User login
Dabigatran also recommended to treat AF
Dabigatran is a useful alternative to warfarin to prevent blood clots and stroke in patients with either paroxysmal or permanent atrial fibrillation (AF), according to an update published in Circulation: Journal of the American Heart Association, the Journal of the American College of Cardiology, and HeartRhythm journal, which focused on emerging antithrombotic agents in AF.
More specifically, the update focused on the changing guidelines released by the 3 organizations in December of last year.
The new guidelines also included patients with atrial fibrillation with risk factors for stroke or blood clotting who do not have a prosthetic heart valve, significant heart valve disease, severe renal failure, or advanced liver disease.
The US Food and Drug administration (FDA) approved the use of dabigatran in AF in October 2010, stating the drug was at least as good as the current standard of care but required less laboratory monitoring than its predecessor, warfarin.
The RE-LY trial suggested that warfarin and dabigatran are comparable at preventing stroke in patients with atrial fibrillation who have previously had a stroke or transient ischemic attack. And the risk of developing intracranial bleeding is lower with dabigatran. ![]()
Dabigatran is a useful alternative to warfarin to prevent blood clots and stroke in patients with either paroxysmal or permanent atrial fibrillation (AF), according to an update published in Circulation: Journal of the American Heart Association, the Journal of the American College of Cardiology, and HeartRhythm journal, which focused on emerging antithrombotic agents in AF.
More specifically, the update focused on the changing guidelines released by the 3 organizations in December of last year.
The new guidelines also included patients with atrial fibrillation with risk factors for stroke or blood clotting who do not have a prosthetic heart valve, significant heart valve disease, severe renal failure, or advanced liver disease.
The US Food and Drug administration (FDA) approved the use of dabigatran in AF in October 2010, stating the drug was at least as good as the current standard of care but required less laboratory monitoring than its predecessor, warfarin.
The RE-LY trial suggested that warfarin and dabigatran are comparable at preventing stroke in patients with atrial fibrillation who have previously had a stroke or transient ischemic attack. And the risk of developing intracranial bleeding is lower with dabigatran. ![]()
Dabigatran is a useful alternative to warfarin to prevent blood clots and stroke in patients with either paroxysmal or permanent atrial fibrillation (AF), according to an update published in Circulation: Journal of the American Heart Association, the Journal of the American College of Cardiology, and HeartRhythm journal, which focused on emerging antithrombotic agents in AF.
More specifically, the update focused on the changing guidelines released by the 3 organizations in December of last year.
The new guidelines also included patients with atrial fibrillation with risk factors for stroke or blood clotting who do not have a prosthetic heart valve, significant heart valve disease, severe renal failure, or advanced liver disease.
The US Food and Drug administration (FDA) approved the use of dabigatran in AF in October 2010, stating the drug was at least as good as the current standard of care but required less laboratory monitoring than its predecessor, warfarin.
The RE-LY trial suggested that warfarin and dabigatran are comparable at preventing stroke in patients with atrial fibrillation who have previously had a stroke or transient ischemic attack. And the risk of developing intracranial bleeding is lower with dabigatran. ![]()
The Triple Crown: Collaboration with clinical documentation specialists can be a win-win for patients, hospitals, and HM
“Doctor, please clarify: Is this type of congestive heart failure acute or chronic, systolic or diastolic?” Most hospitalists have had patients’ charts flagged with these types of queries. And no, the people who write the questions are not trying to be difficult.
In fact, says Karen Bachman, BSN, MHSA, director of clinical documentation at 300-bed Good Samaritan Hospital in Suffern, N.Y., the specialists who place worksheets on hospitalists’ charts are sympathetic to the perceived disconnect between clinical processes and the language of the coding world. Even for nurses, the ICD-9-CM, the manual upon which Medicare bases its reimbursement structure, “is a different language,” she says. “You have to think like a coder.”
And in the coding world, as the saying goes, “if it’s not documented, it didn’t happen.”
That’s where clinical documentation specialists come in. Collaborating with documentation specialists can help boost patient quality, hospital reimbursement, and your hospital’s recognition of the value your HM group adds.
Stephanie Jensen, RN, BSN, coordinator of the Clinical Documentation Integrity (CDI) program at The Nebraska Medical Center in Omaha, summed it up this way: The chart has become more than what it was originally intended. It’s now the repository of “the patient’s story. We’re just trying to help physicians capture the quality of care that they’re giving, and to make sure that, in the medical record, the documentation supports the severity of illness, risk of mortality, and overall clinical picture.”
—Stephanie Jensen, RN, BSN, coordinator, Clinical Documentation Integrity (CDI) program, The Nebraska Medical Center, Omaha
For example, even though nurses can stage a pressure ulcer, the stage must be accompanied by the hospitalist’s diagnosis of decubitus ulcer in order for the coders in the Health Information Management and Services (HIMS) department to properly code the diagnosis, which affects the DRG submitted to Medicare/CMS.
The Challenge
Bachmann thinks the biggest challenge to proper documentation is time. Hospitalists are immersed in caring for their patients. They must balance different coding systems—the ICD-9-CM, as well as CPT and E/M coding for their own billing. They often feel pulled between taking extra time to clarify their working or discharge diagnoses and getting on to the next patient. The catch, though, is that hospital coders can rely only on what the treating physician documents.
At Good Samaritan, documentation specialists see themselves as allies in this process. They use the JA Thomas documentation system and print out worksheets to attach to patients’ charts; it’s intended to be a trigger so that the hospitalist will be as specific with documentation as possible. “As nurses,” Bachmann explains, “we understand what physicians need and what the coders need. We’re an intermediary between the two.”
At The Nebraska Medical Center, the hospital’s mortality committee initiated a systemwide CDI program in November 2009. Jensen explains that every new staff physician at the 689-bed facility now receives a CDI toolkit detailing the documentation program. The six CDI team members wear blue T-shirts, and documentation clarification worksheets are on blue paper.
Further Education
During monthly in-services at hospitalists’ meetings, says Bachmann, “we stress the importance of linking the etiology with the diagnosis. We illustrate how different diagnoses will be given different relative weights for DRGs.” The effort has proven to be an effective educational tool, she says.
Jensen admits that the semantic differences between the clinical and coding worlds can be challenging. But, she says, the more specific physicians can be, the more it will help all indicators in the long run: patient safety, physician profiles, and, yes, hospital reimbursement. And for demonstrating hospitalists’ value, that’s considerable return on investment of the time it takes to write a complete note.
Gretchen Henkel is a freelance writer based in California.
“Doctor, please clarify: Is this type of congestive heart failure acute or chronic, systolic or diastolic?” Most hospitalists have had patients’ charts flagged with these types of queries. And no, the people who write the questions are not trying to be difficult.
In fact, says Karen Bachman, BSN, MHSA, director of clinical documentation at 300-bed Good Samaritan Hospital in Suffern, N.Y., the specialists who place worksheets on hospitalists’ charts are sympathetic to the perceived disconnect between clinical processes and the language of the coding world. Even for nurses, the ICD-9-CM, the manual upon which Medicare bases its reimbursement structure, “is a different language,” she says. “You have to think like a coder.”
And in the coding world, as the saying goes, “if it’s not documented, it didn’t happen.”
That’s where clinical documentation specialists come in. Collaborating with documentation specialists can help boost patient quality, hospital reimbursement, and your hospital’s recognition of the value your HM group adds.
Stephanie Jensen, RN, BSN, coordinator of the Clinical Documentation Integrity (CDI) program at The Nebraska Medical Center in Omaha, summed it up this way: The chart has become more than what it was originally intended. It’s now the repository of “the patient’s story. We’re just trying to help physicians capture the quality of care that they’re giving, and to make sure that, in the medical record, the documentation supports the severity of illness, risk of mortality, and overall clinical picture.”
—Stephanie Jensen, RN, BSN, coordinator, Clinical Documentation Integrity (CDI) program, The Nebraska Medical Center, Omaha
For example, even though nurses can stage a pressure ulcer, the stage must be accompanied by the hospitalist’s diagnosis of decubitus ulcer in order for the coders in the Health Information Management and Services (HIMS) department to properly code the diagnosis, which affects the DRG submitted to Medicare/CMS.
The Challenge
Bachmann thinks the biggest challenge to proper documentation is time. Hospitalists are immersed in caring for their patients. They must balance different coding systems—the ICD-9-CM, as well as CPT and E/M coding for their own billing. They often feel pulled between taking extra time to clarify their working or discharge diagnoses and getting on to the next patient. The catch, though, is that hospital coders can rely only on what the treating physician documents.
At Good Samaritan, documentation specialists see themselves as allies in this process. They use the JA Thomas documentation system and print out worksheets to attach to patients’ charts; it’s intended to be a trigger so that the hospitalist will be as specific with documentation as possible. “As nurses,” Bachmann explains, “we understand what physicians need and what the coders need. We’re an intermediary between the two.”
At The Nebraska Medical Center, the hospital’s mortality committee initiated a systemwide CDI program in November 2009. Jensen explains that every new staff physician at the 689-bed facility now receives a CDI toolkit detailing the documentation program. The six CDI team members wear blue T-shirts, and documentation clarification worksheets are on blue paper.
Further Education
During monthly in-services at hospitalists’ meetings, says Bachmann, “we stress the importance of linking the etiology with the diagnosis. We illustrate how different diagnoses will be given different relative weights for DRGs.” The effort has proven to be an effective educational tool, she says.
Jensen admits that the semantic differences between the clinical and coding worlds can be challenging. But, she says, the more specific physicians can be, the more it will help all indicators in the long run: patient safety, physician profiles, and, yes, hospital reimbursement. And for demonstrating hospitalists’ value, that’s considerable return on investment of the time it takes to write a complete note.
Gretchen Henkel is a freelance writer based in California.
“Doctor, please clarify: Is this type of congestive heart failure acute or chronic, systolic or diastolic?” Most hospitalists have had patients’ charts flagged with these types of queries. And no, the people who write the questions are not trying to be difficult.
In fact, says Karen Bachman, BSN, MHSA, director of clinical documentation at 300-bed Good Samaritan Hospital in Suffern, N.Y., the specialists who place worksheets on hospitalists’ charts are sympathetic to the perceived disconnect between clinical processes and the language of the coding world. Even for nurses, the ICD-9-CM, the manual upon which Medicare bases its reimbursement structure, “is a different language,” she says. “You have to think like a coder.”
And in the coding world, as the saying goes, “if it’s not documented, it didn’t happen.”
That’s where clinical documentation specialists come in. Collaborating with documentation specialists can help boost patient quality, hospital reimbursement, and your hospital’s recognition of the value your HM group adds.
Stephanie Jensen, RN, BSN, coordinator of the Clinical Documentation Integrity (CDI) program at The Nebraska Medical Center in Omaha, summed it up this way: The chart has become more than what it was originally intended. It’s now the repository of “the patient’s story. We’re just trying to help physicians capture the quality of care that they’re giving, and to make sure that, in the medical record, the documentation supports the severity of illness, risk of mortality, and overall clinical picture.”
—Stephanie Jensen, RN, BSN, coordinator, Clinical Documentation Integrity (CDI) program, The Nebraska Medical Center, Omaha
For example, even though nurses can stage a pressure ulcer, the stage must be accompanied by the hospitalist’s diagnosis of decubitus ulcer in order for the coders in the Health Information Management and Services (HIMS) department to properly code the diagnosis, which affects the DRG submitted to Medicare/CMS.
The Challenge
Bachmann thinks the biggest challenge to proper documentation is time. Hospitalists are immersed in caring for their patients. They must balance different coding systems—the ICD-9-CM, as well as CPT and E/M coding for their own billing. They often feel pulled between taking extra time to clarify their working or discharge diagnoses and getting on to the next patient. The catch, though, is that hospital coders can rely only on what the treating physician documents.
At Good Samaritan, documentation specialists see themselves as allies in this process. They use the JA Thomas documentation system and print out worksheets to attach to patients’ charts; it’s intended to be a trigger so that the hospitalist will be as specific with documentation as possible. “As nurses,” Bachmann explains, “we understand what physicians need and what the coders need. We’re an intermediary between the two.”
At The Nebraska Medical Center, the hospital’s mortality committee initiated a systemwide CDI program in November 2009. Jensen explains that every new staff physician at the 689-bed facility now receives a CDI toolkit detailing the documentation program. The six CDI team members wear blue T-shirts, and documentation clarification worksheets are on blue paper.
Further Education
During monthly in-services at hospitalists’ meetings, says Bachmann, “we stress the importance of linking the etiology with the diagnosis. We illustrate how different diagnoses will be given different relative weights for DRGs.” The effort has proven to be an effective educational tool, she says.
Jensen admits that the semantic differences between the clinical and coding worlds can be challenging. But, she says, the more specific physicians can be, the more it will help all indicators in the long run: patient safety, physician profiles, and, yes, hospital reimbursement. And for demonstrating hospitalists’ value, that’s considerable return on investment of the time it takes to write a complete note.
Gretchen Henkel is a freelance writer based in California.
Rewards and Challenges of Two-Physician Marriages
For hospitalist Kirsten N. Kangelaris, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California at San Francisco (UCSF), there are several benefits to being married to a physician. "It's nice to be able to relate with your spouse on a professional, as well as a personal, level," she says.
Although coordinating schedules can be challenging, one of the pluses of being married to another physician is that your spouse understands the lifestyle, says Sarina B. Schrager, MD, associate professor in the Department of Family Medicine at the University of Wisconsin School of Medicine and Public Health in Madison. In 2007, Dr. Schrager surveyed female physicians (WMJ. 106(5);251-255) and found that most reported that there were benefits to having a physician partner.
Making Work Work
Keith Ashby, MD, is a hospitalist and intensivist at Rapides Regional Medical Center in Alexandria, La., and regional director for Hospitalists Management Group (HMG), supervising three other hospitals from Lafayette to Houston. He and his wife, Agnes, a rheumatologist in private practice, met in Chicago 17 years ago, when he was an attending and she a resident in rheumatology. "It truly does help to have your best friend as a support and also a colleague," he says, though the scheduling can sometimes be daunting. "It takes some creative planning and ingenuity to figure out how to couple work and family responsibilities so that neither comes up short."
One way Dr. Kangelaris and her husband, Gerald, a fourth-year resident in otolaryngology/head and neck surgery at UCSF, manage is to avoid compartmentalizing tasks: Each takes a part in childcare, preparing meals, and other household duties when the other is on duty at the hospital. On the advice of a mentor, Dr. Kangelaris and her husband hired a weekly housecleaning service—a boon for mental health and relationship time, she says.
Contingency Plans
Dr. Ashby and his wife moved away from "the comfort of family" when they left Chicago to embark on their dual careers. Without aunts, uncles, or grandparents to turn to for sharing the childcare load, they built a strong support network of friends and other working parents to help bridge the gap.
Dr. Kangelaris and her husband enrolled their now-2-year-old daughter in a university-sponsored childcare center when she was an infant. They also make an effort to stagger their clinical duties. She admits that most of the flexibility in work schedules is coming from her direction right now because her husband's time is "not his own.". There are many young families in the division at UCSF, and Dr. Kangelaris says most of her scheduling requests are honored.
"In a lot of ways, academic medicine does provide more flexibility," Dr. Schrager says. She advises job-seeking residents to anticipate future goals. "Look for a place that, regardless of what your life situation is now, might be flexible for you in the future."
Gretchen Henkel is a freelance writer based in California.
Protect Relationship Time
Instituting a “date night” is one popular strategy for staying in touch with your partner. Now that their teenagers have full social schedules, weekly date nights are a little bit challenging, Dr. Ashby admits, so he and his physician wife plan getaways: If one partner travels to a medical meeting, the other tags along; if the kids are at summer camp, they take an extended trip.
With a 2-year-old and a husband who is a surgical resident, Dr. Kangelaris says they struggle to reach a work-life balance, and look forward to a time when they can reinstitute their own date night.
Just be sure, advises Jim Bird, president and CEO of Atlanta-based training firm WorkLifeBalance.com, that you don’t inadvertently turn date night into meeting night. Table the conversations about work and bills until another time.
Dr. Schrager couldn’t agree more, noting most female physicians in her survey of dual-physician couples noted that they try to limit talk about work, then turn to other subjects.—GH
For hospitalist Kirsten N. Kangelaris, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California at San Francisco (UCSF), there are several benefits to being married to a physician. "It's nice to be able to relate with your spouse on a professional, as well as a personal, level," she says.
Although coordinating schedules can be challenging, one of the pluses of being married to another physician is that your spouse understands the lifestyle, says Sarina B. Schrager, MD, associate professor in the Department of Family Medicine at the University of Wisconsin School of Medicine and Public Health in Madison. In 2007, Dr. Schrager surveyed female physicians (WMJ. 106(5);251-255) and found that most reported that there were benefits to having a physician partner.
Making Work Work
Keith Ashby, MD, is a hospitalist and intensivist at Rapides Regional Medical Center in Alexandria, La., and regional director for Hospitalists Management Group (HMG), supervising three other hospitals from Lafayette to Houston. He and his wife, Agnes, a rheumatologist in private practice, met in Chicago 17 years ago, when he was an attending and she a resident in rheumatology. "It truly does help to have your best friend as a support and also a colleague," he says, though the scheduling can sometimes be daunting. "It takes some creative planning and ingenuity to figure out how to couple work and family responsibilities so that neither comes up short."
One way Dr. Kangelaris and her husband, Gerald, a fourth-year resident in otolaryngology/head and neck surgery at UCSF, manage is to avoid compartmentalizing tasks: Each takes a part in childcare, preparing meals, and other household duties when the other is on duty at the hospital. On the advice of a mentor, Dr. Kangelaris and her husband hired a weekly housecleaning service—a boon for mental health and relationship time, she says.
Contingency Plans
Dr. Ashby and his wife moved away from "the comfort of family" when they left Chicago to embark on their dual careers. Without aunts, uncles, or grandparents to turn to for sharing the childcare load, they built a strong support network of friends and other working parents to help bridge the gap.
Dr. Kangelaris and her husband enrolled their now-2-year-old daughter in a university-sponsored childcare center when she was an infant. They also make an effort to stagger their clinical duties. She admits that most of the flexibility in work schedules is coming from her direction right now because her husband's time is "not his own.". There are many young families in the division at UCSF, and Dr. Kangelaris says most of her scheduling requests are honored.
"In a lot of ways, academic medicine does provide more flexibility," Dr. Schrager says. She advises job-seeking residents to anticipate future goals. "Look for a place that, regardless of what your life situation is now, might be flexible for you in the future."
Gretchen Henkel is a freelance writer based in California.
Protect Relationship Time
Instituting a “date night” is one popular strategy for staying in touch with your partner. Now that their teenagers have full social schedules, weekly date nights are a little bit challenging, Dr. Ashby admits, so he and his physician wife plan getaways: If one partner travels to a medical meeting, the other tags along; if the kids are at summer camp, they take an extended trip.
With a 2-year-old and a husband who is a surgical resident, Dr. Kangelaris says they struggle to reach a work-life balance, and look forward to a time when they can reinstitute their own date night.
Just be sure, advises Jim Bird, president and CEO of Atlanta-based training firm WorkLifeBalance.com, that you don’t inadvertently turn date night into meeting night. Table the conversations about work and bills until another time.
Dr. Schrager couldn’t agree more, noting most female physicians in her survey of dual-physician couples noted that they try to limit talk about work, then turn to other subjects.—GH
For hospitalist Kirsten N. Kangelaris, MD, assistant clinical professor in the Division of Hospital Medicine at the University of California at San Francisco (UCSF), there are several benefits to being married to a physician. "It's nice to be able to relate with your spouse on a professional, as well as a personal, level," she says.
Although coordinating schedules can be challenging, one of the pluses of being married to another physician is that your spouse understands the lifestyle, says Sarina B. Schrager, MD, associate professor in the Department of Family Medicine at the University of Wisconsin School of Medicine and Public Health in Madison. In 2007, Dr. Schrager surveyed female physicians (WMJ. 106(5);251-255) and found that most reported that there were benefits to having a physician partner.
Making Work Work
Keith Ashby, MD, is a hospitalist and intensivist at Rapides Regional Medical Center in Alexandria, La., and regional director for Hospitalists Management Group (HMG), supervising three other hospitals from Lafayette to Houston. He and his wife, Agnes, a rheumatologist in private practice, met in Chicago 17 years ago, when he was an attending and she a resident in rheumatology. "It truly does help to have your best friend as a support and also a colleague," he says, though the scheduling can sometimes be daunting. "It takes some creative planning and ingenuity to figure out how to couple work and family responsibilities so that neither comes up short."
One way Dr. Kangelaris and her husband, Gerald, a fourth-year resident in otolaryngology/head and neck surgery at UCSF, manage is to avoid compartmentalizing tasks: Each takes a part in childcare, preparing meals, and other household duties when the other is on duty at the hospital. On the advice of a mentor, Dr. Kangelaris and her husband hired a weekly housecleaning service—a boon for mental health and relationship time, she says.
Contingency Plans
Dr. Ashby and his wife moved away from "the comfort of family" when they left Chicago to embark on their dual careers. Without aunts, uncles, or grandparents to turn to for sharing the childcare load, they built a strong support network of friends and other working parents to help bridge the gap.
Dr. Kangelaris and her husband enrolled their now-2-year-old daughter in a university-sponsored childcare center when she was an infant. They also make an effort to stagger their clinical duties. She admits that most of the flexibility in work schedules is coming from her direction right now because her husband's time is "not his own.". There are many young families in the division at UCSF, and Dr. Kangelaris says most of her scheduling requests are honored.
"In a lot of ways, academic medicine does provide more flexibility," Dr. Schrager says. She advises job-seeking residents to anticipate future goals. "Look for a place that, regardless of what your life situation is now, might be flexible for you in the future."
Gretchen Henkel is a freelance writer based in California.
Protect Relationship Time
Instituting a “date night” is one popular strategy for staying in touch with your partner. Now that their teenagers have full social schedules, weekly date nights are a little bit challenging, Dr. Ashby admits, so he and his physician wife plan getaways: If one partner travels to a medical meeting, the other tags along; if the kids are at summer camp, they take an extended trip.
With a 2-year-old and a husband who is a surgical resident, Dr. Kangelaris says they struggle to reach a work-life balance, and look forward to a time when they can reinstitute their own date night.
Just be sure, advises Jim Bird, president and CEO of Atlanta-based training firm WorkLifeBalance.com, that you don’t inadvertently turn date night into meeting night. Table the conversations about work and bills until another time.
Dr. Schrager couldn’t agree more, noting most female physicians in her survey of dual-physician couples noted that they try to limit talk about work, then turn to other subjects.—GH
Results of a Multicenter Open-Label Randomized Trial Evaluating Infusion Duration of Zoledronic Acid in Multiple Myeloma Patients (the ZMAX Trial)
Original research
James R. Berenson MD![]()
![]()
Abstract
Zoledronic acid, an intravenous (IV) bisphosphonate, is a standard treatment for multiple myeloma (MM) but may exacerbate preexisting renal dysfunction. The incidence of zoledronic acid–induced renal dysfunction may correlate with infusion duration. In this randomized, multicenter, open-label study, 176 patients with MM, at least one bone lesion, and stable renal function with a serum creatinine (SCr) level <3 mg/dL received zoledronic acid 4 mg (in 250 mL) as a 15- or 30-minute IV infusion every 3–4 weeks. At month 12, 20% (17 patients) in the 15-minute and 16% (13 patients) in the 30-minute arm experienced a clinically relevant but nonsignificant SCr-level increase (P = 0.44). By 24 months, the proportion of patients with a clinically relevant SCr-level increase was similar between arms (15-minute 28% [24 patients] vs 30-minute 27% [23 patients], P = 0.9014). Median zoledronic acid end-of-infusion concentrations were higher with the shorter infusion (15-minute 249 ng/mL vs 30-minute 172 ng/mL), and prolonging the infusion beyond 15 minutes did not influence adverse events related to zoledronic acid. For patients with MM, the safety profile of IV zoledronic acid is similar between those receiving a 15- or 30-minute infusion; therefore, determining the appropriate infusion duration of zoledronic acid should be based on individual patient considerations.
Article Outline
Considerable research has focused on preventive and/or treatment strategies to reduce bone complications in MM patients. In a large, international, randomized, phase III trial of MM patients with at least one osteolytic bone lesion, zoledronic acid (Zometa), a potent intravenous (IV) bisphosphonate that inhibits osteoclast-mediated bone resorption, reduced the overall risk of developing skeletally related events (SREs) including HCM by 16% (P = 0.03) compared with standard-dose pamidronate 90 mg (Aredia), another less potent IV bisphosphonate.[5] and [6] As a result of this study and others, monthly infusion of zoledronic acid at 4 mg over at least 15 minutes has become a common treatment for MM patients with bone involvement.
The U.S. Food and Drug Administration (FDA) has approved zoledronic acid use for patients with MM, documented bone metastases from solid tumors, or HCM.[5], [6], [7] and [8] The FDA-approved dose for MM patients is 4 mg administered as an IV infusion over at least 15 minutes every 3–4 weeks for patients with a creatinine clearance (CrCl) of >60 mL/min; when treating HCM, zoledronic acid 4 mg is administered as a single IV infusion.[5], [6], [7] and [8]
Zoledronic acid is primarily excreted intact through the kidney.9 Preexisting kidney disease and receipt of multiple cycles of bisphosphonate therapy are risk factors for subsequent kidney injury.7 In animal studies, IV bisphosphonates have been shown by histology to precipitate renal tubular injury when administered as a single high dose or when administered more frequently at lower doses.[10] and [11] Additionally, renal dysfunction, as evidenced by increased serum creatinine (SCr) levels, was reported among patients treated at a dose of 4 mg with an infusion time of 5 minutes.[7] and [12] When 4 mg zoledronic acid was administered with a longer infusion time of 15 minutes in large randomized trials, no significant difference between the renal safety profiles of zoledronic acid and pamidronate was reported.6
One hypothesis about the development of kidney injury associated with zoledronic acid is that it may be related to the peak plasma concentration as determined by infusion time. Results of a study evaluating patients with MM or other cancer types and bone metastases demonstrated that prolonging the infusion time of zoledronic acid reduced the end-of-infusion peak plasma concentration (Cmax) by 35%.9 Another theory about the development of kidney dysfunction is that insoluble precipitates may form when the blood is exposed to high concentrations of bisphosphonates as this has been shown to occur in vitro.[9] and [13] Therefore, the current management of renal adverse events (AEs) related to IV bisphosphonates is based on these theories so that reducing the peak plasma concentration of zoledronic acid may prevent the possible formation of insoluble precipitates through (1) lowering the dose, (2) slowing the infusion rate, or (3) increasing the volume of infusate.[5], [12] and [14]
Because MM patients are predisposed to experience deterioration of renal function, it is critical to ensure that zoledronic acid does not contribute to, or exacerbate, a decline in kidney function. To determine if increasing the duration of zoledronic acid infusion further results in improved renal safety, a multicenter, open-label, randomized study was designed to compare a 15-minute vs a 30-minute infusion time with an increased volume of infusate from 100 to 250 mL administered every 3–4 weeks to MM patients with osteolytic bone disease.
Patients and Methods
Patient Population
Men and women (≥18 years of age) with a diagnosis of MM, at least one bone lesion on plain film radiographs, stable kidney function (defined as two SCr level determinations of <3 mg/dL obtained at least 7 days apart during the screening period), calculated CrCl of at least 30 mL/min, Eastern Cooperative Oncology Group (ECOG) performance status of 1 or less, and a life expectancy of at least 9 months were eligible. The study excluded patients with prolonged IV bisphosphonate use (defined as use of zoledronic acid longer than 3 years or pamidronate longer than 1 year [total bisphosphonate duration could not exceed 3 years]), corrected serum calcium level at first visit of <8 or ≥12 mg/dL, or diagnosis of amyloidosis. Additionally, patients who had known hypersensitivity to zoledronic acid or other bisphosphonates; were pregnant or lactating; had uncontrolled cardiovascular disease, hypertension, or type 2 diabetes mellitus; or had a history of noncompliance with medical regimens were not eligible.
Study Design
This open-label, randomized pilot study was conducted at 45 centers in the United States. Before randomization, patients were stratified based on length of time of prior bisphosphonate treatment (bisphosphonate-naive vs ≤1 year prior bisphosphonate therapy vs >1 year prior bisphosphonate therapy) and baseline calculated CrCl (>75 vs >60–75 vs ≥30–≤60 mL/min).
Treatment and Evaluation
Patients were randomized to receive zoledronic acid 4 mg as either a 15- or a 30-minute IV infusion. The volume of infusate was increased from the standard 100 to 250 mL to provide additional hydration; infusions were administered every 3–4 weeks for up to 24 months. At the time this study was developed, the 4 mg dose was used because the dose adjustments for renal dysfunction in the current FDA labeling for zoledronic acid were not yet available.7 Patients were required to take a calcium supplement containing 500 mg of calcium and a multivitamin containing 400–500 IU of vitamin D, orally, once daily, for the duration of zoledronic acid therapy.
HCM during the trial was defined as a corrected serum calcium level ≥12 mg/dL or a lower level of hypercalcemia accompanied by symptoms and/or requiring active treatment other than rehydration. If HCM occurred more than 14 days after a zoledronic acid infusion, patients could receive a zoledronic acid infusion as treatment for HCM, even if this required administration before the next scheduled dose. Patients were allowed to remain in the study provided that HCM did not persist or recur. However, zoledronic acid treatment was immediately discontinued if patients developed HCM ≤14 days after study drug infusion; these patients received HCM treatment at the discretion of their treating physician. Also, patients experiencing HCM discontinued calcium and vitamin D supplements.
Within 2 weeks before each dose, enrolled patients were assessed for increase in SCr levels. For patients experiencing a clinically relevant increase in SCr level (defined as a rise of 0.5 mg/dL or more or a doubling of baseline SCr levels), administration of zoledronic acid was suspended until the SCr level fell to within 10% of the baseline value. During the delay, SCr levels were monitored at each regularly scheduled study visit (every 3–4 weeks) or more frequently if deemed necessary by the investigator. If the SCr level fell to within 10% of the baseline value within the subsequent 12 weeks, zoledronic acid was restarted with an infusion time that was increased by 15 minutes over the starting duration. If the rise in SCr level did not resolve within 12 weeks or if the patient experienced a second clinically relevant increase in SCr level after modification of the infusion time, treatment was permanently discontinued. Otherwise, patients were followed for 24 months. A final safety assessment, including a full hematology and chemistry profile, was performed 28 days after the last infusion.
A pretreatment dental examination with appropriate preventive dentistry was suggested for all patients with known risk factors for the development of osteonecrosis of the jaw (ONJ) (eg, cancer chemotherapy, corticosteroids, poor oral hygiene, dental extraction, or dental implants). Throughout the study, patients reporting symptoms that could be consistent with ONJ were referred to a dental professional for assessment; if exposed bone was noted on dental examination, the patient was referred to an oral surgeon for further evaluation, diagnosis, and treatment. A diagnosis of ONJ required cessation of zoledronic acid therapy and study discontinuation.
Pharmacokinetic Sampling
At the first infusion visit (visit 2), pharmacokinetic (PK) parameters were measured. If PK samples were not obtained at visit 2, they could be obtained at visit 3 (otherwise, they were recorded as not done). All blood samples for PK analysis were drawn from the contralateral arm. For patients receiving the 15-minute zoledronic acid infusion, the protocol specified that PK samples were to be drawn at exactly 10 and 15 minutes from the start of the infusion; patients receiving the 30-minute zoledronic acid infusion were to have blood samples drawn at exactly 25 and 30 minutes from the start of the infusion. The second blood sample for PK analysis was taken before the study drug infusion was stopped in both groups. PK analysis was performed by Novartis Pharmaceuticals Corporation Drug Metabolism and Pharmacokinetics France (Rueil-Malmaison, France) and SGS Cephac (Geneva Switzerland), using a competitive radioimmunoassay that has a lower limit of quantification of 0.04 ng/mL and an upper limit of quantification of 40 ng/mL.
Statistical Analysis
The primary study end point was the proportion of patients with a clinically relevant increase in SCr level at 12 months. Descriptive statistics were used to summarize the primary end point; in addition, an exploratory analysis with a logistic regression model, using treatment group, prior bisphosphonate therapy, and baseline CrCl, was performed.
Additional secondary safety end points included the proportion of patients with a clinically relevant increase in SCr level at 24 months, time to first clinically relevant increase in SCr level, and the PK profile of zoledronic acid. The proportion of patients with a clinically relevant increase in SCr level at 24 months was summarized using descriptive statistics. Time to first clinically relevant increase in SCr level was analyzed using the Kaplan-Meier method at the time of the primary analysis (12 months) and at 24 months. Plasma concentration data were evaluated by treatment group and baseline kidney function using descriptive statistics. Continuous variables of baseline and demographic characteristics between treatment groups were compared using a two-sample t-test; between-group differences in discrete variables were analyzed using Pearson's chi-squared test.
The primary analysis included all randomized patients who received at least one zoledronic acid infusion and who had valid postbaseline data for assessment. All study subjects who had evaluable PK parameters were included in a secondary PK analysis. Efficacy assessments were not included in this trial.
This pilot trial was designed to obtain additional preliminary data to support the hypothesis that a longer infusion is associated with less kidney dysfunction than a shorter infusion; therefore, a sample size of 90 patients per treatment group was selected. All statistical tests employed a significance level of 0.05 against a two-sided alternative hypothesis.
The institutional review boards of participating institutions approved the study, and all patients provided written informed consent before study entry.
Results
Study Population
Between October 2004 and October 2007, 179 MM patients with SCr <3 mg/dL were randomized to receive either a 15- or a 30-minute infusion of zoledronic acid. Of these, 176 patients (88 in each group) received at least one dose of study drug. Because of protocol violations, postbaseline data from one site were excluded from analyses, leaving 85 assessable patients in the 15-minute group and 84 patients in the 30-minute group.
Overall, the study groups were representative of a general population with MM. About two-thirds of patients had received prior bisphosphonate therapy; the duration of therapy was greater than 1 year for most of these patients (Table 1). The most common concomitant therapies included dexamethasone, thalidomide, and melphalan. Although the median age, proportion of patients who were 65 years of age or older, and ratio of men to women were greater in the 15-minute infusion group, none of the differences in baseline demographics was statistically significant. All other baseline demographics and disease characteristics, including prior bisphosphonate use and baseline CrCl values, were similar between the two groups (see Table 1). During the study, six patients in the 15-minute treatment group and one patient in the 30-minute treatment group experienced HCM. Three of the six patients in the 15-minute treatment group and one patient in the 30-minute treatment group discontinued the study as a result of HCM.
| NUMBER OF PATIENTS (%)a | ||
|---|---|---|
| CHARACTERISTIC | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 88)b | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 88)b |
| Age (years) | ||
| Mean (SD) | 64 | 64 |
| Median | 66 | 64 |
| Range | 37–91 | 27–86 |
| Age category (years) | ||
| <65 | 39 (44) | 47 (53) |
| ≥65 | 49 (56) | 41 (47) |
| Sex | ||
| Male | 56 (64) | 49 (56) |
| Female | 32 (36) | 39 (44) |
| Race | ||
| White | 70 (80) | 69 (78) |
| Black | 9 (10) | 13 (15) |
| Asian | 1 (1) | 1 (1) |
| Other | 8 (9) | 5 (6) |
| Time since diagnosis (months) | ||
| Mean (SD) | 12 (24) (n = 86) | 10 (14) (n = 87) |
| Median | 4 | 6 |
| Range | 0–186 | 0–98c |
| Prior bisphosphonate use | ||
| Naive | 28 (32) | 28 (32) |
| ≤1 year | 12 (14) | 14 (16) |
| >1 year | 48 (55) | 39 (44) |
| Missing | 0 (0) | 7 (8) |
| Calculated CrCl (mL/min) | ||
| Mean (SD) | 87 (33) | 89 (40) |
| Median | 84 | 83 |
| Range | 33–210 | 31–224 |
| Calculated CrCl category (mL/min) | ||
| CrCl ≥75 | 54 (61) | 49 (56) |
| 60 < CrCL < 75 | 13 (15) | 15 (17) |
| 30 < CrCl ≤ 60 | 21 (24) | 24 (27) |
| CrCl <30 | 0 (0) | 0 (0) |
CrCl = creatinine clearance; IV = intravenous; SD = standard deviation
a Unless otherwise notedb Safety populationc One patient had a screening visit date before the date of initial diagnosis
Protocol violations and/or deviations (n = 658) occurred during this study, affecting 139 patients. The types of protocol violations/deviations were related to protocol adherence (n = 404), timing of visits (n = 210), protocol adherence/timing of visits (n = 2), exclusion criteria (n = 22), inclusion criteria (n = 10), and informed consent (n = 1); 9 violations were unclassified. Notably, one protocol adherence deviation that occurred was incorrect infusion duration despite the patient having a stable SCr level. In the 15-minute treatment group, 15% of infusions administered were longer than 15 minutes. Among the longer infusions, 7% of the infusions correctly occurred per protocol following an SCr-level increase, whereas 7% of the prolonged infusions were 20 minutes or longer in the absence of an SCr-level increase. Similarly, in the 30-minute treatment group, 5% of patients received infusions lasting at least 35 minutes in the absence of an SCr-level increase.
Renal Safety
At 12 months, slightly fewer patients (n = 13 [16%]) in the 30-minute infusion group had a clinically relevant increase in SCr level than in the 15-minute infusion group (n = 17 [20%]); but this difference was not statistically significant, and for approximately 35% of patients in each group there were no SCr data available (Table 2). The median time to a clinically relevant increase in SCr by Kaplain-Meier was not reached in either group (data not shown). Neither previous bisphosphonate use nor baseline CrCl significantly affected the results (P = 0.5837 and P = 0.9371, respectively).
| NUMBER OF PATIENTS (%) | |||
|---|---|---|---|
| CLINICALLY RELEVANT INCREASE IN SCR | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 85)a | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 84)a | P VALUEb |
| 12 Months | 0.6892 | ||
| Yes | 17 (20) | 13 (16) | |
| No | 38 (45) | 42 (50) | |
| Unknown | 30 (35) | 29 (35) | |
| 24 Months | 0.9750 | ||
| Yes | 24 (28) | 23 (27) | |
| No | 22 (26) | 23 (27) | |
| Unknown | 39 (46) | 38 (45) | |
CI = confidence interval; IV = intravenous; SCr = serum creatinine
a Safety population, excluding patients with protocol violationsb P value calculated based on chi-squared test
After 24 months of treatment, the proportion of patients experiencing a clinically relevant increase in SCr level was similar between treatment groups, although for approximately 45% of patients in each group there were no SCr data available (see Table 2). Moreover, the difference in time to first clinically relevant increase in SCr level was not statistically significant between the two groups (P = 0.55) (Figure 1). However, among patients with a clinically significant rise in SCr level, the median time to SCr rise was slightly longer in the 30-minute group than in the 15-minute group (22 vs 24 weeks), but this was not statistically significant.
Increases in SCr relative to baseline led to treatment discontinuation in 20 patients (24%) receiving a 15-minute infusion and 14 patients (17%) receiving a 30-minute infusion. In these cases, the treating physician either considered the SCr level too high for continued treatment or the SCr level was persistently high despite treatment interruption.
Pharmacokinetics
Median zoledronic acid concentrations, as anticipated, were higher with the 15-minute infusion time at both sampling time points (during infusion: 15-minute group 231 ng/mL [at 10 minutes] vs 30-minute group 186 ng/mL [at 25 minutes]; end-of-infusion: 15-minute group, 249 ng/mL vs 30-minute group 172 ng/mL).
Adverse Events
Overall, the incidence and severity of AEs were as anticipated for MM patients. The most commonly reported AEs included fatigue, anemia, nausea, constipation, and back pain (Table 3). Although many AEs were reported more frequently in the 30-minute infusion group, the incidence rates of AEs suspected to be related to zoledronic acid were similar between the two groups. Toxicities were graded as mild, moderate, or severe; proportions of AEs categorized by these grades were comparable. Nonfatal serious AEs (SAEs) occurred in 26% of patients receiving the 15-minute infusion and 35% of patients receiving the 30-minute infusion; however, only one patient in the 15-minute group and two patients in the 30-minute group had SAEs suspected to be related to study medication.
| NUMBER OF PATIENTS (%) | |||
|---|---|---|---|
| TYPE OF AE | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 85) | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 84) | TOTAL (N = 169) |
| Blood and lymphatic system disorders | |||
| Anemia | 19 (22) | 27 (32) | 46 (27) |
| Neutropenia | 6 (7) | 12 (14) | 18 (11) |
| Gastrointestinal disorders | |||
| Constipation | 20 (24) | 21 (25) | 41 (24) |
| Diarrhea | 14 (17) | 20 (24) | 34 (20) |
| Nausea | 18 (21) | 27 (32) | 45 (27) |
| Vomiting | 10 (12) | 14 (17) | 24 (14) |
| General disorders | |||
| Fatigue | 30 (35) | 41 (49) | 71 (42) |
| Pain | 7 (8) | 10 (12) | 17 (10) |
| Pain in extremity | 14 (17) | 16 (19) | 30 (18) |
| Peripheral edema | 13 (15) | 20 (24) | 33 (20) |
| Pyrexia | 15 (18) | 19 (23) | 34 (20) |
| Infections and infestations | |||
| Pneumonia | 11 (13) | 7 (8) | 18 (11) |
| Upper respiratory tract infection | 13 (15) | 13 (16) | 26 (15) |
| Metabolism and nutrition disorders | |||
| Anorexia | 8 (9) | 9 (11) | 17 (10) |
| Hypokalemia | 12 (14) | 13 (15) | 25 (14) |
| Musculoskeletal and connective tissue disorders | |||
| Arthralgia | 10 (11) | 16 (19) | 26 (15) |
| Asthenia | 9 (10) | 13 (16) | 22 (13) |
| Back pain | 19 (22) | 20 (24) | 39 (23) |
| Bone pain | 10 (12) | 11 (13) | 21 (12) |
| Nervous system disorders | |||
| Dizziness | 11 (13) | 10 (12) | 21 (12) |
| Peripheral neuropathy | 7 (8) | 15 (18) | 22 (13) |
| Psychiatric disorders | |||
| Insomnia | 10 (12) | 14 (17) | 24 (14) |
| Respiratory, thoracic, and mediastinal disorders | |||
| Cough | 13 (15) | 15 (18) | 28 (17) |
| Dyspnea | 15 (18) | 17 (20) | 32 (19) |
| Skin and subcutaneous tissue disorders | |||
| Rash | 9 (11) | 12 (14) | 21 (12) |
AE = adverse event; IV = intravenous
a Safety population excluding patients with protocol violations
The numbers of deaths, trial discontinuations, and treatment interruptions due to AEs were similar between the two groups as well. Deaths (9 [10.6%] 15-minute group vs 6 [7.1%] 30-minute group) were not suspected to be related to zoledronic acid. Eight patients in each treatment group discontinued therapy because of an AE; events leading to treatment discontinuation that were suspected to be related to zoledronic acid occurred in two patients in the 15-minute group (skeletal pain and ONJ) and one patient in the 30-minute group (jaw pain). AEs that required treatment interruption occurred in eight and nine patients in the 15-minute and 30-minute groups, respectively.
AEs of special interest included those related to kidney dysfunction, cardiac arrhythmias, SREs, and ONJ. The number of patients reporting overall kidney and urinary disorders was the same in the two treatment groups (14 patients in each group); however, acute renal failure was reported more frequently in patients receiving the 15-minute infusion compared with the 30-minute infusion (four patients [5%] vs one patient [1%] in 30-minute group). Details of these five patients are presented in Table 4. AEs related to cardiac rhythm occurred in 20 patients while on study; however, only one case of bradycardia was suspected to be related to zoledronic acid therapy (in the 30-minute group). The incidence of SREs at 2 years was comparable in the two groups (19% in 15-minute group vs 21% in 30-minute group). The time to onset of SREs was longer in the 15-minute group (222 vs 158 days), but this was not statistically significant. A total of 10 patients with suspected ONJ were identified, with three patients in the 15-minute group (all moderate) and seven patients in the 30-minute group (mild [n = 5], moderate [n = 1], severe [n = 1]). Six of these patients received bisphosphonates before entering the study (four patients received no prior bisphosphonates), but the length of previous bisphosphonate therapy varied (0–30 months). Patients with suspected ONJ were assessed by clinicians and referred to dental professionals for further evaluation.
| PATIENT DEMOGRAPHICS | TYPE OF MM | MEDICAL HISTORY | CONCURRENT MEDICATIONSa | ACUTE RENAL FAILURE DETAILS | OUTCOME |
|---|---|---|---|---|---|
| Zoledronic acid 4 mg IV for 15 minutes | |||||
| 73-year-old female Caucasian | IgG | Anemia, cardiomyopathy, CHF, cholecystectomy, benign breast lump removal, CAD, DM, dyslipidemia, central venous catheterization, chronic renal failure, GERD, hypercholesterolemia, HTN, hysterectomy, mycobacterial infection, hemorrhoids, B-cell lymphoma, seborrheic keratosis, tonsillectomy | At start of study: aspirin, losartan, digoxin, hydrochlorothiazide/lorsartan, fluconazole, folic acid, atorvastatin, vitamins, warfarinDuring study: ethambutol dihydrochloride, moxifloxacin, rifabutin, fenofibrate, omeprazole, diuretics, nitroglycerin patch, angiotensin-converting enzyme inhibitors, hydroxyzine, loratadine, furosemide, vancomycin, pantoprozole, piperacillin/tazobactam, clarithromycin | Myeloma kidney mass consistent with myeloma kidney found during study; approximately 2 weeks later the patient developed severe infection that culminated in septic shock, with acute renal failure | Nephrologist considered renal insufficiency to be partly related to past history of large-cell lymphoma and chemotherapy; patient was discharged to hospice and died of acute renal failure secondary to myeloma |
| 71-year-old female Caucasian | IgA | Back pain, cholecystectomy, constipation, CAD, NIDDM, hypercholesterolemia, HTN, insomnia, left knee operation, neuralgia, obesity, osteoarthritis, hysterectomy, hypoacusis, seasonal allergies, urinary incontinence | At start of study: zolpidem, amitriptyline, loratidine, tolterodine l-tartrate, valsartan, metrotoprolol, furosemide, ibuprofen, clonazepam, gabapentin, liodcaine, hydrocodone/acetaminophen, quinine sulfate, simvastatin During study: calcium, multivitamins, lactulose, trazodone, hydromorphone, cyclobenzaprine, glipizide, macrogol, lorazepam, methadone, potassium, lisinopril, furosemide, meperidine, promethazine | Developed moderate acute renal failure on the day of her first dose; considered not associated with zoledronic acid | Renal ultrasound showed arterial stenosis; resolved approximately 1 month after diagnosis |
| 65-year-old male Caucasian | IgG | Oxycodone hypersensitivity, anemia, back pain, spine metastases, spinal compression fracture, depression, fatigue, inguinal hernia repair, spinal fusion (L1–L3) surgery, bilateral hip arthroplasty, pain, pneumonia, staphylococcal infection | At start of study: fluconazole, morphine sulfate, oxycodone/acetaminophen During study: naproxen, darbepoietin alfa, sodium ferrifluconate, calcium with vitamin D, cephalexin, dexamethasone, alginic acid, docusate, heparin, sodium polystyrene, levofloxacin, filgrastim, lansoprazole | After 5 doses of zoledronic acid, patient developed severe acute renal failure with elevated SCr; not suspected to be related to zoledronic acid | Resolved 9 days later following treatment with cephalexin and dexamethasone |
| 56-year-old female Caucasian | IgA | Osteolysis, cataract surgery, constipation, bone lesions, hypercholesterolemia, HTN, musculoskeletal pain, anorexia | At start of study: ibuprofen, oxycodone, propoxyphene/acetaminophen, hydrocodone/acetaminophen, valsartan, calcium/vitamin D, potassium chloride, docusate sodiumDuring study: vancomycin, acyclovir | Approximately 1 week after 9th zoledronic acid dose, patient developed acute renal failure with an increased SCr (12.5 mg/dL); not suspected to be related to zoledronic acid | Resulted from myeloma progression to plasma cell leukemia; emergency dialysis performed; catheter-related sepsis occurred approximately 1 month later, and patient died of sepsis and disease progression |
| Zoledronic acid 4 mg IV for 30 minutes | |||||
| 80-year-old male African American | IgG | Anemia, arteriosclerotic heart disease, bilateral ankle swelling/pain, degenerative joint disease, dyspnea on exertion, fatigue, GERD, HTN, neutropenia, shoulder pain, vasovagal syncope | At start of study: aspirin, atenolol, multivitamin, doxazosin, fosinopril, hydrochlorothiazide, amlodipine besylate, simvastatinDuring study: darbepoietin alfa, warfarin sodium, furosemide, omeprazole, calcium carbonate | Approximately 1 month after 2nd dose, patient experienced increased SCr (2.9 mg/dL, 53% increase from baseline); relationship to zoledronic acid unknown | Discontinued from study after 2nd dose, and SCr remained elevated for 2 months following discontinuation |
CAD = coronary artery disease; CHF = congestive heart failure; DM = diabetes mellitus; GERD = gastroesophageal reflux disease; HTN = hypertension; MM = multiple myeloma; NIDDM = non-insulin-dependent diabetes mellitus; SCr = serum creatinine
Discussion
During the past decade, bisphosphonate therapy has become an important adjunctive treatment to prevent the emergence, or worsening, of SREs in patients with MM involving the bone.15 Kidney failure is a common and severe complication of MM that may be exacerbated by chronic administration of zoledronic acid.7 A study evaluating zoledronic acid in patients with cancer and bone metastases suggests that increasing the infusion time decreases the Cmax, which may result in fewer renal AEs.[9] and [12] This study was designed to assess whether prolonging the infusion time of zoledronic acid from the recommended 15 to 30 minutes would improve kidney safety in MM patients, as evidenced by fewer rises in SCr levels. To our knowledge, this is the only trial that has been designed to evaluate the impact of infusion duration on renal effects in this population.
The 12-month results of this pilot study showed a trend toward improved renal safety with the longer infusion time, this difference not being statistically significant. By 24 months, however, there were no differences in SCr level elevations between the two groups. The clinically relevant SCr increases observed in our study, however, differ from those reported by Rosen and colleagues,[5] and [6] who first evaluated zoledronic acid for patients with MM. In that study, 4%–11% of patients experienced kidney function deterioration, manifested by SCr increases, which is much lower than the rate observed in our study. However, several differences exist between our trial and the Rosen study. The Rosen study included both breast cancer patients with at least one bone metastasis and Durie-Salmon stage 3 MM patients with at least one osteolytic lesion, whereas our study only included MM patients with at least one bone lesion. Additionally, the criteria for defining a clinically relevant SCr increase differ between the two studies; therefore, one cannot directly compare the incidence of kidney dysfunction between these two studies. Although in our study the sample size was small, confidence intervals were wide, and protocol deviations did not permit a robust comparison, the results of this pilot study suggest that the longer infusion time of 30 minutes every 3–4 weeks for 2 years for MM patients with bone disease is also safe and well-tolerated.
As expected, PK data showed that the median zoledronic acid concentrations were greater in the samples obtained from the 15-minute group compared to those from the 30-minute group. This effect was observed in samples obtained both 5 minutes before the end of infusion and at the end of infusion.
Increasing the infusion time did not significantly alter the AE profile and was not associated with any new or unexpected AEs. The incidence rates of deaths, SAEs, treatment-related AEs, and overall AEs were generally comparable between treatment groups. Overall, the incidence rates of reported SREs and ONJ were as expected for this patient population, which are important factors when considering zoledronic acid for patients with MM, where the goal of ongoing monthly IV bisphosphonate therapy is to prevent the development of new SREs without increasing the risk of AEs, such as ONJ.
Finally, the FDA-approved current labeling for zoledronic acid recommends decreasing the dose of this bisphosphonate based on baseline kidney function.7 Because these recommendations were not in place at the time that this study was designed, whether the implementation of these dosing guidelines for patients with MM along with varying infusion durations would have impacted the results observed in our study cannot be ascertained.
In summary, the results of this study suggest that the safety profile of IV zoledronic acid is similar regardless of a 15-minute or a 30-minute infusion duration. However, because the study was not powered to detect statistical significance and the current renal dosing guidelines for zoledronic acid were not used in this study, large randomized studies, using current dosing recommendations, will be required to further assess the effects on kidney safety of prolonging the infusion time of ongoing monthly IV zoledronic acid therapy for patients with MM.
Acknowledgments
The authors thank Syntaxx Communications, Inc., specifically, Kristin Hennenfent, PharmD, MBA, BCPS, and Lisa Holle, PharmD, BCOP, who provided manuscript development and medical writing services, and Holly Matthews, BS, who provided editorial services, with support from Novartis Pharmaceuticals Corporation. We also thank all participating patients and study personnel. Research support was provided by Novartis Pharmaceuticals Corporation (East Hanover, NJ).
References
1 A. Jemal, R. Siegel and J. Xu et al., Cancer statistics, 2010, CA Cancer J Clin 60 (2010), pp. 277–300. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (543)
2 R.A. Kyle, M.A. Gertz and T.E. Witzig et al., Review of 1027 patients with newly diagnosed multiple myeloma, Mayo Clin Proc 78 (1) (2003), pp. 21–33. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (396)
3 A. Corso, P. Zappasodi and C. Pascutto et al., Urinary proteins in multiple myeloma: correlation with clinical parameters and diagnostic implications, Ann Hematol 82 (8) (2003), pp. 487–491. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
4 V. Eleutherakis-Papaiakovou, A. Bamias and D. Gika et al., Renal failure in multiple myeloma: incidence, correlations, and prognostic significance, Leuk Lymphoma 48 (2) (2007), pp. 337–341. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (35)
5 L.S. Rosen, D. Gordon and M. Kaminski et al., Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial, Cancer J 7 (5) (2001), pp. 377–387. View Record in Scopus | Cited By in Scopus (461)
6 L.S. Rosen, D. Gordon and M. Kaminski et al., Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized, double-blind, multicenter, comparative trial, Cancer 98 (8) (2003), pp. 1735–1744. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (329)
7 , Zometa (package insert), Novartis Pharmaceuticals, Corporation, East Hanover, NJ (2008).
8 P. Major, A. Lortholary and J. Han et al., Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials, J Clin Oncol 19 (2) (2001), pp. 558–567. View Record in Scopus | Cited By in Scopus (325)
9 T. Chen, J. Berenson and R. Vescio et al., Pharmacokinetics and pharmacodynamics of zoledronic acid in cancer patients with bone metastases, J Clin Pharmacol 42 (11) (2002), pp. 1228–1236. View Record in Scopus | Cited By in Scopus (139)
10 T. Pfister, E. Atzpodien and F. Bauss, The renal effects of minimally nephrotoxic doses of ibandronate and zoledronate following single and intermittent intravenous administration in rats, Toxicology 191 (2003), pp. 159–167. Article |

11 T. Pfister, E. Aztpodien, B. Bohrmann and F. Bauss, Acute renal effects of intravenous bisphosphonates in the rat, Basic Clin Pharmacol Toxicol 97 (2005), pp. 374–381. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (17)
12 F. Saad, D.M. Gleason and R. Murray et al., A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma, J Natl Cancer Inst 94 (19) (2002), pp. 1458–1468. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (650)
13 S. Kautiainen, S. Luurila, P. Ylitalo and R. Ylitalo, Transformation of bisphosphonates into insoluble material in human blood in vitro, Methods Find Exp Clin Pharmacol 20 (4) (1998), pp. 289–295. View Record in Scopus | Cited By in Scopus (5)
14 L.S. Rosen, D. Gordon and S. Tchekmedyian et al., Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial—the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group, J Clin Oncol 21 (16) (2003), pp. 3150–3157. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (251)
15 M.A. Hussein, Multiple myeloma: most common end-organ damage and management, J Natl Compr Canc Netw 5 (2) (2007), pp. 170–178. View Record in Scopus | Cited By in Scopus (4)
Appendix
The following ZMAX Trial principal investigators participated in this study: Bart Barlogie, MD, Myeloma Institute For Research and Therapy; James Berenson, MD, Oncotherapeutics; Robert Bloom, MD, Providence Cancer Center, Clinical Trials Department; Ralph Boccia, MD, Center for Cancer and Blood Disorders; Donald Brooks, MD, Arizona Clinical Research Center, Inc.; Robert Brouillard, MD, Robert P. Brouillard, MD, and Delvyn Case, MD, Maine Center for Cancer Medicine and Blood Disorders, Pharmacy; Veena Charu, MD, Pacific Cancer Medical Center; Naveed Chowhan, MD, Cancer Care Center, Inc; Robert Collins, MD, University of Texas Southwestern Medical Center at Dallas; Thomas Cosgriff, MD, Hematology and Oncology Specialists, LLC; Jose Cruz, MD, Joe Arrington Cancer Research and Treatment Center; Surrinder Dang, MD, Oncology Specialties; Sheldon Davidson, MD, North Valley H/O; Tracy Dobbs, MD, Baptist Regional Cancer Center; Luke Dreisbach, MD, Desert Hematology Oncology Medical Group; Isaac Esseesse, MD, Hematology Oncology Associates of Central Brevard, Laboratory; Mark Fesen, MD, Hutchinson Clinic, PA; George Geils, Jr., MD, Charleston Hematology Oncology Associates, PA; Michael Greenhawt, MD, South Florida Oncology-Hematology; Manuel Guerra, MD, ORA; Rita Gupta, MD, Oncology-Hematology Associates, PA; Vicram Gupta, MD, Saint Joseph Oncology; Alexandre Hageboutros, MD, Cancer Institute of New Jersey at Cooper Hospital; Vincent Hansen, MD, Utah Hematology Oncology; David Henry, MD, Pennsylvania Oncology Hematology Associates; Benjamin Himpler, MD, Syracuse Hematology/Oncology PC; Winston Ho, MD, Hematology/Oncology Group of Orange County; William Horvath, MD, Haematology Oncology Associates of Ohio and Michigan, PC; Paul Hyman, MD, Hematology Oncology Associates of Western Suffolk; Min Kang, MD, Western Washington Oncology; Mark Keaton, MD, Augusta Oncology Associates, PC; Howard Kesselheim, MD, The Center for Cancer and Hematologic Disease; Kapisthalam Kumar, MD, Pasco Hernando Oncology Associates, PA; Edward Lee, MD, Maryland Oncology-Hematology, PA; André Liem, MD, Pacific Shore Medical Group; Timothy Lopez, MD, New Mexico Cancer Care Associates, Cancer Institute of New Mexico; Paul Michael, MD, Comprehensive Cancer Centers of Nevada; Michael Milder, MD, Swedish Cancer Institute; Barry Mirtsching, MD, Center for Oncology Research & Treatment, PA; Ruben Niesvizky, MD, New York Presbyterian Hospital; Jorge Otoya, MD, Osceola Cancer Center; Joseph Pascuzzo, MD, California Oncology of the Central Valley; Ravi Patel, MD, Comprehensive Blood and Cancer Center Lab; Allen Patton, MD, Hematology Oncology Associates, PA; Kelly Pendergrass, MD, Kansas City Cancer Center, LLC; Anthony Phillips, MD, Fox Valley Hematolgy Oncology, SC; Robert Raju, MD, Dayton Oncology and Hematology, PA; Harry Ramsey, MD, Berks Hematology Oncology Associates; Ritesh Rathore, MD, Roger Williams Hospital Medical Center; Phillip Reid, MD, Central Jersey Oncology Center; Robert Robles, MD, Bay Area Cancer Research Group, LLC; Stephen Rosenoff, MD, Oncology and Hematology Associates of Southwest Virginia, Inc; Martin Rubenstein, MD, Southbay Oncology Hematology Partners; Mansoor Saleh, MD, Georgia Cancer Specialists; Sundaresan Sambandam, MD, Hematology and Oncology Associates of RI; Mukund Shah, MD, Antelope Valley Cancer Center; David Siegel, MD, Hackensack University Medical Center; Nelida Sjak-Shie, MD, The Center for Cancer Care and Research; Michael Stone, MD, Greeley Medical Clinic; Stefano Tarantolo, MD, Nebraska Methodist Hospital; Joseph Volk, MD, Palo Verde Hematology Oncology, Ltd; Mitchell Weisberg, MD, MetCare Oncology; Ann Wierman, MD, Nevada Cancer Center; Donald Woytowitz, Jr., MD, Florida Cancer Specialists; Peter Yu, MD, Camino Medical Group.

Original research
James R. Berenson MD![]()
![]()
Abstract
Zoledronic acid, an intravenous (IV) bisphosphonate, is a standard treatment for multiple myeloma (MM) but may exacerbate preexisting renal dysfunction. The incidence of zoledronic acid–induced renal dysfunction may correlate with infusion duration. In this randomized, multicenter, open-label study, 176 patients with MM, at least one bone lesion, and stable renal function with a serum creatinine (SCr) level <3 mg/dL received zoledronic acid 4 mg (in 250 mL) as a 15- or 30-minute IV infusion every 3–4 weeks. At month 12, 20% (17 patients) in the 15-minute and 16% (13 patients) in the 30-minute arm experienced a clinically relevant but nonsignificant SCr-level increase (P = 0.44). By 24 months, the proportion of patients with a clinically relevant SCr-level increase was similar between arms (15-minute 28% [24 patients] vs 30-minute 27% [23 patients], P = 0.9014). Median zoledronic acid end-of-infusion concentrations were higher with the shorter infusion (15-minute 249 ng/mL vs 30-minute 172 ng/mL), and prolonging the infusion beyond 15 minutes did not influence adverse events related to zoledronic acid. For patients with MM, the safety profile of IV zoledronic acid is similar between those receiving a 15- or 30-minute infusion; therefore, determining the appropriate infusion duration of zoledronic acid should be based on individual patient considerations.
Article Outline
Considerable research has focused on preventive and/or treatment strategies to reduce bone complications in MM patients. In a large, international, randomized, phase III trial of MM patients with at least one osteolytic bone lesion, zoledronic acid (Zometa), a potent intravenous (IV) bisphosphonate that inhibits osteoclast-mediated bone resorption, reduced the overall risk of developing skeletally related events (SREs) including HCM by 16% (P = 0.03) compared with standard-dose pamidronate 90 mg (Aredia), another less potent IV bisphosphonate.[5] and [6] As a result of this study and others, monthly infusion of zoledronic acid at 4 mg over at least 15 minutes has become a common treatment for MM patients with bone involvement.
The U.S. Food and Drug Administration (FDA) has approved zoledronic acid use for patients with MM, documented bone metastases from solid tumors, or HCM.[5], [6], [7] and [8] The FDA-approved dose for MM patients is 4 mg administered as an IV infusion over at least 15 minutes every 3–4 weeks for patients with a creatinine clearance (CrCl) of >60 mL/min; when treating HCM, zoledronic acid 4 mg is administered as a single IV infusion.[5], [6], [7] and [8]
Zoledronic acid is primarily excreted intact through the kidney.9 Preexisting kidney disease and receipt of multiple cycles of bisphosphonate therapy are risk factors for subsequent kidney injury.7 In animal studies, IV bisphosphonates have been shown by histology to precipitate renal tubular injury when administered as a single high dose or when administered more frequently at lower doses.[10] and [11] Additionally, renal dysfunction, as evidenced by increased serum creatinine (SCr) levels, was reported among patients treated at a dose of 4 mg with an infusion time of 5 minutes.[7] and [12] When 4 mg zoledronic acid was administered with a longer infusion time of 15 minutes in large randomized trials, no significant difference between the renal safety profiles of zoledronic acid and pamidronate was reported.6
One hypothesis about the development of kidney injury associated with zoledronic acid is that it may be related to the peak plasma concentration as determined by infusion time. Results of a study evaluating patients with MM or other cancer types and bone metastases demonstrated that prolonging the infusion time of zoledronic acid reduced the end-of-infusion peak plasma concentration (Cmax) by 35%.9 Another theory about the development of kidney dysfunction is that insoluble precipitates may form when the blood is exposed to high concentrations of bisphosphonates as this has been shown to occur in vitro.[9] and [13] Therefore, the current management of renal adverse events (AEs) related to IV bisphosphonates is based on these theories so that reducing the peak plasma concentration of zoledronic acid may prevent the possible formation of insoluble precipitates through (1) lowering the dose, (2) slowing the infusion rate, or (3) increasing the volume of infusate.[5], [12] and [14]
Because MM patients are predisposed to experience deterioration of renal function, it is critical to ensure that zoledronic acid does not contribute to, or exacerbate, a decline in kidney function. To determine if increasing the duration of zoledronic acid infusion further results in improved renal safety, a multicenter, open-label, randomized study was designed to compare a 15-minute vs a 30-minute infusion time with an increased volume of infusate from 100 to 250 mL administered every 3–4 weeks to MM patients with osteolytic bone disease.
Patients and Methods
Patient Population
Men and women (≥18 years of age) with a diagnosis of MM, at least one bone lesion on plain film radiographs, stable kidney function (defined as two SCr level determinations of <3 mg/dL obtained at least 7 days apart during the screening period), calculated CrCl of at least 30 mL/min, Eastern Cooperative Oncology Group (ECOG) performance status of 1 or less, and a life expectancy of at least 9 months were eligible. The study excluded patients with prolonged IV bisphosphonate use (defined as use of zoledronic acid longer than 3 years or pamidronate longer than 1 year [total bisphosphonate duration could not exceed 3 years]), corrected serum calcium level at first visit of <8 or ≥12 mg/dL, or diagnosis of amyloidosis. Additionally, patients who had known hypersensitivity to zoledronic acid or other bisphosphonates; were pregnant or lactating; had uncontrolled cardiovascular disease, hypertension, or type 2 diabetes mellitus; or had a history of noncompliance with medical regimens were not eligible.
Study Design
This open-label, randomized pilot study was conducted at 45 centers in the United States. Before randomization, patients were stratified based on length of time of prior bisphosphonate treatment (bisphosphonate-naive vs ≤1 year prior bisphosphonate therapy vs >1 year prior bisphosphonate therapy) and baseline calculated CrCl (>75 vs >60–75 vs ≥30–≤60 mL/min).
Treatment and Evaluation
Patients were randomized to receive zoledronic acid 4 mg as either a 15- or a 30-minute IV infusion. The volume of infusate was increased from the standard 100 to 250 mL to provide additional hydration; infusions were administered every 3–4 weeks for up to 24 months. At the time this study was developed, the 4 mg dose was used because the dose adjustments for renal dysfunction in the current FDA labeling for zoledronic acid were not yet available.7 Patients were required to take a calcium supplement containing 500 mg of calcium and a multivitamin containing 400–500 IU of vitamin D, orally, once daily, for the duration of zoledronic acid therapy.
HCM during the trial was defined as a corrected serum calcium level ≥12 mg/dL or a lower level of hypercalcemia accompanied by symptoms and/or requiring active treatment other than rehydration. If HCM occurred more than 14 days after a zoledronic acid infusion, patients could receive a zoledronic acid infusion as treatment for HCM, even if this required administration before the next scheduled dose. Patients were allowed to remain in the study provided that HCM did not persist or recur. However, zoledronic acid treatment was immediately discontinued if patients developed HCM ≤14 days after study drug infusion; these patients received HCM treatment at the discretion of their treating physician. Also, patients experiencing HCM discontinued calcium and vitamin D supplements.
Within 2 weeks before each dose, enrolled patients were assessed for increase in SCr levels. For patients experiencing a clinically relevant increase in SCr level (defined as a rise of 0.5 mg/dL or more or a doubling of baseline SCr levels), administration of zoledronic acid was suspended until the SCr level fell to within 10% of the baseline value. During the delay, SCr levels were monitored at each regularly scheduled study visit (every 3–4 weeks) or more frequently if deemed necessary by the investigator. If the SCr level fell to within 10% of the baseline value within the subsequent 12 weeks, zoledronic acid was restarted with an infusion time that was increased by 15 minutes over the starting duration. If the rise in SCr level did not resolve within 12 weeks or if the patient experienced a second clinically relevant increase in SCr level after modification of the infusion time, treatment was permanently discontinued. Otherwise, patients were followed for 24 months. A final safety assessment, including a full hematology and chemistry profile, was performed 28 days after the last infusion.
A pretreatment dental examination with appropriate preventive dentistry was suggested for all patients with known risk factors for the development of osteonecrosis of the jaw (ONJ) (eg, cancer chemotherapy, corticosteroids, poor oral hygiene, dental extraction, or dental implants). Throughout the study, patients reporting symptoms that could be consistent with ONJ were referred to a dental professional for assessment; if exposed bone was noted on dental examination, the patient was referred to an oral surgeon for further evaluation, diagnosis, and treatment. A diagnosis of ONJ required cessation of zoledronic acid therapy and study discontinuation.
Pharmacokinetic Sampling
At the first infusion visit (visit 2), pharmacokinetic (PK) parameters were measured. If PK samples were not obtained at visit 2, they could be obtained at visit 3 (otherwise, they were recorded as not done). All blood samples for PK analysis were drawn from the contralateral arm. For patients receiving the 15-minute zoledronic acid infusion, the protocol specified that PK samples were to be drawn at exactly 10 and 15 minutes from the start of the infusion; patients receiving the 30-minute zoledronic acid infusion were to have blood samples drawn at exactly 25 and 30 minutes from the start of the infusion. The second blood sample for PK analysis was taken before the study drug infusion was stopped in both groups. PK analysis was performed by Novartis Pharmaceuticals Corporation Drug Metabolism and Pharmacokinetics France (Rueil-Malmaison, France) and SGS Cephac (Geneva Switzerland), using a competitive radioimmunoassay that has a lower limit of quantification of 0.04 ng/mL and an upper limit of quantification of 40 ng/mL.
Statistical Analysis
The primary study end point was the proportion of patients with a clinically relevant increase in SCr level at 12 months. Descriptive statistics were used to summarize the primary end point; in addition, an exploratory analysis with a logistic regression model, using treatment group, prior bisphosphonate therapy, and baseline CrCl, was performed.
Additional secondary safety end points included the proportion of patients with a clinically relevant increase in SCr level at 24 months, time to first clinically relevant increase in SCr level, and the PK profile of zoledronic acid. The proportion of patients with a clinically relevant increase in SCr level at 24 months was summarized using descriptive statistics. Time to first clinically relevant increase in SCr level was analyzed using the Kaplan-Meier method at the time of the primary analysis (12 months) and at 24 months. Plasma concentration data were evaluated by treatment group and baseline kidney function using descriptive statistics. Continuous variables of baseline and demographic characteristics between treatment groups were compared using a two-sample t-test; between-group differences in discrete variables were analyzed using Pearson's chi-squared test.
The primary analysis included all randomized patients who received at least one zoledronic acid infusion and who had valid postbaseline data for assessment. All study subjects who had evaluable PK parameters were included in a secondary PK analysis. Efficacy assessments were not included in this trial.
This pilot trial was designed to obtain additional preliminary data to support the hypothesis that a longer infusion is associated with less kidney dysfunction than a shorter infusion; therefore, a sample size of 90 patients per treatment group was selected. All statistical tests employed a significance level of 0.05 against a two-sided alternative hypothesis.
The institutional review boards of participating institutions approved the study, and all patients provided written informed consent before study entry.
Results
Study Population
Between October 2004 and October 2007, 179 MM patients with SCr <3 mg/dL were randomized to receive either a 15- or a 30-minute infusion of zoledronic acid. Of these, 176 patients (88 in each group) received at least one dose of study drug. Because of protocol violations, postbaseline data from one site were excluded from analyses, leaving 85 assessable patients in the 15-minute group and 84 patients in the 30-minute group.
Overall, the study groups were representative of a general population with MM. About two-thirds of patients had received prior bisphosphonate therapy; the duration of therapy was greater than 1 year for most of these patients (Table 1). The most common concomitant therapies included dexamethasone, thalidomide, and melphalan. Although the median age, proportion of patients who were 65 years of age or older, and ratio of men to women were greater in the 15-minute infusion group, none of the differences in baseline demographics was statistically significant. All other baseline demographics and disease characteristics, including prior bisphosphonate use and baseline CrCl values, were similar between the two groups (see Table 1). During the study, six patients in the 15-minute treatment group and one patient in the 30-minute treatment group experienced HCM. Three of the six patients in the 15-minute treatment group and one patient in the 30-minute treatment group discontinued the study as a result of HCM.
| NUMBER OF PATIENTS (%)a | ||
|---|---|---|
| CHARACTERISTIC | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 88)b | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 88)b |
| Age (years) | ||
| Mean (SD) | 64 | 64 |
| Median | 66 | 64 |
| Range | 37–91 | 27–86 |
| Age category (years) | ||
| <65 | 39 (44) | 47 (53) |
| ≥65 | 49 (56) | 41 (47) |
| Sex | ||
| Male | 56 (64) | 49 (56) |
| Female | 32 (36) | 39 (44) |
| Race | ||
| White | 70 (80) | 69 (78) |
| Black | 9 (10) | 13 (15) |
| Asian | 1 (1) | 1 (1) |
| Other | 8 (9) | 5 (6) |
| Time since diagnosis (months) | ||
| Mean (SD) | 12 (24) (n = 86) | 10 (14) (n = 87) |
| Median | 4 | 6 |
| Range | 0–186 | 0–98c |
| Prior bisphosphonate use | ||
| Naive | 28 (32) | 28 (32) |
| ≤1 year | 12 (14) | 14 (16) |
| >1 year | 48 (55) | 39 (44) |
| Missing | 0 (0) | 7 (8) |
| Calculated CrCl (mL/min) | ||
| Mean (SD) | 87 (33) | 89 (40) |
| Median | 84 | 83 |
| Range | 33–210 | 31–224 |
| Calculated CrCl category (mL/min) | ||
| CrCl ≥75 | 54 (61) | 49 (56) |
| 60 < CrCL < 75 | 13 (15) | 15 (17) |
| 30 < CrCl ≤ 60 | 21 (24) | 24 (27) |
| CrCl <30 | 0 (0) | 0 (0) |
CrCl = creatinine clearance; IV = intravenous; SD = standard deviation
a Unless otherwise notedb Safety populationc One patient had a screening visit date before the date of initial diagnosis
Protocol violations and/or deviations (n = 658) occurred during this study, affecting 139 patients. The types of protocol violations/deviations were related to protocol adherence (n = 404), timing of visits (n = 210), protocol adherence/timing of visits (n = 2), exclusion criteria (n = 22), inclusion criteria (n = 10), and informed consent (n = 1); 9 violations were unclassified. Notably, one protocol adherence deviation that occurred was incorrect infusion duration despite the patient having a stable SCr level. In the 15-minute treatment group, 15% of infusions administered were longer than 15 minutes. Among the longer infusions, 7% of the infusions correctly occurred per protocol following an SCr-level increase, whereas 7% of the prolonged infusions were 20 minutes or longer in the absence of an SCr-level increase. Similarly, in the 30-minute treatment group, 5% of patients received infusions lasting at least 35 minutes in the absence of an SCr-level increase.
Renal Safety
At 12 months, slightly fewer patients (n = 13 [16%]) in the 30-minute infusion group had a clinically relevant increase in SCr level than in the 15-minute infusion group (n = 17 [20%]); but this difference was not statistically significant, and for approximately 35% of patients in each group there were no SCr data available (Table 2). The median time to a clinically relevant increase in SCr by Kaplain-Meier was not reached in either group (data not shown). Neither previous bisphosphonate use nor baseline CrCl significantly affected the results (P = 0.5837 and P = 0.9371, respectively).
| NUMBER OF PATIENTS (%) | |||
|---|---|---|---|
| CLINICALLY RELEVANT INCREASE IN SCR | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 85)a | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 84)a | P VALUEb |
| 12 Months | 0.6892 | ||
| Yes | 17 (20) | 13 (16) | |
| No | 38 (45) | 42 (50) | |
| Unknown | 30 (35) | 29 (35) | |
| 24 Months | 0.9750 | ||
| Yes | 24 (28) | 23 (27) | |
| No | 22 (26) | 23 (27) | |
| Unknown | 39 (46) | 38 (45) | |
CI = confidence interval; IV = intravenous; SCr = serum creatinine
a Safety population, excluding patients with protocol violationsb P value calculated based on chi-squared test
After 24 months of treatment, the proportion of patients experiencing a clinically relevant increase in SCr level was similar between treatment groups, although for approximately 45% of patients in each group there were no SCr data available (see Table 2). Moreover, the difference in time to first clinically relevant increase in SCr level was not statistically significant between the two groups (P = 0.55) (Figure 1). However, among patients with a clinically significant rise in SCr level, the median time to SCr rise was slightly longer in the 30-minute group than in the 15-minute group (22 vs 24 weeks), but this was not statistically significant.
Increases in SCr relative to baseline led to treatment discontinuation in 20 patients (24%) receiving a 15-minute infusion and 14 patients (17%) receiving a 30-minute infusion. In these cases, the treating physician either considered the SCr level too high for continued treatment or the SCr level was persistently high despite treatment interruption.
Pharmacokinetics
Median zoledronic acid concentrations, as anticipated, were higher with the 15-minute infusion time at both sampling time points (during infusion: 15-minute group 231 ng/mL [at 10 minutes] vs 30-minute group 186 ng/mL [at 25 minutes]; end-of-infusion: 15-minute group, 249 ng/mL vs 30-minute group 172 ng/mL).
Adverse Events
Overall, the incidence and severity of AEs were as anticipated for MM patients. The most commonly reported AEs included fatigue, anemia, nausea, constipation, and back pain (Table 3). Although many AEs were reported more frequently in the 30-minute infusion group, the incidence rates of AEs suspected to be related to zoledronic acid were similar between the two groups. Toxicities were graded as mild, moderate, or severe; proportions of AEs categorized by these grades were comparable. Nonfatal serious AEs (SAEs) occurred in 26% of patients receiving the 15-minute infusion and 35% of patients receiving the 30-minute infusion; however, only one patient in the 15-minute group and two patients in the 30-minute group had SAEs suspected to be related to study medication.
| NUMBER OF PATIENTS (%) | |||
|---|---|---|---|
| TYPE OF AE | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 85) | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 84) | TOTAL (N = 169) |
| Blood and lymphatic system disorders | |||
| Anemia | 19 (22) | 27 (32) | 46 (27) |
| Neutropenia | 6 (7) | 12 (14) | 18 (11) |
| Gastrointestinal disorders | |||
| Constipation | 20 (24) | 21 (25) | 41 (24) |
| Diarrhea | 14 (17) | 20 (24) | 34 (20) |
| Nausea | 18 (21) | 27 (32) | 45 (27) |
| Vomiting | 10 (12) | 14 (17) | 24 (14) |
| General disorders | |||
| Fatigue | 30 (35) | 41 (49) | 71 (42) |
| Pain | 7 (8) | 10 (12) | 17 (10) |
| Pain in extremity | 14 (17) | 16 (19) | 30 (18) |
| Peripheral edema | 13 (15) | 20 (24) | 33 (20) |
| Pyrexia | 15 (18) | 19 (23) | 34 (20) |
| Infections and infestations | |||
| Pneumonia | 11 (13) | 7 (8) | 18 (11) |
| Upper respiratory tract infection | 13 (15) | 13 (16) | 26 (15) |
| Metabolism and nutrition disorders | |||
| Anorexia | 8 (9) | 9 (11) | 17 (10) |
| Hypokalemia | 12 (14) | 13 (15) | 25 (14) |
| Musculoskeletal and connective tissue disorders | |||
| Arthralgia | 10 (11) | 16 (19) | 26 (15) |
| Asthenia | 9 (10) | 13 (16) | 22 (13) |
| Back pain | 19 (22) | 20 (24) | 39 (23) |
| Bone pain | 10 (12) | 11 (13) | 21 (12) |
| Nervous system disorders | |||
| Dizziness | 11 (13) | 10 (12) | 21 (12) |
| Peripheral neuropathy | 7 (8) | 15 (18) | 22 (13) |
| Psychiatric disorders | |||
| Insomnia | 10 (12) | 14 (17) | 24 (14) |
| Respiratory, thoracic, and mediastinal disorders | |||
| Cough | 13 (15) | 15 (18) | 28 (17) |
| Dyspnea | 15 (18) | 17 (20) | 32 (19) |
| Skin and subcutaneous tissue disorders | |||
| Rash | 9 (11) | 12 (14) | 21 (12) |
AE = adverse event; IV = intravenous
a Safety population excluding patients with protocol violations
The numbers of deaths, trial discontinuations, and treatment interruptions due to AEs were similar between the two groups as well. Deaths (9 [10.6%] 15-minute group vs 6 [7.1%] 30-minute group) were not suspected to be related to zoledronic acid. Eight patients in each treatment group discontinued therapy because of an AE; events leading to treatment discontinuation that were suspected to be related to zoledronic acid occurred in two patients in the 15-minute group (skeletal pain and ONJ) and one patient in the 30-minute group (jaw pain). AEs that required treatment interruption occurred in eight and nine patients in the 15-minute and 30-minute groups, respectively.
AEs of special interest included those related to kidney dysfunction, cardiac arrhythmias, SREs, and ONJ. The number of patients reporting overall kidney and urinary disorders was the same in the two treatment groups (14 patients in each group); however, acute renal failure was reported more frequently in patients receiving the 15-minute infusion compared with the 30-minute infusion (four patients [5%] vs one patient [1%] in 30-minute group). Details of these five patients are presented in Table 4. AEs related to cardiac rhythm occurred in 20 patients while on study; however, only one case of bradycardia was suspected to be related to zoledronic acid therapy (in the 30-minute group). The incidence of SREs at 2 years was comparable in the two groups (19% in 15-minute group vs 21% in 30-minute group). The time to onset of SREs was longer in the 15-minute group (222 vs 158 days), but this was not statistically significant. A total of 10 patients with suspected ONJ were identified, with three patients in the 15-minute group (all moderate) and seven patients in the 30-minute group (mild [n = 5], moderate [n = 1], severe [n = 1]). Six of these patients received bisphosphonates before entering the study (four patients received no prior bisphosphonates), but the length of previous bisphosphonate therapy varied (0–30 months). Patients with suspected ONJ were assessed by clinicians and referred to dental professionals for further evaluation.
| PATIENT DEMOGRAPHICS | TYPE OF MM | MEDICAL HISTORY | CONCURRENT MEDICATIONSa | ACUTE RENAL FAILURE DETAILS | OUTCOME |
|---|---|---|---|---|---|
| Zoledronic acid 4 mg IV for 15 minutes | |||||
| 73-year-old female Caucasian | IgG | Anemia, cardiomyopathy, CHF, cholecystectomy, benign breast lump removal, CAD, DM, dyslipidemia, central venous catheterization, chronic renal failure, GERD, hypercholesterolemia, HTN, hysterectomy, mycobacterial infection, hemorrhoids, B-cell lymphoma, seborrheic keratosis, tonsillectomy | At start of study: aspirin, losartan, digoxin, hydrochlorothiazide/lorsartan, fluconazole, folic acid, atorvastatin, vitamins, warfarinDuring study: ethambutol dihydrochloride, moxifloxacin, rifabutin, fenofibrate, omeprazole, diuretics, nitroglycerin patch, angiotensin-converting enzyme inhibitors, hydroxyzine, loratadine, furosemide, vancomycin, pantoprozole, piperacillin/tazobactam, clarithromycin | Myeloma kidney mass consistent with myeloma kidney found during study; approximately 2 weeks later the patient developed severe infection that culminated in septic shock, with acute renal failure | Nephrologist considered renal insufficiency to be partly related to past history of large-cell lymphoma and chemotherapy; patient was discharged to hospice and died of acute renal failure secondary to myeloma |
| 71-year-old female Caucasian | IgA | Back pain, cholecystectomy, constipation, CAD, NIDDM, hypercholesterolemia, HTN, insomnia, left knee operation, neuralgia, obesity, osteoarthritis, hysterectomy, hypoacusis, seasonal allergies, urinary incontinence | At start of study: zolpidem, amitriptyline, loratidine, tolterodine l-tartrate, valsartan, metrotoprolol, furosemide, ibuprofen, clonazepam, gabapentin, liodcaine, hydrocodone/acetaminophen, quinine sulfate, simvastatin During study: calcium, multivitamins, lactulose, trazodone, hydromorphone, cyclobenzaprine, glipizide, macrogol, lorazepam, methadone, potassium, lisinopril, furosemide, meperidine, promethazine | Developed moderate acute renal failure on the day of her first dose; considered not associated with zoledronic acid | Renal ultrasound showed arterial stenosis; resolved approximately 1 month after diagnosis |
| 65-year-old male Caucasian | IgG | Oxycodone hypersensitivity, anemia, back pain, spine metastases, spinal compression fracture, depression, fatigue, inguinal hernia repair, spinal fusion (L1–L3) surgery, bilateral hip arthroplasty, pain, pneumonia, staphylococcal infection | At start of study: fluconazole, morphine sulfate, oxycodone/acetaminophen During study: naproxen, darbepoietin alfa, sodium ferrifluconate, calcium with vitamin D, cephalexin, dexamethasone, alginic acid, docusate, heparin, sodium polystyrene, levofloxacin, filgrastim, lansoprazole | After 5 doses of zoledronic acid, patient developed severe acute renal failure with elevated SCr; not suspected to be related to zoledronic acid | Resolved 9 days later following treatment with cephalexin and dexamethasone |
| 56-year-old female Caucasian | IgA | Osteolysis, cataract surgery, constipation, bone lesions, hypercholesterolemia, HTN, musculoskeletal pain, anorexia | At start of study: ibuprofen, oxycodone, propoxyphene/acetaminophen, hydrocodone/acetaminophen, valsartan, calcium/vitamin D, potassium chloride, docusate sodiumDuring study: vancomycin, acyclovir | Approximately 1 week after 9th zoledronic acid dose, patient developed acute renal failure with an increased SCr (12.5 mg/dL); not suspected to be related to zoledronic acid | Resulted from myeloma progression to plasma cell leukemia; emergency dialysis performed; catheter-related sepsis occurred approximately 1 month later, and patient died of sepsis and disease progression |
| Zoledronic acid 4 mg IV for 30 minutes | |||||
| 80-year-old male African American | IgG | Anemia, arteriosclerotic heart disease, bilateral ankle swelling/pain, degenerative joint disease, dyspnea on exertion, fatigue, GERD, HTN, neutropenia, shoulder pain, vasovagal syncope | At start of study: aspirin, atenolol, multivitamin, doxazosin, fosinopril, hydrochlorothiazide, amlodipine besylate, simvastatinDuring study: darbepoietin alfa, warfarin sodium, furosemide, omeprazole, calcium carbonate | Approximately 1 month after 2nd dose, patient experienced increased SCr (2.9 mg/dL, 53% increase from baseline); relationship to zoledronic acid unknown | Discontinued from study after 2nd dose, and SCr remained elevated for 2 months following discontinuation |
CAD = coronary artery disease; CHF = congestive heart failure; DM = diabetes mellitus; GERD = gastroesophageal reflux disease; HTN = hypertension; MM = multiple myeloma; NIDDM = non-insulin-dependent diabetes mellitus; SCr = serum creatinine
Discussion
During the past decade, bisphosphonate therapy has become an important adjunctive treatment to prevent the emergence, or worsening, of SREs in patients with MM involving the bone.15 Kidney failure is a common and severe complication of MM that may be exacerbated by chronic administration of zoledronic acid.7 A study evaluating zoledronic acid in patients with cancer and bone metastases suggests that increasing the infusion time decreases the Cmax, which may result in fewer renal AEs.[9] and [12] This study was designed to assess whether prolonging the infusion time of zoledronic acid from the recommended 15 to 30 minutes would improve kidney safety in MM patients, as evidenced by fewer rises in SCr levels. To our knowledge, this is the only trial that has been designed to evaluate the impact of infusion duration on renal effects in this population.
The 12-month results of this pilot study showed a trend toward improved renal safety with the longer infusion time, this difference not being statistically significant. By 24 months, however, there were no differences in SCr level elevations between the two groups. The clinically relevant SCr increases observed in our study, however, differ from those reported by Rosen and colleagues,[5] and [6] who first evaluated zoledronic acid for patients with MM. In that study, 4%–11% of patients experienced kidney function deterioration, manifested by SCr increases, which is much lower than the rate observed in our study. However, several differences exist between our trial and the Rosen study. The Rosen study included both breast cancer patients with at least one bone metastasis and Durie-Salmon stage 3 MM patients with at least one osteolytic lesion, whereas our study only included MM patients with at least one bone lesion. Additionally, the criteria for defining a clinically relevant SCr increase differ between the two studies; therefore, one cannot directly compare the incidence of kidney dysfunction between these two studies. Although in our study the sample size was small, confidence intervals were wide, and protocol deviations did not permit a robust comparison, the results of this pilot study suggest that the longer infusion time of 30 minutes every 3–4 weeks for 2 years for MM patients with bone disease is also safe and well-tolerated.
As expected, PK data showed that the median zoledronic acid concentrations were greater in the samples obtained from the 15-minute group compared to those from the 30-minute group. This effect was observed in samples obtained both 5 minutes before the end of infusion and at the end of infusion.
Increasing the infusion time did not significantly alter the AE profile and was not associated with any new or unexpected AEs. The incidence rates of deaths, SAEs, treatment-related AEs, and overall AEs were generally comparable between treatment groups. Overall, the incidence rates of reported SREs and ONJ were as expected for this patient population, which are important factors when considering zoledronic acid for patients with MM, where the goal of ongoing monthly IV bisphosphonate therapy is to prevent the development of new SREs without increasing the risk of AEs, such as ONJ.
Finally, the FDA-approved current labeling for zoledronic acid recommends decreasing the dose of this bisphosphonate based on baseline kidney function.7 Because these recommendations were not in place at the time that this study was designed, whether the implementation of these dosing guidelines for patients with MM along with varying infusion durations would have impacted the results observed in our study cannot be ascertained.
In summary, the results of this study suggest that the safety profile of IV zoledronic acid is similar regardless of a 15-minute or a 30-minute infusion duration. However, because the study was not powered to detect statistical significance and the current renal dosing guidelines for zoledronic acid were not used in this study, large randomized studies, using current dosing recommendations, will be required to further assess the effects on kidney safety of prolonging the infusion time of ongoing monthly IV zoledronic acid therapy for patients with MM.
Acknowledgments
The authors thank Syntaxx Communications, Inc., specifically, Kristin Hennenfent, PharmD, MBA, BCPS, and Lisa Holle, PharmD, BCOP, who provided manuscript development and medical writing services, and Holly Matthews, BS, who provided editorial services, with support from Novartis Pharmaceuticals Corporation. We also thank all participating patients and study personnel. Research support was provided by Novartis Pharmaceuticals Corporation (East Hanover, NJ).
References
1 A. Jemal, R. Siegel and J. Xu et al., Cancer statistics, 2010, CA Cancer J Clin 60 (2010), pp. 277–300. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (543)
2 R.A. Kyle, M.A. Gertz and T.E. Witzig et al., Review of 1027 patients with newly diagnosed multiple myeloma, Mayo Clin Proc 78 (1) (2003), pp. 21–33. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (396)
3 A. Corso, P. Zappasodi and C. Pascutto et al., Urinary proteins in multiple myeloma: correlation with clinical parameters and diagnostic implications, Ann Hematol 82 (8) (2003), pp. 487–491. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
4 V. Eleutherakis-Papaiakovou, A. Bamias and D. Gika et al., Renal failure in multiple myeloma: incidence, correlations, and prognostic significance, Leuk Lymphoma 48 (2) (2007), pp. 337–341. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (35)
5 L.S. Rosen, D. Gordon and M. Kaminski et al., Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial, Cancer J 7 (5) (2001), pp. 377–387. View Record in Scopus | Cited By in Scopus (461)
6 L.S. Rosen, D. Gordon and M. Kaminski et al., Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized, double-blind, multicenter, comparative trial, Cancer 98 (8) (2003), pp. 1735–1744. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (329)
7 , Zometa (package insert), Novartis Pharmaceuticals, Corporation, East Hanover, NJ (2008).
8 P. Major, A. Lortholary and J. Han et al., Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials, J Clin Oncol 19 (2) (2001), pp. 558–567. View Record in Scopus | Cited By in Scopus (325)
9 T. Chen, J. Berenson and R. Vescio et al., Pharmacokinetics and pharmacodynamics of zoledronic acid in cancer patients with bone metastases, J Clin Pharmacol 42 (11) (2002), pp. 1228–1236. View Record in Scopus | Cited By in Scopus (139)
10 T. Pfister, E. Atzpodien and F. Bauss, The renal effects of minimally nephrotoxic doses of ibandronate and zoledronate following single and intermittent intravenous administration in rats, Toxicology 191 (2003), pp. 159–167. Article |
11 T. Pfister, E. Aztpodien, B. Bohrmann and F. Bauss, Acute renal effects of intravenous bisphosphonates in the rat, Basic Clin Pharmacol Toxicol 97 (2005), pp. 374–381. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (17)
12 F. Saad, D.M. Gleason and R. Murray et al., A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma, J Natl Cancer Inst 94 (19) (2002), pp. 1458–1468. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (650)
13 S. Kautiainen, S. Luurila, P. Ylitalo and R. Ylitalo, Transformation of bisphosphonates into insoluble material in human blood in vitro, Methods Find Exp Clin Pharmacol 20 (4) (1998), pp. 289–295. View Record in Scopus | Cited By in Scopus (5)
14 L.S. Rosen, D. Gordon and S. Tchekmedyian et al., Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial—the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group, J Clin Oncol 21 (16) (2003), pp. 3150–3157. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (251)
15 M.A. Hussein, Multiple myeloma: most common end-organ damage and management, J Natl Compr Canc Netw 5 (2) (2007), pp. 170–178. View Record in Scopus | Cited By in Scopus (4)
Appendix
The following ZMAX Trial principal investigators participated in this study: Bart Barlogie, MD, Myeloma Institute For Research and Therapy; James Berenson, MD, Oncotherapeutics; Robert Bloom, MD, Providence Cancer Center, Clinical Trials Department; Ralph Boccia, MD, Center for Cancer and Blood Disorders; Donald Brooks, MD, Arizona Clinical Research Center, Inc.; Robert Brouillard, MD, Robert P. Brouillard, MD, and Delvyn Case, MD, Maine Center for Cancer Medicine and Blood Disorders, Pharmacy; Veena Charu, MD, Pacific Cancer Medical Center; Naveed Chowhan, MD, Cancer Care Center, Inc; Robert Collins, MD, University of Texas Southwestern Medical Center at Dallas; Thomas Cosgriff, MD, Hematology and Oncology Specialists, LLC; Jose Cruz, MD, Joe Arrington Cancer Research and Treatment Center; Surrinder Dang, MD, Oncology Specialties; Sheldon Davidson, MD, North Valley H/O; Tracy Dobbs, MD, Baptist Regional Cancer Center; Luke Dreisbach, MD, Desert Hematology Oncology Medical Group; Isaac Esseesse, MD, Hematology Oncology Associates of Central Brevard, Laboratory; Mark Fesen, MD, Hutchinson Clinic, PA; George Geils, Jr., MD, Charleston Hematology Oncology Associates, PA; Michael Greenhawt, MD, South Florida Oncology-Hematology; Manuel Guerra, MD, ORA; Rita Gupta, MD, Oncology-Hematology Associates, PA; Vicram Gupta, MD, Saint Joseph Oncology; Alexandre Hageboutros, MD, Cancer Institute of New Jersey at Cooper Hospital; Vincent Hansen, MD, Utah Hematology Oncology; David Henry, MD, Pennsylvania Oncology Hematology Associates; Benjamin Himpler, MD, Syracuse Hematology/Oncology PC; Winston Ho, MD, Hematology/Oncology Group of Orange County; William Horvath, MD, Haematology Oncology Associates of Ohio and Michigan, PC; Paul Hyman, MD, Hematology Oncology Associates of Western Suffolk; Min Kang, MD, Western Washington Oncology; Mark Keaton, MD, Augusta Oncology Associates, PC; Howard Kesselheim, MD, The Center for Cancer and Hematologic Disease; Kapisthalam Kumar, MD, Pasco Hernando Oncology Associates, PA; Edward Lee, MD, Maryland Oncology-Hematology, PA; André Liem, MD, Pacific Shore Medical Group; Timothy Lopez, MD, New Mexico Cancer Care Associates, Cancer Institute of New Mexico; Paul Michael, MD, Comprehensive Cancer Centers of Nevada; Michael Milder, MD, Swedish Cancer Institute; Barry Mirtsching, MD, Center for Oncology Research & Treatment, PA; Ruben Niesvizky, MD, New York Presbyterian Hospital; Jorge Otoya, MD, Osceola Cancer Center; Joseph Pascuzzo, MD, California Oncology of the Central Valley; Ravi Patel, MD, Comprehensive Blood and Cancer Center Lab; Allen Patton, MD, Hematology Oncology Associates, PA; Kelly Pendergrass, MD, Kansas City Cancer Center, LLC; Anthony Phillips, MD, Fox Valley Hematolgy Oncology, SC; Robert Raju, MD, Dayton Oncology and Hematology, PA; Harry Ramsey, MD, Berks Hematology Oncology Associates; Ritesh Rathore, MD, Roger Williams Hospital Medical Center; Phillip Reid, MD, Central Jersey Oncology Center; Robert Robles, MD, Bay Area Cancer Research Group, LLC; Stephen Rosenoff, MD, Oncology and Hematology Associates of Southwest Virginia, Inc; Martin Rubenstein, MD, Southbay Oncology Hematology Partners; Mansoor Saleh, MD, Georgia Cancer Specialists; Sundaresan Sambandam, MD, Hematology and Oncology Associates of RI; Mukund Shah, MD, Antelope Valley Cancer Center; David Siegel, MD, Hackensack University Medical Center; Nelida Sjak-Shie, MD, The Center for Cancer Care and Research; Michael Stone, MD, Greeley Medical Clinic; Stefano Tarantolo, MD, Nebraska Methodist Hospital; Joseph Volk, MD, Palo Verde Hematology Oncology, Ltd; Mitchell Weisberg, MD, MetCare Oncology; Ann Wierman, MD, Nevada Cancer Center; Donald Woytowitz, Jr., MD, Florida Cancer Specialists; Peter Yu, MD, Camino Medical Group.
Original research
James R. Berenson MD![]()
![]()
Abstract
Zoledronic acid, an intravenous (IV) bisphosphonate, is a standard treatment for multiple myeloma (MM) but may exacerbate preexisting renal dysfunction. The incidence of zoledronic acid–induced renal dysfunction may correlate with infusion duration. In this randomized, multicenter, open-label study, 176 patients with MM, at least one bone lesion, and stable renal function with a serum creatinine (SCr) level <3 mg/dL received zoledronic acid 4 mg (in 250 mL) as a 15- or 30-minute IV infusion every 3–4 weeks. At month 12, 20% (17 patients) in the 15-minute and 16% (13 patients) in the 30-minute arm experienced a clinically relevant but nonsignificant SCr-level increase (P = 0.44). By 24 months, the proportion of patients with a clinically relevant SCr-level increase was similar between arms (15-minute 28% [24 patients] vs 30-minute 27% [23 patients], P = 0.9014). Median zoledronic acid end-of-infusion concentrations were higher with the shorter infusion (15-minute 249 ng/mL vs 30-minute 172 ng/mL), and prolonging the infusion beyond 15 minutes did not influence adverse events related to zoledronic acid. For patients with MM, the safety profile of IV zoledronic acid is similar between those receiving a 15- or 30-minute infusion; therefore, determining the appropriate infusion duration of zoledronic acid should be based on individual patient considerations.
Article Outline
Considerable research has focused on preventive and/or treatment strategies to reduce bone complications in MM patients. In a large, international, randomized, phase III trial of MM patients with at least one osteolytic bone lesion, zoledronic acid (Zometa), a potent intravenous (IV) bisphosphonate that inhibits osteoclast-mediated bone resorption, reduced the overall risk of developing skeletally related events (SREs) including HCM by 16% (P = 0.03) compared with standard-dose pamidronate 90 mg (Aredia), another less potent IV bisphosphonate.[5] and [6] As a result of this study and others, monthly infusion of zoledronic acid at 4 mg over at least 15 minutes has become a common treatment for MM patients with bone involvement.
The U.S. Food and Drug Administration (FDA) has approved zoledronic acid use for patients with MM, documented bone metastases from solid tumors, or HCM.[5], [6], [7] and [8] The FDA-approved dose for MM patients is 4 mg administered as an IV infusion over at least 15 minutes every 3–4 weeks for patients with a creatinine clearance (CrCl) of >60 mL/min; when treating HCM, zoledronic acid 4 mg is administered as a single IV infusion.[5], [6], [7] and [8]
Zoledronic acid is primarily excreted intact through the kidney.9 Preexisting kidney disease and receipt of multiple cycles of bisphosphonate therapy are risk factors for subsequent kidney injury.7 In animal studies, IV bisphosphonates have been shown by histology to precipitate renal tubular injury when administered as a single high dose or when administered more frequently at lower doses.[10] and [11] Additionally, renal dysfunction, as evidenced by increased serum creatinine (SCr) levels, was reported among patients treated at a dose of 4 mg with an infusion time of 5 minutes.[7] and [12] When 4 mg zoledronic acid was administered with a longer infusion time of 15 minutes in large randomized trials, no significant difference between the renal safety profiles of zoledronic acid and pamidronate was reported.6
One hypothesis about the development of kidney injury associated with zoledronic acid is that it may be related to the peak plasma concentration as determined by infusion time. Results of a study evaluating patients with MM or other cancer types and bone metastases demonstrated that prolonging the infusion time of zoledronic acid reduced the end-of-infusion peak plasma concentration (Cmax) by 35%.9 Another theory about the development of kidney dysfunction is that insoluble precipitates may form when the blood is exposed to high concentrations of bisphosphonates as this has been shown to occur in vitro.[9] and [13] Therefore, the current management of renal adverse events (AEs) related to IV bisphosphonates is based on these theories so that reducing the peak plasma concentration of zoledronic acid may prevent the possible formation of insoluble precipitates through (1) lowering the dose, (2) slowing the infusion rate, or (3) increasing the volume of infusate.[5], [12] and [14]
Because MM patients are predisposed to experience deterioration of renal function, it is critical to ensure that zoledronic acid does not contribute to, or exacerbate, a decline in kidney function. To determine if increasing the duration of zoledronic acid infusion further results in improved renal safety, a multicenter, open-label, randomized study was designed to compare a 15-minute vs a 30-minute infusion time with an increased volume of infusate from 100 to 250 mL administered every 3–4 weeks to MM patients with osteolytic bone disease.
Patients and Methods
Patient Population
Men and women (≥18 years of age) with a diagnosis of MM, at least one bone lesion on plain film radiographs, stable kidney function (defined as two SCr level determinations of <3 mg/dL obtained at least 7 days apart during the screening period), calculated CrCl of at least 30 mL/min, Eastern Cooperative Oncology Group (ECOG) performance status of 1 or less, and a life expectancy of at least 9 months were eligible. The study excluded patients with prolonged IV bisphosphonate use (defined as use of zoledronic acid longer than 3 years or pamidronate longer than 1 year [total bisphosphonate duration could not exceed 3 years]), corrected serum calcium level at first visit of <8 or ≥12 mg/dL, or diagnosis of amyloidosis. Additionally, patients who had known hypersensitivity to zoledronic acid or other bisphosphonates; were pregnant or lactating; had uncontrolled cardiovascular disease, hypertension, or type 2 diabetes mellitus; or had a history of noncompliance with medical regimens were not eligible.
Study Design
This open-label, randomized pilot study was conducted at 45 centers in the United States. Before randomization, patients were stratified based on length of time of prior bisphosphonate treatment (bisphosphonate-naive vs ≤1 year prior bisphosphonate therapy vs >1 year prior bisphosphonate therapy) and baseline calculated CrCl (>75 vs >60–75 vs ≥30–≤60 mL/min).
Treatment and Evaluation
Patients were randomized to receive zoledronic acid 4 mg as either a 15- or a 30-minute IV infusion. The volume of infusate was increased from the standard 100 to 250 mL to provide additional hydration; infusions were administered every 3–4 weeks for up to 24 months. At the time this study was developed, the 4 mg dose was used because the dose adjustments for renal dysfunction in the current FDA labeling for zoledronic acid were not yet available.7 Patients were required to take a calcium supplement containing 500 mg of calcium and a multivitamin containing 400–500 IU of vitamin D, orally, once daily, for the duration of zoledronic acid therapy.
HCM during the trial was defined as a corrected serum calcium level ≥12 mg/dL or a lower level of hypercalcemia accompanied by symptoms and/or requiring active treatment other than rehydration. If HCM occurred more than 14 days after a zoledronic acid infusion, patients could receive a zoledronic acid infusion as treatment for HCM, even if this required administration before the next scheduled dose. Patients were allowed to remain in the study provided that HCM did not persist or recur. However, zoledronic acid treatment was immediately discontinued if patients developed HCM ≤14 days after study drug infusion; these patients received HCM treatment at the discretion of their treating physician. Also, patients experiencing HCM discontinued calcium and vitamin D supplements.
Within 2 weeks before each dose, enrolled patients were assessed for increase in SCr levels. For patients experiencing a clinically relevant increase in SCr level (defined as a rise of 0.5 mg/dL or more or a doubling of baseline SCr levels), administration of zoledronic acid was suspended until the SCr level fell to within 10% of the baseline value. During the delay, SCr levels were monitored at each regularly scheduled study visit (every 3–4 weeks) or more frequently if deemed necessary by the investigator. If the SCr level fell to within 10% of the baseline value within the subsequent 12 weeks, zoledronic acid was restarted with an infusion time that was increased by 15 minutes over the starting duration. If the rise in SCr level did not resolve within 12 weeks or if the patient experienced a second clinically relevant increase in SCr level after modification of the infusion time, treatment was permanently discontinued. Otherwise, patients were followed for 24 months. A final safety assessment, including a full hematology and chemistry profile, was performed 28 days after the last infusion.
A pretreatment dental examination with appropriate preventive dentistry was suggested for all patients with known risk factors for the development of osteonecrosis of the jaw (ONJ) (eg, cancer chemotherapy, corticosteroids, poor oral hygiene, dental extraction, or dental implants). Throughout the study, patients reporting symptoms that could be consistent with ONJ were referred to a dental professional for assessment; if exposed bone was noted on dental examination, the patient was referred to an oral surgeon for further evaluation, diagnosis, and treatment. A diagnosis of ONJ required cessation of zoledronic acid therapy and study discontinuation.
Pharmacokinetic Sampling
At the first infusion visit (visit 2), pharmacokinetic (PK) parameters were measured. If PK samples were not obtained at visit 2, they could be obtained at visit 3 (otherwise, they were recorded as not done). All blood samples for PK analysis were drawn from the contralateral arm. For patients receiving the 15-minute zoledronic acid infusion, the protocol specified that PK samples were to be drawn at exactly 10 and 15 minutes from the start of the infusion; patients receiving the 30-minute zoledronic acid infusion were to have blood samples drawn at exactly 25 and 30 minutes from the start of the infusion. The second blood sample for PK analysis was taken before the study drug infusion was stopped in both groups. PK analysis was performed by Novartis Pharmaceuticals Corporation Drug Metabolism and Pharmacokinetics France (Rueil-Malmaison, France) and SGS Cephac (Geneva Switzerland), using a competitive radioimmunoassay that has a lower limit of quantification of 0.04 ng/mL and an upper limit of quantification of 40 ng/mL.
Statistical Analysis
The primary study end point was the proportion of patients with a clinically relevant increase in SCr level at 12 months. Descriptive statistics were used to summarize the primary end point; in addition, an exploratory analysis with a logistic regression model, using treatment group, prior bisphosphonate therapy, and baseline CrCl, was performed.
Additional secondary safety end points included the proportion of patients with a clinically relevant increase in SCr level at 24 months, time to first clinically relevant increase in SCr level, and the PK profile of zoledronic acid. The proportion of patients with a clinically relevant increase in SCr level at 24 months was summarized using descriptive statistics. Time to first clinically relevant increase in SCr level was analyzed using the Kaplan-Meier method at the time of the primary analysis (12 months) and at 24 months. Plasma concentration data were evaluated by treatment group and baseline kidney function using descriptive statistics. Continuous variables of baseline and demographic characteristics between treatment groups were compared using a two-sample t-test; between-group differences in discrete variables were analyzed using Pearson's chi-squared test.
The primary analysis included all randomized patients who received at least one zoledronic acid infusion and who had valid postbaseline data for assessment. All study subjects who had evaluable PK parameters were included in a secondary PK analysis. Efficacy assessments were not included in this trial.
This pilot trial was designed to obtain additional preliminary data to support the hypothesis that a longer infusion is associated with less kidney dysfunction than a shorter infusion; therefore, a sample size of 90 patients per treatment group was selected. All statistical tests employed a significance level of 0.05 against a two-sided alternative hypothesis.
The institutional review boards of participating institutions approved the study, and all patients provided written informed consent before study entry.
Results
Study Population
Between October 2004 and October 2007, 179 MM patients with SCr <3 mg/dL were randomized to receive either a 15- or a 30-minute infusion of zoledronic acid. Of these, 176 patients (88 in each group) received at least one dose of study drug. Because of protocol violations, postbaseline data from one site were excluded from analyses, leaving 85 assessable patients in the 15-minute group and 84 patients in the 30-minute group.
Overall, the study groups were representative of a general population with MM. About two-thirds of patients had received prior bisphosphonate therapy; the duration of therapy was greater than 1 year for most of these patients (Table 1). The most common concomitant therapies included dexamethasone, thalidomide, and melphalan. Although the median age, proportion of patients who were 65 years of age or older, and ratio of men to women were greater in the 15-minute infusion group, none of the differences in baseline demographics was statistically significant. All other baseline demographics and disease characteristics, including prior bisphosphonate use and baseline CrCl values, were similar between the two groups (see Table 1). During the study, six patients in the 15-minute treatment group and one patient in the 30-minute treatment group experienced HCM. Three of the six patients in the 15-minute treatment group and one patient in the 30-minute treatment group discontinued the study as a result of HCM.
| NUMBER OF PATIENTS (%)a | ||
|---|---|---|
| CHARACTERISTIC | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 88)b | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 88)b |
| Age (years) | ||
| Mean (SD) | 64 | 64 |
| Median | 66 | 64 |
| Range | 37–91 | 27–86 |
| Age category (years) | ||
| <65 | 39 (44) | 47 (53) |
| ≥65 | 49 (56) | 41 (47) |
| Sex | ||
| Male | 56 (64) | 49 (56) |
| Female | 32 (36) | 39 (44) |
| Race | ||
| White | 70 (80) | 69 (78) |
| Black | 9 (10) | 13 (15) |
| Asian | 1 (1) | 1 (1) |
| Other | 8 (9) | 5 (6) |
| Time since diagnosis (months) | ||
| Mean (SD) | 12 (24) (n = 86) | 10 (14) (n = 87) |
| Median | 4 | 6 |
| Range | 0–186 | 0–98c |
| Prior bisphosphonate use | ||
| Naive | 28 (32) | 28 (32) |
| ≤1 year | 12 (14) | 14 (16) |
| >1 year | 48 (55) | 39 (44) |
| Missing | 0 (0) | 7 (8) |
| Calculated CrCl (mL/min) | ||
| Mean (SD) | 87 (33) | 89 (40) |
| Median | 84 | 83 |
| Range | 33–210 | 31–224 |
| Calculated CrCl category (mL/min) | ||
| CrCl ≥75 | 54 (61) | 49 (56) |
| 60 < CrCL < 75 | 13 (15) | 15 (17) |
| 30 < CrCl ≤ 60 | 21 (24) | 24 (27) |
| CrCl <30 | 0 (0) | 0 (0) |
CrCl = creatinine clearance; IV = intravenous; SD = standard deviation
a Unless otherwise notedb Safety populationc One patient had a screening visit date before the date of initial diagnosis
Protocol violations and/or deviations (n = 658) occurred during this study, affecting 139 patients. The types of protocol violations/deviations were related to protocol adherence (n = 404), timing of visits (n = 210), protocol adherence/timing of visits (n = 2), exclusion criteria (n = 22), inclusion criteria (n = 10), and informed consent (n = 1); 9 violations were unclassified. Notably, one protocol adherence deviation that occurred was incorrect infusion duration despite the patient having a stable SCr level. In the 15-minute treatment group, 15% of infusions administered were longer than 15 minutes. Among the longer infusions, 7% of the infusions correctly occurred per protocol following an SCr-level increase, whereas 7% of the prolonged infusions were 20 minutes or longer in the absence of an SCr-level increase. Similarly, in the 30-minute treatment group, 5% of patients received infusions lasting at least 35 minutes in the absence of an SCr-level increase.
Renal Safety
At 12 months, slightly fewer patients (n = 13 [16%]) in the 30-minute infusion group had a clinically relevant increase in SCr level than in the 15-minute infusion group (n = 17 [20%]); but this difference was not statistically significant, and for approximately 35% of patients in each group there were no SCr data available (Table 2). The median time to a clinically relevant increase in SCr by Kaplain-Meier was not reached in either group (data not shown). Neither previous bisphosphonate use nor baseline CrCl significantly affected the results (P = 0.5837 and P = 0.9371, respectively).
| NUMBER OF PATIENTS (%) | |||
|---|---|---|---|
| CLINICALLY RELEVANT INCREASE IN SCR | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 85)a | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 84)a | P VALUEb |
| 12 Months | 0.6892 | ||
| Yes | 17 (20) | 13 (16) | |
| No | 38 (45) | 42 (50) | |
| Unknown | 30 (35) | 29 (35) | |
| 24 Months | 0.9750 | ||
| Yes | 24 (28) | 23 (27) | |
| No | 22 (26) | 23 (27) | |
| Unknown | 39 (46) | 38 (45) | |
CI = confidence interval; IV = intravenous; SCr = serum creatinine
a Safety population, excluding patients with protocol violationsb P value calculated based on chi-squared test
After 24 months of treatment, the proportion of patients experiencing a clinically relevant increase in SCr level was similar between treatment groups, although for approximately 45% of patients in each group there were no SCr data available (see Table 2). Moreover, the difference in time to first clinically relevant increase in SCr level was not statistically significant between the two groups (P = 0.55) (Figure 1). However, among patients with a clinically significant rise in SCr level, the median time to SCr rise was slightly longer in the 30-minute group than in the 15-minute group (22 vs 24 weeks), but this was not statistically significant.
Increases in SCr relative to baseline led to treatment discontinuation in 20 patients (24%) receiving a 15-minute infusion and 14 patients (17%) receiving a 30-minute infusion. In these cases, the treating physician either considered the SCr level too high for continued treatment or the SCr level was persistently high despite treatment interruption.
Pharmacokinetics
Median zoledronic acid concentrations, as anticipated, were higher with the 15-minute infusion time at both sampling time points (during infusion: 15-minute group 231 ng/mL [at 10 minutes] vs 30-minute group 186 ng/mL [at 25 minutes]; end-of-infusion: 15-minute group, 249 ng/mL vs 30-minute group 172 ng/mL).
Adverse Events
Overall, the incidence and severity of AEs were as anticipated for MM patients. The most commonly reported AEs included fatigue, anemia, nausea, constipation, and back pain (Table 3). Although many AEs were reported more frequently in the 30-minute infusion group, the incidence rates of AEs suspected to be related to zoledronic acid were similar between the two groups. Toxicities were graded as mild, moderate, or severe; proportions of AEs categorized by these grades were comparable. Nonfatal serious AEs (SAEs) occurred in 26% of patients receiving the 15-minute infusion and 35% of patients receiving the 30-minute infusion; however, only one patient in the 15-minute group and two patients in the 30-minute group had SAEs suspected to be related to study medication.
| NUMBER OF PATIENTS (%) | |||
|---|---|---|---|
| TYPE OF AE | ZOLEDRONIC ACID 4 MG IV FOR 15 MINUTES (N = 85) | ZOLEDRONIC ACID 4 MG IV FOR 30 MINUTES (N = 84) | TOTAL (N = 169) |
| Blood and lymphatic system disorders | |||
| Anemia | 19 (22) | 27 (32) | 46 (27) |
| Neutropenia | 6 (7) | 12 (14) | 18 (11) |
| Gastrointestinal disorders | |||
| Constipation | 20 (24) | 21 (25) | 41 (24) |
| Diarrhea | 14 (17) | 20 (24) | 34 (20) |
| Nausea | 18 (21) | 27 (32) | 45 (27) |
| Vomiting | 10 (12) | 14 (17) | 24 (14) |
| General disorders | |||
| Fatigue | 30 (35) | 41 (49) | 71 (42) |
| Pain | 7 (8) | 10 (12) | 17 (10) |
| Pain in extremity | 14 (17) | 16 (19) | 30 (18) |
| Peripheral edema | 13 (15) | 20 (24) | 33 (20) |
| Pyrexia | 15 (18) | 19 (23) | 34 (20) |
| Infections and infestations | |||
| Pneumonia | 11 (13) | 7 (8) | 18 (11) |
| Upper respiratory tract infection | 13 (15) | 13 (16) | 26 (15) |
| Metabolism and nutrition disorders | |||
| Anorexia | 8 (9) | 9 (11) | 17 (10) |
| Hypokalemia | 12 (14) | 13 (15) | 25 (14) |
| Musculoskeletal and connective tissue disorders | |||
| Arthralgia | 10 (11) | 16 (19) | 26 (15) |
| Asthenia | 9 (10) | 13 (16) | 22 (13) |
| Back pain | 19 (22) | 20 (24) | 39 (23) |
| Bone pain | 10 (12) | 11 (13) | 21 (12) |
| Nervous system disorders | |||
| Dizziness | 11 (13) | 10 (12) | 21 (12) |
| Peripheral neuropathy | 7 (8) | 15 (18) | 22 (13) |
| Psychiatric disorders | |||
| Insomnia | 10 (12) | 14 (17) | 24 (14) |
| Respiratory, thoracic, and mediastinal disorders | |||
| Cough | 13 (15) | 15 (18) | 28 (17) |
| Dyspnea | 15 (18) | 17 (20) | 32 (19) |
| Skin and subcutaneous tissue disorders | |||
| Rash | 9 (11) | 12 (14) | 21 (12) |
AE = adverse event; IV = intravenous
a Safety population excluding patients with protocol violations
The numbers of deaths, trial discontinuations, and treatment interruptions due to AEs were similar between the two groups as well. Deaths (9 [10.6%] 15-minute group vs 6 [7.1%] 30-minute group) were not suspected to be related to zoledronic acid. Eight patients in each treatment group discontinued therapy because of an AE; events leading to treatment discontinuation that were suspected to be related to zoledronic acid occurred in two patients in the 15-minute group (skeletal pain and ONJ) and one patient in the 30-minute group (jaw pain). AEs that required treatment interruption occurred in eight and nine patients in the 15-minute and 30-minute groups, respectively.
AEs of special interest included those related to kidney dysfunction, cardiac arrhythmias, SREs, and ONJ. The number of patients reporting overall kidney and urinary disorders was the same in the two treatment groups (14 patients in each group); however, acute renal failure was reported more frequently in patients receiving the 15-minute infusion compared with the 30-minute infusion (four patients [5%] vs one patient [1%] in 30-minute group). Details of these five patients are presented in Table 4. AEs related to cardiac rhythm occurred in 20 patients while on study; however, only one case of bradycardia was suspected to be related to zoledronic acid therapy (in the 30-minute group). The incidence of SREs at 2 years was comparable in the two groups (19% in 15-minute group vs 21% in 30-minute group). The time to onset of SREs was longer in the 15-minute group (222 vs 158 days), but this was not statistically significant. A total of 10 patients with suspected ONJ were identified, with three patients in the 15-minute group (all moderate) and seven patients in the 30-minute group (mild [n = 5], moderate [n = 1], severe [n = 1]). Six of these patients received bisphosphonates before entering the study (four patients received no prior bisphosphonates), but the length of previous bisphosphonate therapy varied (0–30 months). Patients with suspected ONJ were assessed by clinicians and referred to dental professionals for further evaluation.
| PATIENT DEMOGRAPHICS | TYPE OF MM | MEDICAL HISTORY | CONCURRENT MEDICATIONSa | ACUTE RENAL FAILURE DETAILS | OUTCOME |
|---|---|---|---|---|---|
| Zoledronic acid 4 mg IV for 15 minutes | |||||
| 73-year-old female Caucasian | IgG | Anemia, cardiomyopathy, CHF, cholecystectomy, benign breast lump removal, CAD, DM, dyslipidemia, central venous catheterization, chronic renal failure, GERD, hypercholesterolemia, HTN, hysterectomy, mycobacterial infection, hemorrhoids, B-cell lymphoma, seborrheic keratosis, tonsillectomy | At start of study: aspirin, losartan, digoxin, hydrochlorothiazide/lorsartan, fluconazole, folic acid, atorvastatin, vitamins, warfarinDuring study: ethambutol dihydrochloride, moxifloxacin, rifabutin, fenofibrate, omeprazole, diuretics, nitroglycerin patch, angiotensin-converting enzyme inhibitors, hydroxyzine, loratadine, furosemide, vancomycin, pantoprozole, piperacillin/tazobactam, clarithromycin | Myeloma kidney mass consistent with myeloma kidney found during study; approximately 2 weeks later the patient developed severe infection that culminated in septic shock, with acute renal failure | Nephrologist considered renal insufficiency to be partly related to past history of large-cell lymphoma and chemotherapy; patient was discharged to hospice and died of acute renal failure secondary to myeloma |
| 71-year-old female Caucasian | IgA | Back pain, cholecystectomy, constipation, CAD, NIDDM, hypercholesterolemia, HTN, insomnia, left knee operation, neuralgia, obesity, osteoarthritis, hysterectomy, hypoacusis, seasonal allergies, urinary incontinence | At start of study: zolpidem, amitriptyline, loratidine, tolterodine l-tartrate, valsartan, metrotoprolol, furosemide, ibuprofen, clonazepam, gabapentin, liodcaine, hydrocodone/acetaminophen, quinine sulfate, simvastatin During study: calcium, multivitamins, lactulose, trazodone, hydromorphone, cyclobenzaprine, glipizide, macrogol, lorazepam, methadone, potassium, lisinopril, furosemide, meperidine, promethazine | Developed moderate acute renal failure on the day of her first dose; considered not associated with zoledronic acid | Renal ultrasound showed arterial stenosis; resolved approximately 1 month after diagnosis |
| 65-year-old male Caucasian | IgG | Oxycodone hypersensitivity, anemia, back pain, spine metastases, spinal compression fracture, depression, fatigue, inguinal hernia repair, spinal fusion (L1–L3) surgery, bilateral hip arthroplasty, pain, pneumonia, staphylococcal infection | At start of study: fluconazole, morphine sulfate, oxycodone/acetaminophen During study: naproxen, darbepoietin alfa, sodium ferrifluconate, calcium with vitamin D, cephalexin, dexamethasone, alginic acid, docusate, heparin, sodium polystyrene, levofloxacin, filgrastim, lansoprazole | After 5 doses of zoledronic acid, patient developed severe acute renal failure with elevated SCr; not suspected to be related to zoledronic acid | Resolved 9 days later following treatment with cephalexin and dexamethasone |
| 56-year-old female Caucasian | IgA | Osteolysis, cataract surgery, constipation, bone lesions, hypercholesterolemia, HTN, musculoskeletal pain, anorexia | At start of study: ibuprofen, oxycodone, propoxyphene/acetaminophen, hydrocodone/acetaminophen, valsartan, calcium/vitamin D, potassium chloride, docusate sodiumDuring study: vancomycin, acyclovir | Approximately 1 week after 9th zoledronic acid dose, patient developed acute renal failure with an increased SCr (12.5 mg/dL); not suspected to be related to zoledronic acid | Resulted from myeloma progression to plasma cell leukemia; emergency dialysis performed; catheter-related sepsis occurred approximately 1 month later, and patient died of sepsis and disease progression |
| Zoledronic acid 4 mg IV for 30 minutes | |||||
| 80-year-old male African American | IgG | Anemia, arteriosclerotic heart disease, bilateral ankle swelling/pain, degenerative joint disease, dyspnea on exertion, fatigue, GERD, HTN, neutropenia, shoulder pain, vasovagal syncope | At start of study: aspirin, atenolol, multivitamin, doxazosin, fosinopril, hydrochlorothiazide, amlodipine besylate, simvastatinDuring study: darbepoietin alfa, warfarin sodium, furosemide, omeprazole, calcium carbonate | Approximately 1 month after 2nd dose, patient experienced increased SCr (2.9 mg/dL, 53% increase from baseline); relationship to zoledronic acid unknown | Discontinued from study after 2nd dose, and SCr remained elevated for 2 months following discontinuation |
CAD = coronary artery disease; CHF = congestive heart failure; DM = diabetes mellitus; GERD = gastroesophageal reflux disease; HTN = hypertension; MM = multiple myeloma; NIDDM = non-insulin-dependent diabetes mellitus; SCr = serum creatinine
Discussion
During the past decade, bisphosphonate therapy has become an important adjunctive treatment to prevent the emergence, or worsening, of SREs in patients with MM involving the bone.15 Kidney failure is a common and severe complication of MM that may be exacerbated by chronic administration of zoledronic acid.7 A study evaluating zoledronic acid in patients with cancer and bone metastases suggests that increasing the infusion time decreases the Cmax, which may result in fewer renal AEs.[9] and [12] This study was designed to assess whether prolonging the infusion time of zoledronic acid from the recommended 15 to 30 minutes would improve kidney safety in MM patients, as evidenced by fewer rises in SCr levels. To our knowledge, this is the only trial that has been designed to evaluate the impact of infusion duration on renal effects in this population.
The 12-month results of this pilot study showed a trend toward improved renal safety with the longer infusion time, this difference not being statistically significant. By 24 months, however, there were no differences in SCr level elevations between the two groups. The clinically relevant SCr increases observed in our study, however, differ from those reported by Rosen and colleagues,[5] and [6] who first evaluated zoledronic acid for patients with MM. In that study, 4%–11% of patients experienced kidney function deterioration, manifested by SCr increases, which is much lower than the rate observed in our study. However, several differences exist between our trial and the Rosen study. The Rosen study included both breast cancer patients with at least one bone metastasis and Durie-Salmon stage 3 MM patients with at least one osteolytic lesion, whereas our study only included MM patients with at least one bone lesion. Additionally, the criteria for defining a clinically relevant SCr increase differ between the two studies; therefore, one cannot directly compare the incidence of kidney dysfunction between these two studies. Although in our study the sample size was small, confidence intervals were wide, and protocol deviations did not permit a robust comparison, the results of this pilot study suggest that the longer infusion time of 30 minutes every 3–4 weeks for 2 years for MM patients with bone disease is also safe and well-tolerated.
As expected, PK data showed that the median zoledronic acid concentrations were greater in the samples obtained from the 15-minute group compared to those from the 30-minute group. This effect was observed in samples obtained both 5 minutes before the end of infusion and at the end of infusion.
Increasing the infusion time did not significantly alter the AE profile and was not associated with any new or unexpected AEs. The incidence rates of deaths, SAEs, treatment-related AEs, and overall AEs were generally comparable between treatment groups. Overall, the incidence rates of reported SREs and ONJ were as expected for this patient population, which are important factors when considering zoledronic acid for patients with MM, where the goal of ongoing monthly IV bisphosphonate therapy is to prevent the development of new SREs without increasing the risk of AEs, such as ONJ.
Finally, the FDA-approved current labeling for zoledronic acid recommends decreasing the dose of this bisphosphonate based on baseline kidney function.7 Because these recommendations were not in place at the time that this study was designed, whether the implementation of these dosing guidelines for patients with MM along with varying infusion durations would have impacted the results observed in our study cannot be ascertained.
In summary, the results of this study suggest that the safety profile of IV zoledronic acid is similar regardless of a 15-minute or a 30-minute infusion duration. However, because the study was not powered to detect statistical significance and the current renal dosing guidelines for zoledronic acid were not used in this study, large randomized studies, using current dosing recommendations, will be required to further assess the effects on kidney safety of prolonging the infusion time of ongoing monthly IV zoledronic acid therapy for patients with MM.
Acknowledgments
The authors thank Syntaxx Communications, Inc., specifically, Kristin Hennenfent, PharmD, MBA, BCPS, and Lisa Holle, PharmD, BCOP, who provided manuscript development and medical writing services, and Holly Matthews, BS, who provided editorial services, with support from Novartis Pharmaceuticals Corporation. We also thank all participating patients and study personnel. Research support was provided by Novartis Pharmaceuticals Corporation (East Hanover, NJ).
References
1 A. Jemal, R. Siegel and J. Xu et al., Cancer statistics, 2010, CA Cancer J Clin 60 (2010), pp. 277–300. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (543)
2 R.A. Kyle, M.A. Gertz and T.E. Witzig et al., Review of 1027 patients with newly diagnosed multiple myeloma, Mayo Clin Proc 78 (1) (2003), pp. 21–33. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (396)
3 A. Corso, P. Zappasodi and C. Pascutto et al., Urinary proteins in multiple myeloma: correlation with clinical parameters and diagnostic implications, Ann Hematol 82 (8) (2003), pp. 487–491. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
4 V. Eleutherakis-Papaiakovou, A. Bamias and D. Gika et al., Renal failure in multiple myeloma: incidence, correlations, and prognostic significance, Leuk Lymphoma 48 (2) (2007), pp. 337–341. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (35)
5 L.S. Rosen, D. Gordon and M. Kaminski et al., Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial, Cancer J 7 (5) (2001), pp. 377–387. View Record in Scopus | Cited By in Scopus (461)
6 L.S. Rosen, D. Gordon and M. Kaminski et al., Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized, double-blind, multicenter, comparative trial, Cancer 98 (8) (2003), pp. 1735–1744. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (329)
7 , Zometa (package insert), Novartis Pharmaceuticals, Corporation, East Hanover, NJ (2008).
8 P. Major, A. Lortholary and J. Han et al., Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials, J Clin Oncol 19 (2) (2001), pp. 558–567. View Record in Scopus | Cited By in Scopus (325)
9 T. Chen, J. Berenson and R. Vescio et al., Pharmacokinetics and pharmacodynamics of zoledronic acid in cancer patients with bone metastases, J Clin Pharmacol 42 (11) (2002), pp. 1228–1236. View Record in Scopus | Cited By in Scopus (139)
10 T. Pfister, E. Atzpodien and F. Bauss, The renal effects of minimally nephrotoxic doses of ibandronate and zoledronate following single and intermittent intravenous administration in rats, Toxicology 191 (2003), pp. 159–167. Article |
11 T. Pfister, E. Aztpodien, B. Bohrmann and F. Bauss, Acute renal effects of intravenous bisphosphonates in the rat, Basic Clin Pharmacol Toxicol 97 (2005), pp. 374–381. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (17)
12 F. Saad, D.M. Gleason and R. Murray et al., A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma, J Natl Cancer Inst 94 (19) (2002), pp. 1458–1468. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (650)
13 S. Kautiainen, S. Luurila, P. Ylitalo and R. Ylitalo, Transformation of bisphosphonates into insoluble material in human blood in vitro, Methods Find Exp Clin Pharmacol 20 (4) (1998), pp. 289–295. View Record in Scopus | Cited By in Scopus (5)
14 L.S. Rosen, D. Gordon and S. Tchekmedyian et al., Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial—the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group, J Clin Oncol 21 (16) (2003), pp. 3150–3157. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (251)
15 M.A. Hussein, Multiple myeloma: most common end-organ damage and management, J Natl Compr Canc Netw 5 (2) (2007), pp. 170–178. View Record in Scopus | Cited By in Scopus (4)
Appendix
The following ZMAX Trial principal investigators participated in this study: Bart Barlogie, MD, Myeloma Institute For Research and Therapy; James Berenson, MD, Oncotherapeutics; Robert Bloom, MD, Providence Cancer Center, Clinical Trials Department; Ralph Boccia, MD, Center for Cancer and Blood Disorders; Donald Brooks, MD, Arizona Clinical Research Center, Inc.; Robert Brouillard, MD, Robert P. Brouillard, MD, and Delvyn Case, MD, Maine Center for Cancer Medicine and Blood Disorders, Pharmacy; Veena Charu, MD, Pacific Cancer Medical Center; Naveed Chowhan, MD, Cancer Care Center, Inc; Robert Collins, MD, University of Texas Southwestern Medical Center at Dallas; Thomas Cosgriff, MD, Hematology and Oncology Specialists, LLC; Jose Cruz, MD, Joe Arrington Cancer Research and Treatment Center; Surrinder Dang, MD, Oncology Specialties; Sheldon Davidson, MD, North Valley H/O; Tracy Dobbs, MD, Baptist Regional Cancer Center; Luke Dreisbach, MD, Desert Hematology Oncology Medical Group; Isaac Esseesse, MD, Hematology Oncology Associates of Central Brevard, Laboratory; Mark Fesen, MD, Hutchinson Clinic, PA; George Geils, Jr., MD, Charleston Hematology Oncology Associates, PA; Michael Greenhawt, MD, South Florida Oncology-Hematology; Manuel Guerra, MD, ORA; Rita Gupta, MD, Oncology-Hematology Associates, PA; Vicram Gupta, MD, Saint Joseph Oncology; Alexandre Hageboutros, MD, Cancer Institute of New Jersey at Cooper Hospital; Vincent Hansen, MD, Utah Hematology Oncology; David Henry, MD, Pennsylvania Oncology Hematology Associates; Benjamin Himpler, MD, Syracuse Hematology/Oncology PC; Winston Ho, MD, Hematology/Oncology Group of Orange County; William Horvath, MD, Haematology Oncology Associates of Ohio and Michigan, PC; Paul Hyman, MD, Hematology Oncology Associates of Western Suffolk; Min Kang, MD, Western Washington Oncology; Mark Keaton, MD, Augusta Oncology Associates, PC; Howard Kesselheim, MD, The Center for Cancer and Hematologic Disease; Kapisthalam Kumar, MD, Pasco Hernando Oncology Associates, PA; Edward Lee, MD, Maryland Oncology-Hematology, PA; André Liem, MD, Pacific Shore Medical Group; Timothy Lopez, MD, New Mexico Cancer Care Associates, Cancer Institute of New Mexico; Paul Michael, MD, Comprehensive Cancer Centers of Nevada; Michael Milder, MD, Swedish Cancer Institute; Barry Mirtsching, MD, Center for Oncology Research & Treatment, PA; Ruben Niesvizky, MD, New York Presbyterian Hospital; Jorge Otoya, MD, Osceola Cancer Center; Joseph Pascuzzo, MD, California Oncology of the Central Valley; Ravi Patel, MD, Comprehensive Blood and Cancer Center Lab; Allen Patton, MD, Hematology Oncology Associates, PA; Kelly Pendergrass, MD, Kansas City Cancer Center, LLC; Anthony Phillips, MD, Fox Valley Hematolgy Oncology, SC; Robert Raju, MD, Dayton Oncology and Hematology, PA; Harry Ramsey, MD, Berks Hematology Oncology Associates; Ritesh Rathore, MD, Roger Williams Hospital Medical Center; Phillip Reid, MD, Central Jersey Oncology Center; Robert Robles, MD, Bay Area Cancer Research Group, LLC; Stephen Rosenoff, MD, Oncology and Hematology Associates of Southwest Virginia, Inc; Martin Rubenstein, MD, Southbay Oncology Hematology Partners; Mansoor Saleh, MD, Georgia Cancer Specialists; Sundaresan Sambandam, MD, Hematology and Oncology Associates of RI; Mukund Shah, MD, Antelope Valley Cancer Center; David Siegel, MD, Hackensack University Medical Center; Nelida Sjak-Shie, MD, The Center for Cancer Care and Research; Michael Stone, MD, Greeley Medical Clinic; Stefano Tarantolo, MD, Nebraska Methodist Hospital; Joseph Volk, MD, Palo Verde Hematology Oncology, Ltd; Mitchell Weisberg, MD, MetCare Oncology; Ann Wierman, MD, Nevada Cancer Center; Donald Woytowitz, Jr., MD, Florida Cancer Specialists; Peter Yu, MD, Camino Medical Group.
Management Of Tyrosine Kinase Inhibitor–Induced Hand–Foot Skin Reaction: Viewpoints from the Medical Oncologist, Dermatologist, and Oncology Nurse
How we do it
Elizabeth Manchen RN, MS, OCN![]()
![]()
Abstract
One significant toxicity associated with the anticancer tyrosine kinase inhibitors (TKIs) is hand–foot skin reaction (HFSR). We provide an overview of HFSR, emphasizing experience-based prevention techniques and nursing management strategies from the viewpoints of a medical oncologist, a dermatologist, and an oncology nurse. Supporting data include (1) published preclinical and phase I–III clinical studies and (2) published abstracts of phase II–III clinical trials of sorafenib and sunitinib. HFSR has been reported in up to 60% of patients treated with sorafenib or sunitinib. TKI-induced HFSR may lead to dose reductions or treatment interruptions and reduced quality of life. Symptoms of TKI-associated HFSR can be managed by implementing supportive measures and aggressive dose modification. Patients educated about HFSR can work with their health-care teams to proactively detect and help manage this cutaneous toxicity, thus preventing or reducing the severity of TKI-associated HFSR. Successful prevention and management of TKI-associated HFSR can help to ensure that patients achieve optimal therapeutic outcomes. Implementation of such measures may increase the likelihood that therapy is continued for the appropriate interval at an appropriate dose for each patient. Optimal management of TKI-associated HFSR is predicated on establishing appropriate partnerships among medical oncologists, dermatologists, oncology nurses, and patients.
Article Outline
This article reviews the mechanism of action, clinical trial results, and adverse effects of two molecularly targeted anticancer agents, the tyrosine kinase inhibitors (TKIs) sorafenib (Nexavar®; Bayer HealthCare Pharmaceuticals, Montville, NJ, and Onyx Pharmaceuticals, Emeryville, CA) and sunitinib (Sutent®; Pfizer Pharmaceuticals, New York, NY). This article specifically focuses on the diagnosis and management of TKI-associated hand–foot skin reaction (HFSR) from the perspectives of the medical oncologist, the dermatologist, and the oncology nurse. Data were derived from (1) published reports of preclinical and phase I–III clinical studies of sorafenib and sunitinib and (2) published abstracts of phase II–III clinical trials of sorafenib and sunitinib.
The Medical Oncologist's Viewpoint
Molecularly Targeted Agents
Molecularly targeted therapies are directed at specific mechanisms involved in cell division, invasion, and metastasis, as well as in cell survival mediated by avoidance of apoptosis and resistance to conventional treatments. Clinical trials in several cancer types have shown that these TKIs can inhibit these activities of cancer cells by either cytostatic or cytotoxic mechanisms.1 However, the ability of these agents to inhibit multiple cancer cell pathways via novel mechanisms of action may explain, at least in part, their apparent direct toxic effects.2 These include adverse events that, from a medical viewpoint, must be anticipated, promptly recognized, and properly treated. Doing so can help minimize disruption to the patient's quality of life and may reduce the need for dose reduction or treatment interruption.1
Both sorafenib and sunitinib are orally administered, small-molecule inhibitors of multiple kinases, some of which are common to both agents (Figure 2).3 Sorafenib has known effects on tumor-cell proliferation and angiogenesis. Its antiproliferative effects are exerted via inhibition of serine/threonine kinases of the RAF/MEK/ERK signaling pathway (also called the MAP-kinase pathway) that is found within tumor cells; specifically, sorafenib targets wild-type RAF gene products (CRAF, BRAF) and mutant BRAF. The antiangiogenic effects of sorafenib are exerted via its inhibition of extracellular vascular endothelial growth factor (VEGF) receptors 2 and 3 (VEGFR-2 and VEGFR-3) and platelet-derived growth factor receptor beta (PDGFR-β), which is found mainly in the tumor vasculature. Sorafenib also exerts broad-spectrum activity against the stem-cell growth factor receptor (c-KIT), FMS-like tyrosine kinase 3 (Flt3), and the receptor encoded by the ret proto-oncogene (RET).[4], [5], [6] and [7] Sunitinib has demonstrated effects on the growth, pathologic angiogenesis, and metastatic progression of cancer by inhibiting PDGFR-α and -β; VEGFR-1, -2, and -3; and colony-stimulating factor receptor (CSF-1R), c-KIT, Flt3, and RET.8
Mechanisms of Action of Sorafenib and Sunitinib
Sorafenib and sunitinib specifically recognize and inhibit c-KIT, VEGFR, PDGFR-β, and Flt3 receptor tyrosine kinases. Sorafenib also inhibits RAF, a serine/threonine kinase involved in the RAF/MEK/ERK kinase pathway
c-KIT = stem-cell growth factor receptor (a cytokine receptor expressed on the surface of hematopoietic stem cells as well as other cell types); ERK = extracellular signal–regulated kinase; Flt3 = FMS-like tyrosine kinase 3 (a cytokine receptor expressed on the surface of hematopoietic progenitor cells); Flt3L = FMS-like tyrosine kinase 3 ligand (Flt3 ligand); MEK = (MAPK/ERK) kinase; PDGF-ΒΒ = platelet-derived growth factor BB; PDGFR-β = platelet-derived growth factor receptor beta; RAF = a gene that encodes for a protein kinase (Raf1) that functions in the mitogen-activated protein kinase/extracellular signal–regulated kinase (MAPK/ERK) signal-transduction pathway as part of a protein kinase cascade; RAS = a superfamily of genes that encode small GTPases involved in cellular signal transduction; SCF = stem-cell factor; VEGF = vascular endothelial growth factor; VEGFR = vascular endothelial growth factor receptor
Adapted with permission from Lacouture et al3
Sorafenib was approved for the treatment of advanced renal cell carcinoma (RCC) in 2005 and for unresectable hepatocellular carcinoma (HCC) in 2007. The efficacy of sorafenib in 903 patients with advanced RCC was demonstrated in the phase III Treatment Approaches in Renal Cancer Global Evaluation Trial (TARGET), the largest phase III trial ever conducted in the second-line setting in patients with advanced RCC. Sorafenib significantly enhanced median progression-free survival (PFS) compared with placebo (24 vs 12 weeks),9 which led to early termination of the study and crossover from placebo to active drug. A preplanned analysis, which did not include patients who received placebo (who had crossed over to active treatment), ultimately demonstrated that sorafenib significantly prolonged overall survival (OS).10 Furthermore, 84% of sorafenib-treated patients experienced a clinical benefit, defined as objective response or disease stabilization.9 These results have been confirmed in larger, “real-world” patient populations in expanded-access programs conducted in North America (n = 2504)11 and the European Union (n = 118).12
Definitive data supporting the efficacy of sorafenib in HCC were provided by the randomized, double-blind, placebo-controlled Sorafenib CCC Assessment Randomized Protocol (SHARP) trial, the largest phase III trial ever conducted in patients with advanced HCC (n = 599) and the first phase III study to demonstrate a significant survival advantage with a systemic treatment in advanced HCC. In this trial, patients treated with sorafenib experienced a 44% increase in median OS (10.7 vs 7.9 months, hazard ratio [HR] = 0.69, 95% confidence interval [CI] 0.55–0.87, P < 0.001) and a 73% prolongation in median time to radiographic progression (5.5 vs 2.8 months, P < 0.001) compared with patients who received placebo.13 These results were confirmed in a separate phase III, randomized, double-blind, placebo-controlled study conducted in 226 patients from the Asia-Pacific region with advanced HCC.14 In this trial also, sorafenib significantly prolonged median OS (6.5 vs 4.2 months, HR = 0.68, 95% CI 0.50–0.93, P = 0.014) and time to progression (TTP) (2.8 vs 1.4 months, HR = 0.57, 95% CI 0.42–0.79, P = 0.0005) compared with placebo.
Sunitinib received approval in 2006 for use in patients with gastrointestinal stromal tumor (GIST) whose disease is refractory to imatinib (Gleevec®; Novartis Pharmaceuticals, East Hanover, NJ) or who are intolerant to the drug and in those with advanced RCC. Approval of sunitinib for the treatment of GIST was based on data from a randomized, placebo-controlled, phase III trial of 312 patients with imatinib-refractory GIST.15 In that study, sunitinib treatment increased median PFS (24.1 vs 6.0 weeks, HR = 0.33, 95% CI 0.24–0.47, P < 0.0001) and median TTP (27.3 vs 6.4 weeks, HR = 0.33, 95% CI 0.23–0.47, P < 0.0001) compared with placebo. The trial was unblinded early when a planned interim analysis revealed significantly longer TTP with sunitinib than with placebo. A subsequent analysis showed that median OS with sunitinib was about twice that with placebo (73.9 vs 35.7 weeks, P < 0.001).16 In an ongoing, worldwide treatment-use program to provide expanded access to sunitinib for patients with advanced GIST intolerant of or resistant to imatinib,17 sunitinib treatment resulted in a median estimated TTP of 41 weeks and a median estimated OS of 75 weeks in the population analyzed (n = 1,117).
A separate phase III randomized controlled trial was conducted in 750 patients with advanced RCC and no history of systemic therapy for RCC.[18] and [19] The active comparator in this trial was interferon-alfa (IFN-α). Compared with IFN-α, sunitinib significantly increased median PFS (11 vs 5 months, HR = 0.539, 95% CI 0.451–0.643, P < 0.001) and was associated with a greater objective response rate (47% vs 12%, P < 0.001). Median OS was greater in the sunitinib group (26.4 vs 21.8 months), but the difference was not significant (P = 0.051). Data from expanded-access programs in patients with RCC and GIST support the phase III trial data for sunitinib.20 Efficacy data for sorafenib and sunitinib are summarized in Table 1.[9], [10], [11], [12], [13], [14], [15], [17], [18] and [20]
| DRUG, DISEASE, AND STUDY | EFFICACY DATA |
|---|---|
| Sorafenib | |
| Advanced RCC | |
| Phase III TARGET[9] and [10] | |
| Expanded-access programs[11] and [12] | Data from expanded-access programs in community-based populations (NA- and EU-ARCCS) were consistent with data from TARGET |
| Unresectable HCC | |
| Phase III SHARP trial13 | • First phase III trial to demonstrate a significant survival advantage for a systemic therapy in advanced HCC • Median OS was 10.7 months in sorafenib group vs 7.9 months in placebo group (HR = 0.69, 95% CI 0.55–0.87, P < 0.001) |
| Phase III Asia-Pacific trial14 | |
| Sunitinib | |
| Advanced RCC | |
| Phase III registration trial18 | • Median PFS was 11 months in sunitinib group vs 5 months in interferon-α group (HR = 0.539, 95% CI 0.451–0.643, P < 0.001) |
| Expanded-access program20 | |
| Imatinib-resistant GIST | |
| Phase III registration trial15 | • Median TTP was 27.3 weeks in sunitinib group vs 6.4 weeks in placebo group (HR = 0.33, 95% CI 0.23–0.47, P < 0.0001) |
| Expanded-access program17 |
CI = confidence interval; CR = complete response; EU-ARCCS = European Union Advanced Renal Cell Carcinoma Sorafenib; GIST = gastrointestinal stromal tumor; HCC = hepatocellular carcinoma; HR = hazard ratio; NA-ARCCS = North American ARCCS; OS = overall survival; PFS = progression-free survival; PR = partial response; RCC = renal cell carcinoma; SD = stable disease; SHARP = Sorafenib CCC Assessment Randomized Protocol; TARGET = Treatment Approaches in Renal Cancer Global Evaluation Trial; TTP = time to progression; TTRP = time to radiologic progression
Characteristics of Hand–Foot Skin Reaction
Data from the clinical trials for sorafenib and sunitinib indicate that both agents are generally well-tolerated; common treatment-related adverse reactions include diarrhea, alopecia, nausea, fatigue, rash, and hypertension, as well as palmar–plantar erythrodysesthesia (PPE) syndrome, also known as hand–foot skin reaction (HFSR) (Table 2).[10] and [19] HFSR is a dermatologic toxicity that has been reported in 14%–62% of patients treated with sorafenib or sunitinib (Table 3).[9], [11], [12], [13], [14], [15], [17], [18], [20], [21], [22], [23], [24] and [25] In general, the term HFSR refers to a group of signs and symptoms affecting the hands and feet of patients taking sorafenib, sunitinib, or, to a lesser extent, other TKIs such as pazopanib (Votrient™; GlaxoSmithKline, Research Triangle Park, NC)[26] and [27] and axitinib (AG013736).[28], [29], [30] and [31]
| ADVERSE EVENT | SORAFENIB 400 MG BID | SUNITINIB 50 MG QD | ||
|---|---|---|---|---|
| ALL GRADES (%) | GRADE 3/4 (%) | ALL GRADES (%) | GRADE 3/4 (%) | |
| Diarrhea | 48 | 3 | 61 | 9 |
| Rash | 41 | 1 | 24 | 2 |
| Hand–foot skin reaction | 33 | 6 | 29 | 9 |
| Alopecia | 31 | 0 | 12 | 0 |
| Fatigue | 29 | 3 | 54 | 11 |
| Nausea | 19 | <1 | 52 | 5 |
| Hypertension | 17 | 4 | 30 | 12 |
| Dry skin | 13 | 0 | 21 | <1 |
| Vomiting | 12 | 1 | 31 | 4 |
| Mucositis | 5 | 0 | 26 | 2 |
| REFERENCE | STUDY | ALL GRADES (%) | GRADE 3 (%) | GRADE 4 (%) |
|---|---|---|---|---|
| Sorafenib | ||||
| 9 | Phase III TARGETa | 30 | 6 (grade 3/4) | |
| 13 | Phase III SHARPa | 21 | 8 | 0 |
| 11 | NA-ARCCS, first-linea | 19 (≥2) | 11 (grade 3/4) | |
| 11 | NA-ARCCS, second-linec | 17 (≥2) | 8 (grade 3/4) | |
| 12 | EU-ARCCSa | 47 | 12 (grade 3/4) | |
| 14 | Phase III Asia-Pacifica | 45 | 11 (grade 3/4) | |
| 24 | Phase II randomized discontinuation trial in advanced RCCb | 62 | 13 | 0 |
| 25 | Phase II study in advanced HCCb | 31 | 5 | 0 |
| 21 | Phase II, uncontrolled study in relapsed/refractory NSCLCa | 37 | 10 (grade 3/4) | |
| Sunitinib | ||||
| 18 | Phase III registration trial in advanced RCCa | 20 | 5 | 0 |
| 20 | Expanded access program in advanced RCCc | 5 (grade 3/4) | ||
| 15 | Phase III registration trial in imatinib-resistant GISTa | 14 | 4 | 0 |
| [17] and [22] | Expanded access program in imatinib-resistant GISTc | N/A | 8 (grade 3/4) | |
| 23 | Phase II trial of second-line treatment in advanced RCCa | 15 | 7 | 0 |
EU-ARCCS = European Union Advanced Renal Cell Carcinoma Sorafenib; GIST = gastrointestinal stromal tumor; HCC = hepatocellular carcinoma; N/A = data not available; NA-ARCCS = North American ARCCS; NSCLC = non-small-cell lung cancer; RCC = renal cell carcinoma; SHARP = Sorafenib CCC Assessment Randomized Protocol; TARGET = Treatment Approaches in Renal Cancer Global Evaluation Trial
a Used version 3.0 of National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE)b Used version 2.0 of NCI-CTCAEc Version of NCI-CTCAE used not specified
HFSR is typically characterized by redness, marked discomfort, swelling, and tingling in the palms of the hands and/or soles of the feet.32 HFSR can be painful enough to interfere profoundly with activities of daily living (ADLs). In fact, patients may report symptoms after as few as 2 weeks on TKI therapy, at which point they may present to the health-care provider (HCP) wearing slippers, unable to walk, and having difficulty in performing ADLs such as eating, dressing, and bathing.[1] and [33] Although HFSR can lead to TKI dose modification or treatment discontinuation, preventive measures can be taken before TKIs are initiated to reduce the likelihood of HFSR. In addition, early treatment of symptoms may prevent HFSR from progressing to the point at which the patient's ability to receive the full potential benefit of therapy is compromised.[3], [34], [35] and [36]
Signs and symptoms of HFSR may appear concomitantly or sequentially and can affect both hands and both feet. Although symptoms are most prominent on the palms and soles, other areas of the hands and feet may also be involved, including the tips of the fingers and toes, the heels, and metatarsophalangeal skin; areas of flexure; and skin overlying the metacarpophalangeal and interphalangeal joints.3 These “pressure areas” are where the most severe symptoms are typically seen. Common symptoms include dysesthesia and paresthesia, described as “tingling, prickling, or creeping sensations” and/or sensitivity or intolerance to hot or warm objects (which may occur before other symptoms are apparent); erythema; edema; hyperkeratosis; and dry and/or cracked skin.[1] and [34] Actual HFSR lesions are described as tender and scaling, with a peripheral halo of erythema, yellowish and hyperkeratotic plaques, or callous-like blisters (which usually do not contain fluid), typically localized to areas of pressure.[3] and [35] Desquamation, particularly with sunitinib treatment, may also be present.37
Since both sorafenib and sunitinib inhibit the VEGFRs, PDGFRs, c-KIT, and Flt3,38 it is likely that inhibition of one or more of these receptors and/or pathways plays a role in HFSR development.36 Differences in the relative appearance of HFSR symptoms are dependent on whether sorafenib or sunitinib is used. Sunitinib use is more often associated with desquamation, whereas sorafenib is more often associated with areas of hyperkeratosis, particularly formation of thick calluses on the soles of the feet.37 The timing of the first appearance of symptoms may also vary according to the TKI used. HFSR usually develops within the first 2–4 weeks of treatment with a TKI and almost always within the first 6 weeks.35 However, because the severity of HFSR appears to be dose-dependent,3 signs and symptoms may present later rather than sooner in patients treated with sunitinib. This is likely due to the recommended sunitinib dosing schedule, which incorporates a 2-week period during which no drug is administered. Although HFSR frequently decreases in intensity during treatment, even without dose modifications or treatment interruption, prompt treatment of HFSR is recommended to prevent rapid progression. Early symptoms can usually be resolved easily by appropriate treatment, which often allows continuation of full-dose therapy for the prescribed length of time.
It is important to note what HFSR is not. TKI-associated HFSR is not the same clinical entity as the hand–foot syndrome (HFS) traditionally seen with cytotoxic agents such as infusional 5-fluorouracil (5-FU); capecitabine, the oral prodrug of 5-FU; and pegylated liposomal doxorubicin. Although HFSR and HFS share several clinical and pathological aspects—each previously has been called “acral erythema” and “PPE”—they clearly are not the same clinical or pathologic entity. HFSR is neither an allergic reaction to a drug nor an indication that a patient may be intolerant to a drug. Finally, HFSR does not indicate drug efficacy, as may be the case with skin rash in patients with non-small-cell lung cancer treated with erlotinib.[3] and [39]
Grading HFSR
In published reports, the severity of HFSR is usually graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE),32 a three-grade classification system. However, modified criteria are considered by some to be a better fit for routine clinical practice.1 What distinguishes the modified criteria from the NCI criteria (version 4.02) is the inclusion of HFSR-specific clinical characteristics plus certain patient-defined considerations used to categorize severity. The modified criteria expressly define the degree to which HFSR discomfort affects the patient's normal activities, an improvement over version 4.02 used alone. The NCI-CTCAE version 4.02 criteria, the modified criteria, and corresponding patient photographs are presented in Figure 3.[1] and [32]
Recommendations for the treatment of grade 1 HFSR include early and appropriate dermatologic management and active collaboration among HCPs.40
The Dermatologist's Viewpoint
Although the exact pathogenesis of HFSR has not been fully elucidated, research into its cause(s) is ongoing. Theoretically, traditional HFS is thought to be due to the direct toxic effects of drugs or their ability to invoke a “host-vs-host” response. In contrast, a unique mechanism has been proposed for TKI-associated HFSR: simultaneous blockage of VEGFRs and PDGFRs.2
Three histopathologic features have been found to predominate in HFSR: dyskeratotic keratinocytes at various states of necrosis (Figure 441), basal layer vacuolar degeneration, and mild perivascular or lichenoid lymphocyte-predominant infiltrate.2 Immunohistochemistry with a variety of skin-cell markers has shown a significant modification of normal maturation of keratinocytes, which are often apoptotic. Minor modifications of blood vessels are also seen, but no signs of intense vasculitis are evident. This is important because HFSR is suspected of being a “class effect” of TKIs that target VEGFRs. HFSR is not seen in patients treated with single-agent bevacizumab, and the lack of histologic evidence of significant damage to blood vessels suggests that HFSR does not result from the general inhibition of angiogenesis. A retrospective analysis found that HFSR rates were higher when patients were treated with sorafenib and bevacizumab in combination, supporting the hypothesis that HSFR is due to the anti-VEGF properties of sorafenib.42 Other possible causes of HFSR include activation by a ligand other than VEGF and/or inhibition of one of the other protein targets inhibited by both sorafenib and sunitinib.[3] and [35]
Layers of the Epidermis
The epidermis is composed of a very sophisticated arrangement of keratinocytes, which originate as stem cells in the stratum germinatum (not shown). The stem cells constantly multiply, creating daughter cells that progressively mature over approximately 28 days and move to the surface of the epidermis. As they move, they change their function and shape. In the stratum spinosum, interactions between cells resemble spines; mature cells move through the stratum granulosum, which has a very important secretory function, until finally the cells reach the stratum corneum and die. Thus, the stratum corneum is the layer of skin containing dead skin cells that have lost their nuclei; it is the part of the epidermis that ensures the barrier function of skin and is the layer most affected by HFSR. The layer beneath the epidermis is called the “papillary dermis.” The papillary dermis contains nerves and blood vessels and supplies the epidermis with nutrients. The fibroblasts and fibers located here give skin its strength and resistance
Adapted with permission from Gawkrodger41
Incidence and Severity of HFSR With TKI
To determine the incidence and severity of HFSR specific to sorafenib, a double-blind, prospective, dermatologic substudy was performed in patients enrolled in the phase III TARGET trial.35 Eighty-five patients with RCC were randomized to receive either sorafenib (n = 43) or placebo (n = 42). Dermatologic examinations were performed before and during treatment. Ninety-one percent of sorafenib-treated patients experienced at least one cutaneous reaction compared with 7% of those in the placebo group. A variant of HFSR clinically distinct from chemotherapy-induced HFS was observed in 60% of sorafenib-treated patients. Reversible grade 3 HFSR leading to dose reduction occurred in two sorafenib-treated patients. Additional cutaneous reactions were facial erythema, scalp dysesthesia, alopecia, and subungual splinter hemorrhages.
HFSR (of any grade) has been shown to occur in approximately 30% of patients treated with sorafenib and 20% of those who received sunitinib in clinical studies.43 Grade 3/4 HFSR has been observed in approximately 6% of sorafenib-treated and 5% of sunitinib-treated patients. HFSR was not reported in a phase II study of 142 patients with relapsed or refractory soft-tissue sarcoma treated with pazopanib.44 In a phase III randomized, double-blind, placebo-controlled trial of pazopanib in patients with advanced RCC, the incidence of HFSR was <10%, while the incidence of grade 3/4 HFSR was <1%. Potential differences may be explained by variations in the potency and selectivity of the TKIs.27
Management Strategies
Our work at the Dermatology Center at the Gustave-Roussy Institute has shown that early intervention against the dermatologic adverse effects of these TKIs can inhibit patient progression to a more serious form of HFSR.[34] and [38]
Effective management of HFSR can begin prior to initiation of treatment with sorafenib or sunitinib. Patients should be advised to remove any preexisting hyperkeratotic areas or calluses, keep skin well-moisturized with appropriate creams, and cushion pressure points with cotton socks, soft shoes, and/or insoles. Dose modification is typically not required for grade 1 HFSR; symptomatic treatments should be employed instead.
If HFSR symptoms progress to grade 2 or 3, with pain and a decrease in quality of life, the dose of sorafenib or sunitinib can be modified until symptoms recede, after which the patient can be brought back to the full dose. Very often, the patient can tolerate the full-dose treatment simply by decreasing the dose briefly.3 A recommended dose-modification scheme is shown in Figure 5.3
Management of Hand–Foot Skin Reaction by Grade
MKI = multikinase inhibitor
Adapted with permission from Lacouture et al3
TKIs are being studied in patients with additional types of tumor, possibly in the adjuvant setting, as well as in combinations. Because these drugs are administered orally, with a decreased (compared with conventional cytotoxic agents) frequency of nurse– or doctor–patient interactions, patients must be very well-informed of any potential toxicities with the TKIs.
At present, there are no evidence-based treatment guidelines for the prevention or management of HFSR. However, HCPs most involved in the day-to-day care of patients with HFSR have made great progress in establishing preventive and treatment strategies and in identifying ancillary products likely to decrease the incidence and/or severity of symptoms. Prevention, which includes preventing HFSR entirely as well as preventing progression from its initial appearance, is a key component of HFSR management.
The Oncology Nurse's Viewpoint
The nurse's viewpoint begins with patient education and empowerment. The goal is to prevent adverse effects from occurring while managing any adverse effects that do occur so that the patient has the best chance of staying on anticancer therapy. This requires a strong partnership between the HCP team and the patient. Although not all cases of HFSR can be prevented, experience suggests that symptom incidence and severity can be alleviated by educating patients to recognize the signs and symptoms of HFSR and report these to their HCPs. HFSR typically occurs early in the course of therapy, so it is prudent to be especially vigilant during the first 6 weeks. Providing the patient with a brochure about HFSR to refer to at home may facilitate identification of HFSR.
To address the lack of evidence-based guidelines to prevent or treat HFSR, an international, interdisciplinary expert panel has provided a set of consensus recommendations for the management of TKI-associated HFSR.45 One component of these recommendations can be phrased simply for the patients as a “3C” approach to management: control calluses, comfort with cushions, and cover with creams.
Prior to treatment, the patient should receive a full-body examination, with emphasis on the condition of the hands and feet. Evaluation should be performed by a qualified HCP who can determine whether there are physical conditions that may predispose a patient to areas of increased friction or rubbing. For all patients, especially those with comorbid conditions (eg, diabetes, poor circulation), a pretreatment pedicure is highly recommended. Patients should also be educated on the proper use of tools (eg, a pumice stone) to aid in callus removal. Such tools are considered beneficial because patients can control the frequency of their use and the extent of skin removed. However, because areas of hyperkeratosis are often extremely tender and painful, patients are cautioned against overuse of these tools, including the aggressive “paring” or “cutting” of callused areas. Finally, patients should be advised of the need for clean tools to guard against infection.
Other protective measures include the use of thick cotton gloves and/or socks, which may also help the skin to retain moisture, and avoidance of warm and/or hot water or objects, tight-fitting shoes, or other items that may rub, pinch, or cause friction in affected areas. Tender areas, pressure points, and pressure-sensitive areas of the hands and feet should be protected. For example, weight lifters might be advised to wear gloves. These recommendations hold true both before and after development of HFSR.[3], [33] and [35] Well-padded but nonconstrictive footwear should be worn, and the use of insole cushions or inserts (eg, silicone or gel) should be encouraged. Foot soaks with lukewarm water and magnesium sulfate may be soothing. Tender areas should be protected at all times, and patients should be encouraged not to walk barefoot.
Use of over-the-counter and prescription-strength creams and moisturizers during treatment with TKIs has also been recommended (Table 4).[40], [45], [46], [47], [48] and [49] Moisturizing agents should be applied liberally, immediately after bathing. Cotton gloves and/or socks can also be worn, to help retain moisture and to provide an additional layer of protection. When applied liberally, these products soften areas of thick and hardened skin, help keep the skin pliable, and may prevent cracks or breaks in skin integrity, which could cause additional discomfort. Prescription-strength topical agents have also shown anecdotal benefit (Table 4). These topical agents are typically applied twice daily to affected areas only because they may irritate unaffected skin. Data on the use of topical/systemic corticosteroids in the treatment of HFS remain inconclusive; the literature primarily includes case studies in patients with PPE treated with chemotherapeutic agents including pegylated liposomal doxorubicin.2 Finally, a qualified HCP must always be consulted to ensure proper diagnosis and treatment of HFSR.
Adapted with permission from Anderson et al40
| PRODUCTS | PRODUCT INFORMATION |
|---|---|
| Over-the-counter[40], [45] and [46] | |
| Cetaphil® (Galderma Laboratories, Ft. Worth, TX) skin cleaners, Aveeno® (Johnson & Johnson, New Brunswick, NJ) shower gel | Nondeodorant, fragrance-free products |
| Udderly Smooth® (Redex Industries, Salem, OH), Gold Bond® (Chattem, Chattanooga, TN), Aveeno® | Thicker products with more intense moisturizing properties than basic lotions; anti-itch formulations are available |
| Norwegian Formula: Smoothing Relief Anti-Itch Moisturizer (Neutrogena, Los Angeles, CA) | Contains dimethicone 1%, camphor 0.1%, and lidocaine |
| Norwegian Formula: Foot Cream (Neutrogena) | Contains cetearyl alcohol, dimethicone, menthol, and urea |
| Bag Balm® (Dairy Association, Lyndonville, VT) | May provide “cooling” effect from eucalyptus |
| Eucerin® (Beiersdorf, Hamburg, Germany) Cream | Best used at night due to greasy formulation |
| Eucerin® Dry Skin Therapy | Contains urea and alpha-hydroxy acid |
| Aquaphor® (Beiersdorf) Healing Ointment | Petrolatum 41% |
| Kerasal® (Alterna, Whippany, NJ) | Salicylic acid 5% exfoliates and softens skin; urea 10% moisturizes skin |
| Blue Lizard® (Crown Laboratories, Johnson City, TN) | UV A and B sunblock, water-resistant |
| Prescription47–49 | |
| Urea 40% cream (Carmol 40®; Doak Dermatologics, Fairfield, NJ) | Softens hyperkeratosis, decreases epidermal thickness, proliferation |
| Tazarotene 0.1% cream (Tazorac®; Allergan Dermatology, Irvine, CA) | Retinoid decreases proliferation, reduces dermal inflammation |
| Fluorouracil 5% cream (Carac®; Dermik Laboratories, Bridgewater, NJ) | Antifolate inhibits proliferation; has shown anecdotal benefit in certain conditions characterized by hyperkeratotic lesions on the palms and soles |
Summary
The addition of molecularly targeted agents to anticancer treatment has been found to cause both common and novel adverse reactions. HFSR is being increasingly recognized as a potential dose-limiting toxicity associated with sorafenib or sunitinib treatment that can result in discomfort, pain, decreased quality of life, and premature termination of a potentially effective cancer treatment. It is important to educate patients about potential dermatologic adverse effects associated with TKIs because limiting toxicity can help avoid treatment interruptions or dose reductions while improving ADLs.
The precise pathogenic mechanism of HFSR is currently not known, and there is no evidence-based protocol for treatment of HFSR. However, the increased clinical experience with these agents has resulted in a wealth of published articles describing empiric and symptomatic approaches that appear to help to prevent and manage HFSR. Frequent communication is necessary between the physician and patient, particularly 2–4 weeks from the initiation of therapy. Symptoms of HFSR should be recognized as early as possible. Providing the patient with a brochure about HFSR to refer to at home may facilitate the early identification of HFSR.
Patients should be advised of the “3C” approach to the management of TKI-associated HFSR: control calluses, comfort with cushions, and cover with creams. Creams should be applied after bathing and before going to bed; cotton gloves and socks should be worn to keep the cream on the hands and feet during the night.
Symptoms of HFSR typically are manageable with the implementation of supportive measures. If symptoms worsen, dose modification or interruption will result in a return to grade 0/1. Many patients can successfully be rechallenged with the full dose. Observations across multiple viewpoints have consistently shown that HFSR severity can be reduced in patients who are educated about HFSR and proactive about its detection and management.
Acknowledgments
All authors contributed equally to the development of this report. Editorial support was provided by Katherine Wright, PharmD, RPh, ISD, Wrighter Medical Education and Training, West Hills, CA; John A. Ibelli, CMPP, BelMed Professional Resources, New Rochelle, NY; and John D. Zoidis, MD, Bayer HealthCare Pharmaceuticals, Montville, NJ.
References1
1 C. Porta, C. Paglino, I. Imarisio and L. Bonomi, Uncovering Pandora's vase: the growing problem of new toxicities from novel anticancer agents: The case of sorafenib and sunitinib, Clin Exp Med 7 (2007), pp. 127–134. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
2 A.D. Lipworth, C. Robert and A.X. Zhu, Hand–foot syndrome (hand–foot skin reaction, palmar–plantar erythrodysesthesia): focus on sorafenib and sunitinib, Oncology 77 (2009), pp. 257–271 [19923864]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
3 M.E. Lacouture, S. Wu and C. Robert et al., Evolving strategies for the management of hand–foot skin reaction associated with the multitargeted kinase inhibitors sorafenib and sunitinib, Oncologist 13 (2008), pp. 1001–1011 [18779536]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (57)
4 S.M. Wilhelm, L. Adnane, P. Newell, A. Villanueva, J.M. Llovet and M. Lynch, Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signaling, Mol Cancer Ther 7 (2008), pp. 3129–3140 [18852116]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (119)
5 D. Auclair, D. Miller and V. Yatsula et al., Antitumor activity of sorafenib in FLT3-driven leukemic cells, Leukemia 21 (2007), pp. 439–445 [17205056]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (40)
6 F. Carlomagno, S. Anaganti and T. Guida et al., BAY 43-9006 inhibition of oncogenic RET mutants, J Natl Cancer Inst 98 (2006), pp. 326–334 [16507829]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (169)
7 S.M. Wilhelm, C. Carter and L. Tang et al., BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis, Cancer Res 64 (2004), pp. 7099–7109 [15466206]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1142)
8 J.G. Christensen, A preclinical review of sunitinib, a multitargeted receptor tyrosine kinase inhibitor with anti-angiogenic and antitumour activities, Ann Oncol 10 (2007), pp. x3–x10 [17761721]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (29)
9 B. Escudier, T. Eisen and W.M. Stadler et al., Sorafenib in advanced clear-cell renal-cell carcinoma, N Engl J Med 356 (2007), pp. 125–134 [17215530]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1425)
10 B. Escudier, T. Eisen and W.M. Stadler et al., Sorafenib for treatment of renal cell carcinoma: final efficacy and safety results of the phase III Treatment Approaches in Renal Cancer Global Evaluation Trial, J Clin Oncol 27 (2009), pp. 3312–3318 [19451442]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (123)
11 W.M. Stadler, R.A. Figlin and D.F. McDermott et al., Safety and efficacy results of the advanced renal cell carcinoma sorafenib expanded access program in North America, Cancer 116 (2010), pp. 1272–1280 [20082451]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (22)
12 J. Beck, E. Bajetta and B. Escudier et al., A large open-label, non-comparative, phase III study of the multi-targeted kinase inhibitor sorafenib in European patients with advanced renal cell carcinoma, Eur J Cancer (suppl) (2007), p. 5 Abstract 4506. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (7)
13 J.M. Llovet, S. Ricci and V. Mazzaferro et al., Sorafenib in advanced hepatocellular carcinoma, N Engl J Med 359 (2008), pp. 378–390 [18650514]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (989)
14 A.L. Cheng, Y.K. Kang and Z. Chen et al., Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial, Lancet Oncol 10 (2009), pp. 25–34 [19095497]. Article |
15 G.D. Demetri, A.T. van Oosterom and C.R. Garrett et al., Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial, Lancet 368 (2006), pp. 1329–1338 [17046465]. Article |
16 G.D. Demetri, X. Huang and C.R. Garrett et al., Novel statistical analysis of long-term survival to account for crossover in a phase III trial of sunitinib (SU) vs placebo (PL) in advanced GIST after imatinib (IM) failure, J Clin Oncol (suppl) (2008), p. 26 Abstract 10524.
17 P. Reichardt, Y. Kang and W. Ruka et al., Detailed analysis of survival and safety with sunitinib (SU) in a worldwide treatment-use trial of patients with advanced GIST, J Clin Oncol (suppl) (2008), p. 26 Abstract 10548.
18 R.J. Motzer, T.E. Hutson and P. Tomczak et al., Sunitinib versus interferon alfa in metastatic renal-cell carcinoma, N Engl J Med 356 (2007), pp. 115–124 [17215529]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1520)
19R.J. Motzer, T.E. Hutson and P. Tomczak et al., Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma, J Clin Oncol 27 (2009), pp. 3584–3590 [19487381]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (194)
20 M.E. Gore, C. Szczylik and C. Porta et al., Safety and efficacy of sunitinib for metastatic renal-cell carcinoma: an expanded-access trial, Lancet Oncol 10 (2009), pp. 757–763 [19615940]. Article |
21 G.R. Blumenschein Jr, U. Gatzemeier and F. Fossella et al., Phase II, multicenter, uncontrolled trial of single-agent sorafenib in patients with relapsed or refractory, advanced non-small-cell lung cancer, J Clin Oncol 27 (2009), pp. 4274–4280 [19652055]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
22 H.J. Schütte, M. Schlemmer, C. Wendtner, P. Reichardt and G.D. Demetri, Sunitinib (SU) in a worldwide treatment-use trial of pts with advanced gastrointestinal stromal tumours (GIST): analysis of survival and safety data, Onkologie (suppl 4) (2008), p. 201 Abstract V582.
23 R.J. Motzer, B.I. Rini and R.M. Bukowski et al., Sunitinib in patients with metastatic renal cell carcinoma, JAMA 295 (2006), pp. 2516–2524 [16757724]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (586)
24 M.J. Ratain, T. Eisen and W.M. Stadler et al., Phase II placebo-controlled randomized discontinuation trial of sorafenib in patients with metastatic renal cell carcinoma, J Clin Oncol 24 (2006), pp. 2505–2512 [16636341]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (544)
25 G.K. Abou-Alfa, L. Schwartz and S. Ricci et al., Phase II study of sorafenib in patients with advanced hepatocellular carcinoma, J Clin Oncol 24 (2006), pp. 4293–4300 [16908937]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (418)
26 T.E. Hutson, I.D. Davis and J.P. Machiels et al., Efficacy and safety of pazopanib in patients with metastatic renal cell carcinoma, J Clin Oncol 28 (2010), pp. 475–480 [20008644]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (31)
27 C.N. Sternberg, I.D. Davis and J. Mardiak et al., Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial, J Clin Oncol 28 (2010), pp. 1061–1068 [20100962]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (100)
28 O. Rixe, R.M. Bukowski and M.D. Michaelson et al., Axitinib treatment in patients with cytokine-refractory metastatic renal-cell cancer: a phase II study, Lancet Oncol 8 (2007), pp. 975–984 [17959415]. Article |
29 B.I. Rini, I. Tamaskar and P. Shaheen et al., Hypothyroidism in patients with metastatic renal cell carcinoma treated with sunitinib, J Natl Cancer Inst 99 (2007), pp. 81–83 [17202116]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (159)
30 B.I. Rini, G. Wilding and G. Hudes et al., Phase II study of axitinib in sorafenib-refractory metastatic renal cell carcinoma, J Clin Oncol 27 (2009), pp. 4462–4468 [19652060]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (49)
31 H.S. Rugo, R.S. Herbst and G. Liu et al., Phase I trial of the oral antiangiogenesis agent AG-013736 in patients with advanced solid tumors: pharmacokinetic and clinical results, J Clin Oncol 23 (2005), pp. 5474–5483 [16027439]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (161)
32 National Cancer Institute, National Institutes of Health, US Department of Health and Human Services, Common Terminology Criteria for Adverse Events (CTCAE) Version 4.02. NIH publication 03-5410, National Institutes of Health, Bethesda, MD (2009).
33 L.S. Wood and B. Manchen, Sorafenib: a promising new targeted therapy for renal cell carcinoma, Clin J Oncol Nurs 11 (2007), pp. 649–656 [17962173]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (15)
34 C. Robert, C. Mateus, A. Spatz, J. Wechsler and B. Escudier, Dermatologic symptoms associated with the multikinase inhibitor sorafenib, J Am Acad Dermatol 60 (2009), pp. 299–305 [19028406]. Article |
35 J. Autier, B. Escudier, J. Wechsler, A. Spatz and C. Robert, Prospective study of the cutaneous adverse effects of sorafenib, a novel multikinase inhibitor, Arch Dermatol 144 (2008), pp. 886–892 [18645140]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (50)
36 M.E. Lacouture, L.M. Reilly, P. Gerami and J. Guitart, Hand foot skin reaction in cancer patients treated with the multikinase inhibitors sorafenib and sunitinib, Ann Oncol 19 (2008), pp. 1955–1961 [18550575]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (35)
37 L.S. Wood, Managing the side effects of sorafenib and sunitinib, Community Oncol 3 (2006), pp. 558–562. View Record in Scopus | Cited By in Scopus (19)
38 C. Robert, J.C. Soria and A. Spatz et al., Cutaneous side-effects of kinase inhibitors and blocking antibodies, Lancet Oncol 6 (2005), pp. 491–500 [15992698]. Article |
39 M.W. Saif, I. Merikas, S. Tsimboukis and K. Syrigos, Erlotinib-induced skin rash: Pathogenesis, clinical significance and management in pancreatic cancer patients, JOP 9 (2008), pp. 267–274 [18469438]. View Record in Scopus | Cited By in Scopus (11)
40 R. Anderson, A. Jatoi, C. Robert, L.S. Wood, K.N. Keating and M.E. Lacouture, Search for evidence-based approaches for the prevention and palliation of hand–foot skin reaction (HFSR) caused by the multikinase inhibitors (MKIs), Oncologist 14 (2009), pp. 291–302 [19276294]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (11)
41 D.J. Gawkrodger, Dermatology: An Illustrated Colour Text, 4th ed, Churchill Livingstone Elsevier, Edinburgh (2008).
42 N.S. Azad, J.B. Aragon-Ching and W.L. Dahut et al., Hand–foot skin reaction increases with cumulative sorafenib dose and with combination anti-vascular endothelial growth factor therapy, Clin Cancer Res 15 (2009), pp. 1411–1416 [19228742]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (31)
43 N. Bhojani, C. Jeldres and J.J. Patard et al., Toxicities associated with the administration of sorafenib, sunitinib, and temsirolimus and their management in patients with metastatic renal cell carcinoma, Eur Urol 53 (2008), pp. 917–930 [18054825]. Article |
44 S. Sleijfer, I. Ray-Coquard and Z. Papai et al., Pazopanib, a multikinase angiogenesis inhibitor, in patients with relapsed or refractory advanced soft tissue sarcoma: a phase II study from the European Organisation for Research and Treatment of Cancer–Soft Tissue and Bone Sarcoma Group (EORTC study 62043), J Clin Oncol 27 (2009), pp. 3126–3132 [19451427]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (55)
45 L.S. Wood, H. Lemont and A. Jatoi et al., Practical considerations in the management of hand–foot skin reaction caused by multikinase inhibitors, Community Oncol 7 (2010), pp. 23–29. View Record in Scopus | Cited By in Scopus (3)
46 P. Esper, D. Gale and P. Muehlbauer, What kind of rash is it?: Deciphering the dermatologic toxicities of biologic and targeted therapies, Clin J Oncol Nurs 11 (2007), pp. 659–666 [17962174]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
47 I. Hagemann and E. Proksch, Topical treatment by urea reduces epidermal hyperproliferation and induces differentiation in psoriasis, Acta Derm Venereol 76 (1996), pp. 353–356 [8891006]. View Record in Scopus | Cited By in Scopus (41)
48 M. Duvic, A.T. Asano, C. Hager and S. Mays, The pathogenesis of psoriasis and the mechanism of action of tazarotene, J Am Acad Dermatol 39 (1998), pp. S129–S133 [9777790]. Article |
49 W. Scheithauer, J. McKendrick and S. Begbie et al., Oral capecitabine as an alternative to i.v. 5-fluorouracil-based adjuvant therapy for colon cancer: safety results of a randomized, phase III trial, Ann Oncol 14 (2003), pp. 1735–1743 [14630678]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (172)
How we do it
Elizabeth Manchen RN, MS, OCN![]()
![]()
Abstract
One significant toxicity associated with the anticancer tyrosine kinase inhibitors (TKIs) is hand–foot skin reaction (HFSR). We provide an overview of HFSR, emphasizing experience-based prevention techniques and nursing management strategies from the viewpoints of a medical oncologist, a dermatologist, and an oncology nurse. Supporting data include (1) published preclinical and phase I–III clinical studies and (2) published abstracts of phase II–III clinical trials of sorafenib and sunitinib. HFSR has been reported in up to 60% of patients treated with sorafenib or sunitinib. TKI-induced HFSR may lead to dose reductions or treatment interruptions and reduced quality of life. Symptoms of TKI-associated HFSR can be managed by implementing supportive measures and aggressive dose modification. Patients educated about HFSR can work with their health-care teams to proactively detect and help manage this cutaneous toxicity, thus preventing or reducing the severity of TKI-associated HFSR. Successful prevention and management of TKI-associated HFSR can help to ensure that patients achieve optimal therapeutic outcomes. Implementation of such measures may increase the likelihood that therapy is continued for the appropriate interval at an appropriate dose for each patient. Optimal management of TKI-associated HFSR is predicated on establishing appropriate partnerships among medical oncologists, dermatologists, oncology nurses, and patients.
Article Outline
This article reviews the mechanism of action, clinical trial results, and adverse effects of two molecularly targeted anticancer agents, the tyrosine kinase inhibitors (TKIs) sorafenib (Nexavar®; Bayer HealthCare Pharmaceuticals, Montville, NJ, and Onyx Pharmaceuticals, Emeryville, CA) and sunitinib (Sutent®; Pfizer Pharmaceuticals, New York, NY). This article specifically focuses on the diagnosis and management of TKI-associated hand–foot skin reaction (HFSR) from the perspectives of the medical oncologist, the dermatologist, and the oncology nurse. Data were derived from (1) published reports of preclinical and phase I–III clinical studies of sorafenib and sunitinib and (2) published abstracts of phase II–III clinical trials of sorafenib and sunitinib.
The Medical Oncologist's Viewpoint
Molecularly Targeted Agents
Molecularly targeted therapies are directed at specific mechanisms involved in cell division, invasion, and metastasis, as well as in cell survival mediated by avoidance of apoptosis and resistance to conventional treatments. Clinical trials in several cancer types have shown that these TKIs can inhibit these activities of cancer cells by either cytostatic or cytotoxic mechanisms.1 However, the ability of these agents to inhibit multiple cancer cell pathways via novel mechanisms of action may explain, at least in part, their apparent direct toxic effects.2 These include adverse events that, from a medical viewpoint, must be anticipated, promptly recognized, and properly treated. Doing so can help minimize disruption to the patient's quality of life and may reduce the need for dose reduction or treatment interruption.1
Both sorafenib and sunitinib are orally administered, small-molecule inhibitors of multiple kinases, some of which are common to both agents (Figure 2).3 Sorafenib has known effects on tumor-cell proliferation and angiogenesis. Its antiproliferative effects are exerted via inhibition of serine/threonine kinases of the RAF/MEK/ERK signaling pathway (also called the MAP-kinase pathway) that is found within tumor cells; specifically, sorafenib targets wild-type RAF gene products (CRAF, BRAF) and mutant BRAF. The antiangiogenic effects of sorafenib are exerted via its inhibition of extracellular vascular endothelial growth factor (VEGF) receptors 2 and 3 (VEGFR-2 and VEGFR-3) and platelet-derived growth factor receptor beta (PDGFR-β), which is found mainly in the tumor vasculature. Sorafenib also exerts broad-spectrum activity against the stem-cell growth factor receptor (c-KIT), FMS-like tyrosine kinase 3 (Flt3), and the receptor encoded by the ret proto-oncogene (RET).[4], [5], [6] and [7] Sunitinib has demonstrated effects on the growth, pathologic angiogenesis, and metastatic progression of cancer by inhibiting PDGFR-α and -β; VEGFR-1, -2, and -3; and colony-stimulating factor receptor (CSF-1R), c-KIT, Flt3, and RET.8
Mechanisms of Action of Sorafenib and Sunitinib
Sorafenib and sunitinib specifically recognize and inhibit c-KIT, VEGFR, PDGFR-β, and Flt3 receptor tyrosine kinases. Sorafenib also inhibits RAF, a serine/threonine kinase involved in the RAF/MEK/ERK kinase pathway
c-KIT = stem-cell growth factor receptor (a cytokine receptor expressed on the surface of hematopoietic stem cells as well as other cell types); ERK = extracellular signal–regulated kinase; Flt3 = FMS-like tyrosine kinase 3 (a cytokine receptor expressed on the surface of hematopoietic progenitor cells); Flt3L = FMS-like tyrosine kinase 3 ligand (Flt3 ligand); MEK = (MAPK/ERK) kinase; PDGF-ΒΒ = platelet-derived growth factor BB; PDGFR-β = platelet-derived growth factor receptor beta; RAF = a gene that encodes for a protein kinase (Raf1) that functions in the mitogen-activated protein kinase/extracellular signal–regulated kinase (MAPK/ERK) signal-transduction pathway as part of a protein kinase cascade; RAS = a superfamily of genes that encode small GTPases involved in cellular signal transduction; SCF = stem-cell factor; VEGF = vascular endothelial growth factor; VEGFR = vascular endothelial growth factor receptor
Adapted with permission from Lacouture et al3
Sorafenib was approved for the treatment of advanced renal cell carcinoma (RCC) in 2005 and for unresectable hepatocellular carcinoma (HCC) in 2007. The efficacy of sorafenib in 903 patients with advanced RCC was demonstrated in the phase III Treatment Approaches in Renal Cancer Global Evaluation Trial (TARGET), the largest phase III trial ever conducted in the second-line setting in patients with advanced RCC. Sorafenib significantly enhanced median progression-free survival (PFS) compared with placebo (24 vs 12 weeks),9 which led to early termination of the study and crossover from placebo to active drug. A preplanned analysis, which did not include patients who received placebo (who had crossed over to active treatment), ultimately demonstrated that sorafenib significantly prolonged overall survival (OS).10 Furthermore, 84% of sorafenib-treated patients experienced a clinical benefit, defined as objective response or disease stabilization.9 These results have been confirmed in larger, “real-world” patient populations in expanded-access programs conducted in North America (n = 2504)11 and the European Union (n = 118).12
Definitive data supporting the efficacy of sorafenib in HCC were provided by the randomized, double-blind, placebo-controlled Sorafenib CCC Assessment Randomized Protocol (SHARP) trial, the largest phase III trial ever conducted in patients with advanced HCC (n = 599) and the first phase III study to demonstrate a significant survival advantage with a systemic treatment in advanced HCC. In this trial, patients treated with sorafenib experienced a 44% increase in median OS (10.7 vs 7.9 months, hazard ratio [HR] = 0.69, 95% confidence interval [CI] 0.55–0.87, P < 0.001) and a 73% prolongation in median time to radiographic progression (5.5 vs 2.8 months, P < 0.001) compared with patients who received placebo.13 These results were confirmed in a separate phase III, randomized, double-blind, placebo-controlled study conducted in 226 patients from the Asia-Pacific region with advanced HCC.14 In this trial also, sorafenib significantly prolonged median OS (6.5 vs 4.2 months, HR = 0.68, 95% CI 0.50–0.93, P = 0.014) and time to progression (TTP) (2.8 vs 1.4 months, HR = 0.57, 95% CI 0.42–0.79, P = 0.0005) compared with placebo.
Sunitinib received approval in 2006 for use in patients with gastrointestinal stromal tumor (GIST) whose disease is refractory to imatinib (Gleevec®; Novartis Pharmaceuticals, East Hanover, NJ) or who are intolerant to the drug and in those with advanced RCC. Approval of sunitinib for the treatment of GIST was based on data from a randomized, placebo-controlled, phase III trial of 312 patients with imatinib-refractory GIST.15 In that study, sunitinib treatment increased median PFS (24.1 vs 6.0 weeks, HR = 0.33, 95% CI 0.24–0.47, P < 0.0001) and median TTP (27.3 vs 6.4 weeks, HR = 0.33, 95% CI 0.23–0.47, P < 0.0001) compared with placebo. The trial was unblinded early when a planned interim analysis revealed significantly longer TTP with sunitinib than with placebo. A subsequent analysis showed that median OS with sunitinib was about twice that with placebo (73.9 vs 35.7 weeks, P < 0.001).16 In an ongoing, worldwide treatment-use program to provide expanded access to sunitinib for patients with advanced GIST intolerant of or resistant to imatinib,17 sunitinib treatment resulted in a median estimated TTP of 41 weeks and a median estimated OS of 75 weeks in the population analyzed (n = 1,117).
A separate phase III randomized controlled trial was conducted in 750 patients with advanced RCC and no history of systemic therapy for RCC.[18] and [19] The active comparator in this trial was interferon-alfa (IFN-α). Compared with IFN-α, sunitinib significantly increased median PFS (11 vs 5 months, HR = 0.539, 95% CI 0.451–0.643, P < 0.001) and was associated with a greater objective response rate (47% vs 12%, P < 0.001). Median OS was greater in the sunitinib group (26.4 vs 21.8 months), but the difference was not significant (P = 0.051). Data from expanded-access programs in patients with RCC and GIST support the phase III trial data for sunitinib.20 Efficacy data for sorafenib and sunitinib are summarized in Table 1.[9], [10], [11], [12], [13], [14], [15], [17], [18] and [20]
| DRUG, DISEASE, AND STUDY | EFFICACY DATA |
|---|---|
| Sorafenib | |
| Advanced RCC | |
| Phase III TARGET[9] and [10] | |
| Expanded-access programs[11] and [12] | Data from expanded-access programs in community-based populations (NA- and EU-ARCCS) were consistent with data from TARGET |
| Unresectable HCC | |
| Phase III SHARP trial13 | • First phase III trial to demonstrate a significant survival advantage for a systemic therapy in advanced HCC • Median OS was 10.7 months in sorafenib group vs 7.9 months in placebo group (HR = 0.69, 95% CI 0.55–0.87, P < 0.001) |
| Phase III Asia-Pacific trial14 | |
| Sunitinib | |
| Advanced RCC | |
| Phase III registration trial18 | • Median PFS was 11 months in sunitinib group vs 5 months in interferon-α group (HR = 0.539, 95% CI 0.451–0.643, P < 0.001) |
| Expanded-access program20 | |
| Imatinib-resistant GIST | |
| Phase III registration trial15 | • Median TTP was 27.3 weeks in sunitinib group vs 6.4 weeks in placebo group (HR = 0.33, 95% CI 0.23–0.47, P < 0.0001) |
| Expanded-access program17 |
CI = confidence interval; CR = complete response; EU-ARCCS = European Union Advanced Renal Cell Carcinoma Sorafenib; GIST = gastrointestinal stromal tumor; HCC = hepatocellular carcinoma; HR = hazard ratio; NA-ARCCS = North American ARCCS; OS = overall survival; PFS = progression-free survival; PR = partial response; RCC = renal cell carcinoma; SD = stable disease; SHARP = Sorafenib CCC Assessment Randomized Protocol; TARGET = Treatment Approaches in Renal Cancer Global Evaluation Trial; TTP = time to progression; TTRP = time to radiologic progression
Characteristics of Hand–Foot Skin Reaction
Data from the clinical trials for sorafenib and sunitinib indicate that both agents are generally well-tolerated; common treatment-related adverse reactions include diarrhea, alopecia, nausea, fatigue, rash, and hypertension, as well as palmar–plantar erythrodysesthesia (PPE) syndrome, also known as hand–foot skin reaction (HFSR) (Table 2).[10] and [19] HFSR is a dermatologic toxicity that has been reported in 14%–62% of patients treated with sorafenib or sunitinib (Table 3).[9], [11], [12], [13], [14], [15], [17], [18], [20], [21], [22], [23], [24] and [25] In general, the term HFSR refers to a group of signs and symptoms affecting the hands and feet of patients taking sorafenib, sunitinib, or, to a lesser extent, other TKIs such as pazopanib (Votrient™; GlaxoSmithKline, Research Triangle Park, NC)[26] and [27] and axitinib (AG013736).[28], [29], [30] and [31]
| ADVERSE EVENT | SORAFENIB 400 MG BID | SUNITINIB 50 MG QD | ||
|---|---|---|---|---|
| ALL GRADES (%) | GRADE 3/4 (%) | ALL GRADES (%) | GRADE 3/4 (%) | |
| Diarrhea | 48 | 3 | 61 | 9 |
| Rash | 41 | 1 | 24 | 2 |
| Hand–foot skin reaction | 33 | 6 | 29 | 9 |
| Alopecia | 31 | 0 | 12 | 0 |
| Fatigue | 29 | 3 | 54 | 11 |
| Nausea | 19 | <1 | 52 | 5 |
| Hypertension | 17 | 4 | 30 | 12 |
| Dry skin | 13 | 0 | 21 | <1 |
| Vomiting | 12 | 1 | 31 | 4 |
| Mucositis | 5 | 0 | 26 | 2 |
| REFERENCE | STUDY | ALL GRADES (%) | GRADE 3 (%) | GRADE 4 (%) |
|---|---|---|---|---|
| Sorafenib | ||||
| 9 | Phase III TARGETa | 30 | 6 (grade 3/4) | |
| 13 | Phase III SHARPa | 21 | 8 | 0 |
| 11 | NA-ARCCS, first-linea | 19 (≥2) | 11 (grade 3/4) | |
| 11 | NA-ARCCS, second-linec | 17 (≥2) | 8 (grade 3/4) | |
| 12 | EU-ARCCSa | 47 | 12 (grade 3/4) | |
| 14 | Phase III Asia-Pacifica | 45 | 11 (grade 3/4) | |
| 24 | Phase II randomized discontinuation trial in advanced RCCb | 62 | 13 | 0 |
| 25 | Phase II study in advanced HCCb | 31 | 5 | 0 |
| 21 | Phase II, uncontrolled study in relapsed/refractory NSCLCa | 37 | 10 (grade 3/4) | |
| Sunitinib | ||||
| 18 | Phase III registration trial in advanced RCCa | 20 | 5 | 0 |
| 20 | Expanded access program in advanced RCCc | 5 (grade 3/4) | ||
| 15 | Phase III registration trial in imatinib-resistant GISTa | 14 | 4 | 0 |
| [17] and [22] | Expanded access program in imatinib-resistant GISTc | N/A | 8 (grade 3/4) | |
| 23 | Phase II trial of second-line treatment in advanced RCCa | 15 | 7 | 0 |
EU-ARCCS = European Union Advanced Renal Cell Carcinoma Sorafenib; GIST = gastrointestinal stromal tumor; HCC = hepatocellular carcinoma; N/A = data not available; NA-ARCCS = North American ARCCS; NSCLC = non-small-cell lung cancer; RCC = renal cell carcinoma; SHARP = Sorafenib CCC Assessment Randomized Protocol; TARGET = Treatment Approaches in Renal Cancer Global Evaluation Trial
a Used version 3.0 of National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE)b Used version 2.0 of NCI-CTCAEc Version of NCI-CTCAE used not specified
HFSR is typically characterized by redness, marked discomfort, swelling, and tingling in the palms of the hands and/or soles of the feet.32 HFSR can be painful enough to interfere profoundly with activities of daily living (ADLs). In fact, patients may report symptoms after as few as 2 weeks on TKI therapy, at which point they may present to the health-care provider (HCP) wearing slippers, unable to walk, and having difficulty in performing ADLs such as eating, dressing, and bathing.[1] and [33] Although HFSR can lead to TKI dose modification or treatment discontinuation, preventive measures can be taken before TKIs are initiated to reduce the likelihood of HFSR. In addition, early treatment of symptoms may prevent HFSR from progressing to the point at which the patient's ability to receive the full potential benefit of therapy is compromised.[3], [34], [35] and [36]
Signs and symptoms of HFSR may appear concomitantly or sequentially and can affect both hands and both feet. Although symptoms are most prominent on the palms and soles, other areas of the hands and feet may also be involved, including the tips of the fingers and toes, the heels, and metatarsophalangeal skin; areas of flexure; and skin overlying the metacarpophalangeal and interphalangeal joints.3 These “pressure areas” are where the most severe symptoms are typically seen. Common symptoms include dysesthesia and paresthesia, described as “tingling, prickling, or creeping sensations” and/or sensitivity or intolerance to hot or warm objects (which may occur before other symptoms are apparent); erythema; edema; hyperkeratosis; and dry and/or cracked skin.[1] and [34] Actual HFSR lesions are described as tender and scaling, with a peripheral halo of erythema, yellowish and hyperkeratotic plaques, or callous-like blisters (which usually do not contain fluid), typically localized to areas of pressure.[3] and [35] Desquamation, particularly with sunitinib treatment, may also be present.37
Since both sorafenib and sunitinib inhibit the VEGFRs, PDGFRs, c-KIT, and Flt3,38 it is likely that inhibition of one or more of these receptors and/or pathways plays a role in HFSR development.36 Differences in the relative appearance of HFSR symptoms are dependent on whether sorafenib or sunitinib is used. Sunitinib use is more often associated with desquamation, whereas sorafenib is more often associated with areas of hyperkeratosis, particularly formation of thick calluses on the soles of the feet.37 The timing of the first appearance of symptoms may also vary according to the TKI used. HFSR usually develops within the first 2–4 weeks of treatment with a TKI and almost always within the first 6 weeks.35 However, because the severity of HFSR appears to be dose-dependent,3 signs and symptoms may present later rather than sooner in patients treated with sunitinib. This is likely due to the recommended sunitinib dosing schedule, which incorporates a 2-week period during which no drug is administered. Although HFSR frequently decreases in intensity during treatment, even without dose modifications or treatment interruption, prompt treatment of HFSR is recommended to prevent rapid progression. Early symptoms can usually be resolved easily by appropriate treatment, which often allows continuation of full-dose therapy for the prescribed length of time.
It is important to note what HFSR is not. TKI-associated HFSR is not the same clinical entity as the hand–foot syndrome (HFS) traditionally seen with cytotoxic agents such as infusional 5-fluorouracil (5-FU); capecitabine, the oral prodrug of 5-FU; and pegylated liposomal doxorubicin. Although HFSR and HFS share several clinical and pathological aspects—each previously has been called “acral erythema” and “PPE”—they clearly are not the same clinical or pathologic entity. HFSR is neither an allergic reaction to a drug nor an indication that a patient may be intolerant to a drug. Finally, HFSR does not indicate drug efficacy, as may be the case with skin rash in patients with non-small-cell lung cancer treated with erlotinib.[3] and [39]
Grading HFSR
In published reports, the severity of HFSR is usually graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE),32 a three-grade classification system. However, modified criteria are considered by some to be a better fit for routine clinical practice.1 What distinguishes the modified criteria from the NCI criteria (version 4.02) is the inclusion of HFSR-specific clinical characteristics plus certain patient-defined considerations used to categorize severity. The modified criteria expressly define the degree to which HFSR discomfort affects the patient's normal activities, an improvement over version 4.02 used alone. The NCI-CTCAE version 4.02 criteria, the modified criteria, and corresponding patient photographs are presented in Figure 3.[1] and [32]
Recommendations for the treatment of grade 1 HFSR include early and appropriate dermatologic management and active collaboration among HCPs.40
The Dermatologist's Viewpoint
Although the exact pathogenesis of HFSR has not been fully elucidated, research into its cause(s) is ongoing. Theoretically, traditional HFS is thought to be due to the direct toxic effects of drugs or their ability to invoke a “host-vs-host” response. In contrast, a unique mechanism has been proposed for TKI-associated HFSR: simultaneous blockage of VEGFRs and PDGFRs.2
Three histopathologic features have been found to predominate in HFSR: dyskeratotic keratinocytes at various states of necrosis (Figure 441), basal layer vacuolar degeneration, and mild perivascular or lichenoid lymphocyte-predominant infiltrate.2 Immunohistochemistry with a variety of skin-cell markers has shown a significant modification of normal maturation of keratinocytes, which are often apoptotic. Minor modifications of blood vessels are also seen, but no signs of intense vasculitis are evident. This is important because HFSR is suspected of being a “class effect” of TKIs that target VEGFRs. HFSR is not seen in patients treated with single-agent bevacizumab, and the lack of histologic evidence of significant damage to blood vessels suggests that HFSR does not result from the general inhibition of angiogenesis. A retrospective analysis found that HFSR rates were higher when patients were treated with sorafenib and bevacizumab in combination, supporting the hypothesis that HSFR is due to the anti-VEGF properties of sorafenib.42 Other possible causes of HFSR include activation by a ligand other than VEGF and/or inhibition of one of the other protein targets inhibited by both sorafenib and sunitinib.[3] and [35]
Layers of the Epidermis
The epidermis is composed of a very sophisticated arrangement of keratinocytes, which originate as stem cells in the stratum germinatum (not shown). The stem cells constantly multiply, creating daughter cells that progressively mature over approximately 28 days and move to the surface of the epidermis. As they move, they change their function and shape. In the stratum spinosum, interactions between cells resemble spines; mature cells move through the stratum granulosum, which has a very important secretory function, until finally the cells reach the stratum corneum and die. Thus, the stratum corneum is the layer of skin containing dead skin cells that have lost their nuclei; it is the part of the epidermis that ensures the barrier function of skin and is the layer most affected by HFSR. The layer beneath the epidermis is called the “papillary dermis.” The papillary dermis contains nerves and blood vessels and supplies the epidermis with nutrients. The fibroblasts and fibers located here give skin its strength and resistance
Adapted with permission from Gawkrodger41
Incidence and Severity of HFSR With TKI
To determine the incidence and severity of HFSR specific to sorafenib, a double-blind, prospective, dermatologic substudy was performed in patients enrolled in the phase III TARGET trial.35 Eighty-five patients with RCC were randomized to receive either sorafenib (n = 43) or placebo (n = 42). Dermatologic examinations were performed before and during treatment. Ninety-one percent of sorafenib-treated patients experienced at least one cutaneous reaction compared with 7% of those in the placebo group. A variant of HFSR clinically distinct from chemotherapy-induced HFS was observed in 60% of sorafenib-treated patients. Reversible grade 3 HFSR leading to dose reduction occurred in two sorafenib-treated patients. Additional cutaneous reactions were facial erythema, scalp dysesthesia, alopecia, and subungual splinter hemorrhages.
HFSR (of any grade) has been shown to occur in approximately 30% of patients treated with sorafenib and 20% of those who received sunitinib in clinical studies.43 Grade 3/4 HFSR has been observed in approximately 6% of sorafenib-treated and 5% of sunitinib-treated patients. HFSR was not reported in a phase II study of 142 patients with relapsed or refractory soft-tissue sarcoma treated with pazopanib.44 In a phase III randomized, double-blind, placebo-controlled trial of pazopanib in patients with advanced RCC, the incidence of HFSR was <10%, while the incidence of grade 3/4 HFSR was <1%. Potential differences may be explained by variations in the potency and selectivity of the TKIs.27
Management Strategies
Our work at the Dermatology Center at the Gustave-Roussy Institute has shown that early intervention against the dermatologic adverse effects of these TKIs can inhibit patient progression to a more serious form of HFSR.[34] and [38]
Effective management of HFSR can begin prior to initiation of treatment with sorafenib or sunitinib. Patients should be advised to remove any preexisting hyperkeratotic areas or calluses, keep skin well-moisturized with appropriate creams, and cushion pressure points with cotton socks, soft shoes, and/or insoles. Dose modification is typically not required for grade 1 HFSR; symptomatic treatments should be employed instead.
If HFSR symptoms progress to grade 2 or 3, with pain and a decrease in quality of life, the dose of sorafenib or sunitinib can be modified until symptoms recede, after which the patient can be brought back to the full dose. Very often, the patient can tolerate the full-dose treatment simply by decreasing the dose briefly.3 A recommended dose-modification scheme is shown in Figure 5.3
Management of Hand–Foot Skin Reaction by Grade
MKI = multikinase inhibitor
Adapted with permission from Lacouture et al3
TKIs are being studied in patients with additional types of tumor, possibly in the adjuvant setting, as well as in combinations. Because these drugs are administered orally, with a decreased (compared with conventional cytotoxic agents) frequency of nurse– or doctor–patient interactions, patients must be very well-informed of any potential toxicities with the TKIs.
At present, there are no evidence-based treatment guidelines for the prevention or management of HFSR. However, HCPs most involved in the day-to-day care of patients with HFSR have made great progress in establishing preventive and treatment strategies and in identifying ancillary products likely to decrease the incidence and/or severity of symptoms. Prevention, which includes preventing HFSR entirely as well as preventing progression from its initial appearance, is a key component of HFSR management.
The Oncology Nurse's Viewpoint
The nurse's viewpoint begins with patient education and empowerment. The goal is to prevent adverse effects from occurring while managing any adverse effects that do occur so that the patient has the best chance of staying on anticancer therapy. This requires a strong partnership between the HCP team and the patient. Although not all cases of HFSR can be prevented, experience suggests that symptom incidence and severity can be alleviated by educating patients to recognize the signs and symptoms of HFSR and report these to their HCPs. HFSR typically occurs early in the course of therapy, so it is prudent to be especially vigilant during the first 6 weeks. Providing the patient with a brochure about HFSR to refer to at home may facilitate identification of HFSR.
To address the lack of evidence-based guidelines to prevent or treat HFSR, an international, interdisciplinary expert panel has provided a set of consensus recommendations for the management of TKI-associated HFSR.45 One component of these recommendations can be phrased simply for the patients as a “3C” approach to management: control calluses, comfort with cushions, and cover with creams.
Prior to treatment, the patient should receive a full-body examination, with emphasis on the condition of the hands and feet. Evaluation should be performed by a qualified HCP who can determine whether there are physical conditions that may predispose a patient to areas of increased friction or rubbing. For all patients, especially those with comorbid conditions (eg, diabetes, poor circulation), a pretreatment pedicure is highly recommended. Patients should also be educated on the proper use of tools (eg, a pumice stone) to aid in callus removal. Such tools are considered beneficial because patients can control the frequency of their use and the extent of skin removed. However, because areas of hyperkeratosis are often extremely tender and painful, patients are cautioned against overuse of these tools, including the aggressive “paring” or “cutting” of callused areas. Finally, patients should be advised of the need for clean tools to guard against infection.
Other protective measures include the use of thick cotton gloves and/or socks, which may also help the skin to retain moisture, and avoidance of warm and/or hot water or objects, tight-fitting shoes, or other items that may rub, pinch, or cause friction in affected areas. Tender areas, pressure points, and pressure-sensitive areas of the hands and feet should be protected. For example, weight lifters might be advised to wear gloves. These recommendations hold true both before and after development of HFSR.[3], [33] and [35] Well-padded but nonconstrictive footwear should be worn, and the use of insole cushions or inserts (eg, silicone or gel) should be encouraged. Foot soaks with lukewarm water and magnesium sulfate may be soothing. Tender areas should be protected at all times, and patients should be encouraged not to walk barefoot.
Use of over-the-counter and prescription-strength creams and moisturizers during treatment with TKIs has also been recommended (Table 4).[40], [45], [46], [47], [48] and [49] Moisturizing agents should be applied liberally, immediately after bathing. Cotton gloves and/or socks can also be worn, to help retain moisture and to provide an additional layer of protection. When applied liberally, these products soften areas of thick and hardened skin, help keep the skin pliable, and may prevent cracks or breaks in skin integrity, which could cause additional discomfort. Prescription-strength topical agents have also shown anecdotal benefit (Table 4). These topical agents are typically applied twice daily to affected areas only because they may irritate unaffected skin. Data on the use of topical/systemic corticosteroids in the treatment of HFS remain inconclusive; the literature primarily includes case studies in patients with PPE treated with chemotherapeutic agents including pegylated liposomal doxorubicin.2 Finally, a qualified HCP must always be consulted to ensure proper diagnosis and treatment of HFSR.
Adapted with permission from Anderson et al40
| PRODUCTS | PRODUCT INFORMATION |
|---|---|
| Over-the-counter[40], [45] and [46] | |
| Cetaphil® (Galderma Laboratories, Ft. Worth, TX) skin cleaners, Aveeno® (Johnson & Johnson, New Brunswick, NJ) shower gel | Nondeodorant, fragrance-free products |
| Udderly Smooth® (Redex Industries, Salem, OH), Gold Bond® (Chattem, Chattanooga, TN), Aveeno® | Thicker products with more intense moisturizing properties than basic lotions; anti-itch formulations are available |
| Norwegian Formula: Smoothing Relief Anti-Itch Moisturizer (Neutrogena, Los Angeles, CA) | Contains dimethicone 1%, camphor 0.1%, and lidocaine |
| Norwegian Formula: Foot Cream (Neutrogena) | Contains cetearyl alcohol, dimethicone, menthol, and urea |
| Bag Balm® (Dairy Association, Lyndonville, VT) | May provide “cooling” effect from eucalyptus |
| Eucerin® (Beiersdorf, Hamburg, Germany) Cream | Best used at night due to greasy formulation |
| Eucerin® Dry Skin Therapy | Contains urea and alpha-hydroxy acid |
| Aquaphor® (Beiersdorf) Healing Ointment | Petrolatum 41% |
| Kerasal® (Alterna, Whippany, NJ) | Salicylic acid 5% exfoliates and softens skin; urea 10% moisturizes skin |
| Blue Lizard® (Crown Laboratories, Johnson City, TN) | UV A and B sunblock, water-resistant |
| Prescription47–49 | |
| Urea 40% cream (Carmol 40®; Doak Dermatologics, Fairfield, NJ) | Softens hyperkeratosis, decreases epidermal thickness, proliferation |
| Tazarotene 0.1% cream (Tazorac®; Allergan Dermatology, Irvine, CA) | Retinoid decreases proliferation, reduces dermal inflammation |
| Fluorouracil 5% cream (Carac®; Dermik Laboratories, Bridgewater, NJ) | Antifolate inhibits proliferation; has shown anecdotal benefit in certain conditions characterized by hyperkeratotic lesions on the palms and soles |
Summary
The addition of molecularly targeted agents to anticancer treatment has been found to cause both common and novel adverse reactions. HFSR is being increasingly recognized as a potential dose-limiting toxicity associated with sorafenib or sunitinib treatment that can result in discomfort, pain, decreased quality of life, and premature termination of a potentially effective cancer treatment. It is important to educate patients about potential dermatologic adverse effects associated with TKIs because limiting toxicity can help avoid treatment interruptions or dose reductions while improving ADLs.
The precise pathogenic mechanism of HFSR is currently not known, and there is no evidence-based protocol for treatment of HFSR. However, the increased clinical experience with these agents has resulted in a wealth of published articles describing empiric and symptomatic approaches that appear to help to prevent and manage HFSR. Frequent communication is necessary between the physician and patient, particularly 2–4 weeks from the initiation of therapy. Symptoms of HFSR should be recognized as early as possible. Providing the patient with a brochure about HFSR to refer to at home may facilitate the early identification of HFSR.
Patients should be advised of the “3C” approach to the management of TKI-associated HFSR: control calluses, comfort with cushions, and cover with creams. Creams should be applied after bathing and before going to bed; cotton gloves and socks should be worn to keep the cream on the hands and feet during the night.
Symptoms of HFSR typically are manageable with the implementation of supportive measures. If symptoms worsen, dose modification or interruption will result in a return to grade 0/1. Many patients can successfully be rechallenged with the full dose. Observations across multiple viewpoints have consistently shown that HFSR severity can be reduced in patients who are educated about HFSR and proactive about its detection and management.
Acknowledgments
All authors contributed equally to the development of this report. Editorial support was provided by Katherine Wright, PharmD, RPh, ISD, Wrighter Medical Education and Training, West Hills, CA; John A. Ibelli, CMPP, BelMed Professional Resources, New Rochelle, NY; and John D. Zoidis, MD, Bayer HealthCare Pharmaceuticals, Montville, NJ.
References1
1 C. Porta, C. Paglino, I. Imarisio and L. Bonomi, Uncovering Pandora's vase: the growing problem of new toxicities from novel anticancer agents: The case of sorafenib and sunitinib, Clin Exp Med 7 (2007), pp. 127–134. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
2 A.D. Lipworth, C. Robert and A.X. Zhu, Hand–foot syndrome (hand–foot skin reaction, palmar–plantar erythrodysesthesia): focus on sorafenib and sunitinib, Oncology 77 (2009), pp. 257–271 [19923864]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
3 M.E. Lacouture, S. Wu and C. Robert et al., Evolving strategies for the management of hand–foot skin reaction associated with the multitargeted kinase inhibitors sorafenib and sunitinib, Oncologist 13 (2008), pp. 1001–1011 [18779536]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (57)
4 S.M. Wilhelm, L. Adnane, P. Newell, A. Villanueva, J.M. Llovet and M. Lynch, Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signaling, Mol Cancer Ther 7 (2008), pp. 3129–3140 [18852116]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (119)
5 D. Auclair, D. Miller and V. Yatsula et al., Antitumor activity of sorafenib in FLT3-driven leukemic cells, Leukemia 21 (2007), pp. 439–445 [17205056]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (40)
6 F. Carlomagno, S. Anaganti and T. Guida et al., BAY 43-9006 inhibition of oncogenic RET mutants, J Natl Cancer Inst 98 (2006), pp. 326–334 [16507829]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (169)
7 S.M. Wilhelm, C. Carter and L. Tang et al., BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis, Cancer Res 64 (2004), pp. 7099–7109 [15466206]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1142)
8 J.G. Christensen, A preclinical review of sunitinib, a multitargeted receptor tyrosine kinase inhibitor with anti-angiogenic and antitumour activities, Ann Oncol 10 (2007), pp. x3–x10 [17761721]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (29)
9 B. Escudier, T. Eisen and W.M. Stadler et al., Sorafenib in advanced clear-cell renal-cell carcinoma, N Engl J Med 356 (2007), pp. 125–134 [17215530]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1425)
10 B. Escudier, T. Eisen and W.M. Stadler et al., Sorafenib for treatment of renal cell carcinoma: final efficacy and safety results of the phase III Treatment Approaches in Renal Cancer Global Evaluation Trial, J Clin Oncol 27 (2009), pp. 3312–3318 [19451442]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (123)
11 W.M. Stadler, R.A. Figlin and D.F. McDermott et al., Safety and efficacy results of the advanced renal cell carcinoma sorafenib expanded access program in North America, Cancer 116 (2010), pp. 1272–1280 [20082451]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (22)
12 J. Beck, E. Bajetta and B. Escudier et al., A large open-label, non-comparative, phase III study of the multi-targeted kinase inhibitor sorafenib in European patients with advanced renal cell carcinoma, Eur J Cancer (suppl) (2007), p. 5 Abstract 4506. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (7)
13 J.M. Llovet, S. Ricci and V. Mazzaferro et al., Sorafenib in advanced hepatocellular carcinoma, N Engl J Med 359 (2008), pp. 378–390 [18650514]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (989)
14 A.L. Cheng, Y.K. Kang and Z. Chen et al., Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial, Lancet Oncol 10 (2009), pp. 25–34 [19095497]. Article |
15 G.D. Demetri, A.T. van Oosterom and C.R. Garrett et al., Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial, Lancet 368 (2006), pp. 1329–1338 [17046465]. Article |
16 G.D. Demetri, X. Huang and C.R. Garrett et al., Novel statistical analysis of long-term survival to account for crossover in a phase III trial of sunitinib (SU) vs placebo (PL) in advanced GIST after imatinib (IM) failure, J Clin Oncol (suppl) (2008), p. 26 Abstract 10524.
17 P. Reichardt, Y. Kang and W. Ruka et al., Detailed analysis of survival and safety with sunitinib (SU) in a worldwide treatment-use trial of patients with advanced GIST, J Clin Oncol (suppl) (2008), p. 26 Abstract 10548.
18 R.J. Motzer, T.E. Hutson and P. Tomczak et al., Sunitinib versus interferon alfa in metastatic renal-cell carcinoma, N Engl J Med 356 (2007), pp. 115–124 [17215529]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1520)
19R.J. Motzer, T.E. Hutson and P. Tomczak et al., Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma, J Clin Oncol 27 (2009), pp. 3584–3590 [19487381]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (194)
20 M.E. Gore, C. Szczylik and C. Porta et al., Safety and efficacy of sunitinib for metastatic renal-cell carcinoma: an expanded-access trial, Lancet Oncol 10 (2009), pp. 757–763 [19615940]. Article |
21 G.R. Blumenschein Jr, U. Gatzemeier and F. Fossella et al., Phase II, multicenter, uncontrolled trial of single-agent sorafenib in patients with relapsed or refractory, advanced non-small-cell lung cancer, J Clin Oncol 27 (2009), pp. 4274–4280 [19652055]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
22 H.J. Schütte, M. Schlemmer, C. Wendtner, P. Reichardt and G.D. Demetri, Sunitinib (SU) in a worldwide treatment-use trial of pts with advanced gastrointestinal stromal tumours (GIST): analysis of survival and safety data, Onkologie (suppl 4) (2008), p. 201 Abstract V582.
23 R.J. Motzer, B.I. Rini and R.M. Bukowski et al., Sunitinib in patients with metastatic renal cell carcinoma, JAMA 295 (2006), pp. 2516–2524 [16757724]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (586)
24 M.J. Ratain, T. Eisen and W.M. Stadler et al., Phase II placebo-controlled randomized discontinuation trial of sorafenib in patients with metastatic renal cell carcinoma, J Clin Oncol 24 (2006), pp. 2505–2512 [16636341]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (544)
25 G.K. Abou-Alfa, L. Schwartz and S. Ricci et al., Phase II study of sorafenib in patients with advanced hepatocellular carcinoma, J Clin Oncol 24 (2006), pp. 4293–4300 [16908937]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (418)
26 T.E. Hutson, I.D. Davis and J.P. Machiels et al., Efficacy and safety of pazopanib in patients with metastatic renal cell carcinoma, J Clin Oncol 28 (2010), pp. 475–480 [20008644]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (31)
27 C.N. Sternberg, I.D. Davis and J. Mardiak et al., Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial, J Clin Oncol 28 (2010), pp. 1061–1068 [20100962]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (100)
28 O. Rixe, R.M. Bukowski and M.D. Michaelson et al., Axitinib treatment in patients with cytokine-refractory metastatic renal-cell cancer: a phase II study, Lancet Oncol 8 (2007), pp. 975–984 [17959415]. Article |
29 B.I. Rini, I. Tamaskar and P. Shaheen et al., Hypothyroidism in patients with metastatic renal cell carcinoma treated with sunitinib, J Natl Cancer Inst 99 (2007), pp. 81–83 [17202116]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (159)
30 B.I. Rini, G. Wilding and G. Hudes et al., Phase II study of axitinib in sorafenib-refractory metastatic renal cell carcinoma, J Clin Oncol 27 (2009), pp. 4462–4468 [19652060]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (49)
31 H.S. Rugo, R.S. Herbst and G. Liu et al., Phase I trial of the oral antiangiogenesis agent AG-013736 in patients with advanced solid tumors: pharmacokinetic and clinical results, J Clin Oncol 23 (2005), pp. 5474–5483 [16027439]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (161)
32 National Cancer Institute, National Institutes of Health, US Department of Health and Human Services, Common Terminology Criteria for Adverse Events (CTCAE) Version 4.02. NIH publication 03-5410, National Institutes of Health, Bethesda, MD (2009).
33 L.S. Wood and B. Manchen, Sorafenib: a promising new targeted therapy for renal cell carcinoma, Clin J Oncol Nurs 11 (2007), pp. 649–656 [17962173]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (15)
34 C. Robert, C. Mateus, A. Spatz, J. Wechsler and B. Escudier, Dermatologic symptoms associated with the multikinase inhibitor sorafenib, J Am Acad Dermatol 60 (2009), pp. 299–305 [19028406]. Article |
35 J. Autier, B. Escudier, J. Wechsler, A. Spatz and C. Robert, Prospective study of the cutaneous adverse effects of sorafenib, a novel multikinase inhibitor, Arch Dermatol 144 (2008), pp. 886–892 [18645140]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (50)
36 M.E. Lacouture, L.M. Reilly, P. Gerami and J. Guitart, Hand foot skin reaction in cancer patients treated with the multikinase inhibitors sorafenib and sunitinib, Ann Oncol 19 (2008), pp. 1955–1961 [18550575]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (35)
37 L.S. Wood, Managing the side effects of sorafenib and sunitinib, Community Oncol 3 (2006), pp. 558–562. View Record in Scopus | Cited By in Scopus (19)
38 C. Robert, J.C. Soria and A. Spatz et al., Cutaneous side-effects of kinase inhibitors and blocking antibodies, Lancet Oncol 6 (2005), pp. 491–500 [15992698]. Article |
39 M.W. Saif, I. Merikas, S. Tsimboukis and K. Syrigos, Erlotinib-induced skin rash: Pathogenesis, clinical significance and management in pancreatic cancer patients, JOP 9 (2008), pp. 267–274 [18469438]. View Record in Scopus | Cited By in Scopus (11)
40 R. Anderson, A. Jatoi, C. Robert, L.S. Wood, K.N. Keating and M.E. Lacouture, Search for evidence-based approaches for the prevention and palliation of hand–foot skin reaction (HFSR) caused by the multikinase inhibitors (MKIs), Oncologist 14 (2009), pp. 291–302 [19276294]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (11)
41 D.J. Gawkrodger, Dermatology: An Illustrated Colour Text, 4th ed, Churchill Livingstone Elsevier, Edinburgh (2008).
42 N.S. Azad, J.B. Aragon-Ching and W.L. Dahut et al., Hand–foot skin reaction increases with cumulative sorafenib dose and with combination anti-vascular endothelial growth factor therapy, Clin Cancer Res 15 (2009), pp. 1411–1416 [19228742]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (31)
43 N. Bhojani, C. Jeldres and J.J. Patard et al., Toxicities associated with the administration of sorafenib, sunitinib, and temsirolimus and their management in patients with metastatic renal cell carcinoma, Eur Urol 53 (2008), pp. 917–930 [18054825]. Article |
44 S. Sleijfer, I. Ray-Coquard and Z. Papai et al., Pazopanib, a multikinase angiogenesis inhibitor, in patients with relapsed or refractory advanced soft tissue sarcoma: a phase II study from the European Organisation for Research and Treatment of Cancer–Soft Tissue and Bone Sarcoma Group (EORTC study 62043), J Clin Oncol 27 (2009), pp. 3126–3132 [19451427]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (55)
45 L.S. Wood, H. Lemont and A. Jatoi et al., Practical considerations in the management of hand–foot skin reaction caused by multikinase inhibitors, Community Oncol 7 (2010), pp. 23–29. View Record in Scopus | Cited By in Scopus (3)
46 P. Esper, D. Gale and P. Muehlbauer, What kind of rash is it?: Deciphering the dermatologic toxicities of biologic and targeted therapies, Clin J Oncol Nurs 11 (2007), pp. 659–666 [17962174]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
47 I. Hagemann and E. Proksch, Topical treatment by urea reduces epidermal hyperproliferation and induces differentiation in psoriasis, Acta Derm Venereol 76 (1996), pp. 353–356 [8891006]. View Record in Scopus | Cited By in Scopus (41)
48 M. Duvic, A.T. Asano, C. Hager and S. Mays, The pathogenesis of psoriasis and the mechanism of action of tazarotene, J Am Acad Dermatol 39 (1998), pp. S129–S133 [9777790]. Article |
49 W. Scheithauer, J. McKendrick and S. Begbie et al., Oral capecitabine as an alternative to i.v. 5-fluorouracil-based adjuvant therapy for colon cancer: safety results of a randomized, phase III trial, Ann Oncol 14 (2003), pp. 1735–1743 [14630678]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (172)
How we do it
Elizabeth Manchen RN, MS, OCN![]()
![]()
Abstract
One significant toxicity associated with the anticancer tyrosine kinase inhibitors (TKIs) is hand–foot skin reaction (HFSR). We provide an overview of HFSR, emphasizing experience-based prevention techniques and nursing management strategies from the viewpoints of a medical oncologist, a dermatologist, and an oncology nurse. Supporting data include (1) published preclinical and phase I–III clinical studies and (2) published abstracts of phase II–III clinical trials of sorafenib and sunitinib. HFSR has been reported in up to 60% of patients treated with sorafenib or sunitinib. TKI-induced HFSR may lead to dose reductions or treatment interruptions and reduced quality of life. Symptoms of TKI-associated HFSR can be managed by implementing supportive measures and aggressive dose modification. Patients educated about HFSR can work with their health-care teams to proactively detect and help manage this cutaneous toxicity, thus preventing or reducing the severity of TKI-associated HFSR. Successful prevention and management of TKI-associated HFSR can help to ensure that patients achieve optimal therapeutic outcomes. Implementation of such measures may increase the likelihood that therapy is continued for the appropriate interval at an appropriate dose for each patient. Optimal management of TKI-associated HFSR is predicated on establishing appropriate partnerships among medical oncologists, dermatologists, oncology nurses, and patients.
Article Outline
This article reviews the mechanism of action, clinical trial results, and adverse effects of two molecularly targeted anticancer agents, the tyrosine kinase inhibitors (TKIs) sorafenib (Nexavar®; Bayer HealthCare Pharmaceuticals, Montville, NJ, and Onyx Pharmaceuticals, Emeryville, CA) and sunitinib (Sutent®; Pfizer Pharmaceuticals, New York, NY). This article specifically focuses on the diagnosis and management of TKI-associated hand–foot skin reaction (HFSR) from the perspectives of the medical oncologist, the dermatologist, and the oncology nurse. Data were derived from (1) published reports of preclinical and phase I–III clinical studies of sorafenib and sunitinib and (2) published abstracts of phase II–III clinical trials of sorafenib and sunitinib.
The Medical Oncologist's Viewpoint
Molecularly Targeted Agents
Molecularly targeted therapies are directed at specific mechanisms involved in cell division, invasion, and metastasis, as well as in cell survival mediated by avoidance of apoptosis and resistance to conventional treatments. Clinical trials in several cancer types have shown that these TKIs can inhibit these activities of cancer cells by either cytostatic or cytotoxic mechanisms.1 However, the ability of these agents to inhibit multiple cancer cell pathways via novel mechanisms of action may explain, at least in part, their apparent direct toxic effects.2 These include adverse events that, from a medical viewpoint, must be anticipated, promptly recognized, and properly treated. Doing so can help minimize disruption to the patient's quality of life and may reduce the need for dose reduction or treatment interruption.1
Both sorafenib and sunitinib are orally administered, small-molecule inhibitors of multiple kinases, some of which are common to both agents (Figure 2).3 Sorafenib has known effects on tumor-cell proliferation and angiogenesis. Its antiproliferative effects are exerted via inhibition of serine/threonine kinases of the RAF/MEK/ERK signaling pathway (also called the MAP-kinase pathway) that is found within tumor cells; specifically, sorafenib targets wild-type RAF gene products (CRAF, BRAF) and mutant BRAF. The antiangiogenic effects of sorafenib are exerted via its inhibition of extracellular vascular endothelial growth factor (VEGF) receptors 2 and 3 (VEGFR-2 and VEGFR-3) and platelet-derived growth factor receptor beta (PDGFR-β), which is found mainly in the tumor vasculature. Sorafenib also exerts broad-spectrum activity against the stem-cell growth factor receptor (c-KIT), FMS-like tyrosine kinase 3 (Flt3), and the receptor encoded by the ret proto-oncogene (RET).[4], [5], [6] and [7] Sunitinib has demonstrated effects on the growth, pathologic angiogenesis, and metastatic progression of cancer by inhibiting PDGFR-α and -β; VEGFR-1, -2, and -3; and colony-stimulating factor receptor (CSF-1R), c-KIT, Flt3, and RET.8
Mechanisms of Action of Sorafenib and Sunitinib
Sorafenib and sunitinib specifically recognize and inhibit c-KIT, VEGFR, PDGFR-β, and Flt3 receptor tyrosine kinases. Sorafenib also inhibits RAF, a serine/threonine kinase involved in the RAF/MEK/ERK kinase pathway
c-KIT = stem-cell growth factor receptor (a cytokine receptor expressed on the surface of hematopoietic stem cells as well as other cell types); ERK = extracellular signal–regulated kinase; Flt3 = FMS-like tyrosine kinase 3 (a cytokine receptor expressed on the surface of hematopoietic progenitor cells); Flt3L = FMS-like tyrosine kinase 3 ligand (Flt3 ligand); MEK = (MAPK/ERK) kinase; PDGF-ΒΒ = platelet-derived growth factor BB; PDGFR-β = platelet-derived growth factor receptor beta; RAF = a gene that encodes for a protein kinase (Raf1) that functions in the mitogen-activated protein kinase/extracellular signal–regulated kinase (MAPK/ERK) signal-transduction pathway as part of a protein kinase cascade; RAS = a superfamily of genes that encode small GTPases involved in cellular signal transduction; SCF = stem-cell factor; VEGF = vascular endothelial growth factor; VEGFR = vascular endothelial growth factor receptor
Adapted with permission from Lacouture et al3
Sorafenib was approved for the treatment of advanced renal cell carcinoma (RCC) in 2005 and for unresectable hepatocellular carcinoma (HCC) in 2007. The efficacy of sorafenib in 903 patients with advanced RCC was demonstrated in the phase III Treatment Approaches in Renal Cancer Global Evaluation Trial (TARGET), the largest phase III trial ever conducted in the second-line setting in patients with advanced RCC. Sorafenib significantly enhanced median progression-free survival (PFS) compared with placebo (24 vs 12 weeks),9 which led to early termination of the study and crossover from placebo to active drug. A preplanned analysis, which did not include patients who received placebo (who had crossed over to active treatment), ultimately demonstrated that sorafenib significantly prolonged overall survival (OS).10 Furthermore, 84% of sorafenib-treated patients experienced a clinical benefit, defined as objective response or disease stabilization.9 These results have been confirmed in larger, “real-world” patient populations in expanded-access programs conducted in North America (n = 2504)11 and the European Union (n = 118).12
Definitive data supporting the efficacy of sorafenib in HCC were provided by the randomized, double-blind, placebo-controlled Sorafenib CCC Assessment Randomized Protocol (SHARP) trial, the largest phase III trial ever conducted in patients with advanced HCC (n = 599) and the first phase III study to demonstrate a significant survival advantage with a systemic treatment in advanced HCC. In this trial, patients treated with sorafenib experienced a 44% increase in median OS (10.7 vs 7.9 months, hazard ratio [HR] = 0.69, 95% confidence interval [CI] 0.55–0.87, P < 0.001) and a 73% prolongation in median time to radiographic progression (5.5 vs 2.8 months, P < 0.001) compared with patients who received placebo.13 These results were confirmed in a separate phase III, randomized, double-blind, placebo-controlled study conducted in 226 patients from the Asia-Pacific region with advanced HCC.14 In this trial also, sorafenib significantly prolonged median OS (6.5 vs 4.2 months, HR = 0.68, 95% CI 0.50–0.93, P = 0.014) and time to progression (TTP) (2.8 vs 1.4 months, HR = 0.57, 95% CI 0.42–0.79, P = 0.0005) compared with placebo.
Sunitinib received approval in 2006 for use in patients with gastrointestinal stromal tumor (GIST) whose disease is refractory to imatinib (Gleevec®; Novartis Pharmaceuticals, East Hanover, NJ) or who are intolerant to the drug and in those with advanced RCC. Approval of sunitinib for the treatment of GIST was based on data from a randomized, placebo-controlled, phase III trial of 312 patients with imatinib-refractory GIST.15 In that study, sunitinib treatment increased median PFS (24.1 vs 6.0 weeks, HR = 0.33, 95% CI 0.24–0.47, P < 0.0001) and median TTP (27.3 vs 6.4 weeks, HR = 0.33, 95% CI 0.23–0.47, P < 0.0001) compared with placebo. The trial was unblinded early when a planned interim analysis revealed significantly longer TTP with sunitinib than with placebo. A subsequent analysis showed that median OS with sunitinib was about twice that with placebo (73.9 vs 35.7 weeks, P < 0.001).16 In an ongoing, worldwide treatment-use program to provide expanded access to sunitinib for patients with advanced GIST intolerant of or resistant to imatinib,17 sunitinib treatment resulted in a median estimated TTP of 41 weeks and a median estimated OS of 75 weeks in the population analyzed (n = 1,117).
A separate phase III randomized controlled trial was conducted in 750 patients with advanced RCC and no history of systemic therapy for RCC.[18] and [19] The active comparator in this trial was interferon-alfa (IFN-α). Compared with IFN-α, sunitinib significantly increased median PFS (11 vs 5 months, HR = 0.539, 95% CI 0.451–0.643, P < 0.001) and was associated with a greater objective response rate (47% vs 12%, P < 0.001). Median OS was greater in the sunitinib group (26.4 vs 21.8 months), but the difference was not significant (P = 0.051). Data from expanded-access programs in patients with RCC and GIST support the phase III trial data for sunitinib.20 Efficacy data for sorafenib and sunitinib are summarized in Table 1.[9], [10], [11], [12], [13], [14], [15], [17], [18] and [20]
| DRUG, DISEASE, AND STUDY | EFFICACY DATA |
|---|---|
| Sorafenib | |
| Advanced RCC | |
| Phase III TARGET[9] and [10] | |
| Expanded-access programs[11] and [12] | Data from expanded-access programs in community-based populations (NA- and EU-ARCCS) were consistent with data from TARGET |
| Unresectable HCC | |
| Phase III SHARP trial13 | • First phase III trial to demonstrate a significant survival advantage for a systemic therapy in advanced HCC • Median OS was 10.7 months in sorafenib group vs 7.9 months in placebo group (HR = 0.69, 95% CI 0.55–0.87, P < 0.001) |
| Phase III Asia-Pacific trial14 | |
| Sunitinib | |
| Advanced RCC | |
| Phase III registration trial18 | • Median PFS was 11 months in sunitinib group vs 5 months in interferon-α group (HR = 0.539, 95% CI 0.451–0.643, P < 0.001) |
| Expanded-access program20 | |
| Imatinib-resistant GIST | |
| Phase III registration trial15 | • Median TTP was 27.3 weeks in sunitinib group vs 6.4 weeks in placebo group (HR = 0.33, 95% CI 0.23–0.47, P < 0.0001) |
| Expanded-access program17 |
CI = confidence interval; CR = complete response; EU-ARCCS = European Union Advanced Renal Cell Carcinoma Sorafenib; GIST = gastrointestinal stromal tumor; HCC = hepatocellular carcinoma; HR = hazard ratio; NA-ARCCS = North American ARCCS; OS = overall survival; PFS = progression-free survival; PR = partial response; RCC = renal cell carcinoma; SD = stable disease; SHARP = Sorafenib CCC Assessment Randomized Protocol; TARGET = Treatment Approaches in Renal Cancer Global Evaluation Trial; TTP = time to progression; TTRP = time to radiologic progression
Characteristics of Hand–Foot Skin Reaction
Data from the clinical trials for sorafenib and sunitinib indicate that both agents are generally well-tolerated; common treatment-related adverse reactions include diarrhea, alopecia, nausea, fatigue, rash, and hypertension, as well as palmar–plantar erythrodysesthesia (PPE) syndrome, also known as hand–foot skin reaction (HFSR) (Table 2).[10] and [19] HFSR is a dermatologic toxicity that has been reported in 14%–62% of patients treated with sorafenib or sunitinib (Table 3).[9], [11], [12], [13], [14], [15], [17], [18], [20], [21], [22], [23], [24] and [25] In general, the term HFSR refers to a group of signs and symptoms affecting the hands and feet of patients taking sorafenib, sunitinib, or, to a lesser extent, other TKIs such as pazopanib (Votrient™; GlaxoSmithKline, Research Triangle Park, NC)[26] and [27] and axitinib (AG013736).[28], [29], [30] and [31]
| ADVERSE EVENT | SORAFENIB 400 MG BID | SUNITINIB 50 MG QD | ||
|---|---|---|---|---|
| ALL GRADES (%) | GRADE 3/4 (%) | ALL GRADES (%) | GRADE 3/4 (%) | |
| Diarrhea | 48 | 3 | 61 | 9 |
| Rash | 41 | 1 | 24 | 2 |
| Hand–foot skin reaction | 33 | 6 | 29 | 9 |
| Alopecia | 31 | 0 | 12 | 0 |
| Fatigue | 29 | 3 | 54 | 11 |
| Nausea | 19 | <1 | 52 | 5 |
| Hypertension | 17 | 4 | 30 | 12 |
| Dry skin | 13 | 0 | 21 | <1 |
| Vomiting | 12 | 1 | 31 | 4 |
| Mucositis | 5 | 0 | 26 | 2 |
| REFERENCE | STUDY | ALL GRADES (%) | GRADE 3 (%) | GRADE 4 (%) |
|---|---|---|---|---|
| Sorafenib | ||||
| 9 | Phase III TARGETa | 30 | 6 (grade 3/4) | |
| 13 | Phase III SHARPa | 21 | 8 | 0 |
| 11 | NA-ARCCS, first-linea | 19 (≥2) | 11 (grade 3/4) | |
| 11 | NA-ARCCS, second-linec | 17 (≥2) | 8 (grade 3/4) | |
| 12 | EU-ARCCSa | 47 | 12 (grade 3/4) | |
| 14 | Phase III Asia-Pacifica | 45 | 11 (grade 3/4) | |
| 24 | Phase II randomized discontinuation trial in advanced RCCb | 62 | 13 | 0 |
| 25 | Phase II study in advanced HCCb | 31 | 5 | 0 |
| 21 | Phase II, uncontrolled study in relapsed/refractory NSCLCa | 37 | 10 (grade 3/4) | |
| Sunitinib | ||||
| 18 | Phase III registration trial in advanced RCCa | 20 | 5 | 0 |
| 20 | Expanded access program in advanced RCCc | 5 (grade 3/4) | ||
| 15 | Phase III registration trial in imatinib-resistant GISTa | 14 | 4 | 0 |
| [17] and [22] | Expanded access program in imatinib-resistant GISTc | N/A | 8 (grade 3/4) | |
| 23 | Phase II trial of second-line treatment in advanced RCCa | 15 | 7 | 0 |
EU-ARCCS = European Union Advanced Renal Cell Carcinoma Sorafenib; GIST = gastrointestinal stromal tumor; HCC = hepatocellular carcinoma; N/A = data not available; NA-ARCCS = North American ARCCS; NSCLC = non-small-cell lung cancer; RCC = renal cell carcinoma; SHARP = Sorafenib CCC Assessment Randomized Protocol; TARGET = Treatment Approaches in Renal Cancer Global Evaluation Trial
a Used version 3.0 of National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE)b Used version 2.0 of NCI-CTCAEc Version of NCI-CTCAE used not specified
HFSR is typically characterized by redness, marked discomfort, swelling, and tingling in the palms of the hands and/or soles of the feet.32 HFSR can be painful enough to interfere profoundly with activities of daily living (ADLs). In fact, patients may report symptoms after as few as 2 weeks on TKI therapy, at which point they may present to the health-care provider (HCP) wearing slippers, unable to walk, and having difficulty in performing ADLs such as eating, dressing, and bathing.[1] and [33] Although HFSR can lead to TKI dose modification or treatment discontinuation, preventive measures can be taken before TKIs are initiated to reduce the likelihood of HFSR. In addition, early treatment of symptoms may prevent HFSR from progressing to the point at which the patient's ability to receive the full potential benefit of therapy is compromised.[3], [34], [35] and [36]
Signs and symptoms of HFSR may appear concomitantly or sequentially and can affect both hands and both feet. Although symptoms are most prominent on the palms and soles, other areas of the hands and feet may also be involved, including the tips of the fingers and toes, the heels, and metatarsophalangeal skin; areas of flexure; and skin overlying the metacarpophalangeal and interphalangeal joints.3 These “pressure areas” are where the most severe symptoms are typically seen. Common symptoms include dysesthesia and paresthesia, described as “tingling, prickling, or creeping sensations” and/or sensitivity or intolerance to hot or warm objects (which may occur before other symptoms are apparent); erythema; edema; hyperkeratosis; and dry and/or cracked skin.[1] and [34] Actual HFSR lesions are described as tender and scaling, with a peripheral halo of erythema, yellowish and hyperkeratotic plaques, or callous-like blisters (which usually do not contain fluid), typically localized to areas of pressure.[3] and [35] Desquamation, particularly with sunitinib treatment, may also be present.37
Since both sorafenib and sunitinib inhibit the VEGFRs, PDGFRs, c-KIT, and Flt3,38 it is likely that inhibition of one or more of these receptors and/or pathways plays a role in HFSR development.36 Differences in the relative appearance of HFSR symptoms are dependent on whether sorafenib or sunitinib is used. Sunitinib use is more often associated with desquamation, whereas sorafenib is more often associated with areas of hyperkeratosis, particularly formation of thick calluses on the soles of the feet.37 The timing of the first appearance of symptoms may also vary according to the TKI used. HFSR usually develops within the first 2–4 weeks of treatment with a TKI and almost always within the first 6 weeks.35 However, because the severity of HFSR appears to be dose-dependent,3 signs and symptoms may present later rather than sooner in patients treated with sunitinib. This is likely due to the recommended sunitinib dosing schedule, which incorporates a 2-week period during which no drug is administered. Although HFSR frequently decreases in intensity during treatment, even without dose modifications or treatment interruption, prompt treatment of HFSR is recommended to prevent rapid progression. Early symptoms can usually be resolved easily by appropriate treatment, which often allows continuation of full-dose therapy for the prescribed length of time.
It is important to note what HFSR is not. TKI-associated HFSR is not the same clinical entity as the hand–foot syndrome (HFS) traditionally seen with cytotoxic agents such as infusional 5-fluorouracil (5-FU); capecitabine, the oral prodrug of 5-FU; and pegylated liposomal doxorubicin. Although HFSR and HFS share several clinical and pathological aspects—each previously has been called “acral erythema” and “PPE”—they clearly are not the same clinical or pathologic entity. HFSR is neither an allergic reaction to a drug nor an indication that a patient may be intolerant to a drug. Finally, HFSR does not indicate drug efficacy, as may be the case with skin rash in patients with non-small-cell lung cancer treated with erlotinib.[3] and [39]
Grading HFSR
In published reports, the severity of HFSR is usually graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE),32 a three-grade classification system. However, modified criteria are considered by some to be a better fit for routine clinical practice.1 What distinguishes the modified criteria from the NCI criteria (version 4.02) is the inclusion of HFSR-specific clinical characteristics plus certain patient-defined considerations used to categorize severity. The modified criteria expressly define the degree to which HFSR discomfort affects the patient's normal activities, an improvement over version 4.02 used alone. The NCI-CTCAE version 4.02 criteria, the modified criteria, and corresponding patient photographs are presented in Figure 3.[1] and [32]
Recommendations for the treatment of grade 1 HFSR include early and appropriate dermatologic management and active collaboration among HCPs.40
The Dermatologist's Viewpoint
Although the exact pathogenesis of HFSR has not been fully elucidated, research into its cause(s) is ongoing. Theoretically, traditional HFS is thought to be due to the direct toxic effects of drugs or their ability to invoke a “host-vs-host” response. In contrast, a unique mechanism has been proposed for TKI-associated HFSR: simultaneous blockage of VEGFRs and PDGFRs.2
Three histopathologic features have been found to predominate in HFSR: dyskeratotic keratinocytes at various states of necrosis (Figure 441), basal layer vacuolar degeneration, and mild perivascular or lichenoid lymphocyte-predominant infiltrate.2 Immunohistochemistry with a variety of skin-cell markers has shown a significant modification of normal maturation of keratinocytes, which are often apoptotic. Minor modifications of blood vessels are also seen, but no signs of intense vasculitis are evident. This is important because HFSR is suspected of being a “class effect” of TKIs that target VEGFRs. HFSR is not seen in patients treated with single-agent bevacizumab, and the lack of histologic evidence of significant damage to blood vessels suggests that HFSR does not result from the general inhibition of angiogenesis. A retrospective analysis found that HFSR rates were higher when patients were treated with sorafenib and bevacizumab in combination, supporting the hypothesis that HSFR is due to the anti-VEGF properties of sorafenib.42 Other possible causes of HFSR include activation by a ligand other than VEGF and/or inhibition of one of the other protein targets inhibited by both sorafenib and sunitinib.[3] and [35]
Layers of the Epidermis
The epidermis is composed of a very sophisticated arrangement of keratinocytes, which originate as stem cells in the stratum germinatum (not shown). The stem cells constantly multiply, creating daughter cells that progressively mature over approximately 28 days and move to the surface of the epidermis. As they move, they change their function and shape. In the stratum spinosum, interactions between cells resemble spines; mature cells move through the stratum granulosum, which has a very important secretory function, until finally the cells reach the stratum corneum and die. Thus, the stratum corneum is the layer of skin containing dead skin cells that have lost their nuclei; it is the part of the epidermis that ensures the barrier function of skin and is the layer most affected by HFSR. The layer beneath the epidermis is called the “papillary dermis.” The papillary dermis contains nerves and blood vessels and supplies the epidermis with nutrients. The fibroblasts and fibers located here give skin its strength and resistance
Adapted with permission from Gawkrodger41
Incidence and Severity of HFSR With TKI
To determine the incidence and severity of HFSR specific to sorafenib, a double-blind, prospective, dermatologic substudy was performed in patients enrolled in the phase III TARGET trial.35 Eighty-five patients with RCC were randomized to receive either sorafenib (n = 43) or placebo (n = 42). Dermatologic examinations were performed before and during treatment. Ninety-one percent of sorafenib-treated patients experienced at least one cutaneous reaction compared with 7% of those in the placebo group. A variant of HFSR clinically distinct from chemotherapy-induced HFS was observed in 60% of sorafenib-treated patients. Reversible grade 3 HFSR leading to dose reduction occurred in two sorafenib-treated patients. Additional cutaneous reactions were facial erythema, scalp dysesthesia, alopecia, and subungual splinter hemorrhages.
HFSR (of any grade) has been shown to occur in approximately 30% of patients treated with sorafenib and 20% of those who received sunitinib in clinical studies.43 Grade 3/4 HFSR has been observed in approximately 6% of sorafenib-treated and 5% of sunitinib-treated patients. HFSR was not reported in a phase II study of 142 patients with relapsed or refractory soft-tissue sarcoma treated with pazopanib.44 In a phase III randomized, double-blind, placebo-controlled trial of pazopanib in patients with advanced RCC, the incidence of HFSR was <10%, while the incidence of grade 3/4 HFSR was <1%. Potential differences may be explained by variations in the potency and selectivity of the TKIs.27
Management Strategies
Our work at the Dermatology Center at the Gustave-Roussy Institute has shown that early intervention against the dermatologic adverse effects of these TKIs can inhibit patient progression to a more serious form of HFSR.[34] and [38]
Effective management of HFSR can begin prior to initiation of treatment with sorafenib or sunitinib. Patients should be advised to remove any preexisting hyperkeratotic areas or calluses, keep skin well-moisturized with appropriate creams, and cushion pressure points with cotton socks, soft shoes, and/or insoles. Dose modification is typically not required for grade 1 HFSR; symptomatic treatments should be employed instead.
If HFSR symptoms progress to grade 2 or 3, with pain and a decrease in quality of life, the dose of sorafenib or sunitinib can be modified until symptoms recede, after which the patient can be brought back to the full dose. Very often, the patient can tolerate the full-dose treatment simply by decreasing the dose briefly.3 A recommended dose-modification scheme is shown in Figure 5.3
Management of Hand–Foot Skin Reaction by Grade
MKI = multikinase inhibitor
Adapted with permission from Lacouture et al3
TKIs are being studied in patients with additional types of tumor, possibly in the adjuvant setting, as well as in combinations. Because these drugs are administered orally, with a decreased (compared with conventional cytotoxic agents) frequency of nurse– or doctor–patient interactions, patients must be very well-informed of any potential toxicities with the TKIs.
At present, there are no evidence-based treatment guidelines for the prevention or management of HFSR. However, HCPs most involved in the day-to-day care of patients with HFSR have made great progress in establishing preventive and treatment strategies and in identifying ancillary products likely to decrease the incidence and/or severity of symptoms. Prevention, which includes preventing HFSR entirely as well as preventing progression from its initial appearance, is a key component of HFSR management.
The Oncology Nurse's Viewpoint
The nurse's viewpoint begins with patient education and empowerment. The goal is to prevent adverse effects from occurring while managing any adverse effects that do occur so that the patient has the best chance of staying on anticancer therapy. This requires a strong partnership between the HCP team and the patient. Although not all cases of HFSR can be prevented, experience suggests that symptom incidence and severity can be alleviated by educating patients to recognize the signs and symptoms of HFSR and report these to their HCPs. HFSR typically occurs early in the course of therapy, so it is prudent to be especially vigilant during the first 6 weeks. Providing the patient with a brochure about HFSR to refer to at home may facilitate identification of HFSR.
To address the lack of evidence-based guidelines to prevent or treat HFSR, an international, interdisciplinary expert panel has provided a set of consensus recommendations for the management of TKI-associated HFSR.45 One component of these recommendations can be phrased simply for the patients as a “3C” approach to management: control calluses, comfort with cushions, and cover with creams.
Prior to treatment, the patient should receive a full-body examination, with emphasis on the condition of the hands and feet. Evaluation should be performed by a qualified HCP who can determine whether there are physical conditions that may predispose a patient to areas of increased friction or rubbing. For all patients, especially those with comorbid conditions (eg, diabetes, poor circulation), a pretreatment pedicure is highly recommended. Patients should also be educated on the proper use of tools (eg, a pumice stone) to aid in callus removal. Such tools are considered beneficial because patients can control the frequency of their use and the extent of skin removed. However, because areas of hyperkeratosis are often extremely tender and painful, patients are cautioned against overuse of these tools, including the aggressive “paring” or “cutting” of callused areas. Finally, patients should be advised of the need for clean tools to guard against infection.
Other protective measures include the use of thick cotton gloves and/or socks, which may also help the skin to retain moisture, and avoidance of warm and/or hot water or objects, tight-fitting shoes, or other items that may rub, pinch, or cause friction in affected areas. Tender areas, pressure points, and pressure-sensitive areas of the hands and feet should be protected. For example, weight lifters might be advised to wear gloves. These recommendations hold true both before and after development of HFSR.[3], [33] and [35] Well-padded but nonconstrictive footwear should be worn, and the use of insole cushions or inserts (eg, silicone or gel) should be encouraged. Foot soaks with lukewarm water and magnesium sulfate may be soothing. Tender areas should be protected at all times, and patients should be encouraged not to walk barefoot.
Use of over-the-counter and prescription-strength creams and moisturizers during treatment with TKIs has also been recommended (Table 4).[40], [45], [46], [47], [48] and [49] Moisturizing agents should be applied liberally, immediately after bathing. Cotton gloves and/or socks can also be worn, to help retain moisture and to provide an additional layer of protection. When applied liberally, these products soften areas of thick and hardened skin, help keep the skin pliable, and may prevent cracks or breaks in skin integrity, which could cause additional discomfort. Prescription-strength topical agents have also shown anecdotal benefit (Table 4). These topical agents are typically applied twice daily to affected areas only because they may irritate unaffected skin. Data on the use of topical/systemic corticosteroids in the treatment of HFS remain inconclusive; the literature primarily includes case studies in patients with PPE treated with chemotherapeutic agents including pegylated liposomal doxorubicin.2 Finally, a qualified HCP must always be consulted to ensure proper diagnosis and treatment of HFSR.
Adapted with permission from Anderson et al40
| PRODUCTS | PRODUCT INFORMATION |
|---|---|
| Over-the-counter[40], [45] and [46] | |
| Cetaphil® (Galderma Laboratories, Ft. Worth, TX) skin cleaners, Aveeno® (Johnson & Johnson, New Brunswick, NJ) shower gel | Nondeodorant, fragrance-free products |
| Udderly Smooth® (Redex Industries, Salem, OH), Gold Bond® (Chattem, Chattanooga, TN), Aveeno® | Thicker products with more intense moisturizing properties than basic lotions; anti-itch formulations are available |
| Norwegian Formula: Smoothing Relief Anti-Itch Moisturizer (Neutrogena, Los Angeles, CA) | Contains dimethicone 1%, camphor 0.1%, and lidocaine |
| Norwegian Formula: Foot Cream (Neutrogena) | Contains cetearyl alcohol, dimethicone, menthol, and urea |
| Bag Balm® (Dairy Association, Lyndonville, VT) | May provide “cooling” effect from eucalyptus |
| Eucerin® (Beiersdorf, Hamburg, Germany) Cream | Best used at night due to greasy formulation |
| Eucerin® Dry Skin Therapy | Contains urea and alpha-hydroxy acid |
| Aquaphor® (Beiersdorf) Healing Ointment | Petrolatum 41% |
| Kerasal® (Alterna, Whippany, NJ) | Salicylic acid 5% exfoliates and softens skin; urea 10% moisturizes skin |
| Blue Lizard® (Crown Laboratories, Johnson City, TN) | UV A and B sunblock, water-resistant |
| Prescription47–49 | |
| Urea 40% cream (Carmol 40®; Doak Dermatologics, Fairfield, NJ) | Softens hyperkeratosis, decreases epidermal thickness, proliferation |
| Tazarotene 0.1% cream (Tazorac®; Allergan Dermatology, Irvine, CA) | Retinoid decreases proliferation, reduces dermal inflammation |
| Fluorouracil 5% cream (Carac®; Dermik Laboratories, Bridgewater, NJ) | Antifolate inhibits proliferation; has shown anecdotal benefit in certain conditions characterized by hyperkeratotic lesions on the palms and soles |
Summary
The addition of molecularly targeted agents to anticancer treatment has been found to cause both common and novel adverse reactions. HFSR is being increasingly recognized as a potential dose-limiting toxicity associated with sorafenib or sunitinib treatment that can result in discomfort, pain, decreased quality of life, and premature termination of a potentially effective cancer treatment. It is important to educate patients about potential dermatologic adverse effects associated with TKIs because limiting toxicity can help avoid treatment interruptions or dose reductions while improving ADLs.
The precise pathogenic mechanism of HFSR is currently not known, and there is no evidence-based protocol for treatment of HFSR. However, the increased clinical experience with these agents has resulted in a wealth of published articles describing empiric and symptomatic approaches that appear to help to prevent and manage HFSR. Frequent communication is necessary between the physician and patient, particularly 2–4 weeks from the initiation of therapy. Symptoms of HFSR should be recognized as early as possible. Providing the patient with a brochure about HFSR to refer to at home may facilitate the early identification of HFSR.
Patients should be advised of the “3C” approach to the management of TKI-associated HFSR: control calluses, comfort with cushions, and cover with creams. Creams should be applied after bathing and before going to bed; cotton gloves and socks should be worn to keep the cream on the hands and feet during the night.
Symptoms of HFSR typically are manageable with the implementation of supportive measures. If symptoms worsen, dose modification or interruption will result in a return to grade 0/1. Many patients can successfully be rechallenged with the full dose. Observations across multiple viewpoints have consistently shown that HFSR severity can be reduced in patients who are educated about HFSR and proactive about its detection and management.
Acknowledgments
All authors contributed equally to the development of this report. Editorial support was provided by Katherine Wright, PharmD, RPh, ISD, Wrighter Medical Education and Training, West Hills, CA; John A. Ibelli, CMPP, BelMed Professional Resources, New Rochelle, NY; and John D. Zoidis, MD, Bayer HealthCare Pharmaceuticals, Montville, NJ.
References1
1 C. Porta, C. Paglino, I. Imarisio and L. Bonomi, Uncovering Pandora's vase: the growing problem of new toxicities from novel anticancer agents: The case of sorafenib and sunitinib, Clin Exp Med 7 (2007), pp. 127–134. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
2 A.D. Lipworth, C. Robert and A.X. Zhu, Hand–foot syndrome (hand–foot skin reaction, palmar–plantar erythrodysesthesia): focus on sorafenib and sunitinib, Oncology 77 (2009), pp. 257–271 [19923864]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
3 M.E. Lacouture, S. Wu and C. Robert et al., Evolving strategies for the management of hand–foot skin reaction associated with the multitargeted kinase inhibitors sorafenib and sunitinib, Oncologist 13 (2008), pp. 1001–1011 [18779536]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (57)
4 S.M. Wilhelm, L. Adnane, P. Newell, A. Villanueva, J.M. Llovet and M. Lynch, Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signaling, Mol Cancer Ther 7 (2008), pp. 3129–3140 [18852116]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (119)
5 D. Auclair, D. Miller and V. Yatsula et al., Antitumor activity of sorafenib in FLT3-driven leukemic cells, Leukemia 21 (2007), pp. 439–445 [17205056]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (40)
6 F. Carlomagno, S. Anaganti and T. Guida et al., BAY 43-9006 inhibition of oncogenic RET mutants, J Natl Cancer Inst 98 (2006), pp. 326–334 [16507829]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (169)
7 S.M. Wilhelm, C. Carter and L. Tang et al., BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis, Cancer Res 64 (2004), pp. 7099–7109 [15466206]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1142)
8 J.G. Christensen, A preclinical review of sunitinib, a multitargeted receptor tyrosine kinase inhibitor with anti-angiogenic and antitumour activities, Ann Oncol 10 (2007), pp. x3–x10 [17761721]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (29)
9 B. Escudier, T. Eisen and W.M. Stadler et al., Sorafenib in advanced clear-cell renal-cell carcinoma, N Engl J Med 356 (2007), pp. 125–134 [17215530]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1425)
10 B. Escudier, T. Eisen and W.M. Stadler et al., Sorafenib for treatment of renal cell carcinoma: final efficacy and safety results of the phase III Treatment Approaches in Renal Cancer Global Evaluation Trial, J Clin Oncol 27 (2009), pp. 3312–3318 [19451442]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (123)
11 W.M. Stadler, R.A. Figlin and D.F. McDermott et al., Safety and efficacy results of the advanced renal cell carcinoma sorafenib expanded access program in North America, Cancer 116 (2010), pp. 1272–1280 [20082451]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (22)
12 J. Beck, E. Bajetta and B. Escudier et al., A large open-label, non-comparative, phase III study of the multi-targeted kinase inhibitor sorafenib in European patients with advanced renal cell carcinoma, Eur J Cancer (suppl) (2007), p. 5 Abstract 4506. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (7)
13 J.M. Llovet, S. Ricci and V. Mazzaferro et al., Sorafenib in advanced hepatocellular carcinoma, N Engl J Med 359 (2008), pp. 378–390 [18650514]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (989)
14 A.L. Cheng, Y.K. Kang and Z. Chen et al., Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial, Lancet Oncol 10 (2009), pp. 25–34 [19095497]. Article |
15 G.D. Demetri, A.T. van Oosterom and C.R. Garrett et al., Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial, Lancet 368 (2006), pp. 1329–1338 [17046465]. Article |
16 G.D. Demetri, X. Huang and C.R. Garrett et al., Novel statistical analysis of long-term survival to account for crossover in a phase III trial of sunitinib (SU) vs placebo (PL) in advanced GIST after imatinib (IM) failure, J Clin Oncol (suppl) (2008), p. 26 Abstract 10524.
17 P. Reichardt, Y. Kang and W. Ruka et al., Detailed analysis of survival and safety with sunitinib (SU) in a worldwide treatment-use trial of patients with advanced GIST, J Clin Oncol (suppl) (2008), p. 26 Abstract 10548.
18 R.J. Motzer, T.E. Hutson and P. Tomczak et al., Sunitinib versus interferon alfa in metastatic renal-cell carcinoma, N Engl J Med 356 (2007), pp. 115–124 [17215529]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1520)
19R.J. Motzer, T.E. Hutson and P. Tomczak et al., Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma, J Clin Oncol 27 (2009), pp. 3584–3590 [19487381]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (194)
20 M.E. Gore, C. Szczylik and C. Porta et al., Safety and efficacy of sunitinib for metastatic renal-cell carcinoma: an expanded-access trial, Lancet Oncol 10 (2009), pp. 757–763 [19615940]. Article |
21 G.R. Blumenschein Jr, U. Gatzemeier and F. Fossella et al., Phase II, multicenter, uncontrolled trial of single-agent sorafenib in patients with relapsed or refractory, advanced non-small-cell lung cancer, J Clin Oncol 27 (2009), pp. 4274–4280 [19652055]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (37)
22 H.J. Schütte, M. Schlemmer, C. Wendtner, P. Reichardt and G.D. Demetri, Sunitinib (SU) in a worldwide treatment-use trial of pts with advanced gastrointestinal stromal tumours (GIST): analysis of survival and safety data, Onkologie (suppl 4) (2008), p. 201 Abstract V582.
23 R.J. Motzer, B.I. Rini and R.M. Bukowski et al., Sunitinib in patients with metastatic renal cell carcinoma, JAMA 295 (2006), pp. 2516–2524 [16757724]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (586)
24 M.J. Ratain, T. Eisen and W.M. Stadler et al., Phase II placebo-controlled randomized discontinuation trial of sorafenib in patients with metastatic renal cell carcinoma, J Clin Oncol 24 (2006), pp. 2505–2512 [16636341]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (544)
25 G.K. Abou-Alfa, L. Schwartz and S. Ricci et al., Phase II study of sorafenib in patients with advanced hepatocellular carcinoma, J Clin Oncol 24 (2006), pp. 4293–4300 [16908937]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (418)
26 T.E. Hutson, I.D. Davis and J.P. Machiels et al., Efficacy and safety of pazopanib in patients with metastatic renal cell carcinoma, J Clin Oncol 28 (2010), pp. 475–480 [20008644]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (31)
27 C.N. Sternberg, I.D. Davis and J. Mardiak et al., Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial, J Clin Oncol 28 (2010), pp. 1061–1068 [20100962]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (100)
28 O. Rixe, R.M. Bukowski and M.D. Michaelson et al., Axitinib treatment in patients with cytokine-refractory metastatic renal-cell cancer: a phase II study, Lancet Oncol 8 (2007), pp. 975–984 [17959415]. Article |
29 B.I. Rini, I. Tamaskar and P. Shaheen et al., Hypothyroidism in patients with metastatic renal cell carcinoma treated with sunitinib, J Natl Cancer Inst 99 (2007), pp. 81–83 [17202116]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (159)
30 B.I. Rini, G. Wilding and G. Hudes et al., Phase II study of axitinib in sorafenib-refractory metastatic renal cell carcinoma, J Clin Oncol 27 (2009), pp. 4462–4468 [19652060]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (49)
31 H.S. Rugo, R.S. Herbst and G. Liu et al., Phase I trial of the oral antiangiogenesis agent AG-013736 in patients with advanced solid tumors: pharmacokinetic and clinical results, J Clin Oncol 23 (2005), pp. 5474–5483 [16027439]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (161)
32 National Cancer Institute, National Institutes of Health, US Department of Health and Human Services, Common Terminology Criteria for Adverse Events (CTCAE) Version 4.02. NIH publication 03-5410, National Institutes of Health, Bethesda, MD (2009).
33 L.S. Wood and B. Manchen, Sorafenib: a promising new targeted therapy for renal cell carcinoma, Clin J Oncol Nurs 11 (2007), pp. 649–656 [17962173]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (15)
34 C. Robert, C. Mateus, A. Spatz, J. Wechsler and B. Escudier, Dermatologic symptoms associated with the multikinase inhibitor sorafenib, J Am Acad Dermatol 60 (2009), pp. 299–305 [19028406]. Article |
35 J. Autier, B. Escudier, J. Wechsler, A. Spatz and C. Robert, Prospective study of the cutaneous adverse effects of sorafenib, a novel multikinase inhibitor, Arch Dermatol 144 (2008), pp. 886–892 [18645140]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (50)
36 M.E. Lacouture, L.M. Reilly, P. Gerami and J. Guitart, Hand foot skin reaction in cancer patients treated with the multikinase inhibitors sorafenib and sunitinib, Ann Oncol 19 (2008), pp. 1955–1961 [18550575]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (35)
37 L.S. Wood, Managing the side effects of sorafenib and sunitinib, Community Oncol 3 (2006), pp. 558–562. View Record in Scopus | Cited By in Scopus (19)
38 C. Robert, J.C. Soria and A. Spatz et al., Cutaneous side-effects of kinase inhibitors and blocking antibodies, Lancet Oncol 6 (2005), pp. 491–500 [15992698]. Article |
39 M.W. Saif, I. Merikas, S. Tsimboukis and K. Syrigos, Erlotinib-induced skin rash: Pathogenesis, clinical significance and management in pancreatic cancer patients, JOP 9 (2008), pp. 267–274 [18469438]. View Record in Scopus | Cited By in Scopus (11)
40 R. Anderson, A. Jatoi, C. Robert, L.S. Wood, K.N. Keating and M.E. Lacouture, Search for evidence-based approaches for the prevention and palliation of hand–foot skin reaction (HFSR) caused by the multikinase inhibitors (MKIs), Oncologist 14 (2009), pp. 291–302 [19276294]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (11)
41 D.J. Gawkrodger, Dermatology: An Illustrated Colour Text, 4th ed, Churchill Livingstone Elsevier, Edinburgh (2008).
42 N.S. Azad, J.B. Aragon-Ching and W.L. Dahut et al., Hand–foot skin reaction increases with cumulative sorafenib dose and with combination anti-vascular endothelial growth factor therapy, Clin Cancer Res 15 (2009), pp. 1411–1416 [19228742]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (31)
43 N. Bhojani, C. Jeldres and J.J. Patard et al., Toxicities associated with the administration of sorafenib, sunitinib, and temsirolimus and their management in patients with metastatic renal cell carcinoma, Eur Urol 53 (2008), pp. 917–930 [18054825]. Article |
44 S. Sleijfer, I. Ray-Coquard and Z. Papai et al., Pazopanib, a multikinase angiogenesis inhibitor, in patients with relapsed or refractory advanced soft tissue sarcoma: a phase II study from the European Organisation for Research and Treatment of Cancer–Soft Tissue and Bone Sarcoma Group (EORTC study 62043), J Clin Oncol 27 (2009), pp. 3126–3132 [19451427]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (55)
45 L.S. Wood, H. Lemont and A. Jatoi et al., Practical considerations in the management of hand–foot skin reaction caused by multikinase inhibitors, Community Oncol 7 (2010), pp. 23–29. View Record in Scopus | Cited By in Scopus (3)
46 P. Esper, D. Gale and P. Muehlbauer, What kind of rash is it?: Deciphering the dermatologic toxicities of biologic and targeted therapies, Clin J Oncol Nurs 11 (2007), pp. 659–666 [17962174]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (9)
47 I. Hagemann and E. Proksch, Topical treatment by urea reduces epidermal hyperproliferation and induces differentiation in psoriasis, Acta Derm Venereol 76 (1996), pp. 353–356 [8891006]. View Record in Scopus | Cited By in Scopus (41)
48 M. Duvic, A.T. Asano, C. Hager and S. Mays, The pathogenesis of psoriasis and the mechanism of action of tazarotene, J Am Acad Dermatol 39 (1998), pp. S129–S133 [9777790]. Article |
49 W. Scheithauer, J. McKendrick and S. Begbie et al., Oral capecitabine as an alternative to i.v. 5-fluorouracil-based adjuvant therapy for colon cancer: safety results of a randomized, phase III trial, Ann Oncol 14 (2003), pp. 1735–1743 [14630678]. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (172)
Observations on the CATIE Schizophrenia StudyHow Should the Data Be Translated Into Clinical Practice?
How Should the Data Be Translated Into Clinical Practice?
A supplement to Clinical Psychiatry News and supported by Pfizer, Inc.
A panel of experts met in November 2005 in Washington, DC, to discuss the first published results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia study. Participants included several principal study investigators as well as experts in the treatment and management of schizophrenia and bipolar illness. The content of this supplement is based in part on that discussion.

Click Here to view the supplement.
Faculty
Peter F. Buckley, MD
Medical College of Georgia
School of Medicine
Grant/Research Support: Astra/Zeneca, Bristol-Myers Squibb Company, Eli Lilly and Company, Janssen Pharmaceutica, LP, Pfizer Inc., and Solvay Pharmaceuticals, Inc. Consultant/Received Honoraria: Abbott Laboratories, Alamo Pharmaceuticals, LLC, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, and Pfizer.
Joseph P. McEvoy, MD
Duke University
Medical Center
Clinical Grant Support: AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, and Pfizer Inc. Consultant: GlaxoSmithKline, Eli Lilly, and Pfizer.
Topics
• Design
• Overview of Results
• Dosing
• Metabolics
• Clinical Implications of CATIE Phase I
• Beyond Phase I
• Implications of CATIE Beyond Schizophrenia
• Conclusion
A supplement to Clinical Psychiatry News and supported by Pfizer, Inc.
A panel of experts met in November 2005 in Washington, DC, to discuss the first published results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia study. Participants included several principal study investigators as well as experts in the treatment and management of schizophrenia and bipolar illness. The content of this supplement is based in part on that discussion.
Click Here to view the supplement.
Faculty
Peter F. Buckley, MD
Medical College of Georgia
School of Medicine
Grant/Research Support: Astra/Zeneca, Bristol-Myers Squibb Company, Eli Lilly and Company, Janssen Pharmaceutica, LP, Pfizer Inc., and Solvay Pharmaceuticals, Inc. Consultant/Received Honoraria: Abbott Laboratories, Alamo Pharmaceuticals, LLC, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, and Pfizer.
Joseph P. McEvoy, MD
Duke University
Medical Center
Clinical Grant Support: AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, and Pfizer Inc. Consultant: GlaxoSmithKline, Eli Lilly, and Pfizer.
Topics
• Design
• Overview of Results
• Dosing
• Metabolics
• Clinical Implications of CATIE Phase I
• Beyond Phase I
• Implications of CATIE Beyond Schizophrenia
• Conclusion
A supplement to Clinical Psychiatry News and supported by Pfizer, Inc.
A panel of experts met in November 2005 in Washington, DC, to discuss the first published results of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) schizophrenia study. Participants included several principal study investigators as well as experts in the treatment and management of schizophrenia and bipolar illness. The content of this supplement is based in part on that discussion.
Click Here to view the supplement.
Faculty
Peter F. Buckley, MD
Medical College of Georgia
School of Medicine
Grant/Research Support: Astra/Zeneca, Bristol-Myers Squibb Company, Eli Lilly and Company, Janssen Pharmaceutica, LP, Pfizer Inc., and Solvay Pharmaceuticals, Inc. Consultant/Received Honoraria: Abbott Laboratories, Alamo Pharmaceuticals, LLC, AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, and Pfizer.
Joseph P. McEvoy, MD
Duke University
Medical Center
Clinical Grant Support: AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, and Pfizer Inc. Consultant: GlaxoSmithKline, Eli Lilly, and Pfizer.
Topics
• Design
• Overview of Results
• Dosing
• Metabolics
• Clinical Implications of CATIE Phase I
• Beyond Phase I
• Implications of CATIE Beyond Schizophrenia
• Conclusion
How Should the Data Be Translated Into Clinical Practice?
How Should the Data Be Translated Into Clinical Practice?

Bacterial Contamination of Work Wear
In September 2007, the British Department of Health developed guidelines for health care workers regarding uniforms and work wear that banned the traditional white coat and other long‐sleeved garments in an attempt to decrease nosocomial bacterial transmission.1 Similar policies have recently been adopted in Scotland.2 Interestingly, the National Health Service report acknowledged that evidence was lacking that would support that white coats and long‐sleeved garments caused nosocomial infection.1, 3 Although many studies have documented that health care work clothes are contaminated with bacteria, including methicillin‐resistant Staphylococcal aureus (MRSA) and other pathogenic species,413 none have determined whether avoiding white coats and switching to short‐sleeved garments decreases bacterial contamination.
We performed a prospective, randomized, controlled trial designed to compare the extent of bacterial contamination of physicians' white coats with that of newly laundered, standardized short‐sleeved uniforms. Our hypotheses were that infrequently cleaned white coats would have greater bacterial contamination than uniforms, that the extent of contamination would be inversely related to the frequency with which the coats were washed, and that the increased contamination of the cuffs of the white coats would result in increased contamination of the skin of the wrists. Our results led us also to assess the rate at which bacterial contamination of short‐sleeved uniforms occurs during the workday.
Methods
The study was conducted at Denver Health, a university‐affiliated public safety‐net hospital and was approved by the Colorado Multiple Institutional Review Board.
Trial Design
The study was a prospective, randomized, controlled trial. No protocol changes occurred during the study.
Participants
Participants included residents and hospitalists directly caring for patients on internal medicine units between August 1, 2008 and November 15, 2009.
Intervention
Subjects wore either a standard, newly laundered, short‐sleeved uniform or continued to wear their own white coats.
Outcomes
The primary end point was the percentage of subjects contaminated with MRSA. Cultures were collected using a standardized RODAC imprint method14 with BBL RODAC plates containing trypticase soy agar with lecithin and polysorbate 80 (Becton Dickinson, Sparks, MD) 8 hours after the physicians started their work day. All physicians had cultures obtained from the breast pocket and sleeve cuff (long‐sleeved for the white coats, short‐sleeved for the uniforms) and from the skin of the volar surface of the wrist of their dominant hand. Those wearing white coats also had cultures obtained from the mid‐biceps level of the sleeve of the dominant hand, as this location closely approximated the location of the cuffs of the short‐sleeved uniforms.
Cultures were incubated in ambient air at 35C‐37C for 1822 hours. After incubation, visible colonies were counted using a dissecting microscope to a maximum of 200 colonies at the recommendation of the manufacturer. Colonies that were morphologically consistent with Staphylococcus species by colony growth and Gram stain were further tested for coagulase using a BactiStaph rapid latex agglutination test (Remel, Lenexa, KS). If positive, these colonies were subcultured to sheep blood agar (Remel, Lenexa, KS) and BBL MRSA Chromagar (Becton Dickinson, Sparks, MD) and incubated for an additional 1824 hours. Characteristic growth on blood agar that also produced mauve‐colored colonies on chromagar was taken to indicate MRSA.
A separate set of 10 physicians donned newly laundered, short‐sleeved uniforms at 6:30 AM for culturing from the breast pocket and sleeve cuff of the dominant hand prior to and 2.5, 5, and 8 hours after they were donned by the participants (with culturing of each site done on separate days to avoid the effects of obtaining multiple cultures at the same site on the same day). These cultures were not assessed for MRSA.
At the time that consent was obtained, all participants completed an anonymous survey that assessed the frequency with which they normally washed or changed their white coats.
Sample Size
Based on the finding that 20% of our first 20 participants were colonized with MRSA, we determined that to find a 25% difference in the percentage of subjects colonized with MRSA in the 2 groups, with a power of 0.8 and P < 0.05 being significant (2‐sided Fisher's exact test), 50 subjects would be needed in each group.
Randomization
Randomization of potential participants occurred 1 day prior to the study using a computer‐generated table of random numbers. The principal investigator and a coinvestigator enrolled participants. Consent was obtained from those randomized to wear a newly laundered standard short‐sleeved uniform at the time of randomization so that they could don the uniforms when arriving at the hospital the following morning (at approximately 6:30 AM). Physicians in this group were also instructed not to wear their white coats at any time during the day they were wearing the uniforms. Physicians randomized to wear their own white coats were not notified or consented until the day of the study, a few hours prior to the time the cultures were obtained. This approach prevented them from either changing their white coats or washing them prior to the time the cultures were taken.
Because our study included both employees of the hospital and trainees, a number of protection measures were required. No information of any sort was collected about those who agreed or refused to participate in the study. In addition, the request to participate in the study did not come from the person's direct supervisor.
Statistical Methods
All data were collected and entered using Excel for Mac 2004 version 11.5.4. All analyses were performed using SAS Enterprise Guide 4.1 (SAS Institute, Inc., Cary, NC).
The Wilcoxon rank‐sum test and chi square analysis were used to seek differences in colony count and percentage of cultures with MRSA, respectively, in cultures obtained: (1) from the sleeve cuffs and pockets of the white coats compared with those from the sleeve cuffs and pockets of the uniforms, (2) from the sleeve cuffs of the white coats compared with those from the sleeve cuffs of the short‐sleeved uniforms, (3) from the mid‐biceps area of the sleeve sof the white coats compared with those from the sleeve cuffs of the uniforms, and (4) from the skin of the wrists of those wearing white coats compared with those wearing the uniforms. Bonferroni's correction for multiple comparisons was applied, with a P < 0.125 indicating significance.
Friedman's test and repeated‐measures logistic regression were used to seek differences in colony count or of the percentage of cultures with MRSA, respectively, on white coats or uniforms by site of culture on both garments. A P < 0.05 indicated significance for these analyses.
The Kruskal‐Wallis and chi‐square tests were utilized to test the effect of white coat wash frequency on colony count and MRSA contamination, respectively.
All data are presented as medians with 95% confidence intervals or proportions.
Results
Participant Flow
Fifty physicians were studied in each group, all of whom completed the survey. In general, more than 95% of potential participants approached agreed to participate in the study (Figure 1).
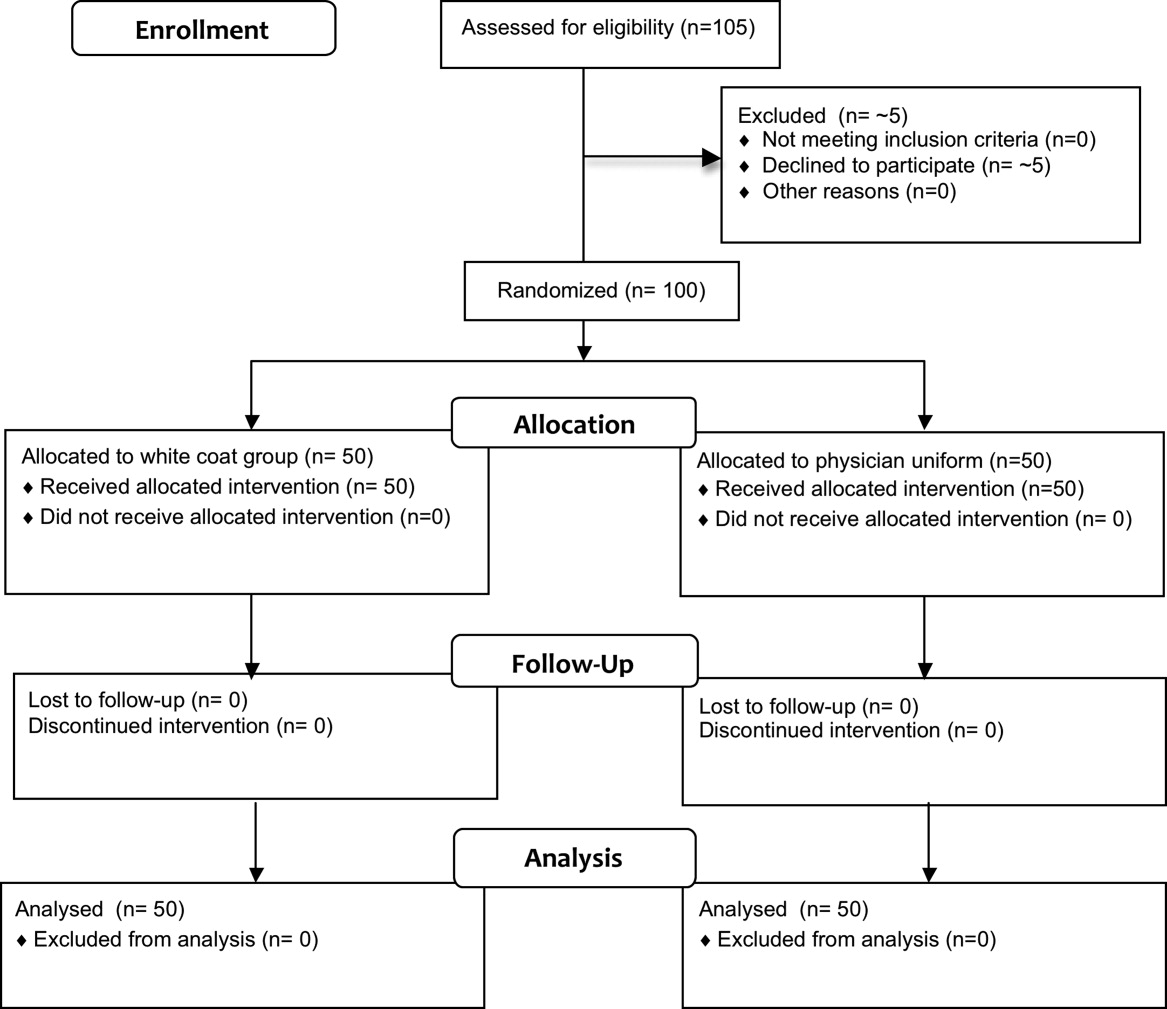
Recruitment
The first and last physicians were studied in August 2008 and November 2009, respectively. The trial ended when the specified number of participants (50 in each group) had been enrolled.
Data on Entry
No data were recorded from the participants at the time of randomization in compliance with institutional review board regulations pertaining to employment issues that could arise when studying members of the workforce.
Outcomes
No significant differences were found between the colony counts cultured from white coats (104 [80127]) versus newly laundered uniforms (142 [83213]), P = 0.61. No significant differences were found between the colony counts cultured from the sleeve cuffs of the white coats (58.5 [4866]) versus the uniforms (37 [2768]), P = 0.07, or between the colony counts cultured from the pockets of the white coats (45.5 [3254]) versus the uniforms (74.5 [4897], P = 0.040. Bonferroni corrections were used for multiple comparisons such that a P < 0.0125 was considered significant. Cultures from at least 1 site of 8 of 50 physicians (16%) wearing white coats and 10 of 50 physicians (20%) wearing short‐sleeved uniforms were positive for MRSA (P = .60).
Colony counts were greater in cultures obtained from the sleeve cuffs of the white coats compared with the pockets or mid‐biceps area (Table 1). For the uniforms, no difference in colony count in cultures from the pockets versus sleeve cuffs was observed. No difference was found when comparing the number of subjects with MRSA contamination of the 3 sites of the white coats or the 2 sites of the uniforms (Table 1).
| White Coat (n = 50) | P | Uniforms (n = 50) | P | |
|---|---|---|---|---|
| Colony count, median (95% CI) | ||||
| Sleeve cuff | 58.5 (4866) | < 0.0001 | 37.0 (2768) | 0.25 |
| 45.5 (3254) | 74.5 (4897) | |||
| Mid‐biceps area of sleeve | 25.5 (2029) | |||
| MRSA contamination, n (%) | ||||
| Sleeve cuff | 4 (8%) | 0.71 | 6 (12%) | 0.18 |
| 5 (10%) | 9 (18%) | |||
| Mid‐biceps area of sleeve | 3 (6%) |
No difference was observed with respect to colony count or the percentage of subjects positive for MRSA in cultures obtained from the mid‐biceps area of the white coats versus those from the cuffs of the short‐sleeved uniforms (Table 2).
| White Coat Mid‐Biceps (n = 50) | Uniform Sleeve Cuff (n = 50) | P | |
|---|---|---|---|
| Colony count, median (95% CI) | 25.5 (2029) | 37.0 (2768) | 0.07 |
| MRSA contamination, n (%) | 3 (6%) | 6 (12%) | 0.49 |
No difference was observed with respect to colony count or the percentage of subjects positive for MRSA in cultures obtained from the volar surface of the wrists of subjects wearing either of the 2 garments (Table 3).
| White Coat (n = 50) | Uniform (n = 50) | P | |
|---|---|---|---|
| Colony count, median (95% CI) | 23.5 (1740) | 40.5 (2859) | 0.09 |
| MRSA Contamination, n (% of subjects) | 3 (6%) | 5 (10%) | 0.72 |
The frequency with which physicians randomized to wearing their white coats admitted to washing or changing their coats varied markedly (Table 4). No significant differences were found with respect to total colony count (P = 0.81), colony count by site (data not shown), or percentage of physicians contaminated with MRSA (P = 0.22) as a function of washing or changing frequency (Table 4).
| White Coat Washing Frequency | Number of Subjects (%) | Total Colony Count (All Sites), Median (95% CI) | Number with MRSA Contamination, n (%) |
|---|---|---|---|
| Weekly | 15 (30%) | 124 (107229) | 1 (7%) |
| Every 2 weeks | 21 (42%) | 156 (90237) | 6 (29%) |
| Every 4 weeks | 8 (16%) | 89 (41206) | 0 (0%) |
| Every 8 weeks | 5 (10%) | 140 (58291) | 2 (40%) |
| Rarely | 1 (2%) | 150 | 0 (0%) |
Sequential culturing showed that the newly laundered uniforms were nearly sterile prior to putting them on. By 3 hours of wear, however, nearly 50% of the colonies counted at 8 hours were already present (Figure 2).

Harms
No adverse events occurred during the course of the study in either group.
Discussion
The important findings of this study are that, contrary to our hypotheses, at the end of an 8‐hour workday, no significant differences were found between the extent of bacterial or MRSA contamination of infrequently washed white coats compared with those of newly laundered uniforms, no difference was observed with respect to the extent of bacterial or MRSA contamination of the wrists of physicians wearing either of the 2 garments, and no association was apparent between the extent of bacterial or MRSA contamination and the frequency with which white coats were washed or changed. In addition, we also found that bacterial contamination of newly laundered uniforms occurred within hours of putting them on.
Interpretation
Numerous studies have demonstrated that white coats and uniforms worn by health care providers are frequently contaminated with bacteria, including both methicillin‐sensitive and ‐resistant Staphylococcus aureus and other pathogens.413 This contamination may come from nasal or perineal carriage of the health care provider, from the environment, and/or from patients who are colonized or infected.11, 15 Although many have suggested that patients can become contaminated from contact with health care providers' clothing and studies employing pulsed‐field gel electrophoresis and other techniques have suggested that cross‐infection can occur,10, 1618 others have not confirmed this contention,19, 20 and Lessing and colleagues16 concluded that transmission from staff to patients was a rare phenomenon. The systematic review reported to the Department of Health in England,3 the British Medical Association guidelines regarding dress codes for doctors,21 and the department's report on which the new clothing guidelines were based1 concluded there was no conclusive evidence indicating that work clothes posed a risk of spreading infection to patients. Despite this, the Working Group and the British Medical Association recommended that white coats should not be worn when providing patient care and that shirts and blouses should be short‐sleeved.1 Recent evidence‐based reviews concluded that there was insufficient evidence to justify this policy,3, 22 and our data indicate that the policy will not decrease bacterial or MRSA contamination of physicians' work clothes or skin.
The recommendation that long‐sleeved clothing should be avoided comes from studies indicating that cuffs of these garments are more heavily contaminated than other areas5, 8 and are more likely to come in contact with patients.1 Wong and colleagues5 reported that cuffs and lower front pockets had greater contamination than did the backs of white coats, but no difference was seen in colony count from cuffs compared with pockets. Loh and colleagues8 found greater bacterial contamination on the cuffs than on the backs of white coats, but their conclusion came from comparing the percentage of subjects with selected colony counts (ie, between 100 and 199 only), and the analysis did not adjust for repeated sampling of each participant. Apparently, colony counts from the cuffs were not different than those from the pockets. Callaghan7 found that contamination of nursing uniforms was equal at all sites. We found that sleeve cuffs of white coats had slightly but significantly more contamination with bacteria than either the pocket or the midsleeve areas, but interestingly, we found no difference in colony count from cultures taken from the skin at the wrists of the subjects wearing either garment. We found no difference in the extent of bacterial contamination by site in the subjects wearing short‐sleeved uniforms or in the percentage of subjects contaminated with MRSA by site of culture of either garment.
Contrary to our hypothesis, we found no association between the frequency with which white coats were changed or washed and the extent of bacterial contamination, despite the physicians having admitted to washing or changing their white coats infrequently (Table 4). Similar findings were reported by Loh and colleagues8 and by Treakle and colleagues.12
Our finding that contamination of clean uniforms happens rapidly is consistent with published data. Speers and colleagues4 found increasing contamination of nurses' aprons and dresses comparing samples obtained early in the day with those taken several hours later. Boyce and colleagues6 found that 65% of nursing uniforms were contaminated with MRSA after performing morning patient‐care activities on patients with MRSA wound or urine infections. Perry and colleagues9 found that 39% of uniforms that were laundered at home were contaminated with MRSA, vancomycin‐resistant enterococci, or Clostridium difficile at the beginning of the work shift, increasing to 54% by the end of a 24‐hour shift, and Babb and colleagues20 found that nearly 100% of nurses' gowns were contaminated within the first day of use (33% with Staphylococcus aureus). Dancer22 recently suggested that if staff were afforded clean coats every day, it is possible that concerns over potential contamination would be less of an issue. Our data suggest, however, that work clothes would have to be changed every few hours if the intent were to reduce bacterial contamination.
Limitations
Our study has a number of potential limitations. The RODAC imprint method only sampled a small area of both the white coats and the uniforms, and accordingly, the culture data might not accurately reflect the total degree of contamination. However, we cultured 3 areas on the white coats and 2 on the uniforms, including areas thought to be more heavily contaminated (sleeve cuffs of white coats). Although this area had greater colony counts, the variation in bacterial and MRSA contamination from all areas was small.
We did not culture the anterior nares to determine if the participants were colonized with MRSA. Normal health care workers have varying degrees of nasal colonization with MRSA, and this could account for some of the 16%‐20% MRSA contamination rate we observed. However, previous studies have shown that nasal colonization of healthcare workers only minimally contributes to uniform contamination.4
Although achieving good hand hygiene compliance has been a major focus at our hospital, we did not track the hand hygiene compliance of the physicians in either group. Accordingly, not finding reduced bacterial contamination in those wearing short‐sleeved uniforms could be explained if physicians in this group had systematically worse hand‐washing compliance than those randomized to wearing their own white coats. Our use of concurrent controls limits this possibility, as does that during the time of this study, hand hygiene compliance (assessed by monthly surreptitious observation) was approximately 90% throughout the hospital.
Despite the infrequent wash frequencies reported, the physicians' responses to the survey could have overestimated the true wash frequency as a result of the Hawthorne effect. The colony count and MRSA contamination rates observed, however, suggest that even if this occurred, it would not have altered our conclusion that bacterial contamination was not associated with wash frequency.
Generalizability
Because data were collected from a single, university‐affiliated public teaching hospital from hospitalists and residents working on the internal medicine service, the results might not be generalizable to other types of institutions, other personnel, or other services.
In conclusion, bacterial contamination of work clothes occurs within the first few hours after donning them. By the end of an 8‐hour work day, we found no data supporting the contention that long‐sleeved white coats were more heavily contaminated than were short‐sleeved uniforms. Our data do not support discarding white coats for uniforms that are changed on a daily basis or for requiring health care workers to avoid long‐sleeved garments.
Acknowledgements
The authors thank Henry Fonseca and his team for providing our physician uniforms. They also thank the Denver Health Department of Medicine Small Grants program for supporting this study.
- Department of Health. Uniforms and workwear: an evidence base for developing local policy. National Health Service, September 17, 2007. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicationspolicyandguidance/DH_078433. Accessed January 29,2010.
- Scottish Government Health Directorates. NHS Scotland Dress Code. Available at: http://www.sehd.scot.nhs.uk/mels/CEL2008_53.pdf. Accessed February 10,2010.
- ,,,.Uniform: an evidence review of the microbiological significance of uniforms and uniform policy in the prevention and control of healthcare‐associated infections. Report to the Department of Health (England).J Hosp Infect.2007;66:301–307.
- ,,,.Contamination of nurses' uniforms with Staphylococcus aureus.Lancet.1969;2:233–235.
- ,,.Microbial flora on doctors' white coats.Brit Med J.1991;303:1602–1604.
- ,,,.Environmental contamination due to methicillin‐resistant Staphylococcus aureus: possible infection control implications.Infect Control Hosp Epidemiol.1997;18:622–627.
- ,Bacterial contamination of nurses' uniforms: a study.Nursing Stand.1998;13:37–42.
- ,,.Bacterial flora on the white coats of medical students.J Hosp Infection.2000;45:65–68.
- ,,.Bacterial contamination of uniforms.J Hosp Infect.2001;48:238–241.
- ,,, et al.Significance of methicillin‐resistant Staphylococcus aureus (MRSA) survey in a university teaching hospital.J Infec Chemother.2003;9:172–177.
- ,,, et al.Detection of methicillin‐resistant Staphylococcus aureus and vancomycin‐resistant enterococci on the gowns and gloves of healthcare workers.Infect Control Hosp Epidemiol2008;29 (7):583–9.
- ,,,,,.Bacterial contamination of health care workers' white coats.Am J Infect Control.2009;37:101–105.
- ,,,,,.Meticillin‐resistant Staphylococcus aureus contamination of healthcare workers' uniforms in long‐term care facilities.J Hosp Infect.2009;71:170–175.
- ,,,,.Comparison of the Rodac imprint method to selective enrichment broth for recovery of vancomycin‐resistant enterococci and drug‐resistant Enterobacteriaceae from environmental surfaces.J Clin Microbiol.2000;38:4646–4648.
- ,,.Effect of clothing on dispersal of Staphylococcus aureus by males and females.Lancet.1974;2:1131–1133.
- ,,.When should healthcare workers be screened for methicillin‐resistant Staphylococcus aureus?J Hosp Infect.1996;34:205–210.
- ,,.Methicillin‐resistant Staphylococcus aureus transmission: the possible importance of unrecognized health care worker carriage.Am J Infect Control.2008;36:93–97.
- ,,, et al.Methicillin‐resistant Staphylococcus aureus carriage, infection and transmission in dialysis patients, healthcare workers and their family members.Nephrol Dial Transplant.2008;23:1659–1665.
- ,,.Are active microbiological surveillance and subsequent isolation needed to prevent the spread of methicillin‐resistant Staphylococcus aureus.Clin Infect Dis.2005;40:405–409.
- ,,.Contamination of protective clothing and nurses' uniforms in an isolation ward.J Hosp Infect.1983;4:149–157.
- British Medical Association. Uniform and dress code for doctors. December 6, 2007. Available at: http://www.bma.org.uk/employmentandcontracts/working_arrangements/CCSCdresscode051207.jsp. Accessed February 9,2010.
- .Pants, policies and paranoia.J Hosp Infect.2010;74:10–15.
In September 2007, the British Department of Health developed guidelines for health care workers regarding uniforms and work wear that banned the traditional white coat and other long‐sleeved garments in an attempt to decrease nosocomial bacterial transmission.1 Similar policies have recently been adopted in Scotland.2 Interestingly, the National Health Service report acknowledged that evidence was lacking that would support that white coats and long‐sleeved garments caused nosocomial infection.1, 3 Although many studies have documented that health care work clothes are contaminated with bacteria, including methicillin‐resistant Staphylococcal aureus (MRSA) and other pathogenic species,413 none have determined whether avoiding white coats and switching to short‐sleeved garments decreases bacterial contamination.
We performed a prospective, randomized, controlled trial designed to compare the extent of bacterial contamination of physicians' white coats with that of newly laundered, standardized short‐sleeved uniforms. Our hypotheses were that infrequently cleaned white coats would have greater bacterial contamination than uniforms, that the extent of contamination would be inversely related to the frequency with which the coats were washed, and that the increased contamination of the cuffs of the white coats would result in increased contamination of the skin of the wrists. Our results led us also to assess the rate at which bacterial contamination of short‐sleeved uniforms occurs during the workday.
Methods
The study was conducted at Denver Health, a university‐affiliated public safety‐net hospital and was approved by the Colorado Multiple Institutional Review Board.
Trial Design
The study was a prospective, randomized, controlled trial. No protocol changes occurred during the study.
Participants
Participants included residents and hospitalists directly caring for patients on internal medicine units between August 1, 2008 and November 15, 2009.
Intervention
Subjects wore either a standard, newly laundered, short‐sleeved uniform or continued to wear their own white coats.
Outcomes
The primary end point was the percentage of subjects contaminated with MRSA. Cultures were collected using a standardized RODAC imprint method14 with BBL RODAC plates containing trypticase soy agar with lecithin and polysorbate 80 (Becton Dickinson, Sparks, MD) 8 hours after the physicians started their work day. All physicians had cultures obtained from the breast pocket and sleeve cuff (long‐sleeved for the white coats, short‐sleeved for the uniforms) and from the skin of the volar surface of the wrist of their dominant hand. Those wearing white coats also had cultures obtained from the mid‐biceps level of the sleeve of the dominant hand, as this location closely approximated the location of the cuffs of the short‐sleeved uniforms.
Cultures were incubated in ambient air at 35C‐37C for 1822 hours. After incubation, visible colonies were counted using a dissecting microscope to a maximum of 200 colonies at the recommendation of the manufacturer. Colonies that were morphologically consistent with Staphylococcus species by colony growth and Gram stain were further tested for coagulase using a BactiStaph rapid latex agglutination test (Remel, Lenexa, KS). If positive, these colonies were subcultured to sheep blood agar (Remel, Lenexa, KS) and BBL MRSA Chromagar (Becton Dickinson, Sparks, MD) and incubated for an additional 1824 hours. Characteristic growth on blood agar that also produced mauve‐colored colonies on chromagar was taken to indicate MRSA.
A separate set of 10 physicians donned newly laundered, short‐sleeved uniforms at 6:30 AM for culturing from the breast pocket and sleeve cuff of the dominant hand prior to and 2.5, 5, and 8 hours after they were donned by the participants (with culturing of each site done on separate days to avoid the effects of obtaining multiple cultures at the same site on the same day). These cultures were not assessed for MRSA.
At the time that consent was obtained, all participants completed an anonymous survey that assessed the frequency with which they normally washed or changed their white coats.
Sample Size
Based on the finding that 20% of our first 20 participants were colonized with MRSA, we determined that to find a 25% difference in the percentage of subjects colonized with MRSA in the 2 groups, with a power of 0.8 and P < 0.05 being significant (2‐sided Fisher's exact test), 50 subjects would be needed in each group.
Randomization
Randomization of potential participants occurred 1 day prior to the study using a computer‐generated table of random numbers. The principal investigator and a coinvestigator enrolled participants. Consent was obtained from those randomized to wear a newly laundered standard short‐sleeved uniform at the time of randomization so that they could don the uniforms when arriving at the hospital the following morning (at approximately 6:30 AM). Physicians in this group were also instructed not to wear their white coats at any time during the day they were wearing the uniforms. Physicians randomized to wear their own white coats were not notified or consented until the day of the study, a few hours prior to the time the cultures were obtained. This approach prevented them from either changing their white coats or washing them prior to the time the cultures were taken.
Because our study included both employees of the hospital and trainees, a number of protection measures were required. No information of any sort was collected about those who agreed or refused to participate in the study. In addition, the request to participate in the study did not come from the person's direct supervisor.
Statistical Methods
All data were collected and entered using Excel for Mac 2004 version 11.5.4. All analyses were performed using SAS Enterprise Guide 4.1 (SAS Institute, Inc., Cary, NC).
The Wilcoxon rank‐sum test and chi square analysis were used to seek differences in colony count and percentage of cultures with MRSA, respectively, in cultures obtained: (1) from the sleeve cuffs and pockets of the white coats compared with those from the sleeve cuffs and pockets of the uniforms, (2) from the sleeve cuffs of the white coats compared with those from the sleeve cuffs of the short‐sleeved uniforms, (3) from the mid‐biceps area of the sleeve sof the white coats compared with those from the sleeve cuffs of the uniforms, and (4) from the skin of the wrists of those wearing white coats compared with those wearing the uniforms. Bonferroni's correction for multiple comparisons was applied, with a P < 0.125 indicating significance.
Friedman's test and repeated‐measures logistic regression were used to seek differences in colony count or of the percentage of cultures with MRSA, respectively, on white coats or uniforms by site of culture on both garments. A P < 0.05 indicated significance for these analyses.
The Kruskal‐Wallis and chi‐square tests were utilized to test the effect of white coat wash frequency on colony count and MRSA contamination, respectively.
All data are presented as medians with 95% confidence intervals or proportions.
Results
Participant Flow
Fifty physicians were studied in each group, all of whom completed the survey. In general, more than 95% of potential participants approached agreed to participate in the study (Figure 1).
Recruitment
The first and last physicians were studied in August 2008 and November 2009, respectively. The trial ended when the specified number of participants (50 in each group) had been enrolled.
Data on Entry
No data were recorded from the participants at the time of randomization in compliance with institutional review board regulations pertaining to employment issues that could arise when studying members of the workforce.
Outcomes
No significant differences were found between the colony counts cultured from white coats (104 [80127]) versus newly laundered uniforms (142 [83213]), P = 0.61. No significant differences were found between the colony counts cultured from the sleeve cuffs of the white coats (58.5 [4866]) versus the uniforms (37 [2768]), P = 0.07, or between the colony counts cultured from the pockets of the white coats (45.5 [3254]) versus the uniforms (74.5 [4897], P = 0.040. Bonferroni corrections were used for multiple comparisons such that a P < 0.0125 was considered significant. Cultures from at least 1 site of 8 of 50 physicians (16%) wearing white coats and 10 of 50 physicians (20%) wearing short‐sleeved uniforms were positive for MRSA (P = .60).
Colony counts were greater in cultures obtained from the sleeve cuffs of the white coats compared with the pockets or mid‐biceps area (Table 1). For the uniforms, no difference in colony count in cultures from the pockets versus sleeve cuffs was observed. No difference was found when comparing the number of subjects with MRSA contamination of the 3 sites of the white coats or the 2 sites of the uniforms (Table 1).
| White Coat (n = 50) | P | Uniforms (n = 50) | P | |
|---|---|---|---|---|
| Colony count, median (95% CI) | ||||
| Sleeve cuff | 58.5 (4866) | < 0.0001 | 37.0 (2768) | 0.25 |
| 45.5 (3254) | 74.5 (4897) | |||
| Mid‐biceps area of sleeve | 25.5 (2029) | |||
| MRSA contamination, n (%) | ||||
| Sleeve cuff | 4 (8%) | 0.71 | 6 (12%) | 0.18 |
| 5 (10%) | 9 (18%) | |||
| Mid‐biceps area of sleeve | 3 (6%) |
No difference was observed with respect to colony count or the percentage of subjects positive for MRSA in cultures obtained from the mid‐biceps area of the white coats versus those from the cuffs of the short‐sleeved uniforms (Table 2).
| White Coat Mid‐Biceps (n = 50) | Uniform Sleeve Cuff (n = 50) | P | |
|---|---|---|---|
| Colony count, median (95% CI) | 25.5 (2029) | 37.0 (2768) | 0.07 |
| MRSA contamination, n (%) | 3 (6%) | 6 (12%) | 0.49 |
No difference was observed with respect to colony count or the percentage of subjects positive for MRSA in cultures obtained from the volar surface of the wrists of subjects wearing either of the 2 garments (Table 3).
| White Coat (n = 50) | Uniform (n = 50) | P | |
|---|---|---|---|
| Colony count, median (95% CI) | 23.5 (1740) | 40.5 (2859) | 0.09 |
| MRSA Contamination, n (% of subjects) | 3 (6%) | 5 (10%) | 0.72 |
The frequency with which physicians randomized to wearing their white coats admitted to washing or changing their coats varied markedly (Table 4). No significant differences were found with respect to total colony count (P = 0.81), colony count by site (data not shown), or percentage of physicians contaminated with MRSA (P = 0.22) as a function of washing or changing frequency (Table 4).
| White Coat Washing Frequency | Number of Subjects (%) | Total Colony Count (All Sites), Median (95% CI) | Number with MRSA Contamination, n (%) |
|---|---|---|---|
| Weekly | 15 (30%) | 124 (107229) | 1 (7%) |
| Every 2 weeks | 21 (42%) | 156 (90237) | 6 (29%) |
| Every 4 weeks | 8 (16%) | 89 (41206) | 0 (0%) |
| Every 8 weeks | 5 (10%) | 140 (58291) | 2 (40%) |
| Rarely | 1 (2%) | 150 | 0 (0%) |
Sequential culturing showed that the newly laundered uniforms were nearly sterile prior to putting them on. By 3 hours of wear, however, nearly 50% of the colonies counted at 8 hours were already present (Figure 2).
Harms
No adverse events occurred during the course of the study in either group.
Discussion
The important findings of this study are that, contrary to our hypotheses, at the end of an 8‐hour workday, no significant differences were found between the extent of bacterial or MRSA contamination of infrequently washed white coats compared with those of newly laundered uniforms, no difference was observed with respect to the extent of bacterial or MRSA contamination of the wrists of physicians wearing either of the 2 garments, and no association was apparent between the extent of bacterial or MRSA contamination and the frequency with which white coats were washed or changed. In addition, we also found that bacterial contamination of newly laundered uniforms occurred within hours of putting them on.
Interpretation
Numerous studies have demonstrated that white coats and uniforms worn by health care providers are frequently contaminated with bacteria, including both methicillin‐sensitive and ‐resistant Staphylococcus aureus and other pathogens.413 This contamination may come from nasal or perineal carriage of the health care provider, from the environment, and/or from patients who are colonized or infected.11, 15 Although many have suggested that patients can become contaminated from contact with health care providers' clothing and studies employing pulsed‐field gel electrophoresis and other techniques have suggested that cross‐infection can occur,10, 1618 others have not confirmed this contention,19, 20 and Lessing and colleagues16 concluded that transmission from staff to patients was a rare phenomenon. The systematic review reported to the Department of Health in England,3 the British Medical Association guidelines regarding dress codes for doctors,21 and the department's report on which the new clothing guidelines were based1 concluded there was no conclusive evidence indicating that work clothes posed a risk of spreading infection to patients. Despite this, the Working Group and the British Medical Association recommended that white coats should not be worn when providing patient care and that shirts and blouses should be short‐sleeved.1 Recent evidence‐based reviews concluded that there was insufficient evidence to justify this policy,3, 22 and our data indicate that the policy will not decrease bacterial or MRSA contamination of physicians' work clothes or skin.
The recommendation that long‐sleeved clothing should be avoided comes from studies indicating that cuffs of these garments are more heavily contaminated than other areas5, 8 and are more likely to come in contact with patients.1 Wong and colleagues5 reported that cuffs and lower front pockets had greater contamination than did the backs of white coats, but no difference was seen in colony count from cuffs compared with pockets. Loh and colleagues8 found greater bacterial contamination on the cuffs than on the backs of white coats, but their conclusion came from comparing the percentage of subjects with selected colony counts (ie, between 100 and 199 only), and the analysis did not adjust for repeated sampling of each participant. Apparently, colony counts from the cuffs were not different than those from the pockets. Callaghan7 found that contamination of nursing uniforms was equal at all sites. We found that sleeve cuffs of white coats had slightly but significantly more contamination with bacteria than either the pocket or the midsleeve areas, but interestingly, we found no difference in colony count from cultures taken from the skin at the wrists of the subjects wearing either garment. We found no difference in the extent of bacterial contamination by site in the subjects wearing short‐sleeved uniforms or in the percentage of subjects contaminated with MRSA by site of culture of either garment.
Contrary to our hypothesis, we found no association between the frequency with which white coats were changed or washed and the extent of bacterial contamination, despite the physicians having admitted to washing or changing their white coats infrequently (Table 4). Similar findings were reported by Loh and colleagues8 and by Treakle and colleagues.12
Our finding that contamination of clean uniforms happens rapidly is consistent with published data. Speers and colleagues4 found increasing contamination of nurses' aprons and dresses comparing samples obtained early in the day with those taken several hours later. Boyce and colleagues6 found that 65% of nursing uniforms were contaminated with MRSA after performing morning patient‐care activities on patients with MRSA wound or urine infections. Perry and colleagues9 found that 39% of uniforms that were laundered at home were contaminated with MRSA, vancomycin‐resistant enterococci, or Clostridium difficile at the beginning of the work shift, increasing to 54% by the end of a 24‐hour shift, and Babb and colleagues20 found that nearly 100% of nurses' gowns were contaminated within the first day of use (33% with Staphylococcus aureus). Dancer22 recently suggested that if staff were afforded clean coats every day, it is possible that concerns over potential contamination would be less of an issue. Our data suggest, however, that work clothes would have to be changed every few hours if the intent were to reduce bacterial contamination.
Limitations
Our study has a number of potential limitations. The RODAC imprint method only sampled a small area of both the white coats and the uniforms, and accordingly, the culture data might not accurately reflect the total degree of contamination. However, we cultured 3 areas on the white coats and 2 on the uniforms, including areas thought to be more heavily contaminated (sleeve cuffs of white coats). Although this area had greater colony counts, the variation in bacterial and MRSA contamination from all areas was small.
We did not culture the anterior nares to determine if the participants were colonized with MRSA. Normal health care workers have varying degrees of nasal colonization with MRSA, and this could account for some of the 16%‐20% MRSA contamination rate we observed. However, previous studies have shown that nasal colonization of healthcare workers only minimally contributes to uniform contamination.4
Although achieving good hand hygiene compliance has been a major focus at our hospital, we did not track the hand hygiene compliance of the physicians in either group. Accordingly, not finding reduced bacterial contamination in those wearing short‐sleeved uniforms could be explained if physicians in this group had systematically worse hand‐washing compliance than those randomized to wearing their own white coats. Our use of concurrent controls limits this possibility, as does that during the time of this study, hand hygiene compliance (assessed by monthly surreptitious observation) was approximately 90% throughout the hospital.
Despite the infrequent wash frequencies reported, the physicians' responses to the survey could have overestimated the true wash frequency as a result of the Hawthorne effect. The colony count and MRSA contamination rates observed, however, suggest that even if this occurred, it would not have altered our conclusion that bacterial contamination was not associated with wash frequency.
Generalizability
Because data were collected from a single, university‐affiliated public teaching hospital from hospitalists and residents working on the internal medicine service, the results might not be generalizable to other types of institutions, other personnel, or other services.
In conclusion, bacterial contamination of work clothes occurs within the first few hours after donning them. By the end of an 8‐hour work day, we found no data supporting the contention that long‐sleeved white coats were more heavily contaminated than were short‐sleeved uniforms. Our data do not support discarding white coats for uniforms that are changed on a daily basis or for requiring health care workers to avoid long‐sleeved garments.
Acknowledgements
The authors thank Henry Fonseca and his team for providing our physician uniforms. They also thank the Denver Health Department of Medicine Small Grants program for supporting this study.
In September 2007, the British Department of Health developed guidelines for health care workers regarding uniforms and work wear that banned the traditional white coat and other long‐sleeved garments in an attempt to decrease nosocomial bacterial transmission.1 Similar policies have recently been adopted in Scotland.2 Interestingly, the National Health Service report acknowledged that evidence was lacking that would support that white coats and long‐sleeved garments caused nosocomial infection.1, 3 Although many studies have documented that health care work clothes are contaminated with bacteria, including methicillin‐resistant Staphylococcal aureus (MRSA) and other pathogenic species,413 none have determined whether avoiding white coats and switching to short‐sleeved garments decreases bacterial contamination.
We performed a prospective, randomized, controlled trial designed to compare the extent of bacterial contamination of physicians' white coats with that of newly laundered, standardized short‐sleeved uniforms. Our hypotheses were that infrequently cleaned white coats would have greater bacterial contamination than uniforms, that the extent of contamination would be inversely related to the frequency with which the coats were washed, and that the increased contamination of the cuffs of the white coats would result in increased contamination of the skin of the wrists. Our results led us also to assess the rate at which bacterial contamination of short‐sleeved uniforms occurs during the workday.
Methods
The study was conducted at Denver Health, a university‐affiliated public safety‐net hospital and was approved by the Colorado Multiple Institutional Review Board.
Trial Design
The study was a prospective, randomized, controlled trial. No protocol changes occurred during the study.
Participants
Participants included residents and hospitalists directly caring for patients on internal medicine units between August 1, 2008 and November 15, 2009.
Intervention
Subjects wore either a standard, newly laundered, short‐sleeved uniform or continued to wear their own white coats.
Outcomes
The primary end point was the percentage of subjects contaminated with MRSA. Cultures were collected using a standardized RODAC imprint method14 with BBL RODAC plates containing trypticase soy agar with lecithin and polysorbate 80 (Becton Dickinson, Sparks, MD) 8 hours after the physicians started their work day. All physicians had cultures obtained from the breast pocket and sleeve cuff (long‐sleeved for the white coats, short‐sleeved for the uniforms) and from the skin of the volar surface of the wrist of their dominant hand. Those wearing white coats also had cultures obtained from the mid‐biceps level of the sleeve of the dominant hand, as this location closely approximated the location of the cuffs of the short‐sleeved uniforms.
Cultures were incubated in ambient air at 35C‐37C for 1822 hours. After incubation, visible colonies were counted using a dissecting microscope to a maximum of 200 colonies at the recommendation of the manufacturer. Colonies that were morphologically consistent with Staphylococcus species by colony growth and Gram stain were further tested for coagulase using a BactiStaph rapid latex agglutination test (Remel, Lenexa, KS). If positive, these colonies were subcultured to sheep blood agar (Remel, Lenexa, KS) and BBL MRSA Chromagar (Becton Dickinson, Sparks, MD) and incubated for an additional 1824 hours. Characteristic growth on blood agar that also produced mauve‐colored colonies on chromagar was taken to indicate MRSA.
A separate set of 10 physicians donned newly laundered, short‐sleeved uniforms at 6:30 AM for culturing from the breast pocket and sleeve cuff of the dominant hand prior to and 2.5, 5, and 8 hours after they were donned by the participants (with culturing of each site done on separate days to avoid the effects of obtaining multiple cultures at the same site on the same day). These cultures were not assessed for MRSA.
At the time that consent was obtained, all participants completed an anonymous survey that assessed the frequency with which they normally washed or changed their white coats.
Sample Size
Based on the finding that 20% of our first 20 participants were colonized with MRSA, we determined that to find a 25% difference in the percentage of subjects colonized with MRSA in the 2 groups, with a power of 0.8 and P < 0.05 being significant (2‐sided Fisher's exact test), 50 subjects would be needed in each group.
Randomization
Randomization of potential participants occurred 1 day prior to the study using a computer‐generated table of random numbers. The principal investigator and a coinvestigator enrolled participants. Consent was obtained from those randomized to wear a newly laundered standard short‐sleeved uniform at the time of randomization so that they could don the uniforms when arriving at the hospital the following morning (at approximately 6:30 AM). Physicians in this group were also instructed not to wear their white coats at any time during the day they were wearing the uniforms. Physicians randomized to wear their own white coats were not notified or consented until the day of the study, a few hours prior to the time the cultures were obtained. This approach prevented them from either changing their white coats or washing them prior to the time the cultures were taken.
Because our study included both employees of the hospital and trainees, a number of protection measures were required. No information of any sort was collected about those who agreed or refused to participate in the study. In addition, the request to participate in the study did not come from the person's direct supervisor.
Statistical Methods
All data were collected and entered using Excel for Mac 2004 version 11.5.4. All analyses were performed using SAS Enterprise Guide 4.1 (SAS Institute, Inc., Cary, NC).
The Wilcoxon rank‐sum test and chi square analysis were used to seek differences in colony count and percentage of cultures with MRSA, respectively, in cultures obtained: (1) from the sleeve cuffs and pockets of the white coats compared with those from the sleeve cuffs and pockets of the uniforms, (2) from the sleeve cuffs of the white coats compared with those from the sleeve cuffs of the short‐sleeved uniforms, (3) from the mid‐biceps area of the sleeve sof the white coats compared with those from the sleeve cuffs of the uniforms, and (4) from the skin of the wrists of those wearing white coats compared with those wearing the uniforms. Bonferroni's correction for multiple comparisons was applied, with a P < 0.125 indicating significance.
Friedman's test and repeated‐measures logistic regression were used to seek differences in colony count or of the percentage of cultures with MRSA, respectively, on white coats or uniforms by site of culture on both garments. A P < 0.05 indicated significance for these analyses.
The Kruskal‐Wallis and chi‐square tests were utilized to test the effect of white coat wash frequency on colony count and MRSA contamination, respectively.
All data are presented as medians with 95% confidence intervals or proportions.
Results
Participant Flow
Fifty physicians were studied in each group, all of whom completed the survey. In general, more than 95% of potential participants approached agreed to participate in the study (Figure 1).
Recruitment
The first and last physicians were studied in August 2008 and November 2009, respectively. The trial ended when the specified number of participants (50 in each group) had been enrolled.
Data on Entry
No data were recorded from the participants at the time of randomization in compliance with institutional review board regulations pertaining to employment issues that could arise when studying members of the workforce.
Outcomes
No significant differences were found between the colony counts cultured from white coats (104 [80127]) versus newly laundered uniforms (142 [83213]), P = 0.61. No significant differences were found between the colony counts cultured from the sleeve cuffs of the white coats (58.5 [4866]) versus the uniforms (37 [2768]), P = 0.07, or between the colony counts cultured from the pockets of the white coats (45.5 [3254]) versus the uniforms (74.5 [4897], P = 0.040. Bonferroni corrections were used for multiple comparisons such that a P < 0.0125 was considered significant. Cultures from at least 1 site of 8 of 50 physicians (16%) wearing white coats and 10 of 50 physicians (20%) wearing short‐sleeved uniforms were positive for MRSA (P = .60).
Colony counts were greater in cultures obtained from the sleeve cuffs of the white coats compared with the pockets or mid‐biceps area (Table 1). For the uniforms, no difference in colony count in cultures from the pockets versus sleeve cuffs was observed. No difference was found when comparing the number of subjects with MRSA contamination of the 3 sites of the white coats or the 2 sites of the uniforms (Table 1).
| White Coat (n = 50) | P | Uniforms (n = 50) | P | |
|---|---|---|---|---|
| Colony count, median (95% CI) | ||||
| Sleeve cuff | 58.5 (4866) | < 0.0001 | 37.0 (2768) | 0.25 |
| 45.5 (3254) | 74.5 (4897) | |||
| Mid‐biceps area of sleeve | 25.5 (2029) | |||
| MRSA contamination, n (%) | ||||
| Sleeve cuff | 4 (8%) | 0.71 | 6 (12%) | 0.18 |
| 5 (10%) | 9 (18%) | |||
| Mid‐biceps area of sleeve | 3 (6%) |
No difference was observed with respect to colony count or the percentage of subjects positive for MRSA in cultures obtained from the mid‐biceps area of the white coats versus those from the cuffs of the short‐sleeved uniforms (Table 2).
| White Coat Mid‐Biceps (n = 50) | Uniform Sleeve Cuff (n = 50) | P | |
|---|---|---|---|
| Colony count, median (95% CI) | 25.5 (2029) | 37.0 (2768) | 0.07 |
| MRSA contamination, n (%) | 3 (6%) | 6 (12%) | 0.49 |
No difference was observed with respect to colony count or the percentage of subjects positive for MRSA in cultures obtained from the volar surface of the wrists of subjects wearing either of the 2 garments (Table 3).
| White Coat (n = 50) | Uniform (n = 50) | P | |
|---|---|---|---|
| Colony count, median (95% CI) | 23.5 (1740) | 40.5 (2859) | 0.09 |
| MRSA Contamination, n (% of subjects) | 3 (6%) | 5 (10%) | 0.72 |
The frequency with which physicians randomized to wearing their white coats admitted to washing or changing their coats varied markedly (Table 4). No significant differences were found with respect to total colony count (P = 0.81), colony count by site (data not shown), or percentage of physicians contaminated with MRSA (P = 0.22) as a function of washing or changing frequency (Table 4).
| White Coat Washing Frequency | Number of Subjects (%) | Total Colony Count (All Sites), Median (95% CI) | Number with MRSA Contamination, n (%) |
|---|---|---|---|
| Weekly | 15 (30%) | 124 (107229) | 1 (7%) |
| Every 2 weeks | 21 (42%) | 156 (90237) | 6 (29%) |
| Every 4 weeks | 8 (16%) | 89 (41206) | 0 (0%) |
| Every 8 weeks | 5 (10%) | 140 (58291) | 2 (40%) |
| Rarely | 1 (2%) | 150 | 0 (0%) |
Sequential culturing showed that the newly laundered uniforms were nearly sterile prior to putting them on. By 3 hours of wear, however, nearly 50% of the colonies counted at 8 hours were already present (Figure 2).
Harms
No adverse events occurred during the course of the study in either group.
Discussion
The important findings of this study are that, contrary to our hypotheses, at the end of an 8‐hour workday, no significant differences were found between the extent of bacterial or MRSA contamination of infrequently washed white coats compared with those of newly laundered uniforms, no difference was observed with respect to the extent of bacterial or MRSA contamination of the wrists of physicians wearing either of the 2 garments, and no association was apparent between the extent of bacterial or MRSA contamination and the frequency with which white coats were washed or changed. In addition, we also found that bacterial contamination of newly laundered uniforms occurred within hours of putting them on.
Interpretation
Numerous studies have demonstrated that white coats and uniforms worn by health care providers are frequently contaminated with bacteria, including both methicillin‐sensitive and ‐resistant Staphylococcus aureus and other pathogens.413 This contamination may come from nasal or perineal carriage of the health care provider, from the environment, and/or from patients who are colonized or infected.11, 15 Although many have suggested that patients can become contaminated from contact with health care providers' clothing and studies employing pulsed‐field gel electrophoresis and other techniques have suggested that cross‐infection can occur,10, 1618 others have not confirmed this contention,19, 20 and Lessing and colleagues16 concluded that transmission from staff to patients was a rare phenomenon. The systematic review reported to the Department of Health in England,3 the British Medical Association guidelines regarding dress codes for doctors,21 and the department's report on which the new clothing guidelines were based1 concluded there was no conclusive evidence indicating that work clothes posed a risk of spreading infection to patients. Despite this, the Working Group and the British Medical Association recommended that white coats should not be worn when providing patient care and that shirts and blouses should be short‐sleeved.1 Recent evidence‐based reviews concluded that there was insufficient evidence to justify this policy,3, 22 and our data indicate that the policy will not decrease bacterial or MRSA contamination of physicians' work clothes or skin.
The recommendation that long‐sleeved clothing should be avoided comes from studies indicating that cuffs of these garments are more heavily contaminated than other areas5, 8 and are more likely to come in contact with patients.1 Wong and colleagues5 reported that cuffs and lower front pockets had greater contamination than did the backs of white coats, but no difference was seen in colony count from cuffs compared with pockets. Loh and colleagues8 found greater bacterial contamination on the cuffs than on the backs of white coats, but their conclusion came from comparing the percentage of subjects with selected colony counts (ie, between 100 and 199 only), and the analysis did not adjust for repeated sampling of each participant. Apparently, colony counts from the cuffs were not different than those from the pockets. Callaghan7 found that contamination of nursing uniforms was equal at all sites. We found that sleeve cuffs of white coats had slightly but significantly more contamination with bacteria than either the pocket or the midsleeve areas, but interestingly, we found no difference in colony count from cultures taken from the skin at the wrists of the subjects wearing either garment. We found no difference in the extent of bacterial contamination by site in the subjects wearing short‐sleeved uniforms or in the percentage of subjects contaminated with MRSA by site of culture of either garment.
Contrary to our hypothesis, we found no association between the frequency with which white coats were changed or washed and the extent of bacterial contamination, despite the physicians having admitted to washing or changing their white coats infrequently (Table 4). Similar findings were reported by Loh and colleagues8 and by Treakle and colleagues.12
Our finding that contamination of clean uniforms happens rapidly is consistent with published data. Speers and colleagues4 found increasing contamination of nurses' aprons and dresses comparing samples obtained early in the day with those taken several hours later. Boyce and colleagues6 found that 65% of nursing uniforms were contaminated with MRSA after performing morning patient‐care activities on patients with MRSA wound or urine infections. Perry and colleagues9 found that 39% of uniforms that were laundered at home were contaminated with MRSA, vancomycin‐resistant enterococci, or Clostridium difficile at the beginning of the work shift, increasing to 54% by the end of a 24‐hour shift, and Babb and colleagues20 found that nearly 100% of nurses' gowns were contaminated within the first day of use (33% with Staphylococcus aureus). Dancer22 recently suggested that if staff were afforded clean coats every day, it is possible that concerns over potential contamination would be less of an issue. Our data suggest, however, that work clothes would have to be changed every few hours if the intent were to reduce bacterial contamination.
Limitations
Our study has a number of potential limitations. The RODAC imprint method only sampled a small area of both the white coats and the uniforms, and accordingly, the culture data might not accurately reflect the total degree of contamination. However, we cultured 3 areas on the white coats and 2 on the uniforms, including areas thought to be more heavily contaminated (sleeve cuffs of white coats). Although this area had greater colony counts, the variation in bacterial and MRSA contamination from all areas was small.
We did not culture the anterior nares to determine if the participants were colonized with MRSA. Normal health care workers have varying degrees of nasal colonization with MRSA, and this could account for some of the 16%‐20% MRSA contamination rate we observed. However, previous studies have shown that nasal colonization of healthcare workers only minimally contributes to uniform contamination.4
Although achieving good hand hygiene compliance has been a major focus at our hospital, we did not track the hand hygiene compliance of the physicians in either group. Accordingly, not finding reduced bacterial contamination in those wearing short‐sleeved uniforms could be explained if physicians in this group had systematically worse hand‐washing compliance than those randomized to wearing their own white coats. Our use of concurrent controls limits this possibility, as does that during the time of this study, hand hygiene compliance (assessed by monthly surreptitious observation) was approximately 90% throughout the hospital.
Despite the infrequent wash frequencies reported, the physicians' responses to the survey could have overestimated the true wash frequency as a result of the Hawthorne effect. The colony count and MRSA contamination rates observed, however, suggest that even if this occurred, it would not have altered our conclusion that bacterial contamination was not associated with wash frequency.
Generalizability
Because data were collected from a single, university‐affiliated public teaching hospital from hospitalists and residents working on the internal medicine service, the results might not be generalizable to other types of institutions, other personnel, or other services.
In conclusion, bacterial contamination of work clothes occurs within the first few hours after donning them. By the end of an 8‐hour work day, we found no data supporting the contention that long‐sleeved white coats were more heavily contaminated than were short‐sleeved uniforms. Our data do not support discarding white coats for uniforms that are changed on a daily basis or for requiring health care workers to avoid long‐sleeved garments.
Acknowledgements
The authors thank Henry Fonseca and his team for providing our physician uniforms. They also thank the Denver Health Department of Medicine Small Grants program for supporting this study.
- Department of Health. Uniforms and workwear: an evidence base for developing local policy. National Health Service, September 17, 2007. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicationspolicyandguidance/DH_078433. Accessed January 29,2010.
- Scottish Government Health Directorates. NHS Scotland Dress Code. Available at: http://www.sehd.scot.nhs.uk/mels/CEL2008_53.pdf. Accessed February 10,2010.
- ,,,.Uniform: an evidence review of the microbiological significance of uniforms and uniform policy in the prevention and control of healthcare‐associated infections. Report to the Department of Health (England).J Hosp Infect.2007;66:301–307.
- ,,,.Contamination of nurses' uniforms with Staphylococcus aureus.Lancet.1969;2:233–235.
- ,,.Microbial flora on doctors' white coats.Brit Med J.1991;303:1602–1604.
- ,,,.Environmental contamination due to methicillin‐resistant Staphylococcus aureus: possible infection control implications.Infect Control Hosp Epidemiol.1997;18:622–627.
- ,Bacterial contamination of nurses' uniforms: a study.Nursing Stand.1998;13:37–42.
- ,,.Bacterial flora on the white coats of medical students.J Hosp Infection.2000;45:65–68.
- ,,.Bacterial contamination of uniforms.J Hosp Infect.2001;48:238–241.
- ,,, et al.Significance of methicillin‐resistant Staphylococcus aureus (MRSA) survey in a university teaching hospital.J Infec Chemother.2003;9:172–177.
- ,,, et al.Detection of methicillin‐resistant Staphylococcus aureus and vancomycin‐resistant enterococci on the gowns and gloves of healthcare workers.Infect Control Hosp Epidemiol2008;29 (7):583–9.
- ,,,,,.Bacterial contamination of health care workers' white coats.Am J Infect Control.2009;37:101–105.
- ,,,,,.Meticillin‐resistant Staphylococcus aureus contamination of healthcare workers' uniforms in long‐term care facilities.J Hosp Infect.2009;71:170–175.
- ,,,,.Comparison of the Rodac imprint method to selective enrichment broth for recovery of vancomycin‐resistant enterococci and drug‐resistant Enterobacteriaceae from environmental surfaces.J Clin Microbiol.2000;38:4646–4648.
- ,,.Effect of clothing on dispersal of Staphylococcus aureus by males and females.Lancet.1974;2:1131–1133.
- ,,.When should healthcare workers be screened for methicillin‐resistant Staphylococcus aureus?J Hosp Infect.1996;34:205–210.
- ,,.Methicillin‐resistant Staphylococcus aureus transmission: the possible importance of unrecognized health care worker carriage.Am J Infect Control.2008;36:93–97.
- ,,, et al.Methicillin‐resistant Staphylococcus aureus carriage, infection and transmission in dialysis patients, healthcare workers and their family members.Nephrol Dial Transplant.2008;23:1659–1665.
- ,,.Are active microbiological surveillance and subsequent isolation needed to prevent the spread of methicillin‐resistant Staphylococcus aureus.Clin Infect Dis.2005;40:405–409.
- ,,.Contamination of protective clothing and nurses' uniforms in an isolation ward.J Hosp Infect.1983;4:149–157.
- British Medical Association. Uniform and dress code for doctors. December 6, 2007. Available at: http://www.bma.org.uk/employmentandcontracts/working_arrangements/CCSCdresscode051207.jsp. Accessed February 9,2010.
- .Pants, policies and paranoia.J Hosp Infect.2010;74:10–15.
- Department of Health. Uniforms and workwear: an evidence base for developing local policy. National Health Service, September 17, 2007. Available at: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicationspolicyandguidance/DH_078433. Accessed January 29,2010.
- Scottish Government Health Directorates. NHS Scotland Dress Code. Available at: http://www.sehd.scot.nhs.uk/mels/CEL2008_53.pdf. Accessed February 10,2010.
- ,,,.Uniform: an evidence review of the microbiological significance of uniforms and uniform policy in the prevention and control of healthcare‐associated infections. Report to the Department of Health (England).J Hosp Infect.2007;66:301–307.
- ,,,.Contamination of nurses' uniforms with Staphylococcus aureus.Lancet.1969;2:233–235.
- ,,.Microbial flora on doctors' white coats.Brit Med J.1991;303:1602–1604.
- ,,,.Environmental contamination due to methicillin‐resistant Staphylococcus aureus: possible infection control implications.Infect Control Hosp Epidemiol.1997;18:622–627.
- ,Bacterial contamination of nurses' uniforms: a study.Nursing Stand.1998;13:37–42.
- ,,.Bacterial flora on the white coats of medical students.J Hosp Infection.2000;45:65–68.
- ,,.Bacterial contamination of uniforms.J Hosp Infect.2001;48:238–241.
- ,,, et al.Significance of methicillin‐resistant Staphylococcus aureus (MRSA) survey in a university teaching hospital.J Infec Chemother.2003;9:172–177.
- ,,, et al.Detection of methicillin‐resistant Staphylococcus aureus and vancomycin‐resistant enterococci on the gowns and gloves of healthcare workers.Infect Control Hosp Epidemiol2008;29 (7):583–9.
- ,,,,,.Bacterial contamination of health care workers' white coats.Am J Infect Control.2009;37:101–105.
- ,,,,,.Meticillin‐resistant Staphylococcus aureus contamination of healthcare workers' uniforms in long‐term care facilities.J Hosp Infect.2009;71:170–175.
- ,,,,.Comparison of the Rodac imprint method to selective enrichment broth for recovery of vancomycin‐resistant enterococci and drug‐resistant Enterobacteriaceae from environmental surfaces.J Clin Microbiol.2000;38:4646–4648.
- ,,.Effect of clothing on dispersal of Staphylococcus aureus by males and females.Lancet.1974;2:1131–1133.
- ,,.When should healthcare workers be screened for methicillin‐resistant Staphylococcus aureus?J Hosp Infect.1996;34:205–210.
- ,,.Methicillin‐resistant Staphylococcus aureus transmission: the possible importance of unrecognized health care worker carriage.Am J Infect Control.2008;36:93–97.
- ,,, et al.Methicillin‐resistant Staphylococcus aureus carriage, infection and transmission in dialysis patients, healthcare workers and their family members.Nephrol Dial Transplant.2008;23:1659–1665.
- ,,.Are active microbiological surveillance and subsequent isolation needed to prevent the spread of methicillin‐resistant Staphylococcus aureus.Clin Infect Dis.2005;40:405–409.
- ,,.Contamination of protective clothing and nurses' uniforms in an isolation ward.J Hosp Infect.1983;4:149–157.
- British Medical Association. Uniform and dress code for doctors. December 6, 2007. Available at: http://www.bma.org.uk/employmentandcontracts/working_arrangements/CCSCdresscode051207.jsp. Accessed February 9,2010.
- .Pants, policies and paranoia.J Hosp Infect.2010;74:10–15.
Copyright © 2011 Society of Hospital Medicine
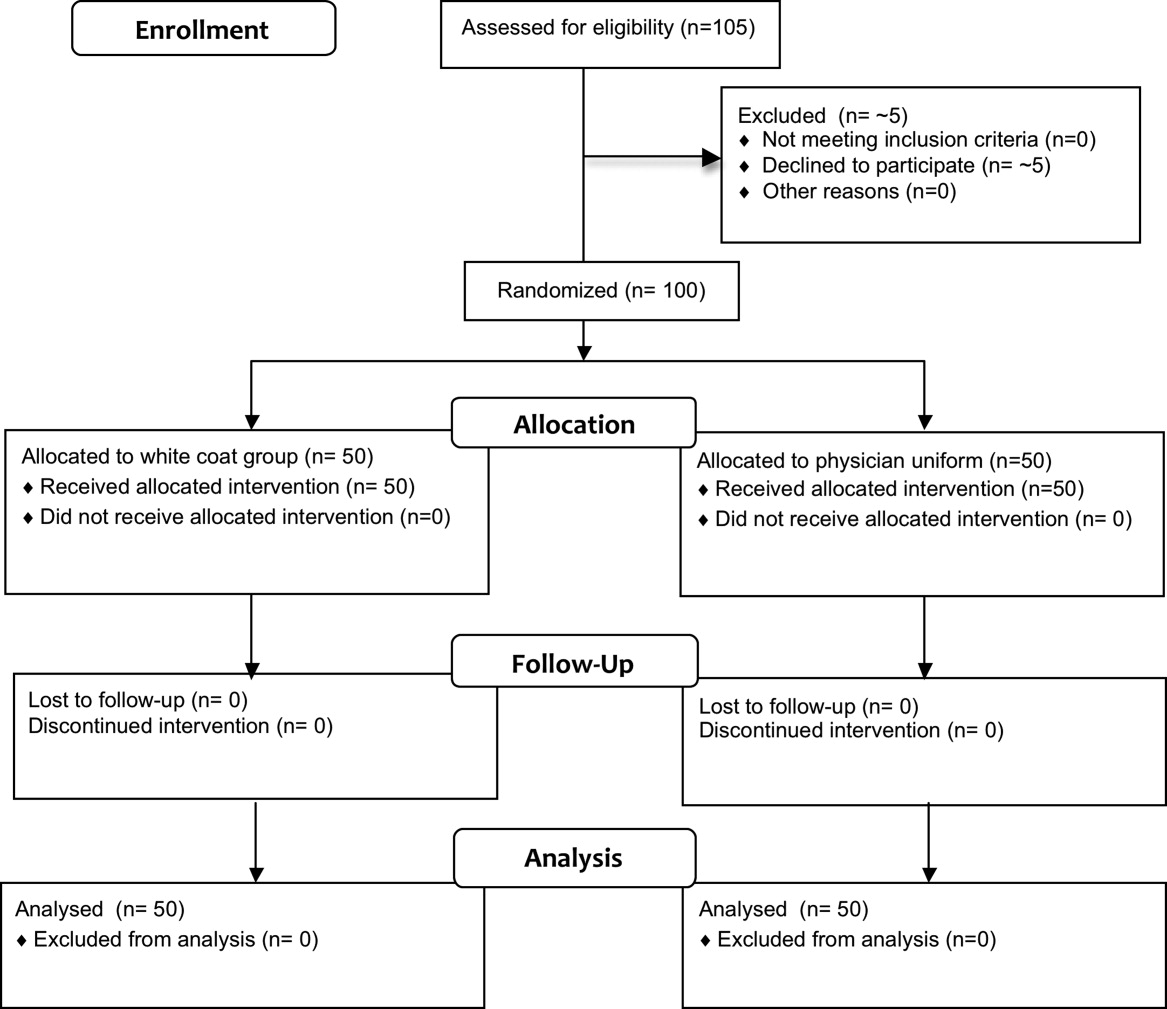
Comparing Collaborative and Toolkit QI
Continuous quality improvement (CQI) methodologies provide a framework for initiating and sustaining improvements in complex systems.1 By definition, CQI engages frontline staff in iterative problem solving using plandostudyact cycles of learning, with decision‐making based on real‐time process measurements.2 The Institute for Healthcare Improvement (IHI) has sponsored Breakthrough Series Collaboratives since 1996 to accelerate the uptake and impact of quality improvement (QI).3, 4 These collaboratives are typically guided by evidence‐based clinical practice guidelines, incorporate change methodologies, and rely on clinical and process improvement subject matter experts. Through the collaborative network, teams share knowledge and ideas about effective and ineffective interventions as well as strategies for overcoming barriers. The collaborative curriculum includes CQI methodology, multidisciplinary teamwork, leadership support, and tools for measurement. Participants are typically required to invest resources and send teams to face‐to‐face goal‐oriented meetings. It is costly for a large healthcare organization to incorporate travel to a learning session conference into its collaborative model. Thus, we attempted virtual learning sessions that make use of webcasts, a Web site, and teleconference calls for tools and networking.5
A recent derivative of collaboratives has been deployment of toolkits for QI. Intuition suggests that such toolkits may help to enable change, and thus some agencies advocate the simpler approach of disseminating toolkits as a change strategy.6 Toolkit dissemination is a passive approach in contrast to collaborative participation, and its effectiveness has not been critically examined in evidence‐based literature.
We sought to compare the virtual collaborative model with the toolkit model for improving care. Recommendations and guidelines for central lineassociated bloodstream infection (CLABSI) and ventilator‐associated pneumonia (VAP) prevention have not been implemented reliably, resulting in unnecessary intensive care unit (ICU) morbidity and mortality and fostering a national call for improvement.7 Our aim was to compare the effectiveness of the virtual collaborative and toolkit approaches on preventing CLABSI and VAP in the ICU.
Methods
This cluster randomized trial included medical centers within the Hospital Corporation of America (HCA), a network of hospitals located primarily in the southern United States. To minimize contamination bias between study groups within the same facility, the unit of randomization was the hospital and implementation was at the level of the ICU. The project received approval from the Vanderbilt University Institutional Review Board.
Leaders of all medical centers with at least 1 adult or pediatric ICU received an invitation from HCA leadership to participate in a QI initiative. Facility clinicians and managers completed baseline surveys (shown in the Supporting Information) on hospital characteristics, types of ICUs, patient safety climate, and QI resources between July and November 2005. Hospital‐level data were extracted from the enterprise‐wide data warehouse. Hospitals willing to participate were matched on geographic location and ICU volume and then randomized into either the Virtual Collaborative (n = 31) or Toolkit (n = 30) groups in December 20058; 1 of the hospitals was sold, yielding 29 hospitals in the Toolkit (n = 29) group. The study lasted 18 months from January 2006 through September 2007, with health careassociated infection data collected through December 2007, and follow‐up data collection through April 2008.
The QI initiative included educational opportunities, evidence‐based clinical prevention interventions, and processes and tools to implement and measure the impact of these interventions. Participants in both groups were offered interactive Web seminars during the study period; 5 of these seminars were on clinical subject matter, and 5 seminars were on patient safety, charting use of statistical process control and QI methods. The interventions were evidence‐based care bundles.9 The key interventions for preventing CLABSI were routine hand hygiene, use of chlorhexidine skin antisepsis, maximal barrier precautions during catheter insertion, catheter site and care, and avoidance of routine replacement of catheters. The key interventions to prevent VAP were routine elevation of head of the bed, regular oral care, daily sedation vacations, daily assessment of readiness to extubate, secretion cleaning, peptic ulcer disease prophylaxis, and deep vein thrombosis prophylaxis.
Toolkit Group
Hospitals randomized to this arm received a toolkit during study month 1 containing a set of evidence‐based guidelines and fact sheets for preventing CLABSI and VAP, a review of QI and teamwork methods, standardized data collection tools, and standardized charting tools. The nurse and quality managers for the Toolkit ICUs were provided ad libitum access to the HCA intranet toolkit Web site containing all of the educational seminars, clinical tools, and QI tools. Otherwise, ICUs in this group were on their own to initiate and implement a local hospital QI initiative to prevent CLABSI and VAP.
Virtual Collaborative Group
In addition to the materials and Web site support described above, facility leaders and managers in this Virtual Collaborative group agreed to participate in a virtual collaborative to develop processes to more reliably implement evidence‐based interventions to prevent CLABSI and VAP. The collaboration differed from the Breakthrough Series model3, 4 in that teams did not come together for face‐to‐face educational and planning sessions but instead attended Web seminars and teleconferences for reporting back to the larger group.5 Teams were supported through monthly educational and troubleshooting conference calls, individual coaching coordinated by the HCA corporate office of quality, safety, and performance improvement, and an e‐mail listserv designed to stimulate interaction among teams.
Clinical Outcome Measures
Although most participating hospitals defined CLABSI and VAP using the Centers for Disease Control and Prevention definitions, data collection and surveillance methods varied across hospitals.10 Education was provided to standardize outcome measurement. A data registry Web application was created as a new tool for infection control data entry, and healthcare‐associated infection data reporting by the infection control personnel was mandated starting the first quarter of 2006. To verify electronic data and correct missing information, the infection control personnel were requested to complete a retrospective data collection sheet providing quarterly reports from January 2005 through December 2007 on ICU infection events as well as total catheter days and ventilator days to allow calculation of event rates. Outcome measures of CLABSI and VAP were at the level of the hospital.
Follow‐Up
The HCA e‐mail distribution and collection routine was employed for the follow‐up survey of ICU nurse and quality managers for all participating medical centers from January 2008 through April 2008. A single survey (shown in the Supporting Information) was requested from each participating ICU. The ICU‐level surveys included questions about the implementation of the CLABSI and VAP process interventions, access of tools, participation in Web seminars, and use of QI strategies.11, 12 The postintervention survey also assessed the character and amount of implementation and teamwork activity expended.
Median CLABSI and VAP rates for a 3‐month baseline and quarterly postintervention periods were compared between the 2 study groups. The CLABSI and VAP infection rates were also analyzed using hierarchical negative binomial regression models to model infection rate changes over time (time in months and group by time interaction effects) and account for clustering of ICUs within hospitals and adjusting for baseline covariates. Baseline and process variables at the hospital and ICU level were compared using chi‐square tests and t tests according to the type of measurement. Time‐to‐event analyses were conducted to compare the groups on time to initiation of a care process. All analyses were conducted using the (R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, 2010).
The power of the study was calculated a priori with a 1‐tailed alpha of 0.05 and group size of 30. We hypothesized a 50% decrease in hospital‐associated infection rates for the Collaborative group vs. a 10% to 15% decrease for the Toolkit group. The calculations yielded power ranging from a low of 82% to a high of 91% for testing group differences.13
Results
Participating facilities included rural (11%), inner city (28%), and suburban (61%) medical centers. The 60 participating sites did not differ in administrative variables from the 113 nonparticipating HCA sites (results not shown). The median hospital size was 177 beds and the median ICU size was 16 beds. The hospitals did not differ between study groups (Table 1). At baseline, 45% of the facilities reported having a CLABSI program and 62% a VAP program.
| Hospital Factors at Baseline | Virtual Collaborative | Toolkit | P Value |
|---|---|---|---|
| |||
| Number of hospitals | 31 | 29* | |
| ICU annual patient volume, median (IQR) | 568 (294, 904) | 578 (244, 1077) | 0.93 |
| ICU patient length of stay days, median (IQR) | 3882 (1758, 5718) | 4228 (1645, 6725) | 0.95 |
| ICU mortality rate, percent (SD) | 5.7% (3.1%) | 7.1% (3.6%) | 0.13 |
| Medicare/Medicaid, percent (SD) | 68.6% (9.5%) | 68.5% (10.1%) | 0.95 |
| Percent admitted to ICU from the Emergency Department (SD) | 71% (15%) | 67% (20%) | 0.27 |
| Percent female (SD) | 49.7% (5.7%) | 50.3% (7.7%) | 0.79 |
| Medicare case‐mix weight, mean (SD) | 1221 (1007) | 1295 (1110) | 0.82 |
| Percent hospitalist ICU management | 47% | 40% | 0.61 |
The baseline and quarterly median and pooled infection rates for the Toolkit and Collaboration groups are shown in Table 2 for CLABSI and in Table 3 for VAP. There were no significant differences in the baseline rates for either CLABSI (P = 0.24) or VAP (P = 0.72) between the Collaborative and Toolkit groups. There was no significant change for either CLABSI or VAP outcomes at either 12 or 18 months of follow‐up. The median bloodstream infection rate for all participating hospitals was 2.27 at baseline, 1.18 at 12 months (P = 0.13), and 2.23 per 1000 catheter days 18 months later (P = 0.95). The median VAP rate for participating hospitals was 2.90 at baseline, 2.67 at 12 months (P = 0.44), and 2.52 per 1000 ventilator days 18 months later (P = 0.84). The hierarchical regression analysis found that neither the Collaborative nor Toolkit groups improved CLABSI (P = 0.75 and P = 0.83, respectively) or VAP (P = 0.61 and P = 0.37, respectively) rates over time, and there was no differential performance between the 2 groups for either outcome (bloodstream infection, P = 0.71; VAP, P = 0.80).
| Overall | Virtual Collaborative | Toolkit | ||||
|---|---|---|---|---|---|---|
| N = 59 Hospitals | N = 30 Hospitals | N = 29 Hospitals | ||||
| Study Period | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals |
| ||||||
| Baseline | 2.27 (0.00‐3.98) | 2.42 | 1.84 (0.00‐3.83) | 1.67 | 2.42 (0.65‐6.80) | 3.05 |
| 3 Month | 2.27 (1.30‐4.69) | 2.61 | 2.24 (0.54‐4.69) | 2.34 | 2.47 (1.48‐5.35) | 2.85 |
| 6 Month | 2.37 (0.00‐4.29) | 2.73 | 2.28 (0.00‐3.73) | 2.35 | 2.54 (0.00‐4.98) | 3.09 |
| 9 Month | 1.66 (0.00‐3.84) | 2.45 | 1.76 (0.00‐3.74) | 2.28 | 1.23 (0.00‐3.93) | 2.59 |
| 12 Month | 1.18 (0.00‐3.10) | 2.17 | 1.18 (0.00‐2.71) | 1.72 | 1.17 (0.00‐3.61) | 2.58 |
| 15 Month | 1.93 (0.00‐4.25) | 2.29 | 2.04 (0.00‐4.91) | 2.53 | 1.77 (0.00‐3.30) | 2.08 |
| 18 Month | 2.23 (0.00‐4.97) | 2.73 | 2.76 (0.00‐4.67) | 2.75 | 1.16 (0.00‐5.46) | 2.72 |
| Study Period | Overall | Virtual Collaborative | Toolkit | |||
|---|---|---|---|---|---|---|
| N = 59 Hospitals | N = 30 Hospitals | N = 29 Hospitals | ||||
| Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | |
| ||||||
| Baseline | 2.90 (0.00‐6.14) | 3.97 | 2.14 (0.00‐6.09) | 3.43 | 3.49 (0.00‐7.04) | 4.36 |
| 3 Month | 3.12 (0.00‐8.40) | 4.46 | 3.01 (0.00‐9.11) | 4.22 | 3.32 (0.00‐8.25) | 4.62 |
| 6 Month | 3.40 (0.00‐7.53) | 4.97 | 2.72 (0.00‐7.09) | 4.81 | 4.61 (0.00‐9.37) | 5.10 |
| 9 Month | 1.49 (0.00‐4.87) | 2.99 | 0 (0.00‐3.94) | 2.51 | 2.27 (0.00‐6.27) | 3.36 |
| 12 Month | 2.67 (0.00‐4.60) | 4.39 | 2.67 (0.00‐4.47) | 3.82 | 2.66 (0.00‐4.82) | 4.95 |
| 15 Month | 3.06 (0.00‐5.10) | 4.03 | 2.40 (0.00‐3.94) | 3.57 | 3.65 (1.15‐6.57) | 4.45 |
| 18 Month | 2.52 (0.00‐7.45) | 4.61 | 2.93 (0.00‐7.63) | 5.02 | 2.06 (0.00‐6.59) | 4.31 |
The poststudy survey was completed by 27 of 31 (87%) of Collaborative group hospitals and 19 of the 29 (66%) Toolkit hospitals. Both groups reported QI improvement efforts to prevent CLABSI (Collaborative 97% vs. Toolkit 88%, P = 0.29) and VAP (Collaborative 97% vs. Toolkit 96%, P = 0.99). Eighty‐three percent of the Collaborative group implemented all components of the bloodstream infection prevention interventions compared with 64% for the Toolkit group (P = 0.13; Figure 1). The Collaborative group implemented daily catheter review more often than the Toolkit group (P = 0.04) and began the process implementation sooner following study implementation (P = 0.006 vs. Toolkit; see Supporting Information Figure). Eighty‐six percent of the Collaborative group implemented the complete VAP prevention interventions vs. 64% of the Toolkit group (P = 0.06; Figure 1) and the Collaborative group conducted the sedation vacation intervention more often (P = 0.03).
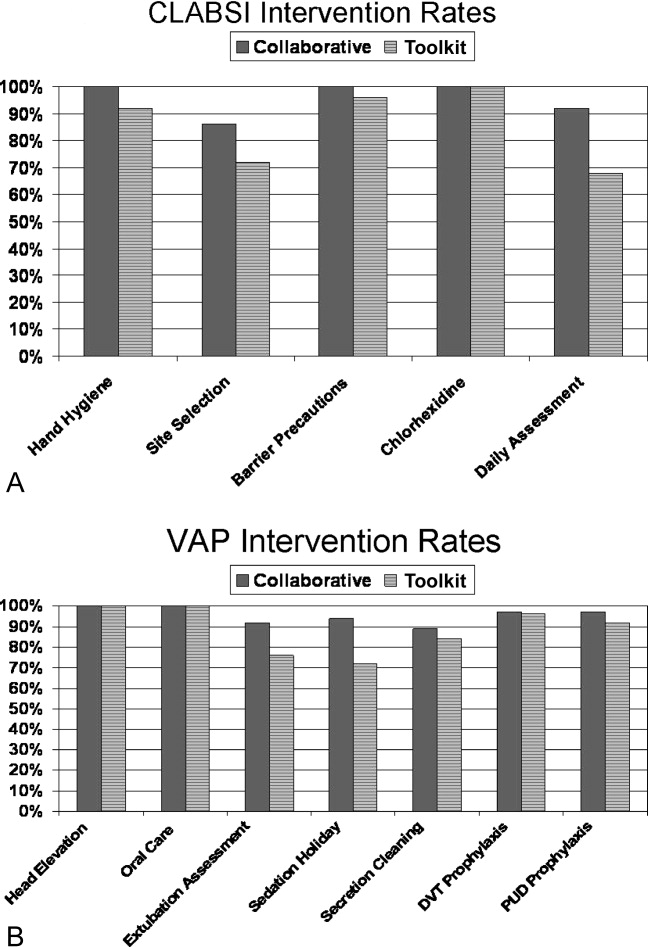
The Collaborative group participated in 57% of the seminars, whereas the Toolkit group participated in 39% (P = 0.014). Members of both groups attended more than half the clinical topics (Collaborative 64% vs. Toolkit 56%, P = 0.37). The Collaborative group had greater participation in the data and method topics (Collaborative 50% vs. Toolkit 22%, P < 0.001). The proportion of hospitals finding the seminars useful to their QI efforts was 49% for the Collaborative and 30% for the Toolkit group (P = 0.017). When restricted to hospitals that participated in the seminars, the usefulness rating was higher for both clinical (91% for the Collaborative and 86% for Toolkit) and Data/Methods (79% for Collaborative and 55% for Toolkit) topics.
A set of 14 tools were produced during the study period (Table 4); 9 clinically related tools (eg, checklists, algorithms, protocols, and flowsheets) and 5 data monitoring and quality improvement tools (eg, easy‐to‐use statistical process control spreadsheet templates, quality improvement tools, and computer tools). The Collaborative group downloaded a median of 10 tools and the Toolkit group a median of 7 (P = 0.051). The groups did not differ in their access to the clinical tools (P = 0.23) but the Collaborative group accessed a greater proportion of the data/methods tools (P = 0.004).
| Tool Access and Strategies | Collaborative Hospitalsa | Tool Kit Hospitalsa | P‐value |
|---|---|---|---|
| N = 36 ICUs | N = 25 ICUs | ||
| |||
| Clinical Tool Use | 61% | 49% | 0.23 |
| BSI Surveillance Guide | 22/36 (61%) | 13/25 (52%) | 0.60 |
| BSI Checklist | 31/36 (86%) | 16/25 (64%) | 0.06 |
| VAP Diagnosis Algorithm | 24/36 (67%) | 15/25 (60%) | 0.60 |
| Ventilator Weaning Protocol | 23/36 (64%) | 11/25 (44%) | 0.18 |
| VAP Surveillance Guide | 21/36 (58%) | 12/25 (48%) | 0.44 |
| VAP Daily Assessment | 17/36 (47%) | 6/25 (24%) | 0.10 |
| Ventilator Weaning Protocol (Flowsheet) | 15/36 (42%) | 11/25 (44%) | 0.99 |
| Data Tools | 56% | 30% | 0.004 |
| QI Implementation Tools | 19/36 (53%) | 6/25 (24%) | 0.03 |
| BSI Statistical Process Control | 23/36 (64%) | 5/25 (20%) | 0.001 |
| VAP Bundle | 23/36 (64%) | 11/25 (44%) | 0.18 |
| VAP Statistical Process Control | 21/36 (58%) | 3/25 (12%) | 0.001 |
| Strategies | 69% | 54% | 0.017 |
| Protocols for BSI | 24/36 (67%) | 19/25 (76%) | 0.57 |
| Protocols for VAP | 22/36 (61%) | 9/25 (36%) | 0.07 |
| Computer Documentation for BSI | 24/36 (67%) | 13/25 (52%) | 0.29 |
| Computer Documentation for VAP | 25/36 (69%) | 15/25 (60%) | 0.58 |
| Increased Staffing | 3/36 (8%) | 0/25 (0%) | 0.26 |
| Written Education for BSI | 31/36 (86%) | 19/25 (76%) | 0.33 |
| Written Education for VAP | 30/36 (83%) | 19/25 (76%) | 0.52 |
| Continuing Education Classes for BSI | 28/36 (78%) | 16/25 (64%) | 0.26 |
| Continuing Education Classes for VAP | 30/36 (83%) | 17/25 (68%) | 0.21 |
| QI teams | 27/36 (75%) | 14/25 (56%) | 0.16 |
| Provider Performance Feedback for BSI | 23/36 (64%) | 11/25 (44%) | 0.18 |
| Provider Performance Feedback for VAP | 24/36 (67%) | 11/25 (44%) | 0.11 |
| Implementation of BSI Checklist | 28/36 (78%) | 15/25 (60%) | 0.16 |
| Implementation of VAP Checklist | 31/36 (86%) | 13/25 (52%) | 0.007 |
Both groups relied primarily on implementation of protocols and informatics approaches (Table 4) without increasing staff levels. The predominant strategy was education; both groups provided written educational materials and classes to their providers. There was a trend for more Collaborative group members to implement QI teams (Table 4, P = 0.16 compared with the Toolkit group). Although the preponderance of both groups provided feedback reports to their hospital leaders and unit managers, Collaborative group hospitals showed a trend for providing feedback to front‐line providers (P = 0.11). With respect to self‐reported interventions, 78% of the Collaborative ICUs reported implementing a CLABSI checklist and 86% a VAP checklist, whereas only 60% of the Toolkit group reported implementation of a CLABSI checklist (P = 0.16) and 52% a VAP checklist (P = 0.007). Once a tool was implemented, both groups reported a high rate of sustaining the implementation (ranging from 86% to 100%). There also seemed to be a pattern of sequencing the interventions. Initial efforts tend to focus on provider education and evidence‐based protocols. Later efforts include more formal formation of QI teams followed by implementation of checklists. The evidence for sequencing of interventions is qualitative; we lacked subgroup sample size to substantiate these results with statistical analysis.
Discussion
In our investigation of Virtual Collaborative and Toolkit strategies for spreading the implementation of safe practices for CLABSI and VAP, ICUs in the Collaborative group had more complete implementation of the processes for prevention of hospital‐associated infections. Although both groups accessed clinical resources consistent with surveillance and clinical education, the Virtual Collaborative group attended to data and implementation methods more likely to lead to systemic CQI and organizational changes. ICUs that engaged these resources believed them useful in implementing QI, and more than 85% of the practices were sustained once integrated into routine care. Although the Collaborative ICUs were about 50% more likely to implement improvement strategies, these differences in implementation and process of care did not translate into group differences or longitudinal changes in infection rates.
In contrast to the context of our investigation, most published QI studies on health careassociated infection prevention report high baseline rates followed by a significant decline in infection rates.1419 The baseline infection rates in our study hospitals were actually below the endpoint found in many prior studies, suggesting that any marginal effects from our intervention would be more difficult to detect. Our study was implemented during the IHI's 100,000 Lives Campaign,20 a trend that may have brought about these lower baseline rates and thus a tighter margin for improvement.
The median CLABSI baseline rate in the well‐publicized Michigan hospital study was 2.7 per 1000 catheter days.21, 22 Although our baseline rate was similar (2.27 per 1000 catheter days), their reported postintervention rate was near zero, inferring nearly total elimination of the risk for CLABSI within 3‐18 months of study implementation. Several other studies using a collaborative approach have similarly reported high‐performance near‐zero results in reducing VAP23, 24 and CLABSI2528 rates. The difference between the present and previously published near‐zero result outcomes raises questions about collaboration‐based studies. We noticed 2 phenomena. First, there was slow uptake of data‐driven QI, and second, there was a differential uptake between general knowledge (clinical evidence and education) and QI implementation knowledge.29, 30
Lack of infrastructure to support data‐driven QI remains a significant barrier throughout the health care system, and teams in collaboratives often must work intensively toward improving their information systems' capability for the purpose of data‐driven decision support.1, 15, 31, 32 Systematic, standardized collection of CLABSI and VAP outcomes was initially lacking in many of our study hospitals,10 and our project expended early effort to deploy a system‐wide standardized infection control database registry.
Both of our study groups gravitated toward educational training and evidence‐based protocol decision‐support strategies. A focus only on established surveillance and education‐based fixes (eg, asking clinicians to follow a protocol within their existing care processes) have produced 32% to 57% reductions in health careacquired infections.3335 These early gains, however, are unlikely to produce the sustained near‐zero results that some collaborative teams have reported.22, 25
The ability to achieve sustained high‐performance results depends on organizational context and requires time.31 A potential benefit of collaboratives might be the return on investment attained by organizational change in quality and safety climate and its influence across the whole organization.19, 31, 36 Participants requiring systems training in the CQI process may not gain these benefits until well into their collaborative.31 For example, accumulating evidence demonstrates that the use of checklists can reduce errors of omission. Although a checklist seems a simple intervention, its effective implementation into routine care processes actually requires time for system redesign that addresses changes in multidisciplinary roles and responsibilities, frontline clinician and mid‐level management buy‐in, new methods of data collection and feedback, unanticipated involvement of ancillary services (eg, medical records, housekeeping), as well as changes to organizational policies, expectations, and priorities that connect silos of care and integrate hierarchical operations. Wall et al.37 and Pronovost and colleagues19, 21, 22, 25 highlighted the strategic effectiveness of embedding a checklist as a behavioral and data collection tool into frontline care process, leading to a redefined role of nursing, as well as new data for further cycles of improvement that collectively reduced infection rates. In our study, the Virtual Collaborative group did not have greater use of CLABSI and VAP checklists until the QI teams had been formed months into the project, consistent with the hypothesis that beneficial translation of desired changes in process of care to observed improvements in patient outcomes may take longer than 18 months to achieve19, 25, 27, 38 as opposed to the remarkable 3 months reported in the Keystone ICU project.21
Our study has several limitations. Our intervention did not mandate fixed specific components of intervention or QI methods. Each medical center was free to tailor its use of tools and change ideas, producing site variation in implementation methods and investment in support of QI. Like other multicomponent, multidimensional intervention studies, we were not able to test the effectiveness of particular QI components or the thoroughness of surveillance for CLABSI and VAP related to efforts to standardize the approach, and we did not have the resources to monitor the intensity with which participants approached QI. Furthermore, our data were dependent on self‐reports and were not verified by independent assessment of the fidelity with which the interventions were implemented, a checklist was embedded into usual care, or practices were enforced by nurses. In addition, the virtual collaborative circumvents the face‐to‐face learning sessions that might play a role in collaborative social networking, peer pressure, and acculturation.31, 36
Despite these limitations, we found that the Virtual Collaborative performed just like a Breakthrough Collaborative with a gradual uptake of implementation science using QI methods, team management, and statistical process control tools. The Toolkit condition had an even slower uptake. From an organization's perspective, the bottom‐line decision is whether a greater and meaningful proportion of collaborative participants will be successful to justify the investment of effort compared to a toolkit‐only approach. Our findings suggest that organizations engaged in change but lacking expertise in implementation science can potentially benefit from the acculturation, experiential learning, and uptake of QI provided by a collaborative.
In summary, although our Virtual Collaborative intervention was more likely to produce changes in ICU processes of care, there were no improvements in patient outcomes over this 18‐month study. The current popularity of evidence‐based guidelines, care protocols, prevention awareness, and surveillance may have produced a background of secular trend, making it difficult to ascertain effects of our QI intervention. Nonetheless, important lessons can be gleaned from this randomized controlled trial. Our study supports the proposition that as long as organizations vary in their capacity for and commitment to the science of QI and systems engineering, we should anticipate variation, uncertainty, and mixed results from short‐term, rapid cycle initiatives.27, 28, 31, 32, 39, 40 The untested, longer‐term benefit produced by a collaborative may be its stimulation of enduring systems engineering that optimizes an environment for QI of health care processes focused on desired outcomes.
Acknowledgements
The authors thank the Agency for Healthcare Research and Quality collaborative investigators for their work in this study: Xu Lei Liu, MS, at Vanderbilt; Laurie Brewer, RN MBA, Jason Hickok, Steve Horner, Susan Littleton, Patsy McFadden, RN BSN MPA CIC, Steve Mok, PharmD, Jonathan Perlin, MD PhD, Joan Reischel, RN BSN CCRN, and Sheri G. Chernestky Tejedor, MD, and all the HCA medical centers that participated in this project.
- ,,.Assessing the impact of continuous quality improvement on clinical practice: What it will take to accelerate progress.Milbank Q.1998;76:593–624.
- .Continuous improvement as an ideal in health care.N Engl J Med.1989;320:53–56.
- .A framework for collaborative improvement: Lessons from the Institute for Healthcare Improvement's Breakthrough Series.Qual Manag Health Care.1998;6(4):1–13.
- ,,,,,.Quality improvement learning collaboratives.Qual Manag Health Care.2005;14:234–237.
- ,,,.Using a virtual breakthrough series collaborative to improve access in primary care.Jt Comm J Qual Patient Saf.2006;32:573–584.
- ,,, et al.Taking the national guideline for care of acute myocardial infarction to the bedside: Developing the guideline applied in practice (GAP) initiative in Southeast Michigan.Jt Comm J Qual Improv.2002;28:5–19.
- ,.Priority Areas for National Action: Transforming Health Care Quality.Washington, DC:The National Academies Press;2003.
- ,,,.Optimal multivariate matching before randomization.Biostatistics.2004;5:263–275.
- Institute for Healthcare Improvement. The 100,000 lives campaign. http://www.ihi.org/IHI/Programs/Campaign.htm;2005.
- ,,, et al.Survey of infection control programs in a large, national healthcare system.Infect Control Hosp Epidemiol.2007;28:1401–1403.
- ,,,. Closing the quality gap: A critical analysis of quality improvement strategies, Volume 1‐Series overview and methodology. Technical Review 9 (Contract No 290–02‐0017 to the Stanford University‐UCSF Evidence‐based Practices Center), 2004. www.ahrq.gov/clinic/tp/qgap1tp.htm. Accessed November 11,2010.
- ,.Improving safety on the front lines: the role of clinical microsystems.Qual Saf Health Care.2002;11:45–50.
- ,,.SamplePower 2.0.Chicago, IL:SPSS Inc.;2001.
- ,,,.Eliminating nosocomial infections at Ascension Health.Jt Comm J Qual Patient Saf.2006;32:612–620.
- ,,, et al.An intensive care unit quality improvement collaborative in nine department of Veterans Affairs hospitals: reducing ventilator‐associated pneumonia and catheter‐related bloodstream infection rates.Jt Comm J Qual Patient Saf.2008;34:639–645.
- ,,, et al.Decreasing ventilator‐associated pneumonia in a trauma ICU.J Trauma.2006;61:122–130.
- ,,,,,.Use of corporate six sigma performance‐improvement strategies to reduce incidence of catheter‐related bloodstream infections in a surgical ICU.J Am Coll Surg.2005;201:349–358.
- ,,,,.Decline in ICU adverse events, nosocomial infections and cost through a quality improvement initiative focusing on teamwork and culture change.Qual Saf Health Care.2006;15:235–239.
- ,,,,,.Using a bundle approach to improve ventilator care processes and reduce ventilator‐associated pneumonia.Jt Comm J Qual Patient Saf.2005;31:243–248.
- ,,,.The 100000 lives campaign: Setting a goal and a deadline for improving health care quality.JAMA.2006;295:324–327.
- ,,.An intervention to decrease catheter‐related bloodstream infections in the ICU.N Engl J Med.2006;355:2725–2732.
- ,,, et al.Improving patient safety units in Michigan.J Crit Care.2008;23:207–221.
- .Toward a zero VAP rate: Personal and team approaches in the ICU.Crit Care Nurs Q.2006;29:108–114.
- ,,, et al.Implementing a ventilator bundle in a community hospital.Jt Comm J Qual Patient Saf.2007;33:219–225.
- ,,, et al.Eliminating catheter‐realted bloodstream infections in the intensive care unit.Crit Care Med.2004;32:2014–2020.
- .Innovative bundle wipes out catheter‐related bloodstream infections.Nursing.2008;38:17–18.
- ,,,,,.The CLABs collaborative: a regionwide effort to improve the quality of care in hospitals.Jt Comm J Qual Patient Saf.2008;34:713–723.
- ,,, et al.Evidence‐based practice to reduce central line infections.Jt Comm J Qual Patient Saf.2006;32:253–260.
- .Learning and improving in quality improvement collaboratives: which collaborative features do participants value most?Health Serv Res.2009;44(2 Pt 1):359–378.
- ,,, et al.Inside the health disparities collaboratives: a detailed exploration of quality improvement at community health centers.Med Care.2008;46:489–496.
- ,,, et al.Quality collaboratives: lessons from research.Qual Saf Health Care.2002;11:345–351.
- ,,, et al.Assessing the implementation of the chronic care model in quality improvement collaboratives.Health Serv Res.2005;40:978–996.
- ,.Prevention of ventilator‐associated pneumonia: Analysis of studies published since 2004.J Hosp Infect.2007;67:1–8.
- ,,,.Effect of comparative data feedback on intensive care unit infection rates in a Veterans Administration Hospital network system.Am J Infect Control.2003;31:397–404.
- ,,, et al.Reducing ventilator‐associated pneumonia rates through a staff education programme.J Hosp Infect.2004;57:223–227.
- ,,,.Does quality improvement implementation affect hospital quality of care?Hosp Top.2007;85:3–12.
- ,,,,,.Using real‐time process measurements to reduce catheter‐related bloodstream infections in the intensive care unit.Qual Saf Health Care.2005;14:295–302.
- ,,,,,.Prevention of ventilator‐associated pneumonia in the Calgary health region: a Canadian success story!Healthcare Qual.2008;11(3 Spec No):129–136.
- .Creating the evidence base for quality improvement collaboratives.Ann Intern Med.2004;140:897–901.
- ,,,,.Evidence for the impact of quality improvement collaboratives: systematic review.Br Med J.2008;336:1491–1494.
Continuous quality improvement (CQI) methodologies provide a framework for initiating and sustaining improvements in complex systems.1 By definition, CQI engages frontline staff in iterative problem solving using plandostudyact cycles of learning, with decision‐making based on real‐time process measurements.2 The Institute for Healthcare Improvement (IHI) has sponsored Breakthrough Series Collaboratives since 1996 to accelerate the uptake and impact of quality improvement (QI).3, 4 These collaboratives are typically guided by evidence‐based clinical practice guidelines, incorporate change methodologies, and rely on clinical and process improvement subject matter experts. Through the collaborative network, teams share knowledge and ideas about effective and ineffective interventions as well as strategies for overcoming barriers. The collaborative curriculum includes CQI methodology, multidisciplinary teamwork, leadership support, and tools for measurement. Participants are typically required to invest resources and send teams to face‐to‐face goal‐oriented meetings. It is costly for a large healthcare organization to incorporate travel to a learning session conference into its collaborative model. Thus, we attempted virtual learning sessions that make use of webcasts, a Web site, and teleconference calls for tools and networking.5
A recent derivative of collaboratives has been deployment of toolkits for QI. Intuition suggests that such toolkits may help to enable change, and thus some agencies advocate the simpler approach of disseminating toolkits as a change strategy.6 Toolkit dissemination is a passive approach in contrast to collaborative participation, and its effectiveness has not been critically examined in evidence‐based literature.
We sought to compare the virtual collaborative model with the toolkit model for improving care. Recommendations and guidelines for central lineassociated bloodstream infection (CLABSI) and ventilator‐associated pneumonia (VAP) prevention have not been implemented reliably, resulting in unnecessary intensive care unit (ICU) morbidity and mortality and fostering a national call for improvement.7 Our aim was to compare the effectiveness of the virtual collaborative and toolkit approaches on preventing CLABSI and VAP in the ICU.
Methods
This cluster randomized trial included medical centers within the Hospital Corporation of America (HCA), a network of hospitals located primarily in the southern United States. To minimize contamination bias between study groups within the same facility, the unit of randomization was the hospital and implementation was at the level of the ICU. The project received approval from the Vanderbilt University Institutional Review Board.
Leaders of all medical centers with at least 1 adult or pediatric ICU received an invitation from HCA leadership to participate in a QI initiative. Facility clinicians and managers completed baseline surveys (shown in the Supporting Information) on hospital characteristics, types of ICUs, patient safety climate, and QI resources between July and November 2005. Hospital‐level data were extracted from the enterprise‐wide data warehouse. Hospitals willing to participate were matched on geographic location and ICU volume and then randomized into either the Virtual Collaborative (n = 31) or Toolkit (n = 30) groups in December 20058; 1 of the hospitals was sold, yielding 29 hospitals in the Toolkit (n = 29) group. The study lasted 18 months from January 2006 through September 2007, with health careassociated infection data collected through December 2007, and follow‐up data collection through April 2008.
The QI initiative included educational opportunities, evidence‐based clinical prevention interventions, and processes and tools to implement and measure the impact of these interventions. Participants in both groups were offered interactive Web seminars during the study period; 5 of these seminars were on clinical subject matter, and 5 seminars were on patient safety, charting use of statistical process control and QI methods. The interventions were evidence‐based care bundles.9 The key interventions for preventing CLABSI were routine hand hygiene, use of chlorhexidine skin antisepsis, maximal barrier precautions during catheter insertion, catheter site and care, and avoidance of routine replacement of catheters. The key interventions to prevent VAP were routine elevation of head of the bed, regular oral care, daily sedation vacations, daily assessment of readiness to extubate, secretion cleaning, peptic ulcer disease prophylaxis, and deep vein thrombosis prophylaxis.
Toolkit Group
Hospitals randomized to this arm received a toolkit during study month 1 containing a set of evidence‐based guidelines and fact sheets for preventing CLABSI and VAP, a review of QI and teamwork methods, standardized data collection tools, and standardized charting tools. The nurse and quality managers for the Toolkit ICUs were provided ad libitum access to the HCA intranet toolkit Web site containing all of the educational seminars, clinical tools, and QI tools. Otherwise, ICUs in this group were on their own to initiate and implement a local hospital QI initiative to prevent CLABSI and VAP.
Virtual Collaborative Group
In addition to the materials and Web site support described above, facility leaders and managers in this Virtual Collaborative group agreed to participate in a virtual collaborative to develop processes to more reliably implement evidence‐based interventions to prevent CLABSI and VAP. The collaboration differed from the Breakthrough Series model3, 4 in that teams did not come together for face‐to‐face educational and planning sessions but instead attended Web seminars and teleconferences for reporting back to the larger group.5 Teams were supported through monthly educational and troubleshooting conference calls, individual coaching coordinated by the HCA corporate office of quality, safety, and performance improvement, and an e‐mail listserv designed to stimulate interaction among teams.
Clinical Outcome Measures
Although most participating hospitals defined CLABSI and VAP using the Centers for Disease Control and Prevention definitions, data collection and surveillance methods varied across hospitals.10 Education was provided to standardize outcome measurement. A data registry Web application was created as a new tool for infection control data entry, and healthcare‐associated infection data reporting by the infection control personnel was mandated starting the first quarter of 2006. To verify electronic data and correct missing information, the infection control personnel were requested to complete a retrospective data collection sheet providing quarterly reports from January 2005 through December 2007 on ICU infection events as well as total catheter days and ventilator days to allow calculation of event rates. Outcome measures of CLABSI and VAP were at the level of the hospital.
Follow‐Up
The HCA e‐mail distribution and collection routine was employed for the follow‐up survey of ICU nurse and quality managers for all participating medical centers from January 2008 through April 2008. A single survey (shown in the Supporting Information) was requested from each participating ICU. The ICU‐level surveys included questions about the implementation of the CLABSI and VAP process interventions, access of tools, participation in Web seminars, and use of QI strategies.11, 12 The postintervention survey also assessed the character and amount of implementation and teamwork activity expended.
Median CLABSI and VAP rates for a 3‐month baseline and quarterly postintervention periods were compared between the 2 study groups. The CLABSI and VAP infection rates were also analyzed using hierarchical negative binomial regression models to model infection rate changes over time (time in months and group by time interaction effects) and account for clustering of ICUs within hospitals and adjusting for baseline covariates. Baseline and process variables at the hospital and ICU level were compared using chi‐square tests and t tests according to the type of measurement. Time‐to‐event analyses were conducted to compare the groups on time to initiation of a care process. All analyses were conducted using the (R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, 2010).
The power of the study was calculated a priori with a 1‐tailed alpha of 0.05 and group size of 30. We hypothesized a 50% decrease in hospital‐associated infection rates for the Collaborative group vs. a 10% to 15% decrease for the Toolkit group. The calculations yielded power ranging from a low of 82% to a high of 91% for testing group differences.13
Results
Participating facilities included rural (11%), inner city (28%), and suburban (61%) medical centers. The 60 participating sites did not differ in administrative variables from the 113 nonparticipating HCA sites (results not shown). The median hospital size was 177 beds and the median ICU size was 16 beds. The hospitals did not differ between study groups (Table 1). At baseline, 45% of the facilities reported having a CLABSI program and 62% a VAP program.
| Hospital Factors at Baseline | Virtual Collaborative | Toolkit | P Value |
|---|---|---|---|
| |||
| Number of hospitals | 31 | 29* | |
| ICU annual patient volume, median (IQR) | 568 (294, 904) | 578 (244, 1077) | 0.93 |
| ICU patient length of stay days, median (IQR) | 3882 (1758, 5718) | 4228 (1645, 6725) | 0.95 |
| ICU mortality rate, percent (SD) | 5.7% (3.1%) | 7.1% (3.6%) | 0.13 |
| Medicare/Medicaid, percent (SD) | 68.6% (9.5%) | 68.5% (10.1%) | 0.95 |
| Percent admitted to ICU from the Emergency Department (SD) | 71% (15%) | 67% (20%) | 0.27 |
| Percent female (SD) | 49.7% (5.7%) | 50.3% (7.7%) | 0.79 |
| Medicare case‐mix weight, mean (SD) | 1221 (1007) | 1295 (1110) | 0.82 |
| Percent hospitalist ICU management | 47% | 40% | 0.61 |
The baseline and quarterly median and pooled infection rates for the Toolkit and Collaboration groups are shown in Table 2 for CLABSI and in Table 3 for VAP. There were no significant differences in the baseline rates for either CLABSI (P = 0.24) or VAP (P = 0.72) between the Collaborative and Toolkit groups. There was no significant change for either CLABSI or VAP outcomes at either 12 or 18 months of follow‐up. The median bloodstream infection rate for all participating hospitals was 2.27 at baseline, 1.18 at 12 months (P = 0.13), and 2.23 per 1000 catheter days 18 months later (P = 0.95). The median VAP rate for participating hospitals was 2.90 at baseline, 2.67 at 12 months (P = 0.44), and 2.52 per 1000 ventilator days 18 months later (P = 0.84). The hierarchical regression analysis found that neither the Collaborative nor Toolkit groups improved CLABSI (P = 0.75 and P = 0.83, respectively) or VAP (P = 0.61 and P = 0.37, respectively) rates over time, and there was no differential performance between the 2 groups for either outcome (bloodstream infection, P = 0.71; VAP, P = 0.80).
| Overall | Virtual Collaborative | Toolkit | ||||
|---|---|---|---|---|---|---|
| N = 59 Hospitals | N = 30 Hospitals | N = 29 Hospitals | ||||
| Study Period | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals |
| ||||||
| Baseline | 2.27 (0.00‐3.98) | 2.42 | 1.84 (0.00‐3.83) | 1.67 | 2.42 (0.65‐6.80) | 3.05 |
| 3 Month | 2.27 (1.30‐4.69) | 2.61 | 2.24 (0.54‐4.69) | 2.34 | 2.47 (1.48‐5.35) | 2.85 |
| 6 Month | 2.37 (0.00‐4.29) | 2.73 | 2.28 (0.00‐3.73) | 2.35 | 2.54 (0.00‐4.98) | 3.09 |
| 9 Month | 1.66 (0.00‐3.84) | 2.45 | 1.76 (0.00‐3.74) | 2.28 | 1.23 (0.00‐3.93) | 2.59 |
| 12 Month | 1.18 (0.00‐3.10) | 2.17 | 1.18 (0.00‐2.71) | 1.72 | 1.17 (0.00‐3.61) | 2.58 |
| 15 Month | 1.93 (0.00‐4.25) | 2.29 | 2.04 (0.00‐4.91) | 2.53 | 1.77 (0.00‐3.30) | 2.08 |
| 18 Month | 2.23 (0.00‐4.97) | 2.73 | 2.76 (0.00‐4.67) | 2.75 | 1.16 (0.00‐5.46) | 2.72 |
| Study Period | Overall | Virtual Collaborative | Toolkit | |||
|---|---|---|---|---|---|---|
| N = 59 Hospitals | N = 30 Hospitals | N = 29 Hospitals | ||||
| Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | |
| ||||||
| Baseline | 2.90 (0.00‐6.14) | 3.97 | 2.14 (0.00‐6.09) | 3.43 | 3.49 (0.00‐7.04) | 4.36 |
| 3 Month | 3.12 (0.00‐8.40) | 4.46 | 3.01 (0.00‐9.11) | 4.22 | 3.32 (0.00‐8.25) | 4.62 |
| 6 Month | 3.40 (0.00‐7.53) | 4.97 | 2.72 (0.00‐7.09) | 4.81 | 4.61 (0.00‐9.37) | 5.10 |
| 9 Month | 1.49 (0.00‐4.87) | 2.99 | 0 (0.00‐3.94) | 2.51 | 2.27 (0.00‐6.27) | 3.36 |
| 12 Month | 2.67 (0.00‐4.60) | 4.39 | 2.67 (0.00‐4.47) | 3.82 | 2.66 (0.00‐4.82) | 4.95 |
| 15 Month | 3.06 (0.00‐5.10) | 4.03 | 2.40 (0.00‐3.94) | 3.57 | 3.65 (1.15‐6.57) | 4.45 |
| 18 Month | 2.52 (0.00‐7.45) | 4.61 | 2.93 (0.00‐7.63) | 5.02 | 2.06 (0.00‐6.59) | 4.31 |
The poststudy survey was completed by 27 of 31 (87%) of Collaborative group hospitals and 19 of the 29 (66%) Toolkit hospitals. Both groups reported QI improvement efforts to prevent CLABSI (Collaborative 97% vs. Toolkit 88%, P = 0.29) and VAP (Collaborative 97% vs. Toolkit 96%, P = 0.99). Eighty‐three percent of the Collaborative group implemented all components of the bloodstream infection prevention interventions compared with 64% for the Toolkit group (P = 0.13; Figure 1). The Collaborative group implemented daily catheter review more often than the Toolkit group (P = 0.04) and began the process implementation sooner following study implementation (P = 0.006 vs. Toolkit; see Supporting Information Figure). Eighty‐six percent of the Collaborative group implemented the complete VAP prevention interventions vs. 64% of the Toolkit group (P = 0.06; Figure 1) and the Collaborative group conducted the sedation vacation intervention more often (P = 0.03).
The Collaborative group participated in 57% of the seminars, whereas the Toolkit group participated in 39% (P = 0.014). Members of both groups attended more than half the clinical topics (Collaborative 64% vs. Toolkit 56%, P = 0.37). The Collaborative group had greater participation in the data and method topics (Collaborative 50% vs. Toolkit 22%, P < 0.001). The proportion of hospitals finding the seminars useful to their QI efforts was 49% for the Collaborative and 30% for the Toolkit group (P = 0.017). When restricted to hospitals that participated in the seminars, the usefulness rating was higher for both clinical (91% for the Collaborative and 86% for Toolkit) and Data/Methods (79% for Collaborative and 55% for Toolkit) topics.
A set of 14 tools were produced during the study period (Table 4); 9 clinically related tools (eg, checklists, algorithms, protocols, and flowsheets) and 5 data monitoring and quality improvement tools (eg, easy‐to‐use statistical process control spreadsheet templates, quality improvement tools, and computer tools). The Collaborative group downloaded a median of 10 tools and the Toolkit group a median of 7 (P = 0.051). The groups did not differ in their access to the clinical tools (P = 0.23) but the Collaborative group accessed a greater proportion of the data/methods tools (P = 0.004).
| Tool Access and Strategies | Collaborative Hospitalsa | Tool Kit Hospitalsa | P‐value |
|---|---|---|---|
| N = 36 ICUs | N = 25 ICUs | ||
| |||
| Clinical Tool Use | 61% | 49% | 0.23 |
| BSI Surveillance Guide | 22/36 (61%) | 13/25 (52%) | 0.60 |
| BSI Checklist | 31/36 (86%) | 16/25 (64%) | 0.06 |
| VAP Diagnosis Algorithm | 24/36 (67%) | 15/25 (60%) | 0.60 |
| Ventilator Weaning Protocol | 23/36 (64%) | 11/25 (44%) | 0.18 |
| VAP Surveillance Guide | 21/36 (58%) | 12/25 (48%) | 0.44 |
| VAP Daily Assessment | 17/36 (47%) | 6/25 (24%) | 0.10 |
| Ventilator Weaning Protocol (Flowsheet) | 15/36 (42%) | 11/25 (44%) | 0.99 |
| Data Tools | 56% | 30% | 0.004 |
| QI Implementation Tools | 19/36 (53%) | 6/25 (24%) | 0.03 |
| BSI Statistical Process Control | 23/36 (64%) | 5/25 (20%) | 0.001 |
| VAP Bundle | 23/36 (64%) | 11/25 (44%) | 0.18 |
| VAP Statistical Process Control | 21/36 (58%) | 3/25 (12%) | 0.001 |
| Strategies | 69% | 54% | 0.017 |
| Protocols for BSI | 24/36 (67%) | 19/25 (76%) | 0.57 |
| Protocols for VAP | 22/36 (61%) | 9/25 (36%) | 0.07 |
| Computer Documentation for BSI | 24/36 (67%) | 13/25 (52%) | 0.29 |
| Computer Documentation for VAP | 25/36 (69%) | 15/25 (60%) | 0.58 |
| Increased Staffing | 3/36 (8%) | 0/25 (0%) | 0.26 |
| Written Education for BSI | 31/36 (86%) | 19/25 (76%) | 0.33 |
| Written Education for VAP | 30/36 (83%) | 19/25 (76%) | 0.52 |
| Continuing Education Classes for BSI | 28/36 (78%) | 16/25 (64%) | 0.26 |
| Continuing Education Classes for VAP | 30/36 (83%) | 17/25 (68%) | 0.21 |
| QI teams | 27/36 (75%) | 14/25 (56%) | 0.16 |
| Provider Performance Feedback for BSI | 23/36 (64%) | 11/25 (44%) | 0.18 |
| Provider Performance Feedback for VAP | 24/36 (67%) | 11/25 (44%) | 0.11 |
| Implementation of BSI Checklist | 28/36 (78%) | 15/25 (60%) | 0.16 |
| Implementation of VAP Checklist | 31/36 (86%) | 13/25 (52%) | 0.007 |
Both groups relied primarily on implementation of protocols and informatics approaches (Table 4) without increasing staff levels. The predominant strategy was education; both groups provided written educational materials and classes to their providers. There was a trend for more Collaborative group members to implement QI teams (Table 4, P = 0.16 compared with the Toolkit group). Although the preponderance of both groups provided feedback reports to their hospital leaders and unit managers, Collaborative group hospitals showed a trend for providing feedback to front‐line providers (P = 0.11). With respect to self‐reported interventions, 78% of the Collaborative ICUs reported implementing a CLABSI checklist and 86% a VAP checklist, whereas only 60% of the Toolkit group reported implementation of a CLABSI checklist (P = 0.16) and 52% a VAP checklist (P = 0.007). Once a tool was implemented, both groups reported a high rate of sustaining the implementation (ranging from 86% to 100%). There also seemed to be a pattern of sequencing the interventions. Initial efforts tend to focus on provider education and evidence‐based protocols. Later efforts include more formal formation of QI teams followed by implementation of checklists. The evidence for sequencing of interventions is qualitative; we lacked subgroup sample size to substantiate these results with statistical analysis.
Discussion
In our investigation of Virtual Collaborative and Toolkit strategies for spreading the implementation of safe practices for CLABSI and VAP, ICUs in the Collaborative group had more complete implementation of the processes for prevention of hospital‐associated infections. Although both groups accessed clinical resources consistent with surveillance and clinical education, the Virtual Collaborative group attended to data and implementation methods more likely to lead to systemic CQI and organizational changes. ICUs that engaged these resources believed them useful in implementing QI, and more than 85% of the practices were sustained once integrated into routine care. Although the Collaborative ICUs were about 50% more likely to implement improvement strategies, these differences in implementation and process of care did not translate into group differences or longitudinal changes in infection rates.
In contrast to the context of our investigation, most published QI studies on health careassociated infection prevention report high baseline rates followed by a significant decline in infection rates.1419 The baseline infection rates in our study hospitals were actually below the endpoint found in many prior studies, suggesting that any marginal effects from our intervention would be more difficult to detect. Our study was implemented during the IHI's 100,000 Lives Campaign,20 a trend that may have brought about these lower baseline rates and thus a tighter margin for improvement.
The median CLABSI baseline rate in the well‐publicized Michigan hospital study was 2.7 per 1000 catheter days.21, 22 Although our baseline rate was similar (2.27 per 1000 catheter days), their reported postintervention rate was near zero, inferring nearly total elimination of the risk for CLABSI within 3‐18 months of study implementation. Several other studies using a collaborative approach have similarly reported high‐performance near‐zero results in reducing VAP23, 24 and CLABSI2528 rates. The difference between the present and previously published near‐zero result outcomes raises questions about collaboration‐based studies. We noticed 2 phenomena. First, there was slow uptake of data‐driven QI, and second, there was a differential uptake between general knowledge (clinical evidence and education) and QI implementation knowledge.29, 30
Lack of infrastructure to support data‐driven QI remains a significant barrier throughout the health care system, and teams in collaboratives often must work intensively toward improving their information systems' capability for the purpose of data‐driven decision support.1, 15, 31, 32 Systematic, standardized collection of CLABSI and VAP outcomes was initially lacking in many of our study hospitals,10 and our project expended early effort to deploy a system‐wide standardized infection control database registry.
Both of our study groups gravitated toward educational training and evidence‐based protocol decision‐support strategies. A focus only on established surveillance and education‐based fixes (eg, asking clinicians to follow a protocol within their existing care processes) have produced 32% to 57% reductions in health careacquired infections.3335 These early gains, however, are unlikely to produce the sustained near‐zero results that some collaborative teams have reported.22, 25
The ability to achieve sustained high‐performance results depends on organizational context and requires time.31 A potential benefit of collaboratives might be the return on investment attained by organizational change in quality and safety climate and its influence across the whole organization.19, 31, 36 Participants requiring systems training in the CQI process may not gain these benefits until well into their collaborative.31 For example, accumulating evidence demonstrates that the use of checklists can reduce errors of omission. Although a checklist seems a simple intervention, its effective implementation into routine care processes actually requires time for system redesign that addresses changes in multidisciplinary roles and responsibilities, frontline clinician and mid‐level management buy‐in, new methods of data collection and feedback, unanticipated involvement of ancillary services (eg, medical records, housekeeping), as well as changes to organizational policies, expectations, and priorities that connect silos of care and integrate hierarchical operations. Wall et al.37 and Pronovost and colleagues19, 21, 22, 25 highlighted the strategic effectiveness of embedding a checklist as a behavioral and data collection tool into frontline care process, leading to a redefined role of nursing, as well as new data for further cycles of improvement that collectively reduced infection rates. In our study, the Virtual Collaborative group did not have greater use of CLABSI and VAP checklists until the QI teams had been formed months into the project, consistent with the hypothesis that beneficial translation of desired changes in process of care to observed improvements in patient outcomes may take longer than 18 months to achieve19, 25, 27, 38 as opposed to the remarkable 3 months reported in the Keystone ICU project.21
Our study has several limitations. Our intervention did not mandate fixed specific components of intervention or QI methods. Each medical center was free to tailor its use of tools and change ideas, producing site variation in implementation methods and investment in support of QI. Like other multicomponent, multidimensional intervention studies, we were not able to test the effectiveness of particular QI components or the thoroughness of surveillance for CLABSI and VAP related to efforts to standardize the approach, and we did not have the resources to monitor the intensity with which participants approached QI. Furthermore, our data were dependent on self‐reports and were not verified by independent assessment of the fidelity with which the interventions were implemented, a checklist was embedded into usual care, or practices were enforced by nurses. In addition, the virtual collaborative circumvents the face‐to‐face learning sessions that might play a role in collaborative social networking, peer pressure, and acculturation.31, 36
Despite these limitations, we found that the Virtual Collaborative performed just like a Breakthrough Collaborative with a gradual uptake of implementation science using QI methods, team management, and statistical process control tools. The Toolkit condition had an even slower uptake. From an organization's perspective, the bottom‐line decision is whether a greater and meaningful proportion of collaborative participants will be successful to justify the investment of effort compared to a toolkit‐only approach. Our findings suggest that organizations engaged in change but lacking expertise in implementation science can potentially benefit from the acculturation, experiential learning, and uptake of QI provided by a collaborative.
In summary, although our Virtual Collaborative intervention was more likely to produce changes in ICU processes of care, there were no improvements in patient outcomes over this 18‐month study. The current popularity of evidence‐based guidelines, care protocols, prevention awareness, and surveillance may have produced a background of secular trend, making it difficult to ascertain effects of our QI intervention. Nonetheless, important lessons can be gleaned from this randomized controlled trial. Our study supports the proposition that as long as organizations vary in their capacity for and commitment to the science of QI and systems engineering, we should anticipate variation, uncertainty, and mixed results from short‐term, rapid cycle initiatives.27, 28, 31, 32, 39, 40 The untested, longer‐term benefit produced by a collaborative may be its stimulation of enduring systems engineering that optimizes an environment for QI of health care processes focused on desired outcomes.
Acknowledgements
The authors thank the Agency for Healthcare Research and Quality collaborative investigators for their work in this study: Xu Lei Liu, MS, at Vanderbilt; Laurie Brewer, RN MBA, Jason Hickok, Steve Horner, Susan Littleton, Patsy McFadden, RN BSN MPA CIC, Steve Mok, PharmD, Jonathan Perlin, MD PhD, Joan Reischel, RN BSN CCRN, and Sheri G. Chernestky Tejedor, MD, and all the HCA medical centers that participated in this project.
Continuous quality improvement (CQI) methodologies provide a framework for initiating and sustaining improvements in complex systems.1 By definition, CQI engages frontline staff in iterative problem solving using plandostudyact cycles of learning, with decision‐making based on real‐time process measurements.2 The Institute for Healthcare Improvement (IHI) has sponsored Breakthrough Series Collaboratives since 1996 to accelerate the uptake and impact of quality improvement (QI).3, 4 These collaboratives are typically guided by evidence‐based clinical practice guidelines, incorporate change methodologies, and rely on clinical and process improvement subject matter experts. Through the collaborative network, teams share knowledge and ideas about effective and ineffective interventions as well as strategies for overcoming barriers. The collaborative curriculum includes CQI methodology, multidisciplinary teamwork, leadership support, and tools for measurement. Participants are typically required to invest resources and send teams to face‐to‐face goal‐oriented meetings. It is costly for a large healthcare organization to incorporate travel to a learning session conference into its collaborative model. Thus, we attempted virtual learning sessions that make use of webcasts, a Web site, and teleconference calls for tools and networking.5
A recent derivative of collaboratives has been deployment of toolkits for QI. Intuition suggests that such toolkits may help to enable change, and thus some agencies advocate the simpler approach of disseminating toolkits as a change strategy.6 Toolkit dissemination is a passive approach in contrast to collaborative participation, and its effectiveness has not been critically examined in evidence‐based literature.
We sought to compare the virtual collaborative model with the toolkit model for improving care. Recommendations and guidelines for central lineassociated bloodstream infection (CLABSI) and ventilator‐associated pneumonia (VAP) prevention have not been implemented reliably, resulting in unnecessary intensive care unit (ICU) morbidity and mortality and fostering a national call for improvement.7 Our aim was to compare the effectiveness of the virtual collaborative and toolkit approaches on preventing CLABSI and VAP in the ICU.
Methods
This cluster randomized trial included medical centers within the Hospital Corporation of America (HCA), a network of hospitals located primarily in the southern United States. To minimize contamination bias between study groups within the same facility, the unit of randomization was the hospital and implementation was at the level of the ICU. The project received approval from the Vanderbilt University Institutional Review Board.
Leaders of all medical centers with at least 1 adult or pediatric ICU received an invitation from HCA leadership to participate in a QI initiative. Facility clinicians and managers completed baseline surveys (shown in the Supporting Information) on hospital characteristics, types of ICUs, patient safety climate, and QI resources between July and November 2005. Hospital‐level data were extracted from the enterprise‐wide data warehouse. Hospitals willing to participate were matched on geographic location and ICU volume and then randomized into either the Virtual Collaborative (n = 31) or Toolkit (n = 30) groups in December 20058; 1 of the hospitals was sold, yielding 29 hospitals in the Toolkit (n = 29) group. The study lasted 18 months from January 2006 through September 2007, with health careassociated infection data collected through December 2007, and follow‐up data collection through April 2008.
The QI initiative included educational opportunities, evidence‐based clinical prevention interventions, and processes and tools to implement and measure the impact of these interventions. Participants in both groups were offered interactive Web seminars during the study period; 5 of these seminars were on clinical subject matter, and 5 seminars were on patient safety, charting use of statistical process control and QI methods. The interventions were evidence‐based care bundles.9 The key interventions for preventing CLABSI were routine hand hygiene, use of chlorhexidine skin antisepsis, maximal barrier precautions during catheter insertion, catheter site and care, and avoidance of routine replacement of catheters. The key interventions to prevent VAP were routine elevation of head of the bed, regular oral care, daily sedation vacations, daily assessment of readiness to extubate, secretion cleaning, peptic ulcer disease prophylaxis, and deep vein thrombosis prophylaxis.
Toolkit Group
Hospitals randomized to this arm received a toolkit during study month 1 containing a set of evidence‐based guidelines and fact sheets for preventing CLABSI and VAP, a review of QI and teamwork methods, standardized data collection tools, and standardized charting tools. The nurse and quality managers for the Toolkit ICUs were provided ad libitum access to the HCA intranet toolkit Web site containing all of the educational seminars, clinical tools, and QI tools. Otherwise, ICUs in this group were on their own to initiate and implement a local hospital QI initiative to prevent CLABSI and VAP.
Virtual Collaborative Group
In addition to the materials and Web site support described above, facility leaders and managers in this Virtual Collaborative group agreed to participate in a virtual collaborative to develop processes to more reliably implement evidence‐based interventions to prevent CLABSI and VAP. The collaboration differed from the Breakthrough Series model3, 4 in that teams did not come together for face‐to‐face educational and planning sessions but instead attended Web seminars and teleconferences for reporting back to the larger group.5 Teams were supported through monthly educational and troubleshooting conference calls, individual coaching coordinated by the HCA corporate office of quality, safety, and performance improvement, and an e‐mail listserv designed to stimulate interaction among teams.
Clinical Outcome Measures
Although most participating hospitals defined CLABSI and VAP using the Centers for Disease Control and Prevention definitions, data collection and surveillance methods varied across hospitals.10 Education was provided to standardize outcome measurement. A data registry Web application was created as a new tool for infection control data entry, and healthcare‐associated infection data reporting by the infection control personnel was mandated starting the first quarter of 2006. To verify electronic data and correct missing information, the infection control personnel were requested to complete a retrospective data collection sheet providing quarterly reports from January 2005 through December 2007 on ICU infection events as well as total catheter days and ventilator days to allow calculation of event rates. Outcome measures of CLABSI and VAP were at the level of the hospital.
Follow‐Up
The HCA e‐mail distribution and collection routine was employed for the follow‐up survey of ICU nurse and quality managers for all participating medical centers from January 2008 through April 2008. A single survey (shown in the Supporting Information) was requested from each participating ICU. The ICU‐level surveys included questions about the implementation of the CLABSI and VAP process interventions, access of tools, participation in Web seminars, and use of QI strategies.11, 12 The postintervention survey also assessed the character and amount of implementation and teamwork activity expended.
Median CLABSI and VAP rates for a 3‐month baseline and quarterly postintervention periods were compared between the 2 study groups. The CLABSI and VAP infection rates were also analyzed using hierarchical negative binomial regression models to model infection rate changes over time (time in months and group by time interaction effects) and account for clustering of ICUs within hospitals and adjusting for baseline covariates. Baseline and process variables at the hospital and ICU level were compared using chi‐square tests and t tests according to the type of measurement. Time‐to‐event analyses were conducted to compare the groups on time to initiation of a care process. All analyses were conducted using the (R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, 2010).
The power of the study was calculated a priori with a 1‐tailed alpha of 0.05 and group size of 30. We hypothesized a 50% decrease in hospital‐associated infection rates for the Collaborative group vs. a 10% to 15% decrease for the Toolkit group. The calculations yielded power ranging from a low of 82% to a high of 91% for testing group differences.13
Results
Participating facilities included rural (11%), inner city (28%), and suburban (61%) medical centers. The 60 participating sites did not differ in administrative variables from the 113 nonparticipating HCA sites (results not shown). The median hospital size was 177 beds and the median ICU size was 16 beds. The hospitals did not differ between study groups (Table 1). At baseline, 45% of the facilities reported having a CLABSI program and 62% a VAP program.
| Hospital Factors at Baseline | Virtual Collaborative | Toolkit | P Value |
|---|---|---|---|
| |||
| Number of hospitals | 31 | 29* | |
| ICU annual patient volume, median (IQR) | 568 (294, 904) | 578 (244, 1077) | 0.93 |
| ICU patient length of stay days, median (IQR) | 3882 (1758, 5718) | 4228 (1645, 6725) | 0.95 |
| ICU mortality rate, percent (SD) | 5.7% (3.1%) | 7.1% (3.6%) | 0.13 |
| Medicare/Medicaid, percent (SD) | 68.6% (9.5%) | 68.5% (10.1%) | 0.95 |
| Percent admitted to ICU from the Emergency Department (SD) | 71% (15%) | 67% (20%) | 0.27 |
| Percent female (SD) | 49.7% (5.7%) | 50.3% (7.7%) | 0.79 |
| Medicare case‐mix weight, mean (SD) | 1221 (1007) | 1295 (1110) | 0.82 |
| Percent hospitalist ICU management | 47% | 40% | 0.61 |
The baseline and quarterly median and pooled infection rates for the Toolkit and Collaboration groups are shown in Table 2 for CLABSI and in Table 3 for VAP. There were no significant differences in the baseline rates for either CLABSI (P = 0.24) or VAP (P = 0.72) between the Collaborative and Toolkit groups. There was no significant change for either CLABSI or VAP outcomes at either 12 or 18 months of follow‐up. The median bloodstream infection rate for all participating hospitals was 2.27 at baseline, 1.18 at 12 months (P = 0.13), and 2.23 per 1000 catheter days 18 months later (P = 0.95). The median VAP rate for participating hospitals was 2.90 at baseline, 2.67 at 12 months (P = 0.44), and 2.52 per 1000 ventilator days 18 months later (P = 0.84). The hierarchical regression analysis found that neither the Collaborative nor Toolkit groups improved CLABSI (P = 0.75 and P = 0.83, respectively) or VAP (P = 0.61 and P = 0.37, respectively) rates over time, and there was no differential performance between the 2 groups for either outcome (bloodstream infection, P = 0.71; VAP, P = 0.80).
| Overall | Virtual Collaborative | Toolkit | ||||
|---|---|---|---|---|---|---|
| N = 59 Hospitals | N = 30 Hospitals | N = 29 Hospitals | ||||
| Study Period | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals |
| ||||||
| Baseline | 2.27 (0.00‐3.98) | 2.42 | 1.84 (0.00‐3.83) | 1.67 | 2.42 (0.65‐6.80) | 3.05 |
| 3 Month | 2.27 (1.30‐4.69) | 2.61 | 2.24 (0.54‐4.69) | 2.34 | 2.47 (1.48‐5.35) | 2.85 |
| 6 Month | 2.37 (0.00‐4.29) | 2.73 | 2.28 (0.00‐3.73) | 2.35 | 2.54 (0.00‐4.98) | 3.09 |
| 9 Month | 1.66 (0.00‐3.84) | 2.45 | 1.76 (0.00‐3.74) | 2.28 | 1.23 (0.00‐3.93) | 2.59 |
| 12 Month | 1.18 (0.00‐3.10) | 2.17 | 1.18 (0.00‐2.71) | 1.72 | 1.17 (0.00‐3.61) | 2.58 |
| 15 Month | 1.93 (0.00‐4.25) | 2.29 | 2.04 (0.00‐4.91) | 2.53 | 1.77 (0.00‐3.30) | 2.08 |
| 18 Month | 2.23 (0.00‐4.97) | 2.73 | 2.76 (0.00‐4.67) | 2.75 | 1.16 (0.00‐5.46) | 2.72 |
| Study Period | Overall | Virtual Collaborative | Toolkit | |||
|---|---|---|---|---|---|---|
| N = 59 Hospitals | N = 30 Hospitals | N = 29 Hospitals | ||||
| Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | Hospital Median (IQR) | Rate Pooled Across Hospitals | |
| ||||||
| Baseline | 2.90 (0.00‐6.14) | 3.97 | 2.14 (0.00‐6.09) | 3.43 | 3.49 (0.00‐7.04) | 4.36 |
| 3 Month | 3.12 (0.00‐8.40) | 4.46 | 3.01 (0.00‐9.11) | 4.22 | 3.32 (0.00‐8.25) | 4.62 |
| 6 Month | 3.40 (0.00‐7.53) | 4.97 | 2.72 (0.00‐7.09) | 4.81 | 4.61 (0.00‐9.37) | 5.10 |
| 9 Month | 1.49 (0.00‐4.87) | 2.99 | 0 (0.00‐3.94) | 2.51 | 2.27 (0.00‐6.27) | 3.36 |
| 12 Month | 2.67 (0.00‐4.60) | 4.39 | 2.67 (0.00‐4.47) | 3.82 | 2.66 (0.00‐4.82) | 4.95 |
| 15 Month | 3.06 (0.00‐5.10) | 4.03 | 2.40 (0.00‐3.94) | 3.57 | 3.65 (1.15‐6.57) | 4.45 |
| 18 Month | 2.52 (0.00‐7.45) | 4.61 | 2.93 (0.00‐7.63) | 5.02 | 2.06 (0.00‐6.59) | 4.31 |
The poststudy survey was completed by 27 of 31 (87%) of Collaborative group hospitals and 19 of the 29 (66%) Toolkit hospitals. Both groups reported QI improvement efforts to prevent CLABSI (Collaborative 97% vs. Toolkit 88%, P = 0.29) and VAP (Collaborative 97% vs. Toolkit 96%, P = 0.99). Eighty‐three percent of the Collaborative group implemented all components of the bloodstream infection prevention interventions compared with 64% for the Toolkit group (P = 0.13; Figure 1). The Collaborative group implemented daily catheter review more often than the Toolkit group (P = 0.04) and began the process implementation sooner following study implementation (P = 0.006 vs. Toolkit; see Supporting Information Figure). Eighty‐six percent of the Collaborative group implemented the complete VAP prevention interventions vs. 64% of the Toolkit group (P = 0.06; Figure 1) and the Collaborative group conducted the sedation vacation intervention more often (P = 0.03).
The Collaborative group participated in 57% of the seminars, whereas the Toolkit group participated in 39% (P = 0.014). Members of both groups attended more than half the clinical topics (Collaborative 64% vs. Toolkit 56%, P = 0.37). The Collaborative group had greater participation in the data and method topics (Collaborative 50% vs. Toolkit 22%, P < 0.001). The proportion of hospitals finding the seminars useful to their QI efforts was 49% for the Collaborative and 30% for the Toolkit group (P = 0.017). When restricted to hospitals that participated in the seminars, the usefulness rating was higher for both clinical (91% for the Collaborative and 86% for Toolkit) and Data/Methods (79% for Collaborative and 55% for Toolkit) topics.
A set of 14 tools were produced during the study period (Table 4); 9 clinically related tools (eg, checklists, algorithms, protocols, and flowsheets) and 5 data monitoring and quality improvement tools (eg, easy‐to‐use statistical process control spreadsheet templates, quality improvement tools, and computer tools). The Collaborative group downloaded a median of 10 tools and the Toolkit group a median of 7 (P = 0.051). The groups did not differ in their access to the clinical tools (P = 0.23) but the Collaborative group accessed a greater proportion of the data/methods tools (P = 0.004).
| Tool Access and Strategies | Collaborative Hospitalsa | Tool Kit Hospitalsa | P‐value |
|---|---|---|---|
| N = 36 ICUs | N = 25 ICUs | ||
| |||
| Clinical Tool Use | 61% | 49% | 0.23 |
| BSI Surveillance Guide | 22/36 (61%) | 13/25 (52%) | 0.60 |
| BSI Checklist | 31/36 (86%) | 16/25 (64%) | 0.06 |
| VAP Diagnosis Algorithm | 24/36 (67%) | 15/25 (60%) | 0.60 |
| Ventilator Weaning Protocol | 23/36 (64%) | 11/25 (44%) | 0.18 |
| VAP Surveillance Guide | 21/36 (58%) | 12/25 (48%) | 0.44 |
| VAP Daily Assessment | 17/36 (47%) | 6/25 (24%) | 0.10 |
| Ventilator Weaning Protocol (Flowsheet) | 15/36 (42%) | 11/25 (44%) | 0.99 |
| Data Tools | 56% | 30% | 0.004 |
| QI Implementation Tools | 19/36 (53%) | 6/25 (24%) | 0.03 |
| BSI Statistical Process Control | 23/36 (64%) | 5/25 (20%) | 0.001 |
| VAP Bundle | 23/36 (64%) | 11/25 (44%) | 0.18 |
| VAP Statistical Process Control | 21/36 (58%) | 3/25 (12%) | 0.001 |
| Strategies | 69% | 54% | 0.017 |
| Protocols for BSI | 24/36 (67%) | 19/25 (76%) | 0.57 |
| Protocols for VAP | 22/36 (61%) | 9/25 (36%) | 0.07 |
| Computer Documentation for BSI | 24/36 (67%) | 13/25 (52%) | 0.29 |
| Computer Documentation for VAP | 25/36 (69%) | 15/25 (60%) | 0.58 |
| Increased Staffing | 3/36 (8%) | 0/25 (0%) | 0.26 |
| Written Education for BSI | 31/36 (86%) | 19/25 (76%) | 0.33 |
| Written Education for VAP | 30/36 (83%) | 19/25 (76%) | 0.52 |
| Continuing Education Classes for BSI | 28/36 (78%) | 16/25 (64%) | 0.26 |
| Continuing Education Classes for VAP | 30/36 (83%) | 17/25 (68%) | 0.21 |
| QI teams | 27/36 (75%) | 14/25 (56%) | 0.16 |
| Provider Performance Feedback for BSI | 23/36 (64%) | 11/25 (44%) | 0.18 |
| Provider Performance Feedback for VAP | 24/36 (67%) | 11/25 (44%) | 0.11 |
| Implementation of BSI Checklist | 28/36 (78%) | 15/25 (60%) | 0.16 |
| Implementation of VAP Checklist | 31/36 (86%) | 13/25 (52%) | 0.007 |
Both groups relied primarily on implementation of protocols and informatics approaches (Table 4) without increasing staff levels. The predominant strategy was education; both groups provided written educational materials and classes to their providers. There was a trend for more Collaborative group members to implement QI teams (Table 4, P = 0.16 compared with the Toolkit group). Although the preponderance of both groups provided feedback reports to their hospital leaders and unit managers, Collaborative group hospitals showed a trend for providing feedback to front‐line providers (P = 0.11). With respect to self‐reported interventions, 78% of the Collaborative ICUs reported implementing a CLABSI checklist and 86% a VAP checklist, whereas only 60% of the Toolkit group reported implementation of a CLABSI checklist (P = 0.16) and 52% a VAP checklist (P = 0.007). Once a tool was implemented, both groups reported a high rate of sustaining the implementation (ranging from 86% to 100%). There also seemed to be a pattern of sequencing the interventions. Initial efforts tend to focus on provider education and evidence‐based protocols. Later efforts include more formal formation of QI teams followed by implementation of checklists. The evidence for sequencing of interventions is qualitative; we lacked subgroup sample size to substantiate these results with statistical analysis.
Discussion
In our investigation of Virtual Collaborative and Toolkit strategies for spreading the implementation of safe practices for CLABSI and VAP, ICUs in the Collaborative group had more complete implementation of the processes for prevention of hospital‐associated infections. Although both groups accessed clinical resources consistent with surveillance and clinical education, the Virtual Collaborative group attended to data and implementation methods more likely to lead to systemic CQI and organizational changes. ICUs that engaged these resources believed them useful in implementing QI, and more than 85% of the practices were sustained once integrated into routine care. Although the Collaborative ICUs were about 50% more likely to implement improvement strategies, these differences in implementation and process of care did not translate into group differences or longitudinal changes in infection rates.
In contrast to the context of our investigation, most published QI studies on health careassociated infection prevention report high baseline rates followed by a significant decline in infection rates.1419 The baseline infection rates in our study hospitals were actually below the endpoint found in many prior studies, suggesting that any marginal effects from our intervention would be more difficult to detect. Our study was implemented during the IHI's 100,000 Lives Campaign,20 a trend that may have brought about these lower baseline rates and thus a tighter margin for improvement.
The median CLABSI baseline rate in the well‐publicized Michigan hospital study was 2.7 per 1000 catheter days.21, 22 Although our baseline rate was similar (2.27 per 1000 catheter days), their reported postintervention rate was near zero, inferring nearly total elimination of the risk for CLABSI within 3‐18 months of study implementation. Several other studies using a collaborative approach have similarly reported high‐performance near‐zero results in reducing VAP23, 24 and CLABSI2528 rates. The difference between the present and previously published near‐zero result outcomes raises questions about collaboration‐based studies. We noticed 2 phenomena. First, there was slow uptake of data‐driven QI, and second, there was a differential uptake between general knowledge (clinical evidence and education) and QI implementation knowledge.29, 30
Lack of infrastructure to support data‐driven QI remains a significant barrier throughout the health care system, and teams in collaboratives often must work intensively toward improving their information systems' capability for the purpose of data‐driven decision support.1, 15, 31, 32 Systematic, standardized collection of CLABSI and VAP outcomes was initially lacking in many of our study hospitals,10 and our project expended early effort to deploy a system‐wide standardized infection control database registry.
Both of our study groups gravitated toward educational training and evidence‐based protocol decision‐support strategies. A focus only on established surveillance and education‐based fixes (eg, asking clinicians to follow a protocol within their existing care processes) have produced 32% to 57% reductions in health careacquired infections.3335 These early gains, however, are unlikely to produce the sustained near‐zero results that some collaborative teams have reported.22, 25
The ability to achieve sustained high‐performance results depends on organizational context and requires time.31 A potential benefit of collaboratives might be the return on investment attained by organizational change in quality and safety climate and its influence across the whole organization.19, 31, 36 Participants requiring systems training in the CQI process may not gain these benefits until well into their collaborative.31 For example, accumulating evidence demonstrates that the use of checklists can reduce errors of omission. Although a checklist seems a simple intervention, its effective implementation into routine care processes actually requires time for system redesign that addresses changes in multidisciplinary roles and responsibilities, frontline clinician and mid‐level management buy‐in, new methods of data collection and feedback, unanticipated involvement of ancillary services (eg, medical records, housekeeping), as well as changes to organizational policies, expectations, and priorities that connect silos of care and integrate hierarchical operations. Wall et al.37 and Pronovost and colleagues19, 21, 22, 25 highlighted the strategic effectiveness of embedding a checklist as a behavioral and data collection tool into frontline care process, leading to a redefined role of nursing, as well as new data for further cycles of improvement that collectively reduced infection rates. In our study, the Virtual Collaborative group did not have greater use of CLABSI and VAP checklists until the QI teams had been formed months into the project, consistent with the hypothesis that beneficial translation of desired changes in process of care to observed improvements in patient outcomes may take longer than 18 months to achieve19, 25, 27, 38 as opposed to the remarkable 3 months reported in the Keystone ICU project.21
Our study has several limitations. Our intervention did not mandate fixed specific components of intervention or QI methods. Each medical center was free to tailor its use of tools and change ideas, producing site variation in implementation methods and investment in support of QI. Like other multicomponent, multidimensional intervention studies, we were not able to test the effectiveness of particular QI components or the thoroughness of surveillance for CLABSI and VAP related to efforts to standardize the approach, and we did not have the resources to monitor the intensity with which participants approached QI. Furthermore, our data were dependent on self‐reports and were not verified by independent assessment of the fidelity with which the interventions were implemented, a checklist was embedded into usual care, or practices were enforced by nurses. In addition, the virtual collaborative circumvents the face‐to‐face learning sessions that might play a role in collaborative social networking, peer pressure, and acculturation.31, 36
Despite these limitations, we found that the Virtual Collaborative performed just like a Breakthrough Collaborative with a gradual uptake of implementation science using QI methods, team management, and statistical process control tools. The Toolkit condition had an even slower uptake. From an organization's perspective, the bottom‐line decision is whether a greater and meaningful proportion of collaborative participants will be successful to justify the investment of effort compared to a toolkit‐only approach. Our findings suggest that organizations engaged in change but lacking expertise in implementation science can potentially benefit from the acculturation, experiential learning, and uptake of QI provided by a collaborative.
In summary, although our Virtual Collaborative intervention was more likely to produce changes in ICU processes of care, there were no improvements in patient outcomes over this 18‐month study. The current popularity of evidence‐based guidelines, care protocols, prevention awareness, and surveillance may have produced a background of secular trend, making it difficult to ascertain effects of our QI intervention. Nonetheless, important lessons can be gleaned from this randomized controlled trial. Our study supports the proposition that as long as organizations vary in their capacity for and commitment to the science of QI and systems engineering, we should anticipate variation, uncertainty, and mixed results from short‐term, rapid cycle initiatives.27, 28, 31, 32, 39, 40 The untested, longer‐term benefit produced by a collaborative may be its stimulation of enduring systems engineering that optimizes an environment for QI of health care processes focused on desired outcomes.
Acknowledgements
The authors thank the Agency for Healthcare Research and Quality collaborative investigators for their work in this study: Xu Lei Liu, MS, at Vanderbilt; Laurie Brewer, RN MBA, Jason Hickok, Steve Horner, Susan Littleton, Patsy McFadden, RN BSN MPA CIC, Steve Mok, PharmD, Jonathan Perlin, MD PhD, Joan Reischel, RN BSN CCRN, and Sheri G. Chernestky Tejedor, MD, and all the HCA medical centers that participated in this project.
- ,,.Assessing the impact of continuous quality improvement on clinical practice: What it will take to accelerate progress.Milbank Q.1998;76:593–624.
- .Continuous improvement as an ideal in health care.N Engl J Med.1989;320:53–56.
- .A framework for collaborative improvement: Lessons from the Institute for Healthcare Improvement's Breakthrough Series.Qual Manag Health Care.1998;6(4):1–13.
- ,,,,,.Quality improvement learning collaboratives.Qual Manag Health Care.2005;14:234–237.
- ,,,.Using a virtual breakthrough series collaborative to improve access in primary care.Jt Comm J Qual Patient Saf.2006;32:573–584.
- ,,, et al.Taking the national guideline for care of acute myocardial infarction to the bedside: Developing the guideline applied in practice (GAP) initiative in Southeast Michigan.Jt Comm J Qual Improv.2002;28:5–19.
- ,.Priority Areas for National Action: Transforming Health Care Quality.Washington, DC:The National Academies Press;2003.
- ,,,.Optimal multivariate matching before randomization.Biostatistics.2004;5:263–275.
- Institute for Healthcare Improvement. The 100,000 lives campaign. http://www.ihi.org/IHI/Programs/Campaign.htm;2005.
- ,,, et al.Survey of infection control programs in a large, national healthcare system.Infect Control Hosp Epidemiol.2007;28:1401–1403.
- ,,,. Closing the quality gap: A critical analysis of quality improvement strategies, Volume 1‐Series overview and methodology. Technical Review 9 (Contract No 290–02‐0017 to the Stanford University‐UCSF Evidence‐based Practices Center), 2004. www.ahrq.gov/clinic/tp/qgap1tp.htm. Accessed November 11,2010.
- ,.Improving safety on the front lines: the role of clinical microsystems.Qual Saf Health Care.2002;11:45–50.
- ,,.SamplePower 2.0.Chicago, IL:SPSS Inc.;2001.
- ,,,.Eliminating nosocomial infections at Ascension Health.Jt Comm J Qual Patient Saf.2006;32:612–620.
- ,,, et al.An intensive care unit quality improvement collaborative in nine department of Veterans Affairs hospitals: reducing ventilator‐associated pneumonia and catheter‐related bloodstream infection rates.Jt Comm J Qual Patient Saf.2008;34:639–645.
- ,,, et al.Decreasing ventilator‐associated pneumonia in a trauma ICU.J Trauma.2006;61:122–130.
- ,,,,,.Use of corporate six sigma performance‐improvement strategies to reduce incidence of catheter‐related bloodstream infections in a surgical ICU.J Am Coll Surg.2005;201:349–358.
- ,,,,.Decline in ICU adverse events, nosocomial infections and cost through a quality improvement initiative focusing on teamwork and culture change.Qual Saf Health Care.2006;15:235–239.
- ,,,,,.Using a bundle approach to improve ventilator care processes and reduce ventilator‐associated pneumonia.Jt Comm J Qual Patient Saf.2005;31:243–248.
- ,,,.The 100000 lives campaign: Setting a goal and a deadline for improving health care quality.JAMA.2006;295:324–327.
- ,,.An intervention to decrease catheter‐related bloodstream infections in the ICU.N Engl J Med.2006;355:2725–2732.
- ,,, et al.Improving patient safety units in Michigan.J Crit Care.2008;23:207–221.
- .Toward a zero VAP rate: Personal and team approaches in the ICU.Crit Care Nurs Q.2006;29:108–114.
- ,,, et al.Implementing a ventilator bundle in a community hospital.Jt Comm J Qual Patient Saf.2007;33:219–225.
- ,,, et al.Eliminating catheter‐realted bloodstream infections in the intensive care unit.Crit Care Med.2004;32:2014–2020.
- .Innovative bundle wipes out catheter‐related bloodstream infections.Nursing.2008;38:17–18.
- ,,,,,.The CLABs collaborative: a regionwide effort to improve the quality of care in hospitals.Jt Comm J Qual Patient Saf.2008;34:713–723.
- ,,, et al.Evidence‐based practice to reduce central line infections.Jt Comm J Qual Patient Saf.2006;32:253–260.
- .Learning and improving in quality improvement collaboratives: which collaborative features do participants value most?Health Serv Res.2009;44(2 Pt 1):359–378.
- ,,, et al.Inside the health disparities collaboratives: a detailed exploration of quality improvement at community health centers.Med Care.2008;46:489–496.
- ,,, et al.Quality collaboratives: lessons from research.Qual Saf Health Care.2002;11:345–351.
- ,,, et al.Assessing the implementation of the chronic care model in quality improvement collaboratives.Health Serv Res.2005;40:978–996.
- ,.Prevention of ventilator‐associated pneumonia: Analysis of studies published since 2004.J Hosp Infect.2007;67:1–8.
- ,,,.Effect of comparative data feedback on intensive care unit infection rates in a Veterans Administration Hospital network system.Am J Infect Control.2003;31:397–404.
- ,,, et al.Reducing ventilator‐associated pneumonia rates through a staff education programme.J Hosp Infect.2004;57:223–227.
- ,,,.Does quality improvement implementation affect hospital quality of care?Hosp Top.2007;85:3–12.
- ,,,,,.Using real‐time process measurements to reduce catheter‐related bloodstream infections in the intensive care unit.Qual Saf Health Care.2005;14:295–302.
- ,,,,,.Prevention of ventilator‐associated pneumonia in the Calgary health region: a Canadian success story!Healthcare Qual.2008;11(3 Spec No):129–136.
- .Creating the evidence base for quality improvement collaboratives.Ann Intern Med.2004;140:897–901.
- ,,,,.Evidence for the impact of quality improvement collaboratives: systematic review.Br Med J.2008;336:1491–1494.
- ,,.Assessing the impact of continuous quality improvement on clinical practice: What it will take to accelerate progress.Milbank Q.1998;76:593–624.
- .Continuous improvement as an ideal in health care.N Engl J Med.1989;320:53–56.
- .A framework for collaborative improvement: Lessons from the Institute for Healthcare Improvement's Breakthrough Series.Qual Manag Health Care.1998;6(4):1–13.
- ,,,,,.Quality improvement learning collaboratives.Qual Manag Health Care.2005;14:234–237.
- ,,,.Using a virtual breakthrough series collaborative to improve access in primary care.Jt Comm J Qual Patient Saf.2006;32:573–584.
- ,,, et al.Taking the national guideline for care of acute myocardial infarction to the bedside: Developing the guideline applied in practice (GAP) initiative in Southeast Michigan.Jt Comm J Qual Improv.2002;28:5–19.
- ,.Priority Areas for National Action: Transforming Health Care Quality.Washington, DC:The National Academies Press;2003.
- ,,,.Optimal multivariate matching before randomization.Biostatistics.2004;5:263–275.
- Institute for Healthcare Improvement. The 100,000 lives campaign. http://www.ihi.org/IHI/Programs/Campaign.htm;2005.
- ,,, et al.Survey of infection control programs in a large, national healthcare system.Infect Control Hosp Epidemiol.2007;28:1401–1403.
- ,,,. Closing the quality gap: A critical analysis of quality improvement strategies, Volume 1‐Series overview and methodology. Technical Review 9 (Contract No 290–02‐0017 to the Stanford University‐UCSF Evidence‐based Practices Center), 2004. www.ahrq.gov/clinic/tp/qgap1tp.htm. Accessed November 11,2010.
- ,.Improving safety on the front lines: the role of clinical microsystems.Qual Saf Health Care.2002;11:45–50.
- ,,.SamplePower 2.0.Chicago, IL:SPSS Inc.;2001.
- ,,,.Eliminating nosocomial infections at Ascension Health.Jt Comm J Qual Patient Saf.2006;32:612–620.
- ,,, et al.An intensive care unit quality improvement collaborative in nine department of Veterans Affairs hospitals: reducing ventilator‐associated pneumonia and catheter‐related bloodstream infection rates.Jt Comm J Qual Patient Saf.2008;34:639–645.
- ,,, et al.Decreasing ventilator‐associated pneumonia in a trauma ICU.J Trauma.2006;61:122–130.
- ,,,,,.Use of corporate six sigma performance‐improvement strategies to reduce incidence of catheter‐related bloodstream infections in a surgical ICU.J Am Coll Surg.2005;201:349–358.
- ,,,,.Decline in ICU adverse events, nosocomial infections and cost through a quality improvement initiative focusing on teamwork and culture change.Qual Saf Health Care.2006;15:235–239.
- ,,,,,.Using a bundle approach to improve ventilator care processes and reduce ventilator‐associated pneumonia.Jt Comm J Qual Patient Saf.2005;31:243–248.
- ,,,.The 100000 lives campaign: Setting a goal and a deadline for improving health care quality.JAMA.2006;295:324–327.
- ,,.An intervention to decrease catheter‐related bloodstream infections in the ICU.N Engl J Med.2006;355:2725–2732.
- ,,, et al.Improving patient safety units in Michigan.J Crit Care.2008;23:207–221.
- .Toward a zero VAP rate: Personal and team approaches in the ICU.Crit Care Nurs Q.2006;29:108–114.
- ,,, et al.Implementing a ventilator bundle in a community hospital.Jt Comm J Qual Patient Saf.2007;33:219–225.
- ,,, et al.Eliminating catheter‐realted bloodstream infections in the intensive care unit.Crit Care Med.2004;32:2014–2020.
- .Innovative bundle wipes out catheter‐related bloodstream infections.Nursing.2008;38:17–18.
- ,,,,,.The CLABs collaborative: a regionwide effort to improve the quality of care in hospitals.Jt Comm J Qual Patient Saf.2008;34:713–723.
- ,,, et al.Evidence‐based practice to reduce central line infections.Jt Comm J Qual Patient Saf.2006;32:253–260.
- .Learning and improving in quality improvement collaboratives: which collaborative features do participants value most?Health Serv Res.2009;44(2 Pt 1):359–378.
- ,,, et al.Inside the health disparities collaboratives: a detailed exploration of quality improvement at community health centers.Med Care.2008;46:489–496.
- ,,, et al.Quality collaboratives: lessons from research.Qual Saf Health Care.2002;11:345–351.
- ,,, et al.Assessing the implementation of the chronic care model in quality improvement collaboratives.Health Serv Res.2005;40:978–996.
- ,.Prevention of ventilator‐associated pneumonia: Analysis of studies published since 2004.J Hosp Infect.2007;67:1–8.
- ,,,.Effect of comparative data feedback on intensive care unit infection rates in a Veterans Administration Hospital network system.Am J Infect Control.2003;31:397–404.
- ,,, et al.Reducing ventilator‐associated pneumonia rates through a staff education programme.J Hosp Infect.2004;57:223–227.
- ,,,.Does quality improvement implementation affect hospital quality of care?Hosp Top.2007;85:3–12.
- ,,,,,.Using real‐time process measurements to reduce catheter‐related bloodstream infections in the intensive care unit.Qual Saf Health Care.2005;14:295–302.
- ,,,,,.Prevention of ventilator‐associated pneumonia in the Calgary health region: a Canadian success story!Healthcare Qual.2008;11(3 Spec No):129–136.
- .Creating the evidence base for quality improvement collaboratives.Ann Intern Med.2004;140:897–901.
- ,,,,.Evidence for the impact of quality improvement collaboratives: systematic review.Br Med J.2008;336:1491–1494.
Copyright © 2011 Society of Hospital Medicine
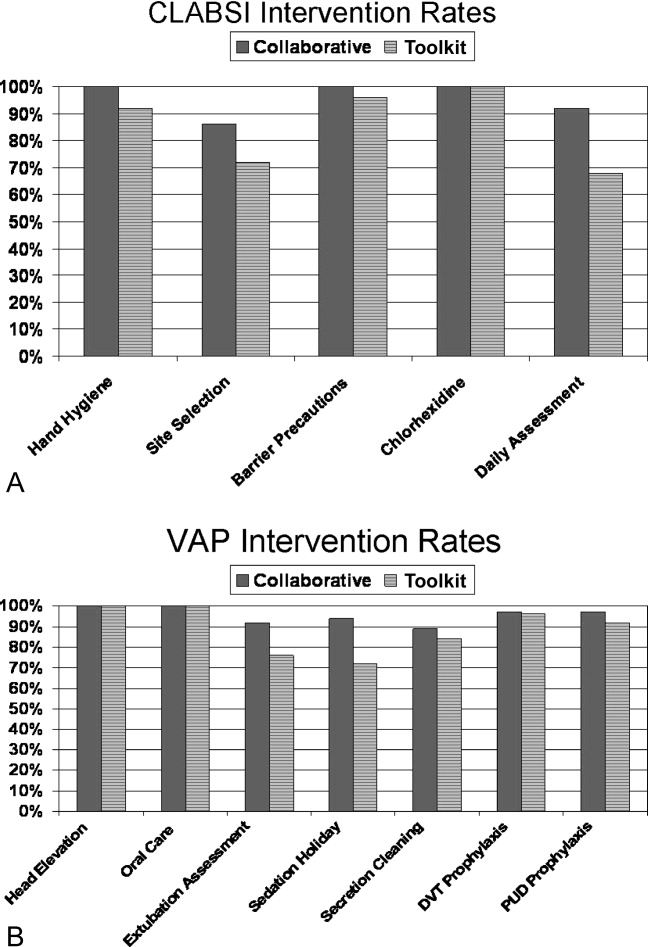
Abuse Potential of Sleeping Agents: Liability Varies Among Agents
A supplement to Clinical Psychiatry News.
This CLINICAL UPDATE is supported by Takeda Pharmaceuticals North America, Inc.
•Introduction
•Topic Highlights

Click Here to view the supplement.
Introduction
Introduction
Roland R. Griffiths, PhD
Professor of Behavioral Biology
Departments of Psychiatry and Neuroscience
Johns Hopkins University
School of Medicine
Baltimore, Md.
Dr. Griffiths has disclosed that he is Principal Investigator of two grants from the National Institute on Drug Abuse (NIDA) (R01 DA03889 and R01 DA03890) and co-investigator on a contract and several other grants from NIDA. During the past 5 years, on issues about drug abuse liability, he has been a consultant to or received grants from the following pharmaceutical companies: Abbott Laboratories, Forest Laboratories Inc., Merck & Co., Inc., Neurocrine Biosciences, Inc., Novartis Pharmaceuticals Corporation, Orphan Medical, Pharmacia Corporation, Pfizer Inc., Takeda Pharmaceuticals, TransOral Pharmaceucticals, Inc., Somaxon Pharmaceuticals Inc., and Wyeth Pharmaceuticals. He has disclosed that he will be discussing non-medical use (ie, abuse) of various hypnotic drugs.
Topic Highlights
• Abuse Potential of Sleeping Agents: Liability Varies Among Agents
Insomnia: A Brief Review
Effects of Insomnia
Pharmacologic Treatment of Insomnia
Patterns of Sedative/Hypnotic Abuse
• Abuse Potential of Hypnotic Agents: Study Evaluates Relative Abuse Liability
Defining Relative Abuse Liability and Toxicity
Relative Abuse Liability Table
Results of Analysis
Copyright © 2006 Elsevier Inc.
A supplement to Clinical Psychiatry News.
This CLINICAL UPDATE is supported by Takeda Pharmaceuticals North America, Inc.
•Introduction
•Topic Highlights
Click Here to view the supplement.
Introduction
Introduction
Roland R. Griffiths, PhD
Professor of Behavioral Biology
Departments of Psychiatry and Neuroscience
Johns Hopkins University
School of Medicine
Baltimore, Md.
Dr. Griffiths has disclosed that he is Principal Investigator of two grants from the National Institute on Drug Abuse (NIDA) (R01 DA03889 and R01 DA03890) and co-investigator on a contract and several other grants from NIDA. During the past 5 years, on issues about drug abuse liability, he has been a consultant to or received grants from the following pharmaceutical companies: Abbott Laboratories, Forest Laboratories Inc., Merck & Co., Inc., Neurocrine Biosciences, Inc., Novartis Pharmaceuticals Corporation, Orphan Medical, Pharmacia Corporation, Pfizer Inc., Takeda Pharmaceuticals, TransOral Pharmaceucticals, Inc., Somaxon Pharmaceuticals Inc., and Wyeth Pharmaceuticals. He has disclosed that he will be discussing non-medical use (ie, abuse) of various hypnotic drugs.
Topic Highlights
• Abuse Potential of Sleeping Agents: Liability Varies Among Agents
Insomnia: A Brief Review
Effects of Insomnia
Pharmacologic Treatment of Insomnia
Patterns of Sedative/Hypnotic Abuse
• Abuse Potential of Hypnotic Agents: Study Evaluates Relative Abuse Liability
Defining Relative Abuse Liability and Toxicity
Relative Abuse Liability Table
Results of Analysis
Copyright © 2006 Elsevier Inc.
A supplement to Clinical Psychiatry News.
This CLINICAL UPDATE is supported by Takeda Pharmaceuticals North America, Inc.
•Introduction
•Topic Highlights
Click Here to view the supplement.
Introduction
Introduction
Roland R. Griffiths, PhD
Professor of Behavioral Biology
Departments of Psychiatry and Neuroscience
Johns Hopkins University
School of Medicine
Baltimore, Md.
Dr. Griffiths has disclosed that he is Principal Investigator of two grants from the National Institute on Drug Abuse (NIDA) (R01 DA03889 and R01 DA03890) and co-investigator on a contract and several other grants from NIDA. During the past 5 years, on issues about drug abuse liability, he has been a consultant to or received grants from the following pharmaceutical companies: Abbott Laboratories, Forest Laboratories Inc., Merck & Co., Inc., Neurocrine Biosciences, Inc., Novartis Pharmaceuticals Corporation, Orphan Medical, Pharmacia Corporation, Pfizer Inc., Takeda Pharmaceuticals, TransOral Pharmaceucticals, Inc., Somaxon Pharmaceuticals Inc., and Wyeth Pharmaceuticals. He has disclosed that he will be discussing non-medical use (ie, abuse) of various hypnotic drugs.
Topic Highlights
• Abuse Potential of Sleeping Agents: Liability Varies Among Agents
Insomnia: A Brief Review
Effects of Insomnia
Pharmacologic Treatment of Insomnia
Patterns of Sedative/Hypnotic Abuse
• Abuse Potential of Hypnotic Agents: Study Evaluates Relative Abuse Liability
Defining Relative Abuse Liability and Toxicity
Relative Abuse Liability Table
Results of Analysis
Copyright © 2006 Elsevier Inc.

Hospitalists Tackle Heart Failure
News that the cost of treating cardiovascular diseases is expected to triple by 2030 comes as a group of hospitalists already are tackling the issue head on.
Vikas Bhalla, MD, a hospitalist at Emory University Hospital in Atlanta, is one of a handful of hospitalists working with the Heart Failure Society of America (HFSA) in an attempt to develop a standardized care plan for HF patients. The approach would risk-stratify patients with the condition and potentially create support protocols to work with outpatient physicians.
Theoretically, Dr. Bhalla says, more outpatient support would ultimately benefit HM by reducing readmissions.
The discussions are "in the very early stages, but we deal with [HF patients] every day," he adds. "There are cardiologists that we invite for a consult on the patients, but there is no heart failure specialist. Nowadays, we have a super-specialty. … If there's a set of guidelines, maybe we can reduce the readmission grade."
The handling of HF patients, and those suffering from other cardiovascular diseases, is even more important in the wake of an American Heart Association (AHA) policy statement last month predicting that treatment costs for cardiovascular diseases would triple to $818 billion in 2030, up from $272 billion last year. The bulk of the costs are tied to hypertension and its "downstream diseases."
If cost-cutting isn't enough, Dr. Bhalla says, hospitalists should be even more motivated to combat HF as future funding rules are likely to not reimburse physicians for readmissions tied to the original case, the so-called bundling of payments. If HM can help solve the problem of readmissions, it can reduce overall costs and improve their own charge capture as well, he adds.
"This immense cost can be at least stopped from escalating, if not decreased, by having a standard of care across the board," Dr. Bhalla says.
News that the cost of treating cardiovascular diseases is expected to triple by 2030 comes as a group of hospitalists already are tackling the issue head on.
Vikas Bhalla, MD, a hospitalist at Emory University Hospital in Atlanta, is one of a handful of hospitalists working with the Heart Failure Society of America (HFSA) in an attempt to develop a standardized care plan for HF patients. The approach would risk-stratify patients with the condition and potentially create support protocols to work with outpatient physicians.
Theoretically, Dr. Bhalla says, more outpatient support would ultimately benefit HM by reducing readmissions.
The discussions are "in the very early stages, but we deal with [HF patients] every day," he adds. "There are cardiologists that we invite for a consult on the patients, but there is no heart failure specialist. Nowadays, we have a super-specialty. … If there's a set of guidelines, maybe we can reduce the readmission grade."
The handling of HF patients, and those suffering from other cardiovascular diseases, is even more important in the wake of an American Heart Association (AHA) policy statement last month predicting that treatment costs for cardiovascular diseases would triple to $818 billion in 2030, up from $272 billion last year. The bulk of the costs are tied to hypertension and its "downstream diseases."
If cost-cutting isn't enough, Dr. Bhalla says, hospitalists should be even more motivated to combat HF as future funding rules are likely to not reimburse physicians for readmissions tied to the original case, the so-called bundling of payments. If HM can help solve the problem of readmissions, it can reduce overall costs and improve their own charge capture as well, he adds.
"This immense cost can be at least stopped from escalating, if not decreased, by having a standard of care across the board," Dr. Bhalla says.
News that the cost of treating cardiovascular diseases is expected to triple by 2030 comes as a group of hospitalists already are tackling the issue head on.
Vikas Bhalla, MD, a hospitalist at Emory University Hospital in Atlanta, is one of a handful of hospitalists working with the Heart Failure Society of America (HFSA) in an attempt to develop a standardized care plan for HF patients. The approach would risk-stratify patients with the condition and potentially create support protocols to work with outpatient physicians.
Theoretically, Dr. Bhalla says, more outpatient support would ultimately benefit HM by reducing readmissions.
The discussions are "in the very early stages, but we deal with [HF patients] every day," he adds. "There are cardiologists that we invite for a consult on the patients, but there is no heart failure specialist. Nowadays, we have a super-specialty. … If there's a set of guidelines, maybe we can reduce the readmission grade."
The handling of HF patients, and those suffering from other cardiovascular diseases, is even more important in the wake of an American Heart Association (AHA) policy statement last month predicting that treatment costs for cardiovascular diseases would triple to $818 billion in 2030, up from $272 billion last year. The bulk of the costs are tied to hypertension and its "downstream diseases."
If cost-cutting isn't enough, Dr. Bhalla says, hospitalists should be even more motivated to combat HF as future funding rules are likely to not reimburse physicians for readmissions tied to the original case, the so-called bundling of payments. If HM can help solve the problem of readmissions, it can reduce overall costs and improve their own charge capture as well, he adds.
"This immense cost can be at least stopped from escalating, if not decreased, by having a standard of care across the board," Dr. Bhalla says.