User login
The renal failure that vanished
A 35‐year‐old African American female presented to her primary care provider with a 4‐day history of progressive nausea, vomiting, and generalized malaise. The patient had been in her usual state of health prior to the onset of these symptoms and had no history of prior hospitalization. She denied any fevers, chills, abdominal pain, or change in diet prior to the onset of her symptoms. She also had no recent exposure to sick contacts, human immunodeficiency virus (HIV) risk factors, or history of recent travel. One week prior to her presentation, the patient had been prescribed rifampin for treatment of chronic hidradenitis suppurativa. She had been taking rifampin for 5 days until she developed her current symptoms. The patient was not taking any other medications and had no other medical problems.
On presentation, the patient was afebrile and her vital signs were within normal limits. She was alert and oriented with no scleral icterus. Cardiopulmonary exam was within normal limits. Her abdomen was nondistended with diffuse nonlocalizing tenderness, normal bowel sounds, and no signs of acute abdomen. No hepatomegaly was noted, and stool was negative for occult blood. No rashes or joint abnormalities were noted on exam, but multiple nodulocystic lesions were noted bilaterally in her axillae. Laboratory findings on presentation were most notable for a blood urea nitrogen level of 38 mg/dL, a creatinine of 5.3 mg/dL, and a calculated fractional excretion of sodium of 2.6%. Urine analysis revealed no significant hematuria, proteinuria, or red blood cell casts, but did demonstrate white blood cells, white blood cell casts, and eosinophils. Blood cultures drawn on admission were negative and the patient had a normal leukocyte count.
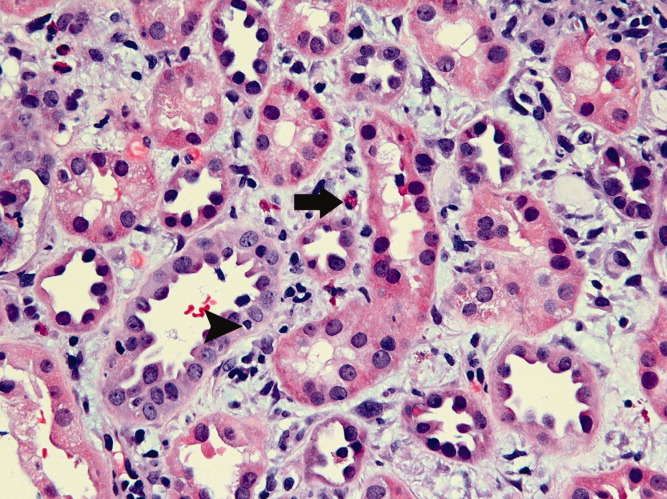
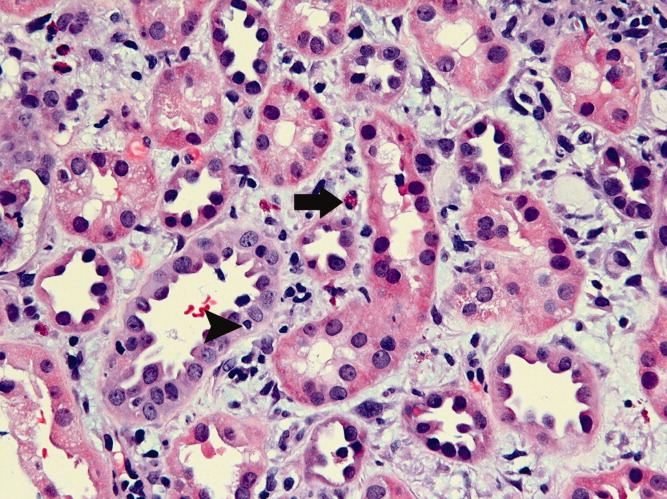
The patient was admitted to the general medicine service and the causes of her acute renal failure were explored. She was treated with intravenous fluids because a component of prerenal azotemia was initially suspected. Rifampin was discontinued. Despite significant hydration, the patient remained oliguric. She was challenged with high‐dose loop diuretics for 3 days but still remained oliguric. Renal ultrasound showed moderately echogenic, large 16‐cm kidneys bilaterally, with no evidence of hydronephrosis or renal calculi. Laboratory evaluation for diabetes and infiltrative disease of the kidneys such as HIV, amyloidosis, and nonspecific gammopathies were negative. The patient's creatinine level steadily increased and eventually peaked at 14.2 mg/dL. When the patient began to develop shortness of breath, lower extremity edema, and abdominal distension on hospital day 4, hemodialysis was initiated. On hospital day 6, the patient underwent a renal biopsy (Figure 1) that demonstrated patchy inflammatory infiltrates with scattered eosinophils and evidence of interstitial edema and tubulitis. Congo red staining was negative for amyloid and no immune deposits were noted. A diagnosis of acute interstitial nephritis (AIN) was made and the patient was started on high‐dose prednisone.
Over the 48 hours following initiation of prednisone therapy, the patient's urine output gradually began to improve and the patient was producing over 2 liters of urine per day. In addition, the patient's axillary cystic lesions became less inflamed and painful. The patient was discharged home with plans to continue hemodialysis as an outpatient. Three days after discharge, when the patient presented for hemodialysis, her creatinine was noted to be 1.2 mg/dL. Due to her improved creatinine and maintenance of good urine output, hemodialysis was discontinued. The patient was slowly tapered off her prednisone over the next several weeks. One month later her creatinine was 0.9 mg/dL. She had required no further hemodialysis since her hospitalization.
DISCUSSION
AIN is an uncommon but significant cause of acute renal failure, and accounts for 2% to 3% of all renal biopsies performed.1 AIN is thought to be an immune‐mediated process, and drug‐induced hypersensitivity is the most common cause of AIN. Nonsteroidal antiinflammatory drug (NSAID) use, antibiotics, proton pump inhibitors, and several other medications have been implicated in the pathogenesis of AIN. Rifampin is a medication that has a known association with AIN, with most cases being described in regions where treatment of endemic tuberculosis is common. The majority of cases of rifampin‐induced AIN occur in the setting of drug reexposure, due to an immunologically‐mediated process that causes tubulointerstitial injury.2
Patients with drug‐induced AIN typically present with oliguria secondary to an acute decline in renal function. The classic clinical triad of fever, rash, and arthralgias is uncommon, and all 3 occur in only 30% of all cases.3 More commonly, patients typically present with vague flu‐like and gastrointestinal symptoms, including fever, abdominal pain, nausea, and vomiting. Urinalysis may be helpful, but hematuria occurs in less than one‐half of all cases, and sterile pyuria is common but not always present. It has been suggested that the presence of eosinophiluria may lead to high suspicion of AIN, but the sensitivity and specificity of eosinophiluria are low, at 40% and 72%, respectively.3 Thus, renal biopsy is often performed to make a confirmatory diagnosis of AIN in the appropriate clinical setting. Histopathologically, the presence of inflammatory infiltrates in the renal tubules and interstitium with conservation of the glomerular structures is visualized.2, 3
A large number of patients who present with AIN may require temporary renal replacement therapy; however, most patients have been observed to recover full renal function. Despite this, review of the literature shows that many patients may have persistent elevations in their serum creatinine. Corticosteroid therapy, although controversial, has commonly been initiated in patients whose renal function does not improve with conservative therapy. To date there are no prospective randomized clinical trials, and data guiding optimal management in AIN is sparse. Some studies have demonstrated no benefit in corticosteroid therapy in lowering serum creatinine levels in patients with AIN,4 but others have observed a significantly increased risk of interstitial fibrosis and failure to return to baseline creatinine in those patients that received delayed treatment with corticosteroids more than 1 week after the withdrawal of the offending agent.5
The patient described in our case did not present with the classic symptoms noted in AIN. Yet she had evidence of eosinophiluria, which increased our suspicion for AIN. Although other potential etiologies of this patient's acute renal failure were considered, given her negative serologic studies and the results of her renal biopsy, AIN was considered the leading diagnosis. Since AIN was recognized early in this patient, the offending medication was discontinued promptly, prednisone therapy was initiated appropriately, and the renal failure that had developed quickly vanished.
- ,.Acute interstitial nephritis.J Am Soc Nephrol.1998;9(3):506–515.
- ,,,,.Rifampicin‐associated acute renal failure: pathophysiologic, immunologic, and clinical features.Am J Kidney Dis.1998;31(1):108–115.
- ,.A reversible cause of acute renal failure.Postgrad Med J.2001;77(909):478–480.
- ,,, et al.Acute interstitial nephritis: clinical features and response to corticosteroid therapy.Nephrol Dial Transplant.2004;19:2778–2783.
- , ,, et al.Early steroid treatment improves the recovery of renal function in patients with drug‐induced acute interstitial nephritis.Kidney Int.2008;73(8):940–946.
A 35‐year‐old African American female presented to her primary care provider with a 4‐day history of progressive nausea, vomiting, and generalized malaise. The patient had been in her usual state of health prior to the onset of these symptoms and had no history of prior hospitalization. She denied any fevers, chills, abdominal pain, or change in diet prior to the onset of her symptoms. She also had no recent exposure to sick contacts, human immunodeficiency virus (HIV) risk factors, or history of recent travel. One week prior to her presentation, the patient had been prescribed rifampin for treatment of chronic hidradenitis suppurativa. She had been taking rifampin for 5 days until she developed her current symptoms. The patient was not taking any other medications and had no other medical problems.
On presentation, the patient was afebrile and her vital signs were within normal limits. She was alert and oriented with no scleral icterus. Cardiopulmonary exam was within normal limits. Her abdomen was nondistended with diffuse nonlocalizing tenderness, normal bowel sounds, and no signs of acute abdomen. No hepatomegaly was noted, and stool was negative for occult blood. No rashes or joint abnormalities were noted on exam, but multiple nodulocystic lesions were noted bilaterally in her axillae. Laboratory findings on presentation were most notable for a blood urea nitrogen level of 38 mg/dL, a creatinine of 5.3 mg/dL, and a calculated fractional excretion of sodium of 2.6%. Urine analysis revealed no significant hematuria, proteinuria, or red blood cell casts, but did demonstrate white blood cells, white blood cell casts, and eosinophils. Blood cultures drawn on admission were negative and the patient had a normal leukocyte count.
The patient was admitted to the general medicine service and the causes of her acute renal failure were explored. She was treated with intravenous fluids because a component of prerenal azotemia was initially suspected. Rifampin was discontinued. Despite significant hydration, the patient remained oliguric. She was challenged with high‐dose loop diuretics for 3 days but still remained oliguric. Renal ultrasound showed moderately echogenic, large 16‐cm kidneys bilaterally, with no evidence of hydronephrosis or renal calculi. Laboratory evaluation for diabetes and infiltrative disease of the kidneys such as HIV, amyloidosis, and nonspecific gammopathies were negative. The patient's creatinine level steadily increased and eventually peaked at 14.2 mg/dL. When the patient began to develop shortness of breath, lower extremity edema, and abdominal distension on hospital day 4, hemodialysis was initiated. On hospital day 6, the patient underwent a renal biopsy (Figure 1) that demonstrated patchy inflammatory infiltrates with scattered eosinophils and evidence of interstitial edema and tubulitis. Congo red staining was negative for amyloid and no immune deposits were noted. A diagnosis of acute interstitial nephritis (AIN) was made and the patient was started on high‐dose prednisone.
Over the 48 hours following initiation of prednisone therapy, the patient's urine output gradually began to improve and the patient was producing over 2 liters of urine per day. In addition, the patient's axillary cystic lesions became less inflamed and painful. The patient was discharged home with plans to continue hemodialysis as an outpatient. Three days after discharge, when the patient presented for hemodialysis, her creatinine was noted to be 1.2 mg/dL. Due to her improved creatinine and maintenance of good urine output, hemodialysis was discontinued. The patient was slowly tapered off her prednisone over the next several weeks. One month later her creatinine was 0.9 mg/dL. She had required no further hemodialysis since her hospitalization.
DISCUSSION
AIN is an uncommon but significant cause of acute renal failure, and accounts for 2% to 3% of all renal biopsies performed.1 AIN is thought to be an immune‐mediated process, and drug‐induced hypersensitivity is the most common cause of AIN. Nonsteroidal antiinflammatory drug (NSAID) use, antibiotics, proton pump inhibitors, and several other medications have been implicated in the pathogenesis of AIN. Rifampin is a medication that has a known association with AIN, with most cases being described in regions where treatment of endemic tuberculosis is common. The majority of cases of rifampin‐induced AIN occur in the setting of drug reexposure, due to an immunologically‐mediated process that causes tubulointerstitial injury.2
Patients with drug‐induced AIN typically present with oliguria secondary to an acute decline in renal function. The classic clinical triad of fever, rash, and arthralgias is uncommon, and all 3 occur in only 30% of all cases.3 More commonly, patients typically present with vague flu‐like and gastrointestinal symptoms, including fever, abdominal pain, nausea, and vomiting. Urinalysis may be helpful, but hematuria occurs in less than one‐half of all cases, and sterile pyuria is common but not always present. It has been suggested that the presence of eosinophiluria may lead to high suspicion of AIN, but the sensitivity and specificity of eosinophiluria are low, at 40% and 72%, respectively.3 Thus, renal biopsy is often performed to make a confirmatory diagnosis of AIN in the appropriate clinical setting. Histopathologically, the presence of inflammatory infiltrates in the renal tubules and interstitium with conservation of the glomerular structures is visualized.2, 3
A large number of patients who present with AIN may require temporary renal replacement therapy; however, most patients have been observed to recover full renal function. Despite this, review of the literature shows that many patients may have persistent elevations in their serum creatinine. Corticosteroid therapy, although controversial, has commonly been initiated in patients whose renal function does not improve with conservative therapy. To date there are no prospective randomized clinical trials, and data guiding optimal management in AIN is sparse. Some studies have demonstrated no benefit in corticosteroid therapy in lowering serum creatinine levels in patients with AIN,4 but others have observed a significantly increased risk of interstitial fibrosis and failure to return to baseline creatinine in those patients that received delayed treatment with corticosteroids more than 1 week after the withdrawal of the offending agent.5
The patient described in our case did not present with the classic symptoms noted in AIN. Yet she had evidence of eosinophiluria, which increased our suspicion for AIN. Although other potential etiologies of this patient's acute renal failure were considered, given her negative serologic studies and the results of her renal biopsy, AIN was considered the leading diagnosis. Since AIN was recognized early in this patient, the offending medication was discontinued promptly, prednisone therapy was initiated appropriately, and the renal failure that had developed quickly vanished.
A 35‐year‐old African American female presented to her primary care provider with a 4‐day history of progressive nausea, vomiting, and generalized malaise. The patient had been in her usual state of health prior to the onset of these symptoms and had no history of prior hospitalization. She denied any fevers, chills, abdominal pain, or change in diet prior to the onset of her symptoms. She also had no recent exposure to sick contacts, human immunodeficiency virus (HIV) risk factors, or history of recent travel. One week prior to her presentation, the patient had been prescribed rifampin for treatment of chronic hidradenitis suppurativa. She had been taking rifampin for 5 days until she developed her current symptoms. The patient was not taking any other medications and had no other medical problems.
On presentation, the patient was afebrile and her vital signs were within normal limits. She was alert and oriented with no scleral icterus. Cardiopulmonary exam was within normal limits. Her abdomen was nondistended with diffuse nonlocalizing tenderness, normal bowel sounds, and no signs of acute abdomen. No hepatomegaly was noted, and stool was negative for occult blood. No rashes or joint abnormalities were noted on exam, but multiple nodulocystic lesions were noted bilaterally in her axillae. Laboratory findings on presentation were most notable for a blood urea nitrogen level of 38 mg/dL, a creatinine of 5.3 mg/dL, and a calculated fractional excretion of sodium of 2.6%. Urine analysis revealed no significant hematuria, proteinuria, or red blood cell casts, but did demonstrate white blood cells, white blood cell casts, and eosinophils. Blood cultures drawn on admission were negative and the patient had a normal leukocyte count.
The patient was admitted to the general medicine service and the causes of her acute renal failure were explored. She was treated with intravenous fluids because a component of prerenal azotemia was initially suspected. Rifampin was discontinued. Despite significant hydration, the patient remained oliguric. She was challenged with high‐dose loop diuretics for 3 days but still remained oliguric. Renal ultrasound showed moderately echogenic, large 16‐cm kidneys bilaterally, with no evidence of hydronephrosis or renal calculi. Laboratory evaluation for diabetes and infiltrative disease of the kidneys such as HIV, amyloidosis, and nonspecific gammopathies were negative. The patient's creatinine level steadily increased and eventually peaked at 14.2 mg/dL. When the patient began to develop shortness of breath, lower extremity edema, and abdominal distension on hospital day 4, hemodialysis was initiated. On hospital day 6, the patient underwent a renal biopsy (Figure 1) that demonstrated patchy inflammatory infiltrates with scattered eosinophils and evidence of interstitial edema and tubulitis. Congo red staining was negative for amyloid and no immune deposits were noted. A diagnosis of acute interstitial nephritis (AIN) was made and the patient was started on high‐dose prednisone.
Over the 48 hours following initiation of prednisone therapy, the patient's urine output gradually began to improve and the patient was producing over 2 liters of urine per day. In addition, the patient's axillary cystic lesions became less inflamed and painful. The patient was discharged home with plans to continue hemodialysis as an outpatient. Three days after discharge, when the patient presented for hemodialysis, her creatinine was noted to be 1.2 mg/dL. Due to her improved creatinine and maintenance of good urine output, hemodialysis was discontinued. The patient was slowly tapered off her prednisone over the next several weeks. One month later her creatinine was 0.9 mg/dL. She had required no further hemodialysis since her hospitalization.
DISCUSSION
AIN is an uncommon but significant cause of acute renal failure, and accounts for 2% to 3% of all renal biopsies performed.1 AIN is thought to be an immune‐mediated process, and drug‐induced hypersensitivity is the most common cause of AIN. Nonsteroidal antiinflammatory drug (NSAID) use, antibiotics, proton pump inhibitors, and several other medications have been implicated in the pathogenesis of AIN. Rifampin is a medication that has a known association with AIN, with most cases being described in regions where treatment of endemic tuberculosis is common. The majority of cases of rifampin‐induced AIN occur in the setting of drug reexposure, due to an immunologically‐mediated process that causes tubulointerstitial injury.2
Patients with drug‐induced AIN typically present with oliguria secondary to an acute decline in renal function. The classic clinical triad of fever, rash, and arthralgias is uncommon, and all 3 occur in only 30% of all cases.3 More commonly, patients typically present with vague flu‐like and gastrointestinal symptoms, including fever, abdominal pain, nausea, and vomiting. Urinalysis may be helpful, but hematuria occurs in less than one‐half of all cases, and sterile pyuria is common but not always present. It has been suggested that the presence of eosinophiluria may lead to high suspicion of AIN, but the sensitivity and specificity of eosinophiluria are low, at 40% and 72%, respectively.3 Thus, renal biopsy is often performed to make a confirmatory diagnosis of AIN in the appropriate clinical setting. Histopathologically, the presence of inflammatory infiltrates in the renal tubules and interstitium with conservation of the glomerular structures is visualized.2, 3
A large number of patients who present with AIN may require temporary renal replacement therapy; however, most patients have been observed to recover full renal function. Despite this, review of the literature shows that many patients may have persistent elevations in their serum creatinine. Corticosteroid therapy, although controversial, has commonly been initiated in patients whose renal function does not improve with conservative therapy. To date there are no prospective randomized clinical trials, and data guiding optimal management in AIN is sparse. Some studies have demonstrated no benefit in corticosteroid therapy in lowering serum creatinine levels in patients with AIN,4 but others have observed a significantly increased risk of interstitial fibrosis and failure to return to baseline creatinine in those patients that received delayed treatment with corticosteroids more than 1 week after the withdrawal of the offending agent.5
The patient described in our case did not present with the classic symptoms noted in AIN. Yet she had evidence of eosinophiluria, which increased our suspicion for AIN. Although other potential etiologies of this patient's acute renal failure were considered, given her negative serologic studies and the results of her renal biopsy, AIN was considered the leading diagnosis. Since AIN was recognized early in this patient, the offending medication was discontinued promptly, prednisone therapy was initiated appropriately, and the renal failure that had developed quickly vanished.
- ,.Acute interstitial nephritis.J Am Soc Nephrol.1998;9(3):506–515.
- ,,,,.Rifampicin‐associated acute renal failure: pathophysiologic, immunologic, and clinical features.Am J Kidney Dis.1998;31(1):108–115.
- ,.A reversible cause of acute renal failure.Postgrad Med J.2001;77(909):478–480.
- ,,, et al.Acute interstitial nephritis: clinical features and response to corticosteroid therapy.Nephrol Dial Transplant.2004;19:2778–2783.
- , ,, et al.Early steroid treatment improves the recovery of renal function in patients with drug‐induced acute interstitial nephritis.Kidney Int.2008;73(8):940–946.
- ,.Acute interstitial nephritis.J Am Soc Nephrol.1998;9(3):506–515.
- ,,,,.Rifampicin‐associated acute renal failure: pathophysiologic, immunologic, and clinical features.Am J Kidney Dis.1998;31(1):108–115.
- ,.A reversible cause of acute renal failure.Postgrad Med J.2001;77(909):478–480.
- ,,, et al.Acute interstitial nephritis: clinical features and response to corticosteroid therapy.Nephrol Dial Transplant.2004;19:2778–2783.
- , ,, et al.Early steroid treatment improves the recovery of renal function in patients with drug‐induced acute interstitial nephritis.Kidney Int.2008;73(8):940–946.
A fall to remember
A healthy 44‐year‐old man presented to the emergency room with buttock pain, 2 days after falling from a 4‐foot table onto a cement floor, striking his right buttock. On presentation he was in moderate distress, with heart rate = 130 beats per minute (bpm) and blood pressure = 80/40 mm Hg. There was a 2‐cm area of erythema on the right flank, and mild tenderness of the right buttock. There was no evidence of skin anesthesia or crepitance. Initial laboratory results were notable for creatinine = 1.5 mg/dl, creatine phosphokinase = 11,500 U/L, lactate = 6.1 mmo/L, and white blood cell count = 10 k/UL, with 93% neutrophils. Plain radiography of the hip and spine were negative for fractures and soft tissue gas. Despite receiving multiple doses of narcotic analgesia, the patient continued to complain of severe pain. Within 2 hours of presentation, the right flank erythema extended proximally up the back and distally to the right thigh (Figure 1). The patient was taken to the operating room for surgical exploration and was diagnosed with necrotizing fasciitis extending from his posterior neck to the right popliteal fossa (Figures 2 and 3). Intraoperative cultures grew Group A streptococcus, confirming a diagnosis of Type II necrotizing fasciitis. The patient required multiple debridements and subsequent reconstructive procedures. After more than 3 months in the hospital and acute rehabilitation, he returned home.



Necrotizing fasciitis is a rapidly progressive infection that spreads along fascial planes, causing necrosis of subcutaneous tissues. Type II necrotizing fasciitis is a monomicrobial infection and occurs in healthy patients, with blunt trauma being a known precipitant. The classic finding in necrotizing fasciitis is pain out of proportion to the physical examination. Additionally, patients will typically present with septic shock and end‐organ dysfunction. Diagnosis requires a strong index of suspicion and surgical exploration is necessary for diagnosis and treatment.
A healthy 44‐year‐old man presented to the emergency room with buttock pain, 2 days after falling from a 4‐foot table onto a cement floor, striking his right buttock. On presentation he was in moderate distress, with heart rate = 130 beats per minute (bpm) and blood pressure = 80/40 mm Hg. There was a 2‐cm area of erythema on the right flank, and mild tenderness of the right buttock. There was no evidence of skin anesthesia or crepitance. Initial laboratory results were notable for creatinine = 1.5 mg/dl, creatine phosphokinase = 11,500 U/L, lactate = 6.1 mmo/L, and white blood cell count = 10 k/UL, with 93% neutrophils. Plain radiography of the hip and spine were negative for fractures and soft tissue gas. Despite receiving multiple doses of narcotic analgesia, the patient continued to complain of severe pain. Within 2 hours of presentation, the right flank erythema extended proximally up the back and distally to the right thigh (Figure 1). The patient was taken to the operating room for surgical exploration and was diagnosed with necrotizing fasciitis extending from his posterior neck to the right popliteal fossa (Figures 2 and 3). Intraoperative cultures grew Group A streptococcus, confirming a diagnosis of Type II necrotizing fasciitis. The patient required multiple debridements and subsequent reconstructive procedures. After more than 3 months in the hospital and acute rehabilitation, he returned home.
Necrotizing fasciitis is a rapidly progressive infection that spreads along fascial planes, causing necrosis of subcutaneous tissues. Type II necrotizing fasciitis is a monomicrobial infection and occurs in healthy patients, with blunt trauma being a known precipitant. The classic finding in necrotizing fasciitis is pain out of proportion to the physical examination. Additionally, patients will typically present with septic shock and end‐organ dysfunction. Diagnosis requires a strong index of suspicion and surgical exploration is necessary for diagnosis and treatment.
A healthy 44‐year‐old man presented to the emergency room with buttock pain, 2 days after falling from a 4‐foot table onto a cement floor, striking his right buttock. On presentation he was in moderate distress, with heart rate = 130 beats per minute (bpm) and blood pressure = 80/40 mm Hg. There was a 2‐cm area of erythema on the right flank, and mild tenderness of the right buttock. There was no evidence of skin anesthesia or crepitance. Initial laboratory results were notable for creatinine = 1.5 mg/dl, creatine phosphokinase = 11,500 U/L, lactate = 6.1 mmo/L, and white blood cell count = 10 k/UL, with 93% neutrophils. Plain radiography of the hip and spine were negative for fractures and soft tissue gas. Despite receiving multiple doses of narcotic analgesia, the patient continued to complain of severe pain. Within 2 hours of presentation, the right flank erythema extended proximally up the back and distally to the right thigh (Figure 1). The patient was taken to the operating room for surgical exploration and was diagnosed with necrotizing fasciitis extending from his posterior neck to the right popliteal fossa (Figures 2 and 3). Intraoperative cultures grew Group A streptococcus, confirming a diagnosis of Type II necrotizing fasciitis. The patient required multiple debridements and subsequent reconstructive procedures. After more than 3 months in the hospital and acute rehabilitation, he returned home.
Necrotizing fasciitis is a rapidly progressive infection that spreads along fascial planes, causing necrosis of subcutaneous tissues. Type II necrotizing fasciitis is a monomicrobial infection and occurs in healthy patients, with blunt trauma being a known precipitant. The classic finding in necrotizing fasciitis is pain out of proportion to the physical examination. Additionally, patients will typically present with septic shock and end‐organ dysfunction. Diagnosis requires a strong index of suspicion and surgical exploration is necessary for diagnosis and treatment.

Pediatric Hospital Medicine Core Competencies
Introduction
The Society of Hospital Medicine (SHM) defines hospitalists as physicians whose primary professional focus is the comprehensive general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to Hospital Medicine.1 It is estimated that there are up to 2500 pediatric hospitalists in the United States, with continued growth due to the converging needs for a dedicated focus on patient safety, quality improvement, hospital throughput, and inpatient teaching.2‐9 (Pediatric Hospital Medicine (PHM), as defined today, has been practiced in the United States for at least 30 years10 and continues to evolve as an area of specialization, with the refinement of a distinct knowledgebase and skill set focused on the provision of high quality general pediatric care in the inpatient setting. PHM is the latest site‐specific specialty to emerge from the field of general pediatrics it's development analogous to the evolution of critical care or emergency medicine during previous decades.11 Adult hospital medicine has defined itself within the field of general internal medicine12 and has recently received approval to provide a recognized focus of practice exam in 2010 for those re‐certifying with the American Board of Internal Medicine,13 PHM is creating an identity as a subspecialty practice with distinct focus on inpatient care for children within the larger context of general pediatric care.8, 14
The Pediatric Hospital Medicine Core Competencies were created to help define the roles and expectations for pediatric hospitalists, regardless of practice setting. The intent is to provide a unified approach toward identifying the specific body of knowledge and measurable skills needed to assure delivery of the highest quality of care for all hospitalized pediatric patients. Most children requiring hospitalization in the United States are hospitalized in community settings where subspecialty support is more limited and many pediatric services may be unavailable. Children with complex, chronic medical problems, however, are more likely to be hospitalized at a tertiary care or academic institutions. In order to unify pediatric hospitalists who work in different practice environments, the PHM Core Competencies were constructed to represent the knowledge, skills, attitudes, and systems improvements that all pediatric hospitalists can be expected to acquire and maintain.
Furthermore, the content of the PHM Core Competencies reflect the fact that children are a vulnerable population. Their care requires attention to many elements which distinguishes it from that given to the majority of the adult population: dependency, differences in developmental physiology and behavior, occurrence of congenital genetic disorders and age‐based clinical conditions, impact of chronic disease states on whole child development, and weight‐based medication dosing often with limited guidance from pediatric studies, to name a few. Awareness of these needs must be heightened when a child enters the hospital where diagnoses, procedures, and treatments often include use of high‐risk modalities and require coordination of care across multiple providers.
Pediatric hospitalists commonly work to improve the systems of care in which they operate and therefore both clinical and non‐clinical topics are included. The 54 chapters address the fundamental and most common components of inpatient care but are not an extensive review of all aspects of inpatient medicine encountered by those caring for hospitalized children. Finally, the PHM Core Competencies are not intended for use in assessing proficiency immediately post‐residency, but do provide a framework for the education and evaluation of both physicians‐in‐training and practicing hospitalists. Meeting these competencies is anticipated to take from one to three years of active practice in pediatric hospital medicine, and may be reached through a combination of practice experience, course work, self‐directed work, and/or formalized training.
Methods
Timeline
In 2002, SHM convened an educational summit from which there was a resolution to create core competencies. Following the summit, the SHM Pediatric Core Curriculum Task Force (CCTF) was created, which included 12 pediatric hospitalists practicing in academic and community facilities, as well as teaching and non‐teaching settings, and occupying leadership positions within institutions of varied size and geographic location. Shortly thereafter, in November 2003, approximately 130 pediatric hospitalists attended the first PHM meeting in San Antonio, Texas.11 At this meeting, with support from leaders in pediatric emergency medicine, first discussions regarding PHM scope of practice were held.
Formal development of the competencies began in 2005 in parallel to but distinct from SHM's adult work, which culminated in The Core Competencies in Hospital Medicine: A Framework for Curriculum Development published in 2006. The CCTF divided into three groups, focused on clinical, procedural, and systems‐based topics. Face‐to‐face meetings were held at the SHM annual meetings, with most work being completed by phone and electronically in the interim periods. In 2007, due to the overlapping interests of the three core pediatric societies, the work was transferred to leaders within the APA. In 2008 the work was transferred back to the leadership within SHM. Since that time, external reviewers were solicited, new chapters created, sections re‐aligned, internal and external reviewer comments incorporated, and final edits for taxonomy, content, and formatting were completed (Table 1).
| Date | Event |
|---|---|
| Feb 2002 | SHM Educational Summit held and CCTF created |
| Oct 2003 | 1st PHM meeting held in San Antonio |
| 2003‐2007 | Chapter focus determined; contributors engaged |
| 2007‐2008 | APA PHM Special Interest Group (SIG) review; creation of separate PHM Fellowship Competencies (not in this document) |
| Aug 2008‐Oct 2008 | SHM Pediatric Committee and CCTF members resume work; editorial review |
| Oct 2008‐Mar 2009 | Internal review: PHM Fellowship Director, AAP, APA, and SHM section/committee leader, and key national PHM leader reviews solicited and returned |
| Mar 2009 | PHM Fellowship Director comments addressed; editorial review |
| Mar‐Apr 2009 | External reviewers solicited from national agencies and societies relevant to PHM |
| Apr‐July 2009 | External reviewer comments returned |
| July‐Oct 2009 | Contributor review of all comments; editorial review, sections revised |
| Oct 2009 | Final review: Chapters to SHM subcommittees and Board |
Areas of Focused Practice
The PHM Core Competencies were conceptualized similarly to the SHM adult core competencies. Initial sections were divided into clinical conditions, procedures, and systems. However as content developed and reviewer comments were addressed, the four final sections were modified to those noted in Table 2. For the Common Clinical Diagnoses and Conditions, the goal was to select conditions most commonly encountered by pediatric hospitalists. Non‐surgical diagnosis‐related group (DRG) conditions were selected from the following sources: The Joint Commission's (TJC) Oryx Performance Measures Report15‐16 (asthma, abdominal pain, acute gastroenteritis, simple pneumonia); Child Health Corporation of America's Pediatric Health Information System Dataset (CHCA PHIS, Shawnee Mission, KS), and relevant publications on common pediatric hospitalizations.17 These data were compared to billing data from randomly‐selected practicing hospitalists representing free‐standing children's and community hospitals, teaching and non‐teaching settings, and urban and rural locations. The 22 clinical conditions chosen by the CCTF were those most relevant to the practice of pediatric hospital medicine.
| Common Clinical Diagnoses and Conditions | Specialized Clinical Services | Core Skills | Healthcare Systems: Supporting and Advancing Child Health | |
|---|---|---|---|---|
| Acute abdominal pain and the acute abdomen | Neonatal fever | Child abuse and neglect | Bladder catheterization/suprapubic bladder tap | Advocacy |
| Apparent life‐threatening event | Neonatal jaundice | Hospice and palliative care | Electrocardiogram interpretation | Business practices |
| Asthma | Pneumonia | Leading a healthcare team | Feeding tubes | Communication |
| Bone and joint infections | Respiratory failure | Newborn care and delivery room management | Fluids and electrolyte management | Continuous quality improvement |
| Bronchiolitis | Seizures | Technology‐dependent children | Intravenous access and phlebotomy | Cost‐effective care |
| Central nervous system infections | Shock | Transport of the critically ill child | Lumbar puncture | Education |
| Diabetes mellitus | Sickle cell disease | Non‐invasive monitoring | Ethics | |
| Failure to thrive | Skin and soft tissue infection | Nutrition | Evidence‐based medicine | |
| Fever of unknown origin | Toxic ingestion | Oxygen delivery and airway management | Health information systems | |
| Gastroenteritis | Upper airway infections | Pain management | Legal issues/risk management | |
| Kawasaki disease | Urinary tract infections | Pediatric advanced life support | Patient safety |
The Specialized Clinical Servicessection addresses important components of care that are not DRG‐based and reflect the unique needs of hospitalized children, as assessed by the CCTF, editors, and contributors. Core Skillswere chosen based on the HCUP Factbook 2 Procedures,18 billing data from randomly‐selected practicing hospitalists representing the same settings listed above, and critical input from reviewers. Depending on the individual setting, pediatric hospitalists may require skills in areas not found in these 11 chapters, such as chest tube placement or ventilator management. The list is therefore not exhaustive, but rather representative of skills most pediatric hospitalists should maintain.
The Healthcare Systems: Supporting and Advancing Child Healthchapters are likely the most dissimilar to any core content taught in traditional residency programs. While residency graduates are versed in some components listed in these chapters, comprehensive education in most of these competencies is currently lacking. Improvement of healthcare systems is an essential element of pediatric hospital medicine, and unifies all pediatric hospitalists regardless of practice environment or patient population. Therefore, this section includes chapters that not only focus on systems of care, but also on advancing child health through advocacy, research, education, evidence‐based medicine, and ethical practice. These chapters were drawn from a combination of several sources: expectations of external agencies (TJC, Center for Medicaid and Medicare) related to the specific nonclinical work in which pediatric hospitalists are integrally involved; expectations for advocacy as best defined by the AAP and the National Association of Children's Hospitals and Related Institutions (NACHRI); the six core competency domains mandated by the Accrediting Council on Graduate Medical Education (ACGME), the American Board of Pediatrics (ABP), and hospital medical staff offices as part of Focused Professional Practice Evaluation (FPPE) and Ongoing Professional Practice Evaluation (OPPE)16; and assessment of responsibilities and leadership roles fulfilled by pediatric hospitalists in all venues. In keeping with the intent of the competencies to be timeless, the competency elements call out the need to attend to the changing goals of these groups as well as those of the Institute of Healthcare Improvement (IHI), the Alliance for Pediatric Quality (which consists of ABP, AAP, TJC, CHCA, NACHRI), and local hospital systems leaders.
Contributors and Review
The CCTF selected section (associate) editors from SHM based on established expertise in each area, with input from the SHM Pediatric and Education Committees and the SHM Board. As a collaborative effort, authors for various chapters were solicited in consultation with experts from the AAP, APA, and SHM, and included non‐hospitalists with reputations as experts in various fields. Numerous SHM Pediatric Committee and CCTF conference calls were held to review hospital and academic appointments, presentations given, and affiliations relevant to the practice of pediatric hospital medicine. This vetting process resulted in a robust author list representing diverse geographic and practice settings. Contributors were provided with structure (Knowledge, Skills, Attitudes, and Systems subsections) and content (timeless, competency based) guidelines.
The review process was rigorous, and included both internal and external reviewers. The APA review in 2007 included the PHM Special Interest Group as well as the PHM Fellowship Directors (Table 1). After return to SHM and further editing, the internal review commenced which focused on content and scope. The editors addressed the resulting suggestions and worked to standardize formatting and use of Bloom's taxonomy.19 A list of common terms and phrases were created to add consistency between chapters. External reviewers were first mailed a letter requesting interest, which was followed up by emails, letters, and phone calls to encourage feedback. External review included 29 solicited agencies and societies (Table 3), with overall response rate of 66% (41% for Groups I and II). Individual contributors then reviewed comments specific to their chapters, with associate editor overview of their respective sections. The editors reviewed each chapter individually multiple times throughout the 2007‐2009 years, contacting individual contributors and reviewers by email and phone. Editors concluded a final comprehensive review of all chapters in late 2009.
| I. Academic and certifying societies |
| Academic Pediatric Association |
| Accreditation Council for Graduate Medical Education, Pediatric Residency Review Committee |
| American Academy of Family Physicians |
| American Academy of Pediatrics Board |
| American Academy of Pediatrics National Committee on Hospital Care |
| American Association of Critical Care Nursing |
| American Board of Family Medicine |
| American Board of Pediatrics |
| American College of Emergency Physicians |
| American Pediatric Society |
| Association of American Medical Colleges |
| Association of Medical School Pediatric Department Chairs (AMSPDC) |
| Association of Pediatric Program Directors |
| Council on Teaching Hospitals |
| Society of Pediatric Research |
| II. Stakeholder agencies |
| Agency for Healthcare Research and Quality |
| American Association of Critical Care Nursing |
| American College of Emergency Physicians |
| American Hospital Association (AHA) |
| American Nurses Association |
| American Society of Health‐System Pharmacists |
| Child Health Corporation of America (CHCA) |
| Institute for Healthcare Improvement |
| National Association for Children's Hospitals and Related Institutions (NACHRI) |
| National Association of Pediatric Nurse Practitioners (NAPNAP) |
| National Initiative for Children's Healthcare Quality (NICHQ) |
| National Quality Forum |
| Quality Resources International |
| Robert Wood Johnson Foundation |
| The Joint Commission for Accreditation of Hospitals and Organizations (TJC) |
| III. Pediatric hospital medicine fellowship directors |
| Boston Children's |
| Children's Hospital Los Angeles |
| Children's National D.C. |
| Emory |
| Hospital for Sick Kids Toronto |
| Rady Children's San Diego University of California San Diego |
| Riley Children's Hospital Indiana |
| University of South Florida, All Children's Hospital |
| Texas Children's Hospital, Baylor College of Medicine |
| IV. SHM, APA, AAP Leadership and committee chairs |
| American Academy of Pediatrics Section on Hospital Medicine |
| Academic Pediatric Association PHM Special Interest Group |
| SHM Board |
| SHM Education Committee |
| SHM Family Practice Committee |
| SHM Hospital Quality and Patient Safety Committee |
| SHM IT Task Force |
| SHM Journal Editorial Board |
| SHM Palliative Care Task Force |
| SHM Practice Analysis Committee |
| SHM Public Policy Committee |
| SHM Research Committee |
Chapter Content
Each of the 54 chapters within the four sections of these competencies is presented in the educational theory of learning domains: Knowledge, Skills, Attitudes, with a final Systems domain added to reflect the emphasis of hospitalist practice on improving healthcare systems. Each chapter is designed to stand alone, which may assist with development of curriculum at individual practice locations. Certain key phrases are apparent throughout, such as lead, coordinate, or participate in and work with hospital and community leaders to which were designed to note the varied roles in different practice settings. Some chapters specifically comment on the application of competency bullets given the unique and differing roles and expectations of pediatric hospitalists, such as research and education. Chapters state specific proficiencies expected wherever possible, with phrases and wording selected to help guide learning activities to achieve the competency.
Application and Future Directions
Although pediatric hospitalists care for children in many settings, these core competencies address the common expectations for any venue. Pediatric hospital medicine requires skills in acute care clinical medicine that attend to the changing needs of hospitalized children. The core of pediatric hospital medicine is dedicated to the care of children in the geographic hospital environment between emergency medicine and tertiary pediatric and neonatal intensive care units. Pediatric hospitalists provide care in related clinical service programs that are linked to hospital systems. In performing these activities, pediatric hospitalists consistently partner with ambulatory providers and subspecialists to render coordinated care across the continuum for a given child. Pediatric hospital medicine is an interdisciplinary practice, with focus on processes of care and clinical quality outcomes based in evidence. Engagement in local, state, and national initiatives to improve child health outcomes is a cornerstone of pediatric hospitalists' practice. These competencies provide the framework for creation of curricula that can reflect local issues and react to changing evidence.
As providers of systems‐based care, pediatric hospitalists are called upon more and more to render care and provide leadership in clinical arenas that are integral to healthcare organizations, such as home health care, sub‐acute care facilities, and hospice and palliative care programs. The practice of pediatric hospital medicine has evolved to its current state through efforts of many represented in the competencies as contributors, associate editors, editors, and reviewers. Pediatric hospitalists are committed to leading change in healthcare for hospitalized children, and are positioned well to address the interests and needs of community and urban, teaching and non‐teaching facilities, and the children and families they serve. These competencies reflect the areas of focused practice which, similar to pediatric emergency medicine, will no doubt be refined but not fundamentally changed in future years. The intent, we hope, is clear: to provide excellence in clinical care, accountability for practice, and lead improvements in healthcare for hospitalized children.
- Society of Hospital Medicine (SHM). Definition of a Hospitalist. http://www.hospitalmedicine.org/AM/Template.cfm?Section=General_Information 2009.
- .Pediatric Hospitalists Membership Numbers. In.Philadelphia:Society of Hospital Medicine, PA 19130;2009.
- , .The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .The future of hospital medicine: evolution or revolution?.Am J Med.2004;117:446–450.
- , .The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- , , , , .Variation in pediatric hospitalists' use of proven and unproven therapies: A study from the Pediatric Research in Inpatient Settings (PRIS) network.J Hosp Med.2008;3(4):292–298.
- , , .Pediatric hospitalists: Training, current practice, and career goals.J Hosp Med.2009;4(3):179–186.
- , .Standardize to excellence: improving the quality and safety of care with clinical pathways.Pediatr Clin North Am.2009;56(4):893–904.
- .Evolution of a new specialty ‐ a twenty year pediatric hospitalist experience [Abstract]. In:National Association of Inpatient Physicians (now Society of Hospital Medicine).New Orleans, Louisiana;1999.
- , , , , , , et al.Pediatric hospitalists: report of a leadership conference.Pediatrics.2006;117(4):1122–1130.
- , , , , e.The core competencies in hospital medicine: a framework for curriculum development.J Hosp Med.2006;1(Suppl 1).
- American Board of Internal Medicine. Questions and answers regarding ABIM recognition of focused practice in hospital medicine through maintenance of certification. http://www.abim.org/news/news/focused‐practice‐hospital‐medicine‐qa.aspx. Published 2010. Accessed January 6,2010.
- .Comprehensive pediatric hospital medicine.N Engl J Med.2008;358(21):2301–2302.
- The Joint Commission. Performance measurement initiatives. http://www. jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/. Published 2010. Accessed December 5,2010.
- The Joint Commission. Standards frequently asked questions: comprehensive accreditation manual for critical access hospitals (CAMCAH). http://www.jointcommission.org/AccreditationPrograms/CriticalAccess Hospitals/Standards/09_FAQs/default.htm. Accessed December 5,2008; December 14, 2009.
- , , , , .Infectious disease hospitalizations among infants in the United States.Pediatrics.2008;121(2):244–252.
- , , , .Procedures in U.S. hospitals, 1997.HCUP fact book no. 2. In:agency for healthcare research and quality,Rockville, MD;2001.
- Anderson L, Krathwohl DR, Airasian PW, Cruikshank KA, Mayer RE, Pintrich PR, et al., editors.A taxonomy for learning, teaching, and assessing. In: A Revision of Bloom's Taxonomy of Educational Objectives.Upper Saddle River, NJ: Addison Wesley Longman, Inc. Pearson Education USA;2001.
Introduction
The Society of Hospital Medicine (SHM) defines hospitalists as physicians whose primary professional focus is the comprehensive general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to Hospital Medicine.1 It is estimated that there are up to 2500 pediatric hospitalists in the United States, with continued growth due to the converging needs for a dedicated focus on patient safety, quality improvement, hospital throughput, and inpatient teaching.2‐9 (Pediatric Hospital Medicine (PHM), as defined today, has been practiced in the United States for at least 30 years10 and continues to evolve as an area of specialization, with the refinement of a distinct knowledgebase and skill set focused on the provision of high quality general pediatric care in the inpatient setting. PHM is the latest site‐specific specialty to emerge from the field of general pediatrics it's development analogous to the evolution of critical care or emergency medicine during previous decades.11 Adult hospital medicine has defined itself within the field of general internal medicine12 and has recently received approval to provide a recognized focus of practice exam in 2010 for those re‐certifying with the American Board of Internal Medicine,13 PHM is creating an identity as a subspecialty practice with distinct focus on inpatient care for children within the larger context of general pediatric care.8, 14
The Pediatric Hospital Medicine Core Competencies were created to help define the roles and expectations for pediatric hospitalists, regardless of practice setting. The intent is to provide a unified approach toward identifying the specific body of knowledge and measurable skills needed to assure delivery of the highest quality of care for all hospitalized pediatric patients. Most children requiring hospitalization in the United States are hospitalized in community settings where subspecialty support is more limited and many pediatric services may be unavailable. Children with complex, chronic medical problems, however, are more likely to be hospitalized at a tertiary care or academic institutions. In order to unify pediatric hospitalists who work in different practice environments, the PHM Core Competencies were constructed to represent the knowledge, skills, attitudes, and systems improvements that all pediatric hospitalists can be expected to acquire and maintain.
Furthermore, the content of the PHM Core Competencies reflect the fact that children are a vulnerable population. Their care requires attention to many elements which distinguishes it from that given to the majority of the adult population: dependency, differences in developmental physiology and behavior, occurrence of congenital genetic disorders and age‐based clinical conditions, impact of chronic disease states on whole child development, and weight‐based medication dosing often with limited guidance from pediatric studies, to name a few. Awareness of these needs must be heightened when a child enters the hospital where diagnoses, procedures, and treatments often include use of high‐risk modalities and require coordination of care across multiple providers.
Pediatric hospitalists commonly work to improve the systems of care in which they operate and therefore both clinical and non‐clinical topics are included. The 54 chapters address the fundamental and most common components of inpatient care but are not an extensive review of all aspects of inpatient medicine encountered by those caring for hospitalized children. Finally, the PHM Core Competencies are not intended for use in assessing proficiency immediately post‐residency, but do provide a framework for the education and evaluation of both physicians‐in‐training and practicing hospitalists. Meeting these competencies is anticipated to take from one to three years of active practice in pediatric hospital medicine, and may be reached through a combination of practice experience, course work, self‐directed work, and/or formalized training.
Methods
Timeline
In 2002, SHM convened an educational summit from which there was a resolution to create core competencies. Following the summit, the SHM Pediatric Core Curriculum Task Force (CCTF) was created, which included 12 pediatric hospitalists practicing in academic and community facilities, as well as teaching and non‐teaching settings, and occupying leadership positions within institutions of varied size and geographic location. Shortly thereafter, in November 2003, approximately 130 pediatric hospitalists attended the first PHM meeting in San Antonio, Texas.11 At this meeting, with support from leaders in pediatric emergency medicine, first discussions regarding PHM scope of practice were held.
Formal development of the competencies began in 2005 in parallel to but distinct from SHM's adult work, which culminated in The Core Competencies in Hospital Medicine: A Framework for Curriculum Development published in 2006. The CCTF divided into three groups, focused on clinical, procedural, and systems‐based topics. Face‐to‐face meetings were held at the SHM annual meetings, with most work being completed by phone and electronically in the interim periods. In 2007, due to the overlapping interests of the three core pediatric societies, the work was transferred to leaders within the APA. In 2008 the work was transferred back to the leadership within SHM. Since that time, external reviewers were solicited, new chapters created, sections re‐aligned, internal and external reviewer comments incorporated, and final edits for taxonomy, content, and formatting were completed (Table 1).
| Date | Event |
|---|---|
| Feb 2002 | SHM Educational Summit held and CCTF created |
| Oct 2003 | 1st PHM meeting held in San Antonio |
| 2003‐2007 | Chapter focus determined; contributors engaged |
| 2007‐2008 | APA PHM Special Interest Group (SIG) review; creation of separate PHM Fellowship Competencies (not in this document) |
| Aug 2008‐Oct 2008 | SHM Pediatric Committee and CCTF members resume work; editorial review |
| Oct 2008‐Mar 2009 | Internal review: PHM Fellowship Director, AAP, APA, and SHM section/committee leader, and key national PHM leader reviews solicited and returned |
| Mar 2009 | PHM Fellowship Director comments addressed; editorial review |
| Mar‐Apr 2009 | External reviewers solicited from national agencies and societies relevant to PHM |
| Apr‐July 2009 | External reviewer comments returned |
| July‐Oct 2009 | Contributor review of all comments; editorial review, sections revised |
| Oct 2009 | Final review: Chapters to SHM subcommittees and Board |
Areas of Focused Practice
The PHM Core Competencies were conceptualized similarly to the SHM adult core competencies. Initial sections were divided into clinical conditions, procedures, and systems. However as content developed and reviewer comments were addressed, the four final sections were modified to those noted in Table 2. For the Common Clinical Diagnoses and Conditions, the goal was to select conditions most commonly encountered by pediatric hospitalists. Non‐surgical diagnosis‐related group (DRG) conditions were selected from the following sources: The Joint Commission's (TJC) Oryx Performance Measures Report15‐16 (asthma, abdominal pain, acute gastroenteritis, simple pneumonia); Child Health Corporation of America's Pediatric Health Information System Dataset (CHCA PHIS, Shawnee Mission, KS), and relevant publications on common pediatric hospitalizations.17 These data were compared to billing data from randomly‐selected practicing hospitalists representing free‐standing children's and community hospitals, teaching and non‐teaching settings, and urban and rural locations. The 22 clinical conditions chosen by the CCTF were those most relevant to the practice of pediatric hospital medicine.
| Common Clinical Diagnoses and Conditions | Specialized Clinical Services | Core Skills | Healthcare Systems: Supporting and Advancing Child Health | |
|---|---|---|---|---|
| Acute abdominal pain and the acute abdomen | Neonatal fever | Child abuse and neglect | Bladder catheterization/suprapubic bladder tap | Advocacy |
| Apparent life‐threatening event | Neonatal jaundice | Hospice and palliative care | Electrocardiogram interpretation | Business practices |
| Asthma | Pneumonia | Leading a healthcare team | Feeding tubes | Communication |
| Bone and joint infections | Respiratory failure | Newborn care and delivery room management | Fluids and electrolyte management | Continuous quality improvement |
| Bronchiolitis | Seizures | Technology‐dependent children | Intravenous access and phlebotomy | Cost‐effective care |
| Central nervous system infections | Shock | Transport of the critically ill child | Lumbar puncture | Education |
| Diabetes mellitus | Sickle cell disease | Non‐invasive monitoring | Ethics | |
| Failure to thrive | Skin and soft tissue infection | Nutrition | Evidence‐based medicine | |
| Fever of unknown origin | Toxic ingestion | Oxygen delivery and airway management | Health information systems | |
| Gastroenteritis | Upper airway infections | Pain management | Legal issues/risk management | |
| Kawasaki disease | Urinary tract infections | Pediatric advanced life support | Patient safety |
The Specialized Clinical Servicessection addresses important components of care that are not DRG‐based and reflect the unique needs of hospitalized children, as assessed by the CCTF, editors, and contributors. Core Skillswere chosen based on the HCUP Factbook 2 Procedures,18 billing data from randomly‐selected practicing hospitalists representing the same settings listed above, and critical input from reviewers. Depending on the individual setting, pediatric hospitalists may require skills in areas not found in these 11 chapters, such as chest tube placement or ventilator management. The list is therefore not exhaustive, but rather representative of skills most pediatric hospitalists should maintain.
The Healthcare Systems: Supporting and Advancing Child Healthchapters are likely the most dissimilar to any core content taught in traditional residency programs. While residency graduates are versed in some components listed in these chapters, comprehensive education in most of these competencies is currently lacking. Improvement of healthcare systems is an essential element of pediatric hospital medicine, and unifies all pediatric hospitalists regardless of practice environment or patient population. Therefore, this section includes chapters that not only focus on systems of care, but also on advancing child health through advocacy, research, education, evidence‐based medicine, and ethical practice. These chapters were drawn from a combination of several sources: expectations of external agencies (TJC, Center for Medicaid and Medicare) related to the specific nonclinical work in which pediatric hospitalists are integrally involved; expectations for advocacy as best defined by the AAP and the National Association of Children's Hospitals and Related Institutions (NACHRI); the six core competency domains mandated by the Accrediting Council on Graduate Medical Education (ACGME), the American Board of Pediatrics (ABP), and hospital medical staff offices as part of Focused Professional Practice Evaluation (FPPE) and Ongoing Professional Practice Evaluation (OPPE)16; and assessment of responsibilities and leadership roles fulfilled by pediatric hospitalists in all venues. In keeping with the intent of the competencies to be timeless, the competency elements call out the need to attend to the changing goals of these groups as well as those of the Institute of Healthcare Improvement (IHI), the Alliance for Pediatric Quality (which consists of ABP, AAP, TJC, CHCA, NACHRI), and local hospital systems leaders.
Contributors and Review
The CCTF selected section (associate) editors from SHM based on established expertise in each area, with input from the SHM Pediatric and Education Committees and the SHM Board. As a collaborative effort, authors for various chapters were solicited in consultation with experts from the AAP, APA, and SHM, and included non‐hospitalists with reputations as experts in various fields. Numerous SHM Pediatric Committee and CCTF conference calls were held to review hospital and academic appointments, presentations given, and affiliations relevant to the practice of pediatric hospital medicine. This vetting process resulted in a robust author list representing diverse geographic and practice settings. Contributors were provided with structure (Knowledge, Skills, Attitudes, and Systems subsections) and content (timeless, competency based) guidelines.
The review process was rigorous, and included both internal and external reviewers. The APA review in 2007 included the PHM Special Interest Group as well as the PHM Fellowship Directors (Table 1). After return to SHM and further editing, the internal review commenced which focused on content and scope. The editors addressed the resulting suggestions and worked to standardize formatting and use of Bloom's taxonomy.19 A list of common terms and phrases were created to add consistency between chapters. External reviewers were first mailed a letter requesting interest, which was followed up by emails, letters, and phone calls to encourage feedback. External review included 29 solicited agencies and societies (Table 3), with overall response rate of 66% (41% for Groups I and II). Individual contributors then reviewed comments specific to their chapters, with associate editor overview of their respective sections. The editors reviewed each chapter individually multiple times throughout the 2007‐2009 years, contacting individual contributors and reviewers by email and phone. Editors concluded a final comprehensive review of all chapters in late 2009.
| I. Academic and certifying societies |
| Academic Pediatric Association |
| Accreditation Council for Graduate Medical Education, Pediatric Residency Review Committee |
| American Academy of Family Physicians |
| American Academy of Pediatrics Board |
| American Academy of Pediatrics National Committee on Hospital Care |
| American Association of Critical Care Nursing |
| American Board of Family Medicine |
| American Board of Pediatrics |
| American College of Emergency Physicians |
| American Pediatric Society |
| Association of American Medical Colleges |
| Association of Medical School Pediatric Department Chairs (AMSPDC) |
| Association of Pediatric Program Directors |
| Council on Teaching Hospitals |
| Society of Pediatric Research |
| II. Stakeholder agencies |
| Agency for Healthcare Research and Quality |
| American Association of Critical Care Nursing |
| American College of Emergency Physicians |
| American Hospital Association (AHA) |
| American Nurses Association |
| American Society of Health‐System Pharmacists |
| Child Health Corporation of America (CHCA) |
| Institute for Healthcare Improvement |
| National Association for Children's Hospitals and Related Institutions (NACHRI) |
| National Association of Pediatric Nurse Practitioners (NAPNAP) |
| National Initiative for Children's Healthcare Quality (NICHQ) |
| National Quality Forum |
| Quality Resources International |
| Robert Wood Johnson Foundation |
| The Joint Commission for Accreditation of Hospitals and Organizations (TJC) |
| III. Pediatric hospital medicine fellowship directors |
| Boston Children's |
| Children's Hospital Los Angeles |
| Children's National D.C. |
| Emory |
| Hospital for Sick Kids Toronto |
| Rady Children's San Diego University of California San Diego |
| Riley Children's Hospital Indiana |
| University of South Florida, All Children's Hospital |
| Texas Children's Hospital, Baylor College of Medicine |
| IV. SHM, APA, AAP Leadership and committee chairs |
| American Academy of Pediatrics Section on Hospital Medicine |
| Academic Pediatric Association PHM Special Interest Group |
| SHM Board |
| SHM Education Committee |
| SHM Family Practice Committee |
| SHM Hospital Quality and Patient Safety Committee |
| SHM IT Task Force |
| SHM Journal Editorial Board |
| SHM Palliative Care Task Force |
| SHM Practice Analysis Committee |
| SHM Public Policy Committee |
| SHM Research Committee |
Chapter Content
Each of the 54 chapters within the four sections of these competencies is presented in the educational theory of learning domains: Knowledge, Skills, Attitudes, with a final Systems domain added to reflect the emphasis of hospitalist practice on improving healthcare systems. Each chapter is designed to stand alone, which may assist with development of curriculum at individual practice locations. Certain key phrases are apparent throughout, such as lead, coordinate, or participate in and work with hospital and community leaders to which were designed to note the varied roles in different practice settings. Some chapters specifically comment on the application of competency bullets given the unique and differing roles and expectations of pediatric hospitalists, such as research and education. Chapters state specific proficiencies expected wherever possible, with phrases and wording selected to help guide learning activities to achieve the competency.
Application and Future Directions
Although pediatric hospitalists care for children in many settings, these core competencies address the common expectations for any venue. Pediatric hospital medicine requires skills in acute care clinical medicine that attend to the changing needs of hospitalized children. The core of pediatric hospital medicine is dedicated to the care of children in the geographic hospital environment between emergency medicine and tertiary pediatric and neonatal intensive care units. Pediatric hospitalists provide care in related clinical service programs that are linked to hospital systems. In performing these activities, pediatric hospitalists consistently partner with ambulatory providers and subspecialists to render coordinated care across the continuum for a given child. Pediatric hospital medicine is an interdisciplinary practice, with focus on processes of care and clinical quality outcomes based in evidence. Engagement in local, state, and national initiatives to improve child health outcomes is a cornerstone of pediatric hospitalists' practice. These competencies provide the framework for creation of curricula that can reflect local issues and react to changing evidence.
As providers of systems‐based care, pediatric hospitalists are called upon more and more to render care and provide leadership in clinical arenas that are integral to healthcare organizations, such as home health care, sub‐acute care facilities, and hospice and palliative care programs. The practice of pediatric hospital medicine has evolved to its current state through efforts of many represented in the competencies as contributors, associate editors, editors, and reviewers. Pediatric hospitalists are committed to leading change in healthcare for hospitalized children, and are positioned well to address the interests and needs of community and urban, teaching and non‐teaching facilities, and the children and families they serve. These competencies reflect the areas of focused practice which, similar to pediatric emergency medicine, will no doubt be refined but not fundamentally changed in future years. The intent, we hope, is clear: to provide excellence in clinical care, accountability for practice, and lead improvements in healthcare for hospitalized children.
Introduction
The Society of Hospital Medicine (SHM) defines hospitalists as physicians whose primary professional focus is the comprehensive general medical care of hospitalized patients. Their activities include patient care, teaching, research, and leadership related to Hospital Medicine.1 It is estimated that there are up to 2500 pediatric hospitalists in the United States, with continued growth due to the converging needs for a dedicated focus on patient safety, quality improvement, hospital throughput, and inpatient teaching.2‐9 (Pediatric Hospital Medicine (PHM), as defined today, has been practiced in the United States for at least 30 years10 and continues to evolve as an area of specialization, with the refinement of a distinct knowledgebase and skill set focused on the provision of high quality general pediatric care in the inpatient setting. PHM is the latest site‐specific specialty to emerge from the field of general pediatrics it's development analogous to the evolution of critical care or emergency medicine during previous decades.11 Adult hospital medicine has defined itself within the field of general internal medicine12 and has recently received approval to provide a recognized focus of practice exam in 2010 for those re‐certifying with the American Board of Internal Medicine,13 PHM is creating an identity as a subspecialty practice with distinct focus on inpatient care for children within the larger context of general pediatric care.8, 14
The Pediatric Hospital Medicine Core Competencies were created to help define the roles and expectations for pediatric hospitalists, regardless of practice setting. The intent is to provide a unified approach toward identifying the specific body of knowledge and measurable skills needed to assure delivery of the highest quality of care for all hospitalized pediatric patients. Most children requiring hospitalization in the United States are hospitalized in community settings where subspecialty support is more limited and many pediatric services may be unavailable. Children with complex, chronic medical problems, however, are more likely to be hospitalized at a tertiary care or academic institutions. In order to unify pediatric hospitalists who work in different practice environments, the PHM Core Competencies were constructed to represent the knowledge, skills, attitudes, and systems improvements that all pediatric hospitalists can be expected to acquire and maintain.
Furthermore, the content of the PHM Core Competencies reflect the fact that children are a vulnerable population. Their care requires attention to many elements which distinguishes it from that given to the majority of the adult population: dependency, differences in developmental physiology and behavior, occurrence of congenital genetic disorders and age‐based clinical conditions, impact of chronic disease states on whole child development, and weight‐based medication dosing often with limited guidance from pediatric studies, to name a few. Awareness of these needs must be heightened when a child enters the hospital where diagnoses, procedures, and treatments often include use of high‐risk modalities and require coordination of care across multiple providers.
Pediatric hospitalists commonly work to improve the systems of care in which they operate and therefore both clinical and non‐clinical topics are included. The 54 chapters address the fundamental and most common components of inpatient care but are not an extensive review of all aspects of inpatient medicine encountered by those caring for hospitalized children. Finally, the PHM Core Competencies are not intended for use in assessing proficiency immediately post‐residency, but do provide a framework for the education and evaluation of both physicians‐in‐training and practicing hospitalists. Meeting these competencies is anticipated to take from one to three years of active practice in pediatric hospital medicine, and may be reached through a combination of practice experience, course work, self‐directed work, and/or formalized training.
Methods
Timeline
In 2002, SHM convened an educational summit from which there was a resolution to create core competencies. Following the summit, the SHM Pediatric Core Curriculum Task Force (CCTF) was created, which included 12 pediatric hospitalists practicing in academic and community facilities, as well as teaching and non‐teaching settings, and occupying leadership positions within institutions of varied size and geographic location. Shortly thereafter, in November 2003, approximately 130 pediatric hospitalists attended the first PHM meeting in San Antonio, Texas.11 At this meeting, with support from leaders in pediatric emergency medicine, first discussions regarding PHM scope of practice were held.
Formal development of the competencies began in 2005 in parallel to but distinct from SHM's adult work, which culminated in The Core Competencies in Hospital Medicine: A Framework for Curriculum Development published in 2006. The CCTF divided into three groups, focused on clinical, procedural, and systems‐based topics. Face‐to‐face meetings were held at the SHM annual meetings, with most work being completed by phone and electronically in the interim periods. In 2007, due to the overlapping interests of the three core pediatric societies, the work was transferred to leaders within the APA. In 2008 the work was transferred back to the leadership within SHM. Since that time, external reviewers were solicited, new chapters created, sections re‐aligned, internal and external reviewer comments incorporated, and final edits for taxonomy, content, and formatting were completed (Table 1).
| Date | Event |
|---|---|
| Feb 2002 | SHM Educational Summit held and CCTF created |
| Oct 2003 | 1st PHM meeting held in San Antonio |
| 2003‐2007 | Chapter focus determined; contributors engaged |
| 2007‐2008 | APA PHM Special Interest Group (SIG) review; creation of separate PHM Fellowship Competencies (not in this document) |
| Aug 2008‐Oct 2008 | SHM Pediatric Committee and CCTF members resume work; editorial review |
| Oct 2008‐Mar 2009 | Internal review: PHM Fellowship Director, AAP, APA, and SHM section/committee leader, and key national PHM leader reviews solicited and returned |
| Mar 2009 | PHM Fellowship Director comments addressed; editorial review |
| Mar‐Apr 2009 | External reviewers solicited from national agencies and societies relevant to PHM |
| Apr‐July 2009 | External reviewer comments returned |
| July‐Oct 2009 | Contributor review of all comments; editorial review, sections revised |
| Oct 2009 | Final review: Chapters to SHM subcommittees and Board |
Areas of Focused Practice
The PHM Core Competencies were conceptualized similarly to the SHM adult core competencies. Initial sections were divided into clinical conditions, procedures, and systems. However as content developed and reviewer comments were addressed, the four final sections were modified to those noted in Table 2. For the Common Clinical Diagnoses and Conditions, the goal was to select conditions most commonly encountered by pediatric hospitalists. Non‐surgical diagnosis‐related group (DRG) conditions were selected from the following sources: The Joint Commission's (TJC) Oryx Performance Measures Report15‐16 (asthma, abdominal pain, acute gastroenteritis, simple pneumonia); Child Health Corporation of America's Pediatric Health Information System Dataset (CHCA PHIS, Shawnee Mission, KS), and relevant publications on common pediatric hospitalizations.17 These data were compared to billing data from randomly‐selected practicing hospitalists representing free‐standing children's and community hospitals, teaching and non‐teaching settings, and urban and rural locations. The 22 clinical conditions chosen by the CCTF were those most relevant to the practice of pediatric hospital medicine.
| Common Clinical Diagnoses and Conditions | Specialized Clinical Services | Core Skills | Healthcare Systems: Supporting and Advancing Child Health | |
|---|---|---|---|---|
| Acute abdominal pain and the acute abdomen | Neonatal fever | Child abuse and neglect | Bladder catheterization/suprapubic bladder tap | Advocacy |
| Apparent life‐threatening event | Neonatal jaundice | Hospice and palliative care | Electrocardiogram interpretation | Business practices |
| Asthma | Pneumonia | Leading a healthcare team | Feeding tubes | Communication |
| Bone and joint infections | Respiratory failure | Newborn care and delivery room management | Fluids and electrolyte management | Continuous quality improvement |
| Bronchiolitis | Seizures | Technology‐dependent children | Intravenous access and phlebotomy | Cost‐effective care |
| Central nervous system infections | Shock | Transport of the critically ill child | Lumbar puncture | Education |
| Diabetes mellitus | Sickle cell disease | Non‐invasive monitoring | Ethics | |
| Failure to thrive | Skin and soft tissue infection | Nutrition | Evidence‐based medicine | |
| Fever of unknown origin | Toxic ingestion | Oxygen delivery and airway management | Health information systems | |
| Gastroenteritis | Upper airway infections | Pain management | Legal issues/risk management | |
| Kawasaki disease | Urinary tract infections | Pediatric advanced life support | Patient safety |
The Specialized Clinical Servicessection addresses important components of care that are not DRG‐based and reflect the unique needs of hospitalized children, as assessed by the CCTF, editors, and contributors. Core Skillswere chosen based on the HCUP Factbook 2 Procedures,18 billing data from randomly‐selected practicing hospitalists representing the same settings listed above, and critical input from reviewers. Depending on the individual setting, pediatric hospitalists may require skills in areas not found in these 11 chapters, such as chest tube placement or ventilator management. The list is therefore not exhaustive, but rather representative of skills most pediatric hospitalists should maintain.
The Healthcare Systems: Supporting and Advancing Child Healthchapters are likely the most dissimilar to any core content taught in traditional residency programs. While residency graduates are versed in some components listed in these chapters, comprehensive education in most of these competencies is currently lacking. Improvement of healthcare systems is an essential element of pediatric hospital medicine, and unifies all pediatric hospitalists regardless of practice environment or patient population. Therefore, this section includes chapters that not only focus on systems of care, but also on advancing child health through advocacy, research, education, evidence‐based medicine, and ethical practice. These chapters were drawn from a combination of several sources: expectations of external agencies (TJC, Center for Medicaid and Medicare) related to the specific nonclinical work in which pediatric hospitalists are integrally involved; expectations for advocacy as best defined by the AAP and the National Association of Children's Hospitals and Related Institutions (NACHRI); the six core competency domains mandated by the Accrediting Council on Graduate Medical Education (ACGME), the American Board of Pediatrics (ABP), and hospital medical staff offices as part of Focused Professional Practice Evaluation (FPPE) and Ongoing Professional Practice Evaluation (OPPE)16; and assessment of responsibilities and leadership roles fulfilled by pediatric hospitalists in all venues. In keeping with the intent of the competencies to be timeless, the competency elements call out the need to attend to the changing goals of these groups as well as those of the Institute of Healthcare Improvement (IHI), the Alliance for Pediatric Quality (which consists of ABP, AAP, TJC, CHCA, NACHRI), and local hospital systems leaders.
Contributors and Review
The CCTF selected section (associate) editors from SHM based on established expertise in each area, with input from the SHM Pediatric and Education Committees and the SHM Board. As a collaborative effort, authors for various chapters were solicited in consultation with experts from the AAP, APA, and SHM, and included non‐hospitalists with reputations as experts in various fields. Numerous SHM Pediatric Committee and CCTF conference calls were held to review hospital and academic appointments, presentations given, and affiliations relevant to the practice of pediatric hospital medicine. This vetting process resulted in a robust author list representing diverse geographic and practice settings. Contributors were provided with structure (Knowledge, Skills, Attitudes, and Systems subsections) and content (timeless, competency based) guidelines.
The review process was rigorous, and included both internal and external reviewers. The APA review in 2007 included the PHM Special Interest Group as well as the PHM Fellowship Directors (Table 1). After return to SHM and further editing, the internal review commenced which focused on content and scope. The editors addressed the resulting suggestions and worked to standardize formatting and use of Bloom's taxonomy.19 A list of common terms and phrases were created to add consistency between chapters. External reviewers were first mailed a letter requesting interest, which was followed up by emails, letters, and phone calls to encourage feedback. External review included 29 solicited agencies and societies (Table 3), with overall response rate of 66% (41% for Groups I and II). Individual contributors then reviewed comments specific to their chapters, with associate editor overview of their respective sections. The editors reviewed each chapter individually multiple times throughout the 2007‐2009 years, contacting individual contributors and reviewers by email and phone. Editors concluded a final comprehensive review of all chapters in late 2009.
| I. Academic and certifying societies |
| Academic Pediatric Association |
| Accreditation Council for Graduate Medical Education, Pediatric Residency Review Committee |
| American Academy of Family Physicians |
| American Academy of Pediatrics Board |
| American Academy of Pediatrics National Committee on Hospital Care |
| American Association of Critical Care Nursing |
| American Board of Family Medicine |
| American Board of Pediatrics |
| American College of Emergency Physicians |
| American Pediatric Society |
| Association of American Medical Colleges |
| Association of Medical School Pediatric Department Chairs (AMSPDC) |
| Association of Pediatric Program Directors |
| Council on Teaching Hospitals |
| Society of Pediatric Research |
| II. Stakeholder agencies |
| Agency for Healthcare Research and Quality |
| American Association of Critical Care Nursing |
| American College of Emergency Physicians |
| American Hospital Association (AHA) |
| American Nurses Association |
| American Society of Health‐System Pharmacists |
| Child Health Corporation of America (CHCA) |
| Institute for Healthcare Improvement |
| National Association for Children's Hospitals and Related Institutions (NACHRI) |
| National Association of Pediatric Nurse Practitioners (NAPNAP) |
| National Initiative for Children's Healthcare Quality (NICHQ) |
| National Quality Forum |
| Quality Resources International |
| Robert Wood Johnson Foundation |
| The Joint Commission for Accreditation of Hospitals and Organizations (TJC) |
| III. Pediatric hospital medicine fellowship directors |
| Boston Children's |
| Children's Hospital Los Angeles |
| Children's National D.C. |
| Emory |
| Hospital for Sick Kids Toronto |
| Rady Children's San Diego University of California San Diego |
| Riley Children's Hospital Indiana |
| University of South Florida, All Children's Hospital |
| Texas Children's Hospital, Baylor College of Medicine |
| IV. SHM, APA, AAP Leadership and committee chairs |
| American Academy of Pediatrics Section on Hospital Medicine |
| Academic Pediatric Association PHM Special Interest Group |
| SHM Board |
| SHM Education Committee |
| SHM Family Practice Committee |
| SHM Hospital Quality and Patient Safety Committee |
| SHM IT Task Force |
| SHM Journal Editorial Board |
| SHM Palliative Care Task Force |
| SHM Practice Analysis Committee |
| SHM Public Policy Committee |
| SHM Research Committee |
Chapter Content
Each of the 54 chapters within the four sections of these competencies is presented in the educational theory of learning domains: Knowledge, Skills, Attitudes, with a final Systems domain added to reflect the emphasis of hospitalist practice on improving healthcare systems. Each chapter is designed to stand alone, which may assist with development of curriculum at individual practice locations. Certain key phrases are apparent throughout, such as lead, coordinate, or participate in and work with hospital and community leaders to which were designed to note the varied roles in different practice settings. Some chapters specifically comment on the application of competency bullets given the unique and differing roles and expectations of pediatric hospitalists, such as research and education. Chapters state specific proficiencies expected wherever possible, with phrases and wording selected to help guide learning activities to achieve the competency.
Application and Future Directions
Although pediatric hospitalists care for children in many settings, these core competencies address the common expectations for any venue. Pediatric hospital medicine requires skills in acute care clinical medicine that attend to the changing needs of hospitalized children. The core of pediatric hospital medicine is dedicated to the care of children in the geographic hospital environment between emergency medicine and tertiary pediatric and neonatal intensive care units. Pediatric hospitalists provide care in related clinical service programs that are linked to hospital systems. In performing these activities, pediatric hospitalists consistently partner with ambulatory providers and subspecialists to render coordinated care across the continuum for a given child. Pediatric hospital medicine is an interdisciplinary practice, with focus on processes of care and clinical quality outcomes based in evidence. Engagement in local, state, and national initiatives to improve child health outcomes is a cornerstone of pediatric hospitalists' practice. These competencies provide the framework for creation of curricula that can reflect local issues and react to changing evidence.
As providers of systems‐based care, pediatric hospitalists are called upon more and more to render care and provide leadership in clinical arenas that are integral to healthcare organizations, such as home health care, sub‐acute care facilities, and hospice and palliative care programs. The practice of pediatric hospital medicine has evolved to its current state through efforts of many represented in the competencies as contributors, associate editors, editors, and reviewers. Pediatric hospitalists are committed to leading change in healthcare for hospitalized children, and are positioned well to address the interests and needs of community and urban, teaching and non‐teaching facilities, and the children and families they serve. These competencies reflect the areas of focused practice which, similar to pediatric emergency medicine, will no doubt be refined but not fundamentally changed in future years. The intent, we hope, is clear: to provide excellence in clinical care, accountability for practice, and lead improvements in healthcare for hospitalized children.
- Society of Hospital Medicine (SHM). Definition of a Hospitalist. http://www.hospitalmedicine.org/AM/Template.cfm?Section=General_Information 2009.
- .Pediatric Hospitalists Membership Numbers. In.Philadelphia:Society of Hospital Medicine, PA 19130;2009.
- , .The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .The future of hospital medicine: evolution or revolution?.Am J Med.2004;117:446–450.
- , .The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- , , , , .Variation in pediatric hospitalists' use of proven and unproven therapies: A study from the Pediatric Research in Inpatient Settings (PRIS) network.J Hosp Med.2008;3(4):292–298.
- , , .Pediatric hospitalists: Training, current practice, and career goals.J Hosp Med.2009;4(3):179–186.
- , .Standardize to excellence: improving the quality and safety of care with clinical pathways.Pediatr Clin North Am.2009;56(4):893–904.
- .Evolution of a new specialty ‐ a twenty year pediatric hospitalist experience [Abstract]. In:National Association of Inpatient Physicians (now Society of Hospital Medicine).New Orleans, Louisiana;1999.
- , , , , , , et al.Pediatric hospitalists: report of a leadership conference.Pediatrics.2006;117(4):1122–1130.
- , , , , e.The core competencies in hospital medicine: a framework for curriculum development.J Hosp Med.2006;1(Suppl 1).
- American Board of Internal Medicine. Questions and answers regarding ABIM recognition of focused practice in hospital medicine through maintenance of certification. http://www.abim.org/news/news/focused‐practice‐hospital‐medicine‐qa.aspx. Published 2010. Accessed January 6,2010.
- .Comprehensive pediatric hospital medicine.N Engl J Med.2008;358(21):2301–2302.
- The Joint Commission. Performance measurement initiatives. http://www. jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/. Published 2010. Accessed December 5,2010.
- The Joint Commission. Standards frequently asked questions: comprehensive accreditation manual for critical access hospitals (CAMCAH). http://www.jointcommission.org/AccreditationPrograms/CriticalAccess Hospitals/Standards/09_FAQs/default.htm. Accessed December 5,2008; December 14, 2009.
- , , , , .Infectious disease hospitalizations among infants in the United States.Pediatrics.2008;121(2):244–252.
- , , , .Procedures in U.S. hospitals, 1997.HCUP fact book no. 2. In:agency for healthcare research and quality,Rockville, MD;2001.
- Anderson L, Krathwohl DR, Airasian PW, Cruikshank KA, Mayer RE, Pintrich PR, et al., editors.A taxonomy for learning, teaching, and assessing. In: A Revision of Bloom's Taxonomy of Educational Objectives.Upper Saddle River, NJ: Addison Wesley Longman, Inc. Pearson Education USA;2001.
- Society of Hospital Medicine (SHM). Definition of a Hospitalist. http://www.hospitalmedicine.org/AM/Template.cfm?Section=General_Information 2009.
- .Pediatric Hospitalists Membership Numbers. In.Philadelphia:Society of Hospital Medicine, PA 19130;2009.
- , .The emerging role of “hospitalists” in the American health care system.N Engl J Med.1996;335:514–517.
- .The future of hospital medicine: evolution or revolution?.Am J Med.2004;117:446–450.
- , .The hospitalist movement 5 years later.JAMA.2002;287:487–494.
- , , , , .Variation in pediatric hospitalists' use of proven and unproven therapies: A study from the Pediatric Research in Inpatient Settings (PRIS) network.J Hosp Med.2008;3(4):292–298.
- , , .Pediatric hospitalists: Training, current practice, and career goals.J Hosp Med.2009;4(3):179–186.
- , .Standardize to excellence: improving the quality and safety of care with clinical pathways.Pediatr Clin North Am.2009;56(4):893–904.
- .Evolution of a new specialty ‐ a twenty year pediatric hospitalist experience [Abstract]. In:National Association of Inpatient Physicians (now Society of Hospital Medicine).New Orleans, Louisiana;1999.
- , , , , , , et al.Pediatric hospitalists: report of a leadership conference.Pediatrics.2006;117(4):1122–1130.
- , , , , e.The core competencies in hospital medicine: a framework for curriculum development.J Hosp Med.2006;1(Suppl 1).
- American Board of Internal Medicine. Questions and answers regarding ABIM recognition of focused practice in hospital medicine through maintenance of certification. http://www.abim.org/news/news/focused‐practice‐hospital‐medicine‐qa.aspx. Published 2010. Accessed January 6,2010.
- .Comprehensive pediatric hospital medicine.N Engl J Med.2008;358(21):2301–2302.
- The Joint Commission. Performance measurement initiatives. http://www. jointcommission.org/PerformanceMeasurement/PerformanceMeasurement/. Published 2010. Accessed December 5,2010.
- The Joint Commission. Standards frequently asked questions: comprehensive accreditation manual for critical access hospitals (CAMCAH). http://www.jointcommission.org/AccreditationPrograms/CriticalAccess Hospitals/Standards/09_FAQs/default.htm. Accessed December 5,2008; December 14, 2009.
- , , , , .Infectious disease hospitalizations among infants in the United States.Pediatrics.2008;121(2):244–252.
- , , , .Procedures in U.S. hospitals, 1997.HCUP fact book no. 2. In:agency for healthcare research and quality,Rockville, MD;2001.
- Anderson L, Krathwohl DR, Airasian PW, Cruikshank KA, Mayer RE, Pintrich PR, et al., editors.A taxonomy for learning, teaching, and assessing. In: A Revision of Bloom's Taxonomy of Educational Objectives.Upper Saddle River, NJ: Addison Wesley Longman, Inc. Pearson Education USA;2001.
Copyright © 2010 Society of Hospital Medicine
Electronic Health Records Get the Green Light
Now that the Centers for Medicare and Medicaid Services (CMS) has defined "meaningful use" of electronic health records (EHR), hospitalists know what's expected of them in order to grab a piece of the $20 billion set aside for doctors and hospitals that adopt new technologies.
CMS’ final rule (PDF) is less restrictive than the proposed rule put forth in January, but it still challenges HM groups and their respective institutions to meet new guidelines to make digital record-keeping routine. Stage-one rules, which take effect next year, require eligible physicians (EPs) and eligible hospitals to meet goals in 15 and 14 categories, respectively. Up to five goals can be deferred, according to CMS. The CMS timeline includes second and third stages, each of which will require goals that are even more advanced.
Some hospitalists feared the rules in stage one would be punitively strict, says Robert Lineberger MD FHM, medical information officer at Durham (N.C.) Regional Hospital, part of the Duke University Health System. “What it means is the government is serious about helping people instead of being as strict as it appeared they were going to be,” says Dr. Lineberger, who serves on SHM's IT Core Committee. “I think people are overall pretty pleased there was a relaxation.”
The road to full adoption of EHR is far from complete, and hospitals that have yet to put in place even the most basic electronic infrastructure might struggle to meet even the lowest thresholds.
And while specific standards for future stages have not been codified, “like everything else that goes on in the hospital, [HM] should be in the middle of that,” Dr. Lineberger says.
Now that the Centers for Medicare and Medicaid Services (CMS) has defined "meaningful use" of electronic health records (EHR), hospitalists know what's expected of them in order to grab a piece of the $20 billion set aside for doctors and hospitals that adopt new technologies.
CMS’ final rule (PDF) is less restrictive than the proposed rule put forth in January, but it still challenges HM groups and their respective institutions to meet new guidelines to make digital record-keeping routine. Stage-one rules, which take effect next year, require eligible physicians (EPs) and eligible hospitals to meet goals in 15 and 14 categories, respectively. Up to five goals can be deferred, according to CMS. The CMS timeline includes second and third stages, each of which will require goals that are even more advanced.
Some hospitalists feared the rules in stage one would be punitively strict, says Robert Lineberger MD FHM, medical information officer at Durham (N.C.) Regional Hospital, part of the Duke University Health System. “What it means is the government is serious about helping people instead of being as strict as it appeared they were going to be,” says Dr. Lineberger, who serves on SHM's IT Core Committee. “I think people are overall pretty pleased there was a relaxation.”
The road to full adoption of EHR is far from complete, and hospitals that have yet to put in place even the most basic electronic infrastructure might struggle to meet even the lowest thresholds.
And while specific standards for future stages have not been codified, “like everything else that goes on in the hospital, [HM] should be in the middle of that,” Dr. Lineberger says.
Now that the Centers for Medicare and Medicaid Services (CMS) has defined "meaningful use" of electronic health records (EHR), hospitalists know what's expected of them in order to grab a piece of the $20 billion set aside for doctors and hospitals that adopt new technologies.
CMS’ final rule (PDF) is less restrictive than the proposed rule put forth in January, but it still challenges HM groups and their respective institutions to meet new guidelines to make digital record-keeping routine. Stage-one rules, which take effect next year, require eligible physicians (EPs) and eligible hospitals to meet goals in 15 and 14 categories, respectively. Up to five goals can be deferred, according to CMS. The CMS timeline includes second and third stages, each of which will require goals that are even more advanced.
Some hospitalists feared the rules in stage one would be punitively strict, says Robert Lineberger MD FHM, medical information officer at Durham (N.C.) Regional Hospital, part of the Duke University Health System. “What it means is the government is serious about helping people instead of being as strict as it appeared they were going to be,” says Dr. Lineberger, who serves on SHM's IT Core Committee. “I think people are overall pretty pleased there was a relaxation.”
The road to full adoption of EHR is far from complete, and hospitals that have yet to put in place even the most basic electronic infrastructure might struggle to meet even the lowest thresholds.
And while specific standards for future stages have not been codified, “like everything else that goes on in the hospital, [HM] should be in the middle of that,” Dr. Lineberger says.
New Study Rebuffs Physician Training Misperceptions
A new study comparing physicians who were trained in the U.S. with those trained in medical schools abroad should offer reassurance to patients, families, and professional peers who hold biases against foreign-born or foreign-trained physicians, the lead author says.
John Norcini, PhD, CEO of the Foundation for Advancement of International Medical Education and Research, and colleagues studied 244,000 hospitalized Pennsylvania patients with congestive heart failure and acute myocardial infarction. They found that mortality rates were slightly lower for physicians who were trained abroad and were not U.S. citizens when they entered medical school. The study showed higher rates for U.S. citizens who went overseas for their medical training.
The Norcini study (Health Affairs. 2010;29:1461-1468) focused on family medicine, internal medicine, and cardiology physicians, but it did not identify hospitalists. One-quarter of all physicians practicing in the U.S. are foreign-trained; however, a greater proportion are found in primary care and internal medicine. For hospitalists, the foreign-trained percentage might be even higher, 40% according to Philip Miller of the physician recruiting firm Merritt Hawkins.
One thing that can be said about international medical graduates is that they are a “crucial and growing part of the hospital medicine workforce, and we welcome them,” says Winthrop Whitcomb, MD, MHM, former SHM president and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. “I find, having worked with physicians trained all over the world, that for the best ones, it’s what they do every day, not where they came from. Are they consistent, careful, compassionate and committed to improving day by day?”
The challenge for hospitalist groups, he adds is to clearly state expectations for physicians, hold them accountable, make sure they understand the group’s goals and standards, and offer the tools they need to improve. An example could be access to English as a Second Language instruction to enhance communication.
A new study comparing physicians who were trained in the U.S. with those trained in medical schools abroad should offer reassurance to patients, families, and professional peers who hold biases against foreign-born or foreign-trained physicians, the lead author says.
John Norcini, PhD, CEO of the Foundation for Advancement of International Medical Education and Research, and colleagues studied 244,000 hospitalized Pennsylvania patients with congestive heart failure and acute myocardial infarction. They found that mortality rates were slightly lower for physicians who were trained abroad and were not U.S. citizens when they entered medical school. The study showed higher rates for U.S. citizens who went overseas for their medical training.
The Norcini study (Health Affairs. 2010;29:1461-1468) focused on family medicine, internal medicine, and cardiology physicians, but it did not identify hospitalists. One-quarter of all physicians practicing in the U.S. are foreign-trained; however, a greater proportion are found in primary care and internal medicine. For hospitalists, the foreign-trained percentage might be even higher, 40% according to Philip Miller of the physician recruiting firm Merritt Hawkins.
One thing that can be said about international medical graduates is that they are a “crucial and growing part of the hospital medicine workforce, and we welcome them,” says Winthrop Whitcomb, MD, MHM, former SHM president and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. “I find, having worked with physicians trained all over the world, that for the best ones, it’s what they do every day, not where they came from. Are they consistent, careful, compassionate and committed to improving day by day?”
The challenge for hospitalist groups, he adds is to clearly state expectations for physicians, hold them accountable, make sure they understand the group’s goals and standards, and offer the tools they need to improve. An example could be access to English as a Second Language instruction to enhance communication.
A new study comparing physicians who were trained in the U.S. with those trained in medical schools abroad should offer reassurance to patients, families, and professional peers who hold biases against foreign-born or foreign-trained physicians, the lead author says.
John Norcini, PhD, CEO of the Foundation for Advancement of International Medical Education and Research, and colleagues studied 244,000 hospitalized Pennsylvania patients with congestive heart failure and acute myocardial infarction. They found that mortality rates were slightly lower for physicians who were trained abroad and were not U.S. citizens when they entered medical school. The study showed higher rates for U.S. citizens who went overseas for their medical training.
The Norcini study (Health Affairs. 2010;29:1461-1468) focused on family medicine, internal medicine, and cardiology physicians, but it did not identify hospitalists. One-quarter of all physicians practicing in the U.S. are foreign-trained; however, a greater proportion are found in primary care and internal medicine. For hospitalists, the foreign-trained percentage might be even higher, 40% according to Philip Miller of the physician recruiting firm Merritt Hawkins.
One thing that can be said about international medical graduates is that they are a “crucial and growing part of the hospital medicine workforce, and we welcome them,” says Winthrop Whitcomb, MD, MHM, former SHM president and medical director of healthcare quality at Baystate Medical Center in Springfield, Mass. “I find, having worked with physicians trained all over the world, that for the best ones, it’s what they do every day, not where they came from. Are they consistent, careful, compassionate and committed to improving day by day?”
The challenge for hospitalist groups, he adds is to clearly state expectations for physicians, hold them accountable, make sure they understand the group’s goals and standards, and offer the tools they need to improve. An example could be access to English as a Second Language instruction to enhance communication.
Inpatient Smoking Cessation Program
In 1992, the Joint Commission on Accreditation of Healthcare Organizations (Joint Commission) introduced standards to make hospital buildings smoke‐free, resulting in the nation's first industry‐wide ban on smoking in the workplace. This hospital smoking ban has led to increased smoking cessation among employees.1 Since 2003, core measures from the Joint Commission and quality indicators from the Centers for Medicare and Medicaid Services have included inpatient smoking cessation counseling for acute myocardial infarction, pneumonia, and heart failure, as national guidelines strongly recommend smoking cessation counseling for patients with these diseases who smoke.25
The Department of Health and Human Services (DHHS) 2008 update on Clinical Practice Guidelines for Treating Tobacco Use and Dependence6 recommends that clinicians use hospitalization as an opportunity to promote smoking cessation and to prescribe medications to alleviate withdrawal symptoms. Hospitalization is an opportune time for smoking cessation because patients are restricted to a smoke‐free environment in the hospital and, increasingly, on hospital campuses.6 The illness leading to hospitalization may be attributable, at least in part, to tobacco use, thereby increasing the patient's receptivity to cessation counseling. Last, medications used in‐hospital to treat nicotine withdrawal symptoms may lead to continued or future use of these medications that, in turn, may ultimately lead to a successful quit attempt.
We report on the outcomes of our hospital's attempt to do this in the context of implementation of a smoke‐free medical campus.7 This study was designed to measure whether an inpatient smoking cessation intervention increases the likelihood of smoking cessation 6 months post‐hospital discharge. Because effectiveness studies are the next step to improving translation of research into health promotion practice,8 we set out to measure what the impact of this intervention would be in routine clinical practice as opposed to a carefully structured efficacy trial.
Methods
Intervention
The Smoking Cessation service for inpatients began on April 3, 2006. Upon admission, all patients were screened regarding their current smoking status. The nurse asked the patient if s/he currently smoked and then entered the responses into the hospital electronic medical record (EMR). A current smoker was defined as smoking every day or some days within the past 30 days. A roster of newly admitted current smokers was electronically transmitted to the Respiratory Care office daily. Only current smokers received counseling. The Smoking Cessation Specialist (SCS) subsequently saw inpatients within a 24‐hour time frame of admission, except for weekends and holidays. Each patient received 1 to 2 intensive follow‐up counseling sessions during hospitalization. An average of 10 patients per day were seen.
The goal of the inpatient smoking cessation service was to counsel patients on the health effects of smoking, address nicotine withdrawal symptoms, explain the different pharmacotherapies available, advise on how to quit, give self‐help materials, counsel family members, and refer to the New York State (NYS) Smokers' Fax‐to‐Quit program.9 Following the consult, the SCS documented the encounter in the patient's chart, including recommendations for nicotine replacement therapy (NRT) or bupropion (varenicline was not addressed as it was not on the formulary). The chart documentation informed the physician and nursing staff of the intervention and included the date/time, stage of change, and support action taken.
The SCS was part‐time, had nursing training, smoking cessation training,10 and was also trained by the Seton Health Cessation Center in the Butt Stops Here Program.11 She also implemented a performance improvement plan to increase the provision of smoking cessation counseling, increase NRT or bupropion prescriptions to smokers admitted to the hospital, and increase referrals to the NYS telephone quitline through the Fax‐to‐Quit program for outpatient resources and help following hospital discharge. The Fax‐to‐Quit program allows health care providers to refer patients to the NYS quitline via fax, with the patient's signature (patient permission) on the fax to quit form. After hospital discharge, the quitline then contacts the patient at a time that the patient requested.
The SCS visited patients with all admitting diagnoses on the medical, surgical, and special care units who were current smokers. Inpatients admitted to psychiatry, obstetrics, and the intensive care unit (ICU) were not seen by the SCS, except for ICU patients referred by a physician. Inpatients who had short stays or who were admitted and discharged in 1 day or during the weekend were not seen.
The intervention included either a brief 3‐minute to 5‐minute intervention or a more intensive intervention, that required 10 to 20 minutes (18 minutes average). The length of the intervention was determined by how receptive the patient was to the intervention. All interventions began with patient identification, an introduction to the SCS, and an explanation of the purpose of the visit. The SCS then inquired about the patient's comfort level vis‐a‐vis nicotine withdrawal and if s/he was receiving any NRT while in the hospital (NRT on the inpatient formulary included the nicotine patch or gum). If the patient was receptive to counseling, the SCS then began to work through the 5 A's, as described in the 2000 DHHS Clinical Practice Guidelines.12 The 2000 DHHS Clinical Practice Guidelines were used because the 2008 update had not been released at the time this study was initiated in 2006. These include: asking about smoking status, advising on how to quit, assessing readiness to quit, and assisting in arranging treatment options that include pharmacotherapy, counseling, as well as referral to the NYS Smokers' Quitline. A workbook was provided to reinforce counseling but was not necessarily used during counseling session. A compact disc (CD) with relaxation exercises5 was provided to those inpatients who were interested in stress reduction. If family members were present, and were also smokers, they were included in the counseling session, if willing. Each patient was offered a referral via the Fax‐to‐Quit program to continue treatment on an outpatient basis.
If the patient was not motivated to quit or declined the consult, the visits were short and focused on the patient's experience with nicotine withdrawal. These patients were also given self‐help materials and, if possible, the relevance of and roadblocks to quitting were reviewed. Patients were prompted to think about why quitting was relevant and often the reason for hospitalization was used to motivate the quitting process.
Upon hospital discharge, the patient's primary care provider was notified of the cessation intervention by a letter from the SCS. The letter described the intervention and stated whether or not the patient agreed to be referred to the Fax‐to‐Quit Program.
Study Participants
Patients were recruited from July 1, 2006 (after the smoking ban went into effect) through June 1, 2008. Inpatients who currently smoked were informed of this study and were asked to sign informed consent to participate after they were seen by the SCS. Current smokers of all admitting diagnoses were recruited into the study. Patients provided informed consent for a telephone interview 6 months posthospital discharge. A written Health Insurance Portability and Accountability Act (HIPAA) release was obtained to allow access to an individual's specific EMR.
A comparison group of inpatients who were also current smokers, but who did not receive the intervention were also contacted six months after hospitalization. Reasons for not receiving the intervention included the fact the SCS was part‐time and also took a leave of absence during the study and therefore could not see all inpatients who currently smoked. Other reasons for not receiving the intervention include too short a stay for the SCS to see the patient or the patient was out of the room for tests or procedures when the SCS was available. These patients provided informed consent to be interviewed 6 months after hospital discharge and HIPAA consent for access to their medical record. Not all inpatients in the comparison group provided written HIPAA release for use of their medical record; therefore, these patients were excluded because their baseline demographic and diagnostic data were missing.
Sample‐size considerations were driven around having adequate numbers of subjects to measure the prevalence of smoking cessation at 6 months post‐hospital discharge with an acceptable degree of precision. Prevalence estimates from previous studies for 6‐month cessation typically range from 20% to 30%, with cessation rates as high as 67% (this estimate applies to postmyocardial infarction patients.)13 For conservative estimation, we used 50% as the 6‐month prevalence of cessation in the current study, which placed binomial variance at its theoretical maximum. In this case, a sample of 300 subjects provides a margin of error of 0.058 for a 95% confidence interval around this point estimate.
Data Sources
The hospital EMR database was used to monitor several components of the program: nursing screening, smoking cessation counseling, and pharmacy dispensing of NRT and bupropion. The screening data were also used to monitor the proportion of current smokers admitted during the study period. Elements of the EMR were used to define the following covariates: patient age, gender, ethnicity, and the primary discharge diagnosis (via International Statistical Classification of Diseases and Related Health Problems, 9th edition [ICD9] codes) and readmission during the six month follow‐up period. Mean length of stay (LOS) was computed. The Elixhauser Comorbidity Index that utilizes ICD9 codes was used for comorbidity risk adjustment.14
Study participants were contacted by phone 6 months posthospital discharge. Data collection began July 1, 2006 and was completed January 1, 2009. The interview focused on self‐reported point prevalence of smoking and 6‐month quit status. The point prevalence for self‐reported abstinence was derived from the question Do you now smoke cigarettes every day, some days, or not at all?15 Self‐reported quit status was derived from question Have you quit smoking since you were discharged from the hospital? In addition, respondents were queried about their number of years smoked, post‐hospital discharge number of quit attempts, and cessation efforts (NRT, self‐help groups, quitline use, etc.). Last, they were surveyed about barriers to cessation (exposure to secondhand smoke, rules about smoking in the home or car), educational level, employment, and health ratings.
To determine the status of those lost to follow‐up, administrative and EMR databases for appointments and follow‐up visits were accessed to determine if the patient was alive during the 6 months between discharge and the follow‐up call. To confirm mortality, we searched the Internet, Ancestry.com, and/or local newspaper obituaries for dates of death for all patients to validate that they had not died during the 6‐month follow‐up. World wide web searches can identify 97% of deaths listed in the Centers for Disease Control and Prevention (CDC)/National Death Index, which is considered the gold standard in epidemiologic studies.16
Analysis
Univariate analysis of all covariates was completed to examine the normal distribution curves for these variables. Bivariate correlation analysis of all the independent variables by study group was performed to assess comparability of the study groups at baseline. The self‐reported cessation outcomes were calculated by dividing the number of patients who said they were not using tobacco or had quit, at 6 months posthospital discharge by the number of individuals in the study group at baseline minus those who had died. Both the intent to treat method, which assumes patients lost to follow‐up were still smoking, and the responder method, which does not include nonresponders in the analysis, were used to adjust the denominators for these outcomes.
Multivariate regression analysis was then used to model receipt of the intervention as predictor of self‐reported quit status adjusted for significant covariates. Statistical significance was defined by a P value of less than 0.05.
Survival analysis was employed to model differences in mortality between the study groups, controlling for any baseline imbalances (eg, comorbidity). Because baseline data were used in this model, the model includes only patients with signed a HIPAA release.
Internal review boards of our hospital and the NYS Department of Health reviewed and approved this study.
Results
From January 1, 2007 to May 30, 2008, 660 inpatients who were current smokers were recruited into the study. Figure 1 summarizes patient flow through the study and explains the final sample size of 607. Exclusions include 52 inpatients from the study who completed the 6‐month interview but who did not return a written HIPAA release. Without a HIPAA release to access the EMR, baseline comparison of the study groups and adjustment for comorbidity could not be completed for these patients. At 6 months posthospital discharge, 53 subjects refused the interview when contacted by telephone.
As might be expected in a quasiexperimental design, the study groups were not equivalent at baseline (Table 1). The intervention and comparison groups differed with regard to age, length of stay (LOS), proportion of acute admissions, and the Elixhauser comorbidity index. These differences suggest that the intervention group was older, had a longer LOS, higher acuity at the time of admission, and more comorbidities. In addition, as a result of the intervention, the intervention group was more likely to receive NRT or bupropion in hospital and a Fax‐to‐Quit referral to the NYS Smokers' Quitline. In the intervention group, most patients received 1 visit from the SCS, only 2% received 2 visits. Family members were included in smoking cessation counseling for 58% of the intervention group.
| Intervention (n = 275) | Comparison (n = 335) (P value) | |
|---|---|---|
| ||
| Sex (% male) | 51 | 51 |
| Mean age (years) | 51.4 | 48.5 (0.03) |
| Ethnicity (% white) | 98 | 97 |
| Marital status (% married) | 48 | 47 |
| Elective admission (vs. acute) (%) | 25 | 31 |
| Inpatient (vs. outpatient observation or outpatient surgical admission) (%) | 86 | 68 (0.00) |
| LOS (days) | 3.80 | 2.68 (0.00) |
| Elixhauser comorbidity index (mean) | 1.66 | 1.17 (0.00) |
| Used NRT in hospital (%) | 37 | 19 (0.00) |
| Used bupropion in hospital (%) | 4 | 1 (0.00) |
| Referred to NYS Smokers' Quitline using Fax‐to‐Quit | 10 | 0 (0.00) |
| Mean cigarettes per day* | 17.7 (n = 213) | 15.9 (n = 192) |
As shown in Table 2, there was a significant amount of diagnostic heterogeneity in the discharge diagnoses codes of patients included in the study. However, there were significantly more patients in the intervention group with a first discharge diagnosis of cardiovascular disease (25%) compared to the comparison group (12%; P = 0.00).
| Intervention (n = 274)* (%) | Comparison (n = 333)* (%) | |
|---|---|---|
| ||
| Cardiovascular | 25 | 12, P = 0.00 |
| Pulmonary | 16 | 7 |
| Orthopedics | 12 | 12 |
| Injury | 10 | 15 |
| GI | 8 | 16 |
| Cancer | 6 | 8 |
| GU | 3 | 6 |
| Endocrine | 3 | 3 |
| Other | 17 | 21 |
Readmission outcomes based on EMR and administrative data were available for 607 inpatients with signed HIPAA releases. The readmission rate was higher for the intervention (41%) than the comparison group (20%). Despite a higher readmission rate, the crude mortality within the 6 months posthospital discharge was lower for the intervention group, ie, 0.02 (6/276), than the comparison group, which had a crude mortality of 0.04 (16/384) during this period.
A multivariate survival model, controlling for age, sex, Elixhauser comorbidity index, LOS, and cardiovascular diagnosis, showed a significantly reduced mortality in the intervention group (hazard ratio [HR] = 0.37; P = 0.04). Although cardiac status (P = 0.09) and LOS (P = 0.15) were not significant in this model, they were retained because both of these variables showed significantly higher levels (along with the Elixhauser Index) at baseline in the intervention group, implying that the intervention group was sicker than the comparison group. The Elixhauser comorbidity index (HR = 1.42; P < 0.00) and age (HR = 1.07; P < 0.00) were the only other significant predictors of mortality in this model.
Among those responding to the interview at 6 months post‐hospital discharge (n = 326), there were no significant differences between the study groups with regard to age first started smoking, gender, educational level, employment status, ethnicity, or physical health status (data not shown). Table 3 summarizes the outcomes by the intervention and comparison groups at 6 months post‐hospital discharge. The point prevalence for abstinence was 27% in the intervention group compared to 19% in the comparison group (P = 0.09). Using the intent to treat analysis, the point prevalence for abstinence was 16% in the intervention group compared to 9.8% in the comparison group (P = 0.02). Self‐reported quit status was 63% in the intervention group vs. 48% in the comparison group (P = 0.00). Using the intent to treat analysis, quit status was 44% in the intervention group vs. 30% in the comparison group (P = 0.00). Exclusion of the 52 patients without signed HIPAA releases (Figure 1) did not significantly alter these outcomes.
| Intervention (n = 161) | Comparison (n = 165) (P value) | |
|---|---|---|
| ||
| Self‐reported now smoking not at all (%) | 16 | 10 (0.02) |
| Self‐reported quit within 6 months (%) | 63 | 48 (0.00 |
| Tried to quit (%) | 68 | 62 |
| Used NRT post‐D/C (%) | 26 | 17 (0.04) |
| Used other intervention (%) | 21 | 14 |
| Heard of the NYS Smokers' Quitline (%) | 92 | 90 |
| Aware that NYS Quitline offers NRT (%) | 73 | 49 (0.00) |
| Received free NRT from NYS Smokers' Quitline (%) | 9 | 6 |
| Used NYS Smokers' Quitline (%) | 15 | 9 |
| Called by the NYS Smokers' Quitline (%) | 11 | 5 |
| Self‐rated health status as fair or poor (%) | 48 | 36 |
| Another smoker living at home (%) | 54 | 48 |
| Mean hours spent in same room where someone else was smoking (n) | 20 | 21 (0.04) |
| Households in which smoking is not allowed in the home (%) | 40 | 33 |
| Patients Still Smoking at the 6‐Month Interview | Intervention (n = 118) | Comparison (n = 134) |
| Mean cigarettes currently smoked (n) | 10.5 | 12.7 |
| Mean quit attempts post‐D/C (n) | 3.2 | 3.5 |
| Mean reduction in smoking* (cigarettes/day) | 5.83 | 4.09 |
Patients who received the inpatient smoking cessation counseling were more likely to be called by or use the NYS Smokers' Quitline; however, these differences were not statistically significant. There was no difference between the study groups in awareness of the Quitline but the intervention group was more aware that free NRT was offered by the NYS Quitline. In terms of quit methods used during the 6‐month period (Table 4), NRT or bupropion use was higher in the intervention group. There were no other significant differences between the study groups, except for the use of acupuncture.
| Intervention (n = 91) | Comparison (n = 93) (P value) | |
|---|---|---|
| ||
| Got help from friends or family (%) | 58 | 50 |
| Used any medication to quit (%) | 44 | 28 (0.02) |
| Used nicotine patch (%) | 43 | 25 (0.00) |
| Used bupropion (%) | 10 | 1 (0.00) |
| Used varenicline (%) | 32 | 25 |
| Cut back (%) | 43 | 46 |
| Quit with a friend (%) | 20 | 13 |
| Switched to lights (%) | 18 | 13 |
| Used print material (%) | 14 | 16 |
| Got help from the NYS Smokers' Quitline (%) | 11 | 9 |
| Called by the NYS Smokers' Quitline (%) | 11 | 5 (0.09) |
| Counseling (%) | 9 | 3 |
| Acupuncture (%) | 5 | 0 (0.02) |
| Switched to chew (%) | 2 | 4 |
| Attended classes (%) | 3 | 1 |
| Used NYS Smokers' Quitline website (%) | 2 | 4 |
Multivariate analysis predicting quit status at 6 months post‐hospital discharge included covariates controlling for age, sex, LOS, study group, and comorbidity. This analysis showed that patients with a cardiovascular discharge diagnosis were more likely to quit than patients who had other discharge diagnoses (odds ratio [OR], 3.02; 95% confidence interval [CI], 1.65.7; P = 0.00). Another statistically significant covariate in this model included sex (men were more likely to quit: OR, 0.61; 95% CI, 0.390.97; P = 0.04). Participating in the inpatient intervention group was marginally significant when controlling for these other variables (OR, 1.54; 95% CI, 0.982.45; P = 0.06). Hospital LOS, age, receipt of NRT in hospital, and the Elixhauser comorbidity index were not predictive of quit status at 6 months.
Discussion
This study demonstrates how effective an inpatient smoking cessation program can be for increasing the success of quitting smoking after hospital discharge. At 6 months posthospital discharge, the intervention group had significantly higher intent to treat outcomes for point prevalence abstinence and quit status as well as lower crude and adjusted mortality than the comparison group.
Although at baseline the intervention group was older, had a longer LOS, more cardiovascular diagnoses, and higher comorbidity index, crude post‐hospital discharge mortality was significantly less in the intervention group (0.02) than in the comparison group (0.04). This finding is more significant in light of the higher comorbidity and acuity of the intervention group at baseline. Our multivariate survival model that controlled for these imbalances at baseline demonstrated that the intervention group had significantly less mortality than the comparison group (HR = 0.37; P = 0.04). Reduction in mortality, as soon as 30 days after inpatient smoking cessation counseling, has been demonstrated postmyocardial infarction.17, 18 Intensive smoking cessation quit services were also linked with lower all cause mortality among cardiovascular disease patients 2 years posthospitalization.19 Our study, despite its relatively small sample size, demonstrates that the intervention retains its impact on mortality in real‐world settings.
Following participation in an inpatient smoking cessation program, self‐reported quit status at 6 months post‐hospital discharge in the intervention group was significantly higher in the intervention group (63%) than the comparison group (48%; P = 0.00). Using the intent to treat method, the differences between the study groups was still significant (44% in the intervention group, 30% in the comparison group; P = 0.00). Given the limitations of self‐report and responder bias, the actual outcomes fall somewhere between these 2 estimates. In an effectiveness study of inpatient smoking cessation involving 6 hospitals in California, self‐reported quit rates of 26% at 6 months were reported; however, different methods were used so the results are not strictly comparable.20
Our multivariate analysis suggests that patients with cardiovascular discharge diagnosis were more likely to quit than patients who had other discharge diagnoses (OR, 3.02; 95% CI, 1.65.7; P = 0.0007). This study extends findings of other studies that show that the success of smoking cessation may vary by diagnosis, particularly for smokers admitted for cardiovascular disease.21, 22 Other studies have shown that smoking cessation rates among patients post‐myocardial infarction were higher in admitting facilities that had hospital‐based smoking cessation programs and for those patients referred to cardiac rehabilitation.23 Thus, the availability of a hospital‐based smoking cessation program may be considered a structural measure of health care quality as suggested by Dawood et al.23
The use of NRT greatly increased in our hospital, coincident with the start of the inpatient cessation program7 and, in this study, NRT use appears to continue after hospital discharge. Some studies show an additive effect of NRT combined with cessation counseling.24, 25 Although a Cochrane review did not find a statistically significant difference, there was a trend toward higher quit rates with the addition of NRT.21, 22
Because hospitalized smokers may be more motivated to stop smoking, the updated 2008 DHHS clinical practice guidelines for Treating Tobacco Use and Dependence now recommend that all inpatients who currently smoke be given medications, advised, counseled, and receive follow‐up after discharge.26 Although our inpatient cessation program was started before these clinical practice guidelines were updated, we have had the opportunity to evaluate the recommended practice of inpatient tobacco cessation counseling. Compared to effects shown in efficacy studies, clinical interventions often lose effect size in daily practice and real‐world settings.27, 28 It is reassuring that, in this effectiveness study, the impact of this intervention is still demonstrable.
Provision of inpatient smoking cessation has been shown to be an effective smoking cessation intervention if combined with outpatient follow‐up.29 Reviews by Rigotti et al.21, 22 recommend that inpatient high‐intensity behavioral interventions should be followed by at least 1 month of supportive contact after discharge to promote smoking cessation among hospitalized patients. In our study, specific cessation‐related outpatient follow‐up was not provided by our program. Although letters were sent to primary care providers describing the cessation service provided during the inpatient stay, our study could not ascertain what specific cessation service was offered by either primary‐care or specialty‐care providers during posthospitalization follow‐up visits. An efficient alternative to outpatient visits may be follow‐up delivered via a quitline. Follow‐up in our study included referrals to the NYS Smokers' Quitline; however, only about 10% of inpatient reported using this service. While feasible, the effectiveness of quitline follow‐up is as yet unknown.30
Limitations
This study targets a later phase in research progression from hypothesis development, pilot studies, efficacy (empirically supported) trials, effectiveness trials (real‐world settings), and dissemination studies.31 Because this study addresses the effectiveness rather than the efficacy of inpatient smoking cessation counseling, the use of a quasiexperimental rather than randomized controlled clinical trial design led to measured differences in the study groups at baseline. An important imbalance arose in the intervention group that had twice the percentage of patients with cardiovascular‐related discharge diagnoses as the comparison group. While we were able to adjust for these differences in our analysis, there may be unmeasured differences due to the fact that the inpatients were not randomized to the study groups.
The outcomes of this study cannot be attributed to any one component of the intervention (eg, NRT) vs. the combined effect of the inpatient smoking cessation program. The program components were implemented simultaneously in order to maximize synergistic effects; therefore, the effects of program components are difficult to disaggregate.
The results are limited by the validity of self‐report of smoking status. It is well known that research studies which validate smoking status biochemically have lower efficacy (OR, 1.44; 95% CI, 0.992.11) than those that do not validate smoking status (OR, 1.92; 95% CI, 1.262.93).32 Although it was impractical in this effectiveness study to biochemically validate smoking status 6 months posthospital discharge, we have documented a significant difference between the study groups that confirms the direction of the effect, if not the effect size.
Self‐reports tend to underestimate smoking status in population studies33; however, the discrepancy between self‐reported smoking and biochemical measurements among clinical trial participants is small.34 However, a small but significant bias toward a socially desirable response in intervention groups compared to control groups of 3% with carbon monoxide and 5% for cotinine has been documented.35 If social desirability bias is operative in this study, and if we apply the above correction factor of 4% to correct this classification error, then the difference between the intervention and comparison group would be 10 percentage points (40% in the intervention group vs. 30% in the comparison group using the intention to treat estimates). That difference is still clinically relevant.
The observed difference between the intervention and comparison group is underestimated because the comparison group was exposed to smoking cessation as well both at the time of admission and following discharge (Table 4). The comparison group in this study could thus be viewed as a usual care group rather than a control group. That exposure does cloud the measurement of quit rates as the comparison group is contaminated to some degree by exposure to various cessation methods. The impact of this exposure is to reduce the effect size observed in this study or underestimate the effect of the inpatient smoking cessation counseling because the comparison group was exposed other cessation methods, although to a lesser extent.
The social desirability bias inherent in self‐reported smoking status may increase the effect size while the use of comparison group that received usual care may decrease the effect size. Because neither of these biases could be measured in this study, it is impossible to say whether they negated each other.
As with any administrative database, use of EMR as a data source in this study led to missing data that precluded use of certain variables in the analysis. In addition, lack of written and signed HIPAA releases also precluded inclusion of several inpatients, mostly in the comparison group, in the analytic database. However, it is reassuring that the results of the 6‐month survey did not differ significantly when these individuals were included or excluded from a separate analysis of the survey data. Last, our study population is almost 100% Caucasian thus limiting how generalizable the results are to more heterogenous patient populations.
Conclusions
This quasiexperimental effectiveness study showed that inpatient smoking cessation intervention improved smoking cessation outcomes, use of NRT, and was associated with a decreased mortality 6 months post‐hospital discharge. The effectiveness of this inpatient intervention is maintained in real world settings but may be improved with posthospital discharge follow‐up.
Acknowledgements
The authors are grateful to the many Mary Imogene Bassett Hospital staff in administration, nursing, inpatient pharmacy, medical education, patient care service, and respiratory care who provided data needed to evaluate this program. They also acknowledge the NYS Smokers' Quitline website for data provided about monthly Fax‐to‐Quit program referrals from our county.
- , , , , , .“Implementing smoking bans in American hospitals: results of a national survey.Tob Control.1998;7(1):47–55.
- The Smoking Cessation Clinical Practice Guideline Panel and Staff: the Agency for Health Care Policy and Research Smoking Cessation Clinical Practice Guideline.JAMA.1996;275(16):1270–1280.
- , , , et al.ACC/AHA clinical performance measures for adults with chronic heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Heart Failure Clinical Performance Measures). Endorsed by the Heart Failure Society of America.J Am Coll Cardiol.2005;46(6):1144–1178.
- , , , et al.ACC/AHA guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction).Circulation.2004;110(9):e82–e292.
- , , , et al.ACC/AHA clinical performance measures for adults with ST‐elevation and non‐ST elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures on ST‐Elevation and Non‐ST‐Elevation Myocardial Infarction).J Am Coll Cardiol.2006;47(1):236–265.
- Treating Tobacco Use and Dependence‐Clinicians Packet. A How‐To Guide For Implementing the Public Health Service Clinical Practice Guideline, March2003. Rockville, MD: U.S. Public Health Service, Agency for Healthcare Research and Quality. Available at: http://www.ahrq.gov/clinic/tobacco. Accessed November 2009.
- , , , .Implementing a smoke‐free medical campus: impact on inpatient and employee outcomes.J Hosp Med.2010;5(1):51–54.
- , , , et al.The future of behavior change research: what is needed to improve translation of research into health promotion practice?Ann Behav Med.2004;27:3–12.
- The New York State Smokers' Quitline. Available at: http://www.nysmokefree.com. Accessed November2009.
- Tobacco Cessation Continuing Education for Healthcare Professionals and Counselors. Available at: http://www.tobaccocme.com. Accessed November2009.
- Seton Health Cessation Center. The Butt Stops Here. Relaxation Exercises for Smoking Cessation. 2001. The Butt Stops Here Program. Available at: http://www.setonhealth.org. Accessed November2009.
- U.S. Department of Health and Human Services.Treating Tobacco Use and Dependence. Clinical Practice Guideline.Rockville, MD:Public Health Service;2000.
- , , , , .A randomized controlled trial of smoking cessation counseling after myocardial infarction.Prev Med.2000;30(4):261–268.
- , , , .Comorbidity measures for use with administrative data.Med Care.1998:36(1):8–27.
- Tobacco Use Supplement to the Current Population Survey (TUS‐CPS). Available at: http://riskfactor.cancer.gov/studies/tus‐cps/info.html. Accessed November 2009.
- , , .Comparison of National Death Index and world wide web death searches.Am J of Epidemiol.2000;152(2):107–111.
- , , , et al.Post‐myocardial infarction smoking cessation counseling: associations with immediate and late mortality in older Medicare patients.Am J Med.2005;118(3):269–275.
- , , .Inpatient smoking‐cessation counseling and all‐cause mortality in patients with acute myocardial infarction.Am Heart J.2007;154(2):213–220.
- , , , et al.Intensive smoking cessation intervention reduces mortality in high‐risk smokers with cardiovascular disease.Chest.2007;131:446–452.
- , , , , .Dissemination of an effective inpatient tobacco use cessation program.Nicotine Tob Res.2005;7(1):129–137.
- , , .Interventions for smoking cessation in hospitalized patients.Cochrane Database Syst Rev.2007;3:CD001837.
- , , .Smoking cessation interventions for hospitalized smokers.Arch Intern Med.2008;168(18):1950–1960.
- , , , et al.Predictors of smoking cessation after a myocardial infarction.Arch Int Med.2008;168(18):1961–1967.
- , , , .The effectiveness of smoking cessation interventions prior to surgery: a systematic review.Nicotine Tob Res.2008;10(3):407–412.
- , , , et al.Clinical trial comparing nicotine replacement therapy (NRT) plus brief counseling, brief counseling alone, and minimal intervention on smoking cessation in hospital inpatients.Thorax.2003;58:484–488.
- Department of Health and Human Services (DHHS). Treating Tobacco Use and Dependence: 2008 Update. Chapter 7. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.section.28504. Accessed November2009.
- , .Implementation of evidence‐based tobacco use cessation guidelines in managed care organizations.Ann Behav Med.2004;27(1):13–21.
- .Decreasing effect sizes for effectiveness studies—implications for the transport of evidence‐based treatments: comment on Curtis, Ronan, and Borduin (2004).J Fam Psychol.2004;18(3):420–423.
- , , , , , .Efficacy of a smoking cessation program for hospital patients.Arch Intern Med.1997;157(22):2653–2660.
- , , , et al.Feasibility, acceptability, and cost of referring surgical patients for postdischarge cessation support from a quitline.Nicotine Tob Res.2008;10(6):1105–1108.
- .Efficacy and effectiveness trials (and other phases of research) in the development of health promotion programs.Prev Med.1986;15:451–474.
- , , .Psychosocial interventions for smoking cessation in patients with coronary heart disease.Cochrane Database Syst Rev.2008;23(1):CD006886.
- , , , , .The accuracy of self‐reported smoking: a systematic review of the relationship between self‐reported and cotinine‐assessed smoking status.Nicotine Tob Res2009;11(1):12–24.
- , , , , .Relations of cotinine and carbon monoxide to self‐reported smoking in a cohort of smokers and ex‐smokers followed over 5 years.Nicotine Tob Res.2002;4(3):287–294.
- , , , .Error in smoking measures: effects of intervention on relations of cotinine and carbon monoxide to self‐reported smoking. The Lung Health Study Research Group.Am J Public Health.1993;83(9):1251–1257.
In 1992, the Joint Commission on Accreditation of Healthcare Organizations (Joint Commission) introduced standards to make hospital buildings smoke‐free, resulting in the nation's first industry‐wide ban on smoking in the workplace. This hospital smoking ban has led to increased smoking cessation among employees.1 Since 2003, core measures from the Joint Commission and quality indicators from the Centers for Medicare and Medicaid Services have included inpatient smoking cessation counseling for acute myocardial infarction, pneumonia, and heart failure, as national guidelines strongly recommend smoking cessation counseling for patients with these diseases who smoke.25
The Department of Health and Human Services (DHHS) 2008 update on Clinical Practice Guidelines for Treating Tobacco Use and Dependence6 recommends that clinicians use hospitalization as an opportunity to promote smoking cessation and to prescribe medications to alleviate withdrawal symptoms. Hospitalization is an opportune time for smoking cessation because patients are restricted to a smoke‐free environment in the hospital and, increasingly, on hospital campuses.6 The illness leading to hospitalization may be attributable, at least in part, to tobacco use, thereby increasing the patient's receptivity to cessation counseling. Last, medications used in‐hospital to treat nicotine withdrawal symptoms may lead to continued or future use of these medications that, in turn, may ultimately lead to a successful quit attempt.
We report on the outcomes of our hospital's attempt to do this in the context of implementation of a smoke‐free medical campus.7 This study was designed to measure whether an inpatient smoking cessation intervention increases the likelihood of smoking cessation 6 months post‐hospital discharge. Because effectiveness studies are the next step to improving translation of research into health promotion practice,8 we set out to measure what the impact of this intervention would be in routine clinical practice as opposed to a carefully structured efficacy trial.
Methods
Intervention
The Smoking Cessation service for inpatients began on April 3, 2006. Upon admission, all patients were screened regarding their current smoking status. The nurse asked the patient if s/he currently smoked and then entered the responses into the hospital electronic medical record (EMR). A current smoker was defined as smoking every day or some days within the past 30 days. A roster of newly admitted current smokers was electronically transmitted to the Respiratory Care office daily. Only current smokers received counseling. The Smoking Cessation Specialist (SCS) subsequently saw inpatients within a 24‐hour time frame of admission, except for weekends and holidays. Each patient received 1 to 2 intensive follow‐up counseling sessions during hospitalization. An average of 10 patients per day were seen.
The goal of the inpatient smoking cessation service was to counsel patients on the health effects of smoking, address nicotine withdrawal symptoms, explain the different pharmacotherapies available, advise on how to quit, give self‐help materials, counsel family members, and refer to the New York State (NYS) Smokers' Fax‐to‐Quit program.9 Following the consult, the SCS documented the encounter in the patient's chart, including recommendations for nicotine replacement therapy (NRT) or bupropion (varenicline was not addressed as it was not on the formulary). The chart documentation informed the physician and nursing staff of the intervention and included the date/time, stage of change, and support action taken.
The SCS was part‐time, had nursing training, smoking cessation training,10 and was also trained by the Seton Health Cessation Center in the Butt Stops Here Program.11 She also implemented a performance improvement plan to increase the provision of smoking cessation counseling, increase NRT or bupropion prescriptions to smokers admitted to the hospital, and increase referrals to the NYS telephone quitline through the Fax‐to‐Quit program for outpatient resources and help following hospital discharge. The Fax‐to‐Quit program allows health care providers to refer patients to the NYS quitline via fax, with the patient's signature (patient permission) on the fax to quit form. After hospital discharge, the quitline then contacts the patient at a time that the patient requested.
The SCS visited patients with all admitting diagnoses on the medical, surgical, and special care units who were current smokers. Inpatients admitted to psychiatry, obstetrics, and the intensive care unit (ICU) were not seen by the SCS, except for ICU patients referred by a physician. Inpatients who had short stays or who were admitted and discharged in 1 day or during the weekend were not seen.
The intervention included either a brief 3‐minute to 5‐minute intervention or a more intensive intervention, that required 10 to 20 minutes (18 minutes average). The length of the intervention was determined by how receptive the patient was to the intervention. All interventions began with patient identification, an introduction to the SCS, and an explanation of the purpose of the visit. The SCS then inquired about the patient's comfort level vis‐a‐vis nicotine withdrawal and if s/he was receiving any NRT while in the hospital (NRT on the inpatient formulary included the nicotine patch or gum). If the patient was receptive to counseling, the SCS then began to work through the 5 A's, as described in the 2000 DHHS Clinical Practice Guidelines.12 The 2000 DHHS Clinical Practice Guidelines were used because the 2008 update had not been released at the time this study was initiated in 2006. These include: asking about smoking status, advising on how to quit, assessing readiness to quit, and assisting in arranging treatment options that include pharmacotherapy, counseling, as well as referral to the NYS Smokers' Quitline. A workbook was provided to reinforce counseling but was not necessarily used during counseling session. A compact disc (CD) with relaxation exercises5 was provided to those inpatients who were interested in stress reduction. If family members were present, and were also smokers, they were included in the counseling session, if willing. Each patient was offered a referral via the Fax‐to‐Quit program to continue treatment on an outpatient basis.
If the patient was not motivated to quit or declined the consult, the visits were short and focused on the patient's experience with nicotine withdrawal. These patients were also given self‐help materials and, if possible, the relevance of and roadblocks to quitting were reviewed. Patients were prompted to think about why quitting was relevant and often the reason for hospitalization was used to motivate the quitting process.
Upon hospital discharge, the patient's primary care provider was notified of the cessation intervention by a letter from the SCS. The letter described the intervention and stated whether or not the patient agreed to be referred to the Fax‐to‐Quit Program.
Study Participants
Patients were recruited from July 1, 2006 (after the smoking ban went into effect) through June 1, 2008. Inpatients who currently smoked were informed of this study and were asked to sign informed consent to participate after they were seen by the SCS. Current smokers of all admitting diagnoses were recruited into the study. Patients provided informed consent for a telephone interview 6 months posthospital discharge. A written Health Insurance Portability and Accountability Act (HIPAA) release was obtained to allow access to an individual's specific EMR.
A comparison group of inpatients who were also current smokers, but who did not receive the intervention were also contacted six months after hospitalization. Reasons for not receiving the intervention included the fact the SCS was part‐time and also took a leave of absence during the study and therefore could not see all inpatients who currently smoked. Other reasons for not receiving the intervention include too short a stay for the SCS to see the patient or the patient was out of the room for tests or procedures when the SCS was available. These patients provided informed consent to be interviewed 6 months after hospital discharge and HIPAA consent for access to their medical record. Not all inpatients in the comparison group provided written HIPAA release for use of their medical record; therefore, these patients were excluded because their baseline demographic and diagnostic data were missing.
Sample‐size considerations were driven around having adequate numbers of subjects to measure the prevalence of smoking cessation at 6 months post‐hospital discharge with an acceptable degree of precision. Prevalence estimates from previous studies for 6‐month cessation typically range from 20% to 30%, with cessation rates as high as 67% (this estimate applies to postmyocardial infarction patients.)13 For conservative estimation, we used 50% as the 6‐month prevalence of cessation in the current study, which placed binomial variance at its theoretical maximum. In this case, a sample of 300 subjects provides a margin of error of 0.058 for a 95% confidence interval around this point estimate.
Data Sources
The hospital EMR database was used to monitor several components of the program: nursing screening, smoking cessation counseling, and pharmacy dispensing of NRT and bupropion. The screening data were also used to monitor the proportion of current smokers admitted during the study period. Elements of the EMR were used to define the following covariates: patient age, gender, ethnicity, and the primary discharge diagnosis (via International Statistical Classification of Diseases and Related Health Problems, 9th edition [ICD9] codes) and readmission during the six month follow‐up period. Mean length of stay (LOS) was computed. The Elixhauser Comorbidity Index that utilizes ICD9 codes was used for comorbidity risk adjustment.14
Study participants were contacted by phone 6 months posthospital discharge. Data collection began July 1, 2006 and was completed January 1, 2009. The interview focused on self‐reported point prevalence of smoking and 6‐month quit status. The point prevalence for self‐reported abstinence was derived from the question Do you now smoke cigarettes every day, some days, or not at all?15 Self‐reported quit status was derived from question Have you quit smoking since you were discharged from the hospital? In addition, respondents were queried about their number of years smoked, post‐hospital discharge number of quit attempts, and cessation efforts (NRT, self‐help groups, quitline use, etc.). Last, they were surveyed about barriers to cessation (exposure to secondhand smoke, rules about smoking in the home or car), educational level, employment, and health ratings.
To determine the status of those lost to follow‐up, administrative and EMR databases for appointments and follow‐up visits were accessed to determine if the patient was alive during the 6 months between discharge and the follow‐up call. To confirm mortality, we searched the Internet, Ancestry.com, and/or local newspaper obituaries for dates of death for all patients to validate that they had not died during the 6‐month follow‐up. World wide web searches can identify 97% of deaths listed in the Centers for Disease Control and Prevention (CDC)/National Death Index, which is considered the gold standard in epidemiologic studies.16
Analysis
Univariate analysis of all covariates was completed to examine the normal distribution curves for these variables. Bivariate correlation analysis of all the independent variables by study group was performed to assess comparability of the study groups at baseline. The self‐reported cessation outcomes were calculated by dividing the number of patients who said they were not using tobacco or had quit, at 6 months posthospital discharge by the number of individuals in the study group at baseline minus those who had died. Both the intent to treat method, which assumes patients lost to follow‐up were still smoking, and the responder method, which does not include nonresponders in the analysis, were used to adjust the denominators for these outcomes.
Multivariate regression analysis was then used to model receipt of the intervention as predictor of self‐reported quit status adjusted for significant covariates. Statistical significance was defined by a P value of less than 0.05.
Survival analysis was employed to model differences in mortality between the study groups, controlling for any baseline imbalances (eg, comorbidity). Because baseline data were used in this model, the model includes only patients with signed a HIPAA release.
Internal review boards of our hospital and the NYS Department of Health reviewed and approved this study.
Results
From January 1, 2007 to May 30, 2008, 660 inpatients who were current smokers were recruited into the study. Figure 1 summarizes patient flow through the study and explains the final sample size of 607. Exclusions include 52 inpatients from the study who completed the 6‐month interview but who did not return a written HIPAA release. Without a HIPAA release to access the EMR, baseline comparison of the study groups and adjustment for comorbidity could not be completed for these patients. At 6 months posthospital discharge, 53 subjects refused the interview when contacted by telephone.
As might be expected in a quasiexperimental design, the study groups were not equivalent at baseline (Table 1). The intervention and comparison groups differed with regard to age, length of stay (LOS), proportion of acute admissions, and the Elixhauser comorbidity index. These differences suggest that the intervention group was older, had a longer LOS, higher acuity at the time of admission, and more comorbidities. In addition, as a result of the intervention, the intervention group was more likely to receive NRT or bupropion in hospital and a Fax‐to‐Quit referral to the NYS Smokers' Quitline. In the intervention group, most patients received 1 visit from the SCS, only 2% received 2 visits. Family members were included in smoking cessation counseling for 58% of the intervention group.
| Intervention (n = 275) | Comparison (n = 335) (P value) | |
|---|---|---|
| ||
| Sex (% male) | 51 | 51 |
| Mean age (years) | 51.4 | 48.5 (0.03) |
| Ethnicity (% white) | 98 | 97 |
| Marital status (% married) | 48 | 47 |
| Elective admission (vs. acute) (%) | 25 | 31 |
| Inpatient (vs. outpatient observation or outpatient surgical admission) (%) | 86 | 68 (0.00) |
| LOS (days) | 3.80 | 2.68 (0.00) |
| Elixhauser comorbidity index (mean) | 1.66 | 1.17 (0.00) |
| Used NRT in hospital (%) | 37 | 19 (0.00) |
| Used bupropion in hospital (%) | 4 | 1 (0.00) |
| Referred to NYS Smokers' Quitline using Fax‐to‐Quit | 10 | 0 (0.00) |
| Mean cigarettes per day* | 17.7 (n = 213) | 15.9 (n = 192) |
As shown in Table 2, there was a significant amount of diagnostic heterogeneity in the discharge diagnoses codes of patients included in the study. However, there were significantly more patients in the intervention group with a first discharge diagnosis of cardiovascular disease (25%) compared to the comparison group (12%; P = 0.00).
| Intervention (n = 274)* (%) | Comparison (n = 333)* (%) | |
|---|---|---|
| ||
| Cardiovascular | 25 | 12, P = 0.00 |
| Pulmonary | 16 | 7 |
| Orthopedics | 12 | 12 |
| Injury | 10 | 15 |
| GI | 8 | 16 |
| Cancer | 6 | 8 |
| GU | 3 | 6 |
| Endocrine | 3 | 3 |
| Other | 17 | 21 |
Readmission outcomes based on EMR and administrative data were available for 607 inpatients with signed HIPAA releases. The readmission rate was higher for the intervention (41%) than the comparison group (20%). Despite a higher readmission rate, the crude mortality within the 6 months posthospital discharge was lower for the intervention group, ie, 0.02 (6/276), than the comparison group, which had a crude mortality of 0.04 (16/384) during this period.
A multivariate survival model, controlling for age, sex, Elixhauser comorbidity index, LOS, and cardiovascular diagnosis, showed a significantly reduced mortality in the intervention group (hazard ratio [HR] = 0.37; P = 0.04). Although cardiac status (P = 0.09) and LOS (P = 0.15) were not significant in this model, they were retained because both of these variables showed significantly higher levels (along with the Elixhauser Index) at baseline in the intervention group, implying that the intervention group was sicker than the comparison group. The Elixhauser comorbidity index (HR = 1.42; P < 0.00) and age (HR = 1.07; P < 0.00) were the only other significant predictors of mortality in this model.
Among those responding to the interview at 6 months post‐hospital discharge (n = 326), there were no significant differences between the study groups with regard to age first started smoking, gender, educational level, employment status, ethnicity, or physical health status (data not shown). Table 3 summarizes the outcomes by the intervention and comparison groups at 6 months post‐hospital discharge. The point prevalence for abstinence was 27% in the intervention group compared to 19% in the comparison group (P = 0.09). Using the intent to treat analysis, the point prevalence for abstinence was 16% in the intervention group compared to 9.8% in the comparison group (P = 0.02). Self‐reported quit status was 63% in the intervention group vs. 48% in the comparison group (P = 0.00). Using the intent to treat analysis, quit status was 44% in the intervention group vs. 30% in the comparison group (P = 0.00). Exclusion of the 52 patients without signed HIPAA releases (Figure 1) did not significantly alter these outcomes.
| Intervention (n = 161) | Comparison (n = 165) (P value) | |
|---|---|---|
| ||
| Self‐reported now smoking not at all (%) | 16 | 10 (0.02) |
| Self‐reported quit within 6 months (%) | 63 | 48 (0.00 |
| Tried to quit (%) | 68 | 62 |
| Used NRT post‐D/C (%) | 26 | 17 (0.04) |
| Used other intervention (%) | 21 | 14 |
| Heard of the NYS Smokers' Quitline (%) | 92 | 90 |
| Aware that NYS Quitline offers NRT (%) | 73 | 49 (0.00) |
| Received free NRT from NYS Smokers' Quitline (%) | 9 | 6 |
| Used NYS Smokers' Quitline (%) | 15 | 9 |
| Called by the NYS Smokers' Quitline (%) | 11 | 5 |
| Self‐rated health status as fair or poor (%) | 48 | 36 |
| Another smoker living at home (%) | 54 | 48 |
| Mean hours spent in same room where someone else was smoking (n) | 20 | 21 (0.04) |
| Households in which smoking is not allowed in the home (%) | 40 | 33 |
| Patients Still Smoking at the 6‐Month Interview | Intervention (n = 118) | Comparison (n = 134) |
| Mean cigarettes currently smoked (n) | 10.5 | 12.7 |
| Mean quit attempts post‐D/C (n) | 3.2 | 3.5 |
| Mean reduction in smoking* (cigarettes/day) | 5.83 | 4.09 |
Patients who received the inpatient smoking cessation counseling were more likely to be called by or use the NYS Smokers' Quitline; however, these differences were not statistically significant. There was no difference between the study groups in awareness of the Quitline but the intervention group was more aware that free NRT was offered by the NYS Quitline. In terms of quit methods used during the 6‐month period (Table 4), NRT or bupropion use was higher in the intervention group. There were no other significant differences between the study groups, except for the use of acupuncture.
| Intervention (n = 91) | Comparison (n = 93) (P value) | |
|---|---|---|
| ||
| Got help from friends or family (%) | 58 | 50 |
| Used any medication to quit (%) | 44 | 28 (0.02) |
| Used nicotine patch (%) | 43 | 25 (0.00) |
| Used bupropion (%) | 10 | 1 (0.00) |
| Used varenicline (%) | 32 | 25 |
| Cut back (%) | 43 | 46 |
| Quit with a friend (%) | 20 | 13 |
| Switched to lights (%) | 18 | 13 |
| Used print material (%) | 14 | 16 |
| Got help from the NYS Smokers' Quitline (%) | 11 | 9 |
| Called by the NYS Smokers' Quitline (%) | 11 | 5 (0.09) |
| Counseling (%) | 9 | 3 |
| Acupuncture (%) | 5 | 0 (0.02) |
| Switched to chew (%) | 2 | 4 |
| Attended classes (%) | 3 | 1 |
| Used NYS Smokers' Quitline website (%) | 2 | 4 |
Multivariate analysis predicting quit status at 6 months post‐hospital discharge included covariates controlling for age, sex, LOS, study group, and comorbidity. This analysis showed that patients with a cardiovascular discharge diagnosis were more likely to quit than patients who had other discharge diagnoses (odds ratio [OR], 3.02; 95% confidence interval [CI], 1.65.7; P = 0.00). Another statistically significant covariate in this model included sex (men were more likely to quit: OR, 0.61; 95% CI, 0.390.97; P = 0.04). Participating in the inpatient intervention group was marginally significant when controlling for these other variables (OR, 1.54; 95% CI, 0.982.45; P = 0.06). Hospital LOS, age, receipt of NRT in hospital, and the Elixhauser comorbidity index were not predictive of quit status at 6 months.
Discussion
This study demonstrates how effective an inpatient smoking cessation program can be for increasing the success of quitting smoking after hospital discharge. At 6 months posthospital discharge, the intervention group had significantly higher intent to treat outcomes for point prevalence abstinence and quit status as well as lower crude and adjusted mortality than the comparison group.
Although at baseline the intervention group was older, had a longer LOS, more cardiovascular diagnoses, and higher comorbidity index, crude post‐hospital discharge mortality was significantly less in the intervention group (0.02) than in the comparison group (0.04). This finding is more significant in light of the higher comorbidity and acuity of the intervention group at baseline. Our multivariate survival model that controlled for these imbalances at baseline demonstrated that the intervention group had significantly less mortality than the comparison group (HR = 0.37; P = 0.04). Reduction in mortality, as soon as 30 days after inpatient smoking cessation counseling, has been demonstrated postmyocardial infarction.17, 18 Intensive smoking cessation quit services were also linked with lower all cause mortality among cardiovascular disease patients 2 years posthospitalization.19 Our study, despite its relatively small sample size, demonstrates that the intervention retains its impact on mortality in real‐world settings.
Following participation in an inpatient smoking cessation program, self‐reported quit status at 6 months post‐hospital discharge in the intervention group was significantly higher in the intervention group (63%) than the comparison group (48%; P = 0.00). Using the intent to treat method, the differences between the study groups was still significant (44% in the intervention group, 30% in the comparison group; P = 0.00). Given the limitations of self‐report and responder bias, the actual outcomes fall somewhere between these 2 estimates. In an effectiveness study of inpatient smoking cessation involving 6 hospitals in California, self‐reported quit rates of 26% at 6 months were reported; however, different methods were used so the results are not strictly comparable.20
Our multivariate analysis suggests that patients with cardiovascular discharge diagnosis were more likely to quit than patients who had other discharge diagnoses (OR, 3.02; 95% CI, 1.65.7; P = 0.0007). This study extends findings of other studies that show that the success of smoking cessation may vary by diagnosis, particularly for smokers admitted for cardiovascular disease.21, 22 Other studies have shown that smoking cessation rates among patients post‐myocardial infarction were higher in admitting facilities that had hospital‐based smoking cessation programs and for those patients referred to cardiac rehabilitation.23 Thus, the availability of a hospital‐based smoking cessation program may be considered a structural measure of health care quality as suggested by Dawood et al.23
The use of NRT greatly increased in our hospital, coincident with the start of the inpatient cessation program7 and, in this study, NRT use appears to continue after hospital discharge. Some studies show an additive effect of NRT combined with cessation counseling.24, 25 Although a Cochrane review did not find a statistically significant difference, there was a trend toward higher quit rates with the addition of NRT.21, 22
Because hospitalized smokers may be more motivated to stop smoking, the updated 2008 DHHS clinical practice guidelines for Treating Tobacco Use and Dependence now recommend that all inpatients who currently smoke be given medications, advised, counseled, and receive follow‐up after discharge.26 Although our inpatient cessation program was started before these clinical practice guidelines were updated, we have had the opportunity to evaluate the recommended practice of inpatient tobacco cessation counseling. Compared to effects shown in efficacy studies, clinical interventions often lose effect size in daily practice and real‐world settings.27, 28 It is reassuring that, in this effectiveness study, the impact of this intervention is still demonstrable.
Provision of inpatient smoking cessation has been shown to be an effective smoking cessation intervention if combined with outpatient follow‐up.29 Reviews by Rigotti et al.21, 22 recommend that inpatient high‐intensity behavioral interventions should be followed by at least 1 month of supportive contact after discharge to promote smoking cessation among hospitalized patients. In our study, specific cessation‐related outpatient follow‐up was not provided by our program. Although letters were sent to primary care providers describing the cessation service provided during the inpatient stay, our study could not ascertain what specific cessation service was offered by either primary‐care or specialty‐care providers during posthospitalization follow‐up visits. An efficient alternative to outpatient visits may be follow‐up delivered via a quitline. Follow‐up in our study included referrals to the NYS Smokers' Quitline; however, only about 10% of inpatient reported using this service. While feasible, the effectiveness of quitline follow‐up is as yet unknown.30
Limitations
This study targets a later phase in research progression from hypothesis development, pilot studies, efficacy (empirically supported) trials, effectiveness trials (real‐world settings), and dissemination studies.31 Because this study addresses the effectiveness rather than the efficacy of inpatient smoking cessation counseling, the use of a quasiexperimental rather than randomized controlled clinical trial design led to measured differences in the study groups at baseline. An important imbalance arose in the intervention group that had twice the percentage of patients with cardiovascular‐related discharge diagnoses as the comparison group. While we were able to adjust for these differences in our analysis, there may be unmeasured differences due to the fact that the inpatients were not randomized to the study groups.
The outcomes of this study cannot be attributed to any one component of the intervention (eg, NRT) vs. the combined effect of the inpatient smoking cessation program. The program components were implemented simultaneously in order to maximize synergistic effects; therefore, the effects of program components are difficult to disaggregate.
The results are limited by the validity of self‐report of smoking status. It is well known that research studies which validate smoking status biochemically have lower efficacy (OR, 1.44; 95% CI, 0.992.11) than those that do not validate smoking status (OR, 1.92; 95% CI, 1.262.93).32 Although it was impractical in this effectiveness study to biochemically validate smoking status 6 months posthospital discharge, we have documented a significant difference between the study groups that confirms the direction of the effect, if not the effect size.
Self‐reports tend to underestimate smoking status in population studies33; however, the discrepancy between self‐reported smoking and biochemical measurements among clinical trial participants is small.34 However, a small but significant bias toward a socially desirable response in intervention groups compared to control groups of 3% with carbon monoxide and 5% for cotinine has been documented.35 If social desirability bias is operative in this study, and if we apply the above correction factor of 4% to correct this classification error, then the difference between the intervention and comparison group would be 10 percentage points (40% in the intervention group vs. 30% in the comparison group using the intention to treat estimates). That difference is still clinically relevant.
The observed difference between the intervention and comparison group is underestimated because the comparison group was exposed to smoking cessation as well both at the time of admission and following discharge (Table 4). The comparison group in this study could thus be viewed as a usual care group rather than a control group. That exposure does cloud the measurement of quit rates as the comparison group is contaminated to some degree by exposure to various cessation methods. The impact of this exposure is to reduce the effect size observed in this study or underestimate the effect of the inpatient smoking cessation counseling because the comparison group was exposed other cessation methods, although to a lesser extent.
The social desirability bias inherent in self‐reported smoking status may increase the effect size while the use of comparison group that received usual care may decrease the effect size. Because neither of these biases could be measured in this study, it is impossible to say whether they negated each other.
As with any administrative database, use of EMR as a data source in this study led to missing data that precluded use of certain variables in the analysis. In addition, lack of written and signed HIPAA releases also precluded inclusion of several inpatients, mostly in the comparison group, in the analytic database. However, it is reassuring that the results of the 6‐month survey did not differ significantly when these individuals were included or excluded from a separate analysis of the survey data. Last, our study population is almost 100% Caucasian thus limiting how generalizable the results are to more heterogenous patient populations.
Conclusions
This quasiexperimental effectiveness study showed that inpatient smoking cessation intervention improved smoking cessation outcomes, use of NRT, and was associated with a decreased mortality 6 months post‐hospital discharge. The effectiveness of this inpatient intervention is maintained in real world settings but may be improved with posthospital discharge follow‐up.
Acknowledgements
The authors are grateful to the many Mary Imogene Bassett Hospital staff in administration, nursing, inpatient pharmacy, medical education, patient care service, and respiratory care who provided data needed to evaluate this program. They also acknowledge the NYS Smokers' Quitline website for data provided about monthly Fax‐to‐Quit program referrals from our county.
In 1992, the Joint Commission on Accreditation of Healthcare Organizations (Joint Commission) introduced standards to make hospital buildings smoke‐free, resulting in the nation's first industry‐wide ban on smoking in the workplace. This hospital smoking ban has led to increased smoking cessation among employees.1 Since 2003, core measures from the Joint Commission and quality indicators from the Centers for Medicare and Medicaid Services have included inpatient smoking cessation counseling for acute myocardial infarction, pneumonia, and heart failure, as national guidelines strongly recommend smoking cessation counseling for patients with these diseases who smoke.25
The Department of Health and Human Services (DHHS) 2008 update on Clinical Practice Guidelines for Treating Tobacco Use and Dependence6 recommends that clinicians use hospitalization as an opportunity to promote smoking cessation and to prescribe medications to alleviate withdrawal symptoms. Hospitalization is an opportune time for smoking cessation because patients are restricted to a smoke‐free environment in the hospital and, increasingly, on hospital campuses.6 The illness leading to hospitalization may be attributable, at least in part, to tobacco use, thereby increasing the patient's receptivity to cessation counseling. Last, medications used in‐hospital to treat nicotine withdrawal symptoms may lead to continued or future use of these medications that, in turn, may ultimately lead to a successful quit attempt.
We report on the outcomes of our hospital's attempt to do this in the context of implementation of a smoke‐free medical campus.7 This study was designed to measure whether an inpatient smoking cessation intervention increases the likelihood of smoking cessation 6 months post‐hospital discharge. Because effectiveness studies are the next step to improving translation of research into health promotion practice,8 we set out to measure what the impact of this intervention would be in routine clinical practice as opposed to a carefully structured efficacy trial.
Methods
Intervention
The Smoking Cessation service for inpatients began on April 3, 2006. Upon admission, all patients were screened regarding their current smoking status. The nurse asked the patient if s/he currently smoked and then entered the responses into the hospital electronic medical record (EMR). A current smoker was defined as smoking every day or some days within the past 30 days. A roster of newly admitted current smokers was electronically transmitted to the Respiratory Care office daily. Only current smokers received counseling. The Smoking Cessation Specialist (SCS) subsequently saw inpatients within a 24‐hour time frame of admission, except for weekends and holidays. Each patient received 1 to 2 intensive follow‐up counseling sessions during hospitalization. An average of 10 patients per day were seen.
The goal of the inpatient smoking cessation service was to counsel patients on the health effects of smoking, address nicotine withdrawal symptoms, explain the different pharmacotherapies available, advise on how to quit, give self‐help materials, counsel family members, and refer to the New York State (NYS) Smokers' Fax‐to‐Quit program.9 Following the consult, the SCS documented the encounter in the patient's chart, including recommendations for nicotine replacement therapy (NRT) or bupropion (varenicline was not addressed as it was not on the formulary). The chart documentation informed the physician and nursing staff of the intervention and included the date/time, stage of change, and support action taken.
The SCS was part‐time, had nursing training, smoking cessation training,10 and was also trained by the Seton Health Cessation Center in the Butt Stops Here Program.11 She also implemented a performance improvement plan to increase the provision of smoking cessation counseling, increase NRT or bupropion prescriptions to smokers admitted to the hospital, and increase referrals to the NYS telephone quitline through the Fax‐to‐Quit program for outpatient resources and help following hospital discharge. The Fax‐to‐Quit program allows health care providers to refer patients to the NYS quitline via fax, with the patient's signature (patient permission) on the fax to quit form. After hospital discharge, the quitline then contacts the patient at a time that the patient requested.
The SCS visited patients with all admitting diagnoses on the medical, surgical, and special care units who were current smokers. Inpatients admitted to psychiatry, obstetrics, and the intensive care unit (ICU) were not seen by the SCS, except for ICU patients referred by a physician. Inpatients who had short stays or who were admitted and discharged in 1 day or during the weekend were not seen.
The intervention included either a brief 3‐minute to 5‐minute intervention or a more intensive intervention, that required 10 to 20 minutes (18 minutes average). The length of the intervention was determined by how receptive the patient was to the intervention. All interventions began with patient identification, an introduction to the SCS, and an explanation of the purpose of the visit. The SCS then inquired about the patient's comfort level vis‐a‐vis nicotine withdrawal and if s/he was receiving any NRT while in the hospital (NRT on the inpatient formulary included the nicotine patch or gum). If the patient was receptive to counseling, the SCS then began to work through the 5 A's, as described in the 2000 DHHS Clinical Practice Guidelines.12 The 2000 DHHS Clinical Practice Guidelines were used because the 2008 update had not been released at the time this study was initiated in 2006. These include: asking about smoking status, advising on how to quit, assessing readiness to quit, and assisting in arranging treatment options that include pharmacotherapy, counseling, as well as referral to the NYS Smokers' Quitline. A workbook was provided to reinforce counseling but was not necessarily used during counseling session. A compact disc (CD) with relaxation exercises5 was provided to those inpatients who were interested in stress reduction. If family members were present, and were also smokers, they were included in the counseling session, if willing. Each patient was offered a referral via the Fax‐to‐Quit program to continue treatment on an outpatient basis.
If the patient was not motivated to quit or declined the consult, the visits were short and focused on the patient's experience with nicotine withdrawal. These patients were also given self‐help materials and, if possible, the relevance of and roadblocks to quitting were reviewed. Patients were prompted to think about why quitting was relevant and often the reason for hospitalization was used to motivate the quitting process.
Upon hospital discharge, the patient's primary care provider was notified of the cessation intervention by a letter from the SCS. The letter described the intervention and stated whether or not the patient agreed to be referred to the Fax‐to‐Quit Program.
Study Participants
Patients were recruited from July 1, 2006 (after the smoking ban went into effect) through June 1, 2008. Inpatients who currently smoked were informed of this study and were asked to sign informed consent to participate after they were seen by the SCS. Current smokers of all admitting diagnoses were recruited into the study. Patients provided informed consent for a telephone interview 6 months posthospital discharge. A written Health Insurance Portability and Accountability Act (HIPAA) release was obtained to allow access to an individual's specific EMR.
A comparison group of inpatients who were also current smokers, but who did not receive the intervention were also contacted six months after hospitalization. Reasons for not receiving the intervention included the fact the SCS was part‐time and also took a leave of absence during the study and therefore could not see all inpatients who currently smoked. Other reasons for not receiving the intervention include too short a stay for the SCS to see the patient or the patient was out of the room for tests or procedures when the SCS was available. These patients provided informed consent to be interviewed 6 months after hospital discharge and HIPAA consent for access to their medical record. Not all inpatients in the comparison group provided written HIPAA release for use of their medical record; therefore, these patients were excluded because their baseline demographic and diagnostic data were missing.
Sample‐size considerations were driven around having adequate numbers of subjects to measure the prevalence of smoking cessation at 6 months post‐hospital discharge with an acceptable degree of precision. Prevalence estimates from previous studies for 6‐month cessation typically range from 20% to 30%, with cessation rates as high as 67% (this estimate applies to postmyocardial infarction patients.)13 For conservative estimation, we used 50% as the 6‐month prevalence of cessation in the current study, which placed binomial variance at its theoretical maximum. In this case, a sample of 300 subjects provides a margin of error of 0.058 for a 95% confidence interval around this point estimate.
Data Sources
The hospital EMR database was used to monitor several components of the program: nursing screening, smoking cessation counseling, and pharmacy dispensing of NRT and bupropion. The screening data were also used to monitor the proportion of current smokers admitted during the study period. Elements of the EMR were used to define the following covariates: patient age, gender, ethnicity, and the primary discharge diagnosis (via International Statistical Classification of Diseases and Related Health Problems, 9th edition [ICD9] codes) and readmission during the six month follow‐up period. Mean length of stay (LOS) was computed. The Elixhauser Comorbidity Index that utilizes ICD9 codes was used for comorbidity risk adjustment.14
Study participants were contacted by phone 6 months posthospital discharge. Data collection began July 1, 2006 and was completed January 1, 2009. The interview focused on self‐reported point prevalence of smoking and 6‐month quit status. The point prevalence for self‐reported abstinence was derived from the question Do you now smoke cigarettes every day, some days, or not at all?15 Self‐reported quit status was derived from question Have you quit smoking since you were discharged from the hospital? In addition, respondents were queried about their number of years smoked, post‐hospital discharge number of quit attempts, and cessation efforts (NRT, self‐help groups, quitline use, etc.). Last, they were surveyed about barriers to cessation (exposure to secondhand smoke, rules about smoking in the home or car), educational level, employment, and health ratings.
To determine the status of those lost to follow‐up, administrative and EMR databases for appointments and follow‐up visits were accessed to determine if the patient was alive during the 6 months between discharge and the follow‐up call. To confirm mortality, we searched the Internet, Ancestry.com, and/or local newspaper obituaries for dates of death for all patients to validate that they had not died during the 6‐month follow‐up. World wide web searches can identify 97% of deaths listed in the Centers for Disease Control and Prevention (CDC)/National Death Index, which is considered the gold standard in epidemiologic studies.16
Analysis
Univariate analysis of all covariates was completed to examine the normal distribution curves for these variables. Bivariate correlation analysis of all the independent variables by study group was performed to assess comparability of the study groups at baseline. The self‐reported cessation outcomes were calculated by dividing the number of patients who said they were not using tobacco or had quit, at 6 months posthospital discharge by the number of individuals in the study group at baseline minus those who had died. Both the intent to treat method, which assumes patients lost to follow‐up were still smoking, and the responder method, which does not include nonresponders in the analysis, were used to adjust the denominators for these outcomes.
Multivariate regression analysis was then used to model receipt of the intervention as predictor of self‐reported quit status adjusted for significant covariates. Statistical significance was defined by a P value of less than 0.05.
Survival analysis was employed to model differences in mortality between the study groups, controlling for any baseline imbalances (eg, comorbidity). Because baseline data were used in this model, the model includes only patients with signed a HIPAA release.
Internal review boards of our hospital and the NYS Department of Health reviewed and approved this study.
Results
From January 1, 2007 to May 30, 2008, 660 inpatients who were current smokers were recruited into the study. Figure 1 summarizes patient flow through the study and explains the final sample size of 607. Exclusions include 52 inpatients from the study who completed the 6‐month interview but who did not return a written HIPAA release. Without a HIPAA release to access the EMR, baseline comparison of the study groups and adjustment for comorbidity could not be completed for these patients. At 6 months posthospital discharge, 53 subjects refused the interview when contacted by telephone.
As might be expected in a quasiexperimental design, the study groups were not equivalent at baseline (Table 1). The intervention and comparison groups differed with regard to age, length of stay (LOS), proportion of acute admissions, and the Elixhauser comorbidity index. These differences suggest that the intervention group was older, had a longer LOS, higher acuity at the time of admission, and more comorbidities. In addition, as a result of the intervention, the intervention group was more likely to receive NRT or bupropion in hospital and a Fax‐to‐Quit referral to the NYS Smokers' Quitline. In the intervention group, most patients received 1 visit from the SCS, only 2% received 2 visits. Family members were included in smoking cessation counseling for 58% of the intervention group.
| Intervention (n = 275) | Comparison (n = 335) (P value) | |
|---|---|---|
| ||
| Sex (% male) | 51 | 51 |
| Mean age (years) | 51.4 | 48.5 (0.03) |
| Ethnicity (% white) | 98 | 97 |
| Marital status (% married) | 48 | 47 |
| Elective admission (vs. acute) (%) | 25 | 31 |
| Inpatient (vs. outpatient observation or outpatient surgical admission) (%) | 86 | 68 (0.00) |
| LOS (days) | 3.80 | 2.68 (0.00) |
| Elixhauser comorbidity index (mean) | 1.66 | 1.17 (0.00) |
| Used NRT in hospital (%) | 37 | 19 (0.00) |
| Used bupropion in hospital (%) | 4 | 1 (0.00) |
| Referred to NYS Smokers' Quitline using Fax‐to‐Quit | 10 | 0 (0.00) |
| Mean cigarettes per day* | 17.7 (n = 213) | 15.9 (n = 192) |
As shown in Table 2, there was a significant amount of diagnostic heterogeneity in the discharge diagnoses codes of patients included in the study. However, there were significantly more patients in the intervention group with a first discharge diagnosis of cardiovascular disease (25%) compared to the comparison group (12%; P = 0.00).
| Intervention (n = 274)* (%) | Comparison (n = 333)* (%) | |
|---|---|---|
| ||
| Cardiovascular | 25 | 12, P = 0.00 |
| Pulmonary | 16 | 7 |
| Orthopedics | 12 | 12 |
| Injury | 10 | 15 |
| GI | 8 | 16 |
| Cancer | 6 | 8 |
| GU | 3 | 6 |
| Endocrine | 3 | 3 |
| Other | 17 | 21 |
Readmission outcomes based on EMR and administrative data were available for 607 inpatients with signed HIPAA releases. The readmission rate was higher for the intervention (41%) than the comparison group (20%). Despite a higher readmission rate, the crude mortality within the 6 months posthospital discharge was lower for the intervention group, ie, 0.02 (6/276), than the comparison group, which had a crude mortality of 0.04 (16/384) during this period.
A multivariate survival model, controlling for age, sex, Elixhauser comorbidity index, LOS, and cardiovascular diagnosis, showed a significantly reduced mortality in the intervention group (hazard ratio [HR] = 0.37; P = 0.04). Although cardiac status (P = 0.09) and LOS (P = 0.15) were not significant in this model, they were retained because both of these variables showed significantly higher levels (along with the Elixhauser Index) at baseline in the intervention group, implying that the intervention group was sicker than the comparison group. The Elixhauser comorbidity index (HR = 1.42; P < 0.00) and age (HR = 1.07; P < 0.00) were the only other significant predictors of mortality in this model.
Among those responding to the interview at 6 months post‐hospital discharge (n = 326), there were no significant differences between the study groups with regard to age first started smoking, gender, educational level, employment status, ethnicity, or physical health status (data not shown). Table 3 summarizes the outcomes by the intervention and comparison groups at 6 months post‐hospital discharge. The point prevalence for abstinence was 27% in the intervention group compared to 19% in the comparison group (P = 0.09). Using the intent to treat analysis, the point prevalence for abstinence was 16% in the intervention group compared to 9.8% in the comparison group (P = 0.02). Self‐reported quit status was 63% in the intervention group vs. 48% in the comparison group (P = 0.00). Using the intent to treat analysis, quit status was 44% in the intervention group vs. 30% in the comparison group (P = 0.00). Exclusion of the 52 patients without signed HIPAA releases (Figure 1) did not significantly alter these outcomes.
| Intervention (n = 161) | Comparison (n = 165) (P value) | |
|---|---|---|
| ||
| Self‐reported now smoking not at all (%) | 16 | 10 (0.02) |
| Self‐reported quit within 6 months (%) | 63 | 48 (0.00 |
| Tried to quit (%) | 68 | 62 |
| Used NRT post‐D/C (%) | 26 | 17 (0.04) |
| Used other intervention (%) | 21 | 14 |
| Heard of the NYS Smokers' Quitline (%) | 92 | 90 |
| Aware that NYS Quitline offers NRT (%) | 73 | 49 (0.00) |
| Received free NRT from NYS Smokers' Quitline (%) | 9 | 6 |
| Used NYS Smokers' Quitline (%) | 15 | 9 |
| Called by the NYS Smokers' Quitline (%) | 11 | 5 |
| Self‐rated health status as fair or poor (%) | 48 | 36 |
| Another smoker living at home (%) | 54 | 48 |
| Mean hours spent in same room where someone else was smoking (n) | 20 | 21 (0.04) |
| Households in which smoking is not allowed in the home (%) | 40 | 33 |
| Patients Still Smoking at the 6‐Month Interview | Intervention (n = 118) | Comparison (n = 134) |
| Mean cigarettes currently smoked (n) | 10.5 | 12.7 |
| Mean quit attempts post‐D/C (n) | 3.2 | 3.5 |
| Mean reduction in smoking* (cigarettes/day) | 5.83 | 4.09 |
Patients who received the inpatient smoking cessation counseling were more likely to be called by or use the NYS Smokers' Quitline; however, these differences were not statistically significant. There was no difference between the study groups in awareness of the Quitline but the intervention group was more aware that free NRT was offered by the NYS Quitline. In terms of quit methods used during the 6‐month period (Table 4), NRT or bupropion use was higher in the intervention group. There were no other significant differences between the study groups, except for the use of acupuncture.
| Intervention (n = 91) | Comparison (n = 93) (P value) | |
|---|---|---|
| ||
| Got help from friends or family (%) | 58 | 50 |
| Used any medication to quit (%) | 44 | 28 (0.02) |
| Used nicotine patch (%) | 43 | 25 (0.00) |
| Used bupropion (%) | 10 | 1 (0.00) |
| Used varenicline (%) | 32 | 25 |
| Cut back (%) | 43 | 46 |
| Quit with a friend (%) | 20 | 13 |
| Switched to lights (%) | 18 | 13 |
| Used print material (%) | 14 | 16 |
| Got help from the NYS Smokers' Quitline (%) | 11 | 9 |
| Called by the NYS Smokers' Quitline (%) | 11 | 5 (0.09) |
| Counseling (%) | 9 | 3 |
| Acupuncture (%) | 5 | 0 (0.02) |
| Switched to chew (%) | 2 | 4 |
| Attended classes (%) | 3 | 1 |
| Used NYS Smokers' Quitline website (%) | 2 | 4 |
Multivariate analysis predicting quit status at 6 months post‐hospital discharge included covariates controlling for age, sex, LOS, study group, and comorbidity. This analysis showed that patients with a cardiovascular discharge diagnosis were more likely to quit than patients who had other discharge diagnoses (odds ratio [OR], 3.02; 95% confidence interval [CI], 1.65.7; P = 0.00). Another statistically significant covariate in this model included sex (men were more likely to quit: OR, 0.61; 95% CI, 0.390.97; P = 0.04). Participating in the inpatient intervention group was marginally significant when controlling for these other variables (OR, 1.54; 95% CI, 0.982.45; P = 0.06). Hospital LOS, age, receipt of NRT in hospital, and the Elixhauser comorbidity index were not predictive of quit status at 6 months.
Discussion
This study demonstrates how effective an inpatient smoking cessation program can be for increasing the success of quitting smoking after hospital discharge. At 6 months posthospital discharge, the intervention group had significantly higher intent to treat outcomes for point prevalence abstinence and quit status as well as lower crude and adjusted mortality than the comparison group.
Although at baseline the intervention group was older, had a longer LOS, more cardiovascular diagnoses, and higher comorbidity index, crude post‐hospital discharge mortality was significantly less in the intervention group (0.02) than in the comparison group (0.04). This finding is more significant in light of the higher comorbidity and acuity of the intervention group at baseline. Our multivariate survival model that controlled for these imbalances at baseline demonstrated that the intervention group had significantly less mortality than the comparison group (HR = 0.37; P = 0.04). Reduction in mortality, as soon as 30 days after inpatient smoking cessation counseling, has been demonstrated postmyocardial infarction.17, 18 Intensive smoking cessation quit services were also linked with lower all cause mortality among cardiovascular disease patients 2 years posthospitalization.19 Our study, despite its relatively small sample size, demonstrates that the intervention retains its impact on mortality in real‐world settings.
Following participation in an inpatient smoking cessation program, self‐reported quit status at 6 months post‐hospital discharge in the intervention group was significantly higher in the intervention group (63%) than the comparison group (48%; P = 0.00). Using the intent to treat method, the differences between the study groups was still significant (44% in the intervention group, 30% in the comparison group; P = 0.00). Given the limitations of self‐report and responder bias, the actual outcomes fall somewhere between these 2 estimates. In an effectiveness study of inpatient smoking cessation involving 6 hospitals in California, self‐reported quit rates of 26% at 6 months were reported; however, different methods were used so the results are not strictly comparable.20
Our multivariate analysis suggests that patients with cardiovascular discharge diagnosis were more likely to quit than patients who had other discharge diagnoses (OR, 3.02; 95% CI, 1.65.7; P = 0.0007). This study extends findings of other studies that show that the success of smoking cessation may vary by diagnosis, particularly for smokers admitted for cardiovascular disease.21, 22 Other studies have shown that smoking cessation rates among patients post‐myocardial infarction were higher in admitting facilities that had hospital‐based smoking cessation programs and for those patients referred to cardiac rehabilitation.23 Thus, the availability of a hospital‐based smoking cessation program may be considered a structural measure of health care quality as suggested by Dawood et al.23
The use of NRT greatly increased in our hospital, coincident with the start of the inpatient cessation program7 and, in this study, NRT use appears to continue after hospital discharge. Some studies show an additive effect of NRT combined with cessation counseling.24, 25 Although a Cochrane review did not find a statistically significant difference, there was a trend toward higher quit rates with the addition of NRT.21, 22
Because hospitalized smokers may be more motivated to stop smoking, the updated 2008 DHHS clinical practice guidelines for Treating Tobacco Use and Dependence now recommend that all inpatients who currently smoke be given medications, advised, counseled, and receive follow‐up after discharge.26 Although our inpatient cessation program was started before these clinical practice guidelines were updated, we have had the opportunity to evaluate the recommended practice of inpatient tobacco cessation counseling. Compared to effects shown in efficacy studies, clinical interventions often lose effect size in daily practice and real‐world settings.27, 28 It is reassuring that, in this effectiveness study, the impact of this intervention is still demonstrable.
Provision of inpatient smoking cessation has been shown to be an effective smoking cessation intervention if combined with outpatient follow‐up.29 Reviews by Rigotti et al.21, 22 recommend that inpatient high‐intensity behavioral interventions should be followed by at least 1 month of supportive contact after discharge to promote smoking cessation among hospitalized patients. In our study, specific cessation‐related outpatient follow‐up was not provided by our program. Although letters were sent to primary care providers describing the cessation service provided during the inpatient stay, our study could not ascertain what specific cessation service was offered by either primary‐care or specialty‐care providers during posthospitalization follow‐up visits. An efficient alternative to outpatient visits may be follow‐up delivered via a quitline. Follow‐up in our study included referrals to the NYS Smokers' Quitline; however, only about 10% of inpatient reported using this service. While feasible, the effectiveness of quitline follow‐up is as yet unknown.30
Limitations
This study targets a later phase in research progression from hypothesis development, pilot studies, efficacy (empirically supported) trials, effectiveness trials (real‐world settings), and dissemination studies.31 Because this study addresses the effectiveness rather than the efficacy of inpatient smoking cessation counseling, the use of a quasiexperimental rather than randomized controlled clinical trial design led to measured differences in the study groups at baseline. An important imbalance arose in the intervention group that had twice the percentage of patients with cardiovascular‐related discharge diagnoses as the comparison group. While we were able to adjust for these differences in our analysis, there may be unmeasured differences due to the fact that the inpatients were not randomized to the study groups.
The outcomes of this study cannot be attributed to any one component of the intervention (eg, NRT) vs. the combined effect of the inpatient smoking cessation program. The program components were implemented simultaneously in order to maximize synergistic effects; therefore, the effects of program components are difficult to disaggregate.
The results are limited by the validity of self‐report of smoking status. It is well known that research studies which validate smoking status biochemically have lower efficacy (OR, 1.44; 95% CI, 0.992.11) than those that do not validate smoking status (OR, 1.92; 95% CI, 1.262.93).32 Although it was impractical in this effectiveness study to biochemically validate smoking status 6 months posthospital discharge, we have documented a significant difference between the study groups that confirms the direction of the effect, if not the effect size.
Self‐reports tend to underestimate smoking status in population studies33; however, the discrepancy between self‐reported smoking and biochemical measurements among clinical trial participants is small.34 However, a small but significant bias toward a socially desirable response in intervention groups compared to control groups of 3% with carbon monoxide and 5% for cotinine has been documented.35 If social desirability bias is operative in this study, and if we apply the above correction factor of 4% to correct this classification error, then the difference between the intervention and comparison group would be 10 percentage points (40% in the intervention group vs. 30% in the comparison group using the intention to treat estimates). That difference is still clinically relevant.
The observed difference between the intervention and comparison group is underestimated because the comparison group was exposed to smoking cessation as well both at the time of admission and following discharge (Table 4). The comparison group in this study could thus be viewed as a usual care group rather than a control group. That exposure does cloud the measurement of quit rates as the comparison group is contaminated to some degree by exposure to various cessation methods. The impact of this exposure is to reduce the effect size observed in this study or underestimate the effect of the inpatient smoking cessation counseling because the comparison group was exposed other cessation methods, although to a lesser extent.
The social desirability bias inherent in self‐reported smoking status may increase the effect size while the use of comparison group that received usual care may decrease the effect size. Because neither of these biases could be measured in this study, it is impossible to say whether they negated each other.
As with any administrative database, use of EMR as a data source in this study led to missing data that precluded use of certain variables in the analysis. In addition, lack of written and signed HIPAA releases also precluded inclusion of several inpatients, mostly in the comparison group, in the analytic database. However, it is reassuring that the results of the 6‐month survey did not differ significantly when these individuals were included or excluded from a separate analysis of the survey data. Last, our study population is almost 100% Caucasian thus limiting how generalizable the results are to more heterogenous patient populations.
Conclusions
This quasiexperimental effectiveness study showed that inpatient smoking cessation intervention improved smoking cessation outcomes, use of NRT, and was associated with a decreased mortality 6 months post‐hospital discharge. The effectiveness of this inpatient intervention is maintained in real world settings but may be improved with posthospital discharge follow‐up.
Acknowledgements
The authors are grateful to the many Mary Imogene Bassett Hospital staff in administration, nursing, inpatient pharmacy, medical education, patient care service, and respiratory care who provided data needed to evaluate this program. They also acknowledge the NYS Smokers' Quitline website for data provided about monthly Fax‐to‐Quit program referrals from our county.
- , , , , , .“Implementing smoking bans in American hospitals: results of a national survey.Tob Control.1998;7(1):47–55.
- The Smoking Cessation Clinical Practice Guideline Panel and Staff: the Agency for Health Care Policy and Research Smoking Cessation Clinical Practice Guideline.JAMA.1996;275(16):1270–1280.
- , , , et al.ACC/AHA clinical performance measures for adults with chronic heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Heart Failure Clinical Performance Measures). Endorsed by the Heart Failure Society of America.J Am Coll Cardiol.2005;46(6):1144–1178.
- , , , et al.ACC/AHA guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction).Circulation.2004;110(9):e82–e292.
- , , , et al.ACC/AHA clinical performance measures for adults with ST‐elevation and non‐ST elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures on ST‐Elevation and Non‐ST‐Elevation Myocardial Infarction).J Am Coll Cardiol.2006;47(1):236–265.
- Treating Tobacco Use and Dependence‐Clinicians Packet. A How‐To Guide For Implementing the Public Health Service Clinical Practice Guideline, March2003. Rockville, MD: U.S. Public Health Service, Agency for Healthcare Research and Quality. Available at: http://www.ahrq.gov/clinic/tobacco. Accessed November 2009.
- , , , .Implementing a smoke‐free medical campus: impact on inpatient and employee outcomes.J Hosp Med.2010;5(1):51–54.
- , , , et al.The future of behavior change research: what is needed to improve translation of research into health promotion practice?Ann Behav Med.2004;27:3–12.
- The New York State Smokers' Quitline. Available at: http://www.nysmokefree.com. Accessed November2009.
- Tobacco Cessation Continuing Education for Healthcare Professionals and Counselors. Available at: http://www.tobaccocme.com. Accessed November2009.
- Seton Health Cessation Center. The Butt Stops Here. Relaxation Exercises for Smoking Cessation. 2001. The Butt Stops Here Program. Available at: http://www.setonhealth.org. Accessed November2009.
- U.S. Department of Health and Human Services.Treating Tobacco Use and Dependence. Clinical Practice Guideline.Rockville, MD:Public Health Service;2000.
- , , , , .A randomized controlled trial of smoking cessation counseling after myocardial infarction.Prev Med.2000;30(4):261–268.
- , , , .Comorbidity measures for use with administrative data.Med Care.1998:36(1):8–27.
- Tobacco Use Supplement to the Current Population Survey (TUS‐CPS). Available at: http://riskfactor.cancer.gov/studies/tus‐cps/info.html. Accessed November 2009.
- , , .Comparison of National Death Index and world wide web death searches.Am J of Epidemiol.2000;152(2):107–111.
- , , , et al.Post‐myocardial infarction smoking cessation counseling: associations with immediate and late mortality in older Medicare patients.Am J Med.2005;118(3):269–275.
- , , .Inpatient smoking‐cessation counseling and all‐cause mortality in patients with acute myocardial infarction.Am Heart J.2007;154(2):213–220.
- , , , et al.Intensive smoking cessation intervention reduces mortality in high‐risk smokers with cardiovascular disease.Chest.2007;131:446–452.
- , , , , .Dissemination of an effective inpatient tobacco use cessation program.Nicotine Tob Res.2005;7(1):129–137.
- , , .Interventions for smoking cessation in hospitalized patients.Cochrane Database Syst Rev.2007;3:CD001837.
- , , .Smoking cessation interventions for hospitalized smokers.Arch Intern Med.2008;168(18):1950–1960.
- , , , et al.Predictors of smoking cessation after a myocardial infarction.Arch Int Med.2008;168(18):1961–1967.
- , , , .The effectiveness of smoking cessation interventions prior to surgery: a systematic review.Nicotine Tob Res.2008;10(3):407–412.
- , , , et al.Clinical trial comparing nicotine replacement therapy (NRT) plus brief counseling, brief counseling alone, and minimal intervention on smoking cessation in hospital inpatients.Thorax.2003;58:484–488.
- Department of Health and Human Services (DHHS). Treating Tobacco Use and Dependence: 2008 Update. Chapter 7. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.section.28504. Accessed November2009.
- , .Implementation of evidence‐based tobacco use cessation guidelines in managed care organizations.Ann Behav Med.2004;27(1):13–21.
- .Decreasing effect sizes for effectiveness studies—implications for the transport of evidence‐based treatments: comment on Curtis, Ronan, and Borduin (2004).J Fam Psychol.2004;18(3):420–423.
- , , , , , .Efficacy of a smoking cessation program for hospital patients.Arch Intern Med.1997;157(22):2653–2660.
- , , , et al.Feasibility, acceptability, and cost of referring surgical patients for postdischarge cessation support from a quitline.Nicotine Tob Res.2008;10(6):1105–1108.
- .Efficacy and effectiveness trials (and other phases of research) in the development of health promotion programs.Prev Med.1986;15:451–474.
- , , .Psychosocial interventions for smoking cessation in patients with coronary heart disease.Cochrane Database Syst Rev.2008;23(1):CD006886.
- , , , , .The accuracy of self‐reported smoking: a systematic review of the relationship between self‐reported and cotinine‐assessed smoking status.Nicotine Tob Res2009;11(1):12–24.
- , , , , .Relations of cotinine and carbon monoxide to self‐reported smoking in a cohort of smokers and ex‐smokers followed over 5 years.Nicotine Tob Res.2002;4(3):287–294.
- , , , .Error in smoking measures: effects of intervention on relations of cotinine and carbon monoxide to self‐reported smoking. The Lung Health Study Research Group.Am J Public Health.1993;83(9):1251–1257.
- , , , , , .“Implementing smoking bans in American hospitals: results of a national survey.Tob Control.1998;7(1):47–55.
- The Smoking Cessation Clinical Practice Guideline Panel and Staff: the Agency for Health Care Policy and Research Smoking Cessation Clinical Practice Guideline.JAMA.1996;275(16):1270–1280.
- , , , et al.ACC/AHA clinical performance measures for adults with chronic heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Heart Failure Clinical Performance Measures). Endorsed by the Heart Failure Society of America.J Am Coll Cardiol.2005;46(6):1144–1178.
- , , , et al.ACC/AHA guidelines for the management of patients with ST‐elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction).Circulation.2004;110(9):e82–e292.
- , , , et al.ACC/AHA clinical performance measures for adults with ST‐elevation and non‐ST elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures on ST‐Elevation and Non‐ST‐Elevation Myocardial Infarction).J Am Coll Cardiol.2006;47(1):236–265.
- Treating Tobacco Use and Dependence‐Clinicians Packet. A How‐To Guide For Implementing the Public Health Service Clinical Practice Guideline, March2003. Rockville, MD: U.S. Public Health Service, Agency for Healthcare Research and Quality. Available at: http://www.ahrq.gov/clinic/tobacco. Accessed November 2009.
- , , , .Implementing a smoke‐free medical campus: impact on inpatient and employee outcomes.J Hosp Med.2010;5(1):51–54.
- , , , et al.The future of behavior change research: what is needed to improve translation of research into health promotion practice?Ann Behav Med.2004;27:3–12.
- The New York State Smokers' Quitline. Available at: http://www.nysmokefree.com. Accessed November2009.
- Tobacco Cessation Continuing Education for Healthcare Professionals and Counselors. Available at: http://www.tobaccocme.com. Accessed November2009.
- Seton Health Cessation Center. The Butt Stops Here. Relaxation Exercises for Smoking Cessation. 2001. The Butt Stops Here Program. Available at: http://www.setonhealth.org. Accessed November2009.
- U.S. Department of Health and Human Services.Treating Tobacco Use and Dependence. Clinical Practice Guideline.Rockville, MD:Public Health Service;2000.
- , , , , .A randomized controlled trial of smoking cessation counseling after myocardial infarction.Prev Med.2000;30(4):261–268.
- , , , .Comorbidity measures for use with administrative data.Med Care.1998:36(1):8–27.
- Tobacco Use Supplement to the Current Population Survey (TUS‐CPS). Available at: http://riskfactor.cancer.gov/studies/tus‐cps/info.html. Accessed November 2009.
- , , .Comparison of National Death Index and world wide web death searches.Am J of Epidemiol.2000;152(2):107–111.
- , , , et al.Post‐myocardial infarction smoking cessation counseling: associations with immediate and late mortality in older Medicare patients.Am J Med.2005;118(3):269–275.
- , , .Inpatient smoking‐cessation counseling and all‐cause mortality in patients with acute myocardial infarction.Am Heart J.2007;154(2):213–220.
- , , , et al.Intensive smoking cessation intervention reduces mortality in high‐risk smokers with cardiovascular disease.Chest.2007;131:446–452.
- , , , , .Dissemination of an effective inpatient tobacco use cessation program.Nicotine Tob Res.2005;7(1):129–137.
- , , .Interventions for smoking cessation in hospitalized patients.Cochrane Database Syst Rev.2007;3:CD001837.
- , , .Smoking cessation interventions for hospitalized smokers.Arch Intern Med.2008;168(18):1950–1960.
- , , , et al.Predictors of smoking cessation after a myocardial infarction.Arch Int Med.2008;168(18):1961–1967.
- , , , .The effectiveness of smoking cessation interventions prior to surgery: a systematic review.Nicotine Tob Res.2008;10(3):407–412.
- , , , et al.Clinical trial comparing nicotine replacement therapy (NRT) plus brief counseling, brief counseling alone, and minimal intervention on smoking cessation in hospital inpatients.Thorax.2003;58:484–488.
- Department of Health and Human Services (DHHS). Treating Tobacco Use and Dependence: 2008 Update. Chapter 7. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.section.28504. Accessed November2009.
- , .Implementation of evidence‐based tobacco use cessation guidelines in managed care organizations.Ann Behav Med.2004;27(1):13–21.
- .Decreasing effect sizes for effectiveness studies—implications for the transport of evidence‐based treatments: comment on Curtis, Ronan, and Borduin (2004).J Fam Psychol.2004;18(3):420–423.
- , , , , , .Efficacy of a smoking cessation program for hospital patients.Arch Intern Med.1997;157(22):2653–2660.
- , , , et al.Feasibility, acceptability, and cost of referring surgical patients for postdischarge cessation support from a quitline.Nicotine Tob Res.2008;10(6):1105–1108.
- .Efficacy and effectiveness trials (and other phases of research) in the development of health promotion programs.Prev Med.1986;15:451–474.
- , , .Psychosocial interventions for smoking cessation in patients with coronary heart disease.Cochrane Database Syst Rev.2008;23(1):CD006886.
- , , , , .The accuracy of self‐reported smoking: a systematic review of the relationship between self‐reported and cotinine‐assessed smoking status.Nicotine Tob Res2009;11(1):12–24.
- , , , , .Relations of cotinine and carbon monoxide to self‐reported smoking in a cohort of smokers and ex‐smokers followed over 5 years.Nicotine Tob Res.2002;4(3):287–294.
- , , , .Error in smoking measures: effects of intervention on relations of cotinine and carbon monoxide to self‐reported smoking. The Lung Health Study Research Group.Am J Public Health.1993;83(9):1251–1257.
Copyright © 2010 Society of Hospital Medicine
Outcomes for Inpatient Gainsharing
Hospitals are challenged to improve quality while reducing costs, yet traditional methods of cost containment have had limited success in aligning the goals of hospitals and physicians. Physicians directly control more than 80% of total medical costs.1 The current fee‐for‐service system encourages procedures and the use of hospital resources. Without the proper incentives to gain active participation and collaboration of the medical staff in improving the efficiency of care, the ability to manage medical costs and improve hospital operational and financial performance is hampered. A further challenge is to encourage physicians to improve the quality of care and maintain safe medical practice. While several examples of pay‐for‐performance (P4P) have previously been attempted to increase efficiency, gainsharing offers real opportunities to achieve these outcomes.
Previous reports regarding the results of gainsharing programs describe its use in outpatient settings and its limited ability to reduce costs for inpatient care for surgical implants such as coronary stents2 or orthopedic prostheses.3 The present study represents the largest series to date using a gainsharing model in a comprehensive program of inpatient care at a tertiary care medical center.
Patients and Methods
Beth Israel Medical Center is a 1000‐bed tertiary care university‐affiliated teaching hospital, located in New York City. The hospital serves a large and ethnically diverse community predominantly located in the lower east side of Manhattan and discharged about 50,000 patients per year during the study period of July 2006 through June 2009.
Applied Medical Software, Inc. (AMS, Collingswood, NJ) analyzed hospital data for case mix and severity. To establish best practice norms (BPNs), AMS used inpatient discharge data (UB‐92) to determine costs by APR‐DRG's4 during calendar year 2005, prior to the inception of the program to establish BPNs. Costs were allocated into specific areas listed in Table 1. A minimum of 10 cases was necessary in each DRG. Cost outliers (as defined by the mean cost of the APR DRG plus 3 standard deviations) were excluded. These data were used to establish a baseline for each physician and a BPN, which was set at the top 25th percentile for each specific APR DRG. BPNs were determined after exclusions using the following criteria:
Each eligible physician had to have at least 10 admissions within their specialty;
Each eligible DRG had to have at least 5 qualifying physicians within a medical specialty;
Each eligible APR DRG had to have at least 3 qualifying admissions;
If the above criteria are met, the BPN was set at the mean of the top 25th percentile of physicians (25% of the physicians with the lowest costs).
| |
| Per diem hospital bed cost | Pharmacy |
| Critical care (ICU and CCU) | Laboratory |
| Medical surgical supplies and implants | Cardiopulmonary care |
| Operating room costs | Blood bank |
| Radiology | Intravenous therapy |
Once BPNs were determined, patients were grouped by physician and compared to the BPN for a particular APR DRG. All patients of participating physicians with qualifying APR DRGs were included in the analysis reports summarizing these results, computed quarterly and distributed to each physician. Obstetrical and psychiatric admissions were excluded in the program. APR DRG data for each physician was compared from year to year to determine whether an individual physician demonstrated measurable improvement in performance.
The gainsharing program was implemented in 2006. Physician participation was voluntary. Payments were made to physicians without any risk or penalties from participation. Incentives were based on individual performance. Incentives for nonsurgical admissions were intended to offset the loss of physician income related to more efficient medical management and a reduced hospital length of stay (LOS). Income for surgical admissions was intended to reward physicians for efficient preoperative and postoperative care.
The methodology provides financial incentives for physicians for each hospital discharge in 2 ways:
Improvement in costs per case against their own historical performance;
Cost per case performance compared to BPN.
In the first year of the gainsharing program, two thirds of the total allowable incentive payments were allocated to physicians' improvement, with one third based on a performance metric. Payments for improvement were phased out over the first 3 years of the gainsharing program, with payments focused fully on performance in Year 3. Cases were adjusted for case‐mix and severity of illness (four levels of APR DRG). Physicians were not penalized for any cases in which costs greatly exceeded BPN. A floor was placed at the BPN and no additional financial incentives were paid for surpassing it. Baselines and BPNs were recalculated yearly.
A key aspect of the gainsharing program was the establishment of specific quality parameters (Table 2) that need to be met before any incentive payments were made. A committee regularly reviewed the quality performance data of each physician to determine eligibility for payments. Physicians were considered to be ineligible for incentive compensation until the next measurement period if there was evidence of failure to adequately meet these measures. At least 80% compliance with core measures (minimum 5 discharges in each domain) was expected. Infectious complication rates were to remain not more than 1 standard deviation above National Healthcare Safety Network rates during the same time period. In addition, payments were withheld from physicians if it was found that the standard of care was not met for any morbidity or mortality that was peer reviewed or if there were any significant patient complaints. Readmission rates were expected to remain at or below the baseline established during the previous 12 months by DRG.
| Quality Measure | Goal |
|---|---|
| |
| Readmissions within 7 days for the same or related diagnosis | Decrease, or less than 10% of discharges |
| Documentationquality and timeliness of medical record and related documentation including date, time, and sign all chart entries | No more than 20% of average monthly discharged medical records incomplete for more than 30 days |
| Consultation with social work/discharge planner within 24 hours of admission for appropriate pts | >80% of all appropriate cases |
| Timely switch from intravenous to oral antibiotics in accordance with hospital policy (%) | >80 |
| Unanticipated return to the operating room | Decrease or < 5% |
| Patient complaints | Decrease |
| Patient satisfaction (HCAHPS) | >75% physician domain |
| Ventilator associated pneumonia | Decrease or < 5% |
| Central line associated blood stream infections | Decrease or < 5 per 1000 catheter days. |
| Surgical site infections | Decrease or within 1 standard deviation of NHSN |
| Antibiotic prophylaxis (%) | >80 |
| Inpatient mortality | Decrease or <1% |
| Medication errors | Decrease or <1% |
| Delinquent medical records | <5 charts delinquent more than 30 days |
| Falls with injury | Decrease or <1% |
| AMI: aspirin on arrival and discharge (%) | >80 |
| AMI‐ACEI or ARB for LVSD (%) | >80 |
| Adult smoking cessation counseling (%) | >80 |
| AMI‐ Beta blocker prescribed at arrival and discharge (%) | >80 |
| CHF: discharge instructions (%) | >80 |
| CHF: Left ventricular function assessment (%) | >80 |
| CHF: ACEI or ARB for left ventricular systolic dysfunction (%) | >80 |
| CHF: smoking cessation counseling (%) | >80 |
| Pneumonia: O2 assessment, pneumococcal vaccine, blood culture and sensitivity before first antibiotic, smoking cessation counseling (%) | >80 |
Employed and private practice community physicians were both eligible for the gainsharing program. Physician participation in the program was voluntary. All patients admitted to the Medical Center received notification on admission about the program. The aggregate costs by DRG were calculated quarterly. Savings over the previous yearif anywere calculated. A total of 20% of the savings was used to administer the program and for incentive payments to physicians.
From July 1, 2006 through September 2008, only commercial managed care cases were eligible for this program. As a result of the approval of the gainsharing program as a demonstration project by the Centers for Medicare and Medicaid Services (CMS), Medicare cases were added to the program starting October 1, 2008.
Physician Payment Calculation Methodology
Performance Incentive
The performance incentive was intended to reward demonstrated levels of performance. Accordingly, a physician's share in hospital savings was in proportion to the relationship between their individual performance and the BPN. This computation was the same for both surgical and medical admissions. The following equation illustrates the computation of performance incentives for participating physicians:
This computation was made at the specific severity level for each hospital discharge. Payment for the performance incentive was made only to physicians at or below the 90th percentile of physicians.
Improvement Incentive
The improvement incentive was intended to encourage positive change. No payments were made from the improvement incentive unless an individual physician demonstrated measurable improvement in operational performance for either surgical or medical admissions. However, because physicians who admitted nonsurgical cases experienced reduced income as they help the hospital to improve operational performance, the methodology for calculating the improvement incentive was different for medical as opposed to surgical cases, as shown below.
For Medical DRGs:
For each severity level the following is calculated:
For Surgical DRGs:
Cost savings were calculated quarterly and defined as the cost per case before the gainsharing program began minus the actual case cost by APR DRG. Student's t‐test was used for continuous data and the categorical data trends were analyzed using Mantel‐Haenszel Chi‐Square.
At least every 6 months, all participating physicians received case‐specific and cost‐centered data about their discharges. They also received a careful explanation of opportunities for financial or quality improvement.
Results
Over the 3‐year period, 184 physicians enrolled, representing 54% of those eligible. The remainder of physicians either decided not to enroll or were not eligible due to inadequate number of index DRG cases or excluded diagnoses. Payer mix was 27% Medicare and 48% of the discharges were commercial and managed care. The remaining cases were a combination of Medicaid and self‐pay. A total of 29,535 commercial and managed care discharges were evaluated from participating physicians (58%) and 20,360 similar discharges from non‐participating physicians. This number of admissions accounted for 29% of all hospital discharges during this time period. Surgical admissions accounted for 43% and nonsurgical admissions for 57%. The distribution of patients by service is shown in Table 3. Pulmonary and cardiology diagnoses were the most frequent reasons for medical admissions. General and head and neck surgery were the most frequent surgical admissions. During the time period of the gainsharing program, the medical center saved $25.1 million for costs attributed to these cases. Participating physicians saved $6.9 million more than non‐participating physicians (P = 0.02, Figure 1), but all discharges demonstrated cost savings during the study period. Cost savings (Figure 2) resulted from savings in medical/surgical supplies and implants (35%), daily hospital costs, (28%), intensive care unit costs (16%) and coronary care unit costs (15%), and operating room costs (8%). Reduction in cost from reduced magnetic resonance imaging (MRI) use was not statistically significant. There were minimal increases in costs due to computed tomography (CT) scan use, cardiopulmonary care, laboratory use, pharmacy and blood bank, but none of these reached statistical significance.
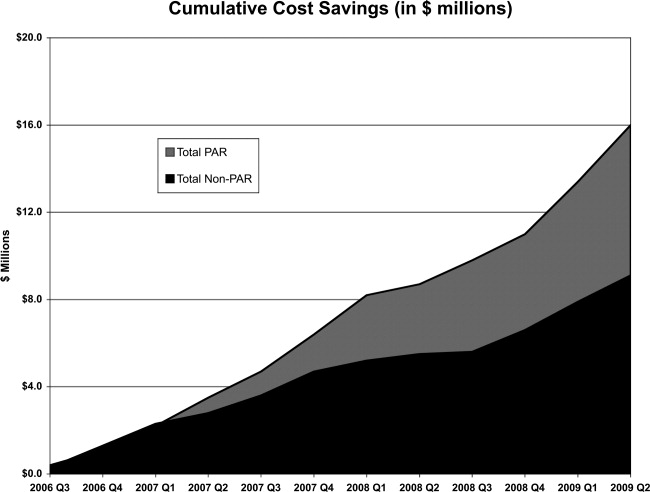
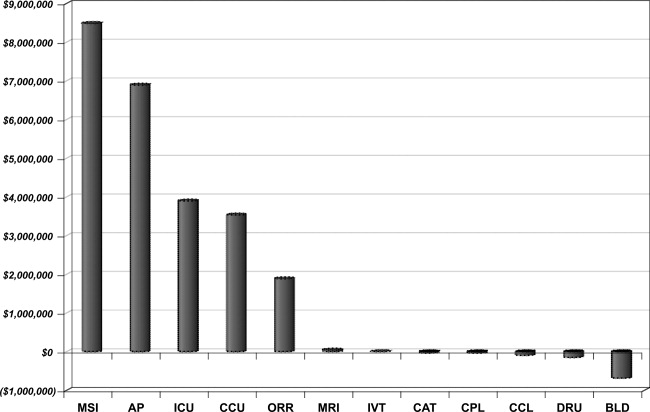
| Admissions by Service | Number (%) |
|---|---|
| |
| Cardiology | 4512 (15.3) |
| Orthopedic surgery | 3994 (13.5) |
| Gastroenterology | 3214 (10.9) |
| General surgery | 2908 (9.8) |
| Cardiovascular surgery | 2432 (8.2) |
| Pulmonary | 2212 (7.5) |
| Neurology | 2064 (7.0) |
| Oncology | 1217 (4.1) |
| Infectious disease | 1171 (4.0) |
| Endocrinology | 906 (3.1) |
| Nephrology | 826 (2.8) |
| Open heart surgery | 656 (2.2) |
| Interventional cardiology | 624 (2.1) |
| Gynecological surgery | 450 (1.5) |
| Urological surgery | 326 (1.1) |
| ENT surgery | 289 (1.0) |
| Obstetrics without delivery | 261 (0.9) |
| Hematology | 253 (0.9) |
| Orthopedicsnonsurgical | 241 (0.8) |
| Rehabilitation | 204 (0.7) |
| Otolaryngology | 183 (0.6) |
| Rheumatology | 165 (0.6) |
| General medicine | 162 (0.5) |
| Neurological surgery | 112 (0.4) |
| Urology | 101 (0.3) |
| Dermatology | 52 (0.2) |
| Grand total | 29535 (100.0) |
Hospital LOS decreased 9.8% from baseline among participating doctors, while LOS decreased 9.0% among non‐participating physicians; this difference was not statistically significant (P = 0.6). Participating physicians reduced costs by an average of $7,871 per quarter, compared to a reduction in costs by $3,018 for admissions by non‐participating physicians (P < 0.0001). The average savings per admission for the participating physicians were $1,835, and for non‐participating physicians were $1,107, a difference of $728 per admission. Overall, cost savings during the three year period averaged $105,000 per physician who participated in the program and $67,000 per physician who did not (P < 0.05). There was not a statistical difference in savings between medical and surgical admissions (P = 0.24).
Deviations from quality thresholds were identified during this time period. Some or all of the gainsharing income was withheld from 8% of participating physicians due to quality issues, incomplete medical records, or administrative reasons. Payouts to participating physicians averaged $1,866 quarterly (range $0‐$27,631). Overall, 9.4% of the hospital savings was directly paid to the participating physicians. Compliance with core measures improved in the following domains from year 2006 to 2009; acute myocardial infarction 94% to 98%, congestive heart failure 76% to 93%, pneumonia 88% to 97%, and surgical care improvement project 90% to 97%, (P = 0.17). There was no measurable increase in 30‐day mortality or readmission by APR‐DRG. The number of incomplete medical records decreased from an average of 43% of the total number of records in the second quarter of 2006 to 30% in the second quarter of 2009 (P < 0.0001). Other quality indicators remained statistically unchanged.
Discussion
The promise of gainsharing may motivate physicians to decrease hospital costs while maintaining quality medical care, since it aligns physician and hospital incentives. Providing a reward to physicians creates positive reinforcement, which is more effective than warnings against poor performing physicians (carrot vs. stick).5, 6 This study is the first and largest of its kind to show the results of a gainsharing program for inpatient medical and surgical admissions and demonstrates that significant cost savings may be achieved. This is similar to previous studies that have shown positive outcomes for pay‐for‐performance programs.7
Participating physicians in the present study accumulated almost $7 million more in savings than non‐participating physicians. Over time this difference has increased, possibly due to a learning curve in educating participating physicians and the way in which information about their performance is given back to them. A significant portion of the hospital's cost savings was through improvements in documentation and completion of medical records. While there was an actual reduction in average length of stay (ALOS), better documentation may also have contributed to adjusting the severity level within each DRG.
Using financial incentives to positively impact on physician behavior is not new. One program in a community‐based hospitalist group reported similar improvements in medical record documentation, as well as improvements in physician meeting attendance and quality goals.8 Another study found that such hospital programs noted improved physician engagement and commitment to best practices and to improving the quality of care.9
There is significant experience in the outpatient setting using pay‐for‐performance programs to enhance quality. Millett et al.10 demonstrated a reduction in smoking among patients with diabetes in a program in the United Kingdom. Another study in Rochester, New York that used pay‐for‐performance incentives demonstrated better diabetes management.11 Mandel and Kotagal12 demonstrated improved asthma care utilizing a quality incentive program.
The use of financial motivation for physicians, as part of a hospital pay‐for‐performance program, has been shown to lead to improvements in quality performance scores when compared to non pay‐for‐performance hospitals.13 Berthiaume demonstrated decreased costs and improvements in risk‐adjusted complications and risk‐adjusted LOS in patents admitted for acute coronary intervention in a pay‐for‐performance program.14 Quality initiatives were integral for the gainsharing program, since measures such as surgical site infections may increase LOS and hospital costs. Core measures related to the care of patients with acute myocardial infarction, heart failure, pneumonia, and surgical prophylaxis steadily improved since the initiation of the gainsharing program. Gainsharing programs also enhance physician compliance with administrative responsibilities such as the completion of medical records.
One unexpected finding of our study was that there was a cost savings per admission even in the patients of physicians who did not participate in the gainsharing program. While the participating physicians showed statistically significant improvements in cost savings, savings were found in both groups. This raises the question as to whether these cost reductions could have been impacted by other factors such as new labor or vendor contracts, better documentation, improved operating room utilization and improved and timely documentation in the medical record. Another possibility is the Hawthorne effect on physicians, who altered their behavior with knowledge that process and outcome measurement were being measured. Physicians who voluntarily sign up for a gainsharing program would be expected to be more committed to the success of this program than physicians who decide to opt out. While this might appear to be a selection bias it does illustrate the point that motivated physicians are more likely to positively change their practice behaviors. However, one might suggest that financial savings directly attributed to the gainsharing program was not the $25.1 million saved during the 3 years overall, but the difference between participating and non‐participating physicians, or $6.9 million.
While the motivation to complete medical records was significant (gainsharing dollars were withheld from doctors with more than 5 incomplete charts for more than 30 days) it was not the only reason why the number of delinquent chart percentage decreased during the study period. While the improvement was significant, there are still more opportunities to reduce the number of incomplete charts. Hospital regulatory inspections and periodic physician education were also likely to have reduced the number of incomplete inpatient charts during this time period and may do so in the future.15
The program focused on the physician activities that have the greatest impact on hospital costs. While optimizing laboratory, blood bank, and pharmacy management decreased hospital costs; we found that improvements in patient LOS, days in an intensive care unit, and management of surgical implants had the greatest impact on costs. Orthopedic surgeons began to use different implants, and all surgeons refrained from opening disposable surgical supplies until needed. Patients in intensive care unit beds stable for transfer were moved to regular medical/surgical rooms earlier. Since the program helped physicians understand the importance of LOS, many physicians increased their rounding on weekends and considered LOS implications before ordering diagnostic procedures that could be performed as an outpatient. Nurses, physician extenders such as physician assistants, and social workers have played an important role in streamlining patient care and hospital discharge; however, they were not directly rewarded under this program.
There are challenges to aligning the incentives of internists compared to procedure‐based specialists. This may be that the result of surgeons receiving payment for bundled care and thus the incentives are already aligned. The incentive of the program for internists, who get paid for each per daily visit, was intended to overcome the lost income resulting from an earlier discharge. Moreover, in the present study, only the discharging physician received incentive payments for each case. Patient care is undoubtedly a team effort and many physicians (radiologists, anesthesiologists, pathologists, emergency medicine physicians, consultant specialty physicians, etc.) are clearly left out in the present gainsharing program. Aligning the incentives of these physicians might be necessary. Furthermore, the actions of other members of the medical team and consultants, by their behaviors, could limit the incentive payments for the discharging physician. The discharging physician is often unable to control the transfer of a patient from a high‐cost or severity unit, or improve the timeliness of consulting physicians. Previous authors have raised the issue as to whether a physician should be prevented from payment because of the actions of another member of the medical team.16
Ensuring a fair and transparent system is important in any pay‐for‐performance program. The present gainsharing program required sophisticated data analysis, which added to the costs of the program. To implement such a program, data must be clear and understandable, segregated by DRG and severity adjusted. But should the highest reward payments go to those who perform the best or improve the most? In the present study, some physicians were consistently unable to meet quality benchmarks. This may be related to several factors, 1 of which might be a particular physician's case mix. Some authors have raised concerns that pay‐for‐performance programs may unfairly impact physicians who care for more challenging or patients from disadvantaged socioeconomic circumstances.17 Other authors have questioned whether widespread implementation of such a program could potentially increase healthcare disparities in the community.18 It has been suggested by Greene and Nash that for a program to be successful, physicians who feel they provide good care yet but are not rewarded should be given an independent review.16 Such a process is important to prevent resentment among physicians who are unable to meet benchmarks for payment, despite hard work.19 Conversely, other studies have found that many physicians who receive payments in a pay‐for‐performance system do not necessarily consciously make improvement to enhance financial performance.20 Only 54% of eligible physicians participated in the present gainsharing program. This is likely due to lack of understanding about the program, misperceptions about the ethics of such programs, perceived possible negative patient outcome, conflict of interest and mistrust.21, 22 This underscores the importance of providing understandable performance results, education, and a physician champion to help facilitate communication and enhanced outcomes. What is clear is that the perception by participating physicians is that this program is worthwhile as the number of participating physicians has steadily increased and it has become an incentive for new providers to choose this medical center over others.
In conclusion, the results of the present study show that physicians can help hospitals reduce inpatients costs while maintaining or improving hospital quality. Improvements in patient LOS, implant costs, overall costs per admission, and medical record completion were noted. Further work is needed to improve physician education and better understand the impact of uneven physician case mix. Further efforts are necessary to allow other members of the health care team to participate and benefit from gainsharing.
- ,,, et al.Guided care and the cost of complex healthcare: a preliminary report.Am J Manag Care.2009;15(8):555–559.
- ,.Hospital‐physician gainsharing in cardiology.Health Aff (Millwood).2008;27(3):803–812.
- ,,,.AOA Symposium. Gainsharing in orthopaedics: passing fancy or wave of the future?J Bone Joint Surg Am.2007;89(9):2075–2083.
- All Patient Defined Diagnosis Related Groups™ ‐ 3M Health Information Systems,St Paul, MN.
- ,,, et al.Guided care and the cost of complex healthcare: a preliminary report.Am J Manag Care.2009;15(8):555–559.
- .Best practices in record completion.J Med Pract Manage.2004;20(1):18–22.
- ,,, et al.Return on investment in pay for performance: a diabetes case study.J Healthc Manag.2006;51(6):365–374; discussion 375‐376.
- .Use of pay for performance in a community hospital private hospitalists group: a preliminary report.Trans Am Clin Climatol Assoc.2007;188:263–272.
- .Making the grade with pay for performance: 7 lessons from best‐performing hospitals.Healthc Financ Manage.2006;60(12):79–85.
- ,,,,.Impact of a pay‐for‐performance incentive on support for smoking cessation and on smoking prevalence among people with diabetes.CMAJ.2007;176(12):1705–1710.
- ,,, et al,Effects of paying physicians based on their relative performance for quality.J Gen Intern Med.2007;22(6):872–876.
- ,.Pay for performance alone cannot drive quality.Arch Pediatr Adolesc Med.2007;161(7):650–655.
- .What's the return? Assessing the effect of “pay‐for‐performance” initiatives on the quality of care delivery.Med Care Res Rev.2006;63(1 suppl)( ):29S–48S.
- ,,,,.Aligning financial incentives with “Get With the Guidelines” to improve cardiovascular care.Am J Manag Care.2004;10(7 pt 2):501–504.
- .Sampling best practices. Managing delinquent records.J AHIMA.1997;68(8):28,30.
- ,.Pay for performance: an overview of the literature.Am J Med Qual.2009;24;140–163.
- ,,.Physician‐level P4P:DOA? Can quality‐based payments be resuscitated?Am J Manag Care.2007;13(5):233–236.
- ,,, et al.Will pay for performance and quality reporting affect health care disparities?Health Aff (Millwood).2007;26(3):w405–w414.
- ,,.The experience of pay for performance in English family practice: a qualitative study.Ann Fam Med.2008;8(3):228–234.
- ,,, et al.Will financial incentives stimulate quality improvement? Reactions from frontline physicians.Am J Med Qual.2006;21(6):367–374.
- ,,.Pay for performance in orthopedic surgery.Clin Orthop Relat Res.2007;457:87–95.
- ,.Pay for performance survey of diagnostic radiology faculty and trainees.J Am Coll Radiol.2007;4(6):411–415.
Hospitals are challenged to improve quality while reducing costs, yet traditional methods of cost containment have had limited success in aligning the goals of hospitals and physicians. Physicians directly control more than 80% of total medical costs.1 The current fee‐for‐service system encourages procedures and the use of hospital resources. Without the proper incentives to gain active participation and collaboration of the medical staff in improving the efficiency of care, the ability to manage medical costs and improve hospital operational and financial performance is hampered. A further challenge is to encourage physicians to improve the quality of care and maintain safe medical practice. While several examples of pay‐for‐performance (P4P) have previously been attempted to increase efficiency, gainsharing offers real opportunities to achieve these outcomes.
Previous reports regarding the results of gainsharing programs describe its use in outpatient settings and its limited ability to reduce costs for inpatient care for surgical implants such as coronary stents2 or orthopedic prostheses.3 The present study represents the largest series to date using a gainsharing model in a comprehensive program of inpatient care at a tertiary care medical center.
Patients and Methods
Beth Israel Medical Center is a 1000‐bed tertiary care university‐affiliated teaching hospital, located in New York City. The hospital serves a large and ethnically diverse community predominantly located in the lower east side of Manhattan and discharged about 50,000 patients per year during the study period of July 2006 through June 2009.
Applied Medical Software, Inc. (AMS, Collingswood, NJ) analyzed hospital data for case mix and severity. To establish best practice norms (BPNs), AMS used inpatient discharge data (UB‐92) to determine costs by APR‐DRG's4 during calendar year 2005, prior to the inception of the program to establish BPNs. Costs were allocated into specific areas listed in Table 1. A minimum of 10 cases was necessary in each DRG. Cost outliers (as defined by the mean cost of the APR DRG plus 3 standard deviations) were excluded. These data were used to establish a baseline for each physician and a BPN, which was set at the top 25th percentile for each specific APR DRG. BPNs were determined after exclusions using the following criteria:
Each eligible physician had to have at least 10 admissions within their specialty;
Each eligible DRG had to have at least 5 qualifying physicians within a medical specialty;
Each eligible APR DRG had to have at least 3 qualifying admissions;
If the above criteria are met, the BPN was set at the mean of the top 25th percentile of physicians (25% of the physicians with the lowest costs).
| |
| Per diem hospital bed cost | Pharmacy |
| Critical care (ICU and CCU) | Laboratory |
| Medical surgical supplies and implants | Cardiopulmonary care |
| Operating room costs | Blood bank |
| Radiology | Intravenous therapy |
Once BPNs were determined, patients were grouped by physician and compared to the BPN for a particular APR DRG. All patients of participating physicians with qualifying APR DRGs were included in the analysis reports summarizing these results, computed quarterly and distributed to each physician. Obstetrical and psychiatric admissions were excluded in the program. APR DRG data for each physician was compared from year to year to determine whether an individual physician demonstrated measurable improvement in performance.
The gainsharing program was implemented in 2006. Physician participation was voluntary. Payments were made to physicians without any risk or penalties from participation. Incentives were based on individual performance. Incentives for nonsurgical admissions were intended to offset the loss of physician income related to more efficient medical management and a reduced hospital length of stay (LOS). Income for surgical admissions was intended to reward physicians for efficient preoperative and postoperative care.
The methodology provides financial incentives for physicians for each hospital discharge in 2 ways:
Improvement in costs per case against their own historical performance;
Cost per case performance compared to BPN.
In the first year of the gainsharing program, two thirds of the total allowable incentive payments were allocated to physicians' improvement, with one third based on a performance metric. Payments for improvement were phased out over the first 3 years of the gainsharing program, with payments focused fully on performance in Year 3. Cases were adjusted for case‐mix and severity of illness (four levels of APR DRG). Physicians were not penalized for any cases in which costs greatly exceeded BPN. A floor was placed at the BPN and no additional financial incentives were paid for surpassing it. Baselines and BPNs were recalculated yearly.
A key aspect of the gainsharing program was the establishment of specific quality parameters (Table 2) that need to be met before any incentive payments were made. A committee regularly reviewed the quality performance data of each physician to determine eligibility for payments. Physicians were considered to be ineligible for incentive compensation until the next measurement period if there was evidence of failure to adequately meet these measures. At least 80% compliance with core measures (minimum 5 discharges in each domain) was expected. Infectious complication rates were to remain not more than 1 standard deviation above National Healthcare Safety Network rates during the same time period. In addition, payments were withheld from physicians if it was found that the standard of care was not met for any morbidity or mortality that was peer reviewed or if there were any significant patient complaints. Readmission rates were expected to remain at or below the baseline established during the previous 12 months by DRG.
| Quality Measure | Goal |
|---|---|
| |
| Readmissions within 7 days for the same or related diagnosis | Decrease, or less than 10% of discharges |
| Documentationquality and timeliness of medical record and related documentation including date, time, and sign all chart entries | No more than 20% of average monthly discharged medical records incomplete for more than 30 days |
| Consultation with social work/discharge planner within 24 hours of admission for appropriate pts | >80% of all appropriate cases |
| Timely switch from intravenous to oral antibiotics in accordance with hospital policy (%) | >80 |
| Unanticipated return to the operating room | Decrease or < 5% |
| Patient complaints | Decrease |
| Patient satisfaction (HCAHPS) | >75% physician domain |
| Ventilator associated pneumonia | Decrease or < 5% |
| Central line associated blood stream infections | Decrease or < 5 per 1000 catheter days. |
| Surgical site infections | Decrease or within 1 standard deviation of NHSN |
| Antibiotic prophylaxis (%) | >80 |
| Inpatient mortality | Decrease or <1% |
| Medication errors | Decrease or <1% |
| Delinquent medical records | <5 charts delinquent more than 30 days |
| Falls with injury | Decrease or <1% |
| AMI: aspirin on arrival and discharge (%) | >80 |
| AMI‐ACEI or ARB for LVSD (%) | >80 |
| Adult smoking cessation counseling (%) | >80 |
| AMI‐ Beta blocker prescribed at arrival and discharge (%) | >80 |
| CHF: discharge instructions (%) | >80 |
| CHF: Left ventricular function assessment (%) | >80 |
| CHF: ACEI or ARB for left ventricular systolic dysfunction (%) | >80 |
| CHF: smoking cessation counseling (%) | >80 |
| Pneumonia: O2 assessment, pneumococcal vaccine, blood culture and sensitivity before first antibiotic, smoking cessation counseling (%) | >80 |
Employed and private practice community physicians were both eligible for the gainsharing program. Physician participation in the program was voluntary. All patients admitted to the Medical Center received notification on admission about the program. The aggregate costs by DRG were calculated quarterly. Savings over the previous yearif anywere calculated. A total of 20% of the savings was used to administer the program and for incentive payments to physicians.
From July 1, 2006 through September 2008, only commercial managed care cases were eligible for this program. As a result of the approval of the gainsharing program as a demonstration project by the Centers for Medicare and Medicaid Services (CMS), Medicare cases were added to the program starting October 1, 2008.
Physician Payment Calculation Methodology
Performance Incentive
The performance incentive was intended to reward demonstrated levels of performance. Accordingly, a physician's share in hospital savings was in proportion to the relationship between their individual performance and the BPN. This computation was the same for both surgical and medical admissions. The following equation illustrates the computation of performance incentives for participating physicians:
This computation was made at the specific severity level for each hospital discharge. Payment for the performance incentive was made only to physicians at or below the 90th percentile of physicians.
Improvement Incentive
The improvement incentive was intended to encourage positive change. No payments were made from the improvement incentive unless an individual physician demonstrated measurable improvement in operational performance for either surgical or medical admissions. However, because physicians who admitted nonsurgical cases experienced reduced income as they help the hospital to improve operational performance, the methodology for calculating the improvement incentive was different for medical as opposed to surgical cases, as shown below.
For Medical DRGs:
For each severity level the following is calculated:
For Surgical DRGs:
Cost savings were calculated quarterly and defined as the cost per case before the gainsharing program began minus the actual case cost by APR DRG. Student's t‐test was used for continuous data and the categorical data trends were analyzed using Mantel‐Haenszel Chi‐Square.
At least every 6 months, all participating physicians received case‐specific and cost‐centered data about their discharges. They also received a careful explanation of opportunities for financial or quality improvement.
Results
Over the 3‐year period, 184 physicians enrolled, representing 54% of those eligible. The remainder of physicians either decided not to enroll or were not eligible due to inadequate number of index DRG cases or excluded diagnoses. Payer mix was 27% Medicare and 48% of the discharges were commercial and managed care. The remaining cases were a combination of Medicaid and self‐pay. A total of 29,535 commercial and managed care discharges were evaluated from participating physicians (58%) and 20,360 similar discharges from non‐participating physicians. This number of admissions accounted for 29% of all hospital discharges during this time period. Surgical admissions accounted for 43% and nonsurgical admissions for 57%. The distribution of patients by service is shown in Table 3. Pulmonary and cardiology diagnoses were the most frequent reasons for medical admissions. General and head and neck surgery were the most frequent surgical admissions. During the time period of the gainsharing program, the medical center saved $25.1 million for costs attributed to these cases. Participating physicians saved $6.9 million more than non‐participating physicians (P = 0.02, Figure 1), but all discharges demonstrated cost savings during the study period. Cost savings (Figure 2) resulted from savings in medical/surgical supplies and implants (35%), daily hospital costs, (28%), intensive care unit costs (16%) and coronary care unit costs (15%), and operating room costs (8%). Reduction in cost from reduced magnetic resonance imaging (MRI) use was not statistically significant. There were minimal increases in costs due to computed tomography (CT) scan use, cardiopulmonary care, laboratory use, pharmacy and blood bank, but none of these reached statistical significance.
| Admissions by Service | Number (%) |
|---|---|
| |
| Cardiology | 4512 (15.3) |
| Orthopedic surgery | 3994 (13.5) |
| Gastroenterology | 3214 (10.9) |
| General surgery | 2908 (9.8) |
| Cardiovascular surgery | 2432 (8.2) |
| Pulmonary | 2212 (7.5) |
| Neurology | 2064 (7.0) |
| Oncology | 1217 (4.1) |
| Infectious disease | 1171 (4.0) |
| Endocrinology | 906 (3.1) |
| Nephrology | 826 (2.8) |
| Open heart surgery | 656 (2.2) |
| Interventional cardiology | 624 (2.1) |
| Gynecological surgery | 450 (1.5) |
| Urological surgery | 326 (1.1) |
| ENT surgery | 289 (1.0) |
| Obstetrics without delivery | 261 (0.9) |
| Hematology | 253 (0.9) |
| Orthopedicsnonsurgical | 241 (0.8) |
| Rehabilitation | 204 (0.7) |
| Otolaryngology | 183 (0.6) |
| Rheumatology | 165 (0.6) |
| General medicine | 162 (0.5) |
| Neurological surgery | 112 (0.4) |
| Urology | 101 (0.3) |
| Dermatology | 52 (0.2) |
| Grand total | 29535 (100.0) |
Hospital LOS decreased 9.8% from baseline among participating doctors, while LOS decreased 9.0% among non‐participating physicians; this difference was not statistically significant (P = 0.6). Participating physicians reduced costs by an average of $7,871 per quarter, compared to a reduction in costs by $3,018 for admissions by non‐participating physicians (P < 0.0001). The average savings per admission for the participating physicians were $1,835, and for non‐participating physicians were $1,107, a difference of $728 per admission. Overall, cost savings during the three year period averaged $105,000 per physician who participated in the program and $67,000 per physician who did not (P < 0.05). There was not a statistical difference in savings between medical and surgical admissions (P = 0.24).
Deviations from quality thresholds were identified during this time period. Some or all of the gainsharing income was withheld from 8% of participating physicians due to quality issues, incomplete medical records, or administrative reasons. Payouts to participating physicians averaged $1,866 quarterly (range $0‐$27,631). Overall, 9.4% of the hospital savings was directly paid to the participating physicians. Compliance with core measures improved in the following domains from year 2006 to 2009; acute myocardial infarction 94% to 98%, congestive heart failure 76% to 93%, pneumonia 88% to 97%, and surgical care improvement project 90% to 97%, (P = 0.17). There was no measurable increase in 30‐day mortality or readmission by APR‐DRG. The number of incomplete medical records decreased from an average of 43% of the total number of records in the second quarter of 2006 to 30% in the second quarter of 2009 (P < 0.0001). Other quality indicators remained statistically unchanged.
Discussion
The promise of gainsharing may motivate physicians to decrease hospital costs while maintaining quality medical care, since it aligns physician and hospital incentives. Providing a reward to physicians creates positive reinforcement, which is more effective than warnings against poor performing physicians (carrot vs. stick).5, 6 This study is the first and largest of its kind to show the results of a gainsharing program for inpatient medical and surgical admissions and demonstrates that significant cost savings may be achieved. This is similar to previous studies that have shown positive outcomes for pay‐for‐performance programs.7
Participating physicians in the present study accumulated almost $7 million more in savings than non‐participating physicians. Over time this difference has increased, possibly due to a learning curve in educating participating physicians and the way in which information about their performance is given back to them. A significant portion of the hospital's cost savings was through improvements in documentation and completion of medical records. While there was an actual reduction in average length of stay (ALOS), better documentation may also have contributed to adjusting the severity level within each DRG.
Using financial incentives to positively impact on physician behavior is not new. One program in a community‐based hospitalist group reported similar improvements in medical record documentation, as well as improvements in physician meeting attendance and quality goals.8 Another study found that such hospital programs noted improved physician engagement and commitment to best practices and to improving the quality of care.9
There is significant experience in the outpatient setting using pay‐for‐performance programs to enhance quality. Millett et al.10 demonstrated a reduction in smoking among patients with diabetes in a program in the United Kingdom. Another study in Rochester, New York that used pay‐for‐performance incentives demonstrated better diabetes management.11 Mandel and Kotagal12 demonstrated improved asthma care utilizing a quality incentive program.
The use of financial motivation for physicians, as part of a hospital pay‐for‐performance program, has been shown to lead to improvements in quality performance scores when compared to non pay‐for‐performance hospitals.13 Berthiaume demonstrated decreased costs and improvements in risk‐adjusted complications and risk‐adjusted LOS in patents admitted for acute coronary intervention in a pay‐for‐performance program.14 Quality initiatives were integral for the gainsharing program, since measures such as surgical site infections may increase LOS and hospital costs. Core measures related to the care of patients with acute myocardial infarction, heart failure, pneumonia, and surgical prophylaxis steadily improved since the initiation of the gainsharing program. Gainsharing programs also enhance physician compliance with administrative responsibilities such as the completion of medical records.
One unexpected finding of our study was that there was a cost savings per admission even in the patients of physicians who did not participate in the gainsharing program. While the participating physicians showed statistically significant improvements in cost savings, savings were found in both groups. This raises the question as to whether these cost reductions could have been impacted by other factors such as new labor or vendor contracts, better documentation, improved operating room utilization and improved and timely documentation in the medical record. Another possibility is the Hawthorne effect on physicians, who altered their behavior with knowledge that process and outcome measurement were being measured. Physicians who voluntarily sign up for a gainsharing program would be expected to be more committed to the success of this program than physicians who decide to opt out. While this might appear to be a selection bias it does illustrate the point that motivated physicians are more likely to positively change their practice behaviors. However, one might suggest that financial savings directly attributed to the gainsharing program was not the $25.1 million saved during the 3 years overall, but the difference between participating and non‐participating physicians, or $6.9 million.
While the motivation to complete medical records was significant (gainsharing dollars were withheld from doctors with more than 5 incomplete charts for more than 30 days) it was not the only reason why the number of delinquent chart percentage decreased during the study period. While the improvement was significant, there are still more opportunities to reduce the number of incomplete charts. Hospital regulatory inspections and periodic physician education were also likely to have reduced the number of incomplete inpatient charts during this time period and may do so in the future.15
The program focused on the physician activities that have the greatest impact on hospital costs. While optimizing laboratory, blood bank, and pharmacy management decreased hospital costs; we found that improvements in patient LOS, days in an intensive care unit, and management of surgical implants had the greatest impact on costs. Orthopedic surgeons began to use different implants, and all surgeons refrained from opening disposable surgical supplies until needed. Patients in intensive care unit beds stable for transfer were moved to regular medical/surgical rooms earlier. Since the program helped physicians understand the importance of LOS, many physicians increased their rounding on weekends and considered LOS implications before ordering diagnostic procedures that could be performed as an outpatient. Nurses, physician extenders such as physician assistants, and social workers have played an important role in streamlining patient care and hospital discharge; however, they were not directly rewarded under this program.
There are challenges to aligning the incentives of internists compared to procedure‐based specialists. This may be that the result of surgeons receiving payment for bundled care and thus the incentives are already aligned. The incentive of the program for internists, who get paid for each per daily visit, was intended to overcome the lost income resulting from an earlier discharge. Moreover, in the present study, only the discharging physician received incentive payments for each case. Patient care is undoubtedly a team effort and many physicians (radiologists, anesthesiologists, pathologists, emergency medicine physicians, consultant specialty physicians, etc.) are clearly left out in the present gainsharing program. Aligning the incentives of these physicians might be necessary. Furthermore, the actions of other members of the medical team and consultants, by their behaviors, could limit the incentive payments for the discharging physician. The discharging physician is often unable to control the transfer of a patient from a high‐cost or severity unit, or improve the timeliness of consulting physicians. Previous authors have raised the issue as to whether a physician should be prevented from payment because of the actions of another member of the medical team.16
Ensuring a fair and transparent system is important in any pay‐for‐performance program. The present gainsharing program required sophisticated data analysis, which added to the costs of the program. To implement such a program, data must be clear and understandable, segregated by DRG and severity adjusted. But should the highest reward payments go to those who perform the best or improve the most? In the present study, some physicians were consistently unable to meet quality benchmarks. This may be related to several factors, 1 of which might be a particular physician's case mix. Some authors have raised concerns that pay‐for‐performance programs may unfairly impact physicians who care for more challenging or patients from disadvantaged socioeconomic circumstances.17 Other authors have questioned whether widespread implementation of such a program could potentially increase healthcare disparities in the community.18 It has been suggested by Greene and Nash that for a program to be successful, physicians who feel they provide good care yet but are not rewarded should be given an independent review.16 Such a process is important to prevent resentment among physicians who are unable to meet benchmarks for payment, despite hard work.19 Conversely, other studies have found that many physicians who receive payments in a pay‐for‐performance system do not necessarily consciously make improvement to enhance financial performance.20 Only 54% of eligible physicians participated in the present gainsharing program. This is likely due to lack of understanding about the program, misperceptions about the ethics of such programs, perceived possible negative patient outcome, conflict of interest and mistrust.21, 22 This underscores the importance of providing understandable performance results, education, and a physician champion to help facilitate communication and enhanced outcomes. What is clear is that the perception by participating physicians is that this program is worthwhile as the number of participating physicians has steadily increased and it has become an incentive for new providers to choose this medical center over others.
In conclusion, the results of the present study show that physicians can help hospitals reduce inpatients costs while maintaining or improving hospital quality. Improvements in patient LOS, implant costs, overall costs per admission, and medical record completion were noted. Further work is needed to improve physician education and better understand the impact of uneven physician case mix. Further efforts are necessary to allow other members of the health care team to participate and benefit from gainsharing.
Hospitals are challenged to improve quality while reducing costs, yet traditional methods of cost containment have had limited success in aligning the goals of hospitals and physicians. Physicians directly control more than 80% of total medical costs.1 The current fee‐for‐service system encourages procedures and the use of hospital resources. Without the proper incentives to gain active participation and collaboration of the medical staff in improving the efficiency of care, the ability to manage medical costs and improve hospital operational and financial performance is hampered. A further challenge is to encourage physicians to improve the quality of care and maintain safe medical practice. While several examples of pay‐for‐performance (P4P) have previously been attempted to increase efficiency, gainsharing offers real opportunities to achieve these outcomes.
Previous reports regarding the results of gainsharing programs describe its use in outpatient settings and its limited ability to reduce costs for inpatient care for surgical implants such as coronary stents2 or orthopedic prostheses.3 The present study represents the largest series to date using a gainsharing model in a comprehensive program of inpatient care at a tertiary care medical center.
Patients and Methods
Beth Israel Medical Center is a 1000‐bed tertiary care university‐affiliated teaching hospital, located in New York City. The hospital serves a large and ethnically diverse community predominantly located in the lower east side of Manhattan and discharged about 50,000 patients per year during the study period of July 2006 through June 2009.
Applied Medical Software, Inc. (AMS, Collingswood, NJ) analyzed hospital data for case mix and severity. To establish best practice norms (BPNs), AMS used inpatient discharge data (UB‐92) to determine costs by APR‐DRG's4 during calendar year 2005, prior to the inception of the program to establish BPNs. Costs were allocated into specific areas listed in Table 1. A minimum of 10 cases was necessary in each DRG. Cost outliers (as defined by the mean cost of the APR DRG plus 3 standard deviations) were excluded. These data were used to establish a baseline for each physician and a BPN, which was set at the top 25th percentile for each specific APR DRG. BPNs were determined after exclusions using the following criteria:
Each eligible physician had to have at least 10 admissions within their specialty;
Each eligible DRG had to have at least 5 qualifying physicians within a medical specialty;
Each eligible APR DRG had to have at least 3 qualifying admissions;
If the above criteria are met, the BPN was set at the mean of the top 25th percentile of physicians (25% of the physicians with the lowest costs).
| |
| Per diem hospital bed cost | Pharmacy |
| Critical care (ICU and CCU) | Laboratory |
| Medical surgical supplies and implants | Cardiopulmonary care |
| Operating room costs | Blood bank |
| Radiology | Intravenous therapy |
Once BPNs were determined, patients were grouped by physician and compared to the BPN for a particular APR DRG. All patients of participating physicians with qualifying APR DRGs were included in the analysis reports summarizing these results, computed quarterly and distributed to each physician. Obstetrical and psychiatric admissions were excluded in the program. APR DRG data for each physician was compared from year to year to determine whether an individual physician demonstrated measurable improvement in performance.
The gainsharing program was implemented in 2006. Physician participation was voluntary. Payments were made to physicians without any risk or penalties from participation. Incentives were based on individual performance. Incentives for nonsurgical admissions were intended to offset the loss of physician income related to more efficient medical management and a reduced hospital length of stay (LOS). Income for surgical admissions was intended to reward physicians for efficient preoperative and postoperative care.
The methodology provides financial incentives for physicians for each hospital discharge in 2 ways:
Improvement in costs per case against their own historical performance;
Cost per case performance compared to BPN.
In the first year of the gainsharing program, two thirds of the total allowable incentive payments were allocated to physicians' improvement, with one third based on a performance metric. Payments for improvement were phased out over the first 3 years of the gainsharing program, with payments focused fully on performance in Year 3. Cases were adjusted for case‐mix and severity of illness (four levels of APR DRG). Physicians were not penalized for any cases in which costs greatly exceeded BPN. A floor was placed at the BPN and no additional financial incentives were paid for surpassing it. Baselines and BPNs were recalculated yearly.
A key aspect of the gainsharing program was the establishment of specific quality parameters (Table 2) that need to be met before any incentive payments were made. A committee regularly reviewed the quality performance data of each physician to determine eligibility for payments. Physicians were considered to be ineligible for incentive compensation until the next measurement period if there was evidence of failure to adequately meet these measures. At least 80% compliance with core measures (minimum 5 discharges in each domain) was expected. Infectious complication rates were to remain not more than 1 standard deviation above National Healthcare Safety Network rates during the same time period. In addition, payments were withheld from physicians if it was found that the standard of care was not met for any morbidity or mortality that was peer reviewed or if there were any significant patient complaints. Readmission rates were expected to remain at or below the baseline established during the previous 12 months by DRG.
| Quality Measure | Goal |
|---|---|
| |
| Readmissions within 7 days for the same or related diagnosis | Decrease, or less than 10% of discharges |
| Documentationquality and timeliness of medical record and related documentation including date, time, and sign all chart entries | No more than 20% of average monthly discharged medical records incomplete for more than 30 days |
| Consultation with social work/discharge planner within 24 hours of admission for appropriate pts | >80% of all appropriate cases |
| Timely switch from intravenous to oral antibiotics in accordance with hospital policy (%) | >80 |
| Unanticipated return to the operating room | Decrease or < 5% |
| Patient complaints | Decrease |
| Patient satisfaction (HCAHPS) | >75% physician domain |
| Ventilator associated pneumonia | Decrease or < 5% |
| Central line associated blood stream infections | Decrease or < 5 per 1000 catheter days. |
| Surgical site infections | Decrease or within 1 standard deviation of NHSN |
| Antibiotic prophylaxis (%) | >80 |
| Inpatient mortality | Decrease or <1% |
| Medication errors | Decrease or <1% |
| Delinquent medical records | <5 charts delinquent more than 30 days |
| Falls with injury | Decrease or <1% |
| AMI: aspirin on arrival and discharge (%) | >80 |
| AMI‐ACEI or ARB for LVSD (%) | >80 |
| Adult smoking cessation counseling (%) | >80 |
| AMI‐ Beta blocker prescribed at arrival and discharge (%) | >80 |
| CHF: discharge instructions (%) | >80 |
| CHF: Left ventricular function assessment (%) | >80 |
| CHF: ACEI or ARB for left ventricular systolic dysfunction (%) | >80 |
| CHF: smoking cessation counseling (%) | >80 |
| Pneumonia: O2 assessment, pneumococcal vaccine, blood culture and sensitivity before first antibiotic, smoking cessation counseling (%) | >80 |
Employed and private practice community physicians were both eligible for the gainsharing program. Physician participation in the program was voluntary. All patients admitted to the Medical Center received notification on admission about the program. The aggregate costs by DRG were calculated quarterly. Savings over the previous yearif anywere calculated. A total of 20% of the savings was used to administer the program and for incentive payments to physicians.
From July 1, 2006 through September 2008, only commercial managed care cases were eligible for this program. As a result of the approval of the gainsharing program as a demonstration project by the Centers for Medicare and Medicaid Services (CMS), Medicare cases were added to the program starting October 1, 2008.
Physician Payment Calculation Methodology
Performance Incentive
The performance incentive was intended to reward demonstrated levels of performance. Accordingly, a physician's share in hospital savings was in proportion to the relationship between their individual performance and the BPN. This computation was the same for both surgical and medical admissions. The following equation illustrates the computation of performance incentives for participating physicians:
This computation was made at the specific severity level for each hospital discharge. Payment for the performance incentive was made only to physicians at or below the 90th percentile of physicians.
Improvement Incentive
The improvement incentive was intended to encourage positive change. No payments were made from the improvement incentive unless an individual physician demonstrated measurable improvement in operational performance for either surgical or medical admissions. However, because physicians who admitted nonsurgical cases experienced reduced income as they help the hospital to improve operational performance, the methodology for calculating the improvement incentive was different for medical as opposed to surgical cases, as shown below.
For Medical DRGs:
For each severity level the following is calculated:
For Surgical DRGs:
Cost savings were calculated quarterly and defined as the cost per case before the gainsharing program began minus the actual case cost by APR DRG. Student's t‐test was used for continuous data and the categorical data trends were analyzed using Mantel‐Haenszel Chi‐Square.
At least every 6 months, all participating physicians received case‐specific and cost‐centered data about their discharges. They also received a careful explanation of opportunities for financial or quality improvement.
Results
Over the 3‐year period, 184 physicians enrolled, representing 54% of those eligible. The remainder of physicians either decided not to enroll or were not eligible due to inadequate number of index DRG cases or excluded diagnoses. Payer mix was 27% Medicare and 48% of the discharges were commercial and managed care. The remaining cases were a combination of Medicaid and self‐pay. A total of 29,535 commercial and managed care discharges were evaluated from participating physicians (58%) and 20,360 similar discharges from non‐participating physicians. This number of admissions accounted for 29% of all hospital discharges during this time period. Surgical admissions accounted for 43% and nonsurgical admissions for 57%. The distribution of patients by service is shown in Table 3. Pulmonary and cardiology diagnoses were the most frequent reasons for medical admissions. General and head and neck surgery were the most frequent surgical admissions. During the time period of the gainsharing program, the medical center saved $25.1 million for costs attributed to these cases. Participating physicians saved $6.9 million more than non‐participating physicians (P = 0.02, Figure 1), but all discharges demonstrated cost savings during the study period. Cost savings (Figure 2) resulted from savings in medical/surgical supplies and implants (35%), daily hospital costs, (28%), intensive care unit costs (16%) and coronary care unit costs (15%), and operating room costs (8%). Reduction in cost from reduced magnetic resonance imaging (MRI) use was not statistically significant. There were minimal increases in costs due to computed tomography (CT) scan use, cardiopulmonary care, laboratory use, pharmacy and blood bank, but none of these reached statistical significance.
| Admissions by Service | Number (%) |
|---|---|
| |
| Cardiology | 4512 (15.3) |
| Orthopedic surgery | 3994 (13.5) |
| Gastroenterology | 3214 (10.9) |
| General surgery | 2908 (9.8) |
| Cardiovascular surgery | 2432 (8.2) |
| Pulmonary | 2212 (7.5) |
| Neurology | 2064 (7.0) |
| Oncology | 1217 (4.1) |
| Infectious disease | 1171 (4.0) |
| Endocrinology | 906 (3.1) |
| Nephrology | 826 (2.8) |
| Open heart surgery | 656 (2.2) |
| Interventional cardiology | 624 (2.1) |
| Gynecological surgery | 450 (1.5) |
| Urological surgery | 326 (1.1) |
| ENT surgery | 289 (1.0) |
| Obstetrics without delivery | 261 (0.9) |
| Hematology | 253 (0.9) |
| Orthopedicsnonsurgical | 241 (0.8) |
| Rehabilitation | 204 (0.7) |
| Otolaryngology | 183 (0.6) |
| Rheumatology | 165 (0.6) |
| General medicine | 162 (0.5) |
| Neurological surgery | 112 (0.4) |
| Urology | 101 (0.3) |
| Dermatology | 52 (0.2) |
| Grand total | 29535 (100.0) |
Hospital LOS decreased 9.8% from baseline among participating doctors, while LOS decreased 9.0% among non‐participating physicians; this difference was not statistically significant (P = 0.6). Participating physicians reduced costs by an average of $7,871 per quarter, compared to a reduction in costs by $3,018 for admissions by non‐participating physicians (P < 0.0001). The average savings per admission for the participating physicians were $1,835, and for non‐participating physicians were $1,107, a difference of $728 per admission. Overall, cost savings during the three year period averaged $105,000 per physician who participated in the program and $67,000 per physician who did not (P < 0.05). There was not a statistical difference in savings between medical and surgical admissions (P = 0.24).
Deviations from quality thresholds were identified during this time period. Some or all of the gainsharing income was withheld from 8% of participating physicians due to quality issues, incomplete medical records, or administrative reasons. Payouts to participating physicians averaged $1,866 quarterly (range $0‐$27,631). Overall, 9.4% of the hospital savings was directly paid to the participating physicians. Compliance with core measures improved in the following domains from year 2006 to 2009; acute myocardial infarction 94% to 98%, congestive heart failure 76% to 93%, pneumonia 88% to 97%, and surgical care improvement project 90% to 97%, (P = 0.17). There was no measurable increase in 30‐day mortality or readmission by APR‐DRG. The number of incomplete medical records decreased from an average of 43% of the total number of records in the second quarter of 2006 to 30% in the second quarter of 2009 (P < 0.0001). Other quality indicators remained statistically unchanged.
Discussion
The promise of gainsharing may motivate physicians to decrease hospital costs while maintaining quality medical care, since it aligns physician and hospital incentives. Providing a reward to physicians creates positive reinforcement, which is more effective than warnings against poor performing physicians (carrot vs. stick).5, 6 This study is the first and largest of its kind to show the results of a gainsharing program for inpatient medical and surgical admissions and demonstrates that significant cost savings may be achieved. This is similar to previous studies that have shown positive outcomes for pay‐for‐performance programs.7
Participating physicians in the present study accumulated almost $7 million more in savings than non‐participating physicians. Over time this difference has increased, possibly due to a learning curve in educating participating physicians and the way in which information about their performance is given back to them. A significant portion of the hospital's cost savings was through improvements in documentation and completion of medical records. While there was an actual reduction in average length of stay (ALOS), better documentation may also have contributed to adjusting the severity level within each DRG.
Using financial incentives to positively impact on physician behavior is not new. One program in a community‐based hospitalist group reported similar improvements in medical record documentation, as well as improvements in physician meeting attendance and quality goals.8 Another study found that such hospital programs noted improved physician engagement and commitment to best practices and to improving the quality of care.9
There is significant experience in the outpatient setting using pay‐for‐performance programs to enhance quality. Millett et al.10 demonstrated a reduction in smoking among patients with diabetes in a program in the United Kingdom. Another study in Rochester, New York that used pay‐for‐performance incentives demonstrated better diabetes management.11 Mandel and Kotagal12 demonstrated improved asthma care utilizing a quality incentive program.
The use of financial motivation for physicians, as part of a hospital pay‐for‐performance program, has been shown to lead to improvements in quality performance scores when compared to non pay‐for‐performance hospitals.13 Berthiaume demonstrated decreased costs and improvements in risk‐adjusted complications and risk‐adjusted LOS in patents admitted for acute coronary intervention in a pay‐for‐performance program.14 Quality initiatives were integral for the gainsharing program, since measures such as surgical site infections may increase LOS and hospital costs. Core measures related to the care of patients with acute myocardial infarction, heart failure, pneumonia, and surgical prophylaxis steadily improved since the initiation of the gainsharing program. Gainsharing programs also enhance physician compliance with administrative responsibilities such as the completion of medical records.
One unexpected finding of our study was that there was a cost savings per admission even in the patients of physicians who did not participate in the gainsharing program. While the participating physicians showed statistically significant improvements in cost savings, savings were found in both groups. This raises the question as to whether these cost reductions could have been impacted by other factors such as new labor or vendor contracts, better documentation, improved operating room utilization and improved and timely documentation in the medical record. Another possibility is the Hawthorne effect on physicians, who altered their behavior with knowledge that process and outcome measurement were being measured. Physicians who voluntarily sign up for a gainsharing program would be expected to be more committed to the success of this program than physicians who decide to opt out. While this might appear to be a selection bias it does illustrate the point that motivated physicians are more likely to positively change their practice behaviors. However, one might suggest that financial savings directly attributed to the gainsharing program was not the $25.1 million saved during the 3 years overall, but the difference between participating and non‐participating physicians, or $6.9 million.
While the motivation to complete medical records was significant (gainsharing dollars were withheld from doctors with more than 5 incomplete charts for more than 30 days) it was not the only reason why the number of delinquent chart percentage decreased during the study period. While the improvement was significant, there are still more opportunities to reduce the number of incomplete charts. Hospital regulatory inspections and periodic physician education were also likely to have reduced the number of incomplete inpatient charts during this time period and may do so in the future.15
The program focused on the physician activities that have the greatest impact on hospital costs. While optimizing laboratory, blood bank, and pharmacy management decreased hospital costs; we found that improvements in patient LOS, days in an intensive care unit, and management of surgical implants had the greatest impact on costs. Orthopedic surgeons began to use different implants, and all surgeons refrained from opening disposable surgical supplies until needed. Patients in intensive care unit beds stable for transfer were moved to regular medical/surgical rooms earlier. Since the program helped physicians understand the importance of LOS, many physicians increased their rounding on weekends and considered LOS implications before ordering diagnostic procedures that could be performed as an outpatient. Nurses, physician extenders such as physician assistants, and social workers have played an important role in streamlining patient care and hospital discharge; however, they were not directly rewarded under this program.
There are challenges to aligning the incentives of internists compared to procedure‐based specialists. This may be that the result of surgeons receiving payment for bundled care and thus the incentives are already aligned. The incentive of the program for internists, who get paid for each per daily visit, was intended to overcome the lost income resulting from an earlier discharge. Moreover, in the present study, only the discharging physician received incentive payments for each case. Patient care is undoubtedly a team effort and many physicians (radiologists, anesthesiologists, pathologists, emergency medicine physicians, consultant specialty physicians, etc.) are clearly left out in the present gainsharing program. Aligning the incentives of these physicians might be necessary. Furthermore, the actions of other members of the medical team and consultants, by their behaviors, could limit the incentive payments for the discharging physician. The discharging physician is often unable to control the transfer of a patient from a high‐cost or severity unit, or improve the timeliness of consulting physicians. Previous authors have raised the issue as to whether a physician should be prevented from payment because of the actions of another member of the medical team.16
Ensuring a fair and transparent system is important in any pay‐for‐performance program. The present gainsharing program required sophisticated data analysis, which added to the costs of the program. To implement such a program, data must be clear and understandable, segregated by DRG and severity adjusted. But should the highest reward payments go to those who perform the best or improve the most? In the present study, some physicians were consistently unable to meet quality benchmarks. This may be related to several factors, 1 of which might be a particular physician's case mix. Some authors have raised concerns that pay‐for‐performance programs may unfairly impact physicians who care for more challenging or patients from disadvantaged socioeconomic circumstances.17 Other authors have questioned whether widespread implementation of such a program could potentially increase healthcare disparities in the community.18 It has been suggested by Greene and Nash that for a program to be successful, physicians who feel they provide good care yet but are not rewarded should be given an independent review.16 Such a process is important to prevent resentment among physicians who are unable to meet benchmarks for payment, despite hard work.19 Conversely, other studies have found that many physicians who receive payments in a pay‐for‐performance system do not necessarily consciously make improvement to enhance financial performance.20 Only 54% of eligible physicians participated in the present gainsharing program. This is likely due to lack of understanding about the program, misperceptions about the ethics of such programs, perceived possible negative patient outcome, conflict of interest and mistrust.21, 22 This underscores the importance of providing understandable performance results, education, and a physician champion to help facilitate communication and enhanced outcomes. What is clear is that the perception by participating physicians is that this program is worthwhile as the number of participating physicians has steadily increased and it has become an incentive for new providers to choose this medical center over others.
In conclusion, the results of the present study show that physicians can help hospitals reduce inpatients costs while maintaining or improving hospital quality. Improvements in patient LOS, implant costs, overall costs per admission, and medical record completion were noted. Further work is needed to improve physician education and better understand the impact of uneven physician case mix. Further efforts are necessary to allow other members of the health care team to participate and benefit from gainsharing.
- ,,, et al.Guided care and the cost of complex healthcare: a preliminary report.Am J Manag Care.2009;15(8):555–559.
- ,.Hospital‐physician gainsharing in cardiology.Health Aff (Millwood).2008;27(3):803–812.
- ,,,.AOA Symposium. Gainsharing in orthopaedics: passing fancy or wave of the future?J Bone Joint Surg Am.2007;89(9):2075–2083.
- All Patient Defined Diagnosis Related Groups™ ‐ 3M Health Information Systems,St Paul, MN.
- ,,, et al.Guided care and the cost of complex healthcare: a preliminary report.Am J Manag Care.2009;15(8):555–559.
- .Best practices in record completion.J Med Pract Manage.2004;20(1):18–22.
- ,,, et al.Return on investment in pay for performance: a diabetes case study.J Healthc Manag.2006;51(6):365–374; discussion 375‐376.
- .Use of pay for performance in a community hospital private hospitalists group: a preliminary report.Trans Am Clin Climatol Assoc.2007;188:263–272.
- .Making the grade with pay for performance: 7 lessons from best‐performing hospitals.Healthc Financ Manage.2006;60(12):79–85.
- ,,,,.Impact of a pay‐for‐performance incentive on support for smoking cessation and on smoking prevalence among people with diabetes.CMAJ.2007;176(12):1705–1710.
- ,,, et al,Effects of paying physicians based on their relative performance for quality.J Gen Intern Med.2007;22(6):872–876.
- ,.Pay for performance alone cannot drive quality.Arch Pediatr Adolesc Med.2007;161(7):650–655.
- .What's the return? Assessing the effect of “pay‐for‐performance” initiatives on the quality of care delivery.Med Care Res Rev.2006;63(1 suppl)( ):29S–48S.
- ,,,,.Aligning financial incentives with “Get With the Guidelines” to improve cardiovascular care.Am J Manag Care.2004;10(7 pt 2):501–504.
- .Sampling best practices. Managing delinquent records.J AHIMA.1997;68(8):28,30.
- ,.Pay for performance: an overview of the literature.Am J Med Qual.2009;24;140–163.
- ,,.Physician‐level P4P:DOA? Can quality‐based payments be resuscitated?Am J Manag Care.2007;13(5):233–236.
- ,,, et al.Will pay for performance and quality reporting affect health care disparities?Health Aff (Millwood).2007;26(3):w405–w414.
- ,,.The experience of pay for performance in English family practice: a qualitative study.Ann Fam Med.2008;8(3):228–234.
- ,,, et al.Will financial incentives stimulate quality improvement? Reactions from frontline physicians.Am J Med Qual.2006;21(6):367–374.
- ,,.Pay for performance in orthopedic surgery.Clin Orthop Relat Res.2007;457:87–95.
- ,.Pay for performance survey of diagnostic radiology faculty and trainees.J Am Coll Radiol.2007;4(6):411–415.
- ,,, et al.Guided care and the cost of complex healthcare: a preliminary report.Am J Manag Care.2009;15(8):555–559.
- ,.Hospital‐physician gainsharing in cardiology.Health Aff (Millwood).2008;27(3):803–812.
- ,,,.AOA Symposium. Gainsharing in orthopaedics: passing fancy or wave of the future?J Bone Joint Surg Am.2007;89(9):2075–2083.
- All Patient Defined Diagnosis Related Groups™ ‐ 3M Health Information Systems,St Paul, MN.
- ,,, et al.Guided care and the cost of complex healthcare: a preliminary report.Am J Manag Care.2009;15(8):555–559.
- .Best practices in record completion.J Med Pract Manage.2004;20(1):18–22.
- ,,, et al.Return on investment in pay for performance: a diabetes case study.J Healthc Manag.2006;51(6):365–374; discussion 375‐376.
- .Use of pay for performance in a community hospital private hospitalists group: a preliminary report.Trans Am Clin Climatol Assoc.2007;188:263–272.
- .Making the grade with pay for performance: 7 lessons from best‐performing hospitals.Healthc Financ Manage.2006;60(12):79–85.
- ,,,,.Impact of a pay‐for‐performance incentive on support for smoking cessation and on smoking prevalence among people with diabetes.CMAJ.2007;176(12):1705–1710.
- ,,, et al,Effects of paying physicians based on their relative performance for quality.J Gen Intern Med.2007;22(6):872–876.
- ,.Pay for performance alone cannot drive quality.Arch Pediatr Adolesc Med.2007;161(7):650–655.
- .What's the return? Assessing the effect of “pay‐for‐performance” initiatives on the quality of care delivery.Med Care Res Rev.2006;63(1 suppl)( ):29S–48S.
- ,,,,.Aligning financial incentives with “Get With the Guidelines” to improve cardiovascular care.Am J Manag Care.2004;10(7 pt 2):501–504.
- .Sampling best practices. Managing delinquent records.J AHIMA.1997;68(8):28,30.
- ,.Pay for performance: an overview of the literature.Am J Med Qual.2009;24;140–163.
- ,,.Physician‐level P4P:DOA? Can quality‐based payments be resuscitated?Am J Manag Care.2007;13(5):233–236.
- ,,, et al.Will pay for performance and quality reporting affect health care disparities?Health Aff (Millwood).2007;26(3):w405–w414.
- ,,.The experience of pay for performance in English family practice: a qualitative study.Ann Fam Med.2008;8(3):228–234.
- ,,, et al.Will financial incentives stimulate quality improvement? Reactions from frontline physicians.Am J Med Qual.2006;21(6):367–374.
- ,,.Pay for performance in orthopedic surgery.Clin Orthop Relat Res.2007;457:87–95.
- ,.Pay for performance survey of diagnostic radiology faculty and trainees.J Am Coll Radiol.2007;4(6):411–415.
Copyright © 2010 Society of Hospital Medicine
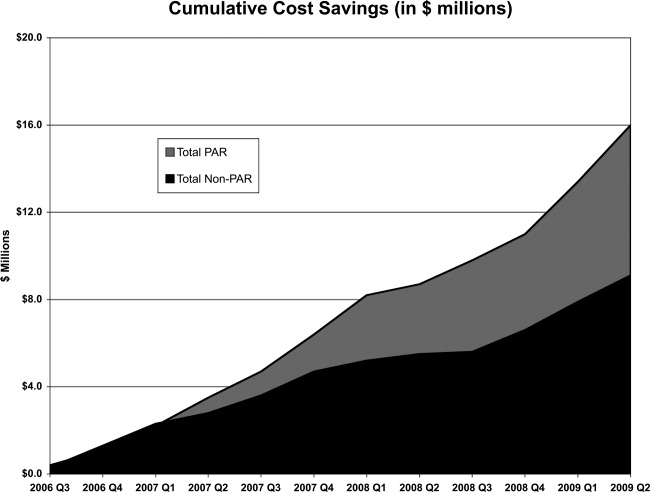
Handoff Efficiency
Transfer of responsibility for patients, or handoff,1 occurs frequently in hospitalist services, requiring excellent and timely communication to ensure patient safety. Communication failure is a major contributor to medical errors.2, 3 Recognizing such findings, a growing body of literature addresses handoff techniques for learners.47
Vidyarthi described the handoff process as traditionally informal, unstructured, and idiosyncratic,4 and many believe efforts to formalize and structure this process are important for patient safety.8 Standardized handoff forms have improved accuracy of information.9 Web‐based sign‐out systems reportedly reduced the number of patients missed on rounds.10
Hospitalists also face challenges with effective communication during service change.11 The Society of Hospital Medicine identified the handoff skill as a core competency for hospitalists, and recommendations based on a systematic review of the literature were published.12 Inpatient medicine programs are increasingly using midlevel providers such as nurse practitioners (NPs) and physician assistants (PAs) along with hospitalists to accommodate workload while maintaining the scholarly enterprise in academic centers.13 To our knowledge there is no literature examining the hospitalist service handoffs involving NP/PAs.
We wished to study the effectiveness and timeliness of the morning handoff from the night coverage providers to the daytime teams consisting of one hospitalist and one NP/PA. Our objectives were to identify deficiencies and to evaluate the effectiveness of a restructured handoff process.
Methods
The Mayo Clinic Institutional Review Board reviewed and approved this study.
Setting
At the time of this study, the Division of Hospital Internal Medicine (HIM) at our institution consisted of 22 hospitalists, 11 NPs and 9 PAs (hereinafter NP/PAs), and 2 clinical assistants (CAs). The CAs assist with clerical duties not covered by Unit Secretaries:
-
Obtaining outside records
-
Clarifying referring physician contact information
-
Scheduling follow‐up outpatient appointments for tests, procedures, and visits
-
Attendance at morning handoff
Each CA can assist 3 or 4 daytime service teams.
Daytime Service Organization
Six HIM services, each managing up to 12 patients, are staffed by a partnership of 1 hospitalist and 1 NP/PA: Four services are primary general medicine services, and 2 consulting (orthopedic comanagement) services.
Night Coverage
Three of 4 primary daytime services and one consult service team transfer care to the (in‐house) night NP/PA. The night NP/PA addresses any acute‐care issues and reports at morning handoff to the 3 primary services and 1 consult service. In a designated conference room the morning handoff occurs, with at least 1 (day team) service representative present. This is usually the NP/PA, as the day team hospitalist concurrently receives a report on new admissions from the (in‐house) night hospitalist (who also covers one service and backs up the night NP/PA).
Improvement Process
An improvement team was formed within the Division of HIM consisting of 3 hospitalists, 3 NP/PAs, and 2 CAs to assess the existing handoff process at 7:45am between the Night NP/PA and daytime services. The improvement team met, reviewed evidence‐based literature on handoffs and discussed our local process. Four problems were identified by consensus:
-
Unpredictable start and finish times
-
Inefficiency (time wasted)
-
Poor environment (room noisy and distracting conversations)
-
Poor communication (overwrought and meandering narratives).
Intervention
The improvement team structured a new handoff process to address these deficiencies.
-
Environment: Moved to a smaller room (lower ceiling, less ambient noise).
-
Identification: table cards designating seats for participants (reduced queries regarding what service are you, today?).
-
Start Times: Each service team assigned a consistent start time (labeled on the table card) within a 15‐minute period, and although earlier reportage could occur, any service team present at their designated time has priority for the attention of the night NP/PA, and the opportunity to ask questions.
-
Quiet and Focus: HIM members were reminded to remain quiet in the handoff room, so the service receiving report has the floor and personal conversations must not impede the principals.
-
Visual Cue: Green Good to go sign placed on team table cards when no verbal was required.
-
Written e‐Material: The improvement team required elements of a brief written report in a specified column of our existing electronic service list (ESL). The ESL is a custom designed template importing laboratory, medication, and demographic data automatically but also capable of free text additions (Figure 1). All providers were instructed to update the ESL every 12 hours.
-
Admission and Progress Notes: After manual electronic medical record search, the CAs printed any notes generated in the preceding 12 hours and placed them by the team table card.
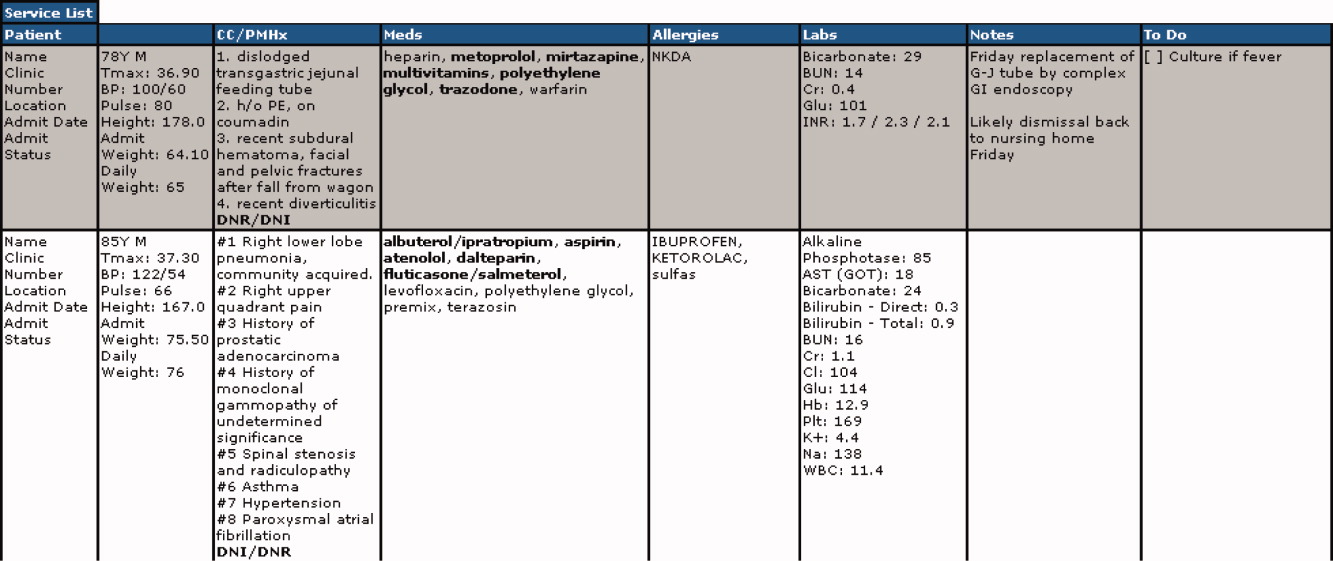
The improvement team provided education for the new process at a division meeting and through e‐mail. The recommended report sequence was night NP/PA reporting and day service teams asking questions and seeking clarifications. We discouraged editorial comments and chit‐chat.
A member of the improvement team monitored the new handoff process for 15 days, and 3 months later for 10 days.
Survey
An anonymous survey (Figure 2) concerning staff satisfaction with handoff was conducted immediately before and 15 days after the intervention. In the e‐mail containing the postintervention survey, providers were asked to respond only if they had been on service the preceding 15 days (and thus eligible to participate in handoff). To help insure this, the first question read, Have you been on service during the past 15 days?
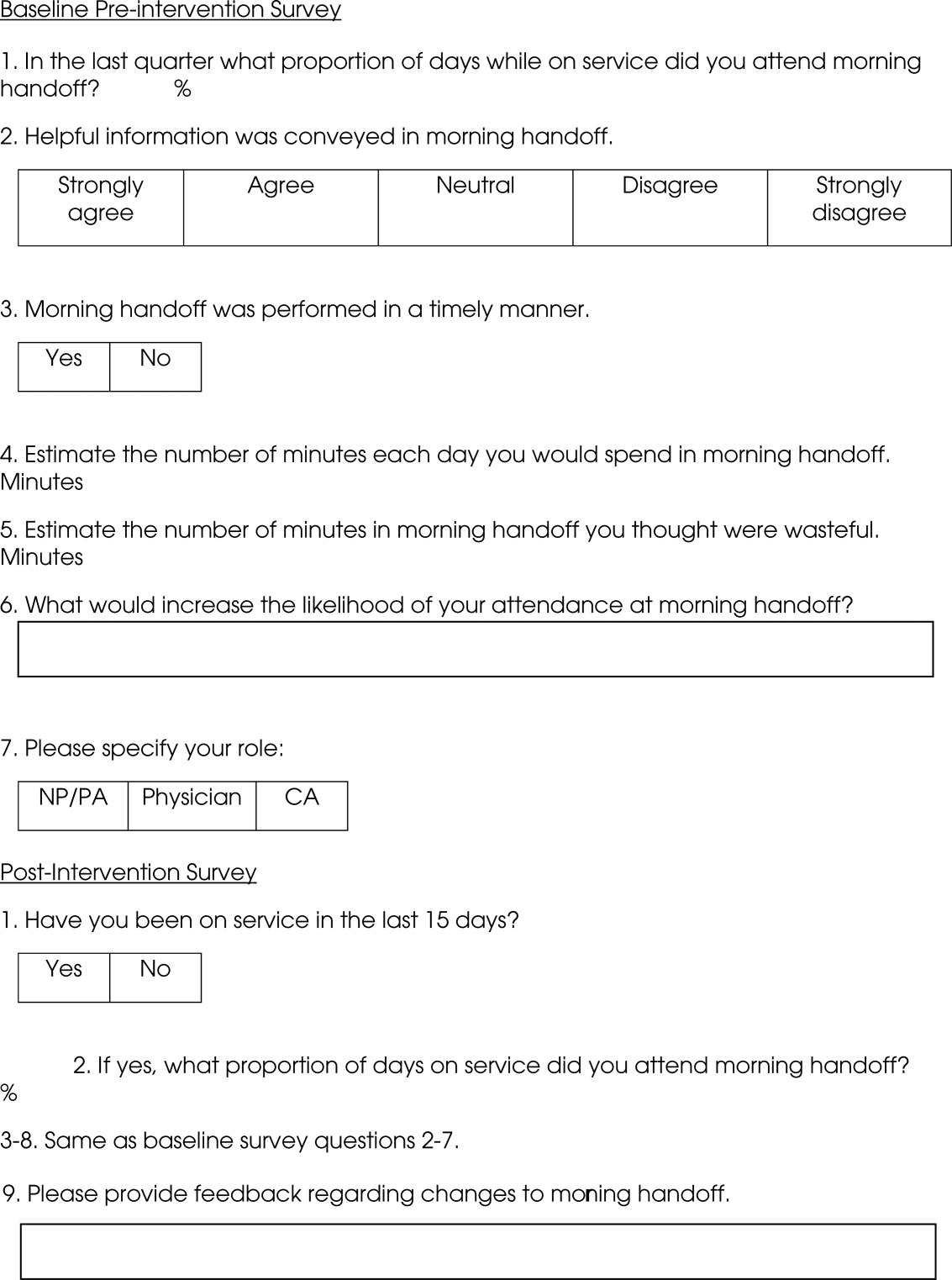
Statistics
To compare the relationship of preintervention and postintervention survey responses, Fisher's exact test was used to compare categorical variables and 2 sample t‐test and Wilcoxon rank sum test were used for continuous variables. Comparisons that adjusted for the possibility of someone responding to both the preintervention and postintervention surveys were not performed since the surveys were anonymous. A P value 0.05 was considered statistically significant. For the item concerning the percentage of days morning report was attended while on service, based on a common standard deviation estimate of 35.3, we had 80% power to detect a difference of 29.1 (pre vs. post). This computation assumes a 2‐sample t‐test of = 0.05 with sample sizes of 36 and 18. We have 59% power to detect a difference of 27% (67% pre vs. 94% post) for those who at least agree that helpful information was conveyed during handoff. This computation is based on a 2‐sided Pearson 2 test with = 0.05.
Qualitative data analysis of respondents' answers to the open‐ended survey questions What would increase the likelihood of your attending handoff? and What feedback do you have regarding the changes to handoff? was performed using the constant comparative method14 associated with grounded theory approaches to identify themes and categories.15 To establish interrater reliability, three investigators (MCB, DTK, LLK) independently identified coding categories for the data set, compared results, redefined coding categories as needed, and reanalyzed the data until 80% agreement was reached.
Results
Thirty‐six of the 44 providers (82%) answered the preintervention survey, including 18 of 22 hospitalists (82%), 17 of 20 NPs/PAs (85%), and 1 of 2 CAs (50%). During the intervention based on our staffing model, 21 providers had the opportunity to participate in handoff, and 18 (86%) answered the postintervention survey, including 5 of 6 hospitalists (83%), 9 of 14 NPs/PAs (64%), and 2 of 2 CAs (100%). All respondents to the postintervention survey reported being on service during the previous 15 days.
As summarized in Table 1, compared to 60.5% of survey participants (n = 38) who thought morning handoff was performed in a timely fashion preintervention, 100% (n = 15) felt it was performed in a timely fashion postintervention (P = 0.005). The average time spent in morning report before the intervention was 11 minutes, as compared to 5 minutes after the intervention (P 0.0028). Prior to the intervention, 6.5 minutes of the handoff were viewed to be wasteful, as compared to 0.5 minutes of the handoff in the postintervention survey (P 0.0001). Attendance and quality of information perceptions did not demonstrate statistically significant change.
| Survey Question | Preintervention | Postintervention | P |
|---|---|---|---|
| What proportion of days while on service did you attend morning report? (%) | 78 | 87 | 0.4119 |
| Helpful information was conveyed in morning report, n (%) | 0.112 | ||
| Strongly agree | 9 (25) | 9 (56) | |
| Agree | 15 (42) | 6 (38) | |
| Neutral | 8 (22) | 1 (6) | |
| Disagree | 4 (11) | 0 | |
| Strongly disagree | 0 | 0 | |
| Morning report was performed in a timely manner, #yes/#no | 23/15 | 15/0 | 0.005 |
| Estimate the number of minutes each day you would spend in morning report (minute) | 11 | 5 | 0.0028 |
| Estimate the number of minutes in morning report you thought were wasteful (minute) | 6.5 | 0.5 | 0.0001 |
During the 15‐day observation period, morning handoff started by 0745 on 14 of 15 (93%) of days and finished by 0800 on 15 of 15 (100%) of days. Table cards, ESL, and progress notes were on the table by 0745 on 15 of 15 (100%) of days following the intervention. Three months after the intervention, the following were observed: morning handoff started by 0745 on 10 of 10 (100%) of days; finished by 0800 on 10 of 10 (100%) of days; and table cards, ESL, and progress notes were on the table by 0745 on 10 of 10 (100%) of days.
Qualitative Data Analysis
Three themes were identified in both preintervention and postintervention surveys: timeliness, quality of report and environment (Table 2). In the preintervention survey, timeliness complaints involved inconsistent start time, prolonged duration of handoff, and inefficiency due to time wasted while teams waited for their handoff report. Comments about report quality mentioned the nonstandardized report process that included nonpertinent information and editorializing. Environmental concerns addressed noise from multiple service team members assembled in 1 large room and chatting while awaiting report. In the postintervention survey, respondents' comments noted improved efficiency, environment, and report quality.
| Deficiency | Pre‐Intervention | Post‐Intervention |
|---|---|---|
| Timeliness | Efficiency needed | I found the changes lead to more concise and valuable time spent in report |
| Timely, scheduled and efficient reports would help increase my attendance | I personally enjoyed having the times set so you are held accountable for a certain handoff | |
| Set report times so I don't have to listen to everyone else's report | More organized and efficient | |
| Too much time wasted | Love the good to go card! Can start on rounds | |
| Environment | Not having to listen to chit chat unrelated to patient carewould improve my attendance | There is less chit chat |
| Services should receive report in a quieter room | Seems less chaotic with less people overall in the room so less distraction | |
| Need a quieter and smaller room | Because the room is quieter, I did not have to repeat information | |
| Too noisy | Quiet and respectful | |
| Quality | I would like a more organized format More information isn't needed, just the correct information in a timely manner | I felt that the amount of information shared was only what was pertinent and important |
| If I first had the opportunity to review ESL and any notes generated in the last 12 hours, this would improve report | Written information on the ESL assured that I didn't forget something important | |
| Less editorializing about events and less adrenaline | I liked having the progress notes generated overnight available for review | |
| Need only meaningful information | Excellent report with prompt dissemination of information |
Discussion
We describe an intervention that set the expectation for formal, structured written and verbal communication in a focused environment involving outgoing and incoming clinicians, resulting in improved satisfaction. Before the intervention, the improvement team identified by consensus 4 problems: unpredictable start time, inefficiency, environment, and report quality. Formal structuring of our handoff process resulted in statistically significant improvement in handoff timeliness and efficiency in the view of the HIM division members. Process improvement included precise team specific start times within a 12‐minute window to improve reliability and predictability and eliminating nonproductive waiting. Additionally, receiving teams were clearly identified with table cards so that no time was wasted locating the appropriate service for report, and minimizing role‐identification challenges. The good to go sign signaled teams that no events had occurred overnight requiring verbal report. Handoff timeliness persisted 3 months after the intervention, suggesting that the process is easily sustainable.
Postintervention survey comments noted the improved environment: a smaller, quieter room with the door closed. Before the intervention, all day team providers, CAs and night provider met in a large, loud room where multiple conversations were commonplace. Previous study of the handoff process supports creating an environment free of distraction.4
Postintervention survey responses to the open‐ended questions suggested improved provider satisfaction with the quality of the report. We believe this occurred for several reasons. First, having a precise start time for each team within a 12‐minute window led to a more focused report. Second, the ESL provided a column for providers to suggest plans of care for anticipated overnight events to improve preparedness and avoid significant omissions. Third, hospital notes generated overnight were made available which allowed daytime providers to review events before handoff, for a more informed update, or just after verbal report to reinforce the information just received, a technique used in other high‐reliability organizations.16 This measure also provided an at‐a‐glance view of each patient, decreasing the complexity of handoff.17
This study has important limitations. We address the handoff process of 1 hospitalist group at a single academic center. NP/PAs are the clinicians with first‐call responsibility for the night coverage of our patients, and the handoff process between the night NP/PA and daytime provider was studied. The handoff between physicians for patients admitted overnight was not assessed. Another limitation is that the time spent in handoff is reported as a participant estimate. There was no objective measurement of time, and respondents may have been biased. An additional limitation of our study concerns the preintervention and postintervention surveys. Both surveys were anonymous, which makes discerning the absolute impact of the intervention difficult due to the lack of paired responses. Lastly, our institution has an ESL. This option may not be available in other hospital systems.
Several deficiencies in the handoff process were addressed by providing key clinical data verbally and in written format, enhancing the physical environment, and defining each team's handoff start time. Our process improvements are consistent with the handoff recommendations endorsed by the Society of Hospital Medicine.12 Subsequent direct observation, subjective reports, and survey results demonstrated improvement in the handoff process.
Future studies might measure the effectiveness of morning handoff by end‐shift interviews of the daytime clinicians. Similarly, a study of evening handoff could measure the efficiency and effectiveness of report given by day teams to night‐coverage colleagues. Furthermore, if the handoff report skill set can be more rigorously defined and measured, a hospitalist clinical competency for hospitalists and NP/PAs could be developed in this core process‐of‐care.12
Acknowledgements
The authors thank Lisa Boucher for preparation of this manuscript.
- , , , et al.Lost in translation: challenges and opportunities in physician‐to‐physician communication during patient handoffs.Acad Med.2005;80:1094–1099.
- , , .Communication failures: an insidious contributor to medical mishaps.Acad Med.2004;79:186–194.
- , , .The human factor: the critical importance of effective teamwork and communication in providing safe care.Quality 13 Suppl 1:i85–90.
- , , , et al.Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign‐out.J Hosp Med.2006;1:257–266.
- , , .Development and implementation of an oral sign‐out skills curriculum.J Gen Intern Med.2007;22:1470–1474.
- , , , et al.The top 10 list for a safe and effective sign‐out.Arch Surg2008;143(10):1008–1010.
- , , , et al.Residents' and attending physicians' handoffs: a systematic review of the literature.Acad Med.2009;84(12):1775–1787.
- , , , et al.A structured handoff program for interns.Acad Med.2009;84:347–352.
- , , , et al.Simple standardized patient handoff system that increases accuracy and completeness.J Surg.2008;65:476–485.
- , , , et al.A randomized, controlled trial evaluation the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200:538–545.
- , , , .Understanding communication during hospitalist service changes: A mixed methods study.J Hosp Med.2009;4(9):535–540.
- , , , , , .Hospitalist handoffs: a systematic review and task force recommendations.J of Hosp Med.2009;4(7):433–440.
- , , , et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3:361–368.
- , .Basics of Qualitiative Research: Grounded Theory Procedures and Techniques.Sage Publications, Inc.Newbury Park, CA.1990.
- , .Naturalistic Inquiry.Sage Publications, Inc.Newbury Park, CA.1985.
- .Communication strategies from high‐reliability organizations.Ann Surg.2007;245(2):170–172.
- , , , et al.Handoff strategies in settings with high consequences for failure: lessons for health care operations.Int J Qual Health Care.2004;16(2):125.
Transfer of responsibility for patients, or handoff,1 occurs frequently in hospitalist services, requiring excellent and timely communication to ensure patient safety. Communication failure is a major contributor to medical errors.2, 3 Recognizing such findings, a growing body of literature addresses handoff techniques for learners.47
Vidyarthi described the handoff process as traditionally informal, unstructured, and idiosyncratic,4 and many believe efforts to formalize and structure this process are important for patient safety.8 Standardized handoff forms have improved accuracy of information.9 Web‐based sign‐out systems reportedly reduced the number of patients missed on rounds.10
Hospitalists also face challenges with effective communication during service change.11 The Society of Hospital Medicine identified the handoff skill as a core competency for hospitalists, and recommendations based on a systematic review of the literature were published.12 Inpatient medicine programs are increasingly using midlevel providers such as nurse practitioners (NPs) and physician assistants (PAs) along with hospitalists to accommodate workload while maintaining the scholarly enterprise in academic centers.13 To our knowledge there is no literature examining the hospitalist service handoffs involving NP/PAs.
We wished to study the effectiveness and timeliness of the morning handoff from the night coverage providers to the daytime teams consisting of one hospitalist and one NP/PA. Our objectives were to identify deficiencies and to evaluate the effectiveness of a restructured handoff process.
Methods
The Mayo Clinic Institutional Review Board reviewed and approved this study.
Setting
At the time of this study, the Division of Hospital Internal Medicine (HIM) at our institution consisted of 22 hospitalists, 11 NPs and 9 PAs (hereinafter NP/PAs), and 2 clinical assistants (CAs). The CAs assist with clerical duties not covered by Unit Secretaries:
-
Obtaining outside records
-
Clarifying referring physician contact information
-
Scheduling follow‐up outpatient appointments for tests, procedures, and visits
-
Attendance at morning handoff
Each CA can assist 3 or 4 daytime service teams.
Daytime Service Organization
Six HIM services, each managing up to 12 patients, are staffed by a partnership of 1 hospitalist and 1 NP/PA: Four services are primary general medicine services, and 2 consulting (orthopedic comanagement) services.
Night Coverage
Three of 4 primary daytime services and one consult service team transfer care to the (in‐house) night NP/PA. The night NP/PA addresses any acute‐care issues and reports at morning handoff to the 3 primary services and 1 consult service. In a designated conference room the morning handoff occurs, with at least 1 (day team) service representative present. This is usually the NP/PA, as the day team hospitalist concurrently receives a report on new admissions from the (in‐house) night hospitalist (who also covers one service and backs up the night NP/PA).
Improvement Process
An improvement team was formed within the Division of HIM consisting of 3 hospitalists, 3 NP/PAs, and 2 CAs to assess the existing handoff process at 7:45am between the Night NP/PA and daytime services. The improvement team met, reviewed evidence‐based literature on handoffs and discussed our local process. Four problems were identified by consensus:
-
Unpredictable start and finish times
-
Inefficiency (time wasted)
-
Poor environment (room noisy and distracting conversations)
-
Poor communication (overwrought and meandering narratives).
Intervention
The improvement team structured a new handoff process to address these deficiencies.
-
Environment: Moved to a smaller room (lower ceiling, less ambient noise).
-
Identification: table cards designating seats for participants (reduced queries regarding what service are you, today?).
-
Start Times: Each service team assigned a consistent start time (labeled on the table card) within a 15‐minute period, and although earlier reportage could occur, any service team present at their designated time has priority for the attention of the night NP/PA, and the opportunity to ask questions.
-
Quiet and Focus: HIM members were reminded to remain quiet in the handoff room, so the service receiving report has the floor and personal conversations must not impede the principals.
-
Visual Cue: Green Good to go sign placed on team table cards when no verbal was required.
-
Written e‐Material: The improvement team required elements of a brief written report in a specified column of our existing electronic service list (ESL). The ESL is a custom designed template importing laboratory, medication, and demographic data automatically but also capable of free text additions (Figure 1). All providers were instructed to update the ESL every 12 hours.
-
Admission and Progress Notes: After manual electronic medical record search, the CAs printed any notes generated in the preceding 12 hours and placed them by the team table card.
The improvement team provided education for the new process at a division meeting and through e‐mail. The recommended report sequence was night NP/PA reporting and day service teams asking questions and seeking clarifications. We discouraged editorial comments and chit‐chat.
A member of the improvement team monitored the new handoff process for 15 days, and 3 months later for 10 days.
Survey
An anonymous survey (Figure 2) concerning staff satisfaction with handoff was conducted immediately before and 15 days after the intervention. In the e‐mail containing the postintervention survey, providers were asked to respond only if they had been on service the preceding 15 days (and thus eligible to participate in handoff). To help insure this, the first question read, Have you been on service during the past 15 days?
Statistics
To compare the relationship of preintervention and postintervention survey responses, Fisher's exact test was used to compare categorical variables and 2 sample t‐test and Wilcoxon rank sum test were used for continuous variables. Comparisons that adjusted for the possibility of someone responding to both the preintervention and postintervention surveys were not performed since the surveys were anonymous. A P value 0.05 was considered statistically significant. For the item concerning the percentage of days morning report was attended while on service, based on a common standard deviation estimate of 35.3, we had 80% power to detect a difference of 29.1 (pre vs. post). This computation assumes a 2‐sample t‐test of = 0.05 with sample sizes of 36 and 18. We have 59% power to detect a difference of 27% (67% pre vs. 94% post) for those who at least agree that helpful information was conveyed during handoff. This computation is based on a 2‐sided Pearson 2 test with = 0.05.
Qualitative data analysis of respondents' answers to the open‐ended survey questions What would increase the likelihood of your attending handoff? and What feedback do you have regarding the changes to handoff? was performed using the constant comparative method14 associated with grounded theory approaches to identify themes and categories.15 To establish interrater reliability, three investigators (MCB, DTK, LLK) independently identified coding categories for the data set, compared results, redefined coding categories as needed, and reanalyzed the data until 80% agreement was reached.
Results
Thirty‐six of the 44 providers (82%) answered the preintervention survey, including 18 of 22 hospitalists (82%), 17 of 20 NPs/PAs (85%), and 1 of 2 CAs (50%). During the intervention based on our staffing model, 21 providers had the opportunity to participate in handoff, and 18 (86%) answered the postintervention survey, including 5 of 6 hospitalists (83%), 9 of 14 NPs/PAs (64%), and 2 of 2 CAs (100%). All respondents to the postintervention survey reported being on service during the previous 15 days.
As summarized in Table 1, compared to 60.5% of survey participants (n = 38) who thought morning handoff was performed in a timely fashion preintervention, 100% (n = 15) felt it was performed in a timely fashion postintervention (P = 0.005). The average time spent in morning report before the intervention was 11 minutes, as compared to 5 minutes after the intervention (P 0.0028). Prior to the intervention, 6.5 minutes of the handoff were viewed to be wasteful, as compared to 0.5 minutes of the handoff in the postintervention survey (P 0.0001). Attendance and quality of information perceptions did not demonstrate statistically significant change.
| Survey Question | Preintervention | Postintervention | P |
|---|---|---|---|
| What proportion of days while on service did you attend morning report? (%) | 78 | 87 | 0.4119 |
| Helpful information was conveyed in morning report, n (%) | 0.112 | ||
| Strongly agree | 9 (25) | 9 (56) | |
| Agree | 15 (42) | 6 (38) | |
| Neutral | 8 (22) | 1 (6) | |
| Disagree | 4 (11) | 0 | |
| Strongly disagree | 0 | 0 | |
| Morning report was performed in a timely manner, #yes/#no | 23/15 | 15/0 | 0.005 |
| Estimate the number of minutes each day you would spend in morning report (minute) | 11 | 5 | 0.0028 |
| Estimate the number of minutes in morning report you thought were wasteful (minute) | 6.5 | 0.5 | 0.0001 |
During the 15‐day observation period, morning handoff started by 0745 on 14 of 15 (93%) of days and finished by 0800 on 15 of 15 (100%) of days. Table cards, ESL, and progress notes were on the table by 0745 on 15 of 15 (100%) of days following the intervention. Three months after the intervention, the following were observed: morning handoff started by 0745 on 10 of 10 (100%) of days; finished by 0800 on 10 of 10 (100%) of days; and table cards, ESL, and progress notes were on the table by 0745 on 10 of 10 (100%) of days.
Qualitative Data Analysis
Three themes were identified in both preintervention and postintervention surveys: timeliness, quality of report and environment (Table 2). In the preintervention survey, timeliness complaints involved inconsistent start time, prolonged duration of handoff, and inefficiency due to time wasted while teams waited for their handoff report. Comments about report quality mentioned the nonstandardized report process that included nonpertinent information and editorializing. Environmental concerns addressed noise from multiple service team members assembled in 1 large room and chatting while awaiting report. In the postintervention survey, respondents' comments noted improved efficiency, environment, and report quality.
| Deficiency | Pre‐Intervention | Post‐Intervention |
|---|---|---|
| Timeliness | Efficiency needed | I found the changes lead to more concise and valuable time spent in report |
| Timely, scheduled and efficient reports would help increase my attendance | I personally enjoyed having the times set so you are held accountable for a certain handoff | |
| Set report times so I don't have to listen to everyone else's report | More organized and efficient | |
| Too much time wasted | Love the good to go card! Can start on rounds | |
| Environment | Not having to listen to chit chat unrelated to patient carewould improve my attendance | There is less chit chat |
| Services should receive report in a quieter room | Seems less chaotic with less people overall in the room so less distraction | |
| Need a quieter and smaller room | Because the room is quieter, I did not have to repeat information | |
| Too noisy | Quiet and respectful | |
| Quality | I would like a more organized format More information isn't needed, just the correct information in a timely manner | I felt that the amount of information shared was only what was pertinent and important |
| If I first had the opportunity to review ESL and any notes generated in the last 12 hours, this would improve report | Written information on the ESL assured that I didn't forget something important | |
| Less editorializing about events and less adrenaline | I liked having the progress notes generated overnight available for review | |
| Need only meaningful information | Excellent report with prompt dissemination of information |
Discussion
We describe an intervention that set the expectation for formal, structured written and verbal communication in a focused environment involving outgoing and incoming clinicians, resulting in improved satisfaction. Before the intervention, the improvement team identified by consensus 4 problems: unpredictable start time, inefficiency, environment, and report quality. Formal structuring of our handoff process resulted in statistically significant improvement in handoff timeliness and efficiency in the view of the HIM division members. Process improvement included precise team specific start times within a 12‐minute window to improve reliability and predictability and eliminating nonproductive waiting. Additionally, receiving teams were clearly identified with table cards so that no time was wasted locating the appropriate service for report, and minimizing role‐identification challenges. The good to go sign signaled teams that no events had occurred overnight requiring verbal report. Handoff timeliness persisted 3 months after the intervention, suggesting that the process is easily sustainable.
Postintervention survey comments noted the improved environment: a smaller, quieter room with the door closed. Before the intervention, all day team providers, CAs and night provider met in a large, loud room where multiple conversations were commonplace. Previous study of the handoff process supports creating an environment free of distraction.4
Postintervention survey responses to the open‐ended questions suggested improved provider satisfaction with the quality of the report. We believe this occurred for several reasons. First, having a precise start time for each team within a 12‐minute window led to a more focused report. Second, the ESL provided a column for providers to suggest plans of care for anticipated overnight events to improve preparedness and avoid significant omissions. Third, hospital notes generated overnight were made available which allowed daytime providers to review events before handoff, for a more informed update, or just after verbal report to reinforce the information just received, a technique used in other high‐reliability organizations.16 This measure also provided an at‐a‐glance view of each patient, decreasing the complexity of handoff.17
This study has important limitations. We address the handoff process of 1 hospitalist group at a single academic center. NP/PAs are the clinicians with first‐call responsibility for the night coverage of our patients, and the handoff process between the night NP/PA and daytime provider was studied. The handoff between physicians for patients admitted overnight was not assessed. Another limitation is that the time spent in handoff is reported as a participant estimate. There was no objective measurement of time, and respondents may have been biased. An additional limitation of our study concerns the preintervention and postintervention surveys. Both surveys were anonymous, which makes discerning the absolute impact of the intervention difficult due to the lack of paired responses. Lastly, our institution has an ESL. This option may not be available in other hospital systems.
Several deficiencies in the handoff process were addressed by providing key clinical data verbally and in written format, enhancing the physical environment, and defining each team's handoff start time. Our process improvements are consistent with the handoff recommendations endorsed by the Society of Hospital Medicine.12 Subsequent direct observation, subjective reports, and survey results demonstrated improvement in the handoff process.
Future studies might measure the effectiveness of morning handoff by end‐shift interviews of the daytime clinicians. Similarly, a study of evening handoff could measure the efficiency and effectiveness of report given by day teams to night‐coverage colleagues. Furthermore, if the handoff report skill set can be more rigorously defined and measured, a hospitalist clinical competency for hospitalists and NP/PAs could be developed in this core process‐of‐care.12
Acknowledgements
The authors thank Lisa Boucher for preparation of this manuscript.
Transfer of responsibility for patients, or handoff,1 occurs frequently in hospitalist services, requiring excellent and timely communication to ensure patient safety. Communication failure is a major contributor to medical errors.2, 3 Recognizing such findings, a growing body of literature addresses handoff techniques for learners.47
Vidyarthi described the handoff process as traditionally informal, unstructured, and idiosyncratic,4 and many believe efforts to formalize and structure this process are important for patient safety.8 Standardized handoff forms have improved accuracy of information.9 Web‐based sign‐out systems reportedly reduced the number of patients missed on rounds.10
Hospitalists also face challenges with effective communication during service change.11 The Society of Hospital Medicine identified the handoff skill as a core competency for hospitalists, and recommendations based on a systematic review of the literature were published.12 Inpatient medicine programs are increasingly using midlevel providers such as nurse practitioners (NPs) and physician assistants (PAs) along with hospitalists to accommodate workload while maintaining the scholarly enterprise in academic centers.13 To our knowledge there is no literature examining the hospitalist service handoffs involving NP/PAs.
We wished to study the effectiveness and timeliness of the morning handoff from the night coverage providers to the daytime teams consisting of one hospitalist and one NP/PA. Our objectives were to identify deficiencies and to evaluate the effectiveness of a restructured handoff process.
Methods
The Mayo Clinic Institutional Review Board reviewed and approved this study.
Setting
At the time of this study, the Division of Hospital Internal Medicine (HIM) at our institution consisted of 22 hospitalists, 11 NPs and 9 PAs (hereinafter NP/PAs), and 2 clinical assistants (CAs). The CAs assist with clerical duties not covered by Unit Secretaries:
-
Obtaining outside records
-
Clarifying referring physician contact information
-
Scheduling follow‐up outpatient appointments for tests, procedures, and visits
-
Attendance at morning handoff
Each CA can assist 3 or 4 daytime service teams.
Daytime Service Organization
Six HIM services, each managing up to 12 patients, are staffed by a partnership of 1 hospitalist and 1 NP/PA: Four services are primary general medicine services, and 2 consulting (orthopedic comanagement) services.
Night Coverage
Three of 4 primary daytime services and one consult service team transfer care to the (in‐house) night NP/PA. The night NP/PA addresses any acute‐care issues and reports at morning handoff to the 3 primary services and 1 consult service. In a designated conference room the morning handoff occurs, with at least 1 (day team) service representative present. This is usually the NP/PA, as the day team hospitalist concurrently receives a report on new admissions from the (in‐house) night hospitalist (who also covers one service and backs up the night NP/PA).
Improvement Process
An improvement team was formed within the Division of HIM consisting of 3 hospitalists, 3 NP/PAs, and 2 CAs to assess the existing handoff process at 7:45am between the Night NP/PA and daytime services. The improvement team met, reviewed evidence‐based literature on handoffs and discussed our local process. Four problems were identified by consensus:
-
Unpredictable start and finish times
-
Inefficiency (time wasted)
-
Poor environment (room noisy and distracting conversations)
-
Poor communication (overwrought and meandering narratives).
Intervention
The improvement team structured a new handoff process to address these deficiencies.
-
Environment: Moved to a smaller room (lower ceiling, less ambient noise).
-
Identification: table cards designating seats for participants (reduced queries regarding what service are you, today?).
-
Start Times: Each service team assigned a consistent start time (labeled on the table card) within a 15‐minute period, and although earlier reportage could occur, any service team present at their designated time has priority for the attention of the night NP/PA, and the opportunity to ask questions.
-
Quiet and Focus: HIM members were reminded to remain quiet in the handoff room, so the service receiving report has the floor and personal conversations must not impede the principals.
-
Visual Cue: Green Good to go sign placed on team table cards when no verbal was required.
-
Written e‐Material: The improvement team required elements of a brief written report in a specified column of our existing electronic service list (ESL). The ESL is a custom designed template importing laboratory, medication, and demographic data automatically but also capable of free text additions (Figure 1). All providers were instructed to update the ESL every 12 hours.
-
Admission and Progress Notes: After manual electronic medical record search, the CAs printed any notes generated in the preceding 12 hours and placed them by the team table card.
The improvement team provided education for the new process at a division meeting and through e‐mail. The recommended report sequence was night NP/PA reporting and day service teams asking questions and seeking clarifications. We discouraged editorial comments and chit‐chat.
A member of the improvement team monitored the new handoff process for 15 days, and 3 months later for 10 days.
Survey
An anonymous survey (Figure 2) concerning staff satisfaction with handoff was conducted immediately before and 15 days after the intervention. In the e‐mail containing the postintervention survey, providers were asked to respond only if they had been on service the preceding 15 days (and thus eligible to participate in handoff). To help insure this, the first question read, Have you been on service during the past 15 days?
Statistics
To compare the relationship of preintervention and postintervention survey responses, Fisher's exact test was used to compare categorical variables and 2 sample t‐test and Wilcoxon rank sum test were used for continuous variables. Comparisons that adjusted for the possibility of someone responding to both the preintervention and postintervention surveys were not performed since the surveys were anonymous. A P value 0.05 was considered statistically significant. For the item concerning the percentage of days morning report was attended while on service, based on a common standard deviation estimate of 35.3, we had 80% power to detect a difference of 29.1 (pre vs. post). This computation assumes a 2‐sample t‐test of = 0.05 with sample sizes of 36 and 18. We have 59% power to detect a difference of 27% (67% pre vs. 94% post) for those who at least agree that helpful information was conveyed during handoff. This computation is based on a 2‐sided Pearson 2 test with = 0.05.
Qualitative data analysis of respondents' answers to the open‐ended survey questions What would increase the likelihood of your attending handoff? and What feedback do you have regarding the changes to handoff? was performed using the constant comparative method14 associated with grounded theory approaches to identify themes and categories.15 To establish interrater reliability, three investigators (MCB, DTK, LLK) independently identified coding categories for the data set, compared results, redefined coding categories as needed, and reanalyzed the data until 80% agreement was reached.
Results
Thirty‐six of the 44 providers (82%) answered the preintervention survey, including 18 of 22 hospitalists (82%), 17 of 20 NPs/PAs (85%), and 1 of 2 CAs (50%). During the intervention based on our staffing model, 21 providers had the opportunity to participate in handoff, and 18 (86%) answered the postintervention survey, including 5 of 6 hospitalists (83%), 9 of 14 NPs/PAs (64%), and 2 of 2 CAs (100%). All respondents to the postintervention survey reported being on service during the previous 15 days.
As summarized in Table 1, compared to 60.5% of survey participants (n = 38) who thought morning handoff was performed in a timely fashion preintervention, 100% (n = 15) felt it was performed in a timely fashion postintervention (P = 0.005). The average time spent in morning report before the intervention was 11 minutes, as compared to 5 minutes after the intervention (P 0.0028). Prior to the intervention, 6.5 minutes of the handoff were viewed to be wasteful, as compared to 0.5 minutes of the handoff in the postintervention survey (P 0.0001). Attendance and quality of information perceptions did not demonstrate statistically significant change.
| Survey Question | Preintervention | Postintervention | P |
|---|---|---|---|
| What proportion of days while on service did you attend morning report? (%) | 78 | 87 | 0.4119 |
| Helpful information was conveyed in morning report, n (%) | 0.112 | ||
| Strongly agree | 9 (25) | 9 (56) | |
| Agree | 15 (42) | 6 (38) | |
| Neutral | 8 (22) | 1 (6) | |
| Disagree | 4 (11) | 0 | |
| Strongly disagree | 0 | 0 | |
| Morning report was performed in a timely manner, #yes/#no | 23/15 | 15/0 | 0.005 |
| Estimate the number of minutes each day you would spend in morning report (minute) | 11 | 5 | 0.0028 |
| Estimate the number of minutes in morning report you thought were wasteful (minute) | 6.5 | 0.5 | 0.0001 |
During the 15‐day observation period, morning handoff started by 0745 on 14 of 15 (93%) of days and finished by 0800 on 15 of 15 (100%) of days. Table cards, ESL, and progress notes were on the table by 0745 on 15 of 15 (100%) of days following the intervention. Three months after the intervention, the following were observed: morning handoff started by 0745 on 10 of 10 (100%) of days; finished by 0800 on 10 of 10 (100%) of days; and table cards, ESL, and progress notes were on the table by 0745 on 10 of 10 (100%) of days.
Qualitative Data Analysis
Three themes were identified in both preintervention and postintervention surveys: timeliness, quality of report and environment (Table 2). In the preintervention survey, timeliness complaints involved inconsistent start time, prolonged duration of handoff, and inefficiency due to time wasted while teams waited for their handoff report. Comments about report quality mentioned the nonstandardized report process that included nonpertinent information and editorializing. Environmental concerns addressed noise from multiple service team members assembled in 1 large room and chatting while awaiting report. In the postintervention survey, respondents' comments noted improved efficiency, environment, and report quality.
| Deficiency | Pre‐Intervention | Post‐Intervention |
|---|---|---|
| Timeliness | Efficiency needed | I found the changes lead to more concise and valuable time spent in report |
| Timely, scheduled and efficient reports would help increase my attendance | I personally enjoyed having the times set so you are held accountable for a certain handoff | |
| Set report times so I don't have to listen to everyone else's report | More organized and efficient | |
| Too much time wasted | Love the good to go card! Can start on rounds | |
| Environment | Not having to listen to chit chat unrelated to patient carewould improve my attendance | There is less chit chat |
| Services should receive report in a quieter room | Seems less chaotic with less people overall in the room so less distraction | |
| Need a quieter and smaller room | Because the room is quieter, I did not have to repeat information | |
| Too noisy | Quiet and respectful | |
| Quality | I would like a more organized format More information isn't needed, just the correct information in a timely manner | I felt that the amount of information shared was only what was pertinent and important |
| If I first had the opportunity to review ESL and any notes generated in the last 12 hours, this would improve report | Written information on the ESL assured that I didn't forget something important | |
| Less editorializing about events and less adrenaline | I liked having the progress notes generated overnight available for review | |
| Need only meaningful information | Excellent report with prompt dissemination of information |
Discussion
We describe an intervention that set the expectation for formal, structured written and verbal communication in a focused environment involving outgoing and incoming clinicians, resulting in improved satisfaction. Before the intervention, the improvement team identified by consensus 4 problems: unpredictable start time, inefficiency, environment, and report quality. Formal structuring of our handoff process resulted in statistically significant improvement in handoff timeliness and efficiency in the view of the HIM division members. Process improvement included precise team specific start times within a 12‐minute window to improve reliability and predictability and eliminating nonproductive waiting. Additionally, receiving teams were clearly identified with table cards so that no time was wasted locating the appropriate service for report, and minimizing role‐identification challenges. The good to go sign signaled teams that no events had occurred overnight requiring verbal report. Handoff timeliness persisted 3 months after the intervention, suggesting that the process is easily sustainable.
Postintervention survey comments noted the improved environment: a smaller, quieter room with the door closed. Before the intervention, all day team providers, CAs and night provider met in a large, loud room where multiple conversations were commonplace. Previous study of the handoff process supports creating an environment free of distraction.4
Postintervention survey responses to the open‐ended questions suggested improved provider satisfaction with the quality of the report. We believe this occurred for several reasons. First, having a precise start time for each team within a 12‐minute window led to a more focused report. Second, the ESL provided a column for providers to suggest plans of care for anticipated overnight events to improve preparedness and avoid significant omissions. Third, hospital notes generated overnight were made available which allowed daytime providers to review events before handoff, for a more informed update, or just after verbal report to reinforce the information just received, a technique used in other high‐reliability organizations.16 This measure also provided an at‐a‐glance view of each patient, decreasing the complexity of handoff.17
This study has important limitations. We address the handoff process of 1 hospitalist group at a single academic center. NP/PAs are the clinicians with first‐call responsibility for the night coverage of our patients, and the handoff process between the night NP/PA and daytime provider was studied. The handoff between physicians for patients admitted overnight was not assessed. Another limitation is that the time spent in handoff is reported as a participant estimate. There was no objective measurement of time, and respondents may have been biased. An additional limitation of our study concerns the preintervention and postintervention surveys. Both surveys were anonymous, which makes discerning the absolute impact of the intervention difficult due to the lack of paired responses. Lastly, our institution has an ESL. This option may not be available in other hospital systems.
Several deficiencies in the handoff process were addressed by providing key clinical data verbally and in written format, enhancing the physical environment, and defining each team's handoff start time. Our process improvements are consistent with the handoff recommendations endorsed by the Society of Hospital Medicine.12 Subsequent direct observation, subjective reports, and survey results demonstrated improvement in the handoff process.
Future studies might measure the effectiveness of morning handoff by end‐shift interviews of the daytime clinicians. Similarly, a study of evening handoff could measure the efficiency and effectiveness of report given by day teams to night‐coverage colleagues. Furthermore, if the handoff report skill set can be more rigorously defined and measured, a hospitalist clinical competency for hospitalists and NP/PAs could be developed in this core process‐of‐care.12
Acknowledgements
The authors thank Lisa Boucher for preparation of this manuscript.
- , , , et al.Lost in translation: challenges and opportunities in physician‐to‐physician communication during patient handoffs.Acad Med.2005;80:1094–1099.
- , , .Communication failures: an insidious contributor to medical mishaps.Acad Med.2004;79:186–194.
- , , .The human factor: the critical importance of effective teamwork and communication in providing safe care.Quality 13 Suppl 1:i85–90.
- , , , et al.Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign‐out.J Hosp Med.2006;1:257–266.
- , , .Development and implementation of an oral sign‐out skills curriculum.J Gen Intern Med.2007;22:1470–1474.
- , , , et al.The top 10 list for a safe and effective sign‐out.Arch Surg2008;143(10):1008–1010.
- , , , et al.Residents' and attending physicians' handoffs: a systematic review of the literature.Acad Med.2009;84(12):1775–1787.
- , , , et al.A structured handoff program for interns.Acad Med.2009;84:347–352.
- , , , et al.Simple standardized patient handoff system that increases accuracy and completeness.J Surg.2008;65:476–485.
- , , , et al.A randomized, controlled trial evaluation the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200:538–545.
- , , , .Understanding communication during hospitalist service changes: A mixed methods study.J Hosp Med.2009;4(9):535–540.
- , , , , , .Hospitalist handoffs: a systematic review and task force recommendations.J of Hosp Med.2009;4(7):433–440.
- , , , et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3:361–368.
- , .Basics of Qualitiative Research: Grounded Theory Procedures and Techniques.Sage Publications, Inc.Newbury Park, CA.1990.
- , .Naturalistic Inquiry.Sage Publications, Inc.Newbury Park, CA.1985.
- .Communication strategies from high‐reliability organizations.Ann Surg.2007;245(2):170–172.
- , , , et al.Handoff strategies in settings with high consequences for failure: lessons for health care operations.Int J Qual Health Care.2004;16(2):125.
- , , , et al.Lost in translation: challenges and opportunities in physician‐to‐physician communication during patient handoffs.Acad Med.2005;80:1094–1099.
- , , .Communication failures: an insidious contributor to medical mishaps.Acad Med.2004;79:186–194.
- , , .The human factor: the critical importance of effective teamwork and communication in providing safe care.Quality 13 Suppl 1:i85–90.
- , , , et al.Managing discontinuity in academic medical centers: strategies for a safe and effective resident sign‐out.J Hosp Med.2006;1:257–266.
- , , .Development and implementation of an oral sign‐out skills curriculum.J Gen Intern Med.2007;22:1470–1474.
- , , , et al.The top 10 list for a safe and effective sign‐out.Arch Surg2008;143(10):1008–1010.
- , , , et al.Residents' and attending physicians' handoffs: a systematic review of the literature.Acad Med.2009;84(12):1775–1787.
- , , , et al.A structured handoff program for interns.Acad Med.2009;84:347–352.
- , , , et al.Simple standardized patient handoff system that increases accuracy and completeness.J Surg.2008;65:476–485.
- , , , et al.A randomized, controlled trial evaluation the impact of a computerized rounding and sign‐out system on continuity of care and resident work hours.J Am Coll Surg.2005;200:538–545.
- , , , .Understanding communication during hospitalist service changes: A mixed methods study.J Hosp Med.2009;4(9):535–540.
- , , , , , .Hospitalist handoffs: a systematic review and task force recommendations.J of Hosp Med.2009;4(7):433–440.
- , , , et al.Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes.J Hosp Med.2008;3:361–368.
- , .Basics of Qualitiative Research: Grounded Theory Procedures and Techniques.Sage Publications, Inc.Newbury Park, CA.1990.
- , .Naturalistic Inquiry.Sage Publications, Inc.Newbury Park, CA.1985.
- .Communication strategies from high‐reliability organizations.Ann Surg.2007;245(2):170–172.
- , , , et al.Handoff strategies in settings with high consequences for failure: lessons for health care operations.Int J Qual Health Care.2004;16(2):125.
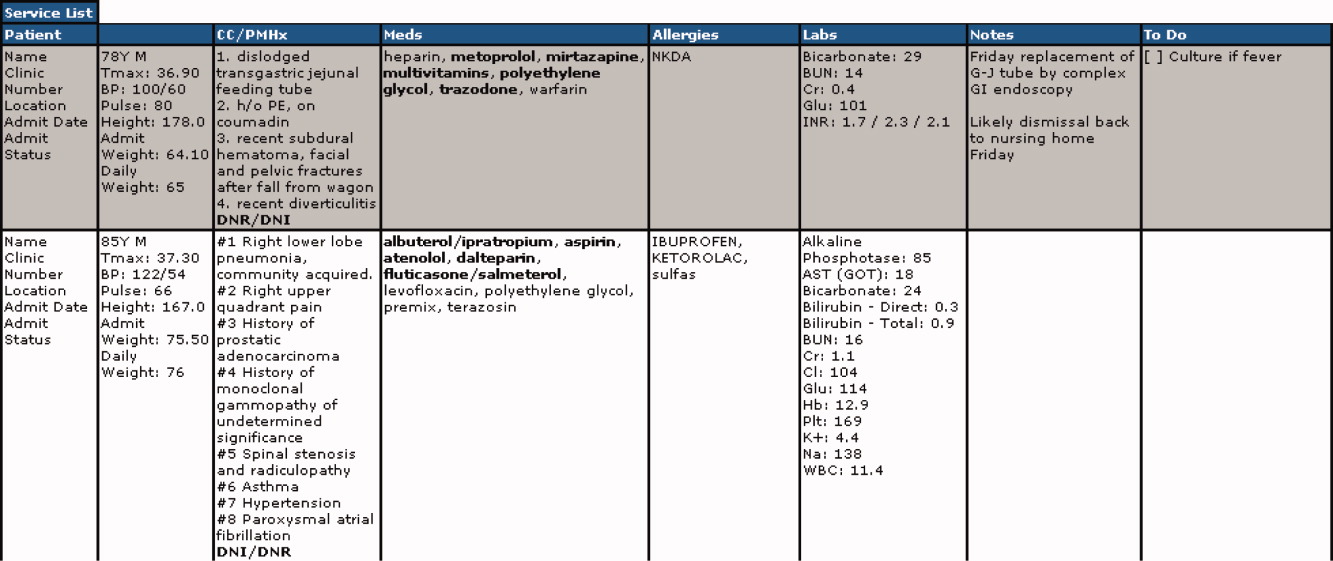
Hospitalist‐Run Observation Unit
Hospitalists play key roles in many types of clinical services, including teaching, nonteaching, consultative, and comanagement services.14 While the impact of hospitalist programs on LOS for inpatient medicine services has been studied,58 less work has focused on the impact of hospitalists in other types of service delivery, such as in short‐stay or observation units.
While many hospitals now have short‐stay units to care for observation patients, most are adjuncts of the emergency department. A Canadian hospitalist‐run short‐stay unit that targeted patients with an expected LOS of less than 3 days has been described.9 The experience of a single, chest‐painspecific service has also been reported.10
In August 2005, we introduced a hospitalist‐run observation unit, the Clinical Decision Unit (CDU), at University Hospital, the primary teaching affiliate of the University of Texas Health Science Center at San Antonio (San Antonio, TX). The rationale was that observation‐level care in a dedicated short‐stay unit would be more efficient than in an inpatient general medicine service. Through the creation of this unit, we consolidated the care of all medical observation patients, including patients previously evaluated in a cardiology‐run chest pain unit.
In this brief report, we present a description of the unit as well as a preliminary analysis of the impact of the unit on LOS for the most common CDU diagnoses.
Methods
CDU Structure
University Hospital is the Bexar County public hospital. It contains 604 acute care beds, and averages 70,000 emergency visits annually. The CDU is a geographically separate, 10‐bed unit, staffed with dedicated nurses in 8‐hour shifts and 24/7 by hospitalists in 12‐hour shifts. Four to five hospitalists rotate through the CDU monthly. About 30% of shifts are staffed through moonlighting by hospitalist faculty or fellows.
For admissions, through examining hospital LOS data, we targeted diagnoses for which patients might be expected to stay less than 24 hours. Potentially appropriate diagnoses were discussed by the group, and general admission guidelines were created based on consensus. These diagnoses included chest pain, cellulitis, pyelonephritis, syncope, asthma exacerbation, chronic obstructive pulmonary disease exacerbation, hyperglycemia, and hepatic encephalopathy. Table 1 lists these guidelines.
| Diagnosis | Guidelines |
|---|---|
| |
| Chest pain | Patients without EKG changes or positive troponins, but for whom stress test was indicated based on history or risk factors |
| Asthma | Patients with oxygen saturation >90% and demonstrating improvement in with ED nebulizer treatment |
| Syncope | Patients without known structural heart disease based on past medical history or exam findings |
| Cellulitis | Patients without suspicion for abscess or osteomyelitis |
| Pyelonephritis | Patients without change from baseline renal function; kidney transplant recipients excluded |
If a patient's stay exceeded 23 hours, the hospitalist could transfer the patient from the CDU to a general medicine team. Formal transfer guidelines were not created, but if patients were expected to be discharged within 12 hours, they generally remained in the CDU to minimize transitions. The census of the general medicine teams could also be a factor in transfer decisions: if they were at admitting capacity, the patient remained in the CDU.
Patients admitted to the general medicine units were cared for by 5 teaching teams, staffed exclusively by hospitalists.
Assessment of CDU Implementation on LOS
To examine the impact of unit implementation on LOS, we performed a retrospective, preimplementation/postimplementation comparison of the LOS of patients discharged 12 months before and after the unit opening on August 1, 2005. To ensure a comparison of similar patients, we identified the top 5 most common CDU discharge diagnoses, and identified people discharged from general medicine with the same diagnoses. Specifically, we compared the LOS of patients discharged from the general medicine units from August 1, 2004 to July 31, 2005, vs. those with the same diagnoses discharged from either the CDU or general medicine units from August 1, 2005 to July 31, 2006.
The 5 most common CDU discharge diagnoses were identified using hospital administrative discharge data. All International Statistical Classification of Diseases and Related Health Problems, 9th edition (ICD‐9) codes associated with CDU discharges were identified and listed in order of frequency. Related ICD‐9 codes were grouped. For example, angina (413.0) and chest pain (786.50, 786.59) were considered related, and were included as chest pain. These ICD‐9 codes were then used to identify patients discharged with these diagnoses in the pre‐CDU and post‐CDU periods. Patients on general medicine units were identified using admission location and admitting attending. Only patients admitted by a hospitalist to a general medicine floor were included. Patients were analyzed according to their admission location. All patients with relevant ICD‐9 codes were included in the analysis. None were excluded. For each patient identified, all data elements were present.
The acuity of patients admitted in the preimplementation and postimplementation periods was compared using the case‐mix index calculated by 3M Incorporated's All Patient RefinedDiagnosis‐Related Group methodology (3M APR‐DRG; 3M, St. Paul, MN). This adjusts administrative data for severity of illness and mortality risk based on primary diagnoses, comorbidities, age, and procedures. Patients are assigned to mortality classes with corresponding scores of 0 or higher.
Statistical Analysis
Statistical analyses were performed using STATA 8.0. LOS and acuity differences were assessed using 2‐sample t tests with equal variances.
Results
Clinical Experience with the CDU
The 5 most common CDU discharge diagnoses accounted for 724 discharges, and included chest pain, asthma, syncope, cellulitis, and pyelonephritis. The ICD‐9 codes, as well as the numbers of patients discharged from the general medicine units and CDU with each diagnosis are listed in Table 2. The average daily census in the unit was 7.2 patients with a standard deviation of 0.8. Overall, 22% of CDU admissions were changed from observation to admission status.
| Diagnosis | ICD‐9 Codes | Pre‐CDU | Post‐CDU | Post‐CDU Admitted to CDU | Post‐CDU Admitted to Ward Team |
|---|---|---|---|---|---|
| |||||
| Top 5 diagnoses | 2240 | 2148 | 724 | 1424 | |
| Cellulitis | 681.0, 682.0‐682.9 | 1002 | 819 | 48 | 771 |
| Asthma | 493.02, 493.12 | 199 | 176 | 71 | 105 |
| Chest pain | 786.50, 786.59, 413.0 | 837 | 917 | 520 | 397 |
| Pyelonephritis | 590.1, 590.8 | 143 | 163 | 61 | 102 |
| Syncope | 780.2 | 59 | 73 | 24 | 49 |
Impact of CDU Implementation on LOS
The overall LOS for patients with the 5 most common diagnoses decreased from 2.4 to 2.2 days (P = 0.05) between the 12‐month preimplementation and postimplementation periods. A significant decrease was seen for patients with cellulitis (2.4‐1.9 days; P 0.001) and asthma (2.2‐1.2 days; P 0.001). Differences in LOS for patients with chest pain, pyelonephritis, and syncope were not statistically significant. These results are summarized in Table 3. The acuity of patients admitted in the pre‐CDU and post‐CDU implementation, shown in Table 4, was not significantly different.
| Diagnosis | Pre‐CDU | Post‐CDU | P Value |
|---|---|---|---|
| |||
| Top 5 diagnoses | 2.4 (3.8) | 2.2 (2.8) | 0.05 |
| Cellulitis | 2.4 (3.2) | 1.9 (2.6) | 0.001 |
| Asthma | 2.2 (1.9) | 1.2 (0.7) | 0.001 |
| Chest pain | 1.5 (1.3) | 1.6 (2.4) | 0.75 |
| Pyelonephritis | 3.3 (4.9) | 2.7 (2.8) | 0.27 |
| Syncope | 2.0 (2.9) | 2.2 (2.0) | 0.68 |
| Diagnosis | All Patients2005 | All Patients2006 |
|---|---|---|
| ||
| Top 5 diagnoses | 0.6987 | 0.7240 |
| Cellulitis | 0.7393 | 0.7630 |
| Asthma | 0.4382 | 0.4622 |
| Chest pain | 0.7428 | 0.7545 |
| Pyelonephritis | 0.7205 | 0.6662 |
| Syncope | 0.6769 | 0.6619 |
Discussion and Conclusions
Implementation of a hospitalist‐run observation unit was associated with an overall decreased LOS for patients with the 5 most common CDU discharge diagnoses of chest pain, cellulitis, asthma, pyelonephritis, and syncope. The lack of statistically significantly differences in patient acuity in the preimplementation and postimplementation periods suggests this result is not due to acuity differences, but rather to unit implementation. We believe this reduction resulted from the greater efficiencies of care that occur from clustering observation patients in a geographically separate unit with dedicated nursing staff and efficient workflow. The reduction of 0.2 days over 2148 patients (total number of postimplementation discharges) led to an additional 429.6 days of capacity without adding additional beds. Thus, what might appear to be a modest LOS reduction has a larger impact when patient volume is considered.
For individual diagnoses, significant differences in LOS were seen for patients with cellulitis and asthma The lack of a difference for chest pain may be related to the fact that these patients were cared for in a chest pain unit prior to CDU creation, which likely fostered similar efficiencies. This finding may suggest that hospitalists are as efficient as cardiologists in assessing patients with chest pain. The lack of a difference in LOS for syncope may have reflected a bottleneck in obtaining echocardiogram tests. Finally, the lack of a difference for pyelonephritis may indicate that it is not a diagnosis for which observation is beneficial.
While our use of administrative data over the year‐long preimplementation and postimplementation periods allows for the inclusion of a large number of discharges, the retrospective study design limits the strength of our results. A prospective study would more definitively reduce the possibility of bias and ensure the validity of our finding of reduced LOS.
The creation of a hospitalist‐run observation unit may represent an alternative to emergency departmentrun units. It allows physicians with greater expertise in inpatient medicine to make admission and discharge decisions, allowing emergency department physicians to concentrate on the care of other patients. This can be particularly critical for high‐volume emergency departments. The CDU also offers an alternative to specialist‐run chest pain units. Because patients either stay for only the observation period or are admitted and typically moved off the unit, there is little need for provider continuity, and the discontinuous shift staffing model works well.
In addition to the geographic localization, several aspects of the CDU model may be critical to the successful implementation of similar hospitalist‐run observation units. Dedicated nursing staff with expertise in caring for high‐turnover patients with a more limited spectrum of diagnoses may be a factor. Another factor may be that the lack of less‐experienced trainees in a nonteaching service leads to more efficient care.
A potential area of further exploration includes understanding the differences between CDU patients who are discharged within 23 hours and those who are later admitted. This understanding may help us better differentiate patients appropriate for CDU admission, allowing the creation of more formal admission criteria.
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
- ,.The role of hospitalists in medical education.Am J Med.1999;107(4):305–309.
- ,,,,.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- ,,, et al.,Hospitalist‐Orthopedic Team Trial Investigators. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141(1):28–38.
- ,,,,,.Implementation of a voluntary hospitalist service at a community teaching hospital: improved efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- ,,,,,.Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357(25):2589–2600.
- ,,,,.Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring.Arch Intern Med.2007;167(17):1869–1874.
- ,,.Comparison of hospital costs and length of stay for community internists, hospitalists, and academicians.J Gen Int Med.2007;22(5):662–667.
- ,,, et al.Effects of physician experience on cost and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;37:866–875.
- ,,,.Program description: a hospitalist‐run, medical short‐stay unit in a teaching hospital.CMAJ.2000;163(11):1477–1480.
- ,,,,.Improving resource utilization in a teaching hospital: development of a nonteaching service for chest pain admissions.Acad Med.2006;81(5):432–435.
Hospitalists play key roles in many types of clinical services, including teaching, nonteaching, consultative, and comanagement services.14 While the impact of hospitalist programs on LOS for inpatient medicine services has been studied,58 less work has focused on the impact of hospitalists in other types of service delivery, such as in short‐stay or observation units.
While many hospitals now have short‐stay units to care for observation patients, most are adjuncts of the emergency department. A Canadian hospitalist‐run short‐stay unit that targeted patients with an expected LOS of less than 3 days has been described.9 The experience of a single, chest‐painspecific service has also been reported.10
In August 2005, we introduced a hospitalist‐run observation unit, the Clinical Decision Unit (CDU), at University Hospital, the primary teaching affiliate of the University of Texas Health Science Center at San Antonio (San Antonio, TX). The rationale was that observation‐level care in a dedicated short‐stay unit would be more efficient than in an inpatient general medicine service. Through the creation of this unit, we consolidated the care of all medical observation patients, including patients previously evaluated in a cardiology‐run chest pain unit.
In this brief report, we present a description of the unit as well as a preliminary analysis of the impact of the unit on LOS for the most common CDU diagnoses.
Methods
CDU Structure
University Hospital is the Bexar County public hospital. It contains 604 acute care beds, and averages 70,000 emergency visits annually. The CDU is a geographically separate, 10‐bed unit, staffed with dedicated nurses in 8‐hour shifts and 24/7 by hospitalists in 12‐hour shifts. Four to five hospitalists rotate through the CDU monthly. About 30% of shifts are staffed through moonlighting by hospitalist faculty or fellows.
For admissions, through examining hospital LOS data, we targeted diagnoses for which patients might be expected to stay less than 24 hours. Potentially appropriate diagnoses were discussed by the group, and general admission guidelines were created based on consensus. These diagnoses included chest pain, cellulitis, pyelonephritis, syncope, asthma exacerbation, chronic obstructive pulmonary disease exacerbation, hyperglycemia, and hepatic encephalopathy. Table 1 lists these guidelines.
| Diagnosis | Guidelines |
|---|---|
| |
| Chest pain | Patients without EKG changes or positive troponins, but for whom stress test was indicated based on history or risk factors |
| Asthma | Patients with oxygen saturation >90% and demonstrating improvement in with ED nebulizer treatment |
| Syncope | Patients without known structural heart disease based on past medical history or exam findings |
| Cellulitis | Patients without suspicion for abscess or osteomyelitis |
| Pyelonephritis | Patients without change from baseline renal function; kidney transplant recipients excluded |
If a patient's stay exceeded 23 hours, the hospitalist could transfer the patient from the CDU to a general medicine team. Formal transfer guidelines were not created, but if patients were expected to be discharged within 12 hours, they generally remained in the CDU to minimize transitions. The census of the general medicine teams could also be a factor in transfer decisions: if they were at admitting capacity, the patient remained in the CDU.
Patients admitted to the general medicine units were cared for by 5 teaching teams, staffed exclusively by hospitalists.
Assessment of CDU Implementation on LOS
To examine the impact of unit implementation on LOS, we performed a retrospective, preimplementation/postimplementation comparison of the LOS of patients discharged 12 months before and after the unit opening on August 1, 2005. To ensure a comparison of similar patients, we identified the top 5 most common CDU discharge diagnoses, and identified people discharged from general medicine with the same diagnoses. Specifically, we compared the LOS of patients discharged from the general medicine units from August 1, 2004 to July 31, 2005, vs. those with the same diagnoses discharged from either the CDU or general medicine units from August 1, 2005 to July 31, 2006.
The 5 most common CDU discharge diagnoses were identified using hospital administrative discharge data. All International Statistical Classification of Diseases and Related Health Problems, 9th edition (ICD‐9) codes associated with CDU discharges were identified and listed in order of frequency. Related ICD‐9 codes were grouped. For example, angina (413.0) and chest pain (786.50, 786.59) were considered related, and were included as chest pain. These ICD‐9 codes were then used to identify patients discharged with these diagnoses in the pre‐CDU and post‐CDU periods. Patients on general medicine units were identified using admission location and admitting attending. Only patients admitted by a hospitalist to a general medicine floor were included. Patients were analyzed according to their admission location. All patients with relevant ICD‐9 codes were included in the analysis. None were excluded. For each patient identified, all data elements were present.
The acuity of patients admitted in the preimplementation and postimplementation periods was compared using the case‐mix index calculated by 3M Incorporated's All Patient RefinedDiagnosis‐Related Group methodology (3M APR‐DRG; 3M, St. Paul, MN). This adjusts administrative data for severity of illness and mortality risk based on primary diagnoses, comorbidities, age, and procedures. Patients are assigned to mortality classes with corresponding scores of 0 or higher.
Statistical Analysis
Statistical analyses were performed using STATA 8.0. LOS and acuity differences were assessed using 2‐sample t tests with equal variances.
Results
Clinical Experience with the CDU
The 5 most common CDU discharge diagnoses accounted for 724 discharges, and included chest pain, asthma, syncope, cellulitis, and pyelonephritis. The ICD‐9 codes, as well as the numbers of patients discharged from the general medicine units and CDU with each diagnosis are listed in Table 2. The average daily census in the unit was 7.2 patients with a standard deviation of 0.8. Overall, 22% of CDU admissions were changed from observation to admission status.
| Diagnosis | ICD‐9 Codes | Pre‐CDU | Post‐CDU | Post‐CDU Admitted to CDU | Post‐CDU Admitted to Ward Team |
|---|---|---|---|---|---|
| |||||
| Top 5 diagnoses | 2240 | 2148 | 724 | 1424 | |
| Cellulitis | 681.0, 682.0‐682.9 | 1002 | 819 | 48 | 771 |
| Asthma | 493.02, 493.12 | 199 | 176 | 71 | 105 |
| Chest pain | 786.50, 786.59, 413.0 | 837 | 917 | 520 | 397 |
| Pyelonephritis | 590.1, 590.8 | 143 | 163 | 61 | 102 |
| Syncope | 780.2 | 59 | 73 | 24 | 49 |
Impact of CDU Implementation on LOS
The overall LOS for patients with the 5 most common diagnoses decreased from 2.4 to 2.2 days (P = 0.05) between the 12‐month preimplementation and postimplementation periods. A significant decrease was seen for patients with cellulitis (2.4‐1.9 days; P 0.001) and asthma (2.2‐1.2 days; P 0.001). Differences in LOS for patients with chest pain, pyelonephritis, and syncope were not statistically significant. These results are summarized in Table 3. The acuity of patients admitted in the pre‐CDU and post‐CDU implementation, shown in Table 4, was not significantly different.
| Diagnosis | Pre‐CDU | Post‐CDU | P Value |
|---|---|---|---|
| |||
| Top 5 diagnoses | 2.4 (3.8) | 2.2 (2.8) | 0.05 |
| Cellulitis | 2.4 (3.2) | 1.9 (2.6) | 0.001 |
| Asthma | 2.2 (1.9) | 1.2 (0.7) | 0.001 |
| Chest pain | 1.5 (1.3) | 1.6 (2.4) | 0.75 |
| Pyelonephritis | 3.3 (4.9) | 2.7 (2.8) | 0.27 |
| Syncope | 2.0 (2.9) | 2.2 (2.0) | 0.68 |
| Diagnosis | All Patients2005 | All Patients2006 |
|---|---|---|
| ||
| Top 5 diagnoses | 0.6987 | 0.7240 |
| Cellulitis | 0.7393 | 0.7630 |
| Asthma | 0.4382 | 0.4622 |
| Chest pain | 0.7428 | 0.7545 |
| Pyelonephritis | 0.7205 | 0.6662 |
| Syncope | 0.6769 | 0.6619 |
Discussion and Conclusions
Implementation of a hospitalist‐run observation unit was associated with an overall decreased LOS for patients with the 5 most common CDU discharge diagnoses of chest pain, cellulitis, asthma, pyelonephritis, and syncope. The lack of statistically significantly differences in patient acuity in the preimplementation and postimplementation periods suggests this result is not due to acuity differences, but rather to unit implementation. We believe this reduction resulted from the greater efficiencies of care that occur from clustering observation patients in a geographically separate unit with dedicated nursing staff and efficient workflow. The reduction of 0.2 days over 2148 patients (total number of postimplementation discharges) led to an additional 429.6 days of capacity without adding additional beds. Thus, what might appear to be a modest LOS reduction has a larger impact when patient volume is considered.
For individual diagnoses, significant differences in LOS were seen for patients with cellulitis and asthma The lack of a difference for chest pain may be related to the fact that these patients were cared for in a chest pain unit prior to CDU creation, which likely fostered similar efficiencies. This finding may suggest that hospitalists are as efficient as cardiologists in assessing patients with chest pain. The lack of a difference in LOS for syncope may have reflected a bottleneck in obtaining echocardiogram tests. Finally, the lack of a difference for pyelonephritis may indicate that it is not a diagnosis for which observation is beneficial.
While our use of administrative data over the year‐long preimplementation and postimplementation periods allows for the inclusion of a large number of discharges, the retrospective study design limits the strength of our results. A prospective study would more definitively reduce the possibility of bias and ensure the validity of our finding of reduced LOS.
The creation of a hospitalist‐run observation unit may represent an alternative to emergency departmentrun units. It allows physicians with greater expertise in inpatient medicine to make admission and discharge decisions, allowing emergency department physicians to concentrate on the care of other patients. This can be particularly critical for high‐volume emergency departments. The CDU also offers an alternative to specialist‐run chest pain units. Because patients either stay for only the observation period or are admitted and typically moved off the unit, there is little need for provider continuity, and the discontinuous shift staffing model works well.
In addition to the geographic localization, several aspects of the CDU model may be critical to the successful implementation of similar hospitalist‐run observation units. Dedicated nursing staff with expertise in caring for high‐turnover patients with a more limited spectrum of diagnoses may be a factor. Another factor may be that the lack of less‐experienced trainees in a nonteaching service leads to more efficient care.
A potential area of further exploration includes understanding the differences between CDU patients who are discharged within 23 hours and those who are later admitted. This understanding may help us better differentiate patients appropriate for CDU admission, allowing the creation of more formal admission criteria.
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
Hospitalists play key roles in many types of clinical services, including teaching, nonteaching, consultative, and comanagement services.14 While the impact of hospitalist programs on LOS for inpatient medicine services has been studied,58 less work has focused on the impact of hospitalists in other types of service delivery, such as in short‐stay or observation units.
While many hospitals now have short‐stay units to care for observation patients, most are adjuncts of the emergency department. A Canadian hospitalist‐run short‐stay unit that targeted patients with an expected LOS of less than 3 days has been described.9 The experience of a single, chest‐painspecific service has also been reported.10
In August 2005, we introduced a hospitalist‐run observation unit, the Clinical Decision Unit (CDU), at University Hospital, the primary teaching affiliate of the University of Texas Health Science Center at San Antonio (San Antonio, TX). The rationale was that observation‐level care in a dedicated short‐stay unit would be more efficient than in an inpatient general medicine service. Through the creation of this unit, we consolidated the care of all medical observation patients, including patients previously evaluated in a cardiology‐run chest pain unit.
In this brief report, we present a description of the unit as well as a preliminary analysis of the impact of the unit on LOS for the most common CDU diagnoses.
Methods
CDU Structure
University Hospital is the Bexar County public hospital. It contains 604 acute care beds, and averages 70,000 emergency visits annually. The CDU is a geographically separate, 10‐bed unit, staffed with dedicated nurses in 8‐hour shifts and 24/7 by hospitalists in 12‐hour shifts. Four to five hospitalists rotate through the CDU monthly. About 30% of shifts are staffed through moonlighting by hospitalist faculty or fellows.
For admissions, through examining hospital LOS data, we targeted diagnoses for which patients might be expected to stay less than 24 hours. Potentially appropriate diagnoses were discussed by the group, and general admission guidelines were created based on consensus. These diagnoses included chest pain, cellulitis, pyelonephritis, syncope, asthma exacerbation, chronic obstructive pulmonary disease exacerbation, hyperglycemia, and hepatic encephalopathy. Table 1 lists these guidelines.
| Diagnosis | Guidelines |
|---|---|
| |
| Chest pain | Patients without EKG changes or positive troponins, but for whom stress test was indicated based on history or risk factors |
| Asthma | Patients with oxygen saturation >90% and demonstrating improvement in with ED nebulizer treatment |
| Syncope | Patients without known structural heart disease based on past medical history or exam findings |
| Cellulitis | Patients without suspicion for abscess or osteomyelitis |
| Pyelonephritis | Patients without change from baseline renal function; kidney transplant recipients excluded |
If a patient's stay exceeded 23 hours, the hospitalist could transfer the patient from the CDU to a general medicine team. Formal transfer guidelines were not created, but if patients were expected to be discharged within 12 hours, they generally remained in the CDU to minimize transitions. The census of the general medicine teams could also be a factor in transfer decisions: if they were at admitting capacity, the patient remained in the CDU.
Patients admitted to the general medicine units were cared for by 5 teaching teams, staffed exclusively by hospitalists.
Assessment of CDU Implementation on LOS
To examine the impact of unit implementation on LOS, we performed a retrospective, preimplementation/postimplementation comparison of the LOS of patients discharged 12 months before and after the unit opening on August 1, 2005. To ensure a comparison of similar patients, we identified the top 5 most common CDU discharge diagnoses, and identified people discharged from general medicine with the same diagnoses. Specifically, we compared the LOS of patients discharged from the general medicine units from August 1, 2004 to July 31, 2005, vs. those with the same diagnoses discharged from either the CDU or general medicine units from August 1, 2005 to July 31, 2006.
The 5 most common CDU discharge diagnoses were identified using hospital administrative discharge data. All International Statistical Classification of Diseases and Related Health Problems, 9th edition (ICD‐9) codes associated with CDU discharges were identified and listed in order of frequency. Related ICD‐9 codes were grouped. For example, angina (413.0) and chest pain (786.50, 786.59) were considered related, and were included as chest pain. These ICD‐9 codes were then used to identify patients discharged with these diagnoses in the pre‐CDU and post‐CDU periods. Patients on general medicine units were identified using admission location and admitting attending. Only patients admitted by a hospitalist to a general medicine floor were included. Patients were analyzed according to their admission location. All patients with relevant ICD‐9 codes were included in the analysis. None were excluded. For each patient identified, all data elements were present.
The acuity of patients admitted in the preimplementation and postimplementation periods was compared using the case‐mix index calculated by 3M Incorporated's All Patient RefinedDiagnosis‐Related Group methodology (3M APR‐DRG; 3M, St. Paul, MN). This adjusts administrative data for severity of illness and mortality risk based on primary diagnoses, comorbidities, age, and procedures. Patients are assigned to mortality classes with corresponding scores of 0 or higher.
Statistical Analysis
Statistical analyses were performed using STATA 8.0. LOS and acuity differences were assessed using 2‐sample t tests with equal variances.
Results
Clinical Experience with the CDU
The 5 most common CDU discharge diagnoses accounted for 724 discharges, and included chest pain, asthma, syncope, cellulitis, and pyelonephritis. The ICD‐9 codes, as well as the numbers of patients discharged from the general medicine units and CDU with each diagnosis are listed in Table 2. The average daily census in the unit was 7.2 patients with a standard deviation of 0.8. Overall, 22% of CDU admissions were changed from observation to admission status.
| Diagnosis | ICD‐9 Codes | Pre‐CDU | Post‐CDU | Post‐CDU Admitted to CDU | Post‐CDU Admitted to Ward Team |
|---|---|---|---|---|---|
| |||||
| Top 5 diagnoses | 2240 | 2148 | 724 | 1424 | |
| Cellulitis | 681.0, 682.0‐682.9 | 1002 | 819 | 48 | 771 |
| Asthma | 493.02, 493.12 | 199 | 176 | 71 | 105 |
| Chest pain | 786.50, 786.59, 413.0 | 837 | 917 | 520 | 397 |
| Pyelonephritis | 590.1, 590.8 | 143 | 163 | 61 | 102 |
| Syncope | 780.2 | 59 | 73 | 24 | 49 |
Impact of CDU Implementation on LOS
The overall LOS for patients with the 5 most common diagnoses decreased from 2.4 to 2.2 days (P = 0.05) between the 12‐month preimplementation and postimplementation periods. A significant decrease was seen for patients with cellulitis (2.4‐1.9 days; P 0.001) and asthma (2.2‐1.2 days; P 0.001). Differences in LOS for patients with chest pain, pyelonephritis, and syncope were not statistically significant. These results are summarized in Table 3. The acuity of patients admitted in the pre‐CDU and post‐CDU implementation, shown in Table 4, was not significantly different.
| Diagnosis | Pre‐CDU | Post‐CDU | P Value |
|---|---|---|---|
| |||
| Top 5 diagnoses | 2.4 (3.8) | 2.2 (2.8) | 0.05 |
| Cellulitis | 2.4 (3.2) | 1.9 (2.6) | 0.001 |
| Asthma | 2.2 (1.9) | 1.2 (0.7) | 0.001 |
| Chest pain | 1.5 (1.3) | 1.6 (2.4) | 0.75 |
| Pyelonephritis | 3.3 (4.9) | 2.7 (2.8) | 0.27 |
| Syncope | 2.0 (2.9) | 2.2 (2.0) | 0.68 |
| Diagnosis | All Patients2005 | All Patients2006 |
|---|---|---|
| ||
| Top 5 diagnoses | 0.6987 | 0.7240 |
| Cellulitis | 0.7393 | 0.7630 |
| Asthma | 0.4382 | 0.4622 |
| Chest pain | 0.7428 | 0.7545 |
| Pyelonephritis | 0.7205 | 0.6662 |
| Syncope | 0.6769 | 0.6619 |
Discussion and Conclusions
Implementation of a hospitalist‐run observation unit was associated with an overall decreased LOS for patients with the 5 most common CDU discharge diagnoses of chest pain, cellulitis, asthma, pyelonephritis, and syncope. The lack of statistically significantly differences in patient acuity in the preimplementation and postimplementation periods suggests this result is not due to acuity differences, but rather to unit implementation. We believe this reduction resulted from the greater efficiencies of care that occur from clustering observation patients in a geographically separate unit with dedicated nursing staff and efficient workflow. The reduction of 0.2 days over 2148 patients (total number of postimplementation discharges) led to an additional 429.6 days of capacity without adding additional beds. Thus, what might appear to be a modest LOS reduction has a larger impact when patient volume is considered.
For individual diagnoses, significant differences in LOS were seen for patients with cellulitis and asthma The lack of a difference for chest pain may be related to the fact that these patients were cared for in a chest pain unit prior to CDU creation, which likely fostered similar efficiencies. This finding may suggest that hospitalists are as efficient as cardiologists in assessing patients with chest pain. The lack of a difference in LOS for syncope may have reflected a bottleneck in obtaining echocardiogram tests. Finally, the lack of a difference for pyelonephritis may indicate that it is not a diagnosis for which observation is beneficial.
While our use of administrative data over the year‐long preimplementation and postimplementation periods allows for the inclusion of a large number of discharges, the retrospective study design limits the strength of our results. A prospective study would more definitively reduce the possibility of bias and ensure the validity of our finding of reduced LOS.
The creation of a hospitalist‐run observation unit may represent an alternative to emergency departmentrun units. It allows physicians with greater expertise in inpatient medicine to make admission and discharge decisions, allowing emergency department physicians to concentrate on the care of other patients. This can be particularly critical for high‐volume emergency departments. The CDU also offers an alternative to specialist‐run chest pain units. Because patients either stay for only the observation period or are admitted and typically moved off the unit, there is little need for provider continuity, and the discontinuous shift staffing model works well.
In addition to the geographic localization, several aspects of the CDU model may be critical to the successful implementation of similar hospitalist‐run observation units. Dedicated nursing staff with expertise in caring for high‐turnover patients with a more limited spectrum of diagnoses may be a factor. Another factor may be that the lack of less‐experienced trainees in a nonteaching service leads to more efficient care.
A potential area of further exploration includes understanding the differences between CDU patients who are discharged within 23 hours and those who are later admitted. This understanding may help us better differentiate patients appropriate for CDU admission, allowing the creation of more formal admission criteria.
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs.
- ,.The role of hospitalists in medical education.Am J Med.1999;107(4):305–309.
- ,,,,.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- ,,, et al.,Hospitalist‐Orthopedic Team Trial Investigators. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141(1):28–38.
- ,,,,,.Implementation of a voluntary hospitalist service at a community teaching hospital: improved efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- ,,,,,.Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357(25):2589–2600.
- ,,,,.Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring.Arch Intern Med.2007;167(17):1869–1874.
- ,,.Comparison of hospital costs and length of stay for community internists, hospitalists, and academicians.J Gen Int Med.2007;22(5):662–667.
- ,,, et al.Effects of physician experience on cost and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;37:866–875.
- ,,,.Program description: a hospitalist‐run, medical short‐stay unit in a teaching hospital.CMAJ.2000;163(11):1477–1480.
- ,,,,.Improving resource utilization in a teaching hospital: development of a nonteaching service for chest pain admissions.Acad Med.2006;81(5):432–435.
- ,.The role of hospitalists in medical education.Am J Med.1999;107(4):305–309.
- ,,,,.Reorganizing an academic medical service: impact on cost, quality, patient satisfaction, and education.JAMA.1998;279:1560–1565.
- ,,, et al.,Hospitalist‐Orthopedic Team Trial Investigators. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.Ann Intern Med.2004;141(1):28–38.
- ,,,,,.Implementation of a voluntary hospitalist service at a community teaching hospital: improved efficiency and patient outcomes.Ann Intern Med.2002;137:859–865.
- ,,,,,.Outcomes of care by hospitalists, general internists, and family physicians.N Engl J Med.2007;357(25):2589–2600.
- ,,,,.Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring.Arch Intern Med.2007;167(17):1869–1874.
- ,,.Comparison of hospital costs and length of stay for community internists, hospitalists, and academicians.J Gen Int Med.2007;22(5):662–667.
- ,,, et al.Effects of physician experience on cost and outcomes on an academic general medicine service: results of a trial of hospitalists.Ann Intern Med.2002;37:866–875.
- ,,,.Program description: a hospitalist‐run, medical short‐stay unit in a teaching hospital.CMAJ.2000;163(11):1477–1480.
- ,,,,.Improving resource utilization in a teaching hospital: development of a nonteaching service for chest pain admissions.Acad Med.2006;81(5):432–435.
Geriatric Train‐The‐Trainer Program
Nearly half of the hospital beds in the United States are occupied by the elderly,1 whose numbers are increasing.2 The odds of a hospitalized Medicare patient being cared for by a hospitalist are increasing by nearly 30% per year.3 Hospitalists require competence in geriatrics to serve their patients and to teach trainees. Train‐the‐Trainer (TTT) programs both educate health care providers and provide educational materials, information, and skills for teaching others.4 This model has been successfully used in geriatrics to impact knowledge, attitudes, and self‐efficacy among health care workers.46
A prominent example of a geriatrics TTT program is the University of Chicago Curriculum for the Hospitalized Aging Medical Patient (CHAMP),7 which requires 48 hours of instruction over 12 sessions. To create a less time‐intensive learning format for busy hospitalists, the University of Chicago developed Mini‐CHAMP, a streamlined 2‐day workshop with web‐based components for hospitalist clinicians, but not necessarily hospitalist educators.7
We created The Donald W. Reynolds Program for Advancing Geriatrics Education (PAGE) at the University of California, San Francisco (UCSF), in light of the time intensity of CHAMP, to integrate geriatric TTT sessions within preexisting hospitalist faculty meetings. This model is consistent with current practices in faculty development.8 This paper describes the evaluation of the PAGE Model, which sought answers to 3 research questions: (1) Does PAGE increase faculty confidence in teaching geriatrics?, (2) Does PAGE increase the frequency of hospitalist teaching geriatrics topics?, and (3) Does PAGE increase residents' practice of geriatrics skills?
Methods
The PAGE Model
The PAGE Model comprises 10 hour‐long monthly seminars held at UCSF from January through December 2008 to teach specific geriatrics principles and clinical skills relevant to providing competent care to a hospitalized older adult. The aims of the PAGE are to:
Give hospitalist physicians knowledge and skills to teach geriatric topics to trainees in a time‐limited environment
Provide exportable teaching modules on geriatric topics for inpatient teaching
Increase teaching about geriatrics received by internal medicine residents
Increase resident use of 15 specific geriatric skills
Create a collaborative environment between the Geriatrics and Hospital Medicine Divisions at UCSF
The PAGE Development Group, which included 2 hospitalists, 2 geriatricians, and an analyst funded by the Donald W. Reynolds Foundation, reviewed American Geriatrics Society core competencies,9 national guidelines and mandates,10, 11 and existing published geriatric curricula.7, 1214 In late 2007, an email‐based needs assessment listing 38 possible topics, drawn from the resources above, was emailed to the 31 hospitalists at UCSF. Each hospitalist identified, in no particular order, 5 topics considered most useful to improve his/her geriatric teaching skills, with write‐in space for additional topic suggestions. The needs assessment also queried what format of teaching tools would be most useful and efficient, such as PowerPoint slides or pocket cards, and interest in session coteaching.
The topics most commonly selected by the respondents (n = 14, response rate 45%) included: home/community resources (64%), delirium/dementia (57%), minimizing medication problems (50%), using prognostic indices to make decisions (43%), and general approach to older inpatients (43%). The Development Group identified less popular topics (falls, pressure ulcers, indwelling catheters/emncontinence) that were gaining significant national attention.15 Finally, a topic suggested by many hospitalists, pain management, was added. Each topic session was mapped to 1 or more of the 15 geriatrics skills in the CHAMP model7 for residents to acquire. The requested and selected topics were then modified to create distinct sessions grouped around a theme, shown in Table 1. For example home and community resources was addressed in the session on Framework on Transitions in Care.
| Topics | Geriatric Skills Addressed for Hospitalized Older Patients |
|---|---|
| |
| 1. Approach to the vulnerable older patient; assessing function; goals of care | Conduct functional status assessmentMobilize early to prevent deconditioning |
| 2. Minimizing medication problems | Reduce polypharmacy and use of high risk/low benefit drugs |
| 3. Framework for transitions in care (including home and community resources) | Develop a safe and appropriate discharge plan, involving communication with other team members, family members and primary care physicians |
| 4. Using prognostics to guide treatment decisions | Give bad news |
| Document advance directives and DNR orders | |
| Discuss hospice care | |
| 5. Falls & immobility | Identify risk factors of hospital falls, including conventional and unconventional types of restraints |
| 6. Delirium | Assess risk and prevent delirium |
| 7. Dementia & depression | Conduct cognitive assessmentScreen for depression |
| Routinely assess pain at bedside in persons with dementia | |
| 8. Pain assessment in the elderly | Routinely assess pain at bedside in persons with dementia |
| Manage pain using the WHO 3‐step ladder and opiate conversion table and manage side effects of opiates | |
| 9. Foley catheters and incontinence | Determine appropriateness for urinary catheter use, discontinuing when inappropriate |
| 10. Pressure ulcers and wound care | Routinely perform a complete skin exam |
Most respondents (86%) wanted teaching materials in a format suitable for attending rounds; 64% preferred teaching cases, 29% PowerPoint presentations, and 29% quality improvement resources. The Development Group, with approval of the Chief of Hospital Medicine, planned 10, 1‐hour monthly sessions during weekly hospitalist meetings to optimize participation. Nine hospitalists agreed to lead sessions with geriatricians; 1 session was co‐led by a hospitalist and urologist.
The Development Group encouraged session leaders to create case‐based PowerPoint teaching modules that could be used during attending rounds, highlighting teaching triggers or teachable moments that modify or reinforce skills.1618 A Development Group hospitalist/geriatrician team cotaught the first session, which modeled the structure and style recommended. A teaching team typically met at least once to define goals and outline their teaching hour; most met repeatedly to refine their presentations. An example of a 1 PAGE session can be found online.19
Evaluation
Evaluation involved data from hospitalist faculty trainees, hospitalist and geriatrician session leaders, and internal medicine residents. The institutional review board approved this study. Self‐report rating scales were used for data collection, which were reviewed by experts in medical education at UCSF and piloted on nonparticipant faculty, or had been previously used by the CHAMP study.7
Hospitalist Trainees' Program Perceptions and Self‐Efficacy
Hospitalist trainees (n = 36) completed paper questionnaires after each session to assess perceived likelihood to use the teaching tools that were presented (1: not at all likely, 5: highly likely), whether they would recommend the program to colleagues (1: do not recommend, 5: highly recommend), and the utility of the PAGE program (Was this experience useful? and Prior to the sessions, did you think it would be useful? 1: definitely not, 5: definitely yes). Change in trainees' perceived self‐efficacy20 to teach geriatrics skills was assessed at the end of the PAGE program, using a posttest and retrospective pretest format with a 12‐items (1: low, 5: high) that was used in the CHAMP study.7 This format was used to avoid response shift bias, or the program‐produced change in a participant's understanding of the construct being measured.21
Faculty Session Leaders' Program Perceptions
After PAGE completion, all faculty session leaders (n = 15) completed an online questionnaire assessing teaching satisfaction (Likert‐type 5‐point scales), experience with coteaching, and years of faculty teaching experience.
Medical Residents
To assess change in hospitalists' teaching about geriatrics and residents' practice of geriatric clinical skills, residents (n = 56; post‐graduate year (PGY)1 = 29, PGY2 = 27) who would not complete residency before the end of PAGE received an online questionnaire, modified from the CHAMP study,7 prior to and after the completion of PAGE. Respondents received monetary gift cards as incentives. Residents gave separate ratings for their inpatient teaching attendings who were hospitalists (80% of inpatient ward attendings) and nonhospitalists (20%, mostly generalists) regarding frequency over the past year of being taught each of 15 geriatric clinical skills. A 3‐point scale was used: (1) never, (2) once, and (3) more than once. Residents also reported the frequency of practicing those skills themselves, using a questionnaire from the CHAMP study,7 with a scale of (1) never to (5) always.
Analysis
Descriptive statistics were computed for all measures. Scale means were constructed from all individual items for the retrospective pretest and posttest measures. Wilcoxon matched‐pairs signed ranks‐tests were used to compare teaching differences between hospitalist and other attendings. For the unmatched pre‐post data on frequency of teaching, Wilcoxon‐Mann‐Whitney tests were used to determine significant differences in instruction, conducting separate tests for hospitalists and nonhospitalist attendings. Effect size22 was calculated using Cohen's d23 to determine the magnitude of increase in self‐efficacy to teach geriatrics; an effect size exceeding 0.8 is considered large. Statistics were performed using PASW Statistics 17.0 (SPSS Inc., Chicago, IL, USA).
Results
The hospitalist group grew from 31 to 36 members in June of 2008. On average, 14 hospitalists (M = 14.40, standard deviation [SD] = 2.41, range 1119) attended each session, with all hospitalists (n = 36) attending 1 session (M = 3.83, SD = 2.35, range 19). At each session, an average of 72% completed a post‐session evaluation form. Overall, faculty were likely to use the PAGE teaching tools (M = 4.61, SD = 0.53) and would recommend PAGE to other hospitalists (M = 4.63, SD = 0.51).
Thirteen hospitalist trainees of 36 (36%) completed a post‐PAGE online questionnaire. Respondents taught on faculty for an average of 5 years (mean (M) = 5.08, SD = 3.52). Faculty perceived self‐efficacy at teaching residents about geriatrics improved significantly with a large effect size (pretest M = 3.05, SD = .60; posttest M = 3.96, SD = .36, d = 1.52; P < 0.001). Session attendance was positively correlated with the increase in geriatrics teaching self‐efficacy (r = .62, P < 0.05), while teaching experience was not (r = 0.05, P = 0.88). Hospitalist trainees found the PAGE model more useful after participating (M = 4.62, SD = 0.65), than they had expected (M = 3.92, SD = 0.76; P < 0.05).
All session leaders (n = 15) completed the questionnaire after PAGE (9 hospitalists, 5 geriatricians, 1 urologist). Two‐thirds had 5 years on faculty; eight had no prior experience as a faculty development trainer. Over 80% indicated that they found their coteaching experience, enjoyable, useful and collaborative. Only 1 participant did not commit to interdisciplinary teaching again. Most hospitalist session leaders reported that coteaching with a geriatrician enhanced their knowledge; they were more likely to consult a geriatrician regarding patients. All but 2 session leaders felt that the model fostered a collaborative environment between their 2 divisions.
Of the 56 residents, 41% (16 PGY1, 7 PGY2) completed a pretest; 43% (15 PGY1, 9 PGY2) completed a posttest. Residents reported receiving inpatient teaching on geriatrics skills significantly more frequently from hospitalists vs. nonhospitalist attendings both before PAGE (hospitalists M = 2.18, SD = 0.37; nonhospitalists M = 2.00, SD = 0.53, P < 0.05), and after (hospitalists M = 2.39, SD = 0.46; nonhospitalists M = 2.05, SD = 0.57, P < 0.05; see Fig. 1). Although hospitalists taught more frequently about geriatrics than nonhospitalists before PAGE, our findings suggest that they increased their teaching by a greater magnitude than nonhospitalists (P < 0.01, P > 0.05, respectively). Residents reported increased geriatric skill practice after PAGE with a medium effect size (pretest M = 2.92, SD = 0.55, posttest M = 3.28, SD = 0.66, P = 0.052, d = 0.66). There was greater mean reported practice for all skills with the exception of hospice care, which already was being performed between often and very often before PAGE. The largest increases in skill practice were (descending order, most increased first): assessing polypharmacy, performing skin exams, prognostication, performing functional assessments and examining Foley catheter use.
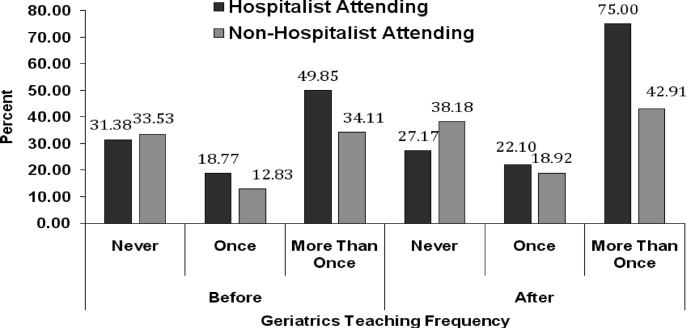
Discussion
Our aging population and a shortage of geriatricians necessitates new, feasible models for geriatric training. Similar to the CHAMP model,7 PAGE had a favorable impact on faculty perceived behavioral change; after the PAGE sessions, faculty reported significantly greater self‐efficacy of teaching geriatrics. However, this study also examined the impact of the PAGE Model on 2 groups not previously reported in the literature: faculty session leaders and medicine residents.
To our knowledge, this is the first study about a hospitalist TTT program codeveloped with nonhospitalists aimed at teaching geriatrics skills to residents, though smaller scale programs for medical students exist.24 We believe codevelopment was important in our model for many reasons. First, using hospitalist peers and local geriatricians likely increased trust in the educational curricula and allowed for strong communication channels between instructors.25, 26 Second, coteaching allowed for hospitalist mentorship. Hospitalists acknowledged their coleaders as mentors and several hospitalists subsequently engaged in new geriatric projects. Third, coteaching was felt to enhance patient care and increase geriatrician consultations. Coteaching may have applicability to other hospitalist faculty development such as intensive care and palliative care, and hospitalist programs may benefit from creating faculty development programs internally with their colleagues, rather than using online resources.
Another important finding of this study is that training hospitalists to teach about geriatrics seems to result in an increase in both the geriatric teaching that residents receive and residents' practice of geriatric skills. This outcome has not been previously demonstrated with geriatric TTT activities.27 This trickle‐down effect to residents likely results from both the increased teaching efficacy of hospitalists after the PAGE Model and the exportable nature of the teaching tools.
Several continuing medical education best practices were used which we believe contributed to the success of PAGE. First, we conducted a needs assessment, which improves knowledge outcomes.28, 29 Second, sessions included cases, lectures, and discussions. Use of multiple educational techniques yields greater knowledge and behavioral change as compared to a single method, such as lecture alone.24, 25, 30, 31 Finally, sessions were sequenced over a year, rather than clustered in short, intensive activity. Sequenced, or learn‐work‐learn opportunities allow education to be translated to practice and reinforced.8, 27, 30, 32
We believe that the PAGE Model is transportable to other hospitalist programs due to its cost and flexible nature. In economically‐lean times, hospitalist divisions can create a program similar to the PAGE Model essentially at no cost, except for donated faculty preparation time. In contrast, CHAMP was expensive, costing nearly $72,000 for 12 faculty to participate in the 48‐hour curriculum,7, 33 and volunteering physicians were compensated for their time. Though Mini‐CHAMP is a streamlined 2‐day workshop that offers free online lectures and slide sets, there may be some benefit to producing a faculty development program internally, as we stated above, and PAGE included additional topics (urinary catheters and decubitus ulcers/wound care) not covered in mini‐CHAMP.
There were several limitations to this study. First, some outcomes of the PAGE Model were assessed by retrospective self‐report, which may allow for recall bias. Although self‐report may or may not correlate with actual behavior,34 faculty and resident perspectives of their teaching and learning experiences are themselves important. Furthermore, a retrospective presurvey allows for content of an educational program or intervention to be explained prior to a survey, so that participants first assess their new level of understanding or skill on the post test, then reflectively assess the level of understanding or skill they had prior to the workshop. This avoids response shift bias and can improve internal validity.21, 35
Second, the small numbers of session leaders, hospitalist trainees, and residents restricted statistical power to detect small effects. The fact that we found significant improvements enhances the likelihood that the differences observed were not due to chance.
Third, the low response rates from the hospitalist trainee post‐intervention questionnaire and the residents' questionnaires may affect the validity of our results. For the resident survey, the subjects were not matched, and we cannot state that an individual's geriatric skill practice changed due to PAGE, though the results suggest the residency program as a whole improved the frequency of geriatric skill practice.
Finally, the residents were required to report the frequency of teaching on and practice of geriatric skills practice over the prior year and accuracy of recall may be an issue. However, frequencies were queried both pre and post intervention and favorable change was noted. Furthermore, because the high end of the 3‐point teaching scale was limited to more than once, the true amount of teaching may have been underestimated if more than once actually represented high frequencies.
Future studies are needed to replicate these findings at other institutions to confirm generalizability. It would be beneficial to measure patient outcomes to determine whether increased teaching and skill practice benefits patients using measures such as reduction in catheter related urinary tract infections, falls, and inadequate pain management. Further investigations of cotaught faculty development programs between hospitalists and other specialists help emphasize why internally created TTT programs are of greater value than online resources.
Conclusions
This time‐sensitive adaptation of a hospitalist geriatric TTT program was successfully implemented at an academic medical center and suggests improved hospitalist faculty self‐efficacy at teaching geriatric skills, increased frequency of inpatient geriatric teaching by hospitalists and increased resident geriatric skill practice. Confidence to care for geriatric patients and a strong skill set to assess risks and manage them appropriately will equip hospitalists and trainees to provide care that reduces geriatric patients' in‐hospital morbidity and costs of care. As hospitalists increasingly care for older adults, the need for time‐efficient methods of teaching geriatrics will continue to grow. The PAGE Model, and other new models of geriatric training for hospitalists, demonstrates that we are beginning to address this urgent need.
Acknowledgements
The authors thank Joan Abrams, MA, MPA, and Patricia O'Sullivan, EdD, whose work was key to the success of this program and this manuscript. They also thank the Donald W. Reynolds Foundation for support of this project.
- ,.2005 National Hospital Discharge Survey.Adv Data.2007;385:1–19.
- ,,,. In:U.S. Census Bureau, Current Population Reports, 65+ in the United States: 2005,Washington, D.C.:U.S. Government Printing Office;2005:23–209.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360(11):1102–1112.
- ,,,.Providing dementia outreach education to rural communities: lessons learned from a train‐the‐trainer program.J Appl Gerontol.2002;21:294–313.
- .Gerontologizing health care: a train‐the‐trainer program for nurses.Gerontol Geriatr Educ.1999;19:47–56.
- ,,.A statewide model detection and prevention program for geriatric alcoholism and alcohol abuse: increased knowledge among service providers.Community Ment Health J.2000;36:137–148.
- ,,, et al.The curriculum for the hospitalized aging medical patient program: a collaborative faculty development program for hospitalists, general internists, and geriatricians.J Hosp Med.2008;3(5):384–393.
- Reframing professional development through understanding authentic professional learning.Rev Educ Res.2009;79:702–739.
- The Education Committee Writing Group of the American Geriatrics Society.Core competencies for the care of older patients: recommendations of the American Geriatrics Society.Acad Med.2000;75:252–255.
- ,,, et al.American Geriatrics Society Task Force on the future of geriatric medicine.J Am Geriatr Soc.2005;53 (6 Suppl):S245–S256.
- Nadzam, Deborah. Preventing patient falls. Joint Commission Resources. Available at: http://www.jcrinc.com/Preventing‐Patient‐Falls. Accessed April2010.
- ,.Curricular recommendations for resident training in nursing home care. A collaborative effort of the Society of General Internal Medicine Task Force on Geriatric Medicine, the Society of Teachers of Family Medicine Geriatrics Task Force, the American Medical Directors Association, and the American Geriatrics Society Education Committee.J Am Geriatr Soc.1994;42:1200–1201.
- ,,,,.Curriculum recommendations for resident training in geriatrics interdisciplinary team care.J Am Geriatr Soc.1999;47:1145–1148.
- ,.ACGME requirements for geriatrics medicine curricula in medical specialties: Progress made and progress needed.Acad Med.2005;80:279–285.
- CMS Office of Public Affairs. CMS Improves Patient Safety for Medicare and Medicaid by Addressing Never Events, August 04, 2008. Available at: http://www.cms.gov/apps/media/press/factsheet.asp?Counter=322434(5):337–343.
- ,.The changing paradigm for continuing medical education: impact of information on the teachable moment.Bull Med Libr Assoc.1990;78(2):173–179.
- ,.Creating the teachable moment.J Nurs Educ.1998;37(6):278–280.
- Society of Hospital Medicine, BOOSTing Care Transitions Resource Room. Mazotti L, Johnston CB. Faculty development: Teaching triggers for transitional care. “A train‐the‐trainer model.” Available at: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/PDFs/Mazotti_UCSF_Transitions.PPT. Accessed April2010.
- .Self‐efficacy: The Exercise of Control.New York:W.H. Freeman and Company;1997.
- .Internal invalidity in pretest‐posttest self‐report evaluations and a re‐evaluation of retrospective pretests.Applied Psychological Measurement.1979;3:1–23.
- ,.A visitor's guide to effect sizes.Adv Health Sci Educ Theory Pract.2004;9:241–249.
- .Statistical Power Analyses for the Behavioral Sciences.2nd ed.Hillsdale, NJ:Lawrence Erlbaum Associates;1988.
- ,,,.Hazards of hospitalization: Hospitalists and geriatricians educating medical students about delirium and falls in geriatric patients.Gerontol Geriatr Educ.2008;28(4):94–104.
- ,,, et al.Continuing medical education, continuing professional development, and knowledge translation: Improving care of older patients by practicing physicians.J Am Geriatr Soc.2006:54(10):1610–1618.
- ,,, et al.Practicing physician education in geriatrics: Lessons learned from a train‐the‐trainer model.J Am Geriatr Soc.2007:55(8):1281–1286.
- ,.CHAMP trains champions: hospitalist‐educators develop new ways to teach care for older patients.J Hosp Med.2008;3(5):357–360.
- ,,,,,.Impact of formal continuing medical education: Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes?JAMA.1999;282(9):867–874.
- ,.Association for the Study of Medical Education Booklet: The effectiveness of continuing professional development.Edinburgh, Scotland:Association for the Study of Medical Education;2000.
- ,,, et al.Effectiveness of continuing medical education.Evid Rep Technol Assess (Full Rep).2007;149:1–69.
- ,,, et al.Continuing education meetings and workshops: effects on professional practice and health care outcomes.Cochrane Database Syst Rev.2009;(2):CD003030.
- ,.Continuing medical education and the physician as learner: guide to the evidence.JAMA.2002;288(9):1057–1060.
- .Care of hospitalized older patients: opportunities for hospital‐based physicians.J Hosp Med.2006;1:42–47.
- ,.What we say and what we do: self‐reported teaching behavior versus performances in written simulations among medical school faculty.Acad Med.1992;67(8):522–527.
- ,.The retrospective pretest and the role of pretest information in evaluation studies.Psychol Rep.1992;70:699–704.
Nearly half of the hospital beds in the United States are occupied by the elderly,1 whose numbers are increasing.2 The odds of a hospitalized Medicare patient being cared for by a hospitalist are increasing by nearly 30% per year.3 Hospitalists require competence in geriatrics to serve their patients and to teach trainees. Train‐the‐Trainer (TTT) programs both educate health care providers and provide educational materials, information, and skills for teaching others.4 This model has been successfully used in geriatrics to impact knowledge, attitudes, and self‐efficacy among health care workers.46
A prominent example of a geriatrics TTT program is the University of Chicago Curriculum for the Hospitalized Aging Medical Patient (CHAMP),7 which requires 48 hours of instruction over 12 sessions. To create a less time‐intensive learning format for busy hospitalists, the University of Chicago developed Mini‐CHAMP, a streamlined 2‐day workshop with web‐based components for hospitalist clinicians, but not necessarily hospitalist educators.7
We created The Donald W. Reynolds Program for Advancing Geriatrics Education (PAGE) at the University of California, San Francisco (UCSF), in light of the time intensity of CHAMP, to integrate geriatric TTT sessions within preexisting hospitalist faculty meetings. This model is consistent with current practices in faculty development.8 This paper describes the evaluation of the PAGE Model, which sought answers to 3 research questions: (1) Does PAGE increase faculty confidence in teaching geriatrics?, (2) Does PAGE increase the frequency of hospitalist teaching geriatrics topics?, and (3) Does PAGE increase residents' practice of geriatrics skills?
Methods
The PAGE Model
The PAGE Model comprises 10 hour‐long monthly seminars held at UCSF from January through December 2008 to teach specific geriatrics principles and clinical skills relevant to providing competent care to a hospitalized older adult. The aims of the PAGE are to:
Give hospitalist physicians knowledge and skills to teach geriatric topics to trainees in a time‐limited environment
Provide exportable teaching modules on geriatric topics for inpatient teaching
Increase teaching about geriatrics received by internal medicine residents
Increase resident use of 15 specific geriatric skills
Create a collaborative environment between the Geriatrics and Hospital Medicine Divisions at UCSF
The PAGE Development Group, which included 2 hospitalists, 2 geriatricians, and an analyst funded by the Donald W. Reynolds Foundation, reviewed American Geriatrics Society core competencies,9 national guidelines and mandates,10, 11 and existing published geriatric curricula.7, 1214 In late 2007, an email‐based needs assessment listing 38 possible topics, drawn from the resources above, was emailed to the 31 hospitalists at UCSF. Each hospitalist identified, in no particular order, 5 topics considered most useful to improve his/her geriatric teaching skills, with write‐in space for additional topic suggestions. The needs assessment also queried what format of teaching tools would be most useful and efficient, such as PowerPoint slides or pocket cards, and interest in session coteaching.
The topics most commonly selected by the respondents (n = 14, response rate 45%) included: home/community resources (64%), delirium/dementia (57%), minimizing medication problems (50%), using prognostic indices to make decisions (43%), and general approach to older inpatients (43%). The Development Group identified less popular topics (falls, pressure ulcers, indwelling catheters/emncontinence) that were gaining significant national attention.15 Finally, a topic suggested by many hospitalists, pain management, was added. Each topic session was mapped to 1 or more of the 15 geriatrics skills in the CHAMP model7 for residents to acquire. The requested and selected topics were then modified to create distinct sessions grouped around a theme, shown in Table 1. For example home and community resources was addressed in the session on Framework on Transitions in Care.
| Topics | Geriatric Skills Addressed for Hospitalized Older Patients |
|---|---|
| |
| 1. Approach to the vulnerable older patient; assessing function; goals of care | Conduct functional status assessmentMobilize early to prevent deconditioning |
| 2. Minimizing medication problems | Reduce polypharmacy and use of high risk/low benefit drugs |
| 3. Framework for transitions in care (including home and community resources) | Develop a safe and appropriate discharge plan, involving communication with other team members, family members and primary care physicians |
| 4. Using prognostics to guide treatment decisions | Give bad news |
| Document advance directives and DNR orders | |
| Discuss hospice care | |
| 5. Falls & immobility | Identify risk factors of hospital falls, including conventional and unconventional types of restraints |
| 6. Delirium | Assess risk and prevent delirium |
| 7. Dementia & depression | Conduct cognitive assessmentScreen for depression |
| Routinely assess pain at bedside in persons with dementia | |
| 8. Pain assessment in the elderly | Routinely assess pain at bedside in persons with dementia |
| Manage pain using the WHO 3‐step ladder and opiate conversion table and manage side effects of opiates | |
| 9. Foley catheters and incontinence | Determine appropriateness for urinary catheter use, discontinuing when inappropriate |
| 10. Pressure ulcers and wound care | Routinely perform a complete skin exam |
Most respondents (86%) wanted teaching materials in a format suitable for attending rounds; 64% preferred teaching cases, 29% PowerPoint presentations, and 29% quality improvement resources. The Development Group, with approval of the Chief of Hospital Medicine, planned 10, 1‐hour monthly sessions during weekly hospitalist meetings to optimize participation. Nine hospitalists agreed to lead sessions with geriatricians; 1 session was co‐led by a hospitalist and urologist.
The Development Group encouraged session leaders to create case‐based PowerPoint teaching modules that could be used during attending rounds, highlighting teaching triggers or teachable moments that modify or reinforce skills.1618 A Development Group hospitalist/geriatrician team cotaught the first session, which modeled the structure and style recommended. A teaching team typically met at least once to define goals and outline their teaching hour; most met repeatedly to refine their presentations. An example of a 1 PAGE session can be found online.19
Evaluation
Evaluation involved data from hospitalist faculty trainees, hospitalist and geriatrician session leaders, and internal medicine residents. The institutional review board approved this study. Self‐report rating scales were used for data collection, which were reviewed by experts in medical education at UCSF and piloted on nonparticipant faculty, or had been previously used by the CHAMP study.7
Hospitalist Trainees' Program Perceptions and Self‐Efficacy
Hospitalist trainees (n = 36) completed paper questionnaires after each session to assess perceived likelihood to use the teaching tools that were presented (1: not at all likely, 5: highly likely), whether they would recommend the program to colleagues (1: do not recommend, 5: highly recommend), and the utility of the PAGE program (Was this experience useful? and Prior to the sessions, did you think it would be useful? 1: definitely not, 5: definitely yes). Change in trainees' perceived self‐efficacy20 to teach geriatrics skills was assessed at the end of the PAGE program, using a posttest and retrospective pretest format with a 12‐items (1: low, 5: high) that was used in the CHAMP study.7 This format was used to avoid response shift bias, or the program‐produced change in a participant's understanding of the construct being measured.21
Faculty Session Leaders' Program Perceptions
After PAGE completion, all faculty session leaders (n = 15) completed an online questionnaire assessing teaching satisfaction (Likert‐type 5‐point scales), experience with coteaching, and years of faculty teaching experience.
Medical Residents
To assess change in hospitalists' teaching about geriatrics and residents' practice of geriatric clinical skills, residents (n = 56; post‐graduate year (PGY)1 = 29, PGY2 = 27) who would not complete residency before the end of PAGE received an online questionnaire, modified from the CHAMP study,7 prior to and after the completion of PAGE. Respondents received monetary gift cards as incentives. Residents gave separate ratings for their inpatient teaching attendings who were hospitalists (80% of inpatient ward attendings) and nonhospitalists (20%, mostly generalists) regarding frequency over the past year of being taught each of 15 geriatric clinical skills. A 3‐point scale was used: (1) never, (2) once, and (3) more than once. Residents also reported the frequency of practicing those skills themselves, using a questionnaire from the CHAMP study,7 with a scale of (1) never to (5) always.
Analysis
Descriptive statistics were computed for all measures. Scale means were constructed from all individual items for the retrospective pretest and posttest measures. Wilcoxon matched‐pairs signed ranks‐tests were used to compare teaching differences between hospitalist and other attendings. For the unmatched pre‐post data on frequency of teaching, Wilcoxon‐Mann‐Whitney tests were used to determine significant differences in instruction, conducting separate tests for hospitalists and nonhospitalist attendings. Effect size22 was calculated using Cohen's d23 to determine the magnitude of increase in self‐efficacy to teach geriatrics; an effect size exceeding 0.8 is considered large. Statistics were performed using PASW Statistics 17.0 (SPSS Inc., Chicago, IL, USA).
Results
The hospitalist group grew from 31 to 36 members in June of 2008. On average, 14 hospitalists (M = 14.40, standard deviation [SD] = 2.41, range 1119) attended each session, with all hospitalists (n = 36) attending 1 session (M = 3.83, SD = 2.35, range 19). At each session, an average of 72% completed a post‐session evaluation form. Overall, faculty were likely to use the PAGE teaching tools (M = 4.61, SD = 0.53) and would recommend PAGE to other hospitalists (M = 4.63, SD = 0.51).
Thirteen hospitalist trainees of 36 (36%) completed a post‐PAGE online questionnaire. Respondents taught on faculty for an average of 5 years (mean (M) = 5.08, SD = 3.52). Faculty perceived self‐efficacy at teaching residents about geriatrics improved significantly with a large effect size (pretest M = 3.05, SD = .60; posttest M = 3.96, SD = .36, d = 1.52; P < 0.001). Session attendance was positively correlated with the increase in geriatrics teaching self‐efficacy (r = .62, P < 0.05), while teaching experience was not (r = 0.05, P = 0.88). Hospitalist trainees found the PAGE model more useful after participating (M = 4.62, SD = 0.65), than they had expected (M = 3.92, SD = 0.76; P < 0.05).
All session leaders (n = 15) completed the questionnaire after PAGE (9 hospitalists, 5 geriatricians, 1 urologist). Two‐thirds had 5 years on faculty; eight had no prior experience as a faculty development trainer. Over 80% indicated that they found their coteaching experience, enjoyable, useful and collaborative. Only 1 participant did not commit to interdisciplinary teaching again. Most hospitalist session leaders reported that coteaching with a geriatrician enhanced their knowledge; they were more likely to consult a geriatrician regarding patients. All but 2 session leaders felt that the model fostered a collaborative environment between their 2 divisions.
Of the 56 residents, 41% (16 PGY1, 7 PGY2) completed a pretest; 43% (15 PGY1, 9 PGY2) completed a posttest. Residents reported receiving inpatient teaching on geriatrics skills significantly more frequently from hospitalists vs. nonhospitalist attendings both before PAGE (hospitalists M = 2.18, SD = 0.37; nonhospitalists M = 2.00, SD = 0.53, P < 0.05), and after (hospitalists M = 2.39, SD = 0.46; nonhospitalists M = 2.05, SD = 0.57, P < 0.05; see Fig. 1). Although hospitalists taught more frequently about geriatrics than nonhospitalists before PAGE, our findings suggest that they increased their teaching by a greater magnitude than nonhospitalists (P < 0.01, P > 0.05, respectively). Residents reported increased geriatric skill practice after PAGE with a medium effect size (pretest M = 2.92, SD = 0.55, posttest M = 3.28, SD = 0.66, P = 0.052, d = 0.66). There was greater mean reported practice for all skills with the exception of hospice care, which already was being performed between often and very often before PAGE. The largest increases in skill practice were (descending order, most increased first): assessing polypharmacy, performing skin exams, prognostication, performing functional assessments and examining Foley catheter use.
Discussion
Our aging population and a shortage of geriatricians necessitates new, feasible models for geriatric training. Similar to the CHAMP model,7 PAGE had a favorable impact on faculty perceived behavioral change; after the PAGE sessions, faculty reported significantly greater self‐efficacy of teaching geriatrics. However, this study also examined the impact of the PAGE Model on 2 groups not previously reported in the literature: faculty session leaders and medicine residents.
To our knowledge, this is the first study about a hospitalist TTT program codeveloped with nonhospitalists aimed at teaching geriatrics skills to residents, though smaller scale programs for medical students exist.24 We believe codevelopment was important in our model for many reasons. First, using hospitalist peers and local geriatricians likely increased trust in the educational curricula and allowed for strong communication channels between instructors.25, 26 Second, coteaching allowed for hospitalist mentorship. Hospitalists acknowledged their coleaders as mentors and several hospitalists subsequently engaged in new geriatric projects. Third, coteaching was felt to enhance patient care and increase geriatrician consultations. Coteaching may have applicability to other hospitalist faculty development such as intensive care and palliative care, and hospitalist programs may benefit from creating faculty development programs internally with their colleagues, rather than using online resources.
Another important finding of this study is that training hospitalists to teach about geriatrics seems to result in an increase in both the geriatric teaching that residents receive and residents' practice of geriatric skills. This outcome has not been previously demonstrated with geriatric TTT activities.27 This trickle‐down effect to residents likely results from both the increased teaching efficacy of hospitalists after the PAGE Model and the exportable nature of the teaching tools.
Several continuing medical education best practices were used which we believe contributed to the success of PAGE. First, we conducted a needs assessment, which improves knowledge outcomes.28, 29 Second, sessions included cases, lectures, and discussions. Use of multiple educational techniques yields greater knowledge and behavioral change as compared to a single method, such as lecture alone.24, 25, 30, 31 Finally, sessions were sequenced over a year, rather than clustered in short, intensive activity. Sequenced, or learn‐work‐learn opportunities allow education to be translated to practice and reinforced.8, 27, 30, 32
We believe that the PAGE Model is transportable to other hospitalist programs due to its cost and flexible nature. In economically‐lean times, hospitalist divisions can create a program similar to the PAGE Model essentially at no cost, except for donated faculty preparation time. In contrast, CHAMP was expensive, costing nearly $72,000 for 12 faculty to participate in the 48‐hour curriculum,7, 33 and volunteering physicians were compensated for their time. Though Mini‐CHAMP is a streamlined 2‐day workshop that offers free online lectures and slide sets, there may be some benefit to producing a faculty development program internally, as we stated above, and PAGE included additional topics (urinary catheters and decubitus ulcers/wound care) not covered in mini‐CHAMP.
There were several limitations to this study. First, some outcomes of the PAGE Model were assessed by retrospective self‐report, which may allow for recall bias. Although self‐report may or may not correlate with actual behavior,34 faculty and resident perspectives of their teaching and learning experiences are themselves important. Furthermore, a retrospective presurvey allows for content of an educational program or intervention to be explained prior to a survey, so that participants first assess their new level of understanding or skill on the post test, then reflectively assess the level of understanding or skill they had prior to the workshop. This avoids response shift bias and can improve internal validity.21, 35
Second, the small numbers of session leaders, hospitalist trainees, and residents restricted statistical power to detect small effects. The fact that we found significant improvements enhances the likelihood that the differences observed were not due to chance.
Third, the low response rates from the hospitalist trainee post‐intervention questionnaire and the residents' questionnaires may affect the validity of our results. For the resident survey, the subjects were not matched, and we cannot state that an individual's geriatric skill practice changed due to PAGE, though the results suggest the residency program as a whole improved the frequency of geriatric skill practice.
Finally, the residents were required to report the frequency of teaching on and practice of geriatric skills practice over the prior year and accuracy of recall may be an issue. However, frequencies were queried both pre and post intervention and favorable change was noted. Furthermore, because the high end of the 3‐point teaching scale was limited to more than once, the true amount of teaching may have been underestimated if more than once actually represented high frequencies.
Future studies are needed to replicate these findings at other institutions to confirm generalizability. It would be beneficial to measure patient outcomes to determine whether increased teaching and skill practice benefits patients using measures such as reduction in catheter related urinary tract infections, falls, and inadequate pain management. Further investigations of cotaught faculty development programs between hospitalists and other specialists help emphasize why internally created TTT programs are of greater value than online resources.
Conclusions
This time‐sensitive adaptation of a hospitalist geriatric TTT program was successfully implemented at an academic medical center and suggests improved hospitalist faculty self‐efficacy at teaching geriatric skills, increased frequency of inpatient geriatric teaching by hospitalists and increased resident geriatric skill practice. Confidence to care for geriatric patients and a strong skill set to assess risks and manage them appropriately will equip hospitalists and trainees to provide care that reduces geriatric patients' in‐hospital morbidity and costs of care. As hospitalists increasingly care for older adults, the need for time‐efficient methods of teaching geriatrics will continue to grow. The PAGE Model, and other new models of geriatric training for hospitalists, demonstrates that we are beginning to address this urgent need.
Acknowledgements
The authors thank Joan Abrams, MA, MPA, and Patricia O'Sullivan, EdD, whose work was key to the success of this program and this manuscript. They also thank the Donald W. Reynolds Foundation for support of this project.
Nearly half of the hospital beds in the United States are occupied by the elderly,1 whose numbers are increasing.2 The odds of a hospitalized Medicare patient being cared for by a hospitalist are increasing by nearly 30% per year.3 Hospitalists require competence in geriatrics to serve their patients and to teach trainees. Train‐the‐Trainer (TTT) programs both educate health care providers and provide educational materials, information, and skills for teaching others.4 This model has been successfully used in geriatrics to impact knowledge, attitudes, and self‐efficacy among health care workers.46
A prominent example of a geriatrics TTT program is the University of Chicago Curriculum for the Hospitalized Aging Medical Patient (CHAMP),7 which requires 48 hours of instruction over 12 sessions. To create a less time‐intensive learning format for busy hospitalists, the University of Chicago developed Mini‐CHAMP, a streamlined 2‐day workshop with web‐based components for hospitalist clinicians, but not necessarily hospitalist educators.7
We created The Donald W. Reynolds Program for Advancing Geriatrics Education (PAGE) at the University of California, San Francisco (UCSF), in light of the time intensity of CHAMP, to integrate geriatric TTT sessions within preexisting hospitalist faculty meetings. This model is consistent with current practices in faculty development.8 This paper describes the evaluation of the PAGE Model, which sought answers to 3 research questions: (1) Does PAGE increase faculty confidence in teaching geriatrics?, (2) Does PAGE increase the frequency of hospitalist teaching geriatrics topics?, and (3) Does PAGE increase residents' practice of geriatrics skills?
Methods
The PAGE Model
The PAGE Model comprises 10 hour‐long monthly seminars held at UCSF from January through December 2008 to teach specific geriatrics principles and clinical skills relevant to providing competent care to a hospitalized older adult. The aims of the PAGE are to:
Give hospitalist physicians knowledge and skills to teach geriatric topics to trainees in a time‐limited environment
Provide exportable teaching modules on geriatric topics for inpatient teaching
Increase teaching about geriatrics received by internal medicine residents
Increase resident use of 15 specific geriatric skills
Create a collaborative environment between the Geriatrics and Hospital Medicine Divisions at UCSF
The PAGE Development Group, which included 2 hospitalists, 2 geriatricians, and an analyst funded by the Donald W. Reynolds Foundation, reviewed American Geriatrics Society core competencies,9 national guidelines and mandates,10, 11 and existing published geriatric curricula.7, 1214 In late 2007, an email‐based needs assessment listing 38 possible topics, drawn from the resources above, was emailed to the 31 hospitalists at UCSF. Each hospitalist identified, in no particular order, 5 topics considered most useful to improve his/her geriatric teaching skills, with write‐in space for additional topic suggestions. The needs assessment also queried what format of teaching tools would be most useful and efficient, such as PowerPoint slides or pocket cards, and interest in session coteaching.
The topics most commonly selected by the respondents (n = 14, response rate 45%) included: home/community resources (64%), delirium/dementia (57%), minimizing medication problems (50%), using prognostic indices to make decisions (43%), and general approach to older inpatients (43%). The Development Group identified less popular topics (falls, pressure ulcers, indwelling catheters/emncontinence) that were gaining significant national attention.15 Finally, a topic suggested by many hospitalists, pain management, was added. Each topic session was mapped to 1 or more of the 15 geriatrics skills in the CHAMP model7 for residents to acquire. The requested and selected topics were then modified to create distinct sessions grouped around a theme, shown in Table 1. For example home and community resources was addressed in the session on Framework on Transitions in Care.
| Topics | Geriatric Skills Addressed for Hospitalized Older Patients |
|---|---|
| |
| 1. Approach to the vulnerable older patient; assessing function; goals of care | Conduct functional status assessmentMobilize early to prevent deconditioning |
| 2. Minimizing medication problems | Reduce polypharmacy and use of high risk/low benefit drugs |
| 3. Framework for transitions in care (including home and community resources) | Develop a safe and appropriate discharge plan, involving communication with other team members, family members and primary care physicians |
| 4. Using prognostics to guide treatment decisions | Give bad news |
| Document advance directives and DNR orders | |
| Discuss hospice care | |
| 5. Falls & immobility | Identify risk factors of hospital falls, including conventional and unconventional types of restraints |
| 6. Delirium | Assess risk and prevent delirium |
| 7. Dementia & depression | Conduct cognitive assessmentScreen for depression |
| Routinely assess pain at bedside in persons with dementia | |
| 8. Pain assessment in the elderly | Routinely assess pain at bedside in persons with dementia |
| Manage pain using the WHO 3‐step ladder and opiate conversion table and manage side effects of opiates | |
| 9. Foley catheters and incontinence | Determine appropriateness for urinary catheter use, discontinuing when inappropriate |
| 10. Pressure ulcers and wound care | Routinely perform a complete skin exam |
Most respondents (86%) wanted teaching materials in a format suitable for attending rounds; 64% preferred teaching cases, 29% PowerPoint presentations, and 29% quality improvement resources. The Development Group, with approval of the Chief of Hospital Medicine, planned 10, 1‐hour monthly sessions during weekly hospitalist meetings to optimize participation. Nine hospitalists agreed to lead sessions with geriatricians; 1 session was co‐led by a hospitalist and urologist.
The Development Group encouraged session leaders to create case‐based PowerPoint teaching modules that could be used during attending rounds, highlighting teaching triggers or teachable moments that modify or reinforce skills.1618 A Development Group hospitalist/geriatrician team cotaught the first session, which modeled the structure and style recommended. A teaching team typically met at least once to define goals and outline their teaching hour; most met repeatedly to refine their presentations. An example of a 1 PAGE session can be found online.19
Evaluation
Evaluation involved data from hospitalist faculty trainees, hospitalist and geriatrician session leaders, and internal medicine residents. The institutional review board approved this study. Self‐report rating scales were used for data collection, which were reviewed by experts in medical education at UCSF and piloted on nonparticipant faculty, or had been previously used by the CHAMP study.7
Hospitalist Trainees' Program Perceptions and Self‐Efficacy
Hospitalist trainees (n = 36) completed paper questionnaires after each session to assess perceived likelihood to use the teaching tools that were presented (1: not at all likely, 5: highly likely), whether they would recommend the program to colleagues (1: do not recommend, 5: highly recommend), and the utility of the PAGE program (Was this experience useful? and Prior to the sessions, did you think it would be useful? 1: definitely not, 5: definitely yes). Change in trainees' perceived self‐efficacy20 to teach geriatrics skills was assessed at the end of the PAGE program, using a posttest and retrospective pretest format with a 12‐items (1: low, 5: high) that was used in the CHAMP study.7 This format was used to avoid response shift bias, or the program‐produced change in a participant's understanding of the construct being measured.21
Faculty Session Leaders' Program Perceptions
After PAGE completion, all faculty session leaders (n = 15) completed an online questionnaire assessing teaching satisfaction (Likert‐type 5‐point scales), experience with coteaching, and years of faculty teaching experience.
Medical Residents
To assess change in hospitalists' teaching about geriatrics and residents' practice of geriatric clinical skills, residents (n = 56; post‐graduate year (PGY)1 = 29, PGY2 = 27) who would not complete residency before the end of PAGE received an online questionnaire, modified from the CHAMP study,7 prior to and after the completion of PAGE. Respondents received monetary gift cards as incentives. Residents gave separate ratings for their inpatient teaching attendings who were hospitalists (80% of inpatient ward attendings) and nonhospitalists (20%, mostly generalists) regarding frequency over the past year of being taught each of 15 geriatric clinical skills. A 3‐point scale was used: (1) never, (2) once, and (3) more than once. Residents also reported the frequency of practicing those skills themselves, using a questionnaire from the CHAMP study,7 with a scale of (1) never to (5) always.
Analysis
Descriptive statistics were computed for all measures. Scale means were constructed from all individual items for the retrospective pretest and posttest measures. Wilcoxon matched‐pairs signed ranks‐tests were used to compare teaching differences between hospitalist and other attendings. For the unmatched pre‐post data on frequency of teaching, Wilcoxon‐Mann‐Whitney tests were used to determine significant differences in instruction, conducting separate tests for hospitalists and nonhospitalist attendings. Effect size22 was calculated using Cohen's d23 to determine the magnitude of increase in self‐efficacy to teach geriatrics; an effect size exceeding 0.8 is considered large. Statistics were performed using PASW Statistics 17.0 (SPSS Inc., Chicago, IL, USA).
Results
The hospitalist group grew from 31 to 36 members in June of 2008. On average, 14 hospitalists (M = 14.40, standard deviation [SD] = 2.41, range 1119) attended each session, with all hospitalists (n = 36) attending 1 session (M = 3.83, SD = 2.35, range 19). At each session, an average of 72% completed a post‐session evaluation form. Overall, faculty were likely to use the PAGE teaching tools (M = 4.61, SD = 0.53) and would recommend PAGE to other hospitalists (M = 4.63, SD = 0.51).
Thirteen hospitalist trainees of 36 (36%) completed a post‐PAGE online questionnaire. Respondents taught on faculty for an average of 5 years (mean (M) = 5.08, SD = 3.52). Faculty perceived self‐efficacy at teaching residents about geriatrics improved significantly with a large effect size (pretest M = 3.05, SD = .60; posttest M = 3.96, SD = .36, d = 1.52; P < 0.001). Session attendance was positively correlated with the increase in geriatrics teaching self‐efficacy (r = .62, P < 0.05), while teaching experience was not (r = 0.05, P = 0.88). Hospitalist trainees found the PAGE model more useful after participating (M = 4.62, SD = 0.65), than they had expected (M = 3.92, SD = 0.76; P < 0.05).
All session leaders (n = 15) completed the questionnaire after PAGE (9 hospitalists, 5 geriatricians, 1 urologist). Two‐thirds had 5 years on faculty; eight had no prior experience as a faculty development trainer. Over 80% indicated that they found their coteaching experience, enjoyable, useful and collaborative. Only 1 participant did not commit to interdisciplinary teaching again. Most hospitalist session leaders reported that coteaching with a geriatrician enhanced their knowledge; they were more likely to consult a geriatrician regarding patients. All but 2 session leaders felt that the model fostered a collaborative environment between their 2 divisions.
Of the 56 residents, 41% (16 PGY1, 7 PGY2) completed a pretest; 43% (15 PGY1, 9 PGY2) completed a posttest. Residents reported receiving inpatient teaching on geriatrics skills significantly more frequently from hospitalists vs. nonhospitalist attendings both before PAGE (hospitalists M = 2.18, SD = 0.37; nonhospitalists M = 2.00, SD = 0.53, P < 0.05), and after (hospitalists M = 2.39, SD = 0.46; nonhospitalists M = 2.05, SD = 0.57, P < 0.05; see Fig. 1). Although hospitalists taught more frequently about geriatrics than nonhospitalists before PAGE, our findings suggest that they increased their teaching by a greater magnitude than nonhospitalists (P < 0.01, P > 0.05, respectively). Residents reported increased geriatric skill practice after PAGE with a medium effect size (pretest M = 2.92, SD = 0.55, posttest M = 3.28, SD = 0.66, P = 0.052, d = 0.66). There was greater mean reported practice for all skills with the exception of hospice care, which already was being performed between often and very often before PAGE. The largest increases in skill practice were (descending order, most increased first): assessing polypharmacy, performing skin exams, prognostication, performing functional assessments and examining Foley catheter use.
Discussion
Our aging population and a shortage of geriatricians necessitates new, feasible models for geriatric training. Similar to the CHAMP model,7 PAGE had a favorable impact on faculty perceived behavioral change; after the PAGE sessions, faculty reported significantly greater self‐efficacy of teaching geriatrics. However, this study also examined the impact of the PAGE Model on 2 groups not previously reported in the literature: faculty session leaders and medicine residents.
To our knowledge, this is the first study about a hospitalist TTT program codeveloped with nonhospitalists aimed at teaching geriatrics skills to residents, though smaller scale programs for medical students exist.24 We believe codevelopment was important in our model for many reasons. First, using hospitalist peers and local geriatricians likely increased trust in the educational curricula and allowed for strong communication channels between instructors.25, 26 Second, coteaching allowed for hospitalist mentorship. Hospitalists acknowledged their coleaders as mentors and several hospitalists subsequently engaged in new geriatric projects. Third, coteaching was felt to enhance patient care and increase geriatrician consultations. Coteaching may have applicability to other hospitalist faculty development such as intensive care and palliative care, and hospitalist programs may benefit from creating faculty development programs internally with their colleagues, rather than using online resources.
Another important finding of this study is that training hospitalists to teach about geriatrics seems to result in an increase in both the geriatric teaching that residents receive and residents' practice of geriatric skills. This outcome has not been previously demonstrated with geriatric TTT activities.27 This trickle‐down effect to residents likely results from both the increased teaching efficacy of hospitalists after the PAGE Model and the exportable nature of the teaching tools.
Several continuing medical education best practices were used which we believe contributed to the success of PAGE. First, we conducted a needs assessment, which improves knowledge outcomes.28, 29 Second, sessions included cases, lectures, and discussions. Use of multiple educational techniques yields greater knowledge and behavioral change as compared to a single method, such as lecture alone.24, 25, 30, 31 Finally, sessions were sequenced over a year, rather than clustered in short, intensive activity. Sequenced, or learn‐work‐learn opportunities allow education to be translated to practice and reinforced.8, 27, 30, 32
We believe that the PAGE Model is transportable to other hospitalist programs due to its cost and flexible nature. In economically‐lean times, hospitalist divisions can create a program similar to the PAGE Model essentially at no cost, except for donated faculty preparation time. In contrast, CHAMP was expensive, costing nearly $72,000 for 12 faculty to participate in the 48‐hour curriculum,7, 33 and volunteering physicians were compensated for their time. Though Mini‐CHAMP is a streamlined 2‐day workshop that offers free online lectures and slide sets, there may be some benefit to producing a faculty development program internally, as we stated above, and PAGE included additional topics (urinary catheters and decubitus ulcers/wound care) not covered in mini‐CHAMP.
There were several limitations to this study. First, some outcomes of the PAGE Model were assessed by retrospective self‐report, which may allow for recall bias. Although self‐report may or may not correlate with actual behavior,34 faculty and resident perspectives of their teaching and learning experiences are themselves important. Furthermore, a retrospective presurvey allows for content of an educational program or intervention to be explained prior to a survey, so that participants first assess their new level of understanding or skill on the post test, then reflectively assess the level of understanding or skill they had prior to the workshop. This avoids response shift bias and can improve internal validity.21, 35
Second, the small numbers of session leaders, hospitalist trainees, and residents restricted statistical power to detect small effects. The fact that we found significant improvements enhances the likelihood that the differences observed were not due to chance.
Third, the low response rates from the hospitalist trainee post‐intervention questionnaire and the residents' questionnaires may affect the validity of our results. For the resident survey, the subjects were not matched, and we cannot state that an individual's geriatric skill practice changed due to PAGE, though the results suggest the residency program as a whole improved the frequency of geriatric skill practice.
Finally, the residents were required to report the frequency of teaching on and practice of geriatric skills practice over the prior year and accuracy of recall may be an issue. However, frequencies were queried both pre and post intervention and favorable change was noted. Furthermore, because the high end of the 3‐point teaching scale was limited to more than once, the true amount of teaching may have been underestimated if more than once actually represented high frequencies.
Future studies are needed to replicate these findings at other institutions to confirm generalizability. It would be beneficial to measure patient outcomes to determine whether increased teaching and skill practice benefits patients using measures such as reduction in catheter related urinary tract infections, falls, and inadequate pain management. Further investigations of cotaught faculty development programs between hospitalists and other specialists help emphasize why internally created TTT programs are of greater value than online resources.
Conclusions
This time‐sensitive adaptation of a hospitalist geriatric TTT program was successfully implemented at an academic medical center and suggests improved hospitalist faculty self‐efficacy at teaching geriatric skills, increased frequency of inpatient geriatric teaching by hospitalists and increased resident geriatric skill practice. Confidence to care for geriatric patients and a strong skill set to assess risks and manage them appropriately will equip hospitalists and trainees to provide care that reduces geriatric patients' in‐hospital morbidity and costs of care. As hospitalists increasingly care for older adults, the need for time‐efficient methods of teaching geriatrics will continue to grow. The PAGE Model, and other new models of geriatric training for hospitalists, demonstrates that we are beginning to address this urgent need.
Acknowledgements
The authors thank Joan Abrams, MA, MPA, and Patricia O'Sullivan, EdD, whose work was key to the success of this program and this manuscript. They also thank the Donald W. Reynolds Foundation for support of this project.
- ,.2005 National Hospital Discharge Survey.Adv Data.2007;385:1–19.
- ,,,. In:U.S. Census Bureau, Current Population Reports, 65+ in the United States: 2005,Washington, D.C.:U.S. Government Printing Office;2005:23–209.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360(11):1102–1112.
- ,,,.Providing dementia outreach education to rural communities: lessons learned from a train‐the‐trainer program.J Appl Gerontol.2002;21:294–313.
- .Gerontologizing health care: a train‐the‐trainer program for nurses.Gerontol Geriatr Educ.1999;19:47–56.
- ,,.A statewide model detection and prevention program for geriatric alcoholism and alcohol abuse: increased knowledge among service providers.Community Ment Health J.2000;36:137–148.
- ,,, et al.The curriculum for the hospitalized aging medical patient program: a collaborative faculty development program for hospitalists, general internists, and geriatricians.J Hosp Med.2008;3(5):384–393.
- Reframing professional development through understanding authentic professional learning.Rev Educ Res.2009;79:702–739.
- The Education Committee Writing Group of the American Geriatrics Society.Core competencies for the care of older patients: recommendations of the American Geriatrics Society.Acad Med.2000;75:252–255.
- ,,, et al.American Geriatrics Society Task Force on the future of geriatric medicine.J Am Geriatr Soc.2005;53 (6 Suppl):S245–S256.
- Nadzam, Deborah. Preventing patient falls. Joint Commission Resources. Available at: http://www.jcrinc.com/Preventing‐Patient‐Falls. Accessed April2010.
- ,.Curricular recommendations for resident training in nursing home care. A collaborative effort of the Society of General Internal Medicine Task Force on Geriatric Medicine, the Society of Teachers of Family Medicine Geriatrics Task Force, the American Medical Directors Association, and the American Geriatrics Society Education Committee.J Am Geriatr Soc.1994;42:1200–1201.
- ,,,,.Curriculum recommendations for resident training in geriatrics interdisciplinary team care.J Am Geriatr Soc.1999;47:1145–1148.
- ,.ACGME requirements for geriatrics medicine curricula in medical specialties: Progress made and progress needed.Acad Med.2005;80:279–285.
- CMS Office of Public Affairs. CMS Improves Patient Safety for Medicare and Medicaid by Addressing Never Events, August 04, 2008. Available at: http://www.cms.gov/apps/media/press/factsheet.asp?Counter=322434(5):337–343.
- ,.The changing paradigm for continuing medical education: impact of information on the teachable moment.Bull Med Libr Assoc.1990;78(2):173–179.
- ,.Creating the teachable moment.J Nurs Educ.1998;37(6):278–280.
- Society of Hospital Medicine, BOOSTing Care Transitions Resource Room. Mazotti L, Johnston CB. Faculty development: Teaching triggers for transitional care. “A train‐the‐trainer model.” Available at: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/PDFs/Mazotti_UCSF_Transitions.PPT. Accessed April2010.
- .Self‐efficacy: The Exercise of Control.New York:W.H. Freeman and Company;1997.
- .Internal invalidity in pretest‐posttest self‐report evaluations and a re‐evaluation of retrospective pretests.Applied Psychological Measurement.1979;3:1–23.
- ,.A visitor's guide to effect sizes.Adv Health Sci Educ Theory Pract.2004;9:241–249.
- .Statistical Power Analyses for the Behavioral Sciences.2nd ed.Hillsdale, NJ:Lawrence Erlbaum Associates;1988.
- ,,,.Hazards of hospitalization: Hospitalists and geriatricians educating medical students about delirium and falls in geriatric patients.Gerontol Geriatr Educ.2008;28(4):94–104.
- ,,, et al.Continuing medical education, continuing professional development, and knowledge translation: Improving care of older patients by practicing physicians.J Am Geriatr Soc.2006:54(10):1610–1618.
- ,,, et al.Practicing physician education in geriatrics: Lessons learned from a train‐the‐trainer model.J Am Geriatr Soc.2007:55(8):1281–1286.
- ,.CHAMP trains champions: hospitalist‐educators develop new ways to teach care for older patients.J Hosp Med.2008;3(5):357–360.
- ,,,,,.Impact of formal continuing medical education: Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes?JAMA.1999;282(9):867–874.
- ,.Association for the Study of Medical Education Booklet: The effectiveness of continuing professional development.Edinburgh, Scotland:Association for the Study of Medical Education;2000.
- ,,, et al.Effectiveness of continuing medical education.Evid Rep Technol Assess (Full Rep).2007;149:1–69.
- ,,, et al.Continuing education meetings and workshops: effects on professional practice and health care outcomes.Cochrane Database Syst Rev.2009;(2):CD003030.
- ,.Continuing medical education and the physician as learner: guide to the evidence.JAMA.2002;288(9):1057–1060.
- .Care of hospitalized older patients: opportunities for hospital‐based physicians.J Hosp Med.2006;1:42–47.
- ,.What we say and what we do: self‐reported teaching behavior versus performances in written simulations among medical school faculty.Acad Med.1992;67(8):522–527.
- ,.The retrospective pretest and the role of pretest information in evaluation studies.Psychol Rep.1992;70:699–704.
- ,.2005 National Hospital Discharge Survey.Adv Data.2007;385:1–19.
- ,,,. In:U.S. Census Bureau, Current Population Reports, 65+ in the United States: 2005,Washington, D.C.:U.S. Government Printing Office;2005:23–209.
- ,,,.Growth in the care of older patients by hospitalists in the United States.N Engl J Med.2009;360(11):1102–1112.
- ,,,.Providing dementia outreach education to rural communities: lessons learned from a train‐the‐trainer program.J Appl Gerontol.2002;21:294–313.
- .Gerontologizing health care: a train‐the‐trainer program for nurses.Gerontol Geriatr Educ.1999;19:47–56.
- ,,.A statewide model detection and prevention program for geriatric alcoholism and alcohol abuse: increased knowledge among service providers.Community Ment Health J.2000;36:137–148.
- ,,, et al.The curriculum for the hospitalized aging medical patient program: a collaborative faculty development program for hospitalists, general internists, and geriatricians.J Hosp Med.2008;3(5):384–393.
- Reframing professional development through understanding authentic professional learning.Rev Educ Res.2009;79:702–739.
- The Education Committee Writing Group of the American Geriatrics Society.Core competencies for the care of older patients: recommendations of the American Geriatrics Society.Acad Med.2000;75:252–255.
- ,,, et al.American Geriatrics Society Task Force on the future of geriatric medicine.J Am Geriatr Soc.2005;53 (6 Suppl):S245–S256.
- Nadzam, Deborah. Preventing patient falls. Joint Commission Resources. Available at: http://www.jcrinc.com/Preventing‐Patient‐Falls. Accessed April2010.
- ,.Curricular recommendations for resident training in nursing home care. A collaborative effort of the Society of General Internal Medicine Task Force on Geriatric Medicine, the Society of Teachers of Family Medicine Geriatrics Task Force, the American Medical Directors Association, and the American Geriatrics Society Education Committee.J Am Geriatr Soc.1994;42:1200–1201.
- ,,,,.Curriculum recommendations for resident training in geriatrics interdisciplinary team care.J Am Geriatr Soc.1999;47:1145–1148.
- ,.ACGME requirements for geriatrics medicine curricula in medical specialties: Progress made and progress needed.Acad Med.2005;80:279–285.
- CMS Office of Public Affairs. CMS Improves Patient Safety for Medicare and Medicaid by Addressing Never Events, August 04, 2008. Available at: http://www.cms.gov/apps/media/press/factsheet.asp?Counter=322434(5):337–343.
- ,.The changing paradigm for continuing medical education: impact of information on the teachable moment.Bull Med Libr Assoc.1990;78(2):173–179.
- ,.Creating the teachable moment.J Nurs Educ.1998;37(6):278–280.
- Society of Hospital Medicine, BOOSTing Care Transitions Resource Room. Mazotti L, Johnston CB. Faculty development: Teaching triggers for transitional care. “A train‐the‐trainer model.” Available at: http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/PDFs/Mazotti_UCSF_Transitions.PPT. Accessed April2010.
- .Self‐efficacy: The Exercise of Control.New York:W.H. Freeman and Company;1997.
- .Internal invalidity in pretest‐posttest self‐report evaluations and a re‐evaluation of retrospective pretests.Applied Psychological Measurement.1979;3:1–23.
- ,.A visitor's guide to effect sizes.Adv Health Sci Educ Theory Pract.2004;9:241–249.
- .Statistical Power Analyses for the Behavioral Sciences.2nd ed.Hillsdale, NJ:Lawrence Erlbaum Associates;1988.
- ,,,.Hazards of hospitalization: Hospitalists and geriatricians educating medical students about delirium and falls in geriatric patients.Gerontol Geriatr Educ.2008;28(4):94–104.
- ,,, et al.Continuing medical education, continuing professional development, and knowledge translation: Improving care of older patients by practicing physicians.J Am Geriatr Soc.2006:54(10):1610–1618.
- ,,, et al.Practicing physician education in geriatrics: Lessons learned from a train‐the‐trainer model.J Am Geriatr Soc.2007:55(8):1281–1286.
- ,.CHAMP trains champions: hospitalist‐educators develop new ways to teach care for older patients.J Hosp Med.2008;3(5):357–360.
- ,,,,,.Impact of formal continuing medical education: Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes?JAMA.1999;282(9):867–874.
- ,.Association for the Study of Medical Education Booklet: The effectiveness of continuing professional development.Edinburgh, Scotland:Association for the Study of Medical Education;2000.
- ,,, et al.Effectiveness of continuing medical education.Evid Rep Technol Assess (Full Rep).2007;149:1–69.
- ,,, et al.Continuing education meetings and workshops: effects on professional practice and health care outcomes.Cochrane Database Syst Rev.2009;(2):CD003030.
- ,.Continuing medical education and the physician as learner: guide to the evidence.JAMA.2002;288(9):1057–1060.
- .Care of hospitalized older patients: opportunities for hospital‐based physicians.J Hosp Med.2006;1:42–47.
- ,.What we say and what we do: self‐reported teaching behavior versus performances in written simulations among medical school faculty.Acad Med.1992;67(8):522–527.
- ,.The retrospective pretest and the role of pretest information in evaluation studies.Psychol Rep.1992;70:699–704.
Copyright © 2010 Society of Hospital Medicine