User login
HM Growth: Phase 2

The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
The growth of our medical specialty is old news. Yes, we now number about 30,000; yes, we now manage the medical care of 50% of hospitalized Medicare patients; yes, hospitalists are in two-thirds of U.S. hospitals. I could go on and on. But recently, I have observed a different type of growth altogether. It is the growth of stability.
In the recent history of HM, the focus was on the increasing number of hospitals that had hospitalists, the growth of SHM’s membership, the growth of our annual meeting, and the ever-increasing number of doctors who, at least when surveyed, called themselves hospitalists. It all looked so impressive.
Many of you know, however, that when you lifted up the hood of our field, it was not always as it seemed. HM actually was a bit unstable. Some doctors who called themselves hospitalists were, in reality, biding time until they moved on to a “real job” or went off to do a fellowship. Multiple groups competed for patients within any given hospital, and also competed for doctors. There were numerous jobs available for any given hospitalist, and, as a result, some groups had substantial turnover despite growth in numbers. In these programs, the group photo from one year to the next had an entirely new set of faces.
Instability did not just affect rank-and-file hospitalists; it also existed within programmatic leadership and entire programs. Annually in many hospitals, the hospitalists had to convince administration that the hospital needed hospitalists and that they were worthy of support. Unfortunately, it was not always successful, so some programs vanished.
Five years ago in Michigan, we were working to create a multihospital safety consortium. We had several participating institutions, all with hospitalist programs. One day, my secretary complained that every time she sent an e-mail to the consortium listserv, a handful would bounce back and indicate a handful of e-mail addresses no longer were in service, or note that an individual had “left the program.” Some of them were HM program directors. Follow-up calls showed that the program had a new director or had folded. In some cases, however, they were just too busy figuring out how to survive instead of focus on safety issues.
Fortunately, that all appears to be changing.
From Unknown to Accepted to Counted On
I have seen the change in my own institution. We, of course, continue to negotiate with hospital administration, but it is no longer about whether we should continue the program or not. Negotiations now center on line items in the budget, how much space we need, where we anticipate future growth, and what quality and safety initiatives we’re working on.
I like to think that the HM program is important infrastructure. Just as you can’t imagine a hospital without an ED or an ICU, the same holds true for the HM program.
Perhaps an even better analogy could be found in technologic innovation. Back when Al Gore invented the Internet, having an Internet connection at home was viewed as a luxury. Now, it nearly is a necessity. Just like HM programs! (OK, maybe that was a stretch.)
There also is stability within the faculty ranks. Many of our faculty have been here for years and plan to stay. Turnover has decreased dramatically. This is not unique to our program, but anecdotally is happening everywhere. In fact, we are in the process of launching additional multihospital HM-based safety projects and collaboratives. And when I reach out to programs to ask them to participate, the directors of these programs are the same ones when I last checked. If they have moved on, it has been to assume a local leadership role. The group photos also show all the same old faces, plus a few new ones. There really has been some stabilization in the field.
New Paradigm Here to Stay
The factors behind this newfound stability are numerous. Among them is the recognized importance of a well-managed HM program. In many institutions, the alternatives to hospitalists (primary-care physicians, surgeons managing all post-operative care, specialists admitting their own patients, etc.) have left the building. There is no going back, and there is no “plan B” if HM programs fold.
The recognition by prospective hospitalists—residents and students—that HM is a viable career path has increased interest in the field, and, in turn, has given many programs more choices among qualified applicants. Hospitalists currently employed in a reasonably functioning program are less likely to jump ship every year looking for something slightly better. And I expect the current economic climate has been a factor as well. As hospitals see operating margins erode, plans for infrastructure growth are delayed, funding for new programs shrinks, and hospitalist groups are asked to do more with less. In other words, they are not hiring as many new hospitalists.
In some sense, the perceived slowing in the growth of hospitalists might be concerning. I see it a different way. Slowing growth in overall numbers allows programs and the field to stabilize a bit, and this growth in stability creates enormous opportunity. Programs formerly struggling to survive can begin to innovate. We’ve seen that in Michigan, as the interest among hospitalist programs that want to participate in QI collaborations has grown. And when we hear what some programs are working on, it’s an impressive list of high-impact projects.
Hospitalists are taking ownership of care transitions, prevention of hospital-acquired complications, and disease-based QI initiatives centered on patients with heart failure, COPD, and diabetes.
Nationally, we have seen hospitalist programs coming together to successfully compete for federal research grants or foundation support targeting important national healthcare priorities. If the current healthcare reform legislation passes, it will better position HM to lead the transformation of healthcare in U.S. hospitals.
My big hope is that 10 to 20 years from now, HM is better known for its second phase of growth. Right now, we are more famous for our rapid growth and, to some extent, our impact on efficiency of care. Efficiency clearly is important; dollars saved from waste can be better put to use improving quality. But I want the field to be judged by our ability to innovate, improve the quality of hospital-care delivery, and to generate new knowledge that advances the care of all patients. Those accomplishments will have a more lasting impact on healthcare.
The stabilization of HM is making all of this possible. Our population expects and deserves great things from the nation’s fastest-growing “specialty,” and I am optimistic we will not let them down. TH
Dr. Flanders is president of SHM.
Insider’s Point of View

Felix Aguirre, MD, entered the field of hospital medicine before the term “hospitalist” had been coined. He didn’t realize how quickly the field would explode, but it didn’t take long to find out. Aguirre helped start an inpatient service in 1994, taking care of patients for about 20 primary-care physicians. Within three years, his service cared for the patients of 360 doctors.
Dr. Aguirre cofounded Hospitalists of San Antonio in 2000, and he served as president of the company until it merged with IPC: The Hospitalist Co. three years later.
A graduate of the U.S. Military Academy at West Point, Dr. Aguirre spent several years as an air-traffic controller before attending medical school. He currently is vice president of medical affairs for California-based IPC, which provides management services to hospitalist practices in more than 400 facilities.
“The biggest reward is being part of a growth industry, helping to mold it and move it forward,” says Dr. Aguirre, who is responsible for medical and leadership oversight, as well as developing IPC’s physicians and providers. “I’m very proud it’s starting to get distinction as a separate specialty, and I really like the idea of getting in on the ground floor. Everybody likes to be one of the pioneers of an industry.”
Question: How did West Point help prepare you for your current career?
Answer: As part of your education at West Point, you need to learn to be a follower before you can learn to be a leader. Coming out of the academy, I was pretty cocky and I thought I could do anything. I’ve learned some pretty humbling lessons, and experience teaches you how to temper that attitude.
Q: How about your time as an air-traffic controller?
A: You have to be able to deal with many things at once and be able to deal with pressure. That experience is great for a career in an emergency room and in hospital medicine, where you’re juggling a lot of information and facing situations that require pretty rapid action.
Q: When you entered HM, did you have a sense of how much—and how quickly—the field would grow?
A: No. It really was in its infancy at that time … but when Dr. (Robert) Wachter (coined the term “hospitalist”), it began to pick up momentum. Before long, we could see there wasn’t going to be any slowing down of this type of medicine. It’s great to be a part of an industry that is still a growing industry, especially in this economic climate. It’s needed now more than ever, so I feel I made the correct decision to enter this field.
Q: Why do you feel it’s needed more now than ever?
A: With healthcare, there needs to be more control, clinically as well as financially. I think hospitalists are well positioned right in the middle of the hospital. They are exposed to every aspect of the hospital’s operation and staff, whether it’s the cleaning service or dietary or physical therapy or talking to specialists or other physicians. Who better to help control what happens than the person who is exposed to it?
Q: What is the biggest challenge you face in your current role?
A: One of the big ones is reduction in variance. Everybody is looking for ways to reduce variance in clinical care, and that’s going to continue to be one of the biggest challenges as we grow. If you’re a small mom-and-pop business, it’s pretty easy to control things. That gets more difficult as you grow. The things that worked when you were smaller don’t work in a medium-sized company, let alone when you become a large company. You have to change the way you manage things, which leads to another challenge—adapting to the change.
Q: Is the fear of a hospitalist shortage on your radar screen?
A: It is. But I can tell you this: We won’t stress about it, because it is going to happen. There will be a shortage—there already is. What we have to try to do is position ourselves as the company, or employer, of choice. We get close to 3,000 applicants a year and hire 200 or so, so we’re fortunate in that we have a tremendous amount of exposure to many of the people who are desiring a hospitalist career.
Q: What do you see as the biggest benefit to the IPC model?
A: There are a couple of things I see, not just as advantages but also as strengths. Number one, IPC has extremely strong leadership. All of the people I work with on the senior leadership level are top-notch people. It’s great to be part of an organization that surrounds itself with talent. The next thing is, it’s a great place to work. IPC was selected as one of the 100 best places to work in healthcare (by Modern Healthcare). We made this list, and a lot of other high-profile names in healthcare did not, so we’re very proud of that.
Q: How does the IPC model translate to increased quality of care?
A: We have resources to educate our physicians. There are hospitals around the country with one-person, two-person, or four-person groups that don’t have the resources to do certain types of training. They acquire it by experience. We’re able to orient them to hospital medicine first … and then bring them along slowly and give them the additional training we think they need to succeed. We also have the resources to do ongoing education and monitor quality measures and efficiency measures as well.
Q: You have been a member of SHM’s Public Policy Committee for about four years. How important is that role?
A: I think it’s incredibly important. The Public Policy Committee gets to be in tune with what the national issues are, and we can help the society foster and create relationships. We had the chance to meet with members of Congress and other national organizations like CMS (Centers for Medicare and Medicaid Services) and AHRQ (Agency for Healthcare Research and Quality), even before healthcare reform became important.
Q: You and other members of the committee went to Washington, D.C., in March. What was the benefit of that trip?
A: We’ve been to Washington several times. We try to do it at least yearly. In previous years, we spent a lot of time just educating people about what hospitalists do. When we first went there, we were surprised by how many members of Congress had never heard of what a hospitalist was. This past year, they were much more aware of what a hospitalist is and how we can help with the goals of healthcare reform.
Q: What’s next for you?
A: I think for now I’m pretty happy with my position and my roles and responsibilities. I help with several different aspects of IPC. I help with some of the risk-management compliance issues. I make presentations to different hospitals and groups we’re thinking of doing business with. I have a varied career, and I enjoy it very much. TH
Mark Leiser is a freelance writer based in New Jersey.
Felix Aguirre, MD, entered the field of hospital medicine before the term “hospitalist” had been coined. He didn’t realize how quickly the field would explode, but it didn’t take long to find out. Aguirre helped start an inpatient service in 1994, taking care of patients for about 20 primary-care physicians. Within three years, his service cared for the patients of 360 doctors.
Dr. Aguirre cofounded Hospitalists of San Antonio in 2000, and he served as president of the company until it merged with IPC: The Hospitalist Co. three years later.
A graduate of the U.S. Military Academy at West Point, Dr. Aguirre spent several years as an air-traffic controller before attending medical school. He currently is vice president of medical affairs for California-based IPC, which provides management services to hospitalist practices in more than 400 facilities.
“The biggest reward is being part of a growth industry, helping to mold it and move it forward,” says Dr. Aguirre, who is responsible for medical and leadership oversight, as well as developing IPC’s physicians and providers. “I’m very proud it’s starting to get distinction as a separate specialty, and I really like the idea of getting in on the ground floor. Everybody likes to be one of the pioneers of an industry.”
Question: How did West Point help prepare you for your current career?
Answer: As part of your education at West Point, you need to learn to be a follower before you can learn to be a leader. Coming out of the academy, I was pretty cocky and I thought I could do anything. I’ve learned some pretty humbling lessons, and experience teaches you how to temper that attitude.
Q: How about your time as an air-traffic controller?
A: You have to be able to deal with many things at once and be able to deal with pressure. That experience is great for a career in an emergency room and in hospital medicine, where you’re juggling a lot of information and facing situations that require pretty rapid action.
Q: When you entered HM, did you have a sense of how much—and how quickly—the field would grow?
A: No. It really was in its infancy at that time … but when Dr. (Robert) Wachter (coined the term “hospitalist”), it began to pick up momentum. Before long, we could see there wasn’t going to be any slowing down of this type of medicine. It’s great to be a part of an industry that is still a growing industry, especially in this economic climate. It’s needed now more than ever, so I feel I made the correct decision to enter this field.
Q: Why do you feel it’s needed more now than ever?
A: With healthcare, there needs to be more control, clinically as well as financially. I think hospitalists are well positioned right in the middle of the hospital. They are exposed to every aspect of the hospital’s operation and staff, whether it’s the cleaning service or dietary or physical therapy or talking to specialists or other physicians. Who better to help control what happens than the person who is exposed to it?
Q: What is the biggest challenge you face in your current role?
A: One of the big ones is reduction in variance. Everybody is looking for ways to reduce variance in clinical care, and that’s going to continue to be one of the biggest challenges as we grow. If you’re a small mom-and-pop business, it’s pretty easy to control things. That gets more difficult as you grow. The things that worked when you were smaller don’t work in a medium-sized company, let alone when you become a large company. You have to change the way you manage things, which leads to another challenge—adapting to the change.
Q: Is the fear of a hospitalist shortage on your radar screen?
A: It is. But I can tell you this: We won’t stress about it, because it is going to happen. There will be a shortage—there already is. What we have to try to do is position ourselves as the company, or employer, of choice. We get close to 3,000 applicants a year and hire 200 or so, so we’re fortunate in that we have a tremendous amount of exposure to many of the people who are desiring a hospitalist career.
Q: What do you see as the biggest benefit to the IPC model?
A: There are a couple of things I see, not just as advantages but also as strengths. Number one, IPC has extremely strong leadership. All of the people I work with on the senior leadership level are top-notch people. It’s great to be part of an organization that surrounds itself with talent. The next thing is, it’s a great place to work. IPC was selected as one of the 100 best places to work in healthcare (by Modern Healthcare). We made this list, and a lot of other high-profile names in healthcare did not, so we’re very proud of that.
Q: How does the IPC model translate to increased quality of care?
A: We have resources to educate our physicians. There are hospitals around the country with one-person, two-person, or four-person groups that don’t have the resources to do certain types of training. They acquire it by experience. We’re able to orient them to hospital medicine first … and then bring them along slowly and give them the additional training we think they need to succeed. We also have the resources to do ongoing education and monitor quality measures and efficiency measures as well.
Q: You have been a member of SHM’s Public Policy Committee for about four years. How important is that role?
A: I think it’s incredibly important. The Public Policy Committee gets to be in tune with what the national issues are, and we can help the society foster and create relationships. We had the chance to meet with members of Congress and other national organizations like CMS (Centers for Medicare and Medicaid Services) and AHRQ (Agency for Healthcare Research and Quality), even before healthcare reform became important.
Q: You and other members of the committee went to Washington, D.C., in March. What was the benefit of that trip?
A: We’ve been to Washington several times. We try to do it at least yearly. In previous years, we spent a lot of time just educating people about what hospitalists do. When we first went there, we were surprised by how many members of Congress had never heard of what a hospitalist was. This past year, they were much more aware of what a hospitalist is and how we can help with the goals of healthcare reform.
Q: What’s next for you?
A: I think for now I’m pretty happy with my position and my roles and responsibilities. I help with several different aspects of IPC. I help with some of the risk-management compliance issues. I make presentations to different hospitals and groups we’re thinking of doing business with. I have a varied career, and I enjoy it very much. TH
Mark Leiser is a freelance writer based in New Jersey.
Felix Aguirre, MD, entered the field of hospital medicine before the term “hospitalist” had been coined. He didn’t realize how quickly the field would explode, but it didn’t take long to find out. Aguirre helped start an inpatient service in 1994, taking care of patients for about 20 primary-care physicians. Within three years, his service cared for the patients of 360 doctors.
Dr. Aguirre cofounded Hospitalists of San Antonio in 2000, and he served as president of the company until it merged with IPC: The Hospitalist Co. three years later.
A graduate of the U.S. Military Academy at West Point, Dr. Aguirre spent several years as an air-traffic controller before attending medical school. He currently is vice president of medical affairs for California-based IPC, which provides management services to hospitalist practices in more than 400 facilities.
“The biggest reward is being part of a growth industry, helping to mold it and move it forward,” says Dr. Aguirre, who is responsible for medical and leadership oversight, as well as developing IPC’s physicians and providers. “I’m very proud it’s starting to get distinction as a separate specialty, and I really like the idea of getting in on the ground floor. Everybody likes to be one of the pioneers of an industry.”
Question: How did West Point help prepare you for your current career?
Answer: As part of your education at West Point, you need to learn to be a follower before you can learn to be a leader. Coming out of the academy, I was pretty cocky and I thought I could do anything. I’ve learned some pretty humbling lessons, and experience teaches you how to temper that attitude.
Q: How about your time as an air-traffic controller?
A: You have to be able to deal with many things at once and be able to deal with pressure. That experience is great for a career in an emergency room and in hospital medicine, where you’re juggling a lot of information and facing situations that require pretty rapid action.
Q: When you entered HM, did you have a sense of how much—and how quickly—the field would grow?
A: No. It really was in its infancy at that time … but when Dr. (Robert) Wachter (coined the term “hospitalist”), it began to pick up momentum. Before long, we could see there wasn’t going to be any slowing down of this type of medicine. It’s great to be a part of an industry that is still a growing industry, especially in this economic climate. It’s needed now more than ever, so I feel I made the correct decision to enter this field.
Q: Why do you feel it’s needed more now than ever?
A: With healthcare, there needs to be more control, clinically as well as financially. I think hospitalists are well positioned right in the middle of the hospital. They are exposed to every aspect of the hospital’s operation and staff, whether it’s the cleaning service or dietary or physical therapy or talking to specialists or other physicians. Who better to help control what happens than the person who is exposed to it?
Q: What is the biggest challenge you face in your current role?
A: One of the big ones is reduction in variance. Everybody is looking for ways to reduce variance in clinical care, and that’s going to continue to be one of the biggest challenges as we grow. If you’re a small mom-and-pop business, it’s pretty easy to control things. That gets more difficult as you grow. The things that worked when you were smaller don’t work in a medium-sized company, let alone when you become a large company. You have to change the way you manage things, which leads to another challenge—adapting to the change.
Q: Is the fear of a hospitalist shortage on your radar screen?
A: It is. But I can tell you this: We won’t stress about it, because it is going to happen. There will be a shortage—there already is. What we have to try to do is position ourselves as the company, or employer, of choice. We get close to 3,000 applicants a year and hire 200 or so, so we’re fortunate in that we have a tremendous amount of exposure to many of the people who are desiring a hospitalist career.
Q: What do you see as the biggest benefit to the IPC model?
A: There are a couple of things I see, not just as advantages but also as strengths. Number one, IPC has extremely strong leadership. All of the people I work with on the senior leadership level are top-notch people. It’s great to be part of an organization that surrounds itself with talent. The next thing is, it’s a great place to work. IPC was selected as one of the 100 best places to work in healthcare (by Modern Healthcare). We made this list, and a lot of other high-profile names in healthcare did not, so we’re very proud of that.
Q: How does the IPC model translate to increased quality of care?
A: We have resources to educate our physicians. There are hospitals around the country with one-person, two-person, or four-person groups that don’t have the resources to do certain types of training. They acquire it by experience. We’re able to orient them to hospital medicine first … and then bring them along slowly and give them the additional training we think they need to succeed. We also have the resources to do ongoing education and monitor quality measures and efficiency measures as well.
Q: You have been a member of SHM’s Public Policy Committee for about four years. How important is that role?
A: I think it’s incredibly important. The Public Policy Committee gets to be in tune with what the national issues are, and we can help the society foster and create relationships. We had the chance to meet with members of Congress and other national organizations like CMS (Centers for Medicare and Medicaid Services) and AHRQ (Agency for Healthcare Research and Quality), even before healthcare reform became important.
Q: You and other members of the committee went to Washington, D.C., in March. What was the benefit of that trip?
A: We’ve been to Washington several times. We try to do it at least yearly. In previous years, we spent a lot of time just educating people about what hospitalists do. When we first went there, we were surprised by how many members of Congress had never heard of what a hospitalist was. This past year, they were much more aware of what a hospitalist is and how we can help with the goals of healthcare reform.
Q: What’s next for you?
A: I think for now I’m pretty happy with my position and my roles and responsibilities. I help with several different aspects of IPC. I help with some of the risk-management compliance issues. I make presentations to different hospitals and groups we’re thinking of doing business with. I have a varied career, and I enjoy it very much. TH
Mark Leiser is a freelance writer based in New Jersey.
Should Hospitalists Report for Service during a Life-Threatening Event?
PRO
When the community is in need, physicians must honor call to duty

As the American Medical Association (AMA) states in its inaugural Code of Ethics from 1847: “When pestilence prevails, it is their duty to face the danger and to continue their labors for the alleviation of the suffering, even at the jeopardy of their own lives.”1 It meant doctors have taken on a calling and social duty to treat sick patients, even at personal expense.
Today, the AMA’s Code of Ethics puts it this way: “Physicians should balance immediate benefits to individual patients with ability to care for patients in future.”2 Over two centuries, the focus remains on the physician’s duty to patient and society.
As a former Air Force physician, I believe in this deontological stance. In the Air Force, we often spoke of our sense of duty, of “service before self, and integrity in everything we do.” This code of conduct applies to combat as well as the peacetime challenges of pandemic flu. If the medical corps’ mantra is to “preserve the fighting force,” the mission of the civilian physician is the community’s survival. This implicit contract with society extends from moments of tranquillity to when the peace is disrupted by either manmade disasters (e.g., war) or biological threats (e.g., pandemic disease).
Having made this assertion, a physician’s obligation is not without its limitations. Doctors have a responsibility to protect themselves and their families from undue harm. We have to stay alive for utilitarian reasons in order to serve others. A society without its physician workforce is imperiled and at enhanced risk, so a physician’s self-preservation is also in the interest of the collective.3
All of this compels doctors to stay alive and remain healthy. Our duty can only be achieved by careful action and avoiding forays into Hollywood heroism. No one asked us to be heroes, only dutiful physicians.4
We have to prepare doctors to meet this challenge. Alexander and Wynia surveyed senior physicians: While 80% were willing to treat high-risk patients, as in bioterrorism or a pandemic, only 21% felt logistically prepared to meet such a challenge in practice.5
If we expect physicians to answer the call, we need to equip them with the knowledge, skills, and equipment necessary to safely and effectively meet their professional responsibilities.
That responsibility is one that society owes its physicians. TH
References
- Code of Medical Ethics of the American Medical Association. American Medical Association Web site. Available at: www.ama-assn.org. Accessed Nov. 30, 2009.
- American Medical Association. Physician Obligation in Disaster Preparedness and Response. Chicago: American Medical Association; 2004.
- Simonds AK, Sokol DK. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur Respir J. 2009;34(2):303-309.
- Sokol D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg Infect Dis. 2006;12(8):1238-1241.
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
CON
Some healthcare providers should be considered exceptions to rule

Infectious illnesses frequently affect healthcare providers disproportionately. Whether physicians are obligated to put themselves at risk is not clear. Many sources argue that participation in infectious epidemic or pandemic events is obligatory, but there is another side to the discussion. Healthcare providers might have risk factors that mitigate this obligation. Two such subgroups are providers with pre-existing health concerns and providers who are caregivers for others.
Studies show that not all providers will report to work in the face of an epidemic. One self-reporting study found that 20% of physicians would report to work.1 Every hospital effected by the SARS epidemic had difficulty with employee attrition.2 Thus, the concern is more than hypothetical.
There is a difference in putting oneself at risk for an illness and putting oneself at risk of death. Providers might be immunosuppressed or have, say, an underlying lung disease. Should higher-risk providers with direct patient contact responsibilities have the same obligation as providers who are not?
Providers who care for others will face different challenges. First, if social distancing becomes widespread and schools and daycare centers are closed, providers will face a dilemma over how to care for their dependents. A second issue for providers with responsibilities to care for others is that those dependent populations are likely to be at higher risk of bad outcomes if they are affected. A provider who is infectious puts their family at risk. Children may be disproportionately affected, and people who require assistance are more likely to have comorbid conditions. Should providers with other responsibilities have the same obligation as providers who do not?
Given that risk is not the same among providers, it is unfair to say that responsibility is the same. Parents simply cannot abandon their children. Risk of death is a serious concern for providers at higher risk. Hospitals should have an explicit plan in place for a pandemic; most do have a plan. The plan needs to consider these issues and have explicit provisions.
Another approach would be to ask providers to state their availability. If the hospital knows that a certain group of providers has specific concerns, the plan can take into account what impact those concerns will have. Transparency in the plan, expectations, and resources will better prepare hospitals.
There is a fundamental duty to provide care to patients who need it, and failure to do so is a violation of a societal and professional trust. However, this duty is not absolute. Giving providers that benefit of the doubt—that they will honor their duty to ill or injured patients—means that providers can be trusted to opt out only for valid reasons. The system must be designed to accommodate special needs. A one-size-fits-all approach is bound to fail. TH
References
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
- Wynia MK. Ethics and public health emergencies: encouraging responsibility. Am J Bioeth. 2007;7(4):1-4.
The opinions expressed herein are those of the authors and do not represent those of the Society of Hospital Medicine or The Hospitalist.
PRO
When the community is in need, physicians must honor call to duty
As the American Medical Association (AMA) states in its inaugural Code of Ethics from 1847: “When pestilence prevails, it is their duty to face the danger and to continue their labors for the alleviation of the suffering, even at the jeopardy of their own lives.”1 It meant doctors have taken on a calling and social duty to treat sick patients, even at personal expense.
Today, the AMA’s Code of Ethics puts it this way: “Physicians should balance immediate benefits to individual patients with ability to care for patients in future.”2 Over two centuries, the focus remains on the physician’s duty to patient and society.
As a former Air Force physician, I believe in this deontological stance. In the Air Force, we often spoke of our sense of duty, of “service before self, and integrity in everything we do.” This code of conduct applies to combat as well as the peacetime challenges of pandemic flu. If the medical corps’ mantra is to “preserve the fighting force,” the mission of the civilian physician is the community’s survival. This implicit contract with society extends from moments of tranquillity to when the peace is disrupted by either manmade disasters (e.g., war) or biological threats (e.g., pandemic disease).
Having made this assertion, a physician’s obligation is not without its limitations. Doctors have a responsibility to protect themselves and their families from undue harm. We have to stay alive for utilitarian reasons in order to serve others. A society without its physician workforce is imperiled and at enhanced risk, so a physician’s self-preservation is also in the interest of the collective.3
All of this compels doctors to stay alive and remain healthy. Our duty can only be achieved by careful action and avoiding forays into Hollywood heroism. No one asked us to be heroes, only dutiful physicians.4
We have to prepare doctors to meet this challenge. Alexander and Wynia surveyed senior physicians: While 80% were willing to treat high-risk patients, as in bioterrorism or a pandemic, only 21% felt logistically prepared to meet such a challenge in practice.5
If we expect physicians to answer the call, we need to equip them with the knowledge, skills, and equipment necessary to safely and effectively meet their professional responsibilities.
That responsibility is one that society owes its physicians. TH
References
- Code of Medical Ethics of the American Medical Association. American Medical Association Web site. Available at: www.ama-assn.org. Accessed Nov. 30, 2009.
- American Medical Association. Physician Obligation in Disaster Preparedness and Response. Chicago: American Medical Association; 2004.
- Simonds AK, Sokol DK. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur Respir J. 2009;34(2):303-309.
- Sokol D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg Infect Dis. 2006;12(8):1238-1241.
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
CON
Some healthcare providers should be considered exceptions to rule
Infectious illnesses frequently affect healthcare providers disproportionately. Whether physicians are obligated to put themselves at risk is not clear. Many sources argue that participation in infectious epidemic or pandemic events is obligatory, but there is another side to the discussion. Healthcare providers might have risk factors that mitigate this obligation. Two such subgroups are providers with pre-existing health concerns and providers who are caregivers for others.
Studies show that not all providers will report to work in the face of an epidemic. One self-reporting study found that 20% of physicians would report to work.1 Every hospital effected by the SARS epidemic had difficulty with employee attrition.2 Thus, the concern is more than hypothetical.
There is a difference in putting oneself at risk for an illness and putting oneself at risk of death. Providers might be immunosuppressed or have, say, an underlying lung disease. Should higher-risk providers with direct patient contact responsibilities have the same obligation as providers who are not?
Providers who care for others will face different challenges. First, if social distancing becomes widespread and schools and daycare centers are closed, providers will face a dilemma over how to care for their dependents. A second issue for providers with responsibilities to care for others is that those dependent populations are likely to be at higher risk of bad outcomes if they are affected. A provider who is infectious puts their family at risk. Children may be disproportionately affected, and people who require assistance are more likely to have comorbid conditions. Should providers with other responsibilities have the same obligation as providers who do not?
Given that risk is not the same among providers, it is unfair to say that responsibility is the same. Parents simply cannot abandon their children. Risk of death is a serious concern for providers at higher risk. Hospitals should have an explicit plan in place for a pandemic; most do have a plan. The plan needs to consider these issues and have explicit provisions.
Another approach would be to ask providers to state their availability. If the hospital knows that a certain group of providers has specific concerns, the plan can take into account what impact those concerns will have. Transparency in the plan, expectations, and resources will better prepare hospitals.
There is a fundamental duty to provide care to patients who need it, and failure to do so is a violation of a societal and professional trust. However, this duty is not absolute. Giving providers that benefit of the doubt—that they will honor their duty to ill or injured patients—means that providers can be trusted to opt out only for valid reasons. The system must be designed to accommodate special needs. A one-size-fits-all approach is bound to fail. TH
References
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
- Wynia MK. Ethics and public health emergencies: encouraging responsibility. Am J Bioeth. 2007;7(4):1-4.
The opinions expressed herein are those of the authors and do not represent those of the Society of Hospital Medicine or The Hospitalist.
PRO
When the community is in need, physicians must honor call to duty
As the American Medical Association (AMA) states in its inaugural Code of Ethics from 1847: “When pestilence prevails, it is their duty to face the danger and to continue their labors for the alleviation of the suffering, even at the jeopardy of their own lives.”1 It meant doctors have taken on a calling and social duty to treat sick patients, even at personal expense.
Today, the AMA’s Code of Ethics puts it this way: “Physicians should balance immediate benefits to individual patients with ability to care for patients in future.”2 Over two centuries, the focus remains on the physician’s duty to patient and society.
As a former Air Force physician, I believe in this deontological stance. In the Air Force, we often spoke of our sense of duty, of “service before self, and integrity in everything we do.” This code of conduct applies to combat as well as the peacetime challenges of pandemic flu. If the medical corps’ mantra is to “preserve the fighting force,” the mission of the civilian physician is the community’s survival. This implicit contract with society extends from moments of tranquillity to when the peace is disrupted by either manmade disasters (e.g., war) or biological threats (e.g., pandemic disease).
Having made this assertion, a physician’s obligation is not without its limitations. Doctors have a responsibility to protect themselves and their families from undue harm. We have to stay alive for utilitarian reasons in order to serve others. A society without its physician workforce is imperiled and at enhanced risk, so a physician’s self-preservation is also in the interest of the collective.3
All of this compels doctors to stay alive and remain healthy. Our duty can only be achieved by careful action and avoiding forays into Hollywood heroism. No one asked us to be heroes, only dutiful physicians.4
We have to prepare doctors to meet this challenge. Alexander and Wynia surveyed senior physicians: While 80% were willing to treat high-risk patients, as in bioterrorism or a pandemic, only 21% felt logistically prepared to meet such a challenge in practice.5
If we expect physicians to answer the call, we need to equip them with the knowledge, skills, and equipment necessary to safely and effectively meet their professional responsibilities.
That responsibility is one that society owes its physicians. TH
References
- Code of Medical Ethics of the American Medical Association. American Medical Association Web site. Available at: www.ama-assn.org. Accessed Nov. 30, 2009.
- American Medical Association. Physician Obligation in Disaster Preparedness and Response. Chicago: American Medical Association; 2004.
- Simonds AK, Sokol DK. Lives on the line? Ethics and practicalities of duty of care in pandemics and disasters. Eur Respir J. 2009;34(2):303-309.
- Sokol D. Virulent epidemics and scope of healthcare workers’ duty of care. Emerg Infect Dis. 2006;12(8):1238-1241.
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
CON
Some healthcare providers should be considered exceptions to rule
Infectious illnesses frequently affect healthcare providers disproportionately. Whether physicians are obligated to put themselves at risk is not clear. Many sources argue that participation in infectious epidemic or pandemic events is obligatory, but there is another side to the discussion. Healthcare providers might have risk factors that mitigate this obligation. Two such subgroups are providers with pre-existing health concerns and providers who are caregivers for others.
Studies show that not all providers will report to work in the face of an epidemic. One self-reporting study found that 20% of physicians would report to work.1 Every hospital effected by the SARS epidemic had difficulty with employee attrition.2 Thus, the concern is more than hypothetical.
There is a difference in putting oneself at risk for an illness and putting oneself at risk of death. Providers might be immunosuppressed or have, say, an underlying lung disease. Should higher-risk providers with direct patient contact responsibilities have the same obligation as providers who are not?
Providers who care for others will face different challenges. First, if social distancing becomes widespread and schools and daycare centers are closed, providers will face a dilemma over how to care for their dependents. A second issue for providers with responsibilities to care for others is that those dependent populations are likely to be at higher risk of bad outcomes if they are affected. A provider who is infectious puts their family at risk. Children may be disproportionately affected, and people who require assistance are more likely to have comorbid conditions. Should providers with other responsibilities have the same obligation as providers who do not?
Given that risk is not the same among providers, it is unfair to say that responsibility is the same. Parents simply cannot abandon their children. Risk of death is a serious concern for providers at higher risk. Hospitals should have an explicit plan in place for a pandemic; most do have a plan. The plan needs to consider these issues and have explicit provisions.
Another approach would be to ask providers to state their availability. If the hospital knows that a certain group of providers has specific concerns, the plan can take into account what impact those concerns will have. Transparency in the plan, expectations, and resources will better prepare hospitals.
There is a fundamental duty to provide care to patients who need it, and failure to do so is a violation of a societal and professional trust. However, this duty is not absolute. Giving providers that benefit of the doubt—that they will honor their duty to ill or injured patients—means that providers can be trusted to opt out only for valid reasons. The system must be designed to accommodate special needs. A one-size-fits-all approach is bound to fail. TH
References
- Alexander GC, Wynia MK. Ready and willing? Physicians’ sense of preparedness for bioterrorism. Health Aff (Millwood). 2003;22(5):189-197.
- Wynia MK. Ethics and public health emergencies: encouraging responsibility. Am J Bioeth. 2007;7(4):1-4.
The opinions expressed herein are those of the authors and do not represent those of the Society of Hospital Medicine or The Hospitalist.
Smooth Moves
Accepting a job in a new city, state, or country can be invigorating for professional and personal reasons, but making the actual move often is stressful, irritating, and more than a little overwhelming. Multiple factors are involved when you transition from one community to another.
For hospitalists relocating for a new job, the good news is it’s almost a given you will receive financial assistance and more than a little guidance to make the move as smooth and hassle-free as possible, says Tommy Bohannon, vice president of hospital-based recruiting for Merritt Hawkins & Associates, a recruitment firm that specializes in the placement of permanent physicians. Ninety-eight percent of physician and certified registered nurse anesthetists are provided relocation assistance, according to a Merritt Hawkins review of recruiting incentives conducted from April 2008 to March 2009. The Irving, Texas-based firm found that the average relocation allowance is $10,427, the highest amount offered since it began tracking recruiting incentives in 2005.
The Upper Hand: HM Still in Demand
While the struggling economy has put a damper on relocation allowances in other professions, it has not had a similar effect on HM, says Cheryl Slack, vice president of human resources for Cogent Healthcare, a Brentwood, Tenn.-based company that partners with hospitals to build and manage hospitalist programs. Hospitalists have become harder and harder to recruit as demand for their services continues to far outpace their supply, she says.
“Relocation assistance is the nature of the beast,” says Slack, whose company typically covers a hospitalist’s move from Point A to Point B, storage fees for a few months, and sometimes travel costs to and from their former home to tie up loose ends. “We see it as the cost of doing business.”
Because most relocation allowances are not tied to a time or service commitment, hospitalists can use the money to facilitate their move without the worry of having to pay some of it back if the job doesn’t work out. They can get the most mileage out of the assistance by comparison shopping (see “Internet Resources for Relocations,” right) or using companies that have a relationship with their recruiter or employer. “We actually have an in-house relocation team and a preferred-rate contract with a national moving company,” Bohannon says. “The vast majority of our candidates work with the in-house team. We help them with the physical move itself. We assist them in taking an inventory of their belongings to get an idea of how much it will cost to move, and we get the moving company in contact with them.”
Temporary vs. Permanent Decisions
Hospitalists might want to consider renting or taking advantage of temporary housing, if offered by the new employer, in order to get acclimated with the new community and its neighborhoods, says Christian Rutherford, president and CEO of Kendall & Davis, a St. Louis-based physician recruitment firm. In the current housing market, renting or using temporary housing might be the best option for hospitalists who are still trying to sell their last home.
When hospitalists are ready to buy a home in their new community, they should check with people at their new job or their recruiter to get names of real estate agents who have considerable insight into the community and local property values. “When we first discuss an opportunity with a candidate, we will pass along pretty detailed information about neighborhoods, schools, housing costs, churches, local clubs that cater to their interests, and hobbies,” Bohannon says. “The market has changed to where the candidate is interviewing the opportunity. We’re pretty hands-on to make sure they have access to the information they need to make a good decision.”
Community Comes First
—Tommy Bohannon, vice president of hospital-based recruiting, Merritt Hawkins & Associates, Irving, Texas
For most job candidates, 50% of the “sale”—the decision to relocate—is the community in which they will work and live, says Mark Dotson, Cogent Healthcare’s senior director of recruitment. Candidates want to know about the neighborhoods, school systems, and cost of living, and nearby entertainment, cultural, and social amenities. Even though a lot of information is available on the Internet, it is not always dependable. Recruiters and potential employers often provide comprehensive community information packets for hospitalists; many organize a community tour while hospitalists are in town for their on-site interview. Some employers and recruiters schedule meetings with real estate agents, school administrators, even Chamber of Commerce representatives.
“I’ve talked to hospitals about providers’ spouses and where they might be able to find work. It’s all part of the recruitment process and determining what the individual provider’s needs are,” says Mimi Hagan, regional director of hospitalist accounts for Hospital Physician Partners of Fort Lauderdale, Fla., a medical management company that partners with hospitals to build emergency and hospitalist practices. “The last thing we want is for a provider to walk into the hospital thinking this isn’t the right fit for them. It’s not good for the provider, it’s not good for the hospital, and it’s not good for us.”
Hagan and Rutherford advise hospitalists who are seriously contemplating relocating and have families to bring their partners with them for the on-site interview. They might want to consider making another trip to their new community with the children in tow. “Relocating to a different area is a really big cultural change. Candidates have to make sure their spouse is as excited about the change as they are,” Rutherford says. “Don’t ever underestimate how much of a strain this can be on the kids and the spouse.” TH
Lisa Ryan is a freelance writer based in New Jersey.
Accepting a job in a new city, state, or country can be invigorating for professional and personal reasons, but making the actual move often is stressful, irritating, and more than a little overwhelming. Multiple factors are involved when you transition from one community to another.
For hospitalists relocating for a new job, the good news is it’s almost a given you will receive financial assistance and more than a little guidance to make the move as smooth and hassle-free as possible, says Tommy Bohannon, vice president of hospital-based recruiting for Merritt Hawkins & Associates, a recruitment firm that specializes in the placement of permanent physicians. Ninety-eight percent of physician and certified registered nurse anesthetists are provided relocation assistance, according to a Merritt Hawkins review of recruiting incentives conducted from April 2008 to March 2009. The Irving, Texas-based firm found that the average relocation allowance is $10,427, the highest amount offered since it began tracking recruiting incentives in 2005.
The Upper Hand: HM Still in Demand
While the struggling economy has put a damper on relocation allowances in other professions, it has not had a similar effect on HM, says Cheryl Slack, vice president of human resources for Cogent Healthcare, a Brentwood, Tenn.-based company that partners with hospitals to build and manage hospitalist programs. Hospitalists have become harder and harder to recruit as demand for their services continues to far outpace their supply, she says.
“Relocation assistance is the nature of the beast,” says Slack, whose company typically covers a hospitalist’s move from Point A to Point B, storage fees for a few months, and sometimes travel costs to and from their former home to tie up loose ends. “We see it as the cost of doing business.”
Because most relocation allowances are not tied to a time or service commitment, hospitalists can use the money to facilitate their move without the worry of having to pay some of it back if the job doesn’t work out. They can get the most mileage out of the assistance by comparison shopping (see “Internet Resources for Relocations,” right) or using companies that have a relationship with their recruiter or employer. “We actually have an in-house relocation team and a preferred-rate contract with a national moving company,” Bohannon says. “The vast majority of our candidates work with the in-house team. We help them with the physical move itself. We assist them in taking an inventory of their belongings to get an idea of how much it will cost to move, and we get the moving company in contact with them.”
Temporary vs. Permanent Decisions
Hospitalists might want to consider renting or taking advantage of temporary housing, if offered by the new employer, in order to get acclimated with the new community and its neighborhoods, says Christian Rutherford, president and CEO of Kendall & Davis, a St. Louis-based physician recruitment firm. In the current housing market, renting or using temporary housing might be the best option for hospitalists who are still trying to sell their last home.
When hospitalists are ready to buy a home in their new community, they should check with people at their new job or their recruiter to get names of real estate agents who have considerable insight into the community and local property values. “When we first discuss an opportunity with a candidate, we will pass along pretty detailed information about neighborhoods, schools, housing costs, churches, local clubs that cater to their interests, and hobbies,” Bohannon says. “The market has changed to where the candidate is interviewing the opportunity. We’re pretty hands-on to make sure they have access to the information they need to make a good decision.”
Community Comes First
—Tommy Bohannon, vice president of hospital-based recruiting, Merritt Hawkins & Associates, Irving, Texas
For most job candidates, 50% of the “sale”—the decision to relocate—is the community in which they will work and live, says Mark Dotson, Cogent Healthcare’s senior director of recruitment. Candidates want to know about the neighborhoods, school systems, and cost of living, and nearby entertainment, cultural, and social amenities. Even though a lot of information is available on the Internet, it is not always dependable. Recruiters and potential employers often provide comprehensive community information packets for hospitalists; many organize a community tour while hospitalists are in town for their on-site interview. Some employers and recruiters schedule meetings with real estate agents, school administrators, even Chamber of Commerce representatives.
“I’ve talked to hospitals about providers’ spouses and where they might be able to find work. It’s all part of the recruitment process and determining what the individual provider’s needs are,” says Mimi Hagan, regional director of hospitalist accounts for Hospital Physician Partners of Fort Lauderdale, Fla., a medical management company that partners with hospitals to build emergency and hospitalist practices. “The last thing we want is for a provider to walk into the hospital thinking this isn’t the right fit for them. It’s not good for the provider, it’s not good for the hospital, and it’s not good for us.”
Hagan and Rutherford advise hospitalists who are seriously contemplating relocating and have families to bring their partners with them for the on-site interview. They might want to consider making another trip to their new community with the children in tow. “Relocating to a different area is a really big cultural change. Candidates have to make sure their spouse is as excited about the change as they are,” Rutherford says. “Don’t ever underestimate how much of a strain this can be on the kids and the spouse.” TH
Lisa Ryan is a freelance writer based in New Jersey.
Accepting a job in a new city, state, or country can be invigorating for professional and personal reasons, but making the actual move often is stressful, irritating, and more than a little overwhelming. Multiple factors are involved when you transition from one community to another.
For hospitalists relocating for a new job, the good news is it’s almost a given you will receive financial assistance and more than a little guidance to make the move as smooth and hassle-free as possible, says Tommy Bohannon, vice president of hospital-based recruiting for Merritt Hawkins & Associates, a recruitment firm that specializes in the placement of permanent physicians. Ninety-eight percent of physician and certified registered nurse anesthetists are provided relocation assistance, according to a Merritt Hawkins review of recruiting incentives conducted from April 2008 to March 2009. The Irving, Texas-based firm found that the average relocation allowance is $10,427, the highest amount offered since it began tracking recruiting incentives in 2005.
The Upper Hand: HM Still in Demand
While the struggling economy has put a damper on relocation allowances in other professions, it has not had a similar effect on HM, says Cheryl Slack, vice president of human resources for Cogent Healthcare, a Brentwood, Tenn.-based company that partners with hospitals to build and manage hospitalist programs. Hospitalists have become harder and harder to recruit as demand for their services continues to far outpace their supply, she says.
“Relocation assistance is the nature of the beast,” says Slack, whose company typically covers a hospitalist’s move from Point A to Point B, storage fees for a few months, and sometimes travel costs to and from their former home to tie up loose ends. “We see it as the cost of doing business.”
Because most relocation allowances are not tied to a time or service commitment, hospitalists can use the money to facilitate their move without the worry of having to pay some of it back if the job doesn’t work out. They can get the most mileage out of the assistance by comparison shopping (see “Internet Resources for Relocations,” right) or using companies that have a relationship with their recruiter or employer. “We actually have an in-house relocation team and a preferred-rate contract with a national moving company,” Bohannon says. “The vast majority of our candidates work with the in-house team. We help them with the physical move itself. We assist them in taking an inventory of their belongings to get an idea of how much it will cost to move, and we get the moving company in contact with them.”
Temporary vs. Permanent Decisions
Hospitalists might want to consider renting or taking advantage of temporary housing, if offered by the new employer, in order to get acclimated with the new community and its neighborhoods, says Christian Rutherford, president and CEO of Kendall & Davis, a St. Louis-based physician recruitment firm. In the current housing market, renting or using temporary housing might be the best option for hospitalists who are still trying to sell their last home.
When hospitalists are ready to buy a home in their new community, they should check with people at their new job or their recruiter to get names of real estate agents who have considerable insight into the community and local property values. “When we first discuss an opportunity with a candidate, we will pass along pretty detailed information about neighborhoods, schools, housing costs, churches, local clubs that cater to their interests, and hobbies,” Bohannon says. “The market has changed to where the candidate is interviewing the opportunity. We’re pretty hands-on to make sure they have access to the information they need to make a good decision.”
Community Comes First
—Tommy Bohannon, vice president of hospital-based recruiting, Merritt Hawkins & Associates, Irving, Texas
For most job candidates, 50% of the “sale”—the decision to relocate—is the community in which they will work and live, says Mark Dotson, Cogent Healthcare’s senior director of recruitment. Candidates want to know about the neighborhoods, school systems, and cost of living, and nearby entertainment, cultural, and social amenities. Even though a lot of information is available on the Internet, it is not always dependable. Recruiters and potential employers often provide comprehensive community information packets for hospitalists; many organize a community tour while hospitalists are in town for their on-site interview. Some employers and recruiters schedule meetings with real estate agents, school administrators, even Chamber of Commerce representatives.
“I’ve talked to hospitals about providers’ spouses and where they might be able to find work. It’s all part of the recruitment process and determining what the individual provider’s needs are,” says Mimi Hagan, regional director of hospitalist accounts for Hospital Physician Partners of Fort Lauderdale, Fla., a medical management company that partners with hospitals to build emergency and hospitalist practices. “The last thing we want is for a provider to walk into the hospital thinking this isn’t the right fit for them. It’s not good for the provider, it’s not good for the hospital, and it’s not good for us.”
Hagan and Rutherford advise hospitalists who are seriously contemplating relocating and have families to bring their partners with them for the on-site interview. They might want to consider making another trip to their new community with the children in tow. “Relocating to a different area is a really big cultural change. Candidates have to make sure their spouse is as excited about the change as they are,” Rutherford says. “Don’t ever underestimate how much of a strain this can be on the kids and the spouse.” TH
Lisa Ryan is a freelance writer based in New Jersey.
How Should Hospitalized Patients with Long QT Syndrome Be Managed?
Case
You are asked to admit a 63-year-old male with a history of hypertension and osteoarthritis. The patient, who fell at home, is scheduled for open repair of his femoral neck fracture the following day. The patient reports tripping over his granddaughter’s toys and denies any associated symptoms around the time of his fall. An electrocardiogram (ECG) reveals a QTc (QT) interval of 480 ms. How should this hospitalized patient’s prolonged QT interval be managed?
Overview
Patients with a prolonged QT interval on routine ECG present an interesting dilemma for clinicians. Although QT prolongation—either congenital or acquired—has been associated with dysrhythmias, the risk of torsades de pointes and sudden cardiac death varies considerably based on myriad underlying factors.1 Therefore, the principle job of the clinician who has recognized QT prolongation is to assess and minimize the risk of the development of clinically significant dysrhythmias, and to be prepared to manage them should they arise.
The QT interval encompasses ventricular depolarization and repolarization. This ventricular action potential proceeds through five phases. The initial upstroke (phase 0) of depolarization occurs with the opening of Na+ channels, triggering the inward Na+ current (INa), and causes the interior of the myocytes to become positively charged. This is followed by initial repolarization (phase 1) when the opening of K+ channels causes an outward K+ current (Ito). Next, the plateau phase (phase 2) of the action potential follows with a balance of inward current through Ca2+channels (Ica-L) and outward current through slow rectifier K+ channels (IKs), and then later through delayed, rapid K+ rectifier channels (IKr). Then, the inward current is deactivated, while the outward current increases through the rapid delayed rectifier (IKr) and opening of inward rectifier channels (IK1) to complete repolarization (phase 3). Finally, the action potential returns to baseline (phase 4) and Na+ begins to enter the cell again (see Figure 1, above).
The long QT syndrome (LQTS) is defined by a defect in these cardiac ion channels, which leads to abnormal repolarization, usually lengthening the QT interval and thus predisposing to ventricular dysrhythmias.2 It is estimated that as many as 85% of these syndromes are inherited, and up to 15% are acquired or sporadic.3 Depending on the underlying etiology of the LQTS, manifestations might first be appreciated at any time from in utero through adulthood.4 Symptoms including palpitations, syncope, seizures, or cardiac arrest bring these patients to medical attention.3 These symptoms frequently elicit physical or emotional stress, but they can occur without obvious inciting triggers.5 A 20% mortality risk exists in patients who are symptomatic and untreated in the first year following diagnosis, and up to 50% within 10 years following diagnosis.4
How is Long QT Syndrome Diagnosed?
The LQTS diagnosis is based on clinical history in combination with ECG abnormalities.6 Important historical elements include symptoms of palpitations, syncope, seizures, or cardiac arrest.3 In addition, a family history of unexplained syncope or sudden death, especially at a young age, should raise LQTS suspicion.5
A variety of ECG findings can be witnessed in LQTS patients.4,5 Although the majority of patients have a QTc >440 ms, approximately one-third have a QTc ≤460 ms, and about 10% have normal QTc intervals.5 Other ECG abnormalities include notched, biphasic, or prolonged T-waves, and the presence of U-waves.4,5 Schwartz et al used these elements to publish criteria (see Table 1, right) that physicians can use to assess the probability that a patient has LQTS.7
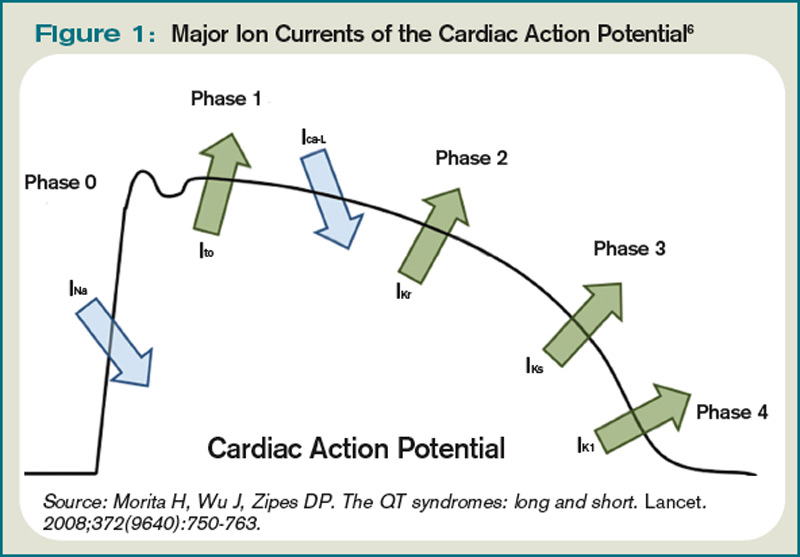
Types of Long QT Syndromes
Because the risk of developing significant dysrhythmias with LQTS is dependent on both the actual QT interval, with risk for sudden cardiac death increased two to three times with QT >440 ms compared with QT <440 ms and the specific underlying genotype, it is important to have an understanding of congenital and acquired LQTS and the associated triggers for torsades de pointes.
Congenital LQTS
Congenital LQTS is caused by mutations in cardiac ion channel proteins, primarily sodium, and potassium channels.5,6 These defects either slow depolarization or lengthen repolarization, leading to heterogeneity of repolarization of the membrane.5 This, in turn, predisposes to ventricular dysrhythmias, including torsades de pointes and subsequent ventricular fibrillation and death.2 Currently, 12 genetic defects have been identified in LQTS. Hundreds of mutations have been described to cause these defects (see Table 2, right).8 Approximately 70% of congenital LQTS are caused by mutations in three genes and are classified as LQTS 1, LQTS 2, and LQTS 3.8 The other seven mutation types account for about 5% of cases; a quarter of LQTS cases have no identified genetic mutations.8
LQTS usually can be distinguished by clinical features and some ECG characteristics, but diagnosis of the specific type requires genetic testing.8,9 The most common types of LQTS are discussed below.
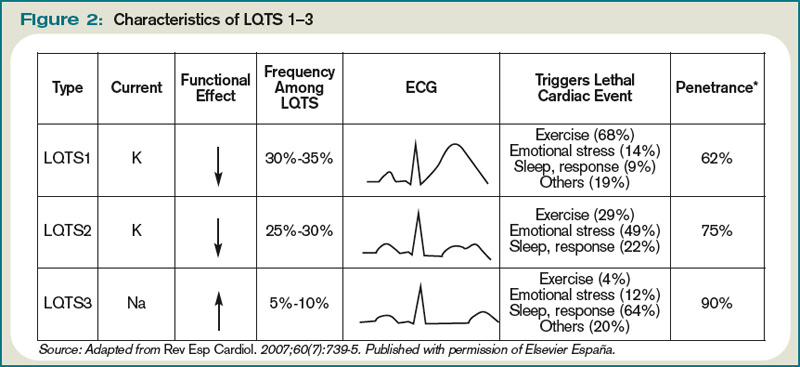
- Long QT1 is the most common type, occurring in approximately 40% to 50% of patients diagnosed with LQTS. It is characterized by a defect in the potassium channel alpha subunit leading to IKs reduction.9 These patients typically present with syncope or adrenergic-induced torsades, might have wide, broad-based T-waves on ECG, and respond well to beta-blocker therapy.6 Triggers for these patients include physical exertion or emotional stressors, particularly exercise and swimming. These patients typically present in early childhood.1
- Long QT2 occurs in 35% to 40% of patients and is characterized by a different defect in the alpha subunit of the potassium channel, which leads to reduced IKr.9 ECGs in LQTS2 can demonstrate low-amplitude and notched T-waves. Sudden catecholamine surges related to emotional stress or loud noises and bradycardia can trigger dysrhythmias in Long QT2.6 Thus, beta blockers reduce overall cardiac events in LQTS2 but less effectively than in LQTS1.6 These patients also present in childhood but typically are older than patients with LQTS1.6
- Long QT3 is less common than LQTS1 or LQTS2, at 2% to 8% of LQTS patients, but carries a higher mortality and is not treated effectively with beta blockers. LQTS3 is characterized by a defect in a sodium channel, causing a gain-of-function in the INa.4,9 These patients are more likely to have a fatal dysrhythmia while sleeping, are less susceptible to exercise-induced events, and have increased morbidity and mortality associated with bradycardia.4,9 ECG frequently reveals a relatively long ST segment, followed by a peaked and tall T-wave. Beta-blocker therapy can predispose to dysrhythmias in these patients; therefore, many of these patients will have pacemakers implanted as first-line therapy.6
While less common, Jervell and Lange Nielson syndrome is an autosomal recessive form of LQTS in which affected patients have homozygous mutations in the KCNQ1 or KCNE1 genes. This syndrome occurs in approximately 1% to 7% of LQTS patients, displays a typical QTc >550 ms, can be triggered by exercise and emotional stress, is associated with deafness, and carries a high risk of cardiac events at a young age.6
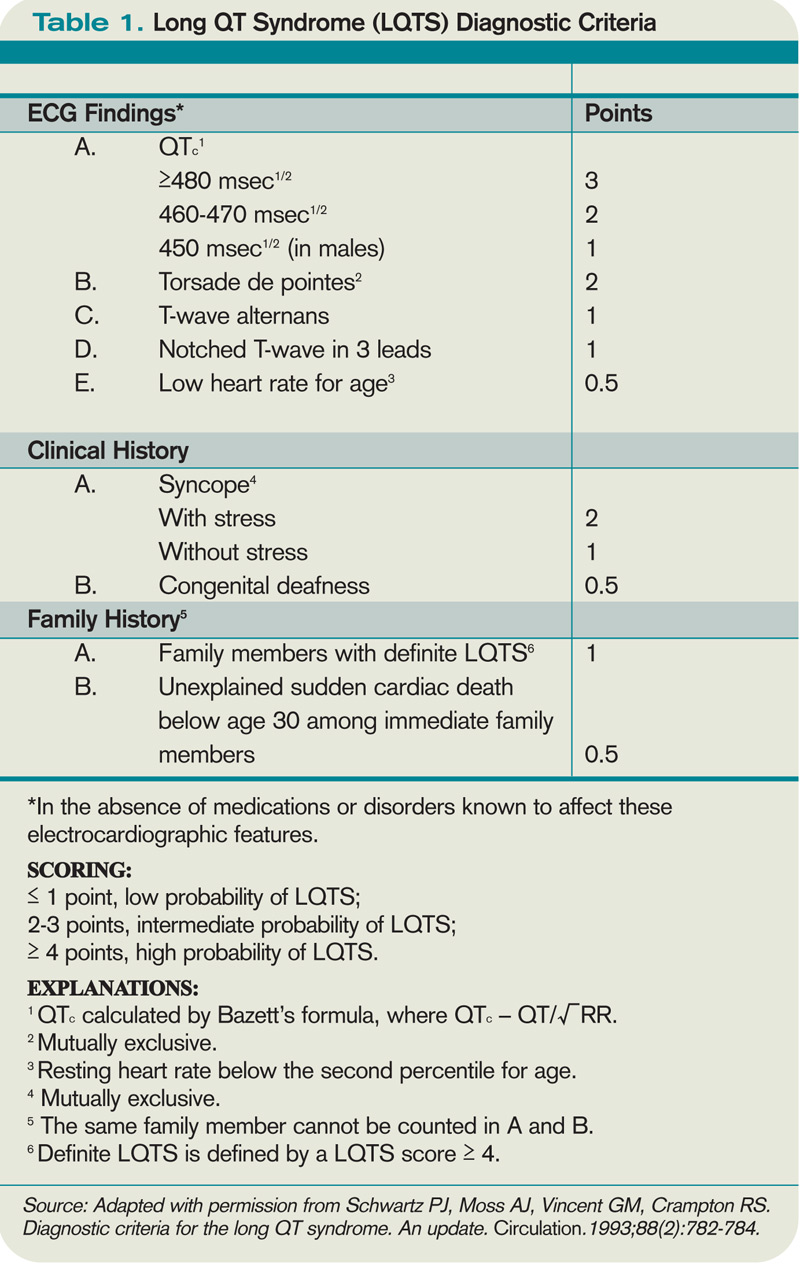
Acquired Syndromes
In addition to congenital LQTS, certain patients can acquire LQTS after being treated with particular drugs or having metabolic abnormalities, namely hypomagnesemia, hypocalcemia, and hypokalemia. Most experts think patients who “acquire” LQTS that predisposes to torsades de pointes have underlying structural heart disease or LQTS genetic carrier mutations that combine with transient initiating events (e.g., drugs or metabolic abnormalities) to induce dysrhythmias.1 In addition to certain drugs, cardiac ischemia, and electrolyte abnormalities, cocaine abuse, HIV, and subarachnoid hemorrhage can induce dysrhythmias in susceptible patients.5
Many types of drugs can cause a prolonged QT interval, and others should be avoided in patients with pre-existing prolonged QT (see Table 3, p. 17). Potentially offending drugs that are frequently encountered by inpatient physicians include amiodarone, diltiazem, erythromycin, clarithromycin, ciprofloxacin, fluoxetine, paroxetine, sertraline, haloperidol, ritonavir, and methadone.1 Additionally, drugs that cause electrolyte abnormalities (e.g., diuretics and lithium) should be monitored closely.
Overall, the goals of therapy in LQTS are:
- Decrease the risk of dysrhythmic events;
- Minimize adrenergic response;
- Shorten the QTc;
- Decrease the dispersion of refractoriness; and
- Improve the function of the ion channels.3
Supportive measures should be taken for patients who are acutely symptomatic from LQTS and associated torsades de pointes. In addition to immediate cardioversion for ongoing and hemodynamically significant torsades, intravenous magnesium should be administered, electrolytes corrected, and offending drugs discontinued.5 Temporary transvenous pacing at rates of approximately 100 beats per minute is highly effective in preventing short-term recurrence of torsades in congenital and acquired LQTS, especially in bradycardic patients.5 Isoproterenol infusion increases the heart rate and effectively prevents acute recurrence of torsades in patients with acquired LQTS, but it should be used with caution in patients with structural heart disease.5
Long-term strategies to manage LQTS include:
- Minimizing the risk of triggering cardiac events via adrenergic stimulation;
- Preventing ongoing dysrhythmias;
- Avoiding medications known to prolong the QT interval; and
- Maintaining normal electrolytes and minerals.5
Most patients with congenital long QT should be discouraged from participating in competitive sports, and patients should attempt to eliminate exposures to stress or sudden awakening, though this is not practical in all cases.5 Beta blockers generally are the first-line therapy and are more effective for LQT1 than LQT2 or LQT3.4,5 If patients are still symptomatic despite adequate medical therapy, or have survived cardiac arrest, they should be considered for ICD therapy.4,5 In addition, patients with profound bradycardia benefit from pacemaker implantation.5 Patients who remain symptomatic despite both beta blockade and ICD placement might find cervicothoracic sympathectomy curative.4,5
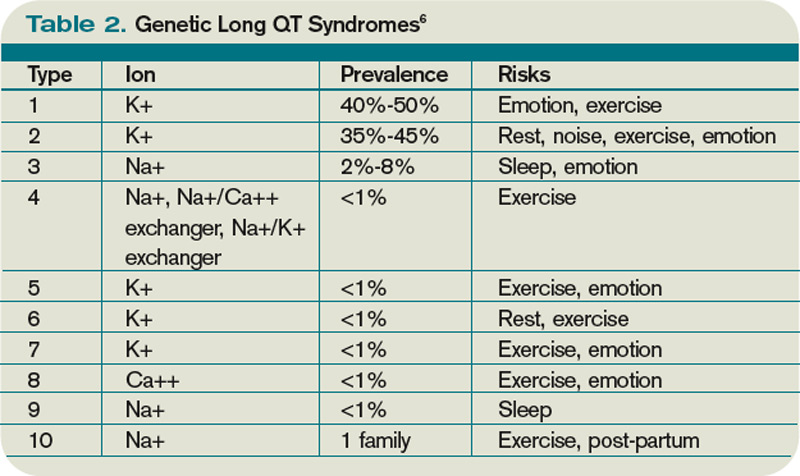
Perioperative Considerations
Although little data is available to guide physicians in the prevention of torsades de pointes during the course of anesthesia, there are a number of considerations that may reduce the chances of symptomatic dysrhythmias.
First, care should be taken to avoid dysrhythmia triggers in LQTS by providing a calm, quiet environment during induction, monitoring, and treating metabolic abnormalities, and providing an appropriate level of anesthesia.10 Beta-blocker therapy should be continued and potentially measured preoperatively by assessing heart rate response during stress testing.5 An implantable cardioverter-defibrillator (AICD) should be interrogated prior to surgery and inactivated during the operation.5
Finally, Kies et al have recommended general anesthesia with propofol for induction (or throughout), isoflurane as the volatile agent, vecuronium for muscle relaxation, and intravenous fentanyl for analgesia when possible.10
Back to the Case
While the patient had no genetic testing for LQTS, evaluation of previous ECGs demonstrated a prolonged QT interval. The hip fracture repair was considered an urgent procedure, which precluded the ability to undertake genetic testing and consideration for device implantation. The only medication that was known to increase the risk for dysrhythmias in this patient was his diuretic, with the attendant risk of electrolyte abnormalities.
Thus, the patient’s hydrochlorothiazide was discontinued and his pre-existing atenolol continued. The patient’s electrolytes and minerals were monitored closely, and magnesium was administered on the day of surgery. Anesthesia was made aware of the prolonged QT interval, such that they were able to minimize the risk for and anticipate the treatment of dysrhythmias. The patient tolerated the surgery and post-operative period without complication and was scheduled for an outpatient workup and management for his prolonged QT interval.
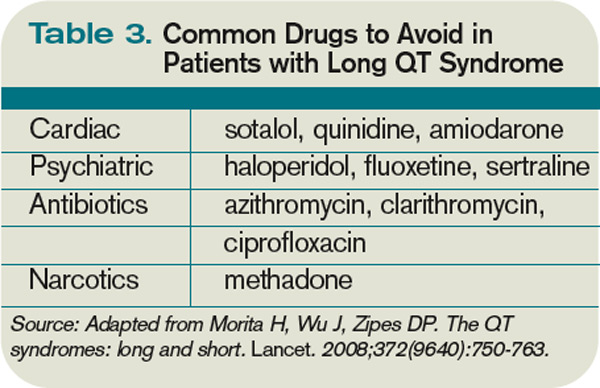
Bottom Line
Long QT syndrome is frequently genetic in origin, but it can be caused by certain medications and perturbations of electrolytes. Beta blockers are the first-line therapy for the majority of LQTS cases, along with discontinuation of drugs that might induce or aggravate the QT prolongation.
Patients who have had cardiac arrest or who remain symptomatic despite beta-blocker therapy should have an ICD implanted.
In the perioperative period, patients’ electrolytes should be monitored and kept within normal limits. If the patient is on a beta blocker, it should be continued, and the anesthesiologist should be made aware of the diagnosis so that the anesthethic plan can be optimized to prevent arrhythmic complications. TH
Dr. Kamali is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Veterans Affairs Medical Center in Denver and an instructor of medicine at UC Denver. Dr. Prochazka is director of ambulatory care at the Denver VA and professor of medicine at UC Denver. Dr. Varosy is director of cardiac electrophysiology at the Denver VA and assistant professor of medicine at UC Denver.
References
- Kao LW, Furbee BR. Drug-induced q-T prolongation. Med Clin North Am. 2005;89(6):1125-1144.
- Marchlinski F. Chapter 226, The Tachyarrhythmias; Harrison's Principles of Internal Medicine, 17e. Available at: www.accessmedicine.com/resourceTOC .aspx?resourceID=4. Accessed Nov. 21, 2009.
- Zareba W, Cygankiewicz I. Long QT syndrome and short QT syndrome. Prog Cardiovasc Dis. 2008; 51(3):264-278.
- Booker PD, Whyte SD, Ladusans EJ. Long QT syndrome and anaesthesia. Br J Anaesth. 2003;90(3):349-366.
- Khan IA. Long QT syndrome: diagnosis and management. Am Heart J. 2002;143(1):7-14.
- Morita H, Wu J, Zipes DP. The QT syndromes: long and short. Lancet. 2008;372(9640):750-763.
- Schwartz PJ, Moss AJ, Vincent GM, Crampton RS. Diagnostic criteria for the long QT syndrome. An update. Circulation. 1993;88(2):782-784.
- Kapa S, Tester DJ, Salisbury BA, et al. Genetic testing for long-QT syndrome: distinguishing pathogenic mutations from benign variants. Circulation. 2009;120(18):1752-1760.
- Modell SM, Lehmann MH. The long QT syndrome family of cardiac ion channelopathies: a HuGE review. Genet Med. 2006;8(3):143-155.
- Kies SJ, Pabelick CM, Hurley HA, White RD, Ackerman MJ. Anesthesia for patients with congenital long QT syndrome. Anesthesiology. 2005;102(1):204-210.
- Wisely NA, Shipton EA. Long QT syndrome and anaesthesia. Eur J Anaesthesiol. 2002;19(12):853-859.
Case
You are asked to admit a 63-year-old male with a history of hypertension and osteoarthritis. The patient, who fell at home, is scheduled for open repair of his femoral neck fracture the following day. The patient reports tripping over his granddaughter’s toys and denies any associated symptoms around the time of his fall. An electrocardiogram (ECG) reveals a QTc (QT) interval of 480 ms. How should this hospitalized patient’s prolonged QT interval be managed?
Overview
Patients with a prolonged QT interval on routine ECG present an interesting dilemma for clinicians. Although QT prolongation—either congenital or acquired—has been associated with dysrhythmias, the risk of torsades de pointes and sudden cardiac death varies considerably based on myriad underlying factors.1 Therefore, the principle job of the clinician who has recognized QT prolongation is to assess and minimize the risk of the development of clinically significant dysrhythmias, and to be prepared to manage them should they arise.
The QT interval encompasses ventricular depolarization and repolarization. This ventricular action potential proceeds through five phases. The initial upstroke (phase 0) of depolarization occurs with the opening of Na+ channels, triggering the inward Na+ current (INa), and causes the interior of the myocytes to become positively charged. This is followed by initial repolarization (phase 1) when the opening of K+ channels causes an outward K+ current (Ito). Next, the plateau phase (phase 2) of the action potential follows with a balance of inward current through Ca2+channels (Ica-L) and outward current through slow rectifier K+ channels (IKs), and then later through delayed, rapid K+ rectifier channels (IKr). Then, the inward current is deactivated, while the outward current increases through the rapid delayed rectifier (IKr) and opening of inward rectifier channels (IK1) to complete repolarization (phase 3). Finally, the action potential returns to baseline (phase 4) and Na+ begins to enter the cell again (see Figure 1, above).
The long QT syndrome (LQTS) is defined by a defect in these cardiac ion channels, which leads to abnormal repolarization, usually lengthening the QT interval and thus predisposing to ventricular dysrhythmias.2 It is estimated that as many as 85% of these syndromes are inherited, and up to 15% are acquired or sporadic.3 Depending on the underlying etiology of the LQTS, manifestations might first be appreciated at any time from in utero through adulthood.4 Symptoms including palpitations, syncope, seizures, or cardiac arrest bring these patients to medical attention.3 These symptoms frequently elicit physical or emotional stress, but they can occur without obvious inciting triggers.5 A 20% mortality risk exists in patients who are symptomatic and untreated in the first year following diagnosis, and up to 50% within 10 years following diagnosis.4
How is Long QT Syndrome Diagnosed?
The LQTS diagnosis is based on clinical history in combination with ECG abnormalities.6 Important historical elements include symptoms of palpitations, syncope, seizures, or cardiac arrest.3 In addition, a family history of unexplained syncope or sudden death, especially at a young age, should raise LQTS suspicion.5
A variety of ECG findings can be witnessed in LQTS patients.4,5 Although the majority of patients have a QTc >440 ms, approximately one-third have a QTc ≤460 ms, and about 10% have normal QTc intervals.5 Other ECG abnormalities include notched, biphasic, or prolonged T-waves, and the presence of U-waves.4,5 Schwartz et al used these elements to publish criteria (see Table 1, right) that physicians can use to assess the probability that a patient has LQTS.7
Types of Long QT Syndromes
Because the risk of developing significant dysrhythmias with LQTS is dependent on both the actual QT interval, with risk for sudden cardiac death increased two to three times with QT >440 ms compared with QT <440 ms and the specific underlying genotype, it is important to have an understanding of congenital and acquired LQTS and the associated triggers for torsades de pointes.
Congenital LQTS
Congenital LQTS is caused by mutations in cardiac ion channel proteins, primarily sodium, and potassium channels.5,6 These defects either slow depolarization or lengthen repolarization, leading to heterogeneity of repolarization of the membrane.5 This, in turn, predisposes to ventricular dysrhythmias, including torsades de pointes and subsequent ventricular fibrillation and death.2 Currently, 12 genetic defects have been identified in LQTS. Hundreds of mutations have been described to cause these defects (see Table 2, right).8 Approximately 70% of congenital LQTS are caused by mutations in three genes and are classified as LQTS 1, LQTS 2, and LQTS 3.8 The other seven mutation types account for about 5% of cases; a quarter of LQTS cases have no identified genetic mutations.8
LQTS usually can be distinguished by clinical features and some ECG characteristics, but diagnosis of the specific type requires genetic testing.8,9 The most common types of LQTS are discussed below.
- Long QT1 is the most common type, occurring in approximately 40% to 50% of patients diagnosed with LQTS. It is characterized by a defect in the potassium channel alpha subunit leading to IKs reduction.9 These patients typically present with syncope or adrenergic-induced torsades, might have wide, broad-based T-waves on ECG, and respond well to beta-blocker therapy.6 Triggers for these patients include physical exertion or emotional stressors, particularly exercise and swimming. These patients typically present in early childhood.1
- Long QT2 occurs in 35% to 40% of patients and is characterized by a different defect in the alpha subunit of the potassium channel, which leads to reduced IKr.9 ECGs in LQTS2 can demonstrate low-amplitude and notched T-waves. Sudden catecholamine surges related to emotional stress or loud noises and bradycardia can trigger dysrhythmias in Long QT2.6 Thus, beta blockers reduce overall cardiac events in LQTS2 but less effectively than in LQTS1.6 These patients also present in childhood but typically are older than patients with LQTS1.6
- Long QT3 is less common than LQTS1 or LQTS2, at 2% to 8% of LQTS patients, but carries a higher mortality and is not treated effectively with beta blockers. LQTS3 is characterized by a defect in a sodium channel, causing a gain-of-function in the INa.4,9 These patients are more likely to have a fatal dysrhythmia while sleeping, are less susceptible to exercise-induced events, and have increased morbidity and mortality associated with bradycardia.4,9 ECG frequently reveals a relatively long ST segment, followed by a peaked and tall T-wave. Beta-blocker therapy can predispose to dysrhythmias in these patients; therefore, many of these patients will have pacemakers implanted as first-line therapy.6
While less common, Jervell and Lange Nielson syndrome is an autosomal recessive form of LQTS in which affected patients have homozygous mutations in the KCNQ1 or KCNE1 genes. This syndrome occurs in approximately 1% to 7% of LQTS patients, displays a typical QTc >550 ms, can be triggered by exercise and emotional stress, is associated with deafness, and carries a high risk of cardiac events at a young age.6
Acquired Syndromes
In addition to congenital LQTS, certain patients can acquire LQTS after being treated with particular drugs or having metabolic abnormalities, namely hypomagnesemia, hypocalcemia, and hypokalemia. Most experts think patients who “acquire” LQTS that predisposes to torsades de pointes have underlying structural heart disease or LQTS genetic carrier mutations that combine with transient initiating events (e.g., drugs or metabolic abnormalities) to induce dysrhythmias.1 In addition to certain drugs, cardiac ischemia, and electrolyte abnormalities, cocaine abuse, HIV, and subarachnoid hemorrhage can induce dysrhythmias in susceptible patients.5
Many types of drugs can cause a prolonged QT interval, and others should be avoided in patients with pre-existing prolonged QT (see Table 3, p. 17). Potentially offending drugs that are frequently encountered by inpatient physicians include amiodarone, diltiazem, erythromycin, clarithromycin, ciprofloxacin, fluoxetine, paroxetine, sertraline, haloperidol, ritonavir, and methadone.1 Additionally, drugs that cause electrolyte abnormalities (e.g., diuretics and lithium) should be monitored closely.
Overall, the goals of therapy in LQTS are:
- Decrease the risk of dysrhythmic events;
- Minimize adrenergic response;
- Shorten the QTc;
- Decrease the dispersion of refractoriness; and
- Improve the function of the ion channels.3
Supportive measures should be taken for patients who are acutely symptomatic from LQTS and associated torsades de pointes. In addition to immediate cardioversion for ongoing and hemodynamically significant torsades, intravenous magnesium should be administered, electrolytes corrected, and offending drugs discontinued.5 Temporary transvenous pacing at rates of approximately 100 beats per minute is highly effective in preventing short-term recurrence of torsades in congenital and acquired LQTS, especially in bradycardic patients.5 Isoproterenol infusion increases the heart rate and effectively prevents acute recurrence of torsades in patients with acquired LQTS, but it should be used with caution in patients with structural heart disease.5
Long-term strategies to manage LQTS include:
- Minimizing the risk of triggering cardiac events via adrenergic stimulation;
- Preventing ongoing dysrhythmias;
- Avoiding medications known to prolong the QT interval; and
- Maintaining normal electrolytes and minerals.5
Most patients with congenital long QT should be discouraged from participating in competitive sports, and patients should attempt to eliminate exposures to stress or sudden awakening, though this is not practical in all cases.5 Beta blockers generally are the first-line therapy and are more effective for LQT1 than LQT2 or LQT3.4,5 If patients are still symptomatic despite adequate medical therapy, or have survived cardiac arrest, they should be considered for ICD therapy.4,5 In addition, patients with profound bradycardia benefit from pacemaker implantation.5 Patients who remain symptomatic despite both beta blockade and ICD placement might find cervicothoracic sympathectomy curative.4,5
Perioperative Considerations
Although little data is available to guide physicians in the prevention of torsades de pointes during the course of anesthesia, there are a number of considerations that may reduce the chances of symptomatic dysrhythmias.
First, care should be taken to avoid dysrhythmia triggers in LQTS by providing a calm, quiet environment during induction, monitoring, and treating metabolic abnormalities, and providing an appropriate level of anesthesia.10 Beta-blocker therapy should be continued and potentially measured preoperatively by assessing heart rate response during stress testing.5 An implantable cardioverter-defibrillator (AICD) should be interrogated prior to surgery and inactivated during the operation.5
Finally, Kies et al have recommended general anesthesia with propofol for induction (or throughout), isoflurane as the volatile agent, vecuronium for muscle relaxation, and intravenous fentanyl for analgesia when possible.10
Back to the Case
While the patient had no genetic testing for LQTS, evaluation of previous ECGs demonstrated a prolonged QT interval. The hip fracture repair was considered an urgent procedure, which precluded the ability to undertake genetic testing and consideration for device implantation. The only medication that was known to increase the risk for dysrhythmias in this patient was his diuretic, with the attendant risk of electrolyte abnormalities.
Thus, the patient’s hydrochlorothiazide was discontinued and his pre-existing atenolol continued. The patient’s electrolytes and minerals were monitored closely, and magnesium was administered on the day of surgery. Anesthesia was made aware of the prolonged QT interval, such that they were able to minimize the risk for and anticipate the treatment of dysrhythmias. The patient tolerated the surgery and post-operative period without complication and was scheduled for an outpatient workup and management for his prolonged QT interval.
Bottom Line
Long QT syndrome is frequently genetic in origin, but it can be caused by certain medications and perturbations of electrolytes. Beta blockers are the first-line therapy for the majority of LQTS cases, along with discontinuation of drugs that might induce or aggravate the QT prolongation.
Patients who have had cardiac arrest or who remain symptomatic despite beta-blocker therapy should have an ICD implanted.
In the perioperative period, patients’ electrolytes should be monitored and kept within normal limits. If the patient is on a beta blocker, it should be continued, and the anesthesiologist should be made aware of the diagnosis so that the anesthethic plan can be optimized to prevent arrhythmic complications. TH
Dr. Kamali is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Veterans Affairs Medical Center in Denver and an instructor of medicine at UC Denver. Dr. Prochazka is director of ambulatory care at the Denver VA and professor of medicine at UC Denver. Dr. Varosy is director of cardiac electrophysiology at the Denver VA and assistant professor of medicine at UC Denver.
References
- Kao LW, Furbee BR. Drug-induced q-T prolongation. Med Clin North Am. 2005;89(6):1125-1144.
- Marchlinski F. Chapter 226, The Tachyarrhythmias; Harrison's Principles of Internal Medicine, 17e. Available at: www.accessmedicine.com/resourceTOC .aspx?resourceID=4. Accessed Nov. 21, 2009.
- Zareba W, Cygankiewicz I. Long QT syndrome and short QT syndrome. Prog Cardiovasc Dis. 2008; 51(3):264-278.
- Booker PD, Whyte SD, Ladusans EJ. Long QT syndrome and anaesthesia. Br J Anaesth. 2003;90(3):349-366.
- Khan IA. Long QT syndrome: diagnosis and management. Am Heart J. 2002;143(1):7-14.
- Morita H, Wu J, Zipes DP. The QT syndromes: long and short. Lancet. 2008;372(9640):750-763.
- Schwartz PJ, Moss AJ, Vincent GM, Crampton RS. Diagnostic criteria for the long QT syndrome. An update. Circulation. 1993;88(2):782-784.
- Kapa S, Tester DJ, Salisbury BA, et al. Genetic testing for long-QT syndrome: distinguishing pathogenic mutations from benign variants. Circulation. 2009;120(18):1752-1760.
- Modell SM, Lehmann MH. The long QT syndrome family of cardiac ion channelopathies: a HuGE review. Genet Med. 2006;8(3):143-155.
- Kies SJ, Pabelick CM, Hurley HA, White RD, Ackerman MJ. Anesthesia for patients with congenital long QT syndrome. Anesthesiology. 2005;102(1):204-210.
- Wisely NA, Shipton EA. Long QT syndrome and anaesthesia. Eur J Anaesthesiol. 2002;19(12):853-859.
Case
You are asked to admit a 63-year-old male with a history of hypertension and osteoarthritis. The patient, who fell at home, is scheduled for open repair of his femoral neck fracture the following day. The patient reports tripping over his granddaughter’s toys and denies any associated symptoms around the time of his fall. An electrocardiogram (ECG) reveals a QTc (QT) interval of 480 ms. How should this hospitalized patient’s prolonged QT interval be managed?
Overview
Patients with a prolonged QT interval on routine ECG present an interesting dilemma for clinicians. Although QT prolongation—either congenital or acquired—has been associated with dysrhythmias, the risk of torsades de pointes and sudden cardiac death varies considerably based on myriad underlying factors.1 Therefore, the principle job of the clinician who has recognized QT prolongation is to assess and minimize the risk of the development of clinically significant dysrhythmias, and to be prepared to manage them should they arise.
The QT interval encompasses ventricular depolarization and repolarization. This ventricular action potential proceeds through five phases. The initial upstroke (phase 0) of depolarization occurs with the opening of Na+ channels, triggering the inward Na+ current (INa), and causes the interior of the myocytes to become positively charged. This is followed by initial repolarization (phase 1) when the opening of K+ channels causes an outward K+ current (Ito). Next, the plateau phase (phase 2) of the action potential follows with a balance of inward current through Ca2+channels (Ica-L) and outward current through slow rectifier K+ channels (IKs), and then later through delayed, rapid K+ rectifier channels (IKr). Then, the inward current is deactivated, while the outward current increases through the rapid delayed rectifier (IKr) and opening of inward rectifier channels (IK1) to complete repolarization (phase 3). Finally, the action potential returns to baseline (phase 4) and Na+ begins to enter the cell again (see Figure 1, above).
The long QT syndrome (LQTS) is defined by a defect in these cardiac ion channels, which leads to abnormal repolarization, usually lengthening the QT interval and thus predisposing to ventricular dysrhythmias.2 It is estimated that as many as 85% of these syndromes are inherited, and up to 15% are acquired or sporadic.3 Depending on the underlying etiology of the LQTS, manifestations might first be appreciated at any time from in utero through adulthood.4 Symptoms including palpitations, syncope, seizures, or cardiac arrest bring these patients to medical attention.3 These symptoms frequently elicit physical or emotional stress, but they can occur without obvious inciting triggers.5 A 20% mortality risk exists in patients who are symptomatic and untreated in the first year following diagnosis, and up to 50% within 10 years following diagnosis.4
How is Long QT Syndrome Diagnosed?
The LQTS diagnosis is based on clinical history in combination with ECG abnormalities.6 Important historical elements include symptoms of palpitations, syncope, seizures, or cardiac arrest.3 In addition, a family history of unexplained syncope or sudden death, especially at a young age, should raise LQTS suspicion.5
A variety of ECG findings can be witnessed in LQTS patients.4,5 Although the majority of patients have a QTc >440 ms, approximately one-third have a QTc ≤460 ms, and about 10% have normal QTc intervals.5 Other ECG abnormalities include notched, biphasic, or prolonged T-waves, and the presence of U-waves.4,5 Schwartz et al used these elements to publish criteria (see Table 1, right) that physicians can use to assess the probability that a patient has LQTS.7
Types of Long QT Syndromes
Because the risk of developing significant dysrhythmias with LQTS is dependent on both the actual QT interval, with risk for sudden cardiac death increased two to three times with QT >440 ms compared with QT <440 ms and the specific underlying genotype, it is important to have an understanding of congenital and acquired LQTS and the associated triggers for torsades de pointes.
Congenital LQTS
Congenital LQTS is caused by mutations in cardiac ion channel proteins, primarily sodium, and potassium channels.5,6 These defects either slow depolarization or lengthen repolarization, leading to heterogeneity of repolarization of the membrane.5 This, in turn, predisposes to ventricular dysrhythmias, including torsades de pointes and subsequent ventricular fibrillation and death.2 Currently, 12 genetic defects have been identified in LQTS. Hundreds of mutations have been described to cause these defects (see Table 2, right).8 Approximately 70% of congenital LQTS are caused by mutations in three genes and are classified as LQTS 1, LQTS 2, and LQTS 3.8 The other seven mutation types account for about 5% of cases; a quarter of LQTS cases have no identified genetic mutations.8
LQTS usually can be distinguished by clinical features and some ECG characteristics, but diagnosis of the specific type requires genetic testing.8,9 The most common types of LQTS are discussed below.
- Long QT1 is the most common type, occurring in approximately 40% to 50% of patients diagnosed with LQTS. It is characterized by a defect in the potassium channel alpha subunit leading to IKs reduction.9 These patients typically present with syncope or adrenergic-induced torsades, might have wide, broad-based T-waves on ECG, and respond well to beta-blocker therapy.6 Triggers for these patients include physical exertion or emotional stressors, particularly exercise and swimming. These patients typically present in early childhood.1
- Long QT2 occurs in 35% to 40% of patients and is characterized by a different defect in the alpha subunit of the potassium channel, which leads to reduced IKr.9 ECGs in LQTS2 can demonstrate low-amplitude and notched T-waves. Sudden catecholamine surges related to emotional stress or loud noises and bradycardia can trigger dysrhythmias in Long QT2.6 Thus, beta blockers reduce overall cardiac events in LQTS2 but less effectively than in LQTS1.6 These patients also present in childhood but typically are older than patients with LQTS1.6
- Long QT3 is less common than LQTS1 or LQTS2, at 2% to 8% of LQTS patients, but carries a higher mortality and is not treated effectively with beta blockers. LQTS3 is characterized by a defect in a sodium channel, causing a gain-of-function in the INa.4,9 These patients are more likely to have a fatal dysrhythmia while sleeping, are less susceptible to exercise-induced events, and have increased morbidity and mortality associated with bradycardia.4,9 ECG frequently reveals a relatively long ST segment, followed by a peaked and tall T-wave. Beta-blocker therapy can predispose to dysrhythmias in these patients; therefore, many of these patients will have pacemakers implanted as first-line therapy.6
While less common, Jervell and Lange Nielson syndrome is an autosomal recessive form of LQTS in which affected patients have homozygous mutations in the KCNQ1 or KCNE1 genes. This syndrome occurs in approximately 1% to 7% of LQTS patients, displays a typical QTc >550 ms, can be triggered by exercise and emotional stress, is associated with deafness, and carries a high risk of cardiac events at a young age.6
Acquired Syndromes
In addition to congenital LQTS, certain patients can acquire LQTS after being treated with particular drugs or having metabolic abnormalities, namely hypomagnesemia, hypocalcemia, and hypokalemia. Most experts think patients who “acquire” LQTS that predisposes to torsades de pointes have underlying structural heart disease or LQTS genetic carrier mutations that combine with transient initiating events (e.g., drugs or metabolic abnormalities) to induce dysrhythmias.1 In addition to certain drugs, cardiac ischemia, and electrolyte abnormalities, cocaine abuse, HIV, and subarachnoid hemorrhage can induce dysrhythmias in susceptible patients.5
Many types of drugs can cause a prolonged QT interval, and others should be avoided in patients with pre-existing prolonged QT (see Table 3, p. 17). Potentially offending drugs that are frequently encountered by inpatient physicians include amiodarone, diltiazem, erythromycin, clarithromycin, ciprofloxacin, fluoxetine, paroxetine, sertraline, haloperidol, ritonavir, and methadone.1 Additionally, drugs that cause electrolyte abnormalities (e.g., diuretics and lithium) should be monitored closely.
Overall, the goals of therapy in LQTS are:
- Decrease the risk of dysrhythmic events;
- Minimize adrenergic response;
- Shorten the QTc;
- Decrease the dispersion of refractoriness; and
- Improve the function of the ion channels.3
Supportive measures should be taken for patients who are acutely symptomatic from LQTS and associated torsades de pointes. In addition to immediate cardioversion for ongoing and hemodynamically significant torsades, intravenous magnesium should be administered, electrolytes corrected, and offending drugs discontinued.5 Temporary transvenous pacing at rates of approximately 100 beats per minute is highly effective in preventing short-term recurrence of torsades in congenital and acquired LQTS, especially in bradycardic patients.5 Isoproterenol infusion increases the heart rate and effectively prevents acute recurrence of torsades in patients with acquired LQTS, but it should be used with caution in patients with structural heart disease.5
Long-term strategies to manage LQTS include:
- Minimizing the risk of triggering cardiac events via adrenergic stimulation;
- Preventing ongoing dysrhythmias;
- Avoiding medications known to prolong the QT interval; and
- Maintaining normal electrolytes and minerals.5
Most patients with congenital long QT should be discouraged from participating in competitive sports, and patients should attempt to eliminate exposures to stress or sudden awakening, though this is not practical in all cases.5 Beta blockers generally are the first-line therapy and are more effective for LQT1 than LQT2 or LQT3.4,5 If patients are still symptomatic despite adequate medical therapy, or have survived cardiac arrest, they should be considered for ICD therapy.4,5 In addition, patients with profound bradycardia benefit from pacemaker implantation.5 Patients who remain symptomatic despite both beta blockade and ICD placement might find cervicothoracic sympathectomy curative.4,5
Perioperative Considerations
Although little data is available to guide physicians in the prevention of torsades de pointes during the course of anesthesia, there are a number of considerations that may reduce the chances of symptomatic dysrhythmias.
First, care should be taken to avoid dysrhythmia triggers in LQTS by providing a calm, quiet environment during induction, monitoring, and treating metabolic abnormalities, and providing an appropriate level of anesthesia.10 Beta-blocker therapy should be continued and potentially measured preoperatively by assessing heart rate response during stress testing.5 An implantable cardioverter-defibrillator (AICD) should be interrogated prior to surgery and inactivated during the operation.5
Finally, Kies et al have recommended general anesthesia with propofol for induction (or throughout), isoflurane as the volatile agent, vecuronium for muscle relaxation, and intravenous fentanyl for analgesia when possible.10
Back to the Case
While the patient had no genetic testing for LQTS, evaluation of previous ECGs demonstrated a prolonged QT interval. The hip fracture repair was considered an urgent procedure, which precluded the ability to undertake genetic testing and consideration for device implantation. The only medication that was known to increase the risk for dysrhythmias in this patient was his diuretic, with the attendant risk of electrolyte abnormalities.
Thus, the patient’s hydrochlorothiazide was discontinued and his pre-existing atenolol continued. The patient’s electrolytes and minerals were monitored closely, and magnesium was administered on the day of surgery. Anesthesia was made aware of the prolonged QT interval, such that they were able to minimize the risk for and anticipate the treatment of dysrhythmias. The patient tolerated the surgery and post-operative period without complication and was scheduled for an outpatient workup and management for his prolonged QT interval.
Bottom Line
Long QT syndrome is frequently genetic in origin, but it can be caused by certain medications and perturbations of electrolytes. Beta blockers are the first-line therapy for the majority of LQTS cases, along with discontinuation of drugs that might induce or aggravate the QT prolongation.
Patients who have had cardiac arrest or who remain symptomatic despite beta-blocker therapy should have an ICD implanted.
In the perioperative period, patients’ electrolytes should be monitored and kept within normal limits. If the patient is on a beta blocker, it should be continued, and the anesthesiologist should be made aware of the diagnosis so that the anesthethic plan can be optimized to prevent arrhythmic complications. TH
Dr. Kamali is a medical resident at the University of Colorado Denver. Dr. Stickrath is a hospitalist at the Veterans Affairs Medical Center in Denver and an instructor of medicine at UC Denver. Dr. Prochazka is director of ambulatory care at the Denver VA and professor of medicine at UC Denver. Dr. Varosy is director of cardiac electrophysiology at the Denver VA and assistant professor of medicine at UC Denver.
References
- Kao LW, Furbee BR. Drug-induced q-T prolongation. Med Clin North Am. 2005;89(6):1125-1144.
- Marchlinski F. Chapter 226, The Tachyarrhythmias; Harrison's Principles of Internal Medicine, 17e. Available at: www.accessmedicine.com/resourceTOC .aspx?resourceID=4. Accessed Nov. 21, 2009.
- Zareba W, Cygankiewicz I. Long QT syndrome and short QT syndrome. Prog Cardiovasc Dis. 2008; 51(3):264-278.
- Booker PD, Whyte SD, Ladusans EJ. Long QT syndrome and anaesthesia. Br J Anaesth. 2003;90(3):349-366.
- Khan IA. Long QT syndrome: diagnosis and management. Am Heart J. 2002;143(1):7-14.
- Morita H, Wu J, Zipes DP. The QT syndromes: long and short. Lancet. 2008;372(9640):750-763.
- Schwartz PJ, Moss AJ, Vincent GM, Crampton RS. Diagnostic criteria for the long QT syndrome. An update. Circulation. 1993;88(2):782-784.
- Kapa S, Tester DJ, Salisbury BA, et al. Genetic testing for long-QT syndrome: distinguishing pathogenic mutations from benign variants. Circulation. 2009;120(18):1752-1760.
- Modell SM, Lehmann MH. The long QT syndrome family of cardiac ion channelopathies: a HuGE review. Genet Med. 2006;8(3):143-155.
- Kies SJ, Pabelick CM, Hurley HA, White RD, Ackerman MJ. Anesthesia for patients with congenital long QT syndrome. Anesthesiology. 2005;102(1):204-210.
- Wisely NA, Shipton EA. Long QT syndrome and anaesthesia. Eur J Anaesthesiol. 2002;19(12):853-859.
Market Watch
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
New Generics
- Fentanyl citrate troche/lozenge (generic Actiq) transmucosal lollipop1,2
- Perindopril erbumine (generic Aceon) tablets3
New Drugs, Indications, Label Changes, and Dosage Forms
- Capsaicin 8% patch (Qutenza) has been approved by the U.S. Food and Drug Administration (FDA) as a prescription medication to treat pain associated with post-herpetic neuralgia.4 The patch is a higher concentration than over-the-counter (OTC) products. The most common side effects in clinical trials were pain, swelling, itching, redness, and bumps at the application site, as well as blood pressure increases.5 Patch placement requires the use of a topical anesthetic and additional pain relief (ice or opioid pain relievers). Therefore, patch placement must be performed by a healthcare professional. Once the patch is applied, the patient must be observed for at least an hour, as there could be a significant increase in blood pressure.
- Diclofenac sodium topical (Pennsaid) has been approved by the FDA as a topical treatment to manage knee osteoarthritis.6 The transdermal carrier dimethylsulfoxide (DMSO) is utilized to deliver active diclofenac sodium through the skin to the pain site.7
- Exenatide injection (Byetta) has been approved by the FDA as monotherapy for treating patients with Type 2 diabetes mellitus, along with diet and exercise.8
- Human papilloma virus (HPV) vaccine (Gardasil) has been approved by the FDA for preventing condyloma acuminata due to HPV types 6 and 11 in males ages 9 to 26.9 The makers hope that this vaccine will decrease the need to treat genital warts. Clinical studies showed that in males not infected with HPV at the beginning of the study, the vaccine was close to 90% effective in preventing genital warts caused by infection of HPV types 6 and 11. The manufacturer plans to obtain additional safety and effectiveness information in this patient population.
- Lansoprazole 24HR (Prevacid OTC) 15-mg delayed-release capsules are available for treating frequent heartburn.10 The capsules will be available by prescription in both the 15-mg and 30-mg dosage strengths.
- Metoclopramide HCl orally disintegrating tablet (Metozolv ODT) has been approved by the FDA for treating both acute and recurrent diabetic gastroparesis and for the short-term management (four to 12 weeks) of adults with documented symptomatic gastroesophageal reflux disease who do not respond to conventional therapy.11
- Peramivir intravenous will be made available by the Centers for Disease Control (CDC) as an emergency treatment for children and adult patients who develop H1N1 influenza and are nonresponsive to oral or inhaled antiviral therapies.12
- Rosuvastatin (Crestor) has been approved by the FDA for treating heterozygous familial cholesterolemia in children ages 10-17.13
- Telmisartan 80-mg tablets (Micardis) have been approved by the FDA for risk reduction of myocardial infarction, stroke, or death from cardiovascular causes in patients 55 years and older who are at high risk for major cardiovascular events, or who are not able to take angiotensin-converting enzyme inhibitors.14
- Telmisartan/amlodipine tablets (Twynsta) have been approved by the FDA as a new combination for treating hypertension, either alone or in combination with other antihypertensive agents. This combination is not indicated for cardiovascular risk reduction. The tablets are available in the following strengths of telmisartan/amlodipine, respectively: 40 mg/5 mg, 40 mg/10 mg, 80 mg/5 mg, and 80 mg/10 mg.
- Tranexamic acid (Lysteda) has been approved by the FDA for the treatment of menorrhagia.15 This is the first nonhormonal, oral therapeutic agent approved to treat this condition.16
Pipeline
- Indacaterol is being investigated as a once-daily bronchodilator for treating adults with chronic obstructive pulmonary disease (COPD).17 Novartis has received a complete response letter from the FDA requesting additional data on the dosing of the agent. The company is working with the FDA to resolve these issues.
- Rituximab injection (Rituxan) is approved for treating moderate to severe rheumatoid arthritis after patients have been treated with methotrexate, as well as non-Hodgkin’s lymphoma.18 Genentech/Biogen is attempting to expand rituximab use to treat patients earlier in the course of their disease. The FDA recently rejected this application, citing the rare but serious safety risk of developing progressive multifocal leukoencephalopathy.
Safety Information
Use of omeprazole and clopidogrel combination therapy should be avoided, according to new data from the FDA.18 Current data suggest that clopidogrel’s antiplatelet effect may be hindered by 50% with concomitant omeprazole therapy. Omeprazole blocks the conversion of clopidogrel to its active, antiplatelet form, thus significantly decreasing its effectiveness. It is not known if other proton-pump inhibitors interfere with clopidogrel’s effectiveness. Other drugs that should not be used with clopidogrel include esomeprazole (Nexium), cimetidine (Tagamet and Tagamet HB), fluconazole (Diflucan), ketoconazole (Nizoral), voriconazole (VFEND), etravirine (Intelence), felbamate (Felbatol), fluoxetine (Prozac, Sarafem, and Symbyax), fluvoxamine (Luvox), and ticlopidine (Ticlid). TH
Michele B. Kaufman is a freelance medical writer based in New York City and a clinical pharmacist at New York Downtown Hospital.
References
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/docs/obdetail.cfm?Appl_No=077312&TABLE1=OB_Rx. Accessed Nov. 19, 2009.
- Covidien gets approval of generic pain drug. Forbes.com Web site. Available at: http://www.forbes.com/feeds/ap/2009/10/30/business-health-care-us-covidien-actiq_7069457.html. Accessed Nov. 19, 2009.
- Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. FDA Web site. Available at: www.accessdata.fda.gov/scripts/cder/ob/default.cfm Accessed Nov. 19, 2009.
- Riley K. FDA Approves New Drug Treatment for Long-Term Pain Relief after Shingles Attacks. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191003.htm. Accessed Nov. 19, 2009.
- Qutenza Approved for Post-Shingles Nerve Pain. U.S. News and World Report Web site. Available at: health.usnews.com/articles/health/healthday/2009/11/17/qutenza-approved-for-post-shingles-nerve-pain.html. Accessed Nov. 19, 2009.
- Nuvo shares surge on FDA pain cream approval. Reuters Web site. Available at: www.reuters.com/article/email/idUSN0543459820091105. Accessed Nov. 19, 2009.
- Pennsaid. Nuvo Web site. Available at: www.nuvoresearch.com/pipeline/pennsaid.asp. Accessed Nov. 19, 2009.
- BYETTA Approved For Expanded Use As First-Line Treatment For Type 2 Diabetes. Medical News Today Web site. Available at: www.medicalnewstoday.com/articles/169396.php. Accessed Nov. 19, 2009.
- Burgess S. FDA Approves New Indication for Gardasil to Prevent Genital Warts in Men and Boys. FDA Web site. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm187003.htm Accessed Nov. 19, 2009.
- Prevacid 24hr available over-the-counter. Monthly Prescribing Reference Web site. Available at: www.empr.com/prevacid-24hr-available-over-the-counter/article/157592/. Accessed Nov. 19, 2009.
- FDA Approves New Salix Product Exclusively in Catalent’s Zydis Fast Dissolve Technology. Catalent Web site. Available at: www.catalent.com/about-us/news/45. Accessed Nov. 19, 2009.
- Peramivir to be Used for Special Swine Flu Cases. Pharmaceutical-Technology.com Web site. Available at: www.pharmaceutical-technology.com/News/News68102.html. Accessed Nov. 19, 2009.
- Dennis M. AstraZeneca’s Crestor approved in US for paediatric use; Vimovo filed in Europe. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=41E54BF434C54C8E903A9EB4EF0839AA&logRowId=332380. Accessed Nov. 19, 2009.
- FDA Approves New Use for Micardis in Cardiovascular Risk Reduction and Twynsta as New Combination Treatment for High Blood Pressure. Boehringer Ingelheim Web site. Available at: us.boehringer-ingelheim.com/newsroom/2009/files/micardis_twynsta_approve_10-19-09.pdf. Accessed Nov. 19, 2009.
- Todoruk M. FDA approves Xanodyne’s Lysteda for menorrhaegia. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=8FCB424A8E7147A08CEC9BFCD8A450D2&logRowId=337054. Accessed Nov. 19, 2009.
- Xanodyne announces FDA approval of Lysteda for treatment of women with heavy menstrual bleeding. Xanodyne Web site. Available at: www.xanodyne.com/newsroom_details.asp?NewsId=61. Accessed Nov. 19, 2009.
- Todoruk M. FDA requests additional data for Novartis’ COPD drug indacaterol. FirstWord Web site. Available at: www.firstwordplus.com/Fws.do?articleid=B426F5ED30AB43A89338DAD0124168A7&logRowId=332718. Accessed Nov. 19, 2009.
- Genentech and Biogen Idec Receive a Complete Response from FDA for Earlier Use of Rituxan for Rheumatoid Arthritis. Genentech Web site. Available at: www.gene.com/gene/news/press-releases/display.do?method=detail&id=12407. Accessed Nov. 19, 2009.
- Walsh S. FDA Announces New Warning on Plavix: Avoid Use with Prilosec/Prilosec OTC. FDA Web site. Available at www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm191169.htm. Accessed Nov. 19, 2009.
In the Literature: February 2010
In This Edition
Literature at a Glance
A guide to this month’s studies
- Perioperative oxygen use and infection rate.
- Effects of adverse events and healthcare costs
- Impact of DVT on PE rates in trauma
- VTE prevention and treatment in cancer patients
- Effect of perioperative beta-blocker discontinuation
- Endovascular vs. open AAA repair
- OTC analgesics in patients with hepatic dysfunction
- Cardiovascular disease and risk of hip fracture
High Perioperative Oxygen Fraction Does Not Improve Surgical-Site Infection Frequency after Abdominal Surgery
Clinical question: Does the use of 80% oxygen perioperatively in abdominal surgery decrease the frequency of surgical-site infection within 14 days without increasing the rate of pulmonary complications?
Background: Low oxygen tension in wounds can negatively impact immune response and healing. Increasing inspiratory oxygen fraction during the perioperative period translates into higher wound oxygen tension. However, the benefit of increased oxygen fraction therapy in abdominal surgery healing and complications is not clear, nor is the frequency of pulmonary complications.
Study design: Patient- and observer-blinded clinical trial.
Setting: Fourteen Danish hospitals from October 2006 to October 2008.
Synopsis: Patients were randomized to receive a fraction of inspired oxygen (FIO2) of 0.80 or 0.30. The primary outcome—surgical-site infection in the superficial or deep wound or intra-abdominal cavity within 14 days of surgery—was defined using Centers for Disease Control and Prevention (CDC) criteria. Secondary outcomes included pulmonary complications within 14 days (pneumonia, atelectasis, or respiratory failure), 30-day mortality, duration of post-op course, ICU stay within 14 days post-op, and any abdominal operation within 14 days. The 1,386 patients were enrolled in the intention-to-treat analysis.
Infection occurred in 19.1% of patients given 0.80 FIO2 and in 20.1% of patients given 0.30 FIO2; odds ratio of 0.94 (95% CI 0.72 to 1.22; P=0.64). Numbers of pulmonary complications were not significantly different between the groups.
This trial included acute and nonacute laparotomies with followup for adverse outcomes. Study limitations included the inability to ensure that both groups received timely antibiotics and prevention for hypothermia. Of patients in the 30% FIO2 group, 7.3% required higher oxygen administration. Additionally, infection might have been underestimated in 11.3% of patients who were not followed up on between days 13 and 30.
Bottom line: High oxygen concentration administered during and after laparotomy did not lead to fewer surgical site infections, nor did it significantly increase the frequency of pulmonary complications or death.
Citation: Meyhoff CS, Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009;302(14):1543-1550.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Trauma Patients with Pulmonary Embolism Might Not Have DVT on Imaging of Lower Extremities
Clinical question: What is the relationship between acute DVT and pulmonary embolism (PE) in trauma patients?
Background: Major trauma is associated with an increased risk of acute DVT and PE. It is assumed that the majority of PEs arise from DVTs in the lower extremities. Definitive evidence demonstrating that PEs form in situ rather than embolize from leg veins could impact indications for inferior vena cava filters.
Study design: Retrospective chart review.
Setting: Academic Level 1 trauma center in Boston.
Synopsis: The medical records of 247 trauma patients with suspected PE who underwent CT angiography of the lungs and simultaneous CT venography of the pelvis and lower extremities from January 2004 to December 2007 were reviewed. High-risk patients also underwent weekly screening with duplex ultrasonagraphy of the legs.
PE was diagnosed in 46 patients (19%) and DVT in 18 patients (7%). Anticoagulant prophylaxis had been administered to 96% and 78% of the patients with PE and DVT, respectively. PE was diagnosed a median of 5.5 days after admission (range 0-40 days) and the majority (61%) were in segmental or subsegmental branches, rather than in the main or lobar pulmonary arteries (39%). Only seven of the 46 patients (15%) diagnosed with PE also had a pelvic or lower-extremity DVT on simultaneous imaging with CT venography.
Bottom line: Trauma patients with PE often do not have a DVT at the time of diagnosis, though it remains unknown whether this is due to in-situ pulmonary thrombosis or complete embolization from the lower extremities.
Citation: Velmahos GC, Spaniolas K, Tabbara M, et al. Pulmonary embolism and deep venous thrombosis in trauma: are they related? Arch Surg. 2009;144:928-932.
Cancer Guideline for VTE Prophylaxis for Inpatients and Long-Term Treatment With Low-Molecular-Weight Heparin for Acute VTE
Clinical question: On what aspects of VTE management in cancer patients are there consensus among the major guideline panels?
Background: VTE is a common and serious complication of cancer. Patients might be hypercoagulable due to prothrombotic mediators released or mediated by tumor cells, chemotherapeutic agents, debility, central venous catheters, hospitalizations, or surgical procedures. The optimal management often is problematic due to uncertain benefit and risk of bleeding.
Study design: Review of major guideline statements.
Synopsis: The authors examined five VTE guidelines of American and European cancer societies. Each guideline was reviewed to determine the main recommendations and whether there was consensus on key aspects of anticoagulant management.
The study authors concluded that consensus was reached on most key recommendations:
- VTE prophylaxis in hospitalized medical patients. All five guidelines recommend the use of prophylaxis, though some guidelines recommend anticoagulant prophylaxis for all inpatients in the absence of contraindications and some recommend limiting prophylaxis to immobilized patients. All five recommend the use of either unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.
- VTE prevention in cancer patients undergoing surgery. All five guidelines recommend anticoagulant prophylaxis in the absence of contraindications and extending prophylaxis approximately four weeks after major surgery.
- VTE prophylaxis in cancer patients with central venous catheters. Not recommended.
- VTE prophylaxis in ambulatory cancer patients without central venous catheters. Recommended only for multiple myeloma patients receiving a thalidomide-lenalidomide regimen.
- Long-term treatment of acute VTE in cancer patients. All five guidelines recommend initial treatment with LMWH for at least three to six months, followed by indefinite treatment with LMWH or a vitamin K antagonist.
Bottom line: Major guideline panels agree on key aspects of VTE management for cancer patients, including the use of prophylaxis for hospitalized medical and surgical patients and the use of long-term LMWH treatment for cancer patients with acute VTE.
Citation: Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009; 27(29):4919-4926.
Discontinuation of Beta Blockers Increases Risk of Postoperative Myocardial Infarction and Death
Clinical question: Does perioperative beta-blocker discontinuation affect postoperative myocardial infarction (MI) in low-risk patients undergoing joint arthroplasty?
Background: Recent trials show no benefit of perioperative beta blockers in reducing the incidence of perioperative myocardial infarctions (POMI) in low-risk patients. This retrospective study examined the impact of continuing or discontinuing beta blockers and the occurrence of POMI in patients undergoing elective joint arthroplasties.
Study design: Retrospective chart review.
Setting: Large academic center in Ottawa, Canada.
Synopsis: Medical records for 5,178 patients undergoing elective hip or knee arthroplasty from January 2002 to June 2006 were included in the review. The primary outcome was POMI, defined as an increased troponin level. Patients were divided into three groups: beta blocker prescribed on post-operative day (POD) zero and continued for one week or until discharge; beta blocker prescribed on POD zero and discontinued at any time in the first week; and no beta blocker on POD 0.
Beta blockers were continued in 992 patients and discontinued in 252 patients. The rate of POMI and death increased in the beta-blocker discontinuation group (odds ratio 2.0 [1.1-3.9] and 2.0 [1.1-3.9], respectively). This association persisted after adjustment for cardiac risk using a validated risk score.
The study was limited by the fact that the control group did not include patients who were on a beta blocker at home, thus potentially increasing the number of events in this group. The discontinuation beta blocker group had an increased baseline risk for POMI. The reason for discontinuing the beta blocker was not known, and cessation of beta blocker could have been due to an acute event.
Bottom line: This study adds support to the American College of Cardiology and American Heart Association (ACC/AHA) guidelines, which recommend continuation of beta-blocker therapy in the perioperative period.
Citation: Van Klei WA, Bryson GL, Yang H, Forster AJ. Effect of beta-blocker prescription on the incidence of postoperative myocardial infarction after hip and knee arthroplasty. Anesthesiology. 2009;111(4):717-724.
Lower Perioperative Mortality with Endovascular Vs. Open Abdominal Aortic Aneurysm Repair
Clinical question: How do perioperative and long-term morbidity and mortality compare in endovascular and open repair of abdominal aortic aneurysm (AAA)?
Background: Open AAA repair has relatively high perioperative mortality. Endovascular repair was developed as a less-invasive option and has been shown to reduce inpatient perioperative mortality, length of hospital stay, and ICU requirement. However, data suggest it leads to more frequent reinterventions and the same mortality rate as open repair at two years.
Study design: Randomized clinical trial.
Setting: Veterans Affairs medical centers.
Synopsis: The study randomized 881 veterans who planned to have elective AAA repair and were eligible for both endovascular and open repair. This is a planned, two-year interim report in a nine-year study.
Perioperative mortality was 0.5% in the endovascular repair group, compared with 3.0% in the open repair group. However, this difference in mortality was not statistically significant at two years. The endovascular repair group experienced shorter procedure and mechanical ventilation time, decreased hospital and ICU stay, and lower rate of blood transfusions.
Overall, there was no difference between the groups for major morbidity, procedure failure, need for secondary therapeutic intervention, quality of life, or erectile dysfunction. More data on long-term comparison of these two interventions will be available at the conclusion of this study.
Bottom line: Endovascular repair of AAA has lower perioperative mortality than open repair but did not lead to improved morbidity or mortality at two years.
Citation: Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs. open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302 (14):1535-1542.
OTC Analgesics Not Associated with Acute Decompensation in Cirrhotic Patients
Clinical question: Do over-the-counter (OTC) analgesics lead to acute hepatic decompensation among patients with cirrhosis?
Background: In theory, intake of acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs) can worsen hepatic function and lead to complications among cirrhotic patients. The role of OTC analgesics in potentially triggering acute hepatic decompensation among cirrhotic patients has not been studied.
Study design: Prospective case-control study.
Setting: Two tertiary-care hospitals.
Synopsis: Cirrhotic patients hospitalized for acute liver decompensation were compared with compensated cirrhotic patients in the liver clinic (cirrhotic controls) and with randomly selected, noncirrhotic patients who were simultaneously hospitalized (noncirrhotic controls). Data collected through questionnaires included quantity and dose of OTC analgesics used and alcohol consumption in the past 30 days.
Thirty-five percent of the hospitalized cirrhotic patients, 52% of the cirrhotic controls, and 70% of the noncirrhotic controls used OTC analgesics. At doses lower than those recommended, acetaminophen is not associated with acute liver decompensation among cirrhotic patients, even with recent alcohol use. However, NSAIDs taken by the cirrhotic patients, when compared to control subjects, were in larger doses and used for a longer duration, suggesting NSAIDs may have contributed to the acute decompensation.
Study limitations include the nature of the study design, reliance on the patient’s recall of OTC analgesic use, and obtaining other possible causes of decompensation, such as herbal supplement intake or compliance with diuretics or dietary indiscretion.
Bottom line: Acetaminophen at doses lower than recommended is not associated with adverse complications in cirrhotic patients, but NSAIDs are possibly associated with acute decompensation.
Citation: Khalid SK, Lane J, Navarro V, Garcia-Tsao G. Use of over-the-counter analgesics is not associated with acute decompensation in patients with cirrhosis. Clin Gastroenterol Hepatol. 2009;7(9):994-999.
Cardiovascular Disease and Risk of Hip Fracture
Clinical question: Is the diagnosis of cardiovascular disease (CVD) associated with the risk of subsequent hip fracture?
Background: Osteoporosis and CVD are regarded as independent, age-related conditions. However, recent research suggests that the bone and vascular systems share common regulatory mechanisms. Stroke is a known risk factor for hip fractures, and bisphosphonates have been shown to prevent atherosclerosis and reduce total mortality rate.
Study design: Cohort study.
Setting: Swedish National Patient Registry.
Synopsis: The study identified 31,936 Swedish twins born from 1914 to 1944. This cohort was followed up to age 50, and time-dependent exposures using Cox-proportional hazard regression models were evaluated.
Times to hip fracture after CVD diagnosis were isolated. Crude absolute rate of hip fractures (per 1,000 person-years) was 12.6 after diagnosis of heart failure, 12.6 after a stroke, 6.6 after peripheral atherosclerosis, and 5.2 after ischemic heart disease (IHD), compared with 1.2 per 1,000 person-years without a CVD diagnosis. Multivariable-adjusted hazard ratio (HR) of hip fracture after heart failure was 4.40 (95% CI, 3.43-5.63); after a stroke was 5.09 (95% CI, 4.18-6.20); after peripheral atherosclerosis was 3.20 (CI, 2.28-4.50); and after an IHD event was 2.32 (CI, 1.91-2.84).
Identical twins even without heart failure and stroke also had an increased risk of hip fracture if their twin had been diagnosed with these diseases.
Bottom line: Cardiovascular disease is significantly associated with risk of subsequent hip fracture, and genetic factors probably play a role in the association.
Citation: Sennerby U, Melhus H, Gedeborg R, et al. Cardiovascular diseases and risk of hip fracture. JAMA. 2009;302(15):1666-1673. TH
PEDIATRIC HM Literature
By Mark Shen, MD
Variation in the Treatment of Henoch-Schönlein Purpura

Clinical question: What is the degree of variation in the inpatient management of Henoch-Schönlein purpura (HSP)?
Background: HSP is the most common pediatric vasculitis, but there are no consensus recommendations or guidelines for treatment. The amount of variation in the pharmacologic management of this disease is unknown.
Study design: Retrospective database analysis.
Setting: Thirty-six children’s hospitals affiliated with the Child Health Corporation of America.
Synopsis: The Pediatric Health Information (PHIS) database was sampled for children younger than 18 years of age with an ICD-9-CM code of HSP and discharge from a hospital that submitted appropriate data from 2000 to 2007. Only index admissions were included, and children with coexisting rheumatic conditions were excluded, for a total of 1,988 subjects.
Logistic regression analysis was used to examine the effects of patient-level standardization on hospital-level rates of therapy and the degree to which variation across hospitals occurred beyond what would be expected after standardization.
Hospital-level variation in medication use was significant (P<0.001) for corticosteroids, opiates, and nonsteroidal anti-inflammatory drugs (NSAIDs), even after adjustment for severity and age at presentation.
Although variation in management is not surprising, the significant degree to which this occurred at the hospital level suggests that local institutional culture plays a dominant role in decision-making. The use of the PHIS database allows for analysis of a large population that would be otherwise difficult to study. However, significant numbers of HSP patients do not require hospitalization, and the study results might substantially over- or underestimate practice patterns. Collaborative efforts to better define optimal management of HSP are needed.
Bottom line: A significant degree of hospital-level variation exists in the inpatient management of HSP.
Citation: Weiss PF, Klink AJ, Hexem K, et al. Variation in inpatient therapy and diagnostic evaluation of children with henoch schönlein purpura. J Pediatr. 2009;155(6):812-818.e1.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Perioperative oxygen use and infection rate.
- Effects of adverse events and healthcare costs
- Impact of DVT on PE rates in trauma
- VTE prevention and treatment in cancer patients
- Effect of perioperative beta-blocker discontinuation
- Endovascular vs. open AAA repair
- OTC analgesics in patients with hepatic dysfunction
- Cardiovascular disease and risk of hip fracture
High Perioperative Oxygen Fraction Does Not Improve Surgical-Site Infection Frequency after Abdominal Surgery
Clinical question: Does the use of 80% oxygen perioperatively in abdominal surgery decrease the frequency of surgical-site infection within 14 days without increasing the rate of pulmonary complications?
Background: Low oxygen tension in wounds can negatively impact immune response and healing. Increasing inspiratory oxygen fraction during the perioperative period translates into higher wound oxygen tension. However, the benefit of increased oxygen fraction therapy in abdominal surgery healing and complications is not clear, nor is the frequency of pulmonary complications.
Study design: Patient- and observer-blinded clinical trial.
Setting: Fourteen Danish hospitals from October 2006 to October 2008.
Synopsis: Patients were randomized to receive a fraction of inspired oxygen (FIO2) of 0.80 or 0.30. The primary outcome—surgical-site infection in the superficial or deep wound or intra-abdominal cavity within 14 days of surgery—was defined using Centers for Disease Control and Prevention (CDC) criteria. Secondary outcomes included pulmonary complications within 14 days (pneumonia, atelectasis, or respiratory failure), 30-day mortality, duration of post-op course, ICU stay within 14 days post-op, and any abdominal operation within 14 days. The 1,386 patients were enrolled in the intention-to-treat analysis.
Infection occurred in 19.1% of patients given 0.80 FIO2 and in 20.1% of patients given 0.30 FIO2; odds ratio of 0.94 (95% CI 0.72 to 1.22; P=0.64). Numbers of pulmonary complications were not significantly different between the groups.
This trial included acute and nonacute laparotomies with followup for adverse outcomes. Study limitations included the inability to ensure that both groups received timely antibiotics and prevention for hypothermia. Of patients in the 30% FIO2 group, 7.3% required higher oxygen administration. Additionally, infection might have been underestimated in 11.3% of patients who were not followed up on between days 13 and 30.
Bottom line: High oxygen concentration administered during and after laparotomy did not lead to fewer surgical site infections, nor did it significantly increase the frequency of pulmonary complications or death.
Citation: Meyhoff CS, Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009;302(14):1543-1550.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Trauma Patients with Pulmonary Embolism Might Not Have DVT on Imaging of Lower Extremities
Clinical question: What is the relationship between acute DVT and pulmonary embolism (PE) in trauma patients?
Background: Major trauma is associated with an increased risk of acute DVT and PE. It is assumed that the majority of PEs arise from DVTs in the lower extremities. Definitive evidence demonstrating that PEs form in situ rather than embolize from leg veins could impact indications for inferior vena cava filters.
Study design: Retrospective chart review.
Setting: Academic Level 1 trauma center in Boston.
Synopsis: The medical records of 247 trauma patients with suspected PE who underwent CT angiography of the lungs and simultaneous CT venography of the pelvis and lower extremities from January 2004 to December 2007 were reviewed. High-risk patients also underwent weekly screening with duplex ultrasonagraphy of the legs.
PE was diagnosed in 46 patients (19%) and DVT in 18 patients (7%). Anticoagulant prophylaxis had been administered to 96% and 78% of the patients with PE and DVT, respectively. PE was diagnosed a median of 5.5 days after admission (range 0-40 days) and the majority (61%) were in segmental or subsegmental branches, rather than in the main or lobar pulmonary arteries (39%). Only seven of the 46 patients (15%) diagnosed with PE also had a pelvic or lower-extremity DVT on simultaneous imaging with CT venography.
Bottom line: Trauma patients with PE often do not have a DVT at the time of diagnosis, though it remains unknown whether this is due to in-situ pulmonary thrombosis or complete embolization from the lower extremities.
Citation: Velmahos GC, Spaniolas K, Tabbara M, et al. Pulmonary embolism and deep venous thrombosis in trauma: are they related? Arch Surg. 2009;144:928-932.
Cancer Guideline for VTE Prophylaxis for Inpatients and Long-Term Treatment With Low-Molecular-Weight Heparin for Acute VTE
Clinical question: On what aspects of VTE management in cancer patients are there consensus among the major guideline panels?
Background: VTE is a common and serious complication of cancer. Patients might be hypercoagulable due to prothrombotic mediators released or mediated by tumor cells, chemotherapeutic agents, debility, central venous catheters, hospitalizations, or surgical procedures. The optimal management often is problematic due to uncertain benefit and risk of bleeding.
Study design: Review of major guideline statements.
Synopsis: The authors examined five VTE guidelines of American and European cancer societies. Each guideline was reviewed to determine the main recommendations and whether there was consensus on key aspects of anticoagulant management.
The study authors concluded that consensus was reached on most key recommendations:
- VTE prophylaxis in hospitalized medical patients. All five guidelines recommend the use of prophylaxis, though some guidelines recommend anticoagulant prophylaxis for all inpatients in the absence of contraindications and some recommend limiting prophylaxis to immobilized patients. All five recommend the use of either unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.
- VTE prevention in cancer patients undergoing surgery. All five guidelines recommend anticoagulant prophylaxis in the absence of contraindications and extending prophylaxis approximately four weeks after major surgery.
- VTE prophylaxis in cancer patients with central venous catheters. Not recommended.
- VTE prophylaxis in ambulatory cancer patients without central venous catheters. Recommended only for multiple myeloma patients receiving a thalidomide-lenalidomide regimen.
- Long-term treatment of acute VTE in cancer patients. All five guidelines recommend initial treatment with LMWH for at least three to six months, followed by indefinite treatment with LMWH or a vitamin K antagonist.
Bottom line: Major guideline panels agree on key aspects of VTE management for cancer patients, including the use of prophylaxis for hospitalized medical and surgical patients and the use of long-term LMWH treatment for cancer patients with acute VTE.
Citation: Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009; 27(29):4919-4926.
Discontinuation of Beta Blockers Increases Risk of Postoperative Myocardial Infarction and Death
Clinical question: Does perioperative beta-blocker discontinuation affect postoperative myocardial infarction (MI) in low-risk patients undergoing joint arthroplasty?
Background: Recent trials show no benefit of perioperative beta blockers in reducing the incidence of perioperative myocardial infarctions (POMI) in low-risk patients. This retrospective study examined the impact of continuing or discontinuing beta blockers and the occurrence of POMI in patients undergoing elective joint arthroplasties.
Study design: Retrospective chart review.
Setting: Large academic center in Ottawa, Canada.
Synopsis: Medical records for 5,178 patients undergoing elective hip or knee arthroplasty from January 2002 to June 2006 were included in the review. The primary outcome was POMI, defined as an increased troponin level. Patients were divided into three groups: beta blocker prescribed on post-operative day (POD) zero and continued for one week or until discharge; beta blocker prescribed on POD zero and discontinued at any time in the first week; and no beta blocker on POD 0.
Beta blockers were continued in 992 patients and discontinued in 252 patients. The rate of POMI and death increased in the beta-blocker discontinuation group (odds ratio 2.0 [1.1-3.9] and 2.0 [1.1-3.9], respectively). This association persisted after adjustment for cardiac risk using a validated risk score.
The study was limited by the fact that the control group did not include patients who were on a beta blocker at home, thus potentially increasing the number of events in this group. The discontinuation beta blocker group had an increased baseline risk for POMI. The reason for discontinuing the beta blocker was not known, and cessation of beta blocker could have been due to an acute event.
Bottom line: This study adds support to the American College of Cardiology and American Heart Association (ACC/AHA) guidelines, which recommend continuation of beta-blocker therapy in the perioperative period.
Citation: Van Klei WA, Bryson GL, Yang H, Forster AJ. Effect of beta-blocker prescription on the incidence of postoperative myocardial infarction after hip and knee arthroplasty. Anesthesiology. 2009;111(4):717-724.
Lower Perioperative Mortality with Endovascular Vs. Open Abdominal Aortic Aneurysm Repair
Clinical question: How do perioperative and long-term morbidity and mortality compare in endovascular and open repair of abdominal aortic aneurysm (AAA)?
Background: Open AAA repair has relatively high perioperative mortality. Endovascular repair was developed as a less-invasive option and has been shown to reduce inpatient perioperative mortality, length of hospital stay, and ICU requirement. However, data suggest it leads to more frequent reinterventions and the same mortality rate as open repair at two years.
Study design: Randomized clinical trial.
Setting: Veterans Affairs medical centers.
Synopsis: The study randomized 881 veterans who planned to have elective AAA repair and were eligible for both endovascular and open repair. This is a planned, two-year interim report in a nine-year study.
Perioperative mortality was 0.5% in the endovascular repair group, compared with 3.0% in the open repair group. However, this difference in mortality was not statistically significant at two years. The endovascular repair group experienced shorter procedure and mechanical ventilation time, decreased hospital and ICU stay, and lower rate of blood transfusions.
Overall, there was no difference between the groups for major morbidity, procedure failure, need for secondary therapeutic intervention, quality of life, or erectile dysfunction. More data on long-term comparison of these two interventions will be available at the conclusion of this study.
Bottom line: Endovascular repair of AAA has lower perioperative mortality than open repair but did not lead to improved morbidity or mortality at two years.
Citation: Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs. open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302 (14):1535-1542.
OTC Analgesics Not Associated with Acute Decompensation in Cirrhotic Patients
Clinical question: Do over-the-counter (OTC) analgesics lead to acute hepatic decompensation among patients with cirrhosis?
Background: In theory, intake of acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs) can worsen hepatic function and lead to complications among cirrhotic patients. The role of OTC analgesics in potentially triggering acute hepatic decompensation among cirrhotic patients has not been studied.
Study design: Prospective case-control study.
Setting: Two tertiary-care hospitals.
Synopsis: Cirrhotic patients hospitalized for acute liver decompensation were compared with compensated cirrhotic patients in the liver clinic (cirrhotic controls) and with randomly selected, noncirrhotic patients who were simultaneously hospitalized (noncirrhotic controls). Data collected through questionnaires included quantity and dose of OTC analgesics used and alcohol consumption in the past 30 days.
Thirty-five percent of the hospitalized cirrhotic patients, 52% of the cirrhotic controls, and 70% of the noncirrhotic controls used OTC analgesics. At doses lower than those recommended, acetaminophen is not associated with acute liver decompensation among cirrhotic patients, even with recent alcohol use. However, NSAIDs taken by the cirrhotic patients, when compared to control subjects, were in larger doses and used for a longer duration, suggesting NSAIDs may have contributed to the acute decompensation.
Study limitations include the nature of the study design, reliance on the patient’s recall of OTC analgesic use, and obtaining other possible causes of decompensation, such as herbal supplement intake or compliance with diuretics or dietary indiscretion.
Bottom line: Acetaminophen at doses lower than recommended is not associated with adverse complications in cirrhotic patients, but NSAIDs are possibly associated with acute decompensation.
Citation: Khalid SK, Lane J, Navarro V, Garcia-Tsao G. Use of over-the-counter analgesics is not associated with acute decompensation in patients with cirrhosis. Clin Gastroenterol Hepatol. 2009;7(9):994-999.
Cardiovascular Disease and Risk of Hip Fracture
Clinical question: Is the diagnosis of cardiovascular disease (CVD) associated with the risk of subsequent hip fracture?
Background: Osteoporosis and CVD are regarded as independent, age-related conditions. However, recent research suggests that the bone and vascular systems share common regulatory mechanisms. Stroke is a known risk factor for hip fractures, and bisphosphonates have been shown to prevent atherosclerosis and reduce total mortality rate.
Study design: Cohort study.
Setting: Swedish National Patient Registry.
Synopsis: The study identified 31,936 Swedish twins born from 1914 to 1944. This cohort was followed up to age 50, and time-dependent exposures using Cox-proportional hazard regression models were evaluated.
Times to hip fracture after CVD diagnosis were isolated. Crude absolute rate of hip fractures (per 1,000 person-years) was 12.6 after diagnosis of heart failure, 12.6 after a stroke, 6.6 after peripheral atherosclerosis, and 5.2 after ischemic heart disease (IHD), compared with 1.2 per 1,000 person-years without a CVD diagnosis. Multivariable-adjusted hazard ratio (HR) of hip fracture after heart failure was 4.40 (95% CI, 3.43-5.63); after a stroke was 5.09 (95% CI, 4.18-6.20); after peripheral atherosclerosis was 3.20 (CI, 2.28-4.50); and after an IHD event was 2.32 (CI, 1.91-2.84).
Identical twins even without heart failure and stroke also had an increased risk of hip fracture if their twin had been diagnosed with these diseases.
Bottom line: Cardiovascular disease is significantly associated with risk of subsequent hip fracture, and genetic factors probably play a role in the association.
Citation: Sennerby U, Melhus H, Gedeborg R, et al. Cardiovascular diseases and risk of hip fracture. JAMA. 2009;302(15):1666-1673. TH
PEDIATRIC HM Literature
By Mark Shen, MD
Variation in the Treatment of Henoch-Schönlein Purpura
Clinical question: What is the degree of variation in the inpatient management of Henoch-Schönlein purpura (HSP)?
Background: HSP is the most common pediatric vasculitis, but there are no consensus recommendations or guidelines for treatment. The amount of variation in the pharmacologic management of this disease is unknown.
Study design: Retrospective database analysis.
Setting: Thirty-six children’s hospitals affiliated with the Child Health Corporation of America.
Synopsis: The Pediatric Health Information (PHIS) database was sampled for children younger than 18 years of age with an ICD-9-CM code of HSP and discharge from a hospital that submitted appropriate data from 2000 to 2007. Only index admissions were included, and children with coexisting rheumatic conditions were excluded, for a total of 1,988 subjects.
Logistic regression analysis was used to examine the effects of patient-level standardization on hospital-level rates of therapy and the degree to which variation across hospitals occurred beyond what would be expected after standardization.
Hospital-level variation in medication use was significant (P<0.001) for corticosteroids, opiates, and nonsteroidal anti-inflammatory drugs (NSAIDs), even after adjustment for severity and age at presentation.
Although variation in management is not surprising, the significant degree to which this occurred at the hospital level suggests that local institutional culture plays a dominant role in decision-making. The use of the PHIS database allows for analysis of a large population that would be otherwise difficult to study. However, significant numbers of HSP patients do not require hospitalization, and the study results might substantially over- or underestimate practice patterns. Collaborative efforts to better define optimal management of HSP are needed.
Bottom line: A significant degree of hospital-level variation exists in the inpatient management of HSP.
Citation: Weiss PF, Klink AJ, Hexem K, et al. Variation in inpatient therapy and diagnostic evaluation of children with henoch schönlein purpura. J Pediatr. 2009;155(6):812-818.e1.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Perioperative oxygen use and infection rate.
- Effects of adverse events and healthcare costs
- Impact of DVT on PE rates in trauma
- VTE prevention and treatment in cancer patients
- Effect of perioperative beta-blocker discontinuation
- Endovascular vs. open AAA repair
- OTC analgesics in patients with hepatic dysfunction
- Cardiovascular disease and risk of hip fracture
High Perioperative Oxygen Fraction Does Not Improve Surgical-Site Infection Frequency after Abdominal Surgery
Clinical question: Does the use of 80% oxygen perioperatively in abdominal surgery decrease the frequency of surgical-site infection within 14 days without increasing the rate of pulmonary complications?
Background: Low oxygen tension in wounds can negatively impact immune response and healing. Increasing inspiratory oxygen fraction during the perioperative period translates into higher wound oxygen tension. However, the benefit of increased oxygen fraction therapy in abdominal surgery healing and complications is not clear, nor is the frequency of pulmonary complications.
Study design: Patient- and observer-blinded clinical trial.
Setting: Fourteen Danish hospitals from October 2006 to October 2008.
Synopsis: Patients were randomized to receive a fraction of inspired oxygen (FIO2) of 0.80 or 0.30. The primary outcome—surgical-site infection in the superficial or deep wound or intra-abdominal cavity within 14 days of surgery—was defined using Centers for Disease Control and Prevention (CDC) criteria. Secondary outcomes included pulmonary complications within 14 days (pneumonia, atelectasis, or respiratory failure), 30-day mortality, duration of post-op course, ICU stay within 14 days post-op, and any abdominal operation within 14 days. The 1,386 patients were enrolled in the intention-to-treat analysis.
Infection occurred in 19.1% of patients given 0.80 FIO2 and in 20.1% of patients given 0.30 FIO2; odds ratio of 0.94 (95% CI 0.72 to 1.22; P=0.64). Numbers of pulmonary complications were not significantly different between the groups.
This trial included acute and nonacute laparotomies with followup for adverse outcomes. Study limitations included the inability to ensure that both groups received timely antibiotics and prevention for hypothermia. Of patients in the 30% FIO2 group, 7.3% required higher oxygen administration. Additionally, infection might have been underestimated in 11.3% of patients who were not followed up on between days 13 and 30.
Bottom line: High oxygen concentration administered during and after laparotomy did not lead to fewer surgical site infections, nor did it significantly increase the frequency of pulmonary complications or death.
Citation: Meyhoff CS, Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA. 2009;302(14):1543-1550.
Eliminating Adverse Events and Redundant Tests Could Generate U.S. Healthcare Savings
Clinical question: Using available data, what is the estimated cost savings of eliminating adverse events and avoiding redundant tests?
Background: Reimbursement schemes are changing such that hospitals are reimbursed less for some adverse events. This financial disincentive is expected to spark interest in improved patient safety. The authors sought to model the cost savings generated by eliminating redundant testing and adverse events from literature-based estimates.
Study design: Development of conceptual model to identify common or costly adverse events, redundant tests, and simulated costs.
Setting: Literature review, expert opinion, data from safety organizations and epidemiologic studies, and patient data from the 2004 National Inpatient Data Sample.
Synopsis: The conceptual model identified 5.7 million adverse events in U.S. hospitals, of which 3 million were considered preventable. The most common events included hospital-acquired infections (82% preventable), adverse drug events (26%), falls (33%), and iatrogenic thromboembolic events (62%). The calculated cost savings totaled $16.6 billion (5.5% of total inpatient costs) for adverse events and $8.2 billion for the elimination of redundant tests. When looking at hospital subtypes, the greatest savings would come from major teaching hospitals.
This study is limited by its use of published and heterogeneous data spanning a 15-year period. The authors did not include events for which there was no epidemiologic or cost data. As hospital-care changes and technology is adopted, it is uncertain how this changes the costs, prevalence, and the preventable nature of these events. The model was not consistently able to identifying high- and low-risk patients. For instance, in some models, all patients were considered at risk for events.
Bottom line: Based on a conceptual model of 2004 hospitalized patients, eliminating preventable adverse events could have saved $16.6 billion, while eliminating redundant tests could have saved another $8 billion.
Citation: Jha AK, Chan DC, Ridgway AB, Franz C, Bates DW. Improving safety and eliminating redundant tests: cutting costs in U.S. hospitals. Health Aff (Millwood). 2009;28(5):1475-1484.
Trauma Patients with Pulmonary Embolism Might Not Have DVT on Imaging of Lower Extremities
Clinical question: What is the relationship between acute DVT and pulmonary embolism (PE) in trauma patients?
Background: Major trauma is associated with an increased risk of acute DVT and PE. It is assumed that the majority of PEs arise from DVTs in the lower extremities. Definitive evidence demonstrating that PEs form in situ rather than embolize from leg veins could impact indications for inferior vena cava filters.
Study design: Retrospective chart review.
Setting: Academic Level 1 trauma center in Boston.
Synopsis: The medical records of 247 trauma patients with suspected PE who underwent CT angiography of the lungs and simultaneous CT venography of the pelvis and lower extremities from January 2004 to December 2007 were reviewed. High-risk patients also underwent weekly screening with duplex ultrasonagraphy of the legs.
PE was diagnosed in 46 patients (19%) and DVT in 18 patients (7%). Anticoagulant prophylaxis had been administered to 96% and 78% of the patients with PE and DVT, respectively. PE was diagnosed a median of 5.5 days after admission (range 0-40 days) and the majority (61%) were in segmental or subsegmental branches, rather than in the main or lobar pulmonary arteries (39%). Only seven of the 46 patients (15%) diagnosed with PE also had a pelvic or lower-extremity DVT on simultaneous imaging with CT venography.
Bottom line: Trauma patients with PE often do not have a DVT at the time of diagnosis, though it remains unknown whether this is due to in-situ pulmonary thrombosis or complete embolization from the lower extremities.
Citation: Velmahos GC, Spaniolas K, Tabbara M, et al. Pulmonary embolism and deep venous thrombosis in trauma: are they related? Arch Surg. 2009;144:928-932.
Cancer Guideline for VTE Prophylaxis for Inpatients and Long-Term Treatment With Low-Molecular-Weight Heparin for Acute VTE
Clinical question: On what aspects of VTE management in cancer patients are there consensus among the major guideline panels?
Background: VTE is a common and serious complication of cancer. Patients might be hypercoagulable due to prothrombotic mediators released or mediated by tumor cells, chemotherapeutic agents, debility, central venous catheters, hospitalizations, or surgical procedures. The optimal management often is problematic due to uncertain benefit and risk of bleeding.
Study design: Review of major guideline statements.
Synopsis: The authors examined five VTE guidelines of American and European cancer societies. Each guideline was reviewed to determine the main recommendations and whether there was consensus on key aspects of anticoagulant management.
The study authors concluded that consensus was reached on most key recommendations:
- VTE prophylaxis in hospitalized medical patients. All five guidelines recommend the use of prophylaxis, though some guidelines recommend anticoagulant prophylaxis for all inpatients in the absence of contraindications and some recommend limiting prophylaxis to immobilized patients. All five recommend the use of either unfractionated heparin, low-molecular-weight heparin (LMWH), or fondaparinux.
- VTE prevention in cancer patients undergoing surgery. All five guidelines recommend anticoagulant prophylaxis in the absence of contraindications and extending prophylaxis approximately four weeks after major surgery.
- VTE prophylaxis in cancer patients with central venous catheters. Not recommended.
- VTE prophylaxis in ambulatory cancer patients without central venous catheters. Recommended only for multiple myeloma patients receiving a thalidomide-lenalidomide regimen.
- Long-term treatment of acute VTE in cancer patients. All five guidelines recommend initial treatment with LMWH for at least three to six months, followed by indefinite treatment with LMWH or a vitamin K antagonist.
Bottom line: Major guideline panels agree on key aspects of VTE management for cancer patients, including the use of prophylaxis for hospitalized medical and surgical patients and the use of long-term LMWH treatment for cancer patients with acute VTE.
Citation: Khorana AA, Streiff MB, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol. 2009; 27(29):4919-4926.
Discontinuation of Beta Blockers Increases Risk of Postoperative Myocardial Infarction and Death
Clinical question: Does perioperative beta-blocker discontinuation affect postoperative myocardial infarction (MI) in low-risk patients undergoing joint arthroplasty?
Background: Recent trials show no benefit of perioperative beta blockers in reducing the incidence of perioperative myocardial infarctions (POMI) in low-risk patients. This retrospective study examined the impact of continuing or discontinuing beta blockers and the occurrence of POMI in patients undergoing elective joint arthroplasties.
Study design: Retrospective chart review.
Setting: Large academic center in Ottawa, Canada.
Synopsis: Medical records for 5,178 patients undergoing elective hip or knee arthroplasty from January 2002 to June 2006 were included in the review. The primary outcome was POMI, defined as an increased troponin level. Patients were divided into three groups: beta blocker prescribed on post-operative day (POD) zero and continued for one week or until discharge; beta blocker prescribed on POD zero and discontinued at any time in the first week; and no beta blocker on POD 0.
Beta blockers were continued in 992 patients and discontinued in 252 patients. The rate of POMI and death increased in the beta-blocker discontinuation group (odds ratio 2.0 [1.1-3.9] and 2.0 [1.1-3.9], respectively). This association persisted after adjustment for cardiac risk using a validated risk score.
The study was limited by the fact that the control group did not include patients who were on a beta blocker at home, thus potentially increasing the number of events in this group. The discontinuation beta blocker group had an increased baseline risk for POMI. The reason for discontinuing the beta blocker was not known, and cessation of beta blocker could have been due to an acute event.
Bottom line: This study adds support to the American College of Cardiology and American Heart Association (ACC/AHA) guidelines, which recommend continuation of beta-blocker therapy in the perioperative period.
Citation: Van Klei WA, Bryson GL, Yang H, Forster AJ. Effect of beta-blocker prescription on the incidence of postoperative myocardial infarction after hip and knee arthroplasty. Anesthesiology. 2009;111(4):717-724.
Lower Perioperative Mortality with Endovascular Vs. Open Abdominal Aortic Aneurysm Repair
Clinical question: How do perioperative and long-term morbidity and mortality compare in endovascular and open repair of abdominal aortic aneurysm (AAA)?
Background: Open AAA repair has relatively high perioperative mortality. Endovascular repair was developed as a less-invasive option and has been shown to reduce inpatient perioperative mortality, length of hospital stay, and ICU requirement. However, data suggest it leads to more frequent reinterventions and the same mortality rate as open repair at two years.
Study design: Randomized clinical trial.
Setting: Veterans Affairs medical centers.
Synopsis: The study randomized 881 veterans who planned to have elective AAA repair and were eligible for both endovascular and open repair. This is a planned, two-year interim report in a nine-year study.
Perioperative mortality was 0.5% in the endovascular repair group, compared with 3.0% in the open repair group. However, this difference in mortality was not statistically significant at two years. The endovascular repair group experienced shorter procedure and mechanical ventilation time, decreased hospital and ICU stay, and lower rate of blood transfusions.
Overall, there was no difference between the groups for major morbidity, procedure failure, need for secondary therapeutic intervention, quality of life, or erectile dysfunction. More data on long-term comparison of these two interventions will be available at the conclusion of this study.
Bottom line: Endovascular repair of AAA has lower perioperative mortality than open repair but did not lead to improved morbidity or mortality at two years.
Citation: Lederle FA, Freischlag JA, Kyriakides TC, et al. Outcomes following endovascular vs. open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009;302 (14):1535-1542.
OTC Analgesics Not Associated with Acute Decompensation in Cirrhotic Patients
Clinical question: Do over-the-counter (OTC) analgesics lead to acute hepatic decompensation among patients with cirrhosis?
Background: In theory, intake of acetaminophen and/or nonsteroidal anti-inflammatory drugs (NSAIDs) can worsen hepatic function and lead to complications among cirrhotic patients. The role of OTC analgesics in potentially triggering acute hepatic decompensation among cirrhotic patients has not been studied.
Study design: Prospective case-control study.
Setting: Two tertiary-care hospitals.
Synopsis: Cirrhotic patients hospitalized for acute liver decompensation were compared with compensated cirrhotic patients in the liver clinic (cirrhotic controls) and with randomly selected, noncirrhotic patients who were simultaneously hospitalized (noncirrhotic controls). Data collected through questionnaires included quantity and dose of OTC analgesics used and alcohol consumption in the past 30 days.
Thirty-five percent of the hospitalized cirrhotic patients, 52% of the cirrhotic controls, and 70% of the noncirrhotic controls used OTC analgesics. At doses lower than those recommended, acetaminophen is not associated with acute liver decompensation among cirrhotic patients, even with recent alcohol use. However, NSAIDs taken by the cirrhotic patients, when compared to control subjects, were in larger doses and used for a longer duration, suggesting NSAIDs may have contributed to the acute decompensation.
Study limitations include the nature of the study design, reliance on the patient’s recall of OTC analgesic use, and obtaining other possible causes of decompensation, such as herbal supplement intake or compliance with diuretics or dietary indiscretion.
Bottom line: Acetaminophen at doses lower than recommended is not associated with adverse complications in cirrhotic patients, but NSAIDs are possibly associated with acute decompensation.
Citation: Khalid SK, Lane J, Navarro V, Garcia-Tsao G. Use of over-the-counter analgesics is not associated with acute decompensation in patients with cirrhosis. Clin Gastroenterol Hepatol. 2009;7(9):994-999.
Cardiovascular Disease and Risk of Hip Fracture
Clinical question: Is the diagnosis of cardiovascular disease (CVD) associated with the risk of subsequent hip fracture?
Background: Osteoporosis and CVD are regarded as independent, age-related conditions. However, recent research suggests that the bone and vascular systems share common regulatory mechanisms. Stroke is a known risk factor for hip fractures, and bisphosphonates have been shown to prevent atherosclerosis and reduce total mortality rate.
Study design: Cohort study.
Setting: Swedish National Patient Registry.
Synopsis: The study identified 31,936 Swedish twins born from 1914 to 1944. This cohort was followed up to age 50, and time-dependent exposures using Cox-proportional hazard regression models were evaluated.
Times to hip fracture after CVD diagnosis were isolated. Crude absolute rate of hip fractures (per 1,000 person-years) was 12.6 after diagnosis of heart failure, 12.6 after a stroke, 6.6 after peripheral atherosclerosis, and 5.2 after ischemic heart disease (IHD), compared with 1.2 per 1,000 person-years without a CVD diagnosis. Multivariable-adjusted hazard ratio (HR) of hip fracture after heart failure was 4.40 (95% CI, 3.43-5.63); after a stroke was 5.09 (95% CI, 4.18-6.20); after peripheral atherosclerosis was 3.20 (CI, 2.28-4.50); and after an IHD event was 2.32 (CI, 1.91-2.84).
Identical twins even without heart failure and stroke also had an increased risk of hip fracture if their twin had been diagnosed with these diseases.
Bottom line: Cardiovascular disease is significantly associated with risk of subsequent hip fracture, and genetic factors probably play a role in the association.
Citation: Sennerby U, Melhus H, Gedeborg R, et al. Cardiovascular diseases and risk of hip fracture. JAMA. 2009;302(15):1666-1673. TH
PEDIATRIC HM Literature
By Mark Shen, MD
Variation in the Treatment of Henoch-Schönlein Purpura
Clinical question: What is the degree of variation in the inpatient management of Henoch-Schönlein purpura (HSP)?
Background: HSP is the most common pediatric vasculitis, but there are no consensus recommendations or guidelines for treatment. The amount of variation in the pharmacologic management of this disease is unknown.
Study design: Retrospective database analysis.
Setting: Thirty-six children’s hospitals affiliated with the Child Health Corporation of America.
Synopsis: The Pediatric Health Information (PHIS) database was sampled for children younger than 18 years of age with an ICD-9-CM code of HSP and discharge from a hospital that submitted appropriate data from 2000 to 2007. Only index admissions were included, and children with coexisting rheumatic conditions were excluded, for a total of 1,988 subjects.
Logistic regression analysis was used to examine the effects of patient-level standardization on hospital-level rates of therapy and the degree to which variation across hospitals occurred beyond what would be expected after standardization.
Hospital-level variation in medication use was significant (P<0.001) for corticosteroids, opiates, and nonsteroidal anti-inflammatory drugs (NSAIDs), even after adjustment for severity and age at presentation.
Although variation in management is not surprising, the significant degree to which this occurred at the hospital level suggests that local institutional culture plays a dominant role in decision-making. The use of the PHIS database allows for analysis of a large population that would be otherwise difficult to study. However, significant numbers of HSP patients do not require hospitalization, and the study results might substantially over- or underestimate practice patterns. Collaborative efforts to better define optimal management of HSP are needed.
Bottom line: A significant degree of hospital-level variation exists in the inpatient management of HSP.
Citation: Weiss PF, Klink AJ, Hexem K, et al. Variation in inpatient therapy and diagnostic evaluation of children with henoch schönlein purpura. J Pediatr. 2009;155(6):812-818.e1.
HM Heads to Washington
Hospital Medicine 2010—HM10, in hospitalist parlance—is coming soon. SHM’s annual meeting continues to exceed expectations for educational content, networking opportunities, professional advancement, and fun.
HM10, which runs April 8-11, has an additional attraction this year: With the conference center just miles from Washington, D.C., HM10 will bring hospitalists closer than ever to the heart of the continued national debate over healthcare reform and delivery. Between now and then, the details of healthcare policy will no doubt change, but the intensity and impact of the decisions made in our nation’s capital are unlikely to fade.
“Washington, D.C., is always an exciting place to visit, but it’s even more attractive now for hospitalists and others involved in healthcare,” says Geri Barnes, SHM’s senior director for education and meetings. “The discussions happening in Washington now are likely to affect every corner of the healthcare sector.”
As in years past, HM10 offerings will be wide-ranging enough to include topics that will satisfy physicians, nonphysician practitioners (NPPs), and HM administrators alike.
Registration for HM09 sold out in advance—an additional incentive for early HM10 registration.
“Last year’s conference set new records and generated real excitement within the specialty,” Barnes says. “We’re confident that the program we’ve created for 2010 will do it again.”
Featured Speakers: The Stars of Hospital Care
This year’s featured presenters represent a mix of fresh, outside perspectives and familiar favorites.
Kicking off the formal agenda will be Paul Levy, president and CEO of Beth Israel Deaconess Medical Center, a 621-bed academic hospital center in Boston. In 2009, it was one of three American Hospital Association McKesson Quest for Quality Prize honorees for its efforts in eliminating preventable harm.

Levy says he expects to expound on the patient-safety theme during his HM10 presentation. He’ll speak about his center’s “journey in preventable harm—what we’ve learned, ideas for the future, the role of transparency, and the different approaches to process improvement,” he says. Check out his blog at http://runningahospital.blogspot.com.
To wrap up the conference, HM pioneer Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World (www.wachters world.com), will bring his perspective on HM and healthcare reform in a presentation called “How Health Care Reform Changes the Hospitalist Field . . . And Vice Versa.”
More Pre-Courses
In response to increased demand for educational content, HM10 will offer the most pre-courses ever. The pre-courses emphasize a hands-on approach to professional development. This year’s eight pre-courses—two more than last year—will run concurrently all day April 8. “Hospitalists are always looking for ways to enhance their knowledge of the specialty and sharpen their skills,” Barnes says. “The new pre-courses at HM10 were added specifically because of demand from hospitalists.”
The two new additions represent the changing needs within HM. The “Essential Neurology for the Hospitalist” pre-course, taught by David Likosky, MD, FHM, a hospitalist at Evergreen Hospital Medical Center in Kirkland, Wash., recognizes hospitalists often serve as the primary health providers for hospitalized patients with neurological disorders. The pre-course will cover the basics of neurological exams, diagnosis, and management of many of the conditions hospitalists encounter on a regular basis.
SHM Teams With Epocrates
New partnership will deliver HM content to mobile platforms; Chad Whelan will serve as mobile resource center’s editor

During work hours, hospitalists rarely find themselves behind a desk. Rather, they are on their feet, tending to patients and collaborating with hospital care teams.
That’s why SHM and Epocrates, one of the industry leaders in providing medical information on mobile platforms, have teamed up to create the first HM resource center for Palm, Windows Mobile, and iPhone platforms. Every two weeks, the new mobile platform will deliver new, exclusive commentary on the latest news and research in HM and hospitalist practice management. The free service is expected to be available in March.
Hospitalists can sign up at SHM’s Web site—www.hospitalmedicine.org/epocrates—and receive an e-mail alert when the new application goes live.
Dr. Chad Whelan, MD, FHM, director of the division of hospital medicine and associate professor at Loyola University’s Stritch School of Medicine in Chicago, will serve as the editor of the HM mobile resource center.
“This combines two of the defining characteristics of the modern hospitalist: the need for latest news and information in the specialty in an on-the-go format,” explains Dr. Whelan, chair of SHM’s Career Satisfaction Task Force. “This is more than recycled content; this is fresh thinking in a fresh new package.”
The second new pre-course addresses some of the daunting challenges that new hospitalists face. “Early Career Hospitalist: Skills for Success,” led by Efren Manjarrez, MD, FHM, of the University of Miami School of Medicine, will lead new hospitalists through such day-to-day issues as communicating with patients and families, coding, quality improvement (QI) efforts, and legal considerations in their practice.
Although the pre-course on the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) isn’t new, it will include new information about the process for applying to ABIM’s new Recognition of Focused Practice in Hospital Medicine program.
Inaugural Year for Senior Fellows
SHM’s Fellows in Hospital Medicine Program will take center stage again, as the society welcomes the first class of Senior Fellows in Hospital Medicine (SFHM) and the second class of Fellows in Hospital Medicine (FHM). Now in its second year, the fellows program recognizes hospitalists for their commitment to excellence.
At HM09, SHM inducted more than 500 hospitalists as fellows. Candidates must have at least five years’ experience as a hospitalist and demonstrate their work in QI, teamwork, and leadership. This year, SHM expects to induct even more fellows.
The requirements for the SHFM are similar to those of the FHM program but demand more experience in each category. Hospitalists applying for SFHM also must be an SHM member in good standing for at least five years.
New Educational Options: Breakout Sessions and RIV Competition
The HM10 educational program features new breakout sessions and the annual Research, Innovations, and Clinical Vignettes (RIV) competition. The new tracks include:
- Academic;
- Clinical 1;
- Clinical 2;
- Evidence-Based Rapid Fire;
- Palliative Care;
- Pediatric;
- Practice Management;
- Quality;
- Research; and
- Workshops (educational format for the annual conference).
Hundreds of hospitalists will submit abstracts for the RIV competition. Of those, dozens will be chosen for the HM10 poster session; a panel of experts will judge the entries on Saturday, April 10. The winners will be announced at the conference and claim a $250 cash prize.
High-Visibility Exhibits
HM’s growth has spurred a burgeoning industry of products and service providers that help hospitalists do their jobs more effectively and efficiently. HM10 brings the best of the industry directly to hospitalists, and this year, SHM is making it easier than ever for hospitalists to find the experts on the exhibit floor. For the first time, HM10’s agenda includes time to allow attendees to browse the exhibit hall without competing workshops or plenary sessions. Plus, attendees will win prizes for visiting exhibit booths.
“HM10 is all about bringing the leaders in hospital medicine together. That includes the leaders in organizations that support hospital medicine,” says Todd Von Deak, vice president of membership and marketing for SHM. “Just like other parts of HM10, innovation and synergy happen on the exhibition floor.”
—Geri Barnes, SHM senior director of education and meetings
Bring the Family
Washington, D.C., is a prime destination for vacationers from around the world, and SHM has organized tours for families and spouses of hospitalists at HM10. Each tour departs directly from the Gaylord National Hotel & Convention Center and takes participants to some of the most famous attractions in the nation’s capital.
Never been to Washington? Then start with the all-day DC IT ALL! Tour, which takes visitors on a guided bus tour to many major monuments, museums, and other city sights.
For those more familiar with Washington, tours of the National Air & Space Museum, a Segway tour of Old Town Alexandria, Va., and George Washington’s Mount Vernon via water cruise are also scheduled.
For more information, visit the “Family Activities” section of the HM10 Web site. To register for a tour, call SHM at 800-843-3360. TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Update
Piedmont Chapter

Fellow in Hospital Medicine Spotlight
Tomas Villanueva, DO, MBA, CPE, FACPE, FHM

Dr. Villanueva is vice chairman of medicine and medical director of the HM program at Baptist Hospital of Miami. He also is an associate professor of medicine at Nova Southeastern University, and a volunteer associate professor of medicine at the University of Miami. He is president of the South Florida chapter of SHM.
Undergraduate education: Saint Thomas University, Miami
Medical school: Nova Southeastern University College of Osteopathic Medicine, North Miami Beach
Notable: Dr. Villanueva’s program started with four physicians in 2003 and has grown to 25 physicians. He says the greatest struggle when he was starting his practice was trying to convince people just how much he was needed.
FYI: Dr. Villanueva is an avid runner. He is training to run the ING Miami Half Marathon later this month.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
ACADEMIC HM LEADERSHIP SUMMIT AT HM10
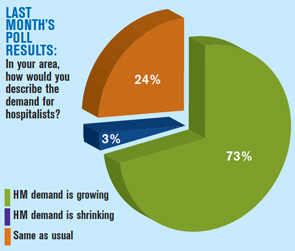
Respected leaders in academic HM will offer a unique opportunity to advance the field April 8 at HM10 in Washington, D.C. The Academic Hospital Medicine Leadership Summit will help shape the direction of educational, scholarship, and clinical practice enterprises in academic HM through interaction, strategic planning, and faculty development activities.
Faculty will be drawn from academic leaders across the country, including SHM President Scott Flanders, president-elect Jeff Wiese, and board member Joe Li. Also scheduled to attend are Journal of Hospital Medicine Editor Mark A. Williams and The Hospitalist Physician Editor Jeff Glasheen.
For academic leaders, the summit is a full-day program. The morning session, for senior faculty only, will use breakout sessions to build a consensus for action in three key areas: clinical operations, scholarly work, and education initiatives. Junior faculty will join the summit for a mentoring lunch, afternoon sessions, and evening poster reception.
For more information about the program, visit www.hospital medicine.org/AcademicSummit, or e-mail SHM education manager Claudia Stahl at [email protected] or [email protected].
Hospital Medicine 2010—HM10, in hospitalist parlance—is coming soon. SHM’s annual meeting continues to exceed expectations for educational content, networking opportunities, professional advancement, and fun.
HM10, which runs April 8-11, has an additional attraction this year: With the conference center just miles from Washington, D.C., HM10 will bring hospitalists closer than ever to the heart of the continued national debate over healthcare reform and delivery. Between now and then, the details of healthcare policy will no doubt change, but the intensity and impact of the decisions made in our nation’s capital are unlikely to fade.
“Washington, D.C., is always an exciting place to visit, but it’s even more attractive now for hospitalists and others involved in healthcare,” says Geri Barnes, SHM’s senior director for education and meetings. “The discussions happening in Washington now are likely to affect every corner of the healthcare sector.”
As in years past, HM10 offerings will be wide-ranging enough to include topics that will satisfy physicians, nonphysician practitioners (NPPs), and HM administrators alike.
Registration for HM09 sold out in advance—an additional incentive for early HM10 registration.
“Last year’s conference set new records and generated real excitement within the specialty,” Barnes says. “We’re confident that the program we’ve created for 2010 will do it again.”
Featured Speakers: The Stars of Hospital Care
This year’s featured presenters represent a mix of fresh, outside perspectives and familiar favorites.
Kicking off the formal agenda will be Paul Levy, president and CEO of Beth Israel Deaconess Medical Center, a 621-bed academic hospital center in Boston. In 2009, it was one of three American Hospital Association McKesson Quest for Quality Prize honorees for its efforts in eliminating preventable harm.
Levy says he expects to expound on the patient-safety theme during his HM10 presentation. He’ll speak about his center’s “journey in preventable harm—what we’ve learned, ideas for the future, the role of transparency, and the different approaches to process improvement,” he says. Check out his blog at http://runningahospital.blogspot.com.
To wrap up the conference, HM pioneer Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World (www.wachters world.com), will bring his perspective on HM and healthcare reform in a presentation called “How Health Care Reform Changes the Hospitalist Field . . . And Vice Versa.”
More Pre-Courses
In response to increased demand for educational content, HM10 will offer the most pre-courses ever. The pre-courses emphasize a hands-on approach to professional development. This year’s eight pre-courses—two more than last year—will run concurrently all day April 8. “Hospitalists are always looking for ways to enhance their knowledge of the specialty and sharpen their skills,” Barnes says. “The new pre-courses at HM10 were added specifically because of demand from hospitalists.”
The two new additions represent the changing needs within HM. The “Essential Neurology for the Hospitalist” pre-course, taught by David Likosky, MD, FHM, a hospitalist at Evergreen Hospital Medical Center in Kirkland, Wash., recognizes hospitalists often serve as the primary health providers for hospitalized patients with neurological disorders. The pre-course will cover the basics of neurological exams, diagnosis, and management of many of the conditions hospitalists encounter on a regular basis.
SHM Teams With Epocrates
New partnership will deliver HM content to mobile platforms; Chad Whelan will serve as mobile resource center’s editor
During work hours, hospitalists rarely find themselves behind a desk. Rather, they are on their feet, tending to patients and collaborating with hospital care teams.
That’s why SHM and Epocrates, one of the industry leaders in providing medical information on mobile platforms, have teamed up to create the first HM resource center for Palm, Windows Mobile, and iPhone platforms. Every two weeks, the new mobile platform will deliver new, exclusive commentary on the latest news and research in HM and hospitalist practice management. The free service is expected to be available in March.
Hospitalists can sign up at SHM’s Web site—www.hospitalmedicine.org/epocrates—and receive an e-mail alert when the new application goes live.
Dr. Chad Whelan, MD, FHM, director of the division of hospital medicine and associate professor at Loyola University’s Stritch School of Medicine in Chicago, will serve as the editor of the HM mobile resource center.
“This combines two of the defining characteristics of the modern hospitalist: the need for latest news and information in the specialty in an on-the-go format,” explains Dr. Whelan, chair of SHM’s Career Satisfaction Task Force. “This is more than recycled content; this is fresh thinking in a fresh new package.”
The second new pre-course addresses some of the daunting challenges that new hospitalists face. “Early Career Hospitalist: Skills for Success,” led by Efren Manjarrez, MD, FHM, of the University of Miami School of Medicine, will lead new hospitalists through such day-to-day issues as communicating with patients and families, coding, quality improvement (QI) efforts, and legal considerations in their practice.
Although the pre-course on the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) isn’t new, it will include new information about the process for applying to ABIM’s new Recognition of Focused Practice in Hospital Medicine program.
Inaugural Year for Senior Fellows
SHM’s Fellows in Hospital Medicine Program will take center stage again, as the society welcomes the first class of Senior Fellows in Hospital Medicine (SFHM) and the second class of Fellows in Hospital Medicine (FHM). Now in its second year, the fellows program recognizes hospitalists for their commitment to excellence.
At HM09, SHM inducted more than 500 hospitalists as fellows. Candidates must have at least five years’ experience as a hospitalist and demonstrate their work in QI, teamwork, and leadership. This year, SHM expects to induct even more fellows.
The requirements for the SHFM are similar to those of the FHM program but demand more experience in each category. Hospitalists applying for SFHM also must be an SHM member in good standing for at least five years.
New Educational Options: Breakout Sessions and RIV Competition
The HM10 educational program features new breakout sessions and the annual Research, Innovations, and Clinical Vignettes (RIV) competition. The new tracks include:
- Academic;
- Clinical 1;
- Clinical 2;
- Evidence-Based Rapid Fire;
- Palliative Care;
- Pediatric;
- Practice Management;
- Quality;
- Research; and
- Workshops (educational format for the annual conference).
Hundreds of hospitalists will submit abstracts for the RIV competition. Of those, dozens will be chosen for the HM10 poster session; a panel of experts will judge the entries on Saturday, April 10. The winners will be announced at the conference and claim a $250 cash prize.
High-Visibility Exhibits
HM’s growth has spurred a burgeoning industry of products and service providers that help hospitalists do their jobs more effectively and efficiently. HM10 brings the best of the industry directly to hospitalists, and this year, SHM is making it easier than ever for hospitalists to find the experts on the exhibit floor. For the first time, HM10’s agenda includes time to allow attendees to browse the exhibit hall without competing workshops or plenary sessions. Plus, attendees will win prizes for visiting exhibit booths.
“HM10 is all about bringing the leaders in hospital medicine together. That includes the leaders in organizations that support hospital medicine,” says Todd Von Deak, vice president of membership and marketing for SHM. “Just like other parts of HM10, innovation and synergy happen on the exhibition floor.”
—Geri Barnes, SHM senior director of education and meetings
Bring the Family
Washington, D.C., is a prime destination for vacationers from around the world, and SHM has organized tours for families and spouses of hospitalists at HM10. Each tour departs directly from the Gaylord National Hotel & Convention Center and takes participants to some of the most famous attractions in the nation’s capital.
Never been to Washington? Then start with the all-day DC IT ALL! Tour, which takes visitors on a guided bus tour to many major monuments, museums, and other city sights.
For those more familiar with Washington, tours of the National Air & Space Museum, a Segway tour of Old Town Alexandria, Va., and George Washington’s Mount Vernon via water cruise are also scheduled.
For more information, visit the “Family Activities” section of the HM10 Web site. To register for a tour, call SHM at 800-843-3360. TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Update
Piedmont Chapter
Fellow in Hospital Medicine Spotlight
Tomas Villanueva, DO, MBA, CPE, FACPE, FHM
Dr. Villanueva is vice chairman of medicine and medical director of the HM program at Baptist Hospital of Miami. He also is an associate professor of medicine at Nova Southeastern University, and a volunteer associate professor of medicine at the University of Miami. He is president of the South Florida chapter of SHM.
Undergraduate education: Saint Thomas University, Miami
Medical school: Nova Southeastern University College of Osteopathic Medicine, North Miami Beach
Notable: Dr. Villanueva’s program started with four physicians in 2003 and has grown to 25 physicians. He says the greatest struggle when he was starting his practice was trying to convince people just how much he was needed.
FYI: Dr. Villanueva is an avid runner. He is training to run the ING Miami Half Marathon later this month.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
ACADEMIC HM LEADERSHIP SUMMIT AT HM10
Respected leaders in academic HM will offer a unique opportunity to advance the field April 8 at HM10 in Washington, D.C. The Academic Hospital Medicine Leadership Summit will help shape the direction of educational, scholarship, and clinical practice enterprises in academic HM through interaction, strategic planning, and faculty development activities.
Faculty will be drawn from academic leaders across the country, including SHM President Scott Flanders, president-elect Jeff Wiese, and board member Joe Li. Also scheduled to attend are Journal of Hospital Medicine Editor Mark A. Williams and The Hospitalist Physician Editor Jeff Glasheen.
For academic leaders, the summit is a full-day program. The morning session, for senior faculty only, will use breakout sessions to build a consensus for action in three key areas: clinical operations, scholarly work, and education initiatives. Junior faculty will join the summit for a mentoring lunch, afternoon sessions, and evening poster reception.
For more information about the program, visit www.hospital medicine.org/AcademicSummit, or e-mail SHM education manager Claudia Stahl at [email protected] or [email protected].
Hospital Medicine 2010—HM10, in hospitalist parlance—is coming soon. SHM’s annual meeting continues to exceed expectations for educational content, networking opportunities, professional advancement, and fun.
HM10, which runs April 8-11, has an additional attraction this year: With the conference center just miles from Washington, D.C., HM10 will bring hospitalists closer than ever to the heart of the continued national debate over healthcare reform and delivery. Between now and then, the details of healthcare policy will no doubt change, but the intensity and impact of the decisions made in our nation’s capital are unlikely to fade.
“Washington, D.C., is always an exciting place to visit, but it’s even more attractive now for hospitalists and others involved in healthcare,” says Geri Barnes, SHM’s senior director for education and meetings. “The discussions happening in Washington now are likely to affect every corner of the healthcare sector.”
As in years past, HM10 offerings will be wide-ranging enough to include topics that will satisfy physicians, nonphysician practitioners (NPPs), and HM administrators alike.
Registration for HM09 sold out in advance—an additional incentive for early HM10 registration.
“Last year’s conference set new records and generated real excitement within the specialty,” Barnes says. “We’re confident that the program we’ve created for 2010 will do it again.”
Featured Speakers: The Stars of Hospital Care
This year’s featured presenters represent a mix of fresh, outside perspectives and familiar favorites.
Kicking off the formal agenda will be Paul Levy, president and CEO of Beth Israel Deaconess Medical Center, a 621-bed academic hospital center in Boston. In 2009, it was one of three American Hospital Association McKesson Quest for Quality Prize honorees for its efforts in eliminating preventable harm.
Levy says he expects to expound on the patient-safety theme during his HM10 presentation. He’ll speak about his center’s “journey in preventable harm—what we’ve learned, ideas for the future, the role of transparency, and the different approaches to process improvement,” he says. Check out his blog at http://runningahospital.blogspot.com.
To wrap up the conference, HM pioneer Robert Wachter, MD, FHM, chief of the hospital medicine division, professor, and associate chair of the Department of Medicine at the University of California at San Francisco, a former SHM president, and author of the blog Wachter’s World (www.wachters world.com), will bring his perspective on HM and healthcare reform in a presentation called “How Health Care Reform Changes the Hospitalist Field . . . And Vice Versa.”
More Pre-Courses
In response to increased demand for educational content, HM10 will offer the most pre-courses ever. The pre-courses emphasize a hands-on approach to professional development. This year’s eight pre-courses—two more than last year—will run concurrently all day April 8. “Hospitalists are always looking for ways to enhance their knowledge of the specialty and sharpen their skills,” Barnes says. “The new pre-courses at HM10 were added specifically because of demand from hospitalists.”
The two new additions represent the changing needs within HM. The “Essential Neurology for the Hospitalist” pre-course, taught by David Likosky, MD, FHM, a hospitalist at Evergreen Hospital Medical Center in Kirkland, Wash., recognizes hospitalists often serve as the primary health providers for hospitalized patients with neurological disorders. The pre-course will cover the basics of neurological exams, diagnosis, and management of many of the conditions hospitalists encounter on a regular basis.
SHM Teams With Epocrates
New partnership will deliver HM content to mobile platforms; Chad Whelan will serve as mobile resource center’s editor
During work hours, hospitalists rarely find themselves behind a desk. Rather, they are on their feet, tending to patients and collaborating with hospital care teams.
That’s why SHM and Epocrates, one of the industry leaders in providing medical information on mobile platforms, have teamed up to create the first HM resource center for Palm, Windows Mobile, and iPhone platforms. Every two weeks, the new mobile platform will deliver new, exclusive commentary on the latest news and research in HM and hospitalist practice management. The free service is expected to be available in March.
Hospitalists can sign up at SHM’s Web site—www.hospitalmedicine.org/epocrates—and receive an e-mail alert when the new application goes live.
Dr. Chad Whelan, MD, FHM, director of the division of hospital medicine and associate professor at Loyola University’s Stritch School of Medicine in Chicago, will serve as the editor of the HM mobile resource center.
“This combines two of the defining characteristics of the modern hospitalist: the need for latest news and information in the specialty in an on-the-go format,” explains Dr. Whelan, chair of SHM’s Career Satisfaction Task Force. “This is more than recycled content; this is fresh thinking in a fresh new package.”
The second new pre-course addresses some of the daunting challenges that new hospitalists face. “Early Career Hospitalist: Skills for Success,” led by Efren Manjarrez, MD, FHM, of the University of Miami School of Medicine, will lead new hospitalists through such day-to-day issues as communicating with patients and families, coding, quality improvement (QI) efforts, and legal considerations in their practice.
Although the pre-course on the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) isn’t new, it will include new information about the process for applying to ABIM’s new Recognition of Focused Practice in Hospital Medicine program.
Inaugural Year for Senior Fellows
SHM’s Fellows in Hospital Medicine Program will take center stage again, as the society welcomes the first class of Senior Fellows in Hospital Medicine (SFHM) and the second class of Fellows in Hospital Medicine (FHM). Now in its second year, the fellows program recognizes hospitalists for their commitment to excellence.
At HM09, SHM inducted more than 500 hospitalists as fellows. Candidates must have at least five years’ experience as a hospitalist and demonstrate their work in QI, teamwork, and leadership. This year, SHM expects to induct even more fellows.
The requirements for the SHFM are similar to those of the FHM program but demand more experience in each category. Hospitalists applying for SFHM also must be an SHM member in good standing for at least five years.
New Educational Options: Breakout Sessions and RIV Competition
The HM10 educational program features new breakout sessions and the annual Research, Innovations, and Clinical Vignettes (RIV) competition. The new tracks include:
- Academic;
- Clinical 1;
- Clinical 2;
- Evidence-Based Rapid Fire;
- Palliative Care;
- Pediatric;
- Practice Management;
- Quality;
- Research; and
- Workshops (educational format for the annual conference).
Hundreds of hospitalists will submit abstracts for the RIV competition. Of those, dozens will be chosen for the HM10 poster session; a panel of experts will judge the entries on Saturday, April 10. The winners will be announced at the conference and claim a $250 cash prize.
High-Visibility Exhibits
HM’s growth has spurred a burgeoning industry of products and service providers that help hospitalists do their jobs more effectively and efficiently. HM10 brings the best of the industry directly to hospitalists, and this year, SHM is making it easier than ever for hospitalists to find the experts on the exhibit floor. For the first time, HM10’s agenda includes time to allow attendees to browse the exhibit hall without competing workshops or plenary sessions. Plus, attendees will win prizes for visiting exhibit booths.
“HM10 is all about bringing the leaders in hospital medicine together. That includes the leaders in organizations that support hospital medicine,” says Todd Von Deak, vice president of membership and marketing for SHM. “Just like other parts of HM10, innovation and synergy happen on the exhibition floor.”
—Geri Barnes, SHM senior director of education and meetings
Bring the Family
Washington, D.C., is a prime destination for vacationers from around the world, and SHM has organized tours for families and spouses of hospitalists at HM10. Each tour departs directly from the Gaylord National Hotel & Convention Center and takes participants to some of the most famous attractions in the nation’s capital.
Never been to Washington? Then start with the all-day DC IT ALL! Tour, which takes visitors on a guided bus tour to many major monuments, museums, and other city sights.
For those more familiar with Washington, tours of the National Air & Space Museum, a Segway tour of Old Town Alexandria, Va., and George Washington’s Mount Vernon via water cruise are also scheduled.
For more information, visit the “Family Activities” section of the HM10 Web site. To register for a tour, call SHM at 800-843-3360. TH
Brendon Shank is a freelance writer based in Philadelphia.
Chapter Update
Piedmont Chapter
Fellow in Hospital Medicine Spotlight
Tomas Villanueva, DO, MBA, CPE, FACPE, FHM
Dr. Villanueva is vice chairman of medicine and medical director of the HM program at Baptist Hospital of Miami. He also is an associate professor of medicine at Nova Southeastern University, and a volunteer associate professor of medicine at the University of Miami. He is president of the South Florida chapter of SHM.
Undergraduate education: Saint Thomas University, Miami
Medical school: Nova Southeastern University College of Osteopathic Medicine, North Miami Beach
Notable: Dr. Villanueva’s program started with four physicians in 2003 and has grown to 25 physicians. He says the greatest struggle when he was starting his practice was trying to convince people just how much he was needed.
FYI: Dr. Villanueva is an avid runner. He is training to run the ING Miami Half Marathon later this month.
For more information about the FHM designation, visit www.hospitalmedicine.org/fellows.
ACADEMIC HM LEADERSHIP SUMMIT AT HM10
Respected leaders in academic HM will offer a unique opportunity to advance the field April 8 at HM10 in Washington, D.C. The Academic Hospital Medicine Leadership Summit will help shape the direction of educational, scholarship, and clinical practice enterprises in academic HM through interaction, strategic planning, and faculty development activities.
Faculty will be drawn from academic leaders across the country, including SHM President Scott Flanders, president-elect Jeff Wiese, and board member Joe Li. Also scheduled to attend are Journal of Hospital Medicine Editor Mark A. Williams and The Hospitalist Physician Editor Jeff Glasheen.
For academic leaders, the summit is a full-day program. The morning session, for senior faculty only, will use breakout sessions to build a consensus for action in three key areas: clinical operations, scholarly work, and education initiatives. Junior faculty will join the summit for a mentoring lunch, afternoon sessions, and evening poster reception.
For more information about the program, visit www.hospital medicine.org/AcademicSummit, or e-mail SHM education manager Claudia Stahl at [email protected] or [email protected].
An Officer and a Physician
Imagine being transferred to a hospital where the temperature is 20 below outside, and 40 inches of snow fill the parking lot. Few physicians would sign on for such an assignment. For a brave few, it’s all in a day’s work.
Maj. Ramey Wilson, MD, is a U.S. Army physician who encountered such conditions during his 15-month experience in Afghanistan. “A couple of times, when we couldn’t get helicopters [for evacuation], we had to turn my aid station into a mini-hospital. There were no nurses, labs, or X-ray,” he says. “With only basic supplies and my combat medics, we had to provide all the patient care until the weather broke.”
Not quite the circumstances most hospitalists encounter in their daily practice.
Hospitalists in the military face daunting odds, and at the same time are blessed with some unexpected advantages. On the plus side, military physicians cite the camaraderie, teamwork, honor of caring for soldiers, and the opportunity to train other providers, both in traditional, U.S.-based residencies and while deployed. Among the minuses, they mention a lack of equipment and supplies when they are assigned to forward-deployed soldiers on foreign soil, the heartache of being separated from family, and lower compensation. Most military physicians, however, say that the lower compensation can be offset by generous government benefits and the absence of medical school debt.
All in all, hospitalists in the military have a unique—and sometimes adventurous—story to tell.
Challenges Met, Success Exemplified
Dr. Wilson is a hospitalist and Army physician assigned to Fort Bragg, N.C. Until this past summer, he was the chief of internal medicine at Womack Army Medical Center, one of eight full-service hospitals in the U.S. Army Medical Command. Because the Army is still familiarizing itself with the HM model and the role hospitalists play in the delivery of healthcare, resident house staff meet many of the operational needs, including night and weekend coverage. “The Army doesn’t have a good system for 24-hour continuous care at busy hospitals without residents,” Dr. Wilson says, “and we’ve worked hard to get hospitalists into our system.”
While other Army medical centers have internal-medicine residencies, Womack has only a family medicine residency program. Residents once provided extensive coverage for the hospital, but decreasing numbers (only four interns this year) and work-hour restrictions have shifted the inpatient responsibilities to the internal-medicine staff. “All of the military general internists have functionally become hospitalists to support the inpatient medicine and ICU services,” Dr. Wilson says. “Our family medicine house staff coverage has evaporated.”
The conditions he sees at Womack are similar to what he sees at FirstHealth Moore Regional Hospital, the civilian community hospital in Pinehurst, N.C., where he practices part time. Womack serves two major military populations: those on active duty and their family members, and those no longer on active duty or retired (and not a part of the Veterans Administration program).

—Col. Walt Franz, MD, U.S. Army Medical Corps, Amarah/Al Kut, Iraq
Dr. Wilson, who served in the Ghazni province in eastern Afghanistan, was the only American physician in an area of 8,800 square miles. He and his physician-assistant staff were tasked with keeping U.S. soldiers healthy, serving acute resuscitative trauma care and “basic sick call.” In addition to caring for U.S. and coalition soldiers, he partnered with the Ghazni Ministry of Health to improve the delivery of healthcare to residents of the province.
“Afghanistan has a great plan for medical care through its ‘basic’ package of health services and ‘essential’ package hospital services, developed with assistance from the U.S. Agency for International Development [USAID], and which we used as our road map for the Afghan public health service,” Dr. Wilson says. He and a nurse practitioner from the nearby provincial reconstruction team worked out of a forward operating base outside Ghazni’s provincial capital—the city of Ghazni—and the nearby provincial hospital. He says his hospitalist background was helpful when it came to working with and teaching the Afghan physicians and nurses at the hospital, which served as the referral center for several surrounding provinces.
“There was no infection-control program; their hospital and clinics were heated by wood stoves; and they were using the one endotracheal tube that had been left by the International Red Cross years earlier,” he says, noting that during his tour, the U.S. military dropped basic medical equipment and supplies—which were shared with the local hospital—into his forward operating base. “They were doing anesthesia without monitors. We trained them with an initial focus of making surgery safer. … To say that it was challenging is an understatement, and for many different reasons.”
Almost every other week, Dr. Wilson hosted a medical conference at his base for 10 to 20 Afghan physicians. Due to local customs, female providers were not allowed to travel without a male relative, so Dr. Wilson’s team videotaped the classes, had them translated into the Pashto language, and arranged with the hospital directors to distribute them to female physicians.
The needs in both army and civilian circumstances are huge in Afghanistan. Most Afghan hospitals and clinics are without Internet access, so decision support and telemedicine consultative service is out of the question. Textbooks are in short supply, too. Because the Taliban decreed that no image of a human being is allowed in print, they confiscated and destroyed all of the country’s anatomy books.
In terms of training, the key to success with locals is demonstrating what success can look like.
“Most of these providers have practiced in a system that they think is as good as it can be given the lack of advanced machinery and equipment,” Dr. Wilson says.
Physicians who visit U.S. military or Western hospitals and witness the successes possible in infection control, nursing care, medication administration, and medical documentation return to Afghanistan excited about the skills introduced to them. “They see that the provision of really good medical care is more dependent on having a clean space, a well-organized system, good communication, and solid basic medical care,” Dr. Wilson says.
Contrast to Care Continuity
Col. Walt Franz, MD, of U.S. Army Medical Corps headquartered in Amarah/Al Kut, Iraq, has just begun the work of partnering with Iraqi physicians and nurses for the first time since 2003. In 2004, as a public health team leader, his primary task was helping Iraqi providers with hospital and clinic projects. The projects ranged in cost from $40,000 (for securing an X-ray machine) to $5,000 for such smaller repairs and fix-ups as securing parts to make an elevator run. In fact, patients were being carried up several flights of stairs in the local, six-story hospital.
For about five months in 2008, Dr. Franz was deputy commander for clinical services for hospital and outpatient medical care at a combat support hospital. Since the beginning of 2009, he has been the commander of the 945th Forward Surgical Team at a small forward base in Amarah, near the Iraq-Iran border. “Our mission here is to provide urgent surgical resuscitation for the critically wounded and evac[uation] by helo [helicopter],” Dr. Franz says.
When he’s at home and working at the Mayo Clinic in Rochester, Minn., he practices primarily as a family physician. With nearly 30 years of clinical practice under his belt, Dr. Franz also puts in plenty of hours as a hospitalist. He has practiced during four deployments: three to Iraq and one to Germany.
“Active duty in a war zone presents experiences ranging from the inspiring to the absolutely tragic,” Dr. Franz says. “There is nothing worse than a casualty coming in on a medevac. It’s someone’s son or daughter or husband or wife, and nothing approaches the joy of helping a soldier. In fact, as a civilian, we scrupulously follow the Geneva Convention requirements.” (The treaty affords wounded and sick soldiers to be cared for and protected even though they may become prisoners of war.)
After you eliminate the dangers of enemy fire, there are still big differences between combat versus civilian medicine, he says. One is that combat medicine is usually acute care with little or no followup in the theater of operation, Dr. Franz says. Combat medicine has a strong foundation in echelons of care and evacuations away from the initial point of care. It runs concurrent to the civilian premise of continuity, and the limited number of specialists in theater usually means the Army relies on evacuation or electronic consults.
Maysan Province, where Dr. Franz is stationed, is the poorest part of Iraq. Because of its large Shia population, its citizens were devastated during the Iran-Iraq war and brutalized by Saddam Hussein. “The docs here are very street-smart; their work ethic is great and they have done without for a long time,” Dr. Franz says. Providers at the 540-bed hospital in Al Amarah see 200 patients per day in the ED; several hundred outpatients are triaged, and senior staff physicians see 75 or more cases daily. “One young doc told me it was not unusual to have 500 patients present to a regional ED in a 24-hour period, making triage and care almost overwhelming,” he says.
The biggest problem Dr. Franz witnesses in Iraqi hospitals is the lack of specialty nurses. His teams are teaching classes and training trainers in ED triage, basic ICU care, and the ultrasound FAST (Focused Assessment with Sonography in Trauma) exam skills Iraqi providers can use anywhere in the hospital.
Other issues include a lack of continuing medical education; poor infrastructure, which chokes the supply of pharmaceuticals and other medical equipment; and paucity of specialty nursing. Dr. Franz also cites critical staffing issues, such as the large number of physicians who have fled the country and the rising prominence of the private, fee-for-service care system, which can attract physicians and nurses away from the public system.
Care for Female Soldiers
With three other OB hospitalists, also known as laborists, Brook Thomson, MD, spent the summer organizing an OB/GYN hospital medicine program at Saint Alphonsus Regional Medical Center in Boise, Idaho. A veteran of military medicine, Dr. Thomson trained at Uniformed Services University of Health Sciences (USUHS) and completed an OB/GYN residency in 1997, then was stationed in Germany for four years. From 2001 to 2004, he served as chief of obstetrics at Madigan Army Medical Center in Tacoma, Wash., during which time he was deployed to Iraq for 10 months.
The OB/GYN expertise combined with the HM practice model that Dr. Thomson offers is a growing need in the military. “The number of women in the military is increasing, and there just aren’t a lot of people who understand female soldiers’ special needs,” he says.
Supporting women’s health has become an important aspect of battlefield medicine, namely the rooting out of potential sexual abuse. Dr. Thomson has published on the subject.1
In 2003, he was deployed as a general medical officer in Kuwait and assigned to the Basra area of Iraq, treating the gamut of patient needs. Recent Army policy changes, he says, ensure that OB/GYN military physicians now practice within their specialty.
A Canadian Perspective
Brendan James Hughes, MD, CCFP, returned from his military tour of duty and became a family practitioner in Lakefield, Ontario, a small community about 100 miles north of Toronto, and medical director of first-aid services for the Ontario Zone of the Canadian Red Cross.
In 2001, when Dr. Hughes was deployed as a hospitalist to Bosnia-Herzegovina for six months, the unrest from the civil war that involved Bosnians, Croatians, and Serbs (more than 100,000 were killed, and millions were injured or displaced), had settled, and his unit returned home without any loss of life. Upon his return, he transitioned from military life to become a full-time civilian hospitalist for six years in Ontario and Alberta. He now works as a part-time hospitalist.
Dr. Hughes says Canadian military practice is more acute and trauma-based now, as compared to his 2001 deployment in Eastern Europe. He notices many more deaths and major trauma cases in reports from Afghanistan, mostly blast injuries, limb amputations, and acute brain injuries, than there would be in a traditional, nonmilitary HM practice. He also notes that a lot of time and effort was placed on rehabilitation-focused practice that the patients required in the recovery phase.
Military practice differs from civilian hospitalist practice in other ways, he says. “In the military, every patient is essentially a workplace patient where the military is the employer,” Dr. Hughes says. Although clinicians maintain patient confidentiality, they are obliged to the chain of command to provide information on patient abilities. “We are careful not to relay a specific diagnosis without patient consent, but we have to dictate any needed restrictions on duty that are important in a combat situation, for themselves and for others,” he adds.
Such privacy and disclosure concerns are particularly difficult to navigate when it comes to diagnosis and treatment of alcohol and drug abuse, depression, post-traumatic stress, and suicide risk—issues that can lead soldiers to develop such long-term problems as substance abuse, marital discord, and marital abuse. TH
Andrea Sattinger is a freelance writer based in North Carolina.
Reference
- Thomson B, Nielsen P. Women’s healthcare in Operation Iraqi Freedom: a survey of camps with echelon one or two facilities. Mil Med. 2006;171:216-219.
The U.S. Army Medical Command
Each branch of the U.S. armed services—Army, Navy, Air Force, Marines and Coast Guard—has dedicated medical personnel and training programs.
The Army has the largest program, with more than 20,000 physicians, eight large medical centers, and 26 medical department activities; numerous clinics in the U.S., Europe, and Japan are grouped under six major subordinate commands called regional medical commands.
The Army offers training programs in six areas of medicine: dental, medical, medical service, medical specialist, nursing, and veterinary. The Army currently is offering $20,000 sign-on bonuses to medical and dental students, and offers free tuition and generous scholarship opportunities to qualified applicants.
For more information, visit www.armymedicine.army.mil/.
Darnall Army Medical Center

Darnall Army Medical Center is located 60 miles north of Austin and services more than 145,000 beneficiaries. The facility has five primary-care clinics, four troop medical clinics, 22 specialty clinics, and is home to the 1st Cavalry Division and the 4th Infantry Division (Mechanized).
Eisenhower Army Medical Center

The Dwight D. Eisenhower Army Medical Center hosts the Center for Total Access, which features lifelike electronic dummies that respond to stimuli and the effects of administering certain kinds of care and medication in a battlefield situation.
Landstuhl Regional Medical Center

Landstuhl Regional Medical Center is the only Army medical facility to house an Air Force Aero-medical Evacuation Unit. The hospital is also a primary evacuation point for injured soldiers who need further treatment before coming home to the U.S. or returning to their units in theater.
Madigan Army Medical Center

Madigan Army Medical Center is one of only three designated Level Two trauma centers within the U.S. Medical Command. Recently, the hospital's Andersen Simulation Center received a three-year accreditation from the American College of Surgeons, becoming the only Defense Department medical educational institution to attain that status.
San Antonio Military Medical Center

San Antonio Military Medical Center is located in San Antonio, Texas. It plays a critical role in patient care, graduate medical education and research, as well as taking care of wounded service members.
Tripler Army Medical Center

The Tripler Army Medical Center is the largest Army medical treatment facility in the Pacific Basin. The Center of Excellence in Disaster Management and Humanitarian Assistance is also located at the facility. The U.N. Department of Peacekeeping Operations has designated the CE as a Peace Operations Institute, the only United Nations-designated Peace Operations Institute currently in the United States.
Womack Army Medical Center

Womack Army Medial Center personnel use the latest technology to better serve its patients. From interventional radiology techniques to laser eye surgery, its physicians strive keep their fingers on the pulse of modern medicine.
William Beaumont Army Medical Center

The William Beaumont Army Medical Center is affiliated with such institutions as Texas Tech University School of Medicine, University of Texas at El Paso School of Nursing, and El Paso Community College Nursing School. It also provides opportunities for medical students throughout the nation to do rotations at the facility.
Walter Reed Army Medical Center

Walter Reed Army Medical Hospital generates the largest number of ongoing clinical research studies within the Department of Defense. It is often referred to as the flagship of DoD clinical research and is the largest and most diverse biomedical research laboratory in DoD.
Source: www.goarmy.com
Dr. Wilson’s photos from Afghanistan
Click images to enlarge

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|

|
PHOTOS COURTESY OF MAJ. RAMEY WILSON
Imagine being transferred to a hospital where the temperature is 20 below outside, and 40 inches of snow fill the parking lot. Few physicians would sign on for such an assignment. For a brave few, it’s all in a day’s work.
Maj. Ramey Wilson, MD, is a U.S. Army physician who encountered such conditions during his 15-month experience in Afghanistan. “A couple of times, when we couldn’t get helicopters [for evacuation], we had to turn my aid station into a mini-hospital. There were no nurses, labs, or X-ray,” he says. “With only basic supplies and my combat medics, we had to provide all the patient care until the weather broke.”
Not quite the circumstances most hospitalists encounter in their daily practice.
Hospitalists in the military face daunting odds, and at the same time are blessed with some unexpected advantages. On the plus side, military physicians cite the camaraderie, teamwork, honor of caring for soldiers, and the opportunity to train other providers, both in traditional, U.S.-based residencies and while deployed. Among the minuses, they mention a lack of equipment and supplies when they are assigned to forward-deployed soldiers on foreign soil, the heartache of being separated from family, and lower compensation. Most military physicians, however, say that the lower compensation can be offset by generous government benefits and the absence of medical school debt.
All in all, hospitalists in the military have a unique—and sometimes adventurous—story to tell.
Challenges Met, Success Exemplified
Dr. Wilson is a hospitalist and Army physician assigned to Fort Bragg, N.C. Until this past summer, he was the chief of internal medicine at Womack Army Medical Center, one of eight full-service hospitals in the U.S. Army Medical Command. Because the Army is still familiarizing itself with the HM model and the role hospitalists play in the delivery of healthcare, resident house staff meet many of the operational needs, including night and weekend coverage. “The Army doesn’t have a good system for 24-hour continuous care at busy hospitals without residents,” Dr. Wilson says, “and we’ve worked hard to get hospitalists into our system.”
While other Army medical centers have internal-medicine residencies, Womack has only a family medicine residency program. Residents once provided extensive coverage for the hospital, but decreasing numbers (only four interns this year) and work-hour restrictions have shifted the inpatient responsibilities to the internal-medicine staff. “All of the military general internists have functionally become hospitalists to support the inpatient medicine and ICU services,” Dr. Wilson says. “Our family medicine house staff coverage has evaporated.”
The conditions he sees at Womack are similar to what he sees at FirstHealth Moore Regional Hospital, the civilian community hospital in Pinehurst, N.C., where he practices part time. Womack serves two major military populations: those on active duty and their family members, and those no longer on active duty or retired (and not a part of the Veterans Administration program).
—Col. Walt Franz, MD, U.S. Army Medical Corps, Amarah/Al Kut, Iraq
Dr. Wilson, who served in the Ghazni province in eastern Afghanistan, was the only American physician in an area of 8,800 square miles. He and his physician-assistant staff were tasked with keeping U.S. soldiers healthy, serving acute resuscitative trauma care and “basic sick call.” In addition to caring for U.S. and coalition soldiers, he partnered with the Ghazni Ministry of Health to improve the delivery of healthcare to residents of the province.
“Afghanistan has a great plan for medical care through its ‘basic’ package of health services and ‘essential’ package hospital services, developed with assistance from the U.S. Agency for International Development [USAID], and which we used as our road map for the Afghan public health service,” Dr. Wilson says. He and a nurse practitioner from the nearby provincial reconstruction team worked out of a forward operating base outside Ghazni’s provincial capital—the city of Ghazni—and the nearby provincial hospital. He says his hospitalist background was helpful when it came to working with and teaching the Afghan physicians and nurses at the hospital, which served as the referral center for several surrounding provinces.
“There was no infection-control program; their hospital and clinics were heated by wood stoves; and they were using the one endotracheal tube that had been left by the International Red Cross years earlier,” he says, noting that during his tour, the U.S. military dropped basic medical equipment and supplies—which were shared with the local hospital—into his forward operating base. “They were doing anesthesia without monitors. We trained them with an initial focus of making surgery safer. … To say that it was challenging is an understatement, and for many different reasons.”
Almost every other week, Dr. Wilson hosted a medical conference at his base for 10 to 20 Afghan physicians. Due to local customs, female providers were not allowed to travel without a male relative, so Dr. Wilson’s team videotaped the classes, had them translated into the Pashto language, and arranged with the hospital directors to distribute them to female physicians.
The needs in both army and civilian circumstances are huge in Afghanistan. Most Afghan hospitals and clinics are without Internet access, so decision support and telemedicine consultative service is out of the question. Textbooks are in short supply, too. Because the Taliban decreed that no image of a human being is allowed in print, they confiscated and destroyed all of the country’s anatomy books.
In terms of training, the key to success with locals is demonstrating what success can look like.
“Most of these providers have practiced in a system that they think is as good as it can be given the lack of advanced machinery and equipment,” Dr. Wilson says.
Physicians who visit U.S. military or Western hospitals and witness the successes possible in infection control, nursing care, medication administration, and medical documentation return to Afghanistan excited about the skills introduced to them. “They see that the provision of really good medical care is more dependent on having a clean space, a well-organized system, good communication, and solid basic medical care,” Dr. Wilson says.
Contrast to Care Continuity
Col. Walt Franz, MD, of U.S. Army Medical Corps headquartered in Amarah/Al Kut, Iraq, has just begun the work of partnering with Iraqi physicians and nurses for the first time since 2003. In 2004, as a public health team leader, his primary task was helping Iraqi providers with hospital and clinic projects. The projects ranged in cost from $40,000 (for securing an X-ray machine) to $5,000 for such smaller repairs and fix-ups as securing parts to make an elevator run. In fact, patients were being carried up several flights of stairs in the local, six-story hospital.
For about five months in 2008, Dr. Franz was deputy commander for clinical services for hospital and outpatient medical care at a combat support hospital. Since the beginning of 2009, he has been the commander of the 945th Forward Surgical Team at a small forward base in Amarah, near the Iraq-Iran border. “Our mission here is to provide urgent surgical resuscitation for the critically wounded and evac[uation] by helo [helicopter],” Dr. Franz says.
When he’s at home and working at the Mayo Clinic in Rochester, Minn., he practices primarily as a family physician. With nearly 30 years of clinical practice under his belt, Dr. Franz also puts in plenty of hours as a hospitalist. He has practiced during four deployments: three to Iraq and one to Germany.
“Active duty in a war zone presents experiences ranging from the inspiring to the absolutely tragic,” Dr. Franz says. “There is nothing worse than a casualty coming in on a medevac. It’s someone’s son or daughter or husband or wife, and nothing approaches the joy of helping a soldier. In fact, as a civilian, we scrupulously follow the Geneva Convention requirements.” (The treaty affords wounded and sick soldiers to be cared for and protected even though they may become prisoners of war.)
After you eliminate the dangers of enemy fire, there are still big differences between combat versus civilian medicine, he says. One is that combat medicine is usually acute care with little or no followup in the theater of operation, Dr. Franz says. Combat medicine has a strong foundation in echelons of care and evacuations away from the initial point of care. It runs concurrent to the civilian premise of continuity, and the limited number of specialists in theater usually means the Army relies on evacuation or electronic consults.
Maysan Province, where Dr. Franz is stationed, is the poorest part of Iraq. Because of its large Shia population, its citizens were devastated during the Iran-Iraq war and brutalized by Saddam Hussein. “The docs here are very street-smart; their work ethic is great and they have done without for a long time,” Dr. Franz says. Providers at the 540-bed hospital in Al Amarah see 200 patients per day in the ED; several hundred outpatients are triaged, and senior staff physicians see 75 or more cases daily. “One young doc told me it was not unusual to have 500 patients present to a regional ED in a 24-hour period, making triage and care almost overwhelming,” he says.
The biggest problem Dr. Franz witnesses in Iraqi hospitals is the lack of specialty nurses. His teams are teaching classes and training trainers in ED triage, basic ICU care, and the ultrasound FAST (Focused Assessment with Sonography in Trauma) exam skills Iraqi providers can use anywhere in the hospital.
Other issues include a lack of continuing medical education; poor infrastructure, which chokes the supply of pharmaceuticals and other medical equipment; and paucity of specialty nursing. Dr. Franz also cites critical staffing issues, such as the large number of physicians who have fled the country and the rising prominence of the private, fee-for-service care system, which can attract physicians and nurses away from the public system.
Care for Female Soldiers
With three other OB hospitalists, also known as laborists, Brook Thomson, MD, spent the summer organizing an OB/GYN hospital medicine program at Saint Alphonsus Regional Medical Center in Boise, Idaho. A veteran of military medicine, Dr. Thomson trained at Uniformed Services University of Health Sciences (USUHS) and completed an OB/GYN residency in 1997, then was stationed in Germany for four years. From 2001 to 2004, he served as chief of obstetrics at Madigan Army Medical Center in Tacoma, Wash., during which time he was deployed to Iraq for 10 months.
The OB/GYN expertise combined with the HM practice model that Dr. Thomson offers is a growing need in the military. “The number of women in the military is increasing, and there just aren’t a lot of people who understand female soldiers’ special needs,” he says.
Supporting women’s health has become an important aspect of battlefield medicine, namely the rooting out of potential sexual abuse. Dr. Thomson has published on the subject.1
In 2003, he was deployed as a general medical officer in Kuwait and assigned to the Basra area of Iraq, treating the gamut of patient needs. Recent Army policy changes, he says, ensure that OB/GYN military physicians now practice within their specialty.
A Canadian Perspective
Brendan James Hughes, MD, CCFP, returned from his military tour of duty and became a family practitioner in Lakefield, Ontario, a small community about 100 miles north of Toronto, and medical director of first-aid services for the Ontario Zone of the Canadian Red Cross.
In 2001, when Dr. Hughes was deployed as a hospitalist to Bosnia-Herzegovina for six months, the unrest from the civil war that involved Bosnians, Croatians, and Serbs (more than 100,000 were killed, and millions were injured or displaced), had settled, and his unit returned home without any loss of life. Upon his return, he transitioned from military life to become a full-time civilian hospitalist for six years in Ontario and Alberta. He now works as a part-time hospitalist.
Dr. Hughes says Canadian military practice is more acute and trauma-based now, as compared to his 2001 deployment in Eastern Europe. He notices many more deaths and major trauma cases in reports from Afghanistan, mostly blast injuries, limb amputations, and acute brain injuries, than there would be in a traditional, nonmilitary HM practice. He also notes that a lot of time and effort was placed on rehabilitation-focused practice that the patients required in the recovery phase.
Military practice differs from civilian hospitalist practice in other ways, he says. “In the military, every patient is essentially a workplace patient where the military is the employer,” Dr. Hughes says. Although clinicians maintain patient confidentiality, they are obliged to the chain of command to provide information on patient abilities. “We are careful not to relay a specific diagnosis without patient consent, but we have to dictate any needed restrictions on duty that are important in a combat situation, for themselves and for others,” he adds.
Such privacy and disclosure concerns are particularly difficult to navigate when it comes to diagnosis and treatment of alcohol and drug abuse, depression, post-traumatic stress, and suicide risk—issues that can lead soldiers to develop such long-term problems as substance abuse, marital discord, and marital abuse. TH
Andrea Sattinger is a freelance writer based in North Carolina.
Reference
- Thomson B, Nielsen P. Women’s healthcare in Operation Iraqi Freedom: a survey of camps with echelon one or two facilities. Mil Med. 2006;171:216-219.
The U.S. Army Medical Command
Each branch of the U.S. armed services—Army, Navy, Air Force, Marines and Coast Guard—has dedicated medical personnel and training programs.
The Army has the largest program, with more than 20,000 physicians, eight large medical centers, and 26 medical department activities; numerous clinics in the U.S., Europe, and Japan are grouped under six major subordinate commands called regional medical commands.
The Army offers training programs in six areas of medicine: dental, medical, medical service, medical specialist, nursing, and veterinary. The Army currently is offering $20,000 sign-on bonuses to medical and dental students, and offers free tuition and generous scholarship opportunities to qualified applicants.
For more information, visit www.armymedicine.army.mil/.
Darnall Army Medical Center
Darnall Army Medical Center is located 60 miles north of Austin and services more than 145,000 beneficiaries. The facility has five primary-care clinics, four troop medical clinics, 22 specialty clinics, and is home to the 1st Cavalry Division and the 4th Infantry Division (Mechanized).
Eisenhower Army Medical Center
The Dwight D. Eisenhower Army Medical Center hosts the Center for Total Access, which features lifelike electronic dummies that respond to stimuli and the effects of administering certain kinds of care and medication in a battlefield situation.
Landstuhl Regional Medical Center
Landstuhl Regional Medical Center is the only Army medical facility to house an Air Force Aero-medical Evacuation Unit. The hospital is also a primary evacuation point for injured soldiers who need further treatment before coming home to the U.S. or returning to their units in theater.
Madigan Army Medical Center
Madigan Army Medical Center is one of only three designated Level Two trauma centers within the U.S. Medical Command. Recently, the hospital's Andersen Simulation Center received a three-year accreditation from the American College of Surgeons, becoming the only Defense Department medical educational institution to attain that status.
San Antonio Military Medical Center
San Antonio Military Medical Center is located in San Antonio, Texas. It plays a critical role in patient care, graduate medical education and research, as well as taking care of wounded service members.
Tripler Army Medical Center
The Tripler Army Medical Center is the largest Army medical treatment facility in the Pacific Basin. The Center of Excellence in Disaster Management and Humanitarian Assistance is also located at the facility. The U.N. Department of Peacekeeping Operations has designated the CE as a Peace Operations Institute, the only United Nations-designated Peace Operations Institute currently in the United States.
Womack Army Medical Center
Womack Army Medial Center personnel use the latest technology to better serve its patients. From interventional radiology techniques to laser eye surgery, its physicians strive keep their fingers on the pulse of modern medicine.
William Beaumont Army Medical Center
The William Beaumont Army Medical Center is affiliated with such institutions as Texas Tech University School of Medicine, University of Texas at El Paso School of Nursing, and El Paso Community College Nursing School. It also provides opportunities for medical students throughout the nation to do rotations at the facility.
Walter Reed Army Medical Center
Walter Reed Army Medical Hospital generates the largest number of ongoing clinical research studies within the Department of Defense. It is often referred to as the flagship of DoD clinical research and is the largest and most diverse biomedical research laboratory in DoD.
Source: www.goarmy.com
Dr. Wilson’s photos from Afghanistan
Click images to enlarge
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHOTOS COURTESY OF MAJ. RAMEY WILSON
Imagine being transferred to a hospital where the temperature is 20 below outside, and 40 inches of snow fill the parking lot. Few physicians would sign on for such an assignment. For a brave few, it’s all in a day’s work.
Maj. Ramey Wilson, MD, is a U.S. Army physician who encountered such conditions during his 15-month experience in Afghanistan. “A couple of times, when we couldn’t get helicopters [for evacuation], we had to turn my aid station into a mini-hospital. There were no nurses, labs, or X-ray,” he says. “With only basic supplies and my combat medics, we had to provide all the patient care until the weather broke.”
Not quite the circumstances most hospitalists encounter in their daily practice.
Hospitalists in the military face daunting odds, and at the same time are blessed with some unexpected advantages. On the plus side, military physicians cite the camaraderie, teamwork, honor of caring for soldiers, and the opportunity to train other providers, both in traditional, U.S.-based residencies and while deployed. Among the minuses, they mention a lack of equipment and supplies when they are assigned to forward-deployed soldiers on foreign soil, the heartache of being separated from family, and lower compensation. Most military physicians, however, say that the lower compensation can be offset by generous government benefits and the absence of medical school debt.
All in all, hospitalists in the military have a unique—and sometimes adventurous—story to tell.
Challenges Met, Success Exemplified
Dr. Wilson is a hospitalist and Army physician assigned to Fort Bragg, N.C. Until this past summer, he was the chief of internal medicine at Womack Army Medical Center, one of eight full-service hospitals in the U.S. Army Medical Command. Because the Army is still familiarizing itself with the HM model and the role hospitalists play in the delivery of healthcare, resident house staff meet many of the operational needs, including night and weekend coverage. “The Army doesn’t have a good system for 24-hour continuous care at busy hospitals without residents,” Dr. Wilson says, “and we’ve worked hard to get hospitalists into our system.”
While other Army medical centers have internal-medicine residencies, Womack has only a family medicine residency program. Residents once provided extensive coverage for the hospital, but decreasing numbers (only four interns this year) and work-hour restrictions have shifted the inpatient responsibilities to the internal-medicine staff. “All of the military general internists have functionally become hospitalists to support the inpatient medicine and ICU services,” Dr. Wilson says. “Our family medicine house staff coverage has evaporated.”
The conditions he sees at Womack are similar to what he sees at FirstHealth Moore Regional Hospital, the civilian community hospital in Pinehurst, N.C., where he practices part time. Womack serves two major military populations: those on active duty and their family members, and those no longer on active duty or retired (and not a part of the Veterans Administration program).
—Col. Walt Franz, MD, U.S. Army Medical Corps, Amarah/Al Kut, Iraq
Dr. Wilson, who served in the Ghazni province in eastern Afghanistan, was the only American physician in an area of 8,800 square miles. He and his physician-assistant staff were tasked with keeping U.S. soldiers healthy, serving acute resuscitative trauma care and “basic sick call.” In addition to caring for U.S. and coalition soldiers, he partnered with the Ghazni Ministry of Health to improve the delivery of healthcare to residents of the province.
“Afghanistan has a great plan for medical care through its ‘basic’ package of health services and ‘essential’ package hospital services, developed with assistance from the U.S. Agency for International Development [USAID], and which we used as our road map for the Afghan public health service,” Dr. Wilson says. He and a nurse practitioner from the nearby provincial reconstruction team worked out of a forward operating base outside Ghazni’s provincial capital—the city of Ghazni—and the nearby provincial hospital. He says his hospitalist background was helpful when it came to working with and teaching the Afghan physicians and nurses at the hospital, which served as the referral center for several surrounding provinces.
“There was no infection-control program; their hospital and clinics were heated by wood stoves; and they were using the one endotracheal tube that had been left by the International Red Cross years earlier,” he says, noting that during his tour, the U.S. military dropped basic medical equipment and supplies—which were shared with the local hospital—into his forward operating base. “They were doing anesthesia without monitors. We trained them with an initial focus of making surgery safer. … To say that it was challenging is an understatement, and for many different reasons.”
Almost every other week, Dr. Wilson hosted a medical conference at his base for 10 to 20 Afghan physicians. Due to local customs, female providers were not allowed to travel without a male relative, so Dr. Wilson’s team videotaped the classes, had them translated into the Pashto language, and arranged with the hospital directors to distribute them to female physicians.
The needs in both army and civilian circumstances are huge in Afghanistan. Most Afghan hospitals and clinics are without Internet access, so decision support and telemedicine consultative service is out of the question. Textbooks are in short supply, too. Because the Taliban decreed that no image of a human being is allowed in print, they confiscated and destroyed all of the country’s anatomy books.
In terms of training, the key to success with locals is demonstrating what success can look like.
“Most of these providers have practiced in a system that they think is as good as it can be given the lack of advanced machinery and equipment,” Dr. Wilson says.
Physicians who visit U.S. military or Western hospitals and witness the successes possible in infection control, nursing care, medication administration, and medical documentation return to Afghanistan excited about the skills introduced to them. “They see that the provision of really good medical care is more dependent on having a clean space, a well-organized system, good communication, and solid basic medical care,” Dr. Wilson says.
Contrast to Care Continuity
Col. Walt Franz, MD, of U.S. Army Medical Corps headquartered in Amarah/Al Kut, Iraq, has just begun the work of partnering with Iraqi physicians and nurses for the first time since 2003. In 2004, as a public health team leader, his primary task was helping Iraqi providers with hospital and clinic projects. The projects ranged in cost from $40,000 (for securing an X-ray machine) to $5,000 for such smaller repairs and fix-ups as securing parts to make an elevator run. In fact, patients were being carried up several flights of stairs in the local, six-story hospital.
For about five months in 2008, Dr. Franz was deputy commander for clinical services for hospital and outpatient medical care at a combat support hospital. Since the beginning of 2009, he has been the commander of the 945th Forward Surgical Team at a small forward base in Amarah, near the Iraq-Iran border. “Our mission here is to provide urgent surgical resuscitation for the critically wounded and evac[uation] by helo [helicopter],” Dr. Franz says.
When he’s at home and working at the Mayo Clinic in Rochester, Minn., he practices primarily as a family physician. With nearly 30 years of clinical practice under his belt, Dr. Franz also puts in plenty of hours as a hospitalist. He has practiced during four deployments: three to Iraq and one to Germany.
“Active duty in a war zone presents experiences ranging from the inspiring to the absolutely tragic,” Dr. Franz says. “There is nothing worse than a casualty coming in on a medevac. It’s someone’s son or daughter or husband or wife, and nothing approaches the joy of helping a soldier. In fact, as a civilian, we scrupulously follow the Geneva Convention requirements.” (The treaty affords wounded and sick soldiers to be cared for and protected even though they may become prisoners of war.)
After you eliminate the dangers of enemy fire, there are still big differences between combat versus civilian medicine, he says. One is that combat medicine is usually acute care with little or no followup in the theater of operation, Dr. Franz says. Combat medicine has a strong foundation in echelons of care and evacuations away from the initial point of care. It runs concurrent to the civilian premise of continuity, and the limited number of specialists in theater usually means the Army relies on evacuation or electronic consults.
Maysan Province, where Dr. Franz is stationed, is the poorest part of Iraq. Because of its large Shia population, its citizens were devastated during the Iran-Iraq war and brutalized by Saddam Hussein. “The docs here are very street-smart; their work ethic is great and they have done without for a long time,” Dr. Franz says. Providers at the 540-bed hospital in Al Amarah see 200 patients per day in the ED; several hundred outpatients are triaged, and senior staff physicians see 75 or more cases daily. “One young doc told me it was not unusual to have 500 patients present to a regional ED in a 24-hour period, making triage and care almost overwhelming,” he says.
The biggest problem Dr. Franz witnesses in Iraqi hospitals is the lack of specialty nurses. His teams are teaching classes and training trainers in ED triage, basic ICU care, and the ultrasound FAST (Focused Assessment with Sonography in Trauma) exam skills Iraqi providers can use anywhere in the hospital.
Other issues include a lack of continuing medical education; poor infrastructure, which chokes the supply of pharmaceuticals and other medical equipment; and paucity of specialty nursing. Dr. Franz also cites critical staffing issues, such as the large number of physicians who have fled the country and the rising prominence of the private, fee-for-service care system, which can attract physicians and nurses away from the public system.
Care for Female Soldiers
With three other OB hospitalists, also known as laborists, Brook Thomson, MD, spent the summer organizing an OB/GYN hospital medicine program at Saint Alphonsus Regional Medical Center in Boise, Idaho. A veteran of military medicine, Dr. Thomson trained at Uniformed Services University of Health Sciences (USUHS) and completed an OB/GYN residency in 1997, then was stationed in Germany for four years. From 2001 to 2004, he served as chief of obstetrics at Madigan Army Medical Center in Tacoma, Wash., during which time he was deployed to Iraq for 10 months.
The OB/GYN expertise combined with the HM practice model that Dr. Thomson offers is a growing need in the military. “The number of women in the military is increasing, and there just aren’t a lot of people who understand female soldiers’ special needs,” he says.
Supporting women’s health has become an important aspect of battlefield medicine, namely the rooting out of potential sexual abuse. Dr. Thomson has published on the subject.1
In 2003, he was deployed as a general medical officer in Kuwait and assigned to the Basra area of Iraq, treating the gamut of patient needs. Recent Army policy changes, he says, ensure that OB/GYN military physicians now practice within their specialty.
A Canadian Perspective
Brendan James Hughes, MD, CCFP, returned from his military tour of duty and became a family practitioner in Lakefield, Ontario, a small community about 100 miles north of Toronto, and medical director of first-aid services for the Ontario Zone of the Canadian Red Cross.
In 2001, when Dr. Hughes was deployed as a hospitalist to Bosnia-Herzegovina for six months, the unrest from the civil war that involved Bosnians, Croatians, and Serbs (more than 100,000 were killed, and millions were injured or displaced), had settled, and his unit returned home without any loss of life. Upon his return, he transitioned from military life to become a full-time civilian hospitalist for six years in Ontario and Alberta. He now works as a part-time hospitalist.
Dr. Hughes says Canadian military practice is more acute and trauma-based now, as compared to his 2001 deployment in Eastern Europe. He notices many more deaths and major trauma cases in reports from Afghanistan, mostly blast injuries, limb amputations, and acute brain injuries, than there would be in a traditional, nonmilitary HM practice. He also notes that a lot of time and effort was placed on rehabilitation-focused practice that the patients required in the recovery phase.
Military practice differs from civilian hospitalist practice in other ways, he says. “In the military, every patient is essentially a workplace patient where the military is the employer,” Dr. Hughes says. Although clinicians maintain patient confidentiality, they are obliged to the chain of command to provide information on patient abilities. “We are careful not to relay a specific diagnosis without patient consent, but we have to dictate any needed restrictions on duty that are important in a combat situation, for themselves and for others,” he adds.
Such privacy and disclosure concerns are particularly difficult to navigate when it comes to diagnosis and treatment of alcohol and drug abuse, depression, post-traumatic stress, and suicide risk—issues that can lead soldiers to develop such long-term problems as substance abuse, marital discord, and marital abuse. TH
Andrea Sattinger is a freelance writer based in North Carolina.
Reference
- Thomson B, Nielsen P. Women’s healthcare in Operation Iraqi Freedom: a survey of camps with echelon one or two facilities. Mil Med. 2006;171:216-219.
The U.S. Army Medical Command
Each branch of the U.S. armed services—Army, Navy, Air Force, Marines and Coast Guard—has dedicated medical personnel and training programs.
The Army has the largest program, with more than 20,000 physicians, eight large medical centers, and 26 medical department activities; numerous clinics in the U.S., Europe, and Japan are grouped under six major subordinate commands called regional medical commands.
The Army offers training programs in six areas of medicine: dental, medical, medical service, medical specialist, nursing, and veterinary. The Army currently is offering $20,000 sign-on bonuses to medical and dental students, and offers free tuition and generous scholarship opportunities to qualified applicants.
For more information, visit www.armymedicine.army.mil/.
Darnall Army Medical Center
Darnall Army Medical Center is located 60 miles north of Austin and services more than 145,000 beneficiaries. The facility has five primary-care clinics, four troop medical clinics, 22 specialty clinics, and is home to the 1st Cavalry Division and the 4th Infantry Division (Mechanized).
Eisenhower Army Medical Center
The Dwight D. Eisenhower Army Medical Center hosts the Center for Total Access, which features lifelike electronic dummies that respond to stimuli and the effects of administering certain kinds of care and medication in a battlefield situation.
Landstuhl Regional Medical Center
Landstuhl Regional Medical Center is the only Army medical facility to house an Air Force Aero-medical Evacuation Unit. The hospital is also a primary evacuation point for injured soldiers who need further treatment before coming home to the U.S. or returning to their units in theater.
Madigan Army Medical Center
Madigan Army Medical Center is one of only three designated Level Two trauma centers within the U.S. Medical Command. Recently, the hospital's Andersen Simulation Center received a three-year accreditation from the American College of Surgeons, becoming the only Defense Department medical educational institution to attain that status.
San Antonio Military Medical Center
San Antonio Military Medical Center is located in San Antonio, Texas. It plays a critical role in patient care, graduate medical education and research, as well as taking care of wounded service members.
Tripler Army Medical Center
The Tripler Army Medical Center is the largest Army medical treatment facility in the Pacific Basin. The Center of Excellence in Disaster Management and Humanitarian Assistance is also located at the facility. The U.N. Department of Peacekeeping Operations has designated the CE as a Peace Operations Institute, the only United Nations-designated Peace Operations Institute currently in the United States.
Womack Army Medical Center
Womack Army Medial Center personnel use the latest technology to better serve its patients. From interventional radiology techniques to laser eye surgery, its physicians strive keep their fingers on the pulse of modern medicine.
William Beaumont Army Medical Center
The William Beaumont Army Medical Center is affiliated with such institutions as Texas Tech University School of Medicine, University of Texas at El Paso School of Nursing, and El Paso Community College Nursing School. It also provides opportunities for medical students throughout the nation to do rotations at the facility.
Walter Reed Army Medical Center
Walter Reed Army Medical Hospital generates the largest number of ongoing clinical research studies within the Department of Defense. It is often referred to as the flagship of DoD clinical research and is the largest and most diverse biomedical research laboratory in DoD.
Source: www.goarmy.com
Dr. Wilson’s photos from Afghanistan
Click images to enlarge
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHOTOS COURTESY OF MAJ. RAMEY WILSON
The Year Ahead
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM
Rising pressure to contain healthcare costs, increasing demands for safety and quality improvement, more focus on institutional accountability: In 2010, healthcare experts expect several dominant themes to continue converging and moving hospitalists even more to the center of key policy debates.
Peter Pronovost, MD, PhD, medical director of the Center for Innovation in Quality Patient Care and director of the Quality and Safety Research Group at Johns Hopkins University in Baltimore, sees three big themes moving to the fore. One is a greater focus on outcome measurements and accountability for performance, and he expects both carrots and sticks to be wielded. “So, both payment reform and social humiliation, or making things public,” Dr. Pronovost says. “Two, I see a lot more focus on measures that are population-based rather than hospital-based, so looking more at episodes of care.” The shift will force hospitalists to expand their purview beyond the hospital and, he says, partner more with community physicians to develop and monitor performance in such areas as transitions of care and general benchmarks of care.
Dr. Pronovost also expects “significant pressure on both the provider organization and individual clinician being paid less for what they do.” Finding ways to minimize costs will be a priority as payors increase scrutiny on expenses like unnecessary hospital readmissions. But hospitalists, he says, are better positioned than many other physicians to play a key role in the drive toward efficiency while also improving healthcare quality and safety. “I think hospitalists’ roles are going to go up dramatically,” Dr. Pronovost adds, “and I hope the field responds by making sure they put out people who have the skills to lead.”
End-of-Life Issues
Nancy Berlinger, PhD, deputy director and research scholar at The Hastings Center in Garrison, N.Y., cites end-of-life care as another theme likely to gain traction in 2010. As project director of the center’s revised ethical guidelines for end-of-life care, Dr. Berlinger notes how often clinicians in her working group have invoked the hospitalist profession. It’s no accident. “Hospitalists are increasingly associated with the care of patients on Medicare,” she says, adding Medicare beneficiaries are far more likely to be nearing the end of life.
Demographics suggest that connection will continue to grow in 2010 and beyond. Dr. Berlinger points to a 2009 New England Journal of Medicine study showing that the odds of a hospitalized Medicare patient receiving care from a hospitalist increased at a brisk 29.2% annual clip from 1997 through 2006.1 And while the U.S. faces a shortage of geriatricians, HM is growing rapidly as a medical profession. “By default, whether or not hospitalists self-identify as caring for older Americans,” Dr. Berlinger says, “this is their area of practical specialization.”
With that specialization comes added responsibility to assist with advanced-care planning and helping patients to document their wishes. Similarly, she says, it means acknowledging that these patients are more likely to have comorbid conditions and identify with goals of care. “I don’t think there’s any way around this,” she says. “Medicare and hospitalists, whether by accident or design, are increasingly joined at the hip. That is something that hospitalists, as a profession, will always need to keep their eye on.”
A parallel trend is that other doctors increasingly view hospitalists as hospital specialists. “The hospitalist’s responsibilities are not just in terms of the patients they care for, but also in terms of the institution itself,” Dr. Berlinger says. Non-staff physicians, for example, expect hospitalists to know how a hospital’s in-patient care system works. Practically speaking, as electronic medical records (EMR) become more commonplace, hospitalists will be increasingly relied upon to understand a hospital’s information technology.
—Peter Pronovost, MD, PhD, medical director, Center for Innovation in Quality Patient Care, Johns Hopkins University, Baltimore
New Economy, New Hospital Landscape
Douglas Wood, MD, chair of the Division of Health Care Policy and Research at the Mayo Clinic in Rochester, Minn., points to language in the federal healthcare reform legislation as evidence that hospitals and hospitalists will need to be in sync in other ways to avoid future penalties. One provision, for example, would increase the penalties for hospital-acquired infections. Other language seeks to reduce unnecessary readmissions.
Likewise, Dr. Wood says, addressing geographical variations in healthcare payments driven largely by unnecessary overutilization—including excessive use of ICU care, in-patient care, imaging, and specialist services—might mean asking hospitalists to take on more aspects of patient care.
Meanwhile, increased interest in demonstration projects that might achieve savings (e.g., accountable care organizations and bundled payments) suggests that proactive hospitals should again look to hospitalists. The flurry of new proposals won’t fundamentally change hospitalists’ responsibilities to provide effective and efficient care, “but it will put more emphasis on what they’re doing,” Dr. Wood says, “to the degree that hospitalists could take a lead in demonstrating how you can provide better outcomes at a lower overall utilization of resources.”
Regardless of how slowly or quickly these initiatives proceed at the national level, he says, hospitalists should be mindful that several states are well ahead of the curve and are likely to be more aggressive in instituting policy changes.
The Bottom Line
If there’s a single, overriding theme for 2010, Bradley Flansbaum, DO, MPH, FACP, FHM, director of hospitalist services at Lenox Hill Hospital in New York City and a member of SHM’s Public Policy Committee, says it might be that of dealing with the unknown. Squeezing healthcare costs and more tightly regulating inflation will have a greater effect on a hospital’s bottom line and thus impact what’s required of hospitalists. Even so, the profession will have to wait and see whether and how various proposals are codified and implemented. “We don’t know exactly what things are going to look like,” he says.
Nor is there a good sense of how new standards for transparency, quality, and accountability might be measured. “While people want more measurement and they want more report-card-type information, the data that we can acquire right now and how we analyze that data are still fairly primitive,” Dr. Flansbaum says. Even current benchmarks are lacking in how to determine who’s doing a good job and who isn’t, he says.
One big question that must be answered, then: Are we even looking at the right measurements? “Or, do the right measurements exist, or do we have the databases, the registries, the sources, to make the decisions we need to make?” he says.
Any new proposals will require another round of such questions and filling-in of blanks to add workable details to vague and potentially confusing language.
“I think we know that change is afoot, and most smart hospitalists know that the system needs to run leaner,” Dr. Flansbaum says. “But how each one of us is going to function in our hospital, and the kinds of demands that will be placed on us, and what we’re going to need to do with the doctors in the community and the other nonphysician colleagues that we work with, is all really unknown.” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Kuo YF, Sharma G, Freeman JL, Goodwin JS. Growth in the care of older patients by hospitalists in the United States. N Engl J Med. 2009;360(11): 1102-1112.
Image Source: PAGADESIGN, OVERSNAP/ISTOCKPHOTO.COM