User login
Scheduled Admissions and Occupancy
Patient flow in a hospital refers to the management and movement of patients through the facility. Optimizing patient flow is considered of great importance to improvement of quality (including safety, efficiency, timeliness, equity, effectiveness, and patient‐centeredness), as well as finance, staff satisfaction, education and overall healthcare value.18 Central to concerns about patient flow at hospitals is occupancy, which is the census (number of patients at a point in time) divided by the bed capacity. Occupancy that is too high is associated with challenges to quality and access,913 while occupancy that is too low may underutilize resources and be costly.14, 15 Occupancy is determined by the pattern of admission and discharge, thus including length of stay (LOS) as a factor. While all related, admissions, census, occupancy, and LOS convey different aspects of hospital operations and may point to different opportunities to improve patient flow.
Variability in patient flow over time has been noted as a common occurrence in adult hospitals, due to uneven patterns of scheduled (elective) admissions, as well as uncontrollable variability of emergent admissions.2, 45, 16 Typically very few patients are scheduled to enter hospitals over weekends. In addition, when the admission is expected to be 5 days or less, clinical and operational staff may schedule those admissions early in the week to avoid patients staying the weekend. This artificial variability has been shown to lead to uneven levels of occupancy, with crowding on some days of the week more than others.2, 45, 16 As hospital crowding adversely affects access to emergent and elective care, quality and safety of care, and patient and staff satisfaction, many groups are focusing attention on patient flow and strategies to avoid high occupancy.19, 17 This is true for children's hospitals, as well, particularly as these scarce resources have ever increasing demand placed on them.1820
Patient flow improvements can be made by increasing efficiency of throughput, primarily measured by decreased LOS, or by addressing artificial variability in how hospital beds are used. As children's hospitals have short LOSs and are relatively efficient (as measured by standardized LOS ratios), we sought to evaluate how much artificial variability was active at 1 large children's hospital. We did this to both evaluate flow at 1 institution and to create methodology for other hospitals to use in order to better understand and improve their flow.
Our specific aims were to describe daily and monthly variability in admission, discharge, LOS, and occupancy patterns at a large children's hospital and assess the relationship between scheduled admissions and occupancy.
Methods
This retrospective administrative data analysis was performed with admission‐discharge‐transfer (ADT) data for inpatient admissions from one urban, tertiary‐care children's hospital for the period July 1, 2007 to June 30, 2008. The dataset included the date and time of all arrivals and departures from all inpatient units (including observation‐status patients), as entered by the unit clerks into the electronic ADT system. The dataset also included categorization of the admission as emergent, urgent, or elective (hereafter referred to as scheduled.) Registration staff entered these codes at or prior to admission. Using the timestamps, LOS was calculated by subtracting admission date and time from discharge date and time. An SAS macro was applied to the timestamps to calculate a hospital census for every hour of each calendar day. Peak census figures were extracted for each day. Occupancy was calculated as census over number of beds in use (monthly average). Data for the hospital's peak daily census and occupancy were utilized to analyze patterns of occupancy by day of week and month of year. To express variability, coefficient of variation (CV) (standard deviation [SD] divided by its mean) was used, as it is helpful when samples sizes are different.21
Analysis of number of admissions per day of week and month by type was performed with descriptive statistics and t‐tests for significant differences across seasons. We calculated a measure of patient hours generated by day of admission based on the LOS generated by each admission, in which the average number of admissions for each day of the week was multiplied by the average LOS (in hours) for those admissions. In order to remove outliers and focus on patients whose occupancy would affect weekly variation, we analyzed in detail the admissions with LOS 30 days and 7 days, respectively.
Statistical analyses were performed with SAS 9.2 (SAS Institute, Cary, NC), Stata 10.0 (StataCorp, College Station, TX) and Microsoft Excel (Microsoft, Redmond, WA). The study was approved by the Human Subjects Committee of the hospital's Institutional Review Board.
Results
A total of 22,310 patients were admitted over the period July 1, 2007 to June 30, 2008, including 4957 (22%) coded as scheduled and 17,353 (78%) coded as emergent. (Only 200 patients were registered as urgent and these were recoded as emergent for this analysis). Details on admission types and discharging departments are provided in Table 1. Overall, mean LOS was 5.6 days (median 2.29 days). For patients with LOS 30 days, mean LOS was 3.88 days (median 2.22 days). For patients staying 7 days, mean LOS was 2.4 days (median 1.98 days). Among patients with LOS 7 days, mean LOS for scheduled patients was longer for those admitted on Monday than on any other weekday (2.49 vs. 2.08 days, P < 0.0001). In contrast, mean LOS for emergent patients was longer for patients admitted on Friday and Saturday than the rest of the week (2.57 vs. 2.44 days, P < 0.0001).
| All | Scheduled | Emergent | |
|---|---|---|---|
| |||
| Total Admissions, n (%)* | 22,310 | 4957 (22) | 17,353 (78) |
| Median LOS (days) | 2.29 | 1.93 | 2.50 |
| Mean LOS (days) (95% CI) | 5.60 (5.41, 5.79) | 4.20 (3.95, 4.45) | 5.78 (5.596.0) |
| % Patients with LOS 30 days (%) | 97 | 98 | 96 |
| % Patients with LOS 7 days (%) | 84 | 89 | 83 |
| Medical patients at discharge, n (%) | 16,586 (74) | 2363 (48) | 14,403 (83) |
| Surgical patients at discharge, n (%) | 4276 (19) | 2450 (49) | 1826 (10.5) |
| Critical care patients at discharge (NICU, PICU, CICU), n (%) | 1433 (6) | 140 (3) | 1293 (7.5) |
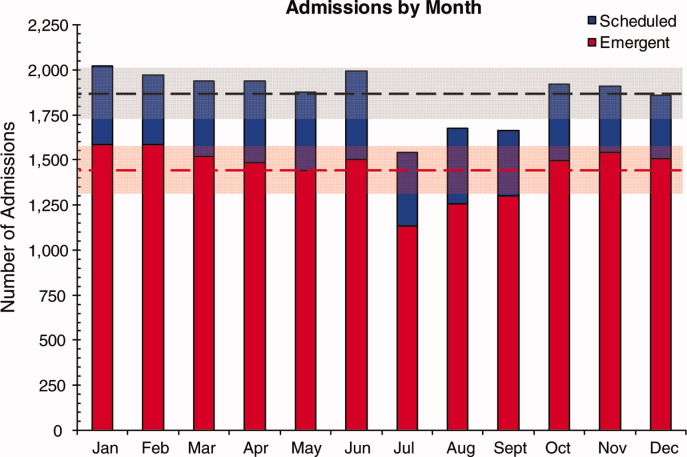
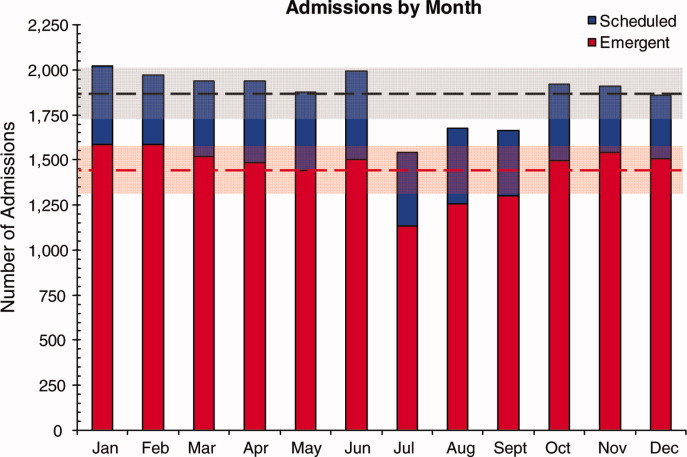
Total admissions per month (Figure 1) averaged 1937 in October through April and 1751 in May through September (P = 0.03). Variation in the number of emergent and scheduled patients over months of the year were similar (CV 10% for each), but emergent admissions did decrease in summer (mean 1299 for June‐September vs. 1520 for the rest of the year, P = 0.003). Conversely, scheduled admissions remained relatively stable all year‐long: mean 423 per month for May through September vs. mean 413 per month for October through April (P = 0.48). Even just the summer months of June‐August, when school‐age children are on vacation, were not significantly different from other months (440 vs. 404, P = 0.2).
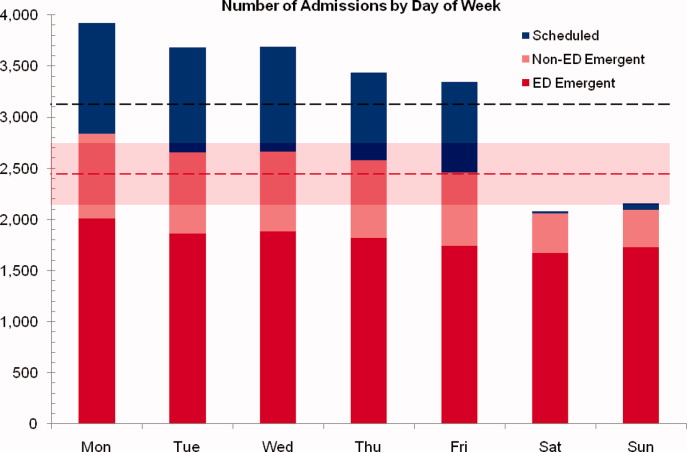
Variation in volume of admissions was large over days of the week, driven primarily by the pattern of scheduled admissions (CV 65.3%), which dropped off completely on weekends (Table 2, Figure 2). In contrast, there was much less variation in the number of emergent admissions across days of the week (CV 12%). For both emergent and scheduled admissions, more patients came in on Mondays than any other day of the week, but even more so for scheduled patients. While emergent admissions did decline on weekends, it was driven primarily by a decrease in physician referrals (ie, direct admission) from clinics (mean 7.48 per weekday vs. 0.73 per weekend day for the entire year, P < 0.001), while emergency department (ED) admissions remained relatively stable (mean 35.8 per weekday vs. 32.7 per weekend day, P = 0.08). Emergency transports were also stable (mean 7.15 per weekday vs. 6.49 per weekend day, P = 0.10).
| All (%) | Scheduled (%) | Emergent (%) | |
|---|---|---|---|
| |||
| CV on admissions by month | 8 | 10 | 10 |
| CV on admissions over days of week (including weekends) | 24 | 65 | 12 |
| CV on admissions over days of week (excluding weekends) | 6 | 10 | 5 |
| CV on monthly occupancy over 12 months | 4 | 14 | 2 |
Although scheduled patients contributed less to the hospital's overall occupancy, they conferred most of the variability by day of week. Over the days of the week, variation for scheduled occupancy was nearly twice that for emergent occupancy (CV 19% vs. 10%). Within the higher‐volume period of October to April, the differential was even more evident (CV 19% for scheduled occupancy versus 6% for emergent).
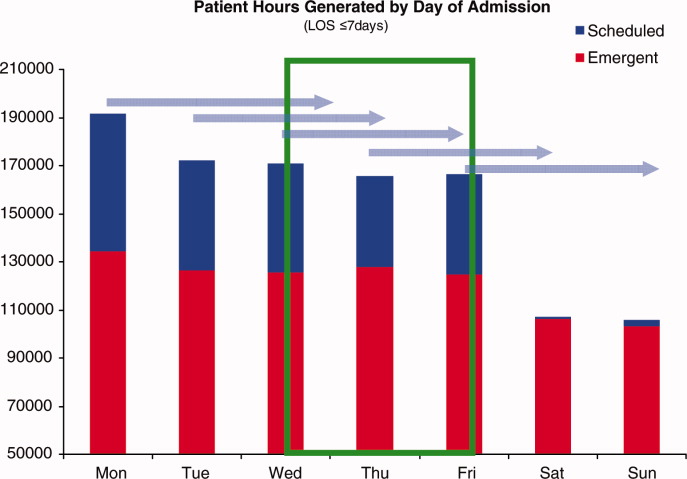
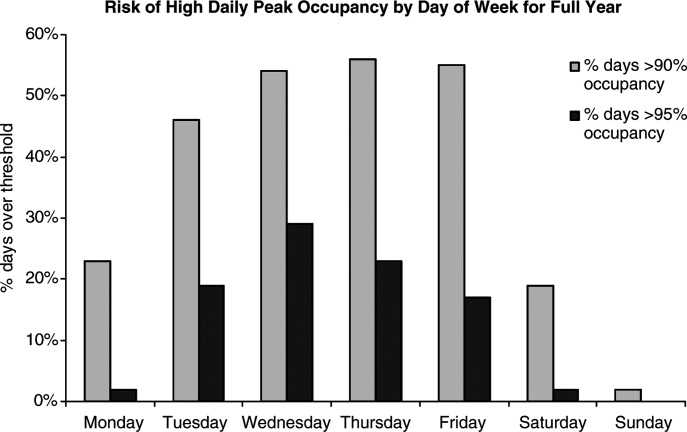
For scheduled patients with LOS 30 days (98% of scheduled patients), Mondays and Tuesdays together accounted for 42.5% of admission volume and 44.7% of the patient‐hours generated. For scheduled patients with LOS 7 days (89% of scheduled patients), Mondays and Tuesdays together accounted for 42% of admission volume and 45.2% of the patient‐hours generated. This combined impact of volume and LOS from admissions earlier in the week (restricted to patients with LOS 7days) is displayed graphically in Figure 3, which depicts the unevenness of scheduled admissions and their time in the hospital, with many patients overlapping in the middle of the week. Together with the more steady flow of emergent patients, this variability in scheduled occupancy contributed to mid‐week crowding, with higher risk of the hospital being >90% and >95% occupied on Wednesday through Friday (Figure 4). Detailed hourly analysis (not displayed) showed this risk to be highest from Wednesday afternoon to Friday afternoon. Due to higher emergent census, certain months also had a higher risk of high occupancy at daily peak. For example, while the entire year had 50% to 60% of Wednesdays and Thursdays with occupancy >90%, during the months of November through February, 70% to 85% of those days had occupancy at that level or higher (all these patterns were seen for both stays with LOS 30 days and 7days).
Discussion
In this study, we found that a large children's hospital was frequently at high occupancy in certain months and on certain days more than others, driven largely by predictable seasonal increases in emergent admissions and variability in scheduled admissions by day of week, respectively. Patient‐hours generated by day of admission varied as a result of both volume and LOS, both of which were larger in the early part of the week and diminished as the week progressed for scheduled admissions. But, the cumulative effect of many admissions with relatively‐longer LOS on Monday through Wednesday contributed to high occupancy on Wednesday afternoon to Friday morning, underscoring the importance of admission patterns on census later in the week. Our finding that the occupancy of scheduled patientsthe result of both the admission pattern and their LOSis also highly variable suggests that managing the inflow of scheduled patients could decrease crowding on weekdays, assure a consistent supply of capacity for regular admissions and surges, and improve the value of the delivery system.18 This inflow management would ideally consider both admissions and associated LOS, since rescheduling patients with a longer LOS (eg, 34 days) would have a greater impact on occupancy than rescheduling patients with a shorter LOS (eg, 12 days).
Not surprisingly, total admissions decreased in summer months, especially in July and August, due primarily to fewer emergent admissions. In fact, scheduled admissions per month remained relatively stable over the entire year. The decrease in summer emergent admissions may present an opportunity to stepwise shift a proportion of scheduled admissions from the spring and fall into the summer months, and winter into spring and fall, to alleviate crowding in the winter (Figure 1). Assuming clinical conditions, families and staff members were amenable to this change, hospitals with similar patterns could use this method to reduce the crowding (eg, days over 90% or 95% occupancy) that occurs in the winter.
Using patient‐hours (or days) generated by day of admission, it is evident that admission of more and longer‐stay patients at the start of the week contributes to higher occupancy later in the week (Figure 4). Mid‐week crowding could potentially contribute to a number of operational issues, including delays of new admissions, decreases in physician referrals and patient satisfaction, and an increased use of nontraditional beds (eg, treatment rooms, playrooms, doubling up single rooms) that lead to excessive patient to staff ratios and burnout for clinical staff.
The reasons for these patterns of admissions may include clinician or patient preference to avoid weekend admissions, lack of availability of particular services or resources on weekends, or concerns about safety and efficiency (due to relatively lower staffing on weekends in many hospitals).2230 While clinicians may prefer to avoid additional work on weekends, there are benefits to smoothing occupancy, including less risk of excessive work mid‐week and potential revenue opportunities. In addition, when contrasted with the estimated $1 million to $2 million cost per bed of construction, the marginal cost of staffing to provide safe, high‐quality care on weekends is dramatically lower than that of adding more beds (when faced with mid‐week crowding and unused weekend capacity). In addition, empty beds also do not generate revenue to cover fixed or variable costs, meaning that hospitals are not matching revenue to cost when there is unused capacity due to artificial variability.15, 31 Hospitals looking to make greater use of weekends, however, must be sensitive to staff concerns and the organizational dynamics of 7‐day operations, including the risk for burn‐out and attrition. Such factors should not be perceived as insurmountable barriers, particularly in light of opportunities for flexible scheduling and gain‐sharing.
Patients' and parents' preferences may partially drive admitting patterns, but a reasonable proportion of them may prefer to minimize the number of work and school days missed by being admitted near or on weekends. For example, an expected 3‐day admission could start on Friday and end on Sunday or Monday, rather than the current practice which appears to be to admit on Monday and discharge before the weekend. This may not only meet preferences among some parents to avoid missing work or school, but also by consideration of educational outcomes for hospitalized children.32
In addition, higher mean LOS for emergent patients on the weekends suggests that some services are currently unavailable on weekends to treat patients who are admitted on Fridays through Sundays.2, 25, 29, 33 More even staffing and provision of diagnostic and therapeutic services on weekends (eg, advanced radiology, consult, and laboratory services) would not only remove the barrier to weekend occupancy, it would also improve efficiency, timeliness, patient‐centeredness, and potentially effectiveness and safety for emergent patients. Running hospitals at full functionality on only 5 days of the week means that 2 out of 7 days puts patients at risk for disparate care, which may be appearing in this analysis as prolonged LOS due to lack of services over the weekenda pattern reported in the literature for adult hospitals.
Operations management and queuing theory suggest that systems function well up to 85% to 90% of capacity.34 Hospitals that plan ahead and ensure a buffer for unscheduled admissions during months or days when that demand is known to rise are less likely to cross into high occupancy. On the other hand, hospitals that do not anticipate increases in unscheduled admissions are more likely to encounter excess capacity problems.35 Aligning incentives with all staff can assist in this planning and maximize control of capacity.
Adopting the use of CV in health care operations would also be of value as a way to better express and track variation in admissions, occupancy, and discharges. Since different patient populations, different units, different hospitals, and different months have different scales, SD is not easily comparable across these settings. CV allows for comparison of variation by normalizing on the mean. In this study, it clearly differentiated the variation in elective admissions (CV 65%) over days of the week from the relative stability of emergent admissions (CV 12%). As variability and its management are important to operations, quality control, and quality improvement, use of CV can play an important role in hospital management and health services research. As days with high levels of activity may put more stress on the system, tracking this variation could lead to improvements in quality and value.
This study has several limitations. Data were analyzed for 1 children's hospital, so the analysis may or may not generally apply to other hospitals. However, in a separate study, we analyzed data from the Pediatric Health Information System database, and observed similar patterns.18 In addition, the proportion of elective patients shown in this study was similar to the national data in Kids Inpatient Database (KID, about 15% of all admissions elective).36 Moreover, the methods are reproducible for other settings, which would be useful to clinical and hospital leadership. Second, the trends depicted in the data only reflected data for one year. Third, coding of the admission as emergent or elective was done by registrars at or before arrival and may not reflect actual clinical need. In addition, those admissions coded as elective included a heterogeneous population (eg, chemotherapy to research studies).
Further studies should analyze trends for other hospitals and evaluate the effect of high peak census and high levels of variation with quality, safety, efficiency, patient satisfaction, financial, and educational outcomes for those receiving care, working, or learning at hospitals. In addition, a qualitative study that develops insights into clinician and patient/parent preferences would help answer questions in regard to usage of weekends for scheduled patients.
Conclusions
Scheduled admissions drive most variability in day‐to‐day occupancy despite the fact that they are a smaller proportion of the inpatient population. Variation in scheduled admissions by day of week provides hospitals with an opportunity to address crowding without adding beds or delaying admissions. Rather, fully utilizing capacity by smoothing occupancy over all days of the week can reduce the risk of high occupancy and thereby improve accessibility and patient/parent satisfaction. While family and staff preferences need to be considered, some combination of within‐week smoothing and shifting admissions towards summer are likely to achieve dramatic improvements in patient flow without large expenditures of capital. The key, then, is to ensure that organizational dynamic factors support these changes, so that staff members do not become stressed working at a 7‐day facility. Taken together, these strategies would better match revenue to capacity, and ultimately increase the quality and value of healthcare operations.
Acknowledgements
Authors' contributions: Study concept and design: Fieldston, Ragavan. Analysis and interpretation of data: Ragavan, Fieldston, Jayaraman, Pati. Drafting of the manuscript: Ragavan, Fieldston. Critical Revision of the manuscript for important intellectual content: Fieldston, Ragavan, Pati, Metlay. Statistical analysis: Fieldston, Jayaraman, Ragavan, Allebach. Study supervision: Fieldston, Pati, Metlay.
Additional contributions: The authors the fellows and faculty of the Robert Wood Johnson Foundation Clinical Scholars Program at the University of Pennsylvania and members of its Community Advisory Board for their suggestions to this work. They also wish to thank Tracy Kish, Jennifer Massenburg, and Brian Smith for assistance with access to and interpretation of hospital census and bed capacity data.
- ,,,,,.Relationship between resident workload and self‐perceived learning on inpatient medicine wards: a longitudinal study.BMC Med Educ.2006;6(1):35.
- AHA Solutions, Patient Flow Challenges Assessment 2009. Chicago, IL.2009.
- ,.Patient flow in hospitals: understanding and controlling it better.Front Health Serv Manage.2004;20:3–15.
- . Managing Variability in Patient Flow is the Key to Improving Access to Care, Nursing Staffing, Quality of Care, and Reducing Its Cost. Paper presented at: Institute of Medicine; June 24,2004.
- ,,,,,.Managing unnecessary variability in patient demand to reduce nursing stress and improve patient safety.Jt Comm J Qual Patient Saf.2005;31(6):330–338.
- ,,.Developing models for patient flow and daily surge capacity research.Acad Emerg Med.2006;13(11):1109–1113.
- Institute for Healthcare Improvement, Flow initiatives. 2008. Available at: http://www.ihi.org/IHI/Topics/Flow. Accessed June2010.
- ,,, et al.Hospital workload and adverse events.Med Care.2007;45(5):448–455.
- ,,,,.Impact of admission‐day crowding on the length of stay of pediatric hospitalizations.Pediatrics.2008;121(4):e718–730.
- ,,,,.Emergency department crowding, Part 1: concept, causes, and moral consequences.Ann Emerg Med.2009;53(5):605–611.
- ,.Emergency department overcrowding and ambulance diversion: the impact and potential solutions of extended boarding of admitted patients in the emergency department.J Emerg Med.2006;30(3):351–356.
- ,,,.A comparison of in‐hospital mortality risk conferred by high hospital occupancy, differences in nurse staffing levels, weekend admission, and seasonal influenza.Medical Care.2010;48(3):224–232.
- .,,.The effect of hospital bed occupancy on throughput in the pediatric emergency department.Ann Emerg Med.2009;53(6):767–776.e763.
- .Interpreting the Volume‐Outcome Relationship in the Context of Health Care Quality: Workshop Summary.Washington, DC:National Academies Press;2000.
- ,.Uncertain demand, the structure of hospital costs, and the cost of empty hospital beds.J Health Econ.1995;14(3):291–317.
- ,,, et al.Variability in surgical caseload and access to intensive care services.Anesthesiology.2003;98(6):1491–1496.
- ,,,,.Effects of hospital care environment on patient mortality and nurse outcomes.J Nurs Adm.2009;39(7/8):S45–S51.
- ,,, et al.Children's hospitals do not acutely respond to high occupancy.Pediatrics.2010;125:974–981.
- ,.Easing the strain on a pediatric tertiary care center: use of a redistribution system.Arch Pediatr Adolesc Med.2007;161(9):870–876.
- ,,.Lengths of stay and costs associated with Children's Hospitals.Pediatrics.2005;115:839–844.
- ,.Matching Supply with Demand: An introduction to operations management.New York:McGraw‐Hill;2006.
- .Do hospitals provide lower quality care on weekends?Health Serv Res.2007;42:1589–1612.
- ,.Waiting for urgent procedures on the weekend among emergently hospitalized patients.Am J Med.2004;117:175–181.
- ,.Mortality among patients admitted to hospitals on weekends as compared with weekdays.N Engl J Med.2001;345:663–668.
- ,.Enhanced weekend service: an affordable means to increased hospital procedure volume.CMAJ.2005;172(4):503–504.
- .Hospital deaths and weekend admissions‐how do we leap across a chasm?Clin Nurse Spec.2002;16:91–92.
- ,.Weekend birth and higher neonatal mortality: a problem of patient acuity or quality of care?J Obstet Gynecol Neonatal Nurs.2003;32(6):724–733.
- ,,, et al.Weekend versus weekday admission and mortality from myocardial infarction.N Engl J Med.2007;356:1099–1109.
- .Weekend admission and treatment of patients with renal colic: a case of avoidable variation?Urology.2009;73(4):720–724.
- ,,.Characteristics of weekday and weekend hospital admissions.HCUP Statistical Brief.2010;87. http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb87.pdf.
- ,. Hospital Costs and the Cost of Empty Hospital Beds (NBER Working Paper No. W3872).1991.
- ,,.The effects of timing of pediatric knee ligament surgery on short‐term academic performance in school‐aged athletes.Am J Sports Med.2009;37(9):1684–1691.
- Institute for Healthcare Improvement, Smoothing Elective Surgical Admissions. Available at: http://www.ihi.org/IHI/Topics/Flow/PatientFlow/EmergingContent/SmoothingElectiveSurgicalAdmissions.htm. Accessed June2010.
- . Institute for Healthcare Improvement, Patient Flow Comments. Available at: http://www.ihi.org/IHI/Topics/Flow. Accessed June2010.
- .OPIM 631: Operations Management.Wharton School, University of Pennsylvania.Philadelphia, PA.2008.
- Agency for Healthcare Research and Quality. HCUP Databases, Healthcare Cost and Utilization Project (HCUP). 2008. Available at: www.hcup‐us.ahrq.gov/kidoverview.jsp. Accessed June2010.
Patient flow in a hospital refers to the management and movement of patients through the facility. Optimizing patient flow is considered of great importance to improvement of quality (including safety, efficiency, timeliness, equity, effectiveness, and patient‐centeredness), as well as finance, staff satisfaction, education and overall healthcare value.18 Central to concerns about patient flow at hospitals is occupancy, which is the census (number of patients at a point in time) divided by the bed capacity. Occupancy that is too high is associated with challenges to quality and access,913 while occupancy that is too low may underutilize resources and be costly.14, 15 Occupancy is determined by the pattern of admission and discharge, thus including length of stay (LOS) as a factor. While all related, admissions, census, occupancy, and LOS convey different aspects of hospital operations and may point to different opportunities to improve patient flow.
Variability in patient flow over time has been noted as a common occurrence in adult hospitals, due to uneven patterns of scheduled (elective) admissions, as well as uncontrollable variability of emergent admissions.2, 45, 16 Typically very few patients are scheduled to enter hospitals over weekends. In addition, when the admission is expected to be 5 days or less, clinical and operational staff may schedule those admissions early in the week to avoid patients staying the weekend. This artificial variability has been shown to lead to uneven levels of occupancy, with crowding on some days of the week more than others.2, 45, 16 As hospital crowding adversely affects access to emergent and elective care, quality and safety of care, and patient and staff satisfaction, many groups are focusing attention on patient flow and strategies to avoid high occupancy.19, 17 This is true for children's hospitals, as well, particularly as these scarce resources have ever increasing demand placed on them.1820
Patient flow improvements can be made by increasing efficiency of throughput, primarily measured by decreased LOS, or by addressing artificial variability in how hospital beds are used. As children's hospitals have short LOSs and are relatively efficient (as measured by standardized LOS ratios), we sought to evaluate how much artificial variability was active at 1 large children's hospital. We did this to both evaluate flow at 1 institution and to create methodology for other hospitals to use in order to better understand and improve their flow.
Our specific aims were to describe daily and monthly variability in admission, discharge, LOS, and occupancy patterns at a large children's hospital and assess the relationship between scheduled admissions and occupancy.
Methods
This retrospective administrative data analysis was performed with admission‐discharge‐transfer (ADT) data for inpatient admissions from one urban, tertiary‐care children's hospital for the period July 1, 2007 to June 30, 2008. The dataset included the date and time of all arrivals and departures from all inpatient units (including observation‐status patients), as entered by the unit clerks into the electronic ADT system. The dataset also included categorization of the admission as emergent, urgent, or elective (hereafter referred to as scheduled.) Registration staff entered these codes at or prior to admission. Using the timestamps, LOS was calculated by subtracting admission date and time from discharge date and time. An SAS macro was applied to the timestamps to calculate a hospital census for every hour of each calendar day. Peak census figures were extracted for each day. Occupancy was calculated as census over number of beds in use (monthly average). Data for the hospital's peak daily census and occupancy were utilized to analyze patterns of occupancy by day of week and month of year. To express variability, coefficient of variation (CV) (standard deviation [SD] divided by its mean) was used, as it is helpful when samples sizes are different.21
Analysis of number of admissions per day of week and month by type was performed with descriptive statistics and t‐tests for significant differences across seasons. We calculated a measure of patient hours generated by day of admission based on the LOS generated by each admission, in which the average number of admissions for each day of the week was multiplied by the average LOS (in hours) for those admissions. In order to remove outliers and focus on patients whose occupancy would affect weekly variation, we analyzed in detail the admissions with LOS 30 days and 7 days, respectively.
Statistical analyses were performed with SAS 9.2 (SAS Institute, Cary, NC), Stata 10.0 (StataCorp, College Station, TX) and Microsoft Excel (Microsoft, Redmond, WA). The study was approved by the Human Subjects Committee of the hospital's Institutional Review Board.
Results
A total of 22,310 patients were admitted over the period July 1, 2007 to June 30, 2008, including 4957 (22%) coded as scheduled and 17,353 (78%) coded as emergent. (Only 200 patients were registered as urgent and these were recoded as emergent for this analysis). Details on admission types and discharging departments are provided in Table 1. Overall, mean LOS was 5.6 days (median 2.29 days). For patients with LOS 30 days, mean LOS was 3.88 days (median 2.22 days). For patients staying 7 days, mean LOS was 2.4 days (median 1.98 days). Among patients with LOS 7 days, mean LOS for scheduled patients was longer for those admitted on Monday than on any other weekday (2.49 vs. 2.08 days, P < 0.0001). In contrast, mean LOS for emergent patients was longer for patients admitted on Friday and Saturday than the rest of the week (2.57 vs. 2.44 days, P < 0.0001).
| All | Scheduled | Emergent | |
|---|---|---|---|
| |||
| Total Admissions, n (%)* | 22,310 | 4957 (22) | 17,353 (78) |
| Median LOS (days) | 2.29 | 1.93 | 2.50 |
| Mean LOS (days) (95% CI) | 5.60 (5.41, 5.79) | 4.20 (3.95, 4.45) | 5.78 (5.596.0) |
| % Patients with LOS 30 days (%) | 97 | 98 | 96 |
| % Patients with LOS 7 days (%) | 84 | 89 | 83 |
| Medical patients at discharge, n (%) | 16,586 (74) | 2363 (48) | 14,403 (83) |
| Surgical patients at discharge, n (%) | 4276 (19) | 2450 (49) | 1826 (10.5) |
| Critical care patients at discharge (NICU, PICU, CICU), n (%) | 1433 (6) | 140 (3) | 1293 (7.5) |
Total admissions per month (Figure 1) averaged 1937 in October through April and 1751 in May through September (P = 0.03). Variation in the number of emergent and scheduled patients over months of the year were similar (CV 10% for each), but emergent admissions did decrease in summer (mean 1299 for June‐September vs. 1520 for the rest of the year, P = 0.003). Conversely, scheduled admissions remained relatively stable all year‐long: mean 423 per month for May through September vs. mean 413 per month for October through April (P = 0.48). Even just the summer months of June‐August, when school‐age children are on vacation, were not significantly different from other months (440 vs. 404, P = 0.2).
Variation in volume of admissions was large over days of the week, driven primarily by the pattern of scheduled admissions (CV 65.3%), which dropped off completely on weekends (Table 2, Figure 2). In contrast, there was much less variation in the number of emergent admissions across days of the week (CV 12%). For both emergent and scheduled admissions, more patients came in on Mondays than any other day of the week, but even more so for scheduled patients. While emergent admissions did decline on weekends, it was driven primarily by a decrease in physician referrals (ie, direct admission) from clinics (mean 7.48 per weekday vs. 0.73 per weekend day for the entire year, P < 0.001), while emergency department (ED) admissions remained relatively stable (mean 35.8 per weekday vs. 32.7 per weekend day, P = 0.08). Emergency transports were also stable (mean 7.15 per weekday vs. 6.49 per weekend day, P = 0.10).
| All (%) | Scheduled (%) | Emergent (%) | |
|---|---|---|---|
| |||
| CV on admissions by month | 8 | 10 | 10 |
| CV on admissions over days of week (including weekends) | 24 | 65 | 12 |
| CV on admissions over days of week (excluding weekends) | 6 | 10 | 5 |
| CV on monthly occupancy over 12 months | 4 | 14 | 2 |
Although scheduled patients contributed less to the hospital's overall occupancy, they conferred most of the variability by day of week. Over the days of the week, variation for scheduled occupancy was nearly twice that for emergent occupancy (CV 19% vs. 10%). Within the higher‐volume period of October to April, the differential was even more evident (CV 19% for scheduled occupancy versus 6% for emergent).
For scheduled patients with LOS 30 days (98% of scheduled patients), Mondays and Tuesdays together accounted for 42.5% of admission volume and 44.7% of the patient‐hours generated. For scheduled patients with LOS 7 days (89% of scheduled patients), Mondays and Tuesdays together accounted for 42% of admission volume and 45.2% of the patient‐hours generated. This combined impact of volume and LOS from admissions earlier in the week (restricted to patients with LOS 7days) is displayed graphically in Figure 3, which depicts the unevenness of scheduled admissions and their time in the hospital, with many patients overlapping in the middle of the week. Together with the more steady flow of emergent patients, this variability in scheduled occupancy contributed to mid‐week crowding, with higher risk of the hospital being >90% and >95% occupied on Wednesday through Friday (Figure 4). Detailed hourly analysis (not displayed) showed this risk to be highest from Wednesday afternoon to Friday afternoon. Due to higher emergent census, certain months also had a higher risk of high occupancy at daily peak. For example, while the entire year had 50% to 60% of Wednesdays and Thursdays with occupancy >90%, during the months of November through February, 70% to 85% of those days had occupancy at that level or higher (all these patterns were seen for both stays with LOS 30 days and 7days).
Discussion
In this study, we found that a large children's hospital was frequently at high occupancy in certain months and on certain days more than others, driven largely by predictable seasonal increases in emergent admissions and variability in scheduled admissions by day of week, respectively. Patient‐hours generated by day of admission varied as a result of both volume and LOS, both of which were larger in the early part of the week and diminished as the week progressed for scheduled admissions. But, the cumulative effect of many admissions with relatively‐longer LOS on Monday through Wednesday contributed to high occupancy on Wednesday afternoon to Friday morning, underscoring the importance of admission patterns on census later in the week. Our finding that the occupancy of scheduled patientsthe result of both the admission pattern and their LOSis also highly variable suggests that managing the inflow of scheduled patients could decrease crowding on weekdays, assure a consistent supply of capacity for regular admissions and surges, and improve the value of the delivery system.18 This inflow management would ideally consider both admissions and associated LOS, since rescheduling patients with a longer LOS (eg, 34 days) would have a greater impact on occupancy than rescheduling patients with a shorter LOS (eg, 12 days).
Not surprisingly, total admissions decreased in summer months, especially in July and August, due primarily to fewer emergent admissions. In fact, scheduled admissions per month remained relatively stable over the entire year. The decrease in summer emergent admissions may present an opportunity to stepwise shift a proportion of scheduled admissions from the spring and fall into the summer months, and winter into spring and fall, to alleviate crowding in the winter (Figure 1). Assuming clinical conditions, families and staff members were amenable to this change, hospitals with similar patterns could use this method to reduce the crowding (eg, days over 90% or 95% occupancy) that occurs in the winter.
Using patient‐hours (or days) generated by day of admission, it is evident that admission of more and longer‐stay patients at the start of the week contributes to higher occupancy later in the week (Figure 4). Mid‐week crowding could potentially contribute to a number of operational issues, including delays of new admissions, decreases in physician referrals and patient satisfaction, and an increased use of nontraditional beds (eg, treatment rooms, playrooms, doubling up single rooms) that lead to excessive patient to staff ratios and burnout for clinical staff.
The reasons for these patterns of admissions may include clinician or patient preference to avoid weekend admissions, lack of availability of particular services or resources on weekends, or concerns about safety and efficiency (due to relatively lower staffing on weekends in many hospitals).2230 While clinicians may prefer to avoid additional work on weekends, there are benefits to smoothing occupancy, including less risk of excessive work mid‐week and potential revenue opportunities. In addition, when contrasted with the estimated $1 million to $2 million cost per bed of construction, the marginal cost of staffing to provide safe, high‐quality care on weekends is dramatically lower than that of adding more beds (when faced with mid‐week crowding and unused weekend capacity). In addition, empty beds also do not generate revenue to cover fixed or variable costs, meaning that hospitals are not matching revenue to cost when there is unused capacity due to artificial variability.15, 31 Hospitals looking to make greater use of weekends, however, must be sensitive to staff concerns and the organizational dynamics of 7‐day operations, including the risk for burn‐out and attrition. Such factors should not be perceived as insurmountable barriers, particularly in light of opportunities for flexible scheduling and gain‐sharing.
Patients' and parents' preferences may partially drive admitting patterns, but a reasonable proportion of them may prefer to minimize the number of work and school days missed by being admitted near or on weekends. For example, an expected 3‐day admission could start on Friday and end on Sunday or Monday, rather than the current practice which appears to be to admit on Monday and discharge before the weekend. This may not only meet preferences among some parents to avoid missing work or school, but also by consideration of educational outcomes for hospitalized children.32
In addition, higher mean LOS for emergent patients on the weekends suggests that some services are currently unavailable on weekends to treat patients who are admitted on Fridays through Sundays.2, 25, 29, 33 More even staffing and provision of diagnostic and therapeutic services on weekends (eg, advanced radiology, consult, and laboratory services) would not only remove the barrier to weekend occupancy, it would also improve efficiency, timeliness, patient‐centeredness, and potentially effectiveness and safety for emergent patients. Running hospitals at full functionality on only 5 days of the week means that 2 out of 7 days puts patients at risk for disparate care, which may be appearing in this analysis as prolonged LOS due to lack of services over the weekenda pattern reported in the literature for adult hospitals.
Operations management and queuing theory suggest that systems function well up to 85% to 90% of capacity.34 Hospitals that plan ahead and ensure a buffer for unscheduled admissions during months or days when that demand is known to rise are less likely to cross into high occupancy. On the other hand, hospitals that do not anticipate increases in unscheduled admissions are more likely to encounter excess capacity problems.35 Aligning incentives with all staff can assist in this planning and maximize control of capacity.
Adopting the use of CV in health care operations would also be of value as a way to better express and track variation in admissions, occupancy, and discharges. Since different patient populations, different units, different hospitals, and different months have different scales, SD is not easily comparable across these settings. CV allows for comparison of variation by normalizing on the mean. In this study, it clearly differentiated the variation in elective admissions (CV 65%) over days of the week from the relative stability of emergent admissions (CV 12%). As variability and its management are important to operations, quality control, and quality improvement, use of CV can play an important role in hospital management and health services research. As days with high levels of activity may put more stress on the system, tracking this variation could lead to improvements in quality and value.
This study has several limitations. Data were analyzed for 1 children's hospital, so the analysis may or may not generally apply to other hospitals. However, in a separate study, we analyzed data from the Pediatric Health Information System database, and observed similar patterns.18 In addition, the proportion of elective patients shown in this study was similar to the national data in Kids Inpatient Database (KID, about 15% of all admissions elective).36 Moreover, the methods are reproducible for other settings, which would be useful to clinical and hospital leadership. Second, the trends depicted in the data only reflected data for one year. Third, coding of the admission as emergent or elective was done by registrars at or before arrival and may not reflect actual clinical need. In addition, those admissions coded as elective included a heterogeneous population (eg, chemotherapy to research studies).
Further studies should analyze trends for other hospitals and evaluate the effect of high peak census and high levels of variation with quality, safety, efficiency, patient satisfaction, financial, and educational outcomes for those receiving care, working, or learning at hospitals. In addition, a qualitative study that develops insights into clinician and patient/parent preferences would help answer questions in regard to usage of weekends for scheduled patients.
Conclusions
Scheduled admissions drive most variability in day‐to‐day occupancy despite the fact that they are a smaller proportion of the inpatient population. Variation in scheduled admissions by day of week provides hospitals with an opportunity to address crowding without adding beds or delaying admissions. Rather, fully utilizing capacity by smoothing occupancy over all days of the week can reduce the risk of high occupancy and thereby improve accessibility and patient/parent satisfaction. While family and staff preferences need to be considered, some combination of within‐week smoothing and shifting admissions towards summer are likely to achieve dramatic improvements in patient flow without large expenditures of capital. The key, then, is to ensure that organizational dynamic factors support these changes, so that staff members do not become stressed working at a 7‐day facility. Taken together, these strategies would better match revenue to capacity, and ultimately increase the quality and value of healthcare operations.
Acknowledgements
Authors' contributions: Study concept and design: Fieldston, Ragavan. Analysis and interpretation of data: Ragavan, Fieldston, Jayaraman, Pati. Drafting of the manuscript: Ragavan, Fieldston. Critical Revision of the manuscript for important intellectual content: Fieldston, Ragavan, Pati, Metlay. Statistical analysis: Fieldston, Jayaraman, Ragavan, Allebach. Study supervision: Fieldston, Pati, Metlay.
Additional contributions: The authors the fellows and faculty of the Robert Wood Johnson Foundation Clinical Scholars Program at the University of Pennsylvania and members of its Community Advisory Board for their suggestions to this work. They also wish to thank Tracy Kish, Jennifer Massenburg, and Brian Smith for assistance with access to and interpretation of hospital census and bed capacity data.
Patient flow in a hospital refers to the management and movement of patients through the facility. Optimizing patient flow is considered of great importance to improvement of quality (including safety, efficiency, timeliness, equity, effectiveness, and patient‐centeredness), as well as finance, staff satisfaction, education and overall healthcare value.18 Central to concerns about patient flow at hospitals is occupancy, which is the census (number of patients at a point in time) divided by the bed capacity. Occupancy that is too high is associated with challenges to quality and access,913 while occupancy that is too low may underutilize resources and be costly.14, 15 Occupancy is determined by the pattern of admission and discharge, thus including length of stay (LOS) as a factor. While all related, admissions, census, occupancy, and LOS convey different aspects of hospital operations and may point to different opportunities to improve patient flow.
Variability in patient flow over time has been noted as a common occurrence in adult hospitals, due to uneven patterns of scheduled (elective) admissions, as well as uncontrollable variability of emergent admissions.2, 45, 16 Typically very few patients are scheduled to enter hospitals over weekends. In addition, when the admission is expected to be 5 days or less, clinical and operational staff may schedule those admissions early in the week to avoid patients staying the weekend. This artificial variability has been shown to lead to uneven levels of occupancy, with crowding on some days of the week more than others.2, 45, 16 As hospital crowding adversely affects access to emergent and elective care, quality and safety of care, and patient and staff satisfaction, many groups are focusing attention on patient flow and strategies to avoid high occupancy.19, 17 This is true for children's hospitals, as well, particularly as these scarce resources have ever increasing demand placed on them.1820
Patient flow improvements can be made by increasing efficiency of throughput, primarily measured by decreased LOS, or by addressing artificial variability in how hospital beds are used. As children's hospitals have short LOSs and are relatively efficient (as measured by standardized LOS ratios), we sought to evaluate how much artificial variability was active at 1 large children's hospital. We did this to both evaluate flow at 1 institution and to create methodology for other hospitals to use in order to better understand and improve their flow.
Our specific aims were to describe daily and monthly variability in admission, discharge, LOS, and occupancy patterns at a large children's hospital and assess the relationship between scheduled admissions and occupancy.
Methods
This retrospective administrative data analysis was performed with admission‐discharge‐transfer (ADT) data for inpatient admissions from one urban, tertiary‐care children's hospital for the period July 1, 2007 to June 30, 2008. The dataset included the date and time of all arrivals and departures from all inpatient units (including observation‐status patients), as entered by the unit clerks into the electronic ADT system. The dataset also included categorization of the admission as emergent, urgent, or elective (hereafter referred to as scheduled.) Registration staff entered these codes at or prior to admission. Using the timestamps, LOS was calculated by subtracting admission date and time from discharge date and time. An SAS macro was applied to the timestamps to calculate a hospital census for every hour of each calendar day. Peak census figures were extracted for each day. Occupancy was calculated as census over number of beds in use (monthly average). Data for the hospital's peak daily census and occupancy were utilized to analyze patterns of occupancy by day of week and month of year. To express variability, coefficient of variation (CV) (standard deviation [SD] divided by its mean) was used, as it is helpful when samples sizes are different.21
Analysis of number of admissions per day of week and month by type was performed with descriptive statistics and t‐tests for significant differences across seasons. We calculated a measure of patient hours generated by day of admission based on the LOS generated by each admission, in which the average number of admissions for each day of the week was multiplied by the average LOS (in hours) for those admissions. In order to remove outliers and focus on patients whose occupancy would affect weekly variation, we analyzed in detail the admissions with LOS 30 days and 7 days, respectively.
Statistical analyses were performed with SAS 9.2 (SAS Institute, Cary, NC), Stata 10.0 (StataCorp, College Station, TX) and Microsoft Excel (Microsoft, Redmond, WA). The study was approved by the Human Subjects Committee of the hospital's Institutional Review Board.
Results
A total of 22,310 patients were admitted over the period July 1, 2007 to June 30, 2008, including 4957 (22%) coded as scheduled and 17,353 (78%) coded as emergent. (Only 200 patients were registered as urgent and these were recoded as emergent for this analysis). Details on admission types and discharging departments are provided in Table 1. Overall, mean LOS was 5.6 days (median 2.29 days). For patients with LOS 30 days, mean LOS was 3.88 days (median 2.22 days). For patients staying 7 days, mean LOS was 2.4 days (median 1.98 days). Among patients with LOS 7 days, mean LOS for scheduled patients was longer for those admitted on Monday than on any other weekday (2.49 vs. 2.08 days, P < 0.0001). In contrast, mean LOS for emergent patients was longer for patients admitted on Friday and Saturday than the rest of the week (2.57 vs. 2.44 days, P < 0.0001).
| All | Scheduled | Emergent | |
|---|---|---|---|
| |||
| Total Admissions, n (%)* | 22,310 | 4957 (22) | 17,353 (78) |
| Median LOS (days) | 2.29 | 1.93 | 2.50 |
| Mean LOS (days) (95% CI) | 5.60 (5.41, 5.79) | 4.20 (3.95, 4.45) | 5.78 (5.596.0) |
| % Patients with LOS 30 days (%) | 97 | 98 | 96 |
| % Patients with LOS 7 days (%) | 84 | 89 | 83 |
| Medical patients at discharge, n (%) | 16,586 (74) | 2363 (48) | 14,403 (83) |
| Surgical patients at discharge, n (%) | 4276 (19) | 2450 (49) | 1826 (10.5) |
| Critical care patients at discharge (NICU, PICU, CICU), n (%) | 1433 (6) | 140 (3) | 1293 (7.5) |
Total admissions per month (Figure 1) averaged 1937 in October through April and 1751 in May through September (P = 0.03). Variation in the number of emergent and scheduled patients over months of the year were similar (CV 10% for each), but emergent admissions did decrease in summer (mean 1299 for June‐September vs. 1520 for the rest of the year, P = 0.003). Conversely, scheduled admissions remained relatively stable all year‐long: mean 423 per month for May through September vs. mean 413 per month for October through April (P = 0.48). Even just the summer months of June‐August, when school‐age children are on vacation, were not significantly different from other months (440 vs. 404, P = 0.2).
Variation in volume of admissions was large over days of the week, driven primarily by the pattern of scheduled admissions (CV 65.3%), which dropped off completely on weekends (Table 2, Figure 2). In contrast, there was much less variation in the number of emergent admissions across days of the week (CV 12%). For both emergent and scheduled admissions, more patients came in on Mondays than any other day of the week, but even more so for scheduled patients. While emergent admissions did decline on weekends, it was driven primarily by a decrease in physician referrals (ie, direct admission) from clinics (mean 7.48 per weekday vs. 0.73 per weekend day for the entire year, P < 0.001), while emergency department (ED) admissions remained relatively stable (mean 35.8 per weekday vs. 32.7 per weekend day, P = 0.08). Emergency transports were also stable (mean 7.15 per weekday vs. 6.49 per weekend day, P = 0.10).
| All (%) | Scheduled (%) | Emergent (%) | |
|---|---|---|---|
| |||
| CV on admissions by month | 8 | 10 | 10 |
| CV on admissions over days of week (including weekends) | 24 | 65 | 12 |
| CV on admissions over days of week (excluding weekends) | 6 | 10 | 5 |
| CV on monthly occupancy over 12 months | 4 | 14 | 2 |
Although scheduled patients contributed less to the hospital's overall occupancy, they conferred most of the variability by day of week. Over the days of the week, variation for scheduled occupancy was nearly twice that for emergent occupancy (CV 19% vs. 10%). Within the higher‐volume period of October to April, the differential was even more evident (CV 19% for scheduled occupancy versus 6% for emergent).
For scheduled patients with LOS 30 days (98% of scheduled patients), Mondays and Tuesdays together accounted for 42.5% of admission volume and 44.7% of the patient‐hours generated. For scheduled patients with LOS 7 days (89% of scheduled patients), Mondays and Tuesdays together accounted for 42% of admission volume and 45.2% of the patient‐hours generated. This combined impact of volume and LOS from admissions earlier in the week (restricted to patients with LOS 7days) is displayed graphically in Figure 3, which depicts the unevenness of scheduled admissions and their time in the hospital, with many patients overlapping in the middle of the week. Together with the more steady flow of emergent patients, this variability in scheduled occupancy contributed to mid‐week crowding, with higher risk of the hospital being >90% and >95% occupied on Wednesday through Friday (Figure 4). Detailed hourly analysis (not displayed) showed this risk to be highest from Wednesday afternoon to Friday afternoon. Due to higher emergent census, certain months also had a higher risk of high occupancy at daily peak. For example, while the entire year had 50% to 60% of Wednesdays and Thursdays with occupancy >90%, during the months of November through February, 70% to 85% of those days had occupancy at that level or higher (all these patterns were seen for both stays with LOS 30 days and 7days).
Discussion
In this study, we found that a large children's hospital was frequently at high occupancy in certain months and on certain days more than others, driven largely by predictable seasonal increases in emergent admissions and variability in scheduled admissions by day of week, respectively. Patient‐hours generated by day of admission varied as a result of both volume and LOS, both of which were larger in the early part of the week and diminished as the week progressed for scheduled admissions. But, the cumulative effect of many admissions with relatively‐longer LOS on Monday through Wednesday contributed to high occupancy on Wednesday afternoon to Friday morning, underscoring the importance of admission patterns on census later in the week. Our finding that the occupancy of scheduled patientsthe result of both the admission pattern and their LOSis also highly variable suggests that managing the inflow of scheduled patients could decrease crowding on weekdays, assure a consistent supply of capacity for regular admissions and surges, and improve the value of the delivery system.18 This inflow management would ideally consider both admissions and associated LOS, since rescheduling patients with a longer LOS (eg, 34 days) would have a greater impact on occupancy than rescheduling patients with a shorter LOS (eg, 12 days).
Not surprisingly, total admissions decreased in summer months, especially in July and August, due primarily to fewer emergent admissions. In fact, scheduled admissions per month remained relatively stable over the entire year. The decrease in summer emergent admissions may present an opportunity to stepwise shift a proportion of scheduled admissions from the spring and fall into the summer months, and winter into spring and fall, to alleviate crowding in the winter (Figure 1). Assuming clinical conditions, families and staff members were amenable to this change, hospitals with similar patterns could use this method to reduce the crowding (eg, days over 90% or 95% occupancy) that occurs in the winter.
Using patient‐hours (or days) generated by day of admission, it is evident that admission of more and longer‐stay patients at the start of the week contributes to higher occupancy later in the week (Figure 4). Mid‐week crowding could potentially contribute to a number of operational issues, including delays of new admissions, decreases in physician referrals and patient satisfaction, and an increased use of nontraditional beds (eg, treatment rooms, playrooms, doubling up single rooms) that lead to excessive patient to staff ratios and burnout for clinical staff.
The reasons for these patterns of admissions may include clinician or patient preference to avoid weekend admissions, lack of availability of particular services or resources on weekends, or concerns about safety and efficiency (due to relatively lower staffing on weekends in many hospitals).2230 While clinicians may prefer to avoid additional work on weekends, there are benefits to smoothing occupancy, including less risk of excessive work mid‐week and potential revenue opportunities. In addition, when contrasted with the estimated $1 million to $2 million cost per bed of construction, the marginal cost of staffing to provide safe, high‐quality care on weekends is dramatically lower than that of adding more beds (when faced with mid‐week crowding and unused weekend capacity). In addition, empty beds also do not generate revenue to cover fixed or variable costs, meaning that hospitals are not matching revenue to cost when there is unused capacity due to artificial variability.15, 31 Hospitals looking to make greater use of weekends, however, must be sensitive to staff concerns and the organizational dynamics of 7‐day operations, including the risk for burn‐out and attrition. Such factors should not be perceived as insurmountable barriers, particularly in light of opportunities for flexible scheduling and gain‐sharing.
Patients' and parents' preferences may partially drive admitting patterns, but a reasonable proportion of them may prefer to minimize the number of work and school days missed by being admitted near or on weekends. For example, an expected 3‐day admission could start on Friday and end on Sunday or Monday, rather than the current practice which appears to be to admit on Monday and discharge before the weekend. This may not only meet preferences among some parents to avoid missing work or school, but also by consideration of educational outcomes for hospitalized children.32
In addition, higher mean LOS for emergent patients on the weekends suggests that some services are currently unavailable on weekends to treat patients who are admitted on Fridays through Sundays.2, 25, 29, 33 More even staffing and provision of diagnostic and therapeutic services on weekends (eg, advanced radiology, consult, and laboratory services) would not only remove the barrier to weekend occupancy, it would also improve efficiency, timeliness, patient‐centeredness, and potentially effectiveness and safety for emergent patients. Running hospitals at full functionality on only 5 days of the week means that 2 out of 7 days puts patients at risk for disparate care, which may be appearing in this analysis as prolonged LOS due to lack of services over the weekenda pattern reported in the literature for adult hospitals.
Operations management and queuing theory suggest that systems function well up to 85% to 90% of capacity.34 Hospitals that plan ahead and ensure a buffer for unscheduled admissions during months or days when that demand is known to rise are less likely to cross into high occupancy. On the other hand, hospitals that do not anticipate increases in unscheduled admissions are more likely to encounter excess capacity problems.35 Aligning incentives with all staff can assist in this planning and maximize control of capacity.
Adopting the use of CV in health care operations would also be of value as a way to better express and track variation in admissions, occupancy, and discharges. Since different patient populations, different units, different hospitals, and different months have different scales, SD is not easily comparable across these settings. CV allows for comparison of variation by normalizing on the mean. In this study, it clearly differentiated the variation in elective admissions (CV 65%) over days of the week from the relative stability of emergent admissions (CV 12%). As variability and its management are important to operations, quality control, and quality improvement, use of CV can play an important role in hospital management and health services research. As days with high levels of activity may put more stress on the system, tracking this variation could lead to improvements in quality and value.
This study has several limitations. Data were analyzed for 1 children's hospital, so the analysis may or may not generally apply to other hospitals. However, in a separate study, we analyzed data from the Pediatric Health Information System database, and observed similar patterns.18 In addition, the proportion of elective patients shown in this study was similar to the national data in Kids Inpatient Database (KID, about 15% of all admissions elective).36 Moreover, the methods are reproducible for other settings, which would be useful to clinical and hospital leadership. Second, the trends depicted in the data only reflected data for one year. Third, coding of the admission as emergent or elective was done by registrars at or before arrival and may not reflect actual clinical need. In addition, those admissions coded as elective included a heterogeneous population (eg, chemotherapy to research studies).
Further studies should analyze trends for other hospitals and evaluate the effect of high peak census and high levels of variation with quality, safety, efficiency, patient satisfaction, financial, and educational outcomes for those receiving care, working, or learning at hospitals. In addition, a qualitative study that develops insights into clinician and patient/parent preferences would help answer questions in regard to usage of weekends for scheduled patients.
Conclusions
Scheduled admissions drive most variability in day‐to‐day occupancy despite the fact that they are a smaller proportion of the inpatient population. Variation in scheduled admissions by day of week provides hospitals with an opportunity to address crowding without adding beds or delaying admissions. Rather, fully utilizing capacity by smoothing occupancy over all days of the week can reduce the risk of high occupancy and thereby improve accessibility and patient/parent satisfaction. While family and staff preferences need to be considered, some combination of within‐week smoothing and shifting admissions towards summer are likely to achieve dramatic improvements in patient flow without large expenditures of capital. The key, then, is to ensure that organizational dynamic factors support these changes, so that staff members do not become stressed working at a 7‐day facility. Taken together, these strategies would better match revenue to capacity, and ultimately increase the quality and value of healthcare operations.
Acknowledgements
Authors' contributions: Study concept and design: Fieldston, Ragavan. Analysis and interpretation of data: Ragavan, Fieldston, Jayaraman, Pati. Drafting of the manuscript: Ragavan, Fieldston. Critical Revision of the manuscript for important intellectual content: Fieldston, Ragavan, Pati, Metlay. Statistical analysis: Fieldston, Jayaraman, Ragavan, Allebach. Study supervision: Fieldston, Pati, Metlay.
Additional contributions: The authors the fellows and faculty of the Robert Wood Johnson Foundation Clinical Scholars Program at the University of Pennsylvania and members of its Community Advisory Board for their suggestions to this work. They also wish to thank Tracy Kish, Jennifer Massenburg, and Brian Smith for assistance with access to and interpretation of hospital census and bed capacity data.
- ,,,,,.Relationship between resident workload and self‐perceived learning on inpatient medicine wards: a longitudinal study.BMC Med Educ.2006;6(1):35.
- AHA Solutions, Patient Flow Challenges Assessment 2009. Chicago, IL.2009.
- ,.Patient flow in hospitals: understanding and controlling it better.Front Health Serv Manage.2004;20:3–15.
- . Managing Variability in Patient Flow is the Key to Improving Access to Care, Nursing Staffing, Quality of Care, and Reducing Its Cost. Paper presented at: Institute of Medicine; June 24,2004.
- ,,,,,.Managing unnecessary variability in patient demand to reduce nursing stress and improve patient safety.Jt Comm J Qual Patient Saf.2005;31(6):330–338.
- ,,.Developing models for patient flow and daily surge capacity research.Acad Emerg Med.2006;13(11):1109–1113.
- Institute for Healthcare Improvement, Flow initiatives. 2008. Available at: http://www.ihi.org/IHI/Topics/Flow. Accessed June2010.
- ,,, et al.Hospital workload and adverse events.Med Care.2007;45(5):448–455.
- ,,,,.Impact of admission‐day crowding on the length of stay of pediatric hospitalizations.Pediatrics.2008;121(4):e718–730.
- ,,,,.Emergency department crowding, Part 1: concept, causes, and moral consequences.Ann Emerg Med.2009;53(5):605–611.
- ,.Emergency department overcrowding and ambulance diversion: the impact and potential solutions of extended boarding of admitted patients in the emergency department.J Emerg Med.2006;30(3):351–356.
- ,,,.A comparison of in‐hospital mortality risk conferred by high hospital occupancy, differences in nurse staffing levels, weekend admission, and seasonal influenza.Medical Care.2010;48(3):224–232.
- .,,.The effect of hospital bed occupancy on throughput in the pediatric emergency department.Ann Emerg Med.2009;53(6):767–776.e763.
- .Interpreting the Volume‐Outcome Relationship in the Context of Health Care Quality: Workshop Summary.Washington, DC:National Academies Press;2000.
- ,.Uncertain demand, the structure of hospital costs, and the cost of empty hospital beds.J Health Econ.1995;14(3):291–317.
- ,,, et al.Variability in surgical caseload and access to intensive care services.Anesthesiology.2003;98(6):1491–1496.
- ,,,,.Effects of hospital care environment on patient mortality and nurse outcomes.J Nurs Adm.2009;39(7/8):S45–S51.
- ,,, et al.Children's hospitals do not acutely respond to high occupancy.Pediatrics.2010;125:974–981.
- ,.Easing the strain on a pediatric tertiary care center: use of a redistribution system.Arch Pediatr Adolesc Med.2007;161(9):870–876.
- ,,.Lengths of stay and costs associated with Children's Hospitals.Pediatrics.2005;115:839–844.
- ,.Matching Supply with Demand: An introduction to operations management.New York:McGraw‐Hill;2006.
- .Do hospitals provide lower quality care on weekends?Health Serv Res.2007;42:1589–1612.
- ,.Waiting for urgent procedures on the weekend among emergently hospitalized patients.Am J Med.2004;117:175–181.
- ,.Mortality among patients admitted to hospitals on weekends as compared with weekdays.N Engl J Med.2001;345:663–668.
- ,.Enhanced weekend service: an affordable means to increased hospital procedure volume.CMAJ.2005;172(4):503–504.
- .Hospital deaths and weekend admissions‐how do we leap across a chasm?Clin Nurse Spec.2002;16:91–92.
- ,.Weekend birth and higher neonatal mortality: a problem of patient acuity or quality of care?J Obstet Gynecol Neonatal Nurs.2003;32(6):724–733.
- ,,, et al.Weekend versus weekday admission and mortality from myocardial infarction.N Engl J Med.2007;356:1099–1109.
- .Weekend admission and treatment of patients with renal colic: a case of avoidable variation?Urology.2009;73(4):720–724.
- ,,.Characteristics of weekday and weekend hospital admissions.HCUP Statistical Brief.2010;87. http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb87.pdf.
- ,. Hospital Costs and the Cost of Empty Hospital Beds (NBER Working Paper No. W3872).1991.
- ,,.The effects of timing of pediatric knee ligament surgery on short‐term academic performance in school‐aged athletes.Am J Sports Med.2009;37(9):1684–1691.
- Institute for Healthcare Improvement, Smoothing Elective Surgical Admissions. Available at: http://www.ihi.org/IHI/Topics/Flow/PatientFlow/EmergingContent/SmoothingElectiveSurgicalAdmissions.htm. Accessed June2010.
- . Institute for Healthcare Improvement, Patient Flow Comments. Available at: http://www.ihi.org/IHI/Topics/Flow. Accessed June2010.
- .OPIM 631: Operations Management.Wharton School, University of Pennsylvania.Philadelphia, PA.2008.
- Agency for Healthcare Research and Quality. HCUP Databases, Healthcare Cost and Utilization Project (HCUP). 2008. Available at: www.hcup‐us.ahrq.gov/kidoverview.jsp. Accessed June2010.
- ,,,,,.Relationship between resident workload and self‐perceived learning on inpatient medicine wards: a longitudinal study.BMC Med Educ.2006;6(1):35.
- AHA Solutions, Patient Flow Challenges Assessment 2009. Chicago, IL.2009.
- ,.Patient flow in hospitals: understanding and controlling it better.Front Health Serv Manage.2004;20:3–15.
- . Managing Variability in Patient Flow is the Key to Improving Access to Care, Nursing Staffing, Quality of Care, and Reducing Its Cost. Paper presented at: Institute of Medicine; June 24,2004.
- ,,,,,.Managing unnecessary variability in patient demand to reduce nursing stress and improve patient safety.Jt Comm J Qual Patient Saf.2005;31(6):330–338.
- ,,.Developing models for patient flow and daily surge capacity research.Acad Emerg Med.2006;13(11):1109–1113.
- Institute for Healthcare Improvement, Flow initiatives. 2008. Available at: http://www.ihi.org/IHI/Topics/Flow. Accessed June2010.
- ,,, et al.Hospital workload and adverse events.Med Care.2007;45(5):448–455.
- ,,,,.Impact of admission‐day crowding on the length of stay of pediatric hospitalizations.Pediatrics.2008;121(4):e718–730.
- ,,,,.Emergency department crowding, Part 1: concept, causes, and moral consequences.Ann Emerg Med.2009;53(5):605–611.
- ,.Emergency department overcrowding and ambulance diversion: the impact and potential solutions of extended boarding of admitted patients in the emergency department.J Emerg Med.2006;30(3):351–356.
- ,,,.A comparison of in‐hospital mortality risk conferred by high hospital occupancy, differences in nurse staffing levels, weekend admission, and seasonal influenza.Medical Care.2010;48(3):224–232.
- .,,.The effect of hospital bed occupancy on throughput in the pediatric emergency department.Ann Emerg Med.2009;53(6):767–776.e763.
- .Interpreting the Volume‐Outcome Relationship in the Context of Health Care Quality: Workshop Summary.Washington, DC:National Academies Press;2000.
- ,.Uncertain demand, the structure of hospital costs, and the cost of empty hospital beds.J Health Econ.1995;14(3):291–317.
- ,,, et al.Variability in surgical caseload and access to intensive care services.Anesthesiology.2003;98(6):1491–1496.
- ,,,,.Effects of hospital care environment on patient mortality and nurse outcomes.J Nurs Adm.2009;39(7/8):S45–S51.
- ,,, et al.Children's hospitals do not acutely respond to high occupancy.Pediatrics.2010;125:974–981.
- ,.Easing the strain on a pediatric tertiary care center: use of a redistribution system.Arch Pediatr Adolesc Med.2007;161(9):870–876.
- ,,.Lengths of stay and costs associated with Children's Hospitals.Pediatrics.2005;115:839–844.
- ,.Matching Supply with Demand: An introduction to operations management.New York:McGraw‐Hill;2006.
- .Do hospitals provide lower quality care on weekends?Health Serv Res.2007;42:1589–1612.
- ,.Waiting for urgent procedures on the weekend among emergently hospitalized patients.Am J Med.2004;117:175–181.
- ,.Mortality among patients admitted to hospitals on weekends as compared with weekdays.N Engl J Med.2001;345:663–668.
- ,.Enhanced weekend service: an affordable means to increased hospital procedure volume.CMAJ.2005;172(4):503–504.
- .Hospital deaths and weekend admissions‐how do we leap across a chasm?Clin Nurse Spec.2002;16:91–92.
- ,.Weekend birth and higher neonatal mortality: a problem of patient acuity or quality of care?J Obstet Gynecol Neonatal Nurs.2003;32(6):724–733.
- ,,, et al.Weekend versus weekday admission and mortality from myocardial infarction.N Engl J Med.2007;356:1099–1109.
- .Weekend admission and treatment of patients with renal colic: a case of avoidable variation?Urology.2009;73(4):720–724.
- ,,.Characteristics of weekday and weekend hospital admissions.HCUP Statistical Brief.2010;87. http://www.hcup‐us.ahrq.gov/reports/statbriefs/sb87.pdf.
- ,. Hospital Costs and the Cost of Empty Hospital Beds (NBER Working Paper No. W3872).1991.
- ,,.The effects of timing of pediatric knee ligament surgery on short‐term academic performance in school‐aged athletes.Am J Sports Med.2009;37(9):1684–1691.
- Institute for Healthcare Improvement, Smoothing Elective Surgical Admissions. Available at: http://www.ihi.org/IHI/Topics/Flow/PatientFlow/EmergingContent/SmoothingElectiveSurgicalAdmissions.htm. Accessed June2010.
- . Institute for Healthcare Improvement, Patient Flow Comments. Available at: http://www.ihi.org/IHI/Topics/Flow. Accessed June2010.
- .OPIM 631: Operations Management.Wharton School, University of Pennsylvania.Philadelphia, PA.2008.
- Agency for Healthcare Research and Quality. HCUP Databases, Healthcare Cost and Utilization Project (HCUP). 2008. Available at: www.hcup‐us.ahrq.gov/kidoverview.jsp. Accessed June2010.
Copyright © 2010 Society of Hospital Medicine
Hospitalist Invention Aims for Infection Prevention
Stethoscopes can be magnets for infectious agents. As many as 1 in 3 stethoscopes used in EDs carry methicillin-resistant Staphylococcus aureus (Prehospital Emergency Care. 2009;13:71-74). Cleaning them with alcohol rubs can be cumbersome, however, and the alcohol doesn’t kill such infections as Clostridium difficile, which is common in hospitals and causes colitis, says Richard Ma, MD, chair of hospital medicine at Saints Memorial Medical Center in Lowell, Mass.
“Being a hospitalist, I see a lot around me that is wasteful and inefficient,” Dr. Ma says. Four years ago, he set out to create a product that would protect against C. diff, and that would meet the challenge of keeping the neck, as well as the business end, of the stethoscope clean.
The solution: a disposable, lightweight, slip-on cover about 12 inches in length, which resembles the transparent plastic bags on rollers found in supermarket produce departments. The cover has a built-in, V-shaped seal into which the stethoscope tip is wedged. Dr. Ma plans to distribute his recently patented invention, called the Stethguard, at Saints, where all staff will be trained in its use, and to other hospitals in the state. He also hopes to license it to a medical supply distributor for wider distribution. He says it only costs pennies per bag, even less when mass-produced.
Demand for the Stethguard could be aided by the current national focus on preventing hospital-acquired infections. But will hospitalists embrace his invention? Perhaps not, Dr. Ma says, given that many doctors resist washing their hands before entering patients’ rooms. But if his idea catches on, consumers will eventually learn to demand it, he adds.
Stethoscopes can be magnets for infectious agents. As many as 1 in 3 stethoscopes used in EDs carry methicillin-resistant Staphylococcus aureus (Prehospital Emergency Care. 2009;13:71-74). Cleaning them with alcohol rubs can be cumbersome, however, and the alcohol doesn’t kill such infections as Clostridium difficile, which is common in hospitals and causes colitis, says Richard Ma, MD, chair of hospital medicine at Saints Memorial Medical Center in Lowell, Mass.
“Being a hospitalist, I see a lot around me that is wasteful and inefficient,” Dr. Ma says. Four years ago, he set out to create a product that would protect against C. diff, and that would meet the challenge of keeping the neck, as well as the business end, of the stethoscope clean.
The solution: a disposable, lightweight, slip-on cover about 12 inches in length, which resembles the transparent plastic bags on rollers found in supermarket produce departments. The cover has a built-in, V-shaped seal into which the stethoscope tip is wedged. Dr. Ma plans to distribute his recently patented invention, called the Stethguard, at Saints, where all staff will be trained in its use, and to other hospitals in the state. He also hopes to license it to a medical supply distributor for wider distribution. He says it only costs pennies per bag, even less when mass-produced.
Demand for the Stethguard could be aided by the current national focus on preventing hospital-acquired infections. But will hospitalists embrace his invention? Perhaps not, Dr. Ma says, given that many doctors resist washing their hands before entering patients’ rooms. But if his idea catches on, consumers will eventually learn to demand it, he adds.
Stethoscopes can be magnets for infectious agents. As many as 1 in 3 stethoscopes used in EDs carry methicillin-resistant Staphylococcus aureus (Prehospital Emergency Care. 2009;13:71-74). Cleaning them with alcohol rubs can be cumbersome, however, and the alcohol doesn’t kill such infections as Clostridium difficile, which is common in hospitals and causes colitis, says Richard Ma, MD, chair of hospital medicine at Saints Memorial Medical Center in Lowell, Mass.
“Being a hospitalist, I see a lot around me that is wasteful and inefficient,” Dr. Ma says. Four years ago, he set out to create a product that would protect against C. diff, and that would meet the challenge of keeping the neck, as well as the business end, of the stethoscope clean.
The solution: a disposable, lightweight, slip-on cover about 12 inches in length, which resembles the transparent plastic bags on rollers found in supermarket produce departments. The cover has a built-in, V-shaped seal into which the stethoscope tip is wedged. Dr. Ma plans to distribute his recently patented invention, called the Stethguard, at Saints, where all staff will be trained in its use, and to other hospitals in the state. He also hopes to license it to a medical supply distributor for wider distribution. He says it only costs pennies per bag, even less when mass-produced.
Demand for the Stethguard could be aided by the current national focus on preventing hospital-acquired infections. But will hospitalists embrace his invention? Perhaps not, Dr. Ma says, given that many doctors resist washing their hands before entering patients’ rooms. But if his idea catches on, consumers will eventually learn to demand it, he adds.
Business Blueprint
When your group needed a director, everybody stepped back except you. Or maybe you’re thinking about transitioning into a hospital administrative leadership role like department chair, patient safety officer, vice president of medical affairs, chief medical officer, or even CEO.
“Over the next 10 years, the single largest source of new CMOs might be hospitalists,” says John Nelson, MD, MHM, medical director at Overlake Hospital in Bellevue, Wash., and principal of the consulting firm Nelson Flores Hospital Medicine Consultants.
You might already have discovered that these responsibilities require skills that weren't taught in medical school, and you could be struggling. The trick is figuring out which skills you need to strengthen, as well as selecting the right training venues.
You'll need financial and business literacy, technical savvy for process and system improvements, planning ability, and emotional intelligence to engineer cooperative relationships between multiple stakeholders. Successful career advancement ultimately requires leadership acumen: proof that you can run a business, manage upstream and downstream communication, and handle administrative and liaison duties within the hospital.
“As healthcare reform begins to financially incentivize things like safe patient handoffs and more evidence-based medicine, the business part of running a practice is going to quickly align with quality and safety outcomes. That’s what hospital medicine leaders should be focusing on,” says Lakshmi K. Halasyamani, MD, SFHM, vice president of quality and systems improvement at Saint Joseph Mercy Hospital in Ann Arbor, Mich., and an SHM board member.
There is no shortage of training options, including books, mentorships, hospital committee membership, workshops, courses, and master’s-level programs in business leadership. And as the healthcare landscape continues to evolve, there will be a growing demand for physicians, particularly hospitalists, with greater procedural and conceptual understanding of healthcare systems.
For more about hospitalists becoming the business leaders in healthcare, check out this month’s cover story, "Business Blueprint."
When your group needed a director, everybody stepped back except you. Or maybe you’re thinking about transitioning into a hospital administrative leadership role like department chair, patient safety officer, vice president of medical affairs, chief medical officer, or even CEO.
“Over the next 10 years, the single largest source of new CMOs might be hospitalists,” says John Nelson, MD, MHM, medical director at Overlake Hospital in Bellevue, Wash., and principal of the consulting firm Nelson Flores Hospital Medicine Consultants.
You might already have discovered that these responsibilities require skills that weren't taught in medical school, and you could be struggling. The trick is figuring out which skills you need to strengthen, as well as selecting the right training venues.
You'll need financial and business literacy, technical savvy for process and system improvements, planning ability, and emotional intelligence to engineer cooperative relationships between multiple stakeholders. Successful career advancement ultimately requires leadership acumen: proof that you can run a business, manage upstream and downstream communication, and handle administrative and liaison duties within the hospital.
“As healthcare reform begins to financially incentivize things like safe patient handoffs and more evidence-based medicine, the business part of running a practice is going to quickly align with quality and safety outcomes. That’s what hospital medicine leaders should be focusing on,” says Lakshmi K. Halasyamani, MD, SFHM, vice president of quality and systems improvement at Saint Joseph Mercy Hospital in Ann Arbor, Mich., and an SHM board member.
There is no shortage of training options, including books, mentorships, hospital committee membership, workshops, courses, and master’s-level programs in business leadership. And as the healthcare landscape continues to evolve, there will be a growing demand for physicians, particularly hospitalists, with greater procedural and conceptual understanding of healthcare systems.
For more about hospitalists becoming the business leaders in healthcare, check out this month’s cover story, "Business Blueprint."
When your group needed a director, everybody stepped back except you. Or maybe you’re thinking about transitioning into a hospital administrative leadership role like department chair, patient safety officer, vice president of medical affairs, chief medical officer, or even CEO.
“Over the next 10 years, the single largest source of new CMOs might be hospitalists,” says John Nelson, MD, MHM, medical director at Overlake Hospital in Bellevue, Wash., and principal of the consulting firm Nelson Flores Hospital Medicine Consultants.
You might already have discovered that these responsibilities require skills that weren't taught in medical school, and you could be struggling. The trick is figuring out which skills you need to strengthen, as well as selecting the right training venues.
You'll need financial and business literacy, technical savvy for process and system improvements, planning ability, and emotional intelligence to engineer cooperative relationships between multiple stakeholders. Successful career advancement ultimately requires leadership acumen: proof that you can run a business, manage upstream and downstream communication, and handle administrative and liaison duties within the hospital.
“As healthcare reform begins to financially incentivize things like safe patient handoffs and more evidence-based medicine, the business part of running a practice is going to quickly align with quality and safety outcomes. That’s what hospital medicine leaders should be focusing on,” says Lakshmi K. Halasyamani, MD, SFHM, vice president of quality and systems improvement at Saint Joseph Mercy Hospital in Ann Arbor, Mich., and an SHM board member.
There is no shortage of training options, including books, mentorships, hospital committee membership, workshops, courses, and master’s-level programs in business leadership. And as the healthcare landscape continues to evolve, there will be a growing demand for physicians, particularly hospitalists, with greater procedural and conceptual understanding of healthcare systems.
For more about hospitalists becoming the business leaders in healthcare, check out this month’s cover story, "Business Blueprint."
Brentuximab and Refractory Hodgkin's Lymphoma
Brentuximab vedotin, an investigational agent, was associated with complete remission in 34% of patients whose Hodgkin's lymphoma recurred after autologous stem cell transplants, based on data from a phase II trial of 102 patients. For the full story, see http://tinyurl.com/2937bbx
Brentuximab vedotin, an investigational agent, was associated with complete remission in 34% of patients whose Hodgkin's lymphoma recurred after autologous stem cell transplants, based on data from a phase II trial of 102 patients. For the full story, see http://tinyurl.com/2937bbx
Brentuximab vedotin, an investigational agent, was associated with complete remission in 34% of patients whose Hodgkin's lymphoma recurred after autologous stem cell transplants, based on data from a phase II trial of 102 patients. For the full story, see http://tinyurl.com/2937bbx
Nilotinib for Myeloid Leukemia
Chronic myeloid leukemia patients who took 400 mg of nilotinib twice daily had a 97% overall survival rate after 3 years, based on data from 73 patients, explains Dr. Gianantonio Rosti. See the Internal Medicine News story at http://tinyurl.com/27nwkcb
Chronic myeloid leukemia patients who took 400 mg of nilotinib twice daily had a 97% overall survival rate after 3 years, based on data from 73 patients, explains Dr. Gianantonio Rosti. See the Internal Medicine News story at http://tinyurl.com/27nwkcb
Chronic myeloid leukemia patients who took 400 mg of nilotinib twice daily had a 97% overall survival rate after 3 years, based on data from 73 patients, explains Dr. Gianantonio Rosti. See the Internal Medicine News story at http://tinyurl.com/27nwkcb
Large gallstone ileus
A 92‐year old man presented with a 5‐day history of obstipation, nausea, and vomiting. A computed tomography (CT) scan of the abdomen revealed a 4.1‐cm gallstone impacted in the sigmoid colon (Figure 1). The proximal colon was diffusely dilated in caliber consistent with obstruction (Figure 1B). The CT also showed a cholecystocolic fistula at the hepatic flexure of the colon (Figure 2) with an edematous gallbladder wall and a residual 3.8‐cm gallstone. Under colonoscopic guidance the stone was fragmented using intraluminal shock wave lithotripsy and other endoscopic techniques. The pieces were retrieved (Figure 3, shown reassembled). Cholecystectomy, common hepatic duct repair, and fistula takedown were electively performed to prevent recurrence.



Gallstone ileus is the mechanical impaction of gallstones within the gastrointestinal (GI) tract. It requires the formation of either a biliary‐enteric fistula or less often a choledocho‐enteric fistula. Usually the stone must be 2 cm or greater to cause obstruction.1 The site of obstruction is typically the terminal ileum or ileocecal valve because of the smaller diameter lumen and less active peristalsis. Although mortality rates approach 15%,2 this patient did remarkably well with early recognition, use of complex endoscopic removal, and avoidance of urgent laparotomy.
- ,.Gallstone ileus: a review of 1001 reported cases.Am Surg.1994;60:441–446.
- ,,,,,.[Gallstone Ileus: results of analysis of a series of 40 patients].Gastroenterol Hepatol.2001;24:489–494. In Spanish.
A 92‐year old man presented with a 5‐day history of obstipation, nausea, and vomiting. A computed tomography (CT) scan of the abdomen revealed a 4.1‐cm gallstone impacted in the sigmoid colon (Figure 1). The proximal colon was diffusely dilated in caliber consistent with obstruction (Figure 1B). The CT also showed a cholecystocolic fistula at the hepatic flexure of the colon (Figure 2) with an edematous gallbladder wall and a residual 3.8‐cm gallstone. Under colonoscopic guidance the stone was fragmented using intraluminal shock wave lithotripsy and other endoscopic techniques. The pieces were retrieved (Figure 3, shown reassembled). Cholecystectomy, common hepatic duct repair, and fistula takedown were electively performed to prevent recurrence.
Gallstone ileus is the mechanical impaction of gallstones within the gastrointestinal (GI) tract. It requires the formation of either a biliary‐enteric fistula or less often a choledocho‐enteric fistula. Usually the stone must be 2 cm or greater to cause obstruction.1 The site of obstruction is typically the terminal ileum or ileocecal valve because of the smaller diameter lumen and less active peristalsis. Although mortality rates approach 15%,2 this patient did remarkably well with early recognition, use of complex endoscopic removal, and avoidance of urgent laparotomy.
A 92‐year old man presented with a 5‐day history of obstipation, nausea, and vomiting. A computed tomography (CT) scan of the abdomen revealed a 4.1‐cm gallstone impacted in the sigmoid colon (Figure 1). The proximal colon was diffusely dilated in caliber consistent with obstruction (Figure 1B). The CT also showed a cholecystocolic fistula at the hepatic flexure of the colon (Figure 2) with an edematous gallbladder wall and a residual 3.8‐cm gallstone. Under colonoscopic guidance the stone was fragmented using intraluminal shock wave lithotripsy and other endoscopic techniques. The pieces were retrieved (Figure 3, shown reassembled). Cholecystectomy, common hepatic duct repair, and fistula takedown were electively performed to prevent recurrence.
Gallstone ileus is the mechanical impaction of gallstones within the gastrointestinal (GI) tract. It requires the formation of either a biliary‐enteric fistula or less often a choledocho‐enteric fistula. Usually the stone must be 2 cm or greater to cause obstruction.1 The site of obstruction is typically the terminal ileum or ileocecal valve because of the smaller diameter lumen and less active peristalsis. Although mortality rates approach 15%,2 this patient did remarkably well with early recognition, use of complex endoscopic removal, and avoidance of urgent laparotomy.
- ,.Gallstone ileus: a review of 1001 reported cases.Am Surg.1994;60:441–446.
- ,,,,,.[Gallstone Ileus: results of analysis of a series of 40 patients].Gastroenterol Hepatol.2001;24:489–494. In Spanish.
- ,.Gallstone ileus: a review of 1001 reported cases.Am Surg.1994;60:441–446.
- ,,,,,.[Gallstone Ileus: results of analysis of a series of 40 patients].Gastroenterol Hepatol.2001;24:489–494. In Spanish.

The Medicaid Gap
Amid the recent focus on Medicare’s spiraling costs and efforts to rein in government spending, media accounts have painted a grim picture of Medicaid financing as well:
- With record enrollment, Kentucky’s Medicaid program is facing a budget shortfall of nearly $500 million. In Arizona, the gap is expected to be $1 billion.
- In September, Washington state announced $112.8 million in Medicaid cuts, a reduction that the state’s Medicaid director described as “devastating.”
- According to the Kaiser Family Foundation, Louisiana cut Medicaid inpatient hospital rates 3.5% in fiscal year 2009, 12.1% in 2010, and an additional 4.6% for 2011 to help close budget gaps.
- Maine politicians are facing off over a $380 million state debt owed to hospitals providing Medicaid services.
Safety-net hospitals that care for a disproportionate share of uninsured and Medicaid patients are likely to feel the most pain. So what does that mean for hospitalists? Experts say they will be increasingly looked to for guidance and leadership in identifying cost-saving measures and in helping hospitals avoid further penalties by focusing on such critical metrics as readmission rates.
Political ‘Hot Potato’
The pressure isn’t likely to ease anytime soon. The American Recovery and Reinvestment Act provided $87 billion to help states pay for Medicaid costs from October 2008 through the end of this year by temporarily boosting the federal Medicaid matching rate, officially known as the Federal Medical Assistance Percentages (FMAP). In August, Congress passed legislation that provided an additional $16.1 billion to provide six more months of scaled-back relief through June, when the fiscal year ends in most states.
That’s when things could get really sticky. According to an annual survey conducted by the Kaiser Family Foundation, average state spending on Medicaid jumped 8.8% last year, the biggest increase in eight years and higher than the initial prediction of 6.3%. State Medicaid officials reported swelling ranks of eligible families due to the recession as a main reason for the rise. The pace is expected to cool slightly next year, but states that had relied heavily on federal aid to meet budget shortfalls are now facing the prospect of doing without amid a continued expansion of Medicaid enrollees.
“That’s the catch-22 that you’re in right now,” says Ellen Kugler, executive director of the National Association of Urban Hospitals, based in Sterling, Va. “There is increased demand and increasing numbers of uninsured. States are still in fiscal crisis, and there’s a delay before new dollars become available.”
New federal funds become available in 2014 to help pay for insuring those who currently lack insurance. That money will flow either through subsidies to state-administered exchanges or through direct Medicaid payments. But that same year, Kugler says, safety-net hospitals will begin seeing hefty reductions in Medicare disproportionate share (DSH) payments and possibly Medicaid DSH payments, too.
In theory, more people will have some form of health insurance by then, lessening the need to pay hospitals to help them recoup the cost of treating uninsured and underinsured patients. However, Kugler is urging caution on the DSH pay cuts, warning that it’s not clear what the ranks of the newly insured will be. Current projections, she says, suggest that half of those insured patients will fall under Medicaid programs, meaning that significant cuts could pose a financial hardship to hospitals that serve those populations.
Beyond reductions in services and reimbursement rates to doctors and hospitals, few politicians have had the stomach to propose major overhauls in how Medicaid is managed and financed. In New York state, however, a suite of proposals by Lt. Gov. Richard Ravitch has earned praise from The New York Times.1 One would streamline management of the program, now administered by 58 local governments and multiple state agencies. Ravitch also supports reducing the political wrangling over how reimbursement fees are calculated by wresting that power away from the state legislature and giving it to the state’s Medicaid director, who would be advised by an expert panel.
Another unresolved issue is how to pay for the long-term care of chronically ill patients, which in New York accounts for nearly half of its Medicaid spending. Kugler says the high incidence of chronic conditions, including mental illness, among patients in urban settings can contribute to the high readmission rates the new law is set to begin penalizing in 2012. Other studies have found that among Medicaid patients at high risk for frequent hospital admissions, substance abuse can be a major contributor.2
The difficult task, then, is to ensure that the hospitals serving these populations don’t lose even more resources through penalties due to subpar quality metrics. “Do the legwork now. Get your IT systems in place to be able to provide the coordinated care,” Kugler advises. Identifying efficiencies while maintaining the appropriate level of care will be key, whether in appropriate reductions in length of stay or in increased focus on communication with outpatient providers and other forms of outreach.
Hope for the Safety Net
Despite the financial and logistical challenges, Lenny Lopez, MD, MPH, a hospitalist at Brigham and Women’s Hospital and an assistant in health policy at Massachusetts General Hospital, both in Boston, says the situation is far from hopeless for safety-net hospitals. “The idea that if you’re a DSH hospital you’re somehow pegged and destined to provide low-quality care—that does not have to be the case,” he says. Nor do problems such as disparities in how patients are treated necessarily require expensive solutions.
In a recent paper in Academic Emergency Medicine, Dr. Lopez and his colleagues found that among patients with chest pain admitted to EDs, blacks, Hispanics, and those who lacked insurance or were on Medicare were less likely to receive urgent triage care.3 “These are problems that are fixable in a low-cost way,” he argues. “We don’t need another fancy machine to diagnose chest pain.” Rather, he suggests, the problem is really one of quality improvement that centers on boosting guidelines, not buying more equipment or involving more personnel.
Properly defining the problem, Dr. Lopez says, can lead to effective measures to boost quality. Amid the continuing budget crunch, pinpointing where interventions could provide the biggest bang for the buck also might prove enormously helpful.
Of the roughly 4,200 acute-care hospitals in the country, Dr. Lopez and his colleagues found that less than 10% care for the bulk of minority patients, and those on Medicaid or lacking insurance. That means such care is concentrated in about 400 hospitals, “which is a huge opportunity for intervention options for this kind of an issue,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- 1. Benefits and burdens of Medicaid. The New York Times website. Available at: www.nytimes.com/2010/09/22/opinion/22wed2.html?_r=2&hp. Accessed Oct. 23, 2010.
- 2. Raven MC, Billings JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urban Health. 2009;86(2):230-241.
- 3. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997-2006. Acad Emerg Med. 2010:17 (8):801-810.
Amid the recent focus on Medicare’s spiraling costs and efforts to rein in government spending, media accounts have painted a grim picture of Medicaid financing as well:
- With record enrollment, Kentucky’s Medicaid program is facing a budget shortfall of nearly $500 million. In Arizona, the gap is expected to be $1 billion.
- In September, Washington state announced $112.8 million in Medicaid cuts, a reduction that the state’s Medicaid director described as “devastating.”
- According to the Kaiser Family Foundation, Louisiana cut Medicaid inpatient hospital rates 3.5% in fiscal year 2009, 12.1% in 2010, and an additional 4.6% for 2011 to help close budget gaps.
- Maine politicians are facing off over a $380 million state debt owed to hospitals providing Medicaid services.
Safety-net hospitals that care for a disproportionate share of uninsured and Medicaid patients are likely to feel the most pain. So what does that mean for hospitalists? Experts say they will be increasingly looked to for guidance and leadership in identifying cost-saving measures and in helping hospitals avoid further penalties by focusing on such critical metrics as readmission rates.
Political ‘Hot Potato’
The pressure isn’t likely to ease anytime soon. The American Recovery and Reinvestment Act provided $87 billion to help states pay for Medicaid costs from October 2008 through the end of this year by temporarily boosting the federal Medicaid matching rate, officially known as the Federal Medical Assistance Percentages (FMAP). In August, Congress passed legislation that provided an additional $16.1 billion to provide six more months of scaled-back relief through June, when the fiscal year ends in most states.
That’s when things could get really sticky. According to an annual survey conducted by the Kaiser Family Foundation, average state spending on Medicaid jumped 8.8% last year, the biggest increase in eight years and higher than the initial prediction of 6.3%. State Medicaid officials reported swelling ranks of eligible families due to the recession as a main reason for the rise. The pace is expected to cool slightly next year, but states that had relied heavily on federal aid to meet budget shortfalls are now facing the prospect of doing without amid a continued expansion of Medicaid enrollees.
“That’s the catch-22 that you’re in right now,” says Ellen Kugler, executive director of the National Association of Urban Hospitals, based in Sterling, Va. “There is increased demand and increasing numbers of uninsured. States are still in fiscal crisis, and there’s a delay before new dollars become available.”
New federal funds become available in 2014 to help pay for insuring those who currently lack insurance. That money will flow either through subsidies to state-administered exchanges or through direct Medicaid payments. But that same year, Kugler says, safety-net hospitals will begin seeing hefty reductions in Medicare disproportionate share (DSH) payments and possibly Medicaid DSH payments, too.
In theory, more people will have some form of health insurance by then, lessening the need to pay hospitals to help them recoup the cost of treating uninsured and underinsured patients. However, Kugler is urging caution on the DSH pay cuts, warning that it’s not clear what the ranks of the newly insured will be. Current projections, she says, suggest that half of those insured patients will fall under Medicaid programs, meaning that significant cuts could pose a financial hardship to hospitals that serve those populations.
Beyond reductions in services and reimbursement rates to doctors and hospitals, few politicians have had the stomach to propose major overhauls in how Medicaid is managed and financed. In New York state, however, a suite of proposals by Lt. Gov. Richard Ravitch has earned praise from The New York Times.1 One would streamline management of the program, now administered by 58 local governments and multiple state agencies. Ravitch also supports reducing the political wrangling over how reimbursement fees are calculated by wresting that power away from the state legislature and giving it to the state’s Medicaid director, who would be advised by an expert panel.
Another unresolved issue is how to pay for the long-term care of chronically ill patients, which in New York accounts for nearly half of its Medicaid spending. Kugler says the high incidence of chronic conditions, including mental illness, among patients in urban settings can contribute to the high readmission rates the new law is set to begin penalizing in 2012. Other studies have found that among Medicaid patients at high risk for frequent hospital admissions, substance abuse can be a major contributor.2
The difficult task, then, is to ensure that the hospitals serving these populations don’t lose even more resources through penalties due to subpar quality metrics. “Do the legwork now. Get your IT systems in place to be able to provide the coordinated care,” Kugler advises. Identifying efficiencies while maintaining the appropriate level of care will be key, whether in appropriate reductions in length of stay or in increased focus on communication with outpatient providers and other forms of outreach.
Hope for the Safety Net
Despite the financial and logistical challenges, Lenny Lopez, MD, MPH, a hospitalist at Brigham and Women’s Hospital and an assistant in health policy at Massachusetts General Hospital, both in Boston, says the situation is far from hopeless for safety-net hospitals. “The idea that if you’re a DSH hospital you’re somehow pegged and destined to provide low-quality care—that does not have to be the case,” he says. Nor do problems such as disparities in how patients are treated necessarily require expensive solutions.
In a recent paper in Academic Emergency Medicine, Dr. Lopez and his colleagues found that among patients with chest pain admitted to EDs, blacks, Hispanics, and those who lacked insurance or were on Medicare were less likely to receive urgent triage care.3 “These are problems that are fixable in a low-cost way,” he argues. “We don’t need another fancy machine to diagnose chest pain.” Rather, he suggests, the problem is really one of quality improvement that centers on boosting guidelines, not buying more equipment or involving more personnel.
Properly defining the problem, Dr. Lopez says, can lead to effective measures to boost quality. Amid the continuing budget crunch, pinpointing where interventions could provide the biggest bang for the buck also might prove enormously helpful.
Of the roughly 4,200 acute-care hospitals in the country, Dr. Lopez and his colleagues found that less than 10% care for the bulk of minority patients, and those on Medicaid or lacking insurance. That means such care is concentrated in about 400 hospitals, “which is a huge opportunity for intervention options for this kind of an issue,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- 1. Benefits and burdens of Medicaid. The New York Times website. Available at: www.nytimes.com/2010/09/22/opinion/22wed2.html?_r=2&hp. Accessed Oct. 23, 2010.
- 2. Raven MC, Billings JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urban Health. 2009;86(2):230-241.
- 3. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997-2006. Acad Emerg Med. 2010:17 (8):801-810.
Amid the recent focus on Medicare’s spiraling costs and efforts to rein in government spending, media accounts have painted a grim picture of Medicaid financing as well:
- With record enrollment, Kentucky’s Medicaid program is facing a budget shortfall of nearly $500 million. In Arizona, the gap is expected to be $1 billion.
- In September, Washington state announced $112.8 million in Medicaid cuts, a reduction that the state’s Medicaid director described as “devastating.”
- According to the Kaiser Family Foundation, Louisiana cut Medicaid inpatient hospital rates 3.5% in fiscal year 2009, 12.1% in 2010, and an additional 4.6% for 2011 to help close budget gaps.
- Maine politicians are facing off over a $380 million state debt owed to hospitals providing Medicaid services.
Safety-net hospitals that care for a disproportionate share of uninsured and Medicaid patients are likely to feel the most pain. So what does that mean for hospitalists? Experts say they will be increasingly looked to for guidance and leadership in identifying cost-saving measures and in helping hospitals avoid further penalties by focusing on such critical metrics as readmission rates.
Political ‘Hot Potato’
The pressure isn’t likely to ease anytime soon. The American Recovery and Reinvestment Act provided $87 billion to help states pay for Medicaid costs from October 2008 through the end of this year by temporarily boosting the federal Medicaid matching rate, officially known as the Federal Medical Assistance Percentages (FMAP). In August, Congress passed legislation that provided an additional $16.1 billion to provide six more months of scaled-back relief through June, when the fiscal year ends in most states.
That’s when things could get really sticky. According to an annual survey conducted by the Kaiser Family Foundation, average state spending on Medicaid jumped 8.8% last year, the biggest increase in eight years and higher than the initial prediction of 6.3%. State Medicaid officials reported swelling ranks of eligible families due to the recession as a main reason for the rise. The pace is expected to cool slightly next year, but states that had relied heavily on federal aid to meet budget shortfalls are now facing the prospect of doing without amid a continued expansion of Medicaid enrollees.
“That’s the catch-22 that you’re in right now,” says Ellen Kugler, executive director of the National Association of Urban Hospitals, based in Sterling, Va. “There is increased demand and increasing numbers of uninsured. States are still in fiscal crisis, and there’s a delay before new dollars become available.”
New federal funds become available in 2014 to help pay for insuring those who currently lack insurance. That money will flow either through subsidies to state-administered exchanges or through direct Medicaid payments. But that same year, Kugler says, safety-net hospitals will begin seeing hefty reductions in Medicare disproportionate share (DSH) payments and possibly Medicaid DSH payments, too.
In theory, more people will have some form of health insurance by then, lessening the need to pay hospitals to help them recoup the cost of treating uninsured and underinsured patients. However, Kugler is urging caution on the DSH pay cuts, warning that it’s not clear what the ranks of the newly insured will be. Current projections, she says, suggest that half of those insured patients will fall under Medicaid programs, meaning that significant cuts could pose a financial hardship to hospitals that serve those populations.
Beyond reductions in services and reimbursement rates to doctors and hospitals, few politicians have had the stomach to propose major overhauls in how Medicaid is managed and financed. In New York state, however, a suite of proposals by Lt. Gov. Richard Ravitch has earned praise from The New York Times.1 One would streamline management of the program, now administered by 58 local governments and multiple state agencies. Ravitch also supports reducing the political wrangling over how reimbursement fees are calculated by wresting that power away from the state legislature and giving it to the state’s Medicaid director, who would be advised by an expert panel.
Another unresolved issue is how to pay for the long-term care of chronically ill patients, which in New York accounts for nearly half of its Medicaid spending. Kugler says the high incidence of chronic conditions, including mental illness, among patients in urban settings can contribute to the high readmission rates the new law is set to begin penalizing in 2012. Other studies have found that among Medicaid patients at high risk for frequent hospital admissions, substance abuse can be a major contributor.2
The difficult task, then, is to ensure that the hospitals serving these populations don’t lose even more resources through penalties due to subpar quality metrics. “Do the legwork now. Get your IT systems in place to be able to provide the coordinated care,” Kugler advises. Identifying efficiencies while maintaining the appropriate level of care will be key, whether in appropriate reductions in length of stay or in increased focus on communication with outpatient providers and other forms of outreach.
Hope for the Safety Net
Despite the financial and logistical challenges, Lenny Lopez, MD, MPH, a hospitalist at Brigham and Women’s Hospital and an assistant in health policy at Massachusetts General Hospital, both in Boston, says the situation is far from hopeless for safety-net hospitals. “The idea that if you’re a DSH hospital you’re somehow pegged and destined to provide low-quality care—that does not have to be the case,” he says. Nor do problems such as disparities in how patients are treated necessarily require expensive solutions.
In a recent paper in Academic Emergency Medicine, Dr. Lopez and his colleagues found that among patients with chest pain admitted to EDs, blacks, Hispanics, and those who lacked insurance or were on Medicare were less likely to receive urgent triage care.3 “These are problems that are fixable in a low-cost way,” he argues. “We don’t need another fancy machine to diagnose chest pain.” Rather, he suggests, the problem is really one of quality improvement that centers on boosting guidelines, not buying more equipment or involving more personnel.
Properly defining the problem, Dr. Lopez says, can lead to effective measures to boost quality. Amid the continuing budget crunch, pinpointing where interventions could provide the biggest bang for the buck also might prove enormously helpful.
Of the roughly 4,200 acute-care hospitals in the country, Dr. Lopez and his colleagues found that less than 10% care for the bulk of minority patients, and those on Medicaid or lacking insurance. That means such care is concentrated in about 400 hospitals, “which is a huge opportunity for intervention options for this kind of an issue,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
References
- 1. Benefits and burdens of Medicaid. The New York Times website. Available at: www.nytimes.com/2010/09/22/opinion/22wed2.html?_r=2&hp. Accessed Oct. 23, 2010.
- 2. Raven MC, Billings JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urban Health. 2009;86(2):230-241.
- 3. López L, Wilper AP, Cervantes MC, Betancourt JR, Green AR. Racial and sex differences in emergency department triage assessment and test ordering for chest pain, 1997-2006. Acad Emerg Med. 2010:17 (8):801-810.
ONLINE EXCLUSIVE: Audio interviews with experts in career advancement, training
Click here to listen to John Nelson, MD, MHM.
Click here to listen to Lakshmi Halasyamani, MD, SFHM.
Click here to listen to Win Whitcomb, MD, MHM.
Click here to listen to John Nelson, MD, MHM.
Click here to listen to Lakshmi Halasyamani, MD, SFHM.
Click here to listen to Win Whitcomb, MD, MHM.
Click here to listen to John Nelson, MD, MHM.
Click here to listen to Lakshmi Halasyamani, MD, SFHM.
Click here to listen to Win Whitcomb, MD, MHM.
Business Blueprint
Perhaps you’ve put in a few years of clinical practice in an HM group. Suddenly, your group needs a director—and everybody stepped back, except you. You now find yourself thrust into an unfamiliar world of bottom-line thinking, budgets, schedules, spreadsheets, decision-making, conflict resolution, recruiting, contract negotiations, and other managerial responsibilities. You’ve tried to learn how to perform most of these duties on the job. But you’ve learned that assuming direct responsibility for the fate of a hospitalist group with millions in annual billing requires skills that weren’t taught in medical school. And you’re struggling.
Maybe you’re a hospitalist residency program director in a teaching hospital setting, and you would like to transition into other hospital administrative leadership roles, such as chair of a medical staff or credentials committee, department chair, vice president of medical affairs, chief medical officer—maybe even CEO. But where do you begin?
The good news is that hospitalists are well positioned for such advancements, there is a core set of skills required for these various leadership positions that you can learn, and there are several places you can turn to for training. The trick is figuring out which skills and aptitudes you already possess, identifying those you need to strengthen, and selecting the training venues that best meet your goals. Your options vary widely, and include simply reading books on management to get up to speed quickly, investing in leadership training seminars and short courses, and pursuing advanced-degree programs in business leadership.
“Over the next 10 years, the single largest source of new CMOs might be hospitalists,” says John Nelson, MD, FACP, MHM, medical director of Overlake Hospital in Bellevue, Wash., and cofounder, past president, and past board member of SHM. “As many specialties focus more of their practice in the ambulatory care setting, that leaves behind those of us who will stay—e.g., hospitalists, radiologists, ER doctors, anesthesiologists—and who think of the hospital as their principal place of work. Of those doctors, hospitalists are probably the most interconnected and networked with all other doctors and all levels of hospital staff. That’s why hospitals are looking toward hospitalists for leadership.”
There is a growing need for HM to develop leaders, Dr. Nelson says, “not just for their own practice, but for various leadership activities within their hospital.”
Start at Self-Assessment
Hospitalist leadership is not for everyone, and you need to find out if you’re making the right decision by pursuing it. For one thing, you’ll need to facilitate consensus among physicians—a notoriously challenging group of professionals who are autonomous by training, conditioned to believe that they always wield veto power and that they don’t have to play by the rules established for everyone else, Dr. Nelson says.

Most daily leadership activities are much more open-ended and far less structured than physicians are used to, entailing simultaneous projects that need to be prioritized, says Dr. Nelson, who splits his time about 30% clinical and 70% administrative. He is a champion for his hospital’s technology initiative, medical director of his institution’s hospitalist practice, physician lead of its palliative-care program, principal of Nelson Flores Hospital Medicine Consultants, and a columnist for The Hospitalist.
How can you find out what you’re good at, what your weaknesses are, and what skills you need to build? There are several personality assessment instruments with which you can appraise your compatibility with leadership culture, says Julia S. Wright, MD, SFHM, FACP, senior medical officer for Canton, Ohio-based Hospitalists Management Group. And there are good self-assessment workbooks to test whether you have an inclination toward leadership, says Mary Jane Kornacki, MS, a partner in the Boston-based consulting firm Amicus Inc. You also can have a personal leadership assessment performed professionally (see “Leadership Self-Assessment,” p. 27).
Identify Core Leadership Requirements

There are various ways to categorize the leadership skills that a hospitalist needs, including these: financial and business literacy, technical savvy for projects like quality and patient safety improvement, planning acumen to identify external trends and implement appropriate change in one’s department or group, and emotional intelligence to engineer cooperative relationships, says Jack Silversin, DMD, DrPH, president of Amicus.
Indeed, the ability to manage the relationships with myriad stakeholders is a hospitalist leader’s central requirement, according to “Hospitalists: A Guide to Building and Sustaining a Successful Program.”1 Stakeholders include patients, families, referring physicians, medical subspecialists and surgeons, the hospital executive team (C-suite), the clinical team (nurses, case management, therapy departments, and others), the HM group itself, and the public.
The hospitalist leader is responsible for many tasks, the authors write, including:
- Blending marketplace needs with those of these various stakeholders;
- Managing budgets, billing and revenue cycles, resources, and performance metrics; and
- Overseeing such operational issues as scheduling, workload, census, staffing, and recruitment.
These duties will likely be time-consuming, but a hospitalist leader should nevertheless maintain a portion of his or her clinical practice to continue to be connected to the core work. “The foundation of your credibility as a leader is that you have excellent clinical skills,” says Winthrop F. Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and SHM cofounder and past president.
Clinical excellence is the foundation of successful leadership because the best quality and safety practices will drive successful hospitalist business practices, according to Lakshmi K. Halasyamani, MD, SFHM, SHM board member and vice president for Quality and Systems Improvement at Saint Joseph Mercy Hospital in Ann Arbor, Mich. “As healthcare reform begins to financially incentivize things like safe patient handoffs and more evidence-based medicine,” she says, “the business part of running a practice is going to quickly align with quality and safety outcomes. That’s what hospital medicine leaders should be focusing on.”
Empathy and communication skills are essential for a leader, who must continually translate messages from hospital administration to rank-and-file physicians, and vice versa, Dr. Whitcomb says. For example, he says, the message that hospitalists want better work conditions and more staff should be presented so that administration hears something like this: “We don’t want care to be unsafe; that would hurt the hospital’s reputation. Some of the hospitalists are burning out, creating the risk of increasing turnover. In fact, length of stay would be lower if the group has better staffing, because they could get the patients earlier in the day and send them home sooner.”
Such “situational awareness” is necessary to win the trust and cooperation of others and avoid becoming marginalized by important allies, says Eric Howell, MD, SFHM, director of the Hospital Medicine Division at Johns Hopkins Bayview Medical Center in Baltimore. “I’ve seen very successful advocates of hospital medicine groups who were not very good leaders,” the SHM board member says, “because they could not see what the leadership above them needed.”
Leadership Self-Assessment

The best way to examine your leadership skills is to take a test, such as the Leadership Effectiveness Analysis (LEA), which scores you on six leadership dimensions: creating a vision, developing followership, implementing the vision, following through, and achieving results, according to Dr. Wright. To understand your personality characteristics a little better, she adds, you can take basic tests like the Minnesota Multiphasic Personality Inventory (MMPI).
Other useful personality surveys that can give you an accurate sense of leadership readiness include the Myers-Briggs Type Indicator assessment and the DiSC personality assessment (the acronym reflects a four-quadrant personality model: Dominance, Influence, Steadiness, and Conscientiousness), says Kornacki.
A good self-assessment workbook to test whether you have an inclination toward leadership is Edgar H. Schein’s “Career Anchor, 3rd Edition,” Kornacki says. The book presents a taxonomy of eight competencies, which people prioritize differently: Technical/Functional, General Managerial, Autonomy/Independence, Security/ Stability, Entrepreneurial Creativity, Service/Dedication to a Cause, Pure Challenge, and Lifestyle. How you prioritize those themes offers insight into your values and motivations as a leader.
You might also consider having a professional assess your leadership strengths and weaknesses. Companies like Personnel Decisions International (www.personneldecisions.com) offer coaches who interact with you to assess your cognitive and experiential skills and make recommendations on what you need to work on, says Dr. Klocke.
Pursue the Right Training Venues
Once you’ve identified your strengths and weaknesses, as well as the core requirements of your leadership duties, you are ready to pursue the right training path. Leadership can be learned, whether you’re thrust into it and find yourself in “damage control” mode, or you want to pursue new leadership opportunities for career advancement, Dr. Howell says.
Your first step might be to develop your leadership skill set through informal self-help training. The easiest way is by reading books that other hospitalist leaders have found to be valuable when they were starting out (see “Self-Training Resources,” below left).
The next step is to find a mentor. This person should be a good leader whom you trust and respect, and from whom you can seek advice. “A leadership position can be awfully lonely,” Dr. Nelson says. “I suggest that people find a confidant and mentor at their local institution, someone who is very accessible, who they see all the time, who works in the same environment and knows the local politics.” The mentor could be someone you trained with, or under, or perhaps a hospitalist program director at another institution. It could be the chief nursing officer at your institution. “It is reassuring to know that others are facing similar problems elsewhere,” Dr. Nelson adds.
A local mentor can help with technical matters like offering you a “crash course” in financial spreadsheets, says Patience Agborbesong, MD, SFHM, medical director of a 17-hospitalist program at Wake Forest University Baptist Medical Center in Winston-Salem, N.C. She notes that SHM provides networking resources to help you connect with other HM leaders (www.hospitalmedicine.org/leadership).
Large hospitalist groups frequently offer mentorship opportunities throughout their chain of operations, says Ethan B. Dunham, MBA, director of organizational development for Brentwood, Tenn.-based Cogent Healthcare. “If you find you’ve received something akin to a ‘battlefield promotion’ and are in over your head, you can turn to someone who has been there,” Dunham says.

Many larger health systems and academic medical centers—and even some community hospitals—offer in-house leadership training and mentorship programs, says David L. Klocke, MD, chair of the Division of Hospital Internal Medicine at Mayo Clinic in Rochester, Minn. In his institution, physician leaders are paired with partners from administration who fill in any gaps in their management or leadership skills, Dr. Klocke says. “You’re mentoring them as well about medical issues and skills,” he adds.
Another way to hone your skills is to join hospital committees. “Build up time in the saddle,” Dunham says. “Indicate your leadership potential and your interest in taking the next steps.” If you seek out committees, you’ll get on them, Dr. Nelson says. “And once on them, if you can distinguish yourself by helping to lead the committee in a good direction, your career will be off and running,” he explains. There are many kinds of hospital committee work to choose from, including peer review, performance improvement, practice guideline development, utilization review, pharmacy, and therapeutics.
Advanced Training

For hospitalists wanting a deeper dive, more formal business and leadership training is available through a variety of workshops and courses, many of which offer CME credit. “My favorite was the SHM Leadership Academy, which is fairly short and very practical. Every minute was directly relevant to me as a hospitalist,” Dr. Howell says of the four-day program. Covered topics include teamwork collaboration, communication strategies, hospital performance metrics, scheduling and compensation, strategic planning, financial reports, recruitment, negotiation, motivating others, and managing physician performance.
The American College of Physician Executives (ACPE) offers leadership training modules with certification, as well as MBA and MMM (master’s in medical management) programs through partnerships with universities, according to Dr. Agborbesong. There are several other organizations that offer leadership training, she notes, including The Institute for Medical Leadership, the Boot Camp on Leadership Fundamentals for Physicians, the Center for Creative Leadership, and the Carolinas Center for Medical Excellence (CCME) Physician Leadership Institute.
An MBA is an appropriate goal for many hospitalist leadership scenarios, such as entry-level program director, lead hospitalist at a healthcare system with multiple hospital medicine programs, or regional coordinator for a hospital medicine staffing company, says Michael Stahl, PhD, director of the Physician Executive MBA Program and professor of Strategy and Business Planning at the University of Tennessee in Knoxville.

“An MBA program is particularly well-suited to the physician who gets invited, all of a sudden, to be a leader and discovers they don’t have the knowledge, skill sets, tools and techniques, and ways of thinking about the business side of healthcare. It’s not unusual to see people at the start of their leadership careers saying, ‘I’m going to make an investment in my own human capital by earning an accredited MBA,’ ” Stahl says.
A rapidly changing healthcare landscape requires greater attention to business planning, capital and budget, revenue, and cost-containment principles, Stahl notes. “There will be incredible pressure on controlling the cost of healthcare in the future,” he says. “New reimbursement models are probably going to yield lower reimbursement. What we’re most interested in is equipping people with the tools and techniques of finance so that they can learn to model those new reimbursement types, whatever they are, and no matter how their regulations change.”
Although an MBA sounds daunting, many programs are tailored to a new leader’s busy schedule. For example, the Physician Executive MBA program at UT-Knoxville takes only one year to complete, focuses entirely on healthcare contexts, and combines four weeklong residence periods on campus with 40 Web-based classes, typically on Saturday mornings.
Traditional MBA programs typically take two years to complete and require more physical presence on campus. But in return, they offer ongoing face-to-face interaction with faculty and peers from a variety of business backgrounds that immerse you in the culture of business leadership, says Guy David, PhD, assistant professor of Healthcare Management at the Wharton School at the University of Pennsylvania in Philadelphia. Coursework includes finance, marketing, management, entrepreneurship, strategic development, data mining, economics, legal issues, IT, and other areas, David says. The coursework, he adds, gives physicians who have been trained to focus on the individual patient a much broader understanding of the system in which they operate.

Successful career advancement ultimately requires managerial and leadership acumen: proof that you can run the business, manage upstream and downstream communication, and handle administrative and liaison duties within the hospital, Dunham says. “An MBA is a shorthand, a way to signal to people that that skill set exists, maybe rather than having to prove it in the trenches,” he adds.
As the healthcare landscape continues to evolve, there will be a growing demand for physicians—particularly hospitalists—with greater procedural and conceptual understanding of healthcare systems and financials.
“Over time, it may become increasingly important to have received formal education in the business discipline,” Dunham says. “That’s something that time will tell.” TH
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Reference
- Miller JA, Nelson JR, Whitcomb WF. Hospitalists: A Guide to Building and Sustaining a Successful Program. Health Administration Press: Chicago; 2008.
Veteran Advice For Aspiring HM leaders

Think carefully about whether you’re appropriately balancing the interests of your employer (i.e. the hospital) and the physicians in your group. Some hospitalist group leaders tilt toward being “union pit bosses” and beat up management, lobbying aggressively for their groups’ interests, Dr. Nelson explains. Other hospitalist leaders tilt too far the opposite way and try to beat the physicians into submitting to whatever the hospital might want. You’re going to be talking to both parties about all kinds of issues on a long-term basis, and you need to forsake adversarial negotiating tactics to cultivate long-term relationships.
Don’t make promises that are hard to keep. A leader often faces a tricky issue and might be tempted to take the easy way out by granting special deals, caving in, or meeting demands (e.g. promising a desirable scheduling arrangement as a recruiting inducement). That’s a rookie mistake, Dr. Nelson says, and others in the practice might resent it.
Advocating for your physicians doesn’t always mean more pay, bigger offices, or better benefits. “Good leadership goes beyond that,” Dr. Howell says, “by having good situational awareness to notice what’s important to other parties and building their trust.” By turning one of his offices into a part-time lactation room for mothers with newborns (half of his hospitalists were women of childbearing age, and five of them gave birth in the same year), Dr. Howell earned their trust and respect for the price of a door lock and a small refrigerator.
Perhaps you’ve put in a few years of clinical practice in an HM group. Suddenly, your group needs a director—and everybody stepped back, except you. You now find yourself thrust into an unfamiliar world of bottom-line thinking, budgets, schedules, spreadsheets, decision-making, conflict resolution, recruiting, contract negotiations, and other managerial responsibilities. You’ve tried to learn how to perform most of these duties on the job. But you’ve learned that assuming direct responsibility for the fate of a hospitalist group with millions in annual billing requires skills that weren’t taught in medical school. And you’re struggling.
Maybe you’re a hospitalist residency program director in a teaching hospital setting, and you would like to transition into other hospital administrative leadership roles, such as chair of a medical staff or credentials committee, department chair, vice president of medical affairs, chief medical officer—maybe even CEO. But where do you begin?
The good news is that hospitalists are well positioned for such advancements, there is a core set of skills required for these various leadership positions that you can learn, and there are several places you can turn to for training. The trick is figuring out which skills and aptitudes you already possess, identifying those you need to strengthen, and selecting the training venues that best meet your goals. Your options vary widely, and include simply reading books on management to get up to speed quickly, investing in leadership training seminars and short courses, and pursuing advanced-degree programs in business leadership.
“Over the next 10 years, the single largest source of new CMOs might be hospitalists,” says John Nelson, MD, FACP, MHM, medical director of Overlake Hospital in Bellevue, Wash., and cofounder, past president, and past board member of SHM. “As many specialties focus more of their practice in the ambulatory care setting, that leaves behind those of us who will stay—e.g., hospitalists, radiologists, ER doctors, anesthesiologists—and who think of the hospital as their principal place of work. Of those doctors, hospitalists are probably the most interconnected and networked with all other doctors and all levels of hospital staff. That’s why hospitals are looking toward hospitalists for leadership.”
There is a growing need for HM to develop leaders, Dr. Nelson says, “not just for their own practice, but for various leadership activities within their hospital.”
Start at Self-Assessment
Hospitalist leadership is not for everyone, and you need to find out if you’re making the right decision by pursuing it. For one thing, you’ll need to facilitate consensus among physicians—a notoriously challenging group of professionals who are autonomous by training, conditioned to believe that they always wield veto power and that they don’t have to play by the rules established for everyone else, Dr. Nelson says.
Most daily leadership activities are much more open-ended and far less structured than physicians are used to, entailing simultaneous projects that need to be prioritized, says Dr. Nelson, who splits his time about 30% clinical and 70% administrative. He is a champion for his hospital’s technology initiative, medical director of his institution’s hospitalist practice, physician lead of its palliative-care program, principal of Nelson Flores Hospital Medicine Consultants, and a columnist for The Hospitalist.
How can you find out what you’re good at, what your weaknesses are, and what skills you need to build? There are several personality assessment instruments with which you can appraise your compatibility with leadership culture, says Julia S. Wright, MD, SFHM, FACP, senior medical officer for Canton, Ohio-based Hospitalists Management Group. And there are good self-assessment workbooks to test whether you have an inclination toward leadership, says Mary Jane Kornacki, MS, a partner in the Boston-based consulting firm Amicus Inc. You also can have a personal leadership assessment performed professionally (see “Leadership Self-Assessment,” p. 27).
Identify Core Leadership Requirements
There are various ways to categorize the leadership skills that a hospitalist needs, including these: financial and business literacy, technical savvy for projects like quality and patient safety improvement, planning acumen to identify external trends and implement appropriate change in one’s department or group, and emotional intelligence to engineer cooperative relationships, says Jack Silversin, DMD, DrPH, president of Amicus.
Indeed, the ability to manage the relationships with myriad stakeholders is a hospitalist leader’s central requirement, according to “Hospitalists: A Guide to Building and Sustaining a Successful Program.”1 Stakeholders include patients, families, referring physicians, medical subspecialists and surgeons, the hospital executive team (C-suite), the clinical team (nurses, case management, therapy departments, and others), the HM group itself, and the public.
The hospitalist leader is responsible for many tasks, the authors write, including:
- Blending marketplace needs with those of these various stakeholders;
- Managing budgets, billing and revenue cycles, resources, and performance metrics; and
- Overseeing such operational issues as scheduling, workload, census, staffing, and recruitment.
These duties will likely be time-consuming, but a hospitalist leader should nevertheless maintain a portion of his or her clinical practice to continue to be connected to the core work. “The foundation of your credibility as a leader is that you have excellent clinical skills,” says Winthrop F. Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and SHM cofounder and past president.
Clinical excellence is the foundation of successful leadership because the best quality and safety practices will drive successful hospitalist business practices, according to Lakshmi K. Halasyamani, MD, SFHM, SHM board member and vice president for Quality and Systems Improvement at Saint Joseph Mercy Hospital in Ann Arbor, Mich. “As healthcare reform begins to financially incentivize things like safe patient handoffs and more evidence-based medicine,” she says, “the business part of running a practice is going to quickly align with quality and safety outcomes. That’s what hospital medicine leaders should be focusing on.”
Empathy and communication skills are essential for a leader, who must continually translate messages from hospital administration to rank-and-file physicians, and vice versa, Dr. Whitcomb says. For example, he says, the message that hospitalists want better work conditions and more staff should be presented so that administration hears something like this: “We don’t want care to be unsafe; that would hurt the hospital’s reputation. Some of the hospitalists are burning out, creating the risk of increasing turnover. In fact, length of stay would be lower if the group has better staffing, because they could get the patients earlier in the day and send them home sooner.”
Such “situational awareness” is necessary to win the trust and cooperation of others and avoid becoming marginalized by important allies, says Eric Howell, MD, SFHM, director of the Hospital Medicine Division at Johns Hopkins Bayview Medical Center in Baltimore. “I’ve seen very successful advocates of hospital medicine groups who were not very good leaders,” the SHM board member says, “because they could not see what the leadership above them needed.”
Leadership Self-Assessment
The best way to examine your leadership skills is to take a test, such as the Leadership Effectiveness Analysis (LEA), which scores you on six leadership dimensions: creating a vision, developing followership, implementing the vision, following through, and achieving results, according to Dr. Wright. To understand your personality characteristics a little better, she adds, you can take basic tests like the Minnesota Multiphasic Personality Inventory (MMPI).
Other useful personality surveys that can give you an accurate sense of leadership readiness include the Myers-Briggs Type Indicator assessment and the DiSC personality assessment (the acronym reflects a four-quadrant personality model: Dominance, Influence, Steadiness, and Conscientiousness), says Kornacki.
A good self-assessment workbook to test whether you have an inclination toward leadership is Edgar H. Schein’s “Career Anchor, 3rd Edition,” Kornacki says. The book presents a taxonomy of eight competencies, which people prioritize differently: Technical/Functional, General Managerial, Autonomy/Independence, Security/ Stability, Entrepreneurial Creativity, Service/Dedication to a Cause, Pure Challenge, and Lifestyle. How you prioritize those themes offers insight into your values and motivations as a leader.
You might also consider having a professional assess your leadership strengths and weaknesses. Companies like Personnel Decisions International (www.personneldecisions.com) offer coaches who interact with you to assess your cognitive and experiential skills and make recommendations on what you need to work on, says Dr. Klocke.
Pursue the Right Training Venues
Once you’ve identified your strengths and weaknesses, as well as the core requirements of your leadership duties, you are ready to pursue the right training path. Leadership can be learned, whether you’re thrust into it and find yourself in “damage control” mode, or you want to pursue new leadership opportunities for career advancement, Dr. Howell says.
Your first step might be to develop your leadership skill set through informal self-help training. The easiest way is by reading books that other hospitalist leaders have found to be valuable when they were starting out (see “Self-Training Resources,” below left).
The next step is to find a mentor. This person should be a good leader whom you trust and respect, and from whom you can seek advice. “A leadership position can be awfully lonely,” Dr. Nelson says. “I suggest that people find a confidant and mentor at their local institution, someone who is very accessible, who they see all the time, who works in the same environment and knows the local politics.” The mentor could be someone you trained with, or under, or perhaps a hospitalist program director at another institution. It could be the chief nursing officer at your institution. “It is reassuring to know that others are facing similar problems elsewhere,” Dr. Nelson adds.
A local mentor can help with technical matters like offering you a “crash course” in financial spreadsheets, says Patience Agborbesong, MD, SFHM, medical director of a 17-hospitalist program at Wake Forest University Baptist Medical Center in Winston-Salem, N.C. She notes that SHM provides networking resources to help you connect with other HM leaders (www.hospitalmedicine.org/leadership).
Large hospitalist groups frequently offer mentorship opportunities throughout their chain of operations, says Ethan B. Dunham, MBA, director of organizational development for Brentwood, Tenn.-based Cogent Healthcare. “If you find you’ve received something akin to a ‘battlefield promotion’ and are in over your head, you can turn to someone who has been there,” Dunham says.
Many larger health systems and academic medical centers—and even some community hospitals—offer in-house leadership training and mentorship programs, says David L. Klocke, MD, chair of the Division of Hospital Internal Medicine at Mayo Clinic in Rochester, Minn. In his institution, physician leaders are paired with partners from administration who fill in any gaps in their management or leadership skills, Dr. Klocke says. “You’re mentoring them as well about medical issues and skills,” he adds.
Another way to hone your skills is to join hospital committees. “Build up time in the saddle,” Dunham says. “Indicate your leadership potential and your interest in taking the next steps.” If you seek out committees, you’ll get on them, Dr. Nelson says. “And once on them, if you can distinguish yourself by helping to lead the committee in a good direction, your career will be off and running,” he explains. There are many kinds of hospital committee work to choose from, including peer review, performance improvement, practice guideline development, utilization review, pharmacy, and therapeutics.
Advanced Training
For hospitalists wanting a deeper dive, more formal business and leadership training is available through a variety of workshops and courses, many of which offer CME credit. “My favorite was the SHM Leadership Academy, which is fairly short and very practical. Every minute was directly relevant to me as a hospitalist,” Dr. Howell says of the four-day program. Covered topics include teamwork collaboration, communication strategies, hospital performance metrics, scheduling and compensation, strategic planning, financial reports, recruitment, negotiation, motivating others, and managing physician performance.
The American College of Physician Executives (ACPE) offers leadership training modules with certification, as well as MBA and MMM (master’s in medical management) programs through partnerships with universities, according to Dr. Agborbesong. There are several other organizations that offer leadership training, she notes, including The Institute for Medical Leadership, the Boot Camp on Leadership Fundamentals for Physicians, the Center for Creative Leadership, and the Carolinas Center for Medical Excellence (CCME) Physician Leadership Institute.
An MBA is an appropriate goal for many hospitalist leadership scenarios, such as entry-level program director, lead hospitalist at a healthcare system with multiple hospital medicine programs, or regional coordinator for a hospital medicine staffing company, says Michael Stahl, PhD, director of the Physician Executive MBA Program and professor of Strategy and Business Planning at the University of Tennessee in Knoxville.
“An MBA program is particularly well-suited to the physician who gets invited, all of a sudden, to be a leader and discovers they don’t have the knowledge, skill sets, tools and techniques, and ways of thinking about the business side of healthcare. It’s not unusual to see people at the start of their leadership careers saying, ‘I’m going to make an investment in my own human capital by earning an accredited MBA,’ ” Stahl says.
A rapidly changing healthcare landscape requires greater attention to business planning, capital and budget, revenue, and cost-containment principles, Stahl notes. “There will be incredible pressure on controlling the cost of healthcare in the future,” he says. “New reimbursement models are probably going to yield lower reimbursement. What we’re most interested in is equipping people with the tools and techniques of finance so that they can learn to model those new reimbursement types, whatever they are, and no matter how their regulations change.”
Although an MBA sounds daunting, many programs are tailored to a new leader’s busy schedule. For example, the Physician Executive MBA program at UT-Knoxville takes only one year to complete, focuses entirely on healthcare contexts, and combines four weeklong residence periods on campus with 40 Web-based classes, typically on Saturday mornings.
Traditional MBA programs typically take two years to complete and require more physical presence on campus. But in return, they offer ongoing face-to-face interaction with faculty and peers from a variety of business backgrounds that immerse you in the culture of business leadership, says Guy David, PhD, assistant professor of Healthcare Management at the Wharton School at the University of Pennsylvania in Philadelphia. Coursework includes finance, marketing, management, entrepreneurship, strategic development, data mining, economics, legal issues, IT, and other areas, David says. The coursework, he adds, gives physicians who have been trained to focus on the individual patient a much broader understanding of the system in which they operate.
Successful career advancement ultimately requires managerial and leadership acumen: proof that you can run the business, manage upstream and downstream communication, and handle administrative and liaison duties within the hospital, Dunham says. “An MBA is a shorthand, a way to signal to people that that skill set exists, maybe rather than having to prove it in the trenches,” he adds.
As the healthcare landscape continues to evolve, there will be a growing demand for physicians—particularly hospitalists—with greater procedural and conceptual understanding of healthcare systems and financials.
“Over time, it may become increasingly important to have received formal education in the business discipline,” Dunham says. “That’s something that time will tell.” TH
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Reference
- Miller JA, Nelson JR, Whitcomb WF. Hospitalists: A Guide to Building and Sustaining a Successful Program. Health Administration Press: Chicago; 2008.
Veteran Advice For Aspiring HM leaders
Think carefully about whether you’re appropriately balancing the interests of your employer (i.e. the hospital) and the physicians in your group. Some hospitalist group leaders tilt toward being “union pit bosses” and beat up management, lobbying aggressively for their groups’ interests, Dr. Nelson explains. Other hospitalist leaders tilt too far the opposite way and try to beat the physicians into submitting to whatever the hospital might want. You’re going to be talking to both parties about all kinds of issues on a long-term basis, and you need to forsake adversarial negotiating tactics to cultivate long-term relationships.
Don’t make promises that are hard to keep. A leader often faces a tricky issue and might be tempted to take the easy way out by granting special deals, caving in, or meeting demands (e.g. promising a desirable scheduling arrangement as a recruiting inducement). That’s a rookie mistake, Dr. Nelson says, and others in the practice might resent it.
Advocating for your physicians doesn’t always mean more pay, bigger offices, or better benefits. “Good leadership goes beyond that,” Dr. Howell says, “by having good situational awareness to notice what’s important to other parties and building their trust.” By turning one of his offices into a part-time lactation room for mothers with newborns (half of his hospitalists were women of childbearing age, and five of them gave birth in the same year), Dr. Howell earned their trust and respect for the price of a door lock and a small refrigerator.
Perhaps you’ve put in a few years of clinical practice in an HM group. Suddenly, your group needs a director—and everybody stepped back, except you. You now find yourself thrust into an unfamiliar world of bottom-line thinking, budgets, schedules, spreadsheets, decision-making, conflict resolution, recruiting, contract negotiations, and other managerial responsibilities. You’ve tried to learn how to perform most of these duties on the job. But you’ve learned that assuming direct responsibility for the fate of a hospitalist group with millions in annual billing requires skills that weren’t taught in medical school. And you’re struggling.
Maybe you’re a hospitalist residency program director in a teaching hospital setting, and you would like to transition into other hospital administrative leadership roles, such as chair of a medical staff or credentials committee, department chair, vice president of medical affairs, chief medical officer—maybe even CEO. But where do you begin?
The good news is that hospitalists are well positioned for such advancements, there is a core set of skills required for these various leadership positions that you can learn, and there are several places you can turn to for training. The trick is figuring out which skills and aptitudes you already possess, identifying those you need to strengthen, and selecting the training venues that best meet your goals. Your options vary widely, and include simply reading books on management to get up to speed quickly, investing in leadership training seminars and short courses, and pursuing advanced-degree programs in business leadership.
“Over the next 10 years, the single largest source of new CMOs might be hospitalists,” says John Nelson, MD, FACP, MHM, medical director of Overlake Hospital in Bellevue, Wash., and cofounder, past president, and past board member of SHM. “As many specialties focus more of their practice in the ambulatory care setting, that leaves behind those of us who will stay—e.g., hospitalists, radiologists, ER doctors, anesthesiologists—and who think of the hospital as their principal place of work. Of those doctors, hospitalists are probably the most interconnected and networked with all other doctors and all levels of hospital staff. That’s why hospitals are looking toward hospitalists for leadership.”
There is a growing need for HM to develop leaders, Dr. Nelson says, “not just for their own practice, but for various leadership activities within their hospital.”
Start at Self-Assessment
Hospitalist leadership is not for everyone, and you need to find out if you’re making the right decision by pursuing it. For one thing, you’ll need to facilitate consensus among physicians—a notoriously challenging group of professionals who are autonomous by training, conditioned to believe that they always wield veto power and that they don’t have to play by the rules established for everyone else, Dr. Nelson says.
Most daily leadership activities are much more open-ended and far less structured than physicians are used to, entailing simultaneous projects that need to be prioritized, says Dr. Nelson, who splits his time about 30% clinical and 70% administrative. He is a champion for his hospital’s technology initiative, medical director of his institution’s hospitalist practice, physician lead of its palliative-care program, principal of Nelson Flores Hospital Medicine Consultants, and a columnist for The Hospitalist.
How can you find out what you’re good at, what your weaknesses are, and what skills you need to build? There are several personality assessment instruments with which you can appraise your compatibility with leadership culture, says Julia S. Wright, MD, SFHM, FACP, senior medical officer for Canton, Ohio-based Hospitalists Management Group. And there are good self-assessment workbooks to test whether you have an inclination toward leadership, says Mary Jane Kornacki, MS, a partner in the Boston-based consulting firm Amicus Inc. You also can have a personal leadership assessment performed professionally (see “Leadership Self-Assessment,” p. 27).
Identify Core Leadership Requirements
There are various ways to categorize the leadership skills that a hospitalist needs, including these: financial and business literacy, technical savvy for projects like quality and patient safety improvement, planning acumen to identify external trends and implement appropriate change in one’s department or group, and emotional intelligence to engineer cooperative relationships, says Jack Silversin, DMD, DrPH, president of Amicus.
Indeed, the ability to manage the relationships with myriad stakeholders is a hospitalist leader’s central requirement, according to “Hospitalists: A Guide to Building and Sustaining a Successful Program.”1 Stakeholders include patients, families, referring physicians, medical subspecialists and surgeons, the hospital executive team (C-suite), the clinical team (nurses, case management, therapy departments, and others), the HM group itself, and the public.
The hospitalist leader is responsible for many tasks, the authors write, including:
- Blending marketplace needs with those of these various stakeholders;
- Managing budgets, billing and revenue cycles, resources, and performance metrics; and
- Overseeing such operational issues as scheduling, workload, census, staffing, and recruitment.
These duties will likely be time-consuming, but a hospitalist leader should nevertheless maintain a portion of his or her clinical practice to continue to be connected to the core work. “The foundation of your credibility as a leader is that you have excellent clinical skills,” says Winthrop F. Whitcomb, MD, MHM, medical director of healthcare quality at Baystate Medical Center in Springfield, Mass., and SHM cofounder and past president.
Clinical excellence is the foundation of successful leadership because the best quality and safety practices will drive successful hospitalist business practices, according to Lakshmi K. Halasyamani, MD, SFHM, SHM board member and vice president for Quality and Systems Improvement at Saint Joseph Mercy Hospital in Ann Arbor, Mich. “As healthcare reform begins to financially incentivize things like safe patient handoffs and more evidence-based medicine,” she says, “the business part of running a practice is going to quickly align with quality and safety outcomes. That’s what hospital medicine leaders should be focusing on.”
Empathy and communication skills are essential for a leader, who must continually translate messages from hospital administration to rank-and-file physicians, and vice versa, Dr. Whitcomb says. For example, he says, the message that hospitalists want better work conditions and more staff should be presented so that administration hears something like this: “We don’t want care to be unsafe; that would hurt the hospital’s reputation. Some of the hospitalists are burning out, creating the risk of increasing turnover. In fact, length of stay would be lower if the group has better staffing, because they could get the patients earlier in the day and send them home sooner.”
Such “situational awareness” is necessary to win the trust and cooperation of others and avoid becoming marginalized by important allies, says Eric Howell, MD, SFHM, director of the Hospital Medicine Division at Johns Hopkins Bayview Medical Center in Baltimore. “I’ve seen very successful advocates of hospital medicine groups who were not very good leaders,” the SHM board member says, “because they could not see what the leadership above them needed.”
Leadership Self-Assessment
The best way to examine your leadership skills is to take a test, such as the Leadership Effectiveness Analysis (LEA), which scores you on six leadership dimensions: creating a vision, developing followership, implementing the vision, following through, and achieving results, according to Dr. Wright. To understand your personality characteristics a little better, she adds, you can take basic tests like the Minnesota Multiphasic Personality Inventory (MMPI).
Other useful personality surveys that can give you an accurate sense of leadership readiness include the Myers-Briggs Type Indicator assessment and the DiSC personality assessment (the acronym reflects a four-quadrant personality model: Dominance, Influence, Steadiness, and Conscientiousness), says Kornacki.
A good self-assessment workbook to test whether you have an inclination toward leadership is Edgar H. Schein’s “Career Anchor, 3rd Edition,” Kornacki says. The book presents a taxonomy of eight competencies, which people prioritize differently: Technical/Functional, General Managerial, Autonomy/Independence, Security/ Stability, Entrepreneurial Creativity, Service/Dedication to a Cause, Pure Challenge, and Lifestyle. How you prioritize those themes offers insight into your values and motivations as a leader.
You might also consider having a professional assess your leadership strengths and weaknesses. Companies like Personnel Decisions International (www.personneldecisions.com) offer coaches who interact with you to assess your cognitive and experiential skills and make recommendations on what you need to work on, says Dr. Klocke.
Pursue the Right Training Venues
Once you’ve identified your strengths and weaknesses, as well as the core requirements of your leadership duties, you are ready to pursue the right training path. Leadership can be learned, whether you’re thrust into it and find yourself in “damage control” mode, or you want to pursue new leadership opportunities for career advancement, Dr. Howell says.
Your first step might be to develop your leadership skill set through informal self-help training. The easiest way is by reading books that other hospitalist leaders have found to be valuable when they were starting out (see “Self-Training Resources,” below left).
The next step is to find a mentor. This person should be a good leader whom you trust and respect, and from whom you can seek advice. “A leadership position can be awfully lonely,” Dr. Nelson says. “I suggest that people find a confidant and mentor at their local institution, someone who is very accessible, who they see all the time, who works in the same environment and knows the local politics.” The mentor could be someone you trained with, or under, or perhaps a hospitalist program director at another institution. It could be the chief nursing officer at your institution. “It is reassuring to know that others are facing similar problems elsewhere,” Dr. Nelson adds.
A local mentor can help with technical matters like offering you a “crash course” in financial spreadsheets, says Patience Agborbesong, MD, SFHM, medical director of a 17-hospitalist program at Wake Forest University Baptist Medical Center in Winston-Salem, N.C. She notes that SHM provides networking resources to help you connect with other HM leaders (www.hospitalmedicine.org/leadership).
Large hospitalist groups frequently offer mentorship opportunities throughout their chain of operations, says Ethan B. Dunham, MBA, director of organizational development for Brentwood, Tenn.-based Cogent Healthcare. “If you find you’ve received something akin to a ‘battlefield promotion’ and are in over your head, you can turn to someone who has been there,” Dunham says.
Many larger health systems and academic medical centers—and even some community hospitals—offer in-house leadership training and mentorship programs, says David L. Klocke, MD, chair of the Division of Hospital Internal Medicine at Mayo Clinic in Rochester, Minn. In his institution, physician leaders are paired with partners from administration who fill in any gaps in their management or leadership skills, Dr. Klocke says. “You’re mentoring them as well about medical issues and skills,” he adds.
Another way to hone your skills is to join hospital committees. “Build up time in the saddle,” Dunham says. “Indicate your leadership potential and your interest in taking the next steps.” If you seek out committees, you’ll get on them, Dr. Nelson says. “And once on them, if you can distinguish yourself by helping to lead the committee in a good direction, your career will be off and running,” he explains. There are many kinds of hospital committee work to choose from, including peer review, performance improvement, practice guideline development, utilization review, pharmacy, and therapeutics.
Advanced Training
For hospitalists wanting a deeper dive, more formal business and leadership training is available through a variety of workshops and courses, many of which offer CME credit. “My favorite was the SHM Leadership Academy, which is fairly short and very practical. Every minute was directly relevant to me as a hospitalist,” Dr. Howell says of the four-day program. Covered topics include teamwork collaboration, communication strategies, hospital performance metrics, scheduling and compensation, strategic planning, financial reports, recruitment, negotiation, motivating others, and managing physician performance.
The American College of Physician Executives (ACPE) offers leadership training modules with certification, as well as MBA and MMM (master’s in medical management) programs through partnerships with universities, according to Dr. Agborbesong. There are several other organizations that offer leadership training, she notes, including The Institute for Medical Leadership, the Boot Camp on Leadership Fundamentals for Physicians, the Center for Creative Leadership, and the Carolinas Center for Medical Excellence (CCME) Physician Leadership Institute.
An MBA is an appropriate goal for many hospitalist leadership scenarios, such as entry-level program director, lead hospitalist at a healthcare system with multiple hospital medicine programs, or regional coordinator for a hospital medicine staffing company, says Michael Stahl, PhD, director of the Physician Executive MBA Program and professor of Strategy and Business Planning at the University of Tennessee in Knoxville.
“An MBA program is particularly well-suited to the physician who gets invited, all of a sudden, to be a leader and discovers they don’t have the knowledge, skill sets, tools and techniques, and ways of thinking about the business side of healthcare. It’s not unusual to see people at the start of their leadership careers saying, ‘I’m going to make an investment in my own human capital by earning an accredited MBA,’ ” Stahl says.
A rapidly changing healthcare landscape requires greater attention to business planning, capital and budget, revenue, and cost-containment principles, Stahl notes. “There will be incredible pressure on controlling the cost of healthcare in the future,” he says. “New reimbursement models are probably going to yield lower reimbursement. What we’re most interested in is equipping people with the tools and techniques of finance so that they can learn to model those new reimbursement types, whatever they are, and no matter how their regulations change.”
Although an MBA sounds daunting, many programs are tailored to a new leader’s busy schedule. For example, the Physician Executive MBA program at UT-Knoxville takes only one year to complete, focuses entirely on healthcare contexts, and combines four weeklong residence periods on campus with 40 Web-based classes, typically on Saturday mornings.
Traditional MBA programs typically take two years to complete and require more physical presence on campus. But in return, they offer ongoing face-to-face interaction with faculty and peers from a variety of business backgrounds that immerse you in the culture of business leadership, says Guy David, PhD, assistant professor of Healthcare Management at the Wharton School at the University of Pennsylvania in Philadelphia. Coursework includes finance, marketing, management, entrepreneurship, strategic development, data mining, economics, legal issues, IT, and other areas, David says. The coursework, he adds, gives physicians who have been trained to focus on the individual patient a much broader understanding of the system in which they operate.
Successful career advancement ultimately requires managerial and leadership acumen: proof that you can run the business, manage upstream and downstream communication, and handle administrative and liaison duties within the hospital, Dunham says. “An MBA is a shorthand, a way to signal to people that that skill set exists, maybe rather than having to prove it in the trenches,” he adds.
As the healthcare landscape continues to evolve, there will be a growing demand for physicians—particularly hospitalists—with greater procedural and conceptual understanding of healthcare systems and financials.
“Over time, it may become increasingly important to have received formal education in the business discipline,” Dunham says. “That’s something that time will tell.” TH
Chris Guadagnino is a freelance medical writer based in Philadelphia.
Reference
- Miller JA, Nelson JR, Whitcomb WF. Hospitalists: A Guide to Building and Sustaining a Successful Program. Health Administration Press: Chicago; 2008.
Veteran Advice For Aspiring HM leaders
Think carefully about whether you’re appropriately balancing the interests of your employer (i.e. the hospital) and the physicians in your group. Some hospitalist group leaders tilt toward being “union pit bosses” and beat up management, lobbying aggressively for their groups’ interests, Dr. Nelson explains. Other hospitalist leaders tilt too far the opposite way and try to beat the physicians into submitting to whatever the hospital might want. You’re going to be talking to both parties about all kinds of issues on a long-term basis, and you need to forsake adversarial negotiating tactics to cultivate long-term relationships.
Don’t make promises that are hard to keep. A leader often faces a tricky issue and might be tempted to take the easy way out by granting special deals, caving in, or meeting demands (e.g. promising a desirable scheduling arrangement as a recruiting inducement). That’s a rookie mistake, Dr. Nelson says, and others in the practice might resent it.
Advocating for your physicians doesn’t always mean more pay, bigger offices, or better benefits. “Good leadership goes beyond that,” Dr. Howell says, “by having good situational awareness to notice what’s important to other parties and building their trust.” By turning one of his offices into a part-time lactation room for mothers with newborns (half of his hospitalists were women of childbearing age, and five of them gave birth in the same year), Dr. Howell earned their trust and respect for the price of a door lock and a small refrigerator.
Infection-prevention professionals, hospital officials suggest steps to simplify and streamline HAI tracking system
Infection-prevention leaders and state hospital association representatives participated in regional meetings sponsored across the country during the summer of 2009 by the U.S. Department of Health and Human Services (HHS) and suggested ways that the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network (NHSN)—a leading federal system for tracking healthcare-associated infections (HAIs)—could be made easier for hospitals. Participants recommended steps to reduce data-collection burdens and to increase usefulness for hospital infection prevention and quality-improvement (QI) programs.
HHS convened the regional meetings to get stakeholders’ input into HHS’ Action Plan to Prevent Healthcare-Associated Infections (www.hhs.gov/ophs/initiatives/hai/index.html), as well as to hear about their experiences with the network. The action plan is a blueprint for HAI prevention and sets specific targets for monitoring and preventing HAIs nationally. Leaders from various HHS agencies, including the Agency for Healthcare Research and Quality (AHRQ), CDC, Centers for Medicare and Medicaid Services (CMS), the National Institutes of Health (NIH), and the Office of Public Health and Science joined me in discussing participants’ concerns at these meetings.
HHS uses NHSN data to help monitor progress toward the action plan goals. Twenty-eight states require hospitals to report HAIs publicly; most use the NHSN (www.cdc.gov/nhsn). Hospital enrollment in the NHSN has increased dramatically, to more than 2,700 hospitals in mid-2010 from 300 in 2005.
Daniel Pollock, MD, the surveillance branch chief for CDC’s Division of Healthcare Quality Promotion, and I reported on CDC’s efforts to update the NHSN and improve its ease of use. Simplifying and streamlining the system, and assuring sufficient technical capacity and user support, are top priorities. For example:
- CDC has instituted changes in data collection requirements for healthcare-associated urinary tract infections into the NHSN application;
- More NHSN staff were hired to perform comprehensive assessments and upgrades of the system’s technical infrastructure and usability, and to provide additional user support for enrollment and training;
- NHSN will begin migrating this fall to a new system of authenticating users; and
- NHSN Web pages are being redesigned to speed response times during peak use.
Dr. Pollock emphasized that the CDC is committed to accelerating the transition from manual to electronic case detection and reporting for the NHSN, and leveraging advances in health information technology as a primary strategy for enhancing the NHSN. As part of that effort, NHSN now is accepting electronic infection records submitted by hospitals that use commercial infection control surveillance systems.
The CDC continues to work closely with AHRQ, CMS, and the Office of the National Coordinator for Health Information Technology to coordinate integration efforts of federal information systems that provide HAI data. That is part of our commitment here in Washington to support hospitals’ efforts to reduce and eliminate HAIs, and to make healthcare safer for patients and families.
Don Wright, MD, MPH,
deputy assistant secretary for healthcare quality,
U.S. Department of Health and Human Services
Infection-prevention leaders and state hospital association representatives participated in regional meetings sponsored across the country during the summer of 2009 by the U.S. Department of Health and Human Services (HHS) and suggested ways that the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network (NHSN)—a leading federal system for tracking healthcare-associated infections (HAIs)—could be made easier for hospitals. Participants recommended steps to reduce data-collection burdens and to increase usefulness for hospital infection prevention and quality-improvement (QI) programs.
HHS convened the regional meetings to get stakeholders’ input into HHS’ Action Plan to Prevent Healthcare-Associated Infections (www.hhs.gov/ophs/initiatives/hai/index.html), as well as to hear about their experiences with the network. The action plan is a blueprint for HAI prevention and sets specific targets for monitoring and preventing HAIs nationally. Leaders from various HHS agencies, including the Agency for Healthcare Research and Quality (AHRQ), CDC, Centers for Medicare and Medicaid Services (CMS), the National Institutes of Health (NIH), and the Office of Public Health and Science joined me in discussing participants’ concerns at these meetings.
HHS uses NHSN data to help monitor progress toward the action plan goals. Twenty-eight states require hospitals to report HAIs publicly; most use the NHSN (www.cdc.gov/nhsn). Hospital enrollment in the NHSN has increased dramatically, to more than 2,700 hospitals in mid-2010 from 300 in 2005.
Daniel Pollock, MD, the surveillance branch chief for CDC’s Division of Healthcare Quality Promotion, and I reported on CDC’s efforts to update the NHSN and improve its ease of use. Simplifying and streamlining the system, and assuring sufficient technical capacity and user support, are top priorities. For example:
- CDC has instituted changes in data collection requirements for healthcare-associated urinary tract infections into the NHSN application;
- More NHSN staff were hired to perform comprehensive assessments and upgrades of the system’s technical infrastructure and usability, and to provide additional user support for enrollment and training;
- NHSN will begin migrating this fall to a new system of authenticating users; and
- NHSN Web pages are being redesigned to speed response times during peak use.
Dr. Pollock emphasized that the CDC is committed to accelerating the transition from manual to electronic case detection and reporting for the NHSN, and leveraging advances in health information technology as a primary strategy for enhancing the NHSN. As part of that effort, NHSN now is accepting electronic infection records submitted by hospitals that use commercial infection control surveillance systems.
The CDC continues to work closely with AHRQ, CMS, and the Office of the National Coordinator for Health Information Technology to coordinate integration efforts of federal information systems that provide HAI data. That is part of our commitment here in Washington to support hospitals’ efforts to reduce and eliminate HAIs, and to make healthcare safer for patients and families.
Don Wright, MD, MPH,
deputy assistant secretary for healthcare quality,
U.S. Department of Health and Human Services
Infection-prevention leaders and state hospital association representatives participated in regional meetings sponsored across the country during the summer of 2009 by the U.S. Department of Health and Human Services (HHS) and suggested ways that the Centers for Disease Control and Prevention’s (CDC) National Healthcare Safety Network (NHSN)—a leading federal system for tracking healthcare-associated infections (HAIs)—could be made easier for hospitals. Participants recommended steps to reduce data-collection burdens and to increase usefulness for hospital infection prevention and quality-improvement (QI) programs.
HHS convened the regional meetings to get stakeholders’ input into HHS’ Action Plan to Prevent Healthcare-Associated Infections (www.hhs.gov/ophs/initiatives/hai/index.html), as well as to hear about their experiences with the network. The action plan is a blueprint for HAI prevention and sets specific targets for monitoring and preventing HAIs nationally. Leaders from various HHS agencies, including the Agency for Healthcare Research and Quality (AHRQ), CDC, Centers for Medicare and Medicaid Services (CMS), the National Institutes of Health (NIH), and the Office of Public Health and Science joined me in discussing participants’ concerns at these meetings.
HHS uses NHSN data to help monitor progress toward the action plan goals. Twenty-eight states require hospitals to report HAIs publicly; most use the NHSN (www.cdc.gov/nhsn). Hospital enrollment in the NHSN has increased dramatically, to more than 2,700 hospitals in mid-2010 from 300 in 2005.
Daniel Pollock, MD, the surveillance branch chief for CDC’s Division of Healthcare Quality Promotion, and I reported on CDC’s efforts to update the NHSN and improve its ease of use. Simplifying and streamlining the system, and assuring sufficient technical capacity and user support, are top priorities. For example:
- CDC has instituted changes in data collection requirements for healthcare-associated urinary tract infections into the NHSN application;
- More NHSN staff were hired to perform comprehensive assessments and upgrades of the system’s technical infrastructure and usability, and to provide additional user support for enrollment and training;
- NHSN will begin migrating this fall to a new system of authenticating users; and
- NHSN Web pages are being redesigned to speed response times during peak use.
Dr. Pollock emphasized that the CDC is committed to accelerating the transition from manual to electronic case detection and reporting for the NHSN, and leveraging advances in health information technology as a primary strategy for enhancing the NHSN. As part of that effort, NHSN now is accepting electronic infection records submitted by hospitals that use commercial infection control surveillance systems.
The CDC continues to work closely with AHRQ, CMS, and the Office of the National Coordinator for Health Information Technology to coordinate integration efforts of federal information systems that provide HAI data. That is part of our commitment here in Washington to support hospitals’ efforts to reduce and eliminate HAIs, and to make healthcare safer for patients and families.
Don Wright, MD, MPH,
deputy assistant secretary for healthcare quality,
U.S. Department of Health and Human Services