User login
Hospitalist Laments Level of Palliative Care
Bradley Flansbaum, DO, MPH, SFHM, director of the hospitalist program at Lenox Hill Hospital in New York City, recently posted "A Hospitalist's Lament," on the SHM-sponsored The Hospitalist Leader blog about the nuances of palliative care and advanced-care-planning discussions for patients nearing the end of life.
Dr. Flansbaum writes that, when asked to name a medical specialty other than HM that he might have enjoyed pursuing, he replies: "pain and palliative care." As he explains, "I didn’t discover that this was an area of interest for me until my career was much advanced," too late to pursue new opportunities for advanced training in palliative-care fellowships.
Yet he views eliciting the needs and wishes of terminally ill hospitalized patients as an art worth mastering. Hospitalists inevitably deal with end-of-life issues as a routine part of their jobs. "It's in our bailiwick. It's what we do, and it behooves us to get better at it," he says.
In his post, Dr. Flansbaum examines the recent medical literature (Sudore RL, Fried TR. Ann Int Med 2010;153:256; Perkins HS. Ann Int Med 2007;147:51-57; Sulmasy DP, Snyder L. JAMA 2010;304:1946-1947) questioning the benefits of advanced-care planning and advance-directive documents, such as living wills, in shaping the care patients want and need at the end of their lives. While these documents are not wasted effort, he says, "too often they're not very useful. We're learning that it's an incredibly dynamic process, contingent on cultural factors, and changing over time. One piece of paper with a static declaration isn't going to cover the bases. I've come to realize that it is about a talking, ongoing process."
Part of his "lament" as a hospitalist is that caring for terminally ill patients can be rife with ambiguities. Meanwhile, "everybody talks about how there's so much money wasted at the end of life, and we should be corralling our healthcare resources in a more efficient way. And yet the solutions we will need to get us to that place are damned hard," he says. (Listen to excerpts from the interview with Dr. Flansbaum [MP3 12.8MB])
Dr. Flansbaum recommends hospitalists make detailed conversations with patients confronting life-limiting illnesses a priority, which requires setting aside enough time for patients and understanding that such conversations are not singular events. He also encourages physicians to consider what their own values and priorities might be in such a situation, an exercise he recently conducted with his residents.
Bradley Flansbaum, DO, MPH, SFHM, director of the hospitalist program at Lenox Hill Hospital in New York City, recently posted "A Hospitalist's Lament," on the SHM-sponsored The Hospitalist Leader blog about the nuances of palliative care and advanced-care-planning discussions for patients nearing the end of life.
Dr. Flansbaum writes that, when asked to name a medical specialty other than HM that he might have enjoyed pursuing, he replies: "pain and palliative care." As he explains, "I didn’t discover that this was an area of interest for me until my career was much advanced," too late to pursue new opportunities for advanced training in palliative-care fellowships.
Yet he views eliciting the needs and wishes of terminally ill hospitalized patients as an art worth mastering. Hospitalists inevitably deal with end-of-life issues as a routine part of their jobs. "It's in our bailiwick. It's what we do, and it behooves us to get better at it," he says.
In his post, Dr. Flansbaum examines the recent medical literature (Sudore RL, Fried TR. Ann Int Med 2010;153:256; Perkins HS. Ann Int Med 2007;147:51-57; Sulmasy DP, Snyder L. JAMA 2010;304:1946-1947) questioning the benefits of advanced-care planning and advance-directive documents, such as living wills, in shaping the care patients want and need at the end of their lives. While these documents are not wasted effort, he says, "too often they're not very useful. We're learning that it's an incredibly dynamic process, contingent on cultural factors, and changing over time. One piece of paper with a static declaration isn't going to cover the bases. I've come to realize that it is about a talking, ongoing process."
Part of his "lament" as a hospitalist is that caring for terminally ill patients can be rife with ambiguities. Meanwhile, "everybody talks about how there's so much money wasted at the end of life, and we should be corralling our healthcare resources in a more efficient way. And yet the solutions we will need to get us to that place are damned hard," he says. (Listen to excerpts from the interview with Dr. Flansbaum [MP3 12.8MB])
Dr. Flansbaum recommends hospitalists make detailed conversations with patients confronting life-limiting illnesses a priority, which requires setting aside enough time for patients and understanding that such conversations are not singular events. He also encourages physicians to consider what their own values and priorities might be in such a situation, an exercise he recently conducted with his residents.
Bradley Flansbaum, DO, MPH, SFHM, director of the hospitalist program at Lenox Hill Hospital in New York City, recently posted "A Hospitalist's Lament," on the SHM-sponsored The Hospitalist Leader blog about the nuances of palliative care and advanced-care-planning discussions for patients nearing the end of life.
Dr. Flansbaum writes that, when asked to name a medical specialty other than HM that he might have enjoyed pursuing, he replies: "pain and palliative care." As he explains, "I didn’t discover that this was an area of interest for me until my career was much advanced," too late to pursue new opportunities for advanced training in palliative-care fellowships.
Yet he views eliciting the needs and wishes of terminally ill hospitalized patients as an art worth mastering. Hospitalists inevitably deal with end-of-life issues as a routine part of their jobs. "It's in our bailiwick. It's what we do, and it behooves us to get better at it," he says.
In his post, Dr. Flansbaum examines the recent medical literature (Sudore RL, Fried TR. Ann Int Med 2010;153:256; Perkins HS. Ann Int Med 2007;147:51-57; Sulmasy DP, Snyder L. JAMA 2010;304:1946-1947) questioning the benefits of advanced-care planning and advance-directive documents, such as living wills, in shaping the care patients want and need at the end of their lives. While these documents are not wasted effort, he says, "too often they're not very useful. We're learning that it's an incredibly dynamic process, contingent on cultural factors, and changing over time. One piece of paper with a static declaration isn't going to cover the bases. I've come to realize that it is about a talking, ongoing process."
Part of his "lament" as a hospitalist is that caring for terminally ill patients can be rife with ambiguities. Meanwhile, "everybody talks about how there's so much money wasted at the end of life, and we should be corralling our healthcare resources in a more efficient way. And yet the solutions we will need to get us to that place are damned hard," he says. (Listen to excerpts from the interview with Dr. Flansbaum [MP3 12.8MB])
Dr. Flansbaum recommends hospitalists make detailed conversations with patients confronting life-limiting illnesses a priority, which requires setting aside enough time for patients and understanding that such conversations are not singular events. He also encourages physicians to consider what their own values and priorities might be in such a situation, an exercise he recently conducted with his residents.
CLINICAL UPDATE: Selected Issues in Psychiatry
This CLINICAL UPDATE is supported by an educational grant from UCB Pharma, Inc., and is a supplement to Clinical Psychiatry News.
This supplement is based on a faculty interview and poster reviews.

Click Here To view the supplement.
Faculty
Joseph F. Goldberg, MD
Director of Bipolar Disorders Research
The Zucker Hillside Hospital-North Shore Long Island Jewish Health System
Glen Oaks, N.Y.
Received Funding for Clinical Grants/Consultant: Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb Company, Eli Lilly and Company, and GlaxoSmithKline. He discusses the off-label use of levetiracetam for the treatment of psychiatric disorders.
Topics
• Anticonvulsants and Psychiatric Disorders
• Treatment of Varied Psychiatric Disorders in an Outpatient Setting
• Prevalence of ADHD in Adults
• Treatment of Mild or Moderate Bipolar Disorder
• Prevalence of Medical Comorbidity in Severe Psychiatric Disorders
• Evaluation of Therapy for Aggression Disorders
• Prevalence of Comorbid Anxiety Disorders
• Evaluation of Therapy for Bipolar Mania
• Evaluation of Add-On Therapy for Bipolar Disorder Therapy
Copyright © 2004 by International Medical News Group
This CLINICAL UPDATE is supported by an educational grant from UCB Pharma, Inc., and is a supplement to Clinical Psychiatry News.
This supplement is based on a faculty interview and poster reviews.
Click Here To view the supplement.
Faculty
Joseph F. Goldberg, MD
Director of Bipolar Disorders Research
The Zucker Hillside Hospital-North Shore Long Island Jewish Health System
Glen Oaks, N.Y.
Received Funding for Clinical Grants/Consultant: Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb Company, Eli Lilly and Company, and GlaxoSmithKline. He discusses the off-label use of levetiracetam for the treatment of psychiatric disorders.
Topics
• Anticonvulsants and Psychiatric Disorders
• Treatment of Varied Psychiatric Disorders in an Outpatient Setting
• Prevalence of ADHD in Adults
• Treatment of Mild or Moderate Bipolar Disorder
• Prevalence of Medical Comorbidity in Severe Psychiatric Disorders
• Evaluation of Therapy for Aggression Disorders
• Prevalence of Comorbid Anxiety Disorders
• Evaluation of Therapy for Bipolar Mania
• Evaluation of Add-On Therapy for Bipolar Disorder Therapy
Copyright © 2004 by International Medical News Group
This CLINICAL UPDATE is supported by an educational grant from UCB Pharma, Inc., and is a supplement to Clinical Psychiatry News.
This supplement is based on a faculty interview and poster reviews.
Click Here To view the supplement.
Faculty
Joseph F. Goldberg, MD
Director of Bipolar Disorders Research
The Zucker Hillside Hospital-North Shore Long Island Jewish Health System
Glen Oaks, N.Y.
Received Funding for Clinical Grants/Consultant: Abbott Laboratories, AstraZeneca, Bristol-Myers Squibb Company, Eli Lilly and Company, and GlaxoSmithKline. He discusses the off-label use of levetiracetam for the treatment of psychiatric disorders.
Topics
• Anticonvulsants and Psychiatric Disorders
• Treatment of Varied Psychiatric Disorders in an Outpatient Setting
• Prevalence of ADHD in Adults
• Treatment of Mild or Moderate Bipolar Disorder
• Prevalence of Medical Comorbidity in Severe Psychiatric Disorders
• Evaluation of Therapy for Aggression Disorders
• Prevalence of Comorbid Anxiety Disorders
• Evaluation of Therapy for Bipolar Mania
• Evaluation of Add-On Therapy for Bipolar Disorder Therapy
Copyright © 2004 by International Medical News Group

BEST PRACTICES IN: Psychosocial Impact of Rosacea
A supplement to Skin & Allergy News. This supplement was sponsored by Galderma Laboratories, L.P.

- NRS Digital Perception Survey
- Presentation And Diagnosis
- Treatment Strategies
Faculty/Faculty Disclosure
Debra B. Luftman, MD
Coauthor of The Beauty Prescription:
The Complete Formula for Looking and Feeling Beautiful Calabasas, California
Dr Luftman has received funding for clinical grants from and is a consultant for Galderma Laboratories, L.P.
Copyright (c) 2011 Elsevier Inc.
A supplement to Skin & Allergy News. This supplement was sponsored by Galderma Laboratories, L.P.
- NRS Digital Perception Survey
- Presentation And Diagnosis
- Treatment Strategies
Faculty/Faculty Disclosure
Debra B. Luftman, MD
Coauthor of The Beauty Prescription:
The Complete Formula for Looking and Feeling Beautiful Calabasas, California
Dr Luftman has received funding for clinical grants from and is a consultant for Galderma Laboratories, L.P.
Copyright (c) 2011 Elsevier Inc.
A supplement to Skin & Allergy News. This supplement was sponsored by Galderma Laboratories, L.P.
- NRS Digital Perception Survey
- Presentation And Diagnosis
- Treatment Strategies
Faculty/Faculty Disclosure
Debra B. Luftman, MD
Coauthor of The Beauty Prescription:
The Complete Formula for Looking and Feeling Beautiful Calabasas, California
Dr Luftman has received funding for clinical grants from and is a consultant for Galderma Laboratories, L.P.
Copyright (c) 2011 Elsevier Inc.

A Rush for Technology Dollars? Not So Fast
HM program directors, particularly those involved in technology upgrades at their institutions, probably have heard a lot about electronic health record (EHR) attestation since the Centers for Medicare & Medicaid Services (CMS) announced that registration was open last month. But while CMS is pushing for physicians and hospitals to register as soon as possible, at least one informatics professional suggests that there is no major hurry to apply for the $20 billion the federal government has set aside for doctors and hospitals that adopt new technologies.
“I’m of the approach there is no rush to sign up even though we know we’re going for the funds,” says Anne M. Bobb, an informatics pharmacist in the Department of Quality and Clinical Informatics at Northwestern Memorial Hospital in Chicago. “We want to do it in a reasonable amount of time.”
Bobb, who works closely with the hospitalists at Northwestern Memorial, says that both “eligible professionals” and “eligible hospitals” have ample time to apply. She says applicants remain eligible for reimbursement as long as they register by fiscal year 2013 (eligible physicians [EP] and eligible hospitals [EH] need only 90 days of reporting for year one; measurements must begin and registration must be completed by EPs on July 3, 2013, and Oct. 3, 2013 for EHs). In addition, groups that register before then and stutter-step in their compliance because their nascent programs are just developing their protocol could jeopardize potential funding.
Those physicians and institutions that want certification must meet “meaningful use” criteria, defined by CMS last summer as meeting prescribed rules for implementation of EHR. Stage 1 rules, which take effect this year, require eligible physicians (EPs) and eligible hospitals to meet goals in 15 and 14 categories, respectively. Up to five goals can be deferred, according to CMS. The CMS timeline includes second and third stages, each of which will require goals that are even more advanced. The thresholds must be met to qualify for funding.
It’s understandable CMS wants to jump-start registration, but individual physicians and hospitals should take their time to determine what works best for them. “If you know you’re not going to make it for fiscal year 2011,” she asks rhetorically, “why go after it now?”
The registration process began Jan. 3 in Alaska, Iowa, Kentucky, Louisiana, Michigan, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. More states, including California, are expected to open the process as early as this month.
For more information on what is needed to register, visit the EHR Incentive Program microsite. The EHR Information Center can be reached at 888-734-6433.
HM program directors, particularly those involved in technology upgrades at their institutions, probably have heard a lot about electronic health record (EHR) attestation since the Centers for Medicare & Medicaid Services (CMS) announced that registration was open last month. But while CMS is pushing for physicians and hospitals to register as soon as possible, at least one informatics professional suggests that there is no major hurry to apply for the $20 billion the federal government has set aside for doctors and hospitals that adopt new technologies.
“I’m of the approach there is no rush to sign up even though we know we’re going for the funds,” says Anne M. Bobb, an informatics pharmacist in the Department of Quality and Clinical Informatics at Northwestern Memorial Hospital in Chicago. “We want to do it in a reasonable amount of time.”
Bobb, who works closely with the hospitalists at Northwestern Memorial, says that both “eligible professionals” and “eligible hospitals” have ample time to apply. She says applicants remain eligible for reimbursement as long as they register by fiscal year 2013 (eligible physicians [EP] and eligible hospitals [EH] need only 90 days of reporting for year one; measurements must begin and registration must be completed by EPs on July 3, 2013, and Oct. 3, 2013 for EHs). In addition, groups that register before then and stutter-step in their compliance because their nascent programs are just developing their protocol could jeopardize potential funding.
Those physicians and institutions that want certification must meet “meaningful use” criteria, defined by CMS last summer as meeting prescribed rules for implementation of EHR. Stage 1 rules, which take effect this year, require eligible physicians (EPs) and eligible hospitals to meet goals in 15 and 14 categories, respectively. Up to five goals can be deferred, according to CMS. The CMS timeline includes second and third stages, each of which will require goals that are even more advanced. The thresholds must be met to qualify for funding.
It’s understandable CMS wants to jump-start registration, but individual physicians and hospitals should take their time to determine what works best for them. “If you know you’re not going to make it for fiscal year 2011,” she asks rhetorically, “why go after it now?”
The registration process began Jan. 3 in Alaska, Iowa, Kentucky, Louisiana, Michigan, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. More states, including California, are expected to open the process as early as this month.
For more information on what is needed to register, visit the EHR Incentive Program microsite. The EHR Information Center can be reached at 888-734-6433.
HM program directors, particularly those involved in technology upgrades at their institutions, probably have heard a lot about electronic health record (EHR) attestation since the Centers for Medicare & Medicaid Services (CMS) announced that registration was open last month. But while CMS is pushing for physicians and hospitals to register as soon as possible, at least one informatics professional suggests that there is no major hurry to apply for the $20 billion the federal government has set aside for doctors and hospitals that adopt new technologies.
“I’m of the approach there is no rush to sign up even though we know we’re going for the funds,” says Anne M. Bobb, an informatics pharmacist in the Department of Quality and Clinical Informatics at Northwestern Memorial Hospital in Chicago. “We want to do it in a reasonable amount of time.”
Bobb, who works closely with the hospitalists at Northwestern Memorial, says that both “eligible professionals” and “eligible hospitals” have ample time to apply. She says applicants remain eligible for reimbursement as long as they register by fiscal year 2013 (eligible physicians [EP] and eligible hospitals [EH] need only 90 days of reporting for year one; measurements must begin and registration must be completed by EPs on July 3, 2013, and Oct. 3, 2013 for EHs). In addition, groups that register before then and stutter-step in their compliance because their nascent programs are just developing their protocol could jeopardize potential funding.
Those physicians and institutions that want certification must meet “meaningful use” criteria, defined by CMS last summer as meeting prescribed rules for implementation of EHR. Stage 1 rules, which take effect this year, require eligible physicians (EPs) and eligible hospitals to meet goals in 15 and 14 categories, respectively. Up to five goals can be deferred, according to CMS. The CMS timeline includes second and third stages, each of which will require goals that are even more advanced. The thresholds must be met to qualify for funding.
It’s understandable CMS wants to jump-start registration, but individual physicians and hospitals should take their time to determine what works best for them. “If you know you’re not going to make it for fiscal year 2011,” she asks rhetorically, “why go after it now?”
The registration process began Jan. 3 in Alaska, Iowa, Kentucky, Louisiana, Michigan, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. More states, including California, are expected to open the process as early as this month.
For more information on what is needed to register, visit the EHR Incentive Program microsite. The EHR Information Center can be reached at 888-734-6433.
In the Literature: Research You Need to Know
Clinical question: Does early initiation of maintenance dialysis for patients with stage 5 chronic kidney disease affect survival?
Background: There is considerable variation in timing of dialysis for patients with chronic kidney disease, with a trend toward early initiation. Observational cohort and case control studies have suggested increased survival and quality of life and decreased complications with early initiation. More recent observational data, however, call this into question.
Study design: Randomized controlled trial.
Setting: Thirty-two centers in Australia and New Zealand.
Synopsis: A total of 828 patients were randomly assigned to the early-start group, in which patients would begin dialysis with an estimated glomerular filtration rate (GFR), using the Cockcroft-Gault Equation, of 10.0 ml to 14.0 ml per minute per 1.72 meters squared, or a late-start group in which dialysis would be initiated at a goal GFR of 5.0 ml/min to 7.0 ml/min.
Though 75.9% of patients in the late-start group initiated dialysis above the target rate due to symptoms or physician recommendation, the mean time to dialysis was still almost six months longer (7.40 months versus 1.80 months).
Patients were followed for a median of 3.59 years. Mortality was similar between the groups: 37.6% and 36.6% of the early-start group and late-start group died, respectively (hazard ratio 1.04, p=0.75). There was no significant difference in other adverse events (cardiovascular events, infections, or complications of dialysis) between the two groups.
The study could not be blinded but the adherence to a definitive endpoint of mortality limits the possibility of observation bias. Post hoc analysis with an alternative method of GFR assessment (the MDRD equation) yielded similar conclusions.
This is the first randomized controlled trial to look at this question, and while concordant with recent observational studies, the conclusions are inconsistent with existing guidelines from national and international groups. Adherence to guidelines recommending early initiation of dialysis is unlikely to improve clinical outcomes while significantly increasing costs.
Bottom line: Early initiation of dialysis is not associated with improved survival in patients with stage 5 chronic kidney disease compared with delaying dialysis to a goal GFR of 7.0 ml/min or the development of symptoms.
Citation: Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619.
Reviewed for TH eWire by Jill Goldenberg, MD, Alan Briones, MD, Chad Craig, MD, Ramiro Jervis, MD, FHM, Brian Markoff, MD, FHM, Andrew Dunn, MD, FACP, FHM, Division of Hospital Medicine, Mount Sinai School of Medicine, New York City.
For more physician reviews of HM-related research, visit our website.
Clinical question: Does early initiation of maintenance dialysis for patients with stage 5 chronic kidney disease affect survival?
Background: There is considerable variation in timing of dialysis for patients with chronic kidney disease, with a trend toward early initiation. Observational cohort and case control studies have suggested increased survival and quality of life and decreased complications with early initiation. More recent observational data, however, call this into question.
Study design: Randomized controlled trial.
Setting: Thirty-two centers in Australia and New Zealand.
Synopsis: A total of 828 patients were randomly assigned to the early-start group, in which patients would begin dialysis with an estimated glomerular filtration rate (GFR), using the Cockcroft-Gault Equation, of 10.0 ml to 14.0 ml per minute per 1.72 meters squared, or a late-start group in which dialysis would be initiated at a goal GFR of 5.0 ml/min to 7.0 ml/min.
Though 75.9% of patients in the late-start group initiated dialysis above the target rate due to symptoms or physician recommendation, the mean time to dialysis was still almost six months longer (7.40 months versus 1.80 months).
Patients were followed for a median of 3.59 years. Mortality was similar between the groups: 37.6% and 36.6% of the early-start group and late-start group died, respectively (hazard ratio 1.04, p=0.75). There was no significant difference in other adverse events (cardiovascular events, infections, or complications of dialysis) between the two groups.
The study could not be blinded but the adherence to a definitive endpoint of mortality limits the possibility of observation bias. Post hoc analysis with an alternative method of GFR assessment (the MDRD equation) yielded similar conclusions.
This is the first randomized controlled trial to look at this question, and while concordant with recent observational studies, the conclusions are inconsistent with existing guidelines from national and international groups. Adherence to guidelines recommending early initiation of dialysis is unlikely to improve clinical outcomes while significantly increasing costs.
Bottom line: Early initiation of dialysis is not associated with improved survival in patients with stage 5 chronic kidney disease compared with delaying dialysis to a goal GFR of 7.0 ml/min or the development of symptoms.
Citation: Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619.
Reviewed for TH eWire by Jill Goldenberg, MD, Alan Briones, MD, Chad Craig, MD, Ramiro Jervis, MD, FHM, Brian Markoff, MD, FHM, Andrew Dunn, MD, FACP, FHM, Division of Hospital Medicine, Mount Sinai School of Medicine, New York City.
For more physician reviews of HM-related research, visit our website.
Clinical question: Does early initiation of maintenance dialysis for patients with stage 5 chronic kidney disease affect survival?
Background: There is considerable variation in timing of dialysis for patients with chronic kidney disease, with a trend toward early initiation. Observational cohort and case control studies have suggested increased survival and quality of life and decreased complications with early initiation. More recent observational data, however, call this into question.
Study design: Randomized controlled trial.
Setting: Thirty-two centers in Australia and New Zealand.
Synopsis: A total of 828 patients were randomly assigned to the early-start group, in which patients would begin dialysis with an estimated glomerular filtration rate (GFR), using the Cockcroft-Gault Equation, of 10.0 ml to 14.0 ml per minute per 1.72 meters squared, or a late-start group in which dialysis would be initiated at a goal GFR of 5.0 ml/min to 7.0 ml/min.
Though 75.9% of patients in the late-start group initiated dialysis above the target rate due to symptoms or physician recommendation, the mean time to dialysis was still almost six months longer (7.40 months versus 1.80 months).
Patients were followed for a median of 3.59 years. Mortality was similar between the groups: 37.6% and 36.6% of the early-start group and late-start group died, respectively (hazard ratio 1.04, p=0.75). There was no significant difference in other adverse events (cardiovascular events, infections, or complications of dialysis) between the two groups.
The study could not be blinded but the adherence to a definitive endpoint of mortality limits the possibility of observation bias. Post hoc analysis with an alternative method of GFR assessment (the MDRD equation) yielded similar conclusions.
This is the first randomized controlled trial to look at this question, and while concordant with recent observational studies, the conclusions are inconsistent with existing guidelines from national and international groups. Adherence to guidelines recommending early initiation of dialysis is unlikely to improve clinical outcomes while significantly increasing costs.
Bottom line: Early initiation of dialysis is not associated with improved survival in patients with stage 5 chronic kidney disease compared with delaying dialysis to a goal GFR of 7.0 ml/min or the development of symptoms.
Citation: Cooper BA, Branley P, Bulfone L, et al. A randomized, controlled trial of early versus late initiation of dialysis. N Engl J Med. 2010;363(7):609-619.
Reviewed for TH eWire by Jill Goldenberg, MD, Alan Briones, MD, Chad Craig, MD, Ramiro Jervis, MD, FHM, Brian Markoff, MD, FHM, Andrew Dunn, MD, FACP, FHM, Division of Hospital Medicine, Mount Sinai School of Medicine, New York City.
For more physician reviews of HM-related research, visit our website.
Hospitalists in Disaster Response
In the last decade, natural disasters such as the Indonesian tsunami of 2004, Hurricane Katrina in 2004, and the Pakistani earthquake of 2005 have brought attention to the importance of diverse but complementary medical professional roles in humanitarian medical aid.14 Natural disasters that cause significant physical trauma to large populations often necessitate initial multidisciplinary responder teams comprised of surgeons, anesthesiologists, emergency medicine physicians, surgical technologists, nurses, psychiatrists, and public health specialists. Their roles are to manage life‐threatening injuries, provide immediate triage, help affected individuals deal with intense psychological shock, and address critical population‐based needs such as water, food, and sanitation. Meanwhile, general medical, pediatric, rehabilitative, and long‐term psychiatric services often constitute a secondary tier of disaster response, providing postsurgical care, managing acute medical illnesses, mitigating psychological trauma, rehabilitating injuries, and providing vaccinations to at‐risk individuals. Hospitalists can play an important role in postcatastrophe recovery services as experts in acute care, stewards of care transitions, and drivers of systems improvement.
The earthquake that occurred January 12, 2010 in Haiti is a dramatic illustration of the importance of a multidisciplinary approach to disaster relief. The 7.0‐magnitude earthquake near Port‐au‐Prince ravaged an already crippled health care system, severely damaging the country's primary academic medical center, and killed the entire class of second‐year nursing students. The death toll has been estimated to be nearly one‐quarter of a million people.5 Victims awaiting surgery, recovering from surgery, or in need of other immediate medical attention quickly inundated any existing health facilities. The following stories describe the authors' respective experiences in Haiti after the earthquake.
JC: I arrived 4 days after the earthquake to a hospital outside of Port‐au‐Prince, spared from destruction, but filled with hundreds of patients with crush injuries and severe fractures. On rounds with the surgical team, I observed that venous thromboembolism (VTE) prophylaxis had not yet been initiated, and I was concerned that patients might die from pulmonary embolism. In the overwhelming urgency of providing life‐saving surgery to as many patients as possible, this simple measure had been overlooked. After discussion with our team and our Haitian medical colleagues, we initiated subcutaneous heparin on all eligible patients and made arrangements to receive further shipments of heparin to accommodate the influx of patients.
A nearby school and church had been annexed into makeshift extensions of the hospital wards. The volume and pace of incoming injuries was such that as soon as a patient was taken to surgery, another patient would often take his or her place in the bed. The rapid movement of patients to and from x‐ray, surgery, and postsurgical care created challenges around effective and accurate communication among multiple care providers. We decided that nonsurgical personnel would triage newly arriving patients and round on patients daily. Each nonsurgical physician was responsible for staffing a particular location. This zone‐defense approach ensured that the surgeons maximized their time in the operating rooms. We also instituted a basic system of portable medical records kept with each patient at all times, allowing personnel to easily and quickly assess care given to date, and to write notes and orders.
Presurgical and postsurgical wound infections became a common event, with the risk of ensuing sepsis. Antibiotic use was dependent on the preferences of individual surgeons and also on the available supply. As a result, antimicrobial treatments were highly variable and sometimes inadequate. The internists on the team proposed standard antibiotic guidelines for open fractures, for contaminated wounds, and for postoperative wounds; these regimens were approved and implemented by Haitian staff and the rest of the team.
Internists recognized the first complications of rhabdomyolysis from crush injuries and delays in receiving medical attention. Malaise, oliguria, and volume overload were often the only clues we had for severe renal failure. We had a functional lab capable of checking complete blood counts, urinalysis and creatinine, but we had a limited supply of serum potassium assays. We only used the latter in confirmed cases of rhabdomyolysis, and on several occasions we diagnosed severe hyperkalemia. Using bedside automated electrical defibrillation devices for monitoring, we sustained these patients on calcium gluconate until they could be transferred to an external dialysis unit run by Mdecins Sans Frontires in Port‐au‐Prince.6 As the number of rhabdomyolysis cases increased, we instigated creatinine rounds on patients arriving with large crush injuries, and we evaluated urine output daily until patients were clinically stable from this threat. We also helped the Haitian staff treat the omnipresent problem of pain and advised renal dosing of medications in renal failure and elderly patients.
GH: The situation 3 months after the earthquake was medically less dire but highlights the evolving importance of generalists in the aftermath of the quake.710 For many Haitian patients, the earthquake had become a universal point of reference for their symptomatology. Anorexia, amenorrhea, headaches, epigastric pain, even fungating soft tissue masses, were all reported to be depi tranbleman t a (since the earthquake) and were often somatic manifestations of a psychologically devastating event. At a hospital in Carrefour, I cared for patients presenting with dramatic sequelae of chronic diseases that had been undertreated due to the destruction of the Haitian medical infrastructurehypertensive coma, diabetic ketoacidosis, cerebral malaria, decompensated liver disease, and severe chronic anemia (including a patient with a hemoglobin of 3 mg/dL). I encountered many patients with infections exacerbated by excessive crowding in tent communities, such as typhoid and tuberculosis. At this particular hospital, priorities appropriately placed on surgical and postsurgical care required the team to devise creative solutions for the care and placement of medical patients, such as restructuring the emergency department and creating a rehabilitation tent on the hospital grounds. While few Haitian internists were present, a number of Haitian obstetricians were on site and helped manage medical conditions within the scope of their experience, such as hypertension, abdominal pain, and genitourinary infections. The expatriate orthopedic surgeons on site sought the consultative skills of hospitalists for preoperative management, postoperative complications, and comorbid conditions.
This hospital was largely sustained by rotating teams of volunteers, which underscored the importance of establishing a flexible system that would accommodate the turnover of personnel and fluctuating levels of professional expertise. The team used a tiered model for acute care delivery designating responsibilities based on the number of nurses, physicians, and other providers available. We collaborated with Haitian physicians to establish a routine of handoff rounds. Finally, we created and centralized documentation such as clinical protocols, contact numbers, and helpful tips for our successors.
Hospitalists have valuable skills to offer in medical responses to natural catastrophes.5 Our fluency with acute care environments becomes a pluripotent asset in disaster relief. Our experiences in assessing acuity are vital in assisting with inpatient triage. Our familiarity with the comanagement model facilitates partnership with other disciplines to optimize the distribution of skill sets without neglecting the overall well‐being of patients. Our clinical expertise in treating the vulnerable elderly, VTE, renal failure, pain management, postoperative infections, sepsis, and many other conditions can bolster medical relief efforts, even when the foremost need is surgical. The hospitalist's core competencies in healthcare systems11 can support recovery initiatives in medical facilities, particularly in the domains of drug safety, resource allocation, information management, team‐based methods, and care transitions. Our respective experiences also suggest the potential value of hospitalists in domestic, in addition to international, disaster response initiatives. Since large‐scale calamities may result in the hospitalization of overwhelming numbers of victims,12 hospitalists may be well‐positioned to assist our emergency medicine and public health colleagues, who currently (and fittingly) lead domestic efforts in disaster relief.
Tragedies like the earthquake in Haiti serve as a sobering reminder that a comprehensive multidisciplinary approach is required as medical disaster relief shifts from a life‐saving focus to one of life‐preserving care.13, 14 Hospitalists can play a vital role in these restorative efforts.
Acknowledgements
The authors thank their hospitalist colleagues at Beth Israel Deaconess who generously covered our shifts and encouraged us to write about our experiences.
- ,.Health impact of the 2004 Andaman Nicobar earthquake and tsunami in Indonesia.Prehosp Disaster Med.2009;24(6):493–499.
- ,,,.Medical response to hurricanes Katrina and Rita: local public health preparedness in action.J Public Health Manag Pract.2007;13(5):441–446.
- .Nephrology in earthquakes: sharing experiences and information.Clin J Am Soc Nephrol.2007;2(4):803–808.
- The Hospitalist. November2005. Hurricane Katrina: tragedy and hope. Available at: http://www.the‐hospitalist.org/details/article/255673/Hurricane_Katrina_Tragedy_and_Hope.html. Accessed August 2010.
- Washington Post. February 10,2010. Haiti raises earthquake toll to 230,000. Available at: http://www.washingtonpost.com/wp‐dyn/content/article/2010/02/09/AR2010020904447.html. Accessed August 2010.
- Médecins sans Frontiéres. About us. Available at: http://www.msf.org/msfinternational/aboutmsf/. Accessed August 2010.
- ,,, et al.Practicing internal medicine onboard the USNS COMFORT in the aftermath of the Haitian earthquake.Ann Intern Med.2010;152(11):733–737.
- Minnesota Medicine. April2010. Help for Haiti. Available at: http://www.minnesotamedicine.com/PastIssues/April2010/CoverstoryApril2010/tabid/3370/Default.aspx. Accessed August 2010.
- The Hospitalist. April2010. Hospitalists in Haiti. Available at: http://www.the‐hospitalist.org/details/article/590287/Hospitalists_in_Haiti.html. Accessed August 2010.
- .Haiti earthquake relief, phase two–long‐term needs and local resources.N Engl J Med.2010;362(20):1858–1861.
- ,,,,.The core competencies in hospital medicine: a framework for curriculum development by the society of hospital medicine. J Hosp Med.2006;(1 Suppl 1):2–95.
- ,,, et al.The impact of the Tsunami on hospitalizations at the tertiary care hospital in the Southern Province of Sri Lanka.Am J Disaster Med.2008;3(3):147–155.
- ,,.Short communication: patterns of chronic and acute diseases after natural disasters ‐ a study from the International Committee of the Red Cross field hospital in Banda Aceh after the 2004 Indian Ocean tsunami.Trop Med Int Health.2007;12(11):1338–1341.
- ,,.Characterisation of patients treated at the Red Cross field hospital in Kashmir during the first three weeks of operation.Emerg Med J.2006;23(8):654–656.
In the last decade, natural disasters such as the Indonesian tsunami of 2004, Hurricane Katrina in 2004, and the Pakistani earthquake of 2005 have brought attention to the importance of diverse but complementary medical professional roles in humanitarian medical aid.14 Natural disasters that cause significant physical trauma to large populations often necessitate initial multidisciplinary responder teams comprised of surgeons, anesthesiologists, emergency medicine physicians, surgical technologists, nurses, psychiatrists, and public health specialists. Their roles are to manage life‐threatening injuries, provide immediate triage, help affected individuals deal with intense psychological shock, and address critical population‐based needs such as water, food, and sanitation. Meanwhile, general medical, pediatric, rehabilitative, and long‐term psychiatric services often constitute a secondary tier of disaster response, providing postsurgical care, managing acute medical illnesses, mitigating psychological trauma, rehabilitating injuries, and providing vaccinations to at‐risk individuals. Hospitalists can play an important role in postcatastrophe recovery services as experts in acute care, stewards of care transitions, and drivers of systems improvement.
The earthquake that occurred January 12, 2010 in Haiti is a dramatic illustration of the importance of a multidisciplinary approach to disaster relief. The 7.0‐magnitude earthquake near Port‐au‐Prince ravaged an already crippled health care system, severely damaging the country's primary academic medical center, and killed the entire class of second‐year nursing students. The death toll has been estimated to be nearly one‐quarter of a million people.5 Victims awaiting surgery, recovering from surgery, or in need of other immediate medical attention quickly inundated any existing health facilities. The following stories describe the authors' respective experiences in Haiti after the earthquake.
JC: I arrived 4 days after the earthquake to a hospital outside of Port‐au‐Prince, spared from destruction, but filled with hundreds of patients with crush injuries and severe fractures. On rounds with the surgical team, I observed that venous thromboembolism (VTE) prophylaxis had not yet been initiated, and I was concerned that patients might die from pulmonary embolism. In the overwhelming urgency of providing life‐saving surgery to as many patients as possible, this simple measure had been overlooked. After discussion with our team and our Haitian medical colleagues, we initiated subcutaneous heparin on all eligible patients and made arrangements to receive further shipments of heparin to accommodate the influx of patients.
A nearby school and church had been annexed into makeshift extensions of the hospital wards. The volume and pace of incoming injuries was such that as soon as a patient was taken to surgery, another patient would often take his or her place in the bed. The rapid movement of patients to and from x‐ray, surgery, and postsurgical care created challenges around effective and accurate communication among multiple care providers. We decided that nonsurgical personnel would triage newly arriving patients and round on patients daily. Each nonsurgical physician was responsible for staffing a particular location. This zone‐defense approach ensured that the surgeons maximized their time in the operating rooms. We also instituted a basic system of portable medical records kept with each patient at all times, allowing personnel to easily and quickly assess care given to date, and to write notes and orders.
Presurgical and postsurgical wound infections became a common event, with the risk of ensuing sepsis. Antibiotic use was dependent on the preferences of individual surgeons and also on the available supply. As a result, antimicrobial treatments were highly variable and sometimes inadequate. The internists on the team proposed standard antibiotic guidelines for open fractures, for contaminated wounds, and for postoperative wounds; these regimens were approved and implemented by Haitian staff and the rest of the team.
Internists recognized the first complications of rhabdomyolysis from crush injuries and delays in receiving medical attention. Malaise, oliguria, and volume overload were often the only clues we had for severe renal failure. We had a functional lab capable of checking complete blood counts, urinalysis and creatinine, but we had a limited supply of serum potassium assays. We only used the latter in confirmed cases of rhabdomyolysis, and on several occasions we diagnosed severe hyperkalemia. Using bedside automated electrical defibrillation devices for monitoring, we sustained these patients on calcium gluconate until they could be transferred to an external dialysis unit run by Mdecins Sans Frontires in Port‐au‐Prince.6 As the number of rhabdomyolysis cases increased, we instigated creatinine rounds on patients arriving with large crush injuries, and we evaluated urine output daily until patients were clinically stable from this threat. We also helped the Haitian staff treat the omnipresent problem of pain and advised renal dosing of medications in renal failure and elderly patients.
GH: The situation 3 months after the earthquake was medically less dire but highlights the evolving importance of generalists in the aftermath of the quake.710 For many Haitian patients, the earthquake had become a universal point of reference for their symptomatology. Anorexia, amenorrhea, headaches, epigastric pain, even fungating soft tissue masses, were all reported to be depi tranbleman t a (since the earthquake) and were often somatic manifestations of a psychologically devastating event. At a hospital in Carrefour, I cared for patients presenting with dramatic sequelae of chronic diseases that had been undertreated due to the destruction of the Haitian medical infrastructurehypertensive coma, diabetic ketoacidosis, cerebral malaria, decompensated liver disease, and severe chronic anemia (including a patient with a hemoglobin of 3 mg/dL). I encountered many patients with infections exacerbated by excessive crowding in tent communities, such as typhoid and tuberculosis. At this particular hospital, priorities appropriately placed on surgical and postsurgical care required the team to devise creative solutions for the care and placement of medical patients, such as restructuring the emergency department and creating a rehabilitation tent on the hospital grounds. While few Haitian internists were present, a number of Haitian obstetricians were on site and helped manage medical conditions within the scope of their experience, such as hypertension, abdominal pain, and genitourinary infections. The expatriate orthopedic surgeons on site sought the consultative skills of hospitalists for preoperative management, postoperative complications, and comorbid conditions.
This hospital was largely sustained by rotating teams of volunteers, which underscored the importance of establishing a flexible system that would accommodate the turnover of personnel and fluctuating levels of professional expertise. The team used a tiered model for acute care delivery designating responsibilities based on the number of nurses, physicians, and other providers available. We collaborated with Haitian physicians to establish a routine of handoff rounds. Finally, we created and centralized documentation such as clinical protocols, contact numbers, and helpful tips for our successors.
Hospitalists have valuable skills to offer in medical responses to natural catastrophes.5 Our fluency with acute care environments becomes a pluripotent asset in disaster relief. Our experiences in assessing acuity are vital in assisting with inpatient triage. Our familiarity with the comanagement model facilitates partnership with other disciplines to optimize the distribution of skill sets without neglecting the overall well‐being of patients. Our clinical expertise in treating the vulnerable elderly, VTE, renal failure, pain management, postoperative infections, sepsis, and many other conditions can bolster medical relief efforts, even when the foremost need is surgical. The hospitalist's core competencies in healthcare systems11 can support recovery initiatives in medical facilities, particularly in the domains of drug safety, resource allocation, information management, team‐based methods, and care transitions. Our respective experiences also suggest the potential value of hospitalists in domestic, in addition to international, disaster response initiatives. Since large‐scale calamities may result in the hospitalization of overwhelming numbers of victims,12 hospitalists may be well‐positioned to assist our emergency medicine and public health colleagues, who currently (and fittingly) lead domestic efforts in disaster relief.
Tragedies like the earthquake in Haiti serve as a sobering reminder that a comprehensive multidisciplinary approach is required as medical disaster relief shifts from a life‐saving focus to one of life‐preserving care.13, 14 Hospitalists can play a vital role in these restorative efforts.
Acknowledgements
The authors thank their hospitalist colleagues at Beth Israel Deaconess who generously covered our shifts and encouraged us to write about our experiences.
In the last decade, natural disasters such as the Indonesian tsunami of 2004, Hurricane Katrina in 2004, and the Pakistani earthquake of 2005 have brought attention to the importance of diverse but complementary medical professional roles in humanitarian medical aid.14 Natural disasters that cause significant physical trauma to large populations often necessitate initial multidisciplinary responder teams comprised of surgeons, anesthesiologists, emergency medicine physicians, surgical technologists, nurses, psychiatrists, and public health specialists. Their roles are to manage life‐threatening injuries, provide immediate triage, help affected individuals deal with intense psychological shock, and address critical population‐based needs such as water, food, and sanitation. Meanwhile, general medical, pediatric, rehabilitative, and long‐term psychiatric services often constitute a secondary tier of disaster response, providing postsurgical care, managing acute medical illnesses, mitigating psychological trauma, rehabilitating injuries, and providing vaccinations to at‐risk individuals. Hospitalists can play an important role in postcatastrophe recovery services as experts in acute care, stewards of care transitions, and drivers of systems improvement.
The earthquake that occurred January 12, 2010 in Haiti is a dramatic illustration of the importance of a multidisciplinary approach to disaster relief. The 7.0‐magnitude earthquake near Port‐au‐Prince ravaged an already crippled health care system, severely damaging the country's primary academic medical center, and killed the entire class of second‐year nursing students. The death toll has been estimated to be nearly one‐quarter of a million people.5 Victims awaiting surgery, recovering from surgery, or in need of other immediate medical attention quickly inundated any existing health facilities. The following stories describe the authors' respective experiences in Haiti after the earthquake.
JC: I arrived 4 days after the earthquake to a hospital outside of Port‐au‐Prince, spared from destruction, but filled with hundreds of patients with crush injuries and severe fractures. On rounds with the surgical team, I observed that venous thromboembolism (VTE) prophylaxis had not yet been initiated, and I was concerned that patients might die from pulmonary embolism. In the overwhelming urgency of providing life‐saving surgery to as many patients as possible, this simple measure had been overlooked. After discussion with our team and our Haitian medical colleagues, we initiated subcutaneous heparin on all eligible patients and made arrangements to receive further shipments of heparin to accommodate the influx of patients.
A nearby school and church had been annexed into makeshift extensions of the hospital wards. The volume and pace of incoming injuries was such that as soon as a patient was taken to surgery, another patient would often take his or her place in the bed. The rapid movement of patients to and from x‐ray, surgery, and postsurgical care created challenges around effective and accurate communication among multiple care providers. We decided that nonsurgical personnel would triage newly arriving patients and round on patients daily. Each nonsurgical physician was responsible for staffing a particular location. This zone‐defense approach ensured that the surgeons maximized their time in the operating rooms. We also instituted a basic system of portable medical records kept with each patient at all times, allowing personnel to easily and quickly assess care given to date, and to write notes and orders.
Presurgical and postsurgical wound infections became a common event, with the risk of ensuing sepsis. Antibiotic use was dependent on the preferences of individual surgeons and also on the available supply. As a result, antimicrobial treatments were highly variable and sometimes inadequate. The internists on the team proposed standard antibiotic guidelines for open fractures, for contaminated wounds, and for postoperative wounds; these regimens were approved and implemented by Haitian staff and the rest of the team.
Internists recognized the first complications of rhabdomyolysis from crush injuries and delays in receiving medical attention. Malaise, oliguria, and volume overload were often the only clues we had for severe renal failure. We had a functional lab capable of checking complete blood counts, urinalysis and creatinine, but we had a limited supply of serum potassium assays. We only used the latter in confirmed cases of rhabdomyolysis, and on several occasions we diagnosed severe hyperkalemia. Using bedside automated electrical defibrillation devices for monitoring, we sustained these patients on calcium gluconate until they could be transferred to an external dialysis unit run by Mdecins Sans Frontires in Port‐au‐Prince.6 As the number of rhabdomyolysis cases increased, we instigated creatinine rounds on patients arriving with large crush injuries, and we evaluated urine output daily until patients were clinically stable from this threat. We also helped the Haitian staff treat the omnipresent problem of pain and advised renal dosing of medications in renal failure and elderly patients.
GH: The situation 3 months after the earthquake was medically less dire but highlights the evolving importance of generalists in the aftermath of the quake.710 For many Haitian patients, the earthquake had become a universal point of reference for their symptomatology. Anorexia, amenorrhea, headaches, epigastric pain, even fungating soft tissue masses, were all reported to be depi tranbleman t a (since the earthquake) and were often somatic manifestations of a psychologically devastating event. At a hospital in Carrefour, I cared for patients presenting with dramatic sequelae of chronic diseases that had been undertreated due to the destruction of the Haitian medical infrastructurehypertensive coma, diabetic ketoacidosis, cerebral malaria, decompensated liver disease, and severe chronic anemia (including a patient with a hemoglobin of 3 mg/dL). I encountered many patients with infections exacerbated by excessive crowding in tent communities, such as typhoid and tuberculosis. At this particular hospital, priorities appropriately placed on surgical and postsurgical care required the team to devise creative solutions for the care and placement of medical patients, such as restructuring the emergency department and creating a rehabilitation tent on the hospital grounds. While few Haitian internists were present, a number of Haitian obstetricians were on site and helped manage medical conditions within the scope of their experience, such as hypertension, abdominal pain, and genitourinary infections. The expatriate orthopedic surgeons on site sought the consultative skills of hospitalists for preoperative management, postoperative complications, and comorbid conditions.
This hospital was largely sustained by rotating teams of volunteers, which underscored the importance of establishing a flexible system that would accommodate the turnover of personnel and fluctuating levels of professional expertise. The team used a tiered model for acute care delivery designating responsibilities based on the number of nurses, physicians, and other providers available. We collaborated with Haitian physicians to establish a routine of handoff rounds. Finally, we created and centralized documentation such as clinical protocols, contact numbers, and helpful tips for our successors.
Hospitalists have valuable skills to offer in medical responses to natural catastrophes.5 Our fluency with acute care environments becomes a pluripotent asset in disaster relief. Our experiences in assessing acuity are vital in assisting with inpatient triage. Our familiarity with the comanagement model facilitates partnership with other disciplines to optimize the distribution of skill sets without neglecting the overall well‐being of patients. Our clinical expertise in treating the vulnerable elderly, VTE, renal failure, pain management, postoperative infections, sepsis, and many other conditions can bolster medical relief efforts, even when the foremost need is surgical. The hospitalist's core competencies in healthcare systems11 can support recovery initiatives in medical facilities, particularly in the domains of drug safety, resource allocation, information management, team‐based methods, and care transitions. Our respective experiences also suggest the potential value of hospitalists in domestic, in addition to international, disaster response initiatives. Since large‐scale calamities may result in the hospitalization of overwhelming numbers of victims,12 hospitalists may be well‐positioned to assist our emergency medicine and public health colleagues, who currently (and fittingly) lead domestic efforts in disaster relief.
Tragedies like the earthquake in Haiti serve as a sobering reminder that a comprehensive multidisciplinary approach is required as medical disaster relief shifts from a life‐saving focus to one of life‐preserving care.13, 14 Hospitalists can play a vital role in these restorative efforts.
Acknowledgements
The authors thank their hospitalist colleagues at Beth Israel Deaconess who generously covered our shifts and encouraged us to write about our experiences.
- ,.Health impact of the 2004 Andaman Nicobar earthquake and tsunami in Indonesia.Prehosp Disaster Med.2009;24(6):493–499.
- ,,,.Medical response to hurricanes Katrina and Rita: local public health preparedness in action.J Public Health Manag Pract.2007;13(5):441–446.
- .Nephrology in earthquakes: sharing experiences and information.Clin J Am Soc Nephrol.2007;2(4):803–808.
- The Hospitalist. November2005. Hurricane Katrina: tragedy and hope. Available at: http://www.the‐hospitalist.org/details/article/255673/Hurricane_Katrina_Tragedy_and_Hope.html. Accessed August 2010.
- Washington Post. February 10,2010. Haiti raises earthquake toll to 230,000. Available at: http://www.washingtonpost.com/wp‐dyn/content/article/2010/02/09/AR2010020904447.html. Accessed August 2010.
- Médecins sans Frontiéres. About us. Available at: http://www.msf.org/msfinternational/aboutmsf/. Accessed August 2010.
- ,,, et al.Practicing internal medicine onboard the USNS COMFORT in the aftermath of the Haitian earthquake.Ann Intern Med.2010;152(11):733–737.
- Minnesota Medicine. April2010. Help for Haiti. Available at: http://www.minnesotamedicine.com/PastIssues/April2010/CoverstoryApril2010/tabid/3370/Default.aspx. Accessed August 2010.
- The Hospitalist. April2010. Hospitalists in Haiti. Available at: http://www.the‐hospitalist.org/details/article/590287/Hospitalists_in_Haiti.html. Accessed August 2010.
- .Haiti earthquake relief, phase two–long‐term needs and local resources.N Engl J Med.2010;362(20):1858–1861.
- ,,,,.The core competencies in hospital medicine: a framework for curriculum development by the society of hospital medicine. J Hosp Med.2006;(1 Suppl 1):2–95.
- ,,, et al.The impact of the Tsunami on hospitalizations at the tertiary care hospital in the Southern Province of Sri Lanka.Am J Disaster Med.2008;3(3):147–155.
- ,,.Short communication: patterns of chronic and acute diseases after natural disasters ‐ a study from the International Committee of the Red Cross field hospital in Banda Aceh after the 2004 Indian Ocean tsunami.Trop Med Int Health.2007;12(11):1338–1341.
- ,,.Characterisation of patients treated at the Red Cross field hospital in Kashmir during the first three weeks of operation.Emerg Med J.2006;23(8):654–656.
- ,.Health impact of the 2004 Andaman Nicobar earthquake and tsunami in Indonesia.Prehosp Disaster Med.2009;24(6):493–499.
- ,,,.Medical response to hurricanes Katrina and Rita: local public health preparedness in action.J Public Health Manag Pract.2007;13(5):441–446.
- .Nephrology in earthquakes: sharing experiences and information.Clin J Am Soc Nephrol.2007;2(4):803–808.
- The Hospitalist. November2005. Hurricane Katrina: tragedy and hope. Available at: http://www.the‐hospitalist.org/details/article/255673/Hurricane_Katrina_Tragedy_and_Hope.html. Accessed August 2010.
- Washington Post. February 10,2010. Haiti raises earthquake toll to 230,000. Available at: http://www.washingtonpost.com/wp‐dyn/content/article/2010/02/09/AR2010020904447.html. Accessed August 2010.
- Médecins sans Frontiéres. About us. Available at: http://www.msf.org/msfinternational/aboutmsf/. Accessed August 2010.
- ,,, et al.Practicing internal medicine onboard the USNS COMFORT in the aftermath of the Haitian earthquake.Ann Intern Med.2010;152(11):733–737.
- Minnesota Medicine. April2010. Help for Haiti. Available at: http://www.minnesotamedicine.com/PastIssues/April2010/CoverstoryApril2010/tabid/3370/Default.aspx. Accessed August 2010.
- The Hospitalist. April2010. Hospitalists in Haiti. Available at: http://www.the‐hospitalist.org/details/article/590287/Hospitalists_in_Haiti.html. Accessed August 2010.
- .Haiti earthquake relief, phase two–long‐term needs and local resources.N Engl J Med.2010;362(20):1858–1861.
- ,,,,.The core competencies in hospital medicine: a framework for curriculum development by the society of hospital medicine. J Hosp Med.2006;(1 Suppl 1):2–95.
- ,,, et al.The impact of the Tsunami on hospitalizations at the tertiary care hospital in the Southern Province of Sri Lanka.Am J Disaster Med.2008;3(3):147–155.
- ,,.Short communication: patterns of chronic and acute diseases after natural disasters ‐ a study from the International Committee of the Red Cross field hospital in Banda Aceh after the 2004 Indian Ocean tsunami.Trop Med Int Health.2007;12(11):1338–1341.
- ,,.Characterisation of patients treated at the Red Cross field hospital in Kashmir during the first three weeks of operation.Emerg Med J.2006;23(8):654–656.
Continuing Medical Education Program in
If you wish to receive credit for this activity, which begins on the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Upon completion of this educational activity, participants will be better able to employ automated bed history data to examine outcomes of intra‐hospital transfers using all hospital admissions as the denominator.
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to
www.blackwellpublishing.com/cme . -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which begins on the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Upon completion of this educational activity, participants will be better able to employ automated bed history data to examine outcomes of intra‐hospital transfers using all hospital admissions as the denominator.
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to
www.blackwellpublishing.com/cme . -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
If you wish to receive credit for this activity, which begins on the next page, please refer to the website:
Accreditation and Designation Statement
Blackwell Futura Media Services designates this educational activity for a 1 AMA PRA Category 1 Credit. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Blackwell Futura Media Services is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Educational Objectives
Upon completion of this educational activity, participants will be better able to employ automated bed history data to examine outcomes of intra‐hospital transfers using all hospital admissions as the denominator.
Continuous participation in the Journal of Hospital Medicine CME program will enable learners to be better able to:
-
Interpret clinical guidelines and their applications for higher quality and more efficient care for all hospitalized patients.
-
Describe the standard of care for common illnesses and conditions treated in the hospital; such as pneumonia, COPD exacerbation, acute coronary syndrome, HF exacerbation, glycemic control, venous thromboembolic disease, stroke, etc.
-
Discuss evidence‐based recommendations involving transitions of care, including the hospital discharge process.
-
Gain insights into the roles of hospitalists as medical educators, researchers, medical ethicists, palliative care providers, and hospital‐based geriatricians.
-
Incorporate best practices for hospitalist administration, including quality improvement, patient safety, practice management, leadership, and demonstrating hospitalist value.
-
Identify evidence‐based best practices and trends for both adult and pediatric hospital medicine.
Instructions on Receiving Credit
For information on applicability and acceptance of continuing medical education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the activity during the valid credit period that is noted on the title page.
Follow these steps to earn credit:
-
Log on to
www.blackwellpublishing.com/cme . -
Read the target audience, learning objectives, and author disclosures.
-
Read the article in print or online format.
-
Reflect on the article.
-
Access the CME Exam, and choose the best answer to each question.
-
Complete the required evaluation component of the activity.
Understanding Hospital Readmissions
Hospital readmissions pose a major problem both to the patient and the fiscal stability of our health care system.1 Many interventions have attempted to tackle this problem. Interventions exist that utilize transition coaches working intensively with hospitalized patients or nurses performing postdischarge home visits or phoning patients.2, 3 Although beneficial, these strategies are costly and require additional, highly trained personnel. Consequently, they have been difficult to sustain financially in a fee‐for‐service environment, and difficult to generalize at other locales. Recent policies to decrease hospital payments for readmissions will incentivize hospitals to implement discharge programs.4 However, all hospital systems will still want to do this in the most efficient manner possible.
One important way to maximize benefits and minimize costs is to target the most intensive, expensive interventions to the highest risk patients who are most likely to be rehospitalized. By targeting the highest risk patients, we could significantly reduce costs. However, models predicting rehospitalization have had limited accuracy, even for condition‐specific models such as heart failure. Two studies in this issue work to better identify high‐risk patients. Mudge and colleagues5 prospectively examined risk factors for recurrent readmissions in an Australian hospital and found that chronic disease, depression, and underweight were independent risk factors for repeat readmission. Allaudeen6 examined risk factors for readmission to their own institution among general medicine patients. In a retrospective analysis of administrative data, they found that several variables predicted hospital readmission, including black race, insurance coverage through Medicaid, prescription of steroids or narcotics, and diagnoses of heart failure, renal disease, cancer, anemia, and weight loss.
These studies raise two questions that are critical if we are to develop better predictive modeling of who will benefit most from intensive interventions to reduce readmissions. First, what are the risk factors for preventable hospitalizations? People with multiple readmissions seem an obvious target on which to focus. However, it may be that these individuals are just very sick with multiple comorbidities, and many of their readmissions may not be preventable. Rich and colleagues reported that a multidisciplinary discharge intervention reduced readmissions for heart failure by 56%.7 What is often forgotten is that in their pilot study they were not able to reduce admissions for the most severely ill, and their final study population excluded the sickest patients. By targeting moderate‐risk patients, they were able to reduce readmissions significantly.8 In the studies by Mudge et al.5 and Allaudeen,6 the fact that chronic diseases predicted rehospitalization is only moderately helpful. It is possible, perhaps likely, that many of the readmissions for heart failure were preventable while many of the readmissions for cancer were not. The challenge for researchers is to develop methods for classifying admissions/readmissions as preventable.9 Using a defined set of diagnostic categories to classify readmissions (eg, ambulatory care sensitive conditions) may misclassify many cases.10 Determining preventable hospitalizations through detailed chart review is expensive and may have limited interobserver reliability. Nevertheless, physician review and classification may be necessary for future research to advance the field.
Second, what predictor variables are causally related to preventable hospitalizations (and presumably actionable), and which are merely markers of true causal factors and therefore harder to interpret and more difficult to act upon? In addition to chronic disease, Mudge et al.5 found that depression and low body mass index were independent risk factors for readmission. These conditions often go hand in hand. Patients who are burdened with chronic disease may be depressed and not eat. Conversely, patients who are depressed may not eat and allow their chronic disease to worsen. But it seems that depression is the more likely of the two to be causal. Depression is an important predictor of medication nonadherence and worsening illness.11, 12 Screening hospitalized patients for depression could provide valuable information on which patients may need treatment or more rigorous postdischarge follow‐up. In contrast, being underweight may not truly cause readmissions, but could be a marker of frailty and difficulty in meeting activities of daily living.
Similarly, Allaudeen6 found that black race, Medicaid use, steroid use, and narcotic use were independently associated with hospital readmission (in addition to chronic diseases and weight loss). Can being on steroids or narcotics cause readmissions? Does enrollment in Medicaid or being of black race cause one to be readmitted? While these may be markers which are statistically significant, they are unlikely to be true causes of rehospitalization. It is more likely that these variables are markers for true causal factors, such as financial barriers to medications or access barriers to primary care. Many other studies have used administrative databases to examine variables linked to readmission. We need to drill deeper to determine what is actually causing readmissions. Did the patient misinterpret how to take their steroid taper or were they so sick that they needed to return to the hospital? Perhaps they decided to wait on taking the steroids until they spoke with their primary care physician. This deeper level of understanding cannot be ascertained through third party administrative data sets. Primary data collection is needed to correctly determine who to target and the specific foci of interventions.
Future research on risk factors for readmissions (and interventions to decrease readmissions) should begin with a theoretical framework that addresses the patient, the hospital, and the receiving outpatient primary care physician or specialist, and the interfaces between each pair that could lead to preventable readmissions (see Figure 1).
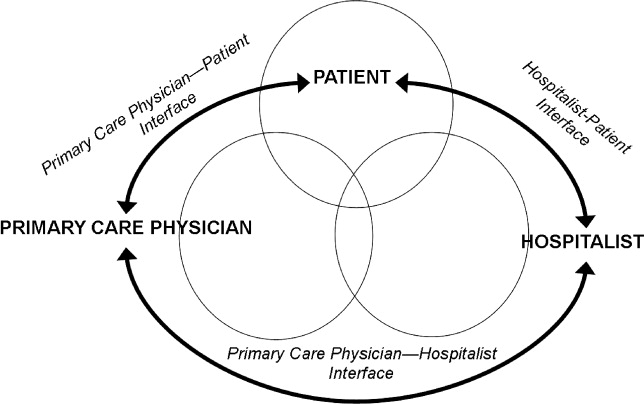
With every potential variable affecting readmission, we need to systematically evaluate whether they are causal and preventable. When a variable is both causal and modifiable, we can then develop interventions to target these variables. We designed Table 1 as a framework to consider when moving forward in creating and implementing interventions.
| Factor | Potential Intervention |
|---|---|
| |
| Patient | |
| Cognition | Screening for cognition at discharge. Increase support at home. Inclusion of surrogate or caregiver in explaining discharge instructions. Additional use of a surrogate in explaining discharge instructions. |
| Depression | Screening for depression during the hospitalization and at discharge. Treatment of depression. Increased outpatient support to monitor depression. |
| Health literacy | Screening for health literacy. Involvement of hospital staff, social support network, and outpatient primary care physician to reinforce discharge instructions. |
| Support at home | Assess home support for patient. Increase phone call and home aid support following discharge for those with inadequate support. |
| Functional ability | Assess physical function throughout hospitalization and at discharge. Involve physical therapy early in the hospitalization and postdischarge. |
| Financial assets | Assess ability to pay for medications and transportation to follow‐up appointments. Work with social work on improving access. |
| Chronic disease (ie, congestive heart failure) | Improve patient education of disease and medications. Increase home support to monitor health status. Increase frequency of outpatient visits as needed. |
| Primary care physician | |
| PatientPCP interface | Via phone call to patient at discharge, reinforce so the patient understands disease process (eg, heart failure exacerbation triggers), will take medications started during hospitalization, and recognizes early precipitants of hospitalization. |
| PCPHospitalist interface | Encourage adequate communication about past medical problems and individualized issues pertinent to care plans. |
| Quality of outpatient primary care | Adhere to guidelines of care recommended by advisory standards. Ensure patients receive optimal outpatient care. |
| Medication reconciliation | Ensure that admission and discharge medication reconciliation is perfect. Update outpatient medication list with inpatient medication changes. |
| Follow‐up of pending tests | Create trigger system of pending tests for recently discharged patients. |
| Access to rapid follow‐up appointments | Incentivize physicians of recently discharged patients to offer follow‐up appointments in 1 week or less. |
| Hospitalist | |
| PatientHospitalist interface | Improve communication with patient on how to access physicians if residual postdischarge questions. |
| HospitalistPCP interface | Encourage adequate communication of hospital course and postdischarge plan. |
| Quality of inpatient hospital care | Ensure patients receive optimal inpatient care. Assess patient clinical stability and determine optimal time for discharge. |
| Written discharge instructions | Create easily understandable discharge instructions. Install checks to limit human errors. Ensure patient has copy on discharge. |
| Verbal discharge instructions | Learn to use teach‐back methodology to assess patient understanding of discharge instructions. Work to eliminate multiple sources (eg, consulting physicians, nurses, therapists) giving conflicting verbal discharge information. |
| Medication reconciliation | Utilize outpatient physician notes and pharmacy records to corroborate patient lists. Ensure that admission and discharge medication reconciliation is perfect. |
| Pending tests | Ensure discharge summary includes information and is communicated to PCP for follow‐up in timely manner. |
| Home services | Arrange for home support and nursing services to assist with patients needs postdischarge. Assess whether the patient knows of pending home services and means of contacting services if they do not occur. |
To advance this area, we need to be stringent about how we perform research and interpret findings. Studies that examine risk factors for readmission to a single hospital may be biased; for example, in the study by Allaudeen,6 it is possible that patients with Medicaid may have been equally likely to be readmitted to any hospital but more likely to be readmitted to the hospital that was the sole source of admission data. Even if findings from a single site are valid, they may not be generalizable. Ideally, studies of risk factors (and interventions to reduce readmissions) should be conducted in multiple sites that can track all hospitalizations and examine differences in risk factors for rehospitalization across hospitals. We have learned a tremendous amount over the last few years about risk markers for all‐cause readmission, and interventions to improve safety and quality of transitions in care. To advance further, multicenter studies are needed that focus on plausible causal variables of preventable readmissions and risk factors beyond the walls of the hospital (eg, access and quality of outpatient care for newly discharged patients). Only then will we better understand which patients can have their readmissions prevented and how to improve upon current strategies to improve outcomes.
- ,,. Nationwide Frequency and Costs of Potentially Preventable Hospitalizations,2006. April 2009. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb72.jsp. Accessed December 8, 2010.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the care transitions intervention.J Am Geriatr Soc.2004;52(11):1817–1825.
- ,,, et al.A reengineered hospital discharge program to decrease rehospitalization: a randomized trial.Ann Int Med.2009;150(3):178–187.
- Sec. 3025.Hospital readmissions reduction program. The Patient Protection and Affordable Care Act. HR 3590. Acts of Congress, 111th second session. January 5,2010.
- ,,,,,,.Recurrent readmissions in medical patients: a prospective study.J Hosp Med.2011;6 (this issue).
- ,,,.Redefining identifiable readmission risk factors for general medicine patients.J Hosp Med.2011;6 (this issue).
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333(18):1190–1195.
- ,,, et al.Prevention of readmission in elderly patients with congestive heart failure: results of a prospective, randomized pilot study.J Gen Intern Med.1993;8(11):585–590.
- ,,,,,.Hospital readmissions and quality of care.Med Care.1999;37(5):490–501.
- ,,,.Ambulatory care sensitive conditions: terminology and disease coding need to be more specific to aid policy makers and clinicians.Public Health.2009;123(2):169–173.
- ,,,,.Depression is an important contributor to low medication adherence in hemodialyzed patients and transplant recipients.Kidney Int.2009;75(11):1223–1229.
- ,,, et al.Depression, medication adherence, and service utilization in systemic lupus erythematosus.Arthritis Rheum.2009;61(2):240–246.
Hospital readmissions pose a major problem both to the patient and the fiscal stability of our health care system.1 Many interventions have attempted to tackle this problem. Interventions exist that utilize transition coaches working intensively with hospitalized patients or nurses performing postdischarge home visits or phoning patients.2, 3 Although beneficial, these strategies are costly and require additional, highly trained personnel. Consequently, they have been difficult to sustain financially in a fee‐for‐service environment, and difficult to generalize at other locales. Recent policies to decrease hospital payments for readmissions will incentivize hospitals to implement discharge programs.4 However, all hospital systems will still want to do this in the most efficient manner possible.
One important way to maximize benefits and minimize costs is to target the most intensive, expensive interventions to the highest risk patients who are most likely to be rehospitalized. By targeting the highest risk patients, we could significantly reduce costs. However, models predicting rehospitalization have had limited accuracy, even for condition‐specific models such as heart failure. Two studies in this issue work to better identify high‐risk patients. Mudge and colleagues5 prospectively examined risk factors for recurrent readmissions in an Australian hospital and found that chronic disease, depression, and underweight were independent risk factors for repeat readmission. Allaudeen6 examined risk factors for readmission to their own institution among general medicine patients. In a retrospective analysis of administrative data, they found that several variables predicted hospital readmission, including black race, insurance coverage through Medicaid, prescription of steroids or narcotics, and diagnoses of heart failure, renal disease, cancer, anemia, and weight loss.
These studies raise two questions that are critical if we are to develop better predictive modeling of who will benefit most from intensive interventions to reduce readmissions. First, what are the risk factors for preventable hospitalizations? People with multiple readmissions seem an obvious target on which to focus. However, it may be that these individuals are just very sick with multiple comorbidities, and many of their readmissions may not be preventable. Rich and colleagues reported that a multidisciplinary discharge intervention reduced readmissions for heart failure by 56%.7 What is often forgotten is that in their pilot study they were not able to reduce admissions for the most severely ill, and their final study population excluded the sickest patients. By targeting moderate‐risk patients, they were able to reduce readmissions significantly.8 In the studies by Mudge et al.5 and Allaudeen,6 the fact that chronic diseases predicted rehospitalization is only moderately helpful. It is possible, perhaps likely, that many of the readmissions for heart failure were preventable while many of the readmissions for cancer were not. The challenge for researchers is to develop methods for classifying admissions/readmissions as preventable.9 Using a defined set of diagnostic categories to classify readmissions (eg, ambulatory care sensitive conditions) may misclassify many cases.10 Determining preventable hospitalizations through detailed chart review is expensive and may have limited interobserver reliability. Nevertheless, physician review and classification may be necessary for future research to advance the field.
Second, what predictor variables are causally related to preventable hospitalizations (and presumably actionable), and which are merely markers of true causal factors and therefore harder to interpret and more difficult to act upon? In addition to chronic disease, Mudge et al.5 found that depression and low body mass index were independent risk factors for readmission. These conditions often go hand in hand. Patients who are burdened with chronic disease may be depressed and not eat. Conversely, patients who are depressed may not eat and allow their chronic disease to worsen. But it seems that depression is the more likely of the two to be causal. Depression is an important predictor of medication nonadherence and worsening illness.11, 12 Screening hospitalized patients for depression could provide valuable information on which patients may need treatment or more rigorous postdischarge follow‐up. In contrast, being underweight may not truly cause readmissions, but could be a marker of frailty and difficulty in meeting activities of daily living.
Similarly, Allaudeen6 found that black race, Medicaid use, steroid use, and narcotic use were independently associated with hospital readmission (in addition to chronic diseases and weight loss). Can being on steroids or narcotics cause readmissions? Does enrollment in Medicaid or being of black race cause one to be readmitted? While these may be markers which are statistically significant, they are unlikely to be true causes of rehospitalization. It is more likely that these variables are markers for true causal factors, such as financial barriers to medications or access barriers to primary care. Many other studies have used administrative databases to examine variables linked to readmission. We need to drill deeper to determine what is actually causing readmissions. Did the patient misinterpret how to take their steroid taper or were they so sick that they needed to return to the hospital? Perhaps they decided to wait on taking the steroids until they spoke with their primary care physician. This deeper level of understanding cannot be ascertained through third party administrative data sets. Primary data collection is needed to correctly determine who to target and the specific foci of interventions.
Future research on risk factors for readmissions (and interventions to decrease readmissions) should begin with a theoretical framework that addresses the patient, the hospital, and the receiving outpatient primary care physician or specialist, and the interfaces between each pair that could lead to preventable readmissions (see Figure 1).
With every potential variable affecting readmission, we need to systematically evaluate whether they are causal and preventable. When a variable is both causal and modifiable, we can then develop interventions to target these variables. We designed Table 1 as a framework to consider when moving forward in creating and implementing interventions.
| Factor | Potential Intervention |
|---|---|
| |
| Patient | |
| Cognition | Screening for cognition at discharge. Increase support at home. Inclusion of surrogate or caregiver in explaining discharge instructions. Additional use of a surrogate in explaining discharge instructions. |
| Depression | Screening for depression during the hospitalization and at discharge. Treatment of depression. Increased outpatient support to monitor depression. |
| Health literacy | Screening for health literacy. Involvement of hospital staff, social support network, and outpatient primary care physician to reinforce discharge instructions. |
| Support at home | Assess home support for patient. Increase phone call and home aid support following discharge for those with inadequate support. |
| Functional ability | Assess physical function throughout hospitalization and at discharge. Involve physical therapy early in the hospitalization and postdischarge. |
| Financial assets | Assess ability to pay for medications and transportation to follow‐up appointments. Work with social work on improving access. |
| Chronic disease (ie, congestive heart failure) | Improve patient education of disease and medications. Increase home support to monitor health status. Increase frequency of outpatient visits as needed. |
| Primary care physician | |
| PatientPCP interface | Via phone call to patient at discharge, reinforce so the patient understands disease process (eg, heart failure exacerbation triggers), will take medications started during hospitalization, and recognizes early precipitants of hospitalization. |
| PCPHospitalist interface | Encourage adequate communication about past medical problems and individualized issues pertinent to care plans. |
| Quality of outpatient primary care | Adhere to guidelines of care recommended by advisory standards. Ensure patients receive optimal outpatient care. |
| Medication reconciliation | Ensure that admission and discharge medication reconciliation is perfect. Update outpatient medication list with inpatient medication changes. |
| Follow‐up of pending tests | Create trigger system of pending tests for recently discharged patients. |
| Access to rapid follow‐up appointments | Incentivize physicians of recently discharged patients to offer follow‐up appointments in 1 week or less. |
| Hospitalist | |
| PatientHospitalist interface | Improve communication with patient on how to access physicians if residual postdischarge questions. |
| HospitalistPCP interface | Encourage adequate communication of hospital course and postdischarge plan. |
| Quality of inpatient hospital care | Ensure patients receive optimal inpatient care. Assess patient clinical stability and determine optimal time for discharge. |
| Written discharge instructions | Create easily understandable discharge instructions. Install checks to limit human errors. Ensure patient has copy on discharge. |
| Verbal discharge instructions | Learn to use teach‐back methodology to assess patient understanding of discharge instructions. Work to eliminate multiple sources (eg, consulting physicians, nurses, therapists) giving conflicting verbal discharge information. |
| Medication reconciliation | Utilize outpatient physician notes and pharmacy records to corroborate patient lists. Ensure that admission and discharge medication reconciliation is perfect. |
| Pending tests | Ensure discharge summary includes information and is communicated to PCP for follow‐up in timely manner. |
| Home services | Arrange for home support and nursing services to assist with patients needs postdischarge. Assess whether the patient knows of pending home services and means of contacting services if they do not occur. |
To advance this area, we need to be stringent about how we perform research and interpret findings. Studies that examine risk factors for readmission to a single hospital may be biased; for example, in the study by Allaudeen,6 it is possible that patients with Medicaid may have been equally likely to be readmitted to any hospital but more likely to be readmitted to the hospital that was the sole source of admission data. Even if findings from a single site are valid, they may not be generalizable. Ideally, studies of risk factors (and interventions to reduce readmissions) should be conducted in multiple sites that can track all hospitalizations and examine differences in risk factors for rehospitalization across hospitals. We have learned a tremendous amount over the last few years about risk markers for all‐cause readmission, and interventions to improve safety and quality of transitions in care. To advance further, multicenter studies are needed that focus on plausible causal variables of preventable readmissions and risk factors beyond the walls of the hospital (eg, access and quality of outpatient care for newly discharged patients). Only then will we better understand which patients can have their readmissions prevented and how to improve upon current strategies to improve outcomes.
Hospital readmissions pose a major problem both to the patient and the fiscal stability of our health care system.1 Many interventions have attempted to tackle this problem. Interventions exist that utilize transition coaches working intensively with hospitalized patients or nurses performing postdischarge home visits or phoning patients.2, 3 Although beneficial, these strategies are costly and require additional, highly trained personnel. Consequently, they have been difficult to sustain financially in a fee‐for‐service environment, and difficult to generalize at other locales. Recent policies to decrease hospital payments for readmissions will incentivize hospitals to implement discharge programs.4 However, all hospital systems will still want to do this in the most efficient manner possible.
One important way to maximize benefits and minimize costs is to target the most intensive, expensive interventions to the highest risk patients who are most likely to be rehospitalized. By targeting the highest risk patients, we could significantly reduce costs. However, models predicting rehospitalization have had limited accuracy, even for condition‐specific models such as heart failure. Two studies in this issue work to better identify high‐risk patients. Mudge and colleagues5 prospectively examined risk factors for recurrent readmissions in an Australian hospital and found that chronic disease, depression, and underweight were independent risk factors for repeat readmission. Allaudeen6 examined risk factors for readmission to their own institution among general medicine patients. In a retrospective analysis of administrative data, they found that several variables predicted hospital readmission, including black race, insurance coverage through Medicaid, prescription of steroids or narcotics, and diagnoses of heart failure, renal disease, cancer, anemia, and weight loss.
These studies raise two questions that are critical if we are to develop better predictive modeling of who will benefit most from intensive interventions to reduce readmissions. First, what are the risk factors for preventable hospitalizations? People with multiple readmissions seem an obvious target on which to focus. However, it may be that these individuals are just very sick with multiple comorbidities, and many of their readmissions may not be preventable. Rich and colleagues reported that a multidisciplinary discharge intervention reduced readmissions for heart failure by 56%.7 What is often forgotten is that in their pilot study they were not able to reduce admissions for the most severely ill, and their final study population excluded the sickest patients. By targeting moderate‐risk patients, they were able to reduce readmissions significantly.8 In the studies by Mudge et al.5 and Allaudeen,6 the fact that chronic diseases predicted rehospitalization is only moderately helpful. It is possible, perhaps likely, that many of the readmissions for heart failure were preventable while many of the readmissions for cancer were not. The challenge for researchers is to develop methods for classifying admissions/readmissions as preventable.9 Using a defined set of diagnostic categories to classify readmissions (eg, ambulatory care sensitive conditions) may misclassify many cases.10 Determining preventable hospitalizations through detailed chart review is expensive and may have limited interobserver reliability. Nevertheless, physician review and classification may be necessary for future research to advance the field.
Second, what predictor variables are causally related to preventable hospitalizations (and presumably actionable), and which are merely markers of true causal factors and therefore harder to interpret and more difficult to act upon? In addition to chronic disease, Mudge et al.5 found that depression and low body mass index were independent risk factors for readmission. These conditions often go hand in hand. Patients who are burdened with chronic disease may be depressed and not eat. Conversely, patients who are depressed may not eat and allow their chronic disease to worsen. But it seems that depression is the more likely of the two to be causal. Depression is an important predictor of medication nonadherence and worsening illness.11, 12 Screening hospitalized patients for depression could provide valuable information on which patients may need treatment or more rigorous postdischarge follow‐up. In contrast, being underweight may not truly cause readmissions, but could be a marker of frailty and difficulty in meeting activities of daily living.
Similarly, Allaudeen6 found that black race, Medicaid use, steroid use, and narcotic use were independently associated with hospital readmission (in addition to chronic diseases and weight loss). Can being on steroids or narcotics cause readmissions? Does enrollment in Medicaid or being of black race cause one to be readmitted? While these may be markers which are statistically significant, they are unlikely to be true causes of rehospitalization. It is more likely that these variables are markers for true causal factors, such as financial barriers to medications or access barriers to primary care. Many other studies have used administrative databases to examine variables linked to readmission. We need to drill deeper to determine what is actually causing readmissions. Did the patient misinterpret how to take their steroid taper or were they so sick that they needed to return to the hospital? Perhaps they decided to wait on taking the steroids until they spoke with their primary care physician. This deeper level of understanding cannot be ascertained through third party administrative data sets. Primary data collection is needed to correctly determine who to target and the specific foci of interventions.
Future research on risk factors for readmissions (and interventions to decrease readmissions) should begin with a theoretical framework that addresses the patient, the hospital, and the receiving outpatient primary care physician or specialist, and the interfaces between each pair that could lead to preventable readmissions (see Figure 1).
With every potential variable affecting readmission, we need to systematically evaluate whether they are causal and preventable. When a variable is both causal and modifiable, we can then develop interventions to target these variables. We designed Table 1 as a framework to consider when moving forward in creating and implementing interventions.
| Factor | Potential Intervention |
|---|---|
| |
| Patient | |
| Cognition | Screening for cognition at discharge. Increase support at home. Inclusion of surrogate or caregiver in explaining discharge instructions. Additional use of a surrogate in explaining discharge instructions. |
| Depression | Screening for depression during the hospitalization and at discharge. Treatment of depression. Increased outpatient support to monitor depression. |
| Health literacy | Screening for health literacy. Involvement of hospital staff, social support network, and outpatient primary care physician to reinforce discharge instructions. |
| Support at home | Assess home support for patient. Increase phone call and home aid support following discharge for those with inadequate support. |
| Functional ability | Assess physical function throughout hospitalization and at discharge. Involve physical therapy early in the hospitalization and postdischarge. |
| Financial assets | Assess ability to pay for medications and transportation to follow‐up appointments. Work with social work on improving access. |
| Chronic disease (ie, congestive heart failure) | Improve patient education of disease and medications. Increase home support to monitor health status. Increase frequency of outpatient visits as needed. |
| Primary care physician | |
| PatientPCP interface | Via phone call to patient at discharge, reinforce so the patient understands disease process (eg, heart failure exacerbation triggers), will take medications started during hospitalization, and recognizes early precipitants of hospitalization. |
| PCPHospitalist interface | Encourage adequate communication about past medical problems and individualized issues pertinent to care plans. |
| Quality of outpatient primary care | Adhere to guidelines of care recommended by advisory standards. Ensure patients receive optimal outpatient care. |
| Medication reconciliation | Ensure that admission and discharge medication reconciliation is perfect. Update outpatient medication list with inpatient medication changes. |
| Follow‐up of pending tests | Create trigger system of pending tests for recently discharged patients. |
| Access to rapid follow‐up appointments | Incentivize physicians of recently discharged patients to offer follow‐up appointments in 1 week or less. |
| Hospitalist | |
| PatientHospitalist interface | Improve communication with patient on how to access physicians if residual postdischarge questions. |
| HospitalistPCP interface | Encourage adequate communication of hospital course and postdischarge plan. |
| Quality of inpatient hospital care | Ensure patients receive optimal inpatient care. Assess patient clinical stability and determine optimal time for discharge. |
| Written discharge instructions | Create easily understandable discharge instructions. Install checks to limit human errors. Ensure patient has copy on discharge. |
| Verbal discharge instructions | Learn to use teach‐back methodology to assess patient understanding of discharge instructions. Work to eliminate multiple sources (eg, consulting physicians, nurses, therapists) giving conflicting verbal discharge information. |
| Medication reconciliation | Utilize outpatient physician notes and pharmacy records to corroborate patient lists. Ensure that admission and discharge medication reconciliation is perfect. |
| Pending tests | Ensure discharge summary includes information and is communicated to PCP for follow‐up in timely manner. |
| Home services | Arrange for home support and nursing services to assist with patients needs postdischarge. Assess whether the patient knows of pending home services and means of contacting services if they do not occur. |
To advance this area, we need to be stringent about how we perform research and interpret findings. Studies that examine risk factors for readmission to a single hospital may be biased; for example, in the study by Allaudeen,6 it is possible that patients with Medicaid may have been equally likely to be readmitted to any hospital but more likely to be readmitted to the hospital that was the sole source of admission data. Even if findings from a single site are valid, they may not be generalizable. Ideally, studies of risk factors (and interventions to reduce readmissions) should be conducted in multiple sites that can track all hospitalizations and examine differences in risk factors for rehospitalization across hospitals. We have learned a tremendous amount over the last few years about risk markers for all‐cause readmission, and interventions to improve safety and quality of transitions in care. To advance further, multicenter studies are needed that focus on plausible causal variables of preventable readmissions and risk factors beyond the walls of the hospital (eg, access and quality of outpatient care for newly discharged patients). Only then will we better understand which patients can have their readmissions prevented and how to improve upon current strategies to improve outcomes.
- ,,. Nationwide Frequency and Costs of Potentially Preventable Hospitalizations,2006. April 2009. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb72.jsp. Accessed December 8, 2010.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the care transitions intervention.J Am Geriatr Soc.2004;52(11):1817–1825.
- ,,, et al.A reengineered hospital discharge program to decrease rehospitalization: a randomized trial.Ann Int Med.2009;150(3):178–187.
- Sec. 3025.Hospital readmissions reduction program. The Patient Protection and Affordable Care Act. HR 3590. Acts of Congress, 111th second session. January 5,2010.
- ,,,,,,.Recurrent readmissions in medical patients: a prospective study.J Hosp Med.2011;6 (this issue).
- ,,,.Redefining identifiable readmission risk factors for general medicine patients.J Hosp Med.2011;6 (this issue).
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333(18):1190–1195.
- ,,, et al.Prevention of readmission in elderly patients with congestive heart failure: results of a prospective, randomized pilot study.J Gen Intern Med.1993;8(11):585–590.
- ,,,,,.Hospital readmissions and quality of care.Med Care.1999;37(5):490–501.
- ,,,.Ambulatory care sensitive conditions: terminology and disease coding need to be more specific to aid policy makers and clinicians.Public Health.2009;123(2):169–173.
- ,,,,.Depression is an important contributor to low medication adherence in hemodialyzed patients and transplant recipients.Kidney Int.2009;75(11):1223–1229.
- ,,, et al.Depression, medication adherence, and service utilization in systemic lupus erythematosus.Arthritis Rheum.2009;61(2):240–246.
- ,,. Nationwide Frequency and Costs of Potentially Preventable Hospitalizations,2006. April 2009. Available at: http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb72.jsp. Accessed December 8, 2010.
- ,,,,,.Preparing patients and caregivers to participate in care delivered across settings: the care transitions intervention.J Am Geriatr Soc.2004;52(11):1817–1825.
- ,,, et al.A reengineered hospital discharge program to decrease rehospitalization: a randomized trial.Ann Int Med.2009;150(3):178–187.
- Sec. 3025.Hospital readmissions reduction program. The Patient Protection and Affordable Care Act. HR 3590. Acts of Congress, 111th second session. January 5,2010.
- ,,,,,,.Recurrent readmissions in medical patients: a prospective study.J Hosp Med.2011;6 (this issue).
- ,,,.Redefining identifiable readmission risk factors for general medicine patients.J Hosp Med.2011;6 (this issue).
- ,,,,,.A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure.N Engl J Med.1995;333(18):1190–1195.
- ,,, et al.Prevention of readmission in elderly patients with congestive heart failure: results of a prospective, randomized pilot study.J Gen Intern Med.1993;8(11):585–590.
- ,,,,,.Hospital readmissions and quality of care.Med Care.1999;37(5):490–501.
- ,,,.Ambulatory care sensitive conditions: terminology and disease coding need to be more specific to aid policy makers and clinicians.Public Health.2009;123(2):169–173.
- ,,,,.Depression is an important contributor to low medication adherence in hemodialyzed patients and transplant recipients.Kidney Int.2009;75(11):1223–1229.
- ,,, et al.Depression, medication adherence, and service utilization in systemic lupus erythematosus.Arthritis Rheum.2009;61(2):240–246.
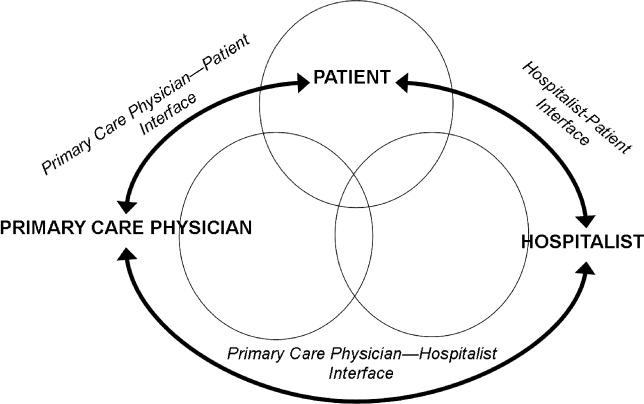
The Ritual: Death Pronouncement
Case
The assessment of the recently arrived critically ill newborn took only seconds: a distended, discolored, and visibly painful abdomen; poor perfusion; assisted ventilation; an intravenous fentanyl drip. I asked the transport nurse practitioner, When did she first show signs of an acute abdomen? Early this morning; she pooped blood, she replied.
In less than 30 minutes, the surgeons were called, antibiotics were on board, fresh frozen plasma and packed red blood cells were being transfused, dobutamine and dopamine were infusing, and a STAT blood gas revealed marked metabolic acidemia with a base deficit of 25, a lactate of 15 mEq/L, and extreme hyperkalemiawould the anesthesiologist even want to put her to sleep for the exploratory laparoscopy?
Where's the family? Have they made it over yet? I asked the team. Mother and her extended family had travelled across town from the hospital where Angel was born and spent the first 18 days of her fragile life to our facility when it became apparent that Angel would require surgery for her abdominal condition. They are talking to the surgeon in the neonatal intensive care unit (NICU) Family Waiting Room, a nurse replied. Organ system failure was rapidly advancing; I requested their presence.
I entered the nearby Family Quiet Room where the single teen mother was surrounded by her extended familynotably, females. I am the neonatologist on call tonight, I started, and I'm afraid your little girl what is her name? Angel. Angel is in a very poor and unstable condition right now. While her young life of not quite 3 weeks has always been somewhat fragile, being born at 27 weeks and less than 2.5 pounds, she is in particular trouble now with her ability to balance her body's pH her blood has too much acid in it. And I believe that this is coming from her bowels. Her bowelsintestinesare very sick and apparently tender, or painful; we have her on pain medication. The x‐rays we have taken reveal a condition known as necrotizing enterocolitis: a bowel problem with circulation, infection, and inflammation. When this happens, germs from inside the bowel leak out into the bloodstream and they have made Angel very unstable. Her blood counts tell us she is trying very hard to fight infection, but both they and her antibiotics may not be enough. Her bowel is sick and dying, and it is releasing toxins and upsetting her balance of blood acids as well as making her potassium too high. This may result in a fatal heart rhythm problem and I don't know that we can successfully put Angel under anesthesia and operate. She may never wake up, or she may die on the operating room table.
Silence. A minute passes and family members express faith, hope, and retell the storied strength of this little girl. She's a fighter. She was doing fine before all this happened. She'll be fine; all we need is a little faith. Yet, mother remained more cautious, and quiet. When will she get to surgery? was all that she asked. The operating room team is here and the surgeons are getting ready, was my reply. Let me get back to her bedside. Can I come see her? she asked. Yes, come with me.
We returned to the bedside. Angel had terminal bradycardia, hypotension, and her perfusion was so poor it left everything but her swollen abdomen pale and mottled. Mother looked on, supported by her own mother. Quietly, efficiently, CPR was continued. An intravenous dose of epinephrine was given. Mother left the room, but some family members remained to watch? To learn what one does in such a predicament? To ensure that everything possible, including CPR, was done for little Angel?
Blood from acute pulmonary hemorrhage gurgled up out of the endotracheal tube; her blood pressure dropped more, and despite epinephrine and bicarbonate, the resuscitation was for naught.
I briefly reentered the Family Quiet Room to inform mother of Angel's progressive decline, and that it was my recommendation that we cease CPR and treat her little body with love and respectI would like to remove her from the life support mechanisms that are not benefiting her, and bring her to you to hold. Do you understand? A tearful head nod affirmed the belief that no mother wants to believe.
Angel's pupils were fixed and dilated, there was no spontaneous respiratory activity, no movement, and a pulse rate of less than 30; I called the code after 12 minutes. I left the NICU nursesthose wonderful agents of care in the best of times and the worst of timesat the bedside to prepare for the continued transition: from life‐supporting critical care toward end‐of‐life care and the bereavement process. I returned again to the Family Quiet Room to speak with Angel's mother.
As you heard before we went back to see Angel, and as you saw at the bedside, her condition would not allow us to proceed toward surgery despite all that had been done for her to attempt to get her stable. I'm sorry to have to tell you this, but Angel is dying and I cannot reverse that reality. Nonetheless, even when she passes away tonight, and I cannot tell you exactly what time that will be, I want you to know that we are all concerned for you, and for your understanding of what has taken place here. I fully recommend that you consider an autopsy to examine and evaluate what Angel went through and provide some answers for us all. Again, a tearful head nod. You don't need to sign anything right now. That can all be handled later. I will ask the nurses to bring Angel here to you.
The NICU nurse brought little Angel, lines and tubes removed, swaddled in a receiving blanket and a cap, to mother. We paused briefly, said our apologies and offered support, while allowing more extended family to stream in. Then, stating we wanted to respect their privacy, we excused ourselves to the nearby bed space and began the documentation process. I looked at my watch about 10 minutes later, knowing it really would not be long before the last remaining vital signa bradycardic heart beat of less than 30would become zero. I knocked on the door, and then opened it slowly. I saw, sitting comfortably in a chair across the room, the young mother holding Angel in her arms. She was surrounded by no less than 8 others, whose eyes moved between her, Angel, and me.
I approached this young mother for the last time that evening. Silently, she opened her arms to allow me access to Angel. I knelt in front of her and slipped the stethoscope under the receiving blanket and onto Angel's chest. I listened, still, quietly, and watched the second hand on my wristwatch. A full minute without a sound; no movement or breathing; a body cool to the touch. Angel has died. She has passed from this life. I am sorry for your loss. One final look in mother's eyesso much more mature than her teen years should have had to allowand I turned to leave the room. See that, I heard from a family member who had previously spoken of Angel's strength, she passed away in your arms. Just like she is supposed to be, in your arms.
Methods
Death pronouncement comes infrequently for the pediatrician. For intensive care specialists in the pediatric or neonatal intensive care units (ICUs), however, it is not an uncommon event.1 For hospitalist physicians, the call to attend and direct a resuscitation, or to decide when it ceases and pronounce a death, may come on any given shift and from almost anywhere in the hospital. How often are our trainees who may be involved in this process actually mentored or shepherded through the death pronouncement after resuscitation ends instead of being thrown to the wolves?2 At a recent speaking engagement addressing pediatric palliative care, this author was asked by a young pediatric resident about just how one goes about death pronouncement. She was left alone to do this on call without any prior experience or instruction, and was even called to do it out of the usual pediatric care environment when she had to pronounce a newborn infant dead following a delivery in an adult ICU where the mother was emergently delivered, though critically ill.
The topic of pediatric death pronouncement is difficult to uncover in the medical literature. Most of it must be gleaned from other reports addressing communication, end‐of‐life care, and the emerging literature on pediatric palliative care.3 Despite efforts to address this in the past 2 decades, resident education in this area is weak by most reports.47 Even in pediatric training programs situated in children's hospitals with palliative care services, the need for continued training and enhancement of communication skills around such matters has been documented.6, 8 As the field of pediatric palliative and hospice medicine matures, the sensitivity to this procedure warrants greater attention, and formal training in communication skills may result in improved resident competence and self‐confidence.9
In consideration of the circumstances around an infant or child's death, it may well be appropriate to inquire about obtaining an autopsy. Although there is an established value to obtaining an autopsy, it may not always follow that every pediatric death should result in an autopsy examination.10, 11 Nonetheless, the conduct of an autopsy, and sharing of its results with appropriate clinical staff and in a conference with family members, may provide many benefits. These include: epidemiologic data, recurrence risk calculations and input to future family planning, contributing to clinical and diagnostic education and accuracy, and assisting with the bereavement process. Autopsy information, even when the examination is limited to certain organ systems (eg, cardiovascular, gastrointestinal tract), may be invaluable to parents and of some comfort as they search for understanding and for answers.12
Given the fact that most children who die in American hospitals die in an intensive care environment, organ donation may not always be an option.13 Nevertheless, most jurisdictions require notification of organ donor or procurement services when a child has died. These are largely operative at state levels, but may have regional or institutional representatives in large medical centers. In some circumstances, family members may actually foresee imminent death and ask about organ donation before their child is removed from life support. The use of organ procurement organizations, consultants, or counselors, separate from the clinical team's management of the patient, and even distinct from the dying process and the family's bereavement care, is generally a positive contributing factor to accomplishing family decisions supportive of organ donation.14
Borrowing from the adult experience as recounted by Hallenbeck,15 and in consideration of practical clinical experience, the following guidelines for pediatric death pronouncement (Table 1) are presented. Additional concepts and exemplary language are noted by Truog and colleagues in their 2006 article titled, Sudden Traumatic Death in Children: We Did Everything, but Your Child Didn't Survive.16
| 1. When in the clinical situation in which you need to pronounce the death of an infant or child unknown to you, quickly gather some information: |
| a. What is the child's name? |
| b. Was this an anticipated death? (eg, following a long‐standing, or known life‐threatening illness) By the clinical team? By the family? |
| c. Was cardiopulmonary resuscitation desired? Performed? Effective? |
| d. Who among concerned family are present, and what is their condition? Are they quiet, in obvious grief, angry, or overwhelmed? |
| e. With whom is information most suitably to be shared? |
| f. Who has decisional responsibility for handling the body and consenting to an autopsy? |
| 2. When entering the room, or coming to the bedside of the deceased child, remind yourself to be calm. |
| 3. Introduce yourself (perhaps you are the physician on call that evening). |
| 4. If there are family members present, assess their reactions to the child's passing. |
| a. Are they actively grieving, or looking anxiously to youwaiting for your evaluation and pronouncement? |
| b. Do not ask family members to leave. Rather, conduct your own brief examination in front of the family: assess the pulse, respirations, and heartbeat. |
| c. Be sensitive to the body's orientation (eg, Muslim families may express a desire for the body to be facing the east, toward Mecca). |
| 5. Clearly communicate that the childcall him/her by namehas died and offer condolences. |
| 6. Pause for the family's immediate grief response and reaction. |
| a. Remain present and available, yet quiet. |
| b. Do not speak too much (unless you have an established relationship with the child and family). |
| c. Respond to the family's immediate reactions in a humanistic manner, and answer their questions simply, without medical jargon or long narratives on the disease. |
| 7. Console the family as you deem appropriateagain, based on any relationship you may or may not have. |
| 8. Allow the family time and privacy and offer your availability and that of other support staff (nursing, social work, child life, chaplain). |
| a. Ask them if there is anyone that they would like to have you contact. |
| b. Give them a time (in so many minutes or hours) when you or another staff member will return and address next steps such as disposition of the body, autopsy, organ donor services notification, and funeral home notification. |
| i. Families vary widely in the expediency with which they may want the body handled and released to a funeral home. |
| ii. Be culturally sensitive to traditions around touching the deceased; some families may choose not to hold the child. |
| iii. Be sensitive to religious stipulations regarding autopsy. |
| 9. Ask the family if it will be all right for you, or someone from the bereavement services office in the hospital, to contact them in the near future. |
| a. Explain that this may serve multiple purposes: |
| i. To determine how they are coping (and, perhaps, make a referral for behavioral health, bereavement or grief support, and counseling). |
| ii. To schedule an autopsy review session (if an autopsy is granted). |
| iii. To schedule a general postmortem counseling session (particularly helpful after an ICU death). |
| 10. In leaving the family, again refer to the child by name, perhaps even saying goodbye to the deceased, as seems appropriate to the circumstances. |
Addressing a patient by name demonstrates respect. Even in the case of a dying newborn, knowing (or asking) this is a matter of demonstrating respect and developing trust. In many cultures, bereaved parents like to hear others remember and speak about their lost infant or child, although this may vary with the time, the context, and the relationship that certain caregivers had with the child. In view of this, a nurse, chaplain, or social worker may be a valuable partner to be present at this time with the family and physician. Proceeding through the initial assessment of the clinical situation in which death takes place, it is important to ascertain who is present (is a parent alone, with family, supported by friends or a member of the clergy?), who knew the child's illness and expected outcome (was death unanticipated or the result of a prolonged illness?), and who has decisional responsibility in the circumstances now before them.
Further assessment of the situation also calls upon the clinician's sense of discerning a family's emotional response to the circumstances of resuscitation and/or death (anger, desperation, grieving, or silent?). It is important to remain calm, focused, and direct your primary attention to the patient and the parent(s)/guardian. Unless someone present is unruly, they need not leave. If someone is so anguished that they cannot hear or attend to your presence or words, quietly excuse yourself and ask for help from a social worker, a colleague, or a chaplain; then return. It is often helpful to acknowledge or validate a family member's emotions, and to show empathy.
Anyone in this circumstance would feel devastated.
Do you have feelings you would like to share?
This must seem very unfair.
For the silent family member, it may be helpful to state,
I know we are often at a loss for words at a time like this, but I would like to express my sorrow for the loss of your [son, daughter] ________ [refer to by name]. I want you to know that we are here to answer your questions and help you in whatever manner possible when you are ready.
In order to move forward, many families need time, privacy, and support. This can be afforded them, even in a busy ICU or Emergency Department. A follow‐up visit to see how the family is doing after a period of 10‐15 minutes may prove opportune in processing what has happened and addressing what happens next. If there is an identified need, or particular problem or difficulty in understanding things, additional resources (social worker, case manager, chaplain, or behavioral health professional) may be helpful. Asking if there is anyone that you can contact is often a simple way to address this.
Attending to cultural sensitivities and practices, religious rituals, and family traditions also requires some initial inquiry of the family, unless there has been a long‐standing, or well‐recognized, interaction pattern. It may be helpful to ask,
How do you and your family deal with crises or difficult decisions? What is important to you at this time?
Sometimes, it may be tempting to stumble into some explanation for the death, or failure of the resuscitation to restore relative stability. But when all of the answers may not yet be forthcoming (eg, laboratory tests may be pending or an autopsy has yet to be performed), this type of effort is potentially confusing or even harmful. It is prudent to state what is known, especially if the death follows a prolonged illness, and note that there may be more information to follow.
In sum, be present, be factual yet empathetic, and be resourceful in eliciting and addressing family member needs.
Resources:
The reader is referred to the following Fast Facts resources on‐line at the end‐of‐life/palliative education resource center (EPERC), at the Medical College of Wisconsin:
Weissman DE, Quill TE, Arnold RM. Responding to Emotions in Family Meetings: #224 Fast Facts and Concepts. January 2010.
http://www.eperc.mcw.edu/fastfact/ff_224. htm . Accessed November 2010.Wang‐Cheng R. Dealing Anger, ed. 2: #59 Fast Facts and Concepts. July 2006.
http://www.eperc.mcw.edu/fastfact/ff_059.htm . Accessed November 2010.Weissman DE, Heidenreich CA. Death Pronouncement in the Hospital, ed. 2: #4 Fast Facts and Concepts. July 2005.
http://www.eperc.mcw.edu/fastfact/ff_004.htm . Accessed November 2010.
- ,.Pediatric death certification.Arch Pediatr Adolesc Med1998;152:852–854.
- .Confidants needed: post‐residency mentoring rare but valuable. Physicians Practice April2003.http://www.physicianspractice.com/index/fuseaction/articles.details/articleID/394/page/1.htm. Accessed November 2010.
- ,,, et al.The death of a child in the emergency department.Ann Emerg Med2003;42:519–529.
- ,,.Death pronouncement: survival tips for residents.Am Fam Physician1998;58:284–285.
- ,.Educational needs among pediatricians regarding caring for terminally ill children.Arch Pediatr Adolesc Med1998;152:909–914.
- ,,.Pediatric resident education in palliative care: a needs assessment.Pediatrics2006;117:1949–1954.
- ,,.Pediatric residents' clinical and educational experiences with end‐of‐life care.Pediatrics2008;121:e731–e737.
- ,,,,.Hospital staff and family perspectives regarding quality of pediatric palliative care.Pediatrics2004;114:1248–1252.
- ,.Pediatric palliative care: an assessment of physicians' confidence in skills, desire for training, and willingness to refer for end‐of‐life care.Am J Hospice Pal Med2008;25:100–105.
- .Clinical aspects of neonatal death and autopsy.Semin Neonatol2004;9:247–254.
- ,.Causes of death, determined by autopsy, in previously healthy (or near‐healthy) children presenting to a children's hospital.Arch Pathol Lab Med2006;130:1780–1785.
- ,.Reorientation of care in the NICU.Semin Fetal Neonatal Med2008;13:305–309.
- American Academy of Pediatrics, Committee on Hospital Care and Section on Surgery.Pediatric organ donation and transplantation.Pediatrics2002;109:982–984.
- ,,,.Factors influencing families' consent for donation of solid organs for transplantation.JAMA2001;286:71–77.
- .Palliative care in the final days of life: “They were expecting it at any time.”JAMA2005;293:2265–2271.
- ,,,.Sudden traumatic death in children: “We did everything, but your child didn't survive.”JAMA2006;295:2646–2654.
Case
The assessment of the recently arrived critically ill newborn took only seconds: a distended, discolored, and visibly painful abdomen; poor perfusion; assisted ventilation; an intravenous fentanyl drip. I asked the transport nurse practitioner, When did she first show signs of an acute abdomen? Early this morning; she pooped blood, she replied.
In less than 30 minutes, the surgeons were called, antibiotics were on board, fresh frozen plasma and packed red blood cells were being transfused, dobutamine and dopamine were infusing, and a STAT blood gas revealed marked metabolic acidemia with a base deficit of 25, a lactate of 15 mEq/L, and extreme hyperkalemiawould the anesthesiologist even want to put her to sleep for the exploratory laparoscopy?
Where's the family? Have they made it over yet? I asked the team. Mother and her extended family had travelled across town from the hospital where Angel was born and spent the first 18 days of her fragile life to our facility when it became apparent that Angel would require surgery for her abdominal condition. They are talking to the surgeon in the neonatal intensive care unit (NICU) Family Waiting Room, a nurse replied. Organ system failure was rapidly advancing; I requested their presence.
I entered the nearby Family Quiet Room where the single teen mother was surrounded by her extended familynotably, females. I am the neonatologist on call tonight, I started, and I'm afraid your little girl what is her name? Angel. Angel is in a very poor and unstable condition right now. While her young life of not quite 3 weeks has always been somewhat fragile, being born at 27 weeks and less than 2.5 pounds, she is in particular trouble now with her ability to balance her body's pH her blood has too much acid in it. And I believe that this is coming from her bowels. Her bowelsintestinesare very sick and apparently tender, or painful; we have her on pain medication. The x‐rays we have taken reveal a condition known as necrotizing enterocolitis: a bowel problem with circulation, infection, and inflammation. When this happens, germs from inside the bowel leak out into the bloodstream and they have made Angel very unstable. Her blood counts tell us she is trying very hard to fight infection, but both they and her antibiotics may not be enough. Her bowel is sick and dying, and it is releasing toxins and upsetting her balance of blood acids as well as making her potassium too high. This may result in a fatal heart rhythm problem and I don't know that we can successfully put Angel under anesthesia and operate. She may never wake up, or she may die on the operating room table.
Silence. A minute passes and family members express faith, hope, and retell the storied strength of this little girl. She's a fighter. She was doing fine before all this happened. She'll be fine; all we need is a little faith. Yet, mother remained more cautious, and quiet. When will she get to surgery? was all that she asked. The operating room team is here and the surgeons are getting ready, was my reply. Let me get back to her bedside. Can I come see her? she asked. Yes, come with me.
We returned to the bedside. Angel had terminal bradycardia, hypotension, and her perfusion was so poor it left everything but her swollen abdomen pale and mottled. Mother looked on, supported by her own mother. Quietly, efficiently, CPR was continued. An intravenous dose of epinephrine was given. Mother left the room, but some family members remained to watch? To learn what one does in such a predicament? To ensure that everything possible, including CPR, was done for little Angel?
Blood from acute pulmonary hemorrhage gurgled up out of the endotracheal tube; her blood pressure dropped more, and despite epinephrine and bicarbonate, the resuscitation was for naught.
I briefly reentered the Family Quiet Room to inform mother of Angel's progressive decline, and that it was my recommendation that we cease CPR and treat her little body with love and respectI would like to remove her from the life support mechanisms that are not benefiting her, and bring her to you to hold. Do you understand? A tearful head nod affirmed the belief that no mother wants to believe.
Angel's pupils were fixed and dilated, there was no spontaneous respiratory activity, no movement, and a pulse rate of less than 30; I called the code after 12 minutes. I left the NICU nursesthose wonderful agents of care in the best of times and the worst of timesat the bedside to prepare for the continued transition: from life‐supporting critical care toward end‐of‐life care and the bereavement process. I returned again to the Family Quiet Room to speak with Angel's mother.
As you heard before we went back to see Angel, and as you saw at the bedside, her condition would not allow us to proceed toward surgery despite all that had been done for her to attempt to get her stable. I'm sorry to have to tell you this, but Angel is dying and I cannot reverse that reality. Nonetheless, even when she passes away tonight, and I cannot tell you exactly what time that will be, I want you to know that we are all concerned for you, and for your understanding of what has taken place here. I fully recommend that you consider an autopsy to examine and evaluate what Angel went through and provide some answers for us all. Again, a tearful head nod. You don't need to sign anything right now. That can all be handled later. I will ask the nurses to bring Angel here to you.
The NICU nurse brought little Angel, lines and tubes removed, swaddled in a receiving blanket and a cap, to mother. We paused briefly, said our apologies and offered support, while allowing more extended family to stream in. Then, stating we wanted to respect their privacy, we excused ourselves to the nearby bed space and began the documentation process. I looked at my watch about 10 minutes later, knowing it really would not be long before the last remaining vital signa bradycardic heart beat of less than 30would become zero. I knocked on the door, and then opened it slowly. I saw, sitting comfortably in a chair across the room, the young mother holding Angel in her arms. She was surrounded by no less than 8 others, whose eyes moved between her, Angel, and me.
I approached this young mother for the last time that evening. Silently, she opened her arms to allow me access to Angel. I knelt in front of her and slipped the stethoscope under the receiving blanket and onto Angel's chest. I listened, still, quietly, and watched the second hand on my wristwatch. A full minute without a sound; no movement or breathing; a body cool to the touch. Angel has died. She has passed from this life. I am sorry for your loss. One final look in mother's eyesso much more mature than her teen years should have had to allowand I turned to leave the room. See that, I heard from a family member who had previously spoken of Angel's strength, she passed away in your arms. Just like she is supposed to be, in your arms.
Methods
Death pronouncement comes infrequently for the pediatrician. For intensive care specialists in the pediatric or neonatal intensive care units (ICUs), however, it is not an uncommon event.1 For hospitalist physicians, the call to attend and direct a resuscitation, or to decide when it ceases and pronounce a death, may come on any given shift and from almost anywhere in the hospital. How often are our trainees who may be involved in this process actually mentored or shepherded through the death pronouncement after resuscitation ends instead of being thrown to the wolves?2 At a recent speaking engagement addressing pediatric palliative care, this author was asked by a young pediatric resident about just how one goes about death pronouncement. She was left alone to do this on call without any prior experience or instruction, and was even called to do it out of the usual pediatric care environment when she had to pronounce a newborn infant dead following a delivery in an adult ICU where the mother was emergently delivered, though critically ill.
The topic of pediatric death pronouncement is difficult to uncover in the medical literature. Most of it must be gleaned from other reports addressing communication, end‐of‐life care, and the emerging literature on pediatric palliative care.3 Despite efforts to address this in the past 2 decades, resident education in this area is weak by most reports.47 Even in pediatric training programs situated in children's hospitals with palliative care services, the need for continued training and enhancement of communication skills around such matters has been documented.6, 8 As the field of pediatric palliative and hospice medicine matures, the sensitivity to this procedure warrants greater attention, and formal training in communication skills may result in improved resident competence and self‐confidence.9
In consideration of the circumstances around an infant or child's death, it may well be appropriate to inquire about obtaining an autopsy. Although there is an established value to obtaining an autopsy, it may not always follow that every pediatric death should result in an autopsy examination.10, 11 Nonetheless, the conduct of an autopsy, and sharing of its results with appropriate clinical staff and in a conference with family members, may provide many benefits. These include: epidemiologic data, recurrence risk calculations and input to future family planning, contributing to clinical and diagnostic education and accuracy, and assisting with the bereavement process. Autopsy information, even when the examination is limited to certain organ systems (eg, cardiovascular, gastrointestinal tract), may be invaluable to parents and of some comfort as they search for understanding and for answers.12
Given the fact that most children who die in American hospitals die in an intensive care environment, organ donation may not always be an option.13 Nevertheless, most jurisdictions require notification of organ donor or procurement services when a child has died. These are largely operative at state levels, but may have regional or institutional representatives in large medical centers. In some circumstances, family members may actually foresee imminent death and ask about organ donation before their child is removed from life support. The use of organ procurement organizations, consultants, or counselors, separate from the clinical team's management of the patient, and even distinct from the dying process and the family's bereavement care, is generally a positive contributing factor to accomplishing family decisions supportive of organ donation.14
Borrowing from the adult experience as recounted by Hallenbeck,15 and in consideration of practical clinical experience, the following guidelines for pediatric death pronouncement (Table 1) are presented. Additional concepts and exemplary language are noted by Truog and colleagues in their 2006 article titled, Sudden Traumatic Death in Children: We Did Everything, but Your Child Didn't Survive.16
| 1. When in the clinical situation in which you need to pronounce the death of an infant or child unknown to you, quickly gather some information: |
| a. What is the child's name? |
| b. Was this an anticipated death? (eg, following a long‐standing, or known life‐threatening illness) By the clinical team? By the family? |
| c. Was cardiopulmonary resuscitation desired? Performed? Effective? |
| d. Who among concerned family are present, and what is their condition? Are they quiet, in obvious grief, angry, or overwhelmed? |
| e. With whom is information most suitably to be shared? |
| f. Who has decisional responsibility for handling the body and consenting to an autopsy? |
| 2. When entering the room, or coming to the bedside of the deceased child, remind yourself to be calm. |
| 3. Introduce yourself (perhaps you are the physician on call that evening). |
| 4. If there are family members present, assess their reactions to the child's passing. |
| a. Are they actively grieving, or looking anxiously to youwaiting for your evaluation and pronouncement? |
| b. Do not ask family members to leave. Rather, conduct your own brief examination in front of the family: assess the pulse, respirations, and heartbeat. |
| c. Be sensitive to the body's orientation (eg, Muslim families may express a desire for the body to be facing the east, toward Mecca). |
| 5. Clearly communicate that the childcall him/her by namehas died and offer condolences. |
| 6. Pause for the family's immediate grief response and reaction. |
| a. Remain present and available, yet quiet. |
| b. Do not speak too much (unless you have an established relationship with the child and family). |
| c. Respond to the family's immediate reactions in a humanistic manner, and answer their questions simply, without medical jargon or long narratives on the disease. |
| 7. Console the family as you deem appropriateagain, based on any relationship you may or may not have. |
| 8. Allow the family time and privacy and offer your availability and that of other support staff (nursing, social work, child life, chaplain). |
| a. Ask them if there is anyone that they would like to have you contact. |
| b. Give them a time (in so many minutes or hours) when you or another staff member will return and address next steps such as disposition of the body, autopsy, organ donor services notification, and funeral home notification. |
| i. Families vary widely in the expediency with which they may want the body handled and released to a funeral home. |
| ii. Be culturally sensitive to traditions around touching the deceased; some families may choose not to hold the child. |
| iii. Be sensitive to religious stipulations regarding autopsy. |
| 9. Ask the family if it will be all right for you, or someone from the bereavement services office in the hospital, to contact them in the near future. |
| a. Explain that this may serve multiple purposes: |
| i. To determine how they are coping (and, perhaps, make a referral for behavioral health, bereavement or grief support, and counseling). |
| ii. To schedule an autopsy review session (if an autopsy is granted). |
| iii. To schedule a general postmortem counseling session (particularly helpful after an ICU death). |
| 10. In leaving the family, again refer to the child by name, perhaps even saying goodbye to the deceased, as seems appropriate to the circumstances. |
Addressing a patient by name demonstrates respect. Even in the case of a dying newborn, knowing (or asking) this is a matter of demonstrating respect and developing trust. In many cultures, bereaved parents like to hear others remember and speak about their lost infant or child, although this may vary with the time, the context, and the relationship that certain caregivers had with the child. In view of this, a nurse, chaplain, or social worker may be a valuable partner to be present at this time with the family and physician. Proceeding through the initial assessment of the clinical situation in which death takes place, it is important to ascertain who is present (is a parent alone, with family, supported by friends or a member of the clergy?), who knew the child's illness and expected outcome (was death unanticipated or the result of a prolonged illness?), and who has decisional responsibility in the circumstances now before them.
Further assessment of the situation also calls upon the clinician's sense of discerning a family's emotional response to the circumstances of resuscitation and/or death (anger, desperation, grieving, or silent?). It is important to remain calm, focused, and direct your primary attention to the patient and the parent(s)/guardian. Unless someone present is unruly, they need not leave. If someone is so anguished that they cannot hear or attend to your presence or words, quietly excuse yourself and ask for help from a social worker, a colleague, or a chaplain; then return. It is often helpful to acknowledge or validate a family member's emotions, and to show empathy.
Anyone in this circumstance would feel devastated.
Do you have feelings you would like to share?
This must seem very unfair.
For the silent family member, it may be helpful to state,
I know we are often at a loss for words at a time like this, but I would like to express my sorrow for the loss of your [son, daughter] ________ [refer to by name]. I want you to know that we are here to answer your questions and help you in whatever manner possible when you are ready.
In order to move forward, many families need time, privacy, and support. This can be afforded them, even in a busy ICU or Emergency Department. A follow‐up visit to see how the family is doing after a period of 10‐15 minutes may prove opportune in processing what has happened and addressing what happens next. If there is an identified need, or particular problem or difficulty in understanding things, additional resources (social worker, case manager, chaplain, or behavioral health professional) may be helpful. Asking if there is anyone that you can contact is often a simple way to address this.
Attending to cultural sensitivities and practices, religious rituals, and family traditions also requires some initial inquiry of the family, unless there has been a long‐standing, or well‐recognized, interaction pattern. It may be helpful to ask,
How do you and your family deal with crises or difficult decisions? What is important to you at this time?
Sometimes, it may be tempting to stumble into some explanation for the death, or failure of the resuscitation to restore relative stability. But when all of the answers may not yet be forthcoming (eg, laboratory tests may be pending or an autopsy has yet to be performed), this type of effort is potentially confusing or even harmful. It is prudent to state what is known, especially if the death follows a prolonged illness, and note that there may be more information to follow.
In sum, be present, be factual yet empathetic, and be resourceful in eliciting and addressing family member needs.
Resources:
The reader is referred to the following Fast Facts resources on‐line at the end‐of‐life/palliative education resource center (EPERC), at the Medical College of Wisconsin:
Weissman DE, Quill TE, Arnold RM. Responding to Emotions in Family Meetings: #224 Fast Facts and Concepts. January 2010.
http://www.eperc.mcw.edu/fastfact/ff_224. htm . Accessed November 2010.Wang‐Cheng R. Dealing Anger, ed. 2: #59 Fast Facts and Concepts. July 2006.
http://www.eperc.mcw.edu/fastfact/ff_059.htm . Accessed November 2010.Weissman DE, Heidenreich CA. Death Pronouncement in the Hospital, ed. 2: #4 Fast Facts and Concepts. July 2005.
http://www.eperc.mcw.edu/fastfact/ff_004.htm . Accessed November 2010.
Case
The assessment of the recently arrived critically ill newborn took only seconds: a distended, discolored, and visibly painful abdomen; poor perfusion; assisted ventilation; an intravenous fentanyl drip. I asked the transport nurse practitioner, When did she first show signs of an acute abdomen? Early this morning; she pooped blood, she replied.
In less than 30 minutes, the surgeons were called, antibiotics were on board, fresh frozen plasma and packed red blood cells were being transfused, dobutamine and dopamine were infusing, and a STAT blood gas revealed marked metabolic acidemia with a base deficit of 25, a lactate of 15 mEq/L, and extreme hyperkalemiawould the anesthesiologist even want to put her to sleep for the exploratory laparoscopy?
Where's the family? Have they made it over yet? I asked the team. Mother and her extended family had travelled across town from the hospital where Angel was born and spent the first 18 days of her fragile life to our facility when it became apparent that Angel would require surgery for her abdominal condition. They are talking to the surgeon in the neonatal intensive care unit (NICU) Family Waiting Room, a nurse replied. Organ system failure was rapidly advancing; I requested their presence.
I entered the nearby Family Quiet Room where the single teen mother was surrounded by her extended familynotably, females. I am the neonatologist on call tonight, I started, and I'm afraid your little girl what is her name? Angel. Angel is in a very poor and unstable condition right now. While her young life of not quite 3 weeks has always been somewhat fragile, being born at 27 weeks and less than 2.5 pounds, she is in particular trouble now with her ability to balance her body's pH her blood has too much acid in it. And I believe that this is coming from her bowels. Her bowelsintestinesare very sick and apparently tender, or painful; we have her on pain medication. The x‐rays we have taken reveal a condition known as necrotizing enterocolitis: a bowel problem with circulation, infection, and inflammation. When this happens, germs from inside the bowel leak out into the bloodstream and they have made Angel very unstable. Her blood counts tell us she is trying very hard to fight infection, but both they and her antibiotics may not be enough. Her bowel is sick and dying, and it is releasing toxins and upsetting her balance of blood acids as well as making her potassium too high. This may result in a fatal heart rhythm problem and I don't know that we can successfully put Angel under anesthesia and operate. She may never wake up, or she may die on the operating room table.
Silence. A minute passes and family members express faith, hope, and retell the storied strength of this little girl. She's a fighter. She was doing fine before all this happened. She'll be fine; all we need is a little faith. Yet, mother remained more cautious, and quiet. When will she get to surgery? was all that she asked. The operating room team is here and the surgeons are getting ready, was my reply. Let me get back to her bedside. Can I come see her? she asked. Yes, come with me.
We returned to the bedside. Angel had terminal bradycardia, hypotension, and her perfusion was so poor it left everything but her swollen abdomen pale and mottled. Mother looked on, supported by her own mother. Quietly, efficiently, CPR was continued. An intravenous dose of epinephrine was given. Mother left the room, but some family members remained to watch? To learn what one does in such a predicament? To ensure that everything possible, including CPR, was done for little Angel?
Blood from acute pulmonary hemorrhage gurgled up out of the endotracheal tube; her blood pressure dropped more, and despite epinephrine and bicarbonate, the resuscitation was for naught.
I briefly reentered the Family Quiet Room to inform mother of Angel's progressive decline, and that it was my recommendation that we cease CPR and treat her little body with love and respectI would like to remove her from the life support mechanisms that are not benefiting her, and bring her to you to hold. Do you understand? A tearful head nod affirmed the belief that no mother wants to believe.
Angel's pupils were fixed and dilated, there was no spontaneous respiratory activity, no movement, and a pulse rate of less than 30; I called the code after 12 minutes. I left the NICU nursesthose wonderful agents of care in the best of times and the worst of timesat the bedside to prepare for the continued transition: from life‐supporting critical care toward end‐of‐life care and the bereavement process. I returned again to the Family Quiet Room to speak with Angel's mother.
As you heard before we went back to see Angel, and as you saw at the bedside, her condition would not allow us to proceed toward surgery despite all that had been done for her to attempt to get her stable. I'm sorry to have to tell you this, but Angel is dying and I cannot reverse that reality. Nonetheless, even when she passes away tonight, and I cannot tell you exactly what time that will be, I want you to know that we are all concerned for you, and for your understanding of what has taken place here. I fully recommend that you consider an autopsy to examine and evaluate what Angel went through and provide some answers for us all. Again, a tearful head nod. You don't need to sign anything right now. That can all be handled later. I will ask the nurses to bring Angel here to you.
The NICU nurse brought little Angel, lines and tubes removed, swaddled in a receiving blanket and a cap, to mother. We paused briefly, said our apologies and offered support, while allowing more extended family to stream in. Then, stating we wanted to respect their privacy, we excused ourselves to the nearby bed space and began the documentation process. I looked at my watch about 10 minutes later, knowing it really would not be long before the last remaining vital signa bradycardic heart beat of less than 30would become zero. I knocked on the door, and then opened it slowly. I saw, sitting comfortably in a chair across the room, the young mother holding Angel in her arms. She was surrounded by no less than 8 others, whose eyes moved between her, Angel, and me.
I approached this young mother for the last time that evening. Silently, she opened her arms to allow me access to Angel. I knelt in front of her and slipped the stethoscope under the receiving blanket and onto Angel's chest. I listened, still, quietly, and watched the second hand on my wristwatch. A full minute without a sound; no movement or breathing; a body cool to the touch. Angel has died. She has passed from this life. I am sorry for your loss. One final look in mother's eyesso much more mature than her teen years should have had to allowand I turned to leave the room. See that, I heard from a family member who had previously spoken of Angel's strength, she passed away in your arms. Just like she is supposed to be, in your arms.
Methods
Death pronouncement comes infrequently for the pediatrician. For intensive care specialists in the pediatric or neonatal intensive care units (ICUs), however, it is not an uncommon event.1 For hospitalist physicians, the call to attend and direct a resuscitation, or to decide when it ceases and pronounce a death, may come on any given shift and from almost anywhere in the hospital. How often are our trainees who may be involved in this process actually mentored or shepherded through the death pronouncement after resuscitation ends instead of being thrown to the wolves?2 At a recent speaking engagement addressing pediatric palliative care, this author was asked by a young pediatric resident about just how one goes about death pronouncement. She was left alone to do this on call without any prior experience or instruction, and was even called to do it out of the usual pediatric care environment when she had to pronounce a newborn infant dead following a delivery in an adult ICU where the mother was emergently delivered, though critically ill.
The topic of pediatric death pronouncement is difficult to uncover in the medical literature. Most of it must be gleaned from other reports addressing communication, end‐of‐life care, and the emerging literature on pediatric palliative care.3 Despite efforts to address this in the past 2 decades, resident education in this area is weak by most reports.47 Even in pediatric training programs situated in children's hospitals with palliative care services, the need for continued training and enhancement of communication skills around such matters has been documented.6, 8 As the field of pediatric palliative and hospice medicine matures, the sensitivity to this procedure warrants greater attention, and formal training in communication skills may result in improved resident competence and self‐confidence.9
In consideration of the circumstances around an infant or child's death, it may well be appropriate to inquire about obtaining an autopsy. Although there is an established value to obtaining an autopsy, it may not always follow that every pediatric death should result in an autopsy examination.10, 11 Nonetheless, the conduct of an autopsy, and sharing of its results with appropriate clinical staff and in a conference with family members, may provide many benefits. These include: epidemiologic data, recurrence risk calculations and input to future family planning, contributing to clinical and diagnostic education and accuracy, and assisting with the bereavement process. Autopsy information, even when the examination is limited to certain organ systems (eg, cardiovascular, gastrointestinal tract), may be invaluable to parents and of some comfort as they search for understanding and for answers.12
Given the fact that most children who die in American hospitals die in an intensive care environment, organ donation may not always be an option.13 Nevertheless, most jurisdictions require notification of organ donor or procurement services when a child has died. These are largely operative at state levels, but may have regional or institutional representatives in large medical centers. In some circumstances, family members may actually foresee imminent death and ask about organ donation before their child is removed from life support. The use of organ procurement organizations, consultants, or counselors, separate from the clinical team's management of the patient, and even distinct from the dying process and the family's bereavement care, is generally a positive contributing factor to accomplishing family decisions supportive of organ donation.14
Borrowing from the adult experience as recounted by Hallenbeck,15 and in consideration of practical clinical experience, the following guidelines for pediatric death pronouncement (Table 1) are presented. Additional concepts and exemplary language are noted by Truog and colleagues in their 2006 article titled, Sudden Traumatic Death in Children: We Did Everything, but Your Child Didn't Survive.16
| 1. When in the clinical situation in which you need to pronounce the death of an infant or child unknown to you, quickly gather some information: |
| a. What is the child's name? |
| b. Was this an anticipated death? (eg, following a long‐standing, or known life‐threatening illness) By the clinical team? By the family? |
| c. Was cardiopulmonary resuscitation desired? Performed? Effective? |
| d. Who among concerned family are present, and what is their condition? Are they quiet, in obvious grief, angry, or overwhelmed? |
| e. With whom is information most suitably to be shared? |
| f. Who has decisional responsibility for handling the body and consenting to an autopsy? |
| 2. When entering the room, or coming to the bedside of the deceased child, remind yourself to be calm. |
| 3. Introduce yourself (perhaps you are the physician on call that evening). |
| 4. If there are family members present, assess their reactions to the child's passing. |
| a. Are they actively grieving, or looking anxiously to youwaiting for your evaluation and pronouncement? |
| b. Do not ask family members to leave. Rather, conduct your own brief examination in front of the family: assess the pulse, respirations, and heartbeat. |
| c. Be sensitive to the body's orientation (eg, Muslim families may express a desire for the body to be facing the east, toward Mecca). |
| 5. Clearly communicate that the childcall him/her by namehas died and offer condolences. |
| 6. Pause for the family's immediate grief response and reaction. |
| a. Remain present and available, yet quiet. |
| b. Do not speak too much (unless you have an established relationship with the child and family). |
| c. Respond to the family's immediate reactions in a humanistic manner, and answer their questions simply, without medical jargon or long narratives on the disease. |
| 7. Console the family as you deem appropriateagain, based on any relationship you may or may not have. |
| 8. Allow the family time and privacy and offer your availability and that of other support staff (nursing, social work, child life, chaplain). |
| a. Ask them if there is anyone that they would like to have you contact. |
| b. Give them a time (in so many minutes or hours) when you or another staff member will return and address next steps such as disposition of the body, autopsy, organ donor services notification, and funeral home notification. |
| i. Families vary widely in the expediency with which they may want the body handled and released to a funeral home. |
| ii. Be culturally sensitive to traditions around touching the deceased; some families may choose not to hold the child. |
| iii. Be sensitive to religious stipulations regarding autopsy. |
| 9. Ask the family if it will be all right for you, or someone from the bereavement services office in the hospital, to contact them in the near future. |
| a. Explain that this may serve multiple purposes: |
| i. To determine how they are coping (and, perhaps, make a referral for behavioral health, bereavement or grief support, and counseling). |
| ii. To schedule an autopsy review session (if an autopsy is granted). |
| iii. To schedule a general postmortem counseling session (particularly helpful after an ICU death). |
| 10. In leaving the family, again refer to the child by name, perhaps even saying goodbye to the deceased, as seems appropriate to the circumstances. |
Addressing a patient by name demonstrates respect. Even in the case of a dying newborn, knowing (or asking) this is a matter of demonstrating respect and developing trust. In many cultures, bereaved parents like to hear others remember and speak about their lost infant or child, although this may vary with the time, the context, and the relationship that certain caregivers had with the child. In view of this, a nurse, chaplain, or social worker may be a valuable partner to be present at this time with the family and physician. Proceeding through the initial assessment of the clinical situation in which death takes place, it is important to ascertain who is present (is a parent alone, with family, supported by friends or a member of the clergy?), who knew the child's illness and expected outcome (was death unanticipated or the result of a prolonged illness?), and who has decisional responsibility in the circumstances now before them.
Further assessment of the situation also calls upon the clinician's sense of discerning a family's emotional response to the circumstances of resuscitation and/or death (anger, desperation, grieving, or silent?). It is important to remain calm, focused, and direct your primary attention to the patient and the parent(s)/guardian. Unless someone present is unruly, they need not leave. If someone is so anguished that they cannot hear or attend to your presence or words, quietly excuse yourself and ask for help from a social worker, a colleague, or a chaplain; then return. It is often helpful to acknowledge or validate a family member's emotions, and to show empathy.
Anyone in this circumstance would feel devastated.
Do you have feelings you would like to share?
This must seem very unfair.
For the silent family member, it may be helpful to state,
I know we are often at a loss for words at a time like this, but I would like to express my sorrow for the loss of your [son, daughter] ________ [refer to by name]. I want you to know that we are here to answer your questions and help you in whatever manner possible when you are ready.
In order to move forward, many families need time, privacy, and support. This can be afforded them, even in a busy ICU or Emergency Department. A follow‐up visit to see how the family is doing after a period of 10‐15 minutes may prove opportune in processing what has happened and addressing what happens next. If there is an identified need, or particular problem or difficulty in understanding things, additional resources (social worker, case manager, chaplain, or behavioral health professional) may be helpful. Asking if there is anyone that you can contact is often a simple way to address this.
Attending to cultural sensitivities and practices, religious rituals, and family traditions also requires some initial inquiry of the family, unless there has been a long‐standing, or well‐recognized, interaction pattern. It may be helpful to ask,
How do you and your family deal with crises or difficult decisions? What is important to you at this time?
Sometimes, it may be tempting to stumble into some explanation for the death, or failure of the resuscitation to restore relative stability. But when all of the answers may not yet be forthcoming (eg, laboratory tests may be pending or an autopsy has yet to be performed), this type of effort is potentially confusing or even harmful. It is prudent to state what is known, especially if the death follows a prolonged illness, and note that there may be more information to follow.
In sum, be present, be factual yet empathetic, and be resourceful in eliciting and addressing family member needs.
Resources:
The reader is referred to the following Fast Facts resources on‐line at the end‐of‐life/palliative education resource center (EPERC), at the Medical College of Wisconsin:
Weissman DE, Quill TE, Arnold RM. Responding to Emotions in Family Meetings: #224 Fast Facts and Concepts. January 2010.
http://www.eperc.mcw.edu/fastfact/ff_224. htm . Accessed November 2010.Wang‐Cheng R. Dealing Anger, ed. 2: #59 Fast Facts and Concepts. July 2006.
http://www.eperc.mcw.edu/fastfact/ff_059.htm . Accessed November 2010.Weissman DE, Heidenreich CA. Death Pronouncement in the Hospital, ed. 2: #4 Fast Facts and Concepts. July 2005.
http://www.eperc.mcw.edu/fastfact/ff_004.htm . Accessed November 2010.
- ,.Pediatric death certification.Arch Pediatr Adolesc Med1998;152:852–854.
- .Confidants needed: post‐residency mentoring rare but valuable. Physicians Practice April2003.http://www.physicianspractice.com/index/fuseaction/articles.details/articleID/394/page/1.htm. Accessed November 2010.
- ,,, et al.The death of a child in the emergency department.Ann Emerg Med2003;42:519–529.
- ,,.Death pronouncement: survival tips for residents.Am Fam Physician1998;58:284–285.
- ,.Educational needs among pediatricians regarding caring for terminally ill children.Arch Pediatr Adolesc Med1998;152:909–914.
- ,,.Pediatric resident education in palliative care: a needs assessment.Pediatrics2006;117:1949–1954.
- ,,.Pediatric residents' clinical and educational experiences with end‐of‐life care.Pediatrics2008;121:e731–e737.
- ,,,,.Hospital staff and family perspectives regarding quality of pediatric palliative care.Pediatrics2004;114:1248–1252.
- ,.Pediatric palliative care: an assessment of physicians' confidence in skills, desire for training, and willingness to refer for end‐of‐life care.Am J Hospice Pal Med2008;25:100–105.
- .Clinical aspects of neonatal death and autopsy.Semin Neonatol2004;9:247–254.
- ,.Causes of death, determined by autopsy, in previously healthy (or near‐healthy) children presenting to a children's hospital.Arch Pathol Lab Med2006;130:1780–1785.
- ,.Reorientation of care in the NICU.Semin Fetal Neonatal Med2008;13:305–309.
- American Academy of Pediatrics, Committee on Hospital Care and Section on Surgery.Pediatric organ donation and transplantation.Pediatrics2002;109:982–984.
- ,,,.Factors influencing families' consent for donation of solid organs for transplantation.JAMA2001;286:71–77.
- .Palliative care in the final days of life: “They were expecting it at any time.”JAMA2005;293:2265–2271.
- ,,,.Sudden traumatic death in children: “We did everything, but your child didn't survive.”JAMA2006;295:2646–2654.
- ,.Pediatric death certification.Arch Pediatr Adolesc Med1998;152:852–854.
- .Confidants needed: post‐residency mentoring rare but valuable. Physicians Practice April2003.http://www.physicianspractice.com/index/fuseaction/articles.details/articleID/394/page/1.htm. Accessed November 2010.
- ,,, et al.The death of a child in the emergency department.Ann Emerg Med2003;42:519–529.
- ,,.Death pronouncement: survival tips for residents.Am Fam Physician1998;58:284–285.
- ,.Educational needs among pediatricians regarding caring for terminally ill children.Arch Pediatr Adolesc Med1998;152:909–914.
- ,,.Pediatric resident education in palliative care: a needs assessment.Pediatrics2006;117:1949–1954.
- ,,.Pediatric residents' clinical and educational experiences with end‐of‐life care.Pediatrics2008;121:e731–e737.
- ,,,,.Hospital staff and family perspectives regarding quality of pediatric palliative care.Pediatrics2004;114:1248–1252.
- ,.Pediatric palliative care: an assessment of physicians' confidence in skills, desire for training, and willingness to refer for end‐of‐life care.Am J Hospice Pal Med2008;25:100–105.
- .Clinical aspects of neonatal death and autopsy.Semin Neonatol2004;9:247–254.
- ,.Causes of death, determined by autopsy, in previously healthy (or near‐healthy) children presenting to a children's hospital.Arch Pathol Lab Med2006;130:1780–1785.
- ,.Reorientation of care in the NICU.Semin Fetal Neonatal Med2008;13:305–309.
- American Academy of Pediatrics, Committee on Hospital Care and Section on Surgery.Pediatric organ donation and transplantation.Pediatrics2002;109:982–984.
- ,,,.Factors influencing families' consent for donation of solid organs for transplantation.JAMA2001;286:71–77.
- .Palliative care in the final days of life: “They were expecting it at any time.”JAMA2005;293:2265–2271.
- ,,,.Sudden traumatic death in children: “We did everything, but your child didn't survive.”JAMA2006;295:2646–2654.
Copyright © 2011 Society of Hospital Medicine
Pregabalin‐induced trismus in a leukemia patient
A 24‐year‐old man with relapsed acute myeloid leukemia and leptomeningeal infiltration (confirmed by magnetic resonance imaging, and leukemic cells in the cerebrospinal fluid) was successful treated with systemic and intrathecal chemotherapy. Concomitantly, he developed an anal fissure, which deteriorated despite treatment with meropenem. The pain was so severe that he required multiple analgesics, with little symptomatic improvement.
Findings
Four weeks afterwards he woke up unable to open his mouth. On physical examination, there was total trismus (Figure 1A). Pharyngeal muscles were also spastic, as he was unable to swallow his saliva or phonate. Respiration was preserved. The anal fissure was inconspicuous with disproportionately excruciating pain. Magnetic resonance imaging of the brain, besides showing resolution of the leptomeningeal leukemia, was unremarkable.
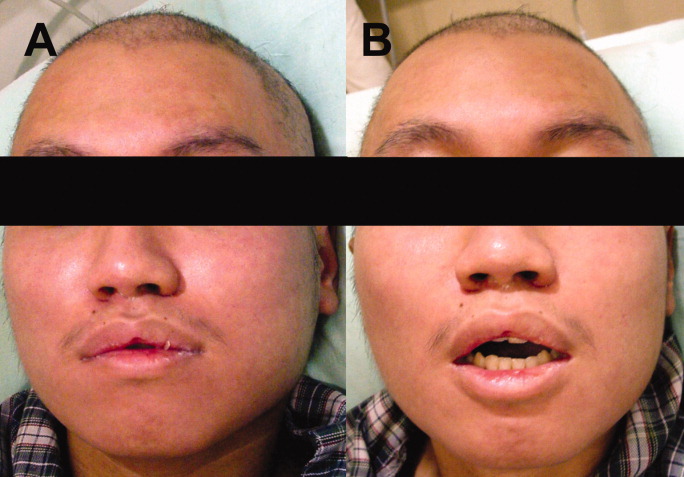
Because the patient grew up in China with an unclear vaccination history, the physical signs were believed to be potentially consistent with localized tetanus. The source of infection was felt to possibly be the anal fissure, although it is unclear if Clostridium tetani can normally be found in gut flora.1 He was given 500 units of human tetanus immune globulin (antitoxin); and metronidazole was commenced. As he was receiving multiple medications (including tramadol, acetaminophen, celecoxib, pregabalin, metronidazole, moxifloxacin and fexofenadine), drug‐induced oromandibular dystonia was also considered. Intravenous diphenhydramine (25 mg) was administered. There was minimal improvement (Figure 1B), and total trismus rapidly recurred.
The patient was admitted into the intensive care unit for airway monitoring. The trismus gradually improved, and completely resolved after 12 hours. His pharyngeal spasm persisted longer, and phonation remained impaired for about 2 days. There was no recurrence of trismus.
Discussion
The clinical course by then was incompatible with tetanus, which would not improve so quickly. Trismus may be caused by dental or pharyngeal infections, temporomandibular joint disorders, and drugs. The trismus in this patient was painless, ruling out infective or inflammatory causes. A review of adverse effects of drugs he was receiving showed that dystonia had not been reported for tramadol, acetaminophen, celecoxib, metronidazole, moxifloxacin and fexofenadine at therapeutic doses. The package insert of pregabalin made no mention of trismus, and a PubMed search failed to show any such association. However, the on‐line drug information of pregabalin from its manufacturer2 actually includes trismus as a rare (1/1000) side effect, without further elaboration on the cumulative dosage required or treatment. In this patient, 6 daily doses of 75 mg of pregabalin had been administered, the last dose 9 hours before the onset of trismus. Pregabalin binds to the alpha 2 delta subunit of voltage‐dependent calcium channels, reducing the release of neurotransmitters including glutamate, noradrenaline, serotonin, dopamine, and substance P.3 The exact mechanism of and antidote to pregabalin‐induced trismus (or oromandibular dystonia in this case, owing to involvement of pharyngeal muscles) is unknown. Diphenhydramine gave partial relief, an early clue that tetanus was not the cause of the trismus, which would not have been expected to respond to this agent. The exact reason why diphenhydramine, an anticholinergic drug, resulted in temporary relaxation remained unclear.
Pregabalin is approved for adult partial‐onset epilepsy, diabetic neuropathic pain, post‐herpetic neuralgia and fibromyalgia. Therefore, this case represented an off‐label use of pregabalin. The effectiveness of pregabalin for postoperative pain relief has been studied,2 but its efficacy in other types of pain remains undefined. In our patient, pregabalin did not appear to be effective.
This case to our knowledge represents the first report of pregabalin‐induced trismus in the peer‐reviewed literature, although the manufacturer was apparently aware that this association had been seen on rare occasions. This underscores the fact that prescribers need to be vigilant for potential adverse drug reactions in the post‐marketing period, both those rarely previously reported as well as those previously unreported.
Acknowledgements
Y.L. Kwong: treated the patient, wrote the manuscript, A.Y.H. Leung: treated the patient, and approved the manuscript, R.T.F. Cheung: treated the patient, and approved the manuscript.
- ,.Clostridium tetani in a metropolitan area: a limited survey incorporating a simplified in vitro identification test.Appl Microbiol.1966;14:993–997.
- Available at: http://www.pfizer.com/files/products/uspi_lyrica.pdf, page 18. Accessed March2010.
- .Pregabalin: its pharmacology and use in pain management.Anesth Analg.2007;105:1805–1815.
A 24‐year‐old man with relapsed acute myeloid leukemia and leptomeningeal infiltration (confirmed by magnetic resonance imaging, and leukemic cells in the cerebrospinal fluid) was successful treated with systemic and intrathecal chemotherapy. Concomitantly, he developed an anal fissure, which deteriorated despite treatment with meropenem. The pain was so severe that he required multiple analgesics, with little symptomatic improvement.
Findings
Four weeks afterwards he woke up unable to open his mouth. On physical examination, there was total trismus (Figure 1A). Pharyngeal muscles were also spastic, as he was unable to swallow his saliva or phonate. Respiration was preserved. The anal fissure was inconspicuous with disproportionately excruciating pain. Magnetic resonance imaging of the brain, besides showing resolution of the leptomeningeal leukemia, was unremarkable.
Because the patient grew up in China with an unclear vaccination history, the physical signs were believed to be potentially consistent with localized tetanus. The source of infection was felt to possibly be the anal fissure, although it is unclear if Clostridium tetani can normally be found in gut flora.1 He was given 500 units of human tetanus immune globulin (antitoxin); and metronidazole was commenced. As he was receiving multiple medications (including tramadol, acetaminophen, celecoxib, pregabalin, metronidazole, moxifloxacin and fexofenadine), drug‐induced oromandibular dystonia was also considered. Intravenous diphenhydramine (25 mg) was administered. There was minimal improvement (Figure 1B), and total trismus rapidly recurred.
The patient was admitted into the intensive care unit for airway monitoring. The trismus gradually improved, and completely resolved after 12 hours. His pharyngeal spasm persisted longer, and phonation remained impaired for about 2 days. There was no recurrence of trismus.
Discussion
The clinical course by then was incompatible with tetanus, which would not improve so quickly. Trismus may be caused by dental or pharyngeal infections, temporomandibular joint disorders, and drugs. The trismus in this patient was painless, ruling out infective or inflammatory causes. A review of adverse effects of drugs he was receiving showed that dystonia had not been reported for tramadol, acetaminophen, celecoxib, metronidazole, moxifloxacin and fexofenadine at therapeutic doses. The package insert of pregabalin made no mention of trismus, and a PubMed search failed to show any such association. However, the on‐line drug information of pregabalin from its manufacturer2 actually includes trismus as a rare (1/1000) side effect, without further elaboration on the cumulative dosage required or treatment. In this patient, 6 daily doses of 75 mg of pregabalin had been administered, the last dose 9 hours before the onset of trismus. Pregabalin binds to the alpha 2 delta subunit of voltage‐dependent calcium channels, reducing the release of neurotransmitters including glutamate, noradrenaline, serotonin, dopamine, and substance P.3 The exact mechanism of and antidote to pregabalin‐induced trismus (or oromandibular dystonia in this case, owing to involvement of pharyngeal muscles) is unknown. Diphenhydramine gave partial relief, an early clue that tetanus was not the cause of the trismus, which would not have been expected to respond to this agent. The exact reason why diphenhydramine, an anticholinergic drug, resulted in temporary relaxation remained unclear.
Pregabalin is approved for adult partial‐onset epilepsy, diabetic neuropathic pain, post‐herpetic neuralgia and fibromyalgia. Therefore, this case represented an off‐label use of pregabalin. The effectiveness of pregabalin for postoperative pain relief has been studied,2 but its efficacy in other types of pain remains undefined. In our patient, pregabalin did not appear to be effective.
This case to our knowledge represents the first report of pregabalin‐induced trismus in the peer‐reviewed literature, although the manufacturer was apparently aware that this association had been seen on rare occasions. This underscores the fact that prescribers need to be vigilant for potential adverse drug reactions in the post‐marketing period, both those rarely previously reported as well as those previously unreported.
Acknowledgements
Y.L. Kwong: treated the patient, wrote the manuscript, A.Y.H. Leung: treated the patient, and approved the manuscript, R.T.F. Cheung: treated the patient, and approved the manuscript.
A 24‐year‐old man with relapsed acute myeloid leukemia and leptomeningeal infiltration (confirmed by magnetic resonance imaging, and leukemic cells in the cerebrospinal fluid) was successful treated with systemic and intrathecal chemotherapy. Concomitantly, he developed an anal fissure, which deteriorated despite treatment with meropenem. The pain was so severe that he required multiple analgesics, with little symptomatic improvement.
Findings
Four weeks afterwards he woke up unable to open his mouth. On physical examination, there was total trismus (Figure 1A). Pharyngeal muscles were also spastic, as he was unable to swallow his saliva or phonate. Respiration was preserved. The anal fissure was inconspicuous with disproportionately excruciating pain. Magnetic resonance imaging of the brain, besides showing resolution of the leptomeningeal leukemia, was unremarkable.
Because the patient grew up in China with an unclear vaccination history, the physical signs were believed to be potentially consistent with localized tetanus. The source of infection was felt to possibly be the anal fissure, although it is unclear if Clostridium tetani can normally be found in gut flora.1 He was given 500 units of human tetanus immune globulin (antitoxin); and metronidazole was commenced. As he was receiving multiple medications (including tramadol, acetaminophen, celecoxib, pregabalin, metronidazole, moxifloxacin and fexofenadine), drug‐induced oromandibular dystonia was also considered. Intravenous diphenhydramine (25 mg) was administered. There was minimal improvement (Figure 1B), and total trismus rapidly recurred.
The patient was admitted into the intensive care unit for airway monitoring. The trismus gradually improved, and completely resolved after 12 hours. His pharyngeal spasm persisted longer, and phonation remained impaired for about 2 days. There was no recurrence of trismus.
Discussion
The clinical course by then was incompatible with tetanus, which would not improve so quickly. Trismus may be caused by dental or pharyngeal infections, temporomandibular joint disorders, and drugs. The trismus in this patient was painless, ruling out infective or inflammatory causes. A review of adverse effects of drugs he was receiving showed that dystonia had not been reported for tramadol, acetaminophen, celecoxib, metronidazole, moxifloxacin and fexofenadine at therapeutic doses. The package insert of pregabalin made no mention of trismus, and a PubMed search failed to show any such association. However, the on‐line drug information of pregabalin from its manufacturer2 actually includes trismus as a rare (1/1000) side effect, without further elaboration on the cumulative dosage required or treatment. In this patient, 6 daily doses of 75 mg of pregabalin had been administered, the last dose 9 hours before the onset of trismus. Pregabalin binds to the alpha 2 delta subunit of voltage‐dependent calcium channels, reducing the release of neurotransmitters including glutamate, noradrenaline, serotonin, dopamine, and substance P.3 The exact mechanism of and antidote to pregabalin‐induced trismus (or oromandibular dystonia in this case, owing to involvement of pharyngeal muscles) is unknown. Diphenhydramine gave partial relief, an early clue that tetanus was not the cause of the trismus, which would not have been expected to respond to this agent. The exact reason why diphenhydramine, an anticholinergic drug, resulted in temporary relaxation remained unclear.
Pregabalin is approved for adult partial‐onset epilepsy, diabetic neuropathic pain, post‐herpetic neuralgia and fibromyalgia. Therefore, this case represented an off‐label use of pregabalin. The effectiveness of pregabalin for postoperative pain relief has been studied,2 but its efficacy in other types of pain remains undefined. In our patient, pregabalin did not appear to be effective.
This case to our knowledge represents the first report of pregabalin‐induced trismus in the peer‐reviewed literature, although the manufacturer was apparently aware that this association had been seen on rare occasions. This underscores the fact that prescribers need to be vigilant for potential adverse drug reactions in the post‐marketing period, both those rarely previously reported as well as those previously unreported.
Acknowledgements
Y.L. Kwong: treated the patient, wrote the manuscript, A.Y.H. Leung: treated the patient, and approved the manuscript, R.T.F. Cheung: treated the patient, and approved the manuscript.
- ,.Clostridium tetani in a metropolitan area: a limited survey incorporating a simplified in vitro identification test.Appl Microbiol.1966;14:993–997.
- Available at: http://www.pfizer.com/files/products/uspi_lyrica.pdf, page 18. Accessed March2010.
- .Pregabalin: its pharmacology and use in pain management.Anesth Analg.2007;105:1805–1815.
- ,.Clostridium tetani in a metropolitan area: a limited survey incorporating a simplified in vitro identification test.Appl Microbiol.1966;14:993–997.
- Available at: http://www.pfizer.com/files/products/uspi_lyrica.pdf, page 18. Accessed March2010.
- .Pregabalin: its pharmacology and use in pain management.Anesth Analg.2007;105:1805–1815.
