User login
Myth: LBBB Masks Hyperkalemia
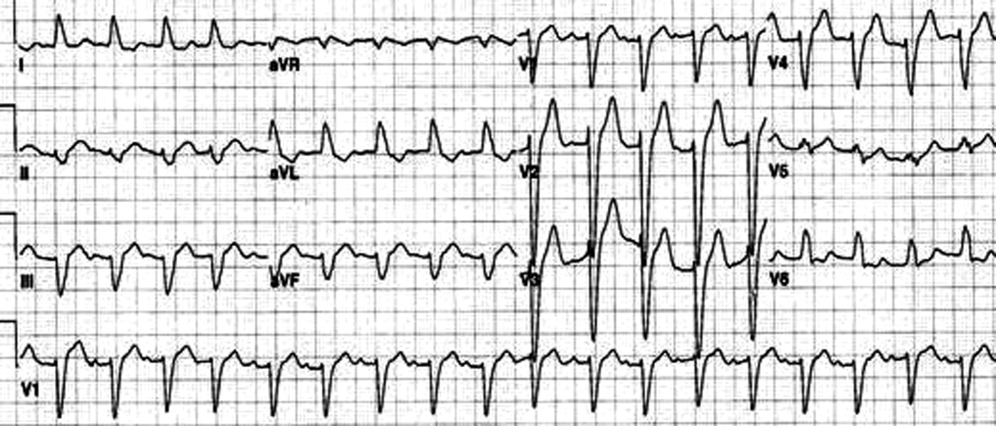
An 80‐year‐old man with end‐stage renal disease requiring maintenance hemodialysis was admitted to the emergency department (ED) with complaints of fever, generalized fatigue, and lethargy. Presenting electrocardiogram (ECG) revealed normal sinus rhythm at 82 beats per minute (bpm), prolonged PR interval, complete left bundle branch block (LBBB) with wide QRS interval and tall T waves (Figure 1). A baseline ECG done 3 months ago also showed LBBB (Figure 2). In view of the underlying LBBB, changes in the presenting ECG were ignored.

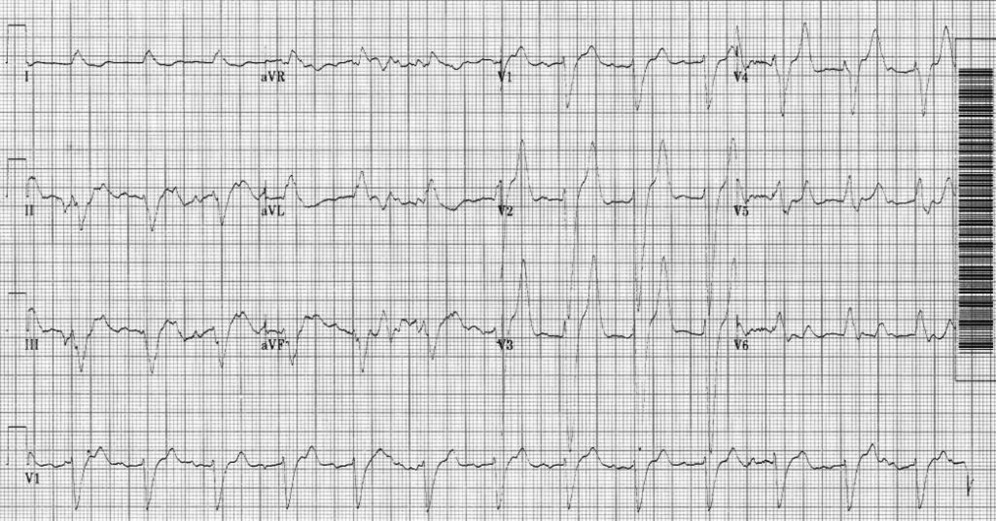
Hemodialysis was planned for the patient. A few hours later, repeat ECG revealed a sine wave pattern suggestive of severe hyperkalemia (Figure 3). Laboratory results were available then and his serum potassium was found to be 6.8 mmol/L. He was started on insulin, dextrose, and calcium gluconate, but he developed cardiorespiratory arrest and died.
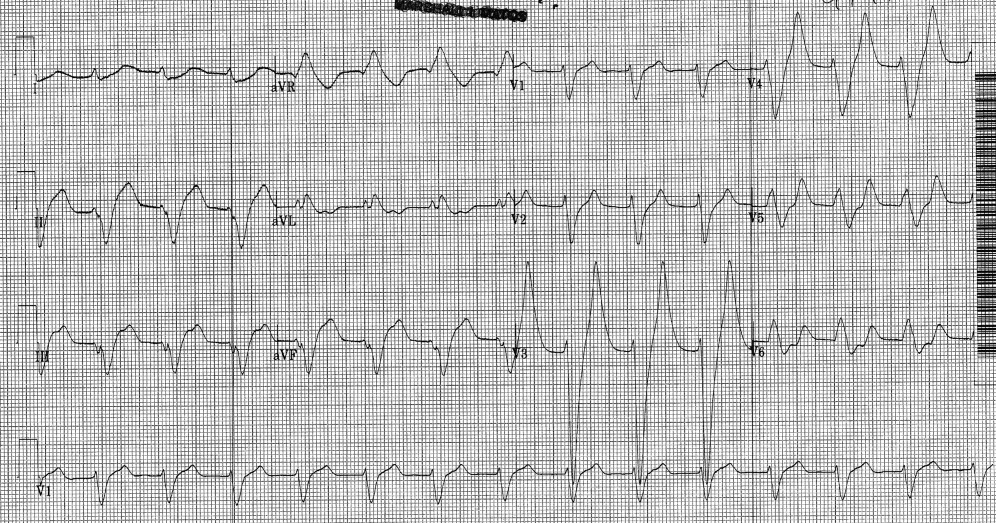
Retrospectively, looking at the presenting ECG (Figure 1), it was found that the PR interval was longer, the QRS was broader, and the T waves were taller and more peaked than the baseline ECG (Figure 2).
Discussion
Hyperkalemia is a true medical emergency with potential lethal consequences that must be treated accordingly.1, 2 It can be difficult to diagnose due to the paucity of distinctive signs and symptoms. Any ECG change due to hyperkalemia becomes an indication for stabilizing the myocardium with calcium infusion.
Often, the sequence of repolarization due to myocardial infarction is altered on ECG in patients with baseline LBBB, making it difficult to diagnose accurately. Although it is thought that changes due to electrolyte imbalances will also be masked by the presence of LBBB, there is no evidence supporting this in the literature. Hence, it is wrongly believed that LBBB masks changes due to hyperkalemia. It is important that in patients with suspected electrolyte imbalance, baseline ECG showing LBBB is compared to the presenting ECG. In our patient, the presenting ECG (Figure 1) might not look too impressive, but in comparison to the baseline ECG (Figure 2), the PR interval is longer, QRS is wider, and T waves are more peaked and taller. If the admitting physician had closely compared the presenting ECG (Figure 1) to the baseline ECG (Figure 2), the suspicion of hyperkalemia would have been high.
- ,,.Electrolyte disturbances. In:Marx JA,Hockberger RS,Walls RM, et al.,Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Vol2.St. Louis:Mosby;2002:1730–1731.
- ,.Hyperkalemia in hospitalized patients.Int Urol Nephrol.2000;32:177–180.
An 80‐year‐old man with end‐stage renal disease requiring maintenance hemodialysis was admitted to the emergency department (ED) with complaints of fever, generalized fatigue, and lethargy. Presenting electrocardiogram (ECG) revealed normal sinus rhythm at 82 beats per minute (bpm), prolonged PR interval, complete left bundle branch block (LBBB) with wide QRS interval and tall T waves (Figure 1). A baseline ECG done 3 months ago also showed LBBB (Figure 2). In view of the underlying LBBB, changes in the presenting ECG were ignored.
Hemodialysis was planned for the patient. A few hours later, repeat ECG revealed a sine wave pattern suggestive of severe hyperkalemia (Figure 3). Laboratory results were available then and his serum potassium was found to be 6.8 mmol/L. He was started on insulin, dextrose, and calcium gluconate, but he developed cardiorespiratory arrest and died.
Retrospectively, looking at the presenting ECG (Figure 1), it was found that the PR interval was longer, the QRS was broader, and the T waves were taller and more peaked than the baseline ECG (Figure 2).
Discussion
Hyperkalemia is a true medical emergency with potential lethal consequences that must be treated accordingly.1, 2 It can be difficult to diagnose due to the paucity of distinctive signs and symptoms. Any ECG change due to hyperkalemia becomes an indication for stabilizing the myocardium with calcium infusion.
Often, the sequence of repolarization due to myocardial infarction is altered on ECG in patients with baseline LBBB, making it difficult to diagnose accurately. Although it is thought that changes due to electrolyte imbalances will also be masked by the presence of LBBB, there is no evidence supporting this in the literature. Hence, it is wrongly believed that LBBB masks changes due to hyperkalemia. It is important that in patients with suspected electrolyte imbalance, baseline ECG showing LBBB is compared to the presenting ECG. In our patient, the presenting ECG (Figure 1) might not look too impressive, but in comparison to the baseline ECG (Figure 2), the PR interval is longer, QRS is wider, and T waves are more peaked and taller. If the admitting physician had closely compared the presenting ECG (Figure 1) to the baseline ECG (Figure 2), the suspicion of hyperkalemia would have been high.
An 80‐year‐old man with end‐stage renal disease requiring maintenance hemodialysis was admitted to the emergency department (ED) with complaints of fever, generalized fatigue, and lethargy. Presenting electrocardiogram (ECG) revealed normal sinus rhythm at 82 beats per minute (bpm), prolonged PR interval, complete left bundle branch block (LBBB) with wide QRS interval and tall T waves (Figure 1). A baseline ECG done 3 months ago also showed LBBB (Figure 2). In view of the underlying LBBB, changes in the presenting ECG were ignored.
Hemodialysis was planned for the patient. A few hours later, repeat ECG revealed a sine wave pattern suggestive of severe hyperkalemia (Figure 3). Laboratory results were available then and his serum potassium was found to be 6.8 mmol/L. He was started on insulin, dextrose, and calcium gluconate, but he developed cardiorespiratory arrest and died.
Retrospectively, looking at the presenting ECG (Figure 1), it was found that the PR interval was longer, the QRS was broader, and the T waves were taller and more peaked than the baseline ECG (Figure 2).
Discussion
Hyperkalemia is a true medical emergency with potential lethal consequences that must be treated accordingly.1, 2 It can be difficult to diagnose due to the paucity of distinctive signs and symptoms. Any ECG change due to hyperkalemia becomes an indication for stabilizing the myocardium with calcium infusion.
Often, the sequence of repolarization due to myocardial infarction is altered on ECG in patients with baseline LBBB, making it difficult to diagnose accurately. Although it is thought that changes due to electrolyte imbalances will also be masked by the presence of LBBB, there is no evidence supporting this in the literature. Hence, it is wrongly believed that LBBB masks changes due to hyperkalemia. It is important that in patients with suspected electrolyte imbalance, baseline ECG showing LBBB is compared to the presenting ECG. In our patient, the presenting ECG (Figure 1) might not look too impressive, but in comparison to the baseline ECG (Figure 2), the PR interval is longer, QRS is wider, and T waves are more peaked and taller. If the admitting physician had closely compared the presenting ECG (Figure 1) to the baseline ECG (Figure 2), the suspicion of hyperkalemia would have been high.
- ,,.Electrolyte disturbances. In:Marx JA,Hockberger RS,Walls RM, et al.,Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Vol2.St. Louis:Mosby;2002:1730–1731.
- ,.Hyperkalemia in hospitalized patients.Int Urol Nephrol.2000;32:177–180.
- ,,.Electrolyte disturbances. In:Marx JA,Hockberger RS,Walls RM, et al.,Rosen's Emergency Medicine: Concepts and Clinical Practice.5th ed. Vol2.St. Louis:Mosby;2002:1730–1731.
- ,.Hyperkalemia in hospitalized patients.Int Urol Nephrol.2000;32:177–180.
Hospitalists in the AHSC
The successful integration of hospitalists in academic health science centers (AHSCs) has been identified as one of the most challenging areas for the hospitalist movement.1, 2 This has been based on a concern that many hospitalists lack academic and research skills, lack mentorship, and may have little time to develop academic careers because of the significant time they spend in clinical care.
A recent survey highlighted that the pediatric hospitalist workforce is in its infancy and additional perspectives, such as from hospitalists themselves, are essential for a more complete picture of the current state of pediatric hospital medicine.3 Hospitalists have had a long history in Canada.4 The Hospital for Sick Children, Toronto, Canada, has had a Division of Pediatric Medicine since 1981, with hospitalists, as we now know them, from inception. This provided a rich resource to explore pediatric hospital medicine in the academic context and from hospitalists themselves. The objective of this survey was to explore the characteristics, practice, and perceptions of pediatric hospital medicine in an AHSC. Locally, we hoped the results would inform the division on program development, training, and faculty career development. Externally, the findings could contribute to a body of knowledge on the evolving role of pediatric hospitalists and provide insight into opportunities for better integration into AHSCs.
Methods
Study Design
This was a cross‐sectional survey of pediatricians who attend on the pediatric medicine inpatient unit at the Hospital for Sick Children, Toronto. The study protocol was approved by Quality and Risk Management at The Hospital for Sick Children.
Setting
The Hospital for Sick Children is a tertiary care children's hospital affiliated with the University of Toronto, Toronto, Canada. The total hospital bed capacity including intensive care unit beds and subspecialty beds is 320. It is the only free‐standing pediatric hospital for the greater Toronto area with a catchment population of 5 million people.
A formal division for general pediatrics, Pediatric Medicine, has been in existence since 1981 with hospital‐based pediatricians (who now are known as hospitalists) who attend on the inpatient unit. The pediatric medicine inpatient unit (PMIU) has a 60‐bed capacity on 3 units. At all times, the PMIU is staffed by 4 to 6 inpatient attendings from a total of 20 full‐time and major part‐time pediatricians. According to Wachter's staging of hospital care, the PMIU is at stage IV of IV in development (mandatory care by hospitalist).5 All attending pediatricians are members of the Division of Pediatric Medicine. Pediatric subspecialists do not attend on the PMIU. Physicians attend for a minimum of 4 weeks at a time. General pediatric house staff including fellows, residents (postgraduate year [PGY] 1, PGY3) and medical students are supervised by the attending pediatricians. Other inpatient clinical services provided include an inpatient general medical consultation team, a complex care team for inpatients with chronic complex conditions, and a consultative and collaborative role with the team of interventional radiologists. An outpatient pediatric consultation program exists for hospital follow‐up, general pediatric consultation, and specialized generalist care for specific populations of children.
In addition to the clinical program, research and education programs exist within the division. The division has had an academic general pediatric fellowship program since 1992, with the majority of most recent graduates obtaining academic hospitalist faculty positions. A formal research group and infrastructure for clinical, outcomes‐based research within the division, known as the Pediatric Outcomes Research Team (PORT), exists.
Study Population
All pediatricians who attend on the PMIU and in the Division of Pediatric Medicine, Hospital for Sick Children in 2007 were eligible for recruitment including the 2 eligible study authors.
Survey Instrument
We constructed a 43‐item structured questionnaire that asked about and explored training and employment characteristics; clinical roles and nonclinical roles (teaching, quality, research, leadership); and perceptions of hospital medicine and a career in this field. Several items were modeled after questions administered to program directors in a survey reported by Freed et al.3 The questionnaire was designed to be completed by the respondent on paper.
Questionnaire Administration
From September to December 2007, eligible pediatricians were sent a letter explaining the study and the questionnaire through interhospital mail by the research coordinator. Questionnaires were deidentified and assigned a unique identification number. Only the research coordinator had access to the list that linked the unique identification numbers with names. Confidentiality of responses and anonymity of responses was explicitly stated in the letter explaining the study to pediatricians. Nonrespondents were contacted by the research assistant at 3‐week intervals with personal reminders.
Data Analysis
During the analysis phase, responses remained deidentified. Descriptive statistics using means, medians, and proportions were calculated for survey items. For open‐ended questions, answers from respondents were summarized into key concepts or themes by the 3 study authors. Excerpts from responses were abstracted to highlight themes.
Results
Eighteen of 20 (90%) faculty responded to the questionnaire. The results are presented by the domains of the questionnaire, as follows.
Training and Employment Characteristics
Due to the requirements of the Royal College of Physicians and Surgeons of Canada, all faculty had a minimum of 4 years of pediatric specialty training leading to certification (Table 1). Seven of 18 (39%) had fellowship and graduate training. Nine of 18 (50%) had been on faculty for greater than 5 years.
| Training after medical schools, median years (range) | 4.8 (46) |
| Fellowship trained, number (%) | 7 (39) |
| Fellowship duration, median years (range) | 2.7 (15) |
| Graduate studies, number (%) | 7 (39) |
| Clinical epidemiology | 5 |
| Education | 2 |
| Duration since first academic appointment | |
| Median, years (range) | 5.5 (030) |
| Mean, years (standard deviation) | 9.9 (10.4) |
| >5 years, number (%) | 9 (50) |
| Academic rank, number (%) | |
| Lecturer | 2 (11) |
| Assistant professor | 10 (56) |
| Associate professor | 4 (22) |
| Full professor | 1 (6) |
Hospitalists: Impact and Definition
Seventeen of 18 (94%) faculty felt that hospitalists reduce cost, increase patient satisfaction, and increase quality of care. Three of 18 (17%) felt that hospitalism adversely affects the primary care physicianpatient relationship. All felt that hospitalists can contribute to the academic mission of an AHSC.
Most (17/18) felt that the Society of Hospital Medicine definition of a hospitalist is useful but 13 of 18 (72%) felt that it was important to develop an international consensus‐based definition.
Clinical Roles
All faculty attended on the PMIU. Other clinical activities included: 13 of 18 (72%) inpatient general medical consultation, 9 of 18 (50%) interventional radiology clinical team, 8 of 18 (44%) attended in the pediatric consultation clinic.
The median number of weeks attending on the PMIU was 16 (range, 440 weeks).
Nine of 18 (50%) provided leadership in clinical programs or the care of specific populations of children. This included leadership in healthcare systems: director of PMIU, director of inpatient general medical consultation, interventional radiology comanagement team; and leadership in patient populations: children with chronic complex conditions, cyclic vomiting, cancer/genetic syndromes, obesity, child abuse and neglect, failure to thrive, and vascular tumors.
Nonclinical and Academic Roles
Sixteen (89%) considered their job to include activities in addition to their role of providing patient care (Table 2). This included primary activity in clinical research, education, quality improvement and health policy.
| Area of Activity | n = 18 [number (%)] |
|---|---|
| |
| QI | |
| Participates in QI activity | 12 (67) |
| Participants who lead in QI activity | 4 (33) |
| Education | |
| Teaching | |
| Medical students | |
| Inpatient unit | 18 (100) |
| Small group sessions | 10 (56) |
| Lectures | 15 (83) |
| Residents | |
| Inpatient unit | 17 (94) |
| Lectures | 12 (67) |
| EBM critical appraisal course | 5 (28) |
| General pediatric fellows | 7 (39) |
| CME | 11 (61) |
| Curriculum or program development | 9 (50) |
| Research | |
| Holds appointment with research institute | 12 (66) |
| Peer review publication in past 12 months | 13 (72) |
| Currently holds research grant | 12 (66) |
| Presented abstract at 2007 PAS meeting | 10 (56) |
Hospitalist Medicine as a Career: Perceptions
Fifteen (83%) felt that it was important to establish an annual minimum time allocation to practicing hospital medicine. A median of 11 weeks per year (range, 816 weeks) was felt to be the minimum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a minimum time for clinical practice in hospital medicine were as follows: maintenance of skills, knowledge, and competency; ensuring quality of care; and efficiency of care. One respondent explained that the main reason to have a minimum time for clinical practice was to keep up clinical skills of acute patients, stay aware of and keep up to date of available facilities in the hospital.
Thirteen (72%) felt that it was important to establish an annual maximum time allocation to practicing hospital medicine. A median of 32 weeks per year (range, 2036 weeks) was felt to be the maximum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a maximum time for clinical practice in hospital medicine were: burnout, balance in career, and desire to develop academic career and to complete nonclinical activities. As this respondent described: I think hospital medicine can be very emotionally difficult and is sustainable if provided time off to pursue other goals such as research, education, creative professional service.
Thirteen (72%) intended to continue their career as a hospitalist and 5 (28%) were unsure. Eleven (61%) felt that a job as a hospitalist was a viable long term career, 6 (33%) were unsure, and 1 (5%) felt that it was not viable. When asked what the barriers to establishing hospital medicine as a long‐term career, the major themes that emerged were as follows: burnout, establishing a nonclinical or academic niche, and the system for career advancement in an academic center. This respondent explained: As long as you have another niche (education for me) that helps provide respite, as well as [you need an] opportunity to have protected time for academic endeavours that are necessary to survive in an academic health science centre.
Another respondent described burnout as a barrier: long hours, emotionally draining with very complex patients, feeling stretchedclinical care and teaching and research and admin.
Perceived advantages to a career as a hospitalist included: working in a team, generalist approach to care, stability relative to community practice, intellectually stimulating and rewarding work, growing area and opportunities for scholarship. One respondent outlined the perceived advantages to a generalist approach: diversity of work, become a generalist specialist, teamwork, develop broad perspective on health.
Others described the perceived advantages over community practice: exciting, interesting, job stability, salary and no worries about administration of the business of community office, stable income, holiday leave.
Perceived disadvantages to a career as a hospitalist included: burnout, recognition and respect, and lack of long‐term relationships with patients. One respondent explained: as an emerging field, we have a lot of growing to do. Although our work (both clinical and academic) seem fundamental to the mission of the hospital and university, we may not feel we receive the respect, support, resources, funding allocated to other areas.
Another response to disadvantages of a career as a hospitalist was, burnout, risk of being seen as a perpetual resident.
Discussion
Freed et al.3 recently conducted a survey of U.S. pediatric hospitalist program directors from a diverse range of settings (ie, teaching vs. nonteaching, free‐standing vs. hospital system, children's hospitals vs. non‐children's hospitals).3 These investigators found that the majority of programs had employed hospitalists for less than 5 years (compared with our program, 30 years); employed 1 to 5 hospitalists (compared with our program, 20); and 25% of programs indicated their hospitalists averaged greater than 5 years on the job (compared with our program, average 10 years on the job). Maniscalco et al.6 conducted a survey in 2007 of hospitalists in a similarly diverse range of settings, found that the mean number of years on the job was 6 and found similar clinical and teaching roles. They also found that the need for advanced training in administration, research, education, and quality improvement was high. Further, we were able to examine academic roles and perceptions of hospital medicine as a career in an AHSC at an individual level. This survey, however, was limited by sampling from a single institution.
Almost all faculty identified an area of focus in addition to clinical care. Educational activities occurred at all levels: undergraduate, residency, fellowship, and continuing medical education. Faculty were engaged in research activities. Hospitalists provide care on all inpatient units as a consultant specialist in general medical care. For example, we have designed a collaborative model of care with the interventional radiology team to comanage children who require image‐guided interventions, such as gastrostomy, chest tube, and central venous line insertions.7 One further area that deserves mention is the leadership of hospitalists in outpatient care of children, especially hospital intense populations, in collaboration with their primary care provider. These groups of children are often medically and socially complex, require repeated and intense hospital resources (including diagnostic testing, subspecialty consultation, and hospitalization), and require generalist care to manage them from a family centered perspective.
A significant proportion of the faculty in this survey acquired advanced academic training. The formal training of hospitalist physicians is in its infancy. A recent work documenting the domains of training for academic general pediatric fellowship in leadership, education, and research seems to be most appropriate for the nonclinical foundation for pediatric academic hospitalists.8
Few studies have examined academic hospitalists' perceptions on the minimum and maximum time per year suitable for clinical service. This undoubtedly will vary depending on the institution, program and financial structure, patient load and complexity, call requirements, academic commitments, and stage of development. Faculty surveyed in this study felt a range of 11 to 32 weeks of clinical inpatient attending per year was ideal. This is consistent with the expert panel recommendations of the Society of Hospital Medicine. What may be equally important to determine is the maximum number of continuous weeks attending on the PMIU.
There have been 3 full‐time faculty who have left the division (all to community hospitalbased generalist practices with academic affiliations) and 1 who has changed from a full‐time to a part‐time role in the division. Most faculty surveyed intended to continue their career as a hospitalist. They identified several positive and satisfying aspects to the career, including relationships with peers, stable salary, numerous opportunities for scholarly work in a young field, and generalist care. Hoff et al.9 described a national US survey of hospitalists in all adult medicine settings that examined personal characteristics, and work‐related attitudes. Similarly, they found that hospital medicine was a source of positive social and professional work experiences related to interactions with peers, patients and families, and coworkers. In the current study, perceived disadvantages to a hospitalist career were burnout, lack of recognition and respect, and lack of long‐term relationships with patients. Hoff et al.9 noted that 37% were burnt out or at risk of burnout, which is less than in the fields of critical care medicine and emergency medicine.
The identified barriers to establishing a career were related to development of an academic focus, balance between clinical and nonclinical time, and the system for career advancement. Few other studies have examined these career issues for hospitalists in the academic setting. Several authors have discussed career issues for clinician‐educators in the US,10, 11 including metrics for promotion and recognition by institutions. Alternate methods have been proposed for promotion, aside from research and education, such as creative professional activity or clinical excellence.12 The developing field of hospital medicine faces similar challenges as individual hospitalists and the specialty itself works to align with the academic mission.1315
The division and hospitalist program have evolved over more than 2 decades to fulfill strategic goals and respond to changing external factors (Table 3). Contextual factors that have supported this evolution and that may be unique to our academic environment merit mention. First, the departments' physicians work in a within a single‐payer universal healthcare system that in some ways is similar to a single‐payer health maintenance organization. The ultimate governance is provided by the provincial Ministry of Health, which is funded through taxation. Second, through an alternative funding plan (AFP) with the provincial government, block funding is providing in lieu of fee for service clinical care that funds physician salaries for clinical work, research, education, and administrative activities.16 Third, the department has a career development compensation program (CDCP) that has an explicit job activity profile which is aligned with the role of hospitaliststhe clinician‐specialist profilewho have a predominate commitment to provide, advance, and promote excellence in clinical care with contributions to education and/or research.16 The compensation and evaluation process for hospitalists is the same as other members in the department. While further refinement of this system is ongoing, this program has demonstrated a support for all roles (ie, clinical, education, and research).17
| Date | Area | Pressure Point | Change |
|---|---|---|---|
| 1981 | Clinical education research | Department priority for academic generalism | Creation of Division of General Pediatrics (now Pediatric Medicine); full‐time hospital‐based pediatricians attending on inpatient unit |
| 1991 | Education | Division priority to foster academic generalism and train future generation of academic generalists | Creation of academic general pediatrics fellowship program |
| 1992 | Research | Division priority to foster clinical, outcomes‐based research | Creation of formal divisional research infrastructure with foundation support for an epidemiologic, outcomes‐based research platform; pediatric outcomes research team (PORT) |
| 1995 | Clinical care | Province‐wide reduction in resident duty hours; division priority to raise the bar for clinical and teaching excellence in hospitalist‐and community‐based pediatrics; need for a financially viable and cost‐effective model for staffing attending pediatricians on inpatient unit | Reorganization of inpatient unit; higher proportion of attending pediatricians who are full‐time, hospital‐based; creation of a staff‐only hospitalist unit19; creation of a section of community pediatrics (2001) |
| 1996 | Clinical care education faculty development | Need to limit attending hospitalists after‐hours clinical care to ensure balance and academic productivity; need for a system of after‐hours physician coverage for inpatient care that is sustainable and financially viable; need for funding sources for academic general pediatrics fellowship | Creation of a clinical departmental fellowship program to fund after hours clinical coverage with qualified pediatricians seeking additional fellowship training20 |
| 1998 | Faculty career development | Need to value and reward all academic contributions, such as the hospitalist role, through an explicit job activity profile within the department16 | Implementation of a career development and compensation program with the clinician specialist role whose primary contributions are to excellence in clinical care |
| 1999 | Clinical care | Expansion of hospital interventional radiology program and need for high quality collaborative care | Comanagement model with hospitalist‐radiologist team7 |
| 20068 | Clinical care research | Division and institution priority to provide high‐quality care for children with complex care health issues and foster a research program21 | Creation of formalized hospitalist complex care program with inpatient and outpatient care22; research support for complex care |
| 2007 | Clinical care | Refinement of inpatient unit organization to improve efficiency of care; increase number of trainees23 | Reorganization of inpatient units to geographic allocation of patients by attending physician; addition of trainees to staff‐only hospitalist unit |
Furthermore, several divisional factors have contributed to the viability of hospitalism within our generalist division. First, hospitalists were integrated into, rather than segregated from the division. Second, hospitalists have the opportunity to engage in diverse clinical activities. Wachter and Goldman18 advocate for hospitalist participation in outpatient care to provide variety and to cement their relationship with their generalist division. Third, a fellowship training program was established in 1992 that integrated principles of academic general pediatrics and hospitalism. Fourth, career development in education, research, and, more recently, quality improvement is fostered.
In summary, the faculty of an established pediatric hospitalist program have diverse and unique clinical, leadership, and scholarly contributions to the academic mission of the department. In order to further promote integration, several issues should be addressed, including optimal training, time allocated to nonclinical activities, systems for career development and promotion of hospitalist faculty, and mentorship. Finally, it is important that leaders in pediatric hospital medicine and general pediatrics engage the larger academic community to strengthen the role and contributions of hospitalists in AHSCs.
Acknowledgements
The authors thank the faculty of the Division of Pediatric Medicine, Hospital for Sick Children for participating in the survey and past and present faculty for their contributions to the development of the division.
- ,.Hospitalists in teaching hospitals: opportunities but not without danger.J Gen Intern Med.2004;19:392–393.
- .The hospitalist movement—time to move on.N Engl J Med.2007;25:2627–2629.
- ,,.Characteristics of the pediatric hospitalist workforce: its roles and work environment.Pediatrics.2007;120:33–39.
- .A Canadian perspective on the American hospitalist movement.Arch Int Med.1999;159:1666–1668.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,,,.Current roles and training needs of pediatric hospitalists: a study from the Pediatric Research in Inpatient Settings (PRIS) network.Paper presented at: Pediatric Academic Society Annual Meeting; May2008;Honolulu, HI. E‐PAS2008:6725.4.
- ,.The pediatric hospitalist and interventional radiologist: a model for clinical care in pediatric interventional radiology.J Vasc Interv Radiol.2006;17:1733–1738.
- ,,, et al.Academic general pediatric fellowships: curriculum design and educational goals and objectives.Ambul Pediatr.2007;7:328–339.
- ,,,,.Characteristics and work experiences of hospitalists in the United States.Arch Intern Med.2001;161:851–858.
- ,.Mission critical—integrating clinician‐educators into academic medical centers.N Engl J Med.1999;341:840–843.
- ,,,.Separate and equitable promotion tracks for clinician‐educators.JAMA.2005;294:1101–1103.
- ,,.Creative professional activity: an additional platform for promotion of faculty.Acad Med.2006;81:568–570.
- .Helping hospitalists achieve academic stature.J Hosp Med.2008;3:285–287.
- ,,,.An innovative approach to supporting hospitalist physicians toward academic success.J Hosp Med.2008;3:314–318.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospitalist medicine research.J Hosp Med.2008;3:308–313.
- ,,,,,.Evaluation of a peer‐reviewed career development and compensation program for physicians at an academic health science centre.Pediatrics.2003;111:e26–e31.
- ,,,,.Performance of a career development and compensation program at an academic health science center.Pediatrics.2007;119:e791–e797.
- ,.Implications of the hospitalist movement for academic departments of medicine: lessons from the UCSF experience.Am J Med.1999;106:127–133.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,.Providing after‐hours on‐call clinical coverage in academic health sciences centres: the Hospital for Sick Children experience.CMAJ.2000;163:298–299.
- ,,,,.A home for medically complex children: the role of hospital programs.J Healthc Qual.2008;30:7–15.
- ,,.Comprehensive care for medically complex children: the pediatric nurse practitioner‐hospitalist model of collaborative care.Hosp Pediatr.2009;1:20–23.
- ,,.Pediatric hospitalist medicine: an overview and a perspective from Toronto, Canada.Clin Pediatr (Phila).2008;47:546–548.
The successful integration of hospitalists in academic health science centers (AHSCs) has been identified as one of the most challenging areas for the hospitalist movement.1, 2 This has been based on a concern that many hospitalists lack academic and research skills, lack mentorship, and may have little time to develop academic careers because of the significant time they spend in clinical care.
A recent survey highlighted that the pediatric hospitalist workforce is in its infancy and additional perspectives, such as from hospitalists themselves, are essential for a more complete picture of the current state of pediatric hospital medicine.3 Hospitalists have had a long history in Canada.4 The Hospital for Sick Children, Toronto, Canada, has had a Division of Pediatric Medicine since 1981, with hospitalists, as we now know them, from inception. This provided a rich resource to explore pediatric hospital medicine in the academic context and from hospitalists themselves. The objective of this survey was to explore the characteristics, practice, and perceptions of pediatric hospital medicine in an AHSC. Locally, we hoped the results would inform the division on program development, training, and faculty career development. Externally, the findings could contribute to a body of knowledge on the evolving role of pediatric hospitalists and provide insight into opportunities for better integration into AHSCs.
Methods
Study Design
This was a cross‐sectional survey of pediatricians who attend on the pediatric medicine inpatient unit at the Hospital for Sick Children, Toronto. The study protocol was approved by Quality and Risk Management at The Hospital for Sick Children.
Setting
The Hospital for Sick Children is a tertiary care children's hospital affiliated with the University of Toronto, Toronto, Canada. The total hospital bed capacity including intensive care unit beds and subspecialty beds is 320. It is the only free‐standing pediatric hospital for the greater Toronto area with a catchment population of 5 million people.
A formal division for general pediatrics, Pediatric Medicine, has been in existence since 1981 with hospital‐based pediatricians (who now are known as hospitalists) who attend on the inpatient unit. The pediatric medicine inpatient unit (PMIU) has a 60‐bed capacity on 3 units. At all times, the PMIU is staffed by 4 to 6 inpatient attendings from a total of 20 full‐time and major part‐time pediatricians. According to Wachter's staging of hospital care, the PMIU is at stage IV of IV in development (mandatory care by hospitalist).5 All attending pediatricians are members of the Division of Pediatric Medicine. Pediatric subspecialists do not attend on the PMIU. Physicians attend for a minimum of 4 weeks at a time. General pediatric house staff including fellows, residents (postgraduate year [PGY] 1, PGY3) and medical students are supervised by the attending pediatricians. Other inpatient clinical services provided include an inpatient general medical consultation team, a complex care team for inpatients with chronic complex conditions, and a consultative and collaborative role with the team of interventional radiologists. An outpatient pediatric consultation program exists for hospital follow‐up, general pediatric consultation, and specialized generalist care for specific populations of children.
In addition to the clinical program, research and education programs exist within the division. The division has had an academic general pediatric fellowship program since 1992, with the majority of most recent graduates obtaining academic hospitalist faculty positions. A formal research group and infrastructure for clinical, outcomes‐based research within the division, known as the Pediatric Outcomes Research Team (PORT), exists.
Study Population
All pediatricians who attend on the PMIU and in the Division of Pediatric Medicine, Hospital for Sick Children in 2007 were eligible for recruitment including the 2 eligible study authors.
Survey Instrument
We constructed a 43‐item structured questionnaire that asked about and explored training and employment characteristics; clinical roles and nonclinical roles (teaching, quality, research, leadership); and perceptions of hospital medicine and a career in this field. Several items were modeled after questions administered to program directors in a survey reported by Freed et al.3 The questionnaire was designed to be completed by the respondent on paper.
Questionnaire Administration
From September to December 2007, eligible pediatricians were sent a letter explaining the study and the questionnaire through interhospital mail by the research coordinator. Questionnaires were deidentified and assigned a unique identification number. Only the research coordinator had access to the list that linked the unique identification numbers with names. Confidentiality of responses and anonymity of responses was explicitly stated in the letter explaining the study to pediatricians. Nonrespondents were contacted by the research assistant at 3‐week intervals with personal reminders.
Data Analysis
During the analysis phase, responses remained deidentified. Descriptive statistics using means, medians, and proportions were calculated for survey items. For open‐ended questions, answers from respondents were summarized into key concepts or themes by the 3 study authors. Excerpts from responses were abstracted to highlight themes.
Results
Eighteen of 20 (90%) faculty responded to the questionnaire. The results are presented by the domains of the questionnaire, as follows.
Training and Employment Characteristics
Due to the requirements of the Royal College of Physicians and Surgeons of Canada, all faculty had a minimum of 4 years of pediatric specialty training leading to certification (Table 1). Seven of 18 (39%) had fellowship and graduate training. Nine of 18 (50%) had been on faculty for greater than 5 years.
| Training after medical schools, median years (range) | 4.8 (46) |
| Fellowship trained, number (%) | 7 (39) |
| Fellowship duration, median years (range) | 2.7 (15) |
| Graduate studies, number (%) | 7 (39) |
| Clinical epidemiology | 5 |
| Education | 2 |
| Duration since first academic appointment | |
| Median, years (range) | 5.5 (030) |
| Mean, years (standard deviation) | 9.9 (10.4) |
| >5 years, number (%) | 9 (50) |
| Academic rank, number (%) | |
| Lecturer | 2 (11) |
| Assistant professor | 10 (56) |
| Associate professor | 4 (22) |
| Full professor | 1 (6) |
Hospitalists: Impact and Definition
Seventeen of 18 (94%) faculty felt that hospitalists reduce cost, increase patient satisfaction, and increase quality of care. Three of 18 (17%) felt that hospitalism adversely affects the primary care physicianpatient relationship. All felt that hospitalists can contribute to the academic mission of an AHSC.
Most (17/18) felt that the Society of Hospital Medicine definition of a hospitalist is useful but 13 of 18 (72%) felt that it was important to develop an international consensus‐based definition.
Clinical Roles
All faculty attended on the PMIU. Other clinical activities included: 13 of 18 (72%) inpatient general medical consultation, 9 of 18 (50%) interventional radiology clinical team, 8 of 18 (44%) attended in the pediatric consultation clinic.
The median number of weeks attending on the PMIU was 16 (range, 440 weeks).
Nine of 18 (50%) provided leadership in clinical programs or the care of specific populations of children. This included leadership in healthcare systems: director of PMIU, director of inpatient general medical consultation, interventional radiology comanagement team; and leadership in patient populations: children with chronic complex conditions, cyclic vomiting, cancer/genetic syndromes, obesity, child abuse and neglect, failure to thrive, and vascular tumors.
Nonclinical and Academic Roles
Sixteen (89%) considered their job to include activities in addition to their role of providing patient care (Table 2). This included primary activity in clinical research, education, quality improvement and health policy.
| Area of Activity | n = 18 [number (%)] |
|---|---|
| |
| QI | |
| Participates in QI activity | 12 (67) |
| Participants who lead in QI activity | 4 (33) |
| Education | |
| Teaching | |
| Medical students | |
| Inpatient unit | 18 (100) |
| Small group sessions | 10 (56) |
| Lectures | 15 (83) |
| Residents | |
| Inpatient unit | 17 (94) |
| Lectures | 12 (67) |
| EBM critical appraisal course | 5 (28) |
| General pediatric fellows | 7 (39) |
| CME | 11 (61) |
| Curriculum or program development | 9 (50) |
| Research | |
| Holds appointment with research institute | 12 (66) |
| Peer review publication in past 12 months | 13 (72) |
| Currently holds research grant | 12 (66) |
| Presented abstract at 2007 PAS meeting | 10 (56) |
Hospitalist Medicine as a Career: Perceptions
Fifteen (83%) felt that it was important to establish an annual minimum time allocation to practicing hospital medicine. A median of 11 weeks per year (range, 816 weeks) was felt to be the minimum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a minimum time for clinical practice in hospital medicine were as follows: maintenance of skills, knowledge, and competency; ensuring quality of care; and efficiency of care. One respondent explained that the main reason to have a minimum time for clinical practice was to keep up clinical skills of acute patients, stay aware of and keep up to date of available facilities in the hospital.
Thirteen (72%) felt that it was important to establish an annual maximum time allocation to practicing hospital medicine. A median of 32 weeks per year (range, 2036 weeks) was felt to be the maximum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a maximum time for clinical practice in hospital medicine were: burnout, balance in career, and desire to develop academic career and to complete nonclinical activities. As this respondent described: I think hospital medicine can be very emotionally difficult and is sustainable if provided time off to pursue other goals such as research, education, creative professional service.
Thirteen (72%) intended to continue their career as a hospitalist and 5 (28%) were unsure. Eleven (61%) felt that a job as a hospitalist was a viable long term career, 6 (33%) were unsure, and 1 (5%) felt that it was not viable. When asked what the barriers to establishing hospital medicine as a long‐term career, the major themes that emerged were as follows: burnout, establishing a nonclinical or academic niche, and the system for career advancement in an academic center. This respondent explained: As long as you have another niche (education for me) that helps provide respite, as well as [you need an] opportunity to have protected time for academic endeavours that are necessary to survive in an academic health science centre.
Another respondent described burnout as a barrier: long hours, emotionally draining with very complex patients, feeling stretchedclinical care and teaching and research and admin.
Perceived advantages to a career as a hospitalist included: working in a team, generalist approach to care, stability relative to community practice, intellectually stimulating and rewarding work, growing area and opportunities for scholarship. One respondent outlined the perceived advantages to a generalist approach: diversity of work, become a generalist specialist, teamwork, develop broad perspective on health.
Others described the perceived advantages over community practice: exciting, interesting, job stability, salary and no worries about administration of the business of community office, stable income, holiday leave.
Perceived disadvantages to a career as a hospitalist included: burnout, recognition and respect, and lack of long‐term relationships with patients. One respondent explained: as an emerging field, we have a lot of growing to do. Although our work (both clinical and academic) seem fundamental to the mission of the hospital and university, we may not feel we receive the respect, support, resources, funding allocated to other areas.
Another response to disadvantages of a career as a hospitalist was, burnout, risk of being seen as a perpetual resident.
Discussion
Freed et al.3 recently conducted a survey of U.S. pediatric hospitalist program directors from a diverse range of settings (ie, teaching vs. nonteaching, free‐standing vs. hospital system, children's hospitals vs. non‐children's hospitals).3 These investigators found that the majority of programs had employed hospitalists for less than 5 years (compared with our program, 30 years); employed 1 to 5 hospitalists (compared with our program, 20); and 25% of programs indicated their hospitalists averaged greater than 5 years on the job (compared with our program, average 10 years on the job). Maniscalco et al.6 conducted a survey in 2007 of hospitalists in a similarly diverse range of settings, found that the mean number of years on the job was 6 and found similar clinical and teaching roles. They also found that the need for advanced training in administration, research, education, and quality improvement was high. Further, we were able to examine academic roles and perceptions of hospital medicine as a career in an AHSC at an individual level. This survey, however, was limited by sampling from a single institution.
Almost all faculty identified an area of focus in addition to clinical care. Educational activities occurred at all levels: undergraduate, residency, fellowship, and continuing medical education. Faculty were engaged in research activities. Hospitalists provide care on all inpatient units as a consultant specialist in general medical care. For example, we have designed a collaborative model of care with the interventional radiology team to comanage children who require image‐guided interventions, such as gastrostomy, chest tube, and central venous line insertions.7 One further area that deserves mention is the leadership of hospitalists in outpatient care of children, especially hospital intense populations, in collaboration with their primary care provider. These groups of children are often medically and socially complex, require repeated and intense hospital resources (including diagnostic testing, subspecialty consultation, and hospitalization), and require generalist care to manage them from a family centered perspective.
A significant proportion of the faculty in this survey acquired advanced academic training. The formal training of hospitalist physicians is in its infancy. A recent work documenting the domains of training for academic general pediatric fellowship in leadership, education, and research seems to be most appropriate for the nonclinical foundation for pediatric academic hospitalists.8
Few studies have examined academic hospitalists' perceptions on the minimum and maximum time per year suitable for clinical service. This undoubtedly will vary depending on the institution, program and financial structure, patient load and complexity, call requirements, academic commitments, and stage of development. Faculty surveyed in this study felt a range of 11 to 32 weeks of clinical inpatient attending per year was ideal. This is consistent with the expert panel recommendations of the Society of Hospital Medicine. What may be equally important to determine is the maximum number of continuous weeks attending on the PMIU.
There have been 3 full‐time faculty who have left the division (all to community hospitalbased generalist practices with academic affiliations) and 1 who has changed from a full‐time to a part‐time role in the division. Most faculty surveyed intended to continue their career as a hospitalist. They identified several positive and satisfying aspects to the career, including relationships with peers, stable salary, numerous opportunities for scholarly work in a young field, and generalist care. Hoff et al.9 described a national US survey of hospitalists in all adult medicine settings that examined personal characteristics, and work‐related attitudes. Similarly, they found that hospital medicine was a source of positive social and professional work experiences related to interactions with peers, patients and families, and coworkers. In the current study, perceived disadvantages to a hospitalist career were burnout, lack of recognition and respect, and lack of long‐term relationships with patients. Hoff et al.9 noted that 37% were burnt out or at risk of burnout, which is less than in the fields of critical care medicine and emergency medicine.
The identified barriers to establishing a career were related to development of an academic focus, balance between clinical and nonclinical time, and the system for career advancement. Few other studies have examined these career issues for hospitalists in the academic setting. Several authors have discussed career issues for clinician‐educators in the US,10, 11 including metrics for promotion and recognition by institutions. Alternate methods have been proposed for promotion, aside from research and education, such as creative professional activity or clinical excellence.12 The developing field of hospital medicine faces similar challenges as individual hospitalists and the specialty itself works to align with the academic mission.1315
The division and hospitalist program have evolved over more than 2 decades to fulfill strategic goals and respond to changing external factors (Table 3). Contextual factors that have supported this evolution and that may be unique to our academic environment merit mention. First, the departments' physicians work in a within a single‐payer universal healthcare system that in some ways is similar to a single‐payer health maintenance organization. The ultimate governance is provided by the provincial Ministry of Health, which is funded through taxation. Second, through an alternative funding plan (AFP) with the provincial government, block funding is providing in lieu of fee for service clinical care that funds physician salaries for clinical work, research, education, and administrative activities.16 Third, the department has a career development compensation program (CDCP) that has an explicit job activity profile which is aligned with the role of hospitaliststhe clinician‐specialist profilewho have a predominate commitment to provide, advance, and promote excellence in clinical care with contributions to education and/or research.16 The compensation and evaluation process for hospitalists is the same as other members in the department. While further refinement of this system is ongoing, this program has demonstrated a support for all roles (ie, clinical, education, and research).17
| Date | Area | Pressure Point | Change |
|---|---|---|---|
| 1981 | Clinical education research | Department priority for academic generalism | Creation of Division of General Pediatrics (now Pediatric Medicine); full‐time hospital‐based pediatricians attending on inpatient unit |
| 1991 | Education | Division priority to foster academic generalism and train future generation of academic generalists | Creation of academic general pediatrics fellowship program |
| 1992 | Research | Division priority to foster clinical, outcomes‐based research | Creation of formal divisional research infrastructure with foundation support for an epidemiologic, outcomes‐based research platform; pediatric outcomes research team (PORT) |
| 1995 | Clinical care | Province‐wide reduction in resident duty hours; division priority to raise the bar for clinical and teaching excellence in hospitalist‐and community‐based pediatrics; need for a financially viable and cost‐effective model for staffing attending pediatricians on inpatient unit | Reorganization of inpatient unit; higher proportion of attending pediatricians who are full‐time, hospital‐based; creation of a staff‐only hospitalist unit19; creation of a section of community pediatrics (2001) |
| 1996 | Clinical care education faculty development | Need to limit attending hospitalists after‐hours clinical care to ensure balance and academic productivity; need for a system of after‐hours physician coverage for inpatient care that is sustainable and financially viable; need for funding sources for academic general pediatrics fellowship | Creation of a clinical departmental fellowship program to fund after hours clinical coverage with qualified pediatricians seeking additional fellowship training20 |
| 1998 | Faculty career development | Need to value and reward all academic contributions, such as the hospitalist role, through an explicit job activity profile within the department16 | Implementation of a career development and compensation program with the clinician specialist role whose primary contributions are to excellence in clinical care |
| 1999 | Clinical care | Expansion of hospital interventional radiology program and need for high quality collaborative care | Comanagement model with hospitalist‐radiologist team7 |
| 20068 | Clinical care research | Division and institution priority to provide high‐quality care for children with complex care health issues and foster a research program21 | Creation of formalized hospitalist complex care program with inpatient and outpatient care22; research support for complex care |
| 2007 | Clinical care | Refinement of inpatient unit organization to improve efficiency of care; increase number of trainees23 | Reorganization of inpatient units to geographic allocation of patients by attending physician; addition of trainees to staff‐only hospitalist unit |
Furthermore, several divisional factors have contributed to the viability of hospitalism within our generalist division. First, hospitalists were integrated into, rather than segregated from the division. Second, hospitalists have the opportunity to engage in diverse clinical activities. Wachter and Goldman18 advocate for hospitalist participation in outpatient care to provide variety and to cement their relationship with their generalist division. Third, a fellowship training program was established in 1992 that integrated principles of academic general pediatrics and hospitalism. Fourth, career development in education, research, and, more recently, quality improvement is fostered.
In summary, the faculty of an established pediatric hospitalist program have diverse and unique clinical, leadership, and scholarly contributions to the academic mission of the department. In order to further promote integration, several issues should be addressed, including optimal training, time allocated to nonclinical activities, systems for career development and promotion of hospitalist faculty, and mentorship. Finally, it is important that leaders in pediatric hospital medicine and general pediatrics engage the larger academic community to strengthen the role and contributions of hospitalists in AHSCs.
Acknowledgements
The authors thank the faculty of the Division of Pediatric Medicine, Hospital for Sick Children for participating in the survey and past and present faculty for their contributions to the development of the division.
The successful integration of hospitalists in academic health science centers (AHSCs) has been identified as one of the most challenging areas for the hospitalist movement.1, 2 This has been based on a concern that many hospitalists lack academic and research skills, lack mentorship, and may have little time to develop academic careers because of the significant time they spend in clinical care.
A recent survey highlighted that the pediatric hospitalist workforce is in its infancy and additional perspectives, such as from hospitalists themselves, are essential for a more complete picture of the current state of pediatric hospital medicine.3 Hospitalists have had a long history in Canada.4 The Hospital for Sick Children, Toronto, Canada, has had a Division of Pediatric Medicine since 1981, with hospitalists, as we now know them, from inception. This provided a rich resource to explore pediatric hospital medicine in the academic context and from hospitalists themselves. The objective of this survey was to explore the characteristics, practice, and perceptions of pediatric hospital medicine in an AHSC. Locally, we hoped the results would inform the division on program development, training, and faculty career development. Externally, the findings could contribute to a body of knowledge on the evolving role of pediatric hospitalists and provide insight into opportunities for better integration into AHSCs.
Methods
Study Design
This was a cross‐sectional survey of pediatricians who attend on the pediatric medicine inpatient unit at the Hospital for Sick Children, Toronto. The study protocol was approved by Quality and Risk Management at The Hospital for Sick Children.
Setting
The Hospital for Sick Children is a tertiary care children's hospital affiliated with the University of Toronto, Toronto, Canada. The total hospital bed capacity including intensive care unit beds and subspecialty beds is 320. It is the only free‐standing pediatric hospital for the greater Toronto area with a catchment population of 5 million people.
A formal division for general pediatrics, Pediatric Medicine, has been in existence since 1981 with hospital‐based pediatricians (who now are known as hospitalists) who attend on the inpatient unit. The pediatric medicine inpatient unit (PMIU) has a 60‐bed capacity on 3 units. At all times, the PMIU is staffed by 4 to 6 inpatient attendings from a total of 20 full‐time and major part‐time pediatricians. According to Wachter's staging of hospital care, the PMIU is at stage IV of IV in development (mandatory care by hospitalist).5 All attending pediatricians are members of the Division of Pediatric Medicine. Pediatric subspecialists do not attend on the PMIU. Physicians attend for a minimum of 4 weeks at a time. General pediatric house staff including fellows, residents (postgraduate year [PGY] 1, PGY3) and medical students are supervised by the attending pediatricians. Other inpatient clinical services provided include an inpatient general medical consultation team, a complex care team for inpatients with chronic complex conditions, and a consultative and collaborative role with the team of interventional radiologists. An outpatient pediatric consultation program exists for hospital follow‐up, general pediatric consultation, and specialized generalist care for specific populations of children.
In addition to the clinical program, research and education programs exist within the division. The division has had an academic general pediatric fellowship program since 1992, with the majority of most recent graduates obtaining academic hospitalist faculty positions. A formal research group and infrastructure for clinical, outcomes‐based research within the division, known as the Pediatric Outcomes Research Team (PORT), exists.
Study Population
All pediatricians who attend on the PMIU and in the Division of Pediatric Medicine, Hospital for Sick Children in 2007 were eligible for recruitment including the 2 eligible study authors.
Survey Instrument
We constructed a 43‐item structured questionnaire that asked about and explored training and employment characteristics; clinical roles and nonclinical roles (teaching, quality, research, leadership); and perceptions of hospital medicine and a career in this field. Several items were modeled after questions administered to program directors in a survey reported by Freed et al.3 The questionnaire was designed to be completed by the respondent on paper.
Questionnaire Administration
From September to December 2007, eligible pediatricians were sent a letter explaining the study and the questionnaire through interhospital mail by the research coordinator. Questionnaires were deidentified and assigned a unique identification number. Only the research coordinator had access to the list that linked the unique identification numbers with names. Confidentiality of responses and anonymity of responses was explicitly stated in the letter explaining the study to pediatricians. Nonrespondents were contacted by the research assistant at 3‐week intervals with personal reminders.
Data Analysis
During the analysis phase, responses remained deidentified. Descriptive statistics using means, medians, and proportions were calculated for survey items. For open‐ended questions, answers from respondents were summarized into key concepts or themes by the 3 study authors. Excerpts from responses were abstracted to highlight themes.
Results
Eighteen of 20 (90%) faculty responded to the questionnaire. The results are presented by the domains of the questionnaire, as follows.
Training and Employment Characteristics
Due to the requirements of the Royal College of Physicians and Surgeons of Canada, all faculty had a minimum of 4 years of pediatric specialty training leading to certification (Table 1). Seven of 18 (39%) had fellowship and graduate training. Nine of 18 (50%) had been on faculty for greater than 5 years.
| Training after medical schools, median years (range) | 4.8 (46) |
| Fellowship trained, number (%) | 7 (39) |
| Fellowship duration, median years (range) | 2.7 (15) |
| Graduate studies, number (%) | 7 (39) |
| Clinical epidemiology | 5 |
| Education | 2 |
| Duration since first academic appointment | |
| Median, years (range) | 5.5 (030) |
| Mean, years (standard deviation) | 9.9 (10.4) |
| >5 years, number (%) | 9 (50) |
| Academic rank, number (%) | |
| Lecturer | 2 (11) |
| Assistant professor | 10 (56) |
| Associate professor | 4 (22) |
| Full professor | 1 (6) |
Hospitalists: Impact and Definition
Seventeen of 18 (94%) faculty felt that hospitalists reduce cost, increase patient satisfaction, and increase quality of care. Three of 18 (17%) felt that hospitalism adversely affects the primary care physicianpatient relationship. All felt that hospitalists can contribute to the academic mission of an AHSC.
Most (17/18) felt that the Society of Hospital Medicine definition of a hospitalist is useful but 13 of 18 (72%) felt that it was important to develop an international consensus‐based definition.
Clinical Roles
All faculty attended on the PMIU. Other clinical activities included: 13 of 18 (72%) inpatient general medical consultation, 9 of 18 (50%) interventional radiology clinical team, 8 of 18 (44%) attended in the pediatric consultation clinic.
The median number of weeks attending on the PMIU was 16 (range, 440 weeks).
Nine of 18 (50%) provided leadership in clinical programs or the care of specific populations of children. This included leadership in healthcare systems: director of PMIU, director of inpatient general medical consultation, interventional radiology comanagement team; and leadership in patient populations: children with chronic complex conditions, cyclic vomiting, cancer/genetic syndromes, obesity, child abuse and neglect, failure to thrive, and vascular tumors.
Nonclinical and Academic Roles
Sixteen (89%) considered their job to include activities in addition to their role of providing patient care (Table 2). This included primary activity in clinical research, education, quality improvement and health policy.
| Area of Activity | n = 18 [number (%)] |
|---|---|
| |
| QI | |
| Participates in QI activity | 12 (67) |
| Participants who lead in QI activity | 4 (33) |
| Education | |
| Teaching | |
| Medical students | |
| Inpatient unit | 18 (100) |
| Small group sessions | 10 (56) |
| Lectures | 15 (83) |
| Residents | |
| Inpatient unit | 17 (94) |
| Lectures | 12 (67) |
| EBM critical appraisal course | 5 (28) |
| General pediatric fellows | 7 (39) |
| CME | 11 (61) |
| Curriculum or program development | 9 (50) |
| Research | |
| Holds appointment with research institute | 12 (66) |
| Peer review publication in past 12 months | 13 (72) |
| Currently holds research grant | 12 (66) |
| Presented abstract at 2007 PAS meeting | 10 (56) |
Hospitalist Medicine as a Career: Perceptions
Fifteen (83%) felt that it was important to establish an annual minimum time allocation to practicing hospital medicine. A median of 11 weeks per year (range, 816 weeks) was felt to be the minimum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a minimum time for clinical practice in hospital medicine were as follows: maintenance of skills, knowledge, and competency; ensuring quality of care; and efficiency of care. One respondent explained that the main reason to have a minimum time for clinical practice was to keep up clinical skills of acute patients, stay aware of and keep up to date of available facilities in the hospital.
Thirteen (72%) felt that it was important to establish an annual maximum time allocation to practicing hospital medicine. A median of 32 weeks per year (range, 2036 weeks) was felt to be the maximum time that should be allocated to practicing hospital medicine. The major themes related to the need to establish a maximum time for clinical practice in hospital medicine were: burnout, balance in career, and desire to develop academic career and to complete nonclinical activities. As this respondent described: I think hospital medicine can be very emotionally difficult and is sustainable if provided time off to pursue other goals such as research, education, creative professional service.
Thirteen (72%) intended to continue their career as a hospitalist and 5 (28%) were unsure. Eleven (61%) felt that a job as a hospitalist was a viable long term career, 6 (33%) were unsure, and 1 (5%) felt that it was not viable. When asked what the barriers to establishing hospital medicine as a long‐term career, the major themes that emerged were as follows: burnout, establishing a nonclinical or academic niche, and the system for career advancement in an academic center. This respondent explained: As long as you have another niche (education for me) that helps provide respite, as well as [you need an] opportunity to have protected time for academic endeavours that are necessary to survive in an academic health science centre.
Another respondent described burnout as a barrier: long hours, emotionally draining with very complex patients, feeling stretchedclinical care and teaching and research and admin.
Perceived advantages to a career as a hospitalist included: working in a team, generalist approach to care, stability relative to community practice, intellectually stimulating and rewarding work, growing area and opportunities for scholarship. One respondent outlined the perceived advantages to a generalist approach: diversity of work, become a generalist specialist, teamwork, develop broad perspective on health.
Others described the perceived advantages over community practice: exciting, interesting, job stability, salary and no worries about administration of the business of community office, stable income, holiday leave.
Perceived disadvantages to a career as a hospitalist included: burnout, recognition and respect, and lack of long‐term relationships with patients. One respondent explained: as an emerging field, we have a lot of growing to do. Although our work (both clinical and academic) seem fundamental to the mission of the hospital and university, we may not feel we receive the respect, support, resources, funding allocated to other areas.
Another response to disadvantages of a career as a hospitalist was, burnout, risk of being seen as a perpetual resident.
Discussion
Freed et al.3 recently conducted a survey of U.S. pediatric hospitalist program directors from a diverse range of settings (ie, teaching vs. nonteaching, free‐standing vs. hospital system, children's hospitals vs. non‐children's hospitals).3 These investigators found that the majority of programs had employed hospitalists for less than 5 years (compared with our program, 30 years); employed 1 to 5 hospitalists (compared with our program, 20); and 25% of programs indicated their hospitalists averaged greater than 5 years on the job (compared with our program, average 10 years on the job). Maniscalco et al.6 conducted a survey in 2007 of hospitalists in a similarly diverse range of settings, found that the mean number of years on the job was 6 and found similar clinical and teaching roles. They also found that the need for advanced training in administration, research, education, and quality improvement was high. Further, we were able to examine academic roles and perceptions of hospital medicine as a career in an AHSC at an individual level. This survey, however, was limited by sampling from a single institution.
Almost all faculty identified an area of focus in addition to clinical care. Educational activities occurred at all levels: undergraduate, residency, fellowship, and continuing medical education. Faculty were engaged in research activities. Hospitalists provide care on all inpatient units as a consultant specialist in general medical care. For example, we have designed a collaborative model of care with the interventional radiology team to comanage children who require image‐guided interventions, such as gastrostomy, chest tube, and central venous line insertions.7 One further area that deserves mention is the leadership of hospitalists in outpatient care of children, especially hospital intense populations, in collaboration with their primary care provider. These groups of children are often medically and socially complex, require repeated and intense hospital resources (including diagnostic testing, subspecialty consultation, and hospitalization), and require generalist care to manage them from a family centered perspective.
A significant proportion of the faculty in this survey acquired advanced academic training. The formal training of hospitalist physicians is in its infancy. A recent work documenting the domains of training for academic general pediatric fellowship in leadership, education, and research seems to be most appropriate for the nonclinical foundation for pediatric academic hospitalists.8
Few studies have examined academic hospitalists' perceptions on the minimum and maximum time per year suitable for clinical service. This undoubtedly will vary depending on the institution, program and financial structure, patient load and complexity, call requirements, academic commitments, and stage of development. Faculty surveyed in this study felt a range of 11 to 32 weeks of clinical inpatient attending per year was ideal. This is consistent with the expert panel recommendations of the Society of Hospital Medicine. What may be equally important to determine is the maximum number of continuous weeks attending on the PMIU.
There have been 3 full‐time faculty who have left the division (all to community hospitalbased generalist practices with academic affiliations) and 1 who has changed from a full‐time to a part‐time role in the division. Most faculty surveyed intended to continue their career as a hospitalist. They identified several positive and satisfying aspects to the career, including relationships with peers, stable salary, numerous opportunities for scholarly work in a young field, and generalist care. Hoff et al.9 described a national US survey of hospitalists in all adult medicine settings that examined personal characteristics, and work‐related attitudes. Similarly, they found that hospital medicine was a source of positive social and professional work experiences related to interactions with peers, patients and families, and coworkers. In the current study, perceived disadvantages to a hospitalist career were burnout, lack of recognition and respect, and lack of long‐term relationships with patients. Hoff et al.9 noted that 37% were burnt out or at risk of burnout, which is less than in the fields of critical care medicine and emergency medicine.
The identified barriers to establishing a career were related to development of an academic focus, balance between clinical and nonclinical time, and the system for career advancement. Few other studies have examined these career issues for hospitalists in the academic setting. Several authors have discussed career issues for clinician‐educators in the US,10, 11 including metrics for promotion and recognition by institutions. Alternate methods have been proposed for promotion, aside from research and education, such as creative professional activity or clinical excellence.12 The developing field of hospital medicine faces similar challenges as individual hospitalists and the specialty itself works to align with the academic mission.1315
The division and hospitalist program have evolved over more than 2 decades to fulfill strategic goals and respond to changing external factors (Table 3). Contextual factors that have supported this evolution and that may be unique to our academic environment merit mention. First, the departments' physicians work in a within a single‐payer universal healthcare system that in some ways is similar to a single‐payer health maintenance organization. The ultimate governance is provided by the provincial Ministry of Health, which is funded through taxation. Second, through an alternative funding plan (AFP) with the provincial government, block funding is providing in lieu of fee for service clinical care that funds physician salaries for clinical work, research, education, and administrative activities.16 Third, the department has a career development compensation program (CDCP) that has an explicit job activity profile which is aligned with the role of hospitaliststhe clinician‐specialist profilewho have a predominate commitment to provide, advance, and promote excellence in clinical care with contributions to education and/or research.16 The compensation and evaluation process for hospitalists is the same as other members in the department. While further refinement of this system is ongoing, this program has demonstrated a support for all roles (ie, clinical, education, and research).17
| Date | Area | Pressure Point | Change |
|---|---|---|---|
| 1981 | Clinical education research | Department priority for academic generalism | Creation of Division of General Pediatrics (now Pediatric Medicine); full‐time hospital‐based pediatricians attending on inpatient unit |
| 1991 | Education | Division priority to foster academic generalism and train future generation of academic generalists | Creation of academic general pediatrics fellowship program |
| 1992 | Research | Division priority to foster clinical, outcomes‐based research | Creation of formal divisional research infrastructure with foundation support for an epidemiologic, outcomes‐based research platform; pediatric outcomes research team (PORT) |
| 1995 | Clinical care | Province‐wide reduction in resident duty hours; division priority to raise the bar for clinical and teaching excellence in hospitalist‐and community‐based pediatrics; need for a financially viable and cost‐effective model for staffing attending pediatricians on inpatient unit | Reorganization of inpatient unit; higher proportion of attending pediatricians who are full‐time, hospital‐based; creation of a staff‐only hospitalist unit19; creation of a section of community pediatrics (2001) |
| 1996 | Clinical care education faculty development | Need to limit attending hospitalists after‐hours clinical care to ensure balance and academic productivity; need for a system of after‐hours physician coverage for inpatient care that is sustainable and financially viable; need for funding sources for academic general pediatrics fellowship | Creation of a clinical departmental fellowship program to fund after hours clinical coverage with qualified pediatricians seeking additional fellowship training20 |
| 1998 | Faculty career development | Need to value and reward all academic contributions, such as the hospitalist role, through an explicit job activity profile within the department16 | Implementation of a career development and compensation program with the clinician specialist role whose primary contributions are to excellence in clinical care |
| 1999 | Clinical care | Expansion of hospital interventional radiology program and need for high quality collaborative care | Comanagement model with hospitalist‐radiologist team7 |
| 20068 | Clinical care research | Division and institution priority to provide high‐quality care for children with complex care health issues and foster a research program21 | Creation of formalized hospitalist complex care program with inpatient and outpatient care22; research support for complex care |
| 2007 | Clinical care | Refinement of inpatient unit organization to improve efficiency of care; increase number of trainees23 | Reorganization of inpatient units to geographic allocation of patients by attending physician; addition of trainees to staff‐only hospitalist unit |
Furthermore, several divisional factors have contributed to the viability of hospitalism within our generalist division. First, hospitalists were integrated into, rather than segregated from the division. Second, hospitalists have the opportunity to engage in diverse clinical activities. Wachter and Goldman18 advocate for hospitalist participation in outpatient care to provide variety and to cement their relationship with their generalist division. Third, a fellowship training program was established in 1992 that integrated principles of academic general pediatrics and hospitalism. Fourth, career development in education, research, and, more recently, quality improvement is fostered.
In summary, the faculty of an established pediatric hospitalist program have diverse and unique clinical, leadership, and scholarly contributions to the academic mission of the department. In order to further promote integration, several issues should be addressed, including optimal training, time allocated to nonclinical activities, systems for career development and promotion of hospitalist faculty, and mentorship. Finally, it is important that leaders in pediatric hospital medicine and general pediatrics engage the larger academic community to strengthen the role and contributions of hospitalists in AHSCs.
Acknowledgements
The authors thank the faculty of the Division of Pediatric Medicine, Hospital for Sick Children for participating in the survey and past and present faculty for their contributions to the development of the division.
- ,.Hospitalists in teaching hospitals: opportunities but not without danger.J Gen Intern Med.2004;19:392–393.
- .The hospitalist movement—time to move on.N Engl J Med.2007;25:2627–2629.
- ,,.Characteristics of the pediatric hospitalist workforce: its roles and work environment.Pediatrics.2007;120:33–39.
- .A Canadian perspective on the American hospitalist movement.Arch Int Med.1999;159:1666–1668.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,,,.Current roles and training needs of pediatric hospitalists: a study from the Pediatric Research in Inpatient Settings (PRIS) network.Paper presented at: Pediatric Academic Society Annual Meeting; May2008;Honolulu, HI. E‐PAS2008:6725.4.
- ,.The pediatric hospitalist and interventional radiologist: a model for clinical care in pediatric interventional radiology.J Vasc Interv Radiol.2006;17:1733–1738.
- ,,, et al.Academic general pediatric fellowships: curriculum design and educational goals and objectives.Ambul Pediatr.2007;7:328–339.
- ,,,,.Characteristics and work experiences of hospitalists in the United States.Arch Intern Med.2001;161:851–858.
- ,.Mission critical—integrating clinician‐educators into academic medical centers.N Engl J Med.1999;341:840–843.
- ,,,.Separate and equitable promotion tracks for clinician‐educators.JAMA.2005;294:1101–1103.
- ,,.Creative professional activity: an additional platform for promotion of faculty.Acad Med.2006;81:568–570.
- .Helping hospitalists achieve academic stature.J Hosp Med.2008;3:285–287.
- ,,,.An innovative approach to supporting hospitalist physicians toward academic success.J Hosp Med.2008;3:314–318.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospitalist medicine research.J Hosp Med.2008;3:308–313.
- ,,,,,.Evaluation of a peer‐reviewed career development and compensation program for physicians at an academic health science centre.Pediatrics.2003;111:e26–e31.
- ,,,,.Performance of a career development and compensation program at an academic health science center.Pediatrics.2007;119:e791–e797.
- ,.Implications of the hospitalist movement for academic departments of medicine: lessons from the UCSF experience.Am J Med.1999;106:127–133.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,.Providing after‐hours on‐call clinical coverage in academic health sciences centres: the Hospital for Sick Children experience.CMAJ.2000;163:298–299.
- ,,,,.A home for medically complex children: the role of hospital programs.J Healthc Qual.2008;30:7–15.
- ,,.Comprehensive care for medically complex children: the pediatric nurse practitioner‐hospitalist model of collaborative care.Hosp Pediatr.2009;1:20–23.
- ,,.Pediatric hospitalist medicine: an overview and a perspective from Toronto, Canada.Clin Pediatr (Phila).2008;47:546–548.
- ,.Hospitalists in teaching hospitals: opportunities but not without danger.J Gen Intern Med.2004;19:392–393.
- .The hospitalist movement—time to move on.N Engl J Med.2007;25:2627–2629.
- ,,.Characteristics of the pediatric hospitalist workforce: its roles and work environment.Pediatrics.2007;120:33–39.
- .A Canadian perspective on the American hospitalist movement.Arch Int Med.1999;159:1666–1668.
- .An introduction to the hospitalist model.Ann Intern Med.1999;130:338–342.
- ,,,,.Current roles and training needs of pediatric hospitalists: a study from the Pediatric Research in Inpatient Settings (PRIS) network.Paper presented at: Pediatric Academic Society Annual Meeting; May2008;Honolulu, HI. E‐PAS2008:6725.4.
- ,.The pediatric hospitalist and interventional radiologist: a model for clinical care in pediatric interventional radiology.J Vasc Interv Radiol.2006;17:1733–1738.
- ,,, et al.Academic general pediatric fellowships: curriculum design and educational goals and objectives.Ambul Pediatr.2007;7:328–339.
- ,,,,.Characteristics and work experiences of hospitalists in the United States.Arch Intern Med.2001;161:851–858.
- ,.Mission critical—integrating clinician‐educators into academic medical centers.N Engl J Med.1999;341:840–843.
- ,,,.Separate and equitable promotion tracks for clinician‐educators.JAMA.2005;294:1101–1103.
- ,,.Creative professional activity: an additional platform for promotion of faculty.Acad Med.2006;81:568–570.
- .Helping hospitalists achieve academic stature.J Hosp Med.2008;3:285–287.
- ,,,.An innovative approach to supporting hospitalist physicians toward academic success.J Hosp Med.2008;3:314–318.
- ,,,.The University of Michigan Specialist‐Hospitalist Allied Research Program: jumpstarting hospitalist medicine research.J Hosp Med.2008;3:308–313.
- ,,,,,.Evaluation of a peer‐reviewed career development and compensation program for physicians at an academic health science centre.Pediatrics.2003;111:e26–e31.
- ,,,,.Performance of a career development and compensation program at an academic health science center.Pediatrics.2007;119:e791–e797.
- ,.Implications of the hospitalist movement for academic departments of medicine: lessons from the UCSF experience.Am J Med.1999;106:127–133.
- ,,,.Evaluation of a staff‐only hospitalist system in a tertiary care, academic children's hospital.Pediatrics.2004;114:1545–1549.
- ,.Providing after‐hours on‐call clinical coverage in academic health sciences centres: the Hospital for Sick Children experience.CMAJ.2000;163:298–299.
- ,,,,.A home for medically complex children: the role of hospital programs.J Healthc Qual.2008;30:7–15.
- ,,.Comprehensive care for medically complex children: the pediatric nurse practitioner‐hospitalist model of collaborative care.Hosp Pediatr.2009;1:20–23.
- ,,.Pediatric hospitalist medicine: an overview and a perspective from Toronto, Canada.Clin Pediatr (Phila).2008;47:546–548.
Copyright © 2010 Society of Hospital Medicine
Treatment of Lactic Acidosis
Lactic acidosis (LA) is common in hospitalized patients and is associated with a high mortality.1, 2 Commonly, it is defined as a lactic acid concentration greater than 5 mmol/L with a pH less than 7.35.3 There are no evidence‐based guidelines for the treatment of LA despite progress in our understanding of its pathophysiology.36 This is not surprising, given the uncertainty regarding the impact of LA itself on clinical outcomes. In this regard, it is interesting to note that, despite its well‐recognized role as a marker of tissue hypoxia, lactate accumulation appears to have beneficial effects and may function as an adaptive mechanism. This raises the possibility that therapy directed at altering this adaptation may be detrimental. Pursuing correction of the pH in LA has been shown to have untoward physiologic effects. These and other ambiguities in the pathophysiology and treatment of LA are the focus of this review.
Lactate Metabolism
The body produces approximately 1400 mmol of lactate daily.7 Lactate is derived from the metabolism of pyruvate through an anaerobic reaction that occurs in all tissues (Figure 1). The liver is the primary site of lactate clearance and can metabolize up to 100 mmol per hour under normal conditions.8 There, lactate is converted to glucose to serve as an energy source during periods of hypoxia (Figure 2).9
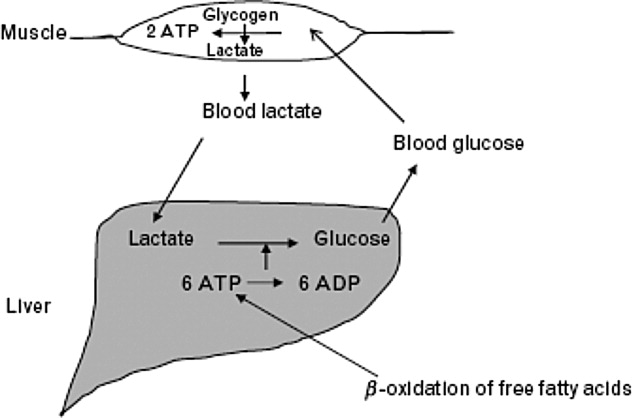
Approximately 20% to 30% of the daily lactate load is metabolized by the kidneys.10, 11 Renal clearance is increased in acidosis12 and is maintained even in the presence of low renal perfusion.10, 12, 13 Renal lactate clearance is primarily through metabolism and not excretion.10, 14
LA Subtypes
Generally, lactic acid accumulation results from excess lactic acid production and not from reduced clearance.15 In cases of fulminant liver failure, it is due to a combination of decreased clearance and tissue hypoxia.16 In the setting of tissue hypoxia, an impairment of mitochondrial oxidative capacity results in the accumulation of pyruvate and generation of lactate. Lactic acid accumulation through this mechanism has historically been described as Type A LA.7 Hence, in critically ill patients lactate has traditionally been viewed as a marker of tissue hypoxia.15, 1721 Hyperlactatemia without tissue hypoxia has been referred to as type B LA. This is seen in a variety of circumstances. In sepsis, for example, several studies have shown lactic acid accumulation, despite adequate oxygen delivery.2224
Hyperlactatemia may also occur in cases of pure mitochondrial dysfunction, which can be induced by commonly prescribed medications such as the biguanides, nucleoside analog reverse‐transcriptase inhibitors (NRTIs), and linezolid.2527 Alternatively, lactate generation from metabolism of agents such as propylene glycol is possible. Finally, excessive lactate generation may occur following stress due to altered carbohydrate metabolism, or with respiratory alkalosis.2831
Lactate: A Metabolic Adaptation
Lactate was traditionally considered only as a marker of tissue hypoxia and anaerobic metabolism.17 This is certainly the case in situations of poor perfusion such as cardiogenic,15, 18 vasopressor‐resistant,19 or hypovolemic shock.20, 21
Alternative explanations for lactic acid accumulation, without tissue hypoperfusion, include catecholamine‐induced alterations in glycolysis,32, 33 mitochondrial disturbances,3436 and increased pyruvate production combined with increased glucose entry into cells.24, 37 In addition, the activity of an enzyme regulating lactate metabolism, pyruvate dehydrogenase kinase, increases in sepsis.38 This enzyme inactivates the pyruvate dehydrogenase (PDH) complex, which metabolizes pyruvate. Pyruvate and lactate may accumulate as a result. These changes partly explain the generation of LA in sepsis, independent of any effect of diminished tissue perfusion.
Recognizing the body's tendency toward homeostasis, it is appealing to speculate that lactate accumulation is adaptive.9 A number of findings support this. For example, lactate may act to shuttle energy between organs, or between cell types in the same organ. The astrocyteneuron lactate shuttle and the spermatogenic lactate shuttle are 2 examples of lactate's valuable effects on cellular metabolism.39 In the astrocyteneuron lactate shuttle, astrocytes support the increased metabolic demands of neurons through lactic acid production.40 Specifically, the neurotransmitter glutamate is released by the neurons and taken up by the astrocytes. Astrocytes produce lactate, which then moves back to the neuron to be used as an energy source. Glutamine, also released by the astrocytes, leads to the regeneration of glutamate and the potential to restart the cycle.39
Animal and human studies have suggested that, in periods of stress, lactate is the preferential energy substrate in the brain.4144 The usefulness of increased lactate production routinely seen in sepsis may thus represent multiple adaptive processes aimed primarily at improving the delivery of energy substrates. Thus, therapeutic strategies aimed specifically at lowering lactic acid levels may prove to have deleterious effects on cellular metabolism.
Impact of LA on Morbidity and Mortality
The poor prognosis in patients with LA is well recognized.2, 4548 For example, in a study of 126 patients with various causes of LA, the median survival was 38.5 hours and 30‐day survival was 17%.2
Studies have revealed that LA with low pH is associated with adverse effects on the cardiovascular system, particularly a decrease in cardiac contractility.49, 50 This effect is particularly prominent with a pH below 7.20. In contrast, acidosis in animal models has been shown to limit myocardial infarct size after reperfusion.51, 52 Variable effects of LA on cell death have been found. A worsening of apoptosis in myocytes has been noted;53 alternatively, protection from hypoxic injury in hepatocytes and myocardium has been observed.52, 54 Thus, although LA is associated with poor outcomes in human studies,2, 4547 it is still unclear to what extent lactic acid accumulation is a marker of severe illness, an independent effector of pathology, or a mechanism with the potential to serve a protective role.
Available data indicate that lactate itself is not harmful. Studies on infusion of lactate solutions to postoperative patients was shown to be safe.55 Also, the fact that lactate generation in states of respiratory alkalosis, stress, or altered carbohydrate metabolism without sepsis is not associated with worse outcomes supports the fact that lactic acid alone may not be maladaptive.2831
Similarly, low pH is not necessarily maladaptive. In the postictal state,56 diabetic ketoacidosis,57 spontaneous respiratory acidosis,58 or permissive hypercapnia,59 low blood pH is not deleterious.
In summary, LA is associated with poor outcomes, and indirect evidence suggests that it is the underlying causative condition rather than the low pH or the lactate that is responsible for the dire outcomes.
Treatment of LA with Sodium Bicarbonate
Since excessive lactic acid generation is accompanied by consumption of plasma bicarbonate and a fall in plasma pH, sodium bicarbonate has been long proposed as a treatment for LA. While theoretically appealing, this strategy has not been validated by studies in animals or humans. Indeed, bicarbonate administration in LA often has been shown to be detrimental.60, 61 The adverse effects of bicarbonate administration in LA, while initially paradoxical, have a number of possible explanations.
First, bicarbonate administration can induce a reduction in intracellular pH.60, 62, 63 The mechanism involves bicarbonate's effect to increase carbon dioxide (CO2) generation through mass action effect. Because the cell membrane is more permeable to CO2 than to bicarbonate, intracellular pH falls.64, 65 In sepsis, this intracellular/extracellular pH discrepancy may be more pronounced due to alterations in blood flow.66 Other reports on outcomes of intracellular pH with bicarbonate therapy show variable effects.6772
Second, to the extent that bicarbonate administration raises extracellular pH, it is associated with a reduction in ionized calcium concentration, since the binding of calcium to albumin is pH dependent.73 A sodium bicarbonate load administered to patients with LA was associated with a significant fall in ionized calcium concentration, whereas a sodium chloride load was not.1 This can affect cardiac function, as the latter varies proportionally with calcium levels.74
Third, bicarbonate administration may reduce tissue oxygen delivery since the affinity of hemoglobin for oxygen increases as pH rises (Bohr effect).75 The administration of bicarbonate worsened systemic oxygen consumption in one study76 and decreased oxygen delivery in another.75
Fourth, bicarbonate administration may indirectly increase intracellular calcium concentration. Low intracellular pH (see above) stimulates proton efflux by way of proton transporters and exchangers, increasing intracellular sodium content.77 A high cell sodium content then may increase intracellular calcium, through the Na/Ca exchanger, impairing cellular function.7779 Compounding this, the reduced function of the Na/H ATPase as a regulator of intracellular sodium in sepsis may not be adequate to limit cell swelling.77
Against this background of mechanistic concerns with the use of bicarbonate treatment, it is not surprising that clinical outcomes have been inconsistent at best. In animal models of LA, the use of sodium bicarbonate has either negative effects on cardiac output60, 72 or no significant hemodynamic effect when compared to sodium chloride infusion.67, 80, 81 One animal study did show some benefit with sodium bicarbonate compared to saline, though all animals subsequently died.50
In humans, sodium bicarbonate was studied in 2 randomized trials of sepsis‐induced LA.1, 82 In a study by Cooper et al.,1 14 critically‐ill patients received sequential infusions of sodium bicarbonate or sodium chloride. Neither solution was superior to the other in terms of hemodynamic improvement. No benefit was noted even when analysis was limited to those with very low pH (7.2). Mathieu et al.82 randomized 10 critically‐ill patients to sequential infusion of either sodium bicarbonate or sodium chloride. Similarly, no significant difference in hemodynamic variables was noted.
When taken together, these studies evaluating sodium bicarbonate in LA fail to show convincing benefit and raise serious questions about its detrimental effects. Extracellular pH may be a misleading marker of success in the treatment of LA, given its direct influence by sodium bicarbonate administration.
Treatment of LA and Use of Other Buffers
Other buffers (Carbicarb, dichloroacetate, and tromethamine [THAM]) have been studied for treatment of LA. Human studies have not shown superiority of any of the buffers as far as improving pH,83, 84 hemodynamics, or survival.85
Treatment of LA by Renal Replacement Therapy
Renal replacement therapy (RRT; dialysis and its variants) has been studied for the treatment of severe acidosis. RRT has a number of theoretical advantages over purely medical therapies in the treatment of LA: it can deliver large quantities of base without contributing to volume overload; it can directly remove lactate from the plasma; and it can mitigate the effect of alkalinization on ionized calcium concentration by delivering calcium.
In critically ill patients with intact liver function, continuous venovenous hemofiltration (CVVH) appears to contribute very little (less then 3%) to overall lactate clearance.86 While outcome studies are limited, continuous dialysis modalities consistently show improved resolution of acidosis of various types when compared to intermittent modalities.87, 88 As described above, this is related to base administration and is not a surprising finding. There are no studies comparing RRT and medical therapy with respect to clinical outcomes in patients with LA.
Special Situations
Biguanides
Biguanide‐induced LA can be due to impairment of hepatic neoglucogenesis, in the case of metformin, or increasing hepatic oxidative phosphorylation, in the case of phenformin.89 This infrequent complication90, 91 is associated with a high mortality.92 Proposed therapy has included the use of sodium bicarbonate infusion.93 In this setting, it is unclear if the use of bicarbonate alone improves clinical outcomes.94
Renal replacement therapy in a wide variety of formats has been used to treat this condition.93, 95101 Metformin has a high clearance during dialysis due to its low molecular weight and lack of protein binding.97, 98, 102 Nonetheless, its high volume of distribution suggests a longer dialysis time would be more beneficial if the main goal is reducing metformin levels.97, 103 The limited prospective literature and lack of conclusive evidence about what levels of metformin induce LA makes generalized recommendations about duration of hemodialysis purely speculative.104
NRTIs
The use of NRTIs is associated with LA due to impairment of mitochondrial oxidative phosphorylation.105108 This uncommon complication, if not recognized early, is associated with a high mortality.101, 109 Investigations are ongoing into agents directed at improving mitochondrial function such as riboflavin, thiamine, and L‐carnitine.110112 As with biguanide‐associated LA, RRT decisions should be individualized based on metabolic circumstances.
Lorazepam
Many intravenous medications are formulated in the alcohol solvent, propylene glycol. Injectable lorazepam has the highest proportional amount of propylene glycol compared with other commonly used agents.113, 114 The kidney normally eliminates 12% to 50% of administered propylene glycol via proximal tubule secretion.115 The remainder is metabolized by the liver to form pyruvate and lactate.114, 116, 117
When propylene glycol accumulates, as in cases of reduced renal function, it results in hyperosmolarity, LA, and can even induce additional kidney injury (probably through proximal tubular cell necrosis).118
LA due to propylene glycol has been reported by many authors and its incidence with high dose intravenous (IV) lorazepam has been estimated to be as high as 19%.114, 116, 119, 120 This disorder can frequently go unrecognized, as many other factors that induce LA often coincide in such patients. But when identified and promptly addressed, its prognosis seems to be favorable.114
The best treatment is prevention, by avoiding the use of IV lorazepam in patients with impaired renal function. Once it is recognized, the drug should be promptly withdrawn. In addition, removal by hemodialysis can quickly lower propylene glycol levels since it is a small, highly water soluble, non‐protein‐bound molecule.121 As no rebound in the level is expected, intermittent dialysis should be an acceptable modality.117
Linezolid
Recently, Gram‐positive bacteria in general and methicillin‐resistant Staphylococcus aureus in particular have emerged as major causes of nosocomial and community‐acquired infections. Linezolid, an oxazolidinone, is increasingly used to treat such infections. Several cases of LA have been associated with linezolid.27, 122, 123 and a survey of the Infectious Diseases Society of America (IDSA) Emerging Infections Network members revealed that this complication was commonly encountered.124 Linezolid causes LA by mitochondrial toxicity125, 126 and risk factors include prolonged exposure and older age. Once the disorder is recognized, the clinician should stop the drug immediately. Chemistries should be monitored frequently in patients on long‐term therapy.
Conclusions
Many studies note the association between LA and adverse outcomes.2, 4547 Though metabolic acidosis from elevated lactate levels may negatively affect organ function, the evidence supporting therapy specifically aimed at increasing pH in these settings is consistently poor.3, 127 Limitations have included small numbers of subjects,1, 82 variable outcomes studied, and the inability to assess intracellular metabolic stability.1, 61 When taking these factors into account it is hard to justify aggressive treatment of LA with mechanisms aimed at raising pH. Literature on the treatment of patients with LA and very low pH (below 7.2) is even more limited.
Moreover, lactate elevations may not represent tissue hypoperfusion. Lactate may have an important role in improving energy metabolism. This represents 1 additional reason to be hesitant when attempting to normalize pH in LA; we may be disrupting the body's physiologic response to sepsis. A conflict for clinicians emerges, however, as lactate is often used to define tissue ischemia. Obviously, more specific markers of tissue hypoperfusion would be ideal.
Bicarbonate therapy is an understandably attractive means to improve the acidemia, but there are serious mechanistic concerns with it use. Moreover, neither animal nor human studies, limited as they may be, show a convincing benefit. LA in the setting of acute kidney injury may be best treated with renal replacement therapy with bicarbonate‐based buffers, but controlled trials are lacking.
A number of commonly used drugs can cause LA. A heightened awareness on the part of clinicians will lead to prompt recognition of these cases, and timely treatment.
- ,,,.Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled clinical study.Ann Intern Med.1990;112(7):492–498.
- ,,, et al.Natural history and course of acquired lactic acidosis in adults. DCA‐Lactic Acidosis Study Group.Am J Med.1994;97(1):47–54.
- ,.Sodium bicarbonate for the treatment of lactic acidosis.Chest.2000;117(1):260–267.
- ,.Management of life‐threatening acid‐base disorders. First of two parts.N Engl J Med.1998;338(1):26–34.
- .Indications for use of bicarbonate in patients with metabolic acidosis.Br J Anaesth.1991;67(2):165–177.
- ,.Bench‐to‐bedside review: treating acid‐base abnormalities in the intensive care unit—the role of buffers.Crit Care.2004;8(4):259–265.
- .Lactic acidosis update for critical care clinicians.J Am Soc Nephrol.2001;12(suppl 17):S15–S19.
- ,.Lactic acidosis: diagnosis and treatment.Clin Endocrinol Metab.1980;9(3):513–541.
- .Lactate and shock state: the metabolic view.Curr Opin Crit Care.2006;12(4):315–321.
- .Bench‐to‐bedside review: lactate and the kidney.Crit Care.2002;6(4):322–326.
- ,,,.The influence of renal function on lactate and glucose metabolism.Biochem J.1984;219(1):73–78.
- ,.The effect of acidosis on lactate removal by the perfused rat kidney.Clin Sci Mol Med.1976;50(3):185–194.
- ,,.Transvisceral lactate fluxes during early endotoxemia.Chest.1996;110(1):198–204.
- ,,,,.Metabolism of lactate by the intact functioning kidney of the dog.Am J Physiol.1973;224(6):1463–1467.
- ,,, et al.Lactate and glucose metabolism in severe sepsis and cardiogenic shock.Crit Care Med.2005;33(10):2235–2240.
- ,,,, et al.Lactic acidosis in fulminant hepatic failure. Some aspects of pathogenesis and prognosis.J Hepatol.1985;1(4):405–416.
- ,.Lactic acidosis in critical illness.Crit Care Med.1992;20(1):80–93.
- ,,, et al.Effects of cardiogenic shock on lactate and glucose metabolism after heart surgery.Crit Care Med.2000;28(12):3784–3791.
- ,,,,,.Evolution of lactate/pyruvate and arterial ketone body ratios in the early course of catecholamine‐treated septic shock.Crit Care Med.2000;28(1):114–119.
- ,,, et al.Oxygen debt and metabolic acidemia as quantitative predictors of mortality and the severity of the ischemic insult in hemorrhagic shock.Crit Care Med.1991;19(2):231–243.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- ,,,.Skeletal muscle partial pressure of oxygen in patients with sepsis.Crit Care Med.1994;22(4):640–650.
- ,.Reevaluation of the role of cellular hypoxia and bioenergetic failure in sepsis.JAMA.1992;267(11):1503–1510.
- ,,,.Lactic acidosis during sepsis is related to increased pyruvate production, not deficits in tissue oxygen availability.Ann Surg.1996;224(1):97–102.
- ,,,.Biguanide‐associated lactic acidosis. Case report and review of the literature.Arch Intern Med.1992;152(11):2333–2336.
- ,,,.Bench‐to‐bedside review: severe lactic acidosis in HIV patients treated with nucleoside analogue reverse transcriptase inhibitors.Crit Care.2003;7(3):226–232.
- ,,,.Lactic acidosis after treatment with linezolid.Infection.2007;35(4):278–281.
- ,,,.Isotopic evaluation of the metabolism of pyruvate and related substrates in normal adult volunteers and severely burned children: effect of dichloroacetate and glucose infusion.Surgery.1991;110(1):54–67.
- .Alterations in carbohydrate metabolism during stress: a review of the literature.Am J Med.1995;98(1):75–84.
- .,,,.Lactic acid kinetics in respiratory alkalosis.Crit Care Med.1991;19(9):1120–1124.
- .Significance of hyperlactatemia without acidosis during hypermetabolic stress.Crit Care Med.1997;25(11):1780–1781.
- ,,,.Lactate is an unreliable indicator of tissue hypoxia in injury or sepsis.Lancet.1999;354(9177):505–508.
- ,,,,.Relation between muscle Na+K+ ATPase activity and raised lactate concentrations in septic shock: a prospective study.Lancet.2005;365(9462):871–875.
- ,.Sepsis induces diaphragm electron transport chain dysfunction and protein depletion.Am J Respir Crit Care Med.2005;172(7):861–868.
- ,,, et al.Association between mitochondrial dysfunction and severity and outcome of septic shock.Lancet.2002;360(9328):219–223.
- ,.Mitochondrial dysfunction in sepsis.Biochem Soc Symp.1999;66:149–166.
- ,,, et al.Altered glucose transporter mRNA abundance in a rat model of endotoxic shock.Biochem Biophys Res Commun.1991;176(1):535–540.
- .Increased pyruvate dehydrogenase kinase activity in response to sepsis.Am J Physiol.1991;260(5 Pt 1):E669–E674.
- .Lactate metabolism: a new paradigm for the third millennium.J Physiol.2004;558(Pt 1):5–30.
- ,,, et al.Evidence supporting the existence of an activity‐dependent astrocyte‐neuron lactate shuttle.Dev Neurosci.1998;20(4–5):291–299.
- ,,,.Brain lactate is an obligatory aerobic energy substrate for functional recovery after hypoxia: further in vitro validation.J Neurochem.1997;69(1):423–426.
- .Bench‐to‐bedside review: a possible resolution of the glucose paradox of cerebral ischemia.Crit Care.2002;6(4):330–334.
- ,,,,,.Intravenous lactate prevents cerebral dysfunction during hypoglycaemia in insulin‐dependent diabetes mellitus.Clin Sci (Lond).1998;94(2):157–163.
- ,,,.Brain lactate, not glucose, fuels the recovery of synaptic function from hypoxia upon reoxygenation: an in vitro study.Brain Res.1997;744(1):105–111.
- ,,,,,.Clinical prognostic markers in patients with severe sepsis: a prospective analysis of 139 consecutive cases.J Infect.2003;47(4):300–306.
- ,,, et al.Serum lactate as a predictor of mortality in patients with infection.Intensive Care Med.2007;33(6):970–977.
- ,,,.Lactate versus non‐lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients.Crit Care.2006;10(1):R22.
- .Abnormal resting blood lactate. I. The significance of hyperlactatemia in hospitalized patients.Am J Med.1961;30:840–848.
- ,,,,.Effect of lactic acidosis on canine hemodynamics and left ventricular function.Am J Physiol.1990;258(4 Pt 2):H1193–H1199.
- ,,,.Alkali therapy extends the period of survival during hypoxia: studies in rats.Am J Physiol.1996;271(2 Pt 2):R381–R387.
- ,,.Acidosis during early reperfusion prevents myocardial stunning in perfused ferret hearts.J Clin Invest.1988;82(3):920–927.
- ,,, et al.Effect of acidotic blood reperfusion on reperfusion injury after coronary artery occlusion in the dog heart.J Cardiovasc Pharmacol.1998;31(2):179–186.
- ,,,.Hypoxia and acidosis activate cardiac myocyte death through the Bcl‐2 family protein BNIP3.Proc Natl Acad Sci U S A.2002;99(20):12825–12830.
- ,,,,,.Extracellular acidosis delays onset of cell death in ATP‐depleted hepatocytes.Am J Physiol.1988;255(3 Pt 1):C315–C322.
- ,.Metabolic and hemodynamic effects of hypertonic solutions: sodium‐lactate versus sodium chloride infusion in postoperative patients.Shock.2002;18(4):306–310.
- .Medical complications of status epilepticus.Adv Neurol.1983;34:395–398.
- ,,,,,.Bicarbonate therapy in severe diabetic ketoacidosis. A double blind, randomized, placebo controlled trial.Rev Invest Clin.1991;43(3):234–238.
- ,,.Supercarbia in children: clinical course and outcome.Crit Care Med.1990;18(2):166–168.
- ,,,.Low mortality rate in adult respiratory distress syndrome using low‐volume, pressure‐limited ventilation with permissive hypercapnia: a prospective study.Crit Care Med.1994;22(10):1568–1578.
- ,,,.Systemic effects of NaHCO3 in experimental lactic acidosis in dogs.Am J Physiol.1982;242(6):F586–F591.
- ,,,,.Lactic acidosis: effect of treatment on intracellular pH and energetics in living rat heart.Am J Physiol.1992;262(5 Pt 2):H1572–H1578.
- ,,,,,.Effect of sodium bicarbonate on intracellular pH under different buffering conditions.Kidney Int.1996;49(5):1262–1267.
- ,,.Hemodynamic and hepatic pH responses to sodium bicarbonate and Carbicarb during systemic acidosis.Magn Reson Med.1990;16(3):403–410.
- ,,, et al.The increase in CO2 production induced by NaHCO3 depends on blood albumin and hemoglobin concentrations.Intensive Care Med.2000;26(5):558–564.
- ,,, et al.Initial effect of sodium bicarbonate on intracellular pH depends on the extracellular nonbicarbonate buffering capacity.Crit Care Med.2001;29(5):1033–1039.
- ,,,,,.Dynamic study of the distribution of microcirculatory blood flow in multiple splanchnic organs in septic shock.Crit Care Med.2000;28(9):3233–3241.
- ,,,,,.The effects of sodium bicarbonate and a mixture of sodium bicarbonate and carbonate (“Carbicarb”) on skeletal muscle pH and hemodynamic status in rats with hypovolemic shock.Metabolism.1994;43(4):518–522.
- ,,, et al.Haemodynamic and metabolic effects in diabetic ketoacidosis in rats of treatment with sodium bicarbonate or a mixture of sodium bicarbonate and sodium carbonate.Diabetologia.1995;38(8):889–898.
- ,,,,,.Effects of sodium bicarbonate on striated muscle metabolism and intracellular pH during endotoxic shock.Shock.1994;1(3):196–200.
- ,,,,.Carbicarb, sodium bicarbonate, and sodium chloride in hypoxic lactic acidosis. Effect on arterial blood gases, lactate concentrations, hemodynamic variables, and myocardial intracellular pH.Chest.1993;104(3):913–918.
- ,.Improved hemodynamic function during hypoxia with Carbicarb, a new agent for the management of acidosis.Circulation.1988;77(1):227–233.
- ,,.Metabolic effects of sodium bicarbonate in hypoxic lactic acidosis in dogs.Am J Physiol.1985;249(5 Pt 2):F630–F635.
- .Binding of calcium to serum albumin. II. Effect of pH via competitive hydrogen and calcium ion binding to the imidazole groups of albumin.Scand J Clin Lab Invest.1972;29(1):75–83.
- ,,,,.Left ventricular contractility varies directly with blood ionized calcium.Ann Intern Med.1988;108(4):524–529.
- ,,.Regulatory mechanisms of hemoglobin oxygen affinity in acidosis and alkalosis.J Clin Invest.1971;50(3):700–706.
- ,,.Metabolic and hemodynamic consequences of sodium bicarbonate administration in patients with heart disease.Am J Med.1989;87(1):7–14.
- ,,.Sodium ion/hydrogen ion exchange inhibition: a new pharmacologic approach to myocardial ischemia and reperfusion injury.J Clin Pharmacol.1998;38(10):887–897.
- ,.SEA0400: a novel sodium‐calcium exchange inhibitor with cardioprotective properties.Cardiovasc Drug Rev.2004;22(4):334–347.
- ,,,.Elevation in cytosolic free calcium concentration early in myocardial ischemia in perfused rat heart.Circ Res.1987;60(5):700–707.
- ,.Acute haemodynamic effects of sodium bicarbonate administration in respiratory and metabolic acidosis in anaesthetized dogs.Anaesth Intensive Care.1997;25(6):615–620.
- ,,,.Bicarbonate does not increase left ventricular contractility during L‐lactic acidemia in pigs.Am Rev Respir Dis.1993;148(2):317–322.
- ,,,,.Effects of bicarbonate therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis: a prospective, controlled clinical study.Crit Care Med.1991;19(11):1352–1356.
- ,,, et al.Safety and efficacy of intravenous Carbicarb in patients undergoing surgery: comparison with sodium bicarbonate in the treatment of mild metabolic acidosis. SPI Research Group. Study of Perioperative Ischemia.Crit Care Med.1994;22(10):1540–1549.
- ,,, et al.Sodium bicarbonate versus THAM in ICU patients with mild metabolic acidosis.J Nephrol.2005;18(3):303–307.
- ,,, et al.A controlled clinical trial of dichloroacetate for treatment of lactic acidosis in adults. The Dichloroacetate‐Lactic Acidosis Study Group.N Engl J Med.1992;327(22):1564–1569.
- ,,,,,.Effect of continuous venovenous hemofiltration with dialysis on lactate clearance in critically ill patients.Crit Care Med.1997;25(1):58–62.
- ,,,,.A pilot randomised controlled comparison of continuous veno‐venous haemofiltration and extended daily dialysis with filtration: effect on small solutes and acid‐base balance.Intensive Care Med.2007;33(5):830–835.
- ,,.Intermittent versus continuous renal replacement therapy in the ICU: impact on electrolyte and acid‐base balance.Intensive Care Med.2001;27(6):1037–1043.
- ,,,.Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus: systematic review and meta‐analysis.Arch Intern Med.2003;163(21):2594–2602.
- ,,,,.Severe acidosis in patients taking metformin—rapid reversal and survival despite high APACHE score.Diabet Med.2006;23(4):432–435.
- ,,.Incidence of lactic acidosis in metformin users.Diabetes Care.1999;22(6):925–927.
- ,.Lactic acidosis in metformin‐treated patients. Prognostic value of arterial lactate levels and plasma metformin concentrations.Drug Saf.1999;20(4):377–384.
- ,,,.The management of metformin overdose.Anaesthesia.1998;53(7):698–701.
- ,,.Lactic acidosis in biguanide‐treated diabetics: a review of 330 cases.Diabetologia.1978;14(2):75–87.
- ,,,,.Treatment of metformin‐associated lactic acidosis with closed recirculation bicarbonate‐buffered hemodialysis.Arch Intern Med.1984;144(1):203–205.
- ,,,.High anion gap metabolic acidosis in suicide: don't forget metformin intoxication—two patients' experiences.Ren Fail.2002;24(5):671–675.
- ,,, et al.Hemodialysis in the treatment of lactic acidosis in diabetics treated by metformin: a study of metformin elimination.Int J Clin Pharmacol Ther Toxicol.1989;27(6):285–288.
- ,,.Bicarbonate haemodialysis as a treatment of metformin overdose.Nephrol Dial Transplant.1997;12(5):1046–1047.
- ,,,.Combination of intermittent haemodialysis and high‐volume continuous haemofiltration for the treatment of severe metformin‐induced lactic acidosis.Nephrol Dial Transplant.2004;19(8):2157–2158.
- ,,,.When a friend can become an enemy! Recognition and management of metformin‐associated lactic acidosis.Kidney Int.2007;72(9):1157–1160.
- .,, et al.Severe nucleoside‐associated lactic acidosis in human immunodeficiency virus‐infected patients: report of 12 cases and review of the literature.Clin Infect Dis.2002;34(6):838–846.
- ,,.Clearance of metformin by hemofiltration in overdose.J Toxicol Clin Toxicol.2002;40(2):177–180.
- .Metformin‐associated lactic acidosis.J Emerg Med.2001;20(3):267–272.
- ,.Contraindications to use of metformin. Blanket banning of metformin two days before surgery may not be a good idea.BMJ.2003;326(7392):762; author reply 762.
- ,,, et al.Hepatic failure and lactic acidosis due to fialuridine (FIAU), an investigational nucleoside analogue for chronic hepatitis B.N Engl J Med.1995;333(17):1099–1105.
- ,,,.Zidovudine‐induced fatal lactic acidosis and hepatic failure in patients with acquired immunodeficiency syndrome: report of two patients and review of the literature.Crit Care Med.1997;25(8):1425–1430.
- ,.Mitochondrial toxicity of antiviral drugs.Nat Med.1995;1(5):417–422.
- ,.Mitochondrial toxicity of nucleoside analogue reverse transcriptase inhibitors: a looming obstacle for long‐term antiretroviral therapy?Curr Opin Infect Dis.2000;13(1):5–11.
- ,,, et al.Treatment for adult HIV infection: 2006 recommendations of the International AIDS Society‐USA panel.JAMA.2006;296(7):827–843.
- ,,.Riboflavin to treat nucleoside analogue‐induced lactic acidosis.Lancet.1998;352(9124):291–292.
- ,,,,,.Severe lactic acidosis and thiamine administration in an HIV‐infected patient on HAART.Int J STD AIDS.2001;12(6):407–409.
- ,,, et al.Detecting life‐threatening lactic acidosis related to nucleoside‐analog treatment of human immunodeficiency virus‐infected patients, and treatment with L‐carnitine.Crit Care Med.2003;31(4):1042–1047.
- ,.Hyperosmolar metabolic acidosis and intravenous Lorazepam.N Engl J Med.2002;347(11):857–858; author reply 857–858.
- ,,,.Propylene glycol toxicity: a severe iatrogenic illness in ICU patients receiving IV benzodiazepines: a case series and prospective, observational pilot study.Chest.2005;128(3):1674–1681.
- ,,, et al.Propylene glycol pharmacokinetics and effects after intravenous infusion in humans.Ther Drug Monit.1987;9(3):255–258.
- .Short‐term lorazepam infusion and concern for propylene glycol toxicity: case report and review.Pharmacotherapy.2001;21(9):1140–1144.
- ,,.Recognition, treatment, and prevention of propylene glycol toxicity.Semin Dial.2007;20(3):217–219.
- ,,.Propylene glycol‐mediated cell injury in a primary culture of human proximal tubule cells.Toxicol Sci.1998;46(2):410–417.
- ,.Osmolar gap metabolic acidosis in a 60‐year‐old man treated for hypoxemic respiratory failure.Chest.2000;118(2):545–546.
- ,,,.Relationship of continuous infusion lorazepam to serum propylene glycol concentration in critically ill adults.Crit Care Med.2004;32(8):1709–1714.
- ,,,.Removal of propylene glycol and correction of increased osmolar gap by hemodialysis in a patient on high dose lorazepam infusion therapy.Intensive Care Med.2002;28(1):81–84.
- ,,.Linezolid use associated with lactic acidosis.Scand J Infect Dis.2005;37(2):153–154.
- ,.Linezolid‐induced lactic acidosis.N Engl J Med.2003;348(1):86–87.
- ,,.Toxicity of extended courses of linezolid: results of an Infectious Diseases Society of America Emerging Infections Network survey.Diagn Microbiol Infect Dis.2008;62(4):407–410.
- ,,.Mitochondrial toxicity associated with linezolid.N Engl J Med.2005;353(21):2305–2306.
- ,,, et al.Linezolid‐induced inhibition of mitochondrial protein synthesis.Clin Infect Dis.2006;42(8):1111–1117.
- ,.Use of base in the treatment of severe acidemic states.Am J Kidney Dis.2001;38(4):703–727.
Lactic acidosis (LA) is common in hospitalized patients and is associated with a high mortality.1, 2 Commonly, it is defined as a lactic acid concentration greater than 5 mmol/L with a pH less than 7.35.3 There are no evidence‐based guidelines for the treatment of LA despite progress in our understanding of its pathophysiology.36 This is not surprising, given the uncertainty regarding the impact of LA itself on clinical outcomes. In this regard, it is interesting to note that, despite its well‐recognized role as a marker of tissue hypoxia, lactate accumulation appears to have beneficial effects and may function as an adaptive mechanism. This raises the possibility that therapy directed at altering this adaptation may be detrimental. Pursuing correction of the pH in LA has been shown to have untoward physiologic effects. These and other ambiguities in the pathophysiology and treatment of LA are the focus of this review.
Lactate Metabolism
The body produces approximately 1400 mmol of lactate daily.7 Lactate is derived from the metabolism of pyruvate through an anaerobic reaction that occurs in all tissues (Figure 1). The liver is the primary site of lactate clearance and can metabolize up to 100 mmol per hour under normal conditions.8 There, lactate is converted to glucose to serve as an energy source during periods of hypoxia (Figure 2).9
Approximately 20% to 30% of the daily lactate load is metabolized by the kidneys.10, 11 Renal clearance is increased in acidosis12 and is maintained even in the presence of low renal perfusion.10, 12, 13 Renal lactate clearance is primarily through metabolism and not excretion.10, 14
LA Subtypes
Generally, lactic acid accumulation results from excess lactic acid production and not from reduced clearance.15 In cases of fulminant liver failure, it is due to a combination of decreased clearance and tissue hypoxia.16 In the setting of tissue hypoxia, an impairment of mitochondrial oxidative capacity results in the accumulation of pyruvate and generation of lactate. Lactic acid accumulation through this mechanism has historically been described as Type A LA.7 Hence, in critically ill patients lactate has traditionally been viewed as a marker of tissue hypoxia.15, 1721 Hyperlactatemia without tissue hypoxia has been referred to as type B LA. This is seen in a variety of circumstances. In sepsis, for example, several studies have shown lactic acid accumulation, despite adequate oxygen delivery.2224
Hyperlactatemia may also occur in cases of pure mitochondrial dysfunction, which can be induced by commonly prescribed medications such as the biguanides, nucleoside analog reverse‐transcriptase inhibitors (NRTIs), and linezolid.2527 Alternatively, lactate generation from metabolism of agents such as propylene glycol is possible. Finally, excessive lactate generation may occur following stress due to altered carbohydrate metabolism, or with respiratory alkalosis.2831
Lactate: A Metabolic Adaptation
Lactate was traditionally considered only as a marker of tissue hypoxia and anaerobic metabolism.17 This is certainly the case in situations of poor perfusion such as cardiogenic,15, 18 vasopressor‐resistant,19 or hypovolemic shock.20, 21
Alternative explanations for lactic acid accumulation, without tissue hypoperfusion, include catecholamine‐induced alterations in glycolysis,32, 33 mitochondrial disturbances,3436 and increased pyruvate production combined with increased glucose entry into cells.24, 37 In addition, the activity of an enzyme regulating lactate metabolism, pyruvate dehydrogenase kinase, increases in sepsis.38 This enzyme inactivates the pyruvate dehydrogenase (PDH) complex, which metabolizes pyruvate. Pyruvate and lactate may accumulate as a result. These changes partly explain the generation of LA in sepsis, independent of any effect of diminished tissue perfusion.
Recognizing the body's tendency toward homeostasis, it is appealing to speculate that lactate accumulation is adaptive.9 A number of findings support this. For example, lactate may act to shuttle energy between organs, or between cell types in the same organ. The astrocyteneuron lactate shuttle and the spermatogenic lactate shuttle are 2 examples of lactate's valuable effects on cellular metabolism.39 In the astrocyteneuron lactate shuttle, astrocytes support the increased metabolic demands of neurons through lactic acid production.40 Specifically, the neurotransmitter glutamate is released by the neurons and taken up by the astrocytes. Astrocytes produce lactate, which then moves back to the neuron to be used as an energy source. Glutamine, also released by the astrocytes, leads to the regeneration of glutamate and the potential to restart the cycle.39
Animal and human studies have suggested that, in periods of stress, lactate is the preferential energy substrate in the brain.4144 The usefulness of increased lactate production routinely seen in sepsis may thus represent multiple adaptive processes aimed primarily at improving the delivery of energy substrates. Thus, therapeutic strategies aimed specifically at lowering lactic acid levels may prove to have deleterious effects on cellular metabolism.
Impact of LA on Morbidity and Mortality
The poor prognosis in patients with LA is well recognized.2, 4548 For example, in a study of 126 patients with various causes of LA, the median survival was 38.5 hours and 30‐day survival was 17%.2
Studies have revealed that LA with low pH is associated with adverse effects on the cardiovascular system, particularly a decrease in cardiac contractility.49, 50 This effect is particularly prominent with a pH below 7.20. In contrast, acidosis in animal models has been shown to limit myocardial infarct size after reperfusion.51, 52 Variable effects of LA on cell death have been found. A worsening of apoptosis in myocytes has been noted;53 alternatively, protection from hypoxic injury in hepatocytes and myocardium has been observed.52, 54 Thus, although LA is associated with poor outcomes in human studies,2, 4547 it is still unclear to what extent lactic acid accumulation is a marker of severe illness, an independent effector of pathology, or a mechanism with the potential to serve a protective role.
Available data indicate that lactate itself is not harmful. Studies on infusion of lactate solutions to postoperative patients was shown to be safe.55 Also, the fact that lactate generation in states of respiratory alkalosis, stress, or altered carbohydrate metabolism without sepsis is not associated with worse outcomes supports the fact that lactic acid alone may not be maladaptive.2831
Similarly, low pH is not necessarily maladaptive. In the postictal state,56 diabetic ketoacidosis,57 spontaneous respiratory acidosis,58 or permissive hypercapnia,59 low blood pH is not deleterious.
In summary, LA is associated with poor outcomes, and indirect evidence suggests that it is the underlying causative condition rather than the low pH or the lactate that is responsible for the dire outcomes.
Treatment of LA with Sodium Bicarbonate
Since excessive lactic acid generation is accompanied by consumption of plasma bicarbonate and a fall in plasma pH, sodium bicarbonate has been long proposed as a treatment for LA. While theoretically appealing, this strategy has not been validated by studies in animals or humans. Indeed, bicarbonate administration in LA often has been shown to be detrimental.60, 61 The adverse effects of bicarbonate administration in LA, while initially paradoxical, have a number of possible explanations.
First, bicarbonate administration can induce a reduction in intracellular pH.60, 62, 63 The mechanism involves bicarbonate's effect to increase carbon dioxide (CO2) generation through mass action effect. Because the cell membrane is more permeable to CO2 than to bicarbonate, intracellular pH falls.64, 65 In sepsis, this intracellular/extracellular pH discrepancy may be more pronounced due to alterations in blood flow.66 Other reports on outcomes of intracellular pH with bicarbonate therapy show variable effects.6772
Second, to the extent that bicarbonate administration raises extracellular pH, it is associated with a reduction in ionized calcium concentration, since the binding of calcium to albumin is pH dependent.73 A sodium bicarbonate load administered to patients with LA was associated with a significant fall in ionized calcium concentration, whereas a sodium chloride load was not.1 This can affect cardiac function, as the latter varies proportionally with calcium levels.74
Third, bicarbonate administration may reduce tissue oxygen delivery since the affinity of hemoglobin for oxygen increases as pH rises (Bohr effect).75 The administration of bicarbonate worsened systemic oxygen consumption in one study76 and decreased oxygen delivery in another.75
Fourth, bicarbonate administration may indirectly increase intracellular calcium concentration. Low intracellular pH (see above) stimulates proton efflux by way of proton transporters and exchangers, increasing intracellular sodium content.77 A high cell sodium content then may increase intracellular calcium, through the Na/Ca exchanger, impairing cellular function.7779 Compounding this, the reduced function of the Na/H ATPase as a regulator of intracellular sodium in sepsis may not be adequate to limit cell swelling.77
Against this background of mechanistic concerns with the use of bicarbonate treatment, it is not surprising that clinical outcomes have been inconsistent at best. In animal models of LA, the use of sodium bicarbonate has either negative effects on cardiac output60, 72 or no significant hemodynamic effect when compared to sodium chloride infusion.67, 80, 81 One animal study did show some benefit with sodium bicarbonate compared to saline, though all animals subsequently died.50
In humans, sodium bicarbonate was studied in 2 randomized trials of sepsis‐induced LA.1, 82 In a study by Cooper et al.,1 14 critically‐ill patients received sequential infusions of sodium bicarbonate or sodium chloride. Neither solution was superior to the other in terms of hemodynamic improvement. No benefit was noted even when analysis was limited to those with very low pH (7.2). Mathieu et al.82 randomized 10 critically‐ill patients to sequential infusion of either sodium bicarbonate or sodium chloride. Similarly, no significant difference in hemodynamic variables was noted.
When taken together, these studies evaluating sodium bicarbonate in LA fail to show convincing benefit and raise serious questions about its detrimental effects. Extracellular pH may be a misleading marker of success in the treatment of LA, given its direct influence by sodium bicarbonate administration.
Treatment of LA and Use of Other Buffers
Other buffers (Carbicarb, dichloroacetate, and tromethamine [THAM]) have been studied for treatment of LA. Human studies have not shown superiority of any of the buffers as far as improving pH,83, 84 hemodynamics, or survival.85
Treatment of LA by Renal Replacement Therapy
Renal replacement therapy (RRT; dialysis and its variants) has been studied for the treatment of severe acidosis. RRT has a number of theoretical advantages over purely medical therapies in the treatment of LA: it can deliver large quantities of base without contributing to volume overload; it can directly remove lactate from the plasma; and it can mitigate the effect of alkalinization on ionized calcium concentration by delivering calcium.
In critically ill patients with intact liver function, continuous venovenous hemofiltration (CVVH) appears to contribute very little (less then 3%) to overall lactate clearance.86 While outcome studies are limited, continuous dialysis modalities consistently show improved resolution of acidosis of various types when compared to intermittent modalities.87, 88 As described above, this is related to base administration and is not a surprising finding. There are no studies comparing RRT and medical therapy with respect to clinical outcomes in patients with LA.
Special Situations
Biguanides
Biguanide‐induced LA can be due to impairment of hepatic neoglucogenesis, in the case of metformin, or increasing hepatic oxidative phosphorylation, in the case of phenformin.89 This infrequent complication90, 91 is associated with a high mortality.92 Proposed therapy has included the use of sodium bicarbonate infusion.93 In this setting, it is unclear if the use of bicarbonate alone improves clinical outcomes.94
Renal replacement therapy in a wide variety of formats has been used to treat this condition.93, 95101 Metformin has a high clearance during dialysis due to its low molecular weight and lack of protein binding.97, 98, 102 Nonetheless, its high volume of distribution suggests a longer dialysis time would be more beneficial if the main goal is reducing metformin levels.97, 103 The limited prospective literature and lack of conclusive evidence about what levels of metformin induce LA makes generalized recommendations about duration of hemodialysis purely speculative.104
NRTIs
The use of NRTIs is associated with LA due to impairment of mitochondrial oxidative phosphorylation.105108 This uncommon complication, if not recognized early, is associated with a high mortality.101, 109 Investigations are ongoing into agents directed at improving mitochondrial function such as riboflavin, thiamine, and L‐carnitine.110112 As with biguanide‐associated LA, RRT decisions should be individualized based on metabolic circumstances.
Lorazepam
Many intravenous medications are formulated in the alcohol solvent, propylene glycol. Injectable lorazepam has the highest proportional amount of propylene glycol compared with other commonly used agents.113, 114 The kidney normally eliminates 12% to 50% of administered propylene glycol via proximal tubule secretion.115 The remainder is metabolized by the liver to form pyruvate and lactate.114, 116, 117
When propylene glycol accumulates, as in cases of reduced renal function, it results in hyperosmolarity, LA, and can even induce additional kidney injury (probably through proximal tubular cell necrosis).118
LA due to propylene glycol has been reported by many authors and its incidence with high dose intravenous (IV) lorazepam has been estimated to be as high as 19%.114, 116, 119, 120 This disorder can frequently go unrecognized, as many other factors that induce LA often coincide in such patients. But when identified and promptly addressed, its prognosis seems to be favorable.114
The best treatment is prevention, by avoiding the use of IV lorazepam in patients with impaired renal function. Once it is recognized, the drug should be promptly withdrawn. In addition, removal by hemodialysis can quickly lower propylene glycol levels since it is a small, highly water soluble, non‐protein‐bound molecule.121 As no rebound in the level is expected, intermittent dialysis should be an acceptable modality.117
Linezolid
Recently, Gram‐positive bacteria in general and methicillin‐resistant Staphylococcus aureus in particular have emerged as major causes of nosocomial and community‐acquired infections. Linezolid, an oxazolidinone, is increasingly used to treat such infections. Several cases of LA have been associated with linezolid.27, 122, 123 and a survey of the Infectious Diseases Society of America (IDSA) Emerging Infections Network members revealed that this complication was commonly encountered.124 Linezolid causes LA by mitochondrial toxicity125, 126 and risk factors include prolonged exposure and older age. Once the disorder is recognized, the clinician should stop the drug immediately. Chemistries should be monitored frequently in patients on long‐term therapy.
Conclusions
Many studies note the association between LA and adverse outcomes.2, 4547 Though metabolic acidosis from elevated lactate levels may negatively affect organ function, the evidence supporting therapy specifically aimed at increasing pH in these settings is consistently poor.3, 127 Limitations have included small numbers of subjects,1, 82 variable outcomes studied, and the inability to assess intracellular metabolic stability.1, 61 When taking these factors into account it is hard to justify aggressive treatment of LA with mechanisms aimed at raising pH. Literature on the treatment of patients with LA and very low pH (below 7.2) is even more limited.
Moreover, lactate elevations may not represent tissue hypoperfusion. Lactate may have an important role in improving energy metabolism. This represents 1 additional reason to be hesitant when attempting to normalize pH in LA; we may be disrupting the body's physiologic response to sepsis. A conflict for clinicians emerges, however, as lactate is often used to define tissue ischemia. Obviously, more specific markers of tissue hypoperfusion would be ideal.
Bicarbonate therapy is an understandably attractive means to improve the acidemia, but there are serious mechanistic concerns with it use. Moreover, neither animal nor human studies, limited as they may be, show a convincing benefit. LA in the setting of acute kidney injury may be best treated with renal replacement therapy with bicarbonate‐based buffers, but controlled trials are lacking.
A number of commonly used drugs can cause LA. A heightened awareness on the part of clinicians will lead to prompt recognition of these cases, and timely treatment.
Lactic acidosis (LA) is common in hospitalized patients and is associated with a high mortality.1, 2 Commonly, it is defined as a lactic acid concentration greater than 5 mmol/L with a pH less than 7.35.3 There are no evidence‐based guidelines for the treatment of LA despite progress in our understanding of its pathophysiology.36 This is not surprising, given the uncertainty regarding the impact of LA itself on clinical outcomes. In this regard, it is interesting to note that, despite its well‐recognized role as a marker of tissue hypoxia, lactate accumulation appears to have beneficial effects and may function as an adaptive mechanism. This raises the possibility that therapy directed at altering this adaptation may be detrimental. Pursuing correction of the pH in LA has been shown to have untoward physiologic effects. These and other ambiguities in the pathophysiology and treatment of LA are the focus of this review.
Lactate Metabolism
The body produces approximately 1400 mmol of lactate daily.7 Lactate is derived from the metabolism of pyruvate through an anaerobic reaction that occurs in all tissues (Figure 1). The liver is the primary site of lactate clearance and can metabolize up to 100 mmol per hour under normal conditions.8 There, lactate is converted to glucose to serve as an energy source during periods of hypoxia (Figure 2).9
Approximately 20% to 30% of the daily lactate load is metabolized by the kidneys.10, 11 Renal clearance is increased in acidosis12 and is maintained even in the presence of low renal perfusion.10, 12, 13 Renal lactate clearance is primarily through metabolism and not excretion.10, 14
LA Subtypes
Generally, lactic acid accumulation results from excess lactic acid production and not from reduced clearance.15 In cases of fulminant liver failure, it is due to a combination of decreased clearance and tissue hypoxia.16 In the setting of tissue hypoxia, an impairment of mitochondrial oxidative capacity results in the accumulation of pyruvate and generation of lactate. Lactic acid accumulation through this mechanism has historically been described as Type A LA.7 Hence, in critically ill patients lactate has traditionally been viewed as a marker of tissue hypoxia.15, 1721 Hyperlactatemia without tissue hypoxia has been referred to as type B LA. This is seen in a variety of circumstances. In sepsis, for example, several studies have shown lactic acid accumulation, despite adequate oxygen delivery.2224
Hyperlactatemia may also occur in cases of pure mitochondrial dysfunction, which can be induced by commonly prescribed medications such as the biguanides, nucleoside analog reverse‐transcriptase inhibitors (NRTIs), and linezolid.2527 Alternatively, lactate generation from metabolism of agents such as propylene glycol is possible. Finally, excessive lactate generation may occur following stress due to altered carbohydrate metabolism, or with respiratory alkalosis.2831
Lactate: A Metabolic Adaptation
Lactate was traditionally considered only as a marker of tissue hypoxia and anaerobic metabolism.17 This is certainly the case in situations of poor perfusion such as cardiogenic,15, 18 vasopressor‐resistant,19 or hypovolemic shock.20, 21
Alternative explanations for lactic acid accumulation, without tissue hypoperfusion, include catecholamine‐induced alterations in glycolysis,32, 33 mitochondrial disturbances,3436 and increased pyruvate production combined with increased glucose entry into cells.24, 37 In addition, the activity of an enzyme regulating lactate metabolism, pyruvate dehydrogenase kinase, increases in sepsis.38 This enzyme inactivates the pyruvate dehydrogenase (PDH) complex, which metabolizes pyruvate. Pyruvate and lactate may accumulate as a result. These changes partly explain the generation of LA in sepsis, independent of any effect of diminished tissue perfusion.
Recognizing the body's tendency toward homeostasis, it is appealing to speculate that lactate accumulation is adaptive.9 A number of findings support this. For example, lactate may act to shuttle energy between organs, or between cell types in the same organ. The astrocyteneuron lactate shuttle and the spermatogenic lactate shuttle are 2 examples of lactate's valuable effects on cellular metabolism.39 In the astrocyteneuron lactate shuttle, astrocytes support the increased metabolic demands of neurons through lactic acid production.40 Specifically, the neurotransmitter glutamate is released by the neurons and taken up by the astrocytes. Astrocytes produce lactate, which then moves back to the neuron to be used as an energy source. Glutamine, also released by the astrocytes, leads to the regeneration of glutamate and the potential to restart the cycle.39
Animal and human studies have suggested that, in periods of stress, lactate is the preferential energy substrate in the brain.4144 The usefulness of increased lactate production routinely seen in sepsis may thus represent multiple adaptive processes aimed primarily at improving the delivery of energy substrates. Thus, therapeutic strategies aimed specifically at lowering lactic acid levels may prove to have deleterious effects on cellular metabolism.
Impact of LA on Morbidity and Mortality
The poor prognosis in patients with LA is well recognized.2, 4548 For example, in a study of 126 patients with various causes of LA, the median survival was 38.5 hours and 30‐day survival was 17%.2
Studies have revealed that LA with low pH is associated with adverse effects on the cardiovascular system, particularly a decrease in cardiac contractility.49, 50 This effect is particularly prominent with a pH below 7.20. In contrast, acidosis in animal models has been shown to limit myocardial infarct size after reperfusion.51, 52 Variable effects of LA on cell death have been found. A worsening of apoptosis in myocytes has been noted;53 alternatively, protection from hypoxic injury in hepatocytes and myocardium has been observed.52, 54 Thus, although LA is associated with poor outcomes in human studies,2, 4547 it is still unclear to what extent lactic acid accumulation is a marker of severe illness, an independent effector of pathology, or a mechanism with the potential to serve a protective role.
Available data indicate that lactate itself is not harmful. Studies on infusion of lactate solutions to postoperative patients was shown to be safe.55 Also, the fact that lactate generation in states of respiratory alkalosis, stress, or altered carbohydrate metabolism without sepsis is not associated with worse outcomes supports the fact that lactic acid alone may not be maladaptive.2831
Similarly, low pH is not necessarily maladaptive. In the postictal state,56 diabetic ketoacidosis,57 spontaneous respiratory acidosis,58 or permissive hypercapnia,59 low blood pH is not deleterious.
In summary, LA is associated with poor outcomes, and indirect evidence suggests that it is the underlying causative condition rather than the low pH or the lactate that is responsible for the dire outcomes.
Treatment of LA with Sodium Bicarbonate
Since excessive lactic acid generation is accompanied by consumption of plasma bicarbonate and a fall in plasma pH, sodium bicarbonate has been long proposed as a treatment for LA. While theoretically appealing, this strategy has not been validated by studies in animals or humans. Indeed, bicarbonate administration in LA often has been shown to be detrimental.60, 61 The adverse effects of bicarbonate administration in LA, while initially paradoxical, have a number of possible explanations.
First, bicarbonate administration can induce a reduction in intracellular pH.60, 62, 63 The mechanism involves bicarbonate's effect to increase carbon dioxide (CO2) generation through mass action effect. Because the cell membrane is more permeable to CO2 than to bicarbonate, intracellular pH falls.64, 65 In sepsis, this intracellular/extracellular pH discrepancy may be more pronounced due to alterations in blood flow.66 Other reports on outcomes of intracellular pH with bicarbonate therapy show variable effects.6772
Second, to the extent that bicarbonate administration raises extracellular pH, it is associated with a reduction in ionized calcium concentration, since the binding of calcium to albumin is pH dependent.73 A sodium bicarbonate load administered to patients with LA was associated with a significant fall in ionized calcium concentration, whereas a sodium chloride load was not.1 This can affect cardiac function, as the latter varies proportionally with calcium levels.74
Third, bicarbonate administration may reduce tissue oxygen delivery since the affinity of hemoglobin for oxygen increases as pH rises (Bohr effect).75 The administration of bicarbonate worsened systemic oxygen consumption in one study76 and decreased oxygen delivery in another.75
Fourth, bicarbonate administration may indirectly increase intracellular calcium concentration. Low intracellular pH (see above) stimulates proton efflux by way of proton transporters and exchangers, increasing intracellular sodium content.77 A high cell sodium content then may increase intracellular calcium, through the Na/Ca exchanger, impairing cellular function.7779 Compounding this, the reduced function of the Na/H ATPase as a regulator of intracellular sodium in sepsis may not be adequate to limit cell swelling.77
Against this background of mechanistic concerns with the use of bicarbonate treatment, it is not surprising that clinical outcomes have been inconsistent at best. In animal models of LA, the use of sodium bicarbonate has either negative effects on cardiac output60, 72 or no significant hemodynamic effect when compared to sodium chloride infusion.67, 80, 81 One animal study did show some benefit with sodium bicarbonate compared to saline, though all animals subsequently died.50
In humans, sodium bicarbonate was studied in 2 randomized trials of sepsis‐induced LA.1, 82 In a study by Cooper et al.,1 14 critically‐ill patients received sequential infusions of sodium bicarbonate or sodium chloride. Neither solution was superior to the other in terms of hemodynamic improvement. No benefit was noted even when analysis was limited to those with very low pH (7.2). Mathieu et al.82 randomized 10 critically‐ill patients to sequential infusion of either sodium bicarbonate or sodium chloride. Similarly, no significant difference in hemodynamic variables was noted.
When taken together, these studies evaluating sodium bicarbonate in LA fail to show convincing benefit and raise serious questions about its detrimental effects. Extracellular pH may be a misleading marker of success in the treatment of LA, given its direct influence by sodium bicarbonate administration.
Treatment of LA and Use of Other Buffers
Other buffers (Carbicarb, dichloroacetate, and tromethamine [THAM]) have been studied for treatment of LA. Human studies have not shown superiority of any of the buffers as far as improving pH,83, 84 hemodynamics, or survival.85
Treatment of LA by Renal Replacement Therapy
Renal replacement therapy (RRT; dialysis and its variants) has been studied for the treatment of severe acidosis. RRT has a number of theoretical advantages over purely medical therapies in the treatment of LA: it can deliver large quantities of base without contributing to volume overload; it can directly remove lactate from the plasma; and it can mitigate the effect of alkalinization on ionized calcium concentration by delivering calcium.
In critically ill patients with intact liver function, continuous venovenous hemofiltration (CVVH) appears to contribute very little (less then 3%) to overall lactate clearance.86 While outcome studies are limited, continuous dialysis modalities consistently show improved resolution of acidosis of various types when compared to intermittent modalities.87, 88 As described above, this is related to base administration and is not a surprising finding. There are no studies comparing RRT and medical therapy with respect to clinical outcomes in patients with LA.
Special Situations
Biguanides
Biguanide‐induced LA can be due to impairment of hepatic neoglucogenesis, in the case of metformin, or increasing hepatic oxidative phosphorylation, in the case of phenformin.89 This infrequent complication90, 91 is associated with a high mortality.92 Proposed therapy has included the use of sodium bicarbonate infusion.93 In this setting, it is unclear if the use of bicarbonate alone improves clinical outcomes.94
Renal replacement therapy in a wide variety of formats has been used to treat this condition.93, 95101 Metformin has a high clearance during dialysis due to its low molecular weight and lack of protein binding.97, 98, 102 Nonetheless, its high volume of distribution suggests a longer dialysis time would be more beneficial if the main goal is reducing metformin levels.97, 103 The limited prospective literature and lack of conclusive evidence about what levels of metformin induce LA makes generalized recommendations about duration of hemodialysis purely speculative.104
NRTIs
The use of NRTIs is associated with LA due to impairment of mitochondrial oxidative phosphorylation.105108 This uncommon complication, if not recognized early, is associated with a high mortality.101, 109 Investigations are ongoing into agents directed at improving mitochondrial function such as riboflavin, thiamine, and L‐carnitine.110112 As with biguanide‐associated LA, RRT decisions should be individualized based on metabolic circumstances.
Lorazepam
Many intravenous medications are formulated in the alcohol solvent, propylene glycol. Injectable lorazepam has the highest proportional amount of propylene glycol compared with other commonly used agents.113, 114 The kidney normally eliminates 12% to 50% of administered propylene glycol via proximal tubule secretion.115 The remainder is metabolized by the liver to form pyruvate and lactate.114, 116, 117
When propylene glycol accumulates, as in cases of reduced renal function, it results in hyperosmolarity, LA, and can even induce additional kidney injury (probably through proximal tubular cell necrosis).118
LA due to propylene glycol has been reported by many authors and its incidence with high dose intravenous (IV) lorazepam has been estimated to be as high as 19%.114, 116, 119, 120 This disorder can frequently go unrecognized, as many other factors that induce LA often coincide in such patients. But when identified and promptly addressed, its prognosis seems to be favorable.114
The best treatment is prevention, by avoiding the use of IV lorazepam in patients with impaired renal function. Once it is recognized, the drug should be promptly withdrawn. In addition, removal by hemodialysis can quickly lower propylene glycol levels since it is a small, highly water soluble, non‐protein‐bound molecule.121 As no rebound in the level is expected, intermittent dialysis should be an acceptable modality.117
Linezolid
Recently, Gram‐positive bacteria in general and methicillin‐resistant Staphylococcus aureus in particular have emerged as major causes of nosocomial and community‐acquired infections. Linezolid, an oxazolidinone, is increasingly used to treat such infections. Several cases of LA have been associated with linezolid.27, 122, 123 and a survey of the Infectious Diseases Society of America (IDSA) Emerging Infections Network members revealed that this complication was commonly encountered.124 Linezolid causes LA by mitochondrial toxicity125, 126 and risk factors include prolonged exposure and older age. Once the disorder is recognized, the clinician should stop the drug immediately. Chemistries should be monitored frequently in patients on long‐term therapy.
Conclusions
Many studies note the association between LA and adverse outcomes.2, 4547 Though metabolic acidosis from elevated lactate levels may negatively affect organ function, the evidence supporting therapy specifically aimed at increasing pH in these settings is consistently poor.3, 127 Limitations have included small numbers of subjects,1, 82 variable outcomes studied, and the inability to assess intracellular metabolic stability.1, 61 When taking these factors into account it is hard to justify aggressive treatment of LA with mechanisms aimed at raising pH. Literature on the treatment of patients with LA and very low pH (below 7.2) is even more limited.
Moreover, lactate elevations may not represent tissue hypoperfusion. Lactate may have an important role in improving energy metabolism. This represents 1 additional reason to be hesitant when attempting to normalize pH in LA; we may be disrupting the body's physiologic response to sepsis. A conflict for clinicians emerges, however, as lactate is often used to define tissue ischemia. Obviously, more specific markers of tissue hypoperfusion would be ideal.
Bicarbonate therapy is an understandably attractive means to improve the acidemia, but there are serious mechanistic concerns with it use. Moreover, neither animal nor human studies, limited as they may be, show a convincing benefit. LA in the setting of acute kidney injury may be best treated with renal replacement therapy with bicarbonate‐based buffers, but controlled trials are lacking.
A number of commonly used drugs can cause LA. A heightened awareness on the part of clinicians will lead to prompt recognition of these cases, and timely treatment.
- ,,,.Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled clinical study.Ann Intern Med.1990;112(7):492–498.
- ,,, et al.Natural history and course of acquired lactic acidosis in adults. DCA‐Lactic Acidosis Study Group.Am J Med.1994;97(1):47–54.
- ,.Sodium bicarbonate for the treatment of lactic acidosis.Chest.2000;117(1):260–267.
- ,.Management of life‐threatening acid‐base disorders. First of two parts.N Engl J Med.1998;338(1):26–34.
- .Indications for use of bicarbonate in patients with metabolic acidosis.Br J Anaesth.1991;67(2):165–177.
- ,.Bench‐to‐bedside review: treating acid‐base abnormalities in the intensive care unit—the role of buffers.Crit Care.2004;8(4):259–265.
- .Lactic acidosis update for critical care clinicians.J Am Soc Nephrol.2001;12(suppl 17):S15–S19.
- ,.Lactic acidosis: diagnosis and treatment.Clin Endocrinol Metab.1980;9(3):513–541.
- .Lactate and shock state: the metabolic view.Curr Opin Crit Care.2006;12(4):315–321.
- .Bench‐to‐bedside review: lactate and the kidney.Crit Care.2002;6(4):322–326.
- ,,,.The influence of renal function on lactate and glucose metabolism.Biochem J.1984;219(1):73–78.
- ,.The effect of acidosis on lactate removal by the perfused rat kidney.Clin Sci Mol Med.1976;50(3):185–194.
- ,,.Transvisceral lactate fluxes during early endotoxemia.Chest.1996;110(1):198–204.
- ,,,,.Metabolism of lactate by the intact functioning kidney of the dog.Am J Physiol.1973;224(6):1463–1467.
- ,,, et al.Lactate and glucose metabolism in severe sepsis and cardiogenic shock.Crit Care Med.2005;33(10):2235–2240.
- ,,,, et al.Lactic acidosis in fulminant hepatic failure. Some aspects of pathogenesis and prognosis.J Hepatol.1985;1(4):405–416.
- ,.Lactic acidosis in critical illness.Crit Care Med.1992;20(1):80–93.
- ,,, et al.Effects of cardiogenic shock on lactate and glucose metabolism after heart surgery.Crit Care Med.2000;28(12):3784–3791.
- ,,,,,.Evolution of lactate/pyruvate and arterial ketone body ratios in the early course of catecholamine‐treated septic shock.Crit Care Med.2000;28(1):114–119.
- ,,, et al.Oxygen debt and metabolic acidemia as quantitative predictors of mortality and the severity of the ischemic insult in hemorrhagic shock.Crit Care Med.1991;19(2):231–243.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- ,,,.Skeletal muscle partial pressure of oxygen in patients with sepsis.Crit Care Med.1994;22(4):640–650.
- ,.Reevaluation of the role of cellular hypoxia and bioenergetic failure in sepsis.JAMA.1992;267(11):1503–1510.
- ,,,.Lactic acidosis during sepsis is related to increased pyruvate production, not deficits in tissue oxygen availability.Ann Surg.1996;224(1):97–102.
- ,,,.Biguanide‐associated lactic acidosis. Case report and review of the literature.Arch Intern Med.1992;152(11):2333–2336.
- ,,,.Bench‐to‐bedside review: severe lactic acidosis in HIV patients treated with nucleoside analogue reverse transcriptase inhibitors.Crit Care.2003;7(3):226–232.
- ,,,.Lactic acidosis after treatment with linezolid.Infection.2007;35(4):278–281.
- ,,,.Isotopic evaluation of the metabolism of pyruvate and related substrates in normal adult volunteers and severely burned children: effect of dichloroacetate and glucose infusion.Surgery.1991;110(1):54–67.
- .Alterations in carbohydrate metabolism during stress: a review of the literature.Am J Med.1995;98(1):75–84.
- .,,,.Lactic acid kinetics in respiratory alkalosis.Crit Care Med.1991;19(9):1120–1124.
- .Significance of hyperlactatemia without acidosis during hypermetabolic stress.Crit Care Med.1997;25(11):1780–1781.
- ,,,.Lactate is an unreliable indicator of tissue hypoxia in injury or sepsis.Lancet.1999;354(9177):505–508.
- ,,,,.Relation between muscle Na+K+ ATPase activity and raised lactate concentrations in septic shock: a prospective study.Lancet.2005;365(9462):871–875.
- ,.Sepsis induces diaphragm electron transport chain dysfunction and protein depletion.Am J Respir Crit Care Med.2005;172(7):861–868.
- ,,, et al.Association between mitochondrial dysfunction and severity and outcome of septic shock.Lancet.2002;360(9328):219–223.
- ,.Mitochondrial dysfunction in sepsis.Biochem Soc Symp.1999;66:149–166.
- ,,, et al.Altered glucose transporter mRNA abundance in a rat model of endotoxic shock.Biochem Biophys Res Commun.1991;176(1):535–540.
- .Increased pyruvate dehydrogenase kinase activity in response to sepsis.Am J Physiol.1991;260(5 Pt 1):E669–E674.
- .Lactate metabolism: a new paradigm for the third millennium.J Physiol.2004;558(Pt 1):5–30.
- ,,, et al.Evidence supporting the existence of an activity‐dependent astrocyte‐neuron lactate shuttle.Dev Neurosci.1998;20(4–5):291–299.
- ,,,.Brain lactate is an obligatory aerobic energy substrate for functional recovery after hypoxia: further in vitro validation.J Neurochem.1997;69(1):423–426.
- .Bench‐to‐bedside review: a possible resolution of the glucose paradox of cerebral ischemia.Crit Care.2002;6(4):330–334.
- ,,,,,.Intravenous lactate prevents cerebral dysfunction during hypoglycaemia in insulin‐dependent diabetes mellitus.Clin Sci (Lond).1998;94(2):157–163.
- ,,,.Brain lactate, not glucose, fuels the recovery of synaptic function from hypoxia upon reoxygenation: an in vitro study.Brain Res.1997;744(1):105–111.
- ,,,,,.Clinical prognostic markers in patients with severe sepsis: a prospective analysis of 139 consecutive cases.J Infect.2003;47(4):300–306.
- ,,, et al.Serum lactate as a predictor of mortality in patients with infection.Intensive Care Med.2007;33(6):970–977.
- ,,,.Lactate versus non‐lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients.Crit Care.2006;10(1):R22.
- .Abnormal resting blood lactate. I. The significance of hyperlactatemia in hospitalized patients.Am J Med.1961;30:840–848.
- ,,,,.Effect of lactic acidosis on canine hemodynamics and left ventricular function.Am J Physiol.1990;258(4 Pt 2):H1193–H1199.
- ,,,.Alkali therapy extends the period of survival during hypoxia: studies in rats.Am J Physiol.1996;271(2 Pt 2):R381–R387.
- ,,.Acidosis during early reperfusion prevents myocardial stunning in perfused ferret hearts.J Clin Invest.1988;82(3):920–927.
- ,,, et al.Effect of acidotic blood reperfusion on reperfusion injury after coronary artery occlusion in the dog heart.J Cardiovasc Pharmacol.1998;31(2):179–186.
- ,,,.Hypoxia and acidosis activate cardiac myocyte death through the Bcl‐2 family protein BNIP3.Proc Natl Acad Sci U S A.2002;99(20):12825–12830.
- ,,,,,.Extracellular acidosis delays onset of cell death in ATP‐depleted hepatocytes.Am J Physiol.1988;255(3 Pt 1):C315–C322.
- ,.Metabolic and hemodynamic effects of hypertonic solutions: sodium‐lactate versus sodium chloride infusion in postoperative patients.Shock.2002;18(4):306–310.
- .Medical complications of status epilepticus.Adv Neurol.1983;34:395–398.
- ,,,,,.Bicarbonate therapy in severe diabetic ketoacidosis. A double blind, randomized, placebo controlled trial.Rev Invest Clin.1991;43(3):234–238.
- ,,.Supercarbia in children: clinical course and outcome.Crit Care Med.1990;18(2):166–168.
- ,,,.Low mortality rate in adult respiratory distress syndrome using low‐volume, pressure‐limited ventilation with permissive hypercapnia: a prospective study.Crit Care Med.1994;22(10):1568–1578.
- ,,,.Systemic effects of NaHCO3 in experimental lactic acidosis in dogs.Am J Physiol.1982;242(6):F586–F591.
- ,,,,.Lactic acidosis: effect of treatment on intracellular pH and energetics in living rat heart.Am J Physiol.1992;262(5 Pt 2):H1572–H1578.
- ,,,,,.Effect of sodium bicarbonate on intracellular pH under different buffering conditions.Kidney Int.1996;49(5):1262–1267.
- ,,.Hemodynamic and hepatic pH responses to sodium bicarbonate and Carbicarb during systemic acidosis.Magn Reson Med.1990;16(3):403–410.
- ,,, et al.The increase in CO2 production induced by NaHCO3 depends on blood albumin and hemoglobin concentrations.Intensive Care Med.2000;26(5):558–564.
- ,,, et al.Initial effect of sodium bicarbonate on intracellular pH depends on the extracellular nonbicarbonate buffering capacity.Crit Care Med.2001;29(5):1033–1039.
- ,,,,,.Dynamic study of the distribution of microcirculatory blood flow in multiple splanchnic organs in septic shock.Crit Care Med.2000;28(9):3233–3241.
- ,,,,,.The effects of sodium bicarbonate and a mixture of sodium bicarbonate and carbonate (“Carbicarb”) on skeletal muscle pH and hemodynamic status in rats with hypovolemic shock.Metabolism.1994;43(4):518–522.
- ,,, et al.Haemodynamic and metabolic effects in diabetic ketoacidosis in rats of treatment with sodium bicarbonate or a mixture of sodium bicarbonate and sodium carbonate.Diabetologia.1995;38(8):889–898.
- ,,,,,.Effects of sodium bicarbonate on striated muscle metabolism and intracellular pH during endotoxic shock.Shock.1994;1(3):196–200.
- ,,,,.Carbicarb, sodium bicarbonate, and sodium chloride in hypoxic lactic acidosis. Effect on arterial blood gases, lactate concentrations, hemodynamic variables, and myocardial intracellular pH.Chest.1993;104(3):913–918.
- ,.Improved hemodynamic function during hypoxia with Carbicarb, a new agent for the management of acidosis.Circulation.1988;77(1):227–233.
- ,,.Metabolic effects of sodium bicarbonate in hypoxic lactic acidosis in dogs.Am J Physiol.1985;249(5 Pt 2):F630–F635.
- .Binding of calcium to serum albumin. II. Effect of pH via competitive hydrogen and calcium ion binding to the imidazole groups of albumin.Scand J Clin Lab Invest.1972;29(1):75–83.
- ,,,,.Left ventricular contractility varies directly with blood ionized calcium.Ann Intern Med.1988;108(4):524–529.
- ,,.Regulatory mechanisms of hemoglobin oxygen affinity in acidosis and alkalosis.J Clin Invest.1971;50(3):700–706.
- ,,.Metabolic and hemodynamic consequences of sodium bicarbonate administration in patients with heart disease.Am J Med.1989;87(1):7–14.
- ,,.Sodium ion/hydrogen ion exchange inhibition: a new pharmacologic approach to myocardial ischemia and reperfusion injury.J Clin Pharmacol.1998;38(10):887–897.
- ,.SEA0400: a novel sodium‐calcium exchange inhibitor with cardioprotective properties.Cardiovasc Drug Rev.2004;22(4):334–347.
- ,,,.Elevation in cytosolic free calcium concentration early in myocardial ischemia in perfused rat heart.Circ Res.1987;60(5):700–707.
- ,.Acute haemodynamic effects of sodium bicarbonate administration in respiratory and metabolic acidosis in anaesthetized dogs.Anaesth Intensive Care.1997;25(6):615–620.
- ,,,.Bicarbonate does not increase left ventricular contractility during L‐lactic acidemia in pigs.Am Rev Respir Dis.1993;148(2):317–322.
- ,,,,.Effects of bicarbonate therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis: a prospective, controlled clinical study.Crit Care Med.1991;19(11):1352–1356.
- ,,, et al.Safety and efficacy of intravenous Carbicarb in patients undergoing surgery: comparison with sodium bicarbonate in the treatment of mild metabolic acidosis. SPI Research Group. Study of Perioperative Ischemia.Crit Care Med.1994;22(10):1540–1549.
- ,,, et al.Sodium bicarbonate versus THAM in ICU patients with mild metabolic acidosis.J Nephrol.2005;18(3):303–307.
- ,,, et al.A controlled clinical trial of dichloroacetate for treatment of lactic acidosis in adults. The Dichloroacetate‐Lactic Acidosis Study Group.N Engl J Med.1992;327(22):1564–1569.
- ,,,,,.Effect of continuous venovenous hemofiltration with dialysis on lactate clearance in critically ill patients.Crit Care Med.1997;25(1):58–62.
- ,,,,.A pilot randomised controlled comparison of continuous veno‐venous haemofiltration and extended daily dialysis with filtration: effect on small solutes and acid‐base balance.Intensive Care Med.2007;33(5):830–835.
- ,,.Intermittent versus continuous renal replacement therapy in the ICU: impact on electrolyte and acid‐base balance.Intensive Care Med.2001;27(6):1037–1043.
- ,,,.Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus: systematic review and meta‐analysis.Arch Intern Med.2003;163(21):2594–2602.
- ,,,,.Severe acidosis in patients taking metformin—rapid reversal and survival despite high APACHE score.Diabet Med.2006;23(4):432–435.
- ,,.Incidence of lactic acidosis in metformin users.Diabetes Care.1999;22(6):925–927.
- ,.Lactic acidosis in metformin‐treated patients. Prognostic value of arterial lactate levels and plasma metformin concentrations.Drug Saf.1999;20(4):377–384.
- ,,,.The management of metformin overdose.Anaesthesia.1998;53(7):698–701.
- ,,.Lactic acidosis in biguanide‐treated diabetics: a review of 330 cases.Diabetologia.1978;14(2):75–87.
- ,,,,.Treatment of metformin‐associated lactic acidosis with closed recirculation bicarbonate‐buffered hemodialysis.Arch Intern Med.1984;144(1):203–205.
- ,,,.High anion gap metabolic acidosis in suicide: don't forget metformin intoxication—two patients' experiences.Ren Fail.2002;24(5):671–675.
- ,,, et al.Hemodialysis in the treatment of lactic acidosis in diabetics treated by metformin: a study of metformin elimination.Int J Clin Pharmacol Ther Toxicol.1989;27(6):285–288.
- ,,.Bicarbonate haemodialysis as a treatment of metformin overdose.Nephrol Dial Transplant.1997;12(5):1046–1047.
- ,,,.Combination of intermittent haemodialysis and high‐volume continuous haemofiltration for the treatment of severe metformin‐induced lactic acidosis.Nephrol Dial Transplant.2004;19(8):2157–2158.
- ,,,.When a friend can become an enemy! Recognition and management of metformin‐associated lactic acidosis.Kidney Int.2007;72(9):1157–1160.
- .,, et al.Severe nucleoside‐associated lactic acidosis in human immunodeficiency virus‐infected patients: report of 12 cases and review of the literature.Clin Infect Dis.2002;34(6):838–846.
- ,,.Clearance of metformin by hemofiltration in overdose.J Toxicol Clin Toxicol.2002;40(2):177–180.
- .Metformin‐associated lactic acidosis.J Emerg Med.2001;20(3):267–272.
- ,.Contraindications to use of metformin. Blanket banning of metformin two days before surgery may not be a good idea.BMJ.2003;326(7392):762; author reply 762.
- ,,, et al.Hepatic failure and lactic acidosis due to fialuridine (FIAU), an investigational nucleoside analogue for chronic hepatitis B.N Engl J Med.1995;333(17):1099–1105.
- ,,,.Zidovudine‐induced fatal lactic acidosis and hepatic failure in patients with acquired immunodeficiency syndrome: report of two patients and review of the literature.Crit Care Med.1997;25(8):1425–1430.
- ,.Mitochondrial toxicity of antiviral drugs.Nat Med.1995;1(5):417–422.
- ,.Mitochondrial toxicity of nucleoside analogue reverse transcriptase inhibitors: a looming obstacle for long‐term antiretroviral therapy?Curr Opin Infect Dis.2000;13(1):5–11.
- ,,, et al.Treatment for adult HIV infection: 2006 recommendations of the International AIDS Society‐USA panel.JAMA.2006;296(7):827–843.
- ,,.Riboflavin to treat nucleoside analogue‐induced lactic acidosis.Lancet.1998;352(9124):291–292.
- ,,,,,.Severe lactic acidosis and thiamine administration in an HIV‐infected patient on HAART.Int J STD AIDS.2001;12(6):407–409.
- ,,, et al.Detecting life‐threatening lactic acidosis related to nucleoside‐analog treatment of human immunodeficiency virus‐infected patients, and treatment with L‐carnitine.Crit Care Med.2003;31(4):1042–1047.
- ,.Hyperosmolar metabolic acidosis and intravenous Lorazepam.N Engl J Med.2002;347(11):857–858; author reply 857–858.
- ,,,.Propylene glycol toxicity: a severe iatrogenic illness in ICU patients receiving IV benzodiazepines: a case series and prospective, observational pilot study.Chest.2005;128(3):1674–1681.
- ,,, et al.Propylene glycol pharmacokinetics and effects after intravenous infusion in humans.Ther Drug Monit.1987;9(3):255–258.
- .Short‐term lorazepam infusion and concern for propylene glycol toxicity: case report and review.Pharmacotherapy.2001;21(9):1140–1144.
- ,,.Recognition, treatment, and prevention of propylene glycol toxicity.Semin Dial.2007;20(3):217–219.
- ,,.Propylene glycol‐mediated cell injury in a primary culture of human proximal tubule cells.Toxicol Sci.1998;46(2):410–417.
- ,.Osmolar gap metabolic acidosis in a 60‐year‐old man treated for hypoxemic respiratory failure.Chest.2000;118(2):545–546.
- ,,,.Relationship of continuous infusion lorazepam to serum propylene glycol concentration in critically ill adults.Crit Care Med.2004;32(8):1709–1714.
- ,,,.Removal of propylene glycol and correction of increased osmolar gap by hemodialysis in a patient on high dose lorazepam infusion therapy.Intensive Care Med.2002;28(1):81–84.
- ,,.Linezolid use associated with lactic acidosis.Scand J Infect Dis.2005;37(2):153–154.
- ,.Linezolid‐induced lactic acidosis.N Engl J Med.2003;348(1):86–87.
- ,,.Toxicity of extended courses of linezolid: results of an Infectious Diseases Society of America Emerging Infections Network survey.Diagn Microbiol Infect Dis.2008;62(4):407–410.
- ,,.Mitochondrial toxicity associated with linezolid.N Engl J Med.2005;353(21):2305–2306.
- ,,, et al.Linezolid‐induced inhibition of mitochondrial protein synthesis.Clin Infect Dis.2006;42(8):1111–1117.
- ,.Use of base in the treatment of severe acidemic states.Am J Kidney Dis.2001;38(4):703–727.
- ,,,.Bicarbonate does not improve hemodynamics in critically ill patients who have lactic acidosis. A prospective, controlled clinical study.Ann Intern Med.1990;112(7):492–498.
- ,,, et al.Natural history and course of acquired lactic acidosis in adults. DCA‐Lactic Acidosis Study Group.Am J Med.1994;97(1):47–54.
- ,.Sodium bicarbonate for the treatment of lactic acidosis.Chest.2000;117(1):260–267.
- ,.Management of life‐threatening acid‐base disorders. First of two parts.N Engl J Med.1998;338(1):26–34.
- .Indications for use of bicarbonate in patients with metabolic acidosis.Br J Anaesth.1991;67(2):165–177.
- ,.Bench‐to‐bedside review: treating acid‐base abnormalities in the intensive care unit—the role of buffers.Crit Care.2004;8(4):259–265.
- .Lactic acidosis update for critical care clinicians.J Am Soc Nephrol.2001;12(suppl 17):S15–S19.
- ,.Lactic acidosis: diagnosis and treatment.Clin Endocrinol Metab.1980;9(3):513–541.
- .Lactate and shock state: the metabolic view.Curr Opin Crit Care.2006;12(4):315–321.
- .Bench‐to‐bedside review: lactate and the kidney.Crit Care.2002;6(4):322–326.
- ,,,.The influence of renal function on lactate and glucose metabolism.Biochem J.1984;219(1):73–78.
- ,.The effect of acidosis on lactate removal by the perfused rat kidney.Clin Sci Mol Med.1976;50(3):185–194.
- ,,.Transvisceral lactate fluxes during early endotoxemia.Chest.1996;110(1):198–204.
- ,,,,.Metabolism of lactate by the intact functioning kidney of the dog.Am J Physiol.1973;224(6):1463–1467.
- ,,, et al.Lactate and glucose metabolism in severe sepsis and cardiogenic shock.Crit Care Med.2005;33(10):2235–2240.
- ,,,, et al.Lactic acidosis in fulminant hepatic failure. Some aspects of pathogenesis and prognosis.J Hepatol.1985;1(4):405–416.
- ,.Lactic acidosis in critical illness.Crit Care Med.1992;20(1):80–93.
- ,,, et al.Effects of cardiogenic shock on lactate and glucose metabolism after heart surgery.Crit Care Med.2000;28(12):3784–3791.
- ,,,,,.Evolution of lactate/pyruvate and arterial ketone body ratios in the early course of catecholamine‐treated septic shock.Crit Care Med.2000;28(1):114–119.
- ,,, et al.Oxygen debt and metabolic acidemia as quantitative predictors of mortality and the severity of the ischemic insult in hemorrhagic shock.Crit Care Med.1991;19(2):231–243.
- ,,, et al.Early goal‐directed therapy in the treatment of severe sepsis and septic shock.N Engl J Med.2001;345(19):1368–1377.
- ,,,.Skeletal muscle partial pressure of oxygen in patients with sepsis.Crit Care Med.1994;22(4):640–650.
- ,.Reevaluation of the role of cellular hypoxia and bioenergetic failure in sepsis.JAMA.1992;267(11):1503–1510.
- ,,,.Lactic acidosis during sepsis is related to increased pyruvate production, not deficits in tissue oxygen availability.Ann Surg.1996;224(1):97–102.
- ,,,.Biguanide‐associated lactic acidosis. Case report and review of the literature.Arch Intern Med.1992;152(11):2333–2336.
- ,,,.Bench‐to‐bedside review: severe lactic acidosis in HIV patients treated with nucleoside analogue reverse transcriptase inhibitors.Crit Care.2003;7(3):226–232.
- ,,,.Lactic acidosis after treatment with linezolid.Infection.2007;35(4):278–281.
- ,,,.Isotopic evaluation of the metabolism of pyruvate and related substrates in normal adult volunteers and severely burned children: effect of dichloroacetate and glucose infusion.Surgery.1991;110(1):54–67.
- .Alterations in carbohydrate metabolism during stress: a review of the literature.Am J Med.1995;98(1):75–84.
- .,,,.Lactic acid kinetics in respiratory alkalosis.Crit Care Med.1991;19(9):1120–1124.
- .Significance of hyperlactatemia without acidosis during hypermetabolic stress.Crit Care Med.1997;25(11):1780–1781.
- ,,,.Lactate is an unreliable indicator of tissue hypoxia in injury or sepsis.Lancet.1999;354(9177):505–508.
- ,,,,.Relation between muscle Na+K+ ATPase activity and raised lactate concentrations in septic shock: a prospective study.Lancet.2005;365(9462):871–875.
- ,.Sepsis induces diaphragm electron transport chain dysfunction and protein depletion.Am J Respir Crit Care Med.2005;172(7):861–868.
- ,,, et al.Association between mitochondrial dysfunction and severity and outcome of septic shock.Lancet.2002;360(9328):219–223.
- ,.Mitochondrial dysfunction in sepsis.Biochem Soc Symp.1999;66:149–166.
- ,,, et al.Altered glucose transporter mRNA abundance in a rat model of endotoxic shock.Biochem Biophys Res Commun.1991;176(1):535–540.
- .Increased pyruvate dehydrogenase kinase activity in response to sepsis.Am J Physiol.1991;260(5 Pt 1):E669–E674.
- .Lactate metabolism: a new paradigm for the third millennium.J Physiol.2004;558(Pt 1):5–30.
- ,,, et al.Evidence supporting the existence of an activity‐dependent astrocyte‐neuron lactate shuttle.Dev Neurosci.1998;20(4–5):291–299.
- ,,,.Brain lactate is an obligatory aerobic energy substrate for functional recovery after hypoxia: further in vitro validation.J Neurochem.1997;69(1):423–426.
- .Bench‐to‐bedside review: a possible resolution of the glucose paradox of cerebral ischemia.Crit Care.2002;6(4):330–334.
- ,,,,,.Intravenous lactate prevents cerebral dysfunction during hypoglycaemia in insulin‐dependent diabetes mellitus.Clin Sci (Lond).1998;94(2):157–163.
- ,,,.Brain lactate, not glucose, fuels the recovery of synaptic function from hypoxia upon reoxygenation: an in vitro study.Brain Res.1997;744(1):105–111.
- ,,,,,.Clinical prognostic markers in patients with severe sepsis: a prospective analysis of 139 consecutive cases.J Infect.2003;47(4):300–306.
- ,,, et al.Serum lactate as a predictor of mortality in patients with infection.Intensive Care Med.2007;33(6):970–977.
- ,,,.Lactate versus non‐lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients.Crit Care.2006;10(1):R22.
- .Abnormal resting blood lactate. I. The significance of hyperlactatemia in hospitalized patients.Am J Med.1961;30:840–848.
- ,,,,.Effect of lactic acidosis on canine hemodynamics and left ventricular function.Am J Physiol.1990;258(4 Pt 2):H1193–H1199.
- ,,,.Alkali therapy extends the period of survival during hypoxia: studies in rats.Am J Physiol.1996;271(2 Pt 2):R381–R387.
- ,,.Acidosis during early reperfusion prevents myocardial stunning in perfused ferret hearts.J Clin Invest.1988;82(3):920–927.
- ,,, et al.Effect of acidotic blood reperfusion on reperfusion injury after coronary artery occlusion in the dog heart.J Cardiovasc Pharmacol.1998;31(2):179–186.
- ,,,.Hypoxia and acidosis activate cardiac myocyte death through the Bcl‐2 family protein BNIP3.Proc Natl Acad Sci U S A.2002;99(20):12825–12830.
- ,,,,,.Extracellular acidosis delays onset of cell death in ATP‐depleted hepatocytes.Am J Physiol.1988;255(3 Pt 1):C315–C322.
- ,.Metabolic and hemodynamic effects of hypertonic solutions: sodium‐lactate versus sodium chloride infusion in postoperative patients.Shock.2002;18(4):306–310.
- .Medical complications of status epilepticus.Adv Neurol.1983;34:395–398.
- ,,,,,.Bicarbonate therapy in severe diabetic ketoacidosis. A double blind, randomized, placebo controlled trial.Rev Invest Clin.1991;43(3):234–238.
- ,,.Supercarbia in children: clinical course and outcome.Crit Care Med.1990;18(2):166–168.
- ,,,.Low mortality rate in adult respiratory distress syndrome using low‐volume, pressure‐limited ventilation with permissive hypercapnia: a prospective study.Crit Care Med.1994;22(10):1568–1578.
- ,,,.Systemic effects of NaHCO3 in experimental lactic acidosis in dogs.Am J Physiol.1982;242(6):F586–F591.
- ,,,,.Lactic acidosis: effect of treatment on intracellular pH and energetics in living rat heart.Am J Physiol.1992;262(5 Pt 2):H1572–H1578.
- ,,,,,.Effect of sodium bicarbonate on intracellular pH under different buffering conditions.Kidney Int.1996;49(5):1262–1267.
- ,,.Hemodynamic and hepatic pH responses to sodium bicarbonate and Carbicarb during systemic acidosis.Magn Reson Med.1990;16(3):403–410.
- ,,, et al.The increase in CO2 production induced by NaHCO3 depends on blood albumin and hemoglobin concentrations.Intensive Care Med.2000;26(5):558–564.
- ,,, et al.Initial effect of sodium bicarbonate on intracellular pH depends on the extracellular nonbicarbonate buffering capacity.Crit Care Med.2001;29(5):1033–1039.
- ,,,,,.Dynamic study of the distribution of microcirculatory blood flow in multiple splanchnic organs in septic shock.Crit Care Med.2000;28(9):3233–3241.
- ,,,,,.The effects of sodium bicarbonate and a mixture of sodium bicarbonate and carbonate (“Carbicarb”) on skeletal muscle pH and hemodynamic status in rats with hypovolemic shock.Metabolism.1994;43(4):518–522.
- ,,, et al.Haemodynamic and metabolic effects in diabetic ketoacidosis in rats of treatment with sodium bicarbonate or a mixture of sodium bicarbonate and sodium carbonate.Diabetologia.1995;38(8):889–898.
- ,,,,,.Effects of sodium bicarbonate on striated muscle metabolism and intracellular pH during endotoxic shock.Shock.1994;1(3):196–200.
- ,,,,.Carbicarb, sodium bicarbonate, and sodium chloride in hypoxic lactic acidosis. Effect on arterial blood gases, lactate concentrations, hemodynamic variables, and myocardial intracellular pH.Chest.1993;104(3):913–918.
- ,.Improved hemodynamic function during hypoxia with Carbicarb, a new agent for the management of acidosis.Circulation.1988;77(1):227–233.
- ,,.Metabolic effects of sodium bicarbonate in hypoxic lactic acidosis in dogs.Am J Physiol.1985;249(5 Pt 2):F630–F635.
- .Binding of calcium to serum albumin. II. Effect of pH via competitive hydrogen and calcium ion binding to the imidazole groups of albumin.Scand J Clin Lab Invest.1972;29(1):75–83.
- ,,,,.Left ventricular contractility varies directly with blood ionized calcium.Ann Intern Med.1988;108(4):524–529.
- ,,.Regulatory mechanisms of hemoglobin oxygen affinity in acidosis and alkalosis.J Clin Invest.1971;50(3):700–706.
- ,,.Metabolic and hemodynamic consequences of sodium bicarbonate administration in patients with heart disease.Am J Med.1989;87(1):7–14.
- ,,.Sodium ion/hydrogen ion exchange inhibition: a new pharmacologic approach to myocardial ischemia and reperfusion injury.J Clin Pharmacol.1998;38(10):887–897.
- ,.SEA0400: a novel sodium‐calcium exchange inhibitor with cardioprotective properties.Cardiovasc Drug Rev.2004;22(4):334–347.
- ,,,.Elevation in cytosolic free calcium concentration early in myocardial ischemia in perfused rat heart.Circ Res.1987;60(5):700–707.
- ,.Acute haemodynamic effects of sodium bicarbonate administration in respiratory and metabolic acidosis in anaesthetized dogs.Anaesth Intensive Care.1997;25(6):615–620.
- ,,,.Bicarbonate does not increase left ventricular contractility during L‐lactic acidemia in pigs.Am Rev Respir Dis.1993;148(2):317–322.
- ,,,,.Effects of bicarbonate therapy on hemodynamics and tissue oxygenation in patients with lactic acidosis: a prospective, controlled clinical study.Crit Care Med.1991;19(11):1352–1356.
- ,,, et al.Safety and efficacy of intravenous Carbicarb in patients undergoing surgery: comparison with sodium bicarbonate in the treatment of mild metabolic acidosis. SPI Research Group. Study of Perioperative Ischemia.Crit Care Med.1994;22(10):1540–1549.
- ,,, et al.Sodium bicarbonate versus THAM in ICU patients with mild metabolic acidosis.J Nephrol.2005;18(3):303–307.
- ,,, et al.A controlled clinical trial of dichloroacetate for treatment of lactic acidosis in adults. The Dichloroacetate‐Lactic Acidosis Study Group.N Engl J Med.1992;327(22):1564–1569.
- ,,,,,.Effect of continuous venovenous hemofiltration with dialysis on lactate clearance in critically ill patients.Crit Care Med.1997;25(1):58–62.
- ,,,,.A pilot randomised controlled comparison of continuous veno‐venous haemofiltration and extended daily dialysis with filtration: effect on small solutes and acid‐base balance.Intensive Care Med.2007;33(5):830–835.
- ,,.Intermittent versus continuous renal replacement therapy in the ICU: impact on electrolyte and acid‐base balance.Intensive Care Med.2001;27(6):1037–1043.
- ,,,.Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus: systematic review and meta‐analysis.Arch Intern Med.2003;163(21):2594–2602.
- ,,,,.Severe acidosis in patients taking metformin—rapid reversal and survival despite high APACHE score.Diabet Med.2006;23(4):432–435.
- ,,.Incidence of lactic acidosis in metformin users.Diabetes Care.1999;22(6):925–927.
- ,.Lactic acidosis in metformin‐treated patients. Prognostic value of arterial lactate levels and plasma metformin concentrations.Drug Saf.1999;20(4):377–384.
- ,,,.The management of metformin overdose.Anaesthesia.1998;53(7):698–701.
- ,,.Lactic acidosis in biguanide‐treated diabetics: a review of 330 cases.Diabetologia.1978;14(2):75–87.
- ,,,,.Treatment of metformin‐associated lactic acidosis with closed recirculation bicarbonate‐buffered hemodialysis.Arch Intern Med.1984;144(1):203–205.
- ,,,.High anion gap metabolic acidosis in suicide: don't forget metformin intoxication—two patients' experiences.Ren Fail.2002;24(5):671–675.
- ,,, et al.Hemodialysis in the treatment of lactic acidosis in diabetics treated by metformin: a study of metformin elimination.Int J Clin Pharmacol Ther Toxicol.1989;27(6):285–288.
- ,,.Bicarbonate haemodialysis as a treatment of metformin overdose.Nephrol Dial Transplant.1997;12(5):1046–1047.
- ,,,.Combination of intermittent haemodialysis and high‐volume continuous haemofiltration for the treatment of severe metformin‐induced lactic acidosis.Nephrol Dial Transplant.2004;19(8):2157–2158.
- ,,,.When a friend can become an enemy! Recognition and management of metformin‐associated lactic acidosis.Kidney Int.2007;72(9):1157–1160.
- .,, et al.Severe nucleoside‐associated lactic acidosis in human immunodeficiency virus‐infected patients: report of 12 cases and review of the literature.Clin Infect Dis.2002;34(6):838–846.
- ,,.Clearance of metformin by hemofiltration in overdose.J Toxicol Clin Toxicol.2002;40(2):177–180.
- .Metformin‐associated lactic acidosis.J Emerg Med.2001;20(3):267–272.
- ,.Contraindications to use of metformin. Blanket banning of metformin two days before surgery may not be a good idea.BMJ.2003;326(7392):762; author reply 762.
- ,,, et al.Hepatic failure and lactic acidosis due to fialuridine (FIAU), an investigational nucleoside analogue for chronic hepatitis B.N Engl J Med.1995;333(17):1099–1105.
- ,,,.Zidovudine‐induced fatal lactic acidosis and hepatic failure in patients with acquired immunodeficiency syndrome: report of two patients and review of the literature.Crit Care Med.1997;25(8):1425–1430.
- ,.Mitochondrial toxicity of antiviral drugs.Nat Med.1995;1(5):417–422.
- ,.Mitochondrial toxicity of nucleoside analogue reverse transcriptase inhibitors: a looming obstacle for long‐term antiretroviral therapy?Curr Opin Infect Dis.2000;13(1):5–11.
- ,,, et al.Treatment for adult HIV infection: 2006 recommendations of the International AIDS Society‐USA panel.JAMA.2006;296(7):827–843.
- ,,.Riboflavin to treat nucleoside analogue‐induced lactic acidosis.Lancet.1998;352(9124):291–292.
- ,,,,,.Severe lactic acidosis and thiamine administration in an HIV‐infected patient on HAART.Int J STD AIDS.2001;12(6):407–409.
- ,,, et al.Detecting life‐threatening lactic acidosis related to nucleoside‐analog treatment of human immunodeficiency virus‐infected patients, and treatment with L‐carnitine.Crit Care Med.2003;31(4):1042–1047.
- ,.Hyperosmolar metabolic acidosis and intravenous Lorazepam.N Engl J Med.2002;347(11):857–858; author reply 857–858.
- ,,,.Propylene glycol toxicity: a severe iatrogenic illness in ICU patients receiving IV benzodiazepines: a case series and prospective, observational pilot study.Chest.2005;128(3):1674–1681.
- ,,, et al.Propylene glycol pharmacokinetics and effects after intravenous infusion in humans.Ther Drug Monit.1987;9(3):255–258.
- .Short‐term lorazepam infusion and concern for propylene glycol toxicity: case report and review.Pharmacotherapy.2001;21(9):1140–1144.
- ,,.Recognition, treatment, and prevention of propylene glycol toxicity.Semin Dial.2007;20(3):217–219.
- ,,.Propylene glycol‐mediated cell injury in a primary culture of human proximal tubule cells.Toxicol Sci.1998;46(2):410–417.
- ,.Osmolar gap metabolic acidosis in a 60‐year‐old man treated for hypoxemic respiratory failure.Chest.2000;118(2):545–546.
- ,,,.Relationship of continuous infusion lorazepam to serum propylene glycol concentration in critically ill adults.Crit Care Med.2004;32(8):1709–1714.
- ,,,.Removal of propylene glycol and correction of increased osmolar gap by hemodialysis in a patient on high dose lorazepam infusion therapy.Intensive Care Med.2002;28(1):81–84.
- ,,.Linezolid use associated with lactic acidosis.Scand J Infect Dis.2005;37(2):153–154.
- ,.Linezolid‐induced lactic acidosis.N Engl J Med.2003;348(1):86–87.
- ,,.Toxicity of extended courses of linezolid: results of an Infectious Diseases Society of America Emerging Infections Network survey.Diagn Microbiol Infect Dis.2008;62(4):407–410.
- ,,.Mitochondrial toxicity associated with linezolid.N Engl J Med.2005;353(21):2305–2306.
- ,,, et al.Linezolid‐induced inhibition of mitochondrial protein synthesis.Clin Infect Dis.2006;42(8):1111–1117.
- ,.Use of base in the treatment of severe acidemic states.Am J Kidney Dis.2001;38(4):703–727.
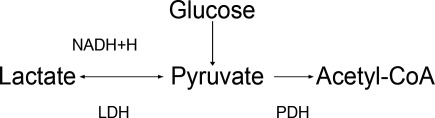
The New Vocabulary of Healthcare Reform
On March 21, 2010, the United States Congress passed the most comprehensive healthcare reform bill since the formation of Medicare. The legislation's greatest impact will be to improve access for nearly 50 million Americans who are presently uninsured. Yet the bill does little to tackle the fundamental problems of the payment and delivery systemsproblems that have resulted in major quality gaps, large numbers of medical errors, fragmented care, and backbreaking costs.
While these tough questions were mostly kicked down the road, the debate did bring many of the key questions and potential solutions into high relief. Our political leaders, pundits, and health policy scholars introduced or popularized a number of terms during the healthcare debates of 2009‐2010 (Table 1). I will attempt to place them in context and discuss their implications for future healthcare reform efforts.
|
| Value‐based purchasing |
| Bending the cost curve |
| Comparative effectiveness research (see also NICE) |
| Dartmouth atlas (see also McAllen, Texas) |
| Death panels (see also rationing) |
| Bundled payments |
| Accountable care organizations (see also Mayo Clinic, Cleveland Clinic, Geisinger; replaces HMOs) |
Some Context for the Healthcare Reform Debate
In our capitalistic economy, we make most purchases based on considerations of value: quality divided by cost. There are few among us wealthy enough to always buy the best product, or cheap enough to always buy the least expensive. Instead, we try to determine value when we purchase a restaurant meal, a house, or a vacation.
Healthcare has traditionally been the major exception to this rule, both because healthcare insurance has partly insulated consumers (patients or their proxies) from the cost consequences of their decisions, and because it is so difficult to determine the quality of healthcare. But, over the past 10 to 15 years, problems with both the numerator and denominator of this equation have created widespread recognition of the need for change.
In the numerator, we now appreciate that there are nearly 100,000 deaths per year from medical mistakes;1 that we deliver evidence‐based care only about half the time,2 and that our healthcare system is extraordinarily fragmented and chaotic. We also know that there are more than 40 million people without healthcare insurance, a uniquely American problem, since other industrialized countries manage to guarantee coverage.
This is the fundamental conundrum that needs to be addressed by healthcare reform: we have a system that produces surprisingly low‐quality, unreliable care at an exorbitant and ever‐increasing cost, and does so while leaving more than 1 out of 8 citizens without coverage. Although government is a large payer (through Medicare, Medicaid, the Veterans Affairs [VA] programs and others), most Americans receive healthcare coverage as an employee benefit; a smaller number pay for health insurance themselves. The government has a key role even in these nongovernment‐sponsored payment systems, by providing tax breaks for healthcare coverage, creating a regulatory framework, and often defining the market through its actions in its public programs.
The end result is that all the involved partiesgovernments, businesses, providers, and patientsare crying out for change. An observer of this situation feels compelled to invoke the popular version of Stein's Law: if a trend can't continue, it won't.
Bending the Cost Curve
Everyone is now familiar with the scary trends (such as in Figure 1) demonstrating the unsustainable rate of healthcare inflation in the US, trends that are projected to lead to the insolvency of the Medicare Trust Fund within a decade. The term bending the cost curve implies that our solvency depends not on lowering total costs (a political impossibility), but rather on simply decreasing the rate of rise. There are only so many ways to do this.
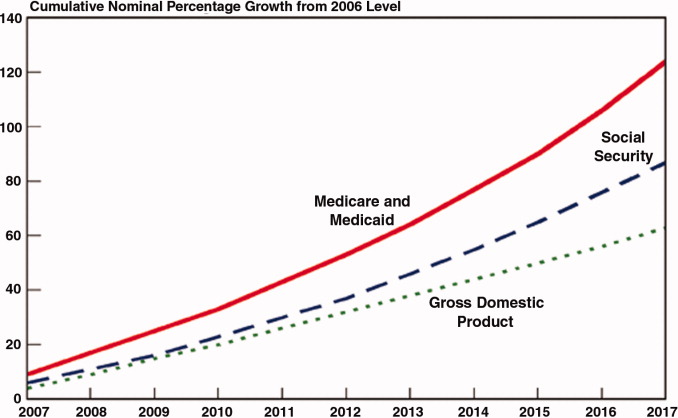
The most attractive, of course, is to stop providing expensive care that adds no or little value in terms of patient outcomes. The term comparative effectiveness research (CER) emerged over the past few years to describe research that pits one approach against another (or, presumably, against no treatment) on both outcomes and cost.3 Obviously, one would favor the less expensive treatment if the efficacy were equal. However, the more common (and politically fraught) question is whether a more expensive but slightly better approach is worth its additional cost.
This, of course, makes complete sense in a world of limited resources, and some countries, mostly notably the United Kingdom, are using CER to inform healthcare coverage decisions. In the United Kingdom, the research is analyzed, and coverage recommendations made, by an organization called the National Institute for Health and Clinical Excellence (NICE).4 While NICE appears to be working well, all signs indicate that the US political system is not ready for such an approach. In fact, although Medicare generally supports CER, most of the healthcare reform proposals considered by Congress explicitly prohibited Medicare from using CER results to influence payment decisions.
If an overall CER approach is too politically difficult for the US, how about focusing on 1 small segment of healthcare: expensive care at the end of life? Over the past 30 years, a group of Dartmouth researchers has examined the costs and quality of care across the entire country, demonstrating a ubiquitous pattern of highly variable costs (varying up to 2‐fold) that is unassociated with quality and outcomes (and sometimes even inversely associated).5 The findings, well known among healthcare researchers but relatively unknown by the public until recently, were brought to public attention by a 2009 New Yorker article that made the border town of McAllen, Texas the poster child for a medical culture that produces high costs without comparable benefits.6 The Dartmouth researchers, who publish their data in a document known as The Dartmouth Atlas, have found striking variations in care at the end of life. For example, even among academic medical centers (which presumably have similarly sick patient populations), the number of hospital days in the last 6 months of life varies strikingly: patients at New York University average 27.1 days, whereas those in my hospital average 11.5 days.7
So promoting better end‐of‐life carebeing sure that patients are aware of their options and that high‐quality palliative care is availableseemed like an obvious solution to part of our cost‐quality conundrum. Some early drafts of reform bills in Congress contained provisions to pay for physicians' time to discuss end‐of‐life options. This, of course, was caricaturized into the now famous Death Panelsproving that American political discourse is not yet mature enough to support realistic discussions about difficult subjects.8
It seems like having payers (government, insurance companies) make formal decisions about which services to cover (ie, rationing) is too hard. Is there another way to force these tough choices but do so without creating a political piata?
Encircling a Population
Rather than explicitly rationing care (using CER results, for example), another way of constraining costs is to place a population of patients on a fixed budget. There is evidence that provider organizations, working within such a budget (structured in a way that permits the providers to pocket any savings), are able to reorganize and change their practice style in a way that can cut costs.9 In the 1990s, we conducted a national experiment by promoting managed care, working through integrated delivery systems called Health Maintenance Organizations (HMOs) that received fixed, capitated payments for every patient. And, in fact, these organizations did cut overall costs.
The problem was that patients neither liked HMOs nor trusted that they were acting in their best interests. Ultimately, managed care became a less important delivery mechanism, and even patients who remained in HMOs had fewer constraints on their choices. Of course, the softening of the managed care market resulted in an uptick in healthcare inflation, contributing to our present predicament.
The concept of fixed payments has resurfaced, but with some modern twists. It appears that organizations that perform best on the Dartmouth measures (namely, they provide high quality care at lower costs) are generally large delivery systems with advanced information technology, strong primary care infrastructures, andprobably most importantlytight integration between physicians and the rest of the organization. During the healthcare debate, the organizations that received the most attention were the Mayo and Cleveland Clinics and the Geisinger system in central Pennsylvania. The problem is that the defining characteristic of these organizations (and others like them) is that they have been at this business of integrated care for more than 50 years! Can the model be emulated?
Two main policy changes have been promoted to try to achieve this integration: one is a change in payment structure, the other a change in organization. The first is known as bundlingin which multiple providers are reimbursed a single sum for all the care related to an episode of illness (such as a hospitalization and a 60‐ or 90‐day period afterwards). You will recognize this as a new form of capitation, but, rather than covering all of a patient's care, a more circumscribed version, focusing on a single illness or procedure. There is some evidence that bundling does reduce costs and may improve quality, by forcing hospitals, post‐acute care facilities, and doctors into collaborative arrangements (both to deliver care and, just as complex, to split the single payment without undue acrimony).10 Fisher et al.11 have promoted a new structure to deliver this kind of bundled care more effectively: The Accountable Care Organization (ACO), which is best thought of as a less ambitious, and potentially more virtual, incarnation of the HMO.
Interestingly, while many healthcare organizations have struggled to remake themselves in Mayo's image in preparation for upcoming pressures to form ACOs, some organizations with hospitalist programs need look no further than these programs to chart a course toward more effective physician‐hospital integration.12 Why? The majority of US hospitals now have hospitalists, and virtually all hospitalist programs receive support payments from their hospital (a sizable minority are on salary from the hospital). Hospitalists recognize that part of their value equation (which justifies the hospital support dollars) is that they help the hospital deliver higher quality care more efficiently. Because of this relationship, a well‐functioning hospitalist program can assume many of the attributes of an ACO, even in organizations with otherwise challenging physician‐hospital relations. It may be that hospitals and doctors need not look to Rochester, Minnesota or Danville, Pennsylvania for positive examples of physician‐hospital integration, but simply to their own local hospitalist groups.
The Bottom Line
While proponents of the Obama reform plan celebrate its passage, virtually all experts agree that it left fundamental problems with the healthcare system unaddressed. Although the 20092010 debate did not solve these problems, the new vocabulary introduced during the debateboth reasonable policy ideas like bundling and ACOs and cynical caricatures like death panelsare here to stay. Understanding these terms and the context that shaped them will be critical for hospitalists and other stakeholders interested in the future of the American healthcare system.
- ,,, eds.To Err is Human: Building a Safer Health System.Washington DC:Committee on Quality of Health Care in America, Institute of Medicine. National Academy Press,2000.
- ,,, et al.The quality of health care delivered to adults in the United States.N Engl J Med.2003;348:2635–2645.
- ,.Health care reform and the need for comparative‐effectiveness research.N Engl J Med.2010;362:e6.
- .Saying no isn't NICE—the travails of Britain's National Institute for health and clinical excellence.N Engl J Med.2008;359:1977–1981.
- .Wrestling with variation: an interview with Jack Wennberg [interviewed by Fitzhugh Mullan].Health Aff (Millwood).2004; Suppl Web Exclsives:VAR73–80.
- .The cost conundrum. What a Texas town can teach us about health care.The New Yorker2009. Available at: http://www.newyorker. com/reporting/2009/06/01/090601fa_fact_gawande. Accessed February 2010.
- .Researchers find huge variations in end‐of‐life treatment.New York Times.2008. Available at: http://www.nytimes.com/2008/04/07/health/policy/07care.html?_r=1. Accessed February 2010.
- .Ending end‐of‐life phobia—a prescription for enlightened health care reform.N Engl J Med.2009. Available at: http://healthcarere form.nejm.org/?p=2580. Accessed February 2010.
- ,.The RAND Health Insurance Experiment and HMOs.Med Care.1990;28:191–200.
- ,,.Cost savings and physician responses to global bundled payments for Medicare heart bypass surgery.Health Care Fin Rev.1997;19:41–57.
- ,,,.Creating accountable care organizations: the extended hospital medical staff.Health Aff (Millwood).2007;26(1):w44–w57.
- . Hospitalists: a little slice of Mayo. Available at: http://community.the‐hospitalist.org/blogs/wachters_world/archive/2009/08/30/hospitalists‐a‐little‐slice‐of‐mayo.aspx. Accessed February 2010.
On March 21, 2010, the United States Congress passed the most comprehensive healthcare reform bill since the formation of Medicare. The legislation's greatest impact will be to improve access for nearly 50 million Americans who are presently uninsured. Yet the bill does little to tackle the fundamental problems of the payment and delivery systemsproblems that have resulted in major quality gaps, large numbers of medical errors, fragmented care, and backbreaking costs.
While these tough questions were mostly kicked down the road, the debate did bring many of the key questions and potential solutions into high relief. Our political leaders, pundits, and health policy scholars introduced or popularized a number of terms during the healthcare debates of 2009‐2010 (Table 1). I will attempt to place them in context and discuss their implications for future healthcare reform efforts.
|
| Value‐based purchasing |
| Bending the cost curve |
| Comparative effectiveness research (see also NICE) |
| Dartmouth atlas (see also McAllen, Texas) |
| Death panels (see also rationing) |
| Bundled payments |
| Accountable care organizations (see also Mayo Clinic, Cleveland Clinic, Geisinger; replaces HMOs) |
Some Context for the Healthcare Reform Debate
In our capitalistic economy, we make most purchases based on considerations of value: quality divided by cost. There are few among us wealthy enough to always buy the best product, or cheap enough to always buy the least expensive. Instead, we try to determine value when we purchase a restaurant meal, a house, or a vacation.
Healthcare has traditionally been the major exception to this rule, both because healthcare insurance has partly insulated consumers (patients or their proxies) from the cost consequences of their decisions, and because it is so difficult to determine the quality of healthcare. But, over the past 10 to 15 years, problems with both the numerator and denominator of this equation have created widespread recognition of the need for change.
In the numerator, we now appreciate that there are nearly 100,000 deaths per year from medical mistakes;1 that we deliver evidence‐based care only about half the time,2 and that our healthcare system is extraordinarily fragmented and chaotic. We also know that there are more than 40 million people without healthcare insurance, a uniquely American problem, since other industrialized countries manage to guarantee coverage.
This is the fundamental conundrum that needs to be addressed by healthcare reform: we have a system that produces surprisingly low‐quality, unreliable care at an exorbitant and ever‐increasing cost, and does so while leaving more than 1 out of 8 citizens without coverage. Although government is a large payer (through Medicare, Medicaid, the Veterans Affairs [VA] programs and others), most Americans receive healthcare coverage as an employee benefit; a smaller number pay for health insurance themselves. The government has a key role even in these nongovernment‐sponsored payment systems, by providing tax breaks for healthcare coverage, creating a regulatory framework, and often defining the market through its actions in its public programs.
The end result is that all the involved partiesgovernments, businesses, providers, and patientsare crying out for change. An observer of this situation feels compelled to invoke the popular version of Stein's Law: if a trend can't continue, it won't.
Bending the Cost Curve
Everyone is now familiar with the scary trends (such as in Figure 1) demonstrating the unsustainable rate of healthcare inflation in the US, trends that are projected to lead to the insolvency of the Medicare Trust Fund within a decade. The term bending the cost curve implies that our solvency depends not on lowering total costs (a political impossibility), but rather on simply decreasing the rate of rise. There are only so many ways to do this.
The most attractive, of course, is to stop providing expensive care that adds no or little value in terms of patient outcomes. The term comparative effectiveness research (CER) emerged over the past few years to describe research that pits one approach against another (or, presumably, against no treatment) on both outcomes and cost.3 Obviously, one would favor the less expensive treatment if the efficacy were equal. However, the more common (and politically fraught) question is whether a more expensive but slightly better approach is worth its additional cost.
This, of course, makes complete sense in a world of limited resources, and some countries, mostly notably the United Kingdom, are using CER to inform healthcare coverage decisions. In the United Kingdom, the research is analyzed, and coverage recommendations made, by an organization called the National Institute for Health and Clinical Excellence (NICE).4 While NICE appears to be working well, all signs indicate that the US political system is not ready for such an approach. In fact, although Medicare generally supports CER, most of the healthcare reform proposals considered by Congress explicitly prohibited Medicare from using CER results to influence payment decisions.
If an overall CER approach is too politically difficult for the US, how about focusing on 1 small segment of healthcare: expensive care at the end of life? Over the past 30 years, a group of Dartmouth researchers has examined the costs and quality of care across the entire country, demonstrating a ubiquitous pattern of highly variable costs (varying up to 2‐fold) that is unassociated with quality and outcomes (and sometimes even inversely associated).5 The findings, well known among healthcare researchers but relatively unknown by the public until recently, were brought to public attention by a 2009 New Yorker article that made the border town of McAllen, Texas the poster child for a medical culture that produces high costs without comparable benefits.6 The Dartmouth researchers, who publish their data in a document known as The Dartmouth Atlas, have found striking variations in care at the end of life. For example, even among academic medical centers (which presumably have similarly sick patient populations), the number of hospital days in the last 6 months of life varies strikingly: patients at New York University average 27.1 days, whereas those in my hospital average 11.5 days.7
So promoting better end‐of‐life carebeing sure that patients are aware of their options and that high‐quality palliative care is availableseemed like an obvious solution to part of our cost‐quality conundrum. Some early drafts of reform bills in Congress contained provisions to pay for physicians' time to discuss end‐of‐life options. This, of course, was caricaturized into the now famous Death Panelsproving that American political discourse is not yet mature enough to support realistic discussions about difficult subjects.8
It seems like having payers (government, insurance companies) make formal decisions about which services to cover (ie, rationing) is too hard. Is there another way to force these tough choices but do so without creating a political piata?
Encircling a Population
Rather than explicitly rationing care (using CER results, for example), another way of constraining costs is to place a population of patients on a fixed budget. There is evidence that provider organizations, working within such a budget (structured in a way that permits the providers to pocket any savings), are able to reorganize and change their practice style in a way that can cut costs.9 In the 1990s, we conducted a national experiment by promoting managed care, working through integrated delivery systems called Health Maintenance Organizations (HMOs) that received fixed, capitated payments for every patient. And, in fact, these organizations did cut overall costs.
The problem was that patients neither liked HMOs nor trusted that they were acting in their best interests. Ultimately, managed care became a less important delivery mechanism, and even patients who remained in HMOs had fewer constraints on their choices. Of course, the softening of the managed care market resulted in an uptick in healthcare inflation, contributing to our present predicament.
The concept of fixed payments has resurfaced, but with some modern twists. It appears that organizations that perform best on the Dartmouth measures (namely, they provide high quality care at lower costs) are generally large delivery systems with advanced information technology, strong primary care infrastructures, andprobably most importantlytight integration between physicians and the rest of the organization. During the healthcare debate, the organizations that received the most attention were the Mayo and Cleveland Clinics and the Geisinger system in central Pennsylvania. The problem is that the defining characteristic of these organizations (and others like them) is that they have been at this business of integrated care for more than 50 years! Can the model be emulated?
Two main policy changes have been promoted to try to achieve this integration: one is a change in payment structure, the other a change in organization. The first is known as bundlingin which multiple providers are reimbursed a single sum for all the care related to an episode of illness (such as a hospitalization and a 60‐ or 90‐day period afterwards). You will recognize this as a new form of capitation, but, rather than covering all of a patient's care, a more circumscribed version, focusing on a single illness or procedure. There is some evidence that bundling does reduce costs and may improve quality, by forcing hospitals, post‐acute care facilities, and doctors into collaborative arrangements (both to deliver care and, just as complex, to split the single payment without undue acrimony).10 Fisher et al.11 have promoted a new structure to deliver this kind of bundled care more effectively: The Accountable Care Organization (ACO), which is best thought of as a less ambitious, and potentially more virtual, incarnation of the HMO.
Interestingly, while many healthcare organizations have struggled to remake themselves in Mayo's image in preparation for upcoming pressures to form ACOs, some organizations with hospitalist programs need look no further than these programs to chart a course toward more effective physician‐hospital integration.12 Why? The majority of US hospitals now have hospitalists, and virtually all hospitalist programs receive support payments from their hospital (a sizable minority are on salary from the hospital). Hospitalists recognize that part of their value equation (which justifies the hospital support dollars) is that they help the hospital deliver higher quality care more efficiently. Because of this relationship, a well‐functioning hospitalist program can assume many of the attributes of an ACO, even in organizations with otherwise challenging physician‐hospital relations. It may be that hospitals and doctors need not look to Rochester, Minnesota or Danville, Pennsylvania for positive examples of physician‐hospital integration, but simply to their own local hospitalist groups.
The Bottom Line
While proponents of the Obama reform plan celebrate its passage, virtually all experts agree that it left fundamental problems with the healthcare system unaddressed. Although the 20092010 debate did not solve these problems, the new vocabulary introduced during the debateboth reasonable policy ideas like bundling and ACOs and cynical caricatures like death panelsare here to stay. Understanding these terms and the context that shaped them will be critical for hospitalists and other stakeholders interested in the future of the American healthcare system.
On March 21, 2010, the United States Congress passed the most comprehensive healthcare reform bill since the formation of Medicare. The legislation's greatest impact will be to improve access for nearly 50 million Americans who are presently uninsured. Yet the bill does little to tackle the fundamental problems of the payment and delivery systemsproblems that have resulted in major quality gaps, large numbers of medical errors, fragmented care, and backbreaking costs.
While these tough questions were mostly kicked down the road, the debate did bring many of the key questions and potential solutions into high relief. Our political leaders, pundits, and health policy scholars introduced or popularized a number of terms during the healthcare debates of 2009‐2010 (Table 1). I will attempt to place them in context and discuss their implications for future healthcare reform efforts.
|
| Value‐based purchasing |
| Bending the cost curve |
| Comparative effectiveness research (see also NICE) |
| Dartmouth atlas (see also McAllen, Texas) |
| Death panels (see also rationing) |
| Bundled payments |
| Accountable care organizations (see also Mayo Clinic, Cleveland Clinic, Geisinger; replaces HMOs) |
Some Context for the Healthcare Reform Debate
In our capitalistic economy, we make most purchases based on considerations of value: quality divided by cost. There are few among us wealthy enough to always buy the best product, or cheap enough to always buy the least expensive. Instead, we try to determine value when we purchase a restaurant meal, a house, or a vacation.
Healthcare has traditionally been the major exception to this rule, both because healthcare insurance has partly insulated consumers (patients or their proxies) from the cost consequences of their decisions, and because it is so difficult to determine the quality of healthcare. But, over the past 10 to 15 years, problems with both the numerator and denominator of this equation have created widespread recognition of the need for change.
In the numerator, we now appreciate that there are nearly 100,000 deaths per year from medical mistakes;1 that we deliver evidence‐based care only about half the time,2 and that our healthcare system is extraordinarily fragmented and chaotic. We also know that there are more than 40 million people without healthcare insurance, a uniquely American problem, since other industrialized countries manage to guarantee coverage.
This is the fundamental conundrum that needs to be addressed by healthcare reform: we have a system that produces surprisingly low‐quality, unreliable care at an exorbitant and ever‐increasing cost, and does so while leaving more than 1 out of 8 citizens without coverage. Although government is a large payer (through Medicare, Medicaid, the Veterans Affairs [VA] programs and others), most Americans receive healthcare coverage as an employee benefit; a smaller number pay for health insurance themselves. The government has a key role even in these nongovernment‐sponsored payment systems, by providing tax breaks for healthcare coverage, creating a regulatory framework, and often defining the market through its actions in its public programs.
The end result is that all the involved partiesgovernments, businesses, providers, and patientsare crying out for change. An observer of this situation feels compelled to invoke the popular version of Stein's Law: if a trend can't continue, it won't.
Bending the Cost Curve
Everyone is now familiar with the scary trends (such as in Figure 1) demonstrating the unsustainable rate of healthcare inflation in the US, trends that are projected to lead to the insolvency of the Medicare Trust Fund within a decade. The term bending the cost curve implies that our solvency depends not on lowering total costs (a political impossibility), but rather on simply decreasing the rate of rise. There are only so many ways to do this.
The most attractive, of course, is to stop providing expensive care that adds no or little value in terms of patient outcomes. The term comparative effectiveness research (CER) emerged over the past few years to describe research that pits one approach against another (or, presumably, against no treatment) on both outcomes and cost.3 Obviously, one would favor the less expensive treatment if the efficacy were equal. However, the more common (and politically fraught) question is whether a more expensive but slightly better approach is worth its additional cost.
This, of course, makes complete sense in a world of limited resources, and some countries, mostly notably the United Kingdom, are using CER to inform healthcare coverage decisions. In the United Kingdom, the research is analyzed, and coverage recommendations made, by an organization called the National Institute for Health and Clinical Excellence (NICE).4 While NICE appears to be working well, all signs indicate that the US political system is not ready for such an approach. In fact, although Medicare generally supports CER, most of the healthcare reform proposals considered by Congress explicitly prohibited Medicare from using CER results to influence payment decisions.
If an overall CER approach is too politically difficult for the US, how about focusing on 1 small segment of healthcare: expensive care at the end of life? Over the past 30 years, a group of Dartmouth researchers has examined the costs and quality of care across the entire country, demonstrating a ubiquitous pattern of highly variable costs (varying up to 2‐fold) that is unassociated with quality and outcomes (and sometimes even inversely associated).5 The findings, well known among healthcare researchers but relatively unknown by the public until recently, were brought to public attention by a 2009 New Yorker article that made the border town of McAllen, Texas the poster child for a medical culture that produces high costs without comparable benefits.6 The Dartmouth researchers, who publish their data in a document known as The Dartmouth Atlas, have found striking variations in care at the end of life. For example, even among academic medical centers (which presumably have similarly sick patient populations), the number of hospital days in the last 6 months of life varies strikingly: patients at New York University average 27.1 days, whereas those in my hospital average 11.5 days.7
So promoting better end‐of‐life carebeing sure that patients are aware of their options and that high‐quality palliative care is availableseemed like an obvious solution to part of our cost‐quality conundrum. Some early drafts of reform bills in Congress contained provisions to pay for physicians' time to discuss end‐of‐life options. This, of course, was caricaturized into the now famous Death Panelsproving that American political discourse is not yet mature enough to support realistic discussions about difficult subjects.8
It seems like having payers (government, insurance companies) make formal decisions about which services to cover (ie, rationing) is too hard. Is there another way to force these tough choices but do so without creating a political piata?
Encircling a Population
Rather than explicitly rationing care (using CER results, for example), another way of constraining costs is to place a population of patients on a fixed budget. There is evidence that provider organizations, working within such a budget (structured in a way that permits the providers to pocket any savings), are able to reorganize and change their practice style in a way that can cut costs.9 In the 1990s, we conducted a national experiment by promoting managed care, working through integrated delivery systems called Health Maintenance Organizations (HMOs) that received fixed, capitated payments for every patient. And, in fact, these organizations did cut overall costs.
The problem was that patients neither liked HMOs nor trusted that they were acting in their best interests. Ultimately, managed care became a less important delivery mechanism, and even patients who remained in HMOs had fewer constraints on their choices. Of course, the softening of the managed care market resulted in an uptick in healthcare inflation, contributing to our present predicament.
The concept of fixed payments has resurfaced, but with some modern twists. It appears that organizations that perform best on the Dartmouth measures (namely, they provide high quality care at lower costs) are generally large delivery systems with advanced information technology, strong primary care infrastructures, andprobably most importantlytight integration between physicians and the rest of the organization. During the healthcare debate, the organizations that received the most attention were the Mayo and Cleveland Clinics and the Geisinger system in central Pennsylvania. The problem is that the defining characteristic of these organizations (and others like them) is that they have been at this business of integrated care for more than 50 years! Can the model be emulated?
Two main policy changes have been promoted to try to achieve this integration: one is a change in payment structure, the other a change in organization. The first is known as bundlingin which multiple providers are reimbursed a single sum for all the care related to an episode of illness (such as a hospitalization and a 60‐ or 90‐day period afterwards). You will recognize this as a new form of capitation, but, rather than covering all of a patient's care, a more circumscribed version, focusing on a single illness or procedure. There is some evidence that bundling does reduce costs and may improve quality, by forcing hospitals, post‐acute care facilities, and doctors into collaborative arrangements (both to deliver care and, just as complex, to split the single payment without undue acrimony).10 Fisher et al.11 have promoted a new structure to deliver this kind of bundled care more effectively: The Accountable Care Organization (ACO), which is best thought of as a less ambitious, and potentially more virtual, incarnation of the HMO.
Interestingly, while many healthcare organizations have struggled to remake themselves in Mayo's image in preparation for upcoming pressures to form ACOs, some organizations with hospitalist programs need look no further than these programs to chart a course toward more effective physician‐hospital integration.12 Why? The majority of US hospitals now have hospitalists, and virtually all hospitalist programs receive support payments from their hospital (a sizable minority are on salary from the hospital). Hospitalists recognize that part of their value equation (which justifies the hospital support dollars) is that they help the hospital deliver higher quality care more efficiently. Because of this relationship, a well‐functioning hospitalist program can assume many of the attributes of an ACO, even in organizations with otherwise challenging physician‐hospital relations. It may be that hospitals and doctors need not look to Rochester, Minnesota or Danville, Pennsylvania for positive examples of physician‐hospital integration, but simply to their own local hospitalist groups.
The Bottom Line
While proponents of the Obama reform plan celebrate its passage, virtually all experts agree that it left fundamental problems with the healthcare system unaddressed. Although the 20092010 debate did not solve these problems, the new vocabulary introduced during the debateboth reasonable policy ideas like bundling and ACOs and cynical caricatures like death panelsare here to stay. Understanding these terms and the context that shaped them will be critical for hospitalists and other stakeholders interested in the future of the American healthcare system.
- ,,, eds.To Err is Human: Building a Safer Health System.Washington DC:Committee on Quality of Health Care in America, Institute of Medicine. National Academy Press,2000.
- ,,, et al.The quality of health care delivered to adults in the United States.N Engl J Med.2003;348:2635–2645.
- ,.Health care reform and the need for comparative‐effectiveness research.N Engl J Med.2010;362:e6.
- .Saying no isn't NICE—the travails of Britain's National Institute for health and clinical excellence.N Engl J Med.2008;359:1977–1981.
- .Wrestling with variation: an interview with Jack Wennberg [interviewed by Fitzhugh Mullan].Health Aff (Millwood).2004; Suppl Web Exclsives:VAR73–80.
- .The cost conundrum. What a Texas town can teach us about health care.The New Yorker2009. Available at: http://www.newyorker. com/reporting/2009/06/01/090601fa_fact_gawande. Accessed February 2010.
- .Researchers find huge variations in end‐of‐life treatment.New York Times.2008. Available at: http://www.nytimes.com/2008/04/07/health/policy/07care.html?_r=1. Accessed February 2010.
- .Ending end‐of‐life phobia—a prescription for enlightened health care reform.N Engl J Med.2009. Available at: http://healthcarere form.nejm.org/?p=2580. Accessed February 2010.
- ,.The RAND Health Insurance Experiment and HMOs.Med Care.1990;28:191–200.
- ,,.Cost savings and physician responses to global bundled payments for Medicare heart bypass surgery.Health Care Fin Rev.1997;19:41–57.
- ,,,.Creating accountable care organizations: the extended hospital medical staff.Health Aff (Millwood).2007;26(1):w44–w57.
- . Hospitalists: a little slice of Mayo. Available at: http://community.the‐hospitalist.org/blogs/wachters_world/archive/2009/08/30/hospitalists‐a‐little‐slice‐of‐mayo.aspx. Accessed February 2010.
- ,,, eds.To Err is Human: Building a Safer Health System.Washington DC:Committee on Quality of Health Care in America, Institute of Medicine. National Academy Press,2000.
- ,,, et al.The quality of health care delivered to adults in the United States.N Engl J Med.2003;348:2635–2645.
- ,.Health care reform and the need for comparative‐effectiveness research.N Engl J Med.2010;362:e6.
- .Saying no isn't NICE—the travails of Britain's National Institute for health and clinical excellence.N Engl J Med.2008;359:1977–1981.
- .Wrestling with variation: an interview with Jack Wennberg [interviewed by Fitzhugh Mullan].Health Aff (Millwood).2004; Suppl Web Exclsives:VAR73–80.
- .The cost conundrum. What a Texas town can teach us about health care.The New Yorker2009. Available at: http://www.newyorker. com/reporting/2009/06/01/090601fa_fact_gawande. Accessed February 2010.
- .Researchers find huge variations in end‐of‐life treatment.New York Times.2008. Available at: http://www.nytimes.com/2008/04/07/health/policy/07care.html?_r=1. Accessed February 2010.
- .Ending end‐of‐life phobia—a prescription for enlightened health care reform.N Engl J Med.2009. Available at: http://healthcarere form.nejm.org/?p=2580. Accessed February 2010.
- ,.The RAND Health Insurance Experiment and HMOs.Med Care.1990;28:191–200.
- ,,.Cost savings and physician responses to global bundled payments for Medicare heart bypass surgery.Health Care Fin Rev.1997;19:41–57.
- ,,,.Creating accountable care organizations: the extended hospital medical staff.Health Aff (Millwood).2007;26(1):w44–w57.
- . Hospitalists: a little slice of Mayo. Available at: http://community.the‐hospitalist.org/blogs/wachters_world/archive/2009/08/30/hospitalists‐a‐little‐slice‐of‐mayo.aspx. Accessed February 2010.
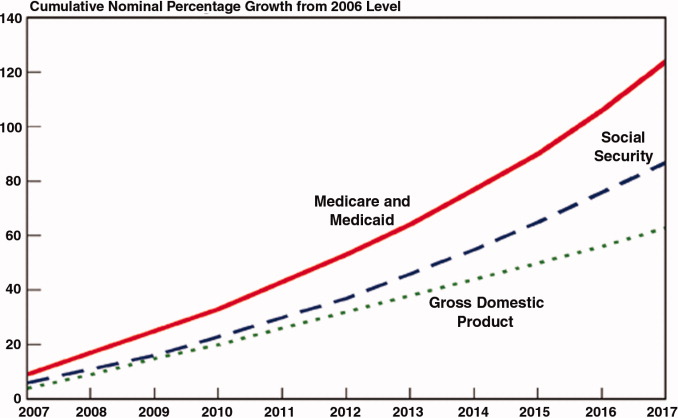
Acute Renal Infarction
A 58‐year‐old man presented with a 1‐day history of left lower quadrant abdominal pain. He had a history of remote tobacco use, hypertension, hypercholesterolemia, deep venous thrombosis, and pulmonary embolism. His white cell count was 18,500/mm,3 and urinalysis revealed hematuria. Contrast‐enhanced abdominal computed tomography (CT) scan showed decreased perfusion of a large section of the lower pole of the left kidney (Figure 1). On day 3, his flank pain persisted, despite hydration, analgesics, and intravenous (IV) antibiotics. His serum lactate dehydrogenase (LDH) was elevated and renal infarction was suspected. Heparin was started and the patient was later discharged on warfarin. One month later, repeat contrast‐enhanced abdominal CT showed a less extensive wedge defect with scarring of the left kidney.
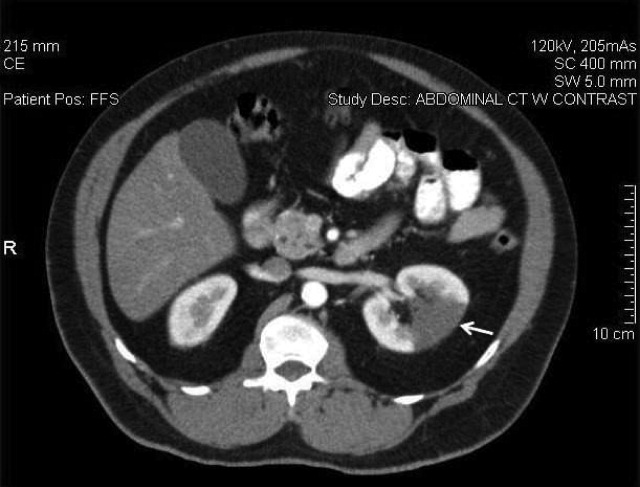
The diagnosis of acute renal infarction is often missed due to its nonspecific symptoms and the fact that it is an uncommon disease. It should be suspected in patients with acute flank pain and risk factors for thromboembolism including: valvular or ischemic heart disease, atrial fibrillation, and previous thromboembolic events.1, 2 Hypertension, which our patient had, is also a risk factor. In the appropriate setting hematuria and elevated LDH strongly suggest the diagnosis.3 Angiography remains the gold‐standard for diagnosis, but contrast‐enhanced CT is an acceptable alternative.3 In the setting of gross hematuria, we recommend that acute renal infarction should be suspected in all patients with the triad of persistent flank pain, high thromboembolic risk, and an increased LDH.
- ,,, et al.ED presentations of acute renal infarction.Am J Emerg Med.2007;25:164–169.
- ,,,.Renal artery embolism: clinical features and long‐term follow‐up of 17 cases.Ann Intern Med.1978;89:477–482.
- ,,, et al.Acute renal infarction. Clinical characteristics of 17 patients.Medicine (Baltimore).1999;78:386–394.
A 58‐year‐old man presented with a 1‐day history of left lower quadrant abdominal pain. He had a history of remote tobacco use, hypertension, hypercholesterolemia, deep venous thrombosis, and pulmonary embolism. His white cell count was 18,500/mm,3 and urinalysis revealed hematuria. Contrast‐enhanced abdominal computed tomography (CT) scan showed decreased perfusion of a large section of the lower pole of the left kidney (Figure 1). On day 3, his flank pain persisted, despite hydration, analgesics, and intravenous (IV) antibiotics. His serum lactate dehydrogenase (LDH) was elevated and renal infarction was suspected. Heparin was started and the patient was later discharged on warfarin. One month later, repeat contrast‐enhanced abdominal CT showed a less extensive wedge defect with scarring of the left kidney.
The diagnosis of acute renal infarction is often missed due to its nonspecific symptoms and the fact that it is an uncommon disease. It should be suspected in patients with acute flank pain and risk factors for thromboembolism including: valvular or ischemic heart disease, atrial fibrillation, and previous thromboembolic events.1, 2 Hypertension, which our patient had, is also a risk factor. In the appropriate setting hematuria and elevated LDH strongly suggest the diagnosis.3 Angiography remains the gold‐standard for diagnosis, but contrast‐enhanced CT is an acceptable alternative.3 In the setting of gross hematuria, we recommend that acute renal infarction should be suspected in all patients with the triad of persistent flank pain, high thromboembolic risk, and an increased LDH.
A 58‐year‐old man presented with a 1‐day history of left lower quadrant abdominal pain. He had a history of remote tobacco use, hypertension, hypercholesterolemia, deep venous thrombosis, and pulmonary embolism. His white cell count was 18,500/mm,3 and urinalysis revealed hematuria. Contrast‐enhanced abdominal computed tomography (CT) scan showed decreased perfusion of a large section of the lower pole of the left kidney (Figure 1). On day 3, his flank pain persisted, despite hydration, analgesics, and intravenous (IV) antibiotics. His serum lactate dehydrogenase (LDH) was elevated and renal infarction was suspected. Heparin was started and the patient was later discharged on warfarin. One month later, repeat contrast‐enhanced abdominal CT showed a less extensive wedge defect with scarring of the left kidney.
The diagnosis of acute renal infarction is often missed due to its nonspecific symptoms and the fact that it is an uncommon disease. It should be suspected in patients with acute flank pain and risk factors for thromboembolism including: valvular or ischemic heart disease, atrial fibrillation, and previous thromboembolic events.1, 2 Hypertension, which our patient had, is also a risk factor. In the appropriate setting hematuria and elevated LDH strongly suggest the diagnosis.3 Angiography remains the gold‐standard for diagnosis, but contrast‐enhanced CT is an acceptable alternative.3 In the setting of gross hematuria, we recommend that acute renal infarction should be suspected in all patients with the triad of persistent flank pain, high thromboembolic risk, and an increased LDH.
- ,,, et al.ED presentations of acute renal infarction.Am J Emerg Med.2007;25:164–169.
- ,,,.Renal artery embolism: clinical features and long‐term follow‐up of 17 cases.Ann Intern Med.1978;89:477–482.
- ,,, et al.Acute renal infarction. Clinical characteristics of 17 patients.Medicine (Baltimore).1999;78:386–394.
- ,,, et al.ED presentations of acute renal infarction.Am J Emerg Med.2007;25:164–169.
- ,,,.Renal artery embolism: clinical features and long‐term follow‐up of 17 cases.Ann Intern Med.1978;89:477–482.
- ,,, et al.Acute renal infarction. Clinical characteristics of 17 patients.Medicine (Baltimore).1999;78:386–394.
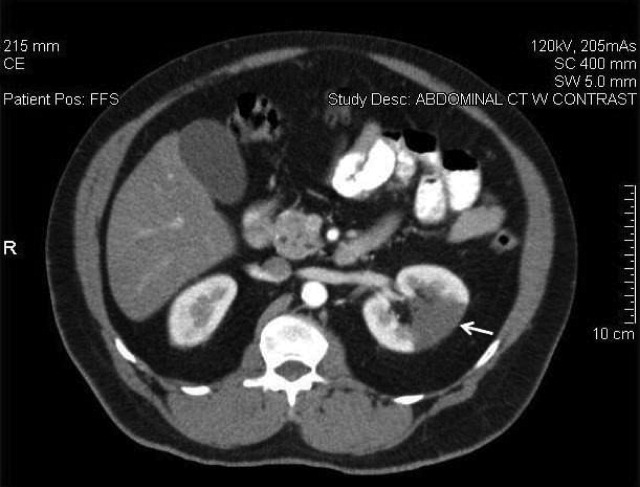
Safety in Numbers
A report that associates lower ICU mortality rates with multidisciplinary team rounding has one thought leader envisioning hospitalists as a key part of future collaborations.
The Feb. 22 study, "The Effect of Multidisciplinary Care Teams on Intensive Care Unit Mortality," included 107,324 patients at 112 hospitals (Arch Intern Med. 2010;170(4):369-376). Overall 30-day mortality was 18.3%. After making adjustments for patient and hospital characteristics, the team reported that multidisciplinary care was associated with significant reductions in the odds of death (odds ratio [OR], 0.84%; 95% confidence interval [CI], 0.76-0.93 [P=0.01]).
J. Perren Cobb, MD, of Massachusetts General Hospital in Boston wrote an accompanying editorial calling for physicians to see quality improvement (QI) projects tied to collaborative care as stepping stones to what he calls "health engineering." He defines the term as the "application of systems science to study how staff, patient, data, and equipment interactions can be engineered to optimize patient outcomes."
Dr. Cobb explains, for example, that hospitalists and intensivists can provide 24/7 care. "Hospitalists can bridge the care of the patient from the ICU to the non-ICU setting," he says.
Dr. Cobb wants competing factions in hospitals to share a "common vision" that studies patient care from both macro and micro perspectives. That encompasses everything from patient handoffs that require brief conversations between shifts to streamlining electronic medical records. His editorial focuses on the potential improvements in ICUs, but he notes that the "engineering of healthcare" can improve efficiency and efficacy across the continuum of care.
"The components are all there; they’ve been there for a long time," Dr. Cobb adds. "But what we're seeing in medicine is we’re evolving from 'seeing one patient at a time' to managing systems."
A report that associates lower ICU mortality rates with multidisciplinary team rounding has one thought leader envisioning hospitalists as a key part of future collaborations.
The Feb. 22 study, "The Effect of Multidisciplinary Care Teams on Intensive Care Unit Mortality," included 107,324 patients at 112 hospitals (Arch Intern Med. 2010;170(4):369-376). Overall 30-day mortality was 18.3%. After making adjustments for patient and hospital characteristics, the team reported that multidisciplinary care was associated with significant reductions in the odds of death (odds ratio [OR], 0.84%; 95% confidence interval [CI], 0.76-0.93 [P=0.01]).
J. Perren Cobb, MD, of Massachusetts General Hospital in Boston wrote an accompanying editorial calling for physicians to see quality improvement (QI) projects tied to collaborative care as stepping stones to what he calls "health engineering." He defines the term as the "application of systems science to study how staff, patient, data, and equipment interactions can be engineered to optimize patient outcomes."
Dr. Cobb explains, for example, that hospitalists and intensivists can provide 24/7 care. "Hospitalists can bridge the care of the patient from the ICU to the non-ICU setting," he says.
Dr. Cobb wants competing factions in hospitals to share a "common vision" that studies patient care from both macro and micro perspectives. That encompasses everything from patient handoffs that require brief conversations between shifts to streamlining electronic medical records. His editorial focuses on the potential improvements in ICUs, but he notes that the "engineering of healthcare" can improve efficiency and efficacy across the continuum of care.
"The components are all there; they’ve been there for a long time," Dr. Cobb adds. "But what we're seeing in medicine is we’re evolving from 'seeing one patient at a time' to managing systems."
A report that associates lower ICU mortality rates with multidisciplinary team rounding has one thought leader envisioning hospitalists as a key part of future collaborations.
The Feb. 22 study, "The Effect of Multidisciplinary Care Teams on Intensive Care Unit Mortality," included 107,324 patients at 112 hospitals (Arch Intern Med. 2010;170(4):369-376). Overall 30-day mortality was 18.3%. After making adjustments for patient and hospital characteristics, the team reported that multidisciplinary care was associated with significant reductions in the odds of death (odds ratio [OR], 0.84%; 95% confidence interval [CI], 0.76-0.93 [P=0.01]).
J. Perren Cobb, MD, of Massachusetts General Hospital in Boston wrote an accompanying editorial calling for physicians to see quality improvement (QI) projects tied to collaborative care as stepping stones to what he calls "health engineering." He defines the term as the "application of systems science to study how staff, patient, data, and equipment interactions can be engineered to optimize patient outcomes."
Dr. Cobb explains, for example, that hospitalists and intensivists can provide 24/7 care. "Hospitalists can bridge the care of the patient from the ICU to the non-ICU setting," he says.
Dr. Cobb wants competing factions in hospitals to share a "common vision" that studies patient care from both macro and micro perspectives. That encompasses everything from patient handoffs that require brief conversations between shifts to streamlining electronic medical records. His editorial focuses on the potential improvements in ICUs, but he notes that the "engineering of healthcare" can improve efficiency and efficacy across the continuum of care.
"The components are all there; they’ve been there for a long time," Dr. Cobb adds. "But what we're seeing in medicine is we’re evolving from 'seeing one patient at a time' to managing systems."
Schedule Solutions
With hospitalist demand outstripping supply, a fine-tuned group schedule can enhance productivity and job satisfaction. Two HM group leaders recently spoke with TH eWire about how they avoid a one-size-fits-all approach.
Stephen Houff, MD, president and CEO of Canton, Ohio-based Hospitalists Management Group, deploys 350 hospitalists to 41 hospitals in 11 states. Groups average eight hospitalists (range four to 20), and have an average daily census (ADC) of 50. Most work a seven-on/seven-off block shift. Dr. Houff says his HM groups create effective schedules in the following ways:
- In an eight-person group, three hospitalists work 7 a.m. to 7 p.m., and one doctor staffs the ED from 11 a.m. to 11 p.m.;
- Members must work four consecutive days;
- After getting established in a location, HM groups find local office-based PCPs to moonlight, covering their malpractice insurance and billing; and
- A dozen HMG hospitalists known as “firefighters” cover emergency or planned short-term leaves, receiving 15% higher pay plus per diems.
Haiwen Ma, MD, PhD, director of Hospitalist Services at South Nassau Communities Hospital in Oceanside, N.Y., has two nocturnists and five hospitalists in the group who work Monday through Friday from 7 a.m. to 7 p.m. The group has an ADC of 45-50 and a 15-patient cap per hospitalist. Here’s how she makes it work:
- Four hospitalists cover admissions in three-hour blocks from 7 a.m. to 7 p.m. and do weekend calls every fourth week;
- The fifth hospitalist performs pre-surgical/post-surgical consults; and
- The group relies on per-diem moonlighters from other hospitals to pick up the slack.
For more scheduling tips, check out practice management articles on our Web site.
With hospitalist demand outstripping supply, a fine-tuned group schedule can enhance productivity and job satisfaction. Two HM group leaders recently spoke with TH eWire about how they avoid a one-size-fits-all approach.
Stephen Houff, MD, president and CEO of Canton, Ohio-based Hospitalists Management Group, deploys 350 hospitalists to 41 hospitals in 11 states. Groups average eight hospitalists (range four to 20), and have an average daily census (ADC) of 50. Most work a seven-on/seven-off block shift. Dr. Houff says his HM groups create effective schedules in the following ways:
- In an eight-person group, three hospitalists work 7 a.m. to 7 p.m., and one doctor staffs the ED from 11 a.m. to 11 p.m.;
- Members must work four consecutive days;
- After getting established in a location, HM groups find local office-based PCPs to moonlight, covering their malpractice insurance and billing; and
- A dozen HMG hospitalists known as “firefighters” cover emergency or planned short-term leaves, receiving 15% higher pay plus per diems.
Haiwen Ma, MD, PhD, director of Hospitalist Services at South Nassau Communities Hospital in Oceanside, N.Y., has two nocturnists and five hospitalists in the group who work Monday through Friday from 7 a.m. to 7 p.m. The group has an ADC of 45-50 and a 15-patient cap per hospitalist. Here’s how she makes it work:
- Four hospitalists cover admissions in three-hour blocks from 7 a.m. to 7 p.m. and do weekend calls every fourth week;
- The fifth hospitalist performs pre-surgical/post-surgical consults; and
- The group relies on per-diem moonlighters from other hospitals to pick up the slack.
For more scheduling tips, check out practice management articles on our Web site.
With hospitalist demand outstripping supply, a fine-tuned group schedule can enhance productivity and job satisfaction. Two HM group leaders recently spoke with TH eWire about how they avoid a one-size-fits-all approach.
Stephen Houff, MD, president and CEO of Canton, Ohio-based Hospitalists Management Group, deploys 350 hospitalists to 41 hospitals in 11 states. Groups average eight hospitalists (range four to 20), and have an average daily census (ADC) of 50. Most work a seven-on/seven-off block shift. Dr. Houff says his HM groups create effective schedules in the following ways:
- In an eight-person group, three hospitalists work 7 a.m. to 7 p.m., and one doctor staffs the ED from 11 a.m. to 11 p.m.;
- Members must work four consecutive days;
- After getting established in a location, HM groups find local office-based PCPs to moonlight, covering their malpractice insurance and billing; and
- A dozen HMG hospitalists known as “firefighters” cover emergency or planned short-term leaves, receiving 15% higher pay plus per diems.
Haiwen Ma, MD, PhD, director of Hospitalist Services at South Nassau Communities Hospital in Oceanside, N.Y., has two nocturnists and five hospitalists in the group who work Monday through Friday from 7 a.m. to 7 p.m. The group has an ADC of 45-50 and a 15-patient cap per hospitalist. Here’s how she makes it work:
- Four hospitalists cover admissions in three-hour blocks from 7 a.m. to 7 p.m. and do weekend calls every fourth week;
- The fifth hospitalist performs pre-surgical/post-surgical consults; and
- The group relies on per-diem moonlighters from other hospitals to pick up the slack.
For more scheduling tips, check out practice management articles on our Web site.
Continuity Conundrum

Editor’s note: Third of a three-part series.
In the two monthly columns preceding this one, I’ve provided an overview of some ways hospitalist groups distribute new referrals among the providers. This month, I’ll review things that cause some groups to make exceptions to their typical method of distributing patients, and turn from how patients are distributed over 24 hours to thoughts about how they might be assigned over the course of consecutive days worked by a doctor.
Equitable Exceptions
There are a number of reasons groups decide to depart from their typical method of assigning patients. These include:
- “Bouncebacks”;
- One hospitalist is at the cap, others aren’t;
- Consult requested of a specific hospitalist;
- Hospitalists with unique skills (e.g., ICU expertise); and
- A patient “fires” the hospitalist.
There isn’t a standard “hospitalist way” of dealing with these issues, and each group will need to work out its own system. The most common of these issues is “bouncebacks.” Every group should try to have patients readmitted within three or four days of discharge go back to the discharging hospitalist. However, this proves difficult in many cases for several reasons, most commonly because the original discharging doctor might not be working when the patient returns.
The Alpha & Omega
Nearly every hospitalist practice makes some effort to maximize continuity between a single hospitalist and patient over the course of a hospital stay. But the effect of the method of patient assignment on continuity often is overlooked.
A reasonable way to think about or measure continuity is to estimate the portion of patients seen by the group that see the same hospitalist for each daytime visit over the course of their stay. (Assume that in most HM groups the same hospitalist can’t make both day and night visits over the course of the hospital stay. So, just for simplicity, I’ve intentionally left night visits, including an initial admission visit at night, out of the continuity calculation.) Plug the numbers for your practice into the formula (see Figure 1, right) and see what you get.
If a hospitalist always works seven consecutive day shifts (e.g., a seven-on/seven-off schedule) and the hospitalist’s patients have an average LOS of 4.2 days, then 54% of patients will see the same hospitalist for all daytime visits, and 46% will experience at least one handoff. (To keep things simple, I’m ignoring the effect on continuity of patients being admitted by an “admitter” or nocturnist who doesn’t see the patient subsequently.)
Changing the number of consecutive day shifts a hospitalist works has the most significant impact on continuity, but just how many consecutive days can one work routinely before fatigue and burnout—not too mention increased errors and decreased patient satisfaction—become a problem? (Many hospitalists make the mistake of trying to stuff what might be a reasonable annual workload into the smallest number of shifts possible with the goal of maximizing the number of days off. That means each worked day will be very busy, making it really hard to work many consecutive days. But you always have the option of titrating out that same annual workload over more days so that each day is less busy and it becomes easier to work more consecutive days.)
An often-overlooked way to improve continuity without having to work more consecutive day shifts is to have a hospitalist who is early in their series of worked days take on more new admissions and consults, and perhaps exempt that doctor from taking on new referrals for the last day or two he or she is on service. Eric Howell, MD, FHM, an SHM board member, calls this method “slam and dwindle.” This has been the approach I’ve experienced my whole career, and it is hard for me to imagine doing it any other way.
Here’s how it might work: Let’s say Dr. Petty always works seven consecutive day shifts, and on the first day he picks up a list of patients remaining from the doctor he’s replacing. To keep things simple, let’s assume he’s not in a large group, and during his first day of seven days on service he accepts and “keeps” all new referrals to the practice. On each successive day, he might assume the care of some new patients, but none on days six and seven. This means he takes on a disproportionately large number of new referrals at the beginning of his consecutive worked days, or “front-loads” new referrals. And because many of these patients will discharge before the end of his seven days and he takes on no new patients on days six and seven, his census will drop a lot before he rotates off, which in turn means there will be few patients who will have to get to know a new doctor on the first day Dr. Petty starts his seven-off schedule.
This system of patient distribution means continuity improved without requiring Dr. Petty to work more consecutive day shifts. Even though he works seven consecutive days and his average (or median) LOS is 4.2, as in the example above, his continuity will be much better than 54%. In fact, as many as 70% to 80% of Dr. Petty’s patients will see him for every daytime visit during their stay.

Other benefits of assigning more patients early and none late in a series of worked days are that on his last day of service, he will have more time to “tee up” patients for the next doctor, including preparing for patients anticipated to discharge the next day (e.g., dictate discharge summary, complete paperwork, etc.), and might be able to wrap up a little earlier that day. And when rotating back on service, he will pick up a small list of patients left by Dr. Tench, maybe fewer than eight, rather than the group’s average daily load of 15 patients per doctor, so he will have the capacity to admit a lot of patients that day.
I think there are three main reasons this isn’t a more common approach:
- Many HM groups just haven’t considered it.
- HM groups might have a schedule that has all doctors rotate off/on the same days each week. For example, all doctors rotate off on Tuesdays and are replaced by new doctors on Wednesday. That makes it impossible to exempt a doctor from taking on new referrals on the last day of service because all of the group’s doctors have their last day on Tuesday. These groups could stagger the day each doctor rotates off—one on Monday, one on Tuesday, and so on.
- Every doctor is so busy each day that it wouldn’t be feasible to exempt any individual doctor from taking on new patients, even if they are off the next day.
Despite the difficulties implementing a system of front-loading new referrals, I think most hospitalists would find that they like it. Because it reduces handoffs, it reduces, at least modestly, the group’s overall workload and probably benefits the group’s quality and patient satisfaction. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: Third of a three-part series.
In the two monthly columns preceding this one, I’ve provided an overview of some ways hospitalist groups distribute new referrals among the providers. This month, I’ll review things that cause some groups to make exceptions to their typical method of distributing patients, and turn from how patients are distributed over 24 hours to thoughts about how they might be assigned over the course of consecutive days worked by a doctor.
Equitable Exceptions
There are a number of reasons groups decide to depart from their typical method of assigning patients. These include:
- “Bouncebacks”;
- One hospitalist is at the cap, others aren’t;
- Consult requested of a specific hospitalist;
- Hospitalists with unique skills (e.g., ICU expertise); and
- A patient “fires” the hospitalist.
There isn’t a standard “hospitalist way” of dealing with these issues, and each group will need to work out its own system. The most common of these issues is “bouncebacks.” Every group should try to have patients readmitted within three or four days of discharge go back to the discharging hospitalist. However, this proves difficult in many cases for several reasons, most commonly because the original discharging doctor might not be working when the patient returns.
The Alpha & Omega
Nearly every hospitalist practice makes some effort to maximize continuity between a single hospitalist and patient over the course of a hospital stay. But the effect of the method of patient assignment on continuity often is overlooked.
A reasonable way to think about or measure continuity is to estimate the portion of patients seen by the group that see the same hospitalist for each daytime visit over the course of their stay. (Assume that in most HM groups the same hospitalist can’t make both day and night visits over the course of the hospital stay. So, just for simplicity, I’ve intentionally left night visits, including an initial admission visit at night, out of the continuity calculation.) Plug the numbers for your practice into the formula (see Figure 1, right) and see what you get.
If a hospitalist always works seven consecutive day shifts (e.g., a seven-on/seven-off schedule) and the hospitalist’s patients have an average LOS of 4.2 days, then 54% of patients will see the same hospitalist for all daytime visits, and 46% will experience at least one handoff. (To keep things simple, I’m ignoring the effect on continuity of patients being admitted by an “admitter” or nocturnist who doesn’t see the patient subsequently.)
Changing the number of consecutive day shifts a hospitalist works has the most significant impact on continuity, but just how many consecutive days can one work routinely before fatigue and burnout—not too mention increased errors and decreased patient satisfaction—become a problem? (Many hospitalists make the mistake of trying to stuff what might be a reasonable annual workload into the smallest number of shifts possible with the goal of maximizing the number of days off. That means each worked day will be very busy, making it really hard to work many consecutive days. But you always have the option of titrating out that same annual workload over more days so that each day is less busy and it becomes easier to work more consecutive days.)
An often-overlooked way to improve continuity without having to work more consecutive day shifts is to have a hospitalist who is early in their series of worked days take on more new admissions and consults, and perhaps exempt that doctor from taking on new referrals for the last day or two he or she is on service. Eric Howell, MD, FHM, an SHM board member, calls this method “slam and dwindle.” This has been the approach I’ve experienced my whole career, and it is hard for me to imagine doing it any other way.
Here’s how it might work: Let’s say Dr. Petty always works seven consecutive day shifts, and on the first day he picks up a list of patients remaining from the doctor he’s replacing. To keep things simple, let’s assume he’s not in a large group, and during his first day of seven days on service he accepts and “keeps” all new referrals to the practice. On each successive day, he might assume the care of some new patients, but none on days six and seven. This means he takes on a disproportionately large number of new referrals at the beginning of his consecutive worked days, or “front-loads” new referrals. And because many of these patients will discharge before the end of his seven days and he takes on no new patients on days six and seven, his census will drop a lot before he rotates off, which in turn means there will be few patients who will have to get to know a new doctor on the first day Dr. Petty starts his seven-off schedule.
This system of patient distribution means continuity improved without requiring Dr. Petty to work more consecutive day shifts. Even though he works seven consecutive days and his average (or median) LOS is 4.2, as in the example above, his continuity will be much better than 54%. In fact, as many as 70% to 80% of Dr. Petty’s patients will see him for every daytime visit during their stay.
Other benefits of assigning more patients early and none late in a series of worked days are that on his last day of service, he will have more time to “tee up” patients for the next doctor, including preparing for patients anticipated to discharge the next day (e.g., dictate discharge summary, complete paperwork, etc.), and might be able to wrap up a little earlier that day. And when rotating back on service, he will pick up a small list of patients left by Dr. Tench, maybe fewer than eight, rather than the group’s average daily load of 15 patients per doctor, so he will have the capacity to admit a lot of patients that day.
I think there are three main reasons this isn’t a more common approach:
- Many HM groups just haven’t considered it.
- HM groups might have a schedule that has all doctors rotate off/on the same days each week. For example, all doctors rotate off on Tuesdays and are replaced by new doctors on Wednesday. That makes it impossible to exempt a doctor from taking on new referrals on the last day of service because all of the group’s doctors have their last day on Tuesday. These groups could stagger the day each doctor rotates off—one on Monday, one on Tuesday, and so on.
- Every doctor is so busy each day that it wouldn’t be feasible to exempt any individual doctor from taking on new patients, even if they are off the next day.
Despite the difficulties implementing a system of front-loading new referrals, I think most hospitalists would find that they like it. Because it reduces handoffs, it reduces, at least modestly, the group’s overall workload and probably benefits the group’s quality and patient satisfaction. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: Third of a three-part series.
In the two monthly columns preceding this one, I’ve provided an overview of some ways hospitalist groups distribute new referrals among the providers. This month, I’ll review things that cause some groups to make exceptions to their typical method of distributing patients, and turn from how patients are distributed over 24 hours to thoughts about how they might be assigned over the course of consecutive days worked by a doctor.
Equitable Exceptions
There are a number of reasons groups decide to depart from their typical method of assigning patients. These include:
- “Bouncebacks”;
- One hospitalist is at the cap, others aren’t;
- Consult requested of a specific hospitalist;
- Hospitalists with unique skills (e.g., ICU expertise); and
- A patient “fires” the hospitalist.
There isn’t a standard “hospitalist way” of dealing with these issues, and each group will need to work out its own system. The most common of these issues is “bouncebacks.” Every group should try to have patients readmitted within three or four days of discharge go back to the discharging hospitalist. However, this proves difficult in many cases for several reasons, most commonly because the original discharging doctor might not be working when the patient returns.
The Alpha & Omega
Nearly every hospitalist practice makes some effort to maximize continuity between a single hospitalist and patient over the course of a hospital stay. But the effect of the method of patient assignment on continuity often is overlooked.
A reasonable way to think about or measure continuity is to estimate the portion of patients seen by the group that see the same hospitalist for each daytime visit over the course of their stay. (Assume that in most HM groups the same hospitalist can’t make both day and night visits over the course of the hospital stay. So, just for simplicity, I’ve intentionally left night visits, including an initial admission visit at night, out of the continuity calculation.) Plug the numbers for your practice into the formula (see Figure 1, right) and see what you get.
If a hospitalist always works seven consecutive day shifts (e.g., a seven-on/seven-off schedule) and the hospitalist’s patients have an average LOS of 4.2 days, then 54% of patients will see the same hospitalist for all daytime visits, and 46% will experience at least one handoff. (To keep things simple, I’m ignoring the effect on continuity of patients being admitted by an “admitter” or nocturnist who doesn’t see the patient subsequently.)
Changing the number of consecutive day shifts a hospitalist works has the most significant impact on continuity, but just how many consecutive days can one work routinely before fatigue and burnout—not too mention increased errors and decreased patient satisfaction—become a problem? (Many hospitalists make the mistake of trying to stuff what might be a reasonable annual workload into the smallest number of shifts possible with the goal of maximizing the number of days off. That means each worked day will be very busy, making it really hard to work many consecutive days. But you always have the option of titrating out that same annual workload over more days so that each day is less busy and it becomes easier to work more consecutive days.)
An often-overlooked way to improve continuity without having to work more consecutive day shifts is to have a hospitalist who is early in their series of worked days take on more new admissions and consults, and perhaps exempt that doctor from taking on new referrals for the last day or two he or she is on service. Eric Howell, MD, FHM, an SHM board member, calls this method “slam and dwindle.” This has been the approach I’ve experienced my whole career, and it is hard for me to imagine doing it any other way.
Here’s how it might work: Let’s say Dr. Petty always works seven consecutive day shifts, and on the first day he picks up a list of patients remaining from the doctor he’s replacing. To keep things simple, let’s assume he’s not in a large group, and during his first day of seven days on service he accepts and “keeps” all new referrals to the practice. On each successive day, he might assume the care of some new patients, but none on days six and seven. This means he takes on a disproportionately large number of new referrals at the beginning of his consecutive worked days, or “front-loads” new referrals. And because many of these patients will discharge before the end of his seven days and he takes on no new patients on days six and seven, his census will drop a lot before he rotates off, which in turn means there will be few patients who will have to get to know a new doctor on the first day Dr. Petty starts his seven-off schedule.
This system of patient distribution means continuity improved without requiring Dr. Petty to work more consecutive day shifts. Even though he works seven consecutive days and his average (or median) LOS is 4.2, as in the example above, his continuity will be much better than 54%. In fact, as many as 70% to 80% of Dr. Petty’s patients will see him for every daytime visit during their stay.
Other benefits of assigning more patients early and none late in a series of worked days are that on his last day of service, he will have more time to “tee up” patients for the next doctor, including preparing for patients anticipated to discharge the next day (e.g., dictate discharge summary, complete paperwork, etc.), and might be able to wrap up a little earlier that day. And when rotating back on service, he will pick up a small list of patients left by Dr. Tench, maybe fewer than eight, rather than the group’s average daily load of 15 patients per doctor, so he will have the capacity to admit a lot of patients that day.
I think there are three main reasons this isn’t a more common approach:
- Many HM groups just haven’t considered it.
- HM groups might have a schedule that has all doctors rotate off/on the same days each week. For example, all doctors rotate off on Tuesdays and are replaced by new doctors on Wednesday. That makes it impossible to exempt a doctor from taking on new referrals on the last day of service because all of the group’s doctors have their last day on Tuesday. These groups could stagger the day each doctor rotates off—one on Monday, one on Tuesday, and so on.
- Every doctor is so busy each day that it wouldn’t be feasible to exempt any individual doctor from taking on new patients, even if they are off the next day.
Despite the difficulties implementing a system of front-loading new referrals, I think most hospitalists would find that they like it. Because it reduces handoffs, it reduces, at least modestly, the group’s overall workload and probably benefits the group’s quality and patient satisfaction. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is also course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Mind Games & Silence

Silence.
Alone, I’m surrounded by strobes of memories—the baby monitor wresting us from sleep … muffled choking sounds … my wife holding our pale, stridorous 2-year-old … desperate attempts to clear his airway … the studied detachment of the 911 operator … paramedics … my wife running from the house without a jacket ... the fading ululations of the ambulance … silence.
I’m left in the bathroom, heart jack-hammering, holding a bloodied towel. Just 20 minutes earlier, I was cloaked in deep sleep. Now I’m shrouded with dread and cold sweat, my wife and son gone—leaving me to tend to our sleeping three-month-old daughter. The night ultimately ends well—perhaps comically, even—but not before being defined by three common cognitive errors.
History of Present Illness
It was a Monday night, and, after putting our kids down, my wife and I retired early to get a good night’s rest. An hour later, we awoke to gasping sounds from the monitor. My son, Grey, who was fine before bedtime, was panting and wheezing, unable to secure a full breath.
I immediately recalled that the night prior he had gagged on a dissolvable “gummy bear” vitamin. As he projected the appearance of someone who had aspirated something, we commenced manual sweeps of his mouth—feeling something in its deepest recesses. Gummy bear? Uvula? After numerous retching attempts to dislodge it, we moved on to Heimlich maneuvers. Nothing.
Just then, the paramedics showed up and took over, hearing this history of present illness.
Momentum Shift
An hour later, having secured a sitter for our sleeping infant, I showed up at the ED. Interestingly, the gummy-bear premise, nothing more than a harried utterance, had gathered the momentum of a boulder rolling downhill. The paramedics had relayed the possibility that our son might have aspirated a vitamin to the ED doctor, who relayed this certainty to the ear, nose, and throat doctor, who was actively scheduling operating-room time to bronchoscopically remove the offending foreign body.
It was all a bit like that childhood game of Telephone, in which the original message gets incrementally distorted with each telling, such that what starts as “Johnny told me he likes Lisa” turns into “Johnny crushed Lisa.”
My inner physician, elbowing the nervous parent aside, asked about the evidence for an aspiration. “The X-ray was negative, as was the exam, but the history suggests aspiration,” the ENT told me.
“What history?” I asked.
“That he has a history of ‘tonguing’ vitamins,” he said.
“Tonguing vitamins?” I responded, incredulously feeling the need to defend my child’s pill-swallowing honor. “Where did that story come from? We aren’t even sure we gave him a vitamin tonight.”
Nonetheless, the ENT was confident that “kids aspirate things all the time.”
Skeptical, I continued the debate. “But what if we hadn’t given that history? Would you still think of aspiration in this case?”
“Probably not, but then you did give us that history,” he replied. “So we need to bronch him.”
Culprit Revealed
Meanwhile, Grey was looking better with supplemental oxygen and a nebulizer’s worth of racemic epinephrine. His stridor took on more of a “barking seal” nature, and 30 minutes later, he developed a fever characteristic of croup. After a dose of steroids and another whiff of racemic epi, he was himself again, laughing the laugh of a wounded seal at the pulse oximeter, which backlit his big toe red. Comedy-club-level laughter replaced the look of death in the matter of an hour, as I was reminded of the resiliency of children. If only Mom and Dad could capture a bit of that.
Feeling a cocktail of relief and embarrassment—how could two physicians misdiagnose croup as an aspirated foreign body?—we readied ourselves for discharge. Just then, the ENT doctor came back in and told us the OR would be ready in a few hours. “But,” I inquired, “isn’t this just croup?”
“Most likely,” he replied, “but we can’t rule out aspiration without a bronchoscopy.”
It was then that I realized we (and our medical team) had fallen victim to some common heuristical errors. Heuristics are those little shortcuts in logic that we utilize to solve common problems. They are bred from years of experience and helpfully get us home every night in time for dinner. Without them, medicine would be a painstaking, Everlasting Gobstopper-like journey through endless differential diagnoses—in other words, your four-hour clerkship patient evaluations in medical school.
These shortcuts allow us to quickly recognize that a diaphoretic, 60-year-old man with diabetes, hyperlipidemia, and substernal chest pain has an acute coronary syndrome. We don’t spend hours thinking of Tietze’s syndrome, Boerhaave’s disease, and their ilk, because our mind quickly takes the shortcut to the right diagnosis. Although helpful, these shortcuts can cut both ways, occasionally resulting in thrombolytic therapy for an aortic dissection.
This is where Grey’s situation went wrong. My wife and I were victimized by the availability bias. This cognitive bias occurs when a recently encountered situation is given undue stature solely because of its proximity in time to the next event—i.e., it is “available.” So, because my son choked on a vitamin the night before, he must be choking on a vitamin the next night. (Even though we didn’t give him a vitamin and hours had passed since we put him to bed.) There is little connection between the two events, outside of the fact that aspiration is at the fore of your mind. This happens to us all the time. Think about the last presentation you attended about an obscure topic, only to amazingly find that the very next day, you had not one but two patients who surely required a workup for acute intermittent porphyria.
Common Practices
Anchoring bias is another common cognitive error in which we overly rely on one piece of information, the “anchor.” This was certainly in play during our ED visit. The mere mention of an aspirated foreign body was latched on to immediately. From there, tidbits of information that supported that diagnosis (something in the back of his throat on our exam, kids aspirate all the time) were kept, while the unsupporting evidence (negative X-ray and exam findings, fever, barking cough that awakes a kid at night) was jettisoned.
We fell prey to the momentum bias. This heuristical hiccup frequently wreaks cross-coverage havoc. You’ve seen this, I’m sure. Because the day team thought the renal failure was due to prerenal azotemia, the night team harmonizes, continuing to treat the patient’s bladder outlet obstruction with volume challenges. That is until someone—in my sphere, it’s usually the third-year medical student—asks if this could all be from the patient’s benign prostatic hyperplasia and medications.
After convincing our well-intentioned ENT colleague to call off the bronch, I was left with the important lesson that the ways in which our minds work, also well-intentioned, can cause us fits of trouble. I was left with the realization that the only way to mitigate the risk these cognitive shortcuts pose is to be constantly vigilant of their presence.
And, perhaps most importantly, I was left with an overstimulated 2-year-old high on the excitement of a hospital visit and large doses of adrenaline—a combination that left me desperately yearning for silence. TH
Dr. Glasheen is The Hospitalist’s physician editor.
Silence.
Alone, I’m surrounded by strobes of memories—the baby monitor wresting us from sleep … muffled choking sounds … my wife holding our pale, stridorous 2-year-old … desperate attempts to clear his airway … the studied detachment of the 911 operator … paramedics … my wife running from the house without a jacket ... the fading ululations of the ambulance … silence.
I’m left in the bathroom, heart jack-hammering, holding a bloodied towel. Just 20 minutes earlier, I was cloaked in deep sleep. Now I’m shrouded with dread and cold sweat, my wife and son gone—leaving me to tend to our sleeping three-month-old daughter. The night ultimately ends well—perhaps comically, even—but not before being defined by three common cognitive errors.
History of Present Illness
It was a Monday night, and, after putting our kids down, my wife and I retired early to get a good night’s rest. An hour later, we awoke to gasping sounds from the monitor. My son, Grey, who was fine before bedtime, was panting and wheezing, unable to secure a full breath.
I immediately recalled that the night prior he had gagged on a dissolvable “gummy bear” vitamin. As he projected the appearance of someone who had aspirated something, we commenced manual sweeps of his mouth—feeling something in its deepest recesses. Gummy bear? Uvula? After numerous retching attempts to dislodge it, we moved on to Heimlich maneuvers. Nothing.
Just then, the paramedics showed up and took over, hearing this history of present illness.
Momentum Shift
An hour later, having secured a sitter for our sleeping infant, I showed up at the ED. Interestingly, the gummy-bear premise, nothing more than a harried utterance, had gathered the momentum of a boulder rolling downhill. The paramedics had relayed the possibility that our son might have aspirated a vitamin to the ED doctor, who relayed this certainty to the ear, nose, and throat doctor, who was actively scheduling operating-room time to bronchoscopically remove the offending foreign body.
It was all a bit like that childhood game of Telephone, in which the original message gets incrementally distorted with each telling, such that what starts as “Johnny told me he likes Lisa” turns into “Johnny crushed Lisa.”
My inner physician, elbowing the nervous parent aside, asked about the evidence for an aspiration. “The X-ray was negative, as was the exam, but the history suggests aspiration,” the ENT told me.
“What history?” I asked.
“That he has a history of ‘tonguing’ vitamins,” he said.
“Tonguing vitamins?” I responded, incredulously feeling the need to defend my child’s pill-swallowing honor. “Where did that story come from? We aren’t even sure we gave him a vitamin tonight.”
Nonetheless, the ENT was confident that “kids aspirate things all the time.”
Skeptical, I continued the debate. “But what if we hadn’t given that history? Would you still think of aspiration in this case?”
“Probably not, but then you did give us that history,” he replied. “So we need to bronch him.”
Culprit Revealed
Meanwhile, Grey was looking better with supplemental oxygen and a nebulizer’s worth of racemic epinephrine. His stridor took on more of a “barking seal” nature, and 30 minutes later, he developed a fever characteristic of croup. After a dose of steroids and another whiff of racemic epi, he was himself again, laughing the laugh of a wounded seal at the pulse oximeter, which backlit his big toe red. Comedy-club-level laughter replaced the look of death in the matter of an hour, as I was reminded of the resiliency of children. If only Mom and Dad could capture a bit of that.
Feeling a cocktail of relief and embarrassment—how could two physicians misdiagnose croup as an aspirated foreign body?—we readied ourselves for discharge. Just then, the ENT doctor came back in and told us the OR would be ready in a few hours. “But,” I inquired, “isn’t this just croup?”
“Most likely,” he replied, “but we can’t rule out aspiration without a bronchoscopy.”
It was then that I realized we (and our medical team) had fallen victim to some common heuristical errors. Heuristics are those little shortcuts in logic that we utilize to solve common problems. They are bred from years of experience and helpfully get us home every night in time for dinner. Without them, medicine would be a painstaking, Everlasting Gobstopper-like journey through endless differential diagnoses—in other words, your four-hour clerkship patient evaluations in medical school.
These shortcuts allow us to quickly recognize that a diaphoretic, 60-year-old man with diabetes, hyperlipidemia, and substernal chest pain has an acute coronary syndrome. We don’t spend hours thinking of Tietze’s syndrome, Boerhaave’s disease, and their ilk, because our mind quickly takes the shortcut to the right diagnosis. Although helpful, these shortcuts can cut both ways, occasionally resulting in thrombolytic therapy for an aortic dissection.
This is where Grey’s situation went wrong. My wife and I were victimized by the availability bias. This cognitive bias occurs when a recently encountered situation is given undue stature solely because of its proximity in time to the next event—i.e., it is “available.” So, because my son choked on a vitamin the night before, he must be choking on a vitamin the next night. (Even though we didn’t give him a vitamin and hours had passed since we put him to bed.) There is little connection between the two events, outside of the fact that aspiration is at the fore of your mind. This happens to us all the time. Think about the last presentation you attended about an obscure topic, only to amazingly find that the very next day, you had not one but two patients who surely required a workup for acute intermittent porphyria.
Common Practices
Anchoring bias is another common cognitive error in which we overly rely on one piece of information, the “anchor.” This was certainly in play during our ED visit. The mere mention of an aspirated foreign body was latched on to immediately. From there, tidbits of information that supported that diagnosis (something in the back of his throat on our exam, kids aspirate all the time) were kept, while the unsupporting evidence (negative X-ray and exam findings, fever, barking cough that awakes a kid at night) was jettisoned.
We fell prey to the momentum bias. This heuristical hiccup frequently wreaks cross-coverage havoc. You’ve seen this, I’m sure. Because the day team thought the renal failure was due to prerenal azotemia, the night team harmonizes, continuing to treat the patient’s bladder outlet obstruction with volume challenges. That is until someone—in my sphere, it’s usually the third-year medical student—asks if this could all be from the patient’s benign prostatic hyperplasia and medications.
After convincing our well-intentioned ENT colleague to call off the bronch, I was left with the important lesson that the ways in which our minds work, also well-intentioned, can cause us fits of trouble. I was left with the realization that the only way to mitigate the risk these cognitive shortcuts pose is to be constantly vigilant of their presence.
And, perhaps most importantly, I was left with an overstimulated 2-year-old high on the excitement of a hospital visit and large doses of adrenaline—a combination that left me desperately yearning for silence. TH
Dr. Glasheen is The Hospitalist’s physician editor.
Silence.
Alone, I’m surrounded by strobes of memories—the baby monitor wresting us from sleep … muffled choking sounds … my wife holding our pale, stridorous 2-year-old … desperate attempts to clear his airway … the studied detachment of the 911 operator … paramedics … my wife running from the house without a jacket ... the fading ululations of the ambulance … silence.
I’m left in the bathroom, heart jack-hammering, holding a bloodied towel. Just 20 minutes earlier, I was cloaked in deep sleep. Now I’m shrouded with dread and cold sweat, my wife and son gone—leaving me to tend to our sleeping three-month-old daughter. The night ultimately ends well—perhaps comically, even—but not before being defined by three common cognitive errors.
History of Present Illness
It was a Monday night, and, after putting our kids down, my wife and I retired early to get a good night’s rest. An hour later, we awoke to gasping sounds from the monitor. My son, Grey, who was fine before bedtime, was panting and wheezing, unable to secure a full breath.
I immediately recalled that the night prior he had gagged on a dissolvable “gummy bear” vitamin. As he projected the appearance of someone who had aspirated something, we commenced manual sweeps of his mouth—feeling something in its deepest recesses. Gummy bear? Uvula? After numerous retching attempts to dislodge it, we moved on to Heimlich maneuvers. Nothing.
Just then, the paramedics showed up and took over, hearing this history of present illness.
Momentum Shift
An hour later, having secured a sitter for our sleeping infant, I showed up at the ED. Interestingly, the gummy-bear premise, nothing more than a harried utterance, had gathered the momentum of a boulder rolling downhill. The paramedics had relayed the possibility that our son might have aspirated a vitamin to the ED doctor, who relayed this certainty to the ear, nose, and throat doctor, who was actively scheduling operating-room time to bronchoscopically remove the offending foreign body.
It was all a bit like that childhood game of Telephone, in which the original message gets incrementally distorted with each telling, such that what starts as “Johnny told me he likes Lisa” turns into “Johnny crushed Lisa.”
My inner physician, elbowing the nervous parent aside, asked about the evidence for an aspiration. “The X-ray was negative, as was the exam, but the history suggests aspiration,” the ENT told me.
“What history?” I asked.
“That he has a history of ‘tonguing’ vitamins,” he said.
“Tonguing vitamins?” I responded, incredulously feeling the need to defend my child’s pill-swallowing honor. “Where did that story come from? We aren’t even sure we gave him a vitamin tonight.”
Nonetheless, the ENT was confident that “kids aspirate things all the time.”
Skeptical, I continued the debate. “But what if we hadn’t given that history? Would you still think of aspiration in this case?”
“Probably not, but then you did give us that history,” he replied. “So we need to bronch him.”
Culprit Revealed
Meanwhile, Grey was looking better with supplemental oxygen and a nebulizer’s worth of racemic epinephrine. His stridor took on more of a “barking seal” nature, and 30 minutes later, he developed a fever characteristic of croup. After a dose of steroids and another whiff of racemic epi, he was himself again, laughing the laugh of a wounded seal at the pulse oximeter, which backlit his big toe red. Comedy-club-level laughter replaced the look of death in the matter of an hour, as I was reminded of the resiliency of children. If only Mom and Dad could capture a bit of that.
Feeling a cocktail of relief and embarrassment—how could two physicians misdiagnose croup as an aspirated foreign body?—we readied ourselves for discharge. Just then, the ENT doctor came back in and told us the OR would be ready in a few hours. “But,” I inquired, “isn’t this just croup?”
“Most likely,” he replied, “but we can’t rule out aspiration without a bronchoscopy.”
It was then that I realized we (and our medical team) had fallen victim to some common heuristical errors. Heuristics are those little shortcuts in logic that we utilize to solve common problems. They are bred from years of experience and helpfully get us home every night in time for dinner. Without them, medicine would be a painstaking, Everlasting Gobstopper-like journey through endless differential diagnoses—in other words, your four-hour clerkship patient evaluations in medical school.
These shortcuts allow us to quickly recognize that a diaphoretic, 60-year-old man with diabetes, hyperlipidemia, and substernal chest pain has an acute coronary syndrome. We don’t spend hours thinking of Tietze’s syndrome, Boerhaave’s disease, and their ilk, because our mind quickly takes the shortcut to the right diagnosis. Although helpful, these shortcuts can cut both ways, occasionally resulting in thrombolytic therapy for an aortic dissection.
This is where Grey’s situation went wrong. My wife and I were victimized by the availability bias. This cognitive bias occurs when a recently encountered situation is given undue stature solely because of its proximity in time to the next event—i.e., it is “available.” So, because my son choked on a vitamin the night before, he must be choking on a vitamin the next night. (Even though we didn’t give him a vitamin and hours had passed since we put him to bed.) There is little connection between the two events, outside of the fact that aspiration is at the fore of your mind. This happens to us all the time. Think about the last presentation you attended about an obscure topic, only to amazingly find that the very next day, you had not one but two patients who surely required a workup for acute intermittent porphyria.
Common Practices
Anchoring bias is another common cognitive error in which we overly rely on one piece of information, the “anchor.” This was certainly in play during our ED visit. The mere mention of an aspirated foreign body was latched on to immediately. From there, tidbits of information that supported that diagnosis (something in the back of his throat on our exam, kids aspirate all the time) were kept, while the unsupporting evidence (negative X-ray and exam findings, fever, barking cough that awakes a kid at night) was jettisoned.
We fell prey to the momentum bias. This heuristical hiccup frequently wreaks cross-coverage havoc. You’ve seen this, I’m sure. Because the day team thought the renal failure was due to prerenal azotemia, the night team harmonizes, continuing to treat the patient’s bladder outlet obstruction with volume challenges. That is until someone—in my sphere, it’s usually the third-year medical student—asks if this could all be from the patient’s benign prostatic hyperplasia and medications.
After convincing our well-intentioned ENT colleague to call off the bronch, I was left with the important lesson that the ways in which our minds work, also well-intentioned, can cause us fits of trouble. I was left with the realization that the only way to mitigate the risk these cognitive shortcuts pose is to be constantly vigilant of their presence.
And, perhaps most importantly, I was left with an overstimulated 2-year-old high on the excitement of a hospital visit and large doses of adrenaline—a combination that left me desperately yearning for silence. TH
Dr. Glasheen is The Hospitalist’s physician editor.
Research Commitment

With the growth of HM has come a major change in the way healthcare is delivered in hospitals across the country: Hospitalists have become one of the major providers of care for hospitalized medical patients. Recent reports suggest that hospitalists care for more than 50% of Medicare patients admitted with a medical diagnosis. In addition to that staggering figure, hospitalists increasingly have assumed care for many surgical patients, have staffed observation units, created procedure services, assumed care of many subspecialty services, and have taken the lead on hospital-based IT and quality-improvement (QI) endeavors, among other key services.
It is hard to argue against the assertion that HM’s emergence over the past decade and a half is one of the most significant game-changers in all of healthcare. Despite this important impact on the structure of care delivery, HM to date has fallen short of the contributions made by many other disciplines over the years in one key area: the generation of new knowledge through research.
New Specialties’ Research Focus
Think for a minute of the contributions of the next two youngest specialties—critical-care medicine and emergency medicine. Both fields have transformed care delivery, as did HM, but in contrast, both critical-care and emergency medicine have well-established investigators and an impressive research agenda. They have had a major impact on the care of patients everywhere.
For example, the critical-care community developed new treatment paradigms for sepsis that grew out of basic science work exploring the roles of cytokines and the inflammatory cascade in infection. Its clinical-research networks have developed and tested new ventilator- and fluid-management strategies for acute respiratory distress syndrome.
Similarly, the emergency medicine community has developed new algorithms for the treatment of cardiac arrest, trauma, and many other common emergency diagnoses that are now implemented in EDs all over the country.
We, the HM community, should aspire to do the same.
By saying we need to do more, I do not mean to undermine the many important contributions we are making. Just pick up any issue of the Journal of Hospital Medicine, and you will find a wealth of literature describing the important work of hospitalists everywhere. But to have a lasting impact, we need to continue to expand on this work to advance the national health research agenda by having hospitalists pursue clinical and comparative-effectiveness research, quality and safety research, health system innovations work, and even basic science research.
Research Assistance
SHM has always prided itself in being at the forefront of training and networking opportunities for hospitalists. It should come as no surprise that SHM continues to lead in the creation of opportunities designed to enhance HM research.
To advance the research agenda, we need to advance researchers. HM researchers struggle to find funding for their work in a federal infrastructure that emphasizes disease- and organ-based investigation. A hospitalist investigator often explores areas that cross disease boundaries, or pursues work that falls into the realm of “quality and safety,” which tends to have fewer funding opportunities. Hospitalist investigators need a hand getting started, and SHM is going to lend that hand.
At HM10 this month in Washington, D.C., we will announce the recipients of the newly created SHM Junior Faculty Development Award. The award will provide two recipients with $25,000 per year for two consecutive years. This award is a mentored research award, which means it is intended to support junior hospitalist faculty as they apply for a research career development award. The goal in creating this award is to fulfill SHM’s mission of promoting excellence in the practice of HM through research, and to build a generation of effective hospitalist researchers who can define and explore questions pertinent to the general medical care of hospitalized patients.
We hope these awards, through funding and mentoring, boost successful hospitalist investigators, grow the number of hospitalist-initiated research projects, and show academic institutions that hospitalist research ideas have merit. It also is likely that, over time, the awards will create a network of SHM-funded investigators whose collaboration and interaction will further accelerate HM research.
Our hope is that this effort benefits not just the investigators receiving the money, but also all practicing hospitalists and their patients by further clarifying the best methods to care for hospitalized patients, by creating new treatment paradigms, and advancing the science of HM for the benefit of all.
Please join me in congratulating the recipients of this important and prestigious award. TH
Dr. Flanders is president of SHM.
With the growth of HM has come a major change in the way healthcare is delivered in hospitals across the country: Hospitalists have become one of the major providers of care for hospitalized medical patients. Recent reports suggest that hospitalists care for more than 50% of Medicare patients admitted with a medical diagnosis. In addition to that staggering figure, hospitalists increasingly have assumed care for many surgical patients, have staffed observation units, created procedure services, assumed care of many subspecialty services, and have taken the lead on hospital-based IT and quality-improvement (QI) endeavors, among other key services.
It is hard to argue against the assertion that HM’s emergence over the past decade and a half is one of the most significant game-changers in all of healthcare. Despite this important impact on the structure of care delivery, HM to date has fallen short of the contributions made by many other disciplines over the years in one key area: the generation of new knowledge through research.
New Specialties’ Research Focus
Think for a minute of the contributions of the next two youngest specialties—critical-care medicine and emergency medicine. Both fields have transformed care delivery, as did HM, but in contrast, both critical-care and emergency medicine have well-established investigators and an impressive research agenda. They have had a major impact on the care of patients everywhere.
For example, the critical-care community developed new treatment paradigms for sepsis that grew out of basic science work exploring the roles of cytokines and the inflammatory cascade in infection. Its clinical-research networks have developed and tested new ventilator- and fluid-management strategies for acute respiratory distress syndrome.
Similarly, the emergency medicine community has developed new algorithms for the treatment of cardiac arrest, trauma, and many other common emergency diagnoses that are now implemented in EDs all over the country.
We, the HM community, should aspire to do the same.
By saying we need to do more, I do not mean to undermine the many important contributions we are making. Just pick up any issue of the Journal of Hospital Medicine, and you will find a wealth of literature describing the important work of hospitalists everywhere. But to have a lasting impact, we need to continue to expand on this work to advance the national health research agenda by having hospitalists pursue clinical and comparative-effectiveness research, quality and safety research, health system innovations work, and even basic science research.
Research Assistance
SHM has always prided itself in being at the forefront of training and networking opportunities for hospitalists. It should come as no surprise that SHM continues to lead in the creation of opportunities designed to enhance HM research.
To advance the research agenda, we need to advance researchers. HM researchers struggle to find funding for their work in a federal infrastructure that emphasizes disease- and organ-based investigation. A hospitalist investigator often explores areas that cross disease boundaries, or pursues work that falls into the realm of “quality and safety,” which tends to have fewer funding opportunities. Hospitalist investigators need a hand getting started, and SHM is going to lend that hand.
At HM10 this month in Washington, D.C., we will announce the recipients of the newly created SHM Junior Faculty Development Award. The award will provide two recipients with $25,000 per year for two consecutive years. This award is a mentored research award, which means it is intended to support junior hospitalist faculty as they apply for a research career development award. The goal in creating this award is to fulfill SHM’s mission of promoting excellence in the practice of HM through research, and to build a generation of effective hospitalist researchers who can define and explore questions pertinent to the general medical care of hospitalized patients.
We hope these awards, through funding and mentoring, boost successful hospitalist investigators, grow the number of hospitalist-initiated research projects, and show academic institutions that hospitalist research ideas have merit. It also is likely that, over time, the awards will create a network of SHM-funded investigators whose collaboration and interaction will further accelerate HM research.
Our hope is that this effort benefits not just the investigators receiving the money, but also all practicing hospitalists and their patients by further clarifying the best methods to care for hospitalized patients, by creating new treatment paradigms, and advancing the science of HM for the benefit of all.
Please join me in congratulating the recipients of this important and prestigious award. TH
Dr. Flanders is president of SHM.
With the growth of HM has come a major change in the way healthcare is delivered in hospitals across the country: Hospitalists have become one of the major providers of care for hospitalized medical patients. Recent reports suggest that hospitalists care for more than 50% of Medicare patients admitted with a medical diagnosis. In addition to that staggering figure, hospitalists increasingly have assumed care for many surgical patients, have staffed observation units, created procedure services, assumed care of many subspecialty services, and have taken the lead on hospital-based IT and quality-improvement (QI) endeavors, among other key services.
It is hard to argue against the assertion that HM’s emergence over the past decade and a half is one of the most significant game-changers in all of healthcare. Despite this important impact on the structure of care delivery, HM to date has fallen short of the contributions made by many other disciplines over the years in one key area: the generation of new knowledge through research.
New Specialties’ Research Focus
Think for a minute of the contributions of the next two youngest specialties—critical-care medicine and emergency medicine. Both fields have transformed care delivery, as did HM, but in contrast, both critical-care and emergency medicine have well-established investigators and an impressive research agenda. They have had a major impact on the care of patients everywhere.
For example, the critical-care community developed new treatment paradigms for sepsis that grew out of basic science work exploring the roles of cytokines and the inflammatory cascade in infection. Its clinical-research networks have developed and tested new ventilator- and fluid-management strategies for acute respiratory distress syndrome.
Similarly, the emergency medicine community has developed new algorithms for the treatment of cardiac arrest, trauma, and many other common emergency diagnoses that are now implemented in EDs all over the country.
We, the HM community, should aspire to do the same.
By saying we need to do more, I do not mean to undermine the many important contributions we are making. Just pick up any issue of the Journal of Hospital Medicine, and you will find a wealth of literature describing the important work of hospitalists everywhere. But to have a lasting impact, we need to continue to expand on this work to advance the national health research agenda by having hospitalists pursue clinical and comparative-effectiveness research, quality and safety research, health system innovations work, and even basic science research.
Research Assistance
SHM has always prided itself in being at the forefront of training and networking opportunities for hospitalists. It should come as no surprise that SHM continues to lead in the creation of opportunities designed to enhance HM research.
To advance the research agenda, we need to advance researchers. HM researchers struggle to find funding for their work in a federal infrastructure that emphasizes disease- and organ-based investigation. A hospitalist investigator often explores areas that cross disease boundaries, or pursues work that falls into the realm of “quality and safety,” which tends to have fewer funding opportunities. Hospitalist investigators need a hand getting started, and SHM is going to lend that hand.
At HM10 this month in Washington, D.C., we will announce the recipients of the newly created SHM Junior Faculty Development Award. The award will provide two recipients with $25,000 per year for two consecutive years. This award is a mentored research award, which means it is intended to support junior hospitalist faculty as they apply for a research career development award. The goal in creating this award is to fulfill SHM’s mission of promoting excellence in the practice of HM through research, and to build a generation of effective hospitalist researchers who can define and explore questions pertinent to the general medical care of hospitalized patients.
We hope these awards, through funding and mentoring, boost successful hospitalist investigators, grow the number of hospitalist-initiated research projects, and show academic institutions that hospitalist research ideas have merit. It also is likely that, over time, the awards will create a network of SHM-funded investigators whose collaboration and interaction will further accelerate HM research.
Our hope is that this effort benefits not just the investigators receiving the money, but also all practicing hospitalists and their patients by further clarifying the best methods to care for hospitalized patients, by creating new treatment paradigms, and advancing the science of HM for the benefit of all.
Please join me in congratulating the recipients of this important and prestigious award. TH
Dr. Flanders is president of SHM.