User login
Stage Presence
For hospitalist Robert Wachter, MD, MHM, the next annual SHM meeting will be particularly poignant, and not just because he’s HM11’s featured speaker.
Next year will mark the 15th anniversary of the New England Journal of Medicine article coauthored by Dr. Wachter that introduced the term “hospitalist” to the American healthcare lexicon. The specialty is growing and developing into adulthood nicely, he says, which will be part of his presentation in Grapevine, Texas.
“At age 15, that’s when you move to adolescence—you’re going to be off on adulthood and on your own,” says Dr. Wachter, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president and author of the blog Wachter’s World (www.wachtersworld.com).

Like a proud father, Dr. Wachter expects that he will reminisce about the past, speculate about HM’s bright future, and encourage hospitalists to continue their work.
“This will be an optimistic talk,” he says. “The growth has been extraordinary.”
At the outset of the specialty, Dr. Wachter says, he and colleagues predicted some of the current trends, but they underestimated how powerful some would become.
“We couldn’t have predicted that the pressures to increase quality and safety would be as intense as they are today, but we did a good job believing that these areas were important before they hit,” he says.
Looking forward, he says, other emerging forces will join quality and safety at the forefront of HM. “The next five years will likely bring similar pressures on efficiency and throughput,” he says. “I’m going to encourage folks to stay ahead of the curve.”
Having attended every annual conference since the beginning, Dr. Wachter looks forward to “polar things” about each meeting: catching up with the founders of the movement and seeing new faces.
“What’s more fun for me is the amount of youthful energy at the meetings,” he says, especially of the hospitalists he has mentored over the years. “When I come with my group from UCSF, it gives me tremendous pride.” TH
Brendon Shank is a freelance writer based in Philadelphia.

Chapter Updates
Lake Erie
The Lake Erie/Northern Ohio chapter met Aug. 24 at Lolita in Cleveland. Joseph G. Verbalis, MD, chief of the Division of Endocrinology and Metabolism and professor in the Department of Medicine at Georgetown University Medical Center in Washington, D.C., was the guest speaker, and his discussion was on hyponatremia. Sixteen area hospitalists attended the meeting, which was sponsored by CME University.
For hospitalist Robert Wachter, MD, MHM, the next annual SHM meeting will be particularly poignant, and not just because he’s HM11’s featured speaker.
Next year will mark the 15th anniversary of the New England Journal of Medicine article coauthored by Dr. Wachter that introduced the term “hospitalist” to the American healthcare lexicon. The specialty is growing and developing into adulthood nicely, he says, which will be part of his presentation in Grapevine, Texas.
“At age 15, that’s when you move to adolescence—you’re going to be off on adulthood and on your own,” says Dr. Wachter, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president and author of the blog Wachter’s World (www.wachtersworld.com).
Like a proud father, Dr. Wachter expects that he will reminisce about the past, speculate about HM’s bright future, and encourage hospitalists to continue their work.
“This will be an optimistic talk,” he says. “The growth has been extraordinary.”
At the outset of the specialty, Dr. Wachter says, he and colleagues predicted some of the current trends, but they underestimated how powerful some would become.
“We couldn’t have predicted that the pressures to increase quality and safety would be as intense as they are today, but we did a good job believing that these areas were important before they hit,” he says.
Looking forward, he says, other emerging forces will join quality and safety at the forefront of HM. “The next five years will likely bring similar pressures on efficiency and throughput,” he says. “I’m going to encourage folks to stay ahead of the curve.”
Having attended every annual conference since the beginning, Dr. Wachter looks forward to “polar things” about each meeting: catching up with the founders of the movement and seeing new faces.
“What’s more fun for me is the amount of youthful energy at the meetings,” he says, especially of the hospitalists he has mentored over the years. “When I come with my group from UCSF, it gives me tremendous pride.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Updates
Lake Erie
The Lake Erie/Northern Ohio chapter met Aug. 24 at Lolita in Cleveland. Joseph G. Verbalis, MD, chief of the Division of Endocrinology and Metabolism and professor in the Department of Medicine at Georgetown University Medical Center in Washington, D.C., was the guest speaker, and his discussion was on hyponatremia. Sixteen area hospitalists attended the meeting, which was sponsored by CME University.
For hospitalist Robert Wachter, MD, MHM, the next annual SHM meeting will be particularly poignant, and not just because he’s HM11’s featured speaker.
Next year will mark the 15th anniversary of the New England Journal of Medicine article coauthored by Dr. Wachter that introduced the term “hospitalist” to the American healthcare lexicon. The specialty is growing and developing into adulthood nicely, he says, which will be part of his presentation in Grapevine, Texas.
“At age 15, that’s when you move to adolescence—you’re going to be off on adulthood and on your own,” says Dr. Wachter, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president and author of the blog Wachter’s World (www.wachtersworld.com).
Like a proud father, Dr. Wachter expects that he will reminisce about the past, speculate about HM’s bright future, and encourage hospitalists to continue their work.
“This will be an optimistic talk,” he says. “The growth has been extraordinary.”
At the outset of the specialty, Dr. Wachter says, he and colleagues predicted some of the current trends, but they underestimated how powerful some would become.
“We couldn’t have predicted that the pressures to increase quality and safety would be as intense as they are today, but we did a good job believing that these areas were important before they hit,” he says.
Looking forward, he says, other emerging forces will join quality and safety at the forefront of HM. “The next five years will likely bring similar pressures on efficiency and throughput,” he says. “I’m going to encourage folks to stay ahead of the curve.”
Having attended every annual conference since the beginning, Dr. Wachter looks forward to “polar things” about each meeting: catching up with the founders of the movement and seeing new faces.
“What’s more fun for me is the amount of youthful energy at the meetings,” he says, especially of the hospitalists he has mentored over the years. “When I come with my group from UCSF, it gives me tremendous pride.” TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Updates
Lake Erie
The Lake Erie/Northern Ohio chapter met Aug. 24 at Lolita in Cleveland. Joseph G. Verbalis, MD, chief of the Division of Endocrinology and Metabolism and professor in the Department of Medicine at Georgetown University Medical Center in Washington, D.C., was the guest speaker, and his discussion was on hyponatremia. Sixteen area hospitalists attended the meeting, which was sponsored by CME University.
Fellow in Hospital Medicine Spotlight

Dr. Sherman, a hospitalist of 15 years, is both chairman and director of quality and performance improvement in the Department of Medicine at Glen Cove (N.Y.) Hospital, part of the North Shore University Health System. He is a clinical associate professor of medicine at New York University School of Medicine and an associate professor of medicine at Hofstra University School of Medicine.
A six-year SHM member, he helped establish the Long Island, N.Y., chapter and led as its president from 2004 to 2007. He served as moderator both for the transitions-in-care discussion and MRSA infections symposium at HM10 in Washington, D.C.
Undergraduate education: Duke University, Durham, N.C.
Graduate education: The Rockefeller University in New York City and New York Medical College in Valhalla, N.Y.
Internship and residency: Northwestern University, Chicago.
Fellowships: Gastroenterology fellowship at University of Pittsburgh from 1994 to 1995; fellowship in quality at Greater New York Hospital Association from 2009 to 2010.
Notable: This year, he completed a 15-month Six Sigma quality project on reducing variation care and standardization for patients admitted with heart failure, as well as a capstone project on reducing 30-day readmissions for patients discharged with heart failure.
Quotable: “Hospital medicine will continue to expand and become an integral part of hospital operations and practice. The comanagement services with surgical specialties will continue to evolve, and hospitalists will be taking a larger role in ensuring that care rendered across the continuum is met at the highest standard, both in and out of the hospital.”
FYI: Dr. Sherman enjoys spending time with his wife and two sons, ages 12 and 9. He is an avid tennis player and a regular at his local gym. —Sarah Gelotte
Dr. Sherman, a hospitalist of 15 years, is both chairman and director of quality and performance improvement in the Department of Medicine at Glen Cove (N.Y.) Hospital, part of the North Shore University Health System. He is a clinical associate professor of medicine at New York University School of Medicine and an associate professor of medicine at Hofstra University School of Medicine.
A six-year SHM member, he helped establish the Long Island, N.Y., chapter and led as its president from 2004 to 2007. He served as moderator both for the transitions-in-care discussion and MRSA infections symposium at HM10 in Washington, D.C.
Undergraduate education: Duke University, Durham, N.C.
Graduate education: The Rockefeller University in New York City and New York Medical College in Valhalla, N.Y.
Internship and residency: Northwestern University, Chicago.
Fellowships: Gastroenterology fellowship at University of Pittsburgh from 1994 to 1995; fellowship in quality at Greater New York Hospital Association from 2009 to 2010.
Notable: This year, he completed a 15-month Six Sigma quality project on reducing variation care and standardization for patients admitted with heart failure, as well as a capstone project on reducing 30-day readmissions for patients discharged with heart failure.
Quotable: “Hospital medicine will continue to expand and become an integral part of hospital operations and practice. The comanagement services with surgical specialties will continue to evolve, and hospitalists will be taking a larger role in ensuring that care rendered across the continuum is met at the highest standard, both in and out of the hospital.”
FYI: Dr. Sherman enjoys spending time with his wife and two sons, ages 12 and 9. He is an avid tennis player and a regular at his local gym. —Sarah Gelotte
Dr. Sherman, a hospitalist of 15 years, is both chairman and director of quality and performance improvement in the Department of Medicine at Glen Cove (N.Y.) Hospital, part of the North Shore University Health System. He is a clinical associate professor of medicine at New York University School of Medicine and an associate professor of medicine at Hofstra University School of Medicine.
A six-year SHM member, he helped establish the Long Island, N.Y., chapter and led as its president from 2004 to 2007. He served as moderator both for the transitions-in-care discussion and MRSA infections symposium at HM10 in Washington, D.C.
Undergraduate education: Duke University, Durham, N.C.
Graduate education: The Rockefeller University in New York City and New York Medical College in Valhalla, N.Y.
Internship and residency: Northwestern University, Chicago.
Fellowships: Gastroenterology fellowship at University of Pittsburgh from 1994 to 1995; fellowship in quality at Greater New York Hospital Association from 2009 to 2010.
Notable: This year, he completed a 15-month Six Sigma quality project on reducing variation care and standardization for patients admitted with heart failure, as well as a capstone project on reducing 30-day readmissions for patients discharged with heart failure.
Quotable: “Hospital medicine will continue to expand and become an integral part of hospital operations and practice. The comanagement services with surgical specialties will continue to evolve, and hospitalists will be taking a larger role in ensuring that care rendered across the continuum is met at the highest standard, both in and out of the hospital.”
FYI: Dr. Sherman enjoys spending time with his wife and two sons, ages 12 and 9. He is an avid tennis player and a regular at his local gym. —Sarah Gelotte
Hospitalists Flock to Free HM App for iPhone, BlackBerry, and Other Handhelds
In less than a year, a smartphone application has attracted the attention of hospitalists across the country. Thousands of individuals have accessed the new “Hospitalist Connection” app since it launched in April.
Developed by Epocrates, one of the leaders in mobile applications in healthcare, “Hospitalist Connection” delivers fresh perspectives and unique content about leading research in hospital medicine. Topics include practice management, quality improvement, and care transitions.
Recent articles have covered the effect that financial incentives can have on HM operations and an editorial from Chad Whelan, MD, FHM, physician editor of “Hospitalist Connection,” about the effects of “presenteeism,” or physicians working when the know they are sick.
“When they are on the job, downtime for hospitalists is rare and valuable,” says Dr. Whelan, director of the Division of Hospital Medicine and associate professor of medicine at Loyola University’s Stritch School of Medicine in Chicago.
“‘Hospitalist Connection’ is an easy way to stay informed on best practices in the field—from anywhere at any time.”
To download and subscribe to “Hospitalist Connection,” visit www.hospitalmedicine.org/epocrates.
For SHM, delivering content to smartphones is a logical move.
“This advances the specialty, and we’re thrilled to make it as easy as possible for our members and others to subscribe,” says Todd Von Deak, MBA, CAE, vice president of operations and general manager of SHM. “This is another tangible way that SHM is helping hospitalists improve the quality, safety, and efficiency of care in the hospital.”
In less than a year, a smartphone application has attracted the attention of hospitalists across the country. Thousands of individuals have accessed the new “Hospitalist Connection” app since it launched in April.
Developed by Epocrates, one of the leaders in mobile applications in healthcare, “Hospitalist Connection” delivers fresh perspectives and unique content about leading research in hospital medicine. Topics include practice management, quality improvement, and care transitions.
Recent articles have covered the effect that financial incentives can have on HM operations and an editorial from Chad Whelan, MD, FHM, physician editor of “Hospitalist Connection,” about the effects of “presenteeism,” or physicians working when the know they are sick.
“When they are on the job, downtime for hospitalists is rare and valuable,” says Dr. Whelan, director of the Division of Hospital Medicine and associate professor of medicine at Loyola University’s Stritch School of Medicine in Chicago.
“‘Hospitalist Connection’ is an easy way to stay informed on best practices in the field—from anywhere at any time.”
To download and subscribe to “Hospitalist Connection,” visit www.hospitalmedicine.org/epocrates.
For SHM, delivering content to smartphones is a logical move.
“This advances the specialty, and we’re thrilled to make it as easy as possible for our members and others to subscribe,” says Todd Von Deak, MBA, CAE, vice president of operations and general manager of SHM. “This is another tangible way that SHM is helping hospitalists improve the quality, safety, and efficiency of care in the hospital.”
In less than a year, a smartphone application has attracted the attention of hospitalists across the country. Thousands of individuals have accessed the new “Hospitalist Connection” app since it launched in April.
Developed by Epocrates, one of the leaders in mobile applications in healthcare, “Hospitalist Connection” delivers fresh perspectives and unique content about leading research in hospital medicine. Topics include practice management, quality improvement, and care transitions.
Recent articles have covered the effect that financial incentives can have on HM operations and an editorial from Chad Whelan, MD, FHM, physician editor of “Hospitalist Connection,” about the effects of “presenteeism,” or physicians working when the know they are sick.
“When they are on the job, downtime for hospitalists is rare and valuable,” says Dr. Whelan, director of the Division of Hospital Medicine and associate professor of medicine at Loyola University’s Stritch School of Medicine in Chicago.
“‘Hospitalist Connection’ is an easy way to stay informed on best practices in the field—from anywhere at any time.”
To download and subscribe to “Hospitalist Connection,” visit www.hospitalmedicine.org/epocrates.
For SHM, delivering content to smartphones is a logical move.
“This advances the specialty, and we’re thrilled to make it as easy as possible for our members and others to subscribe,” says Todd Von Deak, MBA, CAE, vice president of operations and general manager of SHM. “This is another tangible way that SHM is helping hospitalists improve the quality, safety, and efficiency of care in the hospital.”
A New Look at Family Medicine Hospitalists
A new survey spearheaded by SHM’s Family Medicine Task Force gives the first glimpse into the demographics, settings, and scopes of practice of this growing HM segment.
The research found that hospitalists trained in family medicine are experienced physicians who likely work directly for their hospital. More than half (51%) completed residency training more than 10 years ago, although the largest single group of respondents (37%) finished residency six to 10 years ago.
Virtually all respondents (96%) work full-time and a third are hospital employees—the most prevalent staffing model found in the survey. In addition to clinical practice, half of family-medicine-trained hospitalists have teaching and other leadership responsibilities.
The survey is based on responses from 81 of the 263 SHM members registered as family medicine physicians.
“As the number of family-medicine-trained physicians grows within hospital medicine, it’s important for us to understand the people behind it,” said research coauthor Claudia Geyer, MD, FHM.
Family-medicine-trained hospitalists are a growing phenomenon in the specialty. Survey data from 2007 to 2008 revealed that 3.7% of U.S. hospitalists are trained in family medicine; however, SHM’s recent membership data show that more than 6% of SHM members are registered as family medicine physicians.
A new survey spearheaded by SHM’s Family Medicine Task Force gives the first glimpse into the demographics, settings, and scopes of practice of this growing HM segment.
The research found that hospitalists trained in family medicine are experienced physicians who likely work directly for their hospital. More than half (51%) completed residency training more than 10 years ago, although the largest single group of respondents (37%) finished residency six to 10 years ago.
Virtually all respondents (96%) work full-time and a third are hospital employees—the most prevalent staffing model found in the survey. In addition to clinical practice, half of family-medicine-trained hospitalists have teaching and other leadership responsibilities.
The survey is based on responses from 81 of the 263 SHM members registered as family medicine physicians.
“As the number of family-medicine-trained physicians grows within hospital medicine, it’s important for us to understand the people behind it,” said research coauthor Claudia Geyer, MD, FHM.
Family-medicine-trained hospitalists are a growing phenomenon in the specialty. Survey data from 2007 to 2008 revealed that 3.7% of U.S. hospitalists are trained in family medicine; however, SHM’s recent membership data show that more than 6% of SHM members are registered as family medicine physicians.
A new survey spearheaded by SHM’s Family Medicine Task Force gives the first glimpse into the demographics, settings, and scopes of practice of this growing HM segment.
The research found that hospitalists trained in family medicine are experienced physicians who likely work directly for their hospital. More than half (51%) completed residency training more than 10 years ago, although the largest single group of respondents (37%) finished residency six to 10 years ago.
Virtually all respondents (96%) work full-time and a third are hospital employees—the most prevalent staffing model found in the survey. In addition to clinical practice, half of family-medicine-trained hospitalists have teaching and other leadership responsibilities.
The survey is based on responses from 81 of the 263 SHM members registered as family medicine physicians.
“As the number of family-medicine-trained physicians grows within hospital medicine, it’s important for us to understand the people behind it,” said research coauthor Claudia Geyer, MD, FHM.
Family-medicine-trained hospitalists are a growing phenomenon in the specialty. Survey data from 2007 to 2008 revealed that 3.7% of U.S. hospitalists are trained in family medicine; however, SHM’s recent membership data show that more than 6% of SHM members are registered as family medicine physicians.
Fellows Program Application Deadline is Jan. 14
Next year’s annual meeting in Dallas marks the third induction of fellows into the SHM Fellows program. Candidates still have a few weeks to submit an application. The deadline for 2011 applications is Jan. 14.
More than 700 fellows and senior fellows have been inducted since the program began in 2009. “The success and enthusiasm for this program has been incredible,” says Todd Von Deak, SHM’s vice president of operations and general manager. “For individual hospitalists, it’s a simple way to demonstrate to patients and hospitals that you take your profession very seriously. For the specialty, it illustrates the growth and accomplishments of hospital medicine to the rest of the healthcare sector.”
In addition to additional rights and privileges from SHM, fellows can append their designation to their name and credentials.
The SHM Fellows program inducts three levels of fellows every year: Fellow in Hospital Medicine (FHM), Senior Fellow in Hospital Medicine (SFHM), and Master in Hospital Medicine (MHM).
To be nominated, both FHM and SFHM designations require five years as a practicing hospitalist and a demonstrated commitment to quality improvement, teamwork, and leadership. An FHM candidate must be an SHM member for at least three years; SFHM candidates must be members for at least five.
Introduced last year, the MHM designation is by invitation only and reserved for the specialty’s leaders and pioneers. The inaugural MHM designees were John Nelson (pictured left), MD, MHM, Robert Watcher (center), MD, MHM, and Winthrop Whitcomb (right), MD, MHM.
For more information or an application, visit www.hospitalmedicine.org/fellows.
FELLOW IN HOSPITAL MEDICINE SPOTLIGHT
Bradley M. Sherman, MD, FACP, FHM
Dr. Sherman, a hospitalist of 15 years, is both chairman and director of quality and performance improvement in the Department of Medicine at Glen Cove (N.Y.) Hospital, part of the North Shore University Health System. He is a clinical associate professor of medicine at New York University School of Medicine and an associate professor of medicine at Hofstra University School of Medicine.
A six-year SHM member, he helped establish the Long Island, N.Y., chapter and led as its president from 2004 to 2007. He served as moderator both for the transitions-in-care discussion and MRSA infections symposium at HM10 in Washington, D.C.
Undergraduate education: Duke University, Durham, N.C.
Graduate education: The Rockefeller University in New York City and New York Medical College in Valhalla, N.Y.
Internship and residency: Northwestern University, Chicago.
Fellowships: Gastroenterology fellowship at University of Pittsburgh from 1994 to 1995; fellowship in quality at Greater New York Hospital Association from 2009 to 2010.
Notable: This year, he completed a 15-month Six Sigma quality project on reducing variation care and standardization for patients admitted with heart failure, as well as a capstone project on reducing 30-day readmissions for patients discharged with heart failure.
Quotable: “Hospital medicine will continue to expand and become an integral part of hospital operations and practice. The comanagement services with surgical specialties will continue to evolve, and hospitalists will be taking a larger role in ensuring that care rendered across the continuum is met at the highest standard, both in and out of the hospital.”
FYI: Dr. Sherman enjoys spending time with his wife and two sons, ages 12 and 9. He is an avid tennis player and a regular at his local gym. —Sarah Gelotte
Next year’s annual meeting in Dallas marks the third induction of fellows into the SHM Fellows program. Candidates still have a few weeks to submit an application. The deadline for 2011 applications is Jan. 14.
More than 700 fellows and senior fellows have been inducted since the program began in 2009. “The success and enthusiasm for this program has been incredible,” says Todd Von Deak, SHM’s vice president of operations and general manager. “For individual hospitalists, it’s a simple way to demonstrate to patients and hospitals that you take your profession very seriously. For the specialty, it illustrates the growth and accomplishments of hospital medicine to the rest of the healthcare sector.”
In addition to additional rights and privileges from SHM, fellows can append their designation to their name and credentials.
The SHM Fellows program inducts three levels of fellows every year: Fellow in Hospital Medicine (FHM), Senior Fellow in Hospital Medicine (SFHM), and Master in Hospital Medicine (MHM).
To be nominated, both FHM and SFHM designations require five years as a practicing hospitalist and a demonstrated commitment to quality improvement, teamwork, and leadership. An FHM candidate must be an SHM member for at least three years; SFHM candidates must be members for at least five.
Introduced last year, the MHM designation is by invitation only and reserved for the specialty’s leaders and pioneers. The inaugural MHM designees were John Nelson (pictured left), MD, MHM, Robert Watcher (center), MD, MHM, and Winthrop Whitcomb (right), MD, MHM.
For more information or an application, visit www.hospitalmedicine.org/fellows.
FELLOW IN HOSPITAL MEDICINE SPOTLIGHT
Bradley M. Sherman, MD, FACP, FHM
Dr. Sherman, a hospitalist of 15 years, is both chairman and director of quality and performance improvement in the Department of Medicine at Glen Cove (N.Y.) Hospital, part of the North Shore University Health System. He is a clinical associate professor of medicine at New York University School of Medicine and an associate professor of medicine at Hofstra University School of Medicine.
A six-year SHM member, he helped establish the Long Island, N.Y., chapter and led as its president from 2004 to 2007. He served as moderator both for the transitions-in-care discussion and MRSA infections symposium at HM10 in Washington, D.C.
Undergraduate education: Duke University, Durham, N.C.
Graduate education: The Rockefeller University in New York City and New York Medical College in Valhalla, N.Y.
Internship and residency: Northwestern University, Chicago.
Fellowships: Gastroenterology fellowship at University of Pittsburgh from 1994 to 1995; fellowship in quality at Greater New York Hospital Association from 2009 to 2010.
Notable: This year, he completed a 15-month Six Sigma quality project on reducing variation care and standardization for patients admitted with heart failure, as well as a capstone project on reducing 30-day readmissions for patients discharged with heart failure.
Quotable: “Hospital medicine will continue to expand and become an integral part of hospital operations and practice. The comanagement services with surgical specialties will continue to evolve, and hospitalists will be taking a larger role in ensuring that care rendered across the continuum is met at the highest standard, both in and out of the hospital.”
FYI: Dr. Sherman enjoys spending time with his wife and two sons, ages 12 and 9. He is an avid tennis player and a regular at his local gym. —Sarah Gelotte
Next year’s annual meeting in Dallas marks the third induction of fellows into the SHM Fellows program. Candidates still have a few weeks to submit an application. The deadline for 2011 applications is Jan. 14.
More than 700 fellows and senior fellows have been inducted since the program began in 2009. “The success and enthusiasm for this program has been incredible,” says Todd Von Deak, SHM’s vice president of operations and general manager. “For individual hospitalists, it’s a simple way to demonstrate to patients and hospitals that you take your profession very seriously. For the specialty, it illustrates the growth and accomplishments of hospital medicine to the rest of the healthcare sector.”
In addition to additional rights and privileges from SHM, fellows can append their designation to their name and credentials.
The SHM Fellows program inducts three levels of fellows every year: Fellow in Hospital Medicine (FHM), Senior Fellow in Hospital Medicine (SFHM), and Master in Hospital Medicine (MHM).
To be nominated, both FHM and SFHM designations require five years as a practicing hospitalist and a demonstrated commitment to quality improvement, teamwork, and leadership. An FHM candidate must be an SHM member for at least three years; SFHM candidates must be members for at least five.
Introduced last year, the MHM designation is by invitation only and reserved for the specialty’s leaders and pioneers. The inaugural MHM designees were John Nelson (pictured left), MD, MHM, Robert Watcher (center), MD, MHM, and Winthrop Whitcomb (right), MD, MHM.
For more information or an application, visit www.hospitalmedicine.org/fellows.
FELLOW IN HOSPITAL MEDICINE SPOTLIGHT
Bradley M. Sherman, MD, FACP, FHM
Dr. Sherman, a hospitalist of 15 years, is both chairman and director of quality and performance improvement in the Department of Medicine at Glen Cove (N.Y.) Hospital, part of the North Shore University Health System. He is a clinical associate professor of medicine at New York University School of Medicine and an associate professor of medicine at Hofstra University School of Medicine.
A six-year SHM member, he helped establish the Long Island, N.Y., chapter and led as its president from 2004 to 2007. He served as moderator both for the transitions-in-care discussion and MRSA infections symposium at HM10 in Washington, D.C.
Undergraduate education: Duke University, Durham, N.C.
Graduate education: The Rockefeller University in New York City and New York Medical College in Valhalla, N.Y.
Internship and residency: Northwestern University, Chicago.
Fellowships: Gastroenterology fellowship at University of Pittsburgh from 1994 to 1995; fellowship in quality at Greater New York Hospital Association from 2009 to 2010.
Notable: This year, he completed a 15-month Six Sigma quality project on reducing variation care and standardization for patients admitted with heart failure, as well as a capstone project on reducing 30-day readmissions for patients discharged with heart failure.
Quotable: “Hospital medicine will continue to expand and become an integral part of hospital operations and practice. The comanagement services with surgical specialties will continue to evolve, and hospitalists will be taking a larger role in ensuring that care rendered across the continuum is met at the highest standard, both in and out of the hospital.”
FYI: Dr. Sherman enjoys spending time with his wife and two sons, ages 12 and 9. He is an avid tennis player and a regular at his local gym. —Sarah Gelotte
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Continuous insulin infusion in non-ICU patients
- How hospitalists spend their day
- Outcomes of patients leaving against medical advice
- Prediction rule for readmission
- Effects of high- vs. low-dose PPIs for peptic ulcer
- Hospital utilization by generalists before hospitalists
- Effect of hospitalist fragmentation on length of stay
- Medication errors at admissions in older patients
Continuous Insulin Infusion Provides Effective Glycemic Control in Non-ICU Patients
Clinical question: Is continuous insulin infusion (CII) a safe and effective option in the management of hyperglycemia in non-ICU patients?
Background: Hyperglycemia has been associated with worse outcomes in hospitalized patients. Prior research has demonstrated the benefit of CII in managing hyperglycemia in the ICU setting. However, outcomes have not been evaluated in the general medical (non-ICU) setting, where hyperglycemia is often inadequately addressed.
Study design: Retrospective chart review.
Setting: Urban tertiary-care medical center.
Synopsis: Charts of 200 adult patients treated with CII in non-ICU areas were reviewed with the primary outcomes including mean daily blood glucose (BG) levels and number of hyper- and hypoglycemic events occurring on CII. Mean BG dropped from 323 mg/dL to 182 mg/dL by day one, with a BG≤of 150 achieved in 67% of patients by day two of therapy. Twenty-two percent of patients suffered a hypoglycemic event (BG<60), reportedly similar to prior studies of insulin use in ICU and non-ICU settings. Eighty-two percent of patients received some form of nutritional support while on CII. In multivariate analyses, receiving oral nutrition (either a solid or liquid diet) was the only factor associated with increased risk of hyperglycemia and hypoglycemia.
This study was limited by its retrospective analysis in a single center. No comparison was made with basal-bolus or sliding-scale insulin therapy regarding efficacy or safety.
Bottom line: Non-ICU patients with hyperglycemia who received CII were able to achieve effective glycemic control within 48 hours of initiation, with rates of hypoglycemia comparable to those observed in ICU settings.
Citation: Smiley D, Rhee M, Peng L, et al. Safety and efficacy of continuous insulin infusion in noncritical care settings. J Hosp Med. 2010;5(4):212-217.
Hospitalists Spend More Time on Indirect, Rather Than Direct, Patient Care
Clinical question: What are the components of the daily workflow of hospitalists working on a non-housestaff service?
Background: The use of hospitalists is associated with increased efficiency in the hospital setting. However, it is not known how this efficiency is achieved. Prior literature has attempted to address this question, but with increasing demands and patient census, the representativeness of existing data is unclear.
Study design: Observational time-motion study.
Setting: Urban tertiary-care academic medical center.
Synopsis: Twenty-four hospitalists were directly observed for two weekday shifts. An electronic collection tool was developed using initial data on hospitalist activities and piloted prior to formal study data collection. Direct patient care was defined as involving face-to-face interaction between hospitalist and patient, while indirect patient care involved activities relevant to patient care but not performed in the patient’s presence.
Approximately 500 hours of observation were collected. Direct patient care comprised only a mean of 17.4% of the hospitalists’ daily workflow, while more was spent on indirect care, mainly electronic health record (EHR) documentation (mean 34.1%) and communication activities (mean 25.9%). Multitasking occurred 16% of the time, typically during communication or “critical documentation activities” (e.g. writing prescriptions). As patient volume increased, less time was spent in communication, and documentation was deferred to after hours.
These results were consistent with prior observational studies but were limited to a single center and might not represent the workflow of hospitalists in other settings, such as community hospitals, or nocturnists.
Bottom line: Hospitalists on non-housestaff services spend most of their time on indirect patient care and, with increasing patient census, communication is sacrificed. Multitasking is common during periods of communication and critical documentation.
Citation: Tipping MD, Forth VE, O’Leary KJ, et al. Where did the day go?—a time-motion study of hospitalists. J Hosp Med. 2010;5(6):323-328.
Patients Who Leave Against Medical Advice Have Higher Readmission, Mortality Rates
Clinical question: What are the 30-day hospital readmission and mortality rates for Veterans Administration (VA) patients discharged against medical advice (AMA) compared with those appropriately discharged from the hospital?
Background: Patients discharged AMA might be at increased risk of experiencing worse outcomes. Small studies have demonstrated that patients with asthma and acute myocardial infarction (MI) discharged AMA have increased risk of readmission and death. However, it is unclear whether these risks are generalizable to a wider medical population.
Study design: Five-year retrospective cohort study.
Setting: One hundred twenty-nine VA acute-care hospitals.
Synopsis: Of the nearly 2 million patients admitted to the VA from 2004 to 2008, 1.7% were discharged AMA. Patients discharged AMA generally were younger, had lower incomes, and were more likely to be black. Furthermore, patients discharged AMA had statistically significant higher rates of 30-day readmission (17.7% vs. 11%, P<0.001) and higher 30-day mortality rates (0.75% vs. 0.61%, P=0.001) compared with those who had been appropriately discharged. In hazard models, discharge AMA was a significant predictor of 30-day readmission and conferred a nonstatistically significant increase in 30-day mortality.
Because all patients were seen in VA facilities, the results might not be generalizable to other acute-care settings. Although VA patients differ from the general medical population, the characteristics of patients discharged AMA are similar to those in previously published studies. The study utilized administrative data, which are very reliable but limited by little information on clinical factors that could contribute to AMA discharges.
Bottom line: Patients discharged AMA are at increased risk of worse post-hospitalization outcomes, including hospital readmission and death.
Citation: Glasgow JM, Vaughn-Sarrazin M, Kaboli PJ. Leaving against medical advice (AMA): risk of 30-day mortality and hospital readmission. J Gen Intern Med. 2010;25(9): 926-929.
Simple Model Predicts Hospital Readmission
Clinical question: Which patient-level factors can be used in a simple model to predict hospital readmission of medicine patients?
Background: Hospital readmissions are common and costly. Previously published readmission prediction models have had limited utility because they focused on a specific condition, setting, or population, or were too cumbersome for practical use.
Study design: Prospective observational cohort study.
Setting: Six academic medical centers.
Synopsis: Data from nearly 11,000 general medicine patients were included in the analysis. Overall, almost 18% of patients were readmitted within 30 days of discharge.
In the prediction model derived and validated from the data, seven factors were significant predictors of readmission within 30 days of discharge: insurance status, marital status, having a regular healthcare provider, Charlson comorbidity index, SF 12 physical component score, one or more admissions within the last year, and current length of stay greater than two days. Points assigned from each significant predictor were used to create a risk score. The 5% of patients with risk scores of 25 and higher had 30-day readmission rates of approximately 30%, compared to readmission rates of approximately 16% in patients with scores of less than 25.
These results might not be generalizable to small, rural, nonacademic settings. Planned admissions could not be excluded from the data, and readmissions to nonstudy hospitals could not be ascertained. Despite these limitations, this model is easier to use than prior models and relevant to a broad population of patients.
Bottom line: A simple prediction model using patient-level factors can be used to identify patients at higher risk of readmission within 30 days of discharge to home.
Citation: Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2010;25(3):211-219.
No Difference in Outcomes Between High- and Non-High-Dose Proton Pump Inhibitors in Bleeding Peptic Ulcers
Clinical question: Do high-dose proton pump inhibitors (PPIs) decrease the rate of rebleeding, surgical intervention, or mortality in patients with bleeding peptic ulcers who have undergone endoscopic treatment?
Background: Previous studies have demonstrated superiority of both high- and low-dose PPIs to H2 receptor antagonists and placebo in reducing rebleeding rates in patients with peptic ulcers. However, no clear evidence is available to suggest that high-dose PPIs are more effective than non-high-dose PPIs for treatment of bleeding peptic ulcers.
Study design: Systematic review and meta-analysis.
Setting: Multicenter and single-site studies conducted in several countries.
Synopsis: Studies were included if they were randomized controlled trials, compared high- versus non-high-dose PPIs, evaluated endoscopically confirmed bleeding ulcers, gave PPIs after endoscopy, and documented outcomes regarding rates of rebleeding, surgical intervention, or mortality. High-dose PPIs were defined as equivalent to omeprazole 80 mg intravenous bolus followed by continuous intravenous infusion at 8 mg/hr for 72 hours.
Seven studies met inclusion criteria. The pooled odds ratios for rebleeding, surgical intervention, and mortality were 1.30 (95% CI, 0.88-1.91), 1.49 (95% CI, 0.66-3.37), and 0.89 (95% CI, 0.37-2.13), respectively, for high-dose versus non-high-dose PPIs. The authors concluded that high-dose PPIs were not superior to non-high-dose PPIs in reducing the rates of these adverse outcomes after endoscopic treatment of bleeding ulcers. Considering the cost of high-dose PPIs, further studies are indicated to help guide PPI dosing for patients with peptic ulcers.
Major limitations of this study were the small number of studies (1,157 patients in total) and their heterogeneity, and the lack of intention-to-treat analysis. The studies also included a high Asian predominance, and it has been shown that Asian populations have an enhanced PPI effect.
Bottom line: High-dose PPIs did not demonstrate reduced rates of ulcer rebleeding, surgical intervention, or mortality compared with non-high-dose PPIs in this meta-analysis, which included a small number of studies and patients.
Citation: Wang CH, Ma MH, Chou HC, et al. High-dose vs. non-high-dose proton pump inhibitors after endoscopic treatment in patients with bleeding peptic ulcer: a systematic review and meta-analysis of randomized controlled trials. Arch Intern Med. 2010;170(9):751-758.
Hospital Utilization by Practicing Generalists Declined before the Emergence of Hospitalists
Clinical question: What has been the pattern of hospital utilization by generalists before and after the emergence of hospitalists?
Background: It has been proposed that the emergence of hospitalists has “crowded out” generalist physicians from the U.S. hospital setting. This study evaluated the trends of inpatient practice by generalists both before and after the emergence of hospitalists.
Study design: Retrospective analysis of national databases.
Setting: U.S. data from 1980 to 2005.
Synopsis: Utilizing the National Hospital Discharge Survey and the American Medical Association’s Physician Characteristics and Distribution in the U.S., information was extracted to evaluate the average number of annual inpatient encounters relative to generalist workforce from 1980 to 2005. Total inpatient encounters for each year were calculated by multiplying the total number of hospital admissions by the average hospital length of stay. The emergence of hospitalists was defined as beginning in 1994.
Total inpatient encounters by generalists declined by 35% in the pre-hospitalist era but remained essentially unchanged in the hospitalist era. During the pre-hospitalist period, the number of generalists doubled, to more than 200,000 from approximately 100,000, while the number of hospital discharges remained relatively stable and the length of stay declined by a third. The decrease in average inpatient encounters in the pre-hospitalist era is thought to have been secondary to decreased length of stay and increased workforce.
Bottom line: Hospital utilization relative to generalist physician workforce was decreasing prior to the emergence of hospitalists mainly due to decreased length of hospital stay and increased numbers of physicians.
Citation: Meltzer DO, Chung JW. U.S. trends in hospitalization and generalist physician workforce and the emergence of hospitalists. J Gen Intern Med. 2010;25(5):453-459.
Fragmentation of Hospitalist Care Is Associated with Increased Length of Stay
Clinical question: Does fragmentation of care (FOC) by hospitalists affect length of stay (LOS)?
Background: Previous investigations have explored the impact of FOC provided by residency programs on LOS and quality of care. Results of these studies have been mixed. However, there have been no prior studies on the impact of the fragmentation of hospitalist care on LOS.
Study design: Concurrent control study.
Setting: Hospitalist practices all over the country managed by IPC: The Hospitalist Company.
Synopsis: Investigators looked at 10,977 patients admitted with diagnoses of pneumonia or heart failure. The primary endpoint was LOS. The independent variable of interest was a measure of FOC. The FOC was calculated as a quantitative index, by determining the percentage of hospitalist care delivered by a physician other than the primary hospitalist.
Multivariable analyses revealed a statistically significant increase in LOS of 0.39 days for each 10% increase in fragmentation level for pneumonia admissions. Similarly, for patients with heart failure, there was a significant increase in LOS of 0.30 days for each 10% increase in fragmentation level.
The study is a concurrent control study, so conclusions cannot be drawn about causality. Additionally, there are likely unmeasured differences between every hospital and hospitalist practice, which could further confound the relationships between hospitalist care and LOS.
Bottom line: Fragmentation of care provided by hospitalists is associated with an increased LOS in patients hospitalized for pneumonia or heart failure.
Citation: Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
Admission Medication Errors Are Common and Most Harmful in Older Patients Taking Many Medications
Clinical question: What are the risk factors and potential harm associated with medication errors at hospital admission?
Background: Obtaining a medication history from a hospitalized patient is an error-prone process. Several variables can affect the completeness and quality of medication histories, but existing data are limited regarding patient or medication risk factors associated with medication errors at admission.
Study design: Prospective cohort study.
Setting: Academic hospital in Chicago.
Synopsis: Pharmacist and admitting physician medication histories were compared with admission medication orders to identify any unexplained discrepancies. Discrepancies resulting in order changes were defined as medication errors.
Of the 651 adult medical inpatients studied, 234 (35.9%) had medication order errors identified at admission. Errors originated in the medication histories for 85% of these patients. The most frequent type of error was an omission (48.9%). An age of 65 or older (odds ratio [OR]=2.17, 95% confidence interval [CI], 1.09-4.30) and increased number of medications (OR=1.21, 95% CI, 1.14-1.29) were the only risk factors identified by multivariate analysis to be independently associated with increased risk of medication order errors potentially causing harm or requiring monitoring or intervention. Presenting a medication list upon admission was a significant protective factor (OR=0.35, 95% CI, 0.19-0.63).
Though this is the largest study to date evaluating admission medication errors in hospitalized medical patients, it remains limited by its single hospital site. Because the authors were unable to interview patients who were too ill or unwilling to participate and had no caregiver present, they might have underestimated the number of admission errors. Further, the harm assessment was based on potential and not actual harm.
Bottom line: Admission medication order errors are frequent, most commonly originate in the medication histories, and have increased potential to cause adverse outcomes in older patients and those taking higher numbers of medications.
Citation: Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications At Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25(5):441-447.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Continuous insulin infusion in non-ICU patients
- How hospitalists spend their day
- Outcomes of patients leaving against medical advice
- Prediction rule for readmission
- Effects of high- vs. low-dose PPIs for peptic ulcer
- Hospital utilization by generalists before hospitalists
- Effect of hospitalist fragmentation on length of stay
- Medication errors at admissions in older patients
Continuous Insulin Infusion Provides Effective Glycemic Control in Non-ICU Patients
Clinical question: Is continuous insulin infusion (CII) a safe and effective option in the management of hyperglycemia in non-ICU patients?
Background: Hyperglycemia has been associated with worse outcomes in hospitalized patients. Prior research has demonstrated the benefit of CII in managing hyperglycemia in the ICU setting. However, outcomes have not been evaluated in the general medical (non-ICU) setting, where hyperglycemia is often inadequately addressed.
Study design: Retrospective chart review.
Setting: Urban tertiary-care medical center.
Synopsis: Charts of 200 adult patients treated with CII in non-ICU areas were reviewed with the primary outcomes including mean daily blood glucose (BG) levels and number of hyper- and hypoglycemic events occurring on CII. Mean BG dropped from 323 mg/dL to 182 mg/dL by day one, with a BG≤of 150 achieved in 67% of patients by day two of therapy. Twenty-two percent of patients suffered a hypoglycemic event (BG<60), reportedly similar to prior studies of insulin use in ICU and non-ICU settings. Eighty-two percent of patients received some form of nutritional support while on CII. In multivariate analyses, receiving oral nutrition (either a solid or liquid diet) was the only factor associated with increased risk of hyperglycemia and hypoglycemia.
This study was limited by its retrospective analysis in a single center. No comparison was made with basal-bolus or sliding-scale insulin therapy regarding efficacy or safety.
Bottom line: Non-ICU patients with hyperglycemia who received CII were able to achieve effective glycemic control within 48 hours of initiation, with rates of hypoglycemia comparable to those observed in ICU settings.
Citation: Smiley D, Rhee M, Peng L, et al. Safety and efficacy of continuous insulin infusion in noncritical care settings. J Hosp Med. 2010;5(4):212-217.
Hospitalists Spend More Time on Indirect, Rather Than Direct, Patient Care
Clinical question: What are the components of the daily workflow of hospitalists working on a non-housestaff service?
Background: The use of hospitalists is associated with increased efficiency in the hospital setting. However, it is not known how this efficiency is achieved. Prior literature has attempted to address this question, but with increasing demands and patient census, the representativeness of existing data is unclear.
Study design: Observational time-motion study.
Setting: Urban tertiary-care academic medical center.
Synopsis: Twenty-four hospitalists were directly observed for two weekday shifts. An electronic collection tool was developed using initial data on hospitalist activities and piloted prior to formal study data collection. Direct patient care was defined as involving face-to-face interaction between hospitalist and patient, while indirect patient care involved activities relevant to patient care but not performed in the patient’s presence.
Approximately 500 hours of observation were collected. Direct patient care comprised only a mean of 17.4% of the hospitalists’ daily workflow, while more was spent on indirect care, mainly electronic health record (EHR) documentation (mean 34.1%) and communication activities (mean 25.9%). Multitasking occurred 16% of the time, typically during communication or “critical documentation activities” (e.g. writing prescriptions). As patient volume increased, less time was spent in communication, and documentation was deferred to after hours.
These results were consistent with prior observational studies but were limited to a single center and might not represent the workflow of hospitalists in other settings, such as community hospitals, or nocturnists.
Bottom line: Hospitalists on non-housestaff services spend most of their time on indirect patient care and, with increasing patient census, communication is sacrificed. Multitasking is common during periods of communication and critical documentation.
Citation: Tipping MD, Forth VE, O’Leary KJ, et al. Where did the day go?—a time-motion study of hospitalists. J Hosp Med. 2010;5(6):323-328.
Patients Who Leave Against Medical Advice Have Higher Readmission, Mortality Rates
Clinical question: What are the 30-day hospital readmission and mortality rates for Veterans Administration (VA) patients discharged against medical advice (AMA) compared with those appropriately discharged from the hospital?
Background: Patients discharged AMA might be at increased risk of experiencing worse outcomes. Small studies have demonstrated that patients with asthma and acute myocardial infarction (MI) discharged AMA have increased risk of readmission and death. However, it is unclear whether these risks are generalizable to a wider medical population.
Study design: Five-year retrospective cohort study.
Setting: One hundred twenty-nine VA acute-care hospitals.
Synopsis: Of the nearly 2 million patients admitted to the VA from 2004 to 2008, 1.7% were discharged AMA. Patients discharged AMA generally were younger, had lower incomes, and were more likely to be black. Furthermore, patients discharged AMA had statistically significant higher rates of 30-day readmission (17.7% vs. 11%, P<0.001) and higher 30-day mortality rates (0.75% vs. 0.61%, P=0.001) compared with those who had been appropriately discharged. In hazard models, discharge AMA was a significant predictor of 30-day readmission and conferred a nonstatistically significant increase in 30-day mortality.
Because all patients were seen in VA facilities, the results might not be generalizable to other acute-care settings. Although VA patients differ from the general medical population, the characteristics of patients discharged AMA are similar to those in previously published studies. The study utilized administrative data, which are very reliable but limited by little information on clinical factors that could contribute to AMA discharges.
Bottom line: Patients discharged AMA are at increased risk of worse post-hospitalization outcomes, including hospital readmission and death.
Citation: Glasgow JM, Vaughn-Sarrazin M, Kaboli PJ. Leaving against medical advice (AMA): risk of 30-day mortality and hospital readmission. J Gen Intern Med. 2010;25(9): 926-929.
Simple Model Predicts Hospital Readmission
Clinical question: Which patient-level factors can be used in a simple model to predict hospital readmission of medicine patients?
Background: Hospital readmissions are common and costly. Previously published readmission prediction models have had limited utility because they focused on a specific condition, setting, or population, or were too cumbersome for practical use.
Study design: Prospective observational cohort study.
Setting: Six academic medical centers.
Synopsis: Data from nearly 11,000 general medicine patients were included in the analysis. Overall, almost 18% of patients were readmitted within 30 days of discharge.
In the prediction model derived and validated from the data, seven factors were significant predictors of readmission within 30 days of discharge: insurance status, marital status, having a regular healthcare provider, Charlson comorbidity index, SF 12 physical component score, one or more admissions within the last year, and current length of stay greater than two days. Points assigned from each significant predictor were used to create a risk score. The 5% of patients with risk scores of 25 and higher had 30-day readmission rates of approximately 30%, compared to readmission rates of approximately 16% in patients with scores of less than 25.
These results might not be generalizable to small, rural, nonacademic settings. Planned admissions could not be excluded from the data, and readmissions to nonstudy hospitals could not be ascertained. Despite these limitations, this model is easier to use than prior models and relevant to a broad population of patients.
Bottom line: A simple prediction model using patient-level factors can be used to identify patients at higher risk of readmission within 30 days of discharge to home.
Citation: Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2010;25(3):211-219.
No Difference in Outcomes Between High- and Non-High-Dose Proton Pump Inhibitors in Bleeding Peptic Ulcers
Clinical question: Do high-dose proton pump inhibitors (PPIs) decrease the rate of rebleeding, surgical intervention, or mortality in patients with bleeding peptic ulcers who have undergone endoscopic treatment?
Background: Previous studies have demonstrated superiority of both high- and low-dose PPIs to H2 receptor antagonists and placebo in reducing rebleeding rates in patients with peptic ulcers. However, no clear evidence is available to suggest that high-dose PPIs are more effective than non-high-dose PPIs for treatment of bleeding peptic ulcers.
Study design: Systematic review and meta-analysis.
Setting: Multicenter and single-site studies conducted in several countries.
Synopsis: Studies were included if they were randomized controlled trials, compared high- versus non-high-dose PPIs, evaluated endoscopically confirmed bleeding ulcers, gave PPIs after endoscopy, and documented outcomes regarding rates of rebleeding, surgical intervention, or mortality. High-dose PPIs were defined as equivalent to omeprazole 80 mg intravenous bolus followed by continuous intravenous infusion at 8 mg/hr for 72 hours.
Seven studies met inclusion criteria. The pooled odds ratios for rebleeding, surgical intervention, and mortality were 1.30 (95% CI, 0.88-1.91), 1.49 (95% CI, 0.66-3.37), and 0.89 (95% CI, 0.37-2.13), respectively, for high-dose versus non-high-dose PPIs. The authors concluded that high-dose PPIs were not superior to non-high-dose PPIs in reducing the rates of these adverse outcomes after endoscopic treatment of bleeding ulcers. Considering the cost of high-dose PPIs, further studies are indicated to help guide PPI dosing for patients with peptic ulcers.
Major limitations of this study were the small number of studies (1,157 patients in total) and their heterogeneity, and the lack of intention-to-treat analysis. The studies also included a high Asian predominance, and it has been shown that Asian populations have an enhanced PPI effect.
Bottom line: High-dose PPIs did not demonstrate reduced rates of ulcer rebleeding, surgical intervention, or mortality compared with non-high-dose PPIs in this meta-analysis, which included a small number of studies and patients.
Citation: Wang CH, Ma MH, Chou HC, et al. High-dose vs. non-high-dose proton pump inhibitors after endoscopic treatment in patients with bleeding peptic ulcer: a systematic review and meta-analysis of randomized controlled trials. Arch Intern Med. 2010;170(9):751-758.
Hospital Utilization by Practicing Generalists Declined before the Emergence of Hospitalists
Clinical question: What has been the pattern of hospital utilization by generalists before and after the emergence of hospitalists?
Background: It has been proposed that the emergence of hospitalists has “crowded out” generalist physicians from the U.S. hospital setting. This study evaluated the trends of inpatient practice by generalists both before and after the emergence of hospitalists.
Study design: Retrospective analysis of national databases.
Setting: U.S. data from 1980 to 2005.
Synopsis: Utilizing the National Hospital Discharge Survey and the American Medical Association’s Physician Characteristics and Distribution in the U.S., information was extracted to evaluate the average number of annual inpatient encounters relative to generalist workforce from 1980 to 2005. Total inpatient encounters for each year were calculated by multiplying the total number of hospital admissions by the average hospital length of stay. The emergence of hospitalists was defined as beginning in 1994.
Total inpatient encounters by generalists declined by 35% in the pre-hospitalist era but remained essentially unchanged in the hospitalist era. During the pre-hospitalist period, the number of generalists doubled, to more than 200,000 from approximately 100,000, while the number of hospital discharges remained relatively stable and the length of stay declined by a third. The decrease in average inpatient encounters in the pre-hospitalist era is thought to have been secondary to decreased length of stay and increased workforce.
Bottom line: Hospital utilization relative to generalist physician workforce was decreasing prior to the emergence of hospitalists mainly due to decreased length of hospital stay and increased numbers of physicians.
Citation: Meltzer DO, Chung JW. U.S. trends in hospitalization and generalist physician workforce and the emergence of hospitalists. J Gen Intern Med. 2010;25(5):453-459.
Fragmentation of Hospitalist Care Is Associated with Increased Length of Stay
Clinical question: Does fragmentation of care (FOC) by hospitalists affect length of stay (LOS)?
Background: Previous investigations have explored the impact of FOC provided by residency programs on LOS and quality of care. Results of these studies have been mixed. However, there have been no prior studies on the impact of the fragmentation of hospitalist care on LOS.
Study design: Concurrent control study.
Setting: Hospitalist practices all over the country managed by IPC: The Hospitalist Company.
Synopsis: Investigators looked at 10,977 patients admitted with diagnoses of pneumonia or heart failure. The primary endpoint was LOS. The independent variable of interest was a measure of FOC. The FOC was calculated as a quantitative index, by determining the percentage of hospitalist care delivered by a physician other than the primary hospitalist.
Multivariable analyses revealed a statistically significant increase in LOS of 0.39 days for each 10% increase in fragmentation level for pneumonia admissions. Similarly, for patients with heart failure, there was a significant increase in LOS of 0.30 days for each 10% increase in fragmentation level.
The study is a concurrent control study, so conclusions cannot be drawn about causality. Additionally, there are likely unmeasured differences between every hospital and hospitalist practice, which could further confound the relationships between hospitalist care and LOS.
Bottom line: Fragmentation of care provided by hospitalists is associated with an increased LOS in patients hospitalized for pneumonia or heart failure.
Citation: Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
Admission Medication Errors Are Common and Most Harmful in Older Patients Taking Many Medications
Clinical question: What are the risk factors and potential harm associated with medication errors at hospital admission?
Background: Obtaining a medication history from a hospitalized patient is an error-prone process. Several variables can affect the completeness and quality of medication histories, but existing data are limited regarding patient or medication risk factors associated with medication errors at admission.
Study design: Prospective cohort study.
Setting: Academic hospital in Chicago.
Synopsis: Pharmacist and admitting physician medication histories were compared with admission medication orders to identify any unexplained discrepancies. Discrepancies resulting in order changes were defined as medication errors.
Of the 651 adult medical inpatients studied, 234 (35.9%) had medication order errors identified at admission. Errors originated in the medication histories for 85% of these patients. The most frequent type of error was an omission (48.9%). An age of 65 or older (odds ratio [OR]=2.17, 95% confidence interval [CI], 1.09-4.30) and increased number of medications (OR=1.21, 95% CI, 1.14-1.29) were the only risk factors identified by multivariate analysis to be independently associated with increased risk of medication order errors potentially causing harm or requiring monitoring or intervention. Presenting a medication list upon admission was a significant protective factor (OR=0.35, 95% CI, 0.19-0.63).
Though this is the largest study to date evaluating admission medication errors in hospitalized medical patients, it remains limited by its single hospital site. Because the authors were unable to interview patients who were too ill or unwilling to participate and had no caregiver present, they might have underestimated the number of admission errors. Further, the harm assessment was based on potential and not actual harm.
Bottom line: Admission medication order errors are frequent, most commonly originate in the medication histories, and have increased potential to cause adverse outcomes in older patients and those taking higher numbers of medications.
Citation: Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications At Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25(5):441-447.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Continuous insulin infusion in non-ICU patients
- How hospitalists spend their day
- Outcomes of patients leaving against medical advice
- Prediction rule for readmission
- Effects of high- vs. low-dose PPIs for peptic ulcer
- Hospital utilization by generalists before hospitalists
- Effect of hospitalist fragmentation on length of stay
- Medication errors at admissions in older patients
Continuous Insulin Infusion Provides Effective Glycemic Control in Non-ICU Patients
Clinical question: Is continuous insulin infusion (CII) a safe and effective option in the management of hyperglycemia in non-ICU patients?
Background: Hyperglycemia has been associated with worse outcomes in hospitalized patients. Prior research has demonstrated the benefit of CII in managing hyperglycemia in the ICU setting. However, outcomes have not been evaluated in the general medical (non-ICU) setting, where hyperglycemia is often inadequately addressed.
Study design: Retrospective chart review.
Setting: Urban tertiary-care medical center.
Synopsis: Charts of 200 adult patients treated with CII in non-ICU areas were reviewed with the primary outcomes including mean daily blood glucose (BG) levels and number of hyper- and hypoglycemic events occurring on CII. Mean BG dropped from 323 mg/dL to 182 mg/dL by day one, with a BG≤of 150 achieved in 67% of patients by day two of therapy. Twenty-two percent of patients suffered a hypoglycemic event (BG<60), reportedly similar to prior studies of insulin use in ICU and non-ICU settings. Eighty-two percent of patients received some form of nutritional support while on CII. In multivariate analyses, receiving oral nutrition (either a solid or liquid diet) was the only factor associated with increased risk of hyperglycemia and hypoglycemia.
This study was limited by its retrospective analysis in a single center. No comparison was made with basal-bolus or sliding-scale insulin therapy regarding efficacy or safety.
Bottom line: Non-ICU patients with hyperglycemia who received CII were able to achieve effective glycemic control within 48 hours of initiation, with rates of hypoglycemia comparable to those observed in ICU settings.
Citation: Smiley D, Rhee M, Peng L, et al. Safety and efficacy of continuous insulin infusion in noncritical care settings. J Hosp Med. 2010;5(4):212-217.
Hospitalists Spend More Time on Indirect, Rather Than Direct, Patient Care
Clinical question: What are the components of the daily workflow of hospitalists working on a non-housestaff service?
Background: The use of hospitalists is associated with increased efficiency in the hospital setting. However, it is not known how this efficiency is achieved. Prior literature has attempted to address this question, but with increasing demands and patient census, the representativeness of existing data is unclear.
Study design: Observational time-motion study.
Setting: Urban tertiary-care academic medical center.
Synopsis: Twenty-four hospitalists were directly observed for two weekday shifts. An electronic collection tool was developed using initial data on hospitalist activities and piloted prior to formal study data collection. Direct patient care was defined as involving face-to-face interaction between hospitalist and patient, while indirect patient care involved activities relevant to patient care but not performed in the patient’s presence.
Approximately 500 hours of observation were collected. Direct patient care comprised only a mean of 17.4% of the hospitalists’ daily workflow, while more was spent on indirect care, mainly electronic health record (EHR) documentation (mean 34.1%) and communication activities (mean 25.9%). Multitasking occurred 16% of the time, typically during communication or “critical documentation activities” (e.g. writing prescriptions). As patient volume increased, less time was spent in communication, and documentation was deferred to after hours.
These results were consistent with prior observational studies but were limited to a single center and might not represent the workflow of hospitalists in other settings, such as community hospitals, or nocturnists.
Bottom line: Hospitalists on non-housestaff services spend most of their time on indirect patient care and, with increasing patient census, communication is sacrificed. Multitasking is common during periods of communication and critical documentation.
Citation: Tipping MD, Forth VE, O’Leary KJ, et al. Where did the day go?—a time-motion study of hospitalists. J Hosp Med. 2010;5(6):323-328.
Patients Who Leave Against Medical Advice Have Higher Readmission, Mortality Rates
Clinical question: What are the 30-day hospital readmission and mortality rates for Veterans Administration (VA) patients discharged against medical advice (AMA) compared with those appropriately discharged from the hospital?
Background: Patients discharged AMA might be at increased risk of experiencing worse outcomes. Small studies have demonstrated that patients with asthma and acute myocardial infarction (MI) discharged AMA have increased risk of readmission and death. However, it is unclear whether these risks are generalizable to a wider medical population.
Study design: Five-year retrospective cohort study.
Setting: One hundred twenty-nine VA acute-care hospitals.
Synopsis: Of the nearly 2 million patients admitted to the VA from 2004 to 2008, 1.7% were discharged AMA. Patients discharged AMA generally were younger, had lower incomes, and were more likely to be black. Furthermore, patients discharged AMA had statistically significant higher rates of 30-day readmission (17.7% vs. 11%, P<0.001) and higher 30-day mortality rates (0.75% vs. 0.61%, P=0.001) compared with those who had been appropriately discharged. In hazard models, discharge AMA was a significant predictor of 30-day readmission and conferred a nonstatistically significant increase in 30-day mortality.
Because all patients were seen in VA facilities, the results might not be generalizable to other acute-care settings. Although VA patients differ from the general medical population, the characteristics of patients discharged AMA are similar to those in previously published studies. The study utilized administrative data, which are very reliable but limited by little information on clinical factors that could contribute to AMA discharges.
Bottom line: Patients discharged AMA are at increased risk of worse post-hospitalization outcomes, including hospital readmission and death.
Citation: Glasgow JM, Vaughn-Sarrazin M, Kaboli PJ. Leaving against medical advice (AMA): risk of 30-day mortality and hospital readmission. J Gen Intern Med. 2010;25(9): 926-929.
Simple Model Predicts Hospital Readmission
Clinical question: Which patient-level factors can be used in a simple model to predict hospital readmission of medicine patients?
Background: Hospital readmissions are common and costly. Previously published readmission prediction models have had limited utility because they focused on a specific condition, setting, or population, or were too cumbersome for practical use.
Study design: Prospective observational cohort study.
Setting: Six academic medical centers.
Synopsis: Data from nearly 11,000 general medicine patients were included in the analysis. Overall, almost 18% of patients were readmitted within 30 days of discharge.
In the prediction model derived and validated from the data, seven factors were significant predictors of readmission within 30 days of discharge: insurance status, marital status, having a regular healthcare provider, Charlson comorbidity index, SF 12 physical component score, one or more admissions within the last year, and current length of stay greater than two days. Points assigned from each significant predictor were used to create a risk score. The 5% of patients with risk scores of 25 and higher had 30-day readmission rates of approximately 30%, compared to readmission rates of approximately 16% in patients with scores of less than 25.
These results might not be generalizable to small, rural, nonacademic settings. Planned admissions could not be excluded from the data, and readmissions to nonstudy hospitals could not be ascertained. Despite these limitations, this model is easier to use than prior models and relevant to a broad population of patients.
Bottom line: A simple prediction model using patient-level factors can be used to identify patients at higher risk of readmission within 30 days of discharge to home.
Citation: Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2010;25(3):211-219.
No Difference in Outcomes Between High- and Non-High-Dose Proton Pump Inhibitors in Bleeding Peptic Ulcers
Clinical question: Do high-dose proton pump inhibitors (PPIs) decrease the rate of rebleeding, surgical intervention, or mortality in patients with bleeding peptic ulcers who have undergone endoscopic treatment?
Background: Previous studies have demonstrated superiority of both high- and low-dose PPIs to H2 receptor antagonists and placebo in reducing rebleeding rates in patients with peptic ulcers. However, no clear evidence is available to suggest that high-dose PPIs are more effective than non-high-dose PPIs for treatment of bleeding peptic ulcers.
Study design: Systematic review and meta-analysis.
Setting: Multicenter and single-site studies conducted in several countries.
Synopsis: Studies were included if they were randomized controlled trials, compared high- versus non-high-dose PPIs, evaluated endoscopically confirmed bleeding ulcers, gave PPIs after endoscopy, and documented outcomes regarding rates of rebleeding, surgical intervention, or mortality. High-dose PPIs were defined as equivalent to omeprazole 80 mg intravenous bolus followed by continuous intravenous infusion at 8 mg/hr for 72 hours.
Seven studies met inclusion criteria. The pooled odds ratios for rebleeding, surgical intervention, and mortality were 1.30 (95% CI, 0.88-1.91), 1.49 (95% CI, 0.66-3.37), and 0.89 (95% CI, 0.37-2.13), respectively, for high-dose versus non-high-dose PPIs. The authors concluded that high-dose PPIs were not superior to non-high-dose PPIs in reducing the rates of these adverse outcomes after endoscopic treatment of bleeding ulcers. Considering the cost of high-dose PPIs, further studies are indicated to help guide PPI dosing for patients with peptic ulcers.
Major limitations of this study were the small number of studies (1,157 patients in total) and their heterogeneity, and the lack of intention-to-treat analysis. The studies also included a high Asian predominance, and it has been shown that Asian populations have an enhanced PPI effect.
Bottom line: High-dose PPIs did not demonstrate reduced rates of ulcer rebleeding, surgical intervention, or mortality compared with non-high-dose PPIs in this meta-analysis, which included a small number of studies and patients.
Citation: Wang CH, Ma MH, Chou HC, et al. High-dose vs. non-high-dose proton pump inhibitors after endoscopic treatment in patients with bleeding peptic ulcer: a systematic review and meta-analysis of randomized controlled trials. Arch Intern Med. 2010;170(9):751-758.
Hospital Utilization by Practicing Generalists Declined before the Emergence of Hospitalists
Clinical question: What has been the pattern of hospital utilization by generalists before and after the emergence of hospitalists?
Background: It has been proposed that the emergence of hospitalists has “crowded out” generalist physicians from the U.S. hospital setting. This study evaluated the trends of inpatient practice by generalists both before and after the emergence of hospitalists.
Study design: Retrospective analysis of national databases.
Setting: U.S. data from 1980 to 2005.
Synopsis: Utilizing the National Hospital Discharge Survey and the American Medical Association’s Physician Characteristics and Distribution in the U.S., information was extracted to evaluate the average number of annual inpatient encounters relative to generalist workforce from 1980 to 2005. Total inpatient encounters for each year were calculated by multiplying the total number of hospital admissions by the average hospital length of stay. The emergence of hospitalists was defined as beginning in 1994.
Total inpatient encounters by generalists declined by 35% in the pre-hospitalist era but remained essentially unchanged in the hospitalist era. During the pre-hospitalist period, the number of generalists doubled, to more than 200,000 from approximately 100,000, while the number of hospital discharges remained relatively stable and the length of stay declined by a third. The decrease in average inpatient encounters in the pre-hospitalist era is thought to have been secondary to decreased length of stay and increased workforce.
Bottom line: Hospital utilization relative to generalist physician workforce was decreasing prior to the emergence of hospitalists mainly due to decreased length of hospital stay and increased numbers of physicians.
Citation: Meltzer DO, Chung JW. U.S. trends in hospitalization and generalist physician workforce and the emergence of hospitalists. J Gen Intern Med. 2010;25(5):453-459.
Fragmentation of Hospitalist Care Is Associated with Increased Length of Stay
Clinical question: Does fragmentation of care (FOC) by hospitalists affect length of stay (LOS)?
Background: Previous investigations have explored the impact of FOC provided by residency programs on LOS and quality of care. Results of these studies have been mixed. However, there have been no prior studies on the impact of the fragmentation of hospitalist care on LOS.
Study design: Concurrent control study.
Setting: Hospitalist practices all over the country managed by IPC: The Hospitalist Company.
Synopsis: Investigators looked at 10,977 patients admitted with diagnoses of pneumonia or heart failure. The primary endpoint was LOS. The independent variable of interest was a measure of FOC. The FOC was calculated as a quantitative index, by determining the percentage of hospitalist care delivered by a physician other than the primary hospitalist.
Multivariable analyses revealed a statistically significant increase in LOS of 0.39 days for each 10% increase in fragmentation level for pneumonia admissions. Similarly, for patients with heart failure, there was a significant increase in LOS of 0.30 days for each 10% increase in fragmentation level.
The study is a concurrent control study, so conclusions cannot be drawn about causality. Additionally, there are likely unmeasured differences between every hospital and hospitalist practice, which could further confound the relationships between hospitalist care and LOS.
Bottom line: Fragmentation of care provided by hospitalists is associated with an increased LOS in patients hospitalized for pneumonia or heart failure.
Citation: Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-338.
Admission Medication Errors Are Common and Most Harmful in Older Patients Taking Many Medications
Clinical question: What are the risk factors and potential harm associated with medication errors at hospital admission?
Background: Obtaining a medication history from a hospitalized patient is an error-prone process. Several variables can affect the completeness and quality of medication histories, but existing data are limited regarding patient or medication risk factors associated with medication errors at admission.
Study design: Prospective cohort study.
Setting: Academic hospital in Chicago.
Synopsis: Pharmacist and admitting physician medication histories were compared with admission medication orders to identify any unexplained discrepancies. Discrepancies resulting in order changes were defined as medication errors.
Of the 651 adult medical inpatients studied, 234 (35.9%) had medication order errors identified at admission. Errors originated in the medication histories for 85% of these patients. The most frequent type of error was an omission (48.9%). An age of 65 or older (odds ratio [OR]=2.17, 95% confidence interval [CI], 1.09-4.30) and increased number of medications (OR=1.21, 95% CI, 1.14-1.29) were the only risk factors identified by multivariate analysis to be independently associated with increased risk of medication order errors potentially causing harm or requiring monitoring or intervention. Presenting a medication list upon admission was a significant protective factor (OR=0.35, 95% CI, 0.19-0.63).
Though this is the largest study to date evaluating admission medication errors in hospitalized medical patients, it remains limited by its single hospital site. Because the authors were unable to interview patients who were too ill or unwilling to participate and had no caregiver present, they might have underestimated the number of admission errors. Further, the harm assessment was based on potential and not actual harm.
Bottom line: Admission medication order errors are frequent, most commonly originate in the medication histories, and have increased potential to cause adverse outcomes in older patients and those taking higher numbers of medications.
Citation: Gleason KM, McDaniel MR, Feinglass J, et al. Results of the Medications At Transitions and Clinical Handoffs (MATCH) study: an analysis of medication reconciliation errors and risk factors at hospital admission. J Gen Intern Med. 2010;25(5):441-447.
Pediatric HM Literature Review
Clinical question: What is the relationship between duration of intravenous (IV) antibiotic therapy and treatment failure in infants <6 months of age hospitalized with urinary tract infections (UTIs)?
Background: There is an inadequate evidence base to drive decisions regarding duration of IV antibiotic therapy in young infants hospitalized with UTIs. Documented variability exists in length of stay (LOS) and resource utilization for these infants, which might be a direct result of practice variation with respect to IV therapy.
Study design: Retrospective cohort study.
Setting: Twenty-four freestanding children’s hospitals.
Synopsis: The Pediatric Health Information System (PHIS) administrative database was used to identify healthy infants <6 months of age admitted with a primary or secondary diagnosis of UTI or pyelonephritis from 1999 to 2004 to participating hospitals. Duration of IV therapy was defined as a dichotomous variable with three days (short course: three days) selected because it was the median length of therapy. Treatment failure was defined as readmission within 30 days.
More than 12,300 records were analyzed. Male gender, neonatal status, black race, Hispanic ethnicity, nonprivate insurance, severity of illness, known bacteremia, known genitourinary tract disorders, and specific hospital were independently associated with increased likelihood of long-course (four days) therapy.
Unadjusted analysis initially revealed that long-course therapy was significantly associated with a higher rate of treatment failure. After multivariate (to include propensity scores) adjustment, a significant association between treatment duration and failure was no longer identified. Treatment failure association with known genitourinary abnormalities and higher severity of illness remained.
A significant limitation of this study is the potential for multivariate analysis to fail to mitigate a bias toward sicker patients receiving longer duration of antibiotic therapy and, thus, having a higher likelihood of treatment failure. In addition, the greater question of when IV antibiotics (and hospital admission) are indicated in this population was not addressed by the study design.
Nonetheless, the data likely support a limited utility to long-course IV antibiotic therapy in this population. The study also adds to the evolving picture of considerable and widespread variation in physician practice.
Bottom line: Short-course IV therapy for infants with UTIs does not increase risk of treatment failure.
Citation: Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196-203.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the relationship between duration of intravenous (IV) antibiotic therapy and treatment failure in infants <6 months of age hospitalized with urinary tract infections (UTIs)?
Background: There is an inadequate evidence base to drive decisions regarding duration of IV antibiotic therapy in young infants hospitalized with UTIs. Documented variability exists in length of stay (LOS) and resource utilization for these infants, which might be a direct result of practice variation with respect to IV therapy.
Study design: Retrospective cohort study.
Setting: Twenty-four freestanding children’s hospitals.
Synopsis: The Pediatric Health Information System (PHIS) administrative database was used to identify healthy infants <6 months of age admitted with a primary or secondary diagnosis of UTI or pyelonephritis from 1999 to 2004 to participating hospitals. Duration of IV therapy was defined as a dichotomous variable with three days (short course: three days) selected because it was the median length of therapy. Treatment failure was defined as readmission within 30 days.
More than 12,300 records were analyzed. Male gender, neonatal status, black race, Hispanic ethnicity, nonprivate insurance, severity of illness, known bacteremia, known genitourinary tract disorders, and specific hospital were independently associated with increased likelihood of long-course (four days) therapy.
Unadjusted analysis initially revealed that long-course therapy was significantly associated with a higher rate of treatment failure. After multivariate (to include propensity scores) adjustment, a significant association between treatment duration and failure was no longer identified. Treatment failure association with known genitourinary abnormalities and higher severity of illness remained.
A significant limitation of this study is the potential for multivariate analysis to fail to mitigate a bias toward sicker patients receiving longer duration of antibiotic therapy and, thus, having a higher likelihood of treatment failure. In addition, the greater question of when IV antibiotics (and hospital admission) are indicated in this population was not addressed by the study design.
Nonetheless, the data likely support a limited utility to long-course IV antibiotic therapy in this population. The study also adds to the evolving picture of considerable and widespread variation in physician practice.
Bottom line: Short-course IV therapy for infants with UTIs does not increase risk of treatment failure.
Citation: Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196-203.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Clinical question: What is the relationship between duration of intravenous (IV) antibiotic therapy and treatment failure in infants <6 months of age hospitalized with urinary tract infections (UTIs)?
Background: There is an inadequate evidence base to drive decisions regarding duration of IV antibiotic therapy in young infants hospitalized with UTIs. Documented variability exists in length of stay (LOS) and resource utilization for these infants, which might be a direct result of practice variation with respect to IV therapy.
Study design: Retrospective cohort study.
Setting: Twenty-four freestanding children’s hospitals.
Synopsis: The Pediatric Health Information System (PHIS) administrative database was used to identify healthy infants <6 months of age admitted with a primary or secondary diagnosis of UTI or pyelonephritis from 1999 to 2004 to participating hospitals. Duration of IV therapy was defined as a dichotomous variable with three days (short course: three days) selected because it was the median length of therapy. Treatment failure was defined as readmission within 30 days.
More than 12,300 records were analyzed. Male gender, neonatal status, black race, Hispanic ethnicity, nonprivate insurance, severity of illness, known bacteremia, known genitourinary tract disorders, and specific hospital were independently associated with increased likelihood of long-course (four days) therapy.
Unadjusted analysis initially revealed that long-course therapy was significantly associated with a higher rate of treatment failure. After multivariate (to include propensity scores) adjustment, a significant association between treatment duration and failure was no longer identified. Treatment failure association with known genitourinary abnormalities and higher severity of illness remained.
A significant limitation of this study is the potential for multivariate analysis to fail to mitigate a bias toward sicker patients receiving longer duration of antibiotic therapy and, thus, having a higher likelihood of treatment failure. In addition, the greater question of when IV antibiotics (and hospital admission) are indicated in this population was not addressed by the study design.
Nonetheless, the data likely support a limited utility to long-course IV antibiotic therapy in this population. The study also adds to the evolving picture of considerable and widespread variation in physician practice.
Bottom line: Short-course IV therapy for infants with UTIs does not increase risk of treatment failure.
Citation: Brady PW, Conway PH, Goudie A. Length of intravenous antibiotic therapy and treatment failure in infants with urinary tract infections. Pediatrics. 2010;126(2):196-203.
Reviewed by Pediatric Editor Mark Shen, MD, medical director of hospital medicine at Dell Children’s Medical Center, Austin, Texas.
Market Watch
New Generics
- Atomoxetine capsules (Strattera)1
- Clonidine transdermal system USP (catapres-TTS)2
- Enoxaparin sodium injection (Lovenox)3
- Naratriptan hydrochloride 2.5-mg tablets (Amerge)4
New Drugs, Devices, Indications, and Dosage Forms
- A combination tablet containing both aliskiren and amlodipine (Tekamlo) has been approved by the FDA for the treatment of hypertension (HTN).5 Four strengths for once-daily dosing are available.
- Antihemophilic factor VIII (recombinant) injection (Xyntha) for treatment of hemophilia A has been approved by the FDA in a pre-filled, dual-chamber syringe for intravenous (IV) infusion following reconstitution of the freeze-dried powder with 0.9% sodium chloride diluent (both supplied in the dosage form).6 The first dose will be available in the 3,000 international units strength (4 mL). Other dosages will be available in 2011.
- Bimatoprost ophthalmic solution 0.01% (Lumigan) has been approved by the FDA as a first-line treatment for reducing intraocular pressure in patients with open-angle glaucoma or ocular hypertension.7
- Buprenorphine/naloxone sublingual film (Suboxone sublingual) has been approved by the FDA for the treatment of opioid dependence.8
- Coagulation factor VIIa room temperature stable (recombinant) (NovoSeven RT) has been approved by the FDA in an 8-mg vial.9 This larger size allows rapid initiation and administration of this product for patients who need a larger dose. Additionally, this product is approved for an extended shelf life, for all vial sizes, to 36 months at room temperature.
- Donepezil 21-mg tablets (Aricept) have been approved by the FDA for the treatment of moderate to severe Alzheimer’s disease.10
- Glycopyrrolate cherry-flavored oral solution (Cuvposa) has been approved by the FDA as an orphan drug for treating chronic severe drooling in patients ages 3 to 16 with neurological conditions such as cerebral palsy.11
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA for a 24-month shelf life at room temperature when protected from light.12
- Miconazole 50-mg buccal tablets (Oravig) have been approved by the FDA to topically treat oropharyngeal candidiasis in patients 16 and older.13
- Niacin extended release/simvastatin tablets (Simcor) have been approved by the FDA in two new dosage strengths: 500 mg/40 mg and 1000 mg/40 mg.14
- Olmesartan medoxomil, amlodipine besylate, and hydrochlorothiazide tablets (HCTZ) (Tribenzor) have been approved by the FDA in a single tablet to treat hypertension (not initial therapy).15 This combination should not be used in patients with a creatinine clearance <30 mL/minute, or in patients with renal artery stenosis.
- STX-100 has received orphan drug status for treating idiopathic pulmonary fibrosis (IPF) for which there currently are no FDA-approved treatments.16 STX-100 is a humanized, monoclonal antibody that targets integrin vb6, which exhibited major antifibrotic activity in preclinical animal models of the lung and other organs. The FDA previously granted orphan drug designation for STX-100 for chronic allograft nephropathy. A Phase 2 trial in IPF is planned for 2011.
- Docetaxel injection concentrate (Taxotere) has been approved by the FDA in a one-vial system, which eliminates the dilution step.17
- Valganciclovir injection (Valcyte) is FDA-approved for an increased therapy length (200 days) in adult renal transplant patients at high risk of developing cytomegalovirus disease (CMV).18 This extends the length of therapy from 100 days.
Safety, Warnings, and Label Changes
- Carbidopa/levodopa and entacapone tablets (Stalevo) are undergoing a safety review in relation to a possible increased cardiovascular event risk, including myocardial infarction, stroke, and cardiovascular death, compared with patients only taking carbidopa/levodopa.19 An FDA meta-analysis of 15 clinical trials found a small increased risk of cardiovascular events. However, this meta-analysis was not specifically designed to assess cardiovascular safety, and most patients had pre-existing cardiovascular disease risk factors, so even small differences in the level of these risks could significantly affect the study outcomes. Additionally, most negative cardiovascular events occurred in a single trial. The FDA recommends regular evaluation of patients’ cardiovascular status.
- Tigecycline IV injection (Tygacil) has undergone a label change in its “Warnings” and “Precautions” in relation to an increased mortality risk.20 A pooled analysis compared tigecycline use to other similar antibacterials for managing different serious infections. Patients who had a greater increased risk of death were those with hospital-acquired pneumonia, ventilator-associated pneumonia, complicated skin and skin structure infections, diabetic foot infections, and complicated intra-abdominal infections.
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Actavis receives FDA approval of atomoxetine HCI capsules. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/199692.php. Accessed Sept. 2, 2010.
- Mylan receives approval for generic version of Catapres-TTS. Mylan Inc. website. Available at: http://investor.mylan.com/releasedetail.cfm?ReleaseID=489338. Accessed July 20, 2010.
- Riley K. FDA approves first generic enoxaparin sodium injection. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm220092.htm. Accessed Sept. 13, 2010.
- First-time generic approvals August 2010. Formulary website. Available at: http://formularyjournal.modernmedicine.com/formulary/Modern+Medicine+Now/First-time-generic-approvals-Aug.-2010/ArticleStandard/Article/detail/683182?contextCategoryId=44276. Accessed Sept. 7, 2010.
- Novartis receives FDA approval of Tekamlo, a single-pill combination of aliskiren and amlodipine to treat high blood pressure. Novartis Pharmaceuticals Corporation website. Available at: http://www.pharma.us.novartis.com/info/newsroom/press-release.jsp?PRID=2286. Accessed Sept. 13, 2010.
- Xyntha prefilled dual-chamber syringe approved for hemophilia A treatment. Monthly Prescribing Reference website. Available at: http://www.empr.com/xyntha-pre-filled-dual-chamber-syringe-approved-for-hemophilia-a-treatment/article/176666/. Accessed Aug.18, 2010.
- Allergan, Inc. receives FDA approval for Lumigan 0.01% as first-line therapy indicated for the reduction of elevated intraocular pressure in glaucoma patients. MarketWatch website. Available at: http://www.marketwatch.com/story/allergan-inc-receives-fda-approval-for-lumiganr-001-as-first-line-therapy-indicated-for-the-reduction-of-elevated-intraocular-pressure-in-glaucoma-patients-2010-08-31?reflink=MW_news_stmp. Accessed Sept. 2, 2010.
- MonoSol Rx announces Reckitt Benckiser FDA approval of Suboxone sublingual film for treatment of opioid dependence. PR Newswire website. Available at: http://www.prnewswire.com/news-releases/monosol-rx-announces-reckitt-benckiser-fda-approval-of-suboxone-sublingual-film-for-treatment-of-opioid-dependence-101874388.html. Accessed Sept. 14, 2010.
- NovoSeven RT 8mg vial approved for hemophilia A or B. Monthly Prescribing Reference website. Available at: http://www.empr.com/novoseven-rt-8mg-vial-approved-for-hemophilia-a-or-b/printarticle/176743/. Accessed Sept. 13, 2010.
- Eisai announces U.S. FDA approval for new higher dose Aricept 23 mg tablet for the treatment of moderate-to-severe Alzheimer’s disease. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/196410.php. Accessed Sept. 13, 2010.
- Cuvposa approved for chronic severe drooling associated with neurologic conditions. Monthly Prescribing Reference website. Available at: http://www.empr.com/cuvposa-approved-for-chronic-severe-drooling-associated-with-neurologic-conditions/article/175824/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Aug. 2, 2010.
- Shelf life of Hizentra extended from 18 to 24 months. Monthly Prescribing Reference website. Available at: http://www.empr.com/shelf-life-of-hizentra-extended-from-18-to-24-months/article/177068/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Aug. 23, 2010.
- Oravig available for oropharyngeal candidiasis. Monthly Prescribing Reference website. Available at: http://www.empr.com/oravig-available-for-oropharyngeal-candidiasis/article/177492/. Accessed Sept. 13, 2010.
- Additional dosage strengths of Simcor approved. Monthly Prescribing Reference website. Available at: http://www.empr.com/additional-dosage-strengths-of-simcor-approved/article/175825/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Sept. 13, 2010.
- Tribenzor 20/5/12.5mg. Monthly Prescribing Reference website. Available at: http://www.empr.com/tribenzor-205125mg/drugproduct/129/. Accessed Sept. 13, 2010.
- Stromedix receives FDA orphan drug designation for STX-100 for the treatment of idiopathic pulmonary fibrosis. Stromedix website. Available at: http://www.stromedix.com/Stromedix_STX-100_Orphan_Drug_IPF.pdf. Accessed Sept. 13, 2010.
- Dane L. Sanofi-Aventis garners FDA approval for one-vial formulation of Taxotere. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E0B4E517F06C4A9E94DC88EADBA079A8. Accessed Sept. 13, 2010.
- FDA approves longer use of Valcyte for adult kidney transplant patients at high risk of developing cytomegalovirus (CMV) disease. Genentech website. Available at: http://www.gene.com/gene/news/press-releases/display.do?method=detail&id=12907. Accessed Sept. 13, 2010.
- FDA drug safety communication: ongoing safety review of Stalevo and possible increased cardiovascular risk. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm223060.htm. Accessed Sept. 13, 2010.
- FDA drug safety communication: increased risk of death with Tygacil (tigecycline) compared to other antibiotics used to treat similar infections. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm224370.htm. Accessed Sept. 13, 2010.
New Generics
- Atomoxetine capsules (Strattera)1
- Clonidine transdermal system USP (catapres-TTS)2
- Enoxaparin sodium injection (Lovenox)3
- Naratriptan hydrochloride 2.5-mg tablets (Amerge)4
New Drugs, Devices, Indications, and Dosage Forms
- A combination tablet containing both aliskiren and amlodipine (Tekamlo) has been approved by the FDA for the treatment of hypertension (HTN).5 Four strengths for once-daily dosing are available.
- Antihemophilic factor VIII (recombinant) injection (Xyntha) for treatment of hemophilia A has been approved by the FDA in a pre-filled, dual-chamber syringe for intravenous (IV) infusion following reconstitution of the freeze-dried powder with 0.9% sodium chloride diluent (both supplied in the dosage form).6 The first dose will be available in the 3,000 international units strength (4 mL). Other dosages will be available in 2011.
- Bimatoprost ophthalmic solution 0.01% (Lumigan) has been approved by the FDA as a first-line treatment for reducing intraocular pressure in patients with open-angle glaucoma or ocular hypertension.7
- Buprenorphine/naloxone sublingual film (Suboxone sublingual) has been approved by the FDA for the treatment of opioid dependence.8
- Coagulation factor VIIa room temperature stable (recombinant) (NovoSeven RT) has been approved by the FDA in an 8-mg vial.9 This larger size allows rapid initiation and administration of this product for patients who need a larger dose. Additionally, this product is approved for an extended shelf life, for all vial sizes, to 36 months at room temperature.
- Donepezil 21-mg tablets (Aricept) have been approved by the FDA for the treatment of moderate to severe Alzheimer’s disease.10
- Glycopyrrolate cherry-flavored oral solution (Cuvposa) has been approved by the FDA as an orphan drug for treating chronic severe drooling in patients ages 3 to 16 with neurological conditions such as cerebral palsy.11
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA for a 24-month shelf life at room temperature when protected from light.12
- Miconazole 50-mg buccal tablets (Oravig) have been approved by the FDA to topically treat oropharyngeal candidiasis in patients 16 and older.13
- Niacin extended release/simvastatin tablets (Simcor) have been approved by the FDA in two new dosage strengths: 500 mg/40 mg and 1000 mg/40 mg.14
- Olmesartan medoxomil, amlodipine besylate, and hydrochlorothiazide tablets (HCTZ) (Tribenzor) have been approved by the FDA in a single tablet to treat hypertension (not initial therapy).15 This combination should not be used in patients with a creatinine clearance <30 mL/minute, or in patients with renal artery stenosis.
- STX-100 has received orphan drug status for treating idiopathic pulmonary fibrosis (IPF) for which there currently are no FDA-approved treatments.16 STX-100 is a humanized, monoclonal antibody that targets integrin vb6, which exhibited major antifibrotic activity in preclinical animal models of the lung and other organs. The FDA previously granted orphan drug designation for STX-100 for chronic allograft nephropathy. A Phase 2 trial in IPF is planned for 2011.
- Docetaxel injection concentrate (Taxotere) has been approved by the FDA in a one-vial system, which eliminates the dilution step.17
- Valganciclovir injection (Valcyte) is FDA-approved for an increased therapy length (200 days) in adult renal transplant patients at high risk of developing cytomegalovirus disease (CMV).18 This extends the length of therapy from 100 days.
Safety, Warnings, and Label Changes
- Carbidopa/levodopa and entacapone tablets (Stalevo) are undergoing a safety review in relation to a possible increased cardiovascular event risk, including myocardial infarction, stroke, and cardiovascular death, compared with patients only taking carbidopa/levodopa.19 An FDA meta-analysis of 15 clinical trials found a small increased risk of cardiovascular events. However, this meta-analysis was not specifically designed to assess cardiovascular safety, and most patients had pre-existing cardiovascular disease risk factors, so even small differences in the level of these risks could significantly affect the study outcomes. Additionally, most negative cardiovascular events occurred in a single trial. The FDA recommends regular evaluation of patients’ cardiovascular status.
- Tigecycline IV injection (Tygacil) has undergone a label change in its “Warnings” and “Precautions” in relation to an increased mortality risk.20 A pooled analysis compared tigecycline use to other similar antibacterials for managing different serious infections. Patients who had a greater increased risk of death were those with hospital-acquired pneumonia, ventilator-associated pneumonia, complicated skin and skin structure infections, diabetic foot infections, and complicated intra-abdominal infections.
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Actavis receives FDA approval of atomoxetine HCI capsules. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/199692.php. Accessed Sept. 2, 2010.
- Mylan receives approval for generic version of Catapres-TTS. Mylan Inc. website. Available at: http://investor.mylan.com/releasedetail.cfm?ReleaseID=489338. Accessed July 20, 2010.
- Riley K. FDA approves first generic enoxaparin sodium injection. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm220092.htm. Accessed Sept. 13, 2010.
- First-time generic approvals August 2010. Formulary website. Available at: http://formularyjournal.modernmedicine.com/formulary/Modern+Medicine+Now/First-time-generic-approvals-Aug.-2010/ArticleStandard/Article/detail/683182?contextCategoryId=44276. Accessed Sept. 7, 2010.
- Novartis receives FDA approval of Tekamlo, a single-pill combination of aliskiren and amlodipine to treat high blood pressure. Novartis Pharmaceuticals Corporation website. Available at: http://www.pharma.us.novartis.com/info/newsroom/press-release.jsp?PRID=2286. Accessed Sept. 13, 2010.
- Xyntha prefilled dual-chamber syringe approved for hemophilia A treatment. Monthly Prescribing Reference website. Available at: http://www.empr.com/xyntha-pre-filled-dual-chamber-syringe-approved-for-hemophilia-a-treatment/article/176666/. Accessed Aug.18, 2010.
- Allergan, Inc. receives FDA approval for Lumigan 0.01% as first-line therapy indicated for the reduction of elevated intraocular pressure in glaucoma patients. MarketWatch website. Available at: http://www.marketwatch.com/story/allergan-inc-receives-fda-approval-for-lumiganr-001-as-first-line-therapy-indicated-for-the-reduction-of-elevated-intraocular-pressure-in-glaucoma-patients-2010-08-31?reflink=MW_news_stmp. Accessed Sept. 2, 2010.
- MonoSol Rx announces Reckitt Benckiser FDA approval of Suboxone sublingual film for treatment of opioid dependence. PR Newswire website. Available at: http://www.prnewswire.com/news-releases/monosol-rx-announces-reckitt-benckiser-fda-approval-of-suboxone-sublingual-film-for-treatment-of-opioid-dependence-101874388.html. Accessed Sept. 14, 2010.
- NovoSeven RT 8mg vial approved for hemophilia A or B. Monthly Prescribing Reference website. Available at: http://www.empr.com/novoseven-rt-8mg-vial-approved-for-hemophilia-a-or-b/printarticle/176743/. Accessed Sept. 13, 2010.
- Eisai announces U.S. FDA approval for new higher dose Aricept 23 mg tablet for the treatment of moderate-to-severe Alzheimer’s disease. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/196410.php. Accessed Sept. 13, 2010.
- Cuvposa approved for chronic severe drooling associated with neurologic conditions. Monthly Prescribing Reference website. Available at: http://www.empr.com/cuvposa-approved-for-chronic-severe-drooling-associated-with-neurologic-conditions/article/175824/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Aug. 2, 2010.
- Shelf life of Hizentra extended from 18 to 24 months. Monthly Prescribing Reference website. Available at: http://www.empr.com/shelf-life-of-hizentra-extended-from-18-to-24-months/article/177068/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Aug. 23, 2010.
- Oravig available for oropharyngeal candidiasis. Monthly Prescribing Reference website. Available at: http://www.empr.com/oravig-available-for-oropharyngeal-candidiasis/article/177492/. Accessed Sept. 13, 2010.
- Additional dosage strengths of Simcor approved. Monthly Prescribing Reference website. Available at: http://www.empr.com/additional-dosage-strengths-of-simcor-approved/article/175825/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Sept. 13, 2010.
- Tribenzor 20/5/12.5mg. Monthly Prescribing Reference website. Available at: http://www.empr.com/tribenzor-205125mg/drugproduct/129/. Accessed Sept. 13, 2010.
- Stromedix receives FDA orphan drug designation for STX-100 for the treatment of idiopathic pulmonary fibrosis. Stromedix website. Available at: http://www.stromedix.com/Stromedix_STX-100_Orphan_Drug_IPF.pdf. Accessed Sept. 13, 2010.
- Dane L. Sanofi-Aventis garners FDA approval for one-vial formulation of Taxotere. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E0B4E517F06C4A9E94DC88EADBA079A8. Accessed Sept. 13, 2010.
- FDA approves longer use of Valcyte for adult kidney transplant patients at high risk of developing cytomegalovirus (CMV) disease. Genentech website. Available at: http://www.gene.com/gene/news/press-releases/display.do?method=detail&id=12907. Accessed Sept. 13, 2010.
- FDA drug safety communication: ongoing safety review of Stalevo and possible increased cardiovascular risk. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm223060.htm. Accessed Sept. 13, 2010.
- FDA drug safety communication: increased risk of death with Tygacil (tigecycline) compared to other antibiotics used to treat similar infections. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm224370.htm. Accessed Sept. 13, 2010.
New Generics
- Atomoxetine capsules (Strattera)1
- Clonidine transdermal system USP (catapres-TTS)2
- Enoxaparin sodium injection (Lovenox)3
- Naratriptan hydrochloride 2.5-mg tablets (Amerge)4
New Drugs, Devices, Indications, and Dosage Forms
- A combination tablet containing both aliskiren and amlodipine (Tekamlo) has been approved by the FDA for the treatment of hypertension (HTN).5 Four strengths for once-daily dosing are available.
- Antihemophilic factor VIII (recombinant) injection (Xyntha) for treatment of hemophilia A has been approved by the FDA in a pre-filled, dual-chamber syringe for intravenous (IV) infusion following reconstitution of the freeze-dried powder with 0.9% sodium chloride diluent (both supplied in the dosage form).6 The first dose will be available in the 3,000 international units strength (4 mL). Other dosages will be available in 2011.
- Bimatoprost ophthalmic solution 0.01% (Lumigan) has been approved by the FDA as a first-line treatment for reducing intraocular pressure in patients with open-angle glaucoma or ocular hypertension.7
- Buprenorphine/naloxone sublingual film (Suboxone sublingual) has been approved by the FDA for the treatment of opioid dependence.8
- Coagulation factor VIIa room temperature stable (recombinant) (NovoSeven RT) has been approved by the FDA in an 8-mg vial.9 This larger size allows rapid initiation and administration of this product for patients who need a larger dose. Additionally, this product is approved for an extended shelf life, for all vial sizes, to 36 months at room temperature.
- Donepezil 21-mg tablets (Aricept) have been approved by the FDA for the treatment of moderate to severe Alzheimer’s disease.10
- Glycopyrrolate cherry-flavored oral solution (Cuvposa) has been approved by the FDA as an orphan drug for treating chronic severe drooling in patients ages 3 to 16 with neurological conditions such as cerebral palsy.11
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA for a 24-month shelf life at room temperature when protected from light.12
- Miconazole 50-mg buccal tablets (Oravig) have been approved by the FDA to topically treat oropharyngeal candidiasis in patients 16 and older.13
- Niacin extended release/simvastatin tablets (Simcor) have been approved by the FDA in two new dosage strengths: 500 mg/40 mg and 1000 mg/40 mg.14
- Olmesartan medoxomil, amlodipine besylate, and hydrochlorothiazide tablets (HCTZ) (Tribenzor) have been approved by the FDA in a single tablet to treat hypertension (not initial therapy).15 This combination should not be used in patients with a creatinine clearance <30 mL/minute, or in patients with renal artery stenosis.
- STX-100 has received orphan drug status for treating idiopathic pulmonary fibrosis (IPF) for which there currently are no FDA-approved treatments.16 STX-100 is a humanized, monoclonal antibody that targets integrin vb6, which exhibited major antifibrotic activity in preclinical animal models of the lung and other organs. The FDA previously granted orphan drug designation for STX-100 for chronic allograft nephropathy. A Phase 2 trial in IPF is planned for 2011.
- Docetaxel injection concentrate (Taxotere) has been approved by the FDA in a one-vial system, which eliminates the dilution step.17
- Valganciclovir injection (Valcyte) is FDA-approved for an increased therapy length (200 days) in adult renal transplant patients at high risk of developing cytomegalovirus disease (CMV).18 This extends the length of therapy from 100 days.
Safety, Warnings, and Label Changes
- Carbidopa/levodopa and entacapone tablets (Stalevo) are undergoing a safety review in relation to a possible increased cardiovascular event risk, including myocardial infarction, stroke, and cardiovascular death, compared with patients only taking carbidopa/levodopa.19 An FDA meta-analysis of 15 clinical trials found a small increased risk of cardiovascular events. However, this meta-analysis was not specifically designed to assess cardiovascular safety, and most patients had pre-existing cardiovascular disease risk factors, so even small differences in the level of these risks could significantly affect the study outcomes. Additionally, most negative cardiovascular events occurred in a single trial. The FDA recommends regular evaluation of patients’ cardiovascular status.
- Tigecycline IV injection (Tygacil) has undergone a label change in its “Warnings” and “Precautions” in relation to an increased mortality risk.20 A pooled analysis compared tigecycline use to other similar antibacterials for managing different serious infections. Patients who had a greater increased risk of death were those with hospital-acquired pneumonia, ventilator-associated pneumonia, complicated skin and skin structure infections, diabetic foot infections, and complicated intra-abdominal infections.
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Actavis receives FDA approval of atomoxetine HCI capsules. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/199692.php. Accessed Sept. 2, 2010.
- Mylan receives approval for generic version of Catapres-TTS. Mylan Inc. website. Available at: http://investor.mylan.com/releasedetail.cfm?ReleaseID=489338. Accessed July 20, 2010.
- Riley K. FDA approves first generic enoxaparin sodium injection. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm220092.htm. Accessed Sept. 13, 2010.
- First-time generic approvals August 2010. Formulary website. Available at: http://formularyjournal.modernmedicine.com/formulary/Modern+Medicine+Now/First-time-generic-approvals-Aug.-2010/ArticleStandard/Article/detail/683182?contextCategoryId=44276. Accessed Sept. 7, 2010.
- Novartis receives FDA approval of Tekamlo, a single-pill combination of aliskiren and amlodipine to treat high blood pressure. Novartis Pharmaceuticals Corporation website. Available at: http://www.pharma.us.novartis.com/info/newsroom/press-release.jsp?PRID=2286. Accessed Sept. 13, 2010.
- Xyntha prefilled dual-chamber syringe approved for hemophilia A treatment. Monthly Prescribing Reference website. Available at: http://www.empr.com/xyntha-pre-filled-dual-chamber-syringe-approved-for-hemophilia-a-treatment/article/176666/. Accessed Aug.18, 2010.
- Allergan, Inc. receives FDA approval for Lumigan 0.01% as first-line therapy indicated for the reduction of elevated intraocular pressure in glaucoma patients. MarketWatch website. Available at: http://www.marketwatch.com/story/allergan-inc-receives-fda-approval-for-lumiganr-001-as-first-line-therapy-indicated-for-the-reduction-of-elevated-intraocular-pressure-in-glaucoma-patients-2010-08-31?reflink=MW_news_stmp. Accessed Sept. 2, 2010.
- MonoSol Rx announces Reckitt Benckiser FDA approval of Suboxone sublingual film for treatment of opioid dependence. PR Newswire website. Available at: http://www.prnewswire.com/news-releases/monosol-rx-announces-reckitt-benckiser-fda-approval-of-suboxone-sublingual-film-for-treatment-of-opioid-dependence-101874388.html. Accessed Sept. 14, 2010.
- NovoSeven RT 8mg vial approved for hemophilia A or B. Monthly Prescribing Reference website. Available at: http://www.empr.com/novoseven-rt-8mg-vial-approved-for-hemophilia-a-or-b/printarticle/176743/. Accessed Sept. 13, 2010.
- Eisai announces U.S. FDA approval for new higher dose Aricept 23 mg tablet for the treatment of moderate-to-severe Alzheimer’s disease. Medical News Today website. Available at: http://www.medicalnewstoday.com/articles/196410.php. Accessed Sept. 13, 2010.
- Cuvposa approved for chronic severe drooling associated with neurologic conditions. Monthly Prescribing Reference website. Available at: http://www.empr.com/cuvposa-approved-for-chronic-severe-drooling-associated-with-neurologic-conditions/article/175824/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Aug. 2, 2010.
- Shelf life of Hizentra extended from 18 to 24 months. Monthly Prescribing Reference website. Available at: http://www.empr.com/shelf-life-of-hizentra-extended-from-18-to-24-months/article/177068/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Aug. 23, 2010.
- Oravig available for oropharyngeal candidiasis. Monthly Prescribing Reference website. Available at: http://www.empr.com/oravig-available-for-oropharyngeal-candidiasis/article/177492/. Accessed Sept. 13, 2010.
- Additional dosage strengths of Simcor approved. Monthly Prescribing Reference website. Available at: http://www.empr.com/additional-dosage-strengths-of-simcor-approved/article/175825/?DCMP=EMC-MPR_WeeklyNewsbrief. Accessed Sept. 13, 2010.
- Tribenzor 20/5/12.5mg. Monthly Prescribing Reference website. Available at: http://www.empr.com/tribenzor-205125mg/drugproduct/129/. Accessed Sept. 13, 2010.
- Stromedix receives FDA orphan drug designation for STX-100 for the treatment of idiopathic pulmonary fibrosis. Stromedix website. Available at: http://www.stromedix.com/Stromedix_STX-100_Orphan_Drug_IPF.pdf. Accessed Sept. 13, 2010.
- Dane L. Sanofi-Aventis garners FDA approval for one-vial formulation of Taxotere. FirstWord website. Available at: http://www.firstwordplus.com/Fws.do?articleid=E0B4E517F06C4A9E94DC88EADBA079A8. Accessed Sept. 13, 2010.
- FDA approves longer use of Valcyte for adult kidney transplant patients at high risk of developing cytomegalovirus (CMV) disease. Genentech website. Available at: http://www.gene.com/gene/news/press-releases/display.do?method=detail&id=12907. Accessed Sept. 13, 2010.
- FDA drug safety communication: ongoing safety review of Stalevo and possible increased cardiovascular risk. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm223060.htm. Accessed Sept. 13, 2010.
- FDA drug safety communication: increased risk of death with Tygacil (tigecycline) compared to other antibiotics used to treat similar infections. U.S. Food and Drug Administration website. Available at: http://www.fda.gov/Drugs/DrugSafety/ucm224370.htm. Accessed Sept. 13, 2010.
Solution Finder
Kenneth G. Simone, DO, FHM, grew up as the son of a revered pediatrician. As a child, he often accompanied his father on hospital rounds and house calls, developing an appreciation for the “old-fashioned” medicine his father practiced.
Already inspired to follow in his father’s footsteps, Dr. Simone became even more convinced of his calling when the physician-patient roles were reversed: His dad developed a kidney disorder that cut his career—and ultimately his life—short. “His illness and my exposure to hospitals added to my desire to pursue medicine,” Dr. Simone says. “It instilled the drive to help others, to make a difference in someone’s or some family’s life.”
He has done that by developing multiple private medical practices, building the hospitalist program at St. Joseph Hospital in Bangor, Maine, and offering consulting services to more than 100 practices.
“It has always been my nature to challenge myself and put myself in situations that take me out of my comfort zone,” says Dr. Simone, president of Hospitalist and Practice Solutions, a practice-management consultancy in Veazie, Maine. “I enjoy building things from scratch, creating, rebuilding, thinking outside the box, and networking with other healthcare professionals.”
Question: What made you decide to start Hospitalist and Practice Solutions (HPS)?
Answer: HPS was established because of the demand for my services. Initially, word spread locally and then regionally about the work I did at St. Joseph Hospital. As a natural offshoot of my growing interest in helping other programs, HPS became a national consulting firm.
Q: Why did you think this venture could provide a valuable service?
A: I believed there were more effective healthcare delivery systems with which to provide both quality and cost-effective medical care. As time went on, I gained a very unique perspective working as both a hospitalist and referring PCP in private practice. This experience, coupled with my work as an administrative director for a hospitalist program, allowed me to develop applications to help hospitalist programs on a broader basis. I realized the advice I offered to other programs consistently rendered a positive effect.
Q: Which do you find more enjoyable: building a hospitalist program from the ground up or rebuilding a struggling program?
A: I truly enjoy the challenges of both equally. Projects that involve building a program de novo appeal to my creative side. These projects enable me to work with professionals to build a customized program that meets the needs of the community.
Q: What challenges are unique to each?
A: Rebuilding an established program involves critical analysis of the current program to identify what has gone wrong, what has been successful, and what will work in the future. It calls upon one’s skills to build consensus and instill trust in the process because the stakeholders may be apprehensive to have a consultant critically review their program and hospital. In many instances, conflict management is necessary.
In both the creation and rebuilding of an HM program, it is imperative to implement strategies that guide the program to future success. Both projects also require strategic planning and the development of tools and tactics that emphasize collaboration and collegiality.
Q: Do the failing programs you help to rebuild have characteristics in common?
A: Common themes include lack of planning and consensus-building before program start-up, inadequate tools and strategies to support effective practice management, and failure to align the hospitalist practice and sponsoring hospital’s goals and vision. Another common problem is the absence of a hospitalist recruitment and retention plan, which may lead to provider turnover and program instability.
Many programs experience problems due to ineffective leadership, poor implementation and follow-through, and lack of both a short- and long-term strategic plan. Some programs are victims of their own success. The program is not properly prepared to handle the demand for its services and grow accordingly.
Q: You help programs create effective recruitment and retention plans. You also wrote a book on the subject. Why are recruitment and retention challenging for so many programs?
A: The primary contributor is that [hospitalist] supply falls significantly short of physician demand. A secondary contributor is the generational expectations of the younger physician workforce. … In addition, leaders may not prioritize recruitment and retention because they lack an appreciation for the consequences of failed efforts.
Q: What advice would you offer hospitalist program leaders about how they can improve those aspects of their programs?
A: No. 1, create an effective recruitment and retention plan and execute the plan with precision. No. 2, approach recruitment and retention with the same attention to detail as you approach patient care.
Q: You’re offering best-practice advice to help your clients develop and sustain effective programs. What advice do you find yourself giving to your clients that you wish someone gave to you early in your career?
A: From my perspective as a hospitalist administrative director, the advice I would offer is for individuals to believe in themselves and stay engaged. If you feel you have something to offer to the practice or healthcare system as a whole, share it with the appropriate parties. If you experience problems within the workplace, seek resolution in a timely manner. Stay positive and be part of the solution, not part of the problem.
Q: You have written two hospitalist books and coauthored two others. Do you have plans to write another?
A: I wouldn’t say I have immediate plans, but I am always thinking about topics and other projects that would provide value to readers. I’ve got some exciting ideas for future projects, but they are in a very early stage of development.
Q: How would you compare the feeling you get from finishing a book with the satisfaction you derive from other aspects of your career?
A: Writing a book is a highly personal accomplishment for me, while caring for patients is more of a team accomplishment that involves the patient, family, and other healthcare professionals. Typically, the completion of a book is a finite event, while caring for a patient is a long-term commitment.
Q: What is your biggest professional reward?
A: Helping people, whether they are patients in my role as physician, or other professionals—physicians, practice administrators, and hospital administrators—in my role as a practice management consultant. Whenever I reflect on my career, I tell myself how lucky I am. There are not many professions or individuals who have an opportunity to close the door behind them and have other human beings entrust them with their most intimate information. Also, there are very few individuals who are able to impact the delivery of medical care from a systems perspective. I get to do both, and for that I am most grateful.
Q: What is your biggest professional challenge?
A: Saying “no” when someone asks for help. There is nothing more rewarding for me than to help others. With that said, I try not to overextend myself, because that wouldn’t be fair to my family, colleagues, friends, or clients.
Q: What’s next for you professionally?
A: I will continue to concentrate my effort on building my hospitalist consultative practice and expanding the services I offer. In addition, I’m always tempted to explore the valley of the unknown. What excites me is venturing into new areas and to challenge myself to grow as both an individual and professional. TH
Mark Leiser is a freelance writer based in New Jersey.
Kenneth G. Simone, DO, FHM, grew up as the son of a revered pediatrician. As a child, he often accompanied his father on hospital rounds and house calls, developing an appreciation for the “old-fashioned” medicine his father practiced.
Already inspired to follow in his father’s footsteps, Dr. Simone became even more convinced of his calling when the physician-patient roles were reversed: His dad developed a kidney disorder that cut his career—and ultimately his life—short. “His illness and my exposure to hospitals added to my desire to pursue medicine,” Dr. Simone says. “It instilled the drive to help others, to make a difference in someone’s or some family’s life.”
He has done that by developing multiple private medical practices, building the hospitalist program at St. Joseph Hospital in Bangor, Maine, and offering consulting services to more than 100 practices.
“It has always been my nature to challenge myself and put myself in situations that take me out of my comfort zone,” says Dr. Simone, president of Hospitalist and Practice Solutions, a practice-management consultancy in Veazie, Maine. “I enjoy building things from scratch, creating, rebuilding, thinking outside the box, and networking with other healthcare professionals.”
Question: What made you decide to start Hospitalist and Practice Solutions (HPS)?
Answer: HPS was established because of the demand for my services. Initially, word spread locally and then regionally about the work I did at St. Joseph Hospital. As a natural offshoot of my growing interest in helping other programs, HPS became a national consulting firm.
Q: Why did you think this venture could provide a valuable service?
A: I believed there were more effective healthcare delivery systems with which to provide both quality and cost-effective medical care. As time went on, I gained a very unique perspective working as both a hospitalist and referring PCP in private practice. This experience, coupled with my work as an administrative director for a hospitalist program, allowed me to develop applications to help hospitalist programs on a broader basis. I realized the advice I offered to other programs consistently rendered a positive effect.
Q: Which do you find more enjoyable: building a hospitalist program from the ground up or rebuilding a struggling program?
A: I truly enjoy the challenges of both equally. Projects that involve building a program de novo appeal to my creative side. These projects enable me to work with professionals to build a customized program that meets the needs of the community.
Q: What challenges are unique to each?
A: Rebuilding an established program involves critical analysis of the current program to identify what has gone wrong, what has been successful, and what will work in the future. It calls upon one’s skills to build consensus and instill trust in the process because the stakeholders may be apprehensive to have a consultant critically review their program and hospital. In many instances, conflict management is necessary.
In both the creation and rebuilding of an HM program, it is imperative to implement strategies that guide the program to future success. Both projects also require strategic planning and the development of tools and tactics that emphasize collaboration and collegiality.
Q: Do the failing programs you help to rebuild have characteristics in common?
A: Common themes include lack of planning and consensus-building before program start-up, inadequate tools and strategies to support effective practice management, and failure to align the hospitalist practice and sponsoring hospital’s goals and vision. Another common problem is the absence of a hospitalist recruitment and retention plan, which may lead to provider turnover and program instability.
Many programs experience problems due to ineffective leadership, poor implementation and follow-through, and lack of both a short- and long-term strategic plan. Some programs are victims of their own success. The program is not properly prepared to handle the demand for its services and grow accordingly.
Q: You help programs create effective recruitment and retention plans. You also wrote a book on the subject. Why are recruitment and retention challenging for so many programs?
A: The primary contributor is that [hospitalist] supply falls significantly short of physician demand. A secondary contributor is the generational expectations of the younger physician workforce. … In addition, leaders may not prioritize recruitment and retention because they lack an appreciation for the consequences of failed efforts.
Q: What advice would you offer hospitalist program leaders about how they can improve those aspects of their programs?
A: No. 1, create an effective recruitment and retention plan and execute the plan with precision. No. 2, approach recruitment and retention with the same attention to detail as you approach patient care.
Q: You’re offering best-practice advice to help your clients develop and sustain effective programs. What advice do you find yourself giving to your clients that you wish someone gave to you early in your career?
A: From my perspective as a hospitalist administrative director, the advice I would offer is for individuals to believe in themselves and stay engaged. If you feel you have something to offer to the practice or healthcare system as a whole, share it with the appropriate parties. If you experience problems within the workplace, seek resolution in a timely manner. Stay positive and be part of the solution, not part of the problem.
Q: You have written two hospitalist books and coauthored two others. Do you have plans to write another?
A: I wouldn’t say I have immediate plans, but I am always thinking about topics and other projects that would provide value to readers. I’ve got some exciting ideas for future projects, but they are in a very early stage of development.
Q: How would you compare the feeling you get from finishing a book with the satisfaction you derive from other aspects of your career?
A: Writing a book is a highly personal accomplishment for me, while caring for patients is more of a team accomplishment that involves the patient, family, and other healthcare professionals. Typically, the completion of a book is a finite event, while caring for a patient is a long-term commitment.
Q: What is your biggest professional reward?
A: Helping people, whether they are patients in my role as physician, or other professionals—physicians, practice administrators, and hospital administrators—in my role as a practice management consultant. Whenever I reflect on my career, I tell myself how lucky I am. There are not many professions or individuals who have an opportunity to close the door behind them and have other human beings entrust them with their most intimate information. Also, there are very few individuals who are able to impact the delivery of medical care from a systems perspective. I get to do both, and for that I am most grateful.
Q: What is your biggest professional challenge?
A: Saying “no” when someone asks for help. There is nothing more rewarding for me than to help others. With that said, I try not to overextend myself, because that wouldn’t be fair to my family, colleagues, friends, or clients.
Q: What’s next for you professionally?
A: I will continue to concentrate my effort on building my hospitalist consultative practice and expanding the services I offer. In addition, I’m always tempted to explore the valley of the unknown. What excites me is venturing into new areas and to challenge myself to grow as both an individual and professional. TH
Mark Leiser is a freelance writer based in New Jersey.
Kenneth G. Simone, DO, FHM, grew up as the son of a revered pediatrician. As a child, he often accompanied his father on hospital rounds and house calls, developing an appreciation for the “old-fashioned” medicine his father practiced.
Already inspired to follow in his father’s footsteps, Dr. Simone became even more convinced of his calling when the physician-patient roles were reversed: His dad developed a kidney disorder that cut his career—and ultimately his life—short. “His illness and my exposure to hospitals added to my desire to pursue medicine,” Dr. Simone says. “It instilled the drive to help others, to make a difference in someone’s or some family’s life.”
He has done that by developing multiple private medical practices, building the hospitalist program at St. Joseph Hospital in Bangor, Maine, and offering consulting services to more than 100 practices.
“It has always been my nature to challenge myself and put myself in situations that take me out of my comfort zone,” says Dr. Simone, president of Hospitalist and Practice Solutions, a practice-management consultancy in Veazie, Maine. “I enjoy building things from scratch, creating, rebuilding, thinking outside the box, and networking with other healthcare professionals.”
Question: What made you decide to start Hospitalist and Practice Solutions (HPS)?
Answer: HPS was established because of the demand for my services. Initially, word spread locally and then regionally about the work I did at St. Joseph Hospital. As a natural offshoot of my growing interest in helping other programs, HPS became a national consulting firm.
Q: Why did you think this venture could provide a valuable service?
A: I believed there were more effective healthcare delivery systems with which to provide both quality and cost-effective medical care. As time went on, I gained a very unique perspective working as both a hospitalist and referring PCP in private practice. This experience, coupled with my work as an administrative director for a hospitalist program, allowed me to develop applications to help hospitalist programs on a broader basis. I realized the advice I offered to other programs consistently rendered a positive effect.
Q: Which do you find more enjoyable: building a hospitalist program from the ground up or rebuilding a struggling program?
A: I truly enjoy the challenges of both equally. Projects that involve building a program de novo appeal to my creative side. These projects enable me to work with professionals to build a customized program that meets the needs of the community.
Q: What challenges are unique to each?
A: Rebuilding an established program involves critical analysis of the current program to identify what has gone wrong, what has been successful, and what will work in the future. It calls upon one’s skills to build consensus and instill trust in the process because the stakeholders may be apprehensive to have a consultant critically review their program and hospital. In many instances, conflict management is necessary.
In both the creation and rebuilding of an HM program, it is imperative to implement strategies that guide the program to future success. Both projects also require strategic planning and the development of tools and tactics that emphasize collaboration and collegiality.
Q: Do the failing programs you help to rebuild have characteristics in common?
A: Common themes include lack of planning and consensus-building before program start-up, inadequate tools and strategies to support effective practice management, and failure to align the hospitalist practice and sponsoring hospital’s goals and vision. Another common problem is the absence of a hospitalist recruitment and retention plan, which may lead to provider turnover and program instability.
Many programs experience problems due to ineffective leadership, poor implementation and follow-through, and lack of both a short- and long-term strategic plan. Some programs are victims of their own success. The program is not properly prepared to handle the demand for its services and grow accordingly.
Q: You help programs create effective recruitment and retention plans. You also wrote a book on the subject. Why are recruitment and retention challenging for so many programs?
A: The primary contributor is that [hospitalist] supply falls significantly short of physician demand. A secondary contributor is the generational expectations of the younger physician workforce. … In addition, leaders may not prioritize recruitment and retention because they lack an appreciation for the consequences of failed efforts.
Q: What advice would you offer hospitalist program leaders about how they can improve those aspects of their programs?
A: No. 1, create an effective recruitment and retention plan and execute the plan with precision. No. 2, approach recruitment and retention with the same attention to detail as you approach patient care.
Q: You’re offering best-practice advice to help your clients develop and sustain effective programs. What advice do you find yourself giving to your clients that you wish someone gave to you early in your career?
A: From my perspective as a hospitalist administrative director, the advice I would offer is for individuals to believe in themselves and stay engaged. If you feel you have something to offer to the practice or healthcare system as a whole, share it with the appropriate parties. If you experience problems within the workplace, seek resolution in a timely manner. Stay positive and be part of the solution, not part of the problem.
Q: You have written two hospitalist books and coauthored two others. Do you have plans to write another?
A: I wouldn’t say I have immediate plans, but I am always thinking about topics and other projects that would provide value to readers. I’ve got some exciting ideas for future projects, but they are in a very early stage of development.
Q: How would you compare the feeling you get from finishing a book with the satisfaction you derive from other aspects of your career?
A: Writing a book is a highly personal accomplishment for me, while caring for patients is more of a team accomplishment that involves the patient, family, and other healthcare professionals. Typically, the completion of a book is a finite event, while caring for a patient is a long-term commitment.
Q: What is your biggest professional reward?
A: Helping people, whether they are patients in my role as physician, or other professionals—physicians, practice administrators, and hospital administrators—in my role as a practice management consultant. Whenever I reflect on my career, I tell myself how lucky I am. There are not many professions or individuals who have an opportunity to close the door behind them and have other human beings entrust them with their most intimate information. Also, there are very few individuals who are able to impact the delivery of medical care from a systems perspective. I get to do both, and for that I am most grateful.
Q: What is your biggest professional challenge?
A: Saying “no” when someone asks for help. There is nothing more rewarding for me than to help others. With that said, I try not to overextend myself, because that wouldn’t be fair to my family, colleagues, friends, or clients.
Q: What’s next for you professionally?
A: I will continue to concentrate my effort on building my hospitalist consultative practice and expanding the services I offer. In addition, I’m always tempted to explore the valley of the unknown. What excites me is venturing into new areas and to challenge myself to grow as both an individual and professional. TH
Mark Leiser is a freelance writer based in New Jersey.
Are Stress-Dose Steroids Indicated in Patients with Adrenal Insufficiency Hospitalized with Noncritical, Nonsurgical Illness?
Case
A 46-year-old woman with Addison’s disease and type II diabetes presents with one day of right leg pain, swelling, and redness. She has had mild nausea and vomiting over the past week, with an episode of diarrhea three days prior. She takes hydrocortisone 30mg in the morning and 10mg at bedtime, as well as fludrocortisone 0.2mg in the morning. She is afebrile with a pulse of 108 beats per minute. Her initial blood pressure was 74/49 mmHg, which improved to 84/45 mmHg following one liter of normal saline. She is mentating appropriately. The physical exam is significant for a large, tender area of erythema and warmth from the right ankle to mid-calf. She is admitted for cellulitis and intravenous antibiotics are initiated.
Does she require an increase in her glucocorticoid dose during her acute illness?
Overview
Adrenal insufficiency occurs in approximately 5 out of every 10,000 people and results from primary failure of the adrenal gland, or secondary impairment of the hypothalamic-pituitary-adrenal (HPA) axis, which regulates cortisol secretion.1 In developed countries, 90% of primary adrenal insufficiency (Addison’s disease) cases are due to autoimmune adrenalitis, which might occur in isolation or as part of an autoimmune polyglandular syndrome.1,2 Secondary adrenal insufficiency is most commonly the result of chronic glucocorticoid therapy, though lesions involving the hypothalamus or pituitary gland might be implicated.2,3
In a healthy individual, cortisol is secreted in a diurnal pattern from the adrenal glands under the control of corticotropin (ACTH) produced by the pituitary gland and corticotropin-releasing hormone (CRH) produced by the hypothalamus (see Figure 1, p. 19). In the normal state, during periods of such systemic stress as illness, trauma, burns, or surgery, cortisol production increases to a degree roughly proportional to the degree of illness (as much as sixfold).4,5 Patients with adrenal insufficiency are unable to mount an appropriate cortisol response and, therefore, are at risk for adrenal crisis—a life-threatening condition characterized by hypotension and hypovolemic shock.
Although recommendations for high-dose intravenous steroids in adrenally insufficient patients who are critically ill or undergoing surgery have been extensively discussed in the literature, there are relatively few data regarding the appropriate management of adrenal insufficiency in patients hospitalized for noncritical illness.
Several recent studies have investigated the patient characteristics, situations, and conditions most likely to provoke adrenal crisis in order to establish guidelines dictating the use of supra-physiologic steroid dosing.
Review of the Data
Studies have estimated the prevalence of adrenal crisis in patients with underlying insufficiency at 3.3 to 6.3 events per 100 patient years, with 42% of patients reporting at least one crisis.2,5,6 A recent survey of 982 patients with Addison’s disease in the United Kingdom reported an 8% annual frequency.7
A retrospective Japanese study reviewed the medical charts of 137 adult patients receiving steroid replacement for established primary or secondary adrenal insufficiency. The authors noted a significant positive association between adrenal crisis and long-term steroid replacement (>4 years), concomitant mental disorder, and sex hormone deficiency. A combination of any of these factors further increased the risk.8
A more recent survey of 444 patients ages 17-81 assessed independent risk factors for adrenal crisis in the setting of primary (N=254) or secondary (N=190) adrenal insufficiency. The incidence of crisis was higher in primary versus secondary insufficiency. In patients with primary insufficiency, concomitant, non-endocrine disorders increased the risk of adrenal crisis, whereas diabetes insipidus and female gender increased risk in patients with secondary insufficiency. This same study also investigated events leading to a crisis and found gastrointestinal infection to be the most frequent factor, followed by other infectious or febrile illnesses. Overall, infection comprised 45% of all identified triggers.6
A similar study conducted by White and Arlt evaluated 841 Addison’s patients in the United Kingdom, Canada, Australia, and New Zealand.7 Again, gastrointestinal illness was the most common provoking factor, responsible for 56% of all reported crises. Flulike illness followed at 11%, followed by infections and surgical procedures at 6% each. This study found a higher risk of crisis in patients with diabetes (type I or II), premature ovarian failure, and asthma; the presence of multiple comorbidities further increased risk.
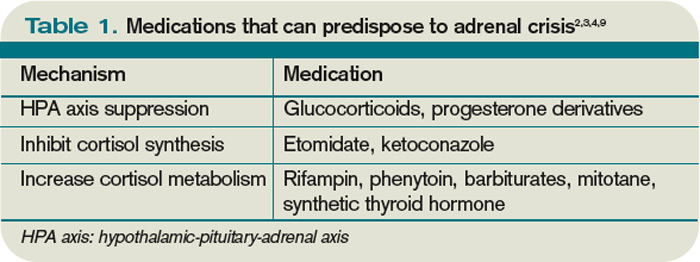
Medications. Glucocorticoid therapy is known to suppress the HPA axis. Although it was once believed that the duration and dose of therapy correlated directly with the degree of HPA suppression, more recent studies have failed to find any definite relationship.9 Patients taking the equivalent of 5mg of prednisone per day should continue to have an intact HPA axis, as this dose mimics physiologic secretion of cortisol in a healthy individual.3
However, the dose and duration of therapy at which suppression occurs is highly variable between patients. In general, patients on 7.5mg of prednisone or more per day for at least three weeks should be considered to be suppressed.3,9 Additionally, progesterone derivatives (i.e., megestrol) have glucocorticoid activity and might suppress HPA function. Other medications that might have related effects are those that inhibit enzymes involved in cortisol synthesis; ketoconazole and etomidate are common examples. Rifampin and several classes of anti-epileptic drugs induce enzymes, which increase hepatic metabolism of cortisol (see Table 1, p. 18).
Hyperthyroidism. Thyroid hormone is involved in the metabolism of cortisol, thus an increase in T4 correlates with lower levels. Adrenal insufficiency and thyroid disease might coexist within the autoimmune polyglandular syndrome. Initiation or uptitration of thyroid replacement should be avoided if acute adrenal insufficiency is suspected, as this might provoke an adrenal crisis. Conversely, any patient with adrenal insufficiency who has uncontrolled hyperthyroidism should receive two to three times their usual glucocorticoid replacement.1,2
Pregnancy. Levels of cortisol-binding globulin increase throughout pregnancy. In women with intact adrenal function, free cortisol levels also rise during the third trimester. Therefore, glucocorticoid replacement should be increased by 50% during the last three months of pregnancy.2
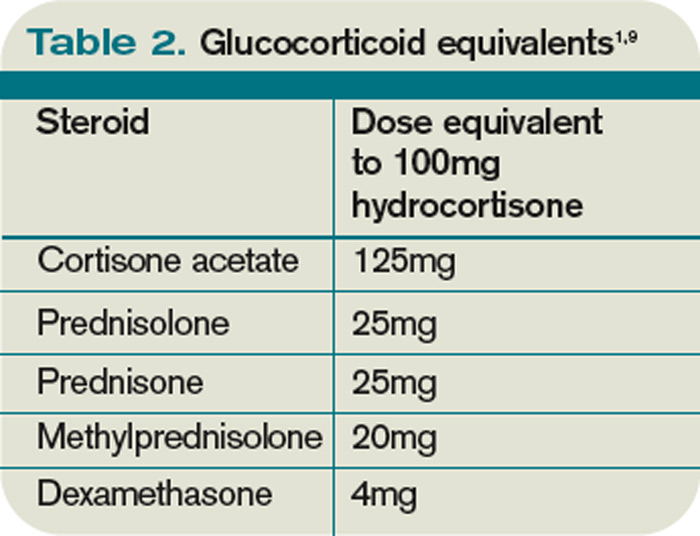
Acute illness. The cortisol response to stress is highly variable and dependent on a number of factors, including age, underlying health, and genetics. In general, most experts recommend doubling or tripling the daily replacement dose during mild to moderate illness until recovery (often referred to as the “sick-day rules”). What constitutes “recovery” is not clearly defined. When oral intake is compromised, as with vomiting or diarrhea, parenteral administration of steroids is recommended.1-5,9,10 Patients with adrenal insufficiency should be provided an emergency injection kit to use and further counseled to seek medical attention. Injection kits typically consist of 100mg of hydrocortisone or 4mg of dexamethasone, although other glucocorticoids may be used (see Table 2, above left, for conversions).
Limited data are available to support guidelines for glucocorticoid adjustment during acute, non-critical illness. Published guidelines vary both in illness categorization and category-specific recommendations (see Table 3, below).
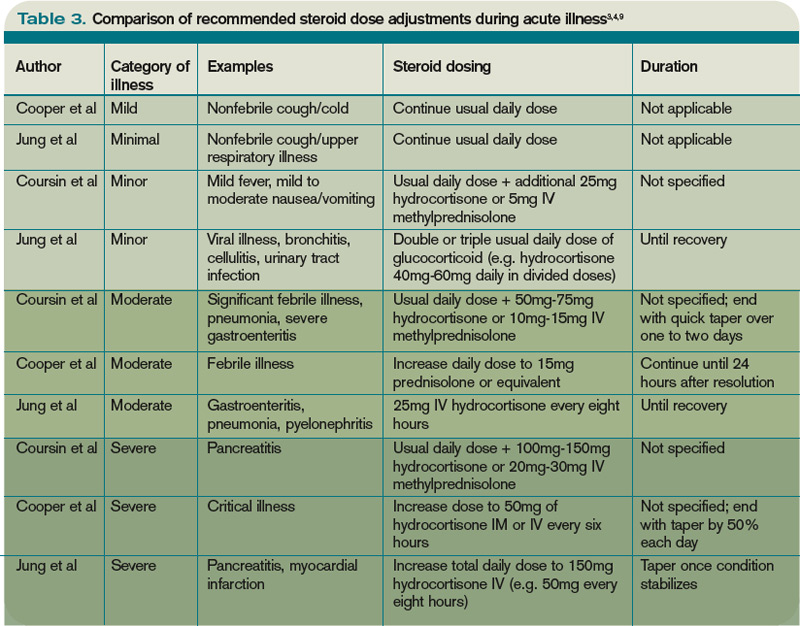
Coursin and Wood devised a set of guidelines based on a literature review and consultation with experts, categorizing medical illness as minor, moderate, severe, and critical (see Table 3).3 For noncritical illness, they recommended continuation of standard replacement therapy with an additional, once-daily dose, which varied according to illness severity.
Cooper and Stewart conducted a similar review, basing their guidelines on a categorization of mild, moderate, severe/critical, or septic shock. These guidelines recommended a total daily dose of glucocorticoid supplementation, rather than an addition of a single dose to current therapy. They also stated that the least severe category of illness (defined as mild) did not require any change to a patient’s regular therapy.4
Jung et al classified illness as minimal, minor, moderate, severe, and critical.9 Under these guidelines, supplemental therapy was not advised for minimal (nonfebrile) illness. Moderate illness, including cellulitis, warranted a doubling or tripling of the outpatient dose until recovery, which was consistent with prior expert recommendation. More severe illness warranted intravenous administration of steroids.
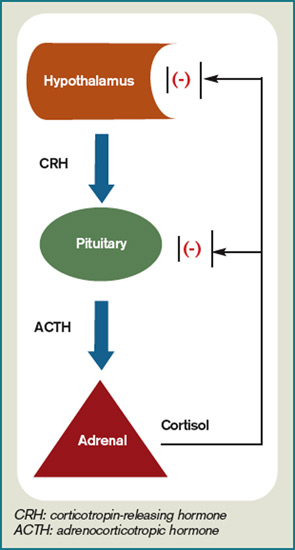
Back to the Case
The patient had a mild case of cellulitis, classified by most experts as moderate illness, which responded well to vancomycin. Her outpatient glucocorticoid dose was doubled on admission and administered orally for the duration of her hospitalization, as she had no further episodes of vomiting or diarrhea.
Review of the patient’s records from prior hospitalizations and ambulatory visits revealed that her systolic blood pressure typically ran in the 80 mmHg to 100 mmHg range. Following initial volume resuscitation, her systolic blood pressure remained in the 90-100 mmHg range.
She was discharged home in stable condition, with instructions to complete a course of oral trimethoprim/sulfamethoxazole, resume her baseline dose of hydrocortisone the day after discharge, and follow up with her PCP for further monitoring and adjustment of her adrenal replacement therapy.
Bottom Line
For adults with adrenal insufficiency hospitalized with noncritical, nonsurgical illness, the expert recommendation is to double or triple the usual outpatient dose of glucocorticoid; however, data to support this is limited, and each patient should be assessed carefully and monitored to determine the optimal dose adjustment. TH
Dr. Shaw is a resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is an assistant professor of medicine in the division of general internal medicine, University of Washington School of Medicine.
References
- Arlt W. The approach to the adult with newly diagnosed adrenal insufficiency. J Clin Endocrinol Metab. 2009;94(4):1059-1067.
- Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003; 361:1881-1893.
- Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002;287:236-240.
- Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003;348:727-734.
- Hahner S, Allolio B. Therapeutic management of adrenal insufficiency. Best Pract Res Clin Endocrinol Metab. 2009;23:167-179.
- Hahner S, Loeffler M, Bleicken B, et al. Epidemiology of adrenal crisis in chronic adrenal insufficiency: the need for new prevention strategies. Eur J Endocrinol. 2010;162:597:602.
- White K, Arlt W. Adrenal crisis in treated Addison’s disease: a predictable but under-managed event. Eur J Endocrinol. 2010;162:115-120.
- Omori K, Nomura K, Shimizu S, Omori N, Takano K. Risk factors for adrenal crises in patients with adrenal insufficiency. Endocr J. 2003;50:745-752.
- Jung C, Inder WJ. Management of adrenal insufficiency during the stress of medical illness and surgery. Med J Aust. 2008;188:409-413.
- Crown A, Lightman S. Why is the management of glucocorticoid deficiency still controversial: a review of the literature. Clin Endocrinol. 2005;63:483-492.
Case
A 46-year-old woman with Addison’s disease and type II diabetes presents with one day of right leg pain, swelling, and redness. She has had mild nausea and vomiting over the past week, with an episode of diarrhea three days prior. She takes hydrocortisone 30mg in the morning and 10mg at bedtime, as well as fludrocortisone 0.2mg in the morning. She is afebrile with a pulse of 108 beats per minute. Her initial blood pressure was 74/49 mmHg, which improved to 84/45 mmHg following one liter of normal saline. She is mentating appropriately. The physical exam is significant for a large, tender area of erythema and warmth from the right ankle to mid-calf. She is admitted for cellulitis and intravenous antibiotics are initiated.
Does she require an increase in her glucocorticoid dose during her acute illness?
Overview
Adrenal insufficiency occurs in approximately 5 out of every 10,000 people and results from primary failure of the adrenal gland, or secondary impairment of the hypothalamic-pituitary-adrenal (HPA) axis, which regulates cortisol secretion.1 In developed countries, 90% of primary adrenal insufficiency (Addison’s disease) cases are due to autoimmune adrenalitis, which might occur in isolation or as part of an autoimmune polyglandular syndrome.1,2 Secondary adrenal insufficiency is most commonly the result of chronic glucocorticoid therapy, though lesions involving the hypothalamus or pituitary gland might be implicated.2,3
In a healthy individual, cortisol is secreted in a diurnal pattern from the adrenal glands under the control of corticotropin (ACTH) produced by the pituitary gland and corticotropin-releasing hormone (CRH) produced by the hypothalamus (see Figure 1, p. 19). In the normal state, during periods of such systemic stress as illness, trauma, burns, or surgery, cortisol production increases to a degree roughly proportional to the degree of illness (as much as sixfold).4,5 Patients with adrenal insufficiency are unable to mount an appropriate cortisol response and, therefore, are at risk for adrenal crisis—a life-threatening condition characterized by hypotension and hypovolemic shock.
Although recommendations for high-dose intravenous steroids in adrenally insufficient patients who are critically ill or undergoing surgery have been extensively discussed in the literature, there are relatively few data regarding the appropriate management of adrenal insufficiency in patients hospitalized for noncritical illness.
Several recent studies have investigated the patient characteristics, situations, and conditions most likely to provoke adrenal crisis in order to establish guidelines dictating the use of supra-physiologic steroid dosing.
Review of the Data
Studies have estimated the prevalence of adrenal crisis in patients with underlying insufficiency at 3.3 to 6.3 events per 100 patient years, with 42% of patients reporting at least one crisis.2,5,6 A recent survey of 982 patients with Addison’s disease in the United Kingdom reported an 8% annual frequency.7
A retrospective Japanese study reviewed the medical charts of 137 adult patients receiving steroid replacement for established primary or secondary adrenal insufficiency. The authors noted a significant positive association between adrenal crisis and long-term steroid replacement (>4 years), concomitant mental disorder, and sex hormone deficiency. A combination of any of these factors further increased the risk.8
A more recent survey of 444 patients ages 17-81 assessed independent risk factors for adrenal crisis in the setting of primary (N=254) or secondary (N=190) adrenal insufficiency. The incidence of crisis was higher in primary versus secondary insufficiency. In patients with primary insufficiency, concomitant, non-endocrine disorders increased the risk of adrenal crisis, whereas diabetes insipidus and female gender increased risk in patients with secondary insufficiency. This same study also investigated events leading to a crisis and found gastrointestinal infection to be the most frequent factor, followed by other infectious or febrile illnesses. Overall, infection comprised 45% of all identified triggers.6
A similar study conducted by White and Arlt evaluated 841 Addison’s patients in the United Kingdom, Canada, Australia, and New Zealand.7 Again, gastrointestinal illness was the most common provoking factor, responsible for 56% of all reported crises. Flulike illness followed at 11%, followed by infections and surgical procedures at 6% each. This study found a higher risk of crisis in patients with diabetes (type I or II), premature ovarian failure, and asthma; the presence of multiple comorbidities further increased risk.
Medications. Glucocorticoid therapy is known to suppress the HPA axis. Although it was once believed that the duration and dose of therapy correlated directly with the degree of HPA suppression, more recent studies have failed to find any definite relationship.9 Patients taking the equivalent of 5mg of prednisone per day should continue to have an intact HPA axis, as this dose mimics physiologic secretion of cortisol in a healthy individual.3
However, the dose and duration of therapy at which suppression occurs is highly variable between patients. In general, patients on 7.5mg of prednisone or more per day for at least three weeks should be considered to be suppressed.3,9 Additionally, progesterone derivatives (i.e., megestrol) have glucocorticoid activity and might suppress HPA function. Other medications that might have related effects are those that inhibit enzymes involved in cortisol synthesis; ketoconazole and etomidate are common examples. Rifampin and several classes of anti-epileptic drugs induce enzymes, which increase hepatic metabolism of cortisol (see Table 1, p. 18).
Hyperthyroidism. Thyroid hormone is involved in the metabolism of cortisol, thus an increase in T4 correlates with lower levels. Adrenal insufficiency and thyroid disease might coexist within the autoimmune polyglandular syndrome. Initiation or uptitration of thyroid replacement should be avoided if acute adrenal insufficiency is suspected, as this might provoke an adrenal crisis. Conversely, any patient with adrenal insufficiency who has uncontrolled hyperthyroidism should receive two to three times their usual glucocorticoid replacement.1,2
Pregnancy. Levels of cortisol-binding globulin increase throughout pregnancy. In women with intact adrenal function, free cortisol levels also rise during the third trimester. Therefore, glucocorticoid replacement should be increased by 50% during the last three months of pregnancy.2
Acute illness. The cortisol response to stress is highly variable and dependent on a number of factors, including age, underlying health, and genetics. In general, most experts recommend doubling or tripling the daily replacement dose during mild to moderate illness until recovery (often referred to as the “sick-day rules”). What constitutes “recovery” is not clearly defined. When oral intake is compromised, as with vomiting or diarrhea, parenteral administration of steroids is recommended.1-5,9,10 Patients with adrenal insufficiency should be provided an emergency injection kit to use and further counseled to seek medical attention. Injection kits typically consist of 100mg of hydrocortisone or 4mg of dexamethasone, although other glucocorticoids may be used (see Table 2, above left, for conversions).
Limited data are available to support guidelines for glucocorticoid adjustment during acute, non-critical illness. Published guidelines vary both in illness categorization and category-specific recommendations (see Table 3, below).
Coursin and Wood devised a set of guidelines based on a literature review and consultation with experts, categorizing medical illness as minor, moderate, severe, and critical (see Table 3).3 For noncritical illness, they recommended continuation of standard replacement therapy with an additional, once-daily dose, which varied according to illness severity.
Cooper and Stewart conducted a similar review, basing their guidelines on a categorization of mild, moderate, severe/critical, or septic shock. These guidelines recommended a total daily dose of glucocorticoid supplementation, rather than an addition of a single dose to current therapy. They also stated that the least severe category of illness (defined as mild) did not require any change to a patient’s regular therapy.4
Jung et al classified illness as minimal, minor, moderate, severe, and critical.9 Under these guidelines, supplemental therapy was not advised for minimal (nonfebrile) illness. Moderate illness, including cellulitis, warranted a doubling or tripling of the outpatient dose until recovery, which was consistent with prior expert recommendation. More severe illness warranted intravenous administration of steroids.
Back to the Case
The patient had a mild case of cellulitis, classified by most experts as moderate illness, which responded well to vancomycin. Her outpatient glucocorticoid dose was doubled on admission and administered orally for the duration of her hospitalization, as she had no further episodes of vomiting or diarrhea.
Review of the patient’s records from prior hospitalizations and ambulatory visits revealed that her systolic blood pressure typically ran in the 80 mmHg to 100 mmHg range. Following initial volume resuscitation, her systolic blood pressure remained in the 90-100 mmHg range.
She was discharged home in stable condition, with instructions to complete a course of oral trimethoprim/sulfamethoxazole, resume her baseline dose of hydrocortisone the day after discharge, and follow up with her PCP for further monitoring and adjustment of her adrenal replacement therapy.
Bottom Line
For adults with adrenal insufficiency hospitalized with noncritical, nonsurgical illness, the expert recommendation is to double or triple the usual outpatient dose of glucocorticoid; however, data to support this is limited, and each patient should be assessed carefully and monitored to determine the optimal dose adjustment. TH
Dr. Shaw is a resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is an assistant professor of medicine in the division of general internal medicine, University of Washington School of Medicine.
References
- Arlt W. The approach to the adult with newly diagnosed adrenal insufficiency. J Clin Endocrinol Metab. 2009;94(4):1059-1067.
- Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003; 361:1881-1893.
- Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002;287:236-240.
- Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003;348:727-734.
- Hahner S, Allolio B. Therapeutic management of adrenal insufficiency. Best Pract Res Clin Endocrinol Metab. 2009;23:167-179.
- Hahner S, Loeffler M, Bleicken B, et al. Epidemiology of adrenal crisis in chronic adrenal insufficiency: the need for new prevention strategies. Eur J Endocrinol. 2010;162:597:602.
- White K, Arlt W. Adrenal crisis in treated Addison’s disease: a predictable but under-managed event. Eur J Endocrinol. 2010;162:115-120.
- Omori K, Nomura K, Shimizu S, Omori N, Takano K. Risk factors for adrenal crises in patients with adrenal insufficiency. Endocr J. 2003;50:745-752.
- Jung C, Inder WJ. Management of adrenal insufficiency during the stress of medical illness and surgery. Med J Aust. 2008;188:409-413.
- Crown A, Lightman S. Why is the management of glucocorticoid deficiency still controversial: a review of the literature. Clin Endocrinol. 2005;63:483-492.
Case
A 46-year-old woman with Addison’s disease and type II diabetes presents with one day of right leg pain, swelling, and redness. She has had mild nausea and vomiting over the past week, with an episode of diarrhea three days prior. She takes hydrocortisone 30mg in the morning and 10mg at bedtime, as well as fludrocortisone 0.2mg in the morning. She is afebrile with a pulse of 108 beats per minute. Her initial blood pressure was 74/49 mmHg, which improved to 84/45 mmHg following one liter of normal saline. She is mentating appropriately. The physical exam is significant for a large, tender area of erythema and warmth from the right ankle to mid-calf. She is admitted for cellulitis and intravenous antibiotics are initiated.
Does she require an increase in her glucocorticoid dose during her acute illness?
Overview
Adrenal insufficiency occurs in approximately 5 out of every 10,000 people and results from primary failure of the adrenal gland, or secondary impairment of the hypothalamic-pituitary-adrenal (HPA) axis, which regulates cortisol secretion.1 In developed countries, 90% of primary adrenal insufficiency (Addison’s disease) cases are due to autoimmune adrenalitis, which might occur in isolation or as part of an autoimmune polyglandular syndrome.1,2 Secondary adrenal insufficiency is most commonly the result of chronic glucocorticoid therapy, though lesions involving the hypothalamus or pituitary gland might be implicated.2,3
In a healthy individual, cortisol is secreted in a diurnal pattern from the adrenal glands under the control of corticotropin (ACTH) produced by the pituitary gland and corticotropin-releasing hormone (CRH) produced by the hypothalamus (see Figure 1, p. 19). In the normal state, during periods of such systemic stress as illness, trauma, burns, or surgery, cortisol production increases to a degree roughly proportional to the degree of illness (as much as sixfold).4,5 Patients with adrenal insufficiency are unable to mount an appropriate cortisol response and, therefore, are at risk for adrenal crisis—a life-threatening condition characterized by hypotension and hypovolemic shock.
Although recommendations for high-dose intravenous steroids in adrenally insufficient patients who are critically ill or undergoing surgery have been extensively discussed in the literature, there are relatively few data regarding the appropriate management of adrenal insufficiency in patients hospitalized for noncritical illness.
Several recent studies have investigated the patient characteristics, situations, and conditions most likely to provoke adrenal crisis in order to establish guidelines dictating the use of supra-physiologic steroid dosing.
Review of the Data
Studies have estimated the prevalence of adrenal crisis in patients with underlying insufficiency at 3.3 to 6.3 events per 100 patient years, with 42% of patients reporting at least one crisis.2,5,6 A recent survey of 982 patients with Addison’s disease in the United Kingdom reported an 8% annual frequency.7
A retrospective Japanese study reviewed the medical charts of 137 adult patients receiving steroid replacement for established primary or secondary adrenal insufficiency. The authors noted a significant positive association between adrenal crisis and long-term steroid replacement (>4 years), concomitant mental disorder, and sex hormone deficiency. A combination of any of these factors further increased the risk.8
A more recent survey of 444 patients ages 17-81 assessed independent risk factors for adrenal crisis in the setting of primary (N=254) or secondary (N=190) adrenal insufficiency. The incidence of crisis was higher in primary versus secondary insufficiency. In patients with primary insufficiency, concomitant, non-endocrine disorders increased the risk of adrenal crisis, whereas diabetes insipidus and female gender increased risk in patients with secondary insufficiency. This same study also investigated events leading to a crisis and found gastrointestinal infection to be the most frequent factor, followed by other infectious or febrile illnesses. Overall, infection comprised 45% of all identified triggers.6
A similar study conducted by White and Arlt evaluated 841 Addison’s patients in the United Kingdom, Canada, Australia, and New Zealand.7 Again, gastrointestinal illness was the most common provoking factor, responsible for 56% of all reported crises. Flulike illness followed at 11%, followed by infections and surgical procedures at 6% each. This study found a higher risk of crisis in patients with diabetes (type I or II), premature ovarian failure, and asthma; the presence of multiple comorbidities further increased risk.
Medications. Glucocorticoid therapy is known to suppress the HPA axis. Although it was once believed that the duration and dose of therapy correlated directly with the degree of HPA suppression, more recent studies have failed to find any definite relationship.9 Patients taking the equivalent of 5mg of prednisone per day should continue to have an intact HPA axis, as this dose mimics physiologic secretion of cortisol in a healthy individual.3
However, the dose and duration of therapy at which suppression occurs is highly variable between patients. In general, patients on 7.5mg of prednisone or more per day for at least three weeks should be considered to be suppressed.3,9 Additionally, progesterone derivatives (i.e., megestrol) have glucocorticoid activity and might suppress HPA function. Other medications that might have related effects are those that inhibit enzymes involved in cortisol synthesis; ketoconazole and etomidate are common examples. Rifampin and several classes of anti-epileptic drugs induce enzymes, which increase hepatic metabolism of cortisol (see Table 1, p. 18).
Hyperthyroidism. Thyroid hormone is involved in the metabolism of cortisol, thus an increase in T4 correlates with lower levels. Adrenal insufficiency and thyroid disease might coexist within the autoimmune polyglandular syndrome. Initiation or uptitration of thyroid replacement should be avoided if acute adrenal insufficiency is suspected, as this might provoke an adrenal crisis. Conversely, any patient with adrenal insufficiency who has uncontrolled hyperthyroidism should receive two to three times their usual glucocorticoid replacement.1,2
Pregnancy. Levels of cortisol-binding globulin increase throughout pregnancy. In women with intact adrenal function, free cortisol levels also rise during the third trimester. Therefore, glucocorticoid replacement should be increased by 50% during the last three months of pregnancy.2
Acute illness. The cortisol response to stress is highly variable and dependent on a number of factors, including age, underlying health, and genetics. In general, most experts recommend doubling or tripling the daily replacement dose during mild to moderate illness until recovery (often referred to as the “sick-day rules”). What constitutes “recovery” is not clearly defined. When oral intake is compromised, as with vomiting or diarrhea, parenteral administration of steroids is recommended.1-5,9,10 Patients with adrenal insufficiency should be provided an emergency injection kit to use and further counseled to seek medical attention. Injection kits typically consist of 100mg of hydrocortisone or 4mg of dexamethasone, although other glucocorticoids may be used (see Table 2, above left, for conversions).
Limited data are available to support guidelines for glucocorticoid adjustment during acute, non-critical illness. Published guidelines vary both in illness categorization and category-specific recommendations (see Table 3, below).
Coursin and Wood devised a set of guidelines based on a literature review and consultation with experts, categorizing medical illness as minor, moderate, severe, and critical (see Table 3).3 For noncritical illness, they recommended continuation of standard replacement therapy with an additional, once-daily dose, which varied according to illness severity.
Cooper and Stewart conducted a similar review, basing their guidelines on a categorization of mild, moderate, severe/critical, or septic shock. These guidelines recommended a total daily dose of glucocorticoid supplementation, rather than an addition of a single dose to current therapy. They also stated that the least severe category of illness (defined as mild) did not require any change to a patient’s regular therapy.4
Jung et al classified illness as minimal, minor, moderate, severe, and critical.9 Under these guidelines, supplemental therapy was not advised for minimal (nonfebrile) illness. Moderate illness, including cellulitis, warranted a doubling or tripling of the outpatient dose until recovery, which was consistent with prior expert recommendation. More severe illness warranted intravenous administration of steroids.
Back to the Case
The patient had a mild case of cellulitis, classified by most experts as moderate illness, which responded well to vancomycin. Her outpatient glucocorticoid dose was doubled on admission and administered orally for the duration of her hospitalization, as she had no further episodes of vomiting or diarrhea.
Review of the patient’s records from prior hospitalizations and ambulatory visits revealed that her systolic blood pressure typically ran in the 80 mmHg to 100 mmHg range. Following initial volume resuscitation, her systolic blood pressure remained in the 90-100 mmHg range.
She was discharged home in stable condition, with instructions to complete a course of oral trimethoprim/sulfamethoxazole, resume her baseline dose of hydrocortisone the day after discharge, and follow up with her PCP for further monitoring and adjustment of her adrenal replacement therapy.
Bottom Line
For adults with adrenal insufficiency hospitalized with noncritical, nonsurgical illness, the expert recommendation is to double or triple the usual outpatient dose of glucocorticoid; however, data to support this is limited, and each patient should be assessed carefully and monitored to determine the optimal dose adjustment. TH
Dr. Shaw is a resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is an assistant professor of medicine in the division of general internal medicine, University of Washington School of Medicine.
References
- Arlt W. The approach to the adult with newly diagnosed adrenal insufficiency. J Clin Endocrinol Metab. 2009;94(4):1059-1067.
- Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003; 361:1881-1893.
- Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002;287:236-240.
- Cooper MS, Stewart PM. Corticosteroid insufficiency in acutely ill patients. N Engl J Med. 2003;348:727-734.
- Hahner S, Allolio B. Therapeutic management of adrenal insufficiency. Best Pract Res Clin Endocrinol Metab. 2009;23:167-179.
- Hahner S, Loeffler M, Bleicken B, et al. Epidemiology of adrenal crisis in chronic adrenal insufficiency: the need for new prevention strategies. Eur J Endocrinol. 2010;162:597:602.
- White K, Arlt W. Adrenal crisis in treated Addison’s disease: a predictable but under-managed event. Eur J Endocrinol. 2010;162:115-120.
- Omori K, Nomura K, Shimizu S, Omori N, Takano K. Risk factors for adrenal crises in patients with adrenal insufficiency. Endocr J. 2003;50:745-752.
- Jung C, Inder WJ. Management of adrenal insufficiency during the stress of medical illness and surgery. Med J Aust. 2008;188:409-413.
- Crown A, Lightman S. Why is the management of glucocorticoid deficiency still controversial: a review of the literature. Clin Endocrinol. 2005;63:483-492.