User login
Hospitalists Should Research Salary Range by Market Before Negotiating a Job Offer

I am a third-year internal-medicine resident and currently looking for a nocturnist opportunity. I have no experience in negotiating a job or salary. When I interview for a job, should I negotiate for salary? How do I know that the salary is correct and what others in the same group are getting? Thanks for the help.
–Santhosh Mannem, New York City
Dr. Hospitalist responds:
Salary discussions are always intriguing, mainly because you won’t really know what everyone else is getting paid. There are several places to get some information. To begin, find out the general salary range for the market in which you want to work. Just because an annual salary might be $240,000 in Emporia, Kan., doesn’t mean a thing if you are looking for a job in Salt Lake City or Seattle. You can use the online resources through SHM (www.hospitalmedicine.org/survey) to paint a pretty good picture of salary by region, but remember that these are ranges only.
When I think of job offers, I like to take total compensation and break it down by category. For example, benefits are not negotiable—your employer cannot vary the health insurance coverage they provide by physician. Still, you need to consider benefits as an important part of the package. A good health insurance plan won’t mean as much to a single physician as it would to one with a family, so consider your individual needs. I strongly encourage you to make a line item for every potential benefit: health, dental, disability, life, continuing medical education (CME), professional dues, retirement plans (potentially with an employer match), malpractice insurance costs, and so on. A job with a “salary” of $300,000 but no benefits would pale in comparison to a job paying $250,000 with full benefits.
Don’t discount the value of benefits; get the numbers and assign a dollar amount. If the group is not being transparent on benefits, walk away.
With strict regard to salary, you probably will get little to no information as to what the rest of the group members are paid. Feel free to ask, but expect some vague answers. Most often, there is a fairly tight convergence of salaries within a given market, and it’s always better to interview for more than one job in the same location. You mentioned that you’d like to work as a nocturnist, which is good. These positions are recruited heavily and tend to command a higher initial salary.
Overall, your ability to negotiate a higher salary is going to be rather limited. However, there is another calculation worth mentioning: You need to find out how much you are being paid per unit of work so you can compare jobs. Here are some of the items to help you figure out a formula that works for you: annual salary, contracted shifts per year/month, pay per shift, admits/census per shift, number of weekends, and potential bonus thresholds. Use these numbers (metrics) to more accurately compare different jobs. There is no magic formula; it just depends on what is important to you, but you will get a much better picture if you combine these metrics with your benefit analysis.
As a nocturnist, I would not expect to hit any productivity metrics. If you are that busy, it’s probably a miserable job. In a business sense, nights almost always lose money.
One thing that can always be negotiated: a signing bonus and/or loan forgiveness. Often, a practice won’t want to continually offer higher starting salaries since eventually this causes wage creep across the practice. However, they can be much more flexible when it comes to “one-time” payments. This keeps the overall salary structure for the practice intact and is usually much more agreeable for your employer. As always, it’s a supply-and-demand issue, but if you are a nocturnist looking at a high-demand area, I would negotiate hard for a signing bonus and maybe even a contract-renewal bonus after your first year.
It never hurts to get creative, either. I remember negotiating my first job; I offered to sign a two-year contract (instead of one) if they would let me take off six months the first year. They said yes, I did some traveling that first year on my new salary, and I stayed with the practice for 11 years. Don’t get so caught up in salary numbers that you lose sight of what’s really important to you and whether the job would be the right fit.
Good luck and welcome to hospital medicine. You’ll love it.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to [email protected].
I am a third-year internal-medicine resident and currently looking for a nocturnist opportunity. I have no experience in negotiating a job or salary. When I interview for a job, should I negotiate for salary? How do I know that the salary is correct and what others in the same group are getting? Thanks for the help.
–Santhosh Mannem, New York City
Dr. Hospitalist responds:
Salary discussions are always intriguing, mainly because you won’t really know what everyone else is getting paid. There are several places to get some information. To begin, find out the general salary range for the market in which you want to work. Just because an annual salary might be $240,000 in Emporia, Kan., doesn’t mean a thing if you are looking for a job in Salt Lake City or Seattle. You can use the online resources through SHM (www.hospitalmedicine.org/survey) to paint a pretty good picture of salary by region, but remember that these are ranges only.
When I think of job offers, I like to take total compensation and break it down by category. For example, benefits are not negotiable—your employer cannot vary the health insurance coverage they provide by physician. Still, you need to consider benefits as an important part of the package. A good health insurance plan won’t mean as much to a single physician as it would to one with a family, so consider your individual needs. I strongly encourage you to make a line item for every potential benefit: health, dental, disability, life, continuing medical education (CME), professional dues, retirement plans (potentially with an employer match), malpractice insurance costs, and so on. A job with a “salary” of $300,000 but no benefits would pale in comparison to a job paying $250,000 with full benefits.
Don’t discount the value of benefits; get the numbers and assign a dollar amount. If the group is not being transparent on benefits, walk away.
With strict regard to salary, you probably will get little to no information as to what the rest of the group members are paid. Feel free to ask, but expect some vague answers. Most often, there is a fairly tight convergence of salaries within a given market, and it’s always better to interview for more than one job in the same location. You mentioned that you’d like to work as a nocturnist, which is good. These positions are recruited heavily and tend to command a higher initial salary.
Overall, your ability to negotiate a higher salary is going to be rather limited. However, there is another calculation worth mentioning: You need to find out how much you are being paid per unit of work so you can compare jobs. Here are some of the items to help you figure out a formula that works for you: annual salary, contracted shifts per year/month, pay per shift, admits/census per shift, number of weekends, and potential bonus thresholds. Use these numbers (metrics) to more accurately compare different jobs. There is no magic formula; it just depends on what is important to you, but you will get a much better picture if you combine these metrics with your benefit analysis.
As a nocturnist, I would not expect to hit any productivity metrics. If you are that busy, it’s probably a miserable job. In a business sense, nights almost always lose money.
One thing that can always be negotiated: a signing bonus and/or loan forgiveness. Often, a practice won’t want to continually offer higher starting salaries since eventually this causes wage creep across the practice. However, they can be much more flexible when it comes to “one-time” payments. This keeps the overall salary structure for the practice intact and is usually much more agreeable for your employer. As always, it’s a supply-and-demand issue, but if you are a nocturnist looking at a high-demand area, I would negotiate hard for a signing bonus and maybe even a contract-renewal bonus after your first year.
It never hurts to get creative, either. I remember negotiating my first job; I offered to sign a two-year contract (instead of one) if they would let me take off six months the first year. They said yes, I did some traveling that first year on my new salary, and I stayed with the practice for 11 years. Don’t get so caught up in salary numbers that you lose sight of what’s really important to you and whether the job would be the right fit.
Good luck and welcome to hospital medicine. You’ll love it.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to [email protected].
I am a third-year internal-medicine resident and currently looking for a nocturnist opportunity. I have no experience in negotiating a job or salary. When I interview for a job, should I negotiate for salary? How do I know that the salary is correct and what others in the same group are getting? Thanks for the help.
–Santhosh Mannem, New York City
Dr. Hospitalist responds:
Salary discussions are always intriguing, mainly because you won’t really know what everyone else is getting paid. There are several places to get some information. To begin, find out the general salary range for the market in which you want to work. Just because an annual salary might be $240,000 in Emporia, Kan., doesn’t mean a thing if you are looking for a job in Salt Lake City or Seattle. You can use the online resources through SHM (www.hospitalmedicine.org/survey) to paint a pretty good picture of salary by region, but remember that these are ranges only.
When I think of job offers, I like to take total compensation and break it down by category. For example, benefits are not negotiable—your employer cannot vary the health insurance coverage they provide by physician. Still, you need to consider benefits as an important part of the package. A good health insurance plan won’t mean as much to a single physician as it would to one with a family, so consider your individual needs. I strongly encourage you to make a line item for every potential benefit: health, dental, disability, life, continuing medical education (CME), professional dues, retirement plans (potentially with an employer match), malpractice insurance costs, and so on. A job with a “salary” of $300,000 but no benefits would pale in comparison to a job paying $250,000 with full benefits.
Don’t discount the value of benefits; get the numbers and assign a dollar amount. If the group is not being transparent on benefits, walk away.
With strict regard to salary, you probably will get little to no information as to what the rest of the group members are paid. Feel free to ask, but expect some vague answers. Most often, there is a fairly tight convergence of salaries within a given market, and it’s always better to interview for more than one job in the same location. You mentioned that you’d like to work as a nocturnist, which is good. These positions are recruited heavily and tend to command a higher initial salary.
Overall, your ability to negotiate a higher salary is going to be rather limited. However, there is another calculation worth mentioning: You need to find out how much you are being paid per unit of work so you can compare jobs. Here are some of the items to help you figure out a formula that works for you: annual salary, contracted shifts per year/month, pay per shift, admits/census per shift, number of weekends, and potential bonus thresholds. Use these numbers (metrics) to more accurately compare different jobs. There is no magic formula; it just depends on what is important to you, but you will get a much better picture if you combine these metrics with your benefit analysis.
As a nocturnist, I would not expect to hit any productivity metrics. If you are that busy, it’s probably a miserable job. In a business sense, nights almost always lose money.
One thing that can always be negotiated: a signing bonus and/or loan forgiveness. Often, a practice won’t want to continually offer higher starting salaries since eventually this causes wage creep across the practice. However, they can be much more flexible when it comes to “one-time” payments. This keeps the overall salary structure for the practice intact and is usually much more agreeable for your employer. As always, it’s a supply-and-demand issue, but if you are a nocturnist looking at a high-demand area, I would negotiate hard for a signing bonus and maybe even a contract-renewal bonus after your first year.
It never hurts to get creative, either. I remember negotiating my first job; I offered to sign a two-year contract (instead of one) if they would let me take off six months the first year. They said yes, I did some traveling that first year on my new salary, and I stayed with the practice for 11 years. Don’t get so caught up in salary numbers that you lose sight of what’s really important to you and whether the job would be the right fit.
Good luck and welcome to hospital medicine. You’ll love it.
Do you have a problem or concern that you’d like Dr. Hospitalist to address? Email your questions to [email protected].
An Encounter With Unflattering Light
ANSWER
The correct answer is dermatoheliosis (choice “d”), also correctly termed photoaging. This condition manifests as a number of specific skin changes, including the items named (choices “a,” “b,” and “c”)—all of which were present on this patient.
DISCUSSION
The consequences of chronic overexposure to UV radiation constitute the most common reason patients present to dermatology practices in the United States. The bulk of this damage takes decades to appear, by which time patients have forgotten about their earlier sun exposure (in fact, they often deny any exposure) and even the painful sunburns that taught them to avoid the sun in the first place.
In general, the effects of sunburns sustained in childhood or young adulthood do not usually manifest until the patient is in his/her 50s or 60s, although patients who are less sun-tolerant (our definition of “fair”) may show signs of damage considerably earlier.
However, with the popularity of artificial tanning among teenagers (and even preteens in some cases), evidence of sun damage is being seen at younger ages than ever. Basal cell carcinomas, once unheard of in teenagers, are being found with increasing frequency in this age-group. In patients ages 12 to 15, there has been a 100-fold increase in the incidence of melanoma—theorized to be due, in part, to the effects of artificial tanning.
This particular patient is typical of cases in which sun damage was obtained more passively. At one time in the US, having a tan was decidedly unfashionable; it marked one as a member of “the lower classes.” But that all began to change after WWI: Hemlines and hairlines rose, Prohibition created a new generation of drinkers and scofflaws, clothing began to be more revealing, and suddenly it was fashionable for women to shave their legs and get a tan.
About that same time, many men began to ignore the long-held tradition of wearing hats and long sleeves when outside, inevitably tanned, and thus gained approval from the opposite sex. Most went off to war in the 1940s, many to the Pacific theater, where they had even more exposure to the sun.
Following WWII, a great number of these men returned to their jobs as farmers, ranchers, or construction workers. Golfing became the “in” sport during leisure time. It’s this generation we’re seeing now for sun-related pathology. Even if they had been inclined to use it, effective sunscreen was not generally available until the early 1970s.
The patient depicted here has a typical collection of the pre-cancerous sun damage known as dermatoheliosis: solar elastosis, actinic keratoses, telangiectasias, and solar atrophy (which affects the arms more than the face). The latter, along with the effects of wind, heat, cold, smoking, and drinking alcohol, constitute the main causes of extrinsic aging.
TREATMENT
Short of heroic efforts, not much will be done for this patient’s dermatoheliosis. However, he was strongly advised to return to dermatology twice a year to watch for the arrival of the basal cell and squamous cell carcinomas that are almost certainly headed his way.
ANSWER
The correct answer is dermatoheliosis (choice “d”), also correctly termed photoaging. This condition manifests as a number of specific skin changes, including the items named (choices “a,” “b,” and “c”)—all of which were present on this patient.
DISCUSSION
The consequences of chronic overexposure to UV radiation constitute the most common reason patients present to dermatology practices in the United States. The bulk of this damage takes decades to appear, by which time patients have forgotten about their earlier sun exposure (in fact, they often deny any exposure) and even the painful sunburns that taught them to avoid the sun in the first place.
In general, the effects of sunburns sustained in childhood or young adulthood do not usually manifest until the patient is in his/her 50s or 60s, although patients who are less sun-tolerant (our definition of “fair”) may show signs of damage considerably earlier.
However, with the popularity of artificial tanning among teenagers (and even preteens in some cases), evidence of sun damage is being seen at younger ages than ever. Basal cell carcinomas, once unheard of in teenagers, are being found with increasing frequency in this age-group. In patients ages 12 to 15, there has been a 100-fold increase in the incidence of melanoma—theorized to be due, in part, to the effects of artificial tanning.
This particular patient is typical of cases in which sun damage was obtained more passively. At one time in the US, having a tan was decidedly unfashionable; it marked one as a member of “the lower classes.” But that all began to change after WWI: Hemlines and hairlines rose, Prohibition created a new generation of drinkers and scofflaws, clothing began to be more revealing, and suddenly it was fashionable for women to shave their legs and get a tan.
About that same time, many men began to ignore the long-held tradition of wearing hats and long sleeves when outside, inevitably tanned, and thus gained approval from the opposite sex. Most went off to war in the 1940s, many to the Pacific theater, where they had even more exposure to the sun.
Following WWII, a great number of these men returned to their jobs as farmers, ranchers, or construction workers. Golfing became the “in” sport during leisure time. It’s this generation we’re seeing now for sun-related pathology. Even if they had been inclined to use it, effective sunscreen was not generally available until the early 1970s.
The patient depicted here has a typical collection of the pre-cancerous sun damage known as dermatoheliosis: solar elastosis, actinic keratoses, telangiectasias, and solar atrophy (which affects the arms more than the face). The latter, along with the effects of wind, heat, cold, smoking, and drinking alcohol, constitute the main causes of extrinsic aging.
TREATMENT
Short of heroic efforts, not much will be done for this patient’s dermatoheliosis. However, he was strongly advised to return to dermatology twice a year to watch for the arrival of the basal cell and squamous cell carcinomas that are almost certainly headed his way.
ANSWER
The correct answer is dermatoheliosis (choice “d”), also correctly termed photoaging. This condition manifests as a number of specific skin changes, including the items named (choices “a,” “b,” and “c”)—all of which were present on this patient.
DISCUSSION
The consequences of chronic overexposure to UV radiation constitute the most common reason patients present to dermatology practices in the United States. The bulk of this damage takes decades to appear, by which time patients have forgotten about their earlier sun exposure (in fact, they often deny any exposure) and even the painful sunburns that taught them to avoid the sun in the first place.
In general, the effects of sunburns sustained in childhood or young adulthood do not usually manifest until the patient is in his/her 50s or 60s, although patients who are less sun-tolerant (our definition of “fair”) may show signs of damage considerably earlier.
However, with the popularity of artificial tanning among teenagers (and even preteens in some cases), evidence of sun damage is being seen at younger ages than ever. Basal cell carcinomas, once unheard of in teenagers, are being found with increasing frequency in this age-group. In patients ages 12 to 15, there has been a 100-fold increase in the incidence of melanoma—theorized to be due, in part, to the effects of artificial tanning.
This particular patient is typical of cases in which sun damage was obtained more passively. At one time in the US, having a tan was decidedly unfashionable; it marked one as a member of “the lower classes.” But that all began to change after WWI: Hemlines and hairlines rose, Prohibition created a new generation of drinkers and scofflaws, clothing began to be more revealing, and suddenly it was fashionable for women to shave their legs and get a tan.
About that same time, many men began to ignore the long-held tradition of wearing hats and long sleeves when outside, inevitably tanned, and thus gained approval from the opposite sex. Most went off to war in the 1940s, many to the Pacific theater, where they had even more exposure to the sun.
Following WWII, a great number of these men returned to their jobs as farmers, ranchers, or construction workers. Golfing became the “in” sport during leisure time. It’s this generation we’re seeing now for sun-related pathology. Even if they had been inclined to use it, effective sunscreen was not generally available until the early 1970s.
The patient depicted here has a typical collection of the pre-cancerous sun damage known as dermatoheliosis: solar elastosis, actinic keratoses, telangiectasias, and solar atrophy (which affects the arms more than the face). The latter, along with the effects of wind, heat, cold, smoking, and drinking alcohol, constitute the main causes of extrinsic aging.
TREATMENT
Short of heroic efforts, not much will be done for this patient’s dermatoheliosis. However, he was strongly advised to return to dermatology twice a year to watch for the arrival of the basal cell and squamous cell carcinomas that are almost certainly headed his way.

During a recent trip, this 77-year-old man stayed in a hotel in which the bathroom lighting was considerably brighter than that at home—allowing him to see a number of skin changes he hadn’t noticed before. As a result, he presents to dermatology for an evaluation. The patient’s forehead, as well as his cheeks and nose, look curiously mottled (pink and white), with a rough, scar-like, pebbly surface that resembles chicken skin. There are also numerous 1- to 3-mm rough, scaly, papular lesions and multiple faint telangiectasias. In sun-exposed areas, such as his hands and arms, the skin is rough, dry, and exceptionally thin, with light and dark color changes; this is in sharp contrast to the relatively pristine texture and uniformly light color of the volar forearms and other areas that are not exposed to the sun. History taking reveals that, as a young man, the patient spent a great deal of time outdoors, both at work and in his free time. He never wore a hat or used any other form of sun protection. Since age 50, he has had several skin cancers removed from his face and back. Despite this, he is not seeing a dermatology provider regularly.

What I wish I'd learned in med school
You might remember from medical school that psychiatrists use a five Axis system when evaluating patients. (Or at least they used to. The recent fifth edition of the Diagnostic and Statistical Manual of Mental Disorders eliminated the Axis system.)
Axis I refers to psychiatric pathology, such as major depressive disorder, bipolar disorder, or generalized anxiety disorder. Axis II refers to personality disorders, such as borderline personality disorder, narcissistic personality disorder, and obsessive-compulsive personality disorder. Axis III covers the medical conditions that the patient has. Axis IV, quite appropriately, lists social and environmental factors contributing to the pathology. Axis V is the global assessment of function.
This five Axis system at the very least reminds us that the individual is more than just the sum of his or her illnesses. Rather than existing in a vacuum, the individual interacts with the world. The system acknowledges that the individual influences the environment (through Axis V) and is influenced by it (Axis IV).
Though we are not psychiatrists, I do think that rheumatologists are generally attuned to the five Axis system anyway. We may not explicitly identify the axes, but we are most definitely interested in our patients’ level of function and how much support is available to them. We are familiar with depression and anxiety, and we don’t shy away from frank discussions with our patients about their emotional well-being.
But where I find my education lacking is in how to manage patients with Axis II (personality) disorders. And yet, I dare say, this is no less important than the other axes. At the very least, it affects my interaction with the patient.
For example, a patient with newly diagnosed rheumatoid arthritis who also has obsessive-compulsive personality disorder was extremely anxious and perseverated on his risk of lymphoma to the point of sleepless nights and frequent phone calls to me. There are patients with narcissistic personality disorder who feel entitled to special treatment and are unhappy even with standard care. Patients with histrionic personality disorder are emotionally labile and have a tendency toward hyperbole.
Most problematic for me are patients with borderline personality disorder. I meet one or two of them every year. By definition they split the world into absolutes, good and bad. They have a pathologic fear of being abandoned, so they heap you with praises that feel contrived and insincere, yet they will roll their eyeballs and speak disparagingly of your colleagues – mostly a bad sign. They are impulsive, argumentative, and frequently self-destructive. These traits make it difficult to manage their care appropriately, with challenges that run the gamut from potential patient noncompliance to exhausting physician goodwill. But they are patients, and we have a responsibility to provide them with the best possible care.
I envy the physician who can talk to these patients, address their concerns, gain their trust, and still be able to set boundaries and maintain objectivity. No one taught me how to do these things. No one even warned me that I would need to do these things. Truthfully, though, these are skills that cannot be taught effectively in a classroom setting. Rather, in this, as in many other situations, experience is the best teacher.
Dr. Chan practices rheumatology in Pawtucket, R.I.
You might remember from medical school that psychiatrists use a five Axis system when evaluating patients. (Or at least they used to. The recent fifth edition of the Diagnostic and Statistical Manual of Mental Disorders eliminated the Axis system.)
Axis I refers to psychiatric pathology, such as major depressive disorder, bipolar disorder, or generalized anxiety disorder. Axis II refers to personality disorders, such as borderline personality disorder, narcissistic personality disorder, and obsessive-compulsive personality disorder. Axis III covers the medical conditions that the patient has. Axis IV, quite appropriately, lists social and environmental factors contributing to the pathology. Axis V is the global assessment of function.
This five Axis system at the very least reminds us that the individual is more than just the sum of his or her illnesses. Rather than existing in a vacuum, the individual interacts with the world. The system acknowledges that the individual influences the environment (through Axis V) and is influenced by it (Axis IV).
Though we are not psychiatrists, I do think that rheumatologists are generally attuned to the five Axis system anyway. We may not explicitly identify the axes, but we are most definitely interested in our patients’ level of function and how much support is available to them. We are familiar with depression and anxiety, and we don’t shy away from frank discussions with our patients about their emotional well-being.
But where I find my education lacking is in how to manage patients with Axis II (personality) disorders. And yet, I dare say, this is no less important than the other axes. At the very least, it affects my interaction with the patient.
For example, a patient with newly diagnosed rheumatoid arthritis who also has obsessive-compulsive personality disorder was extremely anxious and perseverated on his risk of lymphoma to the point of sleepless nights and frequent phone calls to me. There are patients with narcissistic personality disorder who feel entitled to special treatment and are unhappy even with standard care. Patients with histrionic personality disorder are emotionally labile and have a tendency toward hyperbole.
Most problematic for me are patients with borderline personality disorder. I meet one or two of them every year. By definition they split the world into absolutes, good and bad. They have a pathologic fear of being abandoned, so they heap you with praises that feel contrived and insincere, yet they will roll their eyeballs and speak disparagingly of your colleagues – mostly a bad sign. They are impulsive, argumentative, and frequently self-destructive. These traits make it difficult to manage their care appropriately, with challenges that run the gamut from potential patient noncompliance to exhausting physician goodwill. But they are patients, and we have a responsibility to provide them with the best possible care.
I envy the physician who can talk to these patients, address their concerns, gain their trust, and still be able to set boundaries and maintain objectivity. No one taught me how to do these things. No one even warned me that I would need to do these things. Truthfully, though, these are skills that cannot be taught effectively in a classroom setting. Rather, in this, as in many other situations, experience is the best teacher.
Dr. Chan practices rheumatology in Pawtucket, R.I.
You might remember from medical school that psychiatrists use a five Axis system when evaluating patients. (Or at least they used to. The recent fifth edition of the Diagnostic and Statistical Manual of Mental Disorders eliminated the Axis system.)
Axis I refers to psychiatric pathology, such as major depressive disorder, bipolar disorder, or generalized anxiety disorder. Axis II refers to personality disorders, such as borderline personality disorder, narcissistic personality disorder, and obsessive-compulsive personality disorder. Axis III covers the medical conditions that the patient has. Axis IV, quite appropriately, lists social and environmental factors contributing to the pathology. Axis V is the global assessment of function.
This five Axis system at the very least reminds us that the individual is more than just the sum of his or her illnesses. Rather than existing in a vacuum, the individual interacts with the world. The system acknowledges that the individual influences the environment (through Axis V) and is influenced by it (Axis IV).
Though we are not psychiatrists, I do think that rheumatologists are generally attuned to the five Axis system anyway. We may not explicitly identify the axes, but we are most definitely interested in our patients’ level of function and how much support is available to them. We are familiar with depression and anxiety, and we don’t shy away from frank discussions with our patients about their emotional well-being.
But where I find my education lacking is in how to manage patients with Axis II (personality) disorders. And yet, I dare say, this is no less important than the other axes. At the very least, it affects my interaction with the patient.
For example, a patient with newly diagnosed rheumatoid arthritis who also has obsessive-compulsive personality disorder was extremely anxious and perseverated on his risk of lymphoma to the point of sleepless nights and frequent phone calls to me. There are patients with narcissistic personality disorder who feel entitled to special treatment and are unhappy even with standard care. Patients with histrionic personality disorder are emotionally labile and have a tendency toward hyperbole.
Most problematic for me are patients with borderline personality disorder. I meet one or two of them every year. By definition they split the world into absolutes, good and bad. They have a pathologic fear of being abandoned, so they heap you with praises that feel contrived and insincere, yet they will roll their eyeballs and speak disparagingly of your colleagues – mostly a bad sign. They are impulsive, argumentative, and frequently self-destructive. These traits make it difficult to manage their care appropriately, with challenges that run the gamut from potential patient noncompliance to exhausting physician goodwill. But they are patients, and we have a responsibility to provide them with the best possible care.
I envy the physician who can talk to these patients, address their concerns, gain their trust, and still be able to set boundaries and maintain objectivity. No one taught me how to do these things. No one even warned me that I would need to do these things. Truthfully, though, these are skills that cannot be taught effectively in a classroom setting. Rather, in this, as in many other situations, experience is the best teacher.
Dr. Chan practices rheumatology in Pawtucket, R.I.

Anxiety during pregnancy

What is the best treatment for plant-induced contact dermatitis?
IT’S UNCLEAR which treatment is best, because there have been no head-to-head comparisons of treatments for Rhus (plant-induced) contact dermatitis. That said, topical high-potency steroids slightly improve pruritus and the appearance of the rash (strength of recommendation [SOR]: B, small cohort studies).
Neither topical pimecrolimus (an immunomodulatory drug) nor jewelweed extract are helpful (SOR: B, 1 small randomized controlled trial [RCT]).
Oral steroids improve symptoms in severe cases (SOR: C, expert opinion).
It’s unclear which treatment is best, because there have been no head-to-head comparisons of treatments for Rhus (plant-induced) contact dermatitis. That said, topical high-potency steroids slightly improve pruritus and the appearance of the rash (strength of recommendation [SOR]: B, small cohort studies).
Neither topical pimecrolimus (an immunomodulatory drug) nor jewelweed extract are helpful (SOR: B, 1 small randomized controlled trial [RCT]).
Oral steroids improve symptoms in severe cases (SOR: C, expert opinion).
Evidence summary
Two prospective, self-controlled cohort studies (N=30) showed that high-potency topical steroids improved symptoms associated with artificially induced Rhus dermatitis in a group with a history of that type of dermatitis.
The first study found that 0.05% clobetasol propionate ointment applied twice a day significantly reduced overall vesiculation, erythema, induration, and pruritus compared with the control (P<.05, .01, .01, and .05, respectively).1 Investigators evaluated erythema, induration, and pruritus on a scale of 0 to 3 (absent, mild, moderate, or severe) and graded vesiculation on a similar 0- to 3-point scale (a frank bulla was graded 3). They started treatment at 12, 24, and 48 hours after exposure and followed patients for 14 days. The greatest difference in mean scores—a reduction in vesiculation scores of approximately 1 point—occurred between 2 and 7 days of therapy.
The second study compared improvement in symptoms of Rhus dermatitis with daily application of topical steroids of different potencies and a control ointment.2 Investigators evaluated healing using a 0- to 4-point scale (0=clearing and 4=marked edema, erythema, and vesiculation). They found that lower-potency topical steroids such as 1% hydrocortisone and 0.1% triamcinolone were equivalent to the control ointment, but high-potency (class IV) steroid ointments produced significant improvement in symptoms (by a mean of 1.07 points vs the control ointment; supporting statistics not given).
A systematic review of contact dermatitis treatment and prevention identified 4 “good-quality” RCTs that evaluated effective remedies for nickel-induced allergic contact dermatitis in a predominantly female Caucasian population.3 All found that moderately high-potency topical steroid therapy improved symptoms, but heterogeneity among the studies made it impossible to determine the best agent.
Topical immunomodulatory drugs and jewelweed are no help
In a double-blinded RCT of 12 adults with a history of Rhus dermatitis and a significant reaction to tincture of poison ivy, topical pimecrolimus didn’t improve the duration or severity of symptoms (P=nonsignificant).4
A similar RCT from a dermatology clinic of 10 adults with confirmed sensitivity to poison oak or ivy found that topical jewelweed extract didn’t improve symptoms of artificially induced Rhus dermatitis. Investigators didn’t report P values.5
Oral steroids haven’t been studied
No studies have evaluated the effectiveness of oral steroids for Rhus dermatitis. Expert opinion recommends prednisone (60 mg daily, tapered over 14 days) for severe and widespread cases of poison ivy dermatitis.6,7
Recommendations
The American Academy of Allergy, Asthma, and Immunology and the American College of Allergy, Asthma, and Immunology jointly recommend topical corticosteroids as firstline treatment for localized allergic contact dermatitis. They advise giving systemic corticosteroids for lesions covering more than 20% of body surface area (for example, prednisone 0.5-1 mg/kg per day for 5-7 days, then 50% of the dose for another 5-7 days).6
The American Academy of Dermatology hasn’t issued guidelines on plant-induced dermatitis.
A dermatology textbook states that topical steroids are effective during the early stages of an outbreak, when vesicles and blisters aren’t yet present, and that systemic steroids are extremely effective for severe outbreaks. The authors recommend treating weepy lesions with tepid baths, wet to dry soaks, or calamine lotion to dry the lesions.7
1. Vernon HJ, Olsen EA. A controlled trial of clobetasol propionate ointment 0.05% in the treatment of experimentally induced Rhus dermatitis. J Am Acad Dermatol. 1990;23:829-832.
2. Kaidbey KH, Kligman AM. Assay of topical corticosteroids: efficacy of suppression of experimental Rhus dermatitis in humans. Arch Dermatol. 1976;112:808-813.
3. Saary J, Qureshi R, Palda V, et al. A systematic review of contact dermatitis treatment and prevention. J Am Acad Dermatol. 2005;53:845.
4. Amrol D, Keitel D, Hagaman D, et al. Topical pimecrolimus in the treatment of human allergic contact dermatitis. Ann Allergy Asthma Immunol. 2003;91:563-566.
5. Long D, Ballentine NH, Marks JG Jr. Treatment of poison ivy/ oak allergic contact dermatitis with an extract of jewelweed. Am J Contact Dermatol. 1997;8:150-153.
6. American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. Contact dermatitis: a practice parameter. Ann Allergy Asthma Immunol. 2006;97(suppl 2):S1-S38.
7. Habif TP. Contact dermatitis and patch testing. In: Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. St. Louis, Mo: Mosby; 2010:130-153.
IT’S UNCLEAR which treatment is best, because there have been no head-to-head comparisons of treatments for Rhus (plant-induced) contact dermatitis. That said, topical high-potency steroids slightly improve pruritus and the appearance of the rash (strength of recommendation [SOR]: B, small cohort studies).
Neither topical pimecrolimus (an immunomodulatory drug) nor jewelweed extract are helpful (SOR: B, 1 small randomized controlled trial [RCT]).
Oral steroids improve symptoms in severe cases (SOR: C, expert opinion).
It’s unclear which treatment is best, because there have been no head-to-head comparisons of treatments for Rhus (plant-induced) contact dermatitis. That said, topical high-potency steroids slightly improve pruritus and the appearance of the rash (strength of recommendation [SOR]: B, small cohort studies).
Neither topical pimecrolimus (an immunomodulatory drug) nor jewelweed extract are helpful (SOR: B, 1 small randomized controlled trial [RCT]).
Oral steroids improve symptoms in severe cases (SOR: C, expert opinion).
Evidence summary
Two prospective, self-controlled cohort studies (N=30) showed that high-potency topical steroids improved symptoms associated with artificially induced Rhus dermatitis in a group with a history of that type of dermatitis.
The first study found that 0.05% clobetasol propionate ointment applied twice a day significantly reduced overall vesiculation, erythema, induration, and pruritus compared with the control (P<.05, .01, .01, and .05, respectively).1 Investigators evaluated erythema, induration, and pruritus on a scale of 0 to 3 (absent, mild, moderate, or severe) and graded vesiculation on a similar 0- to 3-point scale (a frank bulla was graded 3). They started treatment at 12, 24, and 48 hours after exposure and followed patients for 14 days. The greatest difference in mean scores—a reduction in vesiculation scores of approximately 1 point—occurred between 2 and 7 days of therapy.
The second study compared improvement in symptoms of Rhus dermatitis with daily application of topical steroids of different potencies and a control ointment.2 Investigators evaluated healing using a 0- to 4-point scale (0=clearing and 4=marked edema, erythema, and vesiculation). They found that lower-potency topical steroids such as 1% hydrocortisone and 0.1% triamcinolone were equivalent to the control ointment, but high-potency (class IV) steroid ointments produced significant improvement in symptoms (by a mean of 1.07 points vs the control ointment; supporting statistics not given).
A systematic review of contact dermatitis treatment and prevention identified 4 “good-quality” RCTs that evaluated effective remedies for nickel-induced allergic contact dermatitis in a predominantly female Caucasian population.3 All found that moderately high-potency topical steroid therapy improved symptoms, but heterogeneity among the studies made it impossible to determine the best agent.
Topical immunomodulatory drugs and jewelweed are no help
In a double-blinded RCT of 12 adults with a history of Rhus dermatitis and a significant reaction to tincture of poison ivy, topical pimecrolimus didn’t improve the duration or severity of symptoms (P=nonsignificant).4
A similar RCT from a dermatology clinic of 10 adults with confirmed sensitivity to poison oak or ivy found that topical jewelweed extract didn’t improve symptoms of artificially induced Rhus dermatitis. Investigators didn’t report P values.5
Oral steroids haven’t been studied
No studies have evaluated the effectiveness of oral steroids for Rhus dermatitis. Expert opinion recommends prednisone (60 mg daily, tapered over 14 days) for severe and widespread cases of poison ivy dermatitis.6,7
Recommendations
The American Academy of Allergy, Asthma, and Immunology and the American College of Allergy, Asthma, and Immunology jointly recommend topical corticosteroids as firstline treatment for localized allergic contact dermatitis. They advise giving systemic corticosteroids for lesions covering more than 20% of body surface area (for example, prednisone 0.5-1 mg/kg per day for 5-7 days, then 50% of the dose for another 5-7 days).6
The American Academy of Dermatology hasn’t issued guidelines on plant-induced dermatitis.
A dermatology textbook states that topical steroids are effective during the early stages of an outbreak, when vesicles and blisters aren’t yet present, and that systemic steroids are extremely effective for severe outbreaks. The authors recommend treating weepy lesions with tepid baths, wet to dry soaks, or calamine lotion to dry the lesions.7
IT’S UNCLEAR which treatment is best, because there have been no head-to-head comparisons of treatments for Rhus (plant-induced) contact dermatitis. That said, topical high-potency steroids slightly improve pruritus and the appearance of the rash (strength of recommendation [SOR]: B, small cohort studies).
Neither topical pimecrolimus (an immunomodulatory drug) nor jewelweed extract are helpful (SOR: B, 1 small randomized controlled trial [RCT]).
Oral steroids improve symptoms in severe cases (SOR: C, expert opinion).
It’s unclear which treatment is best, because there have been no head-to-head comparisons of treatments for Rhus (plant-induced) contact dermatitis. That said, topical high-potency steroids slightly improve pruritus and the appearance of the rash (strength of recommendation [SOR]: B, small cohort studies).
Neither topical pimecrolimus (an immunomodulatory drug) nor jewelweed extract are helpful (SOR: B, 1 small randomized controlled trial [RCT]).
Oral steroids improve symptoms in severe cases (SOR: C, expert opinion).
Evidence summary
Two prospective, self-controlled cohort studies (N=30) showed that high-potency topical steroids improved symptoms associated with artificially induced Rhus dermatitis in a group with a history of that type of dermatitis.
The first study found that 0.05% clobetasol propionate ointment applied twice a day significantly reduced overall vesiculation, erythema, induration, and pruritus compared with the control (P<.05, .01, .01, and .05, respectively).1 Investigators evaluated erythema, induration, and pruritus on a scale of 0 to 3 (absent, mild, moderate, or severe) and graded vesiculation on a similar 0- to 3-point scale (a frank bulla was graded 3). They started treatment at 12, 24, and 48 hours after exposure and followed patients for 14 days. The greatest difference in mean scores—a reduction in vesiculation scores of approximately 1 point—occurred between 2 and 7 days of therapy.
The second study compared improvement in symptoms of Rhus dermatitis with daily application of topical steroids of different potencies and a control ointment.2 Investigators evaluated healing using a 0- to 4-point scale (0=clearing and 4=marked edema, erythema, and vesiculation). They found that lower-potency topical steroids such as 1% hydrocortisone and 0.1% triamcinolone were equivalent to the control ointment, but high-potency (class IV) steroid ointments produced significant improvement in symptoms (by a mean of 1.07 points vs the control ointment; supporting statistics not given).
A systematic review of contact dermatitis treatment and prevention identified 4 “good-quality” RCTs that evaluated effective remedies for nickel-induced allergic contact dermatitis in a predominantly female Caucasian population.3 All found that moderately high-potency topical steroid therapy improved symptoms, but heterogeneity among the studies made it impossible to determine the best agent.
Topical immunomodulatory drugs and jewelweed are no help
In a double-blinded RCT of 12 adults with a history of Rhus dermatitis and a significant reaction to tincture of poison ivy, topical pimecrolimus didn’t improve the duration or severity of symptoms (P=nonsignificant).4
A similar RCT from a dermatology clinic of 10 adults with confirmed sensitivity to poison oak or ivy found that topical jewelweed extract didn’t improve symptoms of artificially induced Rhus dermatitis. Investigators didn’t report P values.5
Oral steroids haven’t been studied
No studies have evaluated the effectiveness of oral steroids for Rhus dermatitis. Expert opinion recommends prednisone (60 mg daily, tapered over 14 days) for severe and widespread cases of poison ivy dermatitis.6,7
Recommendations
The American Academy of Allergy, Asthma, and Immunology and the American College of Allergy, Asthma, and Immunology jointly recommend topical corticosteroids as firstline treatment for localized allergic contact dermatitis. They advise giving systemic corticosteroids for lesions covering more than 20% of body surface area (for example, prednisone 0.5-1 mg/kg per day for 5-7 days, then 50% of the dose for another 5-7 days).6
The American Academy of Dermatology hasn’t issued guidelines on plant-induced dermatitis.
A dermatology textbook states that topical steroids are effective during the early stages of an outbreak, when vesicles and blisters aren’t yet present, and that systemic steroids are extremely effective for severe outbreaks. The authors recommend treating weepy lesions with tepid baths, wet to dry soaks, or calamine lotion to dry the lesions.7
1. Vernon HJ, Olsen EA. A controlled trial of clobetasol propionate ointment 0.05% in the treatment of experimentally induced Rhus dermatitis. J Am Acad Dermatol. 1990;23:829-832.
2. Kaidbey KH, Kligman AM. Assay of topical corticosteroids: efficacy of suppression of experimental Rhus dermatitis in humans. Arch Dermatol. 1976;112:808-813.
3. Saary J, Qureshi R, Palda V, et al. A systematic review of contact dermatitis treatment and prevention. J Am Acad Dermatol. 2005;53:845.
4. Amrol D, Keitel D, Hagaman D, et al. Topical pimecrolimus in the treatment of human allergic contact dermatitis. Ann Allergy Asthma Immunol. 2003;91:563-566.
5. Long D, Ballentine NH, Marks JG Jr. Treatment of poison ivy/ oak allergic contact dermatitis with an extract of jewelweed. Am J Contact Dermatol. 1997;8:150-153.
6. American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. Contact dermatitis: a practice parameter. Ann Allergy Asthma Immunol. 2006;97(suppl 2):S1-S38.
7. Habif TP. Contact dermatitis and patch testing. In: Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. St. Louis, Mo: Mosby; 2010:130-153.
1. Vernon HJ, Olsen EA. A controlled trial of clobetasol propionate ointment 0.05% in the treatment of experimentally induced Rhus dermatitis. J Am Acad Dermatol. 1990;23:829-832.
2. Kaidbey KH, Kligman AM. Assay of topical corticosteroids: efficacy of suppression of experimental Rhus dermatitis in humans. Arch Dermatol. 1976;112:808-813.
3. Saary J, Qureshi R, Palda V, et al. A systematic review of contact dermatitis treatment and prevention. J Am Acad Dermatol. 2005;53:845.
4. Amrol D, Keitel D, Hagaman D, et al. Topical pimecrolimus in the treatment of human allergic contact dermatitis. Ann Allergy Asthma Immunol. 2003;91:563-566.
5. Long D, Ballentine NH, Marks JG Jr. Treatment of poison ivy/ oak allergic contact dermatitis with an extract of jewelweed. Am J Contact Dermatol. 1997;8:150-153.
6. American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. Contact dermatitis: a practice parameter. Ann Allergy Asthma Immunol. 2006;97(suppl 2):S1-S38.
7. Habif TP. Contact dermatitis and patch testing. In: Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. St. Louis, Mo: Mosby; 2010:130-153.
Evidence-based answers from the Family Physicians Inquiries Network
Recurrent abdominal pain and vomiting
A 32-year-old man presents to the emergency department with excruciating abdominal pain associated with multiple episodes of vomiting for the past 2 days. He reports no fevers, headaches, diarrhea, constipation, hematochezia, melena, musculoskeletal symptoms, or weight loss. His abdominal pain is generalized and crampy. It does not radiate and has no precipitating factors. The pain is relieved only with intravenous narcotics.
He does not smoke, drink alcohol, or use illicit drugs. He has no known drug or food allergies. He says that his current condition causes him emotional stress that affects his performance at work.
About a year ago, after a complicated surgical procedure, he needed chronic high-dose narcotics. A few months later, he developed multiple bouts of abdominal pain and vomiting that required hospital visits. He now takes oral oxycodone 10–15 mg every 4–6 hours.
On admission, his vital signs are stable, but he is in excruciating pain. He is alert and oriented to person, place, and time. His sclera are anicteric, and the pupils are equal, round, and reactive to light. Lung and heart examinations are normal. The abdomen is soft and nondistended but tender in all four quadrants without guarding; the liver and spleen are not palpable, and no abdominal masses are detected. He has no skin rash, joint swelling or tenderness, or peripheral edema. The neurologic examination is normal. Computed tomography (CT) of the abdomen with contrast shows no signs of bowel obstruction, pancreatic calcifications or edema, cholecystitis, or hepatobiliary disease. Results of initial laboratory testing are shown in Table 1.
1. Based on the information available, which is the least likely cause of his symptoms?
- Acute pancreatitis
- Cyclic vomiting syndrome
- Acute intermittent porphyria
- Gastroparesis
Acute pancreatitis
Acute pancreatitis is the least likely cause of his symptoms. It is commonly caused by gallstones, alcohol, hypertriglyceridemia, and certain drugs.1 The associated abdominal pain is usually epigastric, radiates to the back, and is accompanied by nausea or vomiting, or both. The onset of pain is sudden and rapidly increases in severity within 30 minutes. CT shows enlargement of the pancreas with diffuse edema, heterogeneity of pancreatic parenchyma, peripancreatic stranding, and peripancreatic fluid collections.1 The diagnosis is based on two of the following three criteria: abdominal pain characteristic of acute pancreatitis; a serum amylase or lipase concentration three or more times the upper limit of normal; and characteristic findings of acute pancreatitis on CT.1
Cyclic vomiting syndrome
Cyclic vomiting syndrome is thought to be caused by episodic dysautonomia, mitochondrial DNA mutations, and hypothalamic emetic response oversensitivity,2–4 but the exact pathogenesis is unknown. The syndrome has been strongly linked to migraine and to the chronic excessive use of cannabinoids.5–9 The Rome III diagnostic criteria10 are the following: the vomiting episodes are stereotypical, ie, they are acute and last for less than 1 week; the patient has had three or more episodes in the previous year; and the patient has no nausea or vomiting between episodes. The patient must meet all three criteria. A history of migraine or a family history of migraine further supports the diagnosis.
Acute intermittent porphyria
Acute intermittent porphyria is characterized by neurovisceral symptoms such as convulsions, paresis, autonomic dysfunction, constipation, and diarrhea that result from the overproduction of porphyrin precursors and deficiency of porphobilinogen deaminase.11
Most patients have poorly localized, severe, steady abdominal pain that develops over hours to days and that may persist for days to weeks.11 Since the pain is neuropathic, abdominal tenderness is usually minimal during an acute attack. Other clues include signs of ileus, such as constipation, nausea, abdominal distention, or decreased bowel sounds; bladder dysfunction, eg, urinary retention, incontinence, or dysuria; reddish-brown urine; and sensory neuropathy of the chest, back, and extremities.11 Blistering skin lesions are usually not seen. The presence of porphobilinogen in the urine confirms the diagnosis.11
Gastroparesis
Gastroparesis is a result of discoordination between the sympathetic and parasympathetic nervous systems, neurons, and smooth muscles within the stomach, causing a decrease in gastric motility. Common causes are diabetes,12 scleroderma,13 and neurologic disorders.14 It can also be iatrogenic,15 resulting from visceral nerve injury and drug treatment with narcotics, calcium channel blockers, muscarinic cholinergic antagonists, or certain antidepressants. Symptoms are related to gastric stasis, ie, abdominal pain from gastric distention, bloating, vomiting, and early satiety.15 Abdominal pain may worsen after eating, and vomitus usually consists of recently ingested food. These patients may have abdominal distension or tenderness and succussion splash. After excluding possible mechanical obstruction, a gastric-emptying study may be necessary to make the diagnosis.15
CASE CONTINUED
A serum and urine drug screen in our patient is positive only for opioids. Urine measures of delta-aminolevulinic acid and porphobilinogen are normal. CT angiography of the abdomen shows no signs of mesenteric vascular occlusion. Esophagogastroduodenoscopy shows antral gastritis, but the esophagus and duodenum appear normal, and colonoscopy is normal as well. Histologic study of biopsy specimens obtained during endoscopy is unrevealing. A gastric-emptying study shows delayed emptying. The patient’s abdominal pain and vomiting persist with the initial dose of intravenous narcotic but resolve with escalating doses. When asked, the patient denies an excessive need for hot baths.
2. Which is the most likely diagnosis at this point?
- Narcotic bowel syndrome
- Opioid withdrawal
- Crohn disease
- Chronic pancreatitis
- Chronic mesenteric ischemia
- Cannabinoid hyperemesis
Narcotic bowel syndrome
Narcotic bowel syndrome is the most likely diagnosis. Grunkemeier et al16 described it as chronic or frequently recurring abdominal pain that is treated with narcotics, either chronically or acutely with high doses, and that includes all the following features16:
- The pain worsens or resolves incompletely with continued or increasing doses of narcotics
- The pain markedly worsens when the narcotic dose is decreased, and decreases when the drug is reinstituted (the “soarand-crash” effect)
- The frequency, duration, and intensity of the pain episodes gradually increase
- The nature of the pain and its intensity are not explained by a current or previous gastrointestinal diagnosis.16
This syndrome is common in patients who receive high doses of narcotics for postoperative pain or for other, nonmalignant causes of pain. Patients eventually become dependent on the drugs but are not aware that chronic use activates and facilitates areas in the brain that enhance the perception of pain.16 A study of a rat model of narcotic bowel syndrome17 showed that morphine-induced hyperalgesia depends on central sensitization involving the activation of spinal microglia. This eventually results in concomitant peripheral sensitization involving the colonic mucosal neuroimmune system, and also in central or peripheral activation of opioid kappa-receptors by dynorphin release.17
Patients tend to present with chronic or intermittent colicky abdominal pain that requires escalating doses of narcotics. Eventually, they develop tachyphylaxis and shortened pain-free periods and will require even higher doses of narcotics. This ultimately enhances the perception of pain and worsens opioid bowel symptoms, causing a vicious circle of pain and more narcotic use.16
Laboratory tests are usually normal, and imaging may show only ileus. Gastric emptying may be delayed in patients who have either narcotic bowel syndrome or gastroparesis, but since abdominal pain from narcotic bowel syndrome is a result of central and visceral hypersensitivity, these patients perceive more severe abdominal pain than patients with gastroparesis alone.
Opioid withdrawal
Symptoms of opioid withdrawal may appear as soon as 6 to 24 hours after cessation of the opioid in patients known to be dependent on opioids. These patients present with crampy abdominal pain with nausea.18 Other symptoms include agitation, rhinorrhea, lacrimation, excessive yawning, arthralgias, papillary dilation, and piloerection.18
Our patient did not have the typical signs of opioid withdrawal.
Crohn disease
Crohn disease is a multisystem disorder with specific clinical and pathologic features. It is characterized by focal, asymmetric, transmural, and occasionally granulomatous inflammation primarily affecting the gastrointestinal tract.19 Characteristic symptoms include abdominal pain, chronic diarrhea with or without rectal bleeding, and weight loss. Extraintestinal signs may include anemia and inflammatory changes in the eyes, skin, and joints. The diagnosis is based on endoscopic, radiographic, and pathologic findings.19
Our patient did not have diarrhea or signs of Crohn disease on CT, endoscopy, or histology.
Chronic pancreatitis
Chronic pancreatitis involves progressive inflammatory changes resulting in permanent structural damage to the pancreas and subsequent exocrine and endocrine dysfunction.20 Patients have epigastric abdominal pain that often radiates to the back20; it is associated with eating and is partly relieved with leaning forward. Symptoms of pancreatic insufficiency such as fat malabsorption (resulting in steatorrhea and fat-soluble vitamin deficiency) and diabetes are common. Calcifications within the pancreas on CT suggest chronic pancreatitis.20 Serum lipase and amylase levels may be normal or slightly elevated.20
Our patient’s abdominal pain was not typical of pancreatitis. He had no signs or symptoms of pancreatic insufficiency and no calcifications within the pancreas.
Chronic mesenteric ischemia
Chronic mesenteric ischemia (“intestinal angina”) is caused by a reduction in intestinal blood flow as a result of occlusion, vasospasm, or hypoperfusion of the mesenteric vasculature.21 It is commonly seen in patients who smoke or who have atherosclerotic vascular disease. These patients have chronic dull or crampy abdominal pain that usually occurs within 1 hour after eating.21 To avoid pain, patients avoid eating, resulting in weight loss.21 CT angiography with multi-detector CT is as effective as angiography (the gold standard) in depicting splanchnic arterial anatomy.22
Our patient is young and has no known risk factors for atherosclerosis such as smoking. His abdominal pain is more intermittent than chronic and is not associated with eating.
Cannabinoid hyperemesis
Cannabinoid hyperemesis should be considered in patients with long-term cannabis use presenting with cyclic vomiting, abdominal pain, compulsive use of hot showers, and improvement of symptoms with cannabis cessation.23 Although cannabinoids have been recognized for their antiemetic effects, long-term use may eventually cause autonomic instability and disturbances in the hypothalamic-pituitary-adrenal axis, resulting in cyclic vomiting and thermoregulatory impairment.23
Although our patient presented with multiple episodes of vomiting and abdominal pain, he denied using marijuana, he tested negative for tetrahydrocannabinol, and he did not associate any relief of his symptoms with hot baths.
CASE CONTINUED
Our patient receives intravenous hydration, antiemetics, and a narcotic in tapering intravenous doses, and his symptoms gradually improve. He is discharged from the hospital. However, a few weeks later he is readmitted with the same symptoms of abdominal pain and nausea.
3. What is the cornerstone of treatment for narcotic bowel syndrome?
- Establishing a therapeutic relationship
- Detoxification
- Supportive management with intravenous fluids, antiemetics, and stool-softeners
- Medical management with a short-acting narcotic, clonidine, lorazepam, and desipramine
MANAGEMENT OF NARCOTIC BOWEL SYNDROME
An effective therapeutic relationship with the patient is the cornerstone of treatment and should be established before starting detoxification.17 The physician must first learn to accept that the patient’s condition is real and must show genuine empathy as well as provide information about the pathophysiologic basis of the condition, the rationale for withholding narcotics, and the detrimental role narcotics play in the vicious circle of pain.
Detoxification involves gradually withdrawing the narcotic and substituting a nonnarcotic such as an antidepressant for pain control, as well as prescribing a drug such as a benzodiazepine or clonidine to prevent withdrawal symptoms and a laxative to prevent constipation.17,24 The physician must reassure the patient that he or she will not be abandoned in pain and that all medications will be continuously adjusted as needed to keep him or her comfortable throughout the detoxification process.17,24 The physician must continuously gauge the patient’s willingness to continue with treatment and must also be readily available to address the patient’s concerns in a timely manner.17,24 Involving family members and friends may provide additional support to the patient. Referral to a functional gastrointestinal motility program, a pain specialist, and a psychologist may also be considered.17,24 Follow-up care is essential, even after the withdrawal program has ended.17,24
BACK TO THE PATIENT
After successfully establishing a therapeutic relationship and discussing the treatment plan with our patient, we started him on the same dosage of narcotic that he had been receiving, calculated in intravenous morphine equivalents to achieve maximal comfort, and then decreased the dosage by 10% to 33% daily until he was completely off narcotics. An antidepressant and a benzodiazepine were given simultaneously with narcotic tapering. Oral clonidine (0.1–0.4 mg/day) was given after the narcotic dosage was reduced to about half, and polyethylene glycol was given as needed for constipation. The total duration of detoxification was 7 days.
The patient was referred to a psychologist for cognitive-behavioral and relaxation therapy, as well as for encouragement and support. At 6 months, he had had no recurrence of symptoms.
TAKE-HOME MESSAGE
In the United States, the number of patients taking a narcotic for nonmalignant pain is increasing, 25 and physicians should be more aware of complications such as narcotic bowel syndrome.
Narcotic bowel syndrome should be suspected in any patient with prolonged narcotic use presenting with multiple recurrent episodes of abdominal pain after other causes are ruled out.
Establishing a good therapeutic relationship with the patient is the cornerstone of successful treatment. Patients who understand their condition and are willing to be treated tend to have better outcomes.
Supportive treatment, symptom relief, and emotional support during detoxification increase compliance.
- Banks PA, Freeman ML; Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379–2400.
- Boles RG, Adams K, Ito M, Li BU. Maternal inheritance in cyclic vomiting syndrome with neuromuscular disease. Am J Med Genet A 2003; 120A:474–482.
- Wang Q, Ito M, Adams K, et al. Mitochondrial DNA control region sequence variation in migraine headache and cyclic vomiting syndrome. Am J Med Genet A 2004; 131:50–58.
- Taché Y. Cyclic vomiting syndrome: the corticotropinreleasing-factor hypothesis. Dig Dis Sci 1999; 44(suppl 8):79S–86S.
- Withers GD, Silburn SR, Forbes DA. Precipitants and aetiology of cyclic vomiting syndrome. Acta Paediatr 1998; 87:272–277.
- Whitney HB. Cyclic vomiting. A brief review of this affection as illustrated by a typical case. Arch Pediatr 1898; 15:839–845.
- Stickler GB. Relationship between cyclic vomiting syndrome and migraine. Clin Pediatr (Phila) 2005; 44:505–508.
- Li BU, Murray RD, Heitlinger LA, Robbins JL, Hayes JR. Is cyclic vomiting syndrome related to migraine? J Pediatr 1999; 134:567–572.
- Allen JH, de Moore GM, Heddle R, Twartz JC. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004; 53:1566–1570.
- Rome Foundation. Rome III disorders and diagnostic criteria. http://www.romecriteria.org/criteria/. Accessed February 27, 2013.
- Anderson KE, Bloomer JR, Bonkovsky HL, et al. Recommendations for the diagnosis and treatment of the acute porphyrias. Ann Intern Med 2005; 142:439–450.
- Camilleri M. Clinical practice. Diabetic gastroparesis. N Engl J Med 2007; 356:820–829.
- Maddern GJ, Horowitz M, Jamieson GG, Chatterton BE, Collins PJ, Roberts-Thomson P. Abnormalities of esophageal and gastric emptying in progressive systemic sclerosis. Gastroenterology 1984; 87:922–926.
- Jost WH. Gastrointestinal dysfunction in Parkinson’s disease. J Neurol Sci 2010; 289:69–73.
- Parkman HP, Hasler WL, Fisher RS; American Gastroenterological Association. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004; 127:1592–1622.
- Grunkemeier DM, Cassara JE, Dalton CB, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol Hepatol 2007; 5:1126–1139.
- Agostini S, Eutamene H, Cartier C, et al. Evidence of central and peripheral sensitization in a rat model of narcotic bowel-like syndrome. Gastroenterology 2010; 139:553–563,563.e1–e5.
- Nicholls L, Bragaw L, Ruetsch C. Opioid dependence treatment and guidelines. J Manag Care Pharm 2010; 16(1 suppl B):S14–S21.
- Lichtenstein GR, Hanauer SB, Sandborn WJ; Practice Parameters Committee of American College of Gastroenterology. Management of Crohn’s disease in adults. Am J Gastroenterol 2009; 104:465–483.
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med 1995; 332:1482–1490.
- American Gastroenterological Association Medical Position Statement: guidelines on intestinal ischemia. Gastroenterology 2000; 118:951–953.
- Savastano S, Teso S, Corrà S, Fantozzi O, Miotto D. Multislice CT angiography of the celiac and superior mesenteric arteries: comparison with arteriographic findings. Radiol Med 2002; 103:456–463.
- Simonetto DA, Oxentenko AS, Herman ML, Szostek JH. Cannabinoid hyperemesis: a case series of 98 patients. Mayo Clin Proc 2012; 87:114–119.
- Drossman DA, Morris CB, Edwards H, et al. Diagnosis, characterization, and 3-month outcome after detoxification of 39 patients with narcotic bowel syndrome. Am J Gastroenterol 2012; 107:1426–1440.
- Trescot AM, Boswell MV, Atluri SL, et al. Opioid guidelines in the management of chronic non-cancer pain. Pain Physician 2006; 9:1–39.
A 32-year-old man presents to the emergency department with excruciating abdominal pain associated with multiple episodes of vomiting for the past 2 days. He reports no fevers, headaches, diarrhea, constipation, hematochezia, melena, musculoskeletal symptoms, or weight loss. His abdominal pain is generalized and crampy. It does not radiate and has no precipitating factors. The pain is relieved only with intravenous narcotics.
He does not smoke, drink alcohol, or use illicit drugs. He has no known drug or food allergies. He says that his current condition causes him emotional stress that affects his performance at work.
About a year ago, after a complicated surgical procedure, he needed chronic high-dose narcotics. A few months later, he developed multiple bouts of abdominal pain and vomiting that required hospital visits. He now takes oral oxycodone 10–15 mg every 4–6 hours.
On admission, his vital signs are stable, but he is in excruciating pain. He is alert and oriented to person, place, and time. His sclera are anicteric, and the pupils are equal, round, and reactive to light. Lung and heart examinations are normal. The abdomen is soft and nondistended but tender in all four quadrants without guarding; the liver and spleen are not palpable, and no abdominal masses are detected. He has no skin rash, joint swelling or tenderness, or peripheral edema. The neurologic examination is normal. Computed tomography (CT) of the abdomen with contrast shows no signs of bowel obstruction, pancreatic calcifications or edema, cholecystitis, or hepatobiliary disease. Results of initial laboratory testing are shown in Table 1.
1. Based on the information available, which is the least likely cause of his symptoms?
- Acute pancreatitis
- Cyclic vomiting syndrome
- Acute intermittent porphyria
- Gastroparesis
Acute pancreatitis
Acute pancreatitis is the least likely cause of his symptoms. It is commonly caused by gallstones, alcohol, hypertriglyceridemia, and certain drugs.1 The associated abdominal pain is usually epigastric, radiates to the back, and is accompanied by nausea or vomiting, or both. The onset of pain is sudden and rapidly increases in severity within 30 minutes. CT shows enlargement of the pancreas with diffuse edema, heterogeneity of pancreatic parenchyma, peripancreatic stranding, and peripancreatic fluid collections.1 The diagnosis is based on two of the following three criteria: abdominal pain characteristic of acute pancreatitis; a serum amylase or lipase concentration three or more times the upper limit of normal; and characteristic findings of acute pancreatitis on CT.1
Cyclic vomiting syndrome
Cyclic vomiting syndrome is thought to be caused by episodic dysautonomia, mitochondrial DNA mutations, and hypothalamic emetic response oversensitivity,2–4 but the exact pathogenesis is unknown. The syndrome has been strongly linked to migraine and to the chronic excessive use of cannabinoids.5–9 The Rome III diagnostic criteria10 are the following: the vomiting episodes are stereotypical, ie, they are acute and last for less than 1 week; the patient has had three or more episodes in the previous year; and the patient has no nausea or vomiting between episodes. The patient must meet all three criteria. A history of migraine or a family history of migraine further supports the diagnosis.
Acute intermittent porphyria
Acute intermittent porphyria is characterized by neurovisceral symptoms such as convulsions, paresis, autonomic dysfunction, constipation, and diarrhea that result from the overproduction of porphyrin precursors and deficiency of porphobilinogen deaminase.11
Most patients have poorly localized, severe, steady abdominal pain that develops over hours to days and that may persist for days to weeks.11 Since the pain is neuropathic, abdominal tenderness is usually minimal during an acute attack. Other clues include signs of ileus, such as constipation, nausea, abdominal distention, or decreased bowel sounds; bladder dysfunction, eg, urinary retention, incontinence, or dysuria; reddish-brown urine; and sensory neuropathy of the chest, back, and extremities.11 Blistering skin lesions are usually not seen. The presence of porphobilinogen in the urine confirms the diagnosis.11
Gastroparesis
Gastroparesis is a result of discoordination between the sympathetic and parasympathetic nervous systems, neurons, and smooth muscles within the stomach, causing a decrease in gastric motility. Common causes are diabetes,12 scleroderma,13 and neurologic disorders.14 It can also be iatrogenic,15 resulting from visceral nerve injury and drug treatment with narcotics, calcium channel blockers, muscarinic cholinergic antagonists, or certain antidepressants. Symptoms are related to gastric stasis, ie, abdominal pain from gastric distention, bloating, vomiting, and early satiety.15 Abdominal pain may worsen after eating, and vomitus usually consists of recently ingested food. These patients may have abdominal distension or tenderness and succussion splash. After excluding possible mechanical obstruction, a gastric-emptying study may be necessary to make the diagnosis.15
CASE CONTINUED
A serum and urine drug screen in our patient is positive only for opioids. Urine measures of delta-aminolevulinic acid and porphobilinogen are normal. CT angiography of the abdomen shows no signs of mesenteric vascular occlusion. Esophagogastroduodenoscopy shows antral gastritis, but the esophagus and duodenum appear normal, and colonoscopy is normal as well. Histologic study of biopsy specimens obtained during endoscopy is unrevealing. A gastric-emptying study shows delayed emptying. The patient’s abdominal pain and vomiting persist with the initial dose of intravenous narcotic but resolve with escalating doses. When asked, the patient denies an excessive need for hot baths.
2. Which is the most likely diagnosis at this point?
- Narcotic bowel syndrome
- Opioid withdrawal
- Crohn disease
- Chronic pancreatitis
- Chronic mesenteric ischemia
- Cannabinoid hyperemesis
Narcotic bowel syndrome
Narcotic bowel syndrome is the most likely diagnosis. Grunkemeier et al16 described it as chronic or frequently recurring abdominal pain that is treated with narcotics, either chronically or acutely with high doses, and that includes all the following features16:
- The pain worsens or resolves incompletely with continued or increasing doses of narcotics
- The pain markedly worsens when the narcotic dose is decreased, and decreases when the drug is reinstituted (the “soarand-crash” effect)
- The frequency, duration, and intensity of the pain episodes gradually increase
- The nature of the pain and its intensity are not explained by a current or previous gastrointestinal diagnosis.16
This syndrome is common in patients who receive high doses of narcotics for postoperative pain or for other, nonmalignant causes of pain. Patients eventually become dependent on the drugs but are not aware that chronic use activates and facilitates areas in the brain that enhance the perception of pain.16 A study of a rat model of narcotic bowel syndrome17 showed that morphine-induced hyperalgesia depends on central sensitization involving the activation of spinal microglia. This eventually results in concomitant peripheral sensitization involving the colonic mucosal neuroimmune system, and also in central or peripheral activation of opioid kappa-receptors by dynorphin release.17
Patients tend to present with chronic or intermittent colicky abdominal pain that requires escalating doses of narcotics. Eventually, they develop tachyphylaxis and shortened pain-free periods and will require even higher doses of narcotics. This ultimately enhances the perception of pain and worsens opioid bowel symptoms, causing a vicious circle of pain and more narcotic use.16
Laboratory tests are usually normal, and imaging may show only ileus. Gastric emptying may be delayed in patients who have either narcotic bowel syndrome or gastroparesis, but since abdominal pain from narcotic bowel syndrome is a result of central and visceral hypersensitivity, these patients perceive more severe abdominal pain than patients with gastroparesis alone.
Opioid withdrawal
Symptoms of opioid withdrawal may appear as soon as 6 to 24 hours after cessation of the opioid in patients known to be dependent on opioids. These patients present with crampy abdominal pain with nausea.18 Other symptoms include agitation, rhinorrhea, lacrimation, excessive yawning, arthralgias, papillary dilation, and piloerection.18
Our patient did not have the typical signs of opioid withdrawal.
Crohn disease
Crohn disease is a multisystem disorder with specific clinical and pathologic features. It is characterized by focal, asymmetric, transmural, and occasionally granulomatous inflammation primarily affecting the gastrointestinal tract.19 Characteristic symptoms include abdominal pain, chronic diarrhea with or without rectal bleeding, and weight loss. Extraintestinal signs may include anemia and inflammatory changes in the eyes, skin, and joints. The diagnosis is based on endoscopic, radiographic, and pathologic findings.19
Our patient did not have diarrhea or signs of Crohn disease on CT, endoscopy, or histology.
Chronic pancreatitis
Chronic pancreatitis involves progressive inflammatory changes resulting in permanent structural damage to the pancreas and subsequent exocrine and endocrine dysfunction.20 Patients have epigastric abdominal pain that often radiates to the back20; it is associated with eating and is partly relieved with leaning forward. Symptoms of pancreatic insufficiency such as fat malabsorption (resulting in steatorrhea and fat-soluble vitamin deficiency) and diabetes are common. Calcifications within the pancreas on CT suggest chronic pancreatitis.20 Serum lipase and amylase levels may be normal or slightly elevated.20
Our patient’s abdominal pain was not typical of pancreatitis. He had no signs or symptoms of pancreatic insufficiency and no calcifications within the pancreas.
Chronic mesenteric ischemia
Chronic mesenteric ischemia (“intestinal angina”) is caused by a reduction in intestinal blood flow as a result of occlusion, vasospasm, or hypoperfusion of the mesenteric vasculature.21 It is commonly seen in patients who smoke or who have atherosclerotic vascular disease. These patients have chronic dull or crampy abdominal pain that usually occurs within 1 hour after eating.21 To avoid pain, patients avoid eating, resulting in weight loss.21 CT angiography with multi-detector CT is as effective as angiography (the gold standard) in depicting splanchnic arterial anatomy.22
Our patient is young and has no known risk factors for atherosclerosis such as smoking. His abdominal pain is more intermittent than chronic and is not associated with eating.
Cannabinoid hyperemesis
Cannabinoid hyperemesis should be considered in patients with long-term cannabis use presenting with cyclic vomiting, abdominal pain, compulsive use of hot showers, and improvement of symptoms with cannabis cessation.23 Although cannabinoids have been recognized for their antiemetic effects, long-term use may eventually cause autonomic instability and disturbances in the hypothalamic-pituitary-adrenal axis, resulting in cyclic vomiting and thermoregulatory impairment.23
Although our patient presented with multiple episodes of vomiting and abdominal pain, he denied using marijuana, he tested negative for tetrahydrocannabinol, and he did not associate any relief of his symptoms with hot baths.
CASE CONTINUED
Our patient receives intravenous hydration, antiemetics, and a narcotic in tapering intravenous doses, and his symptoms gradually improve. He is discharged from the hospital. However, a few weeks later he is readmitted with the same symptoms of abdominal pain and nausea.
3. What is the cornerstone of treatment for narcotic bowel syndrome?
- Establishing a therapeutic relationship
- Detoxification
- Supportive management with intravenous fluids, antiemetics, and stool-softeners
- Medical management with a short-acting narcotic, clonidine, lorazepam, and desipramine
MANAGEMENT OF NARCOTIC BOWEL SYNDROME
An effective therapeutic relationship with the patient is the cornerstone of treatment and should be established before starting detoxification.17 The physician must first learn to accept that the patient’s condition is real and must show genuine empathy as well as provide information about the pathophysiologic basis of the condition, the rationale for withholding narcotics, and the detrimental role narcotics play in the vicious circle of pain.
Detoxification involves gradually withdrawing the narcotic and substituting a nonnarcotic such as an antidepressant for pain control, as well as prescribing a drug such as a benzodiazepine or clonidine to prevent withdrawal symptoms and a laxative to prevent constipation.17,24 The physician must reassure the patient that he or she will not be abandoned in pain and that all medications will be continuously adjusted as needed to keep him or her comfortable throughout the detoxification process.17,24 The physician must continuously gauge the patient’s willingness to continue with treatment and must also be readily available to address the patient’s concerns in a timely manner.17,24 Involving family members and friends may provide additional support to the patient. Referral to a functional gastrointestinal motility program, a pain specialist, and a psychologist may also be considered.17,24 Follow-up care is essential, even after the withdrawal program has ended.17,24
BACK TO THE PATIENT
After successfully establishing a therapeutic relationship and discussing the treatment plan with our patient, we started him on the same dosage of narcotic that he had been receiving, calculated in intravenous morphine equivalents to achieve maximal comfort, and then decreased the dosage by 10% to 33% daily until he was completely off narcotics. An antidepressant and a benzodiazepine were given simultaneously with narcotic tapering. Oral clonidine (0.1–0.4 mg/day) was given after the narcotic dosage was reduced to about half, and polyethylene glycol was given as needed for constipation. The total duration of detoxification was 7 days.
The patient was referred to a psychologist for cognitive-behavioral and relaxation therapy, as well as for encouragement and support. At 6 months, he had had no recurrence of symptoms.
TAKE-HOME MESSAGE
In the United States, the number of patients taking a narcotic for nonmalignant pain is increasing, 25 and physicians should be more aware of complications such as narcotic bowel syndrome.
Narcotic bowel syndrome should be suspected in any patient with prolonged narcotic use presenting with multiple recurrent episodes of abdominal pain after other causes are ruled out.
Establishing a good therapeutic relationship with the patient is the cornerstone of successful treatment. Patients who understand their condition and are willing to be treated tend to have better outcomes.
Supportive treatment, symptom relief, and emotional support during detoxification increase compliance.
A 32-year-old man presents to the emergency department with excruciating abdominal pain associated with multiple episodes of vomiting for the past 2 days. He reports no fevers, headaches, diarrhea, constipation, hematochezia, melena, musculoskeletal symptoms, or weight loss. His abdominal pain is generalized and crampy. It does not radiate and has no precipitating factors. The pain is relieved only with intravenous narcotics.
He does not smoke, drink alcohol, or use illicit drugs. He has no known drug or food allergies. He says that his current condition causes him emotional stress that affects his performance at work.
About a year ago, after a complicated surgical procedure, he needed chronic high-dose narcotics. A few months later, he developed multiple bouts of abdominal pain and vomiting that required hospital visits. He now takes oral oxycodone 10–15 mg every 4–6 hours.
On admission, his vital signs are stable, but he is in excruciating pain. He is alert and oriented to person, place, and time. His sclera are anicteric, and the pupils are equal, round, and reactive to light. Lung and heart examinations are normal. The abdomen is soft and nondistended but tender in all four quadrants without guarding; the liver and spleen are not palpable, and no abdominal masses are detected. He has no skin rash, joint swelling or tenderness, or peripheral edema. The neurologic examination is normal. Computed tomography (CT) of the abdomen with contrast shows no signs of bowel obstruction, pancreatic calcifications or edema, cholecystitis, or hepatobiliary disease. Results of initial laboratory testing are shown in Table 1.
1. Based on the information available, which is the least likely cause of his symptoms?
- Acute pancreatitis
- Cyclic vomiting syndrome
- Acute intermittent porphyria
- Gastroparesis
Acute pancreatitis
Acute pancreatitis is the least likely cause of his symptoms. It is commonly caused by gallstones, alcohol, hypertriglyceridemia, and certain drugs.1 The associated abdominal pain is usually epigastric, radiates to the back, and is accompanied by nausea or vomiting, or both. The onset of pain is sudden and rapidly increases in severity within 30 minutes. CT shows enlargement of the pancreas with diffuse edema, heterogeneity of pancreatic parenchyma, peripancreatic stranding, and peripancreatic fluid collections.1 The diagnosis is based on two of the following three criteria: abdominal pain characteristic of acute pancreatitis; a serum amylase or lipase concentration three or more times the upper limit of normal; and characteristic findings of acute pancreatitis on CT.1
Cyclic vomiting syndrome
Cyclic vomiting syndrome is thought to be caused by episodic dysautonomia, mitochondrial DNA mutations, and hypothalamic emetic response oversensitivity,2–4 but the exact pathogenesis is unknown. The syndrome has been strongly linked to migraine and to the chronic excessive use of cannabinoids.5–9 The Rome III diagnostic criteria10 are the following: the vomiting episodes are stereotypical, ie, they are acute and last for less than 1 week; the patient has had three or more episodes in the previous year; and the patient has no nausea or vomiting between episodes. The patient must meet all three criteria. A history of migraine or a family history of migraine further supports the diagnosis.
Acute intermittent porphyria
Acute intermittent porphyria is characterized by neurovisceral symptoms such as convulsions, paresis, autonomic dysfunction, constipation, and diarrhea that result from the overproduction of porphyrin precursors and deficiency of porphobilinogen deaminase.11
Most patients have poorly localized, severe, steady abdominal pain that develops over hours to days and that may persist for days to weeks.11 Since the pain is neuropathic, abdominal tenderness is usually minimal during an acute attack. Other clues include signs of ileus, such as constipation, nausea, abdominal distention, or decreased bowel sounds; bladder dysfunction, eg, urinary retention, incontinence, or dysuria; reddish-brown urine; and sensory neuropathy of the chest, back, and extremities.11 Blistering skin lesions are usually not seen. The presence of porphobilinogen in the urine confirms the diagnosis.11
Gastroparesis
Gastroparesis is a result of discoordination between the sympathetic and parasympathetic nervous systems, neurons, and smooth muscles within the stomach, causing a decrease in gastric motility. Common causes are diabetes,12 scleroderma,13 and neurologic disorders.14 It can also be iatrogenic,15 resulting from visceral nerve injury and drug treatment with narcotics, calcium channel blockers, muscarinic cholinergic antagonists, or certain antidepressants. Symptoms are related to gastric stasis, ie, abdominal pain from gastric distention, bloating, vomiting, and early satiety.15 Abdominal pain may worsen after eating, and vomitus usually consists of recently ingested food. These patients may have abdominal distension or tenderness and succussion splash. After excluding possible mechanical obstruction, a gastric-emptying study may be necessary to make the diagnosis.15
CASE CONTINUED
A serum and urine drug screen in our patient is positive only for opioids. Urine measures of delta-aminolevulinic acid and porphobilinogen are normal. CT angiography of the abdomen shows no signs of mesenteric vascular occlusion. Esophagogastroduodenoscopy shows antral gastritis, but the esophagus and duodenum appear normal, and colonoscopy is normal as well. Histologic study of biopsy specimens obtained during endoscopy is unrevealing. A gastric-emptying study shows delayed emptying. The patient’s abdominal pain and vomiting persist with the initial dose of intravenous narcotic but resolve with escalating doses. When asked, the patient denies an excessive need for hot baths.
2. Which is the most likely diagnosis at this point?
- Narcotic bowel syndrome
- Opioid withdrawal
- Crohn disease
- Chronic pancreatitis
- Chronic mesenteric ischemia
- Cannabinoid hyperemesis
Narcotic bowel syndrome
Narcotic bowel syndrome is the most likely diagnosis. Grunkemeier et al16 described it as chronic or frequently recurring abdominal pain that is treated with narcotics, either chronically or acutely with high doses, and that includes all the following features16:
- The pain worsens or resolves incompletely with continued or increasing doses of narcotics
- The pain markedly worsens when the narcotic dose is decreased, and decreases when the drug is reinstituted (the “soarand-crash” effect)
- The frequency, duration, and intensity of the pain episodes gradually increase
- The nature of the pain and its intensity are not explained by a current or previous gastrointestinal diagnosis.16
This syndrome is common in patients who receive high doses of narcotics for postoperative pain or for other, nonmalignant causes of pain. Patients eventually become dependent on the drugs but are not aware that chronic use activates and facilitates areas in the brain that enhance the perception of pain.16 A study of a rat model of narcotic bowel syndrome17 showed that morphine-induced hyperalgesia depends on central sensitization involving the activation of spinal microglia. This eventually results in concomitant peripheral sensitization involving the colonic mucosal neuroimmune system, and also in central or peripheral activation of opioid kappa-receptors by dynorphin release.17
Patients tend to present with chronic or intermittent colicky abdominal pain that requires escalating doses of narcotics. Eventually, they develop tachyphylaxis and shortened pain-free periods and will require even higher doses of narcotics. This ultimately enhances the perception of pain and worsens opioid bowel symptoms, causing a vicious circle of pain and more narcotic use.16
Laboratory tests are usually normal, and imaging may show only ileus. Gastric emptying may be delayed in patients who have either narcotic bowel syndrome or gastroparesis, but since abdominal pain from narcotic bowel syndrome is a result of central and visceral hypersensitivity, these patients perceive more severe abdominal pain than patients with gastroparesis alone.
Opioid withdrawal
Symptoms of opioid withdrawal may appear as soon as 6 to 24 hours after cessation of the opioid in patients known to be dependent on opioids. These patients present with crampy abdominal pain with nausea.18 Other symptoms include agitation, rhinorrhea, lacrimation, excessive yawning, arthralgias, papillary dilation, and piloerection.18
Our patient did not have the typical signs of opioid withdrawal.
Crohn disease
Crohn disease is a multisystem disorder with specific clinical and pathologic features. It is characterized by focal, asymmetric, transmural, and occasionally granulomatous inflammation primarily affecting the gastrointestinal tract.19 Characteristic symptoms include abdominal pain, chronic diarrhea with or without rectal bleeding, and weight loss. Extraintestinal signs may include anemia and inflammatory changes in the eyes, skin, and joints. The diagnosis is based on endoscopic, radiographic, and pathologic findings.19
Our patient did not have diarrhea or signs of Crohn disease on CT, endoscopy, or histology.
Chronic pancreatitis
Chronic pancreatitis involves progressive inflammatory changes resulting in permanent structural damage to the pancreas and subsequent exocrine and endocrine dysfunction.20 Patients have epigastric abdominal pain that often radiates to the back20; it is associated with eating and is partly relieved with leaning forward. Symptoms of pancreatic insufficiency such as fat malabsorption (resulting in steatorrhea and fat-soluble vitamin deficiency) and diabetes are common. Calcifications within the pancreas on CT suggest chronic pancreatitis.20 Serum lipase and amylase levels may be normal or slightly elevated.20
Our patient’s abdominal pain was not typical of pancreatitis. He had no signs or symptoms of pancreatic insufficiency and no calcifications within the pancreas.
Chronic mesenteric ischemia
Chronic mesenteric ischemia (“intestinal angina”) is caused by a reduction in intestinal blood flow as a result of occlusion, vasospasm, or hypoperfusion of the mesenteric vasculature.21 It is commonly seen in patients who smoke or who have atherosclerotic vascular disease. These patients have chronic dull or crampy abdominal pain that usually occurs within 1 hour after eating.21 To avoid pain, patients avoid eating, resulting in weight loss.21 CT angiography with multi-detector CT is as effective as angiography (the gold standard) in depicting splanchnic arterial anatomy.22
Our patient is young and has no known risk factors for atherosclerosis such as smoking. His abdominal pain is more intermittent than chronic and is not associated with eating.
Cannabinoid hyperemesis
Cannabinoid hyperemesis should be considered in patients with long-term cannabis use presenting with cyclic vomiting, abdominal pain, compulsive use of hot showers, and improvement of symptoms with cannabis cessation.23 Although cannabinoids have been recognized for their antiemetic effects, long-term use may eventually cause autonomic instability and disturbances in the hypothalamic-pituitary-adrenal axis, resulting in cyclic vomiting and thermoregulatory impairment.23
Although our patient presented with multiple episodes of vomiting and abdominal pain, he denied using marijuana, he tested negative for tetrahydrocannabinol, and he did not associate any relief of his symptoms with hot baths.
CASE CONTINUED
Our patient receives intravenous hydration, antiemetics, and a narcotic in tapering intravenous doses, and his symptoms gradually improve. He is discharged from the hospital. However, a few weeks later he is readmitted with the same symptoms of abdominal pain and nausea.
3. What is the cornerstone of treatment for narcotic bowel syndrome?
- Establishing a therapeutic relationship
- Detoxification
- Supportive management with intravenous fluids, antiemetics, and stool-softeners
- Medical management with a short-acting narcotic, clonidine, lorazepam, and desipramine
MANAGEMENT OF NARCOTIC BOWEL SYNDROME
An effective therapeutic relationship with the patient is the cornerstone of treatment and should be established before starting detoxification.17 The physician must first learn to accept that the patient’s condition is real and must show genuine empathy as well as provide information about the pathophysiologic basis of the condition, the rationale for withholding narcotics, and the detrimental role narcotics play in the vicious circle of pain.
Detoxification involves gradually withdrawing the narcotic and substituting a nonnarcotic such as an antidepressant for pain control, as well as prescribing a drug such as a benzodiazepine or clonidine to prevent withdrawal symptoms and a laxative to prevent constipation.17,24 The physician must reassure the patient that he or she will not be abandoned in pain and that all medications will be continuously adjusted as needed to keep him or her comfortable throughout the detoxification process.17,24 The physician must continuously gauge the patient’s willingness to continue with treatment and must also be readily available to address the patient’s concerns in a timely manner.17,24 Involving family members and friends may provide additional support to the patient. Referral to a functional gastrointestinal motility program, a pain specialist, and a psychologist may also be considered.17,24 Follow-up care is essential, even after the withdrawal program has ended.17,24
BACK TO THE PATIENT
After successfully establishing a therapeutic relationship and discussing the treatment plan with our patient, we started him on the same dosage of narcotic that he had been receiving, calculated in intravenous morphine equivalents to achieve maximal comfort, and then decreased the dosage by 10% to 33% daily until he was completely off narcotics. An antidepressant and a benzodiazepine were given simultaneously with narcotic tapering. Oral clonidine (0.1–0.4 mg/day) was given after the narcotic dosage was reduced to about half, and polyethylene glycol was given as needed for constipation. The total duration of detoxification was 7 days.
The patient was referred to a psychologist for cognitive-behavioral and relaxation therapy, as well as for encouragement and support. At 6 months, he had had no recurrence of symptoms.
TAKE-HOME MESSAGE
In the United States, the number of patients taking a narcotic for nonmalignant pain is increasing, 25 and physicians should be more aware of complications such as narcotic bowel syndrome.
Narcotic bowel syndrome should be suspected in any patient with prolonged narcotic use presenting with multiple recurrent episodes of abdominal pain after other causes are ruled out.
Establishing a good therapeutic relationship with the patient is the cornerstone of successful treatment. Patients who understand their condition and are willing to be treated tend to have better outcomes.
Supportive treatment, symptom relief, and emotional support during detoxification increase compliance.
- Banks PA, Freeman ML; Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379–2400.
- Boles RG, Adams K, Ito M, Li BU. Maternal inheritance in cyclic vomiting syndrome with neuromuscular disease. Am J Med Genet A 2003; 120A:474–482.
- Wang Q, Ito M, Adams K, et al. Mitochondrial DNA control region sequence variation in migraine headache and cyclic vomiting syndrome. Am J Med Genet A 2004; 131:50–58.
- Taché Y. Cyclic vomiting syndrome: the corticotropinreleasing-factor hypothesis. Dig Dis Sci 1999; 44(suppl 8):79S–86S.
- Withers GD, Silburn SR, Forbes DA. Precipitants and aetiology of cyclic vomiting syndrome. Acta Paediatr 1998; 87:272–277.
- Whitney HB. Cyclic vomiting. A brief review of this affection as illustrated by a typical case. Arch Pediatr 1898; 15:839–845.
- Stickler GB. Relationship between cyclic vomiting syndrome and migraine. Clin Pediatr (Phila) 2005; 44:505–508.
- Li BU, Murray RD, Heitlinger LA, Robbins JL, Hayes JR. Is cyclic vomiting syndrome related to migraine? J Pediatr 1999; 134:567–572.
- Allen JH, de Moore GM, Heddle R, Twartz JC. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004; 53:1566–1570.
- Rome Foundation. Rome III disorders and diagnostic criteria. http://www.romecriteria.org/criteria/. Accessed February 27, 2013.
- Anderson KE, Bloomer JR, Bonkovsky HL, et al. Recommendations for the diagnosis and treatment of the acute porphyrias. Ann Intern Med 2005; 142:439–450.
- Camilleri M. Clinical practice. Diabetic gastroparesis. N Engl J Med 2007; 356:820–829.
- Maddern GJ, Horowitz M, Jamieson GG, Chatterton BE, Collins PJ, Roberts-Thomson P. Abnormalities of esophageal and gastric emptying in progressive systemic sclerosis. Gastroenterology 1984; 87:922–926.
- Jost WH. Gastrointestinal dysfunction in Parkinson’s disease. J Neurol Sci 2010; 289:69–73.
- Parkman HP, Hasler WL, Fisher RS; American Gastroenterological Association. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004; 127:1592–1622.
- Grunkemeier DM, Cassara JE, Dalton CB, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol Hepatol 2007; 5:1126–1139.
- Agostini S, Eutamene H, Cartier C, et al. Evidence of central and peripheral sensitization in a rat model of narcotic bowel-like syndrome. Gastroenterology 2010; 139:553–563,563.e1–e5.
- Nicholls L, Bragaw L, Ruetsch C. Opioid dependence treatment and guidelines. J Manag Care Pharm 2010; 16(1 suppl B):S14–S21.
- Lichtenstein GR, Hanauer SB, Sandborn WJ; Practice Parameters Committee of American College of Gastroenterology. Management of Crohn’s disease in adults. Am J Gastroenterol 2009; 104:465–483.
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med 1995; 332:1482–1490.
- American Gastroenterological Association Medical Position Statement: guidelines on intestinal ischemia. Gastroenterology 2000; 118:951–953.
- Savastano S, Teso S, Corrà S, Fantozzi O, Miotto D. Multislice CT angiography of the celiac and superior mesenteric arteries: comparison with arteriographic findings. Radiol Med 2002; 103:456–463.
- Simonetto DA, Oxentenko AS, Herman ML, Szostek JH. Cannabinoid hyperemesis: a case series of 98 patients. Mayo Clin Proc 2012; 87:114–119.
- Drossman DA, Morris CB, Edwards H, et al. Diagnosis, characterization, and 3-month outcome after detoxification of 39 patients with narcotic bowel syndrome. Am J Gastroenterol 2012; 107:1426–1440.
- Trescot AM, Boswell MV, Atluri SL, et al. Opioid guidelines in the management of chronic non-cancer pain. Pain Physician 2006; 9:1–39.
- Banks PA, Freeman ML; Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379–2400.
- Boles RG, Adams K, Ito M, Li BU. Maternal inheritance in cyclic vomiting syndrome with neuromuscular disease. Am J Med Genet A 2003; 120A:474–482.
- Wang Q, Ito M, Adams K, et al. Mitochondrial DNA control region sequence variation in migraine headache and cyclic vomiting syndrome. Am J Med Genet A 2004; 131:50–58.
- Taché Y. Cyclic vomiting syndrome: the corticotropinreleasing-factor hypothesis. Dig Dis Sci 1999; 44(suppl 8):79S–86S.
- Withers GD, Silburn SR, Forbes DA. Precipitants and aetiology of cyclic vomiting syndrome. Acta Paediatr 1998; 87:272–277.
- Whitney HB. Cyclic vomiting. A brief review of this affection as illustrated by a typical case. Arch Pediatr 1898; 15:839–845.
- Stickler GB. Relationship between cyclic vomiting syndrome and migraine. Clin Pediatr (Phila) 2005; 44:505–508.
- Li BU, Murray RD, Heitlinger LA, Robbins JL, Hayes JR. Is cyclic vomiting syndrome related to migraine? J Pediatr 1999; 134:567–572.
- Allen JH, de Moore GM, Heddle R, Twartz JC. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004; 53:1566–1570.
- Rome Foundation. Rome III disorders and diagnostic criteria. http://www.romecriteria.org/criteria/. Accessed February 27, 2013.
- Anderson KE, Bloomer JR, Bonkovsky HL, et al. Recommendations for the diagnosis and treatment of the acute porphyrias. Ann Intern Med 2005; 142:439–450.
- Camilleri M. Clinical practice. Diabetic gastroparesis. N Engl J Med 2007; 356:820–829.
- Maddern GJ, Horowitz M, Jamieson GG, Chatterton BE, Collins PJ, Roberts-Thomson P. Abnormalities of esophageal and gastric emptying in progressive systemic sclerosis. Gastroenterology 1984; 87:922–926.
- Jost WH. Gastrointestinal dysfunction in Parkinson’s disease. J Neurol Sci 2010; 289:69–73.
- Parkman HP, Hasler WL, Fisher RS; American Gastroenterological Association. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004; 127:1592–1622.
- Grunkemeier DM, Cassara JE, Dalton CB, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol Hepatol 2007; 5:1126–1139.
- Agostini S, Eutamene H, Cartier C, et al. Evidence of central and peripheral sensitization in a rat model of narcotic bowel-like syndrome. Gastroenterology 2010; 139:553–563,563.e1–e5.
- Nicholls L, Bragaw L, Ruetsch C. Opioid dependence treatment and guidelines. J Manag Care Pharm 2010; 16(1 suppl B):S14–S21.
- Lichtenstein GR, Hanauer SB, Sandborn WJ; Practice Parameters Committee of American College of Gastroenterology. Management of Crohn’s disease in adults. Am J Gastroenterol 2009; 104:465–483.
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med 1995; 332:1482–1490.
- American Gastroenterological Association Medical Position Statement: guidelines on intestinal ischemia. Gastroenterology 2000; 118:951–953.
- Savastano S, Teso S, Corrà S, Fantozzi O, Miotto D. Multislice CT angiography of the celiac and superior mesenteric arteries: comparison with arteriographic findings. Radiol Med 2002; 103:456–463.
- Simonetto DA, Oxentenko AS, Herman ML, Szostek JH. Cannabinoid hyperemesis: a case series of 98 patients. Mayo Clin Proc 2012; 87:114–119.
- Drossman DA, Morris CB, Edwards H, et al. Diagnosis, characterization, and 3-month outcome after detoxification of 39 patients with narcotic bowel syndrome. Am J Gastroenterol 2012; 107:1426–1440.
- Trescot AM, Boswell MV, Atluri SL, et al. Opioid guidelines in the management of chronic non-cancer pain. Pain Physician 2006; 9:1–39.
Postoperative pain: Meeting new expectations
One of the most common questions patients ask when they hear that they need surgery is, “How much pain will I have, and how will you manage it?”
Pain is a common human experience that provokes both fear and anxiety, which in some cases can last a lifetime. The medical community has been slow to meet the challenge of managing it. The US National Institutes of Health states that more than 80% of patients suffer postoperative pain, with fewer than 50% receiving adequate relief.1 Patients have spoken out loudly through the Hospital Consumer Assessment of Healthcare Providers and Systems scores, demonstrating that the issue of inadequate postoperative pain management is real.
Clearly, as the push to tie reimbursement to patient satisfaction grows, clinicians have both a moral and a financial imperative to address postoperative pain.
The management of acute postoperative pain is evolving, and recognition of acute pain has progressed from considering it an afterthought or nuisance to realizing that improperly or inadequately treated postoperative pain can have a number of adverse effects, including debilitating chronic pain syndromes.2 Inadequately treated pain is also contributing to the calamitous rise in addiction to illegal substances and prescription medications.3 The time has come to take responsibility and meet the expectations of our patients.
OPIOIDS HAVE MAJOR DRAWBACKS
Opioid derivatives are potent analgesics and have been the traditional first-line therapy for pain. “Judicious use of opium” for painful maladies has been a mainstay of Western medicine since the 16th century and was described in writings from Mesopotamia and China more than 2,000 years ago.
The ease of administration of these drugs coupled with their efficacy in managing a broad spectrum of pain syndromes has led to their frequent and widespread use, often, unfortunately, without consideration of the potential for negative short-term and long-term consequences. Headache, drowsiness, and pruritus are common adverse effects. Less common is a slowing of bowel motility, leading to constipation, bloating, or nausea. Additionally, in 5% to 10% of patients, narcotics may actually sensitize the nerves and make bowel-related pain worse. This narcotic bowel syndrome, as discussed by Agito and Rizk in this issue of the Journal, may make the patient uncomfortable and may lead to delays in recovery and hospital discharge.4
Opioid-related respiratory depression is especially devastating in the postoperative period, potentially causing respiratory arrest and death. The frequency of drug-induced respiratory depression and clinically significant adverse outcomes prompted the Anesthesia Patient Safety Foundation (APSF) to declare in 2011, “No patient shall be harmed by opioid-induced respiratory depression.”5 The APSF has recommended using new monitoring technology to enhance detection.
While many clinicians have been moving towards aggressive pain-management practice, hospital infrastructure has not kept pace. It is often ill-equipped to adequately monitor breathing patterns and to alert personnel to the need for rapid intervention. In the 21st century, we need to respond to this challenge with a combination of tools and technology, including improved clinical assessment and monitoring equipment that has proven to save lives in the perioperative setting.
A MULTIMODAL APPROACH IS BEST
Pain management professionals have also been moving from a predominantly opioid-based regimen to a more balanced, multimodal approach. The goal is to effectively treat acute postoperative pain while reducing the use of opioids and increasing the use of nonopioid drugs and alternative therapies for both pain management and convalescence.
Studies have shown the benefits of nonopioid drugs such as nonsteroidal anti-inflammatory drugs, paracetamol (intravenous acetaminophen), antidepressants, antiepileptics, and regional or local anesthetics combined with nontraditional treatments such as Reiki, massage therapy, and deep breathing.6
Each patient’s experience of pain is unique and responds to medications and alternative therapies in a distinctly different manner. We should not assume that one intervention is suitable for every patient. It is more beneficial to individualize treatment based on protocols that target different pain pathways. This may lead to better pain management and patient satisfaction while reducing the incidence of drug overdose and unwanted side effects.
WHAT WE NEED TO DO
Although many health care professionals have the authority to prescribe potent anesthetics and analgesics, we believe that there is a lack of adequate education, supervision, and experience, and this exposes patients to risks of prescription drug overdose.7,8 All medical professionals who provide postoperative care need specific education and training to offer the best care to this vulnerable patient population. This includes specific and more extensive training in the appropriate use of controlled medications before receiving their controlled substance registration from the Drug Enforcement Agency. We must also extend education to patients and family members regarding the dangers of drug abuse and the safe use of prescription drugs.8
Finally, we need to engage and communicate more effectively with our patients, especially when they are in acute pain. How long should a patient expect to remain in pain while waiting for an assessment and intervention? The medical community must commit to rapid and consistent coverage throughout the day for all patients experiencing a new or changing pattern of pain not responding to current therapy. Problems do not end at 5 pm or at a shift change. We need to build a process of timely intervention, perhaps by using a model similar to that of the rapid response and resuscitation team, which has been effective in many institutions. When a patient is in pain, minutes spent waiting for relief seem like an eternity. The empathy we show patients by validating, not minimizing, their pain and by following a defined yet tailored therapeutic intervention may not only improve their physical discomfort, but improve their overall patient experience.
Margo McCaffery, RN, a pioneer in pain management nursing, defined pain as “whatever the experiencing person says it is, existing whenever the experiencing person says it does.”9 We have come a long way from the days when attending staff in the post-anesthesia care unit would routinely declare, “Pain never killed anyone.” As caregivers, we need to become engaged, empathetic, and effective as we meet the challenges of managing acute postoperative pain and improving our patients’ experience and outcomes.
- Relieving Pain in America. Institute of Medicine 2011. National Academies Press (US). 2011 ISBN-13: 978-0-309-21484-1.
- Lamacraft G. The link between acute postoperative pain and chronic pain syndromes. South Afr J Anaesth Analg 2012; 18:45–50.
- Binyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician 2008; 11:S105–S120.
- Grunkemeier DMS, Cassara JE, Dalton CB, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol Hepatol 2007; 5:1126–1139.
- Anesthesia Patient Safety Foundation. Proceedings of “Essential Monitoring Strategies to Detect Clinically Significant Drug-Induced Respiratory Depression in the Postoperative Period” Conference, 2011. http://www.apsf.org/newsletters/pdf/fall_2011.pdf. Accessed May 13, 2013.
- So PS, Jiang JY, Qin Y. Touch therapies for pain relief in adults. Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD006535. DOI: 10.1002/14651858.CD006535.pub2.
- Polydorou S, Gunderson EW, Levin FR. Training physicians to treat substance use disorders. Curr Psychiatry Rep 2008; 10:399–404.
- CDC Grand Rounds. Prescription Drug Overdoses – a U.S Epidemic MMWR January 13, 2012/61(01);10–13.
- McCaffery M, Pasero C. Pain: Clinical Manual. 2nd ed. St. Louis: Mosby, 1999.
One of the most common questions patients ask when they hear that they need surgery is, “How much pain will I have, and how will you manage it?”
Pain is a common human experience that provokes both fear and anxiety, which in some cases can last a lifetime. The medical community has been slow to meet the challenge of managing it. The US National Institutes of Health states that more than 80% of patients suffer postoperative pain, with fewer than 50% receiving adequate relief.1 Patients have spoken out loudly through the Hospital Consumer Assessment of Healthcare Providers and Systems scores, demonstrating that the issue of inadequate postoperative pain management is real.
Clearly, as the push to tie reimbursement to patient satisfaction grows, clinicians have both a moral and a financial imperative to address postoperative pain.
The management of acute postoperative pain is evolving, and recognition of acute pain has progressed from considering it an afterthought or nuisance to realizing that improperly or inadequately treated postoperative pain can have a number of adverse effects, including debilitating chronic pain syndromes.2 Inadequately treated pain is also contributing to the calamitous rise in addiction to illegal substances and prescription medications.3 The time has come to take responsibility and meet the expectations of our patients.
OPIOIDS HAVE MAJOR DRAWBACKS
Opioid derivatives are potent analgesics and have been the traditional first-line therapy for pain. “Judicious use of opium” for painful maladies has been a mainstay of Western medicine since the 16th century and was described in writings from Mesopotamia and China more than 2,000 years ago.
The ease of administration of these drugs coupled with their efficacy in managing a broad spectrum of pain syndromes has led to their frequent and widespread use, often, unfortunately, without consideration of the potential for negative short-term and long-term consequences. Headache, drowsiness, and pruritus are common adverse effects. Less common is a slowing of bowel motility, leading to constipation, bloating, or nausea. Additionally, in 5% to 10% of patients, narcotics may actually sensitize the nerves and make bowel-related pain worse. This narcotic bowel syndrome, as discussed by Agito and Rizk in this issue of the Journal, may make the patient uncomfortable and may lead to delays in recovery and hospital discharge.4
Opioid-related respiratory depression is especially devastating in the postoperative period, potentially causing respiratory arrest and death. The frequency of drug-induced respiratory depression and clinically significant adverse outcomes prompted the Anesthesia Patient Safety Foundation (APSF) to declare in 2011, “No patient shall be harmed by opioid-induced respiratory depression.”5 The APSF has recommended using new monitoring technology to enhance detection.
While many clinicians have been moving towards aggressive pain-management practice, hospital infrastructure has not kept pace. It is often ill-equipped to adequately monitor breathing patterns and to alert personnel to the need for rapid intervention. In the 21st century, we need to respond to this challenge with a combination of tools and technology, including improved clinical assessment and monitoring equipment that has proven to save lives in the perioperative setting.
A MULTIMODAL APPROACH IS BEST
Pain management professionals have also been moving from a predominantly opioid-based regimen to a more balanced, multimodal approach. The goal is to effectively treat acute postoperative pain while reducing the use of opioids and increasing the use of nonopioid drugs and alternative therapies for both pain management and convalescence.
Studies have shown the benefits of nonopioid drugs such as nonsteroidal anti-inflammatory drugs, paracetamol (intravenous acetaminophen), antidepressants, antiepileptics, and regional or local anesthetics combined with nontraditional treatments such as Reiki, massage therapy, and deep breathing.6
Each patient’s experience of pain is unique and responds to medications and alternative therapies in a distinctly different manner. We should not assume that one intervention is suitable for every patient. It is more beneficial to individualize treatment based on protocols that target different pain pathways. This may lead to better pain management and patient satisfaction while reducing the incidence of drug overdose and unwanted side effects.
WHAT WE NEED TO DO
Although many health care professionals have the authority to prescribe potent anesthetics and analgesics, we believe that there is a lack of adequate education, supervision, and experience, and this exposes patients to risks of prescription drug overdose.7,8 All medical professionals who provide postoperative care need specific education and training to offer the best care to this vulnerable patient population. This includes specific and more extensive training in the appropriate use of controlled medications before receiving their controlled substance registration from the Drug Enforcement Agency. We must also extend education to patients and family members regarding the dangers of drug abuse and the safe use of prescription drugs.8
Finally, we need to engage and communicate more effectively with our patients, especially when they are in acute pain. How long should a patient expect to remain in pain while waiting for an assessment and intervention? The medical community must commit to rapid and consistent coverage throughout the day for all patients experiencing a new or changing pattern of pain not responding to current therapy. Problems do not end at 5 pm or at a shift change. We need to build a process of timely intervention, perhaps by using a model similar to that of the rapid response and resuscitation team, which has been effective in many institutions. When a patient is in pain, minutes spent waiting for relief seem like an eternity. The empathy we show patients by validating, not minimizing, their pain and by following a defined yet tailored therapeutic intervention may not only improve their physical discomfort, but improve their overall patient experience.
Margo McCaffery, RN, a pioneer in pain management nursing, defined pain as “whatever the experiencing person says it is, existing whenever the experiencing person says it does.”9 We have come a long way from the days when attending staff in the post-anesthesia care unit would routinely declare, “Pain never killed anyone.” As caregivers, we need to become engaged, empathetic, and effective as we meet the challenges of managing acute postoperative pain and improving our patients’ experience and outcomes.
One of the most common questions patients ask when they hear that they need surgery is, “How much pain will I have, and how will you manage it?”
Pain is a common human experience that provokes both fear and anxiety, which in some cases can last a lifetime. The medical community has been slow to meet the challenge of managing it. The US National Institutes of Health states that more than 80% of patients suffer postoperative pain, with fewer than 50% receiving adequate relief.1 Patients have spoken out loudly through the Hospital Consumer Assessment of Healthcare Providers and Systems scores, demonstrating that the issue of inadequate postoperative pain management is real.
Clearly, as the push to tie reimbursement to patient satisfaction grows, clinicians have both a moral and a financial imperative to address postoperative pain.
The management of acute postoperative pain is evolving, and recognition of acute pain has progressed from considering it an afterthought or nuisance to realizing that improperly or inadequately treated postoperative pain can have a number of adverse effects, including debilitating chronic pain syndromes.2 Inadequately treated pain is also contributing to the calamitous rise in addiction to illegal substances and prescription medications.3 The time has come to take responsibility and meet the expectations of our patients.
OPIOIDS HAVE MAJOR DRAWBACKS
Opioid derivatives are potent analgesics and have been the traditional first-line therapy for pain. “Judicious use of opium” for painful maladies has been a mainstay of Western medicine since the 16th century and was described in writings from Mesopotamia and China more than 2,000 years ago.
The ease of administration of these drugs coupled with their efficacy in managing a broad spectrum of pain syndromes has led to their frequent and widespread use, often, unfortunately, without consideration of the potential for negative short-term and long-term consequences. Headache, drowsiness, and pruritus are common adverse effects. Less common is a slowing of bowel motility, leading to constipation, bloating, or nausea. Additionally, in 5% to 10% of patients, narcotics may actually sensitize the nerves and make bowel-related pain worse. This narcotic bowel syndrome, as discussed by Agito and Rizk in this issue of the Journal, may make the patient uncomfortable and may lead to delays in recovery and hospital discharge.4
Opioid-related respiratory depression is especially devastating in the postoperative period, potentially causing respiratory arrest and death. The frequency of drug-induced respiratory depression and clinically significant adverse outcomes prompted the Anesthesia Patient Safety Foundation (APSF) to declare in 2011, “No patient shall be harmed by opioid-induced respiratory depression.”5 The APSF has recommended using new monitoring technology to enhance detection.
While many clinicians have been moving towards aggressive pain-management practice, hospital infrastructure has not kept pace. It is often ill-equipped to adequately monitor breathing patterns and to alert personnel to the need for rapid intervention. In the 21st century, we need to respond to this challenge with a combination of tools and technology, including improved clinical assessment and monitoring equipment that has proven to save lives in the perioperative setting.
A MULTIMODAL APPROACH IS BEST
Pain management professionals have also been moving from a predominantly opioid-based regimen to a more balanced, multimodal approach. The goal is to effectively treat acute postoperative pain while reducing the use of opioids and increasing the use of nonopioid drugs and alternative therapies for both pain management and convalescence.
Studies have shown the benefits of nonopioid drugs such as nonsteroidal anti-inflammatory drugs, paracetamol (intravenous acetaminophen), antidepressants, antiepileptics, and regional or local anesthetics combined with nontraditional treatments such as Reiki, massage therapy, and deep breathing.6
Each patient’s experience of pain is unique and responds to medications and alternative therapies in a distinctly different manner. We should not assume that one intervention is suitable for every patient. It is more beneficial to individualize treatment based on protocols that target different pain pathways. This may lead to better pain management and patient satisfaction while reducing the incidence of drug overdose and unwanted side effects.
WHAT WE NEED TO DO
Although many health care professionals have the authority to prescribe potent anesthetics and analgesics, we believe that there is a lack of adequate education, supervision, and experience, and this exposes patients to risks of prescription drug overdose.7,8 All medical professionals who provide postoperative care need specific education and training to offer the best care to this vulnerable patient population. This includes specific and more extensive training in the appropriate use of controlled medications before receiving their controlled substance registration from the Drug Enforcement Agency. We must also extend education to patients and family members regarding the dangers of drug abuse and the safe use of prescription drugs.8
Finally, we need to engage and communicate more effectively with our patients, especially when they are in acute pain. How long should a patient expect to remain in pain while waiting for an assessment and intervention? The medical community must commit to rapid and consistent coverage throughout the day for all patients experiencing a new or changing pattern of pain not responding to current therapy. Problems do not end at 5 pm or at a shift change. We need to build a process of timely intervention, perhaps by using a model similar to that of the rapid response and resuscitation team, which has been effective in many institutions. When a patient is in pain, minutes spent waiting for relief seem like an eternity. The empathy we show patients by validating, not minimizing, their pain and by following a defined yet tailored therapeutic intervention may not only improve their physical discomfort, but improve their overall patient experience.
Margo McCaffery, RN, a pioneer in pain management nursing, defined pain as “whatever the experiencing person says it is, existing whenever the experiencing person says it does.”9 We have come a long way from the days when attending staff in the post-anesthesia care unit would routinely declare, “Pain never killed anyone.” As caregivers, we need to become engaged, empathetic, and effective as we meet the challenges of managing acute postoperative pain and improving our patients’ experience and outcomes.
- Relieving Pain in America. Institute of Medicine 2011. National Academies Press (US). 2011 ISBN-13: 978-0-309-21484-1.
- Lamacraft G. The link between acute postoperative pain and chronic pain syndromes. South Afr J Anaesth Analg 2012; 18:45–50.
- Binyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician 2008; 11:S105–S120.
- Grunkemeier DMS, Cassara JE, Dalton CB, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol Hepatol 2007; 5:1126–1139.
- Anesthesia Patient Safety Foundation. Proceedings of “Essential Monitoring Strategies to Detect Clinically Significant Drug-Induced Respiratory Depression in the Postoperative Period” Conference, 2011. http://www.apsf.org/newsletters/pdf/fall_2011.pdf. Accessed May 13, 2013.
- So PS, Jiang JY, Qin Y. Touch therapies for pain relief in adults. Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD006535. DOI: 10.1002/14651858.CD006535.pub2.
- Polydorou S, Gunderson EW, Levin FR. Training physicians to treat substance use disorders. Curr Psychiatry Rep 2008; 10:399–404.
- CDC Grand Rounds. Prescription Drug Overdoses – a U.S Epidemic MMWR January 13, 2012/61(01);10–13.
- McCaffery M, Pasero C. Pain: Clinical Manual. 2nd ed. St. Louis: Mosby, 1999.
- Relieving Pain in America. Institute of Medicine 2011. National Academies Press (US). 2011 ISBN-13: 978-0-309-21484-1.
- Lamacraft G. The link between acute postoperative pain and chronic pain syndromes. South Afr J Anaesth Analg 2012; 18:45–50.
- Binyamin R, Trescot AM, Datta S, et al. Opioid complications and side effects. Pain Physician 2008; 11:S105–S120.
- Grunkemeier DMS, Cassara JE, Dalton CB, Drossman DA. The narcotic bowel syndrome: clinical features, pathophysiology, and management. Clin Gastroenterol Hepatol 2007; 5:1126–1139.
- Anesthesia Patient Safety Foundation. Proceedings of “Essential Monitoring Strategies to Detect Clinically Significant Drug-Induced Respiratory Depression in the Postoperative Period” Conference, 2011. http://www.apsf.org/newsletters/pdf/fall_2011.pdf. Accessed May 13, 2013.
- So PS, Jiang JY, Qin Y. Touch therapies for pain relief in adults. Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD006535. DOI: 10.1002/14651858.CD006535.pub2.
- Polydorou S, Gunderson EW, Levin FR. Training physicians to treat substance use disorders. Curr Psychiatry Rep 2008; 10:399–404.
- CDC Grand Rounds. Prescription Drug Overdoses – a U.S Epidemic MMWR January 13, 2012/61(01);10–13.
- McCaffery M, Pasero C. Pain: Clinical Manual. 2nd ed. St. Louis: Mosby, 1999.
Correction: Aspirin
A typographical error appeared in Figure 1 of: Park K, Bavry AA. Aspirin: its risks, benefits, and optimal use in preventing cardiovascular events (Cleve Clin J Med 2013; 80:318–326). The lower left side of the figure, discussing the use of aspirin for primary prevention in men, should read as follows:
Assess risk of myocardial infarction (http://hp2010.nhlbihin.net/atpiii/calculator.asp); give aspirin if:
- Age 45–59 and 10-year risk ≥ 4%
- Age 60–69 and 10-year risk ≥ 9%
- Age 70–79 and 10-year risk ≥ 12%
A typographical error appeared in Figure 1 of: Park K, Bavry AA. Aspirin: its risks, benefits, and optimal use in preventing cardiovascular events (Cleve Clin J Med 2013; 80:318–326). The lower left side of the figure, discussing the use of aspirin for primary prevention in men, should read as follows:
Assess risk of myocardial infarction (http://hp2010.nhlbihin.net/atpiii/calculator.asp); give aspirin if:
- Age 45–59 and 10-year risk ≥ 4%
- Age 60–69 and 10-year risk ≥ 9%
- Age 70–79 and 10-year risk ≥ 12%
A typographical error appeared in Figure 1 of: Park K, Bavry AA. Aspirin: its risks, benefits, and optimal use in preventing cardiovascular events (Cleve Clin J Med 2013; 80:318–326). The lower left side of the figure, discussing the use of aspirin for primary prevention in men, should read as follows:
Assess risk of myocardial infarction (http://hp2010.nhlbihin.net/atpiii/calculator.asp); give aspirin if:
- Age 45–59 and 10-year risk ≥ 4%
- Age 60–69 and 10-year risk ≥ 9%
- Age 70–79 and 10-year risk ≥ 12%
How to interpret surveys in medical research: A practical approach
Surveys are common in medical research. Although survey research may be subject to inherent self-report bias, surveys have a great impact on policies and practices in medicine, often forming the basis for recommendations or new guidelines.1,2 To interpret and use survey research results, clinicians should be familiar with key elements involved in the creation and validation of surveys.
The purpose of this article is to provide readers with a basic framework for evaluating surveys to allow them to be more informed as consumers of survey research.
IMPORTANT TOOLS IN MEDICAL RESEARCH
Surveys are important tools for answering questions on topics that are difficult to assess using other methods.3 They allow us to gather data systematically from subjects by asking questions, in order to make inferences about a larger population.3,4 Clinicians use surveys to explore the opinions, beliefs, and perceptions of a group, or to investigate physician practice patterns and adherence to clinical guidelines. They may also use surveys to better understand why patients are not engaging in recommended behavioral or lifestyle changes.
Survey methods include interviews (in person, by phone) and questionnaires (paper-and-pencil, e-mailed, online).4
A well-constructed, validated survey can provide powerful data that may influence clinical practice, guide future research development, or drive the development and provision of needed programs and services. Surveys have the potential to transform the ways in which we think about and practice medicine.
READER BEWARE
While survey research in health care appears to have grown exponentially, the quality of reported survey research has not necessarily increased over time.
For consumers of survey research, the adage “reader beware” is apt. Although a considerable number of studies have examined the effects of survey methodology on the validity, reliability, and generalizability of the results,4 medical journals differ in their requirements for reporting survey methods.
In an analysis of 117 articles, Bennett et al3 found that more than 80% did not fully describe the survey development process or pretesting methods. They also found limited guidance and lack of consensus about the best way to report survey research. Of 95 surveys requiring scoring, 66% did not report scoring practices.
Duffett et al5 noted that of 127 critical care medicine surveys, only 36% had been pretested or pilot-tested, and half of all surveys reviewed did not include participant demographics or included only minimal information.
Because journal reporting practices differ, physicians may be unaware of the steps involved in survey construction and validation. Knowledge of these steps is helpful not only in constructing surveys but also in assessing published articles that used survey research.
LIMITATIONS OF SURVEY RESEARCH
Indirect measures of attitudes and behaviors
Surveys that rely on participants’ self-reports of behaviors, attitudes, beliefs, or actions are indirect measures and are susceptible to self-report and social-desirability biases. Participants may overestimate their own expertise or knowledge in self-report surveys. They may wish to reduce embarrassment6 or answer in ways that would make them “look better,”7 resulting in social-desirability bias. These issues need to be mentioned in the limitations section in papers reporting survey research.
Questions and response choices
The data derived from surveys are only as good as the questions that are asked.8 Stone9 noted that questions should be intelligible, unambiguous, and unbiased. If respondents do not comprehend questions as researchers intended, if questionnaire response choices are inadequate, or if questions trigger unintended emotional responses,10–14 researchers may unwittingly introduce error, which will affect the validity of results. Even seemingly objective questions, such as those related to clinical algorithm use, practice patterns, or equipment available to hospital staff, may be interpreted differently by different respondents.
In their eagerness to launch a survey, clinician researchers may not realize that it must be carefully constructed. A focus on question development and validation is critical, as the questions determine the quality of the data derived from the survey.8 Even the position of the question or answer in the survey can affect how participants respond,15 as they may be guided to a response choice by preceding questions.16
WHAT DO YOU NEED TO KNOW ABOUT ASSESSING SURVEY RESEARCH?
What follows are questions and a basic framework that can be used to evaluate published survey research. Recommendations are based on the work of survey scientists,4,7,10,14,15,17,18 survey researchers in medicine and the social sciences, and national standards for test and questionnaire construction and validation (Table 1).4,19,20
Who created the survey? How did they do it?
How the survey was created should be sufficiently described to allow readers to judge the adequacy of instrument development.3–5 It is generally recommended that feedback from multiple sources be solicited during survey creation. Both questionnaire-design experts and subject-matter experts are considered critical in the process.4
What question was the survey designed to answer?
Is the objective of the study articulated in the paper? 3,20 To judge survey research, readers need to know if the survey appears to adequately address the research question or questions and the objectives of the study in terms of methods used.4
Was evidence on validity gathered?
Instrument pretesting and field testing are considered best practices by the American Association for Public Opinion Research, a professional organization for US survey scientists.4
Pretesting can include cognitive interviewing, the use of questionnaire appraisal tools, and hybrid methods, all of which are aimed at addressing validity issues.21 Pretesting with a group of participants similar to the target population allows for assessment of item ambiguity, instrument ease of use, adequacy of response categories (response choices), and time to completion.4,12
Cognitive interviewing is designed to explore respondents’ comprehension of questions, response processes, and decision processes governing how they answer questions.4,7,10,11 In cognitive interviewing, respondents are generally interviewed one on one. Techniques vary, but typically include “think alouds” (in which a respondent is asked to verbalize thoughts while responding to questions) and “verbal probing” (in which the respondent answers a question, then is asked follow-up questions as the interviewer probes for information related to the response choice or question itself).7 These techniques can provide evidence that researchers are actually measuring what they set out to measure and not an unrelated construct.4,19
Field testing of a survey under realistic conditions can help to uncover problems in administration, such as issues in standardization of key procedures, and to ensure that the survey was administered as the researchers intended.21,22 Field testing is vital before phone or in-person interviews to ensure standardization of any critical procedures. Pilot testing in a sample similar to the intended population allows for further refinement, with deletion of problem items, before the survey is launched.15
Because even “objective” questions can be somewhat subjective, all research surveys should go through some type of pretesting.4,21 Based on the results of pretesting and field testing, surveys should then be revised before launch.4,21 If an article on a self-report survey makes no mention of survey validation steps, readers may well question the validity of the results.
Are the survey questions and response choices understandable?
Is the meaning of each question unambiguous? Is the reading level appropriate for the sample population (a critical consideration in patient surveys)? Do any of the items actually ask two different questions?13 An example would be: “Was the representative courteous and prompt?” as it is possible to be courteous, but not prompt, and vice versa. If so, respondents may be confused or frustrated in attempting to answer it. If a rating scale is used throughout the questionnaire, are the anchors appropriate? For example, a question may be written in such a way that respondents want to answer “yes/no” or “agree/disagree,” but the scale used may include response options such as “poor,” “marginal,” “good,” and “excellent.” Items with Likert-response formats are commonly used in self-report surveys and allow participants to respond to a statement by choosing from a range of responses (eg, strongly disagree to strongly agree), often spaced horizontally under a line.
It is recommended that surveys also include options for answers beyond the response choices provided,20 such as comment boxes or fill-in-the-blank items. Surveys with a closed-response format may constrain the quality of data collected because investigators may not foresee all possible answers. Surveys need to be available for review either within the article itself, in an appendix, or as supplementary material that is available elsewhere.
Does the sample appear to be appropriate?
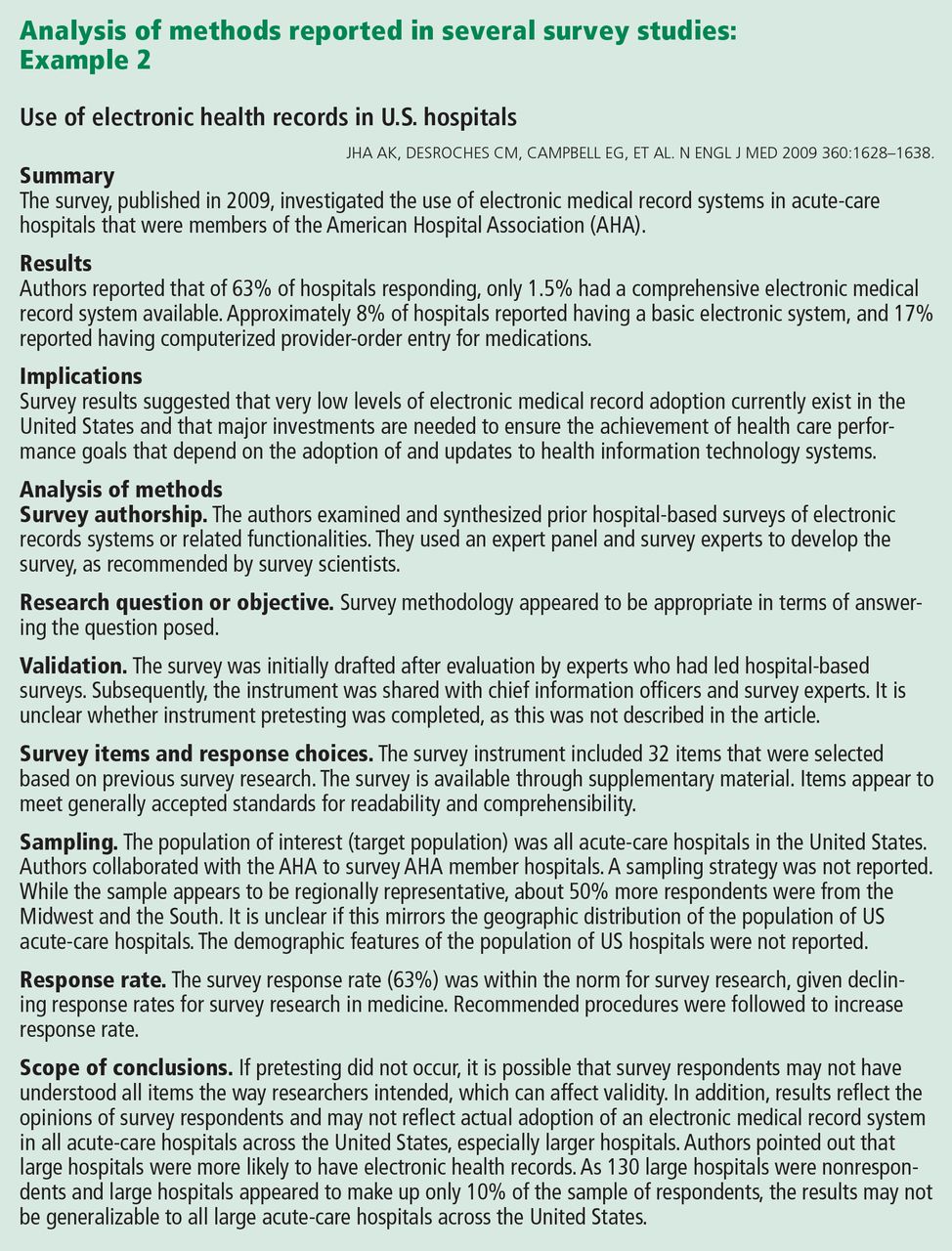
Articles that report the results of surveys should describe the target population, the sample design, and, in a demographic table, respondents and nonrespondents. To judge appropriateness, several questions can be asked regarding sampling:
Target population. Is the population of interest (ie, the target population) described, including regional demographics, if applicable? The relationship between the sample and the target population is important, as a nonrepresentative sample may result in misleading conclusions about the population of interest.
Sampling frame. Who had an opportunity to participate in the survey? At its simplest, the sampling frame establishes who (or what, in the case of institutions) should be included within the sample. This is typically a list of elements (Groves et al4) that acts to “frame” or define the sample to be selected. Where the target population may be all academic internal medicine physicians in the United States, the sampling frame may be all male and female US physicians who are members of particular internal medicine professional organizations, identified by their directory email addresses.
Sample design. How was the sample actually selected?4 For example, did investigators use a convenience sample of colleagues at other institutions or use a stratified random sample, ensuring adequate representation of respondents with certain characteristics?
Description of respondents. How is the sample of respondents described? Are demographic features reported, including statistics on regional or national representativeness?5 Does the sample of survey respondents appear to be representative of the researcher’s population of interest (ie, the target population)?3,23 If not, is this adequately described in the limitations section? Although outcomes will not be available on nonrespondents, demographic and baseline data often are available and should be reported. Are there systematic differences between respondents and nonrespondents?
Was the response rate adequate?
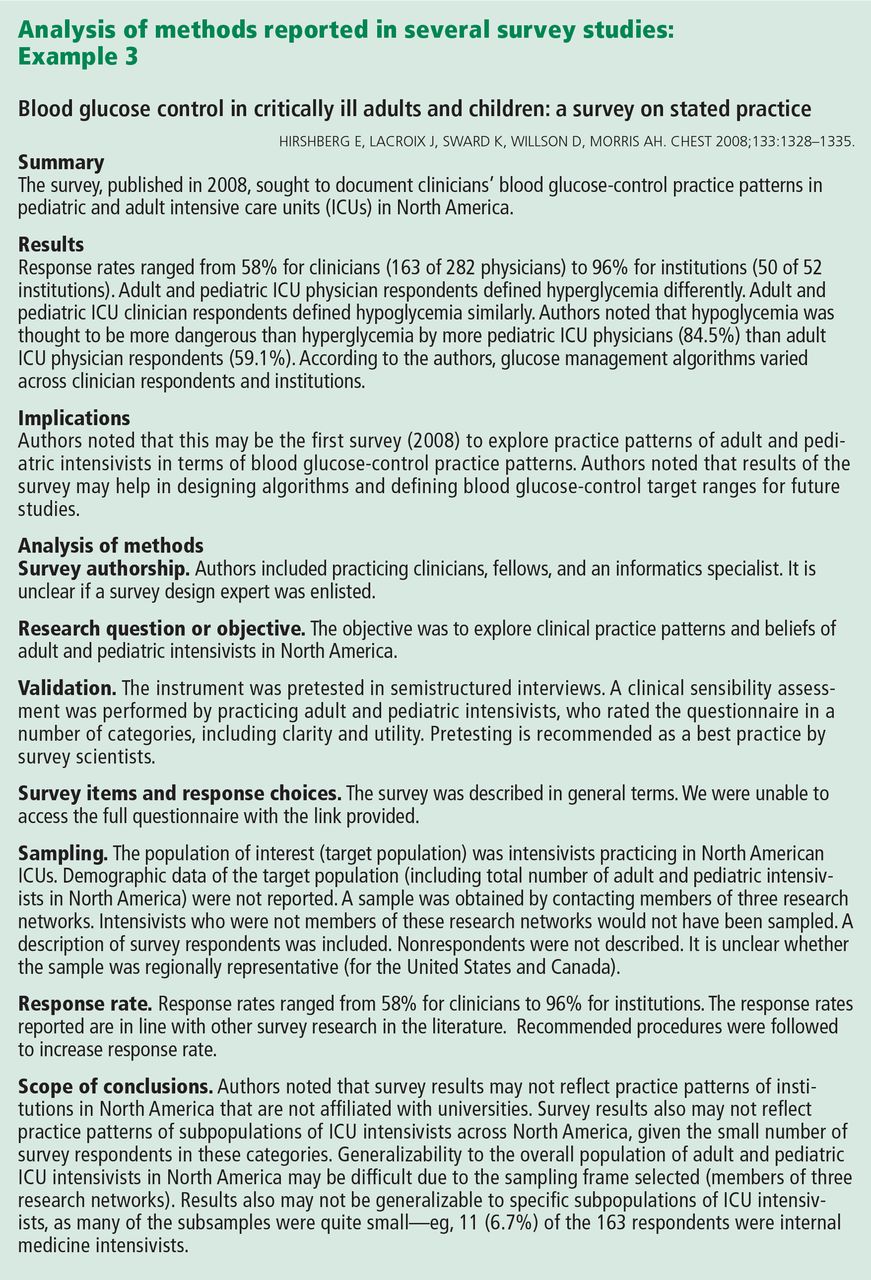
Was the response rate adequate, given the number of participants initially recruited? If the response rate was not adequate, did the researchers discuss this limitation?
Maximum response rate, defined as the total number of surveys returned divided by the total number of surveys sent,18 may be difficult to calculate with electronic or Web-based survey platforms. When the maximum response rate cannot be calculated, this issue needs to be addressed in the article’s limitations section.
The number of surveys has increased across fields over the past few decades, but survey response rates in general have decreased.17,21,24,25 In fields outside of clinical medicine, response rates in the 40% range are common.17 In the 1990s, the mean response rate for surveys published in medical journals (mailed surveys) was approximately 60%.26 A 2001 review of physician questionnaire studies found a similar average response rate (61%), with a 52% response rate for large-sample surveys.27 In 2002, Field et al28 examined the impact of incentives in physician survey studies and found response rates ranging from 8.5% to 80%.
Importantly, electronically delivered surveys (e-mail, Web-based) often have lower response rates than mailed surveys.24,29 Nominal financial incentives have been associated with enhanced response rates.28
A relatively low response rate does not necessarily mean you cannot trust the data. Survey scientists note that the representativeness of the sample may be more critical than response rate alone.17 Studies with small sample sizes may be more representative—and findings more valid—than those with large samples, if large samples are nonrepresentative when considering the target population.17
Do the conclusions go beyond the data?
Are the inferences overreaching, in view of the survey design? In studies with low response rates and nonrepresentative samples, researchers must be careful in interpreting the results. If the results cannot be generalized beyond the research sample, is this clear from the limitations, discussion, and conclusion sections?
In this review, we have summarized the findings of three published surveys1,2,30 and commented on how they appear to meet—or don’t quite meet—recommendations for survey development, validation, and use. The papers chosen were deemed strong examples in particular categories, such as description of survey authorship,1 instrument validation,30 sampling methodology,2 and response rate.1
It should be noted that even when surveys are conducted with the utmost rigor, survey reporting may leave out critical details. Survey methodology may not be adequately described for a variety of reasons, including researchers’ training in survey design and methodology; a lack of universally accepted journal-reporting guidelines3; and even journals’ space limitations. At times, journals may excise descriptions of survey development and validation, deeming these sections superfluous. Limitations sections can be critical to interpreting the results of survey research and evaluating the scope of conclusions.
- Jha AK, DesRoches CM, Campbell EG, et al. Use of electronic health records in US hospitals. N Engl J Med 2009; 360:1628–1638.
- Angus DC, Shorr AF, White A, Dremsizov TT, Schmitz RJ, Kelley MA; Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS). Critical care delivery in the United States: distribution of services and compliance with Leapfrog recommendations. Crit Care Med 2006; 34:1016–1024.
- Bennett C, Khangura S, Brehaut JC, et al. Reporting guidelines for survey research: an analysis of published guidance and reporting practices. PLoS Med 2010; 8:e1001069.
- Groves RM, Fowler FJ, Couper MP, Lepkowski JM, Singer E, Tourangeau R. Survey Methodology. 2nd ed. Hoboken, NJ: John Wiley and Sons, Inc; 2009.
- Duffett M, Burns KE, Adhikari NK, et al. Quality of reporting of surveys in critical care journals: a methodologic review. Crit Care Med 2012; 40:441–449.
- Mattell MS, Jacoby J. Is there an optimal number of alternatives for Likert-scale items? Effects of testing time and scale properties. J Appl Psychol 1972; 56:506–509.
- Willis GB. Cognitive Interviewing. A “How To” Guide. Research Triangle Institute. Presented at the meeting of the American Statistical Association; 1999. http://fog.its.uiowa.edu/~c07b209/interview.pdf. Accessed June 3, 2013.
- Schwarz N. Self-reports. How the questions shape the answers. Amer Psychol 1999; 54:93–105.
- Stone DH. Design a questionnaire. BMJ 1993; 307:1264–1266.
- Willis GB, Royston P, Bercini D. The use of verbal report methods in the development and testing of survey questionnaires. Appl Cogn Psychol 1991; 5:251–267.
- Desimone LM, LeFloch KC. Are we asking the right questions? Using cognitive interviews to improve surveys in education research. Educ Eval Policy Anal 2004; 26:1–22.
- Presser S, Couper MP, Lessler JT, et al. Methods for testing and evaluating survey questions. Public Opin Q 2004; 68:109–130.
- Rogers G. Accreditation Board for Engineering and Technology (ABET), Inc. Sample Protocol for Pilot Testing Survey Items. www.abet.org/WorkArea/DownloadAsset.aspx?id=1299. Accessed January 22, 2013.
- Schwarz N, Oyserman D. Asking questions about behavior: cognition, communication, and questionnaire construction. Am J Eval 2001; 22:127–160.
- Bradburn N, Sudman S, Wansink B. Asking Questions. The Definitive Guide to Questionnaire Design—For Market Research, Political Polls, and Social and Health Questionnaires. San Francisco, CA: Jossey-Bass; 2004.
- Stone AA, Broderick JE, Schwartz JE, Schwarz N. Context effects in survey ratings of health, symptoms, and satisfaction. Med Care 2008; 46:662–667.
- Cook C, Heath F, Thompson RL. A meta-analysis of response rates in Web or internet-based surveys. Educ Psychol Meas 2000; 60:821–836.
- Kaplowitz MD, Hadlock TD, Levine R. A comparison of Web and mail survey response rates. Public Opin Q 2004; 68:94–101.
- American Educational Research Association. Standards for Educational and Psychological Testing/American Educational Research Association, American Psychological Association, National Council on Measurement in Education. Washington, DC: American Educational Research Association; 1999.
- Burns KE, Duffett M, Kho ME, et al; ACCADEMY Group. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ 2008; 179:245–252.
- American Association for Public Opinion Research (AAPOR). http://www.aapor.org/Home.htm. Accessed June 3, 2013.
- National Center for Education Statistics. Planning and Design of Surveys. http://nces.ed.gov/statprog/2002/std2_1.asp. Accessed January 22, 2013.
- Bordens KS, Abbott BB. Research Design and Methods. A Process Approach. 6th ed. New York, NY: McGraw-Hill; 2004.
- Sheehan K. Email survey response rates: a review. JCMC 2001. http://jcmc.indiana.edu/vol6/issue2/sheehan.html. Accessed January 22, 2013.
- Baruch Y, Holtom BC. Survey response rate levels and trends in organizational research. Hum Relat 2008; 61:1139–1160.
- Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol 1997; 50:1129–1136.
- Cummings SM, Savitz LA, Konrad TR. Reported response rates to mailed physician questionnaires. Health Services Res 2001; 35:1347–1355.
- Field TS, Cadoret CA, Brown ML, et al. Surveying physicians. Do components of the “Total Design Approach” to optimizing survey response rates apply to physicians? Med Care 2002; 40:596–606.
- Converse PD, Wolfe EW, Huang X, Oswald FL. Response rates for mixed-mode surveys using mail and e-mail/Web. Am J Eval 2008; 29:99–107.
- Hirshberg E, Lacroix J, Sward K, Willson D, Morris AH. Blood glucose control in critically ill adults and children: a survey on stated practice. Chest 2008; 133:1328–1335.
Surveys are common in medical research. Although survey research may be subject to inherent self-report bias, surveys have a great impact on policies and practices in medicine, often forming the basis for recommendations or new guidelines.1,2 To interpret and use survey research results, clinicians should be familiar with key elements involved in the creation and validation of surveys.
The purpose of this article is to provide readers with a basic framework for evaluating surveys to allow them to be more informed as consumers of survey research.
IMPORTANT TOOLS IN MEDICAL RESEARCH
Surveys are important tools for answering questions on topics that are difficult to assess using other methods.3 They allow us to gather data systematically from subjects by asking questions, in order to make inferences about a larger population.3,4 Clinicians use surveys to explore the opinions, beliefs, and perceptions of a group, or to investigate physician practice patterns and adherence to clinical guidelines. They may also use surveys to better understand why patients are not engaging in recommended behavioral or lifestyle changes.
Survey methods include interviews (in person, by phone) and questionnaires (paper-and-pencil, e-mailed, online).4
A well-constructed, validated survey can provide powerful data that may influence clinical practice, guide future research development, or drive the development and provision of needed programs and services. Surveys have the potential to transform the ways in which we think about and practice medicine.
READER BEWARE
While survey research in health care appears to have grown exponentially, the quality of reported survey research has not necessarily increased over time.
For consumers of survey research, the adage “reader beware” is apt. Although a considerable number of studies have examined the effects of survey methodology on the validity, reliability, and generalizability of the results,4 medical journals differ in their requirements for reporting survey methods.
In an analysis of 117 articles, Bennett et al3 found that more than 80% did not fully describe the survey development process or pretesting methods. They also found limited guidance and lack of consensus about the best way to report survey research. Of 95 surveys requiring scoring, 66% did not report scoring practices.
Duffett et al5 noted that of 127 critical care medicine surveys, only 36% had been pretested or pilot-tested, and half of all surveys reviewed did not include participant demographics or included only minimal information.
Because journal reporting practices differ, physicians may be unaware of the steps involved in survey construction and validation. Knowledge of these steps is helpful not only in constructing surveys but also in assessing published articles that used survey research.
LIMITATIONS OF SURVEY RESEARCH
Indirect measures of attitudes and behaviors
Surveys that rely on participants’ self-reports of behaviors, attitudes, beliefs, or actions are indirect measures and are susceptible to self-report and social-desirability biases. Participants may overestimate their own expertise or knowledge in self-report surveys. They may wish to reduce embarrassment6 or answer in ways that would make them “look better,”7 resulting in social-desirability bias. These issues need to be mentioned in the limitations section in papers reporting survey research.
Questions and response choices
The data derived from surveys are only as good as the questions that are asked.8 Stone9 noted that questions should be intelligible, unambiguous, and unbiased. If respondents do not comprehend questions as researchers intended, if questionnaire response choices are inadequate, or if questions trigger unintended emotional responses,10–14 researchers may unwittingly introduce error, which will affect the validity of results. Even seemingly objective questions, such as those related to clinical algorithm use, practice patterns, or equipment available to hospital staff, may be interpreted differently by different respondents.
In their eagerness to launch a survey, clinician researchers may not realize that it must be carefully constructed. A focus on question development and validation is critical, as the questions determine the quality of the data derived from the survey.8 Even the position of the question or answer in the survey can affect how participants respond,15 as they may be guided to a response choice by preceding questions.16
WHAT DO YOU NEED TO KNOW ABOUT ASSESSING SURVEY RESEARCH?
What follows are questions and a basic framework that can be used to evaluate published survey research. Recommendations are based on the work of survey scientists,4,7,10,14,15,17,18 survey researchers in medicine and the social sciences, and national standards for test and questionnaire construction and validation (Table 1).4,19,20
Who created the survey? How did they do it?
How the survey was created should be sufficiently described to allow readers to judge the adequacy of instrument development.3–5 It is generally recommended that feedback from multiple sources be solicited during survey creation. Both questionnaire-design experts and subject-matter experts are considered critical in the process.4
What question was the survey designed to answer?
Is the objective of the study articulated in the paper? 3,20 To judge survey research, readers need to know if the survey appears to adequately address the research question or questions and the objectives of the study in terms of methods used.4
Was evidence on validity gathered?
Instrument pretesting and field testing are considered best practices by the American Association for Public Opinion Research, a professional organization for US survey scientists.4
Pretesting can include cognitive interviewing, the use of questionnaire appraisal tools, and hybrid methods, all of which are aimed at addressing validity issues.21 Pretesting with a group of participants similar to the target population allows for assessment of item ambiguity, instrument ease of use, adequacy of response categories (response choices), and time to completion.4,12
Cognitive interviewing is designed to explore respondents’ comprehension of questions, response processes, and decision processes governing how they answer questions.4,7,10,11 In cognitive interviewing, respondents are generally interviewed one on one. Techniques vary, but typically include “think alouds” (in which a respondent is asked to verbalize thoughts while responding to questions) and “verbal probing” (in which the respondent answers a question, then is asked follow-up questions as the interviewer probes for information related to the response choice or question itself).7 These techniques can provide evidence that researchers are actually measuring what they set out to measure and not an unrelated construct.4,19
Field testing of a survey under realistic conditions can help to uncover problems in administration, such as issues in standardization of key procedures, and to ensure that the survey was administered as the researchers intended.21,22 Field testing is vital before phone or in-person interviews to ensure standardization of any critical procedures. Pilot testing in a sample similar to the intended population allows for further refinement, with deletion of problem items, before the survey is launched.15
Because even “objective” questions can be somewhat subjective, all research surveys should go through some type of pretesting.4,21 Based on the results of pretesting and field testing, surveys should then be revised before launch.4,21 If an article on a self-report survey makes no mention of survey validation steps, readers may well question the validity of the results.
Are the survey questions and response choices understandable?
Is the meaning of each question unambiguous? Is the reading level appropriate for the sample population (a critical consideration in patient surveys)? Do any of the items actually ask two different questions?13 An example would be: “Was the representative courteous and prompt?” as it is possible to be courteous, but not prompt, and vice versa. If so, respondents may be confused or frustrated in attempting to answer it. If a rating scale is used throughout the questionnaire, are the anchors appropriate? For example, a question may be written in such a way that respondents want to answer “yes/no” or “agree/disagree,” but the scale used may include response options such as “poor,” “marginal,” “good,” and “excellent.” Items with Likert-response formats are commonly used in self-report surveys and allow participants to respond to a statement by choosing from a range of responses (eg, strongly disagree to strongly agree), often spaced horizontally under a line.
It is recommended that surveys also include options for answers beyond the response choices provided,20 such as comment boxes or fill-in-the-blank items. Surveys with a closed-response format may constrain the quality of data collected because investigators may not foresee all possible answers. Surveys need to be available for review either within the article itself, in an appendix, or as supplementary material that is available elsewhere.
Does the sample appear to be appropriate?
Articles that report the results of surveys should describe the target population, the sample design, and, in a demographic table, respondents and nonrespondents. To judge appropriateness, several questions can be asked regarding sampling:
Target population. Is the population of interest (ie, the target population) described, including regional demographics, if applicable? The relationship between the sample and the target population is important, as a nonrepresentative sample may result in misleading conclusions about the population of interest.
Sampling frame. Who had an opportunity to participate in the survey? At its simplest, the sampling frame establishes who (or what, in the case of institutions) should be included within the sample. This is typically a list of elements (Groves et al4) that acts to “frame” or define the sample to be selected. Where the target population may be all academic internal medicine physicians in the United States, the sampling frame may be all male and female US physicians who are members of particular internal medicine professional organizations, identified by their directory email addresses.
Sample design. How was the sample actually selected?4 For example, did investigators use a convenience sample of colleagues at other institutions or use a stratified random sample, ensuring adequate representation of respondents with certain characteristics?
Description of respondents. How is the sample of respondents described? Are demographic features reported, including statistics on regional or national representativeness?5 Does the sample of survey respondents appear to be representative of the researcher’s population of interest (ie, the target population)?3,23 If not, is this adequately described in the limitations section? Although outcomes will not be available on nonrespondents, demographic and baseline data often are available and should be reported. Are there systematic differences between respondents and nonrespondents?
Was the response rate adequate?
Was the response rate adequate, given the number of participants initially recruited? If the response rate was not adequate, did the researchers discuss this limitation?
Maximum response rate, defined as the total number of surveys returned divided by the total number of surveys sent,18 may be difficult to calculate with electronic or Web-based survey platforms. When the maximum response rate cannot be calculated, this issue needs to be addressed in the article’s limitations section.
The number of surveys has increased across fields over the past few decades, but survey response rates in general have decreased.17,21,24,25 In fields outside of clinical medicine, response rates in the 40% range are common.17 In the 1990s, the mean response rate for surveys published in medical journals (mailed surveys) was approximately 60%.26 A 2001 review of physician questionnaire studies found a similar average response rate (61%), with a 52% response rate for large-sample surveys.27 In 2002, Field et al28 examined the impact of incentives in physician survey studies and found response rates ranging from 8.5% to 80%.
Importantly, electronically delivered surveys (e-mail, Web-based) often have lower response rates than mailed surveys.24,29 Nominal financial incentives have been associated with enhanced response rates.28
A relatively low response rate does not necessarily mean you cannot trust the data. Survey scientists note that the representativeness of the sample may be more critical than response rate alone.17 Studies with small sample sizes may be more representative—and findings more valid—than those with large samples, if large samples are nonrepresentative when considering the target population.17
Do the conclusions go beyond the data?
Are the inferences overreaching, in view of the survey design? In studies with low response rates and nonrepresentative samples, researchers must be careful in interpreting the results. If the results cannot be generalized beyond the research sample, is this clear from the limitations, discussion, and conclusion sections?
In this review, we have summarized the findings of three published surveys1,2,30 and commented on how they appear to meet—or don’t quite meet—recommendations for survey development, validation, and use. The papers chosen were deemed strong examples in particular categories, such as description of survey authorship,1 instrument validation,30 sampling methodology,2 and response rate.1
It should be noted that even when surveys are conducted with the utmost rigor, survey reporting may leave out critical details. Survey methodology may not be adequately described for a variety of reasons, including researchers’ training in survey design and methodology; a lack of universally accepted journal-reporting guidelines3; and even journals’ space limitations. At times, journals may excise descriptions of survey development and validation, deeming these sections superfluous. Limitations sections can be critical to interpreting the results of survey research and evaluating the scope of conclusions.
Surveys are common in medical research. Although survey research may be subject to inherent self-report bias, surveys have a great impact on policies and practices in medicine, often forming the basis for recommendations or new guidelines.1,2 To interpret and use survey research results, clinicians should be familiar with key elements involved in the creation and validation of surveys.
The purpose of this article is to provide readers with a basic framework for evaluating surveys to allow them to be more informed as consumers of survey research.
IMPORTANT TOOLS IN MEDICAL RESEARCH
Surveys are important tools for answering questions on topics that are difficult to assess using other methods.3 They allow us to gather data systematically from subjects by asking questions, in order to make inferences about a larger population.3,4 Clinicians use surveys to explore the opinions, beliefs, and perceptions of a group, or to investigate physician practice patterns and adherence to clinical guidelines. They may also use surveys to better understand why patients are not engaging in recommended behavioral or lifestyle changes.
Survey methods include interviews (in person, by phone) and questionnaires (paper-and-pencil, e-mailed, online).4
A well-constructed, validated survey can provide powerful data that may influence clinical practice, guide future research development, or drive the development and provision of needed programs and services. Surveys have the potential to transform the ways in which we think about and practice medicine.
READER BEWARE
While survey research in health care appears to have grown exponentially, the quality of reported survey research has not necessarily increased over time.
For consumers of survey research, the adage “reader beware” is apt. Although a considerable number of studies have examined the effects of survey methodology on the validity, reliability, and generalizability of the results,4 medical journals differ in their requirements for reporting survey methods.
In an analysis of 117 articles, Bennett et al3 found that more than 80% did not fully describe the survey development process or pretesting methods. They also found limited guidance and lack of consensus about the best way to report survey research. Of 95 surveys requiring scoring, 66% did not report scoring practices.
Duffett et al5 noted that of 127 critical care medicine surveys, only 36% had been pretested or pilot-tested, and half of all surveys reviewed did not include participant demographics or included only minimal information.
Because journal reporting practices differ, physicians may be unaware of the steps involved in survey construction and validation. Knowledge of these steps is helpful not only in constructing surveys but also in assessing published articles that used survey research.
LIMITATIONS OF SURVEY RESEARCH
Indirect measures of attitudes and behaviors
Surveys that rely on participants’ self-reports of behaviors, attitudes, beliefs, or actions are indirect measures and are susceptible to self-report and social-desirability biases. Participants may overestimate their own expertise or knowledge in self-report surveys. They may wish to reduce embarrassment6 or answer in ways that would make them “look better,”7 resulting in social-desirability bias. These issues need to be mentioned in the limitations section in papers reporting survey research.
Questions and response choices
The data derived from surveys are only as good as the questions that are asked.8 Stone9 noted that questions should be intelligible, unambiguous, and unbiased. If respondents do not comprehend questions as researchers intended, if questionnaire response choices are inadequate, or if questions trigger unintended emotional responses,10–14 researchers may unwittingly introduce error, which will affect the validity of results. Even seemingly objective questions, such as those related to clinical algorithm use, practice patterns, or equipment available to hospital staff, may be interpreted differently by different respondents.
In their eagerness to launch a survey, clinician researchers may not realize that it must be carefully constructed. A focus on question development and validation is critical, as the questions determine the quality of the data derived from the survey.8 Even the position of the question or answer in the survey can affect how participants respond,15 as they may be guided to a response choice by preceding questions.16
WHAT DO YOU NEED TO KNOW ABOUT ASSESSING SURVEY RESEARCH?
What follows are questions and a basic framework that can be used to evaluate published survey research. Recommendations are based on the work of survey scientists,4,7,10,14,15,17,18 survey researchers in medicine and the social sciences, and national standards for test and questionnaire construction and validation (Table 1).4,19,20
Who created the survey? How did they do it?
How the survey was created should be sufficiently described to allow readers to judge the adequacy of instrument development.3–5 It is generally recommended that feedback from multiple sources be solicited during survey creation. Both questionnaire-design experts and subject-matter experts are considered critical in the process.4
What question was the survey designed to answer?
Is the objective of the study articulated in the paper? 3,20 To judge survey research, readers need to know if the survey appears to adequately address the research question or questions and the objectives of the study in terms of methods used.4
Was evidence on validity gathered?
Instrument pretesting and field testing are considered best practices by the American Association for Public Opinion Research, a professional organization for US survey scientists.4
Pretesting can include cognitive interviewing, the use of questionnaire appraisal tools, and hybrid methods, all of which are aimed at addressing validity issues.21 Pretesting with a group of participants similar to the target population allows for assessment of item ambiguity, instrument ease of use, adequacy of response categories (response choices), and time to completion.4,12
Cognitive interviewing is designed to explore respondents’ comprehension of questions, response processes, and decision processes governing how they answer questions.4,7,10,11 In cognitive interviewing, respondents are generally interviewed one on one. Techniques vary, but typically include “think alouds” (in which a respondent is asked to verbalize thoughts while responding to questions) and “verbal probing” (in which the respondent answers a question, then is asked follow-up questions as the interviewer probes for information related to the response choice or question itself).7 These techniques can provide evidence that researchers are actually measuring what they set out to measure and not an unrelated construct.4,19
Field testing of a survey under realistic conditions can help to uncover problems in administration, such as issues in standardization of key procedures, and to ensure that the survey was administered as the researchers intended.21,22 Field testing is vital before phone or in-person interviews to ensure standardization of any critical procedures. Pilot testing in a sample similar to the intended population allows for further refinement, with deletion of problem items, before the survey is launched.15
Because even “objective” questions can be somewhat subjective, all research surveys should go through some type of pretesting.4,21 Based on the results of pretesting and field testing, surveys should then be revised before launch.4,21 If an article on a self-report survey makes no mention of survey validation steps, readers may well question the validity of the results.
Are the survey questions and response choices understandable?
Is the meaning of each question unambiguous? Is the reading level appropriate for the sample population (a critical consideration in patient surveys)? Do any of the items actually ask two different questions?13 An example would be: “Was the representative courteous and prompt?” as it is possible to be courteous, but not prompt, and vice versa. If so, respondents may be confused or frustrated in attempting to answer it. If a rating scale is used throughout the questionnaire, are the anchors appropriate? For example, a question may be written in such a way that respondents want to answer “yes/no” or “agree/disagree,” but the scale used may include response options such as “poor,” “marginal,” “good,” and “excellent.” Items with Likert-response formats are commonly used in self-report surveys and allow participants to respond to a statement by choosing from a range of responses (eg, strongly disagree to strongly agree), often spaced horizontally under a line.
It is recommended that surveys also include options for answers beyond the response choices provided,20 such as comment boxes or fill-in-the-blank items. Surveys with a closed-response format may constrain the quality of data collected because investigators may not foresee all possible answers. Surveys need to be available for review either within the article itself, in an appendix, or as supplementary material that is available elsewhere.
Does the sample appear to be appropriate?
Articles that report the results of surveys should describe the target population, the sample design, and, in a demographic table, respondents and nonrespondents. To judge appropriateness, several questions can be asked regarding sampling:
Target population. Is the population of interest (ie, the target population) described, including regional demographics, if applicable? The relationship between the sample and the target population is important, as a nonrepresentative sample may result in misleading conclusions about the population of interest.
Sampling frame. Who had an opportunity to participate in the survey? At its simplest, the sampling frame establishes who (or what, in the case of institutions) should be included within the sample. This is typically a list of elements (Groves et al4) that acts to “frame” or define the sample to be selected. Where the target population may be all academic internal medicine physicians in the United States, the sampling frame may be all male and female US physicians who are members of particular internal medicine professional organizations, identified by their directory email addresses.
Sample design. How was the sample actually selected?4 For example, did investigators use a convenience sample of colleagues at other institutions or use a stratified random sample, ensuring adequate representation of respondents with certain characteristics?
Description of respondents. How is the sample of respondents described? Are demographic features reported, including statistics on regional or national representativeness?5 Does the sample of survey respondents appear to be representative of the researcher’s population of interest (ie, the target population)?3,23 If not, is this adequately described in the limitations section? Although outcomes will not be available on nonrespondents, demographic and baseline data often are available and should be reported. Are there systematic differences between respondents and nonrespondents?
Was the response rate adequate?
Was the response rate adequate, given the number of participants initially recruited? If the response rate was not adequate, did the researchers discuss this limitation?
Maximum response rate, defined as the total number of surveys returned divided by the total number of surveys sent,18 may be difficult to calculate with electronic or Web-based survey platforms. When the maximum response rate cannot be calculated, this issue needs to be addressed in the article’s limitations section.
The number of surveys has increased across fields over the past few decades, but survey response rates in general have decreased.17,21,24,25 In fields outside of clinical medicine, response rates in the 40% range are common.17 In the 1990s, the mean response rate for surveys published in medical journals (mailed surveys) was approximately 60%.26 A 2001 review of physician questionnaire studies found a similar average response rate (61%), with a 52% response rate for large-sample surveys.27 In 2002, Field et al28 examined the impact of incentives in physician survey studies and found response rates ranging from 8.5% to 80%.
Importantly, electronically delivered surveys (e-mail, Web-based) often have lower response rates than mailed surveys.24,29 Nominal financial incentives have been associated with enhanced response rates.28
A relatively low response rate does not necessarily mean you cannot trust the data. Survey scientists note that the representativeness of the sample may be more critical than response rate alone.17 Studies with small sample sizes may be more representative—and findings more valid—than those with large samples, if large samples are nonrepresentative when considering the target population.17
Do the conclusions go beyond the data?
Are the inferences overreaching, in view of the survey design? In studies with low response rates and nonrepresentative samples, researchers must be careful in interpreting the results. If the results cannot be generalized beyond the research sample, is this clear from the limitations, discussion, and conclusion sections?
In this review, we have summarized the findings of three published surveys1,2,30 and commented on how they appear to meet—or don’t quite meet—recommendations for survey development, validation, and use. The papers chosen were deemed strong examples in particular categories, such as description of survey authorship,1 instrument validation,30 sampling methodology,2 and response rate.1
It should be noted that even when surveys are conducted with the utmost rigor, survey reporting may leave out critical details. Survey methodology may not be adequately described for a variety of reasons, including researchers’ training in survey design and methodology; a lack of universally accepted journal-reporting guidelines3; and even journals’ space limitations. At times, journals may excise descriptions of survey development and validation, deeming these sections superfluous. Limitations sections can be critical to interpreting the results of survey research and evaluating the scope of conclusions.
- Jha AK, DesRoches CM, Campbell EG, et al. Use of electronic health records in US hospitals. N Engl J Med 2009; 360:1628–1638.
- Angus DC, Shorr AF, White A, Dremsizov TT, Schmitz RJ, Kelley MA; Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS). Critical care delivery in the United States: distribution of services and compliance with Leapfrog recommendations. Crit Care Med 2006; 34:1016–1024.
- Bennett C, Khangura S, Brehaut JC, et al. Reporting guidelines for survey research: an analysis of published guidance and reporting practices. PLoS Med 2010; 8:e1001069.
- Groves RM, Fowler FJ, Couper MP, Lepkowski JM, Singer E, Tourangeau R. Survey Methodology. 2nd ed. Hoboken, NJ: John Wiley and Sons, Inc; 2009.
- Duffett M, Burns KE, Adhikari NK, et al. Quality of reporting of surveys in critical care journals: a methodologic review. Crit Care Med 2012; 40:441–449.
- Mattell MS, Jacoby J. Is there an optimal number of alternatives for Likert-scale items? Effects of testing time and scale properties. J Appl Psychol 1972; 56:506–509.
- Willis GB. Cognitive Interviewing. A “How To” Guide. Research Triangle Institute. Presented at the meeting of the American Statistical Association; 1999. http://fog.its.uiowa.edu/~c07b209/interview.pdf. Accessed June 3, 2013.
- Schwarz N. Self-reports. How the questions shape the answers. Amer Psychol 1999; 54:93–105.
- Stone DH. Design a questionnaire. BMJ 1993; 307:1264–1266.
- Willis GB, Royston P, Bercini D. The use of verbal report methods in the development and testing of survey questionnaires. Appl Cogn Psychol 1991; 5:251–267.
- Desimone LM, LeFloch KC. Are we asking the right questions? Using cognitive interviews to improve surveys in education research. Educ Eval Policy Anal 2004; 26:1–22.
- Presser S, Couper MP, Lessler JT, et al. Methods for testing and evaluating survey questions. Public Opin Q 2004; 68:109–130.
- Rogers G. Accreditation Board for Engineering and Technology (ABET), Inc. Sample Protocol for Pilot Testing Survey Items. www.abet.org/WorkArea/DownloadAsset.aspx?id=1299. Accessed January 22, 2013.
- Schwarz N, Oyserman D. Asking questions about behavior: cognition, communication, and questionnaire construction. Am J Eval 2001; 22:127–160.
- Bradburn N, Sudman S, Wansink B. Asking Questions. The Definitive Guide to Questionnaire Design—For Market Research, Political Polls, and Social and Health Questionnaires. San Francisco, CA: Jossey-Bass; 2004.
- Stone AA, Broderick JE, Schwartz JE, Schwarz N. Context effects in survey ratings of health, symptoms, and satisfaction. Med Care 2008; 46:662–667.
- Cook C, Heath F, Thompson RL. A meta-analysis of response rates in Web or internet-based surveys. Educ Psychol Meas 2000; 60:821–836.
- Kaplowitz MD, Hadlock TD, Levine R. A comparison of Web and mail survey response rates. Public Opin Q 2004; 68:94–101.
- American Educational Research Association. Standards for Educational and Psychological Testing/American Educational Research Association, American Psychological Association, National Council on Measurement in Education. Washington, DC: American Educational Research Association; 1999.
- Burns KE, Duffett M, Kho ME, et al; ACCADEMY Group. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ 2008; 179:245–252.
- American Association for Public Opinion Research (AAPOR). http://www.aapor.org/Home.htm. Accessed June 3, 2013.
- National Center for Education Statistics. Planning and Design of Surveys. http://nces.ed.gov/statprog/2002/std2_1.asp. Accessed January 22, 2013.
- Bordens KS, Abbott BB. Research Design and Methods. A Process Approach. 6th ed. New York, NY: McGraw-Hill; 2004.
- Sheehan K. Email survey response rates: a review. JCMC 2001. http://jcmc.indiana.edu/vol6/issue2/sheehan.html. Accessed January 22, 2013.
- Baruch Y, Holtom BC. Survey response rate levels and trends in organizational research. Hum Relat 2008; 61:1139–1160.
- Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol 1997; 50:1129–1136.
- Cummings SM, Savitz LA, Konrad TR. Reported response rates to mailed physician questionnaires. Health Services Res 2001; 35:1347–1355.
- Field TS, Cadoret CA, Brown ML, et al. Surveying physicians. Do components of the “Total Design Approach” to optimizing survey response rates apply to physicians? Med Care 2002; 40:596–606.
- Converse PD, Wolfe EW, Huang X, Oswald FL. Response rates for mixed-mode surveys using mail and e-mail/Web. Am J Eval 2008; 29:99–107.
- Hirshberg E, Lacroix J, Sward K, Willson D, Morris AH. Blood glucose control in critically ill adults and children: a survey on stated practice. Chest 2008; 133:1328–1335.
- Jha AK, DesRoches CM, Campbell EG, et al. Use of electronic health records in US hospitals. N Engl J Med 2009; 360:1628–1638.
- Angus DC, Shorr AF, White A, Dremsizov TT, Schmitz RJ, Kelley MA; Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS). Critical care delivery in the United States: distribution of services and compliance with Leapfrog recommendations. Crit Care Med 2006; 34:1016–1024.
- Bennett C, Khangura S, Brehaut JC, et al. Reporting guidelines for survey research: an analysis of published guidance and reporting practices. PLoS Med 2010; 8:e1001069.
- Groves RM, Fowler FJ, Couper MP, Lepkowski JM, Singer E, Tourangeau R. Survey Methodology. 2nd ed. Hoboken, NJ: John Wiley and Sons, Inc; 2009.
- Duffett M, Burns KE, Adhikari NK, et al. Quality of reporting of surveys in critical care journals: a methodologic review. Crit Care Med 2012; 40:441–449.
- Mattell MS, Jacoby J. Is there an optimal number of alternatives for Likert-scale items? Effects of testing time and scale properties. J Appl Psychol 1972; 56:506–509.
- Willis GB. Cognitive Interviewing. A “How To” Guide. Research Triangle Institute. Presented at the meeting of the American Statistical Association; 1999. http://fog.its.uiowa.edu/~c07b209/interview.pdf. Accessed June 3, 2013.
- Schwarz N. Self-reports. How the questions shape the answers. Amer Psychol 1999; 54:93–105.
- Stone DH. Design a questionnaire. BMJ 1993; 307:1264–1266.
- Willis GB, Royston P, Bercini D. The use of verbal report methods in the development and testing of survey questionnaires. Appl Cogn Psychol 1991; 5:251–267.
- Desimone LM, LeFloch KC. Are we asking the right questions? Using cognitive interviews to improve surveys in education research. Educ Eval Policy Anal 2004; 26:1–22.
- Presser S, Couper MP, Lessler JT, et al. Methods for testing and evaluating survey questions. Public Opin Q 2004; 68:109–130.
- Rogers G. Accreditation Board for Engineering and Technology (ABET), Inc. Sample Protocol for Pilot Testing Survey Items. www.abet.org/WorkArea/DownloadAsset.aspx?id=1299. Accessed January 22, 2013.
- Schwarz N, Oyserman D. Asking questions about behavior: cognition, communication, and questionnaire construction. Am J Eval 2001; 22:127–160.
- Bradburn N, Sudman S, Wansink B. Asking Questions. The Definitive Guide to Questionnaire Design—For Market Research, Political Polls, and Social and Health Questionnaires. San Francisco, CA: Jossey-Bass; 2004.
- Stone AA, Broderick JE, Schwartz JE, Schwarz N. Context effects in survey ratings of health, symptoms, and satisfaction. Med Care 2008; 46:662–667.
- Cook C, Heath F, Thompson RL. A meta-analysis of response rates in Web or internet-based surveys. Educ Psychol Meas 2000; 60:821–836.
- Kaplowitz MD, Hadlock TD, Levine R. A comparison of Web and mail survey response rates. Public Opin Q 2004; 68:94–101.
- American Educational Research Association. Standards for Educational and Psychological Testing/American Educational Research Association, American Psychological Association, National Council on Measurement in Education. Washington, DC: American Educational Research Association; 1999.
- Burns KE, Duffett M, Kho ME, et al; ACCADEMY Group. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ 2008; 179:245–252.
- American Association for Public Opinion Research (AAPOR). http://www.aapor.org/Home.htm. Accessed June 3, 2013.
- National Center for Education Statistics. Planning and Design of Surveys. http://nces.ed.gov/statprog/2002/std2_1.asp. Accessed January 22, 2013.
- Bordens KS, Abbott BB. Research Design and Methods. A Process Approach. 6th ed. New York, NY: McGraw-Hill; 2004.
- Sheehan K. Email survey response rates: a review. JCMC 2001. http://jcmc.indiana.edu/vol6/issue2/sheehan.html. Accessed January 22, 2013.
- Baruch Y, Holtom BC. Survey response rate levels and trends in organizational research. Hum Relat 2008; 61:1139–1160.
- Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol 1997; 50:1129–1136.
- Cummings SM, Savitz LA, Konrad TR. Reported response rates to mailed physician questionnaires. Health Services Res 2001; 35:1347–1355.
- Field TS, Cadoret CA, Brown ML, et al. Surveying physicians. Do components of the “Total Design Approach” to optimizing survey response rates apply to physicians? Med Care 2002; 40:596–606.
- Converse PD, Wolfe EW, Huang X, Oswald FL. Response rates for mixed-mode surveys using mail and e-mail/Web. Am J Eval 2008; 29:99–107.
- Hirshberg E, Lacroix J, Sward K, Willson D, Morris AH. Blood glucose control in critically ill adults and children: a survey on stated practice. Chest 2008; 133:1328–1335.
KEY POINTS
- Most survey reports do not adequately describe their methods.
- Surveys that rely on participants’ self-reports of behaviors, attitudes, beliefs, or actions are indirect measures and are susceptible to self-report and social-desirability biases.
- Informed readers need to consider a survey’s authorship, objective, validation, items, response choices, sampling representativeness, response rate, generalizability, and scope of the conclusions.
Multiple intracardiac thrombi
A 60-year-old woman presented with sudden swelling and pain in her right arm. She reported progressive lower-extremity edema and abdominal girth over the past month, associated with shortness of breath and orthopnea. She had a remote history of two spontaneous abortions.
Duplex ultrasonography revealed massive venous thrombosis extending from the antecubital fossa to the right atrium. Transthoracic echocardiography revealed severe left ventricular (LV) dysfunction and multiple echo-dense masses in the LV apex, the right ventricle, and the left atrium, as well as at the base of the tricuspid valve (Figure 1). There was no evidence of a structural heart defect, eg, patent foramen ovale, atrial septal defect, or ventricular septal defect. Cardiovascular magnetic resonance imaging (MRI) confirmed the densities as thrombi (Figure 2). Her ejection fraction was 35%.
Blood testing on admission showed a prolonged partial thromboplastin time of 55.0 sec (reference range 22.7–35.6) and a prothrombin time of 13.4 sec (reference range 11.3–14.5). Tissue thromboplastin inhibition at a dilution of 1:50 was elevated at 1.5 sec (reference range 0.7–1.3), as was the tissue thromboplastin inhibition at a dilution of 1:500—ie, 1.6 sec (0.7–1.3). Dilute Russell viper venom testing and anticardiolipin antibody immunoglobulin G and M testing were negative. The lupus antiphospholipid antibody test and the hexagonal lipid neutralization test were positive.
The patient’s clinical presentation of extensive unprovoked venous thrombosis and her laboratory profile together suggested the antiphospholipid antibody syndrome.
SURGICAL TREATMENT NOT AN OPTION
Given her extensive clot burden, surgical thrombectomy was not an option. Instead, warfarin therapy was started and resulted in a progressive diminution of the thrombi. At 4-month follow-up, the thrombi had nearly resolved (Figure 3), and her LV ejection fraction had increased to 45% to 50%. Eighteen months later, she was diagnosed with cholangiocarcinoma. In retrospect, we believe the cancer predisposed the patient to the hypercoagulable state and, subsequently, to thrombosis.
DIAGNOSING AND TREATING LEFT VENTRICULAR THROMBOSIS
Ventricular thrombosis is a serious problem, most commonly associated with extensive myocardial infarction. It is a relatively common complication of myocardial infarction and of ischemic and nonischemic cardiomy-opathies.1 In this population, the incidence of LV thrombosis is reported to be in the range of 10% to 25%, and it increases with increasing LV end-diastolic diameter, lower ejection fraction, and anterior-wall-motion akinesia, and with the presence of apical aneurysms.2 It is an important cause of morbidity and death, whether the thrombus is sessile or mobile.
How diagnostic imaging tests compare
The diagnosis of LV thrombosis requires a certain level of suspicion and has traditionally relied on echocardiography. However, several studies have raised doubt about the sensitivity of echocardiography for the detection of left or right ventricular thrombi.3 In a 2006 report, the sensitivity of transthoracic echocardiography in detecting LV thrombi was 23% and the sensitivity of transesophageal echocardiography was 40%.4 In contrast, delayed-enhancement cardiovascular MRI had a sensitivity near 90%. Similarly, in another study,5 contrast-enhanced echocardiography had a low but higher sensitivity of nearly 60%.5 Therefore, cardiovascular MRI is emerging as the new gold standard test for the detection of this important complication of ventricular dysfunction and myocardial infarction.
Treatment and screening
The optimal management of intraventricular thrombi is poorly defined. It has been suggested from case series that large, mobile, or protruding LV thrombi have more potential for embolization and, therefore, that patients with these findings may benefit from surgical thrombectomy.6 Oral anticoagulation has been reported to dissolve intraventricular thrombi, with success rates from 13% to 59%.7 A prospective study of enoxaparin in 26 patients with LV thrombi reported resolution rates close to 73% at 3-week follow-up.8
There are no guidelines at present on which to base recommendations for screening patients for intracavitary thrombi or for starting empiric anticoagulation in those at risk.
- Weinsaft JW, Kim HW, Shah DJ, et al. Detection of left ventricular thrombus by delayed-enhancement cardiovascular magnetic resonance prevalence and markers in patients with systolic dysfunction. J Am Coll Cardiol 2008; 52:148–157.
- Mollet NR, Dymarkowski S, Volders W, et al. Visualization of ventricular thrombi with contrast-enhanced magnetic resonance imaging in patients with ischemic heart disease. Circulation 2002; 106:2873–2876.
- Tsang BK, Platts DG, Javorsky G, Brown MR. Right ventricular thrombus detection and multimodality imaging using contrast echocardiography and cardiac magnetic resonance imaging. Heart Lung Circ 2012; 21:185–188.
- Srichai MB, Junor C, Rodriguez LL, et al. Clinical, imaging, and pathological characteristics of left ventricular thrombus: a comparison of contrast-enhanced magnetic resonance imaging, transthoracic echocardiography, and transesophageal echocardiography with surgical or pathological validation. Am Heart J 2006; 152:75–84.
- Weinsaft JW, Kim RJ, Ross M, et al. Contrast-enhanced anatomic imaging as compared to contrast-enhanced tissue characterization for detection of left ventricular thrombus. JACC Cardiovasc Imaging 2009; 2:969–979.
- Nili M, Deviri E, Jortner R, Strasberg B, Levy MJ. Surgical removal of a mobile, pedunculated left ventricular thrombus: report of 4 cases. Ann Thorac Surg 1988; 46:396–400.
- Heik SC, Kupper W, Hamm C, et al. Efficacy of high dose intravenous heparin for treatment of left ventricular thrombi with high embolic risk. J Am Coll Cardiol 1994; 24:1305–1309.
- Meurin P, Tabet JY, Renaud N, et al. Treatment of left ventricular thrombi with a low molecular weight heparin. Int J Cardiol 2005; 98:319–323.
A 60-year-old woman presented with sudden swelling and pain in her right arm. She reported progressive lower-extremity edema and abdominal girth over the past month, associated with shortness of breath and orthopnea. She had a remote history of two spontaneous abortions.
Duplex ultrasonography revealed massive venous thrombosis extending from the antecubital fossa to the right atrium. Transthoracic echocardiography revealed severe left ventricular (LV) dysfunction and multiple echo-dense masses in the LV apex, the right ventricle, and the left atrium, as well as at the base of the tricuspid valve (Figure 1). There was no evidence of a structural heart defect, eg, patent foramen ovale, atrial septal defect, or ventricular septal defect. Cardiovascular magnetic resonance imaging (MRI) confirmed the densities as thrombi (Figure 2). Her ejection fraction was 35%.
Blood testing on admission showed a prolonged partial thromboplastin time of 55.0 sec (reference range 22.7–35.6) and a prothrombin time of 13.4 sec (reference range 11.3–14.5). Tissue thromboplastin inhibition at a dilution of 1:50 was elevated at 1.5 sec (reference range 0.7–1.3), as was the tissue thromboplastin inhibition at a dilution of 1:500—ie, 1.6 sec (0.7–1.3). Dilute Russell viper venom testing and anticardiolipin antibody immunoglobulin G and M testing were negative. The lupus antiphospholipid antibody test and the hexagonal lipid neutralization test were positive.
The patient’s clinical presentation of extensive unprovoked venous thrombosis and her laboratory profile together suggested the antiphospholipid antibody syndrome.
SURGICAL TREATMENT NOT AN OPTION
Given her extensive clot burden, surgical thrombectomy was not an option. Instead, warfarin therapy was started and resulted in a progressive diminution of the thrombi. At 4-month follow-up, the thrombi had nearly resolved (Figure 3), and her LV ejection fraction had increased to 45% to 50%. Eighteen months later, she was diagnosed with cholangiocarcinoma. In retrospect, we believe the cancer predisposed the patient to the hypercoagulable state and, subsequently, to thrombosis.
DIAGNOSING AND TREATING LEFT VENTRICULAR THROMBOSIS
Ventricular thrombosis is a serious problem, most commonly associated with extensive myocardial infarction. It is a relatively common complication of myocardial infarction and of ischemic and nonischemic cardiomy-opathies.1 In this population, the incidence of LV thrombosis is reported to be in the range of 10% to 25%, and it increases with increasing LV end-diastolic diameter, lower ejection fraction, and anterior-wall-motion akinesia, and with the presence of apical aneurysms.2 It is an important cause of morbidity and death, whether the thrombus is sessile or mobile.
How diagnostic imaging tests compare
The diagnosis of LV thrombosis requires a certain level of suspicion and has traditionally relied on echocardiography. However, several studies have raised doubt about the sensitivity of echocardiography for the detection of left or right ventricular thrombi.3 In a 2006 report, the sensitivity of transthoracic echocardiography in detecting LV thrombi was 23% and the sensitivity of transesophageal echocardiography was 40%.4 In contrast, delayed-enhancement cardiovascular MRI had a sensitivity near 90%. Similarly, in another study,5 contrast-enhanced echocardiography had a low but higher sensitivity of nearly 60%.5 Therefore, cardiovascular MRI is emerging as the new gold standard test for the detection of this important complication of ventricular dysfunction and myocardial infarction.
Treatment and screening
The optimal management of intraventricular thrombi is poorly defined. It has been suggested from case series that large, mobile, or protruding LV thrombi have more potential for embolization and, therefore, that patients with these findings may benefit from surgical thrombectomy.6 Oral anticoagulation has been reported to dissolve intraventricular thrombi, with success rates from 13% to 59%.7 A prospective study of enoxaparin in 26 patients with LV thrombi reported resolution rates close to 73% at 3-week follow-up.8
There are no guidelines at present on which to base recommendations for screening patients for intracavitary thrombi or for starting empiric anticoagulation in those at risk.
A 60-year-old woman presented with sudden swelling and pain in her right arm. She reported progressive lower-extremity edema and abdominal girth over the past month, associated with shortness of breath and orthopnea. She had a remote history of two spontaneous abortions.
Duplex ultrasonography revealed massive venous thrombosis extending from the antecubital fossa to the right atrium. Transthoracic echocardiography revealed severe left ventricular (LV) dysfunction and multiple echo-dense masses in the LV apex, the right ventricle, and the left atrium, as well as at the base of the tricuspid valve (Figure 1). There was no evidence of a structural heart defect, eg, patent foramen ovale, atrial septal defect, or ventricular septal defect. Cardiovascular magnetic resonance imaging (MRI) confirmed the densities as thrombi (Figure 2). Her ejection fraction was 35%.
Blood testing on admission showed a prolonged partial thromboplastin time of 55.0 sec (reference range 22.7–35.6) and a prothrombin time of 13.4 sec (reference range 11.3–14.5). Tissue thromboplastin inhibition at a dilution of 1:50 was elevated at 1.5 sec (reference range 0.7–1.3), as was the tissue thromboplastin inhibition at a dilution of 1:500—ie, 1.6 sec (0.7–1.3). Dilute Russell viper venom testing and anticardiolipin antibody immunoglobulin G and M testing were negative. The lupus antiphospholipid antibody test and the hexagonal lipid neutralization test were positive.
The patient’s clinical presentation of extensive unprovoked venous thrombosis and her laboratory profile together suggested the antiphospholipid antibody syndrome.
SURGICAL TREATMENT NOT AN OPTION
Given her extensive clot burden, surgical thrombectomy was not an option. Instead, warfarin therapy was started and resulted in a progressive diminution of the thrombi. At 4-month follow-up, the thrombi had nearly resolved (Figure 3), and her LV ejection fraction had increased to 45% to 50%. Eighteen months later, she was diagnosed with cholangiocarcinoma. In retrospect, we believe the cancer predisposed the patient to the hypercoagulable state and, subsequently, to thrombosis.
DIAGNOSING AND TREATING LEFT VENTRICULAR THROMBOSIS
Ventricular thrombosis is a serious problem, most commonly associated with extensive myocardial infarction. It is a relatively common complication of myocardial infarction and of ischemic and nonischemic cardiomy-opathies.1 In this population, the incidence of LV thrombosis is reported to be in the range of 10% to 25%, and it increases with increasing LV end-diastolic diameter, lower ejection fraction, and anterior-wall-motion akinesia, and with the presence of apical aneurysms.2 It is an important cause of morbidity and death, whether the thrombus is sessile or mobile.
How diagnostic imaging tests compare
The diagnosis of LV thrombosis requires a certain level of suspicion and has traditionally relied on echocardiography. However, several studies have raised doubt about the sensitivity of echocardiography for the detection of left or right ventricular thrombi.3 In a 2006 report, the sensitivity of transthoracic echocardiography in detecting LV thrombi was 23% and the sensitivity of transesophageal echocardiography was 40%.4 In contrast, delayed-enhancement cardiovascular MRI had a sensitivity near 90%. Similarly, in another study,5 contrast-enhanced echocardiography had a low but higher sensitivity of nearly 60%.5 Therefore, cardiovascular MRI is emerging as the new gold standard test for the detection of this important complication of ventricular dysfunction and myocardial infarction.
Treatment and screening
The optimal management of intraventricular thrombi is poorly defined. It has been suggested from case series that large, mobile, or protruding LV thrombi have more potential for embolization and, therefore, that patients with these findings may benefit from surgical thrombectomy.6 Oral anticoagulation has been reported to dissolve intraventricular thrombi, with success rates from 13% to 59%.7 A prospective study of enoxaparin in 26 patients with LV thrombi reported resolution rates close to 73% at 3-week follow-up.8
There are no guidelines at present on which to base recommendations for screening patients for intracavitary thrombi or for starting empiric anticoagulation in those at risk.
- Weinsaft JW, Kim HW, Shah DJ, et al. Detection of left ventricular thrombus by delayed-enhancement cardiovascular magnetic resonance prevalence and markers in patients with systolic dysfunction. J Am Coll Cardiol 2008; 52:148–157.
- Mollet NR, Dymarkowski S, Volders W, et al. Visualization of ventricular thrombi with contrast-enhanced magnetic resonance imaging in patients with ischemic heart disease. Circulation 2002; 106:2873–2876.
- Tsang BK, Platts DG, Javorsky G, Brown MR. Right ventricular thrombus detection and multimodality imaging using contrast echocardiography and cardiac magnetic resonance imaging. Heart Lung Circ 2012; 21:185–188.
- Srichai MB, Junor C, Rodriguez LL, et al. Clinical, imaging, and pathological characteristics of left ventricular thrombus: a comparison of contrast-enhanced magnetic resonance imaging, transthoracic echocardiography, and transesophageal echocardiography with surgical or pathological validation. Am Heart J 2006; 152:75–84.
- Weinsaft JW, Kim RJ, Ross M, et al. Contrast-enhanced anatomic imaging as compared to contrast-enhanced tissue characterization for detection of left ventricular thrombus. JACC Cardiovasc Imaging 2009; 2:969–979.
- Nili M, Deviri E, Jortner R, Strasberg B, Levy MJ. Surgical removal of a mobile, pedunculated left ventricular thrombus: report of 4 cases. Ann Thorac Surg 1988; 46:396–400.
- Heik SC, Kupper W, Hamm C, et al. Efficacy of high dose intravenous heparin for treatment of left ventricular thrombi with high embolic risk. J Am Coll Cardiol 1994; 24:1305–1309.
- Meurin P, Tabet JY, Renaud N, et al. Treatment of left ventricular thrombi with a low molecular weight heparin. Int J Cardiol 2005; 98:319–323.
- Weinsaft JW, Kim HW, Shah DJ, et al. Detection of left ventricular thrombus by delayed-enhancement cardiovascular magnetic resonance prevalence and markers in patients with systolic dysfunction. J Am Coll Cardiol 2008; 52:148–157.
- Mollet NR, Dymarkowski S, Volders W, et al. Visualization of ventricular thrombi with contrast-enhanced magnetic resonance imaging in patients with ischemic heart disease. Circulation 2002; 106:2873–2876.
- Tsang BK, Platts DG, Javorsky G, Brown MR. Right ventricular thrombus detection and multimodality imaging using contrast echocardiography and cardiac magnetic resonance imaging. Heart Lung Circ 2012; 21:185–188.
- Srichai MB, Junor C, Rodriguez LL, et al. Clinical, imaging, and pathological characteristics of left ventricular thrombus: a comparison of contrast-enhanced magnetic resonance imaging, transthoracic echocardiography, and transesophageal echocardiography with surgical or pathological validation. Am Heart J 2006; 152:75–84.
- Weinsaft JW, Kim RJ, Ross M, et al. Contrast-enhanced anatomic imaging as compared to contrast-enhanced tissue characterization for detection of left ventricular thrombus. JACC Cardiovasc Imaging 2009; 2:969–979.
- Nili M, Deviri E, Jortner R, Strasberg B, Levy MJ. Surgical removal of a mobile, pedunculated left ventricular thrombus: report of 4 cases. Ann Thorac Surg 1988; 46:396–400.
- Heik SC, Kupper W, Hamm C, et al. Efficacy of high dose intravenous heparin for treatment of left ventricular thrombi with high embolic risk. J Am Coll Cardiol 1994; 24:1305–1309.
- Meurin P, Tabet JY, Renaud N, et al. Treatment of left ventricular thrombi with a low molecular weight heparin. Int J Cardiol 2005; 98:319–323.