpe earned this year’s award for his continued role in teaching at national meetings, presentations at the Academic Hospitalist Academy, multiple peer-reviewed publications, and scholarly work. He has also been recognized with the UCSF Academic Senate Distinction in Teaching Award.
Award for Outstanding Service in Hospital Medicine: Patrick J. Torcson, MD, MMM, SFHM, of St. Tammany Parish Hospital in Covington, La., for his advocacy on behalf of hospitalists and hospitals for quality and performance in health care. Dr. Torcson has distinguished himself as a national leader in hospital value-based purchasing and helped hospitalists better understand the concept through SHM’s Value-Based Toolkit.
Award for Excellence in Hospital Medicine for Nonphysicians: Jeanette Kalupa, DNP, ACNP-BC, APNP, of Hospitalists of Northern Michigan, for her work in improving outcomes for patients and implementing best-practice models in hospitalist programs. Those best-practice models have re-engineered patient-care processes, and her dedication to hospital medicine has paved the way for many other nonphysician providers in the specialty.
Award for Excellence in Teamwork in Quality Improvement: The INTERdisciplinary Approaches to Communication and Teamwork (INTERACT) team at Northwestern Memorial Hospital in Chicago, for improving teamwork among physicians, nurses, and other healthcare providers. The INTERACT team focuses on one of the most common sites of hospital care: medical surgical units, where effective communication is critical but can be difficult.
SHM is accepting nominations for its 2014 Awards of Excellence, which will be presented at the 2014 annual meeting in Las Vegas. For more information, visit www.hospitalmedicine.org/awards.
Brendon Shank is SHM’s associate vice president of communications.
SHM presented its annual Awards of Excellence to five hospitalists and one hospital care team at its annual meeting May 18 just outside Washington, D.C. The awards honor the best practices in the growing specialty in such fields as quality improvement (QI), research, teaching, and teamwork.
“We are thrilled to honor this year’s award winners. Not only do they exemplify the very best in hospital medicine, they are also leading the way for thousands of other of hospitalists across the country,” says Jack Percelay, MD, SFHM, MPH, FAAP, chair of SHM’s Awards Committee. “These are not just personal achievements, they are achievements for the entire specialty—and they are a great representation of the depth and diversity of hospital medicine.”
The 2013 SHM Awards of Excellence recipients are:
Award for Clinical Excellence: Tierza M. Stephan, MD, FACP, SFHM, of Allina Health, for her work in creating new models for improving clinical practices for hospitalists. She has played a vital role in the development and maintenance of a number of tools designed to make a significant impact on the patient experience, including a “Top 10 List to Improve Communication with Patients,” and a monthly patient experience newsletter.
Award for Excellence in Research: Jeffrey Schnipper, MD, MPH, FHM of Harvard Medical School and Brigham & Women’s Hospital, for his track record in uniting the often separate worlds of quality improvement (QI) and clinical trial research. In addition to earning eight Awards of Excellence from Partners Heatlhcare, he has been an investigator on 24 funded studies and served as the Principal Investigator SHM’s first large federal research grant, a $1.5 million grant from the Agency for Healthcare Research and Quality (AHRQ).
Award for Excellence in Teaching: Bradley Sharpe, MD, FACP, SFHM, of the University of California at San Francisco (UCSF). Dr. Sharpe earned this year’s award for his continued role in teaching at national meetings, presentations at the Academic Hospitalist Academy, multiple peer-reviewed publications, and scholarly work. He has also been recognized with the UCSF Academic Senate Distinction in Teaching Award.
Award for Outstanding Service in Hospital Medicine: Patrick J. Torcson, MD, MMM, SFHM, of St. Tammany Parish Hospital in Covington, La., for his advocacy on behalf of hospitalists and hospitals for quality and performance in health care. Dr. Torcson has distinguished himself as a national leader in hospital value-based purchasing and helped hospitalists better understand the concept through SHM’s Value-Based Toolkit.
Award for Excellence in Hospital Medicine for Nonphysicians: Jeanette Kalupa, DNP, ACNP-BC, APNP, of Hospitalists of Northern Michigan, for her work in improving outcomes for patients and implementing best-practice models in hospitalist programs. Those best-practice models have re-engineered patient-care processes, and her dedication to hospital medicine has paved the way for many other nonphysician providers in the specialty.
Award for Excellence in Teamwork in Quality Improvement: The INTERdisciplinary Approaches to Communication and Teamwork (INTERACT) team at Northwestern Memorial Hospital in Chicago, for improving teamwork among physicians, nurses, and other healthcare providers. The INTERACT team focuses on one of the most common sites of hospital care: medical surgical units, where effective communication is critical but can be difficult.
SHM is accepting nominations for its 2014 Awards of Excellence, which will be presented at the 2014 annual meeting in Las Vegas. For more information, visit www.hospitalmedicine.org/awards.
Brendon Shank is SHM’s associate vice president of communications.
SHM Allies with Leading Health Care Groups to Advance Hospital Patient Nutrition
SHM announced in May the launch of a new interdisciplinary partnership, the Alliance to Advance Patient Nutrition, in conjunction with four other organizations. The alliance’s mission is to improve patient outcomes through nutrition intervention in the hospital.
Representing more than 100,000 dietitians, nurses, hospitalists, and other physicians and clinicians from across the nation, the following organizations have come together with SHM to champion for early nutrition screening, assessment, and intervention in hospitals:
- Academy of Medical-Surgical Nurses (AMSN);
- Academy of Nutrition and Dietetics (AND);
- American Society for Parenteral and Enteral Nutrition (ASPEN); and
- Abbott Nutrition.
Malnutrition increases costs, length of stay, and unfavorable outcomes. Properly addressing hospital malnutrition creates an opportunity to improve quality of care while also reducing healthcare costs. Additional clinical research finds that malnourished patients are two times more likely to develop a pressure ulcer, while patients with malnutrition have three times the rate of infection.
Yet when hospitalized patients are provided intervention via oral nutrition supplements, health economic research finds associated benefits:
Nutrition intervention can reduce hospital length of stay by an average of two days, and nutrition intervention has been shown to reduce patient hospitalization costs by 21.6%, or $4,734 per episode.
Additionally, there was a 6.7% reduction in the probability of 30-day readmission with patients who had at least one known subsequent readmission and were offered oral nutrition supplements during hospitalization.
“There is a growing body of evidence supporting the positive impact nutrition has on improving patient outcomes,” says hospitalist Melissa Parkhurst, MD, FHM, who serves as medical director for the University of Kansas Hospital’s hospitalist section and its nutrition support service. “We are seeing that early intervention can make a significant difference. As physicians, we need to work with the entire clinician team to ensure that nutrition is an integral part of our patients’ treatment plans.”
The alliance launched a website at www.malnutrition.org to provide hospital-based clinicians with the following resources:
- Research and fact sheets about malnutrition and the positive impact nutrition intervention has on patient care and outcomes;
- The Alliance Nutrition Toolkit, which facilitates clinician collaboration and nutrition integration; and
- Information about educational events, such as quick learning modules, continuing medical education (CME) programs.
The Alliance to Advance Patient Nutrition is made possible with support from Abbott’s nutrition business.
SHM announced in May the launch of a new interdisciplinary partnership, the Alliance to Advance Patient Nutrition, in conjunction with four other organizations. The alliance’s mission is to improve patient outcomes through nutrition intervention in the hospital.
Representing more than 100,000 dietitians, nurses, hospitalists, and other physicians and clinicians from across the nation, the following organizations have come together with SHM to champion for early nutrition screening, assessment, and intervention in hospitals:
- Academy of Medical-Surgical Nurses (AMSN);
- Academy of Nutrition and Dietetics (AND);
- American Society for Parenteral and Enteral Nutrition (ASPEN); and
- Abbott Nutrition.
Malnutrition increases costs, length of stay, and unfavorable outcomes. Properly addressing hospital malnutrition creates an opportunity to improve quality of care while also reducing healthcare costs. Additional clinical research finds that malnourished patients are two times more likely to develop a pressure ulcer, while patients with malnutrition have three times the rate of infection.
Yet when hospitalized patients are provided intervention via oral nutrition supplements, health economic research finds associated benefits:
Nutrition intervention can reduce hospital length of stay by an average of two days, and nutrition intervention has been shown to reduce patient hospitalization costs by 21.6%, or $4,734 per episode.
Additionally, there was a 6.7% reduction in the probability of 30-day readmission with patients who had at least one known subsequent readmission and were offered oral nutrition supplements during hospitalization.
“There is a growing body of evidence supporting the positive impact nutrition has on improving patient outcomes,” says hospitalist Melissa Parkhurst, MD, FHM, who serves as medical director for the University of Kansas Hospital’s hospitalist section and its nutrition support service. “We are seeing that early intervention can make a significant difference. As physicians, we need to work with the entire clinician team to ensure that nutrition is an integral part of our patients’ treatment plans.”
The alliance launched a website at www.malnutrition.org to provide hospital-based clinicians with the following resources:
- Research and fact sheets about malnutrition and the positive impact nutrition intervention has on patient care and outcomes;
- The Alliance Nutrition Toolkit, which facilitates clinician collaboration and nutrition integration; and
- Information about educational events, such as quick learning modules, continuing medical education (CME) programs.
The Alliance to Advance Patient Nutrition is made possible with support from Abbott’s nutrition business.
SHM announced in May the launch of a new interdisciplinary partnership, the Alliance to Advance Patient Nutrition, in conjunction with four other organizations. The alliance’s mission is to improve patient outcomes through nutrition intervention in the hospital.
Representing more than 100,000 dietitians, nurses, hospitalists, and other physicians and clinicians from across the nation, the following organizations have come together with SHM to champion for early nutrition screening, assessment, and intervention in hospitals:
- Academy of Medical-Surgical Nurses (AMSN);
- Academy of Nutrition and Dietetics (AND);
- American Society for Parenteral and Enteral Nutrition (ASPEN); and
- Abbott Nutrition.
Malnutrition increases costs, length of stay, and unfavorable outcomes. Properly addressing hospital malnutrition creates an opportunity to improve quality of care while also reducing healthcare costs. Additional clinical research finds that malnourished patients are two times more likely to develop a pressure ulcer, while patients with malnutrition have three times the rate of infection.
Yet when hospitalized patients are provided intervention via oral nutrition supplements, health economic research finds associated benefits:
Nutrition intervention can reduce hospital length of stay by an average of two days, and nutrition intervention has been shown to reduce patient hospitalization costs by 21.6%, or $4,734 per episode.
Additionally, there was a 6.7% reduction in the probability of 30-day readmission with patients who had at least one known subsequent readmission and were offered oral nutrition supplements during hospitalization.
“There is a growing body of evidence supporting the positive impact nutrition has on improving patient outcomes,” says hospitalist Melissa Parkhurst, MD, FHM, who serves as medical director for the University of Kansas Hospital’s hospitalist section and its nutrition support service. “We are seeing that early intervention can make a significant difference. As physicians, we need to work with the entire clinician team to ensure that nutrition is an integral part of our patients’ treatment plans.”
The alliance launched a website at www.malnutrition.org to provide hospital-based clinicians with the following resources:
- Research and fact sheets about malnutrition and the positive impact nutrition intervention has on patient care and outcomes;
- The Alliance Nutrition Toolkit, which facilitates clinician collaboration and nutrition integration; and
- Information about educational events, such as quick learning modules, continuing medical education (CME) programs.
The Alliance to Advance Patient Nutrition is made possible with support from Abbott’s nutrition business.
Fellow in Hospital Medicine Spotlight: Efren Manjarrez, MD, SFHM

Dr. Manjarrez is associate chief of the division of hospital medicine, associate chief of patient safety, and quality officer for UHealth, as well as an assistant professor of clinical medicine, all at the University of Miami’s Miller School of Medicine. Additionally, he is a diplomat for the American Board of Internal Medicine (ABIM) and co-chair of SHM’s international hospitalist section.
Undergraduate education: University of California at Irvine.
Medical school: University of California School of Medicine at San Diego, La Jolla, Calif.
Notable: In 1999, Dr. Manjarrez co-founded the first hospitalist group in the nation staffed by internal-medicine and pediatrics-trained physicians. One year later, he became the first director of hospital medicine at the University of Miami School of Medicine. He co-authored “Hospitalist Handoffs: A Systematic Review and Task Force Recommendations,” and a chapter of the recently published “Perioperative Medicine: Medical Consultation and Co-Management” titled “Postoperative Cardiac Complications.”
An active member of SHM, he has been appointed course director of the 2015 annual SHM meeting. Committed to adding international SHM members and supporting hospitalists internationally, Dr. Manjarrez is working to develop HM by maintaining international colleague connections. He hopes to have an overseas SHM meeting someday.
FYI: Dr. Manjarrez loves to travel, especially to Mexico City and Madrid, where his family and his wife’s family live, respectively.
Quotable: “Being an SHM fellow is one of my greatest achievements, and it demonstrates to my colleagues my accomplishments as a hospitalist.”
Dr. Manjarrez is associate chief of the division of hospital medicine, associate chief of patient safety, and quality officer for UHealth, as well as an assistant professor of clinical medicine, all at the University of Miami’s Miller School of Medicine. Additionally, he is a diplomat for the American Board of Internal Medicine (ABIM) and co-chair of SHM’s international hospitalist section.
Undergraduate education: University of California at Irvine.
Medical school: University of California School of Medicine at San Diego, La Jolla, Calif.
Notable: In 1999, Dr. Manjarrez co-founded the first hospitalist group in the nation staffed by internal-medicine and pediatrics-trained physicians. One year later, he became the first director of hospital medicine at the University of Miami School of Medicine. He co-authored “Hospitalist Handoffs: A Systematic Review and Task Force Recommendations,” and a chapter of the recently published “Perioperative Medicine: Medical Consultation and Co-Management” titled “Postoperative Cardiac Complications.”
An active member of SHM, he has been appointed course director of the 2015 annual SHM meeting. Committed to adding international SHM members and supporting hospitalists internationally, Dr. Manjarrez is working to develop HM by maintaining international colleague connections. He hopes to have an overseas SHM meeting someday.
FYI: Dr. Manjarrez loves to travel, especially to Mexico City and Madrid, where his family and his wife’s family live, respectively.
Quotable: “Being an SHM fellow is one of my greatest achievements, and it demonstrates to my colleagues my accomplishments as a hospitalist.”
Dr. Manjarrez is associate chief of the division of hospital medicine, associate chief of patient safety, and quality officer for UHealth, as well as an assistant professor of clinical medicine, all at the University of Miami’s Miller School of Medicine. Additionally, he is a diplomat for the American Board of Internal Medicine (ABIM) and co-chair of SHM’s international hospitalist section.
Undergraduate education: University of California at Irvine.
Medical school: University of California School of Medicine at San Diego, La Jolla, Calif.
Notable: In 1999, Dr. Manjarrez co-founded the first hospitalist group in the nation staffed by internal-medicine and pediatrics-trained physicians. One year later, he became the first director of hospital medicine at the University of Miami School of Medicine. He co-authored “Hospitalist Handoffs: A Systematic Review and Task Force Recommendations,” and a chapter of the recently published “Perioperative Medicine: Medical Consultation and Co-Management” titled “Postoperative Cardiac Complications.”
An active member of SHM, he has been appointed course director of the 2015 annual SHM meeting. Committed to adding international SHM members and supporting hospitalists internationally, Dr. Manjarrez is working to develop HM by maintaining international colleague connections. He hopes to have an overseas SHM meeting someday.
FYI: Dr. Manjarrez loves to travel, especially to Mexico City and Madrid, where his family and his wife’s family live, respectively.
Quotable: “Being an SHM fellow is one of my greatest achievements, and it demonstrates to my colleagues my accomplishments as a hospitalist.”
Hospitalist-Specific Data Shows Rise in Use of Some CPT Codes

Before 2011, hospitalists had only Centers for Medicare & Medicaid Services’ (CMS) specialty-specific CPT distribution data, and no hospitalist-specific data, available when looking for benchmarks against which to compare their billing practices. Thanks to recent State of Hospital Medicine surveys, however, we now have hospitalist-specific data for the distribution of commonly used CPT codes. It’s interesting to analyze how 2011 data compares to 2012, and how the use of high-level codes varies by geographic region, employment model, compensation structure, and practice size.
In 2012, the use of the higher-level inpatient (IP) discharge code (99239) increased to 52% from 48% in 2011 among HM groups serving adults only, and the use of the highest-level IP subsequent code (99233) increased to 33% from 28% in the same comparison. This increase is in keeping with national trends. According to a May 2012 report by the Department of Health and Human Services’ Office of Inspector General, from 2001 to 2010, physicians’ billing shifted from lower-level to higher-level codes. For example, the billing of the lowest-level code (99231) decreased 16%, while the billing of the two higher-level codes (99232 and 99233) increased 6% and 9%, respectively.
Possible drivers of this change include:
- Expanded use of electronic health records (EHRs);
- Increased physician education about documentation requirements; and
- A sicker hospitalized patient population due to expanded outpatient care capabilities.
Although the proportion of high-level subsequent and discharge codes reported by SHM increased in 2012, the percent of highest-level IP admission codes (99223) actually decreased to 66% from 69%. There are many possible reasons for this. First, the elimination of consult codes by CMS in 2010 increased the overall use of admission codes but might have decreased the proportion of highest-level admission codes. Additionally, there may be an increased use of higher RVU-generating critical-care codes preferentially over billing of the highest-level admission codes. Third, there is the possibility that the extra documentation required for high-level admissions is a billing deterrent. Similarly, higher-level codes may be downcoded if documentation is lacking or incomplete.
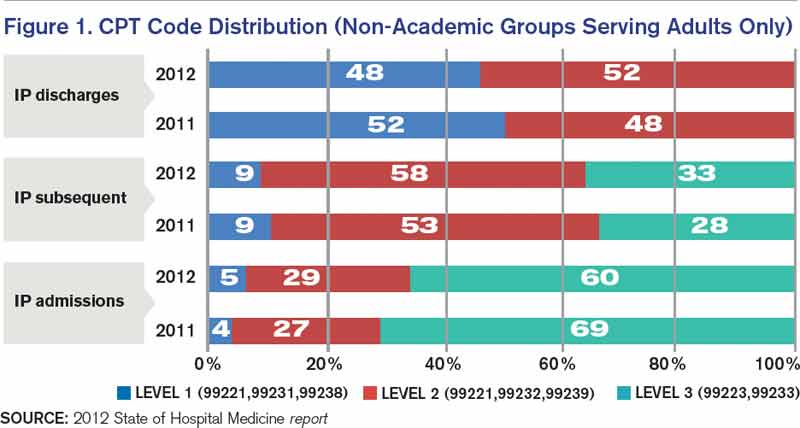
Source: 2012 State of Hospital Medicine report
Comparatively, my health system, Allina Health, showed an increase in the use of highest-level codes for all three CPT codes analyzed.
With the increasing sophistication of EHRs and coding technology tools, it will be interesting to see the future impact on coding distribution as providers adapt to new documentation processes that support health information exchange across systems.
Comparing geographic regions, the West uses the highest proportion of high-level codes for admission, follow-up, and discharge, followed by the Midwest.
Interestingly, variation in billing by group size is only correlated directly to admission codes, but not to follow-up or discharge codes—with larger services tending to bill more of the highest-level admission codes.
Admission code use correlates directly with compensation structure; groups providing 100% of total compensation in the form of salary bill the lowest percentage of high-level admission codes. As compensation trends away from straight salaries, the percentage of high-level admission codes increases. The picture is less clear for high-level follow-up and discharge codes.
Comparing academic and nonacademic HM groups shows greater use of the highest- level admission, follow-up, and discharge codes for nonacademic HM groups. This is likely because academic hospitalists can only bill for their own time and not for time spent by medical residents.
Employment model (e.g. hospital system, private hospitalist-only groups, management companies, etc.) showed no categorical effect on CPT distribution.
Dr. Stephan is regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee.
Before 2011, hospitalists had only Centers for Medicare & Medicaid Services’ (CMS) specialty-specific CPT distribution data, and no hospitalist-specific data, available when looking for benchmarks against which to compare their billing practices. Thanks to recent State of Hospital Medicine surveys, however, we now have hospitalist-specific data for the distribution of commonly used CPT codes. It’s interesting to analyze how 2011 data compares to 2012, and how the use of high-level codes varies by geographic region, employment model, compensation structure, and practice size.
In 2012, the use of the higher-level inpatient (IP) discharge code (99239) increased to 52% from 48% in 2011 among HM groups serving adults only, and the use of the highest-level IP subsequent code (99233) increased to 33% from 28% in the same comparison. This increase is in keeping with national trends. According to a May 2012 report by the Department of Health and Human Services’ Office of Inspector General, from 2001 to 2010, physicians’ billing shifted from lower-level to higher-level codes. For example, the billing of the lowest-level code (99231) decreased 16%, while the billing of the two higher-level codes (99232 and 99233) increased 6% and 9%, respectively.
Possible drivers of this change include:
- Expanded use of electronic health records (EHRs);
- Increased physician education about documentation requirements; and
- A sicker hospitalized patient population due to expanded outpatient care capabilities.
Although the proportion of high-level subsequent and discharge codes reported by SHM increased in 2012, the percent of highest-level IP admission codes (99223) actually decreased to 66% from 69%. There are many possible reasons for this. First, the elimination of consult codes by CMS in 2010 increased the overall use of admission codes but might have decreased the proportion of highest-level admission codes. Additionally, there may be an increased use of higher RVU-generating critical-care codes preferentially over billing of the highest-level admission codes. Third, there is the possibility that the extra documentation required for high-level admissions is a billing deterrent. Similarly, higher-level codes may be downcoded if documentation is lacking or incomplete.
Source: 2012 State of Hospital Medicine report
Comparatively, my health system, Allina Health, showed an increase in the use of highest-level codes for all three CPT codes analyzed.
With the increasing sophistication of EHRs and coding technology tools, it will be interesting to see the future impact on coding distribution as providers adapt to new documentation processes that support health information exchange across systems.
Comparing geographic regions, the West uses the highest proportion of high-level codes for admission, follow-up, and discharge, followed by the Midwest.
Interestingly, variation in billing by group size is only correlated directly to admission codes, but not to follow-up or discharge codes—with larger services tending to bill more of the highest-level admission codes.
Admission code use correlates directly with compensation structure; groups providing 100% of total compensation in the form of salary bill the lowest percentage of high-level admission codes. As compensation trends away from straight salaries, the percentage of high-level admission codes increases. The picture is less clear for high-level follow-up and discharge codes.
Comparing academic and nonacademic HM groups shows greater use of the highest- level admission, follow-up, and discharge codes for nonacademic HM groups. This is likely because academic hospitalists can only bill for their own time and not for time spent by medical residents.
Employment model (e.g. hospital system, private hospitalist-only groups, management companies, etc.) showed no categorical effect on CPT distribution.
Dr. Stephan is regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee.
Before 2011, hospitalists had only Centers for Medicare & Medicaid Services’ (CMS) specialty-specific CPT distribution data, and no hospitalist-specific data, available when looking for benchmarks against which to compare their billing practices. Thanks to recent State of Hospital Medicine surveys, however, we now have hospitalist-specific data for the distribution of commonly used CPT codes. It’s interesting to analyze how 2011 data compares to 2012, and how the use of high-level codes varies by geographic region, employment model, compensation structure, and practice size.
In 2012, the use of the higher-level inpatient (IP) discharge code (99239) increased to 52% from 48% in 2011 among HM groups serving adults only, and the use of the highest-level IP subsequent code (99233) increased to 33% from 28% in the same comparison. This increase is in keeping with national trends. According to a May 2012 report by the Department of Health and Human Services’ Office of Inspector General, from 2001 to 2010, physicians’ billing shifted from lower-level to higher-level codes. For example, the billing of the lowest-level code (99231) decreased 16%, while the billing of the two higher-level codes (99232 and 99233) increased 6% and 9%, respectively.
Possible drivers of this change include:
- Expanded use of electronic health records (EHRs);
- Increased physician education about documentation requirements; and
- A sicker hospitalized patient population due to expanded outpatient care capabilities.
Although the proportion of high-level subsequent and discharge codes reported by SHM increased in 2012, the percent of highest-level IP admission codes (99223) actually decreased to 66% from 69%. There are many possible reasons for this. First, the elimination of consult codes by CMS in 2010 increased the overall use of admission codes but might have decreased the proportion of highest-level admission codes. Additionally, there may be an increased use of higher RVU-generating critical-care codes preferentially over billing of the highest-level admission codes. Third, there is the possibility that the extra documentation required for high-level admissions is a billing deterrent. Similarly, higher-level codes may be downcoded if documentation is lacking or incomplete.
Source: 2012 State of Hospital Medicine report
Comparatively, my health system, Allina Health, showed an increase in the use of highest-level codes for all three CPT codes analyzed.
With the increasing sophistication of EHRs and coding technology tools, it will be interesting to see the future impact on coding distribution as providers adapt to new documentation processes that support health information exchange across systems.
Comparing geographic regions, the West uses the highest proportion of high-level codes for admission, follow-up, and discharge, followed by the Midwest.
Interestingly, variation in billing by group size is only correlated directly to admission codes, but not to follow-up or discharge codes—with larger services tending to bill more of the highest-level admission codes.
Admission code use correlates directly with compensation structure; groups providing 100% of total compensation in the form of salary bill the lowest percentage of high-level admission codes. As compensation trends away from straight salaries, the percentage of high-level admission codes increases. The picture is less clear for high-level follow-up and discharge codes.
Comparing academic and nonacademic HM groups shows greater use of the highest- level admission, follow-up, and discharge codes for nonacademic HM groups. This is likely because academic hospitalists can only bill for their own time and not for time spent by medical residents.
Employment model (e.g. hospital system, private hospitalist-only groups, management companies, etc.) showed no categorical effect on CPT distribution.
Dr. Stephan is regional hospitalist medical director for Allina Health in Minneapolis and the incoming chair of SHM’s Practice Analysis Committee.
Peer Benchmarking Network May Reduce Overutilization in Pediatric Bronchiolitis

Clinical question: What is the impact of a peer benchmarking network on resource utilization in acute bronchiolitis?
Background: Acute bronchiolitis is the most common illness requiring hospitalization in children. Despite the publication of national evidence-based guidelines, variation and overuse of common therapies remains. Despite one report of successful implementation of evidence-based guidelines in a collaborative of freestanding children’s hospitals, most children are hospitalized outside of such institutions, and large-scale, lower-resource efforts have not been described.
Study design: Voluntary, quality-improvement (QI), and benchmarking collaborative.
Setting: Seventeen hospitals, including both community and freestanding children’s facilities.
Synopsis: Over a four-year period, data on 11,568 bronchiolitis hospitalizations were collected. The collaborative facilitated sharing of resources (e.g. scoring tools, guidelines), celebrated high performers on an annual basis, and encouraged regular data collection, primarily via conference calls and email. Notably, a common bundle of interventions were not used; groups worked on local improvement cycles, with only a few groups forming a small subcollaborative utilizing a shared pathway. A significant decrease in bronchodilator utilization and chest physiotherapy was seen over the course of the collaborative, although no change in chest radiography, steroid utilization, and RSV testing was noted.
This voluntary and low-resource effort by similarly motivated peers across a variety of inpatient settings demonstrated improvement over time. It is particularly notable as inpatient collaboratives with face-to-face meeting requirements, and annual fees, become more commonplace.
Study limitations include the lack of a conceptual model for studying contextual factors that might have led to improvement in the varied settings and secular changes over this time period. Additionally, EDs were not included in this initiative, which likely accounted for the lack of improvement in chest radiography and RSV testing. Nonetheless, scalable innovations such as this will become increasingly important as hospitalists search for value in health care.
Bottom line: Creating a national community of practice may reduce overutilization in bronchiolitis.
Citation: Ralston S, Garber M, Narang S, et al. Decreasing unnecessary utilization in acute bronchiolitis care: results from the Value in Inpatient Pediatrics Network. J Hosp Med. 2013;8(1):25-30.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What is the impact of a peer benchmarking network on resource utilization in acute bronchiolitis?
Background: Acute bronchiolitis is the most common illness requiring hospitalization in children. Despite the publication of national evidence-based guidelines, variation and overuse of common therapies remains. Despite one report of successful implementation of evidence-based guidelines in a collaborative of freestanding children’s hospitals, most children are hospitalized outside of such institutions, and large-scale, lower-resource efforts have not been described.
Study design: Voluntary, quality-improvement (QI), and benchmarking collaborative.
Setting: Seventeen hospitals, including both community and freestanding children’s facilities.
Synopsis: Over a four-year period, data on 11,568 bronchiolitis hospitalizations were collected. The collaborative facilitated sharing of resources (e.g. scoring tools, guidelines), celebrated high performers on an annual basis, and encouraged regular data collection, primarily via conference calls and email. Notably, a common bundle of interventions were not used; groups worked on local improvement cycles, with only a few groups forming a small subcollaborative utilizing a shared pathway. A significant decrease in bronchodilator utilization and chest physiotherapy was seen over the course of the collaborative, although no change in chest radiography, steroid utilization, and RSV testing was noted.
This voluntary and low-resource effort by similarly motivated peers across a variety of inpatient settings demonstrated improvement over time. It is particularly notable as inpatient collaboratives with face-to-face meeting requirements, and annual fees, become more commonplace.
Study limitations include the lack of a conceptual model for studying contextual factors that might have led to improvement in the varied settings and secular changes over this time period. Additionally, EDs were not included in this initiative, which likely accounted for the lack of improvement in chest radiography and RSV testing. Nonetheless, scalable innovations such as this will become increasingly important as hospitalists search for value in health care.
Bottom line: Creating a national community of practice may reduce overutilization in bronchiolitis.
Citation: Ralston S, Garber M, Narang S, et al. Decreasing unnecessary utilization in acute bronchiolitis care: results from the Value in Inpatient Pediatrics Network. J Hosp Med. 2013;8(1):25-30.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What is the impact of a peer benchmarking network on resource utilization in acute bronchiolitis?
Background: Acute bronchiolitis is the most common illness requiring hospitalization in children. Despite the publication of national evidence-based guidelines, variation and overuse of common therapies remains. Despite one report of successful implementation of evidence-based guidelines in a collaborative of freestanding children’s hospitals, most children are hospitalized outside of such institutions, and large-scale, lower-resource efforts have not been described.
Study design: Voluntary, quality-improvement (QI), and benchmarking collaborative.
Setting: Seventeen hospitals, including both community and freestanding children’s facilities.
Synopsis: Over a four-year period, data on 11,568 bronchiolitis hospitalizations were collected. The collaborative facilitated sharing of resources (e.g. scoring tools, guidelines), celebrated high performers on an annual basis, and encouraged regular data collection, primarily via conference calls and email. Notably, a common bundle of interventions were not used; groups worked on local improvement cycles, with only a few groups forming a small subcollaborative utilizing a shared pathway. A significant decrease in bronchodilator utilization and chest physiotherapy was seen over the course of the collaborative, although no change in chest radiography, steroid utilization, and RSV testing was noted.
This voluntary and low-resource effort by similarly motivated peers across a variety of inpatient settings demonstrated improvement over time. It is particularly notable as inpatient collaboratives with face-to-face meeting requirements, and annual fees, become more commonplace.
Study limitations include the lack of a conceptual model for studying contextual factors that might have led to improvement in the varied settings and secular changes over this time period. Additionally, EDs were not included in this initiative, which likely accounted for the lack of improvement in chest radiography and RSV testing. Nonetheless, scalable innovations such as this will become increasingly important as hospitalists search for value in health care.
Bottom line: Creating a national community of practice may reduce overutilization in bronchiolitis.
Citation: Ralston S, Garber M, Narang S, et al. Decreasing unnecessary utilization in acute bronchiolitis care: results from the Value in Inpatient Pediatrics Network. J Hosp Med. 2013;8(1):25-30.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
How Can Tumor Lysis Syndrome Be Prevented and Managed in Cancer Patients?
Case
A 25-year-old male with HIV/AIDS and a CD4 count of 65 cells/μL presents to the ED with intractable nausea and vomiting for one week. Laboratory evaluation revealed a white blood cell of 67,000 cells/mm3. An extended chemistry panel reveals creatinine 3.5 mg/dL, potassium 3.0 mmol/L, LDH 250 IU/L, and uric acid 5mg/dL. Calcium and phosphorus were both normal. The patient was admitted for further evaluation and management, and was later diagnosed with Burkitt’s lymphoma.
Overview
Tumor lysis syndrome (TLS) is an acute cell lysis of tumor cells with the release of cell content into circulation either spontaneously or in response to therapy, leading to hyperurecemia, hyperkalemia, hyperphosphatemia, and hypocalcemia.1-3
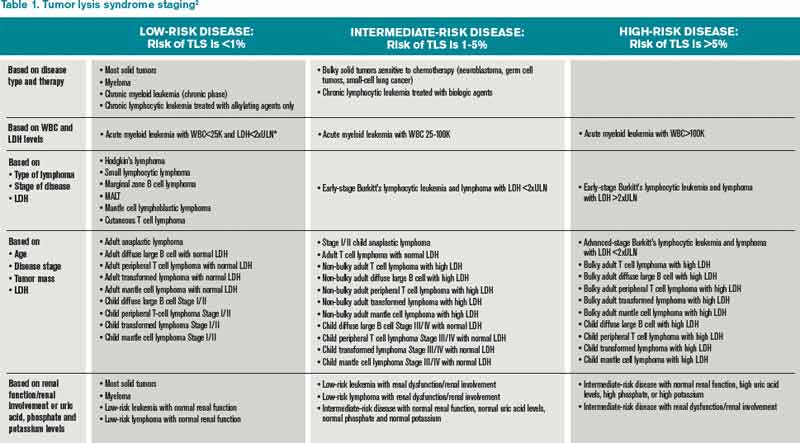
TLS is one of the most common oncology emergencies encountered by hospitalists caring for patients with hematologic malignancies. The incidence and severity of TLS depend on the cell burden, cell proliferation rate, potential for cell lysis or chemo sensitivity, baseline clinical characteristics, and preventive measures taken (see Table 1).2,4
TLS is classified as laboratory or clinical. Laboratory TLS is described as the presence of two or more of the following serum abnormalities at the same time, present within three days before or seven days after the start of therapy.5
- Uric acid >8 mg/dL (475.8 micromole/L) or 25% increase;
- Potassium >6 mEq/L (6 mmol/L) or 25% increase;
- Phosphorus >6.5 mg/dL (2.1 mmol/L) for children or >4.5 mg/dl (1.45 mmol/L) for adults or 25% increase; and
- Calcium >7 mg/dL (1.75 mmol/L) or 25% increase.
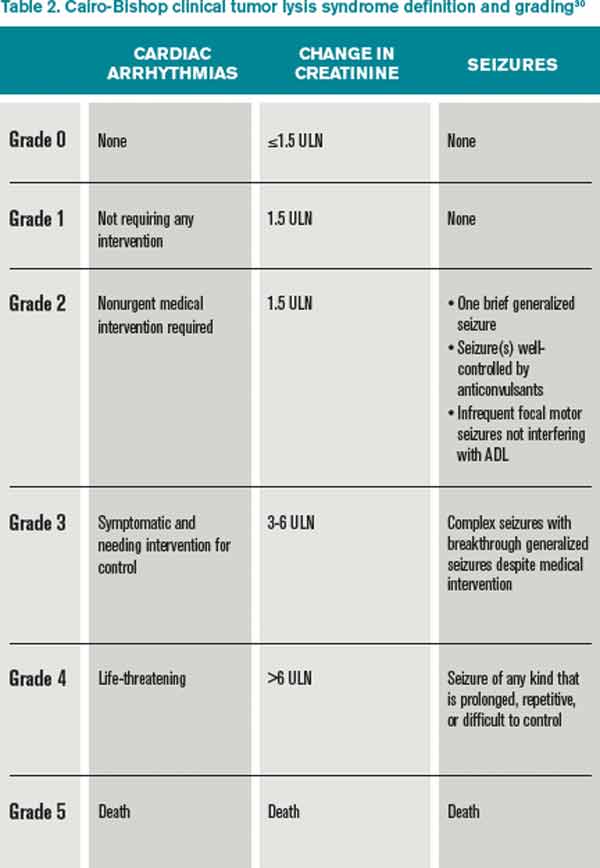
Clinical TLS is defined as laboratory TLS in association with increased creatinine levels, seizures, cardiac arrhythmias, or death (see Table 2).5
Pathogenesis
Tumor cell lysis releases DNA, cytokines, phosphate, and potassium. DNA is metabolized into adenosine and guanosine, which are then converted into xanthines. Xanthines are oxidized by xanthine oxidase into uric acid, which is then excreted through the kidneys.
TLS develops when the accumulation of xanthine, uric acid, potassium, and phosphorus exceeds the kidney’s capacity to excrete them. Cytokines cause hypotension, inflammation, and kidney injury, and worsen the kidney’s excretory capacity. Damage to the kidneys also occurs by renal precipitation of uric acid, xanthine, and calcium phosphate.4
Phosphorus concentrations in tumor cells are four times higher than in normal cells. When the calcium phosphorus product exceeds 60 mg2/dL2, there is an increased risk of calcium phosphate precipitation in the kidney tubules, which could lead to kidney failure. Accumulation of calcium phosphate product may also be cardiotoxic and can lead to cardiac arrhythmias. In addition, hyperphosphatemia can cause secondary hypocalcemia, which may lead to parasthesias, tetany, and cardiac arrhythmias.2,4
TLS is most common in tumors with high proliferative rates and high tumor burden, such as acute lymphoblastic leukemia and Burkitt’s lymphoma, but it can occur with other hematologic malignancies, such as T-cell precursor acute lymphocytic leukemia (ALL), B-cell precursor ALL, acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), anaplastic large cell lymphoma, and plasma cell disorders (e.g. multiple myeloma and plasmacytoma).6,7 TLS has also been reported with the treatment of solid organ nonhematologic tumors (see Table 3).
In hematologic tumors, TLS frequently is associated with cytotoxic chemotherapy, and less frequently with glucocorticoid treatment, monoclonal antibodies (eg, rituximab, bortezomab, imatinib), and radiation therapy.25-29
Patient factors, such as baseline kidney disease or lack of prophylactic/preventive measures for TLS, also increase the risk.4 TLS, however, can develop in patients classified as low risk (see Table 1.
TLS Prevention
Intravenous fluids. Every patient at intermediate or high risk of TLS should receive intravenous fluids (IVF) prior to cancer treatment; those at low risk may receive IVF based on the provider’s clinical judgment.30 The purpose of administering IVF is to generate high urine output to reduce the risk of precipitation of uric acid in the renal tubules.30 Both adults and children should receive approximately 2 to 3 L/m2 per day of IVF,30 and urine output should be maintained at 2 ml/kg/hr (or 4 to 6 ml/kg/hr for children <10kg).30 IVF should be cautiously administered in patients with renal insufficiency or heart failure, and diuretics may be used to maintain goal urine output. Recommended initial fluids are D51/4 normal saline, or normal saline for patients who are dehydrated or hyponatremic.30
Allopurinol. Allopurinol is usually also administered to patients at risk for developing TLS.30 Allopurinol inhibits the metabolism of hypoxanthine and xanthine to uric acid, which decreases the accumulation of uric acid in the renal tubules, thus preventing obstructive renal disease from precipitation of uric acid.4 The recommended dose of allopurinol is 100 mg/m2 every eight hours, and should not exceed 800 mg per day in adults. It should be started one to two days prior to induction chemotherapy and continued for three to seven days after the treatment and until uric acid levels and other electrolyte levels have returned to normal. The dose is adjusted to 50 mg/m2 every eight hours in patients with kidney failure.30
In some cases, allopurinol can lead to increased levels of xanthine crystals in the renal tubules, leading to acute kidney injury. Also, allopurinol does not have any effect on uric acid that has already been formed, so patients with elevated uric acid levels prior to the initiation of cancer therapy will not have any reduction in the levels of uric acid. Allopurinol reduces the degradation of other purines, so it can cause toxicity in patients on azathioprine and 6-mercaptopurine if the doses of these medications are not adjusted.
Rasburicase. Rasburicase is a recombinant urate oxidase, derived from aspergillus favus, which catalyzes the breakdown of uric acid to allantoin, which is a water-soluble product. Rasburicase is recommended as a first-line treatment for patients at high risk for clinical TLS.30 Rasburicase has an earlier onset than allopurinol and rapidly decreases serum levels of uric acid within four hours of administration.30,31 The recommended dose is 0.10 to 0.20 mg/kg once a day for five days in adults.30
A Phase III trial compared the efficiency and safety of rasburicase to rasburicase with allopurinol or allopurinol alone.32 A significantly higher normalization of uric acid was found in patients on rasburicase compared to allopurinol alone. The incidence of laboratory TLS was also significantly lower with rasburicase alone compared to allopurinol alone, and was even lower with allopurinol plus rasburicase. The incidence of acute kidney injury was the same with rasburicase alone or allopurinol alone but was higher with rasburicase plus allopurinol.
Serum uric acid, phosphorus, potassium, and calcium need to be monitored every four hours for 24 hours after the completion of chemotherapy in patients on rasburicase.4 The sample of blood drawn to check the uric acid levels has to be placed on ice and processed within four hours in order to avoid falsely lower levels of uric acid due to the conversion of uric acid to allantoin. Rasburicase is contraindicated in patients with G6PD deficiency and pregnant women, because one of the byproducts of uric acid breakdown is hydrogen peroxide, which can cause severe hemolysis and the formation of methemoglobin in these patients.30
Rasburicase has been approved for use in both children and adults, but there is more evidence for the use in children. Rasburicase has a black-box label for patients with anaphylaxis, methemoglobinemia, hemolysis, and hemoglobinuria, and there is a recommendation to check G6PD deficiency before use in high-risk patients.30
TLS Treatment
Alkalinization. Alkalinization of urine is controversial in the management of TLS. Urine alkalinization increases uric acid solubility but causes hyperphosphatemia and decreases calcium phosphate solubility, which can then deposit in the kidney once cancer treatment starts. Of note, hyperphosphatemia is much more difficult to correct than high levels of uric acid, and there are no clinical trials proving the superiority of urine alkalinization over normal saline.
Normalization of electrolytes. Electrolyte abnormalities should be corrected to avoid arrhythmias and seizures. Phosphorus levels >6.5 mg/dl (2.1 mmol/L) should be managed by restricting phosphorus intake, and by the use of phosphate binders (calcium acetate, calcium carbonate, sevelamer, lanthanum, or aluminum hydroxide). Aluminum hydroxide should be avoided in patients with renal insufficiency. In severe cases of hyperphosphatemia, dialysis should be considered.
Symptomatic hypocalcemia should be treated with calcium gluconate if changes are present on the electrocardiography (ECG). Hypocalcemia in the presence of hyperphosphatemia should be treated only in patients with tetany or cardiac arrhythmias; otherwise, hypocalcemia should not be treated until hyperphosphatemia has been corrected.
In cases of hyperkalemia, patients should be placed on a cardiac monitor and stabilized with calcium gluconate; kayexalate should be administered to reduce total body potassium. Other interventions, such as intravenous insulin given with dextrose, sodium bicarbonate, and albuterol, have a temporary effect on hyperkalemia and can be used as adjunct treatments in patients with severe hyperkalemia (>7). Hemodialysis should be strongly considered in severe cases of hyperkalemia, particularly in patients with persistently elevated potassium levels despite other treatments.
Back to the Case
Our patient was started on IVFs with close monitoring of his urine output. He was considered intermediate risk for developing TLS. Allopurinol, renally dosed, was administered for two days prior to initiating treatment with rituximab plus chemotherapy. His chemistry panel was monitored daily and he did not develop any form of TLS.
Bottom Line
TLS is a common oncology emergency in patients with hematologic malignancies. Preventative measures include starting IVF prior to cancer treatment, and administering allopurinol and/or rasburicase to patients at risk of developing TLS. Treatment should include normalizing electrolytes to avoid arrhythmias and seizures.
Dr. Akwe is assistant professor of medicine at the Emory University School of Medicine and a clinical instructor of medicine at the Morehouse School of Medicine, both in Atlanta. Dr. Smith is an assistant director for education in the division of hospital medicine at Emory. Both work as hospitalists at the Atlanta VA Medical Center.
References
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55:Suppl 3:S1-S13.
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578-586.
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179-180.
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med. 2011;364:1844.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127:3.
- Wössmann W, Schrappe M, Meyer U, et al. Incidence of tumor lysis syndrome in children with advanced stage Burkitt’s lymphoma/leukemia before and after introduction of prophylactic use of urate oxidase. Ann Hematol. 2003;82:160.
- Hussain K, Mazza JJ, Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy Gemici C. Tumor lysis syndrome in solid tumors. J Clin Oncol. 2009;27:2738-2739
- Rostom AY, El-Hussainy G, Kandil A, Allam A. Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer. Ann Oncol. 2000;11:1349.
- Drakos P, Bar-Ziv J, Catane R. Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature. Am J Clin Oncol. 1994;17:502.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51:187.
- Kalemkerian GP, Darwish B, Varterasian ML. Tumor lysis syndrome in small cell carcinoma and other solid tumors. Am J Med. 1997;103:363.
- Noh GY, Choe DH, Kim CH, Lee JC. Fatal tumor lysis syndrome during radiotherapy for non-small-cell lung cancer. J Clin Oncol. 2008;26:6005-6006.
- Pentheroudakis G, O’Neill VJ, Vasey P, Kaye SB. Spontaneous acute tumour lysis syndrome in patients with metastatic germ cell tumours. Report of two cases. Support Care Cancer. 2001;9:554.
- Joshita S, Yoshizawa K, Sano K, et al., A patient with advanced hepatocellular carcinoma treated with sorafenib tosylate showed massive tumor lysis with avoidance of tumor lysis syndrome. Intern Med. 2010;49:991-994.
- Huang WS, Yang CH. Sorafenib-induced tumor lysis syndrome in an advanced hepatocellular carcinoma patient. World J Gastroenterol. 2009;15:4464-4466.
- Bilgrami SF, Fallon BG. Tumor lysis syndrome after combination chemotherapy for ovarian cancer. Med Pediatr Oncol. 1993;21:521.
- Chan JK, Lin SS, McMeekin DS, Berman ML. Patients with malignancy requiring urgent therapy: CASE 3. Tumor lysis syndrome associated with chemotherapy in ovarian cancer. J Clin Oncol. 2005;23:6794.
- Godoy H, Kesterson JP, Lele S. Tumor lysis syndrome associated with carboplatin and paclitaxel in a woman with recurrent endometrial cancer. Int J Gynaecol Obstet. 2010;109:254.
- Shamseddine AI, Khalil AM, Wehbeh MH. Acute tumor lysis syndrome with squamous cell carcinoma of the vulva. Gynecol Oncol 1993;51:258
- Pinder EM, Atwal GS, Ayantunde AA, et al. Tumour lysis syndrome occurring in a patient with metastatic gastrointestinal stromal tumour treated with Glivec (imatinib mesylate, Gleevec, STI571). Sarcoma. 2007;2007:82012.
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406-2408.
- Oztop I, Demirkan B, Yaren A, et al. Rapid tumor lysis syndrome in a patient with metastatic colon cancer as a complication of treatment with 5-fluorouracil/leucoverin and irinotecan. Tumori. 2004;90:514.
- Lin CJ, Lim KH, Cheng YC, et al. Tumor lysis syndrome after treatment with gemcitabine for metastatic transitional cell carcinoma. Med Oncol. 2007;24:455.
- Malik IA, Abubakar S, Alam F, Khan A. Dexamethasone-induced tumor lysis syndrome in high-grade non-Hodgkin’s lymphoma. South Med J. 1994;87:409.
- Jabr FI. Acute tumor lysis syndrome induced by rituximab in diffuse large B-cell lymphoma. Int J Hematol. 2005;82:312.
- Sezer O, Vesole DH, Singhal S, et al. Bortezomib-induced tumor lysis syndrome in multiple myeloma. Clin Lymphoma Myeloma. 2006;7:233.
- Jensen M, Winkler U, Manzke O, et al. Rapid tumor lysis in a patient with B-cell chronic lymphocytic leukemia and lymphocytosis treated with an anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab). Ann Hematol. 1998;77:89.
- Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysis syndrome immediately after 4 Gy fractionated TBI as part of reduced intensity preparative regimen in a patient with T-ALL with high tumor burden. Bone Marrow Transplant. 2003;31:935.
- Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008;26(16):2767-2778. [Erratum, J Clin Oncol. 2010;28:708.]
- Cheuk DK, Chiang AK, Chan GC, Ha SY. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database Syst Rev. 2010;(6):CD006945.
- Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol. 2010;28:4207.
Case
A 25-year-old male with HIV/AIDS and a CD4 count of 65 cells/μL presents to the ED with intractable nausea and vomiting for one week. Laboratory evaluation revealed a white blood cell of 67,000 cells/mm3. An extended chemistry panel reveals creatinine 3.5 mg/dL, potassium 3.0 mmol/L, LDH 250 IU/L, and uric acid 5mg/dL. Calcium and phosphorus were both normal. The patient was admitted for further evaluation and management, and was later diagnosed with Burkitt’s lymphoma.
Overview
Tumor lysis syndrome (TLS) is an acute cell lysis of tumor cells with the release of cell content into circulation either spontaneously or in response to therapy, leading to hyperurecemia, hyperkalemia, hyperphosphatemia, and hypocalcemia.1-3
TLS is one of the most common oncology emergencies encountered by hospitalists caring for patients with hematologic malignancies. The incidence and severity of TLS depend on the cell burden, cell proliferation rate, potential for cell lysis or chemo sensitivity, baseline clinical characteristics, and preventive measures taken (see Table 1).2,4
TLS is classified as laboratory or clinical. Laboratory TLS is described as the presence of two or more of the following serum abnormalities at the same time, present within three days before or seven days after the start of therapy.5
- Uric acid >8 mg/dL (475.8 micromole/L) or 25% increase;
- Potassium >6 mEq/L (6 mmol/L) or 25% increase;
- Phosphorus >6.5 mg/dL (2.1 mmol/L) for children or >4.5 mg/dl (1.45 mmol/L) for adults or 25% increase; and
- Calcium >7 mg/dL (1.75 mmol/L) or 25% increase.
Clinical TLS is defined as laboratory TLS in association with increased creatinine levels, seizures, cardiac arrhythmias, or death (see Table 2).5
Pathogenesis
Tumor cell lysis releases DNA, cytokines, phosphate, and potassium. DNA is metabolized into adenosine and guanosine, which are then converted into xanthines. Xanthines are oxidized by xanthine oxidase into uric acid, which is then excreted through the kidneys.
TLS develops when the accumulation of xanthine, uric acid, potassium, and phosphorus exceeds the kidney’s capacity to excrete them. Cytokines cause hypotension, inflammation, and kidney injury, and worsen the kidney’s excretory capacity. Damage to the kidneys also occurs by renal precipitation of uric acid, xanthine, and calcium phosphate.4
Phosphorus concentrations in tumor cells are four times higher than in normal cells. When the calcium phosphorus product exceeds 60 mg2/dL2, there is an increased risk of calcium phosphate precipitation in the kidney tubules, which could lead to kidney failure. Accumulation of calcium phosphate product may also be cardiotoxic and can lead to cardiac arrhythmias. In addition, hyperphosphatemia can cause secondary hypocalcemia, which may lead to parasthesias, tetany, and cardiac arrhythmias.2,4
TLS is most common in tumors with high proliferative rates and high tumor burden, such as acute lymphoblastic leukemia and Burkitt’s lymphoma, but it can occur with other hematologic malignancies, such as T-cell precursor acute lymphocytic leukemia (ALL), B-cell precursor ALL, acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), anaplastic large cell lymphoma, and plasma cell disorders (e.g. multiple myeloma and plasmacytoma).6,7 TLS has also been reported with the treatment of solid organ nonhematologic tumors (see Table 3).
In hematologic tumors, TLS frequently is associated with cytotoxic chemotherapy, and less frequently with glucocorticoid treatment, monoclonal antibodies (eg, rituximab, bortezomab, imatinib), and radiation therapy.25-29
Patient factors, such as baseline kidney disease or lack of prophylactic/preventive measures for TLS, also increase the risk.4 TLS, however, can develop in patients classified as low risk (see Table 1.
TLS Prevention
Intravenous fluids. Every patient at intermediate or high risk of TLS should receive intravenous fluids (IVF) prior to cancer treatment; those at low risk may receive IVF based on the provider’s clinical judgment.30 The purpose of administering IVF is to generate high urine output to reduce the risk of precipitation of uric acid in the renal tubules.30 Both adults and children should receive approximately 2 to 3 L/m2 per day of IVF,30 and urine output should be maintained at 2 ml/kg/hr (or 4 to 6 ml/kg/hr for children <10kg).30 IVF should be cautiously administered in patients with renal insufficiency or heart failure, and diuretics may be used to maintain goal urine output. Recommended initial fluids are D51/4 normal saline, or normal saline for patients who are dehydrated or hyponatremic.30
Allopurinol. Allopurinol is usually also administered to patients at risk for developing TLS.30 Allopurinol inhibits the metabolism of hypoxanthine and xanthine to uric acid, which decreases the accumulation of uric acid in the renal tubules, thus preventing obstructive renal disease from precipitation of uric acid.4 The recommended dose of allopurinol is 100 mg/m2 every eight hours, and should not exceed 800 mg per day in adults. It should be started one to two days prior to induction chemotherapy and continued for three to seven days after the treatment and until uric acid levels and other electrolyte levels have returned to normal. The dose is adjusted to 50 mg/m2 every eight hours in patients with kidney failure.30
In some cases, allopurinol can lead to increased levels of xanthine crystals in the renal tubules, leading to acute kidney injury. Also, allopurinol does not have any effect on uric acid that has already been formed, so patients with elevated uric acid levels prior to the initiation of cancer therapy will not have any reduction in the levels of uric acid. Allopurinol reduces the degradation of other purines, so it can cause toxicity in patients on azathioprine and 6-mercaptopurine if the doses of these medications are not adjusted.
Rasburicase. Rasburicase is a recombinant urate oxidase, derived from aspergillus favus, which catalyzes the breakdown of uric acid to allantoin, which is a water-soluble product. Rasburicase is recommended as a first-line treatment for patients at high risk for clinical TLS.30 Rasburicase has an earlier onset than allopurinol and rapidly decreases serum levels of uric acid within four hours of administration.30,31 The recommended dose is 0.10 to 0.20 mg/kg once a day for five days in adults.30
A Phase III trial compared the efficiency and safety of rasburicase to rasburicase with allopurinol or allopurinol alone.32 A significantly higher normalization of uric acid was found in patients on rasburicase compared to allopurinol alone. The incidence of laboratory TLS was also significantly lower with rasburicase alone compared to allopurinol alone, and was even lower with allopurinol plus rasburicase. The incidence of acute kidney injury was the same with rasburicase alone or allopurinol alone but was higher with rasburicase plus allopurinol.
Serum uric acid, phosphorus, potassium, and calcium need to be monitored every four hours for 24 hours after the completion of chemotherapy in patients on rasburicase.4 The sample of blood drawn to check the uric acid levels has to be placed on ice and processed within four hours in order to avoid falsely lower levels of uric acid due to the conversion of uric acid to allantoin. Rasburicase is contraindicated in patients with G6PD deficiency and pregnant women, because one of the byproducts of uric acid breakdown is hydrogen peroxide, which can cause severe hemolysis and the formation of methemoglobin in these patients.30
Rasburicase has been approved for use in both children and adults, but there is more evidence for the use in children. Rasburicase has a black-box label for patients with anaphylaxis, methemoglobinemia, hemolysis, and hemoglobinuria, and there is a recommendation to check G6PD deficiency before use in high-risk patients.30
TLS Treatment
Alkalinization. Alkalinization of urine is controversial in the management of TLS. Urine alkalinization increases uric acid solubility but causes hyperphosphatemia and decreases calcium phosphate solubility, which can then deposit in the kidney once cancer treatment starts. Of note, hyperphosphatemia is much more difficult to correct than high levels of uric acid, and there are no clinical trials proving the superiority of urine alkalinization over normal saline.
Normalization of electrolytes. Electrolyte abnormalities should be corrected to avoid arrhythmias and seizures. Phosphorus levels >6.5 mg/dl (2.1 mmol/L) should be managed by restricting phosphorus intake, and by the use of phosphate binders (calcium acetate, calcium carbonate, sevelamer, lanthanum, or aluminum hydroxide). Aluminum hydroxide should be avoided in patients with renal insufficiency. In severe cases of hyperphosphatemia, dialysis should be considered.
Symptomatic hypocalcemia should be treated with calcium gluconate if changes are present on the electrocardiography (ECG). Hypocalcemia in the presence of hyperphosphatemia should be treated only in patients with tetany or cardiac arrhythmias; otherwise, hypocalcemia should not be treated until hyperphosphatemia has been corrected.
In cases of hyperkalemia, patients should be placed on a cardiac monitor and stabilized with calcium gluconate; kayexalate should be administered to reduce total body potassium. Other interventions, such as intravenous insulin given with dextrose, sodium bicarbonate, and albuterol, have a temporary effect on hyperkalemia and can be used as adjunct treatments in patients with severe hyperkalemia (>7). Hemodialysis should be strongly considered in severe cases of hyperkalemia, particularly in patients with persistently elevated potassium levels despite other treatments.
Back to the Case
Our patient was started on IVFs with close monitoring of his urine output. He was considered intermediate risk for developing TLS. Allopurinol, renally dosed, was administered for two days prior to initiating treatment with rituximab plus chemotherapy. His chemistry panel was monitored daily and he did not develop any form of TLS.
Bottom Line
TLS is a common oncology emergency in patients with hematologic malignancies. Preventative measures include starting IVF prior to cancer treatment, and administering allopurinol and/or rasburicase to patients at risk of developing TLS. Treatment should include normalizing electrolytes to avoid arrhythmias and seizures.
Dr. Akwe is assistant professor of medicine at the Emory University School of Medicine and a clinical instructor of medicine at the Morehouse School of Medicine, both in Atlanta. Dr. Smith is an assistant director for education in the division of hospital medicine at Emory. Both work as hospitalists at the Atlanta VA Medical Center.
References
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55:Suppl 3:S1-S13.
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578-586.
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179-180.
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med. 2011;364:1844.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127:3.
- Wössmann W, Schrappe M, Meyer U, et al. Incidence of tumor lysis syndrome in children with advanced stage Burkitt’s lymphoma/leukemia before and after introduction of prophylactic use of urate oxidase. Ann Hematol. 2003;82:160.
- Hussain K, Mazza JJ, Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy Gemici C. Tumor lysis syndrome in solid tumors. J Clin Oncol. 2009;27:2738-2739
- Rostom AY, El-Hussainy G, Kandil A, Allam A. Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer. Ann Oncol. 2000;11:1349.
- Drakos P, Bar-Ziv J, Catane R. Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature. Am J Clin Oncol. 1994;17:502.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51:187.
- Kalemkerian GP, Darwish B, Varterasian ML. Tumor lysis syndrome in small cell carcinoma and other solid tumors. Am J Med. 1997;103:363.
- Noh GY, Choe DH, Kim CH, Lee JC. Fatal tumor lysis syndrome during radiotherapy for non-small-cell lung cancer. J Clin Oncol. 2008;26:6005-6006.
- Pentheroudakis G, O’Neill VJ, Vasey P, Kaye SB. Spontaneous acute tumour lysis syndrome in patients with metastatic germ cell tumours. Report of two cases. Support Care Cancer. 2001;9:554.
- Joshita S, Yoshizawa K, Sano K, et al., A patient with advanced hepatocellular carcinoma treated with sorafenib tosylate showed massive tumor lysis with avoidance of tumor lysis syndrome. Intern Med. 2010;49:991-994.
- Huang WS, Yang CH. Sorafenib-induced tumor lysis syndrome in an advanced hepatocellular carcinoma patient. World J Gastroenterol. 2009;15:4464-4466.
- Bilgrami SF, Fallon BG. Tumor lysis syndrome after combination chemotherapy for ovarian cancer. Med Pediatr Oncol. 1993;21:521.
- Chan JK, Lin SS, McMeekin DS, Berman ML. Patients with malignancy requiring urgent therapy: CASE 3. Tumor lysis syndrome associated with chemotherapy in ovarian cancer. J Clin Oncol. 2005;23:6794.
- Godoy H, Kesterson JP, Lele S. Tumor lysis syndrome associated with carboplatin and paclitaxel in a woman with recurrent endometrial cancer. Int J Gynaecol Obstet. 2010;109:254.
- Shamseddine AI, Khalil AM, Wehbeh MH. Acute tumor lysis syndrome with squamous cell carcinoma of the vulva. Gynecol Oncol 1993;51:258
- Pinder EM, Atwal GS, Ayantunde AA, et al. Tumour lysis syndrome occurring in a patient with metastatic gastrointestinal stromal tumour treated with Glivec (imatinib mesylate, Gleevec, STI571). Sarcoma. 2007;2007:82012.
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406-2408.
- Oztop I, Demirkan B, Yaren A, et al. Rapid tumor lysis syndrome in a patient with metastatic colon cancer as a complication of treatment with 5-fluorouracil/leucoverin and irinotecan. Tumori. 2004;90:514.
- Lin CJ, Lim KH, Cheng YC, et al. Tumor lysis syndrome after treatment with gemcitabine for metastatic transitional cell carcinoma. Med Oncol. 2007;24:455.
- Malik IA, Abubakar S, Alam F, Khan A. Dexamethasone-induced tumor lysis syndrome in high-grade non-Hodgkin’s lymphoma. South Med J. 1994;87:409.
- Jabr FI. Acute tumor lysis syndrome induced by rituximab in diffuse large B-cell lymphoma. Int J Hematol. 2005;82:312.
- Sezer O, Vesole DH, Singhal S, et al. Bortezomib-induced tumor lysis syndrome in multiple myeloma. Clin Lymphoma Myeloma. 2006;7:233.
- Jensen M, Winkler U, Manzke O, et al. Rapid tumor lysis in a patient with B-cell chronic lymphocytic leukemia and lymphocytosis treated with an anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab). Ann Hematol. 1998;77:89.
- Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysis syndrome immediately after 4 Gy fractionated TBI as part of reduced intensity preparative regimen in a patient with T-ALL with high tumor burden. Bone Marrow Transplant. 2003;31:935.
- Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008;26(16):2767-2778. [Erratum, J Clin Oncol. 2010;28:708.]
- Cheuk DK, Chiang AK, Chan GC, Ha SY. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database Syst Rev. 2010;(6):CD006945.
- Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol. 2010;28:4207.
Case
A 25-year-old male with HIV/AIDS and a CD4 count of 65 cells/μL presents to the ED with intractable nausea and vomiting for one week. Laboratory evaluation revealed a white blood cell of 67,000 cells/mm3. An extended chemistry panel reveals creatinine 3.5 mg/dL, potassium 3.0 mmol/L, LDH 250 IU/L, and uric acid 5mg/dL. Calcium and phosphorus were both normal. The patient was admitted for further evaluation and management, and was later diagnosed with Burkitt’s lymphoma.
Overview
Tumor lysis syndrome (TLS) is an acute cell lysis of tumor cells with the release of cell content into circulation either spontaneously or in response to therapy, leading to hyperurecemia, hyperkalemia, hyperphosphatemia, and hypocalcemia.1-3
TLS is one of the most common oncology emergencies encountered by hospitalists caring for patients with hematologic malignancies. The incidence and severity of TLS depend on the cell burden, cell proliferation rate, potential for cell lysis or chemo sensitivity, baseline clinical characteristics, and preventive measures taken (see Table 1).2,4
TLS is classified as laboratory or clinical. Laboratory TLS is described as the presence of two or more of the following serum abnormalities at the same time, present within three days before or seven days after the start of therapy.5
- Uric acid >8 mg/dL (475.8 micromole/L) or 25% increase;
- Potassium >6 mEq/L (6 mmol/L) or 25% increase;
- Phosphorus >6.5 mg/dL (2.1 mmol/L) for children or >4.5 mg/dl (1.45 mmol/L) for adults or 25% increase; and
- Calcium >7 mg/dL (1.75 mmol/L) or 25% increase.
Clinical TLS is defined as laboratory TLS in association with increased creatinine levels, seizures, cardiac arrhythmias, or death (see Table 2).5
Pathogenesis
Tumor cell lysis releases DNA, cytokines, phosphate, and potassium. DNA is metabolized into adenosine and guanosine, which are then converted into xanthines. Xanthines are oxidized by xanthine oxidase into uric acid, which is then excreted through the kidneys.
TLS develops when the accumulation of xanthine, uric acid, potassium, and phosphorus exceeds the kidney’s capacity to excrete them. Cytokines cause hypotension, inflammation, and kidney injury, and worsen the kidney’s excretory capacity. Damage to the kidneys also occurs by renal precipitation of uric acid, xanthine, and calcium phosphate.4
Phosphorus concentrations in tumor cells are four times higher than in normal cells. When the calcium phosphorus product exceeds 60 mg2/dL2, there is an increased risk of calcium phosphate precipitation in the kidney tubules, which could lead to kidney failure. Accumulation of calcium phosphate product may also be cardiotoxic and can lead to cardiac arrhythmias. In addition, hyperphosphatemia can cause secondary hypocalcemia, which may lead to parasthesias, tetany, and cardiac arrhythmias.2,4
TLS is most common in tumors with high proliferative rates and high tumor burden, such as acute lymphoblastic leukemia and Burkitt’s lymphoma, but it can occur with other hematologic malignancies, such as T-cell precursor acute lymphocytic leukemia (ALL), B-cell precursor ALL, acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), anaplastic large cell lymphoma, and plasma cell disorders (e.g. multiple myeloma and plasmacytoma).6,7 TLS has also been reported with the treatment of solid organ nonhematologic tumors (see Table 3).
In hematologic tumors, TLS frequently is associated with cytotoxic chemotherapy, and less frequently with glucocorticoid treatment, monoclonal antibodies (eg, rituximab, bortezomab, imatinib), and radiation therapy.25-29
Patient factors, such as baseline kidney disease or lack of prophylactic/preventive measures for TLS, also increase the risk.4 TLS, however, can develop in patients classified as low risk (see Table 1.
TLS Prevention
Intravenous fluids. Every patient at intermediate or high risk of TLS should receive intravenous fluids (IVF) prior to cancer treatment; those at low risk may receive IVF based on the provider’s clinical judgment.30 The purpose of administering IVF is to generate high urine output to reduce the risk of precipitation of uric acid in the renal tubules.30 Both adults and children should receive approximately 2 to 3 L/m2 per day of IVF,30 and urine output should be maintained at 2 ml/kg/hr (or 4 to 6 ml/kg/hr for children <10kg).30 IVF should be cautiously administered in patients with renal insufficiency or heart failure, and diuretics may be used to maintain goal urine output. Recommended initial fluids are D51/4 normal saline, or normal saline for patients who are dehydrated or hyponatremic.30
Allopurinol. Allopurinol is usually also administered to patients at risk for developing TLS.30 Allopurinol inhibits the metabolism of hypoxanthine and xanthine to uric acid, which decreases the accumulation of uric acid in the renal tubules, thus preventing obstructive renal disease from precipitation of uric acid.4 The recommended dose of allopurinol is 100 mg/m2 every eight hours, and should not exceed 800 mg per day in adults. It should be started one to two days prior to induction chemotherapy and continued for three to seven days after the treatment and until uric acid levels and other electrolyte levels have returned to normal. The dose is adjusted to 50 mg/m2 every eight hours in patients with kidney failure.30
In some cases, allopurinol can lead to increased levels of xanthine crystals in the renal tubules, leading to acute kidney injury. Also, allopurinol does not have any effect on uric acid that has already been formed, so patients with elevated uric acid levels prior to the initiation of cancer therapy will not have any reduction in the levels of uric acid. Allopurinol reduces the degradation of other purines, so it can cause toxicity in patients on azathioprine and 6-mercaptopurine if the doses of these medications are not adjusted.
Rasburicase. Rasburicase is a recombinant urate oxidase, derived from aspergillus favus, which catalyzes the breakdown of uric acid to allantoin, which is a water-soluble product. Rasburicase is recommended as a first-line treatment for patients at high risk for clinical TLS.30 Rasburicase has an earlier onset than allopurinol and rapidly decreases serum levels of uric acid within four hours of administration.30,31 The recommended dose is 0.10 to 0.20 mg/kg once a day for five days in adults.30
A Phase III trial compared the efficiency and safety of rasburicase to rasburicase with allopurinol or allopurinol alone.32 A significantly higher normalization of uric acid was found in patients on rasburicase compared to allopurinol alone. The incidence of laboratory TLS was also significantly lower with rasburicase alone compared to allopurinol alone, and was even lower with allopurinol plus rasburicase. The incidence of acute kidney injury was the same with rasburicase alone or allopurinol alone but was higher with rasburicase plus allopurinol.
Serum uric acid, phosphorus, potassium, and calcium need to be monitored every four hours for 24 hours after the completion of chemotherapy in patients on rasburicase.4 The sample of blood drawn to check the uric acid levels has to be placed on ice and processed within four hours in order to avoid falsely lower levels of uric acid due to the conversion of uric acid to allantoin. Rasburicase is contraindicated in patients with G6PD deficiency and pregnant women, because one of the byproducts of uric acid breakdown is hydrogen peroxide, which can cause severe hemolysis and the formation of methemoglobin in these patients.30
Rasburicase has been approved for use in both children and adults, but there is more evidence for the use in children. Rasburicase has a black-box label for patients with anaphylaxis, methemoglobinemia, hemolysis, and hemoglobinuria, and there is a recommendation to check G6PD deficiency before use in high-risk patients.30
TLS Treatment
Alkalinization. Alkalinization of urine is controversial in the management of TLS. Urine alkalinization increases uric acid solubility but causes hyperphosphatemia and decreases calcium phosphate solubility, which can then deposit in the kidney once cancer treatment starts. Of note, hyperphosphatemia is much more difficult to correct than high levels of uric acid, and there are no clinical trials proving the superiority of urine alkalinization over normal saline.
Normalization of electrolytes. Electrolyte abnormalities should be corrected to avoid arrhythmias and seizures. Phosphorus levels >6.5 mg/dl (2.1 mmol/L) should be managed by restricting phosphorus intake, and by the use of phosphate binders (calcium acetate, calcium carbonate, sevelamer, lanthanum, or aluminum hydroxide). Aluminum hydroxide should be avoided in patients with renal insufficiency. In severe cases of hyperphosphatemia, dialysis should be considered.
Symptomatic hypocalcemia should be treated with calcium gluconate if changes are present on the electrocardiography (ECG). Hypocalcemia in the presence of hyperphosphatemia should be treated only in patients with tetany or cardiac arrhythmias; otherwise, hypocalcemia should not be treated until hyperphosphatemia has been corrected.
In cases of hyperkalemia, patients should be placed on a cardiac monitor and stabilized with calcium gluconate; kayexalate should be administered to reduce total body potassium. Other interventions, such as intravenous insulin given with dextrose, sodium bicarbonate, and albuterol, have a temporary effect on hyperkalemia and can be used as adjunct treatments in patients with severe hyperkalemia (>7). Hemodialysis should be strongly considered in severe cases of hyperkalemia, particularly in patients with persistently elevated potassium levels despite other treatments.
Back to the Case
Our patient was started on IVFs with close monitoring of his urine output. He was considered intermediate risk for developing TLS. Allopurinol, renally dosed, was administered for two days prior to initiating treatment with rituximab plus chemotherapy. His chemistry panel was monitored daily and he did not develop any form of TLS.
Bottom Line
TLS is a common oncology emergency in patients with hematologic malignancies. Preventative measures include starting IVF prior to cancer treatment, and administering allopurinol and/or rasburicase to patients at risk of developing TLS. Treatment should include normalizing electrolytes to avoid arrhythmias and seizures.
Dr. Akwe is assistant professor of medicine at the Emory University School of Medicine and a clinical instructor of medicine at the Morehouse School of Medicine, both in Atlanta. Dr. Smith is an assistant director for education in the division of hospital medicine at Emory. Both work as hospitalists at the Atlanta VA Medical Center.
References
- Abu-Alfa AK, Younes A. Tumor lysis syndrome and acute kidney injury: evaluation, prevention, and management. Am J Kidney Dis. 2010;55:Suppl 3:S1-S13.
- Cairo MS, Coiffier B, Reiter A, Younes A. Recommendations for the evaluation of risk and prophylaxis of tumour lysis syndrome (TLS) in adults and children with malignant diseases: an expert TLS panel consensus. Br J Haematol. 2010;149:578-586.
- Gertz MA. Managing tumor lysis syndrome in 2010. Leuk Lymphoma. 2010;51:179-180.
- Howard SC, Jones DP, Pui CH. The tumor lysis syndrome. N Engl J Med. 2011;364:1844.
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. Br J Haematol. 2004;127:3.
- Wössmann W, Schrappe M, Meyer U, et al. Incidence of tumor lysis syndrome in children with advanced stage Burkitt’s lymphoma/leukemia before and after introduction of prophylactic use of urate oxidase. Ann Hematol. 2003;82:160.
- Hussain K, Mazza JJ, Clouse LH. Tumor lysis syndrome (TLS) following fludarabine therapy Gemici C. Tumor lysis syndrome in solid tumors. J Clin Oncol. 2009;27:2738-2739
- Rostom AY, El-Hussainy G, Kandil A, Allam A. Tumor lysis syndrome following hemi-body irradiation for metastatic breast cancer. Ann Oncol. 2000;11:1349.
- Drakos P, Bar-Ziv J, Catane R. Tumor lysis syndrome in nonhematologic malignancies. Report of a case and review of the literature. Am J Clin Oncol. 1994;17:502.
- Baeksgaard L, Sørensen JB. Acute tumor lysis syndrome in solid tumors—a case report and review of the literature. Cancer Chemother Pharmacol. 2003;51:187.
- Kalemkerian GP, Darwish B, Varterasian ML. Tumor lysis syndrome in small cell carcinoma and other solid tumors. Am J Med. 1997;103:363.
- Noh GY, Choe DH, Kim CH, Lee JC. Fatal tumor lysis syndrome during radiotherapy for non-small-cell lung cancer. J Clin Oncol. 2008;26:6005-6006.
- Pentheroudakis G, O’Neill VJ, Vasey P, Kaye SB. Spontaneous acute tumour lysis syndrome in patients with metastatic germ cell tumours. Report of two cases. Support Care Cancer. 2001;9:554.
- Joshita S, Yoshizawa K, Sano K, et al., A patient with advanced hepatocellular carcinoma treated with sorafenib tosylate showed massive tumor lysis with avoidance of tumor lysis syndrome. Intern Med. 2010;49:991-994.
- Huang WS, Yang CH. Sorafenib-induced tumor lysis syndrome in an advanced hepatocellular carcinoma patient. World J Gastroenterol. 2009;15:4464-4466.
- Bilgrami SF, Fallon BG. Tumor lysis syndrome after combination chemotherapy for ovarian cancer. Med Pediatr Oncol. 1993;21:521.
- Chan JK, Lin SS, McMeekin DS, Berman ML. Patients with malignancy requiring urgent therapy: CASE 3. Tumor lysis syndrome associated with chemotherapy in ovarian cancer. J Clin Oncol. 2005;23:6794.
- Godoy H, Kesterson JP, Lele S. Tumor lysis syndrome associated with carboplatin and paclitaxel in a woman with recurrent endometrial cancer. Int J Gynaecol Obstet. 2010;109:254.
- Shamseddine AI, Khalil AM, Wehbeh MH. Acute tumor lysis syndrome with squamous cell carcinoma of the vulva. Gynecol Oncol 1993;51:258
- Pinder EM, Atwal GS, Ayantunde AA, et al. Tumour lysis syndrome occurring in a patient with metastatic gastrointestinal stromal tumour treated with Glivec (imatinib mesylate, Gleevec, STI571). Sarcoma. 2007;2007:82012.
- Krishnan G, D’Silva K, Al-Janadi A. Cetuximab-related tumor lysis syndrome in metastatic colon carcinoma. J Clin Oncol. 2008;26:2406-2408.
- Oztop I, Demirkan B, Yaren A, et al. Rapid tumor lysis syndrome in a patient with metastatic colon cancer as a complication of treatment with 5-fluorouracil/leucoverin and irinotecan. Tumori. 2004;90:514.
- Lin CJ, Lim KH, Cheng YC, et al. Tumor lysis syndrome after treatment with gemcitabine for metastatic transitional cell carcinoma. Med Oncol. 2007;24:455.
- Malik IA, Abubakar S, Alam F, Khan A. Dexamethasone-induced tumor lysis syndrome in high-grade non-Hodgkin’s lymphoma. South Med J. 1994;87:409.
- Jabr FI. Acute tumor lysis syndrome induced by rituximab in diffuse large B-cell lymphoma. Int J Hematol. 2005;82:312.
- Sezer O, Vesole DH, Singhal S, et al. Bortezomib-induced tumor lysis syndrome in multiple myeloma. Clin Lymphoma Myeloma. 2006;7:233.
- Jensen M, Winkler U, Manzke O, et al. Rapid tumor lysis in a patient with B-cell chronic lymphocytic leukemia and lymphocytosis treated with an anti-CD20 monoclonal antibody (IDEC-C2B8, rituximab). Ann Hematol. 1998;77:89.
- Linck D, Basara N, Tran V, et al. Peracute onset of severe tumor lysis syndrome immediately after 4 Gy fractionated TBI as part of reduced intensity preparative regimen in a patient with T-ALL with high tumor burden. Bone Marrow Transplant. 2003;31:935.
- Coiffier B, Altman A, Pui CH, Younes A, Cairo MS. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. J Clin Oncol. 2008;26(16):2767-2778. [Erratum, J Clin Oncol. 2010;28:708.]
- Cheuk DK, Chiang AK, Chan GC, Ha SY. Urate oxidase for the prevention and treatment of tumor lysis syndrome in children with cancer. Cochrane Database Syst Rev. 2010;(6):CD006945.
- Cortes J, Moore JO, Maziarz RT, et al. Control of plasma uric acid in adults at risk for tumor Lysis syndrome: efficacy and safety of rasburicase alone and rasburicase followed by allopurinol compared with allopurinol alone—results of a multicenter phase III study. J Clin Oncol. 2010;28:4207.
Commemorating Round-the-Clock Hospital Medicine Programs


The steam engine. The telephone. Television. ATMs. The Internet. Smartphones. The 24/7 hospitalist program.
Perhaps the single most important innovation along the road to where we are now in HM has been the development of the hospital-sponsored, 24/7, on-site hospitalist program. And the father of this invention may be the most significant figure in HM you’ve never heard of: John Holbrook, MD, FACEP. An emergency-medicine physician since the mid-1970s, Dr. Holbrook did something in July 1993 that was considered off the wall, yet proved to be revolutionary: From nothing, he launched a 24/7 hospitalist program staffed with board-eligible and board-certified internists at Mercy Hospital in Springfield, Mass. The inpatient physicians (this was before the word “hospitalist” came to be) were employed by a subsidiary of the hospital and worked in place of community primary-care physicians (PCPs), taking care of hospitalized patients who did not have a PCP, or whose PCP chose not to come to the hospital.
Of great significance, from the beginning, and perhaps by unintentional design, these physicians were agents of change and improvement for the hospital itself.
To be sure, in places like Southern California, 24/7, on-site hospitalist programs were in place in the late 1980s. Some claim those programs may have been the birthplace of the hospitalist model. However, such programs came to be in order to help medical groups manage full capitated risk delegated to them from HMOs on a population of patients, and were not supported by the hospital, per se. This is distinct from hospitalist programs—such as Mercy’s—sponsored by hospitals (whether employed or contracted) in predominantly fee-for-service markets, which then comprised the lion’s share of the U.S. market.
I had the extraordinary good fortune to happen along in July 1994, get hired by Dr. Holbrook, and soon after begin serving as medical director for the Mercy program, which I would do for the next decade. To this day, Dr. Holbrook is a mentor and trusted advisor to me. I caught up with him in recognition of the 20th anniversary of the Mercy Inpatient Medicine Service.

Question: What gave you the idea to launch what was, at the time, considered such an unconventional program?
Answer: Before the specialty of emergency medicine, a patient’s private physician would be called in most cases when a patient present in the ED: 25 or 50 doctors might be called over 24 hours, each to see one patient each. The inefficiency and disruption caused by this system was a natural and logical stimulus to develop the specialty of emergency medicine. I saw hospitalist medicine as an exact analogy.
Q: What were you observing in the healthcare environment that drove you to create the Mercy Inpatient Medicine Service?
A: Working for many years in the emergency department of a community hospital without a house staff, the ED docs would admit a patient at night or on the weekend and the attending physician would often plan to see the patient “in the morning.” When the patient would decompensate in the middle of the night, the ED doc would get a call to run to the floor to “Band-Aid” the situation.
Q: How did you convince the board of trustees to fund it?
A: The reasons were primarily economic. No. 1, the hospital was losing market share because local physicians would prefer to admit to the teaching hospital [a nearby competitor], where they were not required to come in during the middle of the night. No. 2, the cost of a hospitalization managed by a hospitalist was less expensive than either a hospital stay managed by house staff or managed over the telephone by a private attending at home.
Q: What was the most difficult operational challenge for the program?
A: Effective and timely communication with the community physicians was the most difficult operational challenge. Access to outpatient medical treatment immediately prior to a hospitalization and timely communication to the community physician were both challenges that we never adequately solved in the early days. I understand that these issues can still be problematic.
Q: How was it received by patients?
A: Overall, patients were very happy with the system. In the old system, with a typical four-physician practice, a patient had only a 1 in 4 chance of being admitted by the doctor who was familiar with the case. The fact that the hospitalist was available in the hospital made the improvement in quality apparent to most patients.
Q: How did you get the medical staff to buy into the program?
A: I personally visited every private physician who participated. Physicians were given the option of not participating, or of part-time participation—for example, on weekends or holidays only. The word spread. Physicians came up to me and told me that the program enabled them to continue practicing for another five years. Physicians’ spouses thanked me.
Q: Are you surprised HM as a field has grown so quickly?
A: I am not really that surprised. It is a better way to organize health care. I am surprised that it did not occur sooner. We talked about instituting this system for 10 years before 1993.
Q: What big challenges remain for hospital medicine? What are some solutions?
A: I believe that the biggest global challenge for hospital medicine remains communication with community-based providers, both before the hospitalization as well as during hospitalization and immediately after discharge. In the era of the EMR, the Internet, and the iPhone and Android, this should be easier. HIPAA has not helped.
The other growing challenge will become apparent as hospitalists age in the profession: Disruption of the diurnal sleep cycle becomes increasingly problematic for many physicians after the age of 50 and can easily lead to burnout. The early hospitalists were all in their 30s. The attractive lifestyle choice for the 30-year-old can lead to burnout for the 55-year-old. The emergency-medicine literature has noted a similar problem of shift work/sleep fragmentation.
Final Thoughts
I believe Dr. Holbrook’s assessments on the future of our specialty are on target. As HM continues to mature, we need to continue to focus on how we communicate with providers outside the four walls of the hospital and how to address barriers to making HM a sustainable career.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
(Editor's note: Updated July 12, 2013.)
The steam engine. The telephone. Television. ATMs. The Internet. Smartphones. The 24/7 hospitalist program.
Perhaps the single most important innovation along the road to where we are now in HM has been the development of the hospital-sponsored, 24/7, on-site hospitalist program. And the father of this invention may be the most significant figure in HM you’ve never heard of: John Holbrook, MD, FACEP. An emergency-medicine physician since the mid-1970s, Dr. Holbrook did something in July 1993 that was considered off the wall, yet proved to be revolutionary: From nothing, he launched a 24/7 hospitalist program staffed with board-eligible and board-certified internists at Mercy Hospital in Springfield, Mass. The inpatient physicians (this was before the word “hospitalist” came to be) were employed by a subsidiary of the hospital and worked in place of community primary-care physicians (PCPs), taking care of hospitalized patients who did not have a PCP, or whose PCP chose not to come to the hospital.
Of great significance, from the beginning, and perhaps by unintentional design, these physicians were agents of change and improvement for the hospital itself.
To be sure, in places like Southern California, 24/7, on-site hospitalist programs were in place in the late 1980s. Some claim those programs may have been the birthplace of the hospitalist model. However, such programs came to be in order to help medical groups manage full capitated risk delegated to them from HMOs on a population of patients, and were not supported by the hospital, per se. This is distinct from hospitalist programs—such as Mercy’s—sponsored by hospitals (whether employed or contracted) in predominantly fee-for-service markets, which then comprised the lion’s share of the U.S. market.
I had the extraordinary good fortune to happen along in July 1994, get hired by Dr. Holbrook, and soon after begin serving as medical director for the Mercy program, which I would do for the next decade. To this day, Dr. Holbrook is a mentor and trusted advisor to me. I caught up with him in recognition of the 20th anniversary of the Mercy Inpatient Medicine Service.
Question: What gave you the idea to launch what was, at the time, considered such an unconventional program?
Answer: Before the specialty of emergency medicine, a patient’s private physician would be called in most cases when a patient present in the ED: 25 or 50 doctors might be called over 24 hours, each to see one patient each. The inefficiency and disruption caused by this system was a natural and logical stimulus to develop the specialty of emergency medicine. I saw hospitalist medicine as an exact analogy.
Q: What were you observing in the healthcare environment that drove you to create the Mercy Inpatient Medicine Service?
A: Working for many years in the emergency department of a community hospital without a house staff, the ED docs would admit a patient at night or on the weekend and the attending physician would often plan to see the patient “in the morning.” When the patient would decompensate in the middle of the night, the ED doc would get a call to run to the floor to “Band-Aid” the situation.
Q: How did you convince the board of trustees to fund it?
A: The reasons were primarily economic. No. 1, the hospital was losing market share because local physicians would prefer to admit to the teaching hospital [a nearby competitor], where they were not required to come in during the middle of the night. No. 2, the cost of a hospitalization managed by a hospitalist was less expensive than either a hospital stay managed by house staff or managed over the telephone by a private attending at home.
Q: What was the most difficult operational challenge for the program?
A: Effective and timely communication with the community physicians was the most difficult operational challenge. Access to outpatient medical treatment immediately prior to a hospitalization and timely communication to the community physician were both challenges that we never adequately solved in the early days. I understand that these issues can still be problematic.
Q: How was it received by patients?
A: Overall, patients were very happy with the system. In the old system, with a typical four-physician practice, a patient had only a 1 in 4 chance of being admitted by the doctor who was familiar with the case. The fact that the hospitalist was available in the hospital made the improvement in quality apparent to most patients.
Q: How did you get the medical staff to buy into the program?
A: I personally visited every private physician who participated. Physicians were given the option of not participating, or of part-time participation—for example, on weekends or holidays only. The word spread. Physicians came up to me and told me that the program enabled them to continue practicing for another five years. Physicians’ spouses thanked me.
Q: Are you surprised HM as a field has grown so quickly?
A: I am not really that surprised. It is a better way to organize health care. I am surprised that it did not occur sooner. We talked about instituting this system for 10 years before 1993.
Q: What big challenges remain for hospital medicine? What are some solutions?
A: I believe that the biggest global challenge for hospital medicine remains communication with community-based providers, both before the hospitalization as well as during hospitalization and immediately after discharge. In the era of the EMR, the Internet, and the iPhone and Android, this should be easier. HIPAA has not helped.
The other growing challenge will become apparent as hospitalists age in the profession: Disruption of the diurnal sleep cycle becomes increasingly problematic for many physicians after the age of 50 and can easily lead to burnout. The early hospitalists were all in their 30s. The attractive lifestyle choice for the 30-year-old can lead to burnout for the 55-year-old. The emergency-medicine literature has noted a similar problem of shift work/sleep fragmentation.
Final Thoughts
I believe Dr. Holbrook’s assessments on the future of our specialty are on target. As HM continues to mature, we need to continue to focus on how we communicate with providers outside the four walls of the hospital and how to address barriers to making HM a sustainable career.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
(Editor's note: Updated July 12, 2013.)
The steam engine. The telephone. Television. ATMs. The Internet. Smartphones. The 24/7 hospitalist program.
Perhaps the single most important innovation along the road to where we are now in HM has been the development of the hospital-sponsored, 24/7, on-site hospitalist program. And the father of this invention may be the most significant figure in HM you’ve never heard of: John Holbrook, MD, FACEP. An emergency-medicine physician since the mid-1970s, Dr. Holbrook did something in July 1993 that was considered off the wall, yet proved to be revolutionary: From nothing, he launched a 24/7 hospitalist program staffed with board-eligible and board-certified internists at Mercy Hospital in Springfield, Mass. The inpatient physicians (this was before the word “hospitalist” came to be) were employed by a subsidiary of the hospital and worked in place of community primary-care physicians (PCPs), taking care of hospitalized patients who did not have a PCP, or whose PCP chose not to come to the hospital.
Of great significance, from the beginning, and perhaps by unintentional design, these physicians were agents of change and improvement for the hospital itself.
To be sure, in places like Southern California, 24/7, on-site hospitalist programs were in place in the late 1980s. Some claim those programs may have been the birthplace of the hospitalist model. However, such programs came to be in order to help medical groups manage full capitated risk delegated to them from HMOs on a population of patients, and were not supported by the hospital, per se. This is distinct from hospitalist programs—such as Mercy’s—sponsored by hospitals (whether employed or contracted) in predominantly fee-for-service markets, which then comprised the lion’s share of the U.S. market.
I had the extraordinary good fortune to happen along in July 1994, get hired by Dr. Holbrook, and soon after begin serving as medical director for the Mercy program, which I would do for the next decade. To this day, Dr. Holbrook is a mentor and trusted advisor to me. I caught up with him in recognition of the 20th anniversary of the Mercy Inpatient Medicine Service.
Question: What gave you the idea to launch what was, at the time, considered such an unconventional program?
Answer: Before the specialty of emergency medicine, a patient’s private physician would be called in most cases when a patient present in the ED: 25 or 50 doctors might be called over 24 hours, each to see one patient each. The inefficiency and disruption caused by this system was a natural and logical stimulus to develop the specialty of emergency medicine. I saw hospitalist medicine as an exact analogy.
Q: What were you observing in the healthcare environment that drove you to create the Mercy Inpatient Medicine Service?
A: Working for many years in the emergency department of a community hospital without a house staff, the ED docs would admit a patient at night or on the weekend and the attending physician would often plan to see the patient “in the morning.” When the patient would decompensate in the middle of the night, the ED doc would get a call to run to the floor to “Band-Aid” the situation.
Q: How did you convince the board of trustees to fund it?
A: The reasons were primarily economic. No. 1, the hospital was losing market share because local physicians would prefer to admit to the teaching hospital [a nearby competitor], where they were not required to come in during the middle of the night. No. 2, the cost of a hospitalization managed by a hospitalist was less expensive than either a hospital stay managed by house staff or managed over the telephone by a private attending at home.
Q: What was the most difficult operational challenge for the program?
A: Effective and timely communication with the community physicians was the most difficult operational challenge. Access to outpatient medical treatment immediately prior to a hospitalization and timely communication to the community physician were both challenges that we never adequately solved in the early days. I understand that these issues can still be problematic.
Q: How was it received by patients?
A: Overall, patients were very happy with the system. In the old system, with a typical four-physician practice, a patient had only a 1 in 4 chance of being admitted by the doctor who was familiar with the case. The fact that the hospitalist was available in the hospital made the improvement in quality apparent to most patients.
Q: How did you get the medical staff to buy into the program?
A: I personally visited every private physician who participated. Physicians were given the option of not participating, or of part-time participation—for example, on weekends or holidays only. The word spread. Physicians came up to me and told me that the program enabled them to continue practicing for another five years. Physicians’ spouses thanked me.
Q: Are you surprised HM as a field has grown so quickly?
A: I am not really that surprised. It is a better way to organize health care. I am surprised that it did not occur sooner. We talked about instituting this system for 10 years before 1993.
Q: What big challenges remain for hospital medicine? What are some solutions?
A: I believe that the biggest global challenge for hospital medicine remains communication with community-based providers, both before the hospitalization as well as during hospitalization and immediately after discharge. In the era of the EMR, the Internet, and the iPhone and Android, this should be easier. HIPAA has not helped.
The other growing challenge will become apparent as hospitalists age in the profession: Disruption of the diurnal sleep cycle becomes increasingly problematic for many physicians after the age of 50 and can easily lead to burnout. The early hospitalists were all in their 30s. The attractive lifestyle choice for the 30-year-old can lead to burnout for the 55-year-old. The emergency-medicine literature has noted a similar problem of shift work/sleep fragmentation.
Final Thoughts
I believe Dr. Holbrook’s assessments on the future of our specialty are on target. As HM continues to mature, we need to continue to focus on how we communicate with providers outside the four walls of the hospital and how to address barriers to making HM a sustainable career.
Dr. Whitcomb is medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. He is a co-founder and past president of SHM. Email him at [email protected].
(Editor's note: Updated July 12, 2013.)
First-Year Medical School Enrollment to Climb to 21,434 by 2017
Estimated number of first-year medical school enrollees in 2017, a 30% increase from 2002, according to the Association of American Medical Colleges.5 Sixty-two percent of this growth will take place at the 125 medical schools that have been accredited for a decade or more. Forty percent of surveyed medical-school deans expressed “major concerns” about enrollment growth outpacing the growth in residency-training positions for the graduates of medical schools.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Stobbe, M. Germ-zapping “robots”: Hospitals combat superbugs. Associated Press website. Available at: http://bigstory.ap.org/article/hospitals-see-surge-superbug-fighting-products. Accessed June 7, 2013.
- Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6209a3.htm?s_cid=mm6209a3_w. Accessed June 7, 2013.
- Wise ME, Scott RD, Baggs JM, et al. National estimates of central line-associated bloodstream infections in critical care patients. Infect Control Hosp Epidemiol, 2013;34(6):547-554.
- Hsu E, Lin D, Evans SJ, et al. Doing well by doing good: assessing the cost savings of an intervention to reduce central line-associated bloodstream infections in a Hawaii hospital. Am J Med Qual, 2013 May 7 [Epub ahead of print].
- Association of American Medical Colleges. Medical school enrollment on pace to reach 30 percent increase by 2017. Association of American Medical Colleges website. Available at: https://www.aamc.org/newsroom/newsreleases/ 335244/050213.html. Accessed June 7, 2013.
Estimated number of first-year medical school enrollees in 2017, a 30% increase from 2002, according to the Association of American Medical Colleges.5 Sixty-two percent of this growth will take place at the 125 medical schools that have been accredited for a decade or more. Forty percent of surveyed medical-school deans expressed “major concerns” about enrollment growth outpacing the growth in residency-training positions for the graduates of medical schools.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Stobbe, M. Germ-zapping “robots”: Hospitals combat superbugs. Associated Press website. Available at: http://bigstory.ap.org/article/hospitals-see-surge-superbug-fighting-products. Accessed June 7, 2013.
- Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6209a3.htm?s_cid=mm6209a3_w. Accessed June 7, 2013.
- Wise ME, Scott RD, Baggs JM, et al. National estimates of central line-associated bloodstream infections in critical care patients. Infect Control Hosp Epidemiol, 2013;34(6):547-554.
- Hsu E, Lin D, Evans SJ, et al. Doing well by doing good: assessing the cost savings of an intervention to reduce central line-associated bloodstream infections in a Hawaii hospital. Am J Med Qual, 2013 May 7 [Epub ahead of print].
- Association of American Medical Colleges. Medical school enrollment on pace to reach 30 percent increase by 2017. Association of American Medical Colleges website. Available at: https://www.aamc.org/newsroom/newsreleases/ 335244/050213.html. Accessed June 7, 2013.
Estimated number of first-year medical school enrollees in 2017, a 30% increase from 2002, according to the Association of American Medical Colleges.5 Sixty-two percent of this growth will take place at the 125 medical schools that have been accredited for a decade or more. Forty percent of surveyed medical-school deans expressed “major concerns” about enrollment growth outpacing the growth in residency-training positions for the graduates of medical schools.
Larry Beresford is a freelance writer in Oakland, Calif.
References
- Stobbe, M. Germ-zapping “robots”: Hospitals combat superbugs. Associated Press website. Available at: http://bigstory.ap.org/article/hospitals-see-surge-superbug-fighting-products. Accessed June 7, 2013.
- Centers for Disease Control and Prevention. Vital Signs: Carbapenem-Resistant Enterobacteriaceae. Centers for Disease Control and Prevention website. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6209a3.htm?s_cid=mm6209a3_w. Accessed June 7, 2013.
- Wise ME, Scott RD, Baggs JM, et al. National estimates of central line-associated bloodstream infections in critical care patients. Infect Control Hosp Epidemiol, 2013;34(6):547-554.
- Hsu E, Lin D, Evans SJ, et al. Doing well by doing good: assessing the cost savings of an intervention to reduce central line-associated bloodstream infections in a Hawaii hospital. Am J Med Qual, 2013 May 7 [Epub ahead of print].
- Association of American Medical Colleges. Medical school enrollment on pace to reach 30 percent increase by 2017. Association of American Medical Colleges website. Available at: https://www.aamc.org/newsroom/newsreleases/ 335244/050213.html. Accessed June 7, 2013.