User login
Market Watch
New Drugs, Indications, Dosage Forms, and Approvals
- Hydromorphone extended-release tablets (Exalgo) have been approved by the FDA as a once-daily treatment for managing moderate to severe pain in opioid-tolerant patients needing continuous opioid analgesia for an extended period of time.1 This formulation uses the OROS osmotic delivery system to control the release rate. It is a CII controlled substance and is accompanied by a comprehensive Risk Evaluation and Mitigation Strategy (REMS) to ensure that the medication’s benefits outweigh its risks.
- IMGN910 has received orphan drug status for treating Merkel cell carcinoma, a skin cancer that usually occurs on the head or neck.2 It is in early-stage clinical trials.
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA as a once-weekly immunoglobulin replacement therapy for patients with primary immunodeficiency.3 It’s the first 20% subcutaneous immunoglobulin to receive FDA approval. This high-concentration product is stabilized with L-proline, a naturally occurring amino acid, which allows it to be stored at room temperature (up to 25°C [77°F]). Some adverse reactions include injection site bruising, pain, cysts, eczema, irritation, headache, cough, diarrhea, and fatigue.4
- Velaglucerase alfa for injection (VPRIV) has been approved by the FDA to treat adults and children with the rare genetic disorder Gaucher disease.5 Patients with Gaucher disease have a deficiency of the glucocerebrosidase enzyme. This enzyme prevents lipids from building up in the liver, spleen, bone marrow, and nervous system, which prevents them from working properly. VPRIV, a long-term replacement therapy, is approved for Type 1 Gaucher disease, the most common form, and is an alternative to imiglucerase (Cerezyme), which is in short supply. The most common reactions seen in clinical trials were allergic reactions, headache, dizziness, abdominal and back pain, nausea, fatigue/weakness, fever, and prolonged activated partial thromboplastin time.
Pipeline
- Betrixaban is a once-daily oral anticoagulant in Phase 2 clinical studies.6 Compared with warfarin in the EXPLORE-Xa study, betrixaban decreased the bleeding incidence in patients with nonvalvular atrial fibrillation or atrial flutter who had at least one stroke risk factor. The major and clinically relevant nonmajor bleeding episodes occurred less frequently in betrixaban-treated patients.
- Dabigatran etexilate is an oral anticoagulant in Phase 3 clinical trials.7 At the recent American College of Cardiology meeting in Ingelheim, Germany, dabigatran demonstrated consistent stroke prevention in patients with atrial fibrillation. It also reduced the number of strokes in patients with atrial fibrillation, compared with warfarin therapy. Additionally, dabigatran etexilate 110 mg and 150 mg twice daily was associated with a lower rate of major bleeding compared with warfarin in atrial fibrillation patients at low risk of stroke.
- Fentanyl sublingual spray (SL Spray) is in Phase 3 clinical trials to treat breakthrough pain in cancer patients. Sublingual administration of this product showed rapid, effective pain relief within five minutes.8
- Ketamine intranasal (Ereska) is a nonopioid NMDA receptor antagonist analgesic, which is undergoing Phase 3 clinical trials for managing moderate to severe acute pain.9 Studies have shown rapid, statistically significant relief of moderate to severe acute postoperative pain following dental surgery, following a variety of major orthopedic surgical procedures, and in cancer breakthrough pain.
- Lu AA21004 and Lu AA24530 are undergoing Phase 3 clinical trials for treating major depressive disorder (MDD).10 Lu AA21004 is a 5-HT3, 5-HT7 and 5-HT1B receptor antagonist, 5HT1A receptor agonist, and 5-HT transporter inhibitor. To date, it has shown a low propensity for drug-drug interactions and is extensively metabolized in the liver. Lu AA24530 has shown activity as a multimodal enhancer with reuptake inhibition at monoamine transporters, and having 5-HT3 and 5-HT2c receptor antagonist activity.
- Lurasidone is an atypical antipsychotic with high affinity and antagonist effects at the dopamine D2, serotonin 5-HT2, and serotonin 5-HT7 receptors.11 It is a partial agonist at serotonin 5HT1A receptor. The NDA was filed for this agent Dec. 30, 2009.
- Mipomersen, an apo-B synthesis inhibitor, is in Phase 3 clinical trials for treating patients with homozygous familial hypercholesterolemia (HoFM).12 This agent is proposed to reduce LDL-C by preventing the development of atherogenic lipids. In a study published in Lancet, mipomersen reduced LDL-C levels by an average of more than 100 mg/dL in HoFM patients.13
- Oxycodone/niacin (Acurox), an abuse deterrent formulation for this popular opioid, has been rejected by the FDA.14 According to the FDA and its review committee, the rejection was due to the “flushing” from the niacin, which was deemed ineffective as an abuse deterrent. In addition, the FDA said the “flushing” could be overcome by food intake or administration with over-the-counter pain relievers.
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol.15 It is in Phase 3 clinical trials for treating asthma. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- FDA approves Exaglo (hydromorphone HCl) extended-release tablets. Drugs.com website. Available at: www.drugs.com/newdrugs/fda-approves-exaglo-hydromorphone-hcl-extended-release-2033.html?printable=1. Accessed April 27, 2010.
- ImmunoGen’s skin cancer drug gets orphan drug status. Reuters website. Available at: www.reuters.com/article/idUSSGE6270L720100308. Accessed April 27, 2010.
- CSL Behring receives FDA approval of Hizentra, first 20 percent subcutaneous immunoglobulin therapy. Drugs.com website. Available at: www.drugs.com/newdrugs/csl-behring-receives-fda-approval-hizentra-first-20-percent-subcutaneous-immunoglobulin-therapy-2037.html. Accessed April 27, 2010.
- Petrochko C. FDA okays 20% skin-injection immunodeficiency treatment. MedPage Today website. Available at: www.medpagetoday.com/tbprint.cfm?tbid=18858. Accessed April 27, 2010.
- Gansz Bobo E. FDA approves therapy to treat Gaucher disease. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm202288.htm. Accessed April 27, 2010.
- Portola Pharmaceuticals and Merck announce that Phase 2 study showed investigational factor Xa inhibitor, betrixaban, reduced incidence of bleeding compared to warfarin in patients with atrial fibrillation. Merck website. Available at: www.merck.com/newsroom/news-release-archive/research-and-development/2010_0315.html. Accessed April 27, 2010.
- Dabigatran etexilate shows greater reductions than warfarin in stroke in patients with atrial fibrillation across all stroke risk groups. Beohringer Ingelheim website. Available at: www.boehringer-ingelheim.com/news/news_releases/press_releases/2010/15_march_2010.html. Accessed April 27, 2010.
- INSYS Therapeutics, Inc. Announces Positive Phase III Efficacy Trial Results for Fentanyl Sublingual Spray. INSYS Therapeutics website. Available at: www.insysrx.com/news.htm. Accessed April 27, 2010.
- Third party reexamination of Javelin Pharmaceuticals’ Phase III trial data for Ereska (intranasal ketamine) yields statistically significant primary endpoint. Javelin website. Available at: ir.javelinpharmaceuticals.com/releasedetail.cfm?ReleaseID=444353. Accessed April 27, 2010.
- Lundbeck and Takeda finalise plans to initiate phase III pivotal clinical trials with Lu AA21004 and Lu AA24530. Takeda Pharmaceutical Company Limited website. Available at: www.takeda.com/press/article_35859.html. Accessed April 27, 2010.
- Dainippon Sumitomo Pharma America announces FDA acceptance of lurasidone new drug application for treatment of schizophrenia. PR Newswire website. Available at: www.prnewswire.com/news-releases/dainippon-sumitomo-pharma-america-announces-fda-acceptance-of-lurasidone-new-drug-application-for-treatment-of-schizophrenia-87265597.html. Accessed April 27, 2010.
- Mipomersen Phase 3 study in HoFH featured in The Lancet. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100315005928. Accessed April 27, 2010.
- Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9719):998-1006.
- US FDA panel rejects King, Acura painkiller. Reuters website. Available at: www.reuters.com/assets/print?aid=USN2223552220100422. Accessed April 27, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed April 27, 2010.
New Drugs, Indications, Dosage Forms, and Approvals
- Hydromorphone extended-release tablets (Exalgo) have been approved by the FDA as a once-daily treatment for managing moderate to severe pain in opioid-tolerant patients needing continuous opioid analgesia for an extended period of time.1 This formulation uses the OROS osmotic delivery system to control the release rate. It is a CII controlled substance and is accompanied by a comprehensive Risk Evaluation and Mitigation Strategy (REMS) to ensure that the medication’s benefits outweigh its risks.
- IMGN910 has received orphan drug status for treating Merkel cell carcinoma, a skin cancer that usually occurs on the head or neck.2 It is in early-stage clinical trials.
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA as a once-weekly immunoglobulin replacement therapy for patients with primary immunodeficiency.3 It’s the first 20% subcutaneous immunoglobulin to receive FDA approval. This high-concentration product is stabilized with L-proline, a naturally occurring amino acid, which allows it to be stored at room temperature (up to 25°C [77°F]). Some adverse reactions include injection site bruising, pain, cysts, eczema, irritation, headache, cough, diarrhea, and fatigue.4
- Velaglucerase alfa for injection (VPRIV) has been approved by the FDA to treat adults and children with the rare genetic disorder Gaucher disease.5 Patients with Gaucher disease have a deficiency of the glucocerebrosidase enzyme. This enzyme prevents lipids from building up in the liver, spleen, bone marrow, and nervous system, which prevents them from working properly. VPRIV, a long-term replacement therapy, is approved for Type 1 Gaucher disease, the most common form, and is an alternative to imiglucerase (Cerezyme), which is in short supply. The most common reactions seen in clinical trials were allergic reactions, headache, dizziness, abdominal and back pain, nausea, fatigue/weakness, fever, and prolonged activated partial thromboplastin time.
Pipeline
- Betrixaban is a once-daily oral anticoagulant in Phase 2 clinical studies.6 Compared with warfarin in the EXPLORE-Xa study, betrixaban decreased the bleeding incidence in patients with nonvalvular atrial fibrillation or atrial flutter who had at least one stroke risk factor. The major and clinically relevant nonmajor bleeding episodes occurred less frequently in betrixaban-treated patients.
- Dabigatran etexilate is an oral anticoagulant in Phase 3 clinical trials.7 At the recent American College of Cardiology meeting in Ingelheim, Germany, dabigatran demonstrated consistent stroke prevention in patients with atrial fibrillation. It also reduced the number of strokes in patients with atrial fibrillation, compared with warfarin therapy. Additionally, dabigatran etexilate 110 mg and 150 mg twice daily was associated with a lower rate of major bleeding compared with warfarin in atrial fibrillation patients at low risk of stroke.
- Fentanyl sublingual spray (SL Spray) is in Phase 3 clinical trials to treat breakthrough pain in cancer patients. Sublingual administration of this product showed rapid, effective pain relief within five minutes.8
- Ketamine intranasal (Ereska) is a nonopioid NMDA receptor antagonist analgesic, which is undergoing Phase 3 clinical trials for managing moderate to severe acute pain.9 Studies have shown rapid, statistically significant relief of moderate to severe acute postoperative pain following dental surgery, following a variety of major orthopedic surgical procedures, and in cancer breakthrough pain.
- Lu AA21004 and Lu AA24530 are undergoing Phase 3 clinical trials for treating major depressive disorder (MDD).10 Lu AA21004 is a 5-HT3, 5-HT7 and 5-HT1B receptor antagonist, 5HT1A receptor agonist, and 5-HT transporter inhibitor. To date, it has shown a low propensity for drug-drug interactions and is extensively metabolized in the liver. Lu AA24530 has shown activity as a multimodal enhancer with reuptake inhibition at monoamine transporters, and having 5-HT3 and 5-HT2c receptor antagonist activity.
- Lurasidone is an atypical antipsychotic with high affinity and antagonist effects at the dopamine D2, serotonin 5-HT2, and serotonin 5-HT7 receptors.11 It is a partial agonist at serotonin 5HT1A receptor. The NDA was filed for this agent Dec. 30, 2009.
- Mipomersen, an apo-B synthesis inhibitor, is in Phase 3 clinical trials for treating patients with homozygous familial hypercholesterolemia (HoFM).12 This agent is proposed to reduce LDL-C by preventing the development of atherogenic lipids. In a study published in Lancet, mipomersen reduced LDL-C levels by an average of more than 100 mg/dL in HoFM patients.13
- Oxycodone/niacin (Acurox), an abuse deterrent formulation for this popular opioid, has been rejected by the FDA.14 According to the FDA and its review committee, the rejection was due to the “flushing” from the niacin, which was deemed ineffective as an abuse deterrent. In addition, the FDA said the “flushing” could be overcome by food intake or administration with over-the-counter pain relievers.
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol.15 It is in Phase 3 clinical trials for treating asthma. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- FDA approves Exaglo (hydromorphone HCl) extended-release tablets. Drugs.com website. Available at: www.drugs.com/newdrugs/fda-approves-exaglo-hydromorphone-hcl-extended-release-2033.html?printable=1. Accessed April 27, 2010.
- ImmunoGen’s skin cancer drug gets orphan drug status. Reuters website. Available at: www.reuters.com/article/idUSSGE6270L720100308. Accessed April 27, 2010.
- CSL Behring receives FDA approval of Hizentra, first 20 percent subcutaneous immunoglobulin therapy. Drugs.com website. Available at: www.drugs.com/newdrugs/csl-behring-receives-fda-approval-hizentra-first-20-percent-subcutaneous-immunoglobulin-therapy-2037.html. Accessed April 27, 2010.
- Petrochko C. FDA okays 20% skin-injection immunodeficiency treatment. MedPage Today website. Available at: www.medpagetoday.com/tbprint.cfm?tbid=18858. Accessed April 27, 2010.
- Gansz Bobo E. FDA approves therapy to treat Gaucher disease. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm202288.htm. Accessed April 27, 2010.
- Portola Pharmaceuticals and Merck announce that Phase 2 study showed investigational factor Xa inhibitor, betrixaban, reduced incidence of bleeding compared to warfarin in patients with atrial fibrillation. Merck website. Available at: www.merck.com/newsroom/news-release-archive/research-and-development/2010_0315.html. Accessed April 27, 2010.
- Dabigatran etexilate shows greater reductions than warfarin in stroke in patients with atrial fibrillation across all stroke risk groups. Beohringer Ingelheim website. Available at: www.boehringer-ingelheim.com/news/news_releases/press_releases/2010/15_march_2010.html. Accessed April 27, 2010.
- INSYS Therapeutics, Inc. Announces Positive Phase III Efficacy Trial Results for Fentanyl Sublingual Spray. INSYS Therapeutics website. Available at: www.insysrx.com/news.htm. Accessed April 27, 2010.
- Third party reexamination of Javelin Pharmaceuticals’ Phase III trial data for Ereska (intranasal ketamine) yields statistically significant primary endpoint. Javelin website. Available at: ir.javelinpharmaceuticals.com/releasedetail.cfm?ReleaseID=444353. Accessed April 27, 2010.
- Lundbeck and Takeda finalise plans to initiate phase III pivotal clinical trials with Lu AA21004 and Lu AA24530. Takeda Pharmaceutical Company Limited website. Available at: www.takeda.com/press/article_35859.html. Accessed April 27, 2010.
- Dainippon Sumitomo Pharma America announces FDA acceptance of lurasidone new drug application for treatment of schizophrenia. PR Newswire website. Available at: www.prnewswire.com/news-releases/dainippon-sumitomo-pharma-america-announces-fda-acceptance-of-lurasidone-new-drug-application-for-treatment-of-schizophrenia-87265597.html. Accessed April 27, 2010.
- Mipomersen Phase 3 study in HoFH featured in The Lancet. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100315005928. Accessed April 27, 2010.
- Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9719):998-1006.
- US FDA panel rejects King, Acura painkiller. Reuters website. Available at: www.reuters.com/assets/print?aid=USN2223552220100422. Accessed April 27, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed April 27, 2010.
New Drugs, Indications, Dosage Forms, and Approvals
- Hydromorphone extended-release tablets (Exalgo) have been approved by the FDA as a once-daily treatment for managing moderate to severe pain in opioid-tolerant patients needing continuous opioid analgesia for an extended period of time.1 This formulation uses the OROS osmotic delivery system to control the release rate. It is a CII controlled substance and is accompanied by a comprehensive Risk Evaluation and Mitigation Strategy (REMS) to ensure that the medication’s benefits outweigh its risks.
- IMGN910 has received orphan drug status for treating Merkel cell carcinoma, a skin cancer that usually occurs on the head or neck.2 It is in early-stage clinical trials.
- Immune globulin subcutaneous (human) 20% liquid (Hizentra) has been approved by the FDA as a once-weekly immunoglobulin replacement therapy for patients with primary immunodeficiency.3 It’s the first 20% subcutaneous immunoglobulin to receive FDA approval. This high-concentration product is stabilized with L-proline, a naturally occurring amino acid, which allows it to be stored at room temperature (up to 25°C [77°F]). Some adverse reactions include injection site bruising, pain, cysts, eczema, irritation, headache, cough, diarrhea, and fatigue.4
- Velaglucerase alfa for injection (VPRIV) has been approved by the FDA to treat adults and children with the rare genetic disorder Gaucher disease.5 Patients with Gaucher disease have a deficiency of the glucocerebrosidase enzyme. This enzyme prevents lipids from building up in the liver, spleen, bone marrow, and nervous system, which prevents them from working properly. VPRIV, a long-term replacement therapy, is approved for Type 1 Gaucher disease, the most common form, and is an alternative to imiglucerase (Cerezyme), which is in short supply. The most common reactions seen in clinical trials were allergic reactions, headache, dizziness, abdominal and back pain, nausea, fatigue/weakness, fever, and prolonged activated partial thromboplastin time.
Pipeline
- Betrixaban is a once-daily oral anticoagulant in Phase 2 clinical studies.6 Compared with warfarin in the EXPLORE-Xa study, betrixaban decreased the bleeding incidence in patients with nonvalvular atrial fibrillation or atrial flutter who had at least one stroke risk factor. The major and clinically relevant nonmajor bleeding episodes occurred less frequently in betrixaban-treated patients.
- Dabigatran etexilate is an oral anticoagulant in Phase 3 clinical trials.7 At the recent American College of Cardiology meeting in Ingelheim, Germany, dabigatran demonstrated consistent stroke prevention in patients with atrial fibrillation. It also reduced the number of strokes in patients with atrial fibrillation, compared with warfarin therapy. Additionally, dabigatran etexilate 110 mg and 150 mg twice daily was associated with a lower rate of major bleeding compared with warfarin in atrial fibrillation patients at low risk of stroke.
- Fentanyl sublingual spray (SL Spray) is in Phase 3 clinical trials to treat breakthrough pain in cancer patients. Sublingual administration of this product showed rapid, effective pain relief within five minutes.8
- Ketamine intranasal (Ereska) is a nonopioid NMDA receptor antagonist analgesic, which is undergoing Phase 3 clinical trials for managing moderate to severe acute pain.9 Studies have shown rapid, statistically significant relief of moderate to severe acute postoperative pain following dental surgery, following a variety of major orthopedic surgical procedures, and in cancer breakthrough pain.
- Lu AA21004 and Lu AA24530 are undergoing Phase 3 clinical trials for treating major depressive disorder (MDD).10 Lu AA21004 is a 5-HT3, 5-HT7 and 5-HT1B receptor antagonist, 5HT1A receptor agonist, and 5-HT transporter inhibitor. To date, it has shown a low propensity for drug-drug interactions and is extensively metabolized in the liver. Lu AA24530 has shown activity as a multimodal enhancer with reuptake inhibition at monoamine transporters, and having 5-HT3 and 5-HT2c receptor antagonist activity.
- Lurasidone is an atypical antipsychotic with high affinity and antagonist effects at the dopamine D2, serotonin 5-HT2, and serotonin 5-HT7 receptors.11 It is a partial agonist at serotonin 5HT1A receptor. The NDA was filed for this agent Dec. 30, 2009.
- Mipomersen, an apo-B synthesis inhibitor, is in Phase 3 clinical trials for treating patients with homozygous familial hypercholesterolemia (HoFM).12 This agent is proposed to reduce LDL-C by preventing the development of atherogenic lipids. In a study published in Lancet, mipomersen reduced LDL-C levels by an average of more than 100 mg/dL in HoFM patients.13
- Oxycodone/niacin (Acurox), an abuse deterrent formulation for this popular opioid, has been rejected by the FDA.14 According to the FDA and its review committee, the rejection was due to the “flushing” from the niacin, which was deemed ineffective as an abuse deterrent. In addition, the FDA said the “flushing” could be overcome by food intake or administration with over-the-counter pain relievers.
- Vilanterol/fluticasone is a combination of the inhaled corticosteroid fluticasone and the long-acting beta-agonist (LABA) vilanterol.15 It is in Phase 3 clinical trials for treating asthma. TH
Michele B. Kaufman, PharmD, BSc, RPh, is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- FDA approves Exaglo (hydromorphone HCl) extended-release tablets. Drugs.com website. Available at: www.drugs.com/newdrugs/fda-approves-exaglo-hydromorphone-hcl-extended-release-2033.html?printable=1. Accessed April 27, 2010.
- ImmunoGen’s skin cancer drug gets orphan drug status. Reuters website. Available at: www.reuters.com/article/idUSSGE6270L720100308. Accessed April 27, 2010.
- CSL Behring receives FDA approval of Hizentra, first 20 percent subcutaneous immunoglobulin therapy. Drugs.com website. Available at: www.drugs.com/newdrugs/csl-behring-receives-fda-approval-hizentra-first-20-percent-subcutaneous-immunoglobulin-therapy-2037.html. Accessed April 27, 2010.
- Petrochko C. FDA okays 20% skin-injection immunodeficiency treatment. MedPage Today website. Available at: www.medpagetoday.com/tbprint.cfm?tbid=18858. Accessed April 27, 2010.
- Gansz Bobo E. FDA approves therapy to treat Gaucher disease. U.S. Food and Drug Administration website. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm202288.htm. Accessed April 27, 2010.
- Portola Pharmaceuticals and Merck announce that Phase 2 study showed investigational factor Xa inhibitor, betrixaban, reduced incidence of bleeding compared to warfarin in patients with atrial fibrillation. Merck website. Available at: www.merck.com/newsroom/news-release-archive/research-and-development/2010_0315.html. Accessed April 27, 2010.
- Dabigatran etexilate shows greater reductions than warfarin in stroke in patients with atrial fibrillation across all stroke risk groups. Beohringer Ingelheim website. Available at: www.boehringer-ingelheim.com/news/news_releases/press_releases/2010/15_march_2010.html. Accessed April 27, 2010.
- INSYS Therapeutics, Inc. Announces Positive Phase III Efficacy Trial Results for Fentanyl Sublingual Spray. INSYS Therapeutics website. Available at: www.insysrx.com/news.htm. Accessed April 27, 2010.
- Third party reexamination of Javelin Pharmaceuticals’ Phase III trial data for Ereska (intranasal ketamine) yields statistically significant primary endpoint. Javelin website. Available at: ir.javelinpharmaceuticals.com/releasedetail.cfm?ReleaseID=444353. Accessed April 27, 2010.
- Lundbeck and Takeda finalise plans to initiate phase III pivotal clinical trials with Lu AA21004 and Lu AA24530. Takeda Pharmaceutical Company Limited website. Available at: www.takeda.com/press/article_35859.html. Accessed April 27, 2010.
- Dainippon Sumitomo Pharma America announces FDA acceptance of lurasidone new drug application for treatment of schizophrenia. PR Newswire website. Available at: www.prnewswire.com/news-releases/dainippon-sumitomo-pharma-america-announces-fda-acceptance-of-lurasidone-new-drug-application-for-treatment-of-schizophrenia-87265597.html. Accessed April 27, 2010.
- Mipomersen Phase 3 study in HoFH featured in The Lancet. Business Wire website. Available at: www.businesswire.com/portal/site/home/email/alert/?ndmViewId=news_view&newsLang=en&newsId=20100315005928. Accessed April 27, 2010.
- Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9719):998-1006.
- US FDA panel rejects King, Acura painkiller. Reuters website. Available at: www.reuters.com/assets/print?aid=USN2223552220100422. Accessed April 27, 2010.
- Dennis M. GlaxoSmithKline begins late-stage clinical programme for asthma drug Relovair. FirstWord website. Available at: www.firstwordplus.com/Fws.do?articleid=E256469FBD8F4A2F80C5DD3E844CC1E1&logRowId=356423. Accessed April 27, 2010.
How Should Hypertensive Emergencies Be Managed?
Case
A 57-year-old male with hypertension and end-stage renal disease is brought into the ED by his family for evaluation of headache, nausea, blurry vision, and confusion. Blood pressure is 235/130 mmHg. He is somnolent but arousable and oriented only to person; the remainder of his neurologic exam is nonfocal. A fundoscopic exam shows retinal hemorrhages, exudates, and papilledema. How should this patient be managed?
Overview
Hypertension (HTN) is a medical problem that affects an estimated 1 in 3 adults in the U.S. and more than 1 billion people worldwide. The Joint National Committee (JNC) 7 Report defines hypertensive emergency as severe hypertension with evidence of impending or progressive end-organ dysfunction.1 Systolic blood pressure (SBP) in these settings often is >180 mm Hg with diastolic blood pressure (DBP) >120 mm Hg. The JNC 7 Report defines hypertensive urgency as severe HTN without acute end-organ dysfunction. Whereas hypertensive urgencies can be treated with oral antihypertensive agents with close outpatient follow-up, hypertensive emergencies require immediate BP reduction to halt the progression of end-organ damage.
Severe HTN causes shear stress and endothelial injury, leading to activation of the coagulation cascade, fibrinoid necrosis, and tissue ischemia.2 Due to adaptive vascular changes, pre-existing hypertension lowers the probability of a hypertensive emergency developing at a particular BP. The rate of BP rise, rather than the absolute level, determines most end-organ damage.3 In previously normotensive patients, end-organ damage can occur at BPs >160/100 mm Hg; however, organ dysfunction is uncommon in chronically hypertensive individuals, unless BP >220/120 mm Hg.
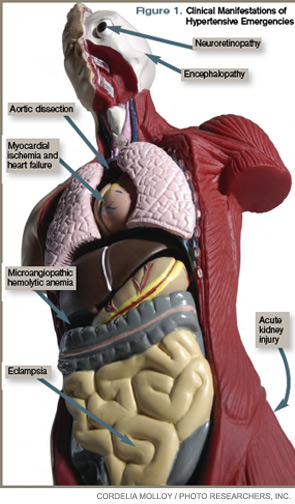
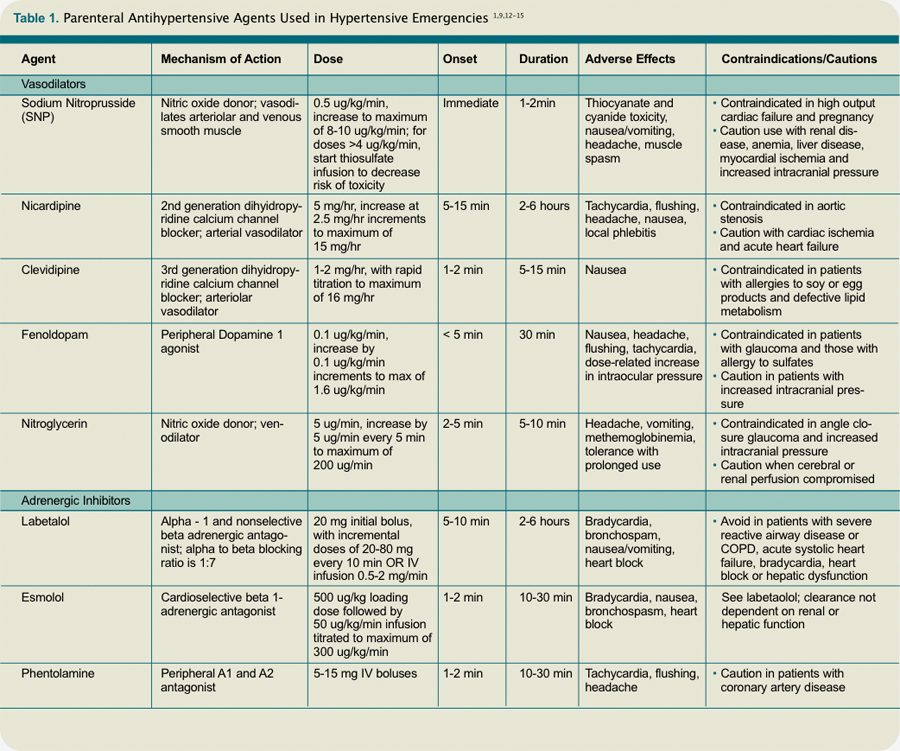
Clinical manifestations of hypertensive emergency depend on the target organs involved (see Figure 1, right). When a patient presents with severe hypertension, a focused evaluation should attempt to identify the presence of end-organ damage. If present, these patients should be admitted to an ICU for close monitoring, and administration of parenteral antihypertensive agents should be started. (Online Exclusive: View a chart of “Parenteral Antihypertensive Agents Used in Hypertensive Emergencies”)
Review of the Data
General principles: The initial therapeutic goal in most hypertensive emergencies is to reduce the mean arterial pressure (MAP) by no more than 25% within the first hour. Precipitous or excessive decreases in BP might worsen renal, cerebral, or coronary ischemia. Due to pressure natriuresis, patients with primary malignant hypertension might be volume-depleted. Restoration of intravascular volume with intravenous (IV) saline can prevent precipitous falls in BP when antihypertensive agents are started.
After the patient stabilizes, the BP can be lowered about 10% per hour to 160/100-110 mm Hg. A gradual reduction to the patient’s baseline BP is targeted over the ensuing 24 to 48 hours. Once there is stable BP control and end-organ damage has ceased, patients can be transitioned to oral therapy.
No large clinical trials have investigated optimal drug therapy in patients with hypertensive emergencies. The choice of pharmacologic agent should be individualized based on drug properties, patient comorbidities, and the end-organ(s) involved.
Selected pharmacologic agents: Sodium nitroprusside (SNP) is a short-acting, potent arterial and venous dilator that has been used extensively in the treatment of hypertensive emergencies. Despite its familiarity, there are several important limitations to its use. SNP can increase intracranial pressure (ICP), worsen myocardial ischemia through coronary steal, and is associated with cyanide and/or thiocyanate toxicity. Although used broadly across many types of hypertensive emergencies, SNP should be considered a first-line agent in acute left ventricular (LV) failure and, when combined with beta-blockers, in acute aortic dissection.
Labetalol is an alpha-1 and nonselective beta-blocker that reduces systemic vascular resistance while preserving cerebral, renal, and coronary blood flow. It is considered a first-line agent in most hypertensive emergencies, with the exception of acute LV failure.
Esmolol is a short-acting, selective beta-blocker that decreases heart rate, myocardial contractility, and cardiac output.
Nicardipine is a second-generation dihydropyridine calcium channel blocker. Although it has a longer duration of action, excess hypotension has not been seen in clinical trials comparing it with SNP.4 Nicardipine is used safely in such hypertensive emergencies as hypertensive encephalopathy, cerebral vascular accidents, and postoperatively.
Fenoldopam creates vasodilation by acting on peripheral dopamine type 1 receptors. It improves creatinine clearance and urine output, and is most useful in acute kidney injury.5 It is a well-tolerated and highly effective agent for use in most hypertensive crises, although is expensive and has limited hard outcome data.
Nitroglycerin is a potent venodilator that is used as an adjunct to other anti-hypertensives in the treatment of acute coronary syndromes and acute pulmonary edema.
Immediate-release nifedipine and clonidine are not recommended; they are long-acting and poorly titratable, with unpredictable hypotensive effects.
Hydralazine may be used in LV failure and in pregnancy.
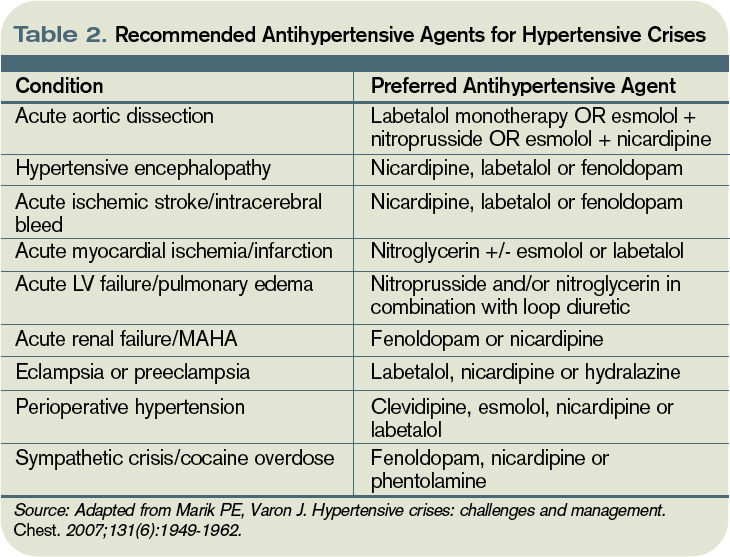
Specific emergencies: Aortic dissection is the most rapidly fatal complication of severe HTN. Untreated, approximately 80% of patients with acute type-A dissections die within two weeks.6 In this specific setting, SBP should be decreased as rapidly as possible to <110 mm Hg in order to halt propagation of the dissection prior to surgery. Therapy should aim to reduce the shear stress on the aortic wall by decreasing both BP and heart rate. This can be accomplished with a combination of esmolol and SNP. Nicardipine and fenoldopam are effective alternatives to SNP. Labetalol is a good single-agent option, provided adequate heart rate suppression is achieved.
LV failure and acute pulmonary edema are associated with high systemic vascular resistance and activation of the Renin Angiotensin Aldosterone (RAAS) system. First-line therapy should consist of arterial vasodilators (e.g., SNP, nicardipine, fenoldopam) in combination with a loop diuretic. Nitroglycerin can be used as an adjunct to reduce LV preload.
In hypertensive encephalopathy, blood pressure exceeds the cerebral autoregulatory threshold, leading to breakthrough vasodilation and the development of cerebral edema. Characteristic symptoms include the insidious onset of headache, nausea, vomiting, and nonlocalizing neurologic signs (e.g., lethargy, confusion, seizures). It is important to exclude stroke, as treatment strategies differ. SNP is used widely in the treatment of hypertensive encephalopathy; it may increase ICP and should be used with caution. Nicardipine and labetalol are effective alternatives with favorable cerebral hemodynamic profiles.
Malignant HTN is characterized by neuroretinopathy: cotton wool spots, flame hemorrhages, and papilledema. Encephalopathy and other evidence of end-organ dysfunction might not be present, although renal disease is common. Preferred drugs are SNP and labetalol, although fenoldopam has been used successfully.
Appropriate BP management following acute ischemic stroke remains controversial. Elevated BP often is a protective physiologic response to maintain cerebral perfusion. The American Heart Association (AHA) recommends initiating IV antihypertensive therapy for thrombolysis candidates when SBP >185 or DBP >110 mm Hg. For those who are not thrombolysis candidates, the recommended threshold for initiating IV antihypertensives is SBP >220 or DBP >120 mm Hg.7 The goal is to lower the BP by 15% to 25% within the first 24 hours. These goals are less aggressive than in patients with hypertensive encephalopathy without stroke.
Spontaneous intracerebral hemorrhage causes a rise in ICP with reflex systemic hypertension. Although a correlation between HTN and hematoma expansion exists, there is no evidence that shows lowering BP is protective. Two clinical trials are evaluating the effects of BP reduction to specified target levels.8 Pending those results, the AHA recommends BP reduction for patients with SBP >200 or MAP >150 mm Hg, or for patients with SBP >180 or MAP >130 mm Hg and evidence of elevated ICP.7 In both ischemic and hemorrhagic stroke, nicardipine and labetalol are appropriate first-line agents.
Most sympathetic crises are related to the recreational use of sympathomimetic drugs, pheochromocytoma, abrupt antihypertensive withdrawal, or concurrent ingestion of monoamine-oxidase inhibitors and tyramine-containing foods. Selective beta-blockers can increase BP and worsen HTN through unopposed alpha effects.
Although labetalol traditionally has been considered the ideal agent—due to its alpha and beta antagonism—studies have failed to support its use in this clinical setting.9 Phentolamine, nicardipine, and fenoldopam are reasonable selections.
Hypertension is common in the early postoperative period following cardiothoracic, vascular, head and neck, and neurosurgical procedures. No consensus exists regarding the treatment of noncardiac surgery patients, but treatment is recommended for BP >140/90 or MAP >105 mmHg in cardiac surgery patients. Nicardipine, clevidipine, and esmolol are proven agents. All three have been shown more effective than SNP in maintaining target BP, and each is associated with less BP variability.10
In patients with pregnancy-induced hypertension, initial therapy for preeclampsia includes magnesium sulfate for seizure prophylaxis and BP control until delivery of the fetus can be safely undertaken. The FDA does not recommend any specific antihypertensive agents; however, ACE inhibitors and SNP are contraindicated. Although hydralazine is used extensively in this setting, a meta-analysis showed increased risk of maternal hypotension, Cesarean section, placental abruptions, and low Apgar scores.11 Labetalol and nicardipine appear to be safe and effective in pregnant hypertensive patients.
Back to the Case
This case represents a classic presentation of malignant hypertension with hypertensive encephalopathy, which is reversible with timely and appropriate management. The patient’s MAP is approximately 165 mmHg, well above the upper threshold of cerebral vascular autoregulation in most patients with chronic hypertension. A brain MRI should be obtained to definitively rule out stroke, as management goals would be considerably different.
If the scan is negative, treatment should be initiated immediately with a goal of reducing the MAP by no more than 25% within the first hour. Nicardipine or labetalol would be appropriate therapeutic choices, administered in an ICU with close hemodynamic monitoring.
Given the patient’s end-stage renal disease and evidence of intracranial hypertension, SNP would be a suboptimal choice. Over hours two through six, BP could be lowered gradually to 160/100, then to his baseline BP over the ensuing 24 to 48 hours, monitoring closely for signs of neurologic deterioration. Once BP is stable and there is no evidence of worsening end-organ damage, he can be safely transitioned to oral agents.
Bottom Line
The therapeutic goal in hypertensive emergencies is to immediately and safely lower BP to halt end-organ damage. Drug selection should be individualized. TH
Dr. Shanahan is a hospitalist and assistant professor at the Denver VA Medical Center. Dr. Linas is professor of medicine in the division of renal diseases and hypertension at the University of Colorado Denver School of Medicine. Dr. Anderson is associate professor and chief of the hospital medicine section at the Denver VA Medical Center.
References
- Lenfant C, Chobanian AV, Jones DW, Roccella EJ. Seventh report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7): resetting the hypertension sails. Hypertension. 2003;41(6):1178-1179.
- Ault MJ, Ellrodt AG. Pathophysiological events leading to the end-organ effects of acute hypertension. Am J Emerg Med. 1985;3(6 Suppl):10-15.
- Vaughan CJ, Delanty N. Hypertensive emergencies. Lancet. 2000;356(9227):411-417.
- Neutel JM, Smith DH, Wallin D, et al. A comparison of intravenous nicardipine and sodium nitroprusside in the immediate treatment of severe hypertension. Am J Hypertens. 1994;7(7 Pt 1):623-628.
- Shusterman NH, Elliott WJ, White WB. Fenoldopam, but not nitroprusside, improves renal function in severely hypertensive patients with impaired renal function. Am J Med. 1993;95(2):161-168.
- Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122(1):311-328.
- Adams HP Jr., del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(20):e478-534.
- Qureshi AI. Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH): rationale and design. Neurocrit Care. 2007;6(1):56-66.
- Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962.
- Aronson S, Dyke CM, Stierer KA, et al. The ECLIPSE trials: comparative studies of clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for acute hypertension treatment in cardiac surgery patients. Anesth Analg. 2008;107(4):1110-1121.
- Magee LA, Cham C, Waterman EJ, Ohlsson A, von Dadelszen P. Hydralazine for treatment of severe hypertension in pregnancy: meta-analysis. BMJ. 2003;327(7421):955-960.
- Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006; 24(1):135-146.
- Rhoney D, Peacock WF. Intravenous therapy for hypertensive emergencies, part 1. Am J Health Syst Pharm. 2009;66(15):1343-1352.
- Rhoney D, Peacock WF. Intravenous therapy for hypertensive emergencies, part 2. Am J Health Syst Pharm. 2009;66(16):1448-1457.
- Varon J. Treatment of acute severe hypertension: current and newer agents. Drugs. 2008;68(3):283-297.
Case
A 57-year-old male with hypertension and end-stage renal disease is brought into the ED by his family for evaluation of headache, nausea, blurry vision, and confusion. Blood pressure is 235/130 mmHg. He is somnolent but arousable and oriented only to person; the remainder of his neurologic exam is nonfocal. A fundoscopic exam shows retinal hemorrhages, exudates, and papilledema. How should this patient be managed?
Overview
Hypertension (HTN) is a medical problem that affects an estimated 1 in 3 adults in the U.S. and more than 1 billion people worldwide. The Joint National Committee (JNC) 7 Report defines hypertensive emergency as severe hypertension with evidence of impending or progressive end-organ dysfunction.1 Systolic blood pressure (SBP) in these settings often is >180 mm Hg with diastolic blood pressure (DBP) >120 mm Hg. The JNC 7 Report defines hypertensive urgency as severe HTN without acute end-organ dysfunction. Whereas hypertensive urgencies can be treated with oral antihypertensive agents with close outpatient follow-up, hypertensive emergencies require immediate BP reduction to halt the progression of end-organ damage.
Severe HTN causes shear stress and endothelial injury, leading to activation of the coagulation cascade, fibrinoid necrosis, and tissue ischemia.2 Due to adaptive vascular changes, pre-existing hypertension lowers the probability of a hypertensive emergency developing at a particular BP. The rate of BP rise, rather than the absolute level, determines most end-organ damage.3 In previously normotensive patients, end-organ damage can occur at BPs >160/100 mm Hg; however, organ dysfunction is uncommon in chronically hypertensive individuals, unless BP >220/120 mm Hg.
Clinical manifestations of hypertensive emergency depend on the target organs involved (see Figure 1, right). When a patient presents with severe hypertension, a focused evaluation should attempt to identify the presence of end-organ damage. If present, these patients should be admitted to an ICU for close monitoring, and administration of parenteral antihypertensive agents should be started. (Online Exclusive: View a chart of “Parenteral Antihypertensive Agents Used in Hypertensive Emergencies”)
Review of the Data
General principles: The initial therapeutic goal in most hypertensive emergencies is to reduce the mean arterial pressure (MAP) by no more than 25% within the first hour. Precipitous or excessive decreases in BP might worsen renal, cerebral, or coronary ischemia. Due to pressure natriuresis, patients with primary malignant hypertension might be volume-depleted. Restoration of intravascular volume with intravenous (IV) saline can prevent precipitous falls in BP when antihypertensive agents are started.
After the patient stabilizes, the BP can be lowered about 10% per hour to 160/100-110 mm Hg. A gradual reduction to the patient’s baseline BP is targeted over the ensuing 24 to 48 hours. Once there is stable BP control and end-organ damage has ceased, patients can be transitioned to oral therapy.
No large clinical trials have investigated optimal drug therapy in patients with hypertensive emergencies. The choice of pharmacologic agent should be individualized based on drug properties, patient comorbidities, and the end-organ(s) involved.
Selected pharmacologic agents: Sodium nitroprusside (SNP) is a short-acting, potent arterial and venous dilator that has been used extensively in the treatment of hypertensive emergencies. Despite its familiarity, there are several important limitations to its use. SNP can increase intracranial pressure (ICP), worsen myocardial ischemia through coronary steal, and is associated with cyanide and/or thiocyanate toxicity. Although used broadly across many types of hypertensive emergencies, SNP should be considered a first-line agent in acute left ventricular (LV) failure and, when combined with beta-blockers, in acute aortic dissection.
Labetalol is an alpha-1 and nonselective beta-blocker that reduces systemic vascular resistance while preserving cerebral, renal, and coronary blood flow. It is considered a first-line agent in most hypertensive emergencies, with the exception of acute LV failure.
Esmolol is a short-acting, selective beta-blocker that decreases heart rate, myocardial contractility, and cardiac output.
Nicardipine is a second-generation dihydropyridine calcium channel blocker. Although it has a longer duration of action, excess hypotension has not been seen in clinical trials comparing it with SNP.4 Nicardipine is used safely in such hypertensive emergencies as hypertensive encephalopathy, cerebral vascular accidents, and postoperatively.
Fenoldopam creates vasodilation by acting on peripheral dopamine type 1 receptors. It improves creatinine clearance and urine output, and is most useful in acute kidney injury.5 It is a well-tolerated and highly effective agent for use in most hypertensive crises, although is expensive and has limited hard outcome data.
Nitroglycerin is a potent venodilator that is used as an adjunct to other anti-hypertensives in the treatment of acute coronary syndromes and acute pulmonary edema.
Immediate-release nifedipine and clonidine are not recommended; they are long-acting and poorly titratable, with unpredictable hypotensive effects.
Hydralazine may be used in LV failure and in pregnancy.
Specific emergencies: Aortic dissection is the most rapidly fatal complication of severe HTN. Untreated, approximately 80% of patients with acute type-A dissections die within two weeks.6 In this specific setting, SBP should be decreased as rapidly as possible to <110 mm Hg in order to halt propagation of the dissection prior to surgery. Therapy should aim to reduce the shear stress on the aortic wall by decreasing both BP and heart rate. This can be accomplished with a combination of esmolol and SNP. Nicardipine and fenoldopam are effective alternatives to SNP. Labetalol is a good single-agent option, provided adequate heart rate suppression is achieved.
LV failure and acute pulmonary edema are associated with high systemic vascular resistance and activation of the Renin Angiotensin Aldosterone (RAAS) system. First-line therapy should consist of arterial vasodilators (e.g., SNP, nicardipine, fenoldopam) in combination with a loop diuretic. Nitroglycerin can be used as an adjunct to reduce LV preload.
In hypertensive encephalopathy, blood pressure exceeds the cerebral autoregulatory threshold, leading to breakthrough vasodilation and the development of cerebral edema. Characteristic symptoms include the insidious onset of headache, nausea, vomiting, and nonlocalizing neurologic signs (e.g., lethargy, confusion, seizures). It is important to exclude stroke, as treatment strategies differ. SNP is used widely in the treatment of hypertensive encephalopathy; it may increase ICP and should be used with caution. Nicardipine and labetalol are effective alternatives with favorable cerebral hemodynamic profiles.
Malignant HTN is characterized by neuroretinopathy: cotton wool spots, flame hemorrhages, and papilledema. Encephalopathy and other evidence of end-organ dysfunction might not be present, although renal disease is common. Preferred drugs are SNP and labetalol, although fenoldopam has been used successfully.
Appropriate BP management following acute ischemic stroke remains controversial. Elevated BP often is a protective physiologic response to maintain cerebral perfusion. The American Heart Association (AHA) recommends initiating IV antihypertensive therapy for thrombolysis candidates when SBP >185 or DBP >110 mm Hg. For those who are not thrombolysis candidates, the recommended threshold for initiating IV antihypertensives is SBP >220 or DBP >120 mm Hg.7 The goal is to lower the BP by 15% to 25% within the first 24 hours. These goals are less aggressive than in patients with hypertensive encephalopathy without stroke.
Spontaneous intracerebral hemorrhage causes a rise in ICP with reflex systemic hypertension. Although a correlation between HTN and hematoma expansion exists, there is no evidence that shows lowering BP is protective. Two clinical trials are evaluating the effects of BP reduction to specified target levels.8 Pending those results, the AHA recommends BP reduction for patients with SBP >200 or MAP >150 mm Hg, or for patients with SBP >180 or MAP >130 mm Hg and evidence of elevated ICP.7 In both ischemic and hemorrhagic stroke, nicardipine and labetalol are appropriate first-line agents.
Most sympathetic crises are related to the recreational use of sympathomimetic drugs, pheochromocytoma, abrupt antihypertensive withdrawal, or concurrent ingestion of monoamine-oxidase inhibitors and tyramine-containing foods. Selective beta-blockers can increase BP and worsen HTN through unopposed alpha effects.
Although labetalol traditionally has been considered the ideal agent—due to its alpha and beta antagonism—studies have failed to support its use in this clinical setting.9 Phentolamine, nicardipine, and fenoldopam are reasonable selections.
Hypertension is common in the early postoperative period following cardiothoracic, vascular, head and neck, and neurosurgical procedures. No consensus exists regarding the treatment of noncardiac surgery patients, but treatment is recommended for BP >140/90 or MAP >105 mmHg in cardiac surgery patients. Nicardipine, clevidipine, and esmolol are proven agents. All three have been shown more effective than SNP in maintaining target BP, and each is associated with less BP variability.10
In patients with pregnancy-induced hypertension, initial therapy for preeclampsia includes magnesium sulfate for seizure prophylaxis and BP control until delivery of the fetus can be safely undertaken. The FDA does not recommend any specific antihypertensive agents; however, ACE inhibitors and SNP are contraindicated. Although hydralazine is used extensively in this setting, a meta-analysis showed increased risk of maternal hypotension, Cesarean section, placental abruptions, and low Apgar scores.11 Labetalol and nicardipine appear to be safe and effective in pregnant hypertensive patients.
Back to the Case
This case represents a classic presentation of malignant hypertension with hypertensive encephalopathy, which is reversible with timely and appropriate management. The patient’s MAP is approximately 165 mmHg, well above the upper threshold of cerebral vascular autoregulation in most patients with chronic hypertension. A brain MRI should be obtained to definitively rule out stroke, as management goals would be considerably different.
If the scan is negative, treatment should be initiated immediately with a goal of reducing the MAP by no more than 25% within the first hour. Nicardipine or labetalol would be appropriate therapeutic choices, administered in an ICU with close hemodynamic monitoring.
Given the patient’s end-stage renal disease and evidence of intracranial hypertension, SNP would be a suboptimal choice. Over hours two through six, BP could be lowered gradually to 160/100, then to his baseline BP over the ensuing 24 to 48 hours, monitoring closely for signs of neurologic deterioration. Once BP is stable and there is no evidence of worsening end-organ damage, he can be safely transitioned to oral agents.
Bottom Line
The therapeutic goal in hypertensive emergencies is to immediately and safely lower BP to halt end-organ damage. Drug selection should be individualized. TH
Dr. Shanahan is a hospitalist and assistant professor at the Denver VA Medical Center. Dr. Linas is professor of medicine in the division of renal diseases and hypertension at the University of Colorado Denver School of Medicine. Dr. Anderson is associate professor and chief of the hospital medicine section at the Denver VA Medical Center.
References
- Lenfant C, Chobanian AV, Jones DW, Roccella EJ. Seventh report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7): resetting the hypertension sails. Hypertension. 2003;41(6):1178-1179.
- Ault MJ, Ellrodt AG. Pathophysiological events leading to the end-organ effects of acute hypertension. Am J Emerg Med. 1985;3(6 Suppl):10-15.
- Vaughan CJ, Delanty N. Hypertensive emergencies. Lancet. 2000;356(9227):411-417.
- Neutel JM, Smith DH, Wallin D, et al. A comparison of intravenous nicardipine and sodium nitroprusside in the immediate treatment of severe hypertension. Am J Hypertens. 1994;7(7 Pt 1):623-628.
- Shusterman NH, Elliott WJ, White WB. Fenoldopam, but not nitroprusside, improves renal function in severely hypertensive patients with impaired renal function. Am J Med. 1993;95(2):161-168.
- Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122(1):311-328.
- Adams HP Jr., del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(20):e478-534.
- Qureshi AI. Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH): rationale and design. Neurocrit Care. 2007;6(1):56-66.
- Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962.
- Aronson S, Dyke CM, Stierer KA, et al. The ECLIPSE trials: comparative studies of clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for acute hypertension treatment in cardiac surgery patients. Anesth Analg. 2008;107(4):1110-1121.
- Magee LA, Cham C, Waterman EJ, Ohlsson A, von Dadelszen P. Hydralazine for treatment of severe hypertension in pregnancy: meta-analysis. BMJ. 2003;327(7421):955-960.
- Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006; 24(1):135-146.
- Rhoney D, Peacock WF. Intravenous therapy for hypertensive emergencies, part 1. Am J Health Syst Pharm. 2009;66(15):1343-1352.
- Rhoney D, Peacock WF. Intravenous therapy for hypertensive emergencies, part 2. Am J Health Syst Pharm. 2009;66(16):1448-1457.
- Varon J. Treatment of acute severe hypertension: current and newer agents. Drugs. 2008;68(3):283-297.
Case
A 57-year-old male with hypertension and end-stage renal disease is brought into the ED by his family for evaluation of headache, nausea, blurry vision, and confusion. Blood pressure is 235/130 mmHg. He is somnolent but arousable and oriented only to person; the remainder of his neurologic exam is nonfocal. A fundoscopic exam shows retinal hemorrhages, exudates, and papilledema. How should this patient be managed?
Overview
Hypertension (HTN) is a medical problem that affects an estimated 1 in 3 adults in the U.S. and more than 1 billion people worldwide. The Joint National Committee (JNC) 7 Report defines hypertensive emergency as severe hypertension with evidence of impending or progressive end-organ dysfunction.1 Systolic blood pressure (SBP) in these settings often is >180 mm Hg with diastolic blood pressure (DBP) >120 mm Hg. The JNC 7 Report defines hypertensive urgency as severe HTN without acute end-organ dysfunction. Whereas hypertensive urgencies can be treated with oral antihypertensive agents with close outpatient follow-up, hypertensive emergencies require immediate BP reduction to halt the progression of end-organ damage.
Severe HTN causes shear stress and endothelial injury, leading to activation of the coagulation cascade, fibrinoid necrosis, and tissue ischemia.2 Due to adaptive vascular changes, pre-existing hypertension lowers the probability of a hypertensive emergency developing at a particular BP. The rate of BP rise, rather than the absolute level, determines most end-organ damage.3 In previously normotensive patients, end-organ damage can occur at BPs >160/100 mm Hg; however, organ dysfunction is uncommon in chronically hypertensive individuals, unless BP >220/120 mm Hg.
Clinical manifestations of hypertensive emergency depend on the target organs involved (see Figure 1, right). When a patient presents with severe hypertension, a focused evaluation should attempt to identify the presence of end-organ damage. If present, these patients should be admitted to an ICU for close monitoring, and administration of parenteral antihypertensive agents should be started. (Online Exclusive: View a chart of “Parenteral Antihypertensive Agents Used in Hypertensive Emergencies”)
Review of the Data
General principles: The initial therapeutic goal in most hypertensive emergencies is to reduce the mean arterial pressure (MAP) by no more than 25% within the first hour. Precipitous or excessive decreases in BP might worsen renal, cerebral, or coronary ischemia. Due to pressure natriuresis, patients with primary malignant hypertension might be volume-depleted. Restoration of intravascular volume with intravenous (IV) saline can prevent precipitous falls in BP when antihypertensive agents are started.
After the patient stabilizes, the BP can be lowered about 10% per hour to 160/100-110 mm Hg. A gradual reduction to the patient’s baseline BP is targeted over the ensuing 24 to 48 hours. Once there is stable BP control and end-organ damage has ceased, patients can be transitioned to oral therapy.
No large clinical trials have investigated optimal drug therapy in patients with hypertensive emergencies. The choice of pharmacologic agent should be individualized based on drug properties, patient comorbidities, and the end-organ(s) involved.
Selected pharmacologic agents: Sodium nitroprusside (SNP) is a short-acting, potent arterial and venous dilator that has been used extensively in the treatment of hypertensive emergencies. Despite its familiarity, there are several important limitations to its use. SNP can increase intracranial pressure (ICP), worsen myocardial ischemia through coronary steal, and is associated with cyanide and/or thiocyanate toxicity. Although used broadly across many types of hypertensive emergencies, SNP should be considered a first-line agent in acute left ventricular (LV) failure and, when combined with beta-blockers, in acute aortic dissection.
Labetalol is an alpha-1 and nonselective beta-blocker that reduces systemic vascular resistance while preserving cerebral, renal, and coronary blood flow. It is considered a first-line agent in most hypertensive emergencies, with the exception of acute LV failure.
Esmolol is a short-acting, selective beta-blocker that decreases heart rate, myocardial contractility, and cardiac output.
Nicardipine is a second-generation dihydropyridine calcium channel blocker. Although it has a longer duration of action, excess hypotension has not been seen in clinical trials comparing it with SNP.4 Nicardipine is used safely in such hypertensive emergencies as hypertensive encephalopathy, cerebral vascular accidents, and postoperatively.
Fenoldopam creates vasodilation by acting on peripheral dopamine type 1 receptors. It improves creatinine clearance and urine output, and is most useful in acute kidney injury.5 It is a well-tolerated and highly effective agent for use in most hypertensive crises, although is expensive and has limited hard outcome data.
Nitroglycerin is a potent venodilator that is used as an adjunct to other anti-hypertensives in the treatment of acute coronary syndromes and acute pulmonary edema.
Immediate-release nifedipine and clonidine are not recommended; they are long-acting and poorly titratable, with unpredictable hypotensive effects.
Hydralazine may be used in LV failure and in pregnancy.
Specific emergencies: Aortic dissection is the most rapidly fatal complication of severe HTN. Untreated, approximately 80% of patients with acute type-A dissections die within two weeks.6 In this specific setting, SBP should be decreased as rapidly as possible to <110 mm Hg in order to halt propagation of the dissection prior to surgery. Therapy should aim to reduce the shear stress on the aortic wall by decreasing both BP and heart rate. This can be accomplished with a combination of esmolol and SNP. Nicardipine and fenoldopam are effective alternatives to SNP. Labetalol is a good single-agent option, provided adequate heart rate suppression is achieved.
LV failure and acute pulmonary edema are associated with high systemic vascular resistance and activation of the Renin Angiotensin Aldosterone (RAAS) system. First-line therapy should consist of arterial vasodilators (e.g., SNP, nicardipine, fenoldopam) in combination with a loop diuretic. Nitroglycerin can be used as an adjunct to reduce LV preload.
In hypertensive encephalopathy, blood pressure exceeds the cerebral autoregulatory threshold, leading to breakthrough vasodilation and the development of cerebral edema. Characteristic symptoms include the insidious onset of headache, nausea, vomiting, and nonlocalizing neurologic signs (e.g., lethargy, confusion, seizures). It is important to exclude stroke, as treatment strategies differ. SNP is used widely in the treatment of hypertensive encephalopathy; it may increase ICP and should be used with caution. Nicardipine and labetalol are effective alternatives with favorable cerebral hemodynamic profiles.
Malignant HTN is characterized by neuroretinopathy: cotton wool spots, flame hemorrhages, and papilledema. Encephalopathy and other evidence of end-organ dysfunction might not be present, although renal disease is common. Preferred drugs are SNP and labetalol, although fenoldopam has been used successfully.
Appropriate BP management following acute ischemic stroke remains controversial. Elevated BP often is a protective physiologic response to maintain cerebral perfusion. The American Heart Association (AHA) recommends initiating IV antihypertensive therapy for thrombolysis candidates when SBP >185 or DBP >110 mm Hg. For those who are not thrombolysis candidates, the recommended threshold for initiating IV antihypertensives is SBP >220 or DBP >120 mm Hg.7 The goal is to lower the BP by 15% to 25% within the first 24 hours. These goals are less aggressive than in patients with hypertensive encephalopathy without stroke.
Spontaneous intracerebral hemorrhage causes a rise in ICP with reflex systemic hypertension. Although a correlation between HTN and hematoma expansion exists, there is no evidence that shows lowering BP is protective. Two clinical trials are evaluating the effects of BP reduction to specified target levels.8 Pending those results, the AHA recommends BP reduction for patients with SBP >200 or MAP >150 mm Hg, or for patients with SBP >180 or MAP >130 mm Hg and evidence of elevated ICP.7 In both ischemic and hemorrhagic stroke, nicardipine and labetalol are appropriate first-line agents.
Most sympathetic crises are related to the recreational use of sympathomimetic drugs, pheochromocytoma, abrupt antihypertensive withdrawal, or concurrent ingestion of monoamine-oxidase inhibitors and tyramine-containing foods. Selective beta-blockers can increase BP and worsen HTN through unopposed alpha effects.
Although labetalol traditionally has been considered the ideal agent—due to its alpha and beta antagonism—studies have failed to support its use in this clinical setting.9 Phentolamine, nicardipine, and fenoldopam are reasonable selections.
Hypertension is common in the early postoperative period following cardiothoracic, vascular, head and neck, and neurosurgical procedures. No consensus exists regarding the treatment of noncardiac surgery patients, but treatment is recommended for BP >140/90 or MAP >105 mmHg in cardiac surgery patients. Nicardipine, clevidipine, and esmolol are proven agents. All three have been shown more effective than SNP in maintaining target BP, and each is associated with less BP variability.10
In patients with pregnancy-induced hypertension, initial therapy for preeclampsia includes magnesium sulfate for seizure prophylaxis and BP control until delivery of the fetus can be safely undertaken. The FDA does not recommend any specific antihypertensive agents; however, ACE inhibitors and SNP are contraindicated. Although hydralazine is used extensively in this setting, a meta-analysis showed increased risk of maternal hypotension, Cesarean section, placental abruptions, and low Apgar scores.11 Labetalol and nicardipine appear to be safe and effective in pregnant hypertensive patients.
Back to the Case
This case represents a classic presentation of malignant hypertension with hypertensive encephalopathy, which is reversible with timely and appropriate management. The patient’s MAP is approximately 165 mmHg, well above the upper threshold of cerebral vascular autoregulation in most patients with chronic hypertension. A brain MRI should be obtained to definitively rule out stroke, as management goals would be considerably different.
If the scan is negative, treatment should be initiated immediately with a goal of reducing the MAP by no more than 25% within the first hour. Nicardipine or labetalol would be appropriate therapeutic choices, administered in an ICU with close hemodynamic monitoring.
Given the patient’s end-stage renal disease and evidence of intracranial hypertension, SNP would be a suboptimal choice. Over hours two through six, BP could be lowered gradually to 160/100, then to his baseline BP over the ensuing 24 to 48 hours, monitoring closely for signs of neurologic deterioration. Once BP is stable and there is no evidence of worsening end-organ damage, he can be safely transitioned to oral agents.
Bottom Line
The therapeutic goal in hypertensive emergencies is to immediately and safely lower BP to halt end-organ damage. Drug selection should be individualized. TH
Dr. Shanahan is a hospitalist and assistant professor at the Denver VA Medical Center. Dr. Linas is professor of medicine in the division of renal diseases and hypertension at the University of Colorado Denver School of Medicine. Dr. Anderson is associate professor and chief of the hospital medicine section at the Denver VA Medical Center.
References
- Lenfant C, Chobanian AV, Jones DW, Roccella EJ. Seventh report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7): resetting the hypertension sails. Hypertension. 2003;41(6):1178-1179.
- Ault MJ, Ellrodt AG. Pathophysiological events leading to the end-organ effects of acute hypertension. Am J Emerg Med. 1985;3(6 Suppl):10-15.
- Vaughan CJ, Delanty N. Hypertensive emergencies. Lancet. 2000;356(9227):411-417.
- Neutel JM, Smith DH, Wallin D, et al. A comparison of intravenous nicardipine and sodium nitroprusside in the immediate treatment of severe hypertension. Am J Hypertens. 1994;7(7 Pt 1):623-628.
- Shusterman NH, Elliott WJ, White WB. Fenoldopam, but not nitroprusside, improves renal function in severely hypertensive patients with impaired renal function. Am J Med. 1993;95(2):161-168.
- Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122(1):311-328.
- Adams HP Jr., del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(20):e478-534.
- Qureshi AI. Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH): rationale and design. Neurocrit Care. 2007;6(1):56-66.
- Marik PE, Varon J. Hypertensive crises: challenges and management. Chest. 2007;131(6):1949-1962.
- Aronson S, Dyke CM, Stierer KA, et al. The ECLIPSE trials: comparative studies of clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for acute hypertension treatment in cardiac surgery patients. Anesth Analg. 2008;107(4):1110-1121.
- Magee LA, Cham C, Waterman EJ, Ohlsson A, von Dadelszen P. Hydralazine for treatment of severe hypertension in pregnancy: meta-analysis. BMJ. 2003;327(7421):955-960.
- Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006; 24(1):135-146.
- Rhoney D, Peacock WF. Intravenous therapy for hypertensive emergencies, part 1. Am J Health Syst Pharm. 2009;66(15):1343-1352.
- Rhoney D, Peacock WF. Intravenous therapy for hypertensive emergencies, part 2. Am J Health Syst Pharm. 2009;66(16):1448-1457.
- Varon J. Treatment of acute severe hypertension: current and newer agents. Drugs. 2008;68(3):283-297.
Raise the ‘Red Flags’
To no one’s surprise, federal legislation doesn’t always do what its architects originally intended. A bill designed to protect consumers from identify theft can instead leave small hospitalist practices and other healthcare businesses in the lurch over whether they must meet stringent antitheft requirements intended for credit-card companies and banks. A bill designed to add millions of patients to the ranks of the insured could instead subtract millions of dollars from the reimbursements hospitals and doctors receive from private insurers.
—Jon Leibowitz, chairman, Federal Trade Commission
So What’s to Be Done?
An effort to correct one of these lingering headaches—known as the “Red Flags Rule”—is again on the table, though not everyone’s convinced it might finally be fixed seven years after it was first enacted. The rule, folded into the Fair and Accurate Credit Transactions Act of 2003, required the Federal Trade Commission (FTC) and other government agencies to come up with specific measures that “creditors” and “financial institutions” would have to design and implement to counter the growing risk of identity theft.
As intended, these measures would help businesses “identify, detect, and respond” to anything that might suggest identity theft. In other words, they could throw up red flags to warn of illegal activity.
But five years later, as the act’s Nov. 1, 2008, enforcement date was approaching, no one seemed to know exactly which businesses should be considered “creditors.” The act’s vague wording, in fact, created widespread fear that a measure designed principally for banks and credit-card companies would also apply to small accounting, legal, and healthcare practices, saddling them with cumbersome and expensive vetting protocols.
Thus began a series of requests by federal legislators that the FTC delay enforcement until the confusion could be sorted out. After three delays, including the latest pushback from June 1 through the end of this year, the commission’s patience is wearing thin. FTC Chairman Jon Leibowitz has been clear about the agency’s frustration over the extensions in lieu of a permanent resolution.
“Congress needs to fix the unintended consequences of the legislation establishing the Red Flags Rule—and to fix this problem quickly,” he said in a May 28 release. “As an agency, we’re charged with enforcing the law, and endless extensions delay enforcement.”
The not-so-subtle jab at Congressional inaction was aimed at one chamber in particular. Bill HR3763, which adds clarifying language to the rule and specifically excludes accounting, legal, and medical practices with 20 or fewer employees, sailed through the House of Representatives last October by a vote of 400-0. And then it promptly hit a giant sandbar in the form of the Senate. On May 25, Sen. John Thune (R-S.D.) and Sen. Mark Begich (D-Alaska) attempted a relaunch with their introduction of S3416, a near carbon copy of the House bill.
The measure is hardly a fait accompli, given the Senate’s recent track record, but a spokesman for Sen. Thune said the senator’s office is expecting a resolution before the FTC’s latest extension expires. Citing the commission’s decision to delay enforcement soon after the Senate bill’s introduction, he said, “We interpret that as an indication that they want to give Congress time to act, so we’re very optimistic that something will happen this year.”
Of course, the enforcement delay also might have something to do with the joint lawsuit filed May 21 by the American Medical Association, American Osteopathic Association, and the Medical Society of the District of Columbia. In their complaint, the three medical associations charged that the FTC’s application of the rule to physicians is “arbitrary, capricious, and contrary to the law.”
It’s now up to the Senate to decide whether that suit will become moot. TH
Bryn Nelson is a freelance medical writer based in Seattle.
To no one’s surprise, federal legislation doesn’t always do what its architects originally intended. A bill designed to protect consumers from identify theft can instead leave small hospitalist practices and other healthcare businesses in the lurch over whether they must meet stringent antitheft requirements intended for credit-card companies and banks. A bill designed to add millions of patients to the ranks of the insured could instead subtract millions of dollars from the reimbursements hospitals and doctors receive from private insurers.
—Jon Leibowitz, chairman, Federal Trade Commission
So What’s to Be Done?
An effort to correct one of these lingering headaches—known as the “Red Flags Rule”—is again on the table, though not everyone’s convinced it might finally be fixed seven years after it was first enacted. The rule, folded into the Fair and Accurate Credit Transactions Act of 2003, required the Federal Trade Commission (FTC) and other government agencies to come up with specific measures that “creditors” and “financial institutions” would have to design and implement to counter the growing risk of identity theft.
As intended, these measures would help businesses “identify, detect, and respond” to anything that might suggest identity theft. In other words, they could throw up red flags to warn of illegal activity.
But five years later, as the act’s Nov. 1, 2008, enforcement date was approaching, no one seemed to know exactly which businesses should be considered “creditors.” The act’s vague wording, in fact, created widespread fear that a measure designed principally for banks and credit-card companies would also apply to small accounting, legal, and healthcare practices, saddling them with cumbersome and expensive vetting protocols.
Thus began a series of requests by federal legislators that the FTC delay enforcement until the confusion could be sorted out. After three delays, including the latest pushback from June 1 through the end of this year, the commission’s patience is wearing thin. FTC Chairman Jon Leibowitz has been clear about the agency’s frustration over the extensions in lieu of a permanent resolution.
“Congress needs to fix the unintended consequences of the legislation establishing the Red Flags Rule—and to fix this problem quickly,” he said in a May 28 release. “As an agency, we’re charged with enforcing the law, and endless extensions delay enforcement.”
The not-so-subtle jab at Congressional inaction was aimed at one chamber in particular. Bill HR3763, which adds clarifying language to the rule and specifically excludes accounting, legal, and medical practices with 20 or fewer employees, sailed through the House of Representatives last October by a vote of 400-0. And then it promptly hit a giant sandbar in the form of the Senate. On May 25, Sen. John Thune (R-S.D.) and Sen. Mark Begich (D-Alaska) attempted a relaunch with their introduction of S3416, a near carbon copy of the House bill.
The measure is hardly a fait accompli, given the Senate’s recent track record, but a spokesman for Sen. Thune said the senator’s office is expecting a resolution before the FTC’s latest extension expires. Citing the commission’s decision to delay enforcement soon after the Senate bill’s introduction, he said, “We interpret that as an indication that they want to give Congress time to act, so we’re very optimistic that something will happen this year.”
Of course, the enforcement delay also might have something to do with the joint lawsuit filed May 21 by the American Medical Association, American Osteopathic Association, and the Medical Society of the District of Columbia. In their complaint, the three medical associations charged that the FTC’s application of the rule to physicians is “arbitrary, capricious, and contrary to the law.”
It’s now up to the Senate to decide whether that suit will become moot. TH
Bryn Nelson is a freelance medical writer based in Seattle.
To no one’s surprise, federal legislation doesn’t always do what its architects originally intended. A bill designed to protect consumers from identify theft can instead leave small hospitalist practices and other healthcare businesses in the lurch over whether they must meet stringent antitheft requirements intended for credit-card companies and banks. A bill designed to add millions of patients to the ranks of the insured could instead subtract millions of dollars from the reimbursements hospitals and doctors receive from private insurers.
—Jon Leibowitz, chairman, Federal Trade Commission
So What’s to Be Done?
An effort to correct one of these lingering headaches—known as the “Red Flags Rule”—is again on the table, though not everyone’s convinced it might finally be fixed seven years after it was first enacted. The rule, folded into the Fair and Accurate Credit Transactions Act of 2003, required the Federal Trade Commission (FTC) and other government agencies to come up with specific measures that “creditors” and “financial institutions” would have to design and implement to counter the growing risk of identity theft.
As intended, these measures would help businesses “identify, detect, and respond” to anything that might suggest identity theft. In other words, they could throw up red flags to warn of illegal activity.
But five years later, as the act’s Nov. 1, 2008, enforcement date was approaching, no one seemed to know exactly which businesses should be considered “creditors.” The act’s vague wording, in fact, created widespread fear that a measure designed principally for banks and credit-card companies would also apply to small accounting, legal, and healthcare practices, saddling them with cumbersome and expensive vetting protocols.
Thus began a series of requests by federal legislators that the FTC delay enforcement until the confusion could be sorted out. After three delays, including the latest pushback from June 1 through the end of this year, the commission’s patience is wearing thin. FTC Chairman Jon Leibowitz has been clear about the agency’s frustration over the extensions in lieu of a permanent resolution.
“Congress needs to fix the unintended consequences of the legislation establishing the Red Flags Rule—and to fix this problem quickly,” he said in a May 28 release. “As an agency, we’re charged with enforcing the law, and endless extensions delay enforcement.”
The not-so-subtle jab at Congressional inaction was aimed at one chamber in particular. Bill HR3763, which adds clarifying language to the rule and specifically excludes accounting, legal, and medical practices with 20 or fewer employees, sailed through the House of Representatives last October by a vote of 400-0. And then it promptly hit a giant sandbar in the form of the Senate. On May 25, Sen. John Thune (R-S.D.) and Sen. Mark Begich (D-Alaska) attempted a relaunch with their introduction of S3416, a near carbon copy of the House bill.
The measure is hardly a fait accompli, given the Senate’s recent track record, but a spokesman for Sen. Thune said the senator’s office is expecting a resolution before the FTC’s latest extension expires. Citing the commission’s decision to delay enforcement soon after the Senate bill’s introduction, he said, “We interpret that as an indication that they want to give Congress time to act, so we’re very optimistic that something will happen this year.”
Of course, the enforcement delay also might have something to do with the joint lawsuit filed May 21 by the American Medical Association, American Osteopathic Association, and the Medical Society of the District of Columbia. In their complaint, the three medical associations charged that the FTC’s application of the rule to physicians is “arbitrary, capricious, and contrary to the law.”
It’s now up to the Senate to decide whether that suit will become moot. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Patients First
Rachel George, MD, MBA, FHM, CPE, acknowledges she found her calling through a fluke. After completing an internal-medicine residency in Chicago in 2002, she knew she wanted to stay in the region. She hadn’t decided much else.
“I was not excited about private practice, and I had thought about a cardiology fellowship,” Dr. George recalls. “I was trying to figure out what I wanted to do when I grew up, so to speak.”
She found a job as the lone hospitalist with OSF Medical Group in Rockford, Ill. Despite knowing she’d see “a ridiculous number of patients”—up to 30 per day on weekends—she liked it enough to sign on. “I decided I’d give it a chance for six months or a year while I figured out what I was really going to do,” she says.
Before long, she realized she already was doing it.
“I absolutely loved it,” says Dr. George, one of six new Team Hospitalist members who joined our reader advisory group in April. She now oversees five hospitalist programs in three states as regional medical director and vice president of operations for Brentwood, Tenn.-based Cogent Healthcare. “It was perfect. It was the niche I was looking for.”
Question: What did you enjoy so much about being a hospitalist?
Answer: The acuity of care, the instant gratification of fixing someone and sending them on their way, the intensity in the hospital, not feeling like I was being pulled in 15 different directions like you are in primary-care practice—all the good things about being a hospitalist.
Q: Within a year of joining OSF, you became medical director of its hospitalist service and oversaw its expansion. Did you always envision yourself moving into a leadership role?
A: When I started, I probably would have said my ultimate goal was to get my MBA and think about hospital administration. That was the 10-year plan, or maybe even the 15- or 20-year plan. But when people at the hospital began talking about expanding the [HM] program, I got thrust into the [medical director] role. By that point, I was hooked.
Q: Within three years, you grew the service from one physician to nine. How did you approach expansion?
A: The goal was sustainable growth—growth without sacrificing quality of patient care. When PCPs approached me about taking over their patient population, I’d say we’d take them on as we hired more people. I didn’t want to take off more than we could chew, and I didn’t want to have ridiculous turnover. That wouldn’t do anybody any good.
Q: You joined Cogent in 2006. What prompted the move?
A: I knew Cogent through SHM, and it was too good of an opportunity to pass up. The chance to expand my management responsibilities also was very appealing.
Q: What do you see as the biggest advantage of Cogent’s model?
A: I was part of an in-house program, and I think they’re great in a lot of ways. What they can’t do is economies of scale. There are certain things you can’t do just because it doesn’t make sense financially.
Q: Can you give an example?
A: The classic example I’ll give is discharge summaries in less than 24 hours. [At OSF], I did everything short of getting on my hands and knees and begging them to transcribe discharge summaries in less than 24 hours. They wouldn’t, and I understand why. It was a financial decision.
Cogent, from its inception, said this is too important and we’re going to make sure PCPs get information at discharge. Those types of economies of scale are very difficult to do in a small program, if you’re trying to do it yourself.
Q: What do you consider your biggest professional reward?
A: Seeing a really high-functioning HM team that I’ve helped make that way.
Q: What are the essential elements of such a team?
A: It’s the culture, that patient-first attitude. If everyone understands getting high-quality care to the patient is the most important thing, and we’re all working together to make sure that happens, everything else—core measure performance, decreasing the length of stay—will follow.
Q: What is your biggest challenge?
A: Trying to revamp broken programs.
Q: How do you begin that process?
A: Once the wrong attitude, wrong vision, and wrong culture have set in, we have to decide “How do we improve this?” It’s very difficult. You can’t just close the service and stop seeing patients until you’ve done what you need to do. It’s like trying to fix an airplane in midair.
Q: Despite an already full plate, you continue to see patients. Why?
A: I do it for myself. I don’t want to quit patient care. I enjoy talking to my patients, figuring out what’s wrong, and trying to help them.
Q: You attended the SHM Leadership Academy and have since facilitated academy sessions. What do you see as its benefit?
A: Hospital medicine is a business, whether we like to accept it or not. It’s important for physicians to understand the business drivers, not only for our own practice but for the hospital as well. The academy gives a great overview of the fundamentals of those business drivers.
Q: Would you recommend it for a physician who doesn’t intend to move into a leadership position?
A: I would. It’s valuable for anyone committed to hospital medicine. It helps them understand how their leaders are thinking and why they’re thinking the way they are.
Q: You are former chair of SHM’s Women in Hospital Medicine Task Force, and you pride yourself on balancing life and work. Is HM conducive to that balance?
A: It absolutely can be. Women sometimes think they have to be all things to all people all the time. It’s really about figuring out what your priorities are. I have two young kids and spending time with them is a bigger priority to me than cooking and cleaning. I’d rather live with a messy house and dishes in the sink than not spend time with them.
As a hospitalist, you have that flexibility, too. Most HM programs would love to have a stable, part-time physician. You can do that if you want, or you can be a nocturnist so you can be home with your kids during the day. You are in control of your own life. Understanding that is important, and you can make your choices accordingly.
Q: How do you think HM fares regarding the inclusion of women?
A: There isn’t as much of a good-old-boys’ club as opposed to other fields, which is really refreshing. Women are very well represented on boards and committees. What strikes me is the percentage of women hospitalist leaders is significantly lower.
Q: Why do you think that is?
A: I haven’t wrapped my mind around whether that’s because they aren’t interested because of the choices they made in their lives—which is perfectly fine—or if it’s a lack of opportunity. I do think some women choose not to have a leadership role because their priorities are different, and that’s wonderful. But I wonder if there are cases when women are being passed over for those positions for men instead. The percentages are something we need to keep an eye on so we can better understand why that’s happening. TH
Mark Leiser is a freelance writer in New Jersey.
Rachel George, MD, MBA, FHM, CPE, acknowledges she found her calling through a fluke. After completing an internal-medicine residency in Chicago in 2002, she knew she wanted to stay in the region. She hadn’t decided much else.
“I was not excited about private practice, and I had thought about a cardiology fellowship,” Dr. George recalls. “I was trying to figure out what I wanted to do when I grew up, so to speak.”
She found a job as the lone hospitalist with OSF Medical Group in Rockford, Ill. Despite knowing she’d see “a ridiculous number of patients”—up to 30 per day on weekends—she liked it enough to sign on. “I decided I’d give it a chance for six months or a year while I figured out what I was really going to do,” she says.
Before long, she realized she already was doing it.
“I absolutely loved it,” says Dr. George, one of six new Team Hospitalist members who joined our reader advisory group in April. She now oversees five hospitalist programs in three states as regional medical director and vice president of operations for Brentwood, Tenn.-based Cogent Healthcare. “It was perfect. It was the niche I was looking for.”
Question: What did you enjoy so much about being a hospitalist?
Answer: The acuity of care, the instant gratification of fixing someone and sending them on their way, the intensity in the hospital, not feeling like I was being pulled in 15 different directions like you are in primary-care practice—all the good things about being a hospitalist.
Q: Within a year of joining OSF, you became medical director of its hospitalist service and oversaw its expansion. Did you always envision yourself moving into a leadership role?
A: When I started, I probably would have said my ultimate goal was to get my MBA and think about hospital administration. That was the 10-year plan, or maybe even the 15- or 20-year plan. But when people at the hospital began talking about expanding the [HM] program, I got thrust into the [medical director] role. By that point, I was hooked.
Q: Within three years, you grew the service from one physician to nine. How did you approach expansion?
A: The goal was sustainable growth—growth without sacrificing quality of patient care. When PCPs approached me about taking over their patient population, I’d say we’d take them on as we hired more people. I didn’t want to take off more than we could chew, and I didn’t want to have ridiculous turnover. That wouldn’t do anybody any good.
Q: You joined Cogent in 2006. What prompted the move?
A: I knew Cogent through SHM, and it was too good of an opportunity to pass up. The chance to expand my management responsibilities also was very appealing.
Q: What do you see as the biggest advantage of Cogent’s model?
A: I was part of an in-house program, and I think they’re great in a lot of ways. What they can’t do is economies of scale. There are certain things you can’t do just because it doesn’t make sense financially.
Q: Can you give an example?
A: The classic example I’ll give is discharge summaries in less than 24 hours. [At OSF], I did everything short of getting on my hands and knees and begging them to transcribe discharge summaries in less than 24 hours. They wouldn’t, and I understand why. It was a financial decision.
Cogent, from its inception, said this is too important and we’re going to make sure PCPs get information at discharge. Those types of economies of scale are very difficult to do in a small program, if you’re trying to do it yourself.
Q: What do you consider your biggest professional reward?
A: Seeing a really high-functioning HM team that I’ve helped make that way.
Q: What are the essential elements of such a team?
A: It’s the culture, that patient-first attitude. If everyone understands getting high-quality care to the patient is the most important thing, and we’re all working together to make sure that happens, everything else—core measure performance, decreasing the length of stay—will follow.
Q: What is your biggest challenge?
A: Trying to revamp broken programs.
Q: How do you begin that process?
A: Once the wrong attitude, wrong vision, and wrong culture have set in, we have to decide “How do we improve this?” It’s very difficult. You can’t just close the service and stop seeing patients until you’ve done what you need to do. It’s like trying to fix an airplane in midair.
Q: Despite an already full plate, you continue to see patients. Why?
A: I do it for myself. I don’t want to quit patient care. I enjoy talking to my patients, figuring out what’s wrong, and trying to help them.
Q: You attended the SHM Leadership Academy and have since facilitated academy sessions. What do you see as its benefit?
A: Hospital medicine is a business, whether we like to accept it or not. It’s important for physicians to understand the business drivers, not only for our own practice but for the hospital as well. The academy gives a great overview of the fundamentals of those business drivers.
Q: Would you recommend it for a physician who doesn’t intend to move into a leadership position?
A: I would. It’s valuable for anyone committed to hospital medicine. It helps them understand how their leaders are thinking and why they’re thinking the way they are.
Q: You are former chair of SHM’s Women in Hospital Medicine Task Force, and you pride yourself on balancing life and work. Is HM conducive to that balance?
A: It absolutely can be. Women sometimes think they have to be all things to all people all the time. It’s really about figuring out what your priorities are. I have two young kids and spending time with them is a bigger priority to me than cooking and cleaning. I’d rather live with a messy house and dishes in the sink than not spend time with them.
As a hospitalist, you have that flexibility, too. Most HM programs would love to have a stable, part-time physician. You can do that if you want, or you can be a nocturnist so you can be home with your kids during the day. You are in control of your own life. Understanding that is important, and you can make your choices accordingly.
Q: How do you think HM fares regarding the inclusion of women?
A: There isn’t as much of a good-old-boys’ club as opposed to other fields, which is really refreshing. Women are very well represented on boards and committees. What strikes me is the percentage of women hospitalist leaders is significantly lower.
Q: Why do you think that is?
A: I haven’t wrapped my mind around whether that’s because they aren’t interested because of the choices they made in their lives—which is perfectly fine—or if it’s a lack of opportunity. I do think some women choose not to have a leadership role because their priorities are different, and that’s wonderful. But I wonder if there are cases when women are being passed over for those positions for men instead. The percentages are something we need to keep an eye on so we can better understand why that’s happening. TH
Mark Leiser is a freelance writer in New Jersey.
Rachel George, MD, MBA, FHM, CPE, acknowledges she found her calling through a fluke. After completing an internal-medicine residency in Chicago in 2002, she knew she wanted to stay in the region. She hadn’t decided much else.
“I was not excited about private practice, and I had thought about a cardiology fellowship,” Dr. George recalls. “I was trying to figure out what I wanted to do when I grew up, so to speak.”
She found a job as the lone hospitalist with OSF Medical Group in Rockford, Ill. Despite knowing she’d see “a ridiculous number of patients”—up to 30 per day on weekends—she liked it enough to sign on. “I decided I’d give it a chance for six months or a year while I figured out what I was really going to do,” she says.
Before long, she realized she already was doing it.
“I absolutely loved it,” says Dr. George, one of six new Team Hospitalist members who joined our reader advisory group in April. She now oversees five hospitalist programs in three states as regional medical director and vice president of operations for Brentwood, Tenn.-based Cogent Healthcare. “It was perfect. It was the niche I was looking for.”
Question: What did you enjoy so much about being a hospitalist?
Answer: The acuity of care, the instant gratification of fixing someone and sending them on their way, the intensity in the hospital, not feeling like I was being pulled in 15 different directions like you are in primary-care practice—all the good things about being a hospitalist.
Q: Within a year of joining OSF, you became medical director of its hospitalist service and oversaw its expansion. Did you always envision yourself moving into a leadership role?
A: When I started, I probably would have said my ultimate goal was to get my MBA and think about hospital administration. That was the 10-year plan, or maybe even the 15- or 20-year plan. But when people at the hospital began talking about expanding the [HM] program, I got thrust into the [medical director] role. By that point, I was hooked.
Q: Within three years, you grew the service from one physician to nine. How did you approach expansion?
A: The goal was sustainable growth—growth without sacrificing quality of patient care. When PCPs approached me about taking over their patient population, I’d say we’d take them on as we hired more people. I didn’t want to take off more than we could chew, and I didn’t want to have ridiculous turnover. That wouldn’t do anybody any good.
Q: You joined Cogent in 2006. What prompted the move?
A: I knew Cogent through SHM, and it was too good of an opportunity to pass up. The chance to expand my management responsibilities also was very appealing.
Q: What do you see as the biggest advantage of Cogent’s model?
A: I was part of an in-house program, and I think they’re great in a lot of ways. What they can’t do is economies of scale. There are certain things you can’t do just because it doesn’t make sense financially.
Q: Can you give an example?
A: The classic example I’ll give is discharge summaries in less than 24 hours. [At OSF], I did everything short of getting on my hands and knees and begging them to transcribe discharge summaries in less than 24 hours. They wouldn’t, and I understand why. It was a financial decision.
Cogent, from its inception, said this is too important and we’re going to make sure PCPs get information at discharge. Those types of economies of scale are very difficult to do in a small program, if you’re trying to do it yourself.
Q: What do you consider your biggest professional reward?
A: Seeing a really high-functioning HM team that I’ve helped make that way.
Q: What are the essential elements of such a team?
A: It’s the culture, that patient-first attitude. If everyone understands getting high-quality care to the patient is the most important thing, and we’re all working together to make sure that happens, everything else—core measure performance, decreasing the length of stay—will follow.
Q: What is your biggest challenge?
A: Trying to revamp broken programs.
Q: How do you begin that process?
A: Once the wrong attitude, wrong vision, and wrong culture have set in, we have to decide “How do we improve this?” It’s very difficult. You can’t just close the service and stop seeing patients until you’ve done what you need to do. It’s like trying to fix an airplane in midair.
Q: Despite an already full plate, you continue to see patients. Why?
A: I do it for myself. I don’t want to quit patient care. I enjoy talking to my patients, figuring out what’s wrong, and trying to help them.
Q: You attended the SHM Leadership Academy and have since facilitated academy sessions. What do you see as its benefit?
A: Hospital medicine is a business, whether we like to accept it or not. It’s important for physicians to understand the business drivers, not only for our own practice but for the hospital as well. The academy gives a great overview of the fundamentals of those business drivers.
Q: Would you recommend it for a physician who doesn’t intend to move into a leadership position?
A: I would. It’s valuable for anyone committed to hospital medicine. It helps them understand how their leaders are thinking and why they’re thinking the way they are.
Q: You are former chair of SHM’s Women in Hospital Medicine Task Force, and you pride yourself on balancing life and work. Is HM conducive to that balance?
A: It absolutely can be. Women sometimes think they have to be all things to all people all the time. It’s really about figuring out what your priorities are. I have two young kids and spending time with them is a bigger priority to me than cooking and cleaning. I’d rather live with a messy house and dishes in the sink than not spend time with them.
As a hospitalist, you have that flexibility, too. Most HM programs would love to have a stable, part-time physician. You can do that if you want, or you can be a nocturnist so you can be home with your kids during the day. You are in control of your own life. Understanding that is important, and you can make your choices accordingly.
Q: How do you think HM fares regarding the inclusion of women?
A: There isn’t as much of a good-old-boys’ club as opposed to other fields, which is really refreshing. Women are very well represented on boards and committees. What strikes me is the percentage of women hospitalist leaders is significantly lower.
Q: Why do you think that is?
A: I haven’t wrapped my mind around whether that’s because they aren’t interested because of the choices they made in their lives—which is perfectly fine—or if it’s a lack of opportunity. I do think some women choose not to have a leadership role because their priorities are different, and that’s wonderful. But I wonder if there are cases when women are being passed over for those positions for men instead. The percentages are something we need to keep an eye on so we can better understand why that’s happening. TH
Mark Leiser is a freelance writer in New Jersey.
Mentorship Matters
As you begin the next phase in your career, whether starting residency, a fellowship, or a new faculty position, it’s likely you have dozens of questions. How do I survive the rigors of residency? What do I need to make the most of my fellowship? What do I need to do to become more efficient in my clinical productivity? How do I succeed in academics? There are many more questions we could add to this list.
While some lessons in life are learned through trial and error, it rarely is the best way. This is especially true when considering your professional future. An essential first step at any phase in your career is finding yourself a mentor. There are many benefits to having someone help you navigate through many of the challenges you will face. A mentor’s experience is invaluable in avoiding potential pitfalls that set many physicians back in their careers, and in giving you the best opportunity to succeed as you begin your desired path.
This might seem like a new idea, but the concept of mentoring has been around for centuries. All of us have been mentored at some point in our lives; you probably just haven’t realized it. It could have been a parent, coach, guidance counselor, or teacher. Mentorship is a mutually beneficial relationship that applies to many areas of life, including your career development in medicine.
Finding a mentor is easier said than done. Many physicians are not sure where to begin. How do you choose? Where do you start? These are common questions, among many others. Some institutions assign mentors for this very reason. However, this is not always an ideal solution, as the mentor/mentee relationship might not be a perfect match.
Here are some ideas to help get you started in your mentor search:
1) Know Thyself: As you begin your search, start by reflecting on yourself. What do you need? What are your current skills? What are your career aspirations? This initial step of introspection is essential in becoming more aware of your own mentoring needs. The more specific you can be in defining your needs and goals, the better equipped you will be to seek out someone who can help guide you on the path to achieve them.
2) Know What to Look for: Having established what you are looking for as a mentee, it is important to consider what makes for a good mentor. A good mentor is experienced, successful, and has the proper skill sets, but also should have the following basic qualities:
- A willingness to mentor. They should want to invest in you and be interested in your career success;
- A commitment to the mentoring relationship. They will spend the time, energy, and resources necessary to help you achieve your goals;
- Availability. They must not be too busy with other responsibilities or other mentees;
- Good communications skills. They need to be a sounding board, and provide honest and constructive advice that is specific to your needs; and
- Professionalism. You should trust them to maintain confidentiality.
3) Start the Search: Now that you understand your needs and the desired qualities in a mentor, start thinking about potential options. You might already have someone in mind based on his or her success or reputation as a mentor. However, by asking around, you might also find other, lesser-known mentors that might be an even better fit for you in the long run.
Don’t limit yourself to your current institution. You might find that the mentors you are looking for are at other institutions. These opportunities are usually found through networking, either through local channels or through regional/national meetings. Although these kinds of mentorship relationships are more difficult to initiate and maintain, the opportunity to collaborate among members at various institutions can end up being more fruitful in the long term.
4) Meet and Greet: After assembling a short list of potential mentors, schedule a meeting with each of them. This may be cumbersome at first, but it is essential in finding out if this is someone you can see working with and learning from over the next few months or years. Finding this natural “fit” is what helps make for a lasting relationship.
At the same time, think of the meetings as interviews for a “position,” which is important to your future. This is the time for communicating your intentions, for making mutual expectations clear, and refining them further. Keep your professional goals in mind, as this will help in narrowing down your list.
5) One Size Does Not Fit All: As you consider potential mentors, keep in mind that it is OK to branch out. You might have many areas (research, education, quality improvement, work-life balance, leadership, clinical productivity, etc.) of interest that need mentoring. One mentor is unlikely to be able to meet all of your needs. This is where developing a core group of mentors could be helpful, each providing their unique insight.
Once you find a good mentor, remember to value their time and respect their expectations for you as a mentee. You are to be as committed to the partnership as you expect them to be. As you develop this mentorship, you will realize that it can become more than a professional relationship—it also can become a lasting alliance that strengthens with time. TH
Dr. LaBrin is an academic hospitalist at Vanderbilt University School of Medicine in Nashville, Tenn.
As you begin the next phase in your career, whether starting residency, a fellowship, or a new faculty position, it’s likely you have dozens of questions. How do I survive the rigors of residency? What do I need to make the most of my fellowship? What do I need to do to become more efficient in my clinical productivity? How do I succeed in academics? There are many more questions we could add to this list.
While some lessons in life are learned through trial and error, it rarely is the best way. This is especially true when considering your professional future. An essential first step at any phase in your career is finding yourself a mentor. There are many benefits to having someone help you navigate through many of the challenges you will face. A mentor’s experience is invaluable in avoiding potential pitfalls that set many physicians back in their careers, and in giving you the best opportunity to succeed as you begin your desired path.
This might seem like a new idea, but the concept of mentoring has been around for centuries. All of us have been mentored at some point in our lives; you probably just haven’t realized it. It could have been a parent, coach, guidance counselor, or teacher. Mentorship is a mutually beneficial relationship that applies to many areas of life, including your career development in medicine.
Finding a mentor is easier said than done. Many physicians are not sure where to begin. How do you choose? Where do you start? These are common questions, among many others. Some institutions assign mentors for this very reason. However, this is not always an ideal solution, as the mentor/mentee relationship might not be a perfect match.
Here are some ideas to help get you started in your mentor search:
1) Know Thyself: As you begin your search, start by reflecting on yourself. What do you need? What are your current skills? What are your career aspirations? This initial step of introspection is essential in becoming more aware of your own mentoring needs. The more specific you can be in defining your needs and goals, the better equipped you will be to seek out someone who can help guide you on the path to achieve them.
2) Know What to Look for: Having established what you are looking for as a mentee, it is important to consider what makes for a good mentor. A good mentor is experienced, successful, and has the proper skill sets, but also should have the following basic qualities:
- A willingness to mentor. They should want to invest in you and be interested in your career success;
- A commitment to the mentoring relationship. They will spend the time, energy, and resources necessary to help you achieve your goals;
- Availability. They must not be too busy with other responsibilities or other mentees;
- Good communications skills. They need to be a sounding board, and provide honest and constructive advice that is specific to your needs; and
- Professionalism. You should trust them to maintain confidentiality.
3) Start the Search: Now that you understand your needs and the desired qualities in a mentor, start thinking about potential options. You might already have someone in mind based on his or her success or reputation as a mentor. However, by asking around, you might also find other, lesser-known mentors that might be an even better fit for you in the long run.
Don’t limit yourself to your current institution. You might find that the mentors you are looking for are at other institutions. These opportunities are usually found through networking, either through local channels or through regional/national meetings. Although these kinds of mentorship relationships are more difficult to initiate and maintain, the opportunity to collaborate among members at various institutions can end up being more fruitful in the long term.
4) Meet and Greet: After assembling a short list of potential mentors, schedule a meeting with each of them. This may be cumbersome at first, but it is essential in finding out if this is someone you can see working with and learning from over the next few months or years. Finding this natural “fit” is what helps make for a lasting relationship.
At the same time, think of the meetings as interviews for a “position,” which is important to your future. This is the time for communicating your intentions, for making mutual expectations clear, and refining them further. Keep your professional goals in mind, as this will help in narrowing down your list.
5) One Size Does Not Fit All: As you consider potential mentors, keep in mind that it is OK to branch out. You might have many areas (research, education, quality improvement, work-life balance, leadership, clinical productivity, etc.) of interest that need mentoring. One mentor is unlikely to be able to meet all of your needs. This is where developing a core group of mentors could be helpful, each providing their unique insight.
Once you find a good mentor, remember to value their time and respect their expectations for you as a mentee. You are to be as committed to the partnership as you expect them to be. As you develop this mentorship, you will realize that it can become more than a professional relationship—it also can become a lasting alliance that strengthens with time. TH
Dr. LaBrin is an academic hospitalist at Vanderbilt University School of Medicine in Nashville, Tenn.
As you begin the next phase in your career, whether starting residency, a fellowship, or a new faculty position, it’s likely you have dozens of questions. How do I survive the rigors of residency? What do I need to make the most of my fellowship? What do I need to do to become more efficient in my clinical productivity? How do I succeed in academics? There are many more questions we could add to this list.
While some lessons in life are learned through trial and error, it rarely is the best way. This is especially true when considering your professional future. An essential first step at any phase in your career is finding yourself a mentor. There are many benefits to having someone help you navigate through many of the challenges you will face. A mentor’s experience is invaluable in avoiding potential pitfalls that set many physicians back in their careers, and in giving you the best opportunity to succeed as you begin your desired path.
This might seem like a new idea, but the concept of mentoring has been around for centuries. All of us have been mentored at some point in our lives; you probably just haven’t realized it. It could have been a parent, coach, guidance counselor, or teacher. Mentorship is a mutually beneficial relationship that applies to many areas of life, including your career development in medicine.
Finding a mentor is easier said than done. Many physicians are not sure where to begin. How do you choose? Where do you start? These are common questions, among many others. Some institutions assign mentors for this very reason. However, this is not always an ideal solution, as the mentor/mentee relationship might not be a perfect match.
Here are some ideas to help get you started in your mentor search:
1) Know Thyself: As you begin your search, start by reflecting on yourself. What do you need? What are your current skills? What are your career aspirations? This initial step of introspection is essential in becoming more aware of your own mentoring needs. The more specific you can be in defining your needs and goals, the better equipped you will be to seek out someone who can help guide you on the path to achieve them.
2) Know What to Look for: Having established what you are looking for as a mentee, it is important to consider what makes for a good mentor. A good mentor is experienced, successful, and has the proper skill sets, but also should have the following basic qualities:
- A willingness to mentor. They should want to invest in you and be interested in your career success;
- A commitment to the mentoring relationship. They will spend the time, energy, and resources necessary to help you achieve your goals;
- Availability. They must not be too busy with other responsibilities or other mentees;
- Good communications skills. They need to be a sounding board, and provide honest and constructive advice that is specific to your needs; and
- Professionalism. You should trust them to maintain confidentiality.
3) Start the Search: Now that you understand your needs and the desired qualities in a mentor, start thinking about potential options. You might already have someone in mind based on his or her success or reputation as a mentor. However, by asking around, you might also find other, lesser-known mentors that might be an even better fit for you in the long run.
Don’t limit yourself to your current institution. You might find that the mentors you are looking for are at other institutions. These opportunities are usually found through networking, either through local channels or through regional/national meetings. Although these kinds of mentorship relationships are more difficult to initiate and maintain, the opportunity to collaborate among members at various institutions can end up being more fruitful in the long term.
4) Meet and Greet: After assembling a short list of potential mentors, schedule a meeting with each of them. This may be cumbersome at first, but it is essential in finding out if this is someone you can see working with and learning from over the next few months or years. Finding this natural “fit” is what helps make for a lasting relationship.
At the same time, think of the meetings as interviews for a “position,” which is important to your future. This is the time for communicating your intentions, for making mutual expectations clear, and refining them further. Keep your professional goals in mind, as this will help in narrowing down your list.
5) One Size Does Not Fit All: As you consider potential mentors, keep in mind that it is OK to branch out. You might have many areas (research, education, quality improvement, work-life balance, leadership, clinical productivity, etc.) of interest that need mentoring. One mentor is unlikely to be able to meet all of your needs. This is where developing a core group of mentors could be helpful, each providing their unique insight.
Once you find a good mentor, remember to value their time and respect their expectations for you as a mentee. You are to be as committed to the partnership as you expect them to be. As you develop this mentorship, you will realize that it can become more than a professional relationship—it also can become a lasting alliance that strengthens with time. TH
Dr. LaBrin is an academic hospitalist at Vanderbilt University School of Medicine in Nashville, Tenn.
Radical vs. Sensible

Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Hospital medicine had grown rapidly and provided the platform for change in our nation’s hospitals long before there was any meaningful healthcare legislation in Washington. With President Obama’s appointment of an innovator—Don Berwick—to head the Centers for Medicare and Medicaid Services (CMS), there is increased opportunity to ramp up revisions, large and small, to provide the incentives and the impetus to create a healthcare system for the 21st century.
With that in mind, I thought I’d offer a few ideas that Don could institute on Day 1, which could start us in the right direction, or throw us all into chaos, depending on how it plays out. While most of my attention is directed to the Medicare population, all of these ideas would be equally applicable to the commercially insured population.
Advanced Directives
We all know that too few people in this country have taken the opportunity to discuss with their families and their personal physicians how they want their care managed at critical junctures, whether it comes on suddenly with an accident or with aging. The suggestion that Medicare would pay for an office visit with your doctor to discuss this imploded with the news media’s fanning of the “death panel” flames first stoked by Sarah Palin, which sidetracked all rational discussion.
Besides setting up people for unwarranted and unwanted assaults and protracted misery, mismanaging the end stages of life leads to an enormous misallocation of physicians’ focus at a time when we all need to be mindful stewards of our limited healthcare resources.
It is acceptable if, after careful consideration, anyone chooses to not have any advanced directive, but it should be a cognitive directed choice, not just a failure to engage.
Therefore, I am proposing that Medicare offer an incentive (e.g., waiving co-payments or deductibles) to have all Medicare beneficiaries complete an advanced directive annually, or sign a form indicating they were offered an advanced directive and declined to have one invoked. In addition, Medicare could set up a system that would allow physicians (or facilities) who would manage the patient’s healthcare to have access to the conditions of the advance directives. The forms could be attached to individual Medicare profiles, possibly on the Web, in addition to being held by a patient’s PCP or medical home, if they have one.
Personal Health Records
Most people in this country can access most of the information about their personal financial status in real time from any computer in the world. Less than 10% of Americans can retrieve meaningful personal medical information. This is in spite of the prevalence of Web-based personal health record (PHR) software from Microsoft, Revolution Health, and other software vendors, along with Kaiser Permanente and a handful of insurance companies.
PHRs allow for an initial baseline set of data to be recorded and updated as new tests, diagnoses, and medications are employed. It allows for a composite knowledge of what has been tried in the past and what is being utilized in the present. This can be under patients’ control, but it would allow for appropriate access at times of acute need (e.g., an ED visit or a hospital admission).
Too often, patients with a long-term relationship with a local PCP present to the hospital and all of the healthcare professionals are forced to make critical decisions in the first few hours with insufficient or inaccurate information. This leads to needless repetition of tests or inability to compare current data with previous data (wouldn’t it be nice to have the last EKG or labs?), or in retrying a treatment regimen that hasn’t worked in the past.
And if you are in another city or if you don’t have a local physician with all of your old records, the information gap is far worse.
Once again, we could incentivize patients to have an up-to-date PHR with reduced premiums, or lower deductibles or copayments. We could look for ways to incentivize PCPs and hospitals to help patients build and maintain their PHR. We could make it a matter of course that a patient’s PHR would be updated at each intersection with healthcare information (e.g., the pharmacy or the lab or each office visit).
Physician Accountability
Somehow, we have evolved into a fragmented health system. We need to repair the disconnect between patients and physicians. The professional pact between the patient and their primary physician needs to be in place until the patient and the “next” physician agree to the handoff of responsibility. As hospitalists, we see this at both ends of the continuum. Patients shouldn’t just be “sent” to the ED or the hospital, especially not when they are acutely ill. Their personal physician, their medical home, should “arrange” for an orderly transfer of care. This would involve a transfer of information (possibly facilitated by an updated PHR), but as much by the assurance that the accepting physician or institution is prepared for the handoff, acknowledges this to the PCP, and that the patient understands the handoff has taken place.
In the same way, patients would not be just “sent out” from the hospital. The treating physician (it could be the hospitalist, but also the surgeon or cardiologist) would remain the doctor of record—the first resource for patients’ question and issues—until another “receiving” physician has accepted the handoff, acknowledges this role, and the patient agrees.
We could rapidly shift this process by allowing the patient to decide when the hospitalization has ended. We could change the system overnight by making one of the conditions for payment for a hospitalization (to the physicians and the hospital) that the patient has signed off that indeed the hospitalization has ended.
This might include a discussion of chronic medications to continue, acute therapies to complete, understanding by the patient of where and when to receive follow-up testing and evaluation, and a clear understanding of which physician is now accountable for future issues and questions as patients travel from acute illness to normal function.
There certainly are economic and societal issues. Not everyone has a PCP or can pay for their outpatient care, and this could be a full-employment plan for liability attorneys, but in the end I am confident medical professionals would create the linkages that would minimize the deep white space patients find themselves in once they are wheeled to the front door of their hospitals.
Creatively Complete the Hospitalization
In a perfect world, everyone would have a functional, robust medical home to return to after an acute hospitalization. Unfortunately, a patient-centered medical home (PCMH) is much more of a hope than a reality for most Americans. While we are working to create a better “horizontal” hospitalization, there are clear gaps in the vertical-care world.
If we are going to be responsible for bundled care that encompasses pre-admit and post-discharge care (e.g., 30 days after discharge), then we must beef up our outpatient capabilities.
Hopefully in the long run, this can be supplied by a reinvigorated and reinvented medical home, but it is still a long way off. If payment and accountability continue to blur just when the hospitalization ends, then hospitals (and hospitalists) and Medicare and insurers will need to be creative in how and who will manage the patient. We’ll need to solve the issues around patients who are no longer sick enough to require a hospital bed but clearly are not back to their steady state.
This ties in with the accountability gap that vexes our patients every day. Very likely, hospitalists will have to assume a role in managing the patients after hospital discharge. This might take the form of a few follow-up visits and continued support systems via the Web and telephone. It will probably require a new class of hospitalist—the ambulist or the subacutist—supported by dedicated ancillary staff and systems.
Once again, Medicare and insurers can drive to a better system of post-acute care by supplying incentives: a more robust discharge payment or rewarding successful completion of a hospitalization, possibly by bundled payment incentives. In addition, there could be clear standards set that would define when this is done well with associated rewards.
I know some of these ideas are radical and make us uncomfortable. They seem to assign more responsibilities to an already overburdened profession. To be successful, these innovations require an active participation and accountability of our patients. We as the providers of healthcare cannot do this alone. It also requires the evolution of the hospital as an institution from just the healthcare provider for the acutely ill, horizontal patient, but as more a part of a continuum from acute illness to return to function. And it cries out for a robust, capable, outpatient partner in a medical home or accountable care organization (ACO) that is equally dedicated, incentivized, and accountable.
We won’t get there tomorrow, even if Dr. Berwick reads this and acts on all of the ideas on his first day at CMS.
But if we don’t get started, we know we definitely won’t get there at any time in our future. TH
Dr. Wellikson is CEO of SHM.
Rise of the Napturnist

The best sleep I ever got was in the winter of 1996. I remember it vividly. It was effortless, natural, blissful. I had swiftly slipped through the early phases of non-REM sleep, skillfully side-stepping alpha and theta waves, leaving myoclonic jerks in my wake. There was a brief hypnagogic dream involving sun-swept landscapes, playful butterflies, and a field of rhythmically blowing lavender that waved me further along on my slumbering voyage. And then, magically, I was basking in the pillowy splendor of stage 4 sleep, delta waves soothingly serenading me into hibernation.
I had found the celebrated state of suspended sensory and motor activity characterized by unconsciousness and loss of voluntary muscle movement.1 I was asleep.
I was an intern, had just worked 36 continuous hours, and was driving a car.
ACGME Outlines Resident Duty-Hours Changes
I was reminded of this incident on June 23, when I reviewed the freshly minted recommendations from the Accreditation Council for Graduate Medical Education (ACGME) task force regarding duty hours.2 This proposal follows on ACGME’s 2003 report, which enacted such national resident duty-hour standards as the 80-hour work week, the maximum 24-hour shift (plus six hours for administrative time), and the requirement for 10 hours off between shifts.
Like the 2003 report, which has played a large role in the rise of academic HM, the 2010 recommendations have major implications for academic hospitalists and our community brethren who will receive our residency graduates. As such, the reaction within the hospitalist community was immediate. Within minutes of ACGME’s notification, I was inundated with e-mail from colleagues both locally and nationally. Everyone was struggling with the repercussions. Was this good for resident education, a boon or bust for HM, a death knell for teaching hospitals?
So What’s in There?
This hotly anticipated report focuses its energy on four key elements of what the ACGME has morphed from “duty hours” into the resident “work environment”: resident supervision, handoffs of patient care, use of systems to enhance patient safety, and the effects of sleep on performance. Much of this is not really controversial and likely good for both residents and HM—an emphasis on systems-based practice, transitions of care, and expectations around communication.
The most discussed and controversial changes regard the move toward supervision and work hours that are customized to trainees’ levels. Unlike in the past, when the intern bore the brunt of the hours and patient duties, this proposal emphasizes graded supervision and duty-hour expectations. Practically, this means first-year residents will require closer supervision (whether by a resident or an attending has yet to be delineated) than more senior residents. Likewise, although all residents can only work a maximum of 80 hours averaged over four weeks (no change from 2003), the maximum shift length for interns will be limited to 16 hours. Upper-level residents will be limited to no more than 24 consecutive hours with an additional four hours for administrative work, but it is “strongly suggested” that residents working longer than 16 hours be provided with opportunities for “strategic napping.”
Read the Tea Leaves
I think these recommendations are rational and reasonable. To be sure, when these go into effect on July 1, 2011, they will have a tremendous impact on my residency program, my hospital, and my hospitalist faculty. My program, like most, likely will move toward a shift system of patient care, instead of overnight call. My hospital likely will have to expend millions of dollars annually to back-fill the work that residents would have done. My hospitalist group likely will have to expand our nonresident coverage both during the day and at night, inducing one of my partners to query, “Does this mean we’ll have to hire napturnists to cover the residents’ strategic nap time?”
It’s easy to deride these work environment changes, especially if we see the world through the uphill-in-the-snow-both-ways lenses most of us use to recollect (fondly?) our residency days. Yes, the field of medicine is losing a rite of passage many of us endured, and I too retrospectively feel the nostalgic tug of the long shifts, the seemingly insurmountable avalanche of admissions, and the autonomy in resident decision-making that made my training so valuable. But are we really against ensuring that residents are properly supervised, handoffs are more standardized, and systems are in place to protect the safety of our patients?
Sleep = Safety
The push behind limiting the maximum duration of work to 16 and 24 hours for interns and residents, respectively, stems from the growing body of literature regarding the detrimental effects of the fatigue and sleep deprivation that comes with long shifts. Not so shockingly, the data show that residents are sleepy. When administered the Epworth Sleepiness Score, residents appear sleepier than sleep apneic patients and nearly as sleepy as narcoleptics.3,4 In fact, they are so sleepy they often don’t even recognize when they are sleeping. One study showed that nearly half the time that anesthesia residents were asleep, they were unaware that they were actually sleeping.5
Further data suggest that residents who sleep less than five hours per night are twice as likely to be sued, and significantly more likely to report adverse events and errors in patient care.6 When comparing traditional, every-third-night call and 24- to 30-hour shifts with 16-hour shifts, the former staffing model is associated with 36% more serious errors than the latter.
Furthermore, there is a five-fold increase in the rate of serious diagnostic errors in the residents in the longer-shift group.7 And to finish where I began, residents who worked shifts that lasted more than 24 hours are more than twice as likely to crash their cars as those working less than 24-hour shifts. In fact, every additional extended-duration shift per month increases the chances of a car crash while commuting by 16%.8
So ask yourself this: If you were designing, from scratch, residency training today, would you really design a system similar to what we had 10 years ago? Like the one we have now? Would you ask residents, many just months out of medical school, to admit a dozen or more patients a day, stay awake for more than 30 hours, and care for the sickest, most frail patients without the assistance of more senior physicians?
The field of medicine is at a crossroads, and it faces many questions, not the least of which is how best to train our future physicians. The ACGME has published its proposal and given the public, including you, until Aug. 9 to voice your comments. These are big issues to ponder.
Maybe you should sleep on it. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Sleep. Wikipedia website. Available at: http://en.wikipedia.org/wiki/Sleep. Accessed July 10, 2010.
- Nasca TJ, Day SH, Amis S. The new recommendations on duty hours from the ACGME task force. New England Journal of Medicine website. Available at: content.nejm.org/cgi/content/full/NEJMsb1005800. Accessed July 2, 2010.
- Mustafa M, Erokwu N, Ebose I, Strohl K. Sleep problems and the risk for sleep disorders in an outpatient veteran population. Sleep & Breathing. 2005;9:57-63.
- Papp KK, Stoller EP, Sage P, et al. The effects of sleep loss and fatigue on resident-physicians: a multi-institutional, mixed-method study. Acad Med. 2005; 79:394-406.
- Howard SK, Gaba DM, Rosekind MR, Zaracone VP. The risks and implications of excessive daytime sleepiness in resident physicians. Acad Med. 2002; 77:1019-1025.
- Baldwin DC, Daugherty SR. Sleep deprivation and fatigue in residency training: results of a national survey of 1st- and 2nd-year residents. Sleep. 2004;27:371-372.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med. 2004;18:1838-1848.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
The best sleep I ever got was in the winter of 1996. I remember it vividly. It was effortless, natural, blissful. I had swiftly slipped through the early phases of non-REM sleep, skillfully side-stepping alpha and theta waves, leaving myoclonic jerks in my wake. There was a brief hypnagogic dream involving sun-swept landscapes, playful butterflies, and a field of rhythmically blowing lavender that waved me further along on my slumbering voyage. And then, magically, I was basking in the pillowy splendor of stage 4 sleep, delta waves soothingly serenading me into hibernation.
I had found the celebrated state of suspended sensory and motor activity characterized by unconsciousness and loss of voluntary muscle movement.1 I was asleep.
I was an intern, had just worked 36 continuous hours, and was driving a car.
ACGME Outlines Resident Duty-Hours Changes
I was reminded of this incident on June 23, when I reviewed the freshly minted recommendations from the Accreditation Council for Graduate Medical Education (ACGME) task force regarding duty hours.2 This proposal follows on ACGME’s 2003 report, which enacted such national resident duty-hour standards as the 80-hour work week, the maximum 24-hour shift (plus six hours for administrative time), and the requirement for 10 hours off between shifts.
Like the 2003 report, which has played a large role in the rise of academic HM, the 2010 recommendations have major implications for academic hospitalists and our community brethren who will receive our residency graduates. As such, the reaction within the hospitalist community was immediate. Within minutes of ACGME’s notification, I was inundated with e-mail from colleagues both locally and nationally. Everyone was struggling with the repercussions. Was this good for resident education, a boon or bust for HM, a death knell for teaching hospitals?
So What’s in There?
This hotly anticipated report focuses its energy on four key elements of what the ACGME has morphed from “duty hours” into the resident “work environment”: resident supervision, handoffs of patient care, use of systems to enhance patient safety, and the effects of sleep on performance. Much of this is not really controversial and likely good for both residents and HM—an emphasis on systems-based practice, transitions of care, and expectations around communication.
The most discussed and controversial changes regard the move toward supervision and work hours that are customized to trainees’ levels. Unlike in the past, when the intern bore the brunt of the hours and patient duties, this proposal emphasizes graded supervision and duty-hour expectations. Practically, this means first-year residents will require closer supervision (whether by a resident or an attending has yet to be delineated) than more senior residents. Likewise, although all residents can only work a maximum of 80 hours averaged over four weeks (no change from 2003), the maximum shift length for interns will be limited to 16 hours. Upper-level residents will be limited to no more than 24 consecutive hours with an additional four hours for administrative work, but it is “strongly suggested” that residents working longer than 16 hours be provided with opportunities for “strategic napping.”
Read the Tea Leaves
I think these recommendations are rational and reasonable. To be sure, when these go into effect on July 1, 2011, they will have a tremendous impact on my residency program, my hospital, and my hospitalist faculty. My program, like most, likely will move toward a shift system of patient care, instead of overnight call. My hospital likely will have to expend millions of dollars annually to back-fill the work that residents would have done. My hospitalist group likely will have to expand our nonresident coverage both during the day and at night, inducing one of my partners to query, “Does this mean we’ll have to hire napturnists to cover the residents’ strategic nap time?”
It’s easy to deride these work environment changes, especially if we see the world through the uphill-in-the-snow-both-ways lenses most of us use to recollect (fondly?) our residency days. Yes, the field of medicine is losing a rite of passage many of us endured, and I too retrospectively feel the nostalgic tug of the long shifts, the seemingly insurmountable avalanche of admissions, and the autonomy in resident decision-making that made my training so valuable. But are we really against ensuring that residents are properly supervised, handoffs are more standardized, and systems are in place to protect the safety of our patients?
Sleep = Safety
The push behind limiting the maximum duration of work to 16 and 24 hours for interns and residents, respectively, stems from the growing body of literature regarding the detrimental effects of the fatigue and sleep deprivation that comes with long shifts. Not so shockingly, the data show that residents are sleepy. When administered the Epworth Sleepiness Score, residents appear sleepier than sleep apneic patients and nearly as sleepy as narcoleptics.3,4 In fact, they are so sleepy they often don’t even recognize when they are sleeping. One study showed that nearly half the time that anesthesia residents were asleep, they were unaware that they were actually sleeping.5
Further data suggest that residents who sleep less than five hours per night are twice as likely to be sued, and significantly more likely to report adverse events and errors in patient care.6 When comparing traditional, every-third-night call and 24- to 30-hour shifts with 16-hour shifts, the former staffing model is associated with 36% more serious errors than the latter.
Furthermore, there is a five-fold increase in the rate of serious diagnostic errors in the residents in the longer-shift group.7 And to finish where I began, residents who worked shifts that lasted more than 24 hours are more than twice as likely to crash their cars as those working less than 24-hour shifts. In fact, every additional extended-duration shift per month increases the chances of a car crash while commuting by 16%.8
So ask yourself this: If you were designing, from scratch, residency training today, would you really design a system similar to what we had 10 years ago? Like the one we have now? Would you ask residents, many just months out of medical school, to admit a dozen or more patients a day, stay awake for more than 30 hours, and care for the sickest, most frail patients without the assistance of more senior physicians?
The field of medicine is at a crossroads, and it faces many questions, not the least of which is how best to train our future physicians. The ACGME has published its proposal and given the public, including you, until Aug. 9 to voice your comments. These are big issues to ponder.
Maybe you should sleep on it. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Sleep. Wikipedia website. Available at: http://en.wikipedia.org/wiki/Sleep. Accessed July 10, 2010.
- Nasca TJ, Day SH, Amis S. The new recommendations on duty hours from the ACGME task force. New England Journal of Medicine website. Available at: content.nejm.org/cgi/content/full/NEJMsb1005800. Accessed July 2, 2010.
- Mustafa M, Erokwu N, Ebose I, Strohl K. Sleep problems and the risk for sleep disorders in an outpatient veteran population. Sleep & Breathing. 2005;9:57-63.
- Papp KK, Stoller EP, Sage P, et al. The effects of sleep loss and fatigue on resident-physicians: a multi-institutional, mixed-method study. Acad Med. 2005; 79:394-406.
- Howard SK, Gaba DM, Rosekind MR, Zaracone VP. The risks and implications of excessive daytime sleepiness in resident physicians. Acad Med. 2002; 77:1019-1025.
- Baldwin DC, Daugherty SR. Sleep deprivation and fatigue in residency training: results of a national survey of 1st- and 2nd-year residents. Sleep. 2004;27:371-372.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med. 2004;18:1838-1848.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
The best sleep I ever got was in the winter of 1996. I remember it vividly. It was effortless, natural, blissful. I had swiftly slipped through the early phases of non-REM sleep, skillfully side-stepping alpha and theta waves, leaving myoclonic jerks in my wake. There was a brief hypnagogic dream involving sun-swept landscapes, playful butterflies, and a field of rhythmically blowing lavender that waved me further along on my slumbering voyage. And then, magically, I was basking in the pillowy splendor of stage 4 sleep, delta waves soothingly serenading me into hibernation.
I had found the celebrated state of suspended sensory and motor activity characterized by unconsciousness and loss of voluntary muscle movement.1 I was asleep.
I was an intern, had just worked 36 continuous hours, and was driving a car.
ACGME Outlines Resident Duty-Hours Changes
I was reminded of this incident on June 23, when I reviewed the freshly minted recommendations from the Accreditation Council for Graduate Medical Education (ACGME) task force regarding duty hours.2 This proposal follows on ACGME’s 2003 report, which enacted such national resident duty-hour standards as the 80-hour work week, the maximum 24-hour shift (plus six hours for administrative time), and the requirement for 10 hours off between shifts.
Like the 2003 report, which has played a large role in the rise of academic HM, the 2010 recommendations have major implications for academic hospitalists and our community brethren who will receive our residency graduates. As such, the reaction within the hospitalist community was immediate. Within minutes of ACGME’s notification, I was inundated with e-mail from colleagues both locally and nationally. Everyone was struggling with the repercussions. Was this good for resident education, a boon or bust for HM, a death knell for teaching hospitals?
So What’s in There?
This hotly anticipated report focuses its energy on four key elements of what the ACGME has morphed from “duty hours” into the resident “work environment”: resident supervision, handoffs of patient care, use of systems to enhance patient safety, and the effects of sleep on performance. Much of this is not really controversial and likely good for both residents and HM—an emphasis on systems-based practice, transitions of care, and expectations around communication.
The most discussed and controversial changes regard the move toward supervision and work hours that are customized to trainees’ levels. Unlike in the past, when the intern bore the brunt of the hours and patient duties, this proposal emphasizes graded supervision and duty-hour expectations. Practically, this means first-year residents will require closer supervision (whether by a resident or an attending has yet to be delineated) than more senior residents. Likewise, although all residents can only work a maximum of 80 hours averaged over four weeks (no change from 2003), the maximum shift length for interns will be limited to 16 hours. Upper-level residents will be limited to no more than 24 consecutive hours with an additional four hours for administrative work, but it is “strongly suggested” that residents working longer than 16 hours be provided with opportunities for “strategic napping.”
Read the Tea Leaves
I think these recommendations are rational and reasonable. To be sure, when these go into effect on July 1, 2011, they will have a tremendous impact on my residency program, my hospital, and my hospitalist faculty. My program, like most, likely will move toward a shift system of patient care, instead of overnight call. My hospital likely will have to expend millions of dollars annually to back-fill the work that residents would have done. My hospitalist group likely will have to expand our nonresident coverage both during the day and at night, inducing one of my partners to query, “Does this mean we’ll have to hire napturnists to cover the residents’ strategic nap time?”
It’s easy to deride these work environment changes, especially if we see the world through the uphill-in-the-snow-both-ways lenses most of us use to recollect (fondly?) our residency days. Yes, the field of medicine is losing a rite of passage many of us endured, and I too retrospectively feel the nostalgic tug of the long shifts, the seemingly insurmountable avalanche of admissions, and the autonomy in resident decision-making that made my training so valuable. But are we really against ensuring that residents are properly supervised, handoffs are more standardized, and systems are in place to protect the safety of our patients?
Sleep = Safety
The push behind limiting the maximum duration of work to 16 and 24 hours for interns and residents, respectively, stems from the growing body of literature regarding the detrimental effects of the fatigue and sleep deprivation that comes with long shifts. Not so shockingly, the data show that residents are sleepy. When administered the Epworth Sleepiness Score, residents appear sleepier than sleep apneic patients and nearly as sleepy as narcoleptics.3,4 In fact, they are so sleepy they often don’t even recognize when they are sleeping. One study showed that nearly half the time that anesthesia residents were asleep, they were unaware that they were actually sleeping.5
Further data suggest that residents who sleep less than five hours per night are twice as likely to be sued, and significantly more likely to report adverse events and errors in patient care.6 When comparing traditional, every-third-night call and 24- to 30-hour shifts with 16-hour shifts, the former staffing model is associated with 36% more serious errors than the latter.
Furthermore, there is a five-fold increase in the rate of serious diagnostic errors in the residents in the longer-shift group.7 And to finish where I began, residents who worked shifts that lasted more than 24 hours are more than twice as likely to crash their cars as those working less than 24-hour shifts. In fact, every additional extended-duration shift per month increases the chances of a car crash while commuting by 16%.8
So ask yourself this: If you were designing, from scratch, residency training today, would you really design a system similar to what we had 10 years ago? Like the one we have now? Would you ask residents, many just months out of medical school, to admit a dozen or more patients a day, stay awake for more than 30 hours, and care for the sickest, most frail patients without the assistance of more senior physicians?
The field of medicine is at a crossroads, and it faces many questions, not the least of which is how best to train our future physicians. The ACGME has published its proposal and given the public, including you, until Aug. 9 to voice your comments. These are big issues to ponder.
Maybe you should sleep on it. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Sleep. Wikipedia website. Available at: http://en.wikipedia.org/wiki/Sleep. Accessed July 10, 2010.
- Nasca TJ, Day SH, Amis S. The new recommendations on duty hours from the ACGME task force. New England Journal of Medicine website. Available at: content.nejm.org/cgi/content/full/NEJMsb1005800. Accessed July 2, 2010.
- Mustafa M, Erokwu N, Ebose I, Strohl K. Sleep problems and the risk for sleep disorders in an outpatient veteran population. Sleep & Breathing. 2005;9:57-63.
- Papp KK, Stoller EP, Sage P, et al. The effects of sleep loss and fatigue on resident-physicians: a multi-institutional, mixed-method study. Acad Med. 2005; 79:394-406.
- Howard SK, Gaba DM, Rosekind MR, Zaracone VP. The risks and implications of excessive daytime sleepiness in resident physicians. Acad Med. 2002; 77:1019-1025.
- Baldwin DC, Daugherty SR. Sleep deprivation and fatigue in residency training: results of a national survey of 1st- and 2nd-year residents. Sleep. 2004;27:371-372.
- Landrigan CP, Rothschild JM, Cronin JW, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med. 2004;18:1838-1848.
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125-134.
ONLINE EXCLUSIVE: Palliative Care Documentation Key to Core Measures
A growing number of publicly reported hospital quality initiatives include severity-adjusted hospital mortality rates. Although individual hospitalists are unlikely to be rated based on their patients’ mortality, this is an important component of how hospitals are evaluated—and thus a natural target for the hospital’s quality-improvement (QI) efforts and for hospitalists’ participation in them.
The challenge is that some hospital-connected deaths are unavoidable, predictable, and even appropriate when care plans focused on maximizing comfort and quality of life replace medical efforts to stave off death. Referring seriously ill patients to the hospital’s palliative-care service or to a community hospice can influence a hospital’s mortality rate, but not always in the same ways.
Where hospice care and palliative care fit in hospital mortality rates, how they are defined and counted, and how predictable deaths are either included or excluded from hospitals’ risk-adjusted mortality tallies vary between the reporting programs, according to J. Brian Cassel, PhD, senior analyst at Virginia Commonwealth University (VCU), a presenter at the National Hospice and Palliative Care Organization’s Management and Leadership Conference in April 2010 in Washington, D.C.
“Hospitals are naturally concerned about mortality rates because they want to be seen as quality health providers,” Dr. Cassel says. “How hospital mortality rates are determined can be quite complex,” with varied data sources and various methods of adjusting for severity and balancing mortality with other quality metrics. Dr. Cassel says he began digging into mortality data when concerns were raised that VCU’s acute-palliative-care unit might be causing the medical center’s overall mortality rates to spike. His research found that the unit’s operation was probably neutral relative to VCU’s overall mortality rates.
Typically, the risk-adjusted mortality rate is for selected diagnoses but counts deaths from all causes, either during the index hospitalization or within 30 days of that admission, Dr. Cassel says. Three examples of QI programs that use mortality data: CMS’ Hospital Compare, which publicly reports data on patient satisfaction and hospital processes and outcomes, including mortality; U.S. News & World Report’s “Best Hospitals” list, for which one-third of total scores are derived from its mortality index; and HealthGrades, a Golden, Colo.-based company that ranks hospitals and other health providers within a region, one condition or procedure at a time.
An ICD-9 billing code, V66.7 for “palliative care encounter,” can flag the involvement of palliative-care consultants on a hospital case, although this code often goes unused and should be among the top nine listed diagnoses in order to turn up in most quality calculations. Palliative-care consultants can help promote the use and higher positioning of this code in hospital billing, along with more complete documentation of comorbidities and symptoms. It also is possible that involving hospice and palliative-care teams with seriously ill patients earlier in their disease progression could help manage their care in community settings, avoiding hospitalizations when death is likely in the next few months.
Some hospitals might choose to refer patients thought to be close to death to contracted hospice programs—and some hospice and palliative-care advocates are using the rates as conversation starters with hospital administrators. Dr. Cassel’s advice for those advocates: Know which quality-measurement systems the hospital’s leadership follows, where adjusted mortality rates fit in those systems, and how hospice and palliative care affect them.
Regardless of mortality metrics, Dr. Cassell says, a clinician’s primary responsibility is to provide the best possible care to patients and families, reflecting their values, hopes, and treatment goals.
A growing number of publicly reported hospital quality initiatives include severity-adjusted hospital mortality rates. Although individual hospitalists are unlikely to be rated based on their patients’ mortality, this is an important component of how hospitals are evaluated—and thus a natural target for the hospital’s quality-improvement (QI) efforts and for hospitalists’ participation in them.
The challenge is that some hospital-connected deaths are unavoidable, predictable, and even appropriate when care plans focused on maximizing comfort and quality of life replace medical efforts to stave off death. Referring seriously ill patients to the hospital’s palliative-care service or to a community hospice can influence a hospital’s mortality rate, but not always in the same ways.
Where hospice care and palliative care fit in hospital mortality rates, how they are defined and counted, and how predictable deaths are either included or excluded from hospitals’ risk-adjusted mortality tallies vary between the reporting programs, according to J. Brian Cassel, PhD, senior analyst at Virginia Commonwealth University (VCU), a presenter at the National Hospice and Palliative Care Organization’s Management and Leadership Conference in April 2010 in Washington, D.C.
“Hospitals are naturally concerned about mortality rates because they want to be seen as quality health providers,” Dr. Cassel says. “How hospital mortality rates are determined can be quite complex,” with varied data sources and various methods of adjusting for severity and balancing mortality with other quality metrics. Dr. Cassel says he began digging into mortality data when concerns were raised that VCU’s acute-palliative-care unit might be causing the medical center’s overall mortality rates to spike. His research found that the unit’s operation was probably neutral relative to VCU’s overall mortality rates.
Typically, the risk-adjusted mortality rate is for selected diagnoses but counts deaths from all causes, either during the index hospitalization or within 30 days of that admission, Dr. Cassel says. Three examples of QI programs that use mortality data: CMS’ Hospital Compare, which publicly reports data on patient satisfaction and hospital processes and outcomes, including mortality; U.S. News & World Report’s “Best Hospitals” list, for which one-third of total scores are derived from its mortality index; and HealthGrades, a Golden, Colo.-based company that ranks hospitals and other health providers within a region, one condition or procedure at a time.
An ICD-9 billing code, V66.7 for “palliative care encounter,” can flag the involvement of palliative-care consultants on a hospital case, although this code often goes unused and should be among the top nine listed diagnoses in order to turn up in most quality calculations. Palliative-care consultants can help promote the use and higher positioning of this code in hospital billing, along with more complete documentation of comorbidities and symptoms. It also is possible that involving hospice and palliative-care teams with seriously ill patients earlier in their disease progression could help manage their care in community settings, avoiding hospitalizations when death is likely in the next few months.
Some hospitals might choose to refer patients thought to be close to death to contracted hospice programs—and some hospice and palliative-care advocates are using the rates as conversation starters with hospital administrators. Dr. Cassel’s advice for those advocates: Know which quality-measurement systems the hospital’s leadership follows, where adjusted mortality rates fit in those systems, and how hospice and palliative care affect them.
Regardless of mortality metrics, Dr. Cassell says, a clinician’s primary responsibility is to provide the best possible care to patients and families, reflecting their values, hopes, and treatment goals.
A growing number of publicly reported hospital quality initiatives include severity-adjusted hospital mortality rates. Although individual hospitalists are unlikely to be rated based on their patients’ mortality, this is an important component of how hospitals are evaluated—and thus a natural target for the hospital’s quality-improvement (QI) efforts and for hospitalists’ participation in them.
The challenge is that some hospital-connected deaths are unavoidable, predictable, and even appropriate when care plans focused on maximizing comfort and quality of life replace medical efforts to stave off death. Referring seriously ill patients to the hospital’s palliative-care service or to a community hospice can influence a hospital’s mortality rate, but not always in the same ways.
Where hospice care and palliative care fit in hospital mortality rates, how they are defined and counted, and how predictable deaths are either included or excluded from hospitals’ risk-adjusted mortality tallies vary between the reporting programs, according to J. Brian Cassel, PhD, senior analyst at Virginia Commonwealth University (VCU), a presenter at the National Hospice and Palliative Care Organization’s Management and Leadership Conference in April 2010 in Washington, D.C.
“Hospitals are naturally concerned about mortality rates because they want to be seen as quality health providers,” Dr. Cassel says. “How hospital mortality rates are determined can be quite complex,” with varied data sources and various methods of adjusting for severity and balancing mortality with other quality metrics. Dr. Cassel says he began digging into mortality data when concerns were raised that VCU’s acute-palliative-care unit might be causing the medical center’s overall mortality rates to spike. His research found that the unit’s operation was probably neutral relative to VCU’s overall mortality rates.
Typically, the risk-adjusted mortality rate is for selected diagnoses but counts deaths from all causes, either during the index hospitalization or within 30 days of that admission, Dr. Cassel says. Three examples of QI programs that use mortality data: CMS’ Hospital Compare, which publicly reports data on patient satisfaction and hospital processes and outcomes, including mortality; U.S. News & World Report’s “Best Hospitals” list, for which one-third of total scores are derived from its mortality index; and HealthGrades, a Golden, Colo.-based company that ranks hospitals and other health providers within a region, one condition or procedure at a time.
An ICD-9 billing code, V66.7 for “palliative care encounter,” can flag the involvement of palliative-care consultants on a hospital case, although this code often goes unused and should be among the top nine listed diagnoses in order to turn up in most quality calculations. Palliative-care consultants can help promote the use and higher positioning of this code in hospital billing, along with more complete documentation of comorbidities and symptoms. It also is possible that involving hospice and palliative-care teams with seriously ill patients earlier in their disease progression could help manage their care in community settings, avoiding hospitalizations when death is likely in the next few months.
Some hospitals might choose to refer patients thought to be close to death to contracted hospice programs—and some hospice and palliative-care advocates are using the rates as conversation starters with hospital administrators. Dr. Cassel’s advice for those advocates: Know which quality-measurement systems the hospital’s leadership follows, where adjusted mortality rates fit in those systems, and how hospice and palliative care affect them.
Regardless of mortality metrics, Dr. Cassell says, a clinician’s primary responsibility is to provide the best possible care to patients and families, reflecting their values, hopes, and treatment goals.
ONLINE EXCLUSIVE: Audio interview with a pediatric hospitalist who is starting a palliative care team
Financial Risk

When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
When I started writing this, Congress hadn’t settled the issue of the 21% cut in Medicare reimbursement for services called for by the sustainable growth rate (SGR) formula. Fortunately, Congress stepped up and passed another extension with a 2.2% pay increase; however, the quick fix only lasts until November.
The process is all too routine: The deadline for these reimbursement cuts looms, Medicare instructs its fiscal intermediaries (the organizations that actually write the checks to providers) to hold claims rather than pay at the lower rate, and, within a few days of the deadline passing, Congress decides to pass an extension, which allows Medicare to continue paying the historical (higher) rate for the time being.
Imagine Medicare reimbursement rates dropping 21% overnight. I suspect it would be cataclysmic. But I hear remarkably little chatter about this possibility. In fact, while with 2,500 other hospitalists for several days at HM10 in April, I didn’t hear a single person bring up the SGR issue.
One reason there isn’t more handwringing about the looming, draconian cuts is that we’ve been there before. In fact, reimbursement cuts required by the SGR have come up every year since 2001. Each time, Congress has chosen not to implement the cuts; and in some years it has approved reimbursement increases instead. So most in healthcare circles basically have come to expect Congress to pass last-minute legislation to avoid the drastic cuts. (SHM and most other medical societies want a repeal of the flawed SGR formula. Visit SHM’s Legislative Action Center, http://capwiz.com/hospitalmedicine/home/, to write your legislators and urge repeal of the SGR. It only takes about two minutes, and you don’t even need to remember who your representatives are; you just need to know your ZIP code.)
Don’t Be Too Smug
There is another reason many hospitalists, and other doctors who are employed and salaried by a large entity like a hospital, might not be more concerned about proposed cuts: They probably think their own salaries will be unaffected by decreases in reimbursement from Medicare and other payors. My experience is that a lot of hospitalists are so unconcerned about payor reimbursement rates that they aren’t even aware of the threatened Medicare cuts.
Their thinking goes something like this: “I’m paid mostly via a fixed annual salary with a small productivity and quality incentive. None of this is connected to the payor mix or collection rates from the patients I see. So if the portion of uninsured patients I see goes up, my compensation is unaffected. Or if payors decrease their rates, my compensation is unaffected. So I don’t need to sweat the possibility of a 21% decrease in Medicare rates. The hospital will have to make up the difference, so my salary is unaffected, and it will be up to bean counters at the hospital to get the numbers to work out.”
In fact, this is true, in theory, for the majority of hospitalists. But I think it is a mistake to assume your salary is untouchable. If Medicare were to cut rates by 21%, you’d better run to your hospital CEO’s office right away, because a long line will form immediately. Every doctor who sees patients at your hospital will be in that line asking the CEO to provide some money to offset the Medicare cuts, and I doubt any hospital will be able to satisfy their doctors without spending so much money that the hospital goes bankrupt or out of business.
Even if you have a valid contract that calls for your compensation to be paid independent of the amount of professional fee collections, a dire shortage of money could lead a hospital to lay off hospitalists or cancel the contract (most contracts would allow the hospital to do this simply by giving a 90-day notice).
I suggest that no hospitalist feel too smug about how well their employment contract protects the group from broader market forces like reimbursement rates. I doubt we’ll ever see an overnight 21% reduction in Medicare rates, but over time, we could see ever-increasing pressure to limit the growth in our incomes.
I believe every hospitalist should spend at least a little time following broader financial issues like this one, and get involved in the political process to let your legislators know your thoughts. For the record, I think the financial underpinnings of our healthcare system are disastrously messed up and something has to be done. And I don’t think anyone’s salary, including mine, is untouchable. But I also believe the SGR is an ineffective way to make the system more financially sound. That said, you don’t need to agree with me; I only recommend that you have a reasonably informed opinion.
One approach might be for your HM group to appoint a “political” or “marketplace” watchdog. This person could be charged with following issues closely and reporting back to the whole group during regular meetings.
“Marketplace” Risk
Medicare rates are only one part of the complex financial ecosystem on which we depend. It is awfully common, and I think pretty reasonable, for hospitalists to have a contractual arrangement with hospitals. The majority of the time, the hospital has most—or all—of the risk for the financial performance of the practice. In fact, most prospective hospitalists, especially those seeking their first jobs out after residency, say one of the most attractive reasons for choosing work as a hospitalist is that many practices provide a salary that is nearly fixed. Any variable components to the salary, such as those based on production or quality, are typically very small.
A hospitalist might think, “I want a practice that pays a fixed salary so I don’t have to worry about any business and financial issues other than when to show up to work.” In fact, a lot of recruitment ads trumpet this very idea (i.e., “you handle the doctoring and get to enjoy the wonderful recreational opportunities and schools our locale provides, and we’ll worry about all the business issues”). That may sound nice, but I worry it is a little short-sighted.
Here is another point of view, which is only slightly more complicated. In most cases, you should try to negotiate a contract that insulates you from “payor risk” (e.g., changes in payor mix and rates paid by payors don’t flow through to your compensation). But you should think twice before asking your employer to assume all the risk for staffing and scheduling decisions, such as whether you get the work done with 10 hospitalists or 11, or whether you have an evening admitter (“swing”) shift. If the employer holds all the risk, then the hospitalists give up nearly all their autonomy to decide how hard they want to work and how they want to schedule themselves. This causes problems for many practices, and is the No. 1 reason I’m called in as a consultant. Contrary to being very risky and stressful, many hospitalists find it liberating to assume financial risk for their staffing and workload decisions.
You should realize that if your employer pays you a fixed compensation, then someone has to ensure that you do enough work to justify that compensation. This can mean that the employer “issues decrees” (i.e., “we won’t add another provide to the practice until we’ve averaged ‘X’ encounters per month for 6 months”). A hospitalist might see this as unreasonable, yet the group has limited recourse since the employer has already guaranteed the compensation.
If you’d rather have more autonomy in your staffing and workload, then you will need to connect your paycheck to these decisions. Although it might sound terribly risky, those who make the switch often say they wouldn’t have it any other way. Most importantly, it ensures hospitalists have much more say in big decisions. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.